Embed Size (px)
Citation preview

A Novel, Non-Prostanoid EP2 Receptor-Selective Prostaglandin E2 AgonistStimulates Local Bone Formation and Enhances Fracture Healing
MEI LI,1,2 HUA ZHU KE,1,2 HONG QI,1 DAVID R HEALY,1 YAN LI,1 D TODD CRAWFORD,1
VISHWAS M PARALKAR,1 THOMAS A OWEN,1 KIMBERLY O CAMERON,1 BRUCE A LEFKER,1
THOMAS A BROWN,1 and DAVID D THOMPSON1
ABSTRACT
CP-533,536, a newly discovered, non-prostanoid EP2 receptor-selective PGE2 agonist, stimulates local boneformation and enhances fracture healing in rat models.
Introduction: There is a significant medical need for agents that can stimulate local bone formation and enhancefracture healing. We tested the effects of CP-533,536, a newly discovered, non-prostanoid EP2 receptor-selectiveprostaglandin E2 (PGE2) agonist, in stimulating local bone formation and enhancing fracture healing in rat models.Materials and Methods: In the first model, a single injection of CP-533,536 at doses of 0.3, 1, or 3 mg/kg to theproximal tibial metaphysis of 6-week-old male rats was given on day 1, and the local bone anabolic effect wasdetermined on day 7. We then tested the effects of this compound in inducing bone formation on rat periosteum ofthe femur. A single dose of 0.3 mg of CP-533,536 incorporated in a poly-(D,L–lactide-co-glycolide) (PLGH) matrixwas injected onto the periosteum of the femur in 3-week-old male rats, and local bone formation was determined onday 14. Finally, the ability of CP-533,536 in PLGH matrix in enhancing fracture healing was tested using the ratfemoral fracture model. CP-533,536 in PLGH matrix at doses of 0.05, 0.5, or 5 mg was delivered to the local fracturesite on the same day of fracture, and its efficacy was evaluated on day 21.Results and Conclusions: A single injection of CP-533,536 at doses of 0.3, 1, or 3 mg/kg to the proximal tibialmetaphysis dose-dependently stimulated local lamellar bone formation on trabecular, endocortical, and periostealsurfaces, and thus increased bone mineral content and bone strength at the injected site. Similarly, a single injectionof 0.3 mg of CP-533,536 incorporated in PLGH matrix onto the periosteum of the femur induced significantly localbone formation. In the rat femoral fracture model, CP-533,536 in PLGH matrix at doses of 0.05, 0.5, and 5 mgdose-dependently increased callus size, density, and strength compared with PLGH matrix alone. These results showthat CP-533,536 stimulates new bone formation on trabecular, endocortical, and periosteal surfaces and enhancesfracture healing. These data reveal that EP2 receptor-selective agonists provide therapeutic potential for local boneaugmentation, bone repair, and bone healing in humans.J Bone Miner Res 2003;18:2033–2042
Key words: prostaglandin E2, EP2 receptor agonist, local bone formation, fracture healing
INTRODUCTION
IN THE UNITED STATES, 7.9 million fractures occur eachyear, and 5–10% of these fractures progress to delayed
union or nonunion.(1–2) Currently, few therapeutic optionsexist for the enhancement of local bone repair. Bone mor-
phogenetic proteins (BMP2 and BMP7) have been investi-gated as pharmacologic agents for enhancing fracturehealing.(3–6) However, the cost effectiveness, degree of clin-ical benefit, and long-term safety of these therapies have notbeen delineated. Furthermore, the disadvantages of proteintherapy include stability of the protein, antibody formation,and complexity of manufacturing. Therefore, a nonpeptide,small molecule may provide advantages over peptides orEvery author owns stock and is an employee of Pfizer Inc.
1Department of Cardiovascular and Metabolic Diseases, Pfizer Global Research and Development, Groton Laboratories, Groton,Connecticut, USA.
2These authors contributed equally to the manuscript.
JOURNAL OF BONE AND MINERAL RESEARCHVolume 18, Number 11, 2003© 2003 American Society for Bone and Mineral Research
2033

proteins as a pharmacologic intervention for initiating orenhancing bone repair.
It has been very well characterized that prostaglandin E2
(PGE2) and prostaglandin F2� stimulate bone formationand increase bone mass and bone strength.(7–10) It has alsobeen reported that endogenous PGE2 increases locally afterfracture,(11) and inhibition of PGE2 production impairs bonehealing.(12–14) In addition, studies have shown that localadministration of PGE2 stimulates bone formation and cal-lus development in animal models.(15,16) However, becauseof side effects that include diarrhea, lethargy, and flushing,PGE2 is an unacceptable therapeutic option for humans. Thepharmacologic activities of PGE2 are mediated through fourreceptor subtypes: EP1–EP4.(17) It has been reported thatthe EP2 receptor mediates PGE2-induced transition of non-adherent to adherent bone marrow mesenchymal precursorcells.(18) Furthermore, the EP2 receptor has also been re-ported to mediate the anabolic effects of prostaglandin onreplication and differentiation of osteoblasts.(19) We haveidentified the EP2 receptor subtype as one of the receptorsassociated with the local bone anabolic activity of PGE2,(20)
and EP1 and EP3 receptor subtypes seem to mediate someof the objectionable side effects. Thus, our efforts werefocused on identifying a small molecule, non-prostanoidEP2 receptor selective agonist that would be expected toincrease local bone formation and enhance fracture healing.These efforts lead to the discovery of CP-533,536 (Fig. 1).CP-533,536 selectively binds to the EP2 receptor with a50% inhibition concentration (IC50) of 11 nM (binding IC50
is greater than 2800 nM for EP1, EP3, and EP4). Similarly,CP-533,536 is selective as an EP2 receptor agonist whenmeasured against other prostanoid receptors including theprostaglandin D2 (DP), prostaglandin F2� (FP), prostacy-clin (IP), and thromboxane receptors (TP) in the prostanoidreceptor family. CP-533,536 stimulates the EP2 receptor-mediated signaling by the cyclic adenosine monophosphate(cAMP) pathway with an 50% effective concentration(EC50) value of 5 nM. Here, we present the in vivo phar-macologic effects of CP-533,536 in several animal modelsto show that EP2 selective agonists have therapeutic poten-tial in stimulating bone formation and enhancing fracturehealing by local administration.
