Embed Size (px)
Citation preview

Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/258859118
AkhtarS,AlkatanH,KiratO,AlmubradT.”UltrastructuralandThree-DimentionalStudyofPost-LasikEctasiaCornea.Micros.Res.Tech.00:000-0002013.
ARTICLEinMICROSCOPYRESEARCHANDTECHNIQUE·JANUARY2013
ImpactFactor:1.15
READS
19
4AUTHORS,INCLUDING:
HindManaaAlkatan
KingSaudUniversity
102PUBLICATIONS191CITATIONS
SEEPROFILE
OmarKirat
KingKhaledEyeSpecialistHospital
14PUBLICATIONS12CITATIONS
SEEPROFILE
Allin-textreferencesunderlinedinbluearelinkedtopublicationsonResearchGate,
lettingyouaccessandreadthemimmediately.
Availablefrom:HindManaaAlkatan
Retrievedon:05February2016

Ultrastructural and Three-Dimensional Study of Post-LASIKEctasia CorneaSAEED AKHTAR,1* HIND ALKATAN,2 OMAR KIRAT,2 AND TURKI ALMUBRAD1
1Department of Optometry, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia2King Khalid Eye Specialist Hospital, Riyadh, Saudi Arabia
KEY WORDS laser in situ keratomileusis; LASIK; collagen fibrils; proteoglycans
ABSTRACT INTRODUCTION: Post-laser in situ keratomileusis (LASIK) corneal ectasia is aserious late postoperative complication. Here, we report the ultrastructural features of the post-LASIK cornea of two patients. METHODS: Two normal corneas (age 24 and 37 years old) andtwo post-LASIK ectaic corneas from two patients (A and B) were studied. The “patient A” (age 27years) underwent penetrating keratoplasty and “patient B” (age 31 years) underwent deep-anterior lamellar keratoplasty. The excised corneas were processed for light and electron micros-copy. A total of 120 images for three-dimensional (3D) reconstruction were taken by using thesoftware “Recorder” and using a bottom mounted camera “Quemesa” attached to a JOEL 1400transmission electron microscope. The 3D images were constructed using “Visual Kai” software.RESULTS: In the post-LASIK cornea, the hemidesmosomes, the basement membrane, andBowman”s layer were abnormal. The stromal lamellae were thin and disorganized. The collagenfibrils (CFs) diameter and interfibrillar spacing had decreased. Aggregated microfibrils werepresent in the Bowman’s layer and all parts of the stroma. A large number of microfilamentswere present at the detachment end of the flap and residual stroma. The 3D images showed thepresence of collagen microfibrils and proteoglycans (PGs) within the CF of the normal and post-LASIK cornea. The collagen microfibrils and PGs within the CFs had degenerated in the post-LASIK cornea. CONCLUSION: Collagen microfibrils and PGs within the CFs were degenerated,leading to the degeneration of CFs, followed by the disorganization of lamellae in post-LASIKcornea. The CFs diameter and interfibrillar spacing decreased. Microsc. Res. Tech. 00:000–000,2013. VC 2013 Wiley Periodicals, Inc.
INTRODUCTION
Laser in situ keratomileusis (LASIK) is widely usedto correct corneal refractive error. Corneal ectasia (alsocalled "kerectasia" or "keratectasia") after laser-assisted in situ keratomileusis (LASIK) surgery is arare but devastating complication that was firstdescribed by Seiler et al. (1998) Keratectasia is definedas a progressive steepening of the corneal curvature,with or without associated central and paracentral cor-neal thinning. Clinically, it presents as the initialappearance of low myopia that progresses over time tohigh myopia and irregular astigmatism, resulting inloss of uncorrected distance visual acuity (UDVA) andcorrected distance visual acuity (CDVA) (Randlemanet al., 2003; Tunc et al., 2011). Two major risk factorsare thought to be responsible for this complication:operating on corneas with preexisting disposition tocorneal ectasia, and removing too much corneal tissue(Flanagan and Binder, 2003). After LASIK, the corneais structurally weakened not only by the laser centralstromal ablation (depending on the attempted correc-tion) but also by the creation of the flap itself (Kymio-nis et al., 2006; Tunc et al., 2011).
