Embed Size (px)
Citation preview

McMillan Rome
Social research and training consultants
An evaluation of the
Community Nurse Consultant Pilot Project
in an NHS Health Board in Scotland

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 2 of 21 McMillan Rome
Social research and training consultants
Report authors
Andrew Rome, McMillan Rome Ltd
Professor Lawrie Elliott, Edinburgh Napier University
Professor Catriona Kennedy, Edinburgh Napier University/University of Limerick
Dr Margaret Currie, The James Hutton Institute
Alison Rome, McMillan Rome Ltd
Correspondence to:
Andrew Rome
Director
McMillan Rome Ltd
33 Strathmartine Road
Dundee, DD3 7RW
Tel. 07789 393864
Email: [email protected]
Website: www.mcmillanrome.co.uk

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 3 of 21 McMillan Rome
Social research and training consultants
Table of Contents
EXECUTIVE SUMMARY ..................................................................................................... 5
CHAPTER 1: INTRODUCTION ........................................................................................... 6
1.1 AIMS AND FOCUS ........................................................................................................................................... 6
1.2 DESIGN AND METHODS ................................................................................................................................. 6
1.2.1 Scope of study ....................................................................................................................................... 6
1.2.2 Methods ................................................................................................................................................. 7
1.3 PROJECT GOVERNANCE ................................................................................................................................. 7
1.4 ANALYSIS...................................................................................................................................................... 7
CHAPTER 2: RESULTS - STRUCTURES AND SUPPORT SYSTEMS ......................... 9
2.1 SUPPORT STRUCTURES .................................................................................................................................. 9
2.1.1 Internal supports and infrastructure ..................................................................................................... 9
2.1.2 External supports ................................................................................................................................ 10
2.2 KEY RELATIONSHIPS AND ELEMENTS OF THE POST ...................................................................................... 10
2.2.1 Response of Colleagues ...................................................................................................................... 11
CHAPTER 3: RESULTS - IMPACT OF COMMUNITY NURSE CONSULTANT
POST ....................................................................................................................................... 13
3.1 PROMOTING HEALTH AND SELF-CARE ........................................................................................................ 13
3.1.1 Utilising tele-care and telehealth ........................................................................................................ 13
3.1.2 Promoting health and addressing inequalities .................................................................................... 13
3.1.3 Enabling and supporting self-care ...................................................................................................... 14
3.2 DEVELOPING SYSTEMS OF CARE ................................................................................................................. 14
3.3 WORKFORCE DEVELOPMENT ...................................................................................................................... 15
3.3.1 Building workforce capacity and capability ....................................................................................... 15
3.3.2 Strengthening leadership and team working ....................................................................................... 16
3.3.3 Achieving an outcome-focused approach ........................................................................................... 17
3.4 WORKING WITH OTHERS ............................................................................................................................. 17
3.4.1 Working with other agencies and disciplines as partners ................................................................... 17
3.4.2 Working with clients, carers and patients as partners ........................................................................ 18
CHAPTER 4: DISCUSSION ................................................................................................ 19
4.1 FRAMING THE RESULTS ............................................................................................................................... 19
4.1.1 Professional impact ............................................................................................................................ 19
4.1.2 Clinical impact .................................................................................................................................... 20
4.2 BARRIERS .................................................................................................................................................... 20

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 4 of 21 McMillan Rome
Social research and training consultants
4.3 FUTURE DIRECTION ..................................................................................................................................... 20
Table of Figures
Table 1: Thematic grouping of MNIC elements ..................................................................................................... 8
Chart 1: Organisational relationships of Community Nurse Consultant post ......................................................... 9

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 5 of 21 McMillan Rome
Social research and training consultants
Executive Summary
The role of Community Nurse Consultant (CNC) was developed by the Queen’s Nursing
Institute Scotland (QNIS) in collaboration with an NHS Health Board in Scotland (The health
board). The post was funded for two years (starting 2011) to commemorate the 150th
anniversary of district nursing.
The aim of the evaluation was to capture the impact of the CNC in regard to the
Modernisation of Nursing in the Community1 and community nursing care for older people
living in their own homes in the Health Board area.
This was a retrospective evaluation that drew upon information and opinion from a range of
stakeholders and the post holder using semi-structure interviews and written documentation
(e.g. job description, minutes of meetings and policy documents). The stakeholders had
worked with the post holder in some capacity and included managers and practitioners within
the health board and from a variety of organisations including local authorities, Scottish
Government, residential care homes and Higher Education Institutions. These were identified
in consultation with the post holder and their line manager, and a final list of 21 individuals
was approved by the contract manager at QNIS.
The data were analysed using the twelve elements contained within the Modernising Nursing
in the Community framework.2
Given the scope of our evaluation it is not possible to determine whether the work of the post
holder led directly to improved outcomes for patients, but it is evident that he/she contributed
visibly to strategic development of the community nursing and provided leadership in the
development of some community-based services for older people in the community. There
was also evidence the post was instrumental in developing partnerships between parts of the
NHS and external organisations.
Some environmental factors facilitated the work of the post holder, notably the support from
senior managers and external organisations and the buy-in from health professionals to the
training and professional development opportunities develop by the post holder. Barriers
included the initial lack of strategic and operational vision (including concerns expressed by
colleagues) during the initial introductory phase of the post and the apparent confused lines of
communication and management. The post also appeared to lack administrative support.
The piloting of a Community Nurse Consultant post has allowed the QNIS and the health
board to evaluate the initial introductory phase of the role. Going forward, there are a number
of issues highlighted through this evaluation which, if addressed, could enhance and support
similar posts.
1 Modernising Nursing in the Community (2012). Available at http://www.scotland.gov.uk/Resource/0039/00396734.pdf
2 Ibid

