Embed Size (px)
Citation preview

Adenoids and Otitis Media With Effusion: A Morphological Study
Mustafa Mete Kiro@u, MD, Kemal azbilgin, MD, Barlas Aydogan, MD, Fikret Kir$lu, MD, Ozgiil Tap, MD, PhD, Mehmet Kaya, MD, PhD, and Can Ozsahinoglu, MD
Purpose: Adenoidectomy, especially for the treatment of suppurative otitis media, has been used for a very long time. In this study, the role of adenoids in the origin of otitis media with effusion was investigated by using light microscopy, immunocytochemistry, enzymechemistry, and electron microscopy. Materials and Methods: A group of 28 children with otitis media with effusion (OME) was identified. Ages ranged from 3 to 12 years. Acontrol group of 10 age-matched children without any middle ear and upper respiratory tract infection served as the basis for comparison. Specimens obtained at surgeries from both groups were divided into groups for light microscopy, immunocytochemistry, enzyme cytochemistry, and electron microscopy and then all were examined blindly. Also, quantitative analysis of antigen-presenting cells was performed blindly on 10 patients and 10 controls. Results: There was an increase in the number of lymphocytes, mast cells, plasma cells, macrophages, dendritic cells, and M cells in the adenoids of patients with OME when compared with the normal cases. Stratified squamous epithelial areas, collagenous fibers, and fibrocytes were also increased in the patient group. Antigen-presenting functions of epithelial cells are shown by major histocompatibilitycomplex (MHC) class II positivity of some ciliated-columnar epithelial cells in the patient group. Conclusion: Adenoid tissues of patients with OME in this study seem to be infectious foci, aggravating immune reactions, which might attack the middle ear through an ascending route. Copyright 0 1998 by W.B. Saunders Company.
Although the adenoids have been recog- nized as a factor in otitis media with effusion (OME) since the definition of the disease, there is still controversy in its treatment, in- cluding adenoidectomy operations.
In fact adenoidectomy, especially for the treatment of suppurative otitis media, has been performed since the beginning of the century. Approximately one million tonsillec- tomy and adenoidectomy procedures were performed in the United States in the 197Os.l In the last 20 years, the number of tonsillec- tomy and adenoidectomy operations decreased dramatically. Discussions about the pros and
From the Departments of Otolaryngology, and Histol- ogy, University of Gukurova School of Medicine, Cuku- rova Universitesi Tip FakOltesi, KBB Anabilim Dali Balcali Adana, Turkey.
Address reprint requests to M. Mete Klroglu, MD, Cukurova Universitesi TIP Fakiiltesi, KBB Anabilim Dali Balcall Adana, Turkey.
Copyright 0 1998 by W.B. Saunders Company 0196-0709/98/1904-0006$8.00/O
cons of the adenoidectomy are still valid to- day.
Morphological studies give clues about the mucociliary transport system, secretory struc- tures, and the infectious and immunological events that take place in the etiopathogenesis of OME. Adenoids are also investigated mor- phologically, but the studies are concerned with comparing the normal and hypertrophic adenoids, without taking OME into consider- ation.2-6
Previously, in our two consecutive studies, morphological changes in the middle ear and nasopharyngeal orifice of the eustachian tube in patients with OME had been showm7J This study is a continuation of these previous stud- ies and investigates the ultrastructure of ad- enoid tissues of patients with OME. The role of adenoids in the origin of OME was investi- gated by using light microscopy, immunocyto- chemistry, enzymechemistry, and electron mi- croscopy.
