Embed Size (px)
Citation preview
Anita Fisher RN, PhDAndrea Baumann RN, PhD
Mabel Hunsberger RN, PhDJennifer Blythe MLS, PhD
Linda Fitzpatrick RN, MHSc
A Collaborative Evaluation of College and Hospital Critical Care
Nursing Programs in Ontario
Critical Care Secretariat,Ministry of Health and Long-Term Care
Nursing Health Services Research Unit, McMaster University SiteOctober, 2007
1A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Anita Fisher, RN, PhD (Principal Investigator)Research Associate, Nursing Health Services Research Unit (McMaster University site)Associate Professor, School of Nursing, Faculty of Health Sciences, McMaster University
Andrea Baumann, RN, PhDAssociate Vice President, Faculty of Health Sciences, International Health, McMaster UniversityDirector, Nursing Health Services Research Unit (McMaster University site)
Mabel Hunsberger, RN, PhDResearch Associate, Nursing Health Services Research Unit (McMaster University site)Associate Professor (Part Time), School of Nursing, Faculty of Health Sciences, McMaster University
Jennifer Blythe, MLS, PHDSenior Scientist, Nursing Health Services Research Unit (McMaster University site)Associate Professor, School of Nursing, Faculty of Health Sciences, McMaster University
Linda Fitzpatrick, RN, MHScResearch Assistant, Nursing Health Services Research Unit, (McMaster University site)
Acknowledgements
The research team would like to acknowledge the valuable contributions of the external expert panel reviewers including:
Nazlin Allidina, Director, Critical Care Education, George Brown College
Elizabeth Gordon, Critical Care Educator, Medical ICU, University Health Network
Glenda Hicks, Critical Care Educator, Sudbury Regional Hospital
Karen Lodato, Critical Care Clinical Nurse Specialist, Hamilton Health Sciences
Mary Runde, Critical Care Educator, Sault Area Hospital
A special thank you goes to Dr. Camille Kolotylo for her expert advice in survey development and Dr. Noori Akhtar-Danesh for his expertise in statistics.
2 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Table of Contents1. EXECUTIVE SUMMARY 3
2. SUMMARY OF RECOMMENDATIONS 4
3. INTRODUCTION 5
4. PURPOSE OF THE STUDY 6
5. METHODOLOGY 6 5.1 Study Design 6 5.2 Sample 6 5.3 Phase 1: Focus Groups 7 5.4 Phase 2: Curriculum Evaluation 7 5.4.1 Survey Development 7 5.4.2 Survey for Self-Evaluation of the Curricula 9 5.4.3 Expert Panel Review of Curricula 9
6. RESULTS 10 6.1. Focus Group Data Collection and Qualitative Analysis 10 6.2 Collaborative Curriculum Evaluation: Demographics and Data Collection 12 6.2.1 Organizational Demographics: Hospitals and Colleges 12 6.2.2 Self-Evaluation Survey 13 6.2.3 Expert Panel Evaluation 13 6.2.4 Hospital and College Rankings of Overall Mean Compliance with Critical Care Nursing Standards 14 6.2.5 College and Hospital Mean Compliance by Groupings 16 6.2.6 Hospital and College Mean Compliance by Item 17 6.2.7 Theoretical/Clinical Content in Critical Care Nursing Curricula 25
7. CONCLUSIONS 26
8. RECOMMENDATIONS 30
9. REFERENCES 32
10. APPENDICES 33 Appendix A. Letter To Focus Group Participants 33 Appendix B. Focus Group Consent Form 34 Appendix C. Focus Group Discussion Guide 35 Appendix D. Focus Group Feedback 36 Appendix E. Survey Instrument: Critical care Collaborative Evaluation 37 Appendix F1. College Demographics Section 55 Appendix F2. Section B: Hospital Demographics Section 57 Appendix G. Letter Critical Care Secretariat: Dr Bernard Lawless 60 Appendix H1. College Demographic Summary 62 Appendix H2. Hospital Demographics 66 Appendix I. Expert Panel Reviewers 70 Appendix J. Intra-class Correlation Coefficients on Expert Panel Reviews 71 Appendix K. Research Ethics Board Approval Letter 72

3A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
1. EXECUTIVE SUMMARYThe Ministry of Health and Long-Term Care through the Critical Care and Nursing Secretariats is committed to providing system supports to improve critical care education for nurses and assist hospitals in meeting their human resource needs for safe and accessible care. Commissioning and supporting the development of new Critical Care Nursing Standards by the Nursing Subcommittee of the Critical Care Expert Panel was the first step in achieving this vision. In order to determine the extent to which these standards were incorporated into college and hospital-based critical care nursing education pro-grams in the province, the Nursing Health Services Research Unit at McMaster University was asked to conduct a collab-orative evaluation of selected programs in Ontario.
The new Ontario Standards of Critical Care Nursing were positively received by critical care nurses in this study as a basis for improving basic critical care nursing education and specialty orientation in the province. Although there were some suggestions for minor changes, they were generally seen as “very thorough and well-framed with inherent specific out-comes.” However, concerns were raised about the professional ownership of and ultimate accountability for consistent implementation of these standards across the province.
Collaborative evaluation of 24 critical care nursing education programs against the new standards of practice demonstrated great variation within and among college and hospital-based curricula in Ontario. The evaluation identified strengths and gaps in compliance at the organizational and Local Health Integration Networks (LHINs) levels. Mean compliance with the standards varied between 25% to 75% compliance levels. These outcomes underscored the need for a standardized curriculum for beginning practitioners in the specialty. If basic preparation in the specialization is to be portable from one hospital to another, all beginning critical care nurses should receive the same educational preparation. Further to this, nurses have consistently identified the lack of formal recognition for the education required to begin work in their specialty area. If educational preparation for the beginning critical care nurse is based on a standardized curriculum, there should be some consideration for formal credit, either towards a baccalaureate in nursing or a critical care nursing certificate. As such, the standardized critical care nursing curriculum should sit in accredited educational institutions in the province that can also assume accountability for the implementation of the standards and ongoing program accreditation through already established processes. For this to be viable and have a provincial impact, strong partnerships between the education and hospital sectors including structures such as the LHINs, are required. Ongoing collaborative planning at the governmental, regional and local level will also be essential in making this a reality.
Precedence has been set at both the undergraduate and postgraduate level with nursing specialization areas such as on-cology, neonatology and primary health care all giving formal educational credit. These programs are offered in various educational institutions and provide a standard approach that can be adopted in other educational institutions. It may be timely to consider such an approach with critical care nurse specialization.

4 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
2. SUMMARY OF RECOMMENDATIONSThe Critical Care Nursing Subcommittee should consider the areas identified by the focus groups for inclusion in the new critical care nursing standards.
A standardized curriculum based on the new Ontario standards should be developed for basic education of new critical care nurses.
The standardized curriculum should be developed under the auspices of the Critical Care Nursing Subcommittee in close collaboration with the Canadian Association of Critical Care Nurses (CACCN), the formal education institutions and the hospitals with whom they work.
The standardized curriculum should be adopted by formal educational institutions which can give course credit, thereby assuring an established accreditation process.
Implementation of this curriculum should be negotiated through a strong partnership between the educational institutions and the hospitals with whom they work.
The teaching strengths of both hospitals and educational institutions should be merged through cross appointments to ensure strong theory and clinical content in the program.
The existing physical space and technical infrastructure of both hospitals and educational institutions should be fully opti-mized.
Ongoing continuing education for critical care nurses is essential to maintain a competent critical care nursing workforce. Based on focus group feedback, the following suggestions are put forward for consideration:
Dedicate budget for continuing education and staffing flexibility for mid-career nurses to maintain competence •and achieve certification.
Funding for certification should be on a shared basis (nurse/employer).•
Create partnerships among hospitals to share educational opportunities and expertise.•
Form a high level multi-sectoral planning committee to strategize integration of a critical care nursing specialty program into existing educational structures in the province.
Individual Local Health Integration Networks (LHINs) should evaluate their critical care nursing education capacity and bring their experts together to discuss strategies for improvement within their own LHIN and provincially.

5A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
3. INTRODUCTIONIn 2004/2005, the Ontario Ministry of Health and Long-Term Care (MOHLTC) launched the Critical Care Transforma-tion Strategy to improve quality of care and system performance in adult critical care services. Strong emphasis was placed on investments to improve access, quality and system level resource management. One of the main recommendations from the Final Report of the Ontario Critical Care Steering Committee (2005, March) was that “professional staff working in critical care should be required to meet provincially recognized standards and core competencies.” The Committee also identified the need for consistency of nurse training in critical care to support the recruitment and retention of critical care nurses. Since training programs vary across the province, all staff who complete training may not have the same competen-cies. The Ministry’s Nursing Secretariat and Critical Care Secretariat have formed a partnership to address issues relating to critical care nursing in a manner consistent with the Nursing Secretariat’s overall leadership for nursing in Ontario. Through this partnership, the Ministry will implement key recommendations of the Ontario Critical Care Steering Com-mittee.
In early 2005, the Critical Care Steering Committee formed the Ontario Critical Care Expert Panel to address specific concerns related to the delivery of critical care. Recognizing that successful recruitment and retention of critical care nurses is at the core of improving access and quality, the Expert Panel established the Critical Care Nurse Training Standards Task Group in October 2005 to more closely assess critical care nursing education needs in the province. The Task Group brought together critical care nurse leaders from across the province. The chief mandate was to identify and articulate adult critical care core competencies and training standards for Ontario. The group conducted an initial survey of all critical care units in the province, and visited selected sites to determine what nursing standards, if any, were being used. Consider-able variation was identified in the duration of didactic and clinical training in both college and hospital-based critical care nurse education programs. Hospital-based programs averaged 3 weeks training in the surveyed critical care units across the province. In most cases, training was not portable from one hospital to another, and critical care nurses were required to repeat training programs when they moved to another hospital. The availability of college–based programs varied by region with the majority of programs located in Southern Ontario. College-based programs also differed in duration, content and teaching methods (Report of the Critical Care Nurse Training Task Group, 2006a). Clearly, there was a need for standard-ization of critical care nursing education programs.
After significant assessment and data gathering, the Task Group developed a set of Standards for Critical Care Nursing (Critical Care Secretariat, 2006b) based on the practice standards of the Canadian Association of Critical Care Nurses (CACCN) (2004) and the College of Nurses of Ontario (CNO) (2005). The Task Group recommended that selected critical care nursing education programs in the province be evaluated against these new standards. It proposed that the evaluation should determine the extent that the new standards had been incorporated into the theoretical and clinical components of selected hospital and college programs. Further, the Task Group suggested that the MOHLTC should provide support for nurses and hospitals to meet the core competencies identified in the standards. It was thought that a made-in-Ontario solution should include a strong, flexible, college-based critical care training program in consultation, coordination and/or partnership with local hospitals to determine the design, content and timing of critical care courses. It was hoped that this approach would reduce the practice-theory gap, decrease duplication of costs and support development and production of a competent, critical care nursing workforce. In August 2006, the Minister of Health accepted the Task Group’s recommendations. The Nursing and Critical Care Secretariats are now working in partnership to implement initia-tives based on the Task Group recommendations. The government is committed to providing system supports to improve critical care education for nurses and assist hospitals in meeting their human resource needs for safe and accessible care.
In March 2007, the Nursing and Critical Care Secretariats commissioned researchers at the Nursing and Health Services Research Unit (NHSRU), McMaster University, to conduct a collaborative evaluation of selected hospital and college-based critical care nursing education programs in the province against the newly formulated Standards of Critical Care Nursing Practice.

6 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
4. PURPOSE OF THE STUDY
The purpose of the study was to determine the extent to which the newly created critical care nursing standards were incor-porated in selected hospital and college-based critical care nursing education programs across the province.
The objectives of the study were to:
Gain stakeholder input into the new standards including their relevance to practice and education, the enablers •and challenges to implementing them and how to evaluate the programs to determine the extent to which the standards exist in current programs.
Develop a survey instrument based on input from the focus groups and the new standards to evaluate all current •college-based and selected hospital-based critical care nursing education programs.
Conduct a survey of all of the identified programs using the new instrument to obtain a self evaluation of their •own individual curriculum against the new standards.
Conduct expert panel evaluations of each curriculum, using the same survey instrument. •
Identify areas of strength and gaps in coverage of the new provincial critical care nursing standards.•
Prepare and submit a policy report based on the study to the Critical Care and Nursing Secretariats, MOHLTC to •assist in policy decisions about critical care nursing education in the province.
5. METHODOLOGY5.1 Study DesignA mixed methods design, including qualitative and quantitative techniques, was developed to conduct this collaborative evaluation of selected critical care curricula in specific provincial hospitals and colleges. Qualitative techniques included focus groups. The purpose of these focus groups was to gain stakeholder input into and feedback on the newly developed standards, and the development of a survey instrument for evaluation of individual curricula against these standards. Quantitative techniques involved a comprehensive evaluation of the curricula of participating organizations to determine the extent to which the new critical care nursing standards were incorporated into each curriculum. To obtain an evalua-tion of their own curriculum, the participating organizations were surveyed using an instrument developed by the research-ers and based on the new standards. Kopcha and Sullivan (2006) have demonstrated the presence of self-evaluation bias, also known as self-presentation bias or social desirability bias, in surveys of curriculum evaluation. They suggest that survey respondents tend to evaluate their own curriculum more positively than that of others. To balance this self-presentation bias, an expert panel of critical care educators and practitioners used the same instrument to conduct other evaluations of these same curricula. Both the self-assessment and the expert panel evaluation were utilized by the researchers in their overall assessment of critical care education programs. The use of quantitative and qualitative techniques and the collection of a wide range of complimentary and confirmatory data facilitated triangulation (Tashakkori & Teddle, 1998). If evidence converges (agrees), one can be reasonably confident that they are capturing a true picture of the phenomena being studied (Gillham, 2000).
5.2 SampleBased on input from the Critical Care Nursing Standards Task Group, the Critical Care Secretariat recommended 27 organizations offering/conducting basic critical care nursing education programs in Ontario as study participants. Fifteen

7A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
organizations were community colleges and the remaining 12 were acute care hospitals, including academic health science centres and community hospitals.
5.3 Phase 1: Focus Groups The purpose of the focus groups was to gain stakeholder input and feedback on the new standards of critical care nursing practice including:
Their relevance and applicability to practice•
Their strengths •
Issues/concerns•
Areas requiring improvement•
Challenges and enablers to implementation•
Feedback on survey development and conduction plans for the next phase of the study•
The 27 selected organizations were stratified according to LHIN and type of organization (i.e., hospitals and colleges). One organization was randomly selected from each of 13 LHINs. One focus group teleconference was conducted in each of the 13 selected organizations. Participating organizations included 8 hospitals and 5 colleges. The Chief Nursing Officer or Dean in each organization was approached through a formal letter from the principle investigator through the Criti-cal Care Secretariat (see Appendix A). The letter explained the study and invited their participation in the focus groups. A copy of the new standards, focus group consent forms (see Appendix B) and focus group discussion guides (see Appendix C) were attached to the letter.
In the following week, the research coordinator phoned and emailed each organizational nurse leader to identify a contact person for the study and initiate planning. Once identified, all participants in the focus groups were asked to give writ-ten consent to participation and were guaranteed anonymity. A teleconferencing schedule was developed. Thirteen focus groups were conducted in the months of April and May, 2007. Focus groups consisted of 3-6 participants including critical care educators, managers and practitioners
The NHSRU at McMaster University initiated the conference calls. Two researchers and a transcriber participated in each call. The researchers explained the critical care collaborative evaluation study and the purpose of the focus groups. Con-sent to tape the focus group discussion was solicited. The researchers emphasized that all tapes would be securely held at the NHSRU, used only for data analysis purposes and destroyed within 3 years of study completion. They reminded the participants that all comments would be confidential and that the final report would be generic in nature. Strict adherence to the focus group guide was maintained.
5.4 Phase 2: Curriculum Evaluation5.4.1 Survey Development
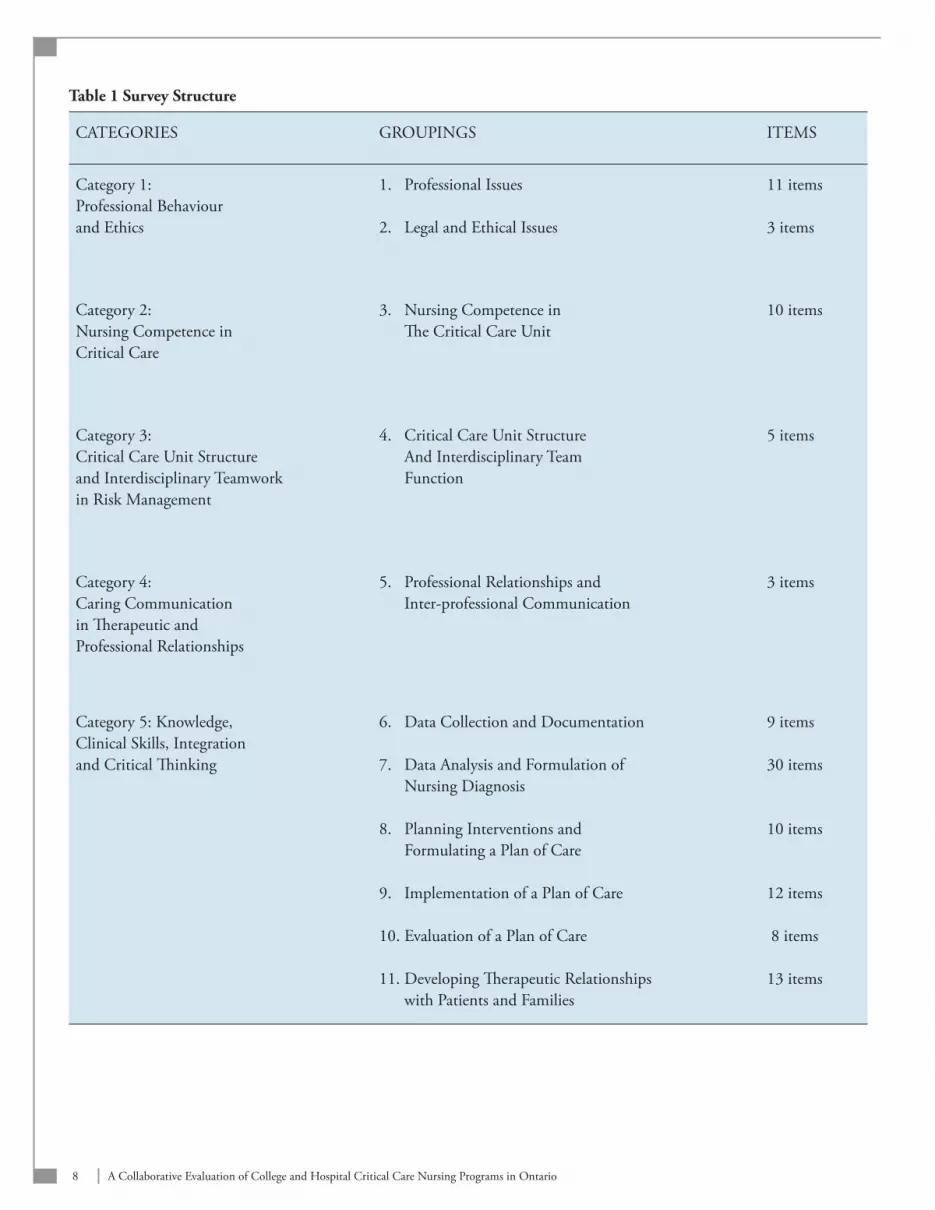
The survey was based on the new Critical Care Nursing Standards in Ontario and on input from the focus group discus-sions (see Appendix D). Its purpose was to determine the extent to which the standards were incorporated in the selected curricula. Following the recommendation of the focus groups, the standards were renumbered and reorganized into five categories to improve logical flow. To facilitate survey development and analysis, the five categories were organized into 11 groupings. A total of 114 items were distributed to their appropriate groupings. Table 1 outlines how the categories were broken down into groupings and the number of items assigned to each category. This structure formed the basis for survey development.
8 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Table 1 Survey Structure
CATEGORIES GROUPINGS ITEMS
Category 1:Professional Behaviour and Ethics
1. Professional Issues
2. Legal and Ethical Issues
11 items
3 items
Category 2:Nursing Competence in Critical Care
3. Nursing Competence in The Critical Care Unit
10 items
Category 3:Critical Care Unit Structure and Interdisciplinary Teamwork in Risk Management
4. Critical Care Unit Structure And Interdisciplinary Team Function
5 items
Category 4:Caring Communication in Therapeutic and Professional Relationships
5. Professional Relationships and Inter-professional Communication
3 items
Category 5: Knowledge, Clinical Skills, Integration and Critical Thinking
6. Data Collection and Documentation
7. Data Analysis and Formulation of Nursing Diagnosis
8. Planning Interventions and Formulating a Plan of Care
9. Implementation of a Plan of Care
10. Evaluation of a Plan of Care
11. Developing Therapeutic Relationships with Patients and Families
9 items
30 items
10 items
12 items
8 items
13 items

9A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Survey participants were asked to identify what percentage (0-100%) of each item they thought was covered in their cur-riculum and whether the item was covered in the theoretical component and/or the clinical component of the curriculum. The survey was developed using Survey Monkey so that it could be administered to the participants in electronic format. The Microsoft Word version of the survey instrument is outlined in Appendix E. Because of differences in the types of programs, separate demographic sections of the survey were developed for hospitals and colleges (see Appendix F).
5.4.2 Survey for Self-Evaluation of the Curricula
Prior to sending out the survey, the Critical Care Secretariat sent a formal letter (see Appendix G) to the Chief Nursing Of-ficers and Deans of the selected organizations inviting their participation in the collaborative curriculum evaluation, both self-evaluation and expert panel evaluation. The letter introduced the survey for self-evaluation and requested organizations to submit their curricular documents to the research team at the NHSRU for blind evaluation by a panel of critical care nursing experts. The process of blinding and expert review was also explained in the letter. Shortly after this letter was sent, the research coordinator sent an electronic version of the survey in Word and Survey Monkey format to all organizational contact persons. Participants were asked to return the completed survey either electronically or by surface mail within 2 weeks. They were provided with contact information for the research team members should they require assistance or clarification. A modified Dillman approach (Dillman, 2007) was used to optimize the survey response rate. After 2 weeks, the research coordinator contacted all institutions that had not responded to offer assistance or encourage completion of the survey. Submission of the completed survey was considered consent to participate in this stage of the study. All partici-pating organizations were asked whether they would be willing to share their individual survey responses and expert panel reviews with the Critical Care Secretariat, MOHLTC by ticking “yes” or “no” on the cover page of the survey.
5.4.3 Expert Panel Review of Curricula
Within one week of the survey distribution, the research coordinator contacted all participating organizations and remind-ed them to submit their curriculum electronically or by surface mail to the NHSRU at McMaster University. A research assistant removed all organizational identifiers from the documents received and coded all the curricula. To guarantee confidentiality, original curricula were secured in a locked file at the NHSRU. Participants were informed that curricula would not leave the NHSRU at any time, that expert panel reviews would take place in the unit and that all curricula used in the review would be destroyed once the study was completed. They were also guaranteed that the final report would not identify individual curricula or their associated facilities and would be generic in nature. Participating organizations were promised a copy of the final report along with an accompanying letter, which confidentially identified their own code number so they could compare their self-evaluation and expert panel review results with those of other participating orga-nizations. Results from organizations that agreed to share their individual information with the MOHLTC were compiled in a confidential addendum to be sent to the MOHLTC along with the main report.
A panel of 8 experts conducted blind evaluations of the submitted curricula to identify the extent to which the new stan-dards were incorporated. Three experts were NHSRU researchers with critical care and curriculum development experi-ence. Five were critical care clinical practitioners and educators from the field recommended by the Critical Care Nursing Subcommittee at the Critical Care Secretariat, MOHLTC. Appendix I contains a list of the expert panel reviewers and their present designations and affiliations. Each reviewer evaluated 6 curricula using the survey instrument intended for self-evaluation by the study participants. Each curriculum underwent independent evaluation by two separate experts. Intraclass correlations were calculated to determine inter-rater reliability (IRR) between the reviewers for each curricu-lum. Laschinger (1992) suggests that intraclass correlation coefficients (ICC) are useful statistics for estimating IRR when knowledge of rater agreement is important and are particularly effective in educational program evaluation research. Al-though Laschinger recommends an ICC of 0.75 or higher, Streiner and Norman (2000) suggest that ICCs of 0.50 to 1.00 indicate satisfactory to excellent inter-rater reliability.