Park and Kim et al. (1999) reported that the parallelarrangement of collagen fibril (CF) lamellae in the cor-neal stroma was not disturbed in the post-LASIK rab-bit cornea. There was also no regeneration of collagen
between the corneal flap and the ablated stromal bedexcept in the wound margin in the post-LASIK rabbitcornea. There was some regeneration of stromal tissuein the wound margin and small increases in the stain-ing of dermatan sulfate within the stroma adjacent tothe interface of the microkeratome incision in the post-LASIK ectatic cornea. Increased staining of hepatocytegrowth factor was found on keratocytes/fibroblasts atthe flap margin in both corneas (Philipp et al., 2003).
Previous authors have described the histopathologyand ultrastructural changes in the epithelium, Bow-man’s layer, and stroma of the post-LASIK ectasiahuman cornea (Anderson et al., 2002; Dawson et al.,2008; Kim et al., 2006; Spirn et al., 2005). Meghparaet al. (2008) reported that there was thinning of theCFs and a decrease in the interfibrillar spacing in thepost-LASIK ectatic cornea. Recently, Abahussin et al.
*Correspondence to: Saeed Akhtar, Department of Optometry, College ofApplied Medical Sciences, King Saud University, Riyadh, Saudi Arabia. E-mailaddress: [email protected]
Received 19 July 2013; accepted in revised form 28 October 2013
REVIEW EDITOR: Prof. Alberto Diaspro
Contract grant sponsors: The authors would like to extend their sincere appre-ciation to the Deanship of Scientific Research at King Saud University for itsfunding of this research through the Research Project no ‘RGP-VPP-219’.
DOI 10.1002/jemt.22316Published online 00 Month 2013 in Wiley Online Library (wileyonlinelibrary.com).
VVC 2013 WILEY PERIODICALS, INC.
MICROSCOPY RESEARCH AND TECHNIQUE 00:00–00 (2013)

(2013) carried out a scanning electron microscopystudy of a cornea 5 years after LASIK surgery. Theauthors observed the flap-bed interface and a largegap at the flap margin. There was lack of connectionbetween lamellae in the interface region.
In this study, we describe the ultrastructural fea-tures of CFs and proteoglycans (PGs) of two humanpost-LASIK ectatic corneas. It is the first time we havedescribed the degeneration of collagen microfibrilswithin the CFs in post-LASIK cornea by using three-dimensional (3D) imaging with electron microscopy.
MATERIALS AND METHODSEthic Statement
Tissue procurement and use was in accordance withthe Declaration of Helsinki and local regulations. Ithas been ethically approved by the Local Ethical Com-mittee; King Saud University, Saudi Arabia; and KingKhalid Eye Specialist Hospital, Riyadh, Saudi Arabia.
Patient DetailsPatient A. A 27-year-old Saudi patient had LASIK
surgery in both eyes. He was diagnosed with post-LASIK ectasia, 7 years following LASIK surgery. HisVisual Acuity in the right eye was 4–5/200 and in theleft Eye was 4–5/200, improved with pinhole to 20/300.Refraction in the right eye was 27.50 3 60 (20/40) andleft eye 21 25.00 3 (20/60). He underwent penetratingkeratoplasty in the right eye.
Patient B. A 33-year-old patient had LASIK sur-gery in both eyes. He developed corneal ectasia in theright eye, 6 years following LASIK surgery. His uncor-
rected visual acuity in the right eye was 10/200 and inthe left eye was 20/60, with corneal steepening andthinning. Refraction in the right eye was 212.2524.00 3 85 (20/60) and in the left eye 10.5 23.75 3140 (20/20). He underwent deep-anterior lamellarkeratoplasty in the right eye.
The cornea was processed for light and electronmicroscopy. To compare the data obtained from post-LASIK cornea specimens of two normal corneas (age24 and 37year) were also processed for electron micros-copy. The normal corneas were obtained from acadaver. The death was caused by an accident. The cor-nea was removed 10 h after death and fixed within 30min.
Light Microscopy
Half of the corneal buttons were fixed in 10% forma-lin. The formalin-fixed specimens were processed bydehydration through a graded series of alcohol solu-tions, cleared with xylene solution, infiltrated withparaffin, and embedded into a paraffin block for sec-tioning. Sections of 5-mm thick were cut and stainedwith hematoxylin–eosin (H&E) or periodic acid-Schiff(PAS) stains according to routine protocols.
