Embed Size (px)
Citation preview

1 23
Cellular and Molecular Life Sciences ISSN 1420-682XVolume 69Number 8 Cell. Mol. Life Sci. (2012) 69:1261-1277DOI 10.1007/s00018-011-0866-4
CD95-mediated cell signaling in cancer:mutations and post-translationalmodulations
Sébastien Tauzin, Laure Debure, Jean-François Moreau & Patrick Legembre

1 23
Your article is protected by copyright and all
rights are held exclusively by Springer Basel
AG. This e-offprint is for personal use only
and shall not be self-archived in electronic
repositories. If you wish to self-archive your
work, please use the accepted author’s
version for posting to your own website or
your institution’s repository. You may further
deposit the accepted author’s version on
a funder’s repository at a funder’s request,
provided it is not made publicly available until
12 months after publication.

REVIEW
CD95-mediated cell signaling in cancer: mutationsand post-translational modulations
Sebastien Tauzin • Laure Debure •
Jean-Francois Moreau • Patrick Legembre
Received: 5 September 2011 / Revised: 10 October 2011 / Accepted: 14 October 2011 / Published online: 1 November 2011
� Springer Basel AG 2011
Abstract Apoptosis has emerged as a fundamental pro-
cess important in tissue homeostasis, immune response,
and during development. CD95 (also known as Fas), a
member of the tumor necrosis factor receptor (TNF-R)
superfamily, has been initially cloned as a death receptor.
Its cognate ligand, CD95L, is mainly found at the plasma
membrane of activated T-lymphocytes and natural killer
cells where it contributes to the elimination of transformed
and infected cells. According to its implication in the
immune homeostasis and immune surveillance, and since
several malignant cells of various histological origins
exhibit loss-of-function mutations, which cause resistance
towards the CD95-mediated apoptotic signal, CD95 has
been classified as a tumor suppressor gene. Nevertheless,
this assumption has been recently challenged, as in certain
pathophysiological contexts, CD95 engagement transmits
non-apoptotic signals that promote inflammation, carcino-
genesis or liver/peripheral nerve regeneration. The focus of
this review is to discuss these apparent contradictions of
the known function(s) of CD95.
Keywords Fas � Oncogene � Tumor suppressor �
Lipid rafts � ALPS
Abbreviations
ASM Acid sphingomyelinase
ADAM A disintegrin and metalloproteinase domain
ALPS Autoimmune lymphoproliferative syndrome
DD Death domain
FADD Fas-associating protein with a death domain
GC Germinal center
LOH Loss of heterozygosity
MAPK Mitogen-activated protein kinase
MMP Matrix metalloproteinase
NF-jB Nuclear factor Kappa B
TNF Tumor necrosis factor
Implementation of a CD95-mediated signaling pathway
CD95: the so-called death receptor
APT-1 (also known as CD95, Fas, or APO-1) gene spans
approximately 25 kb on human chromosome 10 [1]. The
gene consists of nine exons in which exon 6 encodes the
transmembrane domain (Fig. 1a). CD95 is a type I trans-
membrane protein that belongs to the tumor necrosis factor
(TNF) receptor family characterized by cysteine-rich
extracellular domains. CD95 is resolved under denaturing
conditions between 40 and 50 kDa in SDS-PAGE. This
receptor has been initially cloned as a death receptor
[2] bound and activated by the apoptotic-inducing mAb
S. Tauzin
Universite Rennes-1, 2 Avenue du Professeur Leon Bernard,
35043 Rennes, France
L. Debure
IRSET, Team ‘‘Death Receptors and Tumor Escape’’,
2 Av du Prof. Leon Bernard, 35043 Rennes, France
J.-F. Moreau
Universite de Bordeaux-2, UMR CNRS 5164,
146 rue Leo Saignat, 33076 Bordeaux, France
P. Legembre (&)
University of Rennes-1, IRSET (Institut de Recherche sur
la Sante l’Environnement et le Travail), Team ‘‘Death Receptors
and Tumor Escape’’, 2 av Prof Leon Bernard,
35043 Rennes cedex, France
e-mail: [email protected]
Cell. Mol. Life Sci. (2012) 69:1261–1277
DOI 10.1007/s00018-011-0866-4 Cellular and Molecular Life Sciences
123
Author's personal copy

designated APO-1 [3]. Consequently, the death-inducing
activity of the antigen APO-1 has been extensively ana-
lyzed for the last 20 years and the pro-apoptotic role of
CD95 is supported by the fact that the cognate ligand of
CD95, the transmembrane CD95L (CD178/FasL) is present
at the surface of activated lymphocytes [4] and natural
killer cells [5] where it orchestrates the elimination of
transformed and infected cells. In addition, CD95L is
found expressed at the surface of neurons [6], corneal
epithelia, and endothelia [7, 8] and Sertoli cells [9] to
prevent the infiltration of immune cells and thus to prohibit
the spread of inflammation in these sensitive organs (i.e.,
brain, eyes, testis, respectively), which are commonly
called ‘‘immune-privileged’’ sites.
Description of physiological ‘‘immune privilege’’ was
later on followed by tumor-mediated ‘‘immune privileged
area’’ since two groups reported that the ectopic expression
of CD95L by malignant cells participated in the elimina-
tion of infiltrating T lymphocytes and thus could play a role
in the establishment of a tumoral site whose access was
denied to immune effector cells [10, 11]. However, these
observations were rapidly challenged since both allogenic
transplant of b-islets [12, 13] and tumor cells [14]
expressing the membrane-bound CD95L led to a much
rapid elimination of the cells as compared to control islets
and malignant cells, respectively, due to an increase in
infiltration of neutrophils and macrophages endowed with
anti-tumoral activities. Confirming these latter findings,
recent studies revealed that in certain pathophysiological
contexts, engagement of the CD95 receptor promoted pro-
inflammatory [15–17] or even pro-oncogenic processes
[18–20]. In the following parts of this review, we will
discuss how CD95 itself and its ligand organize the
implementation of pro- or anti-apoptotic signals.
CD95-mediated apoptotic signaling pathway(s)
Similarly to the TNF-receptor [21], CD95 has been found
expressed at the plasma membrane as a pre-associated
homotrimer [22, 23]. Binding of CD95L or agonistic anti-
CD95 mAbs to CD95 alters both the conformation and the
extent to which the receptor aggregates at the plasma
1 2 3 4 5 6 7 8
1 347 376 542 680 789 851 914 997 1022 1354 2689 nt mRNA
9exons
1 16 174 190 230 317 335 a.a.PROTEIN
PS TM DD
A
B
COOH5
23 4 1
6
Plasma membrane
Cytosol
α
1α
2
α
3
α
4
α
5
α
6
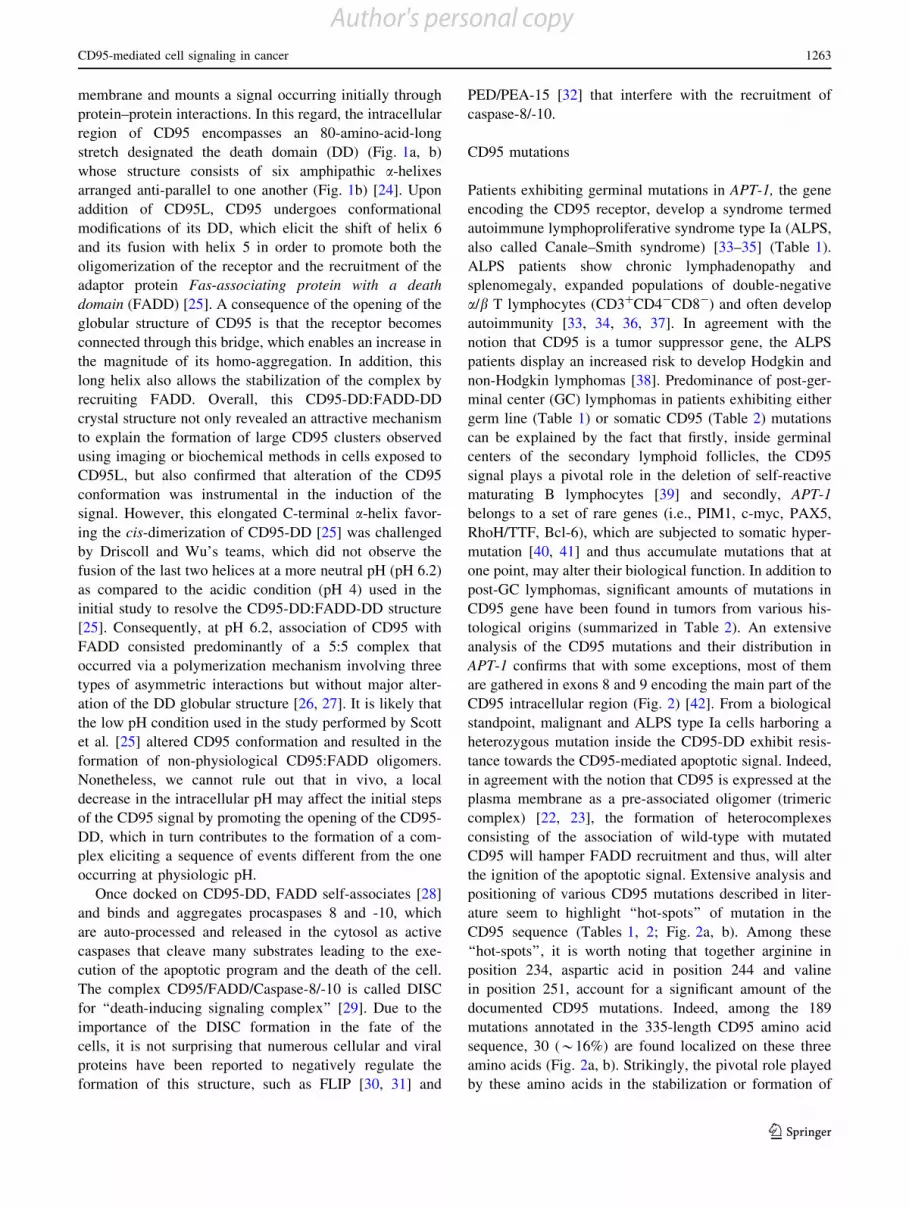
Fig. 1 CD95 structure. a CD95 mRNA consists of 9 exons as
indicated in the upper panel. The CD95 mRNA (upper panel) and
protein (lower panel) are depicted. Numbers on the upper panel stand
for the position of nucleic acids in CD95 mRNA while on the lower
panel, they represent the position of the amino acids in the protein
sequence. The 6 a-helices constituting the CD95-death domain (DD)
are indicated. PS peptide signal, TM transmembrane domain. Num-
bering is applied according to references [2, 59] (NM_000043).
b Nuclear magnetic resonance (NMR) structure of the CD95 death
domain according to 1DDF (Protein data bank) and analyzed using
Jmol version 12.0.18. The rockets stand for the 6 a-helices and the
plasma membrane has been added
1262 S. Tauzin et al.
123
Author's personal copy
membrane and mounts a signal occurring initially through
protein–protein interactions. In this regard, the intracellular
region of CD95 encompasses an 80-amino-acid-long
stretch designated the death domain (DD) (Fig. 1a, b)
whose structure consists of six amphipathic a-helixes
arranged anti-parallel to one another (Fig. 1b) [24]. Upon
addition of CD95L, CD95 undergoes conformational
modifications of its DD, which elicit the shift of helix 6
and its fusion with helix 5 in order to promote both the
oligomerization of the receptor and the recruitment of the
adaptor protein Fas-associating protein with a death
domain (FADD) [25]. A consequence of the opening of the
globular structure of CD95 is that the receptor becomes
connected through this bridge, which enables an increase in
the magnitude of its homo-aggregation. In addition, this
long helix also allows the stabilization of the complex by
recruiting FADD. Overall, this CD95-DD:FADD-DD
crystal structure not only revealed an attractive mechanism
to explain the formation of large CD95 clusters observed
using imaging or biochemical methods in cells exposed to
CD95L, but also confirmed that alteration of the CD95
conformation was instrumental in the induction of the
signal. However, this elongated C-terminal a-helix favor-
ing the cis-dimerization of CD95-DD [25] was challenged
by Driscoll and Wu’s teams, which did not observe the
fusion of the last two helices at a more neutral pH (pH 6.2)
as compared to the acidic condition (pH 4) used in the
initial study to resolve the CD95-DD:FADD-DD structure
[25]. Consequently, at pH 6.2, association of CD95 with
FADD consisted predominantly of a 5:5 complex that
occurred via a polymerization mechanism involving three
types of asymmetric interactions but without major alter-
ation of the DD globular structure [26, 27]. It is likely that
the low pH condition used in the study performed by Scott
et al. [25] altered CD95 conformation and resulted in the
formation of non-physiological CD95:FADD oligomers.
Nonetheless, we cannot rule out that in vivo, a local
decrease in the intracellular pH may affect the initial steps
of the CD95 signal by promoting the opening of the CD95-
DD, which in turn contributes to the formation of a com-
plex eliciting a sequence of events different from the one
occurring at physiologic pH.
Once docked on CD95-DD, FADD self-associates [28]
and binds and aggregates procaspases 8 and -10, which
are auto-processed and released in the cytosol as active
caspases that cleave many substrates leading to the exe-
cution of the apoptotic program and the death of the cell.
The complex CD95/FADD/Caspase-8/-10 is called DISC
for ‘‘death-inducing signaling complex’’ [29]. Due to the
importance of the DISC formation in the fate of the
cells, it is not surprising that numerous cellular and viral
proteins have been reported to negatively regulate the
formation of this structure, such as FLIP [30, 31] and
PED/PEA-15 [32] that interfere with the recruitment of
caspase-8/-10.
CD95 mutations
Patients exhibiting germinal mutations in APT-1, the gene
encoding the CD95 receptor, develop a syndrome termed
autoimmune lymphoproliferative syndrome type Ia (ALPS,
also called Canale–Smith syndrome) [33–35] (Table 1).
ALPS patients show chronic lymphadenopathy and
splenomegaly, expanded populations of double-negative
a/b T lymphocytes (CD3?CD4-CD8-) and often develop
autoimmunity [33, 34, 36, 37]. In agreement with the
notion that CD95 is a tumor suppressor gene, the ALPS
patients display an increased risk to develop Hodgkin and
non-Hodgkin lymphomas [38]. Predominance of post-ger-
minal center (GC) lymphomas in patients exhibiting either
germ line (Table 1) or somatic CD95 (Table 2) mutations
can be explained by the fact that firstly, inside germinal
centers of the secondary lymphoid follicles, the CD95
signal plays a pivotal role in the deletion of self-reactive
maturating B lymphocytes [39] and secondly, APT-1
belongs to a set of rare genes (i.e., PIM1, c-myc, PAX5,
RhoH/TTF, Bcl-6), which are subjected to somatic hyper-
mutation [40, 41] and thus accumulate mutations that at
one point, may alter their biological function. In addition to
post-GC lymphomas, significant amounts of mutations in
CD95 gene have been found in tumors from various his-
tological origins (summarized in Table 2). An extensive
analysis of the CD95 mutations and their distribution in
APT-1 confirms that with some exceptions, most of them
are gathered in exons 8 and 9 encoding the main part of the
CD95 intracellular region (Fig. 2) [42]. From a biological
standpoint, malignant and ALPS type Ia cells harboring a
heterozygous mutation inside the CD95-DD exhibit resis-
tance towards the CD95-mediated apoptotic signal. Indeed,
in agreement with the notion that CD95 is expressed at the
plasma membrane as a pre-associated oligomer (trimeric
complex) [22, 23], the formation of heterocomplexes
consisting of the association of wild-type with mutated
CD95 will hamper FADD recruitment and thus, will alter
the ignition of the apoptotic signal. Extensive analysis and
positioning of various CD95 mutations described in liter-
ature seem to highlight ‘‘hot-spots’’ of mutation in the
CD95 sequence (Tables 1, 2; Fig. 2a, b). Among these
‘‘hot-spots’’, it is worth noting that together arginine in
position 234, aspartic acid in position 244 and valine
in position 251, account for a significant amount of the
documented CD95 mutations. Indeed, among the 189
mutations annotated in the 335-length CD95 amino acid
sequence, 30 (*16%) are found localized on these three
amino acids (Fig. 2a, b). Strikingly, the pivotal role played
by these amino acids in the stabilization or formation of
CD95-mediated cell signaling in cancer 1263
123
Author's personal copy

