Embed Size (px)
Citation preview

Topics in Anti-Cancer Research, Vol. 1, 2012, 113-139 113
Atta-ur Rahman and Khurshid Zaman (Eds) All rights reserved-© 2012 Bentham Science Publishers
CHAPTER 4
Adjuvant Therapy for Renal Cell Carcinoma
Sebastiano Buti1,*, Melissa Bersanelli1, Maddalena Donini2 and Andrea Ardizzoni1
1Operative Unit of Medical Oncology, University Hospital of Parma, Parma, Italy and 2Oncology Division, Istituti Ospitalieri di Cremona, Cremona, Italy
Abstract: Renal cell cancer incidence is fastly growing worldwide. In spite of major advances in the treatment of metastatic disease, to date there is no adjuvant therapy proven feasible in high risk patients after radical resection. An effective adjuvant agent against renal cell cancer should be relatively non toxic, have estabilished efficacy in the metastatic setting and have demonstrated effectiveness against the standard of care in randomized Phase III trials. The development of adjuvant therapy requires the proper identification of patients at highest risk of relapse; our ability to predict the recurrence has much room for improvement. To date, only an autologous vaccine has achieved a significant benefit in the adjuvant setting for renal cell carcinoma. The recent arrival of new drug classes, such as tyrosine kinase inhibitors and monoclonal antibodies, strongly improving overall and progression free survivals in the metastatic disease, has renewed the hopes on the adjuvant treatment of the disease. Several studies have been performed in the past using radiation treatment and systemic agents, including chemotherapy, immunotherapy and hormonal treatments, with adjuvant purpose; new trials are in progress to evaluate the effectiveness of antiangiogenic agents in this setting. An overall review of the completed and upcoming trials and patents on this issue shall be discussed in this chapter.
Keywords: Adjuvant chemoimmunotherapy, adjuvant chemotherapy, adjuvant drugs, adjuvant hormonal therapy, adjuvant immunotherapy, adjuvant radiation therapy, adjuvant targeted therapy, adjuvant therapy, antiangiogenic drugs, chemoimmunotherapy, chemotherapy, hormonal therapy, immunotherapy, kidney cancer, new drugs, postoperative treatment, radiation therapy, RCC, renal cell carcinoma, targeted drugs, vaccine.
1. INTRODUCTION
Renal cell carcinoma (RCC) is responsible for 2 to 3% of all malignant cancers in adults. It is the ninth most common cancer in women and the seventh in men. Its incidence worldwide is 209.000 new cases and 102.000 deaths yearly [1, 2],
*Address correspondence to Sebastiano Buti: Operative Unit of Medical Oncology, University Hospital of Parma,Via Gramsci 14, 43100 Parma, Italy; Tel: 0039 0521 702661; Fax: 0039 0521 995448; E-mail: [email protected]
Send Reprints Orders on [email protected]
114 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
accounting for 3% of deaths due to cancer in the males in the United States in 2008 [2]. The incidence rates have almost doubled over the past 30 years, from 7.1 per 100,000 in 1975 to 13.4 per 100.000 in 2005 [3]; the disease is predominant in men, with a 2:1 incidence ratio and usually occurs during the 6th or 7th decade of life. Among the best known risk factors involved there are active and environmental tobacco smoking [3], obesity and hypertension [4, 5]. Taken together, they account for 49 percent of cases of RCC [6].
While sporadic RCC cases are usually single lesions in individuals in their 60s, genetic-driven cancers are bilateral, multifocal, more aggressive and with an earlier onset [7]. Genetic conditions such as the Von Hippel Lindau (VHL) Syndrome, hereditary papillary renal carcinoma and Birt Hogg Dubé are forms of “inherited” RCC.
1a. Signs, Symptoms and Diagnosis
The clinical onset can be characterized by a myriad of symptoms, hence the popular term “the internist’s tumor” [8]. The classic triad with hematuria, palpable abdominal mass and flank pain is present in less than 10% of patients, and all of them are ominous signs. Probably this small percentage is due to the fact that most of RCC cases were incidentally discovered in early stages [9]. Systemic symptoms can be due to metastases or paraneoplastic syndromes, such as hypertension, pain, hypercalcemia, erythrocytosis, fever and fatigue [10]. Other methods for the diagnosis of genitourinary cancer could be provided in future, such as the thromboxane receptor-β in urine assessment [11].
1b. Stage as Prognosis Factor and Survival
The strongest indicator of prognosis is perhaps the stage at diagnosis. The reported 5-years survival rates using 2010 TNM staging criteria range from 81% in stage I to 8% in stage IV [12].
At diagnosis time, up to 30% of patients with RCC have metastatic disease and recurrence develops in approximately 40% of patients initially treated for a localized disease [13]. The median time to relapse after nephrectomy is 15 to 18 months, and 85% of relapses occur within three years [14].
Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 115
The regional lymph node involvement (stage III/N1 disease) at the time of surgery is strongly related to survival, with reported 5-years survival rates from 11% to 35% in positive cases [15]. Patients with higher stage or higher histologic grade are prone to have earlier recurrences, and rarely metastasize after 2 years of follow up, whilst low nuclear grade and early stage disease may experience later recurrences, even after 5-years of follow up [16]. Other factors are also associated with the issue (see the next section “prognosis factors”), such as histological type, tumor size and necrosis: for example clear cell histology is associated with better outcomes than papillary or chromophobe histology in the metastatic setting, while the opposite being true for localized disease [16, 17].
1c. RCC Initial Management
The main procedure employed in early RCC is surgery, condition almost sine qua non for cure. For smaller tumors the nephron sparing technique should always be envisaged. The partial nephrectomy has been proven equally effective as the radical intervention in carefully selected cases [18, 19]. However, nephron-sparing surgery has been increasingly used in patients with T1a and T1b renal tumors (i.e., up to 7 cm in greatest dimension) and a normal contra lateral kidney, with equivalent outcomes to radical nephrectomy: radical nephrectomies should not be employed when nephron sparing can be achieved [20-23]. Both radical and partial nephrectomy have evolved in later years to be performed by laparoscopy safely [24-26].
Other possible treatment is probe-based thermal ablation, which exploits the tumor exposure to extreme temperatures. This treatment can be performed either as cryoablation or as radiofrequency ablation, by percutaneous or laparoscopic approach [27, 28], with the latter being preferred whenever adjacent organs are involved in the target area. However, the thermal ablation technique results in a much higher recurrence rate than the conventional surgical approach [29], it affects possible future rescue surgery and should not be performed in tumors larger than 3.5 cm. So, this treatment should be very personalised and offered only to patients with contraindications to standard surgery.
1d. Prognosis Factors
The AJCC (American Joint Committee on Cancer) considers five subtypes of RCC: conventional (clear cell), papillary, chromophobe, collecting duct and
116 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
unclassified [30]; currently there are many more known types of kidney cancer [31], giving an idea of the heterogenity of this disease. As the clear cell carcinoma accounts for around 80% of RCCs, it is the most studied in clinical trials, therefore being the best known and used as a “pattern” for therapy and prognosis.
Several factors are associated with a worse prognosis after radical nephrectomy:
Variables related to the patient: A low performance status, the presence of symptoms at the moment of diagnosis, cachexia and alterations in some laboratory parameters (anemia, thrombocytosis, high erythrocyte sedimentation rate, high levels of C-reactive protein, hypercalcemia) are related to a worse prognosis [15].
Stage at diagnosis: Depending on the parameter T defined according to the 2002 TNM system, the probability of 5-years disease-specific survival (DSS) is respectively: 97% for pT1a, 87% for pT1b, 71% for pT2, 53% for pT3a, 44% for pT3b, 37 % for pT3c and 20% for pT4; for pN positive the 5-years DSS decrease to 10-35% [32].
Histological features of the tumor: The Fuhrman nuclear grading, the histological type, the presence of necrosis, microvascular invasion and sarcomatoid features are important variables influencing the risk of relapse [33-37].
Molecular markers: Carbonic anhydrase IX (CAIX) is one of the most studied molecular markers in clear cell RCC; the presence of this trans-membrane anhydrase, involved in the regulation of intra- and extracellular pH during periods of hypoxia, is essential for proliferation and metastasis. A low expression of CAIX (< 85% of cells) is associated with a worse prognosis in patients with localized disease [38-41]; on multivariate analysis low CAIX expression increased the risk of death by 2.5-fold [42]. Despite at least one study showing that CAIX is not an independent predictor of outcome for patients with clear renal cell carcinoma [43], other evidences confirmed its role as independent predictor of improved DFS (disease free survival) for patients with stage

Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 117
I-III disease, while the prognosis is not influenced in metastatic disease [44]. On the other hand, high CAIX expression appears to be related to a greater likelihood of response to systemic treatment for metastatic disease, acquiring in this case a predictive value [45]. The oncofetal protein IMP-3 has been classified as a prognostic marker for cancer in several solid tumors, including RCC [46]; other studies seem to identify a prognostic value of the apoptosis inhibitor protein survivin [47] and the chemokine CXCR3 [48]. A prognostic role in RCC is also described for the B7 glycoproteins family members: B7-H1, a soluble polypeptide present in the serum of patients, and B7-H4, a cell-surface glycoprotein expressed on tumor vasculature [49, 50]. Recently, a molecular signature consisting of five molecular markers has shown the power to predict DFS for localized clear cell RCC: Ki-67, p53, endothelial vascular endothelial growth factor receptor (VEGFR)-1, epithelial VEGFR-1, and epithelial vascular endothelial growth factor (VEGF)-D. The author’s conclusion is that the prognostic ability of the signature and nomogram may even be superior to clinical and pathologic factors alone and may identify a subset of localized tumors with aggressive clinical behavior. Despite no external validation of the nomogram has been done so far [51], this approach is very interesting and remains promising for the future [52]. Other biomarkers such as PTEN, carbonic anhydrase XII and vimentin, have been studied as possible prognostic indicators, but their weight and role are still to be proven [38].
