Embed Size (px)
Citation preview

Chronic Skin-Specific Inflammation PromotesVascular Inflammation and ThrombosisYunmei Wang1,2, Huiyun Gao1,2, Candace M. Loyd3, Wen Fu3, Doina Diaconu3, Shijian Liu1,2,Kevin D. Cooper3,4, Thomas S. McCormick3,4, Daniel I. Simon1,2 and Nicole L. Ward3,4
Patients with psoriasis have systemic and vascular inflammation and are at increased risk for myocardialinfarction, stroke, and cardiovascular death. However, the underlying mechanism(s) mediating the link betweenpsoriasis and vascular disease is incompletely defined. This study sought to determine whether chronicskin-specific inflammation has the capacity to promote vascular inflammation and thrombosis. Using theKC-Tie2 doxycycline-repressible (Dox-off) murine model of psoriasiform skin disease, spontaneous aortic rootinflammation was observed in 33% of KC-Tie2 compared with 0% of control mice by 12 months of age (P¼ 0.04)and was characterized by the accumulation of macrophages, T lymphocytes, and B lymphocytes, as well as byreduced collagen content and increased elastin breaks. Importantly, aortic inflammation was preceded byincreases in serum tumor necrosis factor-a, IL-17A, vascular endothelial growth factor, IL-12, monocytechemotactic protein-1, and S100A8/A9, as well as splenic and circulating CD11bþLy-6Chi pro-inflammatorymonocytes. Doxycycline treatment of old mice with severe skin disease eliminated skin inflammation and thepresence of aortic root lesion in 1-year-old KC-Tie2 animals. Given the bidirectional link between inflammationand thrombosis, arterial thrombosis was assessed in KC-Tie2 and control mice; mean time to occlusivethrombus formation was shortened by 64% (P¼ 0.002) in KC-Tie2 animals; and doxycycline treatment returnedthrombosis clotting times to that of control mice (P¼ 0.69). These findings demonstrate that sustained skin-specific inflammation promotes aortic root inflammation and thrombosis and suggest that aggressive treatmentof skin inflammation may attenuate pro-inflammatory and pro-thrombotic pathways that produce cardiovas-cular disease in psoriasis patients.
Journal of Investigative Dermatology (2012) 132, 2067–2075; doi:10.1038/jid.2012.112; published online 10 May 2012
INTRODUCTIONPsoriasis is a chronic inflammatory skin disease affectingbetween 2.5 and 6 million patients in the United States.Clinical data have convincingly demonstrated that psoriasispatients have an increased risk for developing cardiovasculardisease (CVD), including myocardial infarction and stroke(Gelfand et al., 2006, 2009; Prodanovich et al., 2009; Mehtaet al., 2010, 2011a; Ahlehoff et al., 2011a) and an increasedrisk of thromboembolic events (Ahlehoff et al., 2011b).Psoriasis patients have more established CVD risk factors,including higher levels of serum cholesterol and triglycerides
coupled with low high-density lipoprotein (Pietrzak et al.,2009; Toker et al., 2009), elevated pro-inflammatorymediators (i.e., IL-17, IL-23 (Kryczek et al., 2008) andS100A8/A9 (Benoit et al., 2006)), and lower levels of anti-inflammatory mediators such as IL-10 and adiponectin (Kauret al., 2008; Takahashi et al., 2008), and these correlate withdisease severity (Boehncke et al., 2011c). Psoriasis isaccompanied by impaired endothelial function (Balci et al.,2009) and increased subclinical atherosclerosis as measuredby carotid intimal–medial thickness measurements (Balciet al., 2009), arterial stiffness (Gisondi et al., 2009), andcoronary calcium scores (Ludwig et al., 2007). More recentwork suggests that psoriasis confers an additional 6.2%absolute risk of a 10-year rate of major adverse cardiac eventscompared with the general population (Mehta et al., 2011a).However, these epidemiological studies do not provideinsight as to the etiology of this elevated risk and rely onadjusting for confounders such as hyperlipidemia, hyperten-sion, and diabetes, and thus cannot demonstrate causality.
Common inflammatory cascades have critical roles in theinitiation and maintenance of psoriasis and CVD (Libby,2002; Lowes et al., 2007; Spah, 2008; Alexandroff et al.,2009), including activation of antigen-presenting cells andmacrophages, involvement of Th1, Th17, and regulatory
& 2012 The Society for Investigative Dermatology www.jidonline.org 2067
ORIGINAL ARTICLE
Received 16 November 2011; revised 15 February 2012; accepted 26February 2012; published online 10 May 2012
1Department of Medicine, Division of Cardiovascular Medicine, CaseWestern Reserve University, Cleveland, Ohio, USA; 2The Harrington Heartand Vascular Institute, University Hospitals Case Medical Center, Cleveland,Ohio, USA; 3Department of Dermatology, Case Western Reserve University,Cleveland, Ohio, USA; 4The Murdough Family Center for Psoriasis, UniversityHospitals Case Medical Center, Cleveland, Ohio, USA
Correspondence: Nicole L. Ward, Case Western Reserve University,Department of Dermatology, BRB519, 10900 Euclid Avenue, Cleveland,Ohio 44106, USA. E-mail: [email protected]
Abbreviations: CVD, cardiovascular disease; MCP, monocytechemoattractant protein; TNF-a, tumor necrosis factor alpha

T cells, and a critical role for IL-12p40 and tumor necrosisfactor-a (TNF-a). Psoriasis patients not only have significantinflammation in the skin but also have subclinical inflam-mation in the liver, joints, tendons, and vascular treeeven after adjusting for traditional cardiovascular riskfactors (Mehta et al., 2011b), suggesting that psoriasis itselfpredisposes to pro-inflammation pathways independent oftraditional risk factors. Others have suggested a moredirect hypothesis that psoriasis-initiated skin and systemicinflammation causes insulin resistance, which promotesendothelial cell dysfunction, subsequent atherosclerosis,and, ultimately, myocardial infarction or stroke (Boehnckeet al., 2011c).
Despite the epidemiological association between psoriasisand CVD, the underlying mechanism(s) mediating the linkbetween psoriasis and vascular disease is incompletelydefined. Whether localized, chronic cutaneous inflammationdirectly promotes vascular inflammation and thrombosis isunknown. To address this question, we used the KC-Tie2murine model of psoriasiform skin inflammation, in whichTie2 transgene expression is confined to keratinocytes andwhich recapitulates many characteristics of human plaquepsoriasis (Wolfram et al., 2009; Johnston et al., 2011;Ostrowski et al., 2011; Swindell et al., 2011; Ward et al.,2011). We hypothesized that the presence of sustained skin-confined inflammation would predispose animals to vascularinflammation and thrombosis.
