Embed Size (px)
Citation preview

OTOLOGY
Toxic inner ear lesion following otitis media with effusion:a comparative CT-study regarding the morphologyof the inner ear
Thomas Wilhelm • Tim Stelzer • Susanne Wiegand •
Christian Guldner • Afshin Teymoortash •
Thomas Gunzel • Rudolf Hagen
Received: 8 July 2014 / Accepted: 28 November 2014
� Springer-Verlag Berlin Heidelberg 2014
Abstract Viral infections of the upper respiratory air-
ways can lead to a delayed viral otitis media (VOM) caused
by a diffusion of viruses/virus particles through the round
window membrane and resulting in sensorineural hearing
loss. The treatment of choice is immediate paracentesis,
evacuation of all fluids from the middle ear cavity, and
haemorrheological infusions. However, in some cases,
persistent symptoms may be an indication for a surgical
approach using mastoidectomy. In high-resolution com-
puted tomography, an extended small-sized pneumatisation
of the mastoid cells with complete shading was found in
these non-responsive cases. Therefore, a direct means of
inner ear affliction through weak parts of the labyrinthine
bone may be hypothesised. Patients suffering from a toxic
inner ear lesion (TIEL) following a common cold, treated
over a 10-year period in a Tertiary Care Centre (N = 52,
57 ears), were identified and the morphological character-
istics of the temporal bones of affected patients were
examined by means of high-resolution computed tomog-
raphy (hrCT). The findings were compared with a matched
control group of 64 normal ears (CONT). Measurements
included the grade of pneumatisation, distances within the
temporal bones and Hounsfield units (HU) at defined
anatomical structures. In the TIEL group, we found a
small-sized pneumatisation in 79.4 % and a medium-sized
pneumatisation in 10.9 %, thus differing from the CONT
group and the literature data. Thickness of the bone wall of
the lateral semicircular canal (LSC) and distances within
the aditus ad antrum were significantly reduced in the TIEL
group. HU’s were markedly lower in the TIEL group at the
precochlea, the LSC, and dorsolateral to the promentia of
the LSC. There was a correlation between the HU’s at the
prominentia of the LSC and the hearing loss (p = 0.002).
Persisting interosseous globuli, as described in 1897 by
Paul Manasse, form an osseochondral network within the
otic capsule and may be responsible for a direct means of
toxic inner ear infection. The CT-morphometric results
support this thesis. In the group of these patients (TIEL) a
CT-scan and in non-responders to conservative treatment a
surgical approach by mastoidectomy is recommended.
Keywords Toxic lesion � Inner ear � Subacute
mastoiditis � Otitis media with effusion � Computed
tomography � Sensorineural hearing loss
Introduction
Viral otitis media in most cases is an acute disease of the
middle ear mucosa caused by ascending infection from the
Thomas Wilhelm and Tim Stelzer are both first authors since idea,
conception, and execution of this project derive from both of them
alike.
T. Wilhelm (&) � T. Stelzer
Department of Otolaryngology, Head, Neck and Facial Plastic
Surgery, Kliniken Leipziger Land, Klinikum Borna,
Rudolf-Virchow-Str. 2, 04552 Borna, Germany
e-mail: [email protected]
URL: http://www.kliniken-leipziger-land.de
S. Wiegand � C. Guldner � A. Teymoortash
Department of Otolaryngology, Head and Neck Surgery,
Philipps-University, Marburg, Germany
T. Gunzel
Department of Otolaryngology, Head and Neck Surgery,
Borromaus Hospital, Leer, Germany
R. Hagen
Department of Otolaryngology and Facial Plastic Surgery,
Julius-Maximilians-University, Wurzburg, Germany
123
Eur Arch Otorhinolaryngol
DOI 10.1007/s00405-014-3425-4

nasopharynx. Clinically, patients suffer from ear ache and
hearing loss and otoscopic findings show an inflamed
tympanic membrane with effusions in the middle ear, in
some cases a typical bullous myringitis leading to direct
diagnosis of a viral origin of the disease [1, 2]. A high virus
concentration within the middle ear may lead to a con-
comitant sensorineural hearing loss which, in up to 60 % of
the cases, is caused by penetration of viruses through the
round window membrane [3, 4]. The incidence of viral
otitis is estimated at between 0.5 and 2 % in all common
colds in adults [5].
However, in rare cases middle ear symptoms occur with
some delay after acute rhinosinusitis. Patients report a
‘‘sudden’’ hearing loss up to 4 weeks after a respiratory
tract infection. Otoscopic findings demonstrate middle ear
effusions without acute bacterial infection and audiological
tests reveal a combined sensorineural and conductive
hearing loss. The treatment of choice is a paracentesis with
suction of the middle ear fluid and, in the course of this
particular study period between 2001 and 2011, a so-called
‘‘haemorrheological’’ regime similar to that used in cases
with sudden hearing loss of unknown origin [6] to improve
inner ear function. In cases with persistent symptoms and
missing improvement of inner ear function, computed
tomography demonstrates the involvement of the antrum
and the perilabyrinthine spaces (Fig. 1a).
