Embed Size (px)
Citation preview

Clinical, histological and immunohistochemical features ofectomesenchymal chondromyxoid tumor
Fábio Ramôa Pires, PhD,a Aline Correa Abrahão, DDS, MSc,b
Márcia Grillo Cabral, DDS, PhD,b Rebeca Souza Azevedo, DDS, PhD,c
Martinho Campolina Rebello Horta, DDS, PhD,d Carlos Roberto Martins, DDS, PhD,d
Oslei Paes de Almeida, DDS, PhD,e and Sow-Yeh Chen, DDS, PhD,f Rio de Janeiro,Piracicaba, and Belo Horizonte, Brazil, and Philadelphia, PASTATE UNIVERSITY OF RIO DE JANEIRO, FEDERAL UNIVERSITY OF RIO DE JANEIRO, STATEUNIVERSITY OF CAMPINAS (UNICAMP), PONTIFÍCIA UNIVERSIDADE CATÓLICA DE MINAS GERAIS,AND TEMPLE UNIVERSITY
Objective. Ectomesenchymal chondromyxoid tumor is a rare oral soft tissue neoplasm that should be differentiatedfrom other neural and chondromyxoid entities. The aim of this study was to report the clinical, histological, andimmunohistochemical features of 3 additional cases of this condition.Methods. Clinical data were obtained from the clinical records and all cases were evaluated through light microscopyand immunohistochemistry to cytokeratins, vimentin, S100 protein, desmin, smooth muscle actin, and glial fibrilaryacidic protein.Results. All 3 cases affected the tongue as a long-lasting submucosal swelling and were managed through conservativesurgery. They all showed myxoid and chondroid histological patterns, and vimentin, S100, and glial fibrilary acidicprotein immunoexpression.Conclusions. These findings reinforce the typical features of ectomesenchymal chondromyxoid tumor previouslydescribed, helping to confirm and establish the clinical, histopathological, and immunohistochemical profile of this
uncommon lesion. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:914-919)Ectomesenchymal chondromyxoid tumor (ECT) is arare benign intraoral mesenchymal soft tissue lesionfirst described in 1995.1 All data regarding clinicopath-ological characteristics of ECT are based on 33 previ-ously reported cases in the literature. Therefore, thislesion should be included in the differential diagnosisof several other intraoral soft tissue swellings. As ECTis uncommon, and it can bring difficulties for clinicaland microscopic differential diagnosis, other reports are
aProfessor, Oral Pathology, School of Dentistry, State University ofRio de Janeiro, Rio de Janeiro, RJ, Brazil.bProfessor, Oral Pathology, School of Dentistry, Federal Universityof Rio de Janeiro, Rio de Janeiro, RJ, Brazil.cPhD student, Oral Pathology, Piracicaba Dental School, State Uni-versity of Campinas (UNICAMP), Piracicaba, SP, Brazil.dProfessor, Stomatology and Oral Pathology, School of Dentistry,Pontifícia Universidade Católica de Minas Gerais, Belo Horizonte,MG, Brazil.eProfessor, Oral Pathology, Piracicaba Dental School, State Univer-sity of Campinas (UNICAMP), Piracicaba, SP, Brazil.fProfessor, Department of Pathology and Laboratory Medicine, Tem-ple University School of Medicine.Received for publication Apr 23, 2009; returned for revision Jun 28,2009; accepted for publication Jul 2, 2009.1079-2104/$ - see front matter© 2009 Published by Mosby, Inc.
doi:10.1016/j.tripleo.2009.07.007914
helpful to better understand its biological characteris-tics. The aim of this study was to report the clinical,microscopic, and immunohistochemical features of 3additional cases of ECT.
