Embed Size (px)
Citation preview
CARDIOVASCULAR HEALTH BENEFITS OF VEGETABLES AND THEIR
COMPONENTS
Lauren Blekkenhorst
BHSc (Hons), RNutr
This thesis is presented for the degree of
DOCTOR OF PHILOSOPHY
The University of Western Australia
Medical School
2018
1 THESIS DECLARATION
THESIS DECLARATION I, Lauren Blekkenhorst, certify that:
This thesis has been substantially accomplished during enrolment in the degree.
This thesis does not contain material which has been submitted for the award of any other degree or diploma in my name, in any university or other tertiary institution.
No part of this work will, in the future, be used in a submission in my name, for any other degree or diploma in any university or other tertiary institution without the prior approval of The University of Western Australia and where applicable, any partner institution responsible for the joint-award of this degree.
This thesis does not contain any material previously published or written by another person, except where due reference has been made in the text and, where relevant, in the Declaration that follows.
The work(s) are not in any way a violation or infringement of any copyright, trademark, patent, or other rights whatsoever of any person.
The research involving human data reported in this thesis was assessed and approved by The University of Western Australia Human Research Ethics Committee. Approval #: RA/4/1/6782.
The work described in this thesis was funded by the National Health and Medical Research Council of Australia. Project grant #: 1084922.
This thesis contains published work and/or work prepared for publication, some of which has been co-authored.
Signature:
Date: 15/03/2018

2 ABSTRACT
ABSTRACT BACKGROUND
Despite great advances in cardiovascular medicine and the reduction in cardiovascular disease (CVD) mortality, CVD remains the leading cause of global mortality. Large epidemiological studies have shown plant-based diets, rich in vegetables, are consistently associated with lower CVD risk. Recent evidence suggests greater benefit of some vegetable types, demonstrating substantially larger health benefits in comparison to other vegetables, implying not all vegetables are the same. For example, there is some evidence to suggest leafy green, cruciferous, and allium vegetable types are among the most beneficial.
A second theme in nutrition science is the concept that bioactive compounds found in vegetables may benefit cardiovascular health. One bioactive comound that has gained research interest in the last decade is nitrate.
Nitrate is present in all vegetables; however, the richest sources are leafy green vegetables. Consumption of nitrate-rich vegetables is one strategy to increase nitric oxide (NO). This occurs via the enterosalivary nitrate-nitrite-NO pathway. Nitric oxide plays an important role in vascular tone and integrity, and is a vital molecule for cardiovascular health.
One major physiological measure related to CVD is blood pressure. Although there is strong evidence to suggest nitrate-rich vegetables can lower blood pressure within hours of ingestion, it is yet to be established whether the effects of a sustained increase in nitrate-rich vegetables lowers blood pressure. Furthermore, there are very few epidemiological studies linking nitrate from vegetables with reduced long-term CVD risk.
THIS THESIS
Objectives
The overarching objective of this thesis was to investigate the cardiovascular health benefits of different types of vegetables and their bioactive compounds, in particular, nitrate.
Perth Longitudinal Study of Ageing in Women
The majority of studies reported in this thesis (Chapters 3, 4, 6 and 7) were conducted using data from the Perth Longitudinal Study of Ageing Women (PLSAW). The PLSAW is a 15-year longitudinal study investigating the role of diet and lifestyle factors on health outcomes in a cohort of older women living in Perth, Western Australia.
Outline
Chapter 1 of this thesis is a brief narrative review discussing current literature on the cardiovascular health benefits of different types of vegetables. Vegetable types discussed are leafy green, cruciferous, allium, yellow-orange-red, and legumes. Chapter 2 is a systematic literature review providing an extensive overview of the effects of nitrate ingestion on blood pressure, arterial stiffness, endothelial function, platelet function, and cerebral blood flow in human and animal studies. Observational epidemiologic studies on cardiovascular-related clinical outcomes were also reviewed. The literature was systematically searched using

3 ABSTRACT
Medline and EMBASE databases. Evidence suggests that the beneficial effect of nitrate ingestion in humans at CVD risk is unclear, and that there is a need to investigate the long-term effects of dietary nitrate on CVD clinical endpoints. Chapter 3 reports the results of an epidemiological study investigating the associations of total vegetable intake as well as types of vegetables, grouped according to phytochemical constituents, with atherosclerotic vascular disease (ASVD) mortality over 15 years of follow-up. Higher cruciferous and allium vegetable intakes were independently associated with a lower risk of ASVD mortality. In Chapter 4, we extend on these findings to report on the associations of total vegetable intake and intake of specific types of vegetables, grouped according to phytochemical constituents, with subclinical atherosclerosis. The results of this study indicate that increasing vegetables in the diet with a focus on consuming cruciferous vegetables may have benefits for slowing the progression of atherosclerosis in older women. Chapter 5 reports on the development of a reference database for assessing nitrate in vegetables. Prior to the development of this database there was no assessment tool available to researchers that had systematically collected information on the measured nitrate content of vegetables. The development of this vegetable nitrate database has allowed for the improvement of nitrate intake estimation. In Chapter 6, we use this database and report on the relationship of vegetable nitrate intake and ASVD mortality. Vegetable nitrate intake was inversely associated with ASVD mortality independent of lifestyle and cardiovascular risk factors. These results support the concept that nitrate-rich vegetables may reduce the risk of age-related ASVD mortality in older women. In Chapter 7, we extend on these results and report on the relationship of vegetable nitrate intake with subclinical atherosclerosis and ischaemic cerebrovascular disease events. Independent of other risk factors, higher vegetable nitrate was associated with lower measures of subclinical atherosclerosis and lower risk of ischemic cerebrovascular disease events. These nitrate studies are the first evidence to suggest vegetable nitrate intake lowers the risk of long-term vascular disease. Chapter 8 reports on the results of a 4-week randomised controlled crossover trial investigating the effects of nitrate-rich and nitrate-poor vegetables on blood pressure and arterial stiffness in pre-hypertensive or untreated grade 1 hypertensive individuals. Increased intake of nitrate-rich vegetables did not lower blood pressure or arterial stiffness when compared with increased intake of nitrate-poor vegetables and no increase in vegetables. Chapter 9 provides an overview of the main findings of this thesis. Future directions of research are also discussed.
4 TABLE OF CONTENTS
TABLE OF CONTENTS
THESIS DECLARATION .................................................................................................................................. 1
ABSTRACT ..................................................................................................................................................... 2
ACKNOWLEDGEMENTS ............................................................................................................................... 5
AUTHORSHIP DECLARATION: CO-AUTHORED PUBLICATIONS ............................................................... 6
PUBLICATIONS, PRESENTATIONS AND AWARDS ...................................................................................... 9
CHAPTER 1 .................................................................................................................................................. 14
CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW .... 14
CHAPTER 2 .................................................................................................................................................. 38
NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES ............................................................................................ 38
CHAPTER 3 .................................................................................................................................................. 77
CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN ................................... 77
CHAPTER 4 ................................................................................................................................................ 103
CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN .................................................................................... 103
CHAPTER 5 ................................................................................................................................................ 126
DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES 126
CHAPTER 6 ................................................................................................................................................ 175
ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN ............................................................... 175
CHAPTER 7 ................................................................................................................................................ 194
ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN .............................................................................. 194
CHAPTER 8 ................................................................................................................................................ 212
NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL .......... 212
CHAPTER 9 ................................................................................................................................................ 244
OVERVIEW AND FUTURE DIRECTIONS ................................................................................................... 244
REFERENCES ............................................................................................................................................. 250
5 ACKNOWLEDGEMENTS
ACKNOWLEDGEMENTS
Firstly, my supervisors (Professor Jonathan Hodgson, Professor Richard Prince, Professor Amanda Devine and Dr Joshua Lewis), thank you for your patience, your guidance, your wisdom, your knowledge, and for making this journey possible. You have all taught me so much in so many different areas of nutrition, cardiovascular disease, epidemiology, clinical trials, biostatistics, and the journey of life. You gave me the push when I needed it, the courage to keep going when I thought of giving up, and the determination to try to make this world a better place.
Secondly, I would like to extend my most sincere thanks and appreciation to all my colleagues from the Medical Research Foundation at Royal Perth Hospital. I could not have done this without every single one of you. The list is too long, but you know who you are. I also would like to extend my sincere thanks and appreciation to all my mentors and collaborators that have co-authored the publications in this thesis. Thank you.
Thirdly, the study participants. Without you, this thesis would not be possible.
Fourthly, Michael. You are my rock. Thank you for supporting me. Thank you for loving me.
This research was supported by an Australian Government Research Training Program (RTP) Scholarship and The University of Western Australia Safety Net Top-Up Scholarship.
6 AUTHORSHIP DECLARATION: CO-AUTHORED PUBLICATIONS
AUTHORSHIP DECLARATION: CO-AUTHORED PUBLICATIONS
This thesis contains work that has been published and/or prepared for publication.
Details of the work:
Cardiovascular health benefits of specific vegetable types: a narrative review
Location in thesis:
Chapter 1
Student contribution to work:
Protocol development, literature search, manuscript drafting, and manuscript revisions.
Details of the work:
Nitrate, the oral microbiome and cardiovascular health: a systematic literature review of human and animal studies
Location in thesis:
Chapter 2
Student contribution to work:
Protocol development, systematic literature search, manuscript drafting, manuscript revisions, and manuscript submission (not including oral microbiome and animal sections).
Details of the work:
Cruciferous and allium vegetable intakes are inversely associated with 15-year atherosclerotic vascular disease deaths in older adult women
Location in thesis:
Chapter 3
Student contribution to work:
Study design, protocol development, statistical analyses and interpretation, manuscript drafting, manuscript revisions, and manuscript submission.
Details of the work:
Cruciferous and total vegetable intakes are inversely associated with subclinical atherosclerosis in older adult women
Location in thesis:
Chapter 4
7 AUTHORSHIP DECLARATION: CO-AUTHORED PUBLICATIONS
Student contribution to work:
Study design, protocol development, statistical analyses and interpretation, manuscript drafting, manuscript revisions, and manuscript submission.
Details of the work:
Development of a reference database for assessing dietary nitrate in vegetables
Location in thesis:
Chapter 5
Student contribution to work:
Protocol development, systematic literature search, statistical analyses and interpretation, manuscript drafting, manuscript revisions, and manuscript submission.
Details of the work:
Association of dietary nitrate with atherosclerotic vascular disease mortality: a prospective cohort study of older adult women
Location in thesis:
Chapter 6
Student contribution to work:
Study design, protocol development, statistical analyses and interpretation, manuscript drafting, manuscript revisions, and manuscript submission.
Details of the work:
Association of vegetable nitrate intake with carotid atherosclerosis and ischaemic cerebrovascular disease in older women
Location in thesis:
Chapter 7
Student contribution to work:
Statistical analyses and interpretation, manuscript drafting, manuscript revisions, and manuscript submission.
Details of the work:
Nitrate-rich vegetables do not lower blood pressure in individuals with mildly elevated blood pressure: a 4-week randomised controlled crossover trial
Location in thesis:
Chapter 8
8 AUTHORSHIP DECLARATION: CO-AUTHORED PUBLICATIONS
Student contribution to work:
Study concept and design, ethics application, participant recruitment, study coordination, data acquisition, data analysis and interpretation, manuscript drafting, manuscript revisions, and manuscript submission.
Student signature:
Date: 15/03/2018
I, Professor Jonathan Hodgson, certify that the student statements regarding their contribution to each of the works listed above are correct
Coordinating supervisor signature:
Date: 15/03/2018
9 PUBLICATIONS, PRESENTATIONS AND AWARDS
PUBLICATIONS, PRESENTATIONS AND AWARDS
PUBLICATIONS ARISING FROM THIS THESIS
Blekkenhorst LC, Sim M, Bondonno CP, Bondonno NP, Ward NC, Prince RL, Devine A, Lewis JR, Hodgson JM. Cardiovascular health benefits of specific vegetable types: a narrative review. Nutrients. 2018;10(5):1-24.
Blekkenhorst LC*, Bondonno NP*, Liu AH, Ward NC, Prince RL, Lewis JR, Devine A, Croft KD, Hodgson JM, Bondonno CP. Nitrate, the oral microbiome and cardiovascular health: a systematic literature review of human and animal studies. American Journal of Clinical Nutrition. 2018;107(4):504-522. *Joint first author
Blekkenhorst LC, Bondonno CP, Lewis JR, Devine A, Zhu K, Lim WH, Woodman RJ, Beilin LJ, Prince RL, Hodgson JM. Cruciferous and allium vegetable intakes are inversely associated with 15-year atherosclerotic vascular disease deaths in older adult women. Journal of the American Heart Association. 2017;6(10):1-15.
Blekkenhorst LC, Bondonno CP, Lewis JR, Woodman RJ, Devine A, Bondonno NP, Lim WL, Zhu K, Beilin LJ, Thompson PL, Prince RL, Hodgson JM. Cruciferous and total vegetable intakes are inversely associated with subclinical atherosclerosis in older adult women. Journal of the American Heart Association. 2018;7(8):1-13.
Blekkenhorst LC, Prince RL, Ward NC, Croft KD, Lewis JR, Devine A, Shinde S, Woodman RJ, Hodgson JM, Bondonno CP. Development of a reference database for assessing dietary nitrate in vegetables. Molecular Nutrition & Food Research. 2017;61(8):1-13.
Blekkenhorst LC, Bondonno CP, Lewis JR, Devine A, Woodman RJ, Croft KD, Lim WH, Wong G, Beilin LJ, Prince RL, Hodgson JM. Association of dietary nitrate with atherosclerotic vascular disease mortality: a prospective cohort study of older adult women. American Journal of Clinical Nutrition. 2017;106(1):207-216.
Bondonno CP*, Blekkenhorst LC*, Prince RL, Ivey KL, Lewis JR, Devine A, Woodman RJ, Lundberg JO, Croft KD, Thompson PL, Hodgson JM. Association of vegetable nitrate intake with carotid atherosclerosis and ischemic cerebrovascular disease in older women. Stroke. 2017;48(7):1724-1729. *Joint first author
Bondonno CP, Blekkenhorst LC, Hodgson JM. Response to letter regarding article, "Association of vegetable nitrate intake with carotid atherosclerosis and ischemic cerebrovascular disease in older women". Stroke. 2017;48(10):e305.
Blekkenhorst LC, Lewis JR, Prince RL, Devine A, Bondonno NP, Bondonno CP, Wood LG, Puddey IB, Ward NC, Croft KD, Woodman RJ, Beilin LJ, Hodgson JM. Nitrate-rich vegetables do not lower blood pressure in individuals with mildly elevated blood pressure: a randomised controlled crossover trial. American Journal of Clinical Nutrition. 2018;107(6):894-908.
10 PUBLICATIONS, PRESENTATIONS AND AWARDS
PUBLICATIONS NOT ARISING FROM THIS THESIS BUT PUBLISHED DURING CANDIDATURE
Bondonno CP, Blekkenhorst LC, Liu AH, Bondonno NP, Ward NC, Croft KD, Hodgson JM. Vegetable-derived bioactive nitrate and cardiovascular health. Molecular Aspects of Medicine. 2018;61:83-91.
Bondonno NP, Bondonno CP, Blekkenhorst LC, Considine MJ, Maghzal G, Stocker R, Woodman RJ, Ward NC, Hodgson JM, Croft KD. Flavonoid-rich apple improves endothelial function in individuals at risk for cardiovascular disease: a randomized controlled clinical trial. Molecular Nutrition & Food Research. 2018;62(3):1-10.
Blekkenhorst LC, Hodgson JM, Lewis JR, Devine A, Woodman RJ, Lim WH, Wong G, Zhu K, Bondonno CP, Ward NC, Prince R. Vegetable and fruit intake and fracture-related hospitalisations: a prospective study of older women. Nutrients. 2017;9(5):1-15.
Muka T*, Blekkenhorst LC*, Lewis JR, Prince RL, Erler NS, Hofman A, Franco OH, Rivadeneira F, Kiefte-de Jong JC. Dietary fat composition, total body fat and regional body fat distribution in two Caucasian populations of middle-aged and older adult women. Clinical Nutrition. 2017;36(5):1411-1419. *Joint first author
Bondonno NP, Lewis JR, Blekkenhorst LC, Shivappa N, Woodman RJ, Bondonno CP, Ward NC, Hébert JR, Thompson PL, Prince RL, Hodgson JM. Dietary inflammatory index in relation to sub-clinical atherosclerosis and atherosclerotic vascular disease mortality in older women. British Journal of Nutrition. 2017;117(11):1577-1586.
Blekkenhorst LC, Prince RL, Hodgson JM, Lim WH, Zhu K, Devine A, Thompson PL, Lewis JR. Dietary saturated fat intake and atherosclerotic vascular disease mortality in elderly women: a prospective cohort study. American Journal of Clinical Nutrition. 2015;101(6):1263-1268.
11 PUBLICATIONS, PRESENTATIONS AND AWARDS
PRESENTATIONS
ORAL
2017 10th Asia Pacific Conference on Clinical Nutrition, Adelaide, Australia
Nitrate-rich and nitrate-poor vegetables do not lower blood pressure in individuals with mildly elevated blood pressure: a randomised controlled crossover trial
2017 Sir Charles Gairdner and Osborne Park Health Care Group, Research Week, Perth, Australia
Cruciferous and allium vegetable intakes are inversely associated with 15-year atherosclerotic vascular disease deaths in older adult women
2017 University of Western Australia Institute of Agriculture, Postgraduate Showcase, Frontiers in Agriculture, Perth, Australia
Cardiovascular health benefits of vegetables and their components
2017 Medical Research Foundation Scientific Interchange with Dr Chris Smith of ‘The Naked Scientists’, Perth, Australia
Cardiovascular health benefits of vegetables and their components
2017 Nutrition Society of Australia 2017 Perth Annual General Meeting, Perth, Australia
Cardiovascular health benefits of vegetables and their components
2016 University of Western Australia Medical School, Seminar Series, Perth, Australia
Cardiovascular health benefits of vegetables and their components
2016 Nutrition Society of Australia 2016 Annual Scientific Meeting, Melbourne, Australia
Quantity, type and diversity of vegetable intake and atherosclerotic vascular disease mortality: a prospective cohort study
2016 Royal Perth Hospital & Medical Research Foundation, Research Day, Perth Australia
The association of dietary nitrate with atherosclerotic vascular disease mortality: a prospective cohort study of older women
2016 Australian Society for Medical Research, Medical Research Week, Scientific Symposium, Perth, Australia
Dietary nitrate and cardiovascular mortality in elderly women: a prospective cohort study
2015 Joint Annual Scientific Meeting of the Nutrition Society of New Zealand and the Nutrition Society of Australia, Wellington, New Zealand
Green leafy vegetables and cardiovascular mortality in elderly women: a prospective cohort study
2015 Australian Atherosclerosis Society Annual Scientific Meeting, Perth, Australia
12 PUBLICATIONS, PRESENTATIONS AND AWARDS
Green leafy vegetables and cardiovascular mortality in elderly women: a prospective cohort study
2015 Royal Perth Hospital & Medical Research Foundation, Research Day, Perth, Australia
Green leafy vegetables and cardiovascular mortality in elderly women: a prospective cohort study
POSTER
2017 Sir Charles Gairdner and Osborne Park Health Care Group, Research Week, Perth, Australia
Cruciferous and allium vegetable intakes are inversely associated with 15-year atherosclerotic vascular disease deaths in older adult women
2016 Nutrition Society of Australia 2016 Annual Scientific Meeting, Melbourne, Australia
Nitrate intake and atherosclerotic vascular disease mortality: a prospective cohort study
2016 26th Annual Combined Biological Sciences Meeting, Perth, Australia
Nitrate intake and atherosclerotic vascular disease mortality: a prospective cohort study
Quantity, type and variety of vegetable intake and atherosclerotic vascular disease mortality: a prospective cohort study
13 PUBLICATIONS, PRESENTATIONS AND AWARDS
AWARDS
2017 Edith Cowan University Research Collaboration Travel Grant
2017 Sir Charles Gairdner Hospital New Investigator Award
2017 Nutrition Society of Australia Travel Grant
2016 The University of Western Australia Graduate Research Student Travel Award
2016 Nutrition Society of Australia Travel Grant
2015 Nutrition Society of Australia Travel Grant
2014 Nutrition Society of Australia Travel Grant
2014 The University of Western Australia Top-Up Scholarship
2014 Australian Postgraduate Award
14 CHAPTER 1
CHAPTER 1
CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Manuscript based on this chapter:
Lauren C Blekkenhorst, Marc Sim, Catherine P Bondonno, Nicola P Bondonno, Natalie C Ward, Richard L Prince, Amanda Devine, Joshua R Lewis, Jonathan M Hodgson. Cardiovascular health benefits of specific vegetable types: a narrative review. Nutrients. 2018;10(5):1-24.

15 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
ABSTRACT
Adequate vegetable consumption is one of the cornerstones of a healthy diet. The recommendation to increase vegetable intake is part of most dietary guidelines. Despite widespread and long-running public health messages to increase vegetable intake, similar to other countries worldwide, less than 1 in 10 adult Australians manage to meet target advice. Dietary guidelines are predominantly based on studies linking diets high in vegetables with lower risk of chronic diseases. Identifying vegetables with the strongest health benefits and incorporating these into dietary recommendations may enhance public health initiatives around vegetable intake. These enhanced public health initiatives would be targeted at reducing the risk of chronic diseases, such as cardiovascular diseases (CVD). Specific vegetable types contain high levels of particular nutrients and phytochemicals linked with cardiovascular health benefits. However, it is not clear if increasing intake of these specific vegetable types will result in larger benefits on risk of chronic diseases. This review presents an overview of the evidence for the relationships of specific types of vegetables, including leafy green, cruciferous, allium, yellow-orange-red and legumes, with subclinical and clinical CVD outcomes in observational epidemiological studies.

16 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Introduction
Poor diet is a major contributor to the risk of chronic diseases. Chronic diseases, including cardiovascular diseases (CVD), cancer, chronic respiratory diseases and diabetes, account for 90% of all deaths in Australia (1) and 70% of all deaths worldwide (2). Of these, CVD remains the number one cause of death (2-4). There is abundant evidence supporting public health practice promoting increases in vegetable intake (5-7), which is the cornerstone of dietary approaches for chronic disease primary prevention. Despite widespread and long-running health promotion messages to increase vegetable intake (8), the majority of the world’s population have low vegetable intakes (9-11).
Current dietary guidelines promote an increase in intake of all vegetables (5-7). These guidelines are mainly based on epidemiological evidence linking diets high in vegetables with lower incidence of chronic disease (12), and are supported by data suggesting that individual nutrients found abundantly in vegetables are protective (13-15). Some vegetables may have substantially larger health benefits in comparison to others, implying not all vegetables are the same (16, 17). Therefore, the improvement of dietary guidelines to include targeted advice on consuming specific types of vegetables may enhance population health approaches to increase vegetable intake.
This narrative review focuses on the cardiovascular health benefits of specific vegetable types in observational epidemiological studies. Vegetables can be classified according to their chemical constituents or by biological classifications based on similarities such as evolutionary relationships. Infrequently, these classification systems categorise similar vegetables together. Types of vegetables discussed in this review include leafy green, cruciferous, allium, yellow-orange-red and legumes.
Nutrients and phytochemicals in vegetables
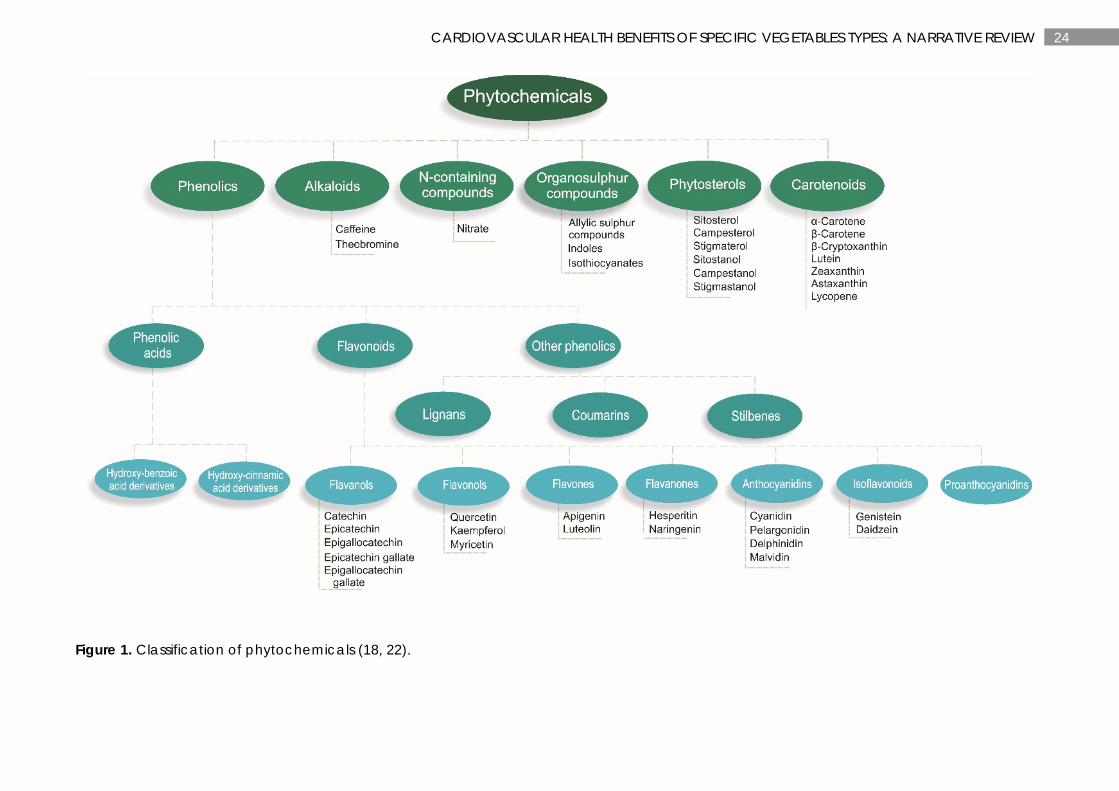
Vegetables contain many nutrients and phytochemicals that have been proposed to have cardiovascular health benefits (18). Phytochemicals are compounds found in plant-based foods that have previously been considered non-essential components of the diet (19). However, emerging evidence suggests phytochemicals extend benefits beyond that of basic nutrients and may be a vital part of a healthy diet (18). Phytochemicals are produced by plants to reduce the risks of environmental stresses, such as insect attacks; however, when consumed by humans they may exhibit a wide range of health benefits (19). While over 20,000 phytochemicals have been identified in plant foods (20), a large percentage remain unknown or are poorly understood (21). Many of these phytochemicals have been isolated to build an understanding of the benefits towards human health (18, 22). For the classification of phytochemicals, see Figure 1.
Meta-analyses have shown nutrients, such as dietary fibre (13), magnesium (15) and potassium (14), and phytochemicals, such as flavonoids (23) and carotenoids (24-27), are associated with benefits on cardiovascular health. Evidence also suggests cardiovascular health benefits of other nutrients, such as vitamin K (28) and vitamin C (29), and phytochemicals, such as nitrate (30, 31) and organosulphur compounds (32). These nutrients and phytochemicals may protect against CVD by a number of mechanisms. These include modulating enzyme activity; altering gene expression and signalling pathways; regulation of blood pressure; regulation of lipid and glucose metabolism; influence on antioxidant, anti-inflammatory, and antiplatelet activity;

17 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
effects on endothelial function; and attenuation of myocardial damage (33). In particular, carotenoids which are phytochemicals found abundantly in yellow-orange-red and dark green leafy vegetables (34), have been postulated to reduce oxidative stress and inflammation. This may be achieved by influencing transcription factors, such as nuclear factor κB (NFκB) or nuclear factor erythroid 2-related factor 2 (Nrf2), and their downstream targets, such as interleukin 8 (IL-8) and prostaglandin E2 (PGE2) or heme oxygenase (Hmox-1) and superoxide dismutase (SOD), respectively (35).
Strong evidence suggests nitrate, found abundantly in leafy green vegetables, beetroot and radish (36), can increase nitric oxide (NO) via the enterosalivary nitrate-nitrite-NO pathway. Nitric oxide is a cell signalling molecule important for vascular homeostasis (37). Nitric oxide is involved in many physiological and pathological processes such as relaxing vascular smooth muscle tissue, increasing regional blood flow, and inhibiting platelet and leukocyte adhesion to vessel walls (38). A combination of all these physiological benefits are likely to slow the progression of atherosclerosis. Evidence suggests organosulphur compounds may also slow the progression of atherosclerosis through anti-inflammatory and antiplatelet effects (39, 40).
Organosulphur compounds are organic sulphur-containing compounds often associated with their foul odours. Glucosinolates, a class of organosulphur compounds, are found almost exclusively in cruciferous vegetables such as cabbage, broccoli, kale and Brussels sprouts. Anti-inflammatory properties of isothiocyanates, a breakdown product of glucosinolates, have been proposed through activation of the redox-sensitive transcription factor Nrf2, which control the expression of antioxidant and phase II enzymes (39). Furthermore, studies have demonstrated in vitro inhibition of platelet aggregation of thiosulfinates, a class of organosulphur compounds found in allium vegetables such as garlic, onions, shallots, leeks and chives (40).
Classification of vegetables
Large observational epidemiological studies have classified vegetable types in different ways. This is usually related to countries having varied accessibility and availability of different vegetable types (41). Some large epidemiological studies have investigated individual vegetables, whilst others have investigated vegetable types grouped together based on botanical families, colours, or plant parts (e.g., stems and stalks, and leaves) (12, 41). The botanical classification of vegetables is based on physiological characteristics and include vegetables grouped under their botanic family name. Examples include Amaryllidaceae (garlic, leek, onion, and scallion), Chenopodiacea (beet and beet greens, spinach, and Swiss chard), Cruciferae/Brassica (broccoli, Brussels sprouts, cauliflower, Chinese broccoli, Chinese cabbage, collards, and kale) and Leguminosae (green peas, kidney beans, lentils, green snap beans, snowpeas, and soybeans) (41). Colour classification reflects the pigments of vegetable plant tissues and can also reflect the presence of phytochemicals such as beta-carotene (deep orange), anthocyanidin (red) and chlorophyll (green) (41). Plant part classification is based on the edible part of the vegetable, including stems and stalks, leaves, legumes, bulbs, and roots and tubers. Stem and stalk vegetables, such as celery, are predominately high in dietary fibre due to their supported structure (41). Leaves of vegetables are the most metabolically active and tend to be the most nutritious part of the vegetable being a good source of folate, carotenoids, vitamin C, flavonols, iron, zinc, calcium and magnesium (41). Legumes are a good source of protein, starch, isoflavones, vitamin B6, folate and iron (41).

18 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Bulbs are a good source of organosulphur compounds, in particular allicin (41). Roots and tubers, such as potatoes, are a good source of resistant starch which may help maintain a healthy gut (42). Gut dysbiosis has been shown to be associated with intestinal inflammation and has been linked to the development of CVD (43).
It has been suggested that grouping vegetables based on food components of public health significance is a way for nutrition professionals to explore health benefits (41). Groupings often include dark green leafy vegetables; cabbage family vegetables; lettuces; allium family bulbs; legumes; deep orange/yellow roots and tubers; and tomatoes and other red vegetables. Despite the comprehensiveness in the development of this grouping system, there are some limitations. One limitation is that vegetable components, such as nitrate and organosulphur compounds, are not taken into consideration. In addition, observational cohort studies are restricted to specific groupings due to limited vegetable items on food frequency questionnaires.
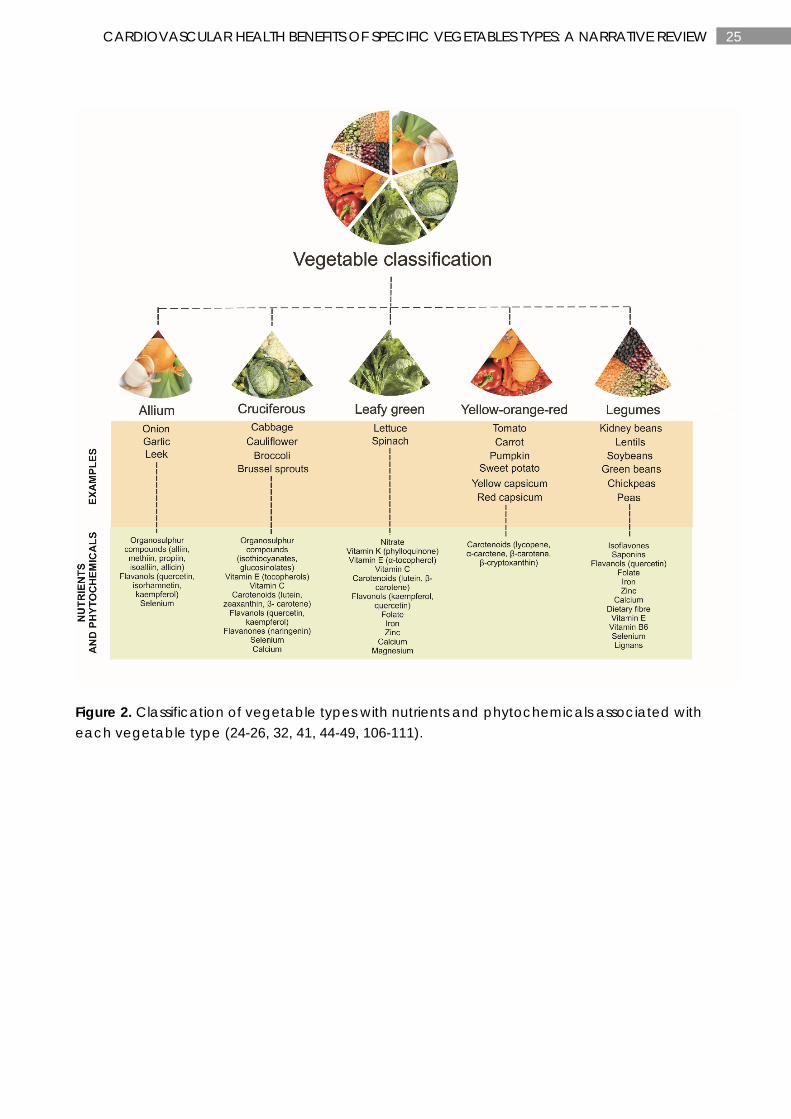
The following sections discuss the associations of specific vegetables types, including leafy green, cruciferous, allium, yellow-orange-red and legumes, with subclinical and clinical CVD. The aforementioned vegetable types are based on the above groupings of vegetables as well as dietary guidelines around the world, and have been modified slightly to align with specific phytochemicals found abundantly in these vegetable types. These include nitrate (leafy green vegetables) (44, 45); organosulphur compounds such as glucosinolates (cruciferous vegetables) (46, 47) and cysteine sulfoxides (allium vegetables) (32); carotenoids such as lycopene and bete-carotene (yellow-orange-red vegetables) (24-26, 48); and polyphenolic compounds such as isoflavones and saponins (legumes) (49). For more information on other nutrients and phytochemicals associated with these vegetable types, see Figure 2.
Subclinical measures of atherosclerosis
Atherosclerosis, the underlying cause of CVD, is a complex multifactorial disorder of the arteries initiated by endothelial dysfunction, inflammation and dyslipidaemia (50, 51). Carotid artery intima-media thickness (IMT) and focal plaques are subclinical measures of atherosclerosis, both of which have been shown to predict CVD outcomes (52-54). Although carotid artery IMT and focal plaques are both interrelated, they may reflect different biological aspects of atherogenesis (55). Carotid artery IMT captures both the atherosclerotic process as well as the compensatory thickening of the carotid wall in response to ageing and hypertension (56), and is strongly related to ischaemic stroke (55). Carotid focal plaques capture the atherosclerotic process, are dependent on the influx of lipids into the plaque, and are more related to hyperlipidaemia and myocardial infarction (55).
Diets rich in vegetables, such as a vegetarian diet and a Mediterranean diet, have been shown to be associated with lower carotid artery IMT (57, 58) and delayed progression of atherosclerotic plaques (59). Very few observational cohort studies have investigated the relationships of vegetable intake alone and/or specific vegetable types with subclinical measures of atherosclerosis (60). To our knowledge, we are the first to publish an association of total vegetable intake, and in particular, intake of cruciferous vegetables, with carotid artery IMT (61). However, no relationship between total vegetable intake and carotid atherosclerotic plaque was observed. This could be due to carotid artery IMT and carotid focal plaques differing in biological aspects of atherogenesis as described above.
19 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Cardiovascular disease clinical endpoints
Increasing vegetable intake is widely recommended for reducing CVD risk, along with other chronic disease. These recommendations are incorporated into dietary guidelines around the world (5-7) and are primarily based on large-scale prospective cohort studies linking diets high in vegetables with lower chronic disease risk. The amount of vegetable intake recommended in dietary guidelines vary globally, but is usually around 5-6 servings/d (375-450 g/d). More than 60 prospective cohort studies have been undertaken to investigate the associations of total vegetable intake and/or intake of specific vegetables with CVD endpoints (12). In a recent meta-analysis, Aune et al (12) showed a summary relative risk (RR) of 0.90 (95%CI 0.87, 0.93) for CVD per 200 g/d increase of vegetable intake. Evidence suggested this relationship was nonlinear (Pnonlinearity=0.04) with steeper inverse associations at lower levels of intake. However, the relationship ‘appeared’ approximately linear with the greatest CVD benefits observed at intakes of 600 g/d, which is slightly higher than most dietary guideline recommendations. For vegetable types, leafy green vegetables, cruciferous vegetables, and tomatoes were inversely associated with CVD risk in nonlinear dose-response analyses. The greatest CVD benefits were observed at intakes of ≥200 g/d for cruciferous vegetable, ≥120 g/d for leafy green vegetables, and ≥200 g/d for tomatoes (12). However, only a few studies were included in these analyses, therefore results need to be interpreted with caution.
Leafy green vegetables
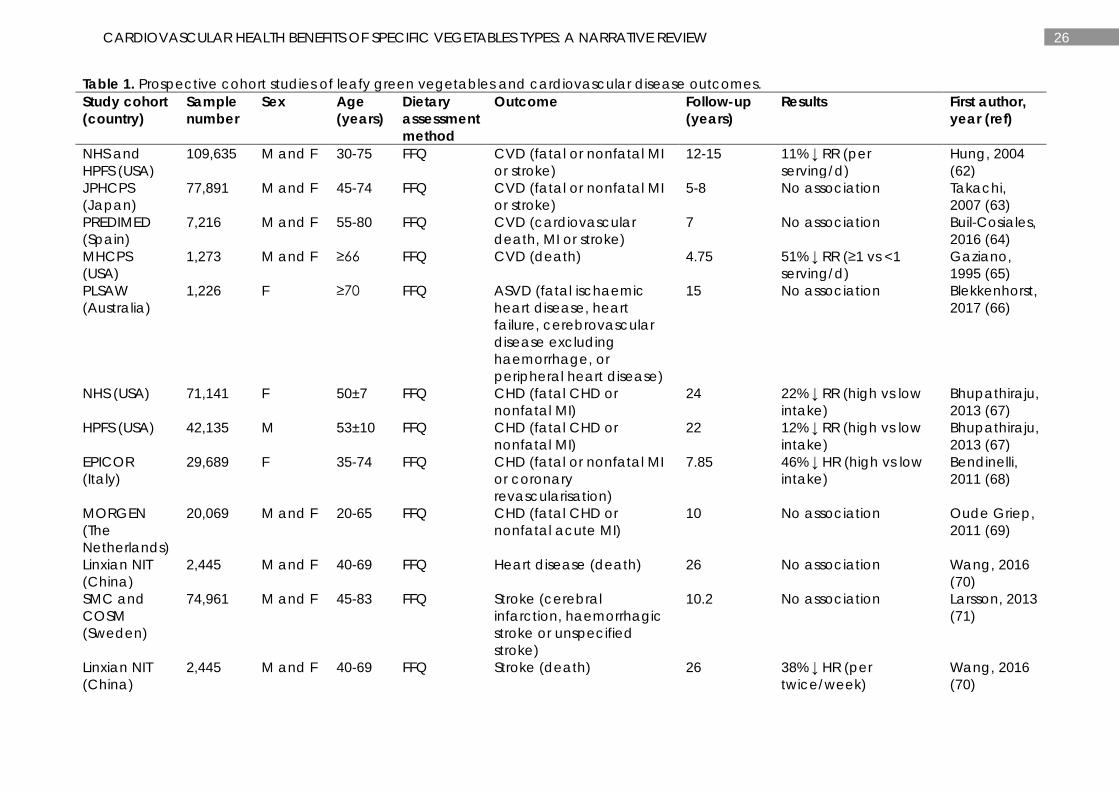
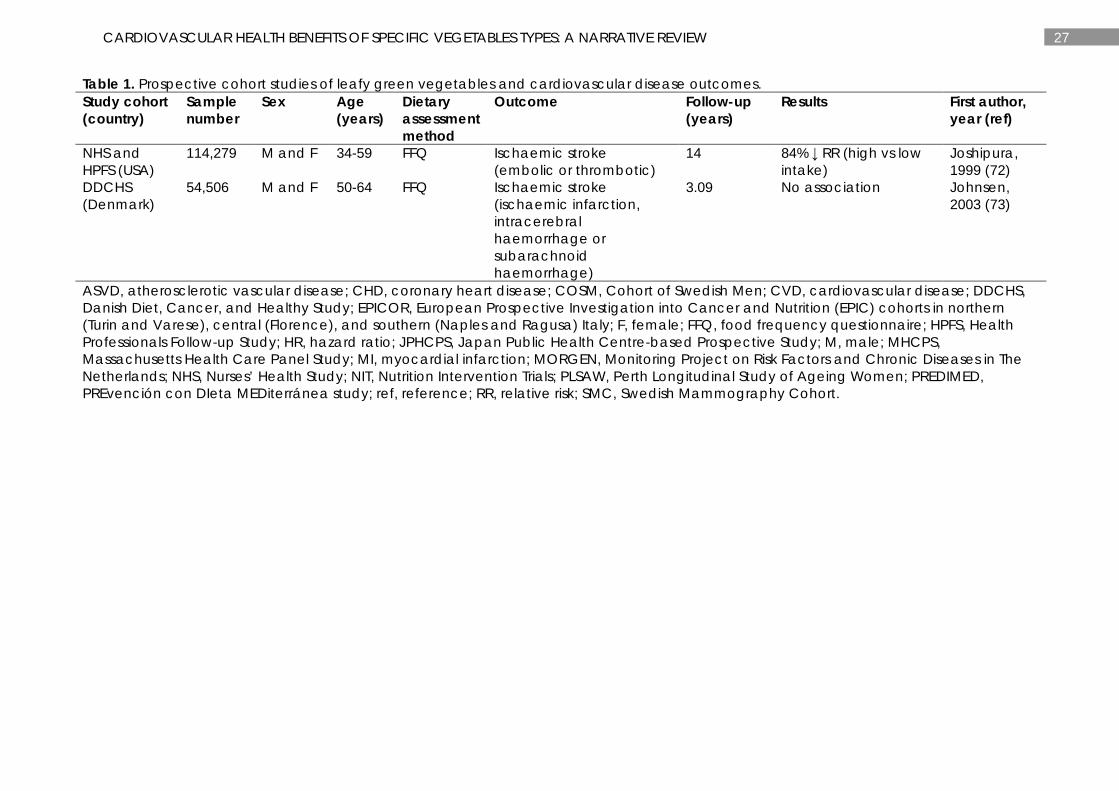
At least 14 studies have reported the associations between intake of leafy green vegetables and CVD (62-65), atherosclerotic vascular disease (ASVD) (66), coronary heart disease (CHD) (67-69), heart disease (70) or stroke (70-73) (Table 1). The most common vegetables included in the classification of leafy green vegetables were spinach and lettuce. Most studies have demonstrated significant inverse associations between intakes of leafy green vegetables and CVD outcomes (62, 65, 67, 68, 70, 72). However, other studies have demonstrated no association (63, 64, 66, 69-71, 73). Most positive studies have been conducted in US cohorts (62, 65, 67, 72), with the exception of one in Italy (68) and another in China (70). Studies demonstrating no associations were conducted in cohorts from Spain (64), Denmark (73), Sweden (71), the Netherlands (69), Japan (63), China (70) and Australia (66).
The US cohorts, Nurses’ Health Study (NHS) and Health Professionals Follow-up Study (HPFS), are the largest cohorts demonstrating an inverse association between intakes of leafy green vegetables and risk of CVD (62), CHD (67) and ischaemic stroke (72). The NHS consists of ~121,700 female registered nurses aged 30-55 years and the NPFS consists of ~51,529 male health professionals aged 40-75 years. Combining these two large cohorts, Hung et al (62) reported an adjusted RR of 0.89 (95%CI 0.83-0.96) for CVD for every one serving increment of leafy green vegetables. Combining the same cohorts, Bhupathiraju et al (67) reported an adjusted RR of 0.83 (95%CI 0.77-0.91) for CHD for the highest (median: ~1.5 servings/d) compared with the lowest (median: ~0.2 servings/d) intakes of leafy green vegetables. For ischaemic stroke, Joshipura et al (72) reported an adjusted RR of 0.76 (95%CI 0.58-0.99) for the highest (median: 1.36 servings/d) versus the lowest (median: 0.16 servings/d) intakes. However, the translation of these findings into practice are limited, as the number of grams in one serving was not reported. In a smaller US cohort (n=1,273), the Massachusetts Health Care Panel Study (MHCPS), Gaziano et al (65) reported a RR of 0.49 (95%CI 0.31-0.77) for CVD mortality for those consuming one or more servings per day of salads and leafy green
20 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
vegetables compared to those consuming less than one serving per day. Again, the number of grams in one serving was not reported, making translation difficult. Importantly, only age and sex were used in the adjusted model, and dietary and lifestyle factors were not taken into consideration. Using the EPICOR study (the European Prospective Investigation into Cancer and Nutrition [EPIC] cohorts in northern [Turin and Varese], central [Florence], and southern [Naples and Ragusa] Italy), Bendinelli et al (68) reported an adjusted hazard ratio (HR) of 0.54 (95%CI 0.33-0.90) for CHD for the highest (>50.8 g/d) compared to the lowest (<17.6 g/d) intakes of leafy green vegetables. This study consisted of 29,689 females aged 35-74 years. Lastly, using the Linxian Nutrition Intervention Trials (NIT) cohort in China, Wang et al (70) reported an adjusted HR of 0.62 (95%CI 0.43-0.91) for stroke mortality for every twice/week increase in leafy green vegetables. However, this relationship was not observed for heart disease mortality.
Cruciferous vegetables
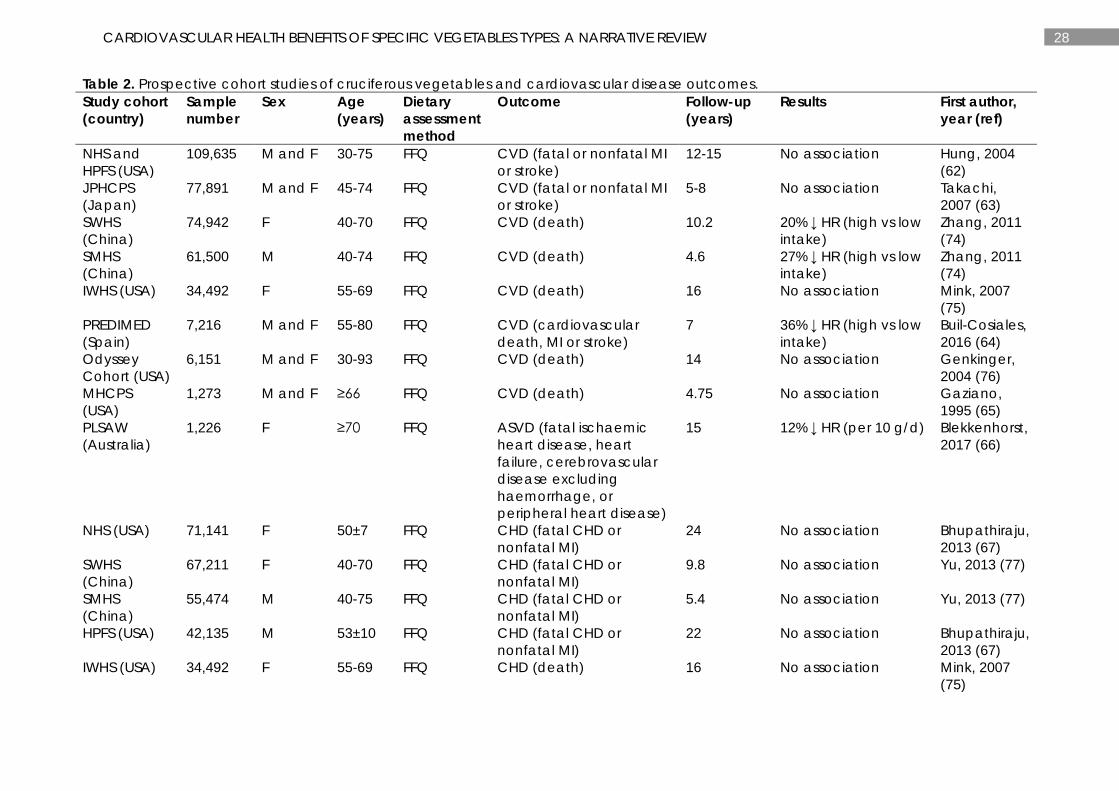
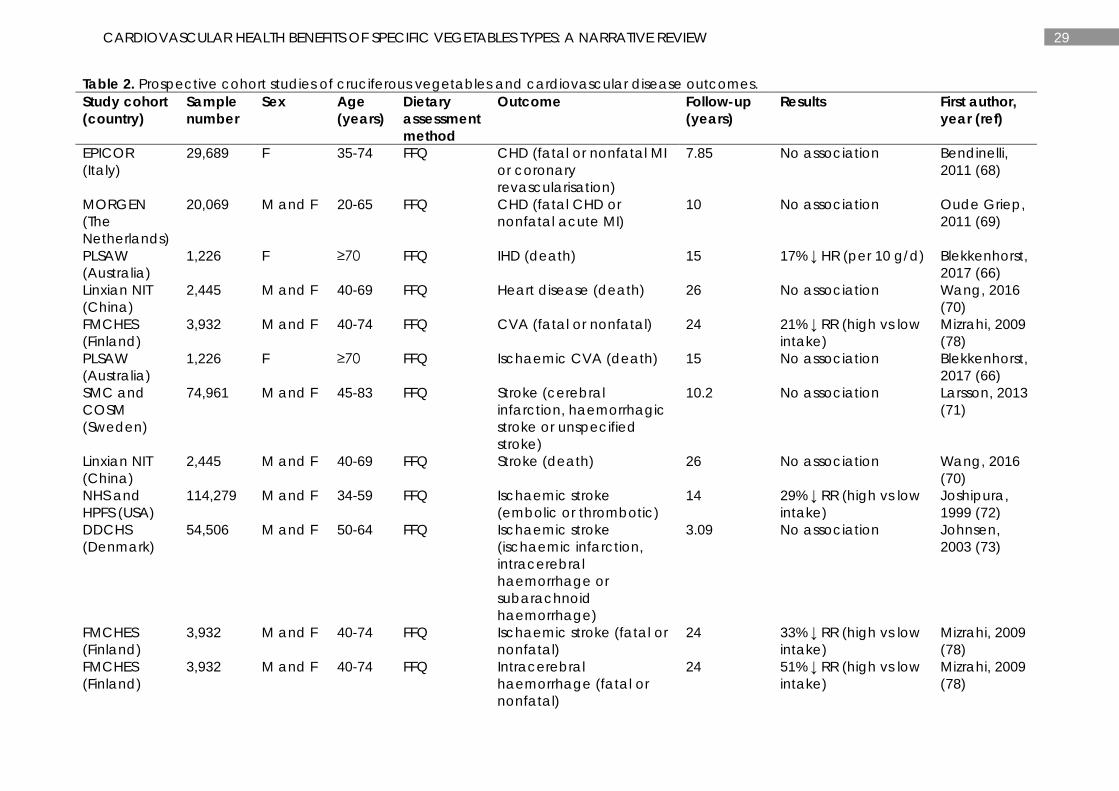
At least 26 studies have reported the associations between intake of cruciferous vegetables and CVD (62-65, 74-76), ASVD (66), CHD (67-70, 75, 77), ischaemic heart disease (IHD) (66), heart disease (70), cerebrovascular disease (CVA) (78), ischaemic CVA (66), stroke (70, 71), ischaemic stroke (72, 73, 78), and intracerebral haemorrhage (78) (Table 2). Broccoli, Brussels sprouts, cabbage, and cauliflower were the most common vegetables grouped as cruciferous vegetables. At least 8 studies have identified an inverse relationship between intake of cruciferous vegetables and 6 separate outcomes: CVD (64, 74), ASVD (66), IHD (66), CVA (78), ischaemic stroke (72, 78) and intracerebral haemorrhage (78). Seventeen studies reporting 5 outcomes (CVD, CHD, ischaemic CVA, ischaemic stroke and stroke) have shown no associations (62, 63, 65-71, 73, 75-77).
In the Shanghai Women’s Health Study (SWHS), Zhang et al (74) reported an adjusted HR of 0.80 (95%CI 0.72-0.89) for CVD for the highest intake (median: 166 g/d) of cruciferous vegetables in comparison to the lowest intake (median: 28 g/d). The SWHS cohort included 74,942 females aged 40-70 years. Similar results were observed in the Shanghai Men’s Health Study (SMHS). An adjusted HR of 0.78 (95%CI 0.71-0.85) was reported for CVD in 61,500 males aged 40-74 years consuming the highest intake (median: 208 g/d) of cruciferous vegetables in comparison to the lowest intake (median: 34 g/d) (74). No relationship was observed with intake of cruciferous vegetables and CHD in the same cohorts (SWHS and SMHS) (77). In the PREvención con DIeta MEDiterránea (PREDIMED) study, Buil-Cosiales et al (64) reported an adjusted HR of 0.64 (95%CI 0.42-0.97) for CVD for the highest cumulative average intake (median: 30 g/d) of cruciferous vegetables in comparison to the lowest cumulative average intake (median: 3.1 g/d). In an Australian cohort, the Perth Longitudinal Study of Ageing Women (PLSAW), we have reported an adjusted HR of 0.88 (95%CI 0.81-0.95) for atherosclerotic vascular disease (ASVD) for every 10 g/d increase in cruciferous vegetables (66). A similar relationship was evident for IHD (adjusted HR=0.83, 95%CI 0.75-0.92), but not for ischaemic CVA (adjusted HR=0.94, 95%CI 0.84-1.05) (66). In the Finnish Mobile Clinic Health Examination Survey (FMCHES) cohort (n=3,939), Mizrahi et al (78) reported an adjusted RR of 0.79 (95%CI 0.63-0.99), 0.67 (95%CI 0.49-0.92), and 0.49 (95%CI 0.25, 0.98) for CVA, ischaemic stroke, and intracerebral haemorrhage, respectively. These results were for the highest intakes (men: 14-269 g/d; women: 16-188 g/d) compared to the lowest intakes (men: 0-1 g/d; women: 0-2 g/d) of cruciferous vegetables. In the NHS and NPFS cohorts, highest (median: 1.0 serving/d) versus lowest (median: 0.14 serving/d) intakes of cruciferous vegetables was
21 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
associated with a lower RR of ischaemic stroke (adjusted RR=0.71, 95%CI 0.55-0.93) (72). However, a similar relationship was not shown for CVD (62) or CHD (67).
Allium vegetables
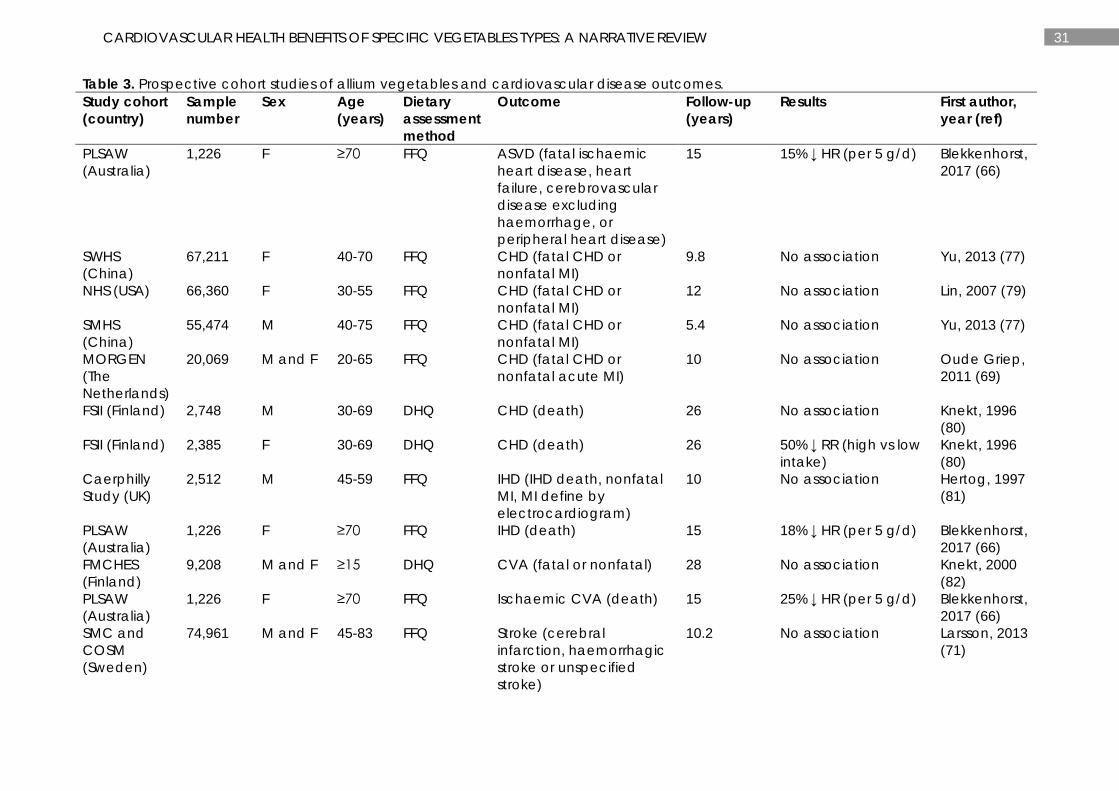
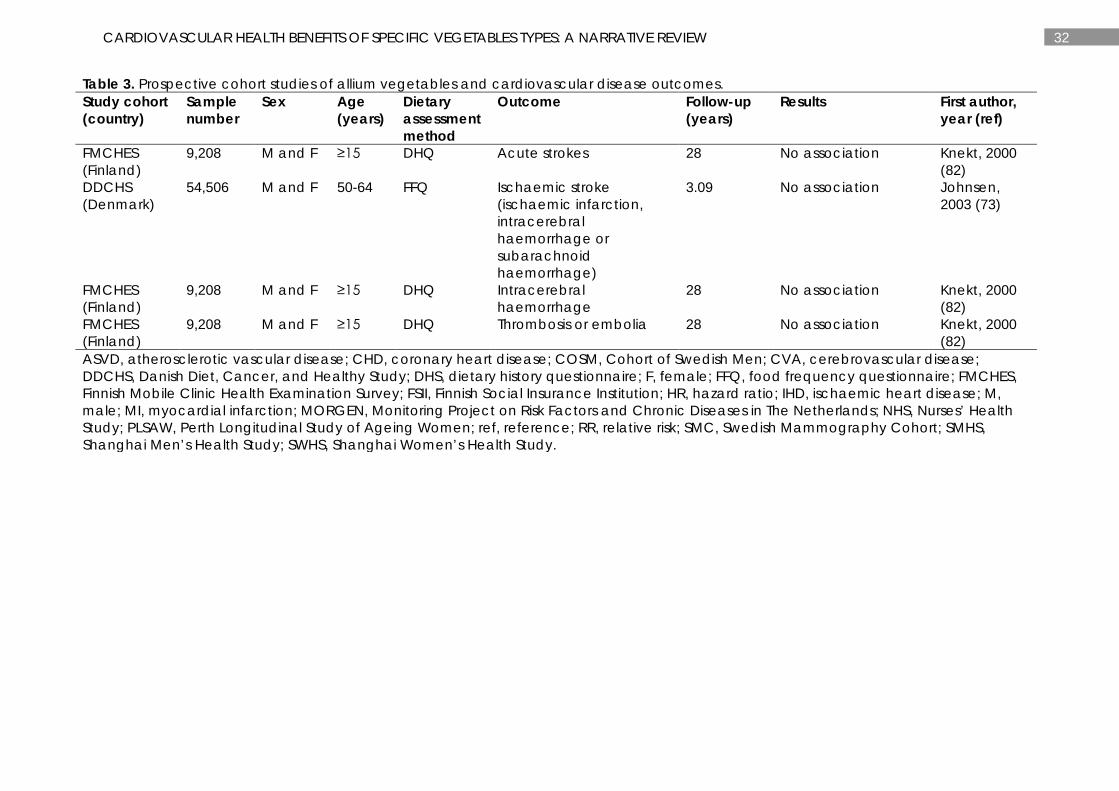
At least 14 studies have investigated the relationships between intake of allium vegetables and ASVD (66), CHD (69, 77, 79, 80), IHD (66, 81), CVA (82), ischaemic CVA (66), stroke (71), acute stroke (82), ischaemic stroke (73), intracerebral haemorrhage (82) and thrombosis or embolia (82) (Table 3). The majority of these studies have investigated the intake of onions. Four studies have reported inverse relationships between intake of allium vegetables and ASVD (66), CHD (80), IHD (66) and ischaemic CVA (66) with all other studies reporting no associations (69, 71, 73, 77, 79, 81, 82).
In the PLSAW cohort (66), we have reported an adjusted HR of 0.85 (95%CI 0.75-0.97) for ASVD for every 5 g/d increase in allium vegetable intake. This relationship remained for IHD (adjusted HR=0.82, 95%CI 0.70-0.97) and ischaemic CVA (adjusted HR=0.75, 95%CI 0.60-0.93). In the Finnish Social Insurance Institution (FSII) cohort, Knekt et al (80) reported an adjusted RR of 0.50 (95%CI 0.30-0.82) for CHD for women (n=2,385) consuming ≥5 g/d compared with <5 g/d of onions. This relationship was not observed in men (n=2,748).
Yellow-orange-red vegetables
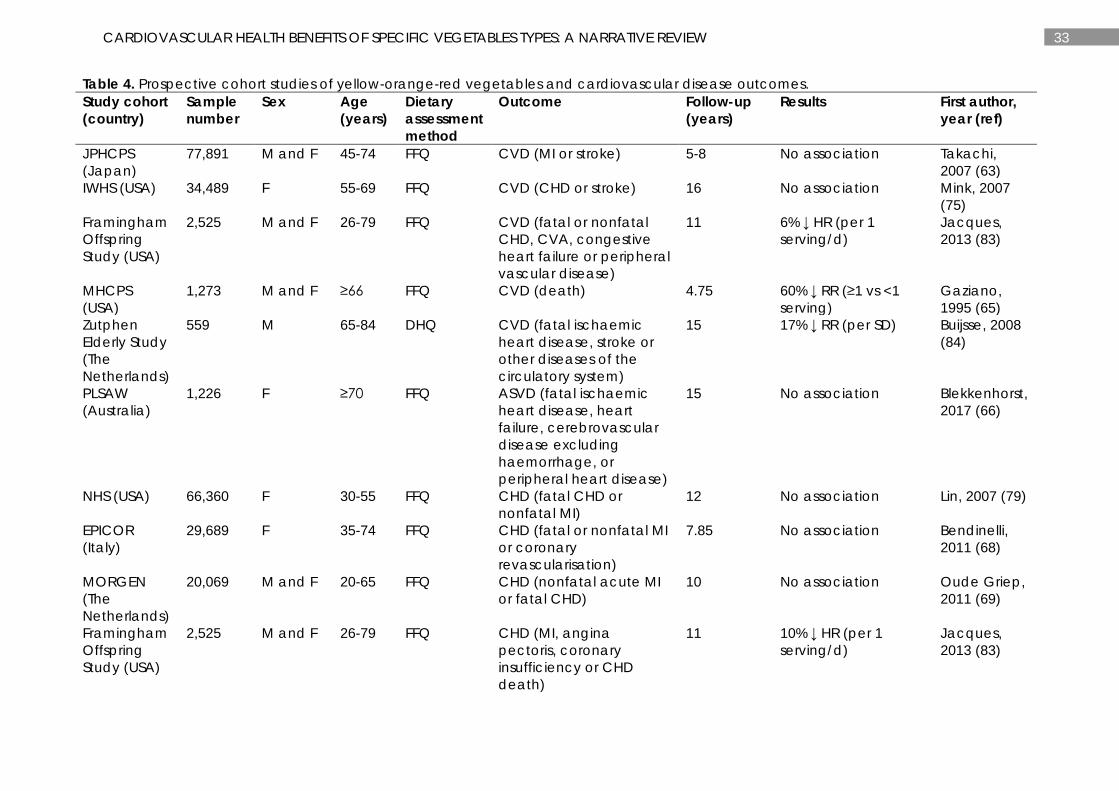
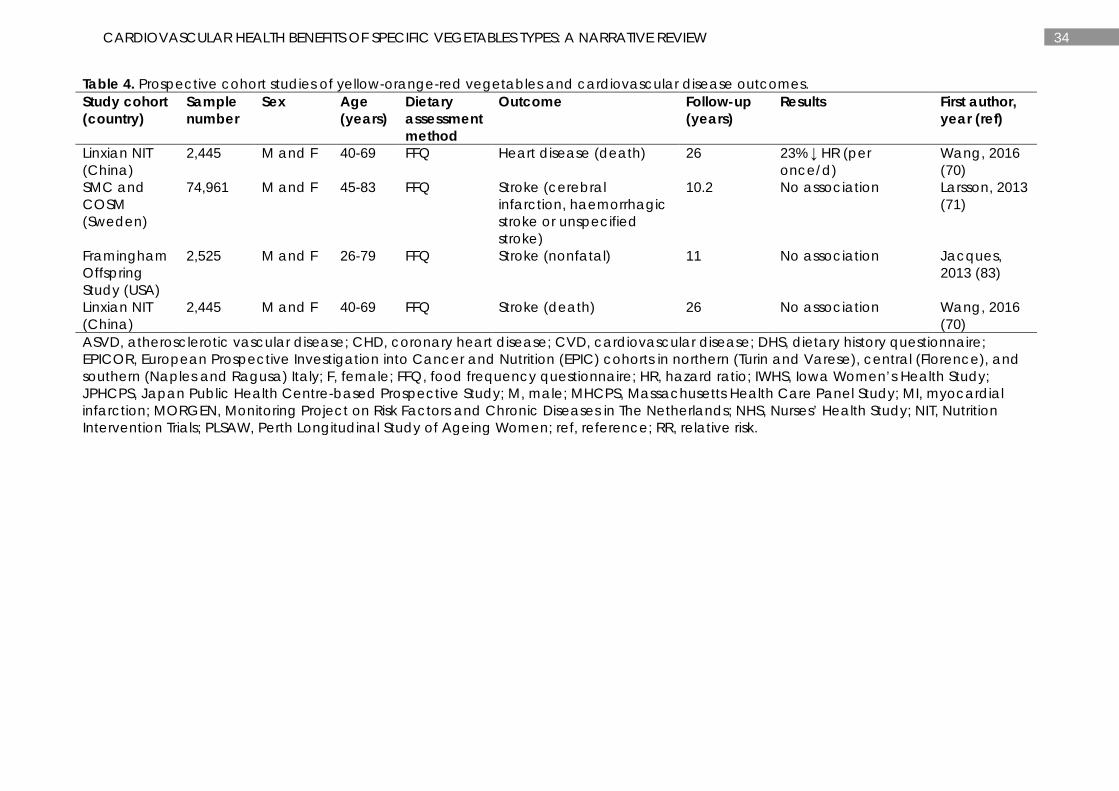
At least 14 studies have reported associations between yellow-orange-red vegetables and CVD (63, 65, 75, 83, 84), ASVD (66), CHD (68, 69, 79, 83), heart disease (70) and stroke (70, 71, 83) (Table 4). Tomato, carrot, sweet potato and pumpkin were the major vegetables studied. Five studies have reported inverse associations between intake of yellow-orange-red vegetables and CVD (65, 83, 84), CHD (83) and heart disease (70). Other studies have reported no associations (63, 66, 68-71, 75, 79, 83).
In the Framingham Offspring Study, Jacques et al (83) reported an inverse relationship for consumption of tomato products (tomatoes, tomato juice and tomato sauce) with an adjusted HR of 0.94 (95%CI 0.88-0.99) for CVD and 0.90 (95%CI 0.83-0.99) for CHD for every one serve increase per day. This relationship was not observed for stroke. In the MHCPS study, Gaziano et al (65) reported an inverse relationship between consumption of carrots and/or squash and CVD mortality. The RR for those who ate one or more servings per day of carrots and squash was 0.40 (95%CI 0.16-0.98), although the number of grams in one serving was not reported. Furthermore, this relationship was not observed for consumption of tomatoes. In the Zutphen Elderly Study, Buijsse et al (84) reported an inverse relationship between consumption of carrots and CVD mortality (per SD, RR=0.83, 95%CI 0.68-1.00). Lastly, in the Linxian NIT study, Wang et al (70) reported consumption of yellow-orange vegetables, such as sweet potatoes, carrots and pumpkins, was inversely associated with heart disease, but not stroke. The adjusted HR for heart disease was 0.77 (95%CI 0.60-0.97) for every once/day increase in consumption of yellow-orange vegetables.
Legumes
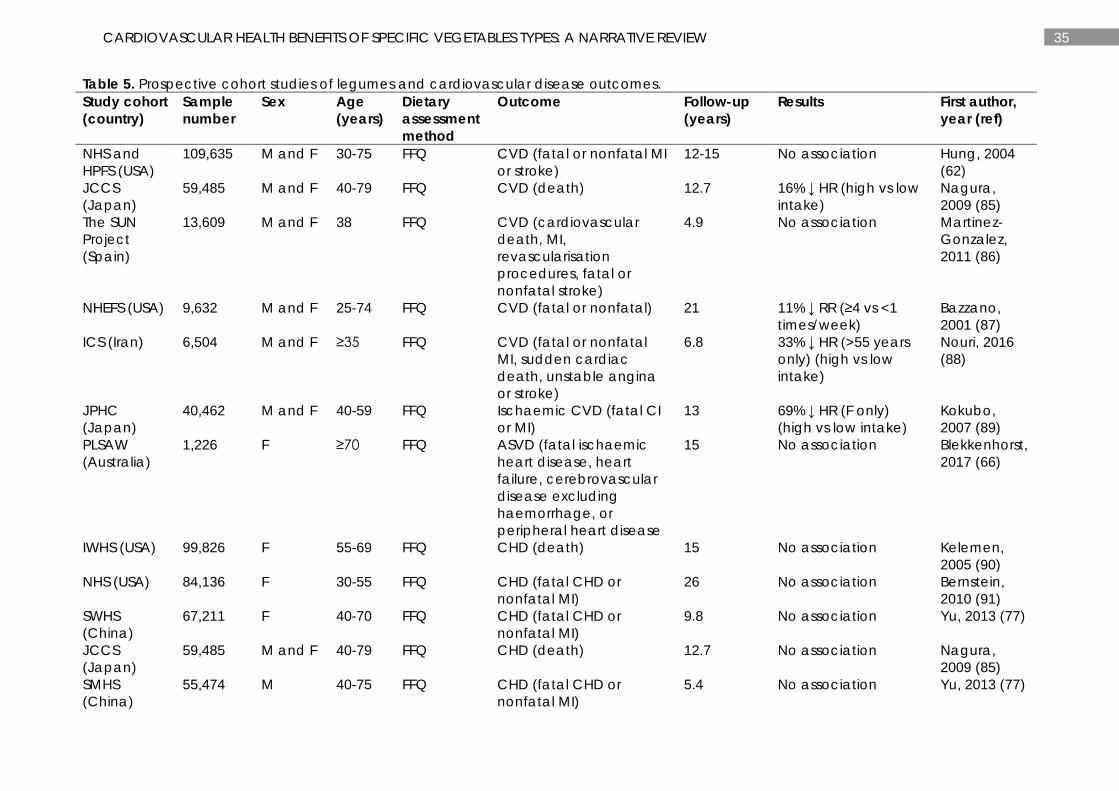
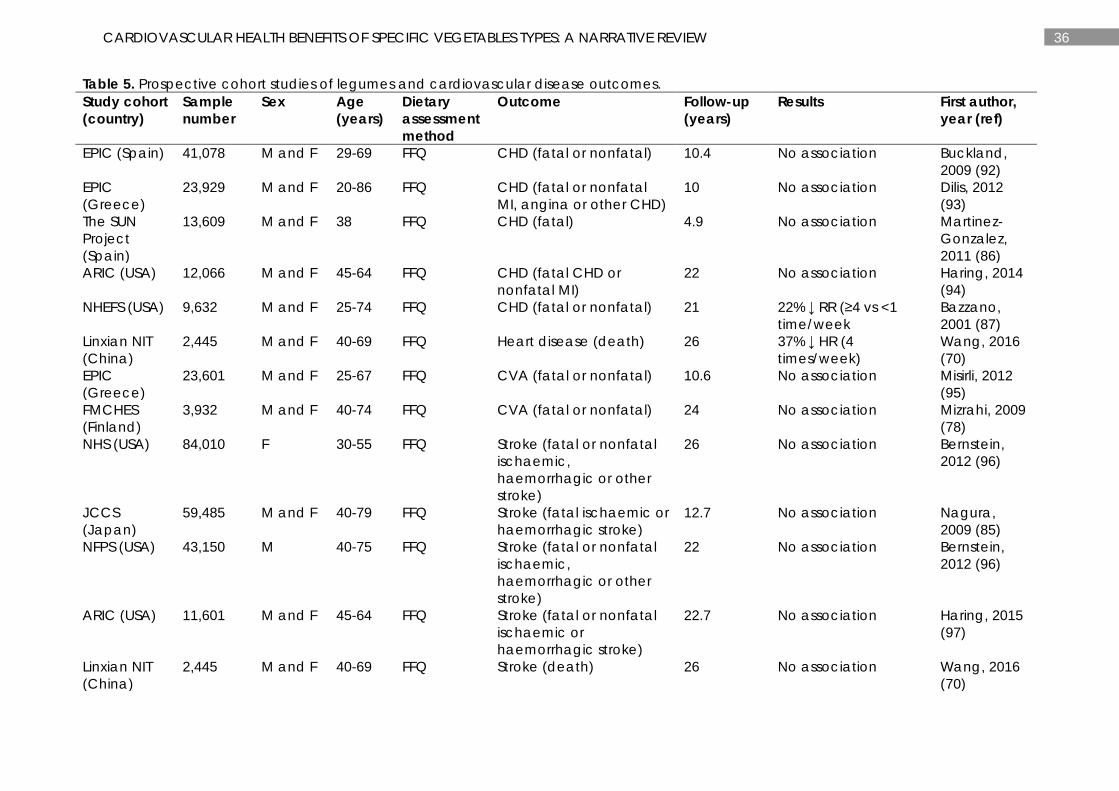
At least 28 studies have reported on the relationships between legume consumption and CVD (62, 85-88), ischaemic CVD (89), ASVD (66), CHD (70, 77, 85-87, 90-94), CVA (78, 95), stroke (70, 85, 96, 97), ischaemic stroke (72, 78) and intracerebral haemorrhage (78) (Table 5). At least 7 studies have reported inverse associations between intakes of legumes and CVD (85, 87, 88),

22 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
ischaemic CVD (89), CHD (87), heart disease (70), and ischaemic stroke (78). However, some studies have demonstrated no relationship (62, 66, 70, 72, 77, 78, 85, 86, 90-97).
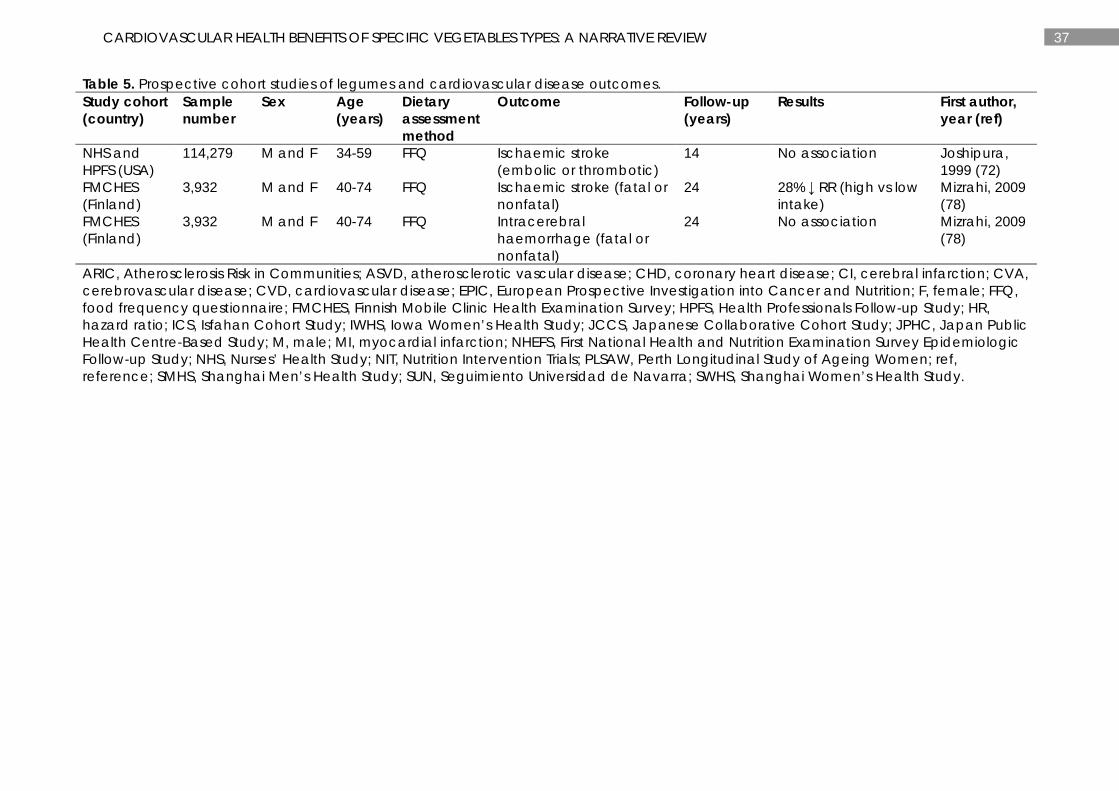
In the Japanese Collaborative Cohort Study (JCCS), Nagura et al (85) reported an inverse relationship between bean intake and CVD with an adjusted HR of 0.84 (95%CI 0.74-0.95) for those consuming the highest (median: 4.5 servings/week) compared to the lowest (median: 0.8 servings/week) bean intake. This relationship was not evident for CHD and stroke. In the First National Health and Nutrition Examination Survey Epidemiologic Follow-up Study (NHEFS), Bazzano et al (87) reported an adjusted RR of 0.89 (95%CI 0.80-0.98) for CVD and 0.78 (95%CI 0.68-0.90) for CHD for those who consumed legumes ≥4 times per week compared to those who consumed legumes less than once per week. In the Isfahan Cohort Study (ICS) in Iran, Nouri et al (88) reported a 33% lower risk of CVD for old-aged individuals consuming high intakes (>3 times per week) compared to low intakes (0-1 time per week) of legumes (HR=0.66, 95%CI 0.45-0.98). In the Japan Public Health Centre-Based (JPHC) Study, Kokubo et al (89) reported an inverse relationship between soy intake and ischaemic CVD mortality. The adjusted HR was 0.31 (95%CI 0.13-0.74) for women consuming high intakes (≥5 days per week) compared to low intakes (0-2 days per week) of soy. This relationship was primarily observed in postmenopausal women and was not observed in men or for dietary intakes of beans. Wang et al (70) reported an inverse relationship between bean intake and heart disease with an adjusted HR of 0.63 (95%CI 0.48-0.83) for increasing bean intake 4 times/week. This relationship was not observed for stroke. In the FMCHES study, Mizrahi et al (78) reported an inverse relationship between consumption of legumes and ischaemic stroke with an adjusted RR of 0.72 (95%CI 0.54-0.96) for those consuming the highest intakes (men: 10-101 g/d; women: 7-43 g/d) compared to the lowest intakes (men: 0-2 g/d; women: 0-1 g/d). Other related outcomes including CVA and intracerebral haemorrhage were not related.
Limitations and future directions
Although nutrition epidemiology has been successful in providing insight into the potential causes and prevention of many health conditions, several important limitations still exist (98). Due to the observational nature of nutrition epidemiological studies, residual confounding is inevitable. Challenges also arise in the accuracy of assessing dietary intake (98). These factors can lead to contradictory findings, especially when comparing results across different populations where dietary assessment methods are sometimes weak and there is large heterogeneity amongst the populations studied. Relationships between vegetable intake and CVD outcomes may be attenuated when large differences in vegetable intake classification and/or categorization exist. There is an urgent need for the international standardization of such variables to limit error, thereby enabling more accurate comparisons between investigations. Such changes if implemented in large cohort studies have the capacity to improve the quality of nutrition research. Technology-based dietary assessment methods in conjunction with recovery biomarkers, such as those that appear in urine, could be used to improve accuracy and are worth considering in future work (99). Finally, adopting STROBE-nut guidelines and checklists will improve reporting of nutritional epidemiological studies and the quality of published literature (99, 100).
Most prospective studies reported in this review were undertaken in older populations. Greater statistical power is present in studies with more events, which occur more frequently in older populations. Therefore, these populations are frequently selected to study disease-related

23 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
outcomes such as CVD. It is clear that dietary changes later in life can significantly reduce the risk of chronic disease within 5 years (101, 102). However, it is likely that the greatest cardiovascular benefit would be to increase vegetable intake throughout the life course. Future studies are needed to evaluate the relationships between intake of specific vegetables and cardiometabolic health outcomes in younger populations. Due to the small number of events that would occur in younger populations, markers of cardiometabolic health are an alternative to study. It is also not known whether the health benefits of increasing vegetable intake is associated with particular racial or ethnic populations, and therefore this should be addressed in future research.
Conclusions
Many large observational follow-up studies have reported the inverse associations of leafy green, cruciferous, allium, yellow-orange-red vegetables, and legumes with CVD outcomes. These vegetables contain many nutrients and phytochemicals that have been postulated to have cardiovascular health benefits. Some studies demonstrate no associations between specific vegetable types and CVD outcomes. This may be due to type II error and/or bias introduced by measurement error and regression dilution, attenuating observed risk estimates (12). Other inherit limitations of observational epidemiological studies may also influence relationships. This presents a major limitation of nutritional epidemiology, making the interpretation and comparison of results difficult (103).
The evidence in this review suggests intake of leafy green and cruciferous vegetables may confer strong cardiovascular health benefits. Increasing vegetable intake, with a focus on consuming leafy green and cruciferous vegetables may provide the greatest cardiovascular health benefits. Incorporating such dietary changes along with other recommended lifestyle changes will optimize health benefits. Lifestyle changes include consuming a diet full of vegetable, fruits, and whole grains; including low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils, and nuts; and limiting intake of saturated and trans fats, sweets, sugar-sweetened beverages, and red meats (104). Other lifestyle changes include increasing physical activity (104), avoiding cigarette smoking (104) and intake of alcohol (105), and maintaining a healthy body weight by consuming appropriate energy requirements (104). There is a need for very large well-designed epidemiological studies investigating the cardiovascular health benefits of different vegetable types. Large long-term randomised controlled trials are needed to establish the causal effects of the specific vegetables found to be most beneficial for cardiovascular health.
24 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Figure 1. Classification of phytochemicals (18, 22).
25 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Figure 2. Classification of vegetable types with nutrients and phytochemicals associated with each vegetable type (24-26, 32, 41, 44-49, 106-111).
26 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Table 1. Prospective cohort studies of leafy green vegetables and cardiovascular disease outcomes. Study cohort (country)
Sample number
Sex Age (years)
Dietary assessment method
Outcome Follow-up (years)
Results First author, year (ref)
NHS and HPFS (USA)
109,635 M and F 30-75 FFQ CVD (fatal or nonfatal MI or stroke)
12-15 11% ↓ RR (per serving/d)
Hung, 2004 (62)
JPHCPS (Japan)
77,891 M and F 45-74 FFQ CVD (fatal or nonfatal MI or stroke)
5-8 No association Takachi, 2007 (63)
PREDIMED (Spain)
7,216 M and F 55-80 FFQ CVD (cardiovascular death, MI or stroke)
7 No association Buil-Cosiales, 2016 (64)
MHCPS (USA)
1,273 M and F ≥66 FFQ CVD (death) 4.75 51% ↓ RR (≥1 vs <1 serving/d)
Gaziano, 1995 (65)
PLSAW (Australia)
1,226 F ≥70 FFQ ASVD (fatal ischaemic heart disease, heart failure, cerebrovascular disease excluding haemorrhage, or peripheral heart disease)
15 No association Blekkenhorst, 2017 (66)
NHS (USA) 71,141 F 50±7 FFQ CHD (fatal CHD or nonfatal MI)
24 22% ↓ RR (high vs low intake)
Bhupathiraju, 2013 (67)
HPFS (USA) 42,135 M 53±10 FFQ CHD (fatal CHD or nonfatal MI)
22 12% ↓ RR (high vs low intake)
Bhupathiraju, 2013 (67)
EPICOR (Italy)
29,689 F 35-74 FFQ CHD (fatal or nonfatal MI or coronary revascularisation)
7.85 46% ↓ HR (high vs low intake)
Bendinelli, 2011 (68)
MORGEN (The Netherlands)
20,069 M and F 20-65 FFQ CHD (fatal CHD or nonfatal acute MI)
10 No association Oude Griep, 2011 (69)
Linxian NIT (China)
2,445 M and F 40-69 FFQ Heart disease (death) 26 No association Wang, 2016 (70)
SMC and COSM (Sweden)
74,961 M and F 45-83 FFQ Stroke (cerebral infarction, haemorrhagic stroke or unspecified stroke)
10.2 No association Larsson, 2013 (71)
Linxian NIT (China)
2,445 M and F 40-69 FFQ Stroke (death) 26 38% ↓ HR (per twice/week)
Wang, 2016 (70)
27 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Table 1. Prospective cohort studies of leafy green vegetables and cardiovascular disease outcomes. Study cohort (country)
Sample number
Sex Age (years)
Dietary assessment method
Outcome Follow-up (years)
Results First author, year (ref)
NHS and HPFS (USA)
114,279 M and F 34-59 FFQ Ischaemic stroke (embolic or thrombotic)
14 84% ↓ RR (high vs low intake)
Joshipura, 1999 (72)
DDCHS (Denmark)
54,506 M and F 50-64 FFQ Ischaemic stroke (ischaemic infarction, intracerebral haemorrhage or subarachnoid haemorrhage)
3.09 No association Johnsen, 2003 (73)
ASVD, atherosclerotic vascular disease; CHD, coronary heart disease; COSM, Cohort of Swedish Men; CVD, cardiovascular disease; DDCHS, Danish Diet, Cancer, and Healthy Study; EPICOR, European Prospective Investigation into Cancer and Nutrition (EPIC) cohorts in northern (Turin and Varese), central (Florence), and southern (Naples and Ragusa) Italy; F, female; FFQ, food frequency questionnaire; HPFS, Health Professionals Follow-up Study; HR, hazard ratio; JPHCPS, Japan Public Health Centre-based Prospective Study; M, male; MHCPS, Massachusetts Health Care Panel Study; MI, myocardial infarction; MORGEN, Monitoring Project on Risk Factors and Chronic Diseases in The Netherlands; NHS, Nurses’ Health Study; NIT, Nutrition Intervention Trials; PLSAW, Perth Longitudinal Study of Ageing Women; PREDIMED, PREvención con DIeta MEDiterránea study; ref, reference; RR, relative risk; SMC, Swedish Mammography Cohort.
28 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Table 2. Prospective cohort studies of cruciferous vegetables and cardiovascular disease outcomes. Study cohort (country)
Sample number
Sex Age (years)
Dietary assessment method
Outcome Follow-up (years)
Results First author, year (ref)
NHS and HPFS (USA)
109,635 M and F 30-75 FFQ CVD (fatal or nonfatal MI or stroke)
12-15 No association Hung, 2004 (62)
JPHCPS (Japan)
77,891 M and F 45-74 FFQ CVD (fatal or nonfatal MI or stroke)
5-8 No association Takachi, 2007 (63)
SWHS (China)
74,942 F 40-70 FFQ CVD (death) 10.2 20% ↓ HR (high vs low intake)
Zhang, 2011 (74)
SMHS (China)
61,500 M 40-74 FFQ CVD (death) 4.6 27% ↓ HR (high vs low intake)
Zhang, 2011 (74)
IWHS (USA) 34,492 F 55-69 FFQ CVD (death) 16 No association Mink, 2007 (75)
PREDIMED (Spain)
7,216 M and F 55-80 FFQ CVD (cardiovascular death, MI or stroke)
7 36% ↓ HR (high vs low intake)
Buil-Cosiales, 2016 (64)
Odyssey Cohort (USA)
6,151 M and F 30-93 FFQ CVD (death) 14 No association Genkinger, 2004 (76)
MHCPS (USA)
1,273 M and F ≥66 FFQ CVD (death) 4.75 No association Gaziano, 1995 (65)
PLSAW (Australia)
1,226 F ≥70 FFQ ASVD (fatal ischaemic heart disease, heart failure, cerebrovascular disease excluding haemorrhage, or peripheral heart disease)
15 12% ↓ HR (per 10 g/d) Blekkenhorst, 2017 (66)
NHS (USA) 71,141 F 50±7 FFQ CHD (fatal CHD or nonfatal MI)
24 No association Bhupathiraju, 2013 (67)
SWHS (China)
67,211 F 40-70 FFQ CHD (fatal CHD or nonfatal MI)
9.8 No association Yu, 2013 (77)
SMHS (China)
55,474 M 40-75 FFQ CHD (fatal CHD or nonfatal MI)
5.4 No association Yu, 2013 (77)
HPFS (USA) 42,135 M 53±10 FFQ CHD (fatal CHD or nonfatal MI)
22 No association Bhupathiraju, 2013 (67)
IWHS (USA) 34,492 F 55-69 FFQ CHD (death) 16 No association Mink, 2007 (75)
29 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Table 2. Prospective cohort studies of cruciferous vegetables and cardiovascular disease outcomes. Study cohort (country)
Sample number
Sex Age (years)
Dietary assessment method
Outcome Follow-up (years)
Results First author, year (ref)
EPICOR (Italy)
29,689 F 35-74 FFQ CHD (fatal or nonfatal MI or coronary revascularisation)
7.85 No association Bendinelli, 2011 (68)
MORGEN (The Netherlands)
20,069 M and F 20-65 FFQ CHD (fatal CHD or nonfatal acute MI)
10 No association Oude Griep, 2011 (69)
PLSAW (Australia)
1,226 F ≥70 FFQ IHD (death) 15 17% ↓ HR (per 10 g/d) Blekkenhorst, 2017 (66)
Linxian NIT (China)
2,445 M and F 40-69 FFQ Heart disease (death) 26 No association Wang, 2016 (70)
FMCHES (Finland)
3,932 M and F 40-74 FFQ CVA (fatal or nonfatal) 24 21% ↓ RR (high vs low intake)
Mizrahi, 2009 (78)
PLSAW (Australia)
1,226 F ≥70 FFQ Ischaemic CVA (death) 15 No association Blekkenhorst, 2017 (66)
SMC and COSM (Sweden)
74,961 M and F 45-83 FFQ Stroke (cerebral infarction, haemorrhagic stroke or unspecified stroke)
10.2 No association Larsson, 2013 (71)
Linxian NIT (China)
2,445 M and F 40-69 FFQ Stroke (death) 26 No association Wang, 2016 (70)
NHS and HPFS (USA)
114,279 M and F 34-59 FFQ Ischaemic stroke (embolic or thrombotic)
14 29% ↓ RR (high vs low intake)
Joshipura, 1999 (72)
DDCHS (Denmark)
54,506 M and F 50-64 FFQ Ischaemic stroke (ischaemic infarction, intracerebral haemorrhage or subarachnoid haemorrhage)
3.09 No association Johnsen, 2003 (73)
FMCHES (Finland)
3,932 M and F 40-74 FFQ Ischaemic stroke (fatal or nonfatal)
24 33% ↓ RR (high vs low intake)
Mizrahi, 2009 (78)
FMCHES (Finland)
3,932 M and F 40-74 FFQ Intracerebral haemorrhage (fatal or nonfatal)
24 51% ↓ RR (high vs low intake)
Mizrahi, 2009 (78)
30 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Table 2. Prospective cohort studies of cruciferous vegetables and cardiovascular disease outcomes. Study cohort (country)
Sample number
Sex Age (years)
Dietary assessment method
Outcome Follow-up (years)
Results First author, year (ref)
ASVD, atherosclerotic vascular disease; CHD, coronary heart disease; COSM, Cohort of Swedish Men; CVA, cerebrovascular disease; CVD, cardiovascular disease; DDCHS, Danish Diet, Cancer, and Healthy Study; EPICOR, European Prospective Investigation into Cancer and Nutrition (EPIC) cohorts in northern (Turin and Varese), central (Florence), and southern (Naples and Ragusa) Italy; F, female; FFQ, food frequency questionnaire; FMCHES, Finnish Mobile Clinic Health Examination Survey; HPFS, Health Professionals Follow-up Study; HR, hazard ratio; IHD, ischaemic heart disease; IWHS, Iowa Women’s Health Study; JPHCPS, Japan Public Health Centre-based Prospective Study; M, male; MHCPS, Massachusetts Health Care Panel Study; MI, myocardial infarction; MORGEN, Monitoring Project on Risk Factors and Chronic Diseases in The Netherlands; NHS, Nurses’ Health Study; NIT, Nutrition Intervention Trials; PLSAW, Perth Longitudinal Study of Ageing Women; PREDIMED, PREvención con DIeta MEDiterránea study; ref, reference; RR, relative risk; SMC, Swedish Mammography Cohort; SMHS, Shanghai Men’s Health Study; SWHS, Shanghai Women’s Health Study.
31 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Table 3. Prospective cohort studies of allium vegetables and cardiovascular disease outcomes. Study cohort (country)
Sample number
Sex Age (years)
Dietary assessment method
Outcome Follow-up (years)
Results First author, year (ref)
PLSAW (Australia)
1,226 F ≥70 FFQ ASVD (fatal ischaemic heart disease, heart failure, cerebrovascular disease excluding haemorrhage, or peripheral heart disease)
15 15% ↓ HR (per 5 g/d) Blekkenhorst, 2017 (66)
SWHS (China)
67,211 F 40-70 FFQ CHD (fatal CHD or nonfatal MI)
9.8 No association Yu, 2013 (77)
NHS (USA) 66,360 F 30-55 FFQ CHD (fatal CHD or nonfatal MI)
12 No association Lin, 2007 (79)
SMHS (China)
55,474 M 40-75 FFQ CHD (fatal CHD or nonfatal MI)
5.4 No association Yu, 2013 (77)
MORGEN (The Netherlands)
20,069 M and F 20-65 FFQ CHD (fatal CHD or nonfatal acute MI)
10 No association Oude Griep, 2011 (69)
FSII (Finland) 2,748 M 30-69 DHQ CHD (death) 26 No association Knekt, 1996 (80)
FSII (Finland) 2,385 F 30-69 DHQ CHD (death) 26 50% ↓ RR (high vs low intake)
Knekt, 1996 (80)
Caerphilly Study (UK)
2,512 M 45-59 FFQ IHD (IHD death, nonfatal MI, MI define by electrocardiogram)
10 No association Hertog, 1997 (81)
PLSAW (Australia)
1,226 F ≥70 FFQ IHD (death) 15 18% ↓ HR (per 5 g/d) Blekkenhorst, 2017 (66)
FMCHES (Finland)
9,208 M and F ≥15 DHQ CVA (fatal or nonfatal) 28 No association Knekt, 2000 (82)
PLSAW (Australia)
1,226 F ≥70 FFQ Ischaemic CVA (death) 15 25% ↓ HR (per 5 g/d) Blekkenhorst, 2017 (66)
SMC and COSM (Sweden)
74,961 M and F 45-83 FFQ Stroke (cerebral infarction, haemorrhagic stroke or unspecified stroke)
10.2 No association Larsson, 2013 (71)
32 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Table 3. Prospective cohort studies of allium vegetables and cardiovascular disease outcomes. Study cohort (country)
Sample number
Sex Age (years)
Dietary assessment method
Outcome Follow-up (years)
Results First author, year (ref)
FMCHES (Finland)
9,208 M and F ≥15 DHQ Acute strokes 28 No association Knekt, 2000 (82)
DDCHS (Denmark)
54,506 M and F 50-64 FFQ Ischaemic stroke (ischaemic infarction, intracerebral haemorrhage or subarachnoid haemorrhage)
3.09 No association Johnsen, 2003 (73)
FMCHES (Finland)
9,208 M and F ≥15 DHQ Intracerebral haemorrhage
28 No association Knekt, 2000 (82)
FMCHES (Finland)
9,208 M and F ≥15 DHQ Thrombosis or embolia 28 No association Knekt, 2000 (82)
ASVD, atherosclerotic vascular disease; CHD, coronary heart disease; COSM, Cohort of Swedish Men; CVA, cerebrovascular disease; DDCHS, Danish Diet, Cancer, and Healthy Study; DHS, dietary history questionnaire; F, female; FFQ, food frequency questionnaire; FMCHES, Finnish Mobile Clinic Health Examination Survey; FSII, Finnish Social Insurance Institution; HR, hazard ratio; IHD, ischaemic heart disease; M, male; MI, myocardial infarction; MORGEN, Monitoring Project on Risk Factors and Chronic Diseases in The Netherlands; NHS, Nurses’ Health Study; PLSAW, Perth Longitudinal Study of Ageing Women; ref, reference; RR, relative risk; SMC, Swedish Mammography Cohort; SMHS, Shanghai Men’s Health Study; SWHS, Shanghai Women’s Health Study.
33 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Table 4. Prospective cohort studies of yellow-orange-red vegetables and cardiovascular disease outcomes. Study cohort (country)
Sample number
Sex Age (years)
Dietary assessment method
Outcome Follow-up (years)
Results First author, year (ref)
JPHCPS (Japan)
77,891 M and F 45-74 FFQ CVD (MI or stroke) 5-8 No association Takachi, 2007 (63)
IWHS (USA) 34,489 F 55-69 FFQ CVD (CHD or stroke) 16 No association Mink, 2007 (75)
Framingham Offspring Study (USA)
2,525 M and F 26-79 FFQ CVD (fatal or nonfatal CHD, CVA, congestive heart failure or peripheral vascular disease)
11 6% ↓ HR (per 1 serving/d)
Jacques, 2013 (83)
MHCPS (USA)
1,273 M and F ≥66 FFQ CVD (death) 4.75 60% ↓ RR (≥1 vs <1 serving)
Gaziano, 1995 (65)
Zutphen Elderly Study (The Netherlands)
559 M 65-84 DHQ CVD (fatal ischaemic heart disease, stroke or other diseases of the circulatory system)
15 17% ↓ RR (per SD) Buijsse, 2008 (84)
PLSAW (Australia)
1,226 F ≥70 FFQ ASVD (fatal ischaemic heart disease, heart failure, cerebrovascular disease excluding haemorrhage, or peripheral heart disease)
15 No association Blekkenhorst, 2017 (66)
NHS (USA) 66,360 F 30-55 FFQ CHD (fatal CHD or nonfatal MI)
12 No association Lin, 2007 (79)
EPICOR (Italy)
29,689 F 35-74 FFQ CHD (fatal or nonfatal MI or coronary revascularisation)
7.85 No association Bendinelli, 2011 (68)
MORGEN (The Netherlands)
20,069 M and F 20-65 FFQ CHD (nonfatal acute MI or fatal CHD)
10 No association Oude Griep, 2011 (69)
Framingham Offspring Study (USA)
2,525 M and F 26-79 FFQ CHD (MI, angina pectoris, coronary insufficiency or CHD death)
11 10% ↓ HR (per 1 serving/d)
Jacques, 2013 (83)
34 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Table 4. Prospective cohort studies of yellow-orange-red vegetables and cardiovascular disease outcomes. Study cohort (country)
Sample number
Sex Age (years)
Dietary assessment method
Outcome Follow-up (years)
Results First author, year (ref)
Linxian NIT (China)
2,445 M and F 40-69 FFQ Heart disease (death) 26 23% ↓ HR (per once/d)
Wang, 2016 (70)
SMC and COSM (Sweden)
74,961 M and F 45-83 FFQ Stroke (cerebral infarction, haemorrhagic stroke or unspecified stroke)
10.2 No association Larsson, 2013 (71)
Framingham Offspring Study (USA)
2,525 M and F 26-79 FFQ Stroke (nonfatal) 11 No association Jacques, 2013 (83)
Linxian NIT (China)
2,445 M and F 40-69 FFQ Stroke (death) 26 No association Wang, 2016 (70)
ASVD, atherosclerotic vascular disease; CHD, coronary heart disease; CVD, cardiovascular disease; DHS, dietary history questionnaire; EPICOR, European Prospective Investigation into Cancer and Nutrition (EPIC) cohorts in northern (Turin and Varese), central (Florence), and southern (Naples and Ragusa) Italy; F, female; FFQ, food frequency questionnaire; HR, hazard ratio; IWHS, Iowa Women’s Health Study; JPHCPS, Japan Public Health Centre-based Prospective Study; M, male; MHCPS, Massachusetts Health Care Panel Study; MI, myocardial infarction; MORGEN, Monitoring Project on Risk Factors and Chronic Diseases in The Netherlands; NHS, Nurses’ Health Study; NIT, Nutrition Intervention Trials; PLSAW, Perth Longitudinal Study of Ageing Women; ref, reference; RR, relative risk.
35 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Table 5. Prospective cohort studies of legumes and cardiovascular disease outcomes. Study cohort (country)
Sample number
Sex Age (years)
Dietary assessment method
Outcome Follow-up (years)
Results First author, year (ref)
NHS and HPFS (USA)
109,635 M and F 30-75 FFQ CVD (fatal or nonfatal MI or stroke)
12-15 No association Hung, 2004 (62)
JCCS (Japan)
59,485 M and F 40-79 FFQ CVD (death) 12.7 16% ↓ HR (high vs low intake)
Nagura, 2009 (85)
The SUN Project (Spain)
13,609 M and F 38 FFQ CVD (cardiovascular death, MI, revascularisation procedures, fatal or nonfatal stroke)
4.9 No association Martinez-Gonzalez, 2011 (86)
NHEFS (USA) 9,632 M and F 25-74 FFQ CVD (fatal or nonfatal) 21 11% ↓ RR (≥4 vs <1 times/week)
Bazzano, 2001 (87)
ICS (Iran) 6,504 M and F ≥35 FFQ CVD (fatal or nonfatal MI, sudden cardiac death, unstable angina or stroke)
6.8 33% ↓ HR (>55 years only) (high vs low intake)
Nouri, 2016 (88)
JPHC (Japan)
40,462 M and F 40-59 FFQ Ischaemic CVD (fatal CI or MI)
13 69% ↓ HR (F only) (high vs low intake)
Kokubo, 2007 (89)
PLSAW (Australia)
1,226 F ≥70 FFQ ASVD (fatal ischaemic heart disease, heart failure, cerebrovascular disease excluding haemorrhage, or peripheral heart disease
15 No association Blekkenhorst, 2017 (66)
IWHS (USA) 99,826 F 55-69 FFQ CHD (death) 15 No association Kelemen, 2005 (90)
NHS (USA) 84,136 F 30-55 FFQ CHD (fatal CHD or nonfatal MI)
26 No association Bernstein, 2010 (91)
SWHS (China)
67,211 F 40-70 FFQ CHD (fatal CHD or nonfatal MI)
9.8 No association Yu, 2013 (77)
JCCS (Japan)
59,485 M and F 40-79 FFQ CHD (death) 12.7 No association Nagura, 2009 (85)
SMHS (China)
55,474 M 40-75 FFQ CHD (fatal CHD or nonfatal MI)
5.4 No association Yu, 2013 (77)
36 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Table 5. Prospective cohort studies of legumes and cardiovascular disease outcomes. Study cohort (country)
Sample number
Sex Age (years)
Dietary assessment method
Outcome Follow-up (years)
Results First author, year (ref)
EPIC (Spain) 41,078 M and F 29-69 FFQ CHD (fatal or nonfatal) 10.4 No association Buckland, 2009 (92)
EPIC (Greece)
23,929 M and F 20-86 FFQ CHD (fatal or nonfatal MI, angina or other CHD)
10 No association Dilis, 2012 (93)
The SUN Project (Spain)
13,609 M and F 38 FFQ CHD (fatal) 4.9 No association Martinez-Gonzalez, 2011 (86)
ARIC (USA) 12,066 M and F 45-64 FFQ CHD (fatal CHD or nonfatal MI)
22 No association Haring, 2014 (94)
NHEFS (USA) 9,632 M and F 25-74 FFQ CHD (fatal or nonfatal) 21 22% ↓ RR (≥4 vs <1 time/week
Bazzano, 2001 (87)
Linxian NIT (China)
2,445 M and F 40-69 FFQ Heart disease (death) 26 37% ↓ HR (4 times/week)
Wang, 2016 (70)
EPIC (Greece)
23,601 M and F 25-67 FFQ CVA (fatal or nonfatal) 10.6 No association Misirli, 2012 (95)
FMCHES (Finland)
3,932 M and F 40-74 FFQ CVA (fatal or nonfatal) 24 No association Mizrahi, 2009 (78)
NHS (USA) 84,010 F 30-55 FFQ Stroke (fatal or nonfatal ischaemic, haemorrhagic or other stroke)
26 No association Bernstein, 2012 (96)
JCCS (Japan)
59,485 M and F 40-79 FFQ Stroke (fatal ischaemic or haemorrhagic stroke)
12.7 No association Nagura, 2009 (85)
NFPS (USA) 43,150 M 40-75 FFQ Stroke (fatal or nonfatal ischaemic, haemorrhagic or other stroke)
22 No association Bernstein, 2012 (96)
ARIC (USA) 11,601 M and F 45-64 FFQ Stroke (fatal or nonfatal ischaemic or haemorrhagic stroke)
22.7 No association Haring, 2015 (97)
Linxian NIT (China)
2,445 M and F 40-69 FFQ Stroke (death) 26 No association Wang, 2016 (70)
37 CARDIOVASCULAR HEALTH BENEFITS OF SPECIFIC VEGETABLES TYPES: A NARRATIVE REVIEW
Table 5. Prospective cohort studies of legumes and cardiovascular disease outcomes. Study cohort (country)
Sample number
Sex Age (years)
Dietary assessment method
Outcome Follow-up (years)
Results First author, year (ref)
NHS and HPFS (USA)
114,279 M and F 34-59 FFQ Ischaemic stroke (embolic or thrombotic)
14 No association Joshipura, 1999 (72)
FMCHES (Finland)
3,932 M and F 40-74 FFQ Ischaemic stroke (fatal or nonfatal)
24 28% ↓ RR (high vs low intake)
Mizrahi, 2009 (78)
FMCHES (Finland)
3,932 M and F 40-74 FFQ Intracerebral haemorrhage (fatal or nonfatal)
24 No association Mizrahi, 2009 (78)
ARIC, Atherosclerosis Risk in Communities; ASVD, atherosclerotic vascular disease; CHD, coronary heart disease; CI, cerebral infarction; CVA, cerebrovascular disease; CVD, cardiovascular disease; EPIC, European Prospective Investigation into Cancer and Nutrition; F, female; FFQ, food frequency questionnaire; FMCHES, Finnish Mobile Clinic Health Examination Survey; HPFS, Health Professionals Follow-up Study; HR, hazard ratio; ICS, Isfahan Cohort Study; IWHS, Iowa Women’s Health Study; JCCS, Japanese Collaborative Cohort Study; JPHC, Japan Public Health Centre-Based Study; M, male; MI, myocardial infarction; NHEFS, First National Health and Nutrition Examination Survey Epidemiologic Follow-up Study; NHS, Nurses’ Health Study; NIT, Nutrition Intervention Trials; PLSAW, Perth Longitudinal Study of Ageing Women; ref, reference; SMHS, Shanghai Men’s Health Study; SUN, Seguimiento Universidad de Navarra; SWHS, Shanghai Women’s Health Study.
38 CHAPTER 2
CHAPTER 2
NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC
LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Manuscript based on this chapter:
Lauren C Blekkenhorst*, Nicola P Bondonno*, Alex H Liu, Natalie C Ward, Richard L Prince, Joshua R Lewis, Amanda Devine, Kevin D Croft, Jonathan M Hodgson, Catherine P Bondonno. Nitrate, the oral microbiome and cardiovascular health: a systematic literature review of human and animal studies. American Journal of Clinical Nutrition. 2018;107(4):504-522. *Joint first author

39 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
ABSTRACT
Background: Dietary nitrate is an important source of nitric oxide (NO), a molecule critical for cardiovascular health. Nitrate is sequentially reduced to NO through an enterosalivary nitrate-nitrite-NO pathway that involves the oral microbiome. This pathway is considered an important adjunct pathway to the classical L-arginine-NO synthase pathway. The objective of this study was to systematically assess the evidence for dietary nitrate intake and improved cardiovascular health from both human and animal studies.
Methods: A systematic literature search was performed according to PRISMA guidelines using key search terms in Medline and EMBASE databases and defined inclusion and exclusion criteria.
Results: Thirty-seven articles were included on humans and fourteen articles on animals from 12,541 screened references. Data on the effects of dietary nitrate on blood pressure, endothelial function, ischaemic reperfusion injury, arterial stiffness, platelet function, and cerebral blood flow in both human and animal models were identified. Beneficial effects of nitrate on vascular health have predominantly been observed in healthy human populations while effects in populations at risk of cardiovascular disease are less clear. Few studies have investigated the long-term effects of dietary nitrate on cardiovascular disease clinical endpoints. In animal studies, there is evidence that nitrate improves blood pressure and endothelial function particularly in animal models with reduced NO bioavailability. Nitrate dose seems to be a critical factor as there is evidence of cross-talk between the two pathways of NO production.
Conclusion: Evidence for a beneficial effect in humans at risk of cardiovascular disease is limited. Furthermore, there is a need to investigate the long-term effects of dietary nitrate on cardiovascular disease clinical endpoints. Further animal studies are required to elucidate the mechanisms behind the observed effects.
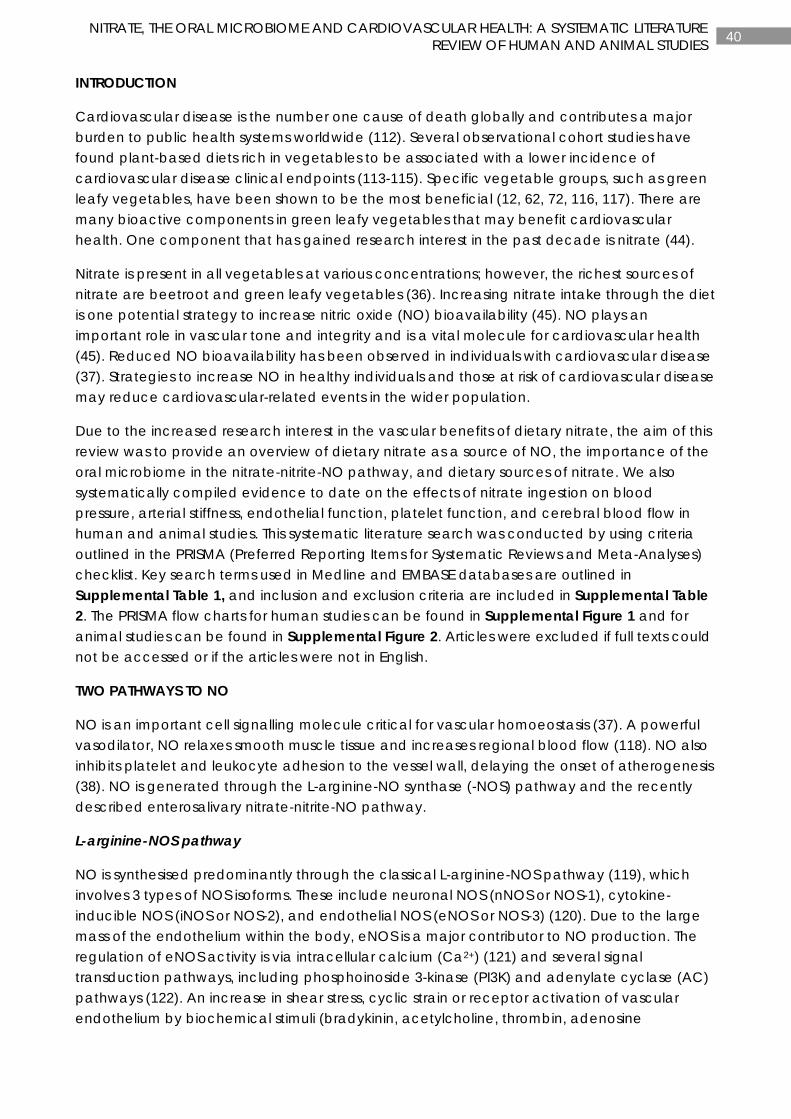
40 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
INTRODUCTION
Cardiovascular disease is the number one cause of death globally and contributes a major burden to public health systems worldwide (112). Several observational cohort studies have found plant-based diets rich in vegetables to be associated with a lower incidence of cardiovascular disease clinical endpoints (113-115). Specific vegetable groups, such as green leafy vegetables, have been shown to be the most beneficial (12, 62, 72, 116, 117). There are many bioactive components in green leafy vegetables that may benefit cardiovascular health. One component that has gained research interest in the past decade is nitrate (44).
Nitrate is present in all vegetables at various concentrations; however, the richest sources of nitrate are beetroot and green leafy vegetables (36). Increasing nitrate intake through the diet is one potential strategy to increase nitric oxide (NO) bioavailability (45). NO plays an important role in vascular tone and integrity and is a vital molecule for cardiovascular health (45). Reduced NO bioavailability has been observed in individuals with cardiovascular disease (37). Strategies to increase NO in healthy individuals and those at risk of cardiovascular disease may reduce cardiovascular-related events in the wider population.
Due to the increased research interest in the vascular benefits of dietary nitrate, the aim of this review was to provide an overview of dietary nitrate as a source of NO, the importance of the oral microbiome in the nitrate-nitrite-NO pathway, and dietary sources of nitrate. We also systematically compiled evidence to date on the effects of nitrate ingestion on blood pressure, arterial stiffness, endothelial function, platelet function, and cerebral blood flow in human and animal studies. This systematic literature search was conducted by using criteria outlined in the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist. Key search terms used in Medline and EMBASE databases are outlined in Supplemental Table 1, and inclusion and exclusion criteria are included in Supplemental Table 2. The PRISMA flow charts for human studies can be found in Supplemental Figure 1 and for animal studies can be found in Supplemental Figure 2. Articles were excluded if full texts could not be accessed or if the articles were not in English.
TWO PATHWAYS TO NO
NO is an important cell signalling molecule critical for vascular homoeostasis (37). A powerful vasodilator, NO relaxes smooth muscle tissue and increases regional blood flow (118). NO also inhibits platelet and leukocyte adhesion to the vessel wall, delaying the onset of atherogenesis (38). NO is generated through the L-arginine-NO synthase (-NOS) pathway and the recently described enterosalivary nitrate-nitrite-NO pathway.
L-arginine-NOS pathway
NO is synthesised predominantly through the classical L-arginine-NOS pathway (119), which involves 3 types of NOS isoforms. These include neuronal NOS (nNOS or NOS-1), cytokine-inducible NOS (iNOS or NOS-2), and endothelial NOS (eNOS or NOS-3) (120). Due to the large mass of the endothelium within the body, eNOS is a major contributor to NO production. The regulation of eNOS activity is via intracellular calcium (Ca2+) (121) and several signal transduction pathways, including phosphoinoside 3-kinase (PI3K) and adenylate cyclase (AC) pathways (122). An increase in shear stress, cyclic strain or receptor activation of vascular endothelium by biochemical stimuli (bradykinin, acetylcholine, thrombin, adenosine
41 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
diphosphate, and serotonin) causes a release of Ca2+ from intracellular stores, stimulating eNOS activity (120, 123). Phosphorylation of several residues on the eNOS dimer is also an important requirement for activation (122). Equimolar amounts of NO and L-citrulline are produced by using L-arginine and molecular oxygen together with tetrahydrobiopterin (BH4) in a complex oxygen-dependent 5-electron-transfer reaction (121, 124).
NO synthesised from L-arginine in the endothelium diffuses across the cell membrane to nearby smooth muscle cells stimulating soluble guanylate cyclase (sGC) (121). This results in the synthesis of cyclic guanosine monophosphate (cGMP) from guanosine triphosphate (GTP), triggering the relaxation of smooth muscle cells (121). Uncoupling of eNOS, by reduced bioavailability of BH4 or the substrate L-arginine, can lead to the production of superoxide or H2O2 (125). Furthermore, studies have shown that reduced tissue concentrations of BH4 and increased superoxide generation are associated with risk factors for atherosclerosis (126-128).
Nitrate-nitrite-NO pathway
Historically, nitrate and nitrite have been considered to be environmental pollutants and potential carcinogenic residues in the food chain (129). Now, however, nitrate and nitrite are considered important molecules for cardiovascular health (130).
Vegetables are a major source of nitrate consumed in the human population (131). When nitrate is ingested, it is absorbed in the proximal area of the small intestine (45). Nitrate then enters the bloodstream and mixes with endogenous sources of nitrate (mainly derived from oxidation of NO through the L-arginine-NOS pathway). Approximately 75% of circulating nitrate is excreted by the kidneys. The rest (~25%) is actively taken up by the salivary glands where nitrate is concentrated in saliva and secreted in the oral cavity (132, 133). Nitrate is then reduced to nitrite by facultative anaerobic bacteria found in the deep clefts on the dorsal surface of the tongue (134). The commensal bacteria in the oral cavity use nitrate as an alternative electron acceptor to oxygen during respiration, reducing nitrate to nitrite by nitrate reductases (135). Once swallowed, a proportion of nitrite is rapidly protonated, forming nitrous acid (HNO2) in the acidic environment of the stomach (136). Nitrous acid decomposes further to form NO, having localised benefits (136). This nonenzymatic reduction of nitrite to NO is enhanced by vitamin C and polyphenols (137, 138). The remaining nitrate and nitrite in the stomach enter the small intestine and are absorbed into the bloodstream where they mix with endogenous forms of nitrate and nitrite (mainly derived from oxidation of NO through the L-arginine-NOS pathway).
The 1-electron reduction of nitrite to NO in the blood and tissues is catalysed by both enzymatic and nonenzymatic pathways (44). Enzymatic pathways include a number of proteins and enzymes, including globins (e.g., haemoglobin, myoglobin, cytoglobin, and neuroglobin), xanthine oxidoreductase, cytochrome P450, mitochondrial proteins, carbonic anhydrase, aldehyde oxidase, and eNOS (44). Nonenzymatic pathways include protons, polyphenols, and vitamin C (44). Both enzymatic and nonenzymatic reductions of nitrite to NO are enhanced during hypoxia and at a low pH (44, 139). Recent evidence suggests that the acidic environment of the stomach plays an important role in the reduction of nitrite to NO (140).
The nitrate-nitrite-NO pathway and the L-arginine-NOS pathway are interconnected through the anions, nitrate and nitrite. Nitrate and nitrite are the oxidation end products of NO
42 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
metabolism through the L-arginine-NOS pathway but can also be derived from the diet (135). Nitrate and nitrite, derived from the diet and derived as oxidation end-products of NO metabolism, are both recycled through the nitrate-nitrite-NO pathway. Both pathways become a storage pool for NO production. Because the L-arginine-NOS pathway requires molecular oxygen to produce NO, nitrite reduction to NO via the nitrate-nitrite-NO pathway may form as a backup system for NO production during hypoxia. A crucial step in the nitrate-nitrite-NO pathway is nitrate to nitrite reduction by the oral microbiome.
THE ORAL MICROBIOME
The oral microbiome is the second most diverse microbial community in the human body comprising 50-100 billion bacteria from >700 prokaryotic taxa, as well as a fungal and viral flora (141). Disturbances to the composition, and therefore function, of the oral microbiome are thought to play a role in a number of diseases, including cardiovascular disease (141). Whether this link is related in part to the nitrate-nitrite-NO pathway is garnering research interest. An important step in the nitrate-nitrite-NO pathway is the reduction of nitrate to nitrite by facultative anaerobic bacteria found in the oral cavity. Reduced oral bacterial nitrate to nitrite reduction, both in the presence and absence of dietary nitrate intake, could have detrimental effects on the circulating NO pool with subsequent vascular effects. In the presence of nitrate intake, interrupting the nitrate-nitrite-NO pathway with an antibacterial mouthwash or spitting out of saliva, prevented the resultant increase in salivary and plasma nitrite and the associated decrease in blood pressure (142, 143). In the absence of dietary nitrate intake, increases in blood pressure with concomitant decreases in salivary and plasma nitrite were observed with daily chlorhexidine-based antibacterial mouthwash use in both healthy volunteers (144) and individuals with treated hypertension (145). This could be explained by the fact that nitrate and nitrite, produced as end-products of NO metabolism, are recycled through the nitrate-nitrite-NO pathway back into the circulating NO pool. Thus nitrate to nitrite reduction by the oral microbiome could play a key role in blood pressure control. The influence on other measures of vascular health has yet to be determined.
The fundamental role of the oral microbiome in the nitrate-nitrite-NO pathway and possibly blood pressure control makes understanding all of the factors that influence oral nitrate to nitrite reduction an important research area. Indeed, there is evidence of a considerable variation between individuals in the nitrate-reducing capacity of the oral microbiome (146). The first set of factors to consider is the use of antibacterial mouthwashes, antibacterial toothpastes, and antibiotics. Given the results of the studies described above, the widespread use of daily mouthwash in the general population is of potential concern. The mouthwash used in these studies, however, contained chlorhexidine, a strong antibacterial agent. Different effects have been observed with other types and strengths of antibacterial mouthwashes (147). To date, only one study to our knowledge has examined the effect of antibacterial toothpaste, which contained triclosan, on oral nitrate to nitrite reduction (148), with no effect observed. These results need to be confirmed in additional studies examining the effect of mouthwash and toothpaste on oral nitrate reduction. Interestingly, epidemiologic studies show that regular tooth brushing and mouthwash use, indicative of good oral hygiene, are associated with a decreased risk of hypertension and cardiovascular disease (149, 150). The effect of antibiotic use on oral nitrate to nitrite reduction has yet to be ascertained.

