Embed Size (px)
Citation preview

REVIEW ARTICLE
Behavioral Interventions to Reduce Incidence of HIV,STD, and Pregnancy Among Adolescents: A Decadein Review
LEAH ROBIN, Ph.D., PATRICIA DITTUS, Ph.D., DANIEL WHITAKER, Ph.D.,
RICHARD CROSBY, Ph.D., KATHLEEN ETHIER, Ph.D., JANE MEZOFF, CHES, Dr.P.H.,
KIM MILLER, Ph.D., AND KATINA PAPPAS-DELUCA, M.A.
Purpose: To review adolescent sexual risk-reductionprograms that were evaluated using quasi-experimentalor experimental methods and published in the 1990s. Wedescribe evaluated programs and identify program andevaluation issues for health educators and researchers.
Methods: We systematically searched seven electronicdatabases and hand-searched journals to identify evalu-ations of behavioral interventions to reduce sexual riskbehaviors among adolescents. Articles were included ifthey were published in the 1990s, provided a theoreticalbasis for the program, information about the interven-tions, clear aims, and quasi-experimental or experimentalevaluation methods. We identified 101 articles, and 24met our criteria for inclusion.
Results: We reviewed these evaluations to assess theirresearch and program characteristics. The majority of
studies included randomized controlled designs andemployed delayed follow-up measures. The most com-monly measured outcomes were delay of initiation ofsexual intercourse, condom use, contraceptive use, andfrequency of sexual intercourse. Programs ranged from 1to 80 sessions, most had adult facilitators, and commonlyincluded skills-building activities about sexual commu-nication, decision-making, and problem solving. Theprograms included a wide range of strategies for contentdelivery such as arts and crafts, school councils, andcommunity service learning.
Conclusions: Analysis of these programs suggest fouroverall factors that may impact program effectivenessincluding the extent to which programs focus on specificskills for reducing sexual risk behaviors; program dura-tion and intensity; what constitutes the content of a totalevaluated program including researchers’ assumptions ofparticipants’ exposure to prior and concurrent programs;and what kind of training is available for facilitators.
KEY WORDS:AdolescentsHIVProgram effectivenessSexual risk-reduction programsSexually transmitted infection
In the 1990s, the prevalence of some sexual riskbehaviors, such as initiation of sexual intercourse,decreased among adolescents, particularly amongmales, African-Americans, and Whites [1]. In addi-tion, the number of adolescents using condoms at
From the Division of Adolescent and School Health, National Centerfor Chronic Disease Prevention and Health Promotion, Centers forDisease Control and Prevention, Atlanta, Georgia (L.R., P.D.); theDivision of HIV/AIDS Prevention, National Center for HIV, STD andTB Prevention, Centers for Disease Control and Prevention, Atlanta,Georgia (D.W., K.M.); the Rollins School of Public Health, EmoryUniversity, Atlanta, Georgia (R.C.); the Division of STD Prevention,National Center for HIV, STD and TB Prevention, Centers for DiseaseControl and Prevention, Atlanta, Georgia (K.E.); and the Division ofReproductive Health, National Center for Chronic Disease Preventionand Health Promotion, Centers for Disease Control and Prevention,Atlanta, Georgia (J.M., K.P-D.).
Address correspondence to: Leah Robin, Ph.D., Division of Adoles-cent and School Health, National Center for Chronic Disease Preventionand Health Promotion, Centers for Disease Control and Prevention,4770 Buford Highway NE, MS K-33, Atlanta, GA 30341. E-mail:[email protected]
Manuscript accepted February 7, 2003.The full text of this article is available via JAH Online at http://
journals.elsevierhealth.com/periodicals/jah
JOURNAL OF ADOLESCENT HEALTH 2004;34:3–26
1054-139X/04/$–see front matterPublished by Elsevier Inc., 360 Park Avenue South, New York, NY 10010 doi:10.1016/S1054-139X(03)00244-1

last intercourse increased. The abundance of sexualrisk-reduction programs during this time may havecontributed to improvements in these behavioraloutcomes [2]. Despite these improvements, however,adolescents continue to be at risk for HIV infection,other sexually transmitted diseases (STD), and preg-nancy. About 50% of new HIV infections occuramong people younger than age 25 years, and 25% ofnew HIV infections occur among people youngerthan age 22 years [3]. One in every four cases of STDdiagnosed annually in the United States occursamong teenagers [4]. In 1997, 840,000 pregnanciesoccurred among 15 to 19 year olds in the UnitedStates [5]. As many as four of every ten youngwomen in the U.S. become pregnant before reachingage 20 years [6].
Several studies have reviewed the characteristicsof effective programs focused on STD and HIV[7–12], teen pregnancy [13–15], and a combination ofthe three [16,17]. Evaluation criteria in most of thesereviews included random assignment, behavioraloutcomes demonstrating reductions in risky behav-ior, comparison data, a required minimum numberof subjects, and limits on attrition. The characteristicsof effective interventions identified by these reviewsare numerous and varied. Among the most com-monly cited are: cultural and community relevance,gender specificity, clear messages about the risks andhow to reduce them, emphasis on both abstinenceand protection from STD and pregnancy, and accessto health and reproductive services in addition tosexual risk-reduction programs. Recent quantitativesystematic literature reviews provide mixed findingsabout the overall effectiveness of sexual risk-reduc-tion interventions in reducing risk behaviors. Mullenet al [18] found that HIV risk-reduction interventionsreduced unprotected sexual intercourse and de-creased overall sexual risk. Other systematic litera-ture reviews of teen pregnancy prevention [19] andgeneral sexuality education [20], however, find nooverall impact of interventions in delaying sexualintercourse, use of condoms or contraceptives, orreducing pregnancy. All of the literature reviewsassess interventions as independent studies; only onereview mentions replications of interventions, andfindings have not been analyzed across interventionsand their variants [13]. Only three reviews includeprograms that simultaneously address HIV, STD,and pregnancy prevention.
In this review we examine common characteristicsand features among sexual risk- reduction programsevaluated during the 1990s. We review individualstudies and compare findings across programs and
their variants. This analysis expands on previouswork by examining interventions implemented at atime when sexual risk behaviors decreased amongadolescents. Furthermore, we look across studies,particularly those that have been replicated, to clarifythe characteristics of effective programs. These find-ings will help health educators and researchers iden-tify important elements to be used in designing moreeffective programs.
MethodsLiterature Searches
Literature searches were performed in six publicresearch databases (Medline, Psychlit, Popline, ERIC,Sociofile, and CHID); in the Prevention EvaluationResearch Registry for Youth (PERRY) at the Centersfor Disease Control and Prevention (CDC); andthrough manual searches of journals. We searchedduring 1999 and 2000 for evaluations of interventionstargeting youth and adolescents published in the1990s.
Standards for Inclusion
Because we aimed to review programs with well-designed evaluations, we set minimum standards forinclusion by reviewing and synthesizing criteriaused in other literature reviews of interventions toreduce sexual risk behaviors among youth and ado-lescents [8,10–12]. Our review criteria were intendedto provide us with a set of studies that would beapplicable to adolescents in the United States andwould allow us to examine the advances made inbehavioral interventions for adolescents in the 1990s.We did not include literature reviews or economicevaluations. We required that studies provide atheoretical basis for the programs, information aboutthe interventions (content, duration, facilitators), andclear aims. Studies were included if they used ran-dom assignment, or matched control groups using aquasi-experimental design that matched unitsthrough stratification of risk behaviors and demo-graphic variables. When analysis revealed inequali-ties among the conditions, studies were included ifresearchers controlled for the differences statistically.Studies were included if they had more than 16participants per condition, followed participants atleast four weeks after the end of the intervention orhad immediate pre- and post-tests for interventionslasting four months or longer, and had attrition ratesof less than 40% at follow-up four weeks after the
4 ROBIN ET AL JOURNAL OF ADOLESCENT HEALTH Vol. 34, No. 1

