Embed Size (px)
Citation preview

M
LQMJa
b
c
d
e
f
g
h
i
j
k
l
m
n
o
p
a
AA
KMTEADBE
T
0d
Acta Tropica 121 (2012) 227– 239
Contents lists available at ScienceDirect
Acta Tropica
journa l h o me pa g e: www.elsev ier .com/ locate /ac ta t ropica
alaria in the Greater Mekong Subregion: Heterogeneity and complexity
iwang Cuia,e,∗, Guiyun Yanb,e, Jetsumon Sattabongkotc, Yaming Caod, Bin Chene, Xiaoguang Chenf,i Fang, Qiang Fangh, Somchai Jongwutiwes i, Daniel Parkera, Jeeraphat Sirichaisinthopj,yat Phone Kyawk, Xin-zhuan Sul, Henglin Yangm, Zhaoqing Yangn, Baomin Wango,
ianwei Xum, Bin Zhengp, Daibin Zhongb, Guofa Zhoub
Department of Entomology, The Pennsylvania State University, 501 ASI Building, University Park, PA 16801, USAProgram in Public Health, University of California at Irvine, Irvine, CA 92697-4050, USADepartment of Entomology, AFRIMS, 315/6 Rajvithi Road, Bangkok 10400, ThailandDepartment of Immunology, College of Basic Medical Sciences, China Medical University, Shenyang, ChinaCollege of Life Sciences, Chongqing Normal University, Chongqing 400047, ChinaDepartment of Etio-biology, School of Public Health and Tropical Medicine, Southern Medical University, Guangzhou 510515, ChinaDalian Institute of Biotechnology, No. 2 Shida Street, Dalian, Liaoning 116024, ChinaDepartment of Microbiology and Parasitology, Bengbu Medical College, 2600 Donghai Avenue, Bengbu, Anhui 233030, ChinaDepartment of Parasitology, Faculty of Medicine, Chulalongkorn University, Bangkok, ThailandVector Borne Disease Training Center, Pra Budhabat, Saraburi 18120, ThailandParasitology Research Division, Department of Medical Research-Lower Myanmar, Yangon 11191, MyanmarLaboratory of Malaria and Vector Research, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD 20892, USAYunnan Institute of Parasitic Diseases, Pu’er, Yunnan 665000, ChinaParasitology Department, Kunming Medical University, Kunming, Yunnan 650031, ChinaCollege of Agronomy and Biotechnology, China Agricultural University, No. 2 Yuanmingyuan Xilu, Beijing 100193, ChinaNational Institute of Parasitic Diseases, Chinese Center for Disease Control and Prevention, 207 Rui Jin Er Rd., Shanghai 200025, China
r t i c l e i n f o
rticle history:vailable online 5 March 2011
eywords:alaria
he Greater Mekong Subregionpidemiologynopheles vectorsrug resistanceorder malarialimination
a b s t r a c t
The Greater Mekong Subregion (GMS), comprised of six countries including Cambodia, China’s YunnanProvince, Lao PDR, Myanmar (Burma), Thailand and Vietnam, is one of the most threatening foci of malaria.Since the initiation of the WHO’s Mekong Malaria Program a decade ago, malaria situation in the GMS hasgreatly improved, reflected in the continuous decline in annual malaria incidence and deaths. However,as many nations are moving towards malaria elimination, the GMS nations still face great challenges.Malaria epidemiology in this region exhibits enormous geographical heterogeneity with Myanmar andCambodia remaining high-burden countries. Within each country, malaria distribution is also patchy,exemplified by ‘border malaria’ and ‘forest malaria’ with high transmission occurring along internationalborders and in forests or forest fringes, respectively. ‘Border malaria’ is extremely difficult to monitor, andfrequent malaria introductions by migratory human populations constitute a major threat to neighboring,malaria-eliminating countries. Therefore, coordination between neighboring countries is essential formalaria elimination from the entire region. In addition to these operational difficulties, malaria controlin the GMS also encounters several technological challenges. Contemporary malaria control measures relyheavily on effective chemotherapy and insecticide control of vector mosquitoes. However, the spread ofmultidrug resistance and potential emergence of artemisinin resistance in Plasmodium falciparum make
resistance management a high priority in the GMS. This situation is further worsened by the circulation ofcounterfeit and substandard artemisinin-related drugs. In most endemic areas of the GMS, P. falciparumxist, and in recent malaria control history, P. vivax has demonstrated remarkable
and Plasmodium vivax coe resilience to control measures. Deployment of the only registered drug (primaquine) for the radical cureof vivax malaria is severely undermined due to high prevalence of glucose-6-phosphate dehydrogenasedeficiency in target human populations. In the GMS, the dramatically different ecologies, diverse vectorsystems, and insecticide resistance render traditional mosquito control less efficient. Here we attempt∗ Corresponding author at: Department of Entomology, The Pennsylvania State University, 501 ASI Building, University Park, PA 16801, USA.el.: +1 814 863 7663; fax: +1 814 865 3048.
E-mail address: [email protected] (L. Cui).
001-706X/$ – see front matter © 2011 Elsevier B.V. All rights reserved.oi:10.1016/j.actatropica.2011.02.016

228 L. Cui et al. / Acta Tropica 121 (2012) 227– 239
to review the changing malaria epidemiology in the GMS, analyze the vector systems and patterns ofmalaria transmission, and identify the major challenges the malaria control community faces on its way
1
mibfmIiasii(mn9o
op(talpdmfttoaviidPfvt(T(oaTi
2e
2
wie
to malaria elimination.
. Introduction
According to World Malaria Report 2010, the estimated annualalaria incidence for 2009 was 225 million cases, resulting
n ∼781,000 deaths (WHO, 2010b). While most of the malariaurden is in sub-Saharan Africa, Southeast (SE) Asia accountedor 10% of the global malaria morbidity and 5% of the global
ortality in 2008. Since the launch of the Roll Back Malarianitiative by WHO in 1998, malaria control has intensifiedn endemic countries, supported by better financial supportnd technological development. A Global Malaria Action Planeeks to eliminate malaria using integrated approaches includ-ng vaccines, insecticide-treated mosquito nets (ITNs), indoornsecticide residue spray (IRS), and improved drug treatmentshttp://www.rollbackmalaria.org/gmap/index.html). Once again,
alaria eradication is on the agenda of the international commu-ity (Feachem and Sabot, 2008; Roberts and Enserink, 2007). Of the9 malaria endemic countries, 32 have declared a national policyf malaria elimination (Feachem et al., 2010).
Within SE Asia, the Greater Mekong Subregion (GMS) has beenne of the most dangerous foci of malaria. The GMS is com-rised of Cambodia, China (Yunnan Province), Lao PDR, MyanmarBurma), Thailand, and Vietnam, which vary in political struc-ure, socio-economic and financial resources, public health system,nd disease ecology. The GMS is one of the most densely popu-ated areas with topographical environments ranging from coastallains to river estuaries and rugged mountainous terrains. Suchivergent ecological systems offer diverse breeding habitats forultiple mosquito vector species with distinctive preferences for
orest edges, foothills, or agricultural fields. Climates range fromemperate conditions with disrupted malaria transmission duringhe harsh winter to tropical climates where malaria transmissionccurs year round. The Mekong River runs through all six countries,nd its watershed plays an important role in the transmission ofector-borne diseases. As such, malaria epidemiology in this regions complex, characterized by immense geographical heterogene-ty in disease distribution with many areas of high endemicity,ifferential prevalence of the two most predominant parasiteslasmodium falciparum and Plasmodium vivax, which require dif-erent drug treatments, and diverse vector systems with differentectorial capacities for these parasites (Socheat et al., 2003). Fur-hermore, the GMS harbors the epicenter of multidrug resistantMDR) P. falciparum in the border area between Cambodia andhailand, which is gradually encompassing the tropical worldHastings, 2004; Wongsrichanalai et al., 2002). Recent detectionf artemisinin resistance in the same area represents a regionalnd global emergency (Dondorp et al., 2009; Noedl et al., 2008).herefore, malaria control in the GMS is not only important for themmediate region, but also for global malaria control (WHO, 2011).
. Malaria situation in the GMS: evidence of changingpidemiology
.1. Overview
Like other malaria-endemic regions of the world, the GMS hasitnessed dramatic changes in its malaria situation. Since malaria
s generally a disease of the poor, the history of malaria, to a largextent, mirrors the broader political environments and economic
© 2011 Elsevier B.V. All rights reserved.
evolution in this region. Between 1950s and 1990s, systematicorganizational efforts saw the gradual elimination or near eradica-tion of major malaria foci from the central plain regions of severalnations in this region, only to see its gradual rise in Cambodia,Myanmar, Vietnam, Thailand, and China due to various precipitat-ing events and conditions. Although regional political and economicinstability is partially blamed for the resurgence of malaria, humanpopulation expansion and mobility into forested regions, and envi-ronmental changes such as urbanization and deforestation haveall contributed to the changing picture of malaria epidemiology(Kidson et al., 2000). Perhaps, the single most important culpritresponsible for the regional and global malaria resurgence is theemergence and spread of MDR falciparum malaria from the GMS.In recent years, the malaria control and elimination campaign facesanother dreadful threat: the emergence of artemisinin resistance(Dondorp et al., 2009; Noedl et al., 2008). Therefore, containmentof the resistant parasites has been and will remain the focus aswell as the greatest challenge of malaria control efforts. Lessonsfrom malaria control history in this region have taught us that thecombination of community organization, exhaustive case detec-tion, management and focus elimination, and strong political willat all levels of the society makes elimination of malaria from largeareas possible. Yet, sustainability of elimination requires collabo-rative political determination of individual nations in this region.In recognition of the need for coordinated efforts, WHO launchedthe Mekong Malaria Program in 1999 with the aims of significantlyreducing malaria-associated morbidity and mortality in this regionand curbing the spread of MDR P. falciparum. Since the inception ofthis program, malaria control in the GMS has made a huge stride,accompanied by the continuous decline in annual malaria incidenceand deaths (Delacollette et al., 2009; Singhasivanon, 1999; Socheatet al., 2003). It was estimated that there was a 25% reduction in thenumber of confirmed malaria cases and 60% reduction in malaria-associated mortality in the GMS from 1998 to 2007 (Delacolletteet al., 2009). Multiple factors, including stronger political will ofthe governments, increasing investments in malaria interventions,and strengthening public health systems have all contributed tothese achievements. Yet, even greater challenges have been laid infront of the malaria control community. Currently, two countriesin the GMS, Myanmar and Cambodia, are still among the countrieswith highest malaria-burden in the world (Fig. 1) (WHO, 2010b). Inparticular, the number of malaria cases and malaria-induced mor-tality in SE Asia has consistently been the highest in Myanmar forthe past three decades.
2.2. Country-specific epidemiology and drug resistance
2.2.1. CambodiaCambodia had 80,644 reported malaria cases in 2008, and this
figure could be significantly higher if malaria cases treated in theprivate sector were taken into account. Malaria incidence is thehighest in the eastern province of Mondulkiri, the most sparselypopulated province. In the western region that borders Thailand,malaria incidence is also high, largely due to the location of the
high-risk groups such as migrant workers clearing forests for land.The Thai–Cambodian border has been an epicenter of antimalarialdrug resistance, and parasites with resistance to chloroquine (CQ)and antifolates have emerged here and spread to the rest of theworld (Anderson and Roper, 2005; Roper et al., 2004; Wootton et al.,
L. Cui et al. / Acta Tropica 121 (2012) 227– 239 229
in the
2sdsaeat
2
pm1e1end
TC
Nmh
Fig. 1. Malaria distribution
002). The emergence of MDR parasites is the most worrisome,ince such parasites may develop resistance to new antimalarialrugs at an accelerated rate (Rathod et al., 1997). It is therefore noturprising that parasites with reduced sensitivity to artemisininnd related drugs have recently been detected in this area (Dondorpt al., 2009; Noedl et al., 2009, 2010). Recently, WHO has developed
five-point action plan that aims to contain the artemisinin-olerant parasites in this region (WHO, 2009, 2011) (Table 1).
