Embed Size (px)
Citation preview

UNCORRECTED PROOF
1
2
3Ž .Journal of Neuroimmunology 4315 2001 xxx45
www.elsevier.comrlocaterjneuroin6
7
8
910
Assessment of HIV-intrathecal humoral immune response in aids-related11
neurological disorders12
13
Enrico Fainardi a,), Carlo Contini b, Natale Benassi c, Andrea Bedetti d,14
Massimiliano Castellazzi a, Luca Vaghi a, Vittorio Govoni a, Ezio Paolino a,15
PierGiorgio Balboni e, Enrico Granieri a1617
a Section of Neurology, UniÕersity of Ferrara, Arcispedale S. Anna, Corso della GioÕecca 203, Ferrara 1-44100, Italy18b Section of Infectious Diseases, UniÕersity of Ferrara, Ferrara, Italy19
c Section of Virology, Azienda Ospedaliera Arcispedale S. Anna, Corso della GioÕecca 203, Ferrara 1-44100, Italy20d Unit of Infectious Diseases, Azienda Ospedaliera Arcispedale S. Anna, Corso della GioÕecca 203, Ferrara 1-44100, Italy21
e Department of Sperimental and Diagnostic Medicine, Section of Microbiology, UniÕersity of Ferrara, Õia Luigi Borsari 46, Ferrara 1-44100, Italy2223
Received 10 January 2001; received in revised form 2 May 2001; accepted 3 July 200124
25
2627
Abstract28
29Ž .Intrathecal synthesis of IgG directed to HIV antigens was investigated by antibody specific index ASI , affinity-mediated immunoblot30
Ž . Ž . Ž .AMI and Western blot WB assay in a group of 88 AIDS patients of which 28 with HIV-associated neurological disorders HAND , 1331Ž . Ž .without associated neurological disorders WAND and 47 with non-HIV-associated neurological disorders non-HAND . CD4q count32
3 Ž . 3 Ž .was above 50 cellsrmm CD4q)50 in 30 and below 50rmm CD4q-50 in 58 patients, respectively. A significantly higher33Ž . Ž .frequency for CSF complete anti-gag profile p-0.001 , and for HIV-specific oligoclonal patterns AmixedB patternsp-0.01 was34
observed in HAND as compared to patterns from the other clinical groups. A decrease in complete anti-env, anti-pol and anti-gag35
reactivity was present in CSF of patients with CD4q-50 as compared to those with CD4q)50. Our findings suggest that AIDS36
appears to be characterized by an anti-HIV intrathecal humoral immune response which is principally directed to env products with a37
prevalence of oligoclonal patterns and CSF complete anti-gag profile in HIV-associated neurological involvement. q 2001 Elsevier38
Science B.V. All rights reserved.39
40Keywords: HIV; Intrathecal IgG synthesis; Specific antibody reactivity; Viral structural proteins41
4243
44
1. Introduction45
46
Converging lines of evidence indicate that neuraxis47
represents a preferential target for Human Immunodefi-48
Ž . Ž .ciency Virus HIV Price, 1996 . A broad spectrum of49
neurological conditions has frequently been documented in50
HIV infected individuals during the various stages of the51
disease in relation to opportunistic infections induced by52
Ž .immunosuppression Price, 1996; Cohen and Berger, 1998 ,53
or as a consequence of virus attack against the nervous54
Ž . Ž .system NS Price, 1996; Gendelman et al., 1997 that55
heralds the onset of central and peripheral neurologic56
complications postulated to have a unified pathogenesis57
Ž .Tan and Guiloff, 1998 . Moreover, HIV has been isolated58
Ž .in cerebrospinal fluid CSF and brain tissue of infected5960
616263
64) Corresponding author. Tel.: q39-532-205525.6566
67
68
Ž .E-mail address: [email protected] E. Fainardi .
69
Žpatients in the different phases of the disease McArthur et 70
.al., 1988; Ho et al., 1985; Chiodi et al., 1988a and it has 71
also been reported that the virus penetrates the intrathecal 72
Žcompartment early in the course of the infection Resnick 73
.et al., 1988; McArthur et al., 1988 . 74
A large number of CSF abnormalities including blood– 75
Ž .brain-barrier B-B-B disturbance and a gradually decreas- 76
ing intrathecal IgG production have been demonstrated 77
Žduring the entire course of the infection Resnick et al., 78
1988; McArthur et al., 1988; Elovaara et al., 1987; Luer et¨ 79.al., 1988; Marshall et al., 1988 . In this setting, the occur- 80
rence of anti-HIV antibodies restricted to CSF compart- 81
ment in asymptomatic carriers has been considered further 82
Žproof that the virus invades the brain early Elovaara et al., 83
.1987 , while in AIDS patients it may represent an active 84
virus replication producing a persistent antigenic stimula- 85
Žtion Luer et al., 1988; Chiodi et al., 1988b; Elovaara et¨ 86.al., 1993 . This HIV-specific CSF-restricted humoral im-
870165-5728r01r$ - see front matter q 2001 Elsevier Science B.V. All rights reserved.88
Ž .PII: S0165-5728 01 00386-1

UNCORRECTED PROOF
( )E. Fainardi et al.rJournal of Neuroimmunology 00 2001 000–000289
mune response has been reported to be markedly poly-90
Žclonal rather than oligoclonal Resnick et al., 1985; Chiodi91
.et al., 1988b . Also, the analysis of antigenic specificity of92
CSF anti-HIV antibodies has shown a progressive decrease93
in anti-pol and anti-gag reactivity in contrast to a perma-94
nent intrathecal anti-env response in asymptomatic stages95
Žas well as in AIDS-mediated conditions Chiodi et al.,96
1988b; Lolli et al., 1990; Goswami et al., 1991; Elovaara97
.et al., 1993 .98
Despite the strong correlation described between intra-99
B-B-B production of anti-HIV antibodies and virus recov-100
Ž .ery from CSF Sonneborg et al., 1989 , no relationship was¨101
detected between HIV-specific antibody response and102
Ž .HIV-associated disorders Goswami et al., 1991 . Thus,103
the recognition of a potential indicator to discriminate the104
different neurological manifestations would be helpful.105
In order to clarify the actual role of virus-specific106
humoral response in the immune deregulation which is107
generated locally in HIV-related NS involvement, we in-108
vestigated intrathecal synthesis of anti-HIV IgG and their109
antigenic specificity in a group of patients suffering from110
AIDS. Since the relationship among HIV-specific oligo-111
clonal IgG, CSF antibody reactivity profiles, clinical pic-112
tures and progression of AIDS has not previously been113
evaluated, we sought to establish whether these anti-HIV114
humoral patterns could contribute to better define some115
pathogenetic aspects of HIV-related neurological manifes-116
tations.117
118
2. Patients and methods119
120
2.1. Patient selection121
122
We conducted a prospective investigation of 88 consec-123
Žutive HIV infected patients 63 men and 25 women; mean124