244 American Journal of Otolaryngology, Vol 19, No 4 (July-August), 1998: pp 244-250

ADENOIDS AND OME 245
MATERIALS AND METHODS
Patients and Specimens
Specimens of adenoid tissue were obtained dur- ing adenoidectomy operations on 28 children with OME; their ages ranged from 3 to 12 years. Diagno- sis of OME was proven with the aspiration of effusion from the middle ear after myringotomy. Also, adenoids were taken with cupped forceps from 10 age-matched control cases who were oper- ated on for foreign bodies in the airway. Informed consent for biopsy was obtained before surgery from the patient’s parents. The normality of the ears of the control group was tested with tympanometry and audiometry before or after the operation, de- pending on the urgency of the case. The adenoid tissue samples were divided into groups for light microscopy, immunocytochemistry, enzyme cyto- chemistry, and electron microscopy. Light micro- scopic and electron microscopic evaluations were performed on 28 patients and 10 controls, blindly. In order to evaluate cytological changes more objec- tively, quantitative analysis of antigen-presenting cells was performed on 10 OME patients and 10 controls.
Light Microscopy
Specimens were fixed with buffered neutral for- malin and after dehydration were embedded in paraffin. Twenty semithin sections at 5-km thick- ness were cut and stained with (1) hematoxylin- eosin or (2) streptavidin-biotin immunoperoxidase. Sections stained with hematoxylin-eosin were evaluated blindly. Also, some tissue samples were frozen in - 70’ C for enzyme-cytochemistry.
lmmunocytochemistry
Streptavidin-biotin immunoperoxidase staining procedures were carried out on the paraffin blocks. After deparafinization, the sections were placed in peroxidase-blocking reagent on each slide for 5 minutes, and the preparations were covered with nonspecific blocking reagent for 28 minutes. After taping off excess reagent, anti-human HLA-DR (Dako 775, Glostrup, Denmark) was incubated for 1 hour. Linking reagents were added to each slide for 30 minutes; subsequently the slides were incubated with streptavidin enzyme labels. Fresh working color reagent was prepared, and the slides were covered with this solution for 15 minutes. This staining procedure was performed at room tempera- ture, and preparations were washed with buffered washing solution at each step. Finally, cells were stained with Mayer hematoxylin (Merck, Darm- stadt, Germany) for 1 to 3 minutes, rinsed with tap water, and mounted in glycerol-jelly.
Enzyme Cytochemistry
On frozen preparations, acid phosphatase (Aph) staining was performed according to Barka.g Incuba-
tion was carried out with a-naphtyl Aph (Sigma 7000, St Louis, MO) for 30 minutes at 37°C. After precipitation of the final reaction product, prepara- tions were rinsed and mounted in glycerol-jelly.
Quantitative Analysis of Antigen-Presenting Cells
The quantitative analysis of antigen-presenting cells was evaluated on the HLA-DR MoAb and u-naphtyl Aph-stained slides. From each group, slides of 10 patients and 10 controls (for a total of 40 slides) were selected for the analysis. On each slide of the series, an interfollicular subepithelial and a follicular area (for a total of 80 areas) were ran- domly chosen and photographed at 400x, original magnification. The antigen-presenting cells (inter- digitating cell, follicular dendritic cell, and macro- phage) and the other cells were counted on these photographs, and the ratio of the antigen-present- ing cells to the total counted cells was calculated. Statistical analysis of the data was performed using Mann-Whitney U test. (PI 85 was considered significant.)
Electron Microscopy
The tissue fragment from each subject was fixed in glutaraldehyde for 4 hours at 4°C and post-fixed in osmic acid for 2 hours at 4°C. The specimens were dehydrated in graded ethanol series and were embedded in araldite. Twenty ultrathin sections were stained with uranyl acetate and lead citrate. Sections were examined with electron microscope blindly (Zeiss EM 900, Carl Zeiss, Oberkochen, Germany).
RESULTS
Light Microscopy
Control group. The surface of adenoids was covered with pseudostratified ciliated columnar epithelium. The epithelium cover- ing the free surface was folded, but no deep crypts were seen. There were several lymph nodules in the subepithelial area. Three kinds of antigen-presenting cells were identified by HLA-DR and Aph positivity: a few epithelial cells; some dendritic cells, which were stained only in perinuclear area; and some macro- phages, which were stained all through their cytoplasm.