Table 1 Germinal mutations in the APT1 gene
Mutations Diseases References Observations
1 Exon 3
Frameshift (-1)
Intron 3 and exon 7:
Splice variants
Exon 9
T225P
Q257X
ALPS Ia [34] Five unrelated ALPS patients
2 Exon 9
D253 (frameshift -2)
L290 (deletion of the last 29 a.a. replaced by YKLHQE)
ALPS Ia [35] Case report of three patients(one sibling and unrelatedpatient)
No surface expression of theL290 mutant
3 Exon 9
K230X (?1 frameshift)
D244Y (father and son)
R234X
ALPS Ia [33] Case report of four patients
4 Exon 1
T12A
Second allele displayed deletion between aa 41 and 96 and exon 6 (no TM)
ALPS Ia in a patient withtype 2 autoimmunehepatitis
[90] Mutation inside exon 1 anddeletion of a part of thePLAD domain
5 Exon 4
R105 W
Exon 9
Y216C
ALPS Ia [91] Autosomal recessive mutations
6 Exon 9
D244 V
ALPS Ia [92]
7 Exon 3
C66R
frameshift
R1X
C47X
Intron 7
S209X
Intron 8
S214X
Exon 9
R234P
D244G
D244Y
T254I
ALPS Ia [93] Cohort of 11 families.
Extracellular mutations (C66R/R1X/C47X) abolished theexpression of the mutatedCD95
8 Exon 3
E63X
Intron 7
splice variant
P201 frameshift
Exon 9
S214 frameshift (?2)
S227 frameshift (?4)
V233L
R234P
G237D
G237S
I243R
T254K
E256K
W265 frameshift
K280 frameshift (-1)
ALPS Ia [37]
1264 S. Tauzin et al.
123
Author's personal copy

Table 1 continued
Mutations Diseases References Observations
9 Intron 3
P49 splice variant
Exon 3
C57X
D62 frameshift (-1)
Intron 4
T131 splice variant
Intron 6
V174 splice variant
Exon 7
K181(del-11)
Intron 7
P201 splice variant
Exon 9
T225P
T225K
R234Q
R234P
A241D
D244V
Q257X
Q260X
L278X
I294S
ALPS Ia [46] Cohort of 155 families
60 Individuals harbor a CD95mutation.
17 different mutations.
Penetrance of one or moreALPS features was 88% forindividuals with intracellularmutations versus 18% forindividuals withextracellular mutations.
Exon 9 encompasses 59% ofmutations causing ALPS
10 Exon 7
K181 (del-11)
P201 frameshift
Exon 9
T225P
R234X
D244V
T254I
E256G
Hodgkin and non-HodgkinLymphomas associatedwith ALPS type Iapatients
[38, 94] Large-scale family case report.
223 members of 39 families,130 individuals possessedheterozygous germline Fasmutations. ALPS patientsdisplayed an increased riskof non-Hodgkin andHodgkin lymphomas (14and 51 times greater,respectively) as compared togeneral population
11 Exon 9
R234Q
ALPS type Ia/HodgkinLymphomas
[95] Family case report
12 Germline mutations (ALPS type Ia)
K181X
P201X
S214X
Somatic mutations (ALPS Type III)
W173X
P201X (3 cases)
S214X
D244V
ALPS Type Ia/Type III [96] Mutation originated inhematopoietic stem cells:6/6 in double negative Tcells from ALPS Type III
0/5 in healthy subjects
13 Exon 9
I246S
ALPS Ia [97]
14 Exon 3
H95R
Exon 7
E195X
Intron 7 (splice mutation/premature stop)
E202X (5 patients)
Exon 8
N207X (del-8)
L208X (del-2)
Exon 9
D244N
V204 (del-2)
D212X (del-5)
Autoimmunelymphoproliferativesyndrome (ALPS typeIII)
[98] 12/31 of double-negative Tcells displayed CD95mutations
CD95-mediated cell signaling in cancer 1265
123
Author's personal copy

Table 2 Somatic mutations in the APT1 gene
Mutations Diseases Mutation frequencies References Observations
1 Exon 9
Y275S
D253Y (2 patients)
K235R
N264H
Multiple myelomas Among 54 patients, 6 did notexpress CD95 and 5–48(10%) displayed mutation.
[99]
2 Exon 2
A(-1)T
Exon 4
C119 (?1) frameshift
Exon 6
L164F
P167L
Exon 7
T182I
L199X
Exon 8
L208X
Exon 9
D244V
N248K (2 patients)
E256K
L262F
K283N
Intron 7
splice variant
Intron 8
splice variant (2 patients)
Non-Hodgkin lymphomas 16/150 non-Hodgkinlymphomas (11%)
3/5 (60%) mucosa-associatedlymphoid tissue (MALT)-type lymphoma
9/43 (21%) diffuse LargeB-cell lymphomas
2/33 (6%) follicle centerlymphomas
1/2 (50%) anaplastic largecell lymphoma
1/17 (6%) B-chroniclymphocytic leukemia
0/5 Burkitt lymphoma
0/9 mantle cell lymphoma
0/35 peripheral T-celllymphoma
[100] Missense mutations withinexon 6 and 7 wereassociated with loss ofheterozygosity (LOH)
3 Exon 9
L213 (frameshift -20)
Adult T cell leukemia Found in an ATL cell line(designated KOB)
[101]
4 Exon 9
A241T
N250S
V251I
Cutaneous malignantmelanoma
3/44 (6.8%) [102] LOH for two patients
5 Exon 6
C162R (2 patients)
Exon 9
V251I (8 patients)
N237K
D244 (?1) stop in 245
Bladder carcinomas 12/43 (28%) [103] 11/12 mutations found inmuscle-invasivetransitional cellcarcinomas
Hotspot mutation in V251
6 Exon 9
I300Va
E323Xa
Hodgkin and Reed–Sternberg lymphomas
1/10 patients (10%) [104]
7 Exon 4
N102S
Exon 6
C162R
Exon 9
N239D
Squamous cell carcinoma 3/21 (14%) burn scar-relatedsquamous cell carcinomadisplayed mutated CD95.
2/6 (33%) with lymph nodemetastasis.
1/15 (7%) without metastasis.
0/50 conventional skinsquamous carcinoma
[105] Mutations are found inmetastatic lesions
1266 S. Tauzin et al.
123
Author's personal copy