.ages36.4"8.5 admitted to the Department of Infectious125
Diseases of Ferrara during the period from March 1993126
to January 1997. Enzyme-linked immunosorbent assay127
Ž . Ž .ELISA and Western blot WB analysis demonstrated128
anti-HIV-1 serology and excluded anti-HIV-2 infection.129
The affected patients enrolled in this study were 61 intra-130
venous drug addicts, 20 heterosexual partners of HIV131
infected subjects, four homosexual men and three transfu-132
sion recipients. All the patients belonged to Group IV of133
Ž .the Centers for Disease Control CDC classification of134
Ž .Atlanta CDC, 1987 : 1 to Group IVA, 19 to Group IVB,135
64 to Group IVC1, 3 to Group IVC2 and 1 to Group IVD.136
Among these patients, 28 showed HIV-associated neuro-137
Ž .logical disorders HAND representing virus-induced brain138
Ždiseases encephalopathys24 cases; peripheral neuropa-139
.thys3 cases; vacuolar myelopathys1 case , 13 were140
AIDS patients without associated neurological disorders141
Ž .WAND and 47 had non-HIV-associated neurological dis-142
Ž .orders non-HAND consisting of bacterial, viral, fungal
143
Žand protozoal opportunistic brain infections Toxoplasma 144
gondii encephalitiss11 cases; Progressive Multifocal Leu- 145
kobencepalopathys11 cases; Cryptococcoccal meningitis 146
s9 cases; Mycobacterial infectionss9 cases; Cytomega- 147
.lovirus encephalitiss4 cases; Aspergillosiss3 cases . 148
Ž 3.Peripheral CD4q cell count means92.3"226.4 mm 1493 Ž . Žwas above 50rmm CD4q)50 in 30 individuals 13 150
HAND, means227.1"166; 5 WAND, means145.2" 151
.96; 12 non-HAND, means145.5"118.5 and below 1523 Ž . Ž50rmm CD4q-50 in 58 subjects 15 HAND, mean 153
s16.5"18.3; 8 WAND, means5.4"6; 35 non-HAND, 154
.means15.4"15.2 . All patients had discontinued the 155
antiretroviral treatment for at least 3 months because of 156
intolerance or therapeutic failure in accordance with the 157
ŽState of Art Consensus Conference criteria Sande et al., 158
.1993 . Samples were obtained before the widespread use 159
of plasma HIV viral load, as a prognostic marker of 160
disease progression. None of these patients had received 161
protease inhibitors or highly active antiretroviral therapy at 162
the moment of sample collection. We also tested as HIV- 163
Žnegative and immunocompetent controls 45 patients 25 164
.women and 20 men, mean ages43q14.2 suffering from 165
Ž .other inflammatory neurological disorders OIND and 39 166
Ž .patients 19 women and 20 men, mean ages45.6q15.9 167
Ž .with non inflammatory neurological disorders NIND . 168
Research protocol was reviewed and approved by the 169
Regional Committee for Medical Ethics in Research.170
171
2.2. Routine CSF and serum examination 172
173
Paired CSF and serum samples were collected under 174
sterile conditions by atraumatic lumbar puncture per- 175
formed for the purpose of diagnosis in the absence of 176
contraindications. Specimens were frozen in aliquots at 177
y70 8C until assay. CSF and serum concentrations were 178
measured nephelometrically with the Beckman Array Pro- 179
Ž .tein System Salden et al., 1988 , while Blood–CSF-Bar- 180
Ž .rier B-CSF-B dysfunction was estimated by CSFral- 181
Ž . Ž .bumin quotient Q following Tibbling et al. 1977 .Alb182
1832.3. Anti-HIV ELISA 184
185
CSF and serum anti-HIV IgG were assayed by ELISA 186
Ž .as previously described Reiber and Lange, 1991 by com- 187
Žmercially available kit for anti-HIV quantitation Genelavia 188
Mixt, Sanofi Diagnostics Pasteur, Marnes-La-Coquette, 189
.France . Adsorbance was read at 490 nm with an auto- 190
Žmated ELISA reader Microline reader DV 920, Poli In- 191
.dustria Chimica , Milano, Italy .192
193
2.4. Calculation of HIV-specific quantitatiÕe index 194
195
Ž .According to Reiber’s formula Reiber and Lange, 1991 196
production of IgG anti-HIV was determined by antibody

UNCORRECTED PROOF
( )E. Fainardi et al.rJournal of Neuroimmunology 00 2001 000–000 3197
Ž .specific index ASI . Reference curve was generated in198
each assay using the standard serial dilutions ranging199
between 0.05 and 2.00 OD. The upper standard titer of200
Ž .each plate was considered as 100 arbitrary units AU . ASI201
means the ratio between CSF and serum AU values, with202
Ž .multiplication by the dilution factor Q and CSFrSpec203Ž .serum total IgG levels expressed as mgrdl Q inIgG204
accordance to the formula205
ASIsQ rQ 1Ž .Spec IgG206
with Q s AU rAU and Q s IgG rSpec CSF serum IgG CSF207IgG .In the case of intrathecal synthesis of total IgG,serum208Q appeared more elevated than Reiber’s hyperbolicIgG209
Ž . Ž .discrimination line Q Reiber and Felgenhauer, 1987 .Lim210Q represented the CSF total IgG fraction completelyLim211blood-derived calculated from the individual Q of aAlb212single patient. Therefore, owing to the introduction of this213
barrier-related correction of the Q , the ratio becameIgG214between Q and Q in agreement with the formulaSpec Lim215Ž .Reiber, 1996216
ASIsQ rQ 2Ž .Spec Lim217
with218
2 y6 y3(Q s0.93 Q q6P10 y1.7P10 .Ž .Lim Alb219
Ž . ŽTherefore, to avoid false-negative results Eq. 1 Q )IgG220.Q is used when no significant intrathecal total IgGLim
221Ž . Ž .synthesis occurs, while Eq. 2 Q -Q was pre-IgG Lim 222
ferred in case of intense brain-derived total IgG production 223
in CSF. 224
HIV-specific intrathecal IgG synthesis was assumed for 225
values of ASI greater than 1.5.226
227
2.5. HIV antigen preparation228
229
Preparation of HIV strain HXBC2 antigens stock was 230
Ž .carried out as described by Destrosiers 1990 . Briefly, 231
Ž 6.CEM-SS cells 1=10 were infected with HIV at a 232
Ž .multiplicity of infection MOI of 0.001 TCID rcell;50 233every week media were collected by centrifugation at 3000 234
rpm for 10 min from virus producing cell cultures. The 235
supernatant was then centrifuged at 17.000 rpm for 3 h at 236
4 8C. Virus pellets were resuspended in PBS-a containing 237
Triton X-100 0.5% to obtain a complete viruses lysis. 238
Antigen stocks were stored aty70 8C. At every collection 239
Ž 7.of media uninfected cells 1=10 were added to virus- 240
producing cell cultures to ensure high levels of virus 241
production. The strain HXBC2, which is HIV-1 IIIB de- 242
rived, has been shown a high affinity for CD4 receptor of 243
T lymphocytes. Thus, its antigens were chosen because 244
representative of all variants, including CD4-indipendent 245
isolates of HIV, and implicated in pathologic effects in 246
Ž .humans La Branche et al., 1999 .
