Embed Size (px)
Citation preview

Aotis
EcMA
c
BCU
5
Biomechanical Evaluation of Arthroscopic Rotator CuffRepairs Over Time
Augustus D. Mazzocca, M.D., M.S., Matthew J. Bollier, M.D., Elifho Obopilwe, M.S.,Joseph P. DeAngelis, M.D., Stephen S. Burkhart, M.D., Russell F. Warren, M.D., and
Robert A. Arciero, M.D.
Purpose: The aim of this study was to assess the contact pressure, force, and area over time for 4common arthroscopic rotator cuff repair techniques. Methods: The transosseous-equivalent, single-row, triangle double-row, and suture-chain transosseous repair techniques were used to repair afull-thickness tear of the supraspinatus in 16 cadaveric shoulders. Continuous data points werecollected immediately after repair and for 160 minutes at set time intervals by use of a custom thinfilm pressure sensor. Results: Each of the 4 rotator cuff repair techniques showed decreased contactforce, pressure, and area 160 minutes after the repair was performed. The transosseous-equivalentconstruct had the highest contact pressure and force initially and at all time points up to 160 minutes.Although the 3 double-row constructs had greater pressure and force at all time points compared withthe single-row repair, only the transosseous-equivalent group showed a statistically greater pressureand force when compared with single-row repair (P � .05). Conclusions: Contact pressure, force,and pressurized footprint area decrease 160 minutes after repair regardless of repair technique. Thetransosseous-equivalent group had the highest contact pressure and force at all time points. ClinicalRelevance: The decrease in contact pressure and force after rotator cuff repair may have importantimplications in evaluating tendon-to-bone healing and determining the optimal rehabilitationprotocol.
oMrbcthr
towatiiimc
rthroscopic rotator cuff repair has become a well-established technique for the surgical treatment
f complete rotator cuff tears.1 Clinical results showhat patients have better functional outcomes withntact repairs than those with recurrent tears.1-3 Recenttudies have shown retear rates as high as 50% after
From the University of Connecticut Medical Center (A.D.M.,.O., R.A.A., M.J.B.), Farmington, Connecticut; Hospital for Spe-ial Surgery (R.F.W.), New York, New York; Beth Israel Deaconessedical Center (J.P.D.), Boston, Massachusetts; and The Sanntonio Orthopaedic Group (S.S.B.), San Antonio, Texas, U.S.A.A.D.M., S.S.B., and R.A.A. received support from Arthrex ex-
eeding the equivalent of US $500 related to this research.Received November 5, 2009; accepted February 19, 2010.Address correspondence and reprint requests to Matthew J.
ollier, M.D., Department of Orthopaedic Surgery, University ofonnecticut, MARB, 263 Farmington Ave, Farmington, CT 06030,.S.A. E-mail: [email protected]© 2010 by the Arthroscopy Association of North America
t0749-8063/10/2605-9663$36.00/0doi:10.1016/j.arthro.2010.02.009
92 Arthroscopy: The Journal of Arthroscopic and Related
pen repair and 89% after arthroscopic repair.2-4
any factors have been blamed for the failure ofotator cuff repair, including blood supply, tendon orone quality, and fatty infiltration of rotator cuff mus-ulature.5-7 There has been much interest in improvinghe success of rotator cuff healing, and much attentionas been directed at finding the optimal biomechanicalepair construct.1,8,9
To restore the footprint area, numerous arthroscopicechniques have been studied. Recently, the transosse-us-equivalent (TOE) technique has become popularith sutures from the medial row of anchors coming
cross the rotator cuff and being secured laterally inhe footprint. It has been hypothesized that maximiz-ng footprint contact pressure, force, and area willmprove tendon-to-bone healing.10-12 However, theres still considerable debate regarding the optimal bio-echanical arthroscopic repair construct. The studies
omparing contact area and pressure for various ar-
hroscopic rotator cuff repair techniques have usedSurgery, Vol 26, No 5 (May), 2010: pp 592-599

pctieitaemaeptrs(a
cwdsatorcgmfawmtdefiwifammdd
la
sbp1tptaspahof5tmoa
wDt(lttftcc
t
FTe
593BIOMECHANICAL EVALUATION OF ROTATOR CUFF REPAIRS
ressure-sensitive film at time 0 only.1,9,13-15 Clini-ally, the viscoelastic properties of the tendon repair atime 0 do not seem to correlate with the final outcomesn a reliable manner.16 Currently, there are no dataxploring contact pressure for rotator cuff repair afternitial fixation. Significant reductions or changes inhese parameters may affect rehabilitation regimensnd tendon-to-bone healing. Biomechanical studiesxamining rotator cuff repairs have concentrated oneasuring contact pressure, force, and area at time 0
fter the initial repair. The purpose of this study was tovaluate contact pressure, force, and pressurized foot-rint area differences between 4 rotator cuff repairechniques over time. We hypothesized that all of theepair techniques will show decreased contact pres-ure and force over time and that the 3 double-rowDR) constructs will have increased pressure, force,nd area compared with the single-row (SR) repair.