The commonly accepted path of infection of the inner
ear in viral otitis media is a diffusion of viruses or toxic
products through the round window membrane or the
annular ligament in the oval niche [4]. In our case series,
the removal of middle ear effusions by paracentesis did not
result in a successful recovery of the inner ear function in
all cases, subsequently leading to the decision to improve
the healing process by removing diseased mucosa via
mastoidectomy (Fig. 1b, c).
The purpose of the present study is the evaluation of
the radiological findings in computed tomography of the
temporal bones in a case series of toxic inner ear lesion
following otitis media with effusion due to viral infec-
tions of the upper airways to identify a typical config-
uration of periantral and perilabyrinthine structures,
which may be responsible for the persistent toxic inner
ear lesion.
Materials and methods
Since 2001, patients suffering from a toxic inner ear lesion
(TIEL) with subacute mastoiditis following a viral infec-
tion of the upper airways 3–4 weeks prior to the hearing
impairment have been treated according to the diagnostic
and therapeutic workflow outlined in Fig. 2. All of these
cases of ‘‘toxic inner ear lesion’’ were included and
evaluated with respect to the hearing outcome, following
conservative or surgical therapy in a Tertiary Care Centre
in a retrospective chart review. Identification of cases
started with a search within the clinical information system
according to the ICD (International Classification of Dis-
eases) classes H83.0 labyrinthitis, H91.0 ototoxic hearing
loss, H65.0/1 acute otitis media with effusion, H66.9 acute
otitis media, H73.0 acute myringitis, J11.8 viral otitis, and
H70.0 acute mastoiditis. Identified cases were checked for
the following inclusion criteria:
Fig. 1 a High-resolution computed tomography of the temporal
bones shows shading of the mastoid cells around the labyrinth.
b Intraoperative findings. c Surgical situs after complete exenteration
of all cells of the temporal bone
Eur Arch Otorhinolaryngol
123

1. Otitis media with effusion following a viral upper
respiratory tract infection with pathological findings in
tympanometry.
2. Combined conductive and sensorineural hearing loss in
the initial audiometric testing.
3. At least one additional audiometric examination during
the treatment period.
4. Either conservative or surgical treatment.
5. No prior history of hearing impairment.
6. No acute bacterial infection (earache, enflamed and
protruding ear drum, purulent secretion by spontaneous
perforation) of the middle ear or the eardrum.
All patients were followed up and re-examined via pure
tone audiometry. Vestibular testing following caloric
stimulation was performed by means of electronystag-
mography in patients reporting dizziness. The directional
and side preponderance were calculated according to the
formula of Jongkees et al. [7]; directional preponderance
exceeding 25 % and side preponderance [15 % were
judged as ‘‘pathological finding’’.
A high-resolution computed tomography (CT) of the
temporal bones was performed on all patients within the
first 5 days. All patients demonstrated signs of an
involvement of the mastoidal mucosa in the CT (shading
and reduced opacity without bone destruction).
A matching group of patients (CONT) from the Picture
Archiving and Communication System of the clinic (PACS
Centricity Enterprise Web, General Electric Medical Sys-
tems, Fairfield/Connecticut, US) was selected for the pur-
pose of comparing morphological features of the temporal
bone configuration. Under the search term ‘‘high-resolution
temporal bone computed tomography’’ a comparable group
with the following exclusion criteria was established: acute
or chronic mastoiditis, previous middle ear or mastoid
surgery, chronic otitis media with meso- or epitympanal
tympanic membrane defect, fracture of the temporal bone.
Indications for the CT-scans in the CONT group were:
exclusion of temporal bone fractures (N = 15), exclusion
of neurological disorders in cases of paresis or tumour
(N = 7), diagnostic workup in cochlear disorders or diz-
ziness of unknown origin (N = 5) or navigational CT-
scans prior to sinus surgery or microvascular decompres-
sion according to JANNETTA (N = 5).
All CT-scans were available as digital scans within the
PACS system from 2002. CT-scans were performed with a
HiSpeed NX/i dual slice CT-scanner and later on with a
BrightSpeed scanner from General Electric Company. The
resolution was 512 9 521 pixels with a pixel size of 0.332
and 0.488 mm, respectively. All CT-scans were done
without contrast medium.