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 6 of 21 McMillan Rome
Social research and training consultants
Chapter 1: Introduction
The role of Community Nurse Consultant (CNC) was developed by the Queen’s Nursing
Institute Scotland (QNIS) in collaboration with an NHS Health Board in Scotland (the health
board). The post was funded for two years (starting 2011) to commemorate the 150th
anniversary of district nursing.
1.1 Aims and focus
The aim of the evaluation is to capture the impact of the CNC in regard to the Modernisation
of Nursing in the Community3 and community nursing care for older people living in their
own homes in the health board area.
From the evidence collected, the evaluation team makes recommendations for the future
development of the CNC role at national and Health Board level.
1.2 Design and Methods
1.2.1 Scope of study
Our methodology is influenced by the work of Gerrish et al4, in terms of the literature review
on the evaluation of Nurse Consultant roles5 and also in the utilisation of their toolkit that was
developed in 20116.
The literature review identified a number of key issues:
It can take up to 5 years for a post to develop fully7
The impact is multi-faceted and hard to capture. For example, Nurse Consultants often
work with others to influence practice8
Previous studies identify perceived (self reported) impact rather than actual (observable)
impact9
3 Ibid
4 Gerrish K., Guillaume L., Kirshbaum M., McDonnell A., Nolan M., Read S. & Tod A. (2007) Empowering Front-Line Staff to Deliver
Evidence-Based Care: The Contribution of Nurses in Advanced Practice Roles. Sheffield Hallam University, Sheffield.
5 Kennedy F, McDonnell A, Gerrish K., Howarth A, Pollard C. & Redman J. (2012) Evaluation of the impact of Nurse Consultant roles in
the United Kingdom: a mixed method systematic literature review. Journal of Advanced Nursing 68(4), 721–742.
6 Gerrish K, McDonnell A, & Kennedy F. (2011) Capturing Impact: A practical toolkit for Nurse Consultants (Sheffield University)
7 National Nursing Research Unit (2007) Advanced Nursing Roles: Survival of the Fittest? Policy plus evidence, issues and options in health
care, Issue 6, National Nursing Research Unit, King’s College London, London.
8 Op. cit. Gerrish (2007)
9 Humphreys A., Johnson S., Richardson J., Stenhouse E. & Watkins M. (2007) A systematic review and meta-synthesis: evaluating the
effectiveness of nurse, midwife/allied health professional consultants. Journal of Clinical Nursing 16(10), 1792–1808.