Electron Microscopy
Each half of the button was then divided into twoquarters. To study the CF diameter, the first quarterwas further divided into 1 mm2 pieces and fixed infreshly prepared 4% paraformaldehyde (PFA) in 0.1 Mphosphate for 2 h at 4�C within 30 min of removal. Tis-sues were washed three times (15 min) in 0.1 M
Fig. 1. Light micrograph of post-LASIK cornea (stained with H&Eand PAS); (A) Part of the post-LASIK cornea showing the detachmentof the flap from the stromal bed (stained with H&E); (B) Part of thepost-LASIK cornea showing thick epithelium, Bowman’s layer, andkeratocytes (stained with PAS); (C) Part of the post-LASIK cornea
showing the detachment of the Bowman’s layer from the epithelium(stained with PAS). An, anterior end of stromal bed; BW, Bowman’slayer; E, epithelium; F, flap; KR, keratocyte; Po, posterior end of flap;S, stromal bed.
2 S. AKHTAR ET AL.
Microscopy Research and Technique

phosphate-buffered saline and dehydrated in 30, 50,70, 90, and 100% ethanol (4�C) for 1 h in each case. Tis-sues were infiltrated in two 1 h changes in a mixture of100% ethanol and LR white (4�C) and three 8 hchanges of LR white (4�C). They were finally polymer-ized in LR white at 4�C for 24 h under ultraviolet light.
To study the ultrastructural features and distribu-tion of PG, the second quarter part was further dividedinto 1 mm2 pieces and fixed in 2.5% glutaraldehydecontaining 0.05% cuprolinic blue (BDH Ltd, Dorset)using a critical electrolyte concentration mode sodiumacetate 1 magnesium chloride buffer overnight atroom temperature (Scott et al., 1981) . The tissue wasthen dehydrated through a graded ethanol series (50–100%) and 100% acetone. They were infiltrated in themixture of acetone and spurr resin for 8 h. The tissueswere further infiltrated in 100% spurr resin 8 h (33)and were polymerized in Spurr resin for 8 h at 70C�.Ultrathin sections were cut from the blocks and col-lected on 200 mesh copper grids. The sections werestained with “uranyl acetate 1 lead citrate” andobserved by transmission electron microscopy Jeol1400 (Jeol Ltd, Akishima, Japan).
Three blocks from each cornea, three sections fromeach block, and three images from each section wereused for the quantitave analysis. The minimum CFdiameter and center-to-center spacing were measuredusing the Soft Imaging System (iTEM, Soft ImagingSystem GmbH, M€unster, Germany) analysis program.We chose to measure the minimum diameter of eachfibril rather than an average value to avoid errors dueto any obliqueness in fibril cross sections. The densityof the CFs was counted using the Soft Imaging System(iTEM, Soft Imaging System GmbH, M€unster, Ger-many) analysis program. The CFs were highlightedand counted automatically by the program.
All statistical analyses were performed with the Sta-tistical Package for the Social Sciences (SPSS GmbH,Munich, Germany). The distribution of data was stat-istically analyzed using the normality test. Once thedata distribution was confirmed, the data were ana-lyzed using nonparametric, Mann Whitney U-test andexpressed as mean 6 standard deviation.
The Mann Whitney U-test (SPSS) was used for sta-tistical analysis because the data were not normallydistributed.
Fig. 2. Electron micrograph of post-LASIK and normal cornea: (A)Part of the post-LASIK cornea showing basal epithelial cell contain-ing large nucleus, basement membrane, and Bowman’s layer; (B)Part of Bowman’s layer of the post-LASIK cornea showing that CFsare replaced by numerous microfibrils; (C) Part of the anterior stromaof the flap of post-LASIK cornea showing the presence of disorganized
lamellae, degenerated CFs, and numerous microfibrils; (D) Part ofthe anterior stroma of the normal cornea showing the presence ofinterlaced lamellae. BE, basal epithelial cell; BM, basement mem-brane; BW, Bowman’s layer; CF, collagen fibrils; L, lamella; MF,microfibrils; N, nucleus; arrowhead, point of interlacing.
STUDY OF POST-LASIK ECTASIA CORNEA 3
Microscopy Research and Technique

3D Imaging
3D images were taken from the 85-nm thick sectionsstained with uranyle acetate and lead citrate. The sec-tions were put in high tilt specimen retainer EM21311HTR and observed on JOEL 1400. The digitalimages were taken by using bottom mounted 11 mega-pixel CCD camera “Quemesa” and software program“Recorder”. The microscope magnification was 40,000and actual magnification on the monitor was 140,000(40,000 3 3.5) magnification. A total of 120 imageswere taken from 260 to 1 60 degree angle. The 3Dimage was reconstructed from the 120 images by usingsoftware program “Composer-364, version 3.4.2.0”(Massachusetts Institute of Technology). The 3D imagewas transferred to the software program “Visual-Kai,version 1.6.3.0” (System in Frontier, INC) to constructcoloured 3D images.