247248
Ž .Fig. 1. Affinity-mediated immunoblot AMI patterns: Asnormal; Bsmirror; Cs local synthesis; Dsmixed; Espatient with multiple sclerosis used249as negative control for non-specific binding. CSFscerebrospinal fluid; Ssserum.
UNCORRECTED PROOF
( )E. Fainardi et al.rJournal of Neuroimmunology 00 2001 000–0004250251
( )2.6. HIV-specific affinity-mediated immunoblotting AMI252
253
Ž .HIV-specific IgG oligoclonal bands OCB were de-254
tected by AMI according to the protocol of Dorries et al.¨255Ž .1989 using a commercially available isoelectric focusing256
Žkit Titan Gel IgG IEF, Helena Laboratories, Gateshead,257
.Tyne and Wear, UK with some modifications. Briefly, 5258
ml of paired undiluted CSF and 1:300 diluted serum259
Ž .samples were applied to the agarose gel pH range 3–10260
and were focused for 85 min at 10 8C in a multiphor unit261
Ž .Isolab, Akron, OH, USA . After IEF run, the gel was262
Ž .blotted onto a nitrocellulose sheet NC previously coated263
overnight at room temperature with HIV antigen solution264
Žin Tris-buffered saline TBS, 50 mM Tris, 200 NaCl, pH265
.7.5 . HIV antigen solution total protein were measured by266
Ž .Markwell procedure Markwell et al., 1981 and were267
diluted with TBS to obtain the optimal concentration of268
100 mgrml per 10 cm3 of NC area. After incubation with269
HIV antigen, the NC membranes were washed in TBS and270
non-specific binding sites were blocked for 1 h in TBS271
Ž .containing 5% bovine serum albumin BSA . The affinity-272
mediated capillary blotting was performed under a uniform273
weight of 1 kg for 30 min at room temperature. After274
washing with PBS, NC papers were incubated for 30 min275
at room temperature with goat anti-human IgG antiserum276
diluted 1:1000 in TBS. The immunoblots were further277
washed with TBS and incubated for 30 min at room278
temperature with peroxidase conjugated rabbit anti-goat279
IgG diluted 1:1000 in TBS. After another washing cycle280
with TBS, the blots were stained using peroxidase conju-281
gated substrate of the kit according to the manufacturer’s282
instructions. The immunoblotting specificity was evaluated283
Žin accordance to the above mentioned protocol Dorries et¨284.al., 1989 . No cross-reactivity to HIV was detected. Ac-285
Žcording to the CSF European Consensus criteria Anders-286
.son et al., 1994 , we identified four different AMI IgG287
banding patterns when comparing CSF and parallel serum288
Ž . Ž .from the same patient Fig. 1 : 1 AnormalBsdiffuse289
polyclonal IgG background in CSF and serum, without any290
Ž .detectable IgG OCB; 2 Alocal synthesisBs two or more291
CSF restricted IgG OCB and absent in the corresponding292
Ž .serum; 3 AmixedBsCSF restricted IgG OCB with addi-293
Ž .tional identical IgG OCB in both CSF and serum; 4294
AmirrorBs identical IgG OCB located at the same isoelec-295
tric point in both CSF and serum. The results were exam-296
ined by two independent investigators. Only the detection297
of AMI profiles 2 and 3 was considered suggestive of298
intrathecal synthesis of oligoclonal anti-HIV IgG.299
300
( )2.7. Western blot WB assay301
302
WB analysis was carried out using a commercially303
Žavailable system Novapath HIV-1 Immunoblot Assay,304
.Bio-Rad Laboratories, CA, USA according to the manu-305
facturer’s instructions. Briefly, 30 ml of undiluted CSF
306
specimen was dispensed onto NC strips containing the 307