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 7 of 21 McMillan Rome
Social research and training consultants
The evaluation also takes cognisance of the findings of the critique of new community
nursing roles conducted by Aranda and Jones which identified political, structural and
personal challenges in establishing such roles.10
Thus, given the scope of the current
evaluation it is not possible to examine the political drivers which shape the new role.
1.2.2 Methods
This was a retrospective evaluation that drew upon information and opinion from a range of
stakeholders and the post holder using semi-structure interviews and written documentation
(e.g. job description, minutes of meetings and policy documents). The stakeholders had
worked with the post holder in some capacity and included managers and practitioners within
the health board and from a variety of organisations including local authorities, Scottish
Government, residential care homes and Higher Education Institutions. These were identified
in consultation with the post holder and their line manager, and a final list of 21 individuals
was approved by the contract manager at QNIS.
Interview data were collected using a digital voice recorder and transferred onto an encrypted
hard drive. All files were transcribed in-house and stored within the same hard drive. No third
party had access to the data at any point of collection, storage or analysis. Data will be stored
on an encrypted hard drive for 5 years after which time it will be destroyed.
1.3 Project Governance
An application was made to the Head of Research, Development and Evaluation at the health
board in October 2012. The submission included all arrangements relating to accessing
participants, both professional and lay, gaining informed consent, and the intended data
collection tools. Written permission was granted on 7th
November 2012 and accompanied by
a letter of access to conduct the evaluation.
Permission to use the data gathering tools contained within ‘Capturing Impact: A practical
toolkit for Nurse Consultants’ was sought from the lead author Professor Kate Gerrish. This
was obtained by email on 01/02/2013.
1.4 Analysis
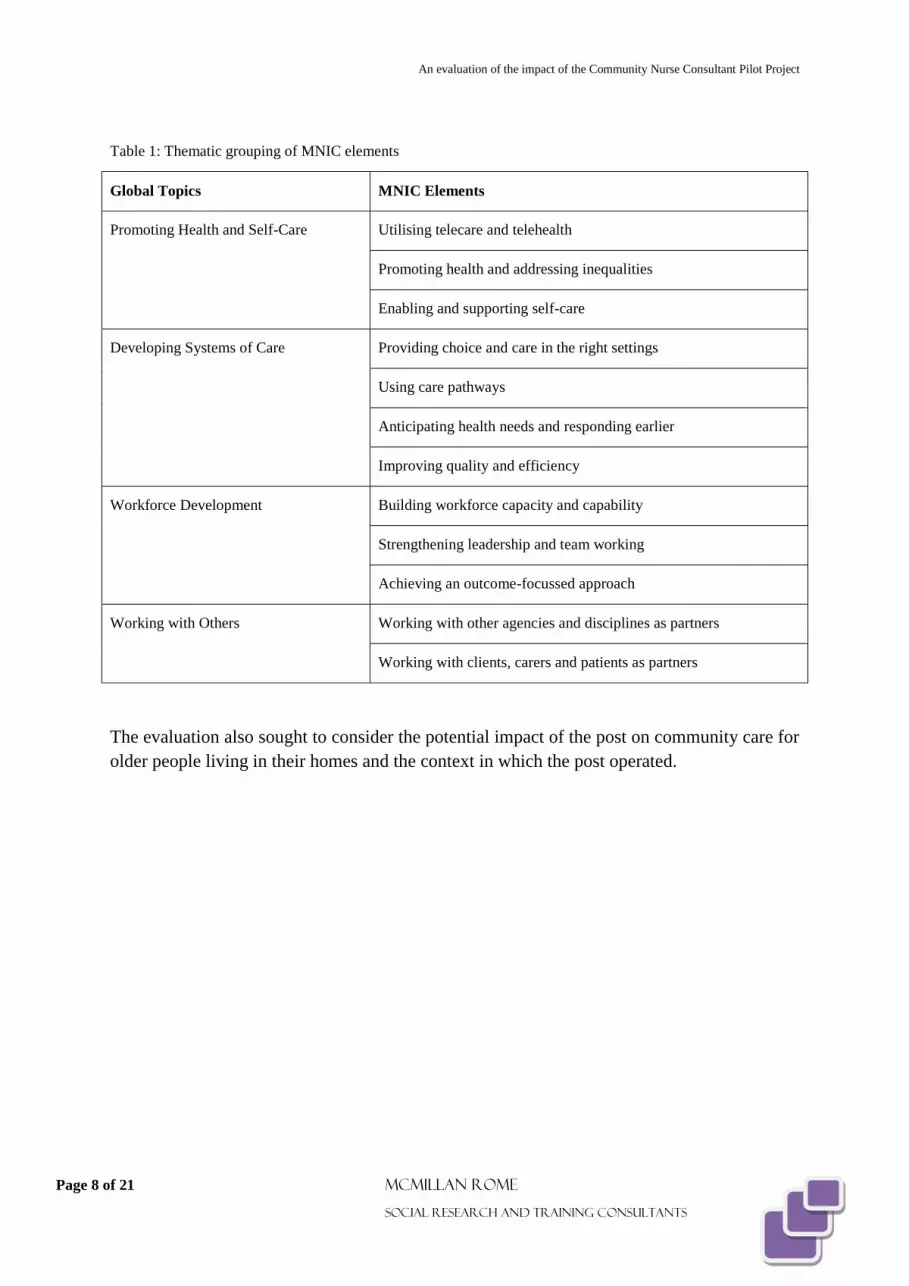
The data were analysed using the twelve elements contained within the Modernising Nursing
in the Community framework.11 These are thematically grouped under 4 global topics as set
out in Table 1 below.
10 Aranda J and Jones A (2008) Exploring new advanced practice roles in community nursing: a critique. Nursing Inquiry 15,
1, 3-10.
11 Op. cit. Modernising Nursing in the Community
An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 8 of 21 McMillan Rome
Social research and training consultants
Table 1: Thematic grouping of MNIC elements
Global Topics MNIC Elements
Promoting Health and Self-Care Utilising telecare and telehealth
Promoting health and addressing inequalities
Enabling and supporting self-care
Developing Systems of Care Providing choice and care in the right settings
Using care pathways
Anticipating health needs and responding earlier
Improving quality and efficiency
Workforce Development Building workforce capacity and capability
Strengthening leadership and team working
Achieving an outcome-focussed approach
Working with Others Working with other agencies and disciplines as partners
Working with clients, carers and patients as partners
The evaluation also sought to consider the potential impact of the post on community care for
older people living in their homes and the context in which the post operated.