10 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
6. RESULTS6.1. Focus Group Data Collection and Qualitative AnalysisThe 13 focus group teleconferences were taped and transcribed. These transcriptions were entered into NVIVO 1.3 and thematic analysis was conducted. The results of the thematic analysis are outlined below.
Qualitative Analysis
Participants believed that the standards were comprehensive and well framed. They liked the detail and appreciated their close alignment with the national standards from CACCN and CNO. Many participants recognized the diligence that went into the development of the new standards and had confidence in their effectiveness as a tool to ensure baseline com-petencies for critical care nurses in Ontario.
StrengthsIn general, participants liked the comprehensiveness of the standards and described them as “all-encompassing.” A particu-lar strength was the inclusion of competencies such as professional behaviour/ethics, continuing competence and research, which emphasized the importance of developing and maintaining skills outside the clinical base. They noted that empha-sizing the importance of these skills in critical care nursing practice, would challenge nurses to think outside the realm of their hands-on clinical practice.
Many participants talked about using the standards as a reference guide in the development and assessment of their cur-riculum, while others described the advantage of using them as a reflective tool to evaluate their current program and improve the quality and relevance of its content.
Credentialing portability was a significant theme that emerged from the interviews. Many participants believed the stan-dards could be used as a catalyst for standardizing critical care curricula across Ontario and increasing nurse movement across organizations.
On a micro level, the standards were seen as a way to normalize expectations within a hospital setting. Participants de-scribed the benefit of having a document that identified expectations for the nurse, members of the health care team and the health care setting.
Participants appreciated the inclusion of an evaluation component in the standards and believed they laid the groundwork for performance reviews. They also suggested that provincial standards would facilitate better performance review that could follow the nurse as she moved across organizations in the province. The standards were considered of great value to hospitals and colleges. Participants believed that the standards allowed them the flexibility to develop a critical care program specific to their organization and provide the structure to ensure content consistency across the province.
Issues/ConcernsIssues raised by participants regarding the new standards of practice included:
The flow and organization of the standards document.•
The relevance of some of the categories and their applicability to all organizations.•
The ambiguity surrounding employer/college responsibility for teaching certain standards. •
11A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Participants were pleased with the detail and depth of the standards, although they believed they could be better organized to enhance the flow and readability of the document. However, this was considered a minor issue rather than a significant weakness.
Many organizations believed that some criteria listed in the standard categories were not applicable to their organization. For example, colleges identified outcome standards 2, 3 and 5 (Structure of the Critical Care Unit) as competencies that would be included in a hospital orientation program but not relevant to college programs. They questioned their role in teaching this competency in their educational programs. Hospitals believed that some of the skills identified (e.g., intra-aortic balloon pumping) were not practiced in all critical care units. Therefore, nurses working in those hospitals would not be able to acquire or maintain competency in those skills. Responsibility/accountability for teaching theoretical versus clinical parts of the curriculum was discussed. Concern was expressed over how accountability would be assigned.
Participants identified gaps in criteria and provided feedback on how to improve these areas. An overview of suggested gaps in the standards is outlined below:
Patient safety should be more clearly identified (outcome standard 4) •
More emphasis should be placed on the role of the critical care nurse in disaster and pandemic planning and emer-•gency preparedness.
More emphasis needs to be placed on infection control in critical care.•
An on going performance appraisal system based on the standards needs to be created to ensure that competencies •are maintained (outcome standard 5.4)
Enhancing criteria to emphasize both the patient and the patient’s family as the client (outcome standard 8)•
A statement that the nurse recognizes the patient as a unique individual, needs to be added to •( outcome standard 7.1)
More attention needs to be given to leadership as a role for the critical care staff nurse.•
More attention needs to be given to the role of the critical care nurse in research.•
Enablers to ImplementationParticipants identified several key factors that would aid in the implementation of the standards across all organizations:
Participants believed that because the standards are so closely aligned with the CACCN standards, implementa-•tion of the new provincial standards should be relatively easy for most organizations.
Forming equitable partnerships between hospitals and colleges was identified as absolutely necessary to enable suc-•cessful implementation of the new standards of practice. If colleges were flexible in scheduling courses and hospi-tals ensured that new hires were required to obtain certification within a set time, they could deliver programs that would satisfy the needs of each organization.
Hiring instructors who are active in clinical practice was seen as a significant factor in ensuring the standards •would be used to develop consistent and effective curricula across the province. By maintaining currency in the clinical setting, instructors would be better equipped to teach the standards and ensure competencies were main-tained in both hospital and educational environments.
Participants were pleased to have a document that clearly defined what is needed to move forward in critical care •education; however, a number of challenges must be addressed.
12 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Challenges to ImplementationResources (both human and fiscal) were identified as a major challenge in implementing the new standards.•
Many nurses cannot take time off work to for continuing education unless financial support is available. Schedul-•ing flexibility and funding is required to enable nurses to take the courses.
Computer/online educational systems are required for nurses to take online courses. •
Supplementary nursing staff is needed to cover shifts for nurses taking courses. •
The time required to address all the standards was seen as a challenge for many organizations, especially hospitals. •
Older nurses refusing to upgrade to meet the new standards of practice. •
New graduates lacking the experience needed to work in critical care units.•
The need to upgrade mentors/preceptors (additional education and training) to bridge the gap between theory and •practice in the clinical teaching environment.
The need for workforce planning to successfully implement the new standards of practice. •
Partnerships Between Colleges and Hospitals Need to be Developed Four key issues were identified:
Size of Student Population: Colleges described the low numbers of students as a challenge in maintaining funding for 1. their programs. They argued that many nurses are trained on-site in hospitals and do not feel compelled to participate in certification programs beyond their hospital orientation.
College based participants believed hospital training was a costly endeavour that should be taken over by educational institutions. Hospital participants argued that the timing of college programs was problematic. Hospitals were forced to provide in-house training because the employment needs of hospitals did not coincide with the academic year.
Curriculum: The curriculum was a contentious issue between colleges and hospitals. Colleges believed that the hos-2. pitals do not have as high curriculum development standards as college-based programs. Conversely, hospitals believe that college programs are too broad based and do not provide nurses with the clinical skills needed to practice in a critical care environment.
Funding Timelines: Limits placed on funding by the MOHLTC are a barrier that both the partnering of hospitals and 3. colleges and the implementation of the new standards in general. For example, if funding is provided in March and hospitals are required to spend it by June, college-based programs which run September to May are not a viable option for nurses.
Technology: A number of colleges around the province are equipped with simulation labs that are used for teach-4. ing clinical skills outside the hospital setting; however, hospitals have difficulty obtaining access to these labs. Due to lack of available space and the costs involved, hospital organizations were interested in using the SIM labs rather than purchasing their own. Hospital participants asked that they be given priority to use the SIM labs as needed and on an equal time basis (i.e., Monday-Friday day time hours).
6.2 Collaborative Curriculum Evaluation: Demographics and Data Collection 6.2.1 Organizational Demographics: Hospitals and Colleges
Twelve hospital organizations participated in the evaluation of critical care nursing curricula. Six were Academic Health Science Centres, 5 were large community hospitals and 1 was a small community-based hospital. Although this organiza-tion did not have a curriculum, they contracted with other centres to provide education as needed. They felt it was impor-tant to be part of the process even though they could not fully participate. All reported having combined medical/surgical critical care units, with the academic health science centres identifying sub specialties as well (i.e., cardiovascular, thoracic
13A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
and trauma). Unit size varied from less than 10 beds to greater than 30 beds. Four centres had greater than 30 beds, 3 had 21-30 beds, 4 had 11-20 beds and 1 had less than 10 beds. Eleven hospitals identified in-house orientation as the method of education and 1 (120) indicated a joint program with their local community college. Total program duration was bro-ken down into total theoretical and total clinical hours. The theoretical component varied from 1 week to 11 weeks, and the clinical component from 3 weeks to 9 weeks. Nine of 12 indicated they had written standards of practice in place and 3 stated that they did not. While eight of 12 hospitals indicated that CNO and CACCN were reflected in their programs to some extent, 4 did not respond to this question. Moreover, these 8 organizations indicated that they updated their unit standards regularly, and time frames for updates varied with each organization. The number of nurses completing the pro-gram on an annual basis varied from less than 10 (1 site), 11-20 (7 sites) and more than 30 (4 sites). Eleven of 12 sites in-dicated their program included an evaluation component and all nurses were continually evaluated, although the frequency varied. Appendix H1 summarizes the demographic analysis of hospital-based programs participating in the survey.
College demographics are summarized in Appendix H2. It was important to identify the kinds of programs that colleges offered and whether they were full or part time. Only 1 college indicated that they had a basic general program, 6 had specialty programs beyond the basic program and 5 had a combination of both. Only 1 college offered full time study, while 8 offered part time study and 3 classified their programs under the “other” category. This category included dis-tance education, continuing education courses and a condensed program. Course completion leading to Critical Care Certification was varied, probably due to the full time/part time status of the programs. The length of time to complete the program ranged from “based on individual needs” to 3 years. The theoretical and clinical components were reported separately in hours. The duration of the theoretical component varied from 100 hours (1 site) to 330 hours (1 site), and the clinical component duration ranged from 84 hours (1 site) to 240 hours (1 site). Total program hours ranged from 297-450 hours. The number of students who had completed the programs to date was reported as “difficult to assess,” and only 4 colleges identified a specific number. Course tuition was reported by 8 of 12 colleges and ranged from $1500.00 to $2,560.00.
6.2.2 Self-Evaluation Survey
Twenty-three out of 27 organizations completed and returned the self-evaluation survey (see Appendix E). One college de-clined to participate in the project, citing short timelines over the summer period as being problematic. Another college no longer offered a critical care program and declined to participate. The third college (112) initially agreed to participate in the self-evaluation survey, but due to the sudden long-term illness of their “critical care expert,” they were unable to com-plete and return the survey. However, they wished to remain a participant in the process and submitted their curriculum for review by the expert panel. One hospital (124) did not have a critical care course because they hired only experienced ICU nurses and utilized the services of a larger teaching hospital in their area when necessary. Those who did not return the survey within 2 weeks of the initial mailing were contacted by phone and by email. All 23 surveys were completed by July 15, 2007 and returned to the NHSRU. Twenty-three organizations responded electronically using the Survey Monkey tool, and one submitted their evaluation in hard copy format.
6.2.3 Expert Panel Evaluation
A panel of 8 experts conducted a blind evaluation of the submitted curricula to identify the extent to which the new standards were incorporated into the programs. Three experts were NHSRU researchers with critical care and curriculum development experience. Five were critical care clinical practitioners and educators from the field recommended by the Critical Care Nursing Subcommittee at the Critical Care Secretariat, MOHLTC. Appendix I contains a list of the expert panel reviewers and their present designations and affiliations. Each reviewer was required to review 6 curricula using the same survey instrument used for the self-evaluation by the participants in the study. If expert reviewers were affiliated with a participating organization, they did not review the curriculum from that organization. Each curriculum underwent independent evaluation by two separate experts. Intraclass correlations were used to determine inter-rater reliability (IRR) between the 2 expert reviewers for each curriculum.
14 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
The expert panel met for 3 days in July 2007. On the first morning, initial training was conducted by the research team on the survey instrument and the evaluation process. In the training session, the 8 experts were given a detailed explanation of the study, a description of their role as expert reviewers, an in-depth overview of the survey instrument and a brief session on the use of intraclass correlation co-efficient to determine inter-rater reliability in the review process. To gain practice in the evaluation process, they all evaluated a section of one curriculum using the corresponding section of the tool. Interclass correlation coefficients were calculated to determine inter-rater reliability. After reaching an ICC of .83 in the practice ses-sion, a highly acceptable inter-rater reliability, the experts were then organized into pairs to begin the blind evaluation of the submitted curricula. Each expert was given 3 curricula. Upon completing an independent evaluation of these 3 cur-ricula, they exchanged curricula with their partner and completed review of the remaining 3 curricula. Each curriculum was reviewed by 2 separate reviewers and each expert reviewed a total of 6 curricula. Intraclass correlation coefficients were calculated on the expert panel review pairs to determine inter-rater reliability for each of the curricula evaluated. The cor-relation coefficients are provided in Appendix J. All but 5 curriculum evaluations achieved satisfactory (ICC= 0.50) to high (ICC= 0.84) inter-rater reliability among the expert reviewers.
Self-evaluation scores were averaged with the scores of the two experts in order to obtain a balanced scoring of each indi-vidual item and overall mean compliance by grouping and by item.
6.2.4 Hospital and College Rankings of Overall Mean Compliance with Critical Care Nursing Standards
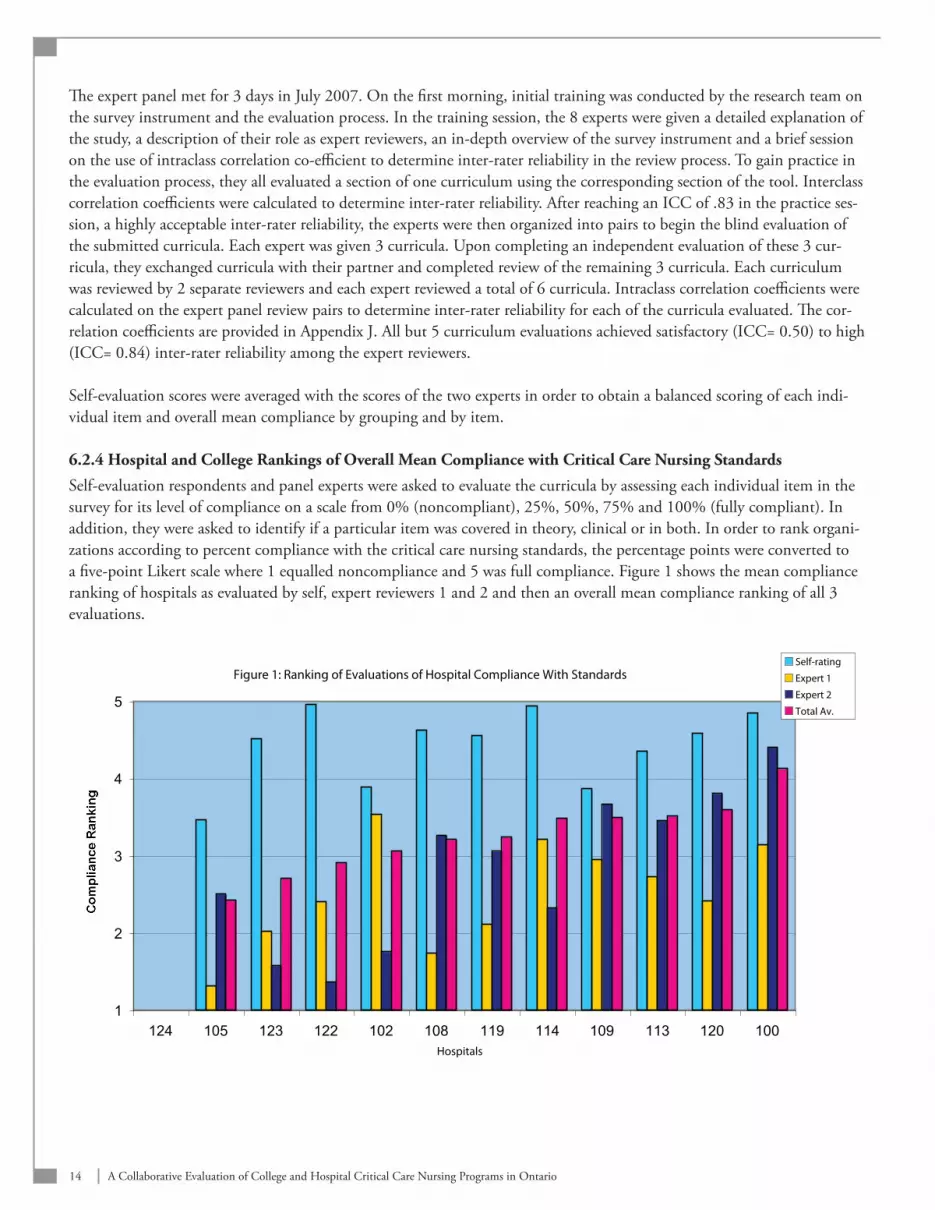
Self-evaluation respondents and panel experts were asked to evaluate the curricula by assessing each individual item in the survey for its level of compliance on a scale from 0% (noncompliant), 25%, 50%, 75% and 100% (fully compliant). In addition, they were asked to identify if a particular item was covered in theory, clinical or in both. In order to rank organi-zations according to percent compliance with the critical care nursing standards, the percentage points were converted to a five-point Likert scale where 1 equalled noncompliance and 5 was full compliance. Figure 1 shows the mean compliance ranking of hospitals as evaluated by self, expert reviewers 1 and 2 and then an overall mean compliance ranking of all 3 evaluations.
Figure 1: Ranking of Evaluations of Hospital Compliance With Standards
1
2
3
4
5
124 105 123 122 102 108 119 114 109 113 120 100Hospitals
Compliance Ranking
Self-rating
Expert 1
Expert 2
Total Av.

15A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Self-ratings in all instances were higher than the experts. This was expected given that individuals know their own pro-grams better than others and self-evaluate with this knowledge. This may have also been attributable to some self-evalua-tion or self-presentation bias. The experts could only evaluate curricula/programs on the information provided in the curri-cula submissions and were not as familiar with them as the self-evaluators. For these reasons it was necessary to average the self-ratings with the expert reviewer ratings. Figure 2 below is extracted from Figure 1 and outlines the ranking of overall mean compliance with the standards by hospital.
Figure 2: Ranking of Overall Mean Compliance With Standards By Hospital
1
2
3
4
5
124 105 123 122 102 108 119 114 109 113 120 100
Hospital
Mean Compliance Ranking
None of the hospital programs are in full compliance with the standards. This may reflect the fact that new standards have only recently become part of the public domain and will require more time for integration into programs. Hospital 124 is an outlier because it is a small community hospital that contracts critical care education to a large teaching centre in the region and does not have a curriculum of its own, but wished to be part of the study.
Figure 3 demonstrates the mean compliance ranking of colleges as evaluated by self, expert reviewers 1 and 2 and then an overall mean compliance ranking of all 3 evaluations.
Figure 3: Ranking of Evaluations of College Compliance With Standards
1
2
3
4
5
112 107 110 104 121 101 118 106 103 115 111 117 116College
Compliance Ranking
Self-rating
Expert 1
Expert 2
Total Av.
16 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
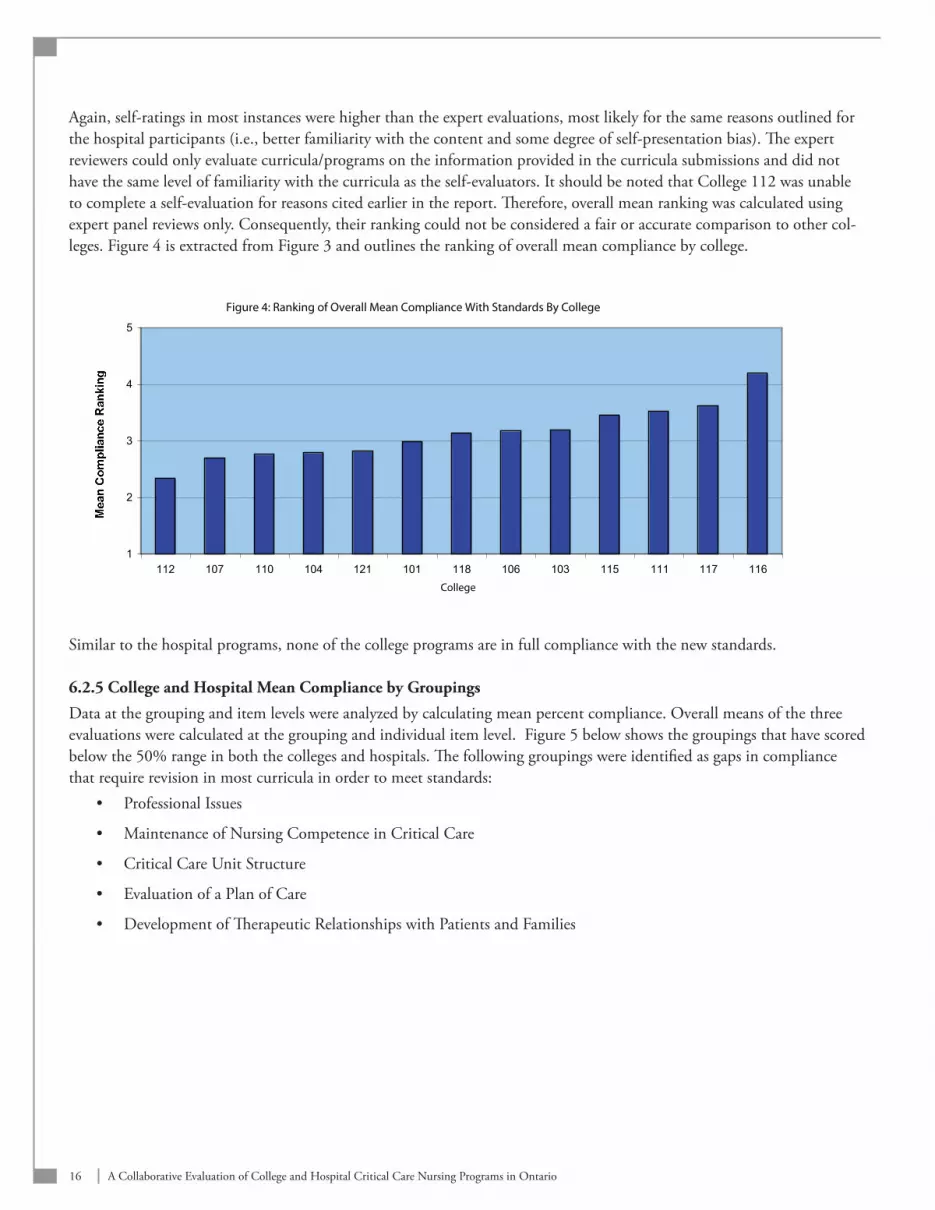
Again, self-ratings in most instances were higher than the expert evaluations, most likely for the same reasons outlined for the hospital participants (i.e., better familiarity with the content and some degree of self-presentation bias). The expert reviewers could only evaluate curricula/programs on the information provided in the curricula submissions and did not have the same level of familiarity with the curricula as the self-evaluators. It should be noted that College 112 was unable to complete a self-evaluation for reasons cited earlier in the report. Therefore, overall mean ranking was calculated using expert panel reviews only. Consequently, their ranking could not be considered a fair or accurate comparison to other col-leges. Figure 4 is extracted from Figure 3 and outlines the ranking of overall mean compliance by college.
Figure 4: Ranking of Overall Mean Compliance With Standards By College
1
2
3
4
5
112 107 110 104 121 101 118 106 103 115 111 117 116
College
Mean Compliance Ranking
Similar to the hospital programs, none of the college programs are in full compliance with the new standards.
6.2.5 College and Hospital Mean Compliance by Groupings
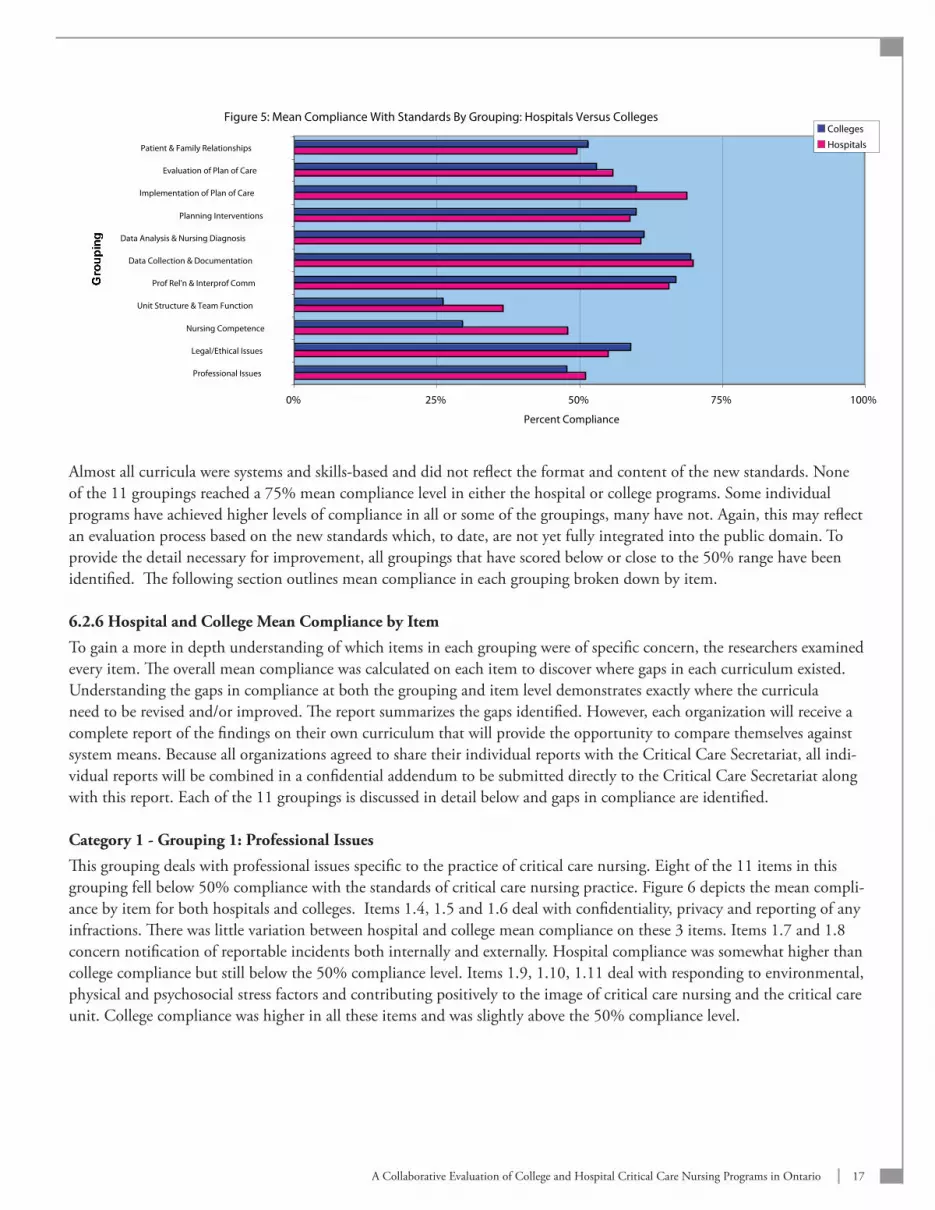
Data at the grouping and item levels were analyzed by calculating mean percent compliance. Overall means of the three evaluations were calculated at the grouping and individual item level. Figure 5 below shows the groupings that have scored below the 50% range in both the colleges and hospitals. The following groupings were identified as gaps in compliance that require revision in most curricula in order to meet standards:
Professional Issues •
Maintenance of Nursing Competence in Critical Care •
Critical Care Unit Structure •
Evaluation of a Plan of Care •
Development of Therapeutic Relationships with Patients and Families•
17A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Figure 5: Mean Compliance With Standards By Grouping: Hospitals Versus Colleges
0% 25% 50% 75% 100%
Professional Issues
Legal/Ethical Issues
Nursing Competence
Unit Structure & Team Function
Prof Rel'n & Interprof Comm
Data Collection & Documentation
Data Analysis & Nursing Diagnosis
Planning Interventions
Implementation of Plan of Care
Evaluation of Plan of Care
Patient & Family Relationships
Grouping
Percent Compliance
Colleges
Hospitals
Almost all curricula were systems and skills-based and did not reflect the format and content of the new standards. None of the 11 groupings reached a 75% mean compliance level in either the hospital or college programs. Some individual programs have achieved higher levels of compliance in all or some of the groupings, many have not. Again, this may reflect an evaluation process based on the new standards which, to date, are not yet fully integrated into the public domain. To provide the detail necessary for improvement, all groupings that have scored below or close to the 50% range have been identified. The following section outlines mean compliance in each grouping broken down by item.
6.2.6 Hospital and College Mean Compliance by Item
To gain a more in depth understanding of which items in each grouping were of specific concern, the researchers examined every item. The overall mean compliance was calculated on each item to discover where gaps in each curriculum existed. Understanding the gaps in compliance at both the grouping and item level demonstrates exactly where the curricula need to be revised and/or improved. The report summarizes the gaps identified. However, each organization will receive a complete report of the findings on their own curriculum that will provide the opportunity to compare themselves against system means. Because all organizations agreed to share their individual reports with the Critical Care Secretariat, all indi-vidual reports will be combined in a confidential addendum to be submitted directly to the Critical Care Secretariat along with this report. Each of the 11 groupings is discussed in detail below and gaps in compliance are identified.
Category 1 - Grouping 1: Professional Issues
This grouping deals with professional issues specific to the practice of critical care nursing. Eight of the 11 items in this grouping fell below 50% compliance with the standards of critical care nursing practice. Figure 6 depicts the mean compli-ance by item for both hospitals and colleges. Items 1.4, 1.5 and 1.6 deal with confidentiality, privacy and reporting of any infractions. There was little variation between hospital and college mean compliance on these 3 items. Items 1.7 and 1.8 concern notification of reportable incidents both internally and externally. Hospital compliance was somewhat higher than college compliance but still below the 50% compliance level. Items 1.9, 1.10, 1.11 deal with responding to environmental, physical and psychosocial stress factors and contributing positively to the image of critical care nursing and the critical care unit. College compliance was higher in all these items and was slightly above the 50% compliance level.

