Embed Size (px)
Citation preview
Assessing cardiometabolic treatment quality in general practice
ParanimfenPeter MolHenk-Jan Bezemer
Druk: Ridderprint, Ridderkerk.
ISBN: 978 94 6070 013 2
Printing of this thesis was supported by:• Dutch Diabetes Research Foundation• Ubbo Emmius Foundation, University of Groningen• Novo Nordisk B.V.
Copyright © 2010 J.VoorhamNiets uit deze uitgave mag worden verveelvoudigd, opgeslagen in een geautom-atiseerd gegevensbestand of openbaar gemaakt in enige vorm of op enige wijze zonder voorafgaande schriftelijke toestemming van de auteur.
RijksuniveRsiteit GRoninGen
Assessing cardiometabolic treatment quality in general practice
Proefschrift
ter verkrijging van het doctoraat in deMedische Wetenschappen
aan de Rijksuniversiteit Groningenop gezag van de
Rector Magnificus, dr. F. Zwarts, in het openbaar te verdedigen op
woensdag 16 juni 2010om 13:15 uur
door
Jaco Voorhamgeboren op 26 juni 1963
te ‘s-Gravenhage
Promotores : Prof. dr. F.M. Haaijer-RuskampProf. dr. B.H.R. Wolffenbuttel
Copromotor : Dr. P. Denig
Beoordelingscommissie : Prof. dr. L.T.W. de Jong-van den BergProf. dr. G. NijpelsProf. dr. C. J. Tack
CONTENTS
Chapter 1 General Introduction 7Chapter 2 Data collection methods 21Chapter 2.1 Computerised extraction of information on the quality of
diabetes care from free text in electronic medical records of general practitioners
23
Chapter 2.2 The GIANTT database - data collection methodology for continuous monitoring of the quality of care of patients with type 2 diabetes in The Netherlands
45
Chapter 3 Quality indicators 63Chapter 3.1 Cross-sectional versus sequential quality indicators of risk
factor management in patients with type 2 diabetes65
Chapter 3.2 A systematic literature review: prescribing indicators related to type 2 diabetes mellitus and cardiovascular risk management
87
Chapter 3.3 Identifying targets to improve treatment in type 2 diabetes: the Groningen Initiative to aNalyse Type 2 diabetes Treatment (GIANTT) observational study 2004-2007
123
Chapter 4 Determinants of treatment intensification 139Chapter 4.1 The influence of elevated cardiometabolic risk factor levels on
treatment changes in type 2 diabetes141
Chapter 4.2 Cardiometabolic treatment decisions in patients with type 2 diabetes: the role of repeated measurements and medication burden
149
Chapter 4.3 Medication adherence affects treatment modifications in type 2 diabetes
167
Chapter 4.4 Competing demands and treatment intensification in type 2 diabetes
187
Chapter 5 General discussion 207Summary 223Samenvatting 229Dankwoord 237Curriculum vitae 241Groningen graduate school of medical sciences - research institute SHARE 245

7Chapter 1 - General introduction

8
Chapter 1 - General Introduction
This thesis covers three intertwined themes of the quality of care for patients with type 2 diabetes in general practice. The first one covers issues related to setting up an observational health care database including a large cohort of such patients in the northern Netherlands. In the second theme, the data from this cohort are used to study several methodological aspects of measuring quality of care. The third theme focuses on medication treatment, and specifically on predictors of (sub)optimal treat-ment quality.
Type 2 diabetesIn the last decades, the world has seen a considerable increase in the number of people with type 2 diabetes mellitus.1-3 It can be seen as a disease of modern life, in-creasing wherever living standards move towards greater availability of high-calorie food and less physical activity. From an evolutionary angle this can be explained by the evolutionary discordance between our ancient biology and the rapid changes that are occurring in our nutritional, cultural and activity patterns.4
Also in the Netherlands the number of people affected is growing steadily. An esti-mate in 2007 showed approximately 740,000 people with diabetes, and predictions estimate this number to become over 1.3 million by the year 2025.5
Patients with diabetes may develop secondary complications, which have consider-able impact on the patients, the health care system, and society as a whole. Diabetes is the leading cause of blindness, end-stage renal disease, and non-traumatic limb amputations in western society. Furthermore, patients with type 2 diabetes mellitus have a risk of coronary heart disease that is two to four times that among persons without diabetes.6-8 Treatment of diabetes aims at reducing risk of complications by means of glucose and blood pressure regulation. In addition, the use of lipid-low-ering medication is advised for all patients with type 2 diabetes. During the 1990s, results became available from large clinical trials showing that intensive treatment with glucose-lowering, antihypertensive, and lipid-lowering drugs can reduce micro- and macrovascular complications considerably.9-13
In the Netherlands, patients with type 2 diabetes are largely treated in general prac-tice. In 1989, the Dutch College of General Practitioners formulated guidelines for the care of patients with type 2 diabetes. Following the appearance of new insights from clinical trials, the diabetes and cardiovascular risk management guidelines have been updated from 1997 onwards, with the last updates in 2006.14,15

9
Chapter 1 - General Introduction
Quality of Care and the GIANTT projectSince the mid 1990’s, diabetes has been identified as one of the priority areas for clinical quality improvement. From a wide variety of locations in the world, gaps have been reported between what clinical guidelines recommend as appropriate care and what is observed in practice.16-21 To improve the quality of diabetes care, many (re-gional) projects have started in various countries, which monitor the processes and outcomes of care. One of such projects is the Groningen Initiative to Analyse Type 2 diabetes Treatment (GIANTT). This project started in 2004 as an initiative of the University Medical Center Groningen, the Martini Hospital Groningen, the General Practitioners of the Groningen region and the Diabetes Facility from the General Practice Laboratory in Groningen. It focuses on the care delivered to patients with type 2 diabetes mellitus in the north of the Netherlands. The goals are to improve the quality of care deliv-ered, through scientific research and benchmarking. To enable this, GIANTT needs a database for continuous monitoring of diabetes care based on routinely registered data.To obtain data for quality of care monitoring, several approaches can be chosen. In The Netherlands, there are several registration networks of general practitioners, which collect information from electronic medical records (EMR).22 Within these net-works agreements are made on what and how to document in the EMR. Maintaining high standards of such registration between and within participating practices re-quires continuous attention. It is expected to result in a selection of practices willing to invest energy into changing their registration habits. Alternatively, one can introduce a dedicated diabetes registration system separate from the general practice’s regu-lar EMR system. Examples in European and Dutch general practice are DiabCare and the diabetes management program developed by Diagnosis4Health.23,24 This also results in a selection of practitioners agreeing to use it. An additional disadvan-tage of a split registration of care is that not everything that occurs at the general practitioners’ office can be divided into diabetes care or not, leading to incomplete data in both registration systems.24 Another method used is to manually collect data from practices.25,26 The Diabeteszorg Beter project used up to recently this method of periodic specific data collection through forms.26 This approach is time consuming, and usually results in a limited dataset.Recently, it became possible to use automatic procedures to collect a limited number of diabetes related data, which are stored in a structured and standardised way in the Dutch EMR systems. It is not yet clear to what extent these procedures will lead to sufficient capture of all relevant data.
10
Chapter 1 - General Introduction
2004
2008
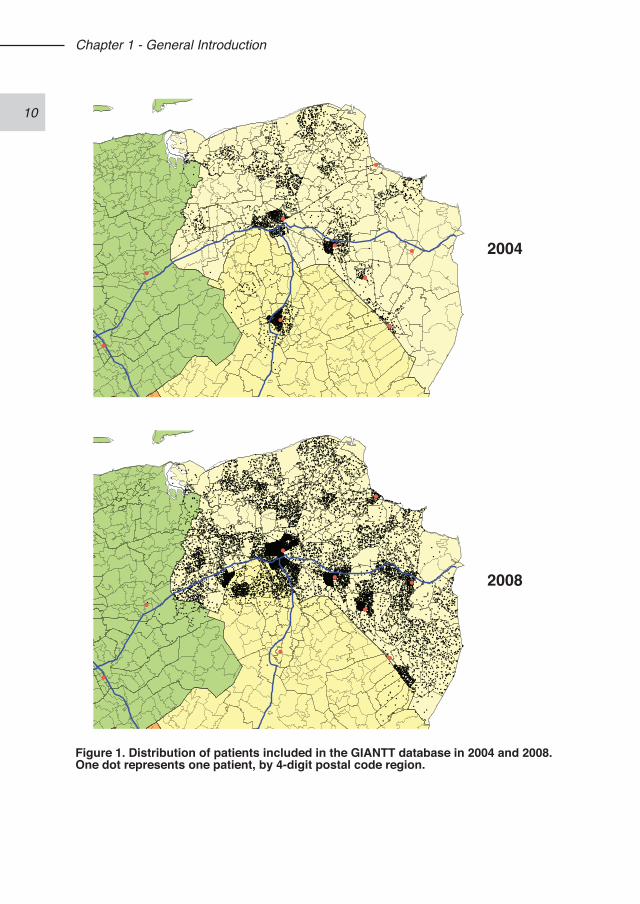
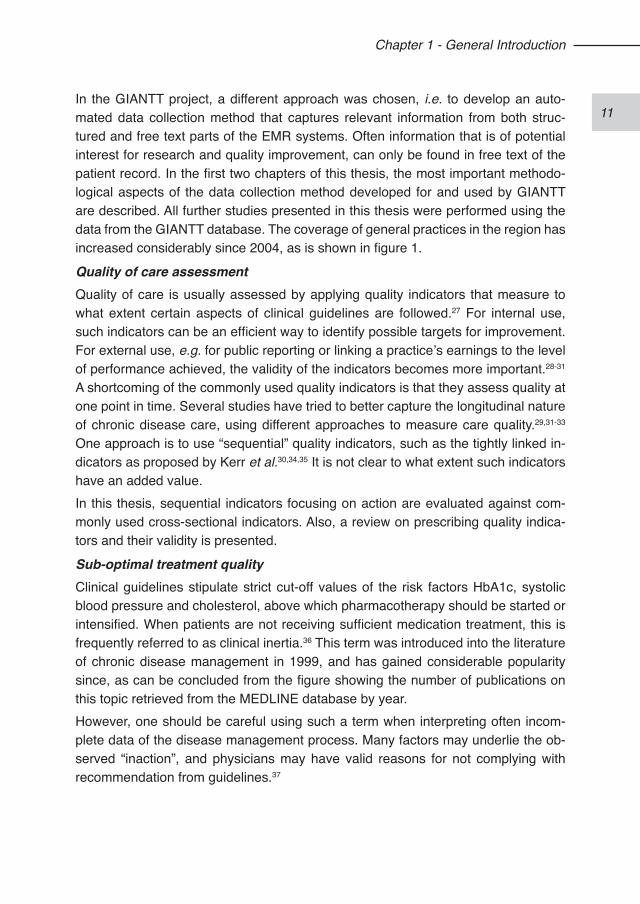
Figure 1. Distribution of patients included in the GIANTT database in 2004 and 2008. One dot represents one patient, by 4-digit postal code region.
11
Chapter 1 - General Introduction
In the GIANTT project, a different approach was chosen, i.e. to develop an auto-mated data collection method that captures relevant information from both struc-tured and free text parts of the EMR systems. Often information that is of potential interest for research and quality improvement, can only be found in free text of the patient record. In the first two chapters of this thesis, the most important methodo-logical aspects of the data collection method developed for and used by GIANTT are described. All further studies presented in this thesis were performed using the data from the GIANTT database. The coverage of general practices in the region has increased considerably since 2004, as is shown in figure 1.
Quality of care assessmentQuality of care is usually assessed by applying quality indicators that measure to what extent certain aspects of clinical guidelines are followed.27 For internal use, such indicators can be an efficient way to identify possible targets for improvement. For external use, e.g. for public reporting or linking a practice’s earnings to the level of performance achieved, the validity of the indicators becomes more important.28-31 A shortcoming of the commonly used quality indicators is that they assess quality at one point in time. Several studies have tried to better capture the longitudinal nature of chronic disease care, using different approaches to measure care quality.29,31-33
One approach is to use “sequential” quality indicators, such as the tightly linked in-dicators as proposed by Kerr et al.30,34,35 It is not clear to what extent such indicators have an added value. In this thesis, sequential indicators focusing on action are evaluated against com-monly used cross-sectional indicators. Also, a review on prescribing quality indica-tors and their validity is presented.
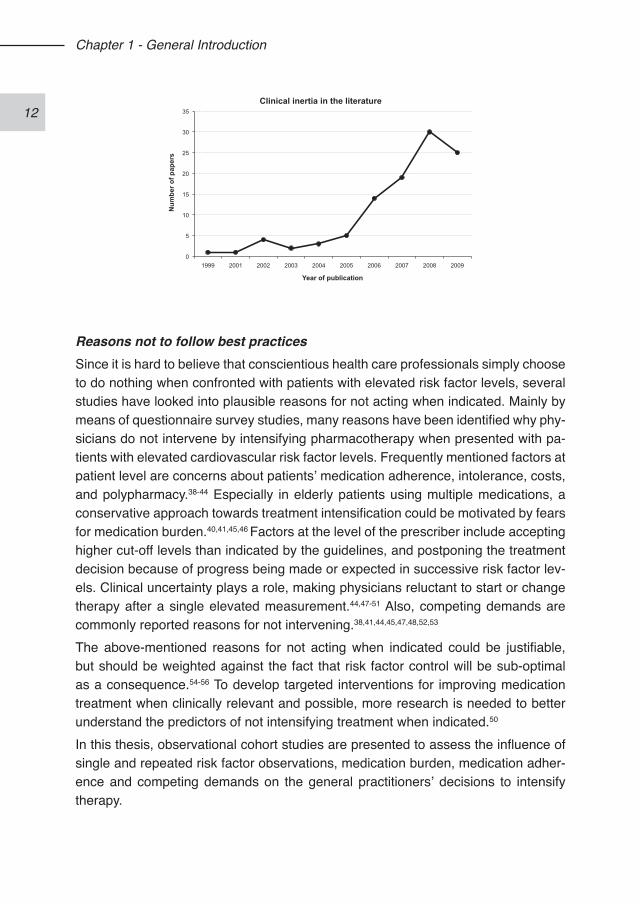
Sub-optimal treatment qualityClinical guidelines stipulate strict cut-off values of the risk factors HbA1c, systolic blood pressure and cholesterol, above which pharmacotherapy should be started or intensified. When patients are not receiving sufficient medication treatment, this is frequently referred to as clinical inertia.36 This term was introduced into the literature of chronic disease management in 1999, and has gained considerable popularity since, as can be concluded from the figure showing the number of publications on this topic retrieved from the MEDLINE database by year. However, one should be careful using such a term when interpreting often incom-plete data of the disease management process. Many factors may underlie the ob-served “inaction”, and physicians may have valid reasons for not complying with recommendation from guidelines.37
12
Chapter 1 - General Introduction
Reasons not to follow best practicesSince it is hard to believe that conscientious health care professionals simply choose to do nothing when confronted with patients with elevated risk factor levels, several studies have looked into plausible reasons for not acting when indicated. Mainly by means of questionnaire survey studies, many reasons have been identified why phy-sicians do not intervene by intensifying pharmacotherapy when presented with pa-tients with elevated cardiovascular risk factor levels. Frequently mentioned factors at patient level are concerns about patients’ medication adherence, intolerance, costs, and polypharmacy.38-44 Especially in elderly patients using multiple medications, a conservative approach towards treatment intensification could be motivated by fears for medication burden.40,41,45,46 Factors at the level of the prescriber include accepting higher cut-off levels than indicated by the guidelines, and postponing the treatment decision because of progress being made or expected in successive risk factor lev-els. Clinical uncertainty plays a role, making physicians reluctant to start or change therapy after a single elevated measurement.44,47-51 Also, competing demands are commonly reported reasons for not intervening.38,41,44,45,47,48,52,53
The above-mentioned reasons for not acting when indicated could be justifiable, but should be weighted against the fact that risk factor control will be sub-optimal as a consequence.54-56 To develop targeted interventions for improving medication treatment when clinically relevant and possible, more research is needed to better understand the predictors of not intensifying treatment when indicated.50
In this thesis, observational cohort studies are presented to assess the influence of single and repeated risk factor observations, medication burden, medication adher-ence and competing demands on the general practitioners’ decisions to intensify therapy.
0
5
10
15
20
25
30
35
1999 2001 2002 2003 2004 2005 2006 2007 2008 2009
Num
ber o
f pap
ers
Year of publication
Clinical inertia in the literature

13
Chapter 1 - General Introduction
AIM AND OUTLINE OF THIS THESISThe aims of this thesis are: 1) To develop and validate methods and tools for collecting data from electronic medical records to build a longitudinal observational database; 2) To improve the assessment of quality of pharmacotherapeutic risk factor manage-ment in patients with type 2 diabetes; and 3) To unravel factors that determine treatment of risk factors in patients with type 2 diabetes.Accordingly, this thesis is divided into three parts.
Chapter 2 describes the data collection methods that have been developed for the GIANTT observational cohort of primary care patients with type 2 diabetes. In Chapter 2.1 the method developed for automated extraction of measurement infor-mation from free text parts of the electronic medical records is described. The choice of the used text recognition approach is explained, and its performance is validated. This extraction method is at the core of the data collection within the GIANTT cohort, and enables the use of relevant clinical information registered in parts of the elec-tronic medical records at the general practices that was not accessible by available automated collection.In Chapter 2.2 the actual data collection process is described at the level of the care provider. This comprises a standardised method to assure consistent patient iden-tification between care providers, data validation, patient confidentiality and patient linkage methods.Chapter 3 focuses on quality indicators. In Chapter 3.1 several indicators of the man-agement of blood glucose, blood pressure and lipids are compared against a refer-ence method. Cross-sectional indicators but also newly developed indicators with different levels of sequentiality, i.e. actions following observations, are compared in an attempt to better incorporate the longitudinal nature of chronic disease manage-ment into quality assessment.A systematic review on prescribing indicators related to type 2 diabetes and cardio-vascular risk management is presented in Chapter 3.2, with the aim to describe the different aspects of validity of existing prescribing indicators.Chapter 3.3 presents a quality assessment of diabetes and cardiovascular risk man-agement between 2004 and 2007 in the northern Netherlands, using different in-dicators. Results from commonly used indicators are contrasted with results from
14
Chapter 1 - General Introduction
indicators that either combine level of control and level of treatment or measure action when indicated. A case is built for incorporating such alternative assessment methods into regular quality evaluations.Chapter 4 focuses on predictors of sub-optimal treatment quality. The first study looks into how treatment start or intensification relates to levels of HbA1c, systolic blood pressure and total cholesterol, in a cohort of more than 3,000 patients in 2004 (Chapter 4.1). The second study looks into to what extent single and repeated meas-urements of HbA1c, systolic blood pressure and total cholesterol predict the decision to start or intensify medication treatment in the same patient cohort (Chapter 4.2). Besides the most recent risk factor level, different aspects of the preceding levels and changes in risk factor level are used as predictors. In addition, the impact of polypharmacy on this is studied. Other factors that could affect the decision to inten-sify therapy are studied in the following chapters in a cohort of over 11,000 patients in 2007. The effect of a patient’s medication adherence on treatment modifications is addressed in Chapter 4.3. Chapter 4.4 presents the last study, which aims at as-sessing how competing demands affect treatment intensification.Finally, in Chapter 5 the main findings of the studies are discussed and put into a broader perspective. Implications of this thesis are discussed for approaches to improve pharmacotherapeutic risk factor management, and the assessment of its quality.
REFERENCES1. King H, Rewers M. Global estimates for prevalence of diabetes mellitus and
impaired glucose tolerance in adults. WHO Ad Hoc Diabetes Reporting Group. Diabetes Care. 1993;16(1):157-77.
2. Amos AF, McCarty DJ, Zimmet P. The rising global burden of diabetes and its complications: estimates and projections to the year 2010. Diabet Med. 1997;14 Suppl 5:S1-85.
3. Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabe-tes: estimates for the year 2000 and projections for 2030. Diabetes Care. 2004;27(5):1047-53.
4. Cordain L, Eaton SB, Sebastian A, Mann N, Lindeberg S, Watkins BA, O’Keefe JH, Brand-Miller J. Origins and evolution of the Western diet: health implications for the 21st century. Am J Clin Nutr. 2005;81(2):341-54.
5. Baan CA, van Baal PH, Jacobs-van der Bruggen MAM, Verkley H, Poos MJJC, Hoogenveen RT, Schoemaker CG. Diabetes mellitus in Nederland: schat-ting van de huidige ziektelast en prognose voor 2025. Ned Tijschr Geneeskd. 2009;153:A580.
6. Barrett-Connor EL, Cohn BA, Wingard DL, EdelsteinL. Why is diabetes mellitus a stronger risk factor for fatal ischemic heart disease in women than in men? The Rancho Bernardo Study. JAMA. 1991;265(5):627-31.
15
Chapter 1 - General Introduction
7. Koskinen P, Manttari M, Manninen V, Huttunen JK, Heinonen OP, Frick MH. Coronary heart disease incidence in NIDDM patients in the Helsinki Heart Study. Diabetes Care. 1992;15(7):820-5.
8. Manson JE, Colditz GA, Stampfer MJ, Willett WC, Krolewski AS, Rosner B, Arky RA, Speizer FE, Hennekens CH. A prospective study of maturity-onset diabetes mellitus and risk of coronary heart disease and stroke in women. Arch Intern Med. 1991;151(6):1141-7.
9. UK Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837-53.
10. UK Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. BMJ. 1998;317(7160):703-13.
11. Pyorala K, Pedersen TR, Kjekshus J, Faergeman O, Olsson AG, Thorgeirsson G. Cholesterol lowering with simvastatin improves prognosis of diabetic pa-tients with coronary heart disease. A subgroup analysis of the Scandinavian Simvastatin Survival Study (4S) Diabetes Care. 1997;20(4):614-20.
12. Ravid M, Lang R, Rachmani R, Lishner M. Long-term renoprotective effect of angiotensin-converting enzyme inhibition in non-insulin-dependent diabetes mellitus. A 7-year follow-up study. Arch Intern Med. 1996;156(3):286-9.
13. Yusuf S, Sleight P, Pogue J, Bosch J, Davies R, Dagenais G. Effects of an angi-otensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med. 2000 ;342(3):145-53.
14. NHG. NHG-Standaard Cardiovasculair risicomanagement. Nederlands Huisartsen Genootschap, Utrecht, 2006. ISBN 9031347213.
15. Rutten GEHM, De Grauw WJC, Nijpels G, Goudswaard AN, Uitewaal PJM, Van der Does FEE, Heine RJ, Van Ballegooie E, Verduijn MM, Bouma M. NHG-Standaard Diabetes mellitus type 2 - Tweede herziening. Huisarts Wet. 2006;49(3):137-152.
16. Brown AF, Gregg EW, Stevens MR, Karter AJ, Weinberger M, Safford MM, Gary TL, Caputo DA, Waitzfelder B, Kim C, Beckles GL. Race, ethnicity, socioeco-nomic position, and quality of care for adults with diabetes enrolled in managed care: The Translating Research Into Action for Diabetes (TRIAD) study. Diabetes Care. 2005;28(12):2864-2870.
17. Wan Q, Harris MF, Jayasinghe UW, Flack J, Georgiou A, Penn DL, Burns JR. Quality of diabetes care and coronary heart disease absolute risk in patients with type 2 diabetes mellitus in Australian general practice. Qual Saf Health Care. 2006;15(2):131-5.
18. Grant RW, Cagliero E, Murphy-Sheehy P, Singer DE, Nathan DM, Meigs JB. Comparison of hyperglycemia, hypertension, and hypercholesterolemia man-agement in patients with type 2 diabetes. Am J Med. 2002;112(8):603-9.
19. McFarlane SI, Jacober SJ, Winer N, Kaur J, Castro JP, Wui MA, Gliwa A, Von Gizycki H, Sowers JR. Control of cardiovascular risk factors in patients with di-
16
Chapter 1 - General Introduction
abetes and hypertension at urban academic medical centers. Diabetes Care. 2002;25(4):718-23.
20. Al Khaja KA, Sequeira RP, Damanhori AH. Comparison of the quality of diabetes care in primary care diabetic clinics and general practice clinics. Diabetes Res Clin Pract. 2005;70(2):174-82.
21. Spann SJ, Nutting PA, Galliher JM, Peterson KA, Pavlik VN, Dickinson LM, Volk RJ. Management of type 2 diabetes in the primary care setting: a practice-based research network study. Ann Fam Med. 2006;4(1):23-31.
22. Metsemakers JFM. Huisartsgeneeskundigen registraties in Nederland. Onderzoeksinstituut voor ExTramurale en Transmurale Gezondheidszorg, editie 3, April 1999.
23. Cleveringa FG, Gorter KJ, van den Donk M, Rutten GEHM. Combined task delegation, computerized decision support, and feedback improve cardiovas-cular risk for type 2 diabetic patients: A cluster randomized trial in primary care. Diabetes Care. 2008;31(12):2273-5.
24. Fokkens AS, Wiegersma PA, Reijneveld SA, 2009. A structured registration pro-gram can be validly used for quality assessment in general practice. BMC Health Serv Res. 2009;9(1):241. doi:10.1186/1472-6963-9-241.
25. Cleveringa FG, Gorter KJ, van den Donk M, Rutten GEHM. Combined task delegation, computerized decision support, and feedback improve cardiovas-cular risk for type 2 diabetic patients: A cluster randomized trial in primary care. Diabetes Care. 2008;31(12):2273-5.
26. Project Diabeteszorg Beter. Samenwerking en samenhang in de keten: Evaluatie en resultaten. Diabeteszorg Beter, Zwolle, 2009.
27. Campbell SM, Braspenning J, Hutchinson A, Marshall M. Research methods used in developing and applying quality indicators in primary care. Qual Saf Health Care. 2002;11(4):358-64.
28. Campbell SM, Roland MO, Buetow SA. Defining quality of care. Soc Sci Med. 2000;51(11):1611-25.
29. Weiner M, Long J. Cross-sectional versus longitudinal performance assess-ments in the management of diabetes. Med Care. 2004;42(2 Suppl):II34-9.
30. Kerr EA, Smith DM, Hogan MM, Hofer TP, Krein SL, Bermann M, Hayward RA. Building a better quality measure: are some patients with ‘poor quality’ actually getting good care? Med Care. 2003;41(10):1173-82.
31. Selby JV, Uratsu CS, Fireman B, Schmittdiel JA, Peng T, Rodondi N, Karter AJ, Kerr EA. Treatment intensification and risk factor control: toward more clinically relevant quality measures. Med Care. 2009;47(4):395-402.
32. Grant RW, Buse JB, Meigs JB. Quality of diabetes care in U.S. academic medical centers: low rates of medical regimen change. Diabetes Care. 2005;28(2):337-442.
33. Andrade SE, Gurwitz JH, Field TS, Kelleher M, Majumdar SR, Reed G, Black R. Hypertension management: the care gap between clinical guidelines and clinical practice. Am J Manag Care. 2004;10(7 Pt 2):481-6.
34. Rodondi N, Peng T, Karter AJ, Baur DC, Vittinghoff E, Tang S, Pettitt D, Kerr EA, Selby JV. Therapy modifications in response to poorly controlled hypertension,
17
Chapter 1 - General Introduction
dyslipidemia, and diabetes mellitus. Ann Intern Med. 2006;144(7):475-4.35. Berlowitz DR, Ash AS, Glickman M, Friedman RH, Pogach LM, Nelson AL, Wong
AT. Developing a quality measure for clinical inertia in diabetes care. Health Serv Res. 2005;40(6 Pt 1):1836-53.
36. Phillips LS, Branch WT, Cook CB, Doyle JP, El-Kebbi IM, Gallina DL, Miller CD, Ziemer DC, Barnes CS. Clinical Inertia. Ann Intern Med. 2001;135(9):825-34.
37. Allen JD, Curtiss FR, Fairman KA. Nonadherence, clinical inertia, or therapeutic inertia? J Manag Care Pharm. 2009;15(8):690-5.
38. Mottur-Pilson C, Snow V, Bartlett K. Physician explanations for failing to comply with “best practices”. Eff Clin Pract. 2001;4(5):207-13.
39. Kedward J, Dakin L. A qualitative study of arriers to the use of statins and the implementation of coronary heart disease prevention in primary care. Br J Gen Pract. 2003;53(494):684-9.
40. Parnes BL, Main DS, Dickinson LM, Niebauer L, Holcomb S, Westfall JM, Pace WDCN - CaReNetCN - HPRN. Clinical decisions regarding HbA1c results in pri-mary care: a report from CaReNet and HPRN. Diabetes Care. 2004;27(1):13-6.
41. Hicks PC, Westfall JM, Van Vorst RF, Bublitz Emsermann C, Dickinson LM, Pace W, Parnes B. Action or inaction? Decision making in patients with diabetes and elevated blood pressure in primary care. Diabetes Care. 2006;29(12):2580-5.
42. Grant RW, Lutfey KE, Gerstenberger E, Link CL, Marceau LD, McKinlay JB. The decision to intensify therapy in patients with type 2 diabetes: results from an ex-periment using a clinical case vignette. J Am Board Fam Med. 2009;22(5):513-20.
43. AB E, Denig P, van Vliet T, Dekker JH. Reasons of general practitioners for not prescribing lipid-lowering medication to patients with diabetes: a qualitative study. BMC Fam Pract. 2009;10:24.
44. Safford MM, Shewchuk R, Qu H, Williams JH, Estrada CA, Ovalle F, Allison JJ. Reasons for not intensifying medications: differentiating “clinical inertia” from ap-propriate care. J Gen Intern Med. 2007;22(12):1648-55.
45. Yarzebski J, Bujor CF, Goldberg RJ, Spencer F, Lessard D, Gore JM. A commu-nity-wide survey of physician practices and attitudes toward cholesterol man-agement in patients with recent acute myocardial infarction. Arch Intern Med. 2002;162(7):797-804.
46. Boyd CM, Darer J, Boult C, FriedLP, Boult L, u AW. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implica-tions for pay for performance. JAMA. 2005;294(6):716-24.
47. Cotton A, Aspy CB, Mold J, Stein H. Clinical decision-making in blood pres-sure management of patients with diabetes mellitus: an Oklahoma Physicians Resource/Research Network (OKPRN) Study. J Am Board Fam Med. 2006;19(3):232-9.
48. Ferrari P, Hess L, Pechere-Bertschi A, Muggli F, Burnier M. Reasons for not intensifying antihypertensive treatment (RIAT): a primary care antihypertensive intervention study. J Hypertens. 2004;22(6):1221-9.
49. Oliveria SA, Lapuerta P, McCarthy BD, L’Italien GJ, Berlowitz DR, Asch SM. Physician-related barriers to the effective management of uncontrolled hyperten-
18
Chapter 1 - General Introduction
sion. Arch Intern Med. 2002;162(4):413-20.50. Kerr EA, Zikmund-Fisher BJ, Klamerus ML, Subramanian U, Hogan MM, Hofer
TP. The role of clinical uncertainty in treatment decisions for diabetic patients with uncontrolled blood pressure. Ann Intern Med. 2008;148(10):717-27.
51. Rose AJ, Shimada SL, Rothendler JA, Reisman JI, Glassman PA, Berlowitz DR, Kressin NR. The Accuracy of Clinician Perceptions of “Usual” Blood Pressure Control. J Gen Intern Med. 2007;10.1007/s11606-007-0464-1.
52. Borzecki AM, Oliveria SA, Berlowitz DR. Barriers to hypertension control. Am Heart J. 2005;149(5):785-94.
53. Persson M, Carlberg B, Tavelin B, Lindholm LH. Doctors’ estimation of cardio-vascular risk and willingness to give drug treatment in hypertension: fair risk as-sessment but defensive treatment policy. J Hypertens. 2004;22(1):65-71.
54. Samuels TA, Bolen S, Yeh HC, Abuid M, Marinopoulos SS, Weiner JP, McGuire M, Brancati FL. Missed opportunities in diabetes management: a longitudinal assessment of factors associated with sub-optimal quality. J Gen Intern Med. 2008;23(11):1770-7.
55. Guthrie B, Inkster M, Fahey T. Tackling therapeutic inertia: role of treatment data in quality indicators. BMJ. 2007;335(7619):542-4.
56. Roumie CL, Elasy TA, Wallston KA, Pratt S, Greevy RA, Liu X, Alvarez V, Dittus RS, Speroff T. Clinical inertia: a common barrier to changing provider prescribing behavior. Jt Comm J Qual Patient Saf. 2007;33(5):277-85.

19

20
21
Chapter 2 - Data collection methods
22
23
Chapter 2.1 - Computerised extraction of information on the quality of diabetes care from free text in electronic medical
records of general practitioners
Jaco Voorham1,2
Petra Denig1
1. Department of Clinical Pharmacology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
2. Department of Epidemiology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
Voorham J, Denig P. Computerized extraction of information on the quality of dia-betes care from free text in electronic patient records of general practitioners. J Am Med Inform Assoc. 2007;14(3):349-354.
24
Chapter 2.1 - Extraction from free text
ABSTRACT Objective. To develop and evaluate a computerised method for extracting numeric clinical measurements related to diabetes care from free text in electronic medical records (EMRs) of general practitioners, using a number-oriented approach.Design. A text recognition algorithm was selected on its ability for recognising the large variation in labels used to identify a set of 13 numeric measurements. This algorithm was used in a text interpretation method for deriving such information from EMRs. The accuracy of the method was compared to manual chart abstraction in-volving 60 EMRs from 6 general practices. Field performance was assessed on two electronic record systems in 10 general practices, involving data extraction for all their 767 patients with type 2 diabetes.Measurements. Sensitivity and positive predictive value were calculated to quantify the accuracy of data extraction. Performance was expressed as the time needed for data collection and processing.Results. Eighty percent of the numeric measurement information could only be found in free text of the EMRs. The extraction method showed a sensitivity of 94-100% and a positive predictive value of 85-100% for 11 of the 13 clinical measurements. Semi-automated post-processing increased sensitivity with several points and posi-tive predictive value to 100%. The field performance showed an average time of 7.8 minutes per 100 patients needed to extract all relevant data.Conclusions. The developed method can convert numeric clinical information to structured data with a high accuracy. This method enables research as well as qual-ity of care assessment in practices that do not comply with structured registration.

25
Chapter 2.1 - Extraction from free text
INTRODUCTIONRoutine entry of clinical information in electronic medical records (“registration”) comprises an important data source for healthcare research and quality improve-ment. The 1990’s saw creation of several European general practice registration networks.1-7 Most such networks collect selected information from structured tables embedded in the electronic medical record (EMR) systems, for example, patients’ prescribing records, diagnostic codes and demographic information. In order to meet sufficient accuracy and completeness, participating practices are required to use consistent, standardised and well-defined registration methods. This approach may restrict research: 1) studies using other information than what is or can be prede-fined are not possible; 2) required registration methods can result in selection bias of both practices and clinical information; 3) forced coding of clinical information may result in artefacts or false certainties, especially when payments depend on the use of specific coding systems as is currently the case in the United Kingdom. In stud-ies using such databases the question always remains whether variations found are due to variation in actual care or to differences in structured registration or lack of uniform coding.8-11
Despite increasing potential and pleas for more structured registration of clinical data, relevant information may be scattered over different parts of the EMR, and much information that is of potential interest for research and quality improvement can only be found in free text of the record.10,12,13 Reasons for physicians to use the free text part of the EMR instead of structured tables include time constraints dur-ing consultation, uncertainty about using or applying certain codes, classification limitations, or inexperience and difficulties with the computer systems.1,2,10,14 Some databases, such as the General Practice Research Database (GPRD)15 and the Integrated Primary Care Information database (IPCI)7 do collect free text information but this can only be used for evaluation and research with large additional costs. Besides technical difficulties of using free text as data source, privacy aspects also play a role. For specific research or quality assessment projects, manual chart re-view or separate data registration is being used but its limitations are obvious, in-cluding time and personnel costs as well as difficulties with standardising the collec-tion procedure. One of the areas in which manual record abstraction is not uncommon involves the quality of diabetes care.16-18 Clinical information that is often needed includes meas-urements of blood pressure, weight, height, and laboratory results.19-21 Although some of these data may be available through administrative or centralised clinical databases, incomplete data registration in such systems necessitates additional pa-tient record review.22 Therefore, there is a need for automated capture of this type of
26
Chapter 2.1 - Extraction from free text
numeric clinical measurement data from EMRs, which can be used across multiple sites that do not have uniform data registration procedures. Many approaches for information retrieval exist,23 and especially Natural Language Processing (NLP) has shown promising results in extracting and structuring clinical information from medical records.24,25 NLP has been used, for example, to classify medical problems lists,26,27 extract disease-related concepts from narrative reports,
28,29 and combine data from multiple discharge summaries.30 NLP techniques are helpful in coping with extracted terms and the related context that is relevant for their meaning, such as negation, degree, or certainty.25 NLP, however, is not well suited to handle some specific problems inherent to the manual data registration of numeric measurements in the free text fields of EMRs. This type of data recording is often ungrammatical and telegraphic in style, and does not follow a fixed structure or a normal text format. Personalised names and abbreviations are common to identify these measurements, which change frequently over time and often contain spell-ing errors, resulting in high variability and ambiguity. Techniques for pre-processing text have been developed to deal with some specific problems,28,31 but these rely on probabilistic relationships or tabular structures that are often lacking in the free text data registration of numeric measurements in EMRs. This makes it worthwhile to de-velop an extraction approach oriented on the numeric values instead of their labels.The aim of this study is to develop and evaluate a computerised extraction method to convert numeric clinical information stored anywhere in the EMRs in general practice to structured data without prerequisites on how and where the information is regis-tered in routine practice.The following issues are addressed: 1) the location of data registration and variation in labelling of numeric clinical measurements relevant for diabetes care; 2) the text recognition method best capable of collecting this information, 3) the field perform-ance of the extraction method and post-processing actions needed to optimise ac-curacy.
METHODS
SettingMost general practices in The Netherlands use computerised medical records, for which there are seven major electronic medical record systems. General practition-ers (GPs) are gatekeepers of the healthcare system, and patients are registered to one GP practice. The average practice size is 2,380 patients. Based on current disease prevalence, 70 of these patients are expected to have type 2 diabetes. GPs routinely collect information on visits in their practice but also other relevant medical details from elsewhere, such as hospitals, laboratories and specialised services.
27
Chapter 2.1 - Extraction from free text
Some of this information is stored in structured tables but most can be found in free text fields of the patient record. Such fields are extremely flexible, containing a varie-ty of notes entered by the GP or the GP’s assistants, including summaries of reports from outside sources. Even laboratory test results which have been received elec-tronically may end up in this free text field instead of the intended structured tables.A set of 13 numeric clinical measurements considered relevant for evaluating the quality of diabetes care was selected.19-21 This set consisted of measurements of systolic (SBP) and diastolic (DBP) blood pressure, weight, height, serum glucose (fasting, non-fasting, unspecified), glycosylated haemoglobin (HbA1c), and serum levels of total cholesterol (TC), high-density lipoprotein (HDL) cholesterol, low-den-sity lipoprotein (LDL) cholesterol, triglycerides, and creatinine.The regional Scientific Advisory Group of the General Practitioners Association ap-proved the anonymous data collection procedure for this project.
Data collectionThe study consisted of three parts: 1. development of the extraction method using a pilot dataset from 6 general practices; 2. assessing the accuracy of the extraction method by comparison with a gold standard dataset of 60 manually coded patient records, and 3. testing the performance of the developed extraction software on two EMR systems in 10 general practices. The pilot dataset was created with a conven-ience sample of practices, all using one EMR system. For each GP practice, we transferred the complete anonymised EMRs of 10 randomly selected patients with type 2 diabetes to the same EMR system in our test environment, using the provided EMR export/import procedures of the system to ensure that no alterations occurred in the content or structure of the EMR. The gold standard dataset was made by manual extraction of data from these complete EMRs for the year 2003. Verification was done by double coding of 30 EMRs by an independent general practitioner, showing excellent agreement between coders (kappa= 0.98).The field performance test was conducted on two EMR systems in actual practice. In this field test, data of 10 GP practices were extracted for all their patients with type 2 diabetes. The two EMR systems (Promedico and MicroHIS) chosen for the field test contribute two-thirds of the market in our region. The GP practices of the field test were different from those contributing to the pilot dataset.
Location of data registrationThe location of data registration in the EMRs for the selected clinical measurements was assessed in both the pilot and the field test. Data entries in free text were only counted if they were not present in the structured part of the EMR as well, to correct for double registration of measurement information. Both EMR systems in our study
28
Chapter 2.1 - Extraction from free text
had structured tables to store clinical measurements using specific measurement codes. In the MicroHIS version studied GPs can define their own codes. Despite this lack of uniform coding, we still considered this structured data storage.
Labelling of numeric dataNumeric data in free text fields of the EMR can be identified by the names and ab-breviations used in practice to label the measurement, and the units or specifications that may be added to the numeric value. The pilot dataset was used to generate an overview of the variability in words used in relation to the 13 selected clinical meas-urements. A vocabulary was generated of all unique words within 2 words distance from a string containing a number, assumed to be potential labels or specifications related to a numeric value. This vocabulary was independently reviewed by the two authors to classify words as 1) belonging to a numeric measurement of interest to be stored in a list for positive recognition, 2) not of interest to be stored in a list for negative recognition.
Text recognition algorithmFive text recognition algorithms were tested: The Levenshtein edit distance, an edit distance algorithm adapted for likelihood of typing errors, bigrams, trigrams, and an algorithm based on character sequences (Appendix A).32,33 For this test, nineteen target words representing labels for various clinical measurements of interest were selected that varied in length, likelihood of different ways of spelling, and possible misinterpretation due to typing errors. The performance of the algorithms was assessed per target word using the vocabu-lary of unique words. All words recognised by an algorithm were ranked on similarity to the target word, and the number of correctly recognised words was counted. We call this the algorithm’s recognition width, which is an indicator of its performance. For each target word, we assessed the recognition width of the five algorithms, and ranked the algorithms accordingly. The algorithm with the highest number of first rankings, allowing for ties in first ranking, over the nineteen target words was consid-ered as most suitable for our purpose.
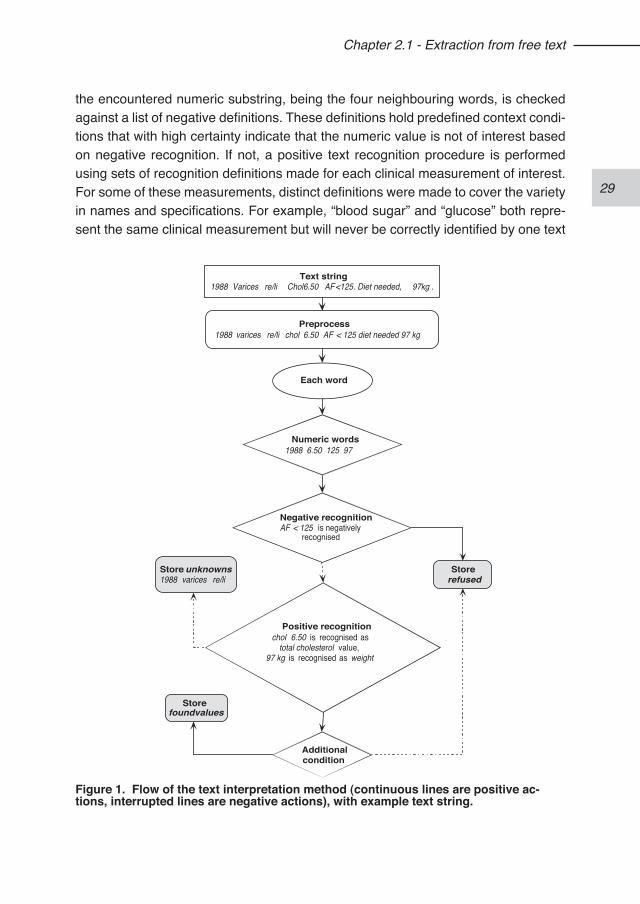
Text interpretation methodA text interpretation method was developed to convert free text numeric measure-ment information into structured data using the best performing text recognition al-gorithm. Several steps are involved (figure 1). Text strings are pre-processed by splitting compound strings and standardising character use, after which they are split into substrings representing individual words. The interpretation method then loops through the substrings, and on each substring containing a numeric value, i.e. infor-mation of potential interest, a sequence of checks is performed. First, the context of
29
Chapter 2.1 - Extraction from free text
the encountered numeric substring, being the four neighbouring words, is checked against a list of negative definitions. These definitions hold predefined context condi-tions that with high certainty indicate that the numeric value is not of interest based on negative recognition. If not, a positive text recognition procedure is performed using sets of recognition definitions made for each clinical measurement of interest. For some of these measurements, distinct definitions were made to cover the variety in names and specifications. For example, “blood sugar” and “glucose” both repre-sent the same clinical measurement but will never be correctly identified by one text
Text string1988 Varices re/li Chol6.50 AF<125. Diet needed, 97kg .
Preprocess1988 varices re/li chol 6.50 AF < 125 diet needed 97 kg
Each word
Numeric words1988 6.50 125 97
Storefoundvalues
Storerefused
Positive recognitionchol 6.50 is recognised as
total cholesterol value,97 kg is recognised as weight
Store unknowns1988 varices re/li
Additionalcondition
Negative recognitionAF < 125 is negatively
recognised
Figure 1. Flow of the text interpretation method (continuous lines are positive ac-tions, interrupted lines are negative actions), with example text string.
30
Chapter 2.1 - Extraction from free text
recognition definition. In case of a match, the numeric value is stored in a structured table together with its context words. Numeric information that is not recognised is stored together with its context in a separate “unknowns” table that is monitored in a post-processing procedure. Since the trigger to start the recognition process is the numeric value, we call this a number-oriented interpretation method, as opposed to a label-oriented approach. The text interpretation method was incorporated into data collection software that accesses all clinical parts, structured and free text, of two EMR systems operating in general practice. Data collection at the GP practice is followed by transmitting the extracted data to a centralised database for further processing. This procedure prevents that the privacy of the patient or the GP is compromised by sending the complete free text fields to a centralised database.
Post-processing procedurePost-processing can be useful in automated data collection to diminish errors in the extracted data. In our case, errors may occur for two reasons. Most of the collected data have originally been entered manually in the EMR by clinical personnel, and may therefore contain data entry errors. In addition, the text interpretation method may be inaccurate. Therefore, a semi-automated post-processing procedure was developed to identify and correct possible errors in the extracted data. Using a stepwise approach, several automated checks were performed, such as checking for numeric values outside specified ranges, unexpected peaks in time-series of a clinical measurement, and specific information in the “unknowns” table. This results in a notification of potential errors that are visually reviewed by a trained registration worker. The reviewer can act on these notifications by correcting the numeric value or its variable allocation, or by deleting erroneous or adding missed data. All such actions are logged, together with the modification reason. Reasons are classified in three types: problems caused by data entry errors in the GP practice (e.g. typing errors), problems introduced by the automated data extraction system (e.g. false positives, cut-off or goal values instead of actual clinical measurements, dates instead of values), and general data problems occurring in electronic databas-es (e.g. unit conversions or bogus values introduced by EMR system conversions).
Evaluation Extraction method accuracy was assessed by comparison with a gold standard da-taset of manually abstracted EMRs.34 Sensitivity, i.e. proportion of correct measure-ments found with the automated data extraction of the total number identified in the gold standard, and positive predictive value, i.e. proportion of correct measurements of the total number of found measurements, were calculated before and after post-
31
Chapter 2.1 - Extraction from free text
processing.In the field evaluation, the time needed for data collection was measured separately for data retrieval and text interpretation by activity logging in the extraction software. The effort to perform the post-processing procedure was measured by activity log-ging in the central database maintenance software.
Statistical analysisMedian and interquartile range of the proportion of numeric data only recorded in free text was calculated per GP practice and per EMR system. The number and proportion of different labels used for each of the 13 selected clinical measurements were assessed in both the pilot and the field test. In the field test, time estimates were calculated per GP practice to collect and process all data for a standardised population of 100 patients and compared by EMR system using Student’s t-test. The mean number of corrective actions taken during post-processing was also calculated for 100 patients per GP practice. In addition, a descriptive analysis was conducted to assess which corrective actions had been made for what reasons.
0
10
20
30
40
50
60
70
80
90
100
DB
P (n
=15,
704)
SB
P (n
=15,
906)
Hei
ght (
n=2,
308)
Wei
ght (
n=6,
210)
TC (n
=4,5
26)
Cre
atin
ine
(n=5
,647
)
Glu
c f (
n=7,
306)
Glu
c nf
(n=3
,826
)
LDL
(n=2
,435
)
Trig
lyce
rides
HD
L (n
=2,9
30)
HbA
1c (n
=9,5
83)
Glu
c ns
(n=6
,023
)
% in
free
text
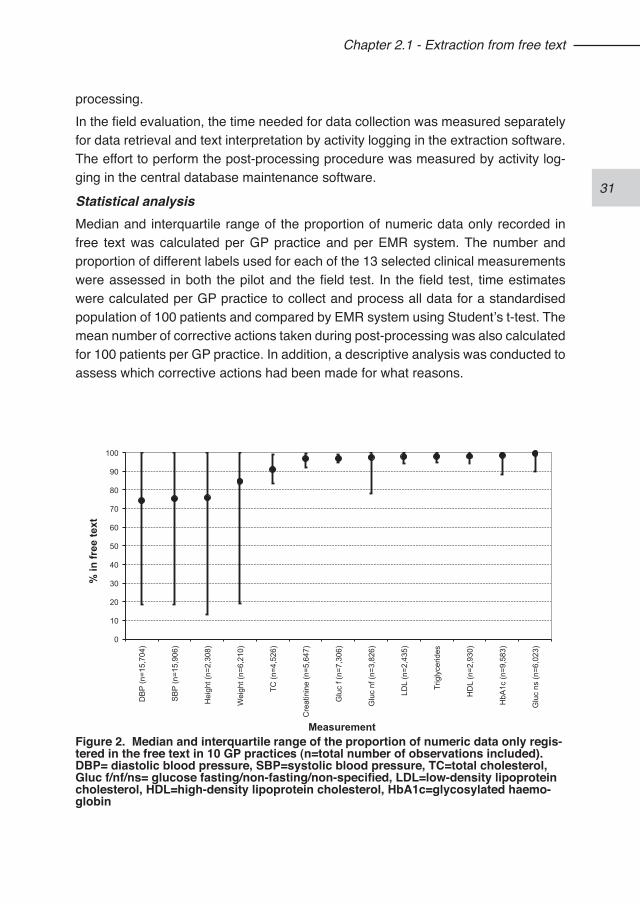
Measurement Figure 2. Median and interquartile range of the proportion of numeric data only regis-tered in the free text in 10 GP practices (n=total number of observations included).DBP= diastolic blood pressure, SBP=systolic blood pressure, TC=total cholesterol, Gluc f/nf/ns= glucose fasting/non-fasting/non-specified, LDL=low-density lipoprotein cholesterol, HDL=high-density lipoprotein cholesterol, HbA1c=glycosylated haemo-globin
32
Chapter 2.1 - Extraction from free text
RESULTS
Location of data registrationThe location of the numeric data registration in the pilot dataset showed that of the 13 selected measurements 80% of the observations could only be found in the free text part of the EMR; for 5 out of the 13 selected measurements this was above 90%. Also, the field test showed considerable variation between GP practices in the use of structured registration of some data (figure 2). Clinical measurements often con-ducted in the practice itself, such as blood pressure, weight and height, were found more frequently in the structured tables in comparison to laboratory results. The overall percentage of observations only available in free text was 96% for MicroHIS and 62% for Promedico indicating that for both systems there is a clear need for a data extraction method that can collect data from free text fields.
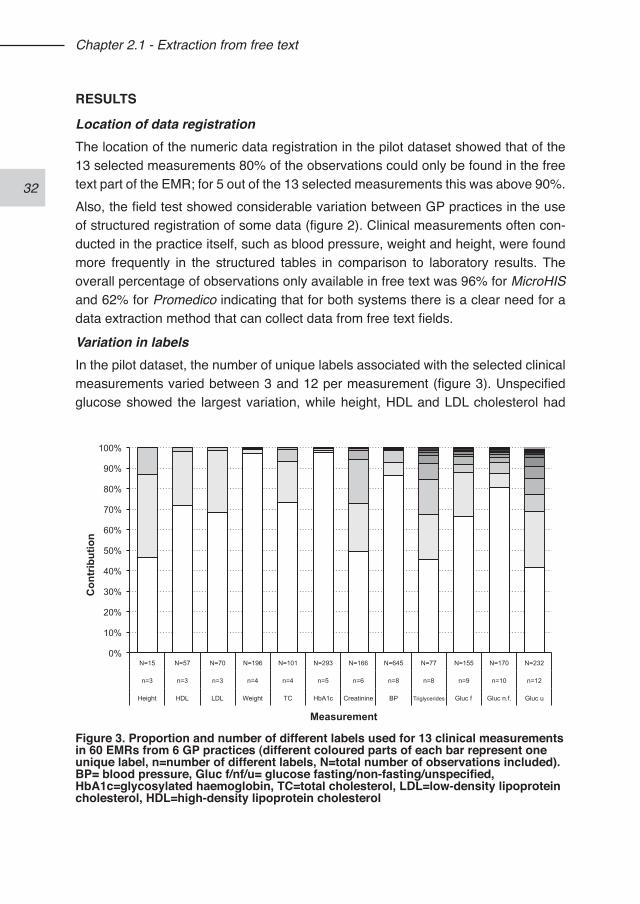
Variation in labelsIn the pilot dataset, the number of unique labels associated with the selected clinical measurements varied between 3 and 12 per measurement (figure 3). Unspecified glucose showed the largest variation, while height, HDL and LDL cholesterol had
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
N=15 N=57 N=70 N=196 N=101 N=293 N=166 N=645 N=77 N=155 N=170 N=232
n=3 n=3 n=3 n=4 n=4 n=5 n=6 n=8 n=8 n=9 n=10 n=12
Height HDL LDL Weight TC HbA1c Creatinine BP Triglycerides Gluc f Gluc n.f. Gluc u
Con
trib
utio
n
Measurement
Figure 3. Proportion and number of different labels used for 13 clinical measurements in 60 EMRs from 6 GP practices (different coloured parts of each bar represent one unique label, n=number of different labels, N=total number of observations included).BP= blood pressure, Gluc f/nf/u= glucose fasting/non-fasting/unspecified, HbA1c=glycosylated haemoglobin, TC=total cholesterol, LDL=low-density lipoprotein cholesterol, HDL=high-density lipoprotein cholesterol
33
Chapter 2.1 - Extraction from free text
the lowest variation. Large variations were found within and between GP practices. In the field test, the total number and variation of observed labels was much larger. For example, there were 39 labels for unspecified glucose, with a range of 5 to 21 within a GP practice. Total cholesterol showed a total of 18 labels, ranging from 2 to 12 within a GP practice. The observed variation was mainly the result of using personalised labels and abbreviations, and to a lesser extent due to typing errors.
Text recognition algorithmWe tested five algorithms for their ability to recognise the large variation in labels used for a set of 19 target words. The Levenshtein edit distance and the adapted edit distance algorithm recognised the largest number of labels for respectively 6 and 5 target words, the bigrams and trigrams algorithms outperformed the others for respectively 8 and 7 target words, and the character sequence algorithm performed best, reaching first ranking on recognition width for 11 target words. Therefore, the character sequence algorithm was selected for the text interpretation method.
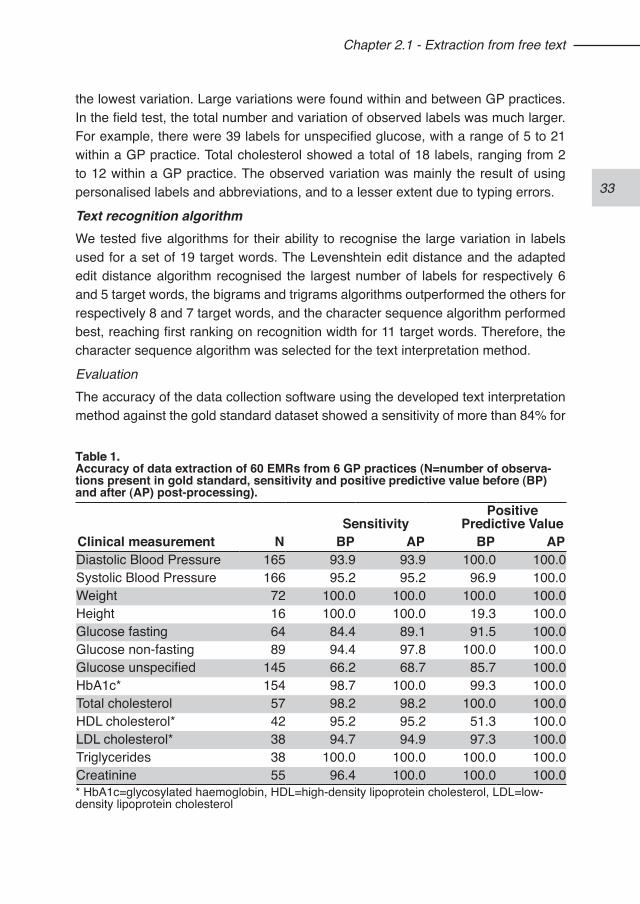
EvaluationThe accuracy of the data collection software using the developed text interpretation method against the gold standard dataset showed a sensitivity of more than 84% for
Table 1. Accuracy of data extraction of 60 EMRs from 6 GP practices (N=number of observa-tions present in gold standard, sensitivity and positive predictive value before (BP) and after (AP) post-processing).
SensitivityPositive
Predictive ValueClinical measurement N BP AP BP APDiastolic Blood Pressure 165 93.9 93.9 100.0 100.0Systolic Blood Pressure 166 95.2 95.2 96.9 100.0Weight 72 100.0 100.0 100.0 100.0Height 16 100.0 100.0 19.3 100.0Glucose fasting 64 84.4 89.1 91.5 100.0Glucose non-fasting 89 94.4 97.8 100.0 100.0Glucose unspecified 145 66.2 68.7 85.7 100.0HbA1c* 154 98.7 100.0 99.3 100.0Total cholesterol 57 98.2 98.2 100.0 100.0HDL cholesterol* 42 95.2 95.2 51.3 100.0LDL cholesterol* 38 94.7 94.9 97.3 100.0Triglycerides 38 100.0 100.0 100.0 100.0Creatinine 55 96.4 100.0 100.0 100.0* HbA1c=glycosylated haemoglobin, HDL=high-density lipoprotein cholesterol, LDL=low-density lipoprotein cholesterol
34
Chapter 2.1 - Extraction from free text
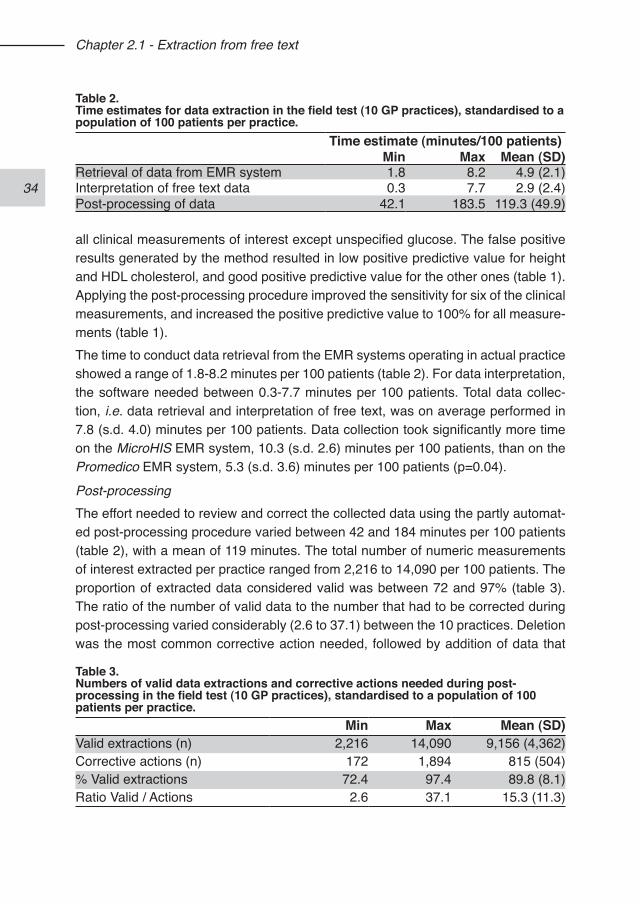
all clinical measurements of interest except unspecified glucose. The false positive results generated by the method resulted in low positive predictive value for height and HDL cholesterol, and good positive predictive value for the other ones (table 1). Applying the post-processing procedure improved the sensitivity for six of the clinical measurements, and increased the positive predictive value to 100% for all measure-ments (table 1).The time to conduct data retrieval from the EMR systems operating in actual practice showed a range of 1.8-8.2 minutes per 100 patients (table 2). For data interpretation, the software needed between 0.3-7.7 minutes per 100 patients. Total data collec-tion, i.e. data retrieval and interpretation of free text, was on average performed in 7.8 (s.d. 4.0) minutes per 100 patients. Data collection took significantly more time on the MicroHIS EMR system, 10.3 (s.d. 2.6) minutes per 100 patients, than on the Promedico EMR system, 5.3 (s.d. 3.6) minutes per 100 patients (p=0.04).
Post-processingThe effort needed to review and correct the collected data using the partly automat-ed post-processing procedure varied between 42 and 184 minutes per 100 patients (table 2), with a mean of 119 minutes. The total number of numeric measurements of interest extracted per practice ranged from 2,216 to 14,090 per 100 patients. The proportion of extracted data considered valid was between 72 and 97% (table 3). The ratio of the number of valid data to the number that had to be corrected during post-processing varied considerably (2.6 to 37.1) between the 10 practices. Deletion was the most common corrective action needed, followed by addition of data that
Table 2.Time estimates for data extraction in the field test (10 GP practices), standardised to a population of 100 patients per practice.
Time estimate (minutes/100 patients)Min Max Mean (SD)
Retrieval of data from EMR system 1.8 8.2 4.9 (2.1)Interpretation of free text data 0.3 7.7 2.9 (2.4)Post-processing of data 42.1 183.5 119.3 (49.9)
Table 3.Numbers of valid data extractions and corrective actions needed during post-processing in the field test (10 GP practices), standardised to a population of 100 patients per practice.
Min Max Mean (SD)Valid extractions (n) 2,216 14,090 9,156 (4,362)Corrective actions (n) 172 1,894 815 (504)% Valid extractions 72.4 97.4 89.8 (8.1)Ratio Valid / Actions 2.6 37.1 15.3 (11.3)
35
Chapter 2.1 - Extraction from free text
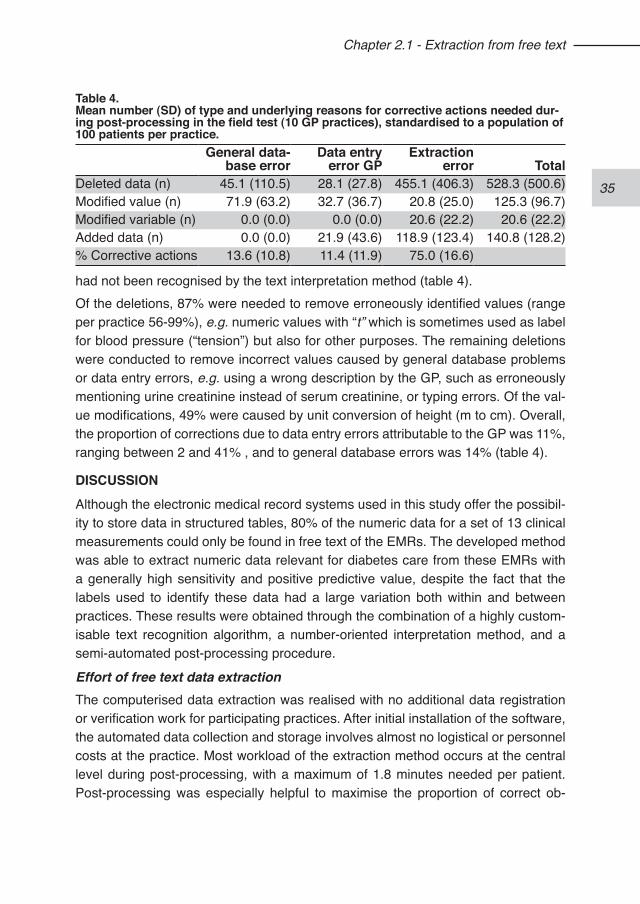
had not been recognised by the text interpretation method (table 4). Of the deletions, 87% were needed to remove erroneously identified values (range per practice 56-99%), e.g. numeric values with “t” which is sometimes used as label for blood pressure (“tension”) but also for other purposes. The remaining deletions were conducted to remove incorrect values caused by general database problems or data entry errors, e.g. using a wrong description by the GP, such as erroneously mentioning urine creatinine instead of serum creatinine, or typing errors. Of the val-ue modifications, 49% were caused by unit conversion of height (m to cm). Overall, the proportion of corrections due to data entry errors attributable to the GP was 11%, ranging between 2 and 41% , and to general database errors was 14% (table 4).
DISCUSSIONAlthough the electronic medical record systems used in this study offer the possibil-ity to store data in structured tables, 80% of the numeric data for a set of 13 clinical measurements could only be found in free text of the EMRs. The developed method was able to extract numeric data relevant for diabetes care from these EMRs with a generally high sensitivity and positive predictive value, despite the fact that the labels used to identify these data had a large variation both within and between practices. These results were obtained through the combination of a highly custom-isable text recognition algorithm, a number-oriented interpretation method, and a semi-automated post-processing procedure.
Effort of free text data extraction The computerised data extraction was realised with no additional data registration or verification work for participating practices. After initial installation of the software, the automated data collection and storage involves almost no logistical or personnel costs at the practice. Most workload of the extraction method occurs at the central level during post-processing, with a maximum of 1.8 minutes needed per patient. Post-processing was especially helpful to maximise the proportion of correct ob-
Table 4.Mean number (SD) of type and underlying reasons for corrective actions needed dur-ing post-processing in the field test (10 GP practices), standardised to a population of 100 patients per practice.
General data-base error
Data entry error GP
Extraction error Total
Deleted data (n) 45.1 (110.5) 28.1 (27.8) 455.1 (406.3) 528.3 (500.6)Modified value (n) 71.9 (63.2) 32.7 (36.7) 20.8 (25.0) 125.3 (96.7)Modified variable (n) 0.0 (0.0) 0.0 (0.0) 20.6 (22.2) 20.6 (22.2)Added data (n) 0.0 (0.0) 21.9 (43.6) 118.9 (123.4) 140.8 (128.2)% Corrective actions 13.6 (10.8) 11.4 (11.9) 75.0 (16.6)
36
Chapter 2.1 - Extraction from free text
servations extracted, which is important for monitoring purposes,35 and was also considered necessary to diminish errors in the extracted data which were caused by data entry errors in general practice. The information obtained from the post-processing procedure can be used to expand the lists for text recognition, resulting in an expected higher accuracy of the automated extraction method, and a decrease in time needed for post-processing. The alternative approach for this type of data extraction is manually collecting and reviewing patient records. In a Dutch project focusing on diabetes care in primary care,36 manually collecting relevant clinical data from patient records showed an estimated minimum effort of 10 minutes per patient.
Requirements of the text recognition algorithmTyping errors, consistently misspelled words, and the use of personal abbreviations and terms are important sources of variation in (medical) text. This is important to consider for the selection of an appropriate text recognition algorithm. The character sequence algorithm that performed best in our pilot is highly customisable. It is more suitable for recognition of short text strings than the bigram or trigram algorithms, and more flexible than the edit-distance algorithms. We found a large variability in labels used to identify numeric data both within and between GP practices. This implies that a label-oriented interpretation approach can be expected to result in poorer accuracy than we obtained using a number-oriented approach. Even making an initial inventory of labels used for the clinical measurements of interest in a prac-tice will not be sufficient to cover the existing variability. Changes in personnel and temporary replacement as well as changes in the use of labels over time will result in a continuous increase of variability. We used a number-oriented approach ensuring the capture of all numeric values of potential interest. Recently, a study was presented abstracting blood pressure measurements from text notes using a label-oriented approach resulting in similar accuracy rates.37 Such a label-oriented approach requires lists with regular expres-sions, and is only feasible in situations where labelling style is constant. When that is not the case, a label-oriented approach can be expected to result in poorer accuracy than obtained using a number-oriented approach.
Structured data registrationStructured data registration and standardisation are often seen as the ultimate solu-tion for getting full benefits of EMRs, although it is also recognised that a combination of free text and structured data registration is needed for keeping adequate patient records.38 An essential feature for any record system is that it is part of the clinician’s workflow, and the efforts required for its correct use are minimal.39 For a general
37
Chapter 2.1 - Extraction from free text
practitioner, the quickest way to record data as well as to get a quick overview of observations is usually in a few lines of free text.11,13 When computer-based support systems are installed to ensure better data registration of specific information in rou-tine practice, they are often faced with incomplete or limited usage.40-42 Navigating through an interface and selecting the applicable items in various screens is usually more time-consuming than entering data in free text. Fixed forms with predefined items may fit the workflow of a specialised environment, but in general practice an-ticipation of data registration is difficult. Our study shows that even though the EMR systems have structured storage mod-ules adapted to clinical protocols used in general practice, their use is not consist-ent. We did found some association between the EMR system and the proportion of structured registration, especially regarding blood pressure and weight. This was caused by the use of a so called “Risk Profile” utility in one of the systems, which ena-bles the GP to quickly store a limited number of data for easy follow-up. Comparable functionality in the other EMR system, however, was not regularly used by the GPs in our study. Increased electronic exchange of laboratory results might be expected to lead to more structured data storage but several logistic, economic and data qual-ity issues still have to be resolved.43 At the moment, much of these electronically exchanged data are still registered in free text in the EMR. Extracting structured and coded data from different information systems is also not without problems. There are technical problems due to local differences of systems, system settings and different versions of coding lists, which necessitate individual customisation of search queries. In addition, some information can be relevant in more than one context, and may be placed in unanticipated parts of the system.10,44 This makes that data extraction of structured data from EMRs is also faced with a continuous need for checking and validation as well as adaptation of the extraction software.14,45
Limitations and generalisabilityWe focused on the extraction of a set of numeric clinical measurements relevant for diabetes care. By including a wide range of measurements coming from physical examination and laboratory results, we have shown that this method is applicable for collecting data from EMRs involving numeric values. This includes clinical informa-tion related to vital signs and test results. Additional functionality is needed to extract categorical information, like lifestyle observations or co-morbidities.Our data collection software was developed for two of the EMR systems used in Dutch general practice, and is therefore not publicly available. Our approach, how-ever, can easily be applied in other settings. The effort needed for free text data
38
Chapter 2.1 - Extraction from free text
extraction may vary for different clinical information as well as different information systems. We observed no difference in the sensitivity of data collection between the two EMR systems used in our study. There is no reason to expect that the method will perform differently with another EMR system regarding this aspect. On the other hand, it is expected that a higher (adequate) use of structured tables will result in a higher positive predictive value before post-processing. Performance in terms of time needed for data extracting and processing can be expected to differ between systems.
ConclusionsThe study extraction method identifies and converts to structured data selected nu-meric clinical information stored anywhere within tested EMR systems. This method offers considerable advantages over existing methods that rely on structured data registration or manual data extraction. The method, through its generality, appears to hold potential value for conducting health services research and quality of care assessments in general practice.
REFERENCES1. Treweek S. The potential of electronic medical record systems to support qual-
ity improvement work and research in Norwegian general practice. BMC Health Serv Res. 2003;3(1):10.
2. Mansson J, Nilsson G, Bjorkelund C, Strender LE. Collection and retrieval of structured clinical data from electronic patient records in general practice. A first-phase study to create a health care database for research and quality assess-ment. Scand J Prim Health Care. 2004;22(1):6-10.
3. Lagasse R, Desmet M, Jamoulle M, Correa G, Roland M, Hoyois P, De Brouwer Ch. European situation of the routine medical data collection and their utilisation for health monitoring. Euro-med-data, final report. 2001.
4. Metsemakers JFM. Huisartsgeneeskundigen registraties in Nederland Onderzoeksinstituut voor ExTramurale en Transmurale Gezondheidszorg, edi-tie 3, April 1999.
5. Jick SS, Kaye JA, Vasilakis-Scaramozza C, Garcia Rodriguez LA, Ruigomez A, Meier CR, Schlienger RG, Black C, Jick H Validity of the general practice research database. Pharmacotherapy. 2003;23(5):686-9.
6. Carey IM, Cook DG, De Wilde S, Bremner SA, Richards N, Caine S, Strachan DP, Hilton SR. Developing a large electronic primary care database (Doctors’ Independent Network) for research. Int J Med Inform. 2004;73(5):443-53.
7. Mosis G, Vlug AE, Mosseveld M, Dieleman JP, Stricker BC, van der Lei J, Sturkenboom MC. A technical infrastructure to conduct randomized database studies facilitated by a general practice research database. J Am Med Inform Assoc. 2005;12(6):602-7.
8. Hippisley-Cox J, O’Hanlon S, Coupland C. Association of deprivation, ethnicity, and sex with quality indicators for diabetes: population based survey of 53,000
39
Chapter 2.1 - Extraction from free text
patients in primary care. BMJ. 2004;329(7477):1267-9.9. Gray J, Orr D, Majeed A. Use of Read codes in diabetes management in a south
London primary care group: implications for establishing disease registers. BMJ. 2003;326(7399):1130.
10. de Lusignan S, Valentin T, Chan T, Hague N, Wood O, van Vlymen J, Dhoul N. Problems with primary care data quality: osteoporosis as an exemplar. Inform Prim Care. 2004;12(3):147-56.
11. Los RK, van Ginneken AM, van der Lei J. OpenSDE: a strategy for expressive and flexible structured data entry. Int J Med Inform. 2005;74:481-90.
12. Prins H, Kruisinga FH, Buller HA, Zwetsloot-Schonk JH. Availability and usability of data for medical practice assessment. Int J Qual Health Care. 2002;14(2):127-37.
13. McDonald CJ. The barriers to electronic medical record systems and how to overcome them. J Am Med Inform Assoc. 1997;4(3):213-21.
14. de Lusignan S, Chan T, Wells S, Cooper A, Harvey M, Brew S, Wright M. Can pa-tients with osteoporosis, who should benefit from implementation of the national service framework for older people, be identified from general practice compu-ter records? A pilot study that illustrates the variability of computerized medical records and problems with searching them. Public Health. 2003;117(6):438-45.
15. GPRD. General practice research database. http://www.gprd.com16. Grant RW, Buse JB, Meigs JBCN - University HealthSystem Consortium (UHC)
Diabetes Benchmarking Project Team. Quality of diabetes care in U.S. aca-demic medical centers: low rates of medical regimen change. Diabetes Care 2005;28(2):337-442.
17. De Berardis G, Pellegrini F, Franciosi M, Belfiglio M, Di Nardo B, Greenfield S, Kaplan SH, Rossi MC, Sacco M, Tognoni G, Valentini M, Nicolucci ACN - for the QuED (Quality of Care and Outcomes in Type 2 Diabetes) Study Group. Quality of diabetes care predicts the development of cardiovascular events: Results of the QuED study. Nutr Metab Cardiovasc Dis. 2008;18(1):57-65.
18. Ackermann RT, Thompson TJ, Selby JV, Safford MM, Stevens M, Brown AF, Narayan KMCN - Translating Research into Action for Diabetes (TRIAD) Study Group. Is the number of documented diabetes process-of-care indicators as-sociated with cardiometabolic risk factor levels, patient satisfaction, or self-rat-ed quality of diabetes care? The Translating Research into Action for Diabetes (TRIAD) study. Diabetes Care. 2006;29(9):2108-13.
19. UK Department of Health. National service framework for diabetes - the delivery strategy. London: 2001.
20. Anonymous. Diabeteszorg Beter. Rapport van de Taakgroep Programma Diabeteszorg. 2005; Ministry of Health, The Netherlands.
21. The Health Plan Employer Data and Information Set (HEDIS). Washington DC: National Committee for Quality Assurance. Accessed at www.ncqa.org/pro-grams/hedis on Oct 10, 2006.
22. Kerr EA, Smith DM, Hogan MM, Krein SL, Pogach L, Hofer TP, Hayward RA. Comparing clinical automated, medical record, and hybrid data sources for dia-betes quality measures. Jt Comm J Qual Improv. 2002;28(10):555-65.
40
Chapter 2.1 - Extraction from free text
23. Wiesman F, Hasman A, van den Herik HJ, 1997. Information retrieval: an over-view of system characteristics. Int J Med Inf. 1997;47(1-2):5-26.
24. Friedman C, Hripcsak G, 1999. Natural language processing and its future in medicine. Acad Med. 1999;74(8):890-5.
25. Friedman C, Shagina L, Lussier Y, Hripcsak G. Automated encoding of clinical documents based on natural language processing. J Am Med Inform Assoc. 2004;11(5):392-402.
26. Meystre S, Haug PJ., 2005. Automation of a problem list using natural language processing. BMC Med Inform Decis Mak. 2005;5-30.
27. Chapman WW, Christensen LM, Wagner MM, Haug PJ, Ivanov O, Dowling JN, Olszewski RT. Classifying free-text triage chief complaints into syndromic cat-egories with natural language processing. Artif Intell Med. 2005;33(1):31-40.
28. Xu H, Anderson K, Grann VR, Friedman C. Facilitating cancer research using natural language processing of pathology reports. Medinfo. 2004;11(Pt 1):565-72.
29. Mendonça EA, Haas J, Shagina L, Larson E, Friedman C. Extracting information on pneumonia in infants using natural language processing of radiology reports. J Biomed Inform. 2005;38(4):314-21.
30. Liu H, Friedman C. CliniViewer: A tool for viewing electronic medical records based on natural language processing and XML. Medinfo. 2004;11(Pt 1):639-43.
31. Xu H, Markatou M, Dimova R, Liu H, Friedman C. Machine learning and word sense disambiguation in the biomedical domain: design and evaluation issues. BMC Bioinformatics. 2006;7:334.
32. Navarro G. A Guided tour to approximate string matching. ACM Computing Surveys. 2001;33(1):31-88.
33. Lovis C, Baud RH. Fast exact string pattern-matching algorithms adapted to the characteristics of the medical language. J Am Med Inform Assoc. 2000;7:378-91.
34. Hogan WR, Wagner MM. Accuracy of data in computer-based patient records. J Am Med Inform Assoc. 1997;4(5):342-55.
35. Andersen M. Is it possible to measure Prescribing quality using only prescription data? Basic Clin Pharmacol Toxicol. 2006;98(3):314-9.
36. Schaars CF, Denig P, Kasje WN, Stewart RE, Wolffenbuttel BHR, Haaijer-Ruskamp FM. Physician, organizational, and patient factors associated with suboptimal blood pressure management in type 2 diabetic patients in primary care. Diabetes Care. 2004;27(1):123-8.
37. Turchin A, Kolatkar NS, Grant RW, Makhni EC, Pendergrass ML, Einbinder JS. Using regular expressions to abstract blood pressure and treatment intensifi-cation information from the text of physician notes. J Am Med Inform Assoc. 2006;13(6):691-5.
38. van Ginneken AM. The computerized patient record: balancing effort and ben-efit. Int J Med Inf. 2002;65(2):97-119.
39. Kawamoto K, Houlihan CA, Balas EA, Lobach DF. Improving clinical practice using CDSS: a systematic review of trials to identify features critical to success. BMJ. 2005;330(7494):740-1.
40. Hetlevik I, Holmen J, Kruger O. Implementing clinical guidelines in the treatment
41
Chapter 2.1 - Extraction from free text
of hypertension in general practice. Evaluation of patient outcome related to implementation of a computer-based clinical decision support system. Scand J Prim Health Care. 1999;17(1):35-40.
41. Montgomery AA, Fahey T, Peters TJ, MacIntosh C, Sharp DJ. Evaluation of com-puter based clinical decision support system and risk chart for management of hypertension in primary care: randomised controlled trial. BMJ. 2000;320:686-90.
42. Balas EA, Krishna S, Kretschmer RA, Cheek TR, Lobach, DF, Boren SA. Computerized knowledge management in diabetes care. Med Care. 2004;42:610-621.
43. Staes CJ, Bennett ST, Evans RS, Narus SP, Huff SM, Sorensen JB. A case for manual entry of structured, coded laboratory data from multiple sources into an ambulatory electronic health record. J Am Med Inform Assoc. 2006;13(1):12-5.
44. Los RK, Roukema J, van Ginneken AM, de Wilde M, van der Lei J. Are struc-tured data structured identically? Investigating the uniformity of pediatric patient data recorded using OpenSDE. Methods Inf Med. 2005;44(5):631-8.
45. Tacken M. Quality of preventive performance in general practice: the use of rou-tinely collected data. 2005. PhD thesis University of Nijmegen, The Netherlands.