MATERIAL AND METHODSThe files of 3 oral pathology laboratories were re-
viewed and 3 cases with final diagnosis of ectomesen-chymal chondromyxoid tumor were selected for thestudy. Clinical and demographic information from eachcase was obtained through review of the laboratoryrecords and clinical charts from the patients. All hema-toxylin and eosin–stained histological slides were re-viewed under light microscopy and all 3 cases weresubmitted to immunohistochemical analysis with anti-bodies directed against pancytokeratins (clone AE1/AE3, Dako A/S, Glostrup, Denmark, dilution 1:500),vimentin (clone vim3B4, Dako A/S, dilution 1:400),S100 protein (policlonal, Dako A/S, dilution1:10.000), desmin (clone D33, Dako A/S, dilution1:1.000), �-smooth-muscle actin (clone 1A4, DakoA/S, dilution 1:400), and glial fibrilary acidic protein(GFAP) (clone, Dako A/S, dilution 1:200) throughan avidin-biotin-peroxidase method. Reactions were
visualized using diaminobenzidine as the chromogen, and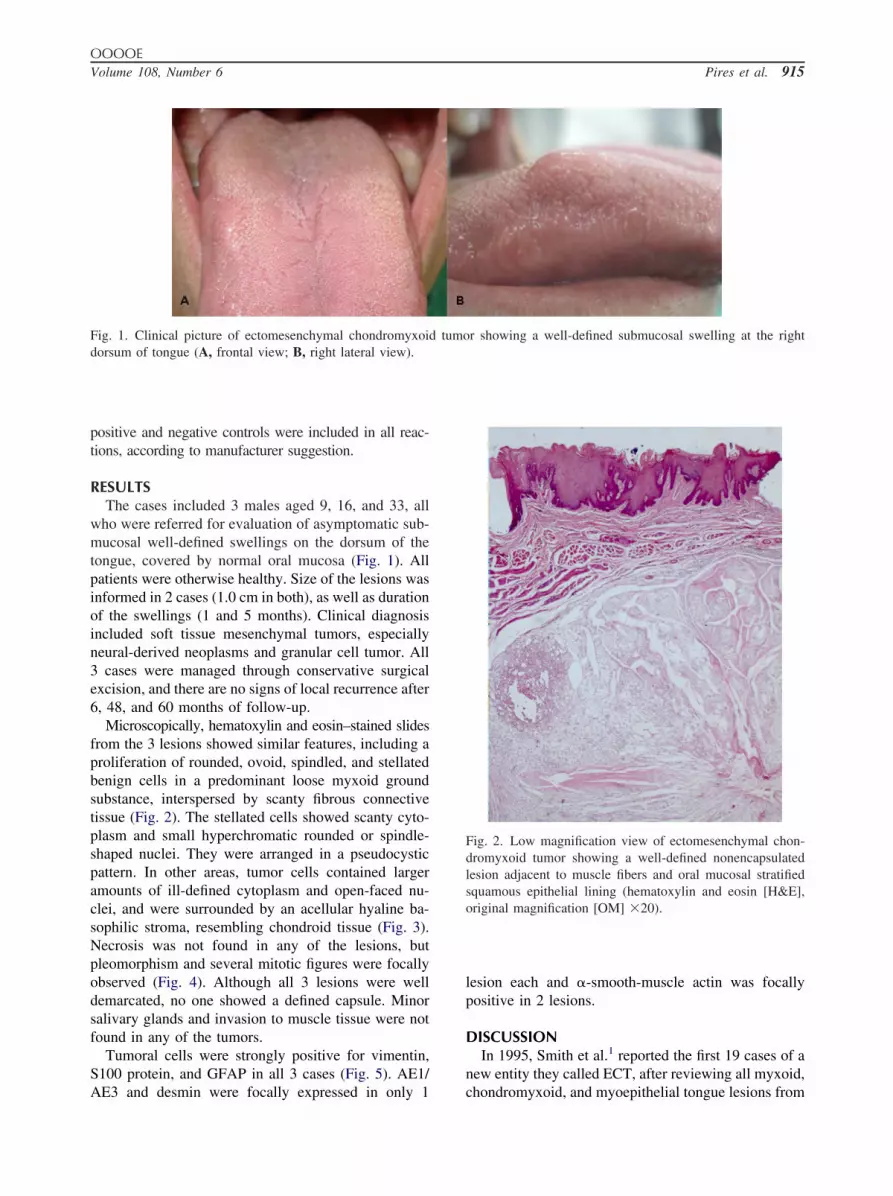
OOOOEVolume 108, Number 6 Pires et al. 915
positive and negative controls were included in all reac-tions, according to manufacturer suggestion.