Table 2 continued
Mutations Diseases Mutation frequencies References Observations
8 Exon 8
Splice variant (deletion codons202–210) 9 6 thyroid lymphoma (TL)and 2 chronic lymphocytic thyroiditis(CLTh)
Exon 9
Y216X
E240V
D244N
D244H
Frameshift exon 9 (?1 codon 285) (9 TLand 1 CLTh)
Thyroid lymphomas 17/26 thyroid lymphomas(65.4%) (consisting of 5/10diffuse large B-celllymphoma; 6/8 low-gradeMALT; 6/8 follicle centercell lymphomas)
3/11 Chronic lymphocyticthyroiditis (27.3%)
[106] Mutation hot-spots in thyroidlymphomas
9 Exon 2
K23R
Exon 3
G50S
Exon 5
D152X
Exon 6
V172A
Exon 9
V229A
284 (Insertion ?1) frameshift
Mucosa associatedlymphoid tissue(MALT)-typelymphomas
4/5 mucosa associatedlymphoid tissue (MALT)-type lymphomas
1/3 DLBLs
[107] Patients display more than 1mutation per gene
10 Exon 9
T254Ab
Q260X
Q260N
N286S
High-grade prostaticintraepithelial neoplasia(HGPIN) and prostaticcancer
4/27 of HGPIN (14.8%) [108]
11 Exon 9
N239D (2 patients)
E240G
D244V
R263H
Gastric cancers 5/43 (11%) [109]
12 Exon 9
D210G
A221G
N239S
H266L
K271M
D276G
I279V
I302V
Testicular germ cell tumor 9/24 patients (37.5%)
A total of 11 mutations werefound in 10 lesions fromthe 9 patients (3 silentmutations)
[110] All mutations in CD95 exon 9were associated with aloss-of-function
13 Exon 2
T24I
Exon 3
C69Y
Exon 4
E98G
Exon 7
Frameshift (-1) E195X
Exon 8
Frameshift (-1) I206X
Exon 9
T203P
Mycosis fungoide (MF)(cutaneous T-celllymphoma)
6/44 (13%) [111] The mutation in CD95 couldexplain the commonresistance of MF tochemotherapy
CD95-mediated cell signaling in cancer 1267
123
Author's personal copy

intra and inter-bridges between CD95 and FADD may
explain these ‘‘hot-spots’’ since for instance, both R234 and
D244 contribute to the homotypic aggregation of the
receptor and the FADD recruitment [24]. Nevertheless, the
observation of death domain ‘‘hot-spots’’ is in contradiction
with the study of Scott and colleagues [25] demonstrating
that the region of the CD95-DD interacting with the
FADD-DD spreads on a disperse surface through weak
binding affinities. Most ALPS type Ia patients affected by
malignancies do not undergo a loss of heterozygosity
(LOH), which let us to hypothesize that this heterozygous
configuration may promote carcinogenesis [43, 44]. Sup-
porting this assumption, we demonstrated that although
conservation of a wild-type allele failed to transmit the
apoptotic signal, it was sufficient and mandatory to elicit
non-apoptotic signals such as NF-jB, MAPK [43, 44],
whose inductions promote invasiveness of tumor cells
[42, 45]. Mutations found in the intracellular CD95-DD
exhibit a higher penetrance of the ALPS phenotype fea-
tures in mutation-bearing relatives than extracellular
mutations, which suggest that these latter mutants require
additional dysfunctions to efficiently abrogate the CD95-
mediated apoptotic signal [46]. Alternatively, it could be
tempting to speculate that in contrast to mutations inside
the death domain, other CD95 mutations somehow prevent
the apoptotic signal but fail to promote non-apoptotic ones,
which may contribute to the disease progression.
Plasma membrane and CD95 signal
In addition to down-regulation of CD95 or accumulation of
heterozygous mutations, the plasma membrane distribution
Table 2 continued
Mutations Diseases Mutation frequencies References Observations
14 Exon 4
C119 frameshift (-1)
Exon 6
S154 frameshift (-1)
Exon 9
A285 frameshift (?1) 2 cases
I246V
L287P
Nasal NK/T-cell lymphoma 7/14 (50%) [112] Insertion in polyA tract fromnucleotide 1,088–1,094(A285 frameshift):mutation hot spot
15 Exon 3
G66D
P84S
Exon 9
Q228X
N250S
Non-small cell lung cancer(NSCLC)
4/80 in NSCLC (5%)
3/43 (7%) in NSCLC withoutmetastasis.
1/37 (2%) in NSCLC withmetastasis
[113] All mutations found inNSCLC patients withmetastasis were onlydetected in the metastaticlesion
16 Exon 2
T27I
S3F
S16P
Intron 3
Splice variant
Intron 8
Splice variant
Exon 9
D244 N
Q260X
Mucosa associatedlymphoid tissue(MALT)-typelymphomas
7 mutations found in 5patients
1/18 (5.6%) Mucosaassociated lymphoid tissue(MALT) lymphomas
4/28 (14.3%) diffuse largeB-cell lymphoma(DLBCL)
[114] Mutations in exon 2 do notimpair the transmission ofthe CD95-mediatedapoptotic signal in T-47D(breast) and Jurkat(lymphocyte) cells
17 50UTR Diffuse large B celllymphomas (DLBCL)
3 of 66 [115]
18 RNA editing
Frame shift (?1)
K284 frameshift (?1)
Systemic lupuserythematosus (SLE)
Mutation accounted for 11%of CD95 cDNA clones inSLE patients and thefrequency of mutant cloneswas less than 1% inhealthy subjects
[116] Transcriptional mRNAediting. Not found in otherhuman death receptormRNAs such as DR5, DR6or TNF receptor 1(TNFR1) or in mouseCD95 mRNA
a Amino acid numbers have been modified according to the regular amino acid annotationb Threonine 256 depicted in this study corresponded in fact to amino acid 254
1268 S. Tauzin et al.
123
Author's personal copy

A
Y275FInternalization (Lee et al, EMBO J, 2006)
TM
Q257K(Beneteau et al, Cancer Research, 2007)
I297D
Open conformation (Scott et al, Nature, 2009)
Mutation/a.a.
CD95L interactions
1 2 3 4 5 6 7 8 9 1011121314
α 1
α 4
α 2
α 3
α 5
α 6
P201
E202
D244
V251
R234
A285
B
TM
Extracellular
Intracellular
Missense mutation
Nonsense mutation
Frameshift and splice variant.
Missense mutation
Nonsense mutation
Frameshift and splice variant.
Somatic
Germinal
Amino acids involved in the binding of CD95L (Starling et al, 1998)
Humanized Lprcg mutation(V238N)
TM
Q257K(Beneteau et al, Cancer Research, 2007)
Transmembrane region
Nucleotides in blue indicate α-helix constituting the CD95-DD
PS
Y275FInternalization (Lee et al, EMBO J, 2006)
I297D open conformationScott et al, Nature , 2009.
N-glycosylation sites (Shatnyeva et al, 2011)
1 5 10 15 1 5 10 15 20
atg ctg ggc atc tgg acc ctc cta cct ctg gtt ctt acg tct gtt gct aga tta tcg tcc aaa agt gtt aat gcc caa gtg act gac atc aac tcc aag gga ttg gaa ttg agg aag act
M L G I W T L L P L V L T S V A R L S S K S V N A Q V T D I N S K G L E L R K T
25 30 35 40 45 55 60
gtt act aca gtt gag act cag aac ttg gaa ggc ctg cat cat gat ggc caa ttc tgc cat aag ccc tgt cct cca ggt gaa agg aaa gct agg gac tgc aca gtc aat ggg gat gaa cca
V T T V E T Q N L E G L H H D G Q F C H K P C P P G E R K A R D C T V N G D E P
65 70 75 80 85 90 95 100
gac tgc gtg ccc tgc caa gaa ggg aag gag tac aca gac aaa gcc cat ttt tct tcc aaa tgc aga aga tgt aga ttg tgt gat gaa gga cat ggc tta gaa gtg gaa ata aac tgc acc
D C V P C Q E G K E Y T D K A H F S S K C R R C R L C D E G H G L E V E I N C T
105 110 115 120 125 130 135 140
cgg acc cag aat acc aag tgc aga tgt aaa cca aac ttt ttt tgt aac tct act gta tgt gaa cac tgt gac cct tgc acc aaa tgt gaa cat gga atc atc aag gaa tgc aca ctc acc
R T Q N T K C R C K P N F F C N S T V C E H C D P C T K C E H G I I K E C T L T
145 150 155 160 165 170 175 180
agc aac acc aag tgc aaa gag gaa gga tcc aga tct aac ttg ggg tgg ctt tgt ctt ctt ctt ttg cca att cca cta att gtt tgg gtg aag aga aag gaa gta cag aaa aca tgc aga
S N T K C K E E G S R S N L G W L C L L L L P I P L I V W V K R K E V Q K T C R
185 190 195 200 205 210 215 220
aag cac aga aag gaa aac caa ggt tct cat gaa tct cca acc tta aat cct gaa aca gtg gca ata aat tta tct gat gtt gac ttg agt aaa tat atc acc act att gct gga gtc atg
K H R K E N Q G S H E S P T L N P E T V A I N L S D V D L S K Y I T T I A G V M
α-1
225 230 235 240 245 250 255 260
aca cta agt caa gtt aaa ggc ttt gtt cga aag aat ggt gtc aat gaa gcc aaa ata gat gag atc aag aat gac aat gtc caa gac aca gca gaa cag aaa gtt caa ctg ctt cgt aat
T L S Q V K G F V R K N G V N E A K I D E I K N D N V Q D T A E Q K V Q L L R N
α-2 α-3 α-4
265 270 275 280 285 290 295 300
tgg cat caa ctt cat gga aag aaa gaa gcg tat gac aca ttg att aaa gat ctc aaa aaa gcc aat ctt tgt act ctt gca gag aaa att cag act atc atc ctc aag gac att act agt
W H Q L H G K K E A Y D T L I K D L K K A N L C T L A E K I Q T I I L K D I T S
850 860 870 880 890 900 910 920 930 940 950
α-5 α-6
305 310 315
gac tca gaa aat tca aac ttc aga aat gaa atc caa agc ttg gtc tag
D S E N S N F R N E I Q S L V *
970 980 990 1000
Fig. 2 Extensive analysis of the loss-of-function CD95 mutations.
a Mutations reported in Tables 1 and 2 have been placed in the
amino-acid sequence of CD95. The 6 a-helices constituting the death
domain and amino acids implicated either in the CD95/CD95L
interaction or the receptor glycosylation are depicted. b Schematic
distribution of CD95 mutations in the CD95 protein. The number of
mutations per amino acid is depicted on CD95 amino-acid sequence.
The death domain and its 6 a-helices are reported
CD95-mediated cell signaling in cancer 1269
123
Author's personal copy

