Embed Size (px)
Citation preview

Accepted Manuscript
Are Procedures Codes in Claims Data a Reliable Indicator of Intraoperative SplenicInjury Compared to Clinical Registry Data?
Anne M. Stey, MD, MSc Clifford Y. Ko, MD, MS, MSHS, FACS Bruce Lee Hall,MD PhD, MBA, FACS Rachel Louie, MS Elise H. Lawson, MD, MSHS Melinda M.Gibbons, MD, MSHS, FACS David S. Zingmond, MD, PhD Marcia M. Russell, MD,FACS
PII: S1072-7515(14)00322-6
DOI: 10.1016/j.jamcollsurg.2014.02.029
Reference: ACS 7367
To appear in: Journal of the American College of Surgeons
Received Date: 10 November 2013
Revised Date: 24 February 2014
Accepted Date: 25 February 2014
Please cite this article as: Stey AM, Ko CY, Lee Hall B, Louie R, Lawson EH, Gibbons MM, ZingmondDS, Russell MM, Are Procedures Codes in Claims Data a Reliable Indicator of Intraoperative SplenicInjury Compared to Clinical Registry Data?, Journal of the American College of Surgeons (2014), doi:10.1016/j.jamcollsurg.2014.02.029.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 1
Are Procedures Codes in Claims Data a Reliable Indicator of Intraoperative Splenic Injury
Compared to Clinical Registry Data?
Anne M Stey, MD, MSc (a, b), Clifford Y Ko, MD, MS, MSHS, FACS (b, c, d), Bruce Lee Hall,
MD PhD, MBA, FACS (c, e), Rachel Louie, MS (b), Elise H Lawson MD, MSHS (b), Melinda
M Gibbons. MD, MSHS, FACS (b), David S Zingmond MD, PhD (b), Marcia M Russell MD,
FACS (b, d)
(a) Icahn School of Medicine at Mount Sinai Medical Center, NY, NY;
(b) David Geffen School of Medicine, University of California Los Angeles, Los Angeles, CA;
(c) American College of Surgeons, Chicago, IL;
(d) VA Greater Los Angeles Healthcare System, Los Angeles, CA;
(e) Washington University in St Louis, Department of Surgery, Olin Business School, and Center
for Health Policy; St Louis VA Medical Center; BJC Healthcare St Louis.
Disclosure Information: Nothing to disclose.
Presented at the American College of Surgeons 99th Annual Clinical Congress, Washington, DC,
October 2013.
Support: Dr Stey’s time was supported for this publication by The Robert Wood Johnson
Foundation Clinical Scholars program and the U.S. Department of Veterans Affairs.
Correspondence address: Anne M. Stey 10940 Wilshire Blvd, Suite 710 Los Angeles, CA 90024. Phone: 310-794-2507
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 2
Fax: 310-794-3288 Email: [email protected]
Running Head: Procedure Codes Capture Iatrogenic Injury

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 3
ABSTRACT
Background: Identifying iatrogenic injuries using existing data sources is important for
improved transparency regarding the occurrence of intraoperative events. There is evidence that
procedure codes are reliably recorded in claims data. The objective of this study was to assess
whether concurrent splenic procedure codes in patients undergoing colectomy procedures are
reliably coded in claims data as compared to clinical registry data.
Study Design: Patients who underwent colectomy procedures in the absence of neoplastic
diagnosis codes were identified from American College of Surgeons National Surgical Quality
Improvement Program (ACS-NSQIP) data linked with Medicare inpatient claims data file (2005-
2008). A kappa statistic was used to assess coding concordance between ACS-NSQIP and
Medicare inpatient claims, with ACS-NSQIP as the reference standard.
Results: A total of 11,367 colectomy patients were identified from 212 hospitals. There were
114 patients (1%) who had a concurrent splenic procedure code recorded in either ACS-NSQIP
or Medicare inpatient claims. There were 7 patients who had a splenic injury diagnosis code
recorded in either data source. Agreement of splenic procedure codes between the data sources
was substantial (kappa statistic 0.72, 95% CI 0.64- 0.79). Medicare inpatient claims identified
81% of the splenic procedure codes recorded in ACS-NSQIP, and 99% of the patients without a
splenic procedure code.
Conclusions: It is feasible to use Medicare claims data to identify splenic injuries occurring
during colectomy procedures as claims data have moderate sensitivity and excellent specificity
for capturing concurrent splenic procedure codes compared to ACS-NSQIP.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 4
INTRODUCTION
The spleen is injured in 0.4-1% of colectomies, affecting a total of 6,000 patients
annually in the United States.(1,2) Such iatrogenic injuries account for approximately 20% of all
splenic procedures performed.(3-6) Patients subsequently have a 5% lifetime risk of
overwhelming post-splenectomy infection with an associated 38-70% mortality rate.(4,7)Despite
these clinical implications, providers and payers have not focused on intraoperative splenic
injury as a target for quality improvement. Yet, how tissue is handled and intraoperative injury to
surrounding organs, such as the spleen, may be viewed as an indicator of poor technical
quality.(8)
Iatrogenic splenic injury may be an identifiable adverse occurrence in administrative
claims data because injury is often treated with an additional procedure to repair or remove the
spleen. Administrative claims data have been used to measure quality for colectomy procedures
by identifying surgical complications based on the presence of diagnosis codes. However, this
use of diagnosis codes for capturing surgical complications in claims data is limited by
variability in coding.(9-13) Additionally, pay-for-performance programs that impose financial
losses on providers based on the presence of surgical complication diagnosis codes may
encourage under-coding of these diagnoses, effectively decreasing transparency within the health
system.(14-16) There is a need for more valid and reliable data elements than the current
diagnosis codes if claims data are to be used for surgical quality measurement.
One such data element that has shown promise in claims data is the procedure code.
Previous studies using claims data have demonstrated that procedure codes may be more reliably
coded than diagnosis codes. (17-19) Some of these authors have postulated that this difference in