.2.2. ChinaSince its launch in 1955, China’s national malaria control
rogram (NMCP) has savoured great success. Prior to its imple-entation, annual malaria incidence totalled 6.79 million cases in
954, accounting for over 60% of recorded acute infectious dis-
ases (Yip, 1998). Despite two major outbreaks in the 1960s and970s, the country saw a steady decrease in the number of cases,specially after the reinstitution of systematic control efforts begin-ing in 1978 (Tang et al., 1991). By the year 2000, malaria casesropped to only 29,039 reported cases. It is noteworthy to mentionable 1ountry-wide malaria incidence in nations of the Greater Mekong Subregion in 1998 and
Country Reported cases A
1998 2008 1
Cambodia 58,874 42,124 4China 27,090 16,650 0Laos 39,031 18,740 7Myanmar 104,753 411,494 3Thailand 131,055 25,449 2Vietnam 72,091 11,354 0
ote: Data were obtained from the following web pages: (1) http://www.wpro.who.intalaria/; (3) http://www.searo.who.int/en/Section10/Section21/Section340 4015.htm
ttp://www.who.int/malaria/publications/country-profiles/en/index.html; (6) http://ww
Greater Mekong Subregion.
that case underreporting may have been high, suggesting signifi-cant underestimation of the disease burden (Zhang, 2005; Zhanget al., 2004). From the most recent malaria distribution map in2008, 110 counties had annual malaria incidence rate exceeding1/10,000. Most of these counties were located in three areas: cen-tral China, Hainan Island, and Yunnan Province (Fig. 1). Among allmalaria cases, vivax malaria accounted for more than 80%, whereasautochthonous falciparum malaria only occurred in subtropicalHainan and Yunnan provinces, which have been historically themost malarious regions in China (Sheng et al., 2003). In addition,the major proportion of falciparum cases happened in young adultmales of 15–50 years of age (Lin et al., 2009), partially attributedto the higher mobility and outdoor activities of this group. OnHainan Island, malaria transmission peaks in May–October and
is distributed in the hilly, forested south-central counties of theisland (Xiao et al., 2010). Similarly, malaria incidences in Yunnanare temporally and spatially clustered (Clements et al., 2009; Huiet al., 2009). Interestingly, before the year 2000, a single malariaincidence peak was observed annually from June through August,2008.
nnual incidence rate/1000 population Proportion of P. falciparum
998 2008 1998 2008
.71 2.87 91.37 35.83
.02 0.01 11.47 7.34
.75 2.96 99.37 25.06
.11 10.15 78.02 87.00
.96 0.55 52.70 47.00
.95 0.13 76.39 78.40
/sites/mvp/data/malaria/; (2) http://www.wpro.who.int/sites/mvp/epidemiology/; (4) http://www.actmalaria.net/home/epidemiological profile.php#base; (5)w.who.int/malaria/publications/country-profiles/2008/en/index.html.

2 pica 1
wiiot2mcevaiiAiwi2HnXcrvtCCgmerm
2
iadurihiWatewir
2
ndTtmdoap(i2S
30 L. Cui et al. / Acta Tro
hereas in 2000–2005 two malaria peaks occurred annually, onen May–July and one in October–November. As expected, high-ncidence counties are clustered at international border areas andverlap with the poverty map of Yunnan, suggesting a correla-ion with socio-economic status (Clements et al., 2009; Hui et al.,009). Yunnan has more than 4000 km of border line with threealarious countries, Myanmar, Laos, and Vietnam, and imported
ases accounted for a large proportion of adult infections (Lint al., 2009). Furthermore, the coexistence of P. falciparum and P.ivax in Yunnan makes disease treatment challenging. Althoughrtemisinin-based combination therapy (ACT) is generally effectiven treating P. falciparum, there is an indication of reduced sensitiv-ty of parasites to artemisinin and its derivatives (Yang et al., 2003).s Yunnan has the longest history of artemisinin usage mostly
n the form of monotherapy, rigorous clinical efficacy studies arearranted in this region. In central China, malaria is character-
zed by temperate-zone P. vivax with a long relapse interval. From000 to 2006, malaria incidence in the central provinces (Anhui,enan, Hunan, Hubei, and Jiangsu) rose steadily, contributing sig-ificantly to nation-wide malaria resurgence (Sleigh et al., 1998;u et al., 2006; Zhou et al., 2007). Spatially, malaria in this region islustered near the Huai River (Zhang et al., 2008). Although envi-onmental changes may be largely responsible for the resurgingivax malaria in central China, other factors such as drug resis-ance may also be held accountable. The clinical efficacy of theQ–primaquine combination has not been evaluated in centralhina, but a recent study at the Yunnan–Myanmar border sug-ested reduced efficacy of this drug combination for treating vivaxalaria (Liang et al., 2009). Since China is embarking on malaria
limination, vivax malaria in central China, prevention of malariaeintroduction, and management of drug resistance are among theajor obstacles.
.2.3. Lao PDRIn recent years, the malaria situation in Lao PDR has notably
mproved, as shown by the reduction in number of malaria casesnd malaria deaths. However, it is noteworthy that the epi-emiology data are based on hospital records, which inevitablynderestimate the actual number of malaria cases, since theate of self-medication is high. Despite great progress maden malaria control, malaria continues to be a serious publicealth problem in southern areas of the country, particularly
n remote areas (Delacollette et al., 2009; Socheat et al., 2003;HO, 2008a). Chloroquine and sulfadoxine-pyrimethamine (SP)
re no longer viable therapy for falciparum malaria, since resis-ance to these drugs is widespread in this country (Mayxayt al., 2003, 2007). Currently ACTs have excellent efficacy, butidespread availability of substandard and counterfeit antimalar-
als is a serious problem and threat to the management of drugesistance.
.2.4. MyanmarThe malaria burden in Myanmar is the heaviest among the GMS
ations. More than half of the malaria cases and ∼75% of the malariaeaths in the GMS in 2007 occurred in Myanmar (WHO, 2008a).he annual malaria incidence in Myanmar decreased from 1998o 2007. Despite this progress, investments in malaria control are
oderate compared to other GMS countries. In 2008, malaria inci-ence rose again from 9.0% to 10.8%. In 2009, 49.3% of the casesccurred in forest and forest-fringe areas of Kachin, Rakhine statesnd Sagaing Division; 74% of reported cases were from P. falci-
arum infections. In the border areas, where poor ethnic minoritiese.g., Wa, Dai, Lahu, Karen, etc.) are concentrated, malaria burdens particularly high and malaria outbreaks occur frequently (WHO,008b). For example, malaria outbreaks in November of 2003 inhan and Kachin states resulted in the death of nearly a thousand21 (2012) 227– 239
people (Li et al., 2005). Kachin State also had the highest malaria-related mortality rate, with 7.8 deaths/1000 people in 2005 (WHO,2008a). Public health infrastructure in the remote states is poorand reported cases may severely underestimate the disease burden.Drug resistance management also makes up an important challengein this country. Resistance to CQ and SP is widespread, whereasresistance to other antimalarials such as mefloquine and quinine isalso on the rise (Meng et al., 2010). Another important impact of themalaria situation in Myanmar is its contribution to malaria in neigh-boring countries, which seriously impedes the progress towardsthe goal of malaria elimination in these countries (Beyrer and Lee,2008).
2.2.5. ThailandSince the implementation of the national malaria control pro-
gram in the 1950s, malaria associated morbidity and mortalityhave been reduced dramatically in Thailand. Like other countries inthis region, malaria displays significant geographical heterogene-ity and is exemplified by the “border malaria” type, with most ofthe malaria cases concentrated along the borders with Myanmarand Cambodia (Childs et al., 2006; Zhou et al., 2005). Many of theborder regions are forested with heavy population migrations, andnon-Thais, mostly migrant workers from the neighboring coun-tries, make a disproportionate contribution to the regional malariaburden. In addition, political unrest among the minorities in Myan-mar has led to significant cross-border population movements, anddisplaced minority populations are at increased risks of malaria(Richards et al., 2009). Moreover, certain life style and behavioralfactors of the hill tribes and migrant workers are also associatedwith increased risks of malaria infection (Chaveepojnkamjorn andPichainarong, 2004, 2005; Pichainarong and Chaveepojnkamjorn,2004). Malaria in Thailand shows a two-peak annual seasonality,often following the patterns of rainfall (Childs et al., 2006; Cuiet al., 2003). The predominant parasite species are P. falciparumand P. vivax, and P. vivax has become more prevalent than P. fal-ciparum at the turn of the century (Sattabongkot et al., 2004).The other two human malaria species, Plasmodium malariae andPlasmodium ovale, are also present at relatively high levels, butare frequently overlooked due to limited sensitivity of the detec-tion methods (Zhou et al., 1998). Furthermore, sporadic zoonoticinfections by the monkey parasite Plasmodium knowlesi were alsoreported (Jongwutiwes et al., 2004; Putaporntip et al., 2009a). Inrecent years, there is also a trend of changing malaria epidemi-ology in Thailand. In some southern provinces, such as Yala andNarathiwat where malaria was largely eliminated decades ago, ithas recently reappeared with sporadic outbreaks occurring in sev-eral districts. Molecular population genetic studies revealed thatthe genetic structure of the parasites, in contrast to being panmicticin the west, is more clonal in the south and likely represents recentexpansion of a limited number of parasite strains (Putaporntip et al.,2009a,b). In eastern areas of Thailand, such as Sa Kaeo Province, P.vivax has replaced the dominant status of falciparum malaria withits relative prevalence increasing from <25% before 1995 to almost90% in recent years. A noticeable change in vector species compo-sition and abundance is a plausible reason for the shift in parasitespecies prevalence (Limrat et al., 2001), but this change in malariaepidemiology still awaits for further investigations. The high pro-portion of MDR P. falciparum parasites near the borders constitutesanother big challenge for the control program. Antimalarial drugpolicy has changed many times in the past in response to the esca-lating problem of drug resistance (Sattabongkot et al., 2004). Since
the switch of the national drug policy to artesunate plus mefloquinein the early 1990s, clinical and parasitological responses to this ACTregimen have dropped considerably (Carrara et al., 2009; WHO,2008a). This problem is especially serious at the Thai–Cambodianborder (Wongsrichanalai and Meshnick, 2008), where measures to
pica 1
cd
2
bscbUd2mtsfctcolsmohv
3
3
dgdecvvimvAeIlclbt(srla2ale
3
t2d
L. Cui et al. / Acta Tro
ontain potential artemisinin-resistant parasite strains are beingeployed (WHO, 2009, 2011).
.2.6. VietnamPrior to the early 1990s, malaria was a major cause of mor-
idity and mortality in Vietnam. As the result of improvedocio-economic conditions, increased government investment, andommunity-based monitoring, the malaria burden in Vietnam haseen dramatically alleviated in recent years (Thang et al., 2009).sing a combination of control strategies such as ITNs and earlyiagnosis and treatment of symptomatic patients (Hung le et al.,002), the number of malaria cases in Vietnam has plunged toerely 11,355 in 2008 (Manh et al., 2011). Much like the situa-
ion in Laos, malaria in Vietnam is distributed in the central andouthern parts of the country, and malaria occurs mostly in theorests or forest edges (Erhart et al., 2005; Sanh et al., 2008). P. fal-iparum remains the predominant species, whereas infections withhe monkey malaria parasite P. knowlesi have also been detected inhildren in the central region (Van den Eede et al., 2009). Becausef the switching of treatment policy from CQ to ACTs, the preva-ence of the pfcrt 76T mutation has dropped, suggesting increasedensitivity to CQ. However, the prevalence of antifolate resistanceutations remains high (Isozumi et al., 2010). Longitudinal surveys
f artemisinin resistance suggest that P. falciparum parasites are stillighly sensitive to the ACTs in this region (Thanh et al., 2010), butigorous clinical studies may be needed to verify such claims.