METHODS
Sixteen cadaveric shoulders with intact rotatoruffs, with a mean age at death of 72.7 � 10.7 years,ere used. After these specimens were thawed, boneensity was measured (Lunar dual-energy X-ray ab-orptiometry; GE Medical Systems, Milwaukee, WI)t a 1 � 1–cm area at the supraspinatus footprint onhe greater tuberosity to assess bone quality at the sitef suture anchor insertion. The deltoid muscle wasemoved from the acromion, providing complete ac-ess to the coracoacromial arch, rotator cuff, andlenohumeral joint. The supraspinatus tendon anduscle were sharply elevated from the supraspinatus
ossa medially and reflected laterally to expose therticular aspect of the anatomic footprint. The processas repeated for the subscapularis and infraspinatususcles. The glenohumeral joint capsule was left in-
act. The individual muscles of the rotator cuff wereissected free from the joint capsule. The circumfer-nce and pennation angle (angle between the musclebers and most centrally located tendon of insertion)ere measured for each rotator cuff muscle. The max-
mum torque (Tmax) was calculated by use of theollowing equation: Tmax � (Muscle cross-sectionalrea cos pennation angle � Specific tension) � Mo-ent arm.17 This allowed us to calculate the actualoment of each rotator cuff muscle so that the shoul-
er would be balanced and have physiologic loadsuring testing.The medial aspects of the supraspinatus, subscapu-
aris, and infraspinatus muscle bellies were individu-
lly secured with strapping for individual loading. The tcapula was trimmed to fit into a custom aluminumox with the glenoid face fixed at 60° to the scapularot, representing 60° of glenohumeral abduction (Fig). The humerus was cut 20 cm from the joint, cen-ered in a polyvinylchloride pipe, and potted withlaster of Paris. The potted cadaveric specimen washen mounted on a custom shoulder testing apparatuss described by Remia et al.18 The scapular box wasecured to a linear bearing system that provided com-ression.19 To center the humeral head in the glenoid,compressive load of 22 N was applied to the gleno-umeral joint by applying a hanging weight at the endf each lever arm underneath the scapular box (11 Nor the supraspinatus, 5.5 N for the subscapularis, and.5 N for the infraspinatus).20 The humerus was cen-ered in a cylinder attached to the jig that allowedultiple positions of rotation and abduction. A goni-
meter was used to ensure neutral humeral rotationnd 0° of abduction.
The intact supraspinatus footprint was measuredith digital calipers for linear measurements (Absoluteigimatic; Mitutoyo, Kawasaki, Japan). The supraspina-
us footprint was measured with a MicroScribe digitizerImmersion, San Jose, CA) before we created the tear byifting the supraspinatus muscle and tracing the outline ofhe attachment.19,21 A complete tear of the supraspinatusendon was sharply created with a No. 15 blade scalpelrom the articular margin of the supraspinatus attachmento the greater tuberosity. At the end of each test, theontact pressure, force, and area were measured andompared with immediate post-repair measurements.
