Embed Size (px)
Citation preview

i
College of Nursing
National Taipei University of Nursing and Health Sciences
Doctoral Dissertation
Effect of Prenatal Childbirth Program on Maternal Anxiety,
Maternal-Fetal Attachment, Childbirth Self-Efficacy and Marital
Satisfaction: A Randomized Controlled Trial Using Roy’s
Adaptation Model
Endang Koni Suryaningsih
Advisor: Professor Meei-Ling Gau, PhD
January 28, 2021

ii

iii
Acknowledgement
All praises to Allah and His Blessing to completion this dissertation. My humble gratitude to the holy Prophet Muhammad (Peace be upon him) whose way of life has been a continuous guidance for me. First and foremost, I would like to sincerely thanks my supervisor Prof. Meei-Ling Gau, PhD for her guidance, understanding, patience and most importantly, she has provided strong and positive encouragement to finish this dissertation. It has been a great pleasure to have her as my supervisor in this PhD journey in which so many against all odd. I would also like to thank my committee members, DR. Chien-Huei Kao, PhD. (NTUNHS), Professor Chieh-Yu Liu (NTUNHS), Professor Shu-Yu Kuo (Taipei Medical University), and Professor Jian-Jiuan Liaw (National Defense Medical Center) who provide me an incredible comments and suggestions and for letting my defense be an enjoyable moment . A special thanks go to my husband, Ns. Wantonoro, S.Kep., M.Kep., Sp.KMB., PhD . for his support and understanding in my up and down. I would also like to thank you to my family. Words cannot express how grateful I am to my father-in-law and mother-in-law for all of the sacrifices that you have made on my behalf, and take care of my son. Thanks to my niece Septi Widya Sari, to help me take care of my children in the last critical moment I almost complete the journey, you come to me in the right time. I dedicated this dissertation and Ph.D title to my beloved son, Muhammad Azam Suryaputra and my beloved daughter Azima Aqilatunnisa, thanks for being such a good boy and girl always cheering me up. My love is never ending for both of you dear. I would especially like to thanks my project manager, Ms. Peggy and Ms. Eunice, my friend Yanuan Ben Olin,. All of you have been there to help me bring my Ph.D title come true. I also would to extend my thanks to Ms. Stefany Preifer for her editing service, thank you for sharing incredible experience. I would especially like thanks to Midwives in the primary health center Mlati II, Midwives in the primary health center Jetis Kota, Midwives in the primary health center Mantrijeron, as the facilitator in the standard childbirth education program. Special thanks also to Siti Nurhayati and Sarah who have been assisted me to recruited participants and collected data for my Ph.D dissertation. For all my participants, thank you for your contributions in this study. I offer my special thanks to all my colleagues in Aisyiyah University of Yogyakarta in Midwifery Diploma III, for my superior, structural management in the health faculty, and my top leaders, for their support, motivation and their sincere help during my study. Finally, thank you for all every single person who involved in this Ph.D journey without I could not mention one-by -one in person, I thank them wholeheartedly. May God shower the above cited personalities with success and honor in their life.

iv
Abstract
Background: As the multifaceted changes during women’s life cycle, pregnancy, is the most crucial period that can affect to her further life process.
Purposes: The aim of this study was to test the effectiveness of childbirth education based on the Roy Adaptation Model through four modes: physiology, self-concept, role function, and interdependence.
Methods: A randomized controlled trial was applied to invite the participant who met the criteria including nullipara pregnant women and their husband, gestational age ranged 24-32 weeks, and married. High-risk pregnancy condition and miscarriage was excluded. The researcher used computer block size to allocate the participants into groups. To measure the potential outcomes of four modes, the following instruments were used: Demographic Data Set, Pregnancy-Related Anxiety Questionnaire Revised, short form of the Childbirth Self-Efficacy Inventory, Prenatal Attachment Inventory, and ENRICH Marital Satisfaction Scale. To produce the Indonesian version of each instruments, the researcher conducted translation and back translation following WHO guideline and measure its reliability using Cronbach’s Alpha. To describe demographic characteristic, a descriptive statistic was calculated. To test the efficacy of the program, general linear model was analyzed.
Results: The mean age of couple were 23.92/ 26.75 (wife/ husband) in the experimental group, and 29.14/ 30.86 (wife/ husband, respectively) in the control group. The mean gestational age week were 29.83 in the experimental group and 31.04 in the control group. In both groups, mostly couple graduated from high school and more than 50% mothers go to work. We loss more than twenty percent of total participants in our study that may due to the pandemic COVID-19 just ran into Indonesia. Consequently, the significance difference between two groups on demographic data include couple’s age, gestational week, husband education level, and wife’s occupation were found. After a-four week intervention, the mean score of maternal anxiety was significantly lower, and the mean score of maternal-fetal attachment, childbirth self-efficacy were significantly higher in the experimental group than that in the control group (p < .001). However, there were no significantly different mean score of marital satisfaction in the two groups. Conclusion and Implications to Nursing Practice: the implemented program in current study was potentially effective in promoting maternal-fetal attachment, childbirth self-efficacy, and decreasing maternal anxiety during pregnancy. Therefore, the modified traditional childbirth education program need to be considered. Recommendations: For the midwife, the flexible intervention may could increase response rate for couple to join the class. For the next researcher, the culture issue need to be consider to establish the feasibility of marital satisfaction tool. Keywords: maternal anxiety, childbirth self-efficacy, maternal-fetal attachment, marital relationship, Roy Adaptation Model, childbirth education, randomized controlled trial

v
TABLE OF CONTENTS
Page
Abstract Iv
Table of Content v
Figures viii
Tables ix
List of Appendices x
CHAPTER I INTRODUCTION
1-1. Background 1
1-2. Conceptual framework: Roy Adaptation Model 3
1-3. Problem statement 7
1-4. Statement of purposes 9
1-5. Research question 9
1-6. Significant of the study 9
CHAPTER II LITERATURE REVIEW
2-1. Description of Roy’s Adaptation Model 11
2-2. Critique of Roy’s Adaptation Model 12
2-3. Roy’s Adaptation Model as a framework 13
2-4. The effectiveness of childbirth education classes 22
2-3. Childbirth education in Indonesia 32
CHAPTER III RESEARCH METHODOLOGY
3-1. Study Design 36
3-2. Study Setting 36
3-3. Population and sample 36
3-4. Data Collection 38
Intervention group 41
Controlled group 42
3-5. Research tools 44
3-6. Data analysis 48
3-7. Ethical consideration 49

vi
CHAPTER IV RESULTs
4-1. Demographic information of the Respondents 51
4-2. Comparison the baseline of the maternal anxiety,
maternal-fetal attachment, childbirth self-efficacy and
marital satisfaction
57
4-3. The relationship among maternal anxiety, maternal-fetal
attachment, childbirth self-efficacy and marital
satisfaction
58
4-4. The effect of childbirth education program on maternal
anxiety, maternal-fetal attachment, childbirth self-
efficacy and marital satisfaction
61
CHAPTER V DISCUSSION
5-1. Descriptive statistic of demographic characteristic of the
participants
68
5-2 The effect of childbirth education program on prenatal
anxiety, childbirth self-efficacy, maternal-fetal
attachment, and marital satisfaction
70
5-2.1 The effect of childbirth education program on
prenatal anxiety
70
5-2.2 The effect of childbirth education program on
maternal-fetal attachment
72
5-2.3 The effect of childbirth education program on
childbirth self-efficacy
73
5-2.4 The effect of childbirth education program on
marital satisfaction
74
CHAPTER VI CONCLUSION and RECOMMENDATIONS
6-1. Conclusion 77
6-2. Study implications 77
6-3. Suggestion for future research 80
REFERENCES
81

vii
APENDIXS 120

viii
Figures
Page
Figure 2.1 The Roy’s Adaptation Model (RAM) 12
Figure 2.2 Model, concept, and operational structures of efficacy on
childbirth education based on Roy’s Adaptation Model
31
Figure 2.3 Scheme of childbirth education class in Indonesia provided by
public sector
33
Figure 3.1 Research design 35
Figure 4.1 CONSORT flow chart 52

ix
TABLES
Page
Table 2.1. The application of RAM for childbirth education classes curriculum 28 Table 3.1 Comparison childbirth education program between experimental and
control group 43
Table 3.2 Reliability of the research instrument 48 Table 3.3 Statistical method 49 Table 4.1 Comparison of the demographic data between missing and non-
missing participants 53
Table 4.2 Comparison of the demographic data between missing and non-missing participants in the control group
54
Table 4.3 Comparison of the demographic characteristics between the
experimental and control groups
56
Table 4.4 Comparison of the baseline pretest test scores between two groups 57 Table 4.5 Pearson correlation for pretest scores within outcome variables 59 Table 4.6 Pearson correlation for posttest scores within outcome variables 60 Table 4.7 Effect of childbirth education program on maternal anxiety 62 Table 4.8 Effect of childbirth education program on maternal-fetal attachment 63 Table 4.9 Effect of childbirth education program on childbirth self-efficacy 64 Table 4.10 Effect of childbirth education program on wife marital satisfaction 65 Table 4.11 Effect of childbirth education program on Husband marital
satisfaction 66

x
APPENDICES
APPENDIX A Random Allocation APPENDIX B Draft of Flyer and Standing Banner APPENDIX C The Plan Curriculum of Childbirth Education Classes Based On Roy’ Model APPENDIX D Instruments APPENDIX E Grant Permission APPENDIX F Institutional Review Board

1
CHAPTER I
INTRODUCTION
This chapter presents a brief summary of the background, the problem statement, and
aims of this study. The chapter also present the research question and addresses the
significance of the study. The conceptual framework of the study, which uses the Roy’s
Adaptation Model, will be explained.
1-1. Background
Changes that come with each stage of women’s lives are commonly accompanied by
anxiety, such as first menstruation, marriage, as well as pregnancy, childbirth, and the
postpartum period up to menopause. Pregnancy is a crucial period in the lives of women with
both short and long-term impacts. Marriage and child bearing bring multifaceted changes
requiring adaptations that are not only physical, but also psychosocial, marital, spiritual, and
financial (Chang, Yu, Chen, & Chen, 2015). Difficulty adapting to those changes may lead to
ineffective reactions such as pregnancy-related anxiety. Anxiety is a common and normal
response to change and is part of normal human experience, but it can also become mental
health problem (Deklava, Lubina, Circenis, Sudraba, & Millere, 2015; Goodman et al., 2014;
June, 2003; Maxson, Edwards, Valentiner, & Miranda, 2016; Wenzel, 2011; Wergeland &
Strand, 1998; Wright & Halfon, 2010). Anxiety during pregnancy is widespread. According
to one study, only seven percent of expectant women do not suffer from anxiety during
pregnancy, particularly in the last trimester (Madhavanprabhakaran, D’Souza, & Nairy,
2015).
Pregnant women with high levels of anxiety are at increased risk of adverse perinatal
outcomes (Abasi, Tahmasebi, Zafari, Gholamreza, & Takami, 2012; Clemens, 2014; Yuksel,

2
Akin, & Durna, 2013) including postpartum depression, preterm birth, low birth weight
(O’Donnell et al., 2012), and fetal growth restriction which in turn, are risk factors for
impaired cognitive and social development children (Buss, Davis, Hobel, & Sandman, 2011;
Fishell, 2010; Qiao, Wang, Li, & Wang, 2012). Another negative effect of anxiety during
pregnancy its effect on the sleep quality (Jamalzehi, Omeidi, Javadi, & Dashipour, 2017).
Anxiety can lead to problem such as sleeping disturbances (Skouteris, Wertheim, Rallis,
Milgrom, & Paxton, 2009), nightmare (Furber, Garrod, Maloney, Lovell, & Mcgowan,
2009), and fatigue (Andersson, Nilsson, & Candidate, 2012). Shortness of breath,
hyperventilation, palpitations, and tremors have also been reported (O’Donnell et al., 2012).
Furthermore, studies have documented the complicated impact of pregnancy-related anxiety,
highlighting somatic complaints such as stomach pain, problems during sexual intercourse,
headaches, dizziness, and pains in the heart or chest, as well as gastrointestinal discomforts,
such as nausea and vomiting (Andersson et al., 2012). Anxiety during pregnancy may
manifest as maladaptive responses to stress, such as denial, self-blame, and self-distraction
(Gourounti, Anagnostopoulos, & Lykeridou, 2013). Anxiety due to fear of specific events,
such as labor, may also contribute to mood swings, short temperedness, panic and discomfort
about the feeling of having a baby living inside (Bayrampour, Ali, McNeil, et al., 2016).
Pregnancy is a period of adaptation to prepare for a new role as a mother (Niska, 1996).
Maternal competence is an important foundation for fulfilling the maternal role which
involves incorporating a set of mothering behaviors into her established identity (Niska,
1996). Mothering behavior include interaction or communication with her unborn baby, such
as calling the unborn baby by name, and preparing things for the baby before giving birth.
Such behaviors are characteristic of maternal-fetal attachment (Muller & Ferketich, 1993).
By contrast, anxiety behavior in women has been shown to have unfavorable impact on the
relationship between mother and fetus. It includes detachment, withholding attachment to the

3
unborn baby, the newborn baby, and later, the child (Fishell, 2010). Manifested problems in
the maternal-fetal relationship manifest as difficulty expressing love and affection towards
the infants, as well as raising the possibility of neglect, rejection, neglection and impulses to
harm the infants (Edhborg, Hogg, & Kabir, 2013). Changes in the marital satisfaction
are frequently reported during pregnancy and the transition to parenthood (Perren, Wyl,
Burgin, Simoni, & Klitzing, 2005). The quality of the marital relationship is recognized as a
significant contributor to maternal mental health during the process of adaptation in
pregnancy (Mutlu, Erkut, Yildirim, & Gundogdu, 2018). A good marital relationship also
contributes to a healthier pregnancy and birth, and creating a supportive family environment
for the new child (Hohmann-marriott, 2009). Consequential characteristics of the marital
relationship include its quality, communication, the intention to get pregnant, and marital
status at the beginning of the pregnancy (Hohmann-marriott, 2009). Previous studies have
reported, the keys to establishing quality of parental relationships are figuring out how to
support one another and to communicate effectively (Mealing, 1991).
1-2. Conceptual framework: The Roy Adaptation Model
Roy Adaptation Model (RAM) has been widely used to help nurses and midwives
provide better care, including developing interventions to overcome physical and
psychological problems such as nausea and vomiting, hypertension, gestational diabetes, and
lack of self-concept as well as impaired body image (Amanak, Sevil, & Karacam, 2019;
Arcamone, 2005; Badr Naga & Al-atiyyat, 2013; Black, 2004; Blake & Beard, 1999; Blamer,
1999; Boucher, 1996; Chou, 2001; Erol Ursavas, Karayurt, & Iseri, 2014; Isbir & Mete,
2013, 2010; Kruszewski, 1999; Lee, Tsang, Wong, & Lee, 2011; Mohammadpour, Najafi,
Tavakkolizadeh, & Mohammadzadeh, 2016; Yaghoubinia, Navidian, Yousefian, & Chaji,
2017; Zhegner, 2003). Roy’s model, focuses on the concept of adaptation, specifically, how a

4
person responds to the stimuli (Alligood & Tomey, 2010). The adaptation model identifies
two subsystems: cognitive and regulation mechanism. Since it is not possible to directly
observe the process of those two subsystems, observable behavioral responses are manifested
through four critical modes: physiology, self-concept, role function, and interdependence
mode (Alligood & Tomey, 2010). The goal of nursing care using the Roy adaptation model is
to promote adaptation in each of those modes (Amanak et al., 2019; Guarino, 1990; Isbir &
Mete, 2010; Jennings, 2017; Mohammadpour et al., 2016). Using Roy’s Adaptation Model as
the conceptual framework, this study will explore behaviors manifested through the four
modes and will be identified as adaptive or ineffective responses to pregnancy.
Ineffective defense mechanisms in one or more of the critical modes affected to a
person’s adaptation level. This adaptation level, will, in turn impact the individual’s ability to
respond effectively to stimuli. Situational demands, as well as previous levels of functioning,
have been noted to affect the ability to adapt the stimuli(Roy, 2009a). Roy uses stimuli as a
way to describe the pregnant woman’s environment, which consists of complex patterns of
interaction, feedback, growth and decline. For instance, expectant pregnant women who feel
well-prepared and who have a good quality marital relationship will respond adaptively
during pregnancy (Cody, Olga, Luciane, Richard, & Paul, 2012). Research has found that
low maternal-fetal attachment, and lack of childbirth self-efficacy are linked to non-adaptive
or ineffective responses to pregnancy (Salomonsson, Berterö, & Alehagen, 2013).
Many projects have shown that prenatal outcomes can be enhanced by reducing
pregnancy-related anxiety and improving childbirth self-efficacy, maternal-fetal attachment,
and marital relationships (Akbarzadeh, Dokuhaki, Joker, Pishva, & Zare, 2016; Arcamone,
2005; Broussard & Weber-Breaux, 1994; Chang, Park, & Chung, 2004; Deave, Johnson, &
Ingram, 2008; Dokuhaki, Akbarzadeh, Pishva, & Zare, 2017; Howharn, 2008; Larsen & Plog,
2012; Suto, Takehara, Yamane, & Ota, 2017). Childbirth education programs are one kind of

5
resource for helping expectant women prepare for the changes they will experience (Larsen
& Plog, 2012). Researchers around the world report interventions that target specific
problems with adapting during pregnancy using different approaches based on the needs of
particular populations. For instance, mindfulness interventions have been used to accomplish
different goals. Two studies in the United States conducted mindfulness-based interventions
to reduce maternal anxiety and depression (Duncan & Bardacke, 2010; Goodman et al.,
2014). In Taiwan, Pan and colleagues developed mindfulness training to enhance the
physiological health of pregnant women (Pan, Gau, Lee, Jou, & Liu, 2018). Larsen and Plog,
2012). In Minnesota, Larsen and Plog developed childbirth classes to enhance self-efficacy
for pregnant women and their support persons (Larsen & Plog, 2012). Dokuhaki and
colleagues (2017) in Iran provided training skills focused on fostering fetal attachment in
mothers and fathers (Dokuhaki et al., 2017). Toosi and colleagues (2017) in Iran conducted
an intervention to increase maternal-fetal attachment using relaxation techniques. In Korea,
Sue, Hee-Sook and Ha-Yoon (2011) used a coaching-based childbirth program to decrease
anxiety and increase childbirth self-efficacy.
Several studies have advocated using Roy’s adaptation model as a guide for
developing antenatal education programs. A project conducted by investigators in Turkey in
2010 tested the effectiveness of prenatal education for promoting maternal prenatal and
postpartum adaptation using Roy’s framework (Sercekus & Mete, 2010). In that study, the
investigators employed only those variables related to two Roy’s adaptation modes: self-
concept and interdependence. The classes consisted of seven weeks with different
educational contents based on women’s needs. The result of that study showed that antenatal
education had a positive effect on prenatal adaptation, but it had no effect on postpartum
adaptation. Therefore, they recommended conducting a review of contents in antenatal
educational that may beneficially impact postpartum adaptation (Sercekus & Mete, 2010).

6
The effectiveness of prenatal education on adaptation to motherhood after vaginal childbirth
in primiparas women following Roy’s four adaptive modes have been also reported
(Arcamone, 2005).
Through the four critical modes described by Roy, it is possible to understand women
who are maladaptive responses to pregnancy (Abasi et al., 2012; Akbarzadeh, Toosi, Zare, &
Sharif, 2011; Cody et al., 2012; Hwang, 2013; Saastad, Israel, Ahlborg, Gunnes, & Frøen,
2011; Yarcheski, Mahon, Yarcheski, Hanks, & Cannella, 2009). For example, physiological
changes contribute to the mother’s complaint and discomfort during pregnancy which may
lead in turn to maternal anxiety (Bayrampour, Ali, McNeil, et al., 2016; Borodulin et al.,
2010; Karaçam & Ançel, 2009). Negative self-concept in pregnancy can decrease a mother’s
childbirth self-efficacy (Bhattacharjee & Banik, 2016; Stern, 1998). Functioning in the
maternal role affects maternal-fetal attachment (Yarcheski et al., 2009) and interdependence
mode can provide insight into improving the marital relationship (Cody et al., 2012; Jang,
Kim, & Lee, 2015; Whisman & Davila, 2011). This phenomena support the hypothesis of the
RAM regarding the four critical modes. Nursing practices informed by Roy’s model promote
adaptation in each of the four modes leading to a more integrated level of functioning (Roy,
2009b).

7
1-3. Problem statement
In the world, in 2017, approximately 810 women died from preventable causes
related to pregnancy and childbirth (World Health Organization, 2019). Two years earlier, in
2015, Indonesia had a 126/100,000 maternal death rate and 25/1,000 neonatal death rate.
These two rates compare unfavorably to other Asian countries such as Singapore (6/100,000),
Thailand (44/100,000), and Malaysia (39/100,000). The majority direct cause of Maternal
Mortality Rate (MMR) in Indonesia is dominated by bleeding (30.3%), pregnancy
hypertension (27.1%), infection (7.3%), prolonged labor (1.8%), abortus (1.6%), and others
(40.8%). To foster knowledge for pregnant women and couples on risk signs of pregnancy
and birth, Indonesia government implemented the national program, provides childbirth
education for free offered by midwives villages. The mother necessary to attend the
childbirth education for three meeting, aimed to acquire mother’s knowledge and skills on the
pregnancy, birth, postpartum, family planning, newborn care and postpartum exercise
(Minsitry of Health, 2014). However, the information on the effectiveness of existing
childbirth education program include learning method as well as the theoretical guidelines,
remain unclear (Fata & Rahmawati, 2016; Lucia, Purwandari, & Pesak, 2013; Nursofyanto &
Cahyanti, 2017).
In 2013, one study reported, roughly 76.8% pregnant women in Indonesia experience
anxiety in their last trimester consist of 80% were nulliparas and 20% were multiparas
(Setyaningsih, Setyowati, & Kuntarti, 2013). Manifested pregnancy-related anxiety among
Indonesian pregnant women affected their childbirth self-efficacy that may lead to prolonged
labor which in turn causing maternal death (Rofi’ah, 2015). Prolonged labor also recognized
as the main cause asphyxia which contribute to the infant mortality among Indonesian
newborn (Prime Minister of Health, 2014).

8
Many Indonesian researchers developed childbirth education on decreasing anxiety
during pregnancy (Aryani, Raden, & Ismarwati, 2016; Fata & Rahmawati, 2016; Lucia et al.,
2013; Nursofyanto & Cahyanti, 2017; Setyaningsih et al., 2013). However, the studies to
investigate the effectiveness of childbirth education to increase maternal-fetal attachment,
childbirth self-efficacy and marital relationship are scarce (Galina & Risti, 2015; Sukriani &
Suryaningsih, 2018). Researchers from other countries emphasized that the method as well as
the content of material of childbirth education contributes on decreasing maternal anxiety,
increasing maternal-fetal attachment, childbirth self-efficacy and marital relationship
(Dokuhaki et al., 2017; Duncan & Bardacke, 2010; Larsen & Plog, 2012; Toosi, Akbarzadeh,
& Ghaemi, 2017). To reach the ultimate purposes of childbirth education, the classes should
be conducted in a sufficient period and appropriate curriculum. The conceptual framework
applied in the childbirth education is also important to be considered (Nichols & Humenick,
2000). Best on our knowledge, there is no study investigated the effectiveness of childbirth
education to addressed four modes outcome based on the Roy Adaptation Model in Indonesia

9
1-4. Statement of purposes
The aim of this study is to explore the effectiveness of a four-week prenatal
childbirth program on prenatal anxiety and childbirth self-efficacy, maternal-fetal
attachment, and marital satisfaction.
1-5. Research questions
Based on the specific aims, the research questions of this study were the following:
1. How the descriptive statistic of demographic characteristic of the participants?
2. Are there any significant differences on the demographic characteristics
between the two groups?
3. How the effect of childbirth education program on prenatal anxiety and
childbirth self-efficacy, maternal-fetal attachment, and marital satisfaction?
1-6. Significance of the study
There are two reasons why using Roy’s Model approach as a framework to
develop the childbirth classes is essential in this study. First, nurses and midwives play
major roles in health-promotion activities. To achieve this critical goal of health
promotion, the nurse and midwives needs an accurate and complete data base. At
present in Indonesia, there is scarce concept of childbirth education class which is
applied the Roy’s Adaptation Model to provide the intervention. Using this model
approach, the appropriate contents and teaching methodology in the prenatal education
will be available as the practice-based practice (Arcamone, 2005). Second, during
pregnancy and preparation for childbirth, pregnant women and spouse seek out
information from various source. Nurse and midwives, in both professional and
personal, encounters, also encourage and interact daily with pregnant women and

10
husband. Therefore, nurse and midwives are in special position to give information to
these couples. Knowledge will gained from this study may afford nurses and midwives
an increased understanding of the physiological aspects of pregnancy and birth. An
increased knowledge base can help mother and husband to optimize the adaptation
during pregnancy and childbirth.
In conclusion, this study will focus on promoting on four modes; prenatal
anxiety, childbirth self-efficacy, maternal-fetal attachment, and marital relationship
during their third trimester of pregnancy in response to gap in existing research and
conflicting theoretical prepositions.

