Embed Size (px)
Citation preview
MISSION STATEMENTOF THE SOUTH AFRICAN
SOCIETY OFPHYSIOTHERAPY
The SASP affirms that:1. It provides a structure withinwhich the needs of its membersare met.2. It strives to ensure the qualityof physiotherapy services to allpeoples throughout South Africa.3. It does not discriminate ongrounds of race, colour, creed,national origins, social status orgender in the practice of physio-therapy or in the administrationof its organisation.4. It safeguards the welfare of itsmembers and makes representa-tion against any form of discrimi-nation against its members.5. It acts as a planning, develop-ment and information resource toits members, to other health pro-fessions, to health planners at alllevels and to the general public.6. It supports unequivocally theprovision of unitary health ser-vice and encourages all progressmade in the integration of healthcare services.
PHYSIOTHERAPY
The deadlines are listed below - late submissions should becleared by telephone. We cannot guarantee the publication ofany late contribution.ISSUE DEADLINEFebruary 2003 13 January 2003
(Special classifieds deadline!)
CLASSIFIEDSPlease use the coupon for placing classified advertisements
CONTRIBUTIONSThe editor accepts contributions from any author, either directlyor through your local PhysioForum representative.
SASP HEAD OFFICETel: (011) 485-1467 or 485-1516, Fax: (011) 485-1613©Physiotherapy Publications, PO Box 92125 Norwood 2117.E-mail: [email protected]
Reproduction in whole or in part without writtenapproval of the publisher is strictly prohibited. The viewsexpressed herein do not necessarily reflect those of theSA Society of Physiotherapy. The advertising of productsdoes not indicate endorsement of those products.
Member of
PUBLISHERPhysiotherapy Publications Tel: (011) 485-1467 Fax: (011) 485-1613
EDITORMandi SmallhorneTel: (011) 672-3555, Fax: (011) 674-3804E-mail: [email protected] Davis Tel / Fax: (011) 884-9776ADVERTISINGTel: (011) 485-1467, Fax: (011) 485-1613E-mail: [email protected] Members: R220 pa incl VAT (7 issues – included in SASP membership fee)DESIGN AND TYPESETTINGKat Graphics Tel / Fax: (012) 653-5813
CIRCULATION MANAGER Fax: (011) 485-1613
DEADLINESPhysioForum is published 7 times a year in February, April,June, July, September, October and December/January
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 1
ContentsPhysioForum
Feature3 Aluta Continua
An interview with Peter Piot, executive director of UNAIDS5 HIV/AIDS - a physio’s story - Little things can help a lot6 Quantum Physics - Insight into CranioSacral therapy9 Skin Deep - Phototherapy and physiotherapy10 Survive December! - Take care of yourself in the holidays34 An island of hope - One hospital confronts the HIV pandemic40 Kid’s stuff - Here’s your chance to work with children!
Society Matters12 Feedback - What was discussed and agreed at Executive Council13 From the President’s Desk - A retrospective from Lynn Fearnhead15 Pay or pain? - Insight on the COID16 The Acupuncture Association
What can this special interest group do for you?17 On My Own Two Feet
How can we all help the first community service graduates?22 Point System - All the gen about CPD
In Focus19 News You Can Use - Info for pirvate practitioners
Smile26 A Christmas Tale - A wry look at Christmas
Student news36 Physio Phun - What the students have been up to!
Regulars27 What’s Up - News from the world of physio42 Course notes - Essential continuing education options43 Classifieds - Sits vac and 4 sale!

2 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
Editor’s Note
which has been badly shaken upand has lost its hold on importantcertainties.
South Africa has weathered - isstill weathering - a massive transitionthat some day people will lookback on with awe, and I believe wewould do well to hold that in mindas we contemplate the other disturb-ing events which have affected usand the rest of the world during2002.
Globally, of course, much of 2002was the offspring of 9/11: the bomb-ing and fighting in Afghanistan and the threat of war against Iraqproviding the dominant colours inthe picture. But then there was theglobal economic uncertainty fol-lowing the end of America’s pro-longed boom and the fallout fromthe fall of Enron, WorldCom andothers; our own rand, on a bungee-jump that seemed to have no end;and disasters in the natural world,such as the floods in Europe andthe drought in southern Africa.
But as there was for Vera Brittainand her contemporaries, there is asilver lining in the dark clouds:more and more people around theworld are stepping out of the ratrace, standing back and looking attheir lives, and asking themselvesthe questions: “What are we doingwrong? Why is there all this angerand hatred in the world? What canwe do about it?”
I will not be sorry to have livedthrough these first years of this century if this process of takingstock bears fruit. During the pasthundred years, it’s as if the devel-oped parts of the world have beentransforming into the very image ofconsumption - a huge, Shrek-likegiant, stomping through the world,stuffing Things into its mouth, cars,cell-phones, clothes, DVDs, crush-ing the living greenery with each
flat-footed step it takes, and shed-ding along the way all the gracesunnecessary to the goal of greed,like compassion, dignity and valuefor things that don’t have a price-tag on them.
More and more people that I meet are coming to reject this wayof being; more and more people areseeking ways to reduce consump-tion in their lives and espouse thevalues which drove great figures ofthe past, such as Ghandi, AlbertSchweitzer, Emily Hobhouse andmany, many others who worked,not for reward, but for the greatergood. If this becomes a major trendaround the world - and I hope itwill - then the dark clouds willhave been worth it.
Likewise, there’s a silver liningfor South Africa in the AIDS pan-demic. Recently I’ve had the greatgood fortune to meet many peopledirectly involved in fighting thedisease, in business and in NGOs.We have so many extraordinarypeople with extraordinarily creativeand practical ideas for fighting thisdisease, so many people who havedecided that a positive status is nota death sentence - it’s very excitingto see all of this come bubbling tothe surface.
Many of the people I have spokento are engaged in research or ‘big-picture thinking’ about AIDS, andover and over again, I hear thesame thoughts repeated: HIV/AIDSrepresents a tremendous opportu-nity for us - to rethink and reworkthe way we run our businesses, and start doing things in ways whichvalue people and their familiesmore than the bottom line; to genuinely reconcile across racialand class barriers; to integratework, family and community sothat each feeds the other and helpsthe other; to show the world the
The silver lining
hat a year it has been, filledwith ‘wars and rumours ofwar’, floods, pestilence and
a whole quiverful of bad news. As I write this, relatives are mourningthe deaths of well over a hundredof the hostages held by Chechenrebels in Moscow, and the Fitz family has just received the per-sonal belongings of their sonGodfrey, killed in the Bali blast.
Of course there was good news as well - babies were born (even toour little publications team!), peoplefell in love, South Africa put on agreat World Summit, and my hus-band and I made it through hisbypass surgery to celebrate ourfifth wedding anniversary on 17October - hardly headline news,but a big deal to us! But on thewhole this year seems to have been shadowed by dark clouds formany people.
Perhaps this is simply becausewe’re in a time of global turbulence.Recently I’ve been re-reading VeraBrittain’s famous autobiographicalbook about the First World War,Testament of Youth, and its lesswell-known sequel, Testament ofExperience, which describes theyears from 1918 to the 1950s. I’vebeen struck by the parallels betweensome of the feelings and nationalmoods she describes in the periodafter World War II - the gloomabout world peace, the widely-heldbelief that another war was justaround the corner, the general pes-simism characteristic of a society
W
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 3
Editor’s Note
way in developing a kinder, gentlerand more human society; to findnew and creative ways to use ourhuman resources through flexi-time,job-sharing and other ways whichenable people who are ill to make acontribution that matters; and so on.
We know the level of infection inSouth Africa - 4.74 million people -and we know from our neighbourswhat kind of fall-out this represents(in Botswana, for example, they arepredicting that, instead of gettingup to 30 working years out of eachadult citizen, they will now only getfive). So we have a great opportu-nity to manage the impact of theepidemic on our economy, our soci-ety and ourselves.
We have to change out mindset toview each positive diagnosis as an opportunity to live - if you are
positive and don’t know it, you aregoing to die fairly soon; but onceyou know your status, you and thosewith a stake in your life (family,employers, churches and the like)can do things to ensure that youlive, live for as long as possible. Ifyou live for ten years after yourdiagnosis instead of two, you haveeight extra years in which to work,save money, bring up your childrenand contribute to society.
I keep meeting HIV-positive people who are cramming oodles oflife into their healthy years, sayingthat if they have a shorter time onearth, they’re going to use it tomake a real difference to the world.I believe this is the way we shouldall live, and that there’s lots we canlearn from these brave people.
So in the New Year, I hope that
we will all take a long hard look atthe dark clouds and say, “Thank youfor the reminder that life is chancyand short. I’m going to use my timeon earth to do things I can be proudof; to make an active contributionto the community I live in, to myprofession and to the lives of thoseI meet; and to make the most ofthose things that don’t have anymonetary value, but are more precious than gold: the love of mychildren and partner in life, thebeauty of the natural world, laughterand song and the joy of using mybody...”
I hope that for you 2003 will befilled achievement and happinessand love.
Feature
Aluta ContinuaThe struggles continues in the fight against HIV/AIDS. Kathryn Strachan of
health-e news talks to Peter Piot, the Executive Director of UNAIDS
n 1982 a young Belgian micro-biologist was working at theInstitute of Tropical Medicine
in the picturesque port-city ofAntwerp when he first noticed anincreasing number of patients fromwhat was then known as Zaire,who were presenting with myste-rious symptoms of an illness thatwas ravaging their bodies.
Belgium, a small country aroundthe size of the Kruger NationalPark, had had a long and bloodyhistory in Africa. Its brutal KingLeopold II had annexed the Congoin 1885 as a personal fiefdom andlater handed it over as a “gift” tothe Belgian people.