RESULTSLesion characterization
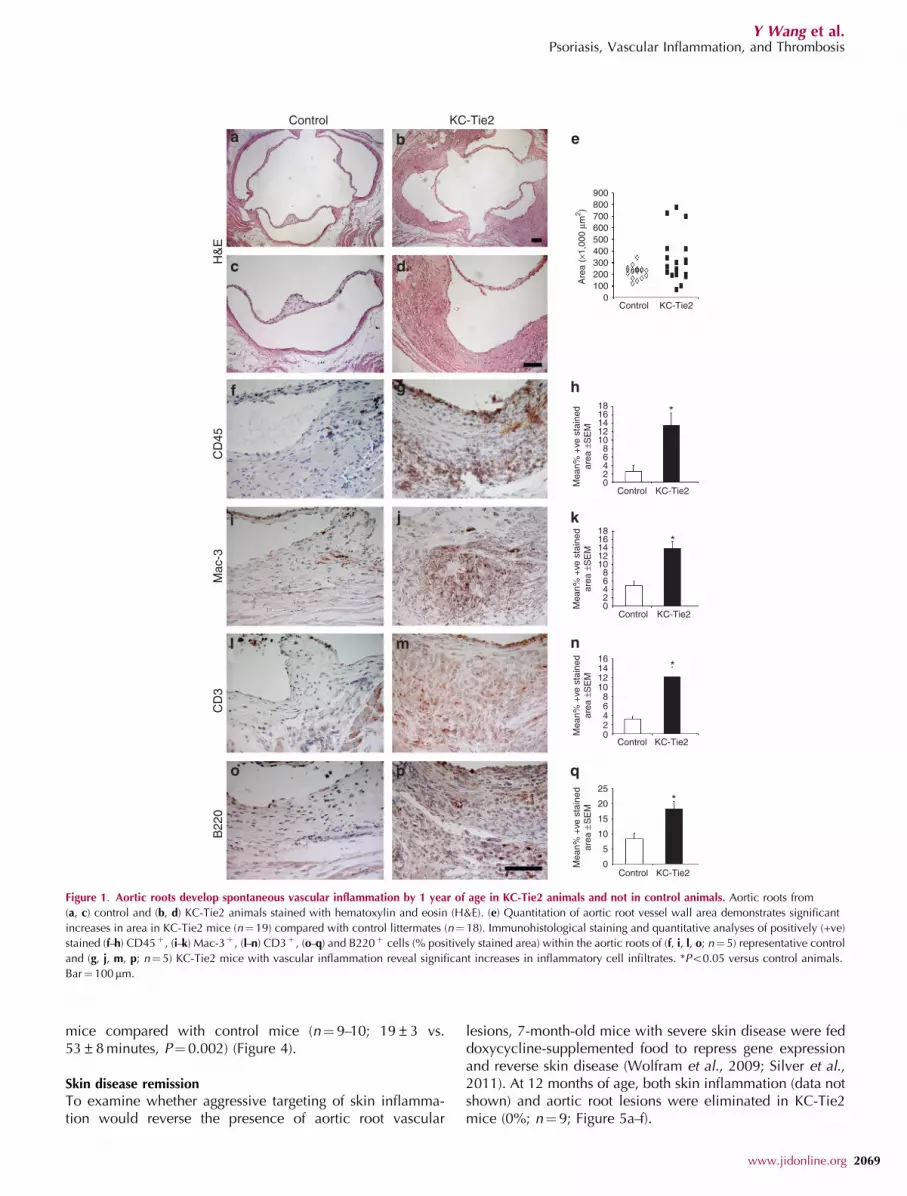
At 12 months of age on a standard chow diet, spontaneousdevelopment of robust aortic root inflammation was observedin 33% of KC-Tie2 mice with psoriasiform skin diseasecompared with 0% of control mice (P¼0. 04) (Figure 1a–d).Lesion formation, quantified by measuring vessel wall area ofthe aortic root at the level of the aortic valve was higher in theKC-Tie2 mice compared with control mice (325±48 mm2 vs.221±12 mm2, n¼ 18–19 per group; P¼ 0.04) (Figure 1e). Nolesions were detected in the descending thoracic orabdominal aorta. Aortic root lesions were also stained withoil-red O and Sudan IV for lipid deposition. There was nosignificant lipid staining in the inflamed aortic roots ofKC-Tie2 mice on a standard chow diet.
Examination of the aortic root revealed significantaccumulation of inflammatory cells (CD45-positive leuko-cytes; Figure 1f–h) in KC-Tie2 mice (13.5±2.9% CD45-positive area) compared with control animals (2.5±1.4%,Po0.001) and affected all layers of the vessel wall. Leukocytesubset analysis was performed by staining for macrophages(Figure 1i–k), T cells (Figure 1l–n), and B cells (Figure 1o–q).Macrophage accumulation was increased 2.8-fold in KC-Tie2mice (13.8±1.7% Mac-3-positive area) compared withcontrols (4.9±1.2%, Po0.0001). The accumulation of bothT cell and B cell in the aortic root was enhanced in KC-Tie2mice, with a 3.9-fold increase in T cells (12.2±2.0% vs.3.2±0.7% CD3-positive area, P¼ 0.0004) and a 2.2-foldincrease in B cells (18.4±2.4% vs. 8.3±1.9% B220-positivearea, P¼0.0003).
Examination of the extracellular matrix (ECM) usingtrichrome staining revealed decreased collagen content inthe lesions in KC-Tie2 animals compared with the densecollagen content observed in control mice (Figure 2a–d).Aortic elastin integrity was investigated by Verhoeffelastin staining and revealed abundant elastin breaks andfragmentation in the aortic root lesions of KC-Tie2 mice(Figure 2e–h).
To verify that transgene expression was limited to the skin,we performed additional matings between the K5tTA drivermouse and nuclear LacZ reporter mouse lines, and analyzedLacZ expression in the skin, spleen, brain, liver, kidney, lung,heart, and aorta of the of KC-LacZ mice (SupplementaryFigures S1 online). Robust LacZ expression was observed inthe skin with little to no expression in the other tissuesincluding the aorta. In addition, we verified the absence ofaberrant Tie2 expression in the aortic roots of KC-Tie2 micethat developed vascular inflammation (SupplementaryFigures S1 online). Taken together, these observationsindicate that chronic, skin-specific inflammation in KC-Tie2mice promotes the de novo development of aortic rootinflammation and alterations in the ECM.