. Malaria vectors in the GMS
.1. Diversity in vector species
One distinct feature of malaria transmission in the GMS is theiversity in vector species and the tremendous spatial hetero-eneity in distribution patterns (WHO, 2007a). Fig. 2 shows theistribution of reported malaria vector species in the GMS. Gen-rally, members of Anopheles minimus, and Anopheles dirus speciesomplexes, as well as Anopheles sinensis are the most importantectors, but the importance of each species in malaria transmissionaries greatly among regions. For example, in tropical and subtrop-cal regions of China (below 25◦N latitude), members of Anopheles
inimus complex and the Anopheles dirus complex are the mainectors, whereas in more temperate regions (above 33◦N latitude),nopheles sinensis is the major malaria vector (Chareonviriyaphapt al., 2000, 2003; Lee et al., 2001; Pinichpongse and Bullner, 1967).n the areas between 25◦N latitude and 33◦N latitude, Anophelesesteri is an important malaria vector. In Thailand, Anopheles dirusomplex, Anopheles minimus complex, Anopheles aconitus, Anophe-es sundaicus complex are the main malaria vectors. Anophelesaimaii and Anopheles pseudowillmori of the Anopheles macula-us group are considered malaria vectors with local importanceChareonviriyahpap et al., 1999). Furthermore, malaria vectorpecies composition varies even among different localities in aegion because vector species exhibit different requirements forarval habitat. For example, Anopheles dirus and Anopheles baimaiire often found in stagnant and shaded waters in forests (Oo et al.,003) whereas Anopheles minimus complex generally uses habitatslong streams in hilly areas (Overgaard et al., 2002), and Anophe-es sinensis is often found in rice fields and irrigation canals (Ruedat al., 2006).
.2. Species complex and molecular identification
It must be noted that many malaria vectors in the region belongo species complexes and groups (Harbach, 2004; Harbach et al.,007), which include closely related species that are difficult toistinguish morphologically, yet often differ in bionomics and
21 (2012) 227– 239 231
capacity for malaria transmission (Manguin et al., 2008). For exam-ple, Anopheles hyrcanus complex includes several important butmorphologically similar malaria vector species such as Anophelessinensis, Anopheles lesteri (syn. Anthropophagus) (WHO, 2007a). Thesympatric occurrence of multiple morphologically indistinguish-able or misidentified vector species complicates our understandingof the roles of individual vector species in malaria transmissionand hampers our ability to optimize vector control strategies. Inthis regard, accurate mosquito identification becomes particularlyimportant. The use of molecular methods has greatly improvedthe accuracy of species identification. PCR-based methods havethe advantage of requiring minute amounts of material for anal-ysis, and ribosomal DNA (rDNA) has been a popular choice fordifferentiating Anopheles species (Collins and Paskewitz, 1996).This is because the rDNA units are typically present in hundredsof copies per genome making them particularly easy to amplify,and the internal transcribed spacers (ITSs) separating ribosomalRNA genes generally exhibit variations among the sibling species(Alves et al., 2005). By designing species-specific primers in the ITS2region, Walton and her colleagues have developed a PCR-basedidentification method to distinguish five species of the Anophelesdirus complex (Anopheles nemophilous, Anopheles dirus [=speciesA], Anopheles cracens [=species B], Anopheles scanloni [=speciesC], and Anopheles baimaii [=species D]) from Thailand (Obsomeret al., 2007; Walton et al., 1999), four species of the Anophelesannularis group (Anopheles annularis, Anopheles nivipes, Anophelesphilippinensis, and Anopheles pallidus) (Walton et al., 2007a), andfive species of the Anopheles maculatus group (Anopheles maculatus,Anopheles dravidicus, Anopheles pseudowillmori, Anopheles sawad-wongporni and species K) (Morgan et al., 2009; Walton et al., 2007b).Similarly, the PCR-based identification method was also used todistinguish mosquitoes of the Anopheles maculatus group in China(Ma et al., 2006). Phuc et al. (2003) reported a multiplex PCR assaybased on ITS2 sequences to identify Anopheles minimus and Anophe-les harrisoni (=species C) of the Anopheles minimus complex (Greenet al., 1990; Phuc et al., 2003). Gao et al. (2004) reported a PCR-RFLPmethod for discriminating Anopheles lesteri and Anopheles sinensis(Gao et al., 2004).
In addition to the PCR-based methods, another potentiallyuseful method for molecular species identification is the loop-mediated isothermal amplification (LAMP) technique (Parida et al.,2008). LAMP is a one step nucleic acid amplification that relies onautocycling strand-displacement DNA synthesis. It is performedunder isothermal conditions using a DNA polymerase with stranddisplacement activity. Moreover, the amplification products can bevisualized directly (Tomita et al., 2008). The LAMP method offershigh sensitivity, requires simple equipment (e.g., a water bath), andno electrophoresis, and thus the method may be suitable for fieldsettings where sophisticated equipment is lacking.
3.3. Insecticide resistance
Currently, long-lasting insecticide treated nets (LLINs) and IRSare the primary vector control tools in the GMS. The insecti-cides of choice for bednet impregnation and IRS are pyrethroidsbecause of their high efficacy, rapid rate of knockdown, strongmosquito exito-repellency, and low mammalian toxicity. Syn-thetic pyrethroids, particularly permethrin and deltamethrin, arewidely used throughout the world. Reducing vector–human con-tact through the use of LLINs has been shown to be effective inreducing malaria prevalence in SE Asia (Sexton, 1994; Li et al.,
1989). Along with the use of insecticides to reduce abundance ofdisease vectors, the application of insecticides for agricultural pur-poses also increases the likelihood and speed at which resistancecan develop (Overgaard et al., 2005). Previous studies in SE Asia sug-gest a patchy distribution of insecticide resistance in four malaria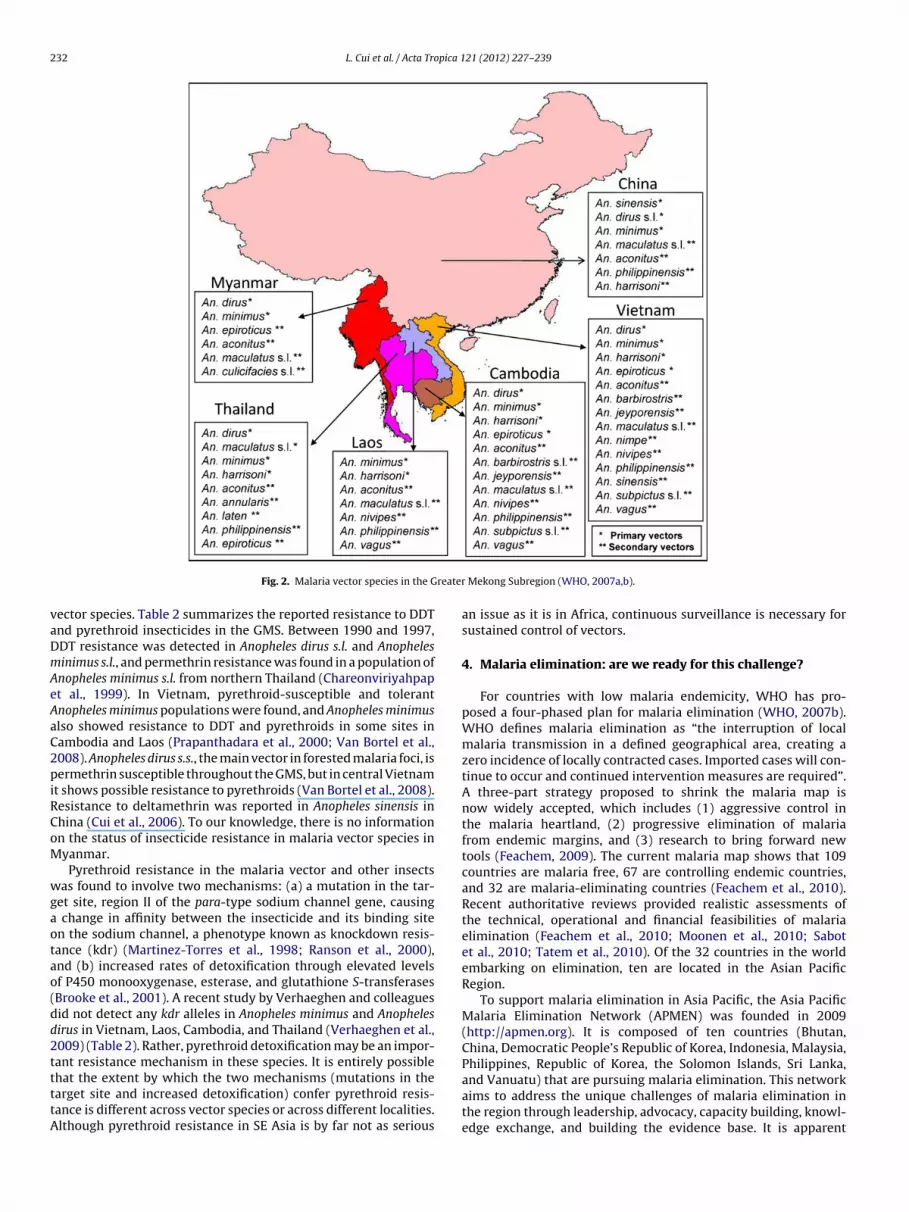
232 L. Cui et al. / Acta Tropica 121 (2012) 227– 239
reater
vaDmAeAaC2piRCoM
wgaotao(dd2ttttA
Fig. 2. Malaria vector species in the G
ector species. Table 2 summarizes the reported resistance to DDTnd pyrethroid insecticides in the GMS. Between 1990 and 1997,DT resistance was detected in Anopheles dirus s.l. and Anophelesinimus s.l., and permethrin resistance was found in a population ofnopheles minimus s.l. from northern Thailand (Chareonviriyahpapt al., 1999). In Vietnam, pyrethroid-susceptible and tolerantnopheles minimus populations were found, and Anopheles minimuslso showed resistance to DDT and pyrethroids in some sites inambodia and Laos (Prapanthadara et al., 2000; Van Bortel et al.,008). Anopheles dirus s.s., the main vector in forested malaria foci, isermethrin susceptible throughout the GMS, but in central Vietnam
t shows possible resistance to pyrethroids (Van Bortel et al., 2008).esistance to deltamethrin was reported in Anopheles sinensis inhina (Cui et al., 2006). To our knowledge, there is no informationn the status of insecticide resistance in malaria vector species inyanmar.Pyrethroid resistance in the malaria vector and other insects
as found to involve two mechanisms: (a) a mutation in the tar-et site, region II of the para-type sodium channel gene, causing
change in affinity between the insecticide and its binding siten the sodium channel, a phenotype known as knockdown resis-ance (kdr) (Martinez-Torres et al., 1998; Ranson et al., 2000),nd (b) increased rates of detoxification through elevated levelsf P450 monooxygenase, esterase, and glutathione S-transferasesBrooke et al., 2001). A recent study by Verhaeghen and colleaguesid not detect any kdr alleles in Anopheles minimus and Anophelesirus in Vietnam, Laos, Cambodia, and Thailand (Verhaeghen et al.,009) (Table 2). Rather, pyrethroid detoxification may be an impor-
ant resistance mechanism in these species. It is entirely possiblehat the extent by which the two mechanisms (mutations in thearget site and increased detoxification) confer pyrethroid resis-ance is different across vector species or across different localities.lthough pyrethroid resistance in SE Asia is by far not as seriousMekong Subregion (WHO, 2007a,b).
an issue as it is in Africa, continuous surveillance is necessary forsustained control of vectors.
4. Malaria elimination: are we ready for this challenge?
For countries with low malaria endemicity, WHO has pro-posed a four-phased plan for malaria elimination (WHO, 2007b).WHO defines malaria elimination as “the interruption of localmalaria transmission in a defined geographical area, creating azero incidence of locally contracted cases. Imported cases will con-tinue to occur and continued intervention measures are required”.A three-part strategy proposed to shrink the malaria map isnow widely accepted, which includes (1) aggressive control inthe malaria heartland, (2) progressive elimination of malariafrom endemic margins, and (3) research to bring forward newtools (Feachem, 2009). The current malaria map shows that 109countries are malaria free, 67 are controlling endemic countries,and 32 are malaria-eliminating countries (Feachem et al., 2010).Recent authoritative reviews provided realistic assessments ofthe technical, operational and financial feasibilities of malariaelimination (Feachem et al., 2010; Moonen et al., 2010; Sabotet al., 2010; Tatem et al., 2010). Of the 32 countries in the worldembarking on elimination, ten are located in the Asian PacificRegion.
To support malaria elimination in Asia Pacific, the Asia PacificMalaria Elimination Network (APMEN) was founded in 2009(http://apmen.org). It is composed of ten countries (Bhutan,China, Democratic People’s Republic of Korea, Indonesia, Malaysia,
Philippines, Republic of Korea, the Solomon Islands, Sri Lanka,and Vanuatu) that are pursuing malaria elimination. This networkaims to address the unique challenges of malaria elimination inthe region through leadership, advocacy, capacity building, knowl-edge exchange, and building the evidence base. It is apparent
L. Cui et al. / Acta Tropica 121 (2012) 227– 239 233
Table 2A summary of DDT and pyrethroid resistance in major malaria vectors in the GMS.