42
Chapter 2.1 - Extraction from free text
APPENDIX AThe character sequence algorithm used for the text recognition part of the data col-lection method uses the following formula to calculate the similarity score V.
t Target stringp Pattern string, to be compared with the targetLt Length of target stringLp Length of pattern stringmseq Maximum similar character sequence in both target and pattern
stringpt Starting position of mseq in target stringpp Starting position of mseq in pattern stringa,b,c,d,e Weighing factors, to adapt recognition behaviour
The flexibility of the algorithm is obtained by using the weighing factors a to e. For each target string, the algorithm can be calibrated to optimise its recognition width using a sample of pattern strings. For instance, by increasing the weighing factor d the similarity between the target and pattern strings is less likely to result in a high score V if the matching string sequence is at the end of the pattern string.
43
44
45
Chapter 2.2 - The GIANTT database - data collection methodology for continuous
monitoring of the quality of care of patients with type 2 diabetes in The
Netherlands
Jaco Voorham1,2
Petra Denig1
Bruce HR Wolffenbuttel3
Flora M Haaijer-Ruskamp1
1. Department of Clinical Pharmacology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
2. Department of Epidemiology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
3. Department of Endocrinology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
46
Chapter 2.2 - GIANTT database
INTRODUCTIONThe GIANTT project (Groningen Initiative to Analyse Type 2 diabetes Treatment) is a regional initiative of health care providers and researchers focussing on the care delivered to ambulant patients with type 2 diabetes mellitus in the Northern Netherlands. The goals are to improve the quality of care delivered to patients with type 2 diabetes mellitus, and reduce complications for these patients.The GIANTT project started in 2003 as an initiative of the University Medical Centre Groningen, the Martini Hospital Groningen, the General Practitioners of the Groningen region and the Regional Diabetes Facility from the General Practice Laboratory.Data collection is based on routinely registered information present in the medical record systems. Automated procedures are used to collect data from the medical records. Distinct methods were developed to collect data of patients with type 2 diabetes from the electronic medical records (EMR) of general practitioners (GPs)1 and from the regional diabetes facility (DF). Important requirements are: 1) validated procedure to select all known patients with type 2 diabetes, 2) method of data col-lection which is not dependent on specific registration routines of the health care provider and does not burden them with separate registration of the needed data, 3) continuous data validation of collected data, and 4) linkage of data from various sources without compromising the patients’ privacy.This chapter describes the methods developed to perform patient selection, data extraction, data cleaning and patient linkage for the two primary diabetes care pro-viders.
DATA COLLECTION AT GP PRACTICESIn the Netherlands, GP records contain much relevant medical information on indi-vidual patients, since patients are registered to a single GP who has a gatekeeper role. The records contain information on patient demographics, physical examina-tions, laboratory measurements, diagnoses, and drug prescriptions (coded accord-ing to the Anatomic Therapeutic Chemical (ATC) classification system2). Clinical information from contacts between the practice and the patient is recorded. In addi-tion, external data coming from laboratories or specialists is often entered manually in the patient records, although electronic communication of especially laboratory data becomes more common.The target was set to develop a method for collecting data from the electronic medi-cal records (EMR) with minimal burden to the participating practices to avoid selec-tion bias caused by anticipated additional workload. Therefore, no agreements were made on how and in what part of the EMR data are recorded, and software was
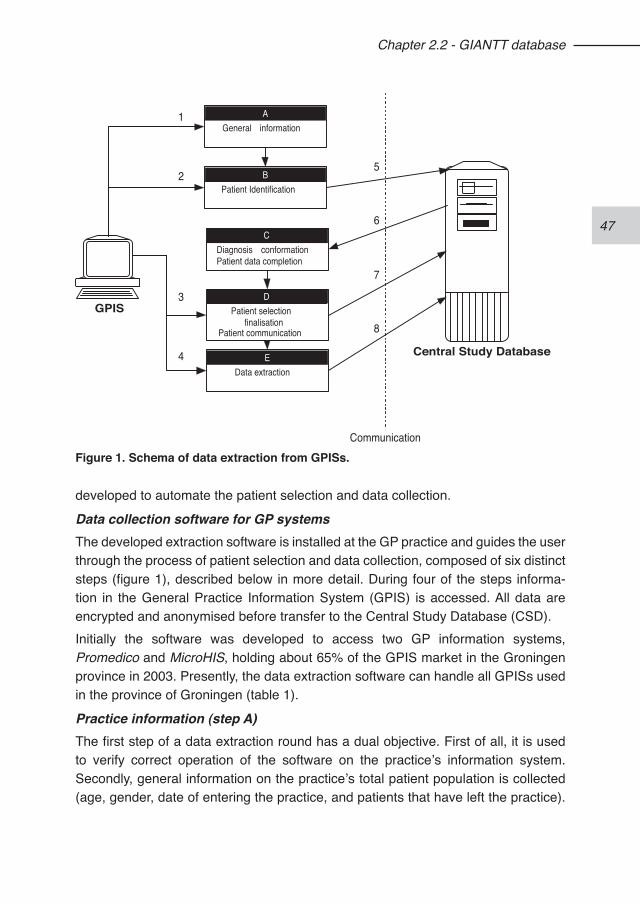
47
Chapter 2.2 - GIANTT database
developed to automate the patient selection and data collection.
Data collection software for GP systems The developed extraction software is installed at the GP practice and guides the user through the process of patient selection and data collection, composed of six distinct steps (figure 1), described below in more detail. During four of the steps informa-tion in the General Practice Information System (GPIS) is accessed. All data are encrypted and anonymised before transfer to the Central Study Database (CSD).Initially the software was developed to access two GP information systems, Promedico and MicroHIS, holding about 65% of the GPIS market in the Groningen province in 2003. Presently, the data extraction software can handle all GPISs used in the province of Groningen (table 1).
Practice information (step A)The first step of a data extraction round has a dual objective. First of all, it is used to verify correct operation of the software on the practice’s information system. Secondly, general information on the practice’s total patient population is collected (age, gender, date of entering the practice, and patients that have left the practice).
GPIS
Central Study Database
BPatient Identification
CDiagnosis conformationPatient data completion
DPatient selection
finalisationPatient communication
EData extraction
AGeneral information
Communication
1
2
3
4
5
6
7
8
Figure 1. Schema of data extraction from GPISs.
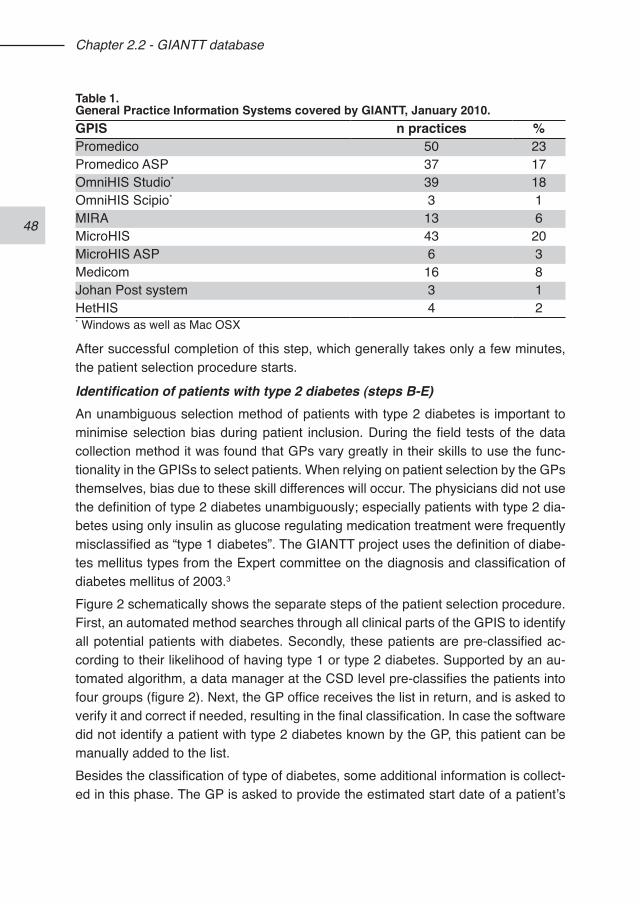
48
Chapter 2.2 - GIANTT database
After successful completion of this step, which generally takes only a few minutes, the patient selection procedure starts.
Identification of patients with type 2 diabetes (steps B-E)An unambiguous selection method of patients with type 2 diabetes is important to minimise selection bias during patient inclusion. During the field tests of the data collection method it was found that GPs vary greatly in their skills to use the func-tionality in the GPISs to select patients. When relying on patient selection by the GPs themselves, bias due to these skill differences will occur. The physicians did not use the definition of type 2 diabetes unambiguously; especially patients with type 2 dia-betes using only insulin as glucose regulating medication treatment were frequently misclassified as “type 1 diabetes”. The GIANTT project uses the definition of diabe-tes mellitus types from the Expert committee on the diagnosis and classification of diabetes mellitus of 2003.3
Figure 2 schematically shows the separate steps of the patient selection procedure. First, an automated method searches through all clinical parts of the GPIS to identify all potential patients with diabetes. Secondly, these patients are pre-classified ac-cording to their likelihood of having type 1 or type 2 diabetes. Supported by an au-tomated algorithm, a data manager at the CSD level pre-classifies the patients into four groups (figure 2). Next, the GP office receives the list in return, and is asked to verify it and correct if needed, resulting in the final classification. In case the software did not identify a patient with type 2 diabetes known by the GP, this patient can be manually added to the list. Besides the classification of type of diabetes, some additional information is collect-ed in this phase. The GP is asked to provide the estimated start date of a patient’s
Table 1.General Practice Information Systems covered by GIANTT, January 2010.GPIS n practices %Promedico 50 23Promedico ASP 37 17OmniHIS Studio* 39 18OmniHIS Scipio* 3 1MIRA 13 6MicroHIS 43 20MicroHIS ASP 6 3Medicom 16 8Johan Post system 3 1HetHIS 4 2* Windows as well as Mac OSX
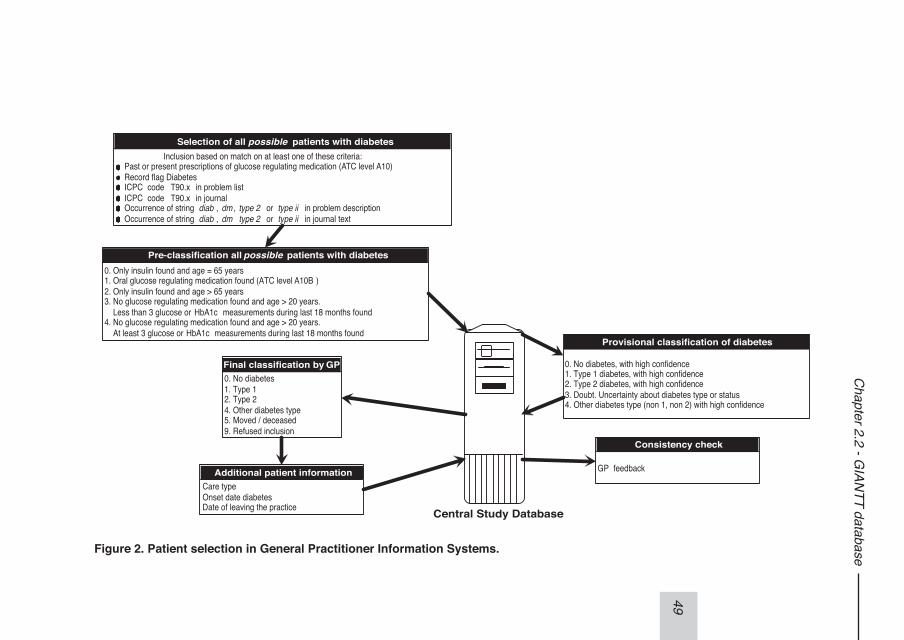
49
Chapter 2.2 - G
IANTT database
Selection of all possible patients with diabetesInclusion based on match on at least one of these criteria:
Past or present prescriptions of glucose regulating medication (ATC level A10)Record flag DiabetesICPC code T90.x in problem listICPC code T90.x in journalOccurrence of string diab , dm , type 2 or type ii in problem descriptionOccurrence of string diab , dm ,type 2 or type ii in journal text
Pre-classification allpossible patients with diabetes0. Only insulin found and age = 65 years1. Oral glucose regulating medication found (ATC level A10B )2. Only insulin found and age > 65 years3. No glucose regulating medication found and age > 20 years. Less than 3 glucose or HbA1c measurements during last 18 months found4. No glucose regulating medication found and age > 20 years. At least 3 glucose or HbA1c measurements during last 18 months found
Central Study Database
Provisional classification of diabetes
0. No diabetes, with high confidence1. Type 1 diabetes, with high confidence2. Type 2 diabetes, with high confidence3. Doubt. Uncertainty about diabetes type or status4. Other diabetes type (non 1, non 2) with high confidence
Final classification by GP0. No diabetes1. Type 12. Type 24. Other diabetes type5. Moved / deceased9. Refused inclusion
Additional patient informationCare typeOnset date diabetesDate of leaving the practice
Consistency check
GP feedback
Figure 2. Patient selection in General Practitioner Information Systems.
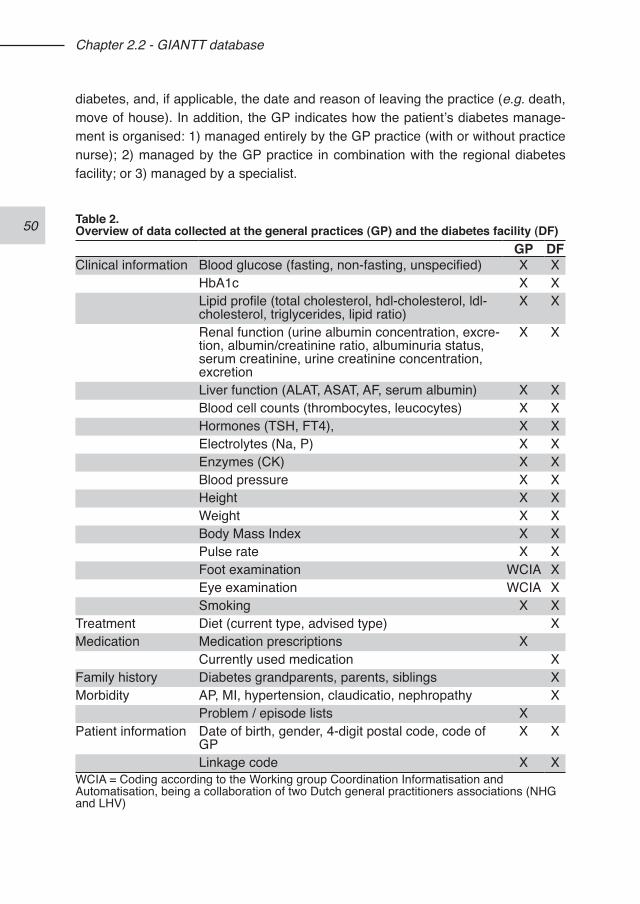
50
Chapter 2.2 - GIANTT database
diabetes, and, if applicable, the date and reason of leaving the practice (e.g. death, move of house). In addition, the GP indicates how the patient’s diabetes manage-ment is organised: 1) managed entirely by the GP practice (with or without practice nurse); 2) managed by the GP practice in combination with the regional diabetes facility; or 3) managed by a specialist.
Table 2.Overview of data collected at the general practices (GP) and the diabetes facility (DF)
GP DFClinical information Blood glucose (fasting, non-fasting, unspecified) X X
HbA1c X XLipid profile (total cholesterol, hdl-cholesterol, ldl-cholesterol, triglycerides, lipid ratio)
X X
Renal function (urine albumin concentration, excre-tion, albumin/creatinine ratio, albuminuria status, serum creatinine, urine creatinine concentration, excretion
X X
Liver function (ALAT, ASAT, AF, serum albumin) X XBlood cell counts (thrombocytes, leucocytes) X XHormones (TSH, FT4), X XElectrolytes (Na, P) X XEnzymes (CK) X XBlood pressure X XHeight X XWeight X XBody Mass Index X XPulse rate X XFoot examination WCIA XEye examination WCIA XSmoking X X
Treatment Diet (current type, advised type) XMedication Medication prescriptions X
Currently used medication XFamily history Diabetes grandparents, parents, siblings XMorbidity AP, MI, hypertension, claudicatio, nephropathy X
Problem / episode lists XPatient information Date of birth, gender, 4-digit postal code, code of
GPX X
Linkage code X XWCIA = Coding according to the Working group Coordination Informatisation and Automatisation, being a collaboration of two Dutch general practitioners associations (NHG and LHV)
51
Chapter 2.2 - GIANTT database
After the practice finalises the patient classification, a final consistency check is performed at the CSD. In case the GP practice deviates from the provisional clas-sifications 1, 2 and 4 (the highly confident ones), clarification is requested from the practice to improve the quality of the provisional classifications and ensure that no classification errors were made in the practice.The general practitioner is responsible for informing identified patients of the prac-tice’s participation in the GIANTT project (see patient confidentiality). The data col-lection software facilitates this by generating a mailing list, which can be merged with a standard information letter for this purpose.
Data collection (step F)An automated method was developed for extracting relevant clinical measurements for diabetes care from unstructured fields in the EMRs. Using the list of selected patients with type 2 diabetes, information relevant for the evaluation of the quality of care of patients with type 2 diabetes is extracted (table 2). For newly included patients all available information is collected, while for patients included during a previous collection round the information from the date of the last collection moment onwards is collected. The data are transmitted to the CSD, where data validation is performed to optimise complete and accurate data storage (see section 4).The dates of the clinical measurements represent the date of registering the obser-vation in the GPIS, while the date of medication is the date of issuing the prescrip-tion. The date of registration in the GPIS is not necessarily the date of the actual observation, especially with regard to external data (e.g. reports of the diabetes facility, or lab results). Also, reference to previous values of a clinical observation can introduce erroneous time allocations. During data validation specific attention is given to this problem (see section 4).
Performance of extraction softwareThe performance of the patient selection procedure was assessed in the first 36 participating GP practices in 2005. The data collection method was tested with the help of 16 general practices, being a convenience sample of practices willing to par-ticipate in the pilot phase of the project.
Performance of patient collectionIn the first 36 practices, including 61 GPs, a total of 6,044 potential patients with diabetes were identified, of which 5,108 had type 2 diabetes confirmed by their GP. In the first selection step (figure 2), the combination of using presence of glucose regulating medication, record flag and/or ICPC code in the problem list showed a sensitivity of 92 - 100% (mean 97.2), and specificity of 38 - 100% (mean 71.1) for
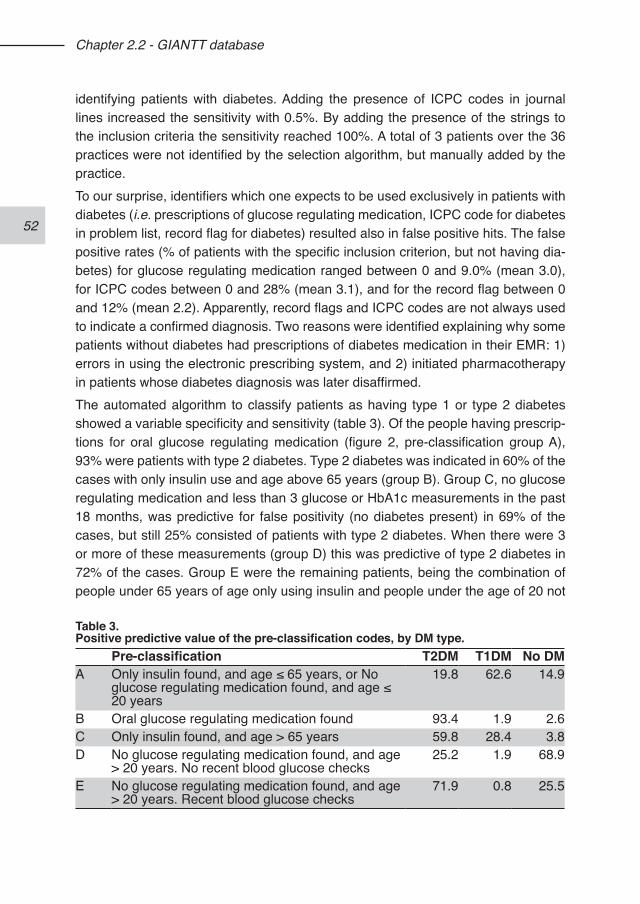
52
Chapter 2.2 - GIANTT database
identifying patients with diabetes. Adding the presence of ICPC codes in journal lines increased the sensitivity with 0.5%. By adding the presence of the strings to the inclusion criteria the sensitivity reached 100%. A total of 3 patients over the 36 practices were not identified by the selection algorithm, but manually added by the practice. To our surprise, identifiers which one expects to be used exclusively in patients with diabetes (i.e. prescriptions of glucose regulating medication, ICPC code for diabetes in problem list, record flag for diabetes) resulted also in false positive hits. The false positive rates (% of patients with the specific inclusion criterion, but not having dia-betes) for glucose regulating medication ranged between 0 and 9.0% (mean 3.0), for ICPC codes between 0 and 28% (mean 3.1), and for the record flag between 0 and 12% (mean 2.2). Apparently, record flags and ICPC codes are not always used to indicate a confirmed diagnosis. Two reasons were identified explaining why some patients without diabetes had prescriptions of diabetes medication in their EMR: 1) errors in using the electronic prescribing system, and 2) initiated pharmacotherapy in patients whose diabetes diagnosis was later disaffirmed. The automated algorithm to classify patients as having type 1 or type 2 diabetes showed a variable specificity and sensitivity (table 3). Of the people having prescrip-tions for oral glucose regulating medication (figure 2, pre-classification group A), 93% were patients with type 2 diabetes. Type 2 diabetes was indicated in 60% of the cases with only insulin use and age above 65 years (group B). Group C, no glucose regulating medication and less than 3 glucose or HbA1c measurements in the past 18 months, was predictive for false positivity (no diabetes present) in 69% of the cases, but still 25% consisted of patients with type 2 diabetes. When there were 3 or more of these measurements (group D) this was predictive of type 2 diabetes in 72% of the cases. Group E were the remaining patients, being the combination of people under 65 years of age only using insulin and people under the age of 20 not
Table 3.Positive predictive value of the pre-classification codes, by DM type.
Pre-classification T2DM T1DM No DMA Only insulin found, and age ≤ 65 years, or No
glucose regulating medication found, and age ≤ 20 years
19.8 62.6 14.9
B Oral glucose regulating medication found 93.4 1.9 2.6C Only insulin found, and age > 65 years 59.8 28.4 3.8D No glucose regulating medication found, and age
> 20 years. No recent blood glucose checks25.2 1.9 68.9
E No glucose regulating medication found, and age > 20 years. Recent blood glucose checks
71.9 0.8 25.5
53
Chapter 2.2 - GIANTT database
using glucose regulating medication. This group was composed of mainly patients with type 1 diabetes, although type 2 was present in 20% of the cases. Shifting the age limits did not improve the predictive values of the classification.This shows that we cannot rely on a fully automated classification procedure, and need verification by the GPs. The automated pre-classification helps to generate provisional classifications and decreases the workload of diabetes status verification.
Performance of data collection methodUsing a pilot dataset of six GP practices an inventory was made of the available data in routine registration of the EMRs, and text recognition algorithms were developed to extract data from free text (see also Chapter 2.1). The data extraction method consists of a fully automated data recognition and interpretation part, and a partially automated data validation part. The automated recognition and interpretation method showed a sensitivity between 94 and 100% for extracting measurements of blood pressure, weight, length, fast-ing/non-fasting glucose, HbA1c, total cholesterol, HDL-cholesterol, LDL-cholesterol, triglycerides, and creatinine. The positive predictive value or precision ranged from 97 to 100% for most measurements, except length, HDL-cholesterol and unspecified glucose. The partially automated data cleaning procedure improved the sensitivity with a few percent, and the precision to 100% for all included measurements. Field tests in 10 general practices showed a mean effort of 80 seconds per patient to ob-tain and clean all data, with minimal burden on the practices.1
DATA COLLECTION AT THE DIABETES FACILITYThe regional diabetes facility (DF) at LabNoord supports the GPs in the province of Groningen, as well as some GPs in the provinces of Friesland and Drenthe. Primary care patients with type 2 diabetes can be referred to the diabetes facility by their GP. This outpatient facility conducts physical examination as well as laboratory tests of blood and urine, during the 3-monthly and yearly diabetes follow-up visits on behalf of the GPs. They report the results back to the GP who remains responsible for further treatment of the patient. The reports to the GPs include, besides listings of laboratory values, specific advise regarding glucose regulating therapy provided by an internist, for instance to start insulin, and general remarks regarding other risk factors, for instance asking attention for blood pressure, cholesterol levels or renal function. The facility can refer patients to a dietician or for a funduscopy, and support patients starting on insulin. Starting in 2006, it is possible that GPs only make use of specific services of the diabetes facility. Since May 2003, patient information is stored in a database developed for the reg-istration of diabetes care (Dimasys). The database contains information on patient
54
Chapter 2.2 - GIANTT database
demographics (birth date, gender, start-date and end-date of registration, GP-code), start-date of diabetes, comorbidity and family history at intake as reported by the GP; smoking and alcohol use as reported by the patient at intake; 3-monthly and/or yearly values of blood pressure, weight, length, feet examination as registered by a practice assistant; 3-monthly and/or yearly laboratory measurements; current and recommended glucose regulating drugs as registered by a practice assistant; yearly registration of other drug use based upon a “brown-bag” method. For this, patients are asked to bring along all of their medication, and the practice assistant copies names of currently used medication. All data included in the Dimasys database in 2004 were screened to determine the methods needed for importing the information into the CSD of the GIANTT project.Much of the patient data are first collected on paper forms and then entered into the Dimasys database. Different forms are available for the intake of a new patient, 3-monthly control visit, and the yearly control visit. The general practitioner usually completes the intake form. Otherwise, data are collected and entered in the informa-tion system by the assistants who conduct the patient contacts. Only new comorbid-ity that assistants expect the GP is not aware of is registered. Laboratory data are imported from the Labosys Database. Only laboratory data, which are used for the reports to the GPs, are transferred to standardised fields (fasting glucose, non-fast-ing glucose, HbA1c, BMI, creatinine, ALAT, AF, total cholesterol). All other laboratory data are dumped in a text field.
Patient selectionAll patients visiting the Diabetes Facility in 2004 and 2005 from the GPs in Groningen who authorised the GIANTT project (85%) to collect their data from the DF were noti-fied and included. Since the DF only serves patients with type 2 diabetes, no other selection criteria were used.
Data collectionFor all authorised patients, a full data dump was made from the Dimasys database for the year 2004 and 2005. Since specific data are always entered in the same fields in the Dimasys system, having limited variability in location and presentation form, a series of mapping methods was developed to convert the data from both structured and text fields. Dimasys includes standardised fields as well as text fields. The structured fields were mapped to the corresponding variable codes in the CSD. For the information residing in text fields, conversion lists were made and recognition algorithms applied in a recursive mapping method. This means that both the posi-tively identified text as well as the mismatches are marked and stored. The unrecog-nised parts are then re-mapped, guaranteeing complete conversion of the Dimasys
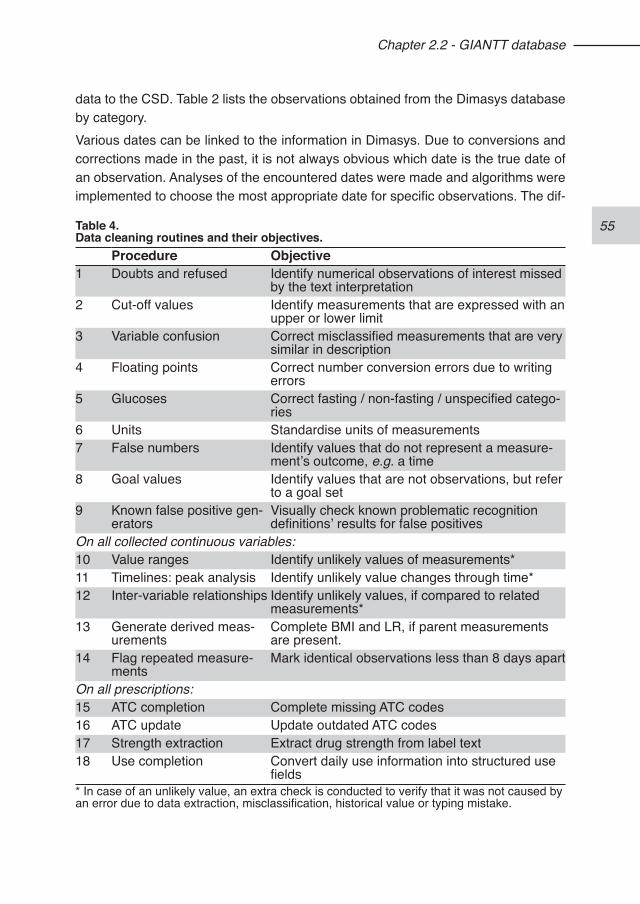
55
Chapter 2.2 - GIANTT database
data to the CSD. Table 2 lists the observations obtained from the Dimasys database by category.Various dates can be linked to the information in Dimasys. Due to conversions and corrections made in the past, it is not always obvious which date is the true date of an observation. Analyses of the encountered dates were made and algorithms were implemented to choose the most appropriate date for specific observations. The dif-
Table 4.Data cleaning routines and their objectives.
Procedure Objective1 Doubts and refused Identify numerical observations of interest missed
by the text interpretation2 Cut-off values Identify measurements that are expressed with an
upper or lower limit3 Variable confusion Correct misclassified measurements that are very
similar in description4 Floating points Correct number conversion errors due to writing
errors5 Glucoses Correct fasting / non-fasting / unspecified catego-
ries6 Units Standardise units of measurements7 False numbers Identify values that do not represent a measure-
ment’s outcome, e.g. a time8 Goal values Identify values that are not observations, but refer
to a goal set9 Known false positive gen-
eratorsVisually check known problematic recognition definitions’ results for false positives
On all collected continuous variables:10 Value ranges Identify unlikely values of measurements*11 Timelines: peak analysis Identify unlikely value changes through time*12 Inter-variable relationships Identify unlikely values, if compared to related
measurements*13 Generate derived meas-
urementsComplete BMI and LR, if parent measurements are present.
14 Flag repeated measure-ments
Mark identical observations less than 8 days apart
On all prescriptions:15 ATC completion Complete missing ATC codes16 ATC update Update outdated ATC codes17 Strength extraction Extract drug strength from label text18 Use completion Convert daily use information into structured use
fields* In case of an unlikely value, an extra check is conducted to verify that it was not caused by an error due to data extraction, misclassification, historical value or typing mistake.
56
Chapter 2.2 - GIANTT database
ferent date types are 1) date of observation, 2) date of registration, 3) date of patient contact, 4) intake date, and 5) date of import in the CSD. Each data record in the CSD contains a code field, which indicates the type of date used.From 2006 onwards, reports and test results from the Diabetes Facility were increas-ingly being received and stored electronically in the general practices, making a separate data extraction of these data from this facility redundant.
DATA VALIDATION PROCEDUREA large part of clinical information in EMRs is manually entered by care providers, and therefore prone to typing and transcription errors. In addition, our data collection method uses highly sensitive text recognition techniques to convert numerical meas-urements from free text to structured measurements. The choice for high sensitivity results in the risk of including false positive observations. Therefore, fixed routines are used to check and correct the data obtained before including them in the CSD. This data cleaning procedure comprises 18 steps (table 4). It starts with looking for missed observations, followed by steps that focus on identifying and correcting spe-cific problems and clear misclassifications.The procedure continues with adding or deriving relevant information before import-ing the data into the CSD. Finally, double registrations, i.e. the occurrence of the same observation within a short time period, are identified and marked. A consider-able portion of measurements with identical values occur within 7 days from each other. These are likely to be duplicates of one observation, partly caused by GPISs that copy structured stored observations to the free text journal, and partly by exter-nal information being dated both on the observation date as well as the registration date of the report.
PATIENT CONFIDENTIALITYData collection within the GIANTT project is done anonymously, and according to Dutch law this does not require fully informed consent from the included patients. However, patients should receive written information explaining the anonymous use of such data for research and benchmark purposes, and be given the opportunity to object to this use.4 Therefore, patients are notified before data collection, and ex-cluded or removed from the database when they object to this anonymous data use.During several stages of the data collection process small pieces of free text infor-mation from the EMRs are collected, which are needed for data checking or patient selection purposes at the central database level. We use an extensive anonymisa-tion procedure replacing any personal information (names, addresses, phone num-bers, security numbers, etc.) as registered in the GPIS for both the patient itself as
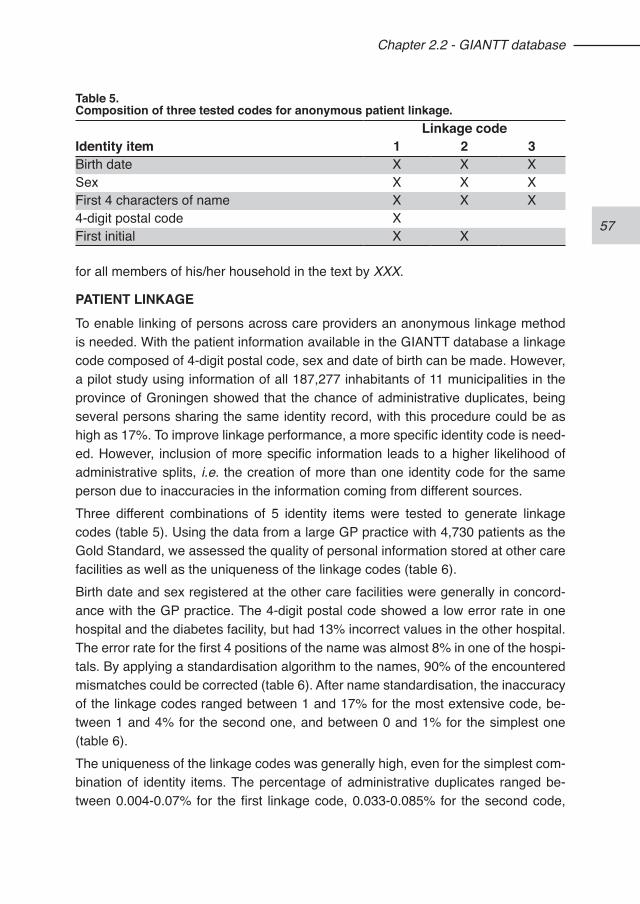
57
Chapter 2.2 - GIANTT database
for all members of his/her household in the text by XXX.
PATIENT LINKAGETo enable linking of persons across care providers an anonymous linkage method is needed. With the patient information available in the GIANTT database a linkage code composed of 4-digit postal code, sex and date of birth can be made. However, a pilot study using information of all 187,277 inhabitants of 11 municipalities in the province of Groningen showed that the chance of administrative duplicates, being several persons sharing the same identity record, with this procedure could be as high as 17%. To improve linkage performance, a more specific identity code is need-ed. However, inclusion of more specific information leads to a higher likelihood of administrative splits, i.e. the creation of more than one identity code for the same person due to inaccuracies in the information coming from different sources.Three different combinations of 5 identity items were tested to generate linkage codes (table 5). Using the data from a large GP practice with 4,730 patients as the Gold Standard, we assessed the quality of personal information stored at other care facilities as well as the uniqueness of the linkage codes (table 6). Birth date and sex registered at the other care facilities were generally in concord-ance with the GP practice. The 4-digit postal code showed a low error rate in one hospital and the diabetes facility, but had 13% incorrect values in the other hospital. The error rate for the first 4 positions of the name was almost 8% in one of the hospi-tals. By applying a standardisation algorithm to the names, 90% of the encountered mismatches could be corrected (table 6). After name standardisation, the inaccuracy of the linkage codes ranged between 1 and 17% for the most extensive code, be-tween 1 and 4% for the second one, and between 0 and 1% for the simplest one (table 6). The uniqueness of the linkage codes was generally high, even for the simplest com-bination of identity items. The percentage of administrative duplicates ranged be-tween 0.004-0.07% for the first linkage code, 0.033-0.085% for the second code,
Table 5.Composition of three tested codes for anonymous patient linkage.
Linkage codeIdentity item 1 2 3Birth date X X XSex X X XFirst 4 characters of name X X X4-digit postal code XFirst initial X X
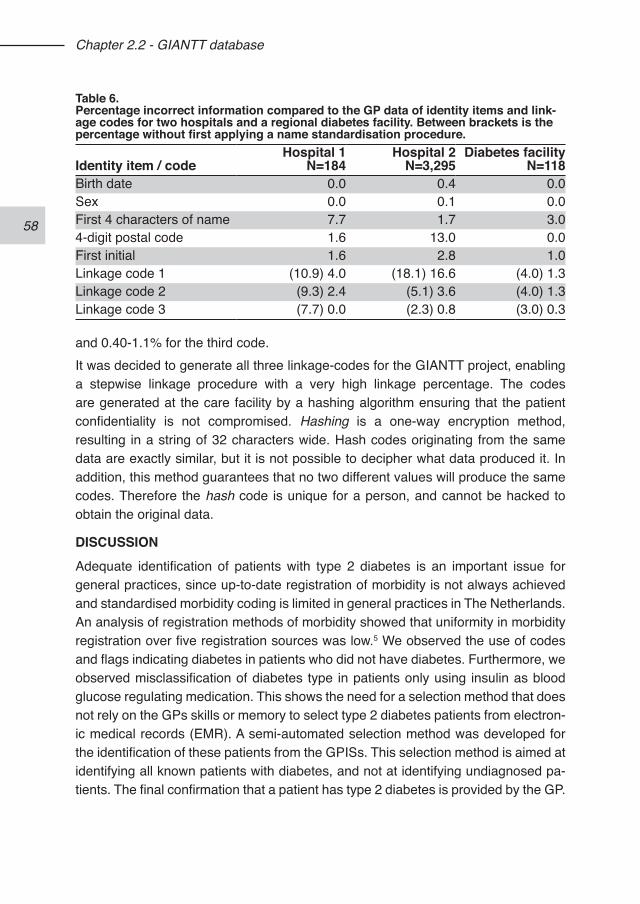
58
Chapter 2.2 - GIANTT database
and 0.40-1.1% for the third code.It was decided to generate all three linkage-codes for the GIANTT project, enabling a stepwise linkage procedure with a very high linkage percentage. The codes are generated at the care facility by a hashing algorithm ensuring that the patient confidentiality is not compromised. Hashing is a one-way encryption method, resulting in a string of 32 characters wide. Hash codes originating from the same data are exactly similar, but it is not possible to decipher what data produced it. In addition, this method guarantees that no two different values will produce the same codes. Therefore the hash code is unique for a person, and cannot be hacked to obtain the original data.
DISCUSSIONAdequate identification of patients with type 2 diabetes is an important issue for general practices, since up-to-date registration of morbidity is not always achieved and standardised morbidity coding is limited in general practices in The Netherlands. An analysis of registration methods of morbidity showed that uniformity in morbidity registration over five registration sources was low.5 We observed the use of codes and flags indicating diabetes in patients who did not have diabetes. Furthermore, we observed misclassification of diabetes type in patients only using insulin as blood glucose regulating medication. This shows the need for a selection method that does not rely on the GPs skills or memory to select type 2 diabetes patients from electron-ic medical records (EMR). A semi-automated selection method was developed for the identification of these patients from the GPISs. This selection method is aimed at identifying all known patients with diabetes, and not at identifying undiagnosed pa-tients. The final confirmation that a patient has type 2 diabetes is provided by the GP.
Table 6.Percentage incorrect information compared to the GP data of identity items and link-age codes for two hospitals and a regional diabetes facility. Between brackets is the percentage without first applying a name standardisation procedure.
Identity item / codeHospital 1
N=184Hospital 2
N=3,295Diabetes facility
N=118Birth date 0.0 0.4 0.0Sex 0.0 0.1 0.0First 4 characters of name 7.7 1.7 3.04-digit postal code 1.6 13.0 0.0First initial 1.6 2.8 1.0Linkage code 1 (10.9) 4.0 (18.1) 16.6 (4.0) 1.3Linkage code 2 (9.3) 2.4 (5.1) 3.6 (4.0) 1.3Linkage code 3 (7.7) 0.0 (2.3) 0.8 (3.0) 0.3

59
Chapter 2.2 - GIANTT database
It is often stated that structured data entry and standardisation will solve many regis-tration problems. However, the quickest way to record data and get a quick overview of observations is often in a few lines of free text.6,7 Structured data entry may fit the workflow of a specialist environment but for a GP, navigating and selecting the ap-propriate items in various screens is usually difficult and time consuming. Computer based systems intended for better data registration are often faced with incomplete or limited use.8 At this moment, there are no broadly used structured patient registra-tion systems for general practice. Therefore, data collection from free text fields com-monly used in EMRs is highly relevant. A text recognition method was developed that converts measurements relevant for diabetes care from free text to structured data with a high accuracy. This enables the collection of data from EMRs without prerequisites of how and where they are registered, and with minimal burden to the participating practices. The price of a highly sensitive data collection method is an initially high data cleaning workload. The information obtained from data cleaning procedure, however, is used to optimise the recognition method, reducing this work-load in the next data collection round. EMRs in general practice contain clinical information, prescriptions, and care proce-dures generated by the practice itself. In a health care system where the GP is the gatekeeper, data originating from other care providers will also be send to the GPs. To what extent such external information is registered in the EMR varies consider-ably between GPs. Besides this, technological characteristics of the practice and the region, e.g. the use of electronic data exchange with other care providers or scan-ning of received documents determines to what degree this external information is accessible for data collection software.In contrast to the EMRs used by GPs, the regional diabetes facility uses a database specifically developed for the (structured) registration of diabetes care. Collecting data from such a system seems straightforward. However, also in this case we en-countered storage of relevant information in free text fields. To enable complete data import from this system, a recursive mapping method was used. In addition, encoun-tered problems with the dating of observations were resolved using decision trees for inclusion of the dates most likely to be accurate. This approach prevents the loss of data but introduces variation regarding the validity of the dating of observations. When selection data for specific research questions, one can choose what informa-tion will be included based on the date types that are recorded.Adequate linkage of data from different sources is important to get a good overview of relevant process and outcome data for diabetes patients that visit several health care providers or institutions. To protect the privacy of individuals, there are strict lim-itations in The Netherlands, as in many other countries, to the use of personal iden-
60
Chapter 2.2 - GIANTT database
tification data. The basic idea is that such personal information is not exchanged or stored when it is not explicitly needed. For research purposes, linkage codes can be generated that aim to be unique while allowing for anonymous data collection. These linkage codes are derived from the personal identification data available at different care providers or institutions. Ideally, this information would be identical enabling (almost) unique linkage codes. We observed, however, considerable variability in the quality of stored information across different health care providers. Therefore, for optimal patient linkage, multiple linkage codes were considered necessary.
CONCLUSIONOur aim was to develop data collection methods based on routinely registered infor-mation with a minimal burden for health care providers. Semi-automated methods were developed to identify patients with type 2 diabetes, and collect data from their medical records in general practice and a regional diabetes facility with a high ac-curacy. Generating three codes based on different identity items enables high link-age probability of data coming from different sources. Patient confidentiality is well guarded by anonymisation, hash-coding, and data encryption.
REFERENCES1. Voorham J, Denig P, on behalf of GIANTT. Computerized extraction of informa-
tion on the quality of diabetes care from free text in electronic patient records of general practitioners. J Am Med Inform Assoc. 2007;14(3):349-54.
2. WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC classification and DDD assignment, 2010. Oslo, 2009..
3. Anonymous. Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care. 2003;26(Suppl 1):S5-20.
4. Code of Conduct: Use of data in health research. The Federation of Dutch Medical Scientific Societies (FDMSS), Rotterdam, 2005. Accessed at http://www.federa.org on December 2009
5. Smith RJA, Hiddema-van der Wal A, van der Werf GTh, Meyboom-de Jong B. Versnippering van morbiditeitsinformatie in het elektronisch medisch dossier. Huisarts Wet. 2000;43:391-4.
6. McDonald CJ. The barriers to electronic medical record systems and how to overcome them. J Am Med Inform Assoc. 1997;4 213-21.
7. Los RK, Roukema J, van Ginneken AM, de Wilde M, van der Lei J. Are struc-tured data structured identically? Investigating the uniformity of pediatric patient data recorded using OpenSDE. Methods Inf Med. 2005;44:631-8.
8. Balas EA, Krishna S, Kretschmer RA, Cheek TR, Lobach, DF, Boren SA. Computerized knowledge management in diabetes care. Med Care. 2004;42:610-621.
61
62
63
Chapter 3 - Quality indicators
64
65
Chapter 3.1 - Cross-sectional versus sequential quality indicators of risk factor
management in patients with type 2 diabetes
Jaco Voorham1,2
Petra Denig1
Bruce HR Wolffenbuttel3
Flora M Haaijer-Ruskamp1
1. Department of Clinical Pharmacology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
2. Department of Epidemiology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
3. Department of Endocrinology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
Voorham J, Denig P, Wolffenbuttel BHR, Haaijer-Ruskamp FM. Cross-sectional ver-sus sequential quality indicators of risk factor management in patients with type 2 diabetes. Med Care. 2008;46(2):133-41.
66
Chapter 3.1 - Cross-sectional versus sequential indicators
ABSTRACTBackground. The fairness of quality assessment methods is under debate. Quality indicators incorporating the longitudinal nature of care have been advocated but their usefulness in comparison to more commonly used cross-sectional measures is not clear.Aims. To compare cross-sectional and sequential quality indicators for risk factor management in patients with type 2 diabetes.Methods. The study population consisted of 1,912 patients who received diabetes care from one of 40 general practitioners in The Netherlands. Clinical outcomes, prescriptions and demographic data were collected from electronic medical records. Quality was assessed for glycaemic, blood pressure and lipid control using indica-tors focusing on clinical outcomes, and treatment in relation to outcomes. Indicator results were compared with a reference method based on national guidelines for general practice.Results. According to the reference method, 76% of the patients received man-agement as recommended for glycaemic control, 58% for blood pressure control, and 67% for lipid control. Cross-sectional indicators looking at patients adequately controlled gave estimates that were 10 - 25% lower than the reference method. Estimates from indicators focusing on uncontrolled patients receiving treatment were 10 - 40% higher than the reference method for blood pressure and glycaemic control. Sequential indicators focusing on improvement in clinical outcomes or as-sessing treatment modifications in response to poor control gave results closer to the reference method.Conclusion. Sequential indicators are valuable for estimating quality of risk factor management in patients with diabetes. Such indicators may provide a more accurate and fair judgment than currently used cross-sectional indicators.

