Embed Size (px)
Citation preview
Future Health Professionals
Running head: FUTURE HEALTH PROFESSIONALS’ HEALTHCARE REFORM
ORIENTATIONS: A QUALITATIVE CONTEXTUALIZATION
Future Health Professionals’ Healthcare Reform Orientations:
A Qualitative Contextualization
Joel B. Goodin, PhD
Vanessa M. D’Brot
1
Future Health Professionals
Submitted to Florida State University Undergraduate Research
Journal
October 31, 2013
Introduction
“Less than a decade away from becoming a doctor, I need to start thinking about my future.
The reform was a change that I had not prepared for.”
~Undergraduate Pre-health Student
One of the most “tangible” ways that Americans show
opposition or support for an idea is through their voting
behavior. For the last 100 years, Republicans and Democrats have
been proposing healthcare reform, but only in 2008 did an actual
legislative push gain substantial traction. The Obama
administration and Congress successfully passed the Patient
Protection and Affordable Care Act (ACA) on March 23, 2010,
despite a divisive vote 219-212 (with 34 Democrats joining the
opposing Republicans), perhaps foreshadowing years of contention,
repeal attempts, and the government shutdown of 2013.
2
Future Health Professionals
The United States’ substantial undersupply of physicians and
other healthcare providers (currently approximately 66%), already
grappling with the increased needs of the aging “Baby Boomer”
generation, will only be exacerbated by an approximated 32
million newly-insured citizens resulting from the ACA.1,2 In the
midst of a changing healthcare landscape, the end goal of the
current research is to provide information that can be used to
better understand factors that affect “potential” (future)
healthcare providers so that the areas of need can be
strengthened.
The importance in understanding the factors that drive and
deter future health providers (e.g., physicians) is essential to
ensuring the success of the healthcare system and to maintaining
or improving the quality of care provided to US citizens. The
political emphasis surrounding healthcare is currently elevated,
with the birth pains of the ACA Individual Mandate and the recent
government shutdown, both in October of 2013. The ACA requires
systemic change as the healthcare system makes strides toward
assisting underserved populations. That shift may require
3
Future Health Professionals
adjustments to Health Education to guide and support students
toward areas of need within their changing career fields.
Health policy and educational researchers have a unique
opportunity to understand and influence health education during a
time of change and great need. The current study is one of many
studies of future healthcare providers facilitated by Author2 and
his colleagues. Their studies have focused on the development and
implementation of a healthcare reform perceptions instrument3,4
and the identification of determinants of specialty choice such
as self-efficacy and a calling to a career,5 community-based
training,6 political alignment,7 and cultural background.8
In contrast to the studies of medical students, the current
study seeks to understand how undergraduate pre-health students'
perceptions and goal-orientations may have changed as a result of
ACA effects on their future professions. It was hypothesized that
the undergraduate students were comparatively less invested
(time, finances, energy) than the medical students in similar
previous studies.3 Perhaps the ACA has spurred more consideration
among pre-health students with regard to alternative career
options. The current qualitative study is a preliminary analysis
4
Future Health Professionals
of undergraduate pre-health students, with the purpose of
providing a valuable analysis of the pre-health students'
cognitions, motivations, and emotions regarding the ACA, as the
foundation for a larger-scale mixed method study.
In the research presented here, the researchers were
interested in understanding how pre-health students’ orientation
to the ACA results in emotions, motivations, and behaviors (i.e.,
Reaction)3,4 toward a health-related career. The researchers were
particularly interested in how each orientation would show
students’ degree (strength of opinion) and direction
(support/opposition) in the operationalization of their views
exhibited by their past and predicted future voting behavior. The
following section includes discussion of relevant theories.
Theoretical Frameworks
The current study was built on Locke’s9 Goal-setting Theory
and Inglehart’s10 Critical Life Event Theory. The pursuit of a
health-related profession is a long-term commitment to a goal
which is often made before a student reaches the undergraduate
level. Based on Author2’s3,4,11 findings, medical students differ
in how they perceive and respond to the ACA. Thus, understanding
5
Future Health Professionals
pre-health students' ACA perceptions is an important factor in
predicting and preparing for a changing healthcare system (i.e.,
adequate supply of physicians).
Goal-setting Theory9 describes how goals and motivations are
interconnected. Goals guide and direct human effort and behavior.
In order to stay on course to goal completion, a person must
overcome obstacles and avoid distractions that may deter them
from their prospective goals.12,13 In the current study, the
effects of ACA implementation on the healthcare system will be
evaluated as a possible “critical event” (deterrent or
attraction) for undergraduate students with health career plans,
such that it may affect their motivation and cause a modification
of goals, as was discussed in previous research by Author2.3,4
Inglehart10 described a critical life event as a positive or
negative event that elicits (a) tension, regardless of the
positive or negative perception of the event;14 (b) appraisal of
the stressor’s relevance and the resources with which to maintain
equilibrium;15 (c) cognitive re-evaluation of goal
attractiveness;16 and (d) stability or decrease of goal
commitment.17 It was unclear to what extent pre-health students
6
Future Health Professionals
might experience tension, appraisal, re-evaluation, and goal
commitment changes in light of the ACA.
Research purpose
The purpose of the current research was to examine the ways
in which undergraduate pre-health students’ retrospective and
current accounts of their political and professional motivations
converge to affect their current ACA perceptions. The goal was to
understand the extent to which the ACA was a relevant issue and
students’ responses to said relevance in terms of attention and
evaluation of the law and its possible personal or social
ramifications. Perceived relevance played a large role in
determining an orientation toward the ACA that was associated
with stimulation of information-seeking behavior, a decision of
ACA support or opposition, or stability/modification of goals to
decrease potential risk or discomfort in students’ future
careers. The researchers were particularly interested in
exploring characteristic differences in the individuals that held
similar philosophical and political ACA orientations, their
career goal stability, and variance in their respective cognitive
7
Future Health Professionals
appraisals (attention and value) of the ACA and its possible
effects on their personal lives, social environments, and
professional careers.
Methods
In order to explore individuals’ ACA orientations from 2012
to present, the researchers took a cross-sectional, retrospective
approach. In doing so, the researchers chose to survey a variety
of undergraduate students who were in the College of Human
Sciences at a large, southeastern university. In particular, the
researchers inquired about students’ career plans, and their
statements regarding ACA-related variables: attention,
importance, knowledge. Additionally, the researchers studied the
students’ responses regarding the influence of the ACA on their
attention, voting behaviors, and their self-regulatory thoughts
and behaviors of redirection processes (e.g., career goal
modification).