The extent of pneumatisation was rated according to the
recommendations of Allam and Schuknecht [8, 9]: mas-
toidal cell diameters below 1.2 mm were rated as small
cells, diameters between 1.2 and 2.5 mm as medium sized,
and all cells with a diameter of more than 2.5 mm as large
cells. The pneumatisation grade was determined for dif-
ferent regions (Fig. 3a) and in each area the smallest cell
diameters were used to determine the classification as a
small-, medium- or large-sized pneumatisation grade.
A second measurement included different distances
within the temporal bone (Fig. 4). The following distances
were evaluated in both the groups (TIEL and CONT):
1. Distance from the suprameatal spine (Henles spine) to
the sigmoid sinus (SpiSin),
2. Thickness of the prominentia of the lateral semicircu-
lar canal (LSC) at the level of the short process of the
incus (PromLat1),
3. Thickness of the labyrinthine bone at a 90� angle
dorsolateral to PromLat1 (PromLat2),
4. Distance from the tympanic sulcus (fibrocartilaginous
sulcus) to the posterior cranial fossa (SulFos),
5. Distances within the aditus ad antrum: medial isthmus
from the prominentia of the LSC to the short process of
the incus (IsthMed),
Fig. 2 Diagnostic and
therapeutic workflow
Eur Arch Otorhinolaryngol
123
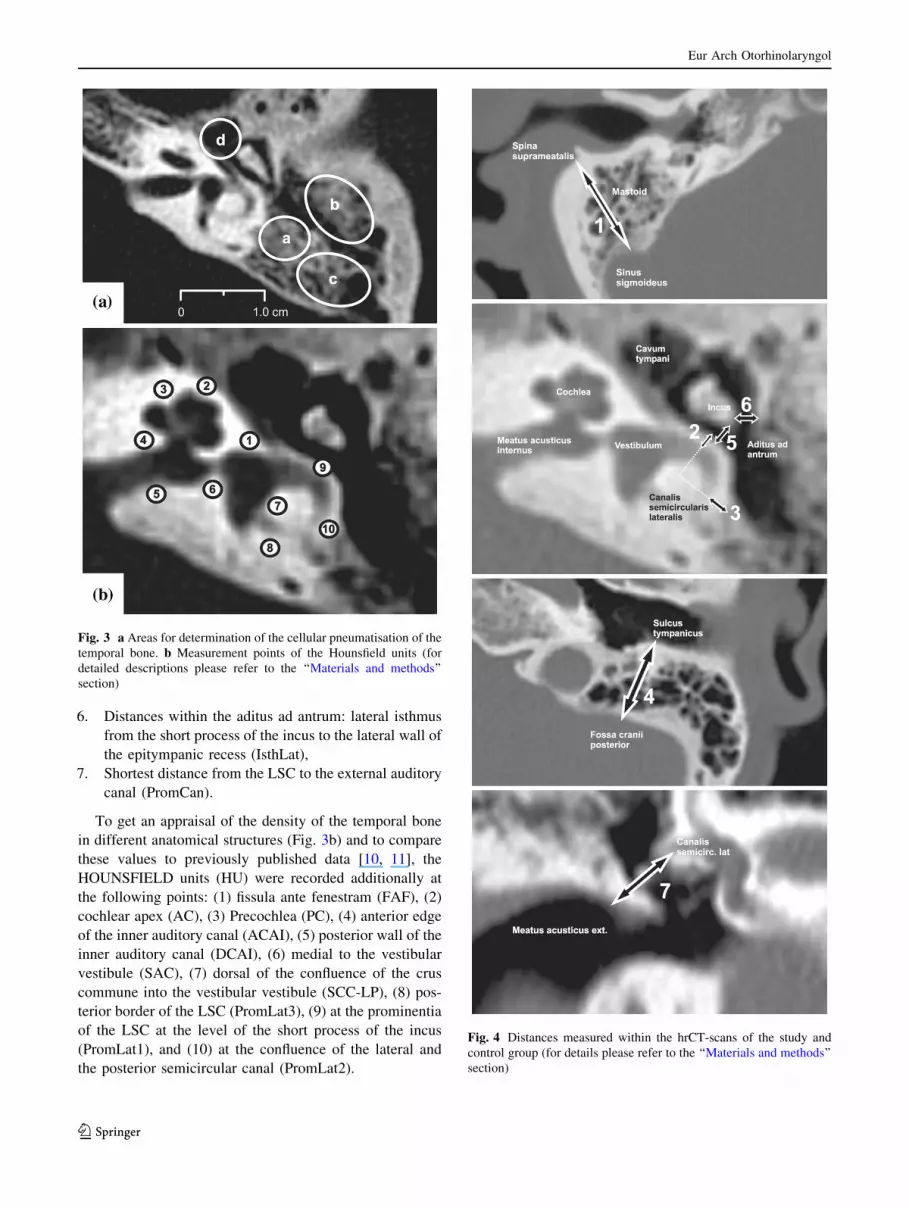
6. Distances within the aditus ad antrum: lateral isthmus
from the short process of the incus to the lateral wall of
the epitympanic recess (IsthLat),
7. Shortest distance from the LSC to the external auditory
canal (PromCan).
