Embed Size (px)
Citation preview

Clinical and hemodynamic course of infants and children with anomalous left coronary artery
The clinical history of all 17 patients with anomalous left coronary artery presenting over the last 20 years was studied, with special emphasis on those who underwent reimplantation of the anomalous coronary artery into the aorta, a procedure that became our “treatment of choice” during this period. These patients were also evaluated for ventricular performance, residual mitral regurgitation, and wall integrity. Early in our experience with reimplantation, two patients died while we waited for them to achieve a more favorable size for surgery. Eight of nine survived reimplantation; three of these were under 1 year of age when operated upon. One of these eight patients has required additional mitral valvuloplasty, but all are doing well clinically up to 12 years after operation. Preoperative left ventricular ejection fraction of 0.37 f 0.16 increased to 0.67 + 0.07 (p < 0.001) by 1 year after surgery, despite ventricular wall abnormalities in four patients. Thus reimplantation of the anomalous left coronary artery should be undertaken upon diagnosis, since surgery can be performed successfully in infancy, with resultant improvement in ventricular function and an adequate clinical condition for at least 12 years. (AM HEART J 1989;118:1176.)
Roger A. Hurwitz, MD, Randall L. Caldwell, MD, Donald A. Girod, MD, John Brown, MD, and Harold King, MD. Indianapolis, Ind.
Anomalous origin of the left coronary artery from the pulmonary artery is an uncommon lesion, associated with major morbidity and mortality. Without surgi- cal intervention, myocardial dysfunction, congestive heart failure, and mitral regurgitation frequently result in a high early morta1ity.r Despite initial surgical procedures in which the coronary artery was ligated at its pulmonary artery “origin,” imme- diate and late mortality was 50% and approached 80% when infants under 1 year of age were operated upon2, 3 Due to this ominous prognosis, alternative surgical procedures were devised to establish a dual coronary system through arterial grafting, construction of an intrapulmonary artery vascular baffle, or coronary artery reimplantation into the aorta.4-6
This communication presents our experience with anomalous left coronary artery, and reviews the clin- ical course, arterial patency, ventricular performance, residual mitral regurgitation, and myocardial wall integrity. The focus is on those patients undergoing coronary artery reimplantation, which became our procedure of choice in 1974.
From the Departments of Pediatrics, Radiology, and Surgery, Indiana Uni- versity Medical School. Received for publication June 15, 1989; accepted July 24, 1989.
Reprint requests: Roger A. Hunvitz, MD, Section of Pediatric Cardiology, Riley Research, Room 126, 702 Barnhill Drive, Indianapolis, IN 46223.
4/l/15938
1176
METHODS Patients. From 1967 to 1987, 17 patients with isolated
anomalous left coronary artery were evaluated (Table I). Presentation was at age 2 months to 15 years. One patient (No. 1) was lost to follow-up 5 years after the initial diag- nosis at 3 years of age. All patients were diagnosed by car- diac catheterization and angiography. Fourteen patients had surgery. Nine of these underwent coronary artery re- implantation at age 3 months to 11 years; three of this group were 9 months old or less at the time of surgery. The eight survivors of reimplantation surgery were followed up clinically for 1 to 12 years; six had postoperative cardiac catheterization and aortography. All eight had evaluation of postoperative ventricular function and wall motion by cardiac catheterization and/or radionuclide angiocardio- gwhy.
Cardiac catheterization. Biplane cineangiography was performed in the right anterior oblique and left anterior oblique projections. Left ventricular function was evalu- ated by measurement of left ventricular ejection fraction by the area-length formula.? Degree of mitral regurgitation was estimated from the left ventriculogram.8 Coronary ar- terial anatomy and patency were determined from arterial root angiography.
