Embed Size (px)
Citation preview
1 23
Cognitive Therapy andResearch ISSN 0147-5916 Cogn Ther ResDOI 10.1007/s10608-011-9381-z
A Latent Profile Analysis of Implicitand Explicit Cognitions Associated withDepression
Wendy J. Phillips, Donald W. Hine &Navjot Bhullar
1 23
Your article is protected by copyright and
all rights are held exclusively by Springer
Science+Business Media, LLC. This e-offprint
is for personal use only and shall not be self-
archived in electronic repositories. If you
wish to self-archive your work, please use the
accepted author’s version for posting to your
own website or your institution’s repository.
You may further deposit the accepted author’s
version on a funder’s repository at a funder’s
request, provided it is not made publicly
available until 12 months after publication.
ORIGINAL ARTICLE
A Latent Profile Analysis of Implicit and Explicit CognitionsAssociated with Depression
Wendy J. Phillips • Donald W. Hine •
Navjot Bhullar
� Springer Science+Business Media, LLC 2011
Abstract Dual-process cognitive profiles associated with
depression were identified in an undergraduate sample
(N = 306) and dysphoric sub-sample (n = 57). Two
Latent Profile Analyses (LPAs) were conducted on four
implicit and four explicit cognitions associated with
depression (self-esteem, negative memory, positive mem-
ory and dysfunctional beliefs). The first LPA, performed on
the total sample, produced a three-profile solution reflect-
ing quantitative shifts from generally negative, through
intermediate, to generally positive biases on both implicit
and explicit indicators. Patterns of biases across the profiles
were associated with incremental decreases in current
depressive symptoms, and logistic regression revealed that
profile membership significantly predicted depression sta-
tus 3 months later. Sequential logistic regression indicated
that implicit self-esteem was the strongest predictor of
subsequent dysphoria. The second LPA, focusing on a
subgroup of dysphoric participants, identified two qualita-
tively distinct profiles that may represent cognitive sub-
types of depression: (1) a schematic profile with multiple
negative biases and (2) a profile dominated by implicit
negative memory. These results are consistent with the
dual-process premise that implicit and explicit cognitive
processes are involved in depression and suggest that
treatment efficacy may be improved by incorporating
strategies that address implicit cognitive biases.
Keywords Depression � Cognitive bias � Dual-process �Implicit � Explicit
Individual responses to stressful or sad events differ
markedly. While some people experience temporary psy-
chological discomfort, others become overwhelmed by
despair. Influential cognitive theories of depression assume
that depression-vulnerable individuals possess negative
self-referential cognitions that precipitate negative
responses to daily stressors, which in turn lead to depres-
sion (Abramson et al. 1989; Beck 1987; Ingram 1984;
Teasdale 1988). Accordingly, an array of negative self-
cognitions have predicted subsequent depressive symp-
tomatology (Abramson et al. 2002; Joormann 2009; Wisco
2009)—including low or unstable self-esteem (e.g., Franck
and De Raedt 2007; Orth et al. 2009), heightened memory
for negative self-referential or emotional stimuli (e.g.,
Bellew and Hill 1991), decreased memory for positive
stimuli (e.g., Johnson et al. 2007), dysfunctional attitudes
(e.g., Reilly-Harrington et al. 1999), and self-deprecating
interpretations of ambiguous information (e.g., Rude et al.
2002). In support of cognitive vulnerability hypotheses,
several self-cognitions have also been found to interact
with stressful events to predict future depression; including
self-esteem, memory bias, and dysfunctional attitudes
(e.g., Bellew and Hill 1991; Haeffel et al. 2007; Reilly-
Harrington et al. 1999).
Recently, theorists have suggested that cognitive vul-
nerability to depression may result from an interaction
between two distinct information processing systems
(Beevers 2005; Carver et al. 2008; Haeffel et al. 2007).
This dual-process perspective recognizes the existence of
an implicit system that is automatic, effortless, affect-
oriented and guided by associative memory, and an explicit
system that is deliberate, motivated, effortful and directed
by rule-based learning (for review, see Evans 2008).
Neurophysiological research suggests that the proposed
cognitive systems map onto two distinct neurological
W. J. Phillips (&) � D. W. Hine � N. Bhullar
School of Behavioural, Cognitive and Social Sciences,
University of New England, Armidale, NSW 2351, Australia
e-mail: [email protected]; [email protected]
123
Cogn Ther Res
DOI 10.1007/s10608-011-9381-z
Author's personal copy

systems (e.g., Lieberman et al. 2004). Dual-process
accounts also tacitly differentiate between explicit output
(i.e., what one thinks) and explicit processes (i.e., how one
thinks). Explicit processing refers to how we interpret a
stimulus (e.g., our cognitive style; Alloy et al. 2000),
whereas explicit output refers to our final conscious inter-
pretation of the stimulus (e.g., our attitude). This distinc-
tion has been empirically supported in relation to
depressive cognitive constructs (Ciesla and Roberts 2007).
As system outputs, implicit and explicit cognitions are
presumed to possess characteristics of their originating
system, which require different modes of assessment.
Measures of explicit cognitions are based on participants’
deliberate consideration (e.g., self-reports) whereas impli-
cit cognitions may be assessed under automatic conditions
(e.g., memory associations). According to Moors et al.
(2010), measures may be automatic in several ways,
including unconscious, uncontrolled, goal-independent,
fast and efficient, and automaticity features may not nec-
essarily co-exist within a particular measure. Traditionally,
researchers have tended to assess depression-related cog-
nitions in the context of predictions made by depression
theories (e.g., Cognitive Theory; Beck 1987). However,
extant research can also be classified according to its
implicit or explicit status. All hypothesised depression-
related cognitions that have been assessed by explicit
measures may be considered explicit depressive cognitions
and all those assessed using implicit methods may be
considered implicit depressive cognitions.
Most dual-process models propose that implicit cogni-
tions reflect initial responses to a stimulus and that explicit
cognitions follow as the result of conscious reflection (see
Evans 2008). Beevers (2005) proposed that depression
occurs when negatively biased implicit processing remains
uncorrected by explicit processing. An initial response to a
negative stimulus is believed to reflect the activation of
negative implicit self-schemas. Effortful explicit process-
ing may perform a corrective function by reinterpreting
stressful stimuli, overriding implicit negative responses and
relieving negative affect. However, if corrective processing
is unsuccessful, negatively biased implicit output will be
reflected in negative explicit cognitions; resulting in
increased dysphoria, depleted cognitive resources and a
downward spiral into depression. Carver et al. (2008)
offered a similar perspective in their review of behavioural,
brain function, and serotonin studies relating to two system
models and depressive vulnerability.
Considerable evidence supports this conceptualisation
(see Beck 2008; Beevers 2005; Carver et al. 2008). For
example, experimental manipulations to deplete cognitive
resources have revealed automatic negative biases amongst
depression-vulnerable individuals that were not otherwise
evident (e.g., Wenzlaff and Bates 1998). Additionally,
neurophysiological evidence suggests that depression may
occur when regulatory functions of top-down (explicit)
processing are undermined and maladaptive bottom-up
(implicit) processing is exposed (see Beck 2008; Carver
et al. 2008; Thase 2009). Haeffel et al. (2007) proposed a
similar dual-process model of depression, but placed
greater emphasis on the influence of explicit processing as
the creator of the final interpretation of an event.
Researchers are currently investigating cognitive
mechanisms that may be involved in an interaction
between processing systems in depression (e.g., Philippot
and Brutoux 2008). However, little research has addressed
the coexistence of multiple implicit and explicit cognitive
biases within individuals, and how they co-exist to predict
current and future depressive symptoms.
One outstanding issue involves determining whether the
structure of dual-process cognitions associated with
depression is best conceptualised as dimensional or cate-
gorical. Specifically, it is not known whether implicit and
explicit cognitive biases coincide to reflect quantitative
differences along one or more continuous dimensions, or
whether these biases co-exist to create qualitatively distinct
subtypes of vulnerable and non-vulnerable individuals.
Only one study has examined the dimensionality of cog-
nitive vulnerability to depression in an unspecified sample.
Gibb and colleagues’ (2004) used taxometric procedures
developed by Meehl and colleagues (see Waller and Meehl
1998) to determine whether the latent structure of dys-
functional attitudes and cognitive styles was dimensional
or categorical. The analysis indicated that explicit cognitive
vulnerability to depression was dimensional amongst
undergraduates. That is, all participants possessed both
explicit depressive cognitions to some degree, and higher
levels of vulnerability were associated with greater
depressive symptomatology. Relatedly, depressive symp-
toms appear to be dimensionally distributed in unspecified
samples (e.g., Ruscio and Ruscio 2002)—although taxons
(i.e., distinct groups of symptoms) have been observed in
depressed samples (e.g., Ruscio et al. 2009).
Such dimensionality of explicit self-referential cogni-
tions and symptoms is consistent with most dual-process
accounts of depression, insofar as they posit that negative
explicit cognitions may emerge as a consequence of un-
curtailed negative implicit output (Beevers 2005; Carver
et al. 2008) and immediately precede and coincide with
depressive symptomatology (Beevers 2005; Carver et al.
2008; Haeffel et al. 2007). To date, no taxometric studies
of implicit cognitive vulnerabilities to depression have
been conducted. However, consistent with a dimensional
structure, significant relationships between negative
implicit cognitive biases and depression have been
observed in various sampled populations (Phillips et al.
2010) and implicit interpretations of ambiguous stories
Cogn Ther Res
123
Author's personal copy
have been found to vary systematically from negative to
positive across depressed, dysphoric and non-depressed
groups (Halberstadt et al. 2008). Therefore, to the extent
that explicit cognitive vulnerability appears to be dimen-
sional, underlying implicit cognitive vulnerabilities may
take a similarly quantitative form that foretells explicit
vulnerabilities and current depressive symptoms.
Alternatively, it is possible that dual-process cognitive
profiles in depression may adopt a qualitative structure.
Logically, four general co-occurrences of depressive cog-
nitions may exist: positive implicit/positive explicit; posi-
tive implicit/negative explicit; negative implicit/positive
explicit; and negative implicit/negative explicit—where
positive and negative refer to levels above and below
average, respectively.