In recent years, identification of patients at different risk of recurrence was made easier by the development of various prognostic nomograms and algorithms, developed to assist both clinicians and patients in estimating the risk of relapse. Among the most used mathematical models to stratify patients with clear cell RCC into different risk groups, should be considered [53]: the Memorial Sloan-Kettering Cancer Center nomogram, which includes pathological stage, Fuhrman nuclear grading, tumor size, necrosis, vascular invasion and clinical presentation [54]; the University of California Los Angeles Integrated Staging System (UISS), based on Eastern Cooperative Oncology Group (ECOG) performance status, Fuhrman nuclear grading and pathological stage according to the 2002 TNM
118 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
staging system [55]; the Mayo Clinic Stage Size Grade and Necrosis (SSIGN) score, considering TNM stage, tumor size, nuclear grade and histological tumor necrosis [56]; the Karakiewicz nomogram, based on TNM stage, Fuhrman grade, histologic subtype, local symptoms, age, and sex [57, 58]; the Leibovich score, including tumor stage, regional lymph node status, tumor size, nuclear grade, and histologic tumor necrosis [59, 60]: a recent supplementation of this last score includes an additional scoring for vascular invasion, with an improvement of the predictive accuracy [61]. There is no universal consensus on which of these nomogram is superior, though two retrospective studies comparing SSIGN and Leibovich scores with UISS score suggested that the SSIGN and Leibovich scores offer a better stratification for clear cell RCC than the UISS model [62, 63]; on the other hand, from recent evidences, the Karakiewicz nomogram emerged as a better clinical predictor for survival outcomes in patients with localized disease when compared to the Leibovich model [63, 64].
Currently, these models are also useful for their ability to educate patients about their prognosis, to run a fair or adequate surveillance and are already used to better select patients to be enrolled in ongoing studies of adjuvant therapy with new molecules.
2. OBJECTIVES & METHODS
The aim of this chapter is to review the most up to date literature in adjuvant treatment for RCC after surgery, considering only Phase III randomized trials, starting from the first performed trials on the issue. Clinical published papers on adjuvant therapy for RCC were obtained from the Pubmed database. The search was manually augmented by reviewing the most important international scientific meetings, abstract databases and online/virtual presentations. The ongoing trials were uploaded on the official website www.clincaltrials.gov, considering only randomized Phase III studies.
3. STATE OF THE ART ON ADJUVANT THERAPY IN RCC
The most recent national cancer center network (NCCN) Guidelines for kidney cancer declared that adjuvant treatment after radical surgery currently has no established role, basing on the absence of any systemic therapy capable to reduce the likelihood of relapse [64]. Actually, observation remains the standard care

Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 119
after nephrectomy, with the only possibility of enrollment in randomized clinical trials for eligible patients [65].
Developing an effective adjuvant therapy requires an evidence-based approach and a knowledge of the molecular and biologic basis of RCC. To classify an agent as an effective adjuvant treatment against RCC it must achieve several goals. It should be relatively non toxic, have established efficacy in the metastatic setting and have demonstrated efficacy against the standard of care in randomized Phase II and III trials. The development of adjuvant therapy requires a proper identification of potential beneficiaries, represented by patients at highest risk of relapse or more sensitive to particular drugs. Our ability to predict the recurrence has much room for improvement: this goal has been made easier by the development of nomograms including the most important prognostic and predictive factors (see previous paragraph). On the other hand, it is important to assert that, probably, patients with low risk of recurrence (small incidentally detected tumors, benign or indolent pathology) should not be candidates to receive an adjuvant treatment.
A systematic review on adjuvant therapy in RCC, with an interesting meta-analysis, was recently performed by Scherr et al. in 2011; the authors considered ten randomized controlled trials comparing adjuvant therapy versus observation after surgery and analyzed the outcomes in terms of overall survival (OS), DFS and severe toxicities. Different strategies of treatment were separately evaluated; as a result, any adjuvant therapy among the considered regimens provided no benefits on OS (HR = 1.07, 95% C.I. 0.89-1.28; p = 0.48; no heterogeneity) or DFS (HR = 1.03, 95% C.I. 0.87-1.21, p = 0.77; heterogeneity measured as I2 = 40%) when compared with observation. Subgroup analysis on different regimens (immunotherapy, hormone therapy, biochemotherapy and vaccines) showed no relevant results. Toxicity evaluations evidenced a higher incidence of adverse events in the adjuvant therapy groups. In conclusion, the performed analysis led to not recommend adjuvant therapy for patients who underwent radical resection for RCC [65].
4. RADIATION THERAPY
Attempts for the use of adjuvant radiotherapy after complete resection of RCC have been performed since the 1970’s; seven controlled trials (five retrospective
120 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
studies and two prospective randomized ones) have been performed until 1997. All of them were included in a recent meta-analysis on post-operative radiotherapy (PORT) in RCC [66-73]: from the results, a significant reduction of loco-regional failure (LRF) emerged in patients treated with PORT (p = 0.0001), in front of no difference in OS (p = 0.29) and DFS (p = 0.14) [73].
Although this strategy failed to show any benefit, in some cases appearing to be even detrimental, with significant complication rate and undesirable side effects such as hepatocyte injury [67], it is important to consider that the majority of patients in the performed studies were treated with old radiation techniques, using large field sizes. This could leave open the possibility of planning new adjuvant trials using the modern conformal and intensity-modulated radiotherapy techniques. Nevertheless, a larger study including 116 patients concluded that the locoregional failure alone is a rare event in RCC, making radiotherapy an unlikely effective tool in minimizing the risk of disease relapse [74]. Since then, this has been a largely abandoned adjuvant strategy.
5. CHEMOTHERAPY
RCC is one of the most chemotherapy resistant solid tumors. This is due to several factors, which involve high expressions of P-glycoprotein (PGP), gamma-glutamyl cysteine synthetase (-GCS) and cis-diamminedichloroplatinum resistance-related gene 9 (CRR9), low expression of vacuolar ATPase and no expression of multidrug resistance-associated protein 1 (MRP1), among others [75]. Hence, chemotherapy regimens have a very limited role whilst treating RCC. Several Phase II trials evaluating chemotherapy regimens in the metastatic setting, considering both monotherapy (in particular capecitabine) and doublets (gemcitabine plus capecitabine or 5-fluorouracil), demonstrated the poor chemosensibility of RCC, leading to the conclusion that it was not even worthy of a Phase III trial [76-78]. Only two randomized trials of chemotherapy associated with immunotherapy in the metastatic setting have been subsequently performed, respectively establishing the safety and improved long-term therapeutic efficacy of subcutaneous interleukin-2 (IL-2) plus interferon-α2a (IFN-α2a) and 5-fluorouracil compared with IFN-a and vinblastine [79], and the lack of survival advantages in favor of capecitabine versus 5-fluorouracil when associated with immunotherapy (IL-2, INF-2a, 13cis-
Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 121
retinoic acid) in advanced renal cell carcinoma [80]. Nevertheless, previous attempts failed to find an effective chemotherapy regimen in RCC, this strategy has been granted the chance to be put under test in the adjuvant setting. In a study from the early 1990’s, vinblastine, doxorubicin and tegafur-uracil (UFT) have been administered in 31 patients with RCC. Even though the 5-years survival rates were significantly better than historical cohorts, this study has received massive criticism upon its methodology, such as low overall risk for chosen patients, small sample size and use of historical controls [81].
Recently, thalidomide has also been evaluated in 46 patients in a randomized Phase III trial conducted by the MD Anderson Cancer Center. After a median of 43.9 months of follow up, it has failed to improve the 2-and 3-years relapse free survival (RFS) rates and the cancer specific death rates [82].
Currently, there are no chemotherapy regimens undergoing evaluation in adjuvant setting for patients with RCC at high risk of relapse.
6. IMMUNOTHERAPY
Immunotherapy for RCC has been available since the 1980’s. The exact mechanism of action of treatment regimens is not completely understood. The best known therapies of this kind are IFN-α and IL-2, used alone or in combination, and the vaccines. The cytokines increased both the activity of cytotoxic lymphocytes and of natural killer (NK) cells, modulating, as vaccines, the immune system of the host in responding to tumor cells; furthermore, IFN-α modulates the growth and cell function, directly inhibiting cell proliferation and regulating the antigenic differentiation and expression of the cell [83].
Several trials have been performed to assess the efficacy of immunotherapy in the adjuvant setting, but unfortunately most of them have failed in showing any survival advantage [84-94]. All randomized trials are indicated in Table 1.
6a. Vaccines
Vaccines with antigens derived from tumor cells have been used in patients with locally advanced or metastatic RCC, with an attempt to increase the immune response against the tumor residual. Several vaccines have been tested, including tumor cell lysates and irradiated and cryopreserved preparations of tumor cells [94].