To measure pressure, force, and area coverage overime, a custom TekScan sensor (TekScan, South Bos-
IGURE 1. Biomechanical setup showing position of shoulder jig,ekscan sensor secured beneath tendon in footprint, and forces onach rotator cuff muscle.
on, MA) for footprint analysis was created. Recently,

aPwbcpttnTtnaBthmpsssnScasastlrttsfiltwsesl
atppdsNMl
apiwtcfbswrTtttastttac
afipTcltcomtrtsra
tsuuSteRsas
594 A. D. MAZZOCCA ET AL.
biomechanical study showed the TekScan I-Scanressure Measurement System to be more accuratehen analyzing contact area, force, and pressure forioengineering applications than the Fuji Film Pres-ale Measuring System (Fuji Photo Film, Tokyo, Ja-an).22 Such superior accuracy, as well as the abilityo continuously collect data points in real time, led uso study multiple arthroscopic rotator cuff repair tech-iques over time using a custom TekScan sensor.23
ekScan sensor model No. 4205 was created to cap-ure data from a normal rotator cuff footprint. Origi-ally, our laboratory was using model No. 4201, withmatrix width of 45.7 mm and height of 21.0 mm.ecause the normal footprint of the supraspinatus
endon averages 23 mm, we increased the matrixeight to 41.9 mm and kept the matrix width at 45.7m. This working area surpasses the average foot-
rint area, thereby allowing us to incorporate the sen-or into our repair, through holes, without losing sen-itivity of our data recording. The Tekscan sensor wasecured in the following manner (with the actual tech-ique for each repair being described later). For theR repair, after the anchors were placed in the rotatoruff footprint on the humerus, 2-mm holes were cre-ted by use of a sharpened leather punch in the Tek-can sensor directly adjacent to the anchors. Thisllowed passage of suture through the Tekscan sensoro that it could be sandwiched between the tendon andhe bone. For the triangle DR repair, 1 medial and 2ateral anchors were placed, and the sutures incorpo-ated both the tendon and the Tekscan sensor so thathe Tekscan sensor was again placed between theendon and the bone. For the TOE repair and theuture-chain repair, the medial anchors were placedrst and sutures tied (for TOE) or passed (for chain
inked), incorporating both the medial aspect of theendon and the Tekscan sensor. The Tekscan sensoras positioned between the tendon and the bone. The
utures or tape was tensioned laterally over the tendondge and brought through a 4-mm hole in the Tekscanensor. The sutures or tape was then fixed with theateral fixation device into bone.
Two main pilot studies were performed to verify theccuracy of the custom Tekscan sensor and to ensurehat no other variable would account for changes inressure or force at the bone-tendon interface. First, ailot study was done to evaluate accuracy and repro-ucibility of the sensors. We preconditioned the sen-or by evenly applying separate loads of 5 N and 100
on a mechanical testing system (MTS, Eden Prairie,N). The sensor continuously recorded the correct
oad value. The sensor was pre-calibrated to a force t
nd pressure consistent with previous rotator cuff re-air studies. To ensure durability, the sensor wasnserted and removed from the data handle 20 timesith a load of 10 N applied to the supraspinatus
endon. Readings were taken each time and wereonsistent. This proved there was no mechanical mal-unction with handling of the sensor. A drift test inoth tension and compression was performed to en-ure accuracy of the sensor over time. A load of 10 Nas applied in both compression and tension and
ecorded in 10-minute intervals for a period of 1 hour.he sensor maintained its recording capability over
he course of 60 minutes in both compression andension, with a correlation of variation of 4.69% inension and 5.85% in compression. The reliability andccuracy of the Tekscan sensor on a curved surfaceuch as the greater tuberosity were compared with theraditional flat surface. Ten Newtons were applied inension and monitored over a period of 1 hour, andhere was no difference in the Tekscan force readoutnd the MTS force applied when comparing a flat or aurved surface.
Suture elongation, knot security, anchor migration,nd tendon deformation were also evaluated to con-rm that these variables would not change force orressure readings at the site of the tendon-bone repair.he sutures were tied onto the MTS fixture, and theonstruct was cycled 1,000 times with no change inength. All anchors were cemented into the greateruberosity by use of standard bone cement, with nohange in anchor position during pilot testing. A loadf 4 N was applied to the tendon, and deformation waseasured over time. We found that the tendon re-
urned to its native state after applied pressure wasemoved and retained its viscoelastic properties. All ofhe pilot studies confirmed that changes in force, pres-ure, or area readings were located at the tendon-boneepair construct and not related to confounding vari-bles.