To get an appraisal of the density of the temporal bone
in different anatomical structures (Fig. 3b) and to compare
these values to previously published data [10, 11], the
HOUNSFIELD units (HU) were recorded additionally at
the following points: (1) fissula ante fenestram (FAF), (2)
cochlear apex (AC), (3) Precochlea (PC), (4) anterior edge
of the inner auditory canal (ACAI), (5) posterior wall of the
inner auditory canal (DCAI), (6) medial to the vestibular
vestibule (SAC), (7) dorsal of the confluence of the crus
commune into the vestibular vestibule (SCC-LP), (8) pos-
terior border of the LSC (PromLat3), (9) at the prominentia
of the LSC at the level of the short process of the incus
(PromLat1), and (10) at the confluence of the lateral and
the posterior semicircular canal (PromLat2).
Fig. 3 a Areas for determination of the cellular pneumatisation of the
temporal bone. b Measurement points of the Hounsfield units (for
detailed descriptions please refer to the ‘‘Materials and methods’’
section)
Fig. 4 Distances measured within the hrCT-scans of the study and
control group (for details please refer to the ‘‘Materials and methods’’
section)
Eur Arch Otorhinolaryngol
123

In the first step, all HU were measured at the described
points: the highest value was chosen for calculation of the
average. In cases of a marked difference between the
averages (PromLat1, PromLat2, and PromLat3), an area
measurement (circular area with at least 5 pixel but without
measuring the outlying areas like mastoidal cells or peri-
and endolymphatic spaces) was performed for calculation
purposes.
Approval for this retrospective study was obtained from
the Ethical Committee of the Saxonian Chamber of Phy-
sicians (22.06.2011, Sign: Prof.Dr.H/Di). The study has
been performed in accordance with the ethical standards
prescribed in the 1964 Declaration of Helsinki in line with
its latest revision. All patients gave their informed consent
to scrutiny of their medical files prior to their inclusion in
the study. Data handling was carried out in accordance
with local data protection laws.
Statistical methods and data analysis
The data were documented in Microsoft Excel 2003�(Redmont, Washington, USA) and evaluated statistically
with SPSS� 14 (Armonk, New York, USA). Standard
deviation and mean variation were calculated for
descriptive statistical means. Data distribution was
checked for normal distribution with the Kolmogorov–
Smirnov test: a p value [0.05 constituted normal distri-
bution. In the case of rejection of the hypothesis of normal
distribution, paired samples were tested using the Wilco-
xon signed-rank test and unpaired samples were tested by
means of a Mann–Whitney test (MWT). Only the com-
parisons of the overall change in hearing level at the
follow-up between the two treatment groups were per-
formed in a confirmatory sense (MWT, significance level
was set to 0.05). A classical Bonferroni transformation
was applied for the purpose of multiple testing: p value
was set at 0.005 for the comparison of the HU (punctual
measurement) and at 0.025 (area measurement); p value
was set at 0.00714 for the distance measurements. The
correlation according to Kendall and Pearson was calcu-
lated to correlate morphological abnormalities with clini-
cal symptoms.
Results
52 patients, including 5 patients affected bilaterally (57
ears), fulfilling the criteria of toxic inner ear lesion fol-
lowing a common cold of the upper air way (TIEL group)
were identified over a 10-year period. 20 of these patients
(21 ears) with a mean age of 54 ± 18.3 years (9 women,
11 men) were treated conservatively (TIEL-CONS) and 32
patients (36 ears) with a mean age of 49 ± 20.1 years (10
women, 22 men) were treated surgically (TIEL-SURG,
Fig. 2). All patients had had a paracentesis on initial pre-
sentation and conservative treatment consisted of haemor-
rheological infusions (500 ml hydroxyethyl starch 6 %
over 4–5 h intravenously ? 300 mg pentoxifylline)
according to the national treatment guidelines which were
valid during the study period (Fig. 2, [6]). All patients were
examined by high-resolution computed tomography during
the first 5 days. The treatment schedule was changed to a
surgical treatment (mastoidectomy) as outlined in the
diagnostic and therapeutic work flow (Fig. 2) in the case of
non-response of the inner ear function.