122 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
Table 1: Adjuvant immunotherapy trials in renal cell cancer.
Author Year Patients Stage Treatment Results
Galligioni et al. [84]
1996 120 pT1-3b, pN1-3 Intradermal vaccination with BCG mixed with irradiated cells
No difference in DFS or OS
Pizzocaro et al. [86]
2001 247 Robson II-III (#) IFN-α-2b No difference in RFS,
no difference in 5 year OS, harmful in N0, possibly protective in pN2-3 in terms of RFS
Clark et al. [88] 2003 69 pT3b-4, pN1-3, resected M1
IL-2 No difference in OS
Messing et al. [89]
2003 294 pT3-T4a, pN1-3 IFN-α No difference in OS
Jocham et al. [85] 2004 558 pT2-3b, pN0-3 Autologus vaccine Slight improvement in the 5 years PFS
Atzpodien et al. [90]
2005 203 pT3b/c-T4, N1-3, resected M1
IL-2 + IFN-α-2a + 5-FU
Significantly decreased OS with treatment
Passalacqua et al. [91]
2007 310 pT1 over 2.5 cm, pT2-T3, pN0-3
IL-2 + IFN-α No difference in RFS or OS
Wood et al. [92] 2008 728 T1b-4, N1-3 Vitespen® (*) No difference in RFS
Hinotsu et al. [93] 2011 107 Stage II and III IFN-α No difference in PFS
Aitchison et al. [104]
2011 309 High risk patients IL-2 + IFN-α + and 5-FU
No difference in DFS or OS
BCG = Bacillus Calmette-Guérin, OS = Overall Survival, RFS = Relapse Free survival, DFS = Disease Free Survival, PFS = Progression Free Survival (intended as recurrence free survival), IL-2 = Interleukin-2, IFN-α = Interpheron-α, 5-FU = 5-Fluorouracil. (#) According to the Robson Staging System [52] (*) An autologous, tumor-derived heat-shock protein "glycoprotein 96-peptide complex".
One of the first studies testing a vaccine in radical resected RCC was published by Galligioni et al. in 1996. In this trial, 120 patients undergoing nephrectomy for RCC were randomized between intradermal injections of irradiated autologous tumor cells and treated with Bacillus of Calmette and Guerin (BCG) versus observation. After a median follow-up of 61 months, there were no differences in OS and in relapse rate between patients who received adjuvant therapy and controls [84].
More recently, German investigators conducted a multicenter Phase III randomized controlled trial using six monthly injections of individually prepared autologous

Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 123
renal tumor cell vaccine as adjuvant treatment for patients undergoing radical nephrectomy [85]. A total of 558 patients with stage pT2-3b RCC, with or without lymph node involvement and without distant metastasis, were enrolled. The primary end point of the trial was the reduction of the risk of tumor progression, defined as progression or death (“PFS” for authors). This autologous vaccine was well tolerated. To our knowledge, this is the only adjuvant trial in RCC to date that shows a potential PFS advantage. A total of 379 patients were included in the analysis, and 5-years PFS was 77.4% and 67.8% (p = 0.02, log-rank test) in vaccine group and control group, respectively. It is important to note, however, that 32% of enrolled patients (174 of 553) were lost after randomization, with a disproportionate number of losses from the treatment group (99 versus 75 from placebo). A criticism of this study, therefore, is that these findings would lose their significance in a true intention-to-treat analysis [95]. Additionally, OS was not reported in the initial analysis. A secondary analysis was subsequently performed on 477 patients to include a greater number of patients; this more inclusive intention-to-treat analysis demonstrated a PFS advantage in favor of the treatment group (p = 0.048), although OS was not significantly different (p = 0.11) [96]. Nevertheless, the use of autologous tumor derived products in patients with high-risk RCC appears to be a promising adjuvant strategy.
An alternative approach was represented by the use of peptides from individual tumors in conjunction with heat-shock proteins to generate a vaccine. The tumor-derived heat-shock protein “glycoprotein 96”-peptide complex (HSPPC-96), called vitespen, was used as an adjuvant agent in a randomized Phase III trial that included 818 patients with high risk of recurrence after resection of locally advanced RCC; the primary endpoint was RFS. After a median follow-up of 1.9 years, in the intention-to-treat population there was no significant difference in the recurrence rate (38% versus 40%; HR 0.92, 95% CI 0.73-1.17). In predefined exploratory analyses by AJCC stage, recurrence events in patients with stage I or II disease were reported in 19 (15%) patients in the vitespen group and 31 (27%) in the observation group (HR 0.57, 95% CI 0.32-1.02; p = 0.056) [92].
Whatever the outcome, all these studies show that the vaccine treatments resulted in a good toxicity profile, a very attractive and promising factor for the adjuvant setting [84, 85, 92].

124 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
6b. Interferon-α
IFN-α was a logical choice as an adjuvant agent for the RCC, since it is one of the active drugs in metastatic disease and has been shown to improve survival (“PFS” for the authors, intended as recurrence free survival), in metastatic patients [83, 97-99]. Two randomized studies of adjuvant therapy were conducted and both led to the same conclusions, with a detrimental trend for treated patients. Pizzocaro et al. in 2001 [86] published the results of a multicenter clinical trial involving patients with stage II or III RCC, randomized to nephrectomy or nephrectomy plus IFN-α2b (6 million IU intramuscularly 3 times per week for 6 months starting within 1 month of surgery; primary endpoint was the comparison of RFS): 51 out of 123 patients in the treatment arm, compared to 38 out of 124 patients in the control arm, had recurrent disease at a median follow-up of 62 months. The study showed no advantage for adjuvant IFN-b therapy over observation in terms of overall and event-free survival.
In another Phase III clinical trial, conducted by ECOG, 294 patients were randomly assigned to receive up to 12 cycles of IFN-α-NL (Wellferon) administered daily for 5 days every 3 weeks (3 million IU/m2 day 1.5 million U/m2 day 2, 20 million IU/m2 days 3, 4, and 5 by intramuscular injection) or to observation until recurrence or progression was identified; primary end point was the comparison of survival. At median follow-up of 10.4 years, median OS was 7.4 years in the observation arm and 5.1 years in the treatment arm (log-rank p = 0.09). Median RFS, defined as time from random assignment of treatment to recurrence or death, although not significant, was longer in observed patients: 3 years in the observation arm versus 2.2 years in the interferon arm [89].
More recently, Hinotsu et al. performed a clinical study of the efficacy of 1-year postoperative administration of natural IFN-α; the results, published in 2011, evidenced a not statistically significant difference for the primary endpoint, represented by the progression free survival (PFS, that for the authors is intended as recurrence free survival), between the groups that received natural IFN-α or follow-up observation (p = 0.456, log-rank test). However, peak hazards of progression in the IFN-α group were delayed for about 6-10 months compared with the observation group [93].
6c. Interleukin-2
IL-2 is a growth factor and activator of both T cells and NK cells. It is produced and released by activated T cells. Based on a study of 255 patients with metastatic
Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 125
RCC treated with bolus high-dose IL-2 (720.000 IU/kg every 8 hours), the Food and Drug Administration (FDA) approved its use for therapy in metastatic RCC in 1992 [100]. Several studies were then conducted by other groups, including some trials comparing different doses of IL-2 [101]. Overall, the median survival of all patients treated with high doses in these studies is approximately 12-15 months, with response rates ranging among 7% and 23%; high dose IL-2 demonstrated to produce durable complete response rate in 5% to 7% of patients [102, 103]. There are no differences in survival between patients treated with different doses or schedules, even if with high doses more objective responses are obtained, and more complete responses are maintained over time [100, 101].
Because of its activity in the metastatic setting, IL-2 high-dose bolus was tested in a single randomized study of adjuvant therapy. In this trial, 69 patients with locally advanced stage after nephrectomy (T3b-4 or N1-N3) or with a single surgically resected metastases, were randomized to observation or to a single cycle of IL-2: 600.000 IU/kg every 8 hours, days 1-5 and 15-19 for a maximum of 28 doses. The study was early interrupted: 15 of 21 patients (71%) with locally advanced disease in the treatment arm and 16 of 23 (69%) in the observation arm relapsed at 2 years, with no significant difference. Even in patients with resected metastatic disease no difference was observed between the two arms [88].