RESULTSLight Microscopy of Post-LASIK Cornea
In patient 1, the post-LASIK flap was separatedfrom the stromal bed. There was a large space betweenthe posterior end of the post-LASIK flap and the ante-rior end of the stromal bed (Fig. 1A). The epithelium of
the post-LASIK cornea was thick (Fig. 1A). It hadcolumnar basal epithelial cells that contained a largenucleus. The Bowman’s layer was thick and it wasdetached from the epithelium in some places (Figs. 1Band 1C). The Stroma was sparse containing wavylamellae and keratocyes (Fig. 1C). In patient 2, thestructure of the flap was very similar to the structureof the flap of patient 1 (not shown).
Ultrastructure of Post-LASIK Cornea
The epithelium of the post-LASIK cornea was thickand appeared normal containing normal large basalepithelial cells (Fig. 2A). The basal epithelial cellswere columnar and contained a large nucleus andother cell organelles (Fig. 2A). The basement mem-brane was thick and the hemidesmosomes had degen-erated (not shown). The Bowman’s layer was thick andin some places the CFs were replaced by numerousmicrofibrils (Fig. 2B). Below the Bowman’s layer, theanterior stroma contained disorganized and degener-ate lamellae (Fig. 2C) unlike the interlacing lamellaeof the normal cornea (Fig. 2D).
The CFs in the anterior stromal lamellae were small,widely spaced, and irregularly distributed (Fig. 3A).
Fig. 3. Electron micrograph of post-LASIK and normal cornea: (A)Part of flap of the post-LASIK cornea containing irregularly distrib-uted CF and microfibrils; (B) Part of flap of the post-LASIK corneashowing randomly running CF; (C) Part of the stromal bed of post-
LASIK cornea containing thin and parallel running lamellae; (D)Part of the middle stroma of the normal cornea containing parallelrunning lamellae. CF, collagen fibrils; L, lamella; MF, microfilaments.
4 S. AKHTAR ET AL.
Microscopy Research and Technique

The PGs were small and most of the CFs lacked theattachment of PGs (Fig. 3A). The CFs in the anteriorstroma were replaced by the aggregates of similarmicrofibrils, which were observed in the Bowman’slayer (Figs. 2B and 3A). In some parts of the anteriorstroma, the CFs were running randomly (Fig. 3B).There were numerous microfibrils present around thelongitudinally running CFs in the stromal bed. In theposterior part of the stromal bed, lamellae were runningparallel to each other (Fig. 3C). These lamellae werevery thin compared with the parallel running lamellaeof the posterior stroma of the normal cornea (Fig. 3D).The mean thickness of the post-LASIK corneal lamellae(524.45 6 167.54nm) was significantly reduced com-pared with the mean thickness of the normal corneallamellae (1499.35 6 79nm). There were large kerato-cytes containing a large nucleus in the stroma (notshown).
The posterior end of the detached flap and anteriorend of the stromal bed did not contain any CFs insteadthey contained a thick layer of microfilaments (Figs. 4Aand 4B). Below the thick layer of microfilaments, widelyspaced degenerate CFs were present (Fig. 4C). TheseCFs were partially electron dense and did not containelectron dense microparticles (Fig. 4C), which wereobserved in the CFs of the normal cornea (Fig. 4D).
Digital Imaging and CF Diameter
The diameter and interfibrillar spacing of CFs of thenormal and post-LASIK cornea were analyzed by digi-
tal imaging (Fig. 5A–5D). The digital image analysis ofCFs showed that the diameters of the normal CFswere from 20 to 30 nm which are shown with blue andyellow colour dots (Fig. 5B). In the post-LASIK stroma,the majority of the CFs have diameters from 15 to 25nm shown with green and blue colour dots (Fig. 5D).
The mean diameter of the normal CFs was24.16 6 2.3 nm and mean interfibrillar spacing was38.378 6 3.8nm. The mean diameter of the CFs of thepost-LASIK flap and stromal bed were 19.09 6 3.16 nmand 21.85 6 2.6 nm, respectively. The mean interfibril-lar spacing of the post-LASIK flap and stromal bedwas 42.09 6 9.16 nm and 38.54 6 6.2 nm, respectively.The diameters of the CF and of post-LASIK cornealflap and stromal bed were significantly (P> 0.001)reduced compared with the diameters of the normalCFs (Table 1). The interfibrillar spacing and density ofthe post-LASIK flap was significantly higher comparedwith the interfibrillar spacing and density of the CF ofthe normal cornea (Table 1). The interfibrillar spacingand density of the CFs in the post-LASIK stromal bedwas not significantly different from those in the nor-mal cornea (Table 1).