Subjects
Purposive sampling was implemented in order to target
subjects that would be able to provide research-related
8
Future Health Professionals
information. In other words, the sampling served the purpose of
gaining information from those who would find the subject of the
study (pre-health ACA orientations) to be most relevant and
would, thus, have the greatest likelihood of having attended to
and evaluated the ACA. Therefore, as part of a larger study of
pre-health students’ goals and beliefs during a time of change in
the healthcare landscape, the researchers were able to obtain
qualitative information in addition to the quantitatively-focused
study through the inclusion of demographics and free response
items. The exploration of retrospective accounts of ACA-related
beliefs and behaviors was used to compliment current beliefs and
behaviors with enhanced clarity and insight.
The researchers collected 44 subjects’ demographics and free
responses to career- and ACA-related prompts. Participants’ ages
ranged between 20 years and 26 years; the mean age was 21.2. Of
the total, 36 of the participants were female (81.8%); eight were
males (18.2%).
Qualitative Responses
As part of the larger, multivariate study of pre-health
9
Future Health Professionals
students, the participants completed the entire survey, including
the qualitative questions, in the days directly after the
government shutdown of 2013. It should be emphasized that
contention surrounding the ACA was considered to be one of the
most influential factors leading to the government shutdown. The
primary research question, “What are the most common orientations
of pre-health students toward the ACA?” had the purpose of
gaining an understanding of how students were attending to and
reacting to the ACA with respect to its relevance to their future
professions. It is important to note that the study’s purpose was
not to identify support or opposition to the ACA, but rather to
ask for open-ended responses to glean the important themes from
students’ statements.
First, given a list of the most common health-oriented
professions, students were asked to indicate their most likely
career choice. They were then asked to respond to the question,
“How has the Health Care Reform affected your current career
plans?” Participants then indicated the political party with
which they usually align, the candidate they voted for in 2012,
the amount of attention they have paid to the ACA, their current
10
Future Health Professionals
level of comfort with the ACA, the extent to which the ACA played
a role in their voting choice in the 2012 Presidential Election,
and the extent to which they believed the ACA would influence
their vote in the 2016 Presidential Election. Finally, with
regard to their vote in 2012 and their predicted vote in 2016,
each participant was asked to respond to the prompt, “Please
explain in 1-2 sentences how the Health Care Reform affected
[will affect] your voting choice.”
Analysis and Results
The demographic data and qualitative statements and answers
were separated from the quantitative data for analysis. Based on
the process described by Strauss and Corbin,18 a grounded theory
approach was used to analyze the data. The first step in the
analysis was “open-coding,” a process that included the
construction of descriptive words or phrases that captured the
meaning of responses. Each code was then grouped into “parent”
(higher-order) categories. Categories, or themes, emerged during
the coding process, such that with each additional participant’s
statements, the researchers were able to reach theoretical
11
Future Health Professionals
saturation, wherein new ideas or content no longer surfaced.18
Rather, themes and phrases began to be repeated.
The major themes that emerged from participants’ interviews
were ACA-related (1) orientations (e.g., ambivalent), (2) degree
of importance (3) degree of knowledge, and (4) career goal
modification. The following sections describe examples of
students’ “orientations,” the emergent categories derived from
their responses, and a comparison across the groups with regard
to each higher order grouping in order to provide a more thorough
understanding of the ACA’s role in the pre-health student’s
cognitions and motivations.
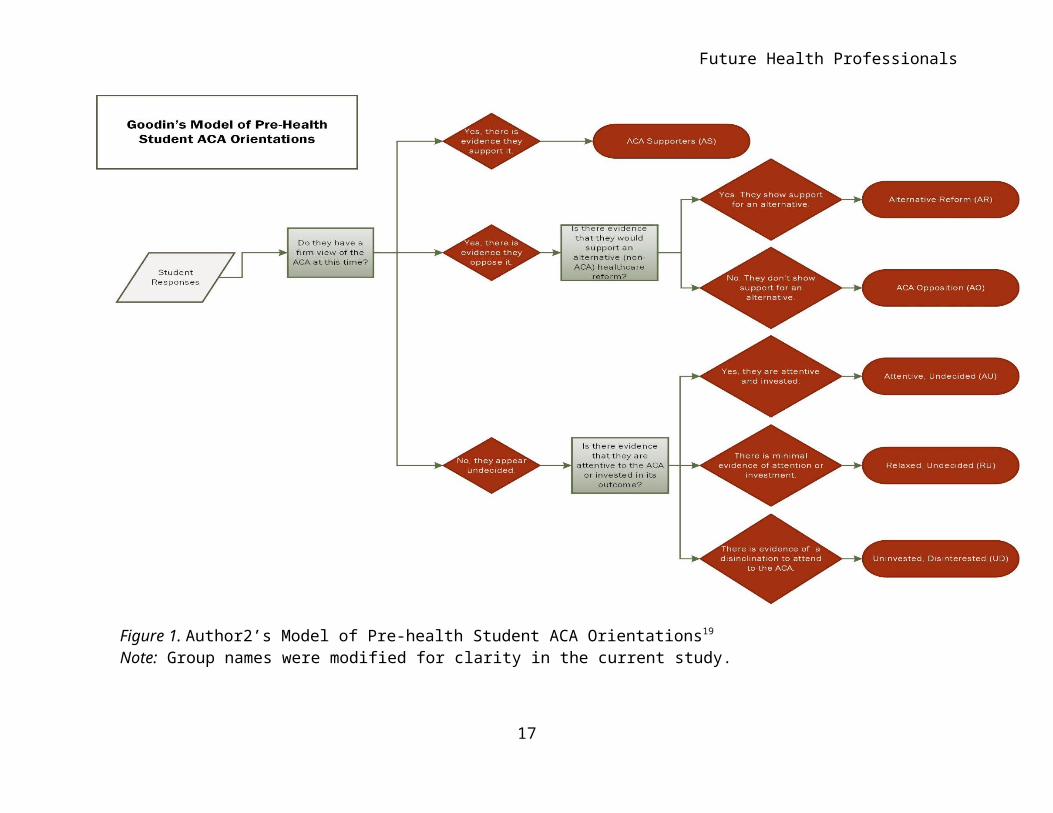
ACA Orientations. Based on the qualitative data collected
via survey, 44 participants’ statements regarding ACA degree of
interest (i.e., how much), direction (i.e., for, against, or
undecided) produced 6 themes or viewpoint categories based on
consistent emphases found in the open coding described above. The
names ascribed to the 6 viewpoints, or “orientations,” are “ACA
Supporters (Support),” “ACA Opposition (Oppose),” “Alternate
Reformers (Alternate),” “Attentive Undecided (Attentive),”
“Relaxed Undecided (Relaxed),” and “Uninvested / Disinterested
12
Future Health Professionals
(Uninvested).” The flowchart model in Figure 119 illustrates the
categorization process based on ACA support/opposition, promotion
of an alternative healthcare reform, and evidence of attention
and investment in the ACA.