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 9 of 21 McMillan Rome
Social research and training consultants
Chapter 2: Results - Structures and Support Systems
The post holder commenced work in January 2011, and moved to part-time (0.5WTE)
working in May 2012. The job purpose, as identified in the description, was to “Improve
outcomes for patients by providing strong, strategic, clinical and professional nursing
leadership to primary care and community services within [the Health Board].”12
2.1 Support structures
The post required to have clearly delineated clinical and managerial relationships and support
structures. This would provide the post holder, the managers and senior clinicians, and the
district nursing workforce with a clear sense of role and responsibility within what was a
changing landscape. Evidence was sought from stakeholders, written documentation and the
post holder, and is described here in terms of internal supports and external supports.
2.1.1 Internal supports and infrastructure
Community nursing services within the health board area are structured under three clinical
directorates. These are Primary Care and Mental Health Services (PCMHS), Integrated Care
and Partner Services (ICPS) and Integrated Care and Emergency Services (ICES).
Chart 1: Organisational relationships of Community Nurse Consultant post13
12 Nurse Consultant (Community Nursing Adults) Job Description (Draft) An NHS Health Board in Scotland (Undated)
13 Adapted from an NHS Health Board in Scotland Organisational Chart and Community Nurse Consultant Job Description

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 10 of 21 McMillan Rome
Social research and training consultants
This arrangement differs from that in other health boards where they would normally be
housed within Community Health Partnerships (CHP) or similar structures14
. In this health
board CHPs are described as being planning structures.
Chart 1 sets out the key relationships of the CNC, in terms of lines of line management and
professional accountability (solid lines) and close working relationships (dotted lines).
The management of the community nursing services sits within Integrated Care and Partner
Services. This includes District Nurses, District Midwives, along with surgical and some in-
patient staff. Professional leadership for these staff is provided by the Associate Nurse
Director (AND) from the Primary Care and Mental Health Services Directorate. This
arrangement was described by stakeholders within the health board as being, ‘A bit weird and
wonderful’ (Manager 1) and, ‘It’s difficult and challenging when I think about the way in
which the services are set up, the way in which the Directorates are set up…’ (Manager 3). In
relation to the cross-cutting nature of community care, ‘It can be quite messy because we’ve
got a number of managers involved’ (Manager 1).
The AND for Primary Care and Mental Health Services has a remit to provide professional
leadership and to modernise the service and therefore ‘Sits to one side of the directorate that
manages the [ICPS] service’ (Manager 1). For this reason, and that the AND was previously
a Nurse Consultant and could provide an understanding to the breadth of the role, the new
post of Community Nurse Consultant was housed within the PCMHS directorate, rather than
ICPS which contains the rest of the District Nursing Services.
2.1.2 External supports
The original aim was to provide academic support to the post holder which enabled the
design and delivery of education and training packages to post-graduate students. This
arrangement failed to materialise for a number of reasons, including the initial absence of the
post holder for several weeks due to compassionate leave and that the nature of the teaching
that was available was out with the post holder’s area of expertise.
It is worthy of note that QNIS provided on-going support to the post holder, in terms of
adopting a flexible approach to the way in which the post evolved and, ultimately ensuring its
continuation when it may otherwise have been halted.
2.2 Key relationships and elements of the post
The primary relationship of the CNC post was between the AND for PC&MH services, who
provided the strategic lead for community nursing (Chart 1). The alignment of this post with
the AND was purposeful, for the reasons set out earlier, and the relationship has been
productive in terms of facilitating the introduction of new ways of delivering nursing care in
the community. However this post holder’s involvement in these activities detracted from the
14 Watt G, Ibe O, McLelland N. Study of Community Health Partnerships. Scottish Government Social Research (2010)