Systemic inflammation
Biomarkers associated with CVD risk were examined in KC-Tie2 mice. Serum levels of MCP-1 (1.7-fold; P¼ 0.038), IL-12p70 (4.3-fold; P¼ 0.048), TNF-a (2.1-fold; P¼ 0.05), IL17a(4.4-fold; P¼0.038), and vascular endothelial growth factor(1.6-fold; P¼0.02) were all elevated in KC-Tie2 micecompared with age-matched littermate controls (Figure 3a).The expression of the pro-inflammatory mediator S100A8/A9(myeloid related protein-8/14, MRP-8/14) was also increasedin the skin and serum of KC-Tie2 mice compared with controlmice (Figure 3b).
Total cholesterol, triglyceride, and low-density lipoproteincholesterol levels were lower in KC-Tie2 mice comparedwith control mice, although not all reached statisticalsignificance. Reduced high-density lipoprotein levels wereobserved in KC-Tie2 mice (Figure 3c).
Specific monocyte subpopulations (i.e., Ly-6Chi) havebeen implicated in monocyte/macrophage vessel wallinfiltration and atherosclerotic lesion formation. Therefore,we evaluated splenic and circulating CD11bþLy-6Chi
monocytes in KC-Tie2 mice at 6 months of age before aorticroot inflammation. Splenic CD11bþLy-6Chi monocyte levelswere increased by 42% (P¼0.009) in KC-Tie2 comparedwith control mice (Figure 3d). Similar results were observedin circulating blood (Supplementary Figures S2 online).
Inflammation and thrombosis
Given the bidirectional link between inflammation andthrombosis, we assessed arterial thrombosis in KC-Tie2 micecompared with control mice using a photochemical (RoseBengal-green light laser) carotid artery injury model, whichproduces thrombosis because of local free-radical release andoxidative endothelial cell injury (Watson et al., 1985; Falatiet al., 2004; Furie and Furie, 2005). The time to occlusivethrombus formation was shortened significantly in KC-Tie2
2068 Journal of Investigative Dermatology (2012), Volume 132
Y Wang et al.Psoriasis, Vascular Inflammation, and Thrombosis
mice compared with control mice (n¼ 9–10; 19±3 vs.53±8 minutes, P¼0.002) (Figure 4).
Skin disease remission
To examine whether aggressive targeting of skin inflamma-tion would reverse the presence of aortic root vascular
lesions, 7-month-old mice with severe skin disease were feddoxycycline-supplemented food to repress gene expressionand reverse skin disease (Wolfram et al., 2009; Silver et al.,2011). At 12 months of age, both skin inflammation (data notshown) and aortic root lesions were eliminated in KC-Tie2mice (0%; n¼ 9; Figure 5a–f).
900
Control
H&
EC
D45
Mac
-3C
D3
B22
0
KC-Tie2
800
Are
a (×
1,00
0 µm
2 )
700600500400300200100
0
024
Mea
n% +
ve s
tain
edar
ea ±
SE
MM
ean%
+ve
sta
ined
area
±S
EM
Mea
n% +
ve s
tain
edar
ea ±
SE
MM
ean%
+ve
sta
ined
area
±S
EM
68
1012
*
*
*
141618
02468
10121416
0
0
5
10
15
20
25*
2468
10121416
18
Control KC-Tie2
Control KC-Tie2
Control KC-Tie2
Control KC-Tie2
Control KC-Tie2
Figure 1. Aortic roots develop spontaneous vascular inflammation by 1 year of age in KC-Tie2 animals and not in control animals. Aortic roots from
(a, c) control and (b, d) KC-Tie2 animals stained with hematoxylin and eosin (H&E). (e) Quantitation of aortic root vessel wall area demonstrates significant
increases in area in KC-Tie2 mice (n¼19) compared with control littermates (n¼ 18). Immunohistological staining and quantitative analyses of positively (+ve)
stained (f–h) CD45þ , (i–k) Mac-3þ , (l–n) CD3þ , (o–q) and B220þ cells (% positively stained area) within the aortic roots of (f, i, l, o; n¼ 5) representative control
and (g, j, m, p; n¼ 5) KC-Tie2 mice with vascular inflammation reveal significant increases in inflammatory cell infiltrates. *Po0.05 versus control animals.
Bar¼100 mm.
www.jidonline.org 2069
Y Wang et al.Psoriasis, Vascular Inflammation, and Thrombosis

To assess the effect of skin disease remission on occlusivethrombosis formation, KC-Tie2 and control animals were feddoxycycline-supplemented food for 6 weeks, and then pho-tochemical carotid artery injury was performed to producethrombosis. Doxycycline treatment returned KC-Tie2 throm-bosis clotting times to control mouse levels (n¼ 10; 31±8controlsþdoxycycline vs. 36±9 KC-Tie2 þ doxycycline;P¼0.69; Figure 5g). Control animals treated with doxycy-cline had slightly shorter clotting times than untreated controlmice; however, this difference was not significant (P¼0.07).
DISCUSSIONIn this study, we have identified that sustained skininflammation itself is sufficient to promote vascular inflam-mation and thrombosis. This conclusion is supported bythe following data: (1) KC-Tie2 mice develop aortic root
inflammatory lesions; (2) collagen content is decreased andelastin fragmentation is increased in the aortic root of KC-Tie2 mice; (3) pro-inflammatory cytokines and chemokinesare increased in the skin and peripheral blood of KC-Tie2mice that precede the development of aortic root inflamma-tory lesions; (4) inflammatory CD11bþ Ly-6Chi monocytesare elevated in KC-Tie2 animals before lesion development;(5) thrombotic occlusion time after photochemical carotidinjury is shortened in KC-Tie2 mice; and (6) aortic rootinflammatory lesions and thrombosis clotting times signifi-cantly improve in KC-Tie2 mice following skin diseaserepression.