Each group title was based on the degree and direction of
ACA support that were consistently common among the same
individuals. The most apparent and predictable groups were the
“Support” group, which was firmly supportive of the ACA, and the
“Oppose” group, which was firmly opposed to the ACA. However, a
third group, “Alternate,” opposed the ACA, but consistently
promoted the need for a “replacement,” or alternative, healthcare
reform in the United States healthcare system. Among those who
were undecided, there was the “Attentive” group, which did not
take a stance for or against the reform, but reported the
importance of watching and learning as the ACA is implemented.
Most in the Attentive group proposed to “wait and see” until it
was time to vote (i.e., 2016; approximately 3 years later) or
until they would begin a health profession (1-5 years later).
The “Relaxed” group showed no evidence of investment or
attention to the ACA, despite indications that the ACA was at
13
Future Health Professionals
least mildly important. In contrast to the Attentive group, The
Relaxed students lacked the motivation to pay attention to the
ACA and continue to evaluate it.
The “Uninvested” group showed complete disregard for the
subject and unwillingness to engage in the topic. Even when
probed a second time on the subject for an opinion, these
students gave repetitive answers that were almost defensive of
their indifference.
Findings
Descriptive analyses and coding of the remainder of the
qualitative data were analyzed for meaningful patterns that could
provide more depth of understanding of each of the six groupings.
Demographics provided important context to the statements of the
students and has implications for future research.
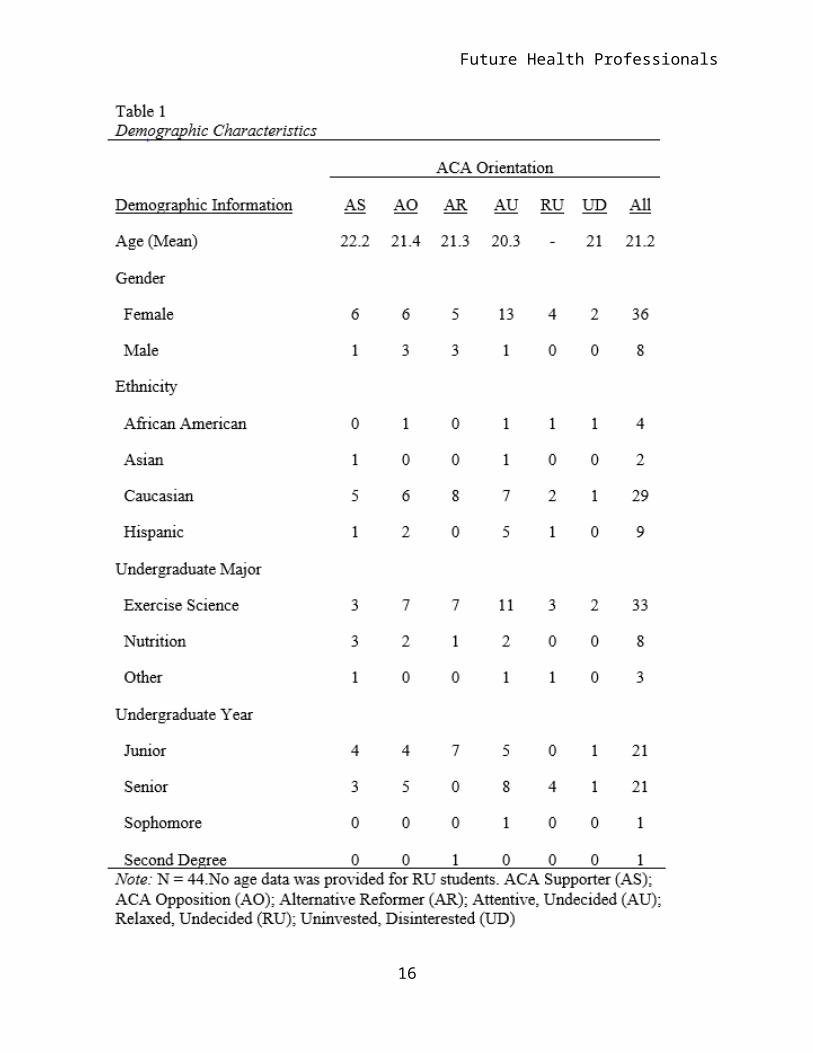
Demographics. The demographics of each ACA Orientation are
described in Table 1. The seven Support students had the highest
mean age of all six groups (M = 22.2). They were primarily
female and were predominantly Caucasian. The nine Oppose students
averaged 21.4 years of age with three females and three ethnic
groups represented. The Oppose group was balanced with four 14
Future Health Professionals
juniors and five seniors. The eight Alternate students average
21.3 years of age and had the highest proportion of males (60%).
Alternate students were solely of Caucasian descent and primarily
Exercise Science majors in their junior year. The 14 Attentive
students had an average age of 20.3 with only one male and
thirteen females. Attentive students were the most diverse,
specifically including the highest proportion of Hispanics (36%).
Attentive students were predominantly Exercise Science majors and
were somewhat balanced by their representation of juniors and
seniors, while including the only sophomore in the sample. The
four Relaxed students gave no age data and all were female
seniors, representing three different ethnicities. Finally, both
Uninvested students were 21-year-old females in the Exercise
Science major. Overall, the average age of the sample was 21.2
years. Males represented only 18% (N = 8).
15
Future Health Professionals
16
Future Health Professionals
Figure 1. Author2’s Model of Pre-health Student ACA Orientations19
Note: Group names were modified for clarity in the current study.
17
Future Health Professionals
18
Future Health Professionals
Qualitative Findings. The six groups of ACA orientations
varied in terms of career commitment and ACA importance,
attention, and knowledge. The next section explores how the
groups varied.
