Embed Size (px)
Citation preview

Cognitive Stimulation Therapy
(CST)
for people with dementia
Dr Aimee Spector
Senior Lecturer in Clinical Psychology
Research Department of Clinical, Education &
Health Psychology,
University College London
E-mail: [email protected]
The context
No cure for dementia. Even when a cure is found, it may
take years to put into practice.
People live 3 - 11 years from diagnosis of dementia to
death (Xie et al, 2008). Priority is improving care and
quality of life for these people.
Drug treatments can be a lifeline, yet are not suitable for
all, have limited effectiveness and can have adverse
effects.
In the past 20 years, non-pharmacological treatments
have increasingly been part of the picture.
Background
Dementia primarily conceptualised from a
medical perspective (Lyman, 1989).
Considered an organic disease for which
assessment, diagnosis and treatment guided by
medical interventions.
Prior to the late 1990’s, no psychological
interventions with a robust evidence-base.
“Tacrine and psychological therapies in
dementia: No contest?” (British Journal of
psychiatry, Orrell & Woods, 1996)
What is CST? A brief, evidence-based group intervention for people
with mild to moderate dementia.
14 themed sessions, typically twice a week for 7 weeks.
Includes word association / categorisation, current
affairs, food, number games.
Key aims: to improve cognitive functioning through using
techniques that exercise different cognitive skills.
Achieved through a variety of means including executive
functioning tasks (e.g. categorisation), multi-sensory
stimulation and reminiscence as an aid to orientation.
Based on concept of ‘use it or lose it’: brain needs to be
exercised in order for skills to be retained.
Improved cognitive functioning is associated with
increased quality of life and independent living.
Aims of Cognitive Stimulation
Therapy (CST) study
To combine elements of past research to create an evidence-based group therapy programme for people with dementia.
To evaluate the effectiveness of this programme as a multi-centre Randomised Controlled Trial (RCT).
Size of trial, methodology and outcome measures to match that of the major drug trials.
Project ran at UCL Department of Psychiatry and Behvavioural Sciences, led by Professor Martin Orrell.
Development of CST: the steps
Stage 1: Cochrane systematic reviews
Stage 2: Literature reviews to guide
development of intervention
Stage 3: Pilot study -> modification
Stage 4: RCT evaluating effectiveness of
CST (including i. cost-effectiveness
analysis and ii. direct comparison with
drugs).
Development of CST: the steps
Stage 5: Implementation work (website,
manuals, training, implementation
research)
Stage 6: Qualitative research
Stage 7: Long-term follow-up (MCST trial)
Stage 8: RCT evaluating individualised
CST (iCST)
Stage 1: Cochrane reviews Two key psychological interventions for dementia
identified in the literature: Reality Orientation and Reminiscence.
Reality Orientation: The presentation and repetition of time, place and person related information. Focuses on rehabilitation through improving orientation.
Cochrane review showed evidence for its effectiveness in cognition and behaviour (Spector et al, 1998).
Reminiscence: Discussion about the past, often using prompts (e.g. pictures, objects, music) with groups or individuals (e.g. life review). Focuses on long-term memory, relatively preserved in dementia.
Cochrane review(s) (Spector et al, 1998; Woods et al, 2005) showed evidence for effectiveness in cognition and mood.
Stage 2: Literature reviews to
develop intervention
We also reviewed evidence on other key psycholologicaltherapies, e.g. Validation Therapy (e.g. Feil, 1992) and Multisensory Stimulation (e.g. Baker et al, 2001).
Evaluated quality of research and focused on papers showing strongest methodology and outcomes.
Attempted to identify best features of each therapy and combine into a single programme.
Named ‘CST’ as it was largely based on Breuil’s
‘Cognitive Stimulation’ (1994)
Stage 3: Pilot study
Pilot programme evaluated with 27 people (17 treatment,
10 controls) in four settings (Spector et al, 2001).
Described 45 minute group sessions(5-8 per group)
Within broad themes there are flexible activities to cater
for group’s needs and abilities.
Positive trends in cognition, anxiety and depression.
Used outcomes to modify programme, including
increasing cognitive element.
Modified into 14 session programme, twice a week for 7
weeks.