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 11 of 21 McMillan Rome
Social research and training consultants
development of relationships between the CNC and the Community Nurse Managers and
wider district nursing workforce who were housed within a parallel management structure.
These had all been identified in the post holder’s job description as being ‘Close working
relationships’.
The work on developing telehealth15
services in the health board has manifested in the
creation of one Community Ward in each of the three local authority areas. Community
Wards are based on the principle of Virtual Wards16
previously implemented in areas of
England e.g. Croydon17
. Each of these Community Wards employed an Advanced Nurse
Practitioner (ANP). The post holder was responsible for the development of a core
competency framework specifically designed to ensure that the staff recruited to these posts
had the knowledge, skills and experience required to deliver care.
Developmentally, this has been the largest single project the CNC was involved in and he/she
provided strong leadership and direction to this new service and to the three ANPs working
within it. More specifically, the post holder was instrumental in organising education,
training and service development for these three practitioners.
2.2.1 Response of Colleagues
As has been noted elsewhere18
there was evidence that the arrangements for responsibility
and accountability were not universally understood by the stakeholders. Specifically there
was a lack of clarity around how the CNC post related to other clinical and managerial posts
within the three-directorate structure.
‘From quite senior nurses to frontline practitioners they have not welcomed the post. They’ve
believed it was unnecessary. So that was something, in terms of that difficulty in bringing in
new roles’ (Manager 2).
‘I think some of these challenges were because of some management resistance within the
community nursing side of things which made that role more challenging. I think if there had
been a better collaborative approach, I think we could have moved things along a lot faster’
(Manager 4).
There were also concerns raised about the ‘lack of vision and lack of leadership’ regarding
the way this post was introduced. This was described by one stakeholder as being, ‘Typical of
[the health board], appoint someone first then get them to write their own job description’
(Practitioner 9).
15 Telehealth is an approach to healthcare delivery that is tailored to an individual’s needs.
16 A Virtual Ward provides the security and the benefits of multi-disciplinary team working associated with hospital wards
for patients living at home. Patients requiring complex disease management are enabled to remain in their own home through
active, intensive monitoring of their physical condition, treatment review and support.
17 Similar facilities are now also in existence in other Scottish Health Board areas
18 Bonsall K. & Cheater F. (2008) What is the impact of advanced primary care nursing roles on patients, nurses and their
colleagues? A literature review. International Journal of Nursing Studies 45, 1090–1102.

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 12 of 21 McMillan Rome
Social research and training consultants
During the initial months of the pilot the lack of clarity regarding management roles and
structures could have been destabilising for the post holder, who had not previously worked
in the health board area. At that time the post holder benefitted from the support of the
Clinical Improvement Manager who also had a remit to develop services relating to primary
care, such as the ‘Living and Dying Well’ project. The Clinical Improvement Manager was
able to assign staff to assist the CNC with this work as well as helping to orientate and advise
the post holder with regard to the many groups and committees that the CNC was invited to
attend.
‘When [the post holder] was doing some piece of work in the Living and Dying Well in the
Community two of my staff that supported that project work as well. So it’s almost like a kind
of negotiation to help her achieve her goals.’ (Manager)
There is documentary evidence which details the discussions between QNIS and the health
board with regard to the joint funding arrangements over the two year pilot period. However
this did not include administrative support. Many stakeholders felt this was to detriment of
the efficiency of the role and to the working arrangements of the individual. This was in
contrast to the position which existed in relation to the three Nurse Consultants with whom
the post holder was co-located. These hospital-based posts, which preceded the Community
Nurse Consultant post, all had administrative support.

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 13 of 21 McMillan Rome
Social research and training consultants
Chapter 3: Results - Impact of Community Nurse Consultant post
3.1 Promoting Health and Self-Care
The CNC had no direct clinical input which differs from the other Nurse Consultant posts in
the health board area and nationally where up to 50% of the post is clinical19
. Although a
recent development has been the allocation of one session per week to work directly with
patients and to support frontline staff in the clinical environment. This said it was clear, that
the post holder worked strategically to influence the practice of others during the pilot period.
3.1.1 Utilising tele-care and telehealth
The post holder chaired a short-life Telehealth working group in 2012 in response to a
request of Scottish Government and QNIS to deliver presentations across Scotland on the
programmes of work related to telehealth and tele-care20
in the health board area.
The objective of the working group was to undertake an evaluation particularly related to
improvements in the quality of care in patients with Long Term Conditions (LTCs) who are
supported by health professional and telehealth equipment in their home. The development of
these initiatives in the health board had been led by a District Nursing Team Leader. The role
of the post holder was to review its progress to date and contribute to the QNIS workshops.
3.1.2 Promoting health and addressing inequalities
An NHS Health Board in Scotland is co-terminus with the three Local Authorities. These
areas have distinctly different socio-economic demographics, with one having a higher
burden of deprivation-related problems.
‘We are one of the highest areas [of social and economic deprivation] in Scotland’
(Practitioner 2).
The three Community Wards and the ANPs that were managed by the post holder were
located within each of these areas. While it is too early to measure impact, it is anticipated
that, as well as the clinical benefits of preventative healthcare, there will be a socio-economic
benefit to patients and carers who live in the more remote and rural parts of the area in terms
of reduced travel time and costs in accessing the Community Wards compared to hospital-
based care.
19 Kennedy op. cit. p1
20 Tele-care – a range of alarms and sensors in the home to enable independent living and linked to a call centre.