11
CHAPTER II
LITERATURE REVIEW
To address the purposes of this study, researcher has been conducted the
literature review in where includes the Roy Adaptation Model include the major
concept and it is in adaptive response to the pregnancy. Roy’s Model critique and
reason why the researcher choose this framework, as well as the conceptual, theoretical
and empirical practices for this approach also has been described.
2-1. Description of Roy’s Adaptation Model
According to Roy (2009), people as part of adaptive system, the environment,
health, and the goal of nursing are the major concepts of her model. People as an
adaptive system defined as a whole with parts that function as a unity for a purpose.
Environment as a stimuli is defined as the condition or surrounding that can affected to
the human as an adaptive system. Health or outcome of adaptation is a state and process
of being and becoming integrated and whole (Roy, 2009b). Adaptation is realized when
an individual shows a positive reaction to stimuli. Roy defined adaptive modes as
physiological and physical, self-concept, role function, and interdependence to evaluate
responses to stimuli as described in the Figure 2.1. The physiological mode refers to
physical maintenance of the integrity of the adaptive system, while the self-concept
mode consist of belief, thought and feeling held about one’s self. The role-function
mode refers to the roles that a person has in her life, and the interdependence mode
consist of establishing and maintaining relationship with significance other. Behavior in
the context aforementioned are classified as adaptive or non-adaptive. Adaptive

12
responses are those that promote the integrity of the human system whereas non-
adaptive modes hinder this purpose (Roy, 2009b).
To derived her adaptation theory, Roy also uses other theory and concept
outside the discipline of nursing. She synthesized her theory from Helson’s
psychophysics theory, who is developed the concept of focal, contextual, and residual
stimuli (Alligood & Tomey, 2010). Roy redefined those concepts within nursing to
form an analysis of factors related to adaptation levels of person. Roy conducted studies
and nursing practice experience of herself, her colleagues, and her students to build her
four adaptive modes. Roy developed a step-by-step model on her conceptual
framework of adaptation and tested its theory to administer nursing care to promote
adaptation in health and illness situation (Roy, 1970).
2-2. Critique of Roy’s Adaptation Model
INPUT CONTROL PROCESS
EFFECTORS OUTPUT
Physiological and physical functions Self-concept Role function Interdependence
Stimuli adaptation level
Coping mechanism Regulator Cognator
Adaptive
Ineffective response
Figure 2.1. The Roy Adaptation Model

13
As grand theory, Roy’s Adaptation Model consist of major concept, sub concept,
and relational statement, therefore it is considered as a complex model. However, this
complexity assist to improve its empirical precision. Researcher has analyze and
criticize the Roy Adaptation Model (Abu & Al, 2012). According to them, in term of
the arrangement, the concept of Roy’s Model is logic, but in term of the word and
concept, inadequate to reflect nursing discipline was remain (Abu & Al, 2012). This
may decreases the clarity of the model when applied in any particular area of practice.
In fact, Roy Adaptation Model is broad in scope, widely accepted and inspired the
development of middle range nursing theories (Abu & Al, 2012). This theory
generalizable to all approaches in nursing practice, education field, and practice-based
research (Abu & Al, 2012; Alligood & Tomey, 2010; Dobratz, 2003).
2-3. Roy’s Adaptation Model as a conceptual framework
Many researchers have used Roy’s model to guide their studies. In this paper,
we have selected following childbearing studies to show their use of that model.
Kiehl and White (2003) conducted the study to test the relationship of maternal
adaptation during pregnancy following Roy’s Model. They invite pregnant women in
the third trimester and complete the questionnaire both during the first recruitment and
again at 6 weeks postpartum. The result reported mother with greater adaptation during
pregnancy have greater adaptation during postpartum. This finding supported the Roy’s
preposition that effective adaptation during pregnancy related with the adaptation after
birth (Kiehl & White, 2003). Serc¸ekus and Mete (2010) also measure the differences
between mother’s adaptation during pregnancy and postpartum, using the same
framework-based quasi experiment. The result in line of previous study that women in
the experimental group were better adapted in the prenatal compared with those in the

14
control. However, in term of prenatal adaptation, that no difference was found in
postpartum adaptation between the groups (Sercekus & Mete, 2010).
Fawcet (2006) used four adaptive modes of Roy’s Model as a guideline to
combined a qualitative and quantitative content analysis of responses to open-ended
interviews. She categorized the word, phrases, and/ or sentences that represent
women’s responses to the five questions which refer to the four adaptive modes
(Fawcet, 2006). Unfortunately, the researcher did not provide clear information on the
quantitative method she calculated.
Isbir and Mete (2010; 2013) followed the Roy’s Model as a framework in their
combined quantitative and qualitative study to explore expectant women with nausea
and vomiting. In 2010, they conduct a quantitative study and provide guidance for
nurse who want to use the model while offering nursing care and conducting research.
Then in 2013, they continued the qualitative study used the four mode to analysis the
content of categories based on transcribed verbatim. They found that the stimuli
causing nausea vomiting during pregnancy differed for each individual (Isbir & Mete,
2013). This result has completely supported the Roy’s Model in which the stimuli can
affecting individual’s adaptation as well as their behavior (Isbir & Mete, 2010, 2013).
A randomized controlled trial study conducted by Mohammadpour and colleagues
(2016) emphasized on self-concept mode in Roy’s Model. They invite expectant
women in the third trimester and join to participate in this study voluntary during four
weeks program. There was a significant self-concept adaptation in both groups before
and after the study. This result completely support that Roy’s Model has positive effect
on primigravida women’s physical and interpersonal self-concept adaptation in
pregnancy (Mohammadpour et al., 2016).

15
In the same way, Amanak, Sevil and Karacam (2019) used the Roy Adaptation
Model to manage mother with gestational hypertension and enhance their adaptation
through prenatal education class. The curriculum was prepared following the four
modes and has been proven effectively to manage the hypertension and promoting
levels of adaptation (Amanak et al., 2019).
Based on some of consideration above, in this study, the Roy Adaptation Model will
also be applied. Researcher will use Roy’s Model to develop the prenatal class based on
four modes to enhance expectant women’s adaptation and will measure each possible
outcome behavior for each modes. In this study, the four modes will be described as
below.
1. Physiological and physical Mode
In this mode, Roy emphasizes the maintenance of physiologic integrity of the
person (Roy, 2009a). The following nine components in physiological mode include:
oxygen, nutrition, elimination, protection, activity and rest, senses, fluid-electrolyte and
acid-base balance, and neurological and endocrine function. According to Roy (2009),
these nine components form the basis of nursing assessment and determined what the
appropriate intervention based on needed. Moreover, a comprehensive physiological
assessment is, indeed, necessary as pregnancy-related physiological changes happen in
almost all the body system. During the third trimester, the physiological changes to the
women’s body become noticeable as she finds its more difficult to find comfort on her
pregnancy. At this point, maternal circulatory system change and raise the physical
complaint and the literature indicates that the following symptoms were experienced by
a significant percentage of women: nausea, heartburn, breast tenderness, shortness of
breath, back pain, sleep disorder, fatigue, and frequency of urination (Beddoe, Lee,
Weiss, Kennedy, & Yang, 2010; Borodulin et al., 2010; Duncan & Bardacke, 2010;

16
Garland, 2017; Greenwood & Stainton, 2001; Milliano, Tabbers, Post, & Benninga,
2012; Yikar, 2019; Zsamboky, 2017).
A review of the related literatures has demonstrated a relationship between
discomfort during pregnancy due to physiological adjustment and pregnancy-related
anxiety as in effective response. For some women who have insufficient knowledge on
her physiology system change, these condition can be assumed as the high pregnancy
risk that can generate anxiety by creating uncertainty about pregnancy and pregnancy
outcome (Bayrampour, Heaman, Duncan, & Tough, 2013; Dako-gyeke, Aikins,
Aryeetey, Mccough, & Adongo, 2013). Through childbirth education program,
midwives could enhance mother’s physiological mode to increase their adaptation
during the transition by providing sufficient information and insight about pregnancy
such as the education of anatomical and physiological adaptation, which in turn, can
help mother to reveal their anxiety during pregnancy (Harpel, 2008). Some best
intervention to reduce maternal anxiety includes relaxation technique such as yoga,
Coping Anxiety trough Living Mindfully (CALM), and hypnotherapy (Baxter,
Hastings, Law, & Glass, 2008; Goodman et al., 2014; Rasouli, Pourheidari, & Gardes,
2019; Tragea, Chrousos, Alexopoulos, & Darviri, 2014).
Pregnancy-related anxiety is defined as worries, concerns and fears about
pregnancy, childbirth, and health of infant and future parenting. The attributes of
pregnancy-related anxiety includes affective response such as emotion: cognition, being
preoccupied with various thoughts; and somatic symptoms such as; physical complaint
(Bayrampour, Ali, Mcneil, et al., 2016). Pregnancy-related anxiety may increase
nausea, poor psychological adaptation, negative perspective of motherhood as well as
the predictor of low birth weight and preterm birth (Glover, 2014; Nicoloro-
SantaBarbara et al., 2017). In Indonesia, out of 15.5/100 live birth newborn were

17
preterm and contribute to the number of infant mortality rate (World Health
Organization, 2019). The deleterious effect of pregnancy-related anxiety has well-
documented in many studies in Indonesia (Alza & Ismarwati, 2017; Eka Roisa
Shodiqoh & Syahrul, 2014; Hayati, Herman, & Agus, 2017; Setyaningsih et al., 2013;
Trisiani, Hikmawati, Bhakti, & Bandung, 2016), and the intervention to decrease the
anxiety in the antenatal class has been developed such as pregnancy exercise (senam
hamil), Dhikr1, belly dance, and counseling to the mother and spouse (Aryani et al.,
2016; Mardhiyah & Khaerani, 2017; Nasir, 2015; Ranita & Hardjanti, 2016;
Setyaningsih et al., 2013). There are number of measures in current use for pregnancy-
related anxiety (Sinesi, Maxwell, Carroll, & Cheyne, 2019), the most appropriate one
for this study is Pregnancy-related Anxiety Questionnaire-revised (PRAQ-R2) consist
of 33 item is designed as screening scale with higher scores indicative of greater
pregnancy-related anxiety. The instrument developed by and characterized by a
pregnancy, the wellbeing of the mother and baby and impending motherhood.
2. Self-concept Mode
The self-concept is defined as the individual’s mixture of beliefs and feeling about
herself or others at a certain time (Roy, 2009b). The variables related to the self-
concept mode in the prenatal period were concern about well-being of self and baby,
fear of helplessness and loss of control during childbirth (Sercekus & Mete, 2010). As
the multidimensional construct, self-concept refers to an individual self-efficacy in
relation any number of characteristics, for instance knowledge, experience, culture,
religion, and belief. Self-efficacy is the antecedent for all motivated behavior (Bandura,
1998). According to Bandura, people with a positive self-efficacy have high motivation
1 are devotional acts in Islam in which short phrases or prayers are repeatedly recited silently within the mind or aloud (Wikipedia, 2019).

18
to accomplish the goal that they have been set up, while people with low self-efficacy
will less effort to fulfill required behavior to achieve the goal. Therefore, women who
predicted has high score on childbirth self-efficacy as low used more epidural analgesia
compared to women with high childbirth self-efficacy (Carlsson, Ziegert, & Nissen,
2014). Similarly, William, Povey and White (2008) also found the level of self-efficacy
was affecting to the intention to use pain relief medication during childbirth (Williams,
Povey, & White, 2008). However, women who planning to have section cesarean (SC)
option reported has lower scores of birth self-efficacy rather than those who are
planning to have vaginal mode (Schwartz et al., 2015; Williams et al., 2008). Obstetric
and psychological factor have been noted as the factor associated with childbirth self-
efficacy (Carlsson et al., 2014; Dilks & Beal, 1997; Drummond & Rickwood, 1997;
Lowe, 1993).
World Health Organization (WHO) determined for cesarean section (CS) indicator
range 10 to 15 % for each country (World Health Organization, 2017). In 2010,
Indonesia has 9.8% delivery birth with CS (Suryati, 2012) and, unfortunately in some
urban area such as Yogyakarta and Jakarta, the number of CS was rather high about
15% and 19.9%, respectively. Bleeding, pre-eclampsia, and infection have been known
as the complication of SC and mostly contribute to the maternal and mortality death in
Indonesia (Ministry of Health, 2018). The evidence on intervention to enhance
maternal self-efficacy for childbirth in Indonesia is lack (Ramie, Afiyanti, & Pujasari,
2004; Sriwenda, 2014). Some are discussed self-efficacy for breastfeeding (Fata &
Rahmawati, 2016; Wardani, Rachmawati, & Gayatri, 2017) hence the reference on the
issue is limit. Senior researcher from China who focus on childbirth self-efficacy
develop the educational intervention to enhance childbirth self-efficacy based on
Bandura’s framework. Out of 110 pregnant women have been recruited to participated

19
in his study. The content includes the biopsychological phenomena of childbirth and
the strategies of coping with childbirth discomfort. Demonstration of coping behavior
including breathing and relaxation techniques to control emotional tensions and pain
during labor have also been applied (Ip, Tang, & Goggins, 2009). They developed the
short form of Childbirths elf-efficacy inventory (CBSEI) to measure the childbirth self-
efficacy.
3. Role function Mode
According to Roy, the role function mode covers the individual’s to her Secondary
roles: different roles (mother, spouse, etc.), and 3. Tertiary roles (as a director or
supervisor in the hospital, etc.). Mercer (2004) reported the first pregnancy task of
prenatal transition to motherhood is commitment which is includes positive and
negative pregnancy effect. However, the positive pregnancy will result the commitment
regarding secondary role; relationship with the unborn baby, spouse and changes in the
women’s daily life (Nichols, Roux, & Harris, 2007). Maternal-fetal attachment is the
concept that can be used to explain the process of bonding (Muller, 1993). Based on the
definitions of maternal and fetal attachment, it could be understood that attachment is
key element in the successful psychological adjustment to pregnancy experience
(Cranley, 1981; Cunningham Facello, 2008; Muller, 1989). According to Muller, this
acquire behavior of attachment includes mimicry or role play such as calling baby with
his name, imagine the baby’s face, communicate with the baby, share her thought and
activity to the baby, and prepare the thing for the baby. Ask the spouse to put his hand
on the belly, as well as ask him to communicate with the baby have been also
recognized as the characteristic of maternal-fetal attachment (Muller, 1993). Evidence
indicate if the mother who have good quality of attachment to their unborn baby, more
engage to take care of their baby after birth, and optimized their interaction (Siddiqui &

20
Hägglöf, 2000), which in turn can enhance the physical, mental, and social health
development of their child (Ainsworth, 1969; Muti’ah, 2009). Mother who performed
high score in maternal-fetal attachment will have positively to their role as the mother
include attend the antenatal care (Lindgren, 2001).
There is a growing studies on maternal-fetal attachment in Indonesia since the
translation of its instrument to measure maternal-fetal attachment: Prenatal Attachment
Inventory (PAI) (Alvianty & Suryaningsih, 2016; Nosrati et al., 1994; Sukriani &
Suryaningsih, 2018; E.K. Suryaningsih, 2015). However, the scarce of intervention to
promote maternal-fetal attachment remain exist in Indonesia, while some
recommendation have been proposed by previous researchers during decade in others
countries (Abasi, Tafazzoli, Esmaily, & Hasanabadi, 2013; Akbarzadeh et al., 2016,
2011; Chang et al., 2004, 2015; Dokuhaki et al., 2017; Nishikawa & Sakakibara, 2013;
Saastad et al., 2011; Toosi et al., 2017) such as mindfulness-based therapy, fetal
movement counting, Leopold’s maneuver, and relaxation techniques. In Japan, a
program to improve maternal-fetal attachment has been selected as the grant project in
2015. The content material includes education on pregnancy, post-partum, relaxation
skills, and communication skill. The opportunity for women to interact with other
pregnant women and allowing them to build their social network also include the
program (Grant, McMahon, & Austin, 2008).
4. Interdependence
According to Roy, this mode is focused on interactions related to love, respect,
giving and receiving value (Roy, 2009a). During pregnancy, different perspective from
men and women in viewing developmental task as a parent can lead conflict, however,
if they can adjust that adaptation process and avoid or resolve conflict sufficiently from
both, so the spouse feel satisfied with the marriage (Ayub, 2014; Mealing, 1991).

21
Interdependence defined as the moment when spouse reach the resolution of parental
relationship conflicts in marital relationship and in turn, couple experience dependence
each other that keep them together. The higher level of couple’s ability to promote their
togetherness and interaction activities include sharing and spend more time together,
the higher level of their interdependence (Mealing, 1991). According to Mealing
(1991), this ability may be change during pregnancy, since upcoming roles as a parent
has been develop. There are two significant indicators in marital relationship: effective
communication, and marital satisfaction. Studies reported, the marital satisfaction as a
predictor of maternal mental health wellbeing during pregnancy, which in turn, affected
to the postpartum mental health such as postpartum stress, anxiety and depression
symptom (Clout & Brown, 2016; Dimitrovsky, 2002; Henriksen & Thuen, 2015). In
line, the latest systematic review reported, studies conducted ranged from 2000 to 2016
have been consistent in result on the relationship between marital satisfaction as well as
quality of marital communication and maternal mental health (Alipour, Kheirabadi,
Kazemi, & Fooladi, 2018).
A longitudinal study in Norway found expectant women who satisfied with their
marriage were more satisfied with their 3 years life after postpartum rather than those
who were less satisfied (Dyrdal & Nes, 2011). This study also found that marriage
satisfaction as a predictor of a future happy life. The intervention includes preparatory
classes or public message is recommended by Dyrdal and Nes (2011). The class aiming
to promote a robust and satisfactory relationship during pregnancy. Classes focus on
the importance of nurturing their relationship and building social support may also can
be considered as the content material of preparation class (Dyrdal & Nes, 2011).
Similarly, other study also recommend productive communication as targeted couple to

22
promote their relationship adjustment during pregnancy (Heyman, Baucom, Katherine,
& Trillingsgaard, 2014).
A mixed method study conducted in Virginia explore the effectiveness of
mindfulness-based relationship education for couples (Gambrel & Piercy, 2015). They
developed the class to improve participant’s relationship satisfaction by inviting 66
expectant parents. The intervention were couple activities and a 15-minute formal daily
mindfulness practices included body scan, mindfulness of breath, and open awareness.
The mindfulness program applied focus on Mindfulness-based Relationship
Enhancement, and Mindfulness-Based Childbirth and Parenting. Mindfulness activities
such as mindful touch, mindful communication, and mindful eye contact also have been
applied. The result findings based on statistical measure that there is a significant
improvement for those in treatment group in relation satisfaction rather than those in
control group. In qualitative result shown men and women have difference of
experience in term of social support, program enrollment, and identity and relational
processes during pregnancy. For men, the program give positive impact for them such
as more deeply connected with their partners. The researcher directed for the future
research to include measure of social support, program expectation, and connecting
with baby (Gambrel & Piercy, 2015).
2-4. The effectiveness of childbirth education classes
The studies on the reducing maternal anxiety, increasing childbirth self-
efficacy, maternal-fetal attachment and marital relationship trough childbirth education
classes are described as below.
Goodman and colleagues (2014) tested the effectivity of Coping with Anxiety
through Living Mindfully (CALM) to the anxious pregnant women during the

23
childbirth classes. They recruited twenty four pregnant women with anxiety symptoms
and conduct interview to test the feasibility of this pilot study. The interviewed
conducted by psychologist to determine the final eligibility of the participants using
Beck Anxiety Inventory (BAI), severity score of ≥ 11 indicating elevated level of
anxiety symptom. The content material of the class include psycho-education
knowledge, mindfulness practices, and cognitive exercises, continued by home practice
for about 30-45 minutes 6 days a week during five weeks. Additionally, the participants
in the experimental group have to read the material which is provided by researchers
from a variety of sources on aspects of mindfulness practices. Goodman and team
found if Mindfulness-Based Cognitive Therapy (MBCT) on form of the CALM
pregnancy intervention holds potential to provide effective treatment for pregnant
women with anxiety (Goodman et al., 2014). This intervention can be considered as the
non-pharmacological treatment and as the promising method to reduce anxiety during
pregnancy, however, the lack of participants is acknowledge as the limitation in this
study.
Larsen and Plog in 2012 developed the childbirth classes aims to enhance self-
efficacy for women and support person. They recruited one hundred fifteen expectant
women and 109 support persons in the small Midwestern hospital who participates in
childbirth education classes. The program conducted during 6 weeks class offered 2.5
hours once a week (Larsen & Plog, 2012). To measure the outcome, initially the
investigators considered using the Childbirth Self-Efficacy Inventory (CBSEI) because
its established reliability and validity (Lowe, 1993). However, they want to evaluated
the impact of the content of these specific classes, therefore they developed the
instrument by themselves: childbirth SE instrument consist of 18-item Likert-type
scale. Before the content of material is pilot tested, initially the investigators invited the
24
experts to review and scored it by rating from 1 (completely lacking in confidence) to 4
(very confident) in performing behaviors associated with communicating needs,
coping, relaxation, working with support person or expectant women, knowledge of
labor and delivery, and overall confidence in coping with labor.
Larsen and Plog (2012) found if both expectant women and support person had
significantly increase in self-efficacy after the childbirth education classes. The
interesting finding result from their study is that additional external hours of
preparation in fact did not significantly affect SE scores for the expectant women but
did not significantly affect SE scores for the expectant women but did have an impact
on support person’s SE. support persons had significantly less outside preparation than
expectant women, which may explain why SE scores were higher following the
childbirth preparation for support person. Therefore, Larsen and Plog recommend for
the childbirth educators to continue to offer various classes to support the learning
needs of expectant families and continue to evaluate both curriculum and pedagogy of
the classes (Larsen & Plog, 2012).
Akbarzadeh and team from Iran in 2016 develop the prenatal class focused on
teaching attachment behavior to pregnant women. In total, 190 pregnant women in their
last trimester, were randomly into two groups (experiment and control group). The
participants in the experiment group attended the six educational class each lasting for
60-90 minutes (Akbarzadeh et al., 2016). The content material includes physiology of
pregnancy and childbirth, awareness of the feelings and perceptions of the embryo, the
concept of attachment, attachment behavior to control the anxiety and negative thought
and patterns of proper sleep, exercise and nutrition during pregnancy. In two
educational sessions in this study, the investigators focused about maternal-fetal

25
attachment, the effects such as attachment on the mother, fetus and baby, and way to
promote trough group discussion and role playing.
The action of maternal-fetal attachment includes: speaking to the fetus, looking
at and caressing the stomach, giving the fetus a name, encouraging other family
members to talk to the fetus, visualizing the face of the fetus, visualizing breastfeeding,
and hugging the baby (Muller, 1993). However, the women in the control group
received routine care delivered by the staff midwife, including assessment of fetal heart
rate and the measurement of uterine growth at each visit. In this group, the women took
public classes in the form of lecturers about prenatal care and breastfeeding. The
investigator found the significance difference of fetal development between mothers
who have poor maternal-fetal attachment and mothers who have good attachment
during pregnancy.
Akbarzadeh and team (2016) provide recommendation for further study to
educate mothers on attachment skilled will encourage the attachment between the
mothers and their unborn babies and reduced anxiety in the babies which, in turn,
improved their mental health at birth and at the age of three months old. Additionally,
they also suggested that educational programs on attachment skills for pregnant women
to be incorporated into routine prenatal care. Tahmabesy et al. (2013) conducted
intervention on prenatal attachment among forty two pregnant women while non-
intervention set up for forty one pregnant women with routine prenatal care. Both
groups of participant were asked to complete a maternal-fetal inventory (Cranley, 1981)
and interview from prior to and after the intervention. The investigators reported that
there is different mean score on attachment between two groups. Therefore, they
concluded that the maternal-fetal attachment intervention lead to an increase in the
mother’s attachment with their fetus, further motivating them to meet the child’s need.