Psoriasis patients have an increased risk for developingCVD, including myocardial infarction and stroke. However,the high prevalence of standard CVD risk factors in patientswith psoriasis required statistical adjustments for the con-founding effects of these variables in psoriasis epidemiologi-cal studies (Gelfand et al., 2006, 2009; Mehta et al., 2010,2011a). Thus, the question of whether inflammatory hyper-plastic disease confined to the skin has the capacity todirectly cause vascular inflammation and thrombosis was,heretofore, unknown. It was highly beneficial to use a murinemodel of psoriasis that recapitulates many aspects of thehuman disease (Wolfram et al., 2009; Johnston et al., 2011;Ostrowski et al., 2011; Swindell et al., 2011; Ward et al.,2011), including the characteristic histological, immunologi-cal, and pro-inflammatory cytokine profiles, as well asdisease attenuation/clearance in response to clinicallyefficacious therapeutics, but without standard CVD riskfactors (i.e., hyperlipidemia, hypertension, diabetes, obesity)to elucidate the effect of the disease itself. Using this model,our findings provide direct evidence linking skin inflamma-tion with the development of vascular inflammation, as wellas an increased propensity for arterial thrombosis afterendothelial redox-mediated injury.
Chronic inflammation and pro-inflammatory cytokineshave significant roles in the pathogenesis of both psoriasisand vascular disease. Evidence suggests that psoriasis andCVD share common pathogenic features (Spah, 2008;Alexandroff et al., 2009), including immunological processes,inflammatory cytokine profiles, and the presence of local andsystemic inflammatory markers (Ross, 1999; Libby, 2002;Hansson, 2005; Lowes et al., 2007; Spah, 2008; Alexandroffet al., 2009; Federman et al., 2009; Gisondi and Girolomoni,2009; Boehncke et al., 2011c). Activation of these inflam-matory cells (dendritic cells, macrophages and T cells)together with the release of pro-inflammatory cytokines(e.g., TNF-a, IFN-g, IL-12) contribute to the development ofpsoriatic lesions (Lowes et al., 2007) and have a major role inthe development and vulnerability of atherosclerotic plaque(Ross, 1999; Libby and Simon, 2001; Libby, 2002; Hansson,2005). The idea that similar mechanisms underlie thedevelopment of both psoriasis and CVD is supported by thefindings of others (Shepherd et al., 2004) such that sustainedIL-1 signaling, accomplished via genomic deletion of the IL-1RA, resulted in three types of strain-dependent inflammatorychanges, including a psoriasiform dermatitis in ear skin,arthritis-like inflammation in the joints, and large-vessel
Control
Tric
hrom
eE
last
in
KC-Tie2
Figure 2. Anatomical characterization of aortic arch lesions. Aortic roots
from (a, c, e, g) control and (b, d, f, h) KC-Tie2 animals stained with (a–d)
trichrome or (e–h) Verhoeff–van Gieson elastin reveal decreased expression of
collagen in trichrome-stained aortic arch tissue from KC-Tie2 mice and
increases in the numbers of elastin breaks in Verhoeff–van Gieson
elastin-stained aortic root tissues. Bar¼ 100mm.
2070 Journal of Investigative Dermatology (2012), Volume 132
Y Wang et al.Psoriasis, Vascular Inflammation, and Thrombosis

arterial inflammation. However, this experimental approachresulted in increased IL-1 signaling throughout the body.The KC-Tie2 mouse has confined gene expression ofthe membrane-bound Tie2 receptor to keratinocytes; thus,our findings provide experimental evidence that keratinocytesignaling and cell–cell interactions within the cutaneousenvironment can initiate inflammation capable of causing
vascular inflammatory foci formation in distant vessels,perhaps as a result of changes in both circulating proin-flammatory cytokines and leukocytes (CD11bþ Ly-6Chi
monocytes). KC-Tie2 mice have higher levels of pro-inflammatory cytokines and chemokines, as well as of splenicand circulating pro-inflammatory CD11bþLy-6Chi monocytes,which precede and are associated with the development of
30
3.0
MCP-1 IL-12p70 TNFα
25
Con
cent
ratio
n(p
g m
l–1)
±SE
MC
once
ntra
tion
(pg
ml–1
) ±S
EM
Con
cent
ratio
n(p
g m
l–1)
±SE
MC
once
ntra
tion
(pg
ml–1
) ±S
EM
Con
cent
ratio
n(p
g m
l–1)
±SE
M
20
15
10
5
0
0
25
20
15
10
5
0
2.5
3.54.04.5
2.01.51.00.5
0Control
IL-17A VEGF8 160140120100806040200
7654321
* *
Control Control
S100A8 S100A9
KC-Tie2
Control
Control
Control
Control
CD11b
100
101
102
103
104
100
101
102
103
104
100 101 102 103 104
CD11b100 101 102 103 104
100 101 102 103 104 100 101 102 103 104
100
101
102
103
104
100
101
102
103
104
Ly6C Ly6C
40
35
30
*
25
20
15
10
5
0
R2
R3
3
5
4
6
R3
3
5
4
6
R2CD
90, B
220,
CD
49,
NK
1.1,
Ly6
GF
4/80
,CD
11C
,I-A
b
F4/
80,C
D11
C,I-
Ab
CD
90, B
220,
CD
49,
NK
1.1,
Ly6
G
% C
D11
bhi L
Y-6C
hi c
ells
HDL LDL Triglyceride Total cholesterol
KC-Tie2
KC-Tie2
KC-Tie2
P-value 0.00757.1±11.797.5±4.9
0.24 0.058.3±3.5 62.7±10.6 70.9±12.1
0.019
117.9±22.4 130.6±18.619.5±8.2
KC-Tie2 Control KC-Tie2
KC-Tie2 KC-Tie2
Serum
Skin
Skin
β Tubulin
** *
Contro
l
KC-Tie2
Contro
l
KC-Tie2
Figure 3. Aortic root vascular inflammation develops in the presence of elevated systemic inflammation and monocytosis, and independent of lower lipid
levels. Proinflammatory cytokines are significantly elevated in (a) KC-Tie2 mouse sera, including levels of monocyte chemoattractant protein 1 (MCP-1),
IL-12p70, tumor necrosis factor alpha (TNFa), IL-17A, and vascular endothelial growth factor (VEGF; mean±SEM; n¼5–11 per group), and (b) S100A8/A9
expression is increased in skin and serum of KC-Tie2 animals. (c) KC-Tie2 animals have significantly less total cholesterol, triglycerides, and high-density
lipoprotein (HDL) compared with control mice (mean±SEM; n¼ 8 per group; P-values indicated for each lipid in table). Four-color flow cytometry reveals
significant increases in splenic pro-atherogenic monocytes (CD90loB220loCD49bloNK1.1loLy6GloCD11cloI-AbloF4/80loCD11bhiLy-6Chi). (d) Representative
flow cytometry and quantification of CD11bþF4/80loLy-6Chi cells (mean±SEM; n¼ 4 spleens per group). *Po0.05 versus control animals. LDL, low-density
lipoprotein.