3D Imaging
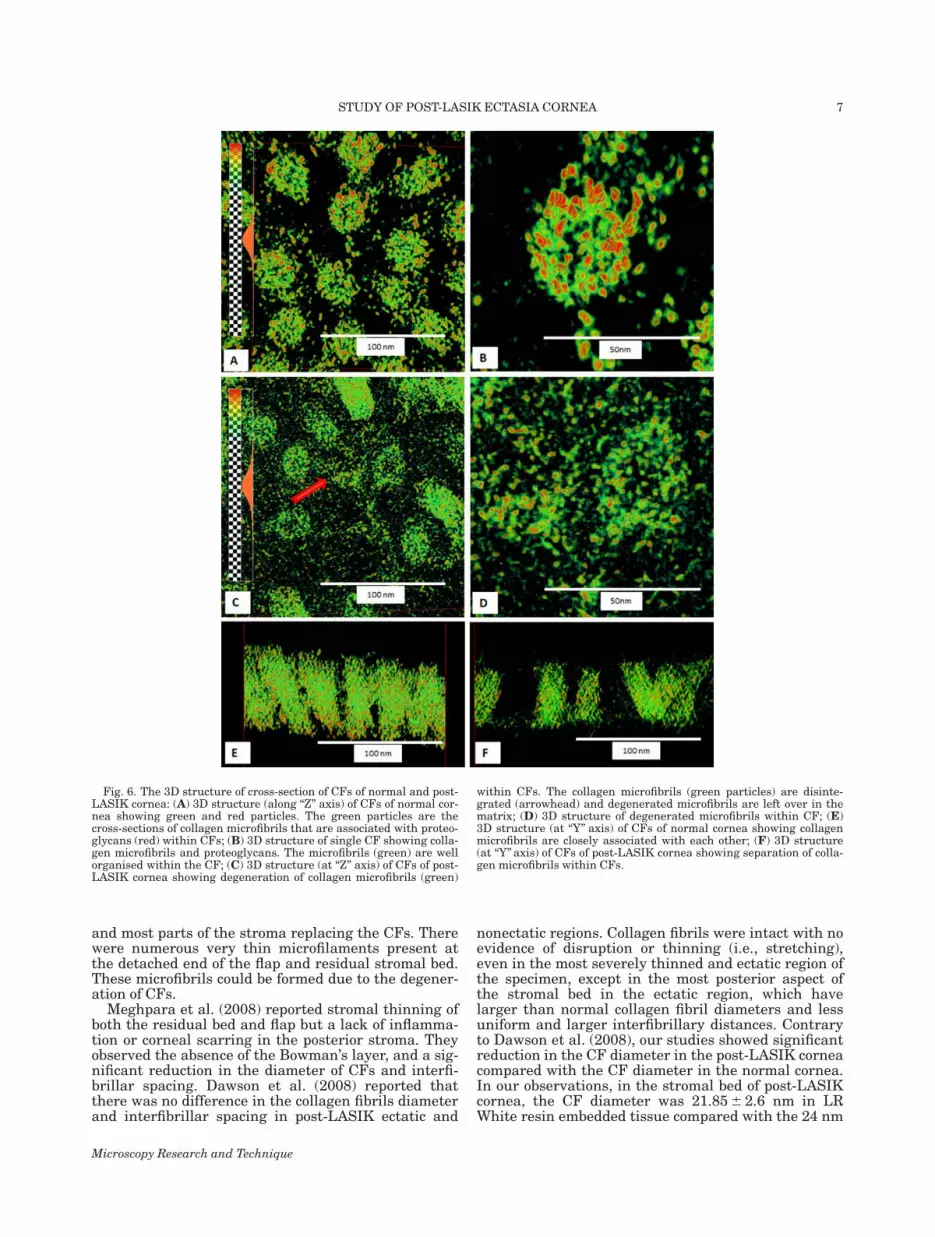
The 3D images of the cross section of the normalCFs showed the presence of collagen microfibrils(green particles) and likely PGs (red particles) withinthe CFs (Fig 6A). The collagen microfibrils (green par-ticles) were arranged in an organized pattern and
Fig. 4. Electron micrograph of post-LASIK and normal cornea; (A)Part of the posterior end of the flap containing microfilament anddegenerate CF; (B) Part of the anterior end of the stromal bed con-taining microfilament and degenerate CF; (C) Distribution of degen-
erate CF in posterior end of flap; (D) Distribution of CF in the normalcornea. CF, collagen fibrils; DCF, degenerate CF; MF, microfilaments;PG, proteoglycans; S, stromal bed.