Patient group. The surface epithelium was similar to that of the control group, but strati- fied squamous epithelium was seen in some
246 KIRO6LU ET AL
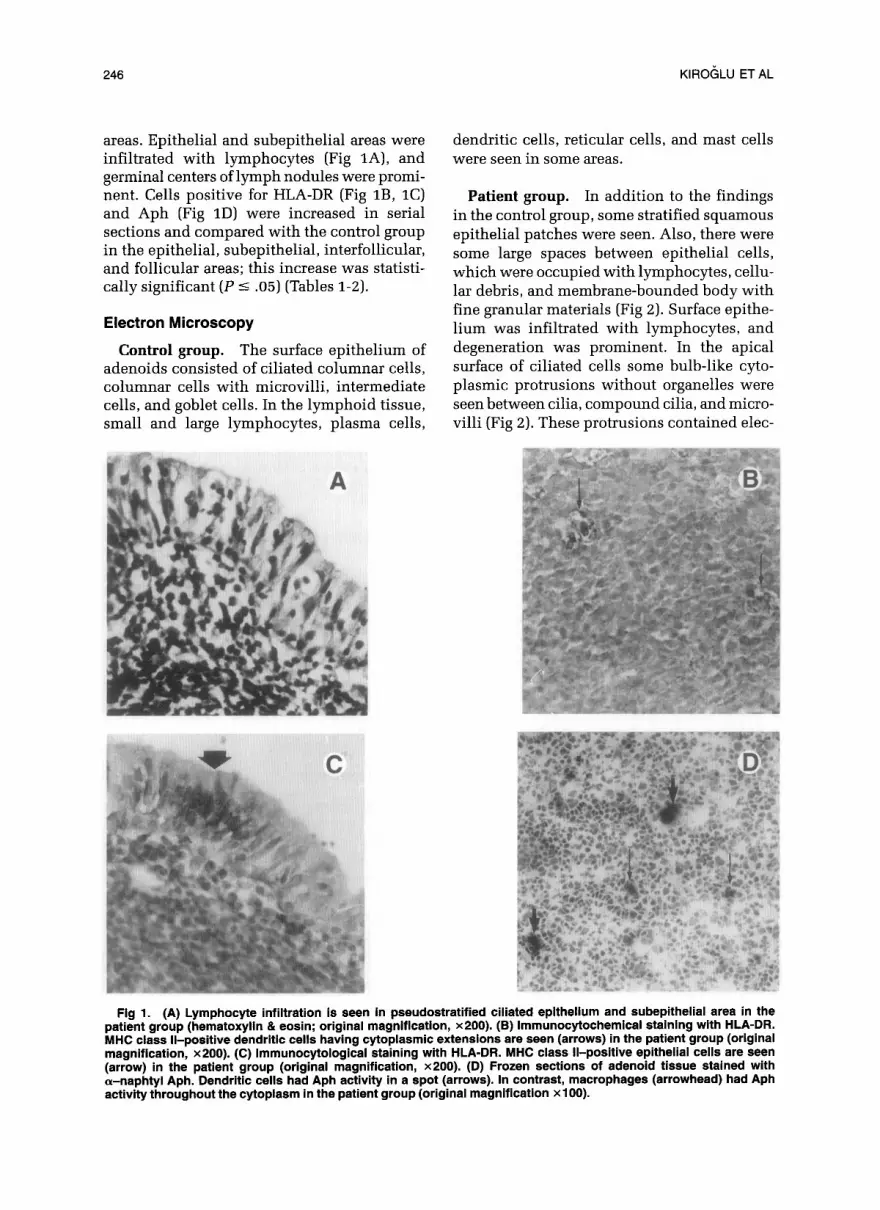
areas. Epithelial and subepithelial areas were infiltrated with lymphocytes (Fig lA), and germinal centers of lymph nodules were promi- nent. Cells positive for HLA-DR (Fig lB, 1C) and Aph (Fig 1D) were increased in serial sections and compared with the control group in the epithelial, subepithelial, interfollicular, and follicular areas: this increase was statisti- cally significant (P 5 .05) (Tables l-2).