of CD95 may also represent an alternative way for tumor
cells to circumvent the apoptotic signal. Indeed, plasma
membrane is a heterogeneous lipid bilayer comprising
compacted or ‘‘liquid-ordered’’ domains called microdo-
mains, lipid rafts or detergent resistant microdomains
(DRMs), which are described as floating in a more fluid or
liquid-disordered 2-D lipid bilayer. Despite the fact that the
composition and the kinetic of formation and disappear-
ance of these plasma membrane structures remain poorly
understood mostly due to limitation in the methodologies
used to characterize them, the lipid rafts play a crucial role
in the modulation of the initial steps induced by death
receptor signaling. For instance, it has been elegantly
reported that while CD95 is mostly excluded from lipid
rafts in activated T lymphocytes, the TCR-dependent re-
activation of these cells leads to the rapid distribution of
the death receptor into lipid rafts [47]. This CD95 com-
partmentalization is crucial to decrease in the apoptotic
threshold leading to the clonotypic elimination of activated
T-lymphocytes through activation of the CD95-mediated
apoptotic signal [47]. Similarly, the reorganization of
CD95 into DRMs can occur independently of its ligand
upon addition of certain chemotherapeutic drugs (e.g., rit-
uximab [48], resveratrol [49, 50], edelfosine [51–53],
aplidin [54], perifosine [53], cisplatin [55]). The intimate
molecular cascades that underlie this process remain to be
elucidated. Nevertheless, the current evidence lead us
to postulate that alteration of intracellular signaling
pathway(s) (e.g., the PI3K signal [51, 56]) may change
biophysical properties of the plasma membrane such as the
membrane fluidity, which may mimic the CD95L-induced
initial steps in promoting the aggregation and clustering of
CD95 into large lipid raft-enriched platforms, which in turn
favor DISC formation and the induction of the apoptotic
program [57]. On the other hand, these signaling pathways
may exert post-translational modifications of the death
receptor itself and thereby may promote or prevent its
redistribution into lipid rafts.
Regulation of the CD95 plasma membrane distribution
Plasma membrane distribution of CD95
Accumulation of CD95 mutations is not the only way by
which malignant cells may impede the extrinsic signaling
pathway elicited by immune cells or chemo- and radio-
therapeutic regimens. Post-translational modifications in
the intracellular tail of CD95 such as reversible oxidations
or covalent attachment of a palmitic acid have been
reported to alter the plasma membrane distribution of
CD95 and thereby its subsequent signaling pathway
(Fig. 3). For instance, S-glutathionylation of mouse CD95
at the cysteine residue 294 promotes the clustering of
CD95 and its distribution into lipid rafts [58] (Fig. 3). This
amino acid is conserved in the human CD95 sequence and
corresponds to cysteine residue at position 304 (C288 in
Internalization
Lipid Rafts
Palmitoylation
S-gluthationylation
α 1
α 4
α 2
α 3
α 5
α 6
P201
E202
D244
V251
R234
A285
TMIntracellular
C288
C183
Y275
S-nitrosylation
SDS-stable
Microaggregates
AP-2 Binding
DISC
NON-APOPTOTIC
SIGNALS (i.e., NFκκB, MAPK, PI3K)
APOPTOSIS
?
?
?
Extracellular
Fig. 3 Post-translational modifications and CD95 internalization.
The main mutations described in Tables 1 and 2 have been placed in
the amino-acid sequence of CD95. The 6 a-helices constituting the
death domain are depicted. CD95 internalization (AP-2 binding)
hampers the implementation of non-apoptotic signaling pathways
while it elicits apoptosis. Question marks indicate experiments that
remain to be conducted to decipher whether similarly to internaliza-
tion, CD95 palmitoylation, S-nitrosylation and S-glutathionylation
inhibit the CD95-mediated non-apoptotic outcomes. Black arrows
indicate activations; red lines (dashed and continuous) stand for
inhibitions
1270 S. Tauzin et al.
123
Author's personal copy

Figs. 2a, 3 whose numbering takes into consideration the
subtraction of the 16-amino acid peptide signal [2, 59]).
Interestingly, Janssen-Heininger Y.M. and colleagues [58]
emphasize that the death receptor glutathionylation occurs
downstream the activation of caspase-8 and -3 whose cat-
alytic activity processes and inhibits the thiol transferases
glutaredoxin 1 (Grx1), an enzyme implicated in the den-
itrosylation of proteins. The consequence of Grx1
inactivation is the accumulation of glutathionylated CD95,
which cluster into lipid rafts sensitizing cells to the CD95-
mediated apoptotic signal. Based on these findings and
counterintuitively, we conclude that caspase-8 activation
occurs prior to aggregation of CD95 and its redistribution
into lipid rafts, which both are mandatory to form the DISC
and subsequently to activate large amounts of caspase-8.
To conciliate these observations, activation of caspase-8
has been reported to occur in a two-step process. First, an
immediate and faint amount of activated caspase-8 (\1%)
is generated when CD95L interacts with CD95 that
orchestrates acid sphingomyelinase (ASM) activation,
ceramide production and CD95 clustering that second,
promote DISC formation and the outburst of caspase-8
processing essential to mount the apoptotic signal [60].
It is noteworthy that S-glutathionylation is not the only
oxidation modulating the CD95 activity. In this regard,
S-nitrosylation has also been reported to cause an augmen-
tation of the plasma membrane expression and the activity
of CD95 [61]. S-nitrosylation of cysteine residues 199
(corresponding to the residue C183 in Figs. 2a, 3) and 304
(C288) in colon and breast tumor cells leads to the redis-
tribution of CD95 into DRMs, the formation of the DISC
and the transmission of the apoptotic signal [61] (Fig. 3).
Two reports have brought to light that covalent coupling
of a 16-carbon fatty acid (palmitic acid) to cysteine residue
at position 199 (C183) elicits the redistribution of CD95
into DRMs, the formation of SDS-stable CD95 microag-
gregates, which resist to denaturing and reducing
treatments and the internalization of the receptor [62, 63]
(Fig. 3). These molecular steps remain to be more finely
ordered but they play critical role in the implementation of
the apoptotic signal (discussed below).
Of note, similarly to S-nitrosylation, both the afore-
mentioned S-glutathionylation at C304 (C288) and
palmitoylation at C199 (C183) promote the partition of
CD95 into lipid rafts and enhance the subsequent apoptotic
signal (Fig. 3). Further investigations addressing if these
post-translational modifications are redundant and occur
simultaneously in dying cells or if they are elicited in a cell
specific and/or in a micro-environmental-specific manner
would be of a great interest to better understand the
molecular mechanisms used by tumor cells to overcome
these post-translational alterations and thereby to resist to
the extrinsic signaling pathway.
Receptor endocytosis
Using an elegant magnetic method to isolate receptor-
containing endocytic vesicles, it has been shown that CD95
is promptly found associated with endosomal and lyso-
somal markers when incubated with an agonistic anti-
CD95 mAb [64]. In addition, expression of a CD95 mutant
in which the tyrosine 291 (Y275 in Figs. 2a, 3) is changed
to phenylalanine does not impinge on FADD binding but
compromises the CD95L-mediated CD95 internalization
occurring through an AP-2/clathrin-driven endocytic
pathway [64]. More strikingly, expression of the internal-
ization defective CD95 mutant (Y291F) abrogates the
transmission of the apoptotic signal while it fails to alter
the non-apoptotic signaling pathways (i.e., NF-jB and Erk)
and even promotes them (Fig. 3). Overall, these findings
provide insight into the presence in the death domain of a
region interacting with AP2 and promoting a clathrin-
dependent endocytic pathway in a FADD-independent
manner. Regarding the role of palmitoylation in the
receptor internalization, the interplay between lipid alter-
ation and AP2/clathrin-driven internalization of CD95
remains to be elucidated.
Implementation of a CD95-mediated non-apoptotic
signaling pathway
CD95L promotes carcinogenesis
Increase rate in malignancies after organ transplantation
represents the major cause of cancer-related mortality in
immunomodulated transplant recipients [65] and provides
the basis for the crucial role played by the immune system
in tumor surveillance. Since among the weapons set at
the disposal of immune cells, CD95L contributes to the
elimination of pre-tumoral cells, it is envisioned that pre-
tumoral cells escaping the immune surveillance will be
shaped to develop resistance to the CD95, a process that
has been termed immunoediting [66]. In other words, the
imprinting of the immune system on pre-tumoral cells
could ultimately select malignant cells with increased
resistance towards the CD95L-induced signal (e.g., down
modulating CD95, expressing dominant negative mutants
of CD95). As heterozygous ‘‘dominant negative’’ muta-
tions of CD95 prevent the CD95-mediated apoptotic signal
triggered by ‘‘weak agonistic’’ molecules such as agonistic
antibodies but do not abrogate the non-apoptotic signals
induced by highly aggregated CD95 ligand (e.g., mem-
brane-embedded CD95L) [67], it is conceivable that these
mutations may increase the apoptotic threshold enough to
switch the signal from apoptotic to non-apoptotic pathways
[44]. Apart from the classical inhibitory effect on apoptosis
CD95-mediated cell signaling in cancer 1271
123
Author's personal copy