18 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Figure 6: Mean Compliance by Item in Professional Issues Grouping: Hospitals Vs Colleges
0%
25%
50%
75%
100%
1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9 1.1 1.11
Items 1.1 to 1.11
Percent Compliance
Hospitals
Colleges
Category 1 - Grouping 2: Legal/Ethical Issues
This grouping contains only 3 items. Figure 7 shows that all 3 items were above the 50% compliance level. Although this area may require attention in future curriculum revision, it does not represent a major gap in the curricula in this aggre-gate analysis. Individual organizations may fall below the 50% compliance level and may need to address this in order to achieve better compliance with the standards.
Figure 7: Mean Compliance by Item in Legal/Ethical Issues Grouping: Hospitals Vs Colleges
0%
25%
50%
75%
100%
1.12 1.13 1.14
Items 1.12 to 1.14
Percent Compliance
HospitalsColleges
Category 2 - Grouping 3: Nursing Competence in Critical Care
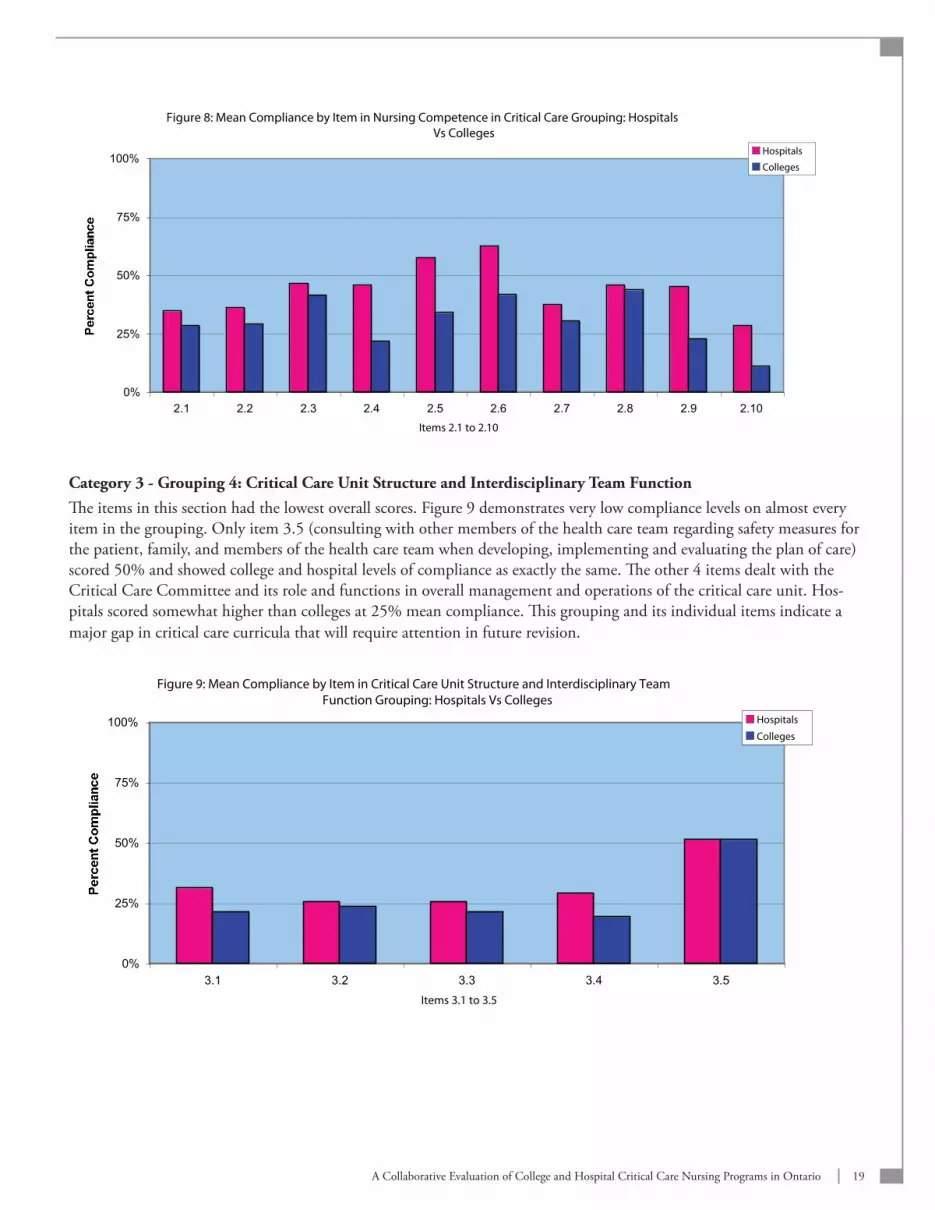
This grouping of 10 items addresses hospital responsibilities in recruiting, hiring and retaining qualified personnel, as well as the responsibility of nurses and hospitals to maintain nursing knowledge and skill and provision of orientation, continu-ing education and regular performance appraisals in critical care areas. As shown in Figure 8, hospitals scored higher than colleges on all of these items, particularly in 2.5 (providing orientation for new critical care nurses where they are supernu-merary) and 2.6 (providing a standards-based orientation for new critical care nurses). The overall average for both colleges and hospitals was below 50%. This represents a gap in compliance and needs to be enhanced in future curriculum revision.
19A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Figure 8: Mean Compliance by Item in Nursing Competence in Critical Care Grouping: Hospitals Vs Colleges
0%
25%
50%
75%
100%
2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8 2.9 2.10
Items 2.1 to 2.10
Percent Compliance
Hospitals
Colleges
Category 3 - Grouping 4: Critical Care Unit Structure and Interdisciplinary Team FunctionThe items in this section had the lowest overall scores. Figure 9 demonstrates very low compliance levels on almost every item in the grouping. Only item 3.5 (consulting with other members of the health care team regarding safety measures for the patient, family, and members of the health care team when developing, implementing and evaluating the plan of care) scored 50% and showed college and hospital levels of compliance as exactly the same. The other 4 items dealt with the Critical Care Committee and its role and functions in overall management and operations of the critical care unit. Hos-pitals scored somewhat higher than colleges at 25% mean compliance. This grouping and its individual items indicate a major gap in critical care curricula that will require attention in future revision.
Figure 9: Mean Compliance by Item in Critical Care Unit Structure and Interdisciplinary Team Function Grouping: Hospitals Vs Colleges
0%
25%
50%
75%
100%
3.1 3.2 3.3 3.4 3.5
Items 3.1 to 3.5
Percent Compliance
Hospitals
Colleges
20 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
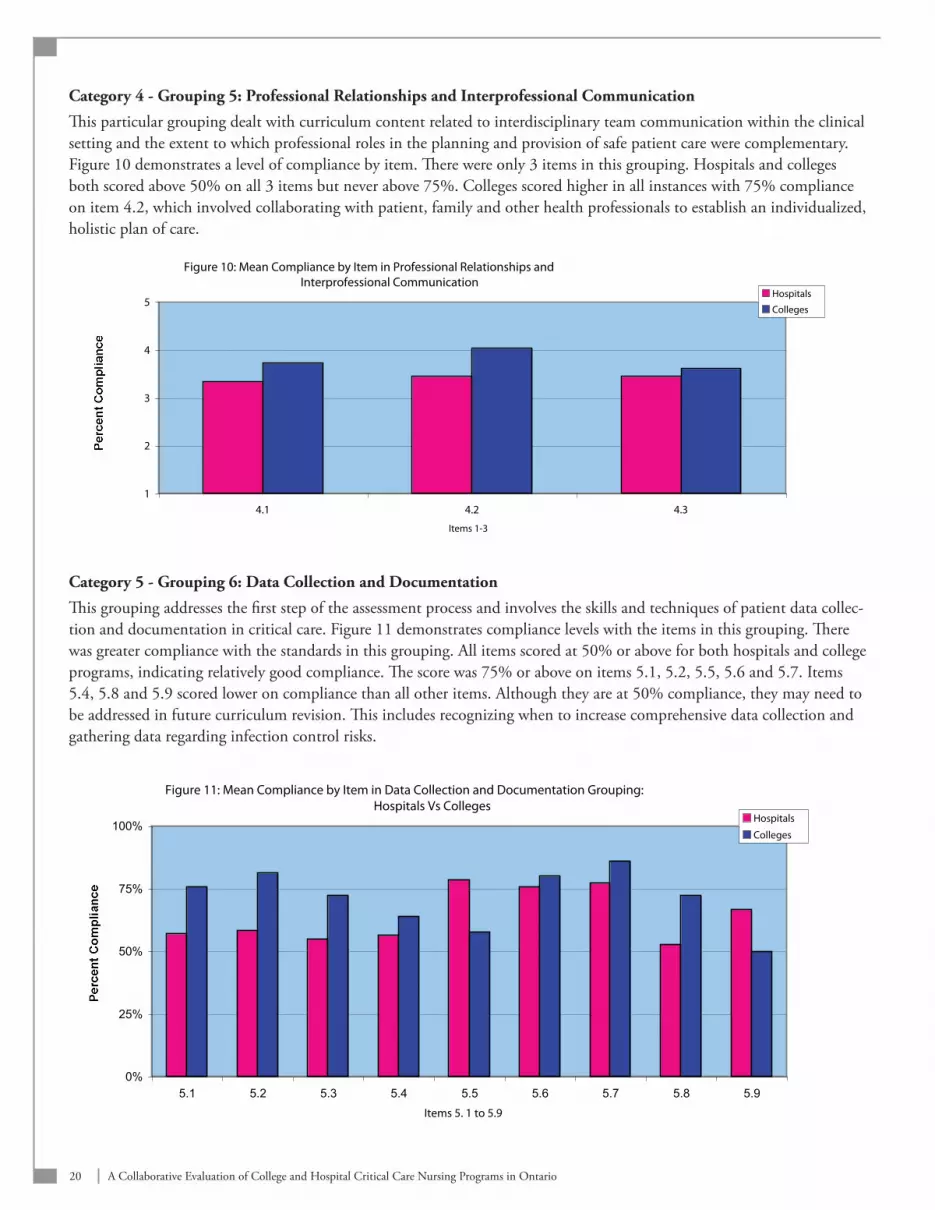
Category 4 - Grouping 5: Professional Relationships and Interprofessional Communication
This particular grouping dealt with curriculum content related to interdisciplinary team communication within the clinical setting and the extent to which professional roles in the planning and provision of safe patient care were complementary. Figure 10 demonstrates a level of compliance by item. There were only 3 items in this grouping. Hospitals and colleges both scored above 50% on all 3 items but never above 75%. Colleges scored higher in all instances with 75% compliance on item 4.2, which involved collaborating with patient, family and other health professionals to establish an individualized, holistic plan of care.
Figure 10: Mean Compliance by Item in Professional Relationships and Interprofessional Communication
1
2
3
4
5
4.1 4.2 4.3
Items 1-3
Percent Compliance
Hospitals
Colleges
Category 5 - Grouping 6: Data Collection and Documentation
This grouping addresses the first step of the assessment process and involves the skills and techniques of patient data collec-tion and documentation in critical care. Figure 11 demonstrates compliance levels with the items in this grouping. There was greater compliance with the standards in this grouping. All items scored at 50% or above for both hospitals and college programs, indicating relatively good compliance. The score was 75% or above on items 5.1, 5.2, 5.5, 5.6 and 5.7. Items 5.4, 5.8 and 5.9 scored lower on compliance than all other items. Although they are at 50% compliance, they may need to be addressed in future curriculum revision. This includes recognizing when to increase comprehensive data collection and gathering data regarding infection control risks.
Figure 11: Mean Compliance by Item in Data Collection and Documentation Grouping: Hospitals Vs Colleges
0%
25%
50%
75%
100%
5.1 5.2 5.3 5.4 5.5 5.6 5.7 5.8 5.9
Items 5. 1 to 5.9
Percent Compliance
Hospitals
Colleges

21A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Category 5 - Grouping 7: Data Analysis and Formulation of Nursing Diagnosis
This particular grouping involves the second step of nursing assessment of critically ill patients. It entails learning of the assessment, documentation and interpretation of all data collected and the analysis of unexpected findings. Based on this analysis, the critical care nurse learns to set priorities for care. This is the largest grouping and contains 30 items. Figures 12a and 12b depict the average level of compliance by item. The overall average for the grouping was above 50%. How-ever, in 10 items in the grouping, either the colleges and/or the hospitals were below the 50% compliance level. Figure 12a shows mean compliance levels for the first 15 items (5.10 to 5.24). Those that fall below the 50% mean compliance level are listed below.
Item 5.18 - Alterations in Integumentary Tissue Perfusion: Hospitals were above 50% compliance, colleges were not.
Item 5.21 - Ineffective Thermoregulation: Hospitals were 50% compliant and colleges were not.
Item 5.24 - Alteration in Immunologic Function: Both hospitals and colleges were below the 50% compliance level.
Figure 12a: Mean Compliance by Item in Data Analysis and Formulation of Nursing Diagnosis Grouping: Hospitals Vs Colleges
0%
20%
40%
60%
80%
100%
5.10 5.11 5.12 5.13 5.14 5.15 5.16 5.17 5.18 5.19 5.20 5.21 5.22 5.23 5.24
Items 5.10 to 5.24
Percent Compliance
Hospitals
Colleges
Figure 12b below outlines the average compliance of items 5.25 to 5.39. All items below 50% compliance are listed below.
Item 5.25 - Alteration in Hematological Function: Colleges were above the 50%, compliance level but hospitals were not.
Item 5.28 - Altered Family Process: Both hospitals and colleges were below the 50% compliance level.
Item 5.30 - Manifestations of Abuse: Both hospitals and colleges were only at the 25% level of compliance.
Item 5.32 - End of Life Withdrawal of treatment and/or the Execution of Advanced Directives: Colleges were above 50% compliance but hospitals were not.
Item 5.33 - Organ Donation and Transplantation: Hospitals scored above 50% compliance and colleges did not.

22 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Item 5.39 - Integrate All Findings From the Assessment to Identify Collaborative and/or Independent Nursing Diagnoses: Colleges above 50% compliance and hospitals were not.
Figure 12b: Mean Compliance by Item in Data Analysis and Formulation of Nursing Diagnosis Grouping: Hospitals Vs Colleges
0%
25%
50%
75%
100%
5.25 5.26 5.27 5.28 5.29 5.30 5.31 5.32 5.33 5.34 5.35 5.36 5.37 5.38 5.39
Items 5.25 to 5.39
Percent Compliance
Hospitals
Colleges
Category 5 - Grouping 8: Planning Interventions and Formulating a Plan of Care
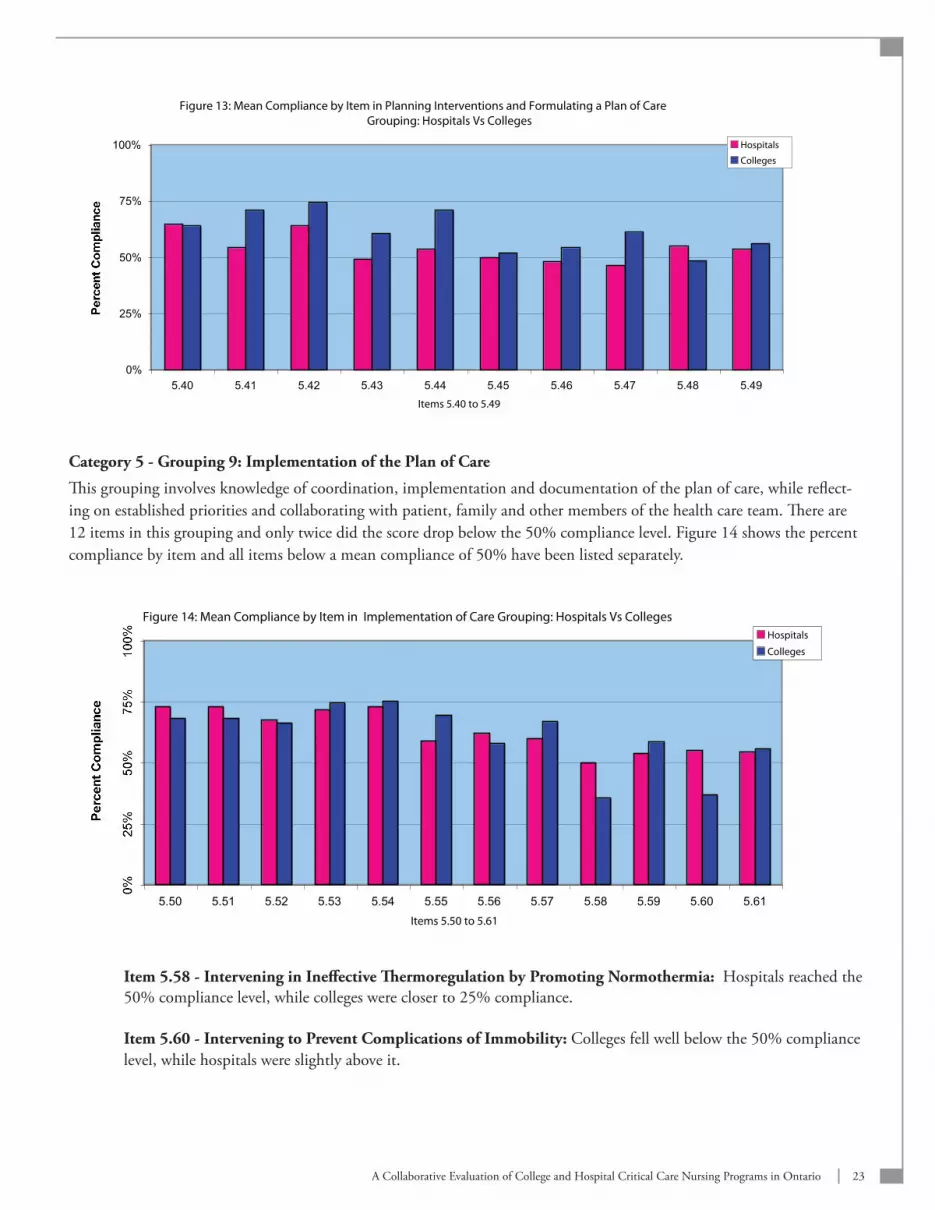
This grouping involves planning interventions for critical care patients based on actual and potential nursing diagnoses and formulating a plan of care in collaboration with other members of the health care team, the patient and the family. The overall average was above 50% compliance for the grouping but individual items fell slightly below this level. As can be seen in Figure 13 the items of concern include 5.43, 5.46, 5.47 and 5.48. These items are outlined and will require atten-tion in any upcoming curriculum revision.
Item 5.43 - Balancing the Science of Curing with the Act of Caring: Hospitals were below the 50% compliance levels and colleges were only slightly above this level.
Item 5.46 - Identifying Realistic and Measurable Expected Patient Outcomes: Hospitals were below the 50% compliance level and colleges were slightly above.
Item 5.47 - Validating the Plan of Care with Patient, Family and Other Members of the Health Care Team: Hospitals were below the 50% compliance level and colleges were slightly above.
Item 5.48 - Identifying Required Resources to Accomplish the Plan of Care: Colleges were below the 50% compliance level and hospitals were not.
23A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Figure 13: Mean Compliance by Item in Planning Interventions and Formulating a Plan of Care Grouping: Hospitals Vs Colleges
0%
25%
50%
75%
100%
5.40 5.41 5.42 5.43 5.44 5.45 5.46 5.47 5.48 5.49
Items 5.40 to 5.49
Percent Compliance
Hospitals
Colleges
Category 5 - Grouping 9: Implementation of the Plan of Care
This grouping involves knowledge of coordination, implementation and documentation of the plan of care, while reflect-ing on established priorities and collaborating with patient, family and other members of the health care team. There are 12 items in this grouping and only twice did the score drop below the 50% compliance level. Figure 14 shows the percent compliance by item and all items below a mean compliance of 50% have been listed separately.
Figure 14: Mean Compliance by Item in Implementation of Care Grouping: Hospitals Vs Colleges
0%
25%
50%
75%
100%
5.50 5.51 5.52 5.53 5.54 5.55 5.56 5.57 5.58 5.59 5.60 5.61
Items 5.50 to 5.61
Percent Compliance
Hospitals
Colleges
Item 5.58 - Intervening in Ineffective Thermoregulation by Promoting Normothermia: Hospitals reached the 50% compliance level, while colleges were closer to 25% compliance.
Item 5.60 - Intervening to Prevent Complications of Immobility: Colleges fell well below the 50% compliance level, while hospitals were slightly above it.
24 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
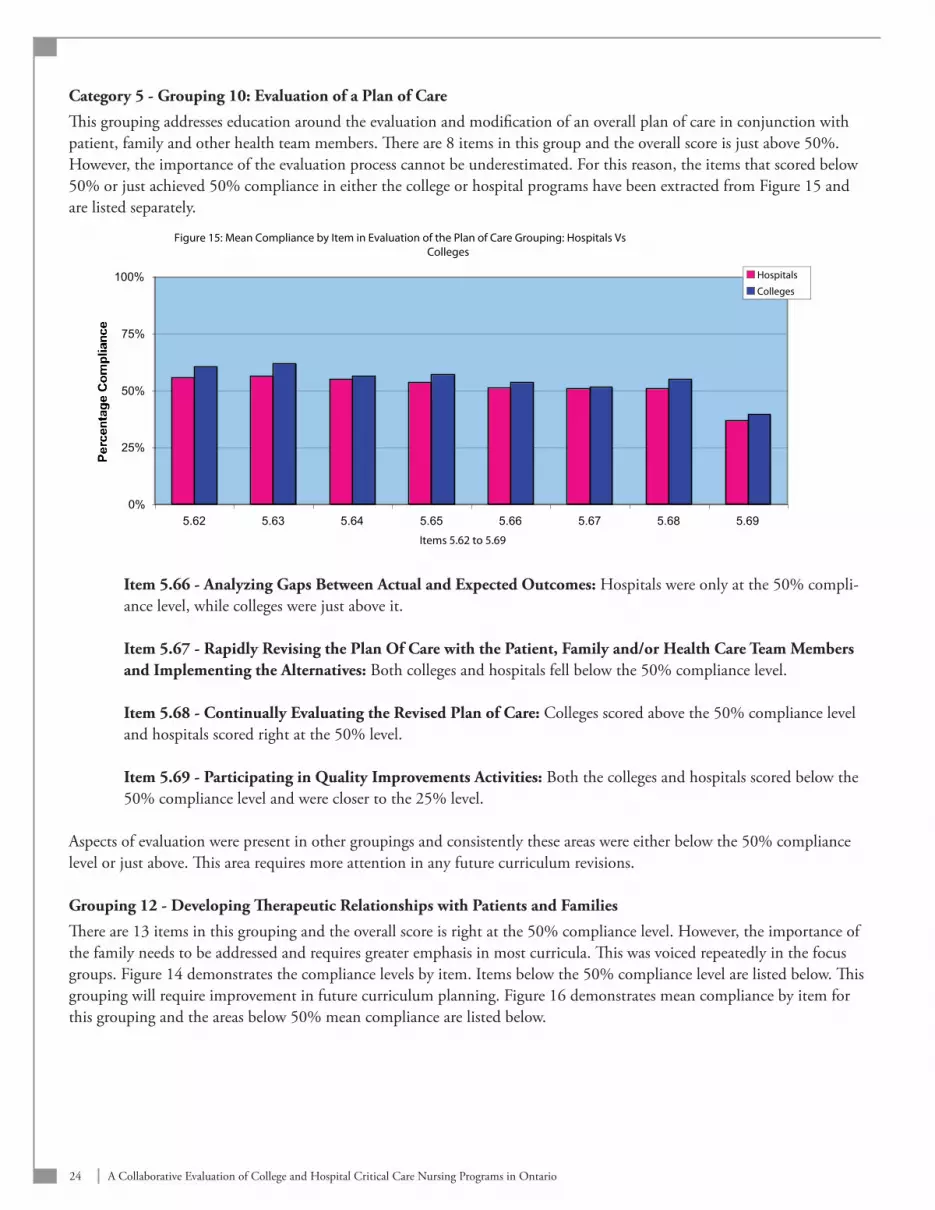
Category 5 - Grouping 10: Evaluation of a Plan of Care
This grouping addresses education around the evaluation and modification of an overall plan of care in conjunction with patient, family and other health team members. There are 8 items in this group and the overall score is just above 50%. However, the importance of the evaluation process cannot be underestimated. For this reason, the items that scored below 50% or just achieved 50% compliance in either the college or hospital programs have been extracted from Figure 15 and are listed separately.
Figure 15: Mean Compliance by Item in Evaluation of the Plan of Care Grouping: Hospitals Vs Colleges
0%
25%
50%
75%
100%
5.62 5.63 5.64 5.65 5.66 5.67 5.68 5.69
Items 5.62 to 5.69
Percentage Compliance
Hospitals
Colleges
Item 5.66 - Analyzing Gaps Between Actual and Expected Outcomes: Hospitals were only at the 50% compli-ance level, while colleges were just above it.
Item 5.67 - Rapidly Revising the Plan Of Care with the Patient, Family and/or Health Care Team Members and Implementing the Alternatives: Both colleges and hospitals fell below the 50% compliance level.
Item 5.68 - Continually Evaluating the Revised Plan of Care: Colleges scored above the 50% compliance level and hospitals scored right at the 50% level.
Item 5.69 - Participating in Quality Improvements Activities: Both the colleges and hospitals scored below the 50% compliance level and were closer to the 25% level.
Aspects of evaluation were present in other groupings and consistently these areas were either below the 50% compliance level or just above. This area requires more attention in any future curriculum revisions.
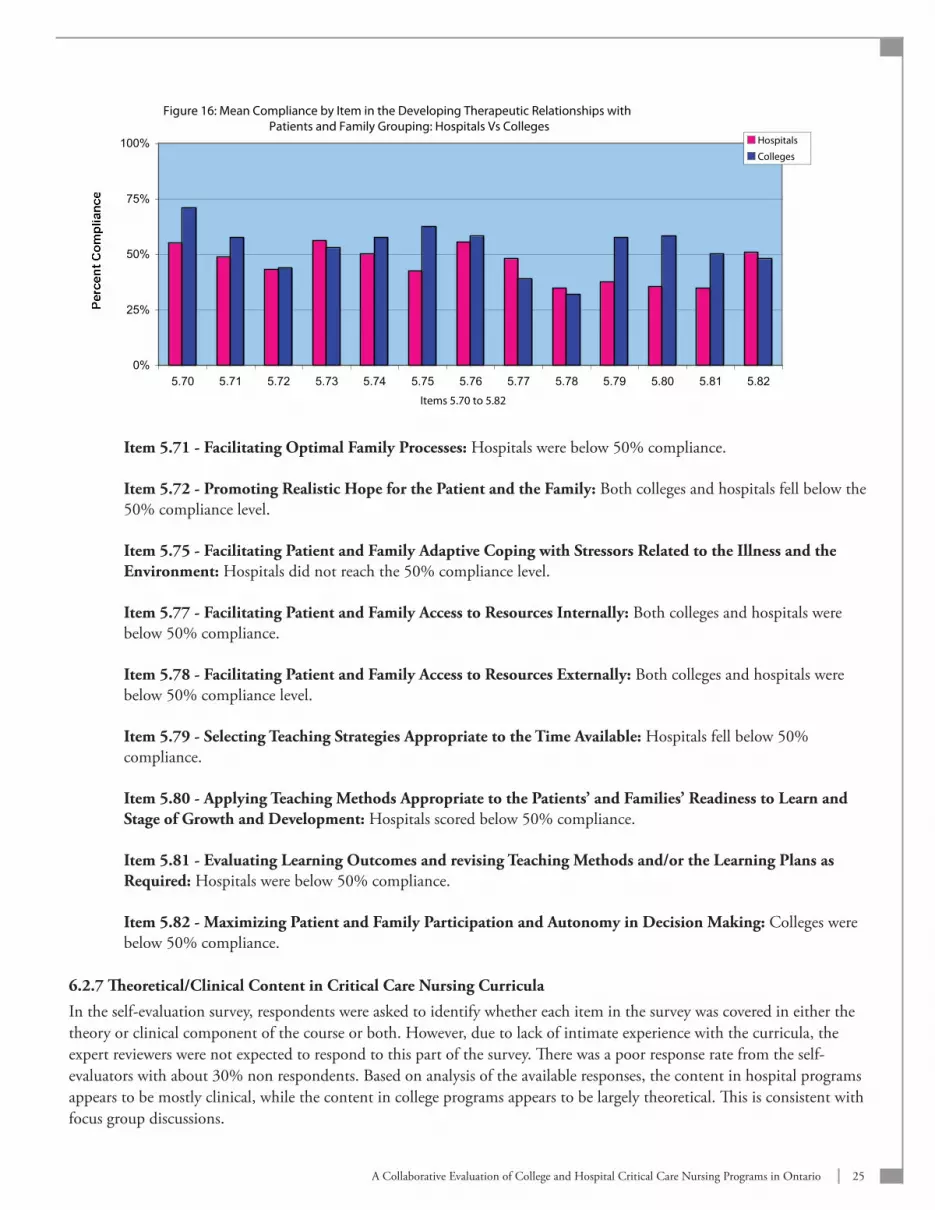
Grouping 12 - Developing Therapeutic Relationships with Patients and Families
There are 13 items in this grouping and the overall score is right at the 50% compliance level. However, the importance of the family needs to be addressed and requires greater emphasis in most curricula. This was voiced repeatedly in the focus groups. Figure 14 demonstrates the compliance levels by item. Items below the 50% compliance level are listed below. This grouping will require improvement in future curriculum planning. Figure 16 demonstrates mean compliance by item for this grouping and the areas below 50% mean compliance are listed below.
25A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Figure 16: Mean Compliance by Item in the Developing Therapeutic Relationships with Patients and Family Grouping: Hospitals Vs Colleges
0%
25%
50%
75%
100%
5.70 5.71 5.72 5.73 5.74 5.75 5.76 5.77 5.78 5.79 5.80 5.81 5.82
Items 5.70 to 5.82
Percent Compliance
Hospitals
Colleges
Item 5.71 - Facilitating Optimal Family Processes: Hospitals were below 50% compliance.
Item 5.72 - Promoting Realistic Hope for the Patient and the Family: Both colleges and hospitals fell below the 50% compliance level.
Item 5.75 - Facilitating Patient and Family Adaptive Coping with Stressors Related to the Illness and the Environment: Hospitals did not reach the 50% compliance level.
Item 5.77 - Facilitating Patient and Family Access to Resources Internally: Both colleges and hospitals were below 50% compliance.
Item 5.78 - Facilitating Patient and Family Access to Resources Externally: Both colleges and hospitals were below 50% compliance level.
Item 5.79 - Selecting Teaching Strategies Appropriate to the Time Available: Hospitals fell below 50% compliance.
Item 5.80 - Applying Teaching Methods Appropriate to the Patients’ and Families’ Readiness to Learn and Stage of Growth and Development: Hospitals scored below 50% compliance.
Item 5.81 - Evaluating Learning Outcomes and revising Teaching Methods and/or the Learning Plans as Required: Hospitals were below 50% compliance.
Item 5.82 - Maximizing Patient and Family Participation and Autonomy in Decision Making: Colleges were below 50% compliance.
6.2.7 Theoretical/Clinical Content in Critical Care Nursing Curricula
In the self-evaluation survey, respondents were asked to identify whether each item in the survey was covered in either the theory or clinical component of the course or both. However, due to lack of intimate experience with the curricula, the expert reviewers were not expected to respond to this part of the survey. There was a poor response rate from the self-evaluators with about 30% non respondents. Based on analysis of the available responses, the content in hospital programs appears to be mostly clinical, while the content in college programs appears to be largely theoretical. This is consistent with focus group discussions.