26
Ultimately, this attachment affected in the social, emotional, ad cognitive growth of the
child (Akbarzadeh et al., 2011).
The study confirms the efficacy of childbirth education of mindfulness-based
program on the psychological health such as self-efficacy, self-perceived stress and
depression (Pan et al., 2018). The eight-week program has been effective to increase
childbirth self-efficacy in the intervention group and decreased self-perceived stress
and depression significantly. The content material has been summarized on the paper,
include yoga, physiology of childbirth from a mind-body perspective, comfort measure
during birth, physiology of breastfeeding to coping breastfeeding challenge.
Childbirth education offers multiple opportunities to reach expectant mothers
with information related to pregnancy, labor, and delivery and as a way of promoting
delivery with the assistance of a skilled health-care provider (Anonymous, 2008).
Based on large study in China (Shi, Wang, Yuan, Jiang, & Zeng, 2015), which is
involved 604 pregnant women to participate in prenatal education curriculum. This
cross-sectional study was collect data on the format of the curriculum: lecture (92.6%),
promotional materials (64.6%), followed by video (60.0%), demonstration and practice
(58.3%) and group discussion (54.3%). In term of the effect of the prenatal education
curriculum provided by the hospitals, the majority of surveyed mothers who
participated in it said they know more about prenatal examination, health care
knowledge during pregnancy, roles of doctors and nurses during delivery, benefits and
approaches of breastfeeding. Therefore, they recommend to should be advocate the
childbirth education for mother and father.
Particularly, childbirth education take place as part of routine prenatal care
based on recommendation from World Health Organization (WHO), and has long been
acknowledged as a crucial component of prenatal care (Bahrami, Simbar, & Bahrami,

27
2013). The goal of childbirth education classes are to help expectant parents become
knowledgeable mothers and fathers, make them actively take part in maintaining health
during pregnancy, delivery, and parenting (Giurgescu & Templin, 2015; Endang Koni
Suryaningsih, 2016). However, the investigators have no provide the information on the
content of the material as the curriculum of the class.
In 1996, Beger and Beaman conducted the evaluation of childbirth education
classes to address the particular issue as the foundation for further researcher who want
to develop curriculum for childbirth education classes (Beger & Beaman, 1996). They
underlined if the timing of an educational interest survey also affects the result of
project. Additionally, expectant parent requested more demonstration and practice, and
breathing, and relaxation techniques to prepare for labor. However, commonly
techniques in childbirth education such as music, imagery, and effleurage have not been
reported useful (Beger & Beaman, 1996).
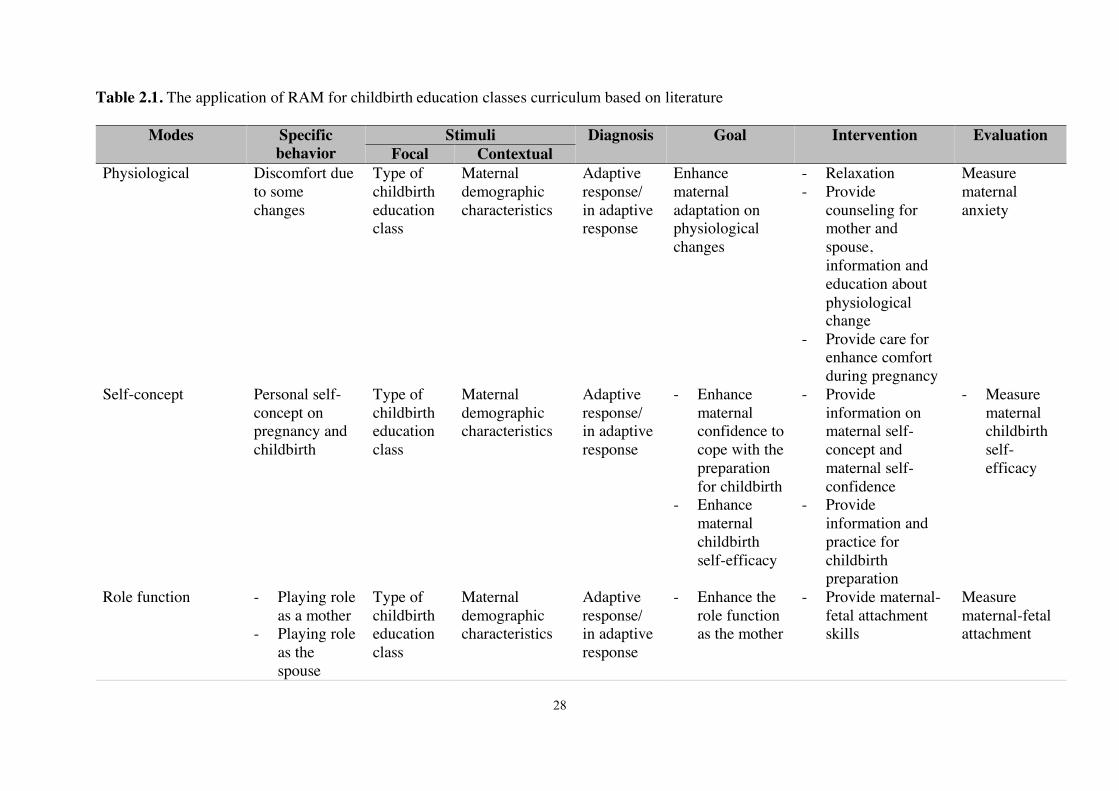
Based on those literature reviews, using RAM as the guidelines, the researcher
has been developed particular intervention to address the specific behavior that
manifest from the four modes as described in the Table 2.1. The goal of those
interventions are to promote mother’s adaptation for each modes and its outcomes can
be measured as the evaluation of the intervention
28
Table 2.1. The application of RAM for childbirth education classes curriculum based on literature
Modes Specific behavior
Stimuli Diagnosis Goal Intervention Evaluation Focal Contextual
Physiological Discomfort due to some changes
Type of childbirth education class
Maternal demographic characteristics
Adaptive response/ in adaptive response
Enhance maternal adaptation on physiological changes
- Relaxation - Provide
counseling for mother and spouse, information and education about physiological change
- Provide care for enhance comfort during pregnancy
Measure maternal anxiety
Self-concept Personal self-concept on pregnancy and childbirth
Type of childbirth education class
Maternal demographic characteristics
Adaptive response/ in adaptive response
- Enhance maternal confidence to cope with the preparation for childbirth
- Enhance maternal childbirth self-efficacy
- Provide information on maternal self-concept and maternal self-confidence
- Provide information and practice for childbirth preparation
- Measure maternal childbirth self-efficacy
Role function - Playing role as a mother
- Playing role as the spouse
Type of childbirth education class
Maternal demographic characteristics
Adaptive response/ in adaptive response
- Enhance the role function as the mother
- Provide maternal-fetal attachment skills
Measure maternal-fetal attachment

29
- Practice the maternal-fetal attachment skills
Interdependence - Relationship
with husband
- Relationship with unborn baby
Type of childbirth education class
Maternal demographic characteristics
Adaptive response/ in adaptive response
- Enhance the quality relationship between mother and spouse
- Provide skill how to communication with husband
- Empower husband to practice comfort measurement during pregnancy and childbirth
Measure marital relationship

30
Since Roy’s Adaptation Model is the complex concept, we need to translate the grant
theory into the practices. Figure 2.2 is the evidence that Roy’s Model can be accepted in this
study in which the gap between theory and empirical indicator can be measured. Adaptive
system in this study is the pregnant women in their third of pregnancy and will be recruited in
this study as the participant. The focal stimuli is childbirth education class that follow Roy’s
Model, and contextual stimuli is the demographic characteristic that may affect to the
mother’s adaptation level. The physiological mode resulted the physic and physiology change
during pregnancy and may lead some discomfort. This condition may resulted either adaptive
or maladaptive response. The indicator of this mode is pregnancy-related anxiety and will be
measured using Pregnancy-Related Anxiety Questionnaire Revised-2 (PRAQ-R2). The self-
concept is the mother’s efficacy to have their childbirth process, therefore the behavior will
be measured using the short form of Childbirth Self-Efficacy Inventory (CBSEI). Role
function mode refers to role function as the mother in which the degree the expectant women
attach to her unborn baby. The indicator behavior will be measure using Prenatal Attachment
Inventory (PAI). Finally, the interdependence mode defined as mother’s relationship with
their husband. Since the indicator variable of marital relationship is marital satisfaction and
communication, therefore ENRICH Marital Satisfaction Scale will be applied to measure the
behavior.

31
Grant theory Roy’s adaptation model
Adaptive system
Empirical stimuli
Adaptation modes
Concept
Pregnant women
Physiological Mode
Role function Mode
Self-concept Mode
Interdependence Mode
Focal
Contextual Nine physiological
change
Operational indicator Participants Experime
nt and control groups
Demographic data sheet
Pregnancy-related anxiety questionnaire (PRAQ-R2)
Short form of
Childbirth Self-
Efficacy Inventory (CBSEI)
Prenatal Attachment Inventory
(PAI)
Developed childbirth education
Maternal demographic characteristic: age, marital status, education, occupation
Discomfort
Adaptive/maladaptive response
Confidence in ability to cope with childbirth process
Role as a mother
Relationship with husband
Figure 2.2 Model, concept, and operational structures of efficacy on childbirth education based on Roy’s Adaptation Model
ENRICH Marital
satisfaction scale (EMS)
32
2-5. Childbirth education in Indonesia
In Indonesia, the program of childbirth education classes has been provide as a part of
midwifery care in the community since 2009 to accelerate the decreasing number of maternal
and infant mortality. The aim of this class is to enhance mother’s knowledge regarding
physiological adjustment and complaint that may rise during pregnancy and post-partum.
Family planning after birth, newborn care, local myth, belief and culture, infection disease as
well as birth certificate, also includes as the major topic of this program (Ministry of Health
Indonesian Republic, 2011). The childbirth educator for this program is the midwives, or
someone who certified as the childbirth educator. Indonesian health authority recommend for
pregnant women after 20 weeks of pregnancy may participate in this program. However,
partner or husband is expected to be involve in the class for at least one time. The participant
limited up to ten person for each class.
In Indonesia, both public and private sector are allowed to provide the childbirth
education class, yet the non-government organization and society. Prior to determine the
content material, need assessment will be conducted by midwives to addressed community’s
demand on the childbirth program. The content of material includes: anatomy and
physiological change during pregnancy, pregnancy care, birth and post-partum. Family
planning after birth, newborn care, local myth, belief and culture, infection disease as well as
birth certificate. The class consist of three time meeting and the number of content based on
the appointment between childbirth educator and the group of pregnant women. After the
program finish, then midwives will report and document the activity as the monitoring
process, and evaluate its effectiveness. The scheme of childbirth education class program in
Indonesia can be seen on the Figure 2.3. Many studies in Indonesia indicate the efficacy of
this program to enhance maternal mental and physical well-being(Agustiningsih, 2017; Faiza,

33
Notobroto, Trijanto, & Soedirham, 2016; Fata & Rahmawati, 2016; Fibriana & Azinar, 2016;
Lucia et al., 2013; Novitasari, Budiningsih, & Mabruri, 2013; Nursofyanto & Cahyanti, 2017;
Septerina, Hastuti, & Fitria, 2014; Setyaningsih et al., 2013).
Figure 2.3 Scheme of childbirth education class in Indonesia provided by public sector
The program has 120-125 minutes for each session, consisted of average four to five
topics. The method delivered by childbirth educator through lecturing, practicing, discussion,
brainstorming, and simulation. Midwives or childbirth educator should made documentation
in the end of the program as the monitoring and evaluation effort that have to be submitted to
ministry of health. Nowadays, the childbirth education class program becoming popular and
provided from private clinic, or hospital, and work independently. One of the most famous
childbirth education training center in Indonesia is Bumi Sehat foundation. As the non-profit
organization, Bumi Sehat, located in Bali, was founded by Robin Lim in 1995 provide a
comprehensive range of allopathic and holistic medicine, as well as pre and post-natal care,
breastfeeding support, infant, child and family health services, nutritional education, pre-natal
yoga and gentle, loving natural birth services (Bumi Sehat, 2019).
Need assessment from society, content material based on demand
Preliminary class
Team is created
Childbirth education class and report
Monitoring
Evaluation

34
Since its development, there are a huge number of facilitator of childbirth prenatal
yoga and gentle birth classes across the province who achieve their certification from this
foundation. They were, then, back to their place and provide childbirth education classes.
One of the private clinic which is provide childbirth education classes is Bidan Kita in Solo,
Center Java. As the one recommended clinic in central Java, Bidan Kita (in English mean:
Our Midwives), provide childbirth education classes for couple and expatriate as well. The
program includes: gentle birth, prenatal yoga, hypnobirthing, childbirth support and healing,
parenting and newborn care (Aprilia, 2019).

35
CHAPTER III
RESEARCH METHODHOLOGY
This chapter describes the research design, study setting, population, sampling and
sample determination, inclusion and exclusion criteria, data collection, childbirth education
curriculum development, data analysis, and ethical considerations.
3-1. Study design
This study was conducted using a randomized controlled trial with pretest-posttest
repeated measurement of pregnancy-related anxiety, maternal-fetal attachment, childbirth
self-efficacy, and the quality of marital relationships in the intervention and control groups.
Allocation concealment was assured by using a sequentially numbered, opaque, sealed
envelopes (SNOSE). This study has covered three aims, some following instruments were
used to measure the outcomes: Demographic questionnaire, Pregnancy-Related Anxiety
Questionnaire Revised (PRAQ-R2), Prenatal Attachment Inventory (PAI), Short Form of
Childbirth Self-Efficacy Inventory (CBSEI), and ENRICH Marital Satisfaction Scale (EMS).
E O1 X O2
Random allocation
C O1 X O2
Note: E= experimental group; C=Control group
O1= pretest Demographic questionnaire, Pregnancy-Related Anxiety Questionnaire
Revised (PRAQ-R2), Prenatal Attachment Inventory (PAI), Short Form of Childbirth
Self-Efficacy Inventory (CBSEI), and ENRICH Marital Satisfaction Scale (EMS)
O2= post PRAQ-R2, PAI, CBSEI, EMS
Figure 3.1 Research design

36
3-2. Study setting
Five health centers (bahasa: puskesmas) have been chosen based on the availability of
regular childbirth education classes. The intervention group, the classes were conducted at
the childbirth education room of health college of Aisyiyah University, Yogyakarta. For the
control group, the classes were conducted at the puskesmas in Yogyakarta Province.
3-3. Population and sample
The study population were pregnant women who attend antenatal care at primary health
care centers in Yogyakarta. Using a G-Power software, repeated measures, between factor,
set effect size = .25 and power= .80. The researcher calculated a sample size of 98 would be
needed for meaningful results (Faul, Erdfelder, Lang, & Buchner, 2007). Assuming a 20%
attrition rate, raises the total number of participants to 122. The researcher was produce a
random allocation list using a computer random allocation block (sequence 4, 6, 8) at five
health centers to ensures equal in size and treatment allocation within each block. The
allocation software using Microsoft Visual Basic 6 version 1.0.0 developed by Saghei from
Anesthesia Department in Isfahan University of Medical Sciences, Iran. This software
installed in the ordinary windows software such as running setup.exe and following on
screen instruction(Saghaei, 2004).
In this study, the inclusion criteria for participation were:
1. First time pregnancy (nullipara)
Prior experience giving birth affects mothers’ anxiety related to pregnancy and
childbirth self-efficacy. Therefore to minimize the threat to internal validity, the
researcher only invited nullipara women for the current study.
37
2. Pregnant women ages 20 to 35
Based on recommendations from the Ministry of Health in Indonesia, the ideal
reproductive range age for a healthy pregnancy is between 20 and 35 years old (Ministry
of Health, 2018). The four most common non-obstetric causes of maternal mortality in
Indonesia are summarized as the 4T conditions: Too young (pregnancy under age 20),
Too old (pregnancy above age 35), Too often (parity of greater than three), and Too close
(pregnancy spacing of less than two years) (Aeni, 2011).
3. Gestational age of 28 to 35 weeks
This program will be conducted during classes held once a week for a period of four
weeks. To prevent the possibility of high-risk pregnancy such as: preterm and posterm
birth, the researcher will invite pregnant women at 28 to 35 weeks of gestation to
participate.
4. Married
This study will invite husbands to accompany their wives during the childbirth
education classes. The classes will enhance the quality of the couples’ marital
relationships through counseling, verbal communication, and touching communication.
Unmarried couples having children are rare in Indonesia and to include marital status in
the model would require a larger number of such couples than are likely to be available.
5. Residents of Yogyakarta
The participants must be residents of Yogyakarta to decrease the possibility of
attrition due to distance from the study setting.
6. Singleton pregnancy
Multiple pregnancies are one of the high-risk pregnancy categories. Women with
multiple pregnancy tend to have shorter average gestation and more complications, such

38
as preterm birth, preeclampsia, diabetes mellitus, and placental problems, than women
with singleton pregnancies. (American Society for Reproductive Medicine, 2012;
Lazarov, Lazarov, & Lazarov, 2016). To minimize risk during this intervention, the
researcher will only invite women with singleton pregnancies.
The exclusion criteria:
Mothers who miss the classes more than two times is considered to be excluded in the
study. The mothers those who miscarry, and those whose pregnancies become high-risk, will
be automatic excluded from the study.
3-4. Data Collection
The researcher was prepare the curriculum, enroll participants, and allocate them into
groups.
1. Curriculum preparation
After a literature review, the researcher selected and modified possible material for
childbirth education based on a Roy’s Adaptation Model approach. The content has been
reviewed by thesis committee members during the proposal defense to get suggestions and
recommendations regarding its content and sequence. Next the researcher invited experts
from Indonesia to evaluate the curriculum. These experts were midwives who have provided
midwifery care for more than two years and who are teaching prenatal classes. They asked to
rate each topic in the curriculum as “not needed,” “a very minor topic,” “a minor topic,” or “a
major topic.” The survey form were open-ended, allowing the experts to add supplementary
topics or to make comments
The researcher recruited two research assistants with a bachelor degrees qualification.
They were participated in a one-day training session to discuss the aims of the study, as well

39
as the procedures and protocols they should use. The rationale for content of the childbirth
education class and the potential outcomes of the intervention also were discussed. The
training were also included a quality control issues relating to biases, fabrication of data,
missing data, and ethical issues, in order to ensure the consistency of the recruitment and data
collection process.
2. Enrolment and allocation
After approval from the Ethical Committee of ‘Aisyiyah University of Yogyakarta
Institutional Review Board, the researcher was prepare materials to approach pregnant
women attending antenatal care clinics for participation in the study. For recruiting purposes,
the researcher was create colorful flyers and standing banners promoting the benefits of
joining the study to put in the waiting rooms of antenatal care clinics in puskesmas. The
program were free of charge and mothers were given incentive for their participation. That
information was provide on the flyers and standing banners. The researcher and the two
trained assistants worn ID cards that include a photo, name, title, and job position for the
current study, along the affiliations name. Name tags for participants also has been provided
by the researcher.
The researcher and assistants were distributed flyers to the mothers who are potential
participants while they are waiting their turn to enter the antenatal care clinic. We were
explained the purpose of the study to all potential participants, as well as the benefits of
participation and the low risk of harm. The confidentiality of results and the right to withdraw
from the study at any time without any consequences will be guaranteed. Additionally,
potential participants also has been allowed to ask questions about the study. Once a
participant agrees, the researcher or a trained assistant will ask them to fill out the informed
consent form and include their cell phone number. The research assistant will give the

40
mothers a card in an opaque and sealed envelope containing a randomly assigned number for
the purpose of allocating them to groups. The research assistants were opened the sealed
envelope and record the number while the women are in the antenatal care room.
There were five intervention group classes and five control group classes held on
different days of the week. Participants were encouraged to choose a class time that is
feasible for them by providing their preferred and second-best available times through
WhatsApp meeting scheduler. The researcher were conducted two classes at a time, repeating
the recruitment and teaching process once the participants were completed due to it was not
possible to recruit enough participants to run five classes simultaneously. Participants who
are randomized to the intervention group were attended a four-week class lasting three hours
each time. Participants randomized to the control group were attended a four-week class
consisting of the existing antenatal education program offered at the puskesmas. The women
were informed of their final assignment to a childbirth education class schedule through
WhatsApp or by phone. The researcher were inquired about how each midwife instructor
normally sets up class times and were provided with a list of participants who have been
allocated to the control group.
The mothers were asked to complete the study questionnaire to establish a baseline
measurement for all instruments, whilst the husbands were asked to complete the
demographic information and the Enrich Marital Satisfaction (EMS) Scale . After four weeks
of classes, the participants were self-administer the same questionnaire again without the
demographic portion. Completing the questionnaire was estimated 15 to 20 minutes.
Intervention group
The participants in the intervention group are pregnant women and their husbands. The
instructors employed teaching methods such as a group discussion, watching videos, and

41
brainstorming, as well as questions and answer periods, demonstrations, childbirth
simulation, and practice. The primary investigator (PI) taught particular sessions, including
maternal-fetal attachment skills, parenting skills, comfort measures, childbirth positions, as
well as knowledge about anatomy and physiology during pregnancy and birth. The prenatal
yoga facilitator were taught pregnancy and relaxation exercises. The materials and learning
methods as the control process are expected to influence the four modes as the effectors that
can reduce maternal anxiety and increase maternal-fetal attachment, childbirth self-efficacy,
as well as marital satisfaction as the outcomes of adaptation level.
The study setting for the intervention group were conducted at antenatal care laboratory
of ‘Aisyiyah University of Yogyakarta. For safety and protocol concern during pandemic
COVID-19 situation, the class was set up in a big classroom and an adequate ventilation that
can accommodate 12 couples and is equipped with yoga mats and pillows, as well as
convenient access to a restroom. The couples and researcher team were required to wear
mask and wash their hand before and after enter the class. The distance from the university to
the five puskesmas or private clinics will range from 2 to 5 km.
Research assistants printed hand outs and lead the group through WhatsApp application to
following up practicing skills at home and also respond the question from the participant at
any time. During the intervention, the health workers from the participating puskesmas have
been invited to observe the intervention. Classes consisted of 180-minute sessions held once
a week for four weeks. Detailed class plans based on RAM are described in Appendix.
Control group
The control group participants in this study have attended standard childbirth education
classes during the same period as the intervention group. The control group classes were
conducted at the puskesmas where they were recruited, not at the university. The facilitators

42
of the control groups were midwives who are already providing prenatal education classes at
the clinics. The classes followed the government curriculum, which consists of three classes
per month and does not invite husbands to participate. However, in this study, participants in
the control group have four classes over a one-month period to better match the program of
the intervention group.
The material for the standard curriculum includes anatomical and physiological changes
during pregnancy, pregnancy care, birth and post-partum care. The classes also address
family planning after giving birth, newborn care, preventing infectious disease, and
procedures for obtaining a birth certificate. The midwives also discuss and debunk unhealthy
local myths, beliefs and cultural practices surrounding pregnancy, childbirth and the post-
partum period. For the fourth class, the control group have a half hour to fill out the
questionnaires and a half hour for feedback and discussion. Then the researcher and assistants
have provided the control group participants with a condensed two-hour class of prenatal
yoga, comfort measures, and maternal-fetal attachment activities.
We conducted online briefing sessions with midwives who are the childbirth education
program facilitator at five health centers. The briefing was discuss about the objectives of the
study, the administration of the questionnaire, and the quality control issues relating to biases,
fabricated data, missing data, and ethical issues. These were established in an effort to ensure
consistency in the process of data collection.
Table 3.1 Comparison childbirth education program between experimental and control group
Experimental group Control group
Content anatomical and physiological
changes during pregnancy and birth,
maternal-fetal attachment skills,
anatomical and physiological
changes during pregnancy,
pregnancy care, birth and post-

43
parenting skills, comfort measures,
childbirth positions, pregnancy and
relaxation exercise during
pregnancy and labor, as well as
couples communication issue.
partum care, family planning
after giving birth, newborn care,
preventing infectious disease,
and procedures for obtaining a
birth certificate.
Learning method Lecturing, round table discussion,
demonstrating, practicing, and
watching the video. Following up
the practical suing group online
discussion.
Lecturing and discussion
Hour 3 hours for each session 2-3 hours for each session
Instructor Researcher Midwives in the health center
Participants Mother and husband or relative Mother
Place Childbirth education room Health center

44
3-5. Research Tools
In this study, researcher applied five different instruments: Demographic
questionnaire, Pregnancy-Related Questionnaires Anxiety Revised-2, Short Form of the
Childbirth Self-Efficacy Inventory, Prenatal Attachment Inventory, and ENRICH Marital
Satisfaction Scale.
Demographic questionnaire
The researcher has developed a demographic data sheet to gain information about
participants’ backgrounds, such as maternal age, religion, ethnicity, education, gestational
week, occupational status, marital status and duration, and monthly income.
Pregnancy-related anxiety questionnaire revised (PRAQ-Q2)
The original instrument, the PRAQ-R1, consisted of 34-items developed by Van Den
Bergh (Bergh, 1990). The revised questionnaire, PRAQ-R2, is shorter and consists of a 10-
item self-report for multipara women, and an 11-item self-report for nulliparas. The scores on
each item range from 1 (definitely not true) to 5 (definitely true) (Huizink, Mulder, Robles de
Medina, Visser, & Buitelaar, 2004). The 10-items consist of three subscales: items 1, 2, 6 and
8 are related to “fear of giving birth,” items 4, 9, 10, and 11 are related to “worries about
bearing a physically or mentally handicapped child,” and items 3, 5, and 7 are related to body
image or “concern about own appearance.” In the revised version, Huizink explains the
awareness for calculate the new version of PRAQ-R2 which is only addressed to measure
pregnancy-anxiety for nulliparous, while PRAQ-R applicable for all pregnant women
regardless of parity. The item 8 (“I am anxious about the delivery because I have never
experience one before”) will apply in this study since all the proposed participant are

45
nulliparous, instead of item 1 (“I am anxious about the delivery”) which is applicable for all
parity. Thus, the minimum and maximum total score are 11 and 55, respectively (Huizink,
Delforterie, Scheinin, & Tolvanen, 2016). The assumption is that, the higher the score, the
higher the level of anxiety in pregnancy. The PRAQ-R2 items are all structurally positive
statement and the questionnaire has no cut-off point. Huizink and team (2016), then tested for
its validity and reliability in a longitudinal study with a large sample size (1144 pregnant
women). The result showed the Cronbach’s Alpha for the total score was good, ranged from
.71 to .85 for the multiparous, and .75 to .84, for the primiparas based on values measured at
different weeks of gestation (Huizink et al., 2016).
Short Form of Childbirth Self-Efficacy Inventory (CBSEI)
Childbirth Self-Efficacy Inventory (CBSEI) was developed by Lowe (1986) to
measure maternal confidence in coping abilities during childbirth. Based on Bandura’s Self-
Efficacy Theory (1977), Lowe create the tool as a self-report instrument consist of 60 items
divided to four subscales; OAL, ESS, OSS and ESS. A total Childbirth Outcome Expectancy
Score (Outcome-Total) is computed by summing the Outcome-AL and Outcome-SS scale
scores. A Total Self-Efficacy Expectancy Score (Efficacy-Total) is computed by summing
the Efficacy-AL and Efficacy-SS scale scores (Lowe, 1989). The example item: “ Relax my
body”, “ tell myself that I can do it”, and “listen to encouragement from the person helping
me.”
Lowe measure the internal consistency ranged from .86 to .95 for all subscales (Lowe,
1993). Many studies reported high validities and reliabilities of CBSEI from different
languages around the world, the Cronbach’s Alpha range were 0.86 -0.93 (Abujilban,
Sinclair, & Kernohan, 2012; Carlsson et al., 2014; Eleonora Björk, Mari Thorildsson, 2007;
46
Gourounti et al., 2013; Gourounti, Kouklaki, & Lykeridou, 2015; Ip, Chan, & Chien, 2005;
Khorsandi et al., 2008; Tanglakmankhong, Perrin, & Lowe, 2011).
In 2005, Ip and colleagues developed the short form of CBSEI consist of 32 items
(OE= 16, and SS=16). They deleting the two repetitive expectancy subscale to producing the
responses across the two stages of labor and reduce the lengthy structure of the original
CBSEI (Ip et al., 2005). In different studies, the short form of CBSEI demonstrates high
internal consistency (á= .90- .96) (Gao, Ip, & Sun, 2011; Ip, Chung, & Tang, 2007;
Khorsandi, Jafarabadi, Farzaneh, & Mohammad, 2013).
Prenatal Attachment Inventory (PAI)
This instrument developed by Muller (1993) to measure the unique relationship
between mothers with their unborn babies. The instrument consist of 21 Likert-type items
ranging from 1 (‘almost never’) to 4 (‘almost always’). All items are summed for a single
score, and the possible range of scores is 21-84 (Muller, 1993). The 21-item PAI was
validated in a Swedish sample of 171 pregnant women by Siddiqui et al (1999), Cronbach’s
alpha coefficient was .86, and the mean was 57.22 (SD = 5.916) (Siddiqui & Hägglöf, 2000).
In 2003, Gau and Lee tested the construct validity of the instrument by using confirmatory
factor analysis (CFA) on a sample of 344 pregnant American women in their third trimesters.
Cronbach’s alpha coefficient was .89 and the mean were 63.7 (Gau & Lee, 2003). The author
have culturally translated, produce the Indonesian version of PAI, and demonstrates high
internal reliability (á= .93) (E.K. Suryaningsih, 2015).