Since independence and a namechange from the Belgian Congo to
Zaire in 1960, a large community ofimmigrants had settled in Belgium,particularly around the capitalBrussels. The first recorded case of what we today know to beHIV/Aids was in 1981 and the 23-year-old bearded and bespectacledPiot had no idea at the time of whatit was that was causing the rapidweight loss in the patients he wasseeing at the Institute.
“We thought if we were seeing so many in Belgium, imagine howmany more there might be back inZaire,” he recalls.
In 1976, the young Dr Piotworked at the Mama Yemo Hospitalin Kinshasa when there was an outbreak of Ebola fever. He is cre-dited with being the first to identify
the Ebola virus. When he visited thesame hospital in 1993, the impact of HIV/Aids was immediately visi-ble. “In 1976, there were hardly anyyoung adults in orthopaedic wards,”Piot said at the time. “Suddenly -boom - I walked in and saw allthese young men and women, emaciated, dying.” Tests then con-firmed his worst fear; the myste-rious new disease was present inAfrica, and its victims were hetero-sexual.
Twenty years later Peter Piot’sbeard is more than flecked withgrey. He is a tall, intense man who, as the Executive Director ofUNAIDS, is still fighting to placeHIV/Aids on top of the inter-national political agenda.
I

4 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
THE MOST IMPORTANT ISSUEHe was in South Africa recently toaddress the World Summit onSustainable Development where hecriticised planners of sidelining“the most important issue facingAfrica’s development - HIV.
“Trying to make the world payattention to Aids is a task that is
often frustrating. It seems that it isnot enough to have eyes to see andnot enough to have ears to listen,”he says of a world that has found iteasier to look the other way. Butwhat keeps him going, he adds, ishis constant contact with people in the communities deeply affectedby Aids.
“I have always been interested in people and in science, and Ialways wanted to know the peoplewe were dealing with. I haveworked in poor rural districts in the Congo and with Aids activistgroups, so I am not easily fooled by bureaucratic words that hidewhat’s going on. Wherever I go Imeet with groups of people livingwith HIV. The work is very oftenfrustrating and I need that personalreality to keep going. It reminds me every time that we are not deal-ing with statistics and economicimpacts,” he said.
He said one of his key frustra-tions was what he described as “the high levels of hypocrisy whenit comes to sex, it touches on ourcollective hang-ups”. The other, headded, are the prejudices that stub-bornly still exist.
“There is still so much blamingand stigmatising. I have to admit it is a mystery to me.” Is he com-pletely free of prejudices himself?
“Well, of course I have my ownprejudices, if someone arrived in aFerrari, for example, I would besuspicious,” he says.
It’s been a long hard road, but hedescribes himself as more of amarathon runner than a sprinter.
“When I was in Mali I was toldthe story of how boys have to sitand watch a chameleon for fivedays as part of their initiation. Andthe lesson they learn is that whilethe chameleon may change colour,and its eyes look all around, itshead never moves from its positionlooking straight ahead. I am likethat in my work. I may have tochange colour and change the wayI talk with people, for example Iwill be different if I am talking tothe Pope or to an activist group,and I have to take in everythingaround me and adapt, but my focus never changes. I keep lookingstraight ahead.”
AIDS ON THE AGENDAThe first years in his job as head ofUNAids were the toughest, he reck-ons. Making different UN organisa-tions put the cause of Aids ahead oftheir own agendas was a challengeand there was a lot of institutionalpolitics to deal with.But there is alot to give him hope.
“Aids is now on the agenda formore people. African leaders arenow convinced of the problemwhich is not how it was in thebeginning. I have even just met thepatriarch of the Russian OrthodoxChurch in Moscow. So there aresome results. If I had the feelingthat this was totally impossible Iwouldn’t be in this job.”
South Africa remains one of themost interesting places for him tovisit. “Nothing here seems to besimple.” Rather than dwelling onthe controversial statements com-ing out of the president’s office, hefocuses instead on what is positivein South Africa.
“South Africa is quite a democra-tic country with strong debate anda strong civil voice and that is a
source of inspiration. I have learntto appreciate that there are manygood things going on here. Thereare excellent prevention pro-grammes such as loveLife whichserve as good examples for othercountries. But the challenge now is to get on to the road of givingtreatment to people. The question is not whether to give treatment,but how. It should not be an all ornothing approach and it must beequitable, otherwise the brutalmarket forces will prevail.”
However, he says there doesseem to be a lack of dialoguebetween different parts of societysuch as government and businessessuch as Anglo American, which isproviding free antiretroviral therapyto all employees who need it. These groups seem to talk to eachother more through news reports,he says.
Faced with such an enormoustask, Piot says he deals with thedanger of burnout from both thedifficult emotions and the toughpolitics of his work by retreating to
his home in a French village, justacross the border from Geneva,where he grows vegetables andcycles.But he feels privileged to beworking in such an important field.“There are few issues in the worldthat are more important than this.There are millions of people infectedand I can’t forget - and I don’t wantto forget.”
Feature
“Trying to make theworld pay attention
to Aids is a task thatis often frustrating.”
“There are fewissues in the
world that aremore important
than this. There aremillions of people
infected and I can’tforget - and I don’t
want to forget.”

PHYSIOFORUM DECEMBER 2002/JANUARY 2003 5
Feature
ast week I examined a patientat a public service hospital inJohannesburg. The 32-year-old
man presented with a right hemi-plegia following a left CVA threeweeks previously. He had been awidower for the past year and theyoungest of his three children hadpassed away six months ago. Hismedical history included ‘rvd’(retroviral disease) as a risk factorfor stroke.
Confronted with this all-too-common scenario one has a feelingof disempowerment. Stroke is dif-ficult enough to deal with but inassociation with HIV/AIDS it ischallenging to be positive aboutphysiotherapy rehabilitation. Itrequires a change in perspective.
It raises the question - what isour role, the role of the physio-therapist, regarding the HIV/AIDSpandemic? 1. Education/Prevention - at
schools/communities re HIV/AIDS - of therapists to preventaccidental transmission in theclinical situation.
2. Treatment to limit disability andenable optimal participation inhis/her community
3. Support for People Living WithAids
Here I believe we potentiallyhave a significant role to play.
I have a close associate who Ihave known for about 15 years. Sheis in her 40s, a mother of three, two older children and a little five-year-old daughter.
After the birth of her daughter wenoticed that she seemed to havedifficulty recovering from relativelyminor infections - an insect bite that became infected, tonsillitis that
became a major throat infection etc.Initially this was thought to be due to the stress in her life but overtime a pattern of limited resistanceto infections became evident. Sherecognized the importance ofensuring that the infection wasappropriately treated as soon aspossible.
Ultimately she was referred to apublic service hospital in Johannes-burg by her GP for a gastroscopy to determine the cause of acutestomach pain associated with weightloss. With very little counseling shewas tested for HIV. The test waspositive, with a CD4 count of 37.Her weight was 48 kg. She lookedand felt awful.
At that time she needed to spendtime with her family. When shereturned to Johannesburg she was referred to the JohannesburgHospital HIV Clinic. Largely becauseshe had always had prompt treat-ment for associated infections andwas able to maintain a healthylifestyle, her health was still stable.The various treatment options werediscussed and she was given a private prescription for anti-retro-virals - the triple therapy - and ahospital prescription for anti-fun-gals and vitamins and iron tablets.She was also able to buy e-pap, afortified porridge. The triple therapyprescription costs in the region ofR850 per month.
The difference has been astonish-ing.
Over eight months her weighthas increased to 61 kg. She hasenergy to spend quality time withher daughter and she is lookinggreat. Her health remains vulne-rable and any minor problem dete-riorates very rapidly. A bout of
gastroenteritis needed antibioticsand rehydration and knocked herflat for a week. However she is tak-ing life a day at a time and at themoment things are looking good.
WHAT HAS MYROLE BEEN?
General health advice, particularlyin terms of recognizing a symptomthat needs treatment and the rela-tive urgency of getting treatment.
EXPLAINING COMPLEXMEDICATION.
I have also encouraged her to bephysically active to the extent thatit has been possible at certainstages, with advice regarding restand exercise.
Supportive - she has been reluc-tant to tell her family formally, andhaving a sounding board on certainissues, particularly with regards toher future and that of her children,has been of value.
I am a great advocate of the anti-retroviral therapy that has undoubt-edly made the difference in thisinstance. It is saving her life and itis also demonstrating to others thatwith proper medication and care agood quality of life can be achieved.However I do recognize that it canonly be prescribed in situationswhere it is specifically medicallyindicated, where there is goodaccess to medical treatment, HIVcounselling and medication educa-tion and that a supportive socialenvironment is essential. Physiothe-rapists can and should be part ofthis support and be much moreactive in the lobby for antiretroviraltherapy to be made available topeople with Aids where it is indi-cated.
HIV/ AIDS - a physiotherapist’s story
How can we make a difference?
L
6 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
Feature
“The body’s energetic potentialto heal itself lies inthe fluid tide of thecerebro-spinal fluid.”
The physicistHeisenberg said,
“When we observewe change what weobserve, and we are
also changed.”
HOW I CAME TO HEAR ABOUTCRANIOSACRAL THERAPY
My original introduction to andfascination with the concept ofCranioSacral Therapy (CST) camefrom reading, specifically an articlein a British physiotherapy journaland pamphlets I collected whenattending the IPPA congress in theUK last year. I also came acrossreports of the phenomenal resultsachieved by the British physiothe-rapist Dr John Cross, who was utilizing a similar procedure ofmanual sensation and energy (viathe meridian system) in the treat-ment of sports injuries. I too hadachieved good results working inthis manner.
What really impressed me initiallywas when I heard that Dr JohnUpledger (the pioneer and earlyteacher of CST, and the author ofthe only books on the subject) hadtaught the technique to the familymembers, caregivers and parents of
children suffering from a myriad ofdisorders (physical, mental andbehavioural) susceptible to benefitsfrom CST. This practice of empower-ing patients and their carers, whichcontinues today, originated whenhe first conducted research at spe-cial schools and realized that he didnot have sufficient therapists totreat the number of children need-ing the technique, or indeed to pro-duce meaningful research.