The duration from the onset of symptoms was
5.9 ± 3.7 days in the TIEL-CONS group and
14.7 ± 12.8 days in the TIEL-SURG group. The audio-
metrical testing results of the inner ear function (bone
conduction thresholds) are displayed in Fig. 5 and the
changes within the hearing classes according to the AAO/
HNS reporting criteria [12] in both groups initially, at the
end of the primary therapy, and at the follow-up are
listed in Table 1. On calculation of the average hearing
loss (250–8,000 Hz), significant improvement in the
TIEL-SURG group was displayed in comparison to the
TIEL-CONS group (Fig. 3, p = 0.025, Mann–Whitney
Test).
14 patients in the TIEL-CONS- and 18 patients in the
TIEL-SURG group complained of dizziness during the
initial phase. In computed nystagmography analysis, 7
patients in the TIEL CONS and 9 patients in the TIEL-
SURG group revealed pathological results: the directional
preponderance was 26.6 ± 15.4 (mean ± standard devia-
tion) in the CONS and 42.9 ± 30.6 in the SURG group;
side preponderance was 22.9 ± 15.4 and 34.2 ± 21.0,
respectively.
As a control group (CONT) patients from the PACS
system of the clinic were matched as described in the
methods ‘‘Materials and methods’’: 32 patients (16 women:
mean age 56.1 ± 24.6 years and 16 men: 52.8 ± 15.4)
were chosen. Both sides were evaluated, giving a total of
64 ears.
A small-sized pneumatisation was found in 79.4 % of
the TIEL group and in 10.9 % of the CONT group while
medium-sized pneumatisation was visible in 20.6 and
62.5 %, respectively. Whereas a large-sized pneumatisa-
tion was absent in the TIEL group, it was present in 26.6 %
of the control group. When compared to literature data
(36.7 % small/41.7 % medium/21.6 % large-sized cells),
the control group matched the data of Turgut and Tos and
the TIEL group showed an increased small-sized pneu-
matisation [13].
The distances measured within the temporal bones are
listed in Table 2. Notable differences between the TIEL
group and the control group were found with regards to
Eur Arch Otorhinolaryngol
123

• The thickness of the bone wall of the LSC at the level
of the short process of the incus (PromLat1,
p = 0.027),
• The thickness of the bone wall of the labyrinthine bone
at a 90� angle dorsolateral to PromLat1 (PromLat2,
p \ 0.005),
• The medial isthmus between the prominentia of the
LSC and the short process of the incus (IsthMed,
p \ 0.005),
• And the shortest distance from the LSC to the external
auditory canal (PromCan, p = 0.008).
The results of the Hounsfield units (HU) measured in
different areas (Fig. 3b) are displayed in Table 3: differ-
ences (two-sided Student’s t test for independent samples
with Bonferroni transformation) with reduced HU’s in the
TIEL group (bold values) were found in the precochlea
(p = 0.016), in the LSC contralateral to the prominentia
(p = 0.014), and dorsolateral of the LSC (p \ 0.005).
Pathologic electronystagmography recordings were
registered in 12 ears in patients reporting dizziness during
their initial visit (N = 32, 2 patients affected bilaterally
resulting in 34 ears). Comparing the HU in the evaluated
CT-scans showed a reduced thickness (bold values) of the
prominentia of the LSC in the group with pathological
results (p = 0.046, Table 4). Correlation analysis
between analysed Hounsfield units, bone thickness at the
LSC and hearing loss, showed a correlation (bold values)
between the HU’s in the prominentia of the LSC and
hearing loss (p = 0.002, Table 5).
Discussion
Toxic inner ear lesions following acute inflammation of
the middle ear are mainly attributed to a permeation of
Fig. 5 Pure tone audiometry pre- and postoperatively following
conservative and surgical treatment (bone conduction thresholds are
displayed): outcome differs markedly (p = 0.025 Mann–Whitney
test,filled circle pre-therapeutic sensorineural hearing threshold, open
square sensorineural hearing threshold on follow-up)
Table 1 Hearing results according to the AAO-HNS reporting cri-
teria (bone conduction thresholds are used for analysis)
Initial EOT Follow-up
CONS
Aver. HL 32.4 ± 15.6 24.3 ± 14.7 20.1 ± 15.0
Class A 10 14 12
Class B 8 5 1
Class C 3 1 1
SURG
Aver. HL 35.4 ± 12.0 28.3 ± 15.1 14.3 ± 9.0
Class A 11 19 21
Class B 20 13 2
Class C 4 3 0
CONS conservative therapy, SURG surgical therapy, EOT end of
primary therapy, aver. HL averaged hearing loss, N patients
Eur Arch Otorhinolaryngol
123

ototoxic substances through the round window membrane
[4, 14, 15]. Yellon and colleagues separated the cytokines
tumour necrosis factor-alpha (TNF-a), gamma-interferon
(IFN-c), interleukin-1-beta (IL-1b), and interleukin-2 (IL-
2) within the inflammatory effusions of chronic otitis
media [16]. Consequently bacteria themselves as well as
metabolic products may transmigrate the round window
membrane and cause direct damage of sensorineural cells
within the cochlea [14].