67
Chapter 3.1 - Cross-sectional versus sequential indicators
INTRODUCTIONQuality of diabetes care has received a lot of attention over the past decade, and room for improvement of glycaemic, blood pressure and lipid management has re-peatedly been shown.1-6 There is, however, debate about the fairness of indicators used to assess quality of care, especially for external accountability.7-10 Many stud-ies looking at quality of care use a cross-sectional approach where processes and outcomes of care are measured at one point in time.2-6,11-13 This approach may be limited, since it does not take the longitudinal nature of chronic patient care into account. One study showed that, although quality of care may seem to improve over time using cross-sectional assessments, a longitudinal approach can show that specific patients groups are not benefiting.9 There are also discrepancies between indicators based on process and outcome measures. It has been shown that only looking at outcomes of care can result in an inaccurate view.14,15 Such indicators do not differentiate between patients receiving suboptimal care and patients that are difficult to manage or non-compliant. Therefore, these indicators are affected by case-mix differences. Indicators reflecting risk factor management in relation to spe-cific outcomes have been advocated to overcome this problem.14,16-20 Especially, the ability to recognise the failure to initiate or intensify treatment when indicated could provide insights important to target interventions.10,18,19,21,22 Rodondi et al.14 have ar-gued that care provided by a physician should be evaluated using a decision tree in which actions and events that do imply appropriate care, despite a target level not being achieved, are acknowledged. To better understand the added value of such an approach, we examined the pos-sible benefits of sequential over cross-sectional quality indicators of risk factor man-agement by comparing both to a reference method. This reference method was based on a detailed assessment of relevant actions and events at the individual patient level.
METHODSIn a cohort study, the quality of glycaemic, blood pressure and lipid management was assessed for patients with type 2 diabetes. We evaluated indicators focusing on clinical outcomes (HbA1c, systolic blood pressure, total cholesterol), and indicators focusing on treatment related to these outcomes, using target levels from national guidelines for clinical practice. Percentages of patients with risk factor management according to these guidelines were determined using a common cross-sectional in-dicator and several newly developed sequential indicators, and compared with the reference method. Calculations were made at the aggregated level, which is com-mon for external quality assessment, and at the individual patient level, because
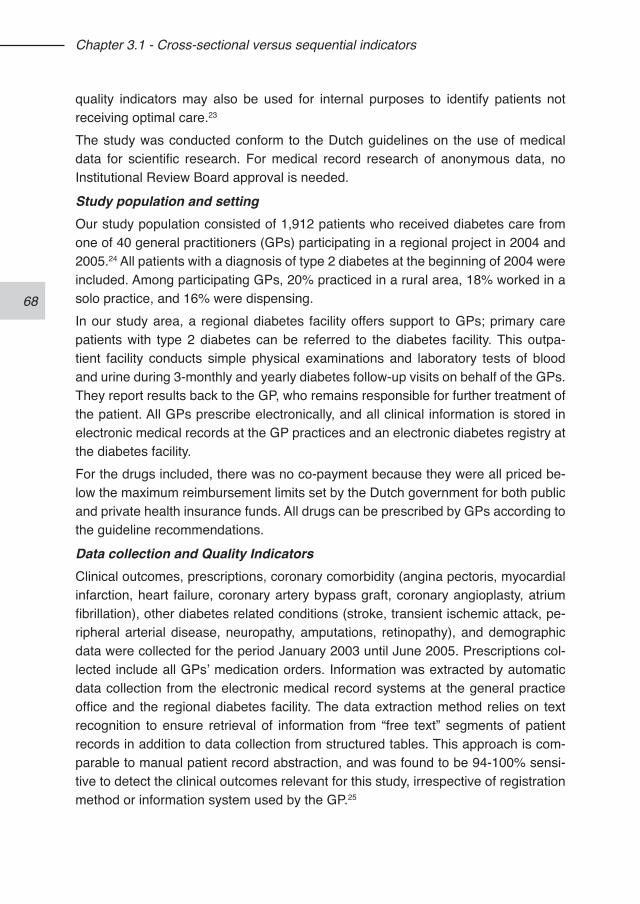
68
Chapter 3.1 - Cross-sectional versus sequential indicators
quality indicators may also be used for internal purposes to identify patients not receiving optimal care.23 The study was conducted conform to the Dutch guidelines on the use of medical data for scientific research. For medical record research of anonymous data, no Institutional Review Board approval is needed.
Study population and settingOur study population consisted of 1,912 patients who received diabetes care from one of 40 general practitioners (GPs) participating in a regional project in 2004 and 2005.24 All patients with a diagnosis of type 2 diabetes at the beginning of 2004 were included. Among participating GPs, 20% practiced in a rural area, 18% worked in a solo practice, and 16% were dispensing.In our study area, a regional diabetes facility offers support to GPs; primary care patients with type 2 diabetes can be referred to the diabetes facility. This outpa-tient facility conducts simple physical examinations and laboratory tests of blood and urine during 3-monthly and yearly diabetes follow-up visits on behalf of the GPs. They report results back to the GP, who remains responsible for further treatment of the patient. All GPs prescribe electronically, and all clinical information is stored in electronic medical records at the GP practices and an electronic diabetes registry at the diabetes facility. For the drugs included, there was no co-payment because they were all priced be-low the maximum reimbursement limits set by the Dutch government for both public and private health insurance funds. All drugs can be prescribed by GPs according to the guideline recommendations.
Data collection and Quality IndicatorsClinical outcomes, prescriptions, coronary comorbidity (angina pectoris, myocardial infarction, heart failure, coronary artery bypass graft, coronary angioplasty, atrium fibrillation), other diabetes related conditions (stroke, transient ischemic attack, pe-ripheral arterial disease, neuropathy, amputations, retinopathy), and demographic data were collected for the period January 2003 until June 2005. Prescriptions col-lected include all GPs’ medication orders. Information was extracted by automatic data collection from the electronic medical record systems at the general practice office and the regional diabetes facility. The data extraction method relies on text recognition to ensure retrieval of information from “free text” segments of patient records in addition to data collection from structured tables. This approach is com-parable to manual patient record abstraction, and was found to be 94-100% sensi-tive to detect the clinical outcomes relevant for this study, irrespective of registration method or information system used by the GP.25
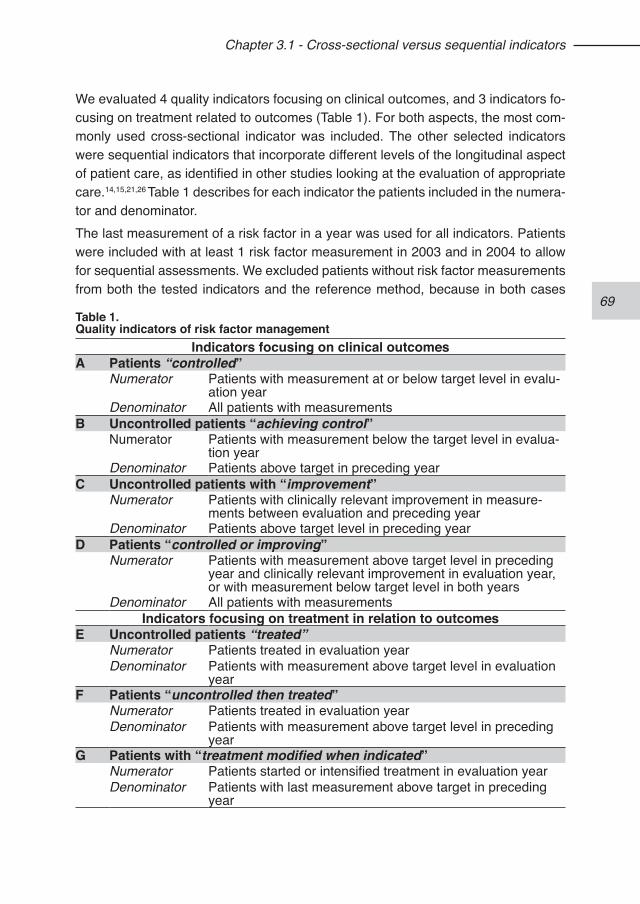
69
Chapter 3.1 - Cross-sectional versus sequential indicators
We evaluated 4 quality indicators focusing on clinical outcomes, and 3 indicators fo-cusing on treatment related to outcomes (Table 1). For both aspects, the most com-monly used cross-sectional indicator was included. The other selected indicators were sequential indicators that incorporate different levels of the longitudinal aspect of patient care, as identified in other studies looking at the evaluation of appropriate care.14,15,21,26 Table 1 describes for each indicator the patients included in the numera-tor and denominator. The last measurement of a risk factor in a year was used for all indicators. Patients were included with at least 1 risk factor measurement in 2003 and in 2004 to allow for sequential assessments. We excluded patients without risk factor measurements from both the tested indicators and the reference method, because in both cases
Table 1.Quality indicators of risk factor management
Indicators focusing on clinical outcomesA Patients “controlled”
Numerator Patients with measurement at or below target level in evalu-ation year
Denominator All patients with measurementsB Uncontrolled patients “achieving control”
Numerator Patients with measurement below the target level in evalua-tion year
Denominator Patients above target in preceding year C Uncontrolled patients with “improvement”
Numerator Patients with clinically relevant improvement in measure-ments between evaluation and preceding year
Denominator Patients above target level in preceding year D Patients “controlled or improving”
Numerator Patients with measurement above target level in preceding year and clinically relevant improvement in evaluation year, or with measurement below target level in both years
Denominator All patients with measurements Indicators focusing on treatment in relation to outcomes
E Uncontrolled patients “treated”Numerator Patients treated in evaluation yearDenominator Patients with measurement above target level in evaluation
year F Patients “uncontrolled then treated”
Numerator Patients treated in evaluation yearDenominator Patients with measurement above target level in preceding
year G Patients with “treatment modified when indicated”
Numerator Patients started or intensified treatment in evaluation yearDenominator Patients with last measurement above target in preceding
year
70
Chapter 3.1 - Cross-sectional versus sequential indicators
they would fall in the same category of inadequate care. Based on the national guidelines for general practice at the time of the study, the following target levels were used to identify controlled risk factors: HbA1c <7.0%, systolic blood pressure <140 mmHg and total cholesterol <5.0 mmol/l. Changes in risk factor level considered clinically relevant were set at 0.3% for HbA1c, 5 mmHg for systolic blood pressure, and 0.5 mmol/l for total cholesterol.The cross-sectional indicator on clinical outcomes is the most widely used measure of patients “controlled” (indicator A) (e.g. in the US, UK and The Netherlands).27-30 This indicator looks at patients below target level as a proportion of all patients. The sequential indicators B and C focus on patients that were previously insufficiently controlled.9,21 Indicator B identifies patients “achieving control”, that is, patients mov-ing from being uncontrolled in the preceding year to controlled in the current year. Indicator C acknowledges patients with any clinically relevant “improvement” in risk factor level. Indicator D is a combined measure identifying patients “controlled or improving” as a proportion of all patients.The indicators looking at treatment in relation to outcomes focus on patients who are in need of treatment, that is, insufficiently controlled patients. The cross-sectional indicator identifies all of such patients concurrently “treated” (indicator E). This is a generic approach for assessing guideline compliance to the recommendation that patients with diabetes with uncontrolled risk factors should receive treatment.1,31 This indicator has been proposed by the Dutch Institute for Healthcare in their recent set of quality indicators for diabetes management.32 Both sequential indicators (F and G) look at treatment in reaction to elevated risk factor levels, thus incorporating the time sequence of observation and action in contrast to the cross-sectional indicator. Patients who receive treatment after being uncontrolled in the preceding period are identified with the “uncontrolled then treated” indicator F. Finally, indicator G also acknowledges cases of “treatment intensified when indicated” by identifying all un-controlled patients not on maximal medication for whom treatment is either initiated or intensified.
Treatment definitionsTreatment modifications were determined by comparing changes in prescriptions during the evaluation year with treatment observed in the final 6 months of the pre-ceding year. A treatment modification was considered intensification when a new drug class was started or added or the dosage of medication was increased. A switch to insulin was considered intensification, but switches to other drug classes without continuation of the original medication were not considered treatment intensification, because such switches could be due to side effects. A prescription was considered
71
Chapter 3.1 - Cross-sectional versus sequential indicators
discontinued if it was not repeated within 120 days from the calculated end date.For glucose lowering medication we included 6 drug classes (insulin, metformin, sulphonylureas, acarbose, thiazolidinediones, and repaglinide), for antihypertensive medication 5 classes (centrally acting antihypertensives, diuretics, beta-blockers, calcium-channel blockers, and renin-angiotensin system inhibitors), and for lipid low-ering medication 5 classes (statins, fibrates, bile acid sequestrants, nicotinic acid derivatives, and ezetimibe). The definitions for maximal medication were derived from treatment recommenda-tions for general practitioners. For glucose-lowering medication, prescription of insu-lin was defined as having reached maximal medication. For blood pressure lowering medication, 3 or more drug classes prescribed at maximum maintenance dosage was considered as maximal medication. For lipid-lowering medication, prescribing the maximum dosage of a drug was considered maximal medication. Combination of lipid lowering drugs is not recommended in general practice. Dosage recommenda-tions were obtained from the Dutch Pharmacotherapy Compendium.33
Reference methodThe reference method involved a stepwise review of care as documented in the electronic medical records. Events and actions were assessed at the individual pa-tient level, using all information on changes in prescriptions and relevant clinical out-comes using an automated procedure (Fig. 1). This method acknowledges to some extent that care can be appropriate in patients not reaching strict target levels, by fo-cusing on the recommended management in relation to outcomes, as has been ad-vocated before.14,16-20 It builds upon the work described by Rodondi et al.14, extended with a follow-up observation to accept management as being in line with guideline recommendations when patients achieved target levels during a monitoring period or medication was modified after a follow-up measurement of the risk factor. Management was assessed for each of the risk factors separately. The following situations were considered as management as recommended in the guidelines:
1. Risk factor was at or below target level, and therefore adequately controlled,2. Risk factor was above target level but medication was started or intensified
within 28 days,3. Risk factor was above target level but maximal medication according to
guideline recommendations for general practice was already being pre-scribed,
4. Risk factor was above target level but target level was achieved during a monitoring period of not more than 120 days,
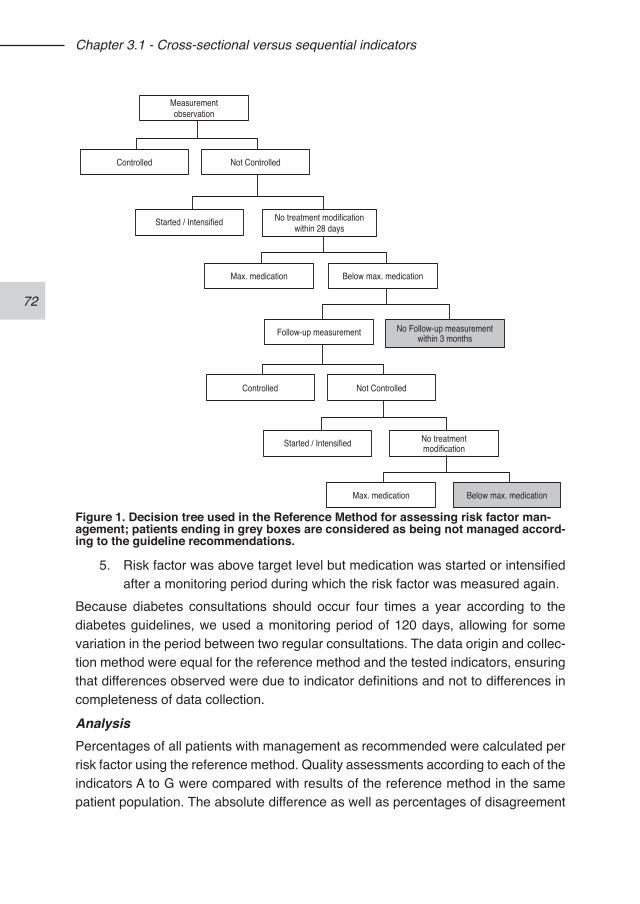
72
Chapter 3.1 - Cross-sectional versus sequential indicators
5. Risk factor was above target level but medication was started or intensified after a monitoring period during which the risk factor was measured again.
Because diabetes consultations should occur four times a year according to the diabetes guidelines, we used a monitoring period of 120 days, allowing for some variation in the period between two regular consultations. The data origin and collec-tion method were equal for the reference method and the tested indicators, ensuring that differences observed were due to indicator definitions and not to differences in completeness of data collection.
AnalysisPercentages of all patients with management as recommended were calculated per risk factor using the reference method. Quality assessments according to each of the indicators A to G were compared with results of the reference method in the same patient population. The absolute difference as well as percentages of disagreement
Measurementobservation
Not ControlledControlled
Started / Intensified No treatment modificationwithin 28 days
Max. medication Below max. medication
Follow-up measurement
Not ControlledControlled
Started / Intensified No treatmentmodification
Max. medication Below max. medication
No Follow-up measurementwithin 3 months
Figure 1. Decision tree used in the Reference Method for assessing risk factor man-agement; patients ending in grey boxes are considered as being not managed accord-ing to the guideline recommendations.
73
Chapter 3.1 - Cross-sectional versus sequential indicators
between both estimates was calculated. Significance of differences was assessed by the McNemar statistic for paired proportions. To test whether the results might be sensitive to the set target levels or population case-mix, we repeated the analyses using levels of poorly controlled patients instead of adequately controlled patients, that is, HbA1c >8.5%, systolic blood pressure >160 mmHg and total cholesterol >6.0 mmol/l, and after stratification on comorbidity (yes/no). Positive and negative likelihood ratios were calculated with 95% confidence inter-vals. These ratios express the ability of an indicator to predict the quality assess-ment at the individual patient level. Likelihood ratios combine sensitivity and spe-cificity into 1 measure, and are insensitive to the underlying probability of risk factor management according to the guidelines. Likelihood ratios between 0.5 and 2 were considered to reflect poor predictors, whereas ratios below 0.2 or above 5 indicate moderate to strong predictors.
RESULTS
Study populationDemographic characteristics, degree of control, and treatment in the study popula-tion are presented in Table 2. Respectively 83%, 88%, and 73% of the 1,912 patients had at least 1 measurement of HbA1c, blood pressure and total cholesterol recorded in 2004. Mean risk factor levels were 7.1% for HbA1c, 146.6 mmHg for systolic blood pressure, and 4.9 mmol/l for total cholesterol. The average 10-year absolute risk for coronary heart disease according to the UK Prospective Diabetes Study risk engine34 was 23.4%. Glucose-lowering medication was prescribed to 83.6%, antihypertensive medication to 71.2%, and lipid-lowering medication to 46.9% of the patients. Coronary comorbidity and other diabetes related conditions were each recorded in 15% of the patients.
Reference methodAccording to the reference method, 75.8% of the patients received management as recommended for glycaemic control, 58.3% for blood pressure control, and 66.4% for lipid control. Of patients with the recommended glycaemic management, 71.5% were already on target, treatment was started or intensified in another 8.8%, 13.8% were on maximal medication, 2.4% returned on target, and 3.5% received a change in medication during follow-up. For blood pressure, 54.3% of such patients were already on target, in 7.4% treatment was started or intensified, 22.9% were already on maximal medication, 11.1% returned to target, and 4.3% received a change in medication during follow-up. For lipid control, 83.6% were on target, treatment was started or intensified in 10.2%, only 0.1% were on maximal medication, 4.1% re-turned to target and 2.0% received a change in medication during follow-up. Of
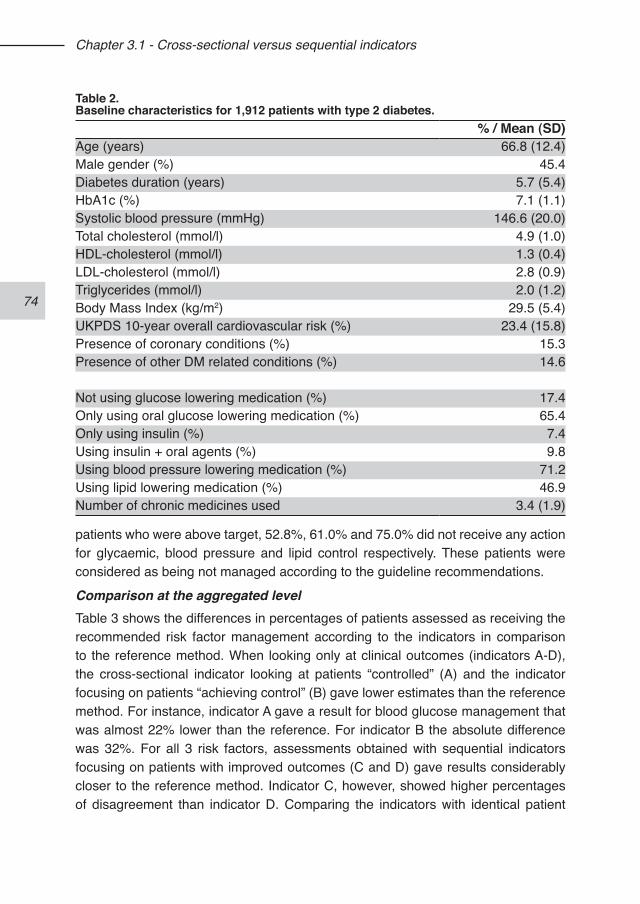
74
Chapter 3.1 - Cross-sectional versus sequential indicators
patients who were above target, 52.8%, 61.0% and 75.0% did not receive any action for glycaemic, blood pressure and lipid control respectively. These patients were considered as being not managed according to the guideline recommendations.
Comparison at the aggregated levelTable 3 shows the differences in percentages of patients assessed as receiving the recommended risk factor management according to the indicators in comparison to the reference method. When looking only at clinical outcomes (indicators A-D), the cross-sectional indicator looking at patients “controlled” (A) and the indicator focusing on patients “achieving control” (B) gave lower estimates than the reference method. For instance, indicator A gave a result for blood glucose management that was almost 22% lower than the reference. For indicator B the absolute difference was 32%. For all 3 risk factors, assessments obtained with sequential indicators focusing on patients with improved outcomes (C and D) gave results considerably closer to the reference method. Indicator C, however, showed higher percentages of disagreement than indicator D. Comparing the indicators with identical patient
Table 2.Baseline characteristics for 1,912 patients with type 2 diabetes.
% / Mean (SD)Age (years) 66.8 (12.4)Male gender (%) 45.4Diabetes duration (years) 5.7 (5.4)HbA1c (%) 7.1 (1.1)Systolic blood pressure (mmHg) 146.6 (20.0)Total cholesterol (mmol/l) 4.9 (1.0)HDL-cholesterol (mmol/l) 1.3 (0.4)LDL-cholesterol (mmol/l) 2.8 (0.9)Triglycerides (mmol/l) 2.0 (1.2)Body Mass Index (kg/m2) 29.5 (5.4)UKPDS 10-year overall cardiovascular risk (%) 23.4 (15.8)Presence of coronary conditions (%) 15.3Presence of other DM related conditions (%) 14.6
Not using glucose lowering medication (%) 17.4Only using oral glucose lowering medication (%) 65.4Only using insulin (%) 7.4Using insulin + oral agents (%) 9.8Using blood pressure lowering medication (%) 71.2Using lipid lowering medication (%) 46.9Number of chronic medicines used 3.4 (1.9)
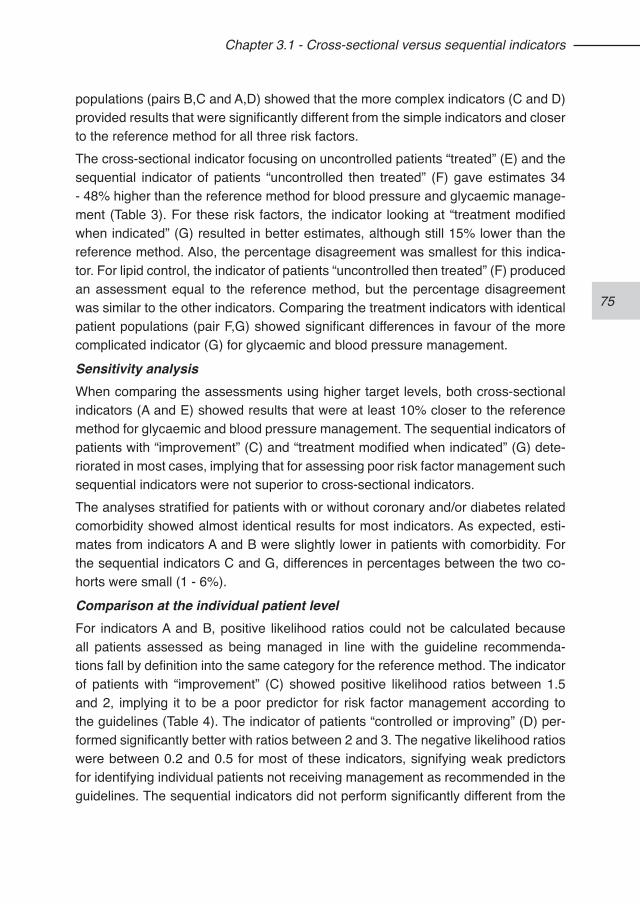
75
Chapter 3.1 - Cross-sectional versus sequential indicators
populations (pairs B,C and A,D) showed that the more complex indicators (C and D) provided results that were significantly different from the simple indicators and closer to the reference method for all three risk factors.The cross-sectional indicator focusing on uncontrolled patients “treated” (E) and the sequential indicator of patients “uncontrolled then treated” (F) gave estimates 34 - 48% higher than the reference method for blood pressure and glycaemic manage-ment (Table 3). For these risk factors, the indicator looking at “treatment modified when indicated” (G) resulted in better estimates, although still 15% lower than the reference method. Also, the percentage disagreement was smallest for this indica-tor. For lipid control, the indicator of patients “uncontrolled then treated” (F) produced an assessment equal to the reference method, but the percentage disagreement was similar to the other indicators. Comparing the treatment indicators with identical patient populations (pair F,G) showed significant differences in favour of the more complicated indicator (G) for glycaemic and blood pressure management.
Sensitivity analysisWhen comparing the assessments using higher target levels, both cross-sectional indicators (A and E) showed results that were at least 10% closer to the reference method for glycaemic and blood pressure management. The sequential indicators of patients with “improvement” (C) and “treatment modified when indicated” (G) dete-riorated in most cases, implying that for assessing poor risk factor management such sequential indicators were not superior to cross-sectional indicators. The analyses stratified for patients with or without coronary and/or diabetes related comorbidity showed almost identical results for most indicators. As expected, esti-mates from indicators A and B were slightly lower in patients with comorbidity. For the sequential indicators C and G, differences in percentages between the two co-horts were small (1 - 6%).
Comparison at the individual patient level For indicators A and B, positive likelihood ratios could not be calculated because all patients assessed as being managed in line with the guideline recommenda-tions fall by definition into the same category for the reference method. The indicator of patients with “improvement” (C) showed positive likelihood ratios between 1.5 and 2, implying it to be a poor predictor for risk factor management according to the guidelines (Table 4). The indicator of patients “controlled or improving” (D) per-formed significantly better with ratios between 2 and 3. The negative likelihood ratios were between 0.2 and 0.5 for most of these indicators, signifying weak predictors for identifying individual patients not receiving management as recommended in the guidelines. The sequential indicators did not perform significantly different from the
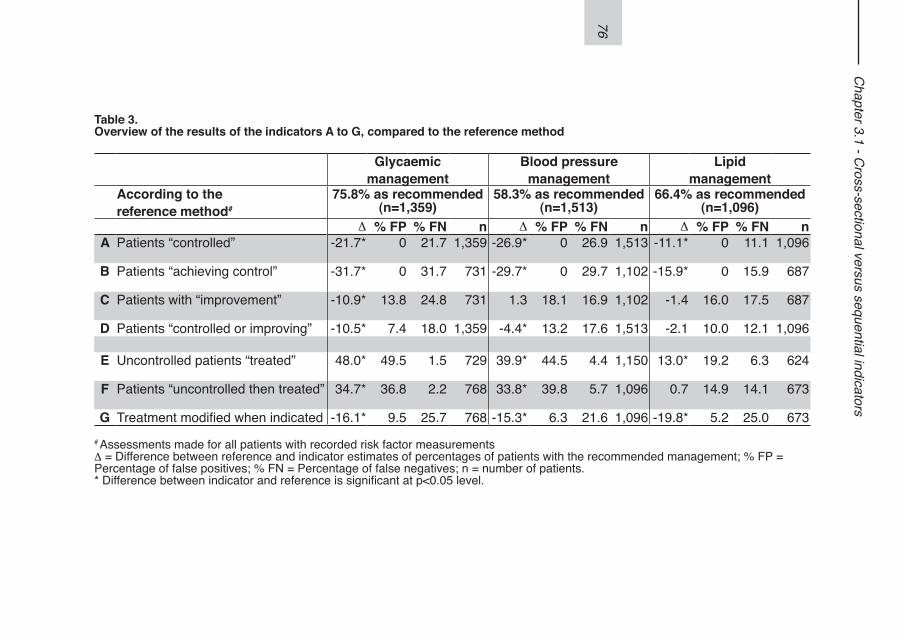
76
Chapter 3.1 - C
ross-sectional versus sequential indicators
Table 3. Overview of the results of the indicators A to G, compared to the reference method
Glycaemicmanagement
Blood pressuremanagement
Lipidmanagement
According to thereference method#
75.8% as recommended (n=1,359)
58.3% as recommended (n=1,513)
66.4% as recommended (n=1,096)
D % FP % FN n D % FP % FN n D % FP % FN nA Patients “controlled” -21.7* 0 21.7 1,359 -26.9* 0 26.9 1,513 -11.1* 0 11.1 1,096
B Patients “achieving control” -31.7* 0 31.7 731 -29.7* 0 29.7 1,102 -15.9* 0 15.9 687
C Patients with “improvement” -10.9* 13.8 24.8 731 1.3 18.1 16.9 1,102 -1.4 16.0 17.5 687
D Patients “controlled or improving” -10.5* 7.4 18.0 1,359 -4.4* 13.2 17.6 1,513 -2.1 10.0 12.1 1,096
E Uncontrolled patients “treated” 48.0* 49.5 1.5 729 39.9* 44.5 4.4 1,150 13.0* 19.2 6.3 624
F Patients “uncontrolled then treated” 34.7* 36.8 2.2 768 33.8* 39.8 5.7 1,096 0.7 14.9 14.1 673
G Treatment modified when indicated -16.1* 9.5 25.7 768 -15.3* 6.3 21.6 1,096 -19.8* 5.2 25.0 673# Assessments made for all patients with recorded risk factor measurements D = Difference between reference and indicator estimates of percentages of patients with the recommended management; % FP = Percentage of false positives; % FN = Percentage of false negatives; n = number of patients.* Difference between indicator and reference is significant at p<0.05 level.
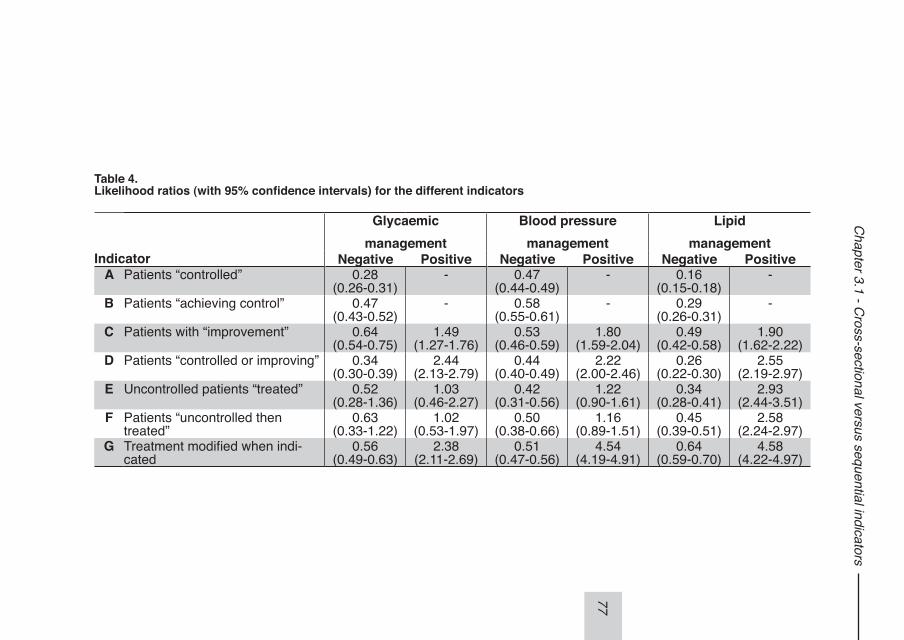
77
Chapter 3.1 - C
ross-sectional versus sequential indicators
Table 4. Likelihood ratios (with 95% confidence intervals) for the different indicators
Glycaemicmanagement
Blood pressuremanagement
Lipidmanagement
Indicator Negative Positive Negative Positive Negative PositiveA Patients “controlled” 0.28
(0.26-0.31)- 0.47
(0.44-0.49)- 0.16
(0.15-0.18)-
B Patients “achieving control” 0.47(0.43-0.52)
- 0.58(0.55-0.61)
- 0.29(0.26-0.31)
-
C Patients with “improvement” 0.64(0.54-0.75)
1.49(1.27-1.76)
0.53(0.46-0.59)
1.80(1.59-2.04)
0.49(0.42-0.58)
1.90(1.62-2.22)
D Patients “controlled or improving” 0.34(0.30-0.39)
2.44(2.13-2.79)
0.44(0.40-0.49)
2.22(2.00-2.46)
0.26(0.22-0.30)
2.55(2.19-2.97)
E Uncontrolled patients “treated” 0.52(0.28-1.36)
1.03(0.46-2.27)
0.42(0.31-0.56)
1.22(0.90-1.61)
0.34(0.28-0.41)
2.93(2.44-3.51)
F Patients “uncontrolled then treated”
0.63(0.33-1.22)
1.02(0.53-1.97)
0.50(0.38-0.66)
1.16(0.89-1.51)
0.45(0.39-0.51)
2.58(2.24-2.97)
G Treatment modified when indi-cated
0.56(0.49-0.63)
2.38(2.11-2.69)
0.51(0.47-0.56)
4.54(4.19-4.91)
0.64(0.59-0.70)
4.58(4.22-4.97)
78
Chapter 3.1 - Cross-sectional versus sequential indicators
cross-sectional indicators regarding these values.For the indicators focusing on treatment, the “treatment modified when indicated” indicator (G) showed positive likelihood ratios between 2 and 5, indicating a weak predictor for identifying patients receiving risk factor management as recommended. The other indicators performed significantly worse, with positive likelihood ratios be-low 2 except for lipid control. For predicting risk factor management not in line with the recommendations at the individual patient level, all indicators performed equally with negative likelihood ratios of around 0.5 (Table 4).
DISCUSSIONThis study showed that the commonly used quality indicator focusing on the number of patients controlled may lead to inaccurate judgments of risk factor management. The simple sequential indicator looking at patients switching from above to below target levels also gave low estimates of the quality of such care, similar to the cross-sectional indicator that only looks at the current risk factor level. More complex indi-cators that focus on uncontrolled patients with clinical improvements provided quality estimates that corresponded better with a detailed evaluation of risk factor manage-ment. Furthermore, our results showed the limited value of the cross-sectional indi-cator looking at uncontrolled patients treated. The observation that a patient with an elevated risk factor level is receiving medication is a poor predictor of management according to guideline recommendations, and will result in high estimates of quality. But again, results of a simple sequential indicator looking at uncontrolled patients subsequently treated were only slightly different from this cross-sectional indicator. Focusing on intensification of treatment in uncontrolled patients led to clearly better quality assessments. At the individual patient level, we observed that the more com-plex sequential indicators were superior in identifying patients receiving risk factor management as recommended. For assessing the quality of treatment focusing on poorly instead of adequately controlled patients, however, simple cross-sectional indicators appeared to be equally sufficient.Ideally, one might want to assess the quality of risk factor management by looking at detailed clinical and therapeutic information for each patient over time. This ap-proach has resulted in the development of clinically detailed indicators that require individual patient chart review.35-37 This is time-consuming and difficult to implement when using automated data for quality assessment. Our reference method involves detailed individual patient assessment over time but is not feasible to conduct on a large scale. Therefore, we evaluated several simpler alternatives on their ability to correspond with this reference method.The quality assessments observed in our study using simple cross-sectional indi-
79
Chapter 3.1 - Cross-sectional versus sequential indicators
cators were similar to those found previously in other studies. The percentages of patients with adequate blood pressure control (32%), lipid control (56%), and gly-caemic control (54%) were within the range of outcomes reported in recent studies with comparable patient groups and target levels in the United Stattes3,6,17,38, Italy39 and The Netherlands.40,41 Also, percentages of patients treated (95%, 79% and 38%) were within ranges observed in other studies for these risk factors.3,6,38
The clear advantage of sequential indicators is that they are capable of quantifying alterations in outcomes and processes of care in response to outcomes. The indica-tor of patients “controlled or improving”, and especially the indicator “treatment modi-fied when indicated” incorporate several factors important to quantify adequate risk factor management, as pointed out by others.14,15,18,21,42 Using these indicators can be expected to result in a reduction of the negative incentives to avoid patients that are more difficult to control. Our study demonstrated that such indicators can be applied in practice using routinely recorded information on treatment and outcomes, and are valuable for estimating quality of diabetes management at the aggregated level. For our primary analyses we used target levels as indicated by the national guide-lines for general practice. However, the use of strict target levels for the entire patient population is under debate.43 We tested the indicators also with high target levels. The proportion of patients that would not benefit from achieving those targets is smaller, and patient case-mix is therefore less important than when focusing on ag-gressive management. We found that the advantage of sequential indicators was larger when using strict target levels. This could imply that sequential indicators may counteract some of the case-mix problems observed in commonly used indicators focusing on strict target levels. The assessed indicators performed comparably for glycaemic and blood pressure control, but for lipid control the differences between the indicators were less pro-nounced. This could be due to physicians reacting less to elevated cholesterol levels than to elevated HbA1c and blood pressure levels. Although the national guidelines at the time of our study recommended that cholesterol levels should guide lipid-low-ering treatment, there were already recommendations that all patients with diabetes are eligible for such treatment.44
LimitationsBoth the reference method and the indicators were tested in a population that in-cluded patients that may not benefit from (aggressive) treatment. This implies that justifiable decisions not to manage risk factors are not captured as being in line with guideline recommendations. We did not have information on contraindications or circumstances, such as patients’ limited life expectancy or treatment refusal, or
80
Chapter 3.1 - Cross-sectional versus sequential indicators
competing demands, which could justify non-intervention. There may be other con-ditions that warrant more immediate attention at a particular visit than risk factor management. Although our reference method allows for an extended period of 120 days in which actions can be taken, some patients may still be incorrectly classified as being in need of additional treatment. This problem is not specific for our study but affects quality assessments in general. When sufficient information is available, it can be solved by excluding these patients from the indicators. For our study, we expect that comparisons between the indicators and the reference method maintain their validity, since this lack of information will affect the tested indicators similarly. The stratified analysis confirmed that our comparative findings were robust for vari-ations in patient population regarding comorbidity. Furthermore, our data did not allow assessing actions taken regarding lifestyle, treat-ment compliance, insulin regime intensifications, or referrals to a medical specialist. Therefore, we considered patients that were uncontrolled but on maximal medica-tion -as defined in this study- as receiving management as recommended. In some cases, however, further actions might have been warranted and possible.The feasibility of using sequential indicators is expected to be good. The data re-quired for their calculation include risk factor measurements and medication treat-ment information in two concurrent years, which are usually registered during regu-lar care.
Implications for quality assessmentQuality indicators can be used for internal quality improvement and for external pur-poses. For internal use, it is helpful to identify patients that possibly receive subop-timal management. Our study showed that for this purpose the simple, commonly used indicators performed as well as the more complex indicators. In other words, to optimise patient care at the individual level sequential indicators do not provide a clear benefit.For external use, such as public accountability, indicators need to provide a fair view of the risk factor management. Indicators looking only at patients below strict target levels may underestimate the quality of care. Substitution of such indicators with the sequential “controlled or improving” indicator, which considers both patients that maintain control and those that achieve clinically relevant improvements, can pro-vide a more meaningful assessment of risk factor management.Indicators focusing on the percentage of uncontrolled patients receiving medication overestimate treatment quality, because they do not take any recommendations for treatment intensification into account. For assessing treatment quality we recom-mend the use of a sequential indicator measuring the modification of treatment when
81
Chapter 3.1 - Cross-sectional versus sequential indicators
indicated. The advantage of including also the “controlled or improving” indicator is that this considers all patients, and not just the ones who are uncontrolled as is done in the treatment oriented indicators. As has been stated before, good quality of risk factor management incorporates achieving control in uncontrolled patients as well as maintaining control in those controlled.9,14
REFERENCES1. Brown AF, Gregg EW, Stevens MR, Karter AJ, Weinberger M, Safford MM,
Gary TL, Caputo DA, Waitzfelder B, Kim C, Beckles GL. Race, Ethnicity, Socioeconomic position, and quality of care for adults with diabetes enrolled in managed care: The translating research Into action for diabetes (TRIAD) study. Diabetes Care. 2005;28(12):2864-2870.
2. Wan Q, Harris MF, Jayasinghe UW, Flack J, Georgiou A, Penn DL, Burns JR. Quality of diabetes care and coronary heart disease absolute risk in patients with type 2 diabetes mellitus in Australian general practice. Qual Saf Health Care. 2006;15(2):131-5.
3. Grant RW, Cagliero E, Murphy-Sheehy P, Singer DE, Nathan DM, Meigs JB. Comparison of hyperglycemia, hypertension, and hypercholesterolemia man-agement in patients with type 2 diabetes. Am J Med. 2002;112(8):603-9.
4. McFarlane SI, Jacober SJ, Winer N, Kaur J, Castro JP, Wui MA, Gliwa A, Von Gizycki H, Sowers JR. Control of cardiovascular risk factors in patients with di-abetes and hypertension at urban academic medical centers. Diabetes Care. 2002;25(4):718-23.
5. Al Khaja KA, Sequeira RP, Damanhori AH. Comparison of the quality of diabetes care in primary care diabetic clinics and general practice clinics. Diabetes Res Clin Pract. 2005;70(2):174-82.
6. Spann SJ, Nutting PA, Galliher JM, Peterson KA, Pavlik VN, Dickinson LM, Volk RJ. Management of type 2 diabetes in the primary care setting: a practice-based research network study. Ann Fam Med. 2006;4(1):23-31.
7. Campbell SM, Roland MO, Buetow SA. Defining quality of care. Soc Sci Med. 2000;51(11):1611-25.
8. Renders CM, Valk GD, Griffin SJ, Wagner EH, van Eijk JT, Assendelft WJ. Interventions to improve the management of diabetes in primary care, outpatient, and community settings: a systematic review. Diabetes Care. 2001;24(10):1821-33.
9. Weiner M, Long J. Cross-sectional versus longitudinal performance assess-ments in the management of diabetes. Med Care. 2004;42(2 Suppl):II34-9.
10. Phillips LS, Branch WT, Cook CB, Doyle JP, El-Kebbi IM, Gallina DL, Miller CD, Ziemer DC, Barnes CS. Clinical Inertia. Ann Intern Med. 2001;135(9):825-34.
11. Frijling BD, Spies TH, Lobo CM, Hulscher ME, van Drenth BB, Braspenning JC, Prins A, van der Wouden JC, Grol RP. Blood pressure control in treated hyper-tensive patients: clinical performance of general practitioners. Br J Gen Pract. 2001;51(462):9-14.
12. Valk GD, Renders CM, Kriegsman DM, Newton KM, Twisk JW, van Eijk JT, van
82
Chapter 3.1 - Cross-sectional versus sequential indicators
der Wal G, Wagner EH. Quality of care for patients with type 2 diabetes mellitus in The Netherlands and the United States: a comparison of two quality improve-ment programs. Health Serv Res. 2004;39(4 Pt 1):709-25.
13. Duggirala MK, Cuddihy RM, Cuddihy MT, Naessens JM, Cha SS, Mandrekar JN, Leibson CL. Predictors of blood pressure control in patients with diabetes and hypertension seen in primary care clinics. Am J Hypertens. 2005;18(6):833-8.
14. Rodondi N, Peng T, Karter AJ, Bauer DC, Vittinghoff E, Tang S, Pettitt D, Kerr EA, Selby JV. Therapy modifications in response to poorly controlled hyperten-sion, dyslipidemia, and diabetes mellitus. Ann Intern Med. 2006;144(7):475-84.
15. Kerr EA, Smith DM, Hogan MM, Hofer TP, Krein SL, Bermann M, Hayward RA. Building a better quality measure: are some patients with ‘poor quality’ actually getting good care? Med Care. 2003;41(10):1173-82.
16. Uitewaal PJ, Bruijnzeels MA, Bernsen RM, Voorham AJ, Hoes AW, Thomas S. Diabetes care in dutch general practice: differences between Turkish immigrants and Dutch patients. Eur J Public Health. 2004;14(1):15-8.
17. Grant RW, Buse JB, Meigs JBCN - University HealthSystem Consortium (UHC) Diabetes Benchmarking Project Team. Quality of diabetes care in U.S. aca-demic medical centers: low rates of medical regimen change. Diabetes Care. 2005;28(2):337-442.
18. Andrade SE, Gurwitz JH, Field TS, Kelleher M, Majumdar SR, Reed G, Black R. Hypertension management: the care gap between clinical guidelines and clinical practice. Am J Manag Care. 2004;10(7 Pt 2):481-6.
19. Berlowitz DR, Ash AS, Glickman M, Friedman RH, Pogach LM, Nelson AL, Wong AT. Developing a quality measure for clinical inertia in diabetes care. Health Serv Res. 2005;40(6 Pt 1):1836-53.
20. Kerr EA, Krein SL, Vijan S, Hofer TP, Hayward RA. Avoiding pitfalls in chronic disease quality measurement: a case for the next generation of technical quality measures. Am J Manag Care. 2001;7(11):1033-43.
21. Grant RW, Cagliero E, Dubey AK, Gildesgame C, Chueh HC, Barry MJ, Singer DE, Nathan DM, Meigs JB. Clinical inertia in the management of Type 2 diabetes metabolic risk factors. Diabet Med. 2004;21(2):150-5.
22. Shah BR, Hux JE, Laupacis A, Zinman B, van Walraven C. Clinical inertia in response to inadequate glycemic control: do specialists differ from primary care physicians? Diabetes Care. 2005;28(3):600-6.
23. Chin MH, Muramatsu N. What is the quality of quality of medical care meas-ures? Rashomon-like relativism and real-world applications. Perspect Biol Med. 2003;46(1):5-20.
24. Groningen Initiative to Analyse Type 2 diabetes Treatment - GIANTT. Available at: http://www.giantt.nl. Accessed Mar 5, 2007.
25. Voorham J, Denig P. Computerized extraction of information on the quality of diabetes care from free text in electronic patient records of general practitioners. J Am Med Inform Assoc. 2007;14(3):349-354.
26. Wetzler HP, Snyder JW. Linking pharmacy and laboratory data to assess the ap-propriateness of care in patients with diabetes. Diabetes Care. 2000;23(11):1637-41.
83
Chapter 3.1 - Cross-sectional versus sequential indicators
27. Diabetes Quality Improvement Project (DQIP). http://www.ncqa.org/dprp/ Accessed on Dec 1 2006.
28. Quality and Outcomes Framework (QOF). http://www.ic.nhs.uk/services/qof. Accessed on Dec 1 2006.
29. CBO. Multidisciplinaire Richtlijn Cardiovasculair risicomanagement. Kwaliteitsinstituut voor de Gezondheidszorg CBO december 2005; Conceptrichtlijn.
30. QUIDS. Final Report of a Development Project Commissioned by NICE, Diabetes UK & NHS Executive - North West 2003; Quality Indicators for Diabetes Services - QUIDS, final report.
31. IDF Clinical Guidelines Task Force. Global guideline for Type 2 diabetes. Brussels 2005.
32. CBO. Kwaliteit van zorg rond diabetes in de etalage - Indicatoren voor dia-betes als onderdeel van het ZonMw project ‘Kwaliteit van zorg in de etalage’. Het Kwaliteitsinstituut voor de Gezondheidszorg CBO, Orde van Medisch Specialisten, 2006.
33. Dutch Pharmacotherapy Compendium (Farmcotherapeutisch Kompas) 2004. Commissie Farmaceutische Hulp (CHF) van het College van Zorgverzekeringen, 2004.
34. Stevens RJ, Kothari V, Adler AI, Stratton IM, Holman RR - United Kingdom Prospective Diabetes Study (UKPDS) Group. The UKPDS risk engine: a model for the risk of coronary heart disease in Type II diabetes (UKPDS 56). Clin Sci. 2001;101(6):671-9.
35. Asch SM, Kerr EA, Lapuerta P, Law A, McGlynn EA. A new approach for meas-uring quality of care for women with hypertension. Arch Intern Med. 2001 28;161(10):1329-35.
36. Higashi T, Shekelle PG, Solomon DH, Knight EL, Roth C, Chang JT, Kamberg CJ, MacLean CH, Young RT, Adams J, Reuben DB, Avorn J, Wenger NS. The quality of pharmacologic care for vulnerable older patients. Ann Intern Med. 2004;140(9):714-20.
37. Shrank WH, Asch SM, Adams J, Setodji C, Kerr EA, Keesey J, Malik S, McGlynn EA. The quality of pharmacologic care for adults in the United States. Med Care. 2006;44(10):936-45.
38. Gill JM, Foy AJ Jr, Ling Y. Quality of outpatient care for diabetes mellitus in a national electronic health record network. Am J Med Qual. 2006;21(1):13-7.
39. De Berardis G, Pellegrini F, Franciosi M, Belfiglio M, Di Nardo B, Greenfield S, Kaplan SH, Rossi MC, Sacco M, Tognoni G, Valentini M, Nicolucci ACN. Quality of care and outcomes in type 2 diabetic patients: a comparison between general practice and diabetes clinics. Diabetes Care. 2004;27(2):398-406.
40. Ubink-Veltmaat LJ, Bilo HJ, Groenier KH, Rischen RO, Meyboom-de Jong B. Challenges in preventing cardiovascular complications in type 2 diabetes in pri-mary care. Eur J Gen Pract. 2005;11(1):11-6.
41. Schaars CF, Denig P, Kasje WN, Stewart RE, Wolffenbuttel BHR, Haaijer-Ruskamp FM. Physician, organizational, and patient factors associated with suboptimal blood pressure management in type 2 diabetic patients in primary
84
Chapter 3.1 - Cross-sectional versus sequential indicators
care. Diabetes Care. 2004;27(1):123-8.42. Thompson W, Wang H, Xie M, Kolassa J, Rajan M, Tseng CL, Crystal S, Zhang Q,
Vardi Y, Pogach L, Safford MM. Assessing quality of diabetes care by measuring longitudinal changes in hemoglobin A1c in the Veterans Health Administration. Health Serv Res. 2005;40(6 Pt 1):1818-35.
43. Pogach LM, Tiwari A, Maney M, Rajan M, Miller DR, Aron D. Should mitigat-ing comorbidities be considered in assessing healthcare plan performance in achieving optimal glycemic control? Am J Manag Care. 2007;13(3):133-40.
44. Farmer JA, Gotto AM Jr. The Heart Protection Study: expanding the boundaries for high-risk coronary disease prevention. Am J Cardiol. 2003;92(1A):3i-9i.
85
86
87
Chapter 3.2 - A systematic literature review: prescribing indicators related
to type 2 diabetes mellitus and cardiovascular risk management
Liana Martirosyan1
Jaco Voorham1,2
Flora M Haaijer-Ruskamp1
Jozé Braspenning3
Bruce HR Wolffenbuttel4
Petra Denig1
1. Department of Clinical Pharmacology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
2. Department of Epidemiology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
3 Scientific Institute for Quality of Healthcare, Radboud University Nijmegen Medical Centre
4. Department of Endocrinology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
Martirosyan L, Voorham J, Haaijer-Ruskamp FM, Braspenning J, Wolffenbuttel BHR, Denig P. A systematic literature review: prescribing indicators related to type 2 diabetes mellitus and cardiovascular risk management. Pharmacoepidemiol Drug Saf. 2010;19(4):319-34.

88
Chapter 3.2 - Review on prescribing quality indicators
ABSTRACTBackground. Valid prescribing indicators (PI) are needed for reliable assessment of prescribing quality. The purpose of this study is to describe the validity of existing PI for type 2 diabetes mellitus and cardiovascular risk management.Methods. We conducted a systematic literature search for studies describing the development and assessment of relevant PIs between January 1990 and January 2009. We grouped identified PI as drug- or disease-oriented, and according to the aspects of prescribing addressed and the additional clinical information included. We reviewed the clinimetric characteristics of the different types of PI. Results. We identified 59 documents describing the clinimetrics of 16 types of PI covering relevant prescribing aspects, including first-choice treatment, safety issues, dosing, costs, sufficient and timely treatment. We identified three types of drug-ori-ented, and five types of disease-oriented PI with proven face and content validity as well as operational feasibility in different settings. PI focusing on treatment modifi-cations were the only indicators that showed concurrent validity. Several solutions were proposed for dealing with case-mix and sample size problems, but their actual effect on PI scores was insufficiently assessed. Predictive validity of individual PI is not yet known. Conclusions. We identified a range of existing PI that are valid for internal quality as-sessment as they are evidence-based, accepted by professionals, and reliable. For external use, problems of patient case-mix and sample size per PI should be better addressed. Further research is needed for selecting indicators that predict clinical outcomes.

89
Chapter 3.2 - Review on prescribing quality indicators
INTRODUCTIONAppropriate drug prescribing has been recognised as an important quality of care issue in the management of chronic conditions. Insight into the quality of prescribing is demanded by health care providers, payers, and the public. Such information is used for internal quality improvement through audit, feedback, and benchmarking in educational contexts.1-3 External stakeholders use prescribing information for com-parison of health care providers, and to implement performance-based reimburse-ment programs that reward health care providers for meeting preset targets.4,5
To measure quality of prescribing, prescribing indicators (PI) have been developed. Distinct types of PI exist that address different aspects of prescribing quality, such as recommended drug-choice, ineffective drugs or timely treatment.6 There are drug-oriented PI which focus on the drugs prescribed irrespective of the indication, and disease-oriented PI looking at the prescriptions in relation to a specific condition.7 Furthermore, there are indicators that link prescribing to clinical outcomes.8,9
Although there are no consensus-based criteria for the development of quality meas-ures, they are expected to reflect the best available evidence, to be relevant, and to be accepted by the professionals in the field.10,11 Effective use of PI requires under-standing of what aspect of prescribing is measured, how the indicators were devel-oped, and whether their clinimetric characteristics, e.g. validity and reliability, were assessed.11 The requirements regarding these characteristics might depend on the aim of the indicator. For internal purposes, PI need to be relevant for healthcare pro-viders: they have to be specific and sufficiently detailed to show potential problems and capture pertinent changes in prescribing. However, to make fair comparisons between health care providers for external use, e.g. by third party payers, there are additional requirements, like adjustment for patient case-mixes and having adequate number of patients per provider.12,13 A large number of PI have been developed in recent years for chronic conditions, such as type 2 diabetes mellitus (T2DM) and cardiovascular risk management. These conditions where one of the first for which disease management programs, as well as quality assurance programs were developed. We have focused on these conditions as they are closely related. While the prevalence of T2DM and cardiovas-cular diseases is dramatically increasing, appropriate pharmacological treatment of risk factors can prevent complications in both diabetic and non-diabetic populations.For reliable measurement of prescribing quality valid indicators are needed. In spite of a large number of existing PI for T2DM and cardiovascular risk management, no information is available on their validity. The purpose of this study is to identify the various types of existing PI, and describe their clinimetric evaluation. The results of
90
Chapter 3.2 - Review on prescribing quality indicators
this study will help health care providers and policy makers to choose the most ap-propriate PI for quality assessment by pointing out their clinimetric values as well as possible limitations.
METHODS
Search and selection strategy We performed a systematic search in MEDLINE and EMBASE databases without language restrictions from January 1990 to January 2009 for studies focusing on the development or assessment of quality indicators including PI related to T2DM or CV risk management (Appendix 1). In addition, we hand searched the WebPages of professional organisations that have sets of quality indicators in English speaking countries and the Netherlands. PI was defined as a measurable element of prescrib-ing that can be used to assess quality or efficiency of treatment at drug, patient or provider level.Two reviewers independently screened the titles and abstracts of 5,121 retrieved manuscripts and excluded papers not focusing on T2DM or CV risk management. Using full copies of the papers, we excluded reviews, letters, commentaries, studies that did not include any PI and studies that merely used indicators to assess pre-scribing quality without assessment of clinimetrics.
Classification of papers and indicatorsAll selected papers were independently reviewed and classified by two researchers in a two-stage process, focusing first on classification of studies, and secondly, on classification of the PI identified from the studies. Disagreement between reviewers was resolved through discussion. On study level, we recorded whether and how clinimetric properties, i.e. face, content, concurrent, and predictive validity, operational feasibility, reliability, robustness to case-mix, and minimal sample size needed, were assessed (Table 1). Furthermore, we recorded the aim and intended setting for the indicators. We classified the identi-fied indicators as drug- or disease-oriented. We further grouped indicators according to the different aspects of prescribing addressed, and the type of clinical information included. As it has been argued that sequential assessment of prescribing in reac-tion to a clinical event or outcome would provide more meaningful indicators than simple cross-sectional assessment of the prescribed treatment,8 we also divided the indicators regarding this aspect. In case of similar indicators, differing slightly in the way of formulation, we provided a general description of the indicator with some typical examples. At this generic indicator level, we reported the studies that have included such an indicator, as well as the outcomes regarding validity, reliability,