exerted by the expression of a dominant-negative mutant of
CD95, which may be sufficient to account for carcino-
genesis, we propose that the switch in the CD95 signal (i.e.,
from apoptotic to non-apoptotic signaling pathway) could
account for malignancy progression. In agreement with this
hypothesis, complete loss of CD95 expression [68] and
LOH are rarely observed in malignant cells [42], which
thereby, are still capable to transmit the CD95-mediated
non-apoptotic signals when exposed to CD95L [44]. In this
regard, recent reports confirmed a role of the couple CD95/
CD95L in carcinogenesis through either the activation of
JNK (C-Jun kinase also called stress-activated protein
kinase) [19], NF-jB (nuclear factor-kappa B) [16] or PI3K
(phosphatidylinositol 3-kinase) [20]. Overall, these recent
studies do not rule out the pro-apoptotic function of the
‘‘death receptor’’ CD95 but they emphasize that in certain
pathophysiological contexts, CD95 engagement enables
the transmission of non-apoptotic and even pro-oncogenic
signaling pathways.
From a molecular standpoint, binding of the membrane-
bound CD95L or homemade generated crosslinked soluble
CD95L to CD95 evokes DISC formation building the
platform for the ignition of the apoptotic signal. On the
other hand, we and others recently observed that once
cleaved by metalloprotease, the soluble version of CD95L
(cl-CD95L) fails to induce DISC formation [17, 20] but it
orchestrates the infiltration and accumulation of activated T
lymphocytes in damaged organs of SLE patients through
the formation of a complex that we called the MISC for
motility inducing signaling complex [17]. This complex is
devoid of FADD and caspase-8/-10 but it encompasses the
c-yes src kinase, whose activity contributes to the activa-
tion of the PI3K signaling pathway [17, 20, 69]. These
studies do not only reveal a molecular link between the
‘‘death receptor’’ CD95 and the class I PI3Ks—p110c (also
known as PIK3CG) and d (PIK3CD) isoforms—in T cells
but they also revisit the biological role of CD95L whose
shedding by metalloproteases, frequently over-expressed in
the inflammatory areas, affects the initial events of the
CD95 signaling pathway.
Likewise, decrease in the plasma membrane level of
CD95 or expression of a mutated CD95 allele as observed
in ALPS patients (Table 1) and various malignant cells
(Table 2) impedes the implementation of the apoptotic
signal but does not affect the transmission of non-apoptotic
signals such as NF-jB, MAPK and PI3K [19, 43, 44]
suggesting that these signals stem from different domains
of CD95 or rely on different thresholds to be elicited. One
important question that remains to be addressed is how the
magnitude of the CD95 aggregation controls the formation
of ‘‘death’’- and/or ‘‘motility’’-ISCs. In other words,
although it is well-accepted that the couple CD95/CD95L
can eliminate malignant cells by the implementation of the
DISC or can promote carcinogenesis by fueling inflam-
mation and/or by inducing metastatic dissemination [15–
20, 45], the molecular mechanism(s) underlying the switch
between these different signaling pathways remains enig-
matic. Addressing this question will bring to light new
therapeutical agents able to contain the spreading of
inflammation or to impede carcinogenesis mechanisms at
least in pathologies in which increase in soluble CD95L
amounts has been reported such as cancers (e.g., pancreatic
cancers [70], large granular lymphocytic leukemia and
natural killer cell lymphoma [71]) or autoimmune disorders
(e.g., rheumatoid arthritis and osteoarthritis [72], graft
versus host disease (GVDH) [73, 74] or SLE patients
[17, 75]).
CD95L stoichiometries elicit different cell signaling
pathways
CD95L is a type II transmembrane protein (carboxy-
terminal extracellular region), which belongs to the TNF
(tumor necrosis factor) family. As aforementioned, CD95L
is mainly found at the surface of immune cells where it
contributes to the elimination of infected or transformed
cells through cell-to-cell contact. CD95L is also detected
on macrophages and dendritic cells upon HIV infection
[76] and on surface of epithelial cells in inflammatory
disorders [77]. It is noteworthy that CD95L can be cleaved
by metalloproteases such as MMP3 [78], MMP7 [79],
MMP9 [80] and ADAM-10 (A disintegrin and metallo-
proteinase 10) [81, 82] and shed from the plasma
membrane to be released in the connective tissue and the
bloodstream as a soluble and homotrimeric ligand. Seminal
studies on the metalloprotease-cleaved CD95L have
revealed that this ligand exhibits a homotrimeric stoichi-
ometry [83, 84]. Considering that hexameric CD95L
represents the minimal stoichiometry required to signal
apoptosis [83], the cleaved form of CD95L (cl-CD95L) has
long been considered as an inert ligand competing with its
membrane-bound counterpart (m-CD95L) to antagonize
the transmission of the apoptotic signal [84, 85].
Strikingly, while the soluble form of CD95L generated
by MMP7 (cleavage site inside the 113ELR115 sequence,
Fig. 4) induces apoptosis [79], its counterpart processed
between the serine126 and the leucine127 does not [16, 17,
84]. To explain this discrepancy, one may postulate that the
different quaternary structures of the naturally processed
CD95L underlie the implementation of ‘‘death’’ or ‘‘non-
death’’-inducing signaling complex and their downstream
signals. In agreement with this notion, it has been reported
that soluble CD95L bathed in bronchoalveolar lavages
(BALs) of patients suffering from acute respiratory distress
syndrome (ARDS) undergoes oxidation of two methionine
residues in position 224 and 225 of CD95L (Fig. 4) that
1272 S. Tauzin et al.
123
Author's personal copy

enhances the aggregation level of the soluble ligand and
thus its cytotoxic activity [86]. The same authors observed
that the stalk region of CD95L corresponding to amino
acids 103–136 and encompassing the metalloprotease
cleavage sites (Fig. 4) is also instrumental in the multi-
merization of CD95L, which accounts for the damage of
lung epithelium in ARDS patients [86]. Of note, in the
ARDS BALs an additional oxidation occurs at methionine
121 (Fig. 4), which in turn prevents the processing of
CD95L by MMP7 and explains why this cytotoxic ligand
keeps its stalk region [86]. Nonetheless, preservation of this
region in soluble CD95L raises the question if a yet
unidentified MMP7-independent cleavage site exists in
the juxtamembrane region of CD95L, near the plasma
membrane, or if the ligand detected in ARDS patients
corresponds in fact to a full length CD95L embedded in
exosomes [87, 88]. Indeed, this peculiar exosome-bound
CD95L can be expressed by human prostate cancer cells
(i.e., LNCaP) and evokes apoptosis in activated T lym-
phocytes [89].
Although the soluble CD95L cleaved between its ser-
ine126 and leucine127 exhibits no apoptotic activity, this
cytokine fueled inflammation and auto-immunity both in a
lupus-prone mouse model [16] and in systemic lupus ery-
thematosus (SLE) patients [17]. Recent findings on CD95L
emphasize that it may be of a great interest in the future to
finely characterize the quaternary structure of the naturally
processed CD95L found increased in sera of patients
affected by cancers or chronic/acute inflammatory disor-
ders to better comprehend the molecular mechanism
engaged by the ligand and its subsequent biological
functions.
Overall, these results indicate that instead of a mono-
lithic and apoptotic function for the couple CD95/CD95L,
the ratio of transmembrane versus cleaved CD95L or the
plasma membrane amounts of functional CD95 may
account for the induction of apoptotic or non-apoptotic
signals and that way, may favor elimination of transformed
cells or promote carcinogenesis, respectively.
Conclusions
The cellular response to CD95 relies on its expression
level, its alteration by post-translational modifications, the
presence or absence of heterozygous mutations and/or the
stoichiometry of the exposed ligand. However, altogether
these features are not sufficient to foresee the main signal
transmitted by CD95. Fifteen years ago, Stuart and col-
leagues already reported that ‘‘immune privilege’’ does not
only result from the expression of CD95L on epithelial and
endothelial corneal cells but also relies on the site itself in
which the CD95L-expressing cells are transplanted.
Indeed, although transplanted corneas display high rate of
acceptance in the eye, allogeneic corneas grafted hetero-
topically to the skin are rapidly rejected [8]. Likewise, the
group of Nabel shed light on the role of TGF-b in the
CD95-mediated recruitment of neutrophils and thus
strengthened the biological effect of the microenvironment
in the modulation of the CD95 signal [14]. We recently
ascertained that the epithelial-mesenchymal transition
(EMT) causes resistance of tumor cells towards the CD95-
mediated apoptotic signal [68]. Indeed, while tumor cells
displaying an epithelial-like signature were sensitive to the
139
CD95-interacting amino-acids
1 28182 102
TM
QLFHLQKELAELRESTSQMHTASSLEKQIGHPSS-RGS
hCD95L
110
P206 Y218 F275L (gld like)
1
MMP3/7/9 & ADAM10
Self
Assembly Domain
137 - 183
Cleavage sites:
120 130103
STALK REGION
oxidation 2 3
YPQDLVMMEGK218
oxidation
Cis-interaction
Fig. 4 Human CD95L protein structure. Different domains (CD95L
self-assembly/CD95 binding sites/Stalk region) of the type II protein
CD95L are depicted in this scheme. In the stalk region, the amino
acids corresponding to the metalloprotease cleavage sites are depicted
in red. Three targets of oxidation (i.e., methionine) are reported and
their role on the CD95L structure is indicated
CD95-mediated cell signaling in cancer 1273
123
Author's personal copy