electrophoresed and transferred viral proteins env, pol and 308
gag. After incubation on a rocking platform for 30 min at 309
room temperature and subsequent two washing cycles, the 310
NC membranes were incubated with secondary antibody 311
for 30 min at room temperature on a rocking platform. 312
After two washing cycles, colour reaction was developed 313
as described in the protocol of the kit. The staining intensi- 314
ties of the bands corresponding to HIV proteins were 315
scored visually by two independent investigators as fol- 316
Ž . Ž . Ž .lows: 1 absent; 2 weak; 3 strong. An immunostaining 317
type 2 or 3 was recorded as positive for each single HIV
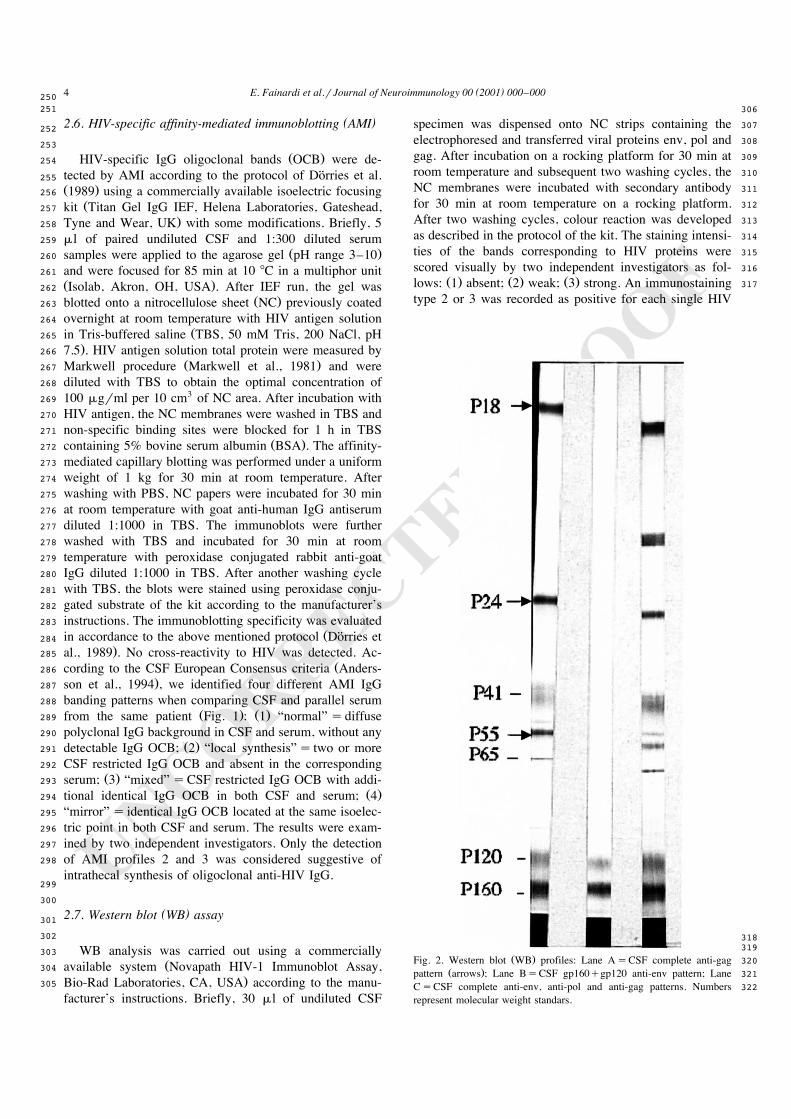
318319
Ž .Fig. 2. Western blot WB profiles: Lane AsCSF complete anti-gag 320Ž .pattern arrows ; Lane BsCSF gp160qgp120 anti-env pattern; Lane 321
CsCSF complete anti-env, anti-pol and anti-gag patterns. Numbers 322represent molecular weight standars.

UNCORRECTED PROOF
( )E. Fainardi et al.rJournal of Neuroimmunology 00 2001 000–000 5323
protein. For each HIV gene, we evaluated the occurrence324
Ž . Ž .of Fig. 2 : a IgG directed to the total of the gene325
Ž .products; b profiles obtained by the combination of IgG326
directed to each single gene product.327
328
2.8. Statistical analysis329
330
The patient group percentages were compared using the331
Ž .Log-Likelihood Ratio Test G . A difference was consid-332
ered significant at p-0.05.333
334
3. Results335
336
3.1. ELISA tests337
338
ASI values above the normal limit were found in 66r88339
Ž . Ž .75% of total AIDS patients. Of these, 21r28 75% were340
Ž . Ž .HAND, 10r13 76.9% were WAND, 35r47 74.5%341
were non-HAND. CD4q values above or below 50rmm3342
Ž . Ž .were found in 23r30 76.7% and in 43r58 74.1%343
patients, respectively, without any statistically significant344
difference among the various groups studied. No signifi-345
cant differences were also observed when the larger sub-346
groups of HAND and non-HAND were compared, since347
Ž .ASI values greater than 1.5 was present in 20r24 83.3%348
Ž . Ž .of HIV encephalopathy HIVE , in 8r11 72.2% of Toxo-349
Ž .plasma gondii encephalitis TE and Progressive Multifo-350
Ž . Ž .cal Leukoencepalopathy PML , in 7r9 77.8% of Cryp-351
Ž .tococcoccal meningitis CM and Mycobacterial infections352
Ž .MI . None of OIND NIND patients displayed an intrathe-353
cal synthesis of anti-HIV antibodies by ASI.354
355
3.2. AMI technique356
357
As summarized in Table 1, in all clinical categories358
examined we detected a relative low frequency of AMI359
oligoclonal IgG profiles indicative of HIV local synthesis
360361
Table 1362Ž .Distribution of affinity-mediated immunoblot AMI intrathecal synthesis363
profiles into 88 total AIDS patients with or without neurological disorders364aITS Local synthesis Mixed
b )Ž . Ž . Ž .HAND 12r28 42% 3r28 10.7% 9r28 32.2% 8c Ž . Ž . Ž .WAND 2r13 15.4% 2r13 15.4% 0r13 0%
d Ž . Ž . Ž .Non-HAND 9r47 19.2% 7r47 19.2% 2r47 14.9%e Ž . Ž . Ž .Total 23r88 26.1% 12r88 13.6% 11r88 12.5%
365
Ž .Mixed profile was significantly more frequent in HAND 8p-0.01 than366in WAND and non-HAND. ITS was significantly more consistent in367
Ž) .HAND p-0.05 than in non-HAND.368a Ž .Intrathecal synthesis patterns local synthesisqmixed .369bHIV-associated neurological disorders.370cWithout associated neurological disorders.371dNon-HIV-associated neurological disorders.372eTotal patients.