Species Country Insecticide Bioassay resistance classificationa kdr genotypingb Reference
Anopheles vagus Cambodia DDT R L1014S 1Pyrethroid PR 1
Laos DDT R L1014S 1Pyrethroid R 1
Vietnam DDT R L1014S 1Pyrethroid R 1
Anopheles sinensis Vietnam DDT R L1014S 1Pyrethroid R 1
China DDT R – 2Pyrethroid R – 2
Anopheles minimus s.l. Cambodia DDT S No kdr mutation 3, 4Pyrethroid S 3, 4
Laos DDT S No kdr mutation 3, 4Pyrethroid S 3, 4
Vietnam DDT S No kdr mutation 3, 4Pyrethroid R 3, 4
Thailand DDT S No kdr mutation 3, 4Pyrethroid S 3, 4
China DDT PR – 2Pyrethroid R – 2
Anopheles lesteri China DDT PR – 2Pyrethroid PR – 2
Anopheles dirus s.l. Cambodia DDT S No kdr mutation 3, 4Pyrethroid S 3, 4
Laos DDT S No kdr mutation 3, 4Pyrethroid S 3, 4
Vietnam DDT S No kdr mutation 3, 4Pyrethroid S 3, 4
Thailand DDT S No kdr mutation 3, 4Pyrethroid S 3, 4
Anopheles epiroticus Cambodia DDT PR No kdr mutation 3, 4Pyrethroid PR 3, 4
Vietnam DDT PR No kdr mutation 3, 4Pyrethroid R 3, 4
Thailand DDT S No kdr mutation 3, 4Pyrethroid S 3, 4
a Bioassay resistance classification is based on WHO (1998): “R”, or resistant (mortality < 80%), “S”, or susceptible (mortality > 98%), and “PR”, or possible resistance (mortalitybetween 80 and 97%) after 60 min of exposure to the discriminate dose of the perspective insecticides.
R 8); 4,
tcmi2crctmipattb
utsecte
b “–” indicates kdr genotyping was not conducted.eferences: 1, Verhaeghen et al. (2010); 2, Cui et al. (2006); 3, Van Bortel et al. (200
hat these malaria-eliminating countries all have country-specificharacteristics in their malaria situations. For those that borderalaria-controlling countries, it is important that measures be
mplemented to curb malaria reintroduction (Tatem and Smith,010). In this aspect, intensified disease surveillance and swiftontrol responses are the basic requirements to prevent theeestablishment of the reintroduced parasites. In some cases,ross-border malaria control, i.e., expansion of malaria con-rol programs from malaria-eliminating countries to neighboring
alaria-controlling countries, might be necessary to create buffer-ng zones to thwart reintroduction of the parasite. For example,ilot trials of cross-border malaria control at the Thai–Myanmarnd Chinese–Myanmar border regions suggest that organized con-rols in these regions are feasible (Richards et al., 2009). Obviously,hese cross-border activities demand coordination of governmentsetween the neighboring nations.
The NMCPs in the nations of the GMS are mostly organizednder the Ministry of Health (MOH) with different organiza-ional structures (WHO, 2008a). For example, the public health
ystem in China is structured mainly through the Centers for Dis-ase Control and Prevention of different municipal levels withoordination of provincial and county health bureaus, whereashe NMCP of Thailand is a division of the Department of Dis-ase Control in the MOH. Depending on the malaria burdenVerhaeghen et al. (2009).
and national goal, the NMCPs have received different levels offinancial support from their governments. In addition, all coun-tries of the GMS have been supported by the Global Fund toFight AIDS, Tuberculosis and Malaria (GFATM), which providedthe majority of international funding for malaria control in theGMS (WHO, 2008a). The GFTAM in China and Thailand focuseson strengthening malaria prevention at the border areas throughimproved surveillance, reporting, and treatment for cross-bordermalaria cases in order to respond to local malaria transmissionand outbreaks. With an improved malaria situation and bet-ter financial support, the NMCPs of GMS nations have revisedtheir national malaria strategies. The following are examples ofnational malaria control strategies in China and Myanmar, respec-tively.
The National Malaria Strategy of China for 2010–2015 aimsto achieve malaria elimination (China MOH, 2009). Specifically,China aims to (1) achieve annual incidence <1/10,000 cases/yearin 70% of endemic counties and eliminate P. falciparum malariafrom Hainan Province by 2015; (2) eliminate malaria in 80% of
counties currently with an incidence ≥1/10,000 cases/year by2015; and (3) prevent reintroduction of malaria in places wherelocal transmission has been interrupted. The Revised MalariaStrategy represents a country-wide intensive effort that coversthe spectrum from intensified control in endemic areas to pre-
2 pica 1
vbteevtbtpasamalo2
iwan(glclnhpa(alitciipe
5
5
dAdmeevgtmdBd2
eh
34 L. Cui et al. / Acta Tro
ention of reintroduction in areas without local transmissionut being prone to malaria epidemics. The main strategies aimo: (1) ensure access to early, accurate diagnosis, and prompt,ffective, safe treatment through public and private sectors; (2)nsure full coverage of the population at risk with appropriateector control measures; (3) strengthen malaria health educa-ion, promotion, and community mobilization efforts and changeehavior to maximize utilization of malaria control and elimina-ion services; (4) ensure comprehensive coverage of vulnerable,oor and marginalized populations at high risk of malaria withppropriate malaria interventions; (5) strengthen the malariaurveillance system by improving case reporting, passive andctive case detection, entomological and antimalarial resistanceonitoring, and ensuring adequate outbreak response capability;
nd (6) provide effective program management, based on firmeadership commitment, to enable high quality implementationf strategies from malaria control to elimination (China MOH,009).
In August 2010, to meet updated malaria situation andnternational opportunities, the Myanmar MOH, in collaboration
ith bilateral and multilateral development partners, nationalnd international non-governmental organizations, developed aew National Strategic Plan for Malaria Prevention and ControlMyanmar MOH, 2010). The goal of the new National Strate-ic Plan is to reduce malaria morbidity and mortality by ateast 50% by 2015 against the baseline level of 2007, and toontribute towards socio-economic development and the Mil-ennium Development Goals. Specifically, the objectives of theew plan are to ensure: (1) at least 80% of the people inigh and moderate risk villages in 180 priority townships arerotected against malaria by using LLINs complemented withnother appropriate vector control methods, where applicable;2) malaria cases in each township receive quality diagnosisnd appropriate treatment in accordance with national guide-ines, preferably within 24 h after appearance of symptoms; (3)n 180 priority townships, the communities at risk actively par-icipate in planning and implementing malaria prevention andontrol interventions; and (4) the Township Health Departmentsn 180 priority townships are capable of planning, implement-ng, monitoring and evaluating the malaria prevention and controlrogram with management and technical support from higher lev-ls.
. Major obstacles and knowledge gaps in malaria control
.1. Geographical heterogeneity and ‘border malaria’
Malaria control in the GMS is confounded by heterogeneousistribution of malaria, both spatially and among populations.t the regional scale, malaria distribution varies greatly amongifferent countries of the GMS. The patchiness is also reflectedicrogeographically within each country. The majority of malaria
ndemic regions lie in forests and their peripheries, with the gen-ral trend being labeled ‘forest malaria’ (Prothero, 1999). Smallillages and communities, with little health infrastructure, areenerally more affected by forest malaria than are urban cen-ers. Furthermore, there is a trend for greater infection and
alaria-related mortality near international borders, making ‘bor-er malaria’ a concern for malaria prevention (WHO, 2008a).ecause of poor accessibility and general negligence, malaria bur-
en in these border areas is the heaviest (Liu et al., 2009; WHO,008a).Border malaria is the result of several socio-cultural, economic,nvironmental, and political factors. Some border regions areeavily forested, making them an ideal environment for malaria
21 (2012) 227– 239
transmission. Along the border regions, many ethnic minorities areconcentrated, some of which are politically, economically, cultur-ally, and geographically marginalized from society. They frequentlyhold occupations or use procurement strategies that increase expo-sure to malaria vectors (Prothero, 1999). In particular, subsistenceactivities that are associated with forest areas, such as loggingand swidden farming, are likely to increase the risk of infection(Erhart et al., 2005). In addition to poor accessibility, border regionsfrequently exhibit cultural and linguistic heterogeneity, makinghealth-care education, prevention, and administration compli-cated. As a result, ethnic minorities and mobile workers on bothsides of the border have little access to routine health care services.In recognition of the disproportionate impact of malaria on ethnicminorities, WHO in its “Strengthening Malaria Control for EthnicMinorities in the Greater Mekong Subregion” program has iden-tified the Wa, Shan-Lahu-Aka, Karen, Brau-Taliang, Kreung, andRaglai as target minorities for malaria control programs (WHO,2008b). Another characteristic of border regions is heavy popu-lation flow. Yunnan Province of China has more than 4000 km ofborder line with Myanmar, Lao PDR, and Vietnam, and popula-tion migration across the border lines exceeds 20 million per year(Hu et al., 1998). Motivations for movement vary: some peoplemove to seek better job opportunities, whereas others move to fleefrom regions afflicted by ethnic tensions, political fighting, wars, ordiseases (Martens and Hall, 2000). The mobile and displaced popu-lations are at increased risk of infection as they are exposed to newenvironments with new vectors and malaria ecologies. Individu-als from these groups often fall through the cracks of public healthefforts. Studies have shown that populations which reside in con-flict zones, such as the Karen, have higher mortality rates regardlessof malaria infection (Lee et al., 2006). Beyond an increased risk ofinfection, migrants may transport malaria parasites to new regions,acting as active transmitters. Reintroduction of malaria is a majorchallenge for countries transitioning towards malaria eliminationwhere malaria transmission in neighboring countries is intense(Tatem and Smith, 2010). This is particularly the case for Chinaand Thailand, which share lengthy land borders with the highlymalaria-endemic Myanmar. For example, in malaria patients over15 years old in Yunnan, imported cases constituted 22% of totalcases in men and 13% in women, and Myanmar was the predomi-nant location of infection for the imported cases (Lin et al., 2009).Since border regions represent the biggest reservoirs for malaria,and frequent malaria introductions by migratory human popula-tions are extremely difficult to monitor, border malaria constitutesone of the biggest obstacles for malaria elimination in these coun-tries. Therefore, ‘border malaria’ is a shared phenomenon in all thenations of the GMS, requiring in-depth studies and coordinatedinternational efforts.