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 14 of 21 McMillan Rome
Social research and training consultants
3.1.3 Enabling and supporting self-care
The post holder played a lead role in the development and implementation of the Community
Wards in the health board area.
This work was overseen by two groups; the Community Wards Clinical Governance
Committee 2, which the post holder co-chaired, and the Community Wards Steering Group.
These groups ran concurrently and met on a two-monthly basis.
The Community Wards Clinical Governance Committee 2 was responsible for overseeing the
development of guidelines, protocols and standard operating procedures and the Steering
Group developed the business case for the initiative, managed the recruitment of the ANPs
and led the development of the competency framework.
‘I think it [Community Wards] might have been set up, but I don’t think the three Advanced
Nurse Practitioners would be performing at the level they are performing at if it hadn’t been
for this post’ (Manager 5).
3.2 Developing Systems of Care
The consensus view of stakeholders was that the post had either led or had contributed
greatly to the planning and delivery of initiatives such as the Anticipatory Care Pathways and
Living & Dying Well and that without this post being in place these would either be at an
earlier stage of development or still in the planning stages. Thus the post was integral to the
success of these initiatives.
The post holder worked with a range of NHS and external colleagues to develop ways of
delivering care in the community in a consistent, auditable and evidence-based way. This
manifested in the development of care pathways to ensure that decisions which affect the way
in which people are cared for and the choices that people make regarding terminal care are
based on patient choice and best practice.
‘I think when it came to the nitty gritty regarding the care and the level of knowledge and
competency of the staff required, then the professional aspect of it in relation to the nursing
staff was very much led by this post’ (Manager 5).
The post holder’s leadership and contribution to the work on ‘Anticipatory Care’ and ‘Living
and Dying Well’ has resulted in people being able to stay in their own homes through the use
of telecare technologies, or continue to reside in Care Homes where otherwise they may have
had to be treated in hospital.
‘There is a growing reduction now in the amount of unplanned admissions to hospital
settings from Care Homes [as a result of the Anticipatory care pathway]’ (External
Stakeholder 5).
‘I think if you took the post out of the equation then…we’d have less well developed and less
well-informed advanced anticipatory care plans' (Manager 1).

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 15 of 21 McMillan Rome
Social research and training consultants
The post holder was also a member of the Significant Event Analysis Review Group as an
expert for care of the acutely unwell patient in the community. The remit of this group was to
undertake a root cause analysis of clinical events. The output of this work was the completion
of a robust and detailed process to identify root cause, the development and submission of a
report including recommendations to senior personnel and other key stakeholders.
3.3 Workforce Development
3.3.1 Building workforce capacity and capability
Over the two-year period there was a significant investment by the post holder in developing
competency frameworks, initially for the post of Advanced Nurse Practitioner. But also
latterly looking at what knowledge and skills other community-based nursing staff need in
order to carry out an increasing range of technical procedures previously undertaken in
hospital.
‘I’m pretty confident that [the post holder’s] position has been in the background driving
various things. As an example, assistance for nurses in care homes to train them up with a
McKinley T34 syringe pump driver and things like that. I’m pretty certain her role has
assisted, if not led the improvements as far as that’s concerned’ (External Stakeholder 5).
The post holder chaired the Task & Finish Group, a multi-disciplinary working group with
the remit to take forward, at local level, recommendations outlined in national strategic
documents such as ‘Living and Dying Well’ and ‘Building on Progress’ documents.
The objectives of the Group were to improve the quality of care to patients receiving
palliative and end of life care within a pilot area with a specific plan to roll out Education and
Training on Advanced Anticipatory Care Planning to key professionals across Acute and
primary care Nursing, Care Homes and GPs, and to reduce avoidable hospital admissions.
‘One of the things that obviously the post holder has been involved in there is the Task and
Finish Group that has been set up there with a particular remit…looking in to the End of Life
and bereavement and palliative care. So that sub-group has come to an end but it has come
to an end very, very successfully…what we are aware of is that there was a big part played in
setting that up and that’s led to a significant joint training exercise that’s going on between
NHS and Social Services’ (External Stakeholder 4).
‘[The post holder] had actually set up the sub-group out of that for that End of Life training.
And as I say now we are offering twenty courses a year between health, social work, older
people services and the private sector and the voluntary sector. So there is quite a
widespread benefit of that having taken place’ (External Stakeholder 4).
Given the problems in linking with the local university the post holder developed links with
colleagues in other Higher Education Institutions, with the aim of developing the
Competency Framework for the Advanced Nurse Practitioners based around the four pillars
of advanced practice; clinical practice, education, research and leadership. This allowed