WHAT IS CRANIOSACRAL THERAPY?
The CranioSacral Therapy Asso-ciation of Chartered Physiothe-rapists describes CST as the treat-ment of body disorder, pain anddysfunction by a gentle touchwhich encourages the body torelease restrictions and rebalanceitself with its own energy ratherthan by imposed forceful inter-ventionist techniques, while alsoencouraging the person to becomemore “connected” to his or herbody. CST has been described as a healing art, and as more anapproach to healing than a tech-nique (see reference 1).
WHAT IS THECRANIOSACRAL RHYTHM?
The rhythm of the CranioSacralsystem is a gentle, subtle wave-likepulse of the body in response to thefluctuations of the cerebro-spinalfluid within the sub-arachnoidspace and ventricles, and passingout into tissue fluids. This rhythmmay be observed, utilised and monitored in every part of the body.
WHAT CONDITIONS CAN BE ADDRESSED WITHCRANIOSACRAL THERAPY?
CST treatment is suitable for anydisorder of the musculo-skeletal,neurological, cardio-vascular, lym-phatic, organic, digestive, excretory,and hormonal systems. It canrelieve acute or chronic conditions,and it is safe for babies as well asthe elderly.
THE CRANIOSACRAL THERAPYCOURSE I ATTENDED
In August 2002 the principal of the Upledger Institute in the UK,John Page, presented the course withtwo teaching assistants. The coursecomprised both theory and practi-cal work, interspersed with wonder-ful British humour, which certainlylifted the energies of the group - notthat those ever really flagged!
The concept, content and presen-tation of the course surpassed myexpectations. It was the most wellorganized and practically struc-tured course I have ever had thepleasure of participating in. Fifteenphysiotherapists of national andinternational repute were amongthe participants, who represented adiversity of professions. All in all,along with acupuncture, this coursein CST has been the best learningopportunity of my whole postgra-duate career.
A REMINDER OF THE ANATOMY RELEVANT TO
CRANIOSACRAL THERAPY.The cranium is connected to thesacrum, not only obviously by the
Quantum Physics - and a Quantum Leap for the
Physiotherapy ProfessionNorma Lederle gives us an insight into CranioSacral Therapy

outcome, and after two months Iam satisfied (as are my patients)that these can be regarded asacceptable evidence.
1. My most profound evidence ofthe success of the technique is inimproving blood supply to thebrain of an 89-year-old patient suf-fering from prolonged giddinessand loss of balance. I plan to write up this case history for ourPhysiotherapy Journal; hence Ishall not detail it here.
2. A 56-year-old female patienthad been suffering for about fiveyears with reflux, anxiety and palpitations as well as strange, dis-turbing chest and abdominal sen-sations, which I believe are relatedto Vagus nerve and autonomicanomalies. Her condition had beenthoroughly investigated and moni-tored - including hospitalisation -and in April this year she had a suc-cessful oesophageal repair for reflux.
Since her first CST treatment shenow has no discomfort in the upperabdominal and chest areas, where-as discomfort had still been presentafter the surgery. She now also hasmore normal bowel function. Therehave also been some unanticipated
benefits, including the cessation ofalmost continuous weeping fromone eye, and an improvement inthe texture of her facial skin.
3. A 43-year-old female academicbeing treated for diverse problemssaid after treatment that the CSThad diverted an incipient cold aswell as improving her chronic
manual contact with the patient’sbody to facilitate the adjustmentsalluded to above. The points of contact include the cranium, theatlo-occipital and sacro-iliac joints,the sacrum, and four further hori-zontal concentrations of fascia suchas the diaphragm.
WHY IS CRANIOSACRALTHERAPY OF
PARTICULAR VALUE TOPHYSIOTHERAPISTS?
As a hands-on method of improv-ing health and functioning, CST is a particularly suitable approach tobe practised by physiotherapists.
Along with our knowledge, ourhands are our greatest assets.Recently, we have been encouragedto develop subtle palpatory andsensory skills, to trust our intuition,and to use gentler techniques andapproaches in our treatments. Thishas been a wonderful paradigm-shift for a profession which has, onthe whole, long been seen by thegeneral public as very active andeven inflicting pain! It is a new andenthralling experience to sit quietlyfor an hour with one’s hands on the fully-clothed supine patient, asthey relax, receive and enjoy the
treatment, while profound releasestake place in their bodies, oftenwithout their being directly awareof it.
CASE EVIDENCE.Note: It is considered that sus-tained amelioration of a conditionconstitutes a favourable treatment
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 7
vertebrae but also by the meningesand the spinal cord. Any part of the system may be utilized to affectthe functioning of the whole per-son. The meninges are extensivelyattached to the skull, to specificpoints in the spinal column, to thesacrum and to the coccyx wherethey blend with the periostium. Thebrain and spinal cord are enclosedby the meninges, which extend withprolongations up to the point ofexit of the nerves of the foramina.Hence, one is able to have an effecton the whole central nervous sys-tem by allowing the sacrum and/orthe skull bones (which are notfixed) to adjust, or reposition.
The intra- and extra-cranial fasciaare also connected. Thus the therapyaffects the fascia by adjustment,releasing, or repositioning. Releasingthe extra-dural fascia - particularlyin the throat, neck and the atlo-occipital junction - may exert a significant positive impact on thecirculation to the cranium (seeexample #1 under patients reports,below). In addition, there may bebenefit to some of the cranialnerves as they exit the base of the skull through the foramina.This occurs as a result of releasingthe fascia, the muscles and the posi-tion of the cranium on the atlas.Dysfunctions in or facilitation ofone area of the system may betransmitted to another, particularlyvia the connective tissue whichfunctions as a unit.
HOW IS CRANIOSACRALTHERAPY PERFORMED?
There is a sound scientific basis for all the techniques practisedwithin CST. Both the therapy andthe therapist are non-invasive andunobtrusive. The contact appliedby the therapist is equivalent toonly 5 grams (about the weight of a 50-cent piece)!
The procedure we came awaywith, which is the initial skillsdevelopment stage of training,involves a 10-step protocol whichthe therapist follows, making
Feature
Norma peersover the headsof her fellow
students.
8 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
sinusitis to the extent that she did-n’t need to take regular medicationand no longer felt anxious aboutthe condition affecting her breath-ing at night. After five sessions, sheno longer experienced premen-strual symptoms or dysmenorrhea.Excessive menstrual flow has alsobeen significantly reduced. In addi-tion, she credits ongoing CST com-bined with acupuncture with havinggiven her increased mental energy,as she can now regularly work 12-hour days at a high intellectuallevel without feeling exhausted.
4. My very first patient, who hadbeen considering neck surgery,experienced a 90% reduction inpain and an increase in her range ofmotion after only one treatment.This improvement has lasted fortwo months already. The dizzinessand tinnitus which had plaguedher disappeared completely, andhave not recurred. She has a 30-yearhistory of lower back pain, which,despite treatment, has limited herability to enjoy strenuous walking,but she reported later that aftertreatment she had been (and still is)able to walk up Table Mountainwith no feeling of weakness in herlegs. Her lasting impression was ofa feeling of well-being.
5. A 66-year-old male patient withextensive responsibilities and com-mitments presented with pain andloss of mobility in his neck, oneshoulder and back (for which hehas twice had surgery as well asphysiotherapy treatment). He hadhad bypass surgery following twomyocardial infarctions. He was alsoexperiencing anxiety and insomnia.After three treatments he reportedthat he had not needed painkillersfor his back. On examination theshoulder was less painful and therewas greatly increased mobility inboth the neck and the shoulder(almost full range). Following thisimprovement acupuncture wasadded to his regimen with conti-nued benefit. He also reported anew sensation of calmness and goodcoping abilities, and compared this
to his brief experience of the bene-ficial effect of prescribed anti-depres-sants. In his case, the unanticipatedbenefits of CST combined withacupuncture included increasedconcentration and memory.
6. A 43-year-old female patientwith a long history of neck patho-logy (diagnosed by a neurologistwho suggested surgery) andreferred pain down her arm hadsustained a fall directly on herneck, resulting in strange sensa-tions, weakness and numbness inthat arm. After one treatment thesensations in the arm were com-pletely relieved. This has beenmaintained for over a month.
7. Before attending the course Ihad needed to have my dentistremove some pieces of dental flossjammed between my right uppermolars. After completing the practi-cals of the course I was able to flossmy teeth without any shearing asthe spacing between the teeth hadreadjusted. (I assume there hadbeen a repositioning of the tempo-ral bones, affecting the temporo-mandibular joint and the maxilla.)
REFLECTIONS ON THE BENEFITS OF CRANIOSACRAL
THERAPYPatients attest to the benefits of CSTand return, asking for more. Inaddition to the obvious improve-ments in respect of specific com-plaints/diagnoses, there arenumerous unanticipated benefits,some of which have been listedabove. The most pronounced ofthese, however, is that CST inducesa deeply relaxed state and relieffrom stress. This is highly signifi-cant, since stress is an underlyingcause of many medical conditions.
CONCLUSIONThe scope and format of my wholepractice has changed, by my ownchoice and that of my patients, tothis new modality. I am indeed for-tunate to have the type of practiceand time-schedule which haveallowed me to incorporate CST.
Since completing the first CSTmodule, I have treated 22 patients,with 48 treatments in total. Theresults of three patients have beeninconclusive or disappointing frommy point of view (though not in allcases from theirs), but these are allpatients with chronic, complexdiagnoses complicated by psycho-logical factors, who have alreadyavailed themselves of the mostadvanced investigations and treat-ments at some of the best health-care facilities in the country
FURTHER OPPORTUNITIESAND CONTACT ADDRESSES
Repeat presentations of the firstmodule (March 2003 in Johannes-burg), as well as follow-up courses,are to be given in South Africa.Details may be obtained fromClaire Waumsley by e-mail:[email protected] or 021 788-5689.The Upledger Institute’s website -www.upledger.co.uk
REFERENCESThe following references are highlyrecommended reading. The jour-nals are available in the media centre at the offices of the SASP -contact (011) 485-1467.1. John Upledger & John Vredevoogd.