5.2. Antimalarial drug resistance
The GMS has been an epicenter of antimalarial drug resistance,and parasite strains with resistance to CQ and SP have emergedhere and spread to Africa (Anderson and Roper, 2005; Roper et al.,2004). In addition, P. falciparum parasites have also developedresistance to other antimalarials such as quinine and mefloquine(Price et al., 2004; Pukrittayakamee et al., 1994). As a result, resis-tance management for effective control of malaria is of paramountimportance. Currently, artemisinins are the only group of anti-malarials that are still effective in all the endemic regions, butit is probably a matter of time that artemisinin resistance will
develop. The emergence of drug resistance de novo is throughspontaneous genetic mutations or gene duplications, which arethen selected and spread as the result of persistent drug pressure(White, 2004). Many factors in this region favor the developmentand spread of antimalarial resistance. In field malaria situations,
pica 1
dprca2s2tFaimniCsmre(waewergrbdaadardtasmfht“tppoamrmr2
5
uammetf
L. Cui et al. / Acta Tro
iagnosis of febrile illness relies mostly on symptoms withoutarasitologic confirmation, and patient adherence to treatmentegimens is often poor (Yeung and White, 2005). Despite advo-acy for using ACTs, artemisinin monotherapy is still very common,nd many manufacturers still ignore the WHO ACT policy (Butler,009). The situation is further worsened by circulation of fake andubstandard quality drugs (Dondorp et al., 2004; Newton et al.,008). As a result, parasites are more often exposed to subcura-ive dosages of the drug, which promotes resistance development.urthermore, many endemic areas in the GMS are hypoendemicnd the resident populations do not develop sufficient levels ofmmunity to kill parasites that might have survived drug treat-
ents (White and Pongtavornpinyo, 2003). Consequently, it isot surprising that parasites in the region have already shown
ncreased tolerance to artemisinins. In vitro studies in westernhina have detected reduced susceptibility of falciparum para-ites to artemisinins (Yang et al., 2003). Historically, artemisininonotherapy has been associated with a baseline recrudescence
ate of 3–5% (Li et al., 1994; Stepniewska et al., 2010); how-ver, this rate has been increased to almost 30% in some regionsWHO, 2010a). Slow parasite clearance has also been reported inestern Thailand (Luxemburger et al., 1998). Three efficacy tri-
ls conducted in Cambodia and Thailand have reported reducedfficacy of artesunate–mefloquine on the Thai–Cambodian border,ith 15–20% recrudescence rates (Denis et al., 2006; Vijaykadga
t al., 2006b). A more recent study in southern Cambodia alsoeported high failure rates of artesunate–mefloquine therapy, sug-esting that this drug combination is beginning to fail in theegion and that resistance is not confined to the Thai–Cambodianorder (Rogers et al., 2009). Studies from the Thai–Myanmar bor-er have similar findings: 13 years (1995–2007) of continuousrtesunate–mefloquine deployment in this area have resulted in
significant decline in efficacy of the three-day regimen of thisrug combination (Carrara et al., 2009). To determine whether par-sites in the GMS are developing resistance to artemisinins, severalecent clinical studies were conducted at the Thai–Cambodian bor-er and in Palin, Cambodia, and they have detected tolerance ofhe parasites to artesunate, which is manifested as prolonged par-site clearance time (Dondorp et al., 2009; Noedl et al., 2008). Thesetudies provided evidence of an early stage of resistance develop-ent in P. falciparum to artemisinins. As efforts are being made
or the containment of the “resistant” strains, data gathered so farighlight the intrinsic genetic difference among parasite popula-ions and provide a rationale for closer resistance surveillance inhotspots” of drug resistance (Noedl, 2005). Meanwhile, it is essen-ial that regional efforts and integrated measures be deployed torevent the spread of MDR, and especially artemisinin-resistant,arasites. WHO has invested significantly in curbing the spreadf artemisinin resistance and recently announced a five-pointction plan: (1) stop the spread of resistant parasites, (2) increaseonitoring and surveillance to evaluate the threat of artemisinin
esistance, (3) improve access to diagnostics and rational treat-ent with ACTs, (4) invest in artemisinin resistance-related
esearch, and (5) motivate action and mobilize resources (WHO,011).
.3. Malaria transmission surveillance and vector control
Accurate identification of vector species is essential to thenderstanding of vectorial systems, as well as to the designnd implementation of vector control methods targeting the
ain vectors in the area. Mosquito identification is achievedostly by using morphologic characteristics; however, the pres-nce of sibling species in anopheline mosquitoes requires newechniques for species differentiation. Furthermore, despite theact that PCR methods have been developed for a number of
21 (2012) 227– 239 235
malaria vector species complexes, methods of molecular diag-nosis for understudied species should be developed. Moreover,simple molecular methods for vector identification that can beused in the field settings can greatly aid malaria vector controlefforts.
Because vector species have their own unique niche require-ments, environmental changes resulting from human activitiesor global climate change can have major impacts on malariavector species, potentially causing shifts in vector communitystructure and malaria transmission dynamics. The impact of envi-ronment and climate changes on vector community structureshould therefore be examined as they contribute to changingmalaria epidemiology. In addition, certain vectors in this regiondisplay exophilic biting behavior, which is responsible for outdoortransmission of malaria. This also raises the issue of vector samplingtechniques. Developing cost-effective vector sampling techniquessuitable to various epidemiological settings (e.g., forest, swamp,and residential) is critical to malaria vector surveillance and eco-logical studies.
5.4. Mosquito resistance to insecticides
Within a single year after the introduction of pyrethroidsas an insecticide in northern Thailand, resistant mutations ofAnopheles minimus were recorded (Chareonviriyahpap et al., 1999).Since then, Anopheles minimus resistance to pyrethroid wasreported in Cambodia, Laos, Vietnam, and China (Cui et al., 2006;Prapanthadara et al., 2000; Van Bortel et al., 2008; Yu et al., 2000).Anopheles dirus likely resistant to pyrethroids has been reported incentral Vietnam (Van Bortel et al., 2008). High level of resistancein Anopheles sinensis was reported in China (Kim et al., 2003). Thepatchy distribution of pyrethroid resistance in the vector popula-tion calls for careful resistance monitoring. Currently, pyrethroidresistance detection is based on the traditional bioassay detec-tion method, kdr mutation or detoxification enzyme activities. Thebioassay method has several limitations: it requires a large num-ber of field-caught live mosquitoes, which is often difficult to obtainin less abundant sites, and mosquito age and physiological condi-tion confound the bioassay results (WHO, 1998). Standardization ofthe bioassay method is often difficult across sentinel sites becausedifferent sites have different temperatures and humidity. Molec-ular or biochemical methods are expected to be more sensitiveand specific; however, the relative importance of kdr mutation ordetoxification enzyme in the resistance phenotype is unknown.Understanding the resistance mechanisms is important for thedevelopment of molecular or biochemical resistance diagnostictools, which are critical to the sustained effectiveness of LLINs andIRS program.
5.5. Counterfeit antimalarial drugs
The WHO defines counterfeit/fake drugs as drugs that are“deliberately and fraudulently mislabeled with respect to iden-tity and/or source.” This includes products with the correct orwrong ingredients, without active ingredients, with insufficientactive ingredients, or with fake packaging. Substandard drugs referto genuine drug products that do not meet quality specificationsset for them. Counterfeit and poor-quality medicines are a majorimpediment to the improvement of public health, and are partic-ularly widespread in developing countries (Caudron et al., 2008).The WHO has estimated that about 25% of the medicines con-
sumed in developing countries are counterfeit (WHO, 2006). Inmany of the developing countries, government agencies such asthe Customs and police lack the capability to stop counterfeit drugsentering the countries, and as a result, counterfeit drugs thrivein private markets. Fake drugs not only reduce treatment effi-
2 pica 1
ciMspcitctiiibnsa1ewoqtpai2bc(stdmtttfwnc
cagocsmiaGioTtti
A
IAN
36 L. Cui et al. / Acta Tro
acy and promote resistance development, but also may resultn life-threatening complications and even death of the patients.
alaria is a potentially fatal disease, which requires early diagno-is and proper treatment with effective antimalarial drugs. As therogression of malaria from mild to severe disease is rapid, espe-ially in young children, giving drugs that contain little or no activengredient is parallel to manslaughter (Newton et al., 2006). Coun-erfeit antimalarial drugs are a huge problem in malaria-endemicountries. Although the situation is slightly better in African coun-ries (Amin and Kokwaro, 2007), Asian countries, especially thosen the GMS, face a much greater challenge to combat the grow-ng threat of counterfeit medicine (Dondorp et al., 2004). Evenn countries such as Thailand, where legislative procedures areetter, substandard antimalarial medicines still constitute a sig-ificant proportion of drugs sold. A survey conducted in 2006 onix antimalarials from 27 government hospitals, 27 malaria clinics,nd 53 drug stores in Thailand revealed that 15.4% of artesunate,1.1% of CQ, and 29.4% of quinine were substandard (Vijaykadgat al., 2006a). In other countries of the GMS, the situation is farorse. In Cambodia, a survey conducted in 2006 found that 79%
f the antimalarial drugs were not registered and 27% failed theuality tests (Lon et al., 2006). Since 1998, an epidemic of mul-iple types of counterfeit artesunate tablets has affected malariaatients in the mainland of SE Asia. In this region, between 38%nd 53% of artesunate blister packages sampled contained no activengredients (Dondorp et al., 2004; Hall et al., 2006; Newton et al.,001, 2003). As many as 14 physical types of fake artesunate haveeen found (Newton et al., 2006, 2007, 2008). In addition, someounterfeits contained dangerously small amounts of artesunateNewton et al., 2008). Even some genuine drugs are often sub-tandard (Keoluangkhot et al., 2008), compromising their expectedherapeutic effect. Another problem associated with substandardrugs is expiration and degradation. Because effective treatment ofalaria is essential for malaria control and elimination, monitoring
he quality of antimalarial drugs needs to be enforced more effec-ively. Recently, USAID entered into a new cooperative agreemento expand their joint efforts to combat the proliferation of counter-eit and substandard medicines (http://www.usp.org/worldwide),hich should greatly strengthen local efforts. In addition, coordi-ation between countries is required to thwart the epidemics ofounterfeiting.
Taken together, increased government investment in malariaontrol in recent years, bolstered by international support suchs the GFATM, has led to intensified malaria control efforts andreatly improved the malaria situations in all GMS nations. More-ver, the adoption of malaria elimination as the ultimate goal inertain nations is encouraging. Despite this, the GMS nations aretill encountering many obstacles on their way towards eliminatingalaria from this entire region. Many of these obstacles includ-
ng ‘border malaria’, MDR P. falciparum parasites, and counterfeitnd substandard antimalarial drugs, are shared phenomena of allMS nations, and require coordinated efforts. In addition, there are
mportant knowledge gaps in malaria epidemiology, vector biol-gy and disease transmission, and mechanisms of drug resistance.herefore, in-depth research on all these urgent topics is neededo provide timely support for effective malaria control activities sohat malaria elimination can ultimately be achieved and sustainedn the GMS.
cknowledgements
This work was supported by National Institute of Allergy andnfectious Diseases (NIAID), National Institutes of Health (NIH) (U19I089672) and partly by the Division of Intramural Research, NIAID,IH.
21 (2012) 227– 239
References
Alves, F.P., Gil, L.H.S., Marrelli, M.T., Ribolla, P.E.M., Camargo, E.P., Pereira DaSilva, L.H., 2005. Asymptomatic carriers of Plasmodium spp. as infection sourcefor malaria vector mosquitoes in the Brazilian Amazon. J. Med. Entomol. 42,777–779.
Amin, A.A., Kokwaro, G.O., 2007. Antimalarial drug quality in Africa. J. Clin. Pharm.Ther. 32, 429–440.
Anderson, T.J., Roper, C., 2005. The origins and spread of antimalarial drug resistance:lessons for policy makers. Acta Trop. 94, 269–280.
Beyrer, C., Lee, T.J., 2008. Responding to infectious diseases in Burma and her borderregions. Conflict Health 2, 2.
Brooke, B.D., Kloke, G., Hunt, R.H., Koekemoer, L.L., Temu, E.A., Taylor, M.E., Small, G.,Hemingway, J., Coetzee, M., 2001. Bioassay and biochemical analyses of insecti-cide resistance in southern African Anopheles funestus (Diptera: Culicidae). Bull.Entomol. Res. 91, 265–272.
Butler, D., 2009. Malaria drug-makers ignore WHO ban. Nature 460, 310–311.Carrara, V.I., Zwang, J., Ashley, E.A., Price, R.N., Stepniewska, K., Barends, M., Brock-
man, A., Anderson, T., McGready, R., Phaiphun, L., Proux, S., van Vugt, M.,Hutagalung, R., Lwin, K.M., Phyo, A.P., Preechapornkul, P., Imwong, M., Pukrit-tayakamee, S., Singhasivanon, P., White, N.J., Nosten, F., 2009. Changes in thetreatment responses to artesunate–mefloquine on the northwestern border ofThailand during 13 years of continuous deployment. PLoS One 4, e4551.
Caudron, J.M., Ford, N., Henkens, M., Mace, C., Kiddle-Monroe, R., Pinel, J., 2008.Substandard medicines in resource-poor settings: a problem that can no longerbe ignored. Trop. Med. Int. Health 13, 1062–1072.
Chareonviriyahpap, T., Aum-Aung, B., Ratanatham, S., 1999. Current insecticideresistance patterns in mosquito vectors in Thailand. Southeast Asian J. Trop.Med. Public Health 30, 184–194.
Chareonviriyaphap, T., Bangs, M.J., Ratanatham, S., 2000. Status ofmalaria in Thailand. Southeast Asian J. Trop. Med. Public Health 31,225–237.
Chareonviriyaphap, T., Prabaripai, A., Bangs, M.J., Aum-Aung, B., 2003. Seasonalabundance and blood feeding activity of Anopheles minimus Theobald (Diptera:Culicidae) in Thailand. J. Med. Entomol. 40, 876–881.
