Embed Size (px)
Citation preview
Adjunctive Intraoperative Photodynamic Therapy in an animal model
M.G. Dilkes MS FRCS FRCS(ORL)
ENT Department, St Bartholomew’s Hospital, West Smithfield,
London EC1Y 0DT, U.K.
Keywords:
Photodynamic Therapy, Adjunctive, Surgery, Foscan
Summary
This experiment was performed by delivering intraoperative
photodynamic therapy to the surgical bed after excision of a
locally invasive, malignant tumour. The aim of the study was to
find out if this led to a reduction in the local recurrence rate
of the tumour. This was a blind, controlled experiment. The
treatment arm involved surgical removal and intraoperative
photodynamic therapy. The control groups were surgery alone,
surgery and photosensitiser diluent, and surgery and laser light.
The results show a statistically significant reduction in the
local tumour recurrence rate up to 4 weeks after surgery (the
experiment end point) in the photodynamic therapy (PDT) group
when compared to the control groups.
Introduction
The local recurrence of malignant disease after surgical removal
is a major cause of morbidity and death. The cause of local
recurrence is usually due to the incomplete removal of tumour, or
burst and spill of malignant cells onto the operative bed, during
surgery. The latter scenario is thought to occur when a viable
cell population is spilt. This cell population re-establishes a
local blood supply, and can continue to grow. Local recurrence is
a particular problem in the treatment of head and neck cancer,
where there is a high rate of positive (tumour involved) margins
due to the proximity of vital structures, and a confined
operative space, which, when faced with large tumours and
necrotic centers, can lead to tumour rupture and spillage.
Photodynamic therapy works by the intracytoplasmic activation of
a previously inert drug (a photosensitiser). Activation is by
light of a specific wavelength. This process causes singlet
oxygen to be released, with consequent intracellular failure and
cell death. This effect mimicks apoptosis, and leaves surrounding
tissue generally intact, although some local damage does occur
when treating a tumour in a bed of normal tissue. The relative
lack of local tissue damage is due to the nature of the healing
that occurs after PDT, and because tumours tend to contain more
photosensitiser than normal tissue does.
The potential value of adjunctive intraoperative photodynamic
therapy (AIOPDT) lies in the fact that by using powerful new
second generation photosensitising drugs and new lasers,
efficient adjunctive treatment can be delivered to the operative
bed following malignant tumour excision, in around 30 minutes.
This means that there is little additional to the overall
operating time, with the potential benefit of reducing the local
recurrence rate.
Material and Methods
This experiment was designed to test the hypothesis that AIOPDT
is effective in reducing the local malignant tumour recurrence
rate in an animal model. The aim of this study was to determine
whether the tumour model HSN fibrosarcoma, which bears a close
resemblance to our target clinical tumour, mucosal squamous cell
carcinoma of the Head and Neck , shows a statistically
significant reduction in local recurrence with the treatment
groups when compared with the control group.
Animal model,Tumour
A rat fibrosarcoma tumour called HSN was used. This cell type was
chosen because it causes an aggressive, locally invasive tumour
that does not widely metastasise or encapsulate. This means that
there should be a reasonably high local recurrence rate if
tumours are removed without wide excision. The animals used were
Chester-Beatty hooded rats, in which this tumour grows.
Tumour preparationFibrosacroma cells were obtained from the Chester-Beatty research
laboratory, The Royal Marsden Hospital, Fulham Road, London.
These were inoculated into the dorsal spine musculature of
Chester Beatty hooded (CBH) rats, in order to grow a solid
tumour. Using a freshly killed donor animal with tumour
previously grown, the tumour periphery (containing viable, non-
necrotic tumour) was excised. Small pieces of tumour
approximately 1mm x 1mm x 1mm were formed by dividing up the
donor tissue. These were then implanted under direct vision into
the flank musculature of further adult CBH rats, under sedation
with Midazolam. Both flank areas were inoculated. Following this
the skin was closed with clips, and the animals were recovered.
Photosensitiser
The photosensitizing drug used was meta-
tetra(hydroxyphenyl)chlorin, mTHPC, or FoscanR. This drug is a
second generation photosensitiser, created to have enhanced
properties over 1st generation compounds. The drug dose of FoscanR
used was 1.0 milligrammes per kilogramme (mg/kg) body weight
delivered intravenously via the tail vein. This compares with the
human dose of 0.15 – 0.3 mg/kg, the higher dose in rats being a
function of their surface area to weight ratio. FoscanR was
obtained from Scotia Pharmaceuticals, Stirling, U.K., as a gift.