MATERIALS AND METHODS
Animals
Male Sprague-Dawley (SD) rats (Taconic Farms Inc.,Germantown, NY, USA) were used in these studies. Theanimals were housed at 24°C with a 12-h light/12-h darkcycle and were allowed free access to water and a commer-cial diet (Purina Laboratory Rodent Chow 5001; Purina-Mills, St Louis, MO, USA) containing 0.95% calcium,0.67% phosphorus, and 4.5 IU/g vitamin D3. The experi-ments were conducted according to Pfizer Animal Care andUse approved protocols and animals were maintained inaccordance with the Institute of Laboratory Animal Re-search Guide for the Care and Use of Laboratory Animals.
Agents
The following agents were tested in the rat marrow in-jection model to determine their ability to stimulate localbone formation: (1) PGE2, which binds to all four EPreceptor subtypes (EP1–EP4) with a 50% inhibition con-centration (IC50) less than 10 nM; (2) 17-phenyl-trinorPGE2, a prostanoid agent that binds to the EP1, EP3, andEP4 receptors with IC50 of 41, 44, and 76 nM, respectively,but does not bind to the EP2 receptor (IC50 � 3200 nM;17-phenyl-trinor PGE2 is an agonist for rat EP4 receptor,because it stimulates the rat EP4 receptor mediated signal-ing by the cAMP pathway with an EC50 value of 2.9 nM);(3) sulprostone, an EP1 and EP3 receptor agonist with abinding IC50 of 18 and 13 nM for the EP1 and EP3 receptorsubtypes, respectively, and �3200 nM for the EP2 and EP4receptor subtypes; and (4) CP-533,536, an EP2 receptorselective PGE2 agonist. The first three agents were pur-chased from Cayman Chemical (Ann Arbor, MI, USA).CP-533,536 [chemical name: (3-{[(4-tert-butyl-benzyl)-(pyridine-3-sulfonyl)-amino]-methyl}-phenoxy)-acetic acidsodium salt; molecular formula: C25H28N2O5SNA; molec-ular weight: 468.56 (free acid) and 490.54 (sodium salt),Fig. 1] was synthesized at Pfizer Global Research andDevelopment (Groton, CT, USA). CP-533,536 was furthertested in rat periosteal injection and femoral fracture modelsto determine its effects on periosteal bone formation andfracture healing.
Rat marrow injection model
We used a rat marrow injection model (Fig. 2A) to testthe local anabolic effect of PGE2, 17-phenyl-trinor PGE2,and sulprostone. Male SD rats at 6 weeks of age wereanesthetized by intraperitoneal injection of a mixture ofketamine/xylazine. The right proximal part of the tibia ofeach rat was shaved and sterilized. A single dose of 10 �l ofaqueous vehicle containing 5% ethanol and 95% injectionwater (n � 10), PGE2 at doses of 3 or 6 mg/kg, 17-phenyl-trinor PGE2 at doses of 1 and 3 mg/kg, or sulprostone atdoses of 1 and 3 mg/kg (n � 10 per subgroup) dissolved in10 �l of the same vehicle were directly injected through thecortex into the marrow cavity of the right proximal tibialmetaphysis (Fig. 2A). At day 7, the animals were killed, andthe injected proximal tibia was harvested. The injected siteswere evaluated using peripheral quantitative computerizedtomography (pQCT; Stratec XCT Research M; Norland
FIG. 1. Chemical structure of CP-533,536.
2034 LI ET AL.

Medical Systems, Fort Atkison, WI, USA) with softwareversion 5.40 as previously described.(21) Volumetric bonemineral content (BMC), density, and bone area were deter-mined for total, trabecular, and cortical bone. In addition,periosteal and endocortical circumferences were deter-mined.
Next, using the same rat marrow injection model, wetested the local anabolic effect of CP-533,536, an EP2receptor selective agonist. CP-533,536 at doses of 0.3, 1, or3 mg/kg (n � 10 per group) dissolved in 10 �l of aqueousvehicle containing 5% ethanol and 95% injection water wasinjected into the marrow cavity of the right proximal tibialmetaphysis. All rats were given a subcutaneous injection of10 mg/kg of calcein (Sigma Chemical Co., St Louis, MO,USA) for fluorescent bone labeling on days 3 and 5 of theexperiment. At day 7, the animals were killed, and theinjected proximal tibia was harvested for analysis by pQCTand microcomputerized tomography (�CT 40; Scanco Med-ical AG, Bassersdorf, Switzerland). Thereafter, 10-�m-thick, undecalcified, methyl methacrylate-embedded longi-tudinal sections of the injected site were prepared.(22) Thesesections were used to measure the newly formed trabecularbone area by histomorphometric method using an ImageAnalysis System (Osteomeasure, Inc., Atlanta, GA, USA).The newly formed trabecular bone was defined as the sumof new trabeculae that were formed on top of the calceinlabels, thus having been formed after calcein was adminis-tered (Fig. 2D). To determine the change in bone strengthafter local administration of CP-533,536, we repeated theabove study, and the injected site was subjected to anindentation test for the initial maximal load and stiffness asdescribed previously.(8)
Rat periosteal injection model
The ability of CP-533,536 to stimulate bone formation onthe periosteum of the long bone diaphysis was tested usinga rat periosteal injection model. The periosteum is a likelysource of chondrocyte and osteoblast precursor cells in-volved in bone healing.(23,24) Our previous studies indicatedthat a longer-term drug exposure is required in this modelfor optimal effects of bone anabolic agents. Thus, CP-533,536 was incorporated into an injectable and biodegrad-able polymer matrix to provide extended drug exposure.The polymer matrix used is based on the ATRIGEL Deliv-ery System (Atrix Laboratories, Inc., Fort Collins, CO,USA) and consists of poly(D,L-lactide-co-glycolide)(PLGH) dissolved in N-methyl-2-pyrrolidone (NMP).(25–27)
After placement in the body, the NMP diffuses out of theimplant, leaving the drug encapsulated in a PLGH matrix.We confirmed that subcutaneous injection of the CP-533,536 in PLGH matrix resulted in an extended release ofCP-533,536 over a period of about 14 days in rats. In thefirst experiment, 20 male SD rats at 3 weeks of age wererandomly divided into two groups with 10 per group andwere subjected to periosteal injection.(28) The rats wereanesthetized by isoflurane inhalation. The right hind limb ofeach rat was shaved and sterilized, and each rat received asingle injection of either PLGH matrix alone or 0.3 mg ofCP-533,536 in a PLGH matrix (6 �l per injection per rat)onto the periosteum of the craniolateral aspect of right
femur on day one. Two weeks later, all rats were killed byCO2 asphyxiation, and the right femurs were harvested.Excised femurs were radiographed, and a pQCT analysiswas performed at the injected site. Total volumetric BMCand bone area were determined. Ten-micrometer-thick, un-decalcified, methyl methacrylate-embedded longitudinalsections were cut from the injected femurs for qualitativeevaluation. In the second experiment, we aimed to investi-gate the fate of the newly formed bone induced by CP-533,536 in this model. The same experimental protocol wasapplied to a second study with 140 male SD rats, one-half ofthem treated with PLGH matrix alone and the other halftreated with CP-533,536 in PLGH matrix. Ten rats fromeach group were necropsied at 2, 3, 4, 6, 8, 10, and 12 weeksafter injection, and the right femurs were harvested. Excisedfemurs were radiographed and scanned by a DXA machine(Hologic QDR 4500/A; Hologic Inc., Waltham, MA, USA)at the region from midshaft to the lesser trochanter of theright femurs. BMC was determined.