Stage 4: RCT
Multi-centre, single-blind, RCT (Spector et al, 2003).
201 participants with dementia in 23 centres (18 residential care homes, 5 day centres)
Results
Significant improvement in cognition using MMSE (p = 0.04) and ADAS-Cog (p = 0.01) (comparing CST with TAU).
ADAS-Cog: trends in all subscales (memory, language, praxis) but only significant subscale was language (including naming, word-finding and comprehension).
Stage 4: RCT Significant improvement in quality of Life using the Qol-
AD (brief, self-rated measure covering 13 areas of QoL) comparing CST to TAU (p = 0.03).
No significant change in functional ability (CAPE-BRS), depression (Cornell) or anxiety (RAID)
Communication (Holden): positive trends (p = 0.09)
CST shown to be comparable to dementia medication (cholinesterase inhibitors – Rivastigmine, Galantamine, Donepezil) using a ‘numbers needed to treat’ analysis.
CST shown to be cost effective, in study run in conjunction with London School of Economics (LSE) (Knapp et al, 2006).
Stage 5: Implementation work
Published 3 manuals (Spector et al 2005,
Spector et al 2006, Aguirre et al 2012)
Developed CST website: www.cstdementia.com
Developed one-day CST training course.
Research trial on implementation (Streater et al,
2014) – looking at effects of manual, training and
outreach support on implementation.

The UK manuals
Stage 6: Qualitative Research
34 participants (people with dementia, carers and staff) participated in individual interviews and focus groups (Spector et al, 2011).
Asked about experiences of CST – positive or negative.
Key themes emerging:
Positive experiences of being in group (e.g. supportive and non-threatening).
Changes generalised into everyday life: improvement in mood and confidence (finding talking easier), changes in concentration and alertness (wanting to attend to things more).
Stage 7: Long-term follow-up
(MCST trial)
Big question: what happens next? (Orrell et al,
2014)
237 people with mild to moderate dementia who
had previously received CST (14 sessions).
Intervention: weekly, 24-session programme of
Maintenance CST (MCST) compared to TAU.
MCST group significantly improved in quality of
life at 3 and 6 months, and in activities of daily
living at 3 months.
Stage 7: Long-term follow-up
(MCST trial)
Cognition was higher in MCST group but the
difference was not significant.
Greatest improvements in the medication plus
MCST group.
Conclusions: There is good evidence for the
benefits of continuing CST beyond the initial
programme. Whilst people are still willing and
able, CST should be continued.
Stage 8: RCT evaluating
individualised CST (iCST)
iCST manual follows similar principles to group
CST manual.
Large trial at UCL, involving family carers and
health professionals.
Results out soon….
iCST manual will be available in November 2014
through Hawker Publications.
What is the outcome of all this
research?
NICE guidelines ( 2006)
“People with mild / moderate dementia should be given the opportunity to participate in a structured group cognitive stimulation programme.
Should be commissioned and provided by a range of health and social care workers with training and supervision.
Should be delivered irrespective of any anti-dementia drug received.”
NHS Institute for Innovation &
Improvement (Matrix Evidence, 2011)
“An economic evaluation of alternatives to antipsychotic
drugs for individuals living with dementia”.
Analysis focused on cost of providing CST.
Combining health care cost savings and QoL
improvements, behavioural interventions generate a net
benefit of nearly £54.9 million per year for NHS.
Use of CST in the UK
National Memory Services Accreditation
programme (NMSAP) audit (2013): CST
used in 66% of UK memory clinics.
CST training : around 104 courses, mainly
commissioned by NHS trusts, around
2400 people trained in CST.
Care home residents – the forgotten
people?
CST internationally
The World Alzheimer’s Report (Alzheimer’s Disease
International, 2012), stated that CST should routinely be
given to people with early stage dementia.
CST manual has been translated into several languages
including Japanese, Spanish, Italian, German,
Portuguese, Dutch, Norwegian and Swahili.
CST is being used in Australia, USA, South Africa, New
Zealand, Germany, Canada, Chile, Italy, Japan, Nepal,
the Philippines, the Netherlands, Tanzania, Brazil, China,
Hong Kong, Indonesia, India, Nigeria, Portugal,
Singapore, South Korea and Turkey.