6d. Interleukin-2 plus Interferon-α
A multicenter randomized GOIRC (Gruppo Oncologico Italiano di Ricerca Clinica) study, comparing the combination of subcutaneous low dose IL-2 plus IFN-α versus observation, was presented at 2007 ASCO (American Society of Clinical Oncology) annual meeting [91]. The peculiarities of this study, compared to other adjuvant therapy trials, are the long duration of immunotherapy treatment, with courses repeated for 4 weeks every 4-6 months up to five years from the surgery, and the inclusion of patients with low risk of relapse, as pT1 (diameter of T > 2,5 cm and < 7 cm) or N0 tumors. The trial enrolled 310 patients and intention-to-treat analysis at a median follow-up of 52 months showed no significant differences between patients and controls. In the first 5-years of observation, RFS curves were similar in the two arms, but thereafter diverged. The actuarial RFS at 5 and 10 years was respectively 73% and 73% in treated

126 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
patients and 73% and 60% in controls (HR 0.84, 95% CI 0.54-1.33, p = 0.47). Efficacy of immunotherapy was more evident in patients with good PS (HR 0.78, 95% CI 0.47-1.30, p = 0.35), age < 60 years (HR 0.61, 95% CI 0.31-1.19, p = 0.15), and low tumor grade (HR 0.70, 95% CI 0.38-1.27, p = 0.24). As for OS, 59 deaths were observed with no differences between the two arms. Toxicity was mild and limited to World Health Organization (WHO) grade 1 or 2 in the majority of cases. However, a not pre-planned subgroups analysis (interaction test 0.24; p = 0.002) has shown a statistically significant benefit in RFS (HR 0.44, 95% CI 0.24-0.82, p < 0.01) and a positive trend in OS (HR 0.66, 95% CI 0.33-1.33, p = 0.25) for patients who had at least two of the following characteristics (60% of patients in the study): pN0, G1-G2, < 60 years and pT3a (tumor involving the renal vein or extending into fatty tissue around the kidney). Even more interesting results, in patients who had only one or none of these characteristics (40% of patients in the study), adjuvant immunotherapy had a not statistically significant detrimental effect on recurrence free survival (HR 1.81, 95% CI 0.89-3.70, p = 0.10) and a significant negative impact on OS (HR 2.28, 95% CI 1.03-5.03, p = 0.042). However, a longer follow-up is needed to confirm these results, arising from unplanned analysis a priori.
7. CHEMOIMMUNOTHERAPY
The combination of cytokines with the concurrent or sequential administration of chemotherapeutic drugs has shown interesting results in metastatic disease and, on this basis, some studies have been conducted in the adjuvant setting with the same approach [94].
In a prospective randomized trial published in 2005, the German Cooperative Renal Carcinoma Chemoimmunotherapy Group tested the combination of IL-2, IFN-α2a and 5-fluorouracil versus observation in the adjuvant treatment of 203 patients at high risk of relapse after nephrectomy. At a median follow-up of 4.3 years, OS was significantly lower in the treated group compared to control group (p = 0.028). Furthermore, the median survival without relapse was 2.75 years in the treated and 4.25 years in the control group. Therefore, this treatment had no advantage, indeed the therapy was detrimental, with an inferior OS in the adjuvant treatment arm [90].

Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 127
A similar Phase III randomized trial was very recently performed by the European Organization for Research and Treatment of Cancer (EORTC, protocol 30955): in this study chemoimmunotherapy was reconsidered in the adjuvant setting for RCC, with a regimen based on IL-2, IFN-and 5-fluorouracil versus observation, in patients with high risk of relapse after surgical treatment. Finally, 309 patients were randomized, with 35% of discontinuation of therapy due to toxicity, with the suggestion of a persistent deficit in fatigue and physical function and a 3 years DFS of 50% in controls versus 61% in the treatment arm (HR = 0.84, 95% C.I. 0.63-1.12). The OS at 5-years was 63% among controls and 70% in treated patients (HR = 0.86, 95% C.I. 0.60-1.22). These final results, not yet published, but presented at the 2011 ASCO Annual Meeting, led to discourage the use of chemoimmunotherapy after radical tumor nephrectomy, reporting significant toxicity with this regimen without any statistically significant benefit for the adjuvant treatment in terms of DFS or OS [104].
8. HORMONAL THERAPY
Only a multicenter Italian Phase III trial has been published more than 20 years ago studying the adjuvant medroxyprogesterone acetate (MPA) three times a week for one year, following radical nephrectomy for category M0 renal cancer [105]. The rationale is due to the ability of MPA to block glucocorticoid receptors on some RCC cells and to produce responses in some patients [106]. In the cited study, 136 patients were randomized to receive MPA 500 mg orally three times per week versus observation; 59 patients had a T1-T2 cancer and the remaining 62, T3 or more advanced; patients with lymph node involvement were included. At a median follow-up of 3 years, 26% of patients in treatment arm showed recurrence, compared with 24% of patients in the control arm. The investigators noted that recurrence was more common in tumors without estrogen receptors. The treatment was associated with significant systemic toxicities without any benefit, hence this strategy was utterly abandoned since then [105].
9. TARGETED THERAPY
In recent years, RCC became from a condition of "orphan disease" because of limited treatment options available [107], to a model of development in vivo for new

128 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
drugs. The cause of this transformation was the discovery of the strong angiogenic pattern linked to the abnormal gene responsible for von Hippel-Lindau (VHL) syndrome in 65-75% of cases of sporadic disease [108]. The altered function of the VHL gene leads, in fact, to an intracellular accumulation of hypoxia inducible factor-1α (HIF-1α), which activates the transcription of a large number of genes coding for growth factors such as platelet derived growth factor alpha (PDGF-α), erythropoietin, transforming growth factor alpha (TGF-α) and, in particular, VEGF, probably the most important angiogenic growth factor strongly implicated in the pathogenesis and progression of RCC [109]. The fact that some studies show the alterations of the VHL gene as an early event in renal lesions of patients with VHL syndrome, and the fact that in the vast majority of sporadic clear cell renal carcinoma VHL gene is mutated and/or contains deletions and/or promoter hypermethylation (resulting in silencing of VHL protein expression) [110], provide a theoretical biologic rationale for the use of antiangiogenic agents in the adjuvant setting [111].
At present, to our knowledge, there are no prospective data that can confer to the status of VHL gene a predictive value for response to tyrosine kinase inhibitors (TKI) treatment in the metastatic disease, nor even in adjuvant setting.
The inhibition of angiogenesis is a promising therapeutic strategy in most solid tumors, but appears to be particularly attractive in RCC, for which, at present, three classes of drugs with antiangiogenic activity have been extensively studied: circulating VEGF inhibitors (bevacizumab) [112], multi-targeted receptor TKIs of VEGFR (sunitinib, sorafenib, pazopanib and axitinib) and inhibitors of mammalian target of rapamycin (mTOR), targets related to protein synthesis and, once again, to angiogenesis (temsirolimus and everolimus). Given the approval of sorafenib [113], sunitinib [13], of the combination of bevacizumab with IFN-α [114], of temsirolimus [115], everolimus [116], and more recently of pazopanib [117] and axitinib [118], one can now envisage a much broader future for metastatic RCC patients.
The next logical step would be to have them tested as adjuvant therapies, and studies are currently being performed to assess this possibility.
On the other hand, a potential negative effect by the use of anti-VEGF therapy in the adjuvant setting has been suggested, including the alteration of the host
Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 129
microenvironment that may facilitate the development of metastases [119]. Furthermore, preclinical studies demonstrated that while TKIs reduce primary tumor growth, they can also promote tumor invasiveness and metastasis [120, 121]. For this reason, targeted agents in the adjuvant setting should be only administered in the context of a clinical trial. No chapter has been published so far with the new targeted drugs, but studies are under way with sorafenib, sunitinib, everolimus and pazopanib (see the next paragraph).
10. ONGOING ADJUVANT TRIALS
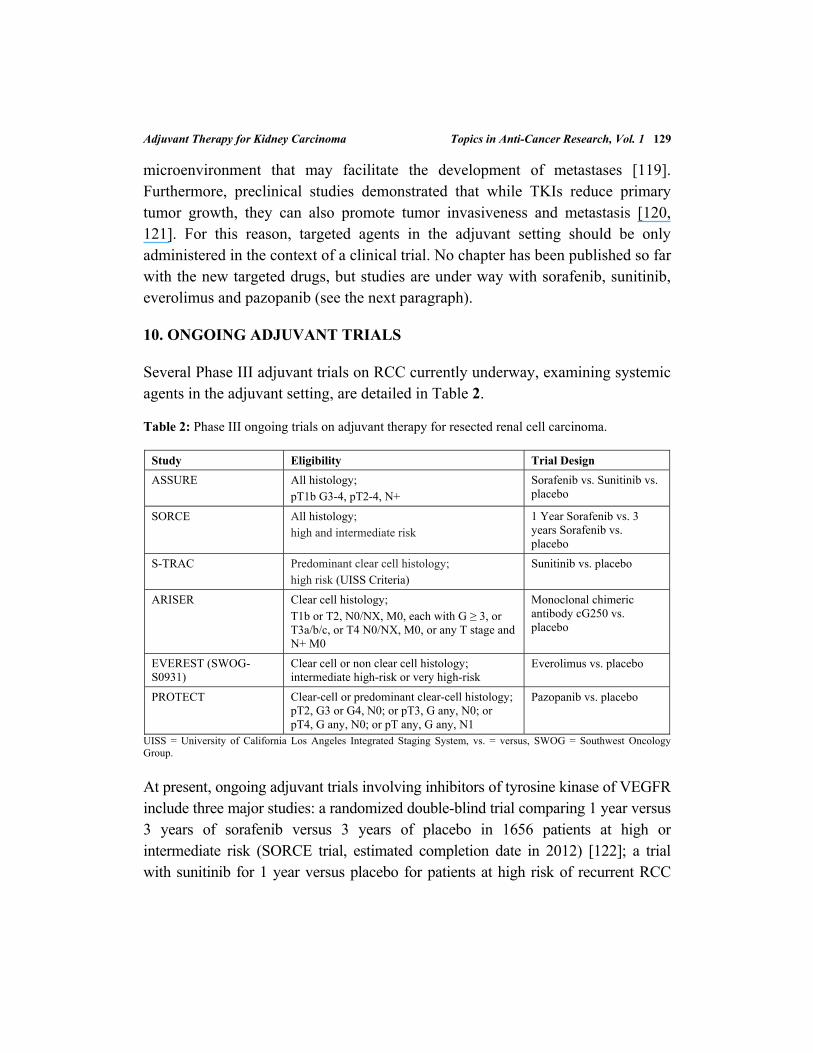
Several Phase III adjuvant trials on RCC currently underway, examining systemic agents in the adjuvant setting, are detailed in Table 2.