CranioSacral Therapy. 1983. EastlandPress. Seattle (22nd printing 2002).
2. John E Upledger. Your Inner Physicianand You. Copyright 1997. North AtlanticBooks, Berkeley, California.
3. Susan Hollenby. “CranioSacral Therapy:An Introduction”. In Touch magazineJanuary 1994. OCPPP.
4. Susan Hollenby. “Looking to the future:An Alternative View.” Physiotherapy,January 1994,vol 80, # A.
5. Susan Hollenby & Maureen Dennis. “An Introduction to CranioSacralTherapy”. Physiotherapy vol.80 #8,August 1994. This includes two case his-tories and other references.
6. Susan Hollenby. “Touching is believing”.In Touch magazine #74, Winter 1995.OCPPP.
7. Susan Hollenby. Olive Sands MemorialLecture. In Touch magazine #89, Spring 1999. Organization of CharteredPhysiotherapists in Private Practice.(OCPPP)
8. Susan Hollenby. Additions to an articleby Louis Gifford. In Touch #99, Spring2002. OCPPP.
Feature

PHYSIOFORUM DECEMBER 2002/JANUARY 2003 9
think it’s so sad that physiothe-rapists should let go of light therapy - it’s not even taught on
some courses now,” says AudreyWeiner. Audrey has made a vocationof treating patients with psoriasis.When last heard of, she had retired,but now she’s back to create a havenfor psoriasis patients at the PsoriasisTotal Care Centre in Pretoria.
Violet Phillips would also like tosee physiotherapists take an inter-est in skin treatments. This fit andbusy lady doesn’t sound like sheshould be thinking of retiring, butsurprisingly, she’s in her 80s, andas she says, she can’t keep work-ing forever. At present she is theonly physiotherapist working atthe Phototherapy Skin TreatmentClinic in Houghton, Johannesburg,and she hopes that a physiothe-rapist can be found to take upwhere she leaves off.
“This kind of work would beideal for retired physios who stillwant to keep their hand in, orphysios who’ve had babies andwant to get back to doing a littlelight work,” she says. (Pardon thepun!) The job entails working fivemornings a week from seven to12:00 pm and two afternoons aweek, from two o’clock to 5:30, with a patient load of about 30 inthe mornings, 55 when full days are
worked. Obviously the work couldbe split, but only one therapist isneeded at a time.
“We treat psoriasis, vitiligo,eczema, mucoids fungoide, hyper-hydrosis and various other skinconditions,” she says. “Treatmentconsists of UV radiation combinedwith tar baths, topical and systemicdrugs, the latter prescribed by oneof the five dermatologists in theclinic. It is satisfying, interestingand exciting work.”
Audrey would agree - she hasseen so many ‘miracles’ in her timetreating psoriasis, it’s no wondershe’s been lured back yet again to
offer holistic care for despairingpatients. At the Psoriasis Total CareCentre, she works closely withphysios Louise Crause and Isabelvan Wielligh. Together they areable to offer physical treatments,including phototherapy and topi-cal and oral medication, as well as counselling, stress reduction,psychoneuroimmunology, self-careguidelines, coping and life-styleskills, and general support for mental and physical health. The
Centre was officially launched on17 October 2002 (Adcock Ingramkindly sponsored the eats and theleaflets). It is undoubtedly a heal-ing place, with soft mauve walls, gentle music and restful plants,sculptures and water features outside.
There is nothing more reward-ing than seeing a patient whooriginally came in with unsightlylesions, and who, thanks in largepart to you, walks away withclear skin, a better understandingof how to prevent recurrences,and improved confidence andself-esteem. If you are interestedin working with skin patients,contact Violet Phillips on (011)
482-4716. If you want to referpatients to the Psoriasis Total CareClinic, contact Audrey Weiner on(012) 343-1762.
Skin DeepPhototherapy and physiotherapy
Feature
“I
Louise Crause, Audrey Weiner andIsabel van Wielligh at the launch of
the Psoriasis Total Care Centre.
NOTICE: Head Office will close on Friday the 20 December 2002 at 12h00. We will re-open Head Office on Wednesday 02 January 2003. Any urgent queries during this period can be directed to Saira Khan, CEO of the Society on 082 3353731 or toMarge Walters, Portfolio secretary on 082 7748426. Head Office wishes our membersa peaceful and joyous vacation and we look forward to providing them with support in the New Year.
Feature
It’s December again - hooray!We all look forward to this lovelytime of summer fun and familytogetherness, a break from routineand a chance to relax. Still, there’salways some fallout, so take ouradvice, and sail through the holidayssmoothly!
Family togetherness translatesinto family fights (I know of somelonglasting feuds which had theirorigins back in the mists of an earlyChristmas); festive fare mutatesinto kilos on the hips and madmood swings; fun in the sun turnsinto a furnace of sunburn; and thatlong drive to the coast could wellbe the biggest disaster of all, as the highways become one longstream of frustrated road rage vic-tims travelling at speed, a recipe for horror if ever there was one.
We’ve collated some tips whichcould help you avoid the worst ofthe festive frenzy!
ONE BIG HAPPY FAMILYWe tend to have this sort of Victo-rian-cum-1950s idealised picture inour minds of the whole family sit-ting together over a groaning table,Grandpapa stroking his whitebeard as he reads the joke from thecracker, Aunty Dot helping to servethe turkey or whatever your foodof preference is, Mom beaming ather beautifully turned-out littleones... but it’s never like that, is it?
So remember:
• Children are at their worst whenover-excited and over-stimulatedby crowds of people. Give thema way to work off their excessenergy while having as littleimpact on the adults as possible.Plan strenuous games, hikes upthe mountain and other activitiesunder the eye of a roster of
adults - if one adult gets stuckwith the kids all the time, there’llbe an explosion sometime!
• Clashes of personality will not goaway under the benign influenceof family togetherness. If thereare two people who always endup in a scrimmage, try to keepthem separate, and intervene atthe first sign of conflict by askingone of them to do something foryou. Never get involved in theirargument!
• Remember that older peoplemay have certain physical limi-tations which might lead to irri-tability and snappiness. I knowan aged gentleman who loves hisgrandchildren dearly but can’tspend hours in their companywithout getting short-tempered.Eventually we discovered hewas concealing a loss of hearing,which meant listening to theirbabbling voices caused immensestrain. And of course, you allknow only too well what kind ofproblems arthritic and otherkinds of chronic pain can cause.Give the older people regulartime to be alone and rest, even ifit’s just sitting in front of the TVwhile everyone else goes out fora swim.
• Never, ever do everything your-self. Family shindigs are hardwork. Lay down the rules beforehand: ask every adult (thatincludes teenagers over the ageof 14) to help in some way. Thelittlies can also help a bit, and it’sgood for them to realise that funtimes have to be ‘earned’, even iftheir contribution is minuscule.
Make absolutely sure that youyourself have some time alone(in a bubble bath with a goodbook, on a long solitary walkwith the dogs, or whateverwould relax you most) or it willall end in tears, mark my words!
FESTIVE FAREAll the goodies that we eat at thistime of year are delicious, but notonly do they pile on the kilos, theyalso may well upset our holiday byupsetting our mood. • Bear in mind that refined sugar
is the worst culprit for raisingblood sugar levels and then mak-ing them plummet. If you want asteady supply of energy, avoidthe sweets and cooldrinks andcakes as much as possible, andopt for complex carbs instead.Think of inventive ways you canuse complex carbs in preferenceto refined white flour, as well.For example, use unpolished ricein your turkey stuffing.
• Don’t skip meals, as we all tendto do at this time of year: “Iwon’t have breakfast becauseI’m going to have a big lunch.”Eating regularly means you’llnever sit down to one of thosefestive meals absolutely starved,ready to stuff yourself! It alsosustains energy levels.
• Plan big meals as marathonsrather than sprints. Who saysyou can’t eat Christmas dinnerover four hours? Alternatively,eat many small meals over theBig Day rather than one hugeone, with a nibble of festive foodat each meal.
Survive December!Holiday fever can cause disaster - so be prepared
10 PHYSIOFORUM DECEMBER 2002/JANUARY 2003

• Avoid alcohol as much as possible- it dulls your mind, takes ages torecover from, and damages yourhealth. Stick to one or two glass-es and see the New Year in sober- you might set a fashion!
ON THE ROADBored with hearing about the acci-dent rate at this time of year? Well,a car accident is the kind of excite-ment you can do without, so let mebore you once more with someshopworn but still excellent adviceabout driving on December’sroads:• Have your car checked before
setting out. A car that doesn’thave brakes as sharp as a knife,that pulls to one side when brak-ing or shudders at speed couldbe a serious liability in an emer-gency. Make sure you have treadon your tyres, the right amountof air in your wheels, fast-actingbrakes and functioning wind-screen wipers.
• Everybody in the car shouldwear a seat belt at all times.Loose people, loose objects andyes, loose animals can causehuge damage if you have to stopsuddenly (let alone the damagethey’ll do to themselves). Don’tkeep sharp or heavy objects onthe same seat as children, or onthe back shelf - video cameras,for instance. If you are in a colli-sion, the object will fly forwardat the same speed as the car wasgoing when you hit, and can kill.
Feature
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 11
• Leave your competitive urges athome. Let other drivers weave inand out of the traffic; you wantto get there safely, so you’ll bedriving at a steady speed appro-priate to the conditions, keepinga safe following distance, andbeing polite and courteous toothers - won’t you?