CD95 signal, the mesenchymal malignant cells resisted to
the transmission of the apoptotic-signaling pathway
through a yet totally unknown process. As TGF-b is the
prototype cytokine contributing to EMT process, it may
correspond to the principal micro-environmental factor,
whose tissue concentration accounts for the CD95 response
both in malignant cells and in innate immune cells. Hith-
erto, it remains to decipher whether the presence of TGF-b
will elicit the expression of factors that hinders the trans-
mission of the CD95 apoptotic signal and promotes the
non-apoptotic signal and/or whether TGF-b will circum-
vent the apoptotic signal and promotes pro-oncogenic
signaling pathways by directly acting on the CD95
expression level and/or the mechanisms of CD95L
cleavage.
Acknowledgments This work was supported by Grants from ANR
(JC07_183182), INCa (projets libres recherche biomedicale), Region
Bretagne, Rennes Metropole and Ligue Contre le Cancer (Comites
d’Ille-et-Vilaine, Comite du Morbihan, Comites de la Dordogne,
Comites des Pyrenees-Atlantiques). S.T. is supported by Ligue Contre
le Cancer (postdoctoral fellowships).
References
1. Behrmann I, Walczak H, Krammer PH (1994) Structure of the
human APO-1 gene. Eur J Immunol 24:3057–3062
2. Itoh N, Yonehara S, Ishii A, Yonehara M, Mizushima S,
Sameshima M, Hase A, Seto Y, Nagata S (1991) The poly-
peptide encoded by the cDNA for human cell surface antigen
Fas can mediate apoptosis. Cell 66:233–243
3. Trauth BC, Klas C, Peters AM, Matzku S, Moller P, Falk W,
Debatin KM, Krammer PH (1989) Monoclonal antibody-medi-
ated tumor regression by induction of apoptosis. Science
245:301–305
4. Takahashi T, Tanaka M, Brannan CI, Jenkins NA, Copeland
NG, Suda T, Nagata S (1994) Generalized lymphoproliferative
disease in mice, caused by a point mutation in the Fas ligand.
Cell 76:969–976
5. Montel AH, Bochan MR, Hobbs JA, Lynch DH, Brahmi Z
(1995) Fas involvement in cytotoxicity mediated by human NK
cells. Cell Immunol 166:236–246
6. Saas P, Walker PR, Hahne M, Quiquerez AL, Schnuriger V,
Perrin G, French L, Van Meir EG, de Tribolet N, Tschopp J,
Dietrich PY (1997) Fas ligand expression by astrocytoma in
vivo: maintaining immune privilege in the brain? J Clin Invest
99:1173–1178
7. Griffith TS, Brunner T, Fletcher SM, Green DR, Ferguson TA
(1995) Fas ligand-induced apoptosis as a mechanism of immune
privilege. Science 270:1189–1192
8. Stuart PM, Griffith TS, Usui N, Pepose J, Yu X, Ferguson TA
(1997) CD95 ligand (FasL)-induced apoptosis is necessary for
corneal allograft survival. J Clin Invest 99:396–402
9. Bellgrau D, Gold D, Selawry H, Moore J, Franzusoff A, Duke
RC (1995) A role for CD95 ligand in preventing graft rejection.
Nature 377:630–632
10. Hahne M, Rimoldi D, Schroter M, Romero P, Schreier M,
French LE, Schneider P, Bornand T, Fontana A, Lienard D,
Cerottini J, Tschopp J, Tschopp J (1996) Melanoma cell
expression of Fas(Apo-1/CD95) ligand: implications for tumor
immune escape. Science 274:1363–1366
11. O’Connell J, O’Sullivan GC, Collins JK, Shanahan F (1996) The
Fas counterattack: Fas-mediated T cell killing by colon cancer
cells expressing Fas ligand. J Exp Med 184:1075–1082
12. Allison J, Georgiou HM, Strasser A, Vaux DL (1997) Trans-
genic expression of CD95 ligand on islet beta cells induces a
granulocytic infiltration but does not confer immune privilege
upon islet allografts. Proc Natl Acad Sci USA 94:3943–3947
13. Kang SM, Schneider DB, Lin Z, Hanahan D, Dichek DA, Stock
PG, Baekkeskov S (1997) Fas ligand expression in islets of
Langerhans does not confer immune privilege and instead tar-
gets them for rapid destruction. Nat Med 3:738–743
14. Chen JJ, Sun Y, Nabel GJ (1998) Regulation of the proinflam-
matory effects of Fas ligand (CD95L). Science 282:1714–1717
15. Letellier E, Kumar S, Sancho-Martinez I, Krauth S, Funke-
Kaiser A, Laudenklos S, Konecki K, Klussmann S, Corsini NS,
Kleber S, Drost N, Neumann A, Levi-Strauss M, Brors B, Gretz
N, Edler L, Fischer C, Hill O, Thiemann M, Biglari B, Karray S,
Martin-Villalba A (2010) CD95-ligand on peripheral myeloid
cells activates Syk kinase to trigger their recruitment to the
inflammatory site. Immunity 32:240–252
16. O’Reilly LA, Tai L, Lee L, Kruse EA, Grabow S, Fairlie WD,
Haynes NM, Tarlinton DM, Zhang JG, Belz GT, Smyth MJ,
Bouillet P, Robb L, Strasser A (2009) Membrane-bound Fas
ligand only is essential for Fas-induced apoptosis. Nature
461:659–663
17. Tauzin S, Chaigne-Delalande B, Selva E, Khadra N, Daburon S,
Contin-Bordes C, Blanco P, Le Seyec J, Ducret T, Counillon L,
Moreau JF, Hofman P, Vacher P, Legembre P (2011) The nat-
urally processed CD95L elicits a c-yes/calcium/PI3K-driven cell
migration pathway. PLoS Biol 9:e1001090
18. Bivona TG, Hieronymus H, Parker J, Chang K, Taron M, Rosell
R, Moonsamy P, Dahlman K, Miller VA, Costa C, Hannon G,
Sawyers CL (2011) FAS and NF-kappaB signalling modulate
dependence of lung cancers on mutant EGFR. Nature
471:523–526
19. Chen L, Park SM, Tumanov AV, Hau A, Sawada K, Feig C,
Turner JR, Fu YX, Romero IL, Lengyel E, Peter ME (2010)
CD95 promotes tumour growth. Nature 465:492–496
20. Kleber S, Sancho-Martinez I, Wiestler B, Beisel A, Gieffers C,
Hill O, Thiemann M, Mueller W, Sykora J, Kuhn A, Schregl-
mann N, Letellier E, Zuliani C, Klussmann S, Teodorczyk M,
Grone HJ, Ganten TM, Sultmann H, Tuttenberg J, von Deimling
A, Regnier-Vigouroux A, Herold-Mende C, Martin-Villalba A
(2008) Yes and PI3K bind CD95 to signal invasion of glio-
blastoma. Cancer Cell 13:235–248
21. Chan FK, Chun HJ, Zheng L, Siegel RM, Bui KL, Lenardo MJ
(2000) A domain in TNF receptors that mediates ligand-inde-
pendent receptor assembly and signaling. Science 288:2351–
2354
22. Papoff G, Hausler P, Eramo A, Pagano MG, Di Leve G, Signore
A, Ruberti G (1999) Identification and characterization of a
ligand-independent oligomerization domain in the extracellular
region of the CD95 death receptor. J Biol Chem 274:38241–
38250
23. Siegel RM, Frederiksen JK, Zacharias DA, Chan FK, Johnson
M, Lynch D, Tsien RY, Lenardo MJ (2000) Fas preassociation
required for apoptosis signaling and dominant inhibition by
pathogenic mutations. Science 288:2354–2357
24. Huang B, Eberstadt M, Olejniczak ET, Meadows RP, Fesik SW
(1996) NMR structure and mutagenesis of the Fas (APO-1/
CD95) death domain. Nature 384:638–641
25. Scott FL, Stec B, Pop C, Dobaczewska MK, Lee JJ, Monosov E,
Robinson H, Salvesen GS, Schwarzenbacher R, Riedl SJ (2009)
1274 S. Tauzin et al.
123
Author's personal copy

The Fas-FADD death domain complex structure unravels sig-
nalling by receptor clustering. Nature 457:1019–1022
26. Esposito D, Sankar A, Morgner N, Robinson CV, Rittinger K,
Driscoll PC (2010) Solution NMR investigation of the CD95/
FADD homotypic death domain complex suggests lack of
engagement of the CD95 C terminus. Structure 18:1378–1390
27. Wang L, Yang JK, Kabaleeswaran V, Rice AJ, Cruz AC, Park
AY, Yin Q, Damko E, Jang SB, Raunser S, Robinson CV, Siegel
RM, Walz T, Wu H (2010) The Fas-FADD death domain
complex structure reveals the basis of DISC assembly and dis-
ease mutations. Nat Struct Mol Biol 17:1324–1329
28. Muppidi JR, Lobito AA, Ramaswamy M, Yang JK, Wang L,
Wu H, Siegel RM (2006) Homotypic FADD interactions
through a conserved RXDLL motif are required for death
receptor-induced apoptosis. Cell Death Differ 13:1641–1650
29. Kischkel FC, Hellbardt S, Behrmann I, Germer M, Pawlita M,
Krammer PH, Peter ME (1995) Cytotoxicity-dependent APO-1
(Fas/CD95)-associated proteins form a death-inducing signaling
complex (DISC) with the receptor. EMBO J 14:5579–5588
30. Irmler M, Thome M, Hahne M, Schneider P, Hofmann K,
Steiner V, Bodmer JL, Schroter M, Burns K, Mattmann C,
Rimoldi D, French LE, Tschopp J (1997) Inhibition of death
receptor signals by cellular FLIP. Nature 388:190–195
31. Thome M, Schneider P, Hofmann K, Fickenscher H, Meinl E,
Neipel F, Mattmann C, Burns K, Bodmer JL, Schroter M,
Scaffidi C, Krammer PH, Peter ME, Tschopp J (1997) Viral
FLICE-inhibitory proteins (FLIPs) prevent apoptosis induced by
death receptors. Nature 386:517–521
32. Condorelli G, Vigliotta G, Cafieri A, Trencia A, Andalo P,
Oriente F, Miele C, Caruso M, Formisano P, Beguinot F (1999)
PED/PEA-15: an anti-apoptotic molecule that regulates FAS/
TNFR1-induced apoptosis. Oncogene 18:4409–4415
33. Drappa J, Vaishnaw AK, Sullivan KE, Chu JL, Elkon KB (1996)
Fas gene mutations in the Canale–Smith syndrome an inherited
lymphoproliferative disorder associated with autoimmunity.
N Engl J Med 335:1643–1649
34. Fisher GH, Rosenberg FJ, Straus SE, Dale JK, Middleton LA,
Lin AY, Strober W, Lenardo MJ, Puck JM (1995) Dominant
interfering Fas gene mutations impair apoptosis in a human
autoimmune lymphoproliferative syndrome. Cell 81:935–946
35. Rieux-Laucat F, Le Deist F, Hivroz C, Roberts IA, Debatin KM,
Fischer A, de Villartay JP (1995) Mutations in Fas associated
with human lymphoproliferative syndrome and autoimmunity.
Science 268:1347–1349
36. Canale VC, Smith CH (1967) Chronic lymphadenopathy simu-
lating malignant lymphoma. J Pediatr 70:891–899
37. Rieux-Laucat F, Blachere S, Danielan S, De Villartay JP,
Oleastro M, Solary E, Bader-Meunier B, Arkwright P, Pondare
C, Bernaudin F, Chapel H, Nielsen S, Berrah M, Fischer A,
Le Deist F (1999) Lymphoproliferative syndrome with auto-
immunity: a possible genetic basis for dominant expression of
the clinical manifestations. Blood 94:2575–2582
38. Straus SE, Jaffe ES, Puck JM, Dale JK, Elkon KB, Rosen-Wolff
A, Peters AM, Sneller MC, Hallahan CW, Wang J, Fischer RE,
Jackson CM, Lin AY, Baumler C, Siegert E, Marx A, Vaishnaw
AK, Grodzicky T, Fleisher TA, Lenardo MJ (2001) The
development of lymphomas in families with autoimmune lym-
phoproliferative syndrome with germline Fas mutations and
defective lymphocyte apoptosis. Blood 98:194–200
39. Hennino A, Berard M, Krammer PH, Defrance T (2001) FLICE-
inhibitory protein is a key regulator of germinal center B cell
apoptosis. J Exp Med 193:447–458
40. Montesinos-Rongen M, Van Roost D, Schaller C, Wiestler OD,
Deckert M (2004) Primary diffuse large B-cell lymphomas of
the central nervous system are targeted by aberrant somatic
hypermutation. Blood 103:1869–1875
41. Muschen M, Rajewsky K, Kronke M, Kuppers R (2002) The
origin of CD95-gene mutations in B-cell lymphoma. Trends
Immunol 23:75–80
42. Peter ME, Legembre P, Barnhart BC (2005) Does CD95 have
tumor promoting activities? Biochim Biophys Acta 1755:25–36
43. Legembre P, Barnhart BC, Peter ME (2004) The relevance of
NF-kappaB for CD95 signaling in tumor cells. Cell Cycle
3:1235–1239
44. Legembre P, Barnhart BC, Zheng L, Vijayan S, Straus SE, Puck
J, Dale JK, Lenardo M, Peter ME (2004) Induction of apoptosis
and activation of NF-kappaB by CD95 require different sig-
nalling thresholds. EMBO Rep 5:1084–1089
45. Barnhart BC, Legembre P, Pietras E, Bubici C, Franzoso G,
Peter ME (2004) CD95 ligand induces motility and invasiveness
of apoptosis-resistant tumor cells. EMBO J 23:3175–3185
46. Jackson CE, Fischer RE, Hsu AP, Anderson SM, Choi Y, Wang
J, Dale JK, Fleisher TA, Middelton LA, Sneller MC, Lenardo
MJ, Straus SE, Puck JM (1999) Autoimmune lymphoprolifera-
tive syndrome with defective Fas: genotype influences
penetrance. Am J Hum Genet 64:1002–1014
47. Muppidi JR, Siegel RM (2004) Ligand-independent redistribu-
tion of Fas (CD95) into lipid rafts mediates clonotypic T cell
death. Nat Immunol 5:182–189
48. Stel AJ, Ten Cate B, Jacobs S, Kok JW, Spierings DC, Dondorff
M, Helfrich W, Kluin-Nelemans HC, de Leij LF, Withoff S,
Kroesen BJ (2007) Fas receptor clustering and involvement of
the death receptor pathway in rituximab-mediated apoptosis
with concomitant sensitization of lymphoma B cells to fas-
induced apoptosis. J Immunol 178:2287–2295
49. Delmas D, Rebe C, Lacour S, Filomenko R, Athias A, Gambert
P, Cherkaoui-Malki M, Jannin B, Dubrez-Daloz L, Latruffe N,
Solary E (2003) Resveratrol-induced apoptosis is associated
with Fas redistribution in the rafts and the formation of a death-
inducing signaling complex in colon cancer cells. J Biol Chem
278:41482–41490
50. Delmas D, Rebe C, Micheau O, Athias A, Gambert P, Grazide S,
Laurent G, Latruffe N, Solary E (2004) Redistribution of CD95,
DR4 and DR5 in rafts accounts for the synergistic toxicity of
resveratrol and death receptor ligands in colon carcinoma cells.
Oncogene 23:8979–8986
51. Beneteau M, Pizon M, Chaigne-Delalande B, Daburon S,
Moreau P, De Giorgi F, Ichas F, Rebillard A, Dimanche-Boitrel
MT, Taupin JL, Moreau JF, Legembre P (2008) Localization of
Fas/CD95 into the lipid rafts on down-modulation of the phos-
phatidylinositol 3-kinase signaling pathway. Mol Cancer Res
MCR 6:604–613
52. Gajate C, Del Canto-Janez E, Acuna AU, Amat-Guerri F, Geijo
E, Santos-Beneit AM, Veldman RJ, Mollinedo F (2004) Intra-
cellular triggering of Fas aggregation and recruitment of
apoptotic molecules into Fas-enriched rafts in selective tumor
cell apoptosis. J Exp Med 200:353–365
53. Gajate C, Mollinedo F (2007) Edelfosine and perifosine induce
selective apoptosis in multiple myeloma by recruitment of death
receptors and downstream signaling molecules into lipid rafts.
Blood 109:711–719
54. Gajate C, Mollinedo F (2005) Cytoskeleton-mediated death
receptor and ligand concentration in lipid rafts forms apoptosis-
promoting clusters in cancer chemotherapy. J Biol Chem
280:11641–11647
55. Lacour S, Hammann A, Grazide S, Lagadic-Gossmann D,
Athias A, Sergent O, Laurent G, Gambert P, Solary E, Diman-
che-Boitrel MT (2004) Cisplatin-induced CD95 redistribution
into membrane lipid rafts of HT29 human colon cancer cells.
Cancer Res 64:3593–3598
56. Pizon M, Rampanarivo H, Tauzin S, Chaigne-Delalande B,
Daburon S, Castroviejo M, Moreau P, Moreau JF, Legembre P
CD95-mediated cell signaling in cancer 1275
123
Author's personal copy