Moreover, it seems that bacterial infections of the
middle ear are not the leading cause in the development of
Table 2 Distances in the temporal bone (mm) and comparison of affected and control ears
Distancea Study Group (N = 34) Control group (N = 64) Mean difference SD 95 % CI p value
PromLatl 0.651 ± 0.114 0.703 ± 0.101 -0.053 0.023 -0.099 to -0.006 0.027
PromLat2 1.080 ± 0.329 1.405 ± 0.382 -0.326 0.074 -0.473 to -0.178 0.000
IsthMed 1.218 ± 0.331 1.459 ± 0.386 -0.241 0.075 -0.389 to -0.093 0.002
IsthLat 1.139 ± 0.405 1.199 ± 0.438 -0.060 0.088 -0.236 to 0.116 0.499
SpiSin 15.342 ± 3.005 15.646 ± 2.724 -0.304 0.618 -1.539 to 0.931 0.625
SulFos 12.909 ± 2.085 12.390 ± 1.958 0.518 0.433 -0.347 to 1.384 0.236
PromCan 6.481 ± 0.908 7.033 ± 1.057 -0.552 0.204 -0.958 to -0.145 0.008
p value tested with the two-sided Student’s t test for independent samples
SD standard deviation, CI confidence intervala For description of the different distances and applied statistical methods please refer to the ‘‘Materials and methods’’ section)
Table 3 Hounsfield units at different measurement points within the temporal bone
Study group
(N = 34)
Min Max Control group
(N = 64)
Min Max Mean
difference
SD 95 % CI p value
Fissula ante fenestram 2,018.4 ± 129.2 1,763 2,306 2,044.5 ± 163.2 1,767 2,511 -26.1 30.1 -86.0 to 33.9 0.390
Apex cochleae 1,861.0 ± 151.1 1,595 2,188 1,898.3 ± 210.5 1,521 2,703 -37.3 36.9 -110.7 to 36.1 0.315
Precochlea 1,948.9 ± 115.6 1,728 2,316 2,024.7 ± 189.9 1,035 2,393 -75.8 30.9 -137.2 to -14.4 0.016
Anterior edge internal
auditory canal
2,034.0 ± 136.4 1,741 2,352 2,012.9 ± 212.8 1,064 2,583 21.1 35.4 -49.2 to 91.4 0.553
Posterior edge internal
auditory canal
1,697.0 ± 85.0 1,527 1,870 1,717.0 ± 108.9 1,452 2,044 -20.0 19.9 -59.6 to 19.7 0.320
Sacculus 1,880.0 ± 120.7 1,500 2,045 1,911.8 ± 167.5 1,675 2,400 -31.8 29.4 -90.3 to 26.7 0.284
Posterior SCC 1,895.2 ± 143.8 1,689 2,482 1,944.6 ± 172.4 1,687 2,367 -49.4 32.8 -114.6 to 15.8 0.136
Lateral SCC
contralateral
to the prominentia
1,661.1 ± 111.0 1,501 1,960 1,718.8 ± 98.8 1,544 2,058 -57.7 22.7 -103.1 to -12.3 0.014
Prominentia of the
lateral SCC
1,410.8 ± 179.8 957 1,738 1,461.4 ± 242.6 948 2,189 -50.6 43.3 -136.6 to 35.4 0.245
Dorsolateral of the
lateral SCC
1,615.1 ± 89.0 1,464 1,935 1,779.0 ± 115.0 1,481 2,051 -163.9 21.0 -205.6 to
-122.2
0.000
p value tested with the two-sided Student’s t test for independent samples; please refer for details of the Bonferroni transformation to the
‘‘Materials and methods’’ section)
SD standard deviation, CI confidence interval, SCC semicircular canal
Table 4 ENG findings related to thickness and Hounsfield units
(HU) of the lateral semicircular canal (LSC) (Prom) and distance to
the outer ear canal (Can; two-sided t test, mean ± standard deviation;
SCC: semicircular canal)
Normal
(N = 22)
Pathologic
(N = 12)
p value
Thickness prominentia
lateral SCC
1.108 ± 0.301 0.883 ± 0.295 0.046
Distance PromCan 6.344 ± 0.960 6.732 ± 0.781 0.214
HU PromLat2 1,613 ± 66.6 1,618 ± 123.7 0.897
Eur Arch Otorhinolaryngol
123

acute otitis media [1]. Infections of the upper airways from
various viruses are accompanied by a virus replication
within the mucosa of the Eustachian tube (ET) with an
expression of cytokines which leads to cytotoxic effects.
This results in a dysfunction of the ET including secretion,
mucosal swelling, impaired mucociliary clearance, and
direct mucosal damage followed by a decrease of middle
ear pressure and a secondary bacterial infection [5].
