Embed Size (px)
Citation preview
Gut, 1977, 18, 786-791
Carcinoembryonic antigen (CEA) in the normalhuman small intestine: a light and electronmicroscopic studyP. ISAACSON AND MARY A. JUDD1
From thze Department ofPathology, Faculty of Medicine, General Hospital, Southampton
SUMMARY An immunoperoxidase method for the demonstration of carcinoembryonic antigen(CEA) in tissues was applied to formalin-fixed paraffin embedded and glutaraldehyde-fixed resinembedded sections of normal human small intestine. CEA could easily be demonstrated coating thesurface of the small intestine, lining the crypts, and in goblet cells, indicating its presence there inconsiderable concentration. At the ultrastructural level CEA was localised in the glycocalyx and inmucin granules of goblet cells but not intracytoplasmically.
After the discovery of carcinoembryonic antigen(CEA) by Gold and Freedman (1965) in the serum ofpatients with colorectal cancer, attention was at firstdirected to the association of the antigen with colonicdisorders. Later, studies of serum levels ofCEA werecarried out in a wide variety of neoplastic and non-neoplastic diseases of various organs (Martin et al.,1976).Immunohistochemical demonstration of CEA in
tissues has, like the studies of serum levels, beenlargely confined to the demonstration of antigen incolonic lesions. This is despite the fact that CEA hasbeen successfully extracted from a number of bothnormal and cancerous tissues (Kupchik andZamcheck, 1972; Khoo et al., 1973; Pusztaszeri andMach, 1973; Goldenberg et al., 1976). In the courseof an immunohistochemical study of CEA inulcerative colitis (Isaacson, 1976), strongly positivestaining was noted in metaplastic Paneth cells and,after this, in sections of ileum from an ileorectalanastamosis, where the antigen appeared to be pre-sent in strong concentration along the mucosal cellborder and in goblet cells, as well as in Paneth cellgranules. These chance observations led to a formalstudy of the localisation of CEA in normal humansmall intestine. During the study the positive stainingof Paneth cells proved to be spurious (Isaacson andJudd, 1977) but it became evident that the entiresurface of the normal jejunum and ileum is coatedwith CEA where it stains with an intensity similar tocolorectal cancer.
'Some of the work described in this paper will form part of athesis for Fellowship of the Institute of Medical LaboratoryScientists.Received for publication 28 February 1977
The ease with which CEA could be demonstrated infreely available normal tissue at the light microscopelevel led to attempts to demonstrate CEA in tissuesat the ultrastructural level. Ultrastructually CEA ispresent in the glycocalyx of the small intestine and inthe mucin granules of immature and mature gobletcells.
Methods
LIGHT MICROSCOPYTwenty-seven biopsies of normal adult small intestine(22 jejunal and five ileal) were studied. These wereobtained either by peroral biopsy or by resection atlaparotomy for disorders not primarily affecting thesmall intestine-for example, gastroenterostomy forpeptic ulcer. Tissues were fixed in formol saline androutinely processed into paraffin blocks; 5 ,um sec-tions were stained for CEA by the indirect immuno-peroxidase technique as described elsewhere(Isaacson and Judd, 1977). Endogenous peroxidaseand non-specific cross-reacting glycoproteins wereinhibited using 1% periodic acid. After demonstrat-ing abolition of staining by absorption of antiCEAwith purified CEA in two cases, negative controlsconsisted of a duplicate section stained with sub-stitution of normal goat serum for goat antiCEA.Positive controls, consisting of the same section ofcolon carcinoma, were included in each staining run.
SEMI-THIN SECTIONS AND ELECTRONMICROSCOPYOf the 27 cases used for light microscopy portions ofsix were cut fresh into 1 mm3 cubes and fixed in 5 %glutaraldehyde at 40 for four to 12 hours. The blocks
786
on February 3, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.18.10.786 on 1 O
ctober 1977. Dow
nloaded from

Carcinoembryonic antigen (CEA) in the normal human small intestine
were dehydrated in several changes of acetone, ~ ...>.... :: .: ~~infiltrated with an acetone/Spurr resin mixture in a AIReichert tissue processr and finally embedded inSpurr resin blocks (Wallis and Griffin, 1973). Tissueswere not treated with osmium tetroxide or uranylacetate at this stage. Sections (1 /.tm) were cut andstained with toluidine blue to locate relevant areas forthin sectioning. These semi-thin sections were also .stained for CEA after removal of the resin by etchingwith sodium methoxide according to the method ofMayor et al. (1961). The staining procedure was thesame as that previously described for light micro-~~~scopy (Isaacson and Judd, 1977) except that the first Vtwo steps were omitted.