• If you go into a skid, rememberto release the brake pedal andsteer in the direction of the skid.It can feel unnatural, especiallywith a front-wheel skid, but it isthe safest thing to do.
• Never pass a car if you feel theleast bit of doubt that you canmake it comfortably. A car travel-ling at 100 kays and one doing 50kays can look almost exactly thesame when you see them head-ing towards you. Better safe thansorry.
• If you have to swerve, head leftrather than right. Almost invari-ably it will be better to land in aditch rather than hit an oncom-ing car.
• Never drive when drowsy. Never.Never, never, never! Better youshould get there late than fallasleep at the wheel. If you do feeldrowsy, stop under the next treeand kip for ten minutes or anhour, whatever your body needs.But, if you absolutely have todrive when a little tired, turn theair-vents onto your face, wipeyour face with a damp cloth, andtake deep breaths every fiveminutes. Tell all your passengersto talk to you.
• Don’t eat a big meal before orduring the journey. Stock the carwith small, high-powered snackslike granola bars, nuts, turkeysandwiches and fruit, and grazeas you go.
• Wear loose clothing for longjourneys. Tight clothes willinduce a feeling of lethargy.
• Never turn a journey into a raceagainst the clock. Set off in goodtime and plan regular stopsalong the way. See if you can findplaces to visit that will take you
out of the lemming rush for anhour or so - caves, game farms,botanical gardens and otherattractions - so that the tripbecomes part of the holiday.
FACE THE SUNOne of the most upsetting things iswhen a holiday is spoiled by healthproblems. The most common ofthese is the incredible discomfort oflobster skin which has roasted toolong under an unfamiliar sun.• Wear tightly-woven, broad
brimmed hats when out between10 in the morning and 4 in theafternoon.
• Sunblock at all other times -preferably SPF 30 or more - andreapply at least every two hours.
• Take a basic first-aid kit with youthat contains:Adhesive tape Antiseptic ointment Adhesive bandages (assortedsizes) Stretch bandage Cotton balls Burn ointment Hydrocortisone cream Liquid antihistamine Aspirin for adults Panado for children Large, square piece of material tomake a basic sling Blanket Cold pack Disposable gloves Gauze pads and roller gauze(assorted sizes) Plastic bags Scissors and tweezers Triangular bandage Prescription medications inchild-proof bottles Eye wash First aid manual, including basicCPR instruction
You could add some antacids forthe invariable indigestion of festiveseason, Imodium for you-know-what, and some apres-sun lotion tocool off any skin which does getburnt.
OK, now go out there and havefun, fun, fun, fun, fun!

12 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
Society Matters
he most recent ExecutiveCouncil (EC) meeting washeld on Saturday 21 September
in Johannesburg. It was precededon the Friday afternoon by a work-shop with Esmé Prins, a lawyerwho specialises in health care legis-lation. She used to work for SAMA,but now runs her own StrategicPlanning Company. The workshopdealt mainly with the NationalHealth Insurance that the govern-ment plans to have in place in 10years and the move to managedhealth care. The aim is to ensurethat everyone in South Africa hasaccess to some kind of health insur-ance. This has great implicationsfor physiotherapy and a strategicplanning workshop is to be held inFebruary 2003 with relevant roleplayers in order that the SASP canplan to meet the needs of its mem-bers and the profession.
PRESIDENT’S REPORTLynn Fearnhead listed the fiveobjectives she had set for 2002 andindicated that most of these hadbeen met. She expressed concernover the lack of commitment ofmembers to service to the profes-sion and several suggestions weremade to improve this. Amongstothers task groups will be set up in the provinces to do strategicplanning, improve communication,involve student members and men-tor new graduates. Daphne Beukes,provincial representative on ECwill coordinate these. Mandi Small-horne, who also attended the meet-ing, will produce an article in Forum.
CEO’S REPORTSaira Khan reported on the cuttingof some of Head Office operational
costs and some staff changes. Herinvolvement with Portfolio Com-mittees and Provinces is also grow-ing and she has been involved innegotiations with COID (WCA)and HPCSA. We had a valuablemeeting with Prof Eales to discusscloser links between the PRC andthe HPCSA. She also has a list ofpersons willing to be involved indrawing up evidence based clinicalguidelines, a priority of the QualityImprovement Portfolio chaired byIna Diener. Any interested personsare asked to contact her or Inaabout their area of interest.
CEO’S FINANCE REPORTA teleconference was held and itwas decided that Income andExpenditure Statements would onlybe submitted twice a year. LorraineJacobs has agreed to assist theFinance Committee, which hasbeen somewhat dormant since shehas resigned and Jean Durell hasagreed to chair it. A finance strategic workshop for chairper-sons and treasurers of provinces,Professional and Special InterestGroups and Portfolio Committeesis in the pipeline. The membershipfees for 2003 were discussed atgreat length. It was agreed thatthere will only be one category offull membership, that PhysioFocuswill be an optional extra like anyProfessional or Special InterestGroup, but will include the Tariffs(“blue”) Book, which would also be an optional extra for all othermembers. I strongly recommend itas it contains essential informationfor all physiotherapists. It is alsoanticipated that malpractice insur-ance will go up to R150. Severalprovincial budgets will have to be
cut in order to keep the members’subscriptions at a reasonable level,and although projects such asSuper Sports, Comrades, ArgusCycle Tour and National Assemblymay be outsourced to provinces,Head Office is still responsible forthe budgets. The major budgets arethose of Publications and PublicRelations, but more funding isalready coming in through adver-tising by the appointment ofAmerico Fernandes Pinheiro, speci-fically to obtain advertising.
SASP NEGOTIATORHester Huysamen will continue inthis post until the end of the year. Ajob description is being drawn upand the post will be advertised.Similarly, the Policy PortfolioCommittee is looking at the needfor the suggested post for a physio-therapist at Head Office, financewill be finalised, some tasks redi-rected and a final decision made atthe next EC meeting.
CHAIRPERSONS FINANCEAND COMMUNICATIONS
PORTFOLIOSSee above for finance. Commu-nications has been split intoPublications, which include theJournal, Forum and the website,chaired by Kelly Davis and assistedby Americo, and Public Relations,which will be headed by RenéGeldenhuys, again assisted byAmerico, until the next NationalAssembly. The Policy Committeewill redraft the Constitution toaccommodate the changes.
COIDA workshop is to be set up soonestwith Saira Khan, Tariffs Committee
FeedbackHere’s a round-up of what was discussed and agreed at the most recent
Executive Council meeting, kindly done for us by Narina Gilder
T

PHYSIOFORUM DECEMBER 2002/JANUARY 2003 13
Society Matters
and PhysioFocus to draft a letter in order to establish physiothera-pists as first line practitioners in thenew Act.
HIV/AIDS TASK GROUPMagda Fourie has been chairingthis as part of the Public ServicePortfolio and has been gathering a lot of information. Alternativechairpersons will be approached.
COMMUNITY SERVICEThe Buddy System seems to be inplace and the Department ofHealth was impressed with physio-therapists being so proactive!Advisory physiotherapists will becovered by malpractice insuranceas this is work undertaken onbehalf of the SASP. An informationbooklet with names and addressesof provincial SASP contact num-bers and addresses, as well as thoseof provincial coordinators of theDepartment of Health has beenproduced and will be issued to allfinal year students. It was also suggested that meetings with finalyear students and these persons beset up. “Buddies” also suggestedthat they should also contact the
new graduates, rather than waitingfor them to make contact whenthey need help and some offered to do on site visits. Some also sug-gested that they will mentor inneighbouring provinces if needed.Application will also be made torecognise such service for CPDpoints.
BHF FEEDBACKNo codes for preventative healthcare had been allocated, only anacross the board 8% increase infees. A press release was supposedto appear during the last week ofSeptember. Any motivation forchange or new codes in 2003 has tobe in to the Tariffs Committee bythe end of 2002. Physiotherapistsare now also allowed to negotiatewith individual medical aids. Atthe workshop with Esmé Prins itwas suggested that we identify keymedical aids.
LEGAL REPRESENTATION AT HPCSA
It was agreed that the SASP cannotset up a fund to assist membersduring a disciplinary enquiry. Itwas also reported that by the time
any complaint reaches the stage ofa disciplinary enquiry, there hasbeen a thorough investigation andlittle chance of being found notguilty.
PRACTICE ACCREDITATIONAfter a teleconference it was agreedthat this has to be scaled down tosuit South Africa and needs to beoutsourced to some agency likeCOHSASA, in cooperation withPhysioFocus.
CONTINUING PROFESSIONALDEVELOPMENT
There was lengthy discussion aboutthis issue. Each CPD “activity” hasto be accredited, i.e. a course, workshop, group discussion, etc.,with its topic, venue, fees and par-ticipants. Although details can besubmitted electronically, the origi-nal attendance register with signa-tures and HPCSA registration numbers also have to be submitted.Multidisciplinary activities are alsoacceptable. It was suggested thatprovinces could sponsor registra-tion of courses, especially for thosein public service and physiotherapyassistants.
hew, it’s been a busy year,and if time flies whenyou’re having fun then we
must have been having lots of fun!The hectic period at the begin-
ning of the year started well withthe membership renewals pouringin. The processes we had put inplace meant that we were muchmore efficient in dealing with ourapproximately 2600 members aswell as about 580 student members.
During 2002 akey focus areahas been imple-menting the new constitu-tion; it’s onething to have asound theoretical document, but itdoes have to prove itself in action.There are a few minor amendmentswe will propose at the 2003 AGM -for example, the splitting of the
Communications Portfolio intoPublic Relations and Publications -but in general it is working well for us.
At the AGM I was able to reportthat the Professional Board hadclarified our status as first line prac-titioners. “Registered physiothera-pists are entitled to practice as firstline practitioners (meaning withoutreferral from a Medical practitioner)in terms of their scopes of practice,
From the President’s DeskA retrospective on the year gone by from President Lynn Fearnhead
W
14 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
competency or outcomes of educa-tion or training.”