Radionuclide studies. Equilibrium ventriculography was performed after in vitro labeling of patients’ red blood cells with 200 &X/kg technetium-99m. Imaging was in the left anterior oblique projection with caudal angulation. Left ventricular function and wall motion were inspected on a continuous loop tine film. Computer-assisted phase, stroke volume, and paradox images helped define chamber borders and identify segmental abnormalities. Left ven-

Volume 118 Number 6 ,4nomalow left coronary artery 1177
Table I. All patients presenting with anomalous left coronary artery, 1967 to 1987
Preop Postop
Patient Age at dr LVEF MR Surgery L VEF MR Wall abn Outcome
1 3 Yr Alive age 8 yr 2 3 mo 0 Died at 1-h yr 3 4 mo 0 Died at 5 mo 4 1 mo Ligation Died 1 day postop 5 2 Yr Ligation Alive age 15 yr 6 4 yr Graft Alive age 17 yr 7 15 yr Ligation Alive age 19 yr 8 2 mo Ligation - Severe Apical dys Alive age 17 yr
MVR 0.47 0 Apical dys Int mammary graft 0.66 0 Apical dys
9 1 yr 0.28 Mod Reimplant Died 1 day postop 10 11 yr 0.61 Mild Reimplant 0.64 Mild N.D. Alive age 14 yr 11 7 yr 0.47 Mild Reimplant 0.53 Mild (1.3) Ant-lat dys Alive age 12 yr
(1.5) 12 8mo 0.36 Mild- Reimplant 0.63 Mild (1.7) None Alive age 10 yr
mod 13 6 mo 0.44 Severe Reimplant 0.51 Severe (4.0) None Alive age 5 yr
0.51 Severe Valvulo 0.68 Mild (1.4) 14 1 yr 0.27 None Reimplant 0.70 None Apical dys Alive age 5 yr 15 1 yr 0.18 Mod Reimplant 0.69 Mod (2.7) Apical dys Alive age 2 yr
(2.4 16 3 mo 0.14 Mod Reimplant 0.68 Mod (3.0) Apical aneurysm Alive age 1 yr
(2.2) 17 1 yr 0.44 Mod Reimplant 0.79 Mild (1.5) None Alive age yr 12
Abn, Abnormality; ant, anterior; dx, diagnosis; dys, dyskinesis; int, internal; lat, lateral; LVEF, left ventricular ejection fraction; mod, moderate; MR, mitral regurgitation; MVR, mitral valve replacement; N.D., not done: postop, postoperative; preop, preoperative; valvulo, valvuloplasty. Number in parentheses in MR is left ventricle:right ventricle stroke volume ratio.
tricular ejection fraction was estimated by standard techniques.g In our laboratory, a left ventricular ejection fraction less than 0.50 is considered abnormal, and a value of 0.50 to 0.55 is borderline. These values reflect the mean of 0.68 f 0.09 established in “normal” children.l” Though these normal values were generated from first-pass studies, our first-pass and equilibrium ventriculographic values are closely correlated. Mitral regurgitation was estimated by quantitating left ventricular:right ventricular stroke vol- ume rati0s.l’ W ith the use of this method, a stroke volume ratio of 1.5 to 2.0 is consistent with mild regurgitation, a stroke volume ratio of more than 2.0 signifies moderate re- gurgitation, and a ratio of more than 3.0 suggests severe regurgitation.
Statistical analysis. Preoperative left ventricular ejec- tion fraction was compared with postoperative left ven- tricular ejection fraction by Student’s t test for paired data.
RESULTS
Clinical course. Three patients underwent no sur- gery. One (No. 1) was asymptomatic until he was lost to follow-up 5 years after diagnosis. Medical man- agement was undertaken in two other patients (Nos. 2 and 3) who were expected to be better candidates for surgery after more growth. One with moderate cardiomegaly and m ild congestive heart failure died
at age 4 months, shortly after diagnosis; the other, with only miid symptoms, died 9 months after diag- nosis at age 1 year.
Surgery was performed in 14 patients. The anom- alous coronary artery was ligated at the pulmonary artery insertion in four patients who were operated upon either before reimplantation was initiated as a surgical procedure (two patients) or in whom the coronary anatomy was considered unfavorable for reimplahtation at operation (two patients). One of these latter patients died early after surgery, with continued low cardiac output associated with myo- cardial infarction and m itral regurgitation, both present before surgery. Following ligation of the anomalous coronary artery, one patient (No. 8) has had numerous problems, necessitating m itral valve replacement on two occasions and internal mammary artery grafting, but this patient is alive and is attending high school full time 17 years after the ini- tial surgery. Two who were treated by ligation of the anomalous artery are asymptomatic 4 and 10 years after surgery. One teenage patient underwent arterial graft anastomosis due to lack of “elasticity of the coronary artery” and did well for 5 years, when con- tact with the patient was lost.