After the blocks had been trimmed, 60-80 nm thinsections were cut and collected on nickle grids. These IY~were etched with 5% 14202 and then stained for CEA ..by floating the grids on the relevant reagents con-tamned in small plastic wells enclosed in a moistchamber. After step 7 of the staining procedure thegrids were stained with -1 04 osmium tetroxide for 10minutes and counterstained with lead citrate. Gridswere then examined using a Phillips 201 electron -microscope.
Controls for semi-thin and thin sections were the -~-same as those used for light microscopy.
~~~~~~Fig 2 Glutaraldehyde-fixed, resin embedded 1 pAmsection of normal ileum stainedfor CEA. Goblet cellstaining is much more marked than in paraffin
- ~~~~~embedded sections. x 100.
Results
~~~ ~~LIGHT MICROSCOPYThere was strongly positive staining over the surfaceof villou s epithelium, intensifying as a lumenal borderin the crypts (Fig. 1). Goblet cells stained variablyand in some sections mucous adherent to the mucosa
~ also showed positive staining. The surface staining of- ~~epithelial cells persisted into high dilutions of goat
- ~~~antiCEA (up to 3200) Positive control sections of
colon carcinoma stained as previously described with
staining -persisting up to a 2 dilution of goat anti-
CEA. No staining was observed in negative controls.
- - ~~~~~SEMI-THIN SECTIONS AND ELECTRON
Fig. 1 Formalin-fixed, paraffin embedded section of MICROSCOPYnormal human jejunum stained for CEA with positive In semi-thin (1 pm) sections the surface of the brushstaining of the epithelial surface, crypt borders and goblet border of the villi stained strongly for CEA withcells. x 100. intensification along the lumenal border of crypts. In
787
on February 3, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.18.10.786 on 1 O
ctober 1977. Dow
nloaded from

Fig. 3 High powtver view of same section illustrated inFig. 2. Note the granular staining ofgoblet cells. CEA ispresent as a band along the surface of the brush border.x 100.
these thinner sections goblet cells always stained,often in a granular fashion (Figs. 2, 3). Despite thefact that 1% periodic acid was not used in the stain-ing procedure, endothelium, red blood cells, andPaneth cell granules did not stain. Negative controlsections did not stain.At the ultrastructural level (Figs. 4, 5, 6) a band of
strong staining was evident along the tips of themicrovilli with incorporation of the tips of the micro-villi into this band. There was intensification ofstaining between the microvilli. Mucin granules inmature and immature goblet cells stained stronglypositive and positively staining granules could beseen streaming out of surface goblet cells. Thus, thepositive band across the tips of microvilli appeared
Fig. 4 (a) Ultrastructural demonstration of CEA injejunal mucosa. Goblet cell granules are strongly positiveand CEA positive material is seen streaming out of thecell. CEA positive glycocalyx fuses with goblet cellcontents. (b) Same area stained, substituting normal goatserum for goat antiCEA, with negative result. The smalldark granules are artefact caused by lead citrate deposits.x 9000.
(a) (b)
on February 3, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.18.10.786 on 1 O
ctober 1977. Dow
nloaded from
Carcinoembryonic antigen (CEA) ini the normal human small intestinel
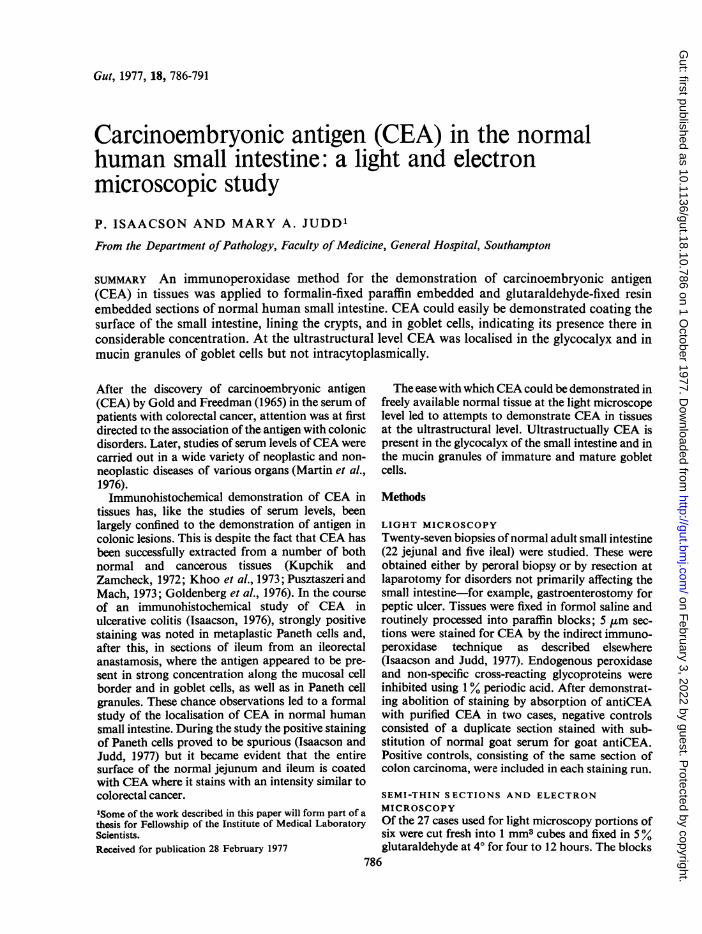
(a) (b)Fig. 5 (a) Intestinal crypt showing less mature goblet cells staining positively for CEA with positive staining ofglycocalyx. (b) Control section stained with normal goat serum is negative. x 2500.