www.jidonline.org 2071
Y Wang et al.Psoriasis, Vascular Inflammation, and Thrombosis

vascular inflammation and disease, and occur independent ofchanges in lipids. The clinical relevance of our observationsin KC-Tie2 mice is supported by highly sensitive, metabolicimaging (i.e., (18F)-fluorodeoxyglucose positron emissiontomography-computed tomography, FDG-PET/CT) in psor-iasis patients showing concomitant aortic inflammation.Coupled with our thrombosis observations, this suggests thatelevated levels of inflammation could potentially be used topredict poor outcomes and adverse cardiovascular events inpatients with psoriasis. Taken together, these findings provideinsight into skin-specific contributions underlying priorepidemiological reports that psoriasis patients are at anincreased risk for myocardial infarction, stroke, venousthromboembolism, and cardiovascular mortality (Gelfand
et al., 2006, 2009; Prodanovich et al., 2009; Mehta et al.,2010, 2011a; Ahlehoff et al., 2011a, b).
There is increasing evidence for an important link betweeninflammation and thrombosis. Leukocyte–platelet interactionsinduce bidirectional signals that amplify pro-inflammatoryand pro-thrombotic cellular responses (Libby and Simon,2001). Activated platelets and platelet-released mediators(e.g., PDGF and PAF) activate leukocytes, thereby enhancingtheir responses such as chemotaxis, reactive oxygen speciesgeneration, phagocytosis, and pro-coagulant activity (Bazzo-ni et al., 1991; Nagata et al., 1993; Kuijper et al., 1997;Lindemann et al., 2001). Conversely, activated leukocytesinduce platelet activation as evidenced by increased plateletP-selectin and activated glycoprotein IIb/IIIa expression(Li et al., 2000). Psoriasis patients have elevated P-selectin,the levels of which correlate with disease severity (Garbar-aviciene et al., 2010). The most compelling observation ofthis study relates to the finding that occlusive thrombusformation was shortened significantly in KC-Tie2 comparedwith control mice and supports recent epidemiological reportsdemonstrating that psoriasis patients had higher incident ratesof venous thromboembolism (Ahlehoff et al., 2011b). Acutemyocardial infarction typically results from atheroscleroticplaque disruption or superficial endothelial cell erosion andthrombosis that cause coronary arterial occlusion (Davies andThomas, 1985; Farb et al., 1996). Yet, molecular events thatprecede acute myocardial infarction in patients with psoriasisremain uncertain. This mouse model provides valuable cluesaddressing this gap area in at-risk psoriasis patients. Forexample, both S100A8/A9 (Figure 3b) and MPO (data notshown), which are elevated in the skin and peripheral bloodof KC-Tie2 mice and psoriasis patients (Benoit et al., 2006),have been implicated in acute coronary syndromes, includ-ing unstable angina and myocardial infarction (Baldus et al.,2003; Healy et al., 2006; Morrow et al., 2008).
Interestingly, most of the literature examining psoriasis andCVD report increases in either cardiovascular risk factors
100
Clo
tting
tim
e (m
inut
es)
908070605040302010
Control
Con
trol
KC-Tie2
KC
-Tie
2
0
Figure 4. KC-Tie2 mice are pro-thrombotic. (a) KC-Tie2 and control mice
underwent experimental thrombosis; carotid artery blood flow was monitored
continuously with a vascular flow probe, and time to occlusion, defined as
cessation of blood flow for 20 minutes, was recorded. Mean time (±SEM) to
occlusive thrombus formation in control mice was 53±8 minutes (n¼ 10),
and was shortened significantly in KC-Tie2 mice (19±3 minutes; n¼9;
P¼ 0.002). Hematoxylin and eosin (H&E)–stained carotid arteries from control
and KC-Tie2 mice following Rose Bengal laser treatment. (b) Note the
fibrin–platelet-rich thrombi with some red blood cells in the lumen of carotid
arteries of KC-Tie2 mice and not control mice. *Po0.05 versus control
animals. Bar¼ 100 mm.
H&E Trichrome Elastin
70
60
Clo
tting
tim
e (m
inut
es)
50
40
30
Control KC-Tie2
+ Dox
20
10
0
Con
trol
+ D
oxK
C-T
ie2
+ D
ox
Figure 5. Repressing skin inflammation improves aortic root lesions and thrombosis clotting times. Seven-month-old KC-Tie2 mice (n¼ 9) and control
littermates (n¼9) were treated with doxycycline to repress transgene expression and to reverse skin inflammation. Aortic roots from (a, c, e) representative
1-year-old control and (b, d, f) KC-Tie2 animals stained with (a, b) hematoxylin and eosin (H&E), (c, d) trichrome, and (e, f) elastin. No aortic root lesions
were observed in any control or KC-Tie2 mice treated with doxycycline. (g) KC-Tie2 and control mice treated with doxycycline for 6 weeks underwent
experimental thrombosis; mean time (±SEM) to occlusive thrombus formation was not significantly different between control mice treated with doxycycline
(31±8 minutes; n¼10) and KC-Tie2 mice treated with doxycycline (36±9 minutes; n¼ 10; P¼0.69). Bar¼ 100mm.
2072 Journal of Investigative Dermatology (2012), Volume 132
Y Wang et al.Psoriasis, Vascular Inflammation, and Thrombosis

(diabetes, hypertension, hyperlipidemia) (Gelfand et al.,2006; Prodanovich et al., 2009; Mehta et al., 2010), changesin CVD surrogate markers (MPO, adiponectin, S100A8/A9)(Benoit et al., 2006; Kaur et al., 2008; Takahashi et al., 2008),or indirect measures of CVD via endothelial function, carotidartery intimal-medial thickness (Balci et al., 2009), andstiffness measurements (Gisondi et al., 2009). KC-Tie2animals have elevated systemic inflammation independentof obesity, hyperglycemia, and hyperlipidemia, demonstrat-ing that skin inflammation alone can elicit systemic levels ofinflammation critical for inflammatory lesion formation in theaortic root and promotion of thrombosis. Our observation oflocalized inflammation in the aortic root is consistent withthe anatomical localization of aortic inflammation previouslyobserved in psoriasis patients (Mehta et al., 2011b), and thisfocus of inflammation appears to be specific rather thanrepresentative of an overall generalized vascular inflamma-tory effect affecting all vessels of the body. Moreover, thelocation of vascular inflammatory lesions also highlycorrelates with sites that develop atherosclerosis in humans.Whether atherosclerosis is in fact elicited by psoriasisremains unclear. We cannot rule out the fact that, with time,these mice would develop atherosclerosis; however, on anon-athero-susceptible genetic background strain, and con-sidering the short life span of a mouse, these experiments arenot likely to yield insightful data addressing this issue. Rather,the usefulness of the murine model lends itself to modelingexperiments whereby variables known to be increasedin psoriasis patients (i.e., dietary choices, very-low-densitylipoprotein levels, ApoB, diabetic state, hypertension) couldbe manipulated in KC-Tie2 animals, and the synergistic oradditive effects of vascular inflammation coupled with theexperimental manipulation on atherosclerotic plaque deve-lopment and thrombosis could be examined.