The tear was fixed with 1 of 4 constructs: SR,riangle DR, TOE, and suture-chain TOE (CL). Theame 5.5-mm bioabsorbable corkscrew anchor wassed in all the repairs double loaded with No. 2ltrahigh-strength suture (Arthrex, Naples, FL) for theR and DR repairs. All anchors were placed by first
apping the hole for the anchor with a punch; deliv-ring polymethyl methacrylate (Dentsply Orthodonticesin; Dentsply, Milford, DE) into the hole, placing a
mall amount on the anchor; and then inserting thenchor. For the TOE repair, the same laterally baseduture anchors were used, 5.5-mm SwiveLock (Ar-
hrex). Arthroscopic knot tying was performed by use
otkmruc2plrpsA
omC
Ft
Fdl
Fli
F
595BIOMECHANICAL EVALUATION OF ROTATOR CUFF REPAIRS
f a standard knot pusher with overhand throws, al-ernating half-hitches and posts to maximize loop andnot security. These were tied by the same surgeon toinimize performance bias. Figure 2 shows the SR
epair with 3 anchors placed 1 cm lateral to the artic-lar margin. The DR repair is shown in Fig 3 andonsists of 1 medial anchor at the articular margin and
laterally based anchors. The medial sutures wereassed in a horizontal mattress configuration and theateral sutures by a simple suture technique. The TOEepair is shown in Fig 4. Two medial anchors werelaced at the articular margin 12.5 mm apart, with theutures passed in a horizontal mattress configuration.
suture limb from each medial anchor was crossed
IGURE 2. SR repair, with 3 double-loaded anchors 1 cm lateral tohe articular cartilage tied in a simple fashion.
IGURE 3. Triangle DR repair, with 1 medial-row anchor and 2
ouble-loaded lateral anchors with no linkage between medial andateral rows.aT
ver the rotator cuff and placed in lateral anchors 10m distal to the lateral edge of the footprint.9,24 TheL repair is shown in Fig 5 and was performed with
IGURE 4. TOE repair, with 2 medial-row anchors with obliqueinkage to 2 lateral-row anchors. There is a crossing pattern ofnterconnection between rows.
IGURE 5. Suture-chain transosseous repair, with 2 medial-row
nchors with FiberChain linearly linked to 2 lateral-row anchors.here is a non-crossing pattern of interconnection between rows.
2tse(wdaltpf
D
pnedmtobsp
S
em2gpiuc
smrh(Whci(F
m(.ccc
6amlNssmllmig(
atstctat
wagwtcrcspceiAtt
596 A. D. MAZZOCCA ET AL.
medial anchors preloaded with an interlocking su-ure chain. The non-linked, free end of the anterioruture chain was passed 15 mm medial to the lateraldge of the tendon with a Scorpion Suture PasserArthrex). The free ends of the FiberChain (Arthrex)ere passed through the terminal link and cinchedown until the suture was flush on the tendon. Thenterior suture chain was placed over the cuff andinked to a lateral screw-in anchor that was placed athe lateral edge of the footprint. Placement of theosterior suture chain was performed in a similarashion.
ata Collection
Immediately after the repair was performed, contactressure, force, and area measurements were taken ineutral rotation (biceps tendon in line with the anteriordge of the acromion) and 0° of abduction. Additionalata points were recorded every minute for the first 10inutes, every 5 minutes for the next 30 minutes, and
hen every 30 minutes until the data collection periodf 160 minutes was reached. We chose 160 minutesecause it was the average time patients spent in oururgery center from the moment the repair was com-lete until discharge.
tatistical Analysis
Power analysis was performed by use of the param-ters of a primary outcome of contact pressure at 160inutes, a 6-psi difference as significant, and an SD ofpsi. It was determined that 16 specimens, 4 in each
roup, were required to provide greater than 95%ower. The mean contact pressure, force, and pressur-zed footprint area for the 4 repairs were compared byse of a 1 � 4 analysis of variance. Statistical signifi-ance was set at P � .05 with a � error at .80 and � � .05.