Chaveepojnkamjorn, W., Pichainarong, N., 2004. Malaria infection among themigrant population along the Thai–Myanmar border area. Southeast Asian J.Trop. Med. Public Health 35, 48–52.
Chaveepojnkamjorn, W., Pichainarong, N., 2005. Behavioral factors and malariainfection among the migrant population, Chiang Rai province. J. Med. Assoc.Thai. 88, 1293–1301.
Childs, D.Z., Cattadori, I.M., Suwonkerd, W., Prajakwong, S., Boots, M., 2006. Spa-tiotemporal patterns of malaria incidence in northern Thailand. Trans. R. Soc.Trop. Med. Hyg. 100, 623–631.
China MOH, 2009. The People’s Republic of China—From Malaria Control to Elimi-nation: A Revised National Malaria Strategy.
Clements, A.C., Barnett, A.G., Cheng, Z.W., Snow, R.W., Zhou, H.N., 2009. Space-timevariation of malaria incidence in Yunnan province, China. Malar. J. 8, 180.
Collins, F.H., Paskewitz, S.M., 1996. A review of the use of ribosomal DNA (rDNA) todifferentiate among cryptic Anopheles species. Insect Mol. Biol. 5, 1–9.
Cui, F., Raymond, M., Qiao, C.L., 2006. Insecticide resistance in vector mosquitoes inChina. Pest Manag. Sci. 62, 1013–1022.
Cui, L., Mascorro, C.N., Fan, Q., Rzomp, K.A., Khuntirat, B., Zhou, G., Chen, H., Yan, G.,Sattabongkot, J., 2003. Genetic diversity and multiple infections of Plasmodiumvivax malaria in Western Thailand. Am. J. Trop. Med. Hyg. 68, 613–619.
Delacollette, C., D’Souza, C., Christophel, E., Thimasarn, K., Abdur, R., Bell, D., Dai, T.C.,Gopinath, D., Lu, S., Mendoza, R., Ortega, L., Rastogi, R., Tantinimitkul, C., Ehren-berg, J., 2009. Malaria trends and challenges in the Greater Mekong Subregion.Southeast Asian J. Trop. Med. Public Health 40, 674–691.
Denis, M.B., Tsuyuoka, R., Lim, P., Lindegardh, N., Yi, P., Top, S.N., Socheat, D.,Fandeur, T., Annerberg, A., Christophel, E.M., Ringwald, P., 2006. Efficacyof artemether-lumefantrine for the treatment of uncomplicated falciparummalaria in northwest Cambodia. Trop. Med. Int. Health 11, 1800–1807.
Dondorp, A.M., Newton, P.N., Mayxay, M., Van Damme, W., Smithuis, F.M., Yeung,S., Petit, A., Lynam, A.J., Johnson, A., Hien, T.T., McGready, R., Farrar, J.J., Looa-reesuwan, S., Day, N.P., Green, M.D., White, N.J., 2004. Fake antimalarials inSoutheast Asia are a major impediment to malaria control: multinational cross-sectional survey on the prevalence of fake antimalarials. Trop. Med. Int. Health9, 1241–1246.
Dondorp, A.M., Nosten, F., Yi, P., Das, D., Phyo, A.P., Tarning, J., Lwin, K.M., Ariey, F.,Hanpithakpong, W., Lee, S.J., Ringwald, P., Silamut, K., Imwong, M., Chotivanich,K., Lim, P., Herdman, T., An, S.S., Yeung, S., Singhasivanon, P., Day, N.P., Linde-gardh, N., Socheat, D., White, N.J., 2009. Artemisinin resistance in Plasmodiumfalciparum malaria. N. Engl. J. Med. 361, 455–467.
Erhart, A., Ngo, D.T., Phan, V.K., Ta, T.T., Van Overmeir, C., Speybroeck, N., Obsomer, V.,Le, X.H., Le, K.T., Coosemans, M., D’Alessandro, U., 2005. Epidemiology of forestmalaria in central Vietnam: a large scale cross-sectional survey. Malar. J. 4, 58.
Feachem, R.G., 2009. The Malaria Elimination Group. Shrinking the Malaria Map: AGuide on Malaria Elimination for Policy Makers. The Global Health Group, GlobalHealth Sciences, University of California, San Francisco, San Francisco.
Feachem, R.G., Sabot, O., 2008. A new global malaria eradication strategy. Lancet371, 1633–1635.
Feachem, R.G., Phillips, A.A., Hwang, J., Cotter, C., Wielgosz, B., Greenwood,B.M., Sabot, O., Rodriguez, M.H., Abeyasinghe, R.R., Ghebreyesus, T.A., Snow,R.W., 2010. Shrinking the malaria map: progress and prospects. Lancet 376,1566–1578.
pica 1
G
G
H
H
H
H
H
H
H
I
J
K
K
K
L
L
L
L
L
L
L
L
L
L
L
M
L. Cui et al. / Acta Tro
ao, Q., Beebe, N.W., Cooper, R.D., 2004. Molecular identification of the malariavectors Anopheles anthropophagus and Anopheles sinensis (Diptera: Culicidae)in central China using polymerase chain reaction and appraisal of their positionwithin the Hyrcanus group. J. Med. Entomol. 41, 5–11.
reen, C.A., Gass, R.F., Munstermann, L.E., Baimai, V., 1990. Population-genetic evi-dence for two species in Anopheles minimus in Thailand. Med. Vet. Entomol. 4,25–34.
all, K.A., Newton, P.N., Green, M.D., De Veij, M., Vandenabeele, P., Pizzanelli, D.,Mayxay, M., Dondorp, A., Fernandez, F.M., 2006. Characterization of counterfeitartesunate antimalarial tablets from southeast Asia. Am. J. Trop. Med. Hyg. 75,804–811.
arbach, R.E., 2004. The classification of genus Anopheles (Diptera: Culicidae):a working hypothesis of phylogenetic relationships. Bull. Entomol. Res. 94,537–553.
arbach, R.E., Garros, C., Nguyen, D.M., Manguin, S., 2007. Formal taxonomy ofspecies C of the Anopheles minimus sibling species complex (Diptera: Culicidae).Zootaxa 1654, 41–54.
astings, I.M., 2004. The origins of antimalarial drug resistance. Trends Parasitol. 20,512–518.
u, H., Singhasivanon, P., Salazar, N.P., Thimasarn, K., Li, X., Wu, Y., Yang, H., Zhu,D., Supavej, S., Looarecsuwan, S., 1998. Factors influencing malaria endemicityin Yunnan Province, PR China (analysis of spatial pattern by GIS). Geograph-ical Information System. Southeast Asian J. Trop. Med. Public Health 29,191–200.
ui, F.M., Xu, B., Chen, Z.W., Cheng, X., Liang, L., Huang, H.B., Fang, L.Q., Yang, H.,Zhou, H.N., Yang, H.L., Zhou, X.N., Cao, W.C., Gong, P., 2009. Spatio-temporaldistribution of malaria in Yunnan Province, China. Am. J. Trop. Med. Hyg. 81,503–509.
ung le, Q., Vries, P.J., Giao, P.T., Nam, N.V., Binh, T.Q., Chong, M.T., Quoc, N.T., Thanh,T.N., Hung, L.N., Kager, P.A., 2002. Control of malaria: a successful experiencefrom Viet Nam. Bull. WHO 80, 660–666.
sozumi, R., Uemura, H., Le, D.D., Truong, V.H., Nguyen, D.G., Ha, V.V., Bui, Q.P.,Nguyen, V.T., Nakazawa, S., 2010. Longitudinal survey of Plasmodium falciparuminfection in Vietnam: characteristics of antimalarial resistance and their associ-ated factors. J. Clin. Microbiol. 48, 70–77.
ongwutiwes, S., Putaporntip, C., Iwasaki, T., Sata, T., Kanbara, H., 2004. Naturallyacquired Plasmodium knowlesi malaria in human, Thailand. Emerg. Infect. Dis.10, 2211–2213.
eoluangkhot, V., Green, M.D., Nyadong, L., Fernandez, F.M., Mayxay, M., New-ton, P.N., 2008. Impaired clinical response in a patient with uncomplicatedfalciparum malaria who received poor-quality and underdosed intramuscularartemether. Am. J. Trop. Med. Hyg. 78, 552–555.
idson, C., Indaratna, K., Looareesuwan, S., 2000. The malaria cauldron of South-east Asia: conflicting strategies of contiguous nation states. Parassitologia 42,101–110.
im, C., Klein, T.A., Song, G.H., Strickman, D., 2003. Molecular confirmation ofAnopheles (Anopheles) lesteri from the Republic of South Korea and its geneticidentity with An. (Ano.) anthropophagus from China (Diptera: Culicidae).Zootaxa 378, 1–14.
ee, H.I., Lee, J.S., Shin, E.H., Lee, W.J., Kim, Y.Y., Lee, K.R., 2001. Malaria transmissionpotential by Anopheles sinensis in the Republic of Korea. Korean J. Parasitol. 39,185–192.
ee, T.J., Mullany, L.C., Richards, A.K., Kuiper, H.K., Maung, C., Beyrer, C., 2006. Mor-tality rates in conflict zones in Karen, Karenni, and Mon states in eastern Burma.Trop. Med. Int. Health 11, 1119–1127.
i, G.Q., Guo, X.B., Fu, L.C., Jian, H.X., Wang, X.H., 1994. Clinical trials of artemisininand its derivatives in the treatment of malaria in China. Trans. R. Soc. Trop. Med.Hyg. 88 (Suppl. 1), 5–6.
i, H., Zhang, Z., Du, Z., Chen, G., Chen, Z., 2005. Investigation into an outbreak ofmalaria in Lincang Prefecture on China–Myanmar border and the neighboringarea outside China. China Trop. Med. 5, 55–60.
i, Z.Z., Zhang, M.C., Wu, Y.G., Zhong, B.L., Lin, G.Y., Huang, H., 1989. Trial ofdeltamethrin impregnated bednets for the control of malaria transmitted byAnopheles sinensis and Anopheles anthropophagus. Am. J. Trop. Med. Hyg. 40,356–359.
iang, G.L., Sun, X.D., Wang, J., Zhang, Z.X., 2009. Sensitivity of Plasmodium vivaxto chloroquine in Laza City, Myanmar. Chin. J. Parasitol. Parasitic Dis. 27,175–176.
imrat, D., Rojruthai, B., Apiwathnasorn, C., Samung, Y., Prommongkol, S., 2001.Anopheles barbirostris/campestris as a probable vector of malaria in Aranyapra-thet, Sa Kaeo Province. Southeast Asian. J. Trop. Med. Public Health 32, 739–744.
in, H., Lu, L., Tian, L., Zhou, S., Wu, H., Bi, Y., Ho, S.C., Liu, Q., 2009. Spatial and temporaldistribution of falciparum malaria in China. Malar. J. 8, 130.
iu, H., Nie, R.-H., Li, C.-F., Sun, Y.-H., Li, G.-S., 2009. Active detection of malaria casesin Myanmar Wa ethnical villages of China–Myanmar border. Parasitoses Infect.Dis. 7, 6–9.
on, C.T., Tsuyuoka, R., Phanouvong, S., Nivanna, N., Socheat, D., Sokhan, C., Blum,N., Christophel, E.M., Smine, A., 2006. Counterfeit and substandard antimalarialdrugs in Cambodia. Trans. R. Soc. Trop. Med. Hyg. 100, 1019–1024.
uxemburger, C., Brockman, A., Silamut, K., Nosten, F., van Vugt, M., Gimenez, F.,
Chongsuphajaisiddhi, T., White, N.J., 1998. Two patients with falciparum malariaand poor in vivo responses to artesunate. Trans. R. Soc. Trop. Med. Hyg. 92,668–669.a, Y., Li, S., Xu, J., 2006. Molecular identification and phylogeny of the Macula-tus group of Anopheles mosquitoes (Diptera: Culicidae) based on nuclear andmitochondrial DNA sequences. Acta Trop. 99, 272–280.
21 (2012) 227– 239 237
Manguin, S., Garros, C., Dusfour, I., Harbach, R.E., Coosemans, M., 2008. Bionomics,taxonomy, and distribution of the major malaria vector taxa of Anophelessubgenus Cellia in Southeast Asia: an updated review. Infect. Genet. Evol. 8,489–503.