(2011) Actin-independent exclusion of CD95 by PI3K/AKT
signalling: implications for apoptosis. Eur J Immunol 41:2368–
2378
57. Segui B, Legembre P (2010) Redistribution of CD95 into the
lipid rafts to treat cancer cells? Recent Pat Anticancer Drug
Discov 5:22–28
58. Anathy V, Aesif SW, Guala AS, Havermans M, Reynaert NL, Ho
YS, Budd RC, Janssen-Heininger YM (2009) Redox amplifica-
tion of apoptosis by caspase-dependent cleavage of glutaredoxin
1 and S-glutathionylation of Fas. J Cell Biol 184:241–252
59. Oehm A, Behrmann I, Falk W, Pawlita M, Maier G, Klas C,
Li-Weber M, Richards S, Dhein J, Trauth BC et al (1992)
Purification and molecular cloning of the APO-1 cell surface
antigen, a member of the tumor necrosis factor/nerve growth
factor receptor superfamily. Sequence identity with the Fas
antigen. J Biol Chem 267:10709–10715
60. Grassme H, Cremesti A, Kolesnick R, Gulbins E (2003) Cera-
mide-mediated clustering is required for CD95-DISC formation.
Oncogene 22:5457–5470
61. Leon-Bollotte L, Subramaniam S, Cauvard O, Plenchette-Colas
S, Paul C, Godard C, Martinez-Ruiz A, Legembre P, Jeannin JF,
Bettaieb A (2011) S-nitrosylation of the death receptor fas
promotes fas ligand-mediated apoptosis in cancer cells. Gas-
troenterology 140:2009–2018 2018 e2001–2004
62. Chakrabandhu K, Herincs Z, Huault S, Dost B, Peng L,
Conchonaud F, Marguet D, He HT, Hueber AO (2007) Palmi-
toylation is required for efficient Fas cell death signaling.
EMBO J 26:209–220
63. Feig C, Tchikov V, Schutze S, Peter ME (2007) Palmitoylation
of CD95 facilitates formation of SDS-stable receptor aggregates
that initiate apoptosis signaling. EMBO J 26:221–231
64. Lee KH, Feig C, Tchikov V, Schickel R, Hallas C, Schutze S,
Peter ME, Chan AC (2006) The role of receptor internalization
in CD95 signaling. EMBO J 25:1009–1023
65. Buell JF, Gross TG, Woodle ES (2005) Malignancy after
transplantation. Transplantation 80:S254–S264
66. Bui JD, Schreiber RD (2007) Cancer immunosurveillance,
immunoediting and inflammation: independent or interdepen-
dent processes? Curr Opin Immunol 19:203–208
67. Beneteau M, Daburon S, Moreau JF, Taupin JL, Legembre P
(2007) Dominant-negative Fas mutation is reversed by down-
expression of c-FLIP. Cancer Res 67:108–115
68. Algeciras-Schimnich A, Pietras EM, Barnhart BC, Legembre P,
Vijayan S, Holbeck SL, Peter ME (2003) Two CD95 tumor
classes with different sensitivities to antitumor drugs. Proc Natl
Acad Sci USA 100:11445–11450
69. Corsini NS, Sancho-Martinez I, Laudenklos S, Glagow D,
Kumar S, Letellier E, Koch P, Teodorczyk M, Kleber S,
Klussmann S, Wiestler B, Brustle O, Mueller W, Gieffers C,
Hill O, Thiemann M, Seedorf M, Gretz N, Sprengel R, Celikel
T, Martin-Villalba A (2009) The death receptor CD95 activates
adult neural stem cells for working memory formation and brain
repair. Cell Stem Cell 5:178–190
70. Bellone G, Smirne C, Carbone A, Mareschi K, Dughera L,
Farina EC, Alabiso O, Valente G, Emanuelli G, Rodeck U
(2000) Production and pro-apoptotic activity of soluble CD95
ligand in pancreatic carcinoma. Clin Cancer Res 6:2448–2455
71. Tanaka M, Suda T, Haze K, Nakamura N, Sato K, Kimura F,
Motoyoshi K, Mizuki M, Tagawa S, Ohga S, Hatake K,
Drummond AH, Nagata S (1996) Fas ligand in human serum.
Nat Med 2:317–322
72. Hashimoto H, Tanaka M, Suda T, Tomita T, Hayashida K,
Takeuchi E, Kaneko M, Takano H, Nagata S, Ochi T (1998)
Soluble Fas ligand in the joints of patients with rheumatoid
arthritis and osteoarthritis. Arthritis Rheum 41:657–662
73. Das H, Imoto S, Murayama T, Kajimoto K, Sugimoto T, Isobe
T, Nakagawa T, Nishimura R, Koizumi T (1999) Levels of
soluble FasL and FasL gene expression during the development
of graft-versus-host disease in DLT-treated patients. Br J Hae-
matol 104:795–800
74. Kanda Y, Tanaka Y, Shirakawa K, Yatomi T, Nakamura N,
Kami M, Saito T, Izutsu K, Asai T, Yuji K, Ogawa S, Honda H,
Mitani K, Chiba S, Yazaki Y, Hirai H (1998) Increased soluble
Fas-ligand in sera of bone marrow transplant recipients with
acute graft-versus-host disease. Bone Marrow Transplant
22:751–754
75. Tomokuni A, Otsuki T, Isozaki Y, Kita S, Ueki H, Kusaka M,
Kishimoto T, Ueki A (1999) Serum levels of soluble Fas ligand
in patients with silicosis. Clin Exp Immunol 118:441–444
76. Strauss G, Lindquist JA, Arhel N, Felder E, Karl S, Haas TL,
Fulda S, Walczak H, Kirchhoff F, Debatin KM (2009) CD95
co-stimulation blocks activation of naive T cells by inhibiting T
cell receptor signaling. J Exp Med 206:1379–1393
77. Le’Negrate G, Selva E, Auberger P, Rossi B, Hofman P (2000)
Sustained polymorphonuclear leukocyte transmigration induces
apoptosis in T84 intestinal epithelial cells. J Cell Biol 150:1479–
1488
78. Matsuno H, Yudoh K, Watanabe Y, Nakazawa F, Aono H,
Kimura T (2001) Stromelysin-1 (MMP-3) in synovial fluid of
patients with rheumatoid arthritis has potential to cleave mem-
brane bound Fas ligand. J Rheumatol 28:22–28
79. Vargo-Gogola T, Crawford HC, Fingleton B, Matrisian LM
(2002) Identification of novel matrix metalloproteinase-7 (ma-
trilysin) cleavage sites in murine and human Fas ligand. Arch
Biochem Biophys 408:155–161
80. Kiaei M, Kipiani K, Calingasan NY, Wille E, Chen J, Heissig B,
Rafii S, Lorenzl S, Beal MF (2007) Matrix metalloproteinase-9
regulates TNF-alpha and FasL expression in neuronal, glial cells
and its absence extends life in a transgenic mouse model of
amyotrophic lateral sclerosis. Exp Neurol 205:74–81
81. Kirkin V, Cahuzac N, Guardiola-Serrano F, Huault S, Luckerath
K, Friedmann E, Novac N, Wels WS, Martoglio B, Hueber AO,
Zornig M (2007) The Fas ligand intracellular domain is released
by ADAM10 and SPPL2a cleavage in T-cells. Cell Death Differ
14:1678–1687
82. Schulte M, Reiss K, Lettau M, Maretzky T, Ludwig A,
Hartmann D, de Strooper B, Janssen O, Saftig P (2007)
ADAM10 regulates FasL cell surface expression and modulates
FasL-induced cytotoxicity and activation-induced cell death.
Cell Death Differ 14:1040–1049
83. Holler N, Tardivel A, Kovacsovics-Bankowski M, Hertig S,
Gaide O, Martinon F, Tinel A, Deperthes D, Calderara S,
Schulthess T, Engel J, Schneider P, Tschopp J (2003) Two
adjacent trimeric Fas ligands are required for Fas signaling and
formation of a death-inducing signaling complex. Mol Cell Biol
23:1428–1440
84. Schneider P, Holler N, Bodmer JL, Hahne M, Frei K, Fontana A,
Tschopp J (1998) Conversion of membrane-bound Fas(CD95)
ligand to its soluble form is associated with downregulation of
its proapoptotic activity and loss of liver toxicity. J Exp Med
187:1205–1213
85. Suda T, Hashimoto H, Tanaka M, Ochi T, Nagata S (1997)
Membrane Fas ligand kills human peripheral blood T lympho-
cytes and soluble Fas ligand blocks the killing. J Exp Med
186:2045–2050
86. Herrero R, Kajikawa O, Matute-Bello G, Wang Y, Hagimoto N,
Mongovin S, Wong V, Park DR, Brot N, Heinecke JW, Rosen
H, Goodman RB, Fu X, Martin TR (2011) The biological
activity of FasL in human and mouse lungs is determined by the
structure of its stalk region. J Clin Invest 121:1174–1190
1276 S. Tauzin et al.
123
Author's personal copy