47
ENRICH Marital Satisfaction Scale (EMS)
Evaluation and Nurturing Relationship Issues, Communication and Happiness
(ENRICH) Marital Satisfaction Scale (EMS) was developed by Fower and Olson (1993)
consist of a 15-item comprising the Idealistic Distortion (5 items) and Marital Satisfaction
Scales (10 items). This scale is a Likert-type ranging from 1 (strongly disagree) to 5 (strongly
agree) which is consist of positive and negative statement that indicate items scored direction
(Fowers & Olson, 1993). Items scored in negative direction would be reverse-scored (i.e if it
is mark 5, it would be scored 1; it is marked 4, it would be scored 2; a 3 remain unchanged).
The example item on Idealistic Distortion scale such as: “ My partner and I understand each
other perfectly”, “ My partner completely understands and sympathizes with my every
mood”. The example item on Marital Satisfaction scale such as : “ I am not pleased with the
personality characteristics and personal habits of my partner”, and “ I am very happy with
how we handle role responsibilities in our marriage”.
The EMS Scale provides a score for each partner. The complete scoring procedures
are available in Appendix D. EMS has been tested and performed high reliability in replica
studies across the countries range between .88 to .92 (Az & Caninsti, 2016; Fowers & Olson,
1993; Handayani & Harsanti, 2017; Salehi & Shahhosseini, 2017).
Translation and back-translation
The researcher will conduct translation and back translation method following
guideline from WHO, to produce the Indonesian version of Pregnancy-Related
Questionnaires Anxiety Revised-2, the Indonesian version of short form of Childbirth Self-
Efficacy Inventory, and the Indonesian version of ENRICH Marital Satisfaction Scale. The
four steps include: forward translation, back translation, pre-testing and cognitive interview
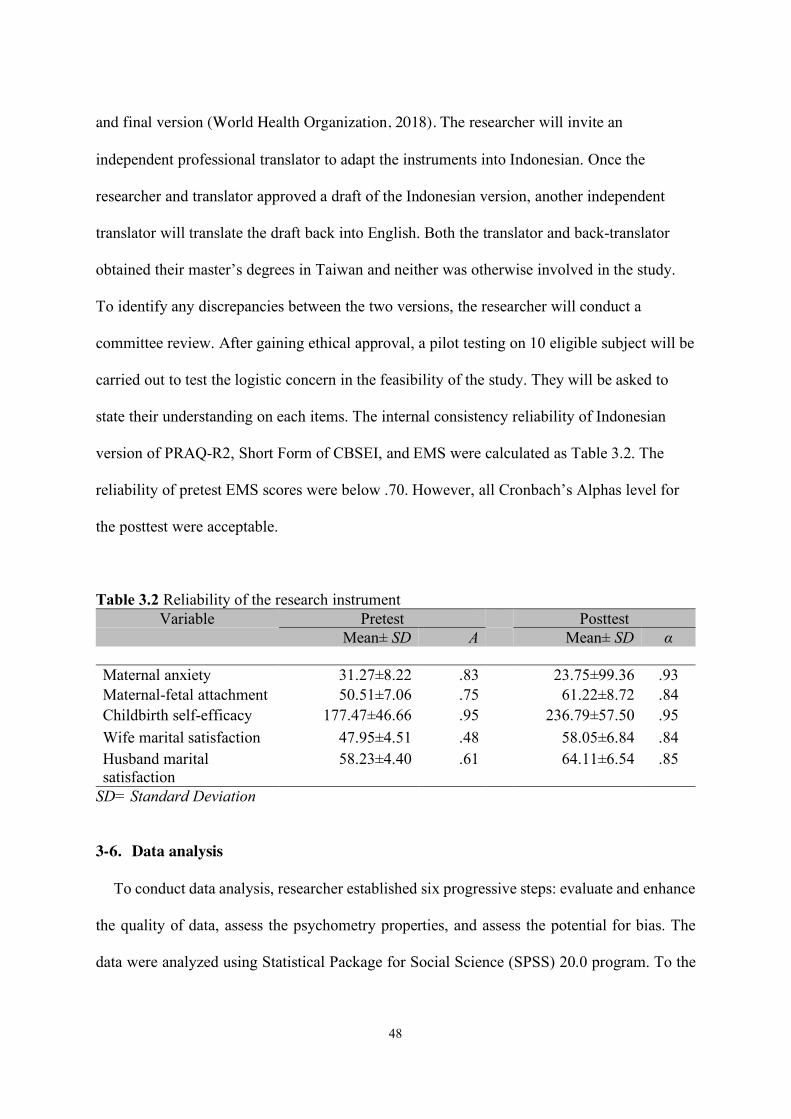
48
and final version (World Health Organization, 2018). The researcher will invite an
independent professional translator to adapt the instruments into Indonesian. Once the
researcher and translator approved a draft of the Indonesian version, another independent
translator will translate the draft back into English. Both the translator and back-translator
obtained their master’s degrees in Taiwan and neither was otherwise involved in the study.
To identify any discrepancies between the two versions, the researcher will conduct a
committee review. After gaining ethical approval, a pilot testing on 10 eligible subject will be
carried out to test the logistic concern in the feasibility of the study. They will be asked to
state their understanding on each items. The internal consistency reliability of Indonesian
version of PRAQ-R2, Short Form of CBSEI, and EMS were calculated as Table 3.2. The
reliability of pretest EMS scores were below .70. However, all Cronbach’s Alphas level for
the posttest were acceptable.
Table 3.2 Reliability of the research instrument Variable Pretest Posttest
Mean± SD Α Mean± SD α
Maternal anxiety 31.27±8.22 .83 23.75±99.36 .93 Maternal-fetal attachment 50.51±7.06 .75 61.22±8.72 .84 Childbirth self-efficacy 177.47±46.66 .95 236.79±57.50 .95 Wife marital satisfaction 47.95±4.51 .48 58.05±6.84 .84 Husband marital satisfaction
58.23±4.40 .61 64.11±6.54 .85
SD= Standard Deviation
3-6. Data analysis
To conduct data analysis, researcher established six progressive steps: evaluate and enhance
the quality of data, assess the psychometry properties, and assess the potential for bias. The
data were analyzed using Statistical Package for Social Science (SPSS) 20.0 program. To the

49
descriptive statistics, the comparison of quantitative data was performed using different
statistical method as described in Table 3.2. The researcher tested the effect of childbirth
education classes on four outcomes: pregnancy-related anxiety, childbirth self-efficacy,
maternal-fetal attachment, and marital relationship.
Table 3.3 Statistical method
No.
Research question
Independent/Dependent Variable
Types of data Analysis method
1. Describe the demographic statistic
Descriptive Percentage Descriptive statistic
2. Compare the demographic characteristic
Maternal age Interval Independent t-test Religion Nominal Chi-square Ethnicity Nominal Chi-square Educational background Ordinal Chi- square Gestational week Interval Independent t-test Occupation Nominal Chi-square Marital duration Interval Independent t-test Monthly income Nominal Chi-square 3. Tested the effect of
childbirth education to the 4 modes in the intervention group
Pregnancy-related anxiety Maternal-fetal attachment Childbirth Self-Efficacy Marital relationship
General Linear Model Per-Protocol
3-7. Ethical consideration
The researcher has obtain grant permission from instruments developers (see
Appendix E). Ethical approval was granted by ‘Aisyiyah University of Yogyakarta
(No.1303/KEP-UNISA/XI/2019). Informed consent from the pregnant women, anonymity
and the administration of questionnaire was conducted privately in the specific room and the
researcher assures the respondents that their information was limited as strictly confidential.
The researcher and assistance research have explained the nature and purpose study to the
respondents, and emphasized that participation was voluntary, and that they can the right to

50
withdraw from the study at any time without penalty. For the publication issue, only the
researcher and those directly involved with the study have access to the data.

51
CHAPTER IV
RESULTS
This chapter contains the result of this study. The contents will be divided into three
sections. The first section described the demographic information of the respondents. The
second section compared the baseline data of the maternal anxiety, maternal-fetal attachment,
childbirth self-efficacy, and marital satisfaction between two groups. The third section
presented the effectivity of the childbirth education program on the maternal anxiety,
maternal-fetal attachment, childbirth self-efficacy, and marital satisfaction between two
groups.
4-1. Demographic Information of the Respondents
The participants for this study were drawn from five public health centers in Yogyakarta,
Indonesia. The places were Mlati II, Jetis Kota, Mantrijeron, Kraton, and Godean I. In total,
there were 122 couples participated in this study consisting of 61 couples belonged to the
experiments group and 61 couples belonged to the control group. In such cases, some
participants were dropped out from the program. The final analysis after 4-weeks intervention
resulted 87 participants consisting of 52 couples in experiment group and 35 couples in
control group (see Figure 4.1).

52
Assessed for eligibility (n=152)
Randomized (n = 122)
Allocated to intervention childbirth education classes
(n=61)
Allocated to standard childbirth education class (n=61)
Enrollment
Allocation
Figure 4.1 CONSORT flow chart
Excluded (n = 60) Refused to participate (n = 15) Concern date and time (n=6) Other reasons (n=9)
Move to other area or cannot afford the schedule (n=12)
Loss of contact (n=14)
Move to another area before the class start (n=2) Premature labor (n=1) Move to other area(n=1) Loss of contact (n=5)
Analyzed (n=35)
Analyzed (n=52)
Analysis
Post-test after 4 weeks
Follow up
Post-test after 4 weeks

53
The missing subjects was about 28.6%. Independent t tests or Chi Square tests was
used to compare the demographic characteristics of the participants and missing subjects. The
results showed that these two groups were quite similar in couple’s occupation, education,
and maternal age. However, the participants had a lower maternal age than the missing
subjects (24.29 vs. 26.17, p<.05, Table 4.1).
Table 4. 1 Comparison of the demographic data between missing and non-missing participants (n=112)
Variables Attrition (n=35) Subject (n=87) Statistics (p) n % n %
Wife’s age (Mean, SD) 24.29 3.61 26.17 3.34 -2.76b (.007) Husband’s age (Mean, SD) 27.46 3.00 28.45 3.11 -1.61b (.110) Gestational week (Mean, SD) 30.23 2.39 30.20 1.76 0.08b (.933) Wife’s Occupation 1.95a(.162)
Unemployed 26 74.3 53 60.9 Employed 9 25.7 34 39.1
Husband’s Occupation Employed 35 100 87 100 ------
Wife’s Education 5.29a(.071) Elementary 15 42.9 23 26.4 High School 11 31.4 47 54.0 College 9 25.7 17 19.5
Husband’s Education 5.29a(.071) Elementary 6 17.1 6 6.9 High School 25 71.4 58 59.2 College 4 11.4 23 19.3
a= Chi Square; b= t test; SD= standard deviation According to table 4.2, there were a significant different in term of wife’s age, gestational
weeks, and couple’s education level in the control group. Mothers who complete the
program were older compare to those mother who missed the program (p < .05). Mothers
with older gestational age have complete the program compare to those mothers in the same
group (p < .001). Mother who graduated from high school were dominantly join the
complete program compare to those mothers who withdrawn from the program (p < .05).
Husband who graduated from high school were dominantly discontinued from the program
compare to those husband who complete the program (p < .05).

54
Table 4. 2 Comparison of the demographic data between missing and non-missing participants in the control groups (n=61)
Variables Attrition (n=26) Subject(n=35) Statistics (p) n % n %
Wife’s age (Mean, SD) 22.35 29.40 -17.07b (.007) Husband’s age (Mean, SD) 26.08 30.86 -9.47b (0.64) Gestational week (Mean, SD) 29.38 30.83 -.0.508b (<.001) Wife’s Occupation 1.95a(.162)
Unemployed 25 10 60.9 Employed 1 25 39.1
Husband’s Occupation Employed 26 100 35 100 ------
Wife’s Education 12.10(.002) Elementary 14 6 High School 6 23 College 6 6
Husband’s Education 4.30(.038) Elementary 2 5 High School 24 17 College 0 13
a= Chi Square; b= t test; SD= standard deviation
The baseline assessment for the demographic information such as couples’ gestational
week, couples’ education level, and couples’ occupation were also presented (Table 4.3).
Husbands were invited in this study since the curriculum address the couple topic including
the maternal-fetal attachment skill and marital relationship. To examine the difference of the
demographic variables between two groups, an independent t-test and Chi Square test were
applied. There was no significant difference mean score for gestational week, couple’s
education level, and couple’s occupation between two groups. However, there was a
significant difference mean score of the mothers’ age in the experiment and control groups (
p<.001). The participant’s age ranged from 20 to 35 years old, mean (SD)=23.92 (1.89) in
the intervention group and 20 to 28 years old, mean (SD)=28.40 (3.07) in the control group.
Husband’s age ranged from 22 to 36 years old in the intervention group and from 24 to 31
age in the control group. The gestational week ranged from 28 week to 33 week in the
intervention group, and from 28 week to 34 week in the control group. The age of the

55
participants and their partners significantly differed between two groups, and there was no
significant different in term of gestational week between two groups.
The Table also compared the frequency and percentage of couples’ education and
occupation across the groups. In the intervention group, almost 50% of the mothers graduated
from elementary-junior high school and senior high school, respectively, whilst mostly the
mothers graduated from senior high school in the control group. The experimental group’s
husband had a lower education level than the control group. The experimental group’s wife
had a higher percentage of the working mothers than the control group.
In summary, there was a significant difference between two groups on the couple’s
age, gestational week, husband’s education level, and mother’s occupation (see Table 4.2).

56
Table 4.3 The comparison of the demographic characteristics between the experimental and control groups
Wife Husband Characteristics Experiment
(n=52) Control (n=35)
t/χ2 p Experiment (n=52)
Control (n=35) t/χ2 p
n(%) n(%) n(%) n(%) Age (M±SD) (23.92±1.89) (29.14±2.10) -
12.08a <.001 (26.75±2.40) (30.86±2.20) -8.11a <.001
Gestational week(M±SD) (29.83±1.45) (31.04±1.80) -.3.45a .001 NA NA NA NA Education level Elementary 18(34.6) 6(17.1) 3.85b .146 1(1.9) 5(1.9) 11.33b <.001 High school 24(46.2) 23(65.7) 42(80.8) 17(48.3) College 10(19.2) 6(17.1) 9(17.3) 13(37.1) Occupation Employed 36(69.2) 22(62.9) 14.94b <.001 52(100) 35(100) NA NA Unemployed 16(30.8) 13(37.1) 0(0) 0(0)
a= t test; b= chi square

57
4-2. The comparison of the baseline of the maternal anxiety, maternal-fetal attachment,
childbirth self-efficacy and marital satisfaction
The comparison of the pretest score of the maternal anxiety, maternal-fetal attachment,
childbirth self-efficacy and marital satisfaction between two groups were presented in Table
4.4. Using independent t test, as the baseline of information presented, the mean score of the
maternal anxiety in the experimental group (28.23) was lower compared to the score in the
control group (35.97). While the wife’s mean score of the marital satisfaction in the
experiment group was higher compared to the wife’s score in the control group
(Experimental= 75.18 vs. Control= 63.09). Thus, there was a significant difference (p < .05)
in term of the maternal anxiety and the wife’s marital satisfaction throughout the groups.
However, as the maternal-fetal attachment, the childbirth self-efficacy, and the husband’s
marital satisfaction pretest score in the experiment group (49.40, 181.44, and 39.93,
respectively) had no significant difference mean with the score in the control group (50.56,
171.51, and 38.27, respectively, p>.05).
Table 4.4. The comparison of the baseline pretest scores between two groups
Variable Experiment (n=52) M±SD
Control (n=35) M±SD
p
Maternal anxiety 28.23±7.70 35.97±6.92 <.001 Maternal fetal-attachment 49.40±7.20 50.56±7.74 .482 Childbirth Self-efficacy 181.44±49.41 171.57±42.24 .336 Marital Satisfaction - Wife 75.18±10.45 63.09±10.89 <.001 - Husband 39.93±6.19 38.27±6.71 .240
M= mean; SD= standard deviation

58
4-3. The relationship among the maternal anxiety, maternal-fetal attachment, childbirth
self-efficacy, and marital satisfaction
The outcome measured were the maternal anxiety using the Pregnancy-Related
Anxiety Questionnaire Revised-2 (PRAQ-R2), the maternal-fetal attachment using the
Prenatal Attachment Inventory (PAI), the childbirth self-efficacy using the Childbirth Self-
Efficacy Inventory (CBSEI), and the marital satisfaction using the Enrich Marital Satisfaction
Scale (EMS scale). In the study, the Pearson’s correlation was used to analyze the
correlation for the outcome variables (Table 4.4). In the pretest measurement, Maternal
Anxiety (MA) had a significant negative correlation to the childbirth self-efficacy (CBSE)
(p<.01), the maternal-fetal attachment (MFA) (p<0.01), the wife’s idealistic distortion marital
(WIDM) (p<.05) and the wife marital satisfaction (WMS) (p<0.01). MA score had a negative
correlation with the score of CBSE, MFA, and WIDM (r =-.572, r = -.287, and r = -.226,
respectively, Table 4.4).
CBSE, had a significant negative correlation to the MA, whilst, it had a significant
positive correlation to the MFA (p<.01 for each). MFA had a significant negative correlation
to the MA, whereas, it had a significant positive correlation to the CBSE (p<.01 for each).
Wife ENRICH marital satisfaction (WEMS) had a positive correlation to its two subscales:
the wife’s idealistic distortion marital (WIDM) and the wife’s marital satisfaction (WMS)
(p<.01, Table 4.4), while WIDM had a significant negative correlation to the MA (r = -.226,
p<.01) (.432, p<.01) and had a positive correlation to the WEMS. Husband ENRICH marital
satisfaction (HEMS) corelated reciprocally to the Husband’s idealistic distortion marital
(HIDM) (r = .536 for each, p<0.01). However, for the husband’s marital satisfaction (HMS)
had no correlation to the others outcome variables including the maternal anxiety, the
maternal-fetal attachment, and the childbirth self-efficacy inventory. The detail information

59
could be seen in the Table 4.4. In the posttest measurement, the result was quite similar. For
detail information it could be seen in Table 4.5.

60
Table 4.5. Pearson correlation for pretest scores within outcome variables in the experimental (n= 52) and control groups (n =35)
MA CBSE MFA WEMS HEMS WIDM WMS HIDM HMS
Maternal Anxiety (MA) 1 Childbirth self-efficacy (CBSE)
-.572*** 1
Maternal-Fetal Attachment (MFA)
-.287** .607** 1
Wife ENRICH Marital Satisfaction (WEMS)
.182 -.060 .042 1
Husband ENRICH Marital Satisfaction (HEMS)
-.203 .098 .024 .050 1
Wife’s Idealistic Distortion Marital (WIDM)
-.226* .020 -.170 .432*** .038 1
Wife’s Marital Satisfaction (WMS)
.337** -.078 .146 .845** .032 -.117 1
Husband’s Idealistic Distortion Marital (HIDM)
-.106 -.015 -.031 -.111 .536** .012 -.129 1
Husband’s Marital Satisfaction (HMS)
-.204 -.018 .092 .060 .109 .029 .049 .185 1
*p < .05 ;** p< .01 ; *** p< .001

61
Table 4.6. Pearson correlation for posttest scores within outcome variables in the experimental (n= 52) and control groups (n =35)
MA CBSE MFA WEMS HEMS WIDM WMS HIDM HMS
Maternal Anxiety (MA)
1
Childbirth self-efficacy (CBSE)
-.857*** 1
Maternal-Fetal Attachment (MFA)
-.564*** .590*** 1
Wife ENRICH Marital Satisfaction (WEMS)
.107 -.086 -.113 1
Husband ENRICH Marital Satisfaction (HEMS)
.413*** -.405** -.241* -0.173 1
Wife’s Idealistic Distortion Marital (WIDM)
-.676*** .699*** .430*** 0.139 -.402*** 1
Wife’s Marital Satisfaction (WMS)
.532*** -.529*** -.376*** .763*** 0.114 -.534*** 1
Husband’s Idealistic Distortion Marital (HIDM)
-0.021 -0.026 0.155 -0.107 .232* 0.077 -0.141 1
Husband’s Marital Satisfaction (HMS)
.548*** -.505*** -.313** -0.163 .881*** -.481*** 0.175 .250* 1
*p < .05 ;** p< .01 ; *** p< .001

62
4.4 The effect of the childbirth education program on the maternal anxiety, maternal-
fetal attachment, childbirth self-efficacy and marital satisfaction
Due to the differences on some demographics data and baseline outcomes data, GLM
(General Linear Model) was used to adjust these demographics and baseline outcomes
variables to analyze the effect of the childbirth education program on the maternal anxiety,
maternal-fetal attachment, childbirth self-efficacy, and couple’s marital satisfaction.
a. The effect of the childbirth education program on the maternal anxiety
Table 4.7 described the effect of childbirth education program on the maternal anxiety.
The intervention group had a lower maternal anxiety score (-16.67) than the control group.
The increase of one point pretest anxiety score would increase 0.19 point of the posttest
maternal anxiety. The couple’s age, couple’s education level, couple’s marital satisfaction,
gestational weeks, maternal-fetal attachment, and childbirth self-efficacy were not related to
the maternal anxiety level.
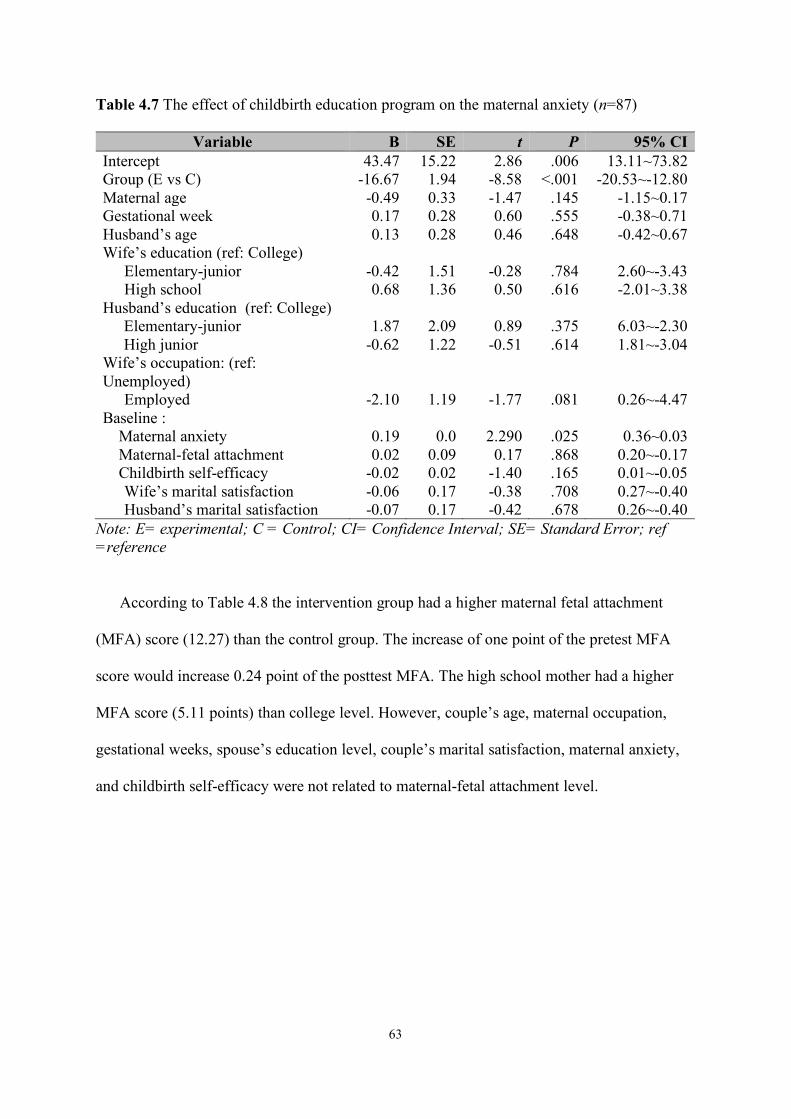
63
Table 4.7 The effect of childbirth education program on the maternal anxiety (n=87)
Variable B SE t P 95% CI Intercept 43.47 15.22 2.86 .006 13.11~73.82 Group (E vs C) -16.67 1.94 -8.58 <.001 -20.53~-12.80 Maternal age -0.49 0.33 -1.47 .145 -1.15~0.17 Gestational week 0.17 0.28 0.60 .555 -0.38~0.71 Husband’s age 0.13 0.28 0.46 .648 -0.42~0.67 Wife’s education (ref: College)
Elementary-junior -0.42 1.51 -0.28 .784 2.60~-3.43 High school 0.68 1.36 0.50 .616 -2.01~3.38
Husband’s education (ref: College) Elementary-junior 1.87 2.09 0.89 .375 6.03~-2.30 High junior -0.62 1.22 -0.51 .614 1.81~-3.04
Wife’s occupation: (ref: Unemployed)
Employed -2.10 1.19 -1.77 .081 0.26~-4.47 Baseline :
Maternal anxiety 0.19 0.0 2.290 .025 0.36~0.03 Maternal-fetal attachment 0.02 0.09 0.17 .868 0.20~-0.17 Childbirth self-efficacy -0.02 0.02 -1.40 .165 0.01~-0.05 Wife’s marital satisfaction -0.06 0.17 -0.38 .708 0.27~-0.40 Husband’s marital satisfaction -0.07 0.17 -0.42 .678 0.26~-0.40
Note: E= experimental; C = Control; CI= Confidence Interval; SE= Standard Error; ref =reference
According to Table 4.8 the intervention group had a higher maternal fetal attachment
(MFA) score (12.27) than the control group. The increase of one point of the pretest MFA
score would increase 0.24 point of the posttest MFA. The high school mother had a higher
MFA score (5.11 points) than college level. However, couple’s age, maternal occupation,
gestational weeks, spouse’s education level, couple’s marital satisfaction, maternal anxiety,
and childbirth self-efficacy were not related to maternal-fetal attachment level.