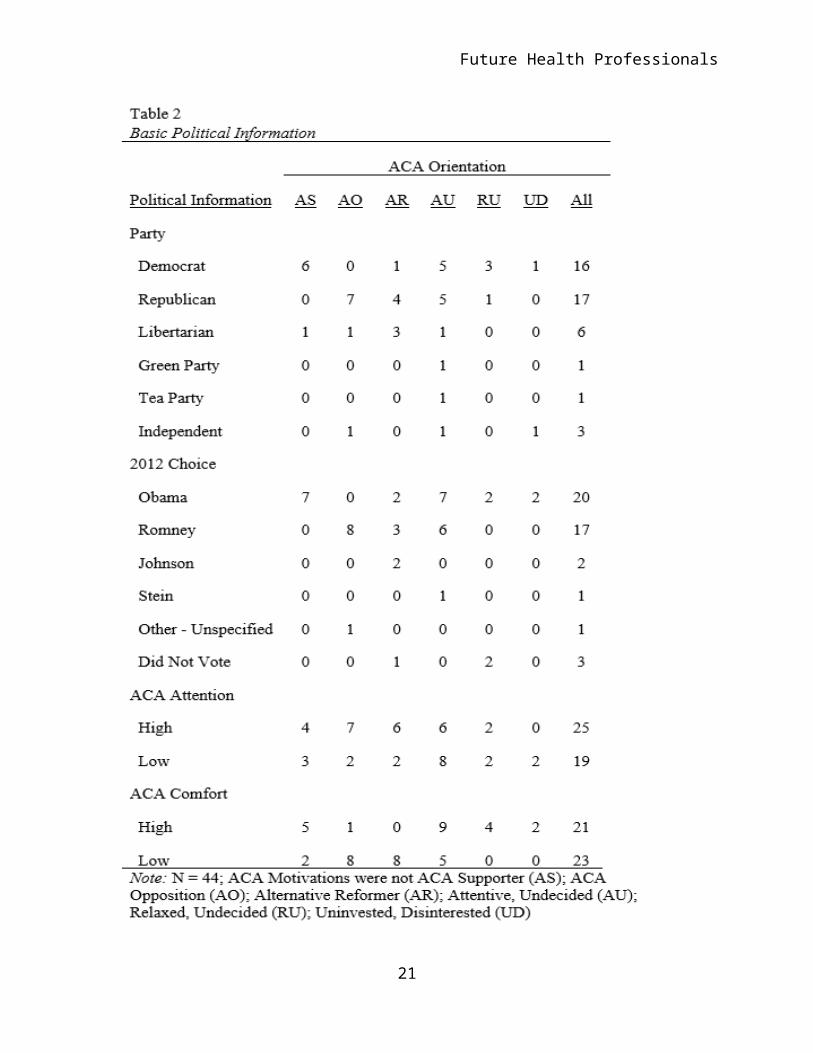
Basic Political Information. The different ACA orientation groups
varied in their basic political information which included their
levels of ACA attention and comfort as seen in Table 2. With
regard to Political Party, the sample was somewhat evenly split
with regard to party affiliations (i.e., Democrats, 36.4%;
Republicans, 38.6%; Libertarians, 13.6%). However, as expected,
the Support group was primarily aligned with the Democratic Party
and the Oppose and Alternate groups were primarily aligned with
the Republican Party. It seemed noteworthy, however, that one
Support student was Libertarian. This “cross-party” behavior is
in accordance with the findings of Author2, Levey, and Author17
in their study of the influence of the ACA on voting behavior.
With regard to the Undecided orientation groups, the
Attentive group was balanced in its political alignments, while
the Relaxed and Uninvested groups were less conservatively
aligned (e.g., Democratic alignment). The Attentive group was the
19
Future Health Professionals
only group to represent all political parties, perhaps
emphasizing the hesitance, concern, and continued evaluation
shared across political parties.
Retrospective accounts of voting choices in the 2012
Presidential Election were mostly consistent with current party
alignment. As will be discussed in the following section,
however, it was clear from student accounts that attention to the
ACA was much lower in 2012 than at present. Nonetheless, Support
students supported Obama, while the entirety of the Oppose group
supported Romney. The Alternate group split its votes between
Obama, Romney, and Johnson. Alternate student responses indicated
that the Romney campaign (i.e., Paul Ryan) did not
20
Future Health Professionals
21
Future Health Professionals
succeed in proposing an acceptable alternative to the ACA. Their
responses indicated that their future voting would be for the
candidate that proposed a viable alternative to the ACA.
Alternate students’ statements included words such as "hoping"
and "curious," and one Alternate student stated, “I will vote for
the party that proposes a better solution for our healthcare
problems.” The Attentive, Relaxed, and Uninvested students voted
along party lines for the most part, though two non-Democrats
voted for Obama and a single non-Republican voted for Romney.
Student responses regarding their attention to the ACA were
categorized as “high” (high attention) and “low” (low attention)
based on evidence found in their statements. An example of high
attention was when an Alternate student stated, “I am curious to
see what the opponents choose to bring to the table and will
decide who has the better plan to fix our now broken health care
system." Conversely, an example of low attention was when an
Uninvested student stated, "I do not know enough about the reform
to let it [a]ffect my decisions."
With regard to ACA Attention, just over half (57%) of
Support students were attentive to the reform, while the Oppose
22
Future Health Professionals
students were the most attentive of any group (78% attentive).
Alternate students were similarly high in their attention to the
ACA (75%). The undecided groups showed lower attention with the
Attentive group (43%) ironically trailing the Relaxed group
(50%). Though the Relaxed group reported slightly greater
attention, their level of overall investment in the ACA (i.e.,
importance and influence) was much higher in their reports.
As with attention to the ACA, students’ responses regarding
their comfort with the reform were categorized as high (high
comfort) and low (low comfort) based on evidence found in their
statements. An example of high comfort was when a Support student
stated, “The [ACA will] be beneficial since [i]t would allow more
people to see a dietician.” An example of low comfort was when an
Oppose student stated, "The reform was a change that I had not
prepared for or am comfortable with [sic]."
ACA comfort was highest for the least decisive groups
(Relaxed and Uninvested) whose members all claimed high comfort
with the ACA. The Support group (71%) was somewhat comfortable
with the ACA as was the Attentive group (64%). Both the Oppose
and Alternate groups were predominantly uncomfortable with the
23
Future Health Professionals
ACA. The influence that the ACA’s relevance had on ACA comfort
and support was reinforced by students’ heightened emotional
responses such as “hoping . . . a better, more affordable and
realistic option involving less government, more private
initiative will evolve.”