373374
Table 2 375Ž .Distribution of affinity-mediated immunoblot AMI intrathecal synthesis 376
Ž .profiles into AIDS patients with HIV encephalopathy HIVE , Toxo- 377Ž .plasma gondii encephalitis TE , Progressive Multifocal Leukoen- 378
Ž . Ž .cepalopathy PML , Cryptococcoccal meningitis CM and Mycobacterial 379Ž .infections MI 380
aITS Local synthesis Mixed') 'Ž . Ž . Ž .HIVE 12r24 45.8% 3r24 12.5% 8r24 33.3% 8
Ž . Ž . Ž .TE 2r11 18.2% 2r11 18.2% 0r11 0%Ž . Ž . Ž .PML 1r11 9.1% 1r11 9.1% 0r11 14.9%Ž . Ž . Ž .CM 1r9 11.1% 1r9 11.1% 0r9 12.5%Ž . Ž . Ž .MI 1r9 11.1% 1r9 11.1% 0r9 12.5%
381
Mixed profile was significantly more frequent in HIVE than in TE, PML, 382Ž . Ž' .MI 8p-0.01 and CM p-0.02 ; ITS was significantly more consis- 383
Ž) . Ž' .tent in HIVE than in PML, CM, MI p-0.05 and TE p-0.02 . 384a Ž .Intrathecal synthesis patterns local synthesisqmixed .
385
within the CSF compartment. AMI oligoclonal patterns 386
supporting an anti-HIV IgG synthesis restricted to brain 387
were slight statistically more frequent in HAND than in 388
Ž .non-HAND p-0.05 and were more represented even in 389
HAND than in WAND, although this difference was not 390
statistically significant. Moreover, HAND had statistically 391
higher percentage of AmixedB profile when compared to 392
Ž .WAND and non-HAND p-0.01 . There were no signif- 393
icant differences for AMI patterns among the different 394
clinical pictures and between CD4q)50 and CD4q- 395
50 lymphocyte count groups. On the other hand, patterns 396
suggestive of systemic oligoclonal IgG production trans- 397
Ž .ferred into brain AmirrorB and AmixedB displayed more 398
Ž .prominent values in HAND 16r28; 57.1% compared to 399
Ž . Ž .WAND 4r13; 30.8% and non-HAND 13r47; 27.6% 400
with a statistically significant difference between HAND 401
Ž .and non-HAND p-0.02 . Finally, as shown in Table 2, 402
the strong discrepancy found between HAND and non- 403
HAND for HIV-specific CSF-restricted oligoclonal re- 404
sponse was confirmed by the evaluation of their larger 405
subgroups. No HIV-specific oligoclonal bands were identi- 406
fied in CSF and serum of OIND and NIND. 407
408
3.3. WB anti-HIV reactiÕity 409
410
3.3.1. CSF total anti-HIV reactiÕity 411
The occurrence of CSF total anti-env, anti-pol and 412
anti-gag response was listed in Table 3. CSF total anti-env 413
specific staining was recognized more frequently than 414
anti-pol and anti-gag IgG bands in the various groups 415
examined with a slight statistically significant prevalence 416
when total anti-pol reactivity of CD4q)50 were com- 417
Ž .pared to CD4q-50 p-0.05 . No anti-HIV specific 418
staining was detected in OIND and NIND. 419
420
3.3.2. CSF anti-HIV patterns 421
In CSF, complete gp160qgp120qgp41 and gp160q 422
gp120 anti-env patterns were remarkably prevalent rather

UNCORRECTED PROOF
( )E. Fainardi et al.rJournal of Neuroimmunology 00 2001 000–0006423424
Table 3425Ž .Frequencies of CSF Western Blot WB total anti-HIV reactivity ob-426
served in 88 AIDS patients divided into various categories427
Anti-env Anti-pol Anti-gaga Ž . Ž . Ž .HAND 28r28 100% 13r28 46.4% 13r28 46.4%b Ž . Ž . Ž .WAND 13r13 100% 6r13 46.1% 6r13 46.1%
c Ž . Ž . Ž .Non-HAND 46r47 97.9% 25r47 53.2% 23r47 48.9%d )Ž . Ž . Ž .CD4q)50 30r30 100% 20r30 66.7% 18r30 60%e Ž . Ž . Ž .CD4q-50 56r58 96.5% 24r58 41.1% 24r58 41.4%
f Ž . Ž . Ž .Total 87r88 98.9% 44r88 50% 42r88 47.7%428
CSF total anti-pol profile was significantly more frequent in CD4q)50429Ž) .p-0.05 than in CD4q-50.430
aHIV-1-associated neurological disorders.431bWithout associated neurological disorders.432cNon-HIV-1-associated neurological disorders.433dPatients with CD4q cell count above 50rmm3.434ePatients with CD4q cell count below 50rmm3.435f Total patients.
436
than those found in all AIDS groups. Significantly more437
increased values were found for CSF complete anti-env438
pattern in CD4q)50 than in CD4q-50 and for gp160439
qgp120 anti-env profile in CD4q-50 than in CD4q440
Ž . Ž .)50 p-0.001 Fig. 3a . In addition, the frequency of
441
CSF complete p65qp32 pattern was significantly more 442
Ž .elevated in CD4q)50 than in CD4q-50 p-0.01 443
Ž .Fig. 3b . When the distinct CSF anti-gag profiles were 444
tested, statistically more pronounced values for complete 445
p55qp24q18 pattern was calculated in HAND in com- 446
Ž .parison to WAND and non-HAND p-0.001 and in 447
Ž . ŽCD4q)50 with respect to CD4q-50 p-0.01 Fig. 448
.3c . The striking predominance of CSF complete anti-gag 449
profile found in HAND than in non-HAND was corrob- 450
orated by significantly greater values obtained in HIVE 451
Ž . Ž10r24; 41.7% with respect to TE and PML 1r11; 9.1%; 452
. Ž .p-0.05 , CM and MI 0r9; 0%; p-0.01 . 453
454
4. Discussion 455
456
The aim of present study was to provide further insights 457
into the effective relevance of anti-HIV IgG restricted 458
production within the brain in a large series of AIDS 459
patients, and to distinguish the different neurological com- 460
plications occurring in the course of AIDS. 461
ŽAccording to prior investigations Resnick et al., 1988; 462
Elovaara et al., 1987; Luer et al., 1988; Chiodi et al.,¨
463464
Fig. 3. Panel A shows the distribution of CSF complete gp160q120q41 and gp160q120 anti-env patterns in patients with CD4q cell count above465Ž . Ž . 3CD4q)50 and below CD4q-50 50rmm with greater rates for complete anti-env profile in CD4q)50 than in CD4q-50 and for466
Ž) .gp160q120 in CD4q-50 than CD4q)50 p-0.001 . Panel B indicates the distribution of CSF complete p65q32 anti-pol pattern in CD4q-50467Ž .and CD4q-50 patients with higher rates in CD4q-50 than CD4q-50 8p)0.01 . Panel C illustrates the distribution of CSF complete468
Ž . Ž .p55q24q18 anti-gag profile in HIV-1-associated neurological disorders HAND , without associated neurological disorders WAND , non-HIV-1-asso-469Ž .ciated neurological disorders non-HAND , CDq)50 and CD4q-50 with more prominent rates in HAND than in non-HAND and WAND470
Ž) . Ž .p-0.001 and in CD4q)50 than in CD4q-50 8p-0.01 .