Rat femoral fracture model
Sixty, 3-month-old male SD rats were randomly dividedinto four groups (n � 15 per group), and each rat wassubjected to a closed transverse fracture on its right fe-mur.(29) Rats were anesthetized with an intraperitoneal in-jection of ketamine hydrochloride and xylazine at doses of50 and 10 mg/kg body weight, respectively. The righthindlimb of each rat was shaved and cleaned. A medialperipatellar incision was made, and the patella was dislo-cated laterally, exposing the femoral condyles. A Kirshnerwire (1.1 mm diameter, 27 mm length) was introduced fromthe intercondylar notch into the intramedullary canal. Afterclosing the knee joints, the mid-diaphysis of the pinnedfemur was fractured by means of a three-point bendingdevice driven by a dropped weight. Immediately after frac-ture, CP-533,536 at doses of 0.05, 0.5, and 5 mg in 100 �lof PLGH matrix or matrix alone was percutaneously in-jected onto the fracture site of each rat in each of therespective groups. The rats were permitted full weight bear-ing and unrestricted activity after recovering from anesthe-sia. Three weeks after injection, all animals were killed afterCO2 asphyxiation, and the right femurs were harvested.Radiographs of the right femurs were taken immediatelyafter necropsy, and the bone samples were frozen and re-tained for torsional testing as described previously.(30) Tostudy the histological changes, the right femurs treated withPLGH matrix alone or with 0.5 mg of CP-533,536 (N � 10per group) collected from a separate study (same studydesign) were fixed, decalcified, and embedded in paraffin.Five-micrometer sections were cut and stained with modi-fied Masson’s trichrome stain. Total callus area, cartilagi-nous callus area, and bony callus area were measured usingan Image Analysis System (Osteomeasure, Inc., Atlanta,GA, USA).
Statistical analysis
Data are expressed as means � SE for each group.Statistics were calculated using StatView 4.0 (Abacus Con-cepts, Inc., Berkeley, CA, USA). Statistical differences be-tween groups were evaluated with ANOVA followed by the
2035EP2 RECEPTOR AGONIST STIMULATES BONE FORMATION AND HEALING

FIG. 2. (A) Diagram of rat marrow injection model. CP-533,536 at doses of 0, 0.3, 1, and 3 mg at 10 �l was injected into the marrow cavityof the proximal tibial metaphysis as shown on day 1. The injected bones were harvested on day 7, and the injected sites were analyzed. (B) pQCTimages of injected sites from vehicle-treated control and CP-533,536 at 3 mg/kg showing CP-533,536 increased both trabecular and cortical bonemass compared with vehicle. (C) �CT images of injected sites from vehicle-treated control and CP-533,536 at 3 mg/kg showing CP-533,536induced new trabecular bone formation compared with vehicle. (D) Micrographs taken from the marrow cavity at the injection site of a rat treatedwith 3 mg/kg of CP-533,536 showing the newly formed trabeculae were well connected and labeled with calcein (green), a fluorescent bonemarker, under the fluorescent light. (E) The same field as shown in D showing lamellae can be observed in the newly formed trabeculae underpolarized light.

Fisher PLSD test for multiple comparisons. Probabilitiesless than 0.05 were considered as significant.
RESULTS
Rat marrow injection model
A single injection of PGE2 at 3 or 6 mg/kg to the marrowcavity of the proximal tibial metaphysis significantly in-creased total mineral content by 5% and 10%, total area by9% and 8%, trabecular content by 20% and 25%, andtrabecular density by 6% and 15%, respectively. However,no significant difference in cortical content, cortical density,and cortical area between PGE2- and vehicle-treated ratswas found. Diarrhea, lethargy, and flushing were observedin all rats who received PGE2. At doses of 1 and 3 mg/kg,both 17-phenyl-trinor PGE2 and sulprostone induced diar-rhea, lethargy, and flushing but did not induce significantbone formation on trabecular, endocortical, or periostealsurfaces around the injection sites as examined by PQCT(data not shown). These results reveal that the EP1 and/orEP3 receptors may mediate undesirable side effects but notthe local bone anabolic effects associated with PGE2.
pQCT images showed that the tibia injected with CP-533,536 had larger tissue cross-sectional area, thicker cor-tex, and higher trabecular density compared with vehiclecontrols (Fig. 2B). CP-533,536 dose-dependently increasedtotal content and density in the injected site (Fig. 3A; Table1). The increases in total content and total density wereachieved through both increased cortical and trabecular
bone, demonstrated by a significant increase in trabecularcontent, trabecular density, cortical content, cortical area,and cortical thickness (Table 1). Furthermore, a significantincrease in periosteal circumference and a significant de-crease in endocortical circumference in CP-533,536–treatedrats were observed (Table 1). All three doses of CP-533,536significantly increased trabecular density and significantlydecreased endocortical circumference, whereas only thehighest dose of CP-533,536 significantly increased perios-teal circumference (Table 1). CP-533,536 induced the for-mation of well-connected trabeculae, determined by �CT(Fig. 2C). Diffused calcein labels were observed on thesenewly formed trabecular surface (Fig. 2D), indicating anactive formation and mineralization of the bone matrixinduced by CP-533,536. In addition, the lamellae in thenewly formed trabeculae were clearly observed using po-larized light (Fig. 2E). Histomorphometric measurementsindicated that there were 6.1- and 12.8-fold increases in thenewly formed trabecular bone area in 1 and 3 mg/kg ofCP-533,536–treated rats, respectively, compared with con-trols (Fig. 3B). Furthermore, measures of bone strength, theinitial maximal load, and stiffness in the injection site of 1and 3 mg/kg of CP-533,536–treated rats increased signifi-cantly compared with controls (Figs. 3C and 3D). In addi-tion, no diarrhea, lethargy, or flushing was observed in ratsinjected with CP-533,536.