end of the intervention. Behavioral and biologicaloutcomes included: abstinence, reduced sexual activ-ity or number of sexual partners, less risky sexualbehaviors, reduced numbers of pregnancies or repeatpregnancies, or reduced STD prevalence. Studiesalso were included if they measured sexual inten-tions for participants 13 years or younger. Positivechanges in these outcomes were not required forinclusion.
Classifying Articles, Studies, and Programs
Out of 101 articles considered for inclusion in thisreview, 24 articles [21–44] met our inclusion criteriaand 77 did not. Of those that did not meet ourinclusion criteria, 60 were evaluations of programs,six were literature reviews or economic analyses, fivefocused on “lessons learned” from evaluation stud-ies, four were evaluations that did not measuresexual risk behaviors or evaluated programs thatwere not behavioral in nature, and two reportedresults found in other articles.
To organize the results we created a classificationsystem that distinguished between studies and pro-grams. Study was defined as an evaluation of anintervention with a unique sample (which couldresult in multiple publications), and program wasdefined as a specific intervention or variant of anintervention (which may have been evaluated inmultiple studies). In all, the 24 articles we includeddescribed 20 studies and 17 programs. Results wereaggregated both at the study level, and across studieson the program level.
Each study was classified as having produced“positive,” “null,” or “negative” effects. A study hadpositive effects if the intervention(s) had a positiveeffect on at least one behavioral or biological out-come and no negative effects relative to the controlgroup. A study had null effects if no differences weredetected among groups for any of the behavioral orbiological outcomes. A study had negative effects ifthe intervention had any negative impact on one ormore of the behavioral or biological outcomes, re-gardless of any positive findings. For programs weadded the category of mixed effects if one or morestudies found positive effects and one or more stud-ies found null effects.
Review Procedures
The eight authors worked in pairs to analyze eacharticle to determine if it met the criteria for inclusion.
All eight authors reviewed three articles beforeworking in pairs to assure consistency in their anal-yses. If they differed in their judgments, all of theauthors discussed the article and arrived at a consen-sus. If the authors could not arrive at a consensus, thearticle was analyzed by a third author and againdiscussed by all of the authors. Two authors thenextracted key features of studies (i.e. population ofinterest, design, theory, attrition, outcome measures,results, limitations), and program characteristics (i.e.duration, facilitators, content, intervention strate-gies).
ResultsKey Features of the Studies
Population of interest. Studies were conducted inschools (n � 9), in community-based venues (n � 2),clinics (n � 2), detention centers (n � 2), participants’homes (n � 1), or some combination of venues (n �4), which generally included schools and clinics orcommunity-based organizations. Some studies fo-cused on broad age ranges during adolescence (suchas Focus on Kids [23,24] which included youth aged9–15 years, and Teen Talk [44] which included youthaged 13–19 years) and others focused on particularages or school grades. Three studies included onlymales. As with age and gender, some studies weretargeted toward a particular ethnic group. Five of theinterventions included only African-Americanparticipants.
Design features. Overall sample sizes ranged fromunder one hundred participants to more than 10,000participants; 13 studies had more than 500 partici-pants (Table 1). Almost all studies used conveniencesampling (18 of 20). Of the 20 studies, 12 employed arandomized, controlled trial design; the remainingstudies had a quasi-experimental design. Of thequasi-experimental studies, almost all evaluated pro-grams that were implemented in schools (n � 6),with only two quasi-experimental studies evaluatingprograms conducted in community settings. Samplesizes within conditions ranged from 43 to 933 partic-ipants, although five studies did not report samplesizes by condition. Nine studies conducted only pre-and post-test measurements; the shortest post-testperiod was 4 weeks, and the longest was 10 months.An additional nine studies conducted follow-upmeasurements at 12 months or later. The remainingtwo studies conducted delayed follow-up measure-ments at less than 1 year.
January 2004 SEXUAL RISK-REDUCTION INTERVENTIONS FOR ADOLESCENTS 5

Table 1. Key Features of 20 Studies With Effects Classified as “Positive,” “Null,” or “Negative”
Program &Citation
Population ofInterest Design Theory Attrition1 Outcome Measures Results for Behavioral Outcomes2,3 Limitations
Positive EffectsBe Proud, Be
Responsible[21]
Convenience samplefrom school, YMCA,and clinic. Mean ageof participants was14.6 yrs.
Participants were:100% male
100% African-American
N � 157. Randomizedtrial with oneintervention group(I; n � 85) and onecontrol group (C;n � 72) that receiveda career planningintervention similarin length and formto BPBR.
Measurement was pre-and post-intervention(3 months).
Nonestated
3% at 3 months Sexual intent Index of riskysexual behavior over last 3months (included ever hadsex, multiple partners,condom use, analintercourse)
• Intent to engage in risky behavior:I � C
• Risk sexual behavior index: I � C;effects were stronger whenfacilitator was female vs. male.
• Frequency of sex, number ofpartners, occasions of sex without acondom, having had anal sex: I � C
None
Making ProudChoices: Asafer-sexapproach
Making aDifference:Anabstinence-basedapproach [22]
(Be Proud, BeResponsibleVariants)
Community basedconveniencesample.
Participants were: ingrades 6 and 7(mean age � 11.8yr, 47% male;
53% female;100% African-
American
N � 659. Randomizedtrial with 3 groups:Abstinence(A; n � 215), Safersex (S; n � 218), andcontrol (C; n � 214)that was a health-promotionintervention focusedon cardiovascularhealth.
Measurement was pre-intervention, 3-, 6-,and 12-month followup.
SocialCognitiveTheory ofPlannedBehavior
5%–7% at 12months
Frequency of: intercourse,condom use, unprotectedsex, and always usedcondoms during past 3months.
• Frequency of intercourse: S � C (6,12 months), A � S (6, 12 months)for sexually experienced at pre-testonly
• Unprotected sex: S � C (3, 6, 12) forsexually experienced only. A � S (3,12 months) for sexually experienced.
• Always used condom: S � C and A� S (3 months)
• Frequency of condom use: S � C (3,6, 12 months), A � C (12 months)
None
6R
OB
INE
TA
LJO
UR
NA
LO
FA
DO
LE
SCE
NT
HE
AL
TH
Vol.34,N
o.1

Table 1. continued
Program &Citation
Population ofInterest Design Theory Attrition1 Outcome Measures Results for Behavioral Outcomes2,3 Limitations
Focus onKids [23,24]
Community basedconveniencesample.
Participants were: 9–15 years old (meanage � 11.4 yr); 56%male; 44% female;100% African-American
N � 383. Randomized trialwith groups of friendsassigned to intervention(I; n � 206) or controlgroup (C; n � 177).
Control group participantswere offered weeklysessions, but not withtheir friendship group.
Measurement was pre- andpost-intervention at 6-,12-, 18- and 24 months.1996 paper reports on 6-& 12-month results only;1997 paper reportscumulative results acrossall assessments.
ProtectionMotivation
22% at 6months
27% at 12months
31% at 18months
31% at 18months
36% at 24months
Intentions, behavior (didvs. did not have sex),condom use
• Condom use and condom useintentions: I � C at 6 months butnot 12 months [23]
• Cumulative prevalence ofunprotected sex: C � 1 at 24months [24]
• Attenuation ofeffects forintentmeasures.
[25] Convenience samplefrom detentionfacility (consecutiveentry into detentioncenter).
Participants were:16–19 years (median
age � 17.8 yr);100% male; 65%Black; 33%Hispanic; 2%White.
N � 157. Quasi-experimental with oneintervention (I; n � 58)and one control group(C; n � 99) who receivednothing.
Measurement was pre andpost-intervention 10months after baseline.
Problemsolvingtherapy
34% at 10months
Multiple partners; riskpartners, anal sex;condom use for vaginal,oral, and anal sex
• Condom use (for intercourse, oralsex/anal sex, and overall) andcondom acceptability: I � C
• No randomassignment
• Recruitmentfrom a singlesetting
January2004
SEX
UA
LR
ISK-R
ED
UC
TIO
NIN
TE
RV
EN
TIO
NS
FOR
AD
OL
ESC
EN
TS
7

Table 1. continued
Program &Citation
Population ofInterest Design Theory Attrition1 Outcome Measures Results for Behavioral Outcomes2,3 Limitations
Reach forHealth[26]
School-basedconveniencesample.
Participantswere: ingrades 7 and8; 47.2% male;52.8% female;15.9%Hispanic;79.2% Black;4.9% “other”
N � 1061. Quasi-experimental with3 groups: 35classrooms at 1school wererandomized intotwo interventiongroups - Reachfor HealthCurriculum only(RHC); Reach forHealth Curriculum,plus theCommunity YouthService (CYS)program. 32classrooms at a2nd schoolcomprised the nointervention control(C). Group n’s notgiven.
HealthBeliefModelSocialLearning
8.3% at 6months
Lifetime sexualexperience; Frequency ofsex in past 3months; Recentcondom use; Recentcontraceptive use;Composite indexof sexual risk.
• Frequency of recent sex;CYS � C at 6 months
• Sex Behavior Index:CYS � C at 6 months
• Included only oneintervention andone control school
• Unit ofrandomization didnot match unit ofanalysis
Measurement waspre- and post-intervention at 6month follow-up.
Reducingthe Risk[27]
School-basedconveniencesample.
Participantswere: ingrades 9–12(mean age �15.3 yr); 47%male; 53%female; 62%White; 20%Latino; 2%African-American;16% “other”
N � 1033. Quasi-experimentalwith 2 groups:Reducing the Riskintervention(RTR; n � 586)& control group(C; n � 447)receiving astandard sexualitycurriculum.
Measurement waspre- and post-intervention at 6and 18 months.
SociallearningSocialinoculationSocialbehavioral
27% at 18months
Ever had sex; Frequencyof sex in past month;Birth control use atfirst and most recent sex;Birth control useall or most of the time;Unprotected sex; Pregnantor caused pregnancy
• Sexual initiation: RTR � control(18 month only). Note that thiswas true when analyzingchange scores, but ns whenusing log regression
• Unprotected sex: RTR � control(18 month only) among youthwho were sexually in-experienced at baseline (truefor change score, but ns whenusing log regression)
• In sub-analyses of lower riskyouth and of females,contraceptive use RTR � C andfor unprotected sex RTR � C(both at 18 m only)
• Potential forcontaminationwithin schools -same teacherstaught some ofthe RTR andcontrol curricula
Interactions nottested to justifysubgroupanalyses, and theonly positiveinterventioneffects from themultivariateanalyses werefound amongsubgroups
8R
OB
INE
TA
LJO
UR
NA
LO
FA
DO
LE
SCE
NT
HE
AL
TH
Vol.34,N
o.1