UNCORRECTED PROOF
( )E. Fainardi et al.rJournal of Neuroimmunology 00 2001 000–000 7471
1988b; Lolli et al., 1990; Goswami et al., 1991; Elovaara472
.et al., 1993 , we observed a high frequency of ASI positive473
values, suggesting an intrathecal synthesis of HIV-specific474
IgG in AIDS clinical groups examined, without any statis-475
tical discrimination among them.476
ŽIn agreement with previous observations Chiodi et al.,477
.1988b; Goswami et al., 1991 and in contrast with others478
Ž .Dorries et al., 1989; Grimaldi et al., 1988 , a small¨479
percentage of AIDS patients was found to be producer of480
CSF restricted oligoclonal IgG bands. However, AMI pro-481
files indicative of anti-HIV intrathecal IgG synthesis, par-482
ticularly AmixedB pattern, were principally associated with483
HAND rather than with the other clinical pictures. Further-484
more, a more elevated frequency of AMI patterns reflect-485
ing blood-derived CSF oligoclonal IgG secretion was486
shown in HAND as compared to non-HAND and, to a487
lesser extent, WAND.488
Antigenic specificity evaluation of CSF and serum anti-489
HIV IgG confirmed the broad spectrum of antibody pro-490
Žduction previously described Ellis et al., 1997; Lolli et al.,491
1990; Goswami et al., 1991; Elovaara et al., 1993; Grimaldi492
.et al., 1988 involving several virus structural proteins as493
targets which are most likely imputable to a different494
Ž .processing of their precursors Chiodi et al., 1988a . Ac-495
cording to some prior studies, we detected a CSF antibody496
response which was mainly directed to env products such497
Žas gp160, gp120 Chiodi et al., 1988a; Lolli et al., 1990;498
.Goswami et al., 1991; Grimaldi et al., 1988 and, to a499
Ž .lesser extent, to gp41 Elovaara et al., 1993 , while the500
high IgG reactivity against pol and gag antigens previously501
Ždocumented in CSF Chiodi et al., 1988a; Goswami et al.,502
.1991; Elovaara et al., 1993 was not found. By examining503
patterns of antibody reactivity to HIV structural proteins,504
we found a greater frequency for CSF complete anti-gag505
profile in HAND than WAND and non-HAND. Generally,506
a slight decrease in CSF anti-pol total response, a strong507
decline in CSF complete env, pol and gag patterns and an508
evident increase in CSF gp160qgp120 reactivity were509
found in patients with advanced AIDS.510
Taken together, these findings support the hypothesis511
that the later stages of the disease are characterized by a512
relatively intense HIV-specific intra-B-B-B antibody re-513
sponse which is predominantly directed toward gp160 and514
Žgp120 env products Chiodi et al., 1988a; Lolli et al.,515
.1990; Goswami et al., 1991; Grimaldi et al., 1988 and516
probably occur in the context of a polyspecific intrathecal517
reaction triggered by immune network interferences and518
persisting even in the absence of the corresponding antigen519
ŽSindic et al., 1994; Conrad et al., 1994; Reiber et al.,520
.1998 .521
This most likely reflects a continual antigenic stimula-522
tion sustained by an active intrathecal virus replication523
ŽLuer et al., 1988; Sonneborg et al., 1989; Elovaara et al.,¨ ¨524.1993 . The low oligoclonal IgG production observed in our525
series may be referred to an overturning of regulatory526
mechanisms which modulate clonal expansion of HIV-
527
Ž .specific antibody producing B cells Chiodi et al., 1988b . 528
This profound dysregulation of brain humoral response 529
may account for the relatively scarce detection of anti-pol 530
and anti-gag IgG bands in comparison to elevated anti-env 531
reactivity shown in CSF by AIDS patients, as well as for 532
the changes occurring to antigenic specificity of CSF 533
anti-HIV IgG with the progression of AIDS. 534
The main result of this study is, however, represented 535
by the remarkable prevalence of AMI AmixedB pattern and 536
CSF complete anti-gag profile in HAND compared to the 537
other clinical groups. In fact, the appearance of this type of 538
response seems to be very specific to recognize HIV-re- 539
lated neurological syndromes due to the influence of virus 540
neuroinvasion indicating potential implications for the in- 541
terpretation of intrathecal immunological events during 542
AIDS. 543
In conclusion, our data underline the possibility that an 544
oligoclonal response directed against the virus, when pre- 545
sent in AIDS patients with neurological disorders induced 546
by HIV, is frequently both intrathecal and systemic. More- 547
over, as previously demonstrated for Toxoplasma gondii 548
Ž .encephalitis Contini et al., 1998 , these findings further 549
confirm that ASI as well as AMI may represent powerful 550
tools for evaluating the specificity of humoral intrathecal 551
immune response in AIDS-related diseases. In addition, an 552
increase in oligoclonal IgG release in HIV-associated neu- 553
rological manifestations seems to corroborate the Aclonal 554
dominance theoryB suggesting that the shift from the nor- 555
mal polyclonal to a restricted anti-HIV response could 556
induce the failure of viral infection control by the immune 557
system with the consequent development of virus variants 558
Ž .escaping antibody reaction Kohler et al., 1992 . 559
The cellular sources of HIV antigenic epitops within the 560
CSF compartment remain to be identified. According to 561
Žobservations recently reported for HIV-1 RNA McArthur 562
.et al., 1997; Ellis et al., 1997, 2000 , we hypothesize that 563
structural virus proteins and their precursors originate both 564
intrathecally and systemically from colonization and de- 565
struction of relatively long-lived host cells as macrophages, 566
microglia and astrocytes by HIV. In addition, the presence, 567
in the brain, of these long-lived infected cells could ac- 568
count for the slow rate of decrease in intrathecal antigenic 569
stimulation despite systemic immunosuppression. 570
Further studies are required to prove whether this ap- 571
proach may contribute to clarify immunological aspects of 572
the pathogenesis of the disease. 573
574
Acknowledgements 575
576
We thank Dr. Tiziana Bellini and Professor Franco 577
Dallocchio of the Biochemistry Department of University 578
of Ferrara for performing total protein measurements of 579
HIV-1 antigen solution, for technical assistance, for help- 580
ful discussions and for substantial intellectual support. The 581
study was supported by a grant of M.U.R.S.T. 1997.