1178 Hurwitz et al.
l.O-
.90-
.80-
.70-
.60-
t; 3 .50-
.40-
.30-
.20-
.lO-
O-
P<O.OOl~,
/
PRE OP EARLY LATE POST-OP POST-OP
Flg. 1. All patients surviving reimplantation of anoma- lous left coronary artery. Left ventricular ejection fraction (LVEF) plotted at initial evaluation (PRE OP) and after surgery (POST OP); EARLY POST-OP is 1 to 2 months following repair and LATE POST-OP is at least 1 year fol- lowing repair.
Nine patients underwent reimplantation of the anomalous coronary artery into the aorta at a mean age of 32 months, with eight survivors. The lone death occurred in a l-year-old patient (No. 9) who presented with congestive heart failure and low car- diac output. Postmortem examination revealed an extensive, old myocardial infarct. Seven of the eight others have been asymptomatic 1.5 to 12.0 years since surgery. One patient (No. 13), with preoperative my- ocardial infarct and papillary muscle dysfunction, has required a second operation for m itral valvulo- plasty and is doing well 6 months later.
Hemodynamics after coronary artery reimplantation Arterial patency. Six patients underwent aortog-
raphy 6 to 12 months after coronary artery reimplan- tation. There was complete coronary artery patency in five; the other patient (No. 14) had a patent, but obstructed coronary artery; she remains asymptom- atic 3 years after initial surgery.
Left ventricular function. Left ventricular ejection fraction increased significantly after reimplantation (0.37 k 0.16 to 0.67 t 0.07, p < 0.001) when esti- mated at least 1 year after surgery (Fig. 1). Each pa- tient had an increase in ejection fraction, though glo-
December 1989 American Heart Journal
bal ejection fraction remained borderline in one. Left ventricular ejection fraction increased further in both patients tested serially; each showed improve- ment early (2 months) and further improvement late (1 year) postoperatively (Fig. 1).
Mitral regurgitation. In the six patients who had preoperative and postoperative left ventricular cin- eangiography, there was only a modest decrease in vis- ually estimated m itral regurgitation. The patient with severe regurgitation continued to have it after successful arterial reimplantation. The left ven- tricular:right ventricular stroke volume ratio esti- mated in three patients before and after surgery showed no significant improvement (Table I). This radionuclide quantitation of m itral regurgitation re- mained constant on serial postoperative studies in one patient with m ild regurgitation and increased slightly in the patient with severe regurgitation. Af- ter m itral valvuloplasty, the stroke volume ratio dropped from 4.0 to 1.4 (near normal) in that patient.
Ventricular wall motion. Preoperative radionu- elide studies in those patients subject to reimplanta- tion identified segmental wall motion abnormalities in two (Nos. 11 and 15). Postoperatively, four pa- tients (Nos. 11, 14, 15, 16) demonstrated abnormal- ities (Figs. 2 to 4).
DISCUSSION
Anomalous left coronary artery is a potentially le- thal condition. When medical therapy is employed, there is an early 20% to 40 % mortality, especially in those with little left-to-right shunt.l” These patients may experience progressive congestive heart failure, ischemia and/or myocardial infarction and m itral re- gurgitation, resulting in sudden death or in a higher risk at surgery. Two of our relatively stable patients died while awaiting “elective” surgery at an older age.
Despite the known attrition during medical man- agement, some authors ls have advised waiting until patients reach 18 months of age before undertaking operation. This was in consideration of the high mortality (75 % ) in those operated upon under 1 year of age3, I3 and was based upon the fact that early sur- gery frequently required ligation of the coronary ar- tery at its pulmonary artery “origin.” However, newer surgical techniques have resulted in higher survival and in many cases have produced a dual coronary artery system.
Attempts to create a two-coronary system were made to promote better myocardial perfusion and to lower the combined early and late mortality associ- ated with coronary artery ligation.2p 3, 13, I4 Though some authors’” report normal perfusion after coro- nary artery ligation, others16 feel that overall prog-

Volume 116
Number 6 Anomalous left coronary artery 1179
Fig. 2. Thall ium-201 perfusion images in patient No. 11, performed in anterior, lateral, and left anterior oblique projections. From top row to bottom are preoperative stress and rest, and postoperative stress and rest. There is an anterolateral wall abnormality (arrows) that improved following surgery.
nosis is still better with a dual coronary artery system. Despite an uncomplicated course in two of four patients in our group following coronary artery ligation, we feel that creation of a two-coronary sys- tem is preferable.