91
Chapter 3.2 - Review on prescribing quality indicators
and operational feasibility. Results on these clinimetrics were classified as “positive” when all referenced studies reported the clinimetric to be present, “negative” when the clinimetric was shown to be absent, and “doubtful” if mixed or inconclusive re-sults were reported.
RESULTSWe identified 46 studies published in peer-reviewed journals. By screening the ref-erences of these papers, we identified six additional published studies. From the WebPages of professional organisations, we found seven relevant documents that had not been formally published. Our final cohort thus included 59 papers focusing on the assessment of PI related to T2DM or CV risk management (Table 2).Many studies described sets of quality indicators including not only PI but also indi-cators focusing on other aspects of care, e.g. screening, referral, etc. In some sets, PI were underrepresented,4,5,14 while others consisted of only PI.3,12,15-22 In general, the assessment of various clinimetric characteristics of some indicator sets, e.g. ACOVE indicators, were described in several studies,23-25 including adaptation of these indicators in different countries.26,27 For sets of indicators that were updated several times, e.g. Beers’ criteria and ACOVE indicators, we have included the latest version.25,28 The development of indicators was described in 37 studies, which always included assessment of face and/or content validity. The other studies focused on the assess-ment of clinimetrics of previously developed PI.
Clinimetrics addressed and methods used in the studies (Table 2)Content validity was addressed in 37 studies. The most common approach to ascer-tain content validity of the PI was using recommendations from clinical guidelines. In two cases, authors first assessed the quality of available guidelines, and used the highest ranking guidelines to propose indicators.29,30 In six studies, authors reviewed randomised controlled trials to propose indicators.2,28,31-34 In three studies a literature review was conducted to identify potential indicators.26,35,36
Face validity was addressed in 36 studies and assessed using different techniques including modified Delphi,2,10,20,25-28,31,32,35-46 nominal group,47,48 focus group discus-sion,1,49 surveys or panels of professionals,1,10,19,29,30,50-53 continuous assessment of indicators using panels of various stakeholders,4,5,12,54 or iterative process.55
Concurrent validity was assessed in four studies by comparing different data sourc-es,24 different PI,8,68 and different data collection methods.57 Medical records pro-vided more detailed clinical information for quality assessment than administrative data, although scores for individual indicators did not change across sources.24
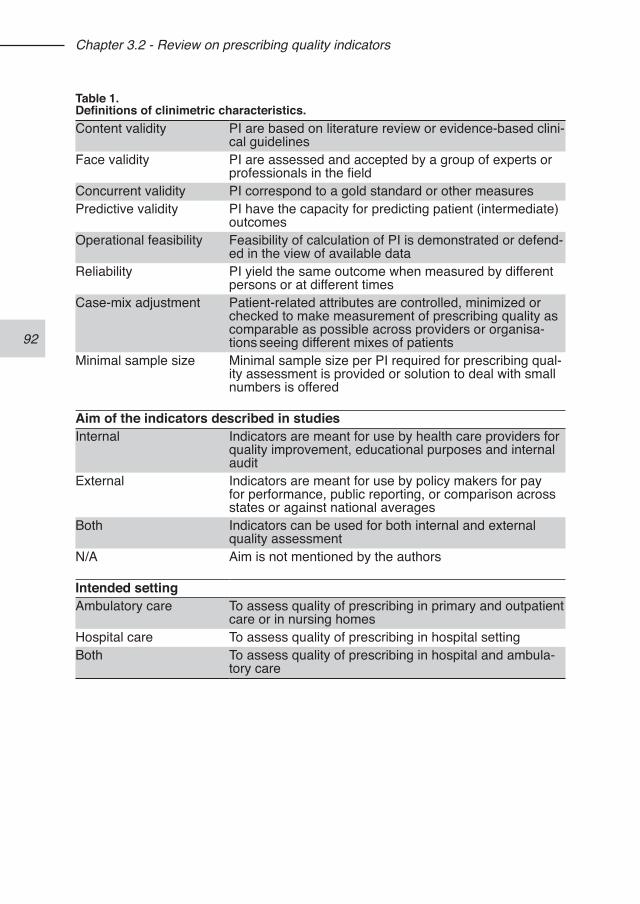
92
Chapter 3.2 - Review on prescribing quality indicators
Table 1.Definitions of clinimetric characteristics.Content validity PI are based on literature review or evidence-based clini-
cal guidelinesFace validity PI are assessed and accepted by a group of experts or
professionals in the fieldConcurrent validity PI correspond to a gold standard or other measuresPredictive validity PI have the capacity for predicting patient (intermediate)
outcomesOperational feasibility Feasibility of calculation of PI is demonstrated or defend-
ed in the view of available dataReliability PI yield the same outcome when measured by different
persons or at different timesCase-mix adjustment Patient-related attributes are controlled, minimized or
checked to make measurement of prescribing quality as comparable as possible across providers or organisa-tions seeing different mixes of patients
Minimal sample size Minimal sample size per PI required for prescribing qual-ity assessment is provided or solution to deal with small numbers is offered
Aim of the indicators described in studiesInternal Indicators are meant for use by health care providers for
quality improvement, educational purposes and internal audit
External Indicators are meant for use by policy makers for pay for performance, public reporting, or comparison across states or against national averages
Both Indicators can be used for both internal and external quality assessment
N/A Aim is not mentioned by the authors
Intended settingAmbulatory care To assess quality of prescribing in primary and outpatient
care or in nursing homesHospital care To assess quality of prescribing in hospital settingBoth To assess quality of prescribing in hospital and ambula-
tory care
93
Chapter 3.2 - Review on prescribing quality indicators
However, frequent misclassifications occurred when using automated measurement in electronic medical records (EMR) in comparison to manual medical record review, because the automated method missed diagnosis or contraindications information registered in free-text notes.57 Sequential quality indicators provided more accurate estimates of quality of care compared to cross-sectional measures.8,68
Predictive validity of PI was assessed in six studies, all using composite indicator scores. In five studies the association between process of care and outcomes was assessed cross-sectionally. Only one study assessed the link between quality of care and survival of patients using a prospective design.23 Three studies used a composite score based on PI,22,65,67 while others also included other process indi-cators. Some concluded that higher scores were associated with better controlled risk factor levels31,67 or better survival,23 while others found at most weak associa-tions.14,22,65
Operational feasibility was the most frequently assessed characteristic (40 studies), using theoretical, implicit and explicit approaches. In case of theoretical assessment, PI requiring information not available in existing databases were excluded during development.4,10,12,16,19,45,53,55 Indicators that were explicitly tested for operational fea-sibility were applied to specific types of datasets or settings, e.g. administrative data, EMR or primary care and hospital settings.9,17,20,21,49,50,52,56,58-60 Implicit assessment of operational feasibility occurred in all other studies when PI were calculated during assessment of other clinimetric characteristics, e.g. reliability or concurrent valid-ity.3,8,14,15,22-24,31,34,37,43,51,57,61-68
The inter-rater reliability was evaluated in studies using manual chart review by means of kappa statistics. In all cases, good reliability was shown for manual data abstraction.19,21-24,37,49,51,57 In some cases reliability was assessed theoretically during the indicator development process.4,17,53,54
Case-mix problems were addressed in nine studies, of which seven included indi-cators with external aim (Table 2). This issue was not addressed in other studies with a clearly mentioned external aim.14,16,22,34,50,57,59,62 Two studies showed the influ-ence of case-mix on performance scores.37,61 Several approaches were proposed to minimise the effect of patient clinical or sociodemographic characteristics on PI out-comes, including statistical adjustment,4,37 exclusion of indicators that are too much affected by such characteristics,53,55 or exclusion of patients for reasons like contrain-dications, perceived side-effects or refusing medication.5,25 Another approach to deal with case-mix was setting lower target levels.70
Sample size was addressed in 13 studies. Two studies showed that sample size can affect performance scores and hinder comparisons between individual provid-
94
Chapter 3.2 - Review on prescribing quality indicators
ers.61,62 Suggested solutions were exclusion of indicators or providers with small numbers,51,55,62,65 use of hierarchical estimates,62 or pooling data from several provid-ers or time periods.1 The minimal sample size suggested per indicator ranged from 5-1049 to 30-60 patients.1 Others suggested to include only providers with a certain number of patients,3,25,52 but did not support this with calculations. A paper related to measures proposed by the National Quality Forum69 provided guidelines for sample size calculations. It was shown that the minimal number of patients to get a reliability of 0.8 depends on the intraclass correlation coefficient (ICC), and could range from 36 for an ICC of 0.10 to 196 for an ICC of 0.02.
Types of PI and their reported clinimetrics We identified in total 16 types of PI, including seven drug-oriented and nine types of disease-oriented PI. The same types of indicators were proposed for internal and external quality assessment. PI for T2DM were typically developed for ambulatory care, whereas PI for cardiac care and more general PI were also developed for hospital care.
Drug-oriented PIThe drug-oriented PI were grouped on different aspects of prescribing: first choice drug (classes), second-step drugs, non-preferred drugs, safety issues, dosing is-sues, redundant prescribing, and cost-conscious prescribing (Table 3). For almost all types, several generic indicators were identified, and five of them were tested in sev-eral studies. Indicators focusing on prescribing of first-choice or non-preferred drugs were both well-studied, and mostly rated as face and content valid, since they were derived from guideline recommendations. Regular updating was deemed necessary to reflect emerging evidence for drug choice. PI expressing currently used ratios and number of prescriptions for specific drugs per prescribing unit (PU) were criticised, since there was no agreement about what defines quality in these cases.10,50
Safety indicators focused on potentially inappropriate drugs or drug combinations to be avoided, and both groups were widely studied. They were considered face and content valid but criticised for reflecting only a limited part of prescribing quality.15,19 Since in specific cases there can be good reasons to use “inappropriate” drugs, these indicators were recommended for internal use to identify potential problems.19 Indicators focusing on redundant prescribing, e.g. number of daily dosing or co-pre-scribing of more than one drug from the same therapeutic group, were studied in two and five studies respectively, which showed that this group of indicators is reliable, face and content valid. Difficulties were encountered regarding the operational feasi-bility of some safety and redundant prescribing indicators because of the absence of eligible patients or lack of information on duration of prescriptions.19,56
95
Chapter 3.2 - Review on prescribing quality indicators
Indicators focusing on cost were seldom assessed for face and content validity47 or doubts were raised for their relation to quality.43 Furthermore, the value of the DU90% focusing on the number of different drugs prescribed within a drug class was disputed, because it does not discriminate between physicians, and high scores can be obtained while prescribing less preferred drugs.43
In summary, the drug-oriented indicators that have repeatedly shown face and con-tent validity focus on: (a) proportions of first choice drugs within a therapeutic class, (b) drugs to be avoided, (c) number of preferred daily dosings. In general, drug-oriented PI have shown good operational feasibility.
Cross-sectional disease-oriented PIWe identified more than 30 generic disease-oriented indicators assessing prescrib-ing in a cross-sectional way. They were grouped reflecting prescribing of: drugs for a specific indication (subdivided for different drugs), drugs for a specific indication unless contra-indicated (subdivided for different drugs), drugs for elevated risk factor levels, first-choice drug for a specific indication, and drugs to be avoided in specific patients (Table 4). From the first group, the indicator “prescription of glucose-lowering treatment in dia-betic patients” was criticised for not reflecting quality.41,53 The other PI from this group were considered face and content valid but adjustment for case-mix was recom-mended to deal with patients that either do not require or should not receive the specified treatment. Alternatively, this could be solved by excluding patients with contraindications to the recommended treatment from the indicator. Several of such PI with exclusion criteria, however, lacked face or content validity across different settings. For example, indicators focusing on prescription of ACE-inhibitors and as-pirin in elderly patients with diabetes unless contra-indicated were accepted as face and content valid by expert panels in the USA and UK, but rejected by a Dutch panel.25-27 Furthermore, the operational feasibility of such indicators was found to be hampered in one study using automated data collection methods, because informa-tion on contraindications entered as text data in medical records was missed.57 Another type of disease-oriented PI that was widely tested consists of indicators that focus on prescribed drugs in patients with an elevated risk factor level (Table 4). The cut-off levels varied depending on the literature used for developing the indicator, and in some cases age-dependent levels were specified.33,51 Face and content va-lidity was considered present but again case-mix problems were mentioned, espe-cially regarding treatment in relation to cholesterol levels. In one case, this resulted in rejecting indicators that were considered too sensitive to patient case-mix.53 We identified relatively few disease-oriented PI focusing on first-choice drugs or drugs
96
Chapter 3.2 - Review on prescribing quality indicators
to be avoided (Table 4). In summary, the most widely assessed disease-oriented PI, showing good clinimet-ric results in different settings, focus on prescribed drugs for a specific indication or elevated risk factor, in particular: (a) statins in high cardiovascular risk patients. (b) aspirin or antiplatelet medication in high cardiovascular risk patients, (c) ACE-inhibitors in T2DM patients with hypertension and/or albuminuria, (d) beta blocker in patients with coronary heart disease or history of myocardial infarction, (e) treatment of patients with elevated HbA1c levels; (f) treatment of patients with elevated blood pressure levels.
Sequential disease-oriented PIAmong the 12 identified generic indicators that incorporate a sequential assessment strategy, we acknowledged four groups: treatment modification after an event, treat-ment modification after an event unless contra-indicated, start of a first-choice drug in specific patients, and continuum of post-discharge treatment (Table 5). These include indicators such as “if a patient has a certain risk factor level, then he should receive a treatment start or intensification”, either with or without a defined maximal time period for such modifications. In two studies, a return to control without treat-ment modification was included in the indicators as adequate care.8,9 Similar to the cross-sectional indicators, sequential indicators incorporated exclusions to deal with patients that have contraindications or already receive maximal treatment. All except one indicator were considered face and content valid. This one focused on treat-ment of elderly patients with an elevated LDL-level, which was considered valid by one panel but rejected by another.25,27 Treatment modification indicators have shown concurrent validity,8,68 and operational feasibility was good for the first three types of PI in this category. For PI focusing on the continuum of hospital through post discharge ambulatory care, the operational feasibility was hampered by the lack of adequate data systems.52 In summary, sequential PI focusing on treatment modifications after elevated risk factors (cholesterol, BP, HbA1c) showed face and content validity in several studies and settings, and are the only PI for which concurrent validity was shown.
DISCUSSIONWe have identified 16 types of PI covering important aspects of drug prescribing related to T2DM and CV risk management, including first-choice treatment, safety issues, dosing, costs, sufficient and timely treatment. Face and content validity, as well as operational feasibility were most frequently assessed. Less attention has been paid to predictive and concurrent validity, and case-mix issues were addressed mostly for PI intended for external use. Sample size problems were discussed for
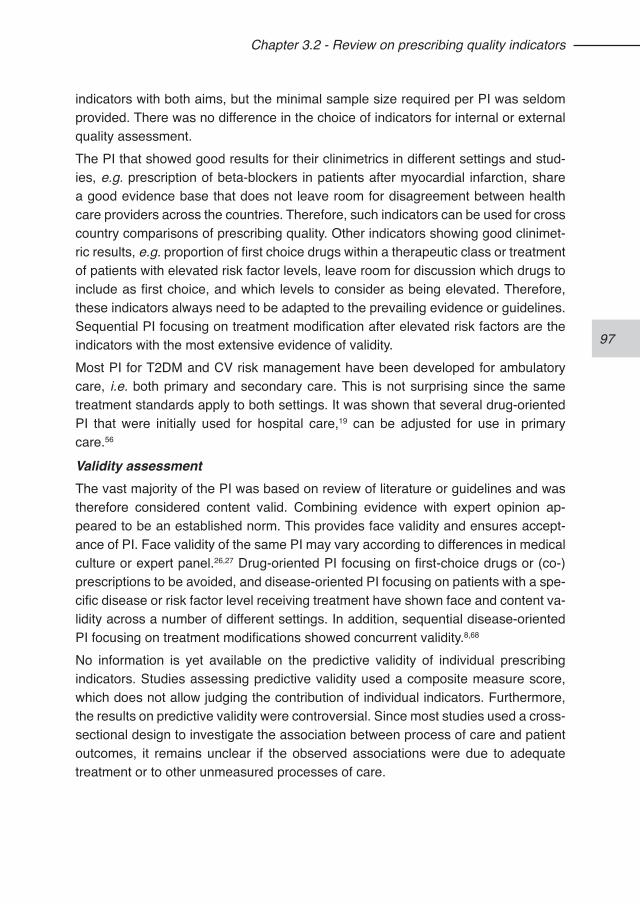
97
Chapter 3.2 - Review on prescribing quality indicators
indicators with both aims, but the minimal sample size required per PI was seldom provided. There was no difference in the choice of indicators for internal or external quality assessment. The PI that showed good results for their clinimetrics in different settings and stud-ies, e.g. prescription of beta-blockers in patients after myocardial infarction, share a good evidence base that does not leave room for disagreement between health care providers across the countries. Therefore, such indicators can be used for cross country comparisons of prescribing quality. Other indicators showing good clinimet-ric results, e.g. proportion of first choice drugs within a therapeutic class or treatment of patients with elevated risk factor levels, leave room for discussion which drugs to include as first choice, and which levels to consider as being elevated. Therefore, these indicators always need to be adapted to the prevailing evidence or guidelines. Sequential PI focusing on treatment modification after elevated risk factors are the indicators with the most extensive evidence of validity. Most PI for T2DM and CV risk management have been developed for ambulatory care, i.e. both primary and secondary care. This is not surprising since the same treatment standards apply to both settings. It was shown that several drug-oriented PI that were initially used for hospital care,19 can be adjusted for use in primary care.56
Validity assessmentThe vast majority of the PI was based on review of literature or guidelines and was therefore considered content valid. Combining evidence with expert opinion ap-peared to be an established norm. This provides face validity and ensures accept-ance of PI. Face validity of the same PI may vary according to differences in medical culture or expert panel.26,27 Drug-oriented PI focusing on first-choice drugs or (co-)prescriptions to be avoided, and disease-oriented PI focusing on patients with a spe-cific disease or risk factor level receiving treatment have shown face and content va-lidity across a number of different settings. In addition, sequential disease-oriented PI focusing on treatment modifications showed concurrent validity.8,68 No information is yet available on the predictive validity of individual prescribing indicators. Studies assessing predictive validity used a composite measure score, which does not allow judging the contribution of individual indicators. Furthermore, the results on predictive validity were controversial. Since most studies used a cross-sectional design to investigate the association between process of care and patient outcomes, it remains unclear if the observed associations were due to adequate treatment or to other unmeasured processes of care.
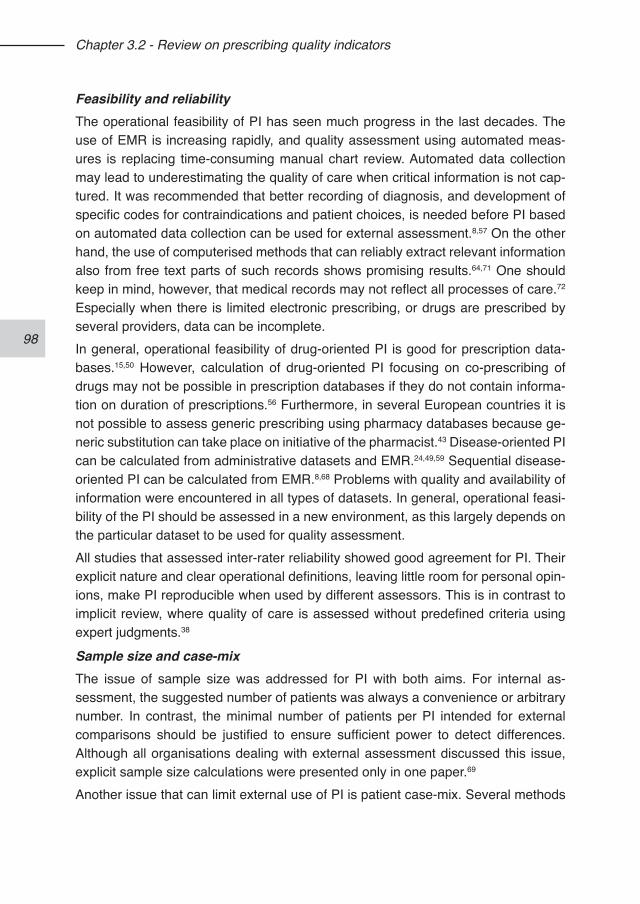
98
Chapter 3.2 - Review on prescribing quality indicators
Feasibility and reliabilityThe operational feasibility of PI has seen much progress in the last decades. The use of EMR is increasing rapidly, and quality assessment using automated meas-ures is replacing time-consuming manual chart review. Automated data collection may lead to underestimating the quality of care when critical information is not cap-tured. It was recommended that better recording of diagnosis, and development of specific codes for contraindications and patient choices, is needed before PI based on automated data collection can be used for external assessment.8,57 On the other hand, the use of computerised methods that can reliably extract relevant information also from free text parts of such records shows promising results.64,71 One should keep in mind, however, that medical records may not reflect all processes of care.72 Especially when there is limited electronic prescribing, or drugs are prescribed by several providers, data can be incomplete.In general, operational feasibility of drug-oriented PI is good for prescription data-bases.15,50 However, calculation of drug-oriented PI focusing on co-prescribing of drugs may not be possible in prescription databases if they do not contain informa-tion on duration of prescriptions.56 Furthermore, in several European countries it is not possible to assess generic prescribing using pharmacy databases because ge-neric substitution can take place on initiative of the pharmacist.43 Disease-oriented PI can be calculated from administrative datasets and EMR.24,49,59 Sequential disease-oriented PI can be calculated from EMR.8,68 Problems with quality and availability of information were encountered in all types of datasets. In general, operational feasi-bility of the PI should be assessed in a new environment, as this largely depends on the particular dataset to be used for quality assessment. All studies that assessed inter-rater reliability showed good agreement for PI. Their explicit nature and clear operational definitions, leaving little room for personal opin-ions, make PI reproducible when used by different assessors. This is in contrast to implicit review, where quality of care is assessed without predefined criteria using expert judgments.38
Sample size and case-mixThe issue of sample size was addressed for PI with both aims. For internal as-sessment, the suggested number of patients was always a convenience or arbitrary number. In contrast, the minimal number of patients per PI intended for external comparisons should be justified to ensure sufficient power to detect differences. Although all organisations dealing with external assessment discussed this issue, explicit sample size calculations were presented only in one paper.69
Another issue that can limit external use of PI is patient case-mix. Several methods
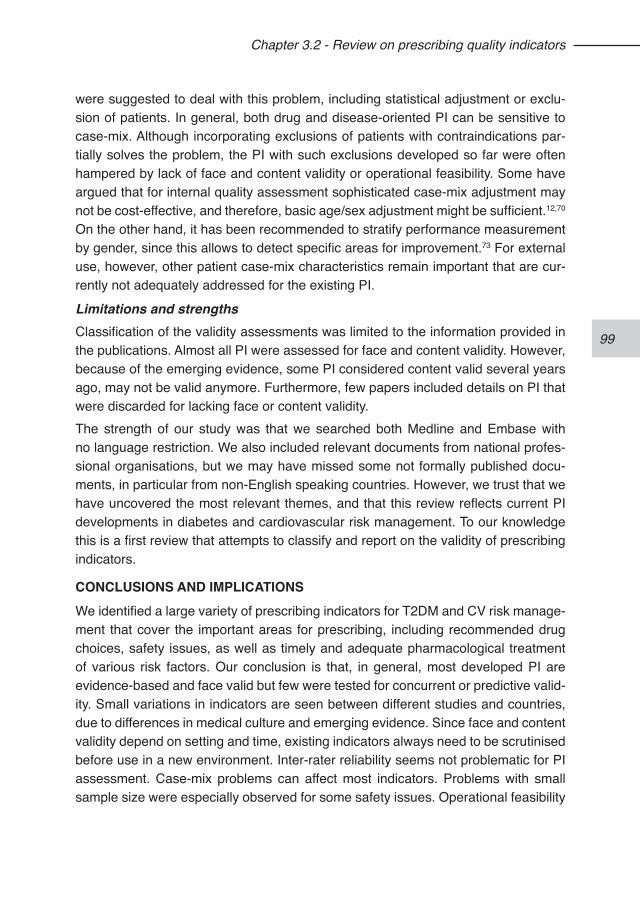
99
Chapter 3.2 - Review on prescribing quality indicators
were suggested to deal with this problem, including statistical adjustment or exclu-sion of patients. In general, both drug and disease-oriented PI can be sensitive to case-mix. Although incorporating exclusions of patients with contraindications par-tially solves the problem, the PI with such exclusions developed so far were often hampered by lack of face and content validity or operational feasibility. Some have argued that for internal quality assessment sophisticated case-mix adjustment may not be cost-effective, and therefore, basic age/sex adjustment might be sufficient.12,70 On the other hand, it has been recommended to stratify performance measurement by gender, since this allows to detect specific areas for improvement.73 For external use, however, other patient case-mix characteristics remain important that are cur-rently not adequately addressed for the existing PI.
Limitations and strengthsClassification of the validity assessments was limited to the information provided in the publications. Almost all PI were assessed for face and content validity. However, because of the emerging evidence, some PI considered content valid several years ago, may not be valid anymore. Furthermore, few papers included details on PI that were discarded for lacking face or content validity.The strength of our study was that we searched both Medline and Embase with no language restriction. We also included relevant documents from national profes-sional organisations, but we may have missed some not formally published docu-ments, in particular from non-English speaking countries. However, we trust that we have uncovered the most relevant themes, and that this review reflects current PI developments in diabetes and cardiovascular risk management. To our knowledge this is a first review that attempts to classify and report on the validity of prescribing indicators.
CONCLUSIONS AND IMPLICATIONS We identified a large variety of prescribing indicators for T2DM and CV risk manage-ment that cover the important areas for prescribing, including recommended drug choices, safety issues, as well as timely and adequate pharmacological treatment of various risk factors. Our conclusion is that, in general, most developed PI are evidence-based and face valid but few were tested for concurrent or predictive valid-ity. Small variations in indicators are seen between different studies and countries, due to differences in medical culture and emerging evidence. Since face and content validity depend on setting and time, existing indicators always need to be scrutinised before use in a new environment. Inter-rater reliability seems not problematic for PI assessment. Case-mix problems can affect most indicators. Problems with small sample size were especially observed for some safety issues. Operational feasibility
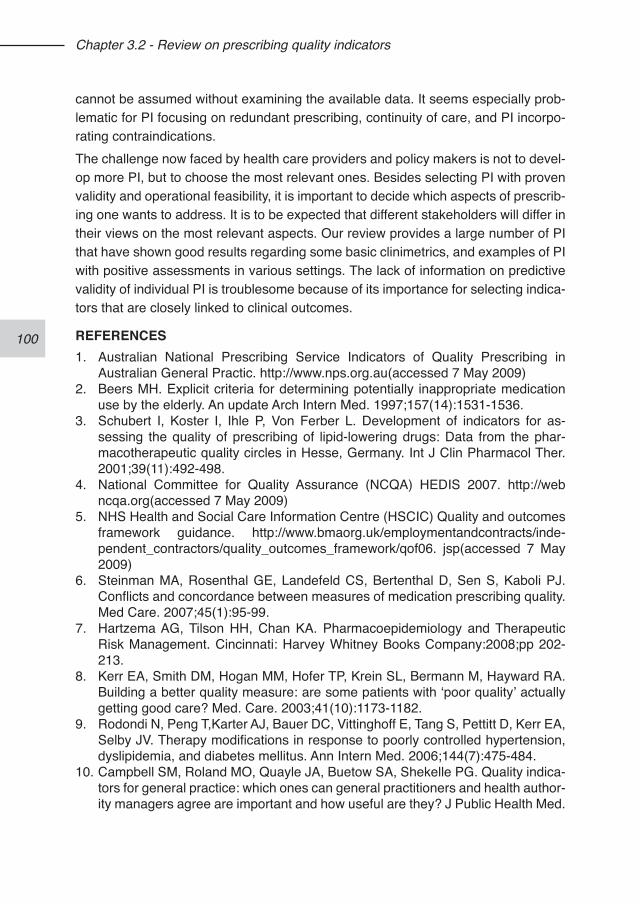
100
Chapter 3.2 - Review on prescribing quality indicators
cannot be assumed without examining the available data. It seems especially prob-lematic for PI focusing on redundant prescribing, continuity of care, and PI incorpo-rating contraindications.The challenge now faced by health care providers and policy makers is not to devel-op more PI, but to choose the most relevant ones. Besides selecting PI with proven validity and operational feasibility, it is important to decide which aspects of prescrib-ing one wants to address. It is to be expected that different stakeholders will differ in their views on the most relevant aspects. Our review provides a large number of PI that have shown good results regarding some basic clinimetrics, and examples of PI with positive assessments in various settings. The lack of information on predictive validity of individual PI is troublesome because of its importance for selecting indica-tors that are closely linked to clinical outcomes.
REFERENCES1. Australian National Prescribing Service Indicators of Quality Prescribing in
Australian General Practic. http://www.nps.org.au(accessed 7 May 2009)2. Beers MH. Explicit criteria for determining potentially inappropriate medication
use by the elderly. An update Arch Intern Med. 1997;157(14):1531-1536.3. Schubert I, Koster I, Ihle P, Von Ferber L. Development of indicators for as-
sessing the quality of prescribing of lipid-lowering drugs: Data from the phar-macotherapeutic quality circles in Hesse, Germany. Int J Clin Pharmacol Ther. 2001;39(11):492-498.
4. National Committee for Quality Assurance (NCQA) HEDIS 2007. http://web ncqa.org(accessed 7 May 2009)
5. NHS Health and Social Care Information Centre (HSCIC) Quality and outcomes framework guidance. http://www.bmaorg.uk/employmentandcontracts/inde-pendent_contractors/quality_outcomes_framework/qof06. jsp(accessed 7 May 2009)
6. Steinman MA, Rosenthal GE, Landefeld CS, Bertenthal D, Sen S, Kaboli PJ. Conflicts and concordance between measures of medication prescribing quality. Med Care. 2007;45(1):95-99.
7. Hartzema AG, Tilson HH, Chan KA. Pharmacoepidemiology and Therapeutic Risk Management. Cincinnati: Harvey Whitney Books Company:2008;pp 202-213.
8. Kerr EA, Smith DM, Hogan MM, Hofer TP, Krein SL, Bermann M, Hayward RA. Building a better quality measure: are some patients with ‘poor quality’ actually getting good care? Med. Care. 2003;41(10):1173-1182.
9. Rodondi N, Peng T,Karter AJ, Bauer DC, Vittinghoff E, Tang S, Pettitt D, Kerr EA, Selby JV. Therapy modifications in response to poorly controlled hypertension, dyslipidemia, and diabetes mellitus. Ann Intern Med. 2006;144(7):475-484.
10. Campbell SM, Roland MO, Quayle JA, Buetow SA, Shekelle PG. Quality indica-tors for general practice: which ones can general practitioners and health author-ity managers agree are important and how useful are they? J Public Health Med.
101
Chapter 3.2 - Review on prescribing quality indicators
1998;20(4):414-421.11. Campbell SM, Braspenning J, Hutchinson A, Marshall M. Research methods
used in developing and applying quality indicators in primary care. Qual Saf Health Care. 2002;11(4):358-364.
12. Prescribing Indicators National Group Quality Prescribing Related Indicators. http://www.ic.nhs.uk(accessed 7 May 2009).
13. Powell AE, Davies HTO, Thomson RG. Using routine comparative data to as-sess the quality of health care: understanding and avoiding common pitfalls. Qual Saf Health Care. 2003;12(2):122-128.
14. Ackermann RT, Thompson TJ, Selby JV, Safford MM, Stevens M, Brown AF, Narayan KMV. Is the number of documented diabetes process-of-care indica-tors associated with cardiometabolic risk factor levels, patient satisfaction, or self-rated quality of diabetes care?: The Translating Research into Action for Diabetes (TRIAD) study. Diabetes Care. 2006;29(9):2108-2113.
15. Anderson GM, Beers MH, Kerluke K. Auditing prescription practice using ex-plicit criteria and computerized drug benefit claims data. J Eval Clin Pract. 1997;3(4):283-294.
16. Ashworth M, Golding S, Majeed A. Prescribing indicators and their use by prima-ry care groups to influence prescribing. J Clin Pharm Ther. 2002;27(3):197-204.
17. Australian National Prescribing Service Indicators of Quality Prescribing in Australian General Practic. http://www.nps.org.au (accessed 7 May 2009)
18. Basger BJ, Chen TF, Moles RJ. Inappropriate medication use and prescribing indicators in elderly Australians: development of a prescribing indicators tool. Drugs Aging. 2008;25(9):777-793.
19. Elliott RA, Woodward MC, Oborne CA. Indicators of prescribing quality for eld-erly hospital inpatients. Aust J Hosp Pharm. 2001;31(1):19-25.
20. Martirosyan L, Braspenning J, Denig P, de Grauw WJ, Bouma M, Storms F, Haaijer-Ruskamp FM. Prescribing quality indicators of type 2 diabetes mellitus ambulatory care. Qual Saf Health Care. 2008;17(5):318-323.
21. Oborne CA, Hooper R, Swift CG, Jackson SH. Explicit, evidence-based crite-ria to assess the quality of prescribing to elderly nursing home residents. Age Ageing. 2003;32(1):102-108.
22. Peterson ED, Bynum DZ, Roe MT. Association of evidence-based care process-es and outcomes among patients with acute coronary syndromes: performance matters. J Cardiovasc Nurs. 2008;23(1):50-55.
23. Higashi T, Shekelle PG, Adams JL, Kamberg CJ, Roth CP, Solomon DH, Reuben DB, Chiang L, Maclean CH, Chang JT, Young RT, Saliba DM, Wenger NS. Quality of care is associated with survival in vulnerable older patients. Ann Intern Med. 2005;143(4):274-281.
24. Maclean CH, Louie R, Shekelle PG, Roth CP, Saliba D, Higashi T, Adams J, Chang JT, Kamberg CJ, Solomon DH, Young RT, Wenger NS. Comparison of administrative data and medical records to measure the quality of medical care provided to vulnerable older patients. Med Care. 2006;44(2):141-148.
25. Wenger NS, Roth CP, Shekelle P. Introduction to the assessing care of vulnera-ble elders-3 quality indicator measurement set. J Am Geriatr Soc. 2007;55(Suppl
102
Chapter 3.2 - Review on prescribing quality indicators
2):S247-S252.26. Steel N, Melzer D, Shekelle PG, Wenger NS, Forsyth D, McWilliams BC.
Developing quality indicators for older adults: transfer from the USA to the UK is feasible. Qual Saf Health Care. 2004;13(4):260-264.
27. van der Ploeg E, Depla MF, Shekelle P, Rigter H, Mackenbach JP. Developing quality indicators for general practice care for vulnerable elders; transfer from US to The Netherlands. Qual Saf Health Care. 2008;17(4):291-295.
28. Fick DM, Cooper JW, Wade WE, Waller JL, Maclean JR, Beers MH. Updating the Beers criteria for potentially inappropriate medication use in older adults: re-sults of a US consensus panel of experts. Arch Intern Med. 2003;163(22):2716-2724.
29. Hutchinson A, McIntosh A, Anderson J, Gilbert C, Field R. Developing primary care review criteria from evidence-based guidelines: Coronary heart disease as a model. Br J Gen Pract. 2003;53(494):690-696.
30. Wens J, Dirven K, Mathieu C, Paulus D, Van RP. Quality indicators for type-2 diabetes care in practice guidelines: an example from six European countries. Prim Care Diabetes. 2007;1(1):17-23.
31. Asch SM, Kerr EA, Lapuerta P, Law A, McGlynn EA. A New Approach for Measuring Quality of Care for Women With Hypertension. Arch Intern Med. 2001;161(10):1329-1335.
32. Burge FI, Bower K, Putnam W, Cox JL. Quality indicators for cardiovascular pri-mary care. Can J Cardiol. 2007;23(5):383-388.
33. Campbell SM, Roland MO, Shekelle PG, Cantrill JA, Buetow SA, Cragg DK. development of review criteria for assessing the quality of management of stable angina, adult asthma, and non-insulin dependent diabetes mellitus in general practice. Qual Health Care. 1999;8(1):6-15.
34. McColl A, Roderick P, Gabbay J, Smith H, Moore M. Performance indicators for pri-mary care groups: An evidence based approach. Br Med J 1998;317(7169):1354-1360.
35. Idanpaan-Heikkila UM, Lambie L, Mattke S, McLaughlin V, Palmer H, Tu JV. Selecting indicators for the quality of cardiac care at the health system level in Organization for Economic Co-operation and Development countries. Int J Qual Health Care. 2006;18(SUPPL. 1):39-44.
36. Cheng EM, Fung CH. Quality indicators for the care of stroke and atrial fibrillation in vulnerable elders. J Am Geriatr Soc. 2007;55(Suppl 2):S431-S437.
37. Asch SM, Kerr EA, Keesey J, Adams JL, Setodji CM, Malik S, McGlynn EA. Who is at greatest risk for receiving poor-quality health care? N Engl J Med. 2006;354(11):1147-1156.
38. Ashton CM, Kuykendall DH, Johnson ML, Wun CC, Wray NP, Carr MJ, Slater CH, Wu L, Bush GR. A method of developing and weighting explicit process of care criteria for quality assessment. Med Care. 1994;32(8):755-770.
39. Campbell SM, Ludt S, Van LJ, Boffin N, Wensing M, Petek D, Grol R, Roland MO. Quality indicators for the prevention and management of cardiovascular dis-ease in primary care in nine European countries. Eur J Cardiovasc Prev Rehabil. 2008;15(5):509-515.
103
Chapter 3.2 - Review on prescribing quality indicators
40. MacKinnon NJ, Hartnell NR, Black EK, Dunbar P, Johnson J, Pattar R, Ur E. Development of clinical indicators for type 2 diabetes. Canadian Pharmacists Journal. 2009;141(2):120-128.
41. Majumdar SR, Johnson JA, Bowker SL, Booth GL, Dolovich L, Ghali W, Harris SB, Hux JE, Holbrook A, Lee HN, Toth EL, Yale GF. A Canadian consensus for the standardized evaluation of quality improvement interventions in type 2 dia-betes. Canadian Journal of Diabetes. 2005;29(3):220-229.
42. Min LC, Mehrotra R, Fung CH. Quality indicators for the care of hypertension in vulnerable elders. J Am Geriatr Soc. 2007;55(Suppl 2):S359-S365.
43. Muijrers PE, Janknegt R, Sijbrandij J, Grol RP, Knottnerus JA. Prescribing indi-cators. Development and validation of guideline-based prescribing indicators as an instrument to measure the variation in the prescribing behaviour of general practitioners. Eur J Clin Pharmacol. 2004;60(10):739-746.
44. Shekelle PG, Vijan S. Quality indicators for the management of diabetes mellitus in vulnerable elders. JAGS. 2007;55:S312-S317.
45. Tu JV, Khalid L, Donovan LR, Ko DT. Indicators of quality of care for patients with acute myocardial infarction. CMAJ. 2008;179(9):909-915.
46. RAND HEALTH Quality of Care Assessment Tools; 2000. http://www.rand.org/health/surveys_tools/qatools/index.html(accessed 7 May 2009)
47. Garjon Parra FJ, Aller Blanco AI, Buisan Giral MJ, Elfau Mairal M, Celaya Lecea MC. Selection of quality indicators for primary care prescription through a con-sensus group. Aten Prim. 2006;38(1):39-44.
48. Milchak JL, Carter BL, Ardery G, Black HR, Bakris GL, Jones DW, Kreiter CD. Development of explicit criteria to measure adherence to hypertension guide-lines. J Hum Hypertens. 2006;20(6):426-433.
49. Katz A, Soodeen RA, Bogdanovic B, De Coster C, Chateau D. Can the quality of care in family practice be measured using administrative data? Health Serv Res. 2006;41(6):2238-2254.
50. Bateman DN, Eccles M, Campbell M, Soutter J, Roberts SJ, Smith JM. Setting standards of prescribing performance in primary care: use of a consensus group of general practitioners and application of standards to practices in the north of England. Br J Gen Pract. 1996;46(402):20-25.
51. Campbell SM, Hann M, Hacker J, Durie A, Thapar A, Roland MO. Quality as-sessment for three common conditions in primary care: validity and reliability of review criteria developed by expert panels for angina, asthma and type 2 diabe-tes. Qual Saf Health Care. 2002;11(2):125-130.
52. DiSalvo TG, Normand SLT, Hauptman PJ, Guadagnoli E, Palmer RH, McNeil BJ. Pitfalls in assessing the quality of care for patients with cardiovascular disease. Am J Med. 2001;111(4):297-303.
53. The Dutch Institute for Health Care Improvement (CBO) Indicatoren voor dia-betes als onderdeel van het ZonMw project ‘Kwaliteit van Zorg in de Etalage’ Registratiegids. http://www.cbo.nl (accessed 7 May 2009)
54. The National Quality Forum Clinical Performance Measures for Ambulatory Care. http://www.ahrq.gov (accessed 7 May 2009)
55. Solberg LI, Engebretson KI, Sperl-Hillen JM, O’Connor PJ, Hroscikoski MC,
104
Chapter 3.2 - Review on prescribing quality indicators
Crain AL. Ambulatory care quality measures for the 6 aims from administrative data. Am J Med Qual. 2006;21(5):310-316.
56. Guptha SH, Mittra R, Puthrasingam S, Johnson GM, Ellis CDW, Hill-Smith I, Jackson SHD. Application of evidence-based prescribing indicators in primary care: A pilot. Qual Prim Care. 2003;11(2):107-116.
57. Persell SD, Wright JM, Thompson JA, Kmetik KS, Baker DW. Assessing the va-lidity of national quality measures for coronary artery disease using an electronic health record. Arch Intern Med. 2006;166(20):2272-2277.
58. Gribben B, Coster G, Pringle M, Simon J. Quality of care indicators for population-based primary care in New Zealand. New Zealand Med J. 2002;115(1151):163-166.
59. McColl A, Roderick P, Smith H, Wilkinson E, Moore M, Exworthy M, Gabbay J. Clinical governance in primary care groups: The feasibility of deriving evidence-based performance indicators. Qual Health Care. 2000;9(2):90-97.
60. Wilkinson EK, McColl A, Exworthy M, Roderick P, Smith H, Moore M, Gabbay J. Reactions to the use of evidence-based performance indicators in primary care: A qualitative study. Qual Health Care. 2000;9(3):166-174.
61. Mehta RH, Liang L, Karve AM, Hernandez AF, Rumsfeld JS, Fonarow GC, Peterson ED. Association of patient case-mix adjustment, hospital process performance rankings, and eligibility for financial incentives. JAMA. 2008;300(16):1897-1903.
62. O’Brien SM, Delong ER, Peterson ED. Impact of case volume on hospital per-formance assessment. Arch Intern Med. 2008;168(12):1277-1284.
63. Pearson ML, Lee JL, Chang BL, Elliott M, Kahn KL, Rubenstein LV. Structured implicit review: a new method for monitoring nursing care quality. Med Care. 2000;38(11):1074-1091.
64. Voorham J, Denig P. Computerized extraction of information on the quality of diabetes care from free text in electronic patient records of general practitioners. J Am Med Inform Assoc. 2007;14(3):349-354.
65. Werner RM, Bradlow ET. Relationship between Medicare’s hospital compare performance measures and mortality rates. JAMA. 2006;296(22):2694-2702.
66. Jencks SF, Cuerdon T, Burwen DR, Fleming B, Houck PM, Kussmaul AE, Nilasena DS, Ordin DL, Arday DR. Quality of medical care delivered to Medicare beneficiaries: A profile at state and national levels. JAMA. 2000;284(13):1670-1676.
67. Torrecilla-Rojas MA, Pedregal-Gonzalez M, Caraballo-Camacho MO, Rodriguez-Papalardo V, Fernandez-Fernandez I. [Definition and validation of quality indica-tors of prescription in primary care]. Aten Primaria. 2006;37(5):273-277.
68. Voorham J, Denig P, Wolffenbuttel BHR, Haaijer-Ruskamp FM. Cross-sectional versus sequential quality indicators of risk factor management in patients with type 2 diabetes. Med Care. 2008;46(2):133-141.
69. Landon BE, Normand SLT. National Voluntary Consensus Standards for Ambulatory Care: Measurement Challenges in Small Group Settings. 2006.
70. The National Quality Forum National Voluntary Consensus Standards for Adult Diabetes Care: 2005 Update. http://www. qualityforum. org/publications/reports/diabetes_update. asp (accessed 7 May 2009).
105
Chapter 3.2 - Review on prescribing quality indicators
71. Turchin A, Kolatkar NS, Grant RW, Makhni EC, Pendergrass ML, Einbinder JS. Using regular expressions to abstract blood pressure and treatment intensifi-cation information from the text of physician notes. J Am Med Inform Assoc. 2006;13(6):691-695.
72. Luck J, Peabody JW, Dresselhaus TR, Lee M, Glassman P. How well does chart abstraction measure quality? A prospective comparison of standardized patients with the medical record. Am J Med. 2000;108(8):642-649.
73. Bird CE, Fremont A, Wickstrom S, Bierman AS, McGlynn E. Improving women’s quality of care for cardiovascular disease and diabetes: the feasibility and desir-ability of stratified reporting of objective performance measures. Womens Health Issues. 2003;13(4):150-157.
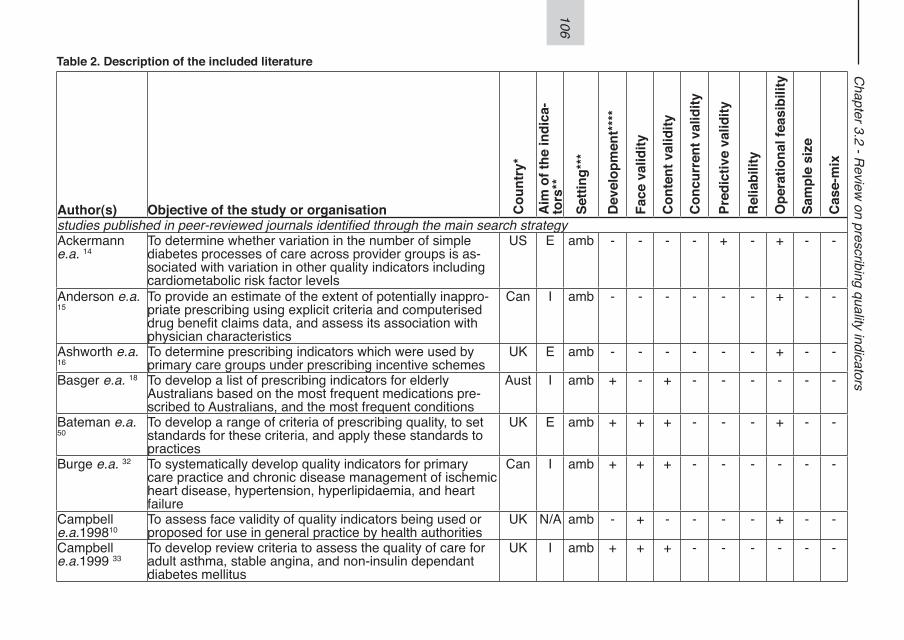
106
Chapter 3.2 - R
eview on prescribing quality indicators
Table 2. Description of the included literature
Author(s) Objective of the study or organisation Cou
ntry
*
Aim
of t
he in
dica
-to
rs**
Setti
ng**
*
Dev
elop
men
t***
*
Face
val
idity
Con
tent
val
idity
Con
curr
ent v
alid
ity
Pred
ictiv
e va
lidity
Rel
iabi
lity
Ope
ratio
nal f
easi
bilit
y
Sam
ple
size
Cas
e-m
ix
studies published in peer-reviewed journals identified through the main search strategyAckermann e.a. 14
To determine whether variation in the number of simple diabetes processes of care across provider groups is as-sociated with variation in other quality indicators including cardiometabolic risk factor levels
US E amb - - - - + - + - -
Anderson e.a. 15
To provide an estimate of the extent of potentially inappro-priate prescribing using explicit criteria and computerised drug benefit claims data, and assess its association with physician characteristics
Can I amb - - - - - - + - -
Ashworth e.a. 16
To determine prescribing indicators which were used by primary care groups under prescribing incentive schemes
UK E amb - - - - - - + - -
Basger e.a. 18 To develop a list of prescribing indicators for elderly Australians based on the most frequent medications pre-scribed to Australians, and the most frequent conditions
Aust I amb + - + - - - - - -
Bateman e.a. 50
To develop a range of criteria of prescribing quality, to set standards for these criteria, and apply these standards to practices
UK E amb + + + - - - + - -
Burge e.a. 32 To systematically develop quality indicators for primary care practice and chronic disease management of ischemic heart disease, hypertension, hyperlipidaemia, and heart failure
Can I amb + + + - - - - - -
Campbell e.a.199810
To assess face validity of quality indicators being used or proposed for use in general practice by health authorities
UK N/A amb - + - - - - + - -
Campbell e.a.1999 33
To develop review criteria to assess the quality of care for adult asthma, stable angina, and non-insulin dependant diabetes mellitus
UK I amb + + + - - - - - -
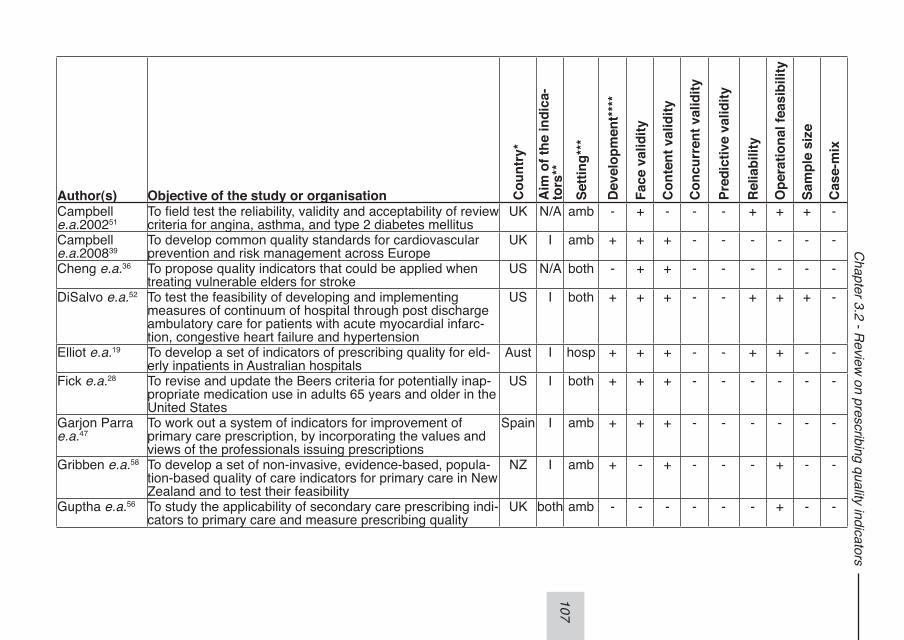
107
Chapter 3.2 - R
eview on prescribing quality indicators
Author(s) Objective of the study or organisation Cou
ntry
*
Aim
of t
he in
dica
-to
rs**
Setti
ng**
*
Dev
elop
men
t***
*
Face
val
idity
Con
tent
val
idity
Con
curr
ent v
alid
ity
Pred
ictiv
e va
lidity
Rel
iabi
lity
Ope
ratio
nal f
easi
bilit
y
Sam
ple
size
Cas
e-m
ix
Campbell e.a.200251
To field test the reliability, validity and acceptability of review criteria for angina, asthma, and type 2 diabetes mellitus
UK N/A amb - + - - - + + + -
Campbell e.a.200839
To develop common quality standards for cardiovascular prevention and risk management across Europe
UK I amb + + + - - - - - -
Cheng e.a.36 To propose quality indicators that could be applied when treating vulnerable elders for stroke
US N/A both - + + - - - - - -
DiSalvo e.a.52 To test the feasibility of developing and implementing measures of continuum of hospital through post discharge ambulatory care for patients with acute myocardial infarc-tion, congestive heart failure and hypertension
US I both + + + - - + + + -
Elliot e.a.19 To develop a set of indicators of prescribing quality for eld-erly inpatients in Australian hospitals
Aust I hosp + + + - - + + - -
Fick e.a.28 To revise and update the Beers criteria for potentially inap-propriate medication use in adults 65 years and older in the United States
US I both + + + - - - - - -
Garjon Parra e.a.47
To work out a system of indicators for improvement of primary care prescription, by incorporating the values and views of the professionals issuing prescriptions
Spain I amb + + + - - - - - -
Gribben e.a.58 To develop a set of non-invasive, evidence-based, popula-tion-based quality of care indicators for primary care in New Zealand and to test their feasibility
NZ I amb + - + - - - + - -
Guptha e.a.56 To study the applicability of secondary care prescribing indi-cators to primary care and measure prescribing quality
UK both amb - - - - - - + - -
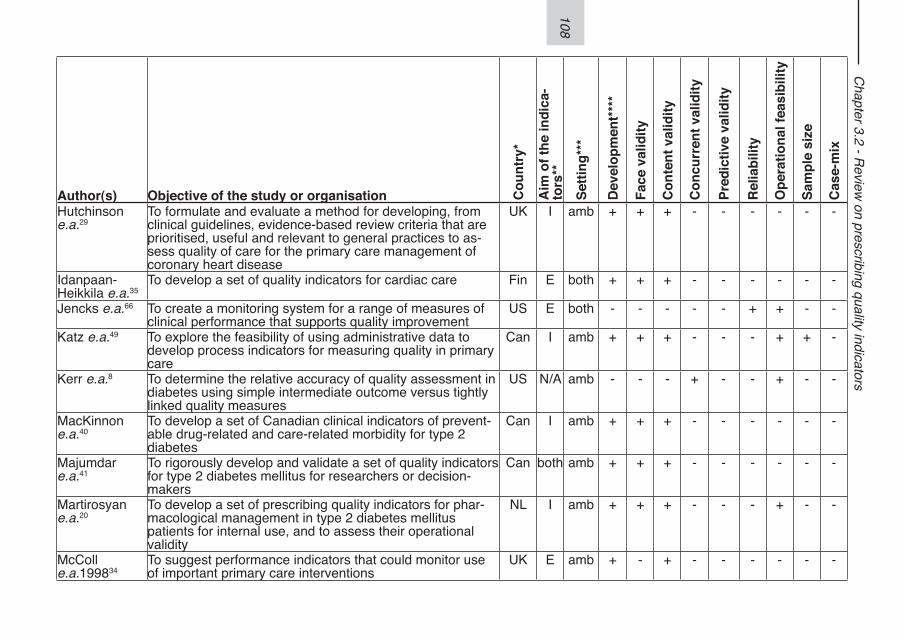
108
Chapter 3.2 - R
eview on prescribing quality indicators
Author(s) Objective of the study or organisation Cou
ntry
*
Aim
of t
he in
dica
-to
rs**
Setti
ng**
*
Dev
elop
men
t***
*
Face
val
idity
Con
tent
val
idity
Con
curr
ent v
alid
ity
Pred
ictiv
e va
lidity
Rel
iabi
lity
Ope
ratio
nal f
easi
bilit
y
Sam
ple
size
Cas
e-m
ix
Hutchinson e.a.29
To formulate and evaluate a method for developing, from clinical guidelines, evidence-based review criteria that are prioritised, useful and relevant to general practices to as-sess quality of care for the primary care management of coronary heart disease
UK I amb + + + - - - - - -
Idanpaan-Heikkila e.a.35
To develop a set of quality indicators for cardiac care Fin E both + + + - - - - - -
Jencks e.a.66 To create a monitoring system for a range of measures of clinical performance that supports quality improvement
US E both - - - - - + + - -
Katz e.a.49 To explore the feasibility of using administrative data to develop process indicators for measuring quality in primary care
Can I amb + + + - - - + + -
Kerr e.a.8 To determine the relative accuracy of quality assessment in diabetes using simple intermediate outcome versus tightly linked quality measures
US N/A amb - - - + - - + - -
MacKinnon e.a.40
To develop a set of Canadian clinical indicators of prevent-able drug-related and care-related morbidity for type 2 diabetes
Can I amb + + + - - - - - -
Majumdar e.a.41
To rigorously develop and validate a set of quality indicators for type 2 diabetes mellitus for researchers or decision-makers
Can both amb + + + - - - - - -
Martirosyan e.a.20
To develop a set of prescribing quality indicators for phar-macological management in type 2 diabetes mellitus patients for internal use, and to assess their operational validity
NL I amb + + + - - - + - -
McColl e.a.199834
To suggest performance indicators that could monitor use of important primary care interventions
UK E amb + - + - - - - - -
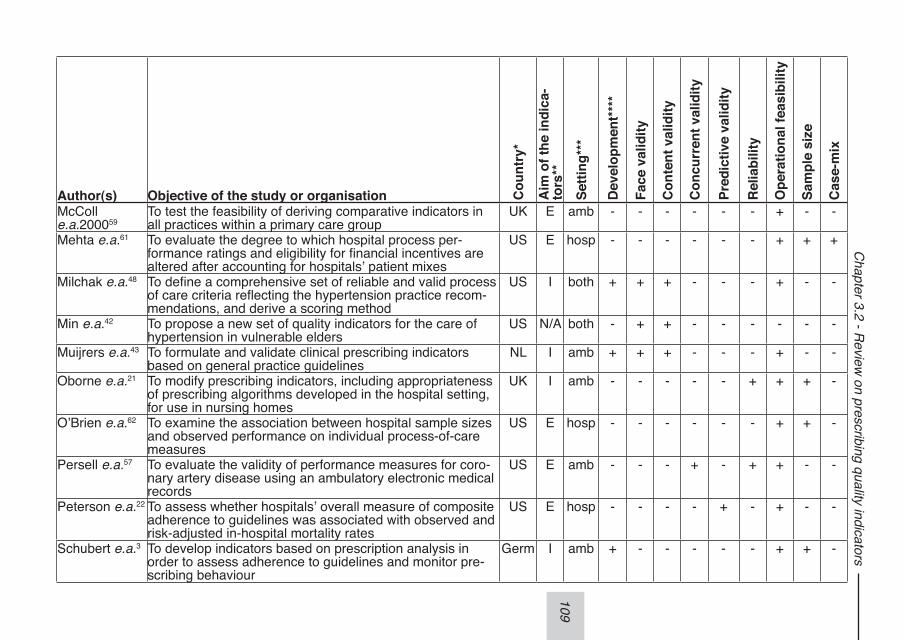
109
Chapter 3.2 - R
eview on prescribing quality indicators
Author(s) Objective of the study or organisation Cou
ntry
*
Aim
of t
he in
dica
-to
rs**
Setti
ng**
*
Dev
elop
men
t***
*
Face
val
idity
Con
tent
val
idity
Con
curr
ent v
alid
ity
Pred
ictiv
e va
lidity
Rel
iabi
lity
Ope
ratio
nal f
easi
bilit
y
Sam
ple
size
Cas
e-m
ix
McColl e.a.200059
To test the feasibility of deriving comparative indicators in all practices within a primary care group
UK E amb - - - - - - + - -
Mehta e.a.61 To evaluate the degree to which hospital process per-formance ratings and eligibility for financial incentives are altered after accounting for hospitals’ patient mixes
US E hosp - - - - - - + + +
Milchak e.a.48 To define a comprehensive set of reliable and valid process of care criteria reflecting the hypertension practice recom-mendations, and derive a scoring method
US I both + + + - - - + - -
Min e.a.42 To propose a new set of quality indicators for the care of hypertension in vulnerable elders
US N/A both - + + - - - - - -
Muijrers e.a.43 To formulate and validate clinical prescribing indicators based on general practice guidelines
NL I amb + + + - - - + - -
Oborne e.a.21 To modify prescribing indicators, including appropriateness of prescribing algorithms developed in the hospital setting, for use in nursing homes
UK I amb - - - - - + + + -
O’Brien e.a.62 To examine the association between hospital sample sizes and observed performance on individual process-of-care measures
US E hosp - - - - - - + + -
Persell e.a.57 To evaluate the validity of performance measures for coro-nary artery disease using an ambulatory electronic medical records
US E amb - - - + - + + - -
Peterson e.a.22 To assess whether hospitals’ overall measure of composite adherence to guidelines was associated with observed and risk-adjusted in-hospital mortality rates
US E hosp - - - - + - + - -
Schubert e.a.3 To develop indicators based on prescription analysis in order to assess adherence to guidelines and monitor pre-scribing behaviour
Germ I amb + - - - - - + + -
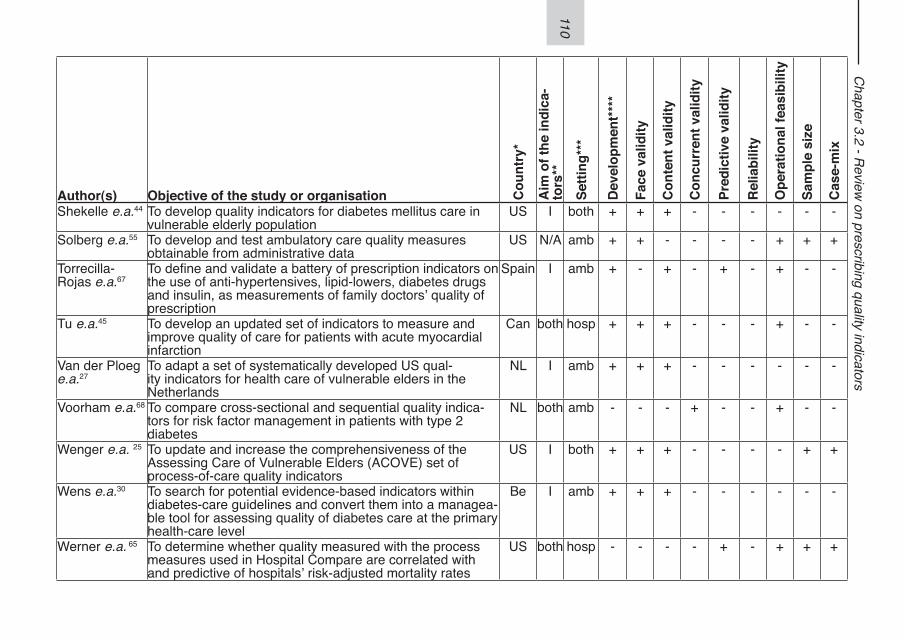
110
Chapter 3.2 - R
eview on prescribing quality indicators
Author(s) Objective of the study or organisation Cou
ntry
*
Aim
of t
he in
dica
-to
rs**
Setti
ng**
*
Dev
elop
men
t***
*
Face
val
idity
Con
tent
val
idity
Con
curr
ent v
alid
ity
Pred
ictiv
e va
lidity
Rel
iabi
lity
Ope
ratio
nal f
easi
bilit
y
Sam
ple
size
Cas
e-m
ix
Shekelle e.a.44 To develop quality indicators for diabetes mellitus care in vulnerable elderly population
US I both + + + - - - - - -
Solberg e.a.55 To develop and test ambulatory care quality measures obtainable from administrative data
US N/A amb + + - - - - + + +
Torrecilla-Rojas e.a.67
To define and validate a battery of prescription indicators on the use of anti-hypertensives, lipid-lowers, diabetes drugs and insulin, as measurements of family doctors’ quality of prescription
Spain I amb + - + - + - + - -
Tu e.a.45 To develop an updated set of indicators to measure and improve quality of care for patients with acute myocardial infarction
Can both hosp + + + - - - + - -
Van der Ploeg e.a.27
To adapt a set of systematically developed US qual-ity indicators for health care of vulnerable elders in the Netherlands
NL I amb + + + - - - - - -
Voorham e.a.68 To compare cross-sectional and sequential quality indica-tors for risk factor management in patients with type 2 diabetes
NL both amb - - - + - - + - -
Wenger e.a. 25 To update and increase the comprehensiveness of the Assessing Care of Vulnerable Elders (ACOVE) set of process-of-care quality indicators
US I both + + + - - - - + +
Wens e.a.30 To search for potential evidence-based indicators within diabetes-care guidelines and convert them into a managea-ble tool for assessing quality of diabetes care at the primary health-care level
Be I amb + + + - - - - - -
Werner e.a. 65 To determine whether quality measured with the process measures used in Hospital Compare are correlated with and predictive of hospitals’ risk-adjusted mortality rates
US both hosp - - - - + - + + +
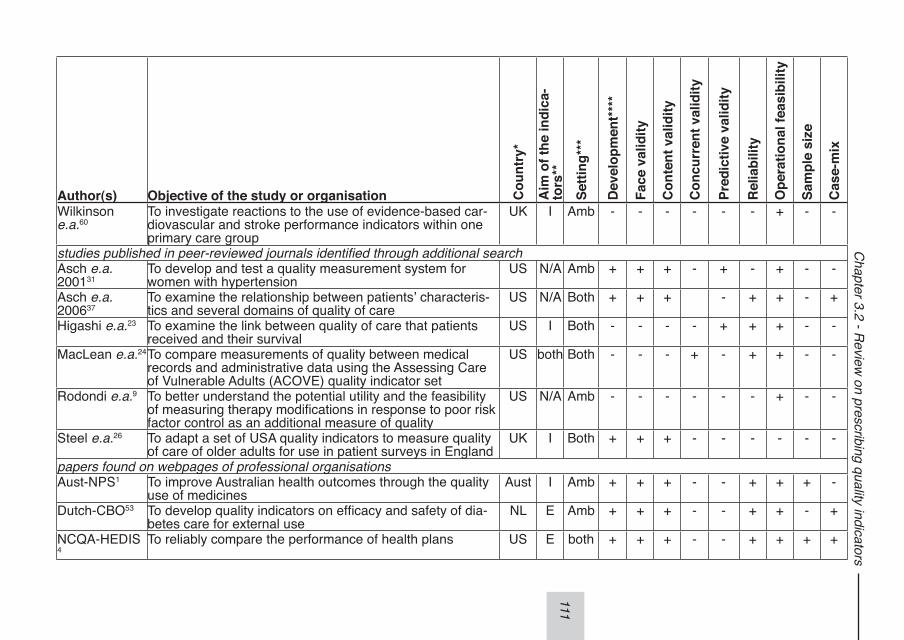
111
Chapter 3.2 - R
eview on prescribing quality indicators
Author(s) Objective of the study or organisation Cou
ntry
*
Aim
of t
he in
dica
-to
rs**
Setti
ng**
*
Dev
elop
men
t***
*
Face
val
idity
Con
tent
val
idity
Con
curr
ent v
alid
ity
Pred
ictiv
e va
lidity
Rel
iabi
lity
Ope
ratio
nal f
easi
bilit
y
Sam
ple
size
Cas
e-m
ix
Wilkinson e.a.60
To investigate reactions to the use of evidence-based car-diovascular and stroke performance indicators within one primary care group
UK I Amb - - - - - - + - -
studies published in peer-reviewed journals identified through additional searchAsch e.a. 200131
To develop and test a quality measurement system for women with hypertension
US N/A Amb + + + - + - + - -
Asch e.a. 200637
To examine the relationship between patients’ characteris-tics and several domains of quality of care
US N/A Both + + + - + + - +
Higashi e.a.23 To examine the link between quality of care that patients received and their survival
US I Both - - - - + + + - -
MacLean e.a.24To compare measurements of quality between medical records and administrative data using the Assessing Care of Vulnerable Adults (ACOVE) quality indicator set
US both Both - - - + - + + - -
Rodondi e.a.9 To better understand the potential utility and the feasibility of measuring therapy modifications in response to poor risk factor control as an additional measure of quality
US N/A Amb - - - - - - + - -
Steel e.a.26 To adapt a set of USA quality indicators to measure quality of care of older adults for use in patient surveys in England
UK I Both + + + - - - - - -
papers found on webpages of professional organisationsAust-NPS1 To improve Australian health outcomes through the quality
use of medicinesAust I Amb + + + - - + + + -
Dutch-CBO53 To develop quality indicators on efficacy and safety of dia-betes care for external use
NL E Amb + + + - - + + - +
NCQA-HEDIS 4
To reliably compare the performance of health plans US E both + + + - - + + + +
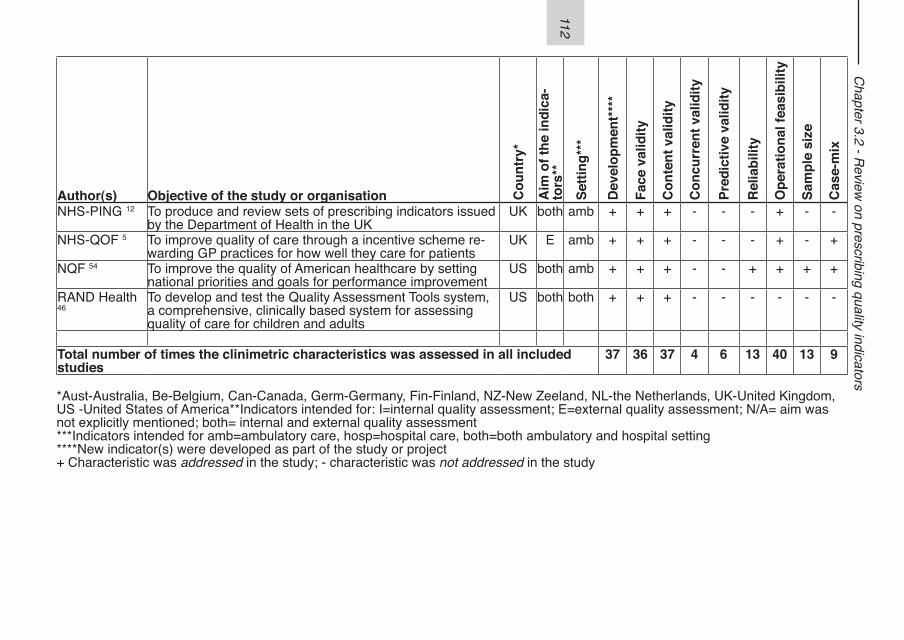
112
Chapter 3.2 - R
eview on prescribing quality indicators
Author(s) Objective of the study or organisation Cou
ntry
*
Aim
of t
he in
dica
-to
rs**
Setti
ng**
*
Dev
elop
men
t***
*
Face
val
idity
Con
tent
val
idity
Con
curr
ent v
alid
ity
Pred
ictiv
e va
lidity
Rel
iabi
lity
Ope
ratio
nal f
easi
bilit
y
Sam
ple
size
Cas
e-m
ix
NHS-PING 12 To produce and review sets of prescribing indicators issued by the Department of Health in the UK
UK both amb + + + - - - + - -
NHS-QOF 5 To improve quality of care through a incentive scheme re-warding GP practices for how well they care for patients
UK E amb + + + - - - + - +
NQF 54 To improve the quality of American healthcare by setting national priorities and goals for performance improvement
US both amb + + + - - + + + +
RAND Health 46
To develop and test the Quality Assessment Tools system, a comprehensive, clinically based system for assessing quality of care for children and adults
US both both + + + - - - - - -
Total number of times the clinimetric characteristics was assessed in all included studies
37 36 37 4 6 13 40 13 9
*Aust-Australia, Be-Belgium, Can-Canada, Germ-Germany, Fin-Finland, NZ-New Zeeland, NL-the Netherlands, UK-United Kingdom, US -United States of America**Indicators intended for: I=internal quality assessment; E=external quality assessment; N/A= aim was not explicitly mentioned; both= internal and external quality assessment***Indicators intended for amb=ambulatory care, hosp=hospital care, both=both ambulatory and hospital setting****New indicator(s) were developed as part of the study or project+ Characteristic was addressed in the study; - characteristic was not addressed in the study
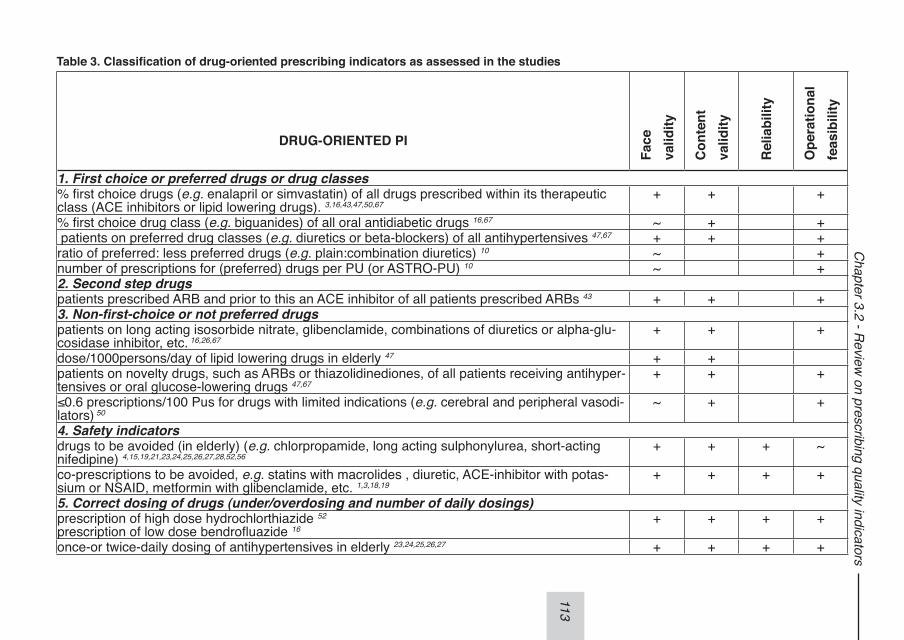
113
Chapter 3.2 - R
eview on prescribing quality indicators
Table 3. Classification of drug-oriented prescribing indicators as assessed in the studies
DRUG-ORIENTED PI
Face
valid
ity
Con
tent
valid
ity
Rel
iabi
lity
Ope
ratio
nal
feas
ibili
ty
1. First choice or preferred drugs or drug classes% first choice drugs (e.g. enalapril or simvastatin) of all drugs prescribed within its therapeutic class (ACE inhibitors or lipid lowering drugs). 3,16,43,47,50,67
+ + +
% first choice drug class (e.g. biguanides) of all oral antidiabetic drugs 16,67 ~ + + patients on preferred drug classes (e.g. diuretics or beta-blockers) of all antihypertensives 47,67 + + +ratio of preferred: less preferred drugs (e.g. plain:combination diuretics) 10 ~ +number of prescriptions for (preferred) drugs per PU (or ASTRO-PU) 10 ~ +2. Second step drugspatients prescribed ARB and prior to this an ACE inhibitor of all patients prescribed ARBs 43 + + +3. Non-first-choice or not preferred drugspatients on long acting isosorbide nitrate, glibenclamide, combinations of diuretics or alpha-glu-cosidase inhibitor, etc. 16,26,67
+ + +
dose/1000persons/day of lipid lowering drugs in elderly 47 + +patients on novelty drugs, such as ARBs or thiazolidinediones, of all patients receiving antihyper-tensives or oral glucose-lowering drugs 47,67
+ + +
≤0.6 prescriptions/100 Pus for drugs with limited indications (e.g. cerebral and peripheral vasodi-lators) 50
~ + +
4. Safety indicatorsdrugs to be avoided (in elderly) (e.g. chlorpropamide, long acting sulphonylurea, short-acting nifedipine) 4,15,19,21,23,24,25,26,27,28,52,56
+ + + ~
co-prescriptions to be avoided, e.g. statins with macrolides , diuretic, ACE-inhibitor with potas-sium or NSAID, metformin with glibenclamide, etc. 1,3,18,19
+ + + +
5. Correct dosing of drugs (under/overdosing and number of daily dosings)prescription of high dose hydrochlorthiazide 52
prescription of low dose bendrofluazide 16 + + + +
once-or twice-daily dosing of antihypertensives in elderly 23,24,25,26,27 + + + +
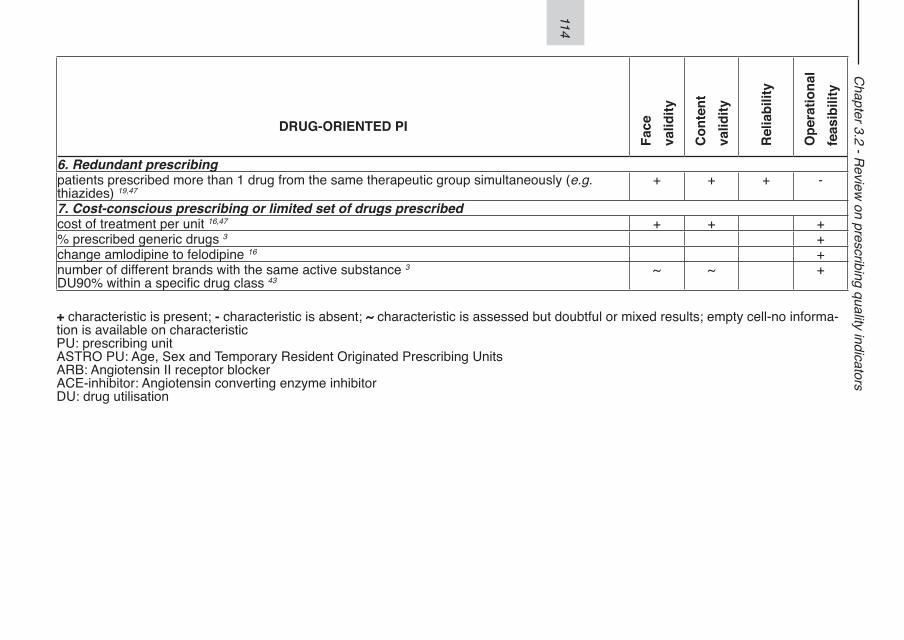
114
Chapter 3.2 - R
eview on prescribing quality indicators
DRUG-ORIENTED PI
Face
valid
ity
Con
tent
valid
ity
Rel
iabi
lity
Ope
ratio
nal
feas
ibili
ty
6. Redundant prescribingpatients prescribed more than 1 drug from the same therapeutic group simultaneously (e.g. thiazides) 19,47
+ + + -
7. Cost-conscious prescribing or limited set of drugs prescribedcost of treatment per unit 16,47 + + +% prescribed generic drugs 3 +change amlodipine to felodipine 16 +number of different brands with the same active substance 3
DU90% within a specific drug class 43 ~ ~ +
+ characteristic is present; - characteristic is absent; ~ characteristic is assessed but doubtful or mixed results; empty cell-no informa-tion is available on characteristicPU: prescribing unitASTRO PU: Age, Sex and Temporary Resident Originated Prescribing UnitsARB: Angiotensin II receptor blockerACE-inhibitor: Angiotensin converting enzyme inhibitorDU: drug utilisation
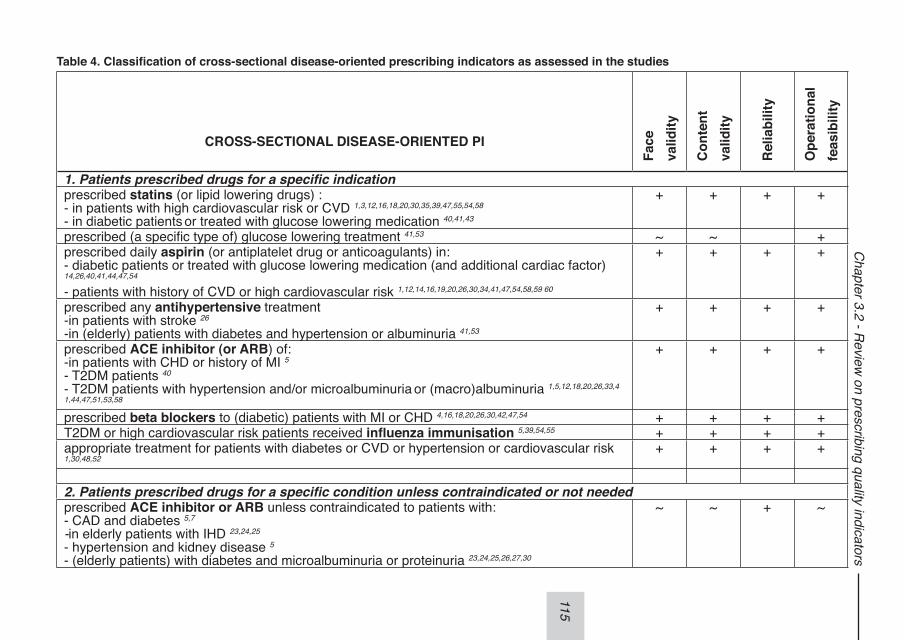
115
Chapter 3.2 - R
eview on prescribing quality indicators
Table 4. Classification of cross-sectional disease-oriented prescribing indicators as assessed in the studies
CROSS-SECTIONAL DISEASE-ORIENTED PI
Face
valid
ity
Con
tent
valid
ity
Rel
iabi
lity
Ope
ratio
nal
feas
ibili
ty
1. Patients prescribed drugs for a specific indication prescribed statins (or lipid lowering drugs) : - in patients with high cardiovascular risk or CVD 1,3,12,16,18,20,30,35,39,47,55,54,58
- in diabetic patients or treated with glucose lowering medication 40,41,43
+ + + +
prescribed (a specific type of) glucose lowering treatment 41,53 ~ ~ +prescribed daily aspirin (or antiplatelet drug or anticoagulants) in:- diabetic patients or treated with glucose lowering medication (and additional cardiac factor) 14,26,40,41,44,47,54 - patients with history of CVD or high cardiovascular risk 1,12,14,16,19,20,26,30,34,41,47,54,58,59 60
+ + + +
prescribed any antihypertensive treatment -in patients with stroke 26
-in (elderly) patients with diabetes and hypertension or albuminuria 41,53
+ + + +
prescribed ACE inhibitor (or ARB) of:-in patients with CHD or history of MI 5
- T2DM patients 40
- T2DM patients with hypertension and/or microalbuminuria or (macro)albuminuria 1,5,12,18,20,26,33,41,44,47,51,53,58
+ + + +
prescribed beta blockers to (diabetic) patients with MI or CHD 4,16,18,20,26,30,42,47,54 + + + +T2DM or high cardiovascular risk patients received influenza immunisation 5,39,54,55 + + + +appropriate treatment for patients with diabetes or CVD or hypertension or cardiovascular risk 1,30,48,52
+ + + +
2. Patients prescribed drugs for a specific condition unless contraindicated or not neededprescribed ACE inhibitor or ARB unless contraindicated to patients with: - CAD and diabetes 5,7 -in elderly patients with IHD 23,24,25
- hypertension and kidney disease 5
- (elderly patients) with diabetes and microalbuminuria or proteinuria 23,24,25,26,27,30
~ ~ + ~
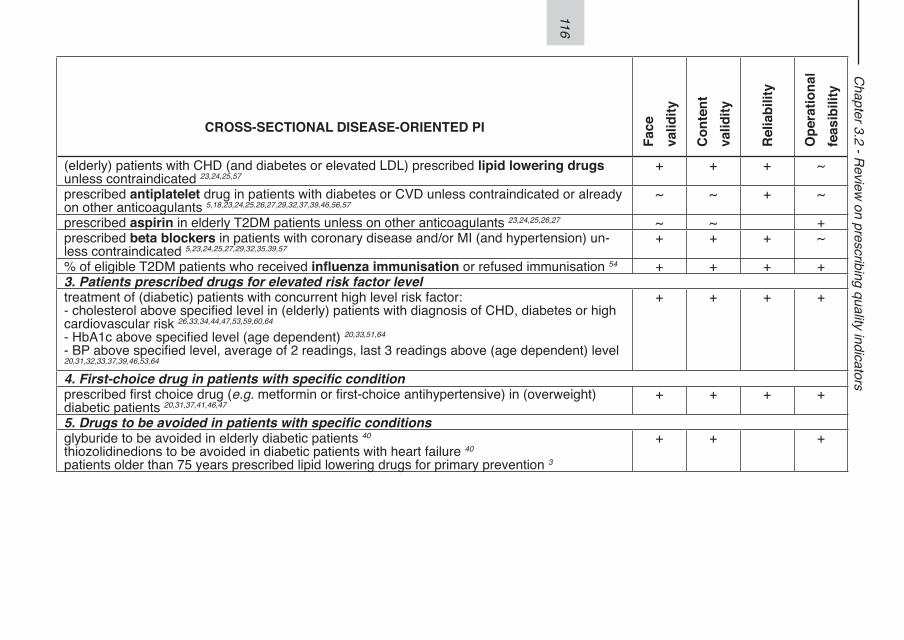
116
Chapter 3.2 - R
eview on prescribing quality indicators
CROSS-SECTIONAL DISEASE-ORIENTED PI
Face
valid
ity
Con
tent
valid
ity
Rel
iabi
lity
Ope
ratio
nal
feas
ibili
ty
(elderly) patients with CHD (and diabetes or elevated LDL) prescribed lipid lowering drugs unless contraindicated 23,24,25,57
+ + + ~
prescribed antiplatelet drug in patients with diabetes or CVD unless contraindicated or already on other anticoagulants 5,18,23,24,25,26,27,29,32,37,39,46,56,57
~ ~ + ~
prescribed aspirin in elderly T2DM patients unless on other anticoagulants 23,24,25,26,27 ~ ~ +prescribed beta blockers in patients with coronary disease and/or MI (and hypertension) un-less contraindicated 5,23,24,25,27,29,32,35,39,57
+ + + ~
% of eligible T2DM patients who received influenza immunisation or refused immunisation 54 + + + +3. Patients prescribed drugs for elevated risk factor leveltreatment of (diabetic) patients with concurrent high level risk factor: - cholesterol above specified level in (elderly) patients with diagnosis of CHD, diabetes or high cardiovascular risk 26,33,34,44,47,53,59,60,64
- HbA1c above specified level (age dependent) 20,33,51,64
- BP above specified level, average of 2 readings, last 3 readings above (age dependent) level 20,31,32,33,37,39,46,53,64
+ + + +
4. First-choice drug in patients with specific conditionprescribed first choice drug (e.g. metformin or first-choice antihypertensive) in (overweight) diabetic patients 20,31,37,41,46,47
+ + + +
5. Drugs to be avoided in patients with specific conditionsglyburide to be avoided in elderly diabetic patients 40
thiozolidinedions to be avoided in diabetic patients with heart failure 40
patients older than 75 years prescribed lipid lowering drugs for primary prevention 3
+ + +
117
Chapter 3.2 - R
eview on prescribing quality indicators
+ characteristic is present; - characteristic is absent; ~ characteristic is assessed but doubtful or mixed results; empty cell-no informa-tion is available on characteristicCVD: cardiovascular diseaseCHD: coronary heart diseaseMI: myocardial infarctionT2DM: type 2 diabetes mellitusHbA1c: glycosylated haemoglobinBP: blood pressureARB: Angiotensin II receptor blockerACE-inhibitor: Angiotensin converting enzyme inhibitorLDL: low density lipoprotein
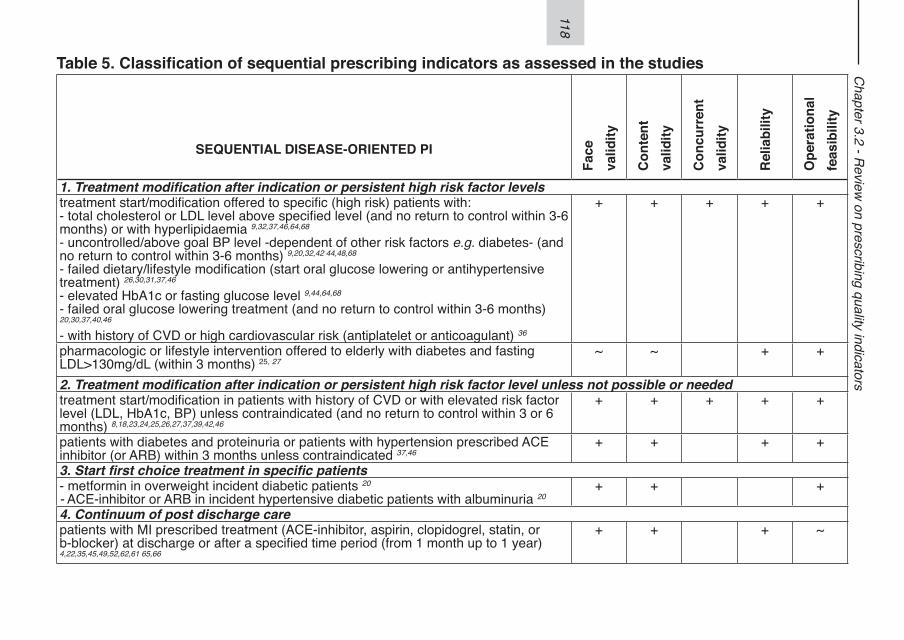
118
Chapter 3.2 - R
eview on prescribing quality indicators
Table 5. Classification of sequential prescribing indicators as assessed in the studies
SEQUENTIAL DISEASE-ORIENTED PI
Face
valid
ity
Con
tent
valid
ity
Con
curr
ent
valid
ity
Rel
iabi
lity
Ope
ratio
nal
feas
ibili
ty
1. Treatment modification after indication or persistent high risk factor levelstreatment start/modification offered to specific (high risk) patients with: - total cholesterol or LDL level above specified level (and no return to control within 3-6 months) or with hyperlipidaemia 9,32,37,46,64,68
- uncontrolled/above goal BP level -dependent of other risk factors e.g. diabetes- (and no return to control within 3-6 months) 9,20,32,42 44,48,68
- failed dietary/lifestyle modification (start oral glucose lowering or antihypertensive treatment) 26,30,31,37,46
- elevated HbA1c or fasting glucose level 9,44,64,68
- failed oral glucose lowering treatment (and no return to control within 3-6 months) 20,30,37,40,46
- with history of CVD or high cardiovascular risk (antiplatelet or anticoagulant) 36
+ + + + +
pharmacologic or lifestyle intervention offered to elderly with diabetes and fasting LDL>130mg/dL (within 3 months) 25, 27
~ ~ + +
2. Treatment modification after indication or persistent high risk factor level unless not possible or neededtreatment start/modification in patients with history of CVD or with elevated risk factor level (LDL, HbA1c, BP) unless contraindicated (and no return to control within 3 or 6 months) 8,18,23,24,25,26,27,37,39,42,46
+ + + + +
patients with diabetes and proteinuria or patients with hypertension prescribed ACE inhibitor (or ARB) within 3 months unless contraindicated 37,46
+ + + +
3. Start first choice treatment in specific patients- metformin in overweight incident diabetic patients 20
- ACE-inhibitor or ARB in incident hypertensive diabetic patients with albuminuria 20+ + +
4. Continuum of post discharge care patients with MI prescribed treatment (ACE-inhibitor, aspirin, clopidogrel, statin, or b-blocker) at discharge or after a specified time period (from 1 month up to 1 year) 4,22,35,45,49,52,62,61 65,66
+ + + ~
119
Chapter 3.2 - R
eview on prescribing quality indicators
+ characteristic is present; - characteristic is absent; ~ characteristic is assessed but doubtful or mixed results; empty cell-no informa-tion is available on characteristicBP: blood pressureHbA1c: glycosylated haemoglobinCVD: cardiovascular diseaseLDL: low density lipoproteinT2DM: type2 diabetes mellitusMI: myocardial infarctionACE-inhibitor: Angiotensin converting enzyme inhibitorARB: Angiotensin II receptor blocker
120
Chapter 3.2 - Review on prescribing quality indicators
APPENDIX 1 SYSTEMATIC SEARCH STRATEGY
Search strategy using embase.com (combined search in Embase and Medline)
1. (EMTREE terms: health care quality OR quality control) AND EMTREE terms: coronary artery atherosclerosis OR cardiovascular disease OR diabetes mellitus OR non insulin dependent diabetes mellitus OR ischem-ic heart disease OR heart infarction OR hypertension OR angina pectoris OR hyperlipidaemia OR chronic disease OR general practice OR primary health care OR general practitionerAND (Title words: (quality AND measure*) OR (quality AND assess*) OR indica-tor* OR perform* OR criteria OR profile*)
2. (EMTREE terms drug utilisation OR prescription)AND (Title words: (quality AND measure*) OR (quality AND assess*) OR indica-tor* OR perform* OR criteria OR profile*)
3. 1 OR 2, for time period from 1990 till January 2009
121
122
123
Chapter 3.3 - Identifying targets to improve treatment in type 2 diabetes:
the Groningen Initiative to aNalyse Type 2 diabetes Treatment (GIANTT)
observational study 2004-2007
Jaco Voorham1,2
Flora M Haaijer-Ruskamp1
Klaas van der Meer3
Dick de Zeeuw1
Bruce HR Wolffenbuttel4
Klaas Hoogenberg5
Petra Denig1
1. Department of Clinical Pharmacology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
2. Department of Epidemiology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
3 Department of General Practice, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
4. Department of Endocrinology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
5 Department of Endocrinology, Martini Hospital, Groningen
Voorham J, Haaijer-Ruskamp FM, van der Meer K, de Zeeuw D, Wolffenbuttel BHR, Hoogenberg K, Denig P. Kwaliteit van behandeling van type 2 diabetes - resultaten van het GIANTT project 2004-2007. Ned Tijdschr Geneeskd. 2010;154:A775.Voorham J, Haaijer-Ruskamp FM, van der Meer K, de Zeeuw D, Wolffenbuttel BHR, Hoogenberg K, Denig P, on behalf of the GIANTT-group Identifying targets to im-prove treatment in type 2 diabetes: the Groningen Initiative to aNalyse Type 2 diabe-tes Treatment (GIANTT) observational study 2004-2007. Submitted.
124
Chapter 3.3 - GIANTT observational study 2004-2007
ABSTRACTAim. Assessment of quality of cardiometabolic risk management in diabetes at the primary care level (2004-2007). Design. Descriptive cohort study. Methods. Using data collected from 124 Dutch general practitioners from the north-ern region, we assessed the medication treatment level in relation to the level of control for HbA1c, systolic blood pressure (SBP) and LDL-cholesterol (LDL-c). Furthermore, we applied a prospective measure of treatment quality by assessing treatment modifications in insufficiently controlled patients.Results. Data were available for 9,646 patients in 2007. The averages for respective-ly HbA1c, SBP and LDL-c were 6.9%, 142mmHg and 2.3mmol/l. Of the patients with an HbA1c>8.5%, 16% were treated with one oral drug and 50% used insulin. In 27% of these patients, therapy modification occurred subsequently. During the 4-year period, a slight decrease in average HbA1c was observed, but no changes in treat-ment level. Over half (56%) of the patients had an SBP≥140mmHg, 19% of whom were not using antihypertensive drugs. In the 13% with a SBP>160mmHg, a quarter (23%) received a therapy modification. During the 4-year period, the average SBP decreased with 6mmHg, but the treatment level showed no substantial increase. For LDL-c, 39% had a level ≥2.5mmol/l, 49% of whom were not using statins. Of the patients with an LDL-c>3.5 mmol/l, only 9% received a therapy modification. Conclusions. The decreasing population averages of HbA1c, SBP and LDL-c values suggest improvement in quality of care. However, the relatively few therapy modifi-cations observed in insufficiently controlled patients shows room for improvement.
125
Chapter 3.3 - GIANTT observational study 2004-2007
INTRODUCTIONCardiovascular risk factor levels in primary care patients with type 2 diabetes appear to have decreased during the period 1999-2006 in The Netherlands.1 It is not clear to what extent this reflects improved quality of care. Quality of care is not necessar-ily shown by measuring population averages of risk factor levels. In general, qual-ity of care is usually assessed by a mixture of process and outcome indicators.2-8 Process indicators focus on performed actions of health care providers, such as the measurement and registration of HbA1c or other recommended tests. Outcome indicators focus on clinical results, such as the percentage of patients who achieved a target HbA1c level. In quality assessments, there is remarkably little attention to how health care providers react to observed test results. This aspect of the medi-cal process can be assessed using treatment indicators. The most commonly used treatment indicators measure whether patients are on recommended medication or not. This provides a limited view on the quality of care. Assessing the rate of starting or intensifying treatment in suboptimally controlled patients provides additional valu-able information.9-11
To improve the quality of diabetes care, many (regional) projects have started in various countries. which monitor the process and outcomes of care. These projects, such as the Groningen Initiative to aNalyse Type 2 diabetes Treatment (GIANTT),12 enable the analysis of trends in quality of care and risk management in primary care. Our aim was to assess diabetes care quality for the risk factors HbA1c, systolic blood pressure (SBP) and LDL-cholesterol with special attention to quality of treatment. To provide more insight in actions taken in patients with suboptimal risk factor control, we assessed not only commonly used process and outcome measures but also new indicators that measure modifications of medical treatment in relation to the level of control. In a subpopulation, we studied how the results of these quality indicators evolved from 2004 to 2007.
METHODS
Study population and settingFor the first part of this observational study, we used data from the 95 general prac-tices (124 general practitioners) that participated in the GIANTT project in 2007. GIANTT provides quality assessments for most general practitioners (GPs) in Groningen province, The Netherlands. The included practices cover a total popula-tion of over 304,000 people. The patient population for 2007 consisted of all patients with a GP-confirmed diagnosis of type 2 diabetes at the beginning of 2007, who were primarily managed by their GP, and not by a specialist (n=9,646). Secondly, the cohort of 23 general practices participating in GIANTT since 2003 was used for
126
Chapter 3.3 - GIANTT observational study 2004-2007
a 4-year quality assessment from 2004 onwards. For each year, all patients with type 2 diabetes managed primarily by their GP were included (n=2,059 in 2004 up to n=2,929 in 2007). The practices of this first cohort had a slightly younger patient population (average 7 months), with a shorter diabetes duration (average 5 months), in comparison to the other practices in 2007. There were, however, no unequivo-cal differences in the averages of the risk factors HbA1c (-0.03 %, p>0.1), SBP (-1.5 mmHg, p<0.01), LDL-cholesterol (+0.05 mmol/l, p<0.05) or in treatment with glucose-regulating drugs (-1.8%, p<0.05), antihypertensive drugs (+0.4%, p>0.7), and statins (-3.1%, p<0.01).
Data collectionWe collected all data on prescriptions and relevant measurements that were regis-tered in structured as well as free text parts of the electronic medical records during the regular care process, using an automated and validated method.13 The data were collected anonymously and concern patients that did not object to the collection.
Process indicatorsWe included commonly used process indicators focusing on the registration level and the treatment level. Registration level is defined as the percentage patients with at least one registered measurement of HbA1c, SBP, or LDL-cholesterol. Treatment level is defined as the percentage patients treated with none, one or more glucose-, blood pressure and lipid-regulating drugs. A patient is considered treated if a drug is prescribed during the last 6 months of a calendar year. As new indicators, we used (A) treatment level in relation to level of risk factor control, and (B) percentage patients for whom medication therapy is started or intensified (increasing the daily dose or adding a new drug class14) within 6 months after the observation of an inap-propriately elevated risk factor level. Patients already on maximal treatment were ex-cluded.14 For lipid-lowering drugs, we considered a switch from simvastatin, fluvas-tatin or pravastatin to atorvastatin or rosuvastatin as possible therapy intensification.
Outcome indicatorsWe included the average level of each risk factor, and the percentage of patients achieving specific target levels as outcome indicators. Both are based on the last recorded measurement in a calendar year. We distinguish the following cut-off points for respectively good, moderate and insufficient risk factor control: HbA1c <7 %, 7-8.5 %, >8.5 %; SBP <140 mmHg, 140-160 mmHg, >160 mmHg; LDL-cholesterol <2.5 mmol/l, 2.5-3.5 mmol/l, >3.5 mmol/l. The target levels for good risk factor con-trol are based on general practice treatment guidelines from 2006.15 The subdivi-sion into classes of moderate and insufficient control was made because it can be expected that prescribers will react differently to levels closer to target compared to
127
Chapter 3.3 - GIANTT observational study 2004-2007
more elevated levels.16 For the 4-year follow-up from 2004 onwards, we used total cholesterol instead of LDL-cholesterol as risk factor in accordance with the prevailing guidelines at that time. The used cut-off points were: <5 mmol/l, 5-7 mmol/l, >7 mmol/l. In this period, the registration level of LDL-cholesterol was limited.Analysis. We performed analyses on the whole population, and stratified for age (below 75 and ≥ 75 years) to enable detection of possible differences in risk manage-ment. Differences between means and percentages were tested using the Student’s t-test and its z-approximation. Differences in class compositions were tested using the chi-square test. We present 95% confidence intervals.
RESULTSIn 2007, the patients were on average 67 years of age, and 52% were women (Table 1). The average time since diabetes diagnosis was almost 6 years. Mean Body Mass Index was 30 kg/m2, and 32% of the patients had albuminuria. The registration level varied from 64% for LDL-cholesterol to 85% for blood pressure. Missing risk factor information was clustered: in 12% of the patients information on all three risk factor levels ( HbA1c, LDL-cholesterol as well as blood pressure) was missing.
Glycaemic controlThe registration level of HbA1c measurements was relatively high (84%) in 2007 (ta-ble 1). The average HbA1c was 6.9%, with 61% of the patient population achieving good glycaemic control, and only 5% having insufficient control. There were no dif-ferences between patients below and above 75 years of age (p>0.1). Of the patients with an HbA1c above 7%, seven percent were not yet using glucose-regulating med-ication (figure 1). Insufficiently controlled patients, the latter group more frequently used oral multitherapy and/or insulin compared to those in moderate glycaemic con-trol (p<0.001). More than a third of the patients with moderate control and 22% of those insufficiently controlled were being prescribed none or just one oral drug. The patients without HbA1c measurements in 2007 were treated less intensively com-pared to the others (figure 1).Therapy modifications. In fewer than 50% of patients with moderate or insufficient control, antihyperglycaemic therapy was started, and in less than a quarter therapy was intensified within six months (figure 2). There were no differences between pa-tients below or above 75 years of age (p>0.1, data not shown).Four years follow-up. In the period 2004-2007, we observed no significant change in the population average of the HbA1c (p>0.2) (figure 3), although there was a reduc-tion of the proportion of moderately controlled patients (p=0.01). During this period,
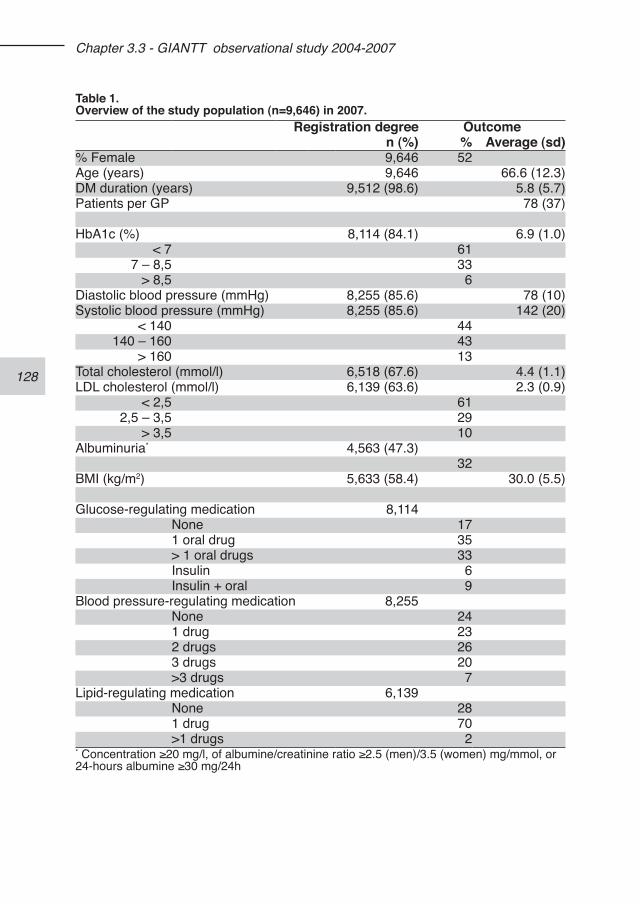
128
Chapter 3.3 - GIANTT observational study 2004-2007
Table 1.Overview of the study population (n=9,646) in 2007.
Registration degree Outcomen (%) % Average (sd)
% Female 9,646 52Age (years) 9,646 66.6 (12.3)DM duration (years) 9,512 (98.6) 5.8 (5.7)Patients per GP 78 (37)
HbA1c (%) 8,114 (84.1) 6.9 (1.0)< 7 61
7 – 8,5 33> 8,5 6
Diastolic blood pressure (mmHg) 8,255 (85.6) 78 (10)Systolic blood pressure (mmHg) 8,255 (85.6) 142 (20)
< 140 44140 – 160 43
> 160 13Total cholesterol (mmol/l) 6,518 (67.6) 4.4 (1.1)LDL cholesterol (mmol/l) 6,139 (63.6) 2.3 (0.9)
< 2,5 612,5 – 3,5 29
> 3,5 10Albuminuria* 4,563 (47.3)
32BMI (kg/m2) 5,633 (58.4) 30.0 (5.5)
Glucose-regulating medication 8,114None 171 oral drug 35> 1 oral drugs 33Insulin 6Insulin + oral 9
Blood pressure-regulating medication 8,255None 241 drug 232 drugs 263 drugs 20>3 drugs 7
Lipid-regulating medication 6,139None 281 drug 70>1 drugs 2
* Concentration ≥20 mg/l, of albumine/creatinine ratio ≥2.5 (men)/3.5 (women) mg/mmol, or 24-hours albumine ≥30 mg/24h
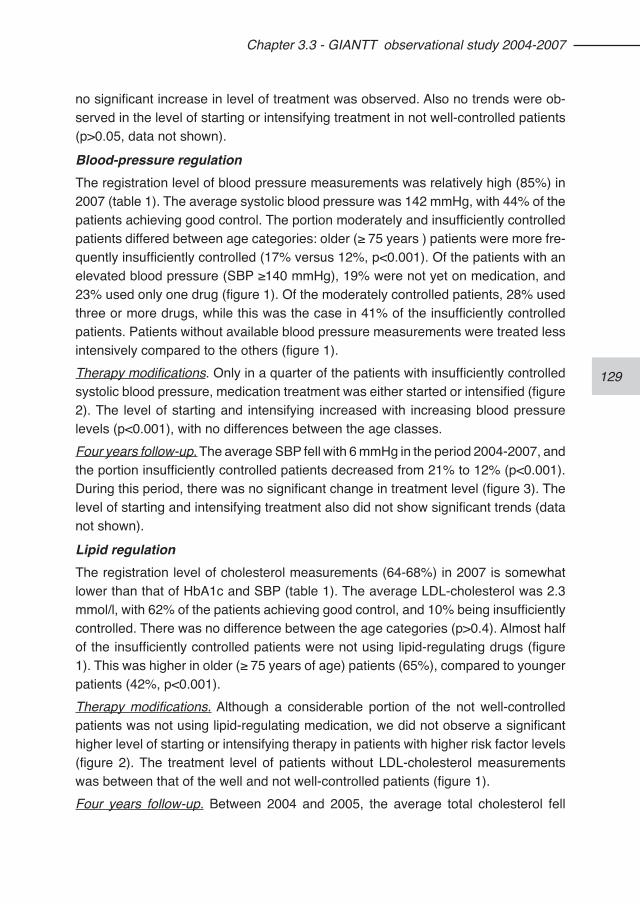
129
Chapter 3.3 - GIANTT observational study 2004-2007
no significant increase in level of treatment was observed. Also no trends were ob-served in the level of starting or intensifying treatment in not well-controlled patients (p>0.05, data not shown).
Blood-pressure regulationThe registration level of blood pressure measurements was relatively high (85%) in 2007 (table 1). The average systolic blood pressure was 142 mmHg, with 44% of the patients achieving good control. The portion moderately and insufficiently controlled patients differed between age categories: older (≥ 75 years ) patients were more fre-quently insufficiently controlled (17% versus 12%, p<0.001). Of the patients with an elevated blood pressure (SBP ≥140 mmHg), 19% were not yet on medication, and 23% used only one drug (figure 1). Of the moderately controlled patients, 28% used three or more drugs, while this was the case in 41% of the insufficiently controlled patients. Patients without available blood pressure measurements were treated less intensively compared to the others (figure 1).Therapy modifications. Only in a quarter of the patients with insufficiently controlled systolic blood pressure, medication treatment was either started or intensified (figure 2). The level of starting and intensifying increased with increasing blood pressure levels (p<0.001), with no differences between the age classes.Four years follow-up. The average SBP fell with 6 mmHg in the period 2004-2007, and the portion insufficiently controlled patients decreased from 21% to 12% (p<0.001). During this period, there was no significant change in treatment level (figure 3). The level of starting and intensifying treatment also did not show significant trends (data not shown).
Lipid regulationThe registration level of cholesterol measurements (64-68%) in 2007 is somewhat lower than that of HbA1c and SBP (table 1). The average LDL-cholesterol was 2.3 mmol/l, with 62% of the patients achieving good control, and 10% being insufficiently controlled. There was no difference between the age categories (p>0.4). Almost half of the insufficiently controlled patients were not using lipid-regulating drugs (figure 1). This was higher in older (≥ 75 years of age) patients (65%), compared to younger patients (42%, p<0.001).Therapy modifications. Although a considerable portion of the not well-controlled patients was not using lipid-regulating medication, we did not observe a significant higher level of starting or intensifying therapy in patients with higher risk factor levels (figure 2). The treatment level of patients without LDL-cholesterol measurements was between that of the well and not well-controlled patients (figure 1).Four years follow-up. Between 2004 and 2005, the average total cholesterol fell
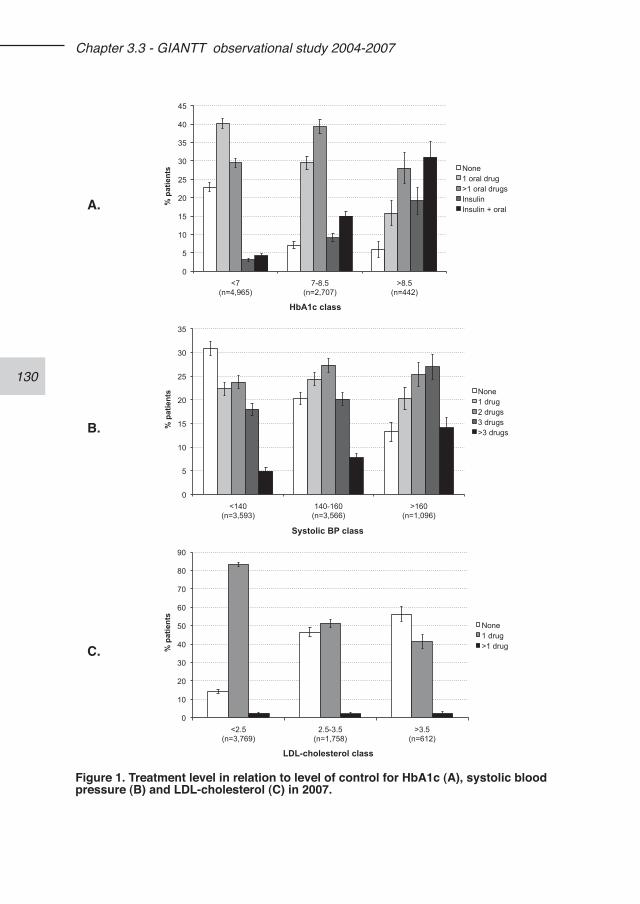
130
Chapter 3.3 - GIANTT observational study 2004-2007
A.
0
5
10
15
20
25
30
35
40
45
<7 (n=4,965)
7-8.5 (n=2,707)
>8.5 (n=442)
% p
atie
nts
HbA1c class
None 1 oral drug >1 oral drugs Insulin Insulin + oral
B.
0
5
10
15
20
25
30
35
<140 (n=3,593)
140-160 (n=3,566)
>160 (n=1,096)
% p
atie
nts
Systolic BP class
None 1 drug 2 drugs 3 drugs >3 drugs
C.
0
10
20
30
40
50
60
70
80
90
<2.5 (n=3,769)
2.5-3.5 (n=1,758)
>3.5 (n=612)
% p
atie
nts
LDL-cholesterol class
None 1 drug >1 drug
Figure 1. Treatment level in relation to level of control for HbA1c (A), systolic blood pressure (B) and LDL-cholesterol (C) in 2007.
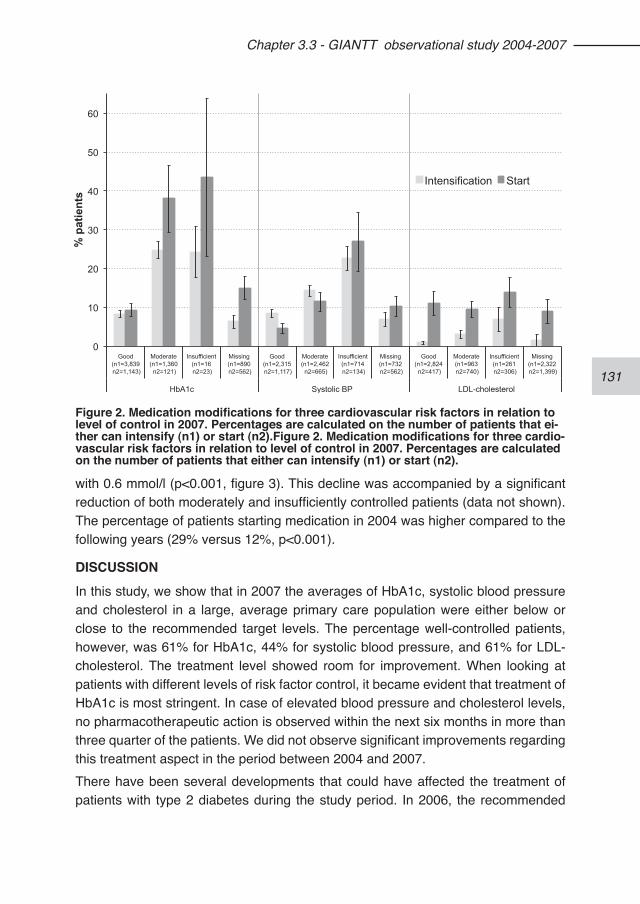
131
Chapter 3.3 - GIANTT observational study 2004-2007
with 0.6 mmol/l (p<0.001, figure 3). This decline was accompanied by a significant reduction of both moderately and insufficiently controlled patients (data not shown). The percentage of patients starting medication in 2004 was higher compared to the following years (29% versus 12%, p<0.001).
DISCUSSIONIn this study, we show that in 2007 the averages of HbA1c, systolic blood pressure and cholesterol in a large, average primary care population were either below or close to the recommended target levels. The percentage well-controlled patients, however, was 61% for HbA1c, 44% for systolic blood pressure, and 61% for LDL-cholesterol. The treatment level showed room for improvement. When looking at patients with different levels of risk factor control, it became evident that treatment of HbA1c is most stringent. In case of elevated blood pressure and cholesterol levels, no pharmacotherapeutic action is observed within the next six months in more than three quarter of the patients. We did not observe significant improvements regarding this treatment aspect in the period between 2004 and 2007.There have been several developments that could have affected the treatment of patients with type 2 diabetes during the study period. In 2006, the recommended
0
10
20
30
40
50
60
Good (n1=3,839 n2=1,143)
Moderate (n1=1,360 n2=121)
Insufficient (n1=16 n2=23)
Missing (n1=890 n2=562)
Good (n1=2,315 n2=1,117)
Moderate (n1=2,462 n2=665)
Insufficient (n1=714 n2=134)
Missing (n1=732 n2=562)
Good (n1=2,824 n2=417)
Moderate (n1=963 n2=740)
Insufficient (n1=261 n2=306)
Missing (n1=2,322 n2=1,399)
HbA1c Systolic BP LDL-cholesterol
% p
atie
nts
Intensification Start
Figure 2. Medication modifications for three cardiovascular risk factors in relation to level of control in 2007. Percentages are calculated on the number of patients that ei-ther can intensify (n1) or start (n2).Figure 2. Medication modifications for three cardio-vascular risk factors in relation to level of control in 2007. Percentages are calculated on the number of patients that either can intensify (n1) or start (n2).
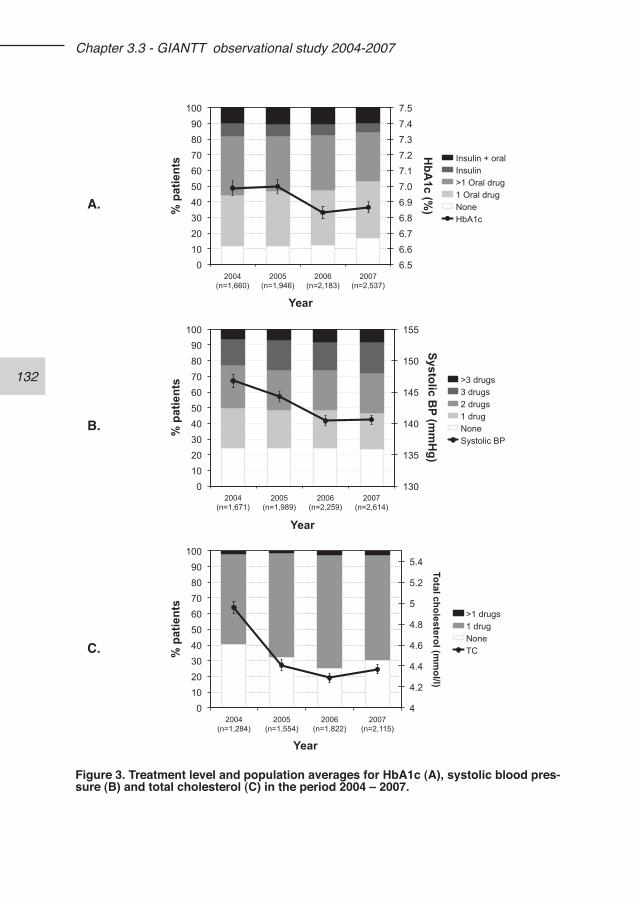
132
Chapter 3.3 - GIANTT observational study 2004-2007
A.
6.5 6.6 6.7 6.8 6.9 7.0 7.1 7.2 7.3 7.4 7.5
0 10 20 30 40 50 60 70 80 90
100
2004 (n=1,660)
2005 (n=1,946)
2006 (n=2,183)
2007 (n=2,537)
HbA
1c (%) %
pat
ient
s
Year
Insulin + oral Insulin >1 Oral drug 1 Oral drug None HbA1c
B.
130
135
140
145
150
155
0 10 20 30 40 50 60 70 80 90
100
2004 (n=1,671)
2005 (n=1,989)
2006 (n=2,259)
2007 (n=2,614)
Systolic BP (m
mH
g)
% p
atie
nts
Year
>3 drugs 3 drugs 2 drugs 1 drug None Systolic BP
C.
4
4.2
4.4
4.6
4.8
5
5.2
5.4
0 10 20 30 40 50 60 70 80 90
100
2004 (n=1,284)
2005 (n=1,554)
2006 (n=1,822)
2007 (n=2,115)
Total cholesterol (mm
ol/l)
% p
atie
nts
Year
>1 drugs 1 drug None TC
Figure 3. Treatment level and population averages for HbA1c (A), systolic blood pres-sure (B) and total cholesterol (C) in the period 2004 – 2007.
133
Chapter 3.3 - GIANTT observational study 2004-2007
risk factor targets in the Dutch clinical guidelines have become more stringent.15 Although one may expect that this would result in tighter control targets after 2006, trends towards this already started before 2006, and levelled off afterwards. The decrease in blood pressure in the beginning of the period is similar to those reported in other Dutch and European studies.17-19 At the regional level, a project was started at the end of 2004 by the Proeftuin Farmacie Groningen to stimulate that all patients with type 2 diabetes were treated with a statin.20 This can partly explain the high percentage of patients that started lipid-regulating drugs in 2004-2005, and the ac-companied decrease in the average total cholesterol.The percentage patients using antihypertensives of around 75% in 2004 is higher than reported elsewhere.17,21 The low percentages of patients that either start medi-cation or receive intensification of glucose-regulating and blood pressure-regulating drugs, are similar to those reported in other studies.17,22,23 Assessing how a prescriber reacts to an elevated risk factor is considered a good method to improve the action when needed.9-11,24 In the whole population, 17% did not yet use glucose-regulating medication. In itself, this finding provides little insight into treatment quality. When leaving the well-controlled patients aside, it becomes apparent that only few insufficiently controlled patients are untreated. On the other hand, the relatively low percentages of treatment start and intensification show room for improvement for the insufficiently controlled patients. Of the patients with elevated blood pressure, 45% use at most one antihypertensive drug, while the UKPDS has shown that often three or more drugs are needed to achieve the target.25 In the case of the 9% patients who, in spite of already using three or more drugs, remain insufficiently controlled, the question is whether the existence of secondary hypertension has been sufficiently investigated.For patients on insulin, the relative high portion insufficiently controlled patients is remarkable. Possibly, some of these patients are difficult to treat due to concomitant problems of a long diabetes duration. The question remains whether enough has been invested in education or specialist referral in these patients.A strong point of this study is that our data reflect an unselected group of general practitioners and patients who did not participate in a specific care organisation or in-tervention program. The population covers all patients with type 2 diabetes who have the general practitioner as their main care provider. The data collection concerns full risk management data as is registered during the care process, enabling assess-ments of treatment start and intensification throughout a year. Presenting treatment indicators that represent an important link between measuring risk factors and their outcomes makes this study innovative.
134
Chapter 3.3 - GIANTT observational study 2004-2007
As for all indicators, the indicators we present here should not be blindly used for external quality assessment.11 A specific limitation of assessing medication modifica-tions is that it ignores those patients already treated adequately. Besides this, these indicators only provide insights into medication treatment, and do not regard justifi-able reasons not to intensify treatment. In a part of these cases, the care provider may try to improve outcomes by lifestyle or adherence advice. Tolerance issues or fear of insulin can further limit medication modification options. A possible limitation of our study lies in its use of patient records. Although the reg-istration degree of HbA1c and blood pressure is high (around 85%), it is lower for LDL-cholesterol (64%). In 12% of the patients all relevant risk information is missing. This clustering makes the existence of a strong association between missing reg-istration and risk factor level improbable. Patients with missing risk information are being treated less intensely, which could indicate that these patients visit their GPs less frequently. We cannot assess whether they need less attention or might be care avoiders.We acknowledged switches from low-potent statins to high potent counterparts as treatment intensification. However, this could have introduced some overestimation, since part of these switches may not be intended as intensification.
CONCLUSIONWe have shown that, despite decreasing trends in levels of cardiovascular risk factors, in over half of insufficiently controlled patients medication treatment is not promptly adjusted. We recommend applying this approach to quality assessment more often in addition to commonly used process and outcome indicators, since it provides a simple way for care providers to identify possible targets for improvement.
REFERENCES1. Rutten GEHM. Zorg voor patiënten met diabetes mellitus type 2 in de 1e lijn. Ned
Tijdschr Geneesk. 2008;152:2389-94.2. Goudswaard AN, Stolk RP, Zuithoff P, Rutten GEHM. Patient characteristics do
not predict poor glycaemic control in type 2 diabetes patients treated in primary care. Eur J Epidemiol. 2004;19:541-5.
3. Meulepas MA, Braspenning JC, de Grauw WJ, Lucas AE, Harms L, Akkermans RP, Grol RP. Logistic support service improves processes and outcomes of dia-betes care in general practice. Fam Pract. 2007;24:20-5.
4. Redekop WK, Koopmanschap MA, Rutten GEHM, Wolffenbuttel BHR, Stolk RP, Niessen LW. Resource consumption and costs in Dutch patients with type 2 dia-betes mellitus. Results from 29 general practices. Diabet Med 2002;19:246-53.
5. Steuten LM, Vrijhoef HJ, Landewe-Cleuren S, Schaper N, Van Merode GG, Spreeuwenberg C. A disease management programme for patients with diabe-
135
Chapter 3.3 - GIANTT observational study 2004-2007
tes mellitus is associated with improved quality of care within existing budgets. Diabet Med. 2007;24:1112-20.
6. Cleveringa FG, Gorter KJ, van den Donk M, Pijman PL, Rutten GEHM. Task delegation and computerized decision support reduce coronary heart disease risk factors in type 2 diabetes patients in primary care. Diabetes Technol Ther. 2007;9:473-81.
7. Cleveringa FG, Gorter KJ, van den Donk M, Rutten GEHM. Combined task delegation, computerized decision support, and feedback improve cardiovas-cular risk for type 2 diabetic patients: A cluster randomized trial in primary care. Diabetes Care. 2008;31:2273-5.
8. Gorter K, van Bruggen R, Stolk R, Zuithoff P, Verhoeven R, Rutten GEHM. Overall quality of diabetes care in a defined geographic region: different sides of the same story. Br J Gen Pract. 2008;58:339-45.
9. Rodondi N, Peng T, Karter AJ, Bauer DC, Vittinghoff E, Tang S, Pettitt D, Kerr EA, Selby JV. Therapy modifications in response to poorly controlled hyperten-sion, dyslipidemia, and diabetes mellitus. Ann Intern Med. 2006;144:475-84.
10. Voorham J, Denig P, Wolffenbuttel BHR, Haaijer-Ruskamp FM. Cross-sectional versus sequential quality indicators of risk factor management in patients with type 2 diabetes. Med Care. 2008;46:133-141.
11. Selby JV, Uratsu CS, Fireman B, Schmittdiel JA, Peng T, Rodondi N, Karter AJ, Kerr EA. Treatment intensification and risk factor control: toward more clinically relevant quality measures. Med Care. 2009;47:395-402.
12. GIANTT, Groningen Initiative to Analyse Type 2 diabetes Treatment. http://www.giantt.nl, accessed on 29dec09.
13. Voorham J, Denig P. Computerized extraction of information on the quality of diabetes care from free text in electronic patient records of general practitioners. J Am Med Inform Assoc. 2007;14:349-354.
14. Voorham J, Haaijer-Ruskamp FM, Stolk RP, Wolffenbuttel BHR, Denig P. Influence of elevated cardiometabolic risk factor levels on treatment changes in type 2 diabetes. Diabetes Care. 2008;31:501-3.
15. Rutten GEHM, De Grauw WJC, Nijpels G, Goudswaard AN, Uitewaal PJM, Van der Does FEE, Heine RJ, Van Ballegooie E, Verduijn MM, Bouma M. ‘Diabetes mellitus type 2’ guideline (second revision) from the Dutch College of General Practitioners. Huisarts Wet. 2006;49:137-152.
16. Hayward RA. All-or-nothing treatment targets make bad performance measures. Am J Manag Care. 2007;13:126-8.
17. Greving JP, Denig P, de Zeeuw D, Bilo H, Haaijer-Ruskamp FM. Trends in hyper-lipidemia and hypertension management in type 2 diabetes patients from 1998-2004: a longitudinal observational study. Cardiovasc Diabetol. 2007;6:25.
18. Kristensen JK, Lauritzen T. Quality indicators of type 2-diabetes monitoring dur-ing 2000-2005. Ugeskr Laeger. 2009;171:130-4.
19. Khunti K, Gadsby R, Millett C, Majeed A, Davies M. Quality of diabetes care in the UK: comparison of published quality-of-care reports with results of the Quality and Outcomes Framework for Diabetes. Diabet Med. 2007;24:1436-41.
20. Proeftuin Farmacie Groningen. http://proeftuinfarmaciegroningen.tmade.nl.
136
Chapter 3.3 - GIANTT observational study 2004-2007
21. Pijman PLW, Timmer SJ, Neter RS, Krasser J. Het diabetes zorgprotocol: Hoe staan de bekende diabetespatiënten ervoor? De resultaten van baseline-data vergaard bij het starten van geprotocolleerde diabeteszorg in de huisartspraktijk. Ned Tijdschr Diabetologie. 2004;2:75-80.
22. Grant RW, Buse JB, Meigs JB. Quality of diabetes care in U.S. academic medical centers: low rates of medical regimen change. Diabetes Care. 2005;28:337-442.
23. Grant RW, Cagliero E, Dubey AK, Gildesgame C, Chueh HC, Barry MJ, Singer DE, Nathan DM, Meigs JB. Clinical inertia in the management of type 2 diabetes metabolic risk factors. Diabet Med. 2004;21:150-5.
24. Guthrie B, Inkster M, Fahey T. Tackling therapeutic inertia: role of treatment data in quality indicators. BMJ. 2007;335:542-4.
25. Anonymous. Tight blood pressure control and risk of macrovascular and micro-vascular complications in type 2 diabetes: UKPDS 38. UK Prospective Diabetes Study Group. BMJ. 1998;317:703-13.
137
138
139
Chapter 4 - Determinants of treatment intensification
140
141
Chapter 4.1 - The influence of elevated cardiometabolic risk factor levels on treatment changes in type 2 diabetes
Jaco Voorham1,2
Flora M Haaijer-Ruskamp1
Ronald P Stolk2
Bruce HR Wolffenbuttel3
Petra Denig1
1. Department of Clinical Pharmacology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
2. Department of Epidemiology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
3. Department of Endocrinology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
Voorham J, Haaijer-Ruskamp FM, Stolk RP, Wolffenbuttel BHR, Denig P; Groningen Initiative to Analyze Type 2 Diabetes Treatment Group. Influence of elevated car-diometabolic risk factor levels on treatment changes in type 2 diabetes. Diabetes Care. 2008;31(3):501-3.
142
Chapter 4.1 - Elevated risk factor levels
ABSTRACTUndertreatment of risk factors in patients with type 2 diabetes is common. We as-sessed the influence of elevated levels of blood pressure, total cholesterol and HbA1c on decisions of Dutch general practitioners to change drug treatment in a cohort of 3,029 patients during a 1-year period. Respectively 58, 71 and 21% of patients re-mained untreated despite poor blood pressure, lipid levels and glycaemic control. Of poorly controlled but already drug-treated patients, 52% did not receive intensifica-tion for antihypertensive medication, 81% not for lipid-lowering medication, and 43% not for glucose-lowering medication. We observed a significantly lower treatment intervention rate in moderately than in poorly controlled patients for blood pressure. This was not seen for decisions on cholesterol or HbA1c results.The relatively low action rates observed for blood pressure can only in part be ex-plained by the use of treatment thresholds higher than those indicated by guidelines. For lipid management, the lack of action cannot be explained by using higher treat-ment thresholds.
143
Chapter 4.1 - Elevated risk factor levels
INTRODUCTIONConsiderable progress has been achieved regarding the quality of diabetes care, but undertreatment remains a topic of concern.1-3 Low rates of starting and intensifying treatment in patients with type 2 diabetes have been observed.4-7 Although accepting higher risk factor levels than indicated by guidelines has been reported as a reason for not changing treatment, few studies have examined differences in treatment in-tervention rates for moderately and poorly controlled patients.8-11 Results from two provider survey studies suggest that physicians treat near-goal HbA1c levels more aggressively than near-goal blood pressure levels.10,12 Our aim was to assess the influence of moderately and highly elevated levels of cardiometabolic risk factors on the decision to change antihypertensive, lipid-lowering and glucose-lowering treat-ment in primary care.
RESEARCH DESIGN AND METHODSWe conducted a cohort study including 3,029 type 2 diabetic patients managed by 62 general practitioners. Clinical measurements and prescriptions were gathered from electronic medical records at the general practitioners’ offices and a regional diabetes facility.13 Of the general practitioners, 20% practiced in a rural area, 18% worked in a private practice, and 16% were allowed to dispense drugs at their prac-tice. We assessed treatment status and risk factor level at baseline (October 1st 2003), using the most recent measurements in the preceding year. Thresholds for moder-ately and highly elevated levels were set, following national guidelines at ≥140 and ≥160 mmHg for systolic blood pressure, ≥85 and ≥95 mmHg for diastolic blood pres-sure, ≥5 and ≥7 mmol/l for total cholesterol, and ≥7 and ≥8.5% for HbA1c. Treatment changes were determined during a follow-up period of 1 year. Patients receiving maximal medication at baseline, as defined by national guidelines for general practi-tioners and the Dutch Pharmacotherapy Compendium, were excluded.14
Treatment change was defined as the start or intensification of drug treatment for antihypertensive, lipid-lowering and glucose-lowering treatment. Patients were con-sidered to start treatment when they received a first prescription during the study period after receiving no prescriptions for this therapeutic group during the previous six months. A treatment change was considered intensification when a new drug class was added or the medication dosage was increased. A switch to another drug class without continuation of the original medication was not considered treatment intensification. A prescription was considered discontinued when it was not repeated within 120 days from the calculated end date.Results are presented as proportions of patients with treatment changes with 95%
144
Chapter 4.1 - Elevated risk factor levels
CIs, and differences were tested by means of z-approximation to the binominal dis-tribution.
RESULTSThe patients were aged 66.4 ± 12.3 years, and 56% were female. At baseline, 14% had a recorded history of coronary disease, and 13% suffered from other macro- or microvascular complications. The number of concurrently prescribed chronic drugs was 4.7 ± 3.1. Annual testing rates were 81.8% for blood pressure, 74.8% for total cholesterol, and 76.9% for HbA1c. The average risk factor levels were 147 ± 20 mmHg for systolic blood pressure, 81 ± 10 mmHg for diastolic blood pressure, 5.1 ± 1.0 mmol/l for total cholesterol, and 7.3 ± 1.3% for HbA1c.
Treatment statusOf the 3,029 patients, 63, 31 and 80%, respectively, were using antihypertensive, lipid-lowering and glucose-lowering medication at baseline, and 22, 16 and 36%, respectively, of untreated patients started treatment during the study period. Of pa-tients treated at baseline, 25, 1 and 17%, respectively, were already on maximal treatment. Of patients not on maximal treatment, 32% received intensification for antihypertensive, 17% for lipid-lowering, and 45% for glucose-lowering medication.Figure 1 shows the percentage of patients starting and intensifying treatment ac-cording to control status. Medication change was significantly more likely in patients with elevated HbA1c levels than with elevated blood pressure or cholesterol levels. Of the patients with poorly controlled systolic or diastolic blood pressure, 58 and 50%, respectively, remained untreated. This was the case for 71% with poorly con-trolled total cholesterol levels (68% in patients <75 years), and for 21% with poorly controlled HbA1c levels. For patients already treated, 52% of the poorly controlled for systolic blood pressure did not receive intensification for antihypertensive medi-cation, whereas this was observed in 81% for lipid-lowering medication and 43% for glucose-lowering medication. We observed a significant difference in treatment intervention rate between moder-ately and poorly controlled patients for blood pressure only. Furthermore, in patients with moderately controlled blood pressure, intervention was less likely in untreated than treated patients.
CONCLUSIONSThis study showed that general practitioners were more likely to change glucose-lowering treatment than antihypertensive or lipid-lowering medication, especially in moderately controlled patients. Regarding blood pressure management, we con-firmed previous findings that treatment changes are less likely in moderately control-
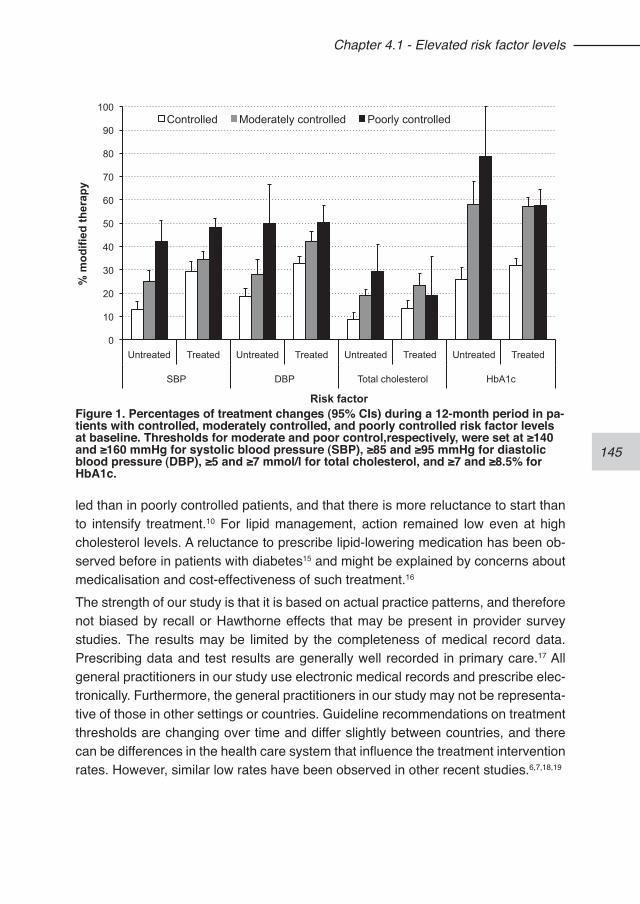
145
Chapter 4.1 - Elevated risk factor levels
led than in poorly controlled patients, and that there is more reluctance to start than to intensify treatment.10 For lipid management, action remained low even at high cholesterol levels. A reluctance to prescribe lipid-lowering medication has been ob-served before in patients with diabetes15 and might be explained by concerns about medicalisation and cost-effectiveness of such treatment.16 The strength of our study is that it is based on actual practice patterns, and therefore not biased by recall or Hawthorne effects that may be present in provider survey studies. The results may be limited by the completeness of medical record data. Prescribing data and test results are generally well recorded in primary care.17 All general practitioners in our study use electronic medical records and prescribe elec-tronically. Furthermore, the general practitioners in our study may not be representa-tive of those in other settings or countries. Guideline recommendations on treatment thresholds are changing over time and differ slightly between countries, and there can be differences in the health care system that influence the treatment intervention rates. However, similar low rates have been observed in other recent studies.6,7,18,19
0
10
20
30
40
50
60
70
80
90
100
Untreated Treated Untreated Treated Untreated Treated Untreated Treated
SBP DBP Total cholesterol HbA1c
% m
odifi
ed th
erap
y
Risk factor
Controlled Moderately controlled Poorly controlled
Figure 1. Percentages of treatment changes (95% CIs) during a 12-month period in pa-tients with controlled, moderately controlled, and poorly controlled risk factor levels at baseline. Thresholds for moderate and poor control,respectively, were set at ≥140 and ≥160 mmHg for systolic blood pressure (SBP), ≥85 and ≥95 mmHg for diastolic blood pressure (DBP), ≥5 and ≥7 mmol/l for total cholesterol, and ≥7 and ≥8.5% for HbA1c.
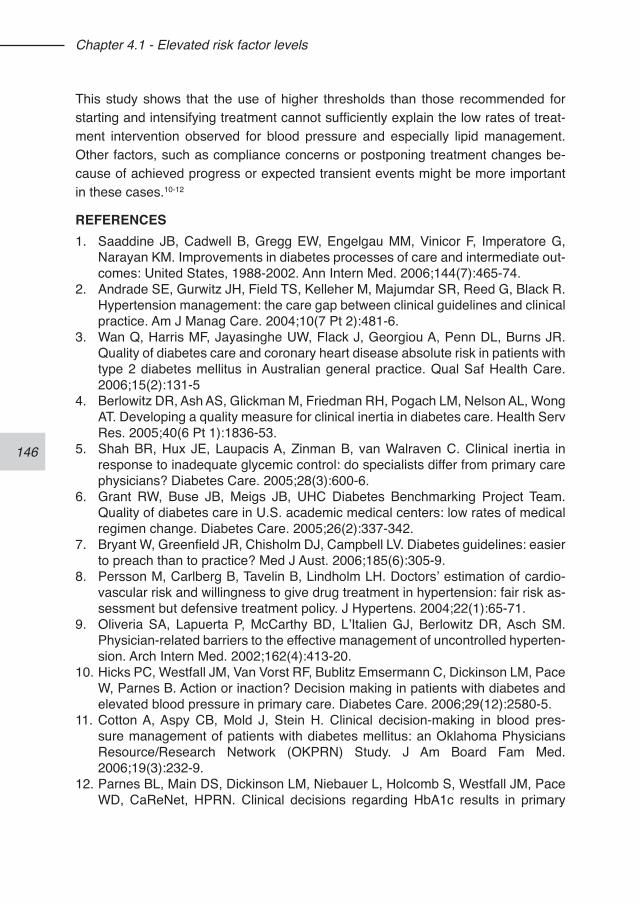
146
Chapter 4.1 - Elevated risk factor levels
This study shows that the use of higher thresholds than those recommended for starting and intensifying treatment cannot sufficiently explain the low rates of treat-ment intervention observed for blood pressure and especially lipid management. Other factors, such as compliance concerns or postponing treatment changes be-cause of achieved progress or expected transient events might be more important in these cases.10-12
REFERENCES1. Saaddine JB, Cadwell B, Gregg EW, Engelgau MM, Vinicor F, Imperatore G,
Narayan KM. Improvements in diabetes processes of care and intermediate out-comes: United States, 1988-2002. Ann Intern Med. 2006;144(7):465-74.
2. Andrade SE, Gurwitz JH, Field TS, Kelleher M, Majumdar SR, Reed G, Black R. Hypertension management: the care gap between clinical guidelines and clinical practice. Am J Manag Care. 2004;10(7 Pt 2):481-6.
3. Wan Q, Harris MF, Jayasinghe UW, Flack J, Georgiou A, Penn DL, Burns JR. Quality of diabetes care and coronary heart disease absolute risk in patients with type 2 diabetes mellitus in Australian general practice. Qual Saf Health Care. 2006;15(2):131-5
4. Berlowitz DR, Ash AS, Glickman M, Friedman RH, Pogach LM, Nelson AL, Wong AT. Developing a quality measure for clinical inertia in diabetes care. Health Serv Res. 2005;40(6 Pt 1):1836-53.
5. Shah BR, Hux JE, Laupacis A, Zinman B, van Walraven C. Clinical inertia in response to inadequate glycemic control: do specialists differ from primary care physicians? Diabetes Care. 2005;28(3):600-6.
6. Grant RW, Buse JB, Meigs JB, UHC Diabetes Benchmarking Project Team. Quality of diabetes care in U.S. academic medical centers: low rates of medical regimen change. Diabetes Care. 2005;26(2):337-342.
7. Bryant W, Greenfield JR, Chisholm DJ, Campbell LV. Diabetes guidelines: easier to preach than to practice? Med J Aust. 2006;185(6):305-9.
8. Persson M, Carlberg B, Tavelin B, Lindholm LH. Doctors’ estimation of cardio-vascular risk and willingness to give drug treatment in hypertension: fair risk as-sessment but defensive treatment policy. J Hypertens. 2004;22(1):65-71.
9. Oliveria SA, Lapuerta P, McCarthy BD, L’Italien GJ, Berlowitz DR, Asch SM. Physician-related barriers to the effective management of uncontrolled hyperten-sion. Arch Intern Med. 2002;162(4):413-20.
10. Hicks PC, Westfall JM, Van Vorst RF, Bublitz Emsermann C, Dickinson LM, Pace W, Parnes B. Action or inaction? Decision making in patients with diabetes and elevated blood pressure in primary care. Diabetes Care. 2006;29(12):2580-5.
11. Cotton A, Aspy CB, Mold J, Stein H. Clinical decision-making in blood pres-sure management of patients with diabetes mellitus: an Oklahoma Physicians Resource/Research Network (OKPRN) Study. J Am Board Fam Med. 2006;19(3):232-9.
12. Parnes BL, Main DS, Dickinson LM, Niebauer L, Holcomb S, Westfall JM, Pace WD, CaReNet, HPRN. Clinical decisions regarding HbA1c results in primary
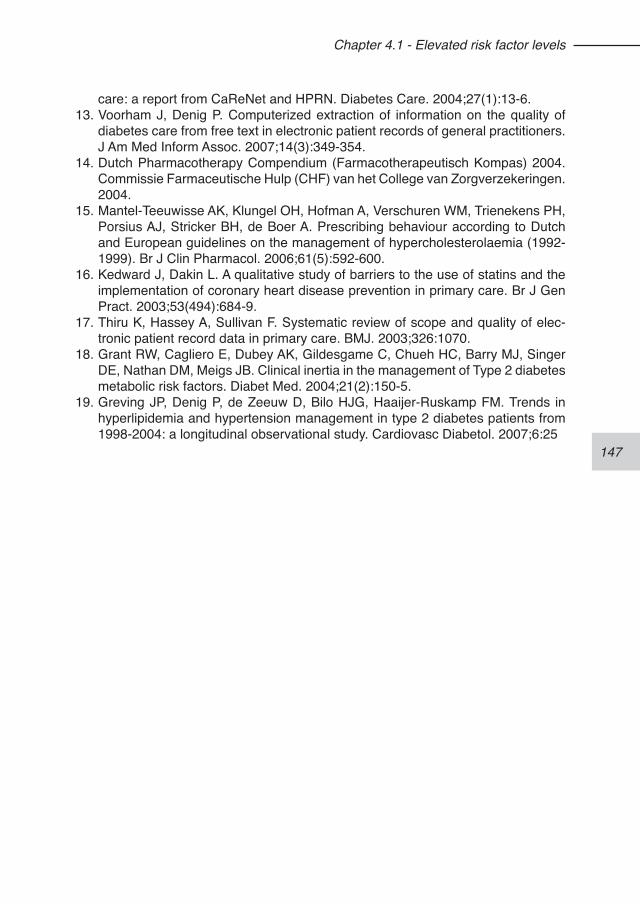
147
Chapter 4.1 - Elevated risk factor levels
care: a report from CaReNet and HPRN. Diabetes Care. 2004;27(1):13-6.13. Voorham J, Denig P. Computerized extraction of information on the quality of
diabetes care from free text in electronic patient records of general practitioners. J Am Med Inform Assoc. 2007;14(3):349-354.
14. Dutch Pharmacotherapy Compendium (Farmacotherapeutisch Kompas) 2004. Commissie Farmaceutische Hulp (CHF) van het College van Zorgverzekeringen. 2004.
15. Mantel-Teeuwisse AK, Klungel OH, Hofman A, Verschuren WM, Trienekens PH, Porsius AJ, Stricker BH, de Boer A. Prescribing behaviour according to Dutch and European guidelines on the management of hypercholesterolaemia (1992-1999). Br J Clin Pharmacol. 2006;61(5):592-600.
16. Kedward J, Dakin L. A qualitative study of barriers to the use of statins and the implementation of coronary heart disease prevention in primary care. Br J Gen Pract. 2003;53(494):684-9.
17. Thiru K, Hassey A, Sullivan F. Systematic review of scope and quality of elec-tronic patient record data in primary care. BMJ. 2003;326:1070.
18. Grant RW, Cagliero E, Dubey AK, Gildesgame C, Chueh HC, Barry MJ, Singer DE, Nathan DM, Meigs JB. Clinical inertia in the management of Type 2 diabetes metabolic risk factors. Diabet Med. 2004;21(2):150-5.
19. Greving JP, Denig P, de Zeeuw D, Bilo HJG, Haaijer-Ruskamp FM. Trends in hyperlipidemia and hypertension management in type 2 diabetes patients from 1998-2004: a longitudinal observational study. Cardiovasc Diabetol. 2007;6:25
148
149
Chapter 4.2 - Cardiometabolic treatment decisions in patients with type 2 diabetes:
the role of repeated measurements and medication burden
Jaco Voorham1,2
Flora M Haaijer-Ruskamp1
Ronald P Stolk2
Bruce HR Wolffenbuttel3
Petra Denig1
1. Department of Clinical Pharmacology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
2. Department of Epidemiology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
3. Department of Endocrinology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
Voorham J, Haaijer-Ruskamp FM, Stolk RP, Wolffenbuttel BHR, Denig P; Groningen Initiative to Analyze Type 2 Diabetes Treatment Group. Cardiometabolic treatment decisions in patients with type 2 diabetes: the role of repeated measurements and medication burden. Qual Saf Health Care. 2010, in press.
150
Chapter 4.2 - Repeated measurements
ABSTRACTBackground. Clinical guidelines for cardiometabolic risk management indicate a sim-ple threshold-based strategy for treatment, but physicians and their patients may be reluctant to modify drug treatment after a single elevated measurement. We deter-mined how repeated measurements of blood pressure, cholesterol and heamoglobin A1c affect general practitioners’ decisions to start or intensify medication in patients with type 2 diabetes. We also evaluated whether medication burden altered these decisions.Methods. We conducted a cohort study in 3,029 patients managed by 62 general practitioners (GPs). We assessed the predictive value of the last risk factor measure-ment, the number of successive measurements above target level, and the percent-age change between the last two measurements. Medication burden was assessed as the number of drugs concurrently used. Effects on treatment decisions were esti-mated by multilevel logistic regression analysis, correcting for clustering at GP level.Results. Repeated high levels of diastolic blood pressure increased the likelihood to start antihypertensive medication (OR=2.08, CI 1.37 to 3.17). Repeated high haemoglobin A1c levels affected intensification of oral glucose-lowering medication (OR=1.71, CI 1.44 to 2.03). Modification of lipid-lowering medication was limited, and only affected by the last total cholesterol level. Starting treatment for all three risk factors, as well as intensifying antihypertensive treatment, was more likely in patients already using more drugs for other chronic diseases.Conclusions. Waiting for the next measurement before deciding to change medica-tion can explain in part the apparent undertreatment for hypertension and hypergly-caemia, but not for hypercholesterolaemia. Medication burden was not a barrier for treatment modification.
151
Chapter 4.2 - Repeated measurements
INTRODUCTIONAdequate treatment of cardiometabolic risk factors in patients with diabetes is impor-tant.1 Clinical guidelines describe strict target levels above which pharmacotherapy should be started or intensified. Although considerable progress has been achieved in the quality of diabetes care, undertreatment still remains a concern.2-5
Several reasons for undertreatment have been identified, including concerns about polypharmacy, medication adherence, intolerance and costs.6-9 Postponing treat-ment intensification because of improvement already being made or competing de-mands are other commonly reported reasons.9-14 Physicians may be reluctant to modify treatment after a single elevated measurement.11,12,15,16 Especially, in patients with low overall risk, this could be the case. Furthermore, in older patients using multiple medications, a conservative approach could be motivated by fears of medi-cation burden.8,9,13,17 Despite this rationale for awaiting a next observation before deciding to intervene, few studies include more than one observation moment to assess appropriate action. Studies that did include a follow-up period suggest that physicians take more than one measurement outcome into account when making treatment decisions.12,18,19
The objective of this study is to investigate the decisions of general practitioners (GPs) to start or intensify medication treatment in patients with type 2 diabetes and determine how repeated measurements of blood pressure, cholesterol and hae-moglobin A1c (HbA1c) levels contribute to these decisions. We evaluated whether the treatment decisions are associated with the number of previous measurements above target level, with recent improvement or worsening of the risk factor, as well as with any other of the three risk factors. This will give insight in the influence of each of these factors on the decision-making process. We further tested whether medication burden affects this decision, and whether the risk factors are weighed differently for patients with a high or low overall risk.
METHODS
Study population and settingOur study population comprised 3,029 patients who where managed for their dia-betes by 1 of 62 GPs participating in a regional diabetes project in the northern Netherlands in 2004 and 2005. Twenty-seven percent of the GPs were female, and the mean age was 49 years for male and 43 years for female patients. Twenty-five (18%) practised alone, six (10%) in a duo practice and 31 (50%) worked in a group practice. Of the 45 general practices, 13 (29%) were located in rural areas and were allowed to dispense drugs. All their patients whom they managed themselves with
152
Chapter 4.2 - Repeated measurements
a diagnosis of type 2 diabetes at the beginning of the study period were included.In The Netherlands, nearly all inhabitants are registered with a GP, who is the gate-keeper of the healthcare system. In our study area, a regional diabetes facility offers support to GPs. Patients can be referred to this facility for physical examination and laboratory tests. The results are reported back to the GPs who remain responsible for further treatment and treatment modifications. Diabetes patients usually visit their GP every 3 months for a check-up and medication refills. During the study period, there were no governmental or insurance restrictions on the prescription or reim-bursement for the drugs included in our study.
Design and data collectionWe conducted a cohort study to assess the influence of repeated risk factor meas-urements on the decision to modify antihypertensive, lipid-lowering and oral blood-glucose-lowering treatment. Clinical measurements, comorbidity, prescriptions, and demographic data were collected from November 2001 until March 2005. All infor-mation was extracted from electronic medical record systems at the GPs’ offices and the regional diabetes facility using a validated software programme.20 All GPs in our study prescribe electronically, ensuring complete prescribing information. For research using anonymous medical records no ethics committee approval is needed in The Netherlands.21
Outcome measuresTreatment modification was the studied endpoint, defined as the first treatment start or intensification between October 2003 and September 2004. Patients were con-sidered to start treatment when they received a first prescription after receiving no prescriptions for that therapeutic group during the previous six months (twice the duration of a standard prescription for chronic medication in The Netherlands). A modification was considered intensification when a new drug class was added or the medication dosage was increased. A switch to another drug class, that is, starting a new drug when the original medication was not continued within 120 days from the calculated end date, was not considered treatment intensification.Patients with incomplete follow-up to assess treatment intensification and patients receiving maximal medication at baseline were excluded from the analyses. The definitions for maximal medication were derived from the Dutch Pharmacotherapy Compendium22 and prevailing national practice guidelines for GPs at the time of the study.23-25 For antihypertensive therapy, three drugs from different classes prescribed at maximum maintenance dosage or more than three drugs was considered maxi-mal medication. For lipid-lowering therapy, prescribing one drug at maximum dosage or more than one drug was considered maximal medication. For glucose-lowering