15 years ago, a subset of patients, who had developed an
otitis media with effusion without acute inflammatory
reaction following a viral infection of the upper airways
and leading to a concomitant sensorineural hearing loss,
was identified. Typically, about 4 weeks following these
common colds, the patients had developed a combined
conductive and sensorineural hearing loss. On admission,
an immediate paracentesis with evacuation of the typically
amber fluids from the middle ear was performed under
local anaesthesia followed by haemorrheological infusions
according to the national treatment guidelines valid during
the study period [6]. In high-resolution CT-scanning of the
temporal bones within the first 5 days, an extended small-
sized pneumatisation of the temporal bone with a shading
of the cells, especially around the semicircular canals, was
found in all cases. In contrast to solely conservative
treatment, surgical therapy in the case of non-response to
conservative treatment resulted in a significant improve-
ment of the inner ear function with complete recovery.
Therefore, the question arose whether a direct perme-
ation through the labyrinthine bone may be responsible for
the toxic inner ear lesion in addition to the classical means
of penetration of toxic agents through the round window or
the ligament of the oval window. This led to a comparison
of the morphological characteristics of the temporal bone
configuration of the affected patients to normal temporal
bone CT-scans displayed by a matched control group.
This analysis revealed characteristic differences
regarding the thickness of the labyrinthine bone at the LSC
and also reduced Hounsfield units within this area. A
notable difference regarding the extent of pneumatisation
and the cell size was also found: the affected patients
showed significant differences in a predominance of small
and medium-sized mastoid cells when compared to the
control group and also to literature data [13].
During the embryologic development of the otic capsule
(consisting of the endosteal, the enchondral, and periosteal
layer) the middle layer is rebuilt by enchondral ossification;
this process of bony reorganisation is incomplete resulting
in interosseal globuli (bone with chondral islands) in var-
ious extensions. Paul Manasse described these interglobu-
lar spaces as remnants of the embryological bone within
the otic capsule in 1897 [17]. In 1933, Lotte Steinberg
published her results on the distribution of the interosseal
globuli [18]: she described a similar arrangement of these
‘‘weak’’ spots around the labyrinth complex and the
cochlea to what was found in the actual study using mea-
surement of Hounsfield Units in CT. These interosseal
globuli are also described in recent literature: Rauchfuss
showed these chondroosseous canals to be persistent after
completion of the ossification and building of the complex
canal system within the otic capsule [19–21]. The
hypothesis, that these channels are a ‘‘weak’’ point for a
possible infectious permeation is at least a reasonable
explanation for the group of patients, who do not improve
following conservative treatment despite immediate para-
centesis with evacuation of all fluids from the middle ear
cavity.
Limitations of the study
A major limitation of this study is the retrospective design
and the missing randomisation of the treatment groups
(conservative vs. surgical treatment); an allocation of
patients to an ongoing conservative treatment in case of
missing recovery seemed to be unethical—therefore, this
retrospective and comparative approach was chosen. The
result of the hearing outcome in favour of the surgically
treated patients supports the point of view of the author’s
opinion.
Another major criticism may be the use of Hounsfield
units to estimate the ‘‘density’’ of the bony structures of the
labyrinthine capsule. Hounsfield units describe an attenu-
ation of X-radiation in the tissue. A density measurement
in a physical definition (kg/m3) is, therefore, not possible.
However, since it is an attenuation of radiation and this
attenuation is compared between the two groups, the value
of the Hounsfield units should correlate with the density of
the measured tissue and probably fulfil the prerequisites for
a realistic comparison. Definitive results regarding the real
density of the bony structures can only be made by quan-
titative computed tomography [22]. Therefore, the
Table 5 Correlation between Hounsfield units (HU), bone thickness
at the lateral semicircular canal (LSC) and hearing loss (HL: bone
conduction thresholds) according to Kendall and Pearson
HU
PromLat2
HL
(dB)
Thickness
LSC
HU
PromLat2
1 Correlation
p value
34 N
HL (dB) -0.561 1 Correlation
0.002 p value
25 25 N
Thickness
LSC
-0.005 0.219 1 Correlation
0.49 0.146 p value
34 25 34 N
Eur Arch Otorhinolaryngol
123

statements regarding the conventional CT-scans used in the
study are only approximate.
Conclusion
On the basis of the embryological development of the otic
capsule with persistent ‘‘interosseous globuli’’ to various
extents and the results of the actual CT-morphological
study, the hypothesis of a direct means of viral infections
through weak parts of the bony labyrinth causing inner ear
afflictions may be realistic. This hypothesis may justify the
surgical approach of mastoidectomy in non-responders to
conservative treatment, particularly in cases of virus-rela-
ted otitis media and persistent sensorineural symptoms
despite of removal of infectious middle ear effusions by
paracentesis. However, these findings should be confirmed
by additional imaging studies of the temporal bone on the
basis of high-resolution CT-scans.