In general, however, the early course of our pa- tients reflects the extent of damage prior to any type of surgery. The two postoperative deaths (one fol- lowing coronary artery ligation and one following re- implantation) occurred in patients who demonstrated large, old myocardial infarcts at postmortem exam- ination. Two with severe m itral regurgitation and papillary muscle dysfunction have required further valve surgery despite “successful” coronary artery surgery. Though two patients with coronary artery ligation have no clinical symptoms (exercise testing
in one was normal), another patient treated by cor- onary artery ligation has had continuing ischemia, with some improvement in angina-like symptoms af- ter recent internal mammary artery bypass grafting.
In an effort to be consistent and develop a two- coronary artery system, we have attempted to reim- plant the coronary artery into the aorta in all patients d iagnosed with anomalous left coronary artery since 1974. Due to anatomic constraints found at surgery, two could not be operated upon by reimplantation. Eight of nine patients survived initial surgery. Three had successful surgery when under 1 year of age, suggesting that age/size is not a ma jor factor. In one of six postoperative patients studied by aortography, there was partial obstruction of the reimplanted ar- tery, but that patient has done well clinically. The
I 180 Hurwitz et al.
Fig. 3. Diastolic (top) and systolic (bottom) radionuclide images of patient No. 16 with apical aneurysm following surgery.
other five demonstrated apparently normal arte- rial patency when studied at least 1 year after sur- gery.
Only one patient was asymptomatic upon diagno- sis. Each of the others experienced major reduction in symptomatology after surgery. All showed signif- icant decrease in cardiomegaly; heart size normalized in five. When left ventricular ejection fraction was estimated by cineangiography or radionuclide angio- cardiography, it was abnormal in all but one patient studied preoperatively. However, ejection fraction became normal in seven and borderline in one by a year after coronary artery reimplantation. Since the radionuclide estimate of left ventricular ejection fraction closely approximates that derived from left
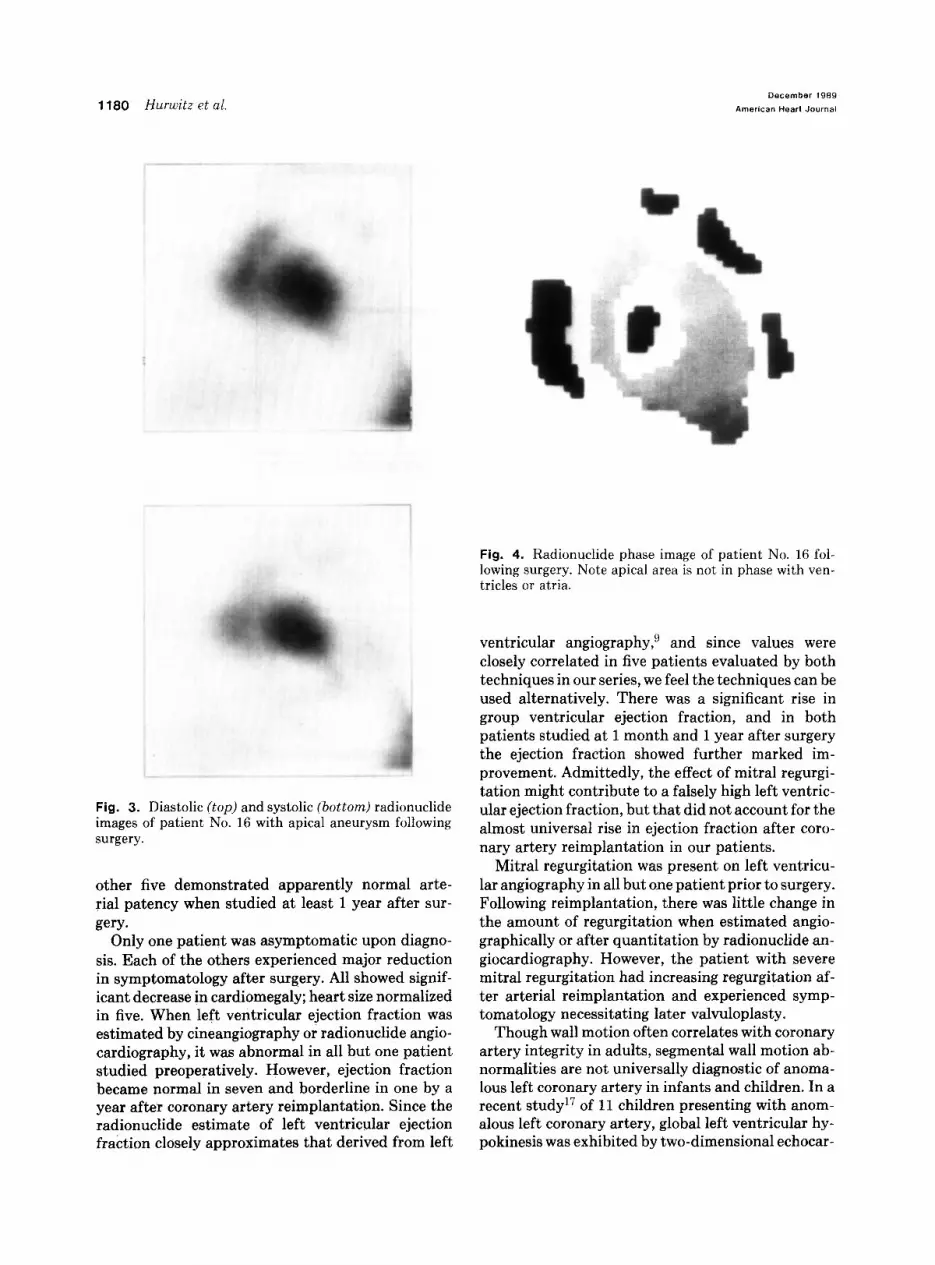
Fig. 4. Radionuclide phase image of patient No. 16 fol- lowing surgery. Note apical area is not in phase with ven- tricles or atria.
ventricular angiography,’ and since values were closely correlated in five patients evaluated by both techniques in our series, we feel the techniques can be used alternatively. There was a significant rise in group ventricular ejection fraction, and in both patients studied at 1 month and 1 year after surgery the ejection fraction showed further marked im- provement. Admittedly, the effect of mitral regurgi- tation might contribute to a falsely high left ventric- ular ejection fraction, but that did not account for the almost universal rise in ejection fraction after coro- nary artery reimplantation in our patients.