CST internationally
‘International research centre at UCL’ currently
being developed.
Our team recently published guidelines for
adapting CST to other cultures (Aguirre et al,
2014).
This draws from our work in Japan (Yamanaka
et al, 2013) Nigeria and Tanzania, and UK
translation into Swahili.
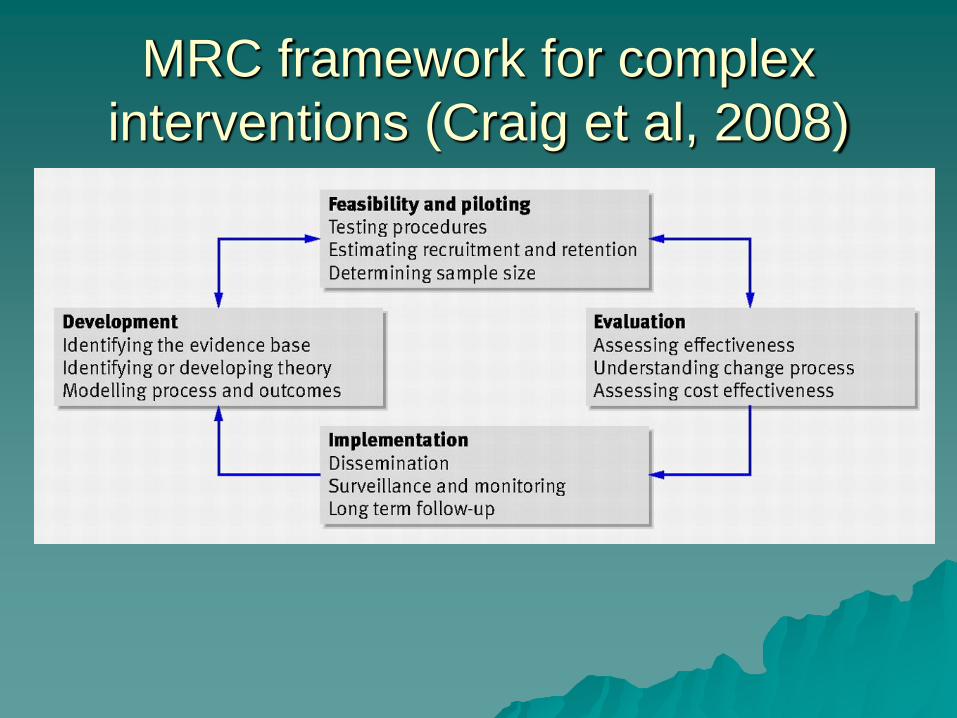
MRC framework for complex
interventions (Craig et al, 2008)
What does CST do?
Aims to be mentally stimulating, yet for people to feel empowered rather than de-skilled
Always encouraging new ideas / new thoughts / new associations.
Stimulate memory through:
Using reminiscence as an aid to the here and now.
Providing triggers to aid recall, e.g. multi-sensory cues, RO board
Continuity and consistency between sessions helps support memory
Implicit (rather than explicit) recall, e.g. famous faces
Using orientation, but sensitively and implicitly
Opinion rather than facts (which supports idea of validation)
What does CST do?Stimulates language through:
Naming of people and objects (e.g. in categorisation) done in implicit way
Thinking about word construction and word association
Stimulates executive functioning through:
Discussion of similarities and differences
Planning and executing stages of a task (e.g. making a cake)
Word association, categorising objects
Can be understood in the context of a Biopsychosocialmodel of dementia (Spector and Orrell, 2010), particularly when considering group factors influencing mood, QoL, social factors, person-centred care, working against a ‘Malignant Social Psychology’ (Kitwood, 1993)
Conclusions
Complex interventions should be developed and
evaluated considering theory, literature and
involve piloting and a full scale trial evaluating
effectiveness and cost-effectiveness.
Many interventions show effectiveness, yet do
not make a clinical impact due to insufficient
implementation.
For all references, see CST website:
www.cstdementia.com


















![[Semantic dementia]](https://img.pdfslide.net/doc/110x75/6356be55debc1859f6037bda/semantic-dementia.jpg)