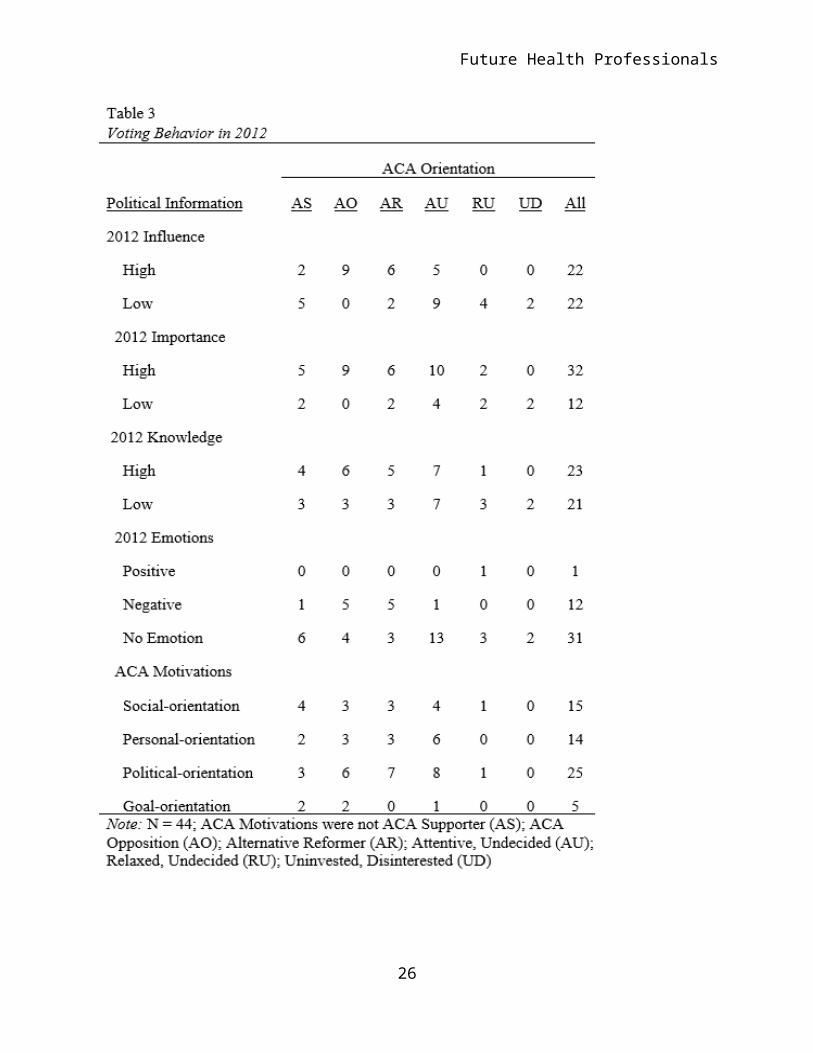
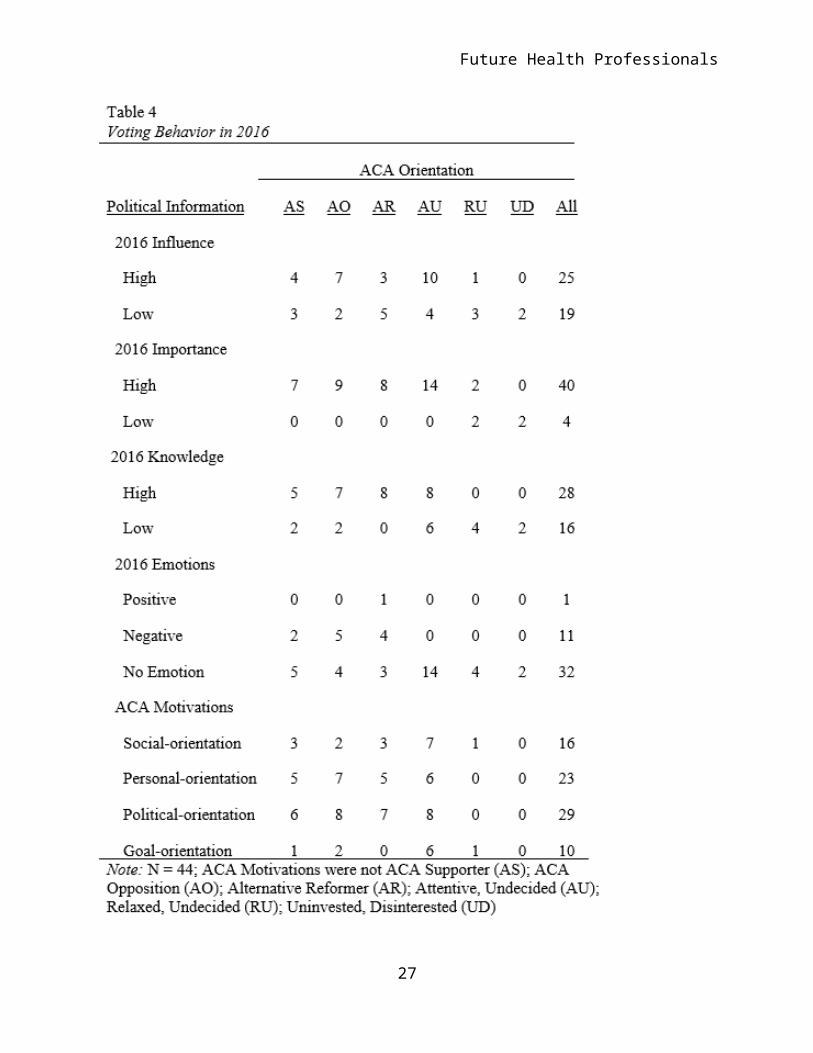
Voting Behavior. As illustrated in Tables 3 and 4, the voting
behaviors and motivations between the ACA orientations varied
between groups and across time with respect to their
retrospective accounts of the 2012 Presidential Election and
their plans for the 2016 Presidential Election. Students’
responses regarding the influence of the ACA on their past and
predicted voting choices were, once again, categorized as high
(high influence) and low (low influence) based on evidence found
in their statements. An example of high influence was when an
Oppose student stated, “[The ACA] is why I didn’t vote for
Obama.” An example of low influence was when an Attentive student
stated, "It did not affect my voting."
An increase in the importance (see influence and importance)
of the reform from 2012 to 2016 was a common theme among all
groups except for the Relaxed and Uninvested. For example, one
24
Future Health Professionals
Attentive student had a significant shift in Influence from 2012
to 2016, as is represented in the statements, "I was unaware to
the details of the Health Care Reform. I wished to be more
educated in it." (low influence in 2012) and "[S]ince it will
affect me greatly I wish to
25
Future Health Professionals
26
Future Health Professionals
27
Future Health Professionals
be more aware of what I'm voting for." (high influence in 2016).
It is important to note that the increase in influence seemed to
be motivated by goal-orientation and its perceived relevance.
Attentive and Uninvested students who did not perceive the
ACA as more important in the 2016 election made abrupt statements
of disregard such as "I don't know yet." Every other group placed
more importance on the reform in 2016, as indicated by statements
such as, "Now that it is in effect, I know more about it.
Depending what happens from now till [sic] the election [in] 2016
[it] will affect my voting choice."
Varying degrees of knowledge about the ACA were apparent
through students’ responses regarding the reform and were
categorized as presence of knowledge (high knowledge) and absence
of knowledge (low knowledge) based on evidence (or lack thereof)
found in their statements. An example of low knowledge was when
an Attentive student stated, “I was unaware of the details of the
Healthcare Reform.” Knowledge about the reform was balanced
within the Attentive group, which was consistent with their
undecided stance on the reform. Attentive student statements
often included non-committal phrases such as "I will have to wait
28
Future Health Professionals
and see." It is important to note the relationship between
knowledge and ACA indecision within the groups.
ACA Motivations. Students’ responses regarding their ACA-
related voting motivations were categorized as social (e.g.,
universal good), personal (e.g., individual relevance),
politically-oriented (e.g., for the good of a political party),
and goal-oriented (e.g., for the good of my future career). An
example of a social motivation was "I believe everyone deserves
health care." An example of a personal motivation was “My family
has been negatively affected by it already especially my
grandparents. I will not . . . vote for it.” “Americans should
[not] be so reliant on the government and its subsidies for care
and help” was considered evidence of a politically-oriented
voting motivation. An example of a goal-oriented motivation was
“Less than a decade away from becoming a doctor, I need to start
thinking about my future. The reform was a change that I had not
prepared for.”