The existence of profiles with compatible implicit and
explicit cognitions is supported by the evidence cited
above. Yet simultaneous possession of conflicting levels of
implicit and explicit depression-related cognitions has also
been observed and associated with a range of adverse
mental health outcomes (see Brinol et al. 2006). For
example, possession of high explicit and low implicit self-
esteem has been associated with poor emotional well-being
(Zelenski and Larsen 2003; cited in Brinol et al. 2006), and
possession of high implicit and low explicit self-esteem has
been associated with depressive cognitive styles and ner-
vousness (Schroder-Abe et al. 2007). Additionally, some
studies have observed relationships between high implicit
self-esteem and depression (e.g., Franck et al. 2007)
despite an overall association with low implicit self-esteem
in the literature (Phillips et al. 2010).
Both possible conflicting cognitive profiles are also
consistent with proposed dual-process mechanisms in
depression. Beevers (2005) and Haeffel et al. (2007) pro-
posed that negative implicit self-cognitions confer cogni-
tive vulnerability to depression. However, individuals with
latent negative implicit biases may escape dysphoria if
explicit processing can override implicit output and create
co-occurring positive explicit cognitions. Accordingly,
negative stressors have precipitated greater activation of a
variety of negative explicit depressive cognitions in for-
merly-dysphoric than in never-dysphoric groups (see Scher
et al. 2005). In contrast, positive implicit and negative
explicit cognitions may co-occur when maladaptive
explicit processing has overridden positive implicit output.
Haeffel et al. (2007) made the additional prediction that the
latter profile may also render an individual vulnerable to
future depression.
Whether dual-process depressive cognitive profiles are
dimensional or categorical, most cognitive theories of
depression predict that individuals who possess negatively
biased self-referential cognitions are particularly likely to
become depressed in the future (Abramson et al. 1989;
Beck 1987; Beevers 2005; Ingram 1984). However, dual-
process theorists differ in their predictions regarding which
type of processing confers the greater vulnerability to
depression. Beevers’ (2005) and Carver et al.’s (2008)
position suggests that individuals whose cognitive profiles
comprise negative implicit self-cognitions are most likely
to experience long-term depressive reactions, whereas
Haeffel et al. (2007) model suggests that cognitive profiles
containing negative explicit cognitions carry greater risk. If
dual-process depressive cognitive profiles are qualitative in
nature, then assessing which profiles confer risk for future
dysphoria has the capacity to shed light on the relative risk
conferred by implicit and explicit cognitions and their
co-occurrence.
A separate but related field of enquiry has investigated
the existence of subtypes of depression. Although taxo-
metric and factor-analytic studies of clinically depressed
samples have tended to identify a melancholic subtype of
depressive symptomatology (e.g., Haslam and Beck 1994),
few have supported the independence of specific clusters of
cognitions predicted by putative depression subtypes, such
as hopelessness (HT; Abramson et al. 1989), autonomous
and sociotropic (CT; Beck 1987), and self-critical (Blatt
and Homann 1992) depression (for reviews, see Adams
et al. 2007; Haslam 2007). For example, a factor analysis
conducted by Reno and Halaris (1989) did not differentiate
explicit cognitions stemming from HT and CT in a sample
of depressed inpatients, where depressive explanatory and
attributional styles (HT) and dysfunctional attitudes (CT)
loaded onto the same factor. Although it should be noted
that factor analytical studies have discriminated between
cognitions associated with putative subtypes (e.g., HT and
CT) in non-clinical, undergraduate, samples (e.g., Hankin
et al. 2007). One shortcoming of extant taxonic research is
the failure to investigate implicit depressive cognitions as
potential discriminators of depressive subtypes. The pos-
sibility that subtypes of depression may reflect differences
in implicit, but not explicit, negative cognitive biases (or
vice versa) has not been assessed.
The Current Study
The current study aimed to identify dual-process cognitive
profiles associated with depression by conducting a Latent
Profile Analysis (LPA) of four implicit and four explicit
cognitions associated with depression (i.e., implicit and
explicit self-esteem, positive and negative memory biases,
and dysfunctional self-beliefs) and to assess their ability to
predict subsequent depression. Our selection of cognitive
indicators was guided by dual-process theory. We selected
four explicit depression-related cognitions that have been
empirically identified as cognitive vulnerabilities for
Cogn Ther Res
123
Author's personal copy

depression1 and paired them with implicit measures that
purport to assess conceptually similar constructs.
LPA is a model-based procedure that groups participants
according to shared responses across multiple measures.
Grouping participants according to their cognitive charac-
teristics may facilitate insight into the relationships
between depression-related implicit and explicit cognitions
and how they co-exist to manifest in depression. In turn,
this may increase our understanding of cognitive vulnera-
bility to depression. Given that interventions for depression
typically address cognitive biases (e.g., Beck et al. 1979),
the results of this study may also inform the refinement of
treatment strategies.
Our primary aim was to determine whether dual-process
cognitive profiles associated with depression would exhibit
a quantitative or qualitative structure in an undergraduate
sample. Guided by dual-process theory and empirical evi-
dence, we hypothesized two alternative outcomes: (1a) At
least two quantitative profiles would emerge—one com-
prising dysphoric individuals with negative biases on all
implicit and explicit cognitions and another comprising
non-dysphoric individuals with positive biases on all cog-
nitions; and (1b) At least four qualitative profiles would
emerge, including profiles comprising: negative implicit
and explicit biases, negative implicit and positive explicit
biases; positive implicit and explicit biases; and positive
implicit and negative explicit biases.
Second, we aimed to investigate whether the profile
solution would predict participants’ depressive status
3 months later. On the basis of Beevers’ (2005) dual-
process theory and extant evidence, we hypothesized that:
(2) Emergent profiles featuring negatively biased implicit
and explicit cognitions or negative implicit and positive
explicit cognitions would predict subsequent depressive
status.
Third, we hoped to identify the relative contributions of
the eight cognitive indicators to future depression status.
We made no predictions regarding specific negatively
biased cognitions, but formed the general hypothesis that:
(3) Implicit biases would represent stronger predictors of
subsequent depressive status than explicit biases.
Fourth, we aimed to analyse a sub-sample of dysphoric
participants to identify dual-process cognitive profiles that
may represent subtypes of depression, and to compare
them with the cognitive profiles of never-depressed
participants.
Method
Participants
Three hundred and six first year undergraduates (57 Males
and 249 Females) at the University of New England par-
ticipated at Time 1 to receive course credits. Ages ranged
from 18 to 66 years (M = 29.91, SD = 10.72;
Median = 27.00).
Cognitive Bias Measures
Implicit Self-Esteem
The Name Letter Preference Task (NLPT; Nuttin 1985)
assesses preferences for one’s own name initials, which
have been shown to reflect self-evaluations that are acti-
vated automatically and without conscious self-reflection
(Koole et al. 2001). All letters of the alphabet were pre-
sented individually, in random order, for (up to) 30 s each.
Participants rated each letter from 1) not at all attractive to
9) very attractive. A practice session involving three
numbers preceded the task. Variable scores were calculated
from participants’ initials using the Z-transformed double-
correction algorithm (LeBel and Gawronski 2009). The
NLPT has previously demonstrated convergent and con-
struct validity (Koole et al. 2001) and test–retest reliability
(Bosson, Swann, and Pennebaker 2000). We assessed
reliability of the NLPT in the current study by calculating
Cronbach’s alpha from all letter scores after replacing each
participant’s own initial scores with the sample mean for
those letters (a = .84).
Explicit Self-Esteem
The Rosenberg Self-Esteem Scale (RSE; Rosenberg 1965)
includes 10 statements of self-worth (e.g., ‘‘On the whole, I
am satisfied with myself’’). Participants indicated agree-
ment with each statement from 1) totally agree to 4) totally
disagree. Scale scores were calculated by summing across
items (a = .91).
Implicit Dysfunctional Beliefs
The Scrambled Sentences Test (SST; Wenzlaff 1993)
measured participants’ tendency to interpret ambiguous
self-referential information (e.g., ‘‘winner born I am loser
a’’) in a positive way (‘‘I am a born winner’’) or a negative
way (‘‘I am a born loser’’). Insofar as interpretations
express underlying beliefs, we are referring to interpreta-
tions as implicit dysfunctional beliefs for ease of compar-
ison with explicit dysfunctional beliefs. Participants
unscrambled 20 sentences in 4 min to form the first
1 We did not include cognitive styles because we believe their
measure assesses explicit processes as well as output and no
conceptually equivalent implicit measure exists.
Cogn Ther Res
123
Author's personal copy

grammatically correct sentences that came to mind. Par-
ticipants simultaneously retained a six-digit number in
memory. The number was presented for 30 s prior to the
scrambled sentences and participants reported it after
unscrambling all sentences. Seventy-nine percent of par-
ticipants correctly recalled at least five digits. Participants
who recalled fewer digits were retained because poor recall
was weakly related to depressive symptoms, r = .06,
p = .28, and did not differ significantly between dysphoric
and non-dysphoric groups, v2 (1) = 2.23, p = .14
(Wenzlaff and Bates 1998). A practice session involving
three neutral sentences with a cognitive load preceded the
task. Proportion of negative to total solutions constituted
the variable scores. The SST has reliably discriminated
between depressed and non-depressed participants in sev-
eral studies (e.g., Rude et al. 2003).
Explicit Dysfunctional Beliefs
The Dysfunctional Attitudes Scale (DAS-A; Weissman and
Beck 1978) includes 40 dysfunctional beliefs that may
influence a person’s self-evaluation (e.g., ‘‘I am nothing if a
person I love doesn’t love me’’). Participants endorsed each
belief on a scale from 1) totally disagree to 9) totally agree.
Variable scores were calculated by summing items
(a = .95).
Implicit Memory Bias
A word-stem completion task (WSCT) using perceptual
encoding assessed implicit memory biases. Two lists of
nine positive state or trait adjectives (e.g., talented) and two
lists of nine negative adjectives (e.g., miserable) were
created from words used in previous research (e.g., Bradley
and Mathews 1983) and matched on numbers of syllables.
One positive and one negative list were combined to form
an encoding list. Following a fixation cross (800 ms),
encoding list words were presented individually on screen
for 7 s in random order. On a scale from 0 to 8, participants
indicated the number of letters in each word that contained
closed parts (e.g., d, p, b, q). After a filler task, all word
lists were presented as three letter word stems. Participants
completed them with the first words that came to mind. The
difference between number of primed and unprimed neg-
ative words completed provided an index of negative
memory bias. Primed minus unprimed positive words
represented an index of positive memory bias.