Our observations of aortic root vascular lesion resolutionand improved thrombosis outcomes following skin-specifictransgene repression provide further evidence demonstratingthat cutaneous inflammation promotes vascular inflammationand thrombosis and suggest that aggressive treatment of skininflammation may attenuate pro-inflammatory and pro-thrombotic pathways that produce CVD in psoriasis patients.Although not skin specific, recent prospective reportsdocument significant improvement in endothelial vasodilatorfunction (Boehncke et al., 2011a) and CVD biomarker levels(Boehncke et al., 2011b) in psoriasis patients following 24weeks of systemic therapeutic treatment.
Evidence linking chronic inflammation to the develop-ment of vascular inflammation is not limited to psoriasis. Forexample, periodontal disease is an important independentcausal risk factor for atherosclerotic disease, includingcoronary heart disease and ischemic stroke (DeStefanoet al., 1993; Humphrey et al., 2008). Importantly, periodontaltherapy has been shown to alter gene expression of peripheralblood monocytes, suggesting that local therapies could havea systemic anti-inflammatory effect (Papapanou et al., 2007).Similar to periodontal disease, rheumatoid arthritis is asso-ciated with increased carotid artery intimal–medial thicken-ing, as well as increased cardiovascular events independent
of traditional cardiac risk factors. Ongoing prospectiveclinical trials are examining the effect of disease-modifyingtherapies, such as anti-TNFa, on cardiovascular complica-tions of rheumatoid arthritis.
The results of our study provide strong evidence of remote,extravascular tissue inflammation promoting induction ofCVD and suggest that suppression of skin inflammation is aviable approach worthy of investigation to favorably impactCVD complications of psoriasis.
MATERIALS AND METHODSAnimals
The KC-specific (K5-tTA) driver line and the TetosTek/Tie2 responder
lines have been described previously (Diamond et al., 2000; Jones
et al., 2001). Matings were performed between the K5tTA line and
the TetosTek/Tie2 line, and offspring were genotyped by PCR using
DNA extracted from ear biopsies as previously described (Wolfram
et al., 2009). We have previously demonstrated that animals
inheriting a single copy of K5tTA and Tetos Tie2 (KC-Tie2
bi-transgenic mice) have B50-fold increase in Tie2 mRNA and
spontaneously develop a psoriasiform skin phenotype (Wolfram
et al., 2009). Male and female KC-Tie2 animals were used in the
current studies, and littermates inheriting one or no transgenes served as
experimental controls. Transgene repression was completed as
previously described (Wolfram et al., 2009; Silver et al., 2011).
All animal protocols were approved by the Case Western Reserve
University institutional animal care and use committee and con-
formed to the American Association for Accreditation of Laboratory
Animal Care guidelines.
Protein analysis
See Supplemental Material online.
Flow cytometry
Four-color flow cytometry was used to stain neutrophils, monocytes,
and macrophages. Cells were incubated with a cocktail of mAbs
against T cells (CD90-PE, 53–2.1), B cells (B220-PE, RA3-6B2), NK
cells (CD49b-PE, DX5 and NK1.1-PE, PK136), neutrophils
(Ly-6G–PE, 1A8), myeloid cells (CD11b-APC, M1/70), and monocyte
subsets (Ly-6C–FITC, AL-21), as described previously (Swirski et al.,
2007; Shi et al., 2008). F4/80 (BM8)-biotin-strep-PerCP, I-Ab (AF6-
120.1)-biotin-strep-PerCP, and CD11c (HL3)-biotin-strep-PerCP
mAbs (BD Biosciences, San Diego, CA) also served to determine
macrophage and dendritic cell differentiation (see also Supplemental
Material online).
Histology and lesion analysis
Mice were perfused transcardially as previously described (Croce
et al., 2009) before dissection of the heart and aorta. For analysis of
the aortic root, the bottom half of the heart was cut off in a plane
parallel to the left and right atria. The top half of heart was
embedded in paraffin after dehydration in ethanol and xylene. Serial
5-mm heart sections were obtained and stained with hematoxylin
and eosin (Sigma, St Louis, MO). Trichrome staining (Sigma) was
performed to visualize collagen. Elastic laminae were visualized
by staining the sections with Verhoeff–van Gieson (Sigma), as
recommended by the manufacturer. Immune cell staining was
performed as described in the Supplemental Material online.
www.jidonline.org 2073
Y Wang et al.Psoriasis, Vascular Inflammation, and Thrombosis

To quantify the size of aortic root lesions, vessel wall area
(including lesional area, if present) was measured using a computer-
assisted image analysis program (Zeiss Axiovision software, Rel 4.5,
Thornwood, NY).
Photochemical carotid artery thrombosis
Ten-week-old male and female KC-Tie2 transgenic and littermate
control mice were anesthetized by intraperitoneal injection with
sodium pentobarbital (62.5 mg kg�1) and placed in the supine
position on a dissecting microscope. Animals at this time point
have established skin disease with abundant inflammatory cell
infiltrate (Wolfram et al., 2009; Ostrowski et al., 2011; Ward et al.,
2011). Animals had a midline surgical incision made to expose the
right common carotid artery, and a Doppler flow probe (MC 0.5PSL
Nanoprobe, Model 0.5 VB, Transonic Systems, Ithaca, NY) was
placed under the exposed artery. The probe was connected to a flow
meter (Transonic Systems Model TS420). Flow data were interpreted
with a computerized data acquisition program (Windaq, DATAQ
Instruments, Akron, OH). Rose Bengal at a concentration of
10 mg ml�1 in phosphate-buffered saline was then injected into
the tail vein to administer a dose of 50 mg kg�1. Following Rose
Bengal injection, the mid portion of the common carotid artery
was illuminated with a 1.5-mW green-light laser source (540 nm;
Melles Griot, Carlsbad, CA) at a distance of 5 cm from the artery.