153
Chapter 4.2 - Repeated measurements
therapy, insulin use was seen as maximal medication.
PredictorsAs predictors of treatment modifications, we included the most recent measurements of systolic and diastolic blood pressure, total serum cholesterol, and HbA1c (called “last value”) and two aspects of previous risk factor information: (1) the number of last successive measurements above target level (called “intensity”) and (2) per cent change in risk factor level, that is, the relative difference between the last two meas-urements (called “change”). Measurements in the preceding year were included for blood pressure and HbA1c, and 2 years for total cholesterol since this was usually measured once a year. Target levels were derived from the practice guidelines at the time of our study: systolic blood pressure <140 mmHg, diastolic blood pressure <90 mmHg, total cholesterol <5.0 mmol/l and HbA1c <7.0 %.23-25
Medication burden was assessed by counting unique drugs prescribed in 6 months up to the medication change, separately for risk factor specific drugs and drugs for other chronic diseases. This included all drugs at the lowest level of the Anatomical Therapeutic Chemical classification system in classes A, B, C, H, L, M, N or R.26 Fixed combinations of drugs were counted as one drug.
AnalysisMultilevel logistic regression was used, correcting for clustering by allowing a ran-dom effect at GP level. We performed complete subject analyses, enabling us to draw conclusions on the influence of the risk factor information when available on the treatment decisions. We constructed separate predictive models for starting and intensifying treatment, adjusted for age, gender, diabetes duration, albuminu-ria, body mass index, coronary comorbidity (angina pectoris, myocardial infarction, heart failure, coronary artery bypass graft, coronary angioplasty, atrium fibrillation), and other diabetes related conditions (stroke, transient ischemic attack, peripheral arterial disease, neuropathy, amputations, retinopathy). Interaction terms between the predictors and sex/age were explored, and regression models where checked for collinearity. Overall models and models stratified on cardiovascular risk were built. Risk stratification was based on UKPDS 10-year cardiovascular risk scores (low-risk<20%, high-risk≥20%).27
RESULTSThe patients were aged 66 (12) years, and 56% were female. At baseline, 14% had a noted history of coronary comorbidity, and 13% suffered from other diabetes-related conditions. The median number of concurrently prescribed chronic drugs was 4. Risk factor measurements were available in 75% to 82% of the cases (table 1).
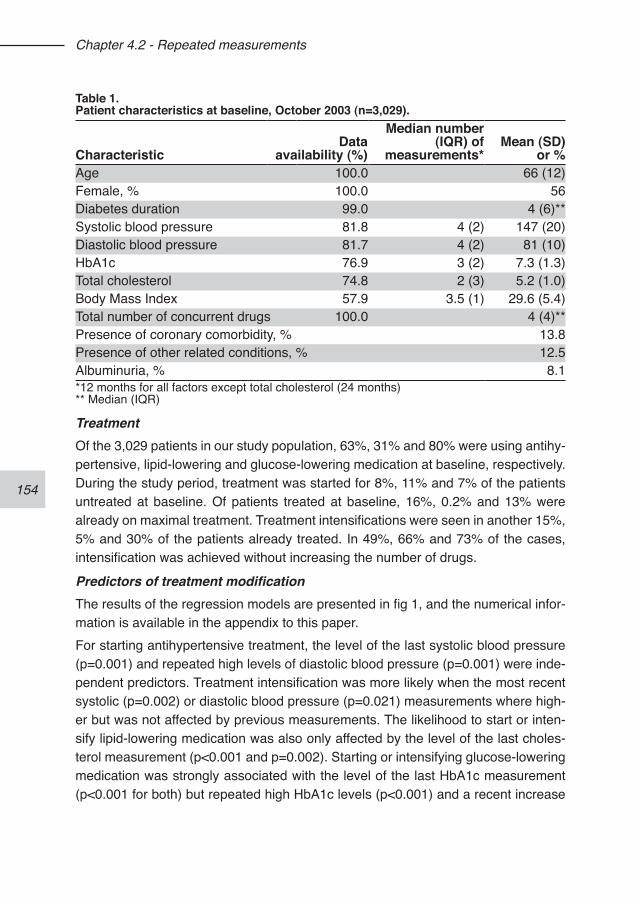
154
Chapter 4.2 - Repeated measurements
TreatmentOf the 3,029 patients in our study population, 63%, 31% and 80% were using antihy-pertensive, lipid-lowering and glucose-lowering medication at baseline, respectively. During the study period, treatment was started for 8%, 11% and 7% of the patients untreated at baseline. Of patients treated at baseline, 16%, 0.2% and 13% were already on maximal treatment. Treatment intensifications were seen in another 15%, 5% and 30% of the patients already treated. In 49%, 66% and 73% of the cases, intensification was achieved without increasing the number of drugs.
Predictors of treatment modificationThe results of the regression models are presented in fig 1, and the numerical infor-mation is available in the appendix to this paper.For starting antihypertensive treatment, the level of the last systolic blood pressure (p=0.001) and repeated high levels of diastolic blood pressure (p=0.001) were inde-pendent predictors. Treatment intensification was more likely when the most recent systolic (p=0.002) or diastolic blood pressure (p=0.021) measurements where high-er but was not affected by previous measurements. The likelihood to start or inten-sify lipid-lowering medication was also only affected by the level of the last choles-terol measurement (p<0.001 and p=0.002). Starting or intensifying glucose-lowering medication was strongly associated with the level of the last HbA1c measurement (p<0.001 for both) but repeated high HbA1c levels (p<0.001) and a recent increase
Table 1. Patient characteristics at baseline, October 2003 (n=3,029).
CharacteristicData
availability (%)
Median number (IQR) of
measurements*Mean (SD)
or %Age 100.0 66 (12)Female, % 100.0 56Diabetes duration 99.0 4 (6)**Systolic blood pressure 81.8 4 (2) 147 (20)Diastolic blood pressure 81.7 4 (2) 81 (10)HbA1c 76.9 3 (2) 7.3 (1.3)Total cholesterol 74.8 2 (3) 5.2 (1.0)Body Mass Index 57.9 3.5 (1) 29.6 (5.4)Total number of concurrent drugs 100.0 4 (4)**Presence of coronary comorbidity, % 13.8Presence of other related conditions, % 12.5Albuminuria, % 8.1*12 months for all factors except total cholesterol (24 months)** Median (IQR)
155
Chapter 4.2 - Repeated measurements
in HbA1c (p=0.002) also increased the likelihood of treatment intensification. There was no significant influence of any of the other risk factor levels on the treatment decisions. In patients already using more drugs for other chronic diseases, starting treatment for all three risk factors (p<0.001), and intensification of antihypertensive treatment (p<0.001) was more likely. The number of risk factor specific drugs already prescribed did not influence the likelihood of treatment modification.The stratified analyses on overall cardiovascular risk showed essentially the same predictors for starting and intensifying medication with some shifts between the stra-ta (appendix). Compared to the associations found in the total patient group, the association of the last value of systolic blood pressure with treatment start increased in the high-risk group, while in the low-risk patients, this association became non-sig-nificant. The effect of repeated diastolic blood pressure measurements showed an opposite shift, increasing in the low-risk group and loosing significance in the high-risk group. For the intensification of blood pressure lowering medication the effect of the last value of diastolic blood pressure on intensification remained significant only in the low-risk stratum. The association between the last value of total cholesterol and treatment intensification of lipid lowering medication increased in the high-risk group, and decreased in the low-risk stratum.
DISCUSSIONThe decision to modify cardiometabolic treatment in patients with diabetes was only, in part, influenced by repeated elevated risk factor levels. Starting antihypertensive treatment and intensifying oral blood-glucose-lowering medication were affected by repeated measurements above target level. Surprisingly, starting treatment for any of the risk factors was more likely in patients with a higher medication burden. The found associations between predictors and outcomes, although they occurred sub-sequent to each other in time, are not necessarily causal.A treatment decision based on the last measurement in combination with recent history acknowledges the intrinsic variation of physiological measurement as well as other variation.28-30 Although it has been suggested that physicians take more than one measurement into account,12,18,19 we could only confirm this for the start of antihypertensive treatment and the intensification of oral blood-glucose-lowering medication. One could expect that a delay in acting on elevated risk factor levels is less desirable in high-risk patients. The models stratified on overall cardiovascular risk indeed showed that the impact of repeated high levels of diastolic blood pres-sure on the decision to start treatment was not significant in high-risk patients. No such differences were observed for the other treatment decisions. We also did not find a significant contribution of other risk factor levels on any of the treatment de-
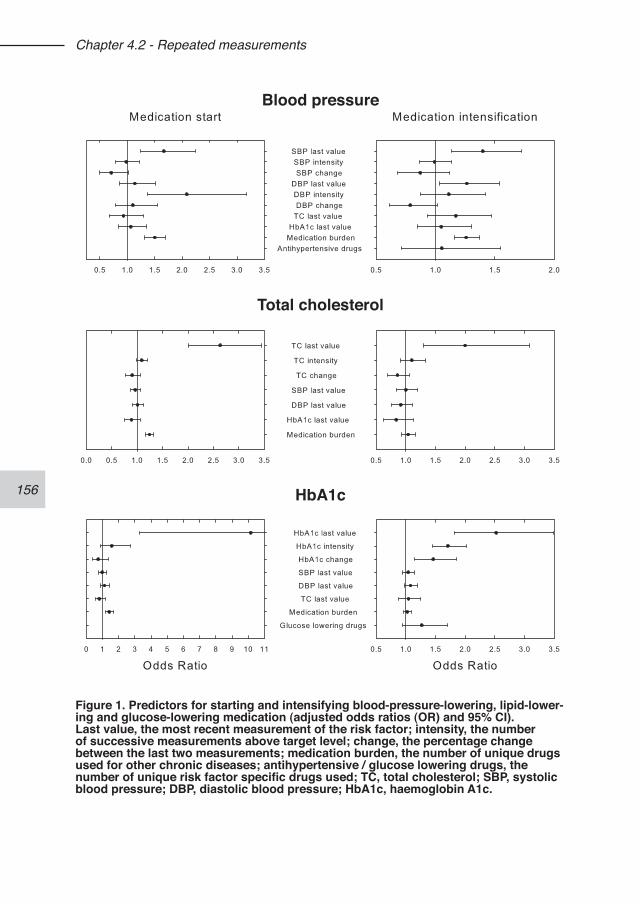
156
Chapter 4.2 - Repeated measurements
Blood pressure
Total cholesterol
HbA1c
Figure 1. Predictors for starting and intensifying blood-pressure-lowering, lipid-lower-ing and glucose-lowering medication (adjusted odds ratios (OR) and 95% CI).Last value, the most recent measurement of the risk factor; intensity, the number of successive measurements above target level; change, the percentage change between the last two measurements; medication burden, the number of unique drugs used for other chronic diseases; antihypertensive / glucose lowering drugs, the number of unique risk factor specific drugs used; TC, total cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure; HbA1c, haemoglobin A1c.
157
Chapter 4.2 - Repeated measurements
cisions, suggesting overall cardiovascular risk was generally not considered. This confirms previous findings showing that treatment changes were mainly determined by elevated levels of the corresponding risk factor.31,32 We observed an influence of both systolic and diastolic blood pressure values on the antihypertensive treatment decisions. Despite the fact that systolic blood pres-sure has become more important for treatment recommendations, diastolic blood pressure appeared still relevant for the GPs in our study. The decision to start treat-ment was influenced by the number of previous diastolic blood pressure measure-ments above target level. Studies looking only at the most recent measurements may therefore have underestimated the influence of diastolic blood pressure on phy-sicians’ decision making.9
According to physicians, concerns about medication burden and compliance are im-portant when deciding to prescribe drug treatment to patients using multiple drugs.8,13 In our study, the number of concurrently used drugs was not a barrier but instead positively associated with the start of medication. Previous studies conducted in the USA showed somewhat conflicting results, where a higher number of concur-rently used other drugs was either found negatively associated or not associated with treatment modifications.9,18 This discrepancy could be explained by differences in drug reimbursement between the countries studied: In The Netherlands there is no financial burden for the patient. Also, our study showed that in many cases drug treatment could be intensified without adding another drug. Furthermore, adding a drug might not be a problem for patients already used to a multiple-drug scheme.33
In contrast to antihypertensives and glucose lowering medication, decisions to start and intensify lipid lowering medication where not influenced by repeated risk fac-tor measurements. Relatively few patients received lipid-lowering medication, and intensification of such medication was uncommon. As was shown in other studies, GPs may have several reservations for prescribing lipid-lowering medication, such as expecting too few benefits in older patients or in patients with near-goal lipid levels.34,35 Also, patients can be reluctant to take them. The results from our study show that the reluctance to prescribe lipid-lowering drugs is not affected by repeated elevated lipid levels and might be seen as a decision of the GP not to prescribe lipid-lowering medication in some of their patients.This study has some limitations. The GPs in our study may not be representative of all GPs in the Netherlands. They participated voluntarily in a regional diabetes project, which could have resulted in a group of GPs included with a higher inter-est in diabetes than in general. The data used in this study come from the first retrospective data collection at these practices, and therefore alteration of the GPs’ prescribing behaviour due to the participation in the regional project was not pos-
158
Chapter 4.2 - Repeated measurements
sible. The level of prescribing in our GP population was similar to other populations in The Netherlands.31,36 It can be questioned whether the results are applicable to other countries. Although similar low rates of treatment and treatment intensification have been observed in other studies,37-39 there may be intrinsic differences in the health care system that influence the motivation and rate of treatment modifications. Furthermore, there can be unmeasured factors at the level of the general practice (e.g. time per consultation, GPs’ workload) and the patient (e.g. social economic status, educational level) that may influence the decisions.Our reliance on data collection from medical records has both strengths and weak-nesses. Incomplete registration may affect our findings. In general, prescribing data and test results are reliably documented in electronic records but underregistration of lifestyle data is common.40 Risk factor measurements, however, are not always routinely assessed by the GPs. In our analyses, we assume that the GPs’ prescrib-ing decisions were not influenced by test results that were not noted in the medical records. Furthermore, we were unable to correct for several potentially relevant confound-ers due to poor registration in the patient files, such as smoking, contraindications or patients’ non-adherence or refusal of treatment, which may have resulted in an underestimation of the effect of risk factor information on the likelihood of treatment modification. One study in the UK showed that a patient’s smoking status may af-fect the GPs’ decision to start lipid lowering medication.41 Medication adherence has been found both positively and negatively related to subsequent treatment modifica-tions.42-44 In a recent study, however, poor medication adherence was found to be irrelevant for the decision to intensify antihypertensive therapy.45
A strength of our study is that it analyses the effect of repeated risk factor measure-ments and concurrent medication on actual prescribing without relying on survey methods that may influence the outcomes.This study shows that waiting for the next measurement before deciding to modify treatment can explain part of the observed undertreatment for hypertension and hyperglycaemia that has been called “clinical inertia”.15,38 The low levels of treatment modification for lipid-lowering drugs, however, can not be explained by an awaiting attitude. Overall cardiovascular risk seems to have some impact on the decision to start or intensify treatment. An alerting system on the combined exposure to el-evated risk factors may be helpful to improve current treatment. Furthermore, quality assessment of physicians’ performance evaluations based only on the most recent measurement of a risk factor may lead to an inaccurate view on the decision making process.
159
Chapter 4.2 - Repeated measurements
REFERENCES1. Bouldin MJ, Low AK, Blackston JW, Duddleston DN, Holman HE, Hicks GS,
Brown CA. Quality of care in diabetes: understanding the guidelines. Am J Med Sci. 2002;324(4):196-206.
2. Saaddine JB, Cadwell B, Gregg EW, Engelgau MM, Vinicor F, Imperatore G, Narayan KM. Improvements in diabetes processes of care and intermediate out-comes: United States, 1988-2002. Ann Intern Med. 2006;144(7):465-74.
3. Andrade SE, Gurwitz JH, Field TS, Kelleher M, Majumdar SR, Reed G, Black R. Hypertension management: the care gap between clinical guidelines and clinical practice. Am J Manag Care. 2004;10(7 Pt 2):481-6.
4. Wan Q, Harris MF, Jayasinghe UW, Flack J, Georgiou A, Penn DL, Burns JR. Quality of diabetes care and coronary heart disease absolute risk in patients with type 2 diabetes mellitus in Australian general practice. Qual Saf Health Care. 2006;15(2):131-5.
5. Voorham J, Haaijer-Ruskamp FM, Stolk RP, Wolffenbuttel BHR, Denig P. Influence of elevated cardiometabolic risk factor levels on treatment changes in type 2 diabetes. Diabetes Care. 2008;31(3):501-3.
6. Parchman ML, Pugh JA, Romero RL, Bowers KW. Competing demands or clinical inertia: the case of elevated glycosylated hemoglobin. Ann Fam Med. 2007;5(3):196-201.
7. Kedward J, Dakin L. A qualitative study of barriers to the use of statins and the implementation of coronary heart disease prevention in primary care. Br J Gen Pract. 2003;53(494):684-9.
8. Parnes BL, Main DS, Dickinson LM, Niebauer L, Holcomb S, Westfall JM, Pace WDCN - CaReNetCN - HPRN. Clinical decisions regarding HbA1c results in pri-mary care: a report from CaReNet and HPRN. Diabetes Care. 2004;27(1):13-6.
9. Hicks PC, Westfall JM, Van Vorst RF, Bublitz Emsermann C, Dickinson LM, Pace W, Parnes B. Action or inaction? Decision making in patients with diabetes and elevated blood pressure in primary care. Diabetes Care. 2006;29(12):2580-5.
10. Borzecki AM, Oliveria SA, Berlowitz DR. Barriers to hypertension control. Am Heart J. 2005;149(5):785-94.
11. Cotton A, Aspy CB, Mold J, Stein H. Clinical decision-making in blood pres-sure management of patients with diabetes mellitus: an Oklahoma Physicians Resource/Research Network (OKPRN) Study. J Am Board Fam Med. 2006;19(3):232-9.
12. Ferrari P, Hess L, Pechere-Bertschi A, Muggli F, Burnier M. Reasons for not intensifying antihypertensive treatment (RIAT): a primary care antihypertensive intervention study. J Hypertens 2004;22(6):1221-9.
13. Yarzebski J, Bujor CF, Goldberg RJ, Spencer F, Lessard D, Gore JM. A commu-nity-wide survey of physician practices and attitudes toward cholesterol man-agement in patients with recent acute myocardial infarction. Arch Intern Med. 2002;162(7):797-804.
14. Persson M, Carlberg B, Tavelin B, Lindholm LH. Doctors’ estimation of cardio-vascular risk and willingness to give drug treatment in hypertension: fair risk as-
160
Chapter 4.2 - Repeated measurements
sessment but defensive treatment policy. J Hypertens. 2004;22(1):65-71.15. Safford MM, Shewchuk R, Qu H, Williams JH, Estrada CA, Ovalle F, Allison JJ.
Reasons for not intensifying medications: differentiating “clinical inertia” from ap-propriate care. J Gen Intern Med. 2007;22(12):1648-55.
16. Oliveria SA, Lapuerta P, McCarthy BD, L’Italien GJ, Berlowitz DR, Asch SM. Physician-related barriers to the effective management of uncontrolled hyperten-sion. Arch Intern Med. 2002;162(4):413-20.
17. Boyd CM, Darer J, Boult C, Fried LP, Boult L, Wu AW. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implica-tions for pay for performance. JAMA. 2005;294(6):716-24.
18. Rodondi N, Peng T, Karter AJ, Bauer DC, Vittinghoff E, Tang S, Pettitt D, Kerr EA, Selby JV. Therapy modifications in response to poorly controlled hyperten-sion, dyslipidemia, and diabetes mellitus. Ann Intern Med. 2006;144(7):475-84.
19. Voorham J, Denig P, Wolffenbuttel BHR, Haaijer-Ruskamp FM. Cross-sectional versus sequential quality indicators of risk factor management in patients with type 2 diabetes. Medical Care. 2008;46(2):133-141.
20. Voorham J, Denig P. Computerized extraction of information on the quality of diabetes care from free text in electronic patient records of general practitioners. J Am Med Inform Assoc. 2007;14(3):349-354.
21. Code of Conduct: Use of data in health research. Stichting FMWV (Federation of Biomedical Scientific Societies), Rotterdam, 2005. Accessed at http://www.federa.org on December 2008.
22. Dutch Pharmacotherapy Compendium (Farmcotherapeutisch Kompas) 2004. Comissie Farmaceutische Hulp (CHF) van het College van Zorgverzekeringen. 2004.
23. Walma EP, Thomas S, Prins A, Grundmeyer HGLM, Van der Laan JR, Wiersma Tj. Practice guideline ‘Hypertension’ (third revision) from the Dutch College of General Practitioners. Huisarts Wet. 2003;46:435-49.
24. Thomas S, van der Weijden T, van Drenth BB, Haverkort AFM, Hooi JD, van der Laan JD. Practice guideline ‘Cholesterol’ (first revision) from the Dutch College of General Practitioners. Huisarts Wet. 1999;42:406-417.
25. Rutten GEHM, Verhoeven S, Heine RJ, de Grauw WJ, Cromme PV,Reenders K, van Ballegooie E, Wiersma Tj: Practice guideline ‘Diabetes mellitus type 2’ (first revision) from the Dutch College of General Practitioners. Huisarts Wet. 1999;42:67-84.
26. WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC classification and DDD assignment, 2010. Oslo, 2009.
27. Stevens R, Adler A, Gray A, Briggs A, Holman R. Life-expectancy projection by modelling and computer simulation (UKPDS 46). Diabetes Res Clin Pract. 2000;50(Suppl 3):S5-13.
28. Houweling ST, Kleefstra N, Lutgers HL, Groenier KH, Meyboom-de Jong B, Bilo HJ. Pitfalls in blood pressure measurement in daily practice. Fam Pract. 2006;23:20-7.
29. Kelly GS. Seasonal variations of selected cardiovascular risk factors. Altern Med Rev. 2005;10(4):307-20.
161
Chapter 4.2 - Repeated measurements
30. Twomey PJ, Wierzbicki AS, Reynolds TM. Issues to consider when attempting to achieve the American Diabetes Association clinical quality requirement for haemoglobin A1c. Curr Med Res Opin. 2003;19(8):719-23.
31. Greving JP, Denig P, de Zeeuw D, Bilo H, Haaijer-Ruskamp FM. Trends in hyper-lipidemia and hypertension management in type 2 diabetes patients from 1998-2004: a longitudinal observational study. Cardiovasc Diabetol. 2007;6:25.
32. Atthobari J, Monster TB, de Jong PE, de Jong-van den Berg LT. The effect of hypertension and hypercholesterolemia screening with subsequent intervention letter on the use of blood pressure and lipid lowering drugs. Br J Clin Pharmacol. 2004;57(3):328-36.
33. Tjia J, Givens JL, Karlawish JH, Okoli-Umeweni A, Barg FK. Beneath the sur-face: discovering the unvoiced concerns of older adults with type 2 diabetes mellitus. Health Educ Res. 2008;23(1):40-52.
34. Hickling J, Rogers S, Nazareth I. Barriers to detecting and treating hypercholes-terolaemia in patients with ischaemic heart disease: primary care perceptions. Br J Gen Pract. 2005;55(516):534-8.
35. Foley KA, Denke MA, Kamal-Bahl S, Simpson R Jr, Berra K, Sajjan S, Alexander CM. The impact of physician attitudes and beliefs on treatment decisions: lipid therapy in high-risk patients. Med Care. 2006;44(5):421-8.
36. Ubink-Veltmaat LJ, Bilo HJ, Groenier KH, Rischen RO, Meyboom-de Jong B. Shared care with task delegation to nurses for type 2 diabetes: prospective ob-servational study. Neth J Med. 2005;63(3):103-10.
37. Grant RW, Buse JB, Meigs JB. Quality of diabetes care in U.S. academic medical centers: low rates of medical regimen change. Diabetes Care. 2005;28(2):337-442.
38. Grant RW, Cagliero E, Dubey AK, Gildesgame C, Chueh HC, Barry MJ, Singer DE, Nathan DM, Meigs JB. Clinical inertia in the management of Type 2 diabetes metabolic risk factors. Diabet Med 2004;21(2):150-5.
39. Bryant W, Greenfield JR, Chisholm DJ, Campbell LV. Diabetes guidelines: easier to preach than to practise? Med J Aust. 2006;185(6):305-9.
40. Thiru K, Hassey A, Sullivan F. Systematic review of scope and quality of elec-tronic patient record data in primary care. BMJ. 2003;326(7398):1070.
41. Evans JS, Harries C, Dennis I, Dean J. General practitioners’ tacit and stated poli-cies in the prescription of lipid lowering agents. Br J Gen Pract. 1995;45(390):15-8.
42. Van Wijk BL, Klungel OH, Heerdink ER, de Boer A. The association between compliance with antihypertensive drugs and modification of antihypertensive drug regimen. J Hypertens. 2004;22(9):1831-7.
43. Grant R, Adams AS, Trinacty CM, Zhang F, Kleinman K, Soumerai SB, Meigs JB, Ross-Degnan D. Relationship between patient medication adherence and subsequent clinical inertia in type 2 diabetes glycemic management. Diabetes Care. 2007;30(4):807-12.
44. Kogut SJ, Andrade SE, Willey C, Larrat EP. Nonadherence as a predictor of an-tidiabetic drug therapy intensification (augmentation). Pharmacoepidemiol Drug Saf. 2004;13(9):591-8.
162
Chapter 4.2 - Repeated measurements
45. Heisler M, Hogan MM, Hofer TP, Schmittdiel JA, Pladevall M, Kerr EA. When more is not better: treatment intensification among hypertensive patients with poor medication adherence. Circulation. 2008;117(22):2884-92.
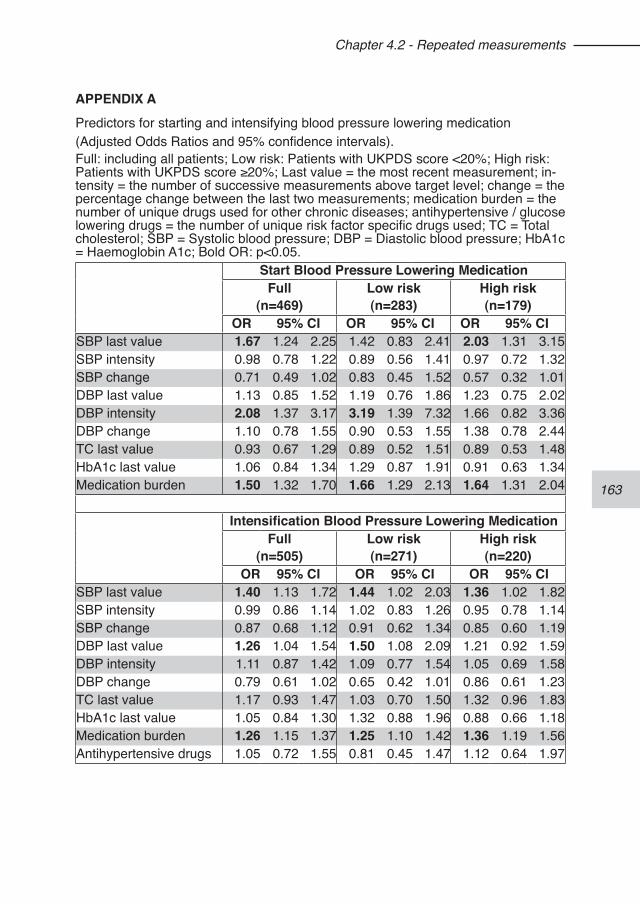
163
Chapter 4.2 - Repeated measurements
APPENDIX APredictors for starting and intensifying blood pressure lowering medication (Adjusted Odds Ratios and 95% confidence intervals).Full: including all patients; Low risk: Patients with UKPDS score <20%; High risk: Patients with UKPDS score ≥20%; Last value = the most recent measurement; in-tensity = the number of successive measurements above target level; change = the percentage change between the last two measurements; medication burden = the number of unique drugs used for other chronic diseases; antihypertensive / glucose lowering drugs = the number of unique risk factor specific drugs used; TC = Total cholesterol; SBP = Systolic blood pressure; DBP = Diastolic blood pressure; HbA1c = Haemoglobin A1c; Bold OR: p<0.05.
Start Blood Pressure Lowering MedicationFull
(n=469)Low risk(n=283)
High risk(n=179)
OR 95% CI OR 95% CI OR 95% CISBP last value 1.67 1.24 2.25 1.42 0.83 2.41 2.03 1.31 3.15SBP intensity 0.98 0.78 1.22 0.89 0.56 1.41 0.97 0.72 1.32SBP change 0.71 0.49 1.02 0.83 0.45 1.52 0.57 0.32 1.01DBP last value 1.13 0.85 1.52 1.19 0.76 1.86 1.23 0.75 2.02DBP intensity 2.08 1.37 3.17 3.19 1.39 7.32 1.66 0.82 3.36DBP change 1.10 0.78 1.55 0.90 0.53 1.55 1.38 0.78 2.44TC last value 0.93 0.67 1.29 0.89 0.52 1.51 0.89 0.53 1.48HbA1c last value 1.06 0.84 1.34 1.29 0.87 1.91 0.91 0.63 1.34Medication burden 1.50 1.32 1.70 1.66 1.29 2.13 1.64 1.31 2.04
Intensification Blood Pressure Lowering MedicationFull
(n=505)Low risk(n=271)
High risk(n=220)
OR 95% CI OR 95% CI OR 95% CISBP last value 1.40 1.13 1.72 1.44 1.02 2.03 1.36 1.02 1.82SBP intensity 0.99 0.86 1.14 1.02 0.83 1.26 0.95 0.78 1.14SBP change 0.87 0.68 1.12 0.91 0.62 1.34 0.85 0.60 1.19DBP last value 1.26 1.04 1.54 1.50 1.08 2.09 1.21 0.92 1.59DBP intensity 1.11 0.87 1.42 1.09 0.77 1.54 1.05 0.69 1.58DBP change 0.79 0.61 1.02 0.65 0.42 1.01 0.86 0.61 1.23TC last value 1.17 0.93 1.47 1.03 0.70 1.50 1.32 0.96 1.83HbA1c last value 1.05 0.84 1.30 1.32 0.88 1.96 0.88 0.66 1.18Medication burden 1.26 1.15 1.37 1.25 1.10 1.42 1.36 1.19 1.56Antihypertensive drugs 1.05 0.72 1.55 0.81 0.45 1.47 1.12 0.64 1.97
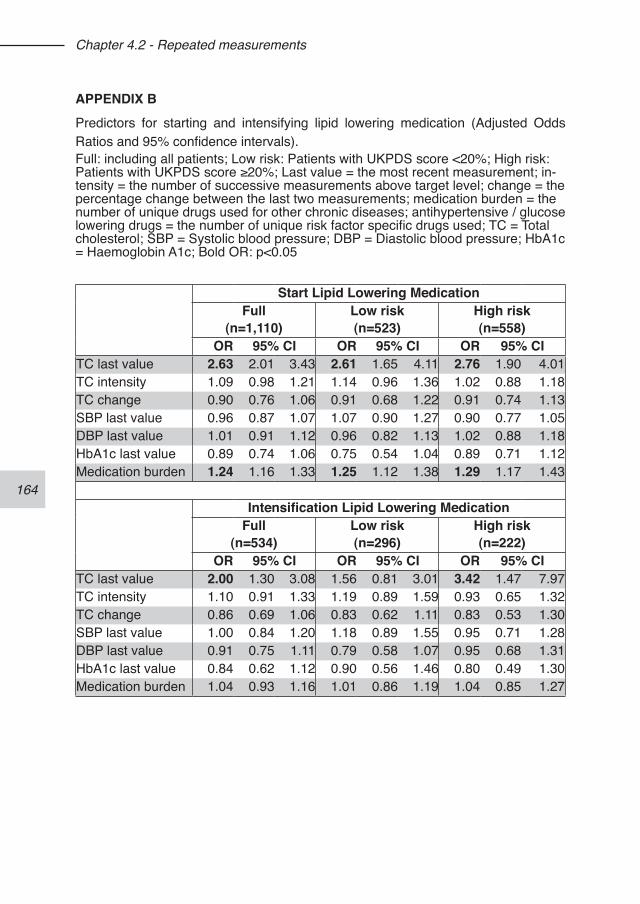
164
Chapter 4.2 - Repeated measurements
APPENDIX BPredictors for starting and intensifying lipid lowering medication (Adjusted Odds Ratios and 95% confidence intervals).Full: including all patients; Low risk: Patients with UKPDS score <20%; High risk: Patients with UKPDS score ≥20%; Last value = the most recent measurement; in-tensity = the number of successive measurements above target level; change = the percentage change between the last two measurements; medication burden = the number of unique drugs used for other chronic diseases; antihypertensive / glucose lowering drugs = the number of unique risk factor specific drugs used; TC = Total cholesterol; SBP = Systolic blood pressure; DBP = Diastolic blood pressure; HbA1c = Haemoglobin A1c; Bold OR: p<0.05
Start Lipid Lowering MedicationFull
(n=1,110)Low risk(n=523)
High risk(n=558)
OR 95% CI OR 95% CI OR 95% CITC last value 2.63 2.01 3.43 2.61 1.65 4.11 2.76 1.90 4.01TC intensity 1.09 0.98 1.21 1.14 0.96 1.36 1.02 0.88 1.18TC change 0.90 0.76 1.06 0.91 0.68 1.22 0.91 0.74 1.13SBP last value 0.96 0.87 1.07 1.07 0.90 1.27 0.90 0.77 1.05DBP last value 1.01 0.91 1.12 0.96 0.82 1.13 1.02 0.88 1.18HbA1c last value 0.89 0.74 1.06 0.75 0.54 1.04 0.89 0.71 1.12Medication burden 1.24 1.16 1.33 1.25 1.12 1.38 1.29 1.17 1.43
Intensification Lipid Lowering MedicationFull
(n=534)Low risk(n=296)
High risk(n=222)
OR 95% CI OR 95% CI OR 95% CITC last value 2.00 1.30 3.08 1.56 0.81 3.01 3.42 1.47 7.97TC intensity 1.10 0.91 1.33 1.19 0.89 1.59 0.93 0.65 1.32TC change 0.86 0.69 1.06 0.83 0.62 1.11 0.83 0.53 1.30SBP last value 1.00 0.84 1.20 1.18 0.89 1.55 0.95 0.71 1.28DBP last value 0.91 0.75 1.11 0.79 0.58 1.07 0.95 0.68 1.31HbA1c last value 0.84 0.62 1.12 0.90 0.56 1.46 0.80 0.49 1.30Medication burden 1.04 0.93 1.16 1.01 0.86 1.19 1.04 0.85 1.27
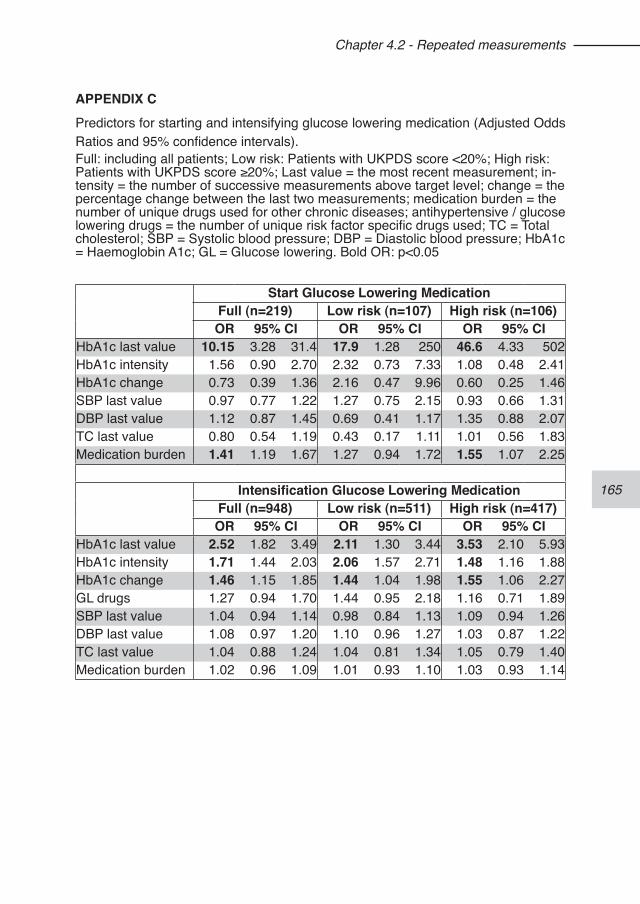
165
Chapter 4.2 - Repeated measurements
APPENDIX CPredictors for starting and intensifying glucose lowering medication (Adjusted Odds Ratios and 95% confidence intervals).Full: including all patients; Low risk: Patients with UKPDS score <20%; High risk: Patients with UKPDS score ≥20%; Last value = the most recent measurement; in-tensity = the number of successive measurements above target level; change = the percentage change between the last two measurements; medication burden = the number of unique drugs used for other chronic diseases; antihypertensive / glucose lowering drugs = the number of unique risk factor specific drugs used; TC = Total cholesterol; SBP = Systolic blood pressure; DBP = Diastolic blood pressure; HbA1c = Haemoglobin A1c; GL = Glucose lowering. Bold OR: p<0.05
Start Glucose Lowering MedicationFull (n=219) Low risk (n=107) High risk (n=106)OR 95% CI OR 95% CI OR 95% CI
HbA1c last value 10.15 3.28 31.4 17.9 1.28 250 46.6 4.33 502HbA1c intensity 1.56 0.90 2.70 2.32 0.73 7.33 1.08 0.48 2.41HbA1c change 0.73 0.39 1.36 2.16 0.47 9.96 0.60 0.25 1.46SBP last value 0.97 0.77 1.22 1.27 0.75 2.15 0.93 0.66 1.31DBP last value 1.12 0.87 1.45 0.69 0.41 1.17 1.35 0.88 2.07TC last value 0.80 0.54 1.19 0.43 0.17 1.11 1.01 0.56 1.83Medication burden 1.41 1.19 1.67 1.27 0.94 1.72 1.55 1.07 2.25
Intensification Glucose Lowering MedicationFull (n=948) Low risk (n=511) High risk (n=417)OR 95% CI OR 95% CI OR 95% CI
HbA1c last value 2.52 1.82 3.49 2.11 1.30 3.44 3.53 2.10 5.93HbA1c intensity 1.71 1.44 2.03 2.06 1.57 2.71 1.48 1.16 1.88HbA1c change 1.46 1.15 1.85 1.44 1.04 1.98 1.55 1.06 2.27GL drugs 1.27 0.94 1.70 1.44 0.95 2.18 1.16 0.71 1.89SBP last value 1.04 0.94 1.14 0.98 0.84 1.13 1.09 0.94 1.26DBP last value 1.08 0.97 1.20 1.10 0.96 1.27 1.03 0.87 1.22TC last value 1.04 0.88 1.24 1.04 0.81 1.34 1.05 0.79 1.40Medication burden 1.02 0.96 1.09 1.01 0.93 1.10 1.03 0.93 1.14
166
167
Chapter 4.3 - Medication adherence affects treatment modifications in type 2 diabetes
Jaco Voorham1,2
Flora M Haaijer-Ruskamp1
Ronald P Stolk2
Bruce HR Wolffenbuttel3
Petra Denig1
1. Department of Clinical Pharmacology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
2. Department of Epidemiology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
3. Department of Endocrinology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
Voorham J, Haaijer-Ruskamp FM, Stolk RP, Wolffenbuttel BHR, Denig P; Groningen Initiative to Analyze Type 2 Diabetes Treatment Group. Medication adherence af-fects treatment modifications in type 2 diabetes. Submitted.
168
Chapter 4.3 - Medication adherence
ABSTRACTBackground. Low rates of treatment modification in patients with insufficiently con-trolled risk factors are common in type 2 diabetes. Although possible adherence problems are often mentioned in surveys as a reason for not intensifying treatment, observational studies have shown inconclusive results regarding this association. Aim. To assess how patients’ medication adherence affects treatment modifications for hypertension and hyperglycaemia. Methods. Cohort study in 11,268 primary care patients with type 2 diabetes. Inclusion criteria were patients prescribed blood pressure or glucose-regulating medica-tion, having at least one elevated measurement in 2007 (systolic blood pressure ≥140mmHg, HbA1c ≥7%), and not on maximal treatment. Treatment modifications were classified as none, dose increase or decrease, class switch, addition or discon-tinuation within 60 days. Refill adherence was assessed as medication possession ratio (MPR), or length of the last gap between refills. We performed multilevel multi-nomial regression analysis to test for associations.Results. We included 4,980 and 2,945 treated patients with elevated blood pressure respectively HbA1c levels. Patients with lower adherence for antihypertensives were more likely to have medication discontinued (odds ratio (OR) for 10% higher MPR: 1.22, 95% CI 1.11-1.33) or dose decreased (OR 1.14, CI 1.01-1.28). For glucose-regulating medication, dose increases (OR 0.92, 95% CI 0.85-0.98) and medication additions (OR 0.90, 95% CI 0.82-0.98) were less likely in patients with lower adher-ence levels.Conclusions. Low adherence inhibits the intensification of glucose-regulating but not antihypertensive medication in insufficiently controlled patients. Adherence affects decisions on drug treatment differently for different therapeutic areas.
169
Chapter 4.3 - Medication adherence
INTRODUCTIONDespite considerable progress in the field of cardiovascular and metabolic risk fac-tor management in type 2 diabetes during the last decade, undertreatment remains a topic of importance.1-3 Since it is hard to believe physicians simply choose to do nothing when confronted with patients with elevated risk factor levels, several stud-ies have looked into plausible reasons for not acting when indicated. Factors at the level of the prescriber as well as at the level of the patient have been identified.4,5 Especially in elderly patients who use multiple medications, there is a fear to in-crease medication burden.6,7 A physician may also be reluctant to intervene with pharmacotherapy when a patient has difficulties with lifestyle modifications,8 or when a patient is reluctant to take medication.9 Poor adherence is considered as a reason not to intensify treatment.10,11 Observational studies, however, demonstrated conflict-ing results on the association between medication adherence and treatment inten-sification.12-17
Some disagreements may be due to the differences in definitions of both medication adherence and treatment intensification. Medication adherence has been assessed using various measures based on prescription refill data.18,19 This often leads to a binary classification of patients collecting sufficient amounts of pills or without large gap periods between prescription refills. Treatment intensification is commonly as-sessed as a binary outcome (intensification or not), including dose increase, addition of a new drug and sometimes even switches within or between classes of drugs16 as intensification. All other therapy modifications are classified as no intensification. In patients with adherence problems it is then considered appropriate not to inten-sify therapy.15-17 There can, however, be other appropriate therapy modifications, depending on the underlying reasons for non-adherence. Patient perceptions about benefits and risks of the treatment are important for their adherence.20 In case of side effects, switching to another class or decreasing the medication dose is warranted. Which action is most appropriate may differ between therapeutic areas with various treatment options. To our knowledge there are no studies on the effect of medication adherence on distinct therapy modifications in different therapeutic areas. The aim of this study is to assess how patients’ medication adherence affects pre-scribing modifications for hypertension and hyperglycaemia in type 2 diabetic pa-tients. Secondary aim is to assess the effect of different adherence estimates and outcome measures. An estimate based on overall period adherence is compared to an estimate based on the length of the last gap between prescription refills. We also assessed possible effects on all distinct treatment modifications in comparison to the commonly used classification of whether or not treatment was intensified.
170
Chapter 4.3 - Medication adherence
METHODSWe conducted a cohort study to assess the influence of medication adherence on prescribing modifications. Clinical measurements, prescriptions, and demographic data for patients with type 2 diabetes were collected from the Groningen Initiative to Analyse Type 2 diabetes Treatment (GIANTT) database. This database contains an-onymised longitudinal information retrieved from electronic medical records of gen-eral practitioners (GPs).21 In the Netherlands, patients are registered with a single GP. The GPs in our study prescribe electronically, ensuring full information on pre-scribed drugs and dosing schemes. For research using anonymous medical records no ethics committee approval is needed in The Netherlands.22
Study populationThe study population consisted of patients with a diagnosis of type 2 diabetes, who were managed by 142 general practitioners. Patients were included if they were di-agnosed before 2007, had at least one risk factor measurement above the treatment target (≥140 mmHg for systolic blood pressure (SBP), ≥7 % for HbA1c) in 2007, and received at least one prescription for an antihypertensive or glucose-regulating drug in the preceding half year. Since our data do not allow for assessing referrals to specialist care nor changes in insulin dose, we excluded patients from the analyses if they already received 3 or more drug classes on maximal maintenance dose for blood pressure lowering, or insulin as glucose-regulating medication (see table 1 for definitions).
Treatment modificationsFor each patient, the first elevated risk factor observation in 2007 is taken as the index observation. The primary outcome in our study is the first therapy modifica-tion after this index observation. Therapy modifications were assessed during a 60 days period starting on the index date. Modifications were classified as: none, dose increase, dose decrease, class switch, addition of a new class, and discontinuation of a class (see table 1 for definitions). For glucose-regulating medication, we also in-cluded start of insulin as a distinct treatment modification. In case of multiple therapy intensifications, insulin start or class addition prevailed, and for multiple reductions, class discontinuation prevailed. Patients with modifications into opposite directions (n=17) were excluded (e.g. a dose increase coinciding with a dose decrease). For comparison, we constructed the commonly used binary outcome: 1) intensification (i.e. dose increase or class added), 2) no intensification (all other cases).
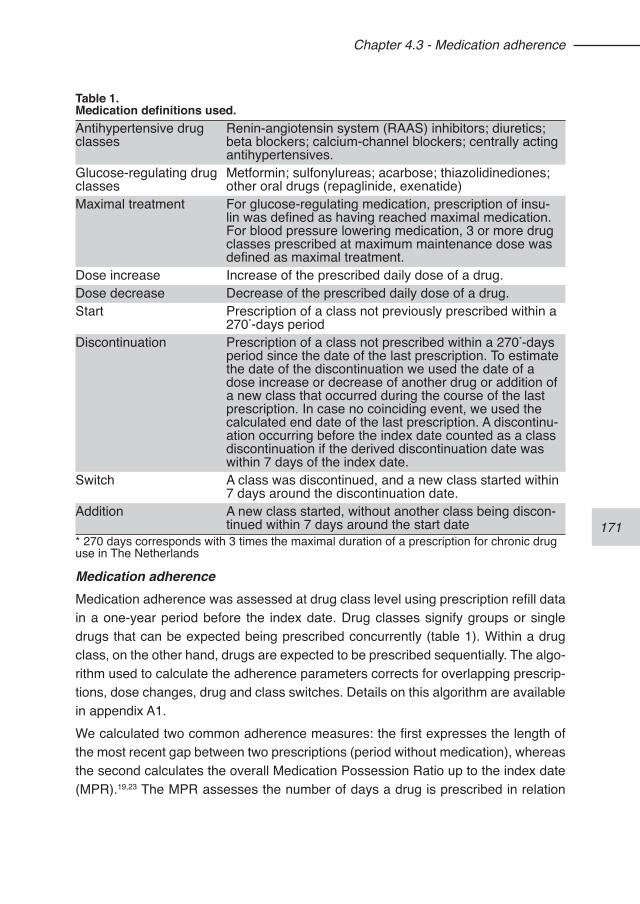
171
Chapter 4.3 - Medication adherence
Medication adherenceMedication adherence was assessed at drug class level using prescription refill data in a one-year period before the index date. Drug classes signify groups or single drugs that can be expected being prescribed concurrently (table 1). Within a drug class, on the other hand, drugs are expected to be prescribed sequentially. The algo-rithm used to calculate the adherence parameters corrects for overlapping prescrip-tions, dose changes, drug and class switches. Details on this algorithm are available in appendix A1.We calculated two common adherence measures: the first expresses the length of the most recent gap between two prescriptions (period without medication), whereas the second calculates the overall Medication Possession Ratio up to the index date (MPR).19,23 The MPR assesses the number of days a drug is prescribed in relation
Table 1. Medication definitions used.Antihypertensive drug classes
Renin-angiotensin system (RAAS) inhibitors; diuretics; beta blockers; calcium-channel blockers; centrally acting antihypertensives.
Glucose-regulating drug classes
Metformin; sulfonylureas; acarbose; thiazolidinediones; other oral drugs (repaglinide, exenatide)
Maximal treatment For glucose-regulating medication, prescription of insu-lin was defined as having reached maximal medication. For blood pressure lowering medication, 3 or more drug classes prescribed at maximum maintenance dose was defined as maximal treatment.
Dose increase Increase of the prescribed daily dose of a drug.Dose decrease Decrease of the prescribed daily dose of a drug.Start Prescription of a class not previously prescribed within a
270*-days periodDiscontinuation Prescription of a class not prescribed within a 270*-days
period since the date of the last prescription. To estimate the date of the discontinuation we used the date of a dose increase or decrease of another drug or addition of a new class that occurred during the course of the last prescription. In case no coinciding event, we used the calculated end date of the last prescription. A discontinu-ation occurring before the index date counted as a class discontinuation if the derived discontinuation date was within 7 days of the index date.
Switch A class was discontinued, and a new class started within 7 days around the discontinuation date.
Addition A new class started, without another class being discon-tinued within 7 days around the start date
* 270 days corresponds with 3 times the maximal duration of a prescription for chronic drug use in The Netherlands
172
Chapter 4.3 - Medication adherence
to the prescribing period, and is a measure of overall medication availability. We expect that the length of the most recent gap can be more visible to the prescribing physicians than a period assessment like the MPR. The latter, on the other hand, may better reflect chronic sub-optimal adherence. We quantified adherence using the largest last gap in any of concurrently prescribed drug classes within either an-tihypertensives or glucose-regulating medication, and analogously used the lowest MPR within each therapeutic group.
Statistical analysisTo analyse the association between adherence and treatment modification, adjust-ed odds ratios (OR) and their 95% confidence intervals (CI) were calculated using multilevel multinomial logistic regression, correcting for clustering at the GP level. Potential confounders added to the models were the index risk factor level, age, sex, DM duration, number of risk factor specific drug classes used, number of other chronic drugs used. Since in glucose-regulating medication it is common practice to increase a drug’s dose until its maximal dose is reached, we included a binary variable indicating whether all drugs used were described at maximal maintenance dose or not.To assess the effect of using different adherence and outcome measures, all analy-ses were conducted using either the last gap or the MPR adherence measure, and using distinct treatment modifications as well as the binary intensification outcome.Odds ratios are presented for 10% increase in MPR or 14 days increase of last gap length. For comparison, we also used categorical adherence measures instead of continuous ones based on commonly used cut-off points of 15 and 30 days for the gap length, and of 70% and 80% for the MPR level.
RESULTSOf the 11,268 patients, respectively 4,980 and 2,945 could be included in the analy-ses for antihypertensive and glucose-regulating medication (figure 1). The patient populations differed slightly with respect to the percentage female, age and diabetes duration (table 2). The most frequently used antihypertensive drug classes were RAAS inhibitors, diu-retics and beta-blockers. One third of the patients were on monotherapy, and 38% used two classes (table 2). The majority of the patients showed high adherence to antihypertensive medication of ≥80% MPR (82% of patients) or last gap<15 days (76%), while low adherence was seen in 6% (MPR below 50%) to 14% (last gap length of at least 30 days).The most frequently used glucose-regulating drugs were metformin and sulfonylu-
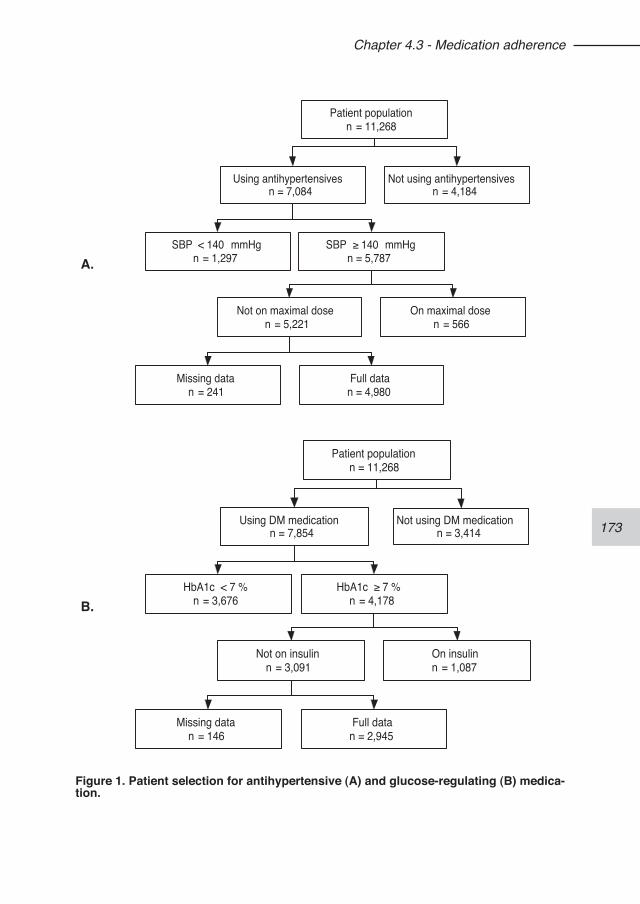
173
Chapter 4.3 - Medication adherence
A.
Patient populationn = 11,268
Using antihypertensivesn = 7,084
Not using antihypertensivesn = 4,184
SBP < 140 mmHgn = 1,297
SBP ≥ 140 mmHgn = 5,787
Not on maximal dosen = 5,221
On maximal dosen = 566
Missing datan = 241
Full datan = 4,980
B.
Patient populationn = 11,268
Using DM medicationn = 7,854
Not using DM medicationn = 3,414
HbA1c < 7 %n = 3,676
HbA1c ≥ 7 %n = 4,178
Not on insulinn = 3,091
On insulinn = 1,087
Missing datan = 146
Full datan = 2,945
Figure 1. Patient selection for antihypertensive (A) and glucose-regulating (B) medica-tion.
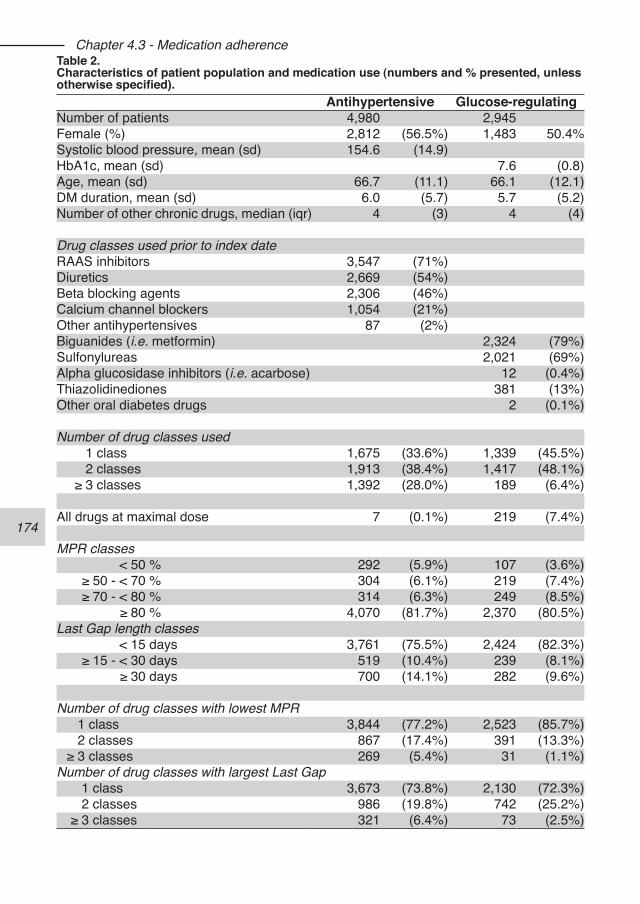
174
Chapter 4.3 - Medication adherenceTable 2. Characteristics of patient population and medication use (numbers and % presented, unless otherwise specified).
Antihypertensive Glucose-regulatingNumber of patients 4,980 2,945Female (%) 2,812 (56.5%) 1,483 50.4%Systolic blood pressure, mean (sd) 154.6 (14.9)HbA1c, mean (sd) 7.6 (0.8)Age, mean (sd) 66.7 (11.1) 66.1 (12.1)DM duration, mean (sd) 6.0 (5.7) 5.7 (5.2)Number of other chronic drugs, median (iqr) 4 (3) 4 (4)
Drug classes used prior to index dateRAAS inhibitors 3,547 (71%)Diuretics 2,669 (54%)Beta blocking agents 2,306 (46%)Calcium channel blockers 1,054 (21%)Other antihypertensives 87 (2%)Biguanides (i.e. metformin) 2,324 (79%)Sulfonylureas 2,021 (69%)Alpha glucosidase inhibitors (i.e. acarbose) 12 (0.4%)Thiazolidinediones 381 (13%)Other oral diabetes drugs 2 (0.1%)
Number of drug classes used1 class 1,675 (33.6%) 1,339 (45.5%)2 classes 1,913 (38.4%) 1,417 (48.1%)
≥ 3 classes 1,392 (28.0%) 189 (6.4%)
All drugs at maximal dose 7 (0.1%) 219 (7.4%)
MPR classes< 50 % 292 (5.9%) 107 (3.6%)
≥ 50 - < 70 % 304 (6.1%) 219 (7.4%)≥ 70 - < 80 % 314 (6.3%) 249 (8.5%)
≥ 80 % 4,070 (81.7%) 2,370 (80.5%)Last Gap length classes
< 15 days 3,761 (75.5%) 2,424 (82.3%)≥ 15 - < 30 days 519 (10.4%) 239 (8.1%)
≥ 30 days 700 (14.1%) 282 (9.6%)
Number of drug classes with lowest MPR1 class 3,844 (77.2%) 2,523 (85.7%)2 classes 867 (17.4%) 391 (13.3%)
≥ 3 classes 269 (5.4%) 31 (1.1%)Number of drug classes with largest Last Gap
1 class 3,673 (73.8%) 2,130 (72.3%)2 classes 986 (19.8%) 742 (25.2%)
≥ 3 classes 321 (6.4%) 73 (2.5%)
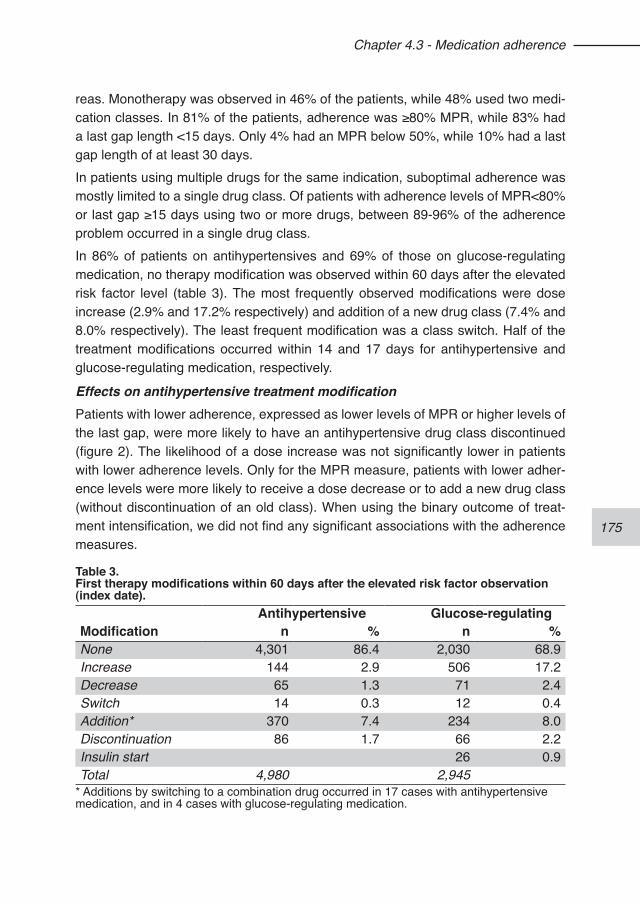
175
Chapter 4.3 - Medication adherence
reas. Monotherapy was observed in 46% of the patients, while 48% used two medi-cation classes. In 81% of the patients, adherence was ≥80% MPR, while 83% had a last gap length <15 days. Only 4% had an MPR below 50%, while 10% had a last gap length of at least 30 days.In patients using multiple drugs for the same indication, suboptimal adherence was mostly limited to a single drug class. Of patients with adherence levels of MPR<80% or last gap ≥15 days using two or more drugs, between 89-96% of the adherence problem occurred in a single drug class.In 86% of patients on antihypertensives and 69% of those on glucose-regulating medication, no therapy modification was observed within 60 days after the elevated risk factor level (table 3). The most frequently observed modifications were dose increase (2.9% and 17.2% respectively) and addition of a new drug class (7.4% and 8.0% respectively). The least frequent modification was a class switch. Half of the treatment modifications occurred within 14 and 17 days for antihypertensive and glucose-regulating medication, respectively.
Effects on antihypertensive treatment modificationPatients with lower adherence, expressed as lower levels of MPR or higher levels of the last gap, were more likely to have an antihypertensive drug class discontinued (figure 2). The likelihood of a dose increase was not significantly lower in patients with lower adherence levels. Only for the MPR measure, patients with lower adher-ence levels were more likely to receive a dose decrease or to add a new drug class (without discontinuation of an old class). When using the binary outcome of treat-ment intensification, we did not find any significant associations with the adherence measures.
Table 3. First therapy modifications within 60 days after the elevated risk factor observation (index date).
Antihypertensive Glucose-regulatingModification n % n %None 4,301 86.4 2,030 68.9Increase 144 2.9 506 17.2Decrease 65 1.3 71 2.4Switch 14 0.3 12 0.4Addition* 370 7.4 234 8.0Discontinuation 86 1.7 66 2.2Insulin start 26 0.9Total 4,980 2,945
* Additions by switching to a combination drug occurred in 17 cases with antihypertensive medication, and in 4 cases with glucose-regulating medication.
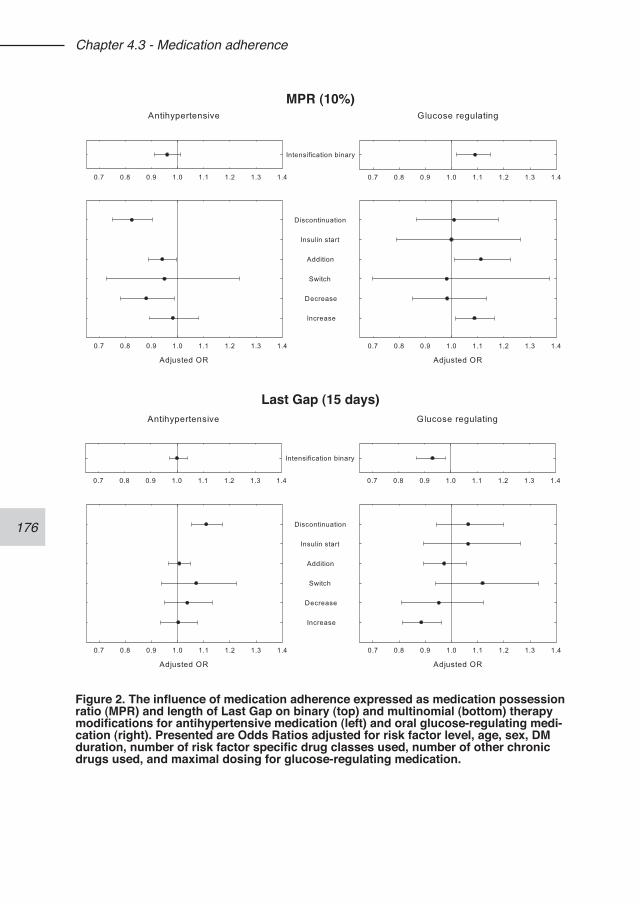
176
Chapter 4.3 - Medication adherence
MPR (10%)
Last Gap (15 days)
Figure 2. The influence of medication adherence expressed as medication possession ratio (MPR) and length of Last Gap on binary (top) and multinomial (bottom) therapy modifications for antihypertensive medication (left) and oral glucose-regulating medi-cation (right). Presented are Odds Ratios adjusted for risk factor level, age, sex, DM duration, number of risk factor specific drug classes used, number of other chronic drugs used, and maximal dosing for glucose-regulating medication.
177
Chapter 4.3 - Medication adherence
Effects on glucose-regulating treatment modificationFor glucose-regulating medication, we observed a lower likelihood for dose increas-es in patients with lower adherence levels using either adherence measure (figure 2). For every 10% decrease in MPR the patients were 8% less likely to have the dose of their medication increased. For the last gap length, this was a 12% reduction in probability for every 14 days increase in gap length. Only for the MPR measure, we found a lower likelihood to add a new class in patients with lower adherence lev-els (figure 2). The level of adherence did not significantly affect starting with insulin. The binary outcome of intensification also showed that a lower level of adherence was associated with a lower probability to intensify treatment.
Categorical adherence measuresFor several associations significance was lost when using categorical adherence measures. For antihypertensives, only the association between the MPR measures and dose decrease or drug class discontinuation remained significant. For glucose-regulating drugs, the associations with class addition and dose increase where lost in the case of both MPR as well as the last gap ≥30 days measure (Appendix A2).
DISCUSSIONTreatment modifications in patients with insufficiently controlled risk factors and sub-optimal adherence differed for the two areas studied. For glucose-regulating medica-tion, a lower adherence was associated with fewer dose increases and additions of a new drug class. This phenomenon was not seen for antihypertensive medication. Instead, in patients with a low adherence to antihypertensive drugs, we observed a higher likelihood to discontinue the drug treatment. More associations with treat-ment modifications were seen using the MPR adherence measure in comparison to the last gap measure. The binary treatment intensification outcome showed similar effects of adherence on treatment modifications for glucose-regulating but not for antihypertensive medication. The inhibitive effect of suboptimal adherence on treatment intensification of glucose-regulating medication has been observed in a study in the US,13 while another study showed an opposite effect.24 This latter study did not correct for the HbA1c level which may explain their unexpected finding. In our study, physicians appear to take adherence into account when confronted with insufficient risk factor control by not intensifying the treatment in patients with low adherence levels. For antihypertensive treatment, however, we found no such association which confirms findings of other studies.14,16 This dissimilar finding can be caused by differences in attention given to adherence, but also in reasons underlying adherence and related possible reactions to non-adherence at physician and patient level. In previous studies, we have found
178
Chapter 4.3 - Medication adherence
indications for a glucose-centred approach to diabetes risk factor management,3,25 which has been reported by other investigators as well.26,27 Such a management strategy may lead to more attention, and thereby higher awareness of adherence problems for glucose-regulating medication. In addition, the link between subop-timal adherence and risk factor levels may be less clear for blood pressure than for HbA1c.13 This can further diminish the physicians’ awareness of the underlying cause of suboptimal blood pressure control. But even when the physician is aware of a potential adherence problem, differences in patients’ reactions can also explain the differences in observed treatment modifications. Self-reported adherence of patients was found to be higher for antihypertensive than for glucose-regulating medication,28 whereas refill rates show opposite results.29,30 This implies that patients either over-estimate adherence or are more reluctant to admit adherence problems for antihy-pertensive medication than for glucose-regulating medication. All these factor will contribute to the pattern we observed, where physicians intensify antihypertensive treatment regardless of low medication adherence levels.We did observe other treatment modifications in patients with low adherence to anti-hypertensive medication. Such patients had a higher probability to discontinue a drug class. This finding of poor adherence to antihypertensives being a strong predictor of discontinuation has been observed before,31 which may indicate a patient-driven pat-tern of non-adherence rather than the decision of the physician to modify the treat-ment. On the other hand, patients with low adherence to antihypertensives tended to receive more dose decreases as well as more additions of a new drug class which are treatment modifications made by physicians. A pharmacy database study in the Netherlands, which focused on first time users of antihypertensive drugs, found a similar association.17 This may be explained by reactions to perceived adverse ef-fects underlying suboptimal adherence. Especially for antihypertensive treatment, there are usually many options to decrease the dose of one drug while adding an-other drug in order to increase effectiveness while reducing adverse effects. Currently, physicians may have trouble to detect non-adherence in daily practice. There is a need for better detection and visibility of adherence,16,32 since correctly distinguishing non-response to therapy from non-adherence is important. When phy-sicians prescribe electronically, tools to support physicians using prescription refill adherence estimates can be implemented as part of the electronic medical record systems. This has however not yet been done in most current GP systems. In our study, the choice of the adherence measure affected our results to some extent. The MPR, which is an overall period adherence estimate, was more strongly related with treatment modifications than an adherence measure based on the last gap between prescription refills. This could indicate that the MPR better reflects adherence judg-
179
Chapter 4.3 - Medication adherence
ments as made by physicians. When looking at treatment modification as a binary outcome, some interesting find-ings are lost. Although the conclusions are similar regarding the effect of adherence on distinct intensifications for glucose-regulating medication (i.e. less intensification in patients with lower adherence levels), they are different for antihypertensive medi-cation. Using a binary outcome, one may conclude that there is no effect of adher-ence on treatment changes, whereas our study showed that adherence levels are related to specific treatment modifications, such as discontinuation, dose decrease and addition of a new drug class. Such modifications could be considered appropri-ate action in patients not adherent to treatment when they have experienced adverse effects. Besides this, by classifying various modifications in the binary outcome as “no intensification”, one could erroneously observe a negative association between adherence and intensification.Using the common cut-off point for adherence (≥80% MPR), the level of adherence observed in our study population is comparable to other studies’ findings,12,15,30 al-though much lower levels have been reported as well.16,18 These differences can be caused by differences in health care system and reimbursement, patient popula-tion, and data source used. We used electronic prescribing data, whereas others have used dispensing data or claims databases. Although these are all related, dif-ferences have been observed.32 When we compare the results obtained from the categorical adherence measures to the ones from the continuous ones, we see that we lose considerable power to detect associations. This can be due to a lower pre-cision of estimates and to the (arbitrary) choice of the cut-off points. As has been recommended before,18 it is therefore better to use continuous measures in studies of adherence.
Strengths and limitationsWe used longitudinal information retrieved from electronic medical records of gen-eral practitioners. This has both advantages and disadvantages. The detailed lon-gitudinal dataset enabled us to consider the first treatment modification within 60 days after an elevated risk factor observation. This is in contrast to other studies that looked at treatment intensifications occurring in longer periods irrespective of wheth-er other modifications preceded these.12,13,15,17,33 Using a short period makes it more likely that the treatment modification is indeed a reaction to the observed elevated risk factor level. The obvious limitation is that we were unable to assess which other actions may have been taken to improve medication adherence. It is possible that in some cases the GPs decided to improve adherence by educating and motivating the patient as well as increase treatment at the same time. This type of action, however, has the risk of predisposing patients to overtreatment.
180
Chapter 4.3 - Medication adherence
Using prescription refill data for calculating adherence has the disadvantage of over-estimating actual adherence, since patients may collect their prescriptions while not actually taking the medication. On the other hand, although these data do not re-flect “true” medication adherence, they reflect prescription refill adherence as can be observed by the GPs from their records. In addition, using prescription data from electronic medical records has the advantage of having a direct measure of the treatment modifications made by the GPs.Finally, there is no best method for measuring adherence using prescription data.19,23 This was the reason for us to use two different adherence measures. There is also no consensus on how to calculate adherence in patients using multiple drugs for the same indication.34 We focused on the drug with the poorest adherence, since we expect this to be relevant information for the prescriber, and patients using multiple drugs can show poor adherence on a single drug.29 Our results confirm that in pa-tients on multitherapy poor adherence occurs predominantly in a single drug class. By averaging adherence measures over concurrently used drugs, the power to as-sess an effect on non-adherence to a single drug is decreased.
ConclusionsAs has been stated before, the real barrier to better risk factor control may not be addressed if treatment is intensified despite low adherence.15,24,35 This study dem-onstrates that low adherence does reduce the chance of intensifying glucose-reg-ulating but not antihypertensive treatment in insufficiently controlled patients. Low adherence may lead to other treatment modifications, which are overlooked when focusing only on whether or not the treatment is intensified. We showed this to be the case for antihypertensive medication. Medication adherence affects decisions regarding drug treatment differently for antihypertensive than for glucose-regulating therapy.
REFERENCES1. Saaddine JB, Cadwell B, Gregg EW, Engelgau MM, Vinicor F, Imperatore G,
Narayan KM. Improvements in diabetes processes of care and intermediate out-comes: United States, 1988-2002. Ann Intern Med. 2006;144(7):465-74.
2. Andrade SE, Gurwitz JH, Field TS, Kelleher M, Majumdar SR, Reed G, Black R. Hypertension management: the care gap between clinical guidelines and clinical practice. Am J Manag Care. 2004;10(7 Pt 2):481-6.
3. Voorham J, Haaijer-Ruskamp FM, Stolk RP, Wolffenbuttel BHR, Denig P, Groningen Initiative to Analyze Type 2 Diabetes Treatment Group. Influence of elevated cardiometabolic risk factor levels on treatment changes in type 2 diabe-tes. Diabetes Care. 2008;31(3):501-3.
4. Borzecki AM, Oliveria SA, Berlowitz DR. Barriers to hypertension control. Am Heart J. 2005;149(5):785-94.
181
Chapter 4.3 - Medication adherence
5. Safford MM, Shewchuk R, Qu H, Williams JH, Estrada CA, Ovalle F, Allison JJ. Reasons for not intensifying medications: differentiating “clinical inertia” from ap-propriate care. J Gen Intern Med. 2007;22(12):1648-55.
6. Hicks PC, Westfall JM, Van Vorst RF, Bublitz Emsermann C, Dickinson LM, Pace W, Parnes B. Action or inaction? Decision making in patients with diabetes and elevated blood pressure in primary care. Diabetes Care. 2006;29(12):2580-5.
7. Boyd CM, Darer J, Boult C, Fried LP, Boult L, Wu AW. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implica-tions for pay for performance. JAMA. 2005;294(6):716-24.
8. Holland N, Segraves D, Nnadi VO, Belletti DA, Wogen J, Arcona S. Identifying barriers to hypertension care: implications for quality improvement initiatives. Dis Manag. 2008;11(2):71-7.
9. Hickling J, Rogers S, Nazareth I. Barriers to detecting and treating hypercholes-terolaemia in patients with ischaemic heart disease: primary care perceptions. Br J Gen Pract. 2005;55(516):534-8.
10. Cotton A, Aspy CB, Mold J, Stein H. Clinical decision-making in blood pres-sure management of patients with diabetes mellitus: an Oklahoma Physicians Resource/Research Network (OKPRN) Study. J Am Board Fam Med. 2006;19(3):232-9.
11. Oliveria SA, Lapuerta P, McCarthy BD, L’Italien GJ, Berlowitz DR, Asch SM. Physician-related barriers to the effective management of uncontrolled hyperten-sion. Arch Intern Med. 2002;162(4):413-20.
12. Schmittdiel JA, Uratsu CS, Karter AJ, Heisler M, Subramanian U, Mangione CM, Selby JV. Why don’t diabetes patients achieve recommended risk factor targets? Poor adherence versus lack of treatment intensification. J Gen Intern Med. 2008;23(5):588-94.
13. Grant R, Adams AS, Trinacty CM, Zhang F, Kleinman K, Soumerai SB, Meigs JB, Ross-Degnan D. Relationship between patient medication adherence and subsequent clinical inertia in type 2 diabetes glycemic management. Diabetes Care. 2007;30(4):807-12.
14. Grant RW, Singer DE, Meigs JB. Medication adherence before an increase in antihypertensive therapy: a cohort study using pharmacy claims data. Clin Ther. 2005;27(6):773-81.
15. Rose AJ, Berlowiz DR, Manze M, Orner MB, Kressin NR. Intensifying therapy for hypertension despite suboptimal adherence. Hypertension. 2009;54(3):524-9.
16. Heisler M, Hogan MM, Hofer TP, Schmittdiel JA, Pladevall M, Kerr EA. When more is not better: treatment intensification among hypertensive patients with poor medication adherence. Circulation. 2008;117(22):2884-92.
17. Van Wijk B, Klungel O, Heerdink E, de Boer A. The association between compli-ance with antihypertensive drugs and modification of antihypertensive drug regi-men. J Hypertens. 2004;22(9):1831-7.
18. Cramer JA, Benedict A, Muszbek N, Keskinaslan A, Khan ZM. The significance of compliance and persistence in the treatment of diabetes, hypertension and dyslipidaemia: a review. Int J Clin Pract. 2008;62(1):76-87.
19. Andrade SE, Kahler KH, Frech F, Chan KA. Methods for evaluation of medication
182
Chapter 4.3 - Medication adherence
adherence and persistence using automated databases. Pharmacoepidemiol Drug Saf. 2006;15(8):565-74.
20. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005; 353(5):487-97.
21. Voorham J, Denig P. Computerized extraction of information on the quality of diabetes are from free text in electronic patient records of general practitioners. J Am Med Inform Assoc. 2007;14(3):349-354.
22. Code of Conduct: Use of data in health research. Stichting FMWV (Federation of Biomedical Scientific Societies), Rotterdam, 2005. Accessed at http://www.federa.org on December 2009.
23. Cramer JA, Roy A Burrell A, Fairchild CJ, Fuldeore MJ, Ollendorf DA, Wong PK. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44-7.
24. Kogut SJ, Andrade SE, Willey C, Larrat EP. Nonadherence as a predictor of an-tidiabetic drug therapy intensification (augmentation). Pharmacoepidemiol Drug Saf. 2004;13(9):591-8.
25. Voorham J, Haaijer-Ruskamp FM, Stolk RP, Wolffenbuttel BHR, Denig P, Groningen Initiative to Analyze Type 2 Diabetes Treatment Group. Cardiometabolic treatment decisions in patients with type 2 diabetes: the role of repeated measurements and medication burden. Qual Saf Health Care. 2010;in press.
26. Brown LC, Johnson JA, Majumdar SR, Tsuyuki RT, McAister FA. Evidence of suboptimal management of cardiovascular risk in patients with type 2 diabetes mellitus and symptomatic atherosclerosis. CMAJ. 2004;171(10):1189-92.
27. Grant RW, Cagliero E, Murphy-Sheehy P, Singer DE, Nathan DM, Meigs JB. Comparison of hyperglycemia, hypertension, and hypercholesterolemia man-agement in patients with type 2 diabetes. Am J Med. 2002;112(8):603-9.
28. Grant RW, Devita NG, Singer DE, Meigs JB. Polypharmacy and medication ad-herence in patients with type 2 diabetes. Diabetes Care. 2003;26(5):1408-12.
29. Vink NM, Klungel OH, Stolk RP, Denig P. Comparison of various measures for as-sessing medication refill adherence using prescription data. Pharmacoepidemiol Drug Saf. 2009;18(2):159-65.
30. van Bruggen R, Gorter K, Stolk RP, Zuithoff P, Klungel OH, Rutten GEHM. Refill adherence and polypharmacy among patients with type 2 diabetes in general practice. Pharmacoepidemiol Drug Saf. 2009;18(11):983-91.
31. Van Wijk BL, Klungel OH, Heerdink ER, de Boer A. Initial non-compliance with antihypertensive monotherapy is followed by complete discontinuation of antihy-pertensive therapy. Pharmacoepidemiol Drug Saf. 2006;15(8):587-93.
32. Mabotuwana T, Warren J, Harrison J, Kenealy T. What can primary care prescrib-ing data tell us about individual adherence to long-term medication? Comparison to pharmacy dispensing data. Pharmacoepidemiol Drug Saf. 2009;18(10):956-64.
33. Ho PM, Magid DJ, Shetterly SM, Olson KL, Peterson PN, Masoudi FA, Rumsfeld JS. Importance of therapy intensification and medication nonadherence for blood pressure control in patients with coronary disease. Arch Intern Med.
183
Chapter 4.3 - Medication adherence
2008;168(3):271-6.34. Choudhry NK, Shrank WH, Levin RL, Lee JL, Jan SA, Brookhart MA Slomon DH.
Measuring concurrent adherence to multiple related medications. Am J Manag Care. 2009;15(7):457-64.
35. Reach G. Patient non-adherence and healthcare-provider inertia are clinical myopia. Diabetes Metab. 2008;34(4 Pt 1):382-5.
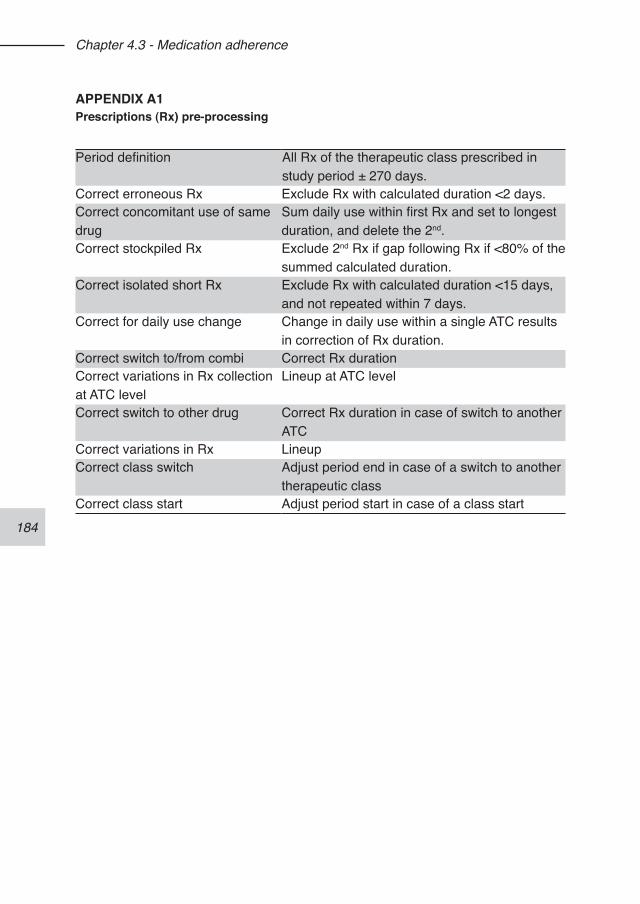
184
Chapter 4.3 - Medication adherence
APPENDIX A1Prescriptions (Rx) pre-processing
Period definition All Rx of the therapeutic class prescribed in study period ± 270 days.
Correct erroneous Rx Exclude Rx with calculated duration <2 days.Correct concomitant use of same drug
Sum daily use within first Rx and set to longest duration, and delete the 2nd.
Correct stockpiled Rx Exclude 2nd Rx if gap following Rx if <80% of the summed calculated duration.
Correct isolated short Rx Exclude Rx with calculated duration <15 days, and not repeated within 7 days.
Correct for daily use change Change in daily use within a single ATC results in correction of Rx duration.
Correct switch to/from combi Correct Rx durationCorrect variations in Rx collection at ATC level
Lineup at ATC level
Correct switch to other drug Correct Rx duration in case of switch to another ATC
Correct variations in Rx LineupCorrect class switch Adjust period end in case of a switch to another
therapeutic classCorrect class start Adjust period start in case of a class start
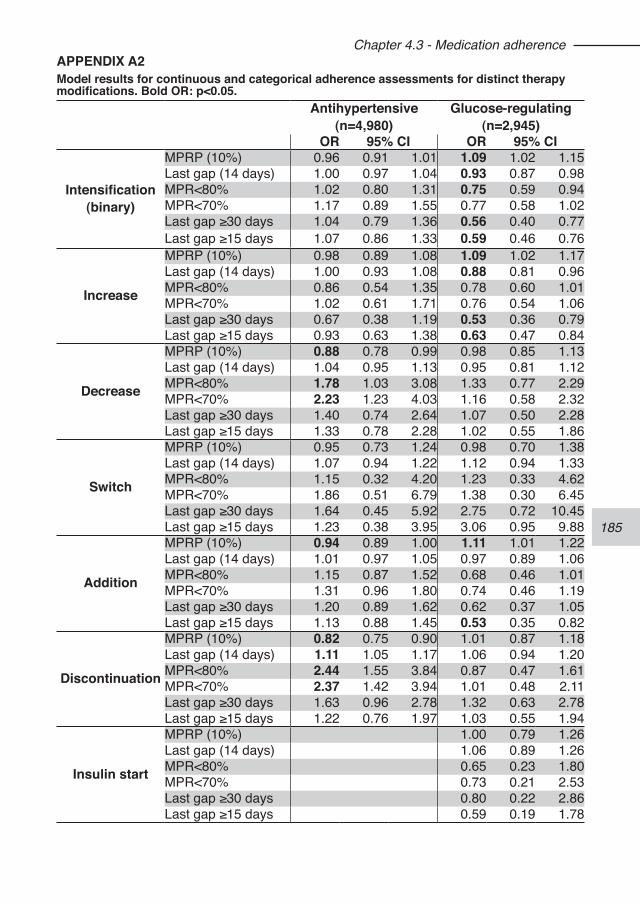
185
Chapter 4.3 - Medication adherenceAPPENDIX A2Model results for continuous and categorical adherence assessments for distinct therapy modifications. Bold OR: p<0.05.
Antihypertensive(n=4,980)
Glucose-regulating(n=2,945)
OR 95% CI OR 95% CI
Intensification(binary)
MPRP (10%) 0.96 0.91 1.01 1.09 1.02 1.15Last gap (14 days) 1.00 0.97 1.04 0.93 0.87 0.98MPR<80% 1.02 0.80 1.31 0.75 0.59 0.94MPR<70% 1.17 0.89 1.55 0.77 0.58 1.02Last gap ≥30 days 1.04 0.79 1.36 0.56 0.40 0.77Last gap ≥15 days 1.07 0.86 1.33 0.59 0.46 0.76
Increase
MPRP (10%) 0.98 0.89 1.08 1.09 1.02 1.17Last gap (14 days) 1.00 0.93 1.08 0.88 0.81 0.96MPR<80% 0.86 0.54 1.35 0.78 0.60 1.01MPR<70% 1.02 0.61 1.71 0.76 0.54 1.06Last gap ≥30 days 0.67 0.38 1.19 0.53 0.36 0.79Last gap ≥15 days 0.93 0.63 1.38 0.63 0.47 0.84
Decrease
MPRP (10%) 0.88 0.78 0.99 0.98 0.85 1.13Last gap (14 days) 1.04 0.95 1.13 0.95 0.81 1.12MPR<80% 1.78 1.03 3.08 1.33 0.77 2.29MPR<70% 2.23 1.23 4.03 1.16 0.58 2.32Last gap ≥30 days 1.40 0.74 2.64 1.07 0.50 2.28Last gap ≥15 days 1.33 0.78 2.28 1.02 0.55 1.86
Switch
MPRP (10%) 0.95 0.73 1.24 0.98 0.70 1.38Last gap (14 days) 1.07 0.94 1.22 1.12 0.94 1.33MPR<80% 1.15 0.32 4.20 1.23 0.33 4.62MPR<70% 1.86 0.51 6.79 1.38 0.30 6.45Last gap ≥30 days 1.64 0.45 5.92 2.75 0.72 10.45Last gap ≥15 days 1.23 0.38 3.95 3.06 0.95 9.88
Addition
MPRP (10%) 0.94 0.89 1.00 1.11 1.01 1.22Last gap (14 days) 1.01 0.97 1.05 0.97 0.89 1.06MPR<80% 1.15 0.87 1.52 0.68 0.46 1.01MPR<70% 1.31 0.96 1.80 0.74 0.46 1.19Last gap ≥30 days 1.20 0.89 1.62 0.62 0.37 1.05Last gap ≥15 days 1.13 0.88 1.45 0.53 0.35 0.82
Discontinuation
MPRP (10%) 0.82 0.75 0.90 1.01 0.87 1.18Last gap (14 days) 1.11 1.05 1.17 1.06 0.94 1.20MPR<80% 2.44 1.55 3.84 0.87 0.47 1.61MPR<70% 2.37 1.42 3.94 1.01 0.48 2.11Last gap ≥30 days 1.63 0.96 2.78 1.32 0.63 2.78Last gap ≥15 days 1.22 0.76 1.97 1.03 0.55 1.94
Insulin start
MPRP (10%) 1.00 0.79 1.26Last gap (14 days) 1.06 0.89 1.26MPR<80% 0.65 0.23 1.80MPR<70% 0.73 0.21 2.53Last gap ≥30 days 0.80 0.22 2.86Last gap ≥15 days 0.59 0.19 1.78
186
187
Chapter 4.4 - Competing demands and treatment intensification in type 2 diabetes
Jaco Voorham1,2
Flora M Haaijer-Ruskamp1
Ronald P Stolk2
Bruce HR Wolffenbuttel3
Petra Denig1
1. Department of Clinical Pharmacology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
2. Department of Epidemiology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
3. Department of Endocrinology, Faculty of Medical Science, University Medical Center Groningen, University of Groningen
Voorham J, Haaijer-Ruskamp FM, Stolk RP, Wolffenbuttel BHR, Denig P; Groningen Initiative to Analyze Type 2 Diabetes Treatment Group. Competing demands and treatment intensification in type 2. Submitted.
188
Chapter 4.4 Competing demands
ABSTRACTObjective. Low rates of treatment modification in patients with uncontrolled risk fac-tors are common in type 2 diabetes. Competing demands are mentioned as justifi-cation but there are conflicting results regarding the impact of other conditions on diabetes care. We assessed the effect of existing comorbidity and incident events on the decision to start or intensify antihypertensive or glucose-regulating medication.Research design and methods. We conducted a cohort study using data from elec-tronic medical records. Patients with type 2 diabetes managed by 142 general prac-titioners were included when they had an elevated measurement in 2007 (systolic blood pressure ≥140mmHg, HbA1c ≥7%), and were not on maximal treatment. As competing demands we considered 1) new symptoms or problems, 2) prescriptions of a new drug, or 3) prevalent chronic conditions. The conditions and events were divided in related or unrelated to diabetes. We performed Cox regression analyses to assess factors associated with treatment intensifications within 120 days.Results. We included 6,839 hypertensive and 3,589 hyperglycaemic patients. The chance to intensify antihypertensive medication was decreased when a new glu-cose-regulating drug was prescribed (HR 0.25, 0.06-1.00). The chance to intensify glucose-regulating medication was decreased in patients with prevalent related con-ditions (HR 0.94, 0.89-1.00). In both areas, incident related comorbidity increased the chance of treatment intensification but unrelated incident or prevalent conditions did not resulted in statistical significantly changes.Conclusions. We found no evidence that incident comorbid conditions in themselves decrease the likelihood to intensify medication treatment. However, starting new diabetes drugs or having diabetes related chronic conditions can compete with the management of hypertension or hyperglycaemia.
189
Chapter 4.4 Competing demands
INTRODUCTIONPreventive treatment of cardiometabolic risk factors in diabetes is important. Although considerable progress has been achieved in the quality of diabetes care, there is a gap between what treatment guidelines indicate as appropriate care and what is observed in daily practice.1-8 Failing to act on insufficient risk factor control is often called “clinical inertia”,9 a term that does not acknowledge justifiable inaction or delay of action at patient level.Many studies have looked at plausible reasons for not acting when indicated. Factors at the level of the prescriber as well as the patient have been identified through sur-veys.10-16 Competing demands during the clinical encounter are reported frequently as reason not to conduct specific actions indicated by treatment guidelines. A study in the USA estimated the time a primary care physician would need to provide all recommended preventive care, and found that time constraints limit the ability of physicians to comply with all preventive services recommendations.17 As a conse-quence, competing demands during primary care encounters require patient and physician to prioritise what is discussed and done, and may defer some actions to subsequent visits.13,18-20
Comorbidity is one of the most obvious competing demands but it is not clear how comorbid conditions interact with diabetes management. One study showed that elderly patients with chronic diseases, such as diabetes, pulmonary emphysema, or psychotic syndromes, receive less treatment for other unrelated disorders.21 With regard to cardiovascular preventive treatment quality, evidence is conflicting. Comorbidity may decrease as well as increase the likelihood of treatment intensifica-tion in insufficiently controlled patients,20,22-28 It seems that comorbidity affects quality of care differently depending on the target condition and the nature of the comorbid condition. 28,29 Also, specific events or actions linked to concurrent conditions can require extra attention, such as starting or changing medication. We expect that the effect of other conditions or events depends on whether or not they are related to diabetes management, and whether they are chronic or non-chronic, and prevalent or incident events.The aim of this study is to assess the effect of competing demands on the decision to intensify antihypertensive or glucose-regulating medication in patients with type 2 diabetes, differentiating for type and nature of the demands.
190
Chapter 4.4 Competing demands
METHODSWe conducted a cohort study to assess the effect of prevalent and incident con-ditions and events on treatment start and intensification. Prescriptions, clinical measurements, morbidity and demographic data for patients with type 2 diabetes were collected from the Groningen Initiative to Analyse Type 2 diabetes Treatment (GIANTT) database. This database contains anonymised longitudinal information retrieved from electronic medical records (EMR) of general practitioners (GPs). The GPs in our study prescribe electronically, ensuring full information on prescribed drugs and dosing schemes. Clinical measurements are collected using a validated computerised extraction method.30 Data on comorbid conditions are collected from the problem/episodes lists in the EMR where the GPs can document symptoms, diagnoses, and (surgical) interventions using either the International Classification for Primary Care version 1 (ICPC)31 coding or text lines, which were recoded into the corresponding ICPC codes or specific additional codes in case a condition or event cannot be classified within the ICPC system. In the Netherlands, patients are reg-istered with a single GP. For research using anonymous medical records no ethics committee approval is needed in The Netherlands.
Study populationThe study population consists of patients with a diagnosis of diabetes type 2, man-aged by 142 general practitioners in the northern Netherlands. Patients were includ-ed if they were diagnosed before 2007, and had a risk factor measurement above the treatment target (≥140 mmHg for systolic blood pressure (SBP), ≥7 % for HbA1c) in 2007. Patients already receiving 3 or more drug classes on maximal maintenance dose for blood pressure lowering, or insulin as glucose-regulating medication were excluded from the analysis (figure 1). Our data do not allow for assessing changes in insulin dose.
Treatment decisionsFor each patient, the first observation of an elevated risk factor level in 2007 is taken as the index observation. Since the occurrence of competing demands can be ex-pected to result in postponing of indicated actions, and the time between regular dia-betes control visits is 3 months in The Netherlands, we assessed treatment changes during a 120-days follow-up period to capture actions that were postponed until the next regular control visit.
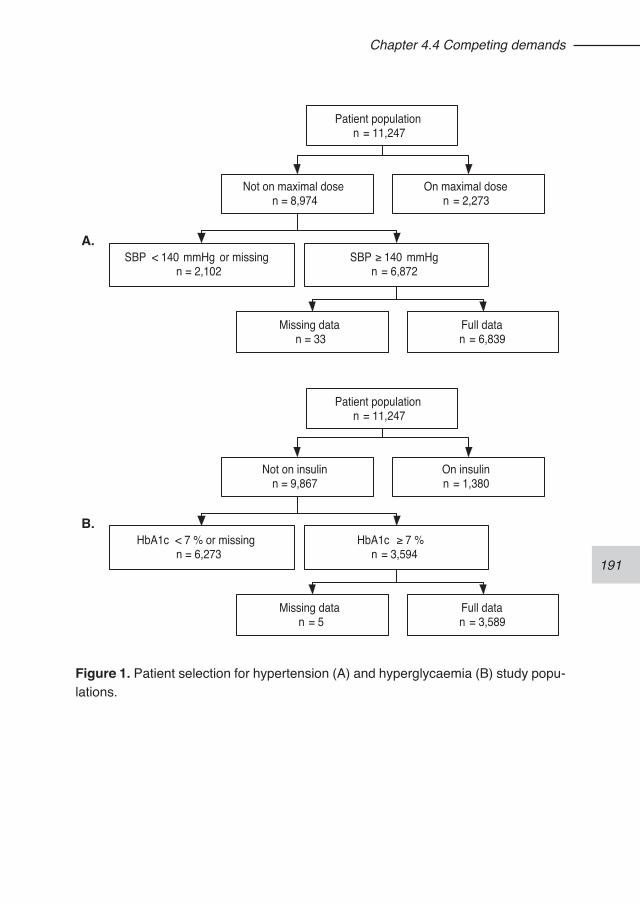
191
Chapter 4.4 Competing demands
A.
Patient populationn = 11,247
Not on maximal dosen = 8,974
On maximal dosen = 2,273
SBP < 140 mmHg or missingn = 2,102
SBP ≥ 140 mmHgn = 6,872
Missing datan = 33
Full datan = 6,839
B.
Patient populationn = 11,247
Not on insulinn = 9,867
On insulinn = 1,380
HbA1c < 7 % or missingn = 6,273
HbA1c ≥ 7 %n = 3,594
Missing datan = 5
Full datan = 3,589
Figure 1. Patient selection for hypertension (A) and hyperglycaemia (B) study popu-lations.
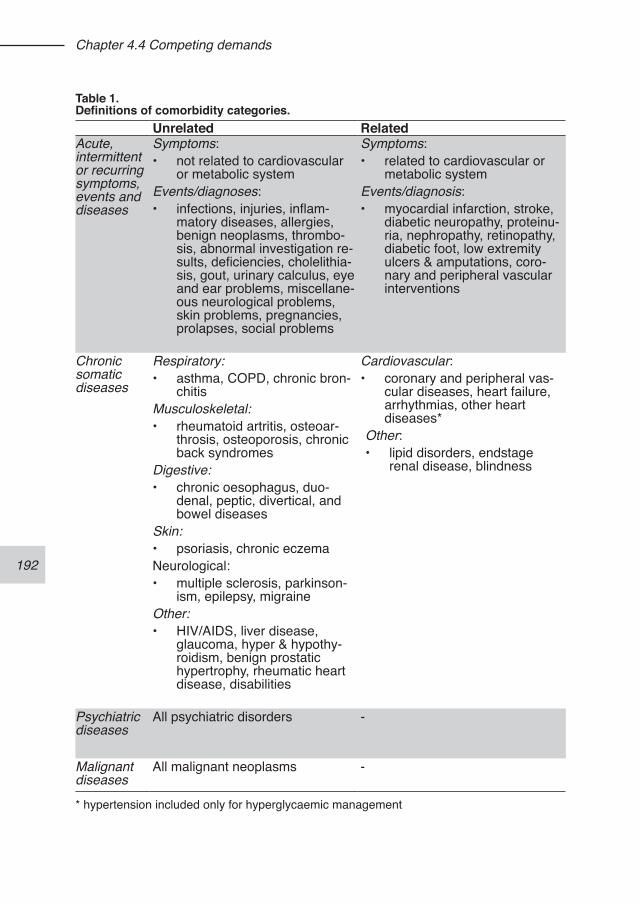
192
Chapter 4.4 Competing demands
Table 1. Definitions of comorbidity categories.
Unrelated RelatedAcute, intermittent or recurring symptoms, events and diseases
Symptoms: • not related to cardiovascular
or metabolic systemEvents/diagnoses:• infections, injuries, inflam-
matory diseases, allergies, benign neoplasms, thrombo-sis, abnormal investigation re-sults, deficiencies, cholelithia-sis, gout, urinary calculus, eye and ear problems, miscellane-ous neurological problems, skin problems, pregnancies, prolapses, social problems
Symptoms: • related to cardiovascular or
metabolic systemEvents/diagnosis: • myocardial infarction, stroke,
diabetic neuropathy, proteinu-ria, nephropathy, retinopathy, diabetic foot, low extremity ulcers & amputations, coro-nary and peripheral vascular interventions
Chronic somatic diseases
Respiratory: • asthma, COPD, chronic bron-
chitisMusculoskeletal: • rheumatoid artritis, osteoar-
throsis, osteoporosis, chronic back syndromes
Digestive: • chronic oesophagus, duo-
denal, peptic, divertical, and bowel diseases
Skin: • psoriasis, chronic eczemaNeurological:• multiple sclerosis, parkinson-
ism, epilepsy, migraineOther: • HIV/AIDS, liver disease,
glaucoma, hyper & hypothy-roidism, benign prostatic hypertrophy, rheumatic heart disease, disabilities
Cardiovascular: • coronary and peripheral vas-
cular diseases, heart failure, arrhythmias, other heart diseases*
Other: • lipid disorders, endstage
renal disease, blindness
Psychiatric diseases
All psychiatric disorders -
Malignant diseases
All malignant neoplasms -
* hypertension included only for hyperglycaemic management
193
Chapter 4.4 Competing demands
Treatment intensification included any dose increase and/or addition of a new drug class. Patients with modifications into opposite directions were excluded (e.g. a dose increase coinciding with a dose decrease).
Competing demandsSince we expect that the effect of other conditions or events depends on their type and nature, we included the following distinct occurrences to compete for attention with regular diabetes care: 1) any new symptom or condition, 2) any prescription of a new drug, or 3) any prevalent or history of a chronic condition. We subdivided all symptoms, conditions, and events as either related to diabetes (cardiovascular or diabetes complication) or unrelated (Table 1). Related drugs were subdivided into antihypertensive, glucose-regulating, lipid-regulating drugs and aspirin (ASA).To define chronic conditions, all disease codes mentioned in the ICPC-1 list were classified by two general practitioners as being (a) chronic diseases in need of con-tinuous attention, or (b) acute, recurring or intermittent diseases (Table 1). The chronic conditions were subdivided in somatic, psychiatric, and malignancies. Chronic somatic diseases are expected to influence current management regardless of when they started. We counted the number of unique chronic somatic conditions as an estimate of comorbidity burden. For psychiatric conditions and malignancies, we included any occurrence in a 10-year period prior to the index date as a binary variable. Incident chronic conditions were defined as any new somatic, psychiatric or malig-nant condition, not yet in the medical history of a patient, occurring during follow-up. Other incident conditions included occurrences of a symptom or acute, recurring or intermittent disease registered as problem or episode in the patient record during follow-up. Such incident non-chronic conditions are expected to compete for atten-tion during a limited time period of not more than 1 week.A prescription for a new drug was defined as a prescription for a drug identified at the lowest ATC-level, which had not been prescribed in the previous 180 days.
Statistical analysisTo assess the association between the possible competing events and treatment start or intensification, we used Cox Proportional Hazard regression analysis with shared frailty at physician level to correct for clustering and time, using STATA ver-sion 11. This approach allows estimating the effect of factors that are not constant during the follow-up period, such as the risk factor that can be measured on several occasions. Patients were censored at 120 days if no intensification occurred.Since results from HbA1c measurements are sent to the practices and can be docu-
194
Chapter 4.4 Competing demands
mented in the EMR after the clinical encounter, the index dates for an elevated HbA1c level in the models for glucose-regulating medication incorporated a back-ward shift of 7 days.All incident non-chronic conditions and events during the follow-up period were add-ed to the models as time-dependent variables with an effect-duration of 7 days. The effect of incident chronic conditions started on the day of their registration in the patient record and lasted until the end of follow-up. The prevalent chronic conditions were added to the models as fixed variables.The following potential confounders were added to the models as fixed covariates scored at the index date: age, diabetes duration, sex, polypharmacy (≥ 4 other chronic drugs), and whether the patient was already using risk factor specific drugs during a 6-months period prior to the index date. The risk factor itself was added to the model as a time-dependent covariate.We performed explorative analyses using subclasses of comorbidity, at the level of ICPC chapters and components, to verify that the predefined comorbidity groups were not composed of conditions with opposite effects on the outcome. We found no indications for this. Furthermore, interaction terms were explored between current use of the risk specific medication and the explaining variables, to establish possible differences in effect between people already on drugs and new users. Results are presented as adjusted Hazard Ratios with 95% confidence intervals.Since the use of problem and episode registration varies between general practices, we conducted a sensitivity analysis to assess the effect of limited morbidity registra-tion habits on the models. For this, we repeated the modelling excluding general practices in the lowest tercile of average number of comorbidity records per patient.
RESULTSOf the 11,248 patients in the study population, respectively 6,839 and 3,589 were included in the models for hypertension and hyperglycaemia (table 2). The rate of treatment start and intensification within 120 days was higher in glycaemic manage-ment compared to hypertension management. The patients in the hyperglycaemic population were younger (mean 1.7 years) than those in the hypertension popula-tion, due to the exclusion of insulin-treated patients. Incident non-chronic comorbidity did not affect the start or intensification of antihy-pertensive medication in patients with elevated SBP levels. Incident chronic related comorbidity increased the chance of a drug start or intensification almost three-fold. The start of a new glucose-regulating drug reduced the chance of a treatment change for hypertension by 75%. The start of other unrelated drugs, lipid-regulating
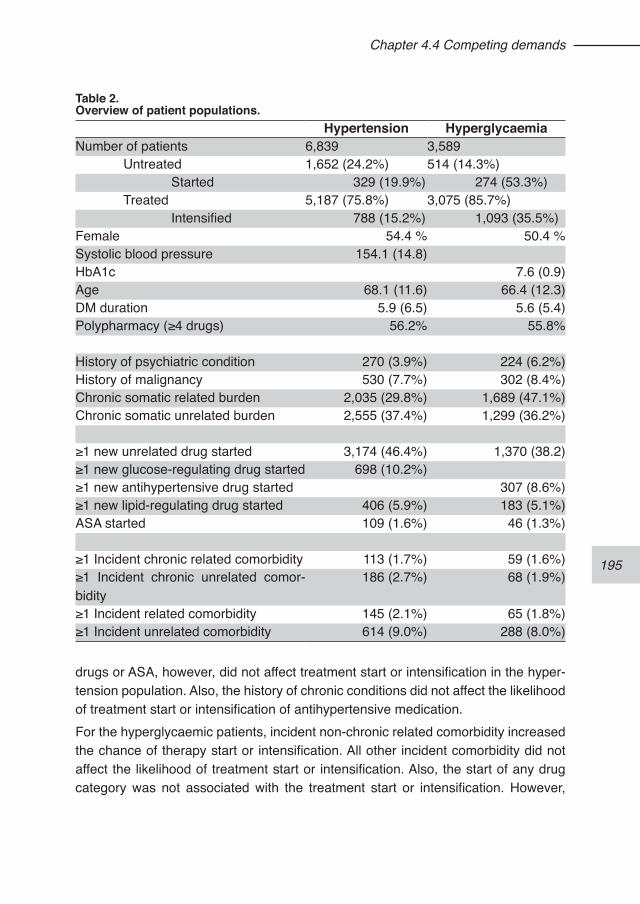
195
Chapter 4.4 Competing demands
drugs or ASA, however, did not affect treatment start or intensification in the hyper-tension population. Also, the history of chronic conditions did not affect the likelihood of treatment start or intensification of antihypertensive medication.For the hyperglycaemic patients, incident non-chronic related comorbidity increased the chance of therapy start or intensification. All other incident comorbidity did not affect the likelihood of treatment start or intensification. Also, the start of any drug category was not associated with the treatment start or intensification. However,
Table 2.Overview of patient populations.
Hypertension HyperglycaemiaNumber of patients 6,839 3,589 Untreated 1,652 (24.2%) 514 (14.3%) Started 329 (19.9%) 274 (53.3%) Treated 5,187 (75.8%) 3,075 (85.7%) Intensified 788 (15.2%) 1,093 (35.5%)Female 54.4 % 50.4 %Systolic blood pressure 154.1 (14.8)HbA1c 7.6 (0.9)Age 68.1 (11.6) 66.4 (12.3)DM duration 5.9 (6.5) 5.6 (5.4)Polypharmacy (≥4 drugs) 56.2% 55.8%
History of psychiatric condition 270 (3.9%) 224 (6.2%)History of malignancy 530 (7.7%) 302 (8.4%)Chronic somatic related burden 2,035 (29.8%) 1,689 (47.1%)Chronic somatic unrelated burden 2,555 (37.4%) 1,299 (36.2%)
≥1 new unrelated drug started 3,174 (46.4%) 1,370 (38.2)≥1 new glucose-regulating drug started 698 (10.2%)≥1 new antihypertensive drug started 307 (8.6%)≥1 new lipid-regulating drug started 406 (5.9%) 183 (5.1%)ASA started 109 (1.6%) 46 (1.3%)
≥1 Incident chronic related comorbidity 113 (1.7%) 59 (1.6%)≥1 Incident chronic unrelated comor-bidity
186 (2.7%) 68 (1.9%)
≥1 Incident related comorbidity 145 (2.1%) 65 (1.8%)≥1 Incident unrelated comorbidity 614 (9.0%) 288 (8.0%)
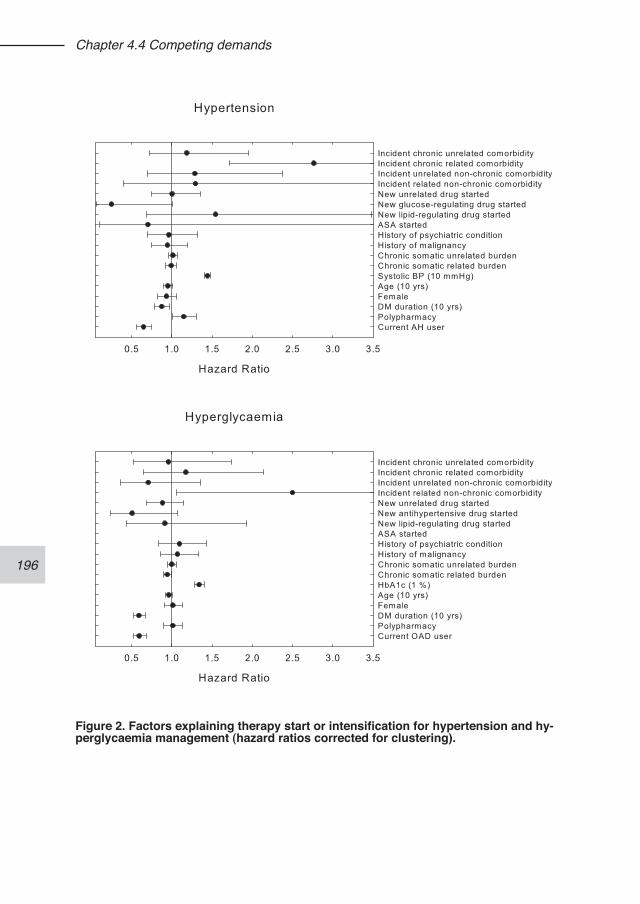
196
Chapter 4.4 Competing demands
Figure 2. Factors explaining therapy start or intensification for hypertension and hy-perglycaemia management (hazard ratios corrected for clustering).