Rat periosteal injection model
In the first experiment, a well-defined area of new boneformation was detected by radiograph and pQCT image(Figs. 4B and 4C) at the site of injection in every femurtreated with CP-533,536. Quantitative measurements bypQCT showed that CP-533,536 in PLGH matrix signifi-cantly increased bone area and BMC of the injected site by25% (p � 0.001) and 18% (p � 0.001), respectively,compared with PLGH matrix alone. Evaluation of histolog-ical sections showed that the newly formed bone containedlamellar trabecular bone with no evidence of woven bone.The later fate of the newly formed bone was determined inthe second experiment. As shown by X-ray (Fig. 5A), thenewly formed bone by CP-533,536 was maximal at 2 weeksafter treatment, and over time, gradually remodeled back tothe shape of controls (6 weeks). BMC of CP-533,536–treated femurs was significantly increased by 18% and 19%compared with those treated with PLGH matrix alone at 2and 3 weeks, respectively (Fig. 5B). There was no differ-ence in BMC between the femurs treated with CP-533,536and PLGH matrix alone at 4, 5, 8, 10, and 12 weeks aftertreatment (Fig. 5B). In addition, no diarrhea, lethargy, orflushing was observed in rats treated with CP-533,536 inPLGH matrix or matrix alone.
Rat femoral fracture model
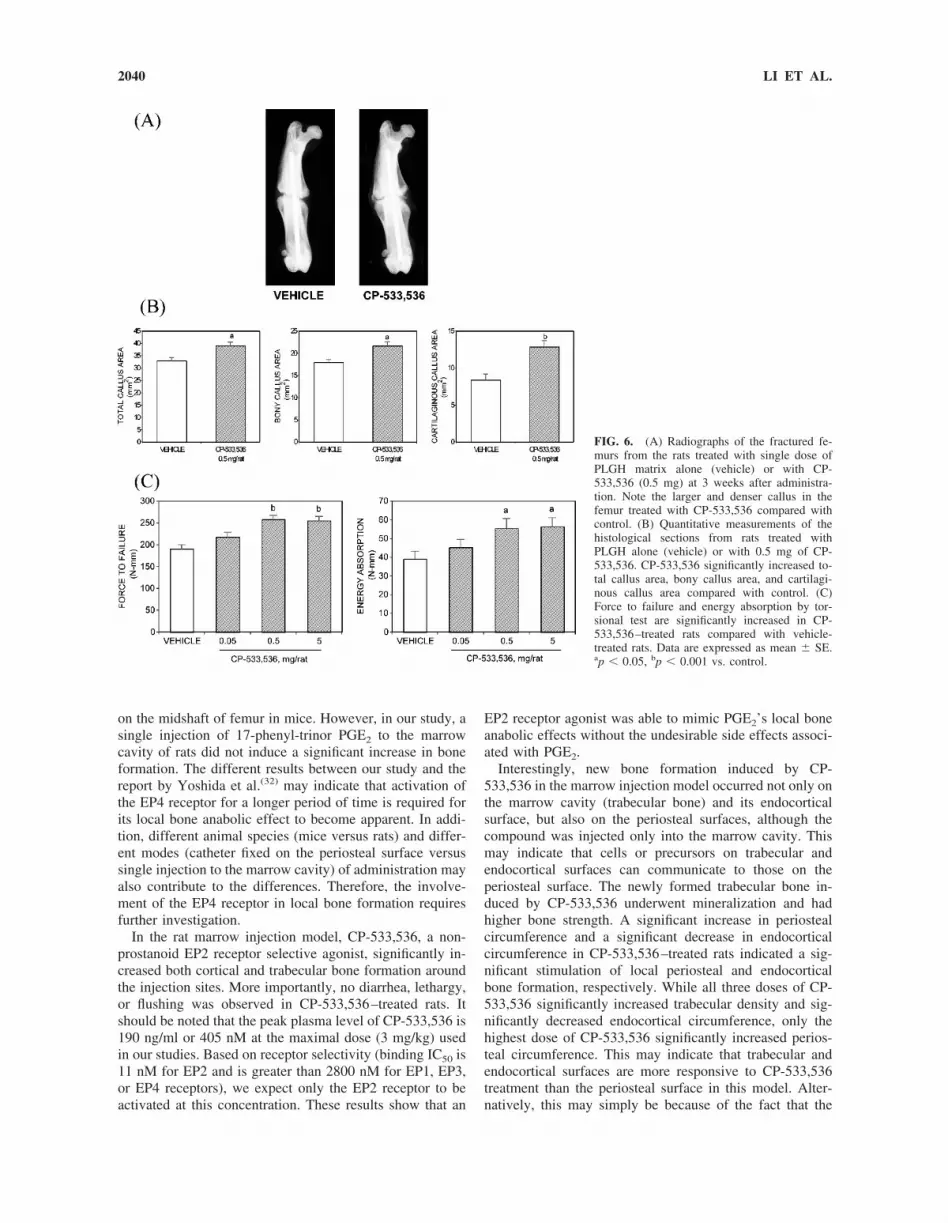
The fractured femurs treated with either PLGH matrixalone or with CP-533,536 demonstrated bone healing (as-sessed by histology and radiography). Histological exami-nation showed that the fracture site consisted of both bonyand soft calluses after 3 weeks of the healing period. How-ever, the femurs from rats treated with CP-533,536 inPLGH matrix had larger and denser calluses than those from
FIG. 3. CP-533,536 at doses of 0 (vehicle), 0.3, 1, and 3 mg at 10 �lwas injected into the marrow cavity of proximal tibial metaphysis of6-week-old male rats. (A) Total density of the injection sites deter-mined by pQCT was dose-dependently increased with CP-533,536treatment. (B) Newly formed bone area in the marrow cavity deter-mined by histomorphometric methods showing an increase of 6.1- and12.8-fold in 1 and 3 mg/kg of CP-533,536–treated rats compared withcontrols, respectively. (C and D) Initial maximal load and stiffnessdetermined by indentation test of the proximal tibial metaphysis show-ing significant increases in 1 and 3 mg/kg of CP-533,536–treated ratscompared with controls. ap � 0.05, bp � 0.001 vs. vehicle.