Mitral regurgitation was present on left ventricu- lar angiography in all but one patient prior to surgery. Following reimplantation, there was little change in the amount of regurgitation when estimated angio- graphically or after quantitation by radionuclide an- giocardiography. However, the patient with severe mitral regurgitation had increasing regurgitation af- ter arterial reimplantation and experienced symp- tomatology necessitating later valvuloplasty.
Though wall motion often correlates with coronary artery integrity in adults, segmental wall motion ab- normalities are not universally diagnostic of anoma- lous left coronary artery in infants and children. In a recent study17 of 11 children presenting with anom- alous left coronary artery, global left ventricular hy- pokinesis was exhibited by two-dimensional echocar-

Volume 118
Number 6
diography; segmental wall abnormalities were not demonstrated. Our experience was somewhat similar; in only one of three patients studied by preoperative radionuclide angiocardiography was regional dyski- nesis noted. Myocardial perfusion imaging can of course identify fixed regional abnormalities, even at rest. Preoperatively, one of our patients had a seg- mental lesion identified on perfusion (thallium-201) scanning. Three of six patients in another study14 that used myocardial perfusion techniques also showed segmental abnormalities. Possible reasons for lack of sensitivity in diagnosing regional wall ab- normalities noninvasively are the technical inability to image infants during stress, and the presence of major subendocardial ischemia, which cannot be vi- sualized by standard diagnostic techniques. Postop- erative regional abnormalities have not been identi- fied on two-dimensional echocardiograms. How- ever, four patients in our series showed dyskinetic apical segments or anterolateral wall abnormalities when evaluated by radionuclide studies. Perhaps such defects can be more readily imaged after the gross ventricular dilatation present preoperatively has receded.
Implications. Though a rare defect, anomalous left coronary artery is a potentially lethal lesion. The condition also carries a significant morbidity, since damage to mitral valve apparatus results in progres- sive mitral regurgitation, necessitating valvuloplasty and/or prosthetic valve replacement. Though a rare patient may have no symptoms or myocardial com- promise for many years, many patients have sudden decompensation, myocardial infarction, or death. Ligation of the anomalous coronary artery at its con- nection to the pulmonary artery is simple and may afford effective palliation; however, it would seem preferable to provide a two-coronary system. We have successfully reimplanted the anomalous coro- nary artery in three infants under 9 months of age, suggesting that the age of the patient is not a major factor that should postpone surgery. Global left ven- tricular systolic function can be expected to normal- ize after surgery, despite severely depressed function preoperatively. Unfortunately, significant reduction in preexisting mitral regurgitation is seldom demon- strated after successful coronary artery reimplanta- tion.