It was stored as a sterile powder in a fridge, and reconstituted
fresh with 1g ethanol and 1g polyethylene glycol 400 made up to 5
ml with sterile water for injection, to make up a solution of 0.5
mg/ml. When reconstituting the drug for injection, meticulous
attention was taken to ensure that the drug had gone into
solution. Invariably this meant 2 or 3 minutes of vigorous
shaking, ensuring no residue was visible on the bottom of the
tube used for reconstitution. The interval between injection of
the drug and delivery of activating laser light (the drug-light
interval, DLI) was 96 hours, as this appears to be a good drug-
light interval (DLI) for normal tissue selectivity and a powerful
tumouricidal effect (Ris et al 1993, Van Geel et al 1993).
Light parametersThe light dose given for photoactivation was 20 joules/square
centimetre (j/cm2) at an intensity of 100 milliwatts/cm2 (mW/cm2).
Laser light was used, at a wavelength of 652 nm, corresponding
with a high peak of absorption for FoscanR. Red light at this
wavelength has good tissue penetration characteristics, which are
beneficial when treating cancer, so as to treat a large volume of
potentially involved tissue. The light intensity was measured
using a calibrated integrating sphere (type INS250), a photodiode
with a flat response filter (type SED100) and a radiometer (type
IL1700), all from International Light Inc., Mass., USA, and was
delivered via a flexible quartz fibre and microlens (Quadra Logic
Technologies, Vancouver, Canada). The laser used was a copper
vapour CU15 system pumping a Rhodamine dye laser, both from
Oxford Lasers Ltd., Abingdon Rd., Oxford, U.K. These light
parameters were used in the first studies with the mTHPC, which
showed excellent necrosis of malignant tissue (Ris et al 1991).
Surgical Technique
Under a general anaesthetic of Hypnorm and Midazolam a single
midline incision was made on the dorsum, between the 2 tumours.
Each tumour was identified and measured separately. Using a No.15
scalpel blade fitted to a scalpel blade holder, the tumour was
excised close to, but not macroscopically involving, its margin.
Macroscopic clearance was confirmed by eye in all cases before
the study could progress. Following adjunctive treatment, the
skin was closed with clips and the animal recovered.
Experimental studies
There were 2 preliminary and 1 definitive studies
The aims of the 2 preliminary studies were to determine:
1) What the feasible maximum size of the tumours was before the
perioperative mortality rate became unacceptable. This was
determined since size of tumour is likely to be directly
proportional to recurrence rate. We wanted as high a target
recurrence rate in controls as possible.
2) What the growth characteristics of the tumour were, in order
to predict the day at which tumours would reach the previously
determined optimum size.
Study 1
Initial studies were performed to determine the optimum size of
tumour in terms of local recurrence rate after macroscopic
excision, and survival of the animal. This was necessary because
the larger the tumour, the more likely it is to recur locally due
to inadequacy of excision, even if the margins are
macroscopically clear. However, resection of very large tumours
will result in a critical loss of fluid, and death of the animal.
Therefore it was necessary to know what the safe maximum size of
the tumours was. Tumours were grown bilaterally until they
reached a size of 1cm, 2cm or 3cm largest diameter as measured
externally with the animal awake. At this stage a general
anaesthetic was administered, and both tumours removed locally,
but with full macroscopic clearance (i.e. no visible tumour
left). The skin was then closed and the animals recovered.
Animals were closely monitored postoperatively for signs of
distress. If any were shown the animals were immediately killed
by a schedule 1 technique. Other animals succumbed shortly after
surgery. All non-survivors were recorded. The survivors were
killed 2 weeks after surgery and the surgical sites examined for
signs of local recurrence, which was recorded.
Study 2
This was performed to determine the predictability of tumour
growth prior to photosensitisation. Once the optimum tumour size
had been determined in study 1, it was important to have an idea
regarding the growth rate of the tumour, since the decision had
been taken to sensitise 4 days prior to treatment. Clearly, a
tumour measured at the safe maximum size at injection would be
significantly above that size 96 hours later, given a doubling
time of x hours, where x is any number less than around 300. Ten
tumours were grown in 10 animals, the same way as above, but
unilaterally. Tumours were implanted on day zero. Alternate daily
measurements of the maximum tumour diameter were taken.
Measurements were taken with the animal awake using a steel ruler
with 1mm gradations. Once the tumour reached around 20mm diameter
(the chosen size for the 3rd experiment on the basis of the first
preliminary study), the animal was killed.