2037EP2 RECEPTOR AGONIST STIMULATES BONE FORMATION AND HEALING

controls as shown by radiograph (Fig. 6A). Quantitativemeasurements of histological sections of the fracture callusshowed significant increases in total callus area (19%), bonycallus area (20%), and cartilaginous callus area (53%) in therats treated with CP-533,536 at 0.5 mg in PLGH matrix
compared with controls (Fig. 6B). Torsional testing showedthat the mean values of force to failure were significantlyincreased by 35% and 34%, respectively, for the femurstreated with either 0.5 or 5 mg of CP-533,536 comparedwith those treated with PLGH matrix alone (Fig. 6C). In
TABLE 1. PQCT ANALYSIS OF INJECTED TIBIAS (RAT MARROW INJECTION MODEL)
Vehicle
CP-533,536
0.3 mg/kg 1 mg/kg 3 mg/kg
Total content (mg/mm) 5.80 � 0.13 5.95 � 0.10 7.33 � 0.23† 8.91 � 0.29†
Trabecular content (mg/mm) 1.00 � 0.04 1.14 � 0.07 1.70 � 0.09† 1.64 � 0.10†
Trabecular density (mg/cm3) 190 � 7.3 226 � 11.4* 320 � 15.3† 328 � 11.5†
Cortical content (mg/mm) 3.73 � 0.08 3.92 � 0.05 5.07 � 0.21† 6.83 � 0.28†
Cortical area (mm2) 5.7 � 0.12 5.92 � 0.08 8.0 � 0.36† 11.0 � 0.48†
Cortical density (mg/cm3) 654 � 6.5 660 � 4.6 634 � 5.7* 623 � 5.8*Cortical thickness (mm) 0.50 � 0.01 0.54 � 0.01* 0.74 � 0.37† 1.00 � 0.04†
Periosteal circumference (mm) 12.9 � 0.12 12.6 � 0.09 13.1 � 0.11 14.1 � 0.26†
Endocortical circumference (mm) 9.7 � 0.13 9.2 � 0.11* 8.54 � 0.23† 7.86 � 0.25†
Data are presented as mean � SEM; n � 10 per group; * p � 0.05, † p � 0.001 vs. vehicle.
FIG. 4. (A) Diagram of rat periosteal injec-tion model. Single dose (6 �l) of PLGH matrixalone (vehicle) or with 0.3 mg of CP-533,536was injected onto the periosteum of the cranio-lateral aspect of femur on day 1. The injectedfemurs were harvested and analyzed on vari-ous days postinjection. (B) Radiographs of fe-murs from the rat treated with PLGH matrixalone (vehicle) or with 0.3 mg of CP-533,536on day 15. Note newly formed bone (arrow) onthe lateral aspect of the femur treated withCP-533,536. (C) pQCT images of injectedsites treated with PLGH matrix alone (vehicle)or with 0.3 mg of CP-533,536 showing thenewly formed bone by CP-533,536.
2038 LI ET AL.

addition, a 42% and 45% increase in energy absorption wasseen in the rats treated with CP-533,536 at 0.5 and 5 mg,respectively, compared with those treated with PLGH ma-trix alone (Fig. 6C). These parameters were not significantlyaltered in the rats treated with 0.05 mg of CP-533,536. Inaddition, no diarrhea, lethargy, or flushing was observed inrats injected with CP-533,536 in PLGH matrix or matrixalone.
DISCUSSION
There is a significant unmet medical need for new agentsthat can stimulate fracture repair and reduce the incidence ofmalunions and nonunions in fracture healings. The resultsfrom our studies show that CP-533,536, a newly discoveredsmall molecular agent, selectively binds to the EP2 receptorsubtype of PGE2 receptors and induces bone formation inthe marrow cavity as well as on endocortical and periostealsurfaces on local delivery to the sites in rat models. Moreimportantly, we found that this agent can increase boneformation and bone strength in the rat femoral fracturemodel.
It has been previously reported that PGE2 increased bonegrowth by local delivery to the rat marrow cavity.(9) Usingthe rat marrow injection model described above, we haveconfirmed that PGE2 induced new bone formation in this
model. However, diarrhea, lethargy, and flushing were ob-served in PGE2-injected rats after administration. Using thesame model, we found that 17-phenyl-trinor PGE2, an EP1,EP3, and EP4 receptor agonist, and sulprostone, an EP1 andEP3 receptor agonist, also induced diarrhea, lethargy, andflushing but did not induce significant bone formationaround the injection sites. These results suggest that the EP1and/or EP3 receptors may mediate undesirable side effectsbut not the local bone anabolic effects associated withPGE2.
The EP4 receptor has been reported to be associated withbone anabolic effects of PGE2.(31–33) However, we did notobserve local anabolic effects by single injection of 17-phenyl-trinor PGE2, which also binds to EP4 receptor.Machwate et al.(31) reported that an EP4 receptor antagonist,given systemically, suppressed the PGE2-induced systemicbone formation. Others have found that the EP4 receptoragonists, given systemically, stimulate bone formation andincrease bone mass in animal models of osteopenia.(32,33)
The reason for this difference between the current study andother studies with EP4 agonists may, at least be in part,caused by the routes (local versus systemic) and regimen(once versus multiple times) of administration. Yoshida etal.(32) reported that local infusion of an EP4 receptor selec-tive agonist for 6 weeks markedly increased bone formation
FIG. 5. (A) Radiographs of femurs from ratstreated with PLGH matrix alone (vehicle) orwith CP-533,536 at 0.3 mg showing CP-533,536stimulated bone formation (arrow) at the injectedsite at 2 weeks (left panel) and the newly formedbone disappeared by 6 weeks (right panel). (B)Time course (2–12 weeks postinjection) changesin BMC by DXA from the femurs treated withCP-533,536. The increased BMC by CP-533,536 peaked around 2–3 weeks and graduallydeclined with time. Data are expressed in per-cent increase compared with age-matched con-trols at each time-point. ap � 0.05, bp � 0.001vs. control.