The situation regarding therequirement for dual registration to practice acupuncture and/or dryneedling has not yet been finalised.We will keep you informed of anydevelopments.
NATIONAL ASSEMBLYThe National Assembly in May wasa real cause for celebration. Thepostal election had taken place and we had a fully representativegoverning body made up of theelected and representative members.We are concerned about issues oftransparency and that we need todevelop mechanisms that allowimportant issues to be taken back tograssroots members for commentand discussion before decisions aretaken. The Policy Portfolio is look-ing into it.
Anna Bizos, who had come to theend of her four-year service as anOffice Bearer of the Society, wasthanked for her significant contri-bution, particularly for creating aclimate that would allow change tooccur. Zola Dantile was welcomedas the new President -Elect.
We tried to fit an AGM, NationalAssembly and EXCO meetings intoa weekend in May and discoveredthat we couldn’t! The EXCO meet-ing was postponed to July. At thatmeeting we realised that we neededto be brought up to date with socio-economic developments inhealth care in South Africa. Wewere fortunate to have a very informative workshop with EsméPrins in September. Topics includedthe proposed National HealthInsurance Plan and ManagedHealth Care.
CPDThe trial year for CPD is wellunderway. Professor Celie Ealesand Helen David are our repre-sentatives on the Wits ConsortiumAccreditation panel, and numerouscourses have already been accre-dited. CPD will bring exciting
opportunities. We are trying tominimise the costs to our membersand appropriately reward peoplefor valuable service to the profes-sion, for instance through studentsupervision and being a ‘buddy’.
Community service is about tobecome a reality in January for our 2002 graduates. SASP CEOSaira Khan has been busy puttingtogether the ‘buddy system’ net-work for anyone needing a helpinghand. There are currently about 450physiotherapists in Public Servicein South Africa. The 245 new com-munity service graduates will con-siderably strengthen the servicedelivery in traditionally under-served areas. I ask all of you to support these new graduates.
OTHERHIGHLIGHTS
We have had a successful BackWeek. Along with the crowds atPretoria University we had fun,hard work and great exposure atthe Supersport Show. Comradeswas also a great success in 2002. In October, I was a signatory at the official South African inauguralmeeting of representatives of orga-nisations committed to promotingthe Bone and Joint Decade 2000 -2010, a project of the WHO.
The Physiotherapy ResearchFoundation has continued to grantfunding to valuable projects byphysiotherapists this year.
OFFICE NEWSUnder Saira’s direction we rede-corated at Head Office, a necessarymove as we had to accommodatethe merging of the SASP andPhysioFocus offices. It is now abright and airy and modern openplan office that is also disability-friendly.
I think we can all congratulateourselves on the way the SASP andPhysioFocus are working togetherto ‘speak with one voice’.
There have been a number of staffchanges. Erica Blom, Michelle daSilva, Lee Partington and recently
Michelle Nair have all moved onbut we are fortunate that we have a core of loyal people committed toyou, the members and the SASP.The stalwarts of the office areMarge, Rosie, Gloria and Florrie. Ithank them on your behalf. AmericoPinheiro has recently joined themand we’re all enjoying having aman in the office. He has been busy taking over the Publicationsand Communications work fromFlorrie and will also spend timesourcing adverts for our variouspublications.
Saira Khan has been with us ayear now and has been able to getaround to most of the Provincialoffices to meet members through-out the country. She has been coordinating the work of portfoliosand provinces from Head Office.She has also been busy networkingwith the Department of Health, the HPCSA and COIDA amongstothers. I think Saira thinks of theSASP as an octopus - just when sheis getting a hold on it a tentacle slipsout! However, I’m sure she agrees,it is never boring!
In South Africa we live in a wonderfully vibrant environmentwith rapid changes occurring inalmost all areas of life. The health-care environment is a typical exam-ple where the implementation ofPHC, service delivery to a popula-tion characterized by vast differ-ences in income, economic pressureson the Medical Aid schemes, tech-nological advances in medicine and pharmaceuticals and the Aidspandemic are a few of the factorsdetermining the changes.
This is our world - help us tograsp the opportunities and buildon the traditions that after over 75years of organized practice in South Africa we have demonstratedthat physiotherapy is a dynamic,innovative, trusted and reliableprofession.
I wish you all a safe, happy andpeaceful festive season and verybest wishes for a prosperous andhealthy 2003.
Society Matters

PHYSIOFORUM DECEMBER 2002/JANUARY 2003 15
Society Matters
he Commission for Occu-pational Injuries and Disease -once known as Workman’s
Compensation, now familiarlyreferred to as COID - has some-thing of a reputation among phy-siotherapists. Pay-out times canvary from thirty days to a couple of months to two years, and forthose whose practice carries a sub-stantial number of COID patients,that can cause serious cash flowproblems. Most at risk are prac-tices in regions with a high levelof industrial employment.
PhysioFocus delegates have hada couple of meetings with COIDthis year. Melanie Skeen says thatCOID has assured them that theirturn-around time is steadily improv-ing. One of the major problems hasbeen delays in opening post con-taining claim forms, and this isbeing attended to. “COID is alsodeveloping an electronic delivery(EDI) system for claims, which willspeed things up considerably,” saysMelanie. “Avoid sending lots ofduplicates, especially if you havereceived confirmation that yourclaim has been captured - this justslows up the system.”
Claims are usually rejected eitherbecause of a dispute about thecause or place of injury, or they arereturned because there is notenough info. Melanie urges physiosto make sure that they have all the right forms - the employer’sreport and the first doctors report -and that they are properly filled in.“Check that everything is filled inadequately and that the two reportscorrelate - that the doctor doesn’tsay anything that contradicts theemployer or vice versa. If there areany errors or any missing informa-tion, then you will have to wait forthe employer to provide a correctedform, and that takes time.”
Melanie suggests that physiosdon’t turn to one of the companies
which offers to speed up claim processing. “COID officials denythat they have any contracts withany such companies, and say theycan see no reasonable way in whichany other party can get the claimprocessed faster - there’s just noroom for it in their system. It isunethical to pay a slice of yourearnings to such companies, and itreally doesn’t benefit you.”
Where there is a dispute as towhether it was an ‘injury on duty’,the claim may never be settled, and in this instance, the patient willbe liable for the cost of treatment,so you should make that clear topeople upfront.
Fanie Kruger, Manager: Medicaland Legal Services at COID, offers
these comments: “The problemwith COID claims is that in manycases the service providers aredoing what is expected of them,and anticipating payment from theCompensation Fund. But it doesnot happen and it is a natural ques-tion to ask “What must I do tospeed up payment?” In many casesthe delay in payment is caused bysomeone else , which you as theservice provider do not know about.There are many stakeholders allinfluencing the payment process.”To speed up the processing ofclaims, Mr Kruger suggests thatyou should:• Ensure that you have confir-
mation from the employer thatthe employee was injured onduty, that is, the Part B of theEmployers Report of an accident.
Although this is not a guaranteeof payment, it is at least an con-firmation by the employer that he is satisfied the employee wasinjured on duty.
• Ensure that you have the refer-ence from the treating doctor andthat there is continued commu-nication with him especially if the therapist is of the opinion thatthe treatment will exceed 20 treatments.
• The first account must be submit-ted to the employer to be submit-ted to COID.
• The second account must be submitted to COID together withcopies of supporting documentssuch as the Part B First MedicalReport and the doctor’s referralto the therapist.
Those are the do’s. The don’ts arethe following:• Do not phone the Compensation
Commissioner for a claim num-ber. The employer will have it ifit was reported to COID. A claimnumber is also not a guarantee ofpayment.
• Do not phone the Office aboutoutstanding accounts. Rather usethe standard form W. Cl 20 ormake an appointment with theenquiry section. Our telephonesystem can handle only so manyincoming calls.Mr Kruger adds, “We have devel-
oped a system that will enable aservice provider to submit anaccount electronically whilst at the same time also submit the sup-porting documents in a scannedformat via the Internet. The systemis still in its pilot phase but you can already access the technicalspecs from our web site atwww.comp.gov.za. As soon as weare satisfied with the pilot and areready for roll-out it will be madeavailable on the website.”
Melanie urges physios to use all the tools at their disposal toensure speedy payment of claims.“And remember, we are constantlyengaged in negotiations on yourbehalf!”
Pay or pain?
T
“And remember,we are constantly
engaged in negotiations on your behalf!”
16 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
cupuncture became part ofSouth African physiothera-pists’ practice in 1983 after
several physiotherapists undertooktheir initial acupuncture trainingunder the tutelage of doctorsGeorge Lewith and Julian Kenyonof Southampton, England. Theseeminent doctors had obtained exten-sive experience of acupuncture andrelated procedures in MainlandChina, and during their visit toSouth Africa, they changed thethinking of a considerable numberof health professionals, includingphysiotherapists, medical doctors,chiropractors and homeopaths.
A demand for acupuncture train-ing of physiotherapists arose in themid-1980s, and course conductedby physiotherapists for physiothe-rapists were instituted in 1985.
The South African Physiothe-rapists’ Acupuncture Associationwas formed in 1986, and thisAssociation evolved into a specialinterest group of the SASP in 1990, with a change of title to theAcupuncture Association of theSouth African Society of Physio-therapy. This process effectivelyrecognised acupuncture and itsvariants (electro-acupuncture, acu-pressure, moxibustion and laserpuncture) as being within the scopeof physiotherapy.