64
Table 4.8 The effect of childbirth education program on the maternal-fetal attachment (n=87)
Variable B SE t P 95% CI Intercept 13.10 22.97 0.57 .570 58.91~-32.71 Group (E vs C) 12.27 2.93 4.19 <.001 6.43~18.11 Maternal age 0.16 0.50 0.31 .757 -0.85~1.16 Gestational week 0.31 0.42 0.75 .458 -0.52~1.14 Husband’s age 0.04 0.42 0.09 .928 -0.79~0.87 Wife’s education: (ref: College)
Elementary-junior 2.75 2.28 1.21 .232 -1.79~7.30 High school 5.11 2.04 2.51 .014 1.04~9.18
Husband’s education : (ref: College) ● Elementary-junior -3.96 3.15 -1.26 .213 -10.25~2.33 ● High junior -1.95 1.84 -1.06 .293 -5.61~1.71
Wife’s occupation: (ref: Unemployed) Employed -0.28 1.79 -0.16 .874 -3.85~3.29
Baseline: Maternal anxiety -0.15 0.13 -1.22 .226 -0.40~0.01 Maternal-fetal attachment 0.24 0.14 1.74 .086 -0.04~0.52 Childbirth self-efficacy -0.02 0.02 -0.66 .514 -0.06~0.03 Wife’s marital satisfaction 0.07 0.25 0.28 .781 -0.44~0.58 Husband’s marital satisfaction 0.30 0.25 1.20 .236 -0.20~0.79
Note: E= experimental; C = Control; CI= Confidence Interval; SE= Standard Error; ref =reference
According to Table 4.9 the intervention group had a higher childbirth self-efficacy
(CSE) score (88.20) than the control group. The increase of one point of the pretest CSE
score would increase 0.39 point of the posttest CSE. The high school mother had a higher
CSE score (20.01 points) than college level. However, the couple’s age, couple’s marital
satisfaction, gestational weeks, maternal occupation, maternal anxiety were not related to the
CSE level.

65
Table 4.9 The effect of childbirth education program on the childbirth self-efficacy (n=87)
Variable B SE t p 95% CI Intercept 242.60 96.52 2.51 .014 50.16~435.05 Group (E vs C) 88.20 12.31 7.16 <.001 63.65~112.75 Maternal age 1.48 2.11 0.70 .485 -2.72~5.69 Gestational week -0.43 1.74 -0.25 .805 -3.91~3.04 Husband’s age -1.75 1.74 -1.00 .319 -5.23~1.73 Wife’s education: (ref: College)
Elementary-junior 13.09 9.58 1.37 .176 -6.01~32.18 High school 20.01 8.57 2.33 .022 2.92~37.09
Husband’s education : (ref: College) Elementary-junior 2.10 13.25 0.16 .875 24.33~-28.52 High junior 1.96 7.71 0.25 .800 13.42~-17.34
Wife’s occupation: (ref: Unemployed) Work 1.99 7.52 0.27 .792 -13.00~16.99
Baseline: Maternal anxiety -0.58 0.53 -1.09 .279 -1.63~0.48 Maternal-fetal attachment -1.09 0.59 -1.85 .069 -2.27~0.09 Childbirth self-efficacy 0.39 0.10 3.94 <.001 0.19~0.59 Wife’s marital satisfaction -0.05 1.07 -0.05 .960 -2.18~2.07 Husband’s marital satisfaction -0.83 1.05 -0.80 .428 -2.92~1.25
Note: E= experimental; C = Control; CI= Confidence Interval; SE= Standard Error; ref =reference
According to Table 4.10 the intervention group had a higher Wife’s Marital
Satisfaction (WMS) score (0.16) than the control group. The increase of one point of the
WMS pretest score would increase 0.24 point of the WMS posttest. The high score mother on
maternal-fetal attachment had a higher WMS score. The couple’s age, couple’s education
level, maternal occupation, maternal anxiety, childbirth self-efficacy, and husband’s marital
satisfaction, were not related to WMS level.

66
Table 4.10 The effect of childbirth education program on the Wife’s marital satisfaction (n=87)
Variable B SE t p 95% CI Intercept 38.29 8.20 4.67 <.001 21.94~54.65 Group (E vs C) 0.16 1.05 0.15 .878 -1.93~2.25 Maternal age 0.22 0.18 1.21 .229 -0.14~0.60 Gestational week 0.09 0.15 0.57 .569 -0.21~0.38 Husband’s age 0.00 0.15 0.02 .988 -0.29~0.30 Wife’s education: (ref: College)
Elementary-junior -0.85 0.81 -1.05 .299 -2.47~0.77 High junior -0.14 0.73 -0.19 .847 -1.59~1.31
Husband’s education : (ref: College) Elementary-junior -0.26 1.13 -0.23 .821 -2.50~1.99 High junior 0.17 0.66 0.26 .797 -1.14~1.48
Wife’s occupation: (ref: Unemployed) Employed 0.18 0.64 0.28 .779 -1.09~1.45
Baseline: Maternal anxiety -0.01 0.05 -0.16 .872 -0.01~0.08 Maternal-fetal attachment -0.11 0.05 -2.23 .029 -0.21~-0.01 Childbirth self-efficacy 0.01 0.01 1.51 .136 -0.00~0.03 Wife’s marital satisfaction 0.24 0.09 2.63 .010 0.06~0.42 Husband’s marital satisfaction -0.10 0.09 -1.10 .273 -0.28~0.08
Note: E= experimental; C = Control; CI= Confidence Interval; SE= Standard Error; ref =reference
According to Table 4.11 the increase of one point of the HMS pretest score would
increase 0.23 point of the posttest HMS. However, there was no significance difference
means score on the Husband’s marital satisfaction between intervention and control group.
The maternal anxiety and childbirth self-efficacy were significant contribution to the score of
HMS. The couple’s age, husband’s education level, maternal occupation, and maternal-fetal
attachment, were not related to HMS level.

67
Table 4.11 The effect of childbirth education program on the Husband’s Marital Satisfaction (n=87)
Variable B SE t P 95% CI Intercept 40.56 8.81 4.61 <.001 22.10~58.11 Group (E vs C) -1.48 1.12 -1.32 .191 -3.72~0.76 Maternal age 0.12 0.19 0.60 .549 -0.27~0.50 Gestational week 0.01 0.16 0.07 .948 -0.31~0.33 Husband’s age 0.16 0.160 0.98 .331 -0.16~0.47 Wife’s education: (ref: College)
Elementary-junior -0.26 0.87 -0.30 .765 -2.00~1.48 High junior -0.33 0.78 -0.42 .677 -1.89~1.23
Husband’s education : (ref: College) Elementary-junior -0.06 1.21 -0.05 .960 -2.47~2.35 High junior -1.44 0.70 -2.04 .045 -2.84~-0.03
Wife’s occupation: (ref: Unemployed)
Employed 0.23 0.69 0.41 .687 -1.09~1.65 Baseline:
Maternal anxiety -0.01 0.05 -2.01 .048 -0.19~-0.00 Maternal-fetal attachment 0.02 0.05 0.39 .696 -0.09~0.13 Childbirth self-efficacy -0.02 0.01 -2.25 .027 -0.04~-0.00 Wife’s marital satisfaction -0.03 0.01 -0.28 .780 -0.22~0.17 Husband’s marital satisfaction 0.23 0.01 2.42 .018 0.04~0.42
Note: E= experimental; C = Control; CI= Confidence Interval; SE= Standard Error; ref =reference

68
CHAPTER V
DISCUSSION
This study answered three research questions. First, the result study on the
demographic characteristics described the mean of the couple’s age were 23.92 and 26.75
(Female and Male, respectively) in the experimental group, and 29.14 and 30.86 (Female and
Male, respectively) in the control group. As for the gestational age, the mean of the week was
29.83 in the experimental group and 31.04 in the control group. In both groups, the couple
mostly graduated from high school and more than 50% of the mothers go to work.
Second, in the study, the researcher found the significance difference between two
groups on the demographic data including the couple’s age, gestational week, husband’s
education level, and wife’s occupation. The researcher lost more than twenty percent
participants in the study. This may due to the Covid-19 pandemic which just began in
Indonesia. Another reason maybe because the missing participants did not gain the
knowledge as their expectation. Moreover, the class in the experimental group was set-up to
be more flexible than in the control group due to some participants who had to adjust with
their working hours. Therefore, maybe there was another cause why the observed group lost
many participants compared to the intervention group.
In this study, the researcher used five instruments to measure the variable outcomes;
Pregnancy-Related Anxiety-2 Revised (PRAQ2-R), Prenatal Attachment Inventory (PAI),
Childbirth Self-Efficacy Inventory (CBSEI), and ENRICH Marital Satisfaction Scale (EMS).
Excluding EMS scale, the researcher used the existing Indonesian version instruments that
had been translated and validated by the author and other researchers. To produce Indonesian
version of EMS scale, translation and back-translation process following WHO guideline
were conducted. The steps included forward translation and backward translation by

69
independent translators to produce the preliminary draft of the Indonesian version of EMS.
Furthermore, committee review by the researcher and those two translators aimed to counter
some discrepancies and cultural context from the draft. Then, three experts in the field had
been invited to provide their judgement using content validity index to determine the validity
content for each item which resulted the final draft of the Indonesian version of EMS. As the
last step, testing the translated version to the targeted subject had been conducted. For the
reliability concern, all the Indonesian version of the instruments are distributed to the mothers
during pre and posttest as well as to the husband for the marital satisfaction measure tool.
5-1. Descriptive statistic of the demographic characteristic of the participants
This study conducted in five health public health centers (Puskesmas), namely
Puskesmas Mlati II, Puskesmas Jetis Kota, Puskesmas Mantrijeron, Puskesmas Godean I, and
Puskesmas Kraton Yogyakarta Province. The participants were recruited based on the block
random allocation for each public health center. In the experiment group, the researcher set
the optional schedule based on the participants’ availability and let them to choose one or
more of their availability time. As for the final confirmation to the participants, the researcher
sent the reminder including the place, date and time through an online group. Husband or
family companion were encouraged to join in the class. The session lasted for 180 minutes
once a week and had been set-up in the well-equipped mini laboratory of ‘Aisyiyah
University lab skill for four weeks. Using the guideline, the topic of the content was flexible
and developed progressively according to the participant’s need and suggestion during the
discussion session. The researcher also created an online group through WhatsApp©
messenger application for communication and to handle issue, while in the control group
there was no such online group. In the control group, the date and time for regular childbirth
education class had been set-up and then confirmed by the midwives during participants’

70
antenatal care examination schedule. The duration and number of weeks were the same as in
the intervention group. The couple was also encouraged to join the class.
In general, following the protocol, the study was conducted while the outbreak of Covid-
19 began to hit Indonesia in the early February 2020. This might be the cause of the attrition
rate is quite high in this current study. Compared to the experiment group, the reduced
number of the participants in the control group were higher. In detail, according to the
comparison between the missing and non-missing subjects, there was a significant difference
mean in some demographic data, such as couple’s age, gestational weeks and mothers’
occupation. The couple’s mean age in the control group was higher compared to the couples’
mean age in the experimental group. The majority of the younger couples discontinued the
program in the control group. Some young expectant mothers decided to stop joining the
class in the control group might be because they move to another area or their hometown to
seek psychological support from their family when delivering the baby.
According to the result, a significant difference mean of the demographic characteristic
also had been found in the term of the mother’s occupation. In the control group, the
presentation of the employed mother was lower than in the experimental group. Time factor
may be the cause of this loss of follow ups since in the experimental group the participants
could reschedule the class according to their availability time. Thus, the sustainability of the
participant’s presence was gained in the experimental group. The result analysis on the
baseline data showed a significant difference on the maternal anxiety and the wife’s marital
satisfaction. In the experiment group, the anxiety level score was lower than in the control
group, while the wife’s marital satisfaction score in the experiment group was higher than in
the control group. Compared to the wife’s marital satisfaction, it was found that the
husband’s marital satisfaction had lower score in both groups.

71
The correlation among outcome variable had been also confirmed in this study. In the
pretest measurement, the maternal anxiety had a negative correlation with the the maternal-
fetal attachment, the childbirth self-efficacy and the husband’s marital satisfaction. The
maternal anxiety correlated positively to the wife’s marital status. The posttest correlation
analysis was quite similar with the pretest result. The finding result had been confirmed by
the previous study conducted by Abazari et al. (Abazari, Pouraboli, Tavakoli, Aflatoonian, &
Kohan, 2019).
5-2. The effect of the childbirth education program on prenatal anxiety, childbirth self-
efficacy, maternal-fetal attachment, and marital satisfaction
In this study, the effectiveness of a four-week childbirth education program to
decrease maternal anxiety, improving maternal-fetal attachment, childbirth self-efficacy and
marital satisfaction were tested. According to the results, the maternal anxiety had decreased
significantly and the maternal-fetal attachment as well as the childbirth self-efficacy had
increased significantly among mothers after the intervention, compared to the mothers who
merely received standard childbirth education program. The marital satisfaction did not
significantly change among mothers and husbands in two groups. To elaborate each variable
outcome, the explanation is presented as follows.
5-2.1 The effect of the childbirth education program on the prenatal anxiety
The result of the covariate test showed that the mothers who participated in the
intervention group had lower score of anxiety in the past 4 weeks program, compared to the
mothers who participated in the control group (p<.001). The finding indicated that the set-up
childbirth education program was effective in decreasing maternal anxiety in the third
trimester of pregnancy. However, mother’s education level, gestational weeks, couple’s
marital satisfaction, maternal-fetal attachment, and childbirth self-efficacy were not related to

72
the maternal anxiety level. Senior researcher, Bastani et al. (2006) reported the congruent
result. They conducted a 7-week class focused on the relaxation practice skill for a-52 first
time expectant mothers in Iran. Furthermore, the study described the importance of relaxation
technique during pregnancy in decreasing anxiety and its impact to the pregnancy outcome.
Mothers who participated in the intervention group performed more normal vaginal delivery
than those in the control group (p <.001). In the study, the mothers who participated in the
intervention group more less likely delivered baby with low birth weight than those in control
group (p<.05). The mothers who participated in the intervention group have higher baby’s
birth weight average than those in the control group (p<.05) (Bastani, Hidarnja, Montgomery,
Aguilar-Vafaei, & Kazemnejad, 2006). However, the conflicting result was found on some
demographic variables compared to the current study. Bastani and colleagues mentioned that
the mothers’ education level and the marital dissatisfaction did not correlate to the maternal
anxiety as well as the maternal-fetal attachment.
Yikar in 2019 conducted a randomize control trial for a-30 first time expectant mothers
who experienced some complains during their pregnancy that may lead to their anxiety.
Yikar created a booklet as a part of the prenatal education to educate 30 pregnant women in
the intervention group containing common complaint during pregnancy, the reason of their
complaint and how to cope with the complaint. While for 30 pregnant women in the control
group, they did not receive any intervention except from routine nursing care in the hospital.
After the program was conducted for the three meetings, mostly women in the intervention
group experienced less anxiety than those in the control group (Yikar, 2019). However, in
the current study, the researcher conducted the learning method to address mothers’ anxiety
during pregnancy. The learning method included the lecturing of anatomy and physiology of
pregnancy, demonstrating and practicing comfort measures to overcome some common
complaints during pregnancy. The program was delivered for four weeks and lasted for 120

73
minutes for every session. To address the maternal anxiety, some relaxation techniques to
release such tension due to discomfort during pregnancy and for labor preparation were
provided.

74
5-2.2 The effect of the childbirth education program on the maternal-fetal attachment
The maternal-fetal attachment can be established during the pregnancy, some particular
behaviors can be applied, for instance calling the baby with name, imagining the baby’s face,
observing and monitoring the baby’s movement, talking to the baby frequently, and buying
some stuffs for the baby. According to the result, the maternal-fetal attachment score in the
experimental group was higher than in the control group (p< .05). The mother’s level of
education correlated with the maternal-fetal attachment score. This result contradicted the
study conducted by Bastani and colleagues in 2006. Their study result showed that there was
no statistically correlation between the maternal fetal-attachment and the mother’s education
level. In the current study, the maternal-fetal attachment did no relate to the couple’s age,
maternal occupation, gestational weeks, spouse’s education level, childbirth-self-efficacy,
couple’s marital satisfaction, maternal anxiety, and childbirth self-efficacy. Gheibi,
Abbaspour, Hosein and Javdifar (2020) tested the effectiveness of childbirth program on the
maternal-fetal attachment. They invited 40 pregnant women to participate in their
randomized study for seven weeks. The childbirth program focused on the mindfulness-based
childbirth and parenting program. The class was set-up for 3 hours for each session once a
week. The participants in the intervention group performed significantly higher mean scores
of maternal-fetal attachment than those in the control group (Gheibi, Abbaspour, & Hossein,
2020). Other study recorded the identical finding (Serçekuş & Başkale, 2016).
Having a baby is a great and challenge phase for the male who are experiencing being a
father for the first time. The father’s emotion needs to be facilitated to gain knowledge and
experience to empower themselves as the wife’s partner during the childbearing process.
Therefore, 52 husbands or mother’s relatives were invited to be trained on the maternal-fetal
attachment in the experimental group, while 35 husbands were invited in the control group.

75
In doing so, the husbands in the experimental group were trained regarding to the attachment
skill and practice the behavior of attachment at home. After the class, as the reminder session,
the husbands were followed up through massage contact and were asked to transfer their
information to their wives. The implication of husband’s involvement in the maternal-fetal
attachment behavior was supported by other study conducted by Akbarzade and colleagues in
2014. They investigated the effectivity of the father’s training regarding attachment skills on
the maternal-fetal attachment. In their randomized trial, 150 qualified pregnant women were
invited to complete the pretest of the maternal-fetal attachment questionnaire as well as the
anxiety measurement. After one month of intervention, the maternal-fetal attachment was
repeated and measured by the researcher and the result indicated that the posttest on the
variables was higher than those in the pretest. The maternal-fetal attachment score also
indicated to be higher in the experimental group than those in the control group (Akbarzade,
Setodeh, & Sharif, 2014). However, in that study, the intervention merely took part in four
90-minutes sessions, while in the current study, the fathers were trained for particular skill in
60-minutes sessions and additional practice at home.
5-2.3 The effect of the childbirth education program on the childbirth self-efficacy
The efficacy, according to Bandura, was from the performance accomplishment,
vicarious experience, social persuasion, and physiological and emotional states. The
childbirth self-efficacy was the mother’s ability to cope with the childbirth process. Using
Bandura’s guideline, this childbirth education material was set-up to address the maternal
efficacy to have childbirth process through four sources of efficacy. This resulted that the
women in the experimental group had higher score of self-efficacy to have childbirth process
than women in the control group. The test indicated that the childbirth education program
was effective to increase the mother’s efficacy on childbirth. The congruent study conducted

76
by Sercekus and Baskale in 2016. They investigated the effectiveness of the antenatal
education on some variables including the maternal self-efficacy on childbirth. The class was
set-up for four to six couples every once a week (120 minutes). The total training was 16
hours and the content material included nutrition during pregnancy and the postpartum
period, physiological and psychological changes during pregnancy and how to cope with
these changes. They also included the content regarding the mechanism of labor and birth and
provided discussion on the feeling about childbirth coping with the labor pain and many
more. After eight weeks education classes, they found that the maternal self-efficacy had
increased significantly compared to the two groups (p value= .002) (Serçekuş & Başkale,
2016).
5-2.3 The effect of the childbirth education program on the marital satisfaction
According to the result, most of the instruments possessed a high internal consistency
at those time points. However, the pretest result of EMS scale for the wife participants solely
possessed low level of internal consistency, while the posttest reliability possessed high level
of internal consistency. In the pretest, some particular items would be resulted in a higher
Cronbach alpha if it was deleted. The items were “I am very pleased about how we express
affection and relate sexually’ and "I am dissatisfied about our relationship with my parents,
in-laws, and/or Friends”. Sexuality is a basic need of physical expression and affection
expression which is belonging and being related with someone (Marlow, Tolley, Kohli, &
Mehendale, 2012). In fact, in our culture, sexuality issue remains vague and taboo (Fujiati,
2016; Susilaningsih & Saluhiyah, 2013; Triani, 2020). Communication about sexuality
between couples rarely happened. In the study, the researcher did not explore whether they
live together with other relatives such as parents, in-laws and/or friends or not. However,
mostly people do not want to share their feeling about their parents, in-laws, and or friend in

77
front of their couple. Culture is the most reason why they possess this attitude. Therefore, in
this item scale, the female participants provided inappropriate answer that may lead to the
low level of Cronbach’s Alpha. This instrument consisted of 15-likert scale composed by two
dimensions; idealistic distortion and marital satisfaction, which had negative and positive
statement. Different from other three tools, EMS scale was solely instruments which had
those negative and positive items. Prior to the questionnaire’s distribution, the researcher
explained to the participants the procedure to fill and asked them to pay attention to the
instruction of each scale. The researcher distributed all of the four scales in the same time just
before the class began. Therefore, it was assumed that the majority of the wife participants
did not fully pay attention to the negative mark on such scale, that may lead to the low level
of internal consistency during the pretest measurement.
The marital satisfaction scores were gained from the wife and the husband. The
finding confirmed that there was no significant difference of the mean score of WMS in the
experimental group and in the control group. This finding was in line with the previous study.
Daley-McCoy et al (2015) conducted a cluster randomized controlled trial to investigate the
couple relationship program during the pregnancy. Using analysis of variance (ANCOVA),
they reported that the women in the intervention group significantly less deterioration in
couple communication compare with women in the control group (Daley-McCoy, Rogers, &
Slade, 2015). However, maternal-fetal attachment, maternal anxiety and husband marital
satisfaction had no contribution to the score of WMS.
In contrast, there was no significant mean difference of HMS in the experimental
group and in the control group. Maternal anxiety and childbirth self-efficacy score had
contributed to the score of HMS, while maternal-fetal attachment had no contribution to the
score of HMS. Interestingly, it was found that the pretest score of HMS was lower than WMS
in both groups. This may due to the culture issue in our country. The researcher considered
78
this issue as the part of the project to enhance the quality of marital relationship. As the
prenatal course was developed in line with the participant’s need, the basic material to
maintain couple communication was modified. For example, the researcher provided “letter
session” for couples to express their feeling, thought and expectation of their partner during
pregnancy following after birth (including sexuality topic and family problem). They were
asked to write down the letter and give it to their partner. Furthermore, the husbands were
allowed to stroke the wife’s head as common love expression in our culture. The glimmer of
light in the room and slow romantic back sound music were adjusted during this session. This
intervention may lead the reliability in the posttest of the wife’s marital satisfaction to be
higher than in the pretest. Another interesting finding in the study was the mean score of the
husband’s marital satisfaction was lower than the mean score of the wife’s marital
satisfaction in both groups.