2039EP2 RECEPTOR AGONIST STIMULATES BONE FORMATION AND HEALING
on the midshaft of femur in mice. However, in our study, asingle injection of 17-phenyl-trinor PGE2 to the marrowcavity of rats did not induce a significant increase in boneformation. The different results between our study and thereport by Yoshida et al.(32) may indicate that activation ofthe EP4 receptor for a longer period of time is required forits local bone anabolic effect to become apparent. In addi-tion, different animal species (mice versus rats) and differ-ent modes (catheter fixed on the periosteal surface versussingle injection to the marrow cavity) of administration mayalso contribute to the differences. Therefore, the involve-ment of the EP4 receptor in local bone formation requiresfurther investigation.
In the rat marrow injection model, CP-533,536, a non-prostanoid EP2 receptor selective agonist, significantly in-creased both cortical and trabecular bone formation aroundthe injection sites. More importantly, no diarrhea, lethargy,or flushing was observed in CP-533,536–treated rats. Itshould be noted that the peak plasma level of CP-533,536 is190 ng/ml or 405 nM at the maximal dose (3 mg/kg) usedin our studies. Based on receptor selectivity (binding IC50 is11 nM for EP2 and is greater than 2800 nM for EP1, EP3,or EP4 receptors), we expect only the EP2 receptor to beactivated at this concentration. These results show that an
EP2 receptor agonist was able to mimic PGE2’s local boneanabolic effects without the undesirable side effects associ-ated with PGE2.
Interestingly, new bone formation induced by CP-533,536 in the marrow injection model occurred not only onthe marrow cavity (trabecular bone) and its endocorticalsurface, but also on the periosteal surfaces, although thecompound was injected only into the marrow cavity. Thismay indicate that cells or precursors on trabecular andendocortical surfaces can communicate to those on theperiosteal surface. The newly formed trabecular bone in-duced by CP-533,536 underwent mineralization and hadhigher bone strength. A significant increase in periostealcircumference and a significant decrease in endocorticalcircumference in CP-533,536–treated rats indicated a sig-nificant stimulation of local periosteal and endocorticalbone formation, respectively. While all three doses of CP-533,536 significantly increased trabecular density and sig-nificantly decreased endocortical circumference, only thehighest dose of CP-533,536 significantly increased perios-teal circumference. This may indicate that trabecular andendocortical surfaces are more responsive to CP-533,536treatment than the periosteal surface in this model. Alter-natively, this may simply be because of the fact that the
FIG. 6. (A) Radiographs of the fractured fe-murs from the rats treated with single dose ofPLGH matrix alone (vehicle) or with CP-533,536 (0.5 mg) at 3 weeks after administra-tion. Note the larger and denser callus in thefemur treated with CP-533,536 compared withcontrol. (B) Quantitative measurements of thehistological sections from rats treated withPLGH alone (vehicle) or with 0.5 mg of CP-533,536. CP-533,536 significantly increased to-tal callus area, bony callus area, and cartilagi-nous callus area compared with control. (C)Force to failure and energy absorption by tor-sional test are significantly increased in CP-533,536–treated rats compared with vehicle-treated rats. Data are expressed as mean � SE.ap � 0.05, bp � 0.001 vs. control.
2040 LI ET AL.

compound was delivered to the trabecular and endocorticalsurfaces and not to the periosteal surface.
The ability of CP-533,536 to stimulate local bone forma-tion in vivo was further investigated in a rat periostealinjection model. Our data showed that CP-533,536 stimu-lated significant bone formation around the injection sitewhen delivered directly onto the periosteal surface, wherethe undifferentiated mesenchymal cell layer is a likelysource of chondrocyte and osteoblast precursor cells in-volved in bone healing.(23,24) The newly formed bone con-sisted of mineralized trabecular bone, without evidence ofcartilage formation. This effect in rats with CP-533,536 issimilar to the effect of continuous delivery of PGE1 or PGE2
onto the periosteum of dogs(34) or mice.(32) Our data suggestthat stimulatory effects of CP-533,536 on periosteal boneformation of an uninjured long bone are mainly throughintramembranous osteogenesis but not chondrogenesis. CP-533,536 simulates the proliferation of mesenchymal cellsthat then differentiate into osteoblasts resulting in new boneformation. The newly formed bone stimulated by CP-533,536 treatment was maximal at 2 weeks, which is con-sistent with the duration of delivery of CP-533,536 in thePLGH matrix. This newly formed bone underwent boneremodeling and the original shape of the bone at the injectedsite was restored. These findings indicated that the newlyformed bone induced by CP-533,536 was gradually remod-eled with time after cessation of the treatments.
With the evidence that CP-533,536 stimulates marrowand periosteal bone formation on local delivery, we soughtto further evaluate this compound for its potential efficacyin fracture healing in a rat femoral fracture model. Our dataclearly showed that CP-533,536 stimulated callus formationwhen delivered at the fracture site. The histological evalu-ation of the site of fracture repair showed more extensiveendochondral and intramembranous ossification in the frac-tured femurs treated with CP-533,536 resulting in a smallerfracture gap, indicating more advanced healing. Interest-ingly, CP-533,536 significantly increased cartilaginous cal-lus area in a fractured bone, while no direct evidence ofchondral bone formation in an uninjured femur was ob-served in the rat periosteal injection model as discussedearlier. It seemed that CP-533,536 enhanced chondral ossi-fication that was initiated by the fracture process. Whetherthis is a direct or an indirect effect is not clear. Moreimportantly, CP-533,536 significantly increased energy ab-sorption and force to failure of the healing fracture calluswhen it was tested to failure in torsion, indicating superiormechanical properties. Taken together, our results show thatCP-533,536 accelerated fracture healing and improved thebiomechanical integrity of the fracture site in rats.