43 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
Other important factors are those inherent to the complex oral microbial community, such as bacterial genetics, the presence and influence of other microorganisms, and environmental pressures. There are a number of potential nitrate-reducing taxa present in the oral microbiome. Doel et al. (151) identified Veillonella spp as the most abundant nitrate-reducing genus followed by Actinomyces, Rothia, and Staphylococcus spp. (151). Hyde et al (152) confirmed Veillonella spp. as the most abundant nitrate-reducing genus present but also detected Prevotella, Neisseria, and Haemophilus at a higher abundance than Actinomyces spp. Nitrate to nitrite reduction by these bacteria is highly variable both within and between bacterial species and needs to be examined in the context of the huge interdependent microbial network in which they exist. This network comprises a heterogeneous microbial community within a biofilm that communicates by using a process called quorum sensing. These communities are highly complex, with all members influencing their health and vitality. Interestingly, the presence of nitrite reducers may prevent the accumulation of nitrite in the saliva and, as such, have a negative influence on the nitrate-nitrite-NO pathway (152). Microbial nitrate metabolism can also be altered by environmental influences such as pH and oxygen tension. A low pH in an oral microenvironment together with increased nitrate and nitrite concentrations, can select for nitrate-reducing bacteria (153). Nitrate-reducing bacteria are facultative anaerobes. A low- or no-oxygen environment will therefore result in the nitrate reductive pathway being utilised for respiration. Other potential factors influencing nitrate to nitrite reduction that require future investigation include host factors such as age, diet, and oral health.
The evidence of the link between oral health and cardiovascular disease being related to the nitrate-nitrite-NO pathway is strongly suggestive. Future studies will need to examine this relation in the context of the large number of factors that could influence oral nitrate to nitrite reduction.
DIETARY SOURCES OF NITRATE AND NITRITE
Vegetables contribute ~80% of dietary nitrate intake in the human population (30, 31, 131, 154, 155). Nitrate ingested in the diet can also be derived from other food sources, such as fruit, grains, and animal products, with the remainder coming from drinking water. Many countries have strict regulations to maintain low amounts of nitrate in drinking water due to underlying health concerns, such as methaemoglobinaemia (156). High amounts, however, have been detected in private wells in rural areas due to nitrogen-based fertiliser use in agricultural areas (157). Another controversial health concern is the addition of nitrate and nitrite to meat and their potential to form N-nitrosoamines, which are potential carcinogens (132). Compounds such as polyphenols, vitamins C and E, and other antioxidants inhibit the formation of N-nitrosoamines (157). These compounds are abundant in vegetables. A large number of countries have also set maximum levels for nitrate in vegetables, particularly for lettuce and spinach, which are known to accumulate high amounts of nitrate (158). These maximum amounts vary across harvest period, being higher in winter and if grown under cover, and lower in summer and if grown in open air (158).
Dietary nitrite, on the other hand, contributes only a small amount to human exposure and is mainly consumed from animal-based foods such as cured meats and bacon (155). Nitrite is added to these products as a preservative and to enhance taste and appearance (155). Although a small amount of nitrite is consumed from these food sources, the majority of nitrite
44 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
exposure (70-90%) is derived from the in vivo conversion of nitrate to nitrite through endogenous pathways (159).
The nitrate content of vegetables depends on many different factors, including the biological properties of plants, fertiliser use, soil conditions, sun exposure, and cooking and storage methods. The biological properties of plants can influence the amount of nitrate that accumulates in that plant. For example, nitrate accumulates in different parts of the plants, with the leaf and stem having the highest concentrations and the bulb and fruit having the lowest (131). In our recently developed reference database for assessing dietary nitrate in vegetables (36), leafy vegetables were found to have the highest nitrate content, with Chinese flat cabbage and arugula containing the highest concentrations of nitrate (3000 mg/kg fresh weight). Corn, mushrooms, and peas had the lowest nitrate content (<50 mg/kg fresh weight). The nitrate concentration in vegetables also differs between varieties. For example, Chinese lettuce has a 3-fold higher nitrate value than iceberg lettuce (36).
Nitrogen-based fertilisers enhance the growth of plants and, thus, have an impact on how much nitrate accumulates in vegetables. Nitrate located in the soil of growing vegetables is transported via the plant xylem system to the leaves of the vegetables (155). Because organic vegetables tend to be grown in fertilisers containing less nitrogen, by comparison, conventionally grown vegetables tend to accumulate higher nitrate concentrations (36, 160).
Other factors, such as handling, storage, and processing, as well as temperature and light intensity, can also influence the amount of nitrate in vegetables (155). Higher nitrate concentrations are observed in vegetables grown in winter than those grown in summer, and vegetables grown under cover contain higher nitrate concentrations than those grown outdoors in the same season and the same region (36, 155).
Storage in ambient temperature can also reduce the nitrate content of fresh vegetables. Under refrigerated and frozen storage conditions, nitrate concentrations appear to be unaffected (155). Endogenous nitrate reductase activity and the amount of bacterial contamination due to postharvest storage and wilting processes reduce nitrate and subsequently increase nitrite in fresh vegetables (155). Being water soluble, nitrate is also reduced with washing and cooking methods by ~10-15% and 50%, respectively (155). Because nitrate is also found in the skin of vegetables, peeling the skin can also reduce nitrate concentrations by ~20-34% (155).
NITRATE INGESTION AND ITS EFFECTS ON VASCULAR FUNCTION
Dietary nitrate is now considered an important alternative source of NO. Human and animal studies to date have focused on the effects of nitrate ingestion on blood pressure, arterial stiffness, endothelial function, platelet function, and cerebral blood flow, as discussed below. A summary of the beneficial effects of nitrate ingestion on these cardiovascular-related outcomes in human and animal studies is shown in Figure 1. Benefits of nitrate ingestion on exercise performance are not covered in this review.
BLOOD PRESSURE
Evidence that decreased NO production was associated with hypertension raised the possibility that nitrate, through the nitrate-nitrite-NO pathway, could partially account for the blood pressure-lowering effects of green leafy vegetables. Randomised controlled trials such
45 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
as the Dietary Approaches to Stop Hypertension (DASH) trial have been shown to reduce blood pressure (161). It has been suggested that the high nitrate content of the DASH diet contributes to the blood pressure-lowering effects observed (131). The DASH diet has been estimated to include as much as 1,222 mg (19.7 mmol) nitrate/d (131). This amount can, however, differ by as much as 700% due to the wide variation in nitrate in vegetables (131). An Acceptable Daily Intake of 3.7 mg nitrate/kg body weight was set by the Joint Food and Agricultural Organisation and WHO (155). For an average person weighing 70 kg, this is calculated to be 259 mg nitrate. The DASH diet can provide ≤500% more nitrate than this Acceptable Daily Intake.
The DASH diet is associated with reductions of 4.5 mmHg in systolic blood pressure (SBP) (162). This blood pressure reduction is similar to that seen in a meta-analysis that showed that consumption of inorganic nitrate and nitrate-rich beetroot juice is associated with an SBP reduction of 4.4 mmHg (163). There is now substantial evidence from human intervention trials to show blood pressure reductions with short-term intake of dietary nitrate in healthy populations (163). However, the effects of chronic nitrate intake on blood pressure in older populations and populations at risk of cardiovascular disease remain uncertain (153, 164-169).
Human studies
Our systematic literature search found 27 acute studies (≤24 h) (Table 1) (143, 153, 164, 170-186) and 15 chronic studies (>1 d) (Table 2) (153, 166-169, 187-194) in 32 publications investigating the effects of nitrate ingestion on blood pressure. Beetroot juice was the most common nitrate source used in both acute and chronic studies. Twenty-four-hour ambulatory blood pressure, the preferred diagnostic method for assessing hypertension (195, 196), was used in 10 studies (166-169, 178, 181-183, 188, 191). Clinic blood pressure was used in 34 studies (143, 153, 164, 166, 168, 170-177, 179, 180, 184-194), and 4 studies used home blood pressure monitoring (167, 168, 188, 191).
Acute studies
The acute effects of nitrate ingestion on blood pressure were investigated between 2 and 24 h with nitrate doses ranging from 68 to 1488 mg (1.1 to 24 mmol) (Table 1). Five studies showed a significant reduction in SBP only (179, 183-186), and 4 studies showed a significant reduction in only diastolic blood pressure (DBP) (172, 178, 180, 181). Eleven studies showed significant reductions in both SBP and DBP (143, 153, 172, 173, 182, 186). Acute reductions in SBP ranged from 2.7 to 22.2 mmHg and from 2.6 to 23.6 mmHg for DBP. Reductions in blood pressure were seen across the entire range of nitrate doses investigated and in subjects who were healthy (143, 172, 173, 178, 179, 181-186), overweight (180), and hypercholesterolaemic (153). Sample sizes of these populations ranged from 6 to 67 participants. Blood pressure reductions were not seen in 7 studies (164, 170, 171, 174-177). These populations consisted of subjects who were healthy (170, 171, 174-177) and subjects with heart failure (164). Sample sizes of these populations ranged from 5 to 40 participants.
Chronic studies
The chronic effects of nitrate ingestion on blood pressure were investigated in 15 studies from 3 to 42 d (6 wk) in duration, with nitrate doses ranging from 155 to 1104 mg/d (2.5 to 17.8 mmol/d) (Table 2). Three studies showed a significant reduction in SBP (189-191), and 3 other
46 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
studies showed a significant reduction in DBP (187, 193, 194). Only one study showed a significant reduction in both SBP and DBP (188). In total, 7 studies showed a significant reduction in blood pressure. It is worth noting that the study conducted by Ashworth et al. (189) was not clear whether the significant reductions in blood pressure were acute or chronic because the subjects were advised to eat high-nitrate vegetables 2-3 h before blood pressure was taken on the final day. Reductions in SBP ranged from 4.0 to 8.1 mmHg and reductions in DBP ranged from 2.4 to 12 mmHg, with nitrate doses ranging from 165 to 1104 mg/d (2.7 to 17.8 mmol/d). Reductions in blood pressure were seen in one study that used 24-h ambulatory blood pressure monitoring (188), 2 studies that used home blood pressure (188, 191), and 6 studies that used clinic blood pressure (187-190, 193, 194). Blood pressure reductions were seen in subjects who were healthy (187, 189, 193, 194), at moderate cardiovascular risk (190), and older and overweight (191), and in those who had grade 1 hypertension (treated and untreated) (188). These studies included a mix of young (mean age: <37 y) (187, 189, 193, 194) and older cohorts (mean age: >56 y) (188, 190, 191). Most studies that showed reductions in blood pressure had low sample sizes (n range: 6-25), except for Kapil et al. (188), which had a sample size of n=64.
Blood pressure reductions were not seen in 8 studies (153, 166-169, 192). These populations consisted of subjects who were older (192), prehypertensive (168), treated hypertensive (167), overweight and obese (166), type 2 diabetic (169), and hypercholesterolemic (153). These populations were all older adult populations (mean age: >60 y) with larger sample sizes (n range: 27-67) (153, 166-169), apart from one study that had a sample size of n=8 (192).
There is now clear and convincing evidence that nitrate reduces blood pressure within hours of ingestion. The evidence of chronic ingestion of nitrate on blood pressure is less clear. Studies suggest that chronic intake of nitrate lowers blood pressure in young healthy individuals; however, these blood pressure-lowering effects are not seen in older individuals and in individuals at risk of cardiovascular disease. Recent evidence suggests possible interactions between sulphate and nitrate, which may explain some of these inconsistencies (197). However, research is needed to further investigate this theory.
Animal studies
We identified 17 studies, in 12 publications, that assessed the effect of nitrate supplementation on blood pressure in an animal model (Table 3). Nitrate sources included NaNO3- (n=10), KNO3- (n=1), and Mg(NO3)2- (n=1) supplemented drinking water. Nitrate doses ranged from 0.1 to 4.27 mmol•kg-1•d-1 and treatment time ranged from 1 wk to 12 mo. The number of animals in each treatment group ranged from 5 to 23. Nine studies reported a decrease in blood pressure after nitrate supplementation and 5 studies reported no change in blood pressure. Only one study reported an increase in blood pressure; Carlström et al. (198) reported a significant increase in mean arterial pressure (MAP) in healthy rats after 8 wk of nitrate supplementation (1 mM•kg-1•d-1). In the same study, a decrease in blood pressure was seen with a 0.1-mM dose of nitrate. In 2 studies in which high blood pressure was induced, either by the use of spontaneously hypertensive rats (199, 200) or by administration of a high-fructose diet (201), nitrate supplementation prevented the increase in blood pressure observed in the control group. In a study by Hezel et al. (202), a decrease in mean arterial pressure and SBP was only seen in old (22 mo) Sprague-Dawley rats and not in young (3 mo) rats. It is important to note that, although both groups were receiving the same concentration of nitrate in their
47 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
drinking water, the younger rats were receiving a much higher dose of nitrate (776 µmol•kg-
1•d-1 compared with 290 µmol•kg-1•d-1), due to their higher water intake and lower body weight. In a study by Khalifi et al. (203), a decrease in SBP was only seen in diabetic Wistar rats and not their healthy counterparts. This may be due to positive effects of nitrate supplementation on NO status and oxidative stress, which would have been compromised in the diabetic rats but not in the healthy rats. Other studies have shown that higher doses of nitrate can reduce blood pressure in animal models that were shown to have reduced NO bioavailability (201, 202, 204).
ENDOTHELIAL FUNCTION
The endothelium lines the entire vascular system and plays an essential role in the maintenance of vascular homeostasis (205). Dysfunction of the endothelium has been identified in the development of atherosclerosis-related diseases (206). Flow-mediated dilatation (FMD) via non-invasive ultrasound measures the endothelial function of the brachial artery (207, 208). It is the gold-standard method for assessing conduit artery endothelial function (207) and is significantly associated with cardiovascular disease events (209, 210). It was previously shown from a meta-analysis of 14 prospective cohort studies that the risk of experiencing a cardiovascular event is reduced by 13% for every 1% increase in FMD (211). The degree of endothelial function is determined by the change in brachial artery diameter before and after a shear stress stimulus, induced by reactive hyperaemia (209). In the forearm vasculature, FMD provides a measure of endothelium-derived NO bioavailability (212).
Human studies
Our systematic literature search found 7 acute studies (≤24 h) (Table 4) (153, 176, 177, 180, 184, 185, 213) and 4 chronic studies (>1 d) (Table 5) (153, 169, 188, 190) in 10 publications investigating the effects of nitrate ingestion on FMD. Beetroot juice was the most common nitrate source used in both acute and chronic studies.
Acute studies
The acute effects of nitrate ingestion on FMD were investigated between 1.5 and 4 h with nitrate doses ranging from 6 to 772 mg (0.1 to 12.4 mmol) (Table 4). The lower nitrate dose in this range was estimated by using the global average body weight of 62 kg, because no average body weight was reported in this study (176). Six studies showed a significant improvement in FMD (153, 176, 177, 180, 184, 213) and one study showed no effect (185). Improvements in FMD ranging from 0.5% to 4.0% were seen across the entire range of nitrate doses investigated. Beetroot juice was also found to attenuate the postprandial impairment of FMD after a high-fat meal (180). Improvements in FMD were seen in mainly healthy populations (176, 177, 184, 213). Other populations in whom improvements in FMD were seen included hypercholesterolaemic (153) and overweight (180) subjects. These healthy and at-risk populations consisted of 3 studies in younger cohorts (mean age: ≤27 y) (176, 177, 213) and 3 studies in older cohorts (mean age: >45 y) (153, 180, 184), with an overall sample size ranging from 5 to 67. No effects on FMD were observed in one healthy population of 14 participants aged 28 y (185).
48 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
Chronic studies
The chronic effects of nitrate ingestion on FMD were investigated in studies with durations that ranged from 14 to 42 d (2 to 6 wk) with nitrate doses ranging from 375 to 577 mg/d (6.0 to 9.3 mmol/d) (Table 5). The higher nitrate dose in this range was estimated by using the global average body weight of 62 kg, because no average body weight was reported in this study (190). Three studies showed a significant improvement in FMD (153, 188, 190), and one study had no effects (169). In particular, Rammos et al. (190) showed that dietary nitrate reversed vascular dysfunction in older adults with moderately increased cardiovascular risk. Improvements in FMD ranged from 0.5% to 1.1% and were seen across the entire range of nitrate doses investigated. Increases in FMD (~1%) were seen in 2 studies (153, 188) by using similar nitrate doses from beetroot juice (375 and 398 mg/d). Ingestion of a slightly higher nitrate dose of 577 mg/d (9.3 mmol/d) with the use of sodium nitrate showed a 0.5% improvement (190). Improvements in FMD were seen in subjects with hypercholesterolemia (153), treated and untreated hypertension (188), and moderate cardiovascular risk (190). All of the populations were older adult populations (mean age: >50 y) with large sample sizes (n>60), except for one study that had a sample size of 11 (190). No effects on FMD were observed after 14 d of nitrate ingestion (beetroot juice) in 27 subjects with type 2 diabetes (169).
Animal studies
Numerous studies reported that blood vessels with a damaged endothelium have impaired vasorelaxation in response to acetylcholine (Table 3) (214, 215). We identified 3 animal studies, from 2 publications, investigating the effects of dietary nitrate supplementation on endothelial function (198, 216). Bakker et al. (216) showed that, although supplementation with very-high-dose nitrate (10 mmol•kg-1•d-1) had no effect on acetylcholine-mediated vessel relaxation in a mouse model of atherosclerosis, low- (0.1 mmol•kg-1•d-1) and moderate- (1 mmol•kg-1•d-1) dose nitrate supplementation significantly improved the endothelial dysfunction associated with this mouse model. In addition, Carlström et al. (198) reported that dietary supplementation with a high dose of nitrate (1 mmol•kg-1•d-1) was associated with attenuated acetylcholine-mediated vasorelaxation. These observations are in support of the theory proposed by Carlström et al. that there is cross-talk between the 2 pathways of NO production. They suggest that high doses of dietary nitrate may inhibit production of NO through the L-arginine-NOS pathway, leading to a net decrease in the amount of NO reaching the smooth muscle cells of the blood vessel (198). Although Bakker et al. showed improvements with a 1 mmol•kg-1•d-1 dose of nitrate and Carlström et al. reported no improvements with the same dose, the animal model used is likely an important factor because the ApoE knockout mice used in the study by Bakker et al (216) have reduced NO bioavailability.
ISCHAEMIC REPERFUSION INJURY
Ischaemic reperfusion injury is tissue damage caused by a period of ischemia or lack of oxygen. Lack of oxygen during an ischaemic period results in inflammation and oxidative damage leading to microvascular dysfunction (217). Local and systemic tissue ischemia remains the major cause of death from cardiovascular disease (112). Because the nitrate-nitrite-NO pathway is enhanced in times of hypoxia, this pathway may provide a back up to the classical L-arginine-NOS pathway.
49 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
Human studies
Our systematic literature search found 3 acute studies (2 publications) investigating the effects of nitrate ingestion on ischaemic reperfusion injury (Table 6) (143, 186). Beetroot juice was the most common nitrate source used. The acute effects of nitrate ingestion on ischaemic reperfusion injury were investigated between 2 and 3 h with nitrate doses ranging from 341 to 1488 mg (5.5 to 24 mmol) (Table 6). Benefits were also seen in all studies in which beetroot juice (143, 186) and potassium nitrate (186) attenuated ischaemia reperfusion-induced endothelial dysfunction measured by using FMD. Improvements were seen in young (mean age: <28 y), healthy populations (143, 186), with an overall sample size ranging from 10 to 12.
Animal studies
We found only one study describing the effects of dietary nitrate supplementation on ischaemia-induced revascularisation in an animal model (Table 3). In a study by Hendgen-Cotta et al. (218), mice were treated with either nitrate (1 g/L NaNO3 in drinking water) or NaCl (control) for 14 d. Perfusion recovery in the ischaemic hind limb was significantly improved in mice treated with nitrate compared with controls via a significant increase in capillary density. These results suggest that dietary nitrate supplementation may represent a strategy to enhance ischaemia-induced revascularisation.
ARTERIAL STIFFNESS
Pulse-wave velocity (PWV) is a measure of aortic stiffness and is a strong predictor of cardiovascular events (219-221). PWV is recognised as the most simple, noninvasive, robust, and reproducible technique to determine arterial stiffness and is considered the gold-standard measurement of arterial stiffness (222). PWV measures arterial stiffness by dividing the estimated distance between the carotid and femoral arteries by the pulse transit time, the time delay between the carotid and femoral waveforms. A tonometer is used to capture the carotid waveform and a cuff is placed around the femoral artery to capture the femoral waveform. The augmentation index (AIx) is another measure of arterial stiffness, which provides a composite measure of elastic plus muscular artery stiffness and wave reflection. The AIx has also been shown to be an independent predictor of future cardiovascular disease events (223).
Human studies
Our systematic literature search found 7 acute studies (≤24 h) (153, 171, 173, 179-181, 185) and 5 chronic studies (>1 d) (153, 166, 168, 188, 190) in 10 publications investigating the effects of nitrate consumption on arterial stiffness (Table 7). Beetroot juice was the most common nitrate source used in both acute and chronic studies.
Acute studies
The acute effects of nitrate ingestion on arterial stiffness were investigated between 2 and 6 h, with nitrate doses ranging from 68 to 583 mg (1.1 to 9.4 mmol) (Table 7). Three studies showed a significant decrease in arterial stiffness (153, 173, 185), and 4 studies showed no effect (171, 179-181). A significant decrease of 0.3 m/s in PWV was observed in 2 studies (153, 185) with a nitrate dose of 375 mg (6 mmol) from beetroot juice (153) and 496 mg (8 mmol) from potassium nitrate (185). The study by Velmurugan et al. (153) consisted of a large sample size
50 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
of 67 hypercholesterolaemic men and women with a mean age of 53 y, whereas the study by Bahra et al. (185) consisted of a smaller sample of 14 healthy individuals with a mean age 28 y. Hughes et al. (173) showed a reduced AIx in young, but not old, adults after a nitrate dose of 583 mg (9.4 mmol). No effect was seen in 4 studies with nitrate doses ranging from 68 to 500 mg (1.1 to 8.1 mmol) with the use of beetroot juice (171, 180), beetroot-enriched bread (181), and spinach (179). These studies consisted of healthy (171, 179, 181) and overweight (180) subjects.
Chronic studies
The chronic effects of nitrate ingestion on arterial stiffness were investigated from 7 to 42 d (1 to 6 wk) with nitrate doses ranging from 300 to 600 mg/d (4.8 to 9.7 mmol/d) (Table 7). Three studies showed a significant decrease in arterial stiffness after nitrate ingestion (153, 188, 190), and 2 studies demonstrated no effect (166, 168). Studies found a significant decrease of 0.2-1.2 m/s in PWV with nitrate doses ranging from 375 to 577 mg/d (6 to 9.3 mmol/d) with the use of beetroot juice and sodium nitrate [577 mg/d was estimated by using the global average body weight of 62 kg because no average body weight was reported in this study (190)]. The populations in whom an effect was observed had moderate cardiovascular risk (190), untreated and treated hypertension (188), and hypercholesterolemia (153). No effect was seen in 2 studies with nitrate doses of 300 mg/d (4.8 mmol/d) from green leafy vegetables (168) and 600 mg/d (9.7 mmol/d) from beetroot juice (166) and in populations who were overweight and obese (166) and prehypertensive (168). It has been shown that for every 3.4-m/s increase in PWV, the risk of experiencing a cardiovascular event is increased by 17% (219). Therefore, a decrease of 0.2-1.2 m/s in PWV is likely to provide a small but significant reduction in the risk of experiencing a cardiovascular disease event.
Animal studies
Upon search of the literature, we found no animal studies investigating the effects of dietary nitrate supplementation on arterial stiffness.
PLATELET FUNCTION
Platelets play a major role in the acute complications of atherosclerosis in the late stages of the disease, which can subsequently lead to atherosclerosis-related events (224). NO has been shown to inhibit platelet aggregation and adhesion to the endothelial wall (225) and there is now evidence to suggest that dietary nitrate may repress platelet reactivity.
Human studies
Our systematic literature search identified 5 acute studies (≤24 h) (143, 226, 227) and one chronic study (>1 d) (153), in 4 publications, investigating the effects of nitrate intake on platelet function (Table 8). Potassium nitrate was the most common nitrate source used in acute studies, and beetroot juice was used in the chronic study.
Acute studies
The acute effects of nitrate ingestion on platelet function were investigated between 2.5 and 3 h with nitrate doses between 31 and 1054 mg (0.5 and 17 mmol) (Table 8). All 5 studies showed reductions in platelet aggregation and reactivity (143, 226, 227). Velmurugan et al.
51 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
(226) showed that nitrate ingestion decreased platelet reactivity in healthy men, but not in healthy women. This was observed with both beetroot juice (192 mg or 3.1 mmol) and potassium nitrate (496 mg or 8 mmol). Further studies that used beetroot juice (1054 mg or 17 mmol) (143) and potassium nitrate (31 and 124 mg or 0.5 and 2 mmol) (227) showed reductions in platelet aggregation. All of the cohorts consisted of young healthy populations and had small sample sizes (n<25). Further acute studies are needed to replicate these findings in older adult populations at risk of developing cardiovascular disease.
Chronic studies
The chronic effects of nitrate ingestion on platelet function were investigated in only one study (Table 8) (153). Velmurugan et al. (153) showed a reduction in platelet-monocyte aggregates after 42 d of daily beetroot juice ingestion with a nitrate dose of 375 mg/d (6 mmol/d). This study had a large sample size (n=67) of older men and women aged 53 y with hypercholesterolemia. There is a strong need for further chronic studies to investigate the effects of nitrate ingestion on platelet function in healthy populations and to replicate findings in older adult populations at risk of cardiovascular disease.
Animal studies
To our knowledge, only one animal study has been published investigating the effects of dietary nitrate supplementation on platelet function (Table 9). In this study, wild-type C57BL/6 mice were supplemented with 1 g NaNO3/L in their drinking water for 1 wk, fed a low-nitrate diet, or continued on standard mouse feed pellets (control) (228). Platelet aggregation was significantly decreased in the group supplemented with nitrate and was significantly increased in the group fed the low-nitrate diet in comparison to the control group. These findings show that the manipulation of nitrate concentrations in blood, via supplementation or dietary restriction, could affect platelet function in mice, although further studies are required to corroborate this finding.
CEREBRAL BLOOD FLOW
The effect of dietary nitrate on cerebral blood flow has been investigated in several studies due to the observed effects of dietary nitrate on vasodilation and increases in blood flow. Diminished blood flow to the brain is likely to contribute to the pathophysiologic processes underlying vascular cognitive impairment (229).
Human studies
Our systematic literature search identified one acute study (≤24 h) (230) and one chronic study (>1 d) (231) in 2 publications investigating the effect of nitrate ingestion on cerebral blood flow (Table 9). Sodium nitrate and a high-nitrate diet were used as nitrate sources.
Acute studies
Presley et al (230) showed that the consumption of a high-nitrate diet (769 mg or 12.4 mmol nitrate) over a 24-h period increased regional cerebral perfusion in frontal lobe white matter in older adults with a mean age of 75 y (Table 9). This was particularly evident in the dorsolateral prefrontal cortex and anterior cingulate cortex. In the same study, however, the acute effects of a high nitrate diet did not modify global cerebral perfusion.
52 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
Chronic studies
Aamand et al. (231) found no effects after 3 d of sodium nitrate ingestion (477 mg or 7.7 mmol nitrate/d, based on a study mean weight of 77kg) on cerebral blood flow in 20 healthy men (Table 9).
Animal studies
No animal studies investigating the effects of dietary nitrate supplementation on blood flow were found.
SUMMARY: NITRATE INGESTION AND ITS EFFECTS ON VASCULAR FUNCTION
Human intervention studies have now shown that the ingestion of nitrate lowers blood pressure and improves endothelial function. These studies were predominantly in healthy populations and of short duration. It is yet to be established whether nitrate ingestion has the same effects in populations at higher risk of cardiovascular disease because few studies have been conducted and findings are inconsistent. Further research is also needed to understand the long-term effects of nitrate intake on cardiovascular clinical endpoints.
EPIDEMIOLOGIC EVIDENCE
Epidemiologic studies have found that plant-based diets rich in vegetables are associated with lower rates of cardiovascular disease (113, 115, 232-237). In particular, cohort studies have shown specific vegetable groups that are high in nitrate, such as green leafy vegetables, to be most beneficial (62, 72, 116, 117). The exact mechanisms for the protective effects shown in these studies are still unknown. A Mediterranean diet (114, 238), the DASH diet (161, 239), and a vegetarian diet (240, 241), all rich in vegetables, have been shown to be particularly beneficial for cardiovascular health. These diets are likely to contain substantially higher amounts of nitrate than the average Western diet. Thus, nitrate is one possible candidate for explaining cardiovascular health benefits seen with higher vegetable intakes (242).
There are very few observational epidemiologic studies investigating nitrate intake and cardiovascular-related health outcomes (Table 10). Although databases have been established to calculate the nitrate intake in observational epidemiologic studies (243-245), there was a strong need for a more comprehensive database with compiled up-to-date data. Our recently developed database on the nitrate content of vegetables (36) now gives researchers the opportunity to conduct more observational epidemiologic studies with an adequate assessment of nitrate intake.
To date, there have been 2 articles published that used the database on the nitrate content of vegetables (36). We have shown nitrate intake to be inversely associated with atherosclerotic vascular disease mortality in a cohort of older women (mean age: 75 ± 3 y) (30). In comparison to lower intakes of nitrate from vegetables of <53 mg/d (median: 39 mg/d), the inverse relationship with atherosclerotic vascular disease mortality reached a plateau at intakes of 53-76 mg/d (median: 63 mg/d) (30). In the same cohort of older women, we also observed an inverse relation between nitrate intakes from vegetables and common carotid artery intima-media thickness, as well as ischaemic cerebrovascular disease events (hospitalisation or death) (31). The inverse relation with ischaemic cerebrovascular disease events also reached a plateau at intakes of 53-76 mg/d (median: 63 mg/d) (31).
53 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
Before these studies were published, the Tehran Lipid and Glucose Study reported on the relation between the consumption of nitrate-containing vegetables and risk of hypertension (246) and chronic kidney disease (CKD) (247), both risk factors for cardiovascular disease. These studies investigated nitrate intake by assessing whole vegetables containing nitrate. The authors further categorised nitrate-containing vegetables into low-nitrate, medium-nitrate, and high-nitrate vegetables. It is worth noting that these studies essentially investigated whole vegetables and then different types of vegetables according to their nitrate contents and not nitrate as a separate entity. It is, however, difficult to separate nitrate intake from vegetable intake because the 2 can be highly correlated, as we have previously shown (r=0.75, P<0.001) (30). Golzarand et al. (246) found a significant inverse association between the intake of nitrate-containing vegetables and 3-y incidence of hypertension in the highest tertile compared with the lowest tertile of nitrate-containing vegetables. There were no significant associations observed between low-nitrate-, medium-nitrate-, and high-nitrate-containing vegetables and 3-y risk of hypertension. Because no associations were found between categories of nitrate-containing vegetables, it is difficult to determine whether the inverse association shown with total nitrate-containing vegetables is due to vegetable intake alone. This cohort consisted of 1,546 Iranian men and women (57% women), aged 38±12 y, without hypertension at baseline. In the same cohort, Mirmiran et al. (247) found that the highest compared with the lowest tertile of intake of nitrate-containing vegetables was associated with a lower estimated glomerular filtration rate and a higher prevalence of CKD at baseline. This could be a demonstration of reverse causality bias in which the diagnosis of chronic disease has altered dietary intake. There was no association with the occurrence of CKD after 3 y of follow-up after excluding patients with CKD at baseline. Last, Bahadoran et al. (248) recently reported findings on the potential effects of dietary nitrate and nitrite on the occurrence of type 2 diabetes in the same cohort of Iranian men and women (Tehran Lipid and Glucose Study). The authors reported on 2,139 adults who were free of type 2 diabetes at baseline, with a median follow-up of 5.8 y. Nitrate and nitrite values were determined from a recent survey conducted on frequently consumed food items among Iranians (249). Nitrate and nitrite concentrations of 87 foods were determined by using spectrophotometric methods. The authors found no associations between nitrate intake and the risk of developing type 2 diabetes. However, they showed an increased risk of type 2 diabetes among participants with higher intakes of total and animal-based nitrite in the presence of low vitamin C intake. The same was not observed in participants with high intakes of vitamin C (>108 mg/d) (248), suggesting that diets high in vitamin C may counteract the suggested adverse effects of nitrite on type 2 diabetes. However, higher intakes of total and animal-based nitrite in the presence of low vitamin C intake may be a marker of an unhealthy diet and lifestyle, which may also be associated with a higher prevalence of type 2 diabetes.
There is a lingering concern that nitrate and nitrite may form cancerous compounds, such as nitrosamines (44). The majority of epidemiologic studies to date have investigated relations between nitrate intake and cancer outcomes. A report compiled by the International Agency for Research on Carcinogenicity concluded “Ingested nitrate or nitrite under conditions that result in endogenous nitrosation is probably carcinogenic to humans (Group 2A)” (250). Conditions that increase endogenous nitrosation are complex but could involve interactions between the amount of nitrate and nitrite consumed, stomach acidity, smoking status, medical conditions, and low intakes of nutrients that are likely to decrease the potential for nitrosation such as polyphenols, vitamin C, and vitamin E (157).

54 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
Now that there is a comprehensive database on the nitrate content of vegetables available, researchers have the opportunity to further investigate the associations between chronic intake of nitrate and health outcomes. Further research is needed to elucidate the relations between different populations, including young and older age groups, low and higher background nitrate intakes, and healthy and at-risk populations.
CONCLUSION
There is now strong evidence to suggest that dietary nitrate derived from vegetables can reduce blood pressure and other markers of vascular function in healthy populations. There is a need for further research to investigate whether similar effects are observed in populations at risk of developing cardiovascular disease. Few studies have investigated the long-term effects of dietary nitrate on cardiovascular disease clinical endpoints; large observational follow-up studies are required to address this. Further animal studies are required to elucidate the mechanisms behind the observed beneficial effects. Increasing nitrate in the diet through the consumption of nitrate-rich vegetables may prove to be an achievable and cost-effective way to reduce the risk of cardiovascular disease.
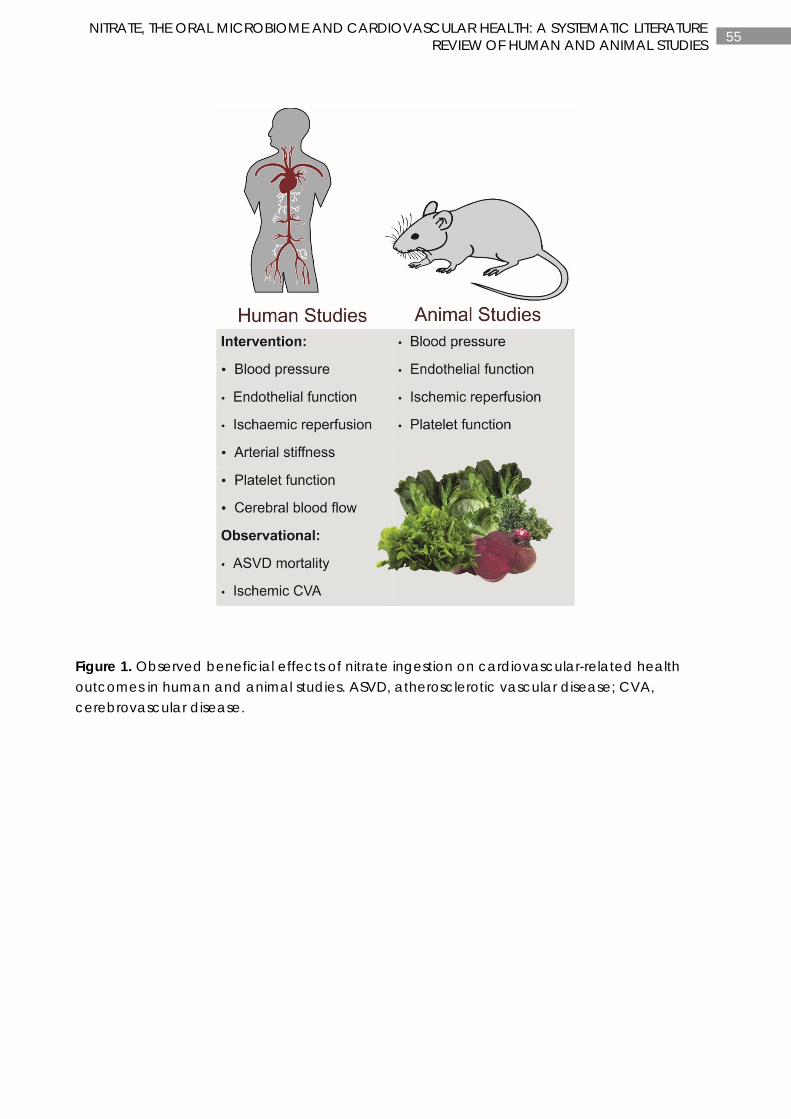
55 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
Figure 1. Observed beneficial effects of nitrate ingestion on cardiovascular-related health outcomes in human and animal studies. ASVD, atherosclerotic vascular disease; CVA, cerebrovascular disease.
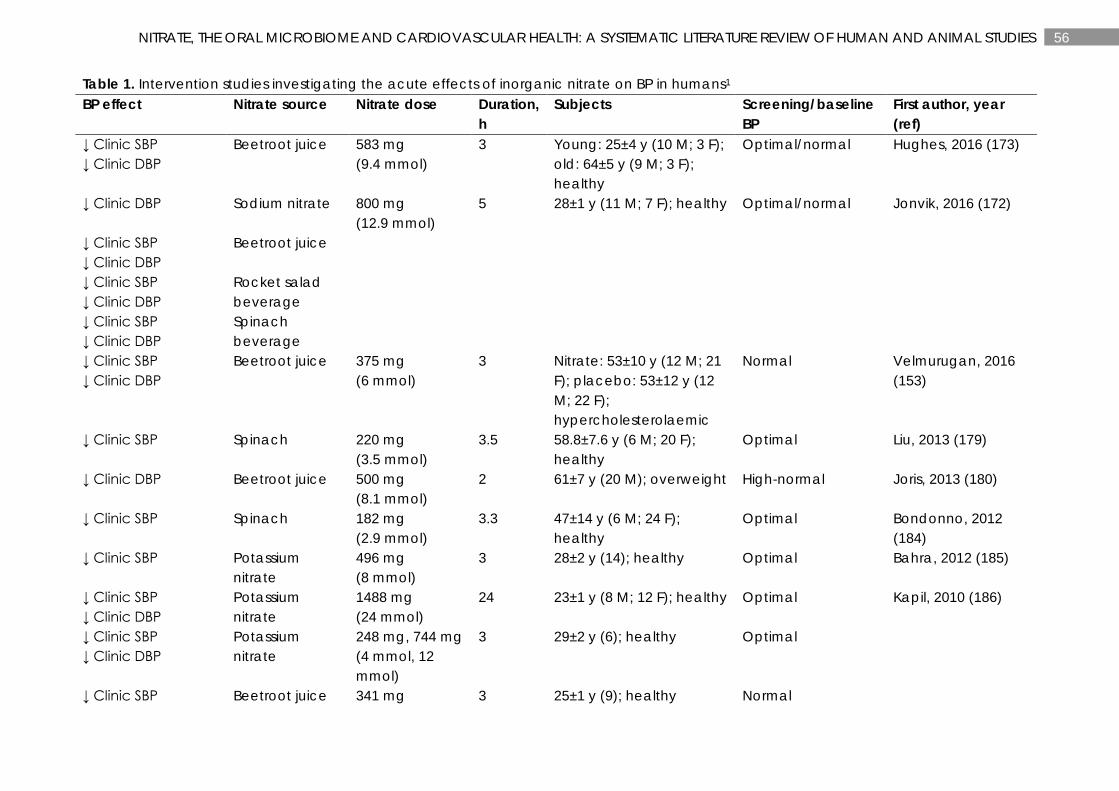
56 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 1. Intervention studies investigating the acute effects of inorganic nitrate on BP in humans1 BP effect Nitrate source Nitrate dose Duration,
h Subjects Screening/baseline
BP First author, year (ref)
↓ Clinic SBP ↓ Clinic DBP
Beetroot juice 583 mg (9.4 mmol)
3 Young: 25±4 y (10 M; 3 F); old: 64±5 y (9 M; 3 F); healthy
Optimal/normal Hughes, 2016 (173)
↓ Clinic DBP
Sodium nitrate 800 mg (12.9 mmol)
5
28±1 y (11 M; 7 F); healthy Optimal/normal Jonvik, 2016 (172)
↓ Clinic SBP ↓ Clinic DBP
Beetroot juice
↓ Clinic SBP ↓ Clinic DBP
Rocket salad beverage
↓ Clinic SBP ↓ Clinic DBP
Spinach beverage
↓ Clinic SBP ↓ Clinic DBP
Beetroot juice 375 mg (6 mmol)
3
Nitrate: 53±10 y (12 M; 21 F); placebo: 53±12 y (12 M; 22 F); hypercholesterolaemic
Normal Velmurugan, 2016 (153)
↓ Clinic SBP Spinach 220 mg (3.5 mmol)
3.5 58.8±7.6 y (6 M; 20 F); healthy
Optimal Liu, 2013 (179)
↓ Clinic DBP Beetroot juice 500 mg (8.1 mmol)
2
61±7 y (20 M); overweight High-normal Joris, 2013 (180)
↓ Clinic SBP Spinach 182 mg (2.9 mmol)
3.3 47±14 y (6 M; 24 F); healthy
Optimal Bondonno, 2012 (184)
↓ Clinic SBP Potassium nitrate
496 mg (8 mmol)
3
28±2 y (14); healthy Optimal Bahra, 2012 (185)
↓ Clinic SBP ↓ Clinic DBP
Potassium nitrate
1488 mg (24 mmol)
24
23±1 y (8 M; 12 F); healthy Optimal Kapil, 2010 (186)
↓ Clinic SBP ↓ Clinic DBP
Potassium nitrate
248 mg, 744 mg (4 mmol, 12 mmol)
3
29±2 y (6); healthy Optimal
↓ Clinic SBP Beetroot juice 341 mg 3 25±1 y (9); healthy Normal
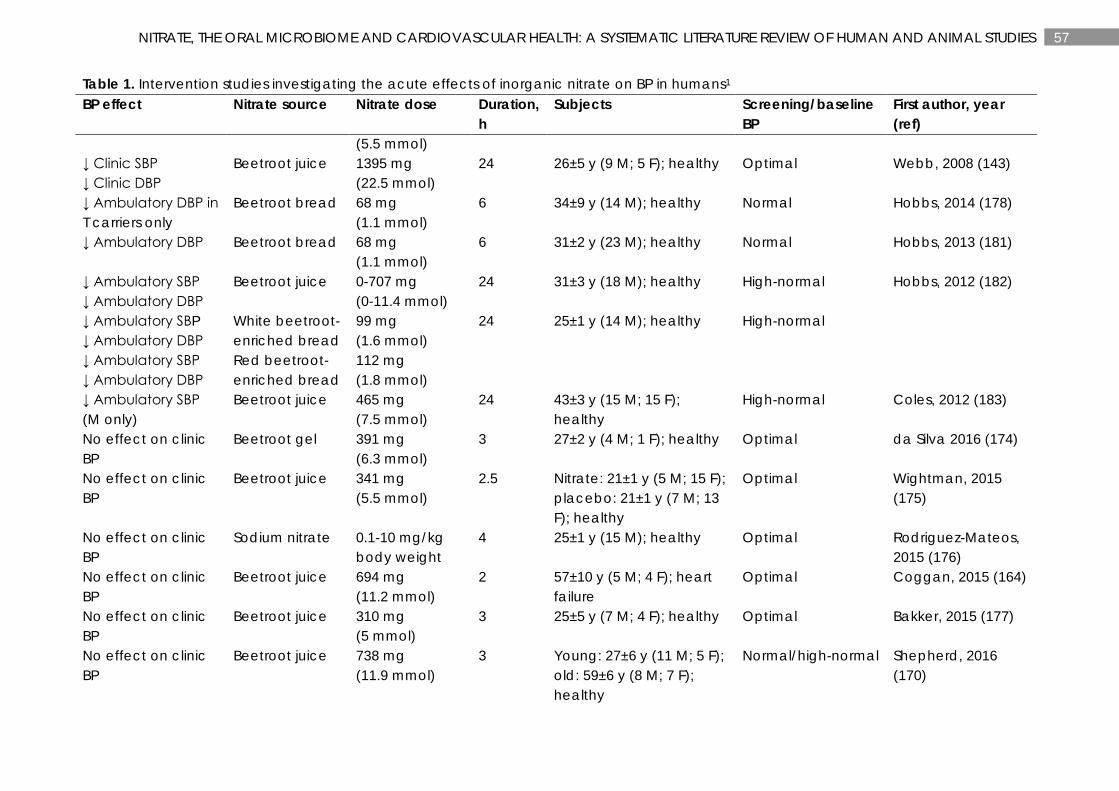
57 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 1. Intervention studies investigating the acute effects of inorganic nitrate on BP in humans1 BP effect Nitrate source Nitrate dose Duration,
h Subjects Screening/baseline
BP First author, year (ref)
(5.5 mmol) ↓ Clinic SBP ↓ Clinic DBP
Beetroot juice 1395 mg (22.5 mmol)
24
26±5 y (9 M; 5 F); healthy Optimal Webb, 2008 (143)
↓ Ambulatory DBP in T carriers only
Beetroot bread 68 mg (1.1 mmol)
6
34±9 y (14 M); healthy Normal Hobbs, 2014 (178)
↓ Ambulatory DBP Beetroot bread 68 mg (1.1 mmol)
6
31±2 y (23 M); healthy Normal Hobbs, 2013 (181)
↓ Ambulatory SBP ↓ Ambulatory DBP
Beetroot juice 0-707 mg (0-11.4 mmol)
24 31±3 y (18 M); healthy High-normal Hobbs, 2012 (182)
↓ Ambulatory SBP ↓ Ambulatory DBP
White beetroot-enriched bread
99 mg (1.6 mmol)
24
25±1 y (14 M); healthy High-normal
↓ Ambulatory SBP ↓ Ambulatory DBP
Red beetroot-enriched bread
112 mg (1.8 mmol)
↓ Ambulatory SBP (M only)
Beetroot juice 465 mg (7.5 mmol)
24
43±3 y (15 M; 15 F); healthy
High-normal Coles, 2012 (183)
No effect on clinic BP
Beetroot gel 391 mg (6.3 mmol)
3 27±2 y (4 M; 1 F); healthy Optimal da Silva 2016 (174)
No effect on clinic BP
Beetroot juice 341 mg (5.5 mmol)
2.5 Nitrate: 21±1 y (5 M; 15 F); placebo: 21±1 y (7 M; 13 F); healthy
Optimal Wightman, 2015 (175)
No effect on clinic BP
Sodium nitrate 0.1-10 mg/kg body weight
4 25±1 y (15 M); healthy Optimal Rodriguez-Mateos, 2015 (176)
No effect on clinic BP
Beetroot juice 694 mg (11.2 mmol)
2 57±10 y (5 M; 4 F); heart failure
Optimal Coggan, 2015 (164)
No effect on clinic BP
Beetroot juice 310 mg (5 mmol)
3 25±5 y (7 M; 4 F); healthy Optimal Bakker, 2015 (177)
No effect on clinic BP
Beetroot juice 738 mg (11.9 mmol)
3 Young: 27±6 y (11 M; 5 F); old: 59±6 y (8 M; 7 F); healthy
Normal/high-normal Shepherd, 2016 (170)
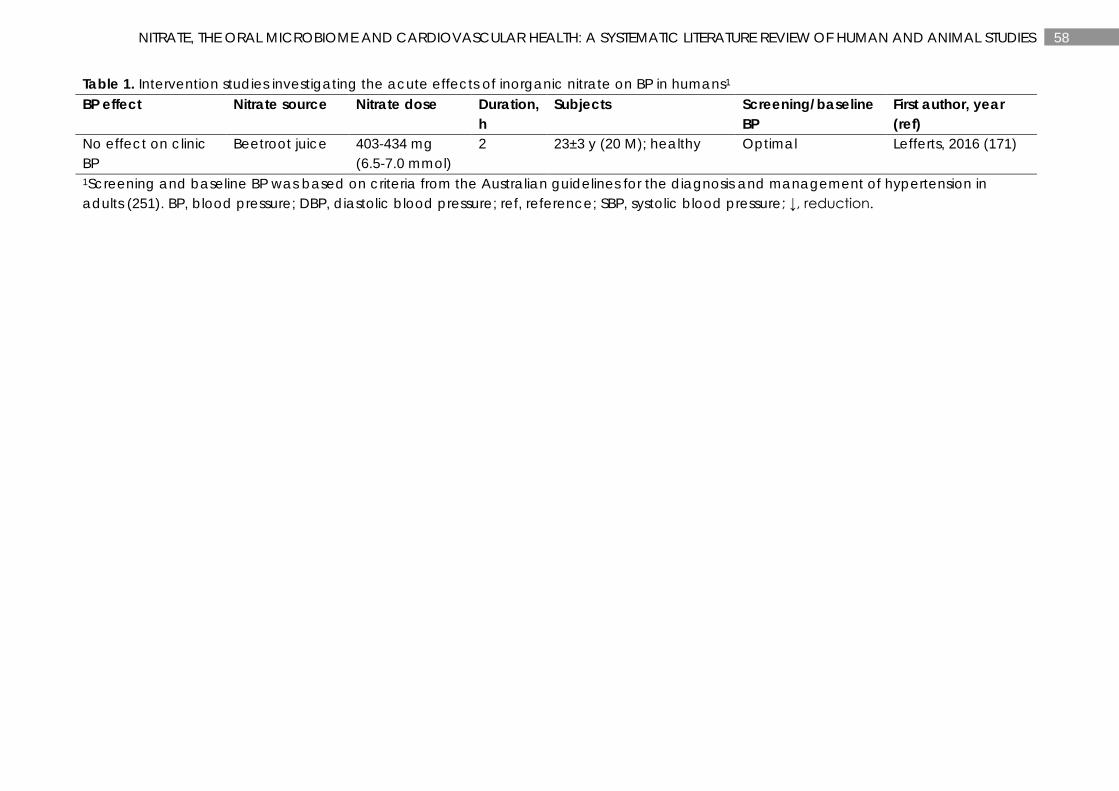
58 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 1. Intervention studies investigating the acute effects of inorganic nitrate on BP in humans1 BP effect Nitrate source Nitrate dose Duration,
h Subjects Screening/baseline
BP First author, year (ref)
No effect on clinic BP
Beetroot juice 403-434 mg (6.5-7.0 mmol)
2 23±3 y (20 M); healthy Optimal Lefferts, 2016 (171)
1Screening and baseline BP was based on criteria from the Australian guidelines for the diagnosis and management of hypertension in adults (251). BP, blood pressure; DBP, diastolic blood pressure; ref, reference; SBP, systolic blood pressure; ↓, reduction.
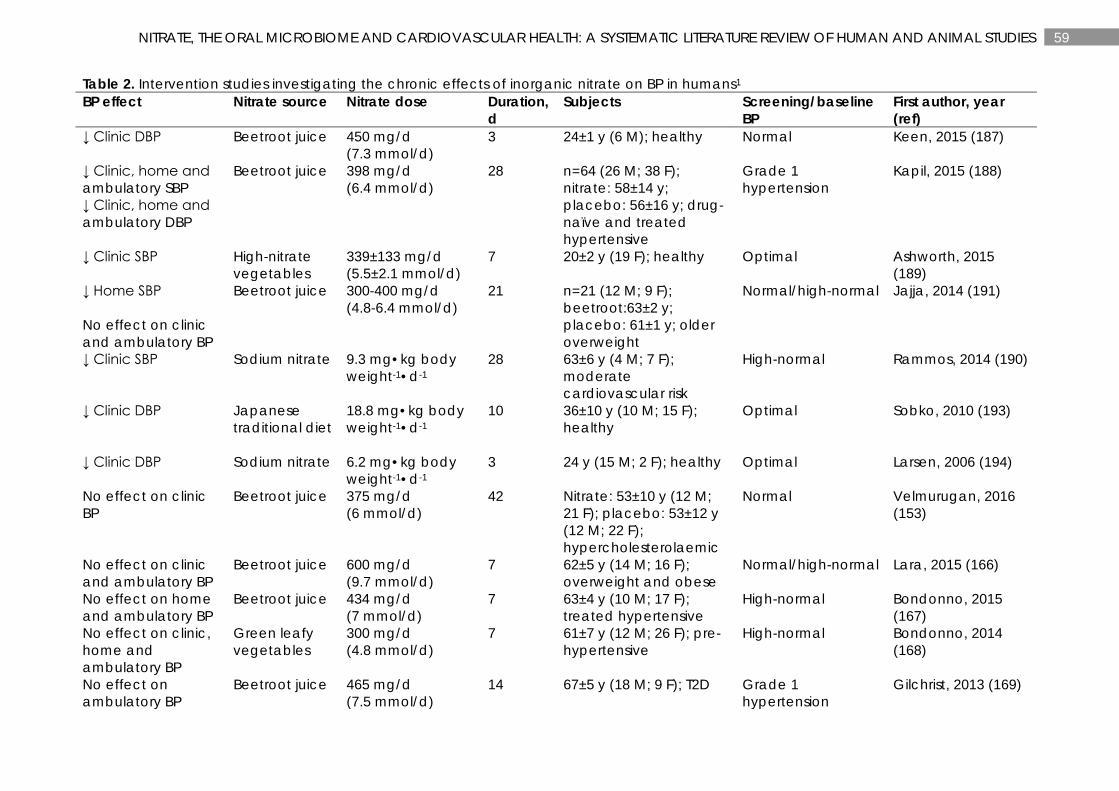
59 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 2. Intervention studies investigating the chronic effects of inorganic nitrate on BP in humans1 BP effect Nitrate source Nitrate dose Duration,
d Subjects Screening/baseline
BP First author, year (ref)
↓ Clinic DBP Beetroot juice 450 mg/d (7.3 mmol/d)
3 24±1 y (6 M); healthy Normal Keen, 2015 (187)
↓ Clinic, home and ambulatory SBP ↓ Clinic, home and ambulatory DBP
Beetroot juice 398 mg/d (6.4 mmol/d)
28
n=64 (26 M; 38 F); nitrate: 58±14 y; placebo: 56±16 y; drug-naïve and treated hypertensive
Grade 1 hypertension
Kapil, 2015 (188)
↓ Clinic SBP High-nitrate vegetables
339±133 mg/d (5.5±2.1 mmol/d)
7
20±2 y (19 F); healthy Optimal Ashworth, 2015 (189)
↓ Home SBP No effect on clinic and ambulatory BP
Beetroot juice 300-400 mg/d (4.8-6.4 mmol/d)
21
n=21 (12 M; 9 F); beetroot:63±2 y; placebo: 61±1 y; older overweight
Normal/high-normal Jajja, 2014 (191)
↓ Clinic SBP
Sodium nitrate 9.3 mg•kg body weight-1•d-1
28
63±6 y (4 M; 7 F); moderate cardiovascular risk
High-normal Rammos, 2014 (190)
↓ Clinic DBP Japanese traditional diet
18.8 mg•kg body weight-1•d-1
10
36±10 y (10 M; 15 F); healthy
Optimal
Sobko, 2010 (193)
↓ Clinic DBP
Sodium nitrate 6.2 mg•kg body weight-1•d-1
3 24 y (15 M; 2 F); healthy Optimal
Larsen, 2006 (194)
No effect on clinic BP
Beetroot juice 375 mg/d (6 mmol/d)
42 Nitrate: 53±10 y (12 M; 21 F); placebo: 53±12 y (12 M; 22 F); hypercholesterolaemic
Normal Velmurugan, 2016 (153)
No effect on clinic and ambulatory BP
Beetroot juice 600 mg/d (9.7 mmol/d)
7 62±5 y (14 M; 16 F); overweight and obese
Normal/high-normal Lara, 2015 (166)
No effect on home and ambulatory BP
Beetroot juice 434 mg/d (7 mmol/d)
7 63±4 y (10 M; 17 F); treated hypertensive
High-normal Bondonno, 2015 (167)
No effect on clinic, home and ambulatory BP
Green leafy vegetables
300 mg/d (4.8 mmol/d)
7 61±7 y (12 M; 26 F); pre-hypertensive
High-normal Bondonno, 2014 (168)
No effect on ambulatory BP
Beetroot juice 465 mg/d (7.5 mmol/d)
14 67±5 y (18 M; 9 F); T2D Grade 1 hypertension
Gilchrist, 2013 (169)
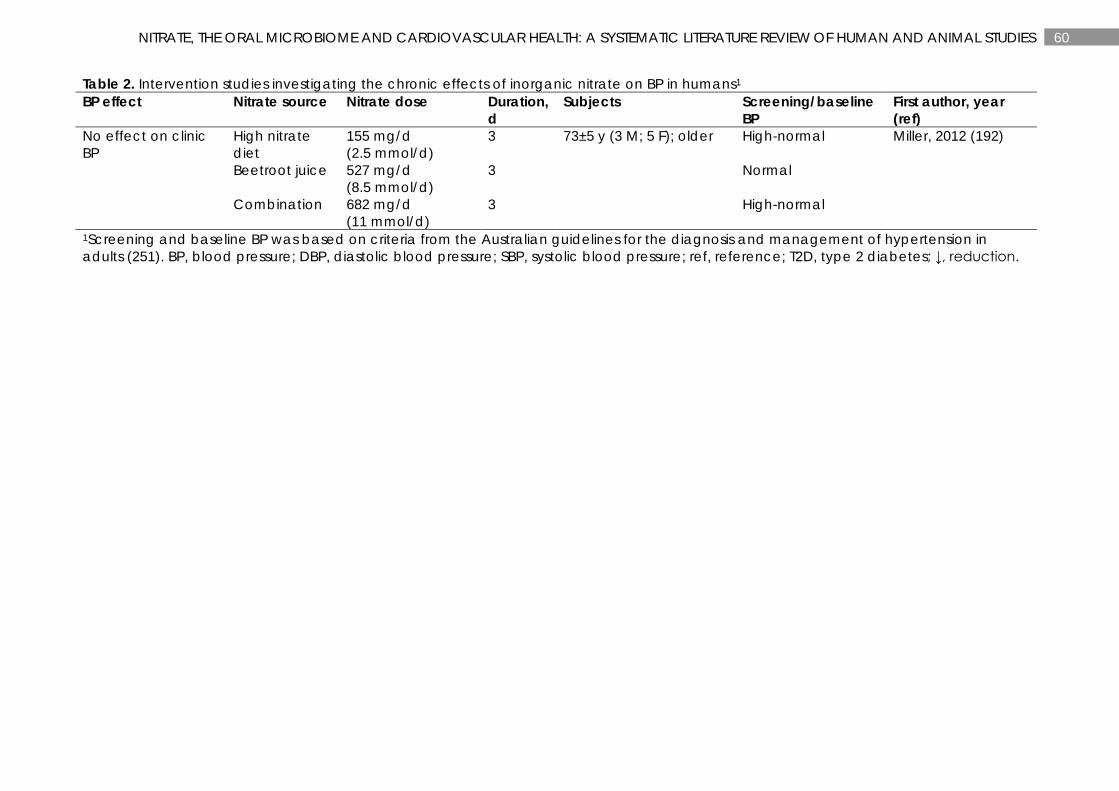
60 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 2. Intervention studies investigating the chronic effects of inorganic nitrate on BP in humans1 BP effect Nitrate source Nitrate dose Duration,
d Subjects Screening/baseline
BP First author, year (ref)
No effect on clinic BP
High nitrate diet
155 mg/d (2.5 mmol/d)
3 73±5 y (3 M; 5 F); older High-normal Miller, 2012 (192)
Beetroot juice 527 mg/d (8.5 mmol/d)
3 Normal
Combination 682 mg/d (11 mmol/d)
3 High-normal
1Screening and baseline BP was based on criteria from the Australian guidelines for the diagnosis and management of hypertension in adults (251). BP, blood pressure; DBP, diastolic blood pressure; SBP, systolic blood pressure; ref, reference; T2D, type 2 diabetes; ↓, reduction.
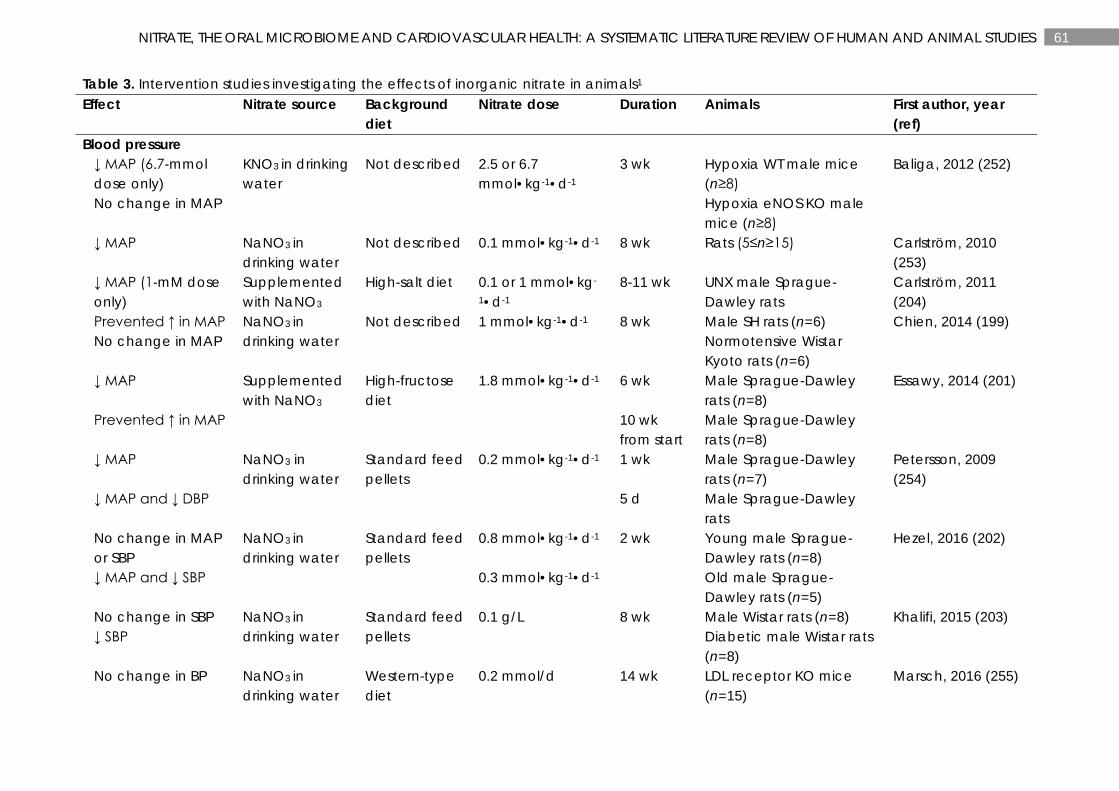
61 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 3. Intervention studies investigating the effects of inorganic nitrate in animals1 Effect Nitrate source Background
diet Nitrate dose Duration Animals First author, year
(ref) Blood pressure
↓ MAP (6.7-mmol dose only)
KNO3 in drinking water
Not described 2.5 or 6.7 mmol•kg-1•d-1
3 wk
Hypoxia WT male mice (n≥8)
Baliga, 2012 (252)
No change in MAP Hypoxia eNOS KO male mice (n≥8)
↓ MAP NaNO3 in drinking water
Not described 0.1 mmol•kg-1•d-1 8 wk Rats (5≤n≥15) Carlström, 2010 (253)
↓ MAP (1-mM dose only)
Supplemented with NaNO3
High-salt diet 0.1 or 1 mmol•kg-
1•d-1 8-11 wk UNX male Sprague-
Dawley rats Carlström, 2011 (204)
Prevented ↑ in MAP NaNO3 in drinking water
Not described 1 mmol•kg-1•d-1 8 wk Male SH rats (n=6) Chien, 2014 (199) No change in MAP Normotensive Wistar
Kyoto rats (n=6)
↓ MAP Supplemented with NaNO3
High-fructose diet
1.8 mmol•kg-1•d-1 6 wk Male Sprague-Dawley rats (n=8)
Essawy, 2014 (201)
Prevented ↑ in MAP 10 wk from start
Male Sprague-Dawley rats (n=8)
↓ MAP NaNO3 in drinking water
Standard feed pellets
0.2 mmol•kg-1•d-1 1 wk Male Sprague-Dawley rats (n=7)
Petersson, 2009 (254)
↓ MAP and ↓ DBP 5 d Male Sprague-Dawley rats
No change in MAP or SBP
NaNO3 in drinking water
Standard feed pellets
0.8 mmol•kg-1•d-1 2 wk Young male Sprague-Dawley rats (n=8)
Hezel, 2016 (202)
↓ MAP and ↓ SBP 0.3 mmol•kg-1•d-1 Old male Sprague-Dawley rats (n=5)
No change in SBP NaNO3 in drinking water
Standard feed pellets
0.1 g/L 8 wk Male Wistar rats (n=8) Khalifi, 2015 (203) ↓ SBP Diabetic male Wistar rats
(n=8)
No change in BP NaNO3 in drinking water
Western-type diet
0.2 mmol/d 14 wk LDL receptor KO mice (n=15)
Marsch, 2016 (255)
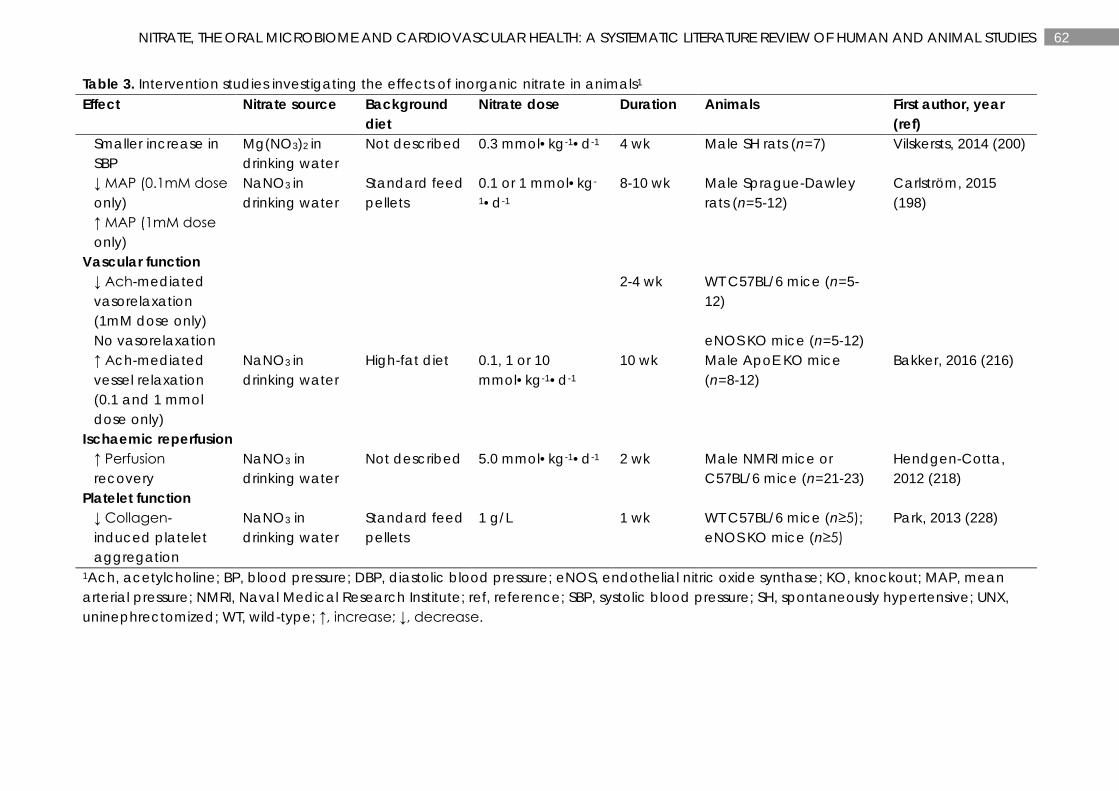
62 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 3. Intervention studies investigating the effects of inorganic nitrate in animals1 Effect Nitrate source Background
diet Nitrate dose Duration Animals First author, year
(ref) Smaller increase in SBP
Mg(NO3)2 in drinking water
Not described 0.3 mmol•kg-1•d-1 4 wk Male SH rats (n=7) Vilskersts, 2014 (200)
↓ MAP (0.1mM dose only) ↑ MAP (1mM dose only)
NaNO3 in drinking water
Standard feed pellets
0.1 or 1 mmol•kg-
1•d-1 8-10 wk Male Sprague-Dawley
rats (n=5-12) Carlström, 2015 (198)
Vascular function ↓ Ach-mediated vasorelaxation (1mM dose only)
2-4 wk WT C57BL/6 mice (n=5-12)
No vasorelaxation eNOS KO mice (n=5-12) ↑ Ach-mediated vessel relaxation (0.1 and 1 mmol dose only)
NaNO3 in drinking water
High-fat diet 0.1, 1 or 10 mmol•kg-1•d-1
10 wk Male ApoE KO mice (n=8-12)
Bakker, 2016 (216)
Ischaemic reperfusion ↑ Perfusion recovery
NaNO3 in drinking water
Not described 5.0 mmol•kg-1•d-1 2 wk Male NMRI mice or C57BL/6 mice (n=21-23)
Hendgen-Cotta, 2012 (218)
Platelet function ↓ Collagen-induced platelet aggregation
NaNO3 in drinking water
Standard feed pellets
1 g/L 1 wk WT C57BL/6 mice (n≥5); eNOS KO mice (n≥5)
Park, 2013 (228)
1Ach, acetylcholine; BP, blood pressure; DBP, diastolic blood pressure; eNOS, endothelial nitric oxide synthase; KO, knockout; MAP, mean arterial pressure; NMRI, Naval Medical Research Institute; ref, reference; SBP, systolic blood pressure; SH, spontaneously hypertensive; UNX, uninephrectomized; WT, wild-type; ↑, increase; ↓, decrease.
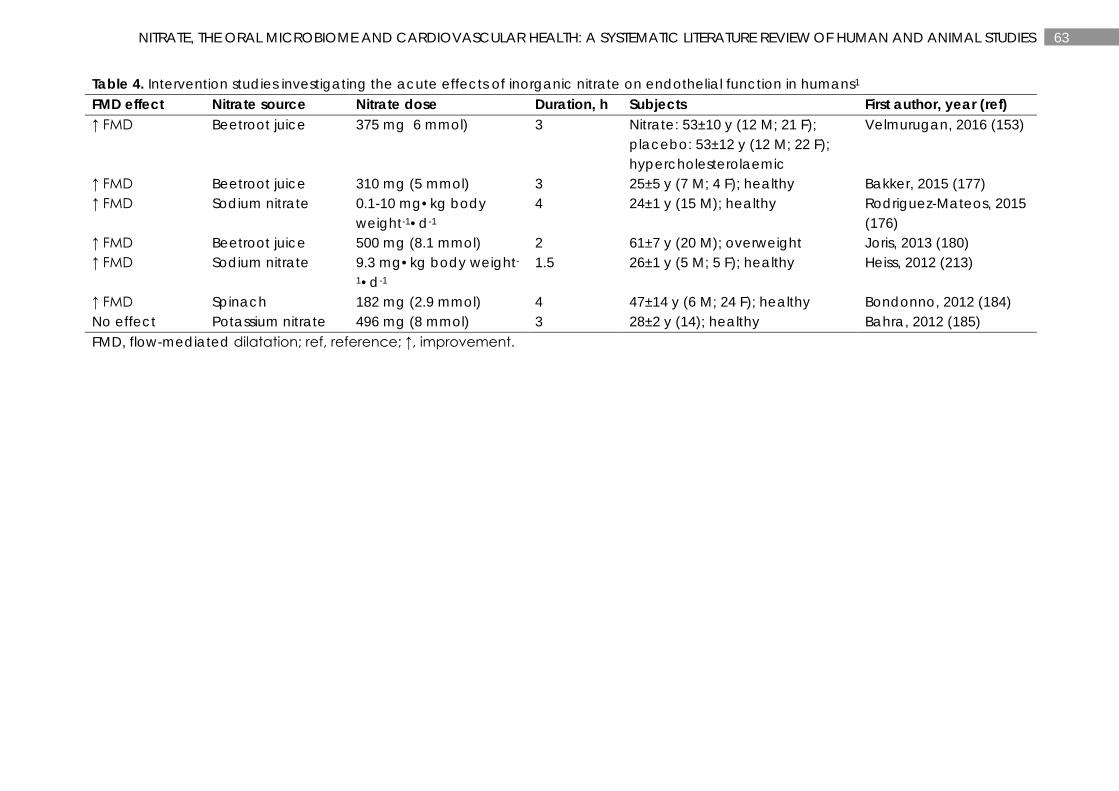
63 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 4. Intervention studies investigating the acute effects of inorganic nitrate on endothelial function in humans1 FMD effect Nitrate source Nitrate dose Duration, h Subjects First author, year (ref) ↑ FMD Beetroot juice 375 mg 6 mmol) 3
Nitrate: 53±10 y (12 M; 21 F); placebo: 53±12 y (12 M; 22 F); hypercholesterolaemic
Velmurugan, 2016 (153)
↑ FMD Beetroot juice 310 mg (5 mmol) 3 25±5 y (7 M; 4 F); healthy Bakker, 2015 (177) ↑ FMD Sodium nitrate 0.1-10 mg•kg body
weight-1•d-1 4 24±1 y (15 M); healthy Rodriguez-Mateos, 2015
(176) ↑ FMD Beetroot juice 500 mg (8.1 mmol) 2 61±7 y (20 M); overweight Joris, 2013 (180) ↑ FMD Sodium nitrate 9.3 mg•kg body weight-
1•d-1 1.5 26±1 y (5 M; 5 F); healthy Heiss, 2012 (213)
↑ FMD Spinach 182 mg (2.9 mmol) 4 47±14 y (6 M; 24 F); healthy Bondonno, 2012 (184) No effect Potassium nitrate 496 mg (8 mmol) 3 28±2 y (14); healthy Bahra, 2012 (185) FMD, flow-mediated dilatation; ref, reference; ↑, improvement.
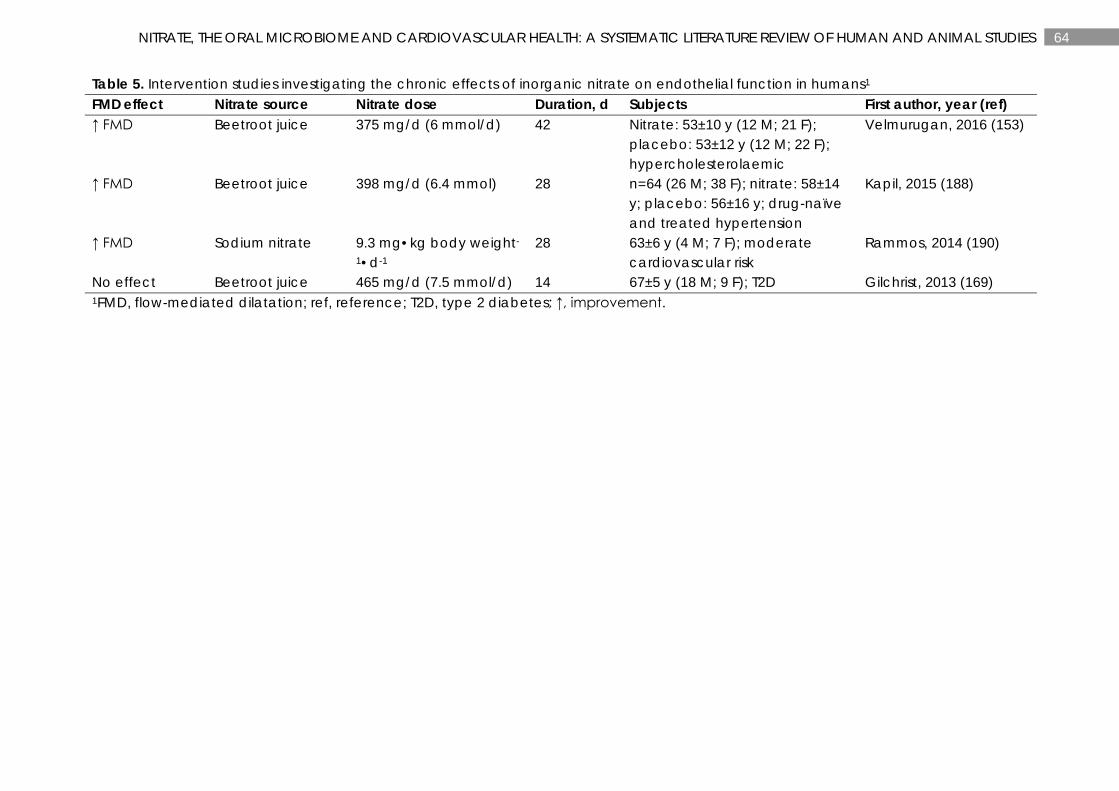
64 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 5. Intervention studies investigating the chronic effects of inorganic nitrate on endothelial function in humans1 FMD effect Nitrate source Nitrate dose Duration, d Subjects First author, year (ref) ↑ FMD Beetroot juice 375 mg/d (6 mmol/d) 42 Nitrate: 53±10 y (12 M; 21 F);
placebo: 53±12 y (12 M; 22 F); hypercholesterolaemic
Velmurugan, 2016 (153)
↑ FMD Beetroot juice 398 mg/d (6.4 mmol) 28 n=64 (26 M; 38 F); nitrate: 58±14 y; placebo: 56±16 y; drug-naïve and treated hypertension
Kapil, 2015 (188)
↑ FMD Sodium nitrate 9.3 mg•kg body weight-
1•d-1 28 63±6 y (4 M; 7 F); moderate
cardiovascular risk Rammos, 2014 (190)
No effect Beetroot juice 465 mg/d (7.5 mmol/d) 14 67±5 y (18 M; 9 F); T2D Gilchrist, 2013 (169) 1FMD, flow-mediated dilatation; ref, reference; T2D, type 2 diabetes; ↑, improvement.
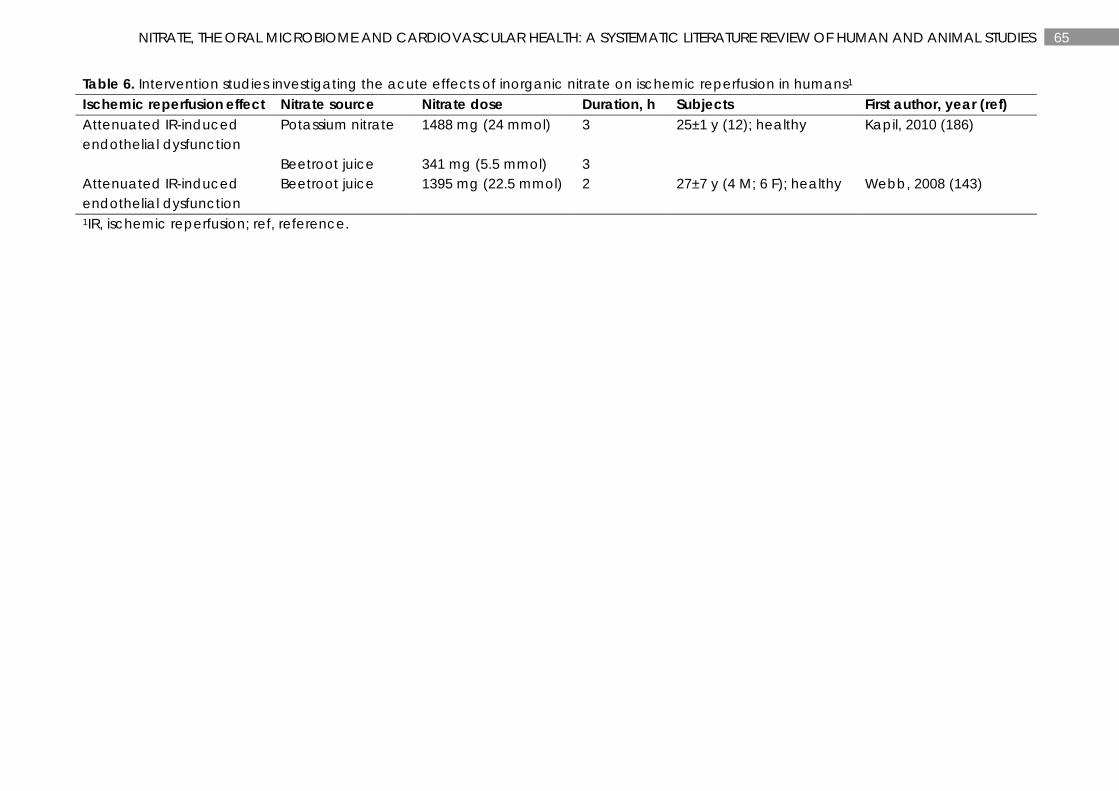
65 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 6. Intervention studies investigating the acute effects of inorganic nitrate on ischemic reperfusion in humans1 Ischemic reperfusion effect Nitrate source Nitrate dose Duration, h Subjects First author, year (ref) Attenuated IR-induced endothelial dysfunction
Potassium nitrate 1488 mg (24 mmol) 3 25±1 y (12); healthy Kapil, 2010 (186)
Beetroot juice 341 mg (5.5 mmol) 3 Attenuated IR-induced endothelial dysfunction
Beetroot juice 1395 mg (22.5 mmol) 2 27±7 y (4 M; 6 F); healthy Webb, 2008 (143)
1IR, ischemic reperfusion; ref, reference.
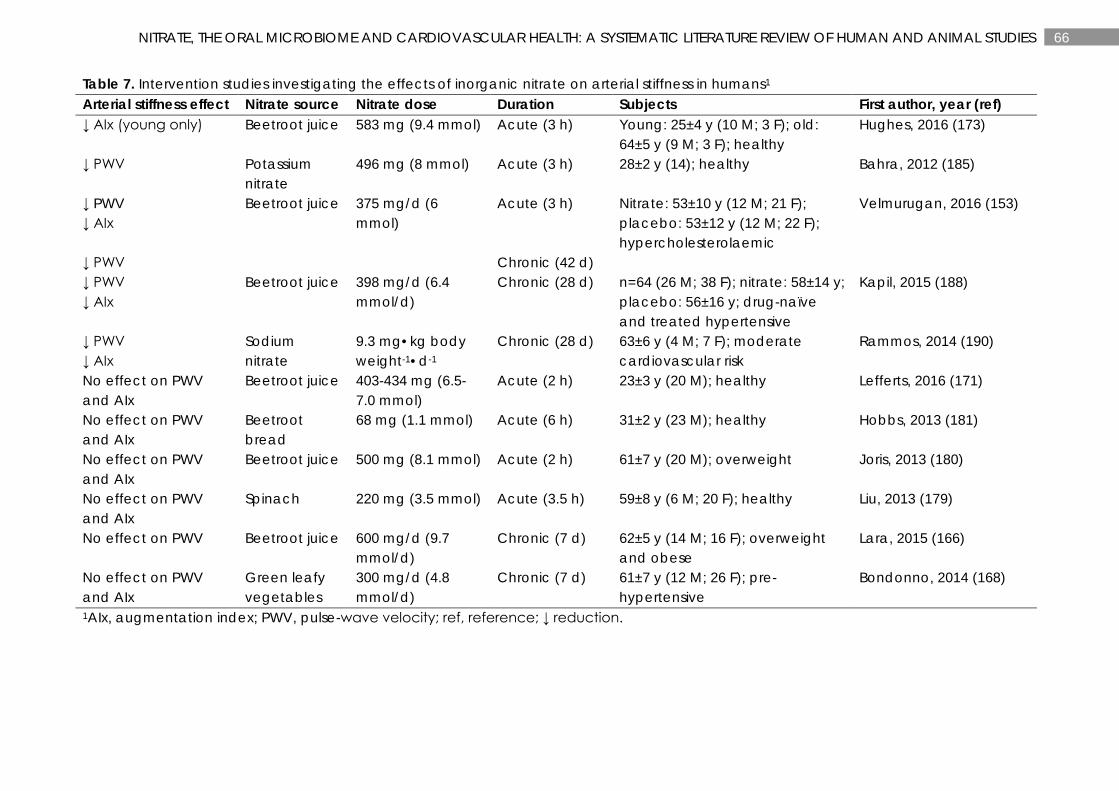
66 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 7. Intervention studies investigating the effects of inorganic nitrate on arterial stiffness in humans1 Arterial stiffness effect Nitrate source Nitrate dose Duration Subjects First author, year (ref) ↓ AIx (young only) Beetroot juice 583 mg (9.4 mmol) Acute (3 h) Young: 25±4 y (10 M; 3 F); old:
64±5 y (9 M; 3 F); healthy Hughes, 2016 (173)
↓ PWV
Potassium nitrate
496 mg (8 mmol) Acute (3 h) 28±2 y (14); healthy Bahra, 2012 (185)
↓ PWV ↓ AIx
Beetroot juice 375 mg/d (6 mmol)
Acute (3 h) Nitrate: 53±10 y (12 M; 21 F); placebo: 53±12 y (12 M; 22 F); hypercholesterolaemic
Velmurugan, 2016 (153)
↓ PWV Chronic (42 d) ↓ PWV ↓ AIx
Beetroot juice 398 mg/d (6.4 mmol/d)
Chronic (28 d) n=64 (26 M; 38 F); nitrate: 58±14 y; placebo: 56±16 y; drug-naïve and treated hypertensive
Kapil, 2015 (188)
↓ PWV ↓ AIx
Sodium nitrate
9.3 mg•kg body weight-1•d-1
Chronic (28 d) 63±6 y (4 M; 7 F); moderate cardiovascular risk
Rammos, 2014 (190)
No effect on PWV and AIx
Beetroot juice 403-434 mg (6.5-7.0 mmol)
Acute (2 h) 23±3 y (20 M); healthy Lefferts, 2016 (171)
No effect on PWV and AIx
Beetroot bread
68 mg (1.1 mmol) Acute (6 h) 31±2 y (23 M); healthy Hobbs, 2013 (181)
No effect on PWV and AIx
Beetroot juice 500 mg (8.1 mmol) Acute (2 h) 61±7 y (20 M); overweight Joris, 2013 (180)
No effect on PWV and AIx
Spinach 220 mg (3.5 mmol) Acute (3.5 h) 59±8 y (6 M; 20 F); healthy Liu, 2013 (179)
No effect on PWV Beetroot juice 600 mg/d (9.7 mmol/d)
Chronic (7 d) 62±5 y (14 M; 16 F); overweight and obese
Lara, 2015 (166)
No effect on PWV and AIx
Green leafy vegetables
300 mg/d (4.8 mmol/d)
Chronic (7 d) 61±7 y (12 M; 26 F); pre-hypertensive
Bondonno, 2014 (168)
1AIx, augmentation index; PWV, pulse-wave velocity; ref, reference; ↓ reduction.
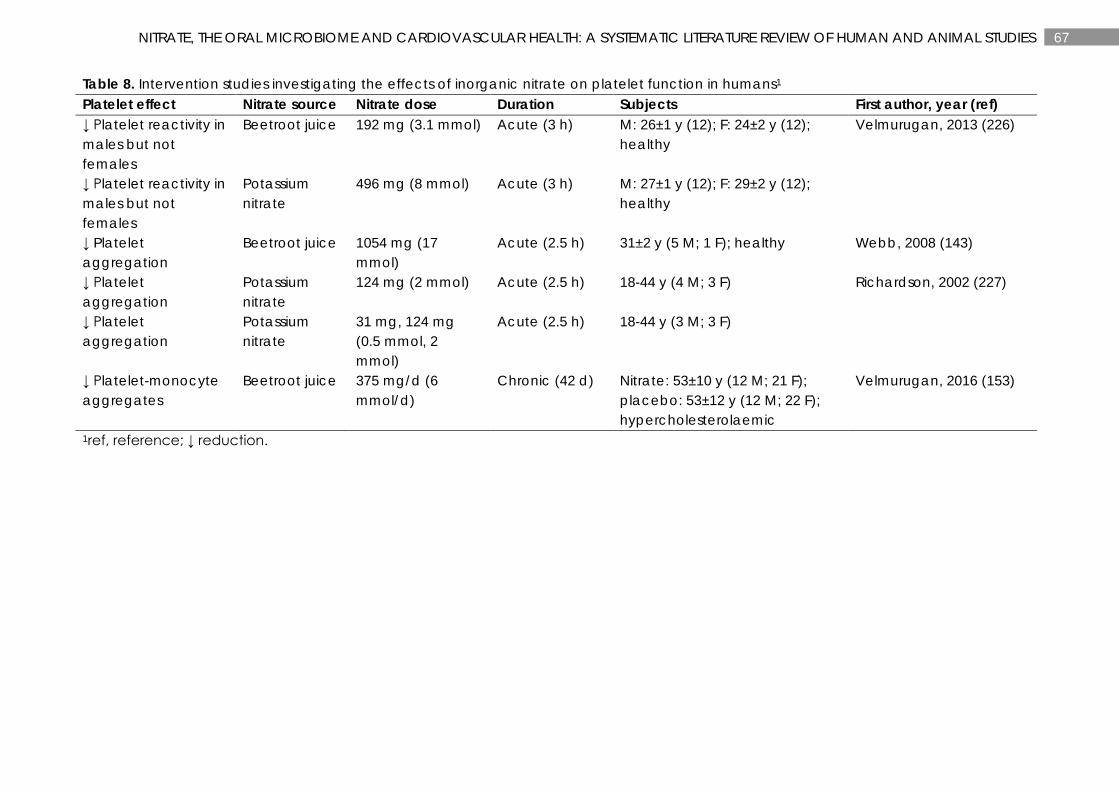
67 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 8. Intervention studies investigating the effects of inorganic nitrate on platelet function in humans1 Platelet effect Nitrate source Nitrate dose Duration Subjects First author, year (ref) ↓ Platelet reactivity in males but not females
Beetroot juice 192 mg (3.1 mmol) Acute (3 h) M: 26±1 y (12); F: 24±2 y (12); healthy
Velmurugan, 2013 (226)
↓ Platelet reactivity in males but not females
Potassium nitrate
496 mg (8 mmol) Acute (3 h) M: 27±1 y (12); F: 29±2 y (12); healthy
↓ Platelet aggregation
Beetroot juice 1054 mg (17 mmol)
Acute (2.5 h) 31±2 y (5 M; 1 F); healthy Webb, 2008 (143)
↓ Platelet aggregation
Potassium nitrate
124 mg (2 mmol) Acute (2.5 h) 18-44 y (4 M; 3 F) Richardson, 2002 (227)
↓ Platelet aggregation
Potassium nitrate
31 mg, 124 mg (0.5 mmol, 2 mmol)
Acute (2.5 h) 18-44 y (3 M; 3 F)
↓ Platelet-monocyte aggregates
Beetroot juice 375 mg/d (6 mmol/d)
Chronic (42 d) Nitrate: 53±10 y (12 M; 21 F); placebo: 53±12 y (12 M; 22 F); hypercholesterolaemic
Velmurugan, 2016 (153)
1ref, reference; ↓ reduction.
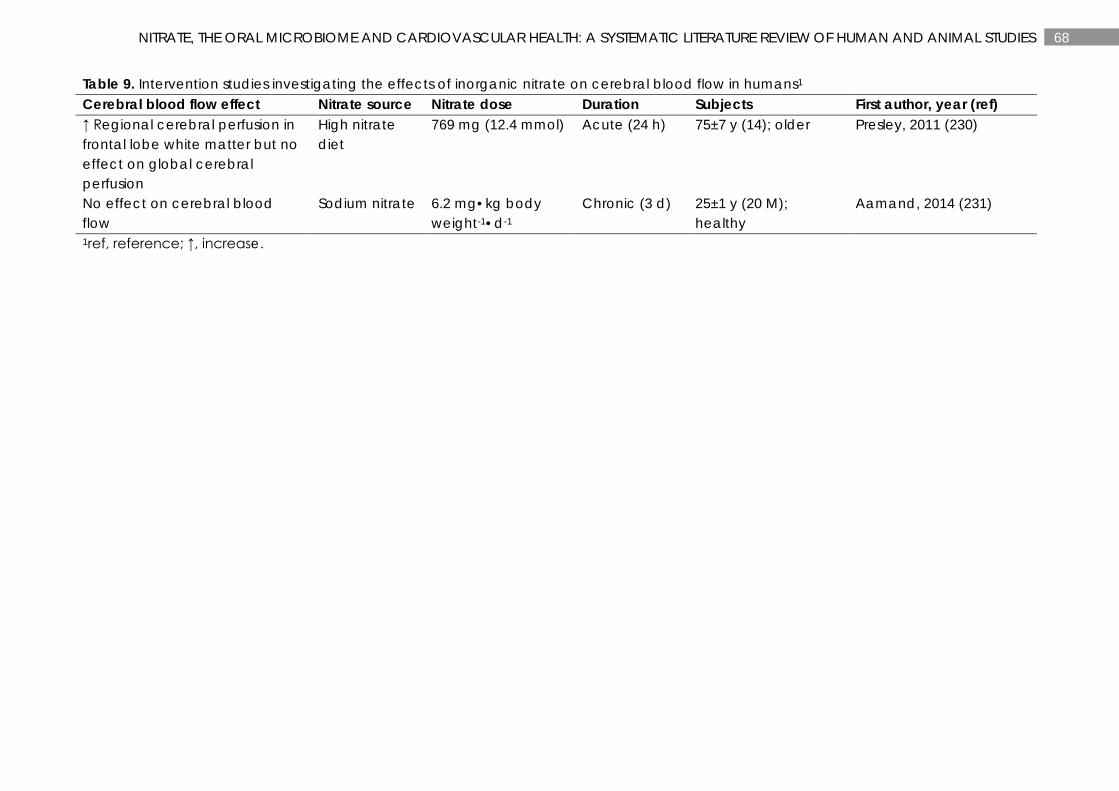
68 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 9. Intervention studies investigating the effects of inorganic nitrate on cerebral blood flow in humans1 Cerebral blood flow effect Nitrate source Nitrate dose Duration Subjects First author, year (ref) ↑ Regional cerebral perfusion in frontal lobe white matter but no effect on global cerebral perfusion
High nitrate diet
769 mg (12.4 mmol) Acute (24 h)
75±7 y (14); older Presley, 2011 (230)
No effect on cerebral blood flow
Sodium nitrate 6.2 mg•kg body weight-1•d-1
Chronic (3 d)
25±1 y (20 M); healthy
Aamand, 2014 (231)
1ref, reference; ↑, increase.
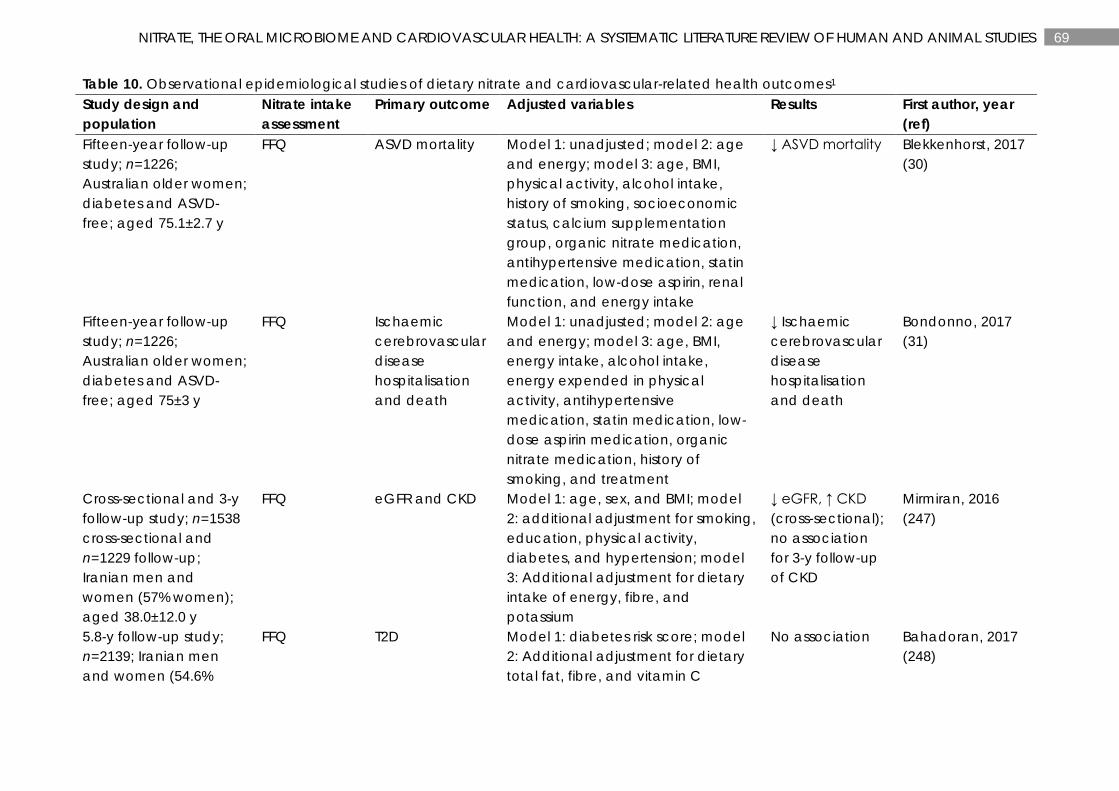
69 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 10. Observational epidemiological studies of dietary nitrate and cardiovascular-related health outcomes1 Study design and population
Nitrate intake assessment
Primary outcome Adjusted variables Results First author, year (ref)
Fifteen-year follow-up study; n=1226; Australian older women; diabetes and ASVD-free; aged 75.1±2.7 y
FFQ ASVD mortality Model 1: unadjusted; model 2: age and energy; model 3: age, BMI, physical activity, alcohol intake, history of smoking, socioeconomic status, calcium supplementation group, organic nitrate medication, antihypertensive medication, statin medication, low-dose aspirin, renal function, and energy intake
↓ ASVD mortality Blekkenhorst, 2017 (30)
Fifteen-year follow-up study; n=1226; Australian older women; diabetes and ASVD-free; aged 75±3 y
FFQ Ischaemic cerebrovascular disease hospitalisation and death
Model 1: unadjusted; model 2: age and energy; model 3: age, BMI, energy intake, alcohol intake, energy expended in physical activity, antihypertensive medication, statin medication, low-dose aspirin medication, organic nitrate medication, history of smoking, and treatment
↓ Ischaemic cerebrovascular disease hospitalisation and death
Bondonno, 2017 (31)
Cross-sectional and 3-y follow-up study; n=1538 cross-sectional and n=1229 follow-up; Iranian men and women (57% women); aged 38.0±12.0 y
FFQ eGFR and CKD Model 1: age, sex, and BMI; model 2: additional adjustment for smoking, education, physical activity, diabetes, and hypertension; model 3: Additional adjustment for dietary intake of energy, fibre, and potassium
↓ eGFR, ↑ CKD (cross-sectional); no association for 3-y follow-up of CKD
Mirmiran, 2016 (247)
5.8-y follow-up study; n=2139; Iranian men and women (54.6%
FFQ T2D Model 1: diabetes risk score; model 2: Additional adjustment for dietary total fat, fibre, and vitamin C
No association
Bahadoran, 2017 (248)
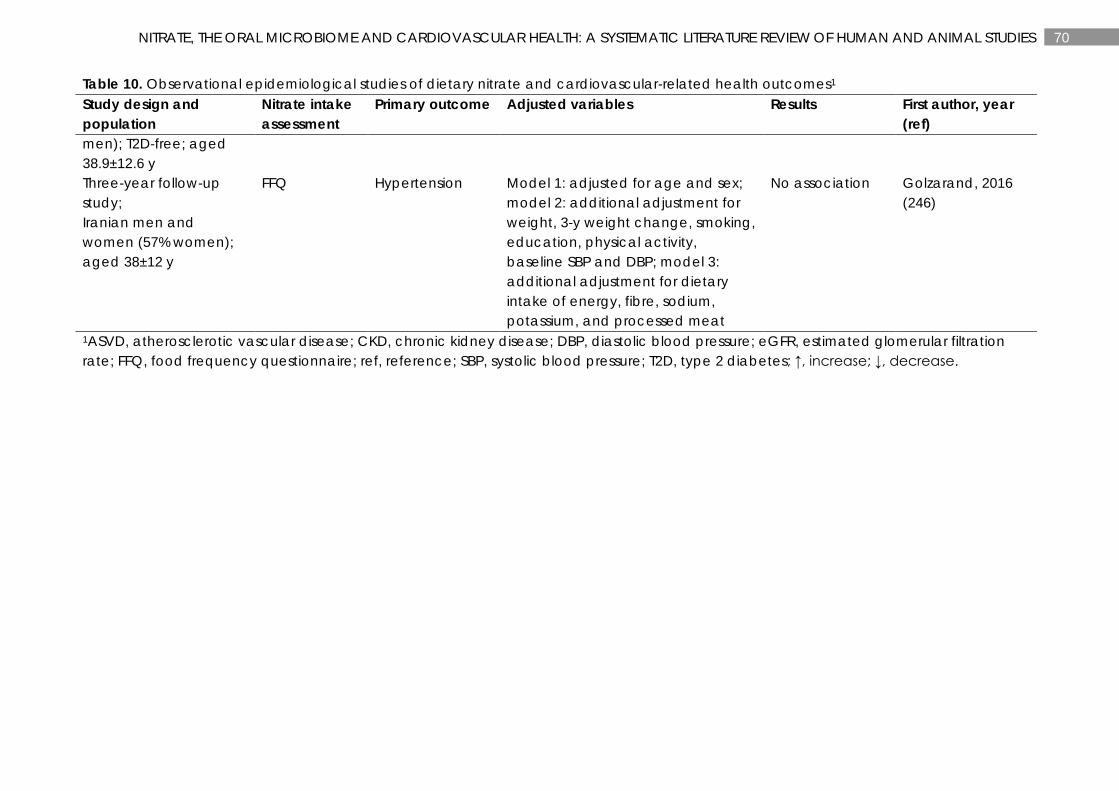
70 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE REVIEW OF HUMAN AND ANIMAL STUDIES
Table 10. Observational epidemiological studies of dietary nitrate and cardiovascular-related health outcomes1 Study design and population
Nitrate intake assessment
Primary outcome Adjusted variables Results First author, year (ref)
men); T2D-free; aged 38.9±12.6 y Three-year follow-up study; Iranian men and women (57% women); aged 38±12 y
FFQ Hypertension Model 1: adjusted for age and sex; model 2: additional adjustment for weight, 3-y weight change, smoking, education, physical activity, baseline SBP and DBP; model 3: additional adjustment for dietary intake of energy, fibre, sodium, potassium, and processed meat
No association Golzarand, 2016 (246)
1ASVD, atherosclerotic vascular disease; CKD, chronic kidney disease; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; FFQ, food frequency questionnaire; ref, reference; SBP, systolic blood pressure; T2D, type 2 diabetes; ↑, increase; ↓, decrease.
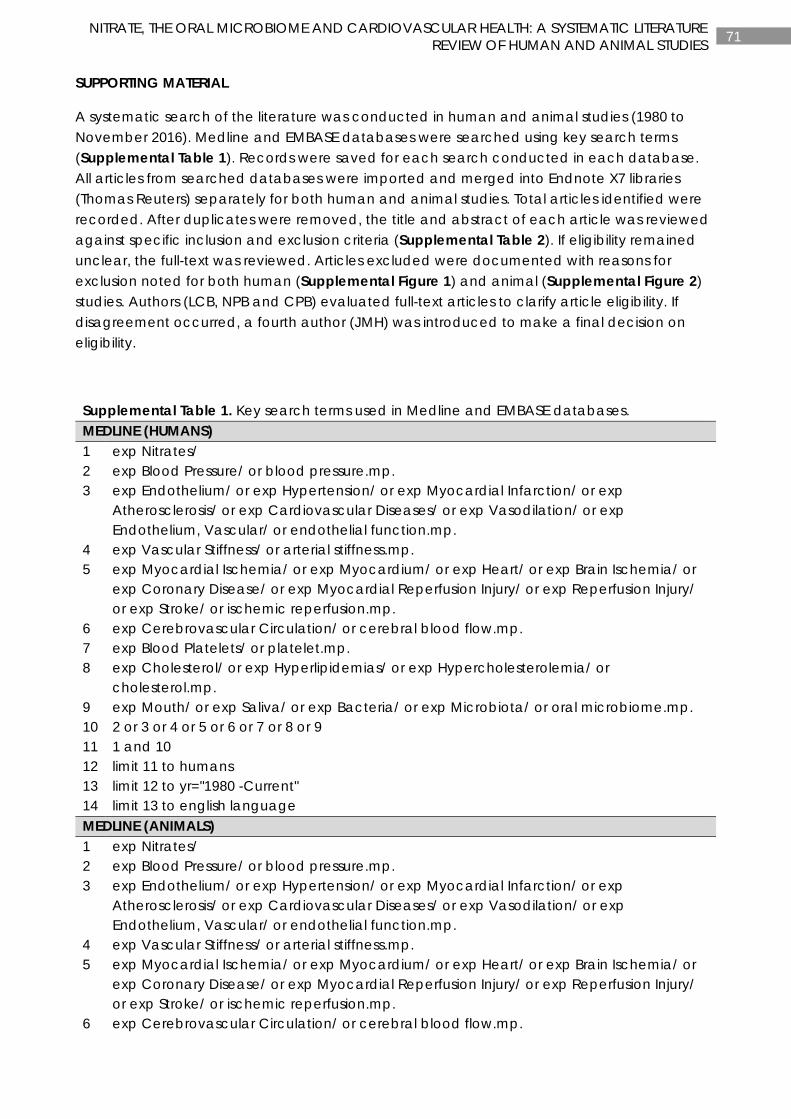
71 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
SUPPORTING MATERIAL
A systematic search of the literature was conducted in human and animal studies (1980 to November 2016). Medline and EMBASE databases were searched using key search terms (Supplemental Table 1). Records were saved for each search conducted in each database. All articles from searched databases were imported and merged into Endnote X7 libraries (Thomas Reuters) separately for both human and animal studies. Total articles identified were recorded. After duplicates were removed, the title and abstract of each article was reviewed against specific inclusion and exclusion criteria (Supplemental Table 2). If eligibility remained unclear, the full-text was reviewed. Articles excluded were documented with reasons for exclusion noted for both human (Supplemental Figure 1) and animal (Supplemental Figure 2) studies. Authors (LCB, NPB and CPB) evaluated full-text articles to clarify article eligibility. If disagreement occurred, a fourth author (JMH) was introduced to make a final decision on eligibility.
Supplemental Table 1. Key search terms used in Medline and EMBASE databases. MEDLINE (HUMANS) 1 exp Nitrates/ 2 exp Blood Pressure/ or blood pressure.mp. 3 exp Endothelium/ or exp Hypertension/ or exp Myocardial Infarction/ or exp
Atherosclerosis/ or exp Cardiovascular Diseases/ or exp Vasodilation/ or exp Endothelium, Vascular/ or endothelial function.mp.
4 exp Vascular Stiffness/ or arterial stiffness.mp. 5 exp Myocardial Ischemia/ or exp Myocardium/ or exp Heart/ or exp Brain Ischemia/ or
exp Coronary Disease/ or exp Myocardial Reperfusion Injury/ or exp Reperfusion Injury/ or exp Stroke/ or ischemic reperfusion.mp.
6 exp Cerebrovascular Circulation/ or cerebral blood flow.mp. 7 exp Blood Platelets/ or platelet.mp. 8 exp Cholesterol/ or exp Hyperlipidemias/ or exp Hypercholesterolemia/ or
cholesterol.mp. 9 exp Mouth/ or exp Saliva/ or exp Bacteria/ or exp Microbiota/ or oral microbiome.mp. 10 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 11 1 and 10 12 limit 11 to humans 13 limit 12 to yr="1980 -Current" 14 limit 13 to english language MEDLINE (ANIMALS) 1 exp Nitrates/ 2 exp Blood Pressure/ or blood pressure.mp. 3 exp Endothelium/ or exp Hypertension/ or exp Myocardial Infarction/ or exp
Atherosclerosis/ or exp Cardiovascular Diseases/ or exp Vasodilation/ or exp Endothelium, Vascular/ or endothelial function.mp.
4 exp Vascular Stiffness/ or arterial stiffness.mp. 5 exp Myocardial Ischemia/ or exp Myocardium/ or exp Heart/ or exp Brain Ischemia/ or
exp Coronary Disease/ or exp Myocardial Reperfusion Injury/ or exp Reperfusion Injury/ or exp Stroke/ or ischemic reperfusion.mp.
6 exp Cerebrovascular Circulation/ or cerebral blood flow.mp.
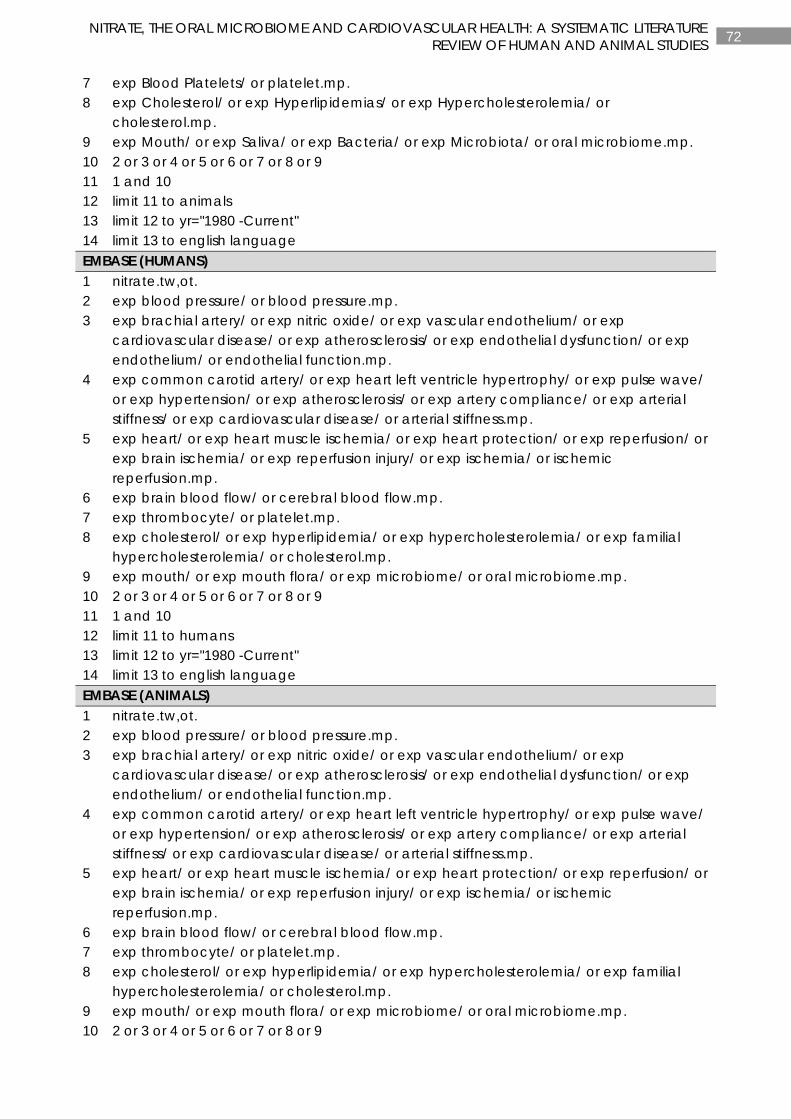
72 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
7 exp Blood Platelets/ or platelet.mp. 8 exp Cholesterol/ or exp Hyperlipidemias/ or exp Hypercholesterolemia/ or
cholesterol.mp. 9 exp Mouth/ or exp Saliva/ or exp Bacteria/ or exp Microbiota/ or oral microbiome.mp. 10 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 11 1 and 10 12 limit 11 to animals 13 limit 12 to yr="1980 -Current" 14 limit 13 to english language EMBASE (HUMANS) 1 nitrate.tw,ot. 2 exp blood pressure/ or blood pressure.mp. 3 exp brachial artery/ or exp nitric oxide/ or exp vascular endothelium/ or exp
cardiovascular disease/ or exp atherosclerosis/ or exp endothelial dysfunction/ or exp endothelium/ or endothelial function.mp.
4 exp common carotid artery/ or exp heart left ventricle hypertrophy/ or exp pulse wave/ or exp hypertension/ or exp atherosclerosis/ or exp artery compliance/ or exp arterial stiffness/ or exp cardiovascular disease/ or arterial stiffness.mp.
5 exp heart/ or exp heart muscle ischemia/ or exp heart protection/ or exp reperfusion/ or exp brain ischemia/ or exp reperfusion injury/ or exp ischemia/ or ischemic reperfusion.mp.
6 exp brain blood flow/ or cerebral blood flow.mp. 7 exp thrombocyte/ or platelet.mp. 8 exp cholesterol/ or exp hyperlipidemia/ or exp hypercholesterolemia/ or exp familial
hypercholesterolemia/ or cholesterol.mp. 9 exp mouth/ or exp mouth flora/ or exp microbiome/ or oral microbiome.mp. 10 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 11 1 and 10 12 limit 11 to humans 13 limit 12 to yr="1980 -Current" 14 limit 13 to english language EMBASE (ANIMALS) 1 nitrate.tw,ot. 2 exp blood pressure/ or blood pressure.mp. 3 exp brachial artery/ or exp nitric oxide/ or exp vascular endothelium/ or exp
cardiovascular disease/ or exp atherosclerosis/ or exp endothelial dysfunction/ or exp endothelium/ or endothelial function.mp.
4 exp common carotid artery/ or exp heart left ventricle hypertrophy/ or exp pulse wave/ or exp hypertension/ or exp atherosclerosis/ or exp artery compliance/ or exp arterial stiffness/ or exp cardiovascular disease/ or arterial stiffness.mp.
5 exp heart/ or exp heart muscle ischemia/ or exp heart protection/ or exp reperfusion/ or exp brain ischemia/ or exp reperfusion injury/ or exp ischemia/ or ischemic reperfusion.mp.
6 exp brain blood flow/ or cerebral blood flow.mp. 7 exp thrombocyte/ or platelet.mp. 8 exp cholesterol/ or exp hyperlipidemia/ or exp hypercholesterolemia/ or exp familial
hypercholesterolemia/ or cholesterol.mp. 9 exp mouth/ or exp mouth flora/ or exp microbiome/ or oral microbiome.mp. 10 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9
73 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
11 1 and 10 12 limit 11 to animals 13 limit 12 to yr="1980 -Current" 14 limit 13 to english language
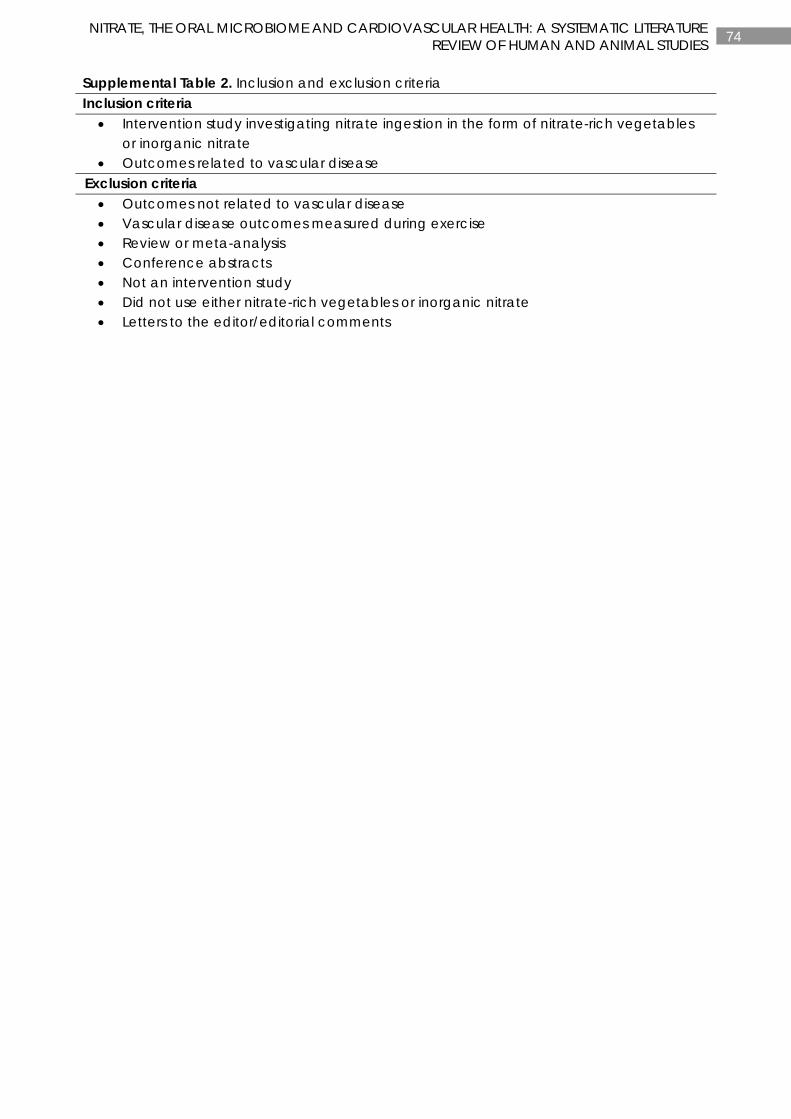
74 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
Supplemental Table 2. Inclusion and exclusion criteria Inclusion criteria
• Intervention study investigating nitrate ingestion in the form of nitrate-rich vegetables or inorganic nitrate
• Outcomes related to vascular disease Exclusion criteria • Outcomes not related to vascular disease • Vascular disease outcomes measured during exercise • Review or meta-analysis • Conference abstracts • Not an intervention study • Did not use either nitrate-rich vegetables or inorganic nitrate • Letters to the editor/editorial comments
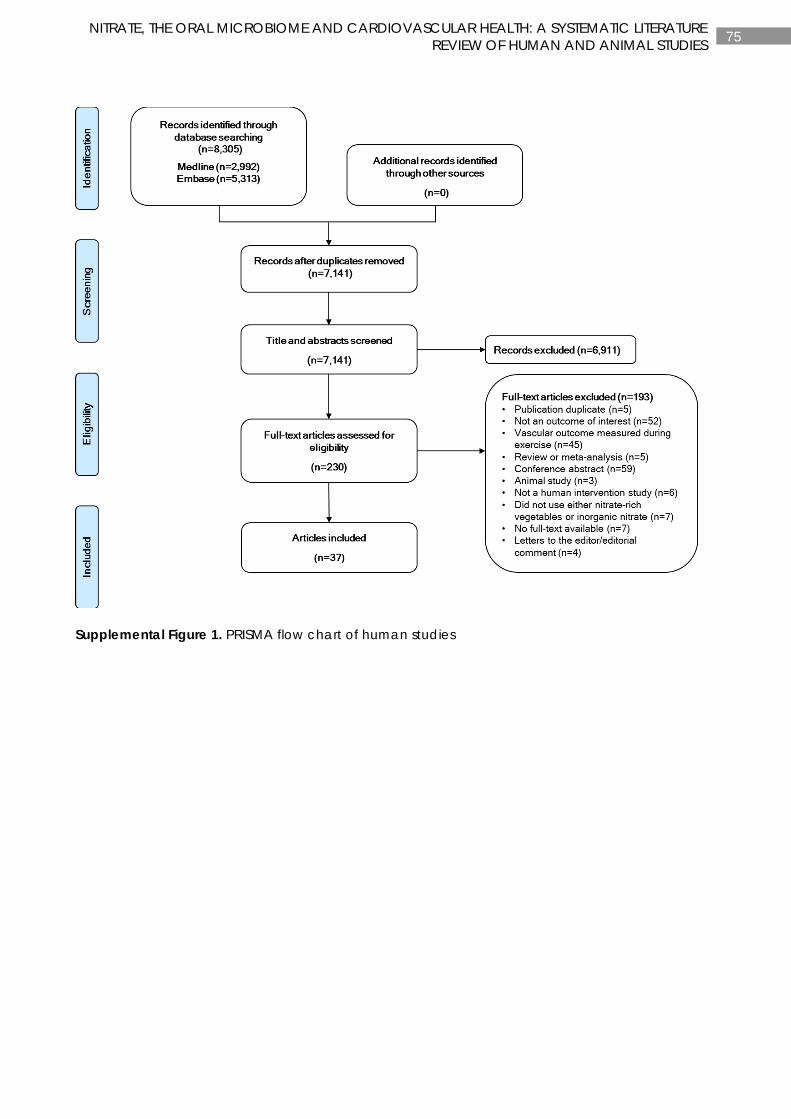
75 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
Supplemental Figure 1. PRISMA flow chart of human studies
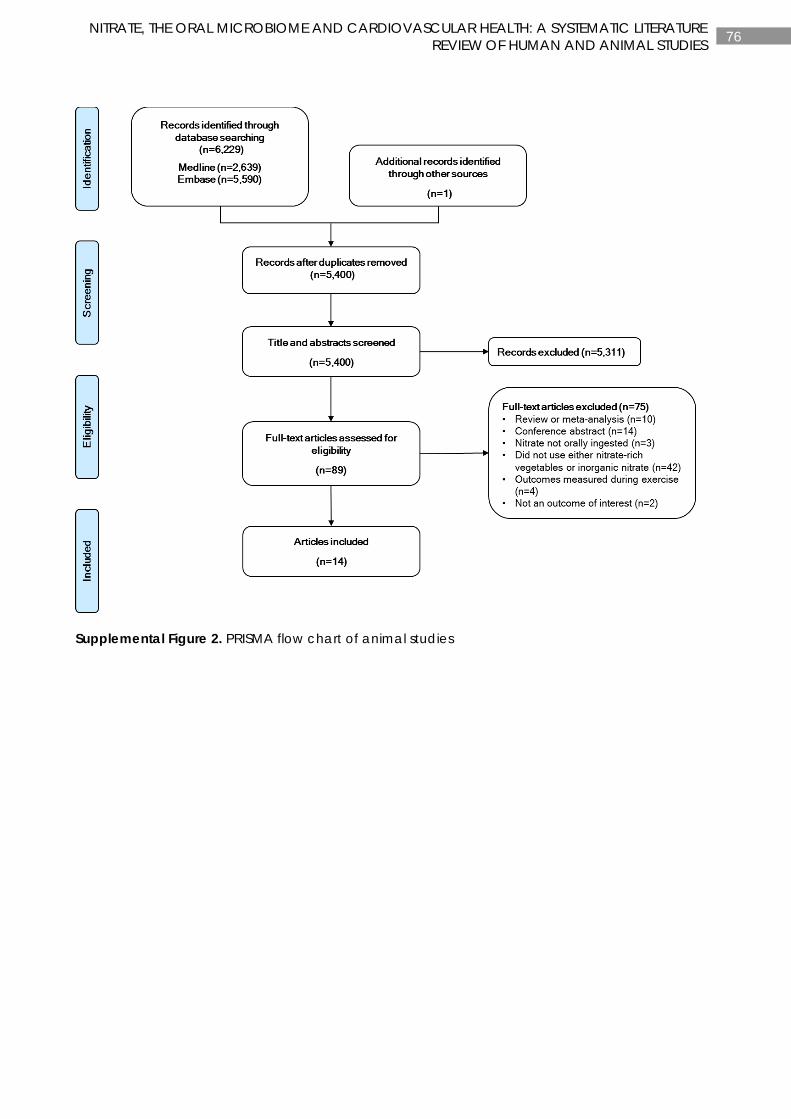
76 NITRATE, THE ORAL MICROBIOME AND CARDIOVASCULAR HEALTH: A SYSTEMATIC LITERATURE
REVIEW OF HUMAN AND ANIMAL STUDIES
Supplemental Figure 2. PRISMA flow chart of animal studies
77 CHAPTER 3
CHAPTER 3
CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
Manuscript based on this chapter:
Lauren C Blekkenhorst, Catherine P Bondonno, Joshua R Lewis, Amanda Devine, Kun Zhu, Wai H Lim, Richard J Woodman, Lawrence J Beilin, Richard L Prince, Jonathan M Hodgson. Cruciferous and allium vegetable intakes are inversely associated with 15-year atherosclerotic vascular disease deaths in older adult women. Journal of the American Heart Association. 2017;6(10):1-15