From 2012 to 2016, all three decided groups displayed strong
political motivation toward the ACA, especially among the Support
students. Support students were slightly more socially motivated
29
Future Health Professionals
than the Oppose and Alternate groups, both of whom were much more
motivated by a political orientation. Attentive students showed
high social, personal, and political motivations, while only five
students in Support, Oppose, and Attentive noted a goal-oriented
motivation, evidencing a connection between their ACA orientation
and their career. One particularly interesting quote from a
forward-thinking Oppose student evidenced a professional
motivation, saying “This will be a major part of my voting
because it will directly affect my profession.” Such forward
thought will be expounded upon in the Discussion.
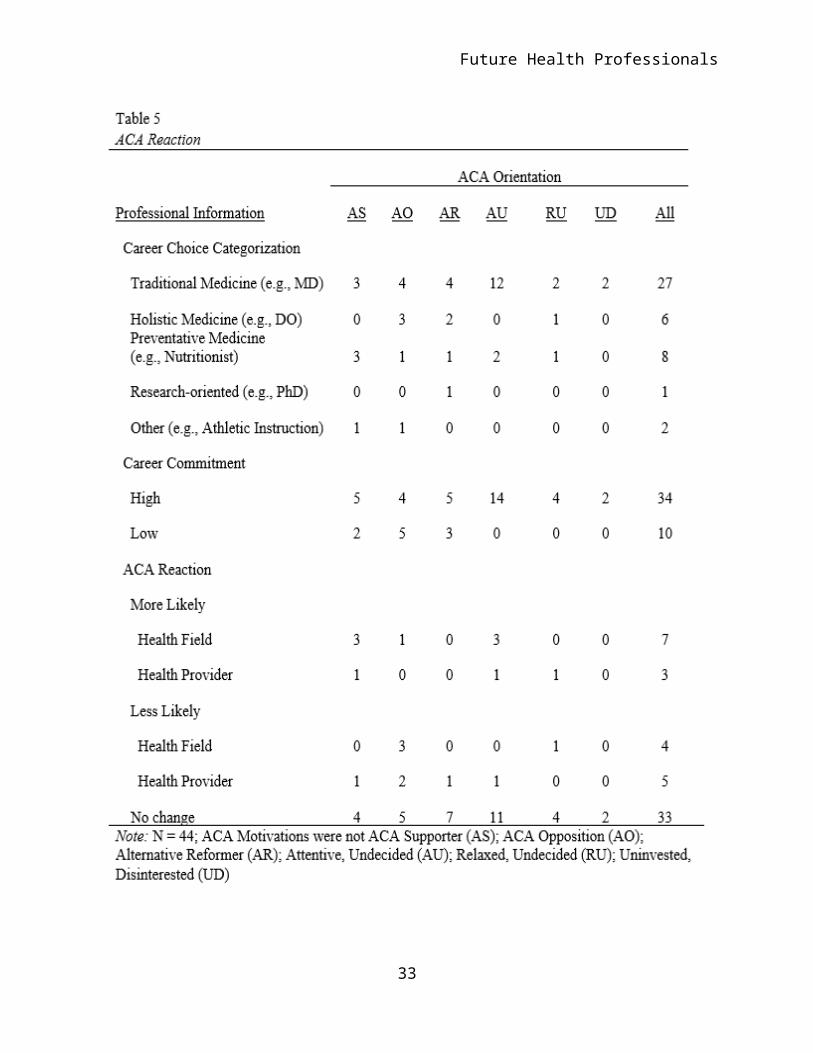
Professional Behavior. Students’ professional behaviors were
discussed in terms of reactions to the reform. Reaction as
described by Author23, 4 was discussed in terms of commitment to
career choice and ACA-related modification of career goals. The
descriptive statistics regarding professional behaviors are
presented in Table 5.
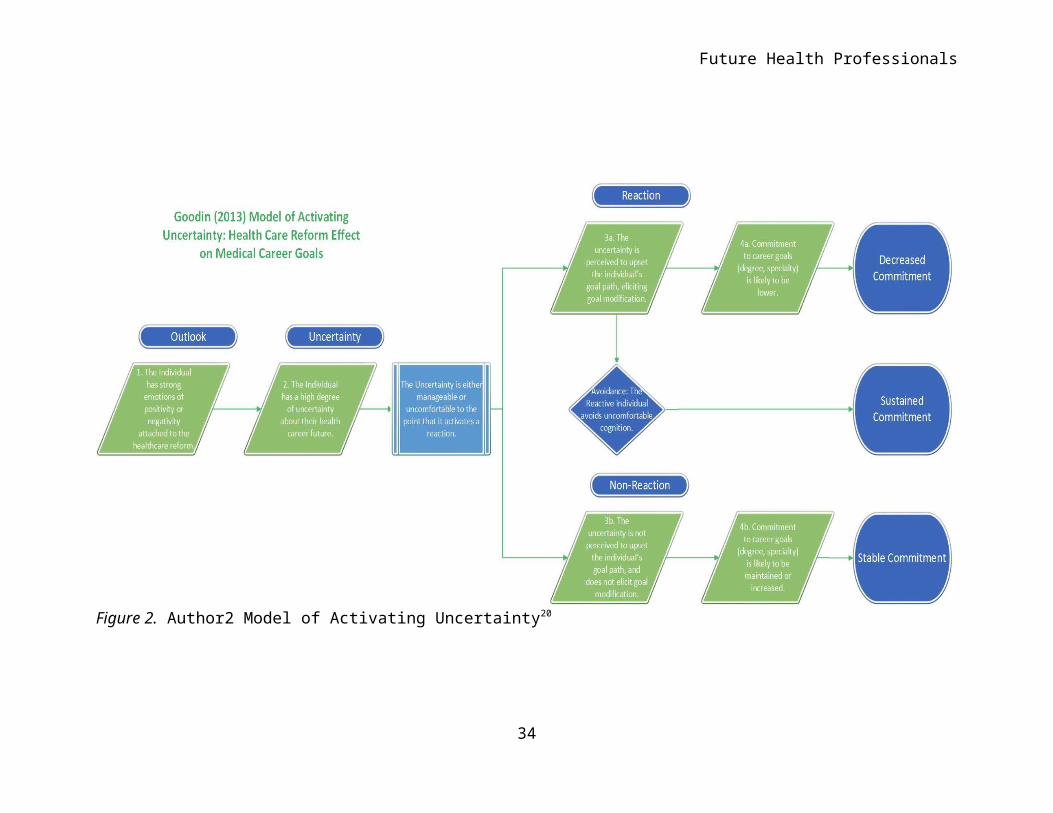
Based on Author2’s4,20 Model of Activating Uncertainty (See
Figure 2), students’ responses to the effect the ACA has on
career plans were categorized by the stability/modification of
their goals in reaction to the ACA. Author2 hypothesized that
30
Future Health Professionals
individuals would be differentially “activated” by varying levels
of uncertainty, such that when an individual meets a subjective
“limit” of discomfort with the uncertainty in their life
situation, they take action (e.g., changing goals) to remediate
uncertainty and the related discomfort. The categories of
stability specified for the current study were “more-likely to
enter a health-related field,” “more likely to become a health
provider,” “less-likely to enter a health-related field,” “less-
likely to become a health provider,” or “no change in goals.”