Table 2: Phase III ongoing trials on adjuvant therapy for resected renal cell carcinoma.
Study Eligibility Trial Design
ASSURE All histology; pT1b G3-4, pT2-4, N+
Sorafenib vs. Sunitinib vs. placebo
SORCE All histology; high and intermediate risk
1 Year Sorafenib vs. 3 years Sorafenib vs. placebo
S-TRAC Predominant clear cell histology; high risk (UISS Criteria)
Sunitinib vs. placebo
ARISER Clear cell histology; T1b or T2, N0/NX, M0, each with G ≥ 3, or T3a/b/c, or T4 N0/NX, M0, or any T stage and N+ M0
Monoclonal chimeric antibody cG250 vs. placebo
EVEREST (SWOG-S0931)
Clear cell or non clear cell histology; intermediate high-risk or very high-risk
Everolimus vs. placebo
PROTECT Clear-cell or predominant clear-cell histology; pT2, G3 or G4, N0; or pT3, G any, N0; or pT4, G any, N0; or pT any, G any, N1
Pazopanib vs. placebo
UISS = University of California Los Angeles Integrated Staging System, vs. = versus, SWOG = Southwest Oncology Group.
At present, ongoing adjuvant trials involving inhibitors of tyrosine kinase of VEGFR include three major studies: a randomized double-blind trial comparing 1 year versus 3 years of sorafenib versus 3 years of placebo in 1656 patients at high or intermediate risk (SORCE trial, estimated completion date in 2012) [122]; a trial with sunitinib for 1 year versus placebo for patients at high risk of recurrent RCC
130 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
after complete resection (S-TRAC, estimated completion in 2015) [123]; a comparison study, called ASSURE trial, with the purpose of establishing how well sunitinib works as compared to sorafenib or placebo in more than 1900 completely resected RCC patients (estimated completion date in April 2016) [124].
About targeted drugs, other two Phase III ongoing clinical trials should be considered. One is the EVEREST study, performed by the Southwest Oncology Group (SWOG-S0931), which is comparing 1-year everolimus versus placebo in high and very high-risk groups, with RFS as primary endpoint, OS and translational studies as secondary endpoints (estimated completion in 2016) [125, 126]. Another study worthy to mention is the PROTECT trial, a randomized, double blind, Phase III study evaluating whether pazopanib compared with placebo can prevent or delay recurrence of RCC in patients with moderately high or high risk of recurrence after surgery; the primary endpoint is represented by DFS, the secondary outcome measures are OS, DFS rates at yearly time points, safety and health outcome (estimated completion date in 2017) [127, 128].
Finally, a currently ongoing clinical trial involves the use of a monoclonal antibody against G250, a transmembrane protein associated with RCC, which is identical to CAIX [129]. The monoclonal immunoglobulin G1 cG250 (WX-G250, Rencarex®, Wilex Pharmaceuticals, Munich, Germany) is an intravenously administered antibody that binds to CAIX on clear cell RCC and may recruit effector cells or activate complement to result in cell death [130]. In 2004, an international randomized Phase III trial, called ARISER (Adjuvant Rencarex Immunotherapy trial to Study Efficacy in non metastatic RCC), opened to accrual to evaluate cG250 versus placebo after nephrectomy in patients with high-risk non-metastatic clear cell RCC. The accrual, at present closed, reached a total of 864 patients [130-132].
It goes without saying that the results of all these trials are eagerly awaited.
11. CURRENT & FUTURE DEVELOPMENTS
In spite of major advances in the treatment of metastatic RCC, with the setting of new standards and the improvement of OS to reach over 17 months [133], to date, there is no adjuvant treatment approved after radical resection for RCC. Among all the systemic therapies tested by clinical trials, only an individual prepared autologous
Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 131
vaccine has achieved some benefit in the adjuvant setting [84], besides a certain benefit obtained with low doses of IL-2 and IFN-α in subgroups of patients at low risk [91].
Attempts have been made spanning a period of more than 30 years without other advances in this field. Unfortunately these few data, although significant, require further validation and still have not changed the standard after radical nephrectomy, since the actual no feasibility of autologous vaccines or other adjuvant approaches outside of research protocols in highly specialized centers. Current knowledge on the issue shows that in the clinical practice, standard care in completely resected cases of RCC is represented by follow up only, without adding any further treatment. The enrollment in randomized clinical trials should be encouraged and offered to all the eligible patients.
The hope to delay the time to relapse and to improve the survival after nephrectomy has actually been renewed with the emerging role of targeted therapies, which currently represent the spearheads of new studies on adjuvant setting in RCC. The results of these new trials are awaited with great enthusiasm, hoping that the hurdle overcame by metastatic disease studies will also be achieved by the adjuvant ones.
Moreover, on the basis of these optimistic perspectives, it is important to better define the prognostic factors which might predict the risk of relapse, in order to improve the selection of patients which should benefit from an adjuvant treatment, tailoring future efforts towards this direction.
ACKNOWLEDGEMENT
Declared none.
CONFLICT OF INTEREST
The authors confirm that this chapter content has no conflict of interest.
DISCLOSURE
The chapter submitted for Patent eBook Series “Topics in Anti-Cancer Research”, Volume 1, is an update of our article "Renal Cell Cancer: State of the Art in
132 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
Adjuvant Therapy", Volume 5, Number 3, November Issue 2010, published in the journal Recent Patents on Anti-Cancer Drug Discovery Page 242 to 250 with modified title, additional text and references.
REFERENCES
[1] Gupta K, Miller JD, Li JZ, Russell MW, Charbonneau C. Epidemiologic and socioeconomic burden of metastatic renal cell carcinoma (mRCC): A literature review. Cancer Treat Rev 2008; 34: 193-205.
[2] Jemal A, Siegel R, Ward E. Cancer statistics, 2008. CA Cancer J Clin 2008; 58: 71-96. [3] Theis RP, Dolwick Grieb SM, Burr D, Siddiqui T, Asal NR. Smoking, environmental tobacco
smoke, and risk of renal cell cancer: A population-based case-control study. BMC Cancer 2008; 8: 387.
[4] Brennan P, van der Hel O, Moore LE. Tobacco smoking, body mass index, hypertension, and kidney cancer risk in central and eastern Europe. Br J Cancer 2008; 99: 1912-5.
[5] Chow WH, Gridley G, Fraumeni IF, Järvholm B. Obesity, hypertension, and the risk of kidney cancer in men. N Engl J Med 2000; 343: 1305-11.
[6] Benichou J, Chow WH, McLaughlin JK, Mandel JS, Fraumeni JF Jr. Population attributable risk of renal cell cancer in Minnesota. Am J Epidemiol 1998; 148: 424-30.
[7] Rosner I, Bratslavsky G, Pinto PA, Linehan WM. The clinical implications of the genetics of renal cell carcinoma. Urol Oncol 2009; 27: 131-6.
[8] McGraw-Hill Concise Dictionary of Modern Medicine. © 2002 by The McGraw-Hill Companies, Inc. 2002.
[9] Beisland C, Medby PC, Beisland HO. Renal cell carcinoma: Gender difference in incidental detection and cancer-specific survival. Scand J Urol Nephrol 2002; 36: 414-8.
[10] Rini BI, Campbell SC, Escudier B. Renal cell carcinoma. Lancet 2009; 373: 1119-32. [11] Moussa, O., Watson, D.K., Halushka, P.V. Methods for the diagnosis of genitourinary cancer.
US20090136972 (2009). [12] AJCC Cancer Staging Handbook. From the AJCC Cancer Staging Manual. Edge SB, Byrd DR,
Compton CC, Fritz AG, Greene FL, Trotti A (Eds.) 6th Printing, 2010; XIV: p 730 p. 130 illus. [13] Motzer RJ, Hutson TE, Tomczak P, Michaelson MD, Bukowski RM, Rixe O, et al. Sunitinib
versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med 2007; 356: 115-24. [14] Motzer RJ, Bander NH, Nanus DM. Renal-cell carcinoma. N Engl J Med 1996; 335: 865-75. [15] Lam JS, Shvarts O, Leppert JT, Figlin RA, Belldegrun AS. Renal cell carcinoma 2005: New
frontiers in staging, prognostication and targeted molecular therapy. J Urol 2005; 173: 1853-62. [16] Frank I, Blute ML, Cheville JC, Lohse CM, Weaver AL, Leibovich BC, et al. A multifactorial
postoperative surveillance model for patients with surgically treated clear cell renal cell carcinoma. J Urol 2003; 170: 2225-32.
[17] Chowdhury S, Larkin JM, Gore ME. Recent advances in the treatment of renal cell carcinoma and the role of targeted therapies. Eur J Cancer 2008; 44: 2152-61.
[18] Butler BP, Novick AC, Miller DP, Campbell SA, Licht MR. Management of small unilateral renal cell carcinomas: Radical versus nephron-sparing surgery. Urology 1995; 45: 34-40.