RESULTSThe cases included 3 males aged 9, 16, and 33, all
who were referred for evaluation of asymptomatic sub-mucosal well-defined swellings on the dorsum of thetongue, covered by normal oral mucosa (Fig. 1). Allpatients were otherwise healthy. Size of the lesions wasinformed in 2 cases (1.0 cm in both), as well as durationof the swellings (1 and 5 months). Clinical diagnosisincluded soft tissue mesenchymal tumors, especiallyneural-derived neoplasms and granular cell tumor. All3 cases were managed through conservative surgicalexcision, and there are no signs of local recurrence after6, 48, and 60 months of follow-up.
Microscopically, hematoxylin and eosin–stained slidesfrom the 3 lesions showed similar features, including aproliferation of rounded, ovoid, spindled, and stellatedbenign cells in a predominant loose myxoid groundsubstance, interspersed by scanty fibrous connectivetissue (Fig. 2). The stellated cells showed scanty cyto-plasm and small hyperchromatic rounded or spindle-shaped nuclei. They were arranged in a pseudocysticpattern. In other areas, tumor cells contained largeramounts of ill-defined cytoplasm and open-faced nu-clei, and were surrounded by an acellular hyaline ba-sophilic stroma, resembling chondroid tissue (Fig. 3).Necrosis was not found in any of the lesions, butpleomorphism and several mitotic figures were focallyobserved (Fig. 4). Although all 3 lesions were welldemarcated, no one showed a defined capsule. Minorsalivary glands and invasion to muscle tissue were notfound in any of the tumors.
Tumoral cells were strongly positive for vimentin,S100 protein, and GFAP in all 3 cases (Fig. 5). AE1/
Fig. 1. Clinical picture of ectomesenchymal chondromyxoidorsum of tongue (A, frontal view; B, right lateral view).
AE3 and desmin were focally expressed in only 1
lesion each and �-smooth-muscle actin was focallypositive in 2 lesions.
DISCUSSIONIn 1995, Smith et al.1 reported the first 19 cases of a
new entity they called ECT, after reviewing all myxoid,
Fig. 2. Low magnification view of ectomesenchymal chon-dromyxoid tumor showing a well-defined nonencapsulatedlesion adjacent to muscle fibers and oral mucosal stratifiedsquamous epithelial lining (hematoxylin and eosin [H&E],original magnification [OM] �20).
r showing a well-defined submucosal swelling at the right
d tumochondromyxoid, and myoepithelial tongue lesions from

OOOOE916 Pires et al. December 2009
the files of the Armed Forces Institute of Pathology ina 24-year period. These 19 cases did not fulfill thediagnostic criteria for any other intraoral soft tissuechondromyxoid lesion. Apart from this initial descrip-tion, only 10 case reports and small series and a veryrecent review were published since then, totaling 33ECT cases reported in the English literature.2-12 Kan-nan et al.2 reported 3 cases selected from the review ofall myxoid, chondromyxoid, and myoepithelial tonguelesions from the files of 2 universities in the UnitedStates. These initial reports1,2 indicated that ECT wasmisinterpreted as other similar soft tissue lesions in thepast, reinforcing the importance of establishing the
Fig. 3. Tumor cells presenting a large ill-defined eosinophiliccytoplasm surrounded by an acellular hyaline stroma resem-bling chondroid tissue in ectomesenchymal chondromyxoidtumor (H&E, OM �160).
Fig. 4. Detail of a myxoid area in ectomesenchymal chon-dromyxoid tumor showing a mild degree of cellular pleomor-phism (H&E, OM �160).
diagnostic criteria for ECT.
Most authors agree that ECT originates from un-differentiated neural crest– derived mesenchymal ce-lls,1-5,9,11,12 although minor salivary gland and muscleorigins have also been considered.1,4,8 The first theoryis supported by the mesenchymal and neural immuno-histochemical phenotype of the lesion.5 Woo et al.8
have suggested that for classification purposes, ECTand myoepithelioma should be considered the samelesion, but this statement is not shared by most of theauthors. Goveas et al.9 have recently demonstrated thatalthough ECT can express general myoepithelial cellimmunomarkers, such as S100 and GFAP, it fails toexpress more specific markers for myoepithelial differ-entiation as calponin, p63, and smooth muscle myosinheavy chain, reinforcing that both lesions are probablydifferent entities.