26 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
7. CONCLUSIONS The new standards of practice were well received by both colleges and hospitals. All participating organizations agreed they were relevant and useful as a tool for developing and maintaining a competent critical care nursing workforce in Ontario. There were suggestions for inclusion of specific items in a future revision, which included:
Patient safety content•
The role of the critical care nurse in disaster and pandemic planning and emergency preparedness•
Enhancement of criteria to emphasize both the patient and the patient’s family as the client•
The clinical leadership role of the critical care staff nurse•
The role of the critical care nurse in clinical and health services research.•
Questions were raised regarding the feasibility of implementation without added support from the Ministry. In particular, the issue of accountability was raised as ownership and maintenance of the standards seem unclear at this point.
Accountability is a complex issue in a single system environment. The involvement of two different Ministries (i.e., the Ministry of Training Colleges and Universities [MTCU] and the MOHLTC) in this process makes it even more difficult to manage. Accountability includes willingness to accept responsibility for one’s actions, and to justify them to others (BCTF, 2006). This suggests that accountability is something that is internal and is related to a nurse’s responsibility to adhere to standards and follow evidence-based, best practice guidelines. However, this may not be sufficient to ensure the delivery of quality service. External accountability mechanisms must also be in place to support operationalization of these standards. External mechanisms (i.e., government, Ministry and LHIN initiatives) are instrumental to support this initiative. In this particular instance, internal and external mechanisms will need to be examined together because health and education are part of the provincial legislation and funding allotments.
Although both hospitals and colleges have respect for the role the other plays in the education of critical care nurses in the province, obstacles impede collaboration between them. Because each is accountable to a different Ministry, they vary in meeting program requirements. They often work independently of one another and sometimes duplicate each another’s ef-forts. Concerns were raised by each organization about their roles and responsibilities in providing an educational program that meets the new standards of practice. In the focus groups, both hospitals and colleges addressed discrepancies in theo-retical and clinical content. Hospitals voiced concern about reductions in clinical hours in college-based programs, while colleges expressed concern about a perceived lack of rigour in curriculum planning and insufficient attention to theoretical content in hospital-based programs. College curricula are reviewed and audited by the Ministry of Training, Colleges and Universities (MTCU) and program survival is based on a successful review. Colleges were concerned about the quality of hospital programs because they are not subjected to the same rigorous review process that their programs undergo. Conversely, hospitals were concerned about their legal responsibility in hiring competent nurses when the MOHLTC does not ensure that standards are being met within college-based programs. Without clear ownership and the creation of an accountability framework to ensure that standards are being met, hospitals feared that colleges would continue to fall short in the education of a clinically-compe-tent critical care nursing workforce. As a result, they must bear the burden of educating nurses to a level that meets both the standards and the needs of their own organization. The resulting duplication of programs is neither efficient nor cost effective. Despite these concerns, most focus groups agreed that there were strengths in both kinds of programs, and any collaboration that brings together these strengths could only benefit critical care nursing and the delivery of quality critical care services in the province. They expressed a willingness to work together in partnership with a view to negotiating a col-laborative program acceptable by all.
27A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Partnerships between the colleges and hospitals will be required to successfully implement the new standards of prac-tice. Hospitals would welcome a partnership with the colleges that involves the use of college space and technology in an equitable manner. Colleges demonstrated an interest in creating partnerships with hospitals that involves the continued support of nurses to enrol and participate in continuing education programs offered by colleges. Both parties agree that a partnership would enhance the level of education and training provided to critical care nurses and decrease the duplication of costs across the system.
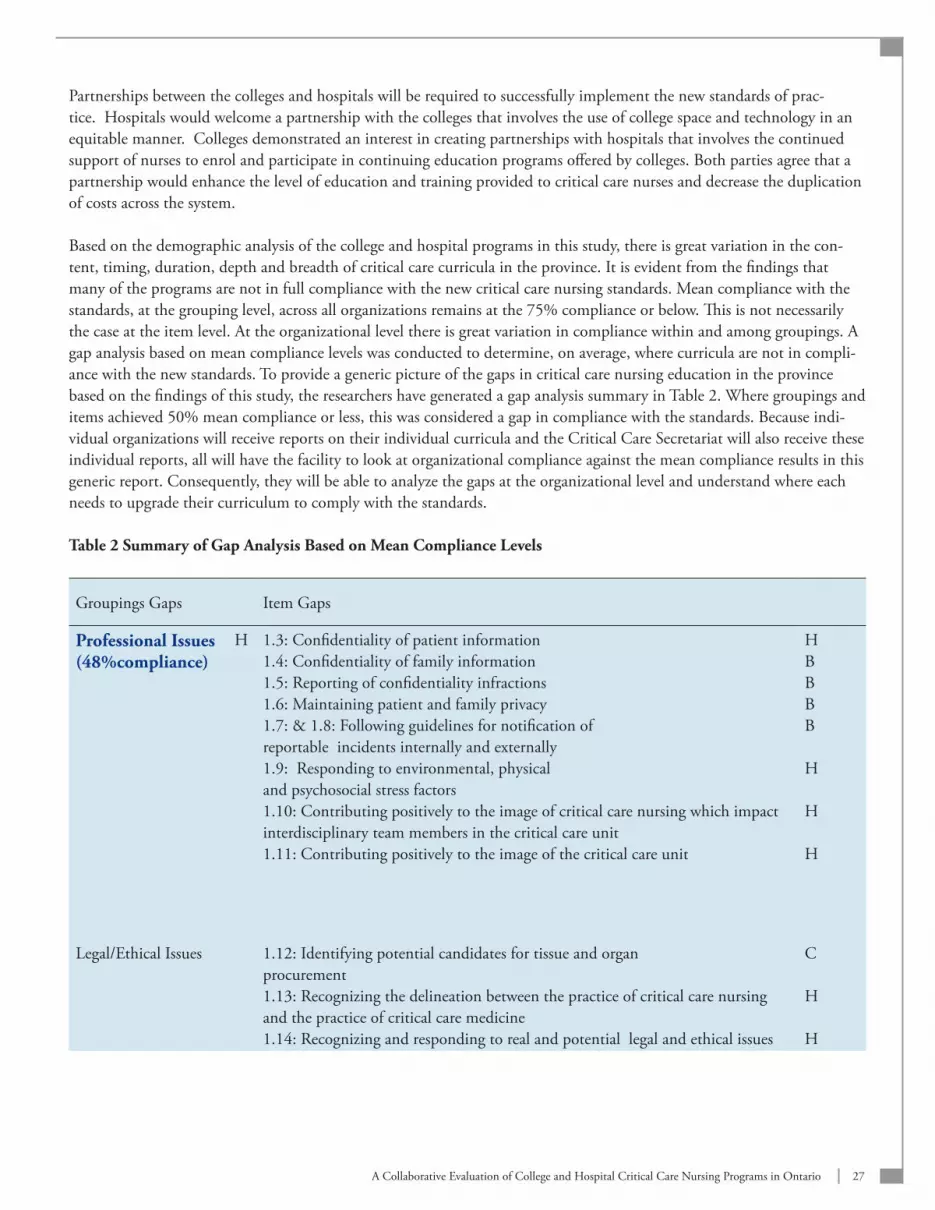
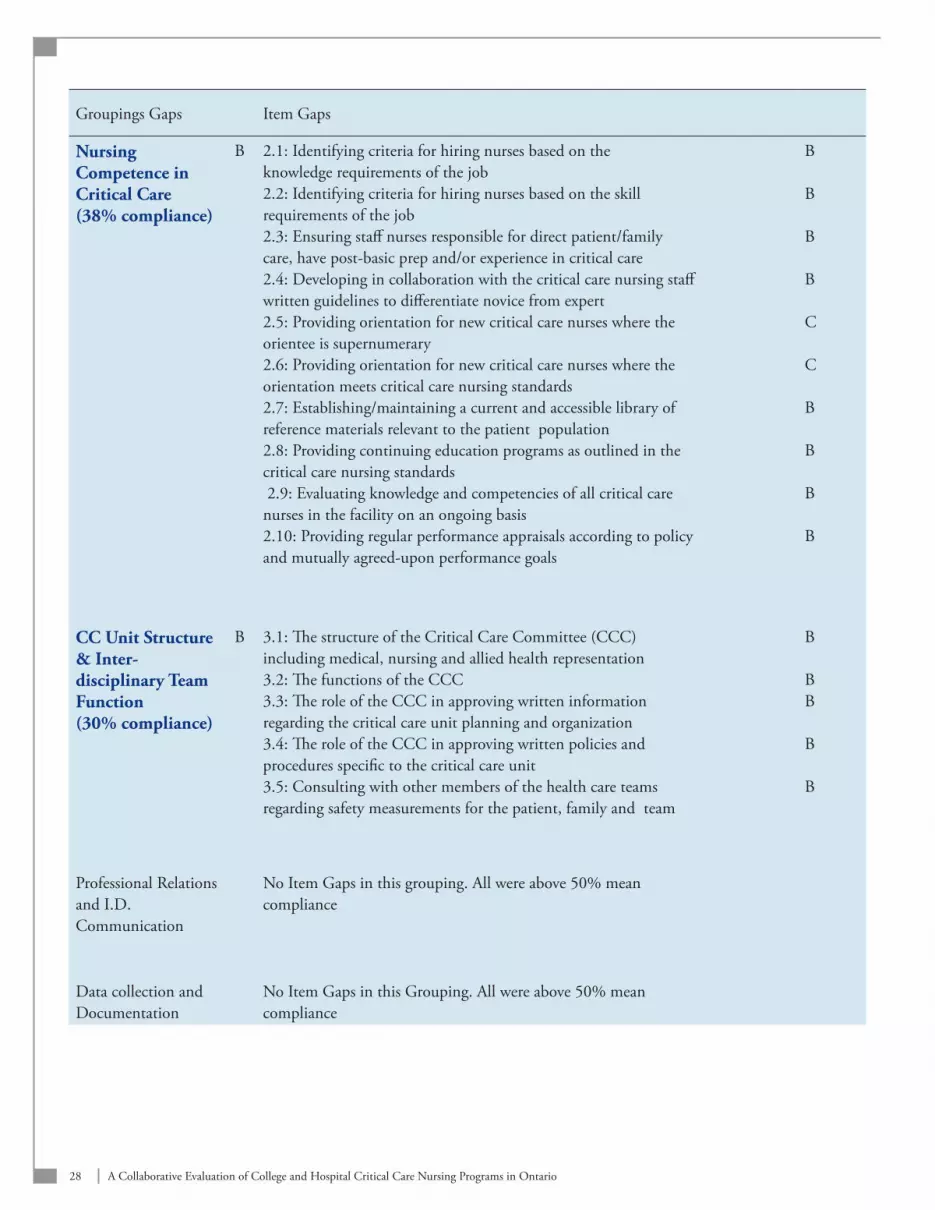
Based on the demographic analysis of the college and hospital programs in this study, there is great variation in the con-tent, timing, duration, depth and breadth of critical care curricula in the province. It is evident from the findings that many of the programs are not in full compliance with the new critical care nursing standards. Mean compliance with the standards, at the grouping level, across all organizations remains at the 75% compliance or below. This is not necessarily the case at the item level. At the organizational level there is great variation in compliance within and among groupings. A gap analysis based on mean compliance levels was conducted to determine, on average, where curricula are not in compli-ance with the new standards. To provide a generic picture of the gaps in critical care nursing education in the province based on the findings of this study, the researchers have generated a gap analysis summary in Table 2. Where groupings and items achieved 50% mean compliance or less, this was considered a gap in compliance with the standards. Because indi-vidual organizations will receive reports on their individual curricula and the Critical Care Secretariat will also receive these individual reports, all will have the facility to look at organizational compliance against the mean compliance results in this generic report. Consequently, they will be able to analyze the gaps at the organizational level and understand where each needs to upgrade their curriculum to comply with the standards.
Table 2 Summary of Gap Analysis Based on Mean Compliance Levels
Groupings Gaps Item Gaps
Professional Issues (48%compliance)
H 1.3: Confidentiality of patient information1.4: Confidentiality of family information1.5: Reporting of confidentiality infractions1.6: Maintaining patient and family privacy1.7: & 1.8: Following guidelines for notification of reportable incidents internally and externally1.9: Responding to environmental, physical and psychosocial stress factors1.10: Contributing positively to the image of critical care nursing which impact interdisciplinary team members in the critical care unit 1.11: Contributing positively to the image of the critical care unit
HBBBB
H
H
H
Legal/Ethical Issues 1.12: Identifying potential candidates for tissue and organ procurement1.13: Recognizing the delineation between the practice of critical care nursing and the practice of critical care medicine1.14: Recognizing and responding to real and potential legal and ethical issues
C
H
H
28 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Groupings Gaps Item Gaps
Nursing Competence in Critical Care (38% compliance)
B 2.1: Identifying criteria for hiring nurses based on the knowledge requirements of the job2.2: Identifying criteria for hiring nurses based on the skill requirements of the job 2.3: Ensuring staff nurses responsible for direct patient/family care, have post-basic prep and/or experience in critical care2.4: Developing in collaboration with the critical care nursing staff written guidelines to differentiate novice from expert 2.5: Providing orientation for new critical care nurses where the orientee is supernumerary2.6: Providing orientation for new critical care nurses where the orientation meets critical care nursing standards2.7: Establishing/maintaining a current and accessible library of reference materials relevant to the patient population 2.8: Providing continuing education programs as outlined in the critical care nursing standards 2.9: Evaluating knowledge and competencies of all critical care nurses in the facility on an ongoing basis2.10: Providing regular performance appraisals according to policy and mutually agreed-upon performance goals
B
B
B
B
C
C
B
B
B
B
CC Unit Structure & Inter-disciplinary Team Function(30% compliance)
B 3.1: The structure of the Critical Care Committee (CCC) including medical, nursing and allied health representation 3.2: The functions of the CCC3.3: The role of the CCC in approving written information regarding the critical care unit planning and organization 3.4: The role of the CCC in approving written policies and procedures specific to the critical care unit3.5: Consulting with other members of the health care teams regarding safety measurements for the patient, family and team
B
BB
B
B
Professional Relations and I.D. Communication
No Item Gaps in this grouping. All were above 50% mean compliance
Data collection and Documentation
No Item Gaps in this Grouping. All were above 50% mean compliance

29A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Groupings Gaps Item Gaps
Data Analysis and Formulation of Nursing Dx
5.18 - Alterations in integumentary tissue perfusion5.21 - Ineffective thermoregulation5.24 - Alteration in immunologic function5.25 - Alteration in hematological function5.28 - Altered family process5.30 - Manifestations of abuse5.32 - End of life withdrawal of treatment and/or the execution of advanced directives5.33 - Organ donation and transplantation5.39 - Integrate all findings from the assessment to identify collaborative and/or independent nursing diagnoses
CCBCBBH
CH
Planning Interventions and Formulating a Plan of Care
5.43 - Balancing the science of curing with the act of caring5.46 - Identifying realistic and measurable expected patient outcomes to be used in the evaluation of formulated goals5.47 - Validating the plan of care with patient, family and other members of the health care team5.48 - Identifying required resources to accomplish the plan of care
HH
H
C
Implementing a Nursing Plan of Care
5.58 - Intervening in ineffective thermoregulation by promoting normo-thermia 5.60 - Intervening to prevent complications of immobility
C
C
Evaluating a Nursing Plan of Care (Just above 50% mean compliance)
B 5.67 - Rapidly revising plan of care with the patient/family and/or ID team members and implementing alternatives 5.68 - Continually evaluating the revised plan of care 5.69 - Participating in quality improvements activities
B
HB
Developing Therapeutic Relationships with Patients and Families(50% compliance)
B 5.72 - Promoting realistic hope for the patient and the family.5.75 - Facilitating patient and family adaptive coping with stressors related to the illness and the environment 5.77 - Facilitating patient and family access to resources internally 5.78 - Facilitating patient and family access to resources externally 5.79 - Selecting teaching strategies appropriate to the time available5.80 - Applying teaching methods appropriate to the patients’/ families’ readiness to learn and stage of growth and development5.81 - Evaluating learning outcomes and revising teaching methods and/or the learning plans as required 5.82 - Maximizing patient and family participation and autonomy in decision making
BH
BBHH
B
B
NOTES: Groupings which have a mean compliance level of 50% or less are in bold blue type face. All items listed as gaps have achieved a 50% mean compliance or less by a hospital, a college or both. In columns 2 and 4, H=Hospitals, C=Colleges and B= Both. This indicates who achieved a 50% compliance level or below.
30 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
In conclusion, the new standards form the template for critical care education in the province. However, curricula in many organizations are not in compliance and there is great variability within and among organizations. Given the variability in the critical care nursing education programs offered in the province, it is not surprising that the credentials are not portable from one organization to another. Consequently, it may be necessary to take standardization to higher level. The variation in curricula and low mean compliance with the new critical care standards highlight the need for some type of standardized curriculum for beginning practitioners in the specialty. If basic preparation in the specialization is to be portable from one place to another, all critical care nurses must receive the same educational preparation. Nurses have consistently identified the lack of formal recognition for the education required to begin work in their specialty areas. If educational preparation for the beginning critical care nurse is based on a standardized curriculum, there should be some consideration for formal educational credit, either towards a baccalaureate in nursing or a critical care nursing certificate.
8. RECOMMENDATIONSCritical Care Nursing StandardsBecause the focus groups have highlighted additional points to be considered for inclusion in the new critical care nursing standards, the following recommendation is put forward:
The Nursing Subcommittee of the Critical Care Expert Panel, at their discretion, should seriously consider the •areas identified by the focus groups for either enhancement or inclusion in the new critical care nursing standards.
Critical Care Nursing Education: The Way ForwardIn the face of a pressing need to develop a strong resilient critical care nursing workforce that can provide care in complex environments, this study has demonstrated considerable variability in critical care curricula across the province. Moreover, specific strengths and weaknesses in both kinds of programs have been identified. In response, the following recommenda-tions are made:
A standardized curriculum based on the new Ontario standards should be developed for basic education of new •critical care nurses and used consistently across the province.
The standardized curriculum should be developed under the auspices of the Critical Care Nursing Subcommittee •in close collaboration with the Canadian Association of Critical Care Nurses, the formal education institutions and the hospitals with whom they work.
The standardized curriculum should be adopted by formal educational institutions which can give course credit, •thereby assuring an established accreditation process.
Implementation of this curriculum should be negotiated through a strong partnership between the educational •institutions and the hospitals with whom they work.
The teaching strengths of both hospitals and educational institutions should be merged through cross appoint-•ments to ensure strong theory and clinical content in the program.
The existing physical space and technical infrastructure of both hospitals and educational institutions should be •fully optimized.
31A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Ongoing continuing education for critical care nurses is essential to maintain a competent critical care nursing •workforce. Based on focus group feedback, the following suggestions are put forward for consideration:
Dedicate budget for continuing education and staffing flexibility for mid-career nurses to maintain * competence and achieve certification.
Funding for certification should be on a shared basis (nurse/employer).*
Create partnerships among hospitals to share educational opportunities and expertise.*
Further Important ConsiderationsExisting critical care nursing education programs and orientation are nested in both educational institutions and the hospital sector with considerable variability across programs. The development of the new critical care standards provides an opportunity to encourage a standardized approach to existing educational programs. Precedence has been set at both the undergraduate and postgraduate level with nursing specialization areas such as oncology, neonatology and primary health care all giving formal educational credit. These programs are offered in various educational institutions and provide a standard approach that can be adopted in other educational institutions. It may be timely to consider such an approach with critical care nurse specialization.
The new Ontario Critical Care Nursing Standards are based on the Canadian Association of Critical Care Nursing Stan-dards. The development of a standardized curriculum for beginning nurses in the specialty provides an opportunity for Ontario to become a leader in championing formal educational credit for specialty education. This process would enhance the adoption of these standards and curriculum across all provinces and nationally.
The standardized critical care nursing curriculum has to sit in already approved and accredited educational institutions. In order for it to be viable and have a provincial impact, there has to be a strong partnership between the educational and hos-pital sector and structures such as the LHINs. There is a process for integrating a curriculum into educational institutions. A higher level critical care educational committee should be formed that has representation from the government (i.e., the MTCU and the MOHLTC), education and hospital sector to provide a blueprint for the adoption of the curriculum into the general education system. This would result in nurses receiving credit for critical care education and would assure stan-dardization across the province between and among different educational institutions. It is essential that hospitals play a strong role in this new structure as their representatives would both advise and possibly teach in this new program. There-fore, as a follow up to this study, additional recommendations would be to:
Form a high level multi-sectoral planning committee to strategize integration of a critical care nursing •specialty program into existing educational structures in the province.
Individual LHINs should evaluate their critical care nursing education capacity and bring their experts •together to discuss strategies for improvement within their own LHIN and provincially.

32 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
REFERENCESBritish Columbia Teachers Federation (BCTF) May 2006. Accountability Update Retrieved October 1, 2007 from http://www.bctf.ca/ Issues in Education.
Bell, R and Robinson, L (2005). Final Report of the Ontario Critical Care Steering Committee. Critical Care Secretariat, Ontario Ministry of Health and Long-Term Care. Toronto, ON. Retrieved March 3, 2007 from http://mohltc.gov.on.ca.
Canadian Association of Critical Care Nurses (2004). Standards of Critical Care Nursing Practice. Retrieved March 3, 2007 from http://www.caccn.ca. Retrieved from http://mohltc.gov.on.ca.
College of Nurses of Ontario, (2005). The Compendium of Nursing Standards of Care. Retrieved June 1, 2007 from http://www.cno.org/pubs/compendium.html.
Critical Care Secretariat (2006a). Critical Care Nurse Standards Task Group Final Report, Retrieved March 3, 2007 from http://mohltc.gov.on.ca.
Critical Care Secretariat, (2006b). Standards for Critical Care Nursing in Ontario. Ontario Retrieved March 3, 2007 from http://www.health.go.on.ca/english/providers/program/critical_care/docs/report_ccn_ccs.pdf.
Dillman, D. A. 2007. Mail and Internet Surveys. John Wiley & Sons: Hoboken, New Jerse
Gillham, B. (2000). Case Study Research Methods: Real World Research Series. London: Continuum Publishers.
Kopcha, T.J. & Sullivan, H. (2006). Self-presentation bias in surveys of teachers’ educational technology practices. Edu-cational Technology Research Development (DOI 10.1007/s11423-006-9011-8) Division of Psychology in Education, Arizona State University, Tempe, AZ.
Streiner, D.L. & Norman, G.R. (2003). Health Measurement Scales: A Practical Guide to their Development and Use. Oxford Medical Publications. New York.
Spence-Laschinger, H (1992). Intraclass correlations as estimates of interrator reliability in nursing research. Western Jour-nal of Nursing Research. 14(2): 246-251.
Tashakkori, A., & Teddle, C. (1998). Mixed methodology: Combining qualitative and quantitative approaches. Applied Social Research Methods Series, 46. Thousand Oaks, CA: Sage Publications.