[19] Lerner SE, Hawkins CA, Blute ML, Grabner A, Wollan PC, Eickholt JT, et al. Disease outcome in patients with low stage renal cell carcinoma treated with nephron sparing or radical surgery. J Urol 1996; 155: 1868-73.
Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 133
[20] Hollingsworth JM, Miller DC, Dunn RL, Montgomery JS, Roberts WW, Hafez KS, et al. Surgical management of low-stage renal cell carcinoma: Technology does not supersede biology. Urology 2006; 67:1175-80. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16765177 (Accessed on: February 27, 2012).
[21] Leibovich BC, Blute ML, Cheville JC, Lohse CM, Weaver AL, Zincke H. Nephron sparing surgery for appropriately selected renal cell carcinoma between 4 and 7 cm results in outcome similar to radical nephrectomy. J Urol 2004; 171: 1066-70.
[22] Shuch B, Lam JS, Belldegrun AS. Open partial nephrectomy for the treatment of renal cell carcinoma. Curr Urol Rep 2006; 7: 31-8.
[23] Chen DY, Uzzo RG. Optimal management of localized renal cell carcinoma: Surgery, ablation, or active surveillance. J Natl Compr Canc Netw 2009; 7: 635-42.
[24] Marszalek M, Meixl H, Polajnar M, Rauchenwald M, Jeschke K, Madersbacher S. Laparoscopic and open partial nephrectomy: A matched-pair comparison of 200 patients. Eur Urol 2009; 181: 170-6.
[25] Breda A, Finelli A, Janetschek G, Porpiglia F, Montorsi F. Complications of laparoscopic surgery for renal masses: Prevention, management, and comparison with the open experience. Eur Urol 2009; 55: 836-50.
[26] Garg S, Batura D, Biyani CS, Gill I. Laparoscopic surgery for cancers of the kidney: Long-term oncological efficacy. BJU Int 2008; 102: 1498-501.
[27] Gill IS, Remer EM, Hasan WA, Strzempkowski B, Spaliviero M, Steinberg AP, et al. Renal cryoablation: Outcome at 3 years. J Urol 2005; 173: 1903-7.
[28] Hafron J, Kaouk JH. Ablative techniques for the management of kidney cancer. Nat Clin Pract Urol 2007; 4: 261-9.
[29] Kunkle DA, Egleston BL, Uzzo RG. Excise, ablate or observe: The small renal mass dilemma. A meta-analysis and review. J Urol 2008; 179: 1227-33.
[30] Gettman MT, Blute ML, Spotts B, Bryant SC, Zincke H. Pathologic staging of renal cell carcinoma: Significance of tumor classification with the 1997 TNM staging system. Cancer 2001; 91: 354-61.
[31] Delahunt B, Eble JN. History of the development of the classification of renal cell neoplasia. Clin Lab Med 2005; 25: 231-46.
[32] Frank I, Blute ML, Leibovich BC, Cheville JC, Lohse CM, Zincke H. Independent validation of the 2002 American Joint Committee on cancer primary tumor classification for renal cell carcinoma using a large, single institution cohort. J Urol 2005; 173: 1889-92.
[33] Fuhrman SA, Lasky LC, Limas C. Prognostic significance of morphologic parameters in renal cell carcinoma. Am J Surg Path 1982; 6: 655-63.
[34] Kontak JA, Campbell SC. Prognostic factors in renal cell carcinoma. Urol Clin North Am 2003; 30: 467-80.
[35] Patard JJ, Leray E, Rioux-Leclercq N, Cindolo L, Ficarra V, Zisman A, et al. Prognostic value of histologic subtypes in renal cell carcinoma: A multicenter experience. J Clin Oncol 2005; 23: 2763-71.
[36] Dall'Oglio MF, Antunes AA, Sarkis AS, Crippa A, Leite KR, Lucon AM, et al. Microvascular tumor invasion in renal cell carcinoma: The most important prognostic factor. BJU Int 2007; 100: 552-5.
[37] Cheville JC, Lohse CM, Zincke H, Weaver AL, Blute ML. Comparisons of outcome and prognostic features among histologic subtypes of renal cell carcinoma. Am J Surg Pathol 2003; 27: 612-24.
134 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
[38] Pantuck AJ, Zeng G, Belldegrun AS, Figlin RA. Pathobiology, prognosis, and targeted therapy for renal cell carcinoma: Exploiting the hypoxia-induced pathway. Clin Cancer Res 2003; 9: 4641-52.
[39] Leppert JT, Lam JS, Pantuck AJ, Figlin RA, Belldegrun AS. Carbonic anhydrase IX and the future of molecular markers in renal cell carcinoma. BJU Int 2005; 96: 281-5.
[40] Bui MH, Seligson D, Han KR, Pantuck AJ, Dorey FJ, Huang Y, et al. Carbonic anhydrase IX is an independent predictor of survival in advanced renal clear cell carcinoma: Implications for prognosis and therapy. Clin Cancer Res 2003; 9: 802-11.
[41] Soyupak, B., Erdogan, S. MN/CA IX/CA9 and renal cancer prognosis. US20090191557 (2009). [42] Patard J, Fergelot P, Karakiewicz PI, Klatte T, Trinh QD, Rioux-Leclercq N, et al. CAIX and
VHL status define two types of clear cell renal cell carcinoma: Low CAIX expression and absence of VHL gene mutation are associated with tumor aggressiveness and poor survival. Int J Cancer 2008; 123(2): 395-400.
[43] Leibovich BC, Sheinin Y, Lohse CM, Thompson RH, Cheville JC, Zavada J, et al. Carbonic anhydrase IX is not an independent predictor of outcome for patients with clear cell renal cell carcinoma. J Clin Oncol 2007; 25: 4757-64.
[44] Sandlund J, Oosterwijk E, Grankvist K, Oosterwijk-Wakka J, Ljungberg B, Rasmuson T. Prognostic impact of carbonic anhydrase IX expression in human renal cell carcinoma. BJU Int 2007; 100: 556-60.
[45] Stillebroer AB, Mulders PF, Boerman OC, Oyen WJ, Oosterwijk E. Carbonic anhydrase IX in renal cell carcinoma: Implications for prognosis, diagnosis, and therapy. Eur Urol 2010; 58(1): 75-83.
[46] Jiang, Z. Use of IMP3 as a prognostic marker for cancer. US20080242606 (2008) & US20110034398 (2011).
[47] Straten, E.P.T., Andersen, M.H. Survivin-derived peptides and use thereof. US20070148194 (2007) & JP2012082213 (2012).
[48] Blatt, L.M. Synthetic chemokine receptor ligands and methods of use thereof. US20070172446 (2007).
[49] Kwon, E.D., Cheville, J. B7-H4 expression on tumor vasculature. US20090176317 (2009). [50] Kwon, E.D., Dong, H., Frigola Baro, X., Inman, B.A. Soluble B7-H1. US20090176317 (2009). [51] Klatte T, Seligson DB, LaRochelle J, Shuch B, Said JW, Riggs SB, et al. Molecular signatures of
localized clear cell renal cell carcinoma to predict disease-free survival after nephrectomy. Cancer Epidemiol Biomarkers Prev 2009; 18: 894-900.
[52] Haab, B., Rhodes, D., Teh, B.T., Takahashi, M. Microarray gene expression profiling in clear cell renal cell carcinoma: Prognosis and drug target identification. US20060088823 (2006).
[53] Galfano A, Novara G, Iafrate M, Cavalleri S, Martignoni G, Gardiman M, et al. Mathematical models for prognostic prediction in patients with renal cell carcinoma. Urol Int 2008; 80: 113-23.
[54] Sorbellini M, Kattan MW, Snyder ME, Reuter V, Motzer R, Goetzl M, et al. A postoperative prognostic nomogram predicting recurrence for patients with conventional clear cell renal cell carcinoma. J Urol 2005; 173: 48-51.
[55] Zisman A, Pantuck AJ, Dorey F, Chao DH, Gitlitz BJ, Moldawer N, et al. Mathematical model to predict individual survival for patients with renal cell carcinoma. J Clin Oncol 2002; 20: 1368-74.
[56] Frank I, Blute ML, Cheville JC, Lohse CM, Weaver AL, Zincke H. An outcome prediction model for patients with clear cell renal cell carcinoma treated with radical nephrectomy based on tumor stage, size, grade and necrosis: The SSIGN score. J Urol 2002; 168: 2395-400.
Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 135
[57] Karakiewicz PI, Briganti A, Chun FK, Trinh QD, Perrotte P, Ficarra V, et al. Multi-institutional validation of a new renal cancer-specific survival nomogram. J Clin Oncol 2007; 25(11): 1316-22.
[58] Leibovich BC, Blute ML, Cheville JC, Lohse CM, Frank I, Kwon ED, et al. Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma: A stratification tool for prospective clinical trials. Cancer 2003; 97(7): 1663-71.
[59] Pichler M, Hutterer GC, Chromecki TF, Jesche J, Kampel-Kettner K, Rehak P, et al. External validation of the Leibovich prognosis score for nonmetastatic clear cell renal cell carcinoma at a single European center applying routine pathology J Urol 2011; 186(5): 1773-7.
[60] Pichler M, Hutterer GC, Chromecki TF, Jesche J, Groselj-Strele A, Kampel-Kettner K, et al. Prognostic Value of the leibovich prognosis score supplemented by vascular invasion for clear cell renal cell carcinoma. J Urol 2012; 187(3): 834-9.