RESULTS
The results for pressure, force, and contact area areummarized in Fig 6. Figures 6A and 6B show theean contact pressure for each of the investigated
epair techniques. The mean contact pressure wasighest for the TOE group immediately after repair13.8 psi) and at all data points up to 160 minutes.
ith the numbers available, this was statisticallyigher than the SR repair (P � .021). The meanontact pressure was lowest for the SR technique bothmmediately after repair (3.6 psi) and at 160 minutes2.4 psi) (P � .021 and P � .028, respectively).
igure 6B shows contact pressure loss over time. The oean pressure loss was highest for the TOE group4.6 psi) and lowest for the SR group (1.2 psi) (P �050). All repair groups had at least a 32% drop inontact pressure over a period of 160 minutes. Thehain-link group showed greater than a 50% drop inontact pressure at 160 minutes (52.0%).
The mean contact force, as shown in Figs 6C andD, was highest for the TOE group both immediatelyfter repair (35.0 N) and at all time points up to 160inutes after repair. The mean contact force was
owest for the SR group immediately after repair (5.4) and at 160 minutes (3.5 N) (P � .006). Figure 6D
hows the mean loss of force among the repair con-tructs over time. The TOE group had the greatestean loss of force (11.6 N), and the SR group had the
owest (1.9 N) (P � .020). All repair groups had ateast a 32% drop in contact force over a period of 160inutes, and these values were not statistically signif-
cant (P � .315). Both the DR and suture-chain TOEroups showed at least a 50% drop in contact force50.0% and 52.0%, respectively).
Figures 6E and 6F show mean area and mean loss ofrea. The TOE group showed the highest initial con-act area (292.3 mm2), and the TOE and DR groupshowed the highest contact area at 160 minutes. Withhe numbers available, these values were not statisti-ally significant (P � .154 and P � .204, respec-ively). The SR group had the smallest loss of contactrea at 160 minutes (20.0 mm2), and the CL group hadhe highest (61.0 mm2) (P � .533).
DISCUSSION
We confirmed our hypothesis that all 4 repairsould show decreased contact pressure, force, and