79
CHAPTER VI
CONCLUSION AND RECOMMENDATIONS
6-1. Conclusion
This study was addressed the research questions. In both groups, mostly the couples
graduated from high school and majority of the mothers go to work. In the current study, the
researcher found the significance difference between two groups in the demographic data
including couple’s age, gestational week, husband education level, and wife’s occupation.
The average mean of the couple’s age in our study who completed the program was younger
than those who missed the program. However, the couple’s occupation, education, and
maternal age were quite similar between two groups. It could be concluded that the childbirth
education program based on Roy Adaptation Model, which included three hours session with
topic and learning method modification, held once a week for four weeks, may be quite
effective in decreasing the maternal anxiety, improving maternal-fetal attachment, childbirth
self-efficacy and marital satisfaction.
6.2 Study Implications
The researcher prepared the prenatal education class following the health authority
guidelines. As an effort to promote the outcome variable according to Roy’s Adaptation
Model and to achieve learning needs of couple’s, the researcher considered to arrange the
material outline according to the participant’s suggestion. As adopted from the guidelines, the
learning method also has been modified according to the outline. The researcher conducted
lecture method for some basic knowledge about pregnancy, labor and delivery. The practice
was conducted for some skills and the discussion was conducted for solving some problems.
The researcher explored the couples’ thought and feeling as well as their expectation to their

80
partner during discussion sessions. The modified class was implied to change the couple’s
perspective on the discussion about sexuality with their partner and discussed the
uncomfortable feeling to their partner.
The husbands or other relative were encouraged to engage in practicing the skills,
such as how to apply the comfort measure, how to bath the baby, how to change baby’s
diaper, and how to establish attachment to the baby. The practice session has implied to the
husband’s motivation to actively take a part during the class. The discussion session had
stimulated the husbands to learn about their role during pregnancy, labor and delivery and
raised many questions from them during the session. Importantly, this program had implied
the mothers to perceive ability to manage their anxiety, increase their efficacy for the birth
process, engage in the maternal-fetal attachment skill, and change the intimate
communication pattern to the couple.
Based on that, the researcher may suggest for the health policy maker to consider that
the standard prenatal education program need to be modified. The prenatal education
program needs to include the material that is sensitive to be discussed between couple. The
prenatal education program also needs to consider the importance of the husband’s
engagement during the class and give them the chance to learn. The variation of the class
learning method also needs to take into account. As valid and reliable instruments are
confirmed in this current study, the researcher also may suggest the policy maker to include
the screening test for all pregnant women in the last trimester using those tools.
The midwives as the facilitator in the prenatal education program are expected to be
more innovative to modify the class to be attractive. Since couple may have different basic
knowledge and expectation and what they want to learn during the class, the Midwives may
conduct a learning contract prior to the class started. The current prenatal education programs
offers the innovation to bridge the gap between the couple and the healthcare provider. In the

81
study, the researcher used free online group discussion for couples to monitor their
attachment skill outside the class and to facilitate them to raise question on such matter and
even for free consultation. Considering that, the Midwives are suggested to provide such
innovation to increase the interaction between couples and certain health care providers
during their participation in the program. The midwives are also suggested to encourage the
husbands or other relative to attend the prenatal class.
As a theory-based intervention, this finding is expected to provide evidence to
enhance the effectivity of the modified childbirth education program. Compared to the
standard childbirth education program, the modified classes were emphasized on the variance
of the learning methods based on the topic and learning outcomes. The researcher also
conducted more discussion sessions with the mothers and their partner to explore their
thought and feeling, including their pregnancy and birth-related concern that may arise during
pregnancy. The community support for the couple during pregnancy was provided through
the participants’ group online. The researcher may underline that this new approach on the
childbirth education program could be effective in broaden the couple’s knowledge and skills
to promote their preparation to get ready for labor and delivery process. All in all,
considering the impact of this finding result, the leadership and the midwives’ perspective to
incorporate this modified classes to the existing program in Indonesia seems to be key to the
application of the research result in the clinical practice.
However, some limitations should be noted in this study. First, each class lasts for
three hours per session. For practicing and discussing session, this duration seems too short
and results in overtime session. In contrast, for lecturing session, the duration seems too long.
Therefore, the researcher would suggest to adjust the duration based on the topic and the
learning method but still has the same total hours as the guidelines (12 hours). Second, as the
pretest of the marital satisfaction indicated low level of the internal consistency, and the

82
possibility that the instrument may not be really appropriate to our population or culture, the
researcher suggests to consider to delete or add some items that are appropriate with the
culture. Third, since the primary investigator functions as the facilitator during the program,
yet as a data collector, the researcher acknowledges this as the limitation in this current study.
Considering that, the bias may arise due to the participants are recruited as an intervention
subject that may lead to the subjective measurement. Fourth, the study was started whilst
situation was normal, however, the ongoing data collection was interrupted by the Covid-19
pandemic in Indonesia. Unfortunately, the facilitators in the control group just began the class
as late as their time availability while the restriction regulation is just released by the
government. This resulted higher attrition rate in the control group compared to the
experimental group.
6-3. Suggestion for the future research
Since the researcher only invited expectant mothers with normal pregnancy and
measured their outcome variables, for the next study it could be considered to invite pregnant
women with complication to test the efficacy of the prenatal education program on the
pregnancy outcomes. The next future study also needs to take into account to measure the
correlation of the variable outcomes to the postnatal event, therefore, longitudinal study
needs to be conducted. As a quantitative approach, the researcher only measured the variable
outcomes based on the questionnaire. Therefore, it is the researcher’s limitation to explore
what participant perceived in the prenatal education program. The future study must consider
to apply a qualitative approach through in-depth interview to gain couples’ understanding and
experience during their participation in the prenatal education program. This study result
functions as a crucial information resource to provide an evidence based to improve a better
prenatal education program in the next future. Importantly, the next study needs to consider

83
the identical study using double or triple blinded method to prevent bias that may affect to the
result. In addition, objective scale to measure the research outcome may consider as the
important recommendation for future research.

84
REFERENCES
Abasi, E., Tafazzoli, M., Esmaily, H., & Hasanabadi, H. (2013). The effect of maternal-fetal attachment education on maternal mental health. Turkish Journal of Medical Sciences, 43(5), 815–820. https://doi.org/10.3906/sag-1204-97
Abasi, E., Tahmasebi, H., Zafari, M., Gholamreza, & Takami, N. (2012). Assessment on effective factors of maternal-fetal attachment in pregnant women. Life Science Journal, 9(1 Supplemen.), 68–75. https://doi.org/10.7537/marslsj0901s12.12
Abazari, F., Pouraboli, B., Tavakoli, P., Aflatoonian, M., & Kohan, M. (2019). Anxiety and its relationship with maternal-fetal attachment in pregnant women in Southeast of Iran. I-Manager’s Journal on Nursing, 7(January), 16–27. https://doi.org/10.26634/jnur.7.3.13788
Abu, G., & Al, M. (2012). A critical analysis of using Roy’s adapatation model in nursing research. International Journal of Academic Research, 4(4), 26–31. https://doi.org/https://doi.org/10.7813/2075-4124.2012/4-4/b.3
Abujilban, S., Sinclair, M., & Kernohan, W. G. (2012). The translation of the childbirth self-efficacy inventory into Arabic. Evidence Based Midwifery, 10(2), 45–49.
Aeni, N. (2011). Risk Factors of Maternal Mortality. Jurnal Kesehatan Masyarakat Nasional, 7(26), 453–459. https://doi.org/https://doi.org/10.21109/kesmas.v7i10.4
Agustiningsih, N. (2017). The efficacy of the childbirth education class program to the knowledge of nutrition, anemia status, chronic energy defisit and low birth weight in Grogol, Sukoharjo. Universitas Muhammadiyah Surakarta.
Ainsworth, M. D. (1969). Object relations, dependency and attachment: A theoretical review of the mother-infant relationship. Child Development, 40, 969–1025. https://doi.org/http://dx.doi.org/10.2307/1127008
Akbarzadeh, M., Dokuhaki, A., Joker, A., Pishva, N., & Zare, N. (2016). Teaching attachment behaviors to pregnant women: a randomized controlled trial of effects on infant mental health from birth to the age of three months Marzieh. Annals of Saudi Medicine, 36(3), 175–183. https://doi.org/10.5144/0256-4947.2016.175
Akbarzadeh, M., Toosi, M., Zare, N., & Sharif, F. (2011). Effect of learning attachment behaviors on anxiety and maternal fetal attachment in first pregnant women. Evidence Based Care, 1(1), 21–34. https://doi.org/10.22038/ebcj.2011.3762
Alipour, Z., Kheirabadi, G. R., Kazemi, A., & Fooladi, M. (2018). The most important risk factors affecting mental health during pregnancy : a systematic review, 24(6). https://doi.org/https://doi.org/10.26719/2018.24.6.549
Alligood, M. ., & Tomey, A. . (2010). Nursing Theories and Their Work 7th Edition (7th ed.). United Stated: Mosby Elsevier.
Alvianty, F. ., & Suryaningsih, E. . (2016). Hubungan dukungan keluarga dengan matrenal-fetal attachment pada ibu hamil trimester III di Puskesmas Jetis kota Yogyakarta. Universitas ’Aisyiyah Yogyakarta, Yogyakarta. Retrieved from http://digilib.unisayogya.ac.id/1992/1/FEenny Nur Alvianty_201510104385_naskah publikasi.pdf
Alza, N., & Ismarwati. (2017). Faktor-faktor yang mempengaruhi kecemasan ibu hamil trimester III (faktors influence mother anxiety in third trimester). Kebidanan Dan Keperawatan, 13(1), 2. https://doi.org/https://doi.org/10.31101/jkk.205
Amanak, K., Sevil, U., & Karacam, Z. (2019). The impact of prenatal education based on the roy adaptation model on gestational hypertension, adaptation to pregnancy and pregnancy outcomes. The Journal of the Pakistan Medical Association., 69(1), 11–17.

85
Retrieved from https://search.proquest.com/docview/2165660119?accountid=8000 American Society for Reproductive Medicine. (2012). Multiple pregnancy and birth : twins ,
triplets , and high-order multiples. In Patient Information Series. Andersson, I., Nilsson, S., & Candidate, R. N. (2012). How women who have experienced
one or more miscarriages manage their feelings and emotions when they become pregnant again – a qualitative interview study, (4). https://doi.org/10.1111/j.1471-6712.2011.00927.x
Anonymous. (2008). ICEA position paper: the role of the childbirth educator and the scope of childbirth education. International Journal of Childbirth Education, 22(4), 34–42. Retrieved from http://search.proquest.com/docview/212806549?accountid=14732%5Cnhttp://bd9jx6as9l.search.serialssolutions.com/?ctx_ver=Z39.88-2004&ctx_enc=info:ofi/enc:UTF-8&rfr_id=info:sid/ProQ:nahs&rft_val_fmt=info:ofi/fmt:kev:mtx:journal&rft.genre=article&rft.jtitle=I
Aprilia, Y. (2019). Pregnancy. Retrieved May 13, 2019, from http://www.bidankita.com/category/pregnancy/
Arcamone, A. . (2005). The effect of prenatal education on adaptation to motherhood after vaginal childbirth in primiparous women as assessed by Roy’s four adaptive modes. Widener University School of Nursing. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=ccm&AN=109846355&site=ehost-live
Aryani, F., Raden, A., & Ismarwati. (2016). Senam hamil berpengaruh terhadap tingkat kecemasan pada primigravida trimester III di rskia sakina idaman sleman (pregnancy exercisei nfluenced the level of anxiety). Indonesian Journal of Nursing and Midwives, 4(3), 129–134. https://doi.org/https://doi.org/10.21927/jnki.2016.4(3).129-134
Ayub, N. (2014). Development of marital satisfaction scale. Pakistan Journal of Clinical Psychology, 9(1), 19–34. Retrieved from https://www.researchgate.net/publication/231026047
Az, S., & Caninsti, R. (2016). Hubungan antara kepuasan pernikahan dengan spiritualitas pada istri bekerja yang berada dalam tahap pernikahan families with school children (Correlation Between marriage satisfaction and spirituality towards working wives in the stages of marriage family. Jurnal Psikogenesis, 4(2), 215–223. https://doi.org/https://doi.org/10.24854/jps.v4i2.351
Badr Naga, B., & Al-atiyyat, N. (2013). Roy adaptation model: a review. Middle East Journal of Nursing, 7(January 2013), 58–61. https://doi.org/https://doi.org/10.5742/mejn.2013.71220
Bahrami, N., Simbar, M., & Bahrami, S. (2013). The effect of prenatal education on mother ’ s quality of life during first year postpartum among iranian Women : a randomized controlled trial. International Journal of Fertility and Sterilisity, 7(3), 169–174. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3914493/pdf/Int-J-Fertil-Steril-7-169.pdf
Bandura. (1998). Self-efficacy. In V. S. Ramachaudran (Ed.), Encyclopedia of human behavior (Vol. 4, pp. 71-81). New York: Academic Press. (Reprinted in H. Friedman [Ed.], Encyclopedia of mental health., 4(1994), 71–81. https://doi.org/10.1002/9780470479216.corpsy0836
Bastani, F., Hidarnja, A., MOntgomery, K., Aguilar-Vafaei, M., & Kazemnejad, A. (2006). Does Relaxation Education in Anxious Primigravid Iranian Women Influence Adverse Pregnancy Outcomes ? Journal Perinatal and Neonatal Nursing, 20(2), 138–146.
Baxter, R., Hastings, N., Law, A., & Glass, E. J. . (2008). Postpartum depression and sleep loss in first time mothers. University of California, San Fransisco.

86
Bayrampour, H., Ali, E., Mcneil, D. A., Benzies, K., Macqueen, G., & Tough, S. (2016). Pregnancy-related anxiety : a concept analysis. International Journal of Nursing Studies, 55, 115–130. https://doi.org/10.1016/j.ijnurstu.2015.10.023
Bayrampour, H., Ali, E., McNeil, D. A., Benzies, K., MacQueen, G., & Tough, S. (2016). Pregnancy-related anxiety: A concept analysis. International Journal of Nursing Studies, 55, 115–130. https://doi.org/10.1016/j.ijnurstu.2015.10.023
Bayrampour, H., Heaman, M., Duncan, K. A., & Tough, S. (2013). Predictors of Perception of Pregnancy Risk among Nulliparous Women. Journal of Obstetric, Gynecologic & Neonatal Nursing, 42(4), 416–427. https://doi.org/https://doi.org/10.1111/1552-6909.12215
Beddoe, A. E., Lee, K. A., Weiss, S. J., Kennedy, H. P., & Yang, C. P. (2010). Effects of mindful yoga on sleep in pregnant women : a pilot study. Biological Research for Nursing, 11(4), 363–370. https://doi.org/10.1177/1099800409356320
Beger, D., & Beaman, M. L. (1996). Childbirth education curriculum: an analysis of parent and educator choices. The Journal of Perinatal Education, 5(4), 29–35. Retrieved from http://turing.library.northwestern.edu/login?url=http://search.proquest.com/docview/203562064?accountid=12861%5Cnhttp://hopper.library.northwestern.edu/sfx?genre=article&sid=ProQ:&atitle=Childbirth+Education+Curriculum:+An+Analysis+of+Parent+and+Educator+
Bergh, V. Den. (1990). The influence of maternal emotions during pregnancy on fetal and neonatal behavior Publication date : Journal of Prenatal & Perinatal Psychology and Health, 5(2), 119–130. Retrieved from https://pure.uvt.nl/ws/portalfiles/portal/1041624/INFLUEN2.PDF
Bhattacharjee, A., & Banik, N. (2016). Self-concept in pregnancy : An exploratory study. Indian Journal of Health and Wellbeing, 7(3), 346–348. Retrieved from http://www.iahrw.com/index.php/home/journal_detail/19#list
Black, K. (2004). Physiologic responses, sense of well-being, self-efficacy for self-monitoring role, perceived availability of social support, and perceived stress in women with pregnancy-induced hypertension. Physiologic Responses, Sense of Well-Being, Self-Efficacy for Self-Monitoring Role, Perceived Availability of Social Support & Perceived Stress in Women With Pregnancy-Induced Hypertension. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=cin20&AN=109844256&site=ehost-live
Blake, J., & Beard, M. (1999). Toward a theory of support during adolescent pregnancy. The Journal of Theory Construction & Testing, 3(2), 48–54.
Blamer, K. (1999). A comparative study of women’s perceptions of vaginal and cesarean births. Grand Valley State University. https://doi.org/10.16953/deusbed.74839
Borodulin, K., Evenson, K. R., Monda, K., Wen, F., Herring, A. H., & Dole, N. (2010). Physical activity and sleep among pregnant women, 45–52. https://doi.org/10.1111/j.1365-3016.2009.01081.x
Boucher, J. S. (1996). Women’s perception of major life changes and family closeness during the pregnancy of a subsequent child in first married and remarried families. Michigan State University. https://doi.org/10.16953/deusbed.74839
Broussard, A., & Weber-Breaux, J. (1994). Application of the childbirth belief-efficacy model in childbirth education classes. Journal of Perinatal Education, 3(1), 7–15. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=rzh&AN=1997010390&site=ehost-live&scope=site
Bumi Sehat. (2019). our history. Retrieved May 13, 2019, from https://bumisehat.org/about/our-team/

87
Buss, C., Davis, E. P., Hobel, C. J., & Sandman, C. A. (2011). Maternal pregnancy-specific anxiety is associated with child executive function at 6–9 years age. Stress, 14(6), 665–676. https://doi.org/10.3109/10253890.2011.623250
Carlsson, I. M., Ziegert, K., & Nissen, E. (2014). Psychometric properties of the Swedish childbirth self-efficacy inventory (Swe-CBSEI). BioMed Central Pregnancy and Childbirth, 14(1), 1–11. https://doi.org/10.1186/1471-2393-14-1
Chang, S. B., Park, S., & Chung, C. W. (2004). Effect of Taegyo-focused prenatal education on maternal-fetal attachment and self-efficacy related to childbirth. Journal of Korean Academy of Nursing, 34(8), 1409–1415. https://doi.org/10.4040/jkan.2004.34.8.1409
Chang, Yu, C. H., Chen, S. Y., & Chen, C. H. (2015). The effects of music listening on psychosocial stress and maternal-fetal attachment during pregnancy. Complementary Therapies in Medicine, 23(4), 509–515. https://doi.org/10.1016/j.ctim.2015.05.002
Chou, F. (2001). The adaptation to pregnancy in Taiwanese women who experience different severities of nausea and vomiting. The University of Texas at Austin. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=rzh&AN=109876399&%5Cnlang=ja&site=ehost-live
Clemens, S. W. (2014). Exploring the component of prenatal anxiety. Morgantown, West Virginia. Retrieved from https://researchrepository.wvu.edu/etd/245
Clout, D., & Brown, R. (2016). Marital relationship and attachment predictors of postpartum stress, anxiety and depression symptoms. Journal of Social and Clinical Psychology, 35(4), 322–341. https://doi.org/https://doi.org/10.1521/jscp.2016.35.4.322
Cody, S., Olga, G., Luciane, M., Richard, B., & Paul, R. (2012). Portuguese translation and validation of the revised dyadic adjustment. Journal of Marital and Family Therapy, 38(s1), 348–358. https://doi.org/10.1111/j.1752-0606.2012.00296.x
Cranley, M. S. (1981). Development of a tool for measurement of maternal attachment during pregnancy. Nursing Research, 30(5), 281–284. https://doi.org/https://doi.org/10.1097/00006199-198109000-00008
Cunningham Facello, D. (2008). Maternal/Fetal Attachment: Associations among Family Relationships, Maternal Health Practices, and Antenatal Attachment. ProQuest Dissertations Publishing, 386. https://doi.org/10.1177/001088048102200214
Dako-gyeke, P., Aikins, M., Aryeetey, R., Mccough, L., & Adongo, P. B. (2013). The influence of socio-cultural interpretations of pregnancy threats on health-seeking behavior among pregnant women in urban Accra , Ghana.
Daley-McCoy, C., Rogers, M., & Slade, P. (2015). Enhancing relationship functioning during the transition to parenthood: a cluster-randomised controlled trial. Archives of Women’s Mental Health, 18(5), 681–692. https://doi.org/10.1007/s00737-015-0510-7
Deave, T., Johnson, D., & Ingram, J. (2008). Transition to parenthood: The needs of parents in pregnancy and early parenthood. BMC Pregnancy and Childbirth, 8, 1–11. https://doi.org/10.1186/1471-2393-8-30
Deklava, L., Lubina, K., Circenis, K., Sudraba, V., & Millere, I. (2015). Causes of anxiety during pregnancy. Procedia - Social and Behavioral Sciences, 205(May), 623–626. https://doi.org/10.1016/j.sbspro.2015.09.097
Dilks, F., & Beal, J. R. (1997). Role of self-efficacy in birth choice. Journal of Perinatal Neonatal Nursing, 11(1), 1–9. https://doi.org/https://doi.org/10.1097/00005237-199706000-00003
Dimitrovsky, L. (2002). Dimensions of depression and perfectionism in pregnant and nonpregnant women: Their level and interrelationship and their relationship to marital satisfaction. The Journal of Psychology, 136(6), 631. https://doi.org/https://doi.org/10.1080/00223980209604824
Dobratz, M. C. (2003). Putting the pieces together : teaching undergraduate research from a

88
theoretical perspective, (Beck 1988), 383–392. https://doi.org/https://doi.org/10.1046/j.1365-2648.2003.02538.x
Dokuhaki, A., Akbarzadeh, M., Pishva, N., & Zare, N. (2017). A study of the effect of training pregnant women about attachment skills on infants’ motor development indices at birth to four months. Family Medicine and Primary Care Review, 19(2), 114–122. https://doi.org/10.5114/fmpcr.2017.67864
Drummond, J., & Rickwood, D. (1997). Childbirth confidence: validating the childbirth self-efficacy inventory (CBSEI) in an Australian sample. Journal Advance Nursing, 26(3), 613–622. https://doi.org/https://doi.org/10.1046/j.1365-2648.1997.t01-24-00999.x
Duncan, L. G., & Bardacke, N. (2010). Mindfulness-Based Childbirth and Parenting Education : Promoting Family Mindfulness During the Perinatal Period. Journal of Child and Family Studies, (19), 190–202. https://doi.org/10.1007/s10826-009-9313-7
Dyrdal, G. M., & Nes, R. B. (2011). Can a Happy Relationship Predict a Happy Life ? A Population-Based Study of Maternal Well-Being During the Life Transition of Pregnancy , Infancy ,. Journal of Happiness Study, 12, 947–962. https://doi.org/10.1007/s10902-010-9238-2
Edhborg, M., Hogg, B., & Kabir, Z. N. (2013). Impact of postnatal maternal depressive symptoms and infant ’ s sex on mother-infant interaction among Bangladeshi women. Health, 5(2), 237–244. https://doi.org/http://dx.doi.org/10.4236/health.2013.52032
Eka Roisa Shodiqoh, & Syahrul, F. (2014). Perbedaan tingkat kecemasan dalam menghadapi persalinan antara primigravida dan multigravida. Jurnal Berkala Epidemologi, 2, 141–150. https://doi.org/DOI: 10.1016/S0376-7388(96)00349-3
Eleonora Björk, Mari Thorildsson, A.-B. R.-A. (2007). Childbirth Self-Efficacy Inventory in Tanzania - a pilot study. Högskolan Dalarna. Retrieved from http://www.diva-portal.se/smash/get/diva2:518410/FULLTEXT01.pdf
Erol Ursavas, F., Karayurt, Ö., & Iseri, Ö. (2014). Nursing Approach Based on Roy Adaptation Model in a Patient Undergoing Breast Conserving Surgery for Breast Cancer. The Journal of Breast Health, 10(3), 134–140. https://doi.org/10.5152/tjbh.2014.1910
Faiza, R., Notobroto, H. B., Trijanto, B., & Soedirham, O. (2016). Influence of Prenatal Class to the Practice of P4K ( Birth Planning and Prevention of Birth Complication ). Airlangga University, 24(Birth Preparedness and Prevention of Birth Complication), 94–99. Retrieved from http://repository.unair.ac.id/id/eprint/45496
Fata, U. H., & Rahmawati, A. (2016). Prenatal education as an effort in enhancing breastfeeding self efficacy. Jurnal Ners Dan Kebidanan, 3(2), 136–141. https://doi.org/10.26699/jnk.v3i2.ART.p136-141
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, (39), 175–191. https://doi.org/https://doi.org/10.3758/bf03193146
Fawcet, J. (2006). The roy adaptation model and content analysis. Revista Aquichan, 6(6), 34–37. Retrieved from http://www.scielo.org.co/pdf/aqui/v6n1/v6n1a04.pdf
Fibriana, A. I., & Azinar, M. (2016). Model kelas ibu hamil untuk pemetaan risiko kehamilan dan pencegahan komplikasi persalinan. Abdimas, 20(1), 11–18.
Fishell, A. (2010). Depression and anxiety in pregnancy. In Journal of population therapeutics and clinical pharmacology = Journal de la therapeutique des populations et de la pharamcologie clinique (Vol. 17, pp. e363-9). Australia. Retrieved from https://pdfs.semanticscholar.org/227d/eef85283dfa0e753af0480b6c031bafdd37f.pdf
Fowers, B. J., & Olson, D. H. (1993). ENRICH Marital Satisfaction Scale : A Brief Research and Clinical Tool. Journal of Family Planning and Reproductive Health Care, 7(2), 176–185. https://doi.org/https://doi.org/10.1037//0893-3200.7.2.176