33A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix A. Letter To Focus Group Participants
February, 2007
Dear Participant,
In follow-up to a letter which you received from the Critical Care Secretariat of the Ontario Ministry of Health and Long Term Care (MOHLTC), we are inviting members of [your organization] to discuss the relevance and applicability of the new critical care nursing standards of practice to current critical care nursing education programmes in the province. The focus group discussions will also invite input into the development of a survey to determine the extent to which college and hospital-based critical care nursing education programmes incorporate these standards into their current curricula.
We would appreciate your help in assisting us by organizing a 1 hour focus group for 3-5 people to meet with 2 of our researchers by teleconference. We plan to use the re-sults of the focus groups in the development of a survey questionnaire for distribution to 14 college-based and 27 hospital-based critical care nursing programmes in the province.
Participants will be free to withdraw from the focus group at any time. Our reports will identify the number of people representing the sectors that participate but people will not be identified or associated with any statements about this study.
This study is funded by the Critical Care Secretariat of the MOHLTC and has received ethics approval from McMaster University Faculty of Health Sciences Ethics Review Board. The attached form provides participant information on the focus groups and a consent form. Each focus group participant will need to read the information/consent form and we will need to receive a signed copy of this information/consent form before their scheduled focus group participation.
We will call you within the next two weeks to discuss your participation in this impor-tant project. Thank you for your assistance in encouraging participation in this study which, in turn, will contribute to critical care nursing education in the province.
Sincerely, Anita Fisher, RN PhD
Nursing
Health
Services
R esearch
Unit
a collaborative project of the University of Toronto Faculty of Nursing and McMaster University School of Nursing
Our mission is to develop, conduct and disseminate research that focuses on:
design•management•utilization•outcomes•provision• •…of nursing.
Faculty of NursingUniversity of Toronto50 St. George StreetToronto, Ontario, CanadaM5S 3H4Tel: (416) 978-1966Fax: (416) 946-7142
McMaster UniversityFaculty of Health SciencesMichael G. DeGroote Centre for Learning and Discovery, MDCL 35001200 Main St. W.Hamilton, Ontario, CanadaL8N 3Z5Tel: (905) 525-9140 x22581Fax: (905) 522-5493
funded by theOntario Ministry of Health &
Long-Term Care2004-2009

34 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix B. Focus Group Consent Form
CONSENT STATEMENT
SIGNATURE OF RESEARCH PARTICIPANT/LEGALLY-AUTHORIZED REPRESENTATIVE
I have read the preceding information thoroughly. I understand whom to contact if I have any questions. I agree to participate in this study.
Name of Participant
Address of Participant
Signature of Participant Date
CONSENT FORM ADMINISTERED BY:
Name and Title
Signature Date
SIGNATURE OF INVESTIGATOR
In my judgement, the participant is voluntarily and knowingly giving informed consent and possesses the legal capacity to give informed consent to participate in this research study.
Signature of Investigator Date
N.B. I will receive a signed copy of this consent form
A Collaborative Evaluation of College and Hospital-Based Critical Care Nursing Education Programs in Ontario

35A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix C. Focus Group Discussion GuideFocus Group Guide: These are a sample of questions which will guide focus group discussion and may be altered depending on focus group discussion
What is your general view on the New Standards of Practice for Critical Care Nursing in the province of Ontario?
Are they relevant to Critical care nursing practice?
What are the strengths of these new standards?
What are the shortcomings, if any?
If you had the opportunity to alter them in any way, how would you change them?
What are the challenges and enablers for implementation of these standards in the practice and educational settings?
We are currently developing a survey for all college-based and selected hospital-based critical care nursing education pro-grams in the province and would invite any input from you on topics for inclusion in the survey?
36 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix D. Focus Group Feedback Suggested Changes or Additions to New Critical Care Standards
FOCUS GROUP FEEDBACK
Participants identified patient safety as an area of weakness in the standards. Specifically, it was noted that drug 5. calculations are absent from the criteria listed under Outcome Standard 4 and should be included as a compo-nent of patient safety.
In providing performance appraisals for critical care nurses, it was suggested that an ongoing performance apprais-6. al system be added to the standards to ensure competencies are maintained. For example, in Outcome Standard 5.4 which states, “the healthcare facility evaluates the knowledge and competencies of the critical care nurse” it was suggested that a specific time frame be added to ensure nurses are maintaining the standards over time. Partici-pants recommended including an evaluation following the orientation period and on an annual basis thereafter.
Participants suggested enhancing criteria under 7. Outcome Standard 8 to recognize not only the patient but also the patient’s family as the client. Engaging family members in the care of the patient was suggested as a way to promote family focused care and provide the nurse with the skills and knowledge necessary to practice holistically. One nurse educator noted: In standard 8.2 it says “the critical care nurse intervenes to facilitate optimal family processes” but I think it would be nice to say “to facilitate family focused care” so that the family is identified as the client and not just the patient.
Under 8. Outcome Standard 7.1 “The critical care nurse collaborates with patient, family, and other health care team members to establish an individualized and holistic plan of care”, it was suggested that a statement regarding the nurse recognizing the patient as a unique individual be included to support the notion that patients are people and understanding them on a personal level aids in the curing and caring process.
Many participants commented on the wording of some of the standards and recommended that they be changed 9. to better represent the role of the nurse. The following suggestions were made:
Outcome standard a 14.9.1, 14.9.2 and 14.9.3: By using the word “manipulate” to describe how a critical care nurse corrects alterations in cardiac output, one participant believed, suggested an advanced competency that her students would not be qualified to do without prior experience in a critical care setting. It was suggested that this word be changed to better represent a baseline competency that could be met through a college-based course rather experience in a clinical setting.
Outcome Standard 8.3, The critical care nurse promotes realistic hope for the patient and family: b Some participants believed that the use of the word “hope” places nurses in a difficult position when dealing with the family and instead suggested that the word “outcome” be substituted in its place.
Outcome Standard 1.9, The critical care nurse responds to environmental, physical, and psychosocial stress cfactors which impact interdisciplinary team members in the critical care setting: It was suggested that this statement be altered to an active standard that describes how the nurse reacts rather the fact that she does react.

37A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix E. Survey Instrument: Critical Care Collaborative EvaluationCritical Care Standard Survey: College Version aThe Critical Care Standards Questionnaire (CCSQ) was designed to determine your impression of the extent to which your basic critical care nursing education curriculum incorporates the Standards for Critical Care Nursing in Ontario (2006). By completing this questionnaire you will conduct a self-evaluation of the extent to which your current critical care nursing education program incorporates the newly developed standards of practice. After completing this question-naire you have been asked to submit a copy of your curriculum to the NHSRU where it will undergo a blind review by an expert panel of reviewers using the exact same instrument being used here for your self evaluation. Both the self evaluation and the expert panel evaluation will be analyzed to determine gaps in meeting the new standards. Data from this question-naire will contribute to the ongoing development of a standardized critical care nurse education and training program and, ultimately, to portable critical care nursing credentials, provincially.
Completion and submission of the questionnaire and voluntary submission of the curriculum documents will constitute implied consent for both the survey and the expert panel review of your curriculum. You have the right to refuse to partici-pate, refuse to answer any questions, or withdraw from the study at any time with no effect to you. Data will be securely stored either in locked cabinets or in password protected computer files.
A generic, aggregate report will be prepared and submitted to the Critical Care Secretariat at the Ontario Ministry of Health and Long Term Care by October, 2007. Each participating institution will receive a copy of the final report which is submitted to the Critical Care Secretariat. You will also receive a report from the research team regarding your individual self evaluation and expert panel review results. If you are willing to share your individual results of your self evaluation and your expert panel review with the Nursing Sub Committee (Chairperson: Ms. Jocelyn Bennett) of the Critical Care Secretariat, please indicate below. Please note that this is voluntary however agreeing to share results provides a baseline for further Ministry decision-making on ongoing allocation of resources for critical care nursing education in the province.
Self-Evaluation Results: Yes r No r
Expert Panel Review Results : Yes r No r
Name of Institution: Date:
Study Contact Information:
Linda FitzpatrickResearch Assistant [email protected] 519-452-7415
Dr. Anita FisherPrincipal Investigator [email protected] 905-525-9140 Ext. 26765

38 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Section A: Standards Evaluation (Category 1-5): For each criterion listed below please indicate to what extent each criterion is incorporated in your curriculum by selecting the appropriate percentage level and whether it is covered as theory or clinical content, or both.
Category 1: Professional Behaviors and Ethics
Outcome Standard 1: The critical care nurse practices within the scope of professional, legal and ethical standards.
Grouping 1 Professional Issues: Critical care nurses are reminded of their professional responsibility for:
0% 25% 50% 75% 100% Theory Clinical
1.1: Maintenance of professional competence through education
1.2: Involvement in and use of evidence-based research in clinical practice
1.3: Confidentiality of patient information
1.4: Confidentiality of family information
1.5: Reporting of confidentiality infractions
1.6: Maintaining patient and family privacy
1.7: Following guidelines for notification of reportable incidents internally
1.8: Following guidelines for notification of report able incidents externally
1.9: Responding to environmental, physical, and psychosocial stress factors which impact interdisciplinary team members in the critical care setting
1.10: Contributing positively to the image of critical care nursing
1.11: Contributing positively to the image of the critical care unit

39A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Grouping 2: Legal and Ethical Issues: Critical care nurses are made aware of their legal and ethical responsibilities in criti-cal care including:
0% 25% 50% 75% 100% Theory Clinical
1.12: Identifying potential candidates for tissue and organ procurement
1.13: Recognizing the delineation between the practice of critical care nursing and the practice of critical care medicine
1.14: Recognizing and responding to real and potential legal and ethical issues
Category 2: Nursing Competence in Critical Care
Outcome Standard 2: Qualified personnel are provided by the health care facility.
Outcome Standard 5: Opportunities for critical care nurse to maintain the knowledge and skill necessary to deliver safe and knowledgeable nursing care, within the chosen conceptual model of nursing practice, are provided by the health care facility.
To what extent is each criterion incorporated in your curriculum; in theory, in clinical, or both:
Grouping 3: Nursing Competence in the Critical Care Unit: Critical care nurses are made aware of the responsibilities of the health facility in:
0% 25% 50% 75% 100% Theory Clinical
2.1: Identifying criteria for hiring nurses based on the knowledge requirements of the job
2.2: Identifying criteria for hiring nurses based on the skill requirements of the job
2.3: Ensuring that staff nurses responsible for direct patient and family care, have post-basic preparation and/or experience in critical care nursing
2.4: Developing, in collaboration with the critical care nursing staff, written guidelines of the skills required to differentiate novice from expert critical care nurses

40 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
0% 25% 50% 75% 100% Theory Clinical
2.5: Providing orientation for new critical care nurses where the orientee is supernumerary
2.6: Providing orientation for new critical care nurses where the orientation meets critical care nursing standards
2.7: Establishing/maintaining a current and accessible library if reference materials relevant to the patient population
2.8: Providing continuing education programs as outlined in the critical care nursing standards
2.9: Evaluating knowledge and competencies of all critical care nurses in the facility on an ongoing basis
2.10: Providing regular performance appraisals directly to each staff member according to policy and based on a written job description resulting in a mutually agreed-upon set of performance goals and objective for the upcoming year
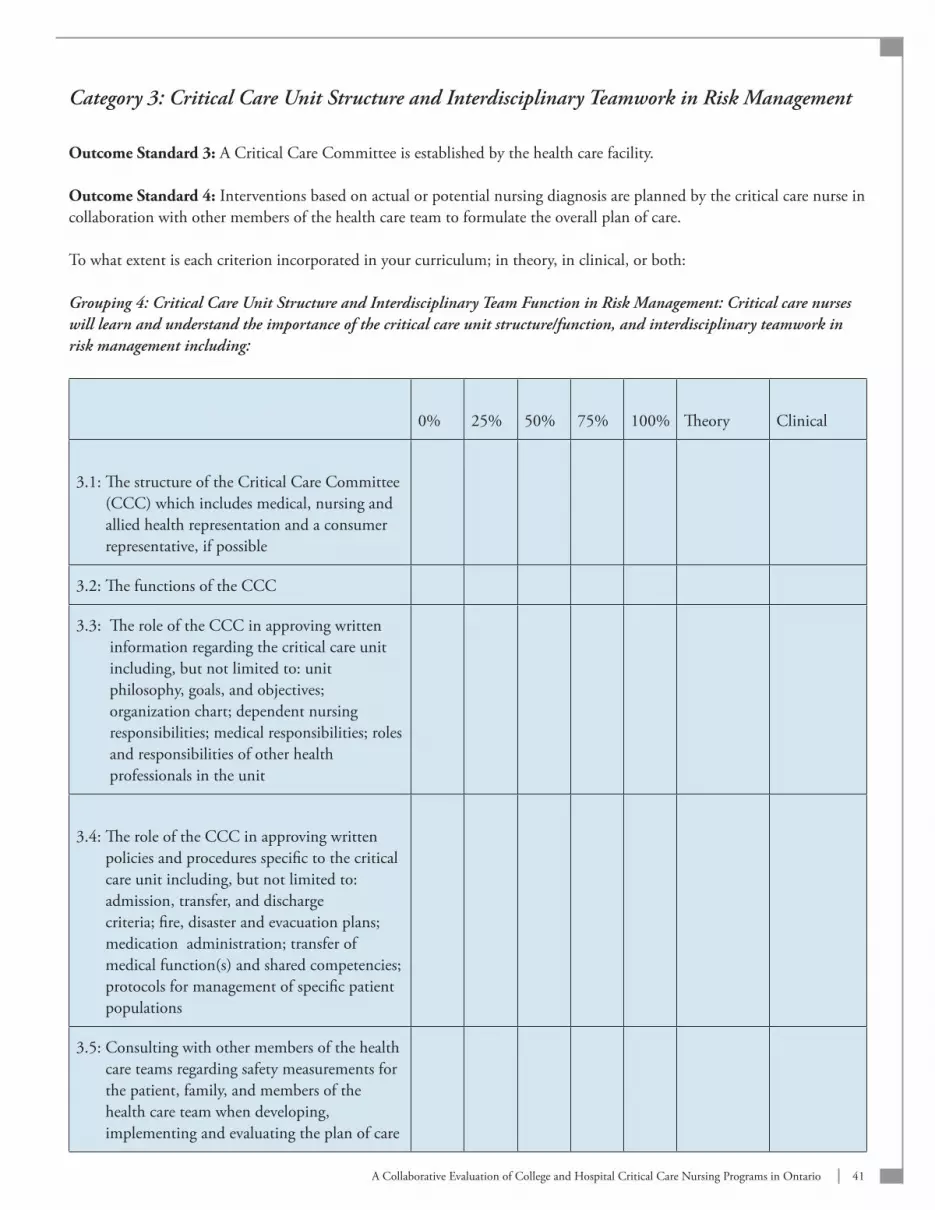
41A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Category 3: Critical Care Unit Structure and Interdisciplinary Teamwork in Risk Management
Outcome Standard 3: A Critical Care Committee is established by the health care facility.
Outcome Standard 4: Interventions based on actual or potential nursing diagnosis are planned by the critical care nurse in collaboration with other members of the health care team to formulate the overall plan of care.
To what extent is each criterion incorporated in your curriculum; in theory, in clinical, or both:
Grouping 4: Critical Care Unit Structure and Interdisciplinary Team Function in Risk Management: Critical care nurses will learn and understand the importance of the critical care unit structure/function, and interdisciplinary teamwork in risk management including:
0% 25% 50% 75% 100% Theory Clinical
3.1: The structure of the Critical Care Committee (CCC) which includes medical, nursing and allied health representation and a consumer representative, if possible
3.2: The functions of the CCC
3.3: The role of the CCC in approving written information regarding the critical care unit including, but not limited to: unit philosophy, goals, and objectives; organization chart; dependent nursing responsibilities; medical responsibilities; roles and responsibilities of other health professionals in the unit
3.4: The role of the CCC in approving written policies and procedures specific to the critical care unit including, but not limited to: admission, transfer, and discharge criteria; fire, disaster and evacuation plans; medication administration; transfer of medical function(s) and shared competencies; protocols for management of specific patient populations
3.5: Consulting with other members of the health care teams regarding safety measurements for the patient, family, and members of the health care team when developing, implementing and evaluating the plan of care

42 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Category 4: Caring/Communication in Therapeutic and Professional Relationships
Outcome Standard 6(12): Based upon knowledge of biological, physical, and behavioral sciences, data are analyzed by the critical care nurse to formulate nursing diagnoses.
Outcome Standard 7(13): Interventional based upon the actual and potential nursing diagnoses are planned by the criti-cal care nurse, in collaboration with other members of the interdisciplinary health care team, to formulate the overall plan of care.
Outcome Standard 8(14): The critical care nurse implements the plan of care including independent and interdependent nursing functions.
Outcome Standard 9(15): The critical care nurse evaluates patient outcomes in accordance with a conceptual model for critical care nursing and consistent with independent nursing functions.
To what extent is each criterion incorporated in your curriculum; in theory, in clinical, or both:
Grouping 5: Professional Relationships and Interprofessional Communication: Critical care nurses are educated on the importance of collaborative interprofessional practice and open, co-operative and clear communication across disciplines including:
0% 25% 50% 75% 100% Theory Clinical
4.1: Reporting and discussing significant findings with other members of the health care team
4.2: Collaborating with patient, family, and other health care team members to establish an individualized, holistic plan of care
4.3: Reporting and discussing significant differences between actual and expected outcomes with the appropriate interdisciplinary team members
Category 5: Knowledge, Clinical Skills, Integration and Critical Thinking
Outcome Standard 6(12): Based upon knowledge of biological, physical, and behavioral sciences, data are analyzed by the critical care nurse to formulate nursing diagnoses.
Outcome Standard 7(13): Interventional based upon the actual and potential nursing diagnoses are planned by the criti-cal care nurse, in collaboration with other members of the interdisciplinary health care team, to formulate the overall plan of care.
Outcome Standard 8(14): The critical care nurse implements the plan of care including independent and interdependent nursing functions.

43A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Outcome Standard 9(15): The critical care nurse evaluates patient outcomes in accordance with a conceptual model for critical care nursing and consistent with independent nursing functions.
Outcome Standard 10: Therapeutic relationships with patients and families are developed and maintained by the critical care nurse.
Outcome Standard 11: The critical care nurse collects and documents data regarding the patient’s physical, emotional, and psychosocial status including any advanced directives at the time of admission to the critical care unit and during the patients stay.
To what extent is each criterion incorporated in your curriculum; in theory, in clinical, or both:
Grouping 6: Data Collection and Documentation: Critical care nurses will learn the skills and techniques of data collection and documentation in critical care including:
0% 25% 50% 75% 100% Theory Clinical
5.1: Obtaining and documenting a comprehensive health history using all available and appropriate sources in the absence of a patient’s ability to communicate
5.2: Gathering pathophysiological, psychosocial, cultural, developmental and spiritual data bases on the patient’s condition
5.3: Documenting pathophysiological, psychosocial, cultural, developmental and spiritual data bases on the patient’s condition
5.4: Collecting data on a continuous basis but recognizing selected times when comprehensive/holistic data collection is necessary
5.5: Collecting laboratory specimens
5.6: Collecting data using invasive techniques
5.7: Collecting data using non-invasive techniques
5.8: Gathering data concerning the family’s needs and responses to the health crisis
5.9: Gathering data regarding infection control risks to patients and staff and takes all the necessary preventative measures to protect against exposure

44 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Outcome Standard 6(12): Based upon knowledge of biological, physical, and behavioral sciences, data are analyzed by the critical care nurse to formulate nursing diagnoses.
To what extent is each criterion incorporated in your curriculum; in theory, in clinical, or both:
Grouping 7: Data Analysis and Formulation of Nursing Diagnosis: Critical care nurses will learn to assess, document and interpret all data collected, analyze unexpected findings and set priorities for care including but not limited to:
0% 25% 50% 75% 100% Theory Clinical
5.10: Ineffective airway clearanceEpiglotitis •Mucous plug•
5.11: Ineffective breathing patternTension pneumothorax• Flail chest•
5.12: Impaired gas exchange including: Upper airway disease
foreign body• croup• epiglottis• postextubation stridor• laryngospasm•
Lower airway disease respiratory distress syndrome• acute respiratory distress syndrome• pulmonary edema• bronchiolitis• status asthmaticus• mixed obstruction and restrictive disease• inhalation injuries•
Ineffective gas exchange pleural effusion•
5.13: Alteration in cardiac outputCongentital heart defects•Cardiac myopathy•Myocardial infarction•Cardiac tamponade•Congestive failure•Cardiac dysrhythmias•

45A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
0% 25% 50% 75% 100% Theory Clinical
5.14: Alteration in cerebral tissue perfusionHead trauma•Cerebral aneurysm•Seizures•Meningitis•Shock•Cerebral vascular accident •Ateriovenous malformation•Cerebral Vasospasm•
5.15: Alteration in gastrointestinal tissue perfusionPancreatitis•
5.16: Alteration renal tissue perfusionAcute renal failure•Congenital•
5.17: Alteration in vascular tissue perfusionCompartment syndrome•Abdominal aortic aneurysm•Thrombosis•
5.18: Alteration in integumentary tissue perfusionBurns•Decubitus ulcer•
5.19: Alteration in fluid balanceSepsis•Ascites•SIADH (Syndrome of Inappropriate •Antidiuretic hormone Secretion)DI (Diabetes Insipidus)•Hemolytic uremia•
5.20: Alteration in motor and sensory functionMyelomeningocele•Guillain-Barre•Spinal cord injury•Neurogenic shock•
5.21: Ineffective thermoregulationMalignant hyperthermia•Hypothermia•

0% 25% 50% 75% 100% Theory Clinical
5.22: Alteration in liver functionHepatitisBiliary atresiaPoisonings
5.23: Alterations in endocrine functionDiabetic ketoacidosis
5.24: Alterations in immunologic functionGraft versus host diseaseTransplantSystemic inflammatory response syndrome
5.25: Alterations in hematologic functionLeukemiaDisseminated intravascular coagulopathyHeparin-induced thrombocytopeniaDeep vein thrombosis
5.26: Altered comfortPainAnxietySleep deprivationDelirium
5.27: Impaired communicationIntubatedNeurological deficitsDevelopmental delaySedation
5.28: Altered family processesGrief/lossGuiltSudden infant death syndrome
5.29: Altered family/patient copingHelplessnessPowerlessness
5.30: Manifestations of abuse (child, spouse, elder)
5.31: Altered nutritional requirements
0% 25% 50% 75% 100% Theory Clinical
5.32: End-of-life withdrawal of treatment and/or the execution of advanced directives
5.33: Organ donation and transplantation
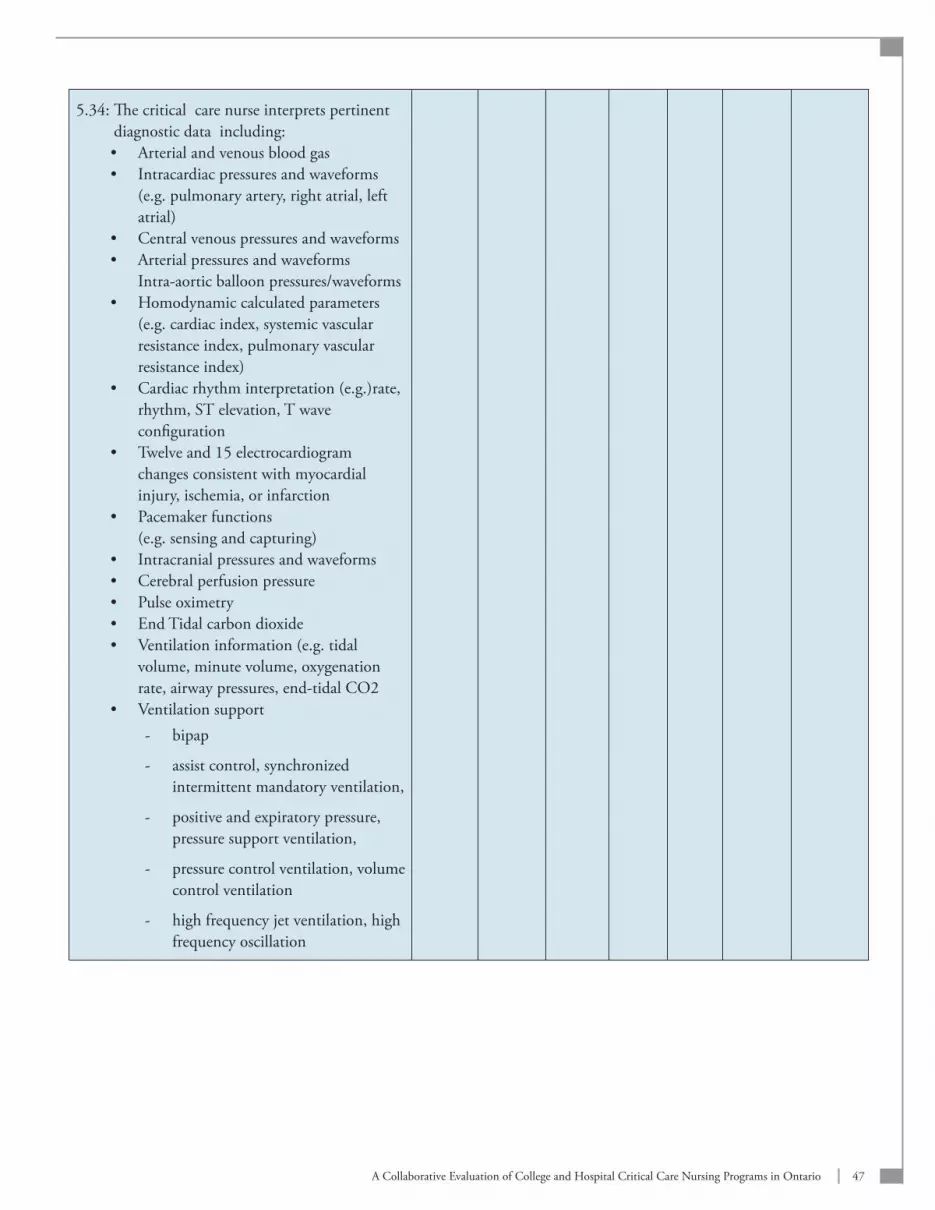
47A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
5.34: The critical care nurse interprets pertinent diagnostic data including:
Arterial and venous blood gas•Intracardiac pressures and waveforms •(e.g. pulmonary artery, right atrial, left atrial)Central venous pressures and waveforms•Arterial pressures and waveforms •Intra-aortic balloon pressures/waveformsHomodynamic calculated parameters •(e.g. cardiac index, systemic vascular resistance index, pulmonary vascular resistance index)Cardiac rhythm interpretation (e.g.)rate, •rhythm, ST elevation, T wave configurationTwelve and 15 electrocardiogram •changes consistent with myocardial injury, ischemia, or infarctionPacemaker functions •(e.g. sensing and capturing)Intracranial pressures and waveforms•Cerebral perfusion pressure•Pulse oximetry•End Tidal carbon dioxide•Ventilation information (e.g. tidal •volume, minute volume, oxygenation rate, airway pressures, end-tidal CO2Ventilation support•
bipap -
assist control, synchronized -intermittent mandatory ventilation,
positive and expiratory pressure, -pressure support ventilation,
pressure control ventilation, volume -control ventilation
high frequency jet ventilation, high -frequency oscillation