Explicit Memory Bias
A free-recall task assessed explicit memory biases. Two
word lists were created as per the lists for the implicit
memory task. The six lists used in both implicit and explicit
memory tasks did not differ in length, usage frequency and
emotionality, all Fs \ 0.50. Following a fixation cross
(800 ms), nine positive and nine negative state or trait
adjectives were presented individually for 7 s in random
order. Participants were asked to memorise the words and to
rate each word’s meaning from 1) very unpleasant to 7) very
pleasant. Following a filler task, participants typed all words
they could remember from the presented series. Numbers of
positive and negative words recalled represented measures
of positive and negative memory bias, respectively.
Depression and Mood Measures
Depression
Severity of current depression symptomatology was
assessed by the Zung Self-Rating Depression Scale (ZDS;
Zung 1965). Participants indicated how often they experi-
enced each of 20 depression symptoms over the previous
two weeks, from 1) a little or none of the time to 4) most or
all of the time. Variable scores were calculated by sum-
ming item scores. The ZDS correlates moderately to highly
with other depression measures and Zung’s (1986) rec-
ommended cut-off score of 50 has reliably discriminated
depressed from non-depressed groups. For example, Turner
and Romano (1984) found the ZDS correlated .86 with the
Beck Depression Inventory and the cut-off score of 50
correctly classified 82% of participants according to clini-
cally diagnosed depression status. The ZDS was highly
reliable in the current study (a = .89 at Times 1 and 2).
Depression Groups and Status
Participants were classified as currently dysphoric if they
scored C50 on the ZDS; never-depressed if they answered
negatively to a yes/no question regarding previous diag-
nosis and scored\50 on the ZDS; and dysphoric at follow-
up if their ZDS-T2 scores were C50.
Sad Mood Induction and Mood Ratings
In accordance with previous cognitive reactivity research,
we included a procedure to sadden participants’ moods (see
Scher et al. 2005). Participants visualised a past unpleasant
event, wrote brief responses to four questions regarding
the event’s sensory, perceptual and semantic elements
(Neumann and Philippot 2007) and graded its degree of
unpleasantness. They then rated their moods on two visual
analogue scales ranging from 1) not at all happy to 100)
extremely happy and 1) not at all sad to 100) extremely sad.
Variable scores were calculated by averaging happy and sad
scores after reverse-scoring sad scores. Mood-ratings pro-
vided by a sub-sample before (M = 62.54) and after
Cogn Ther Res
123
Author's personal copy

(M = 56.82) the induction indicated that it successfully
saddened moods, t(154) = 3.96, p \ .001, d = 0.26. A
‘‘sad mood top-up’’ question seeking further information
about the sad recollection was inserted between the groups
of implicit and explicit measures. To comply with ethical
requirements, 54 individuals who answered affirmatively to
a suicidal ideation question were automatically excluded
from the procedure by the computer software.
Procedure
Data were collected by two web-based surveys. The first
survey contained a series of implicit and explicit measures of
depression-related cognitions. Forward progression through
the survey was enforced. Participants initially completed
measures of current and past depression, followed by the
negative mood induction. Implicit measures were presented
prior to explicit measures because we considered initial
completion of explicit measures may influence subsequent
responses to implicit measures employed in this study
(Wittenbrink and Schwarz 2007). Additionally, we consid-
ered one implicit measure (SST) to be more transparent than
the other implicit measures and likely to influence sub-
sequent responses. Consequently, the NLPT and WSCT
were presented in counterbalanced order prior to the SST. A
filler task was inserted after the implicit measures to mini-
mize cross-priming of subsequent measures. The explicit
measures were then presented in counterbalanced order
following the sad mood top-up. Demographics questions
were inserted as filler items between the encoding and
completion sections of the WSCT and between the learning
and retrieval sections of the free-recall task.
Three months later, participants were invited to com-
plete a follow-up survey that assessed depressive symp-
toms. Drop-out analyses revealed that the 146 individuals
who declined to participate at Time 2 were significantly
younger (M = 27.77) than the 160 follow-up participants,
M = 31.87, t(304) = 3.40, p = .001, d = 0.39, but did not
differ on gender, years of education, relationship status or
on all study variables (i.e., mood, depression and cogni-
tive). They also did not differ on membership of the cog-
nitive profiles that emerged from the initial LPA of the
whole sample (reported below), t(304) = -0.87, p = .38.
The high attrition rate may reflect the absence of incentives
offered for Time 2 participation.
Statistical Methods
LPAs were conducted using MPlus 4.1 (Muthen and Muthen
2006) to classify participants according to patterns in the
strength and valence of their implicit and explicit cognitive
biases. When assessing model fit, particular emphasis was
given to the Bayesian information criterion (BIC, Schwartz
1978), the Lo-Mendell-Rubin likelihood ratio test (LMR,
Lo, Mendell, and Rubin 2001) and the bootstrapped likeli-
hood ratio test (BLRT, McLachlan and Peel 2000). The best
fitting model for a dataset is indicated by the smallest BIC
value generated amongst competing models. The LMR and
BLRT assess difference in goodness-of-fit between model
k and model k - 1, where k refers to the number of retained
profiles. A significant p value indicates that model k fits the
data better than model k - 1. All cognitive variables were
standardized to a mean of 50 with a standard deviation of 10
(T Scores) to facilitate interpretation of the profiles. Using
SPSS 17, we performed logistic regressions to assess the
ability of the sample profile solution and the eight cognitive
indicators to predict future depression, and conducted
ANOVAs to identify characteristics of the profiles that
emerged from both LPAs.
Results
Participants’ self-reported depressive symptoms ranged
from low to moderate (ZDS = 22–65) and the mean ZDS
score of 40 approximated the expected mean of 39 in a
non-clinical sample (Zung 1986). Missing values were
observed on implicit positive and negative memory, and
implicit self esteem (between 1% and 2%). SST responses
were excluded if the valence of an unscrambled sentence
was ambiguous, and total scores were treated as missing
data if less than 60% of the sentences were meaningfully
unscrambled (9.8%). All missing values were imputed
using the expectation maximization algorithm in SPSS 17.
Square root transformations were applied to the ZDS and
SST variables to correct positive skew. Correlations
between the measures are presented in Table 1.
LPA of the Total Sample
Fit indices for one through five profile solutions appear in
Table 2. With the smallest BIC and significant LMR and
BLRT values, the three-profile solution emerged as the best
fitting model for the data. Characteristics of the three
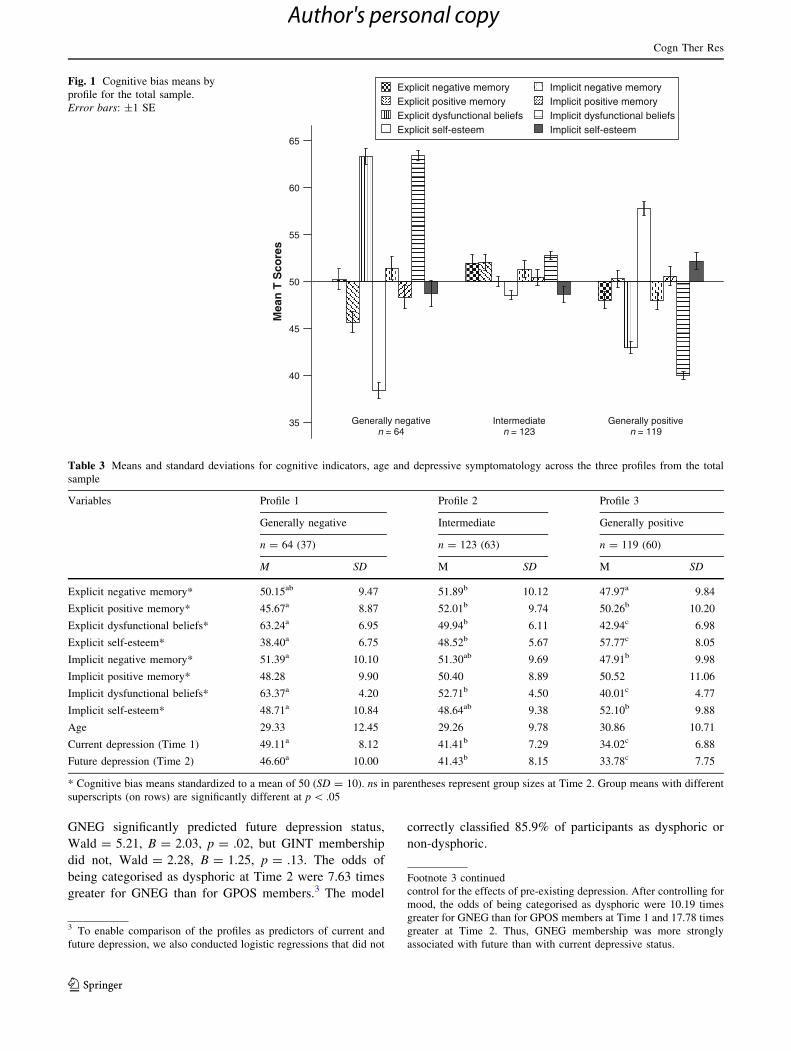
cognitive profiles are depicted in Fig. 1.
Profile 1 comprised 64 (21%) participants who were
characterized by generally negative (GNEG) biases on both
negative (i.e., explicit and implicit negative memory and
dysfunctional beliefs) and positive (i.e., implicit and
explicit positive memory and self-esteem) cognitive indi-
cators. That is, this group scored above average on
most negative indicators and below average on most
positive cognitions. In contrast, the 119 (39%) participants
categorized as Profile 3 demonstrated generally positive
(GPOS) cognitive biases by scoring average or above
average on all positive cognitive indicators and below
Cogn Ther Res
123
Author's personal copy
average on all negative cognitions. Profile 2 contained 123
(40%) participants who displayed an intermediate cogni-
tive profile (GINT), by exhibiting less extreme values on
most cognitive indicators than the other groups. Significant
differences among the three profiles were observed on all
cognitive indicators except implicit positive memory.
Means, standard deviations and group differences are pre-
sented in Table 3.
The Sample Profiles and Depression
ANOVA revealed that membership of the profile solution
was significantly associated with current depressive
symptoms, F(2,303) = 91.54, p \ .001. Participants
belonging to GNEG scored significantly higher on the ZDS
than GINT members, who in turn reported more depressive
symptoms than members of GPOS. Consistent with
hypothesis (1a), GNEG comprised the most severely
dysphoric participants and GPOS included the least dys-
phoric participants. At time 1, GNEG’s mean ZDS score of
49 fell one point short of the cutoff for clinical depression
(Zung 1986). However, score distributions indicated that
52% of this group exceeded the cutoff, including 27% with
moderate levels of depressive symptoms (ZDS 56–65),
whereas mean ZDS scores for the GPOS and GINT groups
were in the non-depressed range and only 4 and 15% of
members reported mild dysphoria (ZDS 50–55 and 50–56),
respectively (Zung 1986).