Once this data had been gathered, a blind, prospective controlled
study (Study 3) was performed to test the hypothesis that AIOPDT
with mTHPC reduces significantly local recurrence after
macroscopic surgical excision in the HSN rat fibrosarcoma model:
Study 3
4 groups of 30 animals were included in the experiment. These
were:
1) Surgery and AIOPDT.
2) Surgery, mTHPC diluent and light only at the above parameters
(no drug).
3) Surgery and drug only
4) Surgery only.
Two independent tumours were grown in each animal, on the back,
to the left and right side of the midline, well separated, using
the method described above. After 10 days, the animals were
admitted into one of the 4 treatment groups. They were kept in
cages of up to 5 animals each, cages were coded according to the
treatment group each animal was in. Each cage was coded following
randomn selection by biological services staff. Those animals due
for drug injection (groups 1 and 2) were weighed and injected
intravenously via the tail vein with 1mg/kg mTHPC that had been
freshly prepared from powder. 4 days later a general anaesthetic
was administered to all animals and the tumours exposed. The
largest diameter was measured. Any tumour of 20mm +/- 2mm largest
diameter was included in the study and resected so that no
macroscopic tumour was left. Tumours beyond these criteria were
not used. At that stage animals due for light administration
(groups 1 and 2) were identified and 20 joules/cm2 of 652 nm
laser light of 100 milliwatts/cm2 intensity was given. The light
was produced by a copper vapour laser pumping a rhodamine dye
laser (Cu 15, Oxford Lasers, Abingdon Rd., Oxford, U.K.).
In all cases a 2.5 cm diameter laser spot was used with the
original tumour site in the middle, giving a margin of normal
tissue treatment, which was approximately 15 % of the original
tumour size. The laser spot diameter was measured using a steel
ruler with 1 mm gradations. The microlens was held steady over
the treatment site by holding it with a clamp fixed to a retort
stand. Following this the skin was closed and the animals were
recovered. At this stage the animals were numbered by puncturing
and marking the ears with Evans Blue dye. Postoperatively the
animals were observed closely. Any animal in distress was killed
immediately and this was recorded. Any animal succumbing to the
immediate effects of surgery was also recorded.
Once obvious macroscopic and potentially distressing tumour
recurrence had occurred in one animal (the experimental end
point), all animals in the groups treated in that session were
killed. This occurred up to 4 weeks post surgery. The flank areas
were opened and examined for tumour recurrence. Any suspicious
areas that were not obviously tumour were biopsied and sent for
histological confirmation of the result, otherwise the diagnosis
of tumour recurrence was made by sight alone. At this stage and
during recording of the results the examining surgeon was blind
to the group the animals were in, only the experiment had been
completed were the codes broken.
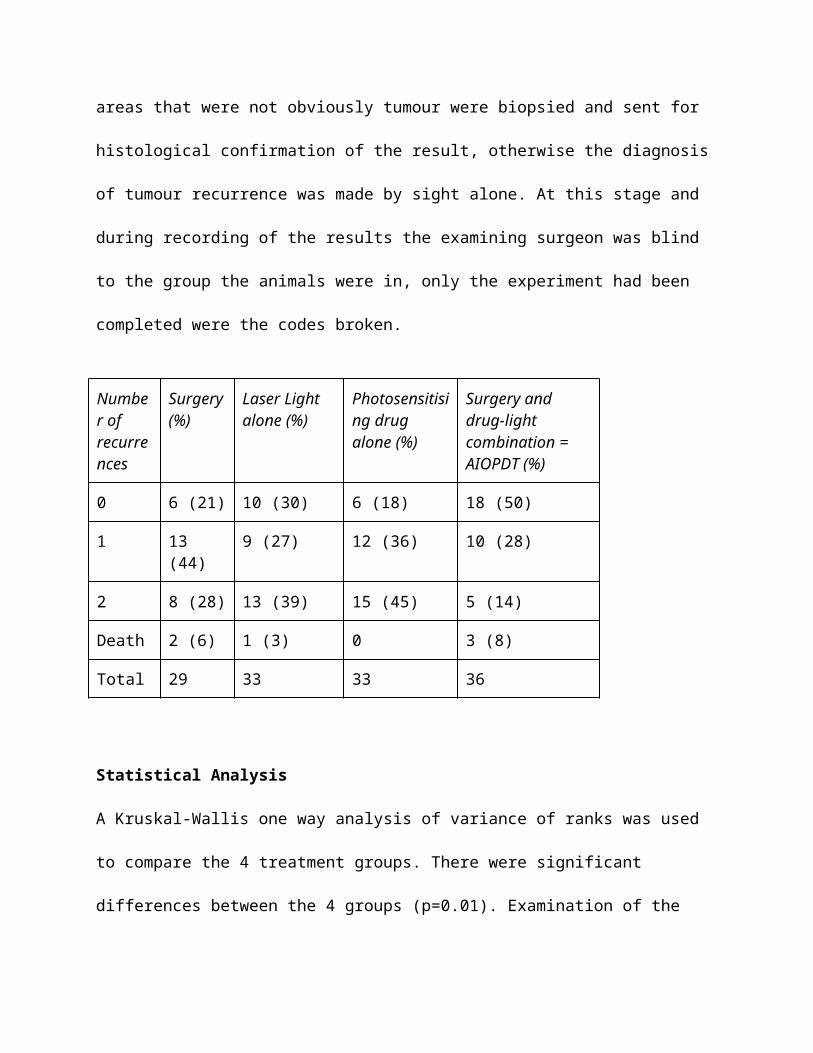
Number ofrecurrences
Surgery(%)
Laser Light alone (%)
Photosensitising drug alone (%)
Surgery and drug-light combination = AIOPDT (%)
0 6 (21) 10 (30) 6 (18) 18 (50)
1 13 (44)
9 (27) 12 (36) 10 (28)
2 8 (28) 13 (39) 15 (45) 5 (14)
Death 2 (6) 1 (3) 0 3 (8)
Total 29 33 33 36
Statistical Analysis
A Kruskal-Wallis one way analysis of variance of ranks was used
to compare the 4 treatment groups. There were significant
differences between the 4 groups (p=0.01). Examination of the
distribution of outcome in the 4 groups suggested that the first
3 groups had similar outcomes. A Kruskal-Wallace anova test was