Sociodemographic data from the 33 previously de-scribed cases and from our additional 3 cases (total of36 cases) revealed a mean age of 36.6 years old, rang-ing from 9.0 to 78.0 years. One of our cases is thesecond reported case with the lower age in the litera-ture, and only 4 (11%) of the 36 cases of affectedpatients in the first 2 decades of life. Males and femaleswere equally affected. Fifteen patients were white, 4were non-white, and the ethnic information was notavailable for the remaining 17 patients (Table I).
Clinically all but one case affected the tongue: theanterior dorsum in 34 cases and the base of the tonguein 1.4 Nigam et al.10 reported a case of ECT involvingthe hard palate and, although the microscopical featureswere not typical for ECT and the authors did notperform any immunohistochemical reaction, we haveincluded this case in our review. Most patients reportedthe presence of an asymptomatic submucosal nodulecovered by normal oral mucosa lasting for an averageof 36.4 months, ranging from 1 month to 20 years.Diameter of the lesions ranged from 3 to 20 mm, witha mean of 11.2 mm, and very few patients reportedminor local complaints, including local pressure (n �1) and purulent discharge (n � 1) (Table I). Our 3 casespresented similar features to those reported in the lit-erature.
Based on the clinical characteristics and differentialdiagnosis, which included granular cell tumor, neu-rofibroma, fibroma, and schwannoma, all 36 reportedlesions were treated by conservative surgery. Meanfollow-up interval was 54.2 months with a range of 2.0months to 20.0 years. Only 2 cases reported by Smith etal.1 showed recurrences, being successfully managedon the second surgical approach (Table I). Although allavailable evidence reinforces the benign nature of ECT,the small number of recurrent cases and the microscop-
ical evidence of foci of pleomorphic hyperchromatic
OOOOEVolume 108, Number 6 Pires et al. 917
cells and sporadic mitotic figures suggest the impor-tance of regular follow-up of patients after treat-ment.2,4,5
Microscopically, ECT is characterized by a prolifer-ation of small rounded, ovoid, spindled, or stellatedcells, arranged in myxoid, loose, and reticular back-grounds.11 Some areas containing dense or hyalinizedconnective tissue can be seen admixed with myxoidareas.7,11 Chondroid areas usually represent a less pro-nounced component and contain large cells with clearto basophilic ill-defined cytoplasm and hyperchromaticnuclei.2,6 Focal areas of cellular atypia can be seen,with hyperchromatic nuclei, prominent nucleoli, nu-clear pseudoinclusions, and binucleated cells.1,2,11
Some authors speculate that these areas of suspected
Fig. 5. Expression of vimentin (A) and S100 protein (B)A, OM �80; B, OM �40).
Table I. Sociodemographic and clinical data from the 3from the literature*
Authors (Reference no.) Year nAge, y
Range (mean)
Smith et al. (1) 1995 19 9-78 (38.5)
Kannan et al. (2) 1996 3 21-51 (35)Van der Wal & Van der Waal (3) 1996 1 25Carlos et al. (4) 1999 1 16De Visscher et al. (5) 2003 2 39-42 (40.5)Ide et al. (6) 2003 1 52Kaplan et al. (7) 2004 2 26-57 (41.5)Woo et al. (8) 2005 1 22Goveas et al. (9) 2006 1 57Nigam et al. (10) 2006 1 30Seckin et al. (11) 2008 1 56Present cases 2009 3 9-33 (19.3)Total — 36 9-78 (36.6)
*Unavailable data from the papers not included in the table.M, male; F, female; NED, no evidence of disease; -, unavailable.