We conducted a logistic regression (LR) to determine
whether profile membership would predict clinical
levels of depressive symptoms assessed 3 months later.
Future depression status was assessed dichotomously,
where 1 = non-dysphoric (ZDS \ 50) and 2 = dysphoric
(ZDS C 50). We treated depression as a dichotomous
variable because theories of cognitive vulnerability to
depression are primarily concerned with factors conferring
risk for future depression onset or escalation, rather than
increases in symptoms that may still be within the normal
range.2 Profile membership was dummy coded with GPOS
serving as the contrast group. After controlling for current
mood and depression status, the future depression model
was statistically reliable, v2 (2) = 6.21, p \ .05, Nage-
lkerke R2 = .35. The latent profile variables explained a
significant 4.4% of the total variance in future depressive
status. Supporting models of cognitive vulnerability to
depression and our second hypothesis, membership of
Table 1 Correlations between cognitive indicator and depression variables
Variables 1 2 3 4 5 6 7 8 9 10
1. Explicit negative memory .37** .01 .06 .01 -.14 .20 .00 .16 .09
2. Explicit positive memory .36** -.24 .20 .06 .14 -.30* .10 -.12 -.17
3. Explicit dysfunctional beliefs .13* -.08 -.64** -.18 -.11 .66** -.14 .55** -.09
4. Explicit self-esteem -.09 .07 -.67** .07 -.06 -.67** .10 -.49** -.10
5. Implicit negative memory .01 .02 .12* -.12* .30* .02 -.08 -.09 .43**
6. Implicit positive memory -.01 .14* -.03 .02 .09 -.01 .04 -.02 .04
7. Implicit dysfunctional beliefs .11* -.12* .63** -.66** .13* -.06 -.15 .61** .22
8. Implicit self-esteem -.03 .01 -.06 .12* -.11 .03 -.12* -.15 -.37*
9. Current depression (Time 1) .08 -.10 .57** -.64** .17** -.09 .61** -.11 .31
10. Future depression (Time 2) .10 -.10 .36** -.50** .20* -.11 .48** -.17* .71**
Values below and above the diagonal refer to the total sample (N = 306) and the depressed sub-sample (n = 57), respectively. * p \ .05,
** p \ .01
Table 2 Model fit indices for profile solutions
Profile solution BIC LMR BLRT
LPA 1: Total sample (N = 306)
1 7,030.69 – –
2 6,780.00 .01 .00
3 6,714.61 \.001 .00
4 6,722.77 .10 .00
5 6,733.01 .13 F
LPA 2: Dysphoric sub-sample (n = 57)
1 1,338.28 – –
2 1,314.19 .04 .00
3 1,319.44 .64 .03
4 1,332.31 .40 .16
5 1,343.01 .46 F
BIC = Bayesian information criterion, LMR = Lo-Mendell-Rubin
likelihood ratio test, BLRT = Bootstrapped likelihood ratio test,
F = failed to converge
2 We also conducted hierarchical multiple regressions predicting
continuous Time 2 depression scores (ZDS-T2) from: (1) the GPOS-
GNEG and GPOS-GINT dummy variables and, (2) the eight cognitive
variables after controlling for ZDS-T1 and mood at the first step. Both
models were significant: (1), R2 = .53, F(4,151) = 42.38, p \ .001;
(2) R2 = .55, F(10,145) = 17.80, p \ .001. However, the dummy
variables and cognitive indicators did not significantly predict ZDS-
T2 at the second steps of their respective models: (1) R2 = .01,
F(2,151) = 1.32, p = .27; (2) R2 = .03, F(8,145) = 1.23, p = .29.
Cogn Ther Res
123
Author's personal copy
GNEG significantly predicted future depression status,
Wald = 5.21, B = 2.03, p = .02, but GINT membership
did not, Wald = 2.28, B = 1.25, p = .13. The odds of
being categorised as dysphoric at Time 2 were 7.63 times
greater for GNEG than for GPOS members.3 The model
correctly classified 85.9% of participants as dysphoric or
non-dysphoric.
Explicit negative memory Explicit positive memory Explicit dysfunctional beliefs Explicit self-esteem
Implicit negative memory Implicit positive memory Implicit dysfunctional beliefs Implicit self-esteem
Generally negative Intermediate Generally positive n = 64 n = 123 n = 119
Mea
n T
Sco
res
65
60
55
50
45
40
35
Fig. 1 Cognitive bias means by
profile for the total sample.
Error bars: ±1 SE
Table 3 Means and standard deviations for cognitive indicators, age and depressive symptomatology across the three profiles from the total
sample
Variables Profile 1 Profile 2 Profile 3
Generally negative Intermediate Generally positive
n = 64 (37) n = 123 (63) n = 119 (60)
M SD M SD M SD
Explicit negative memory* 50.15ab 9.47 51.89b 10.12 47.97a 9.84
Explicit positive memory* 45.67a 8.87 52.01b 9.74 50.26b 10.20
Explicit dysfunctional beliefs* 63.24a 6.95 49.94b 6.11 42.94c 6.98
Explicit self-esteem* 38.40a 6.75 48.52b 5.67 57.77c 8.05
Implicit negative memory* 51.39a 10.10 51.30ab 9.69 47.91b 9.98
Implicit positive memory* 48.28 9.90 50.40 8.89 50.52 11.06
Implicit dysfunctional beliefs* 63.37a 4.20 52.71b 4.50 40.01c 4.77
Implicit self-esteem* 48.71a 10.84 48.64ab 9.38 52.10b 9.88
Age 29.33 12.45 29.26 9.78 30.86 10.71
Current depression (Time 1) 49.11a 8.12 41.41b 7.29 34.02c 6.88
Future depression (Time 2) 46.60a 10.00 41.43b 8.15 33.78c 7.75
* Cognitive bias means standardized to a mean of 50 (SD = 10). ns in parentheses represent group sizes at Time 2. Group means with different
superscripts (on rows) are significantly different at p \ .05
3 To enable comparison of the profiles as predictors of current and
future depression, we also conducted logistic regressions that did not
Footnote 3 continued
control for the effects of pre-existing depression. After controlling for
mood, the odds of being categorised as dysphoric were 10.19 times
greater for GNEG than for GPOS members at Time 1 and 17.78 times
greater at Time 2. Thus, GNEG membership was more strongly
associated with future than with current depressive status.
Cogn Ther Res
123
Author's personal copy
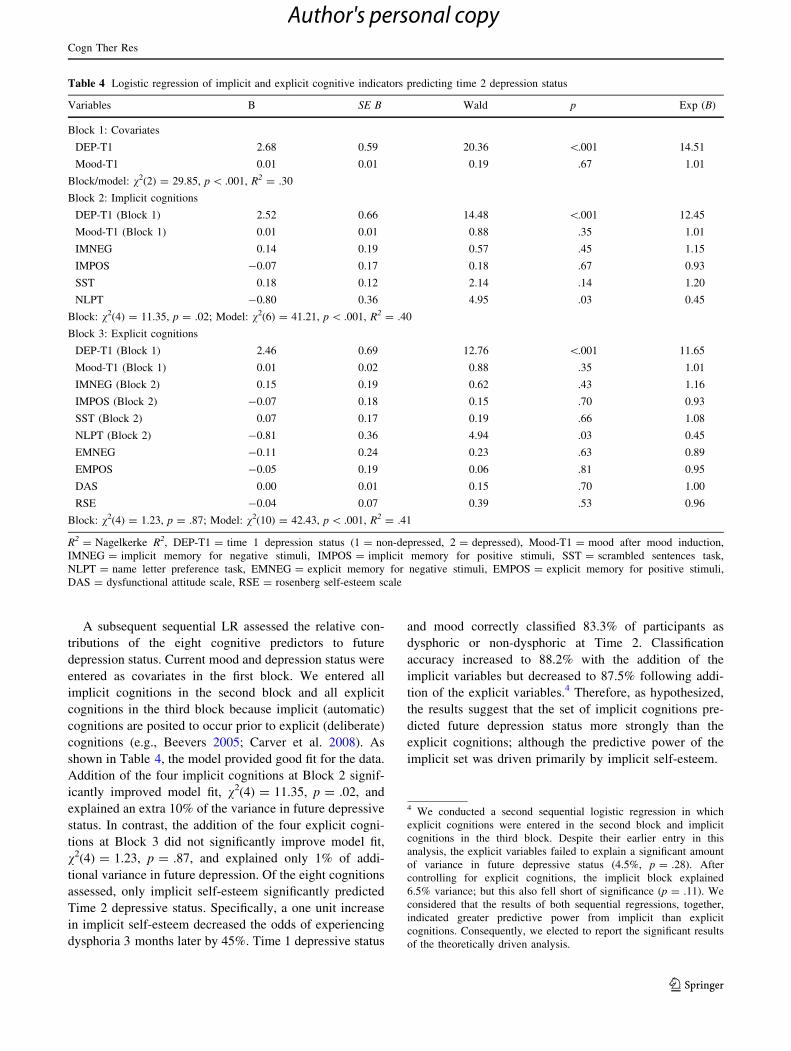
A subsequent sequential LR assessed the relative con-
tributions of the eight cognitive predictors to future
depression status. Current mood and depression status were
entered as covariates in the first block. We entered all
implicit cognitions in the second block and all explicit
cognitions in the third block because implicit (automatic)
cognitions are posited to occur prior to explicit (deliberate)
cognitions (e.g., Beevers 2005; Carver et al. 2008). As
shown in Table 4, the model provided good fit for the data.
Addition of the four implicit cognitions at Block 2 signif-
icantly improved model fit, v2(4) = 11.35, p = .02, and
explained an extra 10% of the variance in future depressive
status. In contrast, the addition of the four explicit cogni-
tions at Block 3 did not significantly improve model fit,
v2(4) = 1.23, p = .87, and explained only 1% of addi-
tional variance in future depression. Of the eight cognitions
assessed, only implicit self-esteem significantly predicted
Time 2 depressive status. Specifically, a one unit increase
in implicit self-esteem decreased the odds of experiencing
dysphoria 3 months later by 45%. Time 1 depressive status
and mood correctly classified 83.3% of participants as
dysphoric or non-dysphoric at Time 2. Classification
accuracy increased to 88.2% with the addition of the
implicit variables but decreased to 87.5% following addi-
tion of the explicit variables.4 Therefore, as hypothesized,
the results suggest that the set of implicit cognitions pre-
dicted future depression status more strongly than the
explicit cognitions; although the predictive power of the
implicit set was driven primarily by implicit self-esteem.