Blood flow was monitored continuously from the onset of injury.
The time to occlusion, determined only after the vessel remained
closed with a cessation of blood flow for 20 minutes, was
recorded.
Statistical analysis
All data are represented as mean±SEM. Between-group compar-
isons were analyzed using either a Student’s t-test or a Mann–
Whitney U-test, and statistical significance was defined as Po0.05.
CONFLICT OF INTERESTThe authors state no conflict if interest.
ACKNOWLEDGMENTSThis work was funded by grants to NLW, TSM, and KDC from the NationalInstitutes of Health (P30AR39750 and P50AR05508) and the MurdoughFamily Center for Psoriasis; to NLW and YW from the National PsoriasisFoundation; to NLW from the American Heart Association and the JuvenileDiabetes Research Foundation; and to DIS from the National Institutes ofHealth (HL85816, HL57506 MERIT Award, and HL73852). The authors thankDr Nehal N. Mehta for his helpful discussions and critical reading of themanuscript.
SUPPLEMENTARY MATERIAL
Supplementary material is linked to the online version of the paper at http://www.nature.com/jid
REFERENCES
Ahlehoff O, Gislason GH, Jorgensen CH et al. (2011a) Psoriasis and risk ofatrial fibrillation and ischaemic stroke: a Danish Nationwide CohortStudy. Eur Heart J; e-pub ahead of print 25 August 2011
Ahlehoff O, Gislason GH, Lindhardsen J et al. (2011b) Psoriasis carries anincreased risk of venous thromboembolism: a Danish NationwideCohort Study. PLoS One 6:e18125
Alexandroff AB, Pauriah M, Camp RD et al. (2009) More than skin deep:atherosclerosis as a systemic manifestation of psoriasis. Br J Dermatol161:1–7
Balci DD, Balci A, Karazincir S et al. (2009) Increased carotid artery intima-media thickness and impaired endothelial function in psoriasis. J EurAcad Dermatol Venereol 23:1–6
Baldus S, Heeschen C, Meinertz T et al. (2003) Myeloperoxidase serum levelspredict risk in patients with acute coronary syndromes. Circulation108:1440–5
Bazzoni G, Dejana E, Del Maschio A (1991) Platelet-neutrophil interactions.Possible relevance in the pathogenesis of thrombosis and inflammation.Haematologica 76:491–9
Benoit S, Toksoy A, Ahlmann M et al. (2006) Elevated serum levels ofcalcium-binding S100 proteins A8 and A9 reflect disease activity andabnormal differentiation of keratinocytes in psoriasis. Br J Dermatol155:62–6
Boehncke S, Fichtlscherer S, Salgo R et al. (2011a) Systemic therapy ofplaque-type psoriasis ameliorates endothelial cell function: results of aprospective longitudinal pilot trial. Arch Dermatol Res 303:381–8
Boehncke S, Salgo R, Garbaraviciene J et al. (2011b) Effective continuoussystemic therapy of severe plaque-type psoriasis is accompanied byamelioration of biomarkers of cardiovascular risk: results of a prospectivelongitudinal observational study. J Eur Acad Dermatol Venereol25:1187–93
Boehncke WH, Boehncke S, Tobin AM et al. (2011c) The ‘psoriatic march’: aconcept of how severe psoriasis may drive cardiovascular comorbidity.Exp Dermatol 20:303–7
Croce K, Gao H, Wang Y et al. (2009) Myeloid-related protein-8/14 iscritical for the biological response to vascular injury. Circulation120:427–36
Davies MJ, Thomas AC (1985) Plaque fissuring–the cause of acute myocardialinfarction, sudden ischaemic death, and crescendo angina. Br Heart J53:363–73
DeStefano F, Anda RF, Kahn HS et al. (1993) Dental disease and risk ofcoronary heart disease and mortality. Br Med J 306:688–91
Diamond I, Owolabi T, Marco M et al. (2000) Conditional gene expression inthe epidermis of transgenic mice using the tetracycline-regulatedtransactivators tTA and rTA linked to the keratin 5 promoter. J InvestDermatol 115:788–94
Falati S, Gross PL, Merrill-Skoloff G et al. (2004) In vivo models of plateletfunction and thrombosis: study of real-time thrombus formation.Methods Mol Biol 272:187–97
Farb A, Burke AP, Tang AL et al. (1996) Coronary plaque erosion withoutrupture into a lipid core. A frequent cause of coronary thrombosis insudden coronary death. Circulation 93:1354–63
Federman DG, Shelling M, Prodanovich S et al. (2009) Psoriasis: anopportunity to identify cardiovascular risk. Br J Dermatol 160:1–7
Furie B, Furie BC (2005) Thrombus formation in vivo. J Clin Invest 115:3355–62
Garbaraviciene J, Diehl S, Varwig D et al. (2010) Platelet P-selectin reflects astate of cutaneous inflammation: possible application to monitortreatment efficacy in psoriasis. Exp Dermatol 19:736–41
Gelfand JM, Dommasch ED, Shin DB et al. (2009) The risk of stroke inpatients with psoriasis. J Invest Dermatol 129:2411–8
Gelfand JM, Neimann AL, Shin DB et al. (2006) Risk of myocardial infarctionin patients with psoriasis. JAMA 296:1735–41
Gisondi P, Fantin F, Del Giglio M et al. (2009) Chronic plaque psoriasis isassociated with increased arterial stiffness. Dermatology 218:110–3
Gisondi P, Girolomoni G (2009) Psoriasis and atherothrombotic diseases:disease-specific and non-disease-specific risk factors. Semin ThrombHemost 35:313–24
Hansson GK (2005) Inflammation, atherosclerosis, and coronary arterydisease. N Engl J Med 352:1685–95
Healy AM, Pickard MD, Pradhan AD et al. (2006) Platelet expression profilingand clinical validation of myeloid-related protein-14 as a noveldeterminant of cardiovascular events. Circulation 113:2278–84
Humphrey LL, Fu R, Buckley DI et al. (2008) Periodontal disease andcoronary heart disease incidence: a systematic review and meta-analysis.J Gen Intern Med 23:2079–86
2074 Journal of Investigative Dermatology (2012), Volume 132
Y Wang et al.Psoriasis, Vascular Inflammation, and Thrombosis