Table 1. continued
Program &Citation
Population ofInterest Design Theory Attrition1 Outcome Measures Results for Behavioral Outcomes2,3 Limitations
Safer Choices[28]
Recruited fromclasses in 20schools.
Participants were: ingrades 9 and 10;48% male; 53%female; 31%White; 27%Hispanic; 17%African-American; 18%Asian.
N � 3869. Randomizedtrial with 2 groups:Safer choices (SC; nnot given) andcomparison program(C; n not given) whichwas a standard HIVknowledge-basedcurriculum.
Measurement was pre-and post-interventionat 7 months.
SocialcognitiveSocialinfluence
5% at 7months
Sexual initiation,frequency ofunprotectedintercourse, # sexpartners, condomuse (1st, last)
• Unprotected sex during past 3months: SC � C
• Condom use at last intercourse:SC � C
• Effective birth control at lastintercourse: SC � C
• None
TeenIncentivesProgram[29]
School-basedconveniencesample.
Participants were:in 9th grade (meanage � 15.1 yr);25.8% male; 74.2%female; 43.3%Black; 30.8% WestIndian; 22.5%Hispanic; 3.3%“other”
N � 120. Randomizedtrial with oneintervention group (I;n � 60) and onecontrol group (C; n �60) that receivedwritten materialsabout contraceptionand decision-makingrelated to risk-takingbehavior.
Measurement was pre-and post-interventionat 6 months afterbaseline.
Nonestated
30%intervention,and 12%Control at 6months
Frequency of sex;Frequency ofcontraceptive use
• Frequency of sex: I � C• Frequency of contraceptive use:
I � C
• Sample recruited fromonly one school
• Differential attritionrate
January2004
SEX
UA
LR
ISK-R
ED
UC
TIO
NIN
TE
RV
EN
TIO
NS
FOR
AD
OL
ESC
EN
TS
9

Table 1. continued
Program &Citation
Population ofInterest Design Theory Attrition1 Outcome Measures Results for Behavioral Outcomes2,3 Limitations
TeenOutreachProject[30]
School-basedconveniencesample.
Participants were:in grades 9–12(mean age � 15.8yr); 15% male;85% female; 68.2%Black; 15.5%White; 11.2%Hispanic; 2.9%“other”
N � 695. Quasi-experimental withone Teen OutreachProject interventiongroup (TOP; n �342) and onecontrol group (C; n� 352) whichreceived regularcurricular offeringsin health or socialstudies. Some siteshad randomassignment atstudent orclassroom level.
Nonestated
5.3% TOP, 8.4%Ctrl at 9months
Ever been pregnant orcaused a pregnancy (orsince baseline)
• Pregnancy rates: TOP � C forfemales only.
• Base line datacollected 2–3weeks into theprogram
• Different units ofrandomassignment acrosssites, so unit ofanalysis did notmatch unit ofrandomization atsome sites.
Measurement was atpre- and post-only(9 months afterbaseline)
[31] Sampling frommatched schoolsin whichclassrooms wererandomlyselected.
Participants were: ingrades 9 and 11(mean age � 15.7yr); 41.5% male;58.5% female;36.7% Black;35.4% Hispanic;27.9% “other”
N � 1316.Randomized with 4schools randomizedto one interventiongroup (I; n � 2with 739 students)or one control (C; n� 2 with 577students) thatreceived no formalAIDS curriculum
Measurement waspre- and post-intervention at 3months
HealthBeliefModelSocialcognitiveSocialinfluence
34% at 3months
AIDS risk behaviors indexincluded sexualinvolvement, condomuse, high risk partner,STD diagnosis
• Risk behavior scores: I � C. • Unit of analysisdid not matchunit ofrandomization
• Low number ofunits randomized
10R
OB
INE
TA
LJO
UR
NA
LO
FA
DO
LE
SCE
NT
HE
AL
TH
Vol.34,N
o.1

Table 1. continued
Program &Citation
Population ofInterest Design Theory Attrition1 Outcome Measures Results for Behavioral Outcomes2,3 Limitations
Youth AIDSPreventionProject(YAPP)[32, 33, 34]
School-basedconveniencesample.
Participants were in7th grade (meanage � 12.6 yr);51% male; 49%female; 22%White; 61%African-American;12% Hispanic; 5%“other”
N � 2392.Randomized trialwith 15 schoolsassigned to 1 of 2interventionsgroups (parent-interactive or PI, n� 770; non-parentinteractive or NP, n� 689) and 1control group (C, n� 933) that receivedbasic AIDSeducation ordinarilyprovided by theschool. Interventiongroups werecombined into onegroup for the 1995banalysis.
SocialcognitiveTheory ofPlannedBehaviorSocialinfluence
As reported in[34]:
At 1 year, C �19.5% NP �28.7 PI � 22.1%
At 2 years, 55.8%overall.C� 50.9%NP� 60.2%PI� 54.9%
Behavioral intentions touse condoms, and to usecondoms with foam
Ever had sex, recent sex(30 days), age of debut,condom use at 1st andlast intercourse (in 9thgrade only), condomuse with foam in past12 months, in past 30days
• Intentions to use condoms withfoam PI and NP � C (at 1 year1995a; among those who becamesexually active between 7th &8th grade, 1995b)
• Intention to use condoms withfoam: PI and NP � C, amongsexually active and not sexuallyactive students (at 2 years)
• Condom use with foam, NP andPI�C (among those who becamesexually active between 7th and8th grade, 1 year, 1995b paper)
• Condom use with foam, ever &at last intercourse, NP�PI amongsexually active students (at 2years)
• Parent-participation wasvery low
• Very high attritionrate at 2 years,and used randomeffects regression,which replacesmissing data so asto include allparticipants—thosewith and withoutdata—in theanalyses
• Unit of analysisdid not matchunit ofrandomization
Measurement wasdone pre- and post-intervention at 1year and 2 years
January2004
SEX
UA
LR
ISK-R
ED
UC
TIO
NIN
TE
RV
EN
TIO
NS
FOR
AD
OL
ESC
EN
TS
11

Table 1. continued
Program &Citation Population of Interest Design Theory Attrition1 Outcome Measures Results for Behavioral Outcomes2,3 Limitations
Becoming aResponsibleTeen [35]
Health Center–basedconvenience sample.
Participants were: 14–18 years (mean age� 15.3 yr); 28%male; 72% female;100% African-American
N � 246. Randomizedtrial with 2 groups:one-time EducationProgram (EC) similarto standard AIDSeducation program,8-wk Education plusBehavioral SkillsTraining (BST). Groupn’s not reported.
Measurement was atpre- and post-intervention, 6- and12-month follow up.
Information,Motivation,BehaviorModel
8.5% at 12months
Frequency of unprotectedvaginal, oral, and analsex; Frequency ofcondom use; Number ofsex partners
• Frequency of condom protectedvaginal intercourse: EC � BST(post, 6m)
• Frequency of condom protectedoral intercourse: EC � BST (6,12 m)
• Composite condom use: BST �EC (post, 6m, 12m) with bothgroups decreasing condom use at1 year
• Rate of sexual activity: BST � ECat 1 year
• Initiation of sexual activity: EC �BST at 1 year among non-sexuallyactive youth
• Some effectsattenuated at oneyear
Null EffectsWorking on
the RightDirection[36]
(Becoming aResponsibleTeenVariant)
State Reformatory–based conveniencesample. Mean age ofparticipants was15.8 years.Participants were100% male; 69.9%African-American;28% White; 1.9%Hispanic
Participants were100% male; 69.9%African-American;28% White; 1.9%Hispanic
N � 361. Randomizedtrial with 2 groups: 6hr intervention basedon 12-hour BARTintervention (ST; n �180), control conditionbased on PACT(Anger Managementintervention; AM, n �181).
Measurement was atpre- and post-intervention, and 6-month follow up.
Information,Motivation,BehaviorModel
14% at 6months
Frequency of unprotectedvaginal, oral, and analsex; Percentage ofintercourse occasionsprotected by condoms;Number of sexpartners—all in past 3months
• No differences on any behavioraloutcomes
• Only 1 institutionincluded in studyso there ispotentialcontamination
[37] School-basedconvenience sample(Phys. Ed. classesfrom 4 schools).
Participants were: in9th grade (mean age� 14.4 yr); 41%male; 59% female;10% White; 16%African-American;20% Latino; 42%Asian; 12% “other”
N � 695. Quasi-experimental withtwo schools assignedto intervention (I; n �210) and two assignedto control (C; n � 303)which received astandard educationalprogram lasting 1class period.
Measurement was pre-and post-interventionat 4 weeks.
Socialcognitive,Heath BeliefModel
26% at 4 weeks Average condom use,sexual risk in pastmonth, condom use inpast month
• No differences on any behavioraloutcomes
• No randomassignment
• Very short followup period andhigh attritiongiven that shortperiod.
12R
OB
INE
TA
LJO
UR
NA
LO
FA
DO
LE
SCE
NT
HE
AL
TH
Vol.34,N
o.1