rea over time and the DR constructs would havereater pressure and force at all time points comparedith the SR repair. This raises the question of whether
he degree of intraoperative fixation using arthros-opic repair techniques is adequately maintained in aeliable fashion. The loss of repair integrity may beoncerning to physicians who believe that the repair isecure in the operating room. Furthermore, lack ofersistent footprint area pressure could diminish theapacity of the tendon to heal to the tuberosity. Weilert al.12,25 have shown that high contact pressures havencreased direct osseous healing between bone and thechilles tendon. Although there has yet to be defini-
ive proof in a rotator cuff repair model, we believehat maximizing contact pressure is beneficial in terms
f tendon-to-bone healing.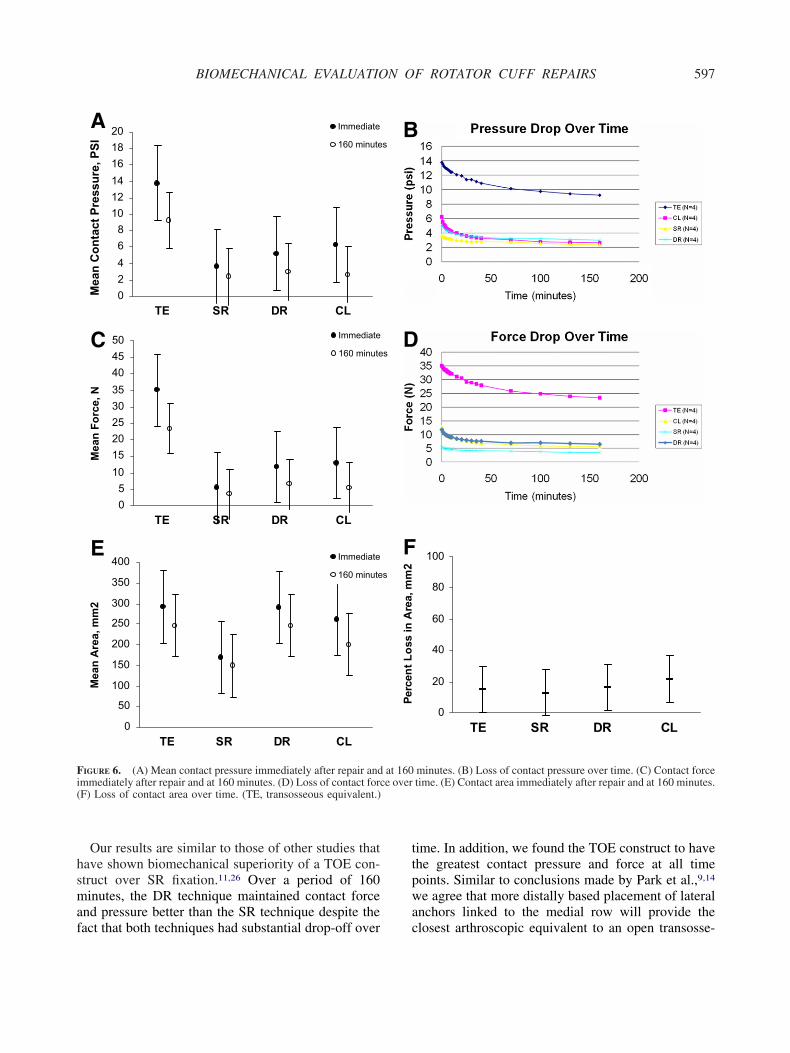
hsmaf
ttpwa
Fi e over(
597BIOMECHANICAL EVALUATION OF ROTATOR CUFF REPAIRS
Our results are similar to those of other studies thatave shown biomechanical superiority of a TOE con-truct over SR fixation.11,26 Over a period of 160inutes, the DR technique maintained contact force
nd pressure better than the SR technique despite the
02468
101214161820
Mea
n C
onta
ct P
ress
ure,
PSI
Immediate
160 minute
TE SR DR CL
05
101520253035404550
Mea
n Fo
rce,
N
Immediate
160 minute
TE SR DR CL
0
50
100
150
200
250
300
350
400
Mea
n A
rea,
mm
2
Immediate
160 minute
TE SR DR CL
A
C
E
IGURE 6. (A) Mean contact pressure immediately after repair andmmediately after repair and at 160 minutes. (D) Loss of contact forcF) Loss of contact area over time. (TE, transosseous equivalent.)
act that both techniques had substantial drop-off over c
ime. In addition, we found the TOE construct to havehe greatest contact pressure and force at all timeoints. Similar to conclusions made by Park et al.,9,14
e agree that more distally based placement of lateralnchors linked to the medial row will provide the
0
20
40
60
80
100
TE SR DR CL
minutes. (B) Loss of contact pressure over time. (C) Contact forcetime. (E) Contact area immediately after repair and at 160 minutes.
s
s
s
Perc
ent L
oss
in A
rea,
mm
2
B
D
F
at 160
losest arthroscopic equivalent to an open transosse-