atypia could in fact be associated with secondary in-
flammatory stimuli or aging of the tumors.2,4 Mitosesare extremely rare and necrosis is virtually absent,unless the lesion is secondarily traumatized or infec-ted.1 Although ECT is usually not encapsulated, bor-ders of the lesion are relatively well defined owing tocondensation of fibrous tissue and muscle fibers aroundthe periphery of the tumor.2 Few muscle fibers can befocally infiltrated by tumor cells, but this seems not torepresent evidence of aggressive behavior.3 Focal areasof inflammation and hemorrhage can be eventuallyfound, as well as flattening of the epithelial projectionsto the connective tissue, especially when the tumor issituated in close proximity to the surface.11 Even con-sidering one of the theories for development of ECTthat originates from minor salivary glands, it is rare to
mesenchymal chondromyxoid tumor (immunoperoxidase,
orted cases of ectomesenchymal chondromyxoid tumor
derF)
Diameter, mmRange (mean)
Symptoms, moRange (mean)
Follow-up, mo Range(mean)
10 3-20 (11.7) 1-120 (38.9) NED – 9; 2-228 (67)Recurrence – 2
1 5-10 (8.3) 1-240 (80.3) —1 15 1.5 NED – 180 20 3 —1 5-18 (11.5) 1-14 (7.5) NED – 2; 12-48 (30)1 — 180 NED – 2401 10-12 (11) 6-12 (9) NED – 2; 24-60 (42)1 — 2 NED – 141 15 1.5 NED – 120 5 48 NED – 241 7 5 NED – 240 10-10 (10) 1-5 (3) NED – 3; 2-60 (37)18 3-20 (11.2) 1-240 (36.4) NED – 22; 2-240 (54.2)
Recurrence – 2
in ecto
6 rep
Gen(M:
9:
2:0:1:1:0:1:0:0:1:0:3:
18:
find these structures in proximity to the tumors.2,3,7

OOOOE918 Pires et al. December 2009
Although the features on light microscopy arehighly suggestive of the condition, immunohisto-chemistry is important for final diagnosis and wasused as an additional diagnostic tool in our 3 casesand in all ECT reported in the literature, except forthe case reported by Nigam et al.10 Vimentin andpolyclonal GFAP proved to be positive in 100% ofthe cases in which they have been performed. Otherimmunomarkers revealed variable expression, in-cluding: S100 (78%), CD57 (76%), monoclonalGFAP (69%), pancytokeratin clone AE1/AE3 (56%),�-smooth-muscle actin (33%), and desmin (15%). Itseems that the most important features when consid-ering diagnosis of ECT are presence of biphasicmyxoid and chondroid patterns, and positivity forvimentin, S100, and, particularly, GFAP by tumorcells.
Several intraoral soft tissue tumors can simulateECT microscopically and should be included in his-topathological differential diagnosis. Two neoplasmsdeserve special attention: myoepithelioma and my-xoid neurofibroma. Although myoepithelioma andECT share some common features, the anatomical lo-calization of ECT as well as the clinical and microscop-ical absence of salivary glands adjacent to ECT isuseful in distinguishing these 2 lesions.3 In addition,myoepitheliomas usually present several different cel-lular patterns in the same tumor, including plasmacy-toid cells, which have not been described in ECT.Interestingly, Handa et al.13 recently evaluated the cy-tohistological correlation in 50 pleomorphic adenomasinvestigated through fine-needle aspiration biopsy. Oneof these cases diagnosed cytologically as a pleomorphicadenoma was histologically an ectomesenchymal chon-dromyxoid tumor of the tongue. Myoepitheliomas alsousually do not show muscle fibers infiltrated by thetumor cells, and this has been reported in some cases ofECT, although our cases did not show this feature.Additionally, myoepitheliomas are commonly positiveto �-smooth-muscle actin, which is expressed in onlyabout 30% of ECTs.1,3,11 Myxoid neurofibroma is theother main differential diagnosis. However, the cyto-morphology of cells with wavy nuclei in neurofibromais not seen in ECT. On the other hand, neither atypianor chondroid areas are seen in myxoid neurofibromas,although both lesions can express vimentin, S100 pro-tein, and GFAP.1,2,8,14
Other reactive and neoplastic lesions should be alsoconsidered. Mucoceles can present myxoid areas butalso show a dense macrophagic infiltrate and are notcommon in the anterior dorsum of tongue. Focal oralmucinosis does not present lobular architecture norchondroid areas as ECT. Soft-tissue myxomas also do
not present chondroid areas. The ossifying fibromyxoidtumor can show myxoid, but not chondroid areas, andpresents peripheral deposition of bone that is not seenin ECT. Extraskeletal myxoid chondrosarcomas usuallyshow more evident areas of cellular atypia. Glial cho-ristomas, even manifesting in the same anatomical re-gion, show the glial component that is not seen in ECT.Chondroid choristomas show an abundant chondroidcomponent, that is, contrary from ECT, mature andwell formed, with no atypia or myxoid areas, eventuallyshowing trabecular bone deposition.2 Peripheral nervesheath myxomas (neurotekeomas) do not present thechondroid pattern seen in ECT.1,2,8 If necessary, in allthe previously mentioned differential diagnoses, immu-nohistochemistry, particularly GFAP, will be veryhelpful.