Table 1. continued
Program &Citation
Population ofInterest Design Theory Attrition1 Outcome Measures Results for Behavioral outcomes2,3 Limitations
Facts &Feelings[38]
Home-basedconveniencesample.
Participants were:in grades 7 and 8(mean age � 13.9yr); gender notreported; 97%White.
N � 548. Randomizedtrial with threegroups: video �newsletter (VN; n �126), video only(VO; n � 132), orcontrol (C, n � 290)which receivednothing.
Nonestated
8% overall at 9months.
VN � 4.7%, VO� 7.5%, C �10%
Teen sexual behavior,intentions
• No differences on any behavioraloutcomes
• Solicited over 6000families and only548 volunteered
• Homogenous andlow risk sample
Measurement waspre- and post-intervention, and9-month follow up.
[39] Clinic-basedsample(consecutiveenrollment ofadolescents withat least 1 STD).
Mean age was 17.6years. Participantswere: 8% male;92% female; 81%Black; 4% White;8% Hispanic; 7%“other”
N � 90. Randomizedtrial with oneintervention group(I; n � 43) and onecontrol group (C; n� 47) whichreceived standardcare at clinic.
Measurement waspre- and post-intervention at 2-months.
Nonestated
8% at 2 months Ever had sex, condom use,number of partners
• No differences on any behavioraloutcomes
• Small N• Recruited from
single clinic.
SNAPP [40] School-basedconveniencesample.
N � 1616.Randomized trialwith classroomsrandomized to oneintervention group(1) or one controlgroup (C) thatreceived didacticinstruction aboutprevention of HIV,STD, andpregnancy. Groupn’s not given
Sociallearning,Health BeliefModel
23% at 17months
Delay of sexual onset,frequency of intercourse,condom use, birthcontrol use. STD andpregnancy rate
• No differences on any behavioraloutcomes
• Randomizationunit wasclassroom notschool
January2004
SEX
UA
LR
ISK-R
ED
UC
TIO
NIN
TE
RV
EN
TIO
NS
FOR
AD
OL
ESC
EN
TS
13

Table 1. continued
Program &Citation
Population ofInterest Design Theory Attrition1 Outcome Measures Results for Behavioral Outcomes2,3 Limitations
Participants were:in 7th grade(mean age � 12.3yr); 46% male;54% female; 64%Latino; 13%Asian; 9%African-American;5% White.
Measurement waspre- and post-intervention at 5and 17 months.
NegativeEffects
PostponingSexualInvolvement[41, 42]
School/Clinicsponsoredconveniencesample.Participants were:in 8th grade; maleand female; 99%Black.
N � 536. Quasi-experimental with 2groups, assigned byschool: oneintervention group(PSI; N � 395 in 24schools) and onecontrol group (C; N� 141 in 29 schools)which receivednothing.
Measurement was atbeginning, middle,& end of 8th gradeand at beginningand end of 9thgrade, and end of12th grade [44].
SocialInfluence
15–19% at 1year; 44–57%at 5 years
Whether or not had sex;Frequency of intercourse;Contraceptive use;Occurrence of pregnancy(females only)
• Sexual initiation: C � PSI (end of8th, 9th, for both males andfemales
• Contraceptive use: PSI � C (endof 9th; only among those whohad not engaged in sex atbaseline)
• Frequency of sex: C � PSI (end of9th only among those who hadnot engaged in sex at baseline)
• Occurrence of pregnancy: C � PSI(end of 9th end of 12th
• Not engaged in sex in past month:C � PSI (males only, end of9th grade)
• No randomassignment
• No effects foryouth sexuallyexperienced atbaseline
• No analysis ofschool leveldifferences
• Significantdifferences atbaseline notcontrolled for
• Attenuation ofmost effects by12th grade.
14R
OB
INE
TA
LJO
UR
NA
LO
FA
DO
LE
SCE
NT
HE
AL
TH
Vol.34,N
o.1

Table 1. continued
Program &Citation Population of Interest Design Theory Attrition1 Outcome Measures Results for Behavioral Outcomes2,3 Limitations
PostponingSexualInvolvement[43]
(Replication ofPostponingSexualInvolvement)
Convenience samplefrom schools, healthdepartments, CBOs.
Participants were: in8th grade (meanage � 12.8 yr); 43%male; 57% female;30% White; 9%Black; 39%Hispanic; 22%“other”.
N � 10,600. Quasi-experimental with 3different designs.One design usedrandom assignmentby classroom, with3 groups: PSI adult-led interventiongroup (PSI-A), PSIpeer-ledintervention group(PSI-P), and noprogram control(C). Second designused randomassignment byschool, with 2groups: PSIintervention whichwas adult-led (PSI-A) plus school-wideactivities in supportof the ENABLinitiative, and a noprogram control(C). Third designrandomly assignedindividuals fromcommunity-basedagencies to adult-led PSI intervention(PSI-A) or a noprogram control(C).
Nonestated
9% at 3 monthsfirst designonly, 31% at 17months
Initiation of sex; Frequencyof sex; Number of sexualpartners; Use ofcontraceptives;Pregnancy rates; Rates ofreported sexuallytransmitted diseases.
• Pregnancy rates: PSI-P � control(major difference among males;relationship holds when examiningsexually active at baseline only).
• STD rates: PSI-A � control.
• Unit ofrandomization didnot match unit ofanalysis
Measurement was atpre-intervention, 3-(1st design only) &17-month followup.
January2004
SEX
UA
LR
ISK-R
ED
UC
TIO
NIN
TE
RV
EN
TIO
NS
FOR
AD
OL
ESC
EN
TS
15

Table 1. continued
Program &Citation
Population ofInterest Design Theory Attrition1 Outcome Measures Results for Behavioral Outcomes2,3 Limitations
Teen Talk[44]
Conveniencesample fromfamily planningagencies andschools.
Participants were:13–19 years; 52%male; 48% female;15% White; 24%Black; 53%Hispanic.
N � 1444. Quasi-experimental withone Teen Talkintervention (TT: N� 722) and onecontrol group (C; N� 722) whichreceived thestandardcurriculum that wasin place at each site(8 differentprograms total).Some sites hadrandom assignmentat student orclassroom level.
HealthBeliefModel,SocialLearningTheory
8% at post; 38%at one year
Ever had sex;Contraceptive use atfirst and most recentsex; Consistency ofcontraceptive use; Indexof contraceptiveefficiency; Occurrenceof pregnancy
• Sexual initiation: TT � Controlat 1 year (males only)
• Contraceptive use at most recent sex:Control � TT at 1 year (femalesonly, sexually inexperienced atbaseline)
• Contraceptive efficiency: Control �TT at 1 year (females only, both forsexually experienced andinexperienced at baseline)
• Contraceptive efficiency: TT �Control at 1 year (males only,sexually experienced at baseline)
• Different units ofrandomassignment acrosssites, so unit ofanalysis did notmatch unit ofrandomization atsome sites.
Measurement was atpre- and post-intervention, andone year follow-up.
1Attrition rates are provided for the longest available follow-up period for which information was available. A single attrition rateindicates that intervention and control group rates did not differ from one another.
2Group abbreviations are defined in the Outcome Measures column. Any effects in which the intervention has a negative impact onadolescents relative to the control group are in italics.
3Results are significant at the p � .05 level unless otherwise indicated.
16R
OB
INE
TA
LJO
UR
NA
LO
FA
DO
LE
SCE
NT
HE
AL
TH
Vol.34,N
o.1