to be largely separate from material escaping fromgoblet cells, although some fusion of positive mat-erial was evident. No intracytoplasmic staining wasevident in any of the epithelial cells and, as in thesemi-thin sections, no endothelial, red blood cell,or Paneth cell staining was observed. In grids usingnormal goat serum there was no staining of the gob-let cells or the tips of the microvilli. A faint band in-corporating the tips of the microvilli could beappreciated.
Discussion
CEA has previously been demonstrated immuno-histochemically in a number of epithelial malignan-cies, including colorectal cancer, and in normal colon(Goldenberg et al., 1976; Huitric et al., 1976;Isaacson, 1976). It has also been extracted from theseand some other normal tissues (Khoo et al., 1973;Goldenberg et al., 1976). While CEA has beendemonstrated in foci of intestinal metaplasia in thestomach (Burtin et al., 1973) there have been no pre-vious attempts to demonstrate CEA in the normal
human small intestine. This is surprising when thelarge amount of CEA present in human faeces isconsidered. Not only is it unlikely that this amountof CEA is derived from the small amounts shown tobe present in colonic epithelium (Khoo et al., 1973),but, if it were, then the presence of colonic carci-noma, which contains 10-100 x more CEA than nor-mal colon, should raise faecal levels of CEA, but, asshown by Elias et al. (1974) this is not the case.Furthermore, Elias et al. found that the CEA con-tent from an ileostomy drainage was equal to that infaeces from normal patients. Additional evidence forthe production ofCEA by small intestinal epitheliumis found in a study of patients with bladder carci-noma. Hall et al. (1973) noted that the urine fromileal conduits contained large amounts of CEA ascompared with urine samples taken directly from theureters of these patients. The ease with which CEAcan be demonstrated in the small intestine is yetanother indication of the high CEA content of thesmall intestine since Goldenberg et al. (1976) haveshown that the ease with which CEA can be demon-strated immunohistochemically is proportional to
789
on February 3, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.18.10.786 on 1 O
ctober 1977. Dow
nloaded from
P. Isaacson and Mary A. Judd
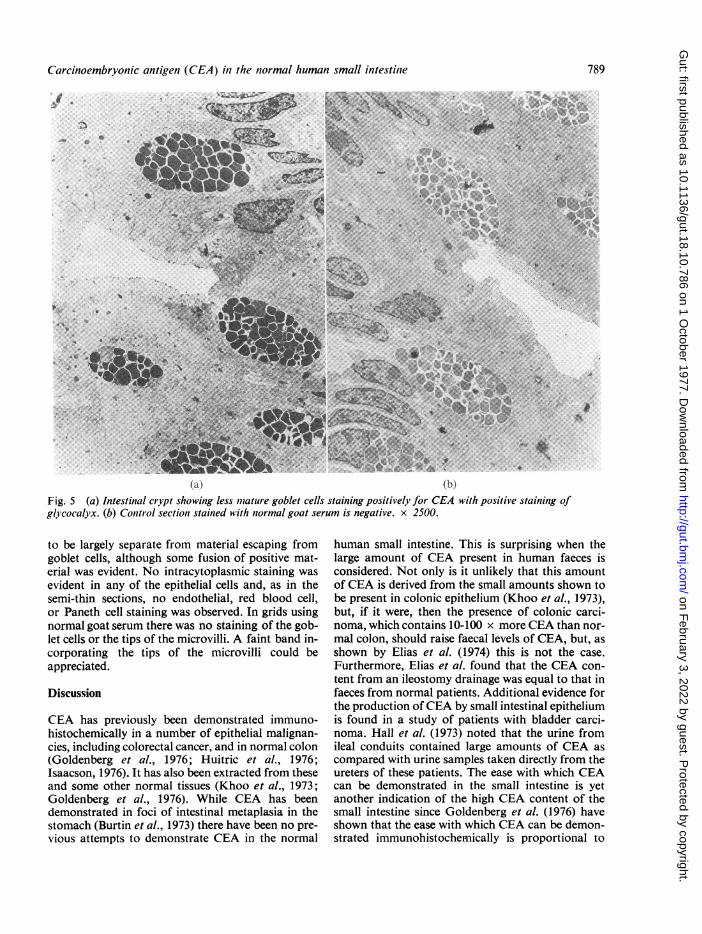
(a) (b)Fig. 6 (a) Microvilli ofjejunum showing incorporation of the tips into a CEA positive band. There is intensification ofstaining between the villi. (b) Control section stained with normal goat serum. A faint electron dense bandincorporates the tips of the microvilli. x 112 000.