Table 4 Logistic regression of implicit and explicit cognitive indicators predicting time 2 depression status
Variables B SE B Wald p Exp (B)
Block 1: Covariates
DEP-T1 2.68 0.59 20.36 \.001 14.51
Mood-T1 0.01 0.01 0.19 .67 1.01
Block/model: v2(2) = 29.85, p \ .001, R2 = .30
Block 2: Implicit cognitions
DEP-T1 (Block 1) 2.52 0.66 14.48 \.001 12.45
Mood-T1 (Block 1) 0.01 0.01 0.88 .35 1.01
IMNEG 0.14 0.19 0.57 .45 1.15
IMPOS -0.07 0.17 0.18 .67 0.93
SST 0.18 0.12 2.14 .14 1.20
NLPT -0.80 0.36 4.95 .03 0.45
Block: v2(4) = 11.35, p = .02; Model: v2(6) = 41.21, p \ .001, R2 = .40
Block 3: Explicit cognitions
DEP-T1 (Block 1) 2.46 0.69 12.76 \.001 11.65
Mood-T1 (Block 1) 0.01 0.02 0.88 .35 1.01
IMNEG (Block 2) 0.15 0.19 0.62 .43 1.16
IMPOS (Block 2) -0.07 0.18 0.15 .70 0.93
SST (Block 2) 0.07 0.17 0.19 .66 1.08
NLPT (Block 2) -0.81 0.36 4.94 .03 0.45
EMNEG -0.11 0.24 0.23 .63 0.89
EMPOS -0.05 0.19 0.06 .81 0.95
DAS 0.00 0.01 0.15 .70 1.00
RSE -0.04 0.07 0.39 .53 0.96
Block: v2(4) = 1.23, p = .87; Model: v2(10) = 42.43, p \ .001, R2 = .41
R2 = Nagelkerke R2, DEP-T1 = time 1 depression status (1 = non-depressed, 2 = depressed), Mood-T1 = mood after mood induction,
IMNEG = implicit memory for negative stimuli, IMPOS = implicit memory for positive stimuli, SST = scrambled sentences task,
NLPT = name letter preference task, EMNEG = explicit memory for negative stimuli, EMPOS = explicit memory for positive stimuli,
DAS = dysfunctional attitude scale, RSE = rosenberg self-esteem scale
4 We conducted a second sequential logistic regression in which
explicit cognitions were entered in the second block and implicit
cognitions in the third block. Despite their earlier entry in this
analysis, the explicit variables failed to explain a significant amount
of variance in future depressive status (4.5%, p = .28). After
controlling for explicit cognitions, the implicit block explained
6.5% variance; but this also fell short of significance (p = .11). We
considered that the results of both sequential regressions, together,
indicated greater predictive power from implicit than explicit
cognitions. Consequently, we elected to report the significant results
of the theoretically driven analysis.
Cogn Ther Res
123
Author's personal copy
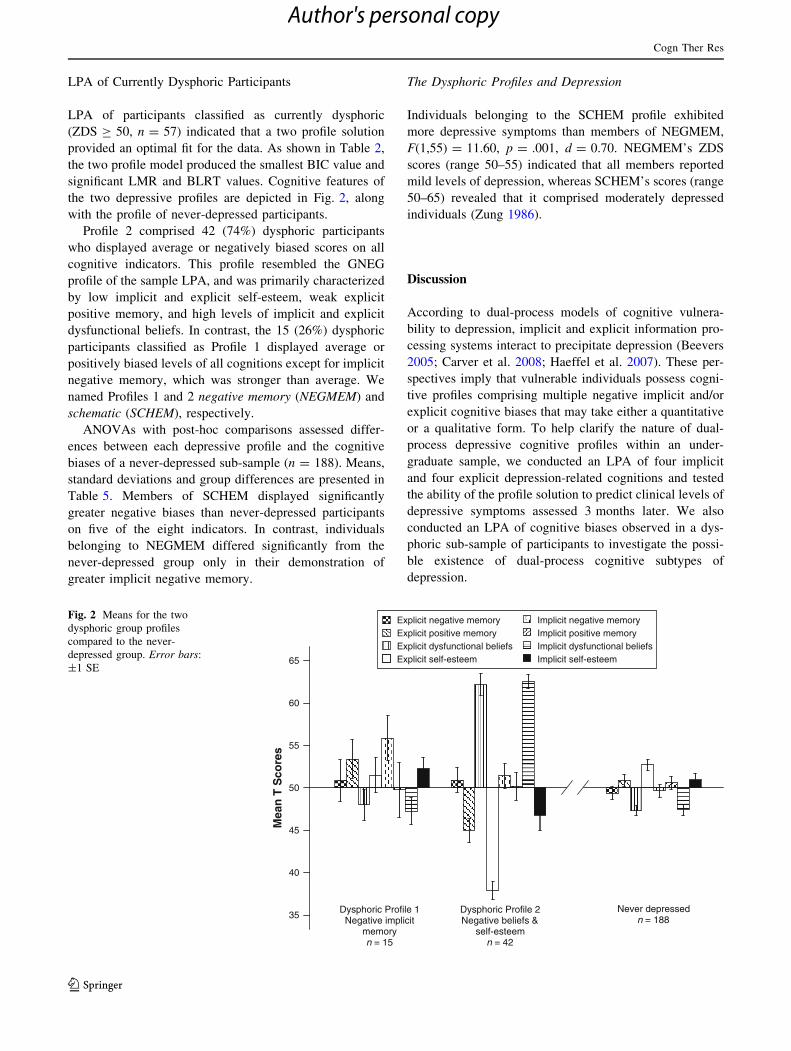
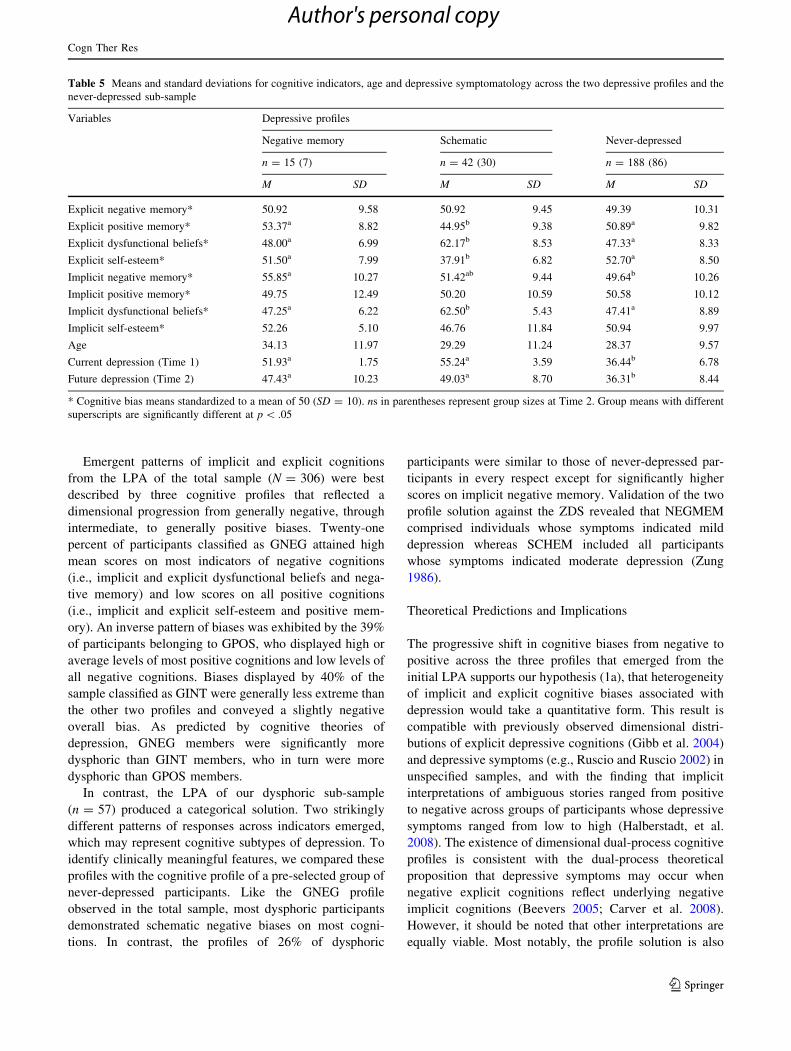
LPA of Currently Dysphoric Participants
LPA of participants classified as currently dysphoric
(ZDS C 50, n = 57) indicated that a two profile solution
provided an optimal fit for the data. As shown in Table 2,
the two profile model produced the smallest BIC value and
significant LMR and BLRT values. Cognitive features of
the two depressive profiles are depicted in Fig. 2, along
with the profile of never-depressed participants.
Profile 2 comprised 42 (74%) dysphoric participants
who displayed average or negatively biased scores on all
cognitive indicators. This profile resembled the GNEG
profile of the sample LPA, and was primarily characterized
by low implicit and explicit self-esteem, weak explicit
positive memory, and high levels of implicit and explicit
dysfunctional beliefs. In contrast, the 15 (26%) dysphoric
participants classified as Profile 1 displayed average or
positively biased levels of all cognitions except for implicit
negative memory, which was stronger than average. We
named Profiles 1 and 2 negative memory (NEGMEM) and
schematic (SCHEM), respectively.
ANOVAs with post-hoc comparisons assessed differ-
ences between each depressive profile and the cognitive
biases of a never-depressed sub-sample (n = 188). Means,
standard deviations and group differences are presented in
Table 5. Members of SCHEM displayed significantly
greater negative biases than never-depressed participants
on five of the eight indicators. In contrast, individuals
belonging to NEGMEM differed significantly from the
never-depressed group only in their demonstration of
greater implicit negative memory.
The Dysphoric Profiles and Depression
Individuals belonging to the SCHEM profile exhibited
more depressive symptoms than members of NEGMEM,
F(1,55) = 11.60, p = .001, d = 0.70. NEGMEM’s ZDS
scores (range 50–55) indicated that all members reported
mild levels of depression, whereas SCHEM’s scores (range
50–65) revealed that it comprised moderately depressed
individuals (Zung 1986).