48 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
0% 25% 50% 75% 100% Theory Clinical
5.35: Weaning parameters (e.g. tidal volume, respiratory rate, minute ventilation, vital capacity, work of breathing, anxiety)
5.36: Oxygen delivery, extraction, consumption
5.37: Laboratory results:Arterial blood gas •Complete blood count•Platelets •Coagulation profiles•Serum and urine electrolytes and •osmolalityLactate •Creatinine•BUN •CK-MB•Cerebral spinal fluid •Glucose•Drug levels •Liver enzymes •
5.38: Compare collected data with expected patient responses and validate unexpected findings
5.39: Integrate all findings from the assessment to identify collaborative and/or independent nursing diagnoses
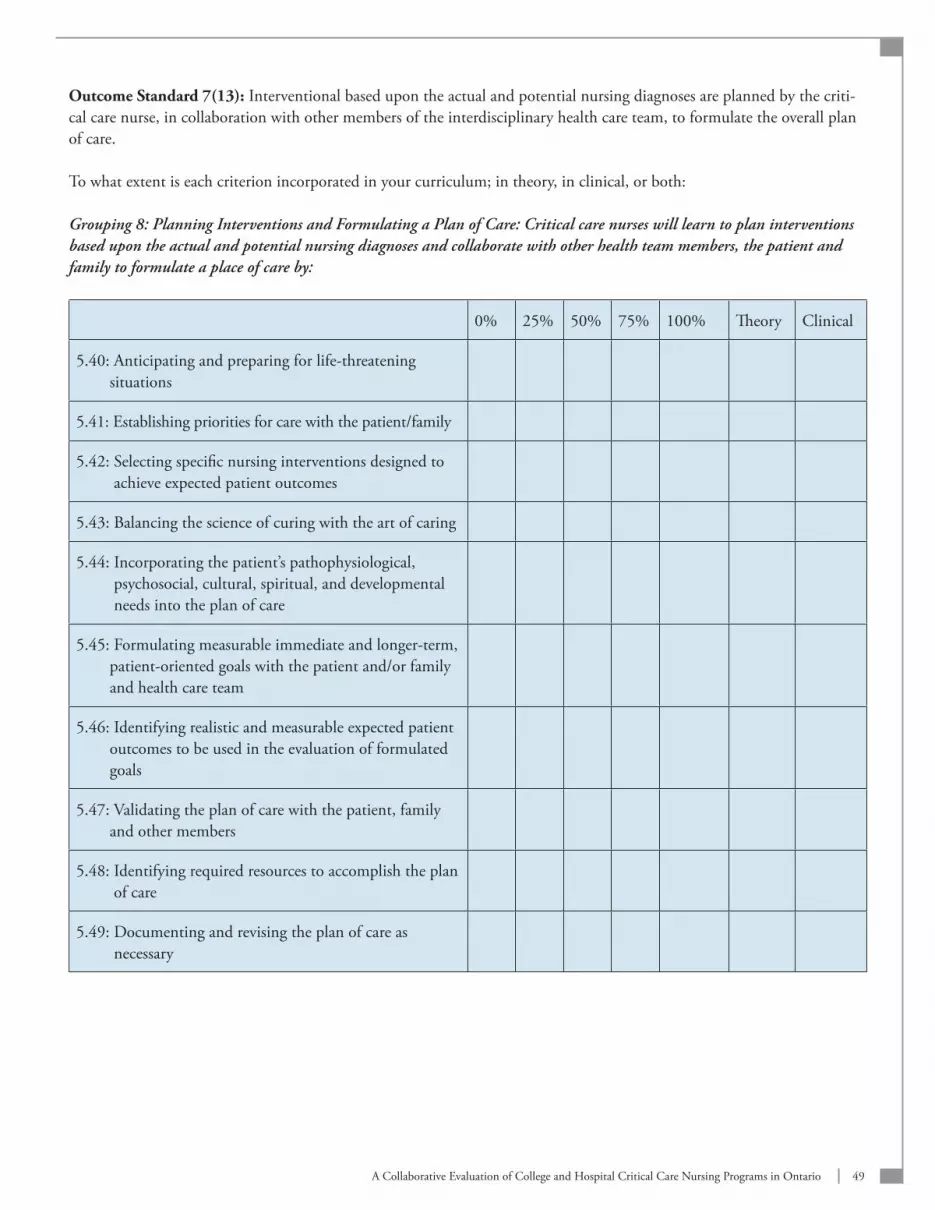
49A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Outcome Standard 7(13): Interventional based upon the actual and potential nursing diagnoses are planned by the criti-cal care nurse, in collaboration with other members of the interdisciplinary health care team, to formulate the overall plan of care.
To what extent is each criterion incorporated in your curriculum; in theory, in clinical, or both:
Grouping 8: Planning Interventions and Formulating a Plan of Care: Critical care nurses will learn to plan interventions based upon the actual and potential nursing diagnoses and collaborate with other health team members, the patient and family to formulate a place of care by:
0% 25% 50% 75% 100% Theory Clinical
5.40: Anticipating and preparing for life-threatening situations
5.41: Establishing priorities for care with the patient/family
5.42: Selecting specific nursing interventions designed to achieve expected patient outcomes
5.43: Balancing the science of curing with the art of caring
5.44: Incorporating the patient’s pathophysiological, psychosocial, cultural, spiritual, and developmental needs into the plan of care
5.45: Formulating measurable immediate and longer-term, patient-oriented goals with the patient and/or family and health care team
5.46: Identifying realistic and measurable expected patient outcomes to be used in the evaluation of formulated goals
5.47: Validating the plan of care with the patient, family and other members
5.48: Identifying required resources to accomplish the plan of care
5.49: Documenting and revising the plan of care as necessary
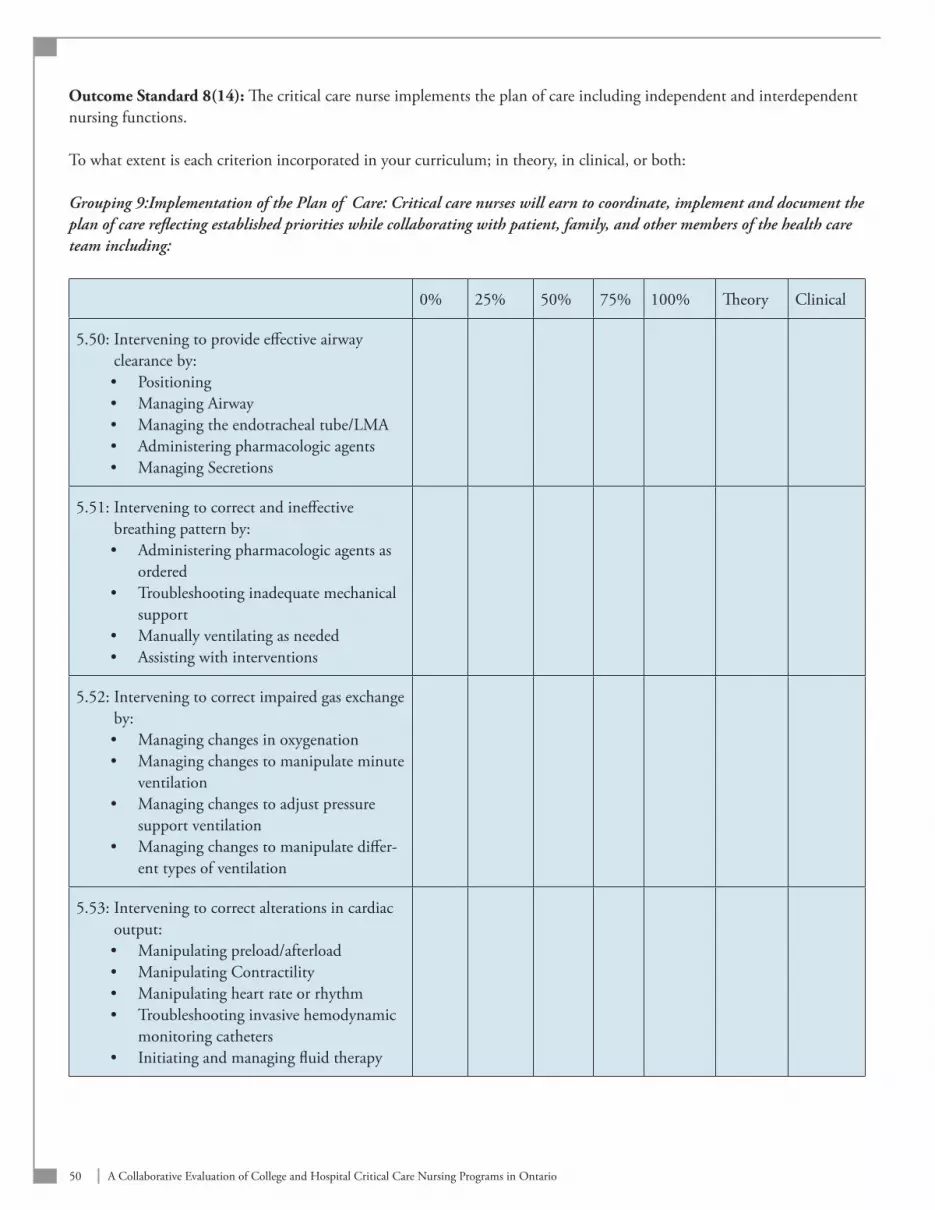
50 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Outcome Standard 8(14): The critical care nurse implements the plan of care including independent and interdependent nursing functions.
To what extent is each criterion incorporated in your curriculum; in theory, in clinical, or both:
Grouping 9:Implementation of the Plan of Care: Critical care nurses will earn to coordinate, implement and document the plan of care reflecting established priorities while collaborating with patient, family, and other members of the health care team including:
0% 25% 50% 75% 100% Theory Clinical
5.50: Intervening to provide effective airway clearance by:
Positioning•Managing Airway•Managing the endotracheal tube/LMA•Administering pharmacologic agents•Managing Secretions•
5.51: Intervening to correct and ineffective breathing pattern by:
Administering pharmacologic agents as •orderedTroubleshooting inadequate mechanical •supportManually ventilating as needed•Assisting with interventions•
5.52: Intervening to correct impaired gas exchange by:
Managing changes in oxygenation•Managing changes to manipulate minute •ventilationManaging changes to adjust pressure •support ventilationManaging changes to manipulate differ-•ent types of ventilation
5.53: Intervening to correct alterations in cardiac output:
Manipulating preload/afterload•Manipulating Contractility•Manipulating heart rate or rhythm•Troubleshooting invasive hemodynamic •monitoring cathetersInitiating and managing fluid therapy•

51A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
0% 25% 50% 75% 100% Theory Clinical
5.54: Intervening to correct alterations in cardiopulmonary tissue perfusion by administration selected pharmacologic agents.
5.55: Intervening to correct alterations in renal perfusion by:
Administering and managing fluids by •calculating total fluid intake/outtakeAdministering pharmacologic agents•Maintaining invasive interventions•Recognizing and minimizing the side •effects of nephrotoxic pharmacologic agents
5.56: Intervening to correct alterations in cerebral perfusion by:
Using techniques to prevent obstruction •and promote venous and cerebral spinal fluid drainageManipulating PaCO2•Minimizing stimulation•Administering pharmacologic agents•Manipulating cerebral perfusion •pressuresManaging seizure activity•Assisting with insertion/maintenance •of intracranial pressure monitoring or ventricular drainage devicesAssisting with insertion of cerebral •oxygenation monitoring devicesTroubleshooting invasive intracranial •parameters/waveformsUsing techniques that minimize •elevations in intrathoracic pressuresAdministering appropriate fluid therapy •to control intracranial hypertensionControlling metabolic rate •Preventing secondary injury•
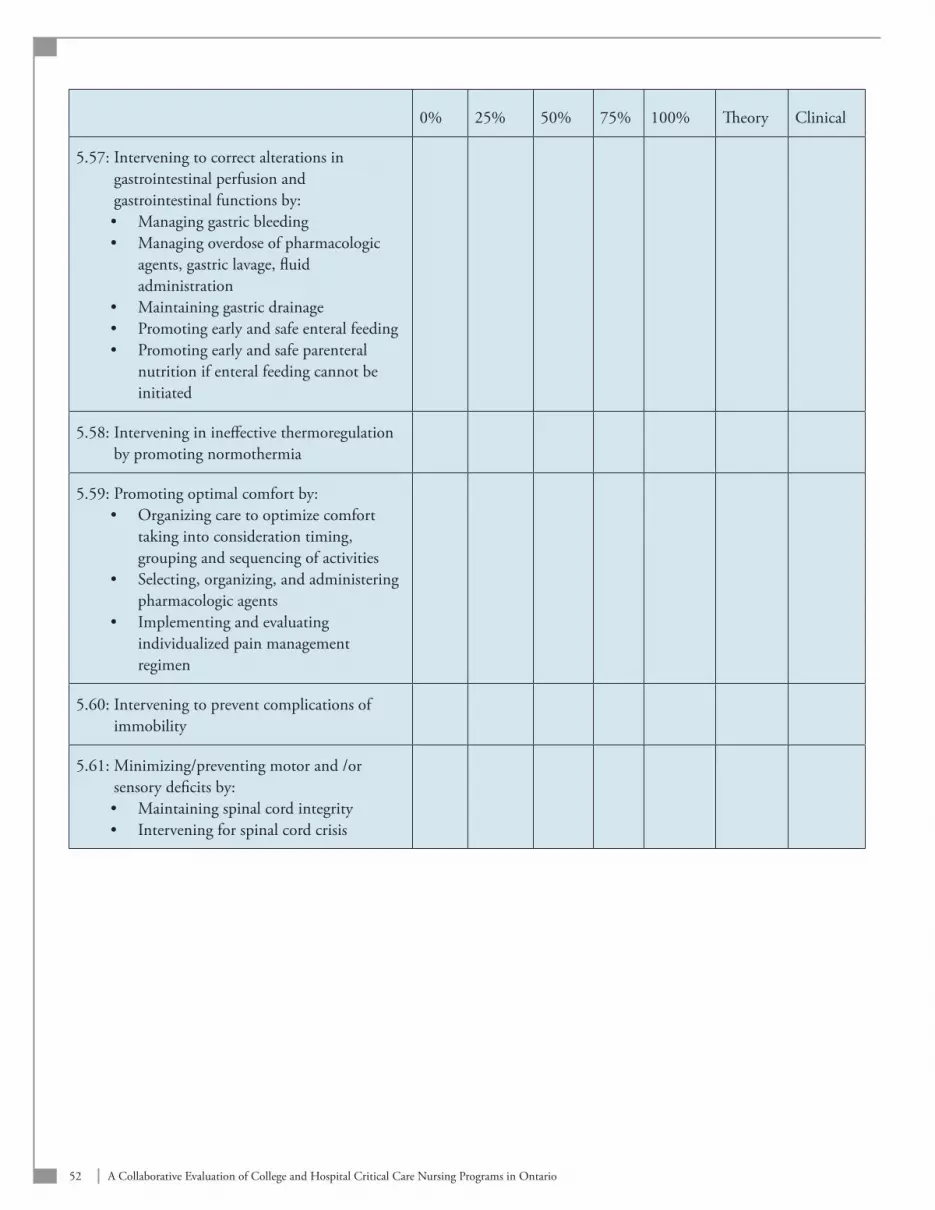
52 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
0% 25% 50% 75% 100% Theory Clinical
5.57: Intervening to correct alterations in gastrointestinal perfusion and gastrointestinal functions by:
Managing gastric bleeding•Managing overdose of pharmacologic •agents, gastric lavage, fluid administrationMaintaining gastric drainage•Promoting early and safe enteral feeding•Promoting early and safe parenteral •nutrition if enteral feeding cannot be initiated
5.58: Intervening in ineffective thermoregulation by promoting normothermia
5.59: Promoting optimal comfort by: Organizing care to optimize comfort •taking into consideration timing, grouping and sequencing of activitiesSelecting, organizing, and administering •pharmacologic agentsImplementing and evaluating •individualized pain management regimen
5.60: Intervening to prevent complications of immobility
5.61: Minimizing/preventing motor and /or sensory deficits by:
Maintaining spinal cord integrity•Intervening for spinal cord crisis•
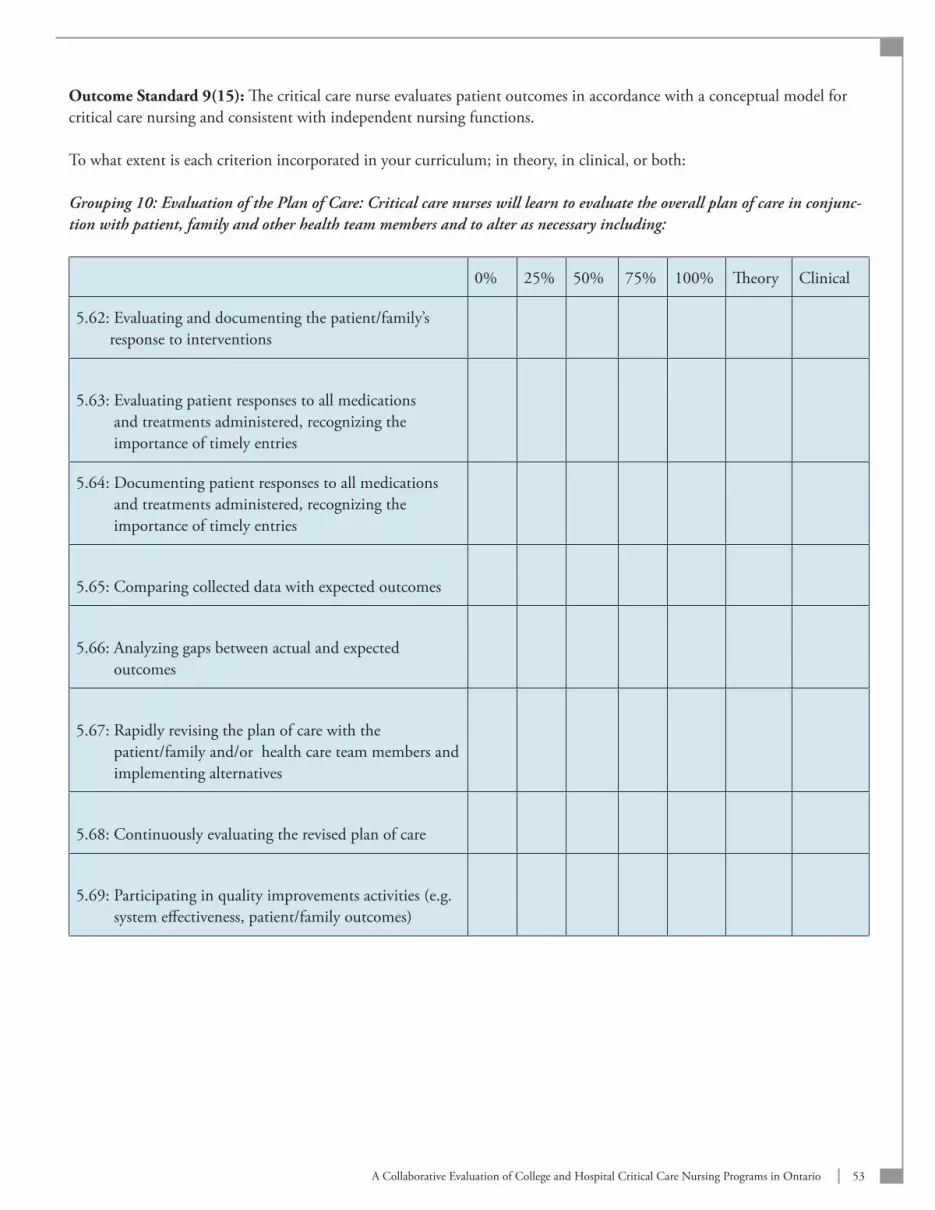
53A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Outcome Standard 9(15): The critical care nurse evaluates patient outcomes in accordance with a conceptual model for critical care nursing and consistent with independent nursing functions.
To what extent is each criterion incorporated in your curriculum; in theory, in clinical, or both:
Grouping 10: Evaluation of the Plan of Care: Critical care nurses will learn to evaluate the overall plan of care in conjunc-tion with patient, family and other health team members and to alter as necessary including:
0% 25% 50% 75% 100% Theory Clinical
5.62: Evaluating and documenting the patient/family’s response to interventions
5.63: Evaluating patient responses to all medications and treatments administered, recognizing the importance of timely entries
5.64: Documenting patient responses to all medications and treatments administered, recognizing the importance of timely entries
5.65: Comparing collected data with expected outcomes
5.66: Analyzing gaps between actual and expected outcomes
5.67: Rapidly revising the plan of care with the patient/family and/or health care team members and implementing alternatives
5.68: Continuously evaluating the revised plan of care
5.69: Participating in quality improvements activities (e.g. system effectiveness, patient/family outcomes)
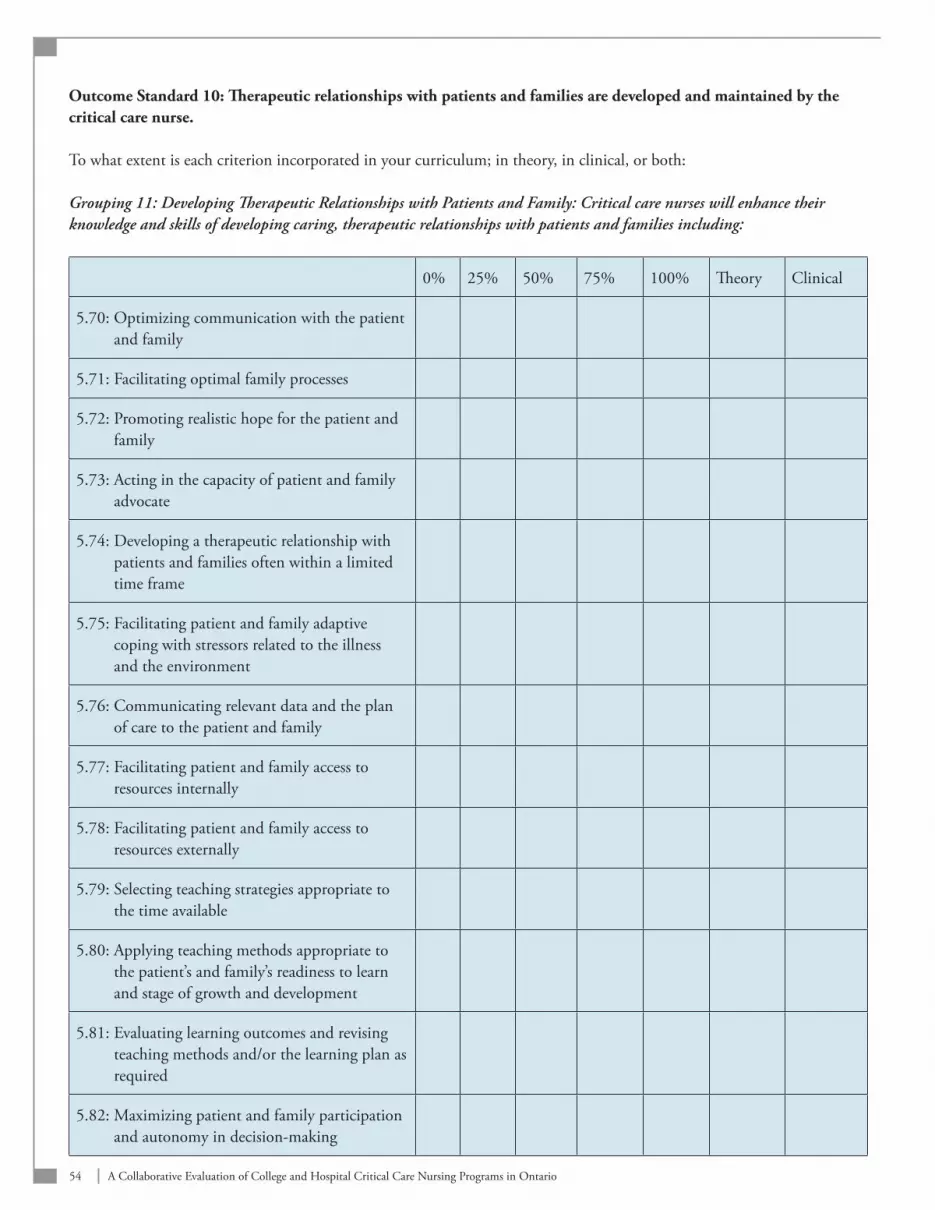
54 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Outcome Standard 10: Therapeutic relationships with patients and families are developed and maintained by the critical care nurse.
To what extent is each criterion incorporated in your curriculum; in theory, in clinical, or both:
Grouping 11: Developing Therapeutic Relationships with Patients and Family: Critical care nurses will enhance their knowledge and skills of developing caring, therapeutic relationships with patients and families including:
0% 25% 50% 75% 100% Theory Clinical
5.70: Optimizing communication with the patient and family
5.71: Facilitating optimal family processes
5.72: Promoting realistic hope for the patient and family
5.73: Acting in the capacity of patient and family advocate
5.74: Developing a therapeutic relationship with patients and families often within a limited time frame
5.75: Facilitating patient and family adaptive coping with stressors related to the illness and the environment
5.76: Communicating relevant data and the plan of care to the patient and family
5.77: Facilitating patient and family access to resources internally
5.78: Facilitating patient and family access to resources externally
5.79: Selecting teaching strategies appropriate to the time available
5.80: Applying teaching methods appropriate to the patient’s and family’s readiness to learn and stage of growth and development
5.81: Evaluating learning outcomes and revising teaching methods and/or the learning plan as required
5.82: Maximizing patient and family participation and autonomy in decision-making
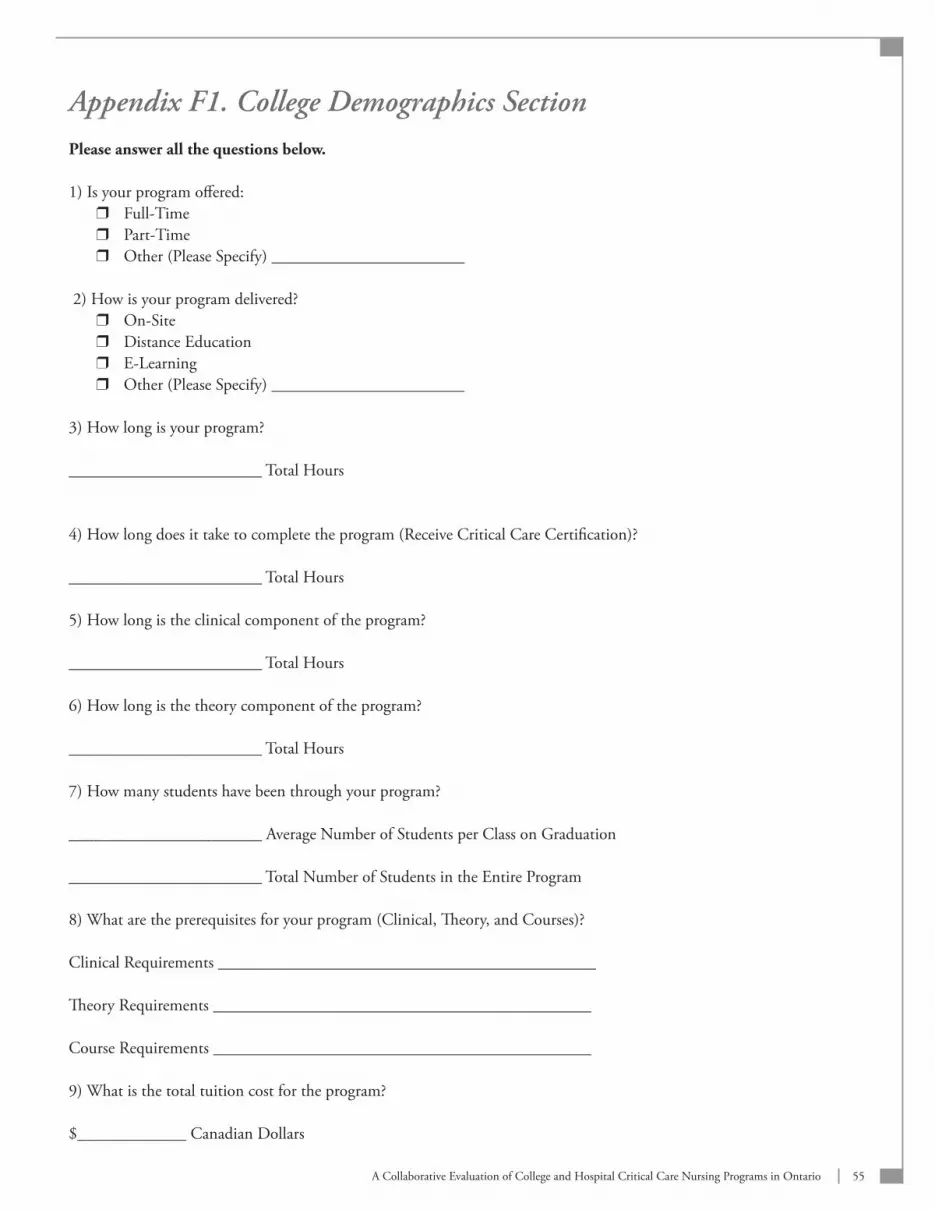
55A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix F1. College Demographics SectionPlease answer all the questions below.
1) Is your program offered: Full-Time r
Part-Time r
Other (Please Specify) _______________________ r
2) How is your program delivered? On-Site r
Distance Education r
E-Learning r
Other (Please Specify) _______________________ r
3) How long is your program?
_______________________ Total Hours
4) How long does it take to complete the program (Receive Critical Care Certification)?
_______________________ Total Hours
5) How long is the clinical component of the program?
_______________________ Total Hours
6) How long is the theory component of the program?
_______________________ Total Hours
7) How many students have been through your program?
_______________________ Average Number of Students per Class on Graduation
_______________________ Total Number of Students in the Entire Program
8) What are the prerequisites for your program (Clinical, Theory, and Courses)?
Clinical Requirements _____________________________________________
Theory Requirements _____________________________________________
Course Requirements _____________________________________________
9) What is the total tuition cost for the program?
$_____________ Canadian Dollars
56 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
10) Is your curriculum: Basic General Program r
Specialty Program (Beyond Basic Preparation i.e. Cardiovascular Surgery, Coronary Care, Neuro-Trauma) r
Combination of Both r
11) We welcome any specific feedback you may have regarding the new Standards for Critical Care Nursing in Ontario (2006). Please share your top three comments/suggestions with us.
I.
II.
II.
12) We welcome any specific feedback you may have on this survey process please share your top 3 comments/suggestions with us.
I.
II.
57A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix F2. Section B: Hospital Demographics SectionPlease answer all the questions below.
1) Which of the following would best describe the type of critical care unit the questionnaire is being completed for? Medical ICU r
Surgical ICU r
Burn Unit r
Trauma Unit r
Combined Medical/Surgical ICU r
Other (Please Specify) _______________________ r
2) What is the total number of beds in this unit? Less than 10 Beds r
11 – 20 Beds r
21 – 30 Beds r
Greater than 30 Beds r
3) On average how many nurses complete your program annually? Less than 10 r
11 – 20 r
21 – 30 r
Greater than 30 r
4) Which of the following training programs does this unit use to prepare nurses new to critical care for practice in that setting? (If a combination of programs is utilized please indicate those that are used.)
College Certification r
In-House Orientation r
Preceptorship r
Other (Please Specify) _______________________ r
5) What is the duration in weeks of theory education?
_______________________ Number of Weeks
6) What is the duration in weeks of clinical education?
_______________________ Number of Weeks
58 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
7) Do you have written standards of practice for nurses in your unit? Yes r
No (Go to Question 10) r
8) If yes: How often does your unit update these specific standards?
_______________________ Number of Years
9) If yes: Which national or provincial standards are most reflected in your documents? (Check all that Apply) I. National or Provincial Standards are reflected in our documents
Very Great Extent r
To Some Extent r
A Small Extent r
Not At All r
II. Canadian Association of Critical Care NursesVery Great Extent r
To Some Extent r
A Small Extent r
Not At All r
III. American Association of Critical Care NursesVery Great ExtentTo Some ExtentA Small ExtentNot At All
IV. College of Nurses of OntarioVery Great Extent r
To Some Extent r
A Small Extent r
Not At All r
Please specify other standards reflected in your documents _______________________
10) Does your program include an evaluation component? Yes r
No (Go to Question 14) r
11) If yes: How frequently are nurses evaluated?
12) If yes: Is documentation provided as that time? Yes r
No r
13) If yes: Is written peer review a required component? Yes r
No r