197
Chapter 4.4 Competing demands
each prevalent chronic related condition reduced the chance of treatment start or intensification by 6% (figure 2).Polypharmacy (concurrent use of ≥4 chronic drugs) did not affect the treatment start or intensification in the hyperglycaemia population, but was positively associated with treatment modification in the hypertension patients (figure 2). In general, the likelihood to start medication was considerably lower than that to intensify medica-tion (resp. 65% and 59% for antihypertensive and glucose-regulating medication). No interaction terms between medication use status at baseline and the competing demands variables were found to contribute significantly to the models. After excluding patients from the practices belonging to the lowest tercile of average number of comorbidity records per patient, the hazard ratios of the comorbidity vari-ables did not change meaningfully (Appendix).
DISCUSSIONOur study shows that incident comorbid conditions in themselves did not compete with regular risk management. The negative effect of the start of new glucose-reg-ulating drugs, though, showed that glycaemic control competes with hypertension management. Of the prevalent chronic conditions, only related comorbidity nega-tively affected glucose-regulating treatment decisions. There were no differences for patients not yet treated, and those already using medication.Indications for the prioritisation of glycaemic control over hypertension control have been reported before, 8,22,32-34 but contrasting results are known as well.23 Our data show that glycaemic management indeed affects hypertension management but also that cardiovascular comorbidity can affect glycaemic management. Although the start of new antihypertensive drugs did not significantly affect the chance of glucose-regulating therapy start or intensification, the number of prevalent chronic somatic conditions related to diabetes, amongst which hypertension, lowered the chance of a therapy modification. This can be due to clinical attention demanded of a different kind than measured by prescription starts alone. It has been shown that discussion of conditions and medication issues, and concerns raised by patients can reduce the likelihood of (indicated) treatment changes.19,20 Other studies looking at prevalent conditions also found comorbidity to negatively affect antihypertensive risk factor management.23,24,26
One would expect that incident comorbid conditions are likely to compete for atten-tion. Our results do not show this. For incident related comorbid conditions, we ob-serve opposite relationships. For hypertension treatment this is not surprising, since the group of related chronic conditions contains mainly cardiovascular conditions for which antihypertensives can also be prescribed. Glycaemic management was
198
Chapter 4.4 Competing demands
increased with the occurrence of new related non-chronic conditions, which includes diabetes related complications such as retinopathy and nephropathy. This indicates that in patients with such complications, GPs are more prone to intensify glucose-regulating treatment. Of the studies that looked into the effect of comorbidity and other competing de-mands on treatment decisions for cardiovascular or glycaemic management, none included incident comorbidity. One study used medication prescription as an acute condition22 and another study quantified topics discussed during clinical visits.20 In these studies, effects of such events were observed as competing demands. Our negative results could be caused by our inability to classify the recorded conditions and comorbidity based on clinical dominance. This could have resulted in a mix-ture of highly relevant and irrelevant conditions within a single comorbidity category, masking possible existing effects.The impact of competing demands on quality assessment is of importance,35 since prioritisation during the care process can easily lead to underestimating quality. On the other hand, two studies looking at the effect of multimorbidity on overall quality scores concluded that multimorbidity may result in better rather than worse quality of care.36,37 This can be explained, however, by overlapping needs between conditions. Our study showed that the effect of comorbidity and the start of new medication can affect the quality of care differently for different risk factors. There is a need for qual-ity indicators that provide fairer quality estimates,38-40 and the resulting delay in action of competing demands should be incorporated. There is a growing interest in the effects of comorbidities on diabetes quality of care, but much remains to be done to better measure comorbidities, and assess their effect on care quality.41
Strength and limitationsTo our knowledge there are no studies outside the US that looked at competing de-mands’ effects on treatment decisions in cardiovascular or glycaemic risk manage-ment.We used only conditions and events registered by the GPs in the problem lists of the EMR. This is likely to be an underestimation of all actual problems or events that may compete with chronic disease management. We have included the start of new drugs as a clear action competing with care but we were not able to incorporate the effect of other interventions, such as discussion of life style issues or medica-tion compliance. We did not include observations of other elevated cardiovascular risk factor as competing demands, since the resulting action will be partly captured by the prescription of a new drug. Also, more frequent risk factor monitoring can be expected to have a strong association with overall care intensity, and could therefore
199
Chapter 4.4 Competing demands
bias the association between these other risk factors and therapy modifications.About half of the GPs in this study worked with a diabetes assistant or nurse practitioner to support diabetes care during the regular diabetes checks. In The Netherlands, this supporting staff is not allowed to change or prescribe medication. However, it is possible that effect of comorbid conditions on treatment modifications is diminished when part of the clinical encounters only focus on diabetes care. We checked this in models where the presence of diabetes support staff was added as a binary covariate, which did not change the outcomes (results not shown).
CONCLUSIONThe decision to start or intensify antihypertensive of glucose-regulating medication in patients with type 2 diabetes is not negatively affected by incident comorbid con-ditions. Management of hyperglycaemia, however, is negatively affected by chronic related conditions. Hypertension management is negatively affected by prescribing of new diabetes drugs.
REFERENCES1. Bouldin MJ, Low AK, Blackston JW, Duddleston DN, Holman HE, Hicks GS,
Brown CA. Quality of care in diabetes: understanding the guidelines. Am J Med Sci. 2002;324(4):196-206.
2. Saaddine JB, Cadwell B, Gregg EW, Engelgau MM, Vinicor F, Imperatore G, Narayan KM. Improvements in diabetes processes of care and intermediate out-comes: United States, 1988-2002. Ann Intern Med. 2006;144(7):465-74.
3. Andrade SE, Gurwitz JH, Field TS, Kelleher M, Majumdar SR, Reed G, Black R. Hypertension management: the care gap between clinical guidelines and clinical practice. Am J Manag Care. 2004;10(7 Pt 2):481-6.
4. Spann SJ, Nutting PA, Galliher JM, Peterson KA, Pavlik VN, Dickinson LM, Volk RJ. Management of type 2 diabetes in the primary care setting: a practice-based research network study. Ann Fam Med. 2006;4(1):23-31.
5. Wan Q, Harris MF, Jayasinghe UW, Flack J, Georgiou A, Penn DL, Burns JR. Quality of diabetes care and coronary heart disease absolute risk in patients with type 2 diabetes mellitus in Australian general practice. Qual Saf Health Care. 2006;15(2):131-5.
6. Asai Y, Heller R, Kajii E. Hypertension control and medication increase in pri-mary care. J Hum Hypertens. 2002;16(5):313-8.
7. Voorham J, Haaijer-Ruskamp FM, van der Meer K, de Zeeuw D, Wolffenbuttel BHR, Hoogenberg K, Denig P, on behalf of the GIANTT-group. Quality of medi-cation treatment in type 2 diabetes - results of the GIANTT project 2004-2007. Ned Tijdschr Geneeskd. 2010;154:A775.
8. Voorham J, Haaijer-Ruskamp FM, Stolk RP, Wolffenbuttel BHR, Denig P, Groningen Initiative to Analyze Type 2 Diabetes Treatment Group. Cardiometabolic treatment decisions in patients with type 2 diabetes: the role of
200
Chapter 4.4 Competing demands
repeated measurements and medication burden. Qual Saf Health Care. 2010;in press.
9. Phillips LS, Branch WT, Cook CB, Doyle JP, El-Kebbi IM, Gallina DL, Miller CD, Ziemer DC,Barnes CS. Clinical Inertia. Ann Intern Med. 2001;135(9):825-34.
10. Borzecki AM, Oliveria SA, Berlowitz DR. Barriers to hypertension control. Am Heart J. 2005;149(5):785-94.
11. Safford MM, Shewchuk R, Qu H, Williams JH, Estrada CA, Ovalle F, Allison JJ. Reasons for not intensifying medications: differentiating “clinical inertia” from ap-propriate care. J Gen Intern Med. 2007;22(12):1648-55.
12. Cotton A, As CB, Mold J, Stein H. Clinical desion-making in blood pressure man-agement of patients with diabetes mellitus: an Oklahoma Physicians Resource/Research Network (OKPRN) Study. J Am Board Fam Med. 2006;19(3):232-9.
13. Oliveria SA, Lapuerta P, McCarthy BD, L’Italien GJ, Berlowitz DR, Asch SM. Physician-related barriers to the effective management of uncontrolled hyperten-sion. Arch Intern Med. 2002 25;162(4):413-20.
14. Parnes BL, Main DS, Dickinson LM, Niebauer L, Holcomb S, Westfall JM, Pace WDCN - CaReNetCN - HPRN. Clinical decisions regarding HbA1c results in pri-mary care: a report from CaReNet and HPRN. Diabetes Care. 2004;27(1):13-6.
15. Ferrari P, Hess L, Pechere-Bertschi A, Muggli F, Burnier M. Reasons for not intensifying antihypertensive treatment (RIAT): a primary care antihypertensive intervention study. J Hypertens 2004;22(6):1221-9.
16. Hicks PC, Westfall JM, Van Vorst RF, Bublitz Emsermann C, Dickinson LM, Pace W, Parnes B. Action or inaction? Decision making in patients with diabetes and elevated blood pressure in primary care. Diabetes Care. 2006;29(12):2580-5.
17. Yarnall KS, Pollak KI, Ostbye T, Krause KM, Michener JL. Primary care: is there enough time for prevention? Am J Public Health. 2003;93(4):635-41.
18. Parchman ML, Romero RL, Pugh JA. Encounters by patients with type 2 di-abetes--complex and demanding: an observational study. Ann Fam Med. 2006;4(1):40-5.
19. Parchman ML, Pugh JA, Romero RL, Bowers KW. Competing demands or clinical inertia: the case of elevated glycosylated hemoglobin. Ann Fam Med. 2007;5(3):196-201.
20. Kerr EA, Zikmund-Fisher BJ, Klamerus ML, Subramanian U, Hogan MM, Hofer TP. The role of clinical uncertainty in treatment decisions for diabetic patients with uncontrolled blood pressure. Ann Intern Med. 2008;148(10):717-27.
21. Redelmeier DA, Tan SH, Booth GL. The treatment of unrelated disorders in pa-tients with chronic medical diseases. N Engl J Med. 1998;338(21):1516-20.
22. Bolen SD, Samuels TA, Yeh HC, Marinopoulos SS, McGuire M, Abuid M, Brancati FL. Failure to intensify antihypertensive treatment by primary care providers: a cohort study in adults with diabetes mellitus and hypertension. J Gen Intern Med. 2008;23(5):543-50.
23. Berlowitz DR, Ash AS, Hickey EC, Glickman M, Friedman R, Kader B. Hypertension management in patients with diabetes: the need for more aggres-sive therapy. Diabetes Care 2003;26(2):355-9.
24. Turner BJ, Hollenbeak CS, Weiner M, Ten Have T, Tang SS. Effect of unre-
201
Chapter 4.4 Competing demands
lated comorbid conditions on hypertension management. Ann Intern Med. 2008;148(8):578-86.
25. Chaudhry SI, Berlowitz DR, Concato J. Do age and comorbidity affect intensity of pharmacological therapy for poorly controlled diabetes mellitus? J Am Geriatr Soc. 2005;53(7):1214-6.
26. Wang PS, Avorn J, Brookhart MA, Mogun H, Schneeweiss S, Fischer MA, Glynn RJ. Effects of noncardiovascular comorbidities on antihypertensive use in elderly hypertensives. Hypertension. 2005;46(2):273-9.
27. Krein SL, Hofer TP, Holleman R, Piette JD, Klamerus ML, Kerr EA. More than a pain in the neck: how discussing chronic pain affects hypertension medication intensification. J Gen Intern Med. 2009;24(8):911-6.
28. Lagu T, Weiner MG, Hollenbeak CS, Eachus S, Roberts CS, Schwartz JS, Turner BJ. The impact of concordant and discordant conditions on the quality of care for hyperlipidemia. J Gen Intern Med. 2008;23(8):1208-13.
29. Piette JD, Kerr EA. The impact of comorbid chronic conditions on diabetes care. Diabetes Care. 2006;29(3):725-31.
30. Voorham J, Denig P. Computerized extraction of information on the quality of diabetes care from free text in electronic patient records of general practitioners. J Am Med Inform Assoc. 2007;14(3):349-354.
31. Lamberts H, Wood M. International Classification of Primary Care. Oxford Medical Publications, 1987; Oxford University Press.
32. Brown LC, Johnson JA, Majumdar SR, Tsuyuki RT, McAlister FA. Evidence of suboptimal management of cardiovascular risk in patients with type 2 diabetes mellitus and symptomatic atherosclerosis. CMAJ. 2004;171(10):1189-92.
33. Grant RW, Cagliero E, Murphy-Sheehy P, Singer DE, Nathan DM, Meigs JB. Comparison of hyperglycemia, hypertension, and hypercholesterolemia man-agement in patients with type 2 diabetes. Am J Med. 2002;112(8):603-9.
34. Voorham J, Haaijer-Ruskamp FM, Stolk RP, Wolffenbuttel BHR, Denig P, Groningen Initiative to Analyze Type 2 Diabetes Treatment Group. Influence of elevated cardiometabolic risk factor levels on treatment changes in type 2 diabe-tes. Diabetes Care. 2008;31(3):501-3.
35. Boyd CM, Darer J, Boult C, Fried LP, Boult L, Wu AW. Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implica-tions for pay for performance. JAMA. 2005;294(6):716-24.
36. Min LC, Wenger NS, Fung C, Chang JT, Ganz DA, Higashi T, Kamberg CJ, MacLean CH, Roth CP, Solomon DH, Young RT, Reuben DB. Multimorbidity is associated with better quality of care among vulnerable elders. Med Care. 2007;45(6):480-8.
37. Higashi T, Wenger NS, Adams JL, Fung C, Roland M, McGlynn EA, Reeves D, Asch SM, Kerr EA, Shekelle PG. Relationship between number of medical con-ditions and quality of care. N Engl J Med. 2007;356(24):2496-504.
38. Kerr EA, Smith DM, Hogan MM, Hofer TP, Krein SL, Bermann M, Hayward RA. Building a better quality measure: are some patients with ‘poor quality’ actually getting good care? Med Care. 2003;41(10):1173-82.
39. Voorham J, Denig P, Wolffenbuttel BHR, Haaijer-Ruskamp FM. Cross-sectional
202
Chapter 4.4 Competing demands
versus sequential quality indicators of risk factor management in patients with type 2 diabetes. Med Care. 2008;46(2):133-41.
40. Martirosyan L, Voorham J, Haaijer-Ruskamp FM, Braspenning J, Wolffenbuttel BHR, Denig P. A systematic literature review: prescribing indicators related to type 2 diabetes mellitus and cardiovascular risk management. Pharmacoepidemiol Drug Saf. 2009;doi 10.1002/pds.1894.
41. Conwell LJ, Boult C. The effects of complications and comorbidities on the quality of preventive diabetes care: a literature review. Popul Health Manag. 2008;11(4):217-28.
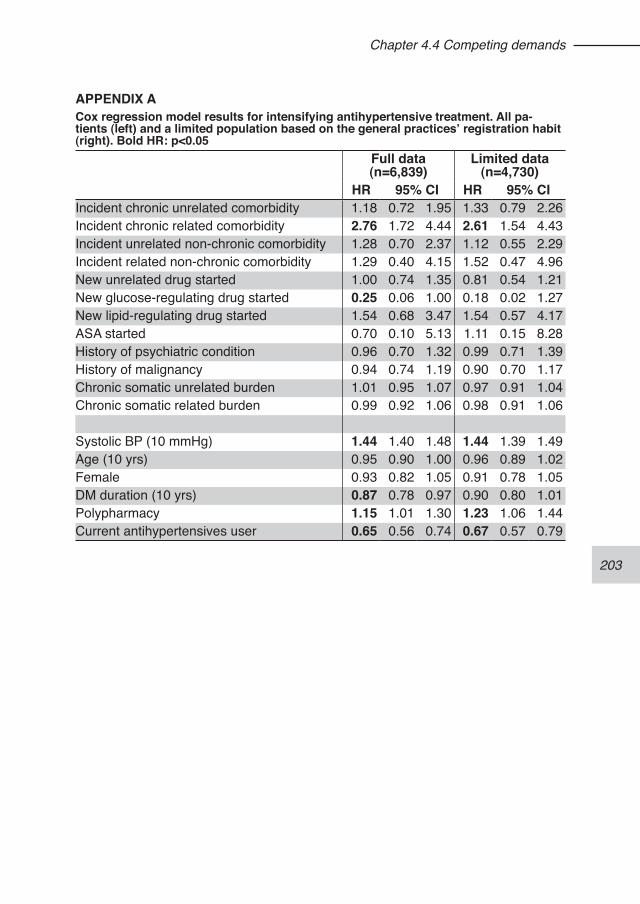
203
Chapter 4.4 Competing demands
APPENDIX ACox regression model results for intensifying antihypertensive treatment. All pa-tients (left) and a limited population based on the general practices’ registration habit (right). Bold HR: p<0.05
Full data (n=6,839)
Limited data (n=4,730)
HR 95% CI HR 95% CIIncident chronic unrelated comorbidity 1.18 0.72 1.95 1.33 0.79 2.26Incident chronic related comorbidity 2.76 1.72 4.44 2.61 1.54 4.43Incident unrelated non-chronic comorbidity 1.28 0.70 2.37 1.12 0.55 2.29Incident related non-chronic comorbidity 1.29 0.40 4.15 1.52 0.47 4.96New unrelated drug started 1.00 0.74 1.35 0.81 0.54 1.21New glucose-regulating drug started 0.25 0.06 1.00 0.18 0.02 1.27New lipid-regulating drug started 1.54 0.68 3.47 1.54 0.57 4.17ASA started 0.70 0.10 5.13 1.11 0.15 8.28History of psychiatric condition 0.96 0.70 1.32 0.99 0.71 1.39History of malignancy 0.94 0.74 1.19 0.90 0.70 1.17Chronic somatic unrelated burden 1.01 0.95 1.07 0.97 0.91 1.04Chronic somatic related burden 0.99 0.92 1.06 0.98 0.91 1.06
Systolic BP (10 mmHg) 1.44 1.40 1.48 1.44 1.39 1.49Age (10 yrs) 0.95 0.90 1.00 0.96 0.89 1.02Female 0.93 0.82 1.05 0.91 0.78 1.05DM duration (10 yrs) 0.87 0.78 0.97 0.90 0.80 1.01Polypharmacy 1.15 1.01 1.30 1.23 1.06 1.44Current antihypertensives user 0.65 0.56 0.74 0.67 0.57 0.79
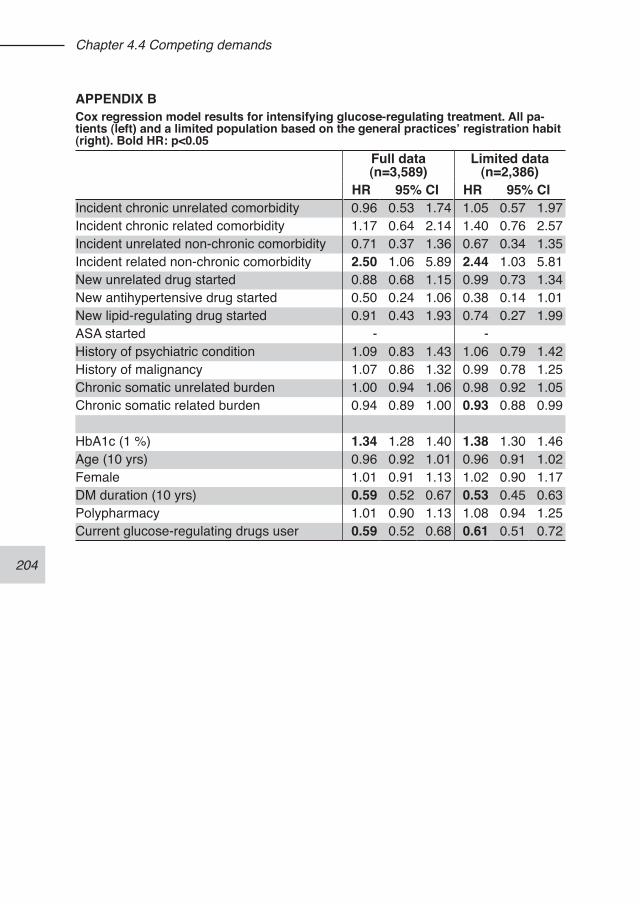
204
Chapter 4.4 Competing demands
APPENDIX BCox regression model results for intensifying glucose-regulating treatment. All pa-tients (left) and a limited population based on the general practices’ registration habit (right). Bold HR: p<0.05
Full data (n=3,589)
Limited data (n=2,386)
HR 95% CI HR 95% CIIncident chronic unrelated comorbidity 0.96 0.53 1.74 1.05 0.57 1.97Incident chronic related comorbidity 1.17 0.64 2.14 1.40 0.76 2.57Incident unrelated non-chronic comorbidity 0.71 0.37 1.36 0.67 0.34 1.35Incident related non-chronic comorbidity 2.50 1.06 5.89 2.44 1.03 5.81New unrelated drug started 0.88 0.68 1.15 0.99 0.73 1.34New antihypertensive drug started 0.50 0.24 1.06 0.38 0.14 1.01New lipid-regulating drug started 0.91 0.43 1.93 0.74 0.27 1.99ASA started - -History of psychiatric condition 1.09 0.83 1.43 1.06 0.79 1.42History of malignancy 1.07 0.86 1.32 0.99 0.78 1.25Chronic somatic unrelated burden 1.00 0.94 1.06 0.98 0.92 1.05Chronic somatic related burden 0.94 0.89 1.00 0.93 0.88 0.99
HbA1c (1 %) 1.34 1.28 1.40 1.38 1.30 1.46Age (10 yrs) 0.96 0.92 1.01 0.96 0.91 1.02Female 1.01 0.91 1.13 1.02 0.90 1.17DM duration (10 yrs) 0.59 0.52 0.67 0.53 0.45 0.63Polypharmacy 1.01 0.90 1.13 1.08 0.94 1.25Current glucose-regulating drugs user 0.59 0.52 0.68 0.61 0.51 0.72
205
206
207
Chapter 5 - General discussion
208
Chapter 5 - General discussion
This thesis describes studies focusing on the assessment of quality of care for pa-tients with type 2 diabetes in general practice. The aims were:1) To develop and validate methods and tools for collecting data from electronic medical records to build a longitudinal observational database; 2) To improve the assessment of quality of pharmacotherapeutic risk factor manage-ment in patients with type 2 diabetes; and 3) To unravel factors which determine treatment of risk factors in patients with type 2 diabetes. The studies presented in this thesis will be discussed in relation to the three themes, and put into a broader perspective. Also, some reflections are presented on the defi-nitions used for treatment modifications and medication adherence. Finally, some suggestions are made for approaches to improve risk factor management, and di-rections for new research are indicated.
MAIN FINDINGS
Data collection methodsData extraction from medical records with partly unstructured data to structured da-tasets poses a challenge. For the studies in this thesis, data from 10 different GP information systems were used, as well as from a specialised diabetes facility. In a perfect world, all components of a healthcare system use the same data structure, and the Dutch GP association clearly has this as a goal.1 However, because the use of electronic medical records is relatively new in the GP offices, the degree of standardisation is currently low. Therefore, one can decide to use only the already standardised portions of the available data or use methods to extract the relevant data from the different formats and structures. Within the GIANTT project it was decided to use both. Two techniques were suc-cessfully developed for restructuring data. The first is an interpretation method using a recognition algorithm, while the second relies on semi-automated evaluation of the data contents and remapping the contents to structured data. The recognition algorithms make use of a “number-oriented” approach to extract numeric clinical measurements from free text medical narratives. As described in Chapter 2.1, this results in complete risk factor data, independent of knowledge on how a certain practice registers this information. This approach, embedded into a process of data collection and post-processing, has proven to be as complete and precise as manual data collection but considerable less labour intensive. It results in what the GP “sees” in the electronic medical record, is what we get into our obser-vational database.
209
Chapter 5 - General discussion
The collected information is complete and accurate, yet, the additional workload for the participating practices is minimal. The data collection at the general practices, as described and evaluated in Chapter 2.2, is now operational for more than 5 years. From our experience, we know that the main workload is to identify which patients should be included for data extraction. Processing the list of possible diabetic pa-tients implies manual checking of the patient lists. Although in theory automated patient identification algorithms could be implemented, e.g. based on absolute val-ues of fasting glucose, issued prescriptions or diagnosis codes, we have shown that blindly relying on such information would result in considerable selection bias.Although we are able to extract all relevant information irrespective of where and how it is registered, this approach cannot extract what is not registered in a digit-ally accessible location. Maintaining paper files next to the electronic records and scanning documents in a picture format are two examples of making information inaccessible. Furthermore, specific registration habits of the practice can be an im-portant determinant of the validity of the information. This is independent of whether a practice registers data in the structured parts of their systems or not. Especially conditional registration of (risk factor) information, e.g. only annotating values out of normal range, is an issue to be aware of when using data obtained from regular registration.2
It has been argued that better and more structured registration is an important as-pect of quality of care. Although this has not been substantiated with evidence,3 there are of course obvious advantages of good registration of patient data. On the other hand, forcing general practitioners to use fixed forms with predefined items could be counterproductive. Such forms may fit the workflow of a specialised or protocolised setting but in case of complex patients with several comorbidities they might hinder optimal care.Until now, our recognition and interpretation efforts have been limited to numerical data. Some time has been invested into piloting text recognition approaches suitable for categorical or non-numerical data (e.g. verbal description of a patient’s smoking status). Although this approach looks promising, more research is needed to have these recognition algorithms fully operational.Other limitations of our approach are related to the post-processing. Although this is done with semi-automated procedures, residual misclassification due to human error remains possible. Although our approach does not result in much workload for the participating practices, currently one full-time data registration functionary is needed for data validation work on annual data collections of about 15,000 patients. A substantial part of the data validation actions are needed to correct typing errors or misclassifications made by the practice itself, and are independent of our data
210
Chapter 5 - General discussion
collection method. Thus, even in a perfect world of entirely structured information storage, post processing of observational data remains necessary.Often it is stated that information registered in free text parts of patient records is not suited for research purposes, as it is the assumption that only data stored in specific structured tables is valid. Using information from free text is then considered according to the GIGO principle often quoted in information technology (Garbage In - Garbage Out). However, this line of reasoning ignores the fact that free text itself follows structures. Moreover, it is also possible to store garbage in a structured way. Given that the waste recycling industry has long discovered the value of what once was classified as garbage, it would be wise to reconsider existing preconceptions regarding free text data, which is more likely a reflection of limitations within organi-sations rather than limitations of technology. “Garbage” can turn out to be a valuable resource.
Quality indicatorsIn assessing the quality of diabetes care, most frequently process indicators (how often are certain actions performed, such as the measurement of a risk factor, or the prescription of a drug) and outcome indicators (such as the mean value of HbA1c) are used. Assessing how a care provider has acted in response to a specific meas-ure links the different processes. When focussing on pharmacotherapy, such indica-tors assess prescribing of medication when indicated.Many quality indicators of treatment assess prescribing cross-sectionally, i.e. they assess whether the indicated or recommended treatment is prescribed for a certain patient population. For identifying poorly controlled patients without treatment such simple cross-sectional indicators can be sufficient (Chapter 3.1). Sequential assess-ment provides more in-depth insight into actions that providers can improve. Several sequential prescribing indicators have been constructed, measuring (changes in) treatment after the observation of an elevated risk factor level. A systematic litera-ture review was conducted to summarize what is known about the validity of the various existing prescribing indicators (Chapter 3.2). From this we concluded that there exists limited knowledge on the validity of many commonly used quality indi-cators for diabetes care. Most indicators have only shown face or content validity. Furthermore, patient case-mix is a problem that is insufficiently addressed in many indicators, which limits their application in external quality assessment. In Chapter 3.1, we compared various indicators with each other and with a reference method. We concluded that sequential assessment provides a better judgment than com-monly used cross-sectional assessments. Focusing on intensification of treatment in patients with uncontrolled risk factors is thus recommended for quality assessment. In addition, such indicators provide important additional information to indicate pos-
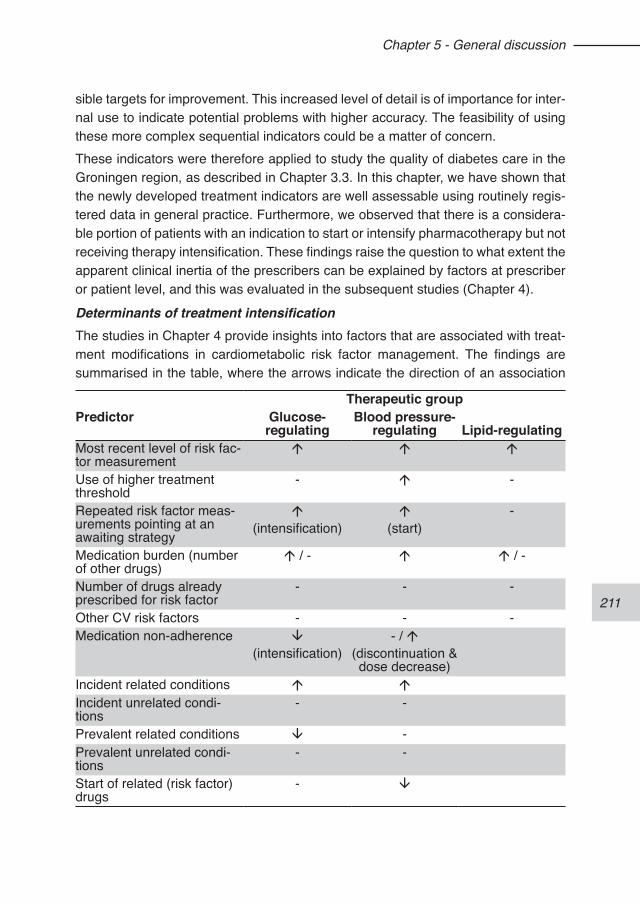
211
Chapter 5 - General discussion
sible targets for improvement. This increased level of detail is of importance for inter-nal use to indicate potential problems with higher accuracy. The feasibility of using these more complex sequential indicators could be a matter of concern. These indicators were therefore applied to study the quality of diabetes care in the Groningen region, as described in Chapter 3.3. In this chapter, we have shown that the newly developed treatment indicators are well assessable using routinely regis-tered data in general practice. Furthermore, we observed that there is a considera-ble portion of patients with an indication to start or intensify pharmacotherapy but not receiving therapy intensification. These findings raise the question to what extent the apparent clinical inertia of the prescribers can be explained by factors at prescriber or patient level, and this was evaluated in the subsequent studies (Chapter 4).
Determinants of treatment intensificationThe studies in Chapter 4 provide insights into factors that are associated with treat-ment modifications in cardiometabolic risk factor management. The findings are summarised in the table, where the arrows indicate the direction of an association
Therapeutic groupPredictor Glucose-
regulatingBlood pressure-
regulating Lipid-regulatingMost recent level of risk fac-tor measurement
á á á
Use of higher treatment threshold
- á -
Repeated risk factor meas-urements pointing at an awaiting strategy
á(intensification)
á(start)
-
Medication burden (number of other drugs)
á / - á á / -
Number of drugs already prescribed for risk factor
- - -
Other CV risk factors - - -Medication non-adherence â
(intensification)- / á
(discontinuation & dose decrease)
Incident related conditions á áIncident unrelated condi-tions
- -
Prevalent related conditions â -Prevalent unrelated condi-tions
- -
Start of related (risk factor) drugs
- â