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 5
the reliability of coding may be due to the higher reimbursement potential associated with
procedures.
The overarching goal of this study was to analyze the reliability of using procedure codes
recorded in Medicare inpatient claims data to identify intraoperative adverse events. We
hypothesized that concurrent splenic procedure codes recorded in Medicare inpatient claims data
for patients undergoing colectomy reliably reflect the concurrent splenic procedures recorded in
the American College of Surgeons National Surgical Quality Improvement Program (ACS-
NSQIP). If procedure codes are as reliable for capturing intraoperative events as hypothesized,
these codes could be a means of improving transparency surrounding intraoperative events. This
increased transparency would allow for the health care system to measure and therefore focus on
reducing the rates of iatrogenic intraoperative adverse events, such as splenic injury.
METHODS
Data Source and Measures
The American College of Surgeons’ National Surgical Quality Improvement Program
(ACS-NSQIP) is a surgical clinical registry that collects high quality clinical data with dedicated
trained clinical abstractors in participating hospitals. The Medicare inpatient claims data file is an
administrative dataset comprised of demographic data, as well as diagnoses and procedures
billed to Medicare for all Medicare beneficiaries. Patient records accrued from the ACS-NSQIP
clinical registry from 2005 to 2008 were linked to the Medicare inpatient claims data file from
the same period using indirect patient identifiers and a deterministic linkage algorithm. The
details of the linkage procedure are provided elsewhere.(20) As a result of the linked data source,
the study sample was restricted to patients 65 years of age and older who underwent a colectomy
at an ACS-NSQIP participating hospital from 2005 to 2008. Colectomy procedures were

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 6
identified by Current Procedures Terminology (CPT) codes recorded in the ACS-NSQIP “CPT
primary procedure” data field (Appendix 1, online only). The exclusion criterion was the
presence of colon cancer diagnoses (due to possibility that the cancer could have invaded the
spleen and therefore splenectomy may have been indicated) in any of the ten Medicare inpatient
claims International Classification of Diseases, 9th edition (ICD-9) diagnosis data fields.
Additionally, colectomies in the setting of trauma admissions were not included in this dataset
because ACS-NSQIP does not accrue any patients who undergo operations as a result of blunt or
penetrating trauma.
The primary occurrence queried was the presence of a concurrent splenic procedure
code. This was determined in ACS-NSQIP based on the presence of designated CPT codes in
any of ACS-NSQIP’s ten “concurrent procedure” or ten “other procedure” data fields. This was
determined in Medicare inpatient claims based on the presence of designated ICD-9 procedure
codes in any of the six Medicare inpatient claims “procedure” data fields. CPT and ICD-9 codes
used to identify splenic procedures are reported in Table 1.
The secondary occurrence queried was the presence of a diagnosis code of splenic injury.
This was determined based on the presence of ICD-9 diagnosis codes denoting splenic injury in
the one “postoperative diagnosis” data field in ACS-NSQIP (Appendix 2, online only). In
Medicare inpatient claims, this was determined based on the presence of the same ICD-9
diagnosis codes in any of the ten “ICD-9 diagnosis” Medicare inpatient claims data fields.
Statistical Analysis
Initial descriptive statistics were performed to compare the demographic and clinical
characteristics of patients who underwent colectomy with concurrent splenic procedure (in ACS-
NSQIP and Medicare inpatient claims) to those who did not. The raw rates of ACS-NSQIP