59A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
14) We welcome any specific feedback you may have regarding the new Standards for Critical Care Nursing in Ontario (2006). Please share your top three comments/suggestions with us.
I.
II.
II.
15) We welcome any specific feedback you may have on this survey process please share your top 3 comments/suggestions with us.
I.
II.
II.
60 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix G. Letter Critical Care Secretariat: Dr Bernard Lawless
Ministry of Health Ministère de la Santé and Long-Term Care et des Soins de longue durée
Critical Care Secretariat Secrétariat des soins aux malades en phase critiqueHealth System Accountability Division de la responsabilisation et de la and Performance Division performance du système de santé77 Wellesley Street W, 2B-74 77, rue Wellesley Ouest, 2B-74Toronto ON M7A 1N3 Toronto ON M7A 1N3
Telephone: 416 340-4800 x 2767 Téléphone : 416 340-4800, poste 2767 Facsimile: 416 340-4920 Télécopieur: 416 340-4920
Wednesday March 21, 2007
Re: Collaborative Evaluation of College/Hospital Critical Care Nurse Training Programs
Dear Colleague:
The Ministry’s Nursing Secretariat and Critical Care Secretariat have formed a partnership to address issues relating to critical care nursing in a manner that is consistent with the Nursing Secretariat’s overall leadership for nursing in Ontario. Through this partnership, the Ministry is moving forward to implement key recommendations of the Ontario Critical Care Steering Committee. In the 2005 Final Report, the Committee identified the need for consistency of nurse training in critical care to support the recruitment and retention of critical care nurses. Currently, training programs vary across the province and it is suspected that staff who complete training may not all have the same competencies.
In October 2005, the Ontario Critical Care Expert Panel established the Critical Care Nurse Training Standards Task Group to identify and articulate adult critical care core competencies and training standards for Ontario. This Task Group brought together critical care nurse leaders from across the province. The Minister of Health accepted the recommenda-tions made by the Task Group in August 2006. Implementation of a set of initiatives which respond to the recommenda-tions of the Task Group are now underway by the Nursing Secretariat and Critical Care Secretariat. The government is committed to providing appropriate and adequate supports to the system to improve critical care education for nurses and to support hospitals in meeting their human resource needs to provide safe and accessible care. A key initiative designed to meet these goals is a collaborative evaluation of all college-based and select hospital-based criti-cal care nursing programs in Ontario to determine the quality and content of didactic and clinical training for nurses. The evaluation will be conducted by the Nursing Health Services Research Unit (NHSRU) under the leadership of Dr. Anita Fisher (Associate Professor, School of Nursing and Co-investigator, NHSRU). The results of the evaluation will be used to support decisions regarding future allocation of funding for training of critical care nurses throughout the province thus contributing to the standardization of critical care nurse training.

61A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
The evaluation process will be conducted in three distinct phases as follows:
Focus groups:• Approximately 13 focus groups, determined by LHIN boundaries, will be conducted by teleconfer-ence with a sample of facilities from the selected sites. Each focus group will consist of 3-5 participants, including critical care educators, managers and practitioners, and last approximately one hour. The purpose of the focus groups is to gain stakeholder input on the new standards including: 1) their relevance to practice and education; 2) the enablers and challenges to implementing these standards and 3) how programs might be evaluated to deter-mine the extent to which these standards exist in current programs. The results of these focus groups will assist in fine-tuning of the new standards and in development of a survey tool.
Survey:• A survey will be developed based on the new Critical Care Nursing Standards in Ontario as well as the input from the focus group discussions. The purpose of the survey is to determine the extent to which these standards have been incorporated in curricula. It is anticipated that this survey will be circulated in May and June, 2007. Participants will be requested to evaluate their own curriculum by completing the survey and to submit, both the completed survey and a copy of their curriculum, to the research team at McMaster University.
Expert Panel: • An expert panel of 3-5 critical care curriculum experts will review all curricula to identify the extent to which the new standards have been incorporated into critical care nursing education across the province. Ex-pert panel reviews of individual curricula will be blind and the results will remain confidential. The final report will not identify individual curricula or the facilities with which they are associated. Individual facilities may request a copy of the expert panel review of their own curriculum by directly contacting the research team.
Analysis of the surveys and the expert panel reviews will be summarized in a generic report, identifying strengths and gaps in critical care nursing education programs in the province. The report will be submitted to the Nursing Subcommittee of the Critical Care Expert Advisory Panel and the Critical Care Secretariat. The evidence will be used to: 1) inform policy decisions to further strengthen critical care nursing education in Ontario; 2) support decisions regarding allocation of funding for educating critical care nurses; and 3) contribute to the creation of a portable critical care nursing credential.
Based on recommendations of the Critical Care Nurse Training Standards Task Group, your institution is being invited to participate in this evaluation. The Nursing Health Services Research Unit will contact you in the next two weeks to request your assistance in identifying focus group participants and to discuss timelines and processes for completing the evaluation for your organization. Please note that participation in this review is voluntary.
Thank you for reviewing this information. We look forward to your participation in a project that will contribute to the advancement of critical care nursing education in Ontario.
Sincerely,
Bernard Lawless MD, MHSc, CHE, FRCSCProvincial Lead, Critical Care and TraumaHealth System Accountability and Performance DivisionMinistry of Health and Long-Term Care
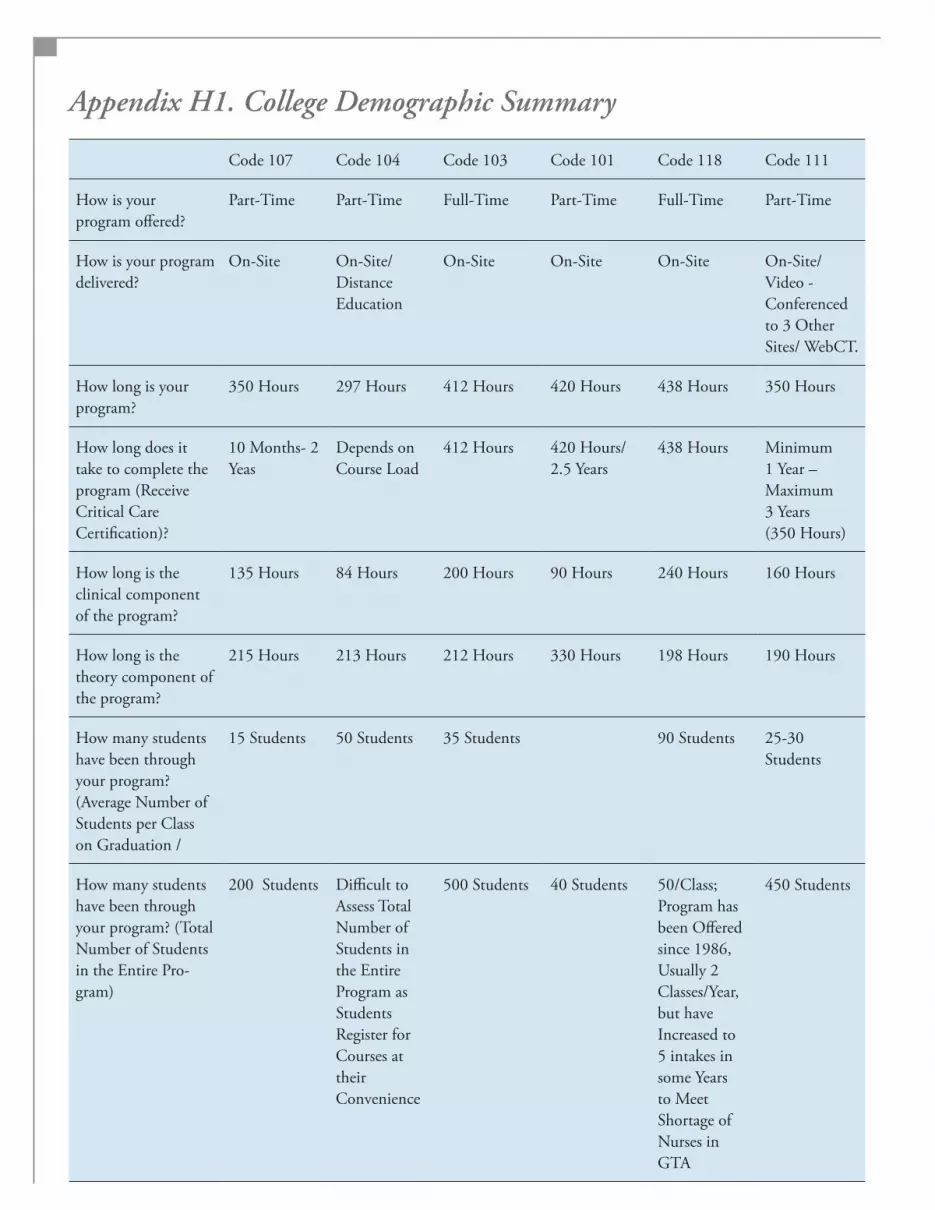
Appendix H1. College Demographic Summary
Code 107 Code 104 Code 103 Code 101 Code 118 Code 111
How is your program offered?
Part-Time Part-Time Full-Time Part-Time Full-Time Part-Time
How is your program delivered?
On-Site On-Site/ Distance Education
On-Site On-Site On-Site On-Site/ Video - Conferenced to 3 Other Sites/ WebCT.
How long is your program?
350 Hours 297 Hours 412 Hours 420 Hours 438 Hours 350 Hours
How long does it take to complete the program (Receive Critical Care Certification)?
10 Months- 2 Yeas
Depends on Course Load
412 Hours 420 Hours/ 2.5 Years
438 Hours Minimum 1 Year –Maximum 3 Years (350 Hours)
How long is the clinical component of the program?
135 Hours 84 Hours 200 Hours 90 Hours 240 Hours 160 Hours
How long is the theory component of the program?
215 Hours 213 Hours 212 Hours 330 Hours 198 Hours 190 Hours
How many students have been through your program? (Average Number of Students per Class on Graduation /
15 Students 50 Students 35 Students 90 Students 25-30Students
How many students have been through your program? (Total Number of Students in the Entire Pro-gram)
200 Students Difficult to Assess Total Number of Students in the Entire Program as Students Register for Courses at their Convenience
500 Students 40 Students 50/Class; Program has been Offered since 1986, Usually 2 Classes/Year, but have Increased to 5 intakes in some Years to Meet Shortage of Nurses in GTA
450 Students
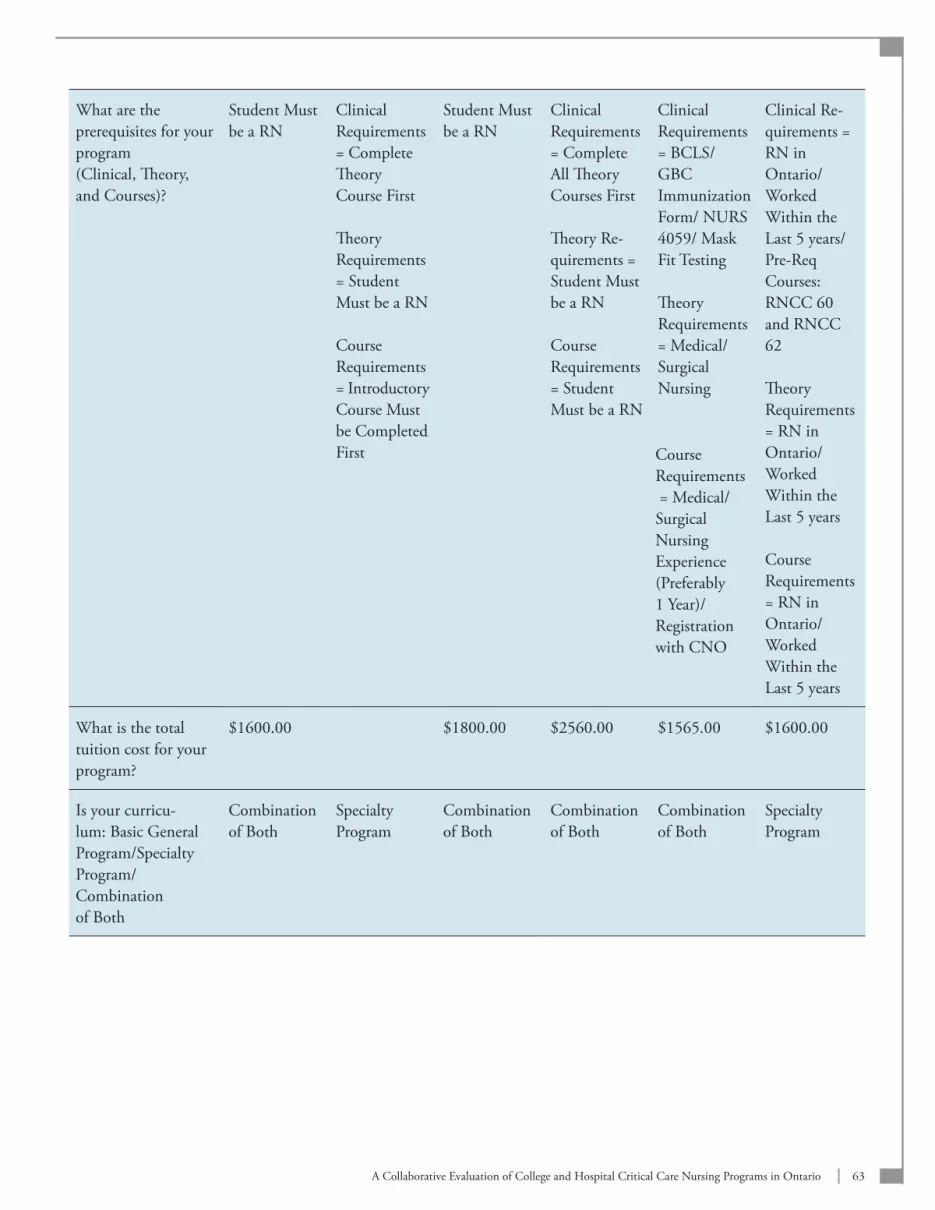
63A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
What are the prerequisites for your program (Clinical, Theory, and Courses)?
Student Must be a RN
Clinical Requirements = Complete Theory Course First
Theory Requirements = Student Must be a RN
Course Requirements = Introductory Course Must be Completed First
Student Must be a RN
Clinical Requirements = Complete All Theory Courses First
Theory Re-quirements = Student Must be a RN
Course Requirements = Student Must be a RN
Clinical Requirements = BCLS/ GBC Immunization Form/ NURS 4059/ Mask Fit Testing
Theory Requirements = Medical/Surgical Nursing
Clinical Re-quirements = RN in Ontario/ Worked Within the Last 5 years/ Pre-Req Courses: RNCC 60 and RNCC 62
Theory Requirements = RN in Ontario/ Worked Within the Last 5 years
Course Requirements = RN in Ontario/ Worked Within the Last 5 years
What is the total tuition cost for your program?
$1600.00 $1800.00 $2560.00 $1565.00 $1600.00
Is your curricu-lum: Basic General Program/Specialty Program/ Combination of Both
Combination of Both
Specialty Program
Combination of Both
Combination of Both
Combination of Both
Specialty Program
Course Requirements = Medical/Surgical Nursing Experience(Preferably 1 Year)/Registration with CNO
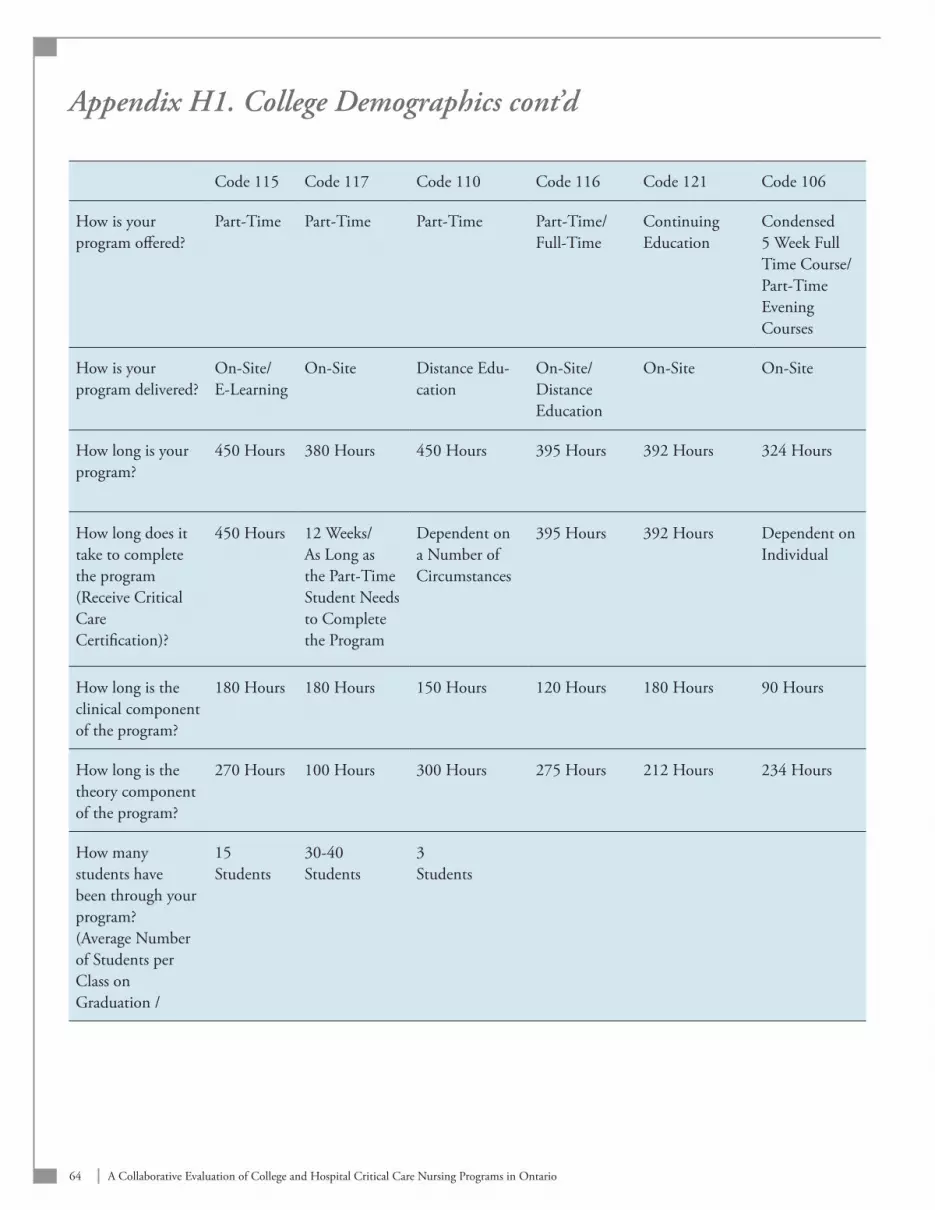
64 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix H1. College Demographics cont’d
Code 115 Code 117 Code 110 Code 116 Code 121 Code 106
How is your program offered?
Part-Time Part-Time Part-Time Part-Time/ Full-Time
Continuing Education
Condensed 5 Week Full Time Course/ Part-Time Evening Courses
How is your program delivered?
On-Site/E-Learning
On-Site Distance Edu-cation
On-Site/Distance Education
On-Site On-Site
How long is your program?
450 Hours 380 Hours 450 Hours 395 Hours 392 Hours 324 Hours
How long does it take to complete the program (Receive Critical Care Certification)?
450 Hours 12 Weeks/As Long as the Part-Time Student Needs to Complete the Program
Dependent on a Number of Circumstances
395 Hours 392 Hours Dependent on Individual
How long is the clinical component of the program?
180 Hours 180 Hours 150 Hours 120 Hours 180 Hours 90 Hours
How long is the theory component of the program?
270 Hours 100 Hours 300 Hours 275 Hours 212 Hours 234 Hours
How many students have been through your program? (Average Number of Students per Class on Graduation /
15 Students
30-40 Students
3 Students
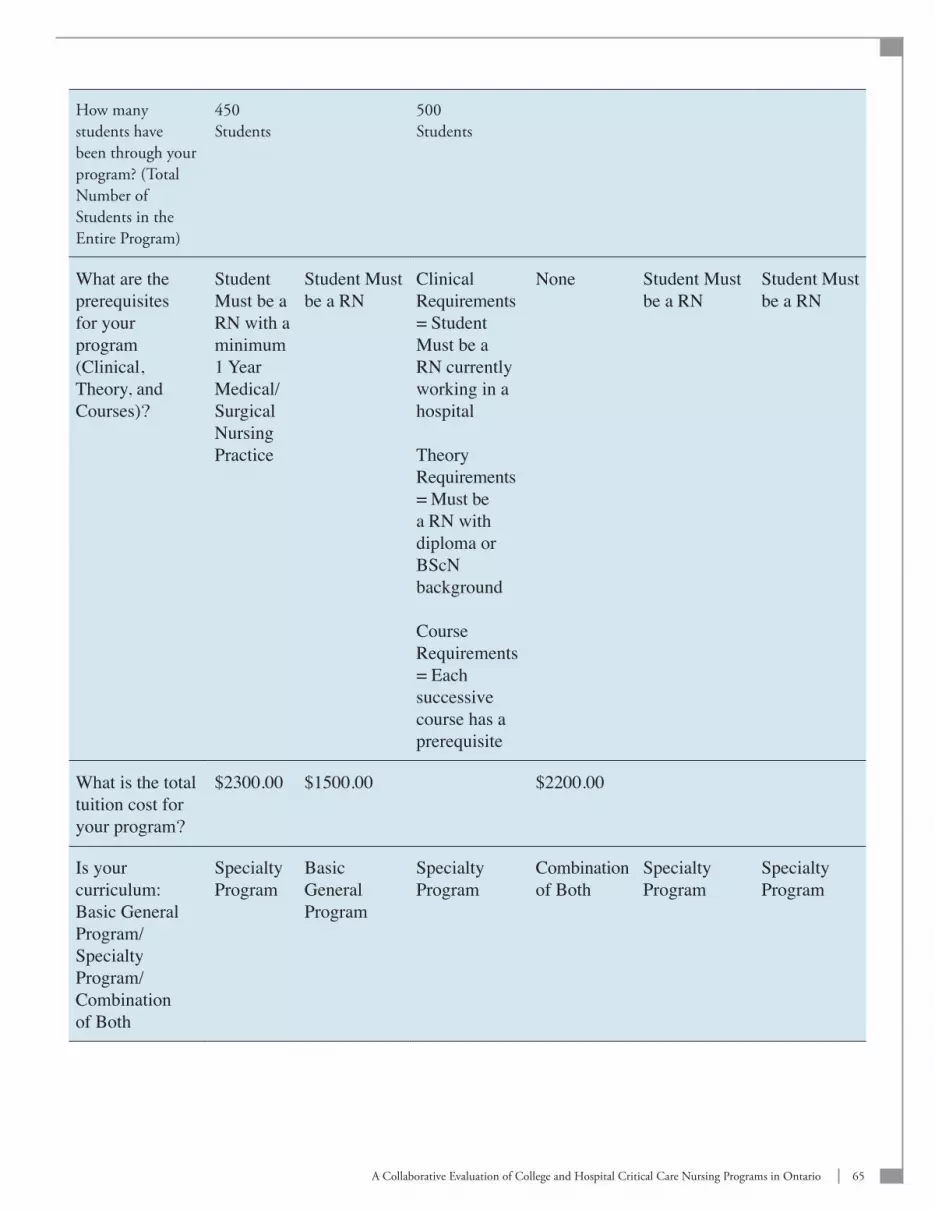
65A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
How many students have been through your program? (Total Number of Students in the Entire Program)
450 Students
500 Students
What are the prerequisites for your program (Clinical, Theory, and Courses)?
Student Must be a RN with a minimum 1 Year Medical/Surgical Nursing Practice
Student Must be a RN
Clinical Requirements = Student Must be a RN currently working in a hospital
Theory Requirements = Must be a RN with diploma or BScN background
Course Requirements = Each successive course has a prerequisite
None
Student Must be a RN
Student Must be a RN
What is the total tuition cost for your program?
$2300.00 $1500.00 $2200.00
Is your curriculum: Basic General Program/Specialty Program/ Combination of Both
Specialty Program
Basic General Program
Specialty Program
Combination of Both
Specialty Program
Specialty Program