Theory. Many interventions were based on a com-bination of theories. Social cognitive theories, theHealth Belief Model, social learning theories, andsocial influence theories were applied most often. Noclear patterns emerged in study methods, year ofpublication, intervention content, or duration withrespect to the theory guiding interventions.
Attrition. Attrition was difficult to assess becauseof differences in follow-up periods and reporting.The average attrition rate was 14.7% among studiesin which any follow-up measurement was conductedbefore 6 months, 13.1% among follow-ups conductedbetween 6 and 12 months, 23% among follow-upsconducted between 1 and 2 years, and 50.5% amongfollow-ups conducted between 2 and 5 years.
Outcome measures. Behavioral measures most fre-quently used were: delay of initiation of sexualintercourse, condom use, contraceptive use, and fre-quency of sexual intercourse. Less frequently mea-sured were cases of teen pregnancy or of STD orsexual risk behaviors such as number of sexualpartners, anal or oral sex, or the perceived riskinessof sexual partners. The time frame for behavioralmeasures varied and included: lifetime, 12 months, 3months, 1 month, most recent sexual intercourse, andfirst intercourse. Many studies used multiple timeframes to measure behavioral outcomes. Of the stud-ies, 50% created a composite index of behavioralmeasures, some of which used multiple time frames.Some studies did not report any time frame for theirmeasures.
Results. Among frequently measured behaviors,condom use (8 studies of 12) was affected mostconsistently, and delayed initiation of sexual inter-course (4 studies of 11) was affected least consis-tently. Among measures less commonly used, themost consistent impact was observed for whetherparticipants became pregnant or impregnated theirsexual partners. Three studies reported negativefindings: (a) increased likelihood of males in theintervention group engaging in sex within the lastmonth relative to the control group [41]; (b) in-creased reports of pregnancy and STD [43]; (c) lesscontraceptive use at most recent sex among femaleswho were sexually inexperienced at baseline [44]; or(d) less contraceptive efficiency (i.e. an index mea-sure combining the consistency of contraceptive useand effectiveness of the selected method of contra-ception) among females in the intervention group[44]. It is worth noting that most studies did not test
the treatment by subgroup interaction before con-ducting subgroup analyses.
Limitations. Common limitations concerning re-cruitment and retention included recruiting all par-ticipants from a single setting (because the potentialfor contamination is higher), differential attritionamong groups, and a high attrition rate in a shortfollow-up period. Common limitations concerninggroup assignment included non-random assignmentto condition and having too few units to randomize.Analytic limitations included differences amonggroups that were reported but not controlled in theanalyses, and the unit of randomization not match-ing the unit of analysis. Finally, the attenuation ofeffect sizes at subsequent follow-up periods consti-tuted a practical limitation. Some study-specific lim-itations also are listed in Table 1. It is important tonote that a lack of limitations for any given studymay result from a lack of information provided in thepaper.
Program Characteristics
Duration and intensity. Programs were of variabledurations (Table 2). The shortest program was onesession (less than an hour) and the longest was 80sessions (over 15 hours). A greater proportion ofprograms that were 15 or more hours long wereevaluated using randomized designs than were pro-grams of shorter duration. About half of programsbetween 2 and 7 hours long were evaluated using aquasi-experimental design (n � 7). Of these, fiveevaluated programs were implemented in a schoolsetting. Further, the program of the shortest durationwas evaluated before 1995, and none evaluated inthat time period were longer than 15 hours. Incontrast, almost half of the studies published after1995 were more than 15 hours long, and none wereless than 7 hours long. In some cases, determiningprogram duration was difficult because other sexualrisk-reduction programs were offered at the sametime as the program of interest and affected thedosage of sexual risk-reduction messages and skillsprovided to youth. Another reason for this difficultywas the failure of some studies to report the totalnumber of hours or the length and number ofsessions. Programs also varied in their intensity. Forexample, Be Proud! Be Responsible! [21] was con-ducted in one 5 hour session, and three programs(Reach for Health [26], Safer Choices [28], and YouthAIDS Prevention Project [32–34]) conducted sessionsover a two year span.
January 2004 SEXUAL RISK-REDUCTION INTERVENTIONS FOR ADOLESCENTS 17

Facilitators. Among the 17 programs, 13 were fa-cilitated by adults and four by peer leaders. Oneprogram was facilitated by only African-Americanadults, and one was facilitated by only males. Adultfacilitators had varied backgrounds and includedparents, counselors, teachers, nursing school stu-dents, university faculty, administrators, communityadults, Masters-level health educators, and medicalprofessionals. Peer leaders also had varied back-grounds and characteristics. Some of the peer leadersin SNAPP [40] (e.g., were teen mothers and personsinfected with HIV).
Intervention content. Program content was diverse.For example, the Teen Outreach Program [30] includedvolunteer work; the Teen Incentives Program [29]included career planning; Reducing the Risk [27] in-cluded activities conducted with parents; and Focuson Kids [23,24] included condom-use skills. Knowl-edge-based content was present in all of the pro-grams and included information on HIV, STDs,pregnancy, violence prevention, alcohol and otherdrug-use prevention, and general youth sexualityinformation. Skills-building activities were also fre-quently addressed, including communication skills(n � 12), problem-solving (n � 8) changing peernorms (n � 8), and decision-making (n � 6). Inter-vention content varied by duration. Programs thatwere more than 15 hours long addressed a greatervariety of knowledge topics (including violence pre-vention and drug and alcohol use) than did those ofshorter duration. In addition, more programs thatwere more than 15 hours long included more generallife skills (such as community service learning, careerplanning, and general problem solving) than pro-grams of shorter duration, and included a greatervariety of general life skills. In contrast, programsbetween 7 and 15 hours were more likely than longeror shorter programs to teach abstinence and con-dom-use skills, and to teach a greater variety of each.
Intervention strategies. Researchers used a varietyof program strategies. For example, Focus on Kids[23,24] included arts and crafts; Reach for Health [26]included community service learning; Safer Choices[28] used a school health promotion council com-posed of teachers, students, administrators, and par-ents; and the Teen Incentives Program [29] includedfamily planning services. The most common strate-gies for content delivery were small group discus-sion, role-playing and interactive and experientialexercises, use of media and interactive media, use ofstructured games, and lecture.
Study Effects
We found that 12 studies had positive effects, fivehad null effects, and three had negative effects. Twostudies classified as having negative effects [41,42]also had positive effects. When we aggregated stud-ies into the 17 programs and their variants, we foundthat 10 programs had positive effects, one had mixedeffects, four had null effects, and two had negativeeffects. Becoming a Responsible Teen [35] was catego-rized as “mixed” because the original curriculumhad positive results, but its variant curriculum, Work-ing on the Right Direction [36], had null results (Table2). We found very few clear differences amongstudies and programs on the basis of their effects.
The majority of studies showing positive effectswere published in 1995 or later, targeted African-American youth, included both males and females,and took place in schools. Three studies with positiveeffects included only African-American participants.Two studies included only male participants. Moststudies with positive effects employed a random-ized, controlled design.
Programs that produced positive effects usedtrained adult facilitators. Two programs demonstrat-ing positive effects, both variants of Be Proud! BeResponsible! [22] and Safer Choices, also used trainedpeer facilitators [28]. Safer Choices also included par-ents and school staff in school-based activities. Pro-grams demonstrating positive effects included con-tent that was specific to reducing sexual riskbehavior such as refusal of unwanted sex and con-dom-use skills. Programs with positive effects mostcommonly employed interactive and participatoryeducational strategies. Although we have found thateffective programs emphasize skills that reduce spe-cific behaviors, interventions more generally tar-geted toward increasing youth resiliency and com-petencies are emerging as promising approaches toreducing sexual risk behavior [13].
An example of a promising youth resiliency pro-gram is the Seattle Social Development Project. In thisprogram, elementary school children received socialcompetence training, and training and support pro-grams were provided for their teachers and parents[45]. This program focused on school bonding, aca-demic success, and the prevention of many healthrisk behaviors. Children receiving the intervention infirst through sixth grades were less likely to reportbeing sexually experienced or having multiple sexpartners by aged 18 years than those in the controlgroup. This program is innovative in its broad,resiliency-based approach and its implementation
18 ROBIN ET AL JOURNAL OF ADOLESCENT HEALTH Vol. 34, No. 1