Discussion
According to dual-process models of cognitive vulnera-
bility to depression, implicit and explicit information pro-
cessing systems interact to precipitate depression (Beevers
2005; Carver et al. 2008; Haeffel et al. 2007). These per-
spectives imply that vulnerable individuals possess cogni-
tive profiles comprising multiple negative implicit and/or
explicit cognitive biases that may take either a quantitative
or a qualitative form. To help clarify the nature of dual-
process depressive cognitive profiles within an under-
graduate sample, we conducted an LPA of four implicit
and four explicit depression-related cognitions and tested
the ability of the profile solution to predict clinical levels of
depressive symptoms assessed 3 months later. We also
conducted an LPA of cognitive biases observed in a dys-
phoric sub-sample of participants to investigate the possi-
ble existence of dual-process cognitive subtypes of
depression.
Mea
n T
Sco
res
65
60
55
50
45
40
35Dysphoric Profile 1 Dysphoric Profile 2 Never depressed Negative implicit Negative beliefs & n = 188
memory self-esteem n = 15 n = 42
Explicit negative memory Explicit positive memory Explicit dysfunctional beliefs Explicit self-esteem
Implicit negative memory Implicit positive memory Implicit dysfunctional beliefs Implicit self-esteem
Fig. 2 Means for the two
dysphoric group profiles
compared to the never-
depressed group. Error bars:
±1 SE
Cogn Ther Res
123
Author's personal copy
Emergent patterns of implicit and explicit cognitions
from the LPA of the total sample (N = 306) were best
described by three cognitive profiles that reflected a
dimensional progression from generally negative, through
intermediate, to generally positive biases. Twenty-one
percent of participants classified as GNEG attained high
mean scores on most indicators of negative cognitions
(i.e., implicit and explicit dysfunctional beliefs and nega-
tive memory) and low scores on all positive cognitions
(i.e., implicit and explicit self-esteem and positive mem-
ory). An inverse pattern of biases was exhibited by the 39%
of participants belonging to GPOS, who displayed high or
average levels of most positive cognitions and low levels of
all negative cognitions. Biases displayed by 40% of the
sample classified as GINT were generally less extreme than
the other two profiles and conveyed a slightly negative
overall bias. As predicted by cognitive theories of
depression, GNEG members were significantly more
dysphoric than GINT members, who in turn were more
dysphoric than GPOS members.
In contrast, the LPA of our dysphoric sub-sample
(n = 57) produced a categorical solution. Two strikingly
different patterns of responses across indicators emerged,
which may represent cognitive subtypes of depression. To
identify clinically meaningful features, we compared these
profiles with the cognitive profile of a pre-selected group of
never-depressed participants. Like the GNEG profile
observed in the total sample, most dysphoric participants
demonstrated schematic negative biases on most cogni-
tions. In contrast, the profiles of 26% of dysphoric
participants were similar to those of never-depressed par-
ticipants in every respect except for significantly higher
scores on implicit negative memory. Validation of the two
profile solution against the ZDS revealed that NEGMEM
comprised individuals whose symptoms indicated mild
depression whereas SCHEM included all participants
whose symptoms indicated moderate depression (Zung
1986).
Theoretical Predictions and Implications
The progressive shift in cognitive biases from negative to
positive across the three profiles that emerged from the
initial LPA supports our hypothesis (1a), that heterogeneity
of implicit and explicit cognitive biases associated with
depression would take a quantitative form. This result is
compatible with previously observed dimensional distri-
butions of explicit depressive cognitions (Gibb et al. 2004)
and depressive symptoms (e.g., Ruscio and Ruscio 2002) in
unspecified samples, and with the finding that implicit
interpretations of ambiguous stories ranged from positive
to negative across groups of participants whose depressive
symptoms ranged from low to high (Halberstadt, et al.
2008). The existence of dimensional dual-process cognitive
profiles is consistent with the dual-process theoretical
proposition that depressive symptoms may occur when
negative explicit cognitions reflect underlying negative
implicit cognitions (Beevers 2005; Carver et al. 2008).
However, it should be noted that other interpretations are
equally viable. Most notably, the profile solution is also
Table 5 Means and standard deviations for cognitive indicators, age and depressive symptomatology across the two depressive profiles and the
never-depressed sub-sample
Variables Depressive profiles
Negative memory Schematic Never-depressed
n = 15 (7) n = 42 (30) n = 188 (86)
M SD M SD M SD
Explicit negative memory* 50.92 9.58 50.92 9.45 49.39 10.31
Explicit positive memory* 53.37a 8.82 44.95b 9.38 50.89a 9.82
Explicit dysfunctional beliefs* 48.00a 6.99 62.17b 8.53 47.33a 8.33
Explicit self-esteem* 51.50a 7.99 37.91b 6.82 52.70a 8.50
Implicit negative memory* 55.85a 10.27 51.42ab 9.44 49.64b 10.26
Implicit positive memory* 49.75 12.49 50.20 10.59 50.58 10.12
Implicit dysfunctional beliefs* 47.25a 6.22 62.50b 5.43 47.41a 8.89
Implicit self-esteem* 52.26 5.10 46.76 11.84 50.94 9.97
Age 34.13 11.97 29.29 11.24 28.37 9.57
Current depression (Time 1) 51.93a 1.75 55.24a 3.59 36.44b 6.78
Future depression (Time 2) 47.43a 10.23 49.03a 8.70 36.31b 8.44
* Cognitive bias means standardized to a mean of 50 (SD = 10). ns in parentheses represent group sizes at Time 2. Group means with different
superscripts are significantly different at p \ .05
Cogn Ther Res
123
Author's personal copy
consistent with the existence of a single system of
depressive processing.
Accordingly, the LPA failed to support our categorical
dual-process hypothesis (1b) which predicted the emer-
gence of qualitatively distinct cognitive profiles, including
a vulnerable profile comprising negative implicit and
positive explicit cognitive biases. This outcome is at odds
with neurophysiological and behavioural evidence sug-
gesting that effortful processing can override negative
implicit processing when sufficient resources are available
(for reviews, see Beck 2008; Beevers 2005; Carver et al.
2008; Scher et al. 2005). The absence of qualitative cog-
nitive profiles is particularly discordant with previous
studies of self-esteem in depression. For example, depres-
sion-related fluctuations in explicit self-esteem (Franck and
De Raedt 2007) and discrepancies between implicit and
explicit self-esteem (Schroder-Abe et al. 2007) support the
notion that some individuals possess conflicting levels of
these constructs. Thus, further research is needed to
investigate the role of implicit and explicit self-esteem in
depression.
An essential feature of all models of cognitive vulner-
ability to depression is that high-risk cognitions can exist in
the absence of symptoms and precede depression onset or
recurrence (Abramson et al. 1989; Beck 1987; Beevers
2005; Haeffel et al. 2007; Ingram 1984). Supporting this
premise and our second hypothesis, logistic regression
revealed that GNEG members were seven times more
likely than GPOS members to experience clinical levels of
depressive symptoms 3 months later, even after controlling
for current depression status and mood. This result suggests
that possession of a GNEG cognitive profile may account
for variance in future depression that cannot be explained
by current depression and mood. Thus, our finding may
offer unique (predictive) support for the theoretical notion
that cognitive vulnerability to depression involves sys-
tematic negative biases in all self-referential thoughts and
information processes (Beck 1987; Bower 1981; Ingram
1984; Teasdale 1988).
Previous research has observed predictive relationships
between individual negative cognitions (e.g., explicit dys-
functional beliefs) and subsequent depression; albeit
inconsistently (for review, see Joormann 2009). However,
to our knowledge, no prior study has simultaneously
assessed as many as eight cognitions. Our sequential
logistic regression of the four implicit and four explicit
cognitive variables revealed that the set of implicit cogni-
tions explained a significant 10% of the variance in future
depressive status over and above the contributions of cur-
rent depression and mood, but adding the set of explicit
cognitions did not significantly improve model fit.
Furthermore, similar (although less pronounced) results
emerged when explicit cognitions were entered prior to
implicit cognitions. Therefore, the results provided some
support for our third hypothesis and the view that negative
implicit cognitions confer greater cognitive vulnerability to
future depression than negative explicit cognitions (e.g.,
Beevers 2005). However, of the eight cognitions assessed,
only implicit self-esteem significantly predicted subsequent
depressive status; where high implicit self-esteem was
associated with reduced likelihood of experiencing dys-
phoria 3 months later. This observed relationship is con-
sistent with most, but not all, previous studies of implicit
self-esteem in depression (see Phillips et al. 2010). Overall,
the results of the sample LPA and logistic regressions
suggest that explicit cognitions are more closely associated
with current depression and implicit cognitions are stronger
predictors of future depression.
The possible identification of a negative memory cog-
nitive subtype of depression is particularly interesting
given the importance of memory in most theories of cog-
nitive vulnerability to depression. Beck (1987) and Bower
(1981) proposed that depressive schemas comprise nega-
tive memory representations that bias information pro-
cessing toward negatively valenced stimuli, and Ingram
(1984) and Teasdale (1988) proposed that depressed mood
increases the accessibility of representations of depressing
experiences and constructs. A variety of empirical studies
support these perspectives. For example, varying mood
inductions (e.g., sad, happy, angry) have been associated
with parallel shifts in mood and representations in working
memory (Siemer 2005). Consequently, mild depression
experienced by individuals belonging to NEGMEM may
reflect activated memory networks associated with low
mood, but may not involve the spreading activation that is
purportedly characteristic of clinical depression (Bower
1981; Ingram 1984; Teasdale 1988).
However, a more intriguing interpretation of the nega-
tive memory profile is suggested by dual-process theories
of cognitive vulnerability to depression (Beevers 2005;
Carver et al. 2008; Haeffel et al. 2007). Memory is an
essential component of these accounts. Depressive cogni-
tions are posited to originate at an implicit level; where
processing is guided by similarities between a current
stimulus and memory associations that have developed
slowly over time through repeated experience (Beevers
2005). These associations are believed to pre-consciously
influence the subsequent processing and interpretation of
new information at both implicit and explicit levels (Smith
and DeCoster 2000). Therefore, although speculative,
NEGMEM may represent the early stages of depressive
onset; where implicit negative memory biases precede or
activate other implicit and explicit depressive cognitions.