STUDY OF POST-LASIK ECTASIA CORNEA 5
Microscopy Research and Technique

attached to the PGs (red particles) within the CFs(Fig. 6B). The 3D image of the cross-section of CFs ofthe post-LASIK ectasia cornea showed that the CFswere degenerated (Fig. 6C). The collagen microfibrils(green particles) were disintegrated and separatedfrom PGs (Fig. 6D). There were degenerated collagenmicrofibrils and PGs left over in the matrix (Fig. 6D).The 3D image of longitudinally running normal colla-gen showed that the collagen microfibrils (greenfibrils) were closely packed and the PGs (red particles)were arranged regularly (Fig. 6E). The 3D image ofthe longitudinally running CFs in the post-LASIK
ectasia cornea showed that the collagen microfibrilswere sparsely arranged (Fig. 6F)
DISCUSSION
The main constituents of the human corneal stromaare CFs and PGs. This specific uniform arrangementof CFs is essential for corneal transparency, a uniquephysical property of the cornea (Maurice, 1957). Themajority of fibril forming collagens of the adult cornealstromal ECM are types I and V (Birk et al., 1990). Thecollagen fibrils of the corneal stroma are heterotypicfibrils: both of these two collagen types are present ineach collagen fibril. Type V is involved in initiatingfibril assembly (Wenstrup et al., 2004) and regulatingfibril diameter (Birk et al., 1990). The cornea also con-tains large amounts of type VI collagen, which formsmicrofibrillar structures by lateral aggregation (Birket al., 1988).
Our study showed that the morphology of the post-LASIK ectasia cornea was different compared with themorphology of the normal cornea. The lamellar organi-sation was disturbed and CFs were of variable diame-ters in the post-LASIK ectasia cornea. There werenumerous microfibrils present in the Bowman’s layer
Fig. 5. Electron micrograph and digital images of normal and post-LASIK cornea; (A) Electron micrograph of CFs of normal cornealstroma; (B) Digital image obtained after processing the image shownin Fig. A; (C) Electron micrograph of CFs of post-LASIK corneal
stroma; (D) Digital image obtained after processing the image shownin (C), showing the presence of the CFs of different diameters. Colourcoding of CF: Red, 10–15 nm; Green, 15–20 nm; Blue, 20–25 nm; Yel-low, 24–30 nm.
TABLE 1. CF diameter, interfibrillar spacing, and density of normaland post-LASIK cornea
CorneaDiameter
(nm)Interfibrillar
spacingDensity(mm2)
Normal Cornea 24.16 6 2.3 38.378 6 3.8 485Post-LASIK
corneal flap19.09 6 3.16a 42.09 6 9.16a 288a
Post-LASIK cornealstoma bed
21.85 6 2.6a 38.54 6 6.2 492
aSignificant different from normal, P<0.001.
6 S. AKHTAR ET AL.
Microscopy Research and Technique
and most parts of the stroma replacing the CFs. Therewere numerous very thin microfilaments present atthe detached end of the flap and residual stromal bed.These microfibrils could be formed due to the degener-ation of CFs.
Meghpara et al. (2008) reported stromal thinning ofboth the residual bed and flap but a lack of inflamma-tion or corneal scarring in the posterior stroma. Theyobserved the absence of the Bowman’s layer, and a sig-nificant reduction in the diameter of CFs and interfi-brillar spacing. Dawson et al. (2008) reported thatthere was no difference in the collagen fibrils diameterand interfibrillar spacing in post-LASIK ectatic and
nonectatic regions. Collagen fibrils were intact with noevidence of disruption or thinning (i.e., stretching),even in the most severely thinned and ectatic region ofthe specimen, except in the most posterior aspect ofthe stromal bed in the ectatic region, which havelarger than normal collagen fibril diameters and lessuniform and larger interfibrillary distances. Contraryto Dawson et al. (2008), our studies showed significantreduction in the CF diameter in the post-LASIK corneacompared with the CF diameter in the normal cornea.In our observations, in the stromal bed of post-LASIKcornea, the CF diameter was 21.85 6 2.6 nm in LRWhite resin embedded tissue compared with the 24 nm
Fig. 6. The 3D structure of cross-section of CFs of normal and post-LASIK cornea: (A) 3D structure (along “Z” axis) of CFs of normal cor-nea showing green and red particles. The green particles are thecross-sections of collagen microfibrils that are associated with proteo-glycans (red) within CFs; (B) 3D structure of single CF showing colla-gen microfibrils and proteoglycans. The microfibrils (green) are wellorganised within the CF; (C) 3D structure (at “Z” axis) of CFs of post-LASIK cornea showing degeneration of collagen microfibrils (green)
within CFs. The collagen microfibrils (green particles) are disinte-grated (arrowhead) and degenerated microfibrils are left over in thematrix; (D) 3D structure of degenerated microfibrils within CF; (E)3D structure (at “Y” axis) of CFs of normal cornea showing collagenmicrofibrils are closely associated with each other; (F) 3D structure(at “Y” axis) of CFs of post-LASIK cornea showing separation of colla-gen microfibrils within CFs.