Table 2. Characteristics of 17 Programs With Effects Classified as “Positive”, “Mixed”, “Null”, and “Negative”
Program Duration/Intensity Facilitators Content Intervention Strategies
Positive EffectsBe Proud Be Responsible!a
[21]5 hour session held on
one SaturdayTrained male and
female adultfacilitators; allwere African-American
Knowledge about HIV/AIDS,education about AIDS-risk activities,condom use skills, negotiation skillsfor safer sex activities
Videos, games, interactive exercises, and role-plays.
Making a Difference: Safer-sex program [22]
(Be Proud Be ResponsibleVariant)a
8 1-hour sessions heldon 2 consecutiveSaturdays.
Trained male andfemale adult andpeer facilitators;adults were allAfrican-American.
Value of condoms, knowledge aboutHIV/STD, enhance beliefs thatcondom use does not adversely affectsexual enjoyment, increase skills andself-efficacy for condom-use, andnegotiating condom-use
Small group discussions, videos, games,brainstorming, experiential exercises, skills-building activities, role-plays.
Making a Difference;Abstinence-focusedprogram [22]
(Be Proud Be ResponsibleVariant)a
8 1-hour sessions heldon 2 consecutiveSaturdays.
Trained male andfemale adult andpeer facilitators;adults were allAfrican-American
HIV/STD knowledge; strengthenbeliefs supporting abstinence,increase self-efficacy and skills toresist pressure to have sexualintercourse and to negotiateabstinence.
Small group discussions, videos, games,brainstorming, experimental exercises,skills-building activities, role-plays.
Focus on Kids [23, 24] 7 1.5-hour sessions of 7weeks, and one 1-dayretreat
Trained adult maleand femalefacilitatorsmatched togender of group;most wereAfrican-American.
Knowledge about STD/AIDS,contraception, communication andnegotiation skills, values clarification,goal setting, prevalence of peer riskbehaviors and condom-use behaviors,condom-use skills.
Small group discussions, lectures, videos,games, role-plays, acting, storytelling, arts,crafts, developing community projects,“family tree” depicting relationships andsituations, “graduation” ceremony.
[25] 4 1-hour sessions, twiceweekly
Adult malecounselors
Knowledge about HIV drug abuseand its consequences, AIDS riskreduction, seeking AIDS-relatedservices in the community.
Small group discussions, role-plays, skillspractice, brainstorming.
Reach for Health [26]O’Donnell et al, 1999
80 sessions over 7thand 8th grade
Teachers, nursingschool students,university facultymembers
2 community service job assignments,instruction in preventingdrug/alcohol use, violence, andrisky sexual behaviors.
A variety of tasks in child daycare centers,nursing homes, and senior centers,including assisting doctors and dentists,clerical work, reading, arts and crafts,exercise; debriefing sessions in classrooms.
Reducing the Risk [27] 15 class periods Teachers whovolunteered toimplement theprogram
Sexual decision-making,communication skills, emphasis onnorms to avoid risky sex throughabstinence or condom-use, parent-adolescent communication
Skills practice, small group discussion, role-plays, parent-child discussion.
January2004
SEX
UA
LR
ISK-R
ED
UC
TIO
NIN
TE
RV
EN
TIO
NS
FOR
AD
OL
ESC
EN
TS
19
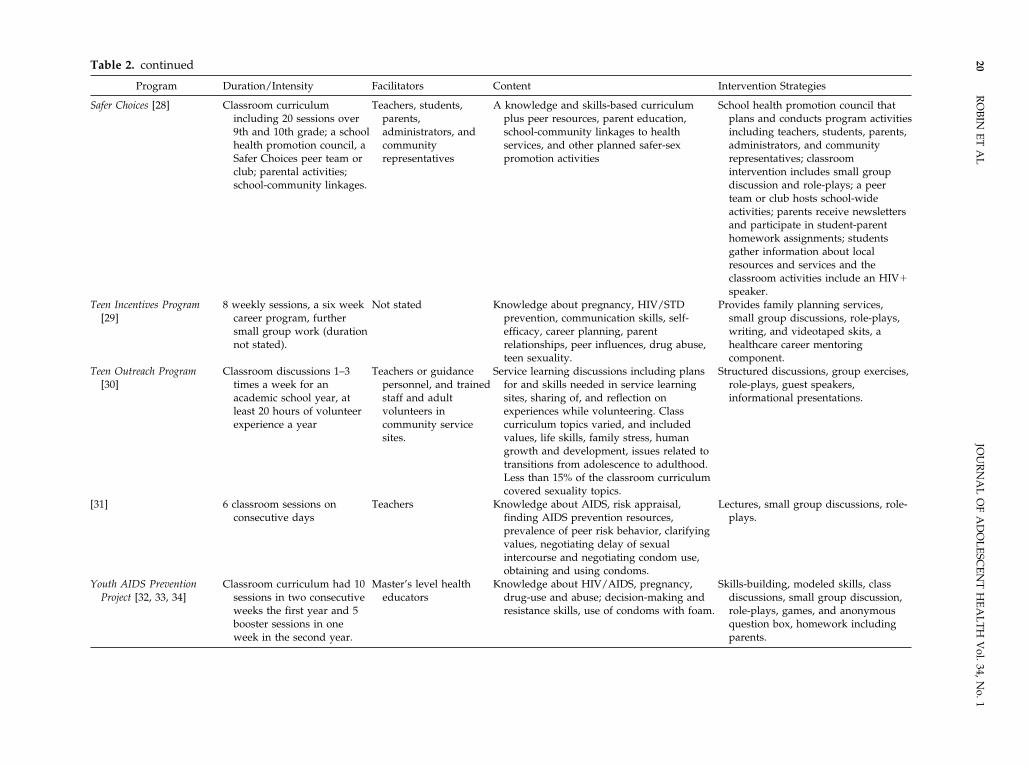
Table 2. continued
Program Duration/Intensity Facilitators Content Intervention Strategies
Safer Choices [28] Classroom curriculumincluding 20 sessions over9th and 10th grade; a schoolhealth promotion council, aSafer Choices peer team orclub; parental activities;school-community linkages.
Teachers, students,parents,administrators, andcommunityrepresentatives
A knowledge and skills-based curriculumplus peer resources, parent education,school-community linkages to healthservices, and other planned safer-sexpromotion activities
School health promotion council thatplans and conducts program activitiesincluding teachers, students, parents,administrators, and communityrepresentatives; classroomintervention includes small groupdiscussion and role-plays; a peerteam or club hosts school-wideactivities; parents receive newslettersand participate in student-parenthomework assignments; studentsgather information about localresources and services and theclassroom activities include an HIV�speaker.
Teen Incentives Program[29]
8 weekly sessions, a six weekcareer program, furthersmall group work (durationnot stated).
Not stated Knowledge about pregnancy, HIV/STDprevention, communication skills, self-efficacy, career planning, parentrelationships, peer influences, drug abuse,teen sexuality.
Provides family planning services,small group discussions, role-plays,writing, and videotaped skits, ahealthcare career mentoringcomponent.
Teen Outreach Program[30]
Classroom discussions 1–3times a week for anacademic school year, atleast 20 hours of volunteerexperience a year
Teachers or guidancepersonnel, and trainedstaff and adultvolunteers incommunity servicesites.
Service learning discussions including plansfor and skills needed in service learningsites, sharing of, and reflection onexperiences while volunteering. Classcurriculum topics varied, and includedvalues, life skills, family stress, humangrowth and development, issues related totransitions from adolescence to adulthood.Less than 15% of the classroom curriculumcovered sexuality topics.
Structured discussions, group exercises,role-plays, guest speakers,informational presentations.
[31] 6 classroom sessions onconsecutive days
Teachers Knowledge about AIDS, risk appraisal,finding AIDS prevention resources,prevalence of peer risk behavior, clarifyingvalues, negotiating delay of sexualintercourse and negotiating condom use,obtaining and using condoms.
Lectures, small group discussions, role-plays.
Youth AIDS PreventionProject [32, 33, 34]
Classroom curriculum had 10sessions in two consecutiveweeks the first year and 5booster sessions in oneweek in the second year.
Master’s level healtheducators
Knowledge about HIV/AIDS, pregnancy,drug-use and abuse; decision-making andresistance skills, use of condoms with foam.
Skills-building, modeled skills, classdiscussions, small group discussion,role-plays, games, and anonymousquestion box, homework includingparents.
20R
OB
INE
TA
LJO
UR
NA
LO
FA
DO
LE
SCE
NT
HE
AL
TH
Vol.34,N
o.1

Table 2. continued
Program Duration/Intensity Facilitators Content Intervention Strategies
A second condition receivedthe curriculum and twoextra assignments withparents in the first year, andone extra assignment withparents the second year
Parent intervention component includedinteractive homework assignments, attendparent meetings, participate in organizingparent networks and participate in AIDSprevention activities in the schools.
Mixed EffectsBecoming a Responsible
Teen [35]a90–120 minute sessions over
8 weeks.Paired male and female
adult facilitatorsKnowledge about STD/AIDS, condom use,
skills, sexual assertiveness, refusal skills,information provision to peers, self-management, and risk recognition.
Small group discussion, videos,modeled skills, skills practice, role-plays, HIV� speakers.
Working on the RightDirection [36[a
(Becoming a ResponsibleTeen Variant)a
6 one-hour sessions over 3weeks
Paired male and femaleadult facilitators
Knowledge about STD/AIDs, condom-useskills refusal skills, information provision topeers, self-management, and condomnegotiation.
Small group discussion, modeled skills,skills practice, videos, role-plays.
Null Effects[37] 3 class periods over 3
consecutive days.Not described Knowledge about HIV/STD, sexual decision-
making skills, problem-solving andcommunication skills.
Interactive slides presentations, videos,classroom and small groupdiscussion, games, role-plays.
Facts & Feelings [38] Six 15–20 minute videos,supplementary printedmaterials and newsletters;intensity was not regulated,families had 3 months toview the tapes.
Self-administered byparents and teens.
Social, emotional, and physical changes frompuberty, sexual values, knowledge ofanatomy, reproduction, prenataldevelopment and birth, sexuality withinrelationships and advantages of postponingintercourse, media influences, consequencesof sexual involvement, and refusal skills.
Videos, printed materials providingsupplementary information andadditional suggestions for discussionsand activities.
[39] 30 minute discussion withadolescent
Physicians HIV risk assessment, condom-use counseling,susceptibility to HIV, HIV prevention,condom efficacy, drug and needle use, freecondoms.
Individualized risk assessment for HIV,counseling on condom use, and HIVpamphlet, an offer of free condoms,and a 20-minute counseling sessionwith a physician to discuss a varietyof HIV prevention issues.
SNAPP [40] 8 sessions over 2 weeks Male and female peereducators, includingteen mothers andHIV� individuals
Identify social influences, gain resistanceskills, knowledge about pregnancy andHIV, learn about risks of unprotected sex,learn decision-making skills andcommunication skills.
Games, role-plays, large- and small-group activities, discussion, andquestion and answer sessions,modeling of skills and skills practice.
January2004
SEX
UA
LR
ISK-R
ED
UC
TIO
NIN
TE
RV
EN
TIO
NS
FOR
AD
OL
ESC
EN
TS
21