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 7
postoperative complications, including 30-day composite morbidity and 30-day mortality were
calculated to understand the clinical implication of concurrent splenic procedures on
postoperative outcomes. Thirty-day composite morbidity was defined as a dichotomous variable
representing the occurrence of any one or more of the following 30-day postoperative
complications: surgical site infection (superficial, deep and/or organ-space), wound disruption,
sepsis, pneumonia, unplanned reintubation, prolonged intubation, bleeding requiring transfusion,
cardiac arrest, myocardial infarction, deep vein thrombosis, pulmonary embolus, coma, stroke,
peripheral nerve injury, renal failure and urinary tract infection.
Next the clinical implication of a splenic injury requiring a splenic procedure was
quantified. This was done by calculating the association between odds of 30-day morbidity and
30-day mortality and a concurrent splenic procedure while controlling for clinical variables. This
association was calculated using a hierarchical multivariate logistic model including, the hospital
as a random intercept, and the following independent variables selected using clinical relevance
and significance on bivariate analysis, p<0.05; splenic procedure, American Society of
Anesthesiologists Classification, functional status, emergent case status, prior surgery,
preoperative open wound, ascites, impaired sensorium, preoperative pneumonia, dyspnea,
ventilator dependence, chronic obstructive pulmonary disease, congestive heart failure,
preoperative renal failure, steroid use, preoperative transfusion, preoperative sepsis, bleeding
disorder and the CPT linear risk variable. The CPT linear risk variable is the linearly scaled
probability of morbidity (or mortality depending on the model) associated with each CPT code
calculated in a previous hierarchical logistic model controlling for age, American Society of
Anesthesiologists Classification and functional status.(21) This is the current standard method of
adjusting for case-mix in ACS-NSQIP semiannual report models.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 8
Subsequently, clinical variables associated with the odds of a splenic procedure were
identified using another hierarchical multivariate logistic model. Initial bivariate analysis was
used to select clinical variables most significantly associated, p<0.05, with splenic procedure for
inclusion in the multivariate model. Emergent case, previous surgery and ascites were included
in the model due to their potential clinical importance. The predictive ability of the model was
determined with the C-statistic.
Finally, the concordance between ACS-NSQIP and Medicare inpatient claims procedure
codes was compared. ACS-NSQIP was treated as the gold-standard as it has been shown to have
a high degree of accuracy when compared to other means of perioperative event capture.(22-26)
Percent agreement was calculated by the ratio of patients who were concordant in both ACS-
NSQIP and Medicare inpatient claims over the total number of patients. In order to calculate the
sensitivity, specificity, positive and negative predictive value of Medicare inpatient claims, the
ACS-NSQIP dataset was designated as the reference standard as has been done in previous
studies.(22,24,25) A Kappa statistic and respective 95% confidence interval was calculated to
assess agreement between the data sources beyond chance. Diagnosis codes recorded in ACS-
NSQIP and Medicare inpatient claims were compared in a similar fashion.
A final sensitivity analysis was performed excluding patients with primary splenic
disorders (Appendix 3, online only). This work was approved by the RAND Corporation
Institutional Review Board. All data management and analyses were performed with SAS
version 9.3 Cary, North Carolina, USA.
RESULTS
A total of 11,367 colectomy procedures were identified from 212 hospitals. A total of 114
(1%) patients underwent a concurrent splenic procedure according to either ACS-NSQIP or

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 9
Medicare inpatient claims. Of those 114 patients, 108 patients (95%) underwent splenectomy and
10 patients (9%) underwent splenorrhaphy. A total of 106 (1.2%) patients undergoing open
colectomy had a splenic procedure compared to 8 (0.3%) patients undergoing laparoscopic
colectomy, p<0.001. There was no difference between the two groups for age or gender (Table
2). Notable statistically significant and clinically relevant differences between patients
undergoing concurrent splenic procedure and those who did not were the proportion of cases that
were emergency (non-trauma) procedures (43% versus 27%, p=0.001), as well as rates of
preoperative ascites (10% versus 4%, p<0.001), and preoperative systemic inflammatory
response or sepsis (38% versus 22% (p<0.001).
The postoperative 30-day outcomes were compared between patients who underwent
concurrent splenic procedure and those who did not while controlling for clinical variables and
case-mix (Table 3). Patients who underwent concurrent splenic procedure had 1.8-fold higher
odds of 30-day morbidity (95% CI 1.1-2.8, p<0.01) when controlling for preoperative
comorbidities and colectomy case-mix. This was likely partly attributable to higher rates of
bleeding requiring intraoperative/postoperative transfusion; 11% versus 1%, p<0.0001. There
was no significant difference in 30-day mortality when controlling for comorbidities and
colectomy case-mix.
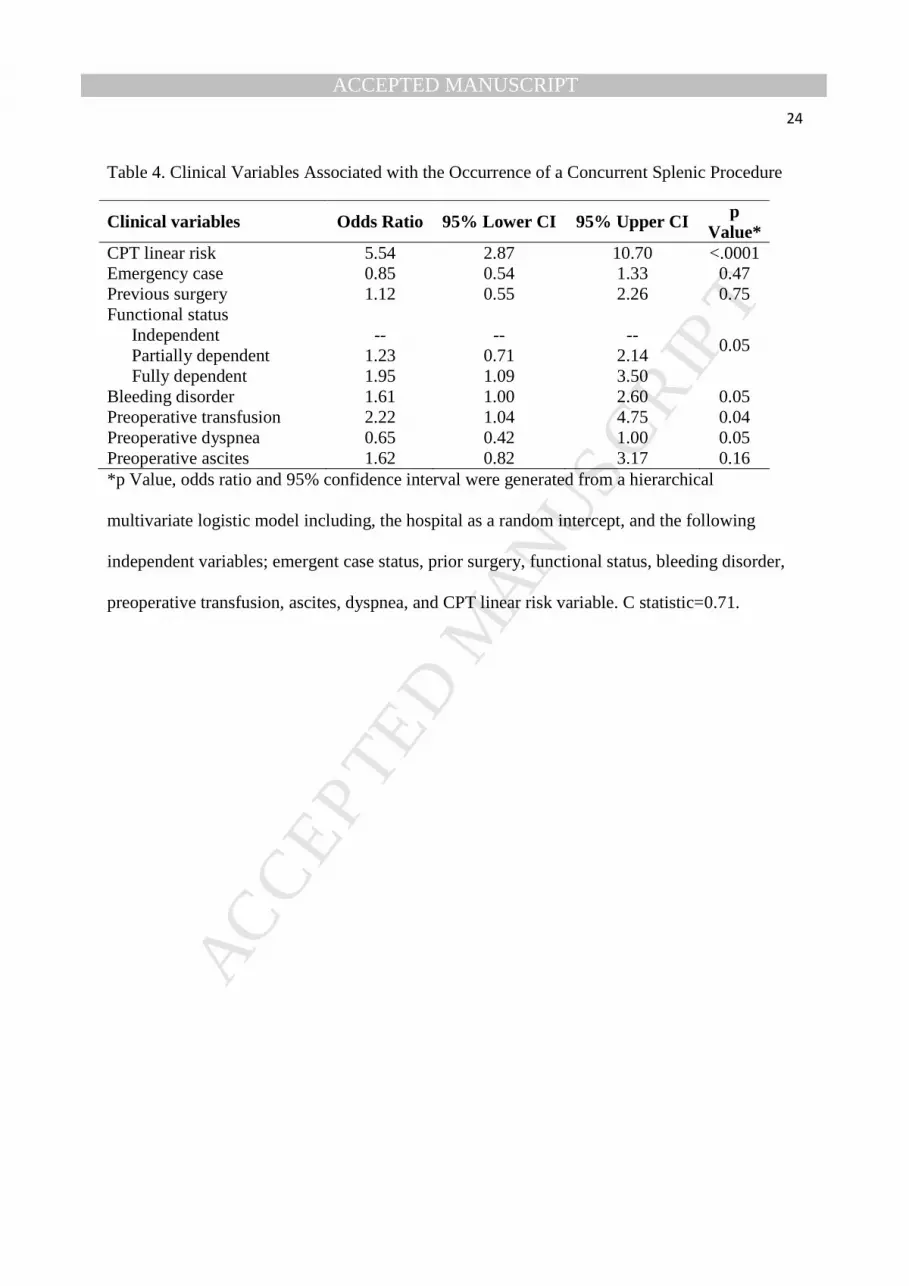
A hierarchical multivariate logistic model demonstrated that two clinical variables were
highly associated with the odds of a splenic procedure. The variable most highly associated was
the colectomy procedure CPT code, odds ratio = 5.54, 95% CI = 2.87-10.70 and having had a
preoperative blood transfusion in the 48 hours prior to colectomy, odds ratio= 2.22, 95% CI =
1.04-4.75 (Table 4). C statistic was 0.71.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 10
Procedure codes captured a rate of splenic events within the incidence range reported in
the literature. Concurrent splenic procedures were reflected in 0.7% of colectomies in ACS-
NSQIP and 0.9% in Medicare inpatient claims (Table 5). Using procedure codes, 64 splenic
injuries were captured in both Medicare inpatient claims and ACS-NSQIP using procedure
codes. A total of 35 splenic injuries were captured in Medicare inpatient claims but not ACS-
NSQIP. Another 15 splenic injuries were captured in ACS-NSQIP but not Medicare inpatient
claims. Percent agreement was 99%. Statistical concordance between the data sources on
recording of splenic procedure codes was substantial (kappa statistic 0.72, 95% CI 0.64-0.79).
Medicare inpatient claims correctly identified 81% of the splenic procedure codes recorded in
ACS-NSQIP, and 99% of the patients without a splenic procedure code. Only 1% of patients
without a splenic procedure code in Medicare claims were false negatives.
Diagnosis codes captured a rate of splenic events below the incidence range reported in
the literature. Seven splenic injuries were captured in Medicare inpatient claims using diagnosis
codes (0.06%). No splenic injuries were captured in ACS-NSQIP and therefore the Kappa
statistic could not be calculated. Of note, 57% or four out of seven patients with a diagnosis code
of splenic injury in Medicare inpatient claims were captured by procedure codes in Medicare
inpatient claims. Conversely, 48% or three out of seven patients with a diagnosis code of splenic
injury in Medicare inpatient claims were captured by procedure code in ACS-NSQIP.
A final sensitivity analysis was performed, excluding patients with diagnoses of primary
splenic disorders (Appendix 3, online only). A total of 35 out of 11,367 patients had portal
hypertension, immune thrombocytopenic purpura, splenomegaly or leukemia/lymphoma. Of the
114 patients who underwent a splenic procedure, 4 of them had one of the above diagnoses. The