STUDY OF POST-LASIK ECTASIA CORNEA 7
Microscopy Research and Technique

fibril diameter of the normal cornea. The fibril diame-ter was further reduced (19.09 6 3.16 nm) in the flapregion.
Meghpara et al. (2011) reported that in the post-LASIK ectasia cornea the CFs in the residual stromalbed may be mechanically stretched, while the sur-rounding extracellular matrix is concurrently com-pressed because of the loss of structural resistance tointraocular pressure. It could be possible in post-LASIK cornea by interlamellar biomechanical slippage(i.e., interlamellar fracture) followed by subsequentinterfibrillar biomechanical slippage (i.e., interfibrillarfracture) as opposed to direct primary collagen fibrilfailure (i.e., fibrillar fracture). This chronic biomechan-ical malfunction in the process is similar to that ofinterlamellar and interfibrillar slippage described inrelation to keratoconus (Bron, 2001; Dawson et al.,2008; Polack, 1976). Our ultrastructural studiesshowed the presence of very thin microfilaments and areduction of CF diameter throughout the stroma of thepost-LASIK ectasia cornea. This reduction in the diam-eter of CFs could be due to a decrease in collagen typeV due to CF fracture because of mechanical stress.
Dawson et al. (2008) suggested that interlamellarslippage is most likely caused by the fracture of colla-gen type VI bridging filament networks that fre-quently join adjacent lamellae together throughout theentire corneal stroma and perhaps fracture of the ante-roposterior lamellar interweaving (composed of hetero-typic collagen type I fibrils) that normally interconnectcorneal stromal lamellar layers together in the ante-rior third of the corneal stroma (Komai and Ushiki,1991). We observed numerous very fine filaments atthe detached end of the flap and of the residual stroma.We presumed that these microfilaments might be colla-gen type VI, which might be fractured or isolated fromthe lamellae junction due to physiological stress.
The presence of keratan sulphate PGs within CFs ofkeratoconus cornea has been suggested by immuno-gold localization of keratan sulphate 5D4 within CFs(Akhtar et al., 2011). In the study, the 3D reconstruc-tion of the CFs of the normal cornea showed the pres-ence of collagen microfibrils and PGs within the CFs.It is presumed that these collagen microfibrils wereassociated with PG. In the post-LASIK cornea, the col-lagen microfibrils and PGs within the CFs were disin-tegrated leading to the degeneration of the CFs.
Our observations showed the random distribution ofPGs. At some places PGs were absent, whereas atother places PGs were very large. This could be relatedto interlamellar slippage. It has been proposed thatinterlamellar slippage might be due to biomechanicalbreakdown of collagen–PGs bonds (Bron, 2001; Daw-son et al., 2008). However, collagen–PG bonds areknown to be weak noncovalent bonds with approxi-mate shear strength on the order of 1025 MPa, whichis too small to withstand normal physiologic stresses(Bron, 2001). Our structural studies suggested thatthe post-LASIK cornea lost the rigidity and biome-chanical strength at the postoperative (flap region)
stress bearing region due to fabrication of microfibrilsand PGs within the CFs. This may lead to the degener-ation of CFs, PGs, and finally lamellae.
REFERENCES
Abahussin M, Hayes S, Edelhauser H, Dawson DG, Meek KM. 2013.A microscopy study of the structural features of post-LASIKhuman corneas. PLoS One 8:e63268.
Akhtar S, Bron AJ, Hayes AJ, Meek KM, Caterson B. 2011. Role ofkeratan sulphate (sulphated poly-N-acetyllactosamine repeats) inkeratoconic cornea, histochemical, and ultrastructural analysis.Graefes Arch Clin Exp Ophthalmol. 249:413–420.