otiifmoestscpOsmwr
iwkivstutlaobisptkmtcdbccetr
1
rctaTfoim1
1
1
1
1
1
598 A. D. MAZZOCCA ET AL.
us repair. This may prove to be beneficial in main-aining appropriate contact for tendon-to-bone heal-ng. Although the CL group is a row-linked construct,t had the greatest percentage drop in contact pressure,orce, and area. The shortcomings of the CL repairay be explained by the linear linkage of rows as
pposed to the oblique linkage of the TOE repair. Parkt al.9 have attributed the superiority of these linkeduture constructs to the fact that oblique suture bridgesraverse a farther distance over the tendon thantraight medial-to-lateral suture bridges. Simple sutureonfigurations tension the tendon itself rather thanrovide a compressive vector toward the footprint.bliquely linking the medial- and lateral-row anchors
eems to add mechanical stability to the repair that isaintained over a period of 160 minutes. It is unclearhether obliquely linking the chain-link rows would
esult in data more comparable to the TOE repair.There are several limitations to this study. First, this
s a cadaveric study with fresh tendons used for repair,hich may not mimic chronic tears in vivo. Second,nots were tied by use of an arthroscopic knot pushern an open environment, which may not replicate an inivo arthroscopic repair. Third, all repairs were ten-ion free, which may not be the case in clinical prac-ice. Although a tension-free repair is desirable, it isnclear what percentage of repairs done clinically isension free. In addition, none of the repairs wasoaded to failure. This was not performed because were currently cycling these repairs at different degreesf abduction and humeral rotation to determine theiomechanical ramifications. By not loading to failure,t is impossible to determine how the individual con-tructs will fail over time. Although all repairs wereerformed by a single surgeon, we did not use aensiometer to ensure equal suture tension when tyingnots for each repair. This may introduce a perfor-ance variable impacting direct comparison across
he different fixation groups. All of the anchors wereemented in place to eliminate any anchor motionuring data collection. However, this may produceetter anchor fixation than could be expected clini-ally. Lastly, we also have a relatively short dataollection period, but we used 160 minutes as thendpoint because this is the average amount of timehat patients are in our surgery center after rotator cuffepair.
CONCLUSIONS
Contact pressure, force, and footprint area decrease
60 minutes after repair regardless of arthroscopicepair technique. The TOE construct had the highestontact pressure and force at all time points. Althoughhe 3 DR constructs had greater pressure and force atll time points compared with the SR repair, only theOE group showed a statistically greater pressure and
orce when compared with SR repair. Oblique linkagef medial-row anchors to lateral-row anchors not onlymproves initial mechanical stability but also bestaintains contact pressure and force over a period of
60 minutes.
REFERENCES
1. Mazzocca AD, Millett PJ, Guanche CA, Santangelo SA, Ar-ciero RA. Arthroscopic single-row versus double-row sutureanchor rotator cuff repair. Am J Sports Med 2005;33:1861-1868.
2. Harryman DT II, Mack LA, Wang KY, Jackins SE, Richard-son ML, Matsen FA III. Repairs of the rotator cuff. Correlationof functional results with integrity of the cuff. J Bone JointSurg Am 1991;73:982-989.
3. Gazielly DF, Gleyze P, Montagnon C. Functional and anatom-ical results after rotator cuff repair. Clin Orthop Relat Res1994:43-53.
4. Galatz LM, Ball CM, Teefey SA, Middleton WD, YamaguchiK. The outcome and repair integrity of completely arthroscopi-cally repaired large and massive rotator cuff tears. J Bone JointSurg Am 2004;86:219-224.
5. Goutallier D, Postel JM, Bernageau J, Lavau L, Voisin MC.Fatty muscle degeneration in cuff ruptures. Pre- and postop-erative evaluation by CT scan. Clin Orthop Relat Res 1994:78-83.
6. Barber FA, Feder SM, Burkhart SS, Ahrens J. The relationshipof suture anchor failure and bone density to proximal humeruslocation: A cadaveric study. Arthroscopy 1997;13:340-345.
7. Liu SH, Baker CL. Arthroscopically assisted rotator cuff re-pair: Correlation of functional results with integrity of the cuff.Arthroscopy 1994;10:54-60.
8. Apreleva M, Ozbaydar M, Fitzgibbons PG, Warner JJ. Rotatorcuff tears: The effect of the reconstruction method on three-dimensional repair site area. Arthroscopy 2002;18:519-526.
9. Park MC, ElAttrache NS, Tibone JE, Ahmad CS, Jun BJ, LeeTQ. Part I: Footprint contact characteristics for a transosseous-equivalent rotator cuff repair technique compared with a dou-ble-row repair technique. J Shoulder Elbow Surg 2007;16:461-468.
0. Lo IK, Burkhart SS. Double-row arthroscopic rotator cuffrepair: Re-establishing the footprint of the rotator cuff. Ar-throscopy 2003;19:1035-1042.