[61] Ficarra V, Novara G, Galfano A, Brunelli M, Cavalleri S, Martignoni G, et al. The 'Stage, Size, Grade and Necrosis' score is more accurate than the University of California Los Angeles Integrated Staging System for predicting cancer-specific survival in patients with clear cell renal cell carcinoma. BJU Int 2009; 103: 165-70.
[62] Tan MH, Kanesvaran R, Li H, Tan HL, Tan PH, Wong CF, et al. Comparison of the UCLA integrated staging system and the Leibovich score in survival prediction for patients with nonmetastatic clear cell renal cell carcinoma. Urology 2010; 75(6): 1365-70.
[63] Tan MH, Li H, Choong CV, Chia KS, Toh CK, Tang T, et al. The Karakiewicz nomogram is the most useful clinical predictor for survival outcomes in patients with localized renal cell carcinoma. Cancer 2011; 117(23): 5314-24.
[64] NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Version 1. 2012. Available at: www.NCCN.org (Accessed on: February 27, 2012)
[65] Scherr AJ, Lima JP, Sasse EC, Lima CS, Sasse AD. Adjuvant therapy for locally advanced renal cell cancer: A systematic review with meta-analysis. BMC Cancer 2011; 11: 115.
[66] Finney R. The value of radiotherapy in the treatment of hypernephroma. A clinical trial. Br J Urol 1973; 45: 258-69.
[67] Kjaer M. Iversen P, Hvidt V, Bruun E, Skaarup P, Bech Hansen J, et al. A randomized trial of postoperative radiotherapy versus observation in stage II and III renal adenocarcinoma. A study by the Copenhagen Renal Cancer Study Group. Scand J Urol Nephrol 1987; 21: 285-9.
[68] Ulutin HC, Aksu G, Fayda M, Kuzhan O, Tahmaz L, Beyzadeoglu M. The value of postoperative radiotherapy in renal cell carcinoma: A single institution experience. Tumori 2006; 92: 202-6.
[69] Safwat A, Shouman T, Hamada E, El-Naggar H, Mohamed NH. Postoperative radiotherapy improves disease free but not overall survival in high risk cell carcinoma patients. J Egypt Nat Cancer Inst 2000; 12: 17-22.
[70] Makarewicz R, Zarzycka M, Kulinska G, Windorbska W. The value of postoperative radiotherapy in advanced renal cell cancer. Neoplasm 1998; 45: 380-3.
[71] Kao G, Malkowicz SB, Whittington R, D'Amico AV, Wein AJ. Locally advanced renal cell carcinoma: Low complication rate and efficacy of postnephrectomy radiation therapy with CT. Radiology 1994; 193: 725-30.
[72] Stein M, Kuten A, Halpern J, Coachman NM, Cohen Y, Robinson E. The value of postoperative irradiation in renal cell cancer. Radiother Oncol 1992; 24: 41-4.
[73] Tunio MA, Hashmi A, Rafi M. Need for a new trial to evaluate postoperative radiotherapy in renal cell carcinoma: A meta-analysis of randomized controlled trials. Ann Oncol 2010; 21: 1839-45.
136 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
[74] Aref I, Bociek RG, Salhani D. Is post-operative radiation for renal cell carcinoma justified? Radiother Oncol 1997; 43: 155-7.
[75] Asakura T, Imai A, Ohkubo-Uraoka N, Kuroda M, Iidaka Y, Uchida K, et al. Relationship between expression of drug-resistance factors and drug sensitivity in normal human renal proximal tubular epithelial cells in comparison with renal cell carcinoma. Oncol Rep 2005; 14: 601-7.
[76] Waters JS, Moss C, Pyle L, James M, Hackett S, A'hern R, et al. Phase II clinical trial of capecitabine and gemcitabine chemotherapy in patients with metastatic renal carcinoma. Br J Cancer 2004; 91: 1763-8.
[77] Stadler WM, Halabi S, Rini BI, Ernstoff MS, Davila E, Picus J, et al. A Phase II study of gemcitabine and capecitabine in metastatic renal cancer: A report of Cancer and Leukemia Group B protocol 90008. Cancer 2006; 107: 1273-9.
[78] Lilleby W, Fossa SD. Chemotherapy in metastatic renal cell cancer. World J Urol 2005; 23: 175-9.
[79] Atzpodien J, Kirchner H, Jonas U, Bergmann L, Schott H, Heynemann H, et al. Interleukin-2-and interferon Alfa-2a-based immunochemotherapy in advanced renal cell carcinoma: A prospectively randomized trial of the German Cooperative Renal Carcinoma Chemoimmunotherapy Group (DGCIN). J Clin Oncol 2004; 22: 1188-94.
[80] Atzpodien J, Kirchner H, Rebmann U, Soder M, Gertenbach U, Siebels M, et al. Interleukin-2/interferon-a2a/13-retinoic acid-based chemoimmunotherapy in advanced renal cell carcinoma: Results of a prospectively randomised trial of the German Cooperative Renal Carcinoma Chemoimmunotherapy Group (DGCIN). British J Cancer 2006; 95: 463-9.
[81] Masuda F, Nakada J, Kondo I, Furuta N. Adjuvant chemotherapy with vinblastine, adriamycin, and UFT for renal-cell carcinoma. Cancer Chemother Pharmacol 1992; 30: 477-9.
[82] Margulis V, Matin SF, Tannir N, Tamboli P, Shen Y, Lozano M, et al. Randomized trial of adjuvant thalidomide versus observation in patients with completely resected high-risk renal cell carcinoma. Urology 2009; 73: 337-41.
[83] Bleumer I, Oosterwijk E, De Mulder P, Mulders PF. Immunotherapy for renal cell carcinoma. Eur Urol 2003; 44: 65-75.
[84] Galligioni E, Quaia M, Merlo A, Carbone A, Spada A, Favaro D, et al. Adjuvant immunotherapy treatment of renal carcinoma patients with autologous tumor cells and bacillus Calmette-Guerin: Five-year results of a prospective randomized study. Cancer 1996; 77: 2560-6.
[85] Jocham D, Richter A, Hoffmann L, Iwig K, Fahlenkamp D, Zakrzewski G, et al. Adjuvant autologous renal tumor cell vaccine and risk of tumor progression in patients with renal-cell carcinoma after radical nephrectomy: Phase III, randomised controlled trial. Lancet 2004; 363: 594-9.
[86] Pizzocaro G, Piva L, Colavita M, Ferri S, Artusi R, Boracchi P, et al. Interferon adjuvant to radical nephrectomy in Robson stages II and III renal cell carcinoma: A multicentric randomized study. J Clin Oncol 2001; 19: 425-31.
[87] Hermanek P, Sigel A, Chlepas S. Combined staging and grading of renal cell carcinoma. Z Krebsforsch Klin Onkol Cancer Res Clin Oncol 1976; 87: 193-6.
[88] Clark JI, Atkins MB, Urba WJ, Creech S, Figlin RA, Dutcher JP, et al. Adjuvant high-dose bolus interleukin-2 for patients with high-risk renal cell carcinoma: A cytokine working group randomized trial. J Clin Oncol 2003; 21: 3133-40.
[89] Messing EM, Manola J, Wilding G, Propert K, Fleischmann J, Crawford ED, et al. Phase III study of interferon alfa-NL as adjuvant treatment for resectable renal cell carcinoma: An Eastern Cooperative Oncology Group/Intergroup trial. J Clin Oncol 2003; 21: 1214-22.
Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 137
[90] Atzpodien J, Schmitt E, Gertenbach U, Fornara P, Heynemann H, Maskow A, et al. Adjuvant treatment with interleukin-2-and interferon-alpha2a-based chemoimmunotherapy in renal cell carcinoma post tumor nephrectomy: Results of a prospectively randomised trial of the German Cooperative Renal Carcinoma Chemoimmunotherapy Group (DGCIN). Br J Cancer 2005; 92: 843-6.
[91] Passalacqua R, Buzio C, Buti S, Labianca R, Porta C, Boni C, et al. Adjuvant low-dose interleukin-2 (IL2) plus interferone-alpha (IFN) in operable renal cell cancer (RCC). A Phase III, randomized, multicenter, independent trial of the Italian Oncology Group for Clinical Research (GOIRC). J Clin Oncol 2007; 25: 965s, Abstract LBA5028.
[92] Wood C, Srivastava P, Bukowski R, Lacombe L, Gorelov AI, Gorelov S, et al. An adjuvant autologous therapeutic vaccine (HSPPC-96; vitespen) versus observation alone for patients at high risk of recurrence after nephrectomy for renal cell carcinoma: A multicentre, open-label, randomised Phase III trial. Lancet 2008; 372: 145-54.
[93] Hinotsu S, Kawai K, Ozono S, Tsushima T, Tokuda N, Nomata K, et al. Randomized controlled study of natural interferon α as adjuvant treatment for stage II or III renal cell carcinoma. Int J Clin Oncol 2011; DOI: 10.1007/s10147-011-0345-9.
[94] Passalacqua R, Buti S, Tomasello G, Longarini R, Brighenti M, Dalla Chiesa M. Immunotherapy options in metastatic renal cell cancer: Where we are and where we are going. Expert Rev Anticancer Ther 2006; 6: 1459-72.