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 16 of 21 McMillan Rome
Social research and training consultants
participants to exit with a Postgraduate Degree in Advanced Nursing Practice or continue
towards an MSc. This work also considered the future educational needs of district nurses
and how best these can be delivered. In addition, the post holder also lent support to
individual nurses such as providing mentorship for a community nurse undertaking an MSc.
‘One of the things that we hadn’t really appreciated was in fact that the teaching element of
[the post holder’s] role would actually be done in a much different way. But in fact the
teaching that she would get involved in would be developing our nurses, the ANPs. So that’s
where the teaching element came in’ (External Stakeholder 1).
The creation of the Community Nurse Consultant role and its introduction at a time of change
and re-structuring within community nursing in the health board area has provided a clinical
career pathway that did not previously exist.
‘I think at the time that role was established there was a lot of uncertainty as to what that
role would achieve. But I think now that things are settled definitely people see the
progression structure. There is a change within; there is a Community Staff Nurse you can
become, there’s a Deputy Team Leader which would lead to a Team Leader, which then
could lead to the Nurse Consultant role. Whereas in community nursing before it was
community staff nurse, charge nurse that was it’ (Practitioner 6).
3.3.2 Strengthening leadership and team working
The introduction of a senior clinical nursing post in the community enabled the development
of services at a pace and direction that was not previously possible.
‘That role has been innovative in leading into places we haven’t gone before’ (Practitioner
6).
It has provided a focal point of change within community nursing and in its relationships with
other key stakeholders.
‘Unless you’ve got this type of role strategically placed in the various areas then the silos
will continue. They might reshape and reform in different ways but they’re will still be loss of
communications and private agendas going on and that’s not going to make things work. At
the end of the day we all know the socio-demographic and financial imperatives that we’ve
got to deal with. You need a role like this to help the catalyst continue to crack the situation…
a good example I would say is that there are various pieces of information gathering and I.T.
packages. But they don’t talk to each other and this type of role can bring the various groups
together to look at the commonalities so that you can get something in that union. You can
work out a system’ (External Stakeholder 5).
There was a consensus view from the stakeholders that the post holder provided clinical
leadership in the development and implementation of the 3 ANP posts within the Community
Wards and continues to provide on-going clinical support, albeit at a reduced level.
Inevitably, in directing a finite resource such as this post to these projects it is at the expense
of other activities which may also have benefitted from this level of clinical leadership. The

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 17 of 21 McMillan Rome
Social research and training consultants
district nursing teams have undergone structural changes as well as a process of role re-
definition. It could be argued that the benefits accrued as a result of the resource attributed to
the Community Wards was at the expense of the clinical leadership of the 200 nurses within
the district nursing teams.
‘Some staff have met with [the post holder], others haven’t. So therefore they know what she
looks like. But as far as having any impact on their practice, no that would be wrong’
(Practitioner 2).
3.3.3 Achieving an outcome-focused approach
Although it is still very early to make causal links between the role of Community Nurse
Consultant and improvements in patient care there are indicators that the work undertaken by
the post holder is having a ‘knock-on effect’ through the improvements in the training of
staff.
‘[It is] very difficult to quantify in terms of what kind of difference it [the training set up by
the CNC] made to reshaping care and shifting the balance about keeping folk out of care
homes and in hospital. But the indication from the training itself was a very high return of
satisfaction from the staff that attended, and for them to go about their business in a much
more professional manner because of it. And again I’ve seen that evidence and I’ve seen that
evaluation from the hospice and the social work side of it. And they are feeling that that is
making a really big impact in the Services that provide it’ (External Stakeholder 4).
‘The End of Life training had been subject to a Change Fund bid. We are actually using the
logic model for the setting up of that. So it’s been recorded in the convalesce system about
the outcomes. So that’s been one of the outcomes that has performed really high’ (External
Stakeholder 4).
3.4 Working with Others
The CNC job description sets out the requirement for the post holder to work in partnership
with GPs, AHPs, nursing colleagues in acute settings, service managers and local
authorities.21
3.4.1 Working with other agencies and disciplines as partners
The Task & Finish Group has a membership list of 28 individuals, 12 of whom were from
outside the NHS. This included representatives from the residential care home sector, the
Care Home Partnership, who recognised the important role of the post holder in, ‘Breaking
down silos’ in order to improve communication and joint working across boundaries.
21 Nurse Consultant (Community Nursing Adults) Job Description (Draft) An NHS Health Board in Scotland (Undated)
An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 18 of 21 McMillan Rome
Social research and training consultants
‘For somebody working in the partnership and working like myself in the middle
management role, again it’s just about having one specific go-to person [the post holder].’
(External Stakeholder 4).
Through the work on Anticipatory Care Pathways and the Community Wards the post holder
worked with colleagues in the Clinical Improvement Team to engage with clinicians in
primary care and the acute hospitals to develop multi-disciplinary systems of working.
‘I would say that since [the post holder] has come into post one of the things that, as a nurse
working in the NHS for many years now, that we are a much closer partnership now with
private sector than we ever had before in my memory’ (Practitioner 5).
The post holder has also contributed to the development of community nursing at a national
level through membership of working groups such as the Modernising Community Nursing
Programme Board (Scottish Government), National Website Development Group (NES) and
the short-life national working group for the development of a District Nursing career
framework.
3.4.2 Working with clients, carers and patients as partners
Evidence from the post holder and the Patient & Public Involvement (PPI) Officers
confirmed that there has been no direct involvement with patients, clients and carers in the
design and delivery of these services. Participation has been limited to the production of
newsletters that are distributed to outlets where patients can access these.