78 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
ABSTRACT
Background: Higher vegetable intake is consistently associated with lower atherosclerotic vascular disease (ASVD) events. However, the components responsible and mechanisms involved are uncertain. Non-nutritive phytochemicals may be involved. The objective of this study was to investigate the associations of total vegetable intake and types of vegetables grouped according to phytochemical constituents with ASVD mortality.
Methods and Results: The cohort consisted of 1,226 Australian women aged ≥70 years without clinical ASVD or diabetes mellitus at baseline (1998). Vegetable intakes were calculated per serving (75 g/d) and were also classified into pre-specified types relating to phytochemical constituents. ASVD-related deaths were ascertained from linked mortality data. During 15 years (15,947 person-years) of follow-up, 238 ASVD-related deaths occurred. A one serving increment of vegetable intake was associated with a 20% lower hazard of ASVD-related death (multivariable-adjusted HR=0.80, 95%CI=0.69, 0.94, P=0.005). In multivariable-adjusted models for vegetable types, cruciferous (per 10 g/d increase, HR=0.87, 95%CI=0.81, 0.94, P<0.001) and allium (per 5 g/d increase, HR=0.82, 95%CI=0.73, 0.94, P=0.003) vegetables were inversely associated with ASVD-related deaths. The inclusion of other vegetable types, as well as lifestyle and cardiovascular risk factors, did not alter these associations. Yellow/orange/red (P=0.463), leafy green (P=0.063) and legume (P=0.379) vegetables were not significant.
Conclusions: Consistent with current evidence, higher cruciferous and allium vegetable intakes were associated with a lower risk of ASVD mortality. In addition, cruciferous and allium vegetables are recognised to be a good source of several non-nutritive phytochemicals such as organosulfur compounds.
79 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
INTRODUCTION
Atherosclerotic vascular disease (ASVD) is the most common cause of death worldwide (4). Higher vegetable intake has been consistently associated with lower risk of ASVD (115). Results from these studies have provided the basis for guideline recommendations around the world to increase vegetable intake (5-7). In recent years further analysis of the role of specific vegetable and fruit species has been undertaken to identify potentially beneficial varieties and thus to allow consideration of the potential nutrient and phytochemical effects on health outcomes. A recent report of the beneficial effects of certain vegetables and fruits on the risks of developing hypertension is an excellent example of the approach required to advance our knowledge of the role of specific vegetable and fruit species on preventing disease (16).
Vegetables contain many important nutrients and phytochemicals that may be cardioprotective (18). For example, recent meta-analyses have identified the beneficial effects on health outcomes of dietary fibre (13) and the micronutrients, potassium (14) and magnesium (15). In addition, specific groups of phytochemicals such as organosulfur compounds, carotenoids, nitrogen-containing compounds and polyphenols have been postulated to have additional benefits towards cardiovascular health (32, 44, 48, 256). Thus, the aim of this study was to investigate the associations of total vegetable intake as well as types of vegetables grouped according to phytochemical constituents with ASVD mortality over 15 years of follow-up in a cohort of older adult women.
METHODS
Ethics statement
The Perth Longitudinal Study of Aging in Women (PLSAW) was approved by the University of Western Australia Human Ethics Committee and complied with the Declaration of Helsinki. Written informed consents were obtained from all participants. Human ethics approval for the use of linked data for the project was provided by the Western Australian Department of Health Human Research Ethics Committee (project #2009/24).
Study population
The population of this prospective cohort study consisted of participants in the PLSAW. This study originated in 1998 as the Calcium Intake Fracture Outcome Study (CAIFOS). The CAIFOS was a 5 year, double-blind, randomised, placebo-controlled trial of daily calcium supplementation (1.2g calcium carbonate) to prevent fractures (257). Women aged 70 years and above (n=1,500) were recruited from the Western Australian general population by mail using the Electoral Roll, which is maintained for all Australian citizens enrolled to vote in Western Australia. After the completion of the CAIFOS, participants were enrolled in a 10-year extension follow-up study. In total, there were 15 years of follow-up (PLSAW).
Eligibility criteria included available data on all exposure and outcome variables. Dietary data was available for 1,485/1,500 (99.0%) participants at baseline. Participants (17/1,485 [1.1%]) with implausible energy intakes (<2,100kJ [500kcal] or >14,700kJ [3,500kcal]) were excluded. Further exclusion of participants with prevalent ASVD (n=152), diabetes mellitus (n=69) or both (n=21) at baseline resulted in 1,226/1,500 (81.7%) participants being included for the analysis of this study. Prevalent ASVD and/or diabetes mellitus at baseline was an a priori exclusion criteria
80 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
because participants with a clinical diagnosis of ASVD or diabetes may have resulted in altered dietary intake and thereby attenuated the association of interest.
History of ASVD at baseline (1998) was determined from principal hospital discharge diagnosis codes from 1980-1998 using the Hospital Morbidity Data Collection, linked via the Western Australian Data Linkage System (WADLS). Diagnosis codes were defined using the Manual of the International Statistical Classification of Diseases, Injuries and Causes of Death, 9th Revision (ICD-9) (258) and the Australian Version of the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) (259). ASVD diagnosis codes included ischaemic heart disease (ICD-9/ICD-9-CM codes 410-414); heart failure (ICD-9/ICD-9-CM code 428); cerebrovascular disease, excluding haemorrhage (ICD-9/ICD-9-CM codes 433-438); and peripheral arterial disease (ICD-9/ICD-9-CM codes 440-444). Baseline history of diabetes mellitus was determined from medication use which was coded (T89001-T90009) using the International Classification of Primary Care – Plus (ICPC-Plus) method (260). This coding methodology allows aggregation of different terms for similar pathologic entities as defined by the ICD-10 coding system.
Atherosclerotic vascular disease mortality assessment
Any death relating to ASVD was the primary outcome of the study. Coded multiple causes of death data over a 15 year period were retrieved from linked mortality data via the WADLS. Multiple causes of death data included the underlying cause of death and all associated causes of death listed on the death certificate. The causes of death were obtained from the coded death certificate using information in Parts 1 and 2 of the death certificate or all diagnosis text fields from the death certificate when coded deaths were not yet available. ASVD deaths were defined using diagnosis codes from the ICD-9-CM (258) and the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM) (261). ASVD-related death diagnosis codes included deaths attributed to ischaemic heart disease (ICD-9-CM codes 410-414 and ICD-10-AM codes I20-I25); heart failure (ICD-9-CM code 428 and ICD-10-AM code I50); cerebrovascular disease, excluding haemorrhage (ICD-9-CM codes 433-438 and ICD-10-AM codes I63-I69, G45.9); and peripheral arterial disease (ICD-9-CM codes 440-444 and ICD-10-AM codes I70-I74).
Dietary intake assessment
A self-administered, semiquantitative food frequency questionnaire developed by the Cancer Council of Victoria was used to assess dietary intake at baseline (1998), 5 years (2003) and 7 years (2005) (262). This questionnaire was designed to assess the usual frequency of dietary intakes over a 12 month period with 10 frequency response options ranging from ‘never’ to ‘3 or more times per day’ and has been validated using 7-day weighed food records (263). Portion size was calculated using photographs of scaled portions of different food types. Energy (kJ/d) and nutrient intakes were calculated by the Cancer Council of Victoria using the NUTTAB95 food composition database (264) and were supplemented by other data where necessary. Individual food items were calculated in g/d by the Cancer Council of Victoria. Participants were supervised by a research assistant whilst completing the food frequency questionnaire. Food models and food charts as well as measuring cups and measuring spoons were provided to ensure the accuracy of reported food consumption.
81 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
Total vegetable intake
Total vegetable intake was calculated in servings per day. Vegetable servings were based on the 2013 Australian Dietary Guidelines of 1 serving of vegetables being equivalent to 75 g (6). Servings per day were calculated as a continuous variable and then categorised as a discrete variable (<2 servings; 2 to <3 servings; ≥3 servings). Vegetable intake was assessed using 24 vegetable items and did not include ‘Potatoes, roasted or fried, including hot chips’ as hot chips are not recommended as part of a healthy diet (6). ‘Potatoes cooked without fat’ were included.
Vegetable type
Classification of vegetable types were based on the 2013 Australian Dietary Guidelines (6) and modified to include the following subgroups of vegetables relating to phytochemical profiles: cruciferous vegetables (cabbage, Brussels sprouts, cauliflower and broccoli) – source of organosulfur compounds (32); allium vegetables (onion, leek and garlic) – source of organosulfur compounds (32); yellow/orange/red vegetables (tomato, capsicum, beetroot, carrot and pumpkin) – source of carotenoids such as lycopene and beta-carotene (48); leafy green vegetables (lettuce and other salad greens, celery, silverbeet and spinach) – source of nitrogen-containing compounds such as nitrate (44); and legumes (peas, greens beans, bean sprouts and alfalfa sprouts, baked beans, soy beans, soy bean curd and tofu, and other beans) – source of polyphenolic compounds such as isoflavonoids and saponins (256).
Nutrient-Rich Foods Index
We assessed overall diet quality using the Nutrient-Rich Foods Index (265). This index was calculated using the Nutrient Reference Values (NRVs) for Australia and New Zealand based on adult females aged >70 y (266) and has been described previously (30).
Baseline demographic and clinical assessment
Body mass index (BMI) (kg/m2) was calculated using body weight (kg) and height (m) which were assessed whilst participants were wearing light clothes without socks and shoes. Body weight was measured using digital scales to the nearest 0.1 kg and height was assessed using a wall-mounted stadiometer to the nearest 0.1 cm. Physical activity was assessed by asking participants about participation in sport, recreation and/or regular physical activities undertaken in the last three months prior to their baseline visit (267). The level of activity (kJ/d) was calculated using a validated method applying the type of activity, time engaged in the activity and body weight (268, 269). Alcohol (g/d) intake was assessed along with other dietary intakes using the validated food frequency questionnaire developed by the Cancer Council of Victoria as described above. Smoking history was collected using a questionnaire and was coded as non-smoker or ex-smoker/current smoker if they had consumed more than 1 cigarette per day for more than 3 months at any time in their life. Socioeconomic status (SES) was calculated using the Socioeconomic Indexes for Areas developed by the Australian Bureau of Statistics (270). The index ranked residential postcodes according to relative socio-economic advantage and disadvantage. Participants were coded into 6 groups from the top 10% most highly disadvantaged to the top 10% least disadvantaged (270).
Participants were asked to provide a detailed medical history and list of medications which were verified by their general practitioner where possible. The ICPC-Plus method was used to
82 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
code medication use (260). Medication use included antihypertensive, statin and low-dose aspirin medications. These medications were used to adjust for ASVD risk factors such as hypertension and dyslipidaemia. Baseline serum creatinine was analysed in 1,106/1,226 (90.2%) participants using an isotope dilution mass spectrometry (IDMS) traceable Jaffe kinetic assay for creatinine on a Hitachi 917 analyser (Roche Diagnostics GmbH, Mannheim, Germany). Estimated glomerular filtration rate (eGFR) was then calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation (271) and was added to the multivariable-adjusted models as this has been shown to predict ASVD in this cohort (272). Total cholesterol, high-density lipoprotein (HDL) cholesterol and triglyceride concentrations were analysed in 895/1,226 (73.0%) participants using a Hitachi 917 auto analyser (Roche Diagnostics, Mannheim, Germany). Low-density lipoprotein (LDL) cholesterol was calculated in 888/1,226 (72.4%) participants using the Friedewald’s method (273).
Framingham 10-year General Cardiovascular Risk Scores (FRS)
The FRS was calculated using body mass index data in 1,188 participants. The FRS included age, sex, previous diabetes, body mass index, current smoking status and treated (prescribed antihypertensives) or the untreated systolic blood pressure using the equation and estimated regression coefficients developed by D'Agostino and others (274).
FRS = 1–0.94833exp(2.72107*ln(Age)+0.51125*ln(BMI)+2.81291*ln(SBP)+0.61868*(Currentsmoker)+0.77763*(Diabetes)-26.0145).
These scores were confirmed using the online calculator developed by D’Agostino and Pencina based on the publication by D’Agostino and others (274).
Statistics
An analytical protocol was produced before analysis began. Statistical significance was set at a 2-sided Type 1 error rate of P<0.05. All data were analysed using IBM SPSS Statistics for Windows, Version 21.0 (2012, Armonk, NY: IBM Corp.) and SAS software, Version 9.4 (Copyright © 2002-2013, SAS Institute Inc. SAS and all other SAS Institute Inc. product or service names are registered trademarks or trademarks of SAS Institute Inc., Cary, NC, USA.). Descriptive statistics of normally distributed continuous variables were expressed as mean ± standard deviation (SD); non-normally distributed continuous variables (physical activity, alcohol intake, allium vegetable intake, nut intake, fish intake, processed meat intake and red meat intake) were expressed as median and interquartile range; and categorical variables as number and proportion (%). Differences in baseline characteristics among vegetable serving categories were tested using one-way ANOVA for normally distributed continuous variables and the Kruskal-Wallis test for non-normally distributed continuous variables. Chi-squared test for independence was used to test for differences in baseline characteristics among vegetable serving categories for categorical variables.
The primary outcome of the study was any death relating to ASVD. Complete follow-up of death records was available for all participants that remained in Western Australia which was likely to be almost all participants given their age. The follow-up time period for each participant was calculated in days from their baseline visit until their last day of follow-up which was their date of death or 15-years of complete follow-up. Cox proportional hazards modelling was used to analyse the associations between vegetable variables and ASVD mortality. Total vegetable intake was analysed per serving (75 g/d) and then further categorised into three

83 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
groups (<2 servings, 2 to <3 servings and ≥3 servings). For vegetable types, intakes of cruciferous, yellow/orange/red, leafy green and legumes were analysed per 10 g/d. Intakes of allium were analysed per 5 g/d. Three models of adjustment were used for the Cox proportional hazards modelling. These models included unadjusted, age and energy-adjusted and multivariable-adjusted models. The multivariable-adjusted models included age, BMI, level of physical activity, alcohol intake, energy intake and CKD-EPI eGFR (entered as continuous variables), and smoking history, SES, the CAIFOS supplementation group of calcium vs. placebo, antihypertensive medication, statin medication and low-dose aspirin (entered as categorical variables). Covariates were selected on an a priori basis as these covariates are known risk factors for ASVD. We also tested for evidence of linear trends across categories of vegetable servings using the median value for each category as a continuous variable in separate Cox proportional hazards models. Cox proportional hazards assumptions were tested using log-log plots which were shown to be parallel indicating that proportional hazards assumptions were not violated.
Sensitivity analyses
Reverse causality bias was explored in multivariable-adjusted analyses, excluding all-cause deaths occurring within the first 24 months, for total vegetable intake (per 75 g/d) and intakes of cruciferous (per 10 g/d), allium (per 5 g/d) and leafy green (per 10 g/d) vegetables.
Since higher vegetable intake may be considered as being a surrogate marker of a healthier diet, we further adjusted for diet quality using the Nutrient-Rich Foods Index in multivariable-adjusted models for total vegetable intake (per 75 g/d) and intakes of cruciferous (per 10 g/d) and allium (per 5 g/d) vegetables. We also considered the impact of possible dietary confounders by including the estimated daily intakes of total fruit (g/d), fish (g/d), nuts (g/d), fibre (g/d), potassium (mg/d), magnesium (mg/d), beta-carotene (ug/d) and saturated fat (g/d) (275). These dietary confounders were entered separately as continuous variables in multivariable-adjusted Cox proportional hazards models on a variable-by-variable basis for total vegetable intake (per 75 g/d) and intakes of cruciferous (per 10 g/d) and allium (per 5 g/d) vegetables.
Subgroups of ASVD-related mortality, including ischaemic heart disease and ischaemic cerebrovascular disease mortality, were investigated in multivariable-adjusted models for total vegetable intake and intakes of cruciferous (per 10 g/d) and allium (per 5 g/d) vegetables. The FRS was used in multivariable-adjusted models to adjust for the estimated 10-year risk of developing cardiovascular disease for total vegetable intake (per 75 g/d) and intakes of cruciferous (per 10 g/d) and allium (per 5 g/d) vegetables. The multivariable-adjusted models included level of physical activity, alcohol intake, SES, the CAIFOS supplementation group of calcium vs. placebo, statin use, low-dose aspirin use, CKD-EPI eGFR and energy intake. Age, BMI, antihypertensive medication and smoking history were not included in this model because the FRS takes into account the participants’ age, body mass index, untreated systolic blood pressure and current smoking status.
The relationship between cruciferous, allium and total vegetables were investigated using Spearman Rank Order Correlation (rho). To examine whether the individual associations of cruciferous and allium vegetables were not due to collinearity and were independent of total vegetable intake, a forward stepwise Cox proportional hazards model with all multivariable-
84 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
adjusted variables as well as total vegetable intake and intakes of cruciferous (per 10 g/d) and allium (per 5 g/d) vegetables was tested.
One-way repeated measures ANOVA was used to test for differences between intakes of cruciferous, allium and total vegetables at baseline (1998), 5 years (2003) and 7 years (2005). The average of the three time points (baseline, 5 years and 7 years) for cruciferous, allium and total vegetables were used separately in multivariable-adjusted Cox proportional hazards models to account for the change in intake.
RESULTS
Participants and their characteristics
The flow diagram for participant selection is shown in Figure 1. In the 15,947 person-years of follow-up there were 238/1,226 (19.4%) ASVD-related deaths, of which 128/1,226 (10.4%) were due to ischaemic heart disease and 92/1,226 (7.5%) due to ischaemic cerebrovascular disease. Participant demographics, medication use and biochemical analyses presented according to all 1,226 study participants and by categories of vegetable servings are presented in Table 1. Nutrient and food intakes are presented in Table 2. Body weight (kg) (Table 1) and all dietary intakes (Table 2) were significantly different among vegetable serving categories (P<0.05 for all). Those consuming more vegetable servings also consumed more of each vegetable type (P<0.001) (Table 2). Mean (SD) vegetable intake was 196.5 (78.8) g/d and vegetable servings was 2.6 (1.0) for all participants. Mean (SD) intake (from highest to lowest) of vegetable types were: yellow/orange/red vegetables 52.4 (27.6) g/d; cruciferous vegetables 32.3 (22.0) g/d; legumes 27.0 (18.7) g/d; and leafy green vegetables 18.8 (12.1) g/d. Median (IQR) intake for allium vegetables was 6.2 (2.9-10.6) g/d (Table 2). Percentage contribution of vegetable types, including potatoes, from all vegetables consumed (g/d) are presented in Figure 2.
Total vegetable intake and atherosclerotic vascular disease mortality
The association of total vegetable intake with ASVD mortality was statistically significant in unadjusted, age and energy-adjusted and multivariable-adjusted models (P<0.01 for all models) (Table 3). Multivariable-adjusted cumulative survival curves for ASVD mortality according to vegetable servings are presented in Figure 3. The survival benefit of higher vegetable intakes diverged after 60 months.
To avoid the potential of reverse causality, participants who died in the first 24 months were excluded. Total vegetable intake remained a statistically significant predictor of ASVD death (per 75 g/d increase, HR=0.81, 95%CI 0.70, 0.95, P=0.008).
Additional adjustment for the Nutrient-Rich Foods Index attenuated the association of total vegetable intake (per 75 g/d increase, HR=0.86, 95%CI 0.73, 1.02, P=0.076). Separate analyses that adjusted for the individual dietary factors, total fruit, fish, nuts and beta-carotene, did not change the association between total vegetable intake and ASVD mortality (Table 4). Adjustment for potassium, magnesium, fibre and saturated fat attenuated the association (Table 4).
85 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
Total vegetable intake was inversely associated with ischaemic heart disease mortality with borderline significance (P=0.050). Ischaemic cerebrovascular disease mortality did not reach significance (P=0.074) (Table 5).
Vegetable types and atherosclerotic vascular disease mortality
The associations between intakes of vegetable types and ASVD mortality are presented in Table 6. Higher intakes of cruciferous and allium vegetables were associated with lower ASVD mortality in unadjusted, age and energy-adjusted and multivariable-adjusted models (P<0.01 for all). These associations were also independent of other vegetable intakes (P<0.05 for both cruciferous and allium). Higher leafy green vegetable intakes were associated with lower ASVD mortality in the unadjusted model (P=0.048), but not in the age and energy-adjusted (P=0.055) and multivariable-adjusted (P=0.063) models. Likewise, higher yellow/orange/red vegetable intakes were associated with lower ASVD mortality in the unadjusted model (P=0.040), but not in adjusted models (P>0.05). Lastly, intakes of legumes were not associated with ASVD mortality in any models (P>0.05).
When excluding participants who died in the first 24 months of the study, cruciferous (per 10 g/d) and allium (per 5 g/d) vegetables remained inversely associated with ASVD mortality, with a multivariable-adjusted HR (95%CI) of 0.87 (0.80, 0.93) and 0.83 (0.73, 0.94), respectively (P<0.01 for both). Although not significant in the initial multivariable-adjusted analysis, intakes of leafy green vegetables (per 10 g/d) were significant after excluding all deaths that occurred in the first 24 months (multivariable-adjusted HR=0.88, 95%CI 0.78, 1.00, P=0.047). The median (IQR) intake for leafy green vegetables for participants excluded in the first 24 months was 12.1 (3.9-25.8) g/d whereas for the cohort excluding these participants it was 17.1 (9.8-25.8) g/d.
Additional adjustment for the Nutrient-Rich Foods Index did not alter the significant associations of cruciferous (per 10 g/d increase, HR=0.89, 95%CI 0.82, 0.95, P=0.002) and allium (per 5 g/d increase, HR=0.84, 95%CI 0.74, 0.95, P=0.006) vegetable intakes. Separate analyses that adjusted for individual dietary factors (total fruit, fish, nuts, fibre, potassium, magnesium, beta-carotene and saturated fat) did not change the associations of both cruciferous and allium vegetable intakes with ASVD mortality (Table 4).
Cruciferous and allium vegetable intakes were inversely associated with ischaemic heart disease mortality (P<0.05 for both), and allium vegetable intake was inversely associated with ischaemic cerebrovascular disease mortality (P=0.011) (Table 5).
Additional sensitivity analyses
Separate analyses that adjusted for the Framingham risk scores did not change the interpretation of the associations between cruciferous (per 10 g/d increase, HR=0.88, 95%CI 0.82, 0.95, P=0.001), allium (per 5 g/d increase, HR=0.81, 95%CI 0.71, 0.92, P=0.001) and total vegetables (per 75 g/d increase, HR=0.81, 95%CI 0.69, 0.94, P=0.006) and ASVD mortality.
There was a weak positive correlation between intakes of cruciferous and allium vegetables (Spearman’s rho=0.12, P<0.001) and a moderate positive correlation between intakes of allium and total vegetables (Spearman’s rho=0.44, P<0.001) and between intakes of cruciferous and total vegetables (Spearman’s rho=0.51, P<0.001). In a forward stepwise Cox proportional hazards model, which included all multivariable-adjusted variables and intakes of cruciferous, allium and total vegetables, age (P<0.001), BMI (P=0.016), antihypertensive medication
86 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
(P<0.001), cruciferous vegetables (P<0.001) and allium vegetables (P=0.014) were independent predictors of ASVD mortality (Table 7).
The mean (SD) of cruciferous, allium and total vegetables at baseline (1998), 5 years (2003) and 7 years (2005) are presented in Table 8. A significant effect for time was observed for intakes of cruciferous, allium and total vegetables using one-way repeated measures ANOVA (Wilks’ Lambda P<0.01 for all). To account for this change the average was individually calculated across all three time points (baseline, 5 years and 7 years) for cruciferous, allium and total vegetable intakes. These average values were then entered separately in multivariable-adjusted Cox proportional hazards models for ASVD mortality. This did not substantively alter the interpretation of the associations between baseline values and ASVD-related mortality (Table 9).
DISCUSSION
This study demonstrates that total vegetable intake was inversely associated with ASVD mortality, supporting current guideline recommendations to increase vegetable consumption (5-7). The major new finding is that both cruciferous and allium vegetables were inversely associated with ASVD mortality. These associations remained after extensive adjustment for other vegetable intakes as well as lifestyle and cardiovascular risk factors. In a forward stepwise model with cruciferous, allium and total vegetable intake, cruciferous and allium vegetables were both independent predictors of ASVD mortality. Total vegetable intake was not considered an independent predictor possibly due to the moderate correlations of allium and cruciferous vegetables with total vegetable intakes. This should not be misinterpreted to indicate a lack of importance for total vegetable intake. If replicated in other studies these data further emphasise the importance of cruciferous and allium vegetables in reducing ASVD.
Emerging evidence suggests a protective role for cruciferous vegetables in cardiovascular health (64, 72, 74, 276). Evidence also suggests allium vegetables such as onions to be protective (80, 277). However, this relationship is inconsistent for garlic (277). The results of some population studies and associated meta-analyses reporting cruciferous and allium vegetable consumption have not always identified an association possibly due to type II error (12). Cruciferous and allium vegetables contain a variety of nutritive and non-nutritive components that may benefit cardiovascular health. We studied the potential effects of nutritive components such as potassium (14) and magnesium (15) on the relationships between cruciferous and allium vegetables and ASVD mortality. This did not substantively alter the associations of interest. Organosulfur compounds, a non-nutritive component of both cruciferous and allium vegetables, may have benefits (32).
Organosulfur compounds are organic sulfur-containing compounds that have the ability to be hydrogen sulfide (H2S) donors (278). H2S is an important gasotransmitter playing an important role in the regulation of vasodilation, angiogenesis, inflammation, oxidative stress and apoptosis (279). Organosulfur compounds found abundantly in cruciferous vegetables are glucosinolates which are a precursor for isothiocyanates. Isothiocyanates have been widely researched due to their anti-cancer properties (280-282). Isothiocyanates also have antioxidant and anti-inflammatory properties, both of which may prevent the progression of atherosclerosis (32, 283, 284). The anti-inflammatory properties of isothiocyanates can be
87 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
supported by a study demonstrating an inverse association between cruciferous vegetables and pro-inflammatory cytokines (285).
Organosulfur compounds found in allium vegetables have been studied in more depth. Although intake of allium vegetables was 6.2 g/d compared to 196.5 g/d in total vegetable intake, the association of allium vegetables and ASVD mortality was strong. There is evidence that organosulfur compounds found in allium vegetables may have the ability to prevent the production of reactive oxygen species, prevent vascular inflammation, inhibit platelet aggregation and increase the bioavailability of nitric oxide (NO) (32). Recent evidence also suggests allicin, an organosulfur compound found in garlic, is readily degraded into organic polysulfides and the subsequent interactions with thiol groups result in the generation of H2S (286). Preclinical studies have demonstrated possible cardioprotective effects of H2S, and cross-talk between H2S and NO signalling may explain these cardioprotective effects (286).
Leafy green vegetables are a rich source of dietary nitrate that can be reduced to NO via the entero-salivary nitrate-nitrite-NO pathway (45). Although significant in the unadjusted analysis, after adjustment for covariates and especially after further adjustment of non-leafy green vegetables which included allium and cruciferous vegetables, the beneficial effect disappeared. This result differs from other studies (12). It should be noted that after excluding all deaths occurring in the first 24 months, leafy green vegetables became significant after adjustment for multiple covariates. While not consistently significant, leafy green vegetables had a consistent suggestive relationship warranting more research (HR between 0.88 to 0.91 and CI between 0.78 and 1.01). This suggests leafy green vegetables may still be an important contributor to the benefits seen with ASVD mortality.
Strengths of this prospective population-based cohort study were that participants were representative of older adult women from the Australian population. The average vegetable intake of participants in this study was 2.6 servings per day, the same for Australian female adults aged 75 years and over (11). Food intake was also assessed at three different time points during the 15 years of follow-up thus reducing measurement error. Given the participants’ age at baseline and the long follow-up period of 15 years, the ASVD death rate was also increased giving the study more power to detect an association. Lastly, loss to follow-up bias was likely minimised having a complete follow-up of death records for all participants that remained in Western Australia which was likely to be the majority of women given their age.
Our findings need to be interpreted carefully in the context of limitations applicable to prospective cohort studies. Classification by one characteristic results in many other differences in other characteristics such as food and nutrients intakes, energy intake and physical activity that may have a substantial effect on the outcome of interest. This problem was addressed by the use of multivariable adjustments that may, however, not have correctly allowed for residual or unknown confounders. For example, it should be noted that the group with the highest vs lowest intake of vegetable servings reported a ~30% higher energy intake and higher proportions of most nutrients and food types despite similar BMI suggesting that they were correspondingly more active. An important consideration to be noted is that physical activity has been shown to be a strong predictor of cardiovascular health (287, 288). To address this concern both total energy intake and self-reported physical activity were included as covariates without affecting the outcome of interest. The self-reported physical

88 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
activity used in this study has been shown to be related to bone mineral density in the same cohort of older adult women (289). Higher intakes of non-vegetable foods such as fish and nuts that have been shown in other studies to have cardiovascular health benefits (290, 291) were observed in participants that consumed higher vegetable servings. Individual adjustments for these foods did not alter the interpretation between cruciferous, allium and total vegetable intakes and ASVD mortality. Dietary intakes in this study were self-reported, and therefore, measurement error and misclassification are possible. We attempted to address measurement error by averaging the intakes of cruciferous, allium and total vegetables across baseline, 5 years (2003) and 7 years (2005), and entering these values individually in multivariable-adjusted Cox proportional hazards models for ASVD mortality. This did not substantively alter the interpretation between baseline values and ASVD-related mortality. Lastly, given the observational nature of this study, a causal relationship between the exposure and ASVD mortality remains uncertain.
Conclusion
Intakes of cruciferous and allium vegetables were inversely associated with ASVD mortality in this cohort of women aged ≥70 years. These findings support a focus on studying the effects of increased cruciferous and allium vegetables on cardiovascular disease risk. They may precipitate greater study of the role and potential mechanisms of organosulfur compounds on ASVD outcomes. If supported by other studies, efforts to increase cruciferous and allium vegetables within the diet may lead to an achievable and cost-effective approach to reduce worldwide cardiovascular morbidity and mortality.
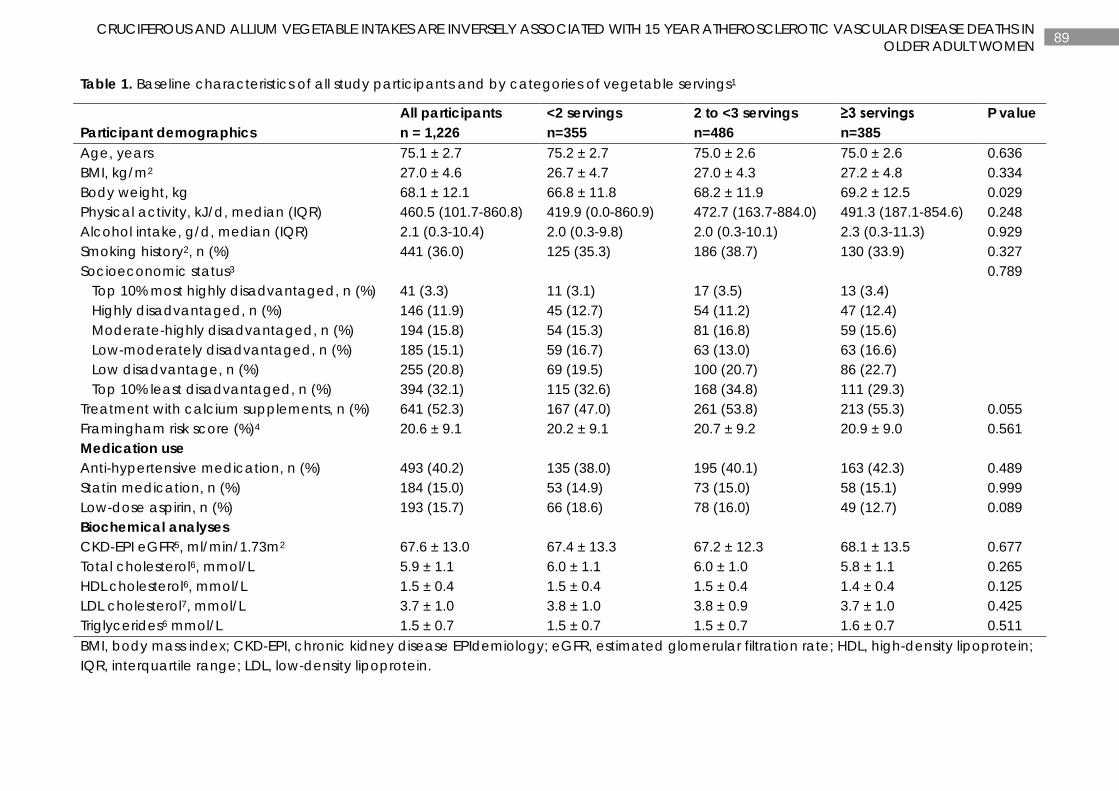
89 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN
OLDER ADULT WOMEN
Table 1. Baseline characteristics of all study participants and by categories of vegetable servings1
Participant demographics All participants n = 1,226
<2 servings n=355
2 to <3 servings n=486
≥3 servings n=385
P value
Age, years 75.1 ± 2.7 75.2 ± 2.7 75.0 ± 2.6 75.0 ± 2.6 0.636 BMI, kg/m2 27.0 ± 4.6 26.7 ± 4.7 27.0 ± 4.3 27.2 ± 4.8 0.334 Body weight, kg 68.1 ± 12.1 66.8 ± 11.8 68.2 ± 11.9 69.2 ± 12.5 0.029 Physical activity, kJ/d, median (IQR) 460.5 (101.7-860.8) 419.9 (0.0-860.9) 472.7 (163.7-884.0) 491.3 (187.1-854.6) 0.248 Alcohol intake, g/d, median (IQR) 2.1 (0.3-10.4) 2.0 (0.3-9.8) 2.0 (0.3-10.1) 2.3 (0.3-11.3) 0.929 Smoking history2, n (%) 441 (36.0) 125 (35.3) 186 (38.7) 130 (33.9) 0.327 Socioeconomic status3 0.789 Top 10% most highly disadvantaged, n (%) 41 (3.3) 11 (3.1) 17 (3.5) 13 (3.4) Highly disadvantaged, n (%) 146 (11.9) 45 (12.7) 54 (11.2) 47 (12.4) Moderate-highly disadvantaged, n (%) 194 (15.8) 54 (15.3) 81 (16.8) 59 (15.6) Low-moderately disadvantaged, n (%) 185 (15.1) 59 (16.7) 63 (13.0) 63 (16.6) Low disadvantage, n (%) 255 (20.8) 69 (19.5) 100 (20.7) 86 (22.7) Top 10% least disadvantaged, n (%) 394 (32.1) 115 (32.6) 168 (34.8) 111 (29.3) Treatment with calcium supplements, n (%) 641 (52.3) 167 (47.0) 261 (53.8) 213 (55.3) 0.055 Framingham risk score (%)4 20.6 ± 9.1 20.2 ± 9.1 20.7 ± 9.2 20.9 ± 9.0 0.561 Medication use Anti-hypertensive medication, n (%) 493 (40.2) 135 (38.0) 195 (40.1) 163 (42.3) 0.489 Statin medication, n (%) 184 (15.0) 53 (14.9) 73 (15.0) 58 (15.1) 0.999 Low-dose aspirin, n (%) 193 (15.7) 66 (18.6) 78 (16.0) 49 (12.7) 0.089 Biochemical analyses CKD-EPI eGFR5, ml/min/1.73m2 67.6 ± 13.0 67.4 ± 13.3 67.2 ± 12.3 68.1 ± 13.5 0.677 Total cholesterol6, mmol/L 5.9 ± 1.1 6.0 ± 1.1 6.0 ± 1.0 5.8 ± 1.1 0.265 HDL cholesterol6, mmol/L 1.5 ± 0.4 1.5 ± 0.4 1.5 ± 0.4 1.4 ± 0.4 0.125 LDL cholesterol7, mmol/L 3.7 ± 1.0 3.8 ± 1.0 3.8 ± 0.9 3.7 ± 1.0 0.425 Triglycerides6 mmol/L 1.5 ± 0.7 1.5 ± 0.7 1.5 ± 0.7 1.6 ± 0.7 0.511 BMI, body mass index; CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate; HDL, high-density lipoprotein; IQR, interquartile range; LDL, low-density lipoprotein.
90 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN
OLDER ADULT WOMEN
1Vegetable servings were calculated based on the 2013 Australian Dietary Guidelines of a vegetable serving equal to 75 g/d. P values are a comparison between groups using ANOVA, Kruskal-Wallis test and Chi-square test where appropriate. Values are presented as mean ± SD unless otherwise stated. 2Measured in 1,218. 3Measured in 1,215. 4Measured in 1,188. 5Measured in 1,106. 6Measured in 895. 7Measured in 888.
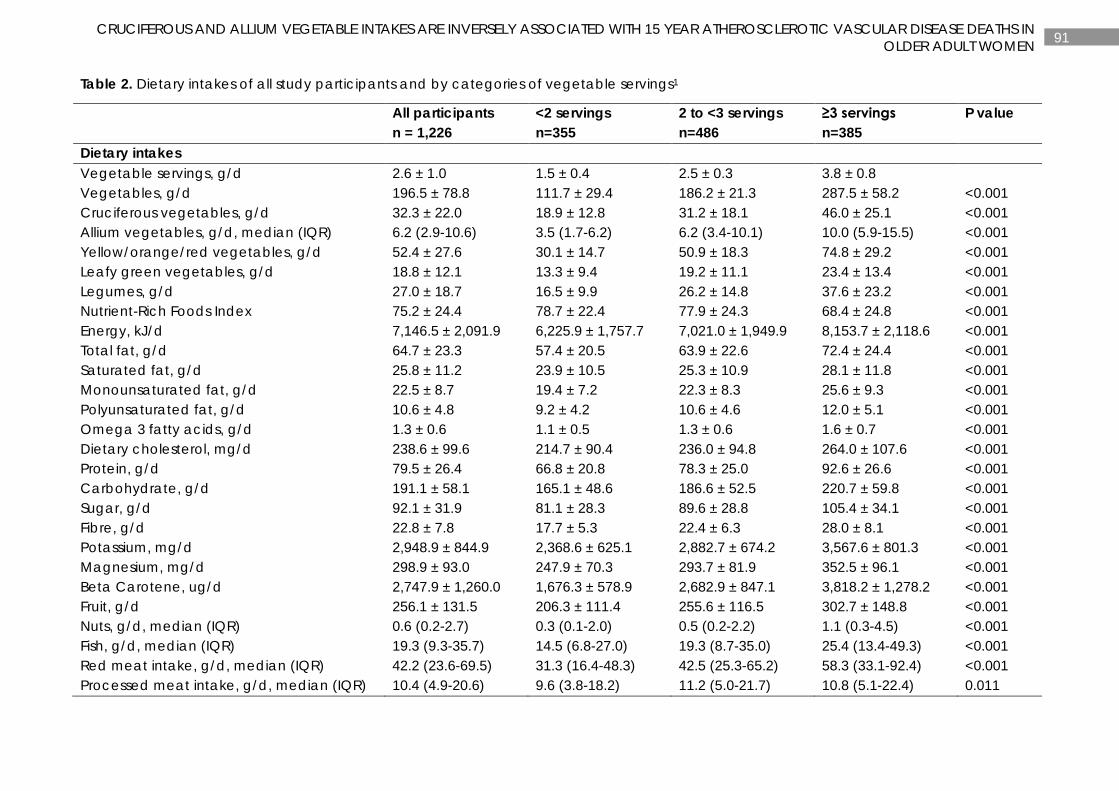
91 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN
OLDER ADULT WOMEN
Table 2. Dietary intakes of all study participants and by categories of vegetable servings1
All participants n = 1,226
<2 servings n=355
2 to <3 servings n=486
≥3 servings n=385
P value
Dietary intakes Vegetable servings, g/d 2.6 ± 1.0 1.5 ± 0.4 2.5 ± 0.3 3.8 ± 0.8 Vegetables, g/d 196.5 ± 78.8 111.7 ± 29.4 186.2 ± 21.3 287.5 ± 58.2 <0.001 Cruciferous vegetables, g/d 32.3 ± 22.0 18.9 ± 12.8 31.2 ± 18.1 46.0 ± 25.1 <0.001 Allium vegetables, g/d, median (IQR) 6.2 (2.9-10.6) 3.5 (1.7-6.2) 6.2 (3.4-10.1) 10.0 (5.9-15.5) <0.001 Yellow/orange/red vegetables, g/d 52.4 ± 27.6 30.1 ± 14.7 50.9 ± 18.3 74.8 ± 29.2 <0.001 Leafy green vegetables, g/d 18.8 ± 12.1 13.3 ± 9.4 19.2 ± 11.1 23.4 ± 13.4 <0.001 Legumes, g/d 27.0 ± 18.7 16.5 ± 9.9 26.2 ± 14.8 37.6 ± 23.2 <0.001 Nutrient-Rich Foods Index 75.2 ± 24.4 78.7 ± 22.4 77.9 ± 24.3 68.4 ± 24.8 <0.001 Energy, kJ/d 7,146.5 ± 2,091.9 6,225.9 ± 1,757.7 7,021.0 ± 1,949.9 8,153.7 ± 2,118.6 <0.001 Total fat, g/d 64.7 ± 23.3 57.4 ± 20.5 63.9 ± 22.6 72.4 ± 24.4 <0.001 Saturated fat, g/d 25.8 ± 11.2 23.9 ± 10.5 25.3 ± 10.9 28.1 ± 11.8 <0.001 Monounsaturated fat, g/d 22.5 ± 8.7 19.4 ± 7.2 22.3 ± 8.3 25.6 ± 9.3 <0.001 Polyunsaturated fat, g/d 10.6 ± 4.8 9.2 ± 4.2 10.6 ± 4.6 12.0 ± 5.1 <0.001 Omega 3 fatty acids, g/d 1.3 ± 0.6 1.1 ± 0.5 1.3 ± 0.6 1.6 ± 0.7 <0.001 Dietary cholesterol, mg/d 238.6 ± 99.6 214.7 ± 90.4 236.0 ± 94.8 264.0 ± 107.6 <0.001 Protein, g/d 79.5 ± 26.4 66.8 ± 20.8 78.3 ± 25.0 92.6 ± 26.6 <0.001 Carbohydrate, g/d 191.1 ± 58.1 165.1 ± 48.6 186.6 ± 52.5 220.7 ± 59.8 <0.001 Sugar, g/d 92.1 ± 31.9 81.1 ± 28.3 89.6 ± 28.8 105.4 ± 34.1 <0.001 Fibre, g/d 22.8 ± 7.8 17.7 ± 5.3 22.4 ± 6.3 28.0 ± 8.1 <0.001 Potassium, mg/d 2,948.9 ± 844.9 2,368.6 ± 625.1 2,882.7 ± 674.2 3,567.6 ± 801.3 <0.001 Magnesium, mg/d 298.9 ± 93.0 247.9 ± 70.3 293.7 ± 81.9 352.5 ± 96.1 <0.001 Beta Carotene, ug/d 2,747.9 ± 1,260.0 1,676.3 ± 578.9 2,682.9 ± 847.1 3,818.2 ± 1,278.2 <0.001 Fruit, g/d 256.1 ± 131.5 206.3 ± 111.4 255.6 ± 116.5 302.7 ± 148.8 <0.001 Nuts, g/d, median (IQR) 0.6 (0.2-2.7) 0.3 (0.1-2.0) 0.5 (0.2-2.2) 1.1 (0.3-4.5) <0.001 Fish, g/d, median (IQR) 19.3 (9.3-35.7) 14.5 (6.8-27.0) 19.3 (8.7-35.0) 25.4 (13.4-49.3) <0.001 Red meat intake, g/d, median (IQR) 42.2 (23.6-69.5) 31.3 (16.4-48.3) 42.5 (25.3-65.2) 58.3 (33.1-92.4) <0.001 Processed meat intake, g/d, median (IQR) 10.4 (4.9-20.6) 9.6 (3.8-18.2) 11.2 (5.0-21.7) 10.8 (5.1-22.4) 0.011
92 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN
OLDER ADULT WOMEN
IQR, interquartile range. 1Vegetable servings were calculated based on the 2013 Australian Dietary Guidelines of a vegetable serving equal to 75 g/d. P values are a comparison between groups using ANOVA and Kruskal-Wallis test where appropriate. Values are presented as mean ± SD unless otherwise stated. Cruciferous vegetables included cabbage, Brussels sprouts, cauliflower and broccoli. Allium vegetables included onion, leek and garlic. Yellow/orange/red vegetables included tomato, capsicum, beetroot, carrot and pumpkin. Leafy green vegetables included lettuce and other salad greens, celery, silverbeet and spinach. Legumes included peas, greens beans, bean sprouts and alfalfa sprouts, baked beans, soy beans, soy bean curd and tofu, and other beans.
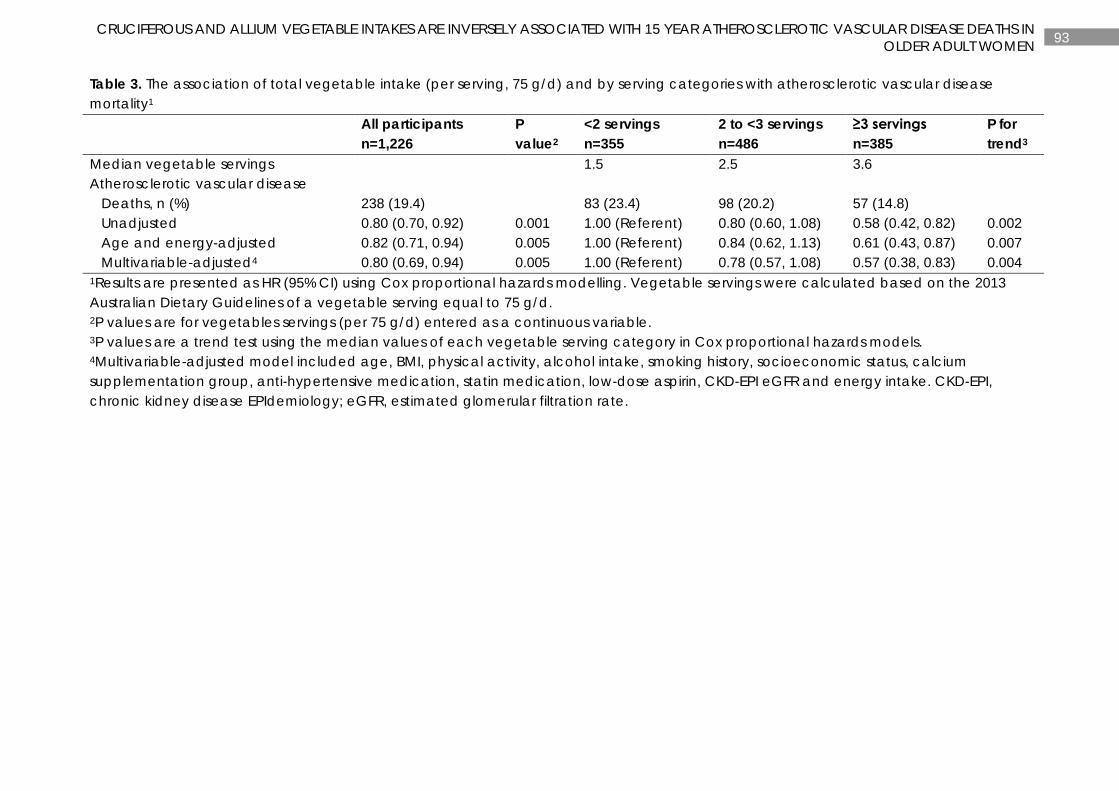
93 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN
OLDER ADULT WOMEN
Table 3. The association of total vegetable intake (per serving, 75 g/d) and by serving categories with atherosclerotic vascular disease mortality1
All participants n=1,226
P value2
<2 servings n=355
2 to <3 servings n=486
≥3 servings n=385
P for trend3
Median vegetable servings 1.5 2.5 3.6 Atherosclerotic vascular disease Deaths, n (%) 238 (19.4) 83 (23.4) 98 (20.2) 57 (14.8) Unadjusted 0.80 (0.70, 0.92) 0.001 1.00 (Referent) 0.80 (0.60, 1.08) 0.58 (0.42, 0.82) 0.002 Age and energy-adjusted 0.82 (0.71, 0.94) 0.005 1.00 (Referent) 0.84 (0.62, 1.13) 0.61 (0.43, 0.87) 0.007 Multivariable-adjusted4 0.80 (0.69, 0.94) 0.005 1.00 (Referent) 0.78 (0.57, 1.08) 0.57 (0.38, 0.83) 0.004 1Results are presented as HR (95% CI) using Cox proportional hazards modelling. Vegetable servings were calculated based on the 2013 Australian Dietary Guidelines of a vegetable serving equal to 75 g/d. 2P values are for vegetables servings (per 75 g/d) entered as a continuous variable. 3P values are a trend test using the median values of each vegetable serving category in Cox proportional hazards models. 4Multivariable-adjusted model included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, calcium supplementation group, anti-hypertensive medication, statin medication, low-dose aspirin, CKD-EPI eGFR and energy intake. CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate.
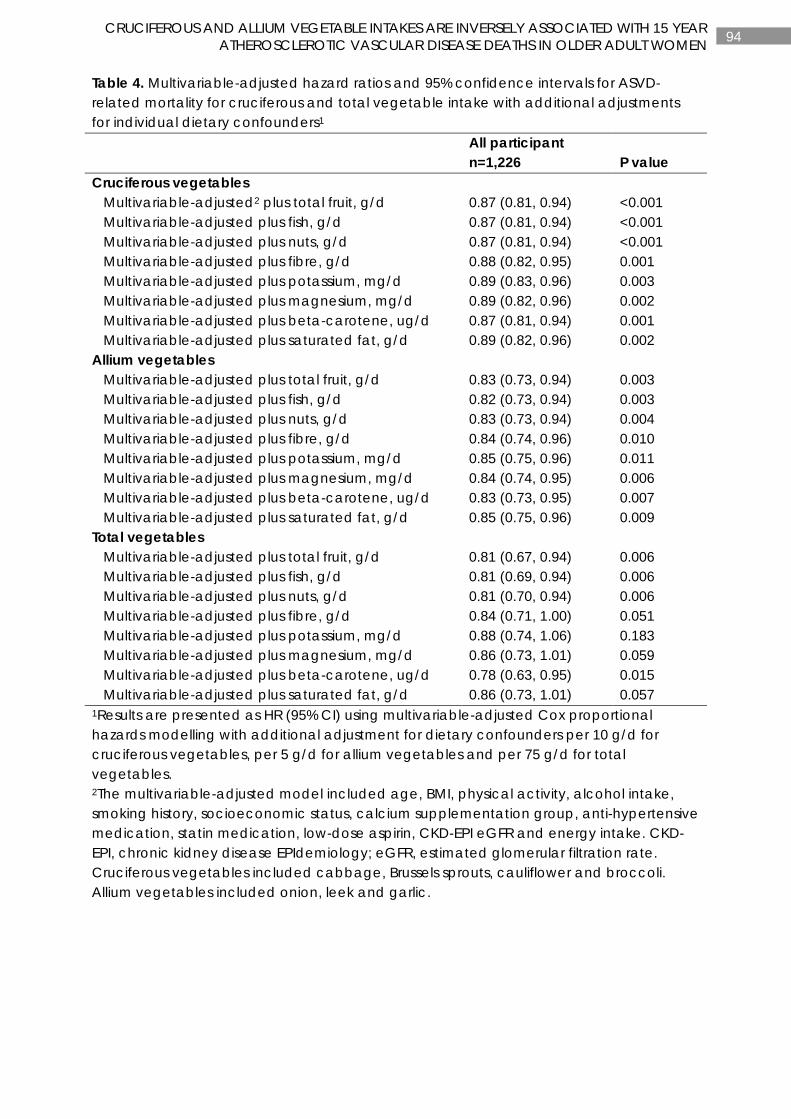
94 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
Table 4. Multivariable-adjusted hazard ratios and 95% confidence intervals for ASVD-related mortality for cruciferous and total vegetable intake with additional adjustments for individual dietary confounders1 All participant
n=1,226 P value Cruciferous vegetables Multivariable-adjusted2 plus total fruit, g/d 0.87 (0.81, 0.94) <0.001 Multivariable-adjusted plus fish, g/d 0.87 (0.81, 0.94) <0.001 Multivariable-adjusted plus nuts, g/d 0.87 (0.81, 0.94) <0.001 Multivariable-adjusted plus fibre, g/d 0.88 (0.82, 0.95) 0.001 Multivariable-adjusted plus potassium, mg/d 0.89 (0.83, 0.96) 0.003 Multivariable-adjusted plus magnesium, mg/d 0.89 (0.82, 0.96) 0.002 Multivariable-adjusted plus beta-carotene, ug/d 0.87 (0.81, 0.94) 0.001 Multivariable-adjusted plus saturated fat, g/d 0.89 (0.82, 0.96) 0.002 Allium vegetables Multivariable-adjusted plus total fruit, g/d 0.83 (0.73, 0.94) 0.003 Multivariable-adjusted plus fish, g/d 0.82 (0.73, 0.94) 0.003 Multivariable-adjusted plus nuts, g/d 0.83 (0.73, 0.94) 0.004 Multivariable-adjusted plus fibre, g/d 0.84 (0.74, 0.96) 0.010 Multivariable-adjusted plus potassium, mg/d 0.85 (0.75, 0.96) 0.011 Multivariable-adjusted plus magnesium, mg/d 0.84 (0.74, 0.95) 0.006 Multivariable-adjusted plus beta-carotene, ug/d 0.83 (0.73, 0.95) 0.007 Multivariable-adjusted plus saturated fat, g/d 0.85 (0.75, 0.96) 0.009 Total vegetables Multivariable-adjusted plus total fruit, g/d 0.81 (0.67, 0.94) 0.006 Multivariable-adjusted plus fish, g/d 0.81 (0.69, 0.94) 0.006 Multivariable-adjusted plus nuts, g/d 0.81 (0.70, 0.94) 0.006 Multivariable-adjusted plus fibre, g/d 0.84 (0.71, 1.00) 0.051 Multivariable-adjusted plus potassium, mg/d 0.88 (0.74, 1.06) 0.183 Multivariable-adjusted plus magnesium, mg/d 0.86 (0.73, 1.01) 0.059 Multivariable-adjusted plus beta-carotene, ug/d 0.78 (0.63, 0.95) 0.015 Multivariable-adjusted plus saturated fat, g/d 0.86 (0.73, 1.01) 0.057 1Results are presented as HR (95% CI) using multivariable-adjusted Cox proportional hazards modelling with additional adjustment for dietary confounders per 10 g/d for cruciferous vegetables, per 5 g/d for allium vegetables and per 75 g/d for total vegetables. 2The multivariable-adjusted model included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, calcium supplementation group, anti-hypertensive medication, statin medication, low-dose aspirin, CKD-EPI eGFR and energy intake. CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate. Cruciferous vegetables included cabbage, Brussels sprouts, cauliflower and broccoli. Allium vegetables included onion, leek and garlic.
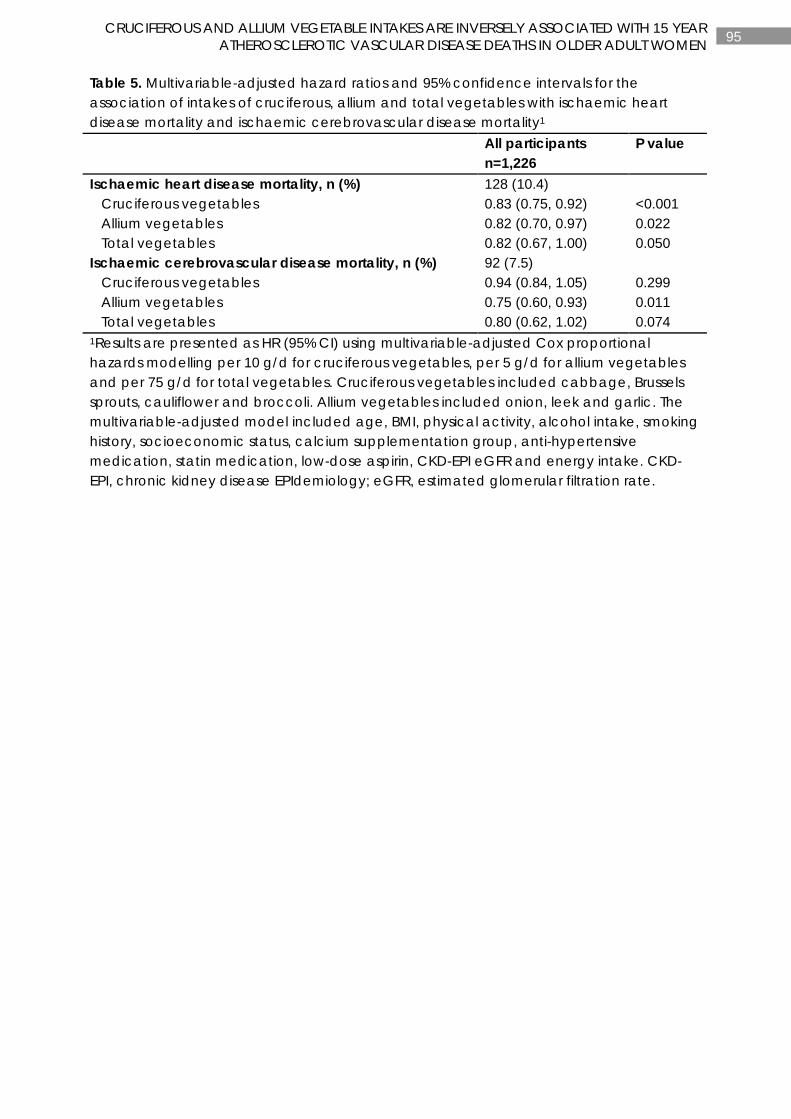
95 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
Table 5. Multivariable-adjusted hazard ratios and 95% confidence intervals for the association of intakes of cruciferous, allium and total vegetables with ischaemic heart disease mortality and ischaemic cerebrovascular disease mortality1
All participants n=1,226
P value
Ischaemic heart disease mortality, n (%) 128 (10.4) Cruciferous vegetables 0.83 (0.75, 0.92) <0.001 Allium vegetables 0.82 (0.70, 0.97) 0.022 Total vegetables 0.82 (0.67, 1.00) 0.050 Ischaemic cerebrovascular disease mortality, n (%) 92 (7.5) Cruciferous vegetables 0.94 (0.84, 1.05) 0.299 Allium vegetables 0.75 (0.60, 0.93) 0.011 Total vegetables 0.80 (0.62, 1.02) 0.074 1Results are presented as HR (95% CI) using multivariable-adjusted Cox proportional hazards modelling per 10 g/d for cruciferous vegetables, per 5 g/d for allium vegetables and per 75 g/d for total vegetables. Cruciferous vegetables included cabbage, Brussels sprouts, cauliflower and broccoli. Allium vegetables included onion, leek and garlic. The multivariable-adjusted model included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, calcium supplementation group, anti-hypertensive medication, statin medication, low-dose aspirin, CKD-EPI eGFR and energy intake. CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate.
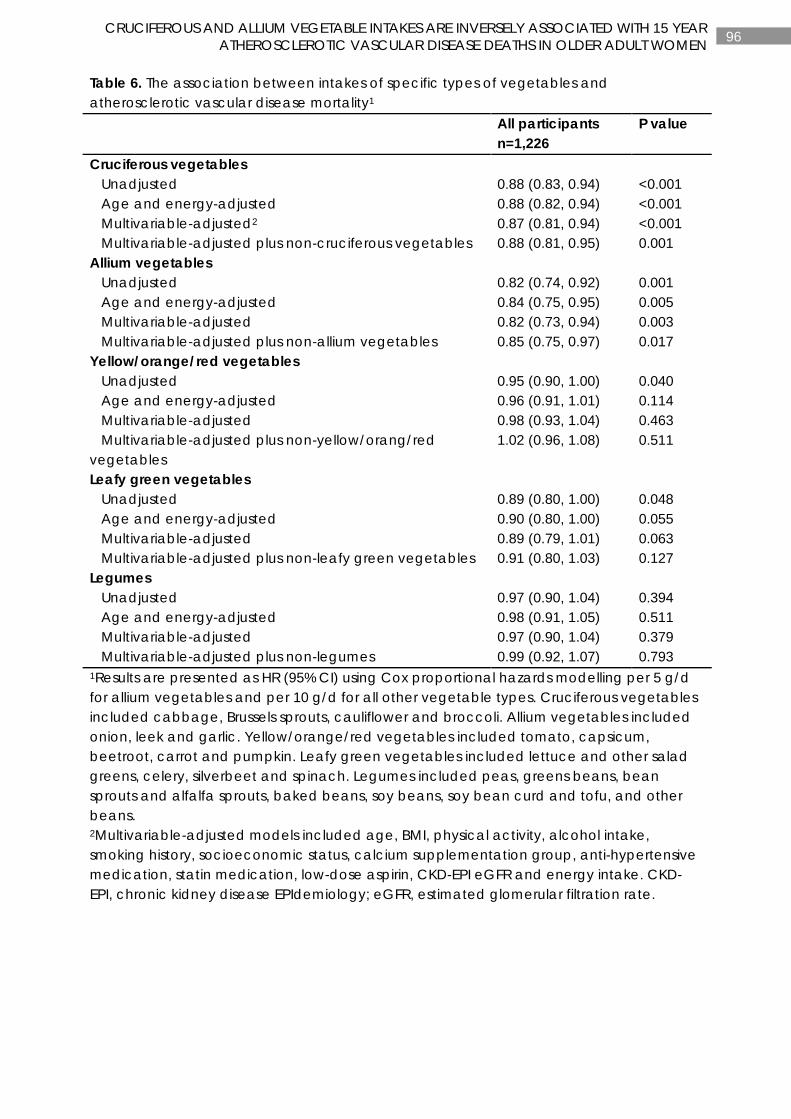
96 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
Table 6. The association between intakes of specific types of vegetables and atherosclerotic vascular disease mortality1
All participants n=1,226
P value
Cruciferous vegetables Unadjusted 0.88 (0.83, 0.94) <0.001 Age and energy-adjusted 0.88 (0.82, 0.94) <0.001 Multivariable-adjusted2 0.87 (0.81, 0.94) <0.001 Multivariable-adjusted plus non-cruciferous vegetables 0.88 (0.81, 0.95) 0.001 Allium vegetables Unadjusted 0.82 (0.74, 0.92) 0.001 Age and energy-adjusted 0.84 (0.75, 0.95) 0.005 Multivariable-adjusted 0.82 (0.73, 0.94) 0.003 Multivariable-adjusted plus non-allium vegetables 0.85 (0.75, 0.97) 0.017 Yellow/orange/red vegetables Unadjusted 0.95 (0.90, 1.00) 0.040 Age and energy-adjusted 0.96 (0.91, 1.01) 0.114 Multivariable-adjusted 0.98 (0.93, 1.04) 0.463 Multivariable-adjusted plus non-yellow/orang/red vegetables
1.02 (0.96, 1.08) 0.511
Leafy green vegetables Unadjusted 0.89 (0.80, 1.00) 0.048 Age and energy-adjusted 0.90 (0.80, 1.00) 0.055 Multivariable-adjusted 0.89 (0.79, 1.01) 0.063 Multivariable-adjusted plus non-leafy green vegetables 0.91 (0.80, 1.03) 0.127 Legumes Unadjusted 0.97 (0.90, 1.04) 0.394 Age and energy-adjusted 0.98 (0.91, 1.05) 0.511 Multivariable-adjusted 0.97 (0.90, 1.04) 0.379 Multivariable-adjusted plus non-legumes 0.99 (0.92, 1.07) 0.793 1Results are presented as HR (95% CI) using Cox proportional hazards modelling per 5 g/d for allium vegetables and per 10 g/d for all other vegetable types. Cruciferous vegetables included cabbage, Brussels sprouts, cauliflower and broccoli. Allium vegetables included onion, leek and garlic. Yellow/orange/red vegetables included tomato, capsicum, beetroot, carrot and pumpkin. Leafy green vegetables included lettuce and other salad greens, celery, silverbeet and spinach. Legumes included peas, greens beans, bean sprouts and alfalfa sprouts, baked beans, soy beans, soy bean curd and tofu, and other beans. 2Multivariable-adjusted models included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, calcium supplementation group, anti-hypertensive medication, statin medication, low-dose aspirin, CKD-EPI eGFR and energy intake. CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate.
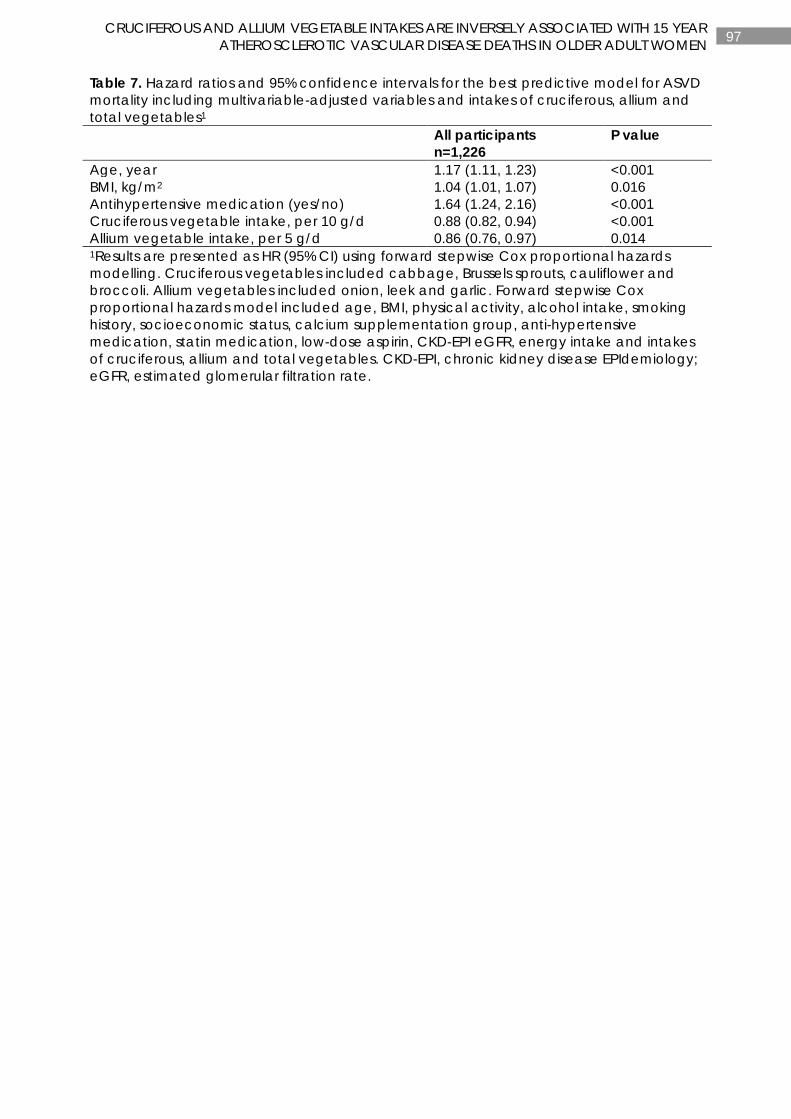
97 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
Table 7. Hazard ratios and 95% confidence intervals for the best predictive model for ASVD mortality including multivariable-adjusted variables and intakes of cruciferous, allium and total vegetables1
All participants n=1,226
P value
Age, year 1.17 (1.11, 1.23) <0.001 BMI, kg/m2 1.04 (1.01, 1.07) 0.016 Antihypertensive medication (yes/no) 1.64 (1.24, 2.16) <0.001 Cruciferous vegetable intake, per 10 g/d 0.88 (0.82, 0.94) <0.001 Allium vegetable intake, per 5 g/d 0.86 (0.76, 0.97) 0.014 1Results are presented as HR (95% CI) using forward stepwise Cox proportional hazards modelling. Cruciferous vegetables included cabbage, Brussels sprouts, cauliflower and broccoli. Allium vegetables included onion, leek and garlic. Forward stepwise Cox proportional hazards model included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, calcium supplementation group, anti-hypertensive medication, statin medication, low-dose aspirin, CKD-EPI eGFR, energy intake and intakes of cruciferous, allium and total vegetables. CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate.

98 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
Table 8. Mean (SD) for intakes of cruciferous, allium and total vegetables at baseline, 5 years (2003) and 7 years (2005)1 Mean SD Cruciferous vegetables, g/d Baseline2 32.3 22.0 5 years (2003)3 32.2 23.0 7 years (2005)4 30.0 21.3 Allium vegetables, g/d Baseline 7.8 6.7 5 years (2003) 6.5 5.5 7 years (2005) 6.0 5.5 Total vegetables, g/d Baseline 196.5 78.9 5 years (2003) 176.3 73.6 7 years (2005) 169.3 68.6 1Cruciferous vegetables included cabbage, Brussels sprouts, cauliflower and broccoli. Allium vegetables included onion, leek and garlic. 2n=1,226. 3n=1,023. 4n=852.
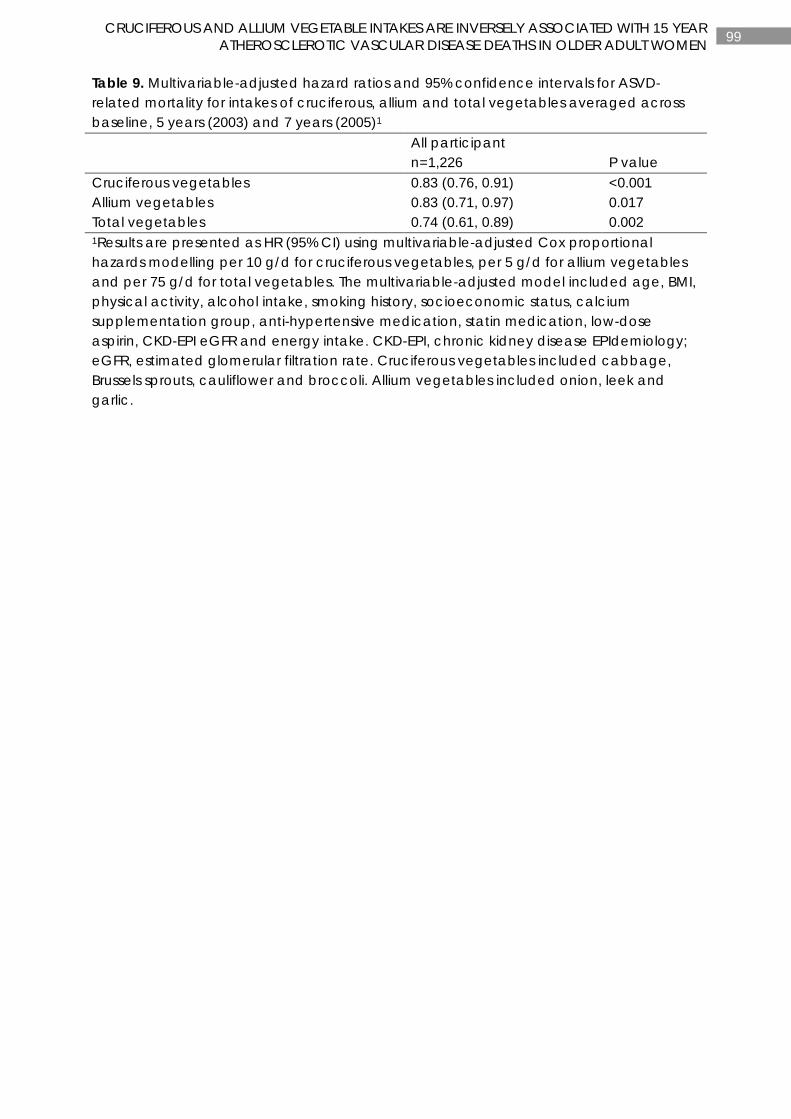
99 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
Table 9. Multivariable-adjusted hazard ratios and 95% confidence intervals for ASVD-related mortality for intakes of cruciferous, allium and total vegetables averaged across baseline, 5 years (2003) and 7 years (2005)1 All participant
n=1,226 P value Cruciferous vegetables 0.83 (0.76, 0.91) <0.001 Allium vegetables 0.83 (0.71, 0.97) 0.017 Total vegetables 0.74 (0.61, 0.89) 0.002 1Results are presented as HR (95% CI) using multivariable-adjusted Cox proportional hazards modelling per 10 g/d for cruciferous vegetables, per 5 g/d for allium vegetables and per 75 g/d for total vegetables. The multivariable-adjusted model included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, calcium supplementation group, anti-hypertensive medication, statin medication, low-dose aspirin, CKD-EPI eGFR and energy intake. CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate. Cruciferous vegetables included cabbage, Brussels sprouts, cauliflower and broccoli. Allium vegetables included onion, leek and garlic.
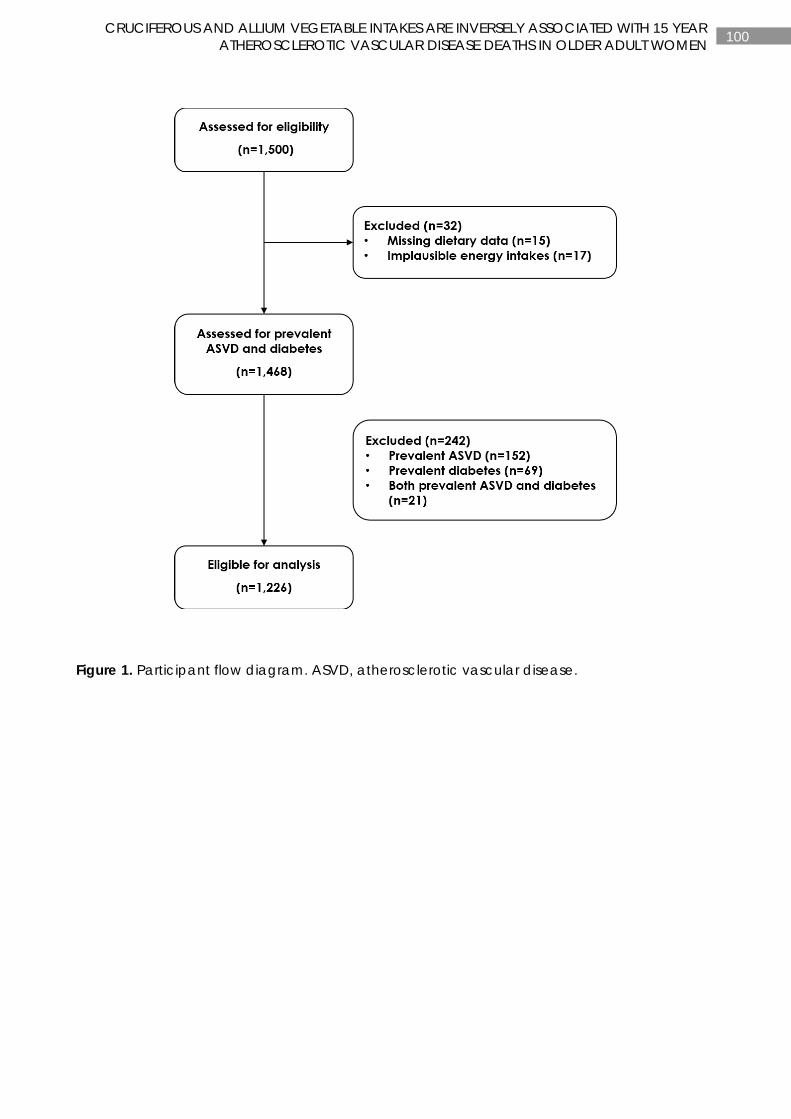
100 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
Figure 1. Participant flow diagram. ASVD, atherosclerotic vascular disease.
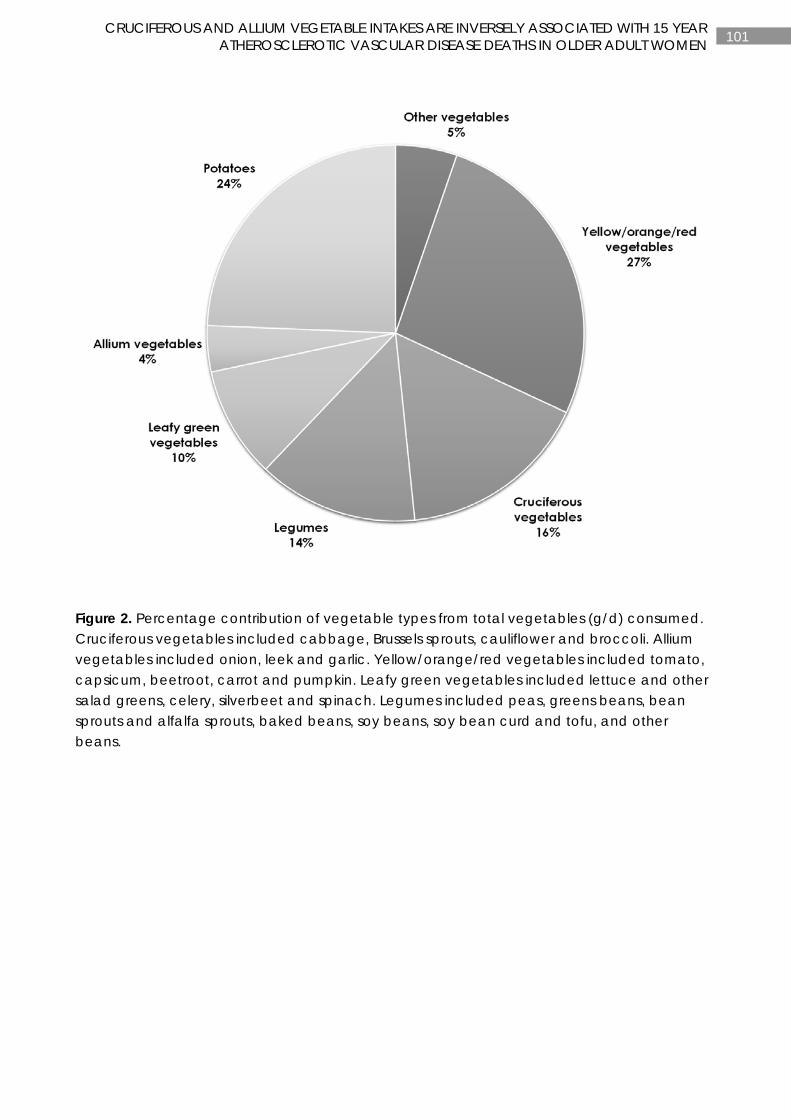
101 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
Figure 2. Percentage contribution of vegetable types from total vegetables (g/d) consumed. Cruciferous vegetables included cabbage, Brussels sprouts, cauliflower and broccoli. Allium vegetables included onion, leek and garlic. Yellow/orange/red vegetables included tomato, capsicum, beetroot, carrot and pumpkin. Leafy green vegetables included lettuce and other salad greens, celery, silverbeet and spinach. Legumes included peas, greens beans, bean sprouts and alfalfa sprouts, baked beans, soy beans, soy bean curd and tofu, and other beans.
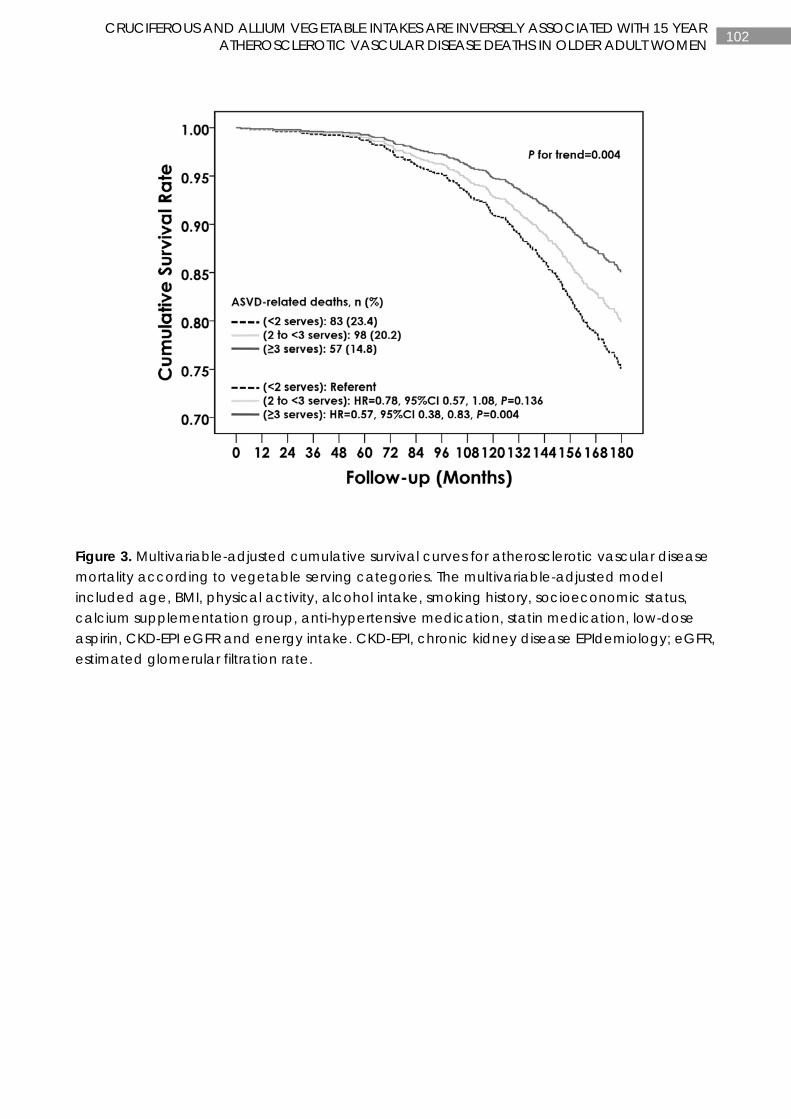
102 CRUCIFEROUS AND ALLIUM VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH 15 YEAR
ATHEROSCLEROTIC VASCULAR DISEASE DEATHS IN OLDER ADULT WOMEN
Figure 3. Multivariable-adjusted cumulative survival curves for atherosclerotic vascular disease mortality according to vegetable serving categories. The multivariable-adjusted model included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, calcium supplementation group, anti-hypertensive medication, statin medication, low-dose aspirin, CKD-EPI eGFR and energy intake. CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate.
103 CHAPTER 4
CHAPTER 4
CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL
ATHEROSCLEROSIS IN OLDER ADULT WOMEN
Manuscript based on this chapter:
Lauren C Blekkenhorst, Catherine P Bondonno, Joshua R Lewis, Richard J Woodman, Amanda Devine, Nicola P Bondonno, Wai H Lim, Kun Zhu, Lawrence J Beilin, Peter L Thompson, Richard L Prince, Jonathan M Hodgson. Cruciferous and total vegetable intakes are inversely associated with subclinical atherosclerosis in older adult women. Journal of the American Heart Association. 2018;7(8):1-13.

104 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH
SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
ABSTRACT
Background: Dietary patterns rich in fruits and vegetables are considered to reduce atherosclerotic disease presentation and are reported to be inversely associated with surrogate markers of atherosclerosis such as carotid artery intima-media thickness and plaque. However, the effect of vegetable intake alone, and relationships to specific types of vegetables containing different phytochemical profiles, are important. The aim of this study was to investigate the associations of total vegetable intake and specific vegetables grouped according to phytochemical constituents with common carotid artery intima-media thickness (CCA-IMT) and carotid plaque severity in a cohort of older adult women aged ≥70 years.
Methods: Total vegetable intake was calculated at baseline (1998) using a validated food frequency questionnaire. Vegetable types included cruciferous, allium, yellow/orange/red, leafy green, and legumes. In 2001, CCA-IMT (n=954) and carotid focal plaque (n=968) were assessed using high-resolution B‐mode carotid ultrasonography.
Results: Mean (SD) total vegetable intake was 199.9 (78.0) g/d. Women consuming ≥3 servings of vegetables each day had approximately 4.6-5.0% lower mean CCA-IMT (P=0.014) and maximum CCA-IMT (P=0.004) compared to participants consuming <2 servings of vegetables. For each 10 g/d higher in cruciferous vegetable intake there was an associated 0.006 mm (0.8%) lower mean CCA-IMT (P<0.01) and 0.007 mm (0.8%) lower maximum CCA-IMT (P<0.01). Other vegetable types were not associated with CCA-IMT (P>0.05). No associations were observed between vegetables and plaque severity (P>0.05).
Conclusions: Increasing vegetables in the diet with a focus on consuming cruciferous vegetables may have benefits for the prevention of subclinical atherosclerosis in older adult women.