66 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix H2. Hospital Demographics
Code 100 Code 102 Code 105 Code 108 Code 109 Code 113
Describe the type of critical care unit the questionnaire is being completed for?
Combined Medical/Surgical Trauma
Combined Medical/Surgical CV/Trauma
Combined Medical/Surgical ICU/CCU
Combined Medical/Surgical ICU
Cardiovascular Thoracic ICU
Combined Medical/Surgical ICU
What is the total number of beds in this unit?
Greater Than 30 Beds
Greater Than 30 Beds
11- 20 Beds 11- 20 Beds 21-30 Beds Greater Than 30 Beds
On average how many nurses complete your program annually?
Greater Than 30 Nurses
Greater Than 30 Nurses
11 – 20 Nurses
11 – 20 Nurses
11 – 20 Nurses Greater Than 30 Nurses
What training programs does this unit use to prepare nurses new to critical care?
In-House Orientation
In-House Orientation
In-House Orientation/ Preceptorship / Vermont Nursing Internship Program
In-House Orientation
In-House Orientation
In-House Orientation
What is the dura-tion in weeks of theory education?
2 Weeks 4 Weeks 2 Weeks 1 Week 2 Weeks 3.5 Weeks
What is the duration in weeks of clinical education?
4 Weeks Tailored to Individual
4-6 Weeks 6 Weeks 5 Weeks 3.5 Weeks
Do you havewritten standards of practice for nurses in your unit and if yes, how often does your unit update these specific standards?
Yes; Every 1-2 Years/ As Necessary
Yes; Every 2 Years
Yes; Annually Yes;CACCN Revisions - Provincial Critical Care Standards
Yes; Every 2 Years
No

67A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
If yes, which of the following standards are most reflected in your documents and specify to what extent (National or Provincial Standards/Canadian Association of Critical Care Nurses/ American Association of Critical Care Nurses/College of Nurses of Ontario)?
National/ Provincial Standards – Not At All
CACCN – Very Great Extent
AACCN – To Some Extent
CNO - Very Great Extent
National/ Provincial Standards – Very Great Extent
CACCN – Very Great Extent
AACCN – Very Great Extent
CNO - Very Great Extent
National/ Provincial Standards – To Some Extent
CACCN – A Small Extent
AACCN – To Some Extent
CNO - To Some Extent
National/ Provincial Standards – Very Great Extent
CACCN – Very Great Extent
AACCN – Not At All
CNO - Very Great Extent
National/ Provincial Standards – To Some Extent
CACCN – To Some Extent
AACCN – To Some Extent
CNO - Very Great Extent
Does your program include an evalu-ation component and if so, how fre-quently are nurses evaluated?
Yes; 3 Months Post-Orientation
Yes; Infor-mally on a Daily Basis
Yes;Weekly While in Orientation
Yes; Daily Yes; After Probation, at 3 Months Probationary Period and Annually
Yes; Throughout and at theEnd of Orientation
If yes: Is documentation provided as that time?
Yes Yes Yes Yes Yes
If yes: Is a written peer review a required component?
Yes No Yes Yes No No
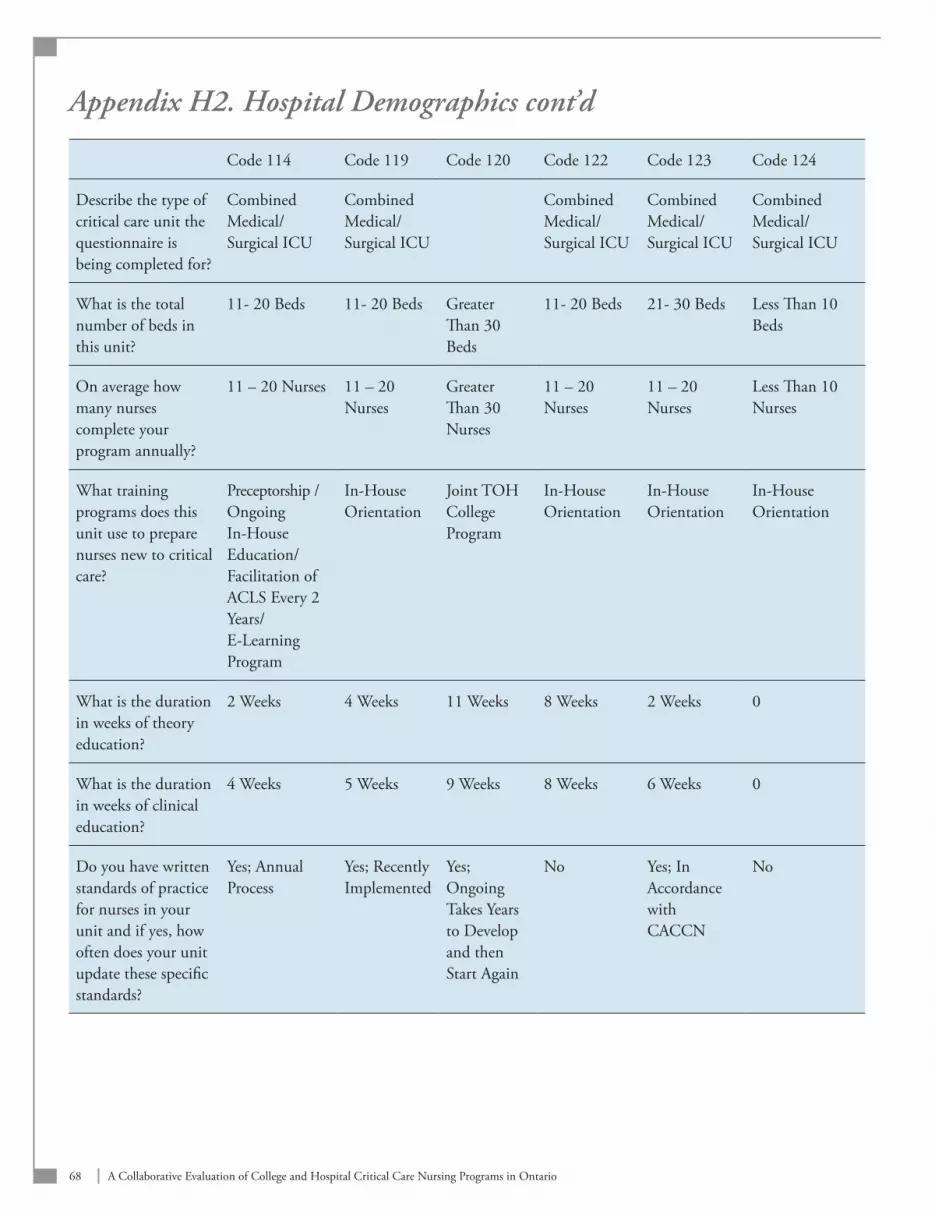
68 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix H2. Hospital Demographics cont’d
Code 114 Code 119 Code 120 Code 122 Code 123 Code 124
Describe the type of critical care unit the questionnaire is being completed for?
Combined Medical/Surgical ICU
Combined Medical/Surgical ICU
Combined Medical/Surgical ICU
Combined Medical/Surgical ICU
Combined Medical/Surgical ICU
What is the total number of beds in this unit?
11- 20 Beds 11- 20 Beds Greater Than 30 Beds
11- 20 Beds 21- 30 Beds Less Than 10 Beds
On average how many nurses complete your program annually?
11 – 20 Nurses 11 – 20 Nurses
Greater Than 30 Nurses
11 – 20 Nurses
11 – 20 Nurses
Less Than 10 Nurses
What training programs does this unit use to prepare nurses new to critical care?
Preceptorship / Ongoing In-House Education/Facilitation of ACLS Every 2 Years/ E-Learning Program
In-House Orientation
Joint TOH College Program
In-House Orientation
In-House Orientation
In-House Orientation
What is the duration in weeks of theory education?
2 Weeks 4 Weeks 11 Weeks 8 Weeks 2 Weeks 0
What is the duration in weeks of clinical education?
4 Weeks 5 Weeks 9 Weeks 8 Weeks 6 Weeks 0
Do you have written standards of practice for nurses in your unit and if yes, how often does your unit update these specific standards?
Yes; Annual Process
Yes; Recently Implemented
Yes; Ongoing Takes Years to Develop and then Start Again
No Yes; In Accordance with CACCN
No
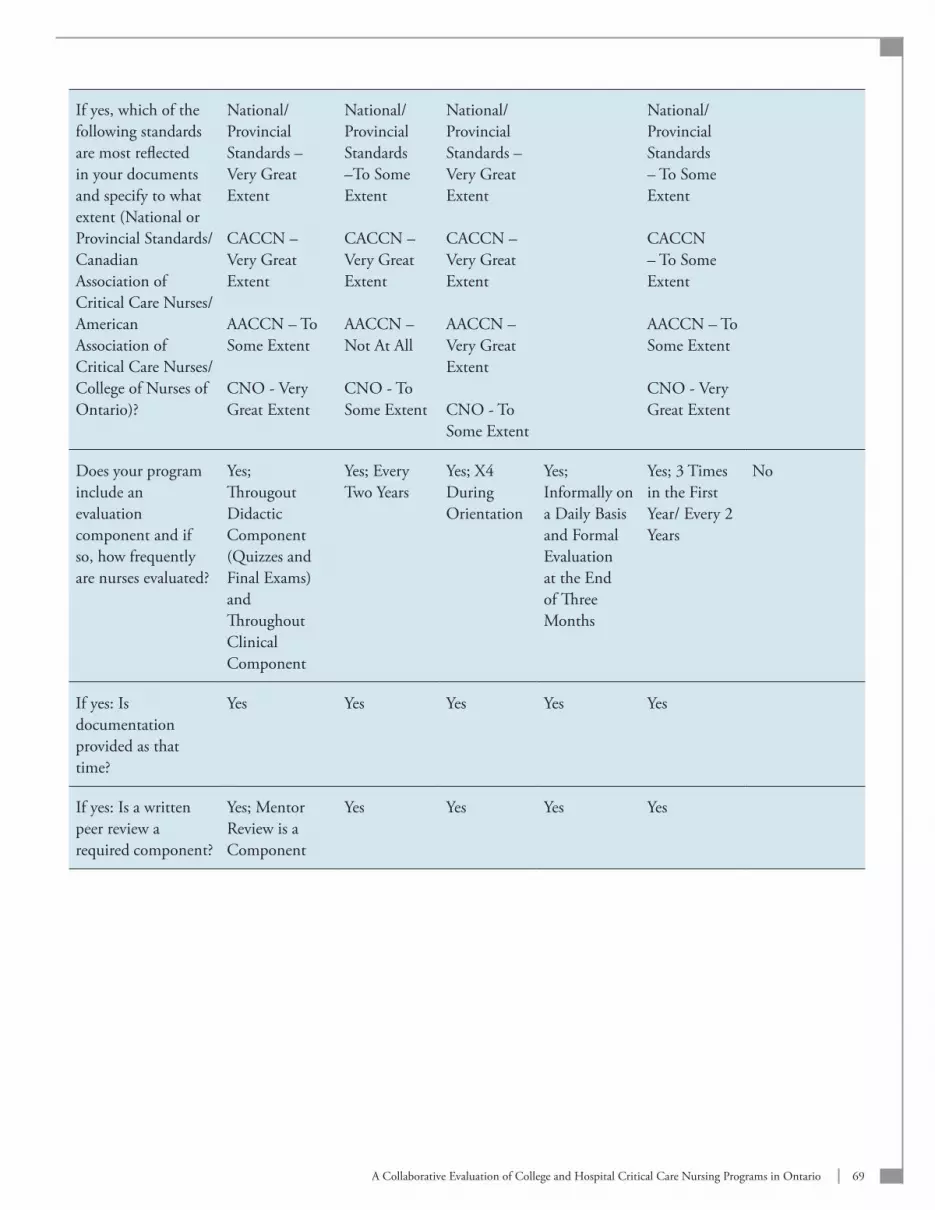
69A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
If yes, which of the following standards are most reflected in your documents and specify to what extent (National or Provincial Standards/Canadian Association of Critical Care Nurses/ American Association of Critical Care Nurses/College of Nurses of Ontario)?
National/ Provincial Standards – Very Great Extent
CACCN – Very Great Extent
AACCN – To Some Extent
CNO - Very Great Extent
National/ Provincial Standards –To Some Extent
CACCN – Very Great Extent
AACCN – Not At All
CNO - To Some Extent
National/ Provincial Standards – Very Great Extent
CACCN – Very Great Extent
AACCN – Very Great Extent
CNO - To Some Extent
National/ Provincial Standards – To Some Extent
CACCN – To Some Extent
AACCN – To Some Extent
CNO - Very Great Extent
Does your program include an evaluation component and if so, how frequently are nurses evaluated?
Yes; Througout Didactic Component (Quizzes and Final Exams) and Throughout Clinical Component
Yes; Every Two Years
Yes; X4 During Orientation
Yes; Informally on a Daily Basis and Formal Evaluation at the End of Three Months
Yes; 3 Times in the First Year/ Every 2 Years
No
If yes: Is documentation provided as that time?
Yes Yes Yes Yes Yes
If yes: Is a written peer review a required component?
Yes; Mentor Review is a Component
Yes Yes Yes Yes
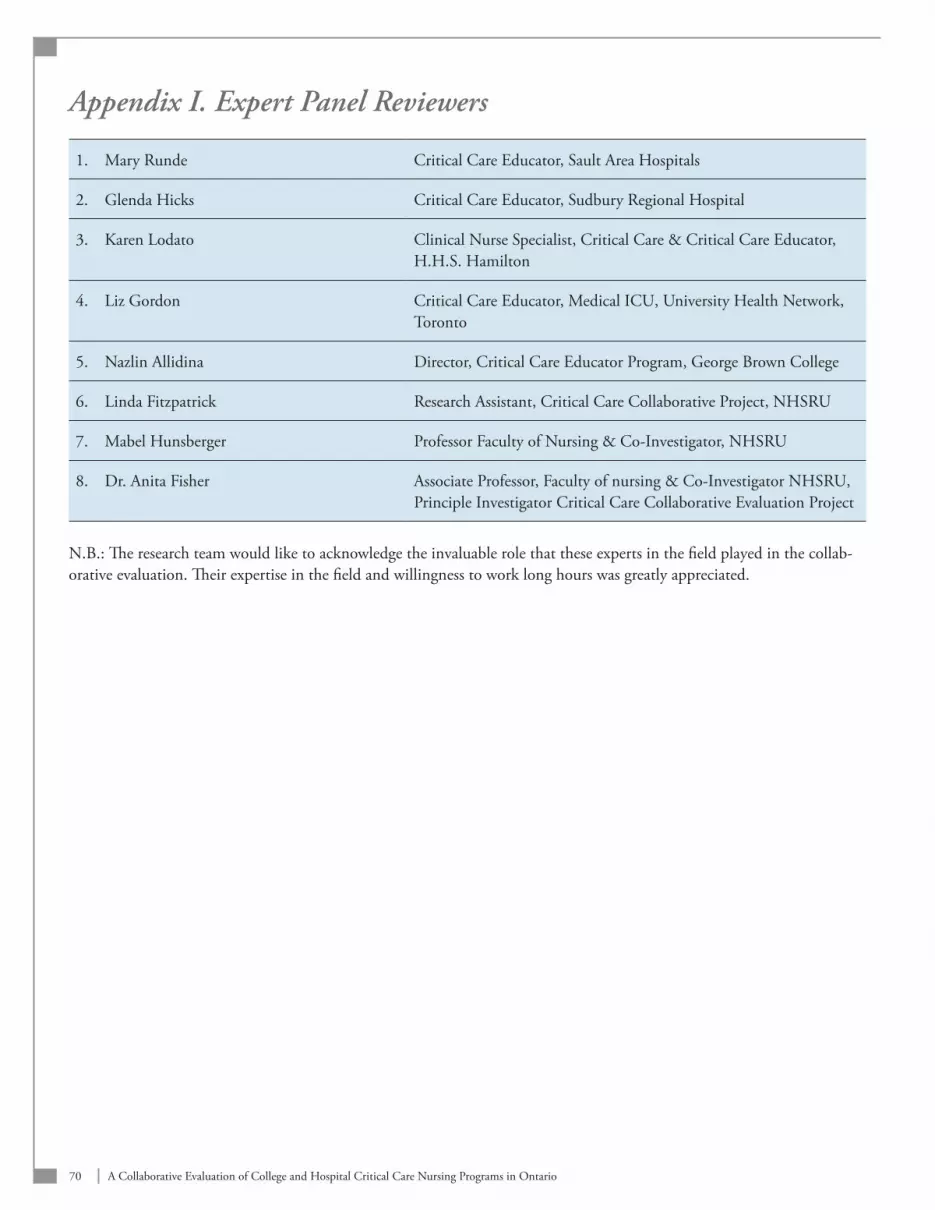
70 A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix I. Expert Panel Reviewers
1. Mary Runde Critical Care Educator, Sault Area Hospitals
2. Glenda Hicks Critical Care Educator, Sudbury Regional Hospital
3. Karen Lodato Clinical Nurse Specialist, Critical Care & Critical Care Educator, H.H.S. Hamilton
4. Liz Gordon Critical Care Educator, Medical ICU, University Health Network, Toronto
5. Nazlin Allidina Director, Critical Care Educator Program, George Brown College
6. Linda Fitzpatrick Research Assistant, Critical Care Collaborative Project, NHSRU
7. Mabel Hunsberger Professor Faculty of Nursing & Co-Investigator, NHSRU
8. Dr. Anita Fisher Associate Professor, Faculty of nursing & Co-Investigator NHSRU, Principle Investigator Critical Care Collaborative Evaluation Project
N.B.: The research team would like to acknowledge the invaluable role that these experts in the field played in the collab-orative evaluation. Their expertise in the field and willingness to work long hours was greatly appreciated.
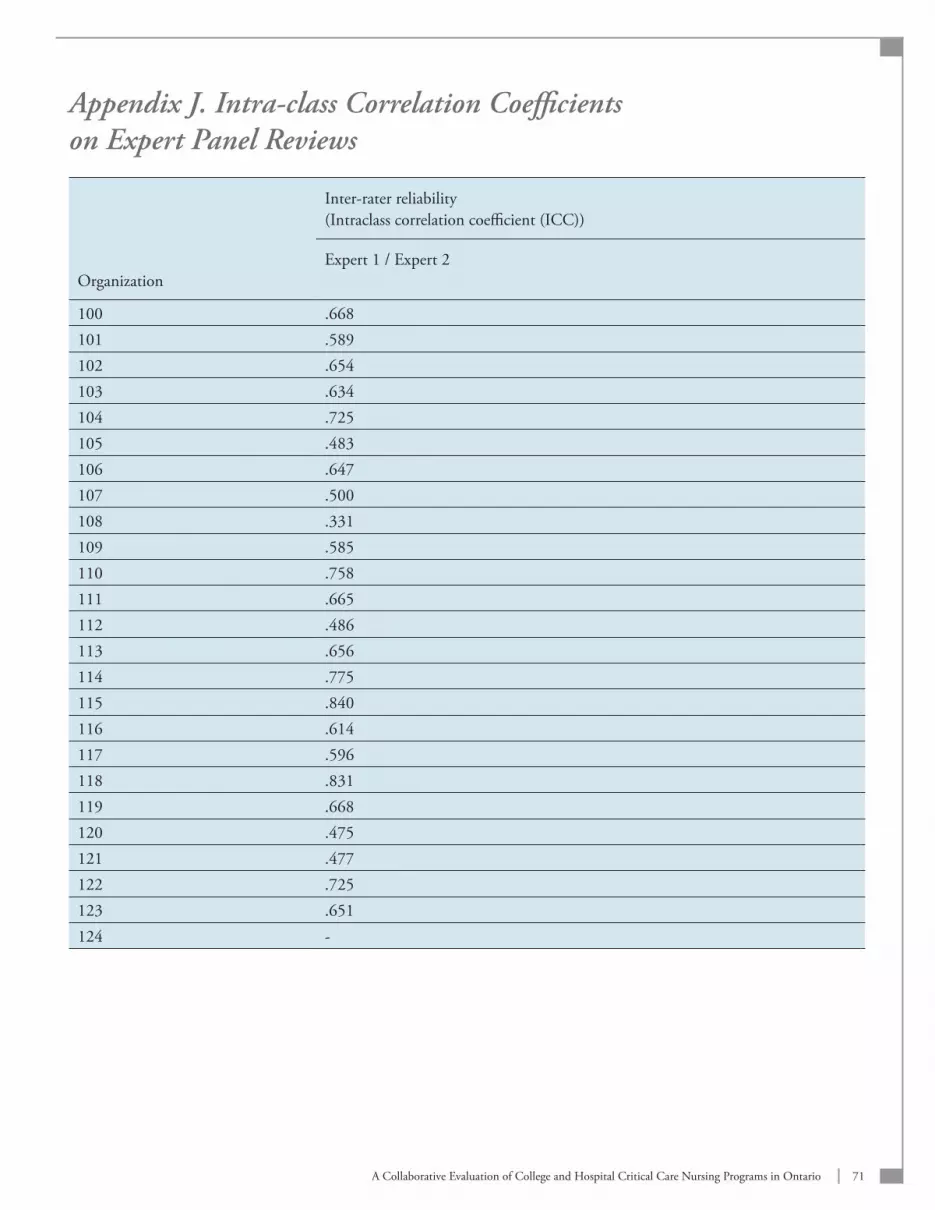
71A Collaborative Evaluation of College and Hospital Critical Care Nursing Programs in Ontario
Appendix J. Intra-class Correlation Coefficients on Expert Panel Reviews
Organization
Inter-rater reliability (Intraclass correlation coefficient (ICC))
Expert 1 / Expert 2
100 .668101 .589102 .654103 .634104 .725105 .483106 .647107 .500108 .331109 .585110 .758111 .665112 .486113 .656114 .775115 .840116 .614117 .596118 .831119 .668120 .475121 .477122 .725123 .651124 -

Appendix K. Research Ethics Board Approval Letter
RESEARCH ETHICS BOARDOffice, 1057 Main St. W., Hamilton, ON L8S 1B7
Telephone: 905-521-2100, Ext. 42013Fax: 905-577-8379
PROJECT NUMBER: 07-037
PROJECT TITLE: Audit of College and Hospital-Based Critical Care Nursing Edu-cation Programmes in Ontario Based on the New Critical Care Nursing Standards of Practice
PRINCIPAL INVESTIGATOR: Dr. Anita Fisher
This will acknowledge receipt of your letter dated March 5, 2007 which enclosed a copy of the revised REB application and the revised Participant Information and Con-sent Form for the above-named study. These issues were raised by the Research Ethics Board at their meeting held on January 15, 2007. Based on this additional informa-tion, we wish to advise your study has been given final approval from the full REB. The revised submission, including the Participant Information and Consent Form was found to be acceptable on both ethical and scientific grounds. Please note attached you will find the Information Sheet/Consent forms with the REB approval affixed; all consent forms and recruitment materials used in this study must be copies of the at-tached materials. We are pleased to issue final approval for the above-named study for a period of 12 months from the date of the REB meeting on January 15, 2007. Continuation be-yond that date will require further review and renewal of REB approval. Any changes or amendments to the protocol or information sheet must be approved by the Research Ethics Board.The Hamilton Health Sciences/McMaster Health Sciences Research Ethics Board oper-ates in compliance with the ICH Guidelines Good Clinical Practice Guidelines, the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans and Division 5 Health Canada Food and Drug Regulations.Investigators in the Project should be aware that they are responsible for ensuring that a complete consent form is inserted in the patient’s health record. In the case of invasive or otherwise risky research, the investigator might consider the advisability of keeping personal copies.A condition of approval is that the physician most responsible for the care of the patient is informed that the patient has agreed to enter the study. Any failure to meet this condition means that Research Ethics Board approval for the project has been withdrawn.
Sincerely,
F. Jack Holland, MD, FRCP, FRCP (C)Chair, Research Ethics Board
Research Ethics Board Membership
Jack Holland MD FRCP FRCP(C) ChairSuzette Salama PhD Vice-Chair/Ethics RepresentativeMary Bedek CCHRA (C) Privacy OfficerMorris Blajchman MD FRCP(C) HematologyJulie Carruthers MLT Research, Transfusion MedicineDavid Clark MD PhD FRCP(C) MedicineJean Crowe MHSc Rehabilitation Science Kavita Dhamanaskar MD Diagnostic ImagingLynn Donohue BA(Hons) Community RepresentativeBrock Easterbrook BA Research Coordinator, AnaesthesiaSylvia Fung BSP LLB Pharmacy/Legal Melanie Griffiths FRCR (UK) Diagnostic ImagingCindy James BScN GastroenterologyNorman Jones MD FRCP FRCPC MedicineRosanne Kent RN BA MHSc(M) CardiologyMadhu Natarajan MD, FRCPC, FACC CardiologyJasim Radhi MB FRCPath, FRCPC Anatomical PathologyKesava Reddy MB BS FRCSC FACS NeurosurgerySusan Shannon BA MSc PhD Clinical Epidemiology & BiostatisticsGita Sobhi BSc Phm Pharmacy Marie Townsend BA(Hons), MBA Administration Graham Turpie MD FRCPC MedicineAlison van Nie MEd Research Ethics OfficerJeff Weitz MD FRCP(C) FACP MedicineJim Wright BSc MD Radiation OncologyEd Younglai PhD Obstetrics/Gynecology
The HHS/FHS REB operates in compliance with the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans; the Health Canada / ICH Good Clinical Practice: Consolidated Guidelines (E6); and the applicable laws and regulations of Ontario. The membership of this REB also complies with the membership requirements for REBs as defined in Canada’sFood and Drug Regulations (Division 5: Drugs for Clinical Trials Involving Humans Subjects).









![NURSING BOARD[655]](https://img.pdfslide.net/doc/110x75/63189d221e5d335f8d0ad250/nursing-board655.jpg)



