Conflict of interest The authors declare that there is no conflict of
interest.
References
1. Chonmaitree T (2006) Acute otitis media is not a pure bacterial
disease. Clin Infect Dis 43:1423–1425
2. Murray LN (2004) Myringitis Bullosa. In: Alper CM, Bluestone
CD, Casselbarnt ML, Dohar J, Mandel EM (eds) Advanced
therapy of otitis media. BC Decker Inc, Hamilton, pp 49–51
3. Hariri MA (1990) Sensorineural hearing loss in bullous myrin-
gitis. A prospective study of eighteen patients. Clin Otolaryngol
Allied Sci 15:351–353
4. Cureoglu S, Schachern PA, Rinaldo A, Tsuprun V, Ferlito A,
Paparella MM (2005) Round window membrane and labyrinthine
pathological changes: an overview. Acta Otolaryngol 125:9–15
5. Hayden FG (2001) Influenza virus and rhinovirus-related otitis
media: potential for antiviral intervention. Vaccine 19(Suppl
1):S66–S70
6. Michel O (2011) The revised version of the German guidelines
‘‘Sudden idiopathic sensorineural hearing loss’’. Laryngo Rhino
Otol 90:290–293
7. Jongkees LB, Maas JP, Philipszoon AJ (1962) Clinical nystag-
mography. A detailed study of electro-nystagmography in 341
patients with vertigo. Pract Otorhinolaryngol (Basel) 24:65–93
8. Allam AF (1969) Pneumatisation of the temporal bone. Ann Otol
Rhinol Laryngol 78:49–64
9. Schuknecht BF (1974) Pathology of the ear. Harvard University
Press, Cambridge, pp 79–92
10. Huizing EH, de Groot JA (1987) Densitometry of the cochlear
capsule and correlation between bone density loss and bone
conduction hearing loss in otosclerosis. Acta Otolaryngol
103:464–468
11. Grayeli AB, Yrieix CS, Imauchi Y, Cyna-Gorse F, Ferrary E,
Sterkers O (2004) Temporal bone density measurements using
CT in otosclerosis. Acta Otolaryngol 124:1136–1140
12. Monsell EM, Balkany TA, Gates GA, Goldenberg RA, Meyer-
hoff WL, House JW (1995) Committee on Hearing and Equi-
librium guidelines for the evaluation of hearing preservation in
acoustic neuroma (vestibular schwannoma). Otolaryngol Head
Neck Surg 113:179–180
13. Turgut S, Tos M (1992) Correlation between temporal bone
pneumatisation, location of lateral sinus and length of the mastoid
process. J Laryngol Otol 106:485–489
14. Kubo T, Anniko M, Stenqvist M, Hsu W (1998) Interleukin-2
affects cochlear function gradually but reversibly. ORL J
Otorhinolaryngol Relat Spec 60:272–277
15. Kim CS, Cho TK, Jinn TH (1990) Permeability of the round
window membrane to horseradish peroxidase in experimental
otitis media. Otolaryngol Head Neck Surg 103:918–925
16. Yellon RF, Leonard G, Marucha PT, Craven R, Carpenter RJ,
Lehmann WB, Burleson JA, Kreutzer DL (1991) Characteriza-
tion of cytokines present in middle ear effusions. Laryngoscope
101:165–169
17. Manasse P (1897) Ueber knorpelhaltige Interglobularraume in
der menschlichen Labyrinthkapsel. Z Ohrenheilk 31:1–10
18. Steinberg L (1933) Uber die Verteilung und Lage der knorpel-
haltigen Interglobularraume in der menschlichen Labyrinthkap-
sel. Arch Ohren Nasen Kehlk Heilk 135:187–196
19. Hildmann H, Haack M (1979) Autoradiographic investigations on
the developing otic capsule of hamsters. Arch Otorhinolaryngol
224:177–186
20. Rauchfuss A (1980) Some morphological details of the endo-
chondral layer of labyrinthine bone. A comparative anatomical
light and transmission electron microscopy study. Arch Otorhi-
nolaryngol 226:239–250
21. Rauchfuss A (1981) On the enchondral ossification of the otic
capsule: formation of the globuli ossei and the interglobular
spaces. Arch Otorhinolaryngol 233:237–250
22. Todisco M, Trisi P (2005) Bone mineral density and bone his-
tomorphometry are statistically related. Int J Oral Maxillofac
Implants 20:898–904
Eur Arch Otorhinolaryngol
123





