The formation of the AASASPhas enabled physiotherapists totake advantage of the trainingcourses organised with the assis-tance of the Association. Since 1986,courses run on a modular basis
have been conducted around thecountry by Charles Liggins andRoy Mitchell, and Charles has run courses in Botswana andZimbabwe. Well over 1000 physio-therapists in this country haveavailed themselves of the opportu-nity to undertake some acupunc-ture training, and a good number of enthusiasts have completed thefull course of five modules.Completion of all five modules hasenabled physiotherapists to qualifyfor registration with the AlliedHealth professions Council ofSouth Africa (AHPCSA) as a practi-
tioner of acupuncture. The practiceof acupuncture in South Africa wasregulated by act of Parliament inNovember 2000 (Act No 50 of 2000published on 1 December 2000 inGovernment Gazette No 21825).Promulgation of the Act had theeffect of recognising acupunctureas part of the general health ser-vices of the country. Physiothe-rapists who had completed theAASASP course were given theopportunity to apply for registra-tion as acupuncturists with the
AHPCSA, and currently about onethird of the AASASP has dual registration (HPSA/AHPCSA).
Recently, Charles Liggins waselected to the Professional Boardfor Ayurvedic, Chinese Medicineand Acupuncture. The inauguralmeeting of several new professionalboards (including this one andTherapeutic Aromatherapy, Thera-peutic Massage Therapy andTherapeutic Reflexology), all underthe jurisdiction of the AHPCSA,was held in Krugersdorp from 30 October to 3 November.
The AASASP became a foundermember of the International Acu-puncture Association of PhysicalTherapists (IAAPT), a sub-group of the World Confederation forPhysical Therapy, in 1991, and has a member (Charles Liggins) on theExecutive and Education Com-mittees of the IAAPT. In addition,Charles is the editor of the IAAPTjournal, Meridian Worldwide.
The Mission of the AASASP is topromote and ensure the integrationand expansion of acupuncture with-in the practice of physiotherapy,and the health delivery systems ofSouthern Africa, through profes-sional and public education, devel-opment of standards of practice,advocacy and research.
The current office bearers of the AASASP are: Charles Liggins(Chairman), Roy Mitchell (Secre-tary) and Dan Dhanraj (Treasurer),with committee members andregional representatives Sue McCall(Gauteng), Narina Gilder (Cape)
The Acupuncture Association of the South African Society of Physiotherapy (AASASP)
We continue our series on the special interest groups with this information from AASASP Chairman, Charles Liggins
Society Matters
A

PHYSIOFORUM DECEMBER 2002/JANUARY 2003 17
Society Matters
and Norma Lederle (Free State).In relation to the wide-ranging
nature of the scope of practice of physiotherapy, the use of the various systems of treatment car-ried on by physiotherapists is alsowide-ranging. With reference toacupuncture, most therapists use itfor pain management, as it isextremely effective in the manage-ment of nociceptive pain. Thisincludes, among many other con-ditions, recent injuries and sport-related injuries, myofascial painsyndromes and the arthritides.
Physiotherapists working in PainManagement Clinics use acupunc-ture for the treatment of a range ofconditions characterised by neuro-genic pain, for example complexregional pain syndromes caused bybullet wound and other injuries.These are just a few examples ofphysiotherapists’ major use ofacupuncture.
This system of treatment also has benefits, and is used, in thephysiotherapeutic management ofneurological conditions (eg hemi-plegia, Parkinson’s disease and
spinal injuries); respiratory condi-tions (eg sinusitis and bronchialasthma); dermatological disorders;stress-related and psychiatric con-ditions and many others which fallwithin the scope of physiotherapy.
The demand from physiothe-rapists for acupuncture training isgrowing and it is the intention of the AASASP to continue themodular courses (both basic andadvanced) and to keep members upto date with trends, research andlegislation through its officialpublication, Meridian.
Please read this extract from a letter from Vanessa Heffer,physiotherapist at a rural hos-pital near Greytown.“I wish people would give the com-munity service idea more support.We really need the therapists inthis region - at our hospital alonewe visit 13 clinics, as well as doing in- and out-patients at the hospitaland home visits where possible. It is quite a load for one person(and two volunteers). The popula-tion we serve is estimated at over amillion people, and most are livingin extreme poverty without runningwater, sewerage and electricity.Disability grants (R640) feed fami-lies of 6-10 people. Most of therural areas tell a similar story, andwe have all heard it before, but it is only when you live in the middleof it that you begin to FEEL thereality of it. For the students whoare feeling unhappy or unsure ofwhere they are going for a year, letthem know this - they are reallyneeded out here, and the ‘little bit’they are doing for the community
will make a huge difference wherethere is nothing...”
I feel sure that the newly qualifiedstudents will be very positive aboutthe contribution they can make tothese desperately needy communi-ties once they get out there.
But if community service is toachieve the goals we believe it can -such as increasing the extent ofphysiotherapy services offeredthroughout the country, enhancingthe profession’s image in the eyesof both our colleagues in healthcare and government, as well asbringing physiotherapy to theattention of a wider public - thenthe newly qualified graduates are goingto need commitment and engagementfrom all of us in the profession.
Our primary tool for offeringsupport will be the Buddy system.What this entails is that graduates,especially in rural areas, will have a “Buddy” (member of the Society),who will be allocated to him or her to offer support in whateverway is most convenient or appro-
priate - whether that’s by telephoneor one-on-one in a clinical setting.(The type of support depends on anumber of factors, chief of which isthe location of the graduate. It’senvisaged that the support wouldmainly be by phone).
Physiotherapists who offer thiskind of assistance will be able to earn Continuing ProfessionalDevelopment (CPD) points in thisway, so there is a benefit in it foryou as well! A maximum of 5 CPDpoints can be earned in this way.(The Health Professions Council ofSouth Africa has agreed to this inprinciple). The physiotherapist andgraduate will both submit confir-mation that the service is being rendered to the Society and thiswill be forwarded to the authoritiesat Wits to capture the CPD points atthe end of 2003.
GET INVOLVEDYour Profession needs you! It is nottoo late to put your name forwardfor this important and valuable service. Look into your heart and
On My Own Two FeetCommunity service is just around the corner for new graduates
- how can we help?

18 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
ask yourself how you would havefelt as a quaking youngster in yourearly twenties, out in a deep ruralarea and perhaps being asked tobear responsibility for a wholedepartment, or even open up a newservice alone. Would you not havebeen hugely grateful to know therewas a voice at the end of a tele-phone, someone whom you couldsound out when in a dilemma?
This is a service which will ridelightly on your shoulders, butwhich could vastly improve the job the graduates are able to do,make all the difference to the pro-fession’s image, and help our coun-try at a time when health servicesare in ever-growing need. Pleasegive it some thought during thisfestive season. If you feel that youcan help, phone CEO Saira Khan on (011) 485-1467 to put your nameforward.
FREQUENTLY ASKEDQUESTIONS ABOUT
COMMUNITY SERVICE
What does a Community ServiceGraduate need to do to benefitfrom the Buddy Programme?• Contact the SA Society of
Physiotherapy Head Office on (011) 4851467 or fax (011) 4851613or on our toll free line 0800001870and provide the Society withyour name, contact telephonenumber, Society membershipnumber and place of appoint-ment (hospital/clinic), so that wecan allocate a buddy to you.Alternatively send us an e-mailproviding us with the aboveinformation to [email protected] attention Saira Khan.
• The Society will then send you aresponse (telephonic, fax or e-mail) providing you with infor-mation and contact details foryour Buddy Physiotherapist.
How does a Buddy support me dur-ing my community service year?• We envisage the support to be
mainly telephonic should dis-tance be a problem; however, it
could well be face-to-face contactif distance is not an issue
• It is difficult to determine howoften the contact would be; thiswould depend very much on theindividuals involved, the level of support within the area ofplacement and the amount ofcontact required by the graduate.We would like the graduate todiscuss this with his or her Buddyto suit individual requirements.
What terms and conditions ofemployment do I need to be awareof as a Community Service Health-care provider?• Firstly, as an employee of the
Department of Health, you aresubject to the terms and condi-tions of employment of the PublicService as well as the Departmentof Health.
• You must be aware of the fact thatprovinces function independentlyof each other and that no twoprovinces are obliged to have the same terms and conditions ofemployment. For example, in oneprovince you may receive anallowance towards your accom-modation as part of your salarywhich could be liable for taxation(as per normal SARS regulations),and in another you may notreceive an allowance but youraccommodation will be paid forby the province.
• At present, rural allowances areonly provided to doctors doingcommunity service and no otherhealthcare professional; however,the department is negotiating to have the rural allowance madeavailable for all Communityservice healthcare workers, asthey believe that there must beparity.
• The commencing grade of remu-neration is Grade F and you are also entitled to all other bene-fits that public servants receive,such as medical aid, housingallowances, and the like.
• Should you for whatever reasonbe unable to complete your community service, you will be
required to firstly tender yourresignation in writing to the hos-pital or clinic citing your reasonsfor non-completion of your com-munity service year. Secondly, ifyou have done less than sixmonths of community service,you will be required to completeanother entire year of communityservice before being allowed tocommence practising indepen-dently. If, however, you have donesix or more months of communi-ty service, you will be required to complete the balance of yourterm when you are able toresume. It must be noted, thatshould your reasons not be justi-fiable, on resuming your commu-nity service, you will be given nopreferences and will be placedlast on the list once the currentselection has been done! Weadvise you to think carefullyabout this.
• As a public servant, you havetwenty two days annual leave andten days sick leave per annum, as per the Basic Conditions ofEmployment Act. You are alsoentitled to maternity/paternityleave and family responsibilityleave as per normal working con-ditions of the Department ofHealth.
• You are not permitted to under-take any post-graduate studiesduring your term of communityservice. The department hasstressed that no leave will be provided for studying post-gra-duate courses.
• The HPCSA (Health ProfessionsCouncil of SA) has also stipulatedthat at present, a community service graduate is also requiredto obtain CPD (ContinuousProfessional Development) points.The SA Society of Physiotherapyis in discussion with HPCSA onthis, as we would like it waivedduring the community serviceyear. The Department of Healthwill provide you with time off,should it be necessary in order toobtain CPD points.
Society Matters
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 19
In Focus
How did you do in our quiz lastissue? If you remember, we askedyou to pick out which of the nameplates on the next page would qua-lify as legal.