212
Chapter 5 - General discussion
and a dash absence of statistical significance. From the results it becomes evident that the factors influencing risk factor manage-ment are not fully similar for glucose, blood pressure, and lipid regulation. The prescribers’ reactions to an elevated HbA1c are the strictest of the three risk fac-tors, but reaction to uncontrolled HbA1c differs for patients already treated with oral glucose-regulating drugs and those not yet using medication. There is a swift action to initiate therapy but prescribers show more reluctance to intensify treatment, where they partly appear to wait for repeated high levels before acting. There was no dif-ference in the rate of therapy intensification between moderately and poorly control-led patients. Concerns about polypharmacy are frequently mentioned in physician surveys as reason for not adding another drug to the treatment. We observed, how-ever, that the number of chronic drugs already taken by a patient was not a factor that inhibits decisions to start or intensify glucose-regulating medication treatment. Also, concerns about adherence are often mentioned, and more importantly, it has been argued that one should not intensify treatment in patients who do not adhere to their medication.4-6 Indeed, we found that low adherence to medication partly inhibits treatment intensification for glucose-regulating drugs. Finally, competing demands have been mentioned as reason not to act when indicated. We observed that pa-tients who already had several related chronic co-morbid conditions were less likely to receive treatment intensification. On the other hand, unrelated conditions were not found to be competing with glycaemic management, and new related conditions enhanced the likelihood of acting.For treatment of high blood pressure in diabetics, there appears to be more reluc-tance to initiate therapy than to intensify already existing therapy. There is a clear as-sociation between the level of blood pressure and the rate of starting or intensifying treatment, which indicates that more action is taken at higher threshold levels than indicated by the clinical guidelines. Furthermore, our studies showed that antihyper-tensive medication was started more often in patients who had repeated high levels of diastolic blood pressure, which is indicative of an awaiting strategy. Similar to gly-caemic management, we did not observe that polypharmacy was a barrier to start or intensify antihypertensive treatment. In contrast with glucose-regulating treatment, however, patients with lower adherence were not less likely to have their treatment intensified compared to adherent patients. There may be several explanations for this. It is tempting to suggest that physicians are less aware of non-adherence to an-tihypertensive treatment. However, sub-optimal adherence did increase the chance of other medication changes, i.e. dose decrease or discontinuation of antihyperten-sive medication, despite elevated blood pressure levels. This could point at alter-native strategies of either the patient or the physician to deal with perceived drug
213
Chapter 5 - General discussion
problems. Finally, we observed that the chance of having antihypertensive treatment intensified was lower at the moment that new glucose-regulating drugs were started. This indicates that glycaemic control competes with hypertension management.Regarding lipid management, the rate of medication initiation or intensification is low. Although there was a significant association between plasma cholesterol levels and the start and intensification of medication treatment, such treatment changes did not occur in the vast majority of patients with elevated cholesterol levels. Previous measurements did not influence treatment modification decisions. Finally, also the level of the other risk factors did not influence these decisions. Because of the low rate of start and intensification of lipid-regulating medication this therapeutic group was not included in the studies on the effect of adherence and competing demands on treatment intensification (Chapters 4.3 and 4.4).
So, from our studies it is apparent that reluctance to start or intensify treatment is of a different nature for the three risk factors studied. In blood glucose manage-ment, the reluctance is seen for maintaining optimal regulation in already treated pa-tients. However, the relation between benefits and harms of tight glycaemic control for all diabetic patients is under discussion.7-9 Therefore, an intervention aiming at improved glycaemic control should consider the patients’ complexity, and possible future definitions of minimum HbA1c values. The awaiting strategy for starting anti-hypertensive medication, in view of the relative low number of drugs used, shows an opportunity for improvement. Polypharmacy appears not to be a barrier, and in many cases intensifications are possible without addition of another pill. In lipid manage-ment, apparently other factors than the risk factor levels dominate in deciding to start or intensify lipid-regulating drugs. From the literature, it seems that both patients and physicians have concerns about benefits and adverse events, which may result in poor adherence and low willingness to use statins.10,11
SOME METHODOLOGICAL CONSIDERATIONS
Defining treatment modificationWhat constitutes a change in treatment can be defined in various ways. In the lit-erature, the focus is often on whether or not the drug treatment is intensified. This binary approach implies that any change in treatment, which does not fit the defini-tion of intensification, will be considered as being similar to no change. We showed in Chapter 4.3 that this approach can obscure relevant findings. Therefore the use of distinct treatment modifications is recommended.In addition, from the studies presented it becomes clear that it is important to dif-ferentiate between patients already or not yet treated for a specific risk factor. The
214
Chapter 5 - General discussion
decision to start medication treatment is not similar to the decision to intensify treat-ment. Studies on treatment changes should therefore consider this in the analyses and presentation of results.
Defining time to treatment modificationThe studies in Chapter 4 used treatment change as outcome. The definitions of the period to assess therapy changes differed between the studies. In the first studies, 4.1 and 4.2, treatment intensification was considered during a fixed one-year period, while the predictors were the last measurements of the risk factors in the preceding year. This approach was chosen to resemble a normal quality indicator, using calen-dar periods. However, this introduces some uncertainty about the link between the risk factor observation and the therapy modification, due to variation in the period in between. Therefore, in the following studies (4.3 and 4.4) therapy modification was assessed within a period relative to a risk factor observation moment. The dura-tion of the follow-up period determines how much distortion by other factors affect-ing therapy intensification is introduced. To minimise this, one can choose a short period, as we did in Chapter 4.3. When it is essential to allow for a longer period to acknowledge postponing of action, as was the case in our study looking at how competing demands affect treatment intensification (Chapter 4.4), distortion can be avoided by modelling the covariates as time dependent variables. Without such cor-rection, the use of longer follow-up periods will produce results that are difficult to interpret, and should be avoided.
Defining treatment adherenceIn our adherence study in Chapter 4.3, the choice of the adherence measure af-fected our results to some extent. The medication possession ratio (MPR), which is an overall period adherence estimate, was more strongly related with treatment modifications than an adherence measure based on the last gap between prescrip-tion refills. We therefore recommend using the MPR as a measure which better reflects prevailing non-adherence problems. In medication adherence research, it is quite common to use a binary adherence measure. We observed a considerable loss of power to detect associations with a binary adherence measure. This can be due to a lower precision of estimates and to the (arbitrary) choice of the cut-off points. It is therefore better to use continuous measures in studies of adherence.
215
Chapter 5 - General discussion
IMPLICATIONS
Data collectionThe data collection methods used in the GIANTT project show that it is possible to reliably extract and use numerical clinical information from free text parts of the medical records for quality assessment and scientific research. It is recommended to use such a flexible approach, because it avoids doubts on whether missing data are caused by the data collection or by the care process.Although electronic medical records are commonplace in Dutch healthcare, their use varies considerably between care providers. The feasibility of implementing se-quential assessment of (treatment) actions depends on the availability of data, and on the ability to process such data correctly. Especially at the secondary care level, longitudinal data on risk factor management are not yet readily available in an ac-cessible format.
Action or no actionThe term “clinical inertia”, as used in the literature, vastly overestimates true lack of clinical attention or activity. What it tries to name, the failure to act when indicated, consists of both justifiable and non-justifiable inaction on a measurable aspect of care. Although the associations found in the multivariate models of the studies in this thesis are difficult to translate into percentages of inaction “explained”, an attempt to this shows interesting results. When applying the reference method of appropriate care (Chapter 3.1) to the cohort study presented in Chapter 4.2, one can evaluate the consequences of an awaiting strategy by allowing decisions to be conditional on the risk factor status of a next observation within a 4-months period. The proportion of initial inaction that can be explained by a follow-up observation of the risk factor having either returned to control or shown a relevant improvement can be as high as 45% in the case of patients with uncontrolled blood pressure (figure 1). After adding the patients with poor adherence levels, and to a lesser extent, those with competing demands, it can be expected that the larger part of the “failure to act when indicated” can be explained by these considerations. Thus, what some classify as clinical iner-tia, actually may avoid unnecessary treatment intensifications. Overtreatment is an often forgotten aspect of prescribing quality in preventive treatment, and should be considered as well.
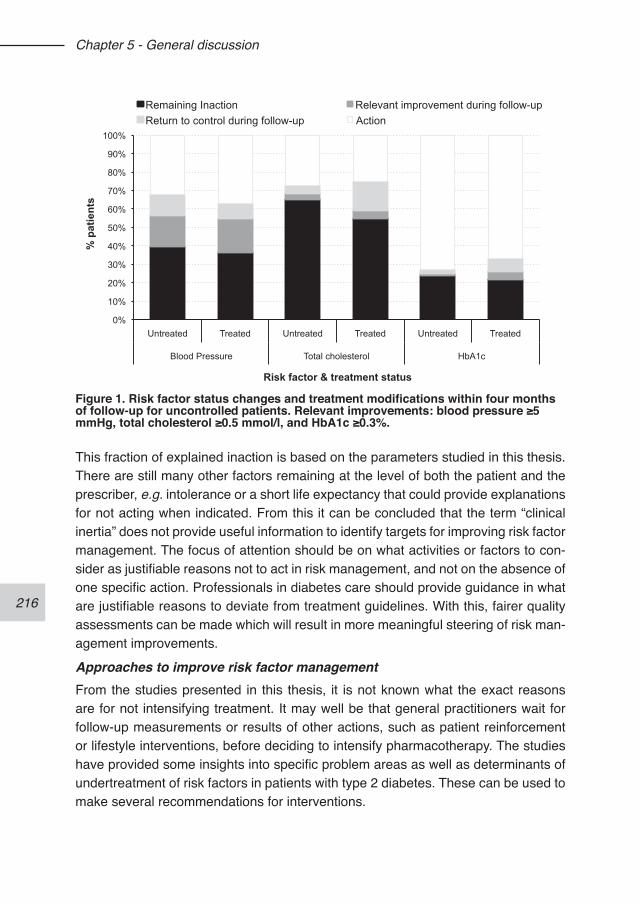
216
Chapter 5 - General discussion
This fraction of explained inaction is based on the parameters studied in this thesis. There are still many other factors remaining at the level of both the patient and the prescriber, e.g. intolerance or a short life expectancy that could provide explanations for not acting when indicated. From this it can be concluded that the term “clinical inertia” does not provide useful information to identify targets for improving risk factor management. The focus of attention should be on what activities or factors to con-sider as justifiable reasons not to act in risk management, and not on the absence of one specific action. Professionals in diabetes care should provide guidance in what are justifiable reasons to deviate from treatment guidelines. With this, fairer quality assessments can be made which will result in more meaningful steering of risk man-agement improvements.
Approaches to improve risk factor managementFrom the studies presented in this thesis, it is not known what the exact reasons are for not intensifying treatment. It may well be that general practitioners wait for follow-up measurements or results of other actions, such as patient reinforcement or lifestyle interventions, before deciding to intensify pharmacotherapy. The studies have provided some insights into specific problem areas as well as determinants of undertreatment of risk factors in patients with type 2 diabetes. These can be used to make several recommendations for interventions.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Untreated Treated Untreated Treated Untreated Treated
Blood Pressure Total cholesterol HbA1c
% p
atie
nts
Risk factor & treatment status
Remaining Inaction Relevant improvement during follow-up Return to control during follow-up Action
Figure 1. Risk factor status changes and treatment modifications within four months of follow-up for uncontrolled patients. Relevant improvements: blood pressure ≥5 mmHg, total cholesterol ≥0.5 mmol/l, and HbA1c ≥0.3%.
217
Chapter 5 - General discussion
Medication adherence showed to affect treatment decisions differently for blood pressure and for blood glucose control. The absence of effect of medication adher-ence on the prescribers’ decision to intensify treatment in hypertension indicates that lack of awareness of non-adherence might be an issue. It is essential to distinguish poor adherence from poor treatment response. Therefore, improving awareness of adherence issues is an important target for intervention. Although most GP informa-tion systems have complete prescription data at their disposal, little information is generated from these data to facilitate the detection of sub-optimal adherence in dai-ly practice. A tool providing an objective estimate of a patient’s prescription refill ad-herence could assist the general. This information combined with other knowledge, such as the patient’s self-reported adherence, can avoid addressing the wrong bar-rier to better risk factor control in patients with poor adherence.What also became clear is that the level of other cardiometabolic risk factors plays a limited role in guiding treatment modifications. In our study population, about 58% of the patients have more than one of the risk factors (HbA1c, systolic blood pressure or LDL-cholesterol) insufficiently controlled. The current guideline on cardiovascular risk management uses a simplified overall cardiovascular risk stratification for pa-tients with type 2 diabetes with regard to the need of treatment.12 Since combined exposure to elevated risk factors is common in patients with type 2 diabetes, an intervention aiming at indicating stacked elevated risk factors could improve overall cardiometabolic risk management.Furthermore, there still seems to be a glucose-centred approach to diabetes risk management, as has been observed in several previous studies,13,14 making this a target for intervention. This topic is closely related to considering overall cardiovas-cular risk for the decisions to intensify treatment. Intensified blood glucose manage-ment which inhibits optimal treatment of high blood pressure is counterproductive with regard to overall cardiovascular risk, because elevated blood pressure may contribute more to the risk for cardiovascular events than hyperglycaemia.15,16
Most of the determinants of treatment intensification studied in this thesis have com-ponents both at the level of the prescriber as of the patient. Therefore, an approach targeting not only the prescriber but also the patient is expected to be an efficient intervention to improve cardiometabolic risk management. Partly built upon the in-sights from our studies, a new research project has started to develop and evaluate a patient-oriented treatment decision aid which focuses on shared goal-setting and decision making. The intervention will need to be tailored to the needs and capacities of a heterogeneous group of patients with type 2 diabetes.