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 11
analyses were re-run with this sample excluding patients with primary splenic diagnoses and all
findings of these analyses were unchanged from those of the larger sample.
DISCUSSION
Using a linked clinical registry and administrative claims database, this study found the
concordance of procedure codes between claims data and a clinical registry was substantial with
a Kappa statistic of 0.72. The sensitivity of concurrent splenic procedure codes in Medicare
inpatient claims for capturing a splenic procedure recorded in ACS-NSQIP was high (0.81),
while the specificity was excellent (0.99). Furthermore, concurrent splenic procedure codes
representing splenic injury were coded in greater frequency than diagnosis codes representing
splenic injury. Finally, concurrent splenic procedures during colectomy were associated with
worse postoperative 30-day morbidity while controlling for comorbidities and colectomy case-
mix. In summary, this study found that there is substantial concordance in procedure codes
between clinical registry and administrative claims data.
Previous work has shown that administrative data unreliably code diagnoses of surgical
complications in certain circumstances.(9,10,13) Other groups have also demonstrated that
procedure codes may be more reliably coded in administrative data than diagnosis codes.(18,19)
As such, procedure codes in administrative claims data may be useful for assessing occurrence of
adverse events during colectomy compared to using diagnosis codes.
This study’s rates of concurrent splenic procedures during colectomy were within the
range of known incidence of splenic injury for both ACS-NSQIP and Medicare inpatient claims.
(1,2) Of note, Medicare inpatient claims data did have slightly higher rates of capture for
concurrent splenic procedures than ACS-NSQIP, but at the same time the false positive rate in