89
Furber, C. M., Garrod, D., Maloney, E., Lovell, K., & Mcgowan, L. (2009). A qualitative study of mild to moderate psychological distress during pregnancy. International Journal of Nursing Studies, 46, 669–677. https://doi.org/10.1016/j.ijnurstu.2008.12.003
Galina, R., & Risti, P. (2015). Efikasi diri menyusui dan asi eksklusif di Wilayah Kecamatan Cimahi Selatan Kota Cimahi tahun 2015 = Breastfeeding self efficacy and exclusive breastfeeding in the Kecamatan Cimahi Selatan 2015, 2, 2–3.
Gambrel, L. E., & Piercy, F. P. (2015). Mindfulness-based relationship education for couples expecting their first child-part 1: a randomized mixed-methods program evaluation. Journal of Marital and Family Therapy, 41(1), 5–24. https://doi.org/10.1111/jmft.12066
Gao, L., Ip, W., & Sun, K. (2011). Validation of the Short Form of the Chinese Childbirth Self-Efficacy Inventory in Mainland China. Research in Nursing and Health, (2004), 49–59. https://doi.org/10.1002/nur.20400
Garland, M. (2017). Physical Activity During Pregnancy : A Prescription for Improved Perinatal. The Journal for Nurse Practitioners, 13(1), 54–58. https://doi.org/10.1016/j.nurpra.2016.07.005
Gau, M., & Lee, T.-Y. (2003). Construct Validity of the Prenatal Attachment Inventory : A Confirmatory Factor Analysis Approach. Journal of Nursing Research, 11(3), 177–187. https://doi.org/https://doi.org/10.1097/01.jnr.0000347634.18218.2f
Gheibi, Z., Abbaspour, Z., & Hossein, M. (2020). Effects of a mindfulness-based childbirth and parenting program on maternal-fetal attachment : A randomized controlled trial among Iranian pregnant women. Complementary Therapies in Clinical Practice, 41(June 2019), 101226. https://doi.org/10.1016/j.ctcp.2020.101226
Giurgescu, C., & Templin, T. N. (2015). Father Involvement and Psychological Well-Being of Pregnant Women. MCN. The American Journal of Maternal Child Nursing, 40(December 2015), 381–387. https://doi.org/10.1097/NMC.0000000000000183.
Glover, V. (2014). Maternal depression, anxiety and stress during pregnancy and child outcome; What needs to be done. Best Practice and Research: Clinical Obstetrics and Gynaecology, 28(1), 25–35. https://doi.org/10.1016/j.bpobgyn.2013.08.017
Goodman, J. H., Guarino, A., Chenausky, K., Klein, L., Prager, J., Petersen, R., … Freeman, M. (2014). CALM Pregnancy: results of a pilot study of mindfulness-based cognitive therapy for perinatal anxiety. Archives of Women’s Mental Health, 17(5), 373–387. https://doi.org/10.1007/s00737-013-0402-7
Gourounti, K., Anagnostopoulos, F., & Lykeridou, K. (2013). Coping strategies as psychological risk factor for antenatal anxiety , worries , and depression among Greek women. Archives of Women’s Mental Health, 16, 353–361. https://doi.org/10.1007/s00737-013-0338-y
Gourounti, K., Kouklaki, E., & Lykeridou, K. (2015). Childbirth efficacy: Validating the childbirth self-efficacy inventory in a Greek sample of pregnant women. Midwifery, 31(7), 742–749. https://doi.org/10.1016/j.midw.2015.03.013
Grant, K. A., McMahon, C., & Austin, M. P. (2008). Maternal anxiety during the transition to parenthood: A prospective study. Journal of Affective Disorders, 108(1–2), 101–111. https://doi.org/10.1016/j.jad.2007.10.002
Greenwood, C. J., & Stainton, M. C. (2001). Back pain/discomfort in pregnancy: invisible and forgotten. The Journal of Perinatal Education, 10(1), 1–12. https://doi.org/10.1624/105812401X88002
Guarino, M. (1990). Adaptation to pregnancy and motherhood : Personality characteristics of primiparas age 30 years and older. Boston University.
Handayani, N. S., & Harsanti, I. (2017). Marital satisfaction: the influence of working jon- family on the working women. Kepuasan pernikahan: studi pengaruh konflik pekerjaan-keluarga pada wanita bekerja -. Psycjology Journal, 10(1), 92–99. Retrieved from

90
https://www.neliti.com/publications/178515/kepuasan-pernikahan-studi-pengaruh-konflik-pekerjan-keluarga-pada-wanita-bekerja
Harpel, T. S. (2008). Fear of the unknown : ultrasound and anxiety about fetal health. An Interdiciplinary Journal for the Social Study of Health, Illness and Medicine, 12(3), 295–312. https://doi.org/10.1177/1363459308090050
Hayati, F., Herman, R. B., & Agus, M. (2017). Perbedaan tingkat kecemasan ibu bersalin di puskesmas dengan di bidan praktik mandiri dan hubungannya dengan lamapersalinan. Jurnal Kesehatan Andalas, 6(3), 564–571.
Henriksen, R. E., & Thuen, F. (2015). Marital quality and stress in pregnancy predict the risk of infectious disease in the offspring : the norwegian mother andchild cohort study. PLOS One, 30, 1–13. https://doi.org/10.1371/journal.pone.0137304
Heyman, R. E., Baucom, Katherine, J., & Trillingsgaard, T. (2014). Predictors of Change in Relationship Satisfaction during the Transition to Parenthood. Family Realations, 63(December), 667–679. https://doi.org/10.1111/fare.12089
Hohmann-marriott, B. (2009). The couple context ofpregnancy and its effects onprenatal care andbirth outcomes. Maternal and Child Health Journal, (13), 745–754. https://doi.org/10.1007/s10995-009-0467-0
Howharn, C. (2008). Effects of childbirth preparation classes on self-efficacy in coping with labor pain in Thai primiparas. The University of Texas at Austin. Retrieved from http://search.ebscohost.com/login.aspx?direct=true&db=cin20&AN=109850307&site=ehost-live
Huizink, A. C., Mulder, E. J., Robles de Medina, P. G., Visser, G. H., & Buitelaar, J. K. (2004). Is pregnancy anxiety a distinctive syndrome? Early Human Development, 79, 81–91. https://doi.org/https://doi.org/10.1016/j.earlhumdev.2004.04.014
Huizink, Delforterie, M. J., Scheinin, N. M., & Tolvanen, M. (2016). Adaption of pregnancy anxiety questionnaire – revised for all pregnant women regardless of parity : PRAQ-R2. Arch Womens Ment Health. https://doi.org/10.1007/s00737-015-0531-2
Hwang, R. H. (2013). Relationship Between Maternal Fetal Attachment and State Anxiety of Pregnant Women in the Preterm Labor. Korean Journal of Women Health Nursing, 19(3), 142. https://doi.org/10.4069/kjwhn.2013.19.3.142
Ip, Chan, D., & Chien, W. . (2005). Chinese version of the childbirth self- efficacy inventory. Journal Advance Nursing Advance Nursing, 51(6), 625–633. https://doi.org/https://doi.org/10.1037/t37483-000
Ip, Chung, T. K. H., & Tang, C. S. K. (2007). The Chinese Childbirth Self-Efficacy Inventory : the development of a short form. Journal of Clinical Nursing, 333–340. https://doi.org/10.1111/j.1365-2702.2006.01919.x
Ip, W. Y., Tang, C. S. K., & Goggins, W. B. (2009). An educational intervention to improve women’s ability to cope with childbirth. Journal of Clinical Nursing, 18(15), 2125–2135. https://doi.org/10.1111/j.1365-2702.2008.02720.x
Isbir, G. G., & Mete, S. (2010). Nursing care of nausea and vomiting in pregnancy: Roy adaptation model. Nursing Science Quarterly, 23(2), 148–155. https://doi.org/doi:http://dx.doi.org/10.1177/0894318410362489
Isbir, G. G., & Mete, S. (2013). Experiences with nausea and vomiting during pregnancy in Turkish women based on Roy adaptation model: A content analysis. Asian Nursing Research, 7(4), 175–181. https://doi.org/10.1016/j.anr.2013.09.006
Jamalzehi, A., Omeidi, K., Javadi, M., & Dashipour, A. (2017). Evaluation of Sleep Quality in Third Trimester of Pregnancy and Its Relation to Birth Characteristics in Women Referred to Gynecology Clinic of Tamin Ejtemaee Hospital of Zahedan. Schlar Research Library, 9(2), 194–201. Retrieved from www.scholarsresearchlibrary.com
Jang, S. H., Kim, I. J., & Lee, S. H. (2015). Relationship between Social Support and

91
Maternal- Fetal Attachment among Unmarried Pregnant Women in Korea : The Mediating Effects of Self-esteem. Advance Science and Technology Letters, 104(2007), 24–28. https://doi.org/https://doi.org/10.14257/astl.2015.104.06
Jennings, K. M. (2017). The Roy adaptation model: A theoretical framework for nurses providing care to individuals with anorexia nervosa. Advances in Nursing Science, 40(4), 370–383. https://doi.org/10.1097/ANS.0000000000000175
June, T. (2003). Pregnancy part six : Minor discomforts : The Journal of the Health Visitors ’ Association. Community Practitioner, 76(9).
Karaçam, Z., & Ançel, G. (2009). Depression, anxiety and influencing factors in pregnancy: a study in a Turkish population. Midwifery, 25(4), 344–356. https://doi.org/10.1016/j.midw.2007.03.006
Khorsandi, M., Ghofranipour, F., Faghihzadeh, S., Hidarnia, A., Akbarzadeh Bagheban, A., & Aguilar-Vafaie, M. E. (2008). Iranian version of childbirth self-efficacy inventory. Journal of Clinical Nursing, 17(21), 2846–2855. https://doi.org/10.1111/j.1365-2702.2008.02385.x
Khorsandi, M., Jafarabadi, M., Farzaneh, J., & Mohammad, R. (2013). Cultural Adaptation and Psychometric Testing of the Short Form of Iranian Childbirth Self Efficacy Inventory. Iranian Red Crescent Medical Journal, 15(11). https://doi.org/10.5812/ircmj.11741
Kiehl, E. M., & White, M. A. (2003). Maternal adaptation during childbearing in Norway, Sweden and the United States. Scandinavian Journal of Caring Sciences, 17(2), 96–103. https://doi.org/10.1046/j.1471-6712.2003.00116.x
Kruszewski, A. (1999). Psychosocial and adaptation to termination of pregnancy for fetal anomaly. Wayne State University, Detroit Michigan.
Larsen, R., & Plog, M. (2012). The Effectiveness of Childbirth Classes for Increasing Self-Efficacy in Women and Support Persons, 2(2), 107–115. https://doi.org/https://doi.org/10.1891/2156-5287.2.2.107
Lazarov, S., Lazarov, L., & Lazarov, N. (2016). Rewiew multiple pregnancy and birth: twins, triplets and high-order multiples. overview. Trakia Journal of Sciences, 14(1), 103–107. https://doi.org/10.15547/tjs.2016.01.015
Lee, L. Y. K., Tsang, A. Y. K., Wong, K. F., & Lee, J. K. L. (2011). Using the roy adaptation model to develop an antenatal assessment instrument. Nursing Science Quarterly, 24(4), 363–369. https://doi.org/10.1177/0894318411419209
Lindgren, K. (2001). Relationships among maternal-fetal attachment, prenatal depression, and health practices in pregnancy. Research in Nursing & Health, 24, 203–217. https://doi.org/https://doi.org/10.1002/nur.1023
Lowe, N. K. (1989). Explaining the pain of active labor: the importance of maternal confidence. Research Nurse Health, 12(4), 237–245. https://doi.org/https://doi.org/10.1002/nur.4770120406
Lowe, N. K. (1993). Maternal confidence for labor: Development of the childbirth self-efficacy inventory. Research in Nursing & Health, 16(2), 141–149. https://doi.org/doi:10.1002/nur.4770160209
Lucia, S., Purwandari, A., & Pesak, E. (2013). Pengaruh Pelaksanaan Kelas Ibu Hamil Terhadap Pengetahuan Tentang Persiapan Persalinan. Jurnl Ilmiah Bidan, 30, 61–65.
Madhavanprabhakaran, G. K., D’Souza, M. S., & Nairy, K. S. (2015). Prevalence of pregnancy anxiety and associated factors. International Journal of Africa Nursing Sciences, 3, 1–7. https://doi.org/10.1016/j.ijans.2015.06.002
Mardhiyah, U., & Khaerani, N. M. (2017). Dzikir training for coping anxiety during pregnancy: pelatihan dzikir untuk menurunkan kecemasan Ibu hamil pertama. Jurnal Psikologi Integratif, 5. Retrieved from http://ejournal.uin-

92
suka.ac.id/isoshum/PI/article/view/1413 Maxson, P. J., Edwards, S. E., Valentiner, E. M., & Miranda, M. L. (2016). A
Multidimensional Approach to Characterizing Psychosocial Health During Pregnancy. Maternal and Child Health Journal, 20(6), 1103–1113. https://doi.org/10.1007/s10995-015-1872-1
Mealing, S. (1991). Marital communication and change during pregnancy : A typological approach. University of Illionis.
Milliano, I. De, Tabbers, M. M., Post, J. A. Van Der, & Benninga, M. A. (2012). Is a multispecies probiotic mixture effective in constipation during pregnancy ? ’ A pilot study ’. Nutrition Journal, 11(1), 1. https://doi.org/10.1186/1475-2891-11-80
Ministry of Health. (2018). Data dan Informasi - Profil Kesehatan Indonesia (Data and Information - Indonesia Health Profil). https://doi.org/10.1037/0022-3514.51.6.1173
Ministry of Health Indonesian Republic. (2011). Pedoman Pelaksanaan Kelas Ibu Hamil. Kementrian Kesehatan RI. https://doi.org/351.077 Ind r
Minsitry of Health. (2014). Peraturan Menteri Kesehatan Republik Indonesia (No. 97 Tahun 2014). Indonesia: Kementrian Kesehatan.
Mohammadpour, A., Najafi, S., Tavakkolizadeh, J., & Mohammadzadeh, F. (2016). The effects of the roy’s adaptation model on primigravida women’s self-concept: A randomized controlled trial. Asian Journal of Pharmaceutical Research and Health Care, 8, 17–23. https://doi.org/10.18311/ajprhc/2016/7717
Muller, M. E. (1989). The development and testing of the Muller prenatal attachment Inventory. Western Journal of Nursing Research. University of California, San Fransisco.
Muller, M. E. (1993). Development of the Prenatal Attachment Inventory. Western Journal of Nursing Research, 15(2), 199–215. https://doi.org/10.1177/019394599301500205
Muller, M. E., & Ferketich, S. (1993). Factor analysis of the maternal-fetal attach ment scale. Nursing Research, 42, 144–147. https://doi.org/https://doi.org/10.1097/00006199-199305000-00004
Muti’ah, T. (2009). Relationship between maternal antenatal attachment, toddler temperament, maternal sensitivity and toddler attachment security in Yogyakarta, Indonesia. University Putra Malaysia.
Mutlu, B., Erkut, Z., Yildirim, Z., & Gundogdu, N. (2018). A review on the relationship between marital adjustment and maternal attachment. Revista Da Associação Médica Brasileira, 64(3), 243–252. https://doi.org/https://doi.org/10.1590/1806-9282.64.03.243
Nasir, N. (2015). Self instruction training (SIT) for decreasing maternal anxiety among primigravida. Ahmad Dahlan University of Yogyakarta.
Nichols, & Humenick, S. S. (2000). Childbirth education practice, research and theory (2nd ed.). United States of America: Saunders Company.
Nichols, M. R., Roux, G. M., & Harris, N. R. (2007). Primigravid and Multigravid Women: Prenatal Perspectives. Journal of Perinatal Education, 16(2), 21–32. https://doi.org/10.1624/105812407X192019
Nicoloro-SantaBarbara, J., Rosenthal, L., Auerbach, M. V., Kocis, C., Busso, C., & Lobel, M. (2017). Patient-provider communication, maternal anxiety, and self-care in pregnancy. Social Science and Medicine, 190, 133–140. https://doi.org/10.1016/j.socscimed.2017.08.011
Nishikawa, M., & Sakakibara, H. (2013). Effect of nursing intervention program using abdominal palpation of Leopold’s maneuvers on maternal-fetal attachment. Reproductive Health, 10(1), 1. https://doi.org/10.1186/1742-4755-10-12
Niska, K. . (1996). Adaptation to parenthood of Mexican AMerican first-time mothers and fathers. Chemical reviews. The University of Mennesota.

93
https://doi.org/10.16953/deusbed.74839 Nosrati, A., Mirzakhani, K., Golmakani, N., Esmaeily, H., Mohsen, S., & Nekah, A. (1994).
The Effect of Expectant Fathers ’ Training on Paternal -fetal Attachment. https://doi.org/10.22038/jmrh.2019.19194.1199
Novitasari, T., Budiningsih, T. E., & Mabruri, M. I. (2013). Keefektivan Konseling Kelompok Pra-Persalinan Untuk Menurunkan Tingkat Kecemasan Primigravida Menghadapi Persalinan. Journal Psychosoc, 1(1), 21–27.
Nursofyanto, R., & Cahyanti, R. . (2017). Hubungan partisipasi kelas ibu hamil terhadap tingkat kecemasan menghadapi persalinan pada ibu hamil risiko tinggi. Jurnal Kedokteran Diponegoro, 6(2), 1166–1177. Retrieved from http://ejournal-s1.undip.ac.id/index.php/medico ISSN Online : 2540-8844%0AR
O’Donnell, K. J., Bugge, A., Freeman, L., Khalife, N., Connor, T. G. O., & Glover, V. (2012). Maternal prenatal anxiety and downregulation of placental 11 b -HSD2. Psychoneuroendocrinology, 37(6), 818–826. https://doi.org/10.1016/j.psyneuen.2011.09.014
Pan, W., Gau, M., Lee, T., Jou, H., & Liu, C. (2018). Mindfulness-based programme on the psychological health of pregnant women $. Women and Birth, 32(1), e102–e109. https://doi.org/10.1016/j.wombi.2018.04.018
Perren, S., Wyl, A. Von, Burgin, D., Simoni, H., & Klitzing, K. Von. (2005). Intergenerational Transmission of Marital Quality Across the Transition to Parenthood. Family Process, 44(4), 441–459. https://doi.org/https://doi.org/10.1111/j.1545-5300.2005.00071.x
Prime Minister of Health. (2014). Infodatin Pusat data dan informasi kementrian kesehatan RI.
Qiao, Y., Wang, J., Li, J., & Wang, J. (2012). Effects of depressive and anxiety symptoms during pregnancy on pregnant, obstetric and neonatal outcomes: A follow-up study. Journal of Obstetrics and Gynaecology, 32(3), 237–240. https://doi.org/10.3109/01443615.2011.647736
Ramie, A., Afiyanti, Y., & Pujasari, H. (2004). Kontrol diri dan efikasi diri meningkatkan kepuasan ibu menjalani proses persalinan. Ners, 9(1), 97–104.
Ranita, B. A., & Hardjanti, T. S. (2016). Pengaruh belly dance terhadap tingkat kecemasan ibu (The efficacy of belly dance on the maternal anxiety). Midwifery Science Journal, 1(3), 26–34. Retrieved from https://www.neliti.com/publications/227212/pengaruh-belly-dance-terhadap-tingkat-kecemasan-ibu-hamil-primigravida-trimester
Rasouli, M., Pourheidari, & Gardes, Z. H. (2019). Effect of Self - care Before and During Pregnancy to Prevention and Control Preeclampsia in High - risk Women. International Journa of Preventive Medicine, 1–10. https://doi.org/10.4103/ijpvm.IJPVM
Rofi’ah, M. (2015). Menghadapi persalinan pada ibu hamil primigravida trisemester ke-Iii di rsnu tuban. Universitas Islam Negeri Maulana Malik Ibrahim. Retrieved from https://core.ac.uk/reader/34003906
Roy. (1970). Adaptation: a conceptual framework for nursing. Nursing Outlook, 18(3), 42–45.
Roy. (2009a). The Roy Adaptation Model (3rd ed.). Upper Saddle River: NJ: Pearson Education, Inc.
Roy, C. (2009b). The Roy Adaptation Model. 3rd ed. Upper Saddle River: NJ: Pearson Education, Inc.
Saastad, E. C. N. M. Ms., Israel, P. D. P. P., Ahlborg, T. C. N. M. P., Gunnes, N. P., & Frøen, J. F. M. D. P. (2011). Fetal Movement Counting - Effects on Maternal-Fetal Attachment: A Multicenter Randomized Controlled Trial. Birth, 38(4), 282. Retrieved from
94
https://search.proquest.com/docview/906397678?accountid=14680%0Ahttp://openurl.ac.uk/?url_ver=Z39.88-2004&rft_val_fmt=info:ofi/fmt:kev:mtx:journal&genre=article&sid=ProQ:ProQ%3Anahs&atitle=Fetal+Movement+Counting+-+Effects+on+Maternal-Fetal+Attachment%3A+
Salehi, F., & Shahhosseini, Z. (2017). Association between women ’ s marital satisfaction andanxiety during pregnancy. Iran Journal Psychiatri Behaviour Science, in Press(e7937), 1–4. https://doi.org/10.17795/ijpbs-7937.Brief
Salomonsson, B., Berterö, C., & Alehagen, S. (2013). Self-Efficacy in Pregnant Women with Severe Fear of Childbirth. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 42(2), 191–202. https://doi.org/10.1111/1552-6909.12024
Schwartz, L., Toohill, J., Creedy, D. K., Baird, K., Gamble, J., & Fenwick, J. (2015). Factors associated with childbirth self-efficacy in Australian childbearing women. BMC Pregnancy and Childbirth, 15(1), 1–10. https://doi.org/10.1186/s12884-015-0465-8
Septerina, P. W., Hastuti, P., & Fitria, Z. (2014). Evaluasi proses pelaksanaaan kelas ibu hamil di kabupaten banyumas. Jurnal Ilmiah Kebidanan, 5(2), 79–84.
Serçekuş, P., & Başkale, H. (2016). Effects of antenatal education on fear of childbirth , maternal self-ef fi cacy and parental attachment. Midwifery, 34, 166–172. https://doi.org/10.1016/j.midw.2015.11.016
Sercekus, P., & Mete, S. (2010). Effects of antenatal education on maternal prenatal and postpartum adaptation. Journal of Advanced Nursing, 999–1010. https://doi.org/10.1111/j.1365-2648.2009.05253.x
Setyaningsih, M. M., Setyowati, S., & Kuntarti, K. (2013). Penurunan Kecemasan Ibu Hamil Risiko Tinggi Dalam Menghadapi Persalinan Melalui Paket “Harmoni.” Jurnal Keperawatan Indonesia, 16(3), 176–182.
Shi, Y., Wang, D., Yuan, Y., Jiang, Y., & Zeng, Q. (2015). The effect of prenatal education curriculum on mother ’ s prenatal examination utilization , delivery mode and recovery status : a cross-sectional survey in China. Environmental Health and Preventive Medicine, 20(6), 397–403. https://doi.org/10.1007/s12199-015-0480-4
Siddiqui, A., & Hägglöf, B. (2000). Does maternal prenatal attachment predict postnatal mother-infant interaction? Early Human Development, 59(1), 13–25. https://doi.org/10.1016/S0378-3782(00)00076-1
Sinesi, A., Maxwell, M., Carroll, R. O., & Cheyne, H. (2019). Anxiety scales used in pregnancy : systematic review, 1–13. https://doi.org/10.1192/bjo.2018.75
Skouteris, H., Wertheim, E. H., Rallis, S., Milgrom, J., & Paxton, S. J. (2009). Depression and anxiety through pregnancy and the early postpartum : An examination of prospective relationships. Journal of Affective Disorders, 113(3), 303–308. https://doi.org/10.1016/j.jad.2008.06.002
Sriwenda, D. (2014). Efektifitas latihan birth ball terhadap efikasi Diri Primipara dengan Persalinan Normal efectivity of birth ball exercise on self efficacy of primiparous with normal labor. Jurnal Ners Dan Kebidanan Indonesia, 4(3), 141–147. https://doi.org/http://dx.doi.org/10.21927/jnki.2016
Stern, D. (1998). Maternal confidence for labor and the use of epidural anesthesia, 8(2), 211. https://doi.org/https://doi.org/10.31979/etd.d6p9-qs6t
Sukriani, W., & Suryaningsih, E. K. (2018). Factor contributed to The Maternal-Fetal Attachment. Jurnal Kesehatan, 9, 185–191. Retrieved from http://ejurnal.poltekkes-tjk.ac.id/index.php/JK%0AFaktor
Suryaningsih, E.K. (2015). Indonesian Version of Prenatal Attachment Inventory (PAI): A Preliminary Study. National Taipei University of Nursing and Health Sciences.
Suryaningsih, Endang Koni. (2016). Father ’ s Involvement During Pregnancy. In 4 th