Manh, B.H., Clements, A.C., Thieu, N.Q., Hung, N.M., Hung, L.X., Hay, S.I., Hien, T.T.,Wertheim, H.F., Snow, R.W., Horby, P., 2011. Social and environmental determi-nants of malaria in space and time in Viet Nam. Int. J. Parasitol. 41, 109–116.
Martens, P., Hall, L., 2000. Malaria on the move: human population movement andmalaria transmission. Emerg. Infect. Dis. 6, 103–109.
Martinez-Torres, D., Chandre, F., Williamson, M.S., Darriet, F., Berge, J.B., Devon-shire, A.L., Guillet, P., Pasteur, N., Pauron, D., 1998. Molecular characterizationof pyrethroid knockdown resistance (kdr) in the major malaria vector Anophelesgambiae s.s. Insect Mol. Biol. 7, 179–184.
Mayxay, M., Nair, S., Sudimack, D., Imwong, M., Tanomsing, N., Pongvongsa, T.,Phompida, S., Phetsouvanh, R., White, N.J., Anderson, T.J., Newton, P.N., 2007.Combined molecular and clinical assessment of Plasmodium falciparum anti-malarial drug resistance in the Lao People’s Democratic Republic (Laos). Am.J. Trop. Med. Hyg. 77, 36–43.
Mayxay, M., Newton, P.N., Khanthavong, M., Tiengkham, P., Phetsouvanh, R.,Phompida, S., Brockman, A., White, N.J., 2003. Chloroquine versus sulfadoxine-pyrimethamine for treatment of Plasmodium falciparum malaria in SavannakhetProvince, Lao People’s Democratic Republic: an assessment of national anti-malarial drug recommendations. Clin. Infect. Dis. 37, 1021–1028.
Meng, H., Zhang, R., Yang, H., Fan, Q., Su, X., Miao, J., Cui, L., Yang, Z., 2010. In vitroSensitivity of Plasmodium falciparum clinical isolates from the China–Myanmarborder area to quinine and association with polymorphism in the Na+/H+exchanger. Antimicrob. Agents Chemother. 54, 4306–4313.
Moonen, B., Cohen, J.M., Snow, R.W., Slutsker, L., Drakeley, C., Smith, D.L.,Abeyasinghe, R.R., Rodriguez, M.H., Maharaj, R., Tanner, M., Targett, G., 2010.Operational strategies to achieve and maintain malaria elimination. Lancet 376,1592–1603.
Morgan, K., O’Loughlin, S.M., Mun-Yik, F., Linton, Y.M., Somboon, P., Min, S., Htun,P.T., Nambanya, S., Weerasinghe, I., Sochantha, T., Prakash, A., Walton, C., 2009.Molecular phylogenetics and biogeography of the Neocellia Series of Anophelesmosquitoes in the Oriental Region. Mol. Phylogenet. Evol. 52, 588–601.
Myanmar MOH, 2010. National Strategic Plan: Malaria Prevention and Control2010–2015, pp. 1–77.
Newton, P., Proux, S., Green, M., Smithuis, F., Rozendaal, J., Prakongpan, S., Choti-vanich, K., Mayxay, M., Looareesuwan, S., Farrar, J., Nosten, F., White, N.J., 2001.Fake artesunate in southeast Asia. Lancet 357, 1948–1950.
Newton, P.N., Dondorp, A., Green, M., Mayxay, M., White, N.J., 2003. Counterfeitartesunate antimalarials in southeast Asia. Lancet 362, 169.
Newton, P.N., Fernandez, F.M., Plancon, A., Mildenhall, D.C., Green, M.D., Ziyong, L.,Christophel, E.M., Phanouvong, S., Howells, S., McIntosh, E., Laurin, P., Blum, N.,Hampton, C.Y., Faure, K., Nyadong, L., Soong, C.W., Santoso, B., Zhiguang, W.,Newton, J., Palmer, K., 2008. A collaborative epidemiological investigation intothe criminal fake artesunate trade in South East Asia. PLoS Med. 5, e32.
Newton, P.N., Green, M.D., Fernandez, F., 2007. Counterfeit artemisinin derivativesand Africa: update from authors. PLoS Med. 4, e139.
Newton, P.N., McGready, R., Fernandez, F., Green, M.D., Sunjio, M., Bruneton, C.,Phanouvong, S., Millet, P., Whitty, C.J., Talisuna, A.O., Proux, S., Christophel, E.M.,Malenga, G., Singhasivanon, P., Bojang, K., Kaur, H., Palmer, K., Day, N.P., Green-wood, B.M., Nosten, F., White, N.J., 2006. Manslaughter by fake artesunate inAsia—will Africa be next? PLoS Med. 3, e197.
Noedl, H., 2005. Artemisinin resistance: how can we find it? Trends Parasitol. 21,404–405.
Noedl, H., Se, Y., Schaecher, K., Smith, B.L., Socheat, D., Fukuda, M.M., 2008. Evi-dence of artemisinin-resistant malaria in western Cambodia. N. Engl. J. Med.359, 2619–2620.
Noedl, H., Se, Y., Sriwichai, S., Schaecher, K., Teja-Isavadharm, P., Smith, B., Rutvi-suttinunt, W., Bethell, D., Surasri, S., Fukuda, M.M., Socheat, D., Chan Thap, L.,2010. Artemisinin resistance in Cambodia: a clinical trial designed to address anemerging problem in Southeast Asia. Clin. Infect. Dis. 51, 82–89.
Noedl, H., Socheat, D., Satimai, W., 2009. Artemisinin-resistant malaria in Asia. N.Engl. J. Med. 361, 540–541.
Obsomer, V., Defourny, P., Coosemans, M., 2007. The Anopheles dirus complex: spatialdistribution and environmental drivers. Malar. J. 6, 26.
Oo, T.T., Storch, V., Becker, N., 2003. Anopheles dirus and its role in malaria transmis-sion in Myanmar. J. Vector Ecol. 28, 175–183.
Overgaard, H.J., Sandve, S.R., Suwonkerd, W., 2005. Evidence of anopheline mosquitoresistance to agrochemicals in northern Thailand. Southeast Asian J. Trop. Med.Public Health 36 (Suppl. 4), 152–157.
Overgaard, H.J., Tsuda, Y., Suwonkerd, W., Takagi, M., 2002. Characteristics ofAnopheles minimus Theobald (Diptera: Culicidae) larval habitats in northernThailand. Environ. Entomol. 31, 134–141.
Parida, M., Sannarangaiah, S., Dash, P.K., Rao, P.V., Morita, K., 2008. Loop mediatedisothermal amplification (LAMP): a new generation of innovative gene amplifi-cation technique; perspectives in clinical diagnosis of infectious diseases. Rev.Med. Virol. 18, 407–421.
Phuc, H.K., Ball, A.J., Son, L., Hanh, N.V., Tu, N.D., Lien, N.G., Verardi, A., Townson,
H., 2003. Multiplex PCR assay for malaria vector Anopheles minimus and fourrelated species in the Myzomyia Series from Southeast Asia. Med. Vet. Entomol.17, 423–428.Pichainarong, N., Chaveepojnkamjorn, W., 2004. Malaria infection and life-style fac-tors among hilltribes along the Thai–Myanmar border area, northern Thailand.Southeast Asian J. Trop. Med. Public Health 35, 834–839.
2 pica 1
P
P
P
P
P
P
P
R
R
R
R
R
R
R
S
S
S
S
S
S
S
S
S
T
T
T
38 L. Cui et al. / Acta Tro
inichpongse, S., Bullner, G.R., 1967. The current status of malaria entomology inThailand. Warasan Mal. 11, 43.
rapanthadara, L., Koottathep, S., Promtet, N., Suwonkerd, W., Ketterman, A.J.,Somboon, P., 2000. Correlation of glutathione S-transferase and DDT dehy-drochlorinase activities with DDT susceptibility in Anopheles and Culexmosquitoes from northern Thailand. Southeast Asian J. Trop. Med. Public Health31 (Suppl. 1), 111–118.
rice, R.N., Uhlemann, A.C., Brockman, A., McGready, R., Ashley, E., Phaipun, L., Patel,R., Laing, K., Looareesuwan, S., White, N.J., Nosten, F., Krishna, S., 2004. Meflo-quine resistance in Plasmodium falciparum and increased pfmdr1 gene copynumber. Lancet 364, 438–447.
rothero, R.M., 1999. Malaria, forests and people in Southeast Asia, Singapore. J.Geography 20, 76–85.
ukrittayakamee, S., Supanaranond, W., Looareesuwan, S., Vanijanonta, S., White,N.J., 1994. Quinine in severe falciparum malaria: evidence of declining efficacyin Thailand. Trans. R. Soc. Trop. Med. Hyg. 88, 324–327.
utaporntip, C., Hongsrimuang, T., Seethamchai, S., Kobasa, T., Limkittikul, K., Cui, L.,Jongwutiwes, S., 2009a. Differential prevalence of Plasmodium infections andcryptic Plasmodium knowlesi malaria in humans in Thailand. J. Infect. Dis. 199,1143–1150.
utaporntip, C., Jongwutiwes, S., Ferreira, M.U., Kanbara, H., Udomsangpetch, R., Cui,L., 2009b. Limited global diversity of the Plasmodium vivax merozoite surfaceprotein 4 gene. Infect. Genet. Evol. 9, 821–826.
anson, H., Jensen, B., Vulule, J.M., Wang, X., Hemingway, J., Collins, F.H., 2000. Identi-fication of a point mutation in the voltage-gated sodium channel gene of KenyanAnopheles gambiae associated with resistance to DDT and pyrethroids. InsectMol. Biol. 9, 491–497.
athod, P.K., McErlean, T., Lee, P.C., 1997. Variations in frequencies of drug resistancein Plasmodium falciparum. Proc. Natl. Acad. Sci. U.S.A. 94, 9389–9393.
ichards, A.K., Banek, K., Mullany, L.C., Lee, C.I., Smith, L., Oo, E.K., Lee, T.J., 2009. Cross-border malaria control for internally displaced persons: observational resultsfrom a pilot programme in eastern Burma/Myanmar. Trop. Med. Int. Health 14,512–521.
oberts, L., Enserink, M., 2007. Malaria. Did they really say eradication? Science 318,1544–1545.
ogers, W.O., Sem, R., Tero, T., Chim, P., Lim, P., Muth, S., Socheat, D., Ariey, F.,Wongsrichanalai, C., 2009. Failure of artesunate–mefloquine combination ther-apy for uncomplicated Plasmodium falciparum malaria in southern Cambodia.Malar. J. 8, 10.
oper, C., Pearce, R., Nair, S., Sharp, B., Nosten, F., Anderson, T., 2004. Intercontinentalspread of pyrimethamine-resistant malaria. Science 305, 1124.
ueda, L.M., Kim, H.C., Klein, T.A., Pecor, J.E., Li, C., Sithiprasasna, R., Debboun, M.,Wilkerson, R.C., 2006. Distribution and larval habitat characteristics of Anopheleshyrcanus group and related mosquito species (Diptera: Culicidae) in South Korea.J. Vector Ecol. 31, 198–205.
abot, O., Cohen, J.M., Hsiang, M.S., Kahn, J.G., Basu, S., Tang, L., Zheng, B., Gao, Q.,Zou, L., Tatarsky, A., Aboobakar, S., Usas, J., Barrett, S., Cohen, J.L., Jamison, D.T.,Feachem, R.G., 2010. Costs and financial feasibility of malaria elimination. Lancet376, 1604–1615.
anh, N.H., Van Dung, N., Thanh, N.X., Trung, T.N., Van Co, T., Cooper, R.D., 2008.Forest malaria in central Vietnam. Am. J. Trop. Med. Hyg. 79, 652–654.
attabongkot, J., Tsuboi, T., Zollner, G.E., Sirichaisinthop, J., Cui, L., 2004. Plasmodiumvivax transmission: chances for control? Trends Parasitol. 20, 192–198.
exton, J.D., 1994. Impregnated bednets for malaria control: biological success andsocial responsibility. Am. J. Trop. Med. Hyg. 50, 72–81.
heng, H.F., Zhou, S.S., Gu, Z.C., Zheng, X., 2003. Malaria situation in the People’sRepublic of China in 2002. Chin. J. Parasitol. Parasitic Dis. 21, 193–196.
inghasivanon, P., 1999. Mekong malaria. Malaria, multi-drug resistance and eco-nomic development in the Greater Mekong Subregion of Southeast Asia.Southeast Asian J. Trop. Med. Public Health 30 (Suppl. 4), 1–101.