105 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH
SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
INTRODUCTION
Higher vegetable intake is consistently associated with a reduced risk of coronary heart disease and stroke (12). The underlying cause of these cardiovascular disease (CVD) subgroups, is atherosclerosis, a complex multifactorial disorder of the arteries initiated by endothelial dysfunction, inflammation and dyslipidaemia (50, 51). Surrogate markers of atherosclerosis include common carotid artery intima-media thickness (CCA-IMT) and carotid atherosclerotic plaques, both of which have been shown to predict myocardial infarction and stroke (52-54).
Diets high in vegetables such as a Mediterranean-style diet and a vegetarian diet have been shown to be associated with lower CCA-IMT (57, 58) and delayed progression of atherosclerotic plaques (59). However, the role of individual dietary components, such as vegetables, is uncertain (60). Furthermore, given the heterogeneity of vegetables, there has been little research investigating whether specific types of vegetables are associated with a reduction in atherosclerosis.
Vegetables contain many nutrients and bioactive compounds such as phytochemicals that may slow the progression of atherosclerosis (18). Some of these naturally occurring compounds include carotenoids, polyphenols, organosulfur compounds, and nitrogen-containing compounds (32, 44, 48, 256). Different types of vegetables contain different levels of these putative protective components. For example, cruciferous vegetables such as cabbage, Brussels sprouts, cauliflower and broccoli, and allium vegetables such as onions, leek and garlic, are rich sources of organosulfur compounds, which are proposed to be beneficial for cardiovascular health (32). Another example is leafy green vegetables such as spinach and lettuce, which are a rich source of the nitrogen-containing compound, nitrate. Nitrate has been shown in clinical trials to lower blood pressure (163, 292), a major risk factor for cardiovascular disease. If specific components have a greater protective role in atherosclerosis, then particular types of vegetables rich in these components may confer a greater cardio-protective effect, as we have previously demonstrated (66).
The primary objective of this study was to investigate the associations of total vegetable intake and intake of specific types of vegetables, grouped according to phytochemical constituents outlined above, with CCA-IMT and carotid plaque severity in a cohort of older adult women. Because of the potential for co-correlation, the effects of individual dietary confounders, including total fruit, fish, nuts, red meat, processed meat, fibre, magnesium, and monounsaturated fat, were studied.
METHODS
Study population
Participants (n=1,500) for this observational study were initially enrolled in 1998 to the Calcium Intake Fracture Outcome Study (CAIFOS). The CAIFOS was a 5-year, double-blinded, randomised, placebo-controlled trial of daily calcium supplementation (1.2 g calcium carbonate) to prevent osteoporotic fracture (257). Participants were recruited in 1998 from the Western Australian general population of women aged ≥70 y. Invitations were sent by mail using the Electoral Roll, which is maintained for all Australian citizens enrolled to vote in Western Australia. All participants recruited into the study were ambulant with an expected survival
106 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH
SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
beyond 5 years and were not receiving any medication known to affect bone metabolism (including hormone replacement therapy). Participants were comparable in terms of disease burden and medication use to the general population of similar age but were more likely to come from a higher socio-economic status (293). A total of 39/1,500 (2.6%) participants of the CAIFOS received 1.2 g calcium carbonate plus 1000 IU of vitamin D (ergocalciferol) as part of a sub-study (294). In 2001, a pre-planned ancillary study was performed to investigate the epidemiological determinants of CCA-IMT and carotid atherosclerosis in 1,154/1,500 (77%) participants. The remaining women (n=346) had either died, withdrew from the study or were unable to be scheduled. Both studies were approved by the Human Ethics Committee at the University of Western Australia and written informed consents were obtained from all participants.
Inclusion criteria for the current observational study included all available exposure and outcome variables. Exclusion criteria included no dietary data, implausible energy intakes and participants with prevalent atherosclerotic vascular disease (ASVD) or diabetes mellitus. Dietary data was available in 1,146/1,154 (99.3%) participants. Implausible energy intakes (<2,100kJ [500kcal] or >14,700kJ [3,500kcal] per day) resulted in 12/1,146 (1.0%) participants being excluded. Participants with prevalent ASVD (n=107), diabetes mellitus (n=44) or both (n=15) at baseline (1998) were excluded, leaving 968 participants for the carotid plaque severity analysis and 954 participants for the CCA-IMT analysis (n=14 with missing CCA-IMT data) (Figure 1). Prevalent ASVD and/or diabetes mellitus at baseline was an a priori exclusion criteria in order to help avoid the possibility of reverse causality which may weaken the true association. Prevalence of ASVD at baseline (1998) was determined from principal hospital discharge diagnosis codes from 1980-1998 using the Hospital Morbidity Data Collection, linked via the Western Australian Data Linkage System. Diagnosis codes for ASVD included ischaemic heart disease (ICD-9/ICD-9-CM codes 410-414); heart failure (ICD-9/ICD-9-CM code 428); cerebrovascular disease, excluding haemorrhage (ICD-9/ICD-9-CM codes 433-438); and peripheral arterial disease (ICD-9/ICD-9-CM codes 440-444). These codes were defined using the Manual of the International Statistical Classification of Diseases, Injuries and Causes of Death, 9th Revision (ICD-9) (258) and the Australian Version of the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) (259). Prevalent diabetes mellitus at baseline (1998) was determined using medication use. Medications were coded (T89001-T90009) using the International Classification of Primary Care – Plus (ICPC-Plus) method (260).
Common carotid artery intima-media thickness and carotid plaque severity
Common carotid artery intima-media thickness and carotid plaque severity were assessed at year 3 (2001) using high-resolution B‐mode carotid ultrasonography. Ultrasounds were conducted by the same sonographer using a standard image acquisition protocol (295). An 8.0‐mHz linear array transducer attached to an Acuson Sequoia 512 ultrasound machine (Mountain View, CA, USA) was used. To account for asymmetrical wall thickening, images were taken from three different angles (anterolateral, lateral and posterolateral) of the far walls of the distal 2 cm of the left and right common carotid arteries. The same technician conducted off-line analyses on all end-diastolic images using a semi-automated edge-detection software program. The mean and maximum CCA‐IMT (mm) from each of the six images (three on either side) were averaged to give an overall mean CCA‐IMT and maximum CCA-IMT. A short-term precision study was undertaken in 20 non-trial subjects using the same sonographer and technician. Repeated IMT measurements were made between 0 and 31
107 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH
SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
days apart (mean 10.3 days). The coefficient of variation for the repeat measures was 5.98% (calculated using the root-mean-square method) (296). Focal plaques were then determined by examining the entire carotid tree (common carotid artery, carotid bulb, internal and external carotid). Carotid plaque severity was categorised according to the degree of stenosis: less advanced (<25% stenosis) or more advanced (≥25% stenosis) (297).
Dietary intake assessment
A semi-quantitative food frequency questionnaire was used to assess dietary intake at baseline (1998). This questionnaire was developed and validated by the Cancer Council of Victoria and was designed to assess usual dietary intake over a period of 12 months (262, 263, 298). Food intake frequency was assessed by 10 frequency options ranging from ‘never’ to ‘3 or more times per day’ and portion size was calculated using photographs of scaled portions of different food types. Energy and nutrient intakes were calculated by the Cancer Council of Victoria using the NUTTAB95 food composition database (264) and were supplemented by other data where necessary. Food items (including 24 vegetable items) were individually calculated in g/d by the Cancer Council of Victoria. A research assistant supervised participants whilst completing the questionnaires and provided food models, photographs, measuring cups and spoons for the accuracy of reported food consumption.
Total vegetable intake
Total vegetable intake was calculated per serving (75 g/d) based on the 2013 Australian Dietary Guidelines (6). Servings per day were then categorised into 3 categories (<2 servings/d, 2 to <3 servings/d, and ≥3 servings/d) with a similar number of participants in each category. ‘Potatoes, roasted or fried, including hot chips’ was not included in total intake of vegetables as hot chips are not recommended as part of a healthy diet (6). ‘Potatoes cooked without fat’ were included.
Vegetable types
Vegetables were grouped based on the 2013 Australian Dietary Guidelines (6) and were modified relating to phytochemical constituents, as previously described (66, 299). Vegetable types included cruciferous (cabbage, Brussels sprouts, cauliflower and broccoli), allium (onion, leek and garlic), yellow/orange/red (tomato, capsicum, beetroot, carrot and pumpkin), leafy green (lettuce and other salad greens, celery, silverbeet and spinach), and legumes (peas, greens beans, bean sprouts and alfalfa sprouts, baked beans, soy beans, soy bean curd and tofu, and other beans).
Baseline demographic and clinical assessment
Body weight (kg) and height (m) were assessed using digital scales and a wall-mounted stadiometer, respectively. Participants were wearing light clothing with no socks and shoes. Body mass index (BMI) (kg/m2) was then calculated. Questionnaires were used to assess physical activity and smoking status. Physical activity (kJ/d) was calculated using a validated method utilising the type of activity, time engaged in the activity and the participants’ weight (268, 269). Smoking status was coded as non-smoker or ex-smoker/current smoker. Ex-smoker/current smoker was defined as consuming >1 cigarette per day for >3 months at any time during the participants’ life. Alcohol intake (g/d) was assessed using the validated food frequency questionnaire as described above. Socioeconomic status (SES) was calculated

108 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH
SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
using the Socioeconomic Indexes for Areas developed by the Australian Bureau of Statistics. These indexes ranked residential postcodes according to relative socio-economic advantage and disadvantage. Participants were coded into 6 groups from the top 10% most highly disadvantaged to the top 10% least disadvantaged (270).
A detailed medical history and list of current medications were obtained from all participants and were verified by their general practitioner where possible. Medication use was coded using the ICPC-Plus method which allows aggregation of different terms for similar pathologic entities as defined by the ICD-10 coding system (260). Use of antihypertensive agents, statin therapy and low-dose aspirin were included in the multivariable models to adjust for atherosclerotic-related risk factors such as hypertension and dyslipidaemia. Baseline serum creatinine was analysed in 875/968 (90.4%) participants using an isotope dilution mass spectrometry traceable Jaffe kinetic assay and Hitachi 917 analyser (Roche Diagnostics GmbH, Mannheim Germany) (272). Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation (271) and was added to the multivariable-adjusted models as this has been shown to predict atherosclerotic disease in this cohort of older adult women (272). Total cholesterol, high-density lipoprotein cholesterol (HDL-C) and triglyceride concentrations were analysed in 895/968 (92.5%) participants using a Hitachi 917 auto analyser (Roche Diagnostics, Mannheim, Germany). Low-density lipoprotein cholesterol (LDL-C) was calculated in 888/968 (91.7%) participants using the Friedewald’s method (273).
Statistics
An analytical protocol was produced prior to analysis. Statistical significance was set at a 2-sided Type 1 error rate of P<0.05. All data were analysed using IBM SPSS Statistics for Windows, version 21.0 (IBM) and SAS software, version 9.4 (SAS Institute Inc). Descriptive statistics of normally distributed continuous variables were expressed as mean ± standard deviation (SD), non-normally distributed continuous variables (physical activity, alcohol intake, allium vegetable intake, nut intake, fish intake, processed meat intake, and red meat intake) were expressed as median and interquartile range, and categorical variables as number and proportion (%). Differences in baseline characteristics and dietary intakes among vegetable serve categories were tested using one-way ANOVA for normally distributed continuous variables and the Kruskal-Wallis test for non-normally distributed continuous variables. Chi-squared test for independence was used to test for differences in baseline characteristics and dietary intakes for categorical variables.
Multivariate linear regression was used to investigate the association between CCA-IMT (mean and maximum) and our primary exposures of interest (total vegetable intake and intake of vegetable types). The association between focal plaque severity (less advanced versus more advanced) and the same exposure variables were investigated using binary logistic regression. Three models of adjustment were used in each analysis: unadjusted, age and energy-adjusted, and multivariable-adjusted (age, BMI, level of physical activity, alcohol intake, smoking history, SES, the CAIFOS supplementation group of calcium vs. calcium plus vitamin D vs. placebo, use of antihypertensive agents, statin therapy and low-dose aspirin, CKD-EPI eGFR, and energy intake). Covariates were entered into the models as continuous variables with the exception of smoking history, SES, the CAIFOS supplementation group of calcium vs. calcium plus vitamin D vs. placebo, use of antihypertensive agents, statin therapy, and low-

109 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH
SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
dose aspirin which were entered as categorical variables. When assessing the association for vegetable types, the total intake from other vegetables was added to the multivariable-adjusted model as an additional analysis. Covariates included in the adjusted models were selected on an a priori basis because of their biological relationship with CVD.
Sensitivity analysis
In addition to the fully adjusted models, we also considered the potential for confounding from other dietary components. Given the potential for multicollinearity between many of these confounders, we considered their impact by entering them into models separately, each as a continuous variable, for mean and maximum CCA-IMT. These included daily intakes of total fruit (g/d) (300), fish (g/d), nuts (g/d), red meat intake (g/d), processed meat intake (g/d), fibre (g/d), potassium (mg/d), magnesium (mg/d), monounsaturated fat (g/d), saturated fat (g/d) (275), and vegetable-derived nitrate (mg/d) (31). In addition, since potato can be classified nutritionally as a starchy food, ‘potatoes cooked without fat’ were excluded from the calculation of total vegetable intake and the fully adjusted models were re-analysed for mean and maximum CCA-IMT. Furthermore, vitamin D has been associated with subclinical atherosclerosis (301), we therefore excluded participants that had received 1.2 g calcium carbonate plus 1000 IU of vitamin D (n=28) and then repeated the fully adjusted models for mean and maximum CCA-IMT. Lastly, since fruit also contains many phytochemicals thought to benefit cardiovascular health (302), we explored the relationship of total fruit intake (per serving, 150 g/d) with CCA-IMT (mean and maximum) and carotid plaque severity using the three models of adjustment described above plus an additional model further adjusting for total vegetable intake (per 75 g/d).
RESULTS
Characteristics of study population
Participant demographics, medication use, and biochemical analyses of all 968 study participants and by categories of vegetable servings are presented in Table 1. Generally, higher intakes of vegetables corresponded to higher intakes of other foods and nutrients. Mean (SD) vegetable intake was 199.9 (78.0) g/d and mean (SD) vegetable servings was 2.7 (1.0) for all participants (Table 2). Proportional intakes of vegetable types (including intake of potatoes and other vegetables) are presented in Figure 2. Mean (SD) mean CCA-IMT was 0.778 (0.129) mm and mean (SD) maximum CCA-IMT was 0.922 (0.152) mm. More advanced carotid stenosis (≥25%) was present in 120/968 (12.4%) of participants and less advanced carotid stenosis (<25%) was present in 848/968 (87.6%).
Common carotid artery intima-media thickness
Total vegetable intake
In linear regression, for all models of adjustment, total vegetable intake was inversely associated with mean CCA-IMT and maximum CCA-IMT (Table 3). For each serving (75 g/d) higher in vegetables there was an associated 0.011 mm (1.4%) lower mean CCA-IMT (P=0.014) and 0.016 mm (1.7%) lower maximum CCA-IMT (P=0.002) after adjusting for lifestyle and cardiovascular risk factors (Table 3). Similarly, participants consuming ≥3 servings of vegetables each day had approximately 0.036 mm (4.6%) lower mean CCA-IMT and 0.047 mm (5.0%)
110 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH
SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
lower maximum CCA-IMT compared to participants consuming <2 servings of vegetables (Table 3).
Vegetable types
In linear regression, for all models of adjustment, intake of cruciferous vegetables was inversely associated with mean CCA-IMT and maximum CCA-IMT (Table 4). This relationship remained significant after further adjustment for non-cruciferous vegetable intakes. Legume intake was not associated with mean CCA-IMT. However, for maximum CCA-IMT, legume intake was inversely associated in unadjusted (P=0.023), and age and energy-adjusted (P=0.044) models, but not the multivariable-adjusted model (P=0.085). Intake of allium, yellow/orange/red, and leafy green vegetables were not significantly associated with mean or maximum CCA-IMT (Table 4).
Carotid plaque severity
Total vegetable intake and intake of vegetable types were not associated with carotid plaque severity (Table 5).
Sensitivity analyses
In the separate linear regression analyses that additionally adjusted for individual dietary confounders, total fruit, fish, nuts, red meat, processed meat, fibre, magnesium, and monounsaturated fat, did not change the interpretation of the association between total vegetable intake and CCA-IMT (Table 6). Adjustment for potassium and vegetable-derived nitrate, however, both attenuated the association between total vegetable intake and CCA-IMT. Adjustment for saturated fat intake attenuated the association between total vegetable intake and mean CCA-IMT, but not maximum CCA-IMT. Similarly, in the separate linear regression analyses that additionally adjusted for individual dietary confounders, total fruit, fish, nuts, fibre, magnesium, monounsaturated fat, and saturated fat, did not change the interpretation of the association between intake of cruciferous vegetables and CCA-IMT (Table 6). Adjustment for potassium and vegetable-derived nitrate both attenuated the association between intake of cruciferous vegetables and maximum CCA-IMT, but not mean CCA-IMT. Exclusion of ‘potatoes cooked without fat’ from total vegetable intake did not change the interpretation of the association between total vegetable intake and mean CCA-IMT (unstandardized ß=-0.018, SE=0.006, P=0.004) and maximum CCA-IMT (unstandardized ß=-0.025, SE=0.007, P=0.001). Furthermore, exclusion of participants that had received 1.2 g calcium carbonate plus 1000IU of vitamin D (n=28) did not change the interpretation of the association of total vegetable intake and intake of cruciferous vegetables with CCA-IMT (mean and maximum) (Table 7).
Total fruit intake (per 150 g/d) was not associated with mean CCA-IMT and carotid plaque severity in all three models of adjustment (P>0.05 for all). There was evidence for an association between total fruit intake (per 150 g/d) and maximum CCA-IMT, but this was only statistically significant in the unadjusted (unstandardized ß=-0.012, SE=0.006, P=0.034) and multivariable-adjusted (unstandardized ß=-0.013, SE=0.006, P=0.042) models. Total fruit intake (per 150 g/d) was not associated with maximum CCA-IMT in the age and energy-adjusted model (unstandardized ß=-0.011, SE=0.006, P=0.072) and in the multivariable-adjusted model after

111 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH
SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
further adjustment for total vegetable intake (per 75 g/d) (unstandardized ß=-0.009, SE=0.006, P=0.166).
DISCUSSION
In this cohort of older adult women, we found that both total vegetable intake and intake of cruciferous vegetables were inversely associated with mean and maximum CCA-IMT. These associations were independent of lifestyle and cardiovascular risk factors as well as other dietary confounders.
We observed a difference of 0.05mm in maximum CCA-IMT between high and low intakes of total vegetables. This is likely to be clinically significant as a 0.1mm decrease in carotid IMT is associated with a 10-18% decrease in risk of myocardial infarction and stroke (53). The results of our study can be supported by a randomised controlled trial reporting a slight regression in CCA-IMT with dietary changes which included an increased intake of fruit and vegetables over a 12 month period (303). However, in observational studies, no associations have been observed between intakes of vegetables alone and carotid intima-media thickness, and suggest fruit intake may be more beneficial (304, 305). Fruit intake, however, did not influence the association between total vegetable intake and CCA-IMT in our study, and was not itself an independent predictor. Individual adjustments for potassium and vegetable-derived nitrate intakes, did however, attenuate the association between total vegetable intake and CCA-IMT. This suggests that at least some of the benefit from total vegetable intake was mediated by these components which are also likely to influence vascular health (14, 31, 306-308).
There are many possible mechanisms to explain the relationship between higher vegetable intake and lower CCA-IMT. Vegetables have many important nutritive and non-nutritive constituents that may contribute to vascular health (18). Phytochemicals have been postulated to have additional benefits beyond basic nutrients. These include polyphenols which may play a role in scavenging free radicals that have the ability to oxidise LDL-C infiltrated in the arterial wall (309). Organosulfur compounds found abundantly in cruciferous vegetables may also play a role. Isothiocyanates are organosulfur compounds that have been extensively researched for their anti-cancer properties (32, 280-282). However, accumulating evidence suggests sulforaphane, a compound within the isothiocyanate group, may have beneficial effects on vascular damage via the blockade of oxidative stress and/or inhibition of advanced glycation end products (283, 284). There was strong evidence that intake of cruciferous vegetables was inversely associated with mean CCA-IMT in this cohort even after further adjustment for non-cruciferous vegetables and other food and nutrients thought to be associated with cardiovascular health.
Focal carotid plaque severity was not associated with vegetable intake in this cohort of older adult women. Although CCA-IMT and carotid plaque are both inter-correlated, they may reflect different biological aspects of atherogenesis and are associations with different clinical vascular outcomes (55). Carotid plaques are strongly related to hyperlipidaemia and myocardial infarction whereas CCA-IMT is more related to hypertension and ischaemic stroke (55). This may be due to focal plaque size being dependent on the influx of lipids into the plaque whereas CCA-IMT captures both the atherosclerotic process as well as the non-atherosclerotic process such as the compensatory thickening of the carotid wall as a response to ageing and hypertension (56).

112 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH
SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
There are several strengths to this observational study. Study participants were representative of older adult females from the Australian population with similar intakes of vegetable servings (11). Furthermore, our study used six repeat measurements for both mean and maximum CCA-IMT and was shown to be highly reproducible thereby reducing the likelihood of measurement error in this variable. However, since 2001 when the carotid ultrasounds were undertaken in the CAIFOS, sonographic characteristic evaluations have advanced (e.g. surface irregularity, ulceration, and echogenicity). These sonographic characteristics along with resistive index were not available to be analysed in this study. In addition, only the common carotid artery was assessed for intima-media thickness and not the bifurcation and internal carotid arteries. Further studies are therefore recommended to replicate the results of this study with these advanced measures. Other limitations include the possible reduced generalizability of study findings due to the study involving 1,154 (77%) of the original 1,500 women recruited at baseline, particularly as this study was done three years after recruitment for the primary randomised controlled trial. In addition, it should be noted that classification by one characteristic results in differences in other characteristics such as food and nutrient intakes. For example, participants consuming the highest servings of vegetables compared to participants consuming the lowest servings of vegetables reported a 32% higher energy intake, as well as most other foods and nutrients. It should also be noted that only marginal weight differences were observed for participants consuming the highest servings of vegetables compared to participants consuming the lowest servings of vegetables even though there was a 32% higher energy intake reported. This suggests either errors in reported food intakes or more likely higher energy utilisation. Lastly, only one measure of food intake and one measure for subclinical atherosclerosis were available; thus, the study resembles a cross-sectional design more than a prospective design. It should also be noted that the study was conducted in older women only, and therefore, results need to be replicated in men and younger cohorts.
Conclusion
We found that both total vegetable intake and intake of cruciferous vegetables were inversely associated with CCA-IMT. These associations were independent of lifestyle and atherosclerotic-related risk factors as well as other dietary confounders. Increasing vegetables within the diet with a focus on consuming cruciferous vegetables may protect against subclinical atherosclerosis in older adult women.
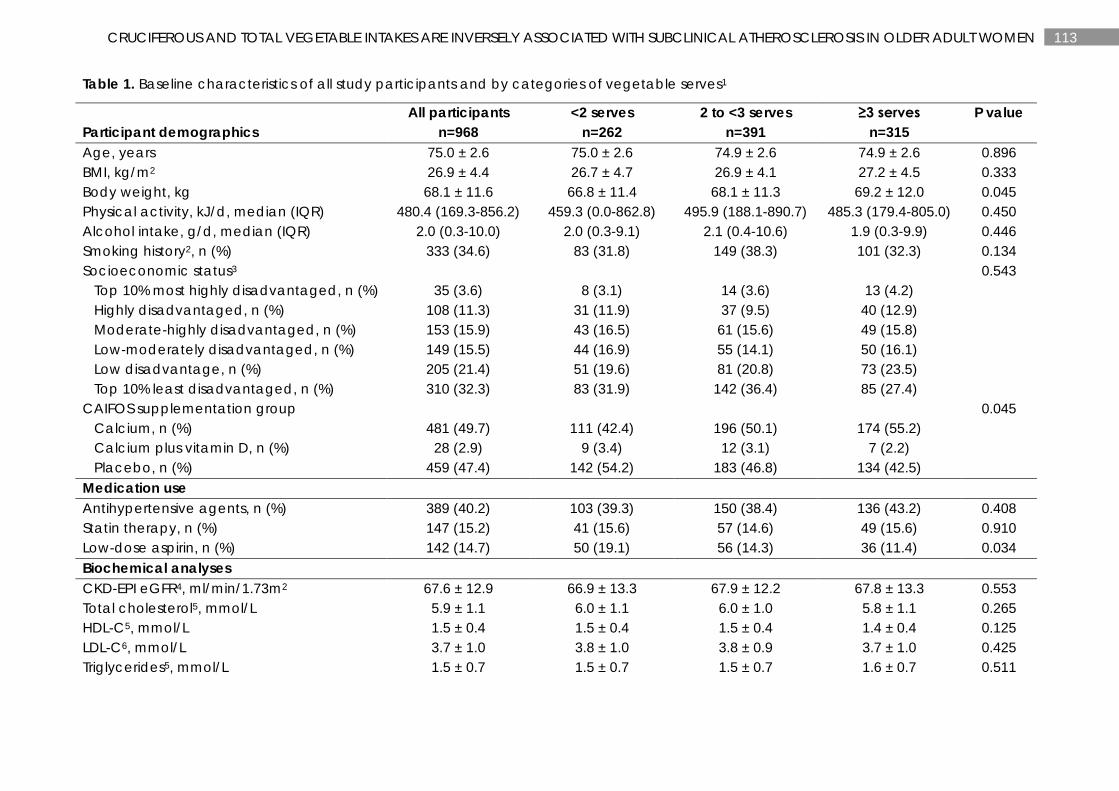
113 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
Table 1. Baseline characteristics of all study participants and by categories of vegetable serves1
Participant demographics All participants
n=968 <2 serves
n=262 2 to <3 serves
n=391 ≥3 serves
n=315 P value
Age, years 75.0 ± 2.6 75.0 ± 2.6 74.9 ± 2.6 74.9 ± 2.6 0.896 BMI, kg/m2 26.9 ± 4.4 26.7 ± 4.7 26.9 ± 4.1 27.2 ± 4.5 0.333 Body weight, kg 68.1 ± 11.6 66.8 ± 11.4 68.1 ± 11.3 69.2 ± 12.0 0.045 Physical activity, kJ/d, median (IQR) 480.4 (169.3-856.2) 459.3 (0.0-862.8) 495.9 (188.1-890.7) 485.3 (179.4-805.0) 0.450 Alcohol intake, g/d, median (IQR) 2.0 (0.3-10.0) 2.0 (0.3-9.1) 2.1 (0.4-10.6) 1.9 (0.3-9.9) 0.446 Smoking history2, n (%) 333 (34.6) 83 (31.8) 149 (38.3) 101 (32.3) 0.134 Socioeconomic status3 0.543 Top 10% most highly disadvantaged, n (%) 35 (3.6) 8 (3.1) 14 (3.6) 13 (4.2) Highly disadvantaged, n (%) 108 (11.3) 31 (11.9) 37 (9.5) 40 (12.9) Moderate-highly disadvantaged, n (%) 153 (15.9) 43 (16.5) 61 (15.6) 49 (15.8) Low-moderately disadvantaged, n (%) 149 (15.5) 44 (16.9) 55 (14.1) 50 (16.1) Low disadvantage, n (%) 205 (21.4) 51 (19.6) 81 (20.8) 73 (23.5) Top 10% least disadvantaged, n (%) 310 (32.3) 83 (31.9) 142 (36.4) 85 (27.4) CAIFOS supplementation group 0.045 Calcium, n (%) 481 (49.7) 111 (42.4) 196 (50.1) 174 (55.2) Calcium plus vitamin D, n (%) 28 (2.9) 9 (3.4) 12 (3.1) 7 (2.2) Placebo, n (%) 459 (47.4) 142 (54.2) 183 (46.8) 134 (42.5) Medication use Antihypertensive agents, n (%) 389 (40.2) 103 (39.3) 150 (38.4) 136 (43.2) 0.408 Statin therapy, n (%) 147 (15.2) 41 (15.6) 57 (14.6) 49 (15.6) 0.910 Low-dose aspirin, n (%) 142 (14.7) 50 (19.1) 56 (14.3) 36 (11.4) 0.034 Biochemical analyses CKD-EPI eGFR4, ml/min/1.73m2 67.6 ± 12.9 66.9 ± 13.3 67.9 ± 12.2 67.8 ± 13.3 0.553 Total cholesterol5, mmol/L 5.9 ± 1.1 6.0 ± 1.1 6.0 ± 1.0 5.8 ± 1.1 0.265 HDL-C5, mmol/L 1.5 ± 0.4 1.5 ± 0.4 1.5 ± 0.4 1.4 ± 0.4 0.125 LDL-C6, mmol/L 3.7 ± 1.0 3.8 ± 1.0 3.8 ± 0.9 3.7 ± 1.0 0.425 Triglycerides5, mmol/L 1.5 ± 0.7 1.5 ± 0.7 1.5 ± 0.7 1.6 ± 0.7 0.511

114 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
1Vegetable serves were calculated based on the 2013 Australian Dietary Guidelines of a vegetable serve equal to 75 g/d. P values are a comparison between groups using ANOVA, Kruskal-Wallis test, and Chi-square test where appropriate. Values are presented as mean ± SD unless otherwise stated. BMI, body mass index; CAIFOS, Calcium Intake Fracture Outcome Study; CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol. 2n=963. 3n=960. 4n=875. 5n=895. 6n=888.
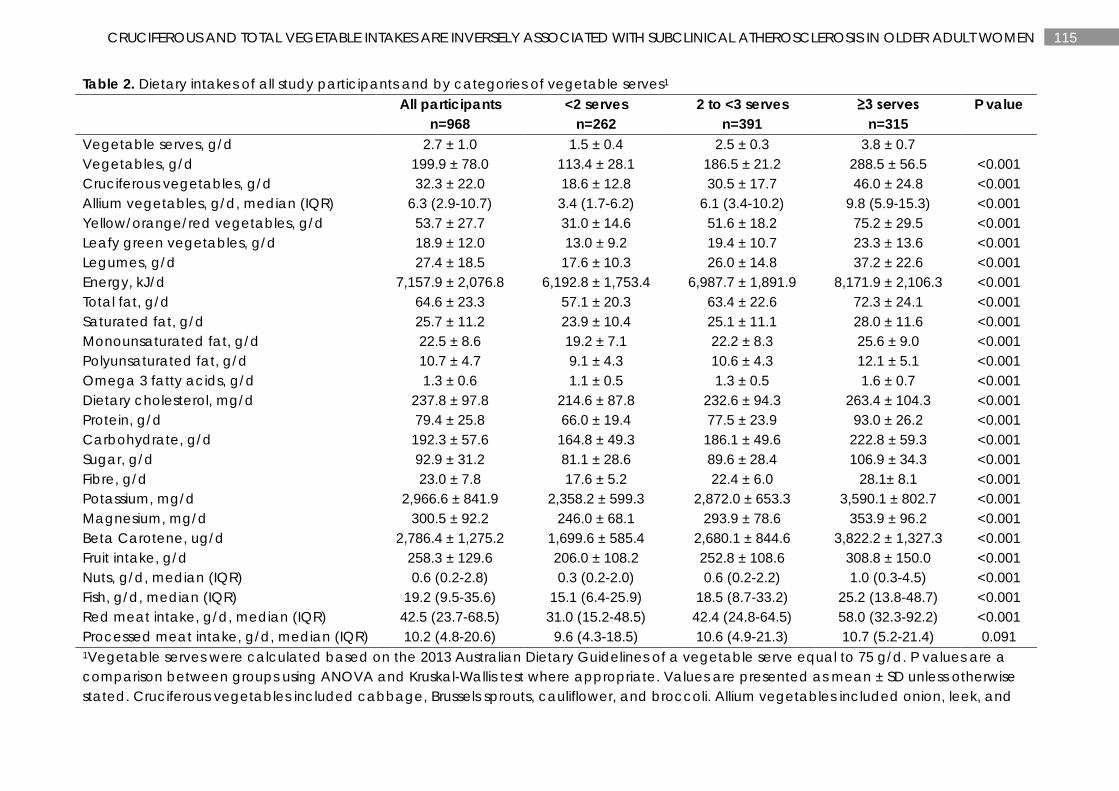
115 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
Table 2. Dietary intakes of all study participants and by categories of vegetable serves1 All participants
n=968 <2 serves
n=262 2 to <3 serves
n=391 ≥3 serves
n=315 P value
Vegetable serves, g/d 2.7 ± 1.0 1.5 ± 0.4 2.5 ± 0.3 3.8 ± 0.7 Vegetables, g/d 199.9 ± 78.0 113.4 ± 28.1 186.5 ± 21.2 288.5 ± 56.5 <0.001 Cruciferous vegetables, g/d 32.3 ± 22.0 18.6 ± 12.8 30.5 ± 17.7 46.0 ± 24.8 <0.001 Allium vegetables, g/d, median (IQR) 6.3 (2.9-10.7) 3.4 (1.7-6.2) 6.1 (3.4-10.2) 9.8 (5.9-15.3) <0.001 Yellow/orange/red vegetables, g/d 53.7 ± 27.7 31.0 ± 14.6 51.6 ± 18.2 75.2 ± 29.5 <0.001 Leafy green vegetables, g/d 18.9 ± 12.0 13.0 ± 9.2 19.4 ± 10.7 23.3 ± 13.6 <0.001 Legumes, g/d 27.4 ± 18.5 17.6 ± 10.3 26.0 ± 14.8 37.2 ± 22.6 <0.001 Energy, kJ/d 7,157.9 ± 2,076.8 6,192.8 ± 1,753.4 6,987.7 ± 1,891.9 8,171.9 ± 2,106.3 <0.001 Total fat, g/d 64.6 ± 23.3 57.1 ± 20.3 63.4 ± 22.6 72.3 ± 24.1 <0.001 Saturated fat, g/d 25.7 ± 11.2 23.9 ± 10.4 25.1 ± 11.1 28.0 ± 11.6 <0.001 Monounsaturated fat, g/d 22.5 ± 8.6 19.2 ± 7.1 22.2 ± 8.3 25.6 ± 9.0 <0.001 Polyunsaturated fat, g/d 10.7 ± 4.7 9.1 ± 4.3 10.6 ± 4.3 12.1 ± 5.1 <0.001 Omega 3 fatty acids, g/d 1.3 ± 0.6 1.1 ± 0.5 1.3 ± 0.5 1.6 ± 0.7 <0.001 Dietary cholesterol, mg/d 237.8 ± 97.8 214.6 ± 87.8 232.6 ± 94.3 263.4 ± 104.3 <0.001 Protein, g/d 79.4 ± 25.8 66.0 ± 19.4 77.5 ± 23.9 93.0 ± 26.2 <0.001 Carbohydrate, g/d 192.3 ± 57.6 164.8 ± 49.3 186.1 ± 49.6 222.8 ± 59.3 <0.001 Sugar, g/d 92.9 ± 31.2 81.1 ± 28.6 89.6 ± 28.4 106.9 ± 34.3 <0.001 Fibre, g/d 23.0 ± 7.8 17.6 ± 5.2 22.4 ± 6.0 28.1± 8.1 <0.001 Potassium, mg/d 2,966.6 ± 841.9 2,358.2 ± 599.3 2,872.0 ± 653.3 3,590.1 ± 802.7 <0.001 Magnesium, mg/d 300.5 ± 92.2 246.0 ± 68.1 293.9 ± 78.6 353.9 ± 96.2 <0.001 Beta Carotene, ug/d 2,786.4 ± 1,275.2 1,699.6 ± 585.4 2,680.1 ± 844.6 3,822.2 ± 1,327.3 <0.001 Fruit intake, g/d 258.3 ± 129.6 206.0 ± 108.2 252.8 ± 108.6 308.8 ± 150.0 <0.001 Nuts, g/d, median (IQR) 0.6 (0.2-2.8) 0.3 (0.2-2.0) 0.6 (0.2-2.2) 1.0 (0.3-4.5) <0.001 Fish, g/d, median (IQR) 19.2 (9.5-35.6) 15.1 (6.4-25.9) 18.5 (8.7-33.2) 25.2 (13.8-48.7) <0.001 Red meat intake, g/d, median (IQR) 42.5 (23.7-68.5) 31.0 (15.2-48.5) 42.4 (24.8-64.5) 58.0 (32.3-92.2) <0.001 Processed meat intake, g/d, median (IQR) 10.2 (4.8-20.6) 9.6 (4.3-18.5) 10.6 (4.9-21.3) 10.7 (5.2-21.4) 0.091 1Vegetable serves were calculated based on the 2013 Australian Dietary Guidelines of a vegetable serve equal to 75 g/d. P values are a comparison between groups using ANOVA and Kruskal-Wallis test where appropriate. Values are presented as mean ± SD unless otherwise stated. Cruciferous vegetables included cabbage, Brussels sprouts, cauliflower, and broccoli. Allium vegetables included onion, leek, and

116 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
garlic. Yellow/orange/red vegetables included tomato, capsicum, beetroot, carrot, and pumpkin. Leafy green vegetables included lettuce and other salad greens, celery, silverbeet, and spinach. Legumes included peas, greens beans, bean sprouts and alfalfa sprouts, baked beans, soy beans, soy bean curd and tofu, and other beans.
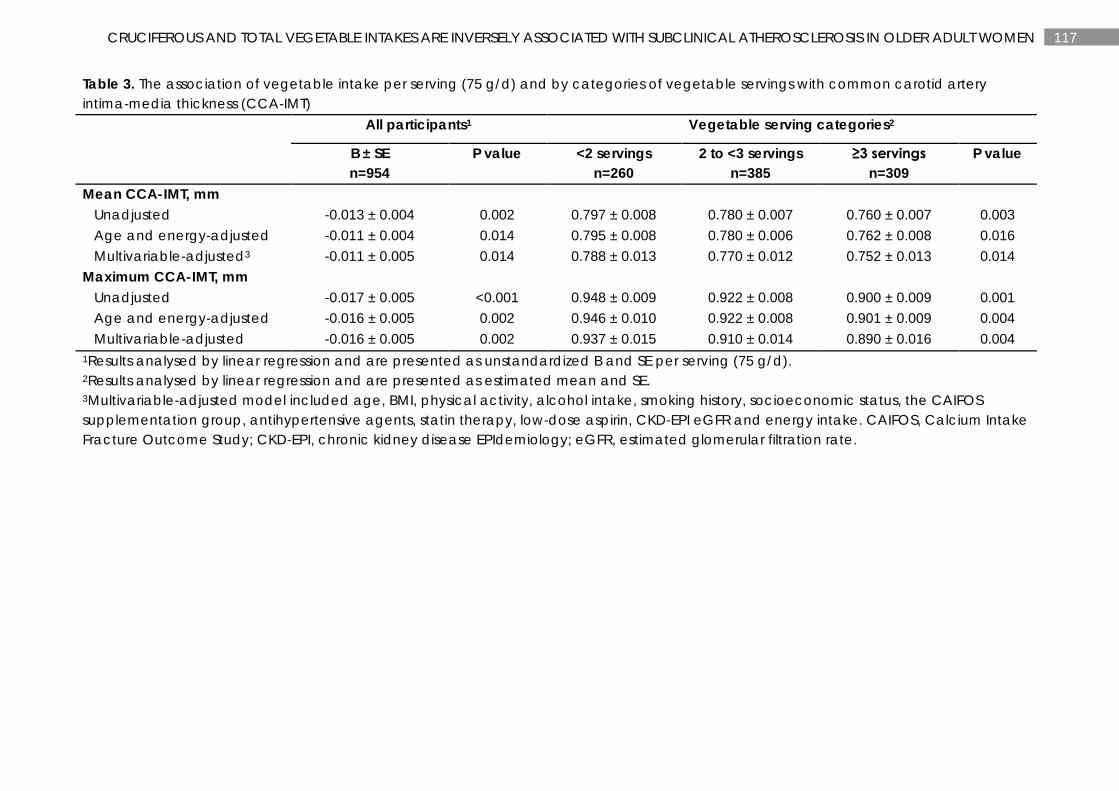
117 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
Table 3. The association of vegetable intake per serving (75 g/d) and by categories of vegetable servings with common carotid artery intima-media thickness (CCA-IMT)
All participants1 Vegetable serving categories2
B ± SE n=954
P value <2 servings n=260
2 to <3 servings n=385
≥3 servings n=309
P value
Mean CCA-IMT, mm Unadjusted -0.013 ± 0.004 0.002 0.797 ± 0.008 0.780 ± 0.007 0.760 ± 0.007 0.003 Age and energy-adjusted -0.011 ± 0.004 0.014 0.795 ± 0.008 0.780 ± 0.006 0.762 ± 0.008 0.016 Multivariable-adjusted3 -0.011 ± 0.005 0.014 0.788 ± 0.013 0.770 ± 0.012 0.752 ± 0.013 0.014 Maximum CCA-IMT, mm Unadjusted -0.017 ± 0.005 <0.001 0.948 ± 0.009 0.922 ± 0.008 0.900 ± 0.009 0.001 Age and energy-adjusted -0.016 ± 0.005 0.002 0.946 ± 0.010 0.922 ± 0.008 0.901 ± 0.009 0.004 Multivariable-adjusted -0.016 ± 0.005 0.002 0.937 ± 0.015 0.910 ± 0.014 0.890 ± 0.016 0.004 1Results analysed by linear regression and are presented as unstandardized B and SE per serving (75 g/d). 2Results analysed by linear regression and are presented as estimated mean and SE. 3Multivariable-adjusted model included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, the CAIFOS supplementation group, antihypertensive agents, statin therapy, low-dose aspirin, CKD-EPI eGFR and energy intake. CAIFOS, Calcium Intake Fracture Outcome Study; CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate.
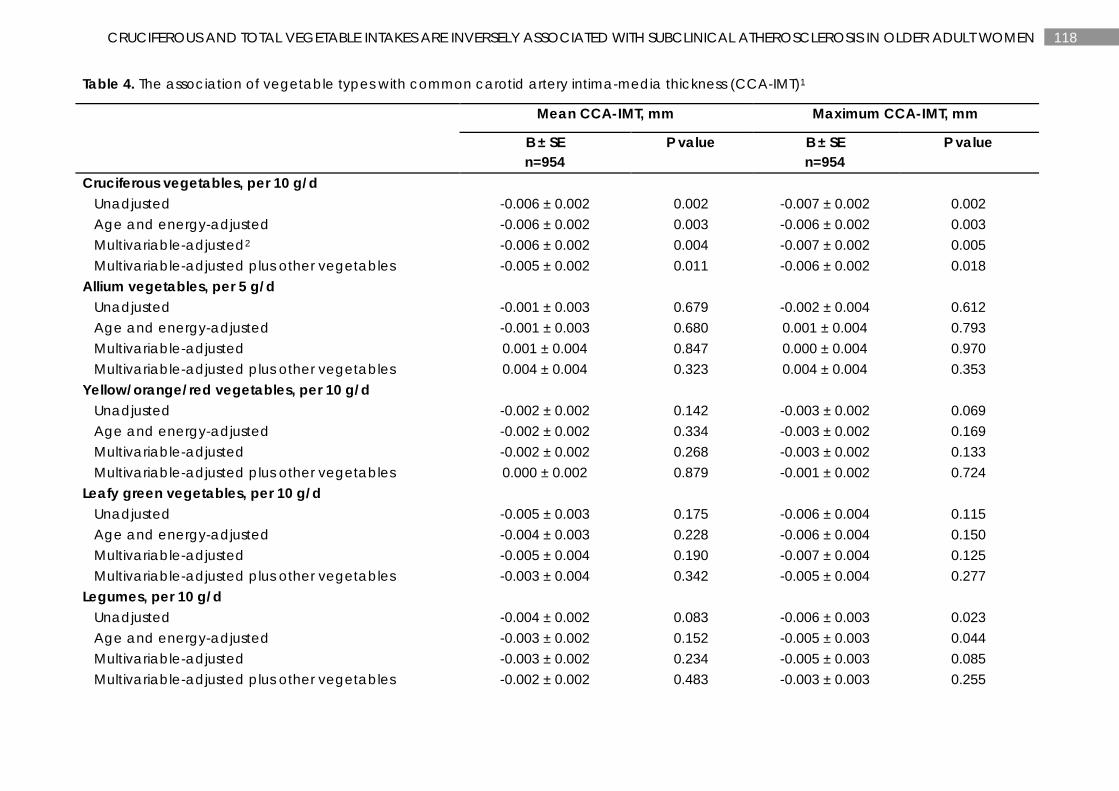
118 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
Table 4. The association of vegetable types with common carotid artery intima-media thickness (CCA-IMT)1
Mean CCA-IMT, mm Maximum CCA-IMT, mm
B ± SE n=954
P value B ± SE n=954
P value
Cruciferous vegetables, per 10 g/d Unadjusted -0.006 ± 0.002 0.002 -0.007 ± 0.002 0.002 Age and energy-adjusted -0.006 ± 0.002 0.003 -0.006 ± 0.002 0.003 Multivariable-adjusted2 -0.006 ± 0.002 0.004 -0.007 ± 0.002 0.005 Multivariable-adjusted plus other vegetables -0.005 ± 0.002 0.011 -0.006 ± 0.002 0.018 Allium vegetables, per 5 g/d Unadjusted -0.001 ± 0.003 0.679 -0.002 ± 0.004 0.612 Age and energy-adjusted -0.001 ± 0.003 0.680 0.001 ± 0.004 0.793 Multivariable-adjusted 0.001 ± 0.004 0.847 0.000 ± 0.004 0.970 Multivariable-adjusted plus other vegetables 0.004 ± 0.004 0.323 0.004 ± 0.004 0.353 Yellow/orange/red vegetables, per 10 g/d Unadjusted -0.002 ± 0.002 0.142 -0.003 ± 0.002 0.069 Age and energy-adjusted -0.002 ± 0.002 0.334 -0.003 ± 0.002 0.169 Multivariable-adjusted -0.002 ± 0.002 0.268 -0.003 ± 0.002 0.133 Multivariable-adjusted plus other vegetables 0.000 ± 0.002 0.879 -0.001 ± 0.002 0.724 Leafy green vegetables, per 10 g/d Unadjusted -0.005 ± 0.003 0.175 -0.006 ± 0.004 0.115 Age and energy-adjusted -0.004 ± 0.003 0.228 -0.006 ± 0.004 0.150 Multivariable-adjusted -0.005 ± 0.004 0.190 -0.007 ± 0.004 0.125 Multivariable-adjusted plus other vegetables -0.003 ± 0.004 0.342 -0.005 ± 0.004 0.277 Legumes, per 10 g/d Unadjusted -0.004 ± 0.002 0.083 -0.006 ± 0.003 0.023 Age and energy-adjusted -0.003 ± 0.002 0.152 -0.005 ± 0.003 0.044 Multivariable-adjusted -0.003 ± 0.002 0.234 -0.005 ± 0.003 0.085 Multivariable-adjusted plus other vegetables -0.002 ± 0.002 0.483 -0.003 ± 0.003 0.255
119 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
1Results analysed by linear regression and are presented as unstandardized B and SE. 2Multivariable-adjusted model included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, the CAIFOS supplementation group, antihypertensive agents, statin therapy, low-dose aspirin, CKD-EPI eGFR and energy intake. CAIFOS, Calcium Intake Fracture Outcome Study; CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate.
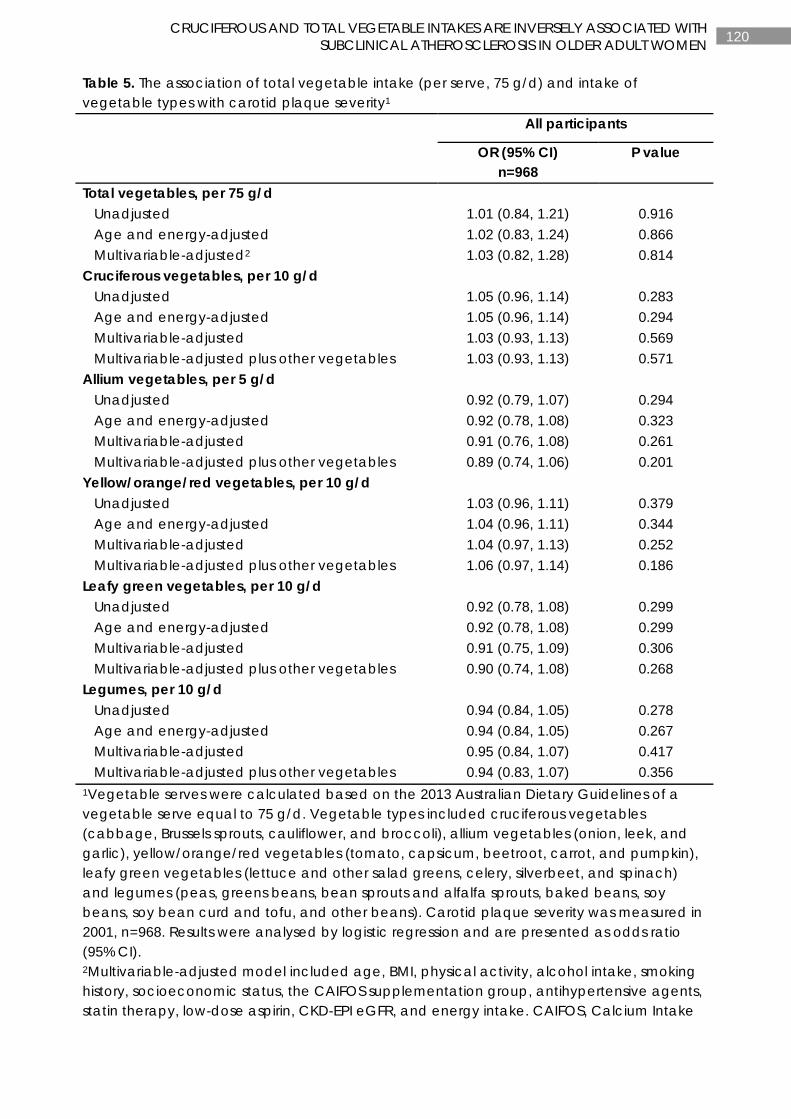
120 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
Table 5. The association of total vegetable intake (per serve, 75 g/d) and intake of vegetable types with carotid plaque severity1
All participants
OR (95% CI)
n=968 P value
Total vegetables, per 75 g/d Unadjusted 1.01 (0.84, 1.21) 0.916 Age and energy-adjusted 1.02 (0.83, 1.24) 0.866 Multivariable-adjusted2 1.03 (0.82, 1.28) 0.814 Cruciferous vegetables, per 10 g/d Unadjusted 1.05 (0.96, 1.14) 0.283 Age and energy-adjusted 1.05 (0.96, 1.14) 0.294 Multivariable-adjusted 1.03 (0.93, 1.13) 0.569 Multivariable-adjusted plus other vegetables 1.03 (0.93, 1.13) 0.571 Allium vegetables, per 5 g/d Unadjusted 0.92 (0.79, 1.07) 0.294 Age and energy-adjusted 0.92 (0.78, 1.08) 0.323 Multivariable-adjusted 0.91 (0.76, 1.08) 0.261 Multivariable-adjusted plus other vegetables 0.89 (0.74, 1.06) 0.201 Yellow/orange/red vegetables, per 10 g/d Unadjusted 1.03 (0.96, 1.11) 0.379 Age and energy-adjusted 1.04 (0.96, 1.11) 0.344 Multivariable-adjusted 1.04 (0.97, 1.13) 0.252 Multivariable-adjusted plus other vegetables 1.06 (0.97, 1.14) 0.186 Leafy green vegetables, per 10 g/d Unadjusted 0.92 (0.78, 1.08) 0.299 Age and energy-adjusted 0.92 (0.78, 1.08) 0.299 Multivariable-adjusted 0.91 (0.75, 1.09) 0.306 Multivariable-adjusted plus other vegetables 0.90 (0.74, 1.08) 0.268 Legumes, per 10 g/d Unadjusted 0.94 (0.84, 1.05) 0.278 Age and energy-adjusted 0.94 (0.84, 1.05) 0.267 Multivariable-adjusted 0.95 (0.84, 1.07) 0.417 Multivariable-adjusted plus other vegetables 0.94 (0.83, 1.07) 0.356 1Vegetable serves were calculated based on the 2013 Australian Dietary Guidelines of a vegetable serve equal to 75 g/d. Vegetable types included cruciferous vegetables (cabbage, Brussels sprouts, cauliflower, and broccoli), allium vegetables (onion, leek, and garlic), yellow/orange/red vegetables (tomato, capsicum, beetroot, carrot, and pumpkin), leafy green vegetables (lettuce and other salad greens, celery, silverbeet, and spinach) and legumes (peas, greens beans, bean sprouts and alfalfa sprouts, baked beans, soy beans, soy bean curd and tofu, and other beans). Carotid plaque severity was measured in 2001, n=968. Results were analysed by logistic regression and are presented as odds ratio (95% CI). 2Multivariable-adjusted model included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, the CAIFOS supplementation group, antihypertensive agents, statin therapy, low-dose aspirin, CKD-EPI eGFR, and energy intake. CAIFOS, Calcium Intake

121 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
Fracture Outcome Study; CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate.
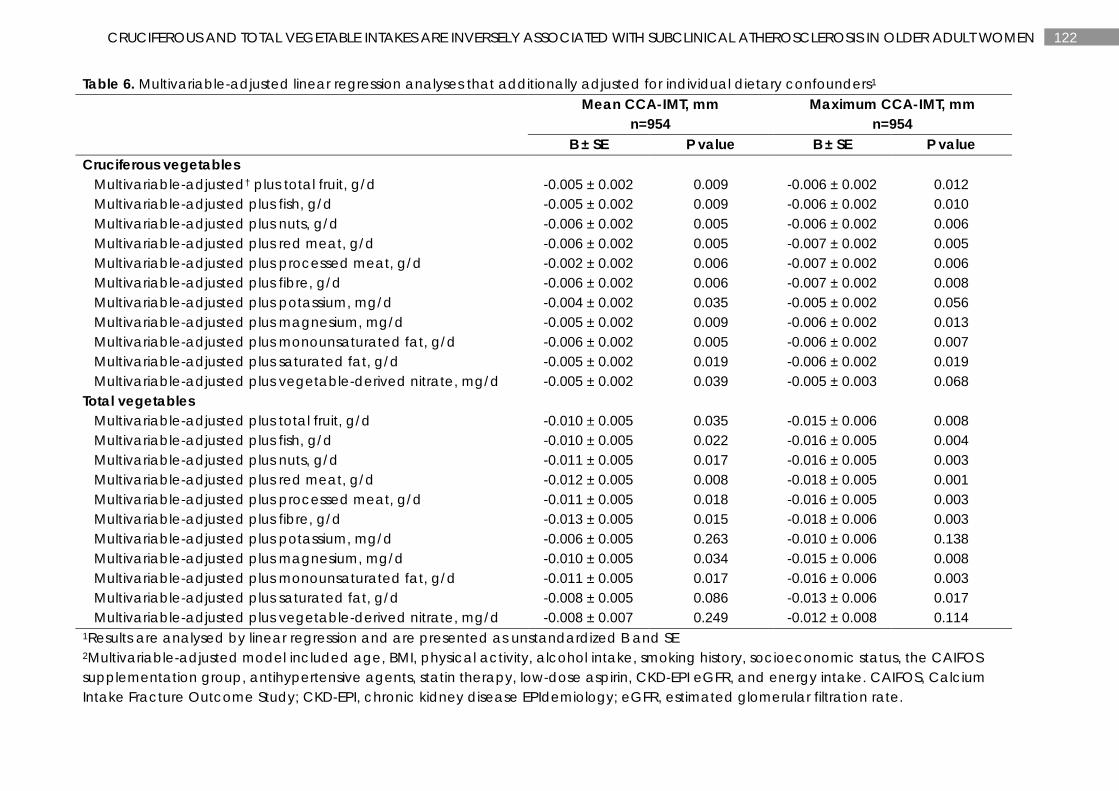
122 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROSCLEROSIS IN OLDER ADULT WOMEN
Table 6. Multivariable-adjusted linear regression analyses that additionally adjusted for individual dietary confounders1
Mean CCA-IMT, mm
n=954 Maximum CCA-IMT, mm
n=954 B ± SE P value B ± SE P value Cruciferous vegetables Multivariable-adjusted† plus total fruit, g/d -0.005 ± 0.002 0.009 -0.006 ± 0.002 0.012 Multivariable-adjusted plus fish, g/d -0.005 ± 0.002 0.009 -0.006 ± 0.002 0.010 Multivariable-adjusted plus nuts, g/d -0.006 ± 0.002 0.005 -0.006 ± 0.002 0.006 Multivariable-adjusted plus red meat, g/d -0.006 ± 0.002 0.005 -0.007 ± 0.002 0.005 Multivariable-adjusted plus processed meat, g/d -0.002 ± 0.002 0.006 -0.007 ± 0.002 0.006 Multivariable-adjusted plus fibre, g/d -0.006 ± 0.002 0.006 -0.007 ± 0.002 0.008 Multivariable-adjusted plus potassium, mg/d -0.004 ± 0.002 0.035 -0.005 ± 0.002 0.056 Multivariable-adjusted plus magnesium, mg/d -0.005 ± 0.002 0.009 -0.006 ± 0.002 0.013 Multivariable-adjusted plus monounsaturated fat, g/d -0.006 ± 0.002 0.005 -0.006 ± 0.002 0.007 Multivariable-adjusted plus saturated fat, g/d -0.005 ± 0.002 0.019 -0.006 ± 0.002 0.019 Multivariable-adjusted plus vegetable-derived nitrate, mg/d -0.005 ± 0.002 0.039 -0.005 ± 0.003 0.068 Total vegetables Multivariable-adjusted plus total fruit, g/d -0.010 ± 0.005 0.035 -0.015 ± 0.006 0.008 Multivariable-adjusted plus fish, g/d -0.010 ± 0.005 0.022 -0.016 ± 0.005 0.004 Multivariable-adjusted plus nuts, g/d -0.011 ± 0.005 0.017 -0.016 ± 0.005 0.003 Multivariable-adjusted plus red meat, g/d -0.012 ± 0.005 0.008 -0.018 ± 0.005 0.001 Multivariable-adjusted plus processed meat, g/d -0.011 ± 0.005 0.018 -0.016 ± 0.005 0.003 Multivariable-adjusted plus fibre, g/d -0.013 ± 0.005 0.015 -0.018 ± 0.006 0.003 Multivariable-adjusted plus potassium, mg/d -0.006 ± 0.005 0.263 -0.010 ± 0.006 0.138 Multivariable-adjusted plus magnesium, mg/d -0.010 ± 0.005 0.034 -0.015 ± 0.006 0.008 Multivariable-adjusted plus monounsaturated fat, g/d -0.011 ± 0.005 0.017 -0.016 ± 0.006 0.003 Multivariable-adjusted plus saturated fat, g/d -0.008 ± 0.005 0.086 -0.013 ± 0.006 0.017 Multivariable-adjusted plus vegetable-derived nitrate, mg/d -0.008 ± 0.007 0.249 -0.012 ± 0.008 0.114 1Results are analysed by linear regression and are presented as unstandardized B and SE 2Multivariable-adjusted model included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, the CAIFOS supplementation group, antihypertensive agents, statin therapy, low-dose aspirin, CKD-EPI eGFR, and energy intake. CAIFOS, Calcium Intake Fracture Outcome Study; CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate.
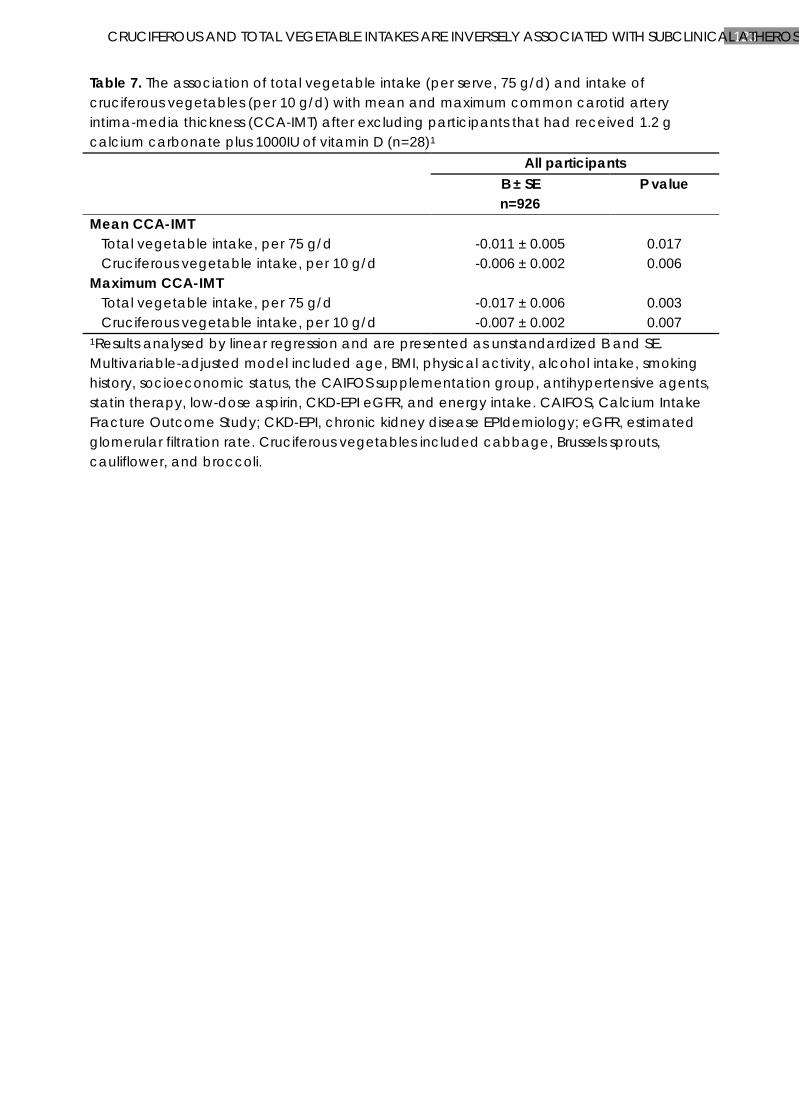
123 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROS
Table 7. The association of total vegetable intake (per serve, 75 g/d) and intake of cruciferous vegetables (per 10 g/d) with mean and maximum common carotid artery intima-media thickness (CCA-IMT) after excluding participants that had received 1.2 g calcium carbonate plus 1000IU of vitamin D (n=28)1 All participants
B ± SE n=926
P value
Mean CCA-IMT Total vegetable intake, per 75 g/d -0.011 ± 0.005 0.017 Cruciferous vegetable intake, per 10 g/d -0.006 ± 0.002 0.006 Maximum CCA-IMT Total vegetable intake, per 75 g/d -0.017 ± 0.006 0.003 Cruciferous vegetable intake, per 10 g/d -0.007 ± 0.002 0.007 1Results analysed by linear regression and are presented as unstandardized B and SE. Multivariable-adjusted model included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, the CAIFOS supplementation group, antihypertensive agents, statin therapy, low-dose aspirin, CKD-EPI eGFR, and energy intake. CAIFOS, Calcium Intake Fracture Outcome Study; CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate. Cruciferous vegetables included cabbage, Brussels sprouts, cauliflower, and broccoli.
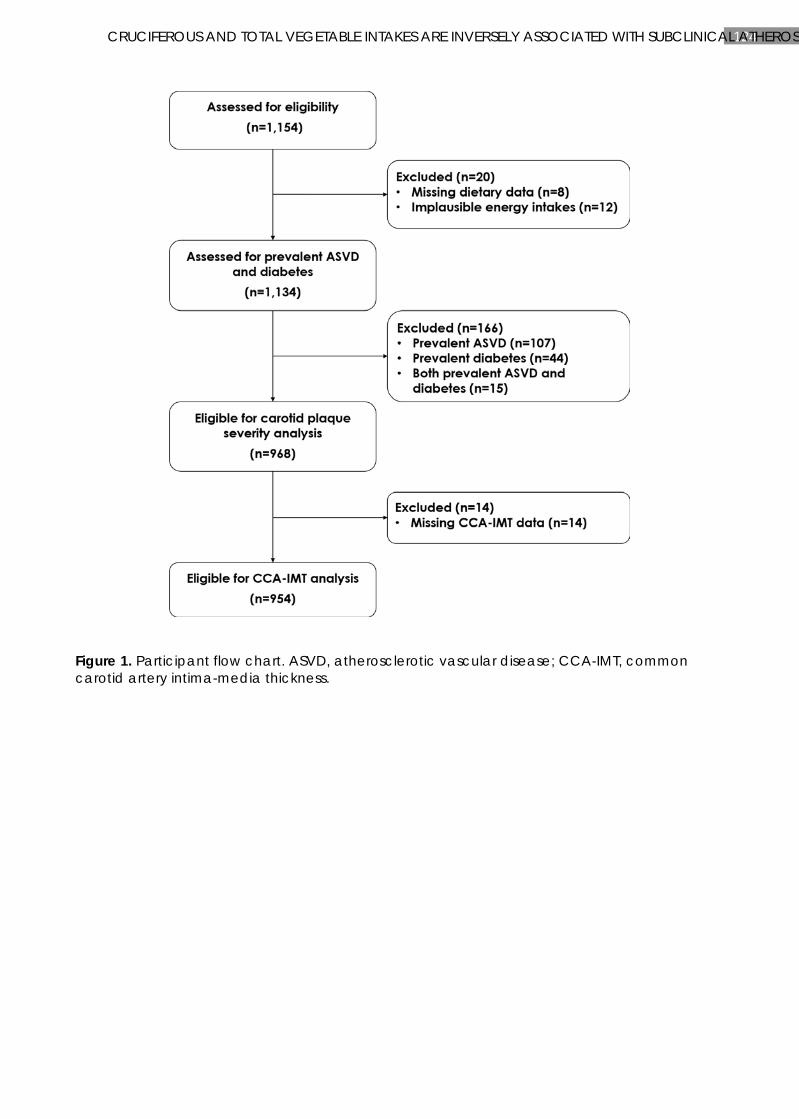
124 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROS
Figure 1. Participant flow chart. ASVD, atherosclerotic vascular disease; CCA-IMT, common carotid artery intima-media thickness.
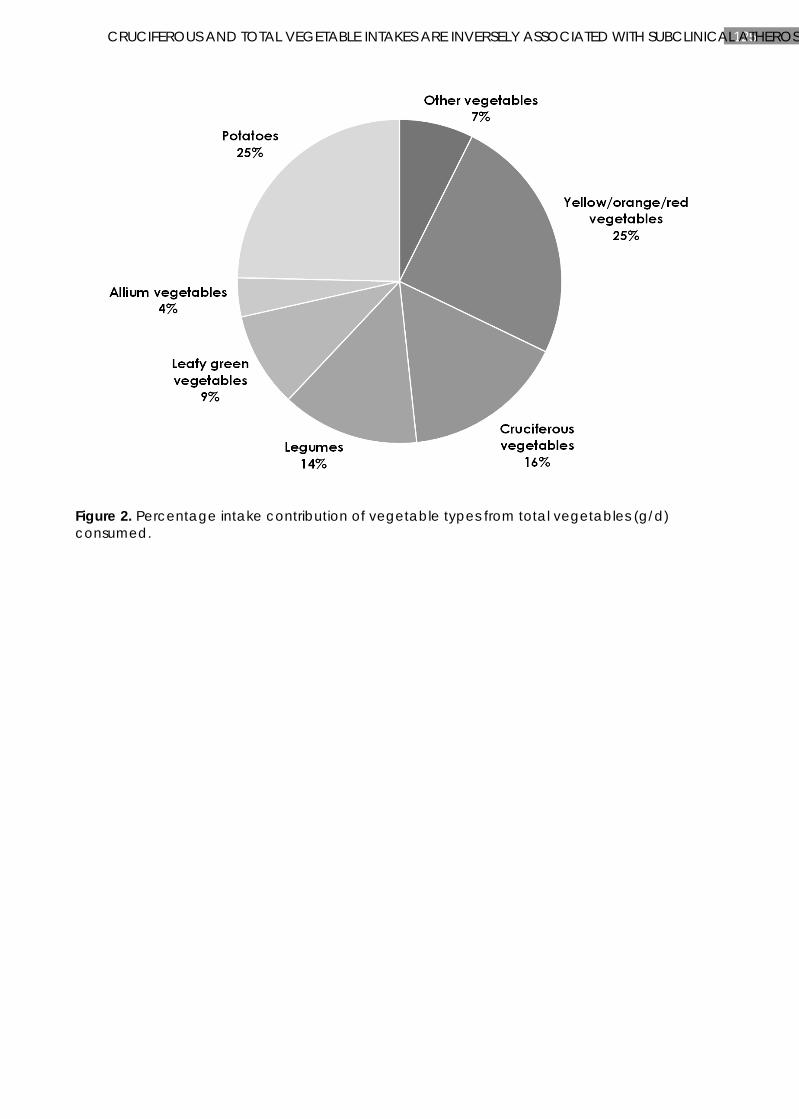
125 CRUCIFEROUS AND TOTAL VEGETABLE INTAKES ARE INVERSELY ASSOCIATED WITH SUBCLINICAL ATHEROS
Figure 2. Percentage intake contribution of vegetable types from total vegetables (g/d) consumed.
126 CHAPTER 5
CHAPTER 5
DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Manuscript based on this chapter:
Lauren C Blekkenhorst, Richard L Prince, Natalie C Ward, Kevin D Croft, Joshua R Lewis, Amanda Devine, Sujata Shinde, Richard J Woodman, Jonathan M Hodgson, Catherine P Bondonno. Development of a reference database for assessing dietary nitrate in vegetables. Molecular Nutrition & Food Research 2017;61(8):1-13.

127 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
ABSTRACT
Scope: Dietary nitrate from vegetables improves vascular health with short term intake. Whether this translates into improved long term health outcomes has yet to be investigated. To enable reliable analysis of nitrate intake from food records there is a strong need for a comprehensive nitrate content of vegetables database.
Methods and results: A systematic literature search (1980-2016) was performed using Medline, Agricola and CAB abstracts databases. The nitrate content of vegetables database contains 4237 records from 255 publications with data on 178 vegetables and 22 herbs and spices. The nitrate content of individual vegetables ranged from Chinese flat cabbage (median; range: 4240; 3004-6310 mg/kg FW) to corn (median; range: 12; 5-1091 mg/kg FW). The database was applied to estimate vegetable nitrate intake using 24-hour dietary recalls (24-HDRs) and food frequency questionnaires (FFQs). Significant correlations were observed between urinary nitrate excretion and 24-HDR (r=0.4, P=0.013); between 24-HDR and 12 month FFQs (r=0.5, P<0.001) as well as two 4 week FFQs administered 8 weeks apart (r=0.86, P<0.001).
Conclusion: This comprehensive nitrate database allows quantification of dietary nitrate from a large variety of vegetables. It can be applied to dietary records to explore the associations between nitrate intake and health outcomes in human studies.
128 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
INTRODUCTION
The understanding of the health effects of dietary nitrate has undergone a recent change. Once considered an environmental pollutant, potential carcinogen and inert end product of endogenous nitric oxide (NO) metabolism, nitrate (obtained primarily from green leafy vegetables and beetroot) is currently a candidate for the cardiovascular benefits of a vegetable-rich diet. The mechanism is via the sequential reduction of nitrate through an enterosalivary circulatory pathway to nitrite and NO, a molecule critical for cardiovascular health (142, 143, 254). NO is a potent vasodilator that plays a key role in maintaining vascular homeostasis (123). Decreased production and/or bioavailability of NO and impairment of endothelial function is a hallmark of a number of cardiovascular disorders including hypertension, atherosclerosis and ischaemic disease. Dietary nitrate, through the nitrate-nitrite-NO pathway, could preserve a healthy vasculature and enhance cardiovascular health. Indeed, over 30 randomised controlled clinical trials examining the benefits of dietary nitrate on blood pressure and vascular function have established cardioprotective benefits (310). In contrast, there is a lingering health concern about nitrate intake and cancer. This is due to the possible formation of carcinogenic N-nitroso compounds when ingested with an amine source. The International Agency for Research on Carcinogenicity (IARC) determined that “ingested nitrate or nitrite under conditions that result in endogenous nitrosation is probably carcinogenic to humans” (250). However, this reaction is inhibited in the presence of antioxidant compounds such as polyphenols, vitamins C and E, which are found in vegetables (311-313). While estimates of the nitrate content of foods, including vegetables, have been generated for observational epidemiology studies in Spain (243) and the US (244, 245), there is a strong need for an accurate, comprehensive and up-to-date database to assess the role of dietary nitrate from vegetables with long term health benefits and risks in multi-national observational studies.
Dietary nitrate is predominantly found in vegetables accounting for ~80% of total nitrate intake (131). Vegetables such as beetroot, lettuce, rocket and spinach are rich in nitrate while other vegetables, such as peas, potato and tomato, contain nitrate at lower concentrations (158). In addition to the effects of different plant species, other factors are recognised as having an effect on nitrate content. These include climate; growing method (for example, open-air vs undercover); cooking and preservation methods; month, season and year of cultivation; and the analytical procedure used to assess nitrate concentration (314-317). There is currently no database in the public or commercial arena that has systematically collected information on the measured nitrate concentration of vegetables including details on factors known to affect nitrate concentration. Such a database will allow for improved estimation of nitrate intake. This is important to determine the relationship between nitrate intake from vegetables and long-term health outcomes in different populations, the next critical step in dietary nitrate research. The standardisation and improved estimation of nitrate intake would lead to increased power to detect nitrate-health outcome relationships in both observational studies and randomised controlled trials. This approach is also vital for developing reference vegetable nitrate intakes that potentially could be included in dietary guidelines.
Here we present details on the construction of a nitrate database that is a systematic, comprehensive evaluation and collation of the currently available data on the nitrate content of vegetables, herbs and spices. For each record in the database, biological (vegetable type, strain or cultivar), environmental/ agricultural (growing method, month, season and year of sampling and country), processing (cooking method and preservation method) and
129 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
measurement information (including variance, sample size and analytical method) is provided where available along with a complete literature citation. In order to highlight the potential utility of the nitrate database, as well as provide an example of the complexities of the variables that can affect nitrate content, the influence of growing method, season and cultivar on the nitrate content of lettuce was investigated. Finally, we used the database to assess the relationship between urinary nitrate excretion and estimated vegetable nitrate intake from 24-hour dietary recalls (24 HDR) in a group of men and women. We also assessed the correlations of vegetable nitrate intake between 24-HDR and 12 month food frequency questionnaires (FFQ) as well as two 4 week FFQs administered 8 weeks apart.
METHODS
Database development
Data collection
A systematic literature search was conducted according to the PRISMA 2009 Statement (Figure 1). Medline, Agricola and CAB (Commonwealth Agricultural Bureaux) abstracts were the major databases searched from January 1980 to January 2016. Key search terms (Supplementary Table 1), comprising subject headings and text words, included nitrate, nitrite, vegetables, food analysis, individual vegetable names and combinations of the listed terms. All searches were fully documented including search terms, search limits and the number of references found. Reports from government agencies were searched in Google Scholar and government agency websites. Additional studies were identified by searching reference lists of reviews and meta-analyses. References were imported into an Endnote® X7.0 (Thomson Reuters) library.
Data evaluation and selection
Titles and abstracts of the imported references were reviewed after the duplicates were removed. Full papers were collected for those meeting the following inclusion criteria: 1) they were published in English; 2) they were published between January 1980 – January 2016; and 3) they reported nitrate and/or nitrite concentration in vegetables. The full-text articles were subsequently assessed for eligibility by two study authors (LB and CB). Disagreement about study inclusion was resolved by consensus between two authors (LB and CB) and further discussion with a third (JH) if necessary. Articles were excluded if 1) the nitrate and/or nitrite concentration was not provided or was unclear; 2) they reported an experimental study with no control or the data was reported under conditions of agricultural practice not conventionally used; 3) they were a nitrate and/or nitrite analysis method development paper with no validated reference method as a comparison; 4) the nitrate and/or nitrite concentrations were measured in vegetables prior to 1980; 5) the nitrate and/or nitrite concentrations were measured during growth of the vegetable prior to harvesting, in an inedible part of the vegetable, in an unknown vegetable or was not assessed in individual vegetables; and 6) the data in the article was compiled or part of a review (Table 1). Articles containing compiled data were used if the original source was not available or was not published in English.
Data compilation
Information on vegetables, sampling, measurement and publication were manually entered into a Microsoft Excel Spreadsheet. The database comprises four main sections:
130 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
1) Vegetable information. This section contains the vegetable name, Latin name, common alternate names, cultivar (if known), cooking method, preservation method and growing method. The codes used are detailed in Supplementary Table 2.
2) Sampling information. This section details month (if available), season (if available), year of sample (if available) and source of data (direct or compiled).
3) Measurement information. This section contains the nitrate and/or nitrite value as mg/kg (the relevant conversions were performed when necessary), type of value (mean, median), variance (SD, SE and/or range), sample size (if reported as a range the lowest number was used; if no sample size was reported or the sample size was unclear then a sample size of 1 was entered) and analytical method.
4) Publication information. This section includes year of publication, authors, title, country and type of publication.
Application of the database to estimate nitrate intake from vegetables
Participants
Participants were recruited by newspaper advertisement from the Perth general population for participation in a clinical trial investigating the effects of nitrate intake from vegetables on blood pressure. This trial was registered on the Australian New Zealand Clinical Trials Registry at www.anzctr.org.au (#ACTRN12615000194561) and ethics approval was obtained from the University of Western Australia Human Research Ethics Committee (RA/4/1/6872). For the purpose of assessing the nitrate database 41 participants consented to complete a FFQ, a 24 hour diet recall (24-HDR) and provide a spot urine sample. Of these participants, 30 also agreed to complete two identical 4 week FFQs 8 weeks apart. Screening was conducted at the University of Western Australia, School of Medicine and Pharmacology Unit, located at Royal Perth Hospital and consisted of a standard health and lifestyle questionnaire, blood pressure measurement, height and weight as well as routine laboratory analysis of a fasting blood sample. Exclusion criteria included: BMI <18.5 kg/m2 or ≥35 kg/m2; age <21 or >75 years; use of antihypertensive medication; diagnosed type 1 or 2 diabetes or fasting glucose >7.0mmol/L; being vegan or vegetarian; use of nitric oxide donors, organic nitrites and nitrates, sildenafil and/or related drugs; use of antibacterial mouthwash; use of antibiotics (with previous 2 months); current or recent (<12 months) smoking; history of symptomatic cardiovascular or peripheral vascular disease, or chronic kidney disease; recent history of a psychiatric illness or other major illness such as cancer; current or recent (within previous 6 months) significant weight loss or gain (>6% of body weight); alcohol intake >140 g per week for women or >210 g per week for men and/or binge drinking behavior; and women who were pregnant, lactating or wishing to become pregnant during the study.
Urine collection
Participants were instructed to collect a spot urine sample the night before their first visit, 60 to 120 minutes after consumption of their last meal of the day. The time of the sample collection was noted and the sample stored at 4ºC overnight.
131 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
24-hour diet recalls
At the first visit participants (n=41) were asked to recall in detail all foods and beverages consumed during the last 24 hours from the time they were interviewed. Emphasis on all vegetables consumed during this period was given. Participants were assisted in recalling portion size of foods and beverages consumed by using food models, photographs, charts, measuring cups and measuring spoons. Vegetable data was extracted from the 24-HDRs and then entered into FoodWorks (FoodWorks 7; Xyris Software) for the calculation of weight in grams. Individual vegetables (g) were then multiplied by the median nitrate content (mg/g) of that vegetable obtained from the nitrate content of vegetables database. The sum of nitrate values from individual vegetables was then calculated.
Food frequency questionnaires
At the first visit, participants (n=41) were also asked to complete a self-administered validated semi-quantitative FFQ developed by the Cancer Council Victoria, Australia (263). This validated FFQ measures the usual frequency of food intake over a period of 12 months and comprises of a food list of 74 items with 10 frequency response options ranging from 'Never' to '3 or more times per day'. The questionnaire calculates portion size using three photographs of scaled portions for four different food types. The process of collection was identical and was supervised by a research assistant/registered nutritionist. Food models, photographs, charts, measuring cups and measuring spoons were provided for accuracy. The FFQ included questions about vegetable intake on 25 vegetables. The Cancer Council of Victoria estimated daily intake of these vegetables in g/day. Each of the weights (g) of the 25 vegetables were multiplied by the median nitrate value (mg/g) of that vegetable. The sum of the nitrate values from individual vegetables was then calculated. A subset of these participants (n=30) also agreed to complete two identical modified versions of the Cancer Council of Victoria FFQ administered 8 weeks apart which assessed dietary intake over the previous 4 weeks instead of 12 months. These FFQs were administered during periods where participants were instructed to limit their intake of green leafy vegetables.
Urine nitrate, nitrite and creatinine
Nitrate and nitrite concentrations in urine were determined in frozen samples using gas chromatography-mass spectrometry (GC-MS) described previously (318). Urinary creatinine measurements were performed by the Department of Clinical Biochemistry at Royal Perth Hospital using a kinetic colorimetric test (Roche, Indianapolis, IN) with an automated analyzer (Roche Hitachi 917).
Statistics
Descriptive statistics including number, mean (SD), median (IQR), minimum and maximum were used to summarise country of sample and individual vegetables. A large proportion of distributions of nitrate values in individual vegetables were not normally distributed therefore both mean and median values were used to describe the nitrate content (mg/kg FW) in Table 2 and 3.
The magnitude of the effect of factors known to potentially influence nitrate content was assessed in lettuce. Nitrate content of lettuce was log-transformed prior to all analyses due to its
132 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
non-normality. Linear mixed models were used in unadjusted and publication ID (a unique number for each publication) adjusted models to investigate the differences of nitrate content amongst growing method (organic vs conventional and undercover vs open air), season and lettuce type. Publication ID was entered as a random factor treating each publication as a separate category rather than as a continuous covariate. This was used to adjust for variation in country, year and method of analysis. Bonferroni method was used to correct for multiple comparisons across categories.
Spearman’s rho correlation coefficient was used to assess the linear relationship between urinary nitrate excretion and vegetable nitrate intake calculated from the 24-HDR (n=41). Agreement in estimated nitrate intake between the 24-HDR and the 12 month FFQ was assessed using Bland & Altman analysis (1986) (n=41). A paired t-test was used to evaluate the presence of fixed bias between methods. We also calculated the intraclass correlation coefficient (ICC) using a one way ANOVA with method of assessment (24-HDR or 12 month FFQ) and participant ID as fixed effects. The Pearson correlation coefficient (r) was used to assess the degree of linearity between the 2 methods. Spearman’s rho correlation coefficient was used to assess the agreement between two 4 week FFQs administered 8 weeks apart (n=30). Statistical analyses were performed using SPSS v22 (SPSS Inc., Chicago, United States of America); SAS software (version 9.3; SAS Institute Inc); and STATA 14 (StataCorp, USA). Statistical significance was set at p<0.05 for all tests.
RESULTS
Nitrate content of vegetables database
The Prisma flow chart showing the selection of included studies is shown in Figure 1. The database contains a total 4237 records, searched from January 1980 to January 2016, sourced from 255 references and includes data on 178 vegetables as well as 22 herbs and spices. The database contains information of the nitrate content of vegetables from 54 countries with a range of 1 - 553 entries per country and 1 - 51 vegetables per country (Supplementary Table 3). Information on cooking, preservation and growing method, month, season and year of sampling as well as analytical method and sample size were recorded where available.
The mean (SD), median (IQR), minimum and maximum nitrate content (mg/kg FW) as well as sample size and number of publications for individual vegetables (raw and fresh) with at least 3 publications are presented in Table 2. The median nitrate content (mg/kg FW) of individual vegetables with at least 3 publications from highest (Chinese flat cabbage: median; range: 4240; 3004-6310 mg/kg FW) to lowest (corn: median; range: 12; 5-1091 mg/kg FW) is shown in Figure 2. The median nitrate content (mg/kg FW) of individual vegetables grouped by family name is shown in Figure 3. The Latin and alternate names of the individual vegetables presented in Table 2 are detailed in Supplementary Table 4. The mean (SD), median (IQR), minimum and maximum nitrate content (mg/kg FW) as well as sample size and number of publications for herbs and spices with at least 3 publications is presented in Table 3.
The mean (SD), median (IQR), minimum and maximum nitrite content (mg/kg FW) as well as sample size and number of publications for individual vegetables (raw and fresh) as well as herbs and spices with at least 3 publications are presented in Supplementary Tables 5 and 6 respectively.
133 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Variables influencing the nitrate content of lettuce
The nitrate concentration of organically grown lettuce was significantly lower than conventionally grown lettuce (P=0.001, Figure 4A). This difference remained significant after adjustment for publication ID (P=0.009, Figure 4B). The nitrate concentration of lettuce grown undercover was significantly higher than lettuce grown open air (P<0.001, Figure 4C). This difference remained significant after adjustment for publication ID (P<0.001, Figure 4D).
The nitrate concentration of lettuce was significantly different among seasons in both unadjusted (Figure 5A) and publication ID adjusted (Figure 5B) models, with the exception of autumn vs. spring (both models) and summer vs. autumn (publication ID adjusted model) which was not significantly different from one another. The lowest nitrate concentration was observed in summer and the highest in winter.
The nitrate concentration varied widely between lettuce types in both unadjusted (Figure 6A) and publication ID adjusted (Figure 6B) models. The highest nitrate content was observed in Chinese lettuce and the lowest in Iceberg lettuce.
Application of the database to estimate nitrate intake from vegetables
The baseline characteristics of the participants (n=41) are presented in Table 4. The median (IQR) urinary nitrate was 81.9 (52.8 – 120.8) µmol/mmol creatinine. The mean (±SD) nitrate intake for the 12-month FFQ and 24-HDR amongst the 41 volunteers were 71.9 ± 33.9 mg/day and 89.3 ± 64.7 mg/day respectively. The mean (±SD) nitrate intake for the two 4 week FFQs, 30 volunteers on a low nitrate diet, administered 8 weeks apart were 45.6 ± 26.8 mg/day and 41.4 ± 40.36 mg/day. There was a positive correlation between urinary nitrate and 24-HDR (r=0.4, P=0.013), a positive correlation between 24-HDR and the 12 month FFQ (r=0.5, P<0.001; Figure 7A) and a positive correlation between the two 4 week FFQs administered 8 weeks apart (r=0.9, P<0.001). Bland Altman analysis and the paired t-test revealed a borderline significant fixed bias with the 12 month FFQ measuring 17.4 mg lower mean nitrate intake (mg/day) (95% CI: -35.9; 1.2, P=0.054) than the 24-HDR. The lower and upper limits of agreement for FFQ versus 24-HDR were -136.2 to +101.4 (Figure 7B). The ICC for reliability estimated from one-way ANOVA was ρ=0.38 (95% CI=0.12 to 0.65).
DISCUSSION
Here we present an up-to-date database of the nitrate content of vegetables. The key strength of this database is the systematic and comprehensive search of currently available literature that has provided important information on the nitrate content of a wide variety of vegetables as well as influencing factors: biological (vegetable type, strain or cultivar); environmental/ agricultural (growing method, month, season and year of sampling and country); processing (cooking method and preservation method); and measurement information (including analytical method). We have highlighted the potential complexities of some of these variables that can affect nitrate content by demonstrating that the nitrate content of lettuce differed significantly between organically and conventionally grown; between undercover and open-air; and across seasons. We have also shown that the database can be used to estimate vegetable nitrate intake as measured by 24-HDRs and FFQs with reasonable consistency.
134 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
The nitrate content of vegetables database is an important tool in better understanding the relationship between nitrate intake from vegetables and health outcomes. It provides reliable values for vegetable nitrate concentrations that can be used in conjunction with other databases to calculate nutrient and non-nutrients from FFQs and/or dietary food records in randomised controlled trials and/or large epidemiological studies. This provides a unique opportunity for researchers to assess the benefits and possible risks of nitrate intake in different populations. The measured nitrate concentration from different countries will allow values to be either generalized or specifically selected to determine nitrate intake. Additionally, the database will increase understanding of factors related to variation of nitrate concentration in vegetables.
Vegetable nitrate content depends on the biological properties of the plant. Nitrate accumulates differently in each part of the plant which can be listed in decreasing order of nitrate content as follows: petiole>leaf>stem>root>inflorescence>tuber>bulb>fruit>seed (131). In our database, green leafy vegetables had the greatest concentration of nitrate with the highest nitrate values observed in Chinese flat cabbage and arugula (> 3000 mg/kg FW). Indeed, all vegetables with a nitrate concentration > 2000 mg/kg FW were green leafy vegetables. Among the stem vegetables, celery had the highest nitrate concentration (> 1000 mg/kg FW). Root vegetables that had the highest nitrate concentration were radish, rutabago, and beet (> 1400 mg/kg FW). Vegetables with a concentration of nitrate > 2000 mg/kg FW belonged to three families: Brassicaceae (Chinese flat cabbage, arugula, false pak-choi, mustard greens, potherb mustard, pak choi, Chinese broccoli and watercress), Amaranthaceae (Swiss chard and sea beet) and Valerianaceae (cornsalad). Nitrate content, however, varied considerably within each family. Nitrate concentration not only varied between vegetable types but also within species, cultivars and even genotype. For example, Chinese lettuce had a 3-fold higher median nitrate content than iceberg lettuce. Where known, details of species and cultivar have been included in the database. Cilantro and basil had the highest nitrate concentration in the herbs and spices (> 1500 mg/kg FW) but given that only a small amount is generally consumed, may not contribute significantly to nitrate intake.
In addition to the biological properties of the vegetable, the accumulation of nitrate is subject to environmental and/or agricultural factors. Fertilizer use, light intensity and temperature have been identified as the major factors that influence nitrate concentration in vegetables (316, 319, 320). Application of fertilizers, in particular nitrogen fertilizers, facilitates the accumulation of nitrate in plant tissues. Thus, conventionally grown vegetables tend to have a higher nitrate content compared to organically grown crops (321, 322). In our database, conventionally grown lettuce had a significantly higher nitrate concentration compared to organically grown lettuce. Light intensity and temperature play a crucial role in nitrate assimilation and variations in nitrate levels are observed in the same vegetable grown in different geographic and climatic conditions (320, 323). Nitrate levels tend to be higher in samples from Northern Europe than those from Mediterranean countries. Additionally, higher nitrate levels are generally observed in winter than in summer and nitrate content in vegetables grown under glass are usually higher than in those grown outdoors in the same season and the same region (324). These differences are recognised by the European Commission (EC Regulation No. 1881/2006) who set maximum limits for the nitrate content in lettuce and spinach according to harvest period and whether grown under cover or grown in open air. Indeed, in our database lettuce grown in winter had the highest nitrate concentration, as did lettuce grown undercover. Growing and preservation
135 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
method, month, season and year of sampling and country of sampling are all included (where available) in the database, therefore researchers have the option of selecting the data relevant to the area and time frame being investigated.
Processing factors also have an effect on the nitrate concentration of vegetables. Nitrates are water-soluble therefore, washing and cooking has been shown to decrease the nitrate content of the vegetable (325-327). Boiling vegetables can reduce the nitrate content up to 75% (325-327); however, information regarding the effect of other cooking methods (microwaving, steaming, frying etc.) is limited. Pickling vegetables can reduce the nitrate content by approximately 45%. In the current database vegetables that have not been analysed as raw and fresh, cooking and preservation methods have been included. Other processing factors influencing the nitrate content of vegetables include storage time and conditions as well as peeling of the vegetables. Storage, particularly at room temperature, can reduce the nitrate content of fresh vegetables possibly due to the action of endogenous nitrate reductases or bacterial contamination (328). Peeling of certain vegetables, for example potatoes, can significantly reduce the nitrate content as the highest concentration is found in and just below the skin (328, 329). Information regarding peeling and storage were not found in the references obtained and thus were not included in this database.
There are several analytical methods for the determination of nitrate in vegetables (330). The best method for nitrate determination in vegetable samples is considered the automated colorimetric method with reduction with cadmium. Other methods include nitrate-selective electrodes, spectrophotometric methods, ion chromatographic methods, polarimetric methods and UV screening methods. All these methods are represented in the database; however, information regarding the degree of accuracy using these methods limited.
There is currently no reliable biomarker to assess nitrate intake. Urinary nitrate levels are affected by the L-arginine-NO synthase pathway as well as dietary nitrate intake, with approximately 70% of dietary nitrate consumed excreted in urine within 24 hours of consumption (331) . Urinary nitrate may provide an indication of short-term intake but may not be good indicator of long-term nitrate intake because of variability in dietary nitrate intake across days. The 24-HDR captured vegetable nitrate intake in the previous 24 hours and the low positive correlation with urinary nitrate is consistent with levels being affected by different endogenous metabolic pathways. While 24-HDRs are recognised as being a more accurate method of assessing dietary intake for most nutrients, large cohort studies usually rely on FFQs as they are cost-effective, quick and easy to administer and are more likely to provide better estimates of nutrient intakes over the long term. In this current study, we have demonstrated a moderate positive correlation between nitrate intakes calculated from 24 HDRs and 12 month FFQs. This correlation is consistent with other nutrient intake method-comparison studies (332). We also observed a strong positive correlation between two 4 week FFQs administered 8 weeks apart demonstrating good reproducibility.
CONCLUSION
There is convincing evidence that intake of vegetables, specifically green leafy vegetables, are associated with positive health outcomes. Clinical trials show that nitrate could be a major cardioprotective component of green leafy vegetables. In light of the new evidence of a potential positive association between dietary nitrate and health outcomes and the lingering

136 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
concern about nitrate and risk of cancer, this comprehensive and up-to-date database of the nitrate content of vegetables presented here will be a timely and invaluable tool for researchers. It allows quantification of dietary nitrate from a comprehensive list of vegetables that can be used to examine the association between nitrate intake and health outcomes in observational studies in which nitrate content is assessed based on recorded food intake and dietary intake recall surveys. These studies are the next critical step in dietary nitrate research and, together with results from randomised controlled clinical trials, could ultimately lead to the development of reference vegetable nitrate intakes that could be included in dietary guidelines.