Anderson NJ, Edelhauser HF, Sharara N, Thompson KP, RubinfeldRS, Devaney DM, Hernault NL, Grossniklaus HE. 2002. Histologicand ultrastructural findings in human corneas after successfullaser in situ keratomileusis. Arch ophthalmol 120:288–293.
Birk DE, Fitch JM, Babiarz JP, Linsenmayer TF. 1988. Collagen typeI and type V are present in the same fibril in the avian cornealstroma. J Cell Biol 106:999–1008.
Birk, DE, Fitch JM, Babiarz JP, Doane KJ, Linsenmayer TF. 1990.Collagen fibrillogenesis in vitro: Interaction of types I and V colla-gen regulates fibril diameter. J. Cell Sci 95:649e–657e.
Bron AJ. 2001. The architecture of the corneal stroma. Br J Ophthal-mol 85:379–381.
Dawson DG, Randleman JB, Grossniklaus HE, O’Brien TP, DubovySR, Schmack I, Stulting RD, Edelhauser HF. 2008. Corneal ectasiaafter excimer laser keratorefractive surgery: Histopathology, ultra-structure, and pathophysiology. Ophthalmology 115:2181–2191.
Flanagan GW, Binder PS. 2003. Estimating residual stromal thick-ness before and after laser in situ keratomileusis. J CataractRefract Surg 29:1674–1683.
Kim H, Song IK, Joo CK. 2006. Keratectasia after laser in situ keratomi-leusis: Clinicopathological case report. Ophthalmologica 220:58–64.
Komai Y, Ushiki T. 1991. The three-dimensional organization of colla-gen fibrils in the human cornea and sclera. Invest Ophthalmol VisSci 32:2244–2258.
Kymionis GD, Tsiklis NS, Pallikaris IG, Kounis G, Diakonis VF,Astyrakakis N, Siganos CS. 2006. Long-term Follow-up of Intacsfor Post-LASIK Corneal Ectasia. Ophthalmology 113:1909–1917.
Maurice DM. 1957. The structure and transparency of the cornea. JPhysiol 136:263–286.
Meghpara B, Nakamura H, Macsai M, Sugar J, Hidayat A, Yue BY,Edward DP. 2008. Keratectasia after laser in situ keratomileusis: Ahistopathologic and immunohistochemical study. Arch Ophthalmol126:1655–1663.
Park CK, Kim JH. 1999. Comparison of wound healing after photore-fractive keratectomy and laser in situ keratomileusis in rabbits. JCataract Refract Surg 25:842–850.
Philipp WE, Speicher L, G€ottinger W. 2003. Histological and immuno-histochemical findings after laser in situ keratomileusis in humancorneas. J Cataract Refract Surg 29:808–820.
Polack FM. 1976. Contributions of electron microscopy to the study ofcorneal pathology. Surv Ophthalmol 20:375–414.
Randleman JB, Russell B, Ward MA, Thompson KP, Stulting RD.2003. Risk factors and prognosis for corneal ectasia after LASIK.Ophthalmology 110:267–275.
Scott JE, Orford CR, Huges EW. 1981. Proteoglycan-collagen arrange-ments in developing rat tail tendon. Biochem J 195:573–581.
Seiler T, Koufala K, Richter G. 1998. Iatrogenic keratectasia afterlaser in situ keratomileusis. J Refract Surg 14:312–317.
Spirn MJ, Dawson DG, Rubinfeld RS, Burris C, Talamo J,Edelhauser HF, Grossniklaus HE. 2005. Histopathological analysisof postlaser assisted in situ keratomileusis corneal ectasia withintrastromal corneal ring segments. Arch Ophthalmol. 123:1604–1607.
Tunc Z, Helvacioglu F, Sencan S. 2011. Evaluation of intrastromalcorneal ring segments for treatment of post-LASIK ectasia patientswith a mechanical implantation technique. Indian J Ophthalmol59:437–443.
Wenstrup RJ, Florer JB, Brunskill EW, Bell SM, Chervoneva I, Birk,DE. 2004. Type V collagen controls the initiation of collagen fibrilassembly. J Biol Chem 279:53331e–53337e.
8 S. AKHTAR ET AL.
Microscopy Research and Technique















![2.1.3 Basic Programming [000] [000] [001] [002] [003]](https://img.pdfslide.net/doc/110x75/632443e2117b4414ec0cb196/213-basic-programming-000-000-001-002-003.jpg)