Johnston A, Xing X, Guzman AM et al. (2011) IL-1F5, -F6, -F8, and -F9: anovel IL-1 family signaling system that is active in psoriasis andpromotes keratinocyte antimicrobial peptide expression. J Immunol186:2613–22
Jones N, Voskas D, Master Z et al. (2001) Rescue of the early vascular defectsin Tek/Tie2 null mice reveals an essential survival function. EMBO Rep2:438–45
Kaur S, Zilmer K, Kairane C et al. (2008) Clear differences in adiponectin leveland glutathione redox status revealed in obese and normal-weightpatients with psoriasis. Br J Dermatol 159:1364–7
Kryczek I, Bruce AT, Gudjonsson JE et al. (2008) Induction of IL-17+ T celltrafficking and development by IFN-gamma: mechanism and patholo-gical relevance in psoriasis. J Immunol 181:4733–41
Kuijper PH, Gallardo Torres HI, Lammers JW et al. (1997) Platelet and fibrindeposition at the damaged vessel wall: cooperative substrates forneutrophil adhesion under flow conditions. Blood 89:166–75
Li N, Hu H, Lindqvist M et al. (2000) Platelet-leukocyte cross talk in wholeblood. Arterioscler Thromb Vasc Biol 20:2702–8
Libby P (2002) Inflammation in atherosclerosis. Nature 420:868–74
Libby P, Simon DI (2001) Inflammation and thrombosis: the clot thickens.Circulation 103:1718–20
Lindemann S, Tolley ND, Dixon DA et al. (2001) Activated platelets mediateinflammatory signaling by regulated interleukin 1beta synthesis. J CellBiol 154:485–90
Lowes MA, Bowcock AM, Krueger JG (2007) Pathogenesis and therapy ofpsoriasis. Nature 445:866–73
Ludwig RJ, Herzog C, Rostock A et al. (2007) Psoriasis: a possible risk factorfor development of coronary artery calcification. Br J Dermatol156:271–6
Mehta NN, Azfar RS, Shin DB et al. (2010) Patients with severe psoriasis are atincreased risk of cardiovascular mortality: cohort study using the GeneralPractice Research Database. Eur Heart J 31:1000–6
Mehta NN, Yu Y, Pinnelas R et al. (2011a) Attributable risk estimate of severepsoriasis on major cardiovascular events. Am J Med 124:775 (e1–6)
Mehta NN, Yu Y, Saboury B et al. (2011b) Systemic and vascularinflammation in patients with moderate to severe psoriasis as measuredby [18F]-fluorodeoxyglucose positron emission tomography-computedtomography (FDG-PET/CT): a pilot study. Arch Dermatol 2011:1031–9
Morrow DA, Wang Y, Croce K et al. (2008) Myeloid-related protein 8/14 andthe risk of cardiovascular death or myocardial infarction after an acutecoronary syndrome in the Pravastatin or Atorvastatin evaluation andInfection Therapy: Thrombolysis in Myocardial Infarction (PROVE IT-TIMI 22) trial. Am Heart J 155:49–55
Nagata K, Tsuji T, Todoroki N et al. (1993) Activated platelets inducesuperoxide anion release by monocytes and neutrophils through P-selectin (CD62). J Immunol 151:3267–73
Ostrowski SM, Belkadi A, Loyd CM et al. (2011) Cutaneous denervation ofpsoriasiform mouse skin improves acanthosis and inflammation in asensory neuropeptide-dependent manner. J Invest Dermatol 131:1530–8
Papapanou PN, Sedaghatfar MH, Demmer RT et al. (2007) Periodontaltherapy alters gene expression of peripheral blood monocytes. J ClinPeriodontol 34:736–47
Pietrzak A, Kadzielewski J, Janowski K et al. (2009) Lipoprotein (a) in patientswith psoriasis: associations with lipid profiles and disease severity. Int JDermatol 48:379–87
Prodanovich S, Kirsner RS, Kravetz JD et al. (2009) Association of psoriasiswith coronary artery, cerebrovascular, and peripheral vascular diseasesand mortality. Arch Dermatol 145:700–3
Ross R (1999) Atherosclerosis—an inflammatory disease. N Engl J Med340:115–26
Shepherd J, Little MC, Nicklin MJ (2004) Psoriasis-like cutaneous inflamma-tion in mice lacking interleukin-1 receptor antagonist. J Invest Dermatol122:665–9
Shi C, Sakuma M, Mooroka T et al. (2008) Down-regulation of the forkheadtranscription factor Foxp1 is required for monocyte differentiation andmacrophage function. Blood 112:4699–711
Silver R, Helms A, Fu W et al. (2011) Using optical coherence tomography forthe longitudinal noninvasive evaluation of epidermal thickness in amurine model of chronic skin inflammation. Skin Res Technol; e-pubahead of print 14 September 2011
Spah F (2008) Inflammation in atherosclerosis and psoriasis: commonpathogenic mechanisms and the potential for an integrated treatmentapproach. Br J Dermatol 159:10–7
Swindell WR, Johnston A, Carbajal S et al. (2011) Genome-wide expressionprofiling of five mouse models identifies similarities and differences withhuman psoriasis. PLoS One 6:e18266
Swirski FK, Libby P, Aikawa E et al. (2007) Ly-6Chi monocytes dominatehypercholesterolemia-associated monocytosis and give rise to macro-phages in atheromata. J Clin Invest 117:195–205
Takahashi H, Tsuji H, Takahashi I et al. (2008) Plasma adiponectin and leptinlevels in Japanese patients with psoriasis. Br J Dermatol 159:1207–8
Toker A, Kadi M, Yildirim AK et al. (2009) Serum lipid profile paraoxonaseand arylesterase activities in psoriasis. Cell Biochem Funct 27:176–80
Ward NL, Loyd CM, Wolfram JA et al. (2011) Depletion of antigen-presentingcells by clodronate liposomes reverses the psoriatic skin phenotype inKC-Tie2 mice. Br J Dermatol 164:750–8
Watson BD, Dietrich WD, Busto R et al. (1985) Induction of reproduciblebrain infarction by photochemically initiated thrombosis. Ann Neurol17:497–504
Wolfram JA, Diaconu D, Hatala DA et al. (2009) Keratinocyte but notendothelial cell specific overexpression of Tie2 leads to the developmentof psoriasis. Am J Pathol 174:1443–58
www.jidonline.org 2075
Y Wang et al.Psoriasis, Vascular Inflammation, and Thrombosis





