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 12
Medicare inpatient claims procedure codes is uncertain. The higher capture rate might in part be
due to the more ambiguous nature of ICD-9 codes, which are less granular than CPT codes.
There are also differences in the training of the personnel collecting data as well as the primary
aims in data collection which may add bias to what is captured in the data.
Diagnosis codes in both ACS-NSQIP and Medicare inpatient claims were much lower
than the known incidence of splenic injury. The diagnoses were coded so infrequently that they
are likely inaccurate as they do not represent known incidence of this complication.(27) Previous
studies have demonstrated that diagnosis coding of postoperative complications may be
unreliable and inaccurate in claims data.(22) In addition, ACS-NSQIP limits ICD-9 codes to one
postoperative diagnosis field, which may underestimate apparent diagnosis rates in registry data.
There has been concern regarding the accuracy of diagnosis codes dating back to the era
of establishment of diagnosis related groups. (17) An advantage of procedure codes in
administrative data is that they may be more reliable in capturing health care related events than
diagnosis codes. Some groups have begun to use procedure codes to define the occurrence of
complications.(28) Intraoperative concurrent splenic procedure codes in claims data may be
useful for identifying intraoperative iatrogenic injuries. Since claims data are available for all
patients, this means providers and payers could work together to improve the transparency of
intraoperative events, which could potentiate subsequent quality improvement activities. For
example, if certain providers are identified as having a large number of iatrogenic injuries,
departments could step in and provide coaching or other support. In this way, claims data could
be used for identifying and monitoring surgical quality within an institution.
Indeed, the major source of iatrogenic splenic injury during colectomy is vigorous tissue
handling near the spleen.(4) As such, the resection of left sided colonic tumors has higher rates

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 13
of iatrogenic splenic injury likely due to mobilization of the splenic flexure.(1) Similarly, any
operation requiring mobilization of the splenic flexure, such as subtotal colectomy may have a
higher rate of splenic injury.(29) Yet, simply because an injury is more likely in this anatomic
location, does not make the injury less significant for the patient. Attention should be focused on
what can be done to prevent splenic injury. Giving feedback to providers has minimized other
perioperative complications.(30-32) This study demonstrates a mechanism for detecting splenic
injury with the ultimate goal of using this data to provide feedback to providers and improve
patient care.
The current study has several limitations. First, ACS-NSQIP during 2005-2008 captured
only one data field for postoperative diagnosis codes. Occasionally, the postoperative diagnosis,
regardless of intraoperative events or findings, is inaccurately recorded as “the same as the
preoperative diagnosis”. As a result, the diagnoses of iatrogenic splenic injuries may be under-
captured. Second, using procedure codes may under-estimate the occurrence of iatrogenic
splenic injury to only those injuries requiring a procedure. However, evidence has demonstrated
that 47% of splenic injuries require a procedure.(33) This is concordant with the findings of this
study; that a splenic procedure was performed in around half of patients with a diagnosis of
splenic injury. It has been recommended that splenic lacerations greater than 1 cm, or multiple
lacerations should be treated with splenectomy or splenorraphy.(4) These more severe injuries
are likely better indicators of poor quality. Therefore the exclusion of smaller injuries controlled
with topical hemostatic may be of little importance to quality measurement. A third limitation is
that the concordance of the CPT and ICD-9 procedure codes is limited by the crosswalk validity.
Since this study used two different types of codes: CPT codes captured ACS-NSQIP concurrent
procedures and ICD-9 codes captured Medicare concurrent procedures, the concordance between

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 14
capture in the two datasets was limited by the fact that the descriptions of ICD-9 codes were less
granular than CPT codes. Therefore matching the codes to generate a crosswalk required some
inference on the part of the researcher. A fully concordant crosswalk may not be possible based
on the differences between the CPT and ICD-9 coding systems and their respective definitions.
A fourth limitation is that no provider characteristics were available to identify and adjust for
differences across providers in rates of splenic injuries. A fifth limitation is that colectomies for
cancer were excluded from this analysis. This was done in order to limit the capture of indicated
splenectomies that would have been necessary for adequate surgical resection. However,
indicated splenectomies even in cancer are very rare, and colon cancer is the most common
indication for colectomy. As such, the generalizability of study findings to the wider population
of colectomy patients may have been limited by this exclusion. Finally, it is possible that ACS-
NSQIP abstractors might collect concurrent procedures variably, as they are not perceived to be
as critical as the index procedure code. Although the rate of splenic procedures were within the
published ranges, it is possible that concurrent procedures were under-captured. Furthermore, the
clinically trained abstractors at ACS-NSQIP may also be more discerning, coding only clinically
relevant procedures as compared to administrative claims coders who may err on the side of
capturing all concurrent procedures. Although, it is beyond scope of this study to assess why
Medicare captured more concurrent procedures than ACS-NSQIP, in this era of large datasets,
this question requires a more extensive study to analyze exactly how diagnosis and procedure
codes are recorded. Standardizing data collection techniques are likely just as important as
standardizing how we care for patients if scientists and policy makers wish to use these data for
quality measurement.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 15
Despite these limitations, the current study adds to the literature by validating the
reliability of procedure codes in administrative claims data for detection of intraoperative events.
Future directions include determining whether procedure codes are useful as a component of
hospital level comparisons. Another important step would be to determine scalability of this
approach, by identifying whether the procedure codes for other iatrogenic injuries during
colectomy can be reliably captured.
CONCLUSION
Procedure codes recorded in claims data for concurrent splenic procedures during
colectomy are more valid and reliable for diagnosing intraoperative splenic injury than diagnosis
codes in claims data. Therefore, in absence of clinical registry data, procedure codes in claims
data may be a means of identifying intraoperative events. Although these intraoperative events
and associated procedure codes are disease-specific, limiting their generalizability, procedure
codes could be extrapolated as an indicator of surgical technical quality. The next steps in this
work include evaluation of other procedure codes that may represent intraoperative
complications, as well as a determination of whether these procedure codes can be used to
evaluate hospital level performance.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 16
REFERENCES
1. McGory ML, Zingmond DS, Sekeris E, Ko CY. The significance of inadvertent
splenectomy during colorectal cancer resection. Arch Surg 2007;142:668-674.
2. Holubar SD, Wang JK, Wolff BG, et al. Splenic salvage after intraoperative splenic
injury during colectomy. Arch Surg 2009;144:1040-1045.
3. Olsen WR, Beaudoin DE. Surgical injury to the spleen. Surg Gynecol Obstet
1970;131:57-62.
4. Peck DA, Jackson FC. Splenectomy after surgical trauma. Arch Surg 1964;89:54-65.
5. Rich NM, Lindner HH, Mathewson C. Splenectomy incidental to iatrogenic trauma. Am
J Surg 1965;110:209-217.
6. Coon WW. Iatrogenic splenic injury. Am J Surg 1990;159:585-588.
7. Kristinsson SY, Gridley G, Hoover RN, et al. Long-term risks after splenectomy among
8,149 cancer-free American veterans: a cohort study with up to 27 years follow-up.
Haematologica 2014;99:392-398.
8. Birkmeyer JD, Finks JF, O'Reilly A, et al. Surgical skill and complication rates after
bariatric surgery. N Engl J Med 2013;369:1434-1442.
9. Hannan EL, Kilburn H, Lindsey ML, Lewis R. Clinical versus administrative data bases
for CABG surgery. Does it matter? Med Care 1992;30:892-907.
10. Hunt JP, Cherr GS, Hunter C, et al. Accuracy of administrative data in trauma: splenic
injuries as an example. J Trauma 2000;49:679-686; discussion 686-688.
11. Best WR, Khuri SF, Phelan M, et al. Identifying patient preoperative risk factors and
postoperative adverse events in administrative databases: results from the Department of