95
ICRIEMS Proceedingsth ICRIEMS Proceedings (pp. 9–14). Yogyakarta. Suryati, T. (2012). Percentage of Sectio Caesaria in Indonesia is Passad the Maximum
Standard , is it in accordance to Medical Indication. Buletin Penelitian Sistem Kesehatan, 15(4), 331–338.
Suto, M., Takehara, K., Yamane, Y., & Ota, E. (2017). Effects of prenatal childbirth education for partners of pregnant women on paternal postnatal mental health and couple relationship: A systematic review. Journal of Affective Disorders, 210(August 2016), 115–121. https://doi.org/10.1016/j.jad.2016.12.025
Tanglakmankhong, K., Perrin, N. A., & Lowe, N. K. (2011). Childbirth self-efficacy inventory and childbirth attitudes questionnaire: psychometric properties of thai language versions. Journal of Advanced Nursing, 67(1), 193–203. https://doi.org/10.1111/j.1365-2648.2010.05479.x
Toosi, M., Akbarzadeh, M., & Ghaemi, Z. (2017). The effect of relaxation on mother’s anxiety and maternal-fetal attachment in primiparous ivf mothers. Journal of the National Medical Association, 109(3), 164–171. https://doi.org/10.1016/j.jnma.2017.03.002
Tragea, C., Chrousos, G. P., Alexopoulos, E. C., & Darviri, C. (2014). A randomized controlled trial of the effects of a stress management programme during pregnancy. Complementary Therapies in Medicine, 22(2), 203–211. https://doi.org/10.1016/j.ctim.2014.01.006
Trisiani, D., Hikmawati, R., Bhakti, S., & Bandung, K. (2016). Hubungan kecemasan ibu hamil terhadap kejadian preeklampsia di rsud majalaya kabupaten Bandung, I(3).
Wardani, D. A., Rachmawati, I. N., & Gayatri, D. (2017). Maternal self-efficacy of pregnant Indonesian teens: development and validation of an Indonesian version of the young adult maternal confidence scale and measurement of its validity and reliability. Comprehensive Child and Adolescent Nursing, 40, 145–151. https://doi.org/10.1080/24694193.2017.1386983
Wenzel, A. (2011). Anxiety in childbearing women: diagnosis and treatment. Washington DC: American Psychological Association. https://doi.org/http://dx.doi.org/10.1037/12302-000
Wergeland, E., & Strand, K. (1998). Need for job adjustment in pregnancy early prediction based on work history. Scandinavian Journal of Primary Health Care, 1994(April 1993), 90–95. https://doi.org/https://doi.org/10.1080/028134398750003232
Whisman, M. A., & Davila, J. (2011). Relationship adjustment, depression, and anxiety during pregnancy and the postpartum period. Journal of Family Psychology, 25(3), 375–383. https://doi.org/http://dx.doi.org/10.1037/a0023790
Wikipedia. (2019). Dhikr. Retrieved May 27, 2019, from https://en.wikipedia.org/wiki/Dhikr Williams, C., Povey, R. C., & White, D. G. (2008). Predicting women’s intentions to use pain
relief medication during childbirth using the Theory of Planned Behaviour and Self-Efficacy Theory. Journal of Reproductive and Infant Psychology, 26(3), 168–179. https://doi.org/10.1080/02646830701691350
World Health Organization. (2017). Country profile, pp. 13–16. Retrieved from http://www.searo.who.int/entity/health_situation_trends/countryprofile_ino.pdf?ua=1
World Health Organization. (2018). Process of translation and adaptation of instruments. Retrieved November 13, 2018, from http://www.who.int/substance_abuse/research_tools/translation/en/
World Health Organization. (2019). Preterm birth. Retrieved May 17, 2019, from https://www.who.int/news-room/fact-sheets/detail/preterm-birth
Wright, K., & Halfon, N. (2010). Closing the black-white gap in birth outcomes: a life-course approach. Ethnicity & Disease, 20(102), 6–72. Retrieved from

96
https://www.ncbi.nlm.nih.gov/pubmed/20629248 Yaghoubinia, F., Navidian, A., Yousefian, N., & Chaji, F. (2017). Effect of care plan based
on Roy adaptation model on physiological adaptation in patients with thalassemia major. Medical-Surgical Nursing Journal, 6(2–3), 37–43.
Yarcheski, A., Mahon, N. E., Yarcheski, T. J., Hanks, M. M., & Cannella, B. L. (2009). A meta-analytic study of predictors of maternal-fetal attachment. International Journal of Nursing Studies, 46(5), 708–715. https://doi.org/10.1016/j.ijnurstu.2008.10.013
Yikar, S. K. (2019). Effects of prenatal education on complaints during pregnancy and on quality of life. Patient Education and Counseling, 102, 119–125. https://doi.org/10.1016/j.pec.2018.08.023
Yuksel, F., Akin, S., & Durna, Z. (2013). Prenatal distress in Turkish pregnant women and factors associated with maternal prenatal distress, (1), 54–64. https://doi.org/10.1111/j.1365-2702.2012.04283.x
Zhegner, D. K. (2003). An exploratory retrospective study usi the Roy Adaptation Model: the adaptive mode variables of physical energy level, self-esteem, marital satisfaction, and parenthood motivation as predictors of coping behaviours in infertile women. Itinerario. Widener University. https://doi.org/10.1016/B978-012397720-5.50034-7
Zsamboky, M. . (2017). Sleep and Pregnancy : Understanding the Importance. International Journal of Childbirth Education, 32(1), 22–25. Retrieved from https://icea.org/wp-content/uploads/2015/12/CBEd-Jan-web-FINAL.pdf

97
APPENDIX A
Place 1
0001: Case 0003: Placebo 0005: Placebo 0007: Case 0002: Placebo 0004: Case 0006: Case 0008: Placebo ============================================================================================================== 0009: Case 0010: Placebo 0011: Case 0012: Placebo ============================================================================================================== 0013: Case 0014: Case 0015: Placebo 0016: Placebo ============================================================================================================== 0017: Case 0018: Placebo 0019: Placebo 0020: Case ==============================================================================================================
Place 2
0001: Case 0003: Placebo 0005: Case 0007: Placebo 0002: Case 0004: Placebo 0006: Placebo 0008: Case ============================================================================================================== 0009: Case 0011: Placebo 0013: Case 0015: Placebo 0010: Case 0012: Placebo 0014: Placebo 0016: Case ============================================================================================================== 0017: Placebo 0018: Case 0019: Placebo 0020: Case ==============================================================================================================
Place 3 0001: Case 0002: Case 0003: Placebo 0004: Placebo 0005: Placebo 0006: Case

98
============================================================================================================== 0007: Placebo 0009: Case 0011: Placebo 0013: Case 0008: Case 0010: Case 0012: Placebo 0014: Placebo ============================================================================================================== 0015: Case 0016: Placebo 0017: Case 0018: Placebo ==============================================================================================================

99
Place 4
0001: Case 0002: Placebo 0003: Placebo 0004: Case 0005: Placebo 0006: Case ============================================================================================================== 0007: Placebo 0008: Case 0009: Case 0010: Placebo 0011: Placebo 0012: Case ============================================================================================================== 0013: Case 0015: Placebo 0017: Case 0019: Placebo 0014: Case 0016: Placebo 0018: Case 0020: Placebo ==========================================================================================================
Place 5
0001: Case 0002: Placebo 0003: Case 0004: Placebo ============================================================================================================== 0005: Placebo 0006: Placebo 0007: Placebo 0008: Case 0009: Case 0010: Case ============================================================================================================== 0011: Case 0012: Placebo 0013: Case 0014: Placebo 0015: Case 0016: Placebo ============================================================================================================== 0017: Case 0019: Placebo 0021: Placebo 0023: Placebo 0018: Case 0020: Case 0022: Case 0024: Placebo ==========================================================================================================

100
APPENDIX B
DRAFT OF FLYER AND STANDING BANNER

101

102
APPENDIX C
THE PROGRAM OUTLINE OF CHILDBIRTH EDUCATION CLASSES
BASED ON ROY’S MODEL

103
Plan curriculum for childbirth education classes
Week/Topic
Content of Topic
Material Duration (min)
Method Media Outcome
I/1 Introduction
● Facilitator will introduce herself as well as the research assistants
● The participants will do so
20 Brainstorming
None To establish the trust relationship
Mother’s blood pressure
Measuring mother’s blood pressure before class
10 Practiced by research assistants
- Stethoscope
- Sphygmomanometer
To measure mother’s blood pressure
I/2 Pretest Questionnaires 15 Self-administered
- Paper - Ballpoi
nt pen
Baseline monitor
Preliminary discussion
● Share mother’s though and feeling as well as her expectation to her partner during pregnancy
● Share father’s thought and feeling during his wife’s pregnancy as well as her expectation to his partner during pregnancy
30 Discussion None Brainstorming
I/3 Fetal heartbeat, Leopold’s palpation and belly mapping
● Father monitors fetal heartbeat
● Father palpates using Leopold’s maneuver
● Father draws a picture to represent baby’s position inside womb
40 Demonstration and practice, led by researcher and assisted by research assistances
- Doppler - Gel - Tissue
To decrease maternal anxiety To enhance parental attachment to the baby
Break 5 Free - Snack Refresh

104
I/4 Introduction of anatomy and physiology during pregnancy and birth
● The comparison of anatomy and physiology before and after pregnancy
● Mother asked to share their discomfort during pregnancy
● Father asked for ideas about dealing with wife’s complaints during pregnancy
25 Discussion and brainstorming led by researcher
- Anatomy poster of pregnancy and birth
To decrease maternal anxiety To enhance marital relationship
I/5 Relaxation technique
Prenatal yoga 35 Practice led by prenatal yoga facilitator
Laptop, audio, aromatherapy, dark light
To increase childbirth self-efficacy
Homework
Mother have to practice the relaxation technique at home Father have to communicate with unborn baby every day before sleep
No limit Checklist To enhance maternal-fetal attachment To decrease anxiety during pregnancy
II/1 Physical
examination
Monitoring mother’s blood pressure before class
10 Done by research assistance
- Stethoscope
- Sphygmomanometer
To measure mother’s blood pressure
Fetal heartbeat
● Monitoring fetal heartbeat
● Father count baby’s movements
20 Demonstration and practice, led by researcher assistants
- Doppler - Gel - Tissue
To enhance parental attachment To decrease maternal anxiety
II/2 Ice breaking and study case
Researcher will ask mother and father to recall previous material in the last class Researcher describes a case and ask the couple how to deal with that situation
35 Led by researcher
None To enhance couple understanding of the material To increase marital relationship

105
II/3 Type of comfort measure and movement to coping labor pain
Researcher will demonstrate movement during labor using phantom and a bottle* - Back massage - Rebozo technique - Slow dance
movement Father practices applying comfort measures to the mother
30 Demonstration and discussion
Phantom pelvic and baby - Two
bottles has been modified to demonstrate the goal Rebozo
- Shock and tennis ball*
- Mats
Increase childbirth self-efficacy Increase marital satisfaction
Movement during labor
Researcher shows a video on how to give birth naturally Couple share feelings and thoughts after watching the video
35 Instruction by the researcher
- LCD,
- Laptop
- Audio
To increase childbirth self-efficacy To decrease pregnancy-related anxiety
Break 5 Free - Snacks Refresh II/4 Commun
ication with unborn baby
Mother and father write a letter to baby and express their feelings about the baby and what they expect for the baby The couple reads each other’s letter
45 Led by researcher
- Paper - Ballpoi
nt pen
To promote parental-fetal attachment
Homework
Mother share to her unborn about her activity for a whole day in a book Father communicate and state his expectation to the baby before sleep
No limit To enhance maternal-fetal attachment To decrease anxiety during pregnancy
III/1 Blood
pressure - Measure the
mother’s blood pressure
10 Done by research assistants
- Stethoscope
- Sphygm
To monitor mother’s blood

106
omanometer
pressure
Fetal heartbeat rate, Leopold’s palpation and belly mapping
Father monitors fetal heartbeat Father palpates using Leopold’s maneuver Father draws a picture to represent baby’s position
30 Demonstration and practice, led by researcher
- Doppler - Gel - Tissue
To decrease maternal anxiety To enhance parental attachment
III/2 Mechanism of labor
Engagement and dilatation process
20 Led by researcher
- Map of labor
- Balloon and ping pong ball*
- Anatomy pictures
To decrease maternal anxiety
Comfort measures during pregnancy and birth
- Birth ball - Acupressure
Father practice applying comfort measures for the mothers
30 Instruction by the researcher
- Birth ball
- Massage tool
Increase childbirth self-efficacy Increase marital satisfaction
Break 5 Free - III/4 Relaxati
on technique
Prenatal yoga
30 Practice led by prenatal yoga facilitator
Laptop, audio, aromatherapy, low lighting
Decrease anxiety during pregnancy
Preparing for breastfeeding
Preparation for breastfeeding Oxytocin massage by husband
30 Demonstration and practice led by researcher
Tools for demonstration
To increase childbirth self-efficacy To increase marital satisfaction
III/5 Reflection
Couple writes a letter to their partners about their expectation as partner and as parent
25 Couple’s Practice
- Audio
- Laptop
- Mats
Increase marital satisfaction

107
Homework
Mother describes her activity for a while day in a book for her unborn child Father communicates and states his expectations for the baby before sleep For next class, couple needs to bring their own towels
Towel
IV/1 Blood
pressure Mother’s blood pressure measurement
10 Done by research assistants
- Stethoscope
- Sphygmomanometer
To measure mother’s blood pressure
IV/2 Ice breaking
Researcher asks mothers and fathers to recall previous material from the last class Couples shares their thoughts and feelings about upcoming delivery date
25 - Decrease maternal anxiety
Relaxation technique
Prenatal yoga
35 practice led by prenatal yoga facilitator
Laptop, audio, aromatherapy, low lighting
Decrease maternal anxiety
IV/3 Movement during birth
Practice movements and positions to open pelvis
20 Practice led by researcher
- Pelvic phantom
To increase childbirth self-efficacy
Parenting preparation
Father practices how to bathe the baby and change diapers Father assists mother to position baby for breastfeeding
40 Practice led by researcher
- Baby’s bathtub
- Soap - Baby’s
cloth - Phanto
m baby
To increase marital relationship
IV/4 Video of labor process and arrange birth plan
Couple watches a video of labor process and discuss as their birth plan
30 Discussion led by researcher
- To increase childbirth self-efficacy

108
IV/5 Posttest 15 Second monitoring
- Questionnaire
- Ballpoint pen

109
*the tools modified
a) Bottles with sand
b) Sock and tennis ball
Tennis ball put inside the socks
c) Balloon and ping pong ball
Ping pong ball put inside the blown balloon
Filled half sand and using tape, tied two bottles
+
+

110
APPENDIX D
INSTRUMENTS

111
The Prenatal Attachment Inventory
The following sentences describe thoughts, feelings, and
situations women may experience during pregnancy. We are
interested in your experiences during the past month. Please
circle the letter under the word that applies to you.
almost
almost
always often sometimes
never
1. I wonder what the baby looks like now..............a. b.
c. d.
2. I imagine calling the baby by name................. a. b.
c. d.
3. I enjoy feeling the baby move...................... a. b.
c. d.
4. I think that my baby already has a personality..... a. b.
c. d.
5. I let other people put their hands on my
tummy to feel the baby move......................... a. b.
c. d.
6. I know things I do make a difference to the baby... a. b.
c. d.
7. I plan the things I will do with my baby........... a. b.
c. d.

112
8. I tell others what the baby does inside me......... a. b.
c. d.
9. I imagine what part of the baby I'm touching.......a. b.
c. d.
10. I know when the baby is asleep..................... a.
b. c. d.
11. I can make my baby move............................ a.
b. c. d.
12. I buy/make things for the baby..................... a.
b. c. d.
13. I feel love for the baby........................... a.
b. c. d.
14. I try to imagine what the baby is doing in there...a. b.
c. d.
15. I like to sit with my arms around my tummy......... a.
b. c. d.
16. I dream about the baby.............................a. b.
c. d.
17. I know why the baby is moving......................a. b.
c. d.
18. I stroke the baby through my tummy.................a. b.
c. d.
19. I share secrets with the baby......................a. b.
c. d.
20. I know the baby hears me...........................a. b.
c. d.

113
21. I get very excited when I think about the baby..... a.
b. c. d.
Copyright Mary E. Muller, PhD 1989
Scoring: A=4, B=3, C=2, D=1. All items are summed for a single score.

114

115

116
EMS

117

118

119
Socio-demographic information questionnaire
1. Personal Information a. Number participation :
b. LMP :…/…/…G…P…A…..Ah…(feel by officer )
c. Gestational week :
d. Mother’s age :
e. Name (initial) :
f. Spouse age :
g. Date of married :
h. Spouse contact number:
i. Education Level : Elementary school ( )
Secondary school ( )
Tertiary school ( )
University ( )
j. Occupation : Housewife ( )
Employee ( )
Entrepreneur ( )
k. Pregnancy complication : Heart ( )
Asthma ( )
Migraine ( )
Bleeding ( )
Hyperemesis ( )%
Anemia/HB <9gr% ( )
Other, specify……………………
None ( )

120
APPENDIX E
GRANT PERMISSION

121

122

123

124
APPENDIX F
INSTITUTIONAL REVIEW BOARD (IRB)

125
IRB application for one semester empirical thesis:
Effect of Prenatal Childbirth Program on Maternal Anxiety, Maternal-Fetal Attachment, Childbirth Self-Efficacy and Marital Relationship: A Randomized
Controlled Trial Using Roy’s Adaptation Model
Endang Koni Suryaningsih konnywae@yah
oo.co.id
Advisor: Professor Meei-Ling Gau

126
Summary and Nature of Intent of Project
Past research has consistently pointed towards the childbirth education classes
as an effective method for alleviating discomfort during pregnancy, enhance self-
concept, role function and interdependence. Using the Roy’s adaptation model, nurse
and midwives can provide intervention through that four modes. This study looks to
determine whether childbirth education program based on the RAM can significantly
impact an individual’s levels of maternal anxiety during pregnancy, improving
maternal-fetal attachment, as well as childbirths elf-efficacy and marital relationship.
The study will consist of nullipara in the third trimester and absence from
pregnancy complication. Half of the participants will receive a session focused on
relaxation, prenatal yoga, maternal-fetal attachment skill, communication skill, and
comfort measure during pregnancy and birth while the other half will receive a
regular prenatal class control intervention. It is predicted that participants receiving
the childbirth education class based on the RAM intervention will have significantly
lower levels of pregnancy-related anxiety, higher level of maternal-fetal attachment,
childbirth self-efficacy, and marital relationship as compared to the participants
receiving the control intervention. The results of this study could aid in providing
evidence towards a framework to develop the childbirth classes based on theory and
provide knowledge that can help mother and husband to optimize the adaptation
during pregnancy and childbirth

127
Procedure Section of Research Proposal
Participants
The sample will be comprised of as many individuals as possible, pulled from
the five puskesmas in Yogyakarta, Java Island. All participants will likely be between
the ages of 20 to 35 years old. Participants will also be recruited using randomized
sampling methods, and will be allocated using computer generating sequence and
opaque and sealed envelopes. Then they will be contacting via WhatsApp application
or phone to date and times for the program.
Materials and Procedure
Participants will sign up for 4-weeks childbirth education classes in the
mornings and/or weekends to come in and take part in the study. Prior to the start of
the study, consent will be taken from all participants (see attached). Participants will
be told that they are taking part in a study focused on measuring the effect of
childbirth education classes on four variables: pregnancy-related anxiety, maternal-
fetal attachment, short form of childbirth self-efficacy, and marital relationship. Each
participant, regardless of the experimental and control intervention condition they are
placed in, will have their initial levels of four variables measured as well as
demographic characteristics. Demographic data set consist of mother’s age,
gestational week, race, religion, education level, monthly income, and marital
duration. Anxiety during pregnancy will be completed using the Pregnancy-Related
Anxiety Questionnaire Revised (PRAQ-R2). This 10-item scale consists of
statements such as “I am afraid the baby will be mentally handicapped or will suffer
from brain damage” , “I am worried about the pain of contractions and the pain
during delivery” and “ I am anxious about the delivery because I have never
experienced one before.” All responses are measured on a five-point Likert scale,

128
where 1 = definitely not true and 5 = definitely true. To measure the maternal-fetal
attachment, the participant will complete the Indonesian version of Prenatal
Attachment Inventory (PAI). The instrument developed by Muller (1993) consist of
21 consisting of Likert-type items ranging from 1 (‘almost never’) to 4 (‘almost
always’). All items are summed for a single score, and the possible range of scores is
21-84 (Muller, 1993).
Short form of Childbirth Self-Efficacy Inventory developed by Ip (2005) will
be used to measure the level of mother’s self-efficacy regarding the childbirth
process. Ip and colleagues created the short form consiste of 32 items divided to two
subscales; Outcome Expectancy and Second Stage Expectancy. To measure the
marital relationship, ENRICH Marital Satisfaction Scale (EMS) will be applied. The
instrument developed by Fower and Olson (1993) consist of 15-item comprising the
Idealistic Distortion (5 items) and Marital Satisfaction Scales (10 items). The
example item on Idealistic Distortion scale such as: “ My partner and I understand
each other perfectly”, “ My partner completely understands and sympathizes with my
every mood”. The example item on Marital Satisfaction scale such as : “ I am not
pleased with the personality characteristics and personal habits of my partner” and “ I
am very happy with how we handle role responsibilities in our marriage”. This scale
is a Likert-type ranging from 1 (strongly disagree) to 5 (strongly agree) which is
consist of positive and negative statement that indicate items scored direction
(Fowers & Olson, 1993). Items scored in negative direction would be reverse-scored
(i.e if it is mark 5, it would be scored 1; it is marked 4, it would be scored 2; a 3
remain unchanged) (Fowers & Olson, 1993).
After completing the questionnaire, the participant will start the program, 4-
week class and 3 hours for each session. Beforehand, the participant will be randomly

129
assigned to one of two conditions and have confirmation when and where they will
have childbirth education classes. In this study, the monitoring of variables will be
measured two times: prior and after the program. All the participants will be
measured their blood pressure and fetal heart beat rate prior the class and they will
also complete the questionnaire. In the experimental condition, participants take part
in a focused program to decrease pregnancy-related anxiety, and increase maternal-
fetal attachment, childbirths elf-efficacy, and marital relationship. Participants will
be facilitated by prenatal yoga instructor, and midwives. During the class, learning
method include lecturer, break session, discussion, practice and demonstration. In the
control condition, participant also will join the program for 4-weeks and 3 hours for
lecturing and some discussion with the midwives regarding the content material such
as anatomy and physiology during pregnancy and birth, postpartum and newborn
care, family planning method, immunization, and birth certificate. In the end of
program, participants in this group will receive prenatal yoga as well as maternal-
fetal attachment skill after they completing the questionnaire as the final monitoring.

130
Debriefing Form Ethical Committee ‘Aisyiyah University of Yogyakarta
Title of the Study: Effect of Prenatal Childbirth Program on Maternal Anxiety, Maternal-Fetal Attachment, Childbirth Self-Efficacy and Marital Relationship: A Randomized Controlled Trial Using Roy’s Adaptation Model
Researcher Name: Endang Koni Suryaningsih, email address: [email protected] Thank you for participating in this research study. We are conducting this study to test the effect of childbirth education on the pregnancy-related anxiety, maternal-fetal attachment, childbirth self-efficacy, and marital relationship. Our main research questions is how the effect of childbirth education program to the pregnancy-related anxiety, childbirth self-efficacy, maternal-fetal attachment and marital relationship? While participating in this study, you will participate in the childbirth education class during 4-weeks and 3 hours per each session. There is no potential harm intervention during this program. Prior the class, your blood pressure and fetal heart rate beat will be measured, and in the first as well as the end of program, you will be asked to complete the questionnaire include demographic data set, maternal anxiety, maternal and fetal attachment, self-efficacy for birth and marital relationship. The program will be conducted indoor, equipment and environment friendly for pregnant women will be provided, such as sufficient ventilation and light, no chemical contact, yoga mat and pillow, and access to restroom. Mineral water and snack for break session as well as T-shirt for couple uniform also will be provided. Additionally, compensate such as parenting book package will be presence for participant who complete the program. We expect to find that the childbirth education program will be effective to reduce pregnancy-related anxiety and increase maternal-fetal attachment, childbirth self-efficacy inventory, as well as marital relationship. If you are interested in learning more about this study, please feel free to ask us questions in person, or contact us using the email address above. If you have any concerns about your rights as a participant in this study, please contact the Ethic Committee ‘of ‘Aisyiyah University of Yogyakarta Institutional Review Board ([email protected]).
Thank you again for participating!

131
Consent Form Title of the Study: Effect of Prenatal Childbirth Program on Maternal Anxiety, Maternal-Fetal Attachment, Childbirth Self-Efficacy and Marital Relationship: A Randomized Controlled Trial Using Roy’s Adaptation Model Research name : Endang Koni Suryaningsih
Contact information : +6285132439488 Advisor : Professor Meei-Ling Gau
The general purpose of this research is to test the effect of childbirth education on the pregnancy-related anxiety, maternal-fetal attachment, childbirth self-efficacy, and marital relationship. Participants in this study will be asked to follow the prenatal class during four weeks, 3 hours per each session. Findings from this study will be used in the thesis for the researcher’s PhD degree. I hereby give my consent to participate in this research study. I acknowledge that the researcher has provided me with: A. An explanation of the study’s general purpose and procedure. B. Answers to any questions I have asked about the study procedure.
I understand that: A. My participation in this study will take approximately four weeks, and 3 hours session. B. The probability and magnitude of harm/discomfort anticipated as a result of participating
in this study are not greater than those ordinarily encountered in daily life or during the performance of the childbirth education classes.
C. The potential benefits of this study include the knowledge beneficial, and the participation husband during the program may increase.
D. I will be compensated for participating in this study with T-shirt as the uniform for the classes, and if I complete the program, the parenting book will be provided.
E. My participation is voluntary, and I may withdraw my consent and discontinue participation in the study at any time. My refusal to participate will not result in any penalty or disadvantage.
F. Some aspects of the study purpose/procedure may be withheld from me until its end. What the investigators hope to learn from this study, the specific nature of and reasons for the procedure employed, and those aspects of my behavior that have been recorded for measurement purposes will all be fully explained to me at the end of the study. After the study’s purpose and procedure have been fully explained to me, I may, for any reason, choose to withhold use of any data provided by my participation, without penalty.
G. My responses in this study will be kept confidential, to the extent permitted by law. The data will be stored in a secure location in hard disk, will be available to the researcher only and research reports will only present findings on a group basis, without any personally identifying information.
Name (printed): __________________________________________________
Signature: _____________________________ Date: ____________________

132

133

134





