137 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Table 1. Summary of full-text articles excluded (n=442)
Reasons for exclusion Number of articles
Nitrate and/or nitrite concentration was not provided or was unclear 114 Experimental study with no control or a control not used in normal agricultural practice
204
Nitrate and/or nitrite analysis method development paper with no validated reference method as a comparison
22
Nitrate and/or nitrite concentration measured prior to 1980 4 Nitrate and/or nitrite concentration measured during growth of the vegetables prior to harvesting, in an inedible part of the vegetable, in an unknown vegetable or was not assessed in individual vegetables
57
Compiled data or part of a review 41
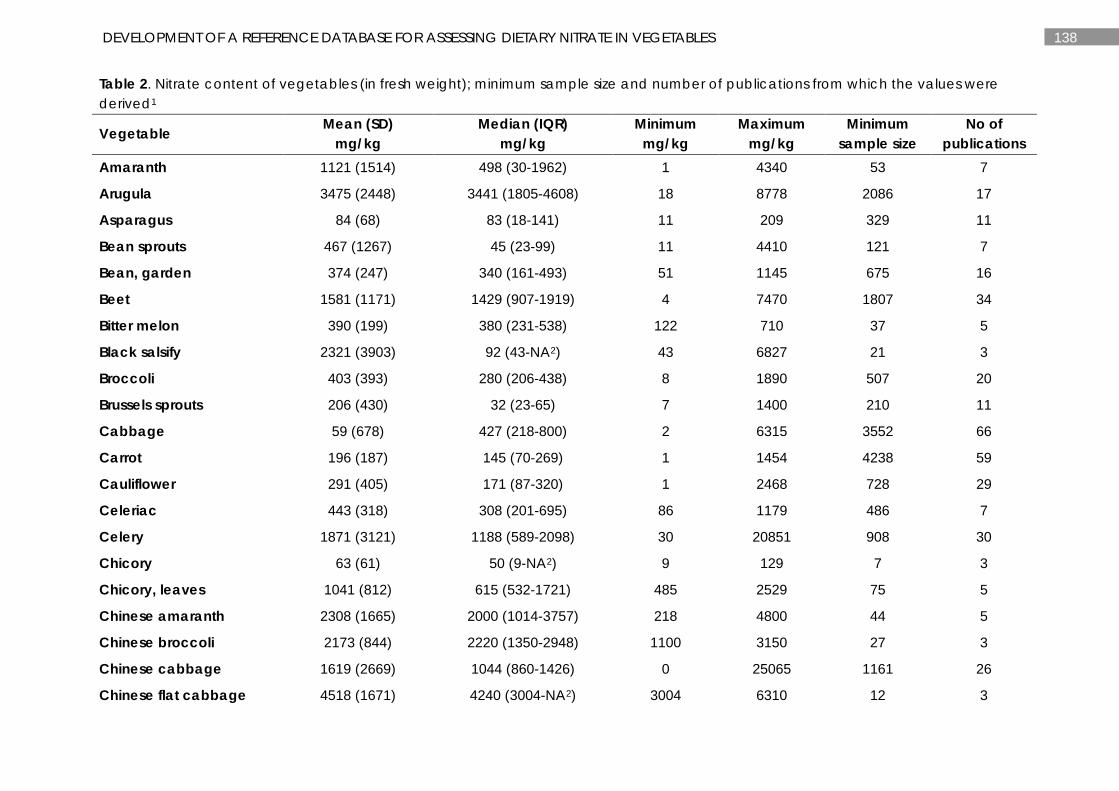
138 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Table 2. Nitrate content of vegetables (in fresh weight); minimum sample size and number of publications from which the values were derived1
Vegetable Mean (SD) mg/kg
Median (IQR) mg/kg
Minimum mg/kg
Maximum mg/kg
Minimum sample size
No of publications
Amaranth 1121 (1514) 498 (30-1962) 1 4340 53 7
Arugula 3475 (2448) 3441 (1805-4608) 18 8778 2086 17
Asparagus 84 (68) 83 (18-141) 11 209 329 11
Bean sprouts 467 (1267) 45 (23-99) 11 4410 121 7
Bean, garden 374 (247) 340 (161-493) 51 1145 675 16
Beet 1581 (1171) 1429 (907-1919) 4 7470 1807 34
Bitter melon 390 (199) 380 (231-538) 122 710 37 5
Black salsify 2321 (3903) 92 (43-NA2) 43 6827 21 3
Broccoli 403 (393) 280 (206-438) 8 1890 507 20
Brussels sprouts 206 (430) 32 (23-65) 7 1400 210 11
Cabbage 59 (678) 427 (218-800) 2 6315 3552 66
Carrot 196 (187) 145 (70-269) 1 1454 4238 59
Cauliflower 291 (405) 171 (87-320) 1 2468 728 29
Celeriac 443 (318) 308 (201-695) 86 1179 486 7
Celery 1871 (3121) 1188 (589-2098) 30 20851 908 30
Chicory 63 (61) 50 (9-NA2) 9 129 7 3
Chicory, leaves 1041 (812) 615 (532-1721) 485 2529 75 5
Chinese amaranth 2308 (1665) 2000 (1014-3757) 218 4800 44 5
Chinese broccoli 2173 (844) 2220 (1350-2948) 1100 3150 27 3
Chinese cabbage 1619 (2669) 1044 (860-1426) 0 25065 1161 26
Chinese flat cabbage 4518 (1671) 4240 (3004-NA2) 3004 6310 12 3
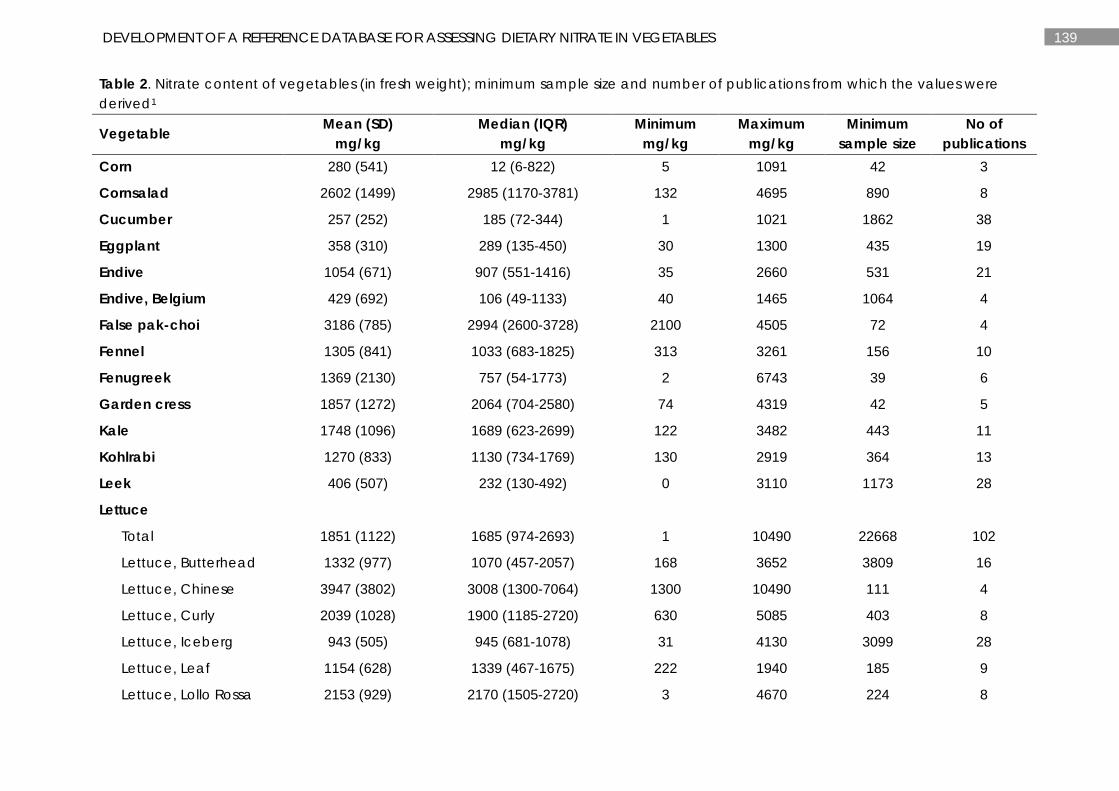
139 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Table 2. Nitrate content of vegetables (in fresh weight); minimum sample size and number of publications from which the values were derived1
Vegetable Mean (SD) mg/kg
Median (IQR) mg/kg
Minimum mg/kg
Maximum mg/kg
Minimum sample size
No of publications
Corn 280 (541) 12 (6-822) 5 1091 42 3
Cornsalad 2602 (1499) 2985 (1170-3781) 132 4695 890 8
Cucumber 257 (252) 185 (72-344) 1 1021 1862 38
Eggplant 358 (310) 289 (135-450) 30 1300 435 19
Endive 1054 (671) 907 (551-1416) 35 2660 531 21
Endive, Belgium 429 (692) 106 (49-1133) 40 1465 1064 4
False pak-choi 3186 (785) 2994 (2600-3728) 2100 4505 72 4
Fennel 1305 (841) 1033 (683-1825) 313 3261 156 10
Fenugreek 1369 (2130) 757 (54-1773) 2 6743 39 6
Garden cress 1857 (1272) 2064 (704-2580) 74 4319 42 5
Kale 1748 (1096) 1689 (623-2699) 122 3482 443 11
Kohlrabi 1270 (833) 1130 (734-1769) 130 2919 364 13
Leek 406 (507) 232 (130-492) 0 3110 1173 28
Lettuce
Total 1851 (1122) 1685 (974-2693) 1 10490 22668 102
Lettuce, Butterhead 1332 (977) 1070 (457-2057) 168 3652 3809 16
Lettuce, Chinese 3947 (3802) 3008 (1300-7064) 1300 10490 111 4
Lettuce, Curly 2039 (1028) 1900 (1185-2720) 630 5085 403 8
Lettuce, Iceberg 943 (505) 945 (681-1078) 31 4130 3099 28
Lettuce, Leaf 1154 (628) 1339 (467-1675) 222 1940 185 9
Lettuce, Lollo Rossa 2153 (929) 2170 (1505-2720) 3 4670 224 8
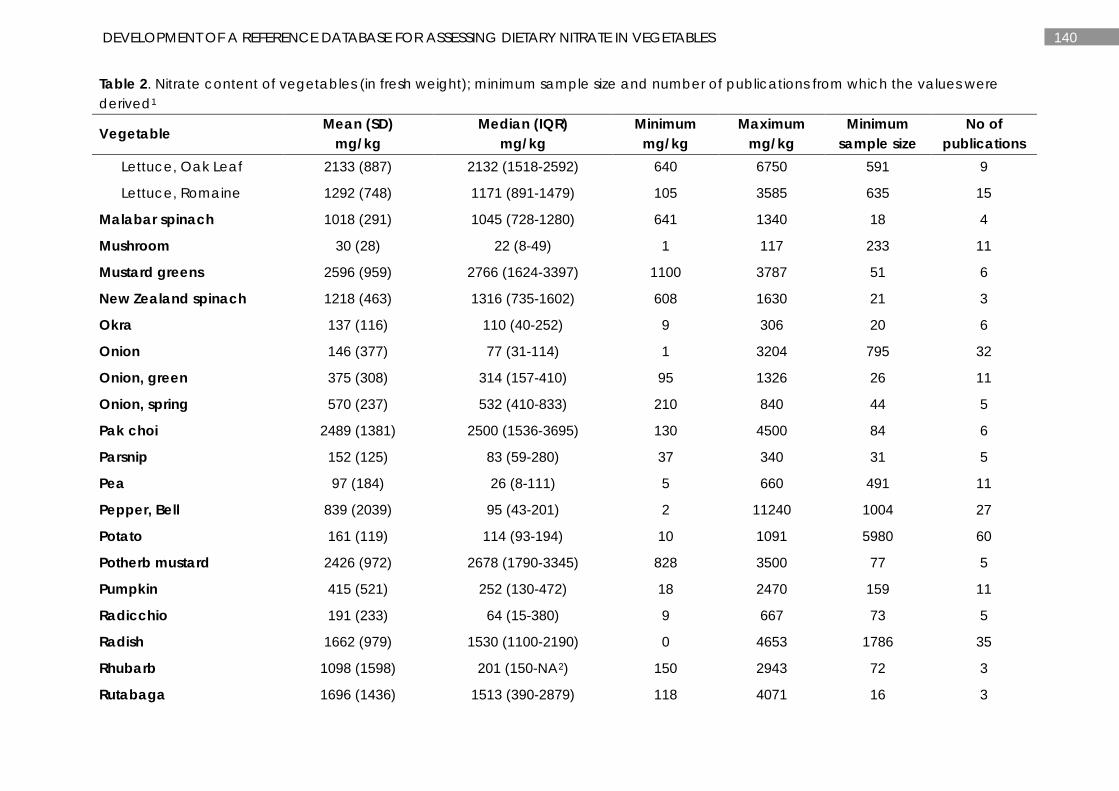
140 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Table 2. Nitrate content of vegetables (in fresh weight); minimum sample size and number of publications from which the values were derived1
Vegetable Mean (SD) mg/kg
Median (IQR) mg/kg
Minimum mg/kg
Maximum mg/kg
Minimum sample size
No of publications
Lettuce, Oak Leaf 2133 (887) 2132 (1518-2592) 640 6750 591 9
Lettuce, Romaine 1292 (748) 1171 (891-1479) 105 3585 635 15
Malabar spinach 1018 (291) 1045 (728-1280) 641 1340 18 4
Mushroom 30 (28) 22 (8-49) 1 117 233 11
Mustard greens 2596 (959) 2766 (1624-3397) 1100 3787 51 6
New Zealand spinach 1218 (463) 1316 (735-1602) 608 1630 21 3
Okra 137 (116) 110 (40-252) 9 306 20 6
Onion 146 (377) 77 (31-114) 1 3204 795 32
Onion, green 375 (308) 314 (157-410) 95 1326 26 11
Onion, spring 570 (237) 532 (410-833) 210 840 44 5
Pak choi 2489 (1381) 2500 (1536-3695) 130 4500 84 6
Parsnip 152 (125) 83 (59-280) 37 340 31 5
Pea 97 (184) 26 (8-111) 5 660 491 11
Pepper, Bell 839 (2039) 95 (43-201) 2 11240 1004 27
Potato 161 (119) 114 (93-194) 10 1091 5980 60
Potherb mustard 2426 (972) 2678 (1790-3345) 828 3500 77 5
Pumpkin 415 (521) 252 (130-472) 18 2470 159 11
Radicchio 191 (233) 64 (15-380) 9 667 73 5
Radish 1662 (979) 1530 (1100-2190) 0 4653 1786 35
Rhubarb 1098 (1598) 201 (150-NA2) 150 2943 72 3
Rutabaga 1696 (1436) 1513 (390-2879) 118 4071 16 3
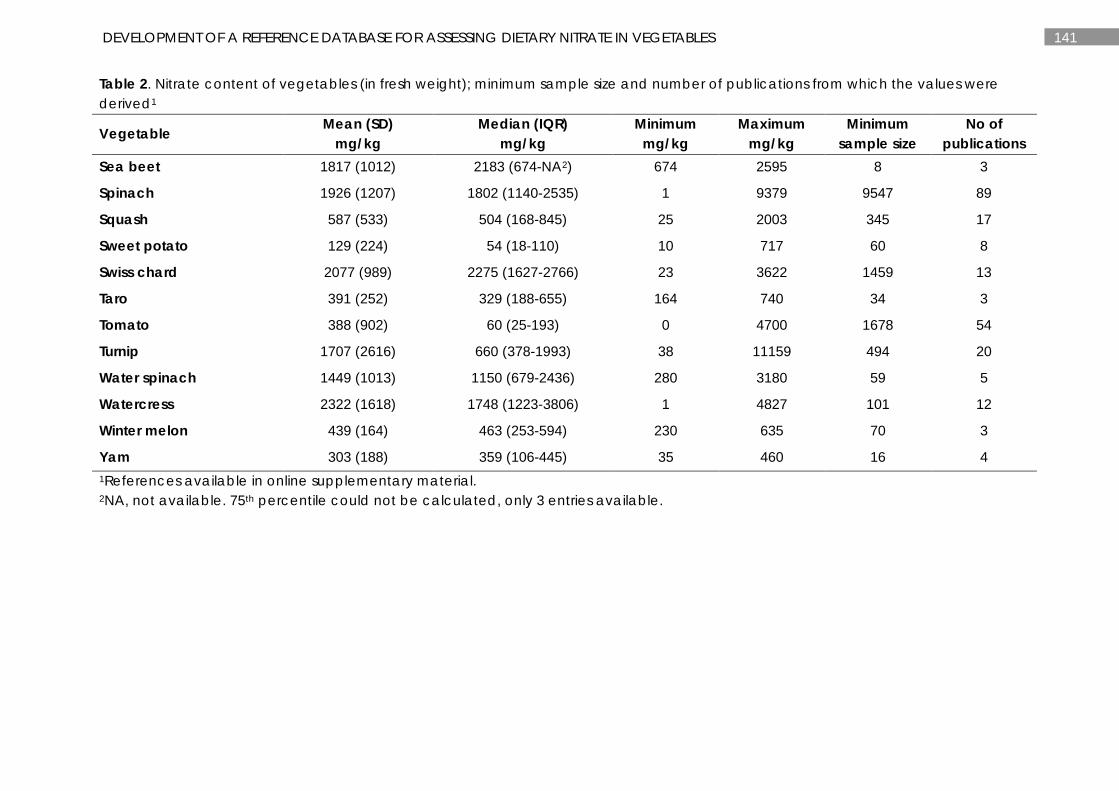
141 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Table 2. Nitrate content of vegetables (in fresh weight); minimum sample size and number of publications from which the values were derived1
Vegetable Mean (SD) mg/kg
Median (IQR) mg/kg
Minimum mg/kg
Maximum mg/kg
Minimum sample size
No of publications
Sea beet 1817 (1012) 2183 (674-NA2) 674 2595 8 3
Spinach 1926 (1207) 1802 (1140-2535) 1 9379 9547 89
Squash 587 (533) 504 (168-845) 25 2003 345 17
Sweet potato 129 (224) 54 (18-110) 10 717 60 8
Swiss chard 2077 (989) 2275 (1627-2766) 23 3622 1459 13
Taro 391 (252) 329 (188-655) 164 740 34 3
Tomato 388 (902) 60 (25-193) 0 4700 1678 54
Turnip 1707 (2616) 660 (378-1993) 38 11159 494 20
Water spinach 1449 (1013) 1150 (679-2436) 280 3180 59 5
Watercress 2322 (1618) 1748 (1223-3806) 1 4827 101 12
Winter melon 439 (164) 463 (253-594) 230 635 70 3
Yam 303 (188) 359 (106-445) 35 460 16 4 1References available in online supplementary material. 2NA, not available. 75th percentile could not be calculated, only 3 entries available.
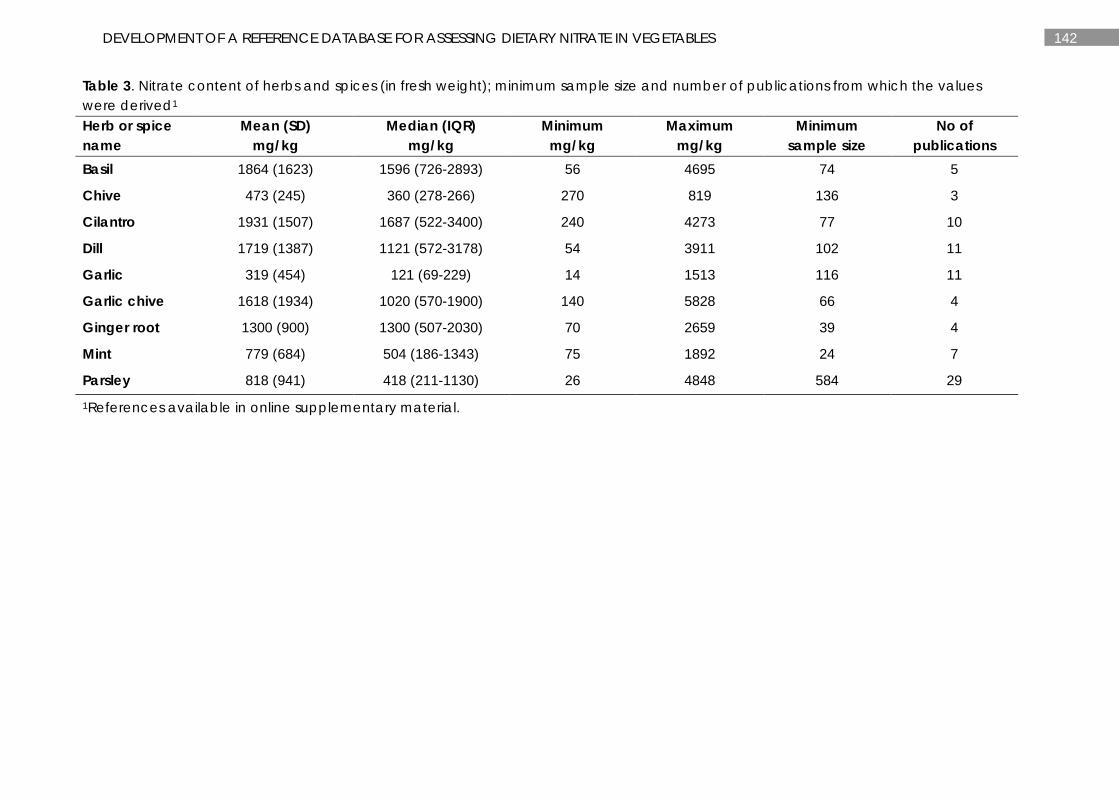
142 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Table 3. Nitrate content of herbs and spices (in fresh weight); minimum sample size and number of publications from which the values were derived1 Herb or spice name
Mean (SD) mg/kg
Median (IQR) mg/kg
Minimum mg/kg
Maximum mg/kg
Minimum sample size
No of publications
Basil 1864 (1623) 1596 (726-2893) 56 4695 74 5
Chive 473 (245) 360 (278-266) 270 819 136 3
Cilantro 1931 (1507) 1687 (522-3400) 240 4273 77 10
Dill 1719 (1387) 1121 (572-3178) 54 3911 102 11
Garlic 319 (454) 121 (69-229) 14 1513 116 11
Garlic chive 1618 (1934) 1020 (570-1900) 140 5828 66 4
Ginger root 1300 (900) 1300 (507-2030) 70 2659 39 4
Mint 779 (684) 504 (186-1343) 75 1892 24 7
Parsley 818 (941) 418 (211-1130) 26 4848 584 29 1References available in online supplementary material.
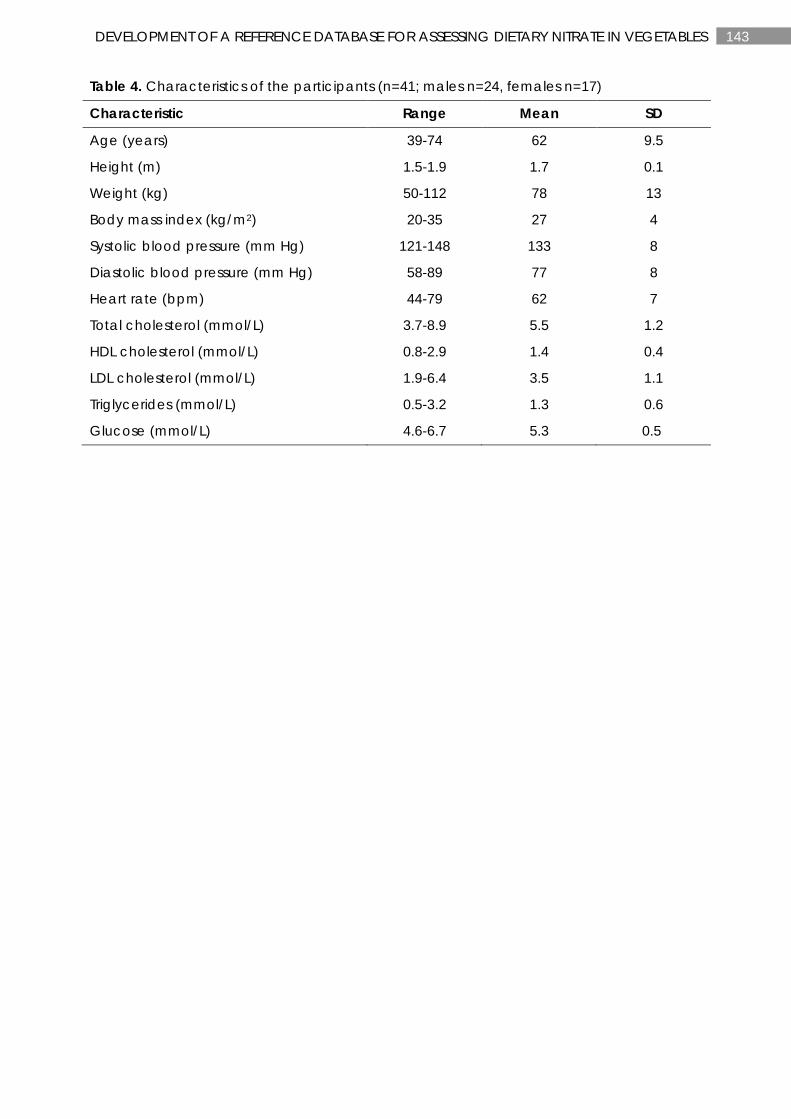
143 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Table 4. Characteristics of the participants (n=41; males n=24, females n=17)
Characteristic Range Mean SD
Age (years) 39-74 62 9.5
Height (m) 1.5-1.9 1.7 0.1
Weight (kg) 50-112 78 13
Body mass index (kg/m2) 20-35 27 4
Systolic blood pressure (mm Hg) 121-148 133 8
Diastolic blood pressure (mm Hg) 58-89 77 8
Heart rate (bpm) 44-79 62 7
Total cholesterol (mmol/L) 3.7-8.9 5.5 1.2
HDL cholesterol (mmol/L) 0.8-2.9 1.4 0.4
LDL cholesterol (mmol/L) 1.9-6.4 3.5 1.1
Triglycerides (mmol/L) 0.5-3.2 1.3 0.6
Glucose (mmol/L) 4.6-6.7 5.3 0.5
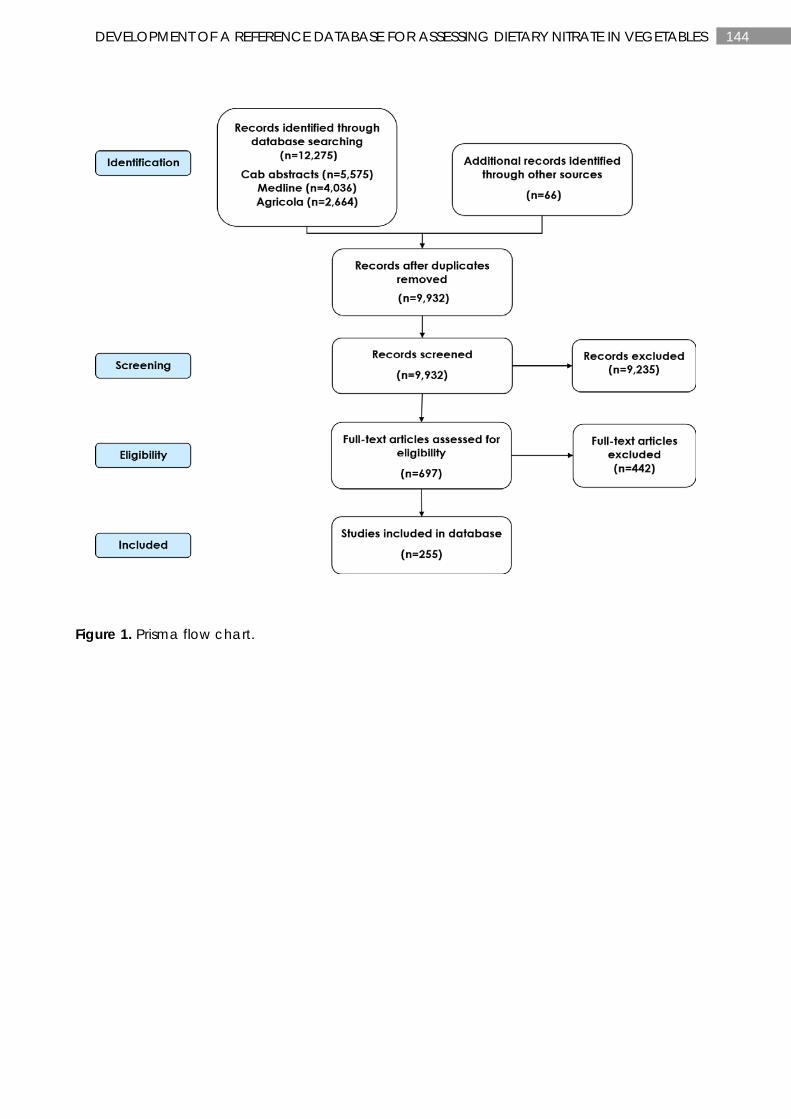
144 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Figure 1. Prisma flow chart.
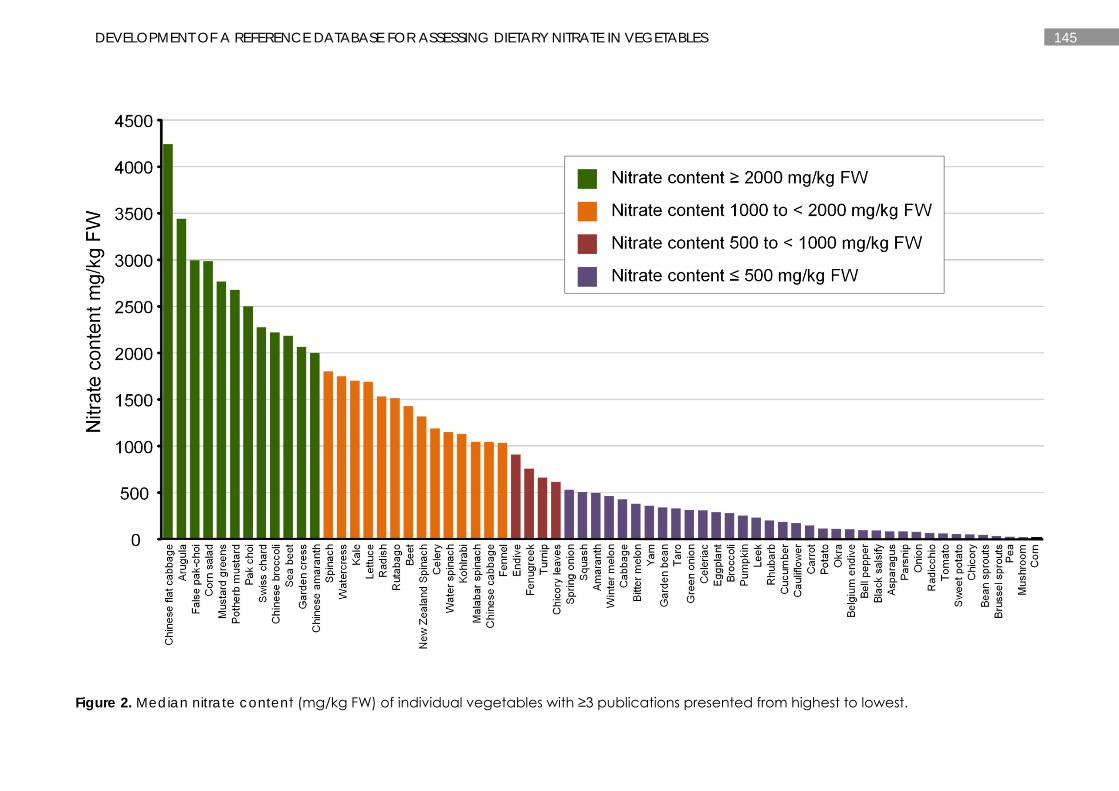
145 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Figure 2. Median nitrate content (mg/kg FW) of individual vegetables with ≥3 publications presented from highest to lowest.
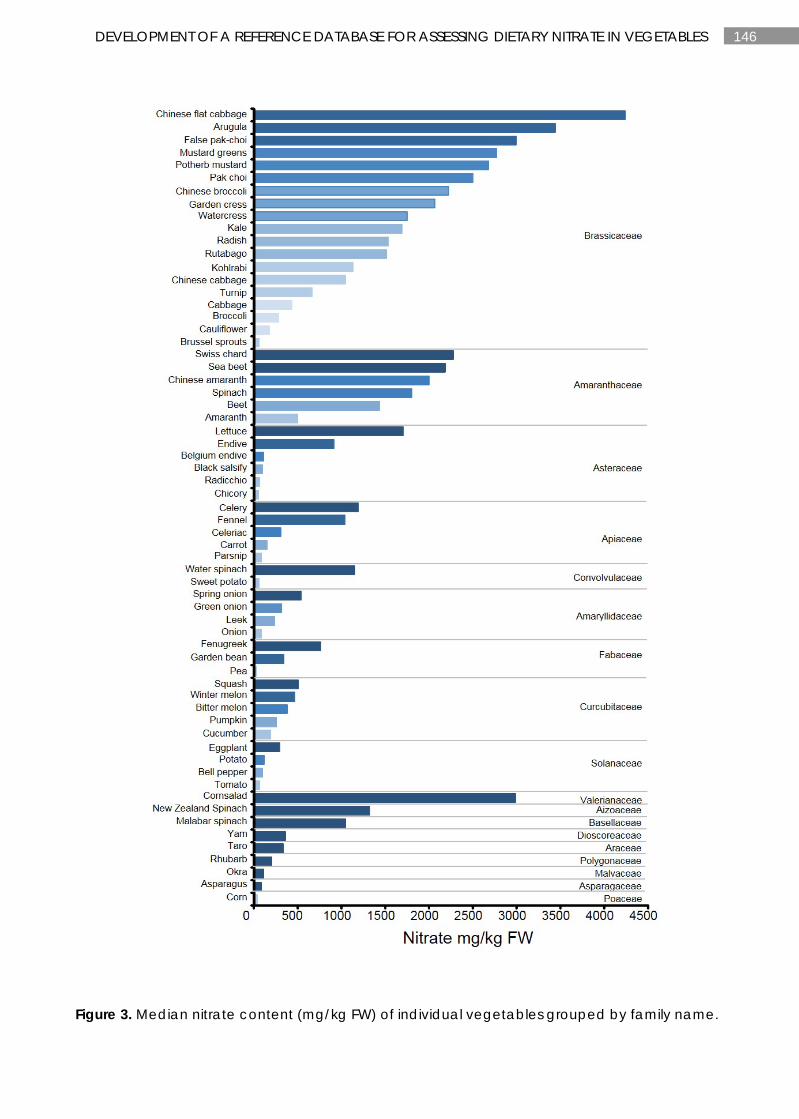
146 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Figure 3. Median nitrate content (mg/kg FW) of individual vegetables grouped by family name.
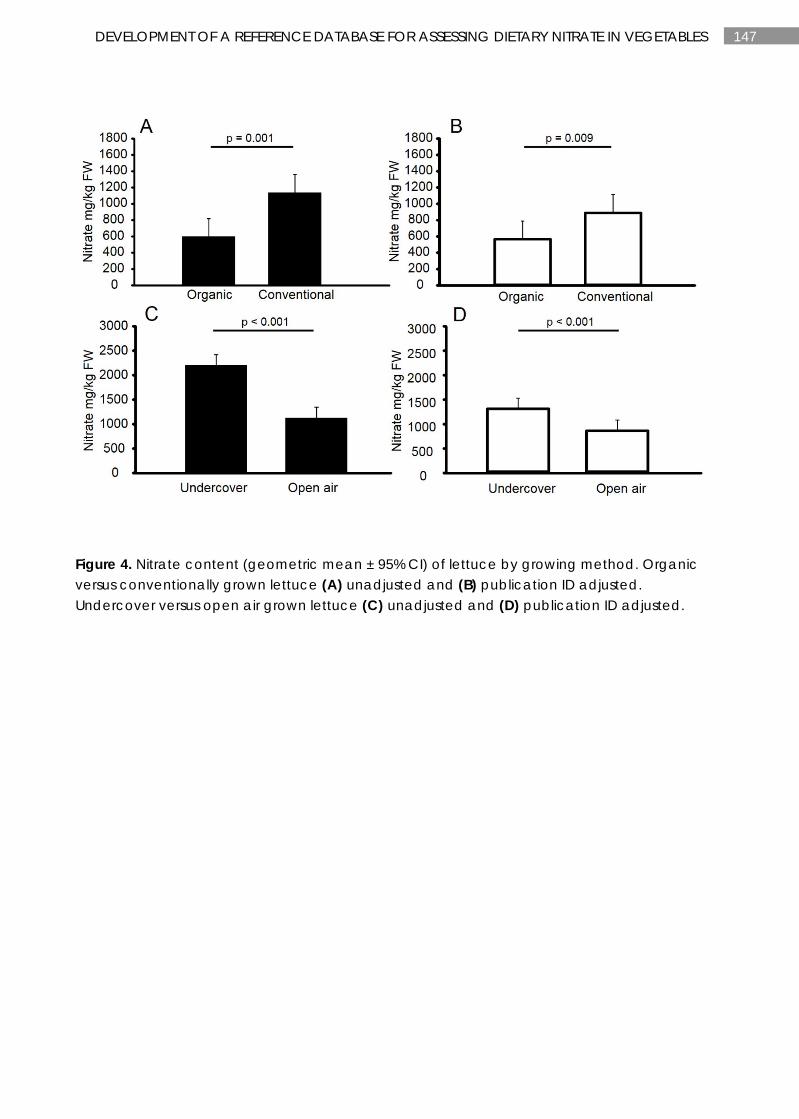
147 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Figure 4. Nitrate content (geometric mean ± 95% CI) of lettuce by growing method. Organic versus conventionally grown lettuce (A) unadjusted and (B) publication ID adjusted. Undercover versus open air grown lettuce (C) unadjusted and (D) publication ID adjusted.
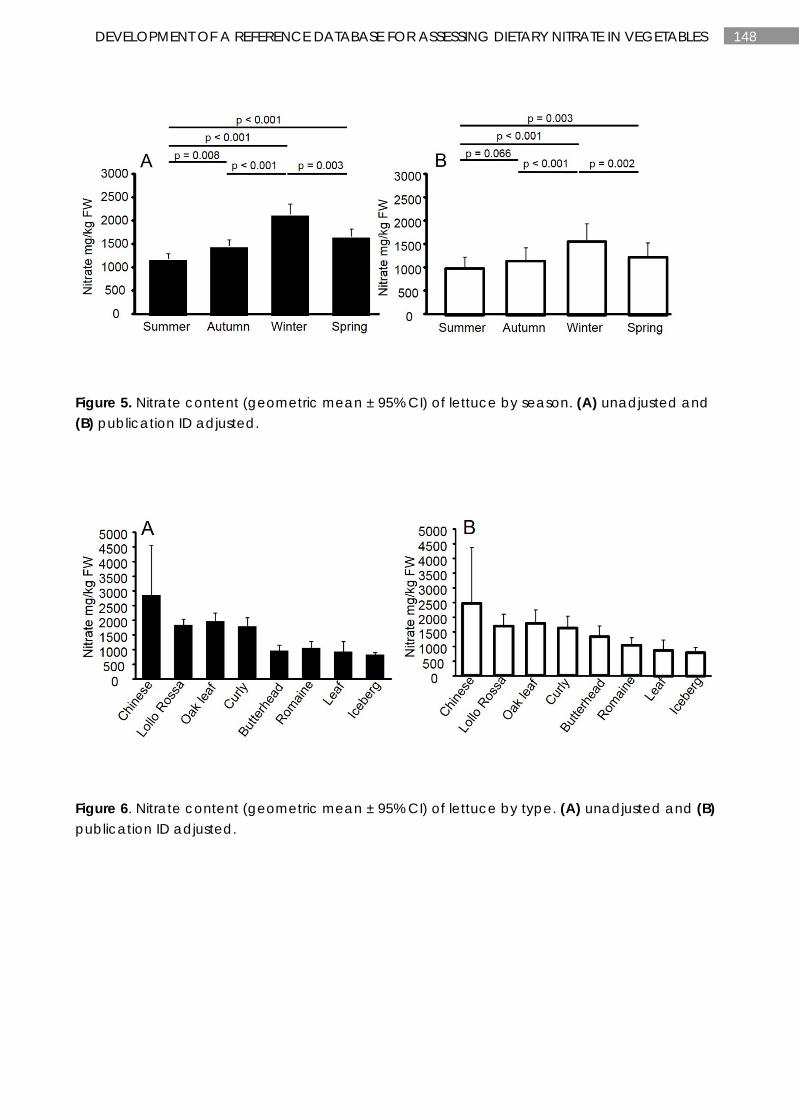
148 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Figure 5. Nitrate content (geometric mean ± 95% CI) of lettuce by season. (A) unadjusted and (B) publication ID adjusted.
Figure 6. Nitrate content (geometric mean ± 95% CI) of lettuce by type. (A) unadjusted and (B) publication ID adjusted.
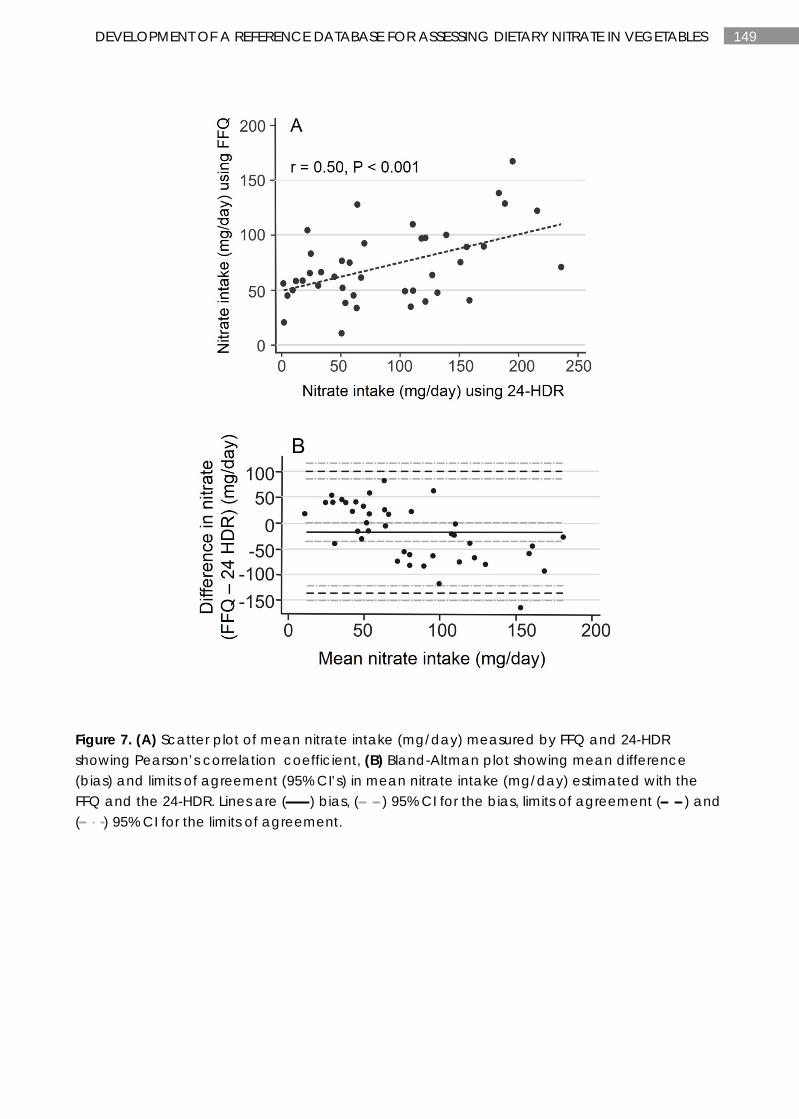
149 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Figure 7. (A) Scatter plot of mean nitrate intake (mg/day) measured by FFQ and 24-HDR showing Pearson’s correlation coefficient, (B) Bland-Altman plot showing mean difference (bias) and limits of agreement (95% CI’s) in mean nitrate intake (mg/day) estimated with the FFQ and the 24-HDR. Lines are ( ) bias, ( ) 95% CI for the bias, limits of agreement ( ) and ( ) 95% CI for the limits of agreement.
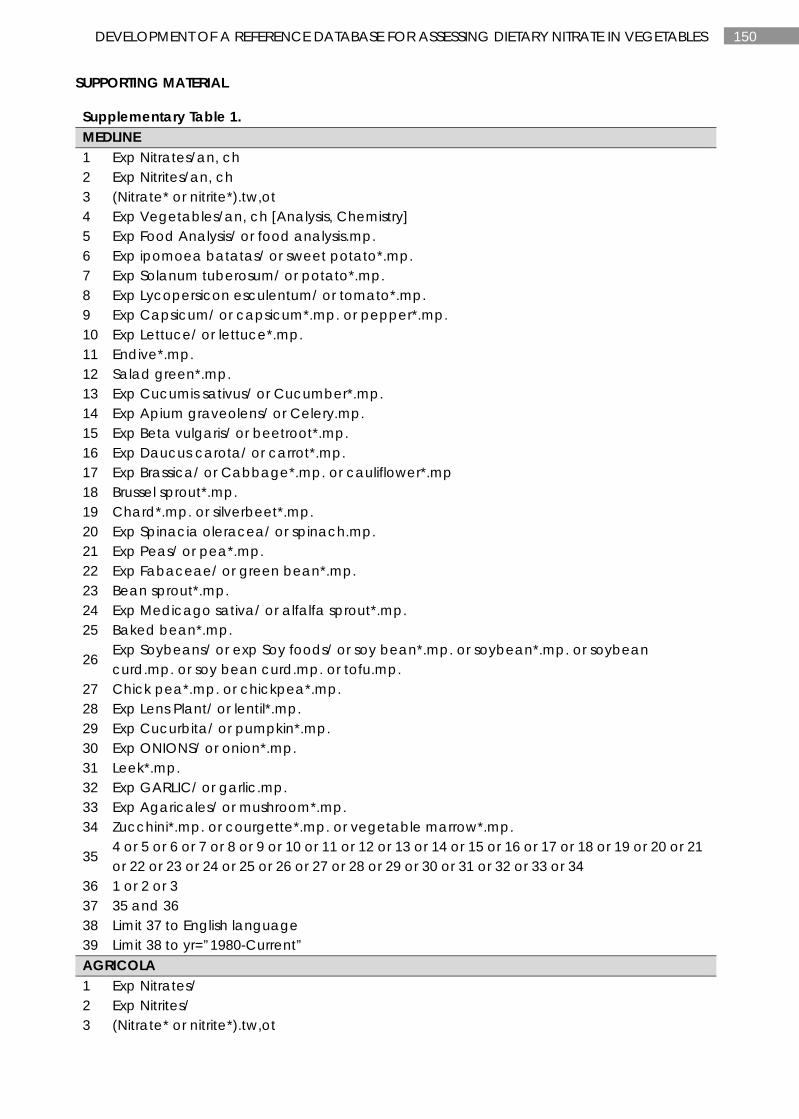
150 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
SUPPORTING MATERIAL
Supplementary Table 1. MEDLINE 1 Exp Nitrates/an, ch 2 Exp Nitrites/an, ch 3 (Nitrate* or nitrite*).tw,ot 4 Exp Vegetables/an, ch [Analysis, Chemistry] 5 Exp Food Analysis/ or food analysis.mp. 6 Exp ipomoea batatas/ or sweet potato*.mp. 7 Exp Solanum tuberosum/ or potato*.mp. 8 Exp Lycopersicon esculentum/ or tomato*.mp. 9 Exp Capsicum/ or capsicum*.mp. or pepper*.mp. 10 Exp Lettuce/ or lettuce*.mp. 11 Endive*.mp. 12 Salad green*.mp. 13 Exp Cucumis sativus/ or Cucumber*.mp. 14 Exp Apium graveolens/ or Celery.mp. 15 Exp Beta vulgaris/ or beetroot*.mp. 16 Exp Daucus carota/ or carrot*.mp. 17 Exp Brassica/ or Cabbage*.mp. or cauliflower*.mp 18 Brussel sprout*.mp. 19 Chard*.mp. or silverbeet*.mp. 20 Exp Spinacia oleracea/ or spinach.mp. 21 Exp Peas/ or pea*.mp. 22 Exp Fabaceae/ or green bean*.mp. 23 Bean sprout*.mp. 24 Exp Medicago sativa/ or alfalfa sprout*.mp. 25 Baked bean*.mp.
26 Exp Soybeans/ or exp Soy foods/ or soy bean*.mp. or soybean*.mp. or soybean curd.mp. or soy bean curd.mp. or tofu.mp.
27 Chick pea*.mp. or chickpea*.mp. 28 Exp Lens Plant/ or lentil*.mp. 29 Exp Cucurbita/ or pumpkin*.mp. 30 Exp ONIONS/ or onion*.mp. 31 Leek*.mp. 32 Exp GARLIC/ or garlic.mp. 33 Exp Agaricales/ or mushroom*.mp. 34 Zucchini*.mp. or courgette*.mp. or vegetable marrow*.mp.
35 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34
36 1 or 2 or 3 37 35 and 36 38 Limit 37 to English language 39 Limit 38 to yr=”1980-Current” AGRICOLA 1 Exp Nitrates/ 2 Exp Nitrites/ 3 (Nitrate* or nitrite*).tw,ot
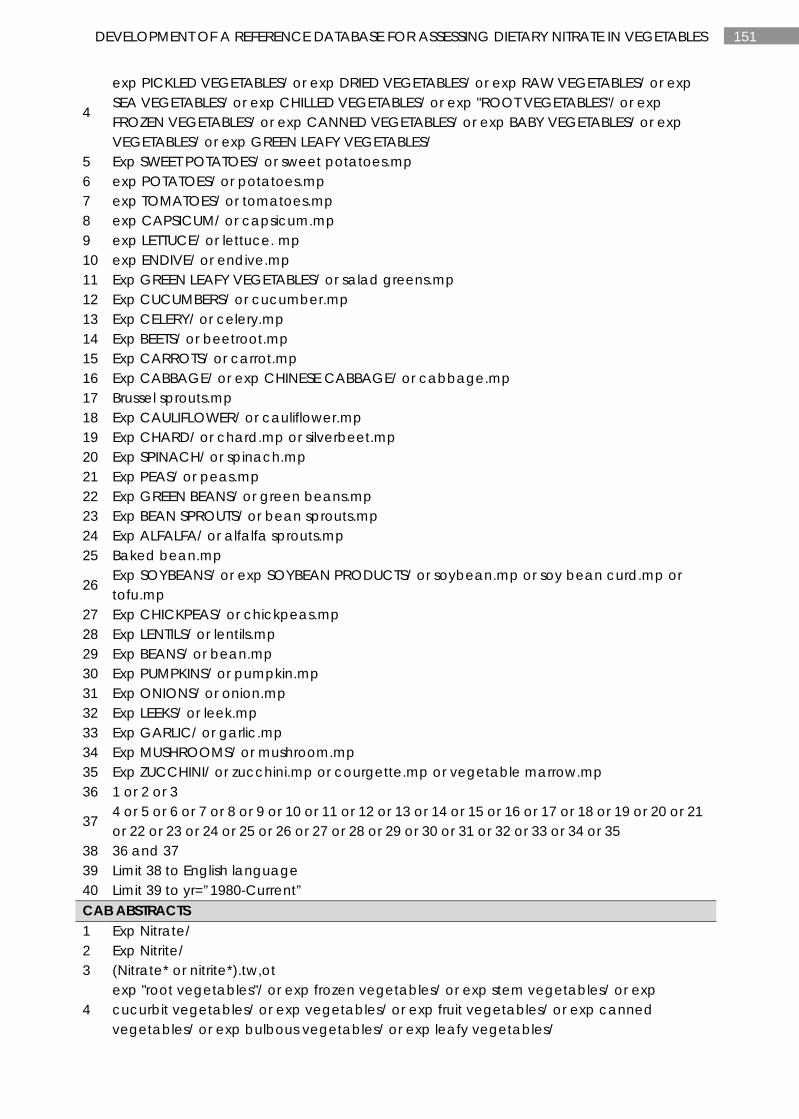
151 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
4
exp PICKLED VEGETABLES/ or exp DRIED VEGETABLES/ or exp RAW VEGETABLES/ or exp SEA VEGETABLES/ or exp CHILLED VEGETABLES/ or exp "ROOT VEGETABLES"/ or exp FROZEN VEGETABLES/ or exp CANNED VEGETABLES/ or exp BABY VEGETABLES/ or exp VEGETABLES/ or exp GREEN LEAFY VEGETABLES/
5 Exp SWEET POTATOES/ or sweet potatoes.mp 6 exp POTATOES/ or potatoes.mp 7 exp TOMATOES/ or tomatoes.mp 8 exp CAPSICUM/ or capsicum.mp 9 exp LETTUCE/ or lettuce. mp 10 exp ENDIVE/ or endive.mp 11 Exp GREEN LEAFY VEGETABLES/ or salad greens.mp 12 Exp CUCUMBERS/ or cucumber.mp 13 Exp CELERY/ or celery.mp 14 Exp BEETS/ or beetroot.mp 15 Exp CARROTS/ or carrot.mp 16 Exp CABBAGE/ or exp CHINESE CABBAGE/ or cabbage.mp 17 Brussel sprouts.mp 18 Exp CAULIFLOWER/ or cauliflower.mp 19 Exp CHARD/ or chard.mp or silverbeet.mp 20 Exp SPINACH/ or spinach.mp 21 Exp PEAS/ or peas.mp 22 Exp GREEN BEANS/ or green beans.mp 23 Exp BEAN SPROUTS/ or bean sprouts.mp 24 Exp ALFALFA/ or alfalfa sprouts.mp 25 Baked bean.mp
26 Exp SOYBEANS/ or exp SOYBEAN PRODUCTS/ or soybean.mp or soy bean curd.mp or tofu.mp
27 Exp CHICKPEAS/ or chickpeas.mp 28 Exp LENTILS/ or lentils.mp 29 Exp BEANS/ or bean.mp 30 Exp PUMPKINS/ or pumpkin.mp 31 Exp ONIONS/ or onion.mp 32 Exp LEEKS/ or leek.mp 33 Exp GARLIC/ or garlic.mp 34 Exp MUSHROOMS/ or mushroom.mp 35 Exp ZUCCHINI/ or zucchini.mp or courgette.mp or vegetable marrow.mp 36 1 or 2 or 3
37 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35
38 36 and 37 39 Limit 38 to English language 40 Limit 39 to yr=”1980-Current” CAB ABSTRACTS 1 Exp Nitrate/ 2 Exp Nitrite/ 3 (Nitrate* or nitrite*).tw,ot
4 exp "root vegetables"/ or exp frozen vegetables/ or exp stem vegetables/ or exp cucurbit vegetables/ or exp vegetables/ or exp fruit vegetables/ or exp canned vegetables/ or exp bulbous vegetables/ or exp leafy vegetables/
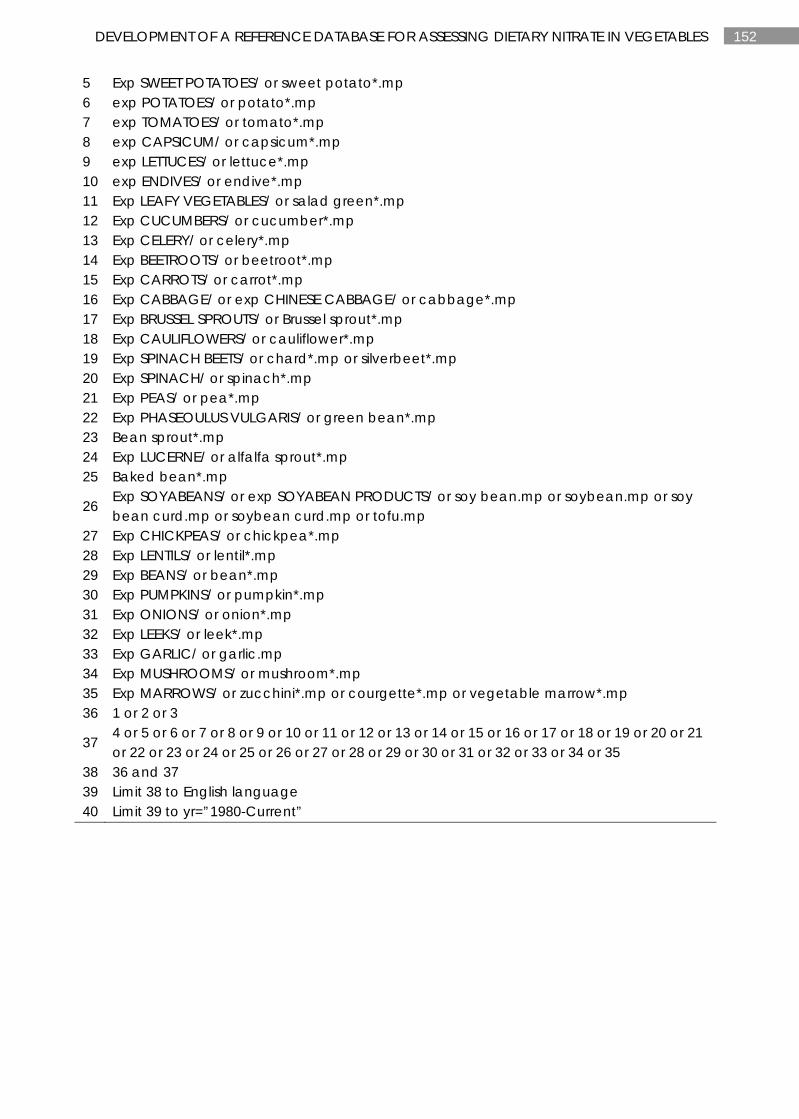
152 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
5 Exp SWEET POTATOES/ or sweet potato*.mp 6 exp POTATOES/ or potato*.mp 7 exp TOMATOES/ or tomato*.mp 8 exp CAPSICUM/ or capsicum*.mp 9 exp LETTUCES/ or lettuce*.mp 10 exp ENDIVES/ or endive*.mp 11 Exp LEAFY VEGETABLES/ or salad green*.mp 12 Exp CUCUMBERS/ or cucumber*.mp 13 Exp CELERY/ or celery*.mp 14 Exp BEETROOTS/ or beetroot*.mp 15 Exp CARROTS/ or carrot*.mp 16 Exp CABBAGE/ or exp CHINESE CABBAGE/ or cabbage*.mp 17 Exp BRUSSEL SPROUTS/ or Brussel sprout*.mp 18 Exp CAULIFLOWERS/ or cauliflower*.mp 19 Exp SPINACH BEETS/ or chard*.mp or silverbeet*.mp 20 Exp SPINACH/ or spinach*.mp 21 Exp PEAS/ or pea*.mp 22 Exp PHASEOULUS VULGARIS/ or green bean*.mp 23 Bean sprout*.mp 24 Exp LUCERNE/ or alfalfa sprout*.mp 25 Baked bean*.mp
26 Exp SOYABEANS/ or exp SOYABEAN PRODUCTS/ or soy bean.mp or soybean.mp or soy bean curd.mp or soybean curd.mp or tofu.mp
27 Exp CHICKPEAS/ or chickpea*.mp 28 Exp LENTILS/ or lentil*.mp 29 Exp BEANS/ or bean*.mp 30 Exp PUMPKINS/ or pumpkin*.mp 31 Exp ONIONS/ or onion*.mp 32 Exp LEEKS/ or leek*.mp 33 Exp GARLIC/ or garlic.mp 34 Exp MUSHROOMS/ or mushroom*.mp 35 Exp MARROWS/ or zucchini*.mp or courgette*.mp or vegetable marrow*.mp 36 1 or 2 or 3
37 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 or 33 or 34 or 35
38 36 and 37 39 Limit 38 to English language 40 Limit 39 to yr=”1980-Current”
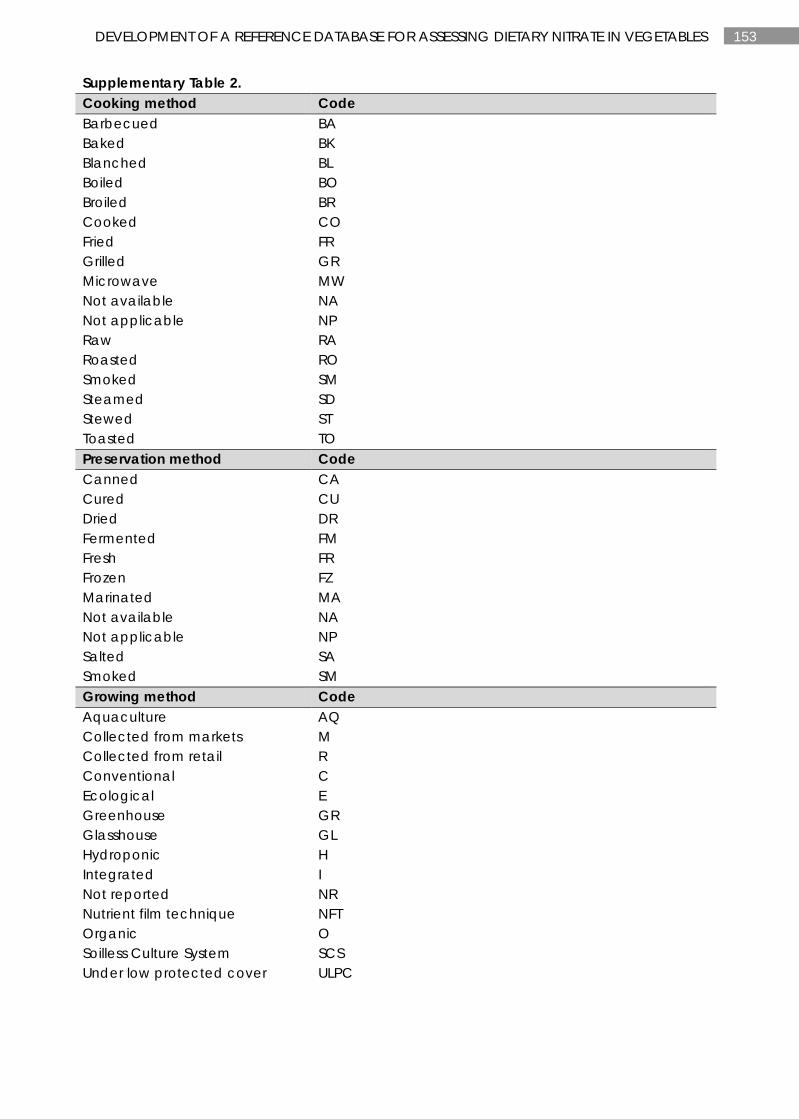
153 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Supplementary Table 2. Cooking method Code Barbecued BA Baked BK Blanched BL Boiled BO Broiled BR Cooked CO Fried FR Grilled GR Microwave MW Not available NA Not applicable NP Raw RA Roasted RO Smoked SM Steamed SD Stewed ST Toasted TO Preservation method Code Canned CA Cured CU Dried DR Fermented FM Fresh FR Frozen FZ Marinated MA Not available NA Not applicable NP Salted SA Smoked SM Growing method Code Aquaculture AQ Collected from markets M Collected from retail R Conventional C Ecological E Greenhouse GR Glasshouse GL Hydroponic H Integrated I Not reported NR Nutrient film technique NFT Organic O Soilless Culture System SCS Under low protected cover ULPC
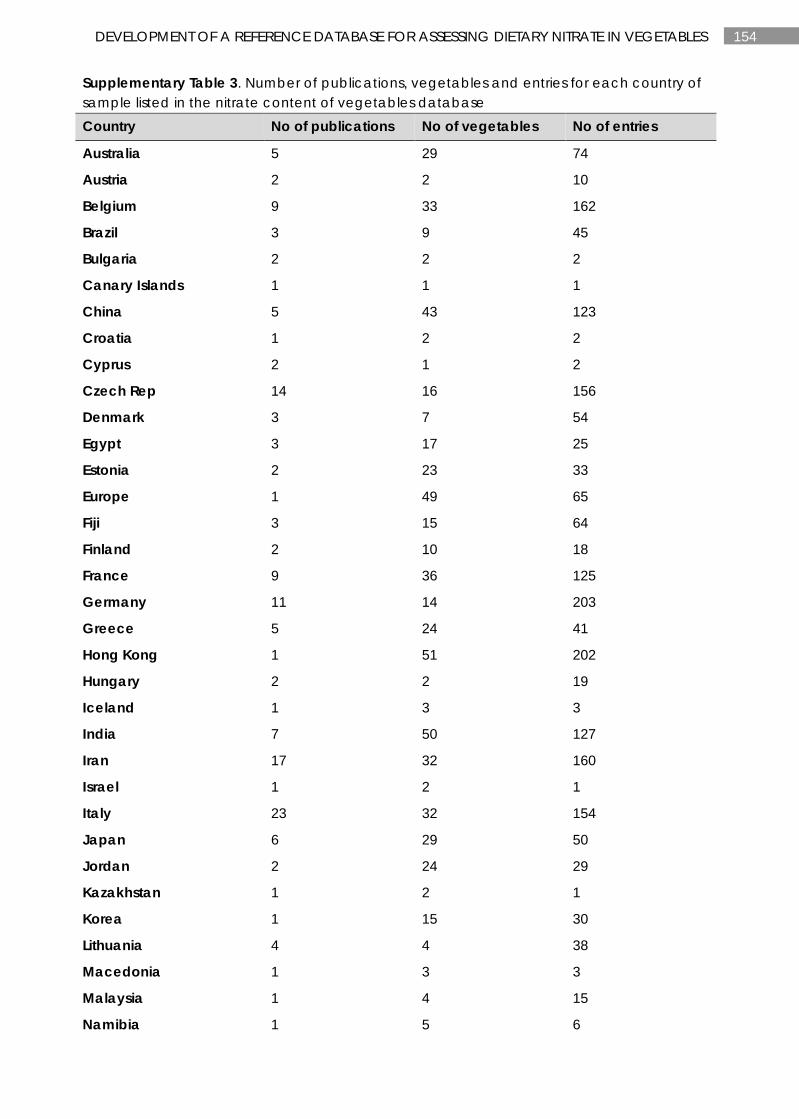
154 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Supplementary Table 3. Number of publications, vegetables and entries for each country of sample listed in the nitrate content of vegetables database Country No of publications No of vegetables No of entries
Australia 5 29 74
Austria 2 2 10
Belgium 9 33 162
Brazil 3 9 45
Bulgaria 2 2 2
Canary Islands 1 1 1
China 5 43 123
Croatia 1 2 2
Cyprus 2 1 2
Czech Rep 14 16 156
Denmark 3 7 54
Egypt 3 17 25
Estonia 2 23 33
Europe 1 49 65
Fiji 3 15 64
Finland 2 10 18
France 9 36 125
Germany 11 14 203
Greece 5 24 41
Hong Kong 1 51 202
Hungary 2 2 19
Iceland 1 3 3
India 7 50 127
Iran 17 32 160
Israel 1 2 1
Italy 23 32 154
Japan 6 29 50
Jordan 2 24 29
Kazakhstan 1 2 1
Korea 1 15 30
Lithuania 4 4 38
Macedonia 1 3 3
Malaysia 1 4 15
Namibia 1 5 6
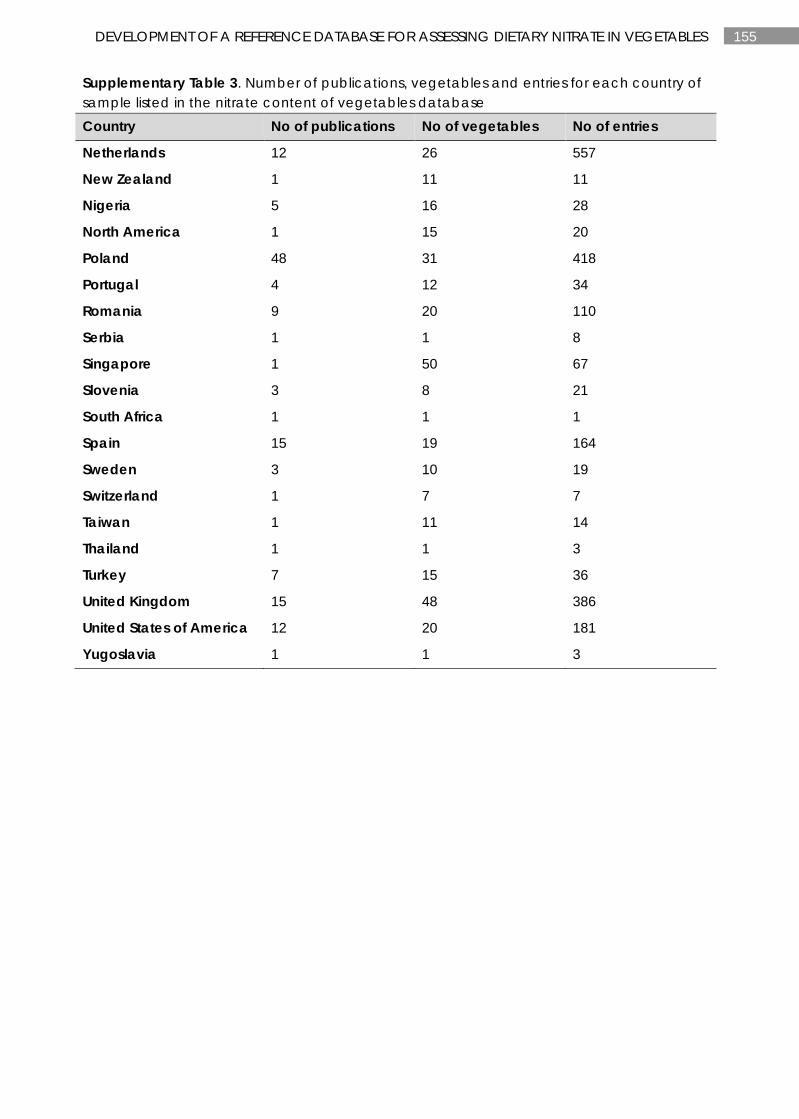
155 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Supplementary Table 3. Number of publications, vegetables and entries for each country of sample listed in the nitrate content of vegetables database Country No of publications No of vegetables No of entries
Netherlands 12 26 557
New Zealand 1 11 11
Nigeria 5 16 28
North America 1 15 20
Poland 48 31 418
Portugal 4 12 34
Romania 9 20 110
Serbia 1 1 8
Singapore 1 50 67
Slovenia 3 8 21
South Africa 1 1 1
Spain 15 19 164
Sweden 3 10 19
Switzerland 1 7 7
Taiwan 1 11 14
Thailand 1 1 3
Turkey 7 15 36
United Kingdom 15 48 386
United States of America 12 20 181
Yugoslavia 1 1 3
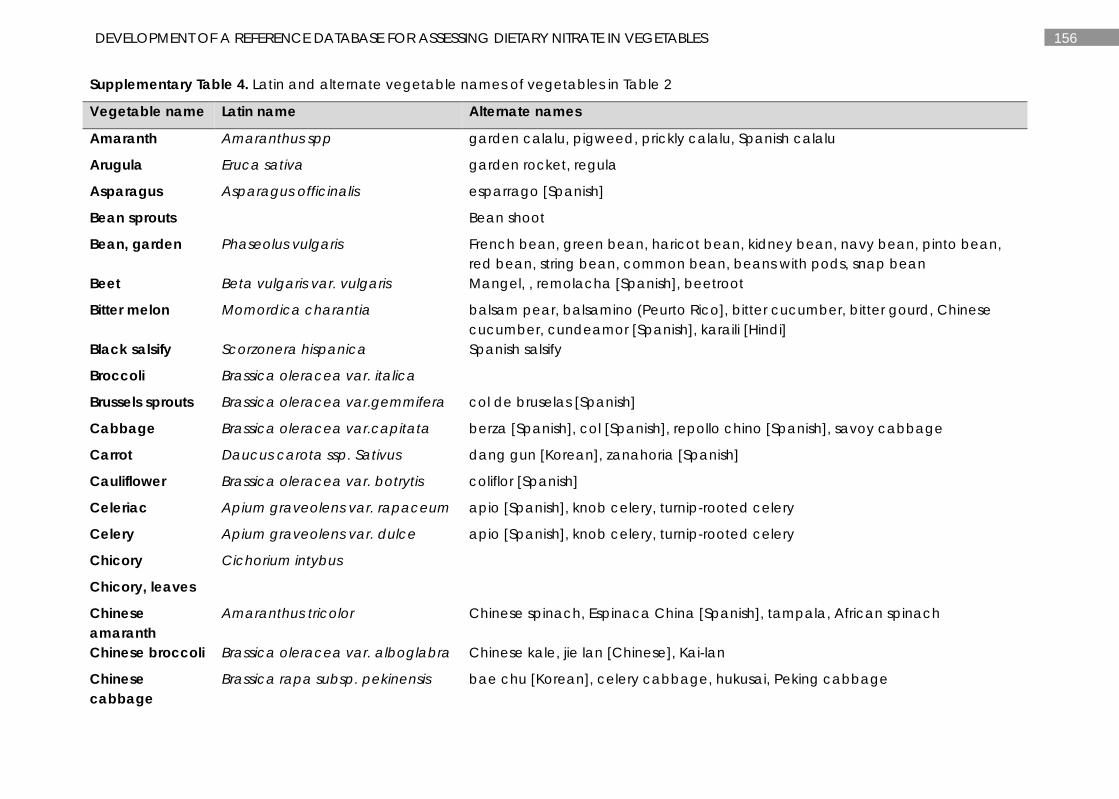
156 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Supplementary Table 4. Latin and alternate vegetable names of vegetables in Table 2
Vegetable name Latin name Alternate names
Amaranth Amaranthus spp garden calalu, pigweed, prickly calalu, Spanish calalu
Arugula Eruca sativa garden rocket, regula
Asparagus Asparagus officinalis esparrago [Spanish]
Bean sprouts Bean shoot
Bean, garden Phaseolus vulgaris French bean, green bean, haricot bean, kidney bean, navy bean, pinto bean, red bean, string bean, common bean, beans with pods, snap bean
Beet Beta vulgaris var. vulgaris Mangel, , remolacha [Spanish], beetroot
Bitter melon Momordica charantia balsam pear, balsamino (Peurto Rico], bitter cucumber, bitter gourd, Chinese cucumber, cundeamor [Spanish], karaili [Hindi]
Black salsify Scorzonera hispanica Spanish salsify
Broccoli Brassica oleracea var. italica
Brussels sprouts Brassica oleracea var.gemmifera col de bruselas [Spanish]
Cabbage Brassica oleracea var.capitata berza [Spanish], col [Spanish], repollo chino [Spanish], savoy cabbage
Carrot Daucus carota ssp. Sativus dang gun [Korean], zanahoria [Spanish]
Cauliflower Brassica oleracea var. botrytis coliflor [Spanish]
Celeriac Apium graveolens var. rapaceum apio [Spanish], knob celery, turnip-rooted celery
Celery Apium graveolens var. dulce apio [Spanish], knob celery, turnip-rooted celery
Chicory Cichorium intybus
Chicory, leaves
Chinese amaranth
Amaranthus tricolor Chinese spinach, Espinaca China [Spanish], tampala, African spinach
Chinese broccoli Brassica oleracea var. alboglabra Chinese kale, jie lan [Chinese], Kai-lan
Chinese cabbage
Brassica rapa subsp. pekinensis bae chu [Korean], celery cabbage, hukusai, Peking cabbage
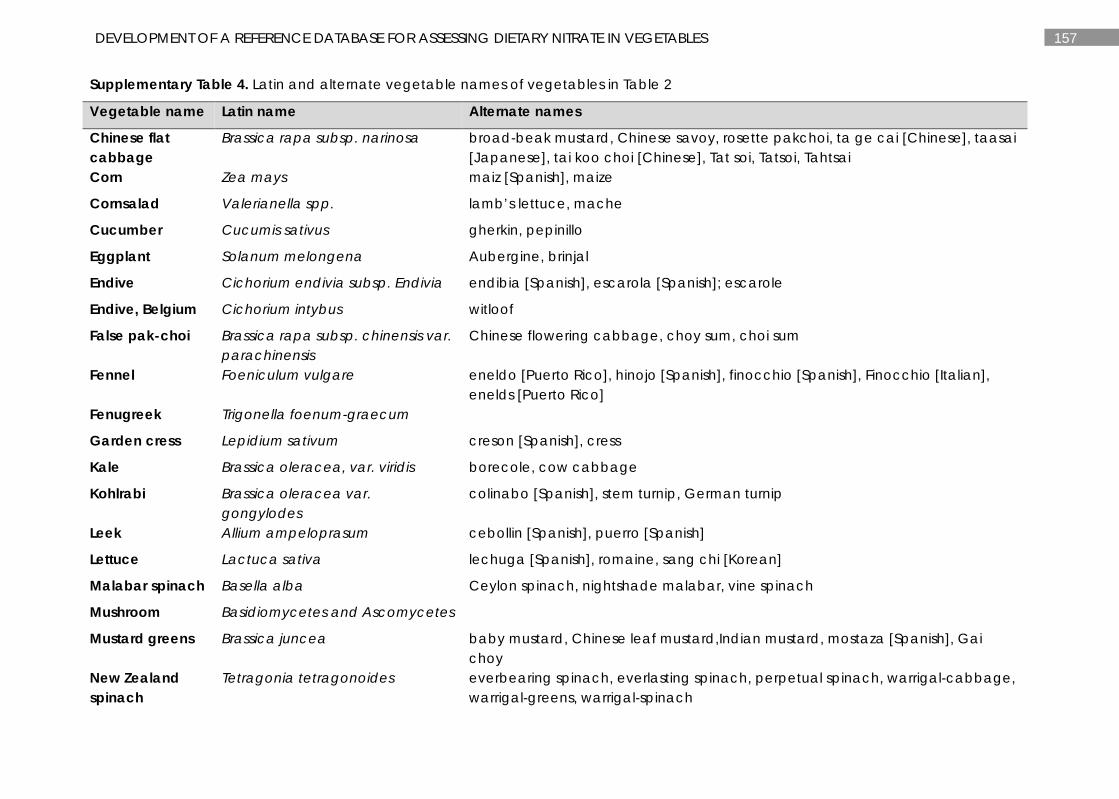
157 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Supplementary Table 4. Latin and alternate vegetable names of vegetables in Table 2
Vegetable name Latin name Alternate names
Chinese flat cabbage
Brassica rapa subsp. narinosa broad-beak mustard, Chinese savoy, rosette pakchoi, ta ge cai [Chinese], taasai [Japanese], tai koo choi [Chinese], Tat soi, Tatsoi, Tahtsai
Corn Zea mays maiz [Spanish], maize
Cornsalad Valerianella spp. lamb’s lettuce, mache
Cucumber Cucumis sativus gherkin, pepinillo
Eggplant Solanum melongena Aubergine, brinjal
Endive Cichorium endivia subsp. Endivia endibia [Spanish], escarola [Spanish]; escarole
Endive, Belgium Cichorium intybus witloof
False pak-choi Brassica rapa subsp. chinensis var. parachinensis
Chinese flowering cabbage, choy sum, choi sum
Fennel Foeniculum vulgare eneldo [Puerto Rico], hinojo [Spanish], finocchio [Spanish], Finocchio [Italian], enelds [Puerto Rico]
Fenugreek Trigonella foenum-graecum
Garden cress Lepidium sativum creson [Spanish], cress
Kale Brassica oleracea, var. viridis borecole, cow cabbage
Kohlrabi Brassica oleracea var. gongylodes
colinabo [Spanish], stem turnip, German turnip
Leek Allium ampeloprasum cebollin [Spanish], puerro [Spanish]
Lettuce Lactuca sativa lechuga [Spanish], romaine, sang chi [Korean]
Malabar spinach Basella alba Ceylon spinach, nightshade malabar, vine spinach
Mushroom Basidiomycetes and Ascomycetes
Mustard greens Brassica juncea baby mustard, Chinese leaf mustard,Indian mustard, mostaza [Spanish], Gai choy
New Zealand spinach
Tetragonia tetragonoides everbearing spinach, everlasting spinach, perpetual spinach, warrigal-cabbage, warrigal-greens, warrigal-spinach
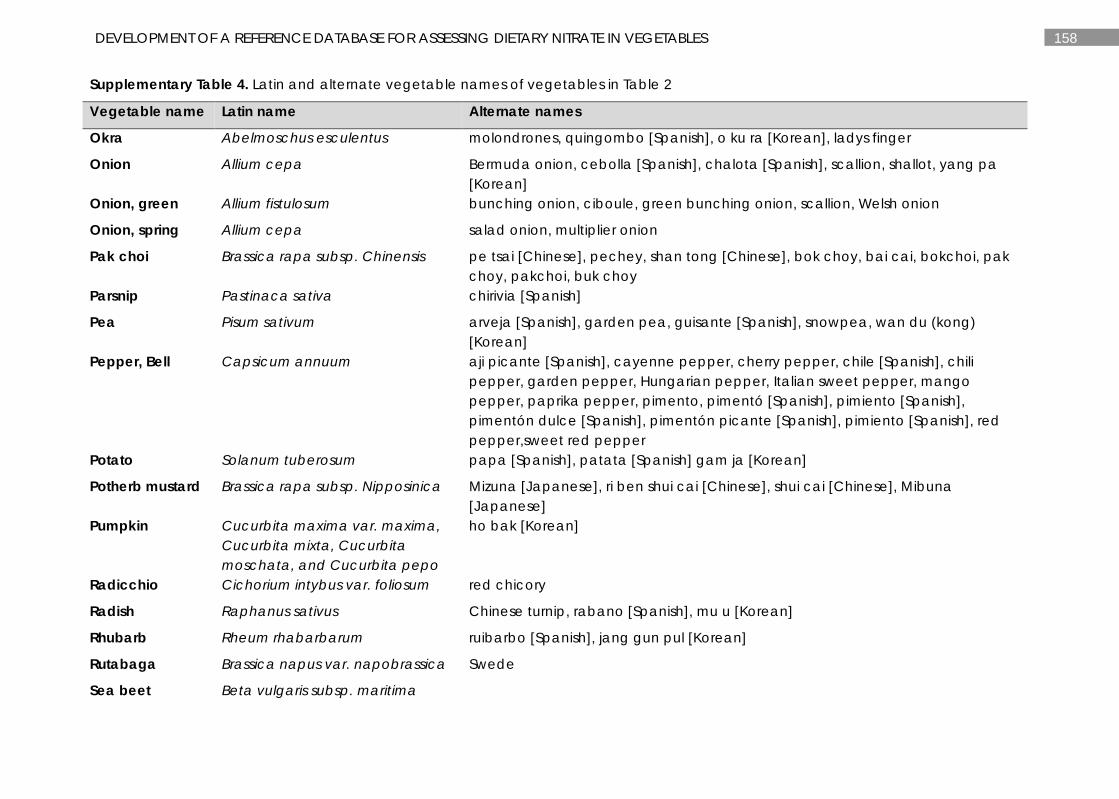
158 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Supplementary Table 4. Latin and alternate vegetable names of vegetables in Table 2
Vegetable name Latin name Alternate names
Okra Abelmoschus esculentus molondrones, quingombo [Spanish], o ku ra [Korean], ladys finger
Onion Allium cepa Bermuda onion, cebolla [Spanish], chalota [Spanish], scallion, shallot, yang pa [Korean]
Onion, green Allium fistulosum bunching onion, ciboule, green bunching onion, scallion, Welsh onion
Onion, spring Allium cepa salad onion, multiplier onion
Pak choi Brassica rapa subsp. Chinensis pe tsai [Chinese], pechey, shan tong [Chinese], bok choy, bai cai, bokchoi, pak choy, pakchoi, buk choy
Parsnip Pastinaca sativa chirivia [Spanish]
Pea Pisum sativum arveja [Spanish], garden pea, guisante [Spanish], snowpea, wan du (kong) [Korean]
Pepper, Bell Capsicum annuum aji picante [Spanish], cayenne pepper, cherry pepper, chile [Spanish], chili pepper, garden pepper, Hungarian pepper, Italian sweet pepper, mango pepper, paprika pepper, pimento, pimentó [Spanish], pimiento [Spanish], pimentón dulce [Spanish], pimentón picante [Spanish], pimiento [Spanish], red pepper,sweet red pepper
Potato Solanum tuberosum papa [Spanish], patata [Spanish] gam ja [Korean]
Potherb mustard Brassica rapa subsp. Nipposinica Mizuna [Japanese], ri ben shui cai [Chinese], shui cai [Chinese], Mibuna [Japanese]
Pumpkin Cucurbita maxima var. maxima, Cucurbita mixta, Cucurbita moschata, and Cucurbita pepo
ho bak [Korean]
Radicchio Cichorium intybus var. foliosum red chicory
Radish Raphanus sativus Chinese turnip, rabano [Spanish], mu u [Korean]
Rhubarb Rheum rhabarbarum ruibarbo [Spanish], jang gun pul [Korean]
Rutabaga Brassica napus var. napobrassica Swede
Sea beet Beta vulgaris subsp. maritima
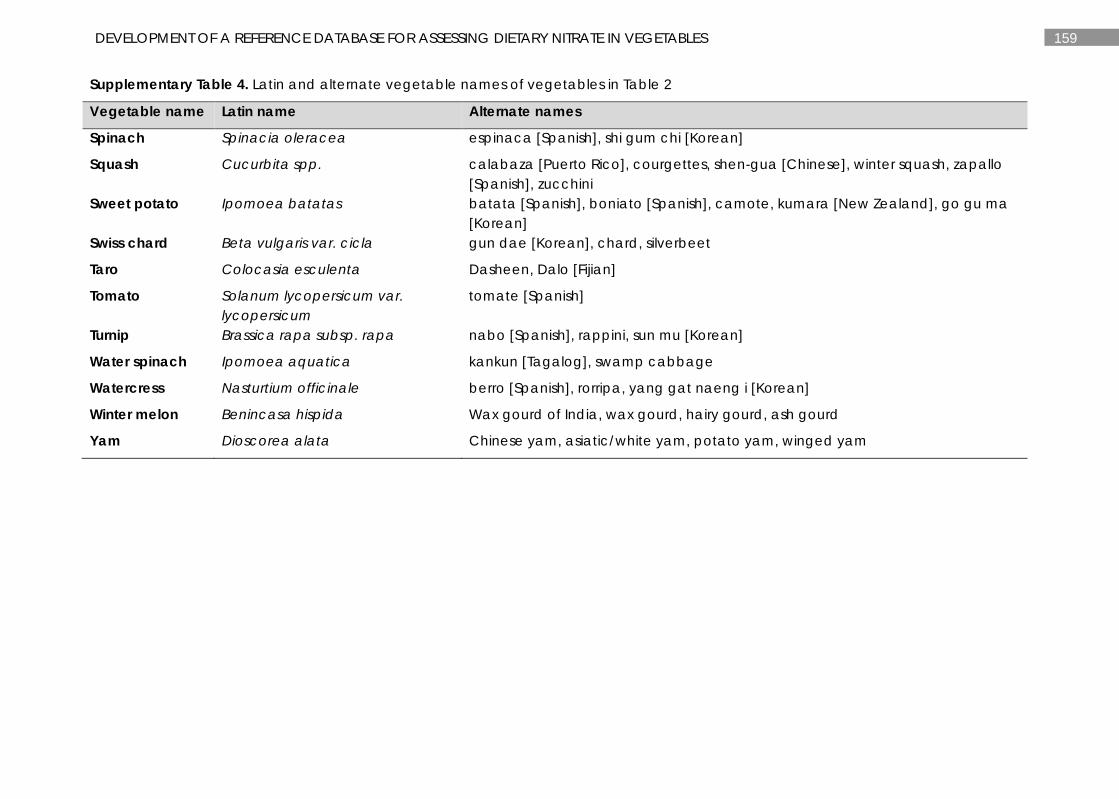
159 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Supplementary Table 4. Latin and alternate vegetable names of vegetables in Table 2
Vegetable name Latin name Alternate names
Spinach Spinacia oleracea espinaca [Spanish], shi gum chi [Korean]
Squash Cucurbita spp. calabaza [Puerto Rico], courgettes, shen-gua [Chinese], winter squash, zapallo [Spanish], zucchini
Sweet potato Ipomoea batatas batata [Spanish], boniato [Spanish], camote, kumara [New Zealand], go gu ma [Korean]
Swiss chard Beta vulgaris var. cicla gun dae [Korean], chard, silverbeet
Taro Colocasia esculenta Dasheen, Dalo [Fijian]
Tomato Solanum lycopersicum var. lycopersicum
tomate [Spanish]
Turnip Brassica rapa subsp. rapa nabo [Spanish], rappini, sun mu [Korean]
Water spinach Ipomoea aquatica kankun [Tagalog], swamp cabbage
Watercress Nasturtium officinale berro [Spanish], rorripa, yang gat naeng i [Korean]
Winter melon Benincasa hispida Wax gourd of India, wax gourd, hairy gourd, ash gourd
Yam Dioscorea alata Chinese yam, asiatic/white yam, potato yam, winged yam
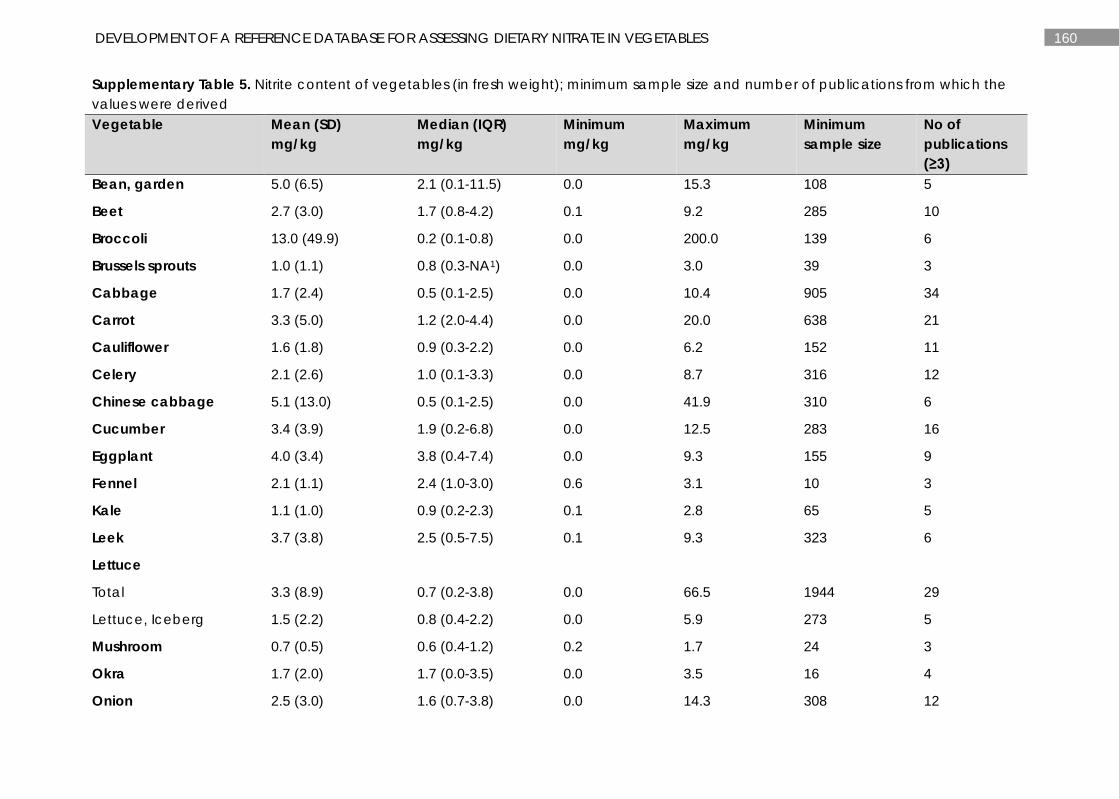
160 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Supplementary Table 5. Nitrite content of vegetables (in fresh weight); minimum sample size and number of publications from which the values were derived Vegetable Mean (SD)
mg/kg Median (IQR) mg/kg
Minimum mg/kg
Maximum mg/kg
Minimum sample size
No of publications (≥3)
Bean, garden 5.0 (6.5) 2.1 (0.1-11.5) 0.0 15.3 108 5
Beet 2.7 (3.0) 1.7 (0.8-4.2) 0.1 9.2 285 10
Broccoli 13.0 (49.9) 0.2 (0.1-0.8) 0.0 200.0 139 6
Brussels sprouts 1.0 (1.1) 0.8 (0.3-NA1) 0.0 3.0 39 3
Cabbage 1.7 (2.4) 0.5 (0.1-2.5) 0.0 10.4 905 34
Carrot 3.3 (5.0) 1.2 (2.0-4.4) 0.0 20.0 638 21
Cauliflower 1.6 (1.8) 0.9 (0.3-2.2) 0.0 6.2 152 11
Celery 2.1 (2.6) 1.0 (0.1-3.3) 0.0 8.7 316 12
Chinese cabbage 5.1 (13.0) 0.5 (0.1-2.5) 0.0 41.9 310 6
Cucumber 3.4 (3.9) 1.9 (0.2-6.8) 0.0 12.5 283 16
Eggplant 4.0 (3.4) 3.8 (0.4-7.4) 0.0 9.3 155 9
Fennel 2.1 (1.1) 2.4 (1.0-3.0) 0.6 3.1 10 3
Kale 1.1 (1.0) 0.9 (0.2-2.3) 0.1 2.8 65 5
Leek 3.7 (3.8) 2.5 (0.5-7.5) 0.1 9.3 323 6
Lettuce
Total 3.3 (8.9) 0.7 (0.2-3.8) 0.0 66.5 1944 29
Lettuce, Iceberg 1.5 (2.2) 0.8 (0.4-2.2) 0.0 5.9 273 5
Mushroom 0.7 (0.5) 0.6 (0.4-1.2) 0.2 1.7 24 3
Okra 1.7 (2.0) 1.7 (0.0-3.5) 0.0 3.5 16 4
Onion 2.5 (3.0) 1.6 (0.7-3.8) 0.0 14.3 308 12
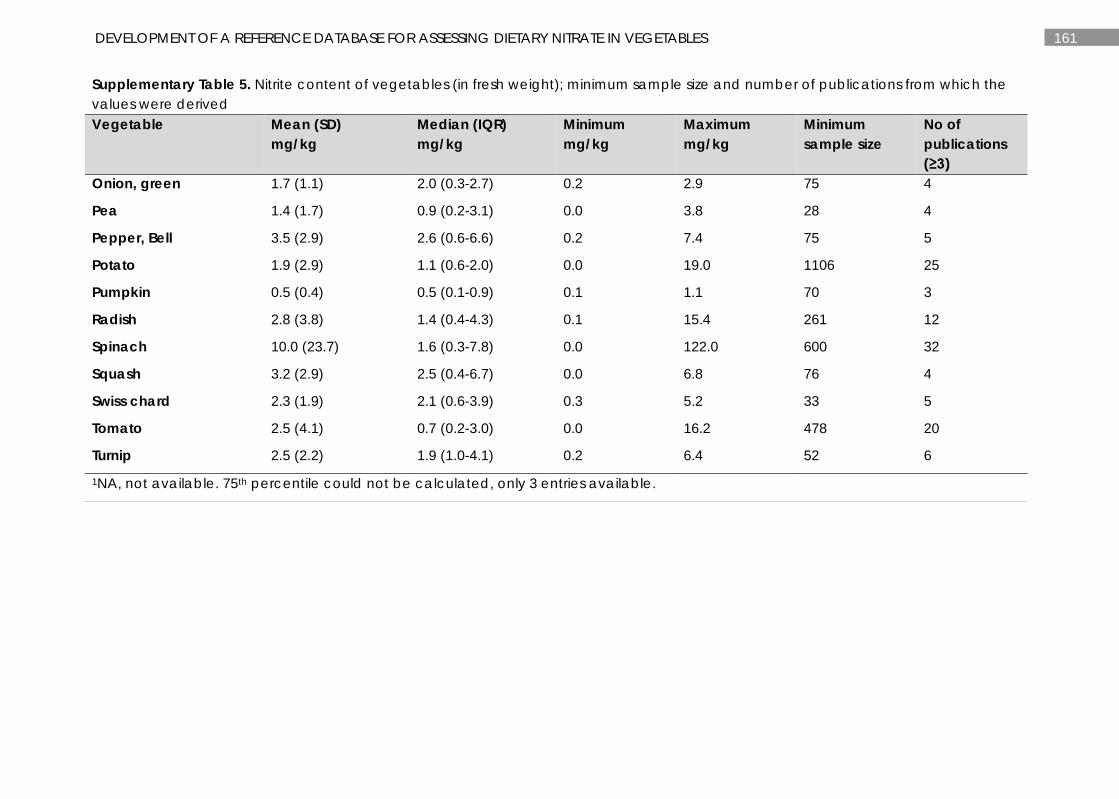
161 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Supplementary Table 5. Nitrite content of vegetables (in fresh weight); minimum sample size and number of publications from which the values were derived Vegetable Mean (SD)
mg/kg Median (IQR) mg/kg
Minimum mg/kg
Maximum mg/kg
Minimum sample size
No of publications (≥3)
Onion, green 1.7 (1.1) 2.0 (0.3-2.7) 0.2 2.9 75 4
Pea 1.4 (1.7) 0.9 (0.2-3.1) 0.0 3.8 28 4
Pepper, Bell 3.5 (2.9) 2.6 (0.6-6.6) 0.2 7.4 75 5
Potato 1.9 (2.9) 1.1 (0.6-2.0) 0.0 19.0 1106 25
Pumpkin 0.5 (0.4) 0.5 (0.1-0.9) 0.1 1.1 70 3
Radish 2.8 (3.8) 1.4 (0.4-4.3) 0.1 15.4 261 12
Spinach 10.0 (23.7) 1.6 (0.3-7.8) 0.0 122.0 600 32
Squash 3.2 (2.9) 2.5 (0.4-6.7) 0.0 6.8 76 4
Swiss chard 2.3 (1.9) 2.1 (0.6-3.9) 0.3 5.2 33 5
Tomato 2.5 (4.1) 0.7 (0.2-3.0) 0.0 16.2 478 20
Turnip 2.5 (2.2) 1.9 (1.0-4.1) 0.2 6.4 52 6
1NA, not available. 75th percentile could not be calculated, only 3 entries available.
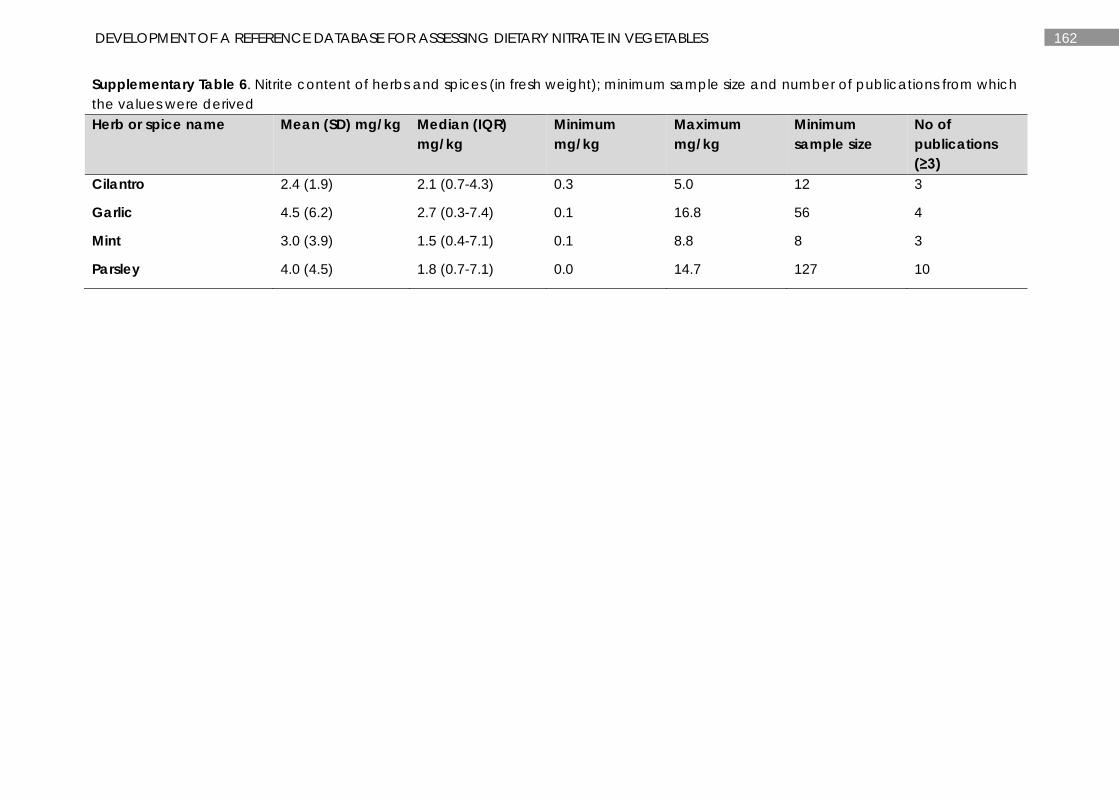
162 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Supplementary Table 6. Nitrite content of herbs and spices (in fresh weight); minimum sample size and number of publications from which the values were derived Herb or spice name Mean (SD) mg/kg Median (IQR)
mg/kg Minimum mg/kg
Maximum mg/kg
Minimum sample size
No of publications (≥3)
Cilantro 2.4 (1.9) 2.1 (0.7-4.3) 0.3 5.0 12 3
Garlic 4.5 (6.2) 2.7 (0.3-7.4) 0.1 16.8 56 4
Mint 3.0 (3.9) 1.5 (0.4-7.1) 0.1 8.8 8 3
Parsley 4.0 (4.5) 1.8 (0.7-7.1) 0.0 14.7 127 10
163 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
Database references:
1. Abah, J., Mashebe, P., Ubwa, S. T., Onjefu, S. A., Assessment of Consumers’ Exposure to Vegetable Dietary Nitrate in Katima Mulilo, Namibia. Journal of Applied Chemistry 2015, 8, 29-34.
2. Abdel-Gawad, S., El-Rify, M. N., El-Geddawy, M. A. H., Sorour, M. A., Changes in the nitrate and nitrite contents of selected Egyptian vegetables during storage and processing. Assiut Journal of Agricultural Sciences 1990, 21, 49-64.
3. Afzali, S. F., Elahi, R., Measuring nitrate and nitrite concentrations in vegetables, fruits in Shiraz. J. Appl. Sci. Environ. Manage. 2014, 18, 451-457.
4. Aghili, F., Khoshgoftarmanesh, A. H., Afyuni, M., Mobli, M., Relationships between fruit mineral nutrients concentrations and some fruit quality attributes in greenhouse cucumber. Journal of Plant Nutrition 2009, 32, 1994-2007.
5. Ahonen, S., Kuokkanen, I., Penttila, P. L., The nitrate concentration of domestic vegetables on Helsinki market in summer and autumn 1984. Journal of Agricultural Science in Finland 1987, 59, 425-430.
6. Aidjanov, M. M., Sharmanov, T., Nitrosamines and their precursors in some Kazakh foodstuffs. IARC Scientific Publications 1982, 267-276.
7. Aires, A., Carvalho, R., Rosa, E. A., Saavedra, M. J., Effects of agriculture production systems on nitrate and nitrite accumulation on baby-leaf salads. Food Sciences and Nutrition 2013, 1, 3-7.
8. Alina, B., Aurel, L., Ersilia, A., Monica, N., Study regarding nitrate and nitrite content in cauliflower, from agro-food markets in Timisoara. Analele Universitatii din Oradea, Fascicula Biologie 2008, 15, 22-23.
9. Amr, A., Hadidi, N., Effect of cultivar and harvest date on nitrate (NO3) and nitrite (NO2) content of selected vegetables grown under open field and greenhouse conditions in Jordan. Journal of Food Composition and Analysis 2001, 14, 59-67.
10. Andac, M., Eren, H., Coldur, F., Determination of nitrate in leafy vegetables by flow injection analysis with potentiometric detection. Journal of Food and Drug Analysis 2011, 19, 457-462.
11. Andrade, R., Viana, C. O., Guadagnin, S. G., Reyes, F. G. R., Rath, S., A flow-injection spectrophotometric method for nitrate and nitrite determination through nitric oxide generation. Food Chemistry 2003, 80, 597-602.
12. Anjana, Shahid, U., Muhammad, I., Abrol, Y. P., Are nitrate concentrations in leafy vegetables within safe limits? Current Science 2007, 92, 355-360.
13. Ayaz, A., Topcu, A., Yurttagul, M., Survey of nitrate and nitrite levels of fresh vegetables in Turkey. Journal of Food Technology 2007, 5, 177-179.
14. Bakowski, J., Kosson, R., Horbowicz, M., Nutritional values of different strains of mushrooms (Agaricus bisporus). Acta Agrobotanica 1986, 39, 111-121.
15. Baldursson, S., Kristjansson, J. K., Analysis of nitrate in food extracts using a thermostable formate linked nitrate reductase enzyme system. Biotechnology Techniques 1990, 4, 211-214.
16. Bartova, V., Divis, J., Barta, J., Brabcova, A., Svajnerova, M., Variation of nitrogenous components in potato (Solanum tuberosum L.) tubers produced under organic and conventional crop management. European Journal of Agronomy 2013, 49, 20-31.
17. Beijaars, P. R., van Dijk, R., van der Horst, G. M., Determination of nitrate in vegetables by continuous flow: interlaboratory study. Journal of AOAC International 1994, 77, 1522-1529.
18. Bianco, V. V., Santamaria, P., Elia, A., Nutritional value and nitrate content in edible wild species used in southern Italy. Acta Horticulturae 1998, 467, 71-87.
19. Biesiada, A., KoLota, E., Adamczewska-Sowinska, K., The effect of maturity stage on nutritional value of leek, zucchini and kohlrabi. Vegetable Crops Research Bulletin 2007, 66, 39-45.
20. Birnin-Yauri, U. A., Yahaya, Y., Bagudo, B. U., Noma, S. S., Seasonal variation in nutrient content of some selected vegetables from Wamakko, Sokoto State, Nigeria. Journal of Soil Science and Environmental Management 2011, 2, 117-125.
21. Boari, F., Cefola, M., Di Gioia, F., Pace, B., et al., Effect of cooking methods on antioxidant activity and nitrate content of selected wild Mediterranean plants. International Journal of Food Sciences & Nutrition 2013, 64, 870-876.
22. Bosch, N. B., Mata, M. G., Penuela, M. J., Ruiz Galan, T., Lopez Ruiz, B., Determination of nitrite levels in refrigerated and frozen spinach by ion chromatography. Journal of Chromatography 1995, 706, 221-228.
164 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
23. Buono, V., Paradiso, A., Serio, F., Gonnella, M., et al., Tuber quality and nutritional components of early potato subjected to chemical haulm desiccation. Journal of Food Composition and Analysis 2009, 22, 556-562.
24. Burns, I. G., Durnford, J., Lynn, J., McClement, S., et al., The influence of genetic variation and nitrogen source on nitrate accumulation and iso-osmotic regulation by lettuce. Plant and Soil 2012, 352, 321-339.
25. Burns, I. G., Zhang, K., Turner, M. K., Lynn, J., et al., Genotype and environment effects on nitrate accumulation in a diversity set of lettuce accessions at commercial maturity: the influence of nitrate uptake and assimilation, osmotic interactions and shoot weight and development. Journal of the Science of Food & Agriculture 2011, 91, 2217-2233.
26. Campeanu, G., Atanasiu, N., Neata, G., Hohan, G., Researches regarding chemical and biochemical components existed in different tomato hybrids. Lucrari Stiintifice Universitatea de Stiinte Agronomice si Medicina Veterinara Bucuresti. Seria B, Horticultura 2008, 51, 33-36.
27. Candido, V., Galgano, F., Castronuovo, D., Miccolis, V., Favati, F., Quality traits of some cauliflower cultivars grown in the "Valle dell'Ofanto" area (Italy) as affected by postharvest storage. Proc VIth on Brassicas and XVIIIth Cruciferous Genetics Workshop. Acta Horticulturae. 1005, ISHS 2013.
28. Chang, A. C., Yang, T. Y., Riskowski, G. L., Ascorbic acid, nitrate, and nitrite concentration relationship to the 24hour light/dark cycle for spinach grown in different conditions. Food Chemistry 2013, 138, 382-388.
29. Chetty, A. A., Surendra, P., Flow injection analysis of nitrate-N determination in root vegetables: study of the effects of cooking. Food Chemistry 2009, 116, 561-566.
30. Chis, A. M., The incidence of nitrates contamination in vegetables during 2002-2008 in the Bihor county. Analele Universitatii din Oradea, Fascicula: Ecotoxicologie, Zootehnie si Tehnologii de Industrie Alimentara 2008, 7, 107-114.
31. Chis, A., Purcarea, C., Animal and vegetal components in relation with the contamination by nitrites and nitrates in complex food. Analele Universitatii din Oradea, Fascicula: Ecotoxicologie, Zootehnie si Tehnologii de Industrie Alimentara 2012, 11, 333-340.
32. Chou, S.-S., Chung, J.-C., Hwang, D.-F., A High Performance Liquid Chromatography Method for Determining Nitrate and Nitrite Levels in Vegetables. Journal of Food and Drug Analysis 2003, 11, 233-238.
33. Chung, S. W. C., Tran, J. C. H., Tong, K. S. K., Chen, M. Y. Y., et al., Nitrate and nitrite levels in commonly consumed vegetables in Hong Kong. Food Additives and Contaminants B, Surveillance 2011, 4, 34-41.
34. Chung, S. Y., Kim, J. S., Kim, M., Hong, M. K., et al., Survey of nitrate and nitrite contents of vegetables grown in Korea. Food Additives & Contaminants 2003, 20, 621-628.
35. Cieslik, E., Effect of the levels of nitrates and nitrites on the nutritional and sensory quality of potato tubers. Hygiene and Nutrition in Foodservice and Catering 1997, 1, 225-230.
36. Cieslik, E., The effect of naturally occurring vitamin C in potato tubers on the levels of nitrates and nitrites. Food Chemistry 1994, 49, 233-235.
37. Cieslik, E., The effect of weather conditions on the level of nitrates in tubers of some potato varieties. Polish Journal of Food and Nutrition Sciences 1995, 4, 11-19.
38. Consalter, A., Rigato, A., Clamor, L., Giandon, P., Determination of nitrate in vegetables using an ion-selective electrode. Journal of Food Composition and Analysis 1992, 5, 252-256.
39. Cornee, J., An estimate of nitrate, nitrite and N-nitrosodimethylamine concentrations in French food products or food groups. Sciences des aliments 1992, 12, 155-197.
40. Correia, M., Barroso, A., Barroso, M. F., Soares, D., et al., Contribution of different vegetable types to exogenous nitrate and nitrite exposure. Food Chemistry 2010, 120, 960-966.
41. Czech, A., Rusinek, E., Content of nitrates V and III and heavy metals in selected Brassica vegetables depending on storage. Journal of Elementology 2012, 17, 201-213.
42. Dambrauskiene, E., Viskelis, P., Bobinas, C., Rubinskiene, M., Influence of lasting storage on biochemical composition of leeks of different earliness. Sodininkyste ir Darzininkyste 2005, 24, 119-126.
43. D'Antuono, L. F., Elementi, S., Neri, R., Post harvest patterns of deltamethrine and nitrates in industrial spinach. Acta Horticulturae 2007, 741, 253-257.
44. Dejonckheere, W., Steurbaut, W., Drieghe, S., Verstraeten, R., Braeckman, H., Nitrate in food commodities of vegetable origin and the total diet in Belgium (1992-1993). MAN Microbiologie, aliments, nutrition 1994, 12, 359-370.
165 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
45. Derolez, J., Vulsteke, G., Accumulation of nitrate: a cultivar-linked property with celeriac (Apium graveolens L. var. rapaceum). Qualitas Plantarum Plant Foods for Human Nutrition 1985, 35, 375-378.
46. Diaper, J., Lawrenson, O., Nitrate content of vegetables commercially grown on land subject to inorganic or organic fertiliser. Environmental Geochemistry & Health 1986, 8, 105-106.
47. Divis, J., Barta, J., Hermanova, V., 3rd International Congress of the European Integrated Project Quality Low Input Food (QLIF), Germany 2007.
48. Djurovka, M., Lazic, B., Markovic, V., General characters of spinach varieties suitable for industrial processing. Acta horticulturae 1998, 220, 159-164.
49. Dorsch, M. M., Calder, I. C., Roder, D. M., Esterman, A. J., Birth defects and the consumption of nitrates in food and water in the Lower South-East of South Australia: An exploratory study. Journal of Food & Nutrition 1984, 41, 30-33.
50. Dutt, M. C., Lim, H. Y., Chew, R. K., Nitrate consumption and the incidence of gastric cancer in Singapore. Food & Chemical Toxicology 1987, 25, 515-520.
51. Escobar-Gutierrez, A. J., Burns, I. G., Lee, A., Edmondson, R. N., Screening lettuce cultivars for low nitrate content during summer and winter production. Journal of Horticultural Science & Biotechnology 2002, 77, 232-237.
52. European Commission, Directorate-General III Industry, Brussels. EU Task 3.2.3. Assessment of dietary intake of nitrates by the population in the European Union as a consequence of the consumption of vegetables. 1997.
53. European Food Safety Authority, Nitrate in vegetables: scientific opinion of the panel on contaminants in the food chain. EFSA Journal 2008, 689, 1-79.
54. Farrington, D., Damant, A. P., Powell, K., Ridsdale, J., et al., A comparison of the extraction methods used in the UK nitrate residues monitoring program. Journal of the Association of Public Analysts 2006, 34, 1-11.
55. Fjelkner-Modig, S., Bengtsson, H., Stegmark, R., Nystrom, S., The influence of organic and integrated production on nutritional, sensory and agricultural aspects of vegetable raw materials for food production. Acta Agriculturae Scandinavica. Section B, Soil and Plant Science 2000, 50, 102-113.
56. Fontana, E., Nicola, S., Traditional and soilless culture systems to produce corn salad (Valerianella olitoria L.) and rocket (Eruca sativa Mill.) with low nitrate content. Journal of Food, Agriculture & Environment 2009, 7, 405-410.
57. Food Standards Agency, UK monitoring programme for nitrate in lettuce and spinach. Food survey Information Sheet No. 16/01 July 2001 (London: Food Standards Agency).
58. Food Standards Australia New Zealand, Survey of nitrates and nitrites in food and beverages in Australia. Canberra, ACT 2013.
59. Forlani, L., Grillenzoni, S., Ori, E., Resca, P., Nitrate levels in vegetables that may be eaten raw. Italian Journal of Food Science 1997, 9, 65-69.
60. Fytianos, K., Zarogiannis, P., Nitrate and nitrite accumulation in fresh vegetables from Greece. Bulletin of Environmental Contamination & Toxicology 1999, 62, 187-192.
61. Gaballa, A. A., Changes in nitrate and nitrite contents of some vegetables during processing. Annals of Agricultural Science 2000, 45, 531-539.
62. Gajc-Wolska, J., Kowalczyk, K., Marcinkowska, M., Radzanowska, J., Bujalski, D., Influence of growth conditions and grafting on the yield, chemical composition and sensory quality of tomato fruit in greenhouse cultivation. Journal of Elementology 2015, 20, 73-81.
63. Gajc-Wolska, J., Kowalczyk, K., Radzanowska, J., Marcinkowska, M., Yield and quality attributes of endive (Cichorum endivia L.) cultivated in rockwool slabs. Acta Horticulturae 2012, 927, 367-372.
64. Gajc-Wolska, J., Lyszkowska, M., Zielony, T., The influence of grafting and biostimulators on the yield and fruit quality of greenhouse tomato cv. (Lycopersicon esculentum Mill.) grown in the field. Vegetable Crops Research Bulletin 2010, 72, 63-70.
65. Gajewski, M., Krawczyk, J., Dabrowska, A., The influence of cold storage on the quality of carrot cultivars. Annales Universitatis Mariae Curie Sklodowska. Sectio EEE, Horticultura 2007, 17, 41-51.
66. Gajewski, M., Radzanowska, J., Danilcenko, H., Jariene, E., Cerniauskiene, J., Quality of pumpkin cultivars in relation to sensory characteristics. Notulae Botanicae, Horti Agrobotanici, Cluj Napoca 2008, 36, 73-79.
166 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
67. Gajewski, M., Smarz, M., Radzanowska, J., Pudzianowska, M., The influence of storage conditions on quality parameters of head cabbage with conical heads. Acta Horticulturae 2015, 1099 233-240.
68. Gajewski, M., Szymczak, P., Bajer, M., Sereda, A., Accumulation of chemical compounds in carrot storage roots under different light conditions. Annals of Warsaw University of Life Sciences SGGW, Horticulture and Landscape Architecture 2011, 32, 15-23.
69. Gajewski, M., Szymczak, P., Bajer, M., The accumulation of chemical compounds in storage roots by carrots of different cultivars during vegetation period. Acta Scientiarum Polonorum Hortorum Cultus 2009, 8, 69-78.
70. Gent, M. P. N., Comparison of diurnal variation of nitrate and sugars in lettuce and predictions of a model based on metabolism. Acta Horticulturae 2011, 893, 739-746.
71. Gent, M. P., Composition of hydroponic lettuce: effect of time of day, plant size, and season. J Sci Food Agric 2012, 92, 542-550.
72. Gonnella, M., Serio, F., Conversa, G., Santamaria, P., Production and nitrate content in lamb's lettuce grown in floating system. Acta Horticulturae 2004, 664, 61-68.
73. Gorenjak, A. H., Koleznik, U. R., Cencic, A., Nitrate content in dandelion (Taraxacum officinale) and lettuce (Lactuca sativa) from organic and conventional origin: intake assessment. Food Additives & Contaminants Part B-Surveillance 2012, 5, 93-99.
74. Gorenjak, A. H., Urih, D., Langerholc, T., Krist, J., Nitrate content in potatoes cultivated in contaminated groundwater areas. Journal of Food Research 2014, 3.
75. Goswami, M., Sarkar, C. R., Das, D., Nitrate and nitrite contents in some vegetables. Journal of the Agricultural Science Society of North East India 2000, 13, 247-250.
76. Grabovtska, A., Kunicki, E., Libik, A., The effect of transplant age and storage time in a cold room on chemical composition of broccoli heads. Folia Horticulturae 2007, 19, 11-22.
77. Grevsen, K., Kaack, K., Quality attributes and morphological characteristics of spinach (Spinacia oleracea L.) cultivars for industrial processing. Journal of Vegetable Crop Production 1996, 2, 15-29.
78. Grzegorzewska, M., Adamicki, F., Elkner, K., Comparison of storage ability of some Chinese cabbage cultivars (Brassica rapa L. var. pekinensis (Lour.) Olsson) from spring, summer and autumn production. Vegetable Crops Research Bulletin 1998, 49, 95-106.
79. Grzeszczuk, M., Jadczak, D., Podsiadlo, C., The effect of blanching, freezing and freeze-storage on changes of some chemical compounds content in New Zealand spinach. Vegetable Crops Research Bulletin 2007, 66, 95-103.
80. Guadagnin, S. G., Rath, S., Reyes, F. G. R., Evaluation of the nitrate content in leaf vegetables produced through different agricultural systems. Food Additives and Contaminants 2005, 22, 1203-1208.
81. Guil-Guerrero, J. L., Martinez-Guirado, C., Rebolloso-Fuentes, M. d. M., Carrique-Perez, A., Nutrient composition and antioxidant activity of 10 pepper (Capsicum annuun) varieties. European Food Research and Technology 2007, 224, 1-9.
82. Guil-Guerrero, J. L., Rebolloso-Fuentes, M. M., Nutrient composition and antioxidant activity of eight tomato (Lycopersicon esculentum) varieties. Journal of Food Composition and Analysis 2009, 22, 123-129.
83. Guillard, K., Allinson, D. W., Seasonal variation in chemical composition of forage Brassicas. II. Mineral imbalances and antiquality constituents. Agronomy Journal 1989, 81, 881-886.
84. Gundimeda, U., Naidu, A. N., Krishnaswamy, K., Dietary intake of nitrate in India. Journal of Food Composition and Analysis 1993, 6, 242-249.
85. Gutezeit, B., Fink, M., Effect of cultivar and harvest date on nitrate content of carrot roots. Journal of Horticultural Science & Biotechnology 1999, 74, 297-300.
86. Haghighi, B., Tavassoli, A., Flow-injection analysis of nitrate by reduction to nitrite and gas-phase molecular absorption spectrometry. Fresenius Journal of Analytical Chemistry 2001, 371, 1113-1118.
87. Hajslova, J., Schulzova, V., Slanina, P., Janne, K., et al., Quality of organically and conventionally grown potatoes: four-year study of micronutrients, metals, secondary metabolites, enzymic browning and organoleptic properties. Food Additives & Contaminants 2005, 22, 514-534.
88. Hamouz, K., Cepl, J., Dvorak, P., Influence of environmental conditions on the quality of potato tubers. Zahradnictvi 2005, 32, 89-95.
167 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
89. Handke, S., Junge, H. Green matter yield and nitrate content in a dioecious spinach genotype with a long vegetative phase. Colloque Eucarpia sur les legumes a feuilles: Versailles, 1894, 28-29.
90. Hertz, J., Baltensperger, U., Determination of nitrate and other inorganic anions (NO2-, PO43-, Cl-, SO42-) in salad and vegetables by ion chromatography. Analytical & Bioanalytical Chemistry 1984, 318, 121-123.
91. Hongsibsong, S., Polyiem, W., Narksen, W., Kerdnoi, T., Prapamontol, T., Determination of nitrate in the edible part of vegetables from markets around Chiang Mai City, Northern Thailand by using high performance liquid chromatography. Asian Journal of Agricultural Research 2014, 8, 204-210.
92. Hord, N. G., Tang, Y. P., Bryan, N. S., Food sources of nitrates and nitrites: the physiologic context for potential health benefits. American Journal of Clinical Nutrition 2009, 90, 1-10.
93. Hsu, J., Arcot, J., Alice Lee, N., Nitrate and nitrite quantification from cured meat and vegetables and their estimated dietary intake in Australians. Food Chemistry 2009, 115, 334-339.
94. Huang, K., Wang, H., Guo, Y., Fan, R., Zhang, H., Spectrofluorimetric determination of trace nitrite in food products with a new fluorescent probe 1,3,5,7-tetramethyl-2,6-dicarbethoxy-8-(3',4'-diaminophenyl)-difluoroboradiaza-s-indacene. Talanta 2006, 69, 73-78.
95. Huang, S. W., Jin, J. Y., Yang, L. P., Bai, Y. L., Li, C. H., Spatial variability of nitrate in cabbage and nitrate-N in soil. Soil Science 2004, 169, 640-649.
96. Hunt, J., Turner, M. K., A survey of nitrite concentrations in retail fresh vegetables. Food Additives & Contaminants 1994, 11, 327-332.
97. Iammarino, M., Taranto, A. d., Cristino, M., Endogenous levels of nitrites and nitrates in wide consumption foodstuffs: results of five years of official controls and monitoring. (Special Issue: Food quality evaluation.). Food Chemistry 2013, 140, 763-771.
98. Iammarino, M., Taranto, A. d., Cristino, M., Monitoring of nitrites and nitrates levels in leafy vegetables (spinach and lettuce): a contribution to risk assessment. Journal of the Science of Food and Agriculture 2014, 94, 773-778.
99. Ierna, A., Influence of harvest date on nitrate contents of three potato varieties for off-season production. (Special Issue: International year of the potato 2008.). Journal of Food Composition and Analysis 2009, 22, 551-555.
100. Ierna, A., Tuber yield and quality characteristics of potatoes for off-season crops in a Mediterranean environment. Journal of the Science of Food & Agriculture 2010, 90, 85-90.
101. Jadczak, D., Grzeszczuk, M., Kosecka, D., Quality characteristics and content of mineral compounds in fruit of some cultivars of sweet pepper (Capsicum annuum L.). Journal of Elementology 2010, 15, 509-515.
102. Jaworska, G., Content of nitrates, nitrites, and oxalates in New Zealand spinach. Food Chemistry 2005, 89, 235-242.
103. Jaworska, G., Kmiecik, W., Comparison of the nutritive value of frozen spinach and New Zealand spinach. Polish Journal of Food and Nutrition Sciences 2000, 9, 79-84.
104. Jaworska, G., Nitrates, nitrites, and oxalates in products of spinach and New Zealand spinach: Effect of technological measures and storage time on the level of nitrates, nitrites, and oxalates in frozen and canned products of spinach and New Zealand spinach. Food Chemistry 2005, 93, 395-401.
105. Jiang, Z.-T., Guo, Y.-X., Li, R., Spectrophotometric determination of trace nitrite with brilliant cresyl blue using o-cyclodextrin as a sensitizer. Food Analytical Methods 2010, 3, 47-53.
106. Jimidar, M., Hartmann, C., Cousement, N., Massart, D. L., Determination of nitrate and nitrite in vegetables by capillary electrophoresis with indirect detection. Journal of Chromatography A 1995, 706, 479-492.
107. Kaack, K., Kjeldsen, G., Mune, L., Changes in quality attributes during growth of leek (Allium porrum L.) for industrial processing. Acta Agriculturae Scandinavica. Section B, Soil and Plant Science 1993, 43, 172-175.
108. Kaminishi, A., Kita, N., Seasonal change of nitrate and oxalate concentration in relation to the growth rate of spinach cultivars. HortScience 2006, 41, 1589-1595.
109. Kaniszewski, S., Rumpel, J., Elkner, K., Yield and quality of leek (Allium porrum) as affected by method of growing. Acta Horticulturae 1989, 244, 229-234.
110. Karkleliene, R., Dambrauskiene, E., Radzevicius, A., Evaluation of the morphological, physiological and biochemical parameters of edible carrot (Daucus sativus Rohl.). Biologija 2008, 54, 101-104.
168 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
111. Karkleliene, R., Viskelis, P., Radzevicius, A., Duchovskiene, L., Evaluation of productivity and biochemical composition of perspective red beet breeding number. Acta Horticulturae 2009, 830, 255-260.
112. Keeton, J. T., Osburn, W. N., Hardin, M. D., Bryan, N. S., Longnecker, M. T., A National Survey of the Nitrite/Nitrate Concentrations in Cured Meat Products and Non-meat Foods Available at Retail. Des Moines: American Meat Institute Foundations 2009.
113. Kharsyntiew, L. S., Bharose, R., Sushil, K., Thomas, T., An analytical study of nitrate-nitrogen on vegetables from different markets of Allahabad. International Journal of Agricultural Sciences 2014, 10, 474-476.
114. Khoshgoftarmanesh, A. H., Aghili, F., Sanaeiostovar, A., Daily intake of heavy metals and nitrate through greenhouse cucumber and bell pepper consumption and potential health risks for human. International Journal of Food Sciences & Nutrition 2009, 60 Suppl 1, 199-208.
115. Kim, S. J., Ishii, G., Effect of storage temperature and duration on glucosinolate, total vitamin C and nitrate contents in rocket salad (Eruca sativa Mill.). Journal of the Science of Food and Agriculture 2007, 87, 966-973.
116. Kirovska-Cigulevska, O., Determination of nitrates in food products. BAU Fen Bil. Enst. Dergisi 2002, 4.2.
117. Koh, E. M., Charoenprasert, S., Mitchell, A. E., Effect of organic and conventional cropping systems on ascorbic acid, vitamin C, flavonoids, nitrate, and oxalate in 27 varieties of spinach (Spinacia oleracea L.). Journal of Agricultural and Food Chemistry 2012, 60, 3144-3150.
118. Kolota, E., Adamczewska-Sowinska, K., The effects of flat covers on overwintering and nutritional value of leeks. Vegetable Crops Research Bulletin 2007, 66, 11-16.
119. Kolton, A., Wojciechowska, R., Leja, M., Effect of maturity stage and short-term storage on the biological quality of sweet pepper fruits. Vegetable Crops Research Bulletin 2011, 74, 143-152.
120. Korus, A., Lisiewska, Z., Effect of cultivar and harvest date of kale (Brassica Oleracea L. var. Acephala) on content of nitrogen compounds. Polish Journal of Environmental Studies 2009, 18, 235-241.
121. Kosson, R., Elkner, K., Szafirowska, A., Quality of fresh and processed red beet from organic and conventional cultivation. Vegetable Crops Research Bulletin 2011, 75, 125-132.
122. Koudela, M., Petrikova, K., Influence of a non-woven textile covering on the content of nutrient compounds of lettuce. Scientia Agriculturae Bohemica 2009, 40, 12-17.
123. Koudela, M., Petrikova, K., Nutrients content and yield in selected cultivars of leaf lettuce (Lactuca sativa L. var. crispa). Horticultural Science 2008, 35, 99-106.
124. Koudela, M., Petrikova, K., Nutritional composition and yield of endive cultivars - Cichorium endivia L. Horticultural Science 2007, 34, 6-10.
125. Koukounaras, A., Yield and quality parameters of two radicchio (Cichorium intubys L.) cultivars as affected by growth season. European Journal of Horticultural Science 2014, 79, 283-287.
126. Krejcova, A., Navesnik, J., Jicinska, J., Cernohorsky, T., An elemental analysis of conventionally, organically and self-grown carrots. Food Chem 2016, 192, 242-249.
127. Krezel, J., Kolota, E., Yield evaluation of some Chinese cabbage cultivars in spring and autumn cultivation. Folia Horticulturae 2003, 15, 11-18.
128. Krusteva, L., Sabeva, M., Lozanov, I., Correlation between nitrate content and some quantitative characters in green bean collection. Acta Horticulturae 1997, 462, 243-248.
129. Kulkarni, S. G., Chauhan, A. S., Ramana, K. V. R., Nitrate and nitrite content in some important South Indian vegetables. Journal of Food Science and Technology 2003, 40, 518-520.
130. Kunicki, E., Grabowska, A., Sekara, A., Wojciechowska, R., The effect of cultivar type, time of cultivation, and biostimulant treatment on the yield of spinach (Spinacia oleracea L.). Folia Horticulturae 2010, 22, 9-13.
131. Lachman, J., Hamouz, K., Dvorak, P., Orsak, M., The effect of selected factors on the content of protein and nitrates in potato tubers. Plant, Soil and Environment 2005, 51, 431-438.
132. Lazic, B., Djurovka, M., Markovic, V., Ilin, Z., VIIth meeting on genetics and breeding on capsicum and eggplant, European Association for Research on Plant Breeding, Kragujevac (Yugoslavia) 1989.
133. Leszczynska, T., Filipiak-Florkiewicz, A., Cieslik, E., Sikora, E., Pisulewski, P. M., Effects of some processing methods on nitrate and nitrite changes in cruciferous vegetables. Journal of Food Composition and Analysis 2009, 22, 315-321.
134. Lu, Z., Liu, L., Li, X., Gong, Y., et al., Analysis and evaluation of nutritional quality in Chinese radish (Raphanus sativus L.). Agricultural Sciences in China 2008, 7, 823-830.
169 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
135. Lucarini, M., D'Evoli, L., Tufi, S., Gabrielli, P., et al., Influence of growing system on nitrate accumulation in two varieties of lettuce and red radicchio of Treviso. Journal of the Science of Food & Agriculture 2012, 92, 2796-2799.
136. Lutynski, R., Steczek-Wojdyla, M., Wojdyla, Z., Kroch, S., The concentrations of nitrates and nitrites in food products and environment and the occurrence of acute toxic methemoglobinemias. Przeglad Lekarski 1996, 53, 351-355.
137. Lyons, D. J., Rayment, G. E., Nobbs, P. E., McCallum, L. E., Nitrate and nitrite in fresh vegetables from Queensland. Journal of the Science of Food and Agriculture 1994, 64, 279-281.
138. MAFF, Department of Health and the Scottish Executive, 1994 Total Diet Study – Nitrate and Nitrite. Joint Food Safety and standards Group Food Surveillance Information Sheet No 137. 1996.
139. MAFF, Department of Health and the Scottish Executive, MAFF UK – 1997 Total Diet Study – Nitrate and Nitrite. Joint Food Safety and standards Group Food Surveillance Information Sheet No 163. 1998.
140. MAFF, Department of Health and the Scottish Executive, MAFF UK – 1997/1998 UK Monitoring Programme for Nitrate in Lettuce and Spinach. Joint Food Safety and standards Group Food Surveillance Information Sheet No 154. 1998.
141. MAFF, Department of Health and the Scottish Executive, MAFF UK – 1996/97 UK Monitoring Programme for Nitrate in Lettuce and Spinach. Joint Food Safety and standards Group Food Surveillance Information Sheet No 121. 1998.
142. MAFF, Department of Health and the Scottish Executive, MAFF UK – Nitrate in Vegetables. Joint Food Safety and standards Group Food Surveillance Information Sheet No 91. 1996.
143. Malmauret, L., Parent-Massin, D., Hardy, J. L., Verger, P., Contaminants in organic and conventional foodstuffs in France. Food Additives & Contaminants 2002, 19, 524-532.
144. Manzocco, L., Foschia, M., Tomasi, N., Maifreni, M., et al., Influence of hydroponic and soil cultivation on quality and shelf life of ready-to-eat lamb's lettuce (Valerianella locusta L. Laterr). Journal of the Science of Food & Agriculture 2011, 91, 1373-1380.
145. Markiewicz, B., Kleiber, T., The effect of Tytanit application on the content of selected microelements and the biological value of tomato fruits. Journal of Elementology 2014, 19, 1065-1072.
146. Martin, S. d., Restani, P., Determination of nitrates by a novel ion chromatographic method: occurrence in leafy vegetables (organic and conventional) and exposure assessment for Italian consumers. Food Additives and Contaminants 2003, 20, 787-792.
147. Martinez, A., Sanchez-Valverde, F., Gil, F., Clerigue, N., et al., Methemoglobinemia induced by vegetable intake in infants in northern Spain. Journal of Pediatric Gastroenterology & Nutrition 2013, 56, 573-577.
148. Matallana Gonzalez, M. C., Martinez-Tome, M. J., Torija Isasa, M. E., Nitrate and nitrite content in organically cultivated vegetables. Food Additives & Contaminants Part B-Surveillance 2010, 3, 19-29.
149. Meah, M. N., Harrison, N., Davies, A., Nitrate and nitrite in foods and the diet. Food Additives & Contaminants 1994, 11, 519-532.
150. Menal-Puey, S., Asensio, E., Validation of a rapid method for detecting nitrate in chard (Beta vulgaris cycla). Analysis of Spanish commercial samples marketed in the Region of Huesca, Spain, and estimation of the daily intake. Spanish Journal of Human Nutrition and Dietetics 2015, 19, 4-11.
151. Menard, C., Heraud, F., Volatier, J. L., Leblanc, J. C., Assessment of dietary exposure of nitrate and nitrite in France. Food Additives & Contaminants. Part A, Chemistry, Analysis, Control, Exposure & Risk Assessment 2008, 25, 971-988.
152. Merino, L., Darnerud, P. O., Edberg, U., Aman, P., Castillo, M. D. P., Levels of nitrate in Swedish lettuce and spinach over the past 10 years. Food Additives and Contaminants 2006, 23, 1283-1289.
153. Mirmohammad-Makki, F., Ziarati, P., Nitrate and nitrite in fresh tomato and tomato derived products. Biomedical & Pharmacology Journal 2015, 8.
154. Mor, F., Sahindokuyucu, F., Erdogan, N., Nitrate and nitrite contents of some vegetables consumed in south province of Turkey. Agricultural Journal 2010, 5, 142-145.
155. Morohashi, M., Enya, N., Suzuki, K., Asada, T., Kawata, K., Nitrate levels in fresh vegetables and berries from central Japan. Toxicological and Environmental Chemistry 2010, 92, 1495-1503.
156. Mozolewski, W., Smoczyñski, S., Effect of Culinary Processes on the Content of Nitrates and Nitrites in Potatoe. Pakistan Journal of Nutrition 2004, 3, 357-361.
170 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
157. Muramoto, J., Comparison of Nitrate Content in Leafy Vegetables from Organic and Conventional Farms in California. Center for Agroecology and Sustainable Food Systems, University of California, Santa Cruz 1999.
158. Musa, A., Ogbadoyi, E. O., Determination of anti-nutrients and toxic substances of selected fresh leafy vegetables obtained from minna town, Nigeria. Nigerian Journal of Basic and Applied Science 2014, 22, 79-83.
159. Negrea, M., Lazureanu, A., Alexa, E., Cozma, A., Olaru, D., Monitoring of nitrates and nitrites content in Allium cepa (onion) from Timisoara food markets and hypermarkets. Agro Buletin AGIR 2010, 2, 38-44.
160. Negrea, M., Lazureanu, A., Ersilia, A., Cozma, A., The monitoring of nitrogen compounds content in the horticultural products from the Timis County. Lucrari Stiintifice, Universitatea de Stiinte Agricole Si Medicina Veterinara "Ion Ionescu de la Brad" Iasi, Seria Horticultura 2007, 50, 937-942.
161. Negrea, M., Patrascoiu, M., Lazureanu, A., Radulov, I., Cocan, I., Studies concerning food safety of vegetables existing on markets and hypermarkets from Timisoara. Journal of Horticulture, Forestry and Biotechnology 2011, 15, 178-183.
162. Negrea, M., Rujescu, C., Alexa, E., Lazureanu, A., Statistics analysis regarding nitrate and nitrite content in lettuce from the west side of Romania. Analele Universitatii din Oradea, Fascicula Biologie 2009, 16, 78-81.
163. Nejatzadeh-Barandozi, F., Gholami-Borujeni, F., Nitrate and nitrite in leek and spinach from urmia district and their changes as affected by boiling. International Journal of Environmental Health Engineering 2013, 2.
164. Netherlands Food and Consumer Product Safety Authority, Report of nitrate monitoring results concerning Regulation EU 466/2001. The Netherlands 2004..
165. Nowrouz, P., Taghipour, H., Dastgiri, S., Bafandeh, Y., Hashemimajd, K., Nitrate Determination of Vegetables in Varzeghan City, North-western Iran. Health Promotion Perspectives 2012, 2, 244-250.
166. Nunez de Gonzalez, M. T., Osburn, W. N., Hardin, M. D., Longnecker, M., et al., A survey of nitrate and nitrite concentrations in conventional and organic-labeled raw vegetables at retail. Journal of Food Science 2015, 00.
167. Oliveira, S. M., Lopes, T. I. M. S., Rangel, A. O. S. S., Sequential injection determination of nitrate in vegetables by spectrophotometry with inline cadmium reduction. Communications in Soil Science and Plant Analysis 2007, 38, 533-544.
168. Ombodi, A., Kosuge, S., Saigusa, M., Effects of polyolefin-coated fertilizer on nutritional quality of spinach plants. Journal of Plant Nutrition 2000, 23, 1495-1504.
169. Onyesom, I., Okoh, P. N., Quantitative analysis of nitrate and nitrite contents in vegetables commonly consumed in Delta State, Nigeria. British Journal of Nutrition 2006, 96, 902-905.
170. Ozdestan, O., Uren, A., Development of a cost-effective method for nitrate and nitrite determination in leafy plants and nitrate and nitrite contents of some green leafy vegetables grown in the Aegean Region of Turkey. Journal of Agricultural and Food Chemistry 2010, 58, 5235-5240.
171. Oztekin, N., Nutku, M. S., Erim, F. B., Simultaneous determination of nitrite and nitrate in meat products and vegetables by capillary electrophoresis. Food Chemistry 2002, 76, 103-106.
172. Pardo-Marin, O., Yusa-Pelecha, V., Villalba-Martin, P., Perez-Dasi, J. A., Monitoring programme on nitrates in vegetables and vegetable-based baby foods marketed in the Region of Valencia, Spain: levels and estimated daily intake. Food Additives & Contaminants. Part A, Chemistry, Analysis, Control, Exposure & Risk Assessment 2010, 27, 478-486.
173. Parks, S. E., Huett, D. O., Campbell, L. C., Spohr, L. J., Nitrate and nitrite in Australian leafy vegetables. Australian Journal of Agricultural Research 2008, 59, 632-638.
174. Penttila, P.-L., Rasanen, L., Kimppa, S., Nitrate, nitrite, and N-nitroso compounds in Finnish and the estimation of the dietary intakes. Zeitschrift für Lebensmittel-Untersuchung und Forschung 1990,190.4: 336-340.
175. Petersen, A., Stoltze, S., Nitrate and nitrite in vegetables on the Danish market: content and intake. Food Additives & Contaminants 1999, 16, 291-299.
176. Peyvast, G., Abbassi, M., Effect of commercial compost on yield and nitrate content of Chinese cabbage. Horticulture, Environment and Biotechnology 2006, 47, 123-125.
177. Pham Hoai, N., Alejandra, B., Frederic, H., Didier, B., et al., A new quantitative and low-cost determination method of nitrate in vegetables, based on deconvolution of UV spectra. Talanta 2008, 76, 936-940.
171 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
178. Phupaibul, P., Chinoim, N., Matoh, T., Nitrate concentration in Chinese kale sold at markets around Bangkok, Thailand. Thai Journal of Agricultural Science 2002, 35, 295-302.
179. Pinto, E., Petisca, C., Amaro, L. F., Pinho, O., Ferreira, I. M. P. L. V. O., Influence of different extraction conditions and sample pretreatments on quantification of nitrate and nitrite in spinach and lettuce. Journal of Liquid Chromatography & Related Technologies 2010, 33, 591-602.
180. Pirsaheb, M., Ahmadian, M., Reshadat, S., Poormohammadi, A., The measurement of nitrite and nitrate contents of tomato from the vast plain of kermanshah state of iran. International Journal of Agriculture and Crop Sciences 2014, 7, 1553-1559.
181. Poberezny, J., The content of nitrates(V) in potato tubers in depending on the cultivation site and storage conditions. Polish Journal of Natural Sciences 2008, 23, 336-346.
182. Pokluda, R., An assessment of the nutritional value of vegetables using an ascorbate-nitrate index. Vegetable Crops Research Bulletin 2006, 64, 29-37.
183. Pokluda, R., Nutritional quality of Chinese cabbage from integrated culture. Horticultural Science 2008, 35, 145-150.
184. Pokluda, R., Petrikova, K., Kopta, T., Jurica, M., et al., The effect of irrigation on the economic and nutritional characteristics of selected vegetables. Acta horticulturae 2014, 1038, 231-238.
185. Pokluda, R., Selected nutritional aspects of field grown root vegetables in the Czech Republic. Acta Horticulturae 2013, 989, 315-322.
186. Prasad, S., Chetty, A. A., Flow injection assessment of nitrate contents in fresh and cooked fruits and vegetables grown in Fiji. Journal of Food Science 2011, 76, C1143-1148.
187. Raczuk, J., Wadas, W., Glozak, K., Nitrates and nitrites in selected vegetables purchased at supermarkets in Siedlce, Poland. Roczniki Panstwowego Zakladu Higieny 2014, 65, 15-20.
188. Radzevicius, A., Karkleliene, R., Bobinas, C., Viskelis, P., Nutrition quality of different tomato cultivars. Zemdirbyste 2009, 96, 67-75.
189. Reinink, K., Groenwold, R., Bootsma, A., Genotypical differences in nitrate content in Lactuca sativa L. and related species and correlation with dry matter content. Euphytica 1987, 36, 11-18.
190. Rembialkowska, E., Comparison of the contents of nitrates, nitrites, lead, cadmium and vitamin C in potatoes from conventional and ecological farms. Polish Journal of Food and Nutrition Sciences 1999, 8, 17-26.
191. Rezaei, M., Fani, A., Moini, A. L., Mirzajani, P., et al., Determining Nitrate and Nitrite Content in Beverages, Fruits, Vegetables, and Stews Marketed in Arak, Iran. International Scholarly Research Notices 2014, 1-5.
192. Roorda van Eysinga, J. P. N. L., Nitrate in vegetables under protected cultivation. Acta Horticulturae 1984, 145, 251-256.
193. Rousta, M. J., Lotfi, E., Shamsalam, N., Mousavi, F., et al., Nitrate situation in some vegetables and the necessity of crop production via organic farming. 19th World Congress of Soil Science, Soil Solutions for a Changing World, Brisbane (Australia) 2010.
194. Rovira, R. F., Bermudo, F. M., Fernández, A. M. C., Sáez, A. C., et al., Report from the Scientific Committee of the Spanish Agency for Food Safety and Nutrition (AESAN) in relation to the risk assessment of infants and young children’s exposure to nitrates resulting from the consumption of chard in Spain. 2011.
195. Rozek, S., Sady, W., Wojciechowska, R., Leja, M., Quality changes in lettuce heads stored in a controlled atmosphere. I. Activity of nitrate and nitrite reductase, content of nitrates and other compounds. Folia Horticulturae 1996, 8, 71-81.
196. Saeedifar, F., Ziarati, P., Ramezan, Y., Nitrate and Heavy Metal Contents In Eggplant (Solanum melongena) cultivated in the farmlands in the south of Tehran-Iran. International Journal of Farming and Allied Sciences 2014, 3, 60-65.
197. Sanchez, C. A., Blount, B. C., Valentin-Blasini, L., Krieger, R. I., Perchlorate, thiocyanate, and nitrate in edible cole crops (Brassica sp.) produced in the lower Colorado River region. Bulletin of Environmental Contamination & Toxicology 2007, 79, 655-659.
198. Sanchez, C. A., Crump, K. S., Krieger, R. I., Khandaker, N. R., Gibbs, J. P., Perchlorate and nitrate in leafy vegetables of North America. Environmental Science & Technology 2005, 39, 9391-9397.
199. Sanni, S. B., A survey of nitrate-nitrite in vegetables in Benin environs. Journal of Plant Foods 1983, 5, 75-79.
200. Santamaria, P., Elia, A., Serio, F., Todaro, E., A survey of nitrate and oxalate content in fresh vegetables. Journal of the Science of Food and Agriculture 1999, 79, 1882-1888.
172 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
201. Sawicka, B., Quality of potato cultivated under the ecological and integrated production system. Sodininkyste ir Darzininkyste 2003, 22, 10-20.
202. Schonbeck, M. W., Rivera, R., O'Brien, J., Ebinger, S., DeGregorio, R. E., Variety selection and cultural methods for lowering nitrate levels in winter greenhouse lettuce and endive. Journal of Sustainable Agriculture 1991, 2, 49-75.
203. Schulzova, V., Hajslova, J., Guziur, J., Velisek, J., in: Hagg, M., Ahvenainen, R., Evers, A. M., Tiilikkala, K. (Eds.), Agri-Food Quality II, The Royal Society of Chemistry, Turku, Finland 1999.
204. Schuster, B. E., Lee, K., Nitrate and nitrite methods of analysis and levels in raw carrots, processed carrots and in selected vegetables and grain products. Journal of Food Science 1987, 52, 1632-1636.
205. Sebecic, B., Vedrina-Dragojevic, I., Nitrate and nitrite in vegetables from areas affected by war-time operations in Croatia. Nahrung 1999, 43, 284-287.
206. Sękara, A., Kalisz, A., Cebula, S., Grabowska, A., The quality and processing usefulness of chosen polish carrot cultivars. Acta Scientiarum Polonorum Hortorum Cultus 2012, 11, 101-112.
207. Sekara, A., Pohl, A., Kalisz, A., Grabowska, A., Cebula, S., Evaluation of selected Polish carrot cultivars for nutritive value and processing - a preliminary study. Annals of Warsaw University of Life Sciences SGGW, Horticulture and Landscape Architecture 2014, 35, 3-14.
208. Shahlaei, A., Ansari, N. A., Dehkordie, F. S., Evaluation of nitrate and nitrite content of Iran southern (Ahwaz) vegetables during winter and spring of 2006. Asian Journal of Plant Sciences 2007, 6, 1197-1203.
209. Shimada, Y., Ko, S., Nitrate in vegetables. Chugoku Gakuen J 2004, 3, 7-10. 210. Shokrzadeh, M., Shokravie, M., Ebadi, A. G., Babaee, Z., Tarighati, A., The measurement of
nitrate and nitrite content in leek and spinach sampled from central cities of Mazandaran state of Iran. American Eurasian Journal of Agricultural and Environmental Science 2007, 2, 169-172.
211. Shokrzadeh, M., Shokravie, M., Saravi, S. S. S., The measurement of nitrate and nitrite content in carrots and onions sampled from central cities of Mazandaran State of Iran. Toxicological and Environmental Chemistry 2008, 90, 603-607.
212. Siddiqi, M., Kumar, R., Fazili, Z., Spiegelhalder, B., Preussmann, R., Increased exposure to dietary amines and nitrate in a population at high risk of oesophageal and gastric cancer in Kashmir (India). Carcinogenesis 1992, 13, 1331-1335.
213. Sikora, E., Bodziarczyk, I., Composition and antioxidant activity of kale (Brassica oleracea L. var. acephala) raw and cooked. Acta Scientiarum Polonorum Technologia Alimentaria 2012, 11, 239-248.
214. Sikora, E., Cieslik, E., Correlation between the levels of nitrates and nitrites and the contents of iron, copper and manganese in potato tubers. Food Chemistry 1999, 67, 301-304.
215. Siomos, A. S., Dogras, C. C., Nitrates in vegetables produced in Greece. Journal of Vegetable Crop Production 1999, 5, 3-13.
216. Skapski, H., Gajc-Wolska, J., Odziemkowski, S., Timing of field production of some salad vegetable crops. Acta Horticulturae 1994, 371, 113-119.
217. Stopes, C., Woodward, L., Forde, G., Vogtmann, H., The nitrate content of vegetable and salad crops offered to the consumer as from "organic" or "conventional" production systems. Biological Agriculture and Horticulture 1988, 5, 215-221.
218. Surendra, P., Chetty, A. A., Nitrate-N determination in leafy vegetables: study of the effects of cooking and freezing. Food Chemistry 2008, 106, 772-780.
219. Susin, J., Kmecl, V., Gregorcic, A., A survey of nitrate and nitrite content of fruit and vegetables grown in Slovenia during 1996-2002. Food Additives & Contaminants 2006, 23, 385-390.
220. Takruri, H. R., Humeid, M. A., Nitrate levels in edible wild herbs and vegetables common in Jordan. Nutrition & Health 1988, 6, 89-98.
221. Tamme, T., Reinik, M., Roasto, M., Juhkam, K., et al., Nitrates and nitrites in vegetables and vegetable-based products and their intakes by the Estonian population. Food Additives & Contaminants 2006, 23, 355-361.
222. Tamme, T., Reinik, M., Roasto, M., Meremae, K., Kiis, A., Nitrate in leafy vegetables, culinary herbs, and cucumber grown under cover in Estonia: content and intake. Food Additives & Contaminants Part B-Surveillance 2010, 3, 108-113.
223. Temme, E. H., Vandevijvere, S., Vinkx, C., Huybrechts, I., et al., Average daily nitrate and nitrite intake in the Belgian population older than 15 years. Food Additives & Contaminants. Part A, Chemistry, Analysis, Control, Exposure & Risk Assessment 2011, 28, 1193-1204.
173 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
224. Tendaj, M., Sawicki, K., Mysiak, B., The content of some chemical compounds in red cabbage (Brassica oleracea L. var. capitata F. rubra) after harvest and long-term storage. Electronic Journal of Polish Agricultural Universities 2013, 16.
225. Teotia, M. S., Berry, S. K., Kulkarni, S. G., Kour, S., Nitrate and nitrite contents in vegetables. Journal of Food Science and Technology 1988, 25, 272-275.
226. Termine, E., Lairon, D., Taupier-Letage, B., Gautier, S., et al., Yield and content in nitrates, minerals and ascorbic acid of leeks and turnips grown under mineral or organic nitrogen fertilizations. Plant Foods for Human Nutrition 1987, 37, 321-332.
227. Thomson, B. M., Nokes, C. J., Cressey, P. J., Intake and risk assessment of nitrate and nitrite from New Zealand foods and drinking water. Food Additives & Contaminants 2007, 24, 113-121.
228. Tokoro, N., Sawada, M., Suganuma, Y., Mochizuki, M., et al., Nitrogen composition of vegetables common to Japan. Journal of Food Composition and Analysis 1987, 1, 18-25.
229. Tomoskozi-Farkas, R., Polgar, Z., Nagy-Gasztonyi, M., Horvath, V., et al., Changes of potentially anti-nutritive components in Hungarian potatoes from organic and conventional farming. Acta Alimentaria 2014, 43, 676-683.
230. Tosun, I., Ustun, N. S., Nitrate content of lettuce grown in the greenhouse. Bulletin of Environmental Contamination & Toxicology 2004, 72, 109-113.
231. Uklanska-Pusz, C. M., Adamczewska-Sowinska, K., Yield and nutritive value of selected endive cultivars grown for spring and autumn harvest. Folia Horticulturae 2011, 23, 111-118.
232. Urrestarazu, M., Postigo, A., Salas, M., Sanchez, A., Carrasco, G., Nitrate accumulation reduction using chloride in the nutrient solution on lettuce growing by NFT in semiarid climate conditions. Journal of Plant Nutrition 1998, 21, 1705-1714.
233. Uwah, E. I., Akan, J. C., Moses, E. A., Abah, J., Ogugbuaja, V. O., Some anion levels in fresh vegetables in Maiduguri, Borno State, Nigeria. Agricultural Journal 2007, 2, 392-396.
234. Vahed, S., Mosafa, L., Mirmohammadi, M., Lakzadeh, L., Effect of some processing methods on nitrate changes in different vegetables. Food Measure 2015.
235. van der Schee, H. A., and A. J. Speek. "Report of nitrate monitoring results concerning Regulation EU 194/97: The Netherlands 2002.
236. van der Schee, H. A., Speek, A. J., . "Report of nitrate monitoring results concerning Regulation EU 194/97: The Netherlands 2000.
237. van der Schee, H. A., Speek, A. J., . "Report of nitrate monitoring results concerning Regulation EU 194/97: The Netherlands 2001.
238. van der Schee, H. A., Speek, A. J., . "Report of nitrate monitoring results concerning Regulation EU 194/97: The Netherlands 2003.
239. van Velzen, A. G., Sips, A. J. A. M., Schothorst, R. C., Lambers, A. C., Meulenbelt, J., The oral bioavailability of nitrate from nitrate-rich vegetables in humans. Toxicology Letters 2008, 181, 177-181.
240. Vasile, G., Artimon, M., Halmajan, H. V., Pele, M., Survey of nitrogen pollutants in horticultural products and their potential toxic implications. Journal of EcoAgriTourism 2010, 6, 67-72.
241. Watanabe, M., Ayugase, J., Effect of low temperature on flavonoids, oxygen radical absorbance capacity values and major components of winter sweet spinach (Spinacia oleracea L.). Journal of the Science of Food and Agriculture 2015, 95, 2095-2104.
242. Weightman, R. M., Dyer, C., Buxton, J., Farrington, D. S., Effects of light level, time of harvest and position within field on the variability of tissue nitrate concentration in commercial crops of lettuce (Lactuca sativa) and endive (Cichorium endiva). Food Additives & Contaminants 2006, 23, 462-469.
243. Weimin, Z., Shijun, L., Lihong, G., Laibing, C., et al., Genetic diversity of nitrate accumulation in vegetable crops. Acta Horticulturae 1998, 467, 119-126.
244. Wierzbicka, B., Kuskowska, M., Majkowska, J., The level of nitrates in edible parts of vegetable species. Sodininkyste ir Darzininkyste 2000, 19, 444-450.
245. Wojciechowska, R., Kolton, A., Comparison of the ability of fifteen onion (Allium cepa L.) cultivars to accumulate nitrates. Acta Agrobotanica 2014, 67, 27-32.
246. Wruss, J., Waldenberger, G., Huemer, S., Uygun, P., et al., Compositional characteristics of commercial beetroot products and beetroot juice prepared from seven beetroot varieties grown in Upper Austria. Journal of Food Composition and Analysis 2015, 42, 46-55.
247. Wrzodak, A., Szwejda-Grzybowska, J., Elkner, K., Babik, I., Comparison of the nutritional value and storage life of carrot roots from organic and conventional cultivation. Vegetable Crops Research Bulletin 2012, 76, 137-150.
174 DEVELOPMENT OF A REFERENCE DATABASE FOR ASSESSING DIETARY NITRATE IN VEGETABLES
248. Ximenes, M. I. N., Rath, S., Reyes, F. G. R., Polarographic determination of nitrate in vegetables. Talanta 2000, 51, 49-56.
249. Ysart, G., Clifford, R., Harrison, N., Monitoring for nitrate in UK-grown lettuce and spinach. Food Additives & Contaminants 1999, 16, 301-306.
250. Ysart, G., Miller, P., Barrett, G., Farrington, D., et al., Dietary exposures to nitrate in the UK. Food Additives & Contaminants 1999, 16, 521-532.
251. Zatar, N. A., Abu-Eid, M. A., Eid, A. F., Spectrophotometric determination of nitrite and nitrate using phosphomolybdenum blue complex. Talanta 1999, 50, 819–826.
252. Zawiska, I., Siwek, P., The effects of PLA biodegradable and polypropylene nonwoven crop mulches on selected components of tomato grown in the field. Folia Horticulturae 2014, 26, 163-167.
253. Zhong, W., Hu, C., Wang, M., Nitrate and nitrite in vegetables from north China: content and intake. Food Additives & Contaminants 2002, 19, 1125-1129.
254. Zhou, Z. Y., Wang, M. J., Wang, J. S., Nitrate and nitrite contamination in vegetables in China. Food Reviews International 2000, 16, 61-76.
255. Ziarati, P., Arbabi-Bidgoli, S., Investigation of cooking method on nitrate and nitrite contents in crops and vegetables and assess the associatied health risk. International Journal of Plant, Animal and Environmental Sciences 2014, 4.
175 CHAPTER 6
CHAPTER 6
ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE
MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
Manuscript based on this chapter:
Lauren C Blekkenhorst, Catherine P Bondonno, Joshua R Lewis, Amanda Devine, Richard J Woodman, Kevin D Croft, Wai H Lim, Germaine Wong, Lawrence J Beilin, Richard L Prince, Jonathan M Hodgson. Association of dietary nitrate with atherosclerotic vascular disease mortality: a prospective cohort study of older adult women. American Journal of Clinical Nutrition 2017;106(1):207-216.