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 17
Veterans Affairs National Surgical Quality Improvement Program. J Am Coll Surg
2002;194:257-266.
12. Shahian DM, Silverstein T, Lovett AF, et al. Comparison of clinical and administrative
data sources for hospital coronary artery bypass graft surgery report cards. Circulation
2007;115:1518-1527.
13. Stevenson KB, Khan Y, Dickman J, et al. Administrative coding data, compared with
CDC/NHSN criteria, are poor indicators of health care-associated infections. Am J Infect
Control 2008;36:155-164.
14. Werner RM, Asch DA. The unintended consequences of publicly reporting quality
information. JAMA 2005;293:1239-1244.
15. McNutt R, Johnson TJ, Odwazny R, et al. Change in MS-DRG assignment and hospital
reimbursement as a result of Centers for Medicare & Medicaid changes in payment for
hospital-acquired conditions: is it coding or quality? Qual Manag Health Care
2010;19:17-24.
16. Stulberg JJ, Delaney CP, Neuhauser DV, et al. Adherence to surgical care improvement
project measures and the association with postoperative infections. JAMA
2010;303:2479-2485.
17. Fisher ES, Whaley FS, Krushat WM, et al. The accuracy of Medicare's hospital claims
data: progress has been made, but problems remain. Am J Public Health 1992;82:243-
248.
18. Romano PS, Mark DH. Bias in the coding of hospital discharge data and its implications
for quality assessment. Med Care 1994;32:81-90.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 18
19. Romano PS, Chan BK, Schembri ME, Rainwater JA. Can administrative data be used to
compare postoperative complication rates across hospitals? Med Care 2002;40:856-867.
20. Lawson EH, Ko CY, Louie R, et al. Linkage of a clinical surgical registry with Medicare
inpatient claims data using indirect identifiers. Surgery 2013;153:423-430.
21. Cohen ME, Ko CY, Bilimoria KY, et al. Optimizing ACS NSQIP modeling for
evaluation of surgical quality and risk: patient risk adjustment, procedure mix adjustment,
shrinkage adjustment, and surgical focus. J Am Coll Surg 2013;217:336-346.e1.
22. Lawson EH, Louie R, Zingmond DS, et al. A comparison of clinical registry versus
administrative claims data for reporting of 30-day surgical complications. Ann Surg
2012;256:973-981.
23. Lawson EH, Wang X, Cohen ME, et al. Morbidity and mortality after colorectal
procedures: comparison of data from the American College of Surgeons case log system
and the ACS NSQIP. J Am Coll Surg 2011;212:1077-1085.
24. Davis CL, Pierce JR, Henderson W, et al. Assessment of the reliability of data collected
for the Department of Veterans Affairs national surgical quality improvement program. J
Am Coll Surg 2007;204:550-560.
25. Lee LC, Reines HD, Sheridan MJ, et al. Apples and oranges: comparison of ACS-NSQIP
observed outcomes with premier's quality manager-predicted outcomes. Am J Med Qual
2011;26:474-479.
26. McVeigh TP, Waters PS, Murphy R, et al. Increasing reporting of adverse events to
improve the educational value of the morbidity and mortality conference. J Am Coll Surg
2013;216:50-56.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 19
27. Wang JK, Holubar SD, Wolff BG, et al. Risk factors for splenic injury during colectomy:
a matched case-control study. World J Surg 2011;35:1123-1129.
28. Reinke CE, Showalter S, Mahmoud NN, Kelz RR. Comparison of anastomotic leak rate
after colorectal surgery using different databases. Dis Colon Rectum 2013;56:638-644.
29. Cioffiro W, Schein CJ, Gliedman ML. Splenic injury during abdominal surgery. Arch
Surg 1976;111:167-171.
30. Khuri SF, Daley J, Henderson WG. The comparative assessment and improvement of
quality of surgical care in the Department of Veterans Affairs. Arch Surg 2002;137:20-
27.
31. Grover FL, Shroyer AL, Hammermeister K, et al. A decade's experience with quality
improvement in cardiac surgery using the Veterans Affairs and Society of Thoracic
Surgeons national databases. Ann Surg 2001;234:464-472; discussion 472-474.
32. O'Connor GT, Plume SK, Olmstead EM, et al. A regional intervention to improve the
hospital mortality associated with coronary artery bypass graft surgery. The Northern
New England Cardiovascular Disease Study Group. JAMA 1996;275:841-846.
33. Langevin JM, Rothenberger DA, Goldberg SM. Accidental splenic injury during surgical
treatment of the colon and rectum. Surg Gynecol Obstet 1984;159:139-144.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 20
Table 1. Procedure Code Crosswalk
Description CPT Procedure Code ICD-9 Procedure Code Total splenectomy 38100, 38120 41.5 Partial splenectomy 38101 41.4, 41.42, 41.43 Other splenectomy 38102 41.9, 41.93, 41.99 Splenorrhaphy 38115, 38129 41.95