Recently, it was reported(35) that cyclo-oxygenenase-2(COX-2) regulates the induction of cbfa1 and osterix and iscritically involved in bone repair as the healing of stabilizedtibial fractures was significantly delayed in mice lackingCOX-2. PGE2 has been shown to upregulate and stabilizeCOX-2 mRNA expression.(36,37) However, the involvementof individual receptor subtypes in regulation of COX-2 isnot completely understood. Faour et al.(36) reported that theupregulation and stabilization of COX-2 mRNA expressionby PGE2 in primary cultures of human synovial fibroblasts
was mediated through the EP4 receptor because butaprost(EP2 agonist) and sulprostone (an EP1/3 agonist) did nothave the effects observed with PGE2 treatment. In contrast,Hinz et al.(37) found that the upregulation of COX-2 expres-sion by PGE2 in lipopolysaccharide-stimulated RAW264.7macrophages was mediated through the EP2 receptor be-cause butaprost (an EP2 agonist) and 11-deoxy PGE1 (anEP2/4 agonist) mimicked the effects of PGE2 in this system.These findings suggest that the upregulation of COX-2 byPGE2 may be mediated by EP2 and/or EP4 receptors. Theinvolvement of individual receptor subtypes probably de-pends on the cell types and the species. Nevertheless, thedirect involvement of COX-2 in PGE2-induced bone heal-ing is not completely understood. In the current studies, wefound that CP-533,536, an EP2 receptor selective agonist,stimulates local bone formation and enhances fracture heal-ing in rat models. Further investigation is required to un-derstand whether CP-533,536 upregulates the expression ofCOX-2.
In summary, CP-533,536, an EP2 receptor agonist, stim-ulates local bone formation and enhances fracture healingon local administration in rats. Our data suggest that such anEP2 receptor selective agonist may provide a potentialtherapeutic for local bone augmentation and bone repair.
ACKNOWLEDGMENTS
The authors thank J Hong, F Dumont, and RW Kors-meyer of Pfizer Global Research and Development, Groton,Connecticut, and M Zhou, RL Dunn, and RL Norton ofAtrix Laboratories, Inc., Fort Collins, Colorado, for theircontributions related to the PLGH matrix formulation. Wealso thank Dr Mark Bolander of Mayo Clinic and Dr VictorShen of Skeletech Inc. for their help in biomechanicaltesting.
REFERENCES
1. Melton LJ III 1995 Epidemiology of fractures. In: Riggs BL,Melton LJ III (eds.) Osteoporosis: Etiology, Diagnosis and Man-agement, 2nd ed. Lippincott-Raven Press, Philadelphia, PA, USA,pp. 225–247.
2. Weitzel PP, Esterhai JL Jr 1994 Delayed union, nonunion, andsynovial pseuarthrosis. In: Brighton CT, Friedlaender GE, LaneJM (eds.) Bone Formation and Repair. American Academy ofOrthopaedic Surgeons, Rosemont, IL, USA, pp. 505–528.
3. Sakou T 1998 Bone morphogenetic proteins: From basic studies toclinical approaches. Bone 22:591–603.
4. Welch RD, Jones AL, Bucholz RW, Reinert CM, Tjia JS, PierceWA, Wozney JM, Li XJ 1998 Effect of recombinant human bonemorphogenetic protein-2 on fracture healing in a goat tibial frac-ture model. J Bone Miner Res 13:1483–1490.
5. Blokhuis TJ, Patka P, Haarman HJTM, Giltaij LR 2002 Osteogenicprotein-1 (OP-1, BMP-7) for stimulation of healing of closedfractures: Evidence based medicine and pre-clinical experience. In:Vukicevic S, Sampath KT (eds.) Bone Morphogenetic Proteins,from Laboratory to Clinical Practice. Birkhauser Verlag, Basel,Switzerland, pp. 145–155.
6. Giltaij LR, Shimmin A, Friedlaender GE 2002 Osteogenicprotein-1 (OP-1) in the repair of bone defects and fractures of longbones: Clinical experience. In: Vukicevic S, Sampath KT (eds.)Bone Morphogenetic Proteins, from Laboratory to Clinical Prac-tice. Birkhauser Verlag, Basel, Switzerland, pp. 193–205.
7. Jee WSS, Ma YF 1997 The in vivo anabolic actions of prostaglan-dins in bone. Bone 21:297–304.
8. Ke HZ, Shen V, Qi H, Crawford DT, Wu DD, Liang XG, Chidsey-Frink KL, Pirie CM, Simmons HA, Thompson DD 1998 Prosta-
2041EP2 RECEPTOR AGONIST STIMULATES BONE FORMATION AND HEALING

glandin E2 increases bone strength in intact rats and in ovariecto-mized rats with established osteopenia. Bone 23:249–255.
9. Yang RS, Liu TK, Lin-Shiau SY 1993 Increased bone growth bylocal prostaglandin E2 in rat. Calcif Tissue Int 52:57–61.
10. Ma YF, Li XJ, Jee WSS, McOsker J, Liang XG, Setterberg R,Chow SY 1995 Effects of prostaglandin E2 and F2� on the skeletonof osteopenic ovariectomized rats. Bone 17:549–554.
11. Dekel S, Lenthall G, Francis MJ 1981 Release of prostaglandinsfrom bone and muscle after tibial fracture. An experimental studyin rabbits. J Bone Joint Surg Br 63:819–921.
12. Elves LW, Bayley I, Royllance PJ 1982 The effect of indomethacinupon experimental fractures in the rat. Acta Orthop Scand 53:35–41.
13. Keller J, Bunger C, Andreassen TT, Bak B, Lucht U 1987 Bonerepair inhibited by indomethacin. Effects on bone metabolism andstrength of rabbit osteotomies. Acta Orthop Scand 58:379–383.
14. Sudmann E, Dregelid E, Bessesen A, Morland J 1979 Inhibition offracture healing by indomethacin in rats. Eur J Clin Invest 9:333–339.
15. Keller J, Klamer A, Bak B, He SZ, Tidd L, Schwartz A, SørensenS, Bunger C 1992 Short-term effect of local application of PGE2on callus in rabbit osteotomy. Eur J Exp Musculoskeletal Res1:86–92.