87. Alonso R, Mazzeo C, Rodriguez MC, Marsh M, Fraile-Ramos
A, Calvo V, Avila-Flores A, Merida I, Izquierdo M (2011)
Diacylglycerol kinase alpha regulates the formation and polar-
isation of mature multivesicular bodies involved in the secretion
of Fas ligand-containing exosomes in T lymphocytes. Cell
Death Differ 18:1161–1173
88. Bianco NR, Kim SH, Morelli AE, Robbins PD (2007) Modu-
lation of the immune response using dendritic cell-derived
exosomes. Methods Mol Biol 380:443–455
89. Abusamra AJ, Zhong Z, Zheng X, Li M, Ichim TE, Chin JL,
Min WP (2005) Tumor exosomes expressing Fas ligand mediate
CD8? T-cell apoptosis. Blood Cells Mol Dis 35:169–173
90. Pensati L, Costanzo A, Ianni A, Accapezzato D, Iorio R, Natoli
G, Nisini R, Almerighi C, Balsano C, Vajro P, Vegnente A,
Levrero M (1997) Fas/Apo1 mutations and autoimmune lym-
phoproliferative syndrome in a patient with type 2 autoimmune
hepatitis. Gastroenterology 113:1384–1389
91. Bettinardi A, Brugnoni D, Quiros-Roldan E, Malagoli A, La
Grutta S, Correra A, Notarangelo LD (1997) Missense mutations
in the Fas gene resulting in autoimmune lymphoproliferative
syndrome: a molecular and immunological analysis. Blood
89:902–909
92. Infante AJ, Britton HA, DeNapoli T, Middelton LA, Lenardo
MJ, Jackson CE, Wang J, Fleisher T, Straus SE, Puck JM (1998)
The clinical spectrum in a large kindred with autoimmune
lymphoproliferative syndrome caused by a Fas mutation that
impairs lymphocyte apoptosis. J Pediatr 133:629–633
93. Vaishnaw AK, Orlinick JR, Chu JL, Krammer PH, Chao MV,
Elkon KB (1999) The molecular basis for apoptotic defects in
patients with CD95 (Fas/Apo-1) mutations. J Clin Invest
103:355–363
94. Peters AM, Kohfink B, Martin H, Griesinger F, Wormann B,
Gahr M, Roesler J (1999) Defective apoptosis due to a point
mutation in the death domain of CD95 associated with auto-
immune lymphoproliferative syndrome T-cell lymphoma, and
Hodgkin’s disease. Exp Hematol 27:868–874
95. van Den Berg A, Maggio E, Diepstra A, de Jong D, van Krieken
J, Poppema S (2002) Germline FAS gene mutation in a case of
ALPS and NLP Hodgkin lymphoma. Blood 99:1492–1494
96. Holzelova E, Vonarbourg C, Stolzenberg MC, Arkwright PD,
Selz F, Prieur AM, Blanche S, Bartunkova J, Vilmer E, Fischer
A, Le Deist F, Rieux-Laucat F (2004) Autoimmune lympho-
proliferative syndrome with somatic Fas mutations. N Engl J
Med 351:1409–1418
97. Del-Rey MJ, Manzanares J, Bosque A, Aguilo JI, Gomez-Rial J,
Roldan E, Serrano A, Anel A, Paz-Artal E, Allende LM (2007)
Autoimmune lymphoproliferative syndrome (ALPS) in a patient
with a new germline Fas gene mutation. Immunobiology
212:73–83
98. Dowdell KC, Niemela JE, Price S, Davis J, Hornung RL, Oli-
veira JB, Puck JM, Jaffe ES, Pittaluga S, Cohen JI, Fleisher TA,
Rao VK (2010) Somatic FAS mutations are common in patients
with genetically undefined autoimmune lymphoproliferative
syndrome. Blood 115:5164–5169
99. Landowski TH, Qu N, Buyuksal I, Painter JS, Dalton WS (1997)
Mutations in the Fas antigen in patients with multiple myeloma.
Blood 90:4266–4270
100. Gronbaek K, Straten PT, Ralfkiaer E, Ahrenkiel V, Andersen
MK, Hansen NE, Zeuthen J, Hou-Jensen K, Guldberg P (1998)
Somatic Fas mutations in non-Hodgkin’s lymphoma: association
with extranodal disease and autoimmunity. Blood 92:3018–3024
101. Maeda T, Yamada Y, Moriuchi R, Sugahara K, Tsuruda K, Joh
T, Atogami S, Tsukasaki K, Tomonaga M, Kamihira S (1999)
Fas gene mutation in the progression of adult T cell leukemia.
J Exp Med 189:1063–1071
102. Shin MS, Park WS, Kim SY, Kim HS, Kang SJ, Song KY, Park
JY, Dong SM, Pi JH, Oh RR, Lee JY, Yoo NJ, Lee SH (1999)
Alterations of Fas (Apo-1/CD95) gene in cutaneous malignant
melanoma. Am J Pathol 154:1785–1791
103. Lee SH, Shin MS, Park WS, Kim SY, Dong SM, Pi JH, Lee HK,
Kim HS, Jang JJ, Kim CS, Kim SH, Lee JY, Yoo NJ (1999)
Alterations of Fas (APO-1/CD95) gene in transitional cell car-
cinomas of urinary bladder. Cancer Res 59:3068–3072
104. Muschen M, Re D, Brauninger A, Wolf J, Hansmann ML, Diehl
V, Kuppers R, Rajewsky K (2000) Somatic mutations of the
CD95 gene in Hodgkin and Reed-Sternberg cells. Cancer Res
60:5640–5643
105. Lee SH, Shin MS, Kim HS, Park WS, Kim SY, Jang JJ, Rhim
KJ, Jang J, Lee HK, Park JY, Oh RR, Han SY, Lee JH, Lee JY,
Yoo NJ (2000) Somatic mutations of Fas (Apo-1/CD95) gene in
cutaneous squamous cell carcinoma arising from a burn scar.
J Invest Dermatol 114:122–126
106. Takakuwa T, Dong Z, Takayama H, Matsuzuka F, Nagata S,
Aozasa K (2001) Frequent mutations of Fas gene in thyroid
lymphoma. Cancer Res 61:1382–1385
107. Seeberger H, Starostik P, Schwarz S, Knorr C, Kalla J, Ott G,
Muller-Hermelink HK, Greiner A (2001) Loss of Fas (CD95/
APO-1) regulatory function is an important step in early MALT-
type lymphoma development. Lab Invest 81:977–986
108. Takayama H, Takakuwa T, Dong Z, Nonomura N, Okuyama A,
Nagata S, Aozasa K (2001) Fas gene mutations in prostatic
intraepithelial neoplasia and concurrent carcinoma: analysis of
laser capture microdissected specimens. Lab Invest 81:283–288
109. Park WS, Oh RR, Kim YS, Park JY, Lee SH, Shin MS, Kim SY,
Kim PJ, Lee HK, Yoo NY, Lee JY (2001) Somatic mutations in
the death domain of the Fas (Apo-1/CD95) gene in gastric
cancer. J Pathol 193:162–168
110. Takayama H, Takakuwa T, Tsujimoto Y, Tani Y, Nonomura N,
Okuyama A, Nagata S, Aozasa K (2002) Frequent Fas gene
mutations in testicular germ cell tumors. Am J Pathol
161:635–641
111. Dereure O, Levi E, Vonderheid EC, Kadin ME (2002) Infre-
quent Fas mutations but no Bax or p53 mutations in early
mycosis fungoides: a possible mechanism for the accumulation
of malignant T lymphocytes in the skin. J Invest Dermatol
118:949–956
112. Takakuwa T, Dong Z, Nakatsuka S, Kojya S, Harabuchi Y,
Yang WI, Nagata S, Aozasa K (2002) Frequent mutations of Fas
gene in nasal NK/T cell lymphoma. Oncogene 21:4702–4705
113. Shin MS, Kim HS, Lee SH, Lee JW, Song YH, Kim YS, Park
WS, Kim SY, Lee SN, Park JY, Lee JH, Xiao W, Jo KH, Wang
YP, Lee KY, Park YG, Kim SH, Lee JY, Yoo NJ (2002)
Alterations of Fas-pathway genes associated with nodal metas-
tasis in non-small cell lung cancer. Oncogene 21:4129–4136
114. Wohlfart S, Sebinger D, Gruber P, Buch J, Polgar D, Krupitza
G, Rosner M, Hengstschlager M, Raderer M, Chott A, Mullauer
L (2004) FAS (CD95) mutations are rare in gastric MALT
lymphoma but occur more frequently in primary gastric diffuse
large B-cell lymphoma. Am J Pathol 164:1081–1089
115. Scholl V, Stefanoff CG, Hassan R, Spector N, Renault IZ (2007)
Mutations within the 50 region of FAS/CD95 gene in nodal
diffuse large B-cell lymphoma. Leuk Lymphoma 48:957–963
116. Wu J, Xie F, Qian K, Gibson AW, Edberg JC, Kimberly RP
(2011) FAS mRNA editing in human systemic lupus erythe-
matosus. Hum Mutat 32:1268–1277
CD95-mediated cell signaling in cancer 1277
123
Author's personal copy





