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 21
Table 2. ACS-NSQIP Characteristics of Medicare Patients Undergoing Colectomy Procedures
with and without a Concurrent Splenic Procedure from 2005-2008 at an ACS-NSQIP
Partipcating Hospital
Preoperative clinical characteristics
Colectomy with
concurrent splenic
procedure
Colectomy without
concurrent splenic
procedure
Total p Value
n=114 n=11,253 n=11,367 n (%) n (%)
Male 56 (49) 4832 (43) 4888 (43) 0.19 Age, y 65-75 75-84 ≥85
51 (45) 48 (42) 15 (13)
5469 (49) 4524 (40) 1260 (11)
5520 (49) 4572 (40) 1275 (11)
0.66
American Society of Anesthesiologists Class 1 or 2 3 4 or 5
27 (24) 49 (43) 38(33)
3533 (31) 5722 (51)
1998 (18)
3568 (31) 5771 (51) 2028 (18)
<0.001
Functional status Independent Partially dependent functional status Fully dependent functional status
69 (61) 19 (16) 26 (23)
9095 (81) 1348(12) 810 (7)
9164 (81) 1367 (12) 836 (7)
<0.001
Approach Open procedure 106 (93) 8835 (79) 8941 (79)
<0.001 Laparoscopic procedure 8 (7) 2418 (21) 2426 (21)
Acuity of illness: Emergency procedure 47 (41) 2995 (27) 3042 (27) 0.001 Previous Surgery within 30 Days 11 (10) 447 (4) 458 (4) 0.002 Preoperative Open Wound 13 (12) 469 (4) 482 (4) <0.001 Recent weight loss >10% 11 (10) 600 (5) 611 (5) 0.04 Body Mass Index >30 28 (25) 2866 (25) 2894 (25) 0.71 Ascites 12 (11) 400 (4) 412 (4) <0.001 Impaired Sensorium 11 (10) 393 (4) 404 (4) <0.001
Pulmonary comorbidities:
Smoker 17 (15) 1349 (12) 1366 (12) 0.34 Chronic obstructive pulmonary disease 21 (18) 1264 (11) 1285 (11) 0.02 Dyspnea 35 (31) 1933 (17) 1968 (17) 0.001 Pneumonia 6 (5) 179 (2) 185 (2) 0.002 Ventilator Dependent 17 (4) 416 (15) 433 (4) <0.001