Author24 noted the importance of modification in either direction
(more or less likely) to be evidence of reaction to the event,
emphasizing the positive valence of reaction (e.g., excitement)
in addition to the negative (e.g., anger).
Similarly to the ACA influence categorizations, students’
responses regarding their commitment to their most-likely career
were categorized as high (high commitment) and low (low
commitment) based on evidence found in their statements. An
example of high commitment was when a student stated, “In 2016 I
will be starting my career as a pharmacist . . .” An example of
low commitment was when a student stated, “I will be a practicing
31
Future Health Professionals
health care professional in 2016, so my view may change after
being directly affected by the reform at that period of time.”
Although, this student stated that they will be a practicing
healthcare professional, his statement was coded as “low
commitment,” due to the uncertainty displayed in his ACA opinions
and the possibility of direct results on the healthcare
professions by "the effects of the reform [in 2016]."
Career goal commitment was more high than low across groups,
especially for the Undecided. Support students were the most
aligned with preventative health career goals, while Oppose and
Alternate students varied somewhat evenly between career goals.
The Attentive students were predominantly invested in traditional
medicine career goals. Most Attentive students evidenced a desire
to manage ACA uncertainty in a logical manner, by watching the
implementation unfold and reserving judgment.
Although more supportive of the ACA than any other group,
Support students were one of the most diverse groups in their
reactions (i.e., career adjustments) to the ACA, second only to
the Oppose group. Support students reported increased likelihood
that they would enter health-
32
Future Health Professionals
33
Future Health Professionals
Figure 2. Author2 Model of Activating Uncertainty20
34
Future Health Professionals
related fields and professions, though one reported a decreased
likelihood that she would become a health provider.
Students’ ACA Orientations seemed to play a large role in
their political and professional behaviors. The high levels of
attention and importance among the Support, Oppose, Alternate,
and Attentive groups seemed to invigorate heightened emotions,
voting responses, and goal modifications that fit uniquely and
differentially with each group’s philosophies and
personal/professional goals.
Discussion
The primary research question and purpose were to identify
the most common orientations of pre-health students toward the
ACA to better understand its relevance and influence in their
lives. The data illustrated that, for undergraduate pre-health
students, the ACA has different roles and influence with regard
to the students voting behavior, career commitments, and career
goal modifications based on six ACA orientations.
The three decided orientations and the Attentive orientation
all reported that the ACA was an important factor in their
35
Future Health Professionals
current and future-oriented thoughts. Their responses
demonstrated differences that can be explained to some extent by
the aforementioned Author2’s4, 20 Model of Activating Uncertainty,
wherein individuals differentially react or remain passive to
uncertainty in their lives. Author2, Levey, and Author1’s7 study
asserted that ACA uncertainty, operationalized as voting choice,
was activated primarily in those with conservative political
alignments. Their findings showed that, while liberally-minded
individuals also felt uncertainty about the ACA, they were more
tolerant of that uncertainty, such that they did not modify their
goals. However, in the current study using a sample of
undergraduate, pre-health students, there seems to be
modification of goals for both opponents, supporters, and those
who are attentive, but undecided regarding the reform. Those who
supported the reform often reported a firmer commitment to
health-related career goals, while those opposed to the reform
often showed decreased commitment to health-related career goals.
Perhaps Husman and Shell’s21 Future Time Perspective (FTP)
Theory provides additional understanding to the findings. FTP
Theory suggests that individuals vary in the extent to which they
36
Future Health Professionals
consider future goals in present-oriented decisions and
behaviors. This concept, called “connectedness,” was evidenced by
statements that indicated that the future (e.g., 3 years ahead)
was relevant. Connectedness was common among Support, Oppose,
Alternate, and Attentive students, who also consistently
indicated more knowledge about the ACA, as opposed to the lacking
evidence of connectedness or ACA knowledge among Relaxed and
Uninvested students.
The connectedness of an individual seems to provide some
explanation for the aforementioned variations in perceived
relevance of the ACA. The Relaxed and Uninvested groups did not
mention the future. It would thus make logical sense that Relaxed
and Uninvested students’ lack of perceived relevance, explained
by limited FTP Connectedness, would result in lower perceived
importance, attention, knowledge, and goal modification. In fact,
Relaxed and Uninvested individuals showed the most consistent
evidence of absolute commitment to their career goals. Though FTP
could not be presumed to explain the full extent of students’
orientations toward the ACA, it makes theoretical sense that
connectedness does play some noteworthy role. Thus, future
37
Future Health Professionals
research may benefit from targeted measurement of FTP variables
such as connectedness to better explain why an individual may
exhibit a specific orientation and the political and social
behaviors that they display among and across different
orientations.
With specific regard to the elevated, unyielding career goal
commitments of the two “Uninvested, Disinterested” students, FTP
connectedness could help explain what the research observed as
indifference that approached a hostile defensiveness. One might
wonder how someone so invested in a career goal could be so
indifferent to what many of their peers consider to be a
significant, relevant issue. Based on Tubbs13 views of goal
commitment maintenance, Author24,20 postulated that those who felt
that the ACA was a threatening or uncomfortable issue might not
always react. Rather, he suggested that due to the high degree of
investment, some students would avoid a realistic evaluation of
the ACA in order to protect their goal from a possible
encumbrance. Thus, Uninvested students may be avoiding cognitions
about the ACA in order to maintain their commitment in light of
their investment. Students who vary in their perceived degree of
38
Future Health Professionals
investment may report disparate levels of comfort with the ACA as
(a) legislation, and (b) change in their career path. Perhaps,
some students with high FTP experience the connectedness to the
future as a sort of “cognitive investment” that increases the
need to modify goals, or avoid the subject altogether.
Conclusion
Future health providers at the undergraduate level, perhaps
due to a lower degree of investment in their careers, seem to
have consider more options than those in graduate medical
training. The ACA presents change and possibility for this
specific sample of the Health Sciences students by emphasizing
preventative health public awareness and career opportunities, a
principal thrust of the reform movement. Understanding the
orientations, perceptions, and reactions of the future
preventative health workforce will be of great importance to the
successful integration of the old and new healthcare system.