Table 2. continued
Program Duration/Intensity Facilitators Content Intervention Strategies
Negative EffectsPostponing Sexual
Involvement [41, 42]a4 45–60 minute sessions in
one week or 4 consecutiveweeks, a fifth session 1–3months later. Preceded by a5 session sexuality course
Male and female older11th and 12th gradestudents.
Knowledge about decision-making, humansexuality, family planning, and STD/HIV;assertiveness skills, resisting social andpeer pressure to have sex, practice inrefusal skills.
5 classroom periods of basic humansexuality information, includingfamily planning, videos, slidepresentations, class discussions.
Sexual Involvement [43](Replication of Postponing
Sexual Involvement)a
4 45–60 minute sessions inone week or 4 consecutiveweek, a fifth session 1–3months later. Preceded by areproductive healtheducation course for 85% ofthe students. Also combinedwith school-wide ENABLproject activities in aclassroom condition
Adult health educatorsand peers.
Knowledge about decision-making, humansexuality, family planning, and STD/HIV;assertiveness skills, resisting social andpeer pressure to have sex, practice inrefusal skills
Class discussions, group activities,videos, slide presentations, and roleplays.
Teen Talk [44] Variable implementationranging from 4 two hoursessions to a total of 12hours.
Adult clinic and schoolstaff
Increase feelings of vulnerability topregnancy, negative consequences of teenparenthood, benefits of delayed sexualinitiation and using contraception, skills toreduce barriers to abstinence andcontraceptive use.
Lectures, simulations, leader-guideddiscussions, role-plays, games, andvideos.
a Aggregated programs and their variants.
22R
OB
INE
TA
LJO
UR
NA
LO
FA
DO
LE
SCE
NT
HE
AL
TH
Vol.34,N
o.1

throughout elementary school. Another youth resil-iency approach is the Teen Outreach Program [30],which focuses on academic success, including ser-vice-learning activities. Little of the Teen OutreachProgram deals specifically with sexual risk-reduction,but the number of pregnancies was reduced amongfemale students participating in the program relativeto the control group.
DiscussionAmong frequently targeted behaviors, the least con-sistent impact was found for delayed initiation ofsexual intercourse and the most consistent for con-dom use. Both the original evaluation of PostponingSexual Involvement [41,42] and the study replicatingthe evaluation [43] focused on delayed initiation ofsexual intercourse and produced negative findings(although the original evaluation produced somepositive findings as well). Only one program focus-ing primarily on delayed initiation of sexual inter-course reported positive effects without also report-ing negative effects [22]. These findings underscorethe need to develop and rigorously evaluate pro-grams that can consistently delay the initiation ofintercourse. The more consistent impact of programson condom use also was reported in a prior literaturereview of HIV prevention programs targeting het-erosexual adolescents [7].
Virtually no key study features or program char-acteristics clearly distinguish studies with positive,null, and negative effects from each other. However,when we aggregate the studies, four implications foreffective programs become apparent: (a) they havefocused on skills that reduce specific sexual riskbehaviors; (b) the duration and intensity of a pro-gram may play a role in its effectiveness; (c) the needfor researchers and health educators to carefullydetermine what constitutes an entire program; and(d) program facilitators’ training may be more im-portant than whether facilitators’ and participants’demographic characteristics match.
The importance of emphasizing skills focusing onreducing specific sexual risk behaviors is under-scored by the fact that, although most of the pro-grams contained skills-building activities (e.g., sex-ual communication, decision-making, problem-solving), programs reporting null and negativeeffects (with the exception of Teen Talk [44]) appearedto emphasize skills that were less specific. We alsofound that many of these programs were likely tohave evaluations published in 1995 or before, and to
be between 7 and 15 hours in duration. These find-ings are consistent with prior literature reviews[9,11,12,13]. Programs for which evaluations werepublished after 1995 were of longer duration, andlonger programs also contained more general typesof skills and knowledge. This may reflect a shifttoward multi-component interventions that target avariety of youth competencies.
Such broad-based programs may be appealingbecause community objections to them are less likelythan objections to programs focused specifically onsexuality and sexual risk-reduction behaviors. How-ever, more narrowly focused programs have beenmore extensively evaluated and their effects arebetter understood. Consequently, health educatorsshould exercise caution in depending solely onbroad-based programs to reduce sexual risk behav-iors among youth.
The second implication of our findings is that theduration of programs may play a role in their effec-tiveness. The three shortest programs (at less than 1hour, 2 hours, and 3 hours) all produced null effects.Becoming a Responsible Teen [35] exhibited mixedeffects. The program was originally effective in re-ducing sexual risk behavior when it was imple-mented in 90–120 minute sessions during 8 weeks. Avariant of the program that produced null effects,Working On the Right Direction [36], was implementedin six 1-hour sessions during 3 weeks. Althoughother aspects of the program were changed, thisreduction in duration may have contributed to itsnull findings.
Similarly, changes in intensity of interventionsmay affect the effectiveness of programs. Rotheram-Borus et al [46] tested two versions of an interventionthat had the same overall duration (10.5 hours) butwere delivered in three or seven sessions to partici-pants. Only the seven session intervention was asso-ciated with reductions in sexual risk behaviorsamong participants. Thus, when the content of anintervention is not changed, a reduction in the num-ber of sessions may reduce the efficacy of an inter-vention even though the overall duration is the same.These findings are supported by previous literaturereviews [9,11,13]. The effect of duration and intensityon interventions results in a particular challenge forschool-based educators because they may have lim-ited time to implement programs within a schoolyear. Community-based organizations also need suf-ficient resources to implement programs in multiplesessions. Rotheram-Borus et al suggest that shortersessions spread over time may better allow adoles-cents to learn and practice sexual risk-reduction
January 2004 SEXUAL RISK-REDUCTION INTERVENTIONS FOR ADOLESCENTS 23

skills [46]. Researchers also should be aware of theseimplications for program intensity in designing pro-grams and should carefully collect dosage data. Thestudy by Rotheram-Borus et al should be replicatedto test the implications of intensity and durationcontrolling for content. The issue of program contentis an especially important one, as we found thatprograms including a greater variety of knowledgeskills and general life skills were longer than pro-grams focused more specifically on abstinence andcondom skills. Researchers performing quantitativesystematic literature reviews should design studiesto untangle the effect of differences in programcontent and program duration, and researchers re-porting evaluation results should carefully reportprogram content and strategies as well as duration.
A third implication of these findings is that healtheducators should be careful when implementingevaluated programs to determine what actually con-stitutes a given program, and how other programsand resources in schools and communities may affectprogram outcomes. The program content of Postpon-ing Sexual Involvement [41,42] and its variant evalu-ated by Kirby et al [43] is difficult to define. Theoriginal program included both the Postponing SexualInvolvement curriculum and a five-session sexualityprogram that preceded it. In an effort to replicatePostponing Sexual Involvement, Kirby et al imple-mented the program along with a reproductivehealth education course and some components of theEducation Now and Babies Later program. As a result,whether the positive and negative outcomes resultfrom the program itself or from the additional cur-riculum elements is not clear. Researchers shouldtherefore give careful consideration to what consti-tutes a particular program. This can be challengingwhen performing an applied evaluation that assessesprograms already offered in a school or communitycontext.
A fourth implication of these findings is thattraining facilitators may be more important thanmatching the demographic characteristics of facilita-tors and participants. Little research has assessed theeffectiveness of peer-led interventions as comparedwith those led by adults. In the only randomizedcontrolled trial to directly compare the effects ofadult versus peer-led interventions, Jemmott et al[22] found no difference in intervention effects. Inanother study, Jemmott et al [47] found that thefacilitators’ race and gender, relative to participants,did not affect the outcomes of the interventions.These findings suggest that the content of the pro-gram and thorough training of facilitators may be
more important than their demographic characteris-tics in producing effective interventions. Educatorsin school and community settings who receivedthorough training could effectively implement pro-grams for youth who are demographically differentfrom them [47]. Kirby also stressed the importance oftraining both adult and peer facilitators [13]. Healtheducators may therefore have more options in thenumber of settings in which they can offer effectiveprograms. Researchers should replicate previousfindings that test the effects of facilitators’ demo-graphic characteristics on the behavioral outcomes ofsexual risk-reduction programs.
Limitations
Our review has several important limitations. Weonly searched through English-language reportspublished in the United States to identify eligibleevaluation studies. Further, we conducted searchesin seven electronic databases and hand-searchedjournals and may have missed studies in our litera-ture review. Additionally, publication bias may haveresulted in the inclusion of more studies with posi-tive results than with null or negative results [48].Published reports may not represent fully all aspectsof any given evaluation study or program, resultingin incomplete information. Finally, our analysis mayhave omitted important research or program designissues. Other research and program issues may ariseas researchers continue to evaluate increasingly so-phisticated interventions.
Conclusions
Health educators are faced with challenges in put-ting researched programs into practice. Our findingsreveal that focusing on appropriate skills, adaptingprograms for length, being clear about what consti-tutes a given program, and deciding who shouldfacilitate them should all be considered. Addition-ally, resiliency-based programs should be furtherexplored to determine their efficacy in reducingsexual risk behaviors among adolescents. Research-ers should also design studies that will clearly revealwhich program characteristics drive positive effectsin sexual risk-reduction. Research in this decade willbuild on the advances in sexual risk-reduction eval-uations and programs of the 1990’s.
We gratefully acknowledge the contributions of Dr. Janet Collinsand Dr. Janet St. Lawrence, both of whose early guidance broughtthe authors together and shaped this project.
24 ROBIN ET AL JOURNAL OF ADOLESCENT HEALTH Vol. 34, No. 1