176 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
ABSTRACT
Background: Nitrate-rich vegetables lower blood pressure and improve endothelial function in humans. However, it is not known if increased consumption of nitrate-rich vegetables translates to lower risk of atherosclerotic vascular disease (ASVD) mortality.
Objective: To investigate the association of nitrate intake from vegetables with ASVD mortality.
Design: 1,226 Australian women without prevalent ASVD and/or diabetes aged 70-85 years were recruited in 1998 and were followed for 15 years. At baseline (1998) demographic and ASVD risk factors were assessed, and a validated food frequency questionnaire was used to evaluate dietary intake. Nitrate intake from vegetables was calculated using a newly developed comprehensive database. The primary outcome was any death attributed to ASVD ascertained using linked data provided via the Western Australian Data Linkage System. Cox proportional hazards modelling was used to examine the association between nitrate intake and ASVD mortality before and after adjustment for lifestyle and cardiovascular risk factors.
Results: Over a follow-up period of 15,947 person-years, 238/1,226 (19.4%) women died from ASVD-related causes. Mean (SD) vegetable nitrate intake was 67.0 (29.2) mg/d. Each SD higher vegetable nitrate intake was associated with a lower risk of ASVD mortality in both unadjusted (HR=0.80, 95%CI 0.70, 0.92, P=0.002) and multivariable-adjusted (HR=0.79, 95%CI 0.68, 0.93, P=0.004) analyses. This relationship was attenuated after further adjustment for diet quality (HR=0.85, 95%CI 0.72, 1.01, P=0.072). Higher vegetable nitrate intake (per SD) was also associated with lower risk of all-cause mortality (multivariable-adjusted HR=0.87, 95%CI 0.78, 0.97, P=0.011).
Conclusion: In this population of older adult women without prevalent ASVD or diabetes, nitrate intake from vegetables was inversely associated with ASVD mortality independent of lifestyle and cardiovascular risk factors. These results support the concept that nitrate-rich vegetables may reduce the risk of age-related ASVD mortality.
177 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
INTRODUCTION
Atherosclerotic vascular disease (ASVD), a collective term for diseases relating to atherosclerosis, remains the leading cause of death worldwide (4). Atherosclerosis is a disease of the arteries initiated by dyslipidaemia and endothelial dysfunction and is characterised by the reduced bioavailability of nitric oxide (NO) (37). NO is an important cell signalling molecule and potent vasodilator, playing a pivotal role in the maintenance of vascular homeostasis (37). Dysfunction of the classical L-arginine-NO pathway and enhanced scavenging of NO underlie the reduced bioavailability of NO in individuals at risk of atherosclerotic diseases (121). Alternative pathways to restore NO levels could provide new therapeutic opportunities.
Dietary nitrate, found abundantly in beetroot and leafy green vegetables, is a precursor of NO via the enterosalivary nitrate-nitrite-NO pathway, a potentially important alternative pathway for NO production (44). Through this pathway, NO is generated via the sequential reduction of the anions nitrate and nitrite by the facultative anaerobic bacteria on the dorsal surface of the tongue, the acidic environment of the stomach and a number of endogenous molecules identified as having nitrite reducing potential (45). This nitrate-nitrite-NO pathway is independent of nitric oxide synthase (NOS) and may be enhanced in times of hypoxia (333). Research on dietary nitrate has undergone a dramatic shift in the last decade. Initially having concerns of being linked with cancer outcomes (250), focus has now shifted to the possible beneficial effects of dietary nitrate on cardiovascular health.
Over 30 human intervention studies have investigated the effects of dietary nitrate in the form of inorganic salts or nitrate-rich vegetables on measures of vascular health (143, 188, 310). These studies have shown increased nitrate intake can reduce blood pressure (163) and improve endothelial function (334). However, it is yet to be determined whether this translates into a reduction in long-term risk of ASVD.
To our knowledge, this prospective cohort study is the first to investigate the hypothesis that nitrate intake from vegetables is inversely associated with ASVD mortality. Nitrate intake from vegetables was the focus of this study as the majority of dietary nitrate consumed in the human population comes from intakes of vegetables (44, 131) and other sources of dietary nitrate such as processed meats have been linked to adverse health outcomes (335-337). Furthermore, there is now strong and up-to-date data on the nitrate concentrations of vegetables (36).
SUBJECTS AND METHODS
Ethics
The Perth Longitudinal Study of Aging in Women (PLSAW) was approved by the Human Ethics Committee of The University of Western Australia. Written informed consents were obtained from all participants. Human ethics approval for the use of linked data for the project was provided by the Human Research Ethics Committee of the Western Australian Department of Health (project #2009/24).
Study population
Participants of this prospective cohort study were originally recruited in 1998 to the Calcium Intake Fracture Outcome Study (CAIFOS). The CAIFOS was a 5 year, double-blind, placebo-
178 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
controlled randomised trial of daily calcium supplementation (1.2g calcium carbonate) to prevent osteoporotic fracture outcomes (257). Participants were ambulant and were included based on an expected survival beyond 5 years and not receiving any medication (including hormone replacement therapy) known to affect bone metabolism. Participants were recruited from the Western Australian general population of women aged 70 years and over by mail using the Electoral Roll, for which Australian citizenship is a requirement. More than 99% of Australians aged 70 years and over are registered on this roll. Of the 5,586 women approached, 1,500 women were recruited. Participants were further followed for an additional 10 years of observation with a total follow-up period of 15 years. This latter 15-year prospective study of older adult women was entitled the PLSAW. The CAIFOS and the PLSAW took place in Perth, Western Australia.
Eligibility criteria for this study included available data on all exposure and outcome variables. Missing dietary data resulted in 15/1,500 (1.0%) of participants being excluded from the analysis. Additionally, implausible scores for total energy intake (<2,100kJ [500kcal] or >14,700kJ [3,500kcal] per day) were excluded in 17/1,500 (1.1%). Participants with a baseline history of ASVD (n=152), diabetes (n=69) or both (n=21) were excluded, 242/1,500 (16.1%). Baseline history of ASVD and/or diabetes was an a priori exclusion criteria as women with a history of clinical ASVD and diabetes may have altered their diet as a result of their diagnosis, and thereby potentially attenuated the strength of the associations of interest. Baseline history of ASVD was determined from principal hospital discharge diagnosis codes from 1980-1998 using the Hospital Morbidity Data Collection, linked via the Western Australian Data Linkage System (WADLS). Diagnosis codes were defined using the Manual of the International Statistical Classification of Diseases, Injuries and Causes of Death, 9th Revision (ICD-9) (258) and the Australian Version of the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) (259). ASVD diagnosis codes included as ischemic heart disease (ICD-9/ICD-9-CM codes 410-414); heart failure (ICD-9/ICD-9-CM code 428); cerebrovascular disease, excluding haemorrhage (ICD-9/ICD-9-CM codes 433-438); and peripheral arterial disease (ICD-9/ICD-9-CM codes 440-444). Baseline history of diabetes was determined from medication use which was coded (T89001-T90009) using the International Classification of Primary Care – Plus (ICPC-Plus) method (260). In total, there were 1,226/1,500 (81.7%) of the original CAIFOS participants who met the entry criteria for this study and were therefore included for analysis (Figure 1).
Atherosclerotic vascular disease mortality assessment
The primary outcome of this study was any ASVD-related death. Fifteen years of multiple cause of death data were retrieved from linked mortality data. Causes of deaths were determined from the coded death certificate using information in Parts 1 and 2 of the death certificate, or all diagnosis text fields from the death certificate where coded death data were not yet available. ASVD deaths were defined using diagnosis codes from the ICD-9-CM (258) and the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM) (261). ASVD death diagnosis codes included as ischemic heart disease (ICD-9-CM codes 410-414 and ICD-10-AM codes I20-I25); heart failure (ICD-9-CM code 428 and ICD-10-AM code I50); cerebrovascular disease, excluding haemorrhage (ICD-9-CM codes 433-438 and ICD-10-AM codes I63-I69, G45.9); and peripheral arterial disease (ICD-9-CM codes 440-444 and ICD-10-AM codes I70-I74).

179 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
Dietary intake assessment
Dietary intake was assessed at baseline using a self-administered semi-quantitative food frequency questionnaire (FFQ) (262). This validated FFQ measures the usual frequency of food intake over a period of 12 months and comprises a food list of 74 items with 10 frequency response options ranging from 'Never' to '3 or more times per day' and is complemented with another 27 food and alcoholic beverage items using various questions such as “what type of milk do you usually use?” (263, 298). The questionnaire calculates portion size using three photographs of scaled portions for four different food types. Nutrient intake calculations were analysed by the Cancer Council of Victoria using the NUTTAB95 food composition database (264) and was supplemented by other data where necessary. The process of collection was identical for each individual, whereby a research assistant supervised the completion of the questionnaire. Food models, cups, spoons and charts were provided for accuracy.
Vegetable nitrate intake
Vegetable intake contributes 60-80% to total nitrate intake consumed in the human population (44). Therefore, for this study, dietary nitrate was calculated from consumed vegetables, which were assessed, using the 24 items listed on the FFQ and quantified in g/d by the Cancer Council of Victoria. Nitrate values for each individual vegetable were obtained from a recently developed comprehensive database on the nitrate content of vegetables (36). This database was compiled using a systematic approach and has nitrate data for 178 vegetables from over 250 publications. Nitrate intake was calculated by multiplying the vegetable consumed (g/d) by the median nitrate value (mg/g) of that vegetable. The sum of daily nitrate values from individual vegetables was then calculated.
Total nitrate intake
Nitrate intake from all other food items (n=77) listed on the FFQ was also determined. Nitrate values of 67 FFQ food items were obtained from Inoue-Choi et al (245), 5 were obtained from the Food Standards Australia New Zealand (FSANZ) survey of nitrates and nitrites in food and beverages in Australia (154), and 3 were obtained from Griesenbeck et al (244). Nitrate intake was calculated by multiplying the FFQ food item consumed (g/d) by the assigned mean nitrate value (mg/g) of that food item. A value of 0 mg/g was applied where no values were available for FFQ food items (Soya milk, vegemite and jam). Total nitrate intake (mg/d) was determined by calculating the sum of daily nitrate values from all other FFQ items together with vegetable items.
The concentration of nitrate in drinking water was assessed using data from the Western Australian Water Corporation Water Quality Management System (2012) from July 1997 to June 2001 for the Perth metropolitan area (24 regions). The absolute maximum value recorded was 0.0022 mg/g with a mean of 0.0003 mg/g. For an individual consuming 2 litres of water (including tea and coffee), this would equate to an estimated intake of 0.6 mg/d. Nitrate intake from drinking water was not included in the estimation of total nitrate intake as this contribution was negligible.
Nutrient-Rich Foods Index
Vegetable nitrate intake may be strongly associated with total vegetable intake and an overall healthy diet. Thus, we assessed overall diet quality by calculated nutrient density scores
180 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
assessed using the Nutrient-Rich Foods Index (265, 338). This index was adapted using the Nutrient Reference Values (NRVs) for Australia and New Zealand based on adult females aged >70 y. Participants were assigned a dietary nutrient density (DND) score, using the following equation DND=[∑(%RDI or AI of beneficial nutrients)] – [∑(%UL or daily intake guide of limit nutrients)] (265, 338). Scores for beneficial nutrients were capped at 100% of the assigned NRV to avoid over-representation of these nutrients in participants who consumed large amounts. Scores for nutrients to limit were not capped. DND scores were standardised for energy intake to give a DND score per 1000kJ/d. Positive scores for beneficial nutrients (protein, fibre, vitamins A, C and E, calcium, iron, potassium and magnesium) and negative scores for nutrients to limit (sodium, saturated fat and added sugars) were based on the percentage of adherence to the reference value for that nutrient. As we could not distinguish added sugar, total sugar was used. For the beneficial nutrients (protein, vitamins A and C, calcium, iron and magnesium) the recommended dietary intake (RDI) was used, and where an RDI was not available the adequate intake (AI) was used (fibre, vitamin E and potassium) (266). For nutrients to limit (sodium), the upper level of intake (UL) was used (266), and where an UL was not available the daily intake guide was used (saturated fat 24 g/d and sugar 90 g/d) (339).
Baseline demographic and clinical assessment
Body weight was measured using digital scales to the nearest 0.1 kg whilst participants were wearing light clothes and no shoes. Height was measured using a wall-mounted stadiometer to the nearest 0.1 cm whilst participants were wearing no socks or shoes. Body mass index (BMI) (kg/m2) was then calculated. Physical activity levels were assessed using a questionnaire asking participants about participation in sport, recreation and/or regular physical activities undertaken in the last three months of their baseline visit (267, 293). Activity levels were calculated in kJ/day using a validated method utilising the type of activity, the length of time engaged in the activity and the participant’s body weight (268, 269). Alcohol (g/d) and total energy intakes (kJ/d) along with all other dietary intakes were assessed using the Cancer Council of Victoria FFQ, which is described above. Data on smoking history was collected using a questionnaire and was coded as non-smoker or ex-smoker/current smoker. Ex-smoker/current smoker was defined as consuming more than 1 cigarette per day for more than 3 months at any time. Socioeconomic status (SES) was calculated using the Socioeconomic Indexes for Areas developed by the Australian Bureau of Statistics. The index ranked residential postcodes according to relative socioeconomic advantage and disadvantage. Participants were coded into 6 groups from the top 10% most highly disadvantaged to the top 10% least disadvantaged (270).
A comprehensive medical history and list of medications were obtained from all participants. The participant’s general practitioner verified accuracy where possible. These data were coded using the International Classification of Primary Care – Plus (ICPC-Plus) method (260). This coding methodology allows aggregation of different terms for similar pathologic entities as defined by the ICD-10 coding system. Cardiovascular medication use included organic nitrate containing medications, antihypertensive, statin and low-dose aspirin medications. These medications were used to adjust for potential risk of cardiovascular risk factors such as hypertension and dyslipidaemia, which may have confounded the association between nitrate intake and ASVD mortality. Baseline serum creatinine was analysed in 1,106/1,226 (90.2%) participants using an isotope dilution mass spectrometry (IDMS) traceable Jaffe kinetic assay for creatinine on a Hitachi 917 analyser (Roche Diagnostics GmbH, Mannheim

181 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
Germany). Estimated glomerular filtration rate (eGFR) was then calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation (271) and was added to the multivariable-adjusted models as this has been shown to be associated with ASVD mortality in this cohort (272).
Statistics
The analytical protocol was determined prior to analysis. Statistical significance was set at a 2-sided Type 1 error rate of p<0.05. All data were analysed using IBM SPSS Statistics for Windows, Version 21.0 (2012, Armonk, NY: IBM Corp.) and SAS software, Version 9.4 (Copyright © 2002-2013, SAS Institute Inc. SAS and all other SAS Institute Inc. product or service names are registered trademarks or trademarks of SAS Institute Inc., Cary, NC, USA.). Descriptive statistics of normally distributed continuous variables were expressed as mean ± standard deviation (SD); non-normally distributed continuous variables (physical activity, alcohol intake, processed meat intake and red meat intake) were expressed as median and interquartile range; and categorical variables as number and proportion (%). Differences in baseline characteristics among tertiles of vegetable nitrate intake were tested using one-way ANOVA for normally distributed continuous variables and the Kruskal-Wallis test for non-normally distributed variables. Chi-squared test for independence was used to test for differences in baseline characteristics among tertiles of vegetable nitrate intake for categorical variables.
The primary outcome of the study was an ASVD-related death. Complete follow-up of death records were available for all participants that remained in Western Australia, which was likely to be the majority of women given their age. The follow-up period for each participant was calculated in days from their baseline clinical visit until death or 15-years of follow-up. Cox proportional hazards models were used to assess the association of nitrate intake (per SD) with ASVD mortality using three models of adjustment: unadjusted; age and energy-adjusted; and multivariable-adjusted (age, BMI, level of physical activity, alcohol intake, smoking history, SES, the CAIFOS supplementation group, organic nitrate medication, antihypertensive medication, statin medication and low-dose aspirin, renal function and energy intake). Covariates were based on an a priori selection process, as these covariates are known risk factors for cardiovascular disease. Covariates were entered into the models as continuous variables with the exception of smoking history, SES, the CAIFOS supplementation group, organic nitrate medication, antihypertensive medication, statin medication, and low-dose aspirin, which were, entered as categorical variables.
To further investigate a dose response association between vegetable nitrate intake and ASVD mortality, tertiles of vegetable nitrate intake were analysed using the three models of adjustment in Cox proportional hazards models with the three tertiles entered as a categorical variable. We also tested for evidence of a trend for vegetable nitrate intakes as continuous variables by using the median vegetable nitrate value within each tertile in separate Cox proportional hazards models. Cox proportional hazards assumptions were tested using log-log plots, which were shown to be parallel. Thus, indicating the proportional hazards assumptions were not violated.
Sensitivity analyses
In a sensitivity analysis, individuals taking medication containing organic nitrates (n=19) were excluded and the multivariable-adjusted analysis was repeated for vegetable nitrate intake

182 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
(per SD) and ASVD mortality. Furthermore, in order to explore possible bias due to reverse-causality, ASVD deaths that occurred within the first 24 months of follow-up were excluded and multivariable-adjusted analyses for nitrate intakes as continuous variables were then repeated.
The relationship between nitrate intake from vegetables and total vegetable intake was investigated using Pearson product-moment correlation coefficient. In the view of multicollinearity, a forward stepwise Cox proportional hazards model was used to assess the most parsimonious model for the prediction of ASVD-related deaths. The potential predictors and confounding variables entered included vegetable nitrate intake (per SD, mg/d), age (years), BMI (kg/m2), level of physical activity (per 100 kJ/d), alcohol intake (g/d), smoking history (yes/no), SES (ordinal), the CAIFOS supplementation group (yes/no), organic nitrate medication (yes/no), antihypertensive medication (yes/no), statin medication (yes/no), low-dose aspirin use (yes/no), renal function (CKD-EPI eGFR, ml/min/1.73m2) and energy intake (kJ/d). To address the limitation that nitrate intake from vegetables may be a surrogate for vegetable intake we also included vegetable intake (g/d) into this model.
Since vegetable nitrate intake may be considered as being a surrogate marker of a healthier diet, in a separate multivariable-adjusted model, we further adjusted for diet quality using the Nutrient-Rich Foods Index. In the view of the importance of co-correlation we also considered the impact of single dietary confounders by including the individual estimated daily intakes of saturated fat (g/d), processed meat (g/d), fibre (g/d), potassium (mg/d), magnesium (mg/d), omega 3 (g/d) and beta-carotene (ug/d) as continuous variables in multivariable-adjusted Cox proportional hazards models on a variable-by-variable basis.
Vegetable intake was also assessed at 5 y (2003) and 7 y (2005) using the same FFQ. Vegetable nitrate intake was therefore calculated at each time point using the same calculation method as for baseline (1998). Differences in vegetable nitrate intake at each time point (baseline, 5 y and 7 y) were tested using one-way repeated measures ANOVA. To account for change in vegetable nitrate intake at 5 y and 7 y, the average of the 3 vegetable nitrate intake values (baseline, 5 y and 7 y) was used in the multivariable-adjusted Cox proportional hazards model.
To explore whether the relationship between vegetable nitrate intake and any ASVD-related death, assessed using multiple cause of death data, was not due to dietary nitrate being associated with other causes of death, all-cause mortality and non-ASVD related mortality were investigated in the multivariable-adjusted Cox proportional hazards models.
RESULTS
Characteristics of study population
Baseline characteristics and dietary intakes for all study participants and by tertiles of vegetable nitrate intakes are shown in Table 1 and Table 2. Mean (SD) nitrate intake from vegetables was 67.0 (29.2) mg/d and nitrate intake from all foods was 79.4 (31.1) mg/d. Vegetables contributed most to total nitrate intake (84%), followed by fruit (6%), grains (3%) and meat (including processed meat) (3%) (Figure 2). Major individual vegetables that contributed to vegetable nitrate intake were lettuce and other salad greens (23%), spinach
183 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
(12%), celery (10%), beetroot (9%) and potatoes (8%). There were differences among tertiles in all dietary intakes (P<0.05) (Table 2).
Atherosclerotic vascular disease mortality
During 15,947 person-years of follow-up, 238/1,226 (19.4%) participants died of an ASVD-related cause (Table 3). The association between baseline nitrate intake from vegetables (per SD, 29.2 mg/d) and ASVD mortality was statistically significant in unadjusted (HR=0.80, 95%CI 0.70, 0.92, P=0.002), age and energy-adjusted (HR=0.81, 95%CI 0.70, 0.93, P=0.004) and multivariable-adjusted models (HR=0.79, 95%CI 0.68, 0.93, P=0.004). Multivariable-adjusted cumulative survival curves for ASVD mortality according to tertiles of vegetable nitrate intakes are presented in Figure 3. In the tertile analysis, there were significant trends between the quantity of vegetable nitrate intakes and ASVD mortality in unadjusted (P=0.013), age and energy-adjusted (P=0.016) and multivariable-adjusted (P=0.016) models (Table 3).
The association between total nitrate intake from all foods (per SD, 31.1 mg/d) and ASVD mortality was statistically significant in unadjusted (HR=0.80, 95%CI 0.70, 0.92, P=0.002), age and energy-adjusted (HR=0.81, 95%CI 0.70, 0.93, P=0.004), and multivariable-adjusted (HR=0.80, 95%CI 0.68, 0.94, P=0.006) models. The association between nitrate intake from non-vegetable sources (per SD, 4.8 mg/d) and ASVD mortality was not statistically significant in unadjusted (HR=0.93, 95%CI 0.81, 1.06, P=0.256), age and energy-adjusted (HR=0.96, 95%CI 0.80, 1.16), P=0.693), and multivariable-adjusted (HR=1.03, 95%CI 0.85, 1.25, P=0.754) models.
Sensitivity analyses
When excluding participants taking medication containing organic nitrates (n=19), the relationship between vegetable nitrate intake and ASVD mortality remained statistically significant (multivariable-adjusted HR=0.80, 95%CI 0.68, 0.94, P=0.006). When all deaths that occurred in the first 24 months were excluded, the association between nitrate intake from vegetables and ASVD mortality remained statistically significant (multivariable-adjusted HR=0.79, 95%CI 0.67, 0.92, P=0.003). Nitrate intake from all foods also remained statistically significant (multivariable-adjusted HR=0.79, 95%CI 0.67, 0.93, P=0.005). Nitrate intake from non-vegetable sources remained non-significant (multivariable-adjusted HR=1.05, 95%CI 0.87, 1.28, P=0.613).
There was a strong, positive correlation between the nitrate intake from vegetables and total vegetable intake, r=0.75, P<0.001. In a multivariable-adjusted forward stepwise Cox proportional hazards model, which included both vegetable nitrate intake and vegetable intake, age (per year increase, HR=1.16, 95%CI 1.11, 1.22, P<0.001), BMI (per kg/m2 increase, HR=1.03, 95%CI 1.00, 1.06, P=0.044), physical activity (per 100 kJ increase, HR=0.97, 95%CI 0.95, 1.00, P=0.040), nitrate medication (HR=2.79, 95%CI 1.47, 5.32, P=0.002), antihypertensive medication (HR=1.57, 95%CI 1.19, 2.07, P=0.001) and vegetable nitrate intake (per SD increase, HR= 0.81, 95%CI 0.70, 0.94, P=0.005) were retained in the final most parsimonious model.
After further adjustment for the Nutrient-Rich Foods Index in the multivariable-adjusted Cox proportional hazards model, the association between baseline nitrate intake from vegetables (per SD, 29.2 mg/d) and ASVD mortality was attenuated (HR=0.85, 95%CI 0.72, 1.01, P=0.072). Separate analyses that adjusted for individual dietary factors (fibre, saturated fat, magnesium, omega 3 fatty acids, beta-carotene and processed meat) did not change the interpretation
184 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
of the association between vegetable nitrate intake and ASVD mortality (P<0.05). However, adjustment for potassium attenuated the association between vegetable nitrate intake and ASVD mortality (multivariable-adjusted HR=0.85, 95%CI 0.72, 1.01, P=0.073).
Nitrate intake from vegetables were compared at baseline (1998), 5 years (2003) and 7 years (2005) in 846 participants. The mean (SD) for each time point was: 68.3 (28.9) for baseline; 62.4 (29.3) for 5 years; and 60.3 (26.9) for 7 years. A one-way repeated measures ANOVA was conducted and confirmed a significant effect for time, Wilks’ Lambda = 0.93, F (2, 844) = 31.39, P<0.001, multivariate partial eta squared = 0.069. Vegetable nitrate intake was 5.9 mg/d lower at 5 years and 8.0 mg/d lower at 7 years compared to baseline. This equated to ~12% statistically significant change in vegetable nitrate intake over 7 years. To account for this change the average vegetable nitrate intake across the 3 time points (baseline, 5 y and 7 y) was entered into the multivariable-adjusted Cox proportional hazards model. This did not substantively alter the observed associations between baseline vegetable nitrate intake and ASVD mortality (multivariable-adjusted HR=0.74, 95%CI 0.60, 0.92, P=0.007).
Lastly, the association of nitrate intake from vegetables (per SD, 29.2 mg/d) with all-cause mortality (n=473 deaths) was statistically significant (multivariable-adjusted HR=0.87, 95%CI 0.78, 0.97, P=0.011). However, the association of nitrate intake from vegetables (per SD, 29.2 mg/d) with non-ASVD related mortality (n=235 deaths) was not significant (multivariable-adjusted HR=0.95, 95%CI 0.82, 1.10, P=0.473).
DISCUSSION
In this 15 y prospective cohort study of older adult women, we demonstrated a significant inverse association of nitrate intake from vegetables with ASVD mortality and all-cause mortality. This inverse relationship remained statistically significant after adjustment risk factors associated with lifestyle and cardiovascular disease.
Evidence from >30, mostly small-scale, randomised controlled trials have established that intake of nitrate-rich vegetables can enhance endogenous NO levels and improve measures of vascular health, including blood pressure and endothelial function (163, 188, 310, 334). There is a need to determine whether these improvements in risk factors may translate into improved long-term clinical cardiovascular outcomes. To our knowledge, this is the first observational study to examine the relationship of nitrate intake with mortality related to cardiovascular diseases and all causes.
Previous epidemiological studies, conducted more than half a century ago, have investigated nitrate intake with predominantly cancer outcomes. This research was based on nitrosamine exposure and the possible pathological consequences in humans (44). The 2010 International Agency for Research on Carcinogenicity (IARC) report concluded “Ingested nitrate or nitrite under conditions that results in endogenous nitrosation is probably carcinogenic to humans (Group 2A)” (250). These conditions, however, are likely to be due to complex interactions between the amount of nitrate and nitrite consumed, stomach acidity, intakes of nutrients likely to decrease the potential for nitrosation (polyphenols, vitamin C and vitamin E), smoking status, and medical conditions likely to increase nitrosation (157).
With the discovery of the enterosalivary nitrate-nitrite-NO pathway focus has now shifted to the possible beneficial effects of dietary nitrate from vegetables (44, 157). In this current
185 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
population, a ~30 mg/d higher nitrate intake from vegetables was associated with a 21% lower risk of ASVD mortality. This nitrate amount equates to ~10-30 g/d of nitrate-rich vegetables (less than ½ serve). When comparing to low nitrate intakes from vegetables <52.7 mg/d (median 39.5 mg/d), this relationship plateaued at intakes of 52.7-76.4 mg/d (median 63.5 mg/d) where participants with intakes of >76.4 mg/d (median 93.8 mg/d) had no additional benefit. Human intervention studies investigating the effects of dietary nitrate on ASVD-related risk factors such as blood pressure have investigated nitrate intakes at much higher doses, ranging from 99 to 1,488 mg (163, 188, 310). A meta-analysis of randomised controlled trials reporting the effects of beetroot juice and inorganic nitrate supplementation found systolic blood pressure was reduced in both acute (<3 d) and chronic (≥3 d) study designs (163). These studies, however, were characterised by small sample sizes, short duration and over-representation of young, healthy men (163).
A number of studies have investigated the effects of dietary nitrate on other measures of vascular health. A meta-analysis of randomised controlled trials reporting the effects of inorganic nitrate and beetroot supplementation found a significant improvement in flow mediated dilatation, but not pulse wave velocity (334). Significant results were only observed in young subjects and in middle-aged drug-naïve and treated hypertensive subjects. The same effect was not observed in older adult obese subjects and individuals with diagnosis of type 2 diabetes and peripheral arterial disease. It is suggested this absence of effect may be due in part to a down regulation of endothelial NOS (eNOS) activity associated with a negative cross-talk between the NOS dependent pathway and the nitrate-nitrite-NO pathway in control of NO homeostasis (198). Carlstrom and colleagues suggest that individual responses to dietary nitrate are dependent on basal eNOS activity, and thus, individuals that are already compromised with eNOS activity, such as the elderly, may have an augmented response to dietary nitrate (198). This augmented response; however, may downregulate NOS dependent pathways resulting in either no effect or an opposite effect to the desired result.
A major strength of this study is the calculation of nitrate intake from vegetables. To date, observational studies have used out-of-date resources with minimal publications to calculate nitrate intake. This is one of the first studies to calculate nitrate intake using an up-to-date comprehensive database with over 250 publications (36). Furthermore, this study had complete follow-up of death records for all participants that remained in Western Australia, which was likely to be almost all women given their age, minimising a major source of bias associated with loss to follow-up. In addition, reverse causality bias was addressed by excluding all ASVD-related deaths that occurred within the first 24 months of follow-up. This resulted in a slightly stronger inverse association between nitrate intakes from vegetables and ASVD mortality. A major limitation of this study is the observational nature, which introduces the possibility for residual confounding and the inability to confirm a causal relationship. The longitudinal nature of this study, does however, suggest a direction of causality. Furthermore, higher nitrate intakes from vegetables may indeed be a surrogate marker for higher vegetable intakes, and therefore, a healthier diet and healthier lifestyle. We attempted to address this by assessing vegetable intake in addition to vegetable nitrate intake in a forward stepwise Cox proportional hazards model. Vegetable nitrate intake was included in preference to vegetable intake as an independent predictor of ASVD mortality and was retained in the final most parsimonious model together with age, BMI, physical activity, use of organic nitrates and use of antihypertensive medications. Even through vegetable intake per se was not an independent predictor included in the final model, nitrate intake from vegetables may still be

186 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
a surrogate for vegetable intake and other healthy diet/lifestyle factors. We attempted to further address this by adjusting for diet quality and other lifestyle factors that could potentially confound the relationship between nitrate intake and ASVD mortality. Lifestyle factors did not affect the relationship seen with nitrate intake and ASVD mortality. However, further adjustment for diet quality or potassium intake did attenuate this relationship, indicating that other constituents of vegetable-rich diets at least partially explain the observed association.
Other residual confounding may be a result of changes in dietary intake over time which may not be completely captured by data collection methods, potentially creating bias due to measurement error. For example we note that total energy intake along with most nutrient and food types was increased in parallel with increasing nitrate intake. Despite this, there were no corresponding increases in BMI or body weight, making it likely that the increased food intake across nitrate tertiles was due to corresponding increases in physical activity. Although the relation between dietary nitrate and ASVD persisted after adjustment for both total energy and reported physical activity, the latter measurement is relatively imprecise in comparison with objective measures. Physical activity is a strong predictor of cardiovascular health (287, 288, 340, 341). Furthermore, it is possible that physical activity associated with higher vegetable and nitrate consumption reflects an overall healthier lifestyle.
To our knowledge, we are the first to demonstrate that nitrate intake from vegetables is inversely associated with mortality related to cardiovascular disease, an association independent of lifestyle and cardiovascular risk factors. Replication of the results of this study are needed in younger female cohorts and male populations. There is also a strong need for further intervention studies to investigate the effects of long-term consumption of nitrate-rich vegetables on cardiovascular-related endpoints in at risk populations.
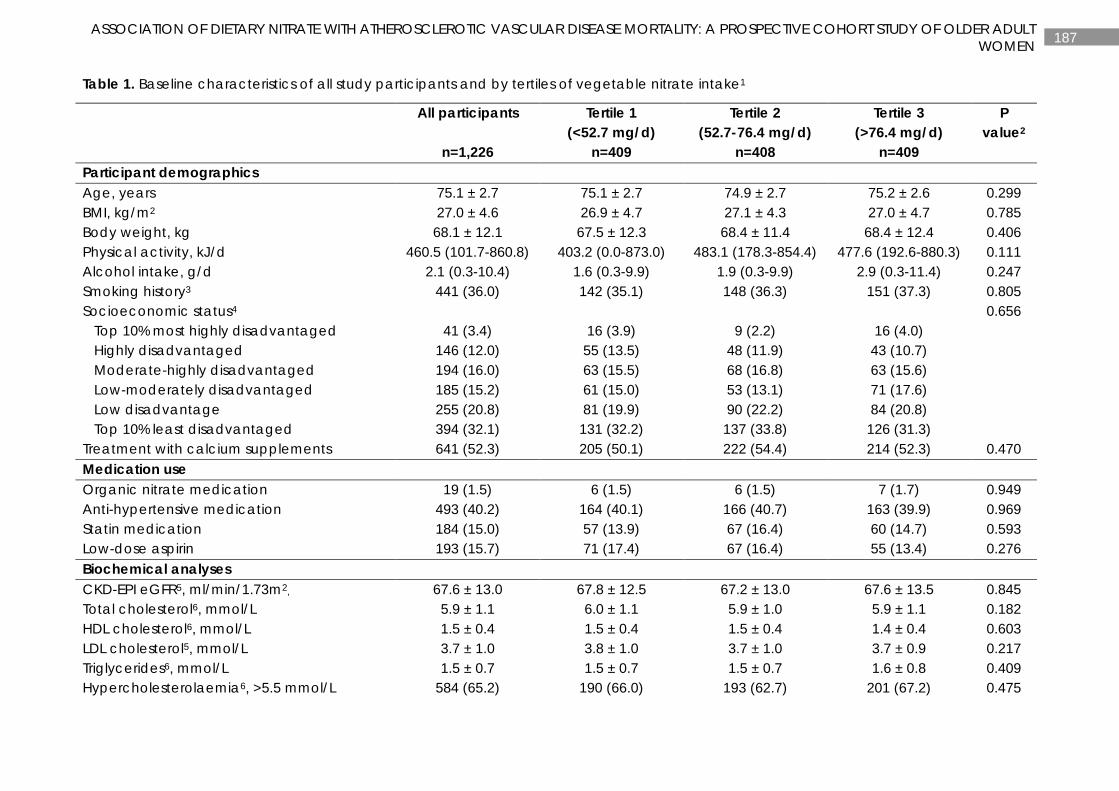
187 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
Table 1. Baseline characteristics of all study participants and by tertiles of vegetable nitrate intake1
All participants
n=1,226
Tertile 1 (<52.7 mg/d)
n=409
Tertile 2 (52.7-76.4 mg/d)
n=408
Tertile 3 (>76.4 mg/d)
n=409
P value2
Participant demographics Age, years 75.1 ± 2.7 75.1 ± 2.7 74.9 ± 2.7 75.2 ± 2.6 0.299 BMI, kg/m2 27.0 ± 4.6 26.9 ± 4.7 27.1 ± 4.3 27.0 ± 4.7 0.785 Body weight, kg 68.1 ± 12.1 67.5 ± 12.3 68.4 ± 11.4 68.4 ± 12.4 0.406 Physical activity, kJ/d 460.5 (101.7-860.8) 403.2 (0.0-873.0) 483.1 (178.3-854.4) 477.6 (192.6-880.3) 0.111 Alcohol intake, g/d 2.1 (0.3-10.4) 1.6 (0.3-9.9) 1.9 (0.3-9.9) 2.9 (0.3-11.4) 0.247 Smoking history3 441 (36.0) 142 (35.1) 148 (36.3) 151 (37.3) 0.805 Socioeconomic status4 0.656 Top 10% most highly disadvantaged 41 (3.4) 16 (3.9) 9 (2.2) 16 (4.0) Highly disadvantaged 146 (12.0) 55 (13.5) 48 (11.9) 43 (10.7) Moderate-highly disadvantaged 194 (16.0) 63 (15.5) 68 (16.8) 63 (15.6) Low-moderately disadvantaged 185 (15.2) 61 (15.0) 53 (13.1) 71 (17.6) Low disadvantage 255 (20.8) 81 (19.9) 90 (22.2) 84 (20.8) Top 10% least disadvantaged 394 (32.1) 131 (32.2) 137 (33.8) 126 (31.3) Treatment with calcium supplements 641 (52.3) 205 (50.1) 222 (54.4) 214 (52.3) 0.470 Medication use Organic nitrate medication 19 (1.5) 6 (1.5) 6 (1.5) 7 (1.7) 0.949 Anti-hypertensive medication 493 (40.2) 164 (40.1) 166 (40.7) 163 (39.9) 0.969 Statin medication 184 (15.0) 57 (13.9) 67 (16.4) 60 (14.7) 0.593 Low-dose aspirin 193 (15.7) 71 (17.4) 67 (16.4) 55 (13.4) 0.276 Biochemical analyses CKD-EPI eGFR5, ml/min/1.73m2, 67.6 ± 13.0 67.8 ± 12.5 67.2 ± 13.0 67.6 ± 13.5 0.845 Total cholesterol6, mmol/L 5.9 ± 1.1 6.0 ± 1.1 5.9 ± 1.0 5.9 ± 1.1 0.182 HDL cholesterol6, mmol/L 1.5 ± 0.4 1.5 ± 0.4 1.5 ± 0.4 1.4 ± 0.4 0.603 LDL cholesterol5, mmol/L 3.7 ± 1.0 3.8 ± 1.0 3.7 ± 1.0 3.7 ± 0.9 0.217 Triglycerides6, mmol/L 1.5 ± 0.7 1.5 ± 0.7 1.5 ± 0.7 1.6 ± 0.8 0.409 Hypercholesterolaemia6, >5.5 mmol/L 584 (65.2) 190 (66.0) 193 (62.7) 201 (67.2) 0.475
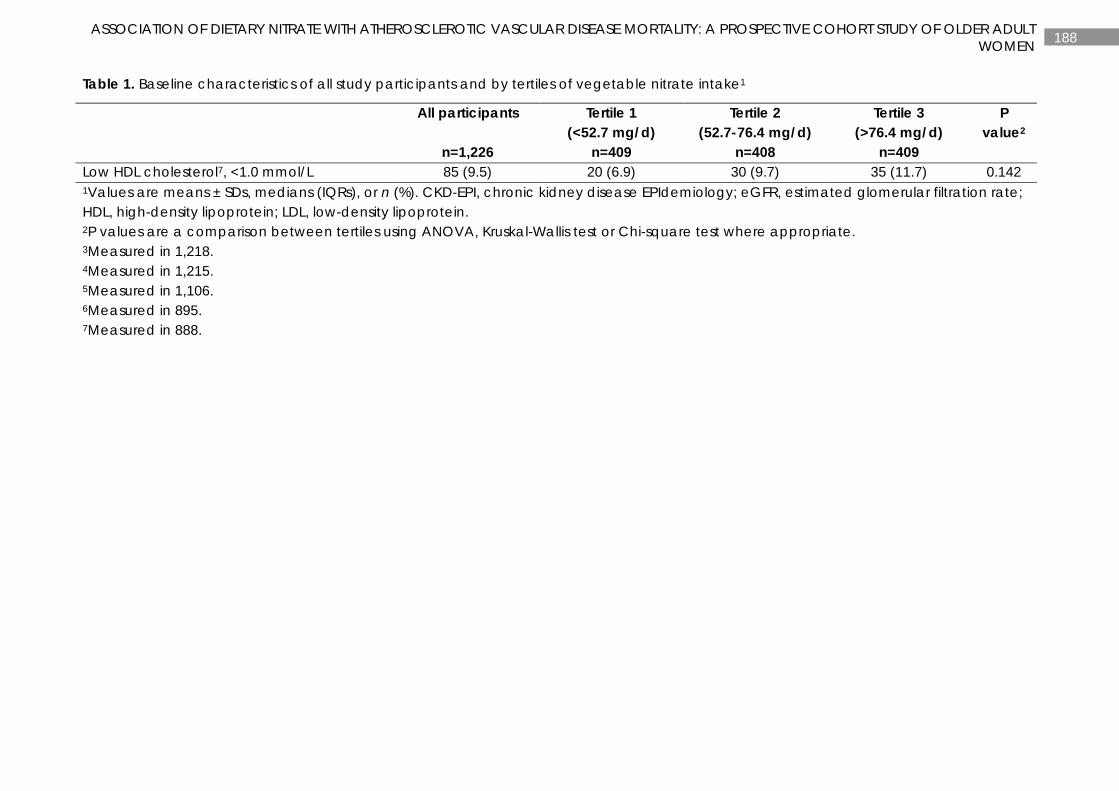
188 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
Table 1. Baseline characteristics of all study participants and by tertiles of vegetable nitrate intake1
All participants
n=1,226
Tertile 1 (<52.7 mg/d)
n=409
Tertile 2 (52.7-76.4 mg/d)
n=408
Tertile 3 (>76.4 mg/d)
n=409
P value2
Low HDL cholesterol7, <1.0 mmol/L 85 (9.5) 20 (6.9) 30 (9.7) 35 (11.7) 0.142 1Values are means ± SDs, medians (IQRs), or n (%). CKD-EPI, chronic kidney disease EPIdemiology; eGFR, estimated glomerular filtration rate; HDL, high-density lipoprotein; LDL, low-density lipoprotein. 2P values are a comparison between tertiles using ANOVA, Kruskal-Wallis test or Chi-square test where appropriate. 3Measured in 1,218. 4Measured in 1,215. 5Measured in 1,106. 6Measured in 895. 7Measured in 888.
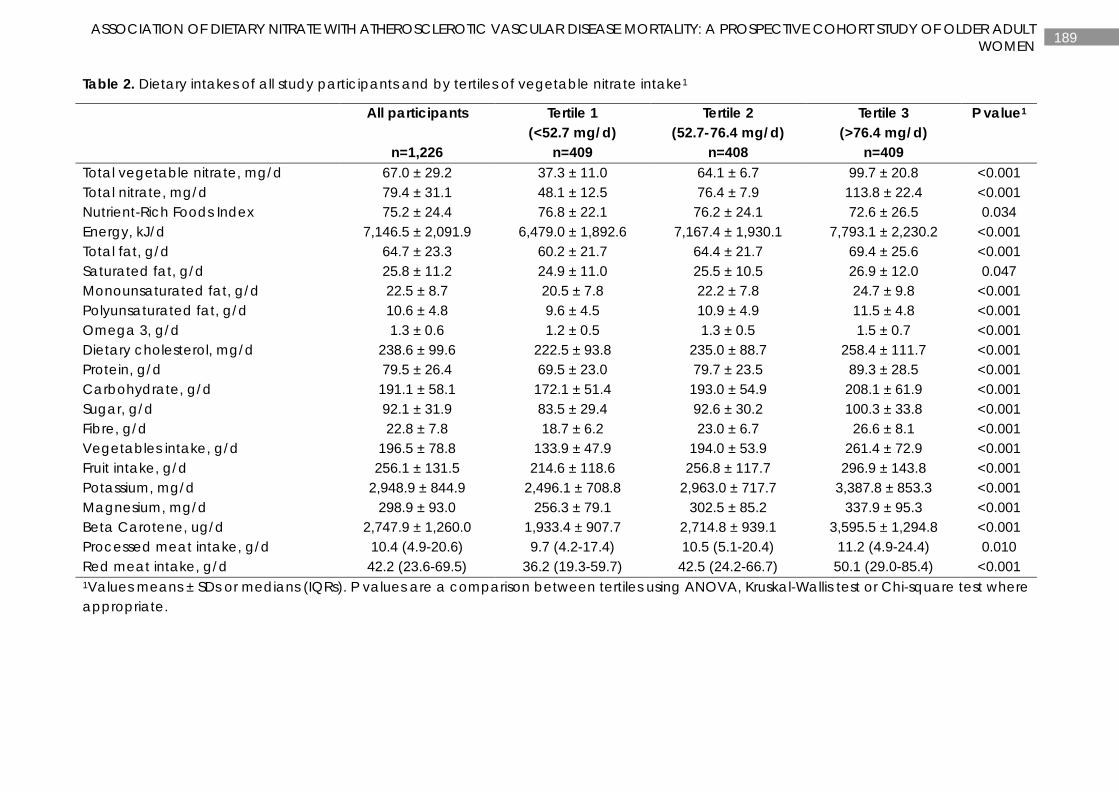
189 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
Table 2. Dietary intakes of all study participants and by tertiles of vegetable nitrate intake1
All participants
n=1,226
Tertile 1 (<52.7 mg/d)
n=409
Tertile 2 (52.7-76.4 mg/d)
n=408
Tertile 3 (>76.4 mg/d)
n=409
P value1
Total vegetable nitrate, mg/d 67.0 ± 29.2 37.3 ± 11.0 64.1 ± 6.7 99.7 ± 20.8 <0.001 Total nitrate, mg/d 79.4 ± 31.1 48.1 ± 12.5 76.4 ± 7.9 113.8 ± 22.4 <0.001 Nutrient-Rich Foods Index 75.2 ± 24.4 76.8 ± 22.1 76.2 ± 24.1 72.6 ± 26.5 0.034 Energy, kJ/d 7,146.5 ± 2,091.9 6,479.0 ± 1,892.6 7,167.4 ± 1,930.1 7,793.1 ± 2,230.2 <0.001 Total fat, g/d 64.7 ± 23.3 60.2 ± 21.7 64.4 ± 21.7 69.4 ± 25.6 <0.001 Saturated fat, g/d 25.8 ± 11.2 24.9 ± 11.0 25.5 ± 10.5 26.9 ± 12.0 0.047 Monounsaturated fat, g/d 22.5 ± 8.7 20.5 ± 7.8 22.2 ± 7.8 24.7 ± 9.8 <0.001 Polyunsaturated fat, g/d 10.6 ± 4.8 9.6 ± 4.5 10.9 ± 4.9 11.5 ± 4.8 <0.001 Omega 3, g/d 1.3 ± 0.6 1.2 ± 0.5 1.3 ± 0.5 1.5 ± 0.7 <0.001 Dietary cholesterol, mg/d 238.6 ± 99.6 222.5 ± 93.8 235.0 ± 88.7 258.4 ± 111.7 <0.001 Protein, g/d 79.5 ± 26.4 69.5 ± 23.0 79.7 ± 23.5 89.3 ± 28.5 <0.001 Carbohydrate, g/d 191.1 ± 58.1 172.1 ± 51.4 193.0 ± 54.9 208.1 ± 61.9 <0.001 Sugar, g/d 92.1 ± 31.9 83.5 ± 29.4 92.6 ± 30.2 100.3 ± 33.8 <0.001 Fibre, g/d 22.8 ± 7.8 18.7 ± 6.2 23.0 ± 6.7 26.6 ± 8.1 <0.001 Vegetables intake, g/d 196.5 ± 78.8 133.9 ± 47.9 194.0 ± 53.9 261.4 ± 72.9 <0.001 Fruit intake, g/d 256.1 ± 131.5 214.6 ± 118.6 256.8 ± 117.7 296.9 ± 143.8 <0.001 Potassium, mg/d 2,948.9 ± 844.9 2,496.1 ± 708.8 2,963.0 ± 717.7 3,387.8 ± 853.3 <0.001 Magnesium, mg/d 298.9 ± 93.0 256.3 ± 79.1 302.5 ± 85.2 337.9 ± 95.3 <0.001 Beta Carotene, ug/d 2,747.9 ± 1,260.0 1,933.4 ± 907.7 2,714.8 ± 939.1 3,595.5 ± 1,294.8 <0.001 Processed meat intake, g/d 10.4 (4.9-20.6) 9.7 (4.2-17.4) 10.5 (5.1-20.4) 11.2 (4.9-24.4) 0.010 Red meat intake, g/d 42.2 (23.6-69.5) 36.2 (19.3-59.7) 42.5 (24.2-66.7) 50.1 (29.0-85.4) <0.001 1Values means ± SDs or medians (IQRs). P values are a comparison between tertiles using ANOVA, Kruskal-Wallis test or Chi-square test where appropriate.
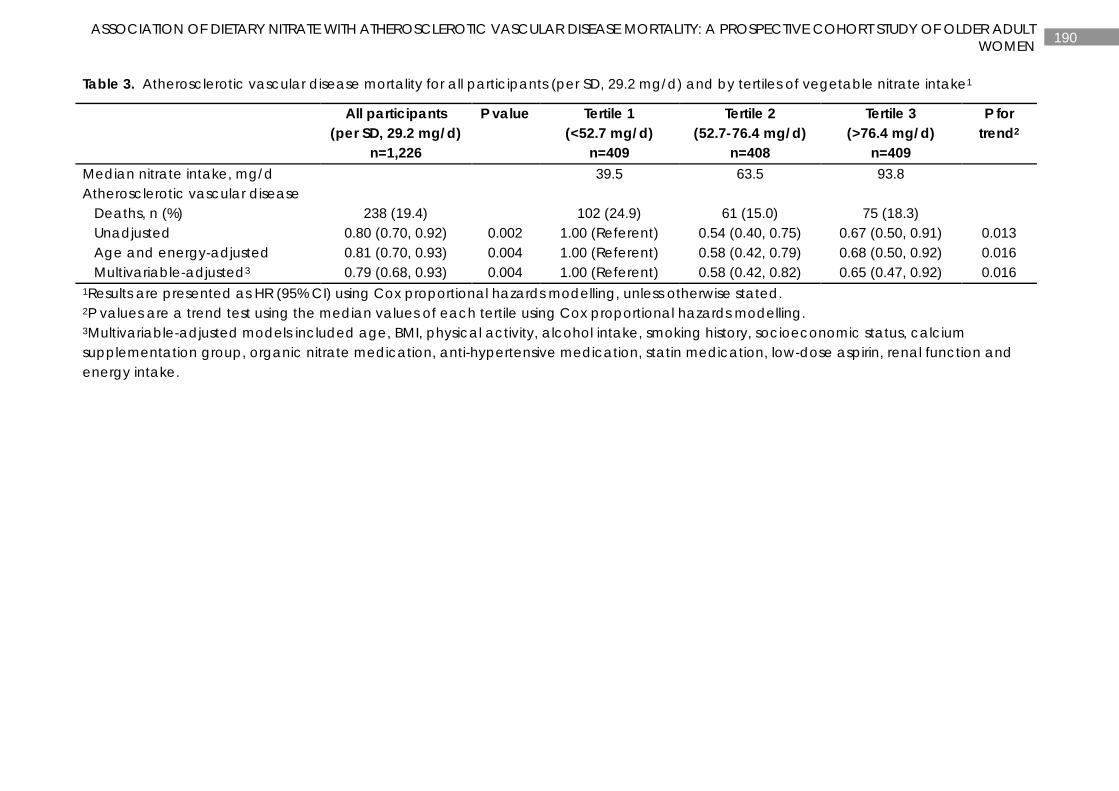
190 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
Table 3. Atherosclerotic vascular disease mortality for all participants (per SD, 29.2 mg/d) and by tertiles of vegetable nitrate intake1
All participants (per SD, 29.2 mg/d)
n=1,226
P value Tertile 1 (<52.7 mg/d)
n=409
Tertile 2 (52.7-76.4 mg/d)
n=408
Tertile 3 (>76.4 mg/d)
n=409
P for trend2
Median nitrate intake, mg/d 39.5 63.5 93.8 Atherosclerotic vascular disease Deaths, n (%) 238 (19.4) 102 (24.9) 61 (15.0) 75 (18.3) Unadjusted 0.80 (0.70, 0.92) 0.002 1.00 (Referent) 0.54 (0.40, 0.75) 0.67 (0.50, 0.91) 0.013 Age and energy-adjusted 0.81 (0.70, 0.93) 0.004 1.00 (Referent) 0.58 (0.42, 0.79) 0.68 (0.50, 0.92) 0.016 Multivariable-adjusted3 0.79 (0.68, 0.93) 0.004 1.00 (Referent) 0.58 (0.42, 0.82) 0.65 (0.47, 0.92) 0.016 1Results are presented as HR (95% CI) using Cox proportional hazards modelling, unless otherwise stated. 2P values are a trend test using the median values of each tertile using Cox proportional hazards modelling. 3Multivariable-adjusted models included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, calcium supplementation group, organic nitrate medication, anti-hypertensive medication, statin medication, low-dose aspirin, renal function and energy intake.
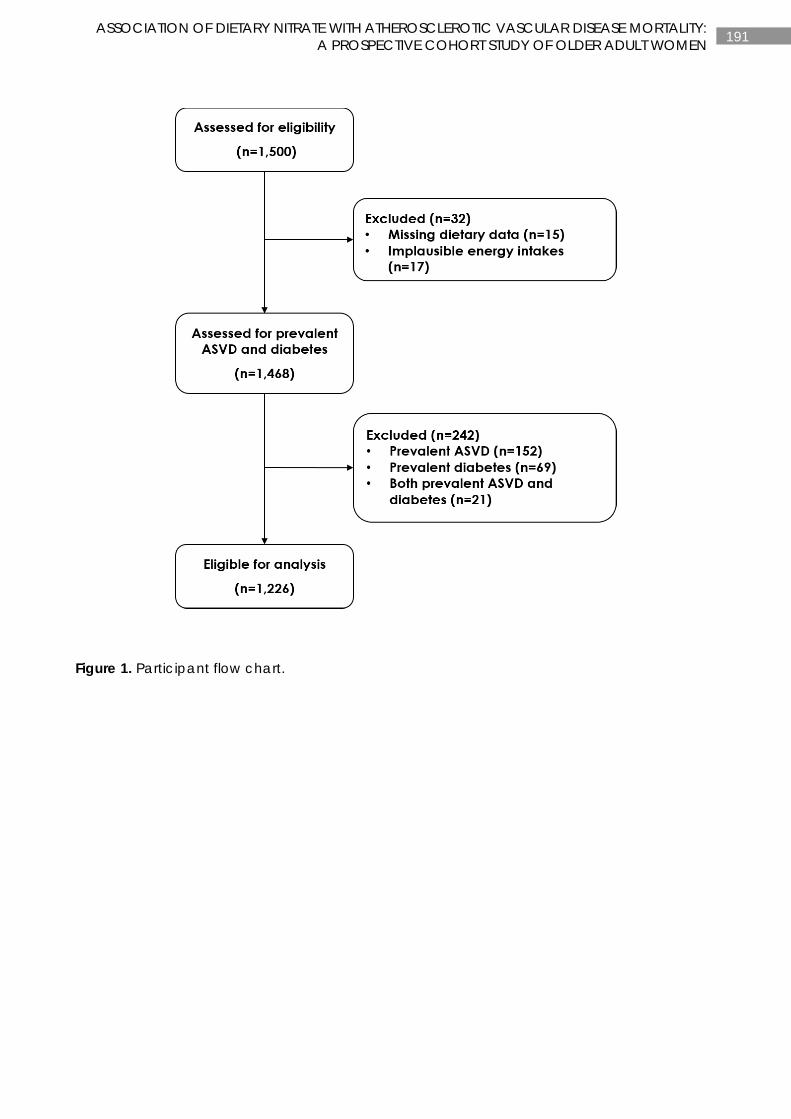
191 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
Figure 1. Participant flow chart.
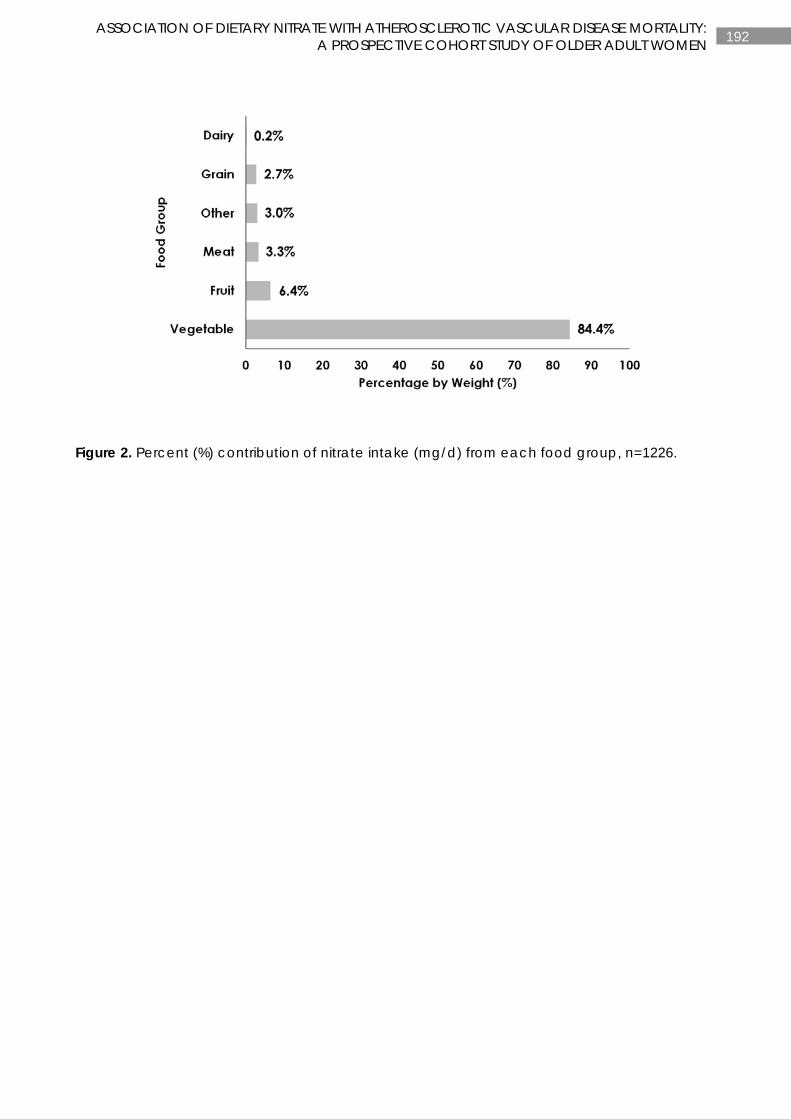
192 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
Figure 2. Percent (%) contribution of nitrate intake (mg/d) from each food group, n=1226.
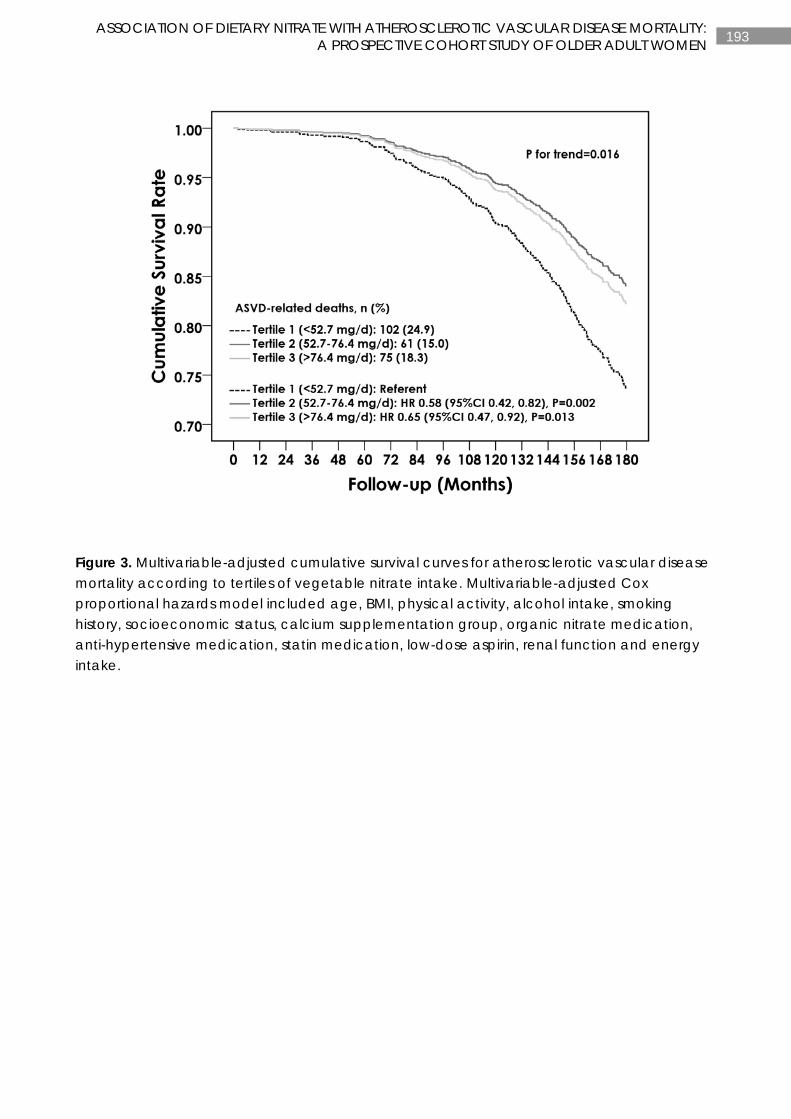
193 ASSOCIATION OF DIETARY NITRATE WITH ATHEROSCLEROTIC VASCULAR DISEASE MORTALITY: A PROSPECTIVE COHORT STUDY OF OLDER ADULT WOMEN
Figure 3. Multivariable-adjusted cumulative survival curves for atherosclerotic vascular disease mortality according to tertiles of vegetable nitrate intake. Multivariable-adjusted Cox proportional hazards model included age, BMI, physical activity, alcohol intake, smoking history, socioeconomic status, calcium supplementation group, organic nitrate medication, anti-hypertensive medication, statin medication, low-dose aspirin, renal function and energy intake.
194 CHAPTER 7
CHAPTER 7
ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC
CEREBROVASCULAR DISEASE IN OLDER WOMEN
Manuscript based on this chapter:
Catherine P Bondonno*, Lauren C Blekkenhorst*, Richard L Prince, Kerry L Ivey, Joshua R Lewis, Amanda Devine, Richard J Woodman, Jon O Lundberg, Kevin D Croft, Peter L Thompson, Jonathan M Hodgson. Association of vegetable nitrate intake with carotid atherosclerosis and ischemic cerebrovascular disease in older women. Stroke 2017;48(8):1-6. *Joint first authors

195 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
ABSTRACT
Background and Purpose: A short-term increase in dietary nitrate (NO3−) improves markers of vascular health via formation of nitric oxide and other bioactive nitrogen oxides. Whether this translates into long-term vascular disease risk reduction has yet to be examined. We investigated the association of vegetable-derived nitrate intake with common carotid artery intima-media thickness (CCA-IMT), plaque severity, and ischemic cerebrovascular disease events in elderly women (n=1226).
Methods: Vegetable nitrate intake, lifestyle factors, and cardiovascular disease risk factors were determined at baseline (1998). CCA-IMT and plaque severity were measured using B-mode carotid ultrasound (2001). Complete ischemic cerebrovascular disease hospitalizations or deaths (events) over 14.5 years (15 032 person-years of follow-up) were obtained from the West Australian Data Linkage System.
Results: Higher vegetable nitrate intake was associated with a lower maximum CCA-IMT (B=−0.015, P=0.002) and lower mean CCA-IMT (B=−0.012, P=0.006). This relationship remained significant after adjustment for lifestyle and cardiovascular risk factors (P≤0.01). Vegetable nitrate intake was not a predictor of plaque severity. In total 186 (15%) women experienced an ischemic cerebrovascular disease event. For every 1 SD (29 mg/d) higher intake of vegetable nitrate, there was an associated 17% lower risk of 14.5-year ischemic cerebrovascular disease events in both unadjusted and fully adjusted models (P=0.02).
Conclusions: Independent of other risk factors, higher vegetable nitrate was associated with a lower CCA-IMT and a lower risk of an ischemic cerebrovascular disease event.
196 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
INTRODUCTION
Our understanding of the health impact of dietary nitrate has recently undergone a radical shift. Originally nitrate was linked with detrimental health outcomes such as cancer, a theory unsupported despite extensive epidemiological research spanning more than 50 years (342). Currently, the potential vascular benefits of dietary nitrate is a major research focus. Dietary nitrate, found predominantly in green leafy vegetables and beetroot, dose-dependently enhances the circulating nitric oxide (NO) pool by increasing levels of circulating nitrite, NO and related nitroso compounds (133, 142, 148, 254). Dietary nitrate, through the enterosalivary nitrate-nitrite-NO pathway, is now recognized as an important alternate source of NO. NO was originally assumed to be solely produced through the oxygen dependent L-arginine-NO synthase pathway. Nitric oxide is a key regulator of vascular homeostasis and integrity, with decreased production and/or bioavailability of NO implicated in a number of cardiovascular disorders (37, 121). More than 30 clinical trials have now demonstrated, via effects on NO, a reduction in blood pressure and/ or improvement in measures of vascular function with a short-term increase in nitrate intake (143, 194, 310). However, epidemiological studies exploring the relationship between nitrate intake and vascular disease risk are scarce.
Common carotid artery intima-media thickness (CCA-IMT) is a surrogate measure of atherosclerosis (55) and is associated with increased vascular risk in general and cerebrovascular disease in particular, independent of conventional risk factors (343). Changes in CCA-IMT are used to assess the success of intervention studies in preventing or reducing the progress of atherosclerotic disease. While specific dietary factors have been associated with CCA-IMT (344), the association of nitrate intake with CCA-IMT has not been studied. Furthermore, the association of nitrate intake with risk of an ischemic cerebrovascular event has yet to be explored.
Thus the primary aim of this study was to investigate the association between intake of nitrate from vegetables and CCA-IMT, plaque severity and risk of an ischemic cerebrovascular disease event in a population-based study of older women rather than total nitrate intake. Our focus on vegetable-derived nitrate is because most dietary nitrate derives from vegetables (131). In addition, processed meat, another source of nitrate in the diet, is strongly linked to detrimental health effects (336). We hypothesized an inverse association between vegetable-derived nitrate intake and CCA-IMT, plaque severity and risk of an ischemic cerebrovascular disease.
SUBJECTS AND METHODS
Ethics statement
The Human Ethics Committee of the University of Western Australia approved the study and written informed consents were obtained from all participants. The study complies with the Declaration of Helsinki.
Participants
In 1998 1500 Western Australian women over the age of 70 were recruited to a 5 year randomised, controlled trial of oral calcium supplements to prevent osteoporotic fractures (ACTRN12615000750583) (257). Of these, 99% (n=1485) had complete food-frequency
197 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
questionnaires (Supplementary Figure 1). After excluding implausible energy intakes < 2100 kJ (500 kcal) or > 14700 kJ (3500 kcal) per day, 1468 (98%) were included. Participants with pre-existing atherosclerotic vascular disease and diabetes were excluded (n=242) leaving n=1226 (82%) for the ischemic cerebrovascular disease analysis. Of these participants, 65% (n=968) had plaque data and 64% (n=954) had CCA-IMT data (Supplementary Figure I). A study of the demographic variables of the recruited women revealed disease burden and pharmaceutical utilization was similar to whole populations of this age group (293).
Baseline assessment
A baseline assessment was performed in 1998. This included weight, height, medical history and lifestyle factors (See Supplementary Material) and completion of a validated Food Frequency Questionnaire (FFQ).
Assessment of nitrate consumption
An estimate of nitrate concentration (mg/g) in each of the vegetable items listed in the Cancer Council of Victoria FFQ was obtained using a recently developed comprehensive nitrate content of vegetables database. This database, compiled using a systematic approach, contains 4254 records sourced from 256 references and includes data on 178 vegetables as well as 22 herbs and spices from 56 countries. The median nitrate value (mg/g) for each vegetable in the FFQ was obtained from the database and multiplied with g/d vegetable consumption to determine nitrate intake. Total nitrate intake from vegetables per day was calculated by totalling the nitrate intake from individual vegetables.
An estimate of nitrate concentration (mg/g) in each of the non-vegetable items listed in the Cancer Council of Victoria FFQ was derived using estimates from three published sources (154, 244, 245) (See Supplementary Material).
Assessment of common carotid artery intima-media thickness (CCA-IMT) and plaque severity
Carotid high-resolution B-mode ultrasonography was used to assess common carotid intima-media thickness and focal carotid plaques at year 3 (2001) of the study (See Supplementary Material).
Assessment of ischemic cerebrovascular disease event
The first episode of ischemic cerebrovascular hospitalizations or death was retrieved from the Western Australian Data Linkage System (WADLS) for each study participant from their baseline clinic visit date in 1998 until 14 ½ years after their baseline visit (See Supplementary Material).
Statistics
A protocol for the statistical analysis of the data was established before analysis began. Data were analysed using IBM SPSS Statistics (version 21; IBM Corp, Armonk, NY) and SAS (version 9.4; SAS Institute Inc, Cary, NC). The relationship between nitrate intake (vegetable total, and non-vegetable nitrate) and CCA-IMT (maximum and mean) was examined using unadjusted, age and energy-adjusted and baseline risk factor-adjusted linear regression. The baseline risk factor-adjusted model included baseline age, body mass index, energy intake, alcohol intake, energy expended in physical activity, antihypertensive medication, statin medication, low-

198 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
dose aspirin medication, organic nitrate medication, history of smoking and supplementation group. Results are presented as unstandardized B ±SE. Vegetable nitrate consumption was then categorized into tertiles for further analysis by analysis of covariance (ANCOVA) with Bonferroni’s adjustment for multiple comparisons. The relationship between tertiles of nitrate intake and CCA-IMT (maximum and mean) was examined using unadjusted, age and energy-adjusted and baseline risk factor-adjusted models as before. The relationship between atherosclerotic plaque severity and nitrate intake was examined using binary logistic regression using unadjusted, age and energy-adjusted and baseline risk factor-adjusted models as before. Cox proportional hazards models were used for ischemic cerebrovascular disease events in unadjusted, age and energy-adjusted and baseline risk factor-adjusted models as before. We tested for evidence of a linear trend for vegetable nitrate intakes as continuous variables by using the median value for each tertile of vegetable nitrate intake in separate Cox proportional hazards models. Cox proportional hazards assumptions were tested using log-log plots, which were shown to be parallel. Thus, the proportional hazards assumptions were not violated. P-values of less than 0.05 in two tailed testing were considered statistically significant.
In a sensitivity analysis we assessed the potential impact of other possible dietary confounders on CCA-IMT and ischemic cerebrovascular disease events. Daily intakes of total fat (g/d), protein (g/d), carbohydrate (g/d) and fibre (g/d) were investigated in multivariable-adjusted Cox proportional hazards models on a variable-by-variable basis. We further explored the relationship of CCA-IMT and plaque severity with ischemic cerebrovascular disease events using Cox regression in unadjusted, age and energy-adjusted and baseline risk factor-adjusted models as described above. As this current cohort excluded older women with prevalent ASVD and diabetes, we repeated the analysis including older women with prevalent ASVD and diabetes.
RESULTS
Baseline characteristics of the study participants are presented in Table 1. Classification of vegetables in the Cancer Council of Victoria FFQ according to nitrate content is presented in Supplementary Table 1. Total nitrate intake from all vegetables was 67±29 mg/d (range: 6-224 mg/d). Total nitrate intake from all foods was 79±31 mg/d (range: 12-231 mg/d). Vegetables accounted for 84% of total nitrate intake (Supplementary Figure 2). After vegetables, fruit and meat were the greatest contributors to total nitrate intake contributing 6% and 3%, respectively. Participants with higher nitrate intake also had higher intakes of energy, total fat, protein, carbohydrate and fibre (Table 1).
Nitrate intake, CCA-IMT and plaque severity
Vegetable nitrate intake
Vegetable nitrate consumption was linearly inversely associated with maximum CCA-IMT and mean CCA-IMT (Table 2). A 29 mg (~1 SD) higher vegetable nitrate intake was associated with a 0.015 mm lower maximum CCA-IMT and a 0.012 mm lower mean CCA-IMT. These effects remained significant after adjustment for age and energy intake as well as after adjustment for baseline risk factors (Table 2).
199 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
The effect of vegetable nitrate intake was explored further by dividing the participants into tertiles: <53 mg/d, 53-76 mg/d and > 76 mg/d vegetable nitrate consumption (Table 2). Participants who consumed >76 mg/d nitrate (top tertile) had a significantly lower CCA-IMT than participants in the bottom tertile with consumption < 53 mg/d. This relationship remained significant after adjustment for age and energy intake for maximum CCA-IMT but was slightly attenuated for mean CCA-IMT. A similar relationship was observed after adjustment for baseline risk factors.
Vegetable nitrate intake (OR= 0.994, 95% CI: 0.806, 1.227; P=1.0) was not a predictor of plaque severity.
Total and non-vegetable nitrate intake
Total nitrate consumption was linearly inversely associated with maximum CCA-IMT and mean CCA-IMT (Supplementary Table 2). This relationship was not observed for non-vegetable nitrate intake (Supplementary Table II).
Neither total nitrate intake (OR= 1.006, 95% CI: 0.810, 1.250; P=0.95) nor non-vegetable nitrate intake (OR= 1.148, 95% CI: 0.865, 1.524; P=0.34) were predictors of plaque severity.
Vegetable nitrate intake and ischemic cerebrovascular disease hospitalizations and deaths
During 15 032 person-years of follow-up, 186 of 1 226 (15%) participants had an ischemic cerebrovascular disease event (hospitalization or death). For every 1 SD (29 mg/d) higher intake of vegetable nitrate there was an associated 17% lower risk of 14.5-y ischemic cerebrovascular disease event in both unadjusted and baseline risk factor-adjusted models (Table 3). A similar relationship was observed for total nitrate intake (P<0.05) but not for non-vegetable nitrate intake (P>0.05).
Across tertiles of vegetable nitrate intake, compared with the lowest tertile (< 53 mg/d), intake of the highest tertile (> 76 mg/d) nitrate from vegetables was associated with a lower risk of an ischemic cerebrovascular disease event (P for trend <0.05 for all models). The multivariable-adjusted cumulative event rate for ischemic cerebrovascular disease according to tertiles of vegetable nitrate intake is presented in Figure 1.
Sensitivity analysis
In separate multivariable-adjusted analyses that adjusted for individual dietary factors, total fat, protein, carbohydrates and fibre, did not change the interpretation of the association of vegetable nitrate intake with maximum and mean CCA-IMT as well as ischemic cerebrovascular disease events (P<0.05).
DISCUSSION
In this study of older women we report an inverse association of vegetable nitrate intake with CCA-IMT and risk of an ischemic cerebrovascular event over 15 years. The relationship remained consistent for total nitrate intake, but not non-vegetable nitrate intake, with CCA-IMT and risk of an ischemic cerebrovascular disease event. These results add weight to the accumulating body of evidence that the vascular benefits associated with a vegetable rich diet are due, in part, to dietary nitrate.

200 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
The observed differences in CCA-IMT, although small, may be clinically important. An increase in CCA-IMT is indicative of arterial wall thickening, a form of atherosclerosis (55) and CCA-IMT is a predictor of future cardiovascular events across all age-groups (343). Vegetable nitrate intake was associated with a 17 % lower risk of an ischemic cerebrovascular disease event per 29 mg/d (1 SD) higher vegetable nitrate intake, found in approximately half a serve (30g) of leafy green vegetable intake. This association was significant before and after adjustment for lifestyle and other cardiovascular risk factors. Our data suggest a nonlinear relationship between nitrate intake and ischemic cerebrovascular events because no additional risk reduction was observed in those consuming > 76 mg/d nitrate (median 100 mg/d) compared to 53 – 76 mg/d nitrate (median 64 mg/d). As little as one serve of nitrate-rich green leafy vegetable per day may provide adequate nitrate intake for ischemic cerebrovascular disease risk reduction.
A possible mechanism for the inverse association of vegetable nitrate intake with CCA-IMT and risk of an ischemic cerebrovascular event is the augmentation of NO status. Through the endogenous nitrate-nitrite-NO pathway, nitrate has the potential to be converted into NO and to form a large and abundant storage pool for this molecule in blood and tissues (130). Recent studies demonstrating beneficial effects on blood pressure, endothelial function, platelet aggregation, ischaemia reperfusion injury and exercise performance after intake of dietary nitrate (310, 345) are consistent with the proposal that nitrate intake contributes to cardiovascular health.
Approximately 80% of dietary nitrate intake is from vegetables (131). In our study population, vegetables accounted for 84% of total dietary nitrate intake. About 85% of vegetable nitrate intake was derived from ten vegetables: lettuce, spinach, celery, beetroot, potatoes, cabbage, pumpkin, green beans, broccoli and carrots. In contrast to other populations (Far Eastern, African, Latin American and European) where potatoes often contribute well over 10% of total nitrate intake (346), potatoes only provided 8% of total nitrate intake in our population. Nitrate intake varies greatly between individuals and populations with mean intakes for populations estimated to be between 0.4 to 2.6 mg/kg or 31 to 185 mg (324), and actual individual daily nitrate intakes ranging from less than 20 mg to greater than 400 mg (316, 317). Our mean intake of nitrate from all food (79 mg/adult/d) fell into this range. It was slightly higher than the WHO estimate of nitrate intake from food in Australia of 67 mg/adult/d (346).
Study strengths and limitations
Our study had several strengths. These included the use of a validated diet assessment tool, detailed information on lifestyle and cardiovascular risk factors as well as the validated measure of CCA-IMT with repeated measurements leading to a high level of precision in measurement of the main outcome. Several potential limitations could be considered. Firstly, a cross-sectional design for the relationship of dietary nitrate with CCA-IMT provides only weak evidence for causality. Secondly, while the possibility of potential reverse causation (changes in diet due to a disease diagnosis) exists, it is unlikely that individuals would knowingly alter their nitrate (or vegetable) intake based on their IMT which is an asymptomatic and pre-clinical marker of atherosclerosis and its value would therefore most likely be unknown to them. Thirdly, high nitrate intake may simply coincide with other lifestyle or dietary patterns that are associated with cardiovascular health. Although we adjusted for multiple lifestyle and

201 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
cardiovascular risk factors as well as dietary factors in our analysis, residual or unmeasured confounders cannot be ruled out. A causal relationship of nitrate intake with CCA-IMT and ischemic cerebrovascular disease events cannot be established because of the observational nature of the study. Fourthly, NO cannot be measured directly and endogenous levels have multifactorial influences (123). There is also no reliable biomarker of nitrate intake. Nitrate levels in plasma, saliva and urine are influenced by factors including dietary nitrate intake; metabolites of the L-arginine-NOS pathway; bacterial synthesis of nitrate within the gastrointestinal tract; denitrifying liver enzymes; and renal function. Fifthly, in this study carotid ultrasound measures were assessed in 2001. Since then there have been numerous advances in the evaluation of sonographic characteristics of carotid plaques, such as surface irregularity, ulceration and echogenicity that were not available for this study. While these newer measures may have provided further insight into how dietary nitrate may affect plaque stability and cerebrovascular events this would not change our overall findings from the study that dietary nitrate is associated with both established measures of carotid atherosclerosis as well as long-term cerebrovascular events. Similarly we did not assess resistive index and we only assessed the common carotid artery intimal medial thickness and not the bifurcation and internal carotid artery intimal medial thickness which have been suggested as better predictors of future cardiovascular events (347). Given this further studies investigating the association of dietary nitrate on newer measures of carotid atherosclerosis and IMT of the three sites are warranted. Finally, the current data is limited to elderly women and needs to be confirmed in men and younger women.
Summary/ Conclusions
Our study found an association of nitrate intake from vegetables with lower maximum and mean CCA-IMT as well as ischemic cerebrovascular disease events in a cohort of older women. The results are consistent with the proposal that increased nitrate consumption, primarily from vegetables, prevents thickening of the common carotid artery-intima-media, and may play a role in stroke and atherosclerosis prevention.
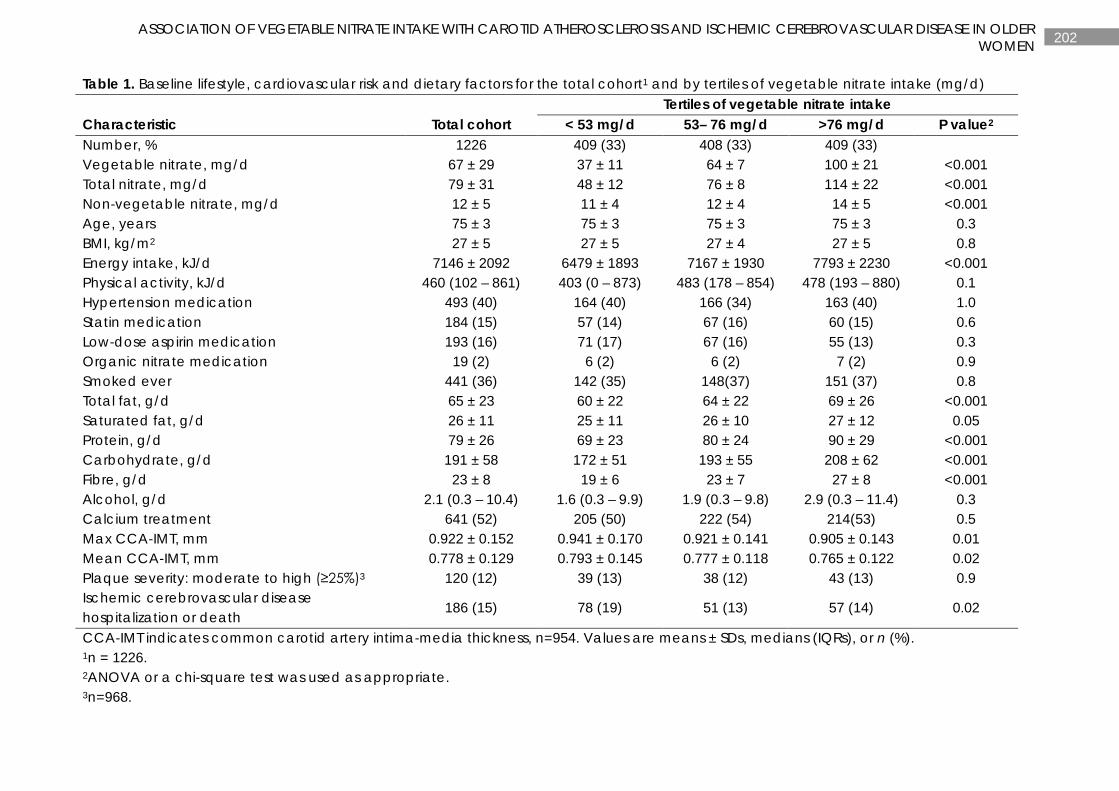
202 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
Table 1. Baseline lifestyle, cardiovascular risk and dietary factors for the total cohort1 and by tertiles of vegetable nitrate intake (mg/d) Tertiles of vegetable nitrate intake Characteristic Total cohort < 53 mg/d 53– 76 mg/d >76 mg/d P value2 Number, % 1226 409 (33) 408 (33) 409 (33) Vegetable nitrate, mg/d 67 ± 29 37 ± 11 64 ± 7 100 ± 21 <0.001 Total nitrate, mg/d 79 ± 31 48 ± 12 76 ± 8 114 ± 22 <0.001 Non-vegetable nitrate, mg/d 12 ± 5 11 ± 4 12 ± 4 14 ± 5 <0.001 Age, years 75 ± 3 75 ± 3 75 ± 3 75 ± 3 0.3 BMI, kg/m2 27 ± 5 27 ± 5 27 ± 4 27 ± 5 0.8 Energy intake, kJ/d 7146 ± 2092 6479 ± 1893 7167 ± 1930 7793 ± 2230 <0.001 Physical activity, kJ/d 460 (102 – 861) 403 (0 – 873) 483 (178 – 854) 478 (193 – 880) 0.1 Hypertension medication 493 (40) 164 (40) 166 (34) 163 (40) 1.0 Statin medication 184 (15) 57 (14) 67 (16) 60 (15) 0.6 Low-dose aspirin medication 193 (16) 71 (17) 67 (16) 55 (13) 0.3 Organic nitrate medication 19 (2) 6 (2) 6 (2) 7 (2) 0.9 Smoked ever 441 (36) 142 (35) 148(37) 151 (37) 0.8 Total fat, g/d 65 ± 23 60 ± 22 64 ± 22 69 ± 26 <0.001 Saturated fat, g/d 26 ± 11 25 ± 11 26 ± 10 27 ± 12 0.05 Protein, g/d 79 ± 26 69 ± 23 80 ± 24 90 ± 29 <0.001 Carbohydrate, g/d 191 ± 58 172 ± 51 193 ± 55 208 ± 62 <0.001 Fibre, g/d 23 ± 8 19 ± 6 23 ± 7 27 ± 8 <0.001 Alcohol, g/d 2.1 (0.3 – 10.4) 1.6 (0.3 – 9.9) 1.9 (0.3 – 9.8) 2.9 (0.3 – 11.4) 0.3 Calcium treatment 641 (52) 205 (50) 222 (54) 214(53) 0.5 Max CCA-IMT, mm 0.922 ± 0.152 0.941 ± 0.170 0.921 ± 0.141 0.905 ± 0.143 0.01 Mean CCA-IMT, mm 0.778 ± 0.129 0.793 ± 0.145 0.777 ± 0.118 0.765 ± 0.122 0.02 Plaque severity: moderate to high (≥25%)3 120 (12) 39 (13) 38 (12) 43 (13) 0.9 Ischemic cerebrovascular disease hospitalization or death
186 (15) 78 (19) 51 (13) 57 (14) 0.02
CCA-IMT indicates common carotid artery intima-media thickness, n=954. Values are means ± SDs, medians (IQRs), or n (%). 1n = 1226. 2ANOVA or a chi-square test was used as appropriate. 3n=968.
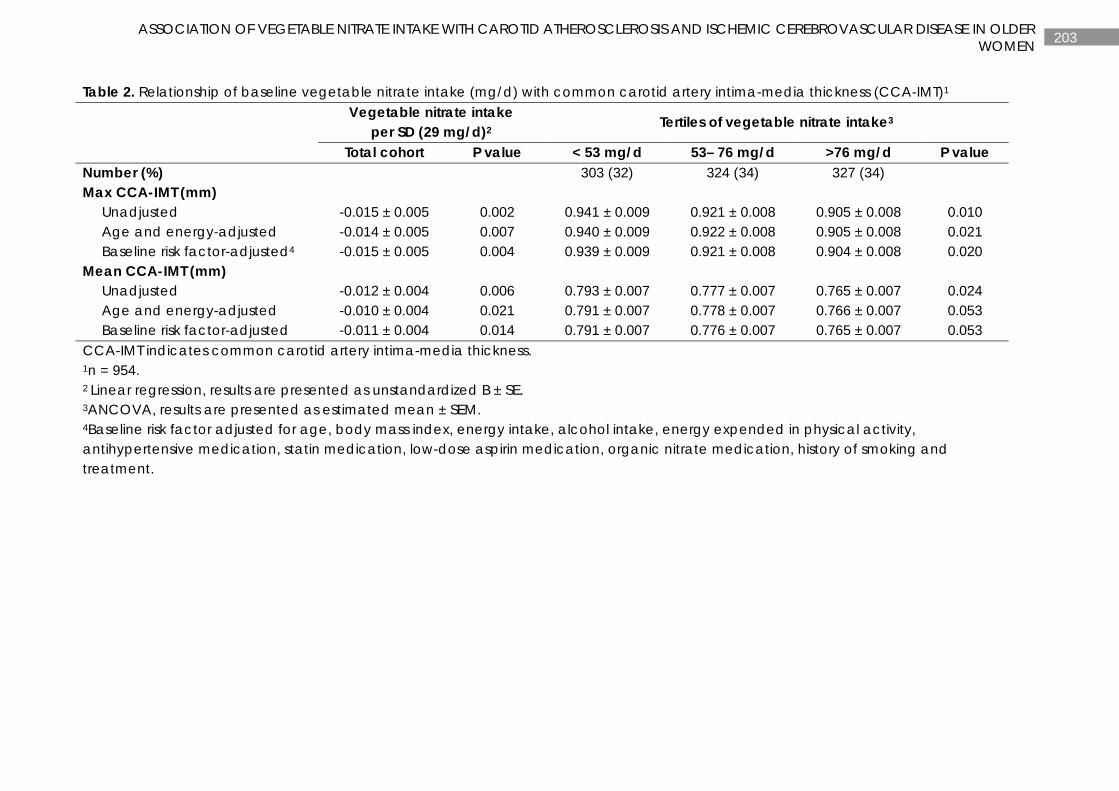
203 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
Table 2. Relationship of baseline vegetable nitrate intake (mg/d) with common carotid artery intima-media thickness (CCA-IMT)1
Vegetable nitrate intake per SD (29 mg/d)2 Tertiles of vegetable nitrate intake3
Total cohort P value < 53 mg/d 53– 76 mg/d >76 mg/d P value Number (%) 303 (32) 324 (34) 327 (34) Max CCA-IMT (mm) Unadjusted -0.015 ± 0.005 0.002 0.941 ± 0.009 0.921 ± 0.008 0.905 ± 0.008 0.010 Age and energy-adjusted -0.014 ± 0.005 0.007 0.940 ± 0.009 0.922 ± 0.008 0.905 ± 0.008 0.021 Baseline risk factor-adjusted4 -0.015 ± 0.005 0.004 0.939 ± 0.009 0.921 ± 0.008 0.904 ± 0.008 0.020 Mean CCA-IMT (mm) Unadjusted -0.012 ± 0.004 0.006 0.793 ± 0.007 0.777 ± 0.007 0.765 ± 0.007 0.024 Age and energy-adjusted -0.010 ± 0.004 0.021 0.791 ± 0.007 0.778 ± 0.007 0.766 ± 0.007 0.053 Baseline risk factor-adjusted -0.011 ± 0.004 0.014 0.791 ± 0.007 0.776 ± 0.007 0.765 ± 0.007 0.053 CCA-IMT indicates common carotid artery intima-media thickness. 1n = 954. 2 Linear regression, results are presented as unstandardized B ± SE. 3ANCOVA, results are presented as estimated mean ± SEM. 4Baseline risk factor adjusted for age, body mass index, energy intake, alcohol intake, energy expended in physical activity, antihypertensive medication, statin medication, low-dose aspirin medication, organic nitrate medication, history of smoking and treatment.
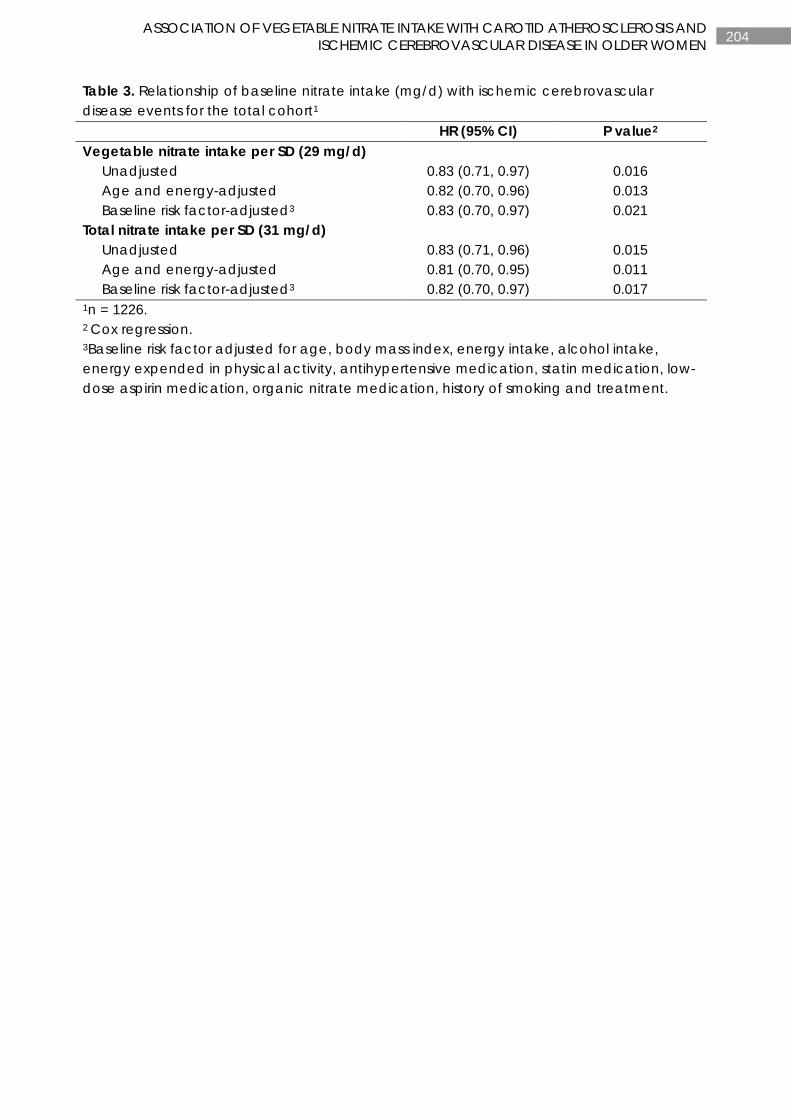
204 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
Table 3. Relationship of baseline nitrate intake (mg/d) with ischemic cerebrovascular disease events for the total cohort1 HR (95% CI) P value2 Vegetable nitrate intake per SD (29 mg/d) Unadjusted 0.83 (0.71, 0.97) 0.016 Age and energy-adjusted 0.82 (0.70, 0.96) 0.013 Baseline risk factor-adjusted3 0.83 (0.70, 0.97) 0.021 Total nitrate intake per SD (31 mg/d) Unadjusted 0.83 (0.71, 0.96) 0.015 Age and energy-adjusted 0.81 (0.70, 0.95) 0.011 Baseline risk factor-adjusted3 0.82 (0.70, 0.97) 0.017 1n = 1226. 2 Cox regression. 3Baseline risk factor adjusted for age, body mass index, energy intake, alcohol intake, energy expended in physical activity, antihypertensive medication, statin medication, low-dose aspirin medication, organic nitrate medication, history of smoking and treatment.
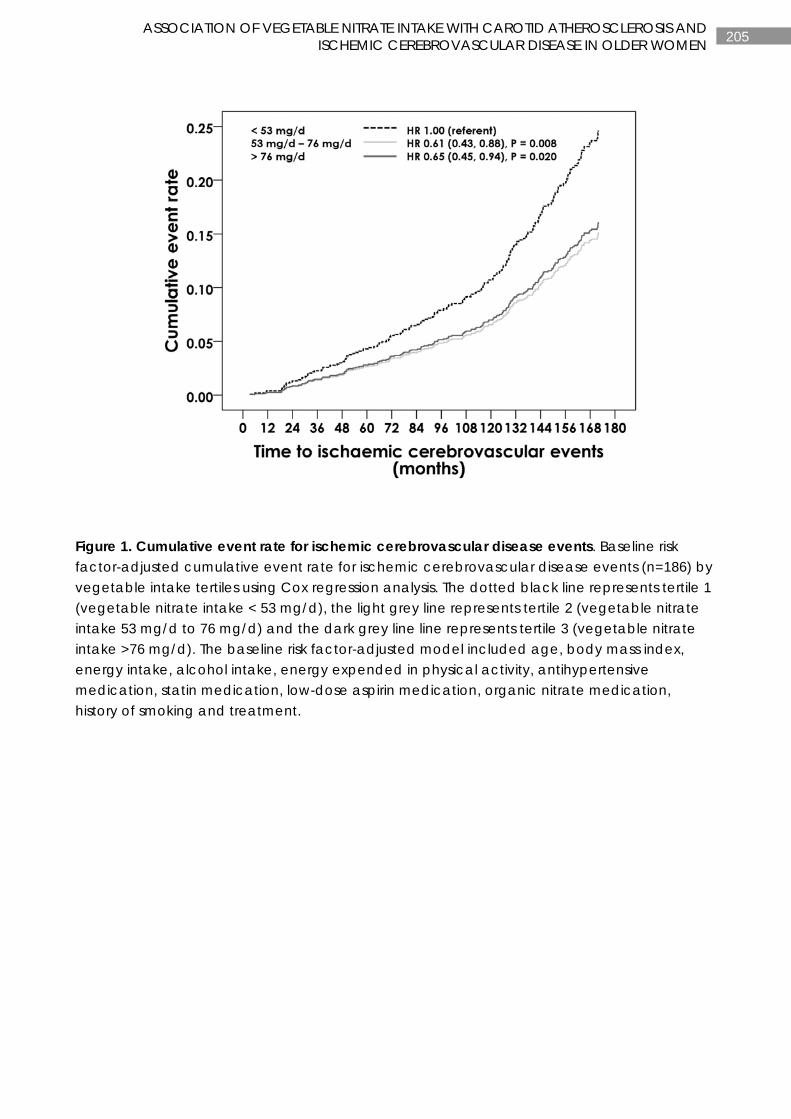
205 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
Figure 1. Cumulative event rate for ischemic cerebrovascular disease events. Baseline risk factor-adjusted cumulative event rate for ischemic cerebrovascular disease events (n=186) by vegetable intake tertiles using Cox regression analysis. The dotted black line represents tertile 1 (vegetable nitrate intake < 53 mg/d), the light grey line represents tertile 2 (vegetable nitrate intake 53 mg/d to 76 mg/d) and the dark grey line line represents tertile 3 (vegetable nitrate intake >76 mg/d). The baseline risk factor-adjusted model included age, body mass index, energy intake, alcohol intake, energy expended in physical activity, antihypertensive medication, statin medication, low-dose aspirin medication, organic nitrate medication, history of smoking and treatment.