[95] Wood CG. Multimodal approaches in the management of locally advanced and metastatic renal cell carcinoma: Combining surgery and systemic therapies to improve patient outcome. Clin Cancer Res 2007; 13: 697-702.
[96] Doehn C, Richter A, Theodor RA, Lehmacher W, Jocham D. An adjuvant vaccination with Reniale® prolongs survival in patients with renal cell carcinoma following radical nephrectomy: Secondary analysis of a multicenter Phase-III trial. J Urol 2007; 177: 167S.
[97] Pyrhonen S, Salminen E, Ruutu M, Lehtonen T, Nurmi M, Tammela T, et al. Prospective randomized trial of interferon alfa-2a plus vinblastine versus vinblastine alone in patients with advanced renal cell cancer. J Clin Oncol 1999; 17: 2859-67.
[98] Medical Research Council Renal Cancer Collaborators. Interferon-alpha and survival in metastatic renal carcinoma: Early results of a randomised controlled trial. Lancet 1999; 353: 14-7.
[99] Amato R. Modest effect of interferon alfa on metastatic renal-cell carcinoma. Lancet 1999; 353: 6-7.
[100] Fisher RI, Rosenberg SA, Sznol M, Parkinson DR, Fyfe G. High-dose aldesleukin in renal cell carcinoma: Long-term survival update. Cancer J Sci Am 1997; 3: S70-S2.
[101] McDermott DF, Regan MM, Clark JI, Flaherty LE, Weiss GR, Logan TF, et al. Randomized Phase III trial of high-dose interleukin-2 versus subcutaneous interleukin-2 and interferon in patients with metastatic renal cell carcinoma. J Clin Oncol 2005; 23: 133-41.
[102] Fyfe GA, Fisher RI, Rosenberg SA, Sznol M, Parkinson DR, Louie AC. Long-term response data for 255 patients with metastatic renal cell carcinoma treated with high-dose recombinant interleukin-2 therapy. J Clin Oncol 1996; 14: 2410-1.
[103] McDermott DF. The application of high-dose interleukin-2 for metastatic renal cell carcinoma. Med Oncol 2009; 26 (Suppl 1): 13-7.
[104] Aitchison M, Bray CA, Van Poppel H, Sylvester R, Graham J, Innes C, et al. Final results from an EORTC (GU Group)/NCRI randomized Phase III trial of adjuvant interleukin-2, interferon alpha, and 5-fluorouracil in patients with a high risk of relapse after nephrectomy for renal cell

138 Topics in Anti-Cancer Research, Vol. 1 Buti et al.
carcinoma (RCC). Oral Abstract Session of American Society of Clinical Oncology -11th Annual Meeting, USA (2011).
[105] Pizzocaro G, Piva L, Di Fronzo G, Giongo A, Cozzoli A, Dormia E, et al. Adjuvant medroxyprogesterone acetate to radical nephrectomy in renal cancer: 5-Years results of a prospective randomized study. J Urol 1987; 138: 1379-81.
[106] Pizzocaro G, Piva L, Salvioni R, Di Fronzo G, Ronchi E, Miodini P. Adjuvant medroxyprogesterone acetate and steroid hormone receptors in category M0 renal cell carcinoma. An interim report of a prospective randomized study. J Urol 1986; 135: 18-21.
[107] Coppin C, Porzsolt F, Awa A, Kumpf J, Coldman A, Wilt T. Immunotherapy for advanced renal cell cancer. Cochrane Database Syst Rev 2005; (1): CD001425.
[108] Patel PH, Chadalavada RS, Chaganti RS, Motzer RJ. Targeting von Hippel-Lindau pathway in renal cell carcinoma. Clin Cancer Res 2006; 12: 7215-20.
[109] Rini BI, Small EJ. Biology and clinical development of vascular endothelial growth factor-targeted therapy in renal cell carcinoma. J Clin Oncol 2005; 23: 1028-43.
[110] Sudarshan S, Linehan WM. Genetic basis of cancer of the kidney. Semin Oncol 2006; 33: 544-51.
[111] Ferrara, N., Korsisaari, N., Mass, R.D. VEGF-specific antagonists for adjuvant and neoadjuvant therapy and the treatment of early stage tumors. WO2008077077 (2008).
[112] Fyfe, G., Holmgren, E., Mass, R.D., Novotny, W. Treatment with anti-VEGF antibodies. US20090191215 (2009).
[113] Escudier B, Eisen T, Stadler WM, Szczylik C, Szczylik C, Oudard S, et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med 2007; 356: 125-34.
[114] Escudier B, Pluzanska A, Koralewski P, Ravaud A, Bracarda S, Szczylik C, et al. Bevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carcinoma: A randomised, double-blind Phase III trial. Lancet 2007; 370: 2103-11.
[115] Hudes G, Carducci M, Tomczak P, Dutcher J, Figlin R, Kapoor A, et al. Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. N Engl J Med 2007; 356: 2271-81.
[116] Motzer RJ, Hutson TE, Tomczak P, Hutson TE, Porta C, Bracarda S, et al. Efficacy of everolimus in advanced renal cell carcinoma: A double-blind, randomised, placebo-controlled Phase III trial. Lancet 2008; 372: 449-56.
[117] Sternberg CN, Davis ID, Mardiak J, Szczylik C, Lee E, Waqstaff J, et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: Results of a randomized Phase III trial. J Clin Oncol 2010; 28: 1061-68.
[118] Rini BI, Escudier B, Tomczak P, Kaprin A, Szczylik C, Huston TE, et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): A randomised Phase 3 trial. Lancet 2011; 378(9807): 1931-9.
[119] Plimack ER, Tannir N, Lin E, Bekele BN, Jonasch E. Patterns of disease progression in metastatic renal cell carcinoma patients treated with antivascular agents and interferon: Impact of therapy on recurrence patterns and outcome measures. Cancer 2009; 115: 1859-66.
[120] Ebos JM, Lee CR, Cruz-Munoz W, Bjarnason GA, Christensen JG, Kerbel RS. Accelerated metastasis after short-term treatment with a potent inhibitor of tumorangiogenesis. Cancer Cell 2009; 15: 232-9.
[121] Paez-Ribes M, Allen E, Hudock J, Takeda T, Okuyama H, Viñals F, et al. Antiangiogenic therapy elicits malignant progression of tumors to increased local invasion and distant metastasis. Cancer Cell 2009; 15: 220-31.
[122] Sorafenib in Treating Patients at Risk of Relapse After Undergoing Surgery to Remove Kidney Cancer. Available at: www.clinicaltrials.gov: NCT00492258. (Accessed on: February 27, 2012).
Adjuvant Therapy for Kidney Carcinoma Topics in Anti-Cancer Research, Vol. 1 139
[123] A Clinical Trial Comparing Efficacy and Safety Of Sunitinib Versus Placebo For The Treatment of Patients at High Risk of Recurrent Renal Cell Cancer (S-TRAC). Available at: www.clinicaltrials.gov: NCT00375674. (Accessed on: February 27, 2012).
[124] Sunitinib or Sorafenib in Treating Patients with Kidney Cancer That Was Removed By Surgery. Available at: www.clinicaltrials.gov: NCT00326898. (Accessed on: February 27, 2012).
[125] Everolimus in Treating Patients with Kidney Cancer Who Have Undergone Surgery. Available at: www.clinicaltrials.gov: NCT01120249. (Accessed on: February 27, 2012).
[126] Homicsko K and Berthold DR. Neoadjuvant and adjuvant strategies in renal cell carcinoma: More questions than answers. Anti-Cancer Drugs 2011; 22 (suppl 1): S4-S8.
[127] A Study to Evaluate Pazopanib as an Adjuvant Treatment for Localized Renal Cell Carcinoma (RCC) (PROTECT). Available at: www.clinicaltrials.gov: NCT01235962. (Accessed on: February 27, 2012).
[128] Rexer H. Adjuvante AUO-Studie beim Nierenzellkarzinom nach (Teil) Nephrektomie. Randomisierte, doppelblinde, placebokontrollierte Phase-III-studie (PROTECT -AN 30/10) zur Untersuchung der Wirksamkeit und Sicherheit von Pazopanib als adjuvante therapie bei Patienten mit lokalisiertem oder lokal fortgeschrittenem Nierenzellkarzinom nach Nephrektomie. Urologe 2011; 50: 489-91.
[129] Liao SY, Aurelio ON, Jan K, Zavada J, Stanbridge EJ. Identification of the MN/CA9 protein as a reliable diagnostic biomarker of clear cell carcinoma of the kidney. Cancer Res 1997; 57: 2827-31.
[130] Lam JS, Leppert JT, Belldegrun AS, Figlin RA. Adjuvant therapy of renal cell carcinoma: Patient selection and therapeutic options. BJU Int 2005; 96: 483-8.
[131] Sokoloff MH, Daneshmand S, Ryan CW. Current clinical trials in renal cell carcinoma. Urol Oncol 2005; 23: 289-92.
[132] Monoclonal Antibody Therapy (Rencarex®) in Treating Patients Who Have Undergone Surgery for Non-metastatic Kidney Cancer. Available at: www.clinicaltrials.gov: NCT00087022. (Accessed on: February 27, 2012).
[133] Reeves DJ, Liu CY. Treatment of metastatic renal cell carcinoma. Cancer Chemother Pharmacol 2009; 64: 11-25.





