39
Future Health Professionals
References
1Association of American Medical Colleges (2007). Medical school expansion plans: results of
the 2006 AAMC survey. Retrieved fromhttps://www.aamc.org/download/105350/data/msep.
pdf.
2Association of American Medical Colleges (2012a). MSAR: Getting started, medical school
admissions requirements. Retrieved from https://www.aamc.org/students/download/278466/
data/gettingstartedpreview.pdf
3Author2 (to be presented 2013, November). Medical Students’ Perceptions of Health
Reform and Implications for Specialty Choice: An Overview. In Author2. (Chair), A Focus
on Medical Education: The Critical Role of Medical Students in the Changing Healthcare
Landscape. Symposium presented at the Florida Educational Research Association, Gainesville,
FL.
4Author2 (In Press). The Health Care Reform as a critical life event: Investigating medical student commitment to medical careergoals in a time of health care reform. (Doctoral dissertation). ProQuest Dissertations and Theses Database. (11230).
5Author2, Duffy, R.D., Borges, N.J., Ulman, C.A., Author1, & Manuel, R.S. (In Press). Medical Students with Low Self-Efficacy Bolstered by a Calling to their Medical Specialty. Perspectives in Medical Education.
6Author2, Johnson, M., Author1, & Levey, B. (to be presented 2013, November). The
Facilitation of Primary Care Pursuit within an Ambulatory Training Atmosphere. In Author2
(Chair), A Focus on Medical Education: The Critical Role of 40
Future Health Professionals
Medical Students in theChanging Healthcare Landscape. Symposium presented at the Florida
Educational ResearchAssociation, Gainesville, FL.
7Author2, Levey, B., & Author1 (to be presented 2013, November). Obama Voting Explained: The influence of Healthcare Reform Perceptions on Medical Students’ Voting in the 2012 Presidential Election. In Author2 (Chair), A Focus on Medical Education: The Critical Role of Medical Students in the Changing Healthcare Landscape. Symposium presented at the Florida Educational Research Association, Gainesville, FL.
8Author2, Author1, and Levey, B. (to be presented 2013, November). A Striking Divergence among Ethnicities in Health Reform Perception and Specialty Choice Commitments. In Author2 (Chair), A Focus on Medical Education: The Critical Role of Medical Students in the Changing Healthcare Landscape. Symposium presented at the Florida Educational Research Association, Gainesville, FL. 9Locke, E. A. (1968). Toward a theory of task motivation incentives. Organizational Behavior and Human Performance, 3, 157-189.
10Inglehart, M.R. (1991). Reactions to Critical Life Events: A Social Psychological Analysis.New York: Praeger Publishers.11Author2 (2011, October). The Health Care Reform Law as a Critical Life Event: Investigating Choice of Medical Specialty Commitment in a time ofHealth Care Reform. Presented at Florida Educational Research Association.
12Klein, H., & Kim, J. (1998). A field study of the influence of situational constraints, leader-member exchange, and goal commitment on performance. The Academy of Management Journal, 41(1), 88-95.
41
Future Health Professionals
13Tubbs, M.E. (1993). Commitment as a moderator of the goal–performance relationship: A case for clearer construct definition. Journal of Applied Psychology, 78, 86–97.
14Selye, H. (1956). The Stress of life. New York: McGraw-Hill.
15Lazarus, R.S., & Folkman, S. (1984). Stress, appraisal, and coping. New York: Spring Publishing Company.
16Wortman, C., & Brehm, J. (1975). Responses to uncontrollable outcomes: An integration ofreactance theory and the learned helplessness model. In L. Berkowitz (Ed.) Advances inexperimental social psychology (Vol. 8, pp. 278-336). New York: Academic Press.
17Klinger, E. (1975). Consequences of commitment to and disengagement from incentives.Psychological Review, 82, 1-25.
18Strauss, A., & Corbin, J. (1990). Basics of qualitative research: Grounded theory procedures and techniques. Newbury Park, CA: Sage.
19Author2 (to be presented 2013, November). Pre-health student ACA orientations: A flowchart for categorizations. In Author2 (Chair), A Focus on Medical Education: The Critical Role of Medical Students in the Changing Healthcare Landscape. Symposium presented at the Florida Educational Research Association, Gainesville, FL.
20Author2 (to be presented 2013, November). A Model of ActivatingUncertainty: Pre-healthStudents Differentially React to Uncertainty. In Author2 (Chair),A Focus on MedicalEducation: The Critical Role of Medical Students in the Changing Healthcare Landscape.Symposium presented at the Florida Educational Research Association, Gainesville, FL.
42
Future Health Professionals
21Husman, J. & Shell, D.F. (2008). Beliefs and Perceptions about the Future: A Measurement ofFuture Time Perspective. Learning and Individual Differences, 18(2), pp 166-175.
43
Future Health Professionals
Key Terms
Future Health Professionals: Also known as pre-health students. Refers to students that are preparing for one of a wide scope of medical and health careers that serve to increase or maintain a person's health. Future Health Professionals can include healthcare providers, nutrition and health maintenance, physical therapists, exercise prescription specialists, and others.
ACA: Patient Protection and Affordable Care Act, also referred toas the PPACA, the healthcare reform, the reform, the healthcare reform law, and "ObamaCare." The legislation initiated the current healthcare reform in the United States.
Preventative health: A field of health providers that focuses on disease prevention and health maintenance to improve overall long-term health status.
Calling: The presence of a feeling that an individual is called to serve in a specific career or career field
Community-based training: Also referred to as ambulatory style medicine. Abbreviated as "CBT," this type of training is emergingin medical schools in order to promote community health practice by connecting future providers to communities by serving in a variety of locations.
Traditional training- A highly structured training environment that has been the prevalent training environment for medical doctors. Medical schools often have a local "training hospital" wherein their students do clerkship experiences, wherein they apprentice under a practicing medical doctor.
Self-efficacy: Refers to an individual's confidence in his/her specific, future tasks.
Reaction: Modification of career goals in response to perceived blockage of goals stemming from a critical life event (e.g., a football player breaks his leg). This theoretical construct was coined by Author2 in 2013.
44
Future Health Professionals
Grounded Theory: A methodology wherein theory is developed by analysis of the data as a process of the analysis. Theoretical tenets emerge as qualitative data is analyzed for consistent themes.
Open Coding: As part of a Grounded Theory approach, qualitative data (i.e., statements and responses) are analyzed for key words and phrases that are repeated by multiple participants.
Parent Categories: Open Coding provides the building blocks of Parent categories, such that words like "energized," "excited," "ready," "prepared," or "focused," might compose a parent category of "active engagement." Parent categories are used to describe overarching themes.
45




