used to compare these first 3 groups and found no significant
difference (p=0.6). The 4th group (AIOPDT) was then compared with
these 3 groups combined. The Kruskal-Wallace anova test result
demonstrated a significant difference (p=0.002) between the
AIOPDT group and the other 3 groups combined.
A rank transformation was also used on the data, and a two way
analysis of variance on the ranks with the factors “treatment
group” and “day” was performed. There were no significant
differences between the 7 days on which the study was performed
(p=0.7).
Discussion
Similar adjunctive intraoperative preclinical studies have been
performed in the past (Davis et al 1990, Van Hillsberg et al,
Abulafi et al). These were different to this study, both in terms
of study design, and tumour type and sensitiser used. In
particular, the studies by Davis, and Van Hillsberg did not have
control groups as in this study. Abulafi used a different tumour
model and photosensitiser have shown this theory to be true,
although the structure of these studies was not fully blind, and
some potential control groups were missing.
The results show a statistically significant reduction in the
local tumour recurrence rate with the treatment group as compared
to the control groups. Although there were more deaths
postoperatively in this group, this was not a significant
finding, and may just represent the relatively small numbers
tested. The variation of numbers within the groups represents
excluded tumours that were outside the treatment parameters. The
control groups tested the hypothesis that the drug and diluent is
toxic to tumours without light (drug only group), although even
in this group there will have been a mild photodynamic effect due
to background theatre illumination and theatre lights during the
excision. However, the total light dose given during the
relatively short (approximately 5 minutes) time that it took for
excision of both tumours is so low that this effect is unlikely
to have been significant. The control groups also tested the
hypothesis that the drug diluent is an active photosensitising
agent (light and diluent only group), although the hypothesis
that 652 nm laser light at non-thermal intensity could be
cytotoxic was not independently tested. This is extremely
unlikely however since there are many publicly available lasers
at around this wavelength (laser light pointers) that have been
shown to be totally safe except when shone directly into the
eyes. The fact that there was no significant difference between
any of the control groups including the surgery alone means that
these hypotheses are invalid.
A study such as this is only valid if the principle that local
tumour recurrence is due to residual disease is agreed. There are
other theories regarding why tumours recur in the excision bed,
such as further metastases from the primary area, or new primary
disease growing in the tumour bed. Studies have shown that after
a macroscopically complete excision, if the tumour bed is washed
with cell growth medium and incubated in the correct conditions
for growth, viable tumour cells can be grown (Harris and Smith
1960). These cells almost certainly come from the excised tumour
area, either due to "burst and spill" or unwittingly cutting
through tumour during the excision, and contaminating the
surgical instruments (Beahrs and Barber 1962). What is not known
is whether these are viable or not in the clinical situation.
Disease recurrence due to residual tumour can also occur because
of involvement of vital structures rendering the tumour
inoperable, or because tumour margins or not clear due to the
disease growing to the defined limits of the operation (Olcott et
al 1981).