the tissue concentration. The present study, there-fore, indicates that the epithelium of the small intes-tine is manufacturing CEA in amounts similar to thatof colorectal cancer, but, unlike CEA from colorectalcancer, some of which finds its way into the bloodstream, small intestinal CEA is mostly shed into thelumen of the gut. Given that the entire adult humansmall inestine is so well coated with CEA, this canhardly be designated an oncofetal antigen. Moreprobably, as has already been suggested by others(Neville and Laurence, 1974), CEA is related to celldivision in some way, being associated with rapidlydividing epithelial tissues. Further study on the bio-logical functions ofCEA would seem to be indicated.CEA has been previously demonstrated in semi-
thin and thin sections of normal colon and coloniccarcinoma (Huitric, 1973; Huitric et al., 1976). Themethods used have been extremely complex, employ-ing special fixatives and, for ultrastructural studies,blocks were prestained as frozen sections beforebeing processed for electron microscopy. For thesestudies undiluted antisera were necessary and the
results, while in some ways similar to those of thepresent study, contained some surprising differences,not the least being the negative staining of coloniccarcinoma in light microscope preparations. Themethods used in our investigation of the small intes-tine are extremely simple and reproducible. We feelthat this is principally because we used Nakane andKawaoi's (1974) method for preparing peroxidaseconjugates, as we found that when we used com-mercially supplied conjugates, prepared byglutaraldehyde coupling, the sensitivity dropped offdramatically.
It is interesting that the preparation of semi-thinand thin sections inhibited the cross-reaction of anti-CEA with other tissue glycoproteins as describedpreviously (Isaacson and Judd, 1977). It was, in fact,this observation that led to the formal study of theimmunohistochemical cross-reactivity of CEA. Re-agents used for etching the resin were tested andfound not to inhibit these reactions. Thus the pro-cess of resin embedding had the same effect as pre-treating sections with 1% periodic acid. As no single
790
on February 3, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.18.10.786 on 1 O
ctober 1977. Dow
nloaded from

Carcinoembryonic antigen (CEA) in the normal human small intestine 791
reagent used in resin embedding was found to act inthis way we must assume that some combination ofreagents or resin polymerisation was responsible.The glycocalyx is usually described as a fuzzy layer
above the microvilli (Toner et al., 1971). No suchlayer was present in our ultrastructural preparationsand instead a band appeared to incorporate the tipsof the microvilli. We feel that this can only be theglycocalyx and that its slightly different position iscaused by the different preparation and subsequentmanipulation of the thin sections. Previous studies,using radiolabelled carbohydrates (Bennett, 1970;Bennett and Leblond, 1970) have indicated that theglyco-protein destined for the glycocalyx is synthe-sised in the Golgi apparatus from which it migratesinto its final position. The restriction ofCEA stainingto the goblet cell and glycocalyx suggests an alterna-tive possibility-namely, that the glycocalyx, or partof it, is derived from the goblet cell. We have beenunable to demonstrate true intracytoplasmic CEA,the glycocalyx and mucin granule being, in effect,extracellular structures. At the light microscopelevel, CEA has been shown to be present intra-cytoplasmically in medullary carcinoma of thethyroid (Isaacson and Judd, 1976) and ultrastructuralstudies of this tumour may be more rewarding inestablishing the site of CEA synthesis.
We are indebted to Professor D. H. Wright for hisadvice and to Mrs Olive Huber for secretarialassistance.