206 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
SUPPORTING MATERIAL
Participants
A population-based approach was used to recruit the women into the study. Letters of invitation were sent to a random selection (n=24800) of women over the age of 70 on the Western Australia electoral roll (a citizenship requirement). Of these women 22% (n=5586) responded to the letter of which 27% (n=1510) were eligible to participate. Exclusion criteria included use of bone active agents, including calcium supplements and hormone replacement therapy, current illness and any medical condition likely to influence 5-year survival.
Baseline assessment
A baseline assessment was performed in 1998. Weight and height was determined using digital scales and a stadiometer while the participant was wearing light clothes and no shoes. BMI was calculated in kg/m2. Vascular disease risk was calculated using previous medical history and current medications, as verified by the participant’s general practitioner. These were coded using the International Classification of Primary Care-Plus (ICPC-Plus) method (260). The occurrence of pre-existing atherosclerotic vascular disease (ASVD) were determined from the complete hospital discharge data from 1980-1998 and were defined using primary diagnosis codes from International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)(258). These codes included ischemic heart disease (ICD-9-CM codes 410-414); heart failure (ICD-9-CM code 428); cerebrovascular disease excluding hemorrhage (ICD-9-CM codes 433-438); and peripheral arterial disease (ICD-9-CM codes 440-444). The presence of baseline vascular disease risk factors included pre-existing diabetes (T89001-90009). Use of cardiovascular medications included β-blockers, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, 3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors as well as antiplatelet agents. These medications were used to provide an estimate of prevalent hypertension and dyslipidaemia, risk factors classically used in calculating cardiovascular risk. Participants were coded as ex-smoker/current smoker (if smoked >1 cigarette/d for >3 months at any time) or non-smoker. The physical activity of participants in the 3 months prior to enrolment in the study was determined using a previously validated questionnaire which included questions relating to the hours spent per week in up to 4 sporting activities, recreational activities as well as other forms of regular physical activity such as walking. Energy costs of activity were used to determine the energy expenditure in kJ/d for these activities (293).
Baseline dietary intake was assessed using a validated semi-quantitative food frequency questionnaire (FFQ) developed by the Cancer Council of Victoria, Australia (262, 263). The completion of the questionnaire was performed in small groups supervised by a research assistant with food models, cups, spoons and frequency charts. Frequency of consumption (servings per day) and an overall estimate of portion size were used to estimate energy and nutrient intakes (262, 263).

207 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
Assessment of nitrate consumption
Total nitrate intake
An estimate of nitrate concentration (mg/g) in each of the non-vegetable items listed in the Cancer Council of Victoria FFQ was obtained using estimates derived from three sources. Nitrate concentration of 67 of the 77 non-vegetable items were obtained from Inoue-Choi et al. (245), 5 values were obtained from the Food Standards Australia New Zealand (FSANZ) survey of nitrates and nitrites in food and beverages in Australia (154) and 3 values from Griesenbeck et al (244). Where no value was available (two foods: vegemite and jam), a value of 0 mg/g was used. These values, together with the nitrate intake from vegetable values were used to determine total dietary nitrate intake as mg/d.
The concentration of nitrate in Perth drinking water was assessed using data from July 1997 to June 2001 for 24 regions around the Perth metropolitan area. The absolute maximum value at any time at any site was 0.0022 mg/g. The absolute 4-year mean (range of means) was 0.0003 mg/g (<0.00005; 0.0022) (the WA Water Corporation Water Quality Management System, personal communication). For a person drinking 2 L of water (including tea and coffee), this would equate to an estimated intake of 0.6 mg/d. These values were not included in the estimation of dietary nitrate intake as their contribution to nitrate intake in this population was negligible. The very low nitrate concentrations in Perth drinking water therefore allowed us to focus on nitrate intake from food.
Assessment of common carotid artery intima-media thickness (CCA-IMT) and presence of plaque
Carotid high-resolution B-mode ultrasonography was used to assess common carotid intima-media thickness and focal carotid plaques at year 3 (2001) of the study. The ultrasonic examinations were performed using an 8.0-MHz linear array transducer fitted to an Acuson Sequoia 512 ultrasound machine and a standard image-acquisition protocol. The far-wall carotid IMT at the distal 2 cm of both the left and right arteries were visualised from 3 different angles: anterolateral, lateral and posterolateral. The images were digitally captured at end-diastole for offline measurement by the same observer using semi-automated edge-detection software. The mean, maximum, minimum and SD was calculated for each of the 3 views from both sides. An overall mean CCA-IMT was determined from the average of the CCA-IMT of each of the 6 images. Plaque was defined as a distinct area of focal increased thickness (≥ 1 mm) of the intima-media layer. The severity of the carotid plaque was further categorised by the degree of carotid stenosis as either none to minimal (<25%) or moderate to high (≥25%) plaque. The precision of these measurements was determined in a previous study which reported a CV of 5.9% (root-mean-square error method) for repeat measures between 7 to 10 days apart (348).
Assessment of ischemic cerebrovascular disease event
The first episode of ischemic cerebrovascular hospitalizations or death was retrieved from the Western Australian Data Linkage System (WADLS) for each of the study participants from their baseline clinic visit date in 1998 until 14 ½ years after their baseline visit. Ischemic cerebrovascular disease hospitalizations were retrieved from the Hospital Morbidity Data Collection (HMDC), which provides a complete record of every participant’s primary diagnosis

208 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
at hospital discharge (hospital separation) using coded data from all hospitals in Western Australia. Ischemic cerebrovascular disease deaths were retrieved from the Death Registry by using the coded death certificate or Parts 1 and 2 of the death certificate where coded cause of death data was not yet available. Both HMDC and Death Registry data are linked through the WADLS. If the women remained in Western Australia, we had complete follow-up for hospitalizations and deaths. Cerebrovascular hospitalization separations and deaths were defined from the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) (258) and the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10- AM) (261). These codes for cerebrovascular disease, excluding hemorrhage, included: ICD-9-CM codes 433-438 and ICD-10-AM, codes I63-I69, G45.9.
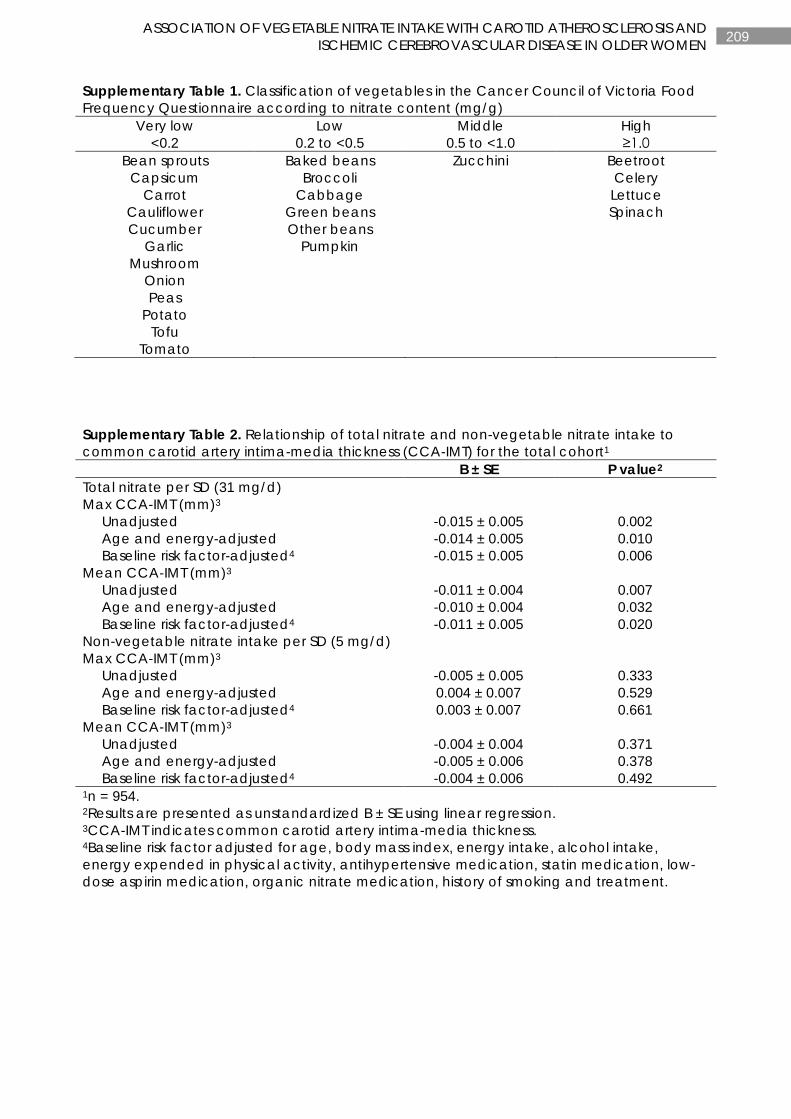
209 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
Supplementary Table 1. Classification of vegetables in the Cancer Council of Victoria Food Frequency Questionnaire according to nitrate content (mg/g)
Very low Low Middle High <0.2 0.2 to <0.5 0.5 to <1.0 ≥1.0
Bean sprouts Capsicum
Carrot Cauliflower Cucumber
Garlic Mushroom
Onion Peas
Potato Tofu
Tomato
Baked beans Broccoli
Cabbage Green beans Other beans
Pumpkin
Zucchini Beetroot Celery Lettuce Spinach
Supplementary Table 2. Relationship of total nitrate and non-vegetable nitrate intake to common carotid artery intima-media thickness (CCA-IMT) for the total cohort1 B ± SE P value2 Total nitrate per SD (31 mg/d) Max CCA-IMT (mm)3 Unadjusted -0.015 ± 0.005 0.002 Age and energy-adjusted -0.014 ± 0.005 0.010 Baseline risk factor-adjusted4 -0.015 ± 0.005 0.006 Mean CCA-IMT (mm)3 Unadjusted -0.011 ± 0.004 0.007 Age and energy-adjusted -0.010 ± 0.004 0.032 Baseline risk factor-adjusted4 -0.011 ± 0.005 0.020 Non-vegetable nitrate intake per SD (5 mg/d) Max CCA-IMT (mm)3 Unadjusted -0.005 ± 0.005 0.333 Age and energy-adjusted 0.004 ± 0.007 0.529 Baseline risk factor-adjusted4 0.003 ± 0.007 0.661 Mean CCA-IMT (mm)3 Unadjusted -0.004 ± 0.004 0.371 Age and energy-adjusted -0.005 ± 0.006 0.378 Baseline risk factor-adjusted4 -0.004 ± 0.006 0.492 1n = 954. 2Results are presented as unstandardized B ± SE using linear regression. 3CCA-IMT indicates common carotid artery intima-media thickness. 4Baseline risk factor adjusted for age, body mass index, energy intake, alcohol intake, energy expended in physical activity, antihypertensive medication, statin medication, low-dose aspirin medication, organic nitrate medication, history of smoking and treatment.
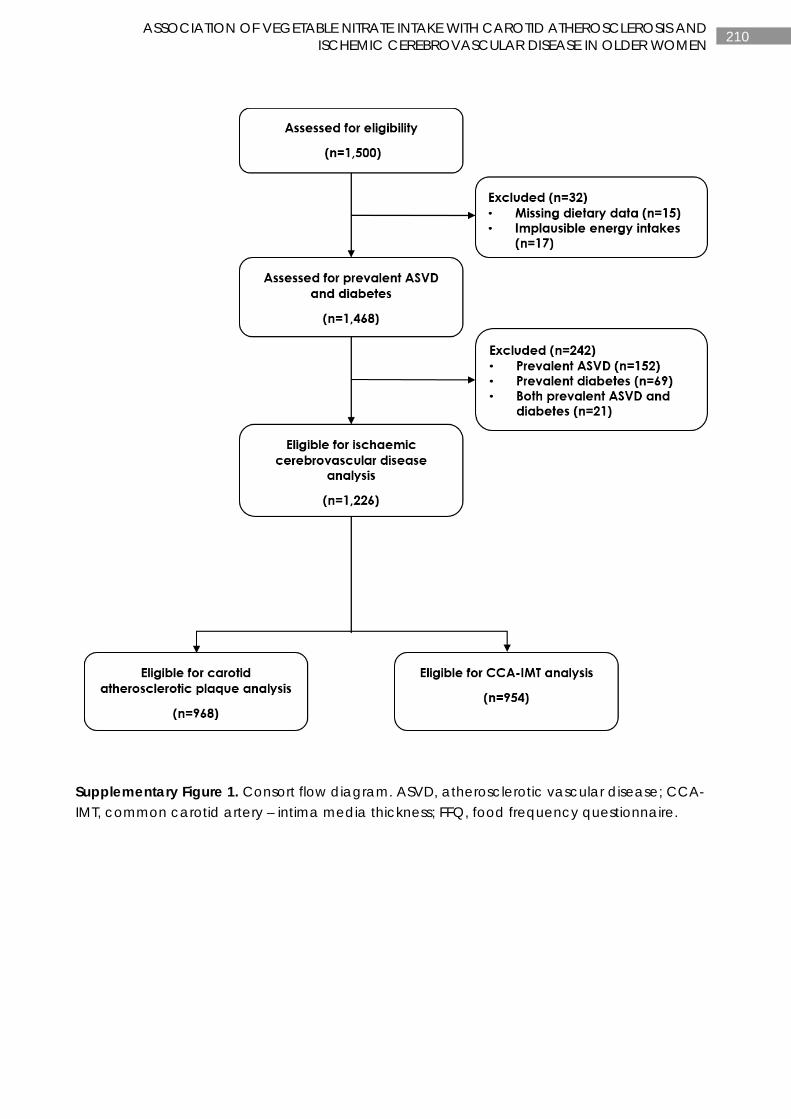
210 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
Supplementary Figure 1. Consort flow diagram. ASVD, atherosclerotic vascular disease; CCA-IMT, common carotid artery – intima media thickness; FFQ, food frequency questionnaire.
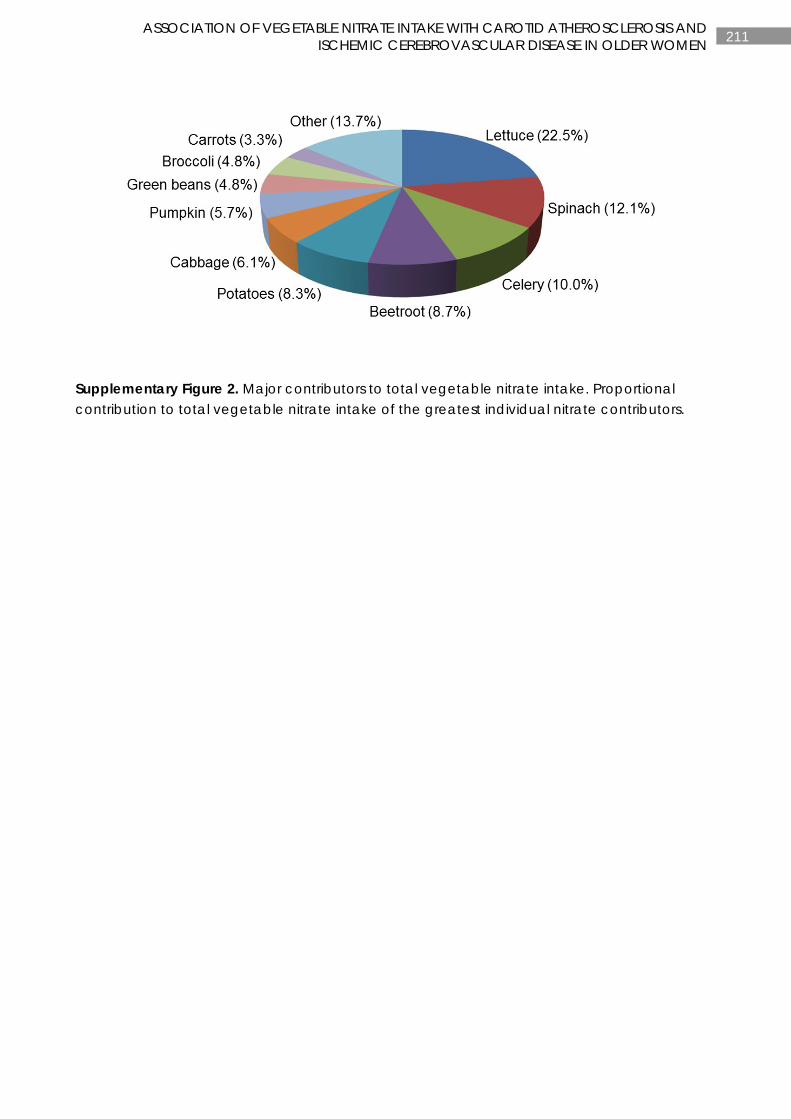
211 ASSOCIATION OF VEGETABLE NITRATE INTAKE WITH CAROTID ATHEROSCLEROSIS AND ISCHEMIC CEREBROVASCULAR DISEASE IN OLDER WOMEN
Supplementary Figure 2. Major contributors to total vegetable nitrate intake. Proportional contribution to total vegetable nitrate intake of the greatest individual nitrate contributors.
212 CHAPTER 8
CHAPTER 8
NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY
ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Manuscript based on this chapter:
Lauren C Blekkenhorst, Joshua R Lewis, Richard L Prince, Amanda Devine, Nicola P Bondonno1, Catherine P Bondonno, Lisa G Wood, Ian B Puddey, Natalie C Ward, Kevin D Croft, Richard J Woodman, Lawrence J Beilin, Jonathan M Hodgson. Nitrate-rich vegetables do not lower blood pressure in individuals with mildly elevated blood pressure: a randomised controlled crossover trial. American Journal of Clinical Nutrition. 2018;107(6):894-908.

213 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
ABSTRACT
Background: Emerging evidence suggests that increasing intakes of nitrate-rich vegetables may be an effective approach to reducing blood pressure.
Objective: Our primary aim was to determine whether daily consumption of nitrate-rich vegetables over 4 weeks would result in lower blood pressure.
Design: Thirty participants with pre-hypertension or untreated grade 1 hypertension were recruited to a randomised, controlled, crossover trial with 4-week treatment periods separated by 4-week washout periods. Participants completed three treatments in random order: (1) increased intake (~200 g/d) of nitrate-rich vegetables (high nitrate, HN, ~150 mg/d nitrate); (2) increased intake (~200 g/d) of nitrate-poor vegetables (low nitrate, LN, ~22 mg/d nitrate); and (3) no increase in vegetables (control, C, ~6 mg/d nitrate). Compliance was assessed using food diaries and by measuring plasma nitrate and carotenoids. Nitrate metabolism was assessed using plasma, salivary, and urinary nitrate and nitrite concentrations. The primary outcome was blood pressure assessed using 24-hour ambulatory, home, and clinic measurements. Secondary outcomes included measures of arterial stiffness.
Results: Plasma nitrate and nitrite concentrations were increased with the HN treatment in comparison to the LN and control treatments (P<0.001). Plasma carotenoids were increased with the HN and LN treatments compared to the control (P<0.01). High nitrate treatment did not reduce systolic blood pressure (24-hour ambulatory: HN 127.4±1.1 mmHg, LN 128.6±1.1 mmHg, C 126.2±1.1 mmHg, P=0.20; home: HN 127.4±0.7 mmHg, LN 128.7±0.7 mmHg, C 128.3±0.7 mmHg, P=0.36; clinic: HN 128.4±1. 3mmHg, LN 130.3±1.3 mmHg, C 129.8±1.3 mmHg, P=0.49) or diastolic blood pressure compared with LN and C treatments (P>0.05) after adjustement for pre-treatment values, treatment period and treatment order. Similarly, no differences were observed between treatments for arterial stiffness measures (P>0.05).
Conclusion: Increased intake of nitrate-rich vegetables did not lower blood pressure in pre-hypertensive or untreated grade 1 hypertensive individuals when compared with increased intake of nitrate-poor vegetables and no increase in vegetables.

214 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
INTRODUCTION
High blood pressure is the leading risk factor for global disease burden (349). The maintenance of a healthy blood pressure and the prevention of hypertension continue to be a public health priority worldwide (350, 351). It is estimated that for every 10 mmHg reduction in systolic blood pressure, there is a 13-28% lower risk of cardiovascular disease events and all-cause mortality (352). Arterial stiffness, which is closely related to hypertension (353, 354), is also a predictor of cardiovascular disease and all-cause mortality (355). Diets rich in vegetables, such as a vegetarian diet (241), Mediterranean diet, Nordic diet, and the Dietary Approaches to Stop Hypertension (DASH) diet (356), have been shown to lower blood pressure. There are many components of a diet rich in vegetables that may benefit cardiovascular health. In particular, emerging evidence suggests that inorganic nitrate found in vegetables can contribute to lowering blood pressure (163, 292).
Inorganic nitrate is a precursor for nitric oxide (NO) (44). NO is an important cell-signalling molecule and potent vasodilator critical for vascular health (37). The enterosalivary nitrate-nitrite-NO pathway generates NO via the sequential reduction in the anions nitrate and nitrite. This is facilitated by facultative anaerobic bacteria in the oral cavity, the acidic environment of the stomach, and numerous endogenous molecules identified as having nitrite-reducing ability (45). Increased scavenging of NO and dysfunction of the L-arginine-NO pathway underlie the reduced bioavailability of NO observed in hypertensive individuals (121). Increasing plasma nitrate through dietary means may provide a new therapeutic measure for restoring NO concentrations.
Vegetables account for ~80% of total nitrate consumed in the general population, with the majority coming from leafy green vegetables and beetroot (44, 131). There is now consistent and convincing evidence that an increase in nitrate salts and nitrate-rich vegetables can result in a decrease in blood pressure within hours of ingestion (143, 163, 188, 292, 310). However, data from short-term trials have yet to provide a clear understanding of the effects of a chronic increase in nitrate intake on blood pressure (292). In particular, there is a need to determine whether increasing nitrate-rich vegetables results in sustained lower blood pressure in individuals with elevated blood pressure. The results of published studies in this population are inconsistent (167, 188).
The objective of this study was to investigate whether increased intakes of nitrate-rich vegetables would result in lower blood pressure and improved arterial stiffness. An increased intake of nitrate-rich vegetables was compared with a matching increase in nitrate-poor vegetables and with no increase in vegetables.
METHODS
Ethics
The Vegetable Intake and Blood Pressure (VIABP) Study (registered at www.anzctr.org.au as ACTRN12615000194561) was approved by the University of Western Australia Human Research Ethics Committee and was carried out in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
215 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Trial design
The VIABP study was a randomised controlled crossover trial with three 4-wk treatment periods, each preceded by a 4-wk washout period (Supplemental Figure 1). The study was conducted at the Royal Perth Hospital Medical Research Foundation, Perth, Australia. Participants were randomly assigned to 1 of 6 sequence orders for the 3 treatments using computer-generated random numbers, assigned upon randomisation. The 3 treatments were as follows: 1) increased intake of nitrate-rich vegetables [high-nitrate (HN) diet; ~200 g/d]; 2) increased intake of nitrate-poor vegetables [low nitrate (LN) diet; ~200 g/d]; and 3) no increase in vegetables (control diet). Throughout the entire 24-wk trial period all of the participants were asked to limit their intake of nitrate-rich vegetables, except while undertaking the HN treatment (Supplemental Table 1).
Participants
Thirty participants with prehypertension or untreated grade 1 hypertension were recruited from the Perth general population with the use of newspaper advertisements between March and July 2015. Participants were ambulant men and women between the ages of 21 and 75 y, with a resting mean systolic blood pressure between 120 and 160 mmHg, inclusive. Participants were excluded if they were diabetic; a smoker; taking antihypertensive medication, NO donors, organic nitrates and nitrites, or related drugs; had a BMI (kg/m2) ≥35 or <18.5; or used antibacterial mouthwash. For a complete list of inclusion and exclusion criteria see Supplemental Table 2. Participants underwent screening procedures consisting of anthropometric measurements (height, weight, waist circumference, and hip circumference), an electrocardiogram, and a fasting blood test, which consisted of a full blood count, lipid profile, and glucose test, analysed by PathWest Laboratories (Royal Perth Hospital, Perth, Australia). Blood pressure was assessed by using a Dinamap 1846SX/P oscillometric recorder (Critikon, Inc.). Participants were asked to rest for 5 min before 5 blood pressure and heart rate readings were taken at 2-min intervals. The first measurement was excluded and the mean of the next 4 consecutive readings was used to determine resting blood pressure. After blood tests confirmed eligibility, participants were asked to return to the research clinic to complete a medical examination by 1 of our physicians (IBP or LJB). Participants provided a list of current medications and supplements and a medical history. At the same visit, participants completed a validated food-frequency questionnaire (Dietary Questionnaire for Epidemiological Studies, version 2) (262, 263, 357) to obtain baseline dietary intake. Participants were supervised by a nutritionist while completing the questionnaire. Food models, food charts, measuring cups, and measuring spoons were provided to ensure the accuracy of reported food consumption.
Dietary interventions
During each 4-wk treatment period, additions were made to participants’ breakfast and dinner, consisting of vegetables blended into juices or a matching control juice. Participants were asked to maintain all meals as usual with the exception of limiting HN vegetables, where possible. In the HN and LN treatment periods, participants were asked to consume 100 g of HN and LN vegetables/d, respectively, before breakfast and dinner. This was equivalent to increasing vegetable intake by ~2.7 servings/d (~200-300 kJ/d) (6). For the control treatment, participants were asked to blend one-quarter of an orange and 8 g maltodextrin in water
216 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
(approximately energy matched to the vegetables consumed in the HN and LN treatments). Before being randomly assigned, participants consumed a sample juice for all 3 treatments and completed a juice acceptability questionnaire to ensure willingness to participate. They were provided with blenders and blended ≥3 different vegetables of approximate equal weight with one-quarter of an orange (for taste) and <1 cup (~200 mL) of water. For the LN treatment, participants were instructed that they could microwave, oven bake, boil, or steam any LN root vegetables before consumption and were asked not to add any condiments (e.g. cooking oil, salt). The HN and LN vegetables consumed by participants are presented in Supplemental Table 3. Participants were asked to freeze a small sample of each treatment juice in a sterile 5-mL tube in the week before their post-treatment visit. Nitrate and nitrite concentrations were determined for each treatment juice. In addition, participants kept a diary of the type and weight of all vegetables (HN and LN) consumed in all prepared juices. Treatment diaries along with plasma concentrations of nitrate, nitrite, and total carotenoids were used to assess compliance.
Clinical measurements
Anthropometric measurements (body weight, waist circumference, and hip circumference) were assessed pre- and post-treatment, with participants wearing minimal clothing and no shoes. Standing height (m) was measured with the use of a wall-mounted stadiometer to the nearest 0.01 m. Fasting body weight (kg) was measured with the use of electronic scales to the nearest 0.01 kg. Waist and hip circumference (cm) were measured by using a steel tape measure (W606PM; Lufkin Executive Thinline). Waist and hip measurements were used to calculate waist-to-hip ratio (waist in cm: hip in cm).
Physical activity was assessed pre- and post-treatment with the use of the validated short form of the International Physical Activity Questionnaire (358). Total physical activity was calculated in metabolic equivalent task minutes per week and then converted to kJ/d. Alcohol intake was assessed pre- and post-treatment with the use of a 7-d alcohol diary. Standard drinks were calculated by multiplying the volume of alcohol consumed (L), the percentage of alcohol consumed (%) and the specific gravity of ethyl alcohol (0.789). Alcohol was converted to g/d.
Blood pressure
Ambulatory blood pressure
Ambulatory blood pressure and heart rate were monitored every 20 min during the day and every 30 min overnight for a 24-h period commencing at the end of the pre- and post-treatment visits, as previously described (359). Measurements that showed an error code or those with a pulse pressure of <20 mmHg were excluded from the analysis. Blood pressure traces that were missing >4 hourly means over the 24 h were also excluded from the analysis. A minimum of 70% successful readings was considered a valid recording. Mean blood pressure was determined for the 24-h, daytime (0600-2159), and nighttime (2200-0559) periods.

217 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Home blood pressure
Participants were provided with a digital blood pressure monitor (UA-767PC; A&D Co., Ltd) and an appropriately sized upper-arm cuff. Participants were given appropriate training and instructions on its use before commencing the study. Home blood pressure was measured and recorded by each participant 3 times daily (shortly after waking and before breakfast, 1-2 h before dinner, and 1-2 h after dinner) for the entire study duration. Participants were instructed to rest for 5 min before commencing 3 blood pressure readings over a 3-min period. The first measurement was excluded from the analysis, and the mean of the second and third measurements was used. Mean blood pressure was determined for the overall 4-wk pre- and post-treatment periods; weeks 1, 2, and 3 of each treatment; the last 7 d of the pre- and post-treatment period; and the morning, afternoon, and evening of the last 7 d of the pre- and post-treatment period.
Clinic blood pressure
Clinic blood pressure was measured pre- and post-treatment with the use of the SphygmoCor XCEL device (2012; AtCor Medical Pty. Ltd.). An appropriately sized blood pressure cuff was fitted to each participant’s non-dominant arm ~2.5 cm above the antecubital fossa. Participants had fasted for ≥12 h and were asked to rest in a supine position for 5 min before 3 blood pressure measurements performed at 60-s intervals. The first blood pressure reading was excluded, and the mean of the second and third measurements was used in analysis.
Arterial stiffness
Pulse-wave analysis (PWA) and pulse-wave velocity (PWV) were measured pre- and post-treatment with the use of the SphygmorCor XCEL device (2012; AtCor Medical Pty. Ltd.). Participants had fasted for ≥12 h, and avoided vigorous exercise and alcohol intake for ≥24 h before assessment. Participants were asked to rest for 5 min in a supine position before 3 blood pressure measurements at 60-s intervals were taken. Clinic blood pressure was followed by one 10-s capture PWA reading, which included central aortic systolic pressure, central aortic diastolic pressure, and augmentation index (%). An appropriately sized cuff was then fitted to each participant’s right thigh. Tubing was attached and a probe placed on the carotid artery. When a pulse was detected, the femoral cuff inflated and captured aortic PWV. Two PWV measurements were taken and the average was used in the analysis. If a difference of >0.5 m/s between the first 2 measurements was observed, a third measurement was taken and the middle value of the 3 measurements was used.
Biochemical analyses
Fasting (≥12 h) blood, saliva, and urine samples were collected pre- and post-treatment. Blood samples were collected by venipuncture into EDTA-coated and lithium heparin plasma gel (LH PST II) tubes. Whole blood was centrifuged at 4⁰C at 3500 rpm for 10 min and plasma aliquots stored at -80⁰C until analysis. Participants expectorated into sterile polystyrene jars for 5 min to obtain saliva samples and saliva aliquots were stored at -80°C until analysis. Spot urine samples were also collected into sterile polystyrene jars and aliquots were stored at -80°C until analysis.
218 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Nitrate and nitrite analysis
Nitrate and nitrite concentrations were measured in plasma, saliva, urine, and juice samples with the use of gas chromatography-mass spectrometry with 15N-labelled nitrate and nitrite as internal standards, as previously described (318).
Plasma carotenoid analysis
HPLC methodology was used to determine plasma carotenoid concentrations of β-carotene, lycopene, α-carotene, β-cryptoxanthin, and lutein and zeaxanthin, as previously described (360). Carotenoids were extracted by using ethanol, ethyl acetate, and hexane, with canthaxanthin as an internal standard. After evaporation of the solvents, the dried extract was reconstituted in dichloromethane:methanol (1:2 vol) and chromatography performed on an Agilent 1200 HPLC system using a Hypersil ODS column (100 mm x 2.1 mm x 5 µm). Carotenoids were analysed by using a mobile phase of acetonitrile: dichloromethane: methanol 0.05% ammonium acetate (85:10:5 vol:vol) at a flow rate of 0.3 mL/min with the use of a diode array detector (450 nm).
Other biochemical analyses
Urinary concentrations of sodium, potassium, and creatinine as well as plasma concentrations of sodium, potassium, creatinine, glucose, total cholesterol, HDL cholesterol, triglycerides, and calculated LDL cholesterol were analysed by PathWest Laboratories (Fiona Stanley Hospital, Perth, Australia).
Statistics
Sample size
The required sample size for the study was based on the primary outcome of blood pressure measured using 24-h ambulatory monitoring. It was estimated that 25 participants would provide >80% power to detect a 2.0-mmHg difference in mean 24-h systolic blood pressure on the basis of data from our previous studies (361, 362). This calculation assumes a type I error rate of 0.05/3 (0.017). In addition, we had >80% power to detect a 2.0-mmHg difference in mean home systolic blood pressure on the basis of data from our previous studies (361, 362).
Statistical methods
Global statistical significance was set at a 2-sided type 1 error rate of P<0.05. All data were analysed by using IBM SPSS Statistics for Windows, version 21.0 (IBM), and SAS software, version 9.4 (SAS Institute, Inc.). Normality of distributions was tested with the use of the Shapiro-Wilk normality test. Descriptive statistics of normally distributed continuous variables were expressed as means ± SDs, nonnormally distributed continuous variables were expressed as medians and IQRs, and categorical variables as numbers and proportions (%). Differences between treatments (HN, LN, and control) were tested for each outcome variable using a repeated-measures mixed-model (Proc Mixed command) with additional adjustments for outcome pretreatment values, treatment period, and treatment order. We tested for any carryover effects between treatment periods by using a treatment x treatment period interaction term.
219 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
RESULTS
Recruitment began on 25 May 2015 and final data were collected on 5 May 2016. Of the 65 participants screened for the study, 32 were randomly assigned, 30 of whom completed the study. Two participants withdrew after randomisation due to medical reasons unrelated to the trial (Figure 1).
Baseline demographic and clinical characteristics for the 30 participants are shown in Table 1. Baseline dietary data are shown in Supplemental Table 4. At baseline, the mean ± SD total nitrate, estimated by using a nitrate content of vegetables database (36) as well as published food-composition data, was 84.7 ± 36.2 mg/d (81.9% from vegetables alone). The mean ± SD total vegetable intake was 181.8 ± 75.8 g/d. With the use of participants’ food diaries from each treatment period, the median (IQR) reported increase in nitrate-rich vegetables for the HN treatment was 201.5 (198.7-204.1) g/d and the increase in nitrate-poor vegetables for the LN treatment was 201.7 (197.0-207.7) g/d. Descriptive statistics for the individual nitrate-rich and nitrate-poor vegetables consumed in both the HN and LN treatments are shown in Supplemental Table 3. The median (IQR) nitrate and nitrite concentrations, from the juice samples provided by participants, and in which the participants were estimated to be consuming, were as follows: 149.1 (118.2-237.0) and 3.96 (2.19-5.20) mg/d for the HN treatment (n=30); 21.5 (13.9-29.9) and 0.31 (0.16-0.48) mg/d for the LN treatment (n=27); and 5.5 (3.7-8.0) and 0.06 (0.05-0.08) mg/d for the control (n=29), respectively. Nitrate and nitrite concentrations were significantly different between treatment juices (P<0.001 for both). HN juices were 27-fold higher in nitrate and 66-fold higher in nitrite concentration than that of the control (P<0.001 for both). In addition, the HN juices were 6.9-fold higher in nitrate and 12.8-fold higher in nitrite concentration than that of the LN juices (P<0.001 for both). The LN and control juices were not different in nitrate (P=0.326) and nitrite (P=0.779) concentrations.
Compliance
Compliance was measured for the 3 treatments with the use of self-reported food diaries. Participants recorded the weight (g) of each vegetable consumed in their juice on a daily basis. Compliance was calculated by dividing the number of days the vegetables were consumed by the number of days the vegetables should have been consumed and then multiplying by 100. On the basis of reported consumption of treatments with the use of food diaries, the median (IQR) compliance was 98.1% (90.6-100.0%) for the HN treatment, 98.1% (92.9-100.0%) for the LN treatment, and 98.1% (96.0-100.0%) for the control treatment. Compliance for the control diet was also measured by dividing the amount (g) of returned maltodextrin by the amount (g) of maltodextrin administered to participants before their treatment period and then multiplying by 100. Based on returned maltodextrin, the median (IQR) compliance was 131.5% (110.7-142.5%). All of the treatment diets were well tolerated. While receiving the control treatment, 1 participant reported constipation symptoms and another reported loose stools. No serious adverse events were reported.
220 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Biomarkers of intake and metabolism
Plasma nitrate and nitrite
Median (IQR) plasma nitrate and nitrite concentrations pre- and post-treatment are shown in Table 2. Plasma nitrate was significantly different between treatments (P<0.001) (Figure 2). There was a 1.7-fold increase in plasma nitrate concentrations for the HN treatment compared with the LN treatment (P<0.001) and a 1.6-fold increase for the HN treatment compared with the control (P<0.001) (Figure 2). Plasma nitrite was significantly different between treatments (P=0.007) (Figure 2). There was a 1.5-fold increase in plasma nitrite concentrations for the HN treatment compared with the LN treatment (P=0.002) and a 1.3-fold increase for the HN treatment compared with the control (P=0.037) (Figure 2).
Salivary nitrate and nitrite
Median (IQR) salivary nitrate and nitrite concentrations for pre- and post-treatment are shown in Table 2. Salivary nitrate was significantly different between treatments (P=0.038) (Figure 2). There was a 1.7-fold increase in salivary nitrate concentrations for the HN treatment compared with the LN treatment (P=0.022) and a 1.6-fold increase for the HN treatment compared with the control (P=0.036) (Figure 2). Salivary nitrite was not significantly different between treatments (P=0.098) (Figure 2).
Urinary nitrate and nitrite
Median (IQR) urinary nitrate and nitrite concentrations adjusted for urinary creatinine are presented in Table 2. Urinary nitrate was significantly different between treatments (P<0.001) (Figure 2). There was a 1.9-fold increase in urinary nitrate concentration for the HN treatment compared with the LN treatment (P<0.001) and a 1.8-fold increase for the HN treatment compared with the control (P<0.001) (Figure 2). Urinary nitrite was not significantly different between treatments (P=0.074) (Figure 2).
Plasma carotenoids
Descriptive statistics for plasma total carotenoids, lutein, β-cryptoxanthin, lycopene, α-carotene, and β-carotene are presented in Table 3. Plasma total carotenoids were significantly different between treatments (P<0.001) (Figure 3). There was a 1.4-fold increase in the HN treatment compared with the control (P<0.001) and a 1.3-fold increase in the LN treatment compared with the control (P=0.002) (Figure 3). Plasma lutein was significantly different between treatments (P<0.001) (Figure 3). There was a 1.6-fold increase in plasma lutein in the HN treatment compared with the LN treatment (P<0.001) and a 1.8-fold increase in the HN treatment compared with the control (P<0.001) (Figure 3). Plasma β-carotene was significantly different between treatments (P=0.002) (Figure 3). There was a 1.6-fold increase in plasma β-carotene in the HN treatment compared with the control (P=0.002) and a 1.6-fold increase in the LN treatment compared with the control (P=0.003) (Figure 3). Plasma β-cryptoxanthin, lycopene, and α-carotene were not significantly different between treatments (Figure 3).
221 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Plasma and urinary sodium and potassium
Plasma and urinary sodium and potassium and urinary sodium to potassium ratio were not significantly different between treatments (Table 4).
Blood pressure
Ambulatory blood pressure
Ambulatory measures of blood pressure were excluded for 2 (6.7%) participants due to equipment malfunction (n=1) and readings that were <70% successful (n=1). The mean ± SD 24-h, daytime, and nighttime ambulatory measures of blood pressure and heart rate pre- and post-treatment are presented in Table 5. There were no significant differences between treatments for mean 24-h, daytime, or nighttime ambulatory blood pressure and heart rate (Figure 4). No carryover effects were observed for 24-h, daytime, and nighttime ambulatory measures of blood pressure and heart rate (P>0.05 for all). In a post hoc sensitivity analysis in which we adjusted for age, sex and BMI, the results were very similar and not substantively changed (data not shown).
Home blood pressure
Home measures of blood pressure were complete for all participants. Mean ± SD home measures of blood pressure and heart rate pre- and post-treatment are presented in Table 5. There were no significant differences between treatments for blood pressure and heart rate for the last 7 d of treatment (Figure 4). There were also no significant differences between treatments for blood pressure and heart rate for week 1, week 2 and week 3 of treatment when analysed separately (Figure 5). In addition, we found no significant differences between treatments for blood pressure and heart rate measured in the morning, afternoon, and evening when analysed separately (data not shown). Mean daily home measures of blood pressure and heart rate are shown in Supplemental Figure 2. No carryover effects were observed for home measures of blood pressure and heart rate (P>0.05 for all).
Clinic blood pressure
Clinic measures of blood pressure were complete for all participants. Mean ± SD clinic measures of blood pressure and heart rate pre- and post-treatment are presented in Table 5. There were no significant differences between treatments for blood pressure and heart rate (Figure 4).
Arterial stiffness
PWA was complete for all participants. PWV was incomplete for 4 (13.3%) participants due to an inability to obtain measurements. Mean ± SD central systolic and diastolic pressures, central augmentation index (%), and PWV for pre- and post-treatment are shown in Table 6. No significant differences were observed between treatments for central systolic blood pressure, central diastolic blood pressure, central augmentation index, and PWV.

222 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Plasma lipids and glucose
Plasma total cholesterol, triglycerides, LDL cholesterol, HDL cholesterol, and glucose were not significantly different between treatments (Table 4).
Anthropometric measures, physical activity, and alcohol intake
Descriptive statistics for anthropometric measures, physical activity, and alcohol intake pre- and post-treatment are presented in Supplemental Table 5. Weight, BMI, waist circumference, hip circumference, and waist-to-hip ratio were not significantly different between treatments. Physical activity expended in kJ/d and alcohol consumed in the last 7 d before to each treatment period were also not significantly different between treatments.
DISCUSSION
In this 4-wk randomised controlled crossover trial, an additional ~200 g/d intake of nitrate-rich vegetables did not alter blood pressure or arterial stiffness in men and women with prehypertension or untreated grade 1 hypertension. There was a significant increase in salivary, urinary, and plasma nitrate as well as plasma nitrite concentrations after the HN treatment, confirming that the dietary interventions were effective in altering nitrate concentrations. In addition, total plasma carotenoids increased with increased consumption of both HN and LN vegetables. Our study findings did not support our hypothesis that an increased intake of HN vegetables would result in lower blood pressure and improved arterial stiffness.
A number of short-term trials have assessed the effects of increased nitrate intake on blood pressure (163, 292). The results of these studies are inconsistent, with several trials finding lower blood pressure with increased nitrate intake (187-191, 193, 194) and others finding no effect (153, 166-169, 192). Our study is unique in that the design assessed the impact of a sustained 4-wk increase in nitrate-rich vegetables in individuals with prehypertension or untreated grade 1 hypertension and that participants were not taking antihypertensive medication that could have modified any effect of nitrate. Many potential factors could influence whether an increase in nitrate intake results in lower blood pressure. The duration of the study appears to be a factor, with acute studies consistently showing blood pressure-lowering effects (143, 153, 172, 173, 178-186). Other factors may include the following: the dose of nitrate provided; the background nitrate and vegetable intake of the study participants, which may alter the effective dose; whether there is an individual threshold level beyond which there is little additional benefit; and the age and health status of the participants.
Only 3 studies investigated the short-term sustained effects of nitrate ingestion on blood pressure and arterial stiffness over a period of ≥4 wk (153, 188, 190). Of these, only 1 investigated the effects in prehypertensive or untreated hypertensive individuals (188). Kapil et al. (188) found that daily consumption of beetroot juice (nitrate dose: 398 mg/d or 6.4 mmol/d) reduced blood pressure and improved arterial stiffness in 64 untreated or treated hypertensive individuals. Although our study does not align with the aforementioned study (188), other short-term intervention studies (3-42 d) have shown no effect of nitrate ingestion on blood pressure (153, 166-169, 192) or arterial stiffness (166, 168). These studies were all in individuals at risk of cardiovascular disease (153, 166-169, 192). Previous trials in which improvements were observed in blood pressure and arterial stiffness with increased nitrate intake have included a
223 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
mix of healthy participants (187, 189, 193, 194) and those at risk of cardiovascular disease (153, 188, 190, 191). There is strong evidence to show that nitrate ingestion reduces blood pressure within hours of ingestion (143, 153, 172, 173, 178-186). The acute effects on arterial stiffness are less clear. Some studies showed improvements (153, 173, 185), whereas others did not (171, 179-181).
Several factors may explain why our study did not show a reduction in blood pressure. As mentioned previously, background diet may have influenced nitrate metabolism, with individuals having sufficient nitrate intake unresponsive to further nitrate supplementation. Possible interactions between nitrate and sulphur-containing dietary constituents have been proposed (197). Nitrate in drinking water was inversely associated with blood pressure at low sulphate concentrations (9-33 mg/L), but this relationship was reversed at medium to high concentrations (34-102 mg/L). Such an interaction would be unlikely to have confounded the results of our study because the calculated mean sulphate concentration in water consumed by our cohort was 13.5 mg/L (data not shown). These data, however, do not fully discount such an interaction because sulphur-containing foods within the diet cannot be calculated due to the absence of adequate nutrient databases. In addition, Montenegro et al. (140) recently showed that acid-suppressing drugs abolished the blood pressure-lowering effects of oral nitrite ingestion despite the increase in plasma nitrite concentration. Only 1 participant in our study reported taking an acid-suppressing drug (rabeprazole) for the treatment of gout. This does not discount the theory that gastric pH may differ between individuals and that it is a possible determinant in influencing blood pressure after nitrate ingestion.
Limitations to this intervention study need to be considered. First, we did not observe differences in urinary potassium concentrations. We may have expected to see an increase of >10% in potassium excretion given the self-reported increases in vegetable intake. This could be the result of using creatinine-adjusted values from a spot urine sample instead of a 24-h urine sample to assess urinary potassium (363). We did, however, observe an increase of ~1.6-fold in plasma nitrate and nitrite with increased nitrate-rich vegetables and an increase of ~1.4-fold in plasma total carotenoids with increased nitrate-rich and nitrate-poor vegetables. The increase in plasma nitrate, nitrite, and total carotenoids gives us confidence the participants were compliant. It should be noted that plasma nitrite concentrations in our study are higher than some reported values in the literature. This could be due to a number of factors; however, it is likely an outcome of the gas chromatography-mass spectrometry method in comparison to gas phase chemiluminescence (318). Second, our study showed no statistical difference in salivary and urinary nitrite concentrations. Circulating nitrate and nitrite concentrations depend on when nitrate is last ingested. The half-life of nitrate in plasma is 5-6 h (333). Nitrite is likely to be similar because new nitrite is being continuously generated from the ingested nitrate. Because participants were asked to fast for ≥12 h before providing samples, this may explain why no increases in salivary and urinary nitrite concentrations were observed. However, other mechanisms may explain this observation and warrant further investigation. Third, the estimated nitrate intake from the measured juice samples was 149 mg/d, whereas the estimated nitrate intake with the use of a comprehensive international nitrate database (36) was 326 mg/d. The nitrate content of vegetables available in Perth may be appreciably lower than in many other regions of the world due to the high intensity of sunlight and longer daylight hours. Vegetables grown in lower light intensity and fewer daylight hours have a tendency to accumulate higher nitrate concentrations (155, 364). Fourth, due to the nature of

224 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
the intervention, participants could not be blinded to the treatments received. Blinding was, however, used for of the laboratory analyses. Last, we cannot rule out any small effects on blood pressure (<2 mmHg).
In summary, our findings suggest no short-term clinically significant effects on blood pressure, arterial stiffness, lipids, or glucose from increasing the intakes of nitrate-rich vegetables in men and women with prehypertension or untreated grade 1 hypertension. There are likely complex issues surrounding why no benefit was seen, including background nitrate intake, the amount of increase in nitrate intake, cross-talk mechanisms, and populations at risk of cardiovascular disease, which may all play a vital role in the differences observed between studies.
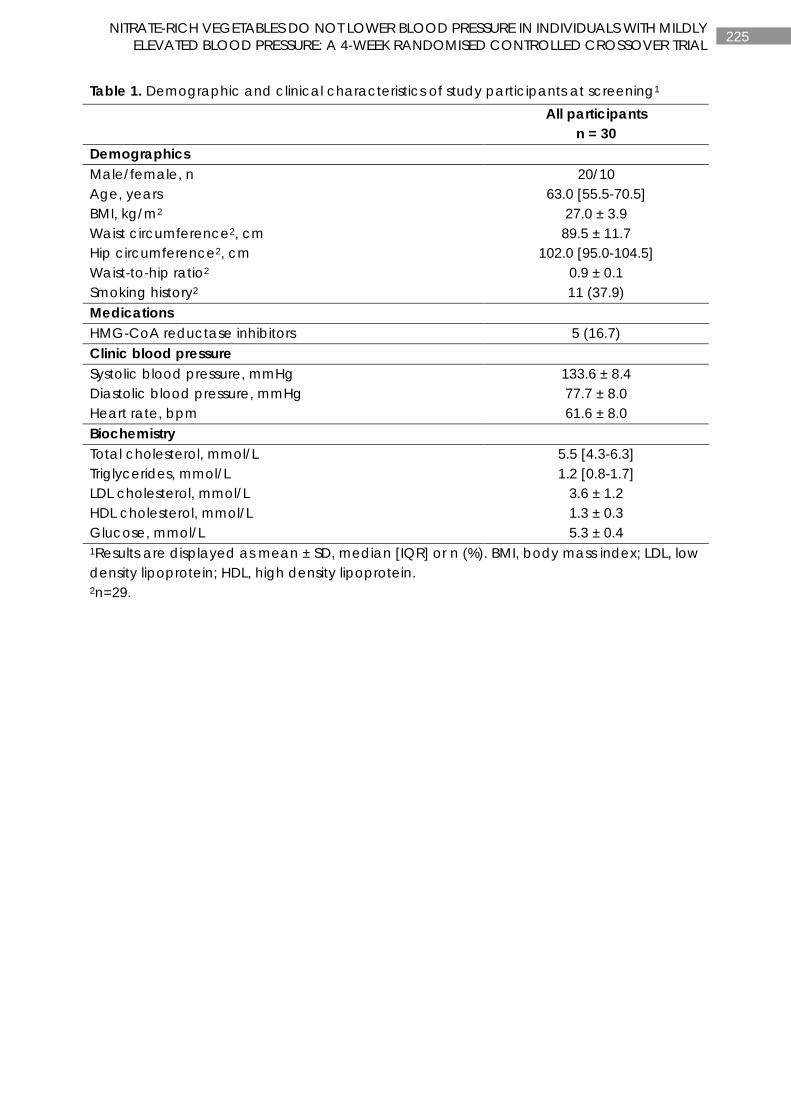
225 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Table 1. Demographic and clinical characteristics of study participants at screening1
All participants
n = 30 Demographics Male/female, n 20/10 Age, years 63.0 [55.5-70.5] BMI, kg/m2 27.0 ± 3.9 Waist circumference2, cm 89.5 ± 11.7 Hip circumference2, cm 102.0 [95.0-104.5] Waist-to-hip ratio2 0.9 ± 0.1 Smoking history2 11 (37.9) Medications HMG-CoA reductase inhibitors 5 (16.7) Clinic blood pressure Systolic blood pressure, mmHg 133.6 ± 8.4 Diastolic blood pressure, mmHg 77.7 ± 8.0 Heart rate, bpm 61.6 ± 8.0 Biochemistry Total cholesterol, mmol/L 5.5 [4.3-6.3] Triglycerides, mmol/L 1.2 [0.8-1.7] LDL cholesterol, mmol/L 3.6 ± 1.2 HDL cholesterol, mmol/L 1.3 ± 0.3 Glucose, mmol/L 5.3 ± 0.4 1Results are displayed as mean ± SD, median [IQR] or n (%). BMI, body mass index; LDL, low density lipoprotein; HDL, high density lipoprotein. 2n=29.
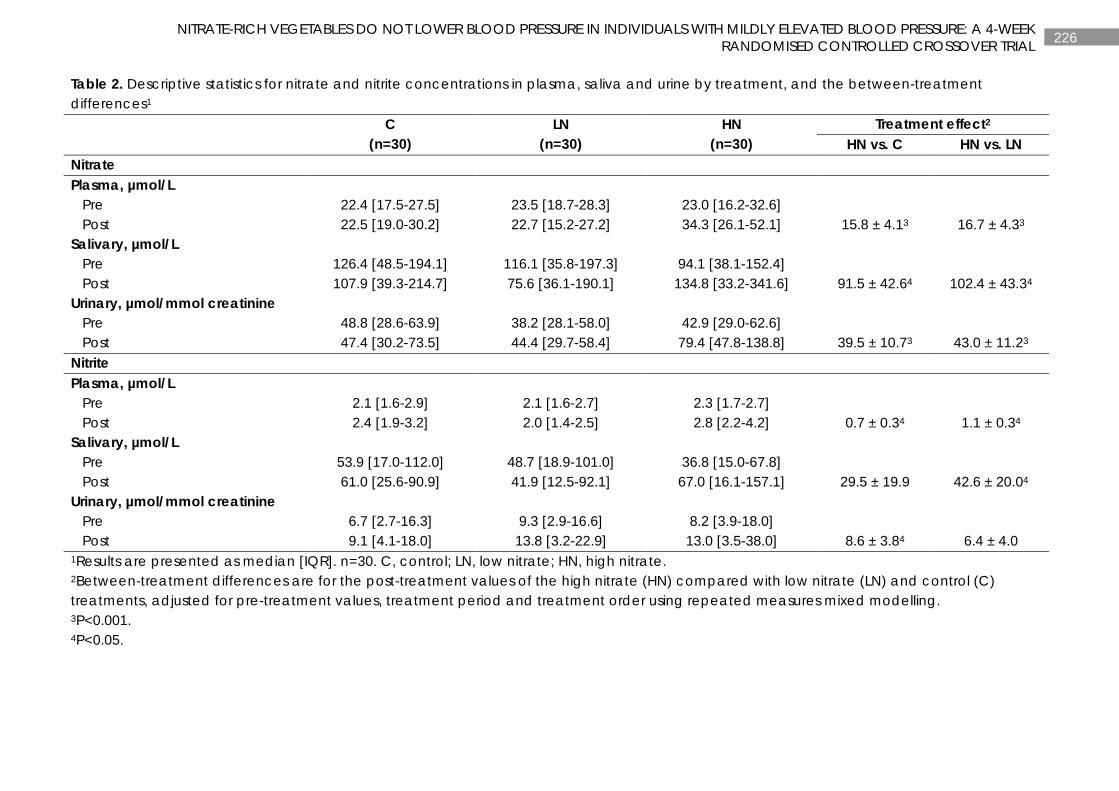
226 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Table 2. Descriptive statistics for nitrate and nitrite concentrations in plasma, saliva and urine by treatment, and the between-treatment differences1
C
(n=30) LN
(n=30) HN
(n=30) Treatment effect2
HN vs. C HN vs. LN Nitrate Plasma, µmol/L Pre 22.4 [17.5-27.5] 23.5 [18.7-28.3] 23.0 [16.2-32.6] Post 22.5 [19.0-30.2] 22.7 [15.2-27.2] 34.3 [26.1-52.1] 15.8 ± 4.13 16.7 ± 4.33 Salivary, µmol/L Pre 126.4 [48.5-194.1] 116.1 [35.8-197.3] 94.1 [38.1-152.4] Post 107.9 [39.3-214.7] 75.6 [36.1-190.1] 134.8 [33.2-341.6] 91.5 ± 42.64 102.4 ± 43.34 Urinary, µmol/mmol creatinine Pre 48.8 [28.6-63.9] 38.2 [28.1-58.0] 42.9 [29.0-62.6] Post 47.4 [30.2-73.5] 44.4 [29.7-58.4] 79.4 [47.8-138.8] 39.5 ± 10.73 43.0 ± 11.23 Nitrite Plasma, µmol/L Pre 2.1 [1.6-2.9] 2.1 [1.6-2.7] 2.3 [1.7-2.7] Post 2.4 [1.9-3.2] 2.0 [1.4-2.5] 2.8 [2.2-4.2] 0.7 ± 0.34 1.1 ± 0.34 Salivary, µmol/L Pre 53.9 [17.0-112.0] 48.7 [18.9-101.0] 36.8 [15.0-67.8] Post 61.0 [25.6-90.9] 41.9 [12.5-92.1] 67.0 [16.1-157.1] 29.5 ± 19.9 42.6 ± 20.04 Urinary, µmol/mmol creatinine Pre 6.7 [2.7-16.3] 9.3 [2.9-16.6] 8.2 [3.9-18.0] Post 9.1 [4.1-18.0] 13.8 [3.2-22.9] 13.0 [3.5-38.0] 8.6 ± 3.84 6.4 ± 4.0 1Results are presented as median [IQR]. n=30. C, control; LN, low nitrate; HN, high nitrate. 2Between-treatment differences are for the post-treatment values of the high nitrate (HN) compared with low nitrate (LN) and control (C) treatments, adjusted for pre-treatment values, treatment period and treatment order using repeated measures mixed modelling. 3P<0.001. 4P<0.05.
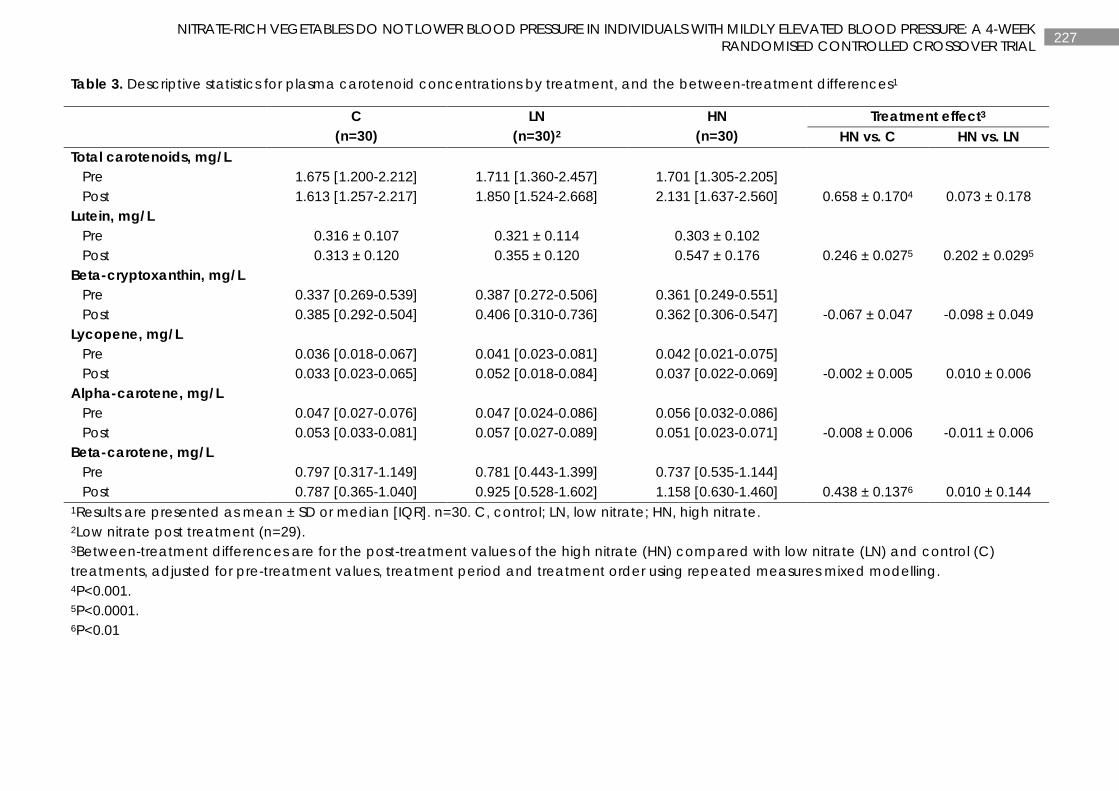
227 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Table 3. Descriptive statistics for plasma carotenoid concentrations by treatment, and the between-treatment differences1
C
(n=30) LN
(n=30)2 HN
(n=30) Treatment effect3
HN vs. C HN vs. LN Total carotenoids, mg/L Pre 1.675 [1.200-2.212] 1.711 [1.360-2.457] 1.701 [1.305-2.205] Post 1.613 [1.257-2.217] 1.850 [1.524-2.668] 2.131 [1.637-2.560] 0.658 ± 0.1704 0.073 ± 0.178 Lutein, mg/L Pre 0.316 ± 0.107 0.321 ± 0.114 0.303 ± 0.102 Post 0.313 ± 0.120 0.355 ± 0.120 0.547 ± 0.176 0.246 ± 0.0275 0.202 ± 0.0295 Beta-cryptoxanthin, mg/L Pre 0.337 [0.269-0.539] 0.387 [0.272-0.506] 0.361 [0.249-0.551] Post 0.385 [0.292-0.504] 0.406 [0.310-0.736] 0.362 [0.306-0.547] -0.067 ± 0.047 -0.098 ± 0.049 Lycopene, mg/L Pre 0.036 [0.018-0.067] 0.041 [0.023-0.081] 0.042 [0.021-0.075] Post 0.033 [0.023-0.065] 0.052 [0.018-0.084] 0.037 [0.022-0.069] -0.002 ± 0.005 0.010 ± 0.006 Alpha-carotene, mg/L Pre 0.047 [0.027-0.076] 0.047 [0.024-0.086] 0.056 [0.032-0.086] Post 0.053 [0.033-0.081] 0.057 [0.027-0.089] 0.051 [0.023-0.071] -0.008 ± 0.006 -0.011 ± 0.006 Beta-carotene, mg/L Pre 0.797 [0.317-1.149] 0.781 [0.443-1.399] 0.737 [0.535-1.144] Post 0.787 [0.365-1.040] 0.925 [0.528-1.602] 1.158 [0.630-1.460] 0.438 ± 0.1376 0.010 ± 0.144 1Results are presented as mean ± SD or median [IQR]. n=30. C, control; LN, low nitrate; HN, high nitrate. 2Low nitrate post treatment (n=29). 3Between-treatment differences are for the post-treatment values of the high nitrate (HN) compared with low nitrate (LN) and control (C) treatments, adjusted for pre-treatment values, treatment period and treatment order using repeated measures mixed modelling. 4P<0.001. 5P<0.0001. 6P<0.01
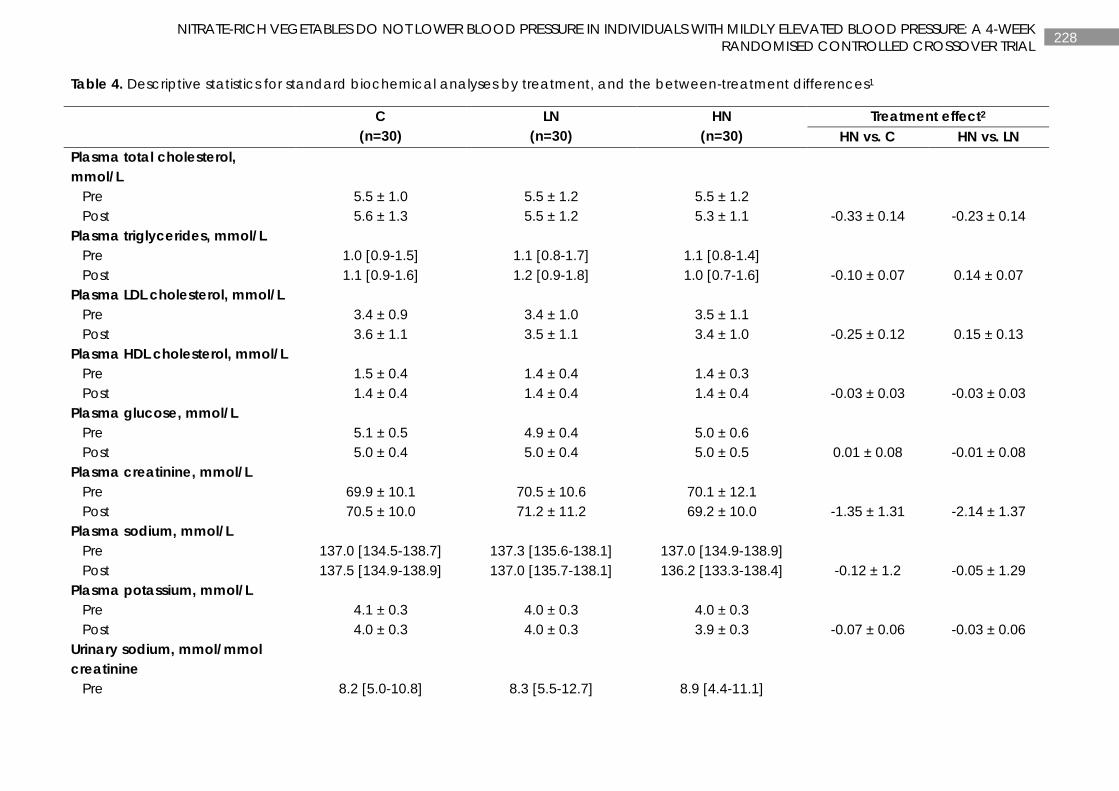
228 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Table 4. Descriptive statistics for standard biochemical analyses by treatment, and the between-treatment differences1
C
(n=30) LN
(n=30) HN
(n=30) Treatment effect2
HN vs. C HN vs. LN Plasma total cholesterol, mmol/L
Pre 5.5 ± 1.0 5.5 ± 1.2 5.5 ± 1.2 Post 5.6 ± 1.3 5.5 ± 1.2 5.3 ± 1.1 -0.33 ± 0.14 -0.23 ± 0.14 Plasma triglycerides, mmol/L Pre 1.0 [0.9-1.5] 1.1 [0.8-1.7] 1.1 [0.8-1.4] Post 1.1 [0.9-1.6] 1.2 [0.9-1.8] 1.0 [0.7-1.6] -0.10 ± 0.07 0.14 ± 0.07 Plasma LDL cholesterol, mmol/L Pre 3.4 ± 0.9 3.4 ± 1.0 3.5 ± 1.1 Post 3.6 ± 1.1 3.5 ± 1.1 3.4 ± 1.0 -0.25 ± 0.12 0.15 ± 0.13 Plasma HDL cholesterol, mmol/L Pre 1.5 ± 0.4 1.4 ± 0.4 1.4 ± 0.3 Post 1.4 ± 0.4 1.4 ± 0.4 1.4 ± 0.4 -0.03 ± 0.03 -0.03 ± 0.03 Plasma glucose, mmol/L Pre 5.1 ± 0.5 4.9 ± 0.4 5.0 ± 0.6 Post 5.0 ± 0.4 5.0 ± 0.4 5.0 ± 0.5 0.01 ± 0.08 -0.01 ± 0.08 Plasma creatinine, mmol/L Pre 69.9 ± 10.1 70.5 ± 10.6 70.1 ± 12.1 Post 70.5 ± 10.0 71.2 ± 11.2 69.2 ± 10.0 -1.35 ± 1.31 -2.14 ± 1.37 Plasma sodium, mmol/L Pre 137.0 [134.5-138.7] 137.3 [135.6-138.1] 137.0 [134.9-138.9] Post 137.5 [134.9-138.9] 137.0 [135.7-138.1] 136.2 [133.3-138.4] -0.12 ± 1.2 -0.05 ± 1.29 Plasma potassium, mmol/L Pre 4.1 ± 0.3 4.0 ± 0.3 4.0 ± 0.3 Post 4.0 ± 0.3 4.0 ± 0.3 3.9 ± 0.3 -0.07 ± 0.06 -0.03 ± 0.06 Urinary sodium, mmol/mmol creatinine
Pre 8.2 [5.0-10.8] 8.3 [5.5-12.7] 8.9 [4.4-11.1]
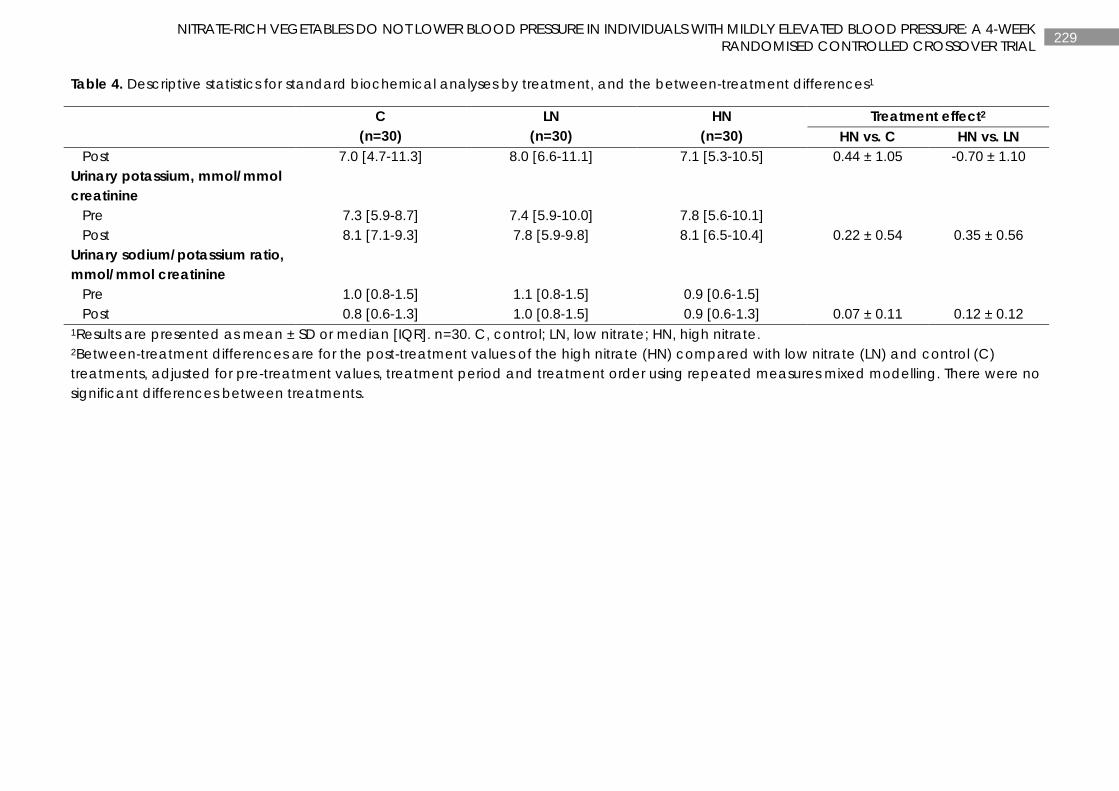
229 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Table 4. Descriptive statistics for standard biochemical analyses by treatment, and the between-treatment differences1
C
(n=30) LN
(n=30) HN
(n=30) Treatment effect2
HN vs. C HN vs. LN Post 7.0 [4.7-11.3] 8.0 [6.6-11.1] 7.1 [5.3-10.5] 0.44 ± 1.05 -0.70 ± 1.10 Urinary potassium, mmol/mmol creatinine
Pre 7.3 [5.9-8.7] 7.4 [5.9-10.0] 7.8 [5.6-10.1] Post 8.1 [7.1-9.3] 7.8 [5.9-9.8] 8.1 [6.5-10.4] 0.22 ± 0.54 0.35 ± 0.56 Urinary sodium/potassium ratio, mmol/mmol creatinine
Pre 1.0 [0.8-1.5] 1.1 [0.8-1.5] 0.9 [0.6-1.5] Post 0.8 [0.6-1.3] 1.0 [0.8-1.5] 0.9 [0.6-1.3] 0.07 ± 0.11 0.12 ± 0.12 1Results are presented as mean ± SD or median [IQR]. n=30. C, control; LN, low nitrate; HN, high nitrate. 2Between-treatment differences are for the post-treatment values of the high nitrate (HN) compared with low nitrate (LN) and control (C) treatments, adjusted for pre-treatment values, treatment period and treatment order using repeated measures mixed modelling. There were no significant differences between treatments.
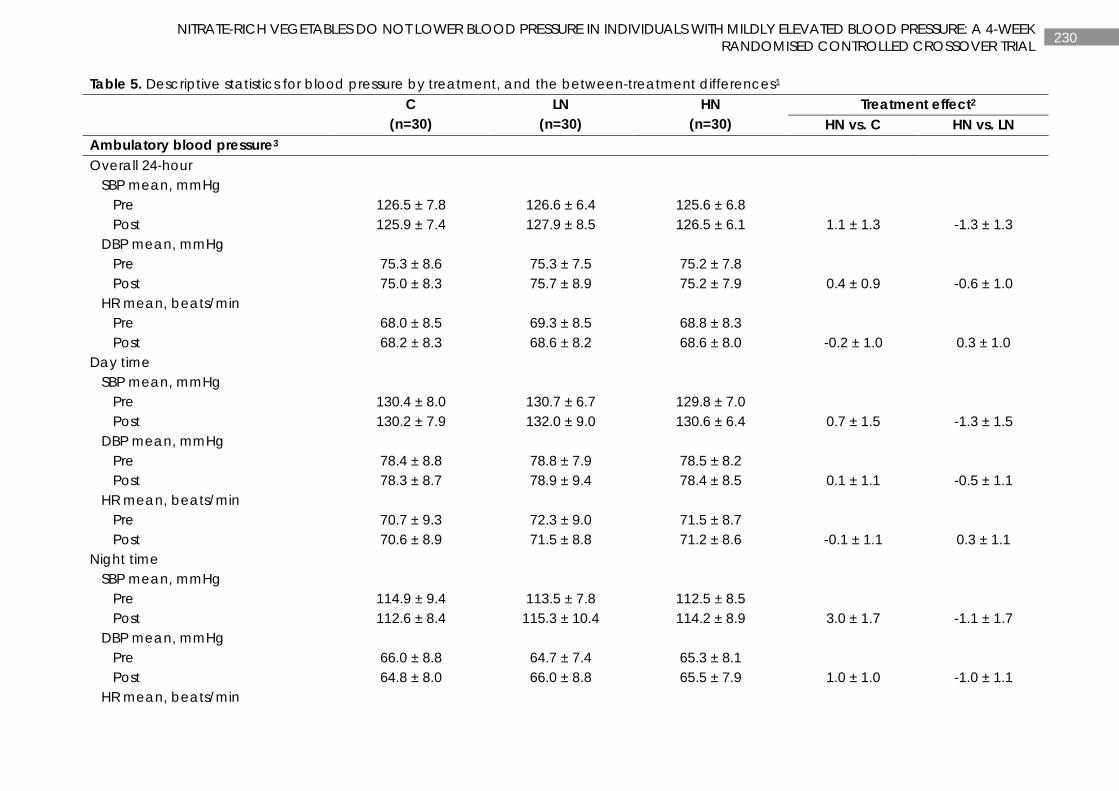
230 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Table 5. Descriptive statistics for blood pressure by treatment, and the between-treatment differences1 C
(n=30) LN
(n=30) HN
(n=30) Treatment effect2
HN vs. C HN vs. LN Ambulatory blood pressure3 Overall 24-hour SBP mean, mmHg Pre 126.5 ± 7.8 126.6 ± 6.4 125.6 ± 6.8 Post 125.9 ± 7.4 127.9 ± 8.5 126.5 ± 6.1 1.1 ± 1.3 -1.3 ± 1.3 DBP mean, mmHg Pre 75.3 ± 8.6 75.3 ± 7.5 75.2 ± 7.8 Post 75.0 ± 8.3 75.7 ± 8.9 75.2 ± 7.9 0.4 ± 0.9 -0.6 ± 1.0 HR mean, beats/min Pre 68.0 ± 8.5 69.3 ± 8.5 68.8 ± 8.3 Post 68.2 ± 8.3 68.6 ± 8.2 68.6 ± 8.0 -0.2 ± 1.0 0.3 ± 1.0 Day time SBP mean, mmHg Pre 130.4 ± 8.0 130.7 ± 6.7 129.8 ± 7.0 Post 130.2 ± 7.9 132.0 ± 9.0 130.6 ± 6.4 0.7 ± 1.5 -1.3 ± 1.5 DBP mean, mmHg Pre 78.4 ± 8.8 78.8 ± 7.9 78.5 ± 8.2 Post 78.3 ± 8.7 78.9 ± 9.4 78.4 ± 8.5 0.1 ± 1.1 -0.5 ± 1.1 HR mean, beats/min Pre 70.7 ± 9.3 72.3 ± 9.0 71.5 ± 8.7 Post 70.6 ± 8.9 71.5 ± 8.8 71.2 ± 8.6 -0.1 ± 1.1 0.3 ± 1.1 Night time SBP mean, mmHg Pre 114.9 ± 9.4 113.5 ± 7.8 112.5 ± 8.5 Post 112.6 ± 8.4 115.3 ± 10.4 114.2 ± 8.9 3.0 ± 1.7 -1.1 ± 1.7 DBP mean, mmHg Pre 66.0 ± 8.8 64.7 ± 7.4 65.3 ± 8.1 Post 64.8 ± 8.0 66.0 ± 8.8 65.5 ± 7.9 1.0 ± 1.0 -1.0 ± 1.1 HR mean, beats/min
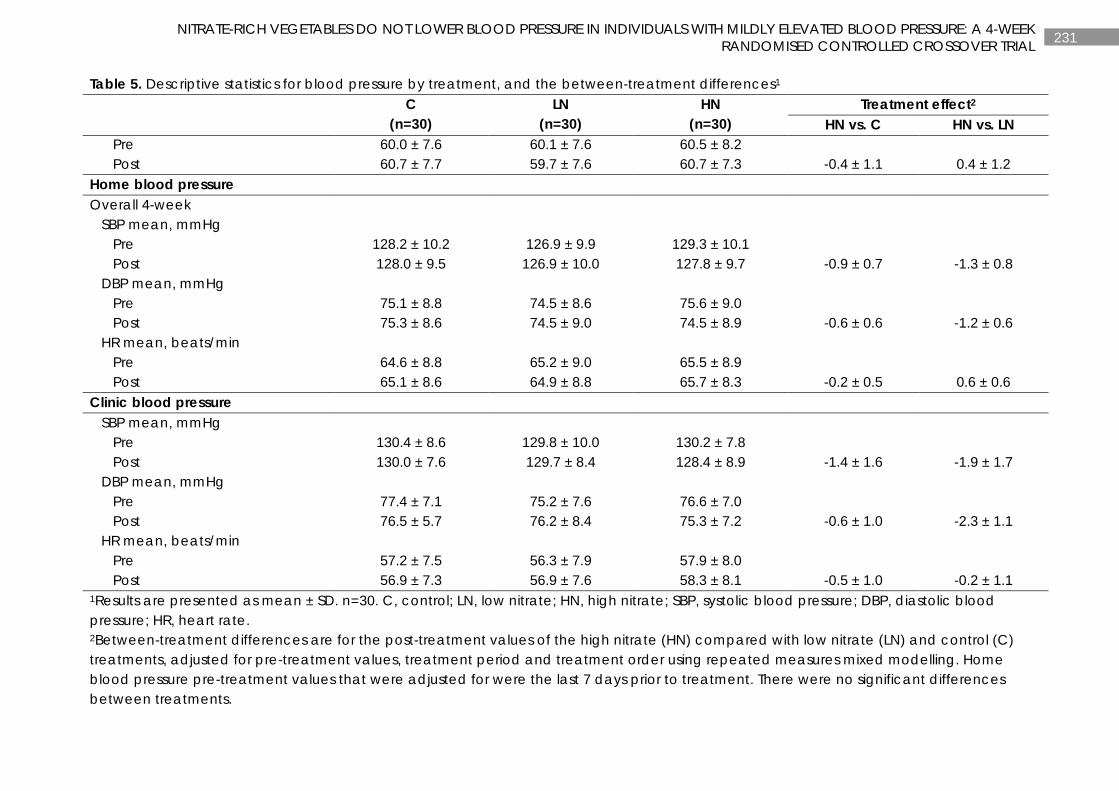
231 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Table 5. Descriptive statistics for blood pressure by treatment, and the between-treatment differences1 C
(n=30) LN
(n=30) HN
(n=30) Treatment effect2
HN vs. C HN vs. LN Pre 60.0 ± 7.6 60.1 ± 7.6 60.5 ± 8.2 Post 60.7 ± 7.7 59.7 ± 7.6 60.7 ± 7.3 -0.4 ± 1.1 0.4 ± 1.2 Home blood pressure Overall 4-week SBP mean, mmHg Pre 128.2 ± 10.2 126.9 ± 9.9 129.3 ± 10.1 Post 128.0 ± 9.5 126.9 ± 10.0 127.8 ± 9.7 -0.9 ± 0.7 -1.3 ± 0.8 DBP mean, mmHg Pre 75.1 ± 8.8 74.5 ± 8.6 75.6 ± 9.0 Post 75.3 ± 8.6 74.5 ± 9.0 74.5 ± 8.9 -0.6 ± 0.6 -1.2 ± 0.6 HR mean, beats/min Pre 64.6 ± 8.8 65.2 ± 9.0 65.5 ± 8.9 Post 65.1 ± 8.6 64.9 ± 8.8 65.7 ± 8.3 -0.2 ± 0.5 0.6 ± 0.6 Clinic blood pressure SBP mean, mmHg Pre 130.4 ± 8.6 129.8 ± 10.0 130.2 ± 7.8 Post 130.0 ± 7.6 129.7 ± 8.4 128.4 ± 8.9 -1.4 ± 1.6 -1.9 ± 1.7 DBP mean, mmHg Pre 77.4 ± 7.1 75.2 ± 7.6 76.6 ± 7.0 Post 76.5 ± 5.7 76.2 ± 8.4 75.3 ± 7.2 -0.6 ± 1.0 -2.3 ± 1.1 HR mean, beats/min Pre 57.2 ± 7.5 56.3 ± 7.9 57.9 ± 8.0 Post 56.9 ± 7.3 56.9 ± 7.6 58.3 ± 8.1 -0.5 ± 1.0 -0.2 ± 1.1 1Results are presented as mean ± SD. n=30. C, control; LN, low nitrate; HN, high nitrate; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate. 2Between-treatment differences are for the post-treatment values of the high nitrate (HN) compared with low nitrate (LN) and control (C) treatments, adjusted for pre-treatment values, treatment period and treatment order using repeated measures mixed modelling. Home blood pressure pre-treatment values that were adjusted for were the last 7 days prior to treatment. There were no significant differences between treatments.
232 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Table 5. Descriptive statistics for blood pressure by treatment, and the between-treatment differences1 C
(n=30) LN
(n=30) HN
(n=30) Treatment effect2
HN vs. C HN vs. LN 3n=28.
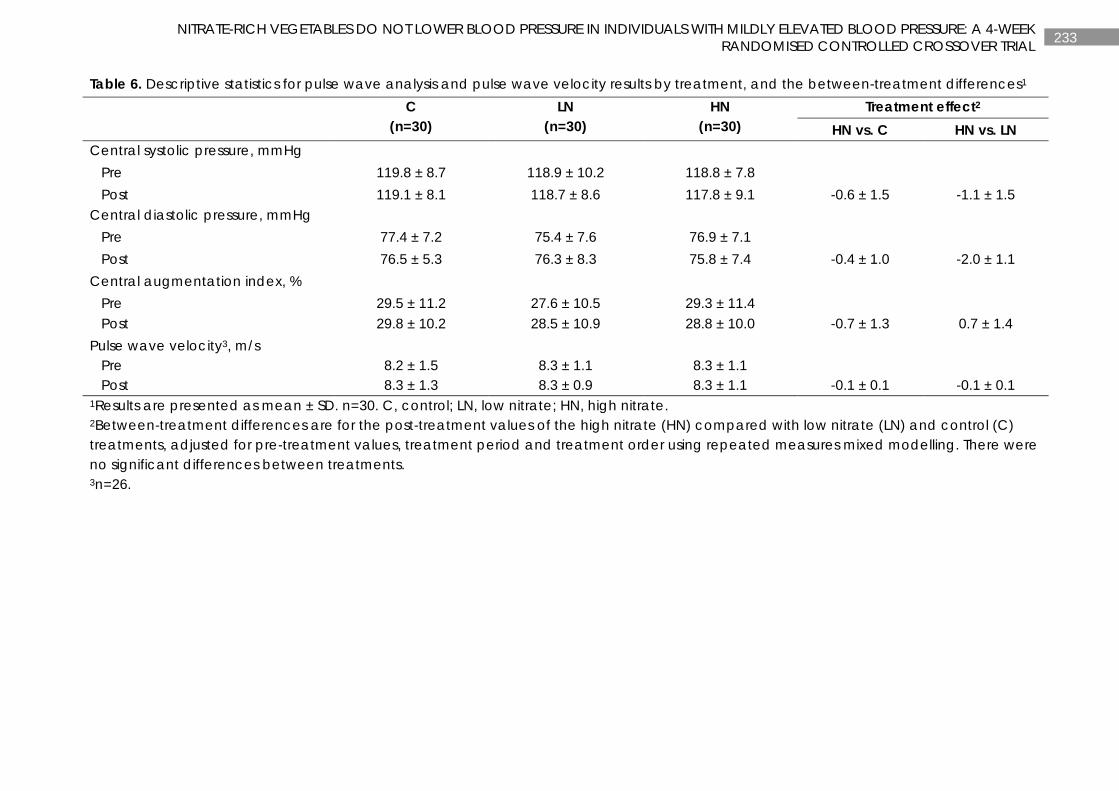
233 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Table 6. Descriptive statistics for pulse wave analysis and pulse wave velocity results by treatment, and the between-treatment differences1 C
(n=30) LN
(n=30) HN
(n=30) Treatment effect2
HN vs. C HN vs. LN Central systolic pressure, mmHg Pre 119.8 ± 8.7 118.9 ± 10.2 118.8 ± 7.8 Post 119.1 ± 8.1 118.7 ± 8.6 117.8 ± 9.1 -0.6 ± 1.5 -1.1 ± 1.5 Central diastolic pressure, mmHg Pre 77.4 ± 7.2 75.4 ± 7.6 76.9 ± 7.1 Post 76.5 ± 5.3 76.3 ± 8.3 75.8 ± 7.4 -0.4 ± 1.0 -2.0 ± 1.1 Central augmentation index, % Pre 29.5 ± 11.2 27.6 ± 10.5 29.3 ± 11.4 Post 29.8 ± 10.2 28.5 ± 10.9 28.8 ± 10.0 -0.7 ± 1.3 0.7 ± 1.4 Pulse wave velocity3, m/s Pre 8.2 ± 1.5 8.3 ± 1.1 8.3 ± 1.1 Post 8.3 ± 1.3 8.3 ± 0.9 8.3 ± 1.1 -0.1 ± 0.1 -0.1 ± 0.1 1Results are presented as mean ± SD. n=30. C, control; LN, low nitrate; HN, high nitrate. 2Between-treatment differences are for the post-treatment values of the high nitrate (HN) compared with low nitrate (LN) and control (C) treatments, adjusted for pre-treatment values, treatment period and treatment order using repeated measures mixed modelling. There were no significant differences between treatments. 3n=26.
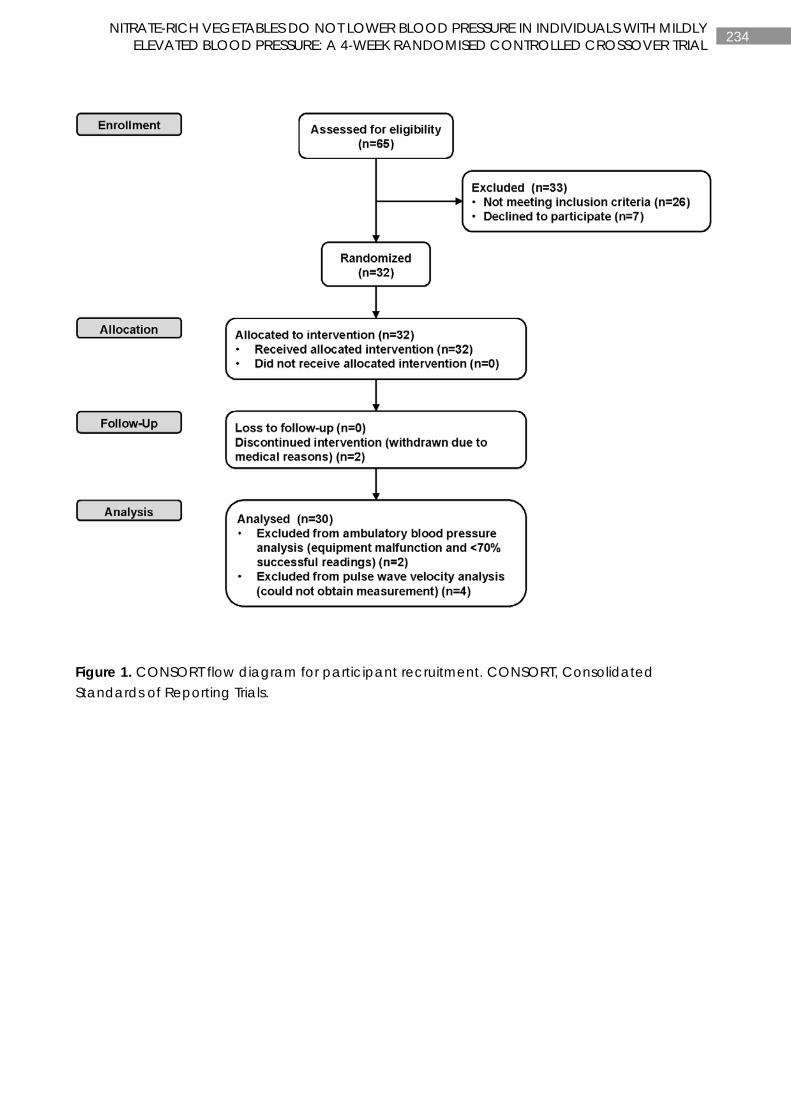
234 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Figure 1. CONSORT flow diagram for participant recruitment. CONSORT, Consolidated Standards of Reporting Trials.
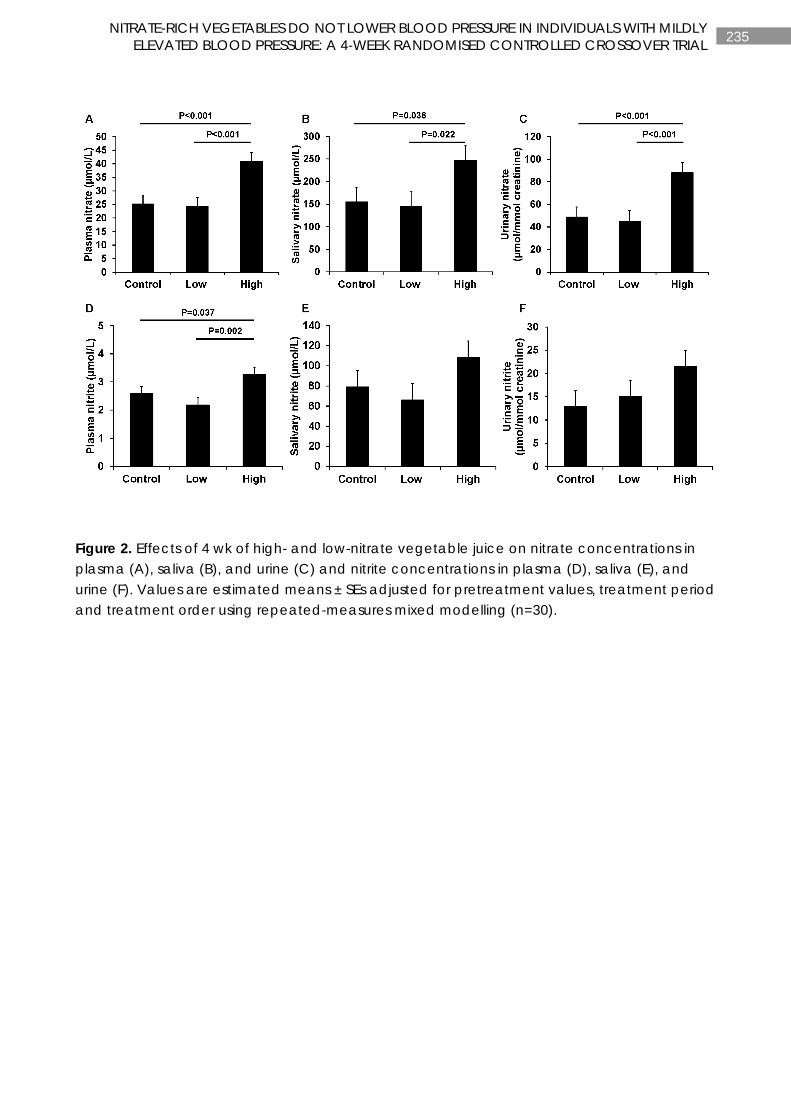
235 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Figure 2. Effects of 4 wk of high- and low-nitrate vegetable juice on nitrate concentrations in plasma (A), saliva (B), and urine (C) and nitrite concentrations in plasma (D), saliva (E), and urine (F). Values are estimated means ± SEs adjusted for pretreatment values, treatment period and treatment order using repeated-measures mixed modelling (n=30).
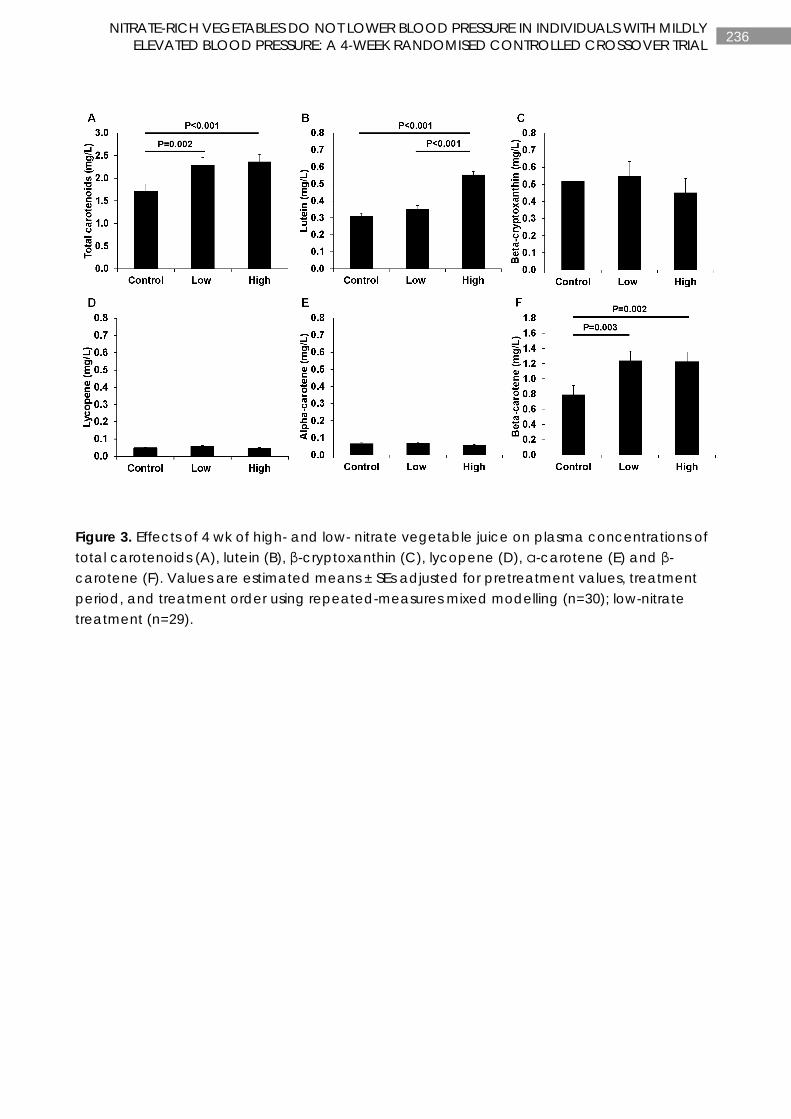
236 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Figure 3. Effects of 4 wk of high- and low- nitrate vegetable juice on plasma concentrations of total carotenoids (A), lutein (B), β-cryptoxanthin (C), lycopene (D), α-carotene (E) and β-carotene (F). Values are estimated means ± SEs adjusted for pretreatment values, treatment period, and treatment order using repeated-measures mixed modelling (n=30); low-nitrate treatment (n=29).
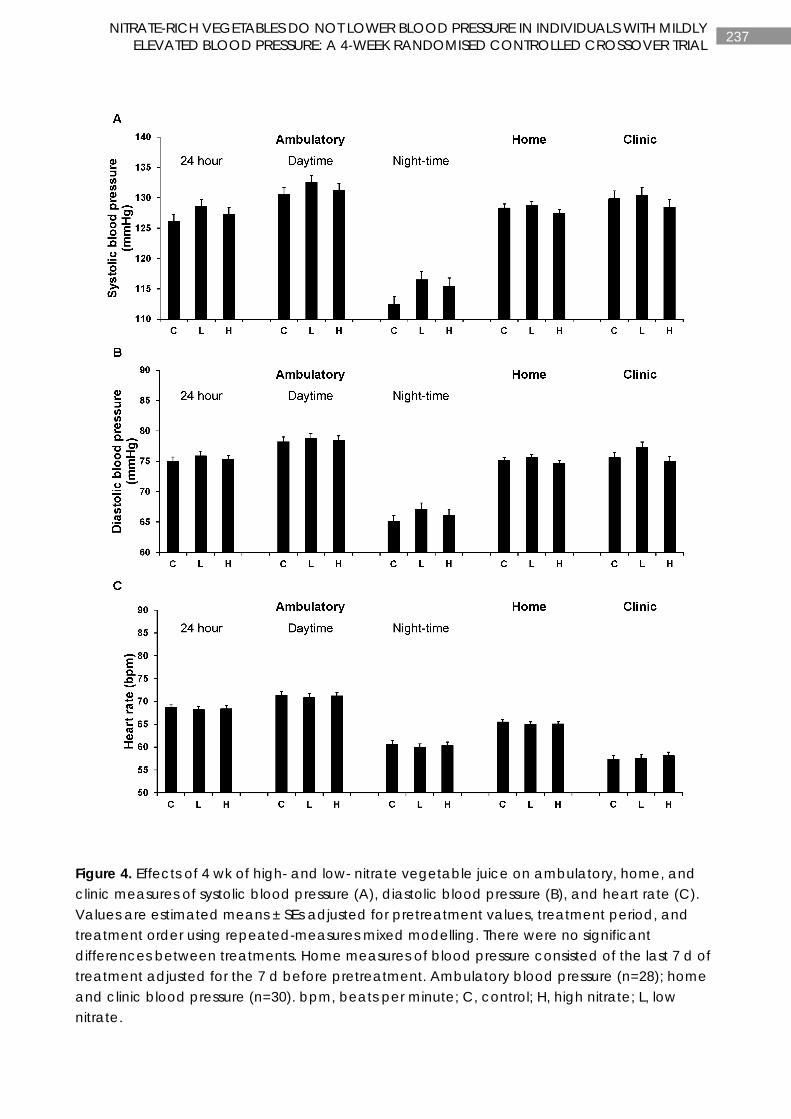
237 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Figure 4. Effects of 4 wk of high- and low- nitrate vegetable juice on ambulatory, home, and clinic measures of systolic blood pressure (A), diastolic blood pressure (B), and heart rate (C). Values are estimated means ± SEs adjusted for pretreatment values, treatment period, and treatment order using repeated-measures mixed modelling. There were no significant differences between treatments. Home measures of blood pressure consisted of the last 7 d of treatment adjusted for the 7 d before pretreatment. Ambulatory blood pressure (n=28); home and clinic blood pressure (n=30). bpm, beats per minute; C, control; H, high nitrate; L, low nitrate.
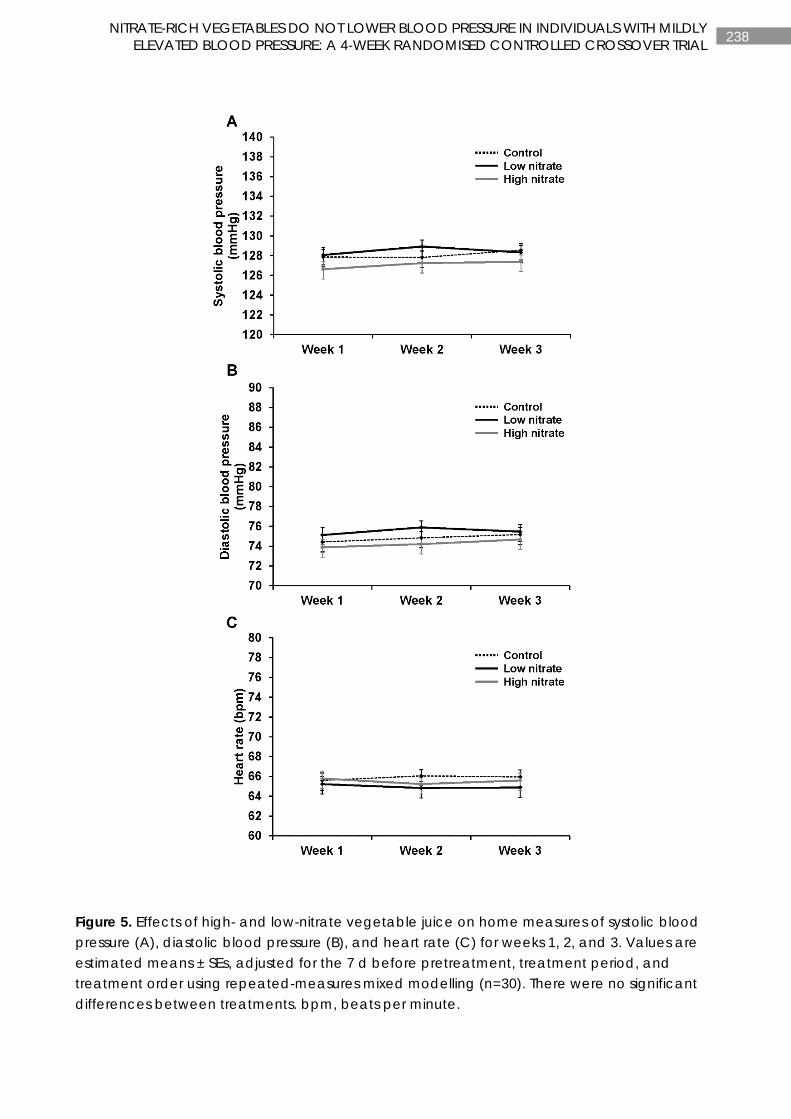
238 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Figure 5. Effects of high- and low-nitrate vegetable juice on home measures of systolic blood pressure (A), diastolic blood pressure (B), and heart rate (C) for weeks 1, 2, and 3. Values are estimated means ± SEs, adjusted for the 7 d before pretreatment, treatment period, and treatment order using repeated-measures mixed modelling (n=30). There were no significant differences between treatments. bpm, beats per minute.
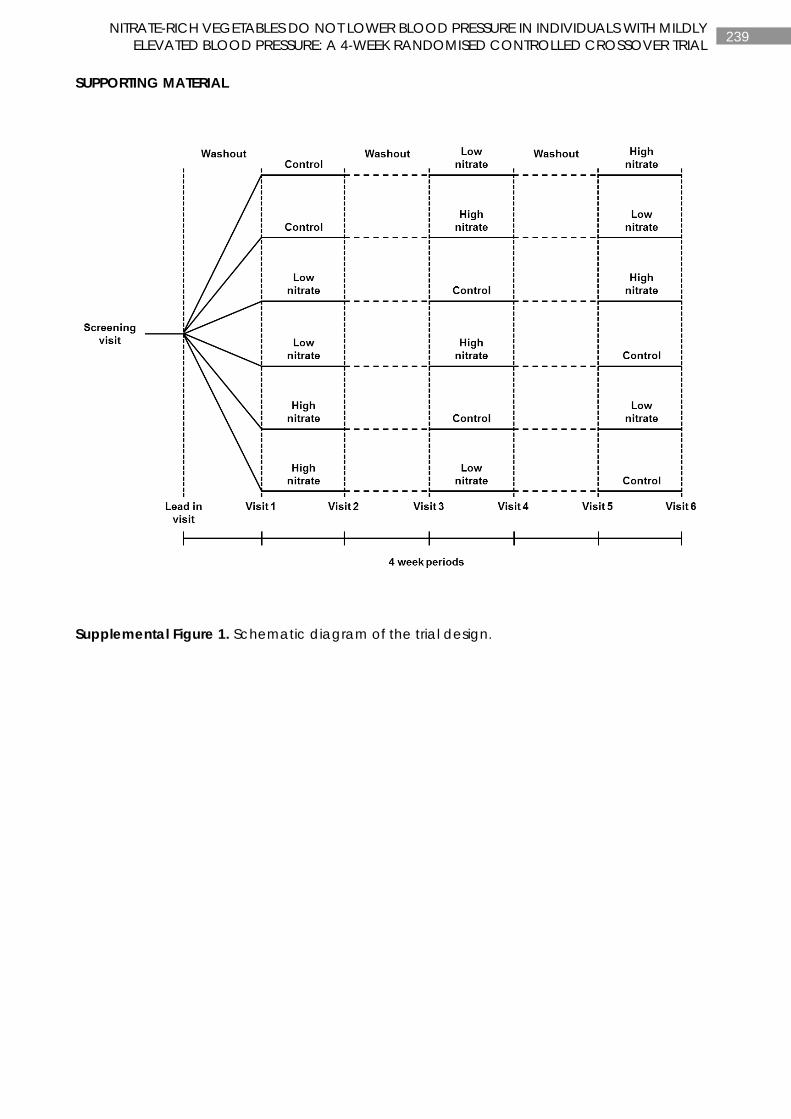
239 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
SUPPORTING MATERIAL
Supplemental Figure 1. Schematic diagram of the trial design.
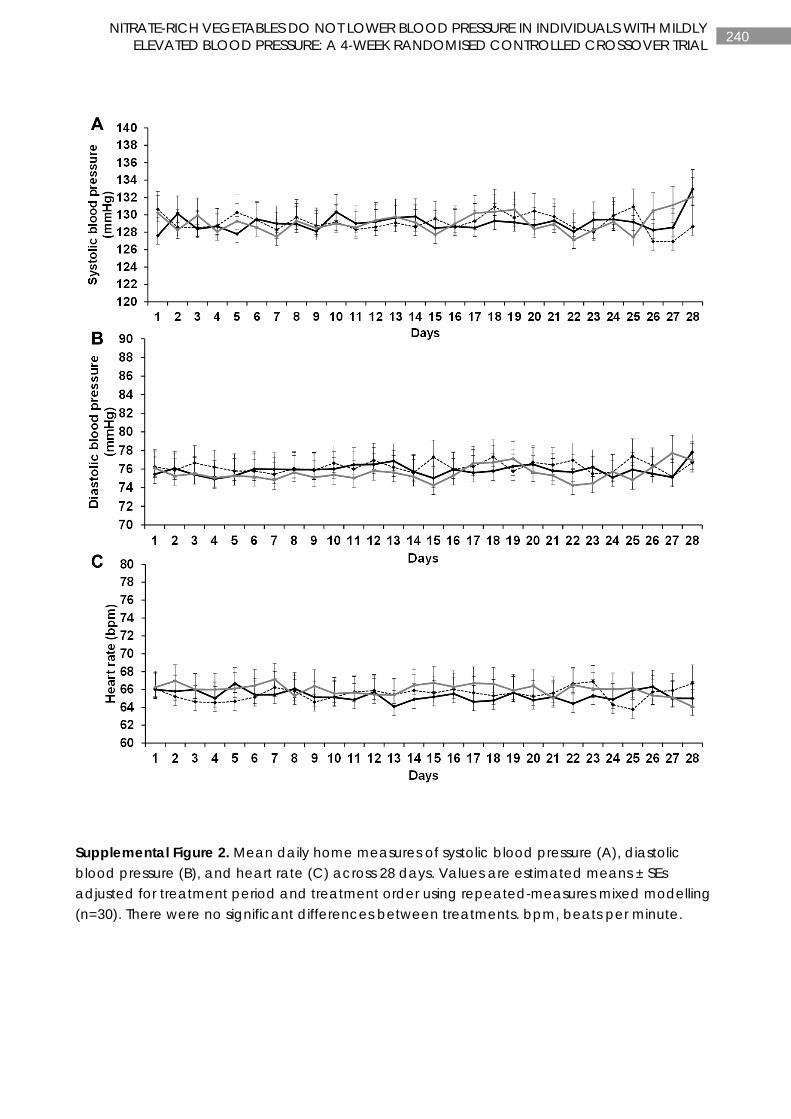
240 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Supplemental Figure 2. Mean daily home measures of systolic blood pressure (A), diastolic blood pressure (B), and heart rate (C) across 28 days. Values are estimated means ± SEs adjusted for treatment period and treatment order using repeated-measures mixed modelling (n=30). There were no significant differences between treatments. bpm, beats per minute.
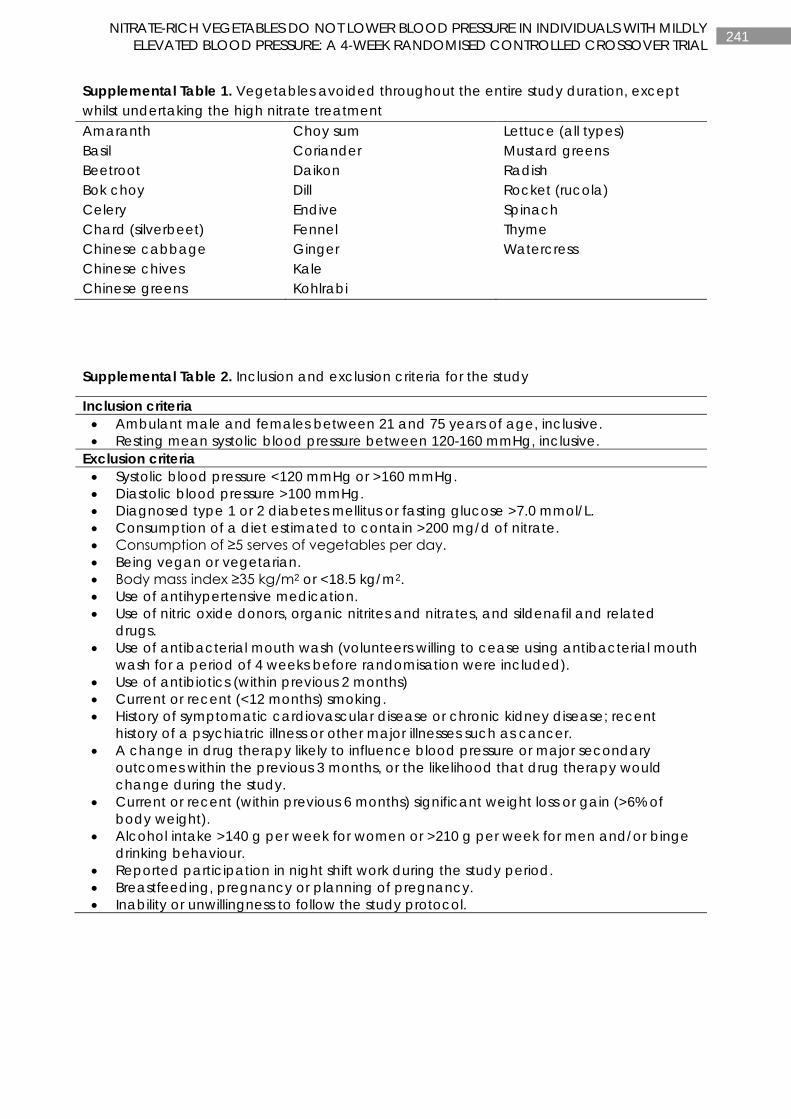
241 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Supplemental Table 1. Vegetables avoided throughout the entire study duration, except whilst undertaking the high nitrate treatment Amaranth Choy sum Lettuce (all types) Basil Coriander Mustard greens Beetroot Daikon Radish Bok choy Dill Rocket (rucola) Celery Endive Spinach Chard (silverbeet) Fennel Thyme Chinese cabbage Ginger Watercress Chinese chives Kale Chinese greens Kohlrabi
Supplemental Table 2. Inclusion and exclusion criteria for the study
Inclusion criteria • Ambulant male and females between 21 and 75 years of age, inclusive. • Resting mean systolic blood pressure between 120-160 mmHg, inclusive.
Exclusion criteria • Systolic blood pressure <120 mmHg or >160 mmHg. • Diastolic blood pressure >100 mmHg. • Diagnosed type 1 or 2 diabetes mellitus or fasting glucose >7.0 mmol/L. • Consumption of a diet estimated to contain >200 mg/d of nitrate. • Consumption of ≥5 serves of vegetables per day. • Being vegan or vegetarian. • Body mass index ≥35 kg/m2 or <18.5 kg/m2. • Use of antihypertensive medication. • Use of nitric oxide donors, organic nitrites and nitrates, and sildenafil and related
drugs. • Use of antibacterial mouth wash (volunteers willing to cease using antibacterial mouth
wash for a period of 4 weeks before randomisation were included). • Use of antibiotics (within previous 2 months) • Current or recent (<12 months) smoking. • History of symptomatic cardiovascular disease or chronic kidney disease; recent
history of a psychiatric illness or other major illnesses such as cancer. • A change in drug therapy likely to influence blood pressure or major secondary
outcomes within the previous 3 months, or the likelihood that drug therapy would change during the study.
• Current or recent (within previous 6 months) significant weight loss or gain (>6% of body weight).
• Alcohol intake >140 g per week for women or >210 g per week for men and/or binge drinking behaviour.
• Reported participation in night shift work during the study period. • Breastfeeding, pregnancy or planning of pregnancy. • Inability or unwillingness to follow the study protocol.
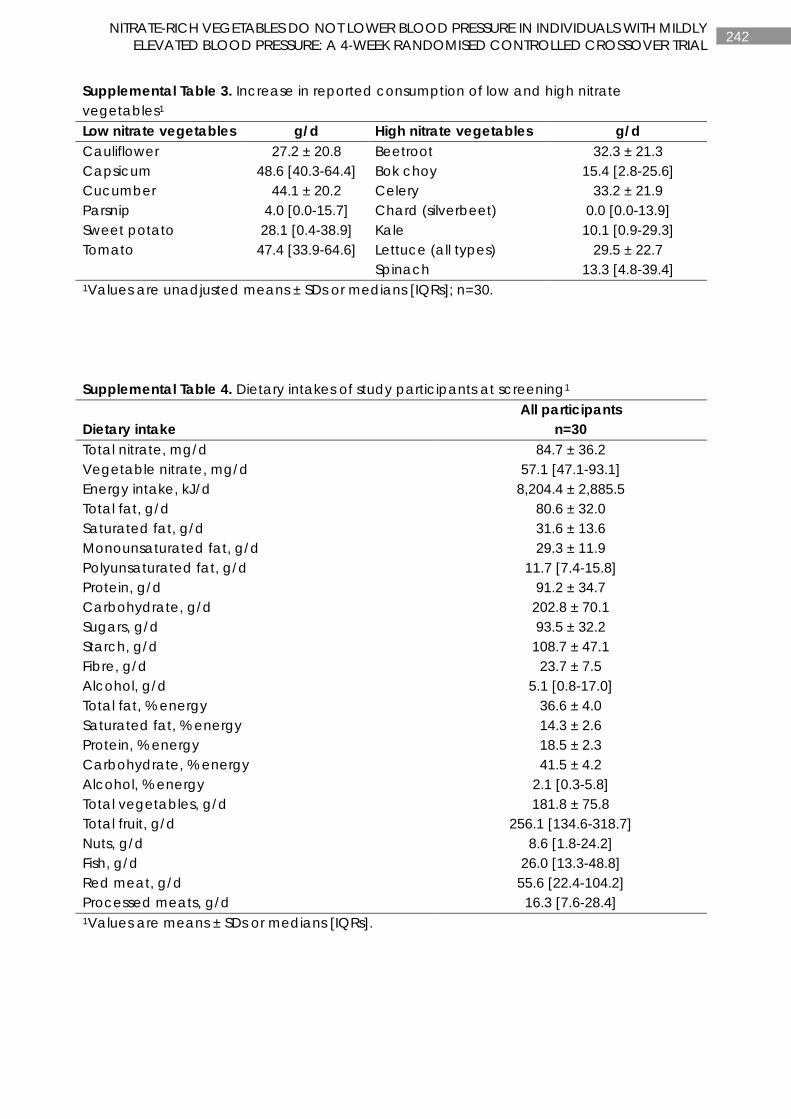
242 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Supplemental Table 3. Increase in reported consumption of low and high nitrate vegetables1 Low nitrate vegetables g/d High nitrate vegetables g/d Cauliflower 27.2 ± 20.8 Beetroot 32.3 ± 21.3 Capsicum 48.6 [40.3-64.4] Bok choy 15.4 [2.8-25.6] Cucumber 44.1 ± 20.2 Celery 33.2 ± 21.9 Parsnip 4.0 [0.0-15.7] Chard (silverbeet) 0.0 [0.0-13.9] Sweet potato 28.1 [0.4-38.9] Kale 10.1 [0.9-29.3] Tomato 47.4 [33.9-64.6] Lettuce (all types) 29.5 ± 22.7 Spinach 13.3 [4.8-39.4] 1Values are unadjusted means ± SDs or medians [IQRs]; n=30.
Supplemental Table 4. Dietary intakes of study participants at screening1
Dietary intake All participants
n=30 Total nitrate, mg/d 84.7 ± 36.2 Vegetable nitrate, mg/d 57.1 [47.1-93.1] Energy intake, kJ/d 8,204.4 ± 2,885.5 Total fat, g/d 80.6 ± 32.0 Saturated fat, g/d 31.6 ± 13.6 Monounsaturated fat, g/d 29.3 ± 11.9 Polyunsaturated fat, g/d 11.7 [7.4-15.8] Protein, g/d 91.2 ± 34.7 Carbohydrate, g/d 202.8 ± 70.1 Sugars, g/d 93.5 ± 32.2 Starch, g/d 108.7 ± 47.1 Fibre, g/d 23.7 ± 7.5 Alcohol, g/d 5.1 [0.8-17.0] Total fat, % energy 36.6 ± 4.0 Saturated fat, % energy 14.3 ± 2.6 Protein, % energy 18.5 ± 2.3 Carbohydrate, % energy 41.5 ± 4.2 Alcohol, % energy 2.1 [0.3-5.8] Total vegetables, g/d 181.8 ± 75.8 Total fruit, g/d 256.1 [134.6-318.7] Nuts, g/d 8.6 [1.8-24.2] Fish, g/d 26.0 [13.3-48.8] Red meat, g/d 55.6 [22.4-104.2] Processed meats, g/d 16.3 [7.6-28.4] 1Values are means ± SDs or medians [IQRs].
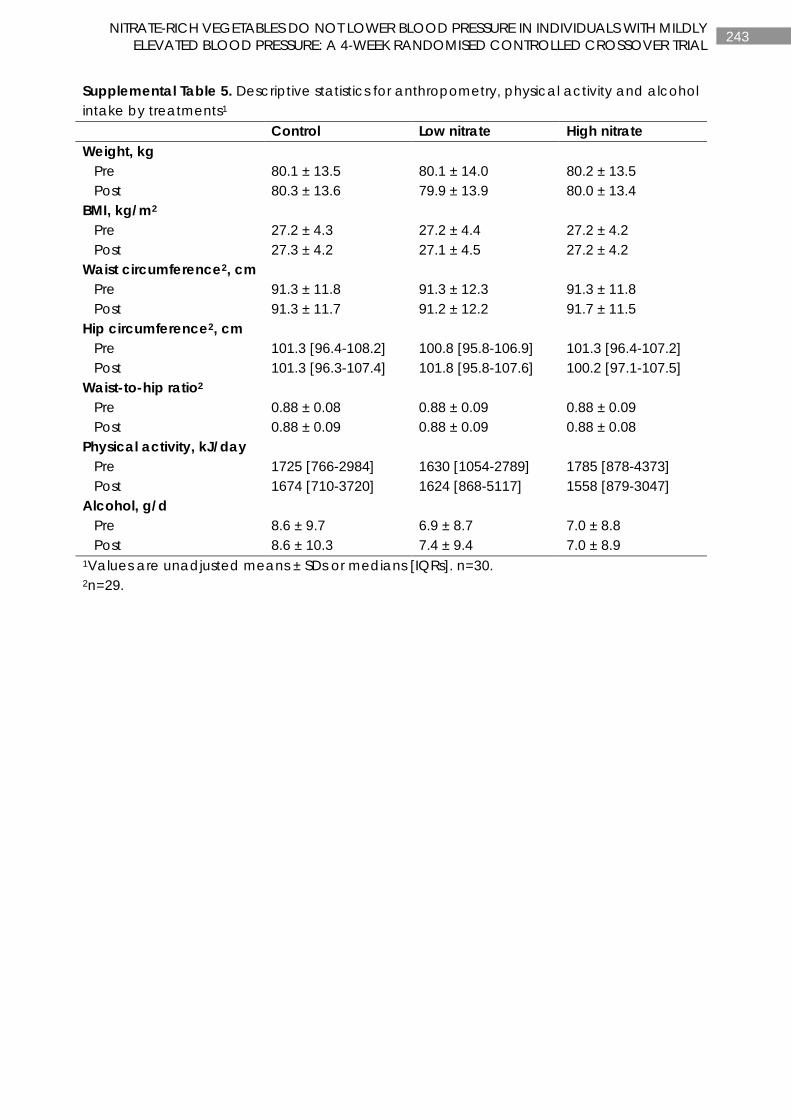
243 NITRATE-RICH VEGETABLES DO NOT LOWER BLOOD PRESSURE IN INDIVIDUALS WITH MILDLY ELEVATED BLOOD PRESSURE: A 4-WEEK RANDOMISED CONTROLLED CROSSOVER TRIAL
Supplemental Table 5. Descriptive statistics for anthropometry, physical activity and alcohol intake by treatments1 Control Low nitrate High nitrate Weight, kg Pre 80.1 ± 13.5 80.1 ± 14.0 80.2 ± 13.5 Post 80.3 ± 13.6 79.9 ± 13.9 80.0 ± 13.4 BMI, kg/m2 Pre 27.2 ± 4.3 27.2 ± 4.4 27.2 ± 4.2 Post 27.3 ± 4.2 27.1 ± 4.5 27.2 ± 4.2 Waist circumference2, cm Pre 91.3 ± 11.8 91.3 ± 12.3 91.3 ± 11.8 Post 91.3 ± 11.7 91.2 ± 12.2 91.7 ± 11.5 Hip circumference2, cm Pre 101.3 [96.4-108.2] 100.8 [95.8-106.9] 101.3 [96.4-107.2] Post 101.3 [96.3-107.4] 101.8 [95.8-107.6] 100.2 [97.1-107.5] Waist-to-hip ratio2 Pre 0.88 ± 0.08 0.88 ± 0.09 0.88 ± 0.09 Post 0.88 ± 0.09 0.88 ± 0.09 0.88 ± 0.08 Physical activity, kJ/day Pre 1725 [766-2984] 1630 [1054-2789] 1785 [878-4373] Post 1674 [710-3720] 1624 [868-5117] 1558 [879-3047] Alcohol, g/d Pre 8.6 ± 9.7 6.9 ± 8.7 7.0 ± 8.8 Post 8.6 ± 10.3 7.4 ± 9.4 7.0 ± 8.9 1Values are unadjusted means ± SDs or medians [IQRs]. n=30. 2n=29.
244 CHAPTER 9
CHAPTER 9
OVERVIEW AND FUTURE DIRECTIONS