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 22
Cardiac comorbidities:
History of myocardial infarction 6 4 (4) 176 (2) 180 (2) 0.10 Congestive heart failure 9 (8) 341(3) 350 (3) 0.003 Recent percutaneous coronary intervention 7 (6) 1069 (10) 1076 (10) 0.22 History of cardiac surgery 15 (13) 1271 (11) 1286 (11) 0.53
Renal comorbidities:
Renal failure 7 (6) 240 (2) 247 (2) 0.004 Dialysis 3 (2) 129 (1) 132(1) 0.14
Hematologic and immunologic comorbidities
Bleeding disorder 28 (25) 1127 (11) 1255 (11) <0.001 Blood transfusion 9 (8) 226 (2) 235 (2) <0.001 Systemic inflammatory response syndrome, sepsis, or septic shock
44 (39) 2435 (22) 2479 (22) <0.001
Steroid use 15 (13) 811 (7) 826 (7) <0.001 All clinical variables were derived from ACS-NSQIP. Concurrent splenic procedure definition
included in Table 1.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 23
Table 3: Association between Occurrence of a Concurrent Splenic Procedure and 30-day Postoperative Morbidity and Mortality for Patients Undergoing Colectomy Procedures
Outcomes
Colectomy with concurrent splenic
procedure
(n=114)
Colectomy without concurrent splenic
procedure
(n=11,253)
30-d postoperative morbidity, n (%) 67 (59) 3794 (34) 30-d postoperative mortality, n (%) 23 (20) 969 (9) Risk-adjusted odds ratio for 30-d postoperative morbidity (95% CI)
1.8 (1.2-2.8)* Reference Group
Risk-adjusted odds ratio for 30-d postoperative mortality (95% CI)
1.1 (0.6-2.0)* Reference Group
*Odds ratio and 95% confidence interval were generated from a hierarchical multivariate logistic
model including, the hospital as a random intercept, and the following independent variables;
splenic procedure, American Society of Anesthesiologists Classification, functional status,
emergent case status, prior surgery, preoperative open wound, ascites, impaired sensorium,
preoperative pneumonia, dyspnea, ventilator dependence, chronic obstructive pulmonary disease,
congestive heart failure, preoperative renal failure, steroid use, preoperative transfusion,
preoperative sepsis, bleeding disorder and CPT linear risk variable. CI= Confidence interval. 30-
day morbidity and mortality variables derived from ACS-NSQIP data. See text for list of
complications included in 30-day morbidity definition. Concurrent splenic procedure defined in
Table 1.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 24
Table 4. Clinical Variables Associated with the Occurrence of a Concurrent Splenic Procedure
Clinical variables Odds Ratio 95% Lower CI 95% Upper CI p Value*
CPT linear risk 5.54 2.87 10.70 <.0001 Emergency case 0.85 0.54 1.33 0.47 Previous surgery 1.12 0.55 2.26 0.75 Functional status
0.05 Independent -- -- -- Partially dependent 1.23 0.71 2.14 Fully dependent 1.95 1.09 3.50
Bleeding disorder 1.61 1.00 2.60 0.05 Preoperative transfusion 2.22 1.04 4.75 0.04 Preoperative dyspnea 0.65 0.42 1.00 0.05 Preoperative ascites 1.62 0.82 3.17 0.16 *p Value, odds ratio and 95% confidence interval were generated from a hierarchical
multivariate logistic model including, the hospital as a random intercept, and the following
independent variables; emergent case status, prior surgery, functional status, bleeding disorder,
preoperative transfusion, ascites, dyspnea, and CPT linear risk variable. C statistic=0.71.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
25
Table 5. Identification of Splenic Injury Occurring during Colectomy Procedures using ACS-NSQIP and Medicare Inpatient Claims
for 11,367 Patients
Type of code used to identify
splenic injury in Medicare inpatient
claims
No. of patients captured with
splenic injury in ACS-NSQIP and
Medicare inpatient claims (sensitivity*)
No. of patients captured without splenic injury in ACS-NSQIP and
Medicare inpatient claims (specificity*)
No. of splenic injuries not captured in
ACS-NSQIP but captured in Medicare
inpatient claims
No. of splenic injuries
captured in ACS-NSQIP
but not captured in Medicare inpatient
claims
Agreement beyond chance of
capturing splenic injury between
ACS-NSQIP and Medicare inpatient
claims Kappa (95% CI)
Procedure codes
64/79 (0.81) 11,253/11,288 (0.99) 35 15 0.72 (0.64-0.79)
Diagnosis codes
0/0 (NA) 11,360/11,367 (NA) 7 0 NA
*Using ACS-NSQIP as the gold standard. NA signifies not applicable because too few observations were captured to calculate an estimate.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT 26
Precis
It is feasible to use Medicare claims data to identify splenic injuries occurring during colectomy
procedures as claims data have moderate sensitivity and excellent specificity for recording of
concurrent splenic procedure codes compared to ACS-NSQIP.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Appendix 1. Current Procedure Terminology (CPT) Codes and Descriptions
CPT Code Case Description
44140 Partial removal of colon 44141 Partial colectomy with ostomy 44143 Partial colectomy with end ostomy 44144 Partial colectomy with mucous fistula 44155 Colectomy with proctectomy 44156 Colectomy with kock pouch 44157 Colectomy with ileoanal anastomosis 44158 Colectomy with pouch anastomosis 44160 Partial colectomy with ileocolostomy 44204 Laparoscopic partial colectomy 44205 Laparoscopic partial colectomy with ileocolostomy 44206 Laparoscopic hartmanns with end colostomy 44207 Laparoscopic colectomy/coloproctostomy 44208 Total colectomy with coloproctostomy 44210 Total colectomy without proctectomy 44211 Total colectomy with proctectomy jpouch 44212 Total colectomy with proctectomy ileostomy 44213 Colectomy take down splenic flexure

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Appendix 2. ICD-9 Diagnosis Codes of Splenic Injury
Description ICD-9 Diagnosis Splenic injury unspecified 865.00 Splenic Injury Hematoma without Rupture 865.01 Splenic injury capsular tear 865.02 Splenic Injury Laceration Extending into the Parenchyma 865.03 Splenic injury complete parenchymal disruption 865.04 Splenic injury open 865.10 Splenic injury open hematoma 865.11 Splenic injury open tear 865.12 Splenic injury open parenchymal disruption 865.14

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Appendix 3. ICD-9 Diagnosis Codes of Primary Splenic Diagnosis
Primary splenic disorder ICD-9 Diagnosis
Portal hypertension 572.3 Immune thrombocytopenic purpura 287.31
Splenomegaly
289.4 289.51 289.52 289.53 789.2
Leukemia/Lymphoma
200.07 200.17 200.27 200.37 200.47 200.57 200.67 200.77 200.87 201.07 201.17 201.27 201.47 201.57 201.67 201.77 201.97 202.07 202.17 202.27 202.37 202.47 202.57 202.67 202.77 202.87 202.97 205.0 205.1 205.2 205.3 205.8 205.9





