Electron Microscopy
Control group. The surface epithelium of adenoids consisted of ciliated columnar cells, columnar cells with microvilli, intermediate cells, and goblet cells. In the lymphoid tissue, small and large lymphocytes, plasma cells,
dendritic cells, reticular cells, and mast cells were seen in some areas.
Patient group. In addition to the findings in the control group, some stratified squamous epithelial patches were seen. Also, there were some large spaces between epithelial cells, which were occupied with lymphocytes, cellu- lar debris, and membrane-bounded body with fine granular materials (Fig 2). Surface epithe- lium was infiltrated with lymphocytes, and degeneration was prominent. In the apical surface of ciliated cells some bulb-like cyto- plasmic protrusions without organelles were seen between cilia, compound cilia, and micro- villi (Fig 2). These protrusions contained elec-
Fig 1. (A) Lymphocyte infiltration is seen in pseudostratified ciliated epithelium and subepithelial area in the patient group (hematoxylin & eosin; original magnification, x200). (B) lmmunocytochemical staining with HLA-DR. MHC class II-positive dendritic cells having cytoplasmic extensions are seen (arrows) in the patient group (original magnification; x200). (C) lmmunocytologi~al &ah-ring with HLA-DR. MHC class II-positive epithelial cells are seen (arrow) in the patient group (original magnification, x200). (D) Frozen sections of adenoid tissue stained with a-naphtyl Aph. Dendritic cells had Aph activity in a spot (arrows). In contrast, macrophages (arrowhead) had Aph activity throughout the cytoplasm in the patient group (original magnification x 100).

ADENOIDS AND OME 247
TABLE 1. Percentages of Antigen-Presenting Ceils as Determinated by HLA-DR MoAB
Control Patient P
lnterfollicular subepithelial area
IDC 1.180 2 0.103 1.810 5 0.168 <.05 M 0.615 ?I 0.133 0.875 k 0.146 <.05
Follicular area FDC l.llO? 0.166 1.535 k 0.342 <.05 M 0.925 5 0.189 1.185 2 0.272 <.05
Abbreviations: IDC, interfollicular dendritic cells; M, macro- phage; FDC, follicular dendritic cells.
tron-dense fine granular materials. Also, there were structures very similar to these, envel- oped with a membrane localized between epithelial cells in close association with inter- mediate and ciliated cells, leading to the con- clusion that these were the eventually pinched- off epithelial protusions described previously. It is interesting to note that these structures were very similar to the cytoplasm of lympho- cytes (Fig 3). In some areas, goblet cells were seen in the epithelium. M cells forming a narrow barrier between the lumen and the lymphocyte were seen in some areas (Fig 4).
Lymphoid tissue consisted of different- sized lymphocytes, mast cells, plasma cells, macrophages, reticular cells, and dendritic cells. In some lymphocytes there were cyto- plasmic protusions with fine granular mate- rial, in some areas these bulgings were con- nected with a thin stalk to the lymphocyte, and in some areas slits developed between lymphocytes and their largely protuding cyto- plasmic compartments (Fig 3). Both pycnotic lymphocytes and remnants of degenerated cells were observed in some areas. The number of plasma cells had increased (Fig 5). Also, mast
TABLE 2. Percentages of Antigen-Presenting Cells as Determined by a-naphtyl Acid Phosphate
Control Patient P
lnterfollicular subepithelial area
IDC 1.090 z 0.151 1.620 + 0.574 <.05 M 0.765 k 0.176 1.185 2 0.910 <.05
Follicular area FDC 1.245 + 0.198 1.560 k 0.126 <.05 M 0.915 + 0.160 1.095 2 0.154 <.05
Abbreviations: IDC, interfollicular dendritic cells; M, macro- phage; FDC, follicular dendritic cells.
Fig 2. At the apical surface of the ciliated ceils bulb-like cytoplasmic bulgings (arrow) and compound cilia (arrowhead) are seen. Lymphocytes (Ly) and mem- brane-bounded cytoplasmic bodies (asterisk) are ob- served between epithelial cells in the patient group (original magnification, x6,300).
cells and macrophages widespread in ad- enoids of the patients. The number of den- dritic cells had increased in the subepithelial, interfollicular, and follicular areas. Dendritic cells had an irregular shape, thin, long cyto- plasmic extensions, and were in close contact with lymphocytes and plasma cells (Fig 6).