16. Voegeli TL, Chapman MW 1985 Utilization of prostaglandin infracture healing. Trans Orthop Res Soc 10:134.
17. Breyer RM, Bagdassarian CK, Myers SA, Breyer MD 2001 Pro-stanoid receptors: Subtypes and signaling. Ann Rev PharmacolToxicol 41:661–690.
18. Scutt A, Zeschnigk M, Bertram P 1995 PGE2 induces the transi-tion from non-adherent to adherent bone marrow mesenchymalprecursor cells via a camp/EP2-mediated mechanism. Prostaglan-dins 49:383–395.
19. Woodiel FN, Fall PM, Raisz LG 1996 Anabolic effects of prosta-glandins in cultured fetal rat calvariae: Structure-activity relationsand signal transduction pathway. J Bone Miner Res 11:1249–1255.
20. Ke HZ, Qi H, Crawford DT, Chidsey-Frink KL, Lefker BA,Paralkar VM, Owen TA, Li M, Lu B, Grasser WA, Yu L, DaSilva-Jardine P, Thompson DD 2000 Discovery of a non-prostanoid EP2receptor selective prostaglandin E2 (PGE2) agonist that mimics thelocal anabolic effects of PGE2. J Bone Miner Res 15:S1;S377.
21. Ke HZ, Qi H, Chidsey-Frink KL, Crawford DT, Thompson DD2001 Lasofoxifene (CP-336, 156) protects against the age-relatedchanges in bone mass, bone strength, and total serum cholesterol inintact aged male rats. J Bone Miner Res 16:765–773.
22. Jee WSS, Li XJ, Inoue J, Jee KW, Haba T, Ke HZ, Setterberg RB,Ma YF 1997 Histomorphometric assay of the growing long bone.In: Takahashi N (ed.) Handbook of Bone Morphology. Nishimusa,Niigata City, Japan, pp. 87–112.
23. Ham AW 1930 A histological study of the early phase of bonerepair. J Bone Joint Surg Am 30:827–844.
24. Tonna EA, Cronkite EO 1963 The periosteum: Autoradiographicstudies on cellular proliferation and transformation utilizing triti-ated thymidine. Clin Orthop Relat Res 30:218–233.
25. Dunn RL 2002 The Atrigel drug delivery system. In: Rathbone MJ,Hagraft J, Roberts MS (eds.) Modified-Release Drug DeliveryTechnology. Marcel Dekker, New York, NY, USA, pp. 647–655.
26. Coonts BA, Whitman SL, O’Donnell M, Polson AM, Bogle G,Garrett S, Swanbom DD, Fulfs JC, Rodgers PW, Southhard GL,Dunn RL 1998 Biodegradation and biocompatibility of a guidedtissue regeneration barrier membrane formed from a liquid poly-mer material. J Biomed Mater Res 42:303–311.
27. Royals MA, Fujita S, Yewey GL, Rodriguez J, Schultheiss PC,Dunn RL 1999 Biocompatibility of a biodegradable in situ formingimplant system in rhesus monkeys. J Biomed Mater Res 45:231–239.
28. Joyce ME, Roberts AB, Sporn MB, Bolander ME 1990 Transform-ing growth factor-� and the initiation of chondrogenesis and os-teogenesis in the rat femur. J Cell Biol 110:2195–2207.
29. Bonnarens F, Einhorn TA 1984 Production of a standard closedfracture in laboratory animal bone. J Orthop Res 2:97–101.
30. White AA III, Panjabi MM, Southwick WO 1997 The four biome-chanical stages of fracture repair. J Bone Jt Surg Am 59:188–192.
31. Machwate M, Harada S, Leu CT, Seedor G, Labelle M, Gallant M,Hutchings S, Lachance N, Sawyer N, Slipetz D, Metters KM,Rodan SB, Young S, Rodan GA 2001 Prostaglandin receptor EP4mediates the bone anabolic effects of PGE2. Mol Pharmocol 60:36–41.
32. Yoshida K, Oida H, Kobayashi T, Maruyama T, Tanaka M, Katay-ama T, Yamaguchi K, Segi E, Tsuboyama T, Matsushita M, Ito K,Ito Y, Sugimoto Y, Ushikubi F, Ohuchida S, Kondo K, NakamuraT, Narumiya S 2002 Stimulation of bone formation and preventionof bone loss by prostaglandin E EP4 receptor activation. Proc NatlAcad Sci USA 899:4580–4585.
33. Ke HZ, Crawford DT, Qi H, Li M, Paralkar VM, Owen TA, PanLC, Brown TA, Cameron KO, Lefker BA, DaSilva-Jardine P, LuB, Grasser WA, Simmons HA, Yu LJ, Scott DO, Thompson DD2002 A non-prostanoid EP4 receptor selective prostaglandin E2(PGE2) agonist stimulates bone formation and restores bone massand strength in ovariectomized rats. J Bone Miner Res 17:S1;S483.
34. Miller SC, Markers SC 1993 Local stimulation of new boneformation by prostaglandin E1: Quantitative histomorphometry andcomparison of delivery by minipumps and controlled-release pel-lets. Bone 14:143–151.
35. Zhang X, Schwarz EM, Young DA, Puzas JE, Rosier RN, O’KeefeRJ 2002 Cyclooxygenase-2 regulates mesenchymal cell differen-tiation into the osteoblast lineage and is critically involved in bonerepair. J Clin Invest 109:1405–1415.
36. Faour WH, He Y, He QW, de Ladurantaye M, Quintero M,Mancini A, Di Battista JA 2001 Prostaglandin E2 regulates thelevel and stability of cyclooxygenase-2 mRNA through activationof p38 mitogen-activated protein kinase in interleukin-1 b-treatedhuman synovial fibroblasts. J Biol Chem 276:31720–31731.
37. Hinz B, Brune K, Pahl A 2000 Prostaglandin E2 upregulatescyclooxygenase-2 expression in lipopolysaccharide-stimulatedRAW 264.7 macrophages. Biochem Biophys Res Commun 272:744–748.
Address reprint requests to:HZ Ke, MD
Osteoporosis ResearchMail Stop 8118W-216
Groton LaboratoriesPfizer Global Research and Development
Groton, CT 06340, USAE-mail: [email protected]
Received in original form March 17, 2003; in revised form June 25,2003; accepted July 8, 2003.
2042 LI ET AL.





