leigh, A.C., Liu, X.L., Jackson, S., Li, P., Shang, L.Y., 1998. Resurgence of vivax malariain Henan Province, China. Bull. WHO 76, 265–270.
ocheat, D., Denis, M.B., Fandeur, T., Zhang, Z., Yang, H., Xu, J., Zhou, X., Phompida,S., Phetsouvanh, R., Lwin, S., Lin, K., Win, T., Than, S.W., Htut, Y., Prajakwong,S., Rojanawatsirivet, C., Tipmontree, R., Vijaykadga, S., Konchom, S., Cong le, D.,Thien, N.T., Thuan le, K., Ringwald, P., Schapira, A., Christophel, E., Palmer, K.,Arbani, P.R., Prasittisuk, C., Rastogi, R., Monti, F., Urbani, C., Tsuyuoka, R., Hoyer, S.,Otega, L., Thimasarn, K., Songcharoen, S., Meert, J.P., Gay, F., Crissman, L., Cho Min,N., Chansuda, W., Darasri, D., Indaratna, K., Singhasivanon, P., Chuprapawan, S.,Looareesuwan, S., Supavej, S., Kidson, C., Baimai, V., Yimsamran, S., Buchachart,K., 2003. Mekong malaria. II. Update of malaria, multi-drug resistance and eco-nomic development in the Mekong region of Southeast Asia. Southeast Asian J.Trop. Med. Public Health 34 (Suppl. 4), 1–102.
tepniewska, K., Ashley, E., Lee, S.J., Anstey, N., Barnes, K.I., Binh, T.Q., D’Alessandro,U., Day, N.P., de Vries, P.J., Dorsey, G., Guthmann, J.P., Mayxay, M., Newton, P.N.,Olliaro, P., Osorio, L., Price, R.N., Rowland, M., Smithuis, F., Taylor, W.R., Nosten, F.,White, N.J., 2010. In vivo parasitological measures of artemisinin susceptibility.J. Infect. Dis. 201, 570–579.
ang, L.H., Qian, H.L., Xu, S.H., 1991. Malaria and its control in the People’s Republicof China. Southeast Asian J. Trop. Med. Public Health 22, 467–476.
atem, A.J., Smith, D.L., 2010. International population movements and regional Plas-modium falciparum malaria elimination strategies. Proc. Natl. Acad. Sci. U.S.A.107, 12222–12227.
atem, A.J., Smith, D.L., Gething, P.W., Kabaria, C.W., Snow, R.W., Hay, S.I., 2010.Ranking of elimination feasibility between malaria-endemic countries. Lancet376, 1579–1591.
21 (2012) 227– 239
Thang, N.D., Erhart, A., Hung le, X., Thuan le, K., Xa, N.X., Thanh, N.N., Ky, P.V., Coose-mans, M., Speybroeck, N., D’Alessandro, U., 2009. Rapid decrease of malariamorbidity following the introduction of community-based monitoring in a ruralarea of central Vietnam. Malar. J. 8, 3.
Thanh, N.V., Toan, T.Q., Cowman, A.F., Casey, G.J., Phuc, B.Q., Tien, N.T., Hung,N.M., Biggs, B.A., 2010. Monitoring for Plasmodium falciparum drug resistanceto artemisinin and artesunate in Binh Phuoc Province, Vietnam: 1998–2009.Malar. J. 9, 181.
Tomita, N., Mori, Y., Kanda, H., Notomi, T., 2008. Loop-mediated isothermal amplifi-cation (LAMP) of gene sequences and simple visual detection of products. Nat.Protoc. 3, 877–882.
Van Bortel, W., Trung, H.D., Thuan, L.K., Sochantha, T., Socheat, D., Sumrandee, C.,Baimai, V., Keokenchanh, K., Samlane, P., Roelants, P., 2008. The insecticide resis-tance status of malaria vectors in the Mekong region. Malar. J. 7, 102.
Van den Eede, P., Van, H.N., Van Overmeir, C., Vythilingam, I., Duc, T.N., Hung le,X., Manh, H.N., Anne, J., D’Alessandro, U., Erhart, A., 2009. Human Plasmodiumknowlesi infections in young children in central Vietnam. Malar. J. 8, 249.
Verhaeghen, K., Van Bortel, W., Trung, H.D., Sochantha, T., Coosemans, M., 2009.Absence of knockdown resistance suggests metabolic resistance in the mainmalaria vectors of the Mekong region. Malar. J. 8, 84.
Verhaeghen, K., Van Bortel, W., Trung, H.D., Sochantha, T., Keokenchanh, K., Coose-mans, M., 2010. Knockdown resistance in Anopheles vagus, An. sinensis, An.paraliae and An. peditaeniatus populations of the Mekong region. Parasite Vectors3, 59.
Vijaykadga, S., Cholpol, S., Sitthimongkol, S., Pawaphutanan, A., Pinyoratanachot, A.,Rojanawatsirivet, C., Kovithvattanapong, R., Thimasarn, K., 2006a. Strengtheningof national capacity in implementation of antimalarial drug quality assurancein Thailand. Southeast Asian J. Trop. Med. Public Health 37 (Suppl. 3), 5–10.
Vijaykadga, S., Rojanawatsirivej, C., Cholpol, S., Phoungmanee, D., Nakavej, A.,Wongsrichanalai, C., 2006b. In vivo sensitivity monitoring of mefloquinemonotherapy and artesunate–mefloquine combinations for the treatment ofuncomplicated falciparum malaria in Thailand in 2003. Trop. Med. Int. Health11, 211–219.
Walton, C., Handley, J.M., Kuvangkadilok, C., Collins, F.H., Harbach, R.E., Baimai, V.,Butlin, R.K., 1999. Identification of five species of the Anopheles dirus complexfrom Thailand, using allele-specific polymerase chain reaction. Med. Vet. Ento-mol. 13, 24–32.
Walton, C., Somboon, P., Harbach, R.E., Zhang, S., Weerasinghe, I., O’Loughlin, S.M.,Phompida, S., Sochantha, T., Tun-Lin, W., Chen, B., Butlin, R.K., 2007a. Molecularidentification of mosquito species in the Anopheles annularis group in southernAsia. Med. Vet. Entomol. 21, 30–35.
Walton, C., Somboon, P., O’Loughlin, S.M., Zhang, S., Harbach, R.E., Linton, Y.M., Chen,B., Nolan, K., Duong, S., Fong, M.Y., Vythilingum, I., Mohammed, Z.D., Trung, H.D.,Butlin, R.K., 2007b. Genetic diversity and molecular identification of mosquitospecies in the Anopheles maculatus group using the ITS2 region of rDNA. Infect.Genet. Evol. 7, 93–102.
White, N.J., 2004. Antimalarial drug resistance. J. Clin. Investig. 113, 1084–1092.White, N.J., Pongtavornpinyo, W., 2003. The de novo selection of drug-resistant
malaria parasites. Proc. Biol. Sci. 270, 545–554.WHO, 1998. Test Procedures for Insecticide Resistance Monitoring in Malaria Vec-
tors, Bio-efficacy and Persistence of Insecticide on Treated Surfaces, Geneva.WHO, 2006. Counterfeit medicines. Fact Sheet No 275.WHO, 2007. Anopheline Species Complexes in South and South-East Asia. SEARO
Technical Publication No. 57, 102.WHO, 2007b. Malaria Elimination: A Field Manual for Lowland and Moderate
Endemic Countries, pp. 1–98.WHO, 2008a. Malaria in the Greater Mekong Subregion: Regional and Country Pro-
files, p. 59 http://www.whothailand.org/EN/Section3/section 113.htm.WHO, 2008b. Strengthening Malaria Control for Ethnic Minorities in the Greater
Mekong Subregion., http://www.wpro.who.int/NR/rdonlyres/4B162E2E-11BE-4C92-8304-A6D129E0AF75/0/ADB FinalProjectReport.pdf.
WHO, 2009. Development of a Strategy Towards Elimination of Plasmodium falci-parum Parasites with Altered Response to Artemisinins, p. 52.
WHO, 2010a. Global Report on Antimalarial Drug Efficacy and Drug Resistance:2000–2010, p. 115.
WHO, 2010b. World Malaria Report 2010., http://www.who.int/malaria/worldmalaria report 2010/en/index.html.
WHO, 2011. Global Plan for Artemisinin Resistance Containment (GPARC), p. 87.Wongsrichanalai, C., Meshnick, S.R., 2008. Declining artesunate–mefloquine efficacy
against falciparum malaria on the Cambodia–Thailand border. Emerg. Infect. Dis.14, 716–719.
Wongsrichanalai, C., Pickard, A.L., Wernsdorfer, W.H., Meshnick, S.R., 2002. Epidemi-ology of drug-resistant malaria. Lancet Infect. Dis. 2, 209–218.
Wootton, J.C., Feng, X., Ferdig, M.T., Cooper, R.A., Mu, J., Baruch, D.I., Magill, A.J., Su,X.Z., 2002. Genetic diversity and chloroquine selective sweeps in Plasmodiumfalciparum. Nature 418, 320–323.
Xiao, D., Long, Y., Wang, S., Fang, L., Xu, D., Wang, G., Li, L., Cao, W., Yan, Y., 2010.Spatiotemporal distribution of malaria and the association between its epidemicand climate factors in Hainan, China. Malar. J. 9, 185.
Xu, B.L., Su, Y.P., Shang, L.Y., Zhang, H.W., 2006. Malaria control in Henan Province,
People’s Republic of China. Am. J. Trop. Med. Hyg. 74, 564–567.Yang, H., Liu, D., Yang, Y., Fan, B., Yang, P., Li, X., Li, C., Dong, Y., Yang, C., 2003.Changes in susceptibility of Plasmodium falciparum to artesunate in vitro inYunnan Province, China. Trans. R. Soc. Trop. Med. Hyg. 97, 226–228.
Yeung, S., White, N.J., 2005. How do patients use antimalarial drugs? A review of theevidence. Trop. Med. Int. Health 10, 121–138.

pica 1
Y
Y
Z
Z
Z
F., 1998. High prevalence of Plasmodium malariae and Plasmodium ovalein malaria patients along the Thai–Myanmar border, as revealed by acri-
L. Cui et al. / Acta Tro
ip, K., 1998. Antimalarial work in China: a historical perspective. Parassitologia 40,29–38.
u, P.H., Zhang, H.X., Zhang, S.Q., Xu, B.Z., 2000. Survey of susceptibility of anophelinevectors to insecticides in a malaria mesoendemic area, Hubei Province. Chin. J.Parasitol. Parasitic Dis. 18, 149–151.
hang, W., Wang, L., Fang, L., Ma, J., Xu, Y., Jiang, J., Hui, F., Wang, J., Liang, S., Yang,H., Cao, W., 2008. Spatial analysis of malaria in Anhui province, China. Malar. J.
7, 206.hang, Z., 2005. Current situation of malaria under-reporting in China. Chin. J. Parasit.Dis. Control 18, 311–312.
hang, Z., Zhou, S., Xu, J., Du, Z., Chen, G., Li, L., Zhou, H., Guo, X., Wu, C., Li, J., Liu, H., Xu,S., Wang, L., Chen, Z., Yang, Y., Xia, M., Li, R., 2004. Investigation on missing-reportof malaria cases in Yunnan, China. Chin. J. Parasit. Dis. Control 17, 25–27.
21 (2012) 227– 239 239
Zhou, G., Sirichaisinthop, J., Sattabongkot, J., Jones, J., Bjornstad, O.N., Yan, G., Cui,L., 2005. Spatio-temporal distribution of Plasmodium falciparum and P. vivaxmalaria in Thailand. Am. J. Trop. Med. Hyg. 72, 256–262.
Zhou, M., Liu, Q., Wongsrichanalai, C., Suwonkerd, W., Panart, K., Prajakwong, S.,Pensiri, A., Kimura, M., Matsuoka, H., Ferreira, M.U., Isomura, S., Kawamoto,
dine orange staining and PCR-based diagnoses. Trop. Med. Int. Health 3,304–312.
Zhou, S.S., Wang, Y., Tang, L.H., 2007. Malaria situation in the People’s Republic ofChina in 2006. Chin. J. Parasitol. Parasitic Dis. 25, 439–441.





