Fig 3. The large lymphocyte (Ly) had an indented nucleus (N), scanty mitochondria (m), membranous whorls (arrowhead), and cytoplasmic bulgings (arrow) in the patient group (original magnification, x8,000).

248 KlROrjLU ET AL
Fig 4. The thin cytoplasm of an M cell (M) on the surface of the epithelium forming a single cell barrier between the lumen and intraepithelial channels. (Cc, ciliated cell; original magnification, x3,000).
Also, collagenous fibers had increased, and the fibroblasts were observed in the fibrocyte form in many micrographs (Fig 7).
DISCUSSION
The current study shows that there is an increase in the number of lymphocytes, mast cells, plasma cells, macrophages, dendritic
Fig 5. Increased plasma cells (PC) in patient group. A nucleus (N), well-developed granular endoplasmic retic- ulum profiles (GER), and Golgi complex (G) in the cytoplasm (original magnification, x7,000).
Fig 6. The dendritic cells (DC) in the patient group were in close contact (arrow) with lymphocytes (Ly). The dendritic cells had an indented nucleus(N), short granu- lar endoplasmic reticulum cisternae (GER), mitochon- dria (m), smooth endoplasmic reticulum (SER), Golgi complex (G), and dense bodies (db) in cytoplasm and a few lipid droplets (L) in their cytoplasmic extensions. (PC, plasma cell; original magnification, x4,400).
cells, and M cells in the adenoids of patients with OME when compared with the normal cases. Although electron microscopic demon- stration of this increase is partly subjective,
Fig 7. The fibroblasts (F) are mostly seen in inactive fibrocyte form in patient group. The collagenous fibers (Col) were increased. Between fibroblasts and collag- enous fibers there are membrane-bound bodies with finely granular material (asterisks) and cellular debris (d) (original magnification, x4,000).

ADENOIDS AND OME 249
objective measurements were performed on 10 patients and 10 controls for antigen-present- ing cells. Also, there was epithelial destruc- tion and a decrease in the number of ciliated cells on the micrographs of the patient group.
We have also shown the immune function of epithelial cells by HLA-DR positivity in serial sections (Fig 1C). This finding (the antigen- presenting activity of epithelial cells) is not supported by all reports,4 but von-Nieuwkerk et a15 showed the presence of major histocom- patibility complex (MHC) class II-positive cili- ated epithelial cells in all adenoid tissues that they studied immunocytochemically. In our opinion, the epithelial cells gain this function in chronic infections; this is probably the reason why we have seen extremely few HLA- DR-positive epithelial cells in the control cases. The similarity between the contents of bulb-like cytoplasmic protusions in the apical surface of the ciliated cells (Fig 2, arrow) and the lymphocyte cytoplasm (Fig 3) seems to be an electron microscopic support of the antigen- presenting activity of epithelial cells. These bulgings (which are very similar to the ones branching from lymphocytes; Fig 3, arrow) might be some useless parts of cytoplasm that are lost in the way of maturation and specifica- tion for antigen. This theory is supported by the demonstration of vesicles that contain horseradish peroxidase in the ciliated cells of infected adenoids by Fujiyoshi et al3 who suggested that immunocompetent M cells de- velop from neighboring ciliated or nonciliated cells under the influence of antigens or lym- phocytes. Nevertheless, our assumption that these cytoplasmic bulgings were related to immune mechanisms needs to be proven with immuno-electron microscopic methods.