UNCORRECTED PROOF
( )E. Fainardi et al.rJournal of Neuroimmunology 00 2001 000–0008582
583
References584
585Andersson, M., Alvarez-Cermeno, J., Bernardi, G., Cogato, I., Fredman,˜586
P., Frederiksen, J., Fredriksonn, S., Gallo, P., Grimaldi, L.M.,587Grønning, M., Keir, G., Lamers, K., Link, H., Magalhaes, A., Mas-˜588
¨saro, A.R., Ohman, S., Reiber, H., Ronnback, L., Schluep, M.,¨ ¨589Shuller, E., Sindic, C.J.M., Thompson, E.J., Trojano, M., Wurster, U.,¨5901994. Cerebrospinal fluid in the diagnosis of multiple sclerosis: a591consensus report. J. Neurol., Neurosurg. Psychiatry 57, 897–902.592
Centers for Disease Control, 1987. Revision of the CDC surveillance case593definition for acquired immunodeficiency syndrome. MMWR 36594Ž .Suppl. 1 , 3–15.595
Chiodi, F., Sonneborg, A., Albert, J., Gaines, H., Norkrans, G., Hagberg,¨596˚ ¨L., Asjo, B., Strannegard, O., Fenyo, E.M., 1988a. Human immunod-¨ ˚ ¨597
eficiency virus infection of the brain: I. Virus isolation and detection598of HIV specific antibodies in the cerebrospinal fluid of patients with599varying clinical conditions. J. Neurol. Sci. 85, 245–257.600
Chiodi, F., Norkrans, G., Hagberg, L., Sonneborg, A., Gaines, H.,¨601Frøland, S., Fenyo, E.M., Morrby, E., Vandvik, B., 1988b. Human¨602immunodeficiency virus infection of the brain: II. Detection of in-603trathecally synthesized antibodies by enzyme linked immunosorbent604assay and imprint immunofixation. J. Neurol. Sci. 87, 37–48.605
Cohen, B.A., Berger, J.R., 1998. Neurologic opportunistic infections in606AIDS. In: Gendelman, H.E., Lipton, S.A., Epstein, L., Swindells, S.607Ž .Eds. , The Neurology of AIDS. Chapman & Hall, New York, pp.608303–332.609
Conrad, A.J., Chiang, E.Y., Andeen, L.E., Avolio, C., Walker, S.M.,610Baumhefner, R.W., Tourtellotte, W.W., 1994. Quantitation of in-611trathecal measles virus IgG antibody synthesis rate: subacute scleros-612ing panencephalitis and multiple sclerosis. J. Neuroimmunol. 54,61399–108.614
Contini, C., Fainardi, E., Cultrera, R., Canipari, R., Peyron, F., Delia, S.,615Paolino, E., Granieri, E., 1998. Advanced laboratory techniques for616diagnosing Toxoplasma gondii encephalitis in AIDS patients: signifi-617cance of intrathecal production and comparison with PCR and ECL-618Western blotting. J. Neuroimmunol. 92, 29–37.619
Destrosiers, R.C., 1990. Virus purification, preparation of infectious virus620Ž .stock and virus storage. In: Aldovini, A., Walker, B.D. Eds. ,621
Techniques in HIV Research. Stockton Press, New York, pp. 121–127.622Dorries, R., Kaiser, R., ter Meulen, V., 1989. Human immunodeficiency¨623
virus infection: affinity-mediated immunoblot detects intrathecal syn-624thesis of oligoclonal IgG specific for individual viral protein. AIDS625Res. Hum. Retroviruses 5, 303–310.626
Ellis, R.J., Hsia, K., Spector, S.A., Nelson, J.A., Heaton, R.K., Wallace,627M.R., Abramson, I., Atkinson, J.H., Grant, I., McCutchan, J.A., 1997.628Cerebrospinal fluid human immunodeficiency virus type 1 RNA629levels are elevated in neurocognitively impaired individuals with630acquired immunodeficiency syndrome. Ann. Neurol. 42, 679–688.631
Ellis, R.J., Gamst, A.C., Capparelli, E., Spector, S.A., Hsia, K., Wolfson,632T., Abramson, I., Grant, I., Mc Cutchan, J.A., 2000. Cerebrospinal633fluid HIV RNA originates from both local CNS and systemic sources.634Neurology 54, 927–936.635
Elovaara, I., Iivanainen, M., Valle, S.L., Suni, J., Tervo, T., Lahdevirta,¨636J., 1987. CSF protein and cellular profiles in various stages of HIV637infection related to neurological manifestation. J. Neurol. Sci. 78,638331–342.639
Elovaara, I., Albert, P.S., Ranki, A., Krohn, K., Seppala, I., 1993. HIV-1¨ ¨640specificity of cerebrospinal fluid and serum IgG, IgM and IgG1-G4641antibodies in relation to clinical disease. J. Neurol. Sci. 117, 111–119.642
Gendelman, H.E., Persidsky, Y., Ghorpade, A., Limoges, J., Stims, M.,643Fiala, M., Morrisett, R., 1997. The neuropathogenesis of the AIDS644
Ž .dementia complex. AIDS 11 Suppl. A , S35–S45.645Goswami, K.K., Kaye, S., Miller, R., Mc Allister, R., Tedder, R., 1991.646
Intrathecal IgG synthesis and specificity of oligoclonal IgG in patients647infected with HIV-1 do not correlate with CNS disease. J. Med. Virol.64833, 106–113.649
Grimaldi, L.M.E., Roos, R.P., Devare, S.G., Robey, W.G., Casey, J.M.,
650Gurney, M.E., Apatoff, B.R., Lazzarin, A., 1988. Restricted hetero- 651geneity of antibody to gp120 and p24 in AIDS. J. Immunol. 141, 652114–117. 653
Ho, D.D., Rota, T.R., Schooley, R.T., Kaplan, J.K., Groopman, J.E., 654Resnick, L., Felsenstein, D., Andrews, C.A., Hirsh, M.S., 1985. 655Isolation of HTLV-III from cerebrospinal fluid and neural tissue of 656patients with neurologic symptoms related to the acquired immunode- 657ficiency syndrome. New Engl. J. Med. 313, 1493–1497. 658