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 19 of 21 McMillan Rome
Social research and training consultants
Chapter 4: Discussion
The ultimate purpose of this role is to “Improve outcomes for patients by providing strong,
strategic, clinical and professional nursing leadership to primary care and community
services within [the health board area].”22
Given the scope of our evaluation it is not
possible to determine whether the work of the post holder lead directly to improved outcomes
for patients, but it is evident that he/she contributed visibly to strategic development of the
community nursing and provided leadership in the development of some community based
services for older people in the community. There was also evidence the post was
instrumental in developing partnerships between parts of the NHS and external organisations.
Some environmental factors facilitated the work of the post holder, notably the support from
senior managers and external organisations and the buy-in from health professionals to the
training and professional development opportunities develop by the post holder. Barriers
included the initial lack of strategic and operational vision (including concerns expressed by
colleagues) during the initial introductory phase of the post and the apparent confused lines of
communication and management. The post also appeared to lack administrative support.
4.1 Framing the results
Nurse Consultant posts traditionally have four key areas of activity; Clinical, Education,
Leadership and Research. To date the greatest proportion of activity has been focussed on
providing clinical leadership to 3 Advanced Nurse Practitioners (ANPs) in the health board
area. There is a degree of crossover therefore between leadership, clinical and education
activities.
4.1.1 Professional impact
The creation of a senior clinical nursing role provides a career pathway for community
nurses.
It is clear that the post holder has been the driving force in the creation and development of
the three Advanced Nurse Practitioner posts. In terms of professional impact, the work of the
post holder, in collaboration with Higher Education Institutions, to design and implement the
competency framework for the ANPs has been the major contribution to professional
advancement. This output is now being used as a blueprint for the benefit of wider
community nursing staff, in terms of the adaptation of the competency framework for Band
5/6 nurses.
It could be argued that there was a need and a role for strong clinical leadership during the
recent re-structuring of district nursing services. There was no evidence to suggest that this
wider workforce has yet benefitted from this post.
22 Ibid

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 20 of 21 McMillan Rome
Social research and training consultants
4.1.2 Clinical impact
It has been established that the post has, until recently, had no direct clinical contact with
patients. The potential clinical impact has therefore been as a result of the post holder’s
contributory or leadership role in bringing a number of initiatives to fruition. It is clear that
the development of the Community Wards, the work on Living and Dying Well in the
community and Anticipatory Care Pathways would not have progressed to the same extent in
the absence of this post.
4.2 Barriers
The post of Community Nurse Consultant was introduced opportunistically rather than part of
a strategic plan for community nursing within the health board area. As such it lacked a clear
remit or direction at the outset.
Within the organisation there was a lack of clarity or understanding about where this post sat
within the managerial/clinical tree and its lines of responsibility and accountability.
The decision to host this post within the PC&MH Services directorate was taken in order that
the AND could provide support and direction to the post. While there is evidence that this
relationship has worked well, it also created a distance between the post and those working in
the district nursing service that were positioned within a parallel management structure.
The lack of administrative support has resulted in an uneconomic use of the Nurse
Consultant’s time which is not commensurate with the function or level of seniority of the
role.
4.3 Future direction
The piloting of a Community Nurse Consultant post has allowed the QNIS and the health
board to evaluate the initial introductory phase of the role. Going forward, there are a number
of issues highlighted through this evaluation which, if addressed, could enhance and support
similar posts.
a) The introduction of a Community Nurse Consultant post should be informed by a strategic
planning process which clearly identifies the need for such a role, in terms of vision and how
the work will contribute to the development of the four key aspects of a Nurse Consultant’s
post namely Clinical, Education, Leadership and Research.
b) The CNC should be housed within the same clinical directorate, or similar structure, as the
branch of nursing to which they are aligned. In this case that means that the Nurse Consultant
should be a visible and accessible resource to all nurses working within district nursing
services.

An evaluation of the impact of the Community Nurse Consultant Pilot Project
Page 21 of 21 McMillan Rome
Social research and training consultants
c) Given the initial reactions by other health professions it would be worth consulting with
key stakeholders prior to the introduction of such a post to assess the level buy-in and work
towards a critical level of acceptance.
d) The sustainability of the post requires some thought including structural support and the
possibility of full-time hours.
Unlike many other Nurse Consultant posts which are ‘disease-specific’ the CNC has a more
reactive role across community care. While this could be regarded as a challenge, it can also
be seen as a flexible resource which can adapt to changing needs and healthcare priorities
within the community.
At this time many of the developmental projects undertaken by the post holder haves reached
a level where they can now be managed by operational managers and practitioners.
e) The evidence suggests that the focus should now be on identifying the support needs of the
district nursing services, particularly in the development of new skills and roles previously
carried out by hospital-based staff. The Nurse Consultant has a key leadership role to play in
the development or adaptation of competency frameworks and training for Band 5/6 nurses.
f) In order to provide ongoing clinical leadership, priority should be given to defining and
establishing a substantive clinical consultancy function for the post.





