Future longitudinal research may investigate this pos-
sibility by reassessing cognitive biases at follow-up to
identify which biases behave like symptoms of disorder
Cogn Ther Res
123
Author's personal copy

(i.e., returning to normal/positive following recovery) and
which cognitions remain relatively stable despite decreases
in depressive symptoms. Stability of negative biases before
and/or after a depressive episode may be indicative of
cognitive vulnerability. Several studies have investigated
the stability of depressive cognitions (e.g., Dozois and
Dobson 2001); however, they did not statistically assess the
relative stability of conceptually similar output from both
processing systems (e.g., implicit vs. explicit self-esteem).
Prospective research that elucidates mechanisms
underlying the hypothesized dual-process interaction is
also needed. To date, two studies have directly addressed
dual-process diathesis-stress hypotheses and found con-
flicting results. Haeffel et al. (2007) found that explicit
cognitive styles conferred greater vulnerability than
implicit self-esteem to depressive symptoms five weeks
later for undergraduates who experienced high life stress.
In contrast, Steinberg et al. (2007) found a greater pre-
dictive contribution from implicit self-esteem assessed by
the Implicit Association Task (Greenwald and Farnham
2000) toward future depression in the presence of life stress
amongst undergraduates who scored highly on measures of
explicit depressive cognitions.5 Study designs employing
participant groups that differ in their capacity to utilise
explicit corrective processing may effectively assess the
hypothesized dual-process interaction.
Treatment Implications
Our initial LPA solution suggests that some cognitive
biases are more reliable discriminators of current depres-
sive symptoms than others. Significant decreases in
depressive symptoms across the profiles were reflected in
dramatic and regular increases in explicit self-esteem and
decreases in implicit and explicit dysfunctional beliefs.
Thus, our results validate the approach of the most widely
used intervention, Cognitive Therapy (Beck et al. 1979),
which aims to modify explicit negative beliefs by inter-
rupting thought patterns associated with depression. How-
ever, although this treatment is strongly associated with
immediate symptomatic improvement, 2 year recurrence
rates can be as high as 73% for certain patient groups (Tang
et al. 2007). We found that participants with cognitive
profiles featuring both implicit and explicit negatively-
biased cognitions were at high risk of experiencing clinical
levels of depressive symptoms 3 months later, and that
possession of negative implicit cognitions, especially low
implicit self-esteem, conferred greater vulnerability to
future depression than negative explicit cognitions. These
results suggest that long-term treatment efficacy may be
improved by incorporating strategies that address implicit
processes.
Beevers (2005) described three ways to target implicit
processing. First, therapies could aim to change conscious
expectancies so that corrective explicit processing is trig-
gered in response to negative implicit responses. For
example, Mindfulness Based Cognitive Therapy (Segal
et al. 2002) aims to help recovered depressed individuals to
become aware of unwanted thoughts, feelings and body
sensations, and to disengage from negative thinking pat-
terns by changing their responses from automatic or
avoidant to intentional and skilful. Second, strategies could
aim to change patterns of activation determined by asso-
ciative network structures by repeatedly engaging in cor-
rective explicit processing. For example, repeatedly
preventing memories from entering awareness has been
shown to impair their subsequent deliberate recollection
(Anderson and Green 2001) and a procedure to train
depressed individuals to forget negative material was
recently developed (Joormann et al. 2009). Third, therapies
could incorporate both affective and cognitive strategies to
relearn implicit associations and explicit interpretations.
For example, Emotion-Focused Therapy (Greenberg and
Watson 2005) and Exposure-Based Cognitive Therapy
(Hayes et al. 2005) aim to generate new cognitive struc-
tures by focussing on emotional experiences and the
meanings attributed to them.
Limitations
Several limitations of this study should be taken into
account when interpreting its results. First, the generalis-
ability of these results may be limited by our relatively
small, predominantly mature-aged, undergraduate sample
and substantial attrition rate at Time 2. It is also probable
that the small follow-up sample underpowered the logistic
regression of the eight cognitive indicators, and that
stronger effects may be observed in a larger sample.
Additionally, the small dysphoric sub-sample may have
limited the power to detect subgroups in the dysphoric
group analysis. Second, control of environmental factors
during survey completion was not possible due to our web-
based data-collection medium. Third, participants’
depression status was determined by self-report because the
preferred method of classification by formal diagnosis was
not practicable. Fourth, this study did not consider the
effects of life stress, which are hypothesized to play an
integral role in models of cognitive vulnerability to
depression. Lastly, we classified the SST as an implicit
measure because it involves the automaticity features of
fast and efficient (see, Moors et al. 2010). However, its
5 Steinberg et al. (2007) found no significant effects when implicit
self-esteem was assessed by the NLPT. However, their scoring
procedure did not include an algorithm to control for individual
differences in baseline responses (LeBel and Gawronski 2009) which
may have affected the measure’s validity.
Cogn Ther Res
123
Author's personal copy

relative transparency may overlap with explicit measures in
the consciousness and control of participants’ responses
(Wenzlaff et al. 2001).6 Thus, its role as an implicit mea-
sure should be considered with caution.
Conclusion
LPA of unselected undergraduates identified three dual-
process cognitive profiles comprising compatible levels of
implicit and explicit cognitive biases ranging from nega-
tive, through intermediate, to positive. This quantitative
distribution is consistent with the dual-process notion that
negative explicit cognitions and depressive symptomatol-
ogy may occur when negative implicit processing remains
uncorrected by explicit processing. The LPA produced
little evidence to support the alternative dual-process
implication that some individuals possess conflicting
implicit and explicit self-cognitions that place them at
greater risk for depression. Patterns of biases across the
profiles were associated with decreases in current depres-
sive symptoms and membership of the negative profile
significantly predicted clinical levels of depressive symp-
toms 3 months later. Implicit self-esteem emerged as the
strongest predictor of subsequent dysphoria, and the like-
lihood of future dysphoria was more strongly influenced by
the set of four implicit self-cognitions than the set of
explicit cognitions. Our dysphoric group LPA identified a
possible cognitive subtype of depression that was charac-
terized by heightened implicit memory for negative stimuli
but was otherwise positive. Further research is needed to
determine whether this profile represents a distinct form of
mild depression or a precursor to more severe forms of
depression. Overall, our results are consistent with the
dual-process premise that two types of cognitive processes
are involved in depression; suggest that cognitive therapies
should incorporate strategies that target implicit cognitions;
and highlight the need for further investigations into the
roles of implicit and explicit processes in depression.
References
Abramson, L. Y., Alloy, L. B., Hogan, M. E., Whitehouse, W. G.,
Donovan, P., Rose, D. T., et al. (2002). Cognitive vulnerability to
depression: Theory and evidence. In R. L. Leahy & E. T. Dowd
(Eds.), Clinical advances in cognitive psychotherapy: Theoryand application (Vol. xiv, pp. 75–92). New York: Springer.
Abramson, L. Y., Metalsky, G. I., & Alloy, L. B. (1989). Hopeless-
ness depression: A theory-based subtype of depression. Psycho-logical Review, 96, 358–372.
Adams, P., Abela, J. R. Z., & Hankin, B. L. (2007). Factorial
categorization of depression-related constructs in early adoles-
cents. Journal of Cognitive Psychotherapy: An InternationalQuarterly, 21, 123–139.
Alloy, L. B., Abramson, L. Y., Hogan, M. F., Whitehouse, W. G.,
Rose, D. T., Robinson, M. S., et al. (2000). The temple–
wisconsin cognitive vulnerability to depression project: Lifetime
history of axis I psychopathology in individuals at high and low
cognitive risk for depression. Journal of Abnormal Psychology,109, 403–418.
Anderson, M. C., & Green, C. (2001). Suppressing unwanted
memories by executive control. Nature, 410, 366–369.
Beck, A. T. (1987). Cognitive model of depression. Journal ofCognitive Psychotherapy, 1, 2–27.
Beck, A. T. (2008). The evolution of the cognitive model of
depression and its neurobiological correlates. The AmericanJournal of Psychiatry, 165, 969–977.
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitivetherapy of depression. New York: Guilford.
Beevers, C. G. (2005). Cognitive vulnerability to depression: A dual
process model. Clinical Psychology Review, 25, 975–1002.
Bellew, M., & Hill, A. B. (1991). Schematic processing and the
prediction of depression following childbirth. Personality andIndividual Differences, 12, 943–949.
Blatt, S. J., & Homann, E. (1992). Parent-child interaction in the
etiology of dependent and self-critical depression. ClinicalPsychology Review, 72, 47–91.
Bosson, J. K., Swann, W. B., & Pennebaker, J. W. (2000). Stalking
the perfect measure of implicit self-esteem: The blind men and
the elephant revisited? Journal of Personality and SocialPsychology, 79, 631–643.
Bower, G. H. (1981). Mood and memory. American Psychologist, 36,
129–148.
Bradley, B., & Mathews, A. (1983). Negative self-schemata in
clinical depression. British Journal of Clinical Psychology, 22,
173–181.
Brinol, P., Petty, R. E., & Wheeler, S. C. (2006). Discrepancies
between explicit and implicit self-concepts: Consequences for
information processing. Journal of Personality and SocialPsychology, 91, 154–170.
Carver, C. S., Johnson, S. L., & Joormann, J. (2008). Serotonergic
function, two-mode models of self-regulation, and vulnerability
to depression: What depression has in common with impulsive
aggression. Psychological Bulletin, 134, 912–943.
Ciesla, J. A., & Roberts, J. E. (2007). Rumination, negative cognition,
and their interactive effects on depressed mood. Emotion, 7,
555–565.
Dozois, D. J. A., & Dobson, K. S. (2001). A longitudinal investigation
of information processing and cognitive organization in depres-
sion: Stability of schematic interconnectedness. Journal ofConsulting and Clinical Psychology, 60, 914–925.
Evans, J. S. B. T. (2008). Dual-processing accounts of reasoning,
judgment and social cognition. Annual Review of Psychology,59, 255–278.
Franck, E., & De Raedt, R. (2007). Self-esteem reconsidered:
Unstable self-esteem outperforms level of self-esteem as
vulnerability marker for depression. Behaviour Research andTherapy, 45, 1531–1541.
Franck, E., De Raedt, R., & De Houwer, J. (2007). Implicit but not
explicit self-esteem predicts future depressive symptomatology.
Behaviour Research and Therapy, 45, 2448–2455.
6 We also conducted a supplementary LPA which excluded the SST.
A similar quantitative three profile solution emerged from the total
sample when the remaining seven cognitive measures were analysed.
Thus, the transparency of the SST did not appear to unduly influence
our results.
Cogn Ther Res
123
Author's personal copy
Gibb, B. E., Alloy, L. B., Abramson, L. Y., Beevers, C. G., & Miller,
I. W. (2004). Cognitive vulnerability to depression: A taxometric
analysis. Journal of Abnormal Psychology, 113, 81–89.