Kohler, H., Goudsmit, J., Nara, P., 1992. Clonal dominance: cause for a 659limited and failing immune response to HIV-1 infection and vaccina- 660tion. J. Acquired Immune Defic. Syndr. 5, 1158–1168. 661
La Branche, C.C., Hoffman, T.L., Romano, J., Haggarty, B.S., Edwards, 662T.G., Matthews, T.J., Doms, R.W., Hoxie, J.A., 1999. Determinants 663of CD4 indipendence for a human immunodeficiency virus type 1 664variant map outside regions required for coreceptor specificita. J.` 665Virol. 73, 10310–10319. 666
Lolli, F., Colao, M.G., De Maio, E., Di Pietro, M., Galli, E., Grippo, A., 667Mazzotta, F., Pinto, F., 1990. Intrathecal synthesis of anti-HIV anti- 668bodies in AIDS patients. J. Neurol. Sci. 99, 281–289. 669
Luer, W., Poser, S., Weber, T., Jurgens, S., Eichenlaub, D., Pohle, H.D.,¨ ¨ 670Felgenhauer, K., 1988. Chronic HIV encephalitis: 1. Cerebrospinal 671fluid diagnosis. Klin. Wochenschr. 66, 21–25. 672
Markwell, M.A.K., Haas, S.M., Tolbert, N.E., Bieber, L.L., 1981. Protein 673determination in membrane and lipoprotein samples: manual and 674automated procedures. Methods Enzymol. 72, 296–300. 675
Marshall, D.W., Brey, R.L., Cahill, W.T., Houk, R.W., Zajac, R.A., 676Boswell, R.N., 1988. Spectrum of cerebrospinal fluid findings in 677various stages of human immunodeficiency virus infection. Arch. 678Neurol. 45, 954–958. 679
McArthur, J.C., Cohen, B.A., Farzedegan, H., Cornblath, D.R., Selnes, 680O.A., Ostrow, D., Johnson, R.T., Phair, J., Polk, B.F., 1988. Cere- 681brospinal fluid abnormalities in homosexual men with and without 682
Ž .neuropsychiatric findings. Ann. Neurol. 23, S34–S37 suppl . 683McArthur, J.C., McClernon, D.R., Cronin, M.F., Nance-Sproson, T.E., 684
Saah, A.J., Clair, M.S., Lanier, E.R., 1997. Relationship between 685human immunodeficiency virus-associated dementia and viral load in 686cerebrospinal fluid and brain. Ann. Neurol. 42, 689–698. 687
Price, R.W., 1996. Neurological complications of HIV infection. Lancet 688348, 445–452. 689
Reiber, H., 1996. Evaluation of blood cerebrospinal fluid barrier function 690and quantification of the humoral immune response within the central 691
Ž .nervous system. In: Thompson, E.J., Trojano, M., Livrea, P. Eds. , 692Cerebrospinal Fluid Analysis in Multiple Sclerosis. Springer, Milano, 693pp. 51–72. 694
Reiber, H., Felgenhauer, K., 1987. Protein tranfer at the blood cere- 695brospinal fluid barrier and the quantitation of the humoral immune 696response within the central nervous system. Clin. Chem. Acta 163, 697319–328. 698
Reiber, H., Lange, P., 1991. Quantification of virus-specific antibodies in 699cerebrospinal fluid and serum: sensitive and specific detection of 700antibody synthesis in brain. Clin. Chem. 37, 1153–1160. 701
Reiber, H., Ungefehr, S., Jacobi, C., 1998. The intrathecal, polyspecific 702and oligoclonal immune response in multiple sclerosis. Mult. Scler. 4, 703111–117. 704
Resnick, L., Di Marzo-Veronese, F., Schupbach, J., Tourtellotte, W.W.,¨ 705Ho, D.D., Muller, F., Shapshak, P., Vogt, M., Groopman, J.E.,¨ 706Markham, P.D., Gallo, R.C., 1985. Intra-blood–brain-barrier synthe- 707sis of HTLV-III-specific IgG in patients with neurological symptoms 708associated with AIDS or AIDS-related complex. N. Engl. J. Med. 709313, 1498–1504. 710
Resnick, L., Berger, J.R., Shapshak, P., Tourtellotte, W.W., 1988. Early 711penetration of the blood–brain-barrier by HIV. Neurology 38, 9–14. 712
Salden, H.J.M., Bas, B.M., Hermas, J.T.H., Janson, P.C.V., 1988. Analyt- 713ical performance of three commercially available nephelomethers 714compared quantifying protein in serum and cerebrospinal fluid. Clin. 715Chem. 34, 1594–1596. 716
Sande, M.A., Carpenter, C.C.J., Cobbs, C.G., Holmes, K.K., Sanford,

UNCORRECTED PROOF
( )E. Fainardi et al.rJournal of Neuroimmunology 00 2001 000–000 9717
J.P., 1993. Antiretroviral therapy for adult HIV-infected patients.718Recommendation from a State-of-the-Art Conference. JAMA 270,7192583–2589.720
Sindic, C.J.M., Monteyne, P., Laterre, E.C., 1994. The intrathecal synthe-721sis of virus-specific oligoclonal IgG in multiple sclerosis. J. Neuroim-722munol. 54, 75–80.723
Sonneborg, A.B., von Sydow, M.A.E., Forsgren, M., Strannegard, O.O.,¨ ˚7241989. Association between intrathecal anti-HIV-1 immunoglobulin G
725synthesis and occurrence of HIV-1 in cerebrospinal fluid. AIDS 3, 726701–705. 727
Tan, S.V., Guiloff, R.J., 1998. Hypothesis on the pathogenesis of vacuo- 728lar myelopathy, dementia, and peripheral neuropathy in AIDS. J. 729Neurol. Neurosurg. Psychiatry 65, 23–28. 730
¨Tibbling, G., Link, H., Ohman, S., 1977. Principles of albumin and IgG 731analyses in neurological disorders: I. Establishment of reference value. 732Scand. J. Clin. Lab. Invest. 37, 385–390.733





