Other adjunctive intraoperative methods have been tried in order
to reduce the local recurrence rate of tumour after Head and Neck
surgery. These include intraoperative external beam radiotherapy,
which was logistically very difficult, time consuming and
damaging to the carotid artery (Freeman et al 1990), and washing
the tumour bed with cytotoxic agents, including distilled,
sterile water which has not been shown to be effective,
presumably because there is little penetration of effect into the
microscopic cracks and crevices on the tumour bed where viable
tumour clumps may lodge.
This tumour model bears a reasonable relationship to the proposed
clinical treatment, namely metastatic neck disease treated by
radical neck dissection. Neither are primary tumour sites, the
animal model being an implanted tumour graft, the clinical model
being a proliferating clump of tumour cells shed from the primary
site into lymphatic channels and caught in the draining lymph
glands. The main difference apart from site of growth is in the
fact that the clinical model lies in a lymph gland, the animal
model in normal surrounding muscle, although this is important
since the tumour is growing in its natural environment, being a
connective tissue tumour (Bown S.G. pers. comm.). It thus is a
more natural model than others used for AIOPDT studies, such as
neuroblastoma in muscle (Davis et al 1990) or adenocarcinoma in
subcutaneous tissue (Abulafi et al 1994). However, by the time
most secondary tumours in the neck have been detected, they have
reached a size of at least 1cm diameter, and have usually
destroyed the lymph node they lie in. The adjacent tissue to most
of the lymph nodes in the neck is mainly muscle, particularly in
the lymph node bed, and fat, which tends to lie superficially.
Thus even in the human situation, the tumour lies in close
proximity to the muscle. This is even more so following radical
neck dissection, since the superficial tissue (mainly fat,
internal jugular vein and the sternocleidomastoid muscle) and
tumour is removed, the deep musculature is left untouched. Thus
the treatment site for AIOPDT in both cases would be a muscle
bed.
The tumour type used, HSN fibrosarcoma was also similar to the
human model: squamous cell carcinoma of the upper aerodigestive
tract. This is because it is a locally invasive, non-
encapsulating tumour (see picture). Clearly an encapsulating
tumour would be easy to shell out with little chance of local
recurrence, whereas a tumour microscopically invading into the
surrounding tissue will recur unless a wide block of apparently
normal tissue is removed with the specimen, which was not done in
this case. The tumour was removed very close to the main tumour
lump, although macroscopic clearance was complete in all cases.
Therefore it is more likely that microscopic tumour residue
occurs, leading to a local recurrence rate in the control groups
of around 70%. The initial studies on survival after excision
also showed this - it would have been useful to have had an even
higher local recurrence rate as occurred with the 3 cm diameter
tumours, but the postoperative mortality rate made this
unacceptable.
The scope of procedures suitable for AIOPDT in surgery is much
greater than just radical neck dissection . It may also have a
role in general surgery (Herrera-Ornelas et al 1986, Nambisan
R.L. et al 1988, Abulafi et al 1993), neurosurgery (Muller and
Wilson 1995) and thoracic surgery (Ris et al 1993). Conservation
surgery in the neck, in vogue since it seems to reduce
postoperative morbidity (Bocca 1975) could be made safer by
treating those retained structures such as the accessory nerve
with PDT to mop up any residual tumour around such structures.
The fact that red light penetrates tissue significantly means
that structures such as the accessory nerve can be completely
treated by illuminating onto and through the nerve. The same may
be true of other vital structures in the neck such as the carotid
tree, although the fact that this is of quite large diameter and
filled with blood means that complete penetration and treatment
of the medial surface is unlikely to be effective. Prior to
clinical studies, safety work is therefore needed, particularly

regarding the effect of PDT on arterial structures.
Conclusion
The scope of adjunctive intraoperative photodynamic therapy is
large, in the Head and Neck as well as other areas. This and
other studies have successfully demonstrated, to the satisfaction
of statisticians, the principle that this treatment reduces the
local recurrence rate of tumour following macroscopically clear
excision to be true on a preclinical basis.
References
(INCOMPLETE)
Abulafi A.M., DeJode M.L, Allardice J.T., Ansell J.K, Williams N.S. (1997) Adjuvant intraoperative photodynamic therapy in experimental colorectal cancer using a new photosensitiser. Br. J. Surg.;84(3):368-71
Van Hillegersberg R., Hekking-Weijma J.M., Wilson J.H.,
Edixhoven-Bosdijk A. and Kort W.J. (1995) Adjuvant intraoperative
photodynamic therapy diminishes the rate of local recurrence in a
rat mammary tumour model. Br. J. Cancer;71(4):733-737





