Greenberg, L. S., & Watson, J. (2005). Emotion-focused therapy ofdepression. Washington, DC: American Psychological
Association.
Greenwald, A. G., & Farnham, S. D. (2000). Using the implicit
association test to measure self-esteem and self-concept. Journalof Personality and Social Psychology, 79, 1022–1038.
Haeffel, G. J., Abramson, L. Y., Brazy, P. C., Shah, J. Y., Teachman,
B. A., & Nosek, B. A. (2007). Explicit and implicit cognition: A
preliminary test of a dual-process theory of cognitive vulnera-
bility to depression. Behaviour Research and Therapy, 45,
1155–1167.
Halberstadt, L., Haeffel, G. J., Abramson, L. Y., Mukherji, B. R.,
Metalsky, G. I., & Dykman, B. M. (2008). Schematic processing:
A comparison of clinically depressed, dysphoric, and nonde-
pressed college students. Cognitive Therapy and Research, 32,
843–855.
Hankin, B. L., Lakdawalla, Z., Carter, I., Abela, J. R. Z., & Adams, P.
(2007). Are neuroticism, cognitive vulnerability and self-esteem
overlapping or distinct risks for depression? Evidence from
exploratory and confirmatory factor analyses. Journal of Socialand Clinical Psychology, 26, 29–63.
Haslam, N. (2007). The latent structure of mental disorders: A
taxometric update on the categorical vs dimensional debate.
Current Psychiatry Reviews, 3, 172–177.
Haslam, N., & Beck, A. T. (1994). Subtyping major depression: A
taxometric analysis. Journal of Abnormal Psychology, 103,
686–692.
Hayes, A. M., Beevers, C., Feldman, G., Laurenceau, J.-P., &
Perlman, C. (2005). Avoidance and emotional processing as
predictors of symptom change and positive growth in an
integrative therapy for depression. International Journal ofBehavioral Medicine, 12, 111–122.
Ingram, R. E. (1984). Toward an information-processing analysis of
depression. Cognitive Therapy and Research, 8, 443–477.
Johnson, S. L., Joormann, J., & Gotlib, I. H. (2007). Does processing
of emotional stimuli predict symptomatic improvement and
diagnostic recovery from major depression? Emotion, 7,
201–206.
Joormann, J. (2009). Cognitive aspects of depression. In I. H. Gotlib
& C. L. Hammen (Eds.), Handbook of depression (2nd ed.,
pp. 298–321). New York: Guilford Press.
Joormann, J., Hertel, P. T., LeMoult, J., & Gotlib, I. H. (2009).
Training forgetting of negative material in depression. Journal ofAbnormal Psychology, 118, 34–43.
Koole, S. L., Dijksterhuis, A., & van Knippenberg, A. (2001). What’s
in a name: Implicit self-esteem and the automatic self. Journal ofPersonality and Social Psychology, 80, 669–685.
LeBel, E. P., & Gawronski, B. (2009). How to find what’s in a
name: Scrutinizing the optimality of five scoring algorithms for
the name-letter task. European Journal of Personality, 32, 85–
106.
Lieberman, M. D., Jarcho, J. M., & Satpute, A. B. (2004). Evidence-
based and intution-based self knowledge: An fMRI study.
Journal of Personality and Social Psychology, 87, 421–435.
Lo, Y., Mendell, N. R., & Rubin, D. B. (2001). Testing the number of
components in a normal mixture. Biometrika, 88, 767–778.
McLachlan, G., & Peel, D. (2000). Finite mixture models. New York:
Wiley.
Moors, A., Spruyt, A., & De Houwer, J. (2010). In search of a measure
that qualifies as implicit: Recommendations based on a decom-
positional view of automaticity. In B. Gawronski & K. B. Payne
(Eds.), Handbook of implicit social cognition: Measurement,theory, and applications. New York: Guilford Press.
Muthen, L. K., & Muthen, B. O. (2006). MPlus 4.1. Los Angeles, CA:Muthen and Muthen.
Neumann, A., & Philippot, P. (2007). Specifying what makes a
personal memory unique enhances emotion regulation. Emotion,7, 566–578.
Nuttin, J. M. (1985). Narcissism beyond Gestalt awareness: The
name letter effect. European Journal of Social Psychology, 15,
353–361.
Orth, U., Robins, R. W., Trzesniewski, K. H., Maes, J., & Schmitt, M.
(2009). Low self-esteem is a risk factor for depressive symptoms
from young adulthood to old age. Journal of AbnormalPsychology, 118, 472–478.
Philippot, P., & Brutoux, F. (2008). Induced rumination dampens
executive processes in dysphoric young adults. Journal ofBehavior Therapy and Experimental Psychiatry, 39, 219–227.
Phillips, W. J., Hine, D. W., & Thorsteinsson, E. B. (2010). Implicit
cognition and depression: A meta-analysis. Clinical PsychologyReview, 30, 691–709.
Reilly-Harrington, N. A., Alloy, L. B., Fresco, D. M., & Whitehouse,
W. G. (1999). Cognitive styles and life events interact to predict
bipolar and unipolar symptomatology. Journal of AbnormalPsychology, 108, 567–578.
Reno, R. M., & Halaris, A. E. (1989). Dimensions of depression: A
comparative longitudinal study. Cognitive Therapy andResearch, 13, 549–563.
Rosenberg, M. (1965). Society and the adolescent self-image.
Princeton, NJ: Princeton University Press.
Rude, S. S., Valdez, C. R., Odom, S., & Ebrahimi, A. (2003).
Negative cognitive biases predict subsequent depression. Cog-nitive Therapy and Research, 27, 415–429.
Rude, S. S., Wenzlaff, R. M., Gibbs, B., Vane, J., & Whitney, T.
(2002). Negative processing biases predict subsequent depres-
sive symptoms. Cognition and Emotion, 16, 423–440.
Ruscio, J., Brown, T. A., & Ruscio, A. M. (2009). A taxometric
investigation of DSM-IV major depression in a large outpatient
sample. Assessment, 16, 127–144.
Ruscio, A. M., & Ruscio, J. (2002). The latent structure of analogue
depression: Should the beck depression inventory be used to
classify groups? Psychological Assessment, 14, 135–145.
Scher, C. D., Ingram, R. E., & Segal, Z. V. (2005). Cognitive
reactivity and vulnerability: Empirical evaluation of construct
activation and cognitive diatheses in unipolar depression.
Clinical Psychology Review, 25, 487–510.
Schroder-Abe, M., Rudolph, A., & Schutz, A. (2007). High implicit
self-esteem is not necessarily advantageous: Discrepancies
between explicit and implicit self-esteem and their relationship
with anger expression and psychological health. EuropeanJournal of Personality, 21, 319–339.
Schwartz, G. (1978). Estimating the dimension of a model. TheAnnals of Statistics, 6, 461–464.
Segal, Z. V., Williams, J. M. G., & Teasdale, J. D. (2002).
Mindfulness based cognitive therapy for depression—A newapproach to preventing relapse. New York: Guilford Press.
Siemer, M. (2005). Mood-congruent cognitions constitute mood
experience. Emotion, 5, 296–308.
Smith, E. R., & DeCoster, J. (2000). Dual-process models in social
and cognitive psychology: Conceptual integration and links to
underlying memory systems. Personality and Social PsychologyReview, 4, 108–131.
Steinberg, J. A., Karpinski, A., & Alloy, L. B. (2007). The exploration
of implicit aspects of self-esteem in vulnerability-stress models
of depression. Self and Identity, 6, 101–117.
Tang, T. Z., DeRubeis, R. J., Hollon, S. D., Shelton, R., &
Amsterdam, J. (2007). Sudden gains in cognitive therapy of
depression and depression relapse/recurrence. Journal of Con-sulting and Clinical Psychology, 75, 404–408.
Cogn Ther Res
123
Author's personal copy

Teasdale, J. D. (1988). Cognitive vulnerability to persistent depres-
sion. Cognition and Emotion, 2, 247–274.
Thase, M. E. (2009). Neurobiological aspects of depression. In
I. H. Gotlib & C. L. Hammen (Eds.), Handbook of depression(pp. 187–217). New York: Guilford Press.
Turner, J. A., & Romano, J. M. (1984). Self-report screening
measures for depression in chronic pain patients. Journal ofClinical Psychology, 40, 909–913.
Waller, N. G., & Meehl, P. E. (1998). Multivariate taxometricprocedures: Distinguishing types from continua. Thousand Oaks,
CA: Sage.
Weissman, A. N., & Beck, A. T. (1978). Development and validationof the dysfunctional attitude scale: A preliminary investigation.
Paper presented at the Annual Meeting of the American
Educational Research Association, 62nd, Toronto, Ontario,
Canada, March 27–31, 1978.
Wenzlaff, R. M. (1993). The mental control of depression: Psycho-
logical obstacles to emotional well-being. In D. M. Wegner &
J. W. Pennebaker (Eds.), Handbook of mental control(pp. 239–257). Englewood Cliffs, NJ: Prentice Hall.
Wenzlaff, R. M., & Bates, D. E. (1998). Unmasking a cognitive
vulnerability to depression: How lapses in mental control reveal
depressive thinking. Journal of Personality and Social Psychol-ogy, 75, 1559–1571.
Wenzlaff, R. M., Rude, S. S., Taylor, C. J., Stultz, C. H., & Sweatt, R.
A. (2001). Beneath the veil of thought suppression: Attentional
bias and depression risk. Cognition and Emotion, 15, 435–452.
Wisco, B. E. (2009). Depressive cognition: Self-reference and depth
of processing. Clinical Psychology Review, 29, 382–392.
Wittenbrink, B., & Schwarz, N. (2007). Implicit measures ofattitudes. New York: Guilford Press.
Zelenski, J. M., & Larsen, R. J. (2003). The importance of knowingwhat we want: How implicit and explicit motives interact topredict well-being. Paper presented at the meeting of the Society
for Personality and Social Psychology, Los Angeles, CA.
Zung, W. W. (1965). A self-rating depression scale. Archives ofGeneral Psychiatry, 12, 63–70.
Zung, W. W. (1986). Zung self-rating depression scale and depression
status inventory. In N. Sartorius & T. A. Ban (Eds.), Assessmentof depression. Berlin: Springer.
Cogn Ther Res
123
Author's personal copy





