1. Millett PJ, Mazzocca A, Guanche CA. Mattress double anchorfootprint repair: A novel, arthroscopic rotator cuff repair tech-nique. Arthroscopy 2004;20:875-879.
2. Weiler A, Hoffmann RF, Bail HJ, Rehm O, Sudkamp NP.Tendon healing in a bone tunnel. Part II: Histologic analysisafter biodegradable interference fit fixation in a model ofanterior cruciate ligament reconstruction in sheep. Arthroscopy2002;18:124-135.
3. Ahmad CS, Stewart AM, Izquierdo R, Bigliani LU. Tendon-bone interface motion in transosseous suture and suture anchorrotator cuff repair techniques. Am J Sports Med 2005;33:1667-1671.
4. Park MC, Tibone JE, ElAttrache NS, Ahmad CS, Jun BJ, Lee
TQ. Part II: Biomechanical assessment for a footprint-restor-ing transosseous-equivalent rotator cuff repair technique com-
1
1
1
1
1
2
2
2
2
2
2
2
599BIOMECHANICAL EVALUATION OF ROTATOR CUFF REPAIRS
pared with a double-row repair technique. J Shoulder ElbowSurg 2007;16:469-476.
5. Tuoheti Y, Itoi E, Yamamoto N, et al. Contact area, contactpressure, and pressure patterns of the tendon-bone interfaceafter rotator cuff repair. Am J Sports Med 2005;33:1869-1874.
6. Lorbach O, Bachelier F, Vees J, Kohn D, Pape D. Cyclicloading of rotator cuff reconstructions: Single-row repair withmodified suture configurations versus double-row repair. Am JSports Med 2008;36:1504-1510.
7. Juul-Kristensen B, Bojsen-Moller F, Finsen L, et al. Musclesizes and moment arms of rotator cuff muscles determined bymagnetic resonance imaging. Cells Tissues Organs 2000;167:214-222.
8. Remia LF, Ravalin RV, Lemly KS, McGarry MH, Kvitne RS,Lee TQ. Biomechanical evaluation of multidirectional gleno-humeral instability and repair. Clin Orthop Relat Res 2003:225-236.
9. Schneider DJ, Tibone JE, McGarry MH, Grossman MG, Ven-eziani S, Lee TQ. Biomechanical evaluation after five and tenmillimeter anterior glenohumeral capsulorrhaphy using anovel shoulder model of increased laxity. J Shoulder ElbowSurg 2005;14:318-323.
0. Halder AM, O’Driscoll SW, Heers G, et al. Biomechanicalcomparison of effects of supraspinatus tendon detachments,
tendon defects, and muscle retractions. J Bone Joint Surg Am2002;84:780-785.
1. Curtis AS, Burbank KM, Tierney JJ, Scheller AD, Curran AR.The insertional footprint of the rotator cuff: An anatomicstudy. Arthroscopy 2006;22:603-609.e1. Available online atwww.arthroscopyjournal.org.
2. Hildebrand KA, Frank CB, Hart DA. Gene intervention inligament and tendon: Current status, challenges, future direc-tions. Gene Ther 2004;11:368-378.
3. Drewniak EI, Crisco JJ, Spenciner DB, Fleming BC. Accuracyof circular contact area measurements with thin-film pressuresensors. J Biomech 2007;40:2569-2572.
4. Caldwell GL, Warner JP, Miller MD, Boardman D, Towers J,Debski R. Strength of fixation with transosseous sutures inrotator cuff repair. J Bone Joint Surg Am 1997;79:1064-1068.
5. Weiler A, Peine R, Pashmineh-Azar A, Abel C, Sudkamp NP,Hoffmann RF. Tendon healing in a bone tunnel. Part I: Bio-mechanical results after biodegradable interference fit fixationin a model of anterior cruciate ligament reconstruction insheep. Arthroscopy 2002;18:113-123.
6. Wall LB, Keener JD, Brophy RH. Double-row vs single-rowrotator cuff repair: A review of the biomechanical evidence. J
Shoulder Elbow Surg 2009;18:933-941.




