It is obvious that persistent infection causes epithelial destruction; this in turn can allow penetration of foreign antigens through epithe- lium that has lost its integrity. Formation of clefts down to the lymphoid tissue may lead antigens to reach lymphocytes easily, augment- ing the immunologic reactions. Also, some large spaces between epithelial cells found in some electron micrographs gave us the impres- sion that these were structural units for a close contact with the outside environment, similar to intraepithelial lymphatic canals described in 1994 by Winther and Innes.6
Our findings support the opinion that there
is no defect in the immune systems of patients with OME. Moreover, increased amounts of immune cells reflect increased antigenic load, probably resulting from infection of the ad- enoid tissue. The identification of the den- dritic cells in contact with the lymphocytes through their cytoplasmic elongations, espe- cially in degenerative areas and in areas resem- bling reparation where collagenous and reticu- lar fibers are present, encourage us to think that around these cells, charged to present antigenic stimuli to lymphocytes, there would be large numbers of antigens and antibodies, which can activate the complement system. The activation of the complement system causes vasodilatation, increase in vascular per- meability, and fluid exudation, all of which precipitate OME.
An epithelial destruction resulting from cy- totoxic activities of intraepithelial lympho- cytes as proposed by Bani et al2 and Gallo et al4 also seems possible. Destruction of ciliated epithelium can lead to OME by mucociliary degeneration because of decreased middle ear clearance. These mucociliary changes are seen in some electron microscopic photographs of the patient group in which compound cilia formation and destruction of ciliated cells are shown (Fig 2); changes in mucociliary trans- port system in OME patients were shown in our two previous electron microscopic stud- ies.7s8 The decrease of ciliated cells, a common finding in enlarged adenoids,3v4 not only af- fects mucociliary clearance adversely, but also decreases local immunity and may lead to secretory cell metaplasia.
In the areas of degenerated cells and cell remnants, fibrosis develops, characterized by the marked proliferation of fibroblasts and the increase of collagen and reticular fibrils. The injured parenchyme, resulting from degenera- tion of cells, was replaced by fibrotic material. Increase of these areas will cause atrophy of adenoids and may be the reason for the recov- ery of the OME patients with or without any therapy in the course of time.
In conclusion, adenoid tissues of patients with OME seem to be infectious foci, aggravat- ing immune reactions, which might attack the middle ear through an ascending route. Future studies are required to shed more light on the multifactorial origins of OME.

250 KlROCiLU ET AL
REFERENCES
1. Maw AR: Otitis media with effusion, in Kerr AG, Evans JNG (eds): Scott-Brown’s Otolaryngology (vol 6; ed 5). Butterworths, London, 1987, pp 158-176
2. Bani D, Gallo 0, Fini-Storchi 0: Intaepithelial lym- phocyte subpopulations and dendritic accessory cells in normal and hypertrophic adenoids. Laryngoscope 104:869- 873,1994
3. Fujiyoshi T, Watanabe T, Chimiyal I, et al: Functional architecture of the nasopharyngeal tonsil. Am J Otolaryn- go110:124-131,1989
4. Gallo 0, Bani D, Rucci L, et al: Does the epithelium play a central role in the immune function of rhinopharyn- geal tonsils. An immunocytochemical and ultrastructural study. Int J Pediatr Otorhinolaryngol22:219-229,1991
5. van-Nieuwkerk EBJ, van-der Baan S, Richters CD, et
al: Isolation and characterization of dendritic cells from adenoids of children with otitis media with effusion. Clin Exp Immunol88:345-349,1992
6. Winther B, Innes DJ: The human adenoid. Arch Otolaryngol12O:144-149, 1994
7. Getik F, Kaya M, Knoglu M, et al: Ultrastructure of the nasopharyngeal orifice of the eustachian tube in otitis media with effusion. In: 15th World Congress of Otorhino- laryngology Head and Neck Surgery, Istanbul, Erol Ofset, 1993,~ 246
8. Knoglu F, Kaya M, 6zgahinoglu C, et al: Changes of middle ear mucosa in secretory otitis media treated with ventilation tubes. Acta Otolaryngol (Stockh) 110:266-273, 1990
9. Williams D: Enzyme histochemistry, in Prophet EB, Mills B, Arrington JB, et al (eds): Laboratory Methods in Histochemistry. Washington, DC, American Registry of Pathology, 1992, pp 242-243





