245 OVERVIEW AND FUTURE DIRECTIONS
OVERVIEW AND FUTURE DIRECTIONS
The studies in this thesis explore the cardiovascular health benefits of different vegetable types and their bioactive compounds, in particular, nitrate. Large epidemiologic studies have shown plant-based diets, rich in vegetables, are consistently associated with lower risk of cardiovascular disease (CVD). Despite this evidence and the widespread and long-running health promotion campaigns to increase population consumption of vegetables, less than 1 in 10 adult Australians achieve the recommended intake (5-6 servings/d or 375-450 g/d). This situation is similar around the world.
Not all vegetables provide equivalent health benefits (12, 66, 299). Targeted advice focusing on specific vegetable types that provide the greatest health benefit may provide a more realistic and achievable strategy to enhance the health benefits of increasing vegetable intake. Findings from this thesis support the idea that intakes of leafy green, cruciferous and allium vegetables may provide greater health benefits for cardiovascular health. Furthermore, the findings suggest vegetable nitrate may be a contributing factor to these benefits.
Chapter 1 of this thesis was a narrative review discussing current literature on the cardiovascular health benefits of different vegetable types in observational epidemiologic studies. Vegetable types discussed were leafy green, cruciferous, allium, yellow-orange-red, and legumes. The evidence suggests intake of leafy green and cruciferous vegetables may confer the most cardiovascular health benefits, while the cardiovascular health benefits for legumes, yellow-orange-red and allium vegetables are less clear. This may be due to type II error and/or bias introduced by measurement error and regression dilution, attenuating observed risk estimates (12).
Although nutrition epidemiology has been successful in providing insight into the potential causes and prevention of many health conditions, several important limitations still exist (98). Due to the observational nature of nutrition epidemiological studies, residual confounding is inevitable. Challenges also arise in the accuracy of assessing dietary intake (98). These factors can lead to contradictory findings, especially when comparing results across different populations where dietary assessment methods are sometimes weak and there is large heterogeneity amongst the populations studied. Relationships between vegetable intake and CVD outcomes may be attenuated when large differences in vegetable intake classification and/or categorization exist. There is a need for the international standardization of such variables to limit error, thereby enabling more accurate comparisons between investigations. Such changes if implemented in large cohort studies have the capacity to improve the quality of nutrition research. Technology-based dietary assessment methods in conjunction with recovery biomarkers, such as those that appear in urine, could be used to improve accuracy and are worth considering in future work (99). Finally, adopting STROBE-nut guidelines and checklists will improve reporting of nutritional epidemiological studies and the quality of published literature (99, 100).
Increasing vegetable intake, with a focus on consuming leafy green and cruciferous vegetables may provide the greatest cardiovascular health benefits. Incorporating such dietary changes along with other recommended lifestyle changes will optimize health benefits. Lifestyle changes include consuming a diet full of vegetable, fruits, and whole grains; including low-fat dairy products, poultry, fish, legumes, nontropical vegetable oils, and nuts;

246 OVERVIEW AND FUTURE DIRECTIONS
and limiting intake of saturated and trans fats, sweets, sugar-sweetened beverages, and red meats (104). Other lifestyle changes include increasing physical activity (104), avoiding cigarette smoking (104) and intake of alcohol (105), and maintaining a healthy body weight by consuming appropriate energy requirements (104). There is a need for very large well-designed epidemiological studies investigating the cardiovascular health benefits of different vegetable types. Large long-term randomised controlled trials are needed to establish the causal effects of the specific vegetables found to be most beneficial for cardiovascular health.
In Chapter 2 of this thesis, the findings of a systematic literature review were reported. Scientific literature was systematically searched on the effects of dietary nitrate ingestion on blood pressure, arterial stiffness, endothelial function, platelet function, and cerebral blood flow in human and animal studies. Medline and EMBASE search databases were used and the reporting of data complied with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). From 12,541 screened references, 37 articles were included for human trials and 14 articles for animal trials.
Beneficial effects of dietary nitrate ingestion on vascular health in human intervention trials were predominantly observed in healthy individuals, whereas effects in individuals that were older and at risk of CVD were less clear. Many potential factors could influence whether ingestion of nitrate results in vascular health benefits. The study duration is likely a factor, with acute studies consistently showing a reduction in blood pressure (143, 153, 172, 173, 178-186). Other factors may include the dose of nitrate provided; the background nitrate intake and vegetable intake of individuals, which may alter the effective dose; whether there is an individual threshold level, beyond which there is little additional benefit; and the age and health status of individuals.
In animal studies, evidence suggests nitrate ingestion improves blood pressure and endothelial function particularly in animal models with reduced nitric oxide (NO) bioavailability. Nitrate dose is likely a factor as evidence of crosstalk between the classical L-arginine-NO synthase pathway and the nitrate-nitrite-NO pathway has been identified with administration of high-nitrate doses. Findings from this systematic literature review also show that in constrast to the observational epidemiologic studies in this thesis, there are no long-term follow-up studies that have investigated the habitual intake of dietary nitrate and cardiovascular disease clinical endpoints.
Chapter 3 of this thesis reports the results of an observational 15-year follow-up study. This study explored the associations of total vegetable intake as well as specific vegetable types, grouped according to phytochemical constituents, with atherosclerotic vascular disease (ASVD) mortality in older women. Higher cruciferous and allium vegetable intakes were independently associated with a lower risk of ASVD mortality. Cruciferous and allium vegetables contain a number of nutrients and phytochemicals that are postulated to have cardiovascular health benefits. Organosulfur compounds, bioactive phytochemicals found almost exclusively in cruciferous and allium vegetables, may contribute to the benefits of these vegetables. Future research is required to establish whether these compounds are directly involved. Furthermore, no studies have investigated these bioactive compounds with long-term CVD risk.

247 OVERVIEW AND FUTURE DIRECTIONS
In Chapter 4, we extended on these findings to report on the associations of total vegetable intake and intake of specific vegetable types, grouped according to phytochemical constituents, with subclinical atherosclerosis. This publication was the first to report an inverse association between total vegetables, in particular cruciferous vegetables, and common carotid artery intima-media thickness (a subclinical measure of atherosclerosis). However, this relationship was not observed for carotid plaque severity. Although carotid plaque and common carotid artery intima-media thickness are intercorrelated, they may reflect different biological aspects of atherogenesis. Carotid plaques are dependent on the influx of lipids into the plaque and are strongly related to high cholesterol and myocardial infarction. Carotid artery intima-media thickness captures the compensatory thickening of the carotid wall and is more related to high blood pressure and stroke. This would suggest cruciferous vegetable intake would be more related to stroke, rather than myocardial infarction. However, the results in Chapter 3 report cruciferous vegetables are related to ischaemic heart disease, rather than ischaemic cerebrovascular disease. Further research is required to elucidate these inconsistencies. Nevertheless, increasing vegetables in the diet with a focus on consuming cruciferous vegetables may have benefits for slowing the progression of atherosclerosis in older women. Future research is required to explore novel phytochemicals found in cruciferous vegetables that may be responsible for the observed health benefits. Human intervention studies are also required to establish causal effects of increasing intake of cruciferous vegetables in the diet.
Chapter 5 reports on the development of a reference database for assessing nitrate in vegetables. Prior to the development of this database there was no such tool available to researchers that had systematically collected information on the measured nitrate content of vegetables. A systematic literature search (1980-2016) was performed using Medline, Agricola and CAB abstracts databases. The development of this vegetable nitrate database has allowed for the improvement in nitrate intake estimation. The vegetable nitrate database contains 4237 records from 255 publications with data on 178 vegetables and 22 herbs and spices. This database has stimulated researchers around the world to investigate the relationships of nitrate intake with a range of health outcomes.
In Chapter 6, we used this database and reported on the relationship of vegetable nitrate intake and ASVD mortality over 15 years of follow-up in a cohort of older women. This study, along with the study reported in Chapter 7, provide the first evidence from observational studies that higher nitrate intake may reduce the risk of vascular disease. Vegetable nitrate intake was inversely associated with ASVD mortality. In comparison to lower intakes of nitrate from vegetables of <53 mg/d (median: 39 mg/d), the inverse relationship observed with ASVD mortality reached a plateau at intakes of 53-76 mg/d (median: 63 mg/d). These results support the concept that consumption of relatively low levels of vegetable nitrate may reduce the risk of age-related ASVD mortality. Replication of these results are required in cohorts of men and younger women. Furthermore, further research is required to explore the optimal dose of nitrate for cardiovascular health benefits.
In Chapter 7, we extended on these results and reported on the relationship of vegetable nitrate intake with subclinical atherosclerosis and ischaemic cerebrovascular disease events in a cohort of older women. Higher vegetable nitrate was associated with lower measures of subclinical atherosclerosis and lower risk of ischemic cerebrovascular disease events. The results suggested a nonlinear relationship between nitrate intake and ischaemic

248 OVERVIEW AND FUTURE DIRECTIONS
cerebrovascular disease events because no additional benefit was observed in those consuming >76 mg/d nitrate (median: 100 mg/d) compared with 53 to 76 mg/d nitrate (median: 64 mg/d). As little as one serving of nitrate-rich green leafy vegetables per day may provide adequate nitrate intake for lowering the risk of ischaemic cerebrovascular disease. As mentioned previously, replication of these results are required to explore the optimal dose of nitrate for lowering the risk of vascular disease. Similar studies are required in other populations.
Lastly, Chapter 8 reports the results of a 4-week randomised controlled crossover trial investigating the effects of nitrate-rich and nitrate-poor vegetables on blood pressure and arterial stiffness in men and women with pre-hypertension or untreated grade 1 hypertension. There is clear evidence that dietary nitrate reduces blood pressure within hours of ingestion. However, short-term and medium-term studies provide mixed results. Evidence suggests blood pressure-lowering effects of dietary nitrate are mainly observed in healthy populations. These benefits seem to be attenuated in at risk populations. Our intervention study demonstrated no benefit of a daily increase in nitrate-rich vegetables compared to a daily increase in nitrate-poor vegetables and no increase in vegetables on blood pressure and arterial stiffness in individuals with slightly elevated blood pressure. Many potential factors could influence whether an increase in nitrate intake results in lower blood pressure. Factors include the dose of nitrate provided; the background nitrate and vegetable intake of the study participants, which may alter the effective dose; whether there is an individual threshold level, beyond which there is little additional benefit; and the age and health status of the participants. Background diet may have influenced nitrate metabolism with individuals having sufficient nitrate intake unresponsive to further nitrate supplementation. Possible interactions between nitrate and sulphur-containing dietary constituents have been proposed (197). The authors of this study reported nitrate in drinking water was inversely associated with blood pressure at low sulphate concentrations (9-33 mg/L), but this relationship reversed at medium to high concentrations (34-102 mg/L). Such an interaction would unlikely to have confounded the results of our study, as the calculated mean sulphate concentration in water consumed by our cohort was 13.5 mg/L. This does not fully discount such an interaction, as sulphur-containing foods within the diet cannot be calculated due to the absence of adequate nutrient databases. A study recently published (365) explored the hypothesis that nitrate-rich vegetable consumption would lower systolic blood pressure but that this effect would be abolished when nitrate-rich and thiocyanate-rich (sulphur-containing) vegetables were co-ingested. The authors found that when vegetables high in nitrate and low in thiocyanate were consumed systolic blood pressure was lowered. However, when vegetables high in nitrate (same dose) and high in thiocyanate were consumed the increase in salivary nitrite was smaller and the blood pressure-lowering effects were abolished. This could be an explanation for the observed results in our intervention study. We observed no increase in salivary nitrite and no blood pressure-lowering effects. Participants were instructed to consume high-nitrate vegetables including Chinese cabbage and kale, which contain sulphur-containing compounds. Following enzymatic breakdown, these sulphur-containing compounds can degrade to form thiocyanate compounds and other breakdown products.
In conclusion, the work in this thesis provides new evidence to improve the identification of vegetable types that may have greater cardiovascular health benefits. The findings direct future research to investigate potential interactions between nitrate-rich and thiocyanate-rich vegetables and have implications for vascular health. Investigation into the possible health

249 OVERVIEW AND FUTURE DIRECTIONS
benefits of novel phytochemicals, such as organosulfur compounds, found almost exclusively in cruciferous and allium vegetables, also warrants future research. The findings from this thesis could have implications for enhancing dietary guidelines aimed at improving cardiovascular health.
250 REFERENCES
REFERENCES 1. Australian Institute of Health and Welfare. Australia's health 2014 [Internet]. Canberra: AIHW;
2014 [Cat. no. AUS 178:[Available from: http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=60129548150].
2. World Health Organization. Global status report on noncommunicable diseases 2014. Geneva, Switzerland; 2014.
3. Celermajer DS, Chow CK, Marijon E, Anstey NM, Woo KS. Cardiovascular disease in the developing world: prevalences, patterns, and the potential of early disease detection. J Am Coll Cardiol. 2012;60(14):1207-16.
4. Medis S, Puska P, Norrving B. Global atlas on cardiovascular disease prevention and control. Internet. Geneva; 2011.
5. World Health Organization. Fruit and vegetables for health: report of a joint FAO/WHO workshop. 2004.
6. National Health and Medical Research Council. Australian Dietary Guidelines. Canberra: National Health and Medical Research Council; 2013.
7. U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. 2015.
8. Carter OB, Pollard CM, Atkins JF, Marie Milliner J, Pratt IS. 'We're not told why-we're just told': qualitative reflections about the Western Australian Go for 2&5(R) fruit and vegetable campaign. Public Health Nutr. 2011;14(6):982-8.
9. National Cancer Institute. Usual dietary intakes: food intakes, US population, 2007-10. Available at http://appliedresearch.cancer.gov/diet/usualintakes/pop/2007-10.
10. Hall JN, Moore S, Harper SB, Lynch JW. Global variability in fruit and vegetable consumption. Am J Prev Med. 2009;36(5):402-9.e5.
11. Australian Bureau of Statistics. National Health Survey: First Results, 2014-15. Commenwealth of Australia; 2015.
12. Aune D, Giovannucci E, Boffetta P, Fadnes LT, Keum N, Norat T, et al. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality: a systematic review and dose-response meta-analysis of prospective studies. Int J Epidemiol. 2017;46(3):1029-56.
13. Threapleton DE, Greenwood DC, Evans CEL, Cleghorn CL, Nykjaer C, Woodhead C, et al. Dietary fibre intake and risk of cardiovascular disease: systematic review and meta-analysis. Br Med J. 2013;347.
14. Aburto NJ, Hanson S, Gutierrez H, Hooper L, Elliott P, Cappuccio FP. Effect of increased potassium intake on cardiovascular risk factors and disease: systematic review and meta-analyses. Br Med J. 2013;346.
15. Del Gobbo LC, Imamura F, Wu JHY, de Oliveira Otto MC, Chiuve SE, Mozaffarian D. Circulating and dietary magnesium and risk of cardiovascular disease: a systematic review and meta-analysis of prospective studies. Am J Clin Nutr. 2013;98(1):160-73.
16. Borgi L, Muraki I, Satija A, Willett WC, Rimm EB, Forman JP. Fruit and vegetable consumption and the incidence of hypertension in three prospective cohort studies. Hypertension. 2016;67(2):288-93.
17. Borgi L, Rimm EB, Willett WC, Forman JP. Potato intake and incidence of hypertension: results from three prospective US cohort studies. BMJ. 2016;353.
18. Liu RH. Health-promoting components of fruits and vegetables in the diet. Adv Nutr. 2013;4:384S-92S.
19. van Breda SGJ, de Kok TMCM. Smart combinations of bioactive compounds in fruits and vegetables may guide new strategies for personalized prevention of chronic diseases. Mol Nutr Food Res. 2018;62(1):1700597-n/a.
20. Scalbert A, Andres-Lacueva C, Arita M, Kroon P, Manach C, Urpi-Sarda M, et al. Databases on food phytochemicals and their health-promoting effects. J Agric Food Chem. 2011;59(9):4331-48.
21. Liu RH. Health benefits of fruit and vegetables are from additive and synergistic combinations of phytochemicals. Am J Clin Nutr. 2003;78(3):517S-20S.
22. Liu RH. Potential synergy of phytochemicals in cancer prevention: mechanism of action. J Nutr. 2004;134:3479s-85s.
251 REFERENCES
23. Kim Y, Je Y. Flavonoid intake and mortality from cardiovascular disease and all causes: A meta-analysis of prospective cohort studies. Clinical Nutrition ESPEN. 2017;20(Supplement C):68-77.
24. Cheng HM, Koutsidis G, Lodge JK, Ashor A, Siervo M, Lara J. Tomato and lycopene supplementation and cardiovascular risk factors: a systematic review and meta-analysis. Atherosclerosis. 2017;257:100-8.
25. Chen J, Song Y, Zhang L. Effect of lycopene supplementation on oxidative stress: an exploratory systematic review and meta-analysis of randomized controlled trials. J Med Food. 2013;16(5):361-74.
26. Li X, Xu J. Dietary and circulating lycopene and stroke risk: a meta-analysis of prospective studies. Sci Rep. 2014;4:5031.
27. Leermakers ETM, Darweesh SKL, Baena CP, Moreira EM, Melo van Lent D, Tielemans MJ, et al. The effects of lutein on cardiometabolic health across the life course: a systematic review and meta-analysis. Am J Clin Nutr. 2016;103(2):481-94.
28. Shea MK, Booth SL, Weiner DE, Brinkley TE, Kanaya AM, Murphy RA, et al. Circulating vitamin K is inversely associated with incident cardiovascular disease risk among those treated for hypertension in the Health, Aging, and Body Composition Study (Health ABC). J Nutr. 2017;147(5):888-95.
29. Moser M, Chun O. Vitamin C and heart health: a review based on findings from epidemiologic studies. Int J Mol Sci. 2016;17(8):1328.
30. Blekkenhorst LC, Bondonno CP, Lewis JR, Devine A, Woodman RJ, Croft KD, et al. Association of dietary nitrate with atherosclerotic vascular disease mortality: a prospective cohort study of older adult women. Am J Clin Nutr. 2017;106(1):207-16.
31. Bondonno CP, Blekkenhorst LC, Prince RL, Ivey KL, Lewis JR, Devine A, et al. Association of vegetable nitrate intake with carotid atherosclerosis and ischemic cerebrovascular disease in older women. Stroke. 2017;48(8):1-6.
32. Vazquez-Prieto MA, Miatello RM. Organosulfur compounds and cardiovascular disease. Mol Aspects Med. 2010;31(6):540-5.
33. Tang G, Meng X, Li Y, Zhao C, Liu Q, Li H. Effects of vegetables on cardiovascular diseases and related mechanisms. Nutrients. 2017;9(857):1-25.
34. Maiani G, Periago Castón MJ, Catasta G, Toti E, Cambrodón IG, Bysted A, et al. Carotenoids: Actual knowledge on food sources, intakes, stability and bioavailability and their protective role in humans. Mol Nutr Food Res. 2009;53(S2):S194-S218.
35. Kaulmann A, Bohn T. Carotenoids, inflammation, and oxidative stress—implications of cellular signaling pathways and relation to chronic disease prevention. Nutr Res. 2014;34(11):907-29.
36. Blekkenhorst LC, Prince RL, Ward NC, Croft KD, Lewis JR, Devine A, et al. Development of a reference database for assessing dietary nitrate in vegetables. Mol Nutr Food Res. 2017;61(8):1-13.
37. Napoli C, Ignarro LJ. Nitric oxide and pathogenic mechanisms involved in the development of vascular diseases. Arch Pharm Res. 2009;32(8):1103-8.
38. Förstermann U, Münzel T. Endothelial nitric oxide synthase in vascular disease. Circulation. 2006;113(13):1708-14.
39. Sturm C, Wagner AE. Brassica-derived plant bioactives as modulators of chemopreventive and inflammatory signaling pathways. Int J Mol Sci. 2017;18(9):1890.
40. Beretta HV, Bannoud F, Insani M, Berli F, Hirschegger P, Galmarini CR, et al. Relationships between bioactive compound content andthe antiplatelet and antioxidant activities of six allium vegetable species. Food Technol Biotechnol. 2017;55(2):266-75.
41. Pennington JAT, Fisher RA. Classification of fruits and vegetables. J Food Compost Anal. 2009;22S:S23-S31.
42. Birt DF, Boylston T, Hendrich S, Jane J-L, Hollis J, Li L, et al. Resistant starch: promise for improving human health. Adv Nutr. 2013;4(6):587-601.
43. Battson ML, Lee DM, Weir TL, Gentile CL. The gut microbiota as a novel regulator of cardiovascular function and disease. J Nutr Biochem. 2017;56:1-15.
44. Weitzberg E, Lundberg JO. Novel aspects of dietary nitrate and human health. Annu Rev Nutr. 2013;33(1):129-59.
45. Bondonno CP, Croft KD, Hodgson JM. Dietary nitrate, nitric oxide, and cardiovascular health. Crit Rev Food Sci Nutr. 2016;56(12):2036-52.
46. Dinkova-Kostova AT, Kostov RV. Glucosinolates and isothiocyanates in health and disease. Trends Mol Med. 2012;18(6):337-47.
252 REFERENCES
47. Raiola A, Errico A, Petruk G, Monti DM, Barone A, Rigano MM. Bioactive compounds in brassicaceae vegetables with a role in the prevention of chronic diseases. Molecules. 2017;23(1):1-10.
48. Voutilainen S, Nurmi T, Mursu J, Rissanen TH. Carotenoids and cardiovascular health. Am J Clin Nutr. 2006;83(6):1265-71.
49. Messina MJ. Legumes and soybeans: overview of their nutritional profiles and health effects. Am J Clin Nutr. 1999;70(3):439s-50s.
50. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352(16):1685-95.
51. Manduteanu I, Simionescu M. Inflammation in atherosclerosis: a cause or a result of vascular disorders? J Cell Mol Med. 2012;16(9):1978-90.
52. Ebrahim S, Papacosta O, Whincup P, Wannamethee G, Walker M, Nicolaides AN, et al. Carotid plaque, intima media thickness, cardiovascular risk factors, and prevalent cardiovascular disease in men and women. Stroke. 1999;30(4):841-50.
53. Lorenz MW, Markus HS, Bots ML, Rosvall M, Sitzer M. Prediction of clinical cardiovascular events with carotid intima-media thickness: a systematic review and meta-analysis. Circulation. 2007;115(4):459-67.
54. Touboul PJ, Hennerici MG, Meairs S, Adams H, Amarenco P, Bornstein N, et al. Mannheim carotid intima-media thickness and plaque consensus (2004–2006–2011). Cerebrovasc Dis. 2012;34(4):290-6.
55. Johnsen SH, Mathiesen EB. Carotid plaque compared with intima-media thickness as a predictor of coronary and cerebrovascular disease. Curr Cardiol Rep. 2009;11(1):21-7.
56. Plichart M, Celermajer DS, Zureik M, Helmer C, Jouven X, Ritchie K, et al. Carotid intima-media thickness in plaque-free site, carotid plaques and coronary heart disease risk prediction in older adults. Atherosclerosis. 2011;219(2):917-24.
57. Murie-Fernandez M, Irimia P, Toledo E, Martínez-Vila E, Buil-Cosiales P, Serrano-Martínez M, et al. Carotid intima-media thickness changes with Mediterranean diet: a randomized trial (PREDIMED-Navarra). Atherosclerosis. 2011;219(1):158-62.
58. Yang S-Y, Li X-J, Zhang W, Liu C-Q, Zhang H-J, Lin J-R, et al. Chinese lacto-vegetarian diet exerts favorable effects on metabolic parameters, intima-media thickness, and cardiovascular risks in healthy men. Nutr Clin Pract. 2012;27(3):392-8.
59. Sala-Vila A, Romero-Mamani E-S, Gilabert R, Núñez I, de la Torre R, Corella D, et al. Changes in ultrasound-assessed carotid intima-media thickness and plaque with a Mediterranean diet: a substudy of the PREDIMED trial. Arterioscler Thromb Vasc Biol. 2014;34(2):439-45.
60. Petersen KS, Clifton PM, Keogh JB. The association between carotid intima media thickness and individual dietary components and patterns. Nutr Metab Cardiovasc Dis. 2014;24(5):495-502.
61. Blekkenhorst LC, Bondonno CP, Lewis JR, Woodman RJ, Devine A, Bondonno NP, et al. Cruciferous and total vegetable intakes are inversely associated with subclinical atherosclerosis in older adult women. J Am Heart Assoc. 2018;7(e008391):1-13.
62. Hung H-C, Joshipura KJ, Jiang R, Hu FB, Hunter D, Smith-Warner SA, et al. Fruit and vegetable intake and risk of major chronic disease. J Natl Cancer Inst. 2004;96(21):1577-84.
63. Takachi R, Inoue M, Ishihara J, Kurahashi N, Iwasaki M, Sasazuki S, et al. Fruit and vegetable intake and risk of total cancer and cardiovascular disease: Japan Public Health Center-based Prospective Study. Am J Epidemiol. 2007;167(1):59-70.
64. Buil-Cosiales P, Toledo E, Salas-Salvadó J, Zazpe I, Farràs M, Basterra-Gortari FJ, et al. Association between dietary fibre intake and fruit, vegetable or whole-grain consumption and the risk of CVD: results from the PREvención con DIeta MEDiterránea (PREDIMED) trial. Br J Nutr. 2016;116(3):534-46.
65. Gaziano JM, Manson JE, Branch LG, Colditz GA, Willett WC, Buring JE. A prospective study of consumption of carotenoids in fruits and vegetables and decreased cardiovascular mortality in the elderly. Ann Epidemiol. 1995;5(4):255-60.
66. Blekkenhorst LC, Bondonno CP, Lewis JR, Devine A, Zhu K, Lim WH, et al. Cruciferous and allium vegetable intakes are inversely associated with 15‐year atherosclerotic vascular disease deaths in older adult women. J Am Heart Assoc. 2017;6(10):1-15.
67. Bhupathiraju SN, Wedick NM, Pan A, Manson JE, Rexrode KM, Willett WC, et al. Quantity and variety in fruit and vegetable intake and risk of coronary heart disease. Am J Clin Nutr. 2013;98(6):1514-23.
253 REFERENCES
68. Bendinelli B, Masala G, Saieva C, Salvini S, Calonico C, Sacerdote C, et al. Fruit, vegetables, and olive oil and risk of coronary heart disease in Italian women: the EPICOR Study. Am J Clin Nutr. 2011;93(2):275-83.
69. Oude Griep LM, Verschuren WM, Kromhout D, Ocke MC, Geleijnse JM. Colours of fruit and vegetables and 10-year incidence of CHD. Br J Nutr. 2011;106(10):1562-9.
70. Wang J-B, Fan J-H, Dawsey SM, Sinha R, Freedman ND, Taylor PR, et al. Dietary components and risk of total, cancer and cardiovascular disease mortality in the Linxian Nutrition Intervention Trials cohort in China. Sci Rep. 2016;6:22619.
71. Larsson SC, Virtamo J, Wolk A. Total and specific fruit and vegetable consumption and risk of stroke: a prospective study. Atherosclerosis. 2013;227(1):147-52.
72. Joshipura KJ, Ascherio A, Manson JE, Stampfer MJ, Rimm EB, Speizer FE, et al. Fruit and vegetable intake in relation to risk of ischemic stroke. J Am Med Assoc. 1999;282(13):1233-9.
73. Johnsen SP, Overvad K, Stripp C, Tjonneland A, Husted SE, Sorensen HT. Intake of fruit and vegetables and the risk of ischemic stroke in a cohort of Danish men and women. Am J Clin Nutr. 2003;78(1):57-64.
74. Zhang X, Shu X-O, Xiang Y-B, Yang G, Li H, Gao J, et al. Cruciferous vegetable consumption is associated with a reduced risk of total and cardiovascular disease mortality. Am J Clin Nutr. 2011.
75. Mink PJ, Scrafford CG, Barraj LM, Harnack L, Hong CP, Nettleton JA, et al. Flavonoid intake and cardiovascular disease mortality: a prospective study in postmenopausal women. Am J Clin Nutr. 2007;85(3):895-909.
76. Genkinger JM, Platz EA, Hoffman SC, Comstock GW, Helzlsouer KJ. Fruit, vegetable, and antioxidant intake and all-cause, cancer, and cardiovascular disease mortality in a community-dwelling population in Washington County, Maryland. Am J Epidemiol. 2004;160(12):1223-33.
77. Yu D, Zhang X, Gao Y-T, Li H, Yang G, Huang J, et al. Fruit and vegetable intake and risk of CHD: results from prospective cohort studies of Chinese adults in Shanghai. Br J Nutr. 2013;111(2):353-62.
78. Mizrahi A, Knekt P, Montonen J, Laaksonen MA, Heliovaara M, Jarvinen R. Plant foods and the risk of cerebrovascular diseases: a potential protection of fruit consumption. Br J Nutr. 2009;102(7):1075-83.
79. Lin J, Rexrode KM, Hu F, Albert CM, Chae CU, Rimm EB, et al. Dietary intakes of flavonols and flavones and coronary heart disease in US women. Am J Epidemiol. 2007;165(11):1305-13.
80. Knekt P, Jarvinen R, Reunanen A, Maatela J. Flavonoid intake and coronary mortality in Finland: a cohort study. Br Med J. 1996;312(7029):478-81.
81. Hertog MG, Sweetnam PM, Fehily AM, Elwood PC, Kromhout D. Antioxidant flavonols and ischemic heart disease in a Welsh population of men: the Caerphilly Study. Am J Clin Nutr. 1997;65(5):1489-94.
82. Knekt P, Isotupa S, Rissanen H, Heliovaara M, Jarvinen R, Hakkinen S, et al. Quercetin intake and the incidence of cerebrovascular disease. Eur J Clin Nutr. 2000;54(5):415-7.
83. Jacques PF, Lyass A, Massaro JM, Vasan RS, D'Agostino RB, Sr. Relationship of lycopene intake and consumption of tomato products to incident CVD. Br J Nutr. 2013;110(3):545-51.
84. Buijsse B, Feskens EJM, Kwape L, Kok FJ, Kromhout D. Both α- and β-carotene, but not tocopherols and vitamin c, are inversely related to 15-year cardiovascular mortality in Dutch elderly men. J Nutr. 2008;138(2):344-50.
85. Nagura J, Iso H, Watanabe Y, Maruyama K, Date C, Toyoshima H, et al. Fruit, vegetable and bean intake and mortality from cardiovascular disease among Japanese men and women: the JACC Study. Br J Nutr. 2009;102(2):285-92.
86. Martínez-González MA, García-López M, Bes-Rastrollo M, Toledo E, Martínez-Lapiscina EH, Delgado-Rodriguez M, et al. Mediterranean diet and the incidence of cardiovascular disease: a Spanish cohort. Nutrition, Metabolism and Cardiovascular Diseases.21(4):237-44.
87. Bazzano LA, He J, Ogden LG, Loria C, Vupputuri S, Myers L, et al. Legume consumption and risk of coronary heart disease in us men and women: NHANES I Epidemiologic Follow-up Study. Arch Intern Med. 2001;161(21):2573-8.
88. Nouri F, Sarrafzadegan N, Mohammadifard N, Sadeghi M, Mansourian M. Intake of legumes and the risk of cardiovascular disease: frailty modeling of a prospective cohort study in the Iranian middle-aged and older population. Eur J Clin Nutr. 2016;70(2):217.
89. Kokubo Y, Iso H, Ishihara J, Okada K, Inoue M, Tsugane S. Association of dietary intake of soy, beans, and isoflavones with risk of cerebral and myocardial infarctions in japanese
254 REFERENCES
populations: the Japan Public Health Center–Based (JPHC) Study Cohort I. Circulation. 2007;116(22):2553-62.
90. Kelemen LE, Kushi LH, Jacobs JDR, Cerhan JR. Associations of dietary protein with disease and mortality in a prospective study of postmenopausal women. Am J Epidemiol. 2005;161(3):239-49.
91. Bernstein AM, Sun Q, Hu FB, Stampfer MJ, Manson JE, Willett WC. Major dietary protein sources and risk of coronary heart disease in women. Circulation. 2010;122(9):876-83.
92. Buckland G, González CA, Agudo A, Vilardell M, Berenguer A, Amiano P, et al. Adherence to the mediterranean diet and risk of coronary heart disease in the Spanish EPIC cohort study. Am J Epidemiol. 2009;170(12):1518-29.
93. Dilis V, Katsoulis M, Lagiou P, Trichopoulos D, Naska A, Trichopoulou A. Mediterranean diet and CHD: the Greek European Prospective Investigation into Cancer and Nutrition cohort. Br J Nutr. 2012;108(4):699-709.
94. Haring B, Gronroos N, Nettleton JA, Von Ballmoos MCW, Selvin E, Alonso A. Dietary protein intake and coronary heart disease in a large community based cohort: results from the Atherosclerosis Risk in Communities (ARIC) Study. PLoS One. 2014;9(10):e109552.
95. Misirli G, Benetou V, Lagiou P, Bamia C, Trichopoulos D, Trichopoulou A. Relation of the traditional Mediterranean diet to cerebrovascular disease in a Mediterranean population. Am J Epidemiol. 2012;176(12):1185-92.
96. Bernstein AM, Pan A, Rexrode KM, Stampfer M, Hu FB, Mozaffarian D, et al. Dietary protein sources and the risk of stroke in men and women. Stroke. 2012;43:1-8.
97. Haring B, Misialek JR, Rebholz CM, Petruski-Ivleva N, Gottesman RF, Mosley TH, et al. Association of dietary protein consumption with incident silent cerebral infarcts and stroke: the Atherosclerosis Risk in Communities (ARIC) Study. Stroke. 2015;46(12):3443-50.
98. Langseth L. Nutritional epidemiology: possibilities and limitations. Brussels, Belgium: International Life Sciences Institute Europe; 1996.
99. Rollo ME, Williams RL, Burrows T, Kirkpatrick SI, Bucher T, Collins CE. What are they really eating? A review on new approaches to dietary intake assessment and validation. Current Nutrition Reports. 2016;5(4):307-14.
100. Lachat C, Hawwash D, Ocké MC, Berg C, Forsum E, Hörnell A, et al. Strengthening the reporting of observational studies in epidemiology – nutritional epidemiology (STROBE‐nut): an extension of the STROBE statement. Nutr Bull. 2016;41(3):240-51.
101. Huang T, Yang B, Zheng J, Li G, Wahlqvist ML, Li D. Cardiovascular disease mortality and cancer incidence in vegetarians: a meta-analysis and systematic review. Ann Nutr Metab. 2012;60(4):233-40.
102. Crowe FL, Appleby PN, Travis RC, Key TJ. Risk of hospitalization or death from ischemic heart disease among British vegetarians and nonvegetarians: results from the EPIC-Oxford cohort study. Am J Clin Nutr. 2013;97(3):597-603.
103. Bazzano LA, Serdula MK, Liu S. Dietary intake of fruits and vegetables and risk of cardiovascular disease. Curr Atheroscler Rep. 2003;5(6):492-9.
104. Eckel RH, Jakicic JM, Ard JD, de Jesus JM, Houston Miller N, Hubbard VS, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. J Am Coll Cardiol. 2014;63(25 Part B):2960-84.
105. Wood AM, Kaptoge S, Butterworth AS, Willeit P, Warnakula S, Bolton T, et al. Risk thresholds for alcohol consumption: combined analysis of individual-participant data for 599 912 current drinkers in 83 prospective studies. Lancet. 2018;391(10129):1513-23.
106. Rodriguez-Casado A. The Health Potential of Fruits and Vegetables Phytochemicals: Notable Examples. Crit Rev Food Sci Nutr. 2016;56(7):1097-107.
107. Bondonno NP, Bondonno CP, Hodgson JM, Ward NC, Croft KD. The efficacy of quercetin in cardiovascular health. Current Nutrition Reports. 2015;4(4):290-303.
108. Bhagwat S, Haytowitz DB, Holden JM. USDA Database for the Flavonoid Content of Selected Foods Release 3.1. Beltsville, Maryland: U.S. Department of Agriculture; 2014.
109. Bhagwat S, Haytowitz DB, Holden JM. USDA Database for the Isoflavone Content of Selected Foods Release 2.0. Beltsville, Maryland: U.S. Department of Agriculture; 2008.
110. Morris MC, Wang Y, Barnes LL, Bennett DA, Dawson-Hughes B, Booth SL. Nutrients and bioactives in green leafy vegetables and cognitive decline: Prospective study. Neurology. 2018;90(3):e214-e22.
255 REFERENCES
111. Papandreou C, Becerra-Tomás N, Bulló M, Martínez-González MÁ, Corella D, Estruch R, et al. Legume consumption and risk of all-cause, cardiovascular, and cancer mortality in the PREDIMED study. Clin Nutr. 2018.
112. World Health Organization. The global burden of disease: 2004 update. Geneva, Switzerland: World Health Organization; 2008.
113. Bazzano LA, He J, Ogden LG, Loria CM, Vupputuri S, Myers L, et al. Fruit and vegetable intake and risk of cardiovascular disease in US adults: the first National Health and Nutrition Examination Survey epidemiologic follow-up study. Am J Clin Nutr. 2002;76(1):93-9.
114. Estruch R, Ros E, Salas-Salvadó J, Covas M-I, Corella D, Arós F, et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N Engl J Med. 2013;368(14):1279-90.
115. Gan Y, Tong X, Li L, Cao S, Yin X, Gao C, et al. Consumption of fruit and vegetable and risk of coronary heart disease: a meta-analysis of prospective cohort studies. Int J Cardiol. 2015;183:129-37.
116. Joshipura KJ, Hu FB, Manson JE, Stampfer MJ, Rimm EB, Speizer FE, et al. The effect of fruit and vegetable intake on risk for coronary heart disease. Ann Intern Med. 2001;134(12):1106-14.
117. Rastogi T, Reddy KS, Vaz M, Spiegelman D, Prabhakaran D, Willett WC, et al. Diet and risk of ischemic heart disease in India. Am J Clin Nutr. 2004;79(4):582-92.
118. Ignarro LJ. Nitric oxide as a unique signaling molecule in the vascular system: a historical overview. J Physiol Pharmacol. 2002;53(4):503-14.
119. Gkaliagkousi E, Douma S, Zamboulis C, Ferro A. Nitric oxide dysfunction in vascular endothelium and platelets: role in essential hypertension. J Hypertens. 2009;27(12):2310-20.
120. Moncada S, Higgs A. The L-arginine-nitric oxide pathway. N Engl J Med. 1993;329(27):2002-12. 121. Lundberg JO, Gladwin MT, Weitzberg E. Strategies to increase nitric oxide signalling in
cardiovascular disease. Nat Rev Drug Discov. 2015;14(9):623-41. 122. Sessa WC. eNOS at a glance. J Cell Sci. 2004;117(12):2427-9. 123. Jin RC, Loscalzo J. Vascular nitric oxide: formation and function. J Blood Med. 2010;1:147-62. 124. Werner ER, Gorren ACF, Heller R, Werner-Felmayer G, Mayer B. Tetrahydrobiopterin and nitric
oxide: mechanistic and pharmacological aspects. Exp Biol Med. 2003;228(11):1291-302. 125. Rabelink TJ, Luscher TF. Endothelial nitric oxide synthase. Arterioscler Thromb Vasc Biol.
2006;26(2):267-71. 126. Meininger CJ, Cai S, Parker JL, Channon KM, Kelly KA, Becker EJ, et al. GTP cyclohydrolase I
gene transfer reverses tetrahydrobiopterin deficiency and increases nitric oxide synthesis in endothelial cells and isolated vessels from diabetic rats. FASEB J. 2004;18(15):1900-2.
127. Stroes E, Kastelein J, Cosentino F, Erkelens W, Wever R, Koomans H, et al. Tetrahydrobiopterin restores endothelial function in hypercholesterolemia. J Clin Invest. 1997;99(1):41-6.
128. d’Uscio LV, Milstien S, Richardson D, Smith L, Katusic ZS. Long-term vitamin C treatment increases vascular tetrahydrobiopterin levels and nitric oxide synthase activity. Circ Res. 2003;92(1):88-95.
129. Mensinga TT, Speijers GJA, Meulenbelt J. Health implications of exposure to environmental nitrogenous compounds. Toxicol Rev. 2003;22(1):41-51.
130. Lundberg JO, Gladwin MT, Ahluwalia A, Benjamin N, Bryan NS, Butler A, et al. Nitrate and nitrite in biology, nutrition and therapeutics. Nat Chem Biol. 2009;5(12):865-9.
131. Hord NG, Tang Y, Bryan NS. Food sources of nitrates and nitrites: the physiologic context for potential health benefits. Am J Clin Nutr. 2009;90(1):1-10.
132. Spiegelhalder B, Eisenbrand G, Preussmann R. Influence of dietary nitrate on nitrite content of human saliva: possible relevance to in vivo formation of N-nitroso compounds. Food Cosmet Toxicol. 1976;14(6):545-8.
133. Lundberg JO, Govoni M. Inorganic nitrate is a possible source for systemic generation of nitric oxide. Free Radic Biol Med. 2004;37(3):395-400.
134. Lundberg JO, Weitzberg E, Cole JA, Benjamin N. Nitrate, bacteria and human health. Nat Rev Microbiol. 2004;2(7):593-602.
135. Lundberg JO, Weitzberg E, Gladwin MT. The nitrate-nitrite-nitric oxide pathway in physiology and therapeutics. Nat Rev Drug Discov. 2008;7(2):156-67.
136. Lundberg JO, Weitzberg E, Lundberg JM, Alving K. Intragastric nitric oxide production in humans: measurements in expelled air. Gut. 1994;35(11):1543-6.
137. Peri L, Pietraforte D, Scorza G, Napolitano A, Fogliano V, Minetti M. Apples increase nitric oxide production by human saliva at the acidic pH of the stomach: a new biological function for polyphenols with a catechol group? Free Radic Biol Med. 2005;39(5):668-81.
256 REFERENCES
138. Gago B, Lundberg JO, Barbosa RM, Laranjinha J. Red wine-dependent reduction of nitrite to nitric oxide in the stomach. Free Radic Biol Med. 2007;43(9):1233-42.
139. van Faassen EE, Bahrami S, Feelisch M, Hogg N, Kelm M, Kim-Shapiro DB, et al. Nitrite as regulator of hypoxic signaling in mammalian physiology. Med Res Rev. 2009;29(5):683-741.
140. Montenegro MF, Sundqvist ML, Larsen FJ, Zhuge Z, Carlström M, Weitzberg E, et al. Blood pressure–lowering effect of orally ingested nitrite is abolished by a proton pump inhibitor. Hypertension. 2017;69(1):23-31.
141. Kilian M, Chapple ILC, Hannig M, Marsh PD, Meuric V, Pedersen AML, et al. The oral microbiome - an update for oral healthcare professionals. Br Dent J. 2016;221(10):657-66.
142. Govoni M, Jansson EÅ, Weitzberg E, Lundberg JO. The increase in plasma nitrite after a dietary nitrate load is markedly attenuated by an antibacterial mouthwash. Nitric Oxide. 2008;19(4):333-7.
143. Webb AJ, Patel N, Loukogeorgakis S, Okorie M, Aboud Z, Misra S, et al. Acute blood pressure lowering, vasoprotective, and antiplatelet properties of dietary nitrate via bioconversion to nitrite. Hypertension. 2008;51(3):784-90.
144. Kapil V, Haydar SMA, Pearl V, Lundberg JO, Weitzberg E, Ahluwalia A. Physiological role for nitrate-reducing oral bacteria in blood pressure control. Free Radic Biol Med. 2013;55:93-100.
145. Bondonno CP, Liu AH, Croft KD, Considine MJ, Puddey IB, Woodman RJ, et al. Antibacterial mouthwash blunts oral nitrate reduction and increases blood pressure in treated hypertensive men and women. Am J Hypertens. 2015;28(5):572-5.
146. Bryan NS, Tribble G, Angelov N. Oral microbiome and nitric oxide: the missing link in the management of blood pressure. Curr Hypertens Rep. 2017;19(4):33.
147. Woessner M, Smoliga JM, Tarzia B, Stabler T, Van Bruggen M, Allen JD. A stepwise reduction in plasma and salivary nitrite with increasing strengths of mouthwash following a dietary nitrate load. Nitric Oxide. 2016;54:1-7.
148. Bondonno CP, Croft KD, Puddey IB, Considine MJ, Yang X, Ward NC, et al. Nitrate causes a dose-dependent augmentation of nitric oxide status in healthy women. Food Funct. 2012;3(5):522-7.
149. Choi HM, Han K, Park Y-G, Park J-B. Associations among oral hygiene behavior and hypertension prevalence and control: the 2008 to 2010 Korea National Health and Nutrition Examination Survey. J Periodontol. 2015;86(7):866-73.
150. Fujita M, Ueno K, Hata A. Lower frequency of daily teeth brushing is related to high prevalence of cardiovascular risk factors. Exp Biol Med. 2009;234(4):387-94.
151. Doel JJ, Benjamin N, Hector MP, Rogers M, Allaker RP. Evaluation of bacterial nitrate reduction in the human oral cavity. Eur J Oral Sci. 2005;113(1):14-9.
152. Hyde ER, Andrade F, Vaksman Z, Parthasarathy K, Jiang H, Parthasarathy DK, et al. Metagenomic analysis of nitrate-reducing bacteria in the oral cavity: implications for nitric oxide homeostasis. PLoS One. 2014;9(3):1-13.
153. Velmurugan S, Gan JM, Rathod KS, Khambata RS, Ghosh SM, Hartley A, et al. Dietary nitrate improves vascular function in patients with hypercholesterolemia: a randomized, double-blind, placebo-controlled study. Am J Clin Nutr. 2016;103(1):25-38.
154. Food Standards Australia New Zealand. Survey of nitrates and nitrites in food and beverages in Australia. Canberra: FSANZ; 2011.
155. European Food Safety Authority. Opinion of the scientific panel on contaminants in the food chain on a request from the European Commission to perform a scientific risk assessment on nitrate in vegetables. The EFSA Journal. 2008;689:1-79.
156. Comly HH. Cyanosis in infants caused by nitrates in well water. J Am Med Assoc. 1945;129(2):112-6.
157. Ahluwalia A, Gladwin M, Coleman GD, Hord N, Howard G, Kim‐Shapiro DB, et al. Dietary nitrate and the epidemiology of cardiovascular disease: report from a national heart, lung, and blood institute workshop. J Am Heart Assoc. 2016;5(7):1-10.
158. Santamaria P. Nitrate in vegetables: toxicity, content, intake and EC regulation. J Sci Food Agric. 2006;86(1):10-7.
159. Kleinbongard P, Dejam A, Lauer T, Rassaf T, Schindler A, Picker O, et al. Plasma nitrite reflects constitutive nitric oxide synthase activity in mammals. Free Radic Biol Med. 2003;35(7):790-6.
160. Garcia JM, Teixeira P. Organic versus conventional food: a comparison regarding food safety. Food Reviews International. 2017;33(4):424-46.
161. Saneei P, Salehi-Abargouei A, Esmaillzadeh A, Azadbakht L. Influence of Dietary Approaches to Stop Hypertension (DASH) diet on blood pressure: a systematic review and meta-analysis on
257 REFERENCES
randomized controlled trials. Nutrition, Metabolism & Cardiovascular Disease. 2014;24(12):1253-61.
162. Siervo M, Lara J, Chowdhury S, Oggioni C, Ashor DA, Mathers JC. Effects of Dietary Approaches to Stop Hypertension (DASH) diet on cardiovascular risk factors: a systematic review and meta-analysis. Proc Nutr Soc. 2015;74(OCE1):E138.
163. Siervo M, Lara J, Ogbonmwan I, Mathers JC. Inorganic nitrate and beetroot juice supplementation reduces blood pressure in adults: a systematic review and meta-analysis. J Nutr. 2013;143(6):818-26.
164. Coggan AR, Leibowitz JL, Spearie CA, Kadkhodayan A, Thomas DP, Ramamurthy S, et al. Acute dietary nitrate intake improves muscle contractile function in patients with heart failure: a double-blind, placebo-controlled, randomized trial. Circ Heart Fail. 2015;8(5):914-20.
165. Siervo M, Lara J, Jajja A, Sutyarjoko A, Ashor AW, Brandt K, et al. Ageing modifies the effects of beetroot juice supplementation on 24-hour blood pressure variability: an individual participant meta-analysis. Nitric Oxide. 2015;47:97-105.
166. Lara J, Ogbonmwan I, Oggioni C, Zheng D, Qadir O, Ashor A, et al. Effects of handgrip exercise or inorganic nitrate supplementation on 24-h ambulatory blood pressure and peripheral arterial function in overweight and obese middle age and older adults: a pilot RCT. Maturitas. 2015;82(2):228-35.
167. Bondonno CP, Liu AH, Croft KD, Ward NC, Shinde S, Moodley Y, et al. Absence of an effect of high nitrate intake from beetroot juice on blood pressure in treated hypertensive individuals: a randomized controlled trial. Am J Clin Nutr. 2015;102(2):368-75.
168. Bondonno CP, Liu AH, Croft KD, Ward NC, Yang X, Considine MJ, et al. Short-term effects of nitrate-rich green leafy vegetables on blood pressure and arterial stiffness in individuals with high-normal blood pressure. Free Radic Biol Med. 2014;77:353-62.
169. Gilchrist M, Winyard PG, Aizawa K, Anning C, Shore A, Benjamin N. Effect of dietary nitrate on blood pressure, endothelial function, and insulin sensitivity in type 2 diabetes. Free Radic Biol Med. 2013;60:89-97.
170. Shepherd AI, Wilkerson DP, Fulford J, Winyard PG, Benjamin N, Shore AC, et al. Effect of nitrate supplementation on hepatic blood flow and glucose homeostasis: a double-blind, placebo-controlled, randomized control trial. Am J Physiol Gastrointest Liver Physiol. 2016;311 (3):G356-G64.
171. Lefferts WK, Hughes WE, Heffernan KS. Effect of acute nitrate ingestion on central hemodynamic load in hypoxia. Nitric Oxide. 2016;52:49-55.
172. Jonvik KL, Nyakayiru J, Pinckaers PJM, Senden JMG, van Loon LJC, Verdijk LB. Nitrate-rich vegetables increase plasma nitrate and nitrite concentrations and lower blood pressure in healthy adults. J Nutr. 2016;146 (5):986-93.
173. Hughes WE, Ueda K, Treichler DP, Casey DP. Effects of acute dietary nitrate supplementation on aortic blood pressure and aortic augmentation index in young and older adults. Nitric Oxide. 2016;59:21-7.
174. da Silva DVT, de Oliveira Silva F, Perrone D, Pierucci APTR, Conte-Junior CA, Da Silveira Alvares T, et al. Physicochemical, nutritional, and sensory analyses of a nitrateenriched beetroot gel and its effects on plasmatic nitric oxide and blood pressure. Food Nutr Res. 2016;60 (no pagination)(29909).
175. Wightman EL, Haskell-Ramsay CF, Thompson KG, Blackwell JR, Winyard PG, Forster J, et al. Dietary nitrate modulates cerebral blood flow parameters and cognitive performance in humans: A double-blind, placebo-controlled, crossover investigation. Physiol Behav. 2015;149:149-58.
176. Rodriguez-Mateos A, Hezel M, Aydin H, Kelm M, Lundberg JO, Weitzberg E, et al. Interactions between cocoa flavanols and inorganic nitrate: additive effects on endothelial function at achievable dietary amounts. Free Radic Biol Med. 2015;80:121-8.
177. Bakker E, Engan H, Patrician A, Schagatay E, Karlsen T, Wisloff U, et al. Acute dietary nitrate supplementation improves arterial endothelial function at high altitude: A double-blinded randomized controlled cross over study. Nitric Oxide. 2015;50:58-64.
178. Hobbs DA, George TW, Lovegrove JA. Differential effect of beetroot bread on postprandial DBP according to Glu298Asp polymorphism in the eNOS gene: a pilot study. J Hum Hypertens. 2014;28(12):726-30.
179. Liu AH, Bondonno CP, Croft KD, Puddey IB, Woodman RJ, Rich L, et al. Effects of a nitrate-rich meal on arterial stiffness and blood pressure in healthy volunteers. Nitric Oxide. 2013;35:123-30.
258 REFERENCES
180. Joris PJ, Mensink RP. Beetroot juice improves in overweight and slightly obese men postprandial endothelial function after consumption of a mixed meal. Atherosclerosis. 2013;231(1):78-83.
181. Hobbs DA, Goulding MG, Nguyen A, Malaver T, Walker CF, George TW, et al. Acute ingestion of beetroot bread increases endothelium-independent vasodilation and lowers diastolic blood pressure in healthy men: a randomized controlled trial. J Nutr. 2013;143(9):1399-405.
182. Hobbs DA, Kaffa N, George TW, Methven L, Lovegrove JA. Blood pressure-lowering effects of beetroot juice and novel beetroot-enriched bread products in normotensive male subjects. Br J Nutr. 2012;108(11):2066-74.
183. Coles LT, Clifton PM. Effect of beetroot juice on lowering blood pressure in free-living, disease-free adults: a randomized, placebo-controlled trial. Nutr J. 2012;11(106):1-6.
184. Bondonno CP, Yang X, Croft KD, Considine MJ, Ward NC, Rich L, et al. Flavonoid-rich apples and nitrate-rich spinach augment nitric oxide status and improve endothelial function in healthy men and women: a randomized controlled trial. Free Radic Biol Med. 2012;52(1):95-102.
185. Bahra M, Kapil V, Pearl V, Ghosh S, Ahluwalia A. Inorganic nitrate ingestion improves vascular compliance but does not alter flow-mediated dilatation in healthy volunteers. Nitric Oxide. 2012;26(4):197-202.
186. Kapil V, Milsom AB, Okorie M, Maleki-Toyserkani S, Akram F, Rehman F, et al. Inorganic nitrate supplementation lowers blood pressure in humans: role for nitrite-derived NO. Hypertension. 2010;56(2):274-81.
187. Keen JT, Levitt EL, Hodges GJ, Wong BJ. Short-term dietary nitrate supplementation augments cutaneous vasodilatation and reduces mean arterial pressure in healthy humans. Microvasc Res. 2015;98:48-53.
188. Kapil V, Khambata RS, Robertson A, Caulfield MJ, Ahluwalia A. Dietary nitrate provides sustained blood pressure lowering in hypertensive patients: a randomized, phase 2, double-blind, placebo-controlled study. Hypertension. 2015;65(2):320-7.
189. Ashworth A, Mitchell K, Blackwell JR, Vanhatalo A, Jones AM. High-nitrate vegetable diet increases plasma nitrate and nitrite concentrations and reduces blood pressure in healthy women. Public Health Nutr. 2015;18(14):2669-78.
190. Rammos C, Hendgen-Cotta UB, Sobierajski J, Bernard A, Kelm M, Rassaf T. Dietary nitrate reverses vascular dysfunction in older adults with moderately increased cardiovascular risk. J Am Coll Cardiol. 2014;63(15):1584-5.
191. Jajja A, Sutyarjoko A, Lara J, Rennie K, Brandt K, Qadir O, et al. Beetroot supplementation lowers daily systolic blood pressure in older, overweight subjects. Nutr Res. 2014;34(10):868-75.
192. Miller GD, Marsh AP, Dove RW, Beavers D, Presley T, Helms C, et al. Plasma nitrate and nitrite are increased by a high-nitrate supplement but not by high-nitrate foods in older adults. Nutr Res. 2012;32(3):160-8.
193. Sobko T, Marcus C, Govoni M, Kamiya S. Dietary nitrate in Japanese traditional foods lowers diastolic blood pressure in healthy volunteers. Nitric Oxide. 2010;22(2):136-40.
194. Larsen FJ, Ekblom B, Sahlin K, Lundberg JO, Weitzberg E. Effects of dietary nitrate on blood pressure in healthy volunteers. N Engl J Med. 2006;355(26):2792-3.
195. Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, et al. Recommendations for blood pressure measurement in humans and experimental animals. Circulation. 2005;111(5):697-716.
196. Turner JR, Viera AJ, Shimbo D. Ambulatory blood pressure monitoring in clinical practice: a review. Am J Med. 2015;128(1):14-20.
197. Kuhnle GG, Luben R, Khaw K-T, Feelisch M. Sulfate, nitrate and blood pressure – an EPIC interaction between sulfur and nitrogen. Pharmacol Res. 2017;122:127-9.
198. Carlström M, Liu M, Yang T, Zollbrecht C, Huang L, Peleli M, et al. Cross-talk between nitrate-nitrite-NO and NO synthase pathways in control of vascular NO homeostasis. Antioxid Redox Sign. 2015;23(4):295-306.
199. Chien S-J, Lin K-M, Kuo H-C, Huang C-F, Lin Y-J, Huang L-T, et al. Two different approaches to restore renal nitric oxide and prevent hypertension in young spontaneously hypertensive rats: l-citrulline and nitrate. Translational Research. 2014;163(1):43-52.
200. Vilskersts R, Kuka J, Liepinsh E, Cirule H, Gulbe A, Kalvinsh I, et al. Magnesium nitrate attenuates blood pressure rise in SHR rats. Magnes Res. 2014;27(1):16-24.
201. Essawy SS, Abdel-Sater KA, Elbaz AA. Comparing the effects of inorganic nitrate and allopurinol in renovascular complications of metabolic syndrome in rats: role of nitric oxide and uric acid. Arch Med Sci. 2014;10(3):537-45.
259 REFERENCES
202. Hezel M, Peleli M, Liu M, Zollbrecht C, Jensen BL, Checa A, et al. Dietary nitrate improves age-related hypertension and metabolic abnormalities in rats via modulation of angiotensin II receptor signaling and inhibition of superoxide generation. Free Radic Biol Med. 2016;99:87-98.
203. Khalifi S, Rahimipour A, Jeddi S, Ghanbari M, Kazerouni F, Ghasemi A. Dietary nitrate improves glucose tolerance and lipid profile in an animal model of hyperglycemia. Nitric Oxide. 2015;44:24-30.
204. Carlström M, Persson AEG, Larsson E, Hezel M, Scheffer PG, Teerlink T, et al. Dietary nitrate attenuates oxidative stress, prevents cardiac and renal injuries, and reduces blood pressure in salt-induced hypertension. Cardiovasc Res. 2011;89(3):574-85.
205. Davignon J, Ganz P. Role of endothelial dysfunction in atherosclerosis. Circulation. 2004;109(23 suppl 1):III-27-III-32.
206. Ross R. Atherosclerosis - an inflammatory disease. N Engl J Med. 1999;340(2):115-26. 207. Celermajer DS, Sorensen KE, Gooch VM, Spiegelhalter DJ, Miller OI, Sullivan ID, et al. Non-
invasive detection of endothelial dysfunction in children and adults at risk of atherosclerosis. Lancet. 1992;340(8828):1111-5.
208. Corretti MC, Anderson TJ, Benjamin EJ, Celermajer D, Charbonneau F, Creager MA, et al. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: a report of the International Brachial Artery Reactivity Task Force. J Am Coll Cardiol. 2002;39(2):257-65.
209. Ras RT, Streppel MT, Draijer R, Zock PL. Flow-mediated dilation and cardiovascular risk prediction: a systematic review with meta-analysis. Int J Cardiol. 2013;168(1):344-51.
210. Yeboah J, Crouse JR, Hsu F-C, Burke GL, Herrington DM. Brachial flow-mediated dilation predicts incident cardiovascular events in older adults. Circulation. 2007;115(18):2390-7.
211. Inaba Y, Chen JA, Bergmann SR. Prediction of future cardiovascular outcomes by flow-mediated vasodilatation of brachial artery: a meta-analysis. Int J Cardiovasc Imaging. 2010;26(6):631-40.
212. Green D. Point: Flow-mediated dilation does reflect nitric oxide-mediated endothelial function. J Appl Physiol. 2005;99(3):1233-4.
213. Heiss C, Meyer C, Totzeck M, Hendgen-Cotta UB, Heinen Y, Luedike P, et al. Dietary inorganic nitrate mobilizes circulating angiogenic cells. Free Radic Biol Med. 2012;52:1767-72.
214. Healy B. Endothelial cell dysfunction: an emerging endocrinopathy linked to coronary disease. J Am Coll Cardiol. 1990;16(2):357-8.
215. Freiman PC, Mitchell GG, Heistad DD, Armstrong ML, Harrison DG. Atherosclerosis impairs endothelium-dependent vascular relaxation to acetylcholine and thrombin in primates. Circ Res. 1986;58(6):783-9.
216. Bakker JR, Bondonno NP, Gaspari TA, Kemp-Harper BK, McCashney AJ, Hodgson JM, et al. Low dose dietary nitrate improves endothelial dysfunction and plaque stability in the ApoE−/− mouse fed a high fat diet. Free Radic Biol Med. 2016;99:189-98.
217. Carden DL, Granger DN. Pathophysiology of ischaemia–reperfusion injury. J Pathol. 2000;190(3):255-66.
218. Hendgen-Cotta UB, Luedike P, Totzeck M, Kropp M, Schicho A, Stock P, et al. Dietary nitrate supplementation improves revascularization in chronic ischemia. Circulation. 2012;126(16):1983-92.
219. Willum Hansen T, Staessen JA, Torp-Pedersen C, Rasmussen S, Thijs L, Ibsen H, et al. Prognostic value of aortic pulse wave velocity as index of arterial stiffness in the general population. Circulation. 2006;113(5):664-70.
220. Mitchell GF, Hwang SJ, Vasan RS, Larson MG, Pencina MJ, Hamburg NM, et al. Arterial stiffness and cardiovascular events: the Framingham Heart Study. Circulation. 2010;121(4):505-11.
221. Ben-Shlomo Y, Spears M, Boustred C, May M, Anderson SG, Benjamin EJ, et al. Aortic pulse wave velocity improves cardiovascular event prediction: an individual participant meta-analysis of prospective observational data from 17,635 subjects. J Am Coll Cardiol. 2014;63(7):636-46.
222. Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, et al. Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J. 2006;27(21):2588-605.
223. Vlachopoulos C, Aznaouridis K, O'Rourke MF, Safar ME, Baou K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with central haemodynamics: a systematic review and meta-analysis. Eur Heart J. 2010;31(15):1865-71.
260 REFERENCES
224. Fuentes Q E, Fuentes Q F, Andrés V, Pello OM, de Mora JF, Palomo G I. Role of platelets as mediators that link inflammation and thrombosis in atherosclerosis. Platelets. 2013;24(4):255-62.
225. Radomski MW, Palmer RMJ, Moncada S. Endogenous nitric oxide inhibits human platelet adhersion to vascualr endothelium. Lancet. 1987;330(8567):1057-8.
226. Velmurugan S, Kapil V, Ghosh SM, Davies S, McKnight A, Aboud Z, et al. Antiplatelet effects of dietary nitrate in healthy volunteers: involvement of cGMP and influence of sex. Free Radic Biol Med. 2013;65:1521-32.
227. Richardson G, Hicks SL, O'Byrne S, Frost MT, Moore K, Benjamin N, et al. The ingestion of inorganic nitrate increases gastric S-nitrosothiol levels and inhibits platelet function in humans. Nitric Oxide. 2002;7(1):24-9.
228. Park JW, Piknova B, Huang PL, Noguchi CT, Schechter AN. Effect of blood nitrite and nitrate levels on murine platelet function. PLoS One. 2013;8(2):1-7.
229. Gorelick PB, Scuteri A, Black SE, DeCarli C, Greenberg SM, Iadecola C, et al. Vascular contributions to cognitive impairment and dementia. Stroke. 2011;42(9):2672-713.
230. Presley TD, Morgan AR, Bechtold E, Clodfelter W, Dove RW, Jennings JM, et al. Acute effect of a high nitrate diet on brain perfusion in older adults. Nitric Oxide. 2011;24(1):34-42.
231. Aamand R, Ho YC, Dalsgaard T, Roepstorff A, Lund TE. Dietary nitrate facilitates an acetazolamide-induced increase in cerebral blood flow during visual stimulation. J Appl Physiol. 2014;116(3):267-73.
232. Damasceno M, de Araújo MF, Freire de Freitas RW, de Almeida PC, Zanetti ML. The association between blood pressure in adolescents and the consumption of fruits, vegetables and fruit juice–an exploratory study. J Clin Nurs. 2011;20(11‐12):1553-60.
233. Radhika G, Sudha V, Mohan Sathya R, Ganesan A, Mohan V. Association of fruit and vegetable intake with cardiovascular risk factors in urban south Indians. Br J Nutr. 2008;99(02):398-405.
234. Dauchet L, Kesse-Guyot E, Czernichow S, Bertrais S, Estaquio C, Péneau S, et al. Dietary patterns and blood pressure change over 5-y follow-up in the SU. VI. MAX cohort. Am J Clin Nutr. 2007;85(6):1650-6.
235. Alonso A, de la Fuente C, Martín-Arnau AM, de Irala J, Alfredo Martínez J, Martínez-González MÁ. Fruit and vegetable consumption is inversely associated with blood pressure in a Mediterranean population with a high vegetable-fat intake: the Seguimiento Universidad de Navarra (SUN) Study. Br J Nutr. 2004;92(02):311-9.
236. Aatola H, Koivistoinen T, Hutri-Kähönen N, Juonala M, Mikkilä V, Lehtimäki T, et al. Lifetime fruit and vegetable consumption and arterial pulse wave velocity in adulthood: the Cardiovascular Risk in Young Finns Study. Circulation. 2010;122(24):2521-8.
237. de Paula TP, Steemburgo T, de Almeida JC, Dall'Alba V, Gross JL, de Azevedo MJ. The role of Dietary Approaches to Stop Hypertension (DASH) diet food groups in blood pressure in type 2 diabetes. Br J Nutr. 2012;108(01):155-62.
238. Nordmann AJ, Suter-Zimmermann K, Bucher HC, Shai I, Tuttle KR, Estruch R, et al. Meta-analysis comparing Mediterranean to low-fat diets for modification of cardiovascular risk factors. Am J Med. 2011;124(9):841-51.
239. Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM, et al. A clinical trial of the effects of dietary patterns on blood pressure. N Engl J Med. 1997;336(16):1117-24.
240. Rouse IL, Armstrong BK, Beilin LJ, Vandongen R. Blood-pressure-lowering effect of a vegetarian diet: controlled trial in normotensive subjects. The Lancet. 1983;321(8314):5-10.
241. Yokoyama Y, Nishimura K, Barnard ND, Takegami M, Watanabe M, Sekikawa A, et al. Vegetarian diets and blood pressure: a meta-analysis. J Am Med Assoc. 2014;174(4):577-87.
242. Lundberg JO, Feelisch M, Björne H, Jansson EÅ, Weitzberg E. Cardioprotective effects of vegetables: is nitrate the answer? Nitric Oxide. 2006;15(4):359-62.
243. Jakszyn P, Agudo A, Ibáñez R, García-Closas R, Pera G, Amiano P, et al. Development of a food database of nitrosamines, heterocyclic amines, and polycyclic aromatic hydrocarbons. J Nutr. 2004;134(8):2011-4.
244. Griesenbeck JS, Steck MD, Huber JC, Sharkey JR, Rene AA, Brender JD. Development of estimates of dietary nitrates, nitrites, and nitrosamines for use with the short willet food frequency questionnaire. Nutr J. 2009;8(16):1-9.
245. Inoue-Choi M, Virk-Baker MK, Aschebrook-Kilfoy B, Cross AJ, Subar AF, Thompson FE, et al. Development and calibration of a dietary nitrate and nitrite database in the NIH–AARP Diet and Health Study. Public Health Nutr. 2016;19(11):1934-43.
261 REFERENCES
246. Golzarand M, Bahadoran Z, Mirmiran P, Zadeh-Vakili A, Azizi F. Consumption of nitrate-containing vegetables is inversely associated with hypertension in adults: a prospective investigation from the Tehran Lipid and Glucose Study. Journal of Nephrology. 2016;29(3):377-84.
247. Mirmiran P, Bahadoran Z, Golzarand M, Asghari G, Azizi F. Consumption of nitrate containing vegetables and the risk of chronic kidney disease: Tehran Lipid and Glucose Study. Ren Fail. 2016;38(6):937-44.
248. Bahadoran Z, Mirmiran P, Ghasemi A, Carlström M, Azizi F, Hadaegh F. Vitamin C intake modify the impact of dietary nitrite on the incidence of type 2 diabetes: a 6-year follow-up in Tehran Lipid and Glucose Study. Nitric Oxide. 2017;62:24-31.
249. Bahadoran Z, Mirmiran P, Jeddi S, Azizi F, Ghasemi A, Hadaegh F. Nitrate and nitrite content of vegetables, fruits, grains, legumes, dairy products, meats and processed meats. J Food Compost Anal. 2016;51:93-105.
250. IARC Working Group on the Evaluation of Carcinogenic Risk to Humans. Ingested nitrate and nitrite, and cyanobacterial peptide toxins. Lyon, France: International Agency for Research on Cancer; 2010. Available from: https://www.ncbi.nlm.nih.gov/books/NBK326535/.
251. National Heart Foundation of Australia. Guidelines for the diagnosis and management of hypertension in adults. Melbourne, Victoria: National Heart Foundation of Australia; 2016.
252. Baliga RS, Milsom AB, Ghosh SM, Trinder SL, MacAllister RJ, Ahluwalia A, et al. Dietary nitrate ameliorates pulmonary hypertension. Circulation. 2012;125(23):2922-32.
253. Carlström M, Larsen FJ, Nyström T, Hezel M, Borniquel S, Weitzberg E, et al. Dietary inorganic nitrate reverses features of metabolic syndrome in endothelial nitric oxide synthase-deficient mice. Proceedings of the National Academy of Sciences. 2010;107(41):17716-20.
254. Petersson J, Carlström M, Schreiber O, Phillipson M, Christoffersson G, Jägare A, et al. Gastroprotective and blood pressure lowering effects of dietary nitrate are abolished by an antiseptic mouthwash. Free Radic Biol Med. 2009;46(8):1068-75.
255. Marsch E, Theelen TL, Janssen BJA, Briede JJ, Haenen GR, Senden JMG, et al. The effect of prolonged dietary nitrate supplementation on atherosclerosis development. Atherosclerosis. 2016;245:212-21.
256. Quiñones M, Miguel M, Aleixandre A. Beneficial effects of polyphenols on cardiovascular disease. Pharmacol Res. 2013;68(1):125-31.
257. Prince RL, Devine A, Dhaliwal SS, Dick IM. Effects of calcium supplementation on clinical fracture and bone structure: results of a 5-year, double-blind, placebo-controlled trial in elderly women. Arch Intern Med. 2006;166(8):869-75.
258. World Health Organization. Manual of the International Statistical Classification of Diseases, Injuries and Causes of Death, 9th Revision (ICD-9). Geneva: World Health Organization; 1977.
259. National Coding Centre. The Australian Version of the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). Sydney: National Coding Centre, Faculty of Health Sciences, University of Sydney; 1996.
260. Britt H, Scahill S, Miller G. ICPC PLUS for community health? A feasibility study. Health Inf Manag. 1997;27(4):171-5.
261. National Centre for Classification in Health. International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Australian Modification (ICD-10-AM). Sydney: National Centre for Classification in Health; 1998.
262. Ireland P, Jolley D, Giles G, O’Dea K, Powles J, Rutishauser I, et al. Development of the Melbourne FFQ: a food frequency questionnaire for use in an Australian prospective study involving an ethnically diverse cohort. Asia Pac J Clin Nutr. 1994;3(1):19-31.
263. Hodge A, Patterson AJ, Brown WJ, Ireland P, Giles G. The Anti Cancer Council of Victoria FFQ: relative validity of nutrient intakes compared with weighed food records in young to middle‐aged women in a study of iron supplementation. Aust N Z J Public Health. 2000;24(6):576-83.
264. Lewis J, Milligan G, Hunt A. NUTTAB95 Nutrient Data Table for Use in Australia. Canberra: Australian Government Publishing Service; 1995.
265. Fulgoni VL, Keast DR, Drewnowski A. Development and validation of the nutrient-rich foods index: a tool to measure nutritional quality of foods. J Nutr. 2009;139(8):1549-54.
266. National Health and Medical Research Council. Nutrient Reference Values for Australia and New Zealand. Canberra2006.
267. Devine A, Dhaliwal SS, Dick IM, Bollerslev J, Prince RL. Physical activity and calcium consumption are important determinants of lower limb bone mass in older women. J Bone Miner Res. 2004;19(10):1634-9.
262 REFERENCES
268. McArdle WD, Katch FI, Katch VL. Energy, nutrition and human performance. Philadelphia: Lea & Febiger; 1991.
269. Pollock ML, Wilmore JH, Fox SM. Health and fitness through physical activity. New York: Wiley; 1978.
270. Australian Bureau of Statistics. Socio-economic indexes for areas. Catalogue Number 2039.0. Canberra: ABS; 1998.
271. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF, Feldman HI, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604-12.
272. Lewis JR, Lim W, Dhaliwal SS, Zhu K, Lim EM, Thompson PL, et al. Estimated glomerular filtration rate as an independent predictor of atherosclerotic vascular disease in older women. BMC Nephrol. 2012;13(58):1-7.
273. Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma without use of the preparative ultracentrifuge. Clin Chem. 1972;18(6):499-502.
274. D’Agostino RB, Vasan RS, Pencina MJ, Wolf PA, Cobain M, Massaro JM, et al. General cardiovascular risk profile for use in primary care: the Framingham Heart Study. Circ J. 2008;117(6):743-53.
275. Blekkenhorst LC, Prince RL, Hodgson JM, Lim WH, Zhu K, Devine A, et al. Dietary saturated fat intake and atherosclerotic vascular disease mortality in elderly women: a prospective cohort study. Am J Clin Nutr. 2015;101(6):1263-8.
276. Cornelis MC, El-Sohemy A, Campos H. GSTT1 genotype modifies the association between cruciferous vegetable intake and the risk of myocardial infarction. Am J Clin Nutr. 2007;86(3):752-8.
277. Galeone C, Tavani A, Pelucchi C, Negri E, La Vecchia C. Allium vegetable intake and risk of acute myocardial infarction in Italy. Eur J Nutr. 2009;48(2):120-3.
278. Gu X, Zhu YZ. Therapeutic applications of organosulfur compounds as novel hydrogen sulfide donors and/or mediators. Expert Rev Clin Pharmacol. 2011;4(1):123-33.
279. Yu XH, Cui LB, Wu K, Zheng XL, Cayabyab FS, Chen ZW, et al. Hydrogen sulfide as a potent cardiovascular protective agent. Clin Chim Acta. 2014;437:78-87.
280. Wu QJ, Yang Y, Vogtmann E, Wang J, Han LH, Li HL, et al. Cruciferous vegetables intake and the risk of colorectal cancer: a meta-analysis of observational studies. Ann Oncol. 2013;24(4):1079-87.
281. Liu X, Lv K. Cruciferous vegetables intake is inversely associated with risk of breast cancer: A meta-analysis. The Breast. 2013;22(3):309-13.
282. Liu B, Mao Q, Cao M, Xie L. Cruciferous vegetables intake and risk of prostate cancer: A meta-analysis. Int J Urol. 2012;19(2):134-41.
283. Bai Y, Wang X, Zhao S, Ma C, Cui J, Zheng Y. Sulforaphane protects against cardiovascular disease via Nrf2 activation. Oxid Med Cell Longev. 2015:1-13.
284. Yamagishi S, Matsui T. Protective role of sulphoraphane against vascular complications in diabetes. Pharm Biol. 2016;54(10):2329-39.
285. Jiang Y, Wu S-H, Shu X-O, Xiang Y-B, Ji B-T, Milne GL, et al. Cruciferous vegetable intake is inversely correlated with circulating levels of proinflammatory markers in women. J Acad Nutr Diet. 2014;114(5):700-8.e2.
286. Bradley JM, Organ CL, Lefer DJ. Garlic-derived organic polysulfides and myocardial protection. The Journal of Nutrition. 2016;146(2):403S-9S.
287. Berlin JA, Colditz GA. A meta-analysis of physical activity in the prevention of coronary heart disease. Am J Epidemiol. 1990;132(4):612-28.
288. Manson JE, Greenland P, LaCroix AZ, Stefanick ML, Mouton CP, Oberman A, et al. Walking compared with vigorous exercise for the prevention of cardiovascular events in women. N Engl J Med. 2002;347(10):716-25.
289. Nurzenski MK, Briffa NK, Price RI, Khoo BCC, Devine A, Beck TJ, et al. Geometric indices of bone strength are associated with physical activity and dietary calcium intake in healthy older women. J Bone Miner Res. 2007;22(3):416-24.
290. He K, Song Y, Daviglus ML, Liu K, Van Horn L, Dyer AR, et al. Accumulated evidence on fish consumption and coronary heart disease mortality: a meta-analysis of cohort studies. Circulation. 2004;109(22):2705-11.
291. Luo C, Zhang Y, Ding Y, Shan Z, Chen S, Yu M, et al. Nut consumption and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality: a systematic review and meta-analysis. Am J Clin Nutr. 2014;100(1):256-69.
263 REFERENCES
292. Ashor AW, Lara J, Siervo M. Medium-term effects of dietary nitrate supplementation on systolic and diastolic blood pressure in adults: a systematic review and meta-analysis. J Hypertens. 2017;35(7):1353-9.
293. Bruce DG, Devine A, Prince RL. Recreational physical activity levels in healthy older women: the importance of fear of falling. J Am Geriatr Soc. 2002;50(1):84-9.
294. Zhu K, Devine A, Dick IM, Wilson SG, Prince RL. Effects of calcium and vitamin D supplementation on hip bone mineral density and calcium-related analytes in elderly ambulatory Australian women: a five-year randomized controlled trial. J Clin Endocrinol Metab. 2008;93(3):743-9.
295. Salonen JT, Salonen R. Ultrasound B-mode imaging in observational studies of atherosclerotic progression. Circulation. 1993;87(3 Suppl):II56-65.
296. Lewis JR, Zhu K, Thompson PL, Prince RL. The effects of 3 years of calcium supplementation on common carotid artery intimal medial thickness and carotid atherosclerosis in older women: an ancillary study of the CAIFOS randomized controlled trial. J Bone Miner Res. 2014;29(3):534-41.
297. Wilson PWF, Hoeg JM, D'Agostino RB, Silbershatz H, Belanger AM, Poehlmann H, et al. Cumulative effects of high cholesterol levels, high blood pressure, and cigarette smoking on carotid stenosis. N Engl J Med. 1997;337(8):516-22.
298. Woods RK, Stoney RM, Ireland PD, Bailey MJ, Raven JM, Thien FCK, et al. A valid food frequency questionnaire for measuring dietary fish intake. Asia Pac J Clin Nutr. 2002;11(1):56-61.
299. Blekkenhorst LC, Hodgson JM, Lewis JR, Devine A, Woodman RJ, Lim WH, et al. Vegetable and fruit intake and fracture-related hospitalisations: a prospective study of older women. Nutrients. 2017;9(5):511.
300. Bondonno N, Lewis J, Prince R, Lim W, Wong G, Schousboe J, et al. Fruit intake and abdominal aortic calcification in elderly women: a prospective cohort study. Nutrients. 2016;8(3):159.
301. Lupoli R, Vaccaro A, Ambrosino P, Poggio P, Amato M, Di Minno MND. Impact of vitamin D deficiency on subclinical carotid atherosclerosis: a pooled analysis of cohort studies. J Clin Endocrinol Metab. 2017;102(7):2146-53.
302. Bondonno NP, Bondonno CP, Ward NC, Hodgson JM, Croft KD. The cardiovascular health benefits of apples: whole fruit vs. isolated compounds. Trends in Food Science & Technology. 2017;69(Part B):243-56.
303. Petersen KS, Clifton PM, Blanch N, Keogh JB, Petersen KS, Clifton PM, et al. Effect of improving dietary quality on carotid intima media thickness in subjects with type 1 and type 2 diabetes: a 12-mo randomized controlled trial. Am J Clin Nutr. 2015;102:771-9.
304. Chan HT, Yiu KH, Wong CY, Li SW, Tam S, Tse HF. Increased dietary fruit intake was associated with lower burden of carotid atherosclerosis in Chinese patients with Type 2 diabetes mellitus. Diabet Med. 2013;30(1):100-8.
305. Buil-Cosiales P, Irimia P, Ros E, Riverol M, Gilabert R, Martinez-Vila E, et al. Dietary fibre intake is inversely associated with carotid intima-media thickness: a cross-sectional assessment in the PREDIMED study. Eur J Clin Nutr. 2009;63(10):1213-9.
306. Whelton PK, He J, Cutler JA, Brancati FL, Appel LJ, Follmann D, et al. Effects of oral potassium on blood pressure: meta-analysis of randomized controlled clinical trials. J Am Med Assoc. 1997;277(20):1624-32.
307. D'Elia L, Barba G, Cappuccio FP, Strazzullo P. Potassium intake, stroke, and cardiovascular disease: a meta-analysis of prospective studies. J Am Coll Cardiol. 2011;57(10):1210-9.
308. D'Elia L, Iannotta C, Sabino P, Ippolito R. Potassium-rich diet and risk of stroke: updated meta-analysis. Nutr Metab Cardiovasc Dis. 2014;24(6):585-7.
309. Sánchez-Moreno C, Jiménez-Escrig A, Saura-Calixto F. Study of low-density lipoprotein oxidizability indexes to measure the antioxidant activity of dietary polyphenols. Nutr Res. 2000;20(7):941-53.
310. Bondonno CP, Croft KD, Ward N, Considine MJ, Hodgson JM. Dietary flavonoids and nitrate: effects on nitric oxide and vascular function. Nutr Rev. 2015;73(4):216-35.
311. Bartsch H, Ohshima H, Pignatelli B. Inhibitors of endogenous nitrosation mechanisms and implications in human cancer prevention. Mutation Research/Fundamental and Molecular Mechanisms of Mutagenesis. 1988;202(2):307-24.
312. Bartsch H, Pignatelli B, Calmels S, Ohshima H. Inhibition of Nitrosation. In: Bronzetti G, Hayatsu H, De Flora S, Waters MD, Shankel DM, editors. Antimutagenesis and Anticarcinogenesis Mechanisms III. Boston, MA: Springer US; 1993. p. 27-44.
264 REFERENCES
313. Helser MA, Hotchkiss JH, Roe DA. Influence of fruit and vegetable juices on the endogenous formation of N-nitrosoproline and N-nitrosothiazolidine-4-carboxylic acid in humans on controlled diets. Carcinogenesis. 1992;13(12):2277-80.
314. Anjana, Umar S, Iqbal M, Abrol YP. Are nitrate concentrations in leafy vegetables within safe limits? Curr Sci. 2007;92(3):355-60.
315. Pennington JAT. Dietary exposure models for nitrates and nitrites. Food Control. 1998;9(6):385-95.
316. Petersen A, Stoltze S. Nitrate and nitrite in vegetables on the Danish market: content and intake. Food Addit Contam. 1999;16(7):291-9.
317. Ysart G, Miller P, Barrett G, Farrington D, Lawrance P, Harrison N. Dietary exposures to nitrate in the UK. Food Addit Contam. 1999;16(12):521-32.
318. Yang X, Bondonno CP, Indrawan A, Hodgson JM, Croft KD. An improved mass spectrometry-based measurement of NO metabolites in biological fluids. Free Radic Biol Med. 2013;56:1-8.
319. Meah MN, Harrison N, Davies A. Nitrate and nitrite in foods and the diet. Food Addit Contam. 1994;11(4):519-32.
320. Breimer T. Environmental factors and cultural measures affecting the nitrate content in spinach. Fertilizer research. 1982;3(3):191-292.
321. Winter CK, Davis SF. Organic Foods. J Food Sci. 2006;71(9):R117-R24. 322. Aires A, Carvalho R, Rosa EAS, Saavedra MJ. Effects of agriculture production systems on
nitrate and nitrite accumulation on baby-leaf salads. Food Science & Nutrition. 2013;1(1):3-7. 323. Kanaan S, Economakis C. Effect of climatic conditions and time of harvest on growth and
tissue nitrate content of lettuce in nutrient film culture. Acta Horticulturae. 1992;323:75-80. 324. Gangolli SD, van den Brandt PA, Feron VJ, Janzowsky C, Koeman JH, Speijers GJA, et al.
Nitrate, nitrite and N-nitroso compounds. European Journal of Pharmacology: Environmental Toxicology and Pharmacology. 1994;292(1):1-38.
325. Dejongheere W, Steurbaut W, Drieghe S, Verstraete R, Braeckman H. Nitrate in food commodities of vegetable origin and the total diet in Belgium (1992-1993). Microbiologie-Aliments-Nutrition. 1994;12:359-70.
326. Leszczyńska T, Filipiak-Florkiewicz A, Cieślik E, Sikora E, Pisulewski PM. Effects of some processing methods on nitrate and nitrite changes in cruciferous vegetables. J Food Compost Anal. 2009;22(4):315-21.
327. Prasad S, Chetty AA. Flow injection assessment of nitrate contents in fresh and cooked fruits and vegetables grown in Fiji. J Food Sci. 2011;76(8):C1143-8.
328. Fernández AMC, Larrañaga MRM, de la Puerta CN, Martínez AP, Rodríguez RL. Report from the Scientific Committee of the Spanish Agency for Food Safety and Nutrition (AESAN) in relation to the risk assess-ment of infants and young children’s exposure to nitrates result-ing from the consumption of chard in Spain. 2011.
329. Pęksa A, Gołubowska G, Aniołowski K, Lisińska G, Rytel E. Changes of glycoalkaloids and nitrate contents in potatoes during chip processing. Food Chem. 2006;97(1):151-6.
330. Sohail M, Adeloju SB. Nitrate biosensors and biological methods for nitrate determination. Talanta. 2016;153:83-98.
331. Pannala AS, Mani AR, Spencer JP, Skinner V, Bruckdorfer KR, Moore KP, et al. The effect of dietary nitrate on salivary, plasma, and urinary nitrate metabolism in humans. Free Radic Biol Med. 2003;34(5):576-84.
332. Hu FB, Rimm E, Smith-Warner SA, Feskanich D, Stampfer MJ, Ascherio A, et al. Reproducibility and validity of dietary patterns assessed with a food-frequency questionnaire. Am J Clin Nutr. 1999;69(2):243-9.
333. Omar SA, Webb AJ, Lundberg JO, Weitzberg E, Omar SA, Webb AJ, et al. Therapeutic effects of inorganic nitrate and nitrite in cardiovascular and metabolic diseases. J Intern Med. 2016;279(4):315-36.
334. Lara J, Ashor AW, Oggioni C, Ahluwalia A, Mathers JC, Siervo M. Effects of inorganic nitrate and beetroot supplementation on endothelial function: a systematic review and meta-analysis. Eur J Nutr. 2016;55:451-9.
335. Larsson SC, Orsini N, Wolk A. Processed meat consumption and stomach cancer risk: a meta-analysis. J Natl Cancer Inst. 2006;98(15):1078-87.
336. Larsson SC, Orsini N. Red meat and processed meat consumption and all-cause mortality: a meta-analysis. Am J Epidemiol. 2014;179(3):282-9.
265 REFERENCES
337. Micha R, Wallace SK, Mozaffarian D. Red and processed meat consumption and risk of incident coronary heart disease, stroke, and diabetes mellitus: a systematic review and meta-analysis. Circulation. 2010;121(21):2271-83.
338. Drewnowski A. Defining nutrient density: development and validation of the nutrient rich foods index. J Am Coll Nutr. 2009;28(4):421S-6S.
339. Australian Food and Grocery Council. Daily intake guide healthy eating made easy [Internet]. ACT: Australian Food and Grocery Council; 2011 [cited 2016 11 Aug]. Available from: http://www.mydailyintake.net/nutrients/.
340. Kodama S, Tanaka S, Heianza Y, Fujihara K, Horikawa C, Shimano H, et al. Association between physical activity and risk of all-cause mortality and cardiovascular disease in patients with diabetes: a meta-analysis. Diabetes Care. 2013;36(2):471-9.
341. Sluik D, Buijsse B, Muckelbauer R, Kaaks R, Teucher B, Johnsen NF, et al. Physical activity and mortality in individuals with diabetes mellitus: a prospective study and meta-analysis. Arch Intern Med. 2012;172(17):1285-95.
342. Speijers G, van den Brandt P. World Health Organization Food Additive Series: 50. Nitrate and potential endogenous formation of N-nitroso compounds. Geneva, Switzerland: World Health Organization; 2003.
343. Lorenz MW, von Kegler S, Steinmetz H, Markus HS, Sitzer M. Carotid intima-media thickening indicates a higher vascular risk across a wide age range: prospective data from the Carotid Atherosclerosis Progression Study (CAPS). Stroke. 2006;37(1):87-92.
344. Ivey KL, Lewis JR, Hodgson JM, Zhu K, Dhaliwal SS, Thompson PL, et al. Association between yogurt, milk, and cheese consumption and common carotid artery intima-media thickness and cardiovascular disease risk factors in elderly women. Am J Clin Nutr. 2011;94(1):234-9.
345. Weitzberg E, Lundberg JO, Weitzberg E, Lundberg JO. Dietary nitrate - a slow train coming. J Physiol. 2011;589(Pt 22):5333-4.
346. Hambridge T. World Health Organization Food Additives Series: 50. Nitrate and Nitrite: Intake Assessment. Geneva, Switzerland: World Health Organization; 2003.
347. Naqvi TZ, Lee M-S. Carotid Intima-Media Thickness and Plaque in Cardiovascular Risk Assessment. JACC Cardiovasc Imaging. 2014;7(10):1025-38.
348. McQuillan BM, Beilby JP, Nidorf M, Thompson PL, Hung J. Hyperhomocysteinemia but not the C677T mutation of methylenetetrahydrofolate reductase is an independent risk determinant of carotid wall thickening. Circulation. 1999;99(18):2383-8.
349. Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224-60.
350. Bromfield S, Muntner P. High blood pressure: the leading global burden of disease risk factor and the need for worldwide prevention programs. Curr Hypertens Rep. 2013;15(3):134-6.
351. World Health Organization. A global brief on hypertension. Geneva: World Health Organization; 2013.
352. Ettehad D, Emdin CA, Kiran A, Anderson SG, Callender T, Emberson J, et al. Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet. 2016;387(10022):957-67.
353. Liao D, Arnett DK, Tyroler HA, Riley WA, Chambless LE, Szklo M, et al. Arterial stiffness and the development of hypertension. Hypertension. 1999;34(2):201-6.
354. Payne RA, Wilkinson IB, Webb DJ. Arterial stiffness and hypertension: emerging concepts. Hypertension. 2010;55(1):9-14.
355. Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;55(13):1318-27.
356. Ndanuko RN, Tapsell LC, Charlton KE, Neale EP, Batterham MJ. Dietary patterns and blood pressure in adults: a systematic review and meta-analysis of randomized controlled trials. Adv Nutr. 2016;7(1):76-89.
357. Giles G, Ireland P. Dietary Questionnaire for Epidemiological Studies (Version 2). Melbourne: Cancer Council Victoria; 1996.
358. Ekelund U, Sepp H, Brage S, Becker W, Jakes R, Hennings M, et al. Criterion-related validity of the last 7-day, short form of the International Physical Activity Questionnaire in Swedish adults. Public Health Nutr. 2006;9.
266 REFERENCES
359. Ward NC, Hodgson JM, Croft KD, Burke V, Beilin LJ, Puddey IB. The combination of vitamin C and grape-seed polyphenols increases blood pressure: a randomized, double-blind, placebo-controlled trial. J Hypertens. 2005;23(2):427-34.
360. Wood LG, Garg ML, Smart JM, Scott HA, Barker D, Gibson PG. Manipulating antioxidant intake in asthma: a randomized controlled trial. Am J Clin Nutr. 2012;96(3):534-43.
361. Lee YP, Mori TA, Puddey IB, Sipsas S, Ackland TR, Beilin LJ, et al. Effects of lupin kernel flour–enriched bread on blood pressure: a controlled intervention study. Am J Clin Nutr. 2009;89(3):766-72.
362. Hodgson JM, Croft KD, Woodman RJ, Puddey IB, Fuchs D, Draijer R, et al. Black tea lowers the rate of blood pressure variation: a randomized controlled trial. Am J Clin Nutr. 2013;97(5):943-50.
363. Ilich Jasminka Z, Blanuša M, Orlić Željka C, Orct T, Kostial K. Comparison of calcium, magnesium, sodium, potassium, zinc, and creatinine concentration in 24-h and spot urine samples in women. Clin Chem Lab Med. 2009;47:216-21.
364. Anjana SU, Iqbal M. Nitrate accumulation in plants, factors affecting the process, and human health implications. A review. Agronomy for Sustainable Development. 2007;27(1):45-57.
365. Dewhurst-Trigg R, Yeates T, Blackwell JR, Thompson C, Linoby A, Morgan PT, et al. Lowering of blood pressure after nitrate-rich vegetable consumption is abolished with the co-ingestion of thiocyanate-rich vegetables in healthy normotensive males. Nitric Oxide. 2018;74:39-46.





