References1. Centers for Disease Control and Prevention. Trends in sexual
risk behaviors among high school students—United States,1991–1997. MMWR 1998;47:749–52.
2. Santelli JS, Lindberg L, Abma J, et al. Adolescent sexualbehavior: Estimates and trends from four nationally represen-tative surveys. Fam Plann Perspect 2000;32:157–95.
3. Centers for Disease Control and Prevention. Young People atrisk: HIV/AIDS among America’s youth. Available at: http://www.cdc.gov/hiv/pubs/facts/youth.htm. (Accessed Decem-ber 12, 2001.)
4. Eng TR, Butler WT (eds). The Hidden Epidemic: ConfrontingSexually Transmitted Diseases. Washington, DC: NationalAcademy Press, 1997.
5. Centers for Disease Control and Prevention. National andstate-specific pregnancy rates among adolescents—UnitedStates, 1995–1997. MMWR 2000;4:605–11.
6. Heneshaw SK. Unintended pregnancy in the United States.Fam Plann Perspect 1998;30:24–9.
7. Jemmott JB III, Jemmott LS. HIV risk reduction behavioralinterventions with heterosexual adolescents. AIDS 2000;14(Suppl 2):S40–52.
8. Centers for Disease Control and Prevention, HIV/AIDS Pre-vention Research Synthesis Project. Compendium of HIVPrevention Interventions with Evidence of Effectiveness, No-vember, 1999.
9. Peersman GV, Levy JA. Focus and effectiveness of HIV-prevention efforts for young people. AIDS 1998;12(SupplA):S191–6.
10. Kim N, Stanton B, Li X, et al. Effectiveness of the 40 adolescentAIDS-risk reduction interventions: A quantitative review. JAdolesc Health 1997;20:204–15.
11. Stanton B, Kim N, Galbraith J, et al. Design issues addressed inpublished evaluations of adolescent HIV-risk reduction inter-ventions: A review. J Adolesc Health 1996;18:387–96.
12. Oakley A, Fullerton D, Holland J. Behavioral interventions forHIV/AIDS prevention. AIDS 1995;9:479–86.
13. Kirby D. Emerging Answers: Research Findings on Programsto Reduce Teen Pregnancy. Washington, DC: National Cam-paign to Prevent Teen Pregnancy, 2001.
14. Card JJ, Niego S, Mallari A, et al. The Program Archive onSexuality, Health & Adolescence: Promising “prevention pro-grams in a box.” Fam Plann Perspect 1996;28:210–20.
15. Philliber S, Namerow P. Trying to maximize the odds: Usingwhat we know to prevent teen pregnancy. Paper presented ata Centers for Disease Control and Prevention technical assis-tance workshop; December 13–15, 1995, Atlanta, Georgia.
16. Grunseit A, Kippax S, Aggleton P, et al. Sexuality educationand young people’s sexual behavior: A review of studies. JAdolesc Res 1997;12:421–53.
17. Kirby D, Short L, Collins J, et al. School-based programs toreduce sexual risk behaviors: A review of effectiveness. PublicHealth Rep 1994;109:339–60.
18. Mullen PD, Ramirez G, Strouse D, et al. Meta-analysis of theeffects of behavioral HIV prevention interventions on thesexual risk behavior of sexually experienced adolescents incontrolled studies in the United States. J Acquir Immune DeficSyndr 2002;30(Suppl 1):S94–S105.
19. DiCenso A, Guyatt G, Willan A, Griffith L. Interventions toreduce unintended pregnancies among adolescents: System-atic review of randomized controlled trials. BMJ 2002;324:1426–34.
20. Wright-DeAguero LK, Smith SJ, Valverde K, et al. A system-atic review of sexuality education interventions for adoles-
cents. Poster presented at XIV International AIDS Conference,July 9, 2002, Barcelona, Spain.
21. Jemmott JB III, Jemmott LS, Fong GT. Reductions in HIVrisk-associated sexual behaviors among black male adoles-cents: Effects of an AIDS prevention intervention. Am J PublicHealth 1992;82:372–77.
22. Jemmott JB III, Jemmott LS, Fong GT. Abstinence and safer sexHIV risk-reduction interventions for African American ado-lescents: A randomized controlled trial. JAMA 1998;279:1529–36.
23. Stanton B, Li X, Ricardo I, et al. A randomized, controlledeffectiveness trial of an AIDS prevention program for low-income African-American youths. Arch Pediatr Adolesc Med1996;150:363–72.
24. Stanton B, Fang X, Li X, et al. Evolution of risk behaviors over2 years among a cohort of urban African American adoles-cents. Arch Pediatr Adolesc Med 1997;151:398–406.
25. Magura S, Kang SY, Shapiro JL. Outcomes of intensive AIDSeducation for male adolescent drug users in jail. J AdolescHealth 1994;15:457–63.
26. O’Donnell L, Stueve A, Doval AS, et al. The effectivenesss ofthe Reach for Health Community Youth Service LearningProgram in reducing early and unprotected sex among urbanmiddle school students. Am J Public Health 1999;89:176–81.
27. Kirby D, Barth RP, Leland N, et al. Reducing the Risk: Impactof a new curriculum on sexual risk taking. Fam Plann Perspect1991;23:254–63.
28. Coyle K, Basen-Enquist K, Kirby D, et al. Short-term impact ofSafer Choices: A multi-component, school-based HIV, otherSTD, and pregnancy prevention program. J Sch Health 1999;69:181–8.
29. Bayne Smith MA. Teen Incentives Program: Evaluation of ahealth promotion model for adolescent pregnancy prevention.J Health Educ 1994;25:24–9.
30. Allen JP, Philliber S, Herling S, et al. Preventing teen preg-nancy and academic failure: Experimental evaluation of adevelopmentally based approach. Child Dev 1997;64:729–42.
31. Walter HJ, Vaughan RD. AIDS risk reduction among a multi-ethnic sample of urban high school students. JAMA 1993;27:725–30.
32. Weeks K, Levy SR, Zhu C, et al. Impact of a school-based AIDSprevention program on young adolescents’ self-efficacy skills.Health Educ Res 1995;10:329–44.
33. Levy SR, Perhats C, Weeks K, et al. Impact of a school-basedAIDS prevention program on risk and protective behavior fornewly sexually active students. J Sch Health 1995;65:145–51.
34. Weeks K, Levy SR, Gordon AK, et al. Does parent involvementmake a difference? The impact of parent interactive activitieson students in a school-based AIDS prevention program.AIDS Educ Prev 1997;9(Suppl 1):90–106.
35. St. Lawrence JS, Brasfield TL, Jefferson KW, et al. Cognitive-behavioral intervention to reduce African American adoles-cents’ risk for HIV infection. J Consult Clin Psychol 1995;63:221–37.
36. St. Lawrence JS, Crosby RA, Belcher L, et al. Sexual riskreduction and anger management interventions for incarcer-ated male adolescents: A randomized controlled trial of twointerventions. J Sex Educ Ther 1999;24:9–17.
37. Boyer CB, Shafer M, Tschann JM. Evaluation of a knowledgeand cognitive-behavioral skills-building intervention to pre-vent STDs and HIV infection in high school students. Adoles-cence 1997;32:25–42.
38. Miller BC, Norton MC, Jenson GO, et al. Impact evaluation ofFacts & Feelings: A home-based video sex education curricu-lum. Fam Relat 1993;42:392–400.
January 2004 SEXUAL RISK-REDUCTION INTERVENTIONS FOR ADOLESCENTS 25

39. Mansfield CJ, Conroy ME, Emans SJ, et al. A pilot study ofAIDS education and counseling of high-risk adolescents in anoffice setting. J Adolesc Health 1993;14:115–9.
40. Kirby D, Korpi M, Adivi C, et al. An impact evaluation ofProject SNAPP: An AIDS and pregnancy prevention middleschool program. AIDS Educ Prev 1997;9(Suppl 1):44–61.
41. Howard M, McCabe JB. Helping teenagers postpone sexualinvolvement. Fam Plann Perspect 1990;22:21–6.
42. Howard M. Delaying the start of intercourse among adoles-cents. Adolesc Med 1992;3:181–93.
43. Kirby D, Korpi M, Barth RP, et al. The impact of the Postpon-ing Sexual Involvement Curriculum among youths in Califor-nia. Fam Plann Perspect 1997;29:100–8.
44. Eisen M, Zellman GL, McAlister AL. Evaluating the impact of
a theory-based sexuality and contraception education pro-gram. Fam Plann Perspect 1990;22:261–71.
45. Hawkins JD, Catalano RF, Kosterman R, et al. Preventingadolescent health-risk behaviors by strengthening protectionduring childhood. Arch Pediatr Adolesc Med 1999;153:226–34.
46. Rotheram-Borus MJ, Gwadz M, Fernandez MI, et al. Timing ofHIV interventions on reductions in sexual risk among adoles-cents. Am J Community Psychol 1998;26:73–96.
47. Jemmott JB III, Jemmott LS, Fong G. Reducing HIV risk-associated sexual behavior among African American adoles-cents: testing the generality of intervention effects. Am JCommunity Psychol 1999;27:161–87.
48. Begg CB. Publication bias. In: Cooper C, Hedges LV (eds). TheHandbook of Research Synthesis. New York: Russell Sage,1994:399–410.
26 ROBIN ET AL JOURNAL OF ADOLESCENT HEALTH Vol. 34, No. 1





