References
Bennett, G. (1970). Migration of glycoprotein from golgiapparatus to cell coat in the columnar cells of the duodenalepithelium. Journal of Cell Biology, 45, 668-673.
Bennett, G., and Leblond, C. P. (1970). Formation of cellcoat material for the whole surface of columnar cells in therat small intestine, as visualized by radioautography withl-Fucose-3H. Journal of Cell Biology, 46, 409-416.
Burtin, P., von Kleist, S., Sabine, M. C., and King, M.(1973). Immunohistological localization of carcinoem-bryonic antigen and non-specific cross-reacting antigen ingastrointestinal normal and tumoral tissues. Cancer Re-search, 33, 3299-3305.
Elias, E. G., Holyoke, E. D., and Chu, T. Ming. (1974).Carcinoembryonic antigen (CEA) in feces and plasma ofnormal subjects and patients with colorectal carcinoma.Diseases of Colon and Rectum, 17, 38-41.
Gold, P., and Freedman, S. 0. (1965). Specific carcino-embryonic antigens of the human digestive system.
Journal of Experimental Medicine, 122, 467-481.Goldenberg, D. M., Sharkey, R. M., and Primus, F. J. (1976).
Carcinoembryonic antigen in histopathology: immuno-peroxidase staining of conventional tissue sections. Journalof the National Cancer Institute, 57, 11-22.
Hall, R. R., Laurence, D. J. R., Neville, A. M., and Wallace,D. M. (1973). Carcinoembryonic antigen and urothelialcarcinoma. British Journal of Urology, 45, 88-92.
Huitric, E. (1973). An ultrastructural study of the localizationof the carcinoembryonic antigen in adenocarcinomas of thehuman colon. Annales d'Immunologie (Institut Pasteur),124 C, 603-608.
Huitric, E., Laumonier, R., Burtin, P., von Kleist, S., andChavanel, G. (1976). An optical and ultrastructural studyof the localization of carcinoembryonic antigen (CEA) innormal and cancerous human rectocolonic mucosa.Laboratory Investigation, 34, 97-107.
Isaacson, P. (1976). Tissue demonstration of carcino-embryonic antigen (CEA) in ulcerative colitis. Gut, 17, 561-567.
Isaacson, P., and Judd, M. A. (1976). Carcinoembryonicantigen in medullary carcinoma of thyroid. Lancet, 2, 1016-1017.
Isaacson, P., and Judd, M. A. (1977). Immunohistochemistryof carcinoembryonic antigen: characterisation of cross-reactions with other glycoproteins. Gut. 18, 779-785.
Khoo, S. K., Warner, N. L., Lie, J. T., and MacKay, I. R.(1973). Carcinoembryonic antigenic activity of tissueextracts: quantitative study of malignant and benign neo-plasms, cirrhotic liver, normal adult and fetal organs.International Journal of Cancer, 11, 681-687.
Kupchik, H. Z., and Zamcheck, N. (1972). Carcinoembryonicantigen(s) in liver diseases. Isolation from human cirrhoticliver and serum and from normal liver. Gastroenterology,63,95-101.
Martin, E. W. Jr., Kibbey, W. E., DiVecchia, L., Anderson,G., Catalano, P., and Minton, J. P. (1976). Carcino-embryonic antigen, clinical and historical aspects. Cancer,37, 62-81.
Mayor, H. D., Hampton, J. C., and Rosario, B. (1961). Asimple method for removing the resin from epoxy-embedded tissue. Journal of Biophysical and BiochemicalCytology, 9, 909-910.
Nakane, P. K., and Kawaoi, A. (1974). Peroxidase-labeledantibody. A new method of conjugation. Journal ofHistochernistry and Cytochemistry, 22, 1084-1091.
Neville, A. M., and Laurence, D. J. R. (1974). Report of theworkshop on the carcinoembryonic antigen (CEA): thepresent position and proposals for future investigation.International Journal of Cancer, 14, 1-18.
Pusztaszeri, G., and Mach, J-P. (1973). Carcinoembryonicantigen (CEA) in non-digestive cancerous and normal tis-sues. Immunochemistry, 10, 197-204.
Toner, P. G., Carr, K. E., and Wyburn, G. M. (1971). TheDigestive System-An Ultrastructural Atlas and Review.Butterworth: London.
Wallis, M. A., and Griffin, R. L. (1973). A routine method forembedding animal tissues in Spurr resin for electronmicroscopy. Journal of Clinical Pathology, 26, 77-78.
on February 3, 2022 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.18.10.786 on 1 O
ctober 1977. Dow
nloaded from





