218
Chapter 5 - General discussion
FUTURE RESEARCHObservational studies with data registered during the care process provide an ef-ficient way to obtain important insight into the quality of cardiometabolic treatment, and targets for improvement. More research is needed to expand the use of avail-able data in electronic medical records. It can be expected that with some creativity and willingness to re-evaluate common practice and attitudes towards data registra-tion and processing, a wealth of information will become available. The value of this approach should be evaluated in other areas of medicine.Sequential indicators on action provide a more meaningful assessment of risk factor management than many of the commonly used indicators, and also combining the level of treatment with the level of control provides additional information on treat-ment quality. A recent report of the Dutch Ministry of Health on diabetes care organi-sation1 cites the advantages of the alternative indicators presented in this thesis. The report states that such indicators will likely be implemented in routine quality of care assessments. Implementation studies are needed to embed these approaches in risk management assessment into regular quality evaluations, with specific attention to feasibility in relation to data availability in different settings. Also, more efforts need to be made to incorporate justifiable reasons to deviate from treatment guidelines into the quality indicators. Additional research is needed to increase our knowledge on what constitutes quality of care for complex patients.17 Simply excluding patients from the quality assessment because they are old, or have dementia, or are socio-economically deprived may not benefit these patients.18,19 Differences in case-mix are clearly important to take into account for external quality assessment. It has been suggested to include the registration of guideline devia-tions in diabetes protocols.20 This will improve identification of barriers to better risk factor management, and provide important information on how to use reasons for not acting in quality assessment. However, the validity of this information should be assessed through independent research, since it is important to know whether the patients were rightly excluded.Related to this is the general recommendation that more research is needed on what aspects of care should be evaluated in quality assessments for different purposes. Such a selection should guide research into the predictive validity of selected indica-tors. We need more evidence that improvements, as measured with quality indica-tors, will in the end lead to better outcomes for patients.
219
Chapter 5 - General discussion
REFERENCES1. Struijs JN, van Til JT, Baan CA. Experimenteren met de keten-dbc diabetes.
NHG. Adequate dossiervorming met het Elektronisch Medisch Dossier. NHG – 2004. Rijksinstituut voor Volksgezondheid en Milieu, RIVM 2009; rapportnum-mer 260014001.
2. Thiru K, Hassey A, Sullivan F. Systematic review of scope and quality of elec-tronic patient record data in primary care. BMJ. 2003;326(7398):1070.
3. Goudswaard AN, Lam K, Stolk RP, Rutten GEHM. Quality of recording of data from patients with type 2 diabetes is not a valid indicator of quality of care. A cross-sectional study. Fam Pract. 2003;20(2):173-7.
4. Rose AJ, Berlowitz DR, Manze M, Orner MB, Kressin NR. Intensifying therapy for hypertension despite suboptimal adherence. Hypertension. 2009;54(3):524-9.
5. Kogut SJ, Andrade SE, Willey C, Larrat EP. Nonadherence as a predictor of an-tidiabetic drug therapy intensification (augmentation). Pharmacoepidemiol Drug Saf. 2004;13(9):591-8.
6. Reach G. Patient non-adherence and healthcare-provider inertia are clinical myopia. Diabetes Metab. 2008;34(4 Pt 1):382-5.
7. Pogach L, Engelgau M, Aron D. Measuring progress toward achieving hemoglob-in A1c goals in diabetes care: pass/fail or partial credit. JAMA. 2007;297(5):520-3.
8. Aron D, Pogach L. Transparency standards for diabetes performance measures. JAMA. 2009;301(2):210-2.
9. Currie CJ, Peters JR, Tynan A, Evans M, Heine RJ, Bracco OL, Zagar T, Poole CD. Survival as a function of HbA(1c) in people with type 2 diabetes: a retrospec-tive cohort study. Lancet. 2010;375:481-89.
10. Kedward J, Dakin L. A qualitative study of barriers to the use of statins and the implementation of coronary heart disease prevention in primary care. Br J Gen Pract. 2003;53(494):684-9.
11. AB E, Denig P, van Vliet T, Dekker JH. Reasons of general practitioners for not prescribing lipid-lowering medication to patients with diabetes: a qualitative study. BMC Fam Pract. 2009;10:24.
12. NHG. NHG-Standard Cardiovasulair risicomanagement. Nederlands Huisartsen Genootschap, Utrecht.
13. Brown LC, Johnson JA, Majumdar SR, Tsuyuki RT, McAlister FA. Evidence of suboptimal management of cardiovascular risk in patients with type 2 diabetes mellitus and symptomatic atherosclerosis. CMAJ. 2004;171(10):1189-92.
14. Grant RW, Cagliero E, Murphy-Sheehy P, Singer DE, Nathan DM, Meigs JB. Comparison of hyperglycemia, hypertension, and hypercholesterolemia man-agement in patients with type 2 diabetes. Am J Med. 2002;112(8):603-9.
15. Stevens RJ, Kothari V, Adler AI, Stratton IM, Holman RR - United Kingdom Prospective Diabetes Study (UKPDS) Group. The UKPDS risk engine: a model for the risk of coronary heart disease in Type II diabetes (UKPDS 56). Clin Sci. 2001;101(6):671-9.
220
Chapter 5 - General discussion
16. Gaede P, Vedel P, Larsen N, Jensen GV, Parving HH, Pedersen O. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med. 2003;348(5):383-93.
17. Heath I, Rubinstein A, Stange KC, van Driel ML. Quality in primary health care: a multidimensional approach to complexity. BMJ. 2009;338:911-3.
18. Sigfrid LA, Turner C, Crook D, Ray S. Using the UK primary care Quality and Outcomes Framework to audit health care equity: preliminary data on diabetes management. J Public Health. 2006;28(3):221-5.
19. Simpson CR, Hannaford PC, McGovern M, Taylor MW, Green PN, Lefevre K, Williams DJ. Are different groups of patients with stroke more likely to be exclud-ed from the new UK general medical services contract? A cross-sectional retro-spective analysis of a large primary care population. BMC Fam Pract. 2007;8:56.
20. Burgers JS. Het meten van behandelaanpassing. Een nieuwe indicator voor kwaliteit van chronische zorg. Ned Tijdschr Geneeskd. 2010;154:A1602
221
222
223
Summary
224
Summary
This dissertation concerns the quality of cardiometabolic treatment in patients with type 2 diabetes in general practice. The aims of this thesis are: 1) To develop and validate methods and tools for collecting clinical data related to diabetes care from electronic medical records; 2) To improve the assessment of quality of pharmaco-therapeutic risk factor management; and 3) To unravel factors that determine treat-ment of risk factors in patients with type 2 diabetes. Accordingly, the thesis is divided into three parts.
In the first part, the data collection methods that have been developed for the Groningen Initiative to Analyse Type 2 diabetes Treatment (GIANTT) project are presented (Chapter 2). The GIANTT project aims at improving the quality of care delivered to patients with type 2 diabetes mellitus. It entails the monitoring of process and outcomes of care in an observational cohort of patients in general practice in the northern Netherlands. Chapter 2.1 describes the development and validation of a computerised method for extracting numeric clinical measurements related to diabe-tes care from free text in electronic medical records of general practitioners. It makes use of a combination of a highly customizable text recognition algorithm, a number-oriented interpretation method, and a semi-automated post-processing procedure. The extraction method showed a sensitivity of 94-100% and a positive predictive value of 85-100% for the evaluated clinical measurements. The field performance showed an average time of 7.8 minutes per 100 patients needed to extract all rel-evant data. Most workload occurs at the central level during post-processing, with a maximum of 1.8 minutes needed per patient. Post-processing is helpful to maximize the proportion of correct observations extracted, and is also considered necessary to diminish errors in the extracted data which are caused by data entry errors in gen-eral practice. It was concluded that the developed extraction method identifies and converts numeric textual to structured data with a high accuracy, independent of how data are registered in the electronic medical records. This method can thus be used to build a longitudinal observational database with information relevant for diabetes care, enabling research as well as quality of care assessment in general practice. Chapter 2.2 describes the overall data collection procedure used within GIANTT, having the text recognition method from the previous chapter at its core. The data collection software, which can be applied to all 10 variants of general practice infor-mation systems in the region, is described. The software first guides the participating general practices through the process of identifying and confirming all patients with type 2 diabetes. This uniform patient identification method ensures consistent inclu-sion of patients over all practices. Next, all relevant data for these patients can be extracted with a push of a button. The post-processing of collected data is presented
225
Summary
in detail. This is needed to correct possible errors in the data. Over the past years, the presented approach showed that it is possible to collect accurate and complete data based on what is registered during the care process with a low burden for the participating general practices.
The second part of the thesis focuses on measuring quality with indicators of risk factor management in DM2 patients (Chapter 3). The fairness of such indicators is under debate, and this part of the dissertation contributes to a better understand-ing of the validity of commonly used indicators. It offers new approaches to assess chronic care quality through indicators that better incorporate the longitudinal nature of care.In Chapter 3.1 several quality indicators of blood glucose, blood pressure and lipid management are compared against a reference method. Commonly used cross-sectional indicators and newly developed “sequential” indicators are compared with regard to how well they predict appropriate care. The sequential indicators meas-ure actions following specific clinical observations, for example, whether treatment is intensified after an elevated HbA1c level was observed. From this study, it was concluded that sequential indicators are valuable for estimating quality of risk factor management in patients with diabetes. Such indicators may provide a more accurate and fair judgment than currently used cross-sectional indicators.A systematic review on prescribing indicators related to type 2 diabetes and cardio-vascular risk management is presented in Chapter 3.2. The aim was to describe the different aspects of validity of existing prescribing indicators. From this we concluded that there exists limited knowledge on the validity of many commonly used quality indicators for diabetes care. Most indicators have only shown face or content validity. Furthermore, patient case-mix is a problem that is insufficiently addressed in many indicators, which limits their application in external quality assessment.In Chapter 3.3, the quality of cardiometabolic risk factor management is presented for the period 2004 – 2007 in the northern Netherlands. Results from commonly used indicators are contrasted with results from indicators that either link the level of treat-ment to the level of control or measure action when indicated, as tested in Chapter 3.1. A case is built for incorporating such alternative assessment methods into reg-ular quality evaluations. This study showed that, although population averages of HbA1c, systolic blood pressure and cholesterol declined during the 4-year follow-up, suggesting improvement of the quality of care, relatively few therapy modifications occurred in insufficiently controlled patients: <45%, <28% and <15% of the patients with insufficiently controlled HbA1c, systolic blood pressure and LDL-cholesterol,
226
Summary
respectively. This approach can help health care professionals to identify specific targets for improvement. The question remains what the reasons are for not acting when indicated.
The third part of this dissertation focuses on factors that are often mentioned as rea-sons why patients with an indication for treatment intensification do not receive such therapy modifications (Chapter 4). In a series of observational studies, the relevance of these factors for decisions to start or intensify antihypertensive, glucose regulat-ing, or lipid regulating medication in general practice is studied.First, it has been suggested that some physicians may use higher thresholds to start or intensify treatment than indicated by the clinical guidelines. The study in Chapter 4.1 looks into how the level of blood pressure, HbA1c, and total cholesterol affect decisions of general practitioners to change drug treatment in a cohort of over 3,000 patients. We observed a significantly lower treatment intervention rate in moderately than in poorly controlled patients for blood pressure, indicating the use of higher threshold level. This was not seen for decisions on HbA1c or cholesterol results.Secondly, physicians may not react to the first elevated risk factor level. The study reported in Chapter 4.2 looks into this aspect of reaction to specific patterns of re-peated risk factor measurements. Besides the level of the most recent risk factor measurement, also the change in risk factor level since the previous measurement, and the number of measurements above treatment target level were considered as predictors of treatment modification. Repeated high levels of blood pressure were positively associated with the start of antihypertensive medication, while repeated high HbA1c levels positively affected the chance of glucose-lowering medication in-tensification. This shows that for blood pressure and HbA1c control a “wait-and-see” attitude could explain part of the reluctance to start or intensify medication treatment. For lipid-lowering medication, though, this was not the case. In the same study, we found that the medication burden (number of already used drugs) was not a barrier for therapy start or intensification for any of the three risk factors.Since medication adherence issues are also mentioned frequently as a reason for not wanting to add another drug to a patient’s medication regime, the association between a patient’s adherence to medication and therapy intensification was stud-ied for hypertension and hyperglycaemia in over 11,000 patients (Chapter 4.3). This study showed that adherence affects decisions on drug treatment differently for dif-ferent therapeutic areas. For glucose-regulating medication, therapy intensification was indeed less likely in patients with lower adherence levels. For antihypertensive medication, however, patients with lower adherence were more likely to have a dose
227
Summary
decreased or a drug discontinued. Thus, low adherence inhibits the intensification of glucose-regulating but not of antihypertensive medication in insufficiently controlled patients. Finally, in Chapter 4.4, the effect of competing demands on the decision to start or intensify antihypertensive or glucose-regulating medication is evaluated. A differen-tiation is made between existing comorbidity and incident events, and between con-ditions or events that are related and unrelated to diabetes. We considered prevalent chronic conditions, new symptoms or problems and prescriptions of a new drug as possibly competing for clinical attention. We found no evidence that incident un-related conditions in themselves decreased the likelihood to intensify medication treatment. However, starting new diabetes drugs competed with the management of hypertension, and having diabetes related chronic conditions competed with the management of hyperglycaemia.
In Chapter 5, the studies are discussed with regard to their outcomes and methodol-ogies. The most important implication following from the presented research on data collection methods is the recommendation to make better use of available data in medical records, and not to rely only on the use of specific registration methods. We have shown that this is quite feasible in Dutch general practice. For the quality indi-cators, the implications are on the application of the proposed sequential quality as-sessment methods. As a result of our research, reflections on the usefulness of this approach and its incorporation into regular quality of care assessment have been given by several Dutch health care quality organisations. Furthermore, we showed the need for more knowledge on the relation between what is measured with qual-ity indicators and the outcomes for patients. The research on the determinants of treatment modification shows possible targets for interventions to improve risk factor management. Finally, the findings from these studies illustrate that the concept of “clinical inertia”, frequently used in the literature on risk factor management, may vastly overestimate true inaction.
228
229
Samenvatting
230
Samenvatting
Deze dissertatie gaat over verscheidene aspecten van de kwaliteit van cardiome-tabole behandeling bij patiënten met type 2 diabetes in de eerstelijn. De doelstel-lingen van dit proefschrift zijn: 1) het ontwikkelen en valideren van methoden voor het geautomatiseerd verzamelen van diabetes gerelateerde klinische gegevens uit elektronische medische dossiers; 2) het ontwikkelen en evalueren van maten voor de kwaliteitsbepaling van cardiometabool risicofactor management; en 3) het evalu-eren van factoren, die de medicamenteuze behandeling van risicofactoren bepalen bij patiënten met type 2 diabetes.In het eerste deel van het proefschrift worden de dataverzamelingsmethoden be-schreven, die zijn ontwikkeld binnen het Groningen Initiative to Analyse Type 2 dia-betes Treatment (GIANTT) project (Hoofdstuk 2). Het GIANTT project heeft als doel de verbetering van de zorg verleend aan patiënten met type 2 diabetes. Hierbinnen worden processen en uitkomsten van zorg gevolgd in een observationeel cohort van patiënten in de eerstelijn in het noorden van Nederland. Hoofdstuk 2.1 beschrijft de ontwikkeling en validatie van een computergestuurde methode om numerieke klinische meetwaarden gerelateerd aan diabeteszorg te ex-traheren uit vrije tekstdelen van elektronische medische dossiers in huisartspraktij-ken. Het gebruikt een combinatie van een flexibel tekstherkenningsalgoritme, een nummer-georiënteerde interpretatiemethode en een half-geautomatiseerde proce-dure voor het controleren van de aldus gevonden gegevens (nabewerking). Deze methode van gegevensextractie liet een sensitiviteit zien tussen de 94 en 100%, en een positieve voorspellende waarde tussen de 85 en 100% voor de relevante klini-sche meetwaarden. Uit een veldtest bleek dat er gemiddeld 7,8 minuten nodig was om alle relevante gegevens voor 100 diabetes patiënten te verzamelen. Het grootste deel van de werkbelasting ligt op centraal niveau bij de nabewerking, met een maxi-maal geschatte tijdsduur van 1,8 minuten per patiënt. De nabewerking is nuttig om het aandeel correcte waarnemingen te maximaliseren, waarbij zonodig ook (type)fouten in de verzamelde gegevens worden gecorrigeerd, die door de huisartsprak-tijk zelf zijn veroorzaakt. We concluderen dat de ontwikkelde extractiemethode in staat is om met hoge accuratesse numerieke gegevens uit tekst te herkennen en om te zetten in gestructureerde gegevens, onafhankelijk van hoe de gegevens in de medische dossiers zijn geregistreerd. Deze methode kan dus gebruikt worden voor het opzetten van een longitudinale observationele database met gegevens, die relevant zijn voor de diabeteszorg. Dit maakt het mogelijk om zowel wetenschap-pelijk onderzoek als kwaliteit-van-zorg bepalingen te doen met routinematig geregi-streerde gegevens in de eerstelijn.Hoofdstuk 2.2 beschrijft de totale dataverzamelingsprocedure, zoals gebruikt bin-nen GIANTT, met de eerder beschreven extractiemethode als kern. De ontwikkelde
231
Samenvatting
extractie–software is toepasbaar op alle 10 varianten van huisarts informatie syste-men (HISsen) in onze regio. Het programma leidt een huisartspraktijk eerst door het proces van het identificeren en bevestigen van alle patiënten met type 2 diabetes. Deze uniforme methode van patiëntidentificatie levert een consistente inclusie van patiënten op voor alle deelnemende praktijken. Vervolgens worden met een druk op de knop de relevante gegevens van deze patiënten verzameld. Daarna wordt door een registratiemedewerker van GIANTT de nabewerking uitgevoerd. Deze nabewer-king bestaat uit verschillende stappen, die in dit hoofdstuk nader worden beschre-ven. Gedurende de afgelopen jaren is gebleken dat het met deze aanpak mogelijk is om, met minimale belasting voor de deelnemende huisartspraktijken, accurate en volledige gegevens te verzamelen, gebaseerd op wat gedurende het normale zorg-proces geregistreerd wordt.
Het tweede deel van het proefschrift richt zich op kwaliteitsindicatoren van risicofac-tor management (Hoofdstuk 3). De redelijkheid van zulke indicatoren staat ter dis-cussie. Dit deel van de dissertatie draagt bij tot een beter inzicht in de validiteit van een aantal veel gebruikte indicatoren. Tevens worden nieuwe benaderingen voor het meten van de kwaliteit van chronische zorg worden gepresenteerd, met behulp van indicatoren die beter rekening houden met het longitudinale aspect van zorg. In Hoofdstuk 3.1 worden verschillende kwaliteitsindicatoren van glucose-, bloed-druk- en cholesterolmanagement vergeleken met een referentiemethode van “ade-quate zorg”. Vaak gebruikte dwarsdoorsnede indicatoren, die de status quo op 1 moment vaststellen, en nieuw ontwikkelde sequentiële indicatoren worden vergele-ken met betrekking tot hoe goed ze adequate zorg kunnen meten. De sequentiële in-dicatoren meten acties, die volgen op specifieke klinische waarnemingen. Ze meten bijvoorbeeld of de medicamenteuze behandeling is geïntensiveerd na de observatie van een verhoogd HbA1c. Deze studie laat zien dat sequentiële indicatoren waar-devol zijn voor het meten van de kwaliteit van risicofactor management in patiënten met diabetes. Deze indicatoren kunnen een rechtvaardiger oordeel geven over de geleverde zorg in vergelijking met de huidig gebruikte dwarsdoorsnede indicatoren.Een systematisch review van voorschrijfindicatoren gerelateerd aan type 2 diabe-tes en cardiovasculair risico management wordt gepresenteerd in Hoofdstuk 3.2. Het doel hiervan was het beschrijven van verschillende aspecten van validiteit van bestaande voorschrijfindicatoren. Op basis hiervan concluderen we dat er beperkte kennis is over de validiteit van veelgebruikte voorschrijfindicatoren voor diabetes-zorg. De meeste indicatoren hebben alleen indruks- en inhoudsvaliditeit (face and content validity), maar geen bewijs van predictieve validiteit. Daarnaast is patiënten case-mix een probleem waarmee veel van de indicatoren onvoldoende rekening
232
Samenvatting
houden, wat de toepasbaarheid voor externe kwaliteitsmeting nadelig beïnvloedt.In Hoofdstuk 3.3 wordt de kwaliteit van het cardiometabole risicofactor management in noord Nederland voor de periode 2004-2007 gepresenteerd. Resultaten van veel-gebruikte kwaliteitsindicatoren worden gecontrasteerd met die van verschillende al-ternatieve indicatoren. Deze alternatieven meten enerzijds het behandelingsniveau in relatie tot de mate van regulering, en anderzijds de actie waar geïndiceerd, met indicatoren zoals beschreven in Hoofdstuk 3.1. Deze studie laat zien dat, hoewel de populatiegemiddelden van HbA1c, systolische bloeddruk en cholesterol zijn gedaald gedurende de 4-jaars follow-up, er relatief weinig therapieaanpassingen plaats vin-den in onvoldoende gereguleerde patiënten: minder dan 45%, 28% en 15% van de patiënten met onvoldoende gereguleerde HbA1c, systolische bloeddruk en LDL-cholesterol, respectievelijk. Er wordt een pleidooi gehouden voor het toevoegen van zulke alternatieve meetmethoden aan reguliere kwaliteitsevaluaties. Deze benade-ring kan zorgverleners helpen bij het identificeren van specifieke verbeterdoelen.
Het derde deel van deze dissertatie richt zich op verscheidene factoren, die vaak genoemd worden als redenen om de (medicamenteuze) behandeling bij patiënten met een verhoogde risicofactor niet te intensiveren (Hoofdstuk 4). In een reeks ob-servationele studies wordt bestudeerd in hoeverre deze factoren de beslissing om behandeling met antihypertensiva, glucoseregulerende medicatie of cholesterolver-lager te starten of the intensiveren beïnvloeden.Allereerst wordt ingegaan op de bewering dat sommige artsen hogere afkapwaar-den gebruiken dan de richtlijnen aangeven om medicatie te starten of te intensi-veren. In de studie in Hoofdstuk 4.1 wordt in een cohort van ruim 3.000 patiënten bekeken hoe het niveau van de bloeddruk, HbA1c en totaal cholesterol de beslis-sing van huisartsen beïnvloedt om medicamenteuze behandeling aan te passen. We constateren dat bij patiënten met een matig gereguleerde bloeddruk minder be-handelaanpassingen plaatsvinden in vergelijking tot slecht gereguleerde patiënten, wat duidt op het gebruik van hogere afkapwaarden. Dit was niet het geval voor de behandelbeslissingen bij niet goed gereguleerde HbA1c of cholesterol waarden.Als tweede is gekeken naar de verklaring dat huisartsen wellicht niet direct reage-ren op een eerste waargenomen verhoogde risicofactor. De studie in Hoofdstuk 4.2 bestudeert dit aspect van het reageren op herhaalde risicofactor metingen. Duidelijk is dat de hoogte van de meest recente meting van invloed is op de behandelbe-slissingen. Daarnaast blijken in sommige gevallen ook de relatieve verandering in een risicofactor of het aantal opeenvolgende metingen boven de streefwaarde rele-vant voor de beslissing om behandeling aan te passen. Zo waren herhaalde hoge
233
Samenvatting
bloeddrukwaarden positief geassocieerd met de start van antihypertensiva, terwijl herhaalde hoge HbA1c waarden de kans op intensivering van glucoseregulerende medicatie positief beïnvloedde. Dit betekent dat voor bloeddruk en HbA1c regule-ring een afwachtende houding van de behandelaar een deel van de vaak gerap-porteerde “onderbehandeling” kan verklaren. Voor cholesterolverlagende medicatie was dit echter niet het geval. In dezelfde studie is ook gekeken naar de invloed van polyfarmacie op de behandelbeslissingen. Er werd gevonden dat voor geen van de drie bestudeerde risicofactoren het aantal al gebruikte medicijnen gerelateerd is met het al dan niet starten of intensiveren van de medicamenteuze behandeling.Aangezien therapietrouw ook vaak genoemd wordt als reden om de medicatie van een patiënt niet uit te breiden, is de associatie tussen therapietrouw en therapie intensivering bestudeerd voor hypertensie en hyperglycemie bij meer dan 11.000 patiënten (Hoofdstuk 4.3). Uit deze studie blijkt dat behandelaanpassingen bij pa-tiënten, die minder therapietrouw zijn, niet hetzelfde zijn voor de verschillende the-rapeutische gebieden. In het geval van glucoseregulering werd, zoals verwacht, de medicatie minder geïntensiveerd in patiënten met slechtere therapietrouw. Bij hypertensie kregen patiënten met slechtere therapietrouw daarentegen vaker een dosisverlaging of werd een middel helemaal gestopt. Onvoldoende therapietrouw houdt dus de intensivering van glucoseregulerende medicatie deels tegen, maar dit lijkt niet het geval bij bloeddrukverlagende medicatie.Tenslotte is in Hoofdstuk 4.4 het effect bestudeerd van concurrerende gebeurtenis-sen (competing demands) op de beslissing medicatie te starten of te intensiveren voor glucose- en bloeddrukregulerende medicatie. We hebben prevalente chroni-sche ziekten, nieuwe symptomen of ziekten en recepten voor een nieuw medicijn beschouwd als mogelijk concurrent voor klinische aandacht. Er is onderscheid ge-maakt tussen ziekten of gebeurtenissen, die gerelateerd of ongerelateerd zijn aan diabetes. In deze studie hebben we geen bewijs gevonden dat incidente, niet aan di-abetes gerelateerde gebeurtenissen de kans op therapieaanpassing verlagen. Wel bleek dat het starten van nieuwe diabetes medicatie concurreerde met bloeddruk management, en daarnaast het hebben van aan diabetes gerelateerde chronische condities concurreerde met glucose management.
In Hoofdstuk 5 volgt een beschouwing van de resultaten en gebruikte methoden uit de verschillende studies. De belangrijkste implicatie van het onderzoek rond nieuwe dataextractie methoden is de aanbeveling om beter gebruik te maken van beschikbare gegevens in medische dossiers en gegevensverzameling niet afhan-kelijk te maken van specifieke registratiemethoden. We hebben laten zien dat dit goed haalbaar is in de Nederlandse huisartspraktijken. Het onderzoek rond de kwa-

234
Samenvatting
liteitsindicatoren heeft geleid tot een voorstel om de nieuw ontwikkelde sequentiële behandelindicatoren in het huidige kwaliteitsmeten te implementeren. Inmiddels is door verschillende partijen in Nederland de bruikbaarheid en mogelijke toepassing hiervan in de reguliere kwaliteitsmetingen beschouwd. Los daarvan is duidelijk ge-worden dat er meer kennis nodig is over de relatie tussen wat wordt gemeten met de kwaliteitsindicatoren en de uitkomsten voor de patiënten. De studies naar de determinanten van behandelaanpassingen tonen mogelijke aangrijpingspunten voor interventies om risicofactor management te verbeteren. Tevens illustreren de bevin-dingen van deze studies dat het concept van “clinical inertia”, veelvuldig gebruikt in de literatuur over risicofactor management, het aandeel daadwerkelijke “behan-delstarheid” flink kan overschatten.
235

236
237
Dankwoord
238
Dankwoord
Dat een niet al te jong persoon met een vreemde achtergrond de kans krijgt om een promotietraject te volgen, lijkt me niet de meest logische keuze voor een onder-zoeksgroep. Floor en Petra, mijn dank voor jullie vertrouwen, en het door jullie mogelijk gemaakte pad om in de wetenschap terug te keren. Er zijn grote verschillen tussen mijn vorige en huidige vakgebied, en ben jullie veel verschuldigd voor de hulp bij deze overgang. Petra, over wat ik aan jou verschuldigd ben zou ik vele zinnen kunnen wijden. Maar, waar we in onze samenwerking goed in zijn geworden is veel zeggen met weinig woorden. Dank je.Bruce, mijn dank voor de immer scherpe beschouwingen over de methoden en de klinische kanten van de vraagstellingen en discussies.Ronald, mijn dank voor jouw inbreng, die de methodologische kanten van de studies heeft versterkt.
Mijn dank gaat uit naar de stuurgroep van GIANTT, bestaande uit:D. de Zeeuw, F.M. Haaijer-Ruskamp, P. Denig (Klinische Farmacologie, Universitair Medisch Centrum Groningen), B.H.R. Wolffenbuttel (Endocrinologie, Universitair Medisch Centrum Groningen), K. van der Meer (Huisartsgeneeskunde, Universitair Medisch Centrum Groningen), K. Hoogenberg (Interne Geneeskunde, Martini Ziekenhuis Groningen), P. Bijster (Diabetesdienst, Huisartsenlaboratorium LabNoord, Groningen), P. Rademaker (Districts Huisartsen Vereniging Groningen, Groninger Huisartsen Coöperatie), R.P. Stolk (Epidemiologie, Universitair Medisch Centrum Groningen), H.J.G. Bilo (Isala Klinieken, Zwolle; Interne Geneeskunde, Universitair Medisch Centrum Groningen), J. Bolt† (Districts Huisartsen Vereniging Groningen).Deze groep, onder voorzitterschap van Dick de Zeeuw, heeft het GIANTT project mogelijk gemaakt, en hun blijvende inzet heeft gezorgd voor continuïteit van het project.
In de beginfase van de methodenontwikkeling voor het GIANTT project zijn een aantal huisartsen van groot belang geweest. Zij hebben het veelvuldig veldtesten van data extractie software mogelijk gemaakt, en geholpen met het uitwerken van de te volgen procedures. Marcel Ingenhut, Arie Booij, Alie Hiddema, Henk Smeenge, Frank Beltman (en Karin), Coos Cijsouw, Bram Luteijn, Jan Huizinga, mijn dank voor jullie tijd en geduld. Hoewel het testen soms e-mailtjes opleverde met @#$%^&* als onderwerp en een enkel boos telefoontje, is de goede samenwerking blijven be-staan. Uiteraard wil ik ook alle andere huisartsen die mee werken aan het GIANTT project bedanken.
239
Dankwoord
Ik dank mijn vroegere collega’s van het TCC, Marco Assmann en Rob Bieringa, voor de goede samenwerking en hulp bij het ontwikkelen van mijn IT competenties.
De GIANTT groep op de werkvloer dank ik voor hun inzet en goede samenwerking: Wessel, Ellen, Judith, Sandra en Ronald.
Peter en Henk-Jan, bedankt dat jullie mijn paranimfen wilden zijn.
Júlia, Luna en Johanna dank ik voor de tijd die ze me hebben gegund om dit proef-schrift te realiseren, maar zeker ook voor de momenten dat ze me het werk lieten vergeten, wat geen makkelijke klus was.
240
241
Curriculum vitae
242
Curriculum vitae
Jaco Voorham werd geboren op 26 juni 1963 te ‘s-Gravenhage. Na het doorlopen van de Theo Thijssen lagere school, en de Simon Stevin Scholengemeenschap in Den Haag begon hij zijn studie Biologie aan de Rijksuniversiteit Leiden in 1981. Tijdens deze studie heeft hij z’n hoofdvak in de Parasitologie gedaan met veldwerk naar malariabestrijdingsmethoden in het binnenland van Suriname. Voortzetting van dit onderzoek onderbrak zijn studie een jaar. Dit vakgebied bleef hem trekken, want bij terugkeer uit Suriname rondde hij zijn studie af met een gedragsstudie met muskieten aan de Landbouw Universiteit Wageningen. Zijn doctoraalexamen werd in augustus 1988 gehaald.In 1989 keerde hij terug naar de binnenlanden van Suriname, ditmaal om de malari-abestrijding op te zetten in het gebied dat door binnenlandse conflicten van de rest van het land was gescheiden, in dienst van het Zeister Zendingsgenootschap. Deze activiteiten duurden 3 jaar.In 1993 trad hij in dienst bij de PAHO (regionale afdeling voor de Amerikas van de WHO) als associate professional officer, binnen een team van malariadeskundigen dat in Brazilië was gestationeerd. In deze twee jaren deed hij zelf onderzoek naar bestrijdingsmethoden, besteedde veel aandacht aan het opleiden van counterparts en het samenbrengen van onderzoeksgroepen in het land.Na het dienstverband met de WHO in 1995 bleef hij Brazilië, en heeft op verschillende plekken in het Amazonegebied gewoond en gewerkt voor lokale overheidsinstan-ties. Deels waren zijn bezigheden gericht op onderzoek naar malariabestrijdings-methoden, en deels op andere gebieden binnen de openbare gezondheidszorg. Dit leverde hem veel ervaring met allerlei aspecten van de openbare gezondheidszorg en overheden op. In 2000 en 2001 heeft hij een uitstap richting Afrika gemaakt, en binnen een malaria onderzoeksproject gewerkt in Mozambique, in dienst van de United States Agency for International Development (USAID).Een belangrijk aspect van zijn activiteiten binnen het toegepaste malariaonderzoek heeft zich gericht op het stimuleren van het gebruik van evidence bij de keuzes van controle strategieën, en het samenvoegen van epidemiologische informatie op het niveau van de parasiet, vector en mens. Ook het optimaal gebruiken van be-schikbare gegevens, en het inzetten van computers daarvoor, heeft altijd een rol gespeeld in zijn bezigheden.In 2002 repatrieerde hij, en vestigde zich in de provincie Groningen. Dit “tweede leven” begon met een tijdelijke baan als onderzoeksmedewerker bij een longfunc-tieonderzoek van de RuG. Eind 2002 trad hij in dienst van het Trial Coordination Center van het UMCG. Daar heeft hij data- en projectmanagement, en software ontwikkeling activiteiten uitgevoerd. In 2003 begon hij vanuit het TCC met het opzet-
243
Curriculum vitae
ten van de dataverzameling en –verwerking in opdracht van het GIANTT project. In december 2005 begon hij zijn promotieonderzoek bij de disciplinegroep Klinische Farmacologie van de RuG, in deeltijd naast de “gewone” ontwikkel, onderhouds en datamanagement werkzaamheden van het GIANTT project.
244
245
Groningen graduate school of medical sciences - research institute SHARE
246
SHARE
This thesis is published within the research program Evidence Based Medicine in Practice of the Research Institute SHARE of the Groningen Graduate School of Medical Sciences (embedded in the University Medical Center Groningen / University of Groningen). More information regarding the institute and its research can be obtained from our internetsite: www.rug.nl/share.
Previous dissertations from the program Evidence Based Medicine in Practice:
Vries R de (2010). Health-economics of interventions aimed at infectious diseases: dynamic modeling inevitable for reliable medical decision making.Supervisors: prof dr MJ Postma, prof dr LTW de Jong-van den Berg
Schorr SG (2010). Drug safety in patients with psychotic disorders.Supervisors: prof dr K Taxis, prof dr JRBJ BrouwersCo-supervisors: dr R Bruggeman, dr CJ Slooff
Doormaal JE van (2009). Medication errors and adverse drug events in hospital-ised patients; methodological issues and computerised intervention.Supervisor: prof dr FM Haaijer-RuskampCo-supervisors: dr PGM Mol, dr JGW Kosterink, dr PLA van den Bemt
Peters-Veluthamaningal C (2009). Corticosteroid injections for the treatment of hand and wrist disorders in general practice.Supervisor: prof dr B Meyboom-de JongCo-supervisor: dr JC Winters
Beinema MJ (2009). The optimalization of coumarin anticoagulant therapy: pharma-cogenetics and computer asisted dose finding.Supervisors: prof dr JRBJ Brouwers, prof dr J van der MeerCo-supervisor: dr B Wilffert
247
SHARE
Boersma C (2009). Health economics of cardiovascular & renal disease prevention.Supervisors: prof dr MJ Postma, prof dr LTW de Jong-van den Berg, prof dr PE de JongCo-supervisor: dr T Gansevoort
Stewart RE (2009). A multilevel perspective of patients and general practitioners.Supervisors: prof dr B Meyboom-de Jong, prof dr TAB Snijders, prof dr FM Haaijer-Ruskamp
Vroom F (2009). Drug use in pregnancy; exploring the field of DMARDs in preg-nancy.Supervisors: prof dr LTW de Jong-van den Berg, prof dr JRBJ Brouwers, prof dr MAFJ van de LaarCo-supervisor: dr HEK de Walle
Hulst, M van (2008). Health economics of blood transfusion safety.Supervisors: prof dr MJ Postma, prof dr CTh Smit Sibinga

Stellingen behorende bij het proefschriftAssessing cardiometabolic treatment quality in general practiceJaco Voorham, 16 juni 2010
1. De dogmatische overtuiging dat Garbage In leidt to Garbage Out resulteert in gemiste kansen.
2. Gestructureerde gegevensregistratie heeft als consequentie dat de aandacht van de zorgverlener steeds meer gericht is op de muis dan op de patiënt.
3. Indicatoren voor behandelaanpassing zijn beter in staat kwaliteit van zorg te meten dan dwarsdoorsneematen (dit proefschrift).
4. De bruikbaarheid van kwaliteitsindicatoren van diabeteszorg voor vergelijking van huisartsen is beperkt, zolang er geen oplossing gevonden wordt voor de lage schattingsprecisie.
5. Bij cardiometabool risicomanagement in de eerstelijn ligt de aandacht teveel op glucoseregulering, ten koste van bloeddruk- en lipidenregulering (dit proefschrift).
6. Een groot deel van wat anderen als Clinical Inertia bestempelen, kan verklaard worden door legitieme redenen voor het niet ophogen van medicatie (dit proefschrift).
7. Het ontbreken van voorspellende validiteit van de meeste voorschrijfindicatoren maakt de relevantie hiervan twijfelachtig (dit proefschrift).
8. Gecombineerde blootstelling aan meerdere te hoge risicofactoren moet meer aandacht krijgen in het risicomanagement.
9. IT-ers zouden zich meer moeten richten op het verwezenlijken van wensen dan het afbakenen en handhaven van grenzen voor wat volgens hun eigen beperkingen mogelijk is.
10. Accountability en cynisme gaan vaak hand in hand.
11. Multidisciplinair werken kan ook alleen.
12. Het is aardig om te zeggen dat je nooit hebt gezegd dat je aardig bent.
13. Het belangrijkste gereedschap van de wetenschapper is de liniaal.





