In conclusion, ECT is an uncommon intraoral long-lasting asymptomatic mesenchymal soft tissue neo-plasm located on the dorsum of the tongue of adults. Itis microscopically characterized by a biphasic myxoidand chondroid pattern. Immunohistochemical expres-sion of vimentin, S100, and GFAP is very helpful inconfirming the diagnosis, indicating its probable mes-enchymal and neural origins.
The authors thank CNPq, FAPERJ, and FAPESP (Brazil)for their financial support.
REFERENCES1. Smith BC, Ellis GL, Meis-Kindblom JM, Williams SB. Ecto-
mesenchymal chondromyxoid tumor of the anterior tongue: nine-teen cases of a new clinicopathologic entity. Am J Surg Pathol1995;19:519-30.
2. Kannan R, Damm DD, White DK, Marsh W, Allen CM. Ecto-mesenchymal chondromyxoid tumor of the anterior tongue: areport of three cases. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1996;82:417-22.
3. Van der Wal JE, Van der Waal I. Ectomesenchymal chondro-myxoid tumor of the anterior tongue. Report of a case. J OralPathol Med 1996;25:456-8.
4. Carlos R, Aguirre JM, Pineda V. Tumor condromixoide ecto-mesenquimal de la lengua. Med Oral 1999;4:361-5.
5. De Visscher JGAM, Kibbelaar RE, Van der Waal I. Ectomesen-chymal chondromyxoid tumor of the anterior tongue. Report oftwo cases. Oral Oncol 2003;39:83-6.
6. Ide F, Mishima K, Saito I. Ectomesenchymal chondromyxoidtumor of the anterior tongue with myxoglobulosislike change.Virchows Arch 2003;442:302-3.
7. Kaplan I, Anavi Y, Calderon S. Ectomesenchymal chondromyx-oid tumour of the anterior tongue. Int J Oral Maxillofac Surg2004;33:404-7.
8. Woo VLK, Angiero F, Fantasia JE. Myoepithelioma of thetongue. Oral Surg Oral Med Oral Pathol Oral Radiol Endod2005;99:581-9.
9. Goveas N, Ethunandan M, Cowlishaw D, Flood TR. Ectomes-enchymal chondromyxoid tumour of the tongue: unlikelyto originate from myoepithelial cells. Oral Oncol 2006;42:1026-8.
10. Nigam S, Dhingra KK, Gulati A. Ectomesenchymal chondro-myxoid tumor of the hard palate—a case report. J Oral Pathol
Med 2006;35:126-8.
OOOOEVolume 108, Number 6 Pires et al. 919
11. Allen C. The ectomesenchymal chondromyxoid tumor: a review.Oral Dis 2008;14:390-5.
12. Seckin D, Demirkesen C, Gurbuz O. Ectomesenchymal chon-dromyxoid tumor of the anterior aspect of the tongue. J Am AcadDermatol 2008;59:S23-S24.
13. Handa U, Dhingra N, Chopra R, Mohan H. Pleomorphic ade-noma: cytologic variations and potential diagnostic pitfalls. Di-agn Cytopathol 2009;37:11-5.
14. Kawahara E, Oda Y, Ooi A, Katsuda S, Nakanishi I, Umeda S.Expression of glial fibrillary acidic protein (GFAP) in peripheralnerve sheath tumors. A comparative study of immunoreactivity
of GFAP, vimentin, S-100 protein, and neurofilament in 38schwannomas and 18 neurofibromas. Am J Surg Pathol 1988;12:115-20.
Reprint requests:
Fábio Ramôa Pires, PhDOral PathologySchool of DentistryState University of Rio de JaneiroBoulevard 28 de Setembro157 - Vila Isabel - CEP: 20550-030Rio de Janeiro/RJ, Brazil
[email protected]




