The clinical condition of our patients suggests that myocardial perfusion at rest and during routine ac- tivities remains adequate for up to 12 years. Further myocardial imaging, with stress intervention studies, will be instructive in ascertaining the long-term
Anomalous left coronary artery 1181
growth of the reimplanted coronary artery and the continued adequacy of myocardial integrity and function.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
Wesselhoeft H, Fawcett JS, Johnson AL. Anomalous origin of the left coronary artery from the pulmonary trunk: its clinical spectrum, pathology and pathophysiology based on a review of 140 cases with seven further cases. Circulation 1968;38:403-25. Burton R, Jonas RA, Lang P, Rein AJ, Castaneda AR. Anom- alous origin of left coronary artery from pulmonary artery. J Thorac Cardiovasc Surg 1987;93:iO3-8. Laborde F. Marchand M. Leca F. Jarreau M. Deauirot A. Hazan E. Surgical treatment of anomalous origin oithe left coronary artery in infancy and childhood. J Thorac Cardiovasc Surg 1981;82:423-8. Neches WH, Mathews RA, Park SC, Lenox CC, Zuberbuhler JR, Siewers RD, Bahnson HT. Anomalous origin of the left coronary artery from the pulmonary artery. Circulation 1974;50:582-7. Takeuchi S, Imamura H, Katsumoto K, Hayashi I, Katonhgi T, Yozu R, Ohkura M, Inoue T. New surgical method for re- pair of anomalous left coronary artery from pulmonary artery. J Thorac Cardiovasc Surg 1979;78:7-11. Grace RR, Angeluni P, Cooley D. Aortic implantation of anomalous left coronary artery arising from pulmonary artery. Am J Cardiol 1977;39:608-13. Dodge HT, Sandler H, Ballew DW, Lord JE Jr. Use of biplane angiocardiography for measurement of left ventricular volume in man. AM HEART J 1960;60:762-3. Sellers RD, Levy MJ, Amplatz K, Lillehei EW. Left retrograde cardioangiography in acquired cardiac disease. Am J Cardiol 1964;14:437-47. Burow RD, Strauss HW, Singleton R, Pond M, Rehn T, Bai- ley IK, Griffith LC, Nickoloff E, Pitt B. Analysis of left ven- tricular function from multiple gated acquisition cardiac blood pool imaging. Comparison to contrast angiography. Cir- culation 1977;56:1024-8. Hurwitz RA, Treves S, Kuruc A. Right ventricular and left ventricular ejection fraction in pediatric patients with normal hearts: first-pass radionuclide angiocardiography. AM HEART J 1984;107:726-32. Hurwitz RA, Treves S, Freed M, Girod DA, Caldwell RL. Quantitation of aortic and mitral regurgitation in the pediat- ric population: evaluation by radionuclide angiocardiography. Am J Cardiol 1983;51:252-5. Askenazi J, Nadas AS. Anomalous left coronary artery origi- nating from the pulmonary artery. Circulation 1975;51:976-87. Driscoll DJ, Nihill MR, Mullins CE, Cooley DA, McNamara DG. Management of symptomatic infants with anomalous or- igin of the left coronary artery from the pulmonary artery. Am J Cardiol 1981;47:642-8. Arciniegas E, Farooki ZQ, Hakimi M, Green EW. Management of anomalous left coronary artery from the pulmonary-artery. Circulation 1980;62(suppl 1)4:180-g. Finley JP, Howman-Giles R, Gilday DL, Olley PM, Rowe RD. Thallium-201 myocardial imaging in anomalous left coronary artery arising from the pulmonary artery. Am J Cardiol 1978;42:675-80.
16. Wilson CL, Diabal PW, McGuire SA. Surgical treatment of anomalous left coronary artery from pulmonary arterv. Fol- low-up in teenagers and adults. AM HEART J 1979;98:440-6.
17. Rein AJ, Colan SD. Parness IA. Sanders SP. Regional and global left ventricular function in infants with anomalous or- igin of the left coronary artery from the pulmonary trunk: pre-operative and post-operative assessment. Circulation 1987;75:115-23.





