Have another look, and then readthrough the rules extracted fromthe HPCSA Guidelines for MakingProfessional Services Known:
10. OUTSIDE SIGNSAND NAMEPLATES
10.1 Signs and nameplates may not be larger than 1 m x 0.5 mand may contain some or allof the following information,but nothing more, namely -
10.1.1 names (initials) and surnameof the health care professional
10.1.2 profession (e.g. medical doc-tor, dentist)
10.1.3 indication of the location of the practice (e.g. roomnumber, street number, nameof the building)
10.1.4 telephone number(s)10.1.5 consulting hours10.1.6 the “red cross” symbol may
not be used by medical prac-titioners: This emblem wasadopted by the InternationalFederation of Red Cross andRed Crescent Societies andmay only be used as autho-rised in terms of the 1991Regulations on the use of theEmblem.
10.2 Logos may not be used onoutside signs and nameplates.
10.3 Only one outside sign maybe used, except in the case ofa large complex with morethan one entrance where asign may be placed at eachentrance. The sign should be placed on the premiseswhere the practice is situated,or, at most, at the street cor-ner closest to the premises.
10.4 A nameplate may be used on the door of the consultingroom.
10.5 In the case of occupants oflarge complexes where spe-cial provision is made in the entrance hall and on thevarious floors to indicate thetenants, it shall be permis-sible to make use of suchprovision.
10.6 If necessary, in large com-plexes, a nameplate with thename of the health care pro-fessional only, may be usedin the corridor for the direc-tion of the patients.
10.7 An outside sign indicating“PRIVATE PARKING FOR............” (indicating the streetname and number only) willbe permissible (for examplePRIVATE PARKING FOR 23 FORD STREET).
10.8 In the event of a change in themembership of a company,partnership, or association,the original nameplate maybe displayed for a period of six months whereafter anameplate with the correctinformation should be dis-played. Should a practicemove to other premises, thename of the practice and the new address may also bedisplayed at the vacatedaddress for six months.
10.9 If an illuminated sign is used,the only sources of illumina-tion may be a constant whitelight.
10.10 Only two colours of ownchoice may be used on out-side signs, one for back-ground and one for lettering.
11. PRACTICE NAMES
11.1 Health care professionalsmay use as the name of apractice, their own namesand/or the names of their
partners, directors or asso-ciates or the name of one orof certain partners or asso-ciates or directors, togetherwith the words “and part-ners”, “incorporated” or “andassociates”, as the case maybe.
11.2 The use of an expressionsuch as “hospital”, “clinic”or “institute” or any otherspecial term which could create the impression that apractice forms part of, or is inassociation with a hospital,clinic or similar institution,should be avoided.
11.3 A building occupied byhealth care professionalswho are registered with theHealth Professions Councilof South Africa may have aname indicating the profes-sion of the occupants only if there are at least two such independent profes-sional practices in the build-ing. Should only one suchprofessional practice (e.g. amedical practitioner, psycho-logist, optometrist) be con-ducted in the building andthe name of the buildingrefers to that profession (e.g.medical centre, psychologycentre, optometry centre) theimpression may be createdthat that single practice ismore important than otherindividual practices. In thecase of registered health careprofessionals of differentprofessions such as a medicalpractitioner, psychologist andoptometrist practicing in the same building, the name“Health Centre”, however,may be used.
11.4 “Section 54A companies”and partnerships falling inthe same category may nolonger be indicated as “prac-tising as” or “trading as”.
By any other name
Mary Jones (Bsc Phys Wits)Physiotherapist
Room 206 second floor(011) 803 2678 082 6590001
Open 7:30 to 18:30
Physiotherapy
PhysiotherapistRoom 206 second floor
Mary JonesPhysiotherapist
Treating:back pain, headaches, sports injuries
Room 206 second floor
Physiotherapy CentreMary Jones • John SmithOrthopaedic rehabilitation
- sports - back pain - chest treatmentHours: 7:30 am to 6:30 pm
Room 613 Ground floor
20 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
In Focus
PhysioFocus
BLUE BOOKJoin PhysioFocus - and you willautomatically get one of the mostuseful tools your practice couldever have, the Blue Book!What is the Blue Book?The textbook for private practice -all you need to know:- All the latest tariffs and rules,- All the ethical and legal require-
ments for starting and running apractice.
- Important telephone numbers andaddresses for info, medical aidsand many other organisations.
- All about third party claims- Our scope of practice and locum
policies- Medico-legal reports - how and
what- Sporting event tariffs- Terms and acronyms- Indemnity forms- HPSCA registration and rules- Information concerning tax
Can anyone afford to be withoutthis? And it all comes in one bookset out in easy-to-find sections - anasset to every private practitionerand even to the public practitioner.
Cost R250 - or receive it free withyour Physiofocus membership fee
TARIFF TIT-BITSAnother year is almost past and wehave had a busy but productiveyear at Tariffs. Here are some of ourachievements:
• Our Tomorrow in Private Prac-tice course is planned for 25thJanuary 2003 at the St George’sHotel. See the application formon page 21.
* Our negotiation meeting withCOID was held on the 10thSeptember. Further motivationswere submitted to back ourmotivations.
• BHF has offered us an 8%increase which we are not satis-fied with so we are re-negotiat-ing.
• Our new tariffs will be out inDecember.
• Mx Health has agreed to pay uswith out a referral from a GPuntil further notice
• BHF have removed the wordsBenchmark tariff from their tariffs
• BHF, Medical aids and othergroups are being investigateddue to a meeting with theCompetitions Commissioner
Remember you may charge a72701 and a 72702 at the first con-sultation, but then you must specifywhich is evaluation and which isadvice or counselling (if both aredone) - you can’t charge for eva-luation, advice and counselling onthe same code!
If you use EDI with DHSwitchplease fill in a peer review authori-sation form (available from them)to enable us to use code informa-tion (all confidentially) in our nego-tiations with medical aids.
As a tariff committee it is our aimto be of service to all our Privatepractitioners. Please contact us withyour suggestions and complaints.Tariffs are our BusinessMelanie Skeen082 565 3745
PS: Please remember that you may notemploy new graduates until they havecompleted their community service asthey are not fully registered with theprofessional board until it is completed.
News you can Use
✘
✘
✘
✔
✔
TOMORROW IN PRIVATE PRACTICE25th January 2003 (only 100 places-Book NOW!)7h30 - 8h00 Registration & view exhibits & Tea 8h00 - 8h10 Opening address:
Saira Khan, CEO SASP8h10 - 8h30 Guest speaker:
Dr Ramakgopa, MEC Health Gauteng8h30 - 9h00 National Health Insurance -
What? When? Where? Esme Prins
9h00 - 9h30 Medico-legal & Informed consent:Hester Huysamen
9h30 - 10h00 Practice ethics: Hester Huysamen10h00 - 10h30 Tea & exhibits10h30 - 11h00 Basic conditions of Employment:
Gerhard Papenfus11h00 - 11h30 Diagnostic Related Groups:
Brian Ruff11h30 - 12h00 Ethical Debt collecting, Performance
Based Reimbursement & PerverseIncentives: Elsebe Klink
12h00 - 12h30 Practice liability planning:Juanita Wantenaar
12h30 -13h30 LUNCH and view exhibitors13h30 -14h00 Tariffs 2003 & Private practice:
Melanie Skeen14h00 - 15h00 Practical tariff OR Ethics workshops15h00 - 15h30 Tea & exhibits15h30 - 16h30 Tariff OR Tax Workshops
STROKE SYMPOSIUM 20031ST ANNOUNCEMENT
The Southern African Stroke Foundation is proud to announce the 3rd Stroke Symposiumwhich will be jointly hosted with The SA Academy of Family Practice/Primary Care
Date: Friday, 6 June 2003 - Sunday, 8 June 2003Venue: Birchwood Executive Hotel (5 minutes from Johannesburg International Airport)Highlights Include: - International Satellite symposium and dinner- Poster presentations - Workshops will include the following topics (Please select your interest)
❑ Risk Factors ❑ Stroke Units ❑ Ethics & Stroke/Legal Aspects ❑ Clinical Evaluation ❑ Rehabilitation ❑ Cerebral Hemorrhage❑ Acute Stroke Management ❑ Cost Implications ❑ Psychiatric Complications ❑ Chronic Stroke Management ❑ Lacunes ❑ Long Term Stroke Care
Join us for a truly unique opportunity to learn more about all aspects of Stroke! Participation in our exciting workshops will provide a forum for the exchange of mutual experiences. CPD Points will be issued for all HealthProfessionals.If you wish to receive further notices about the meeting, details regarding poster presentations and registrationplease complete the following information and fax to: (011) 803 4997 or email [email protected] : -
YES! I want to be there! To be accredited for 6 C.P.D. points (2 for ethics)
When: 25th January 2003Where: St George’s Hotel Old Kempton Park road Cost: R450 S.A.S.P. members, R750 non-membersName:S.A.S.P. no:Cell no:Pr.No:
Deposit money to :Account Name: S.A.S.P. Tariff committeeBank: First National BankBranch: PretoriaBranch Code: 251445Account number: 51461168995And fax application form & deposit slip to(012) 347 -5033 before 8 January 2003OR post to: Suite 323, Postnet x4, Menlo Park, 0102
Workshop choices: Please choose 2!Chests: ❑ Yes/No ❑Ortho: ❑ Yes/No ❑Neuro: ❑ Yes/No ❑Ethics ❑ Yes/No ❑Tax ❑ Yes/No ❑
Any enquiries Call Melanie on 082 565 3745
Last Name: First Name:HPCSA Number: Title:Professional Discipline: (Family/General Practitioner/Specialist/Therapist) Please specify:
Address:Email: Cell No:Tel No: Fax No:
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 21
22 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
Society Matters
here is still some confusionand uncertainty surround-ing Continuing Professional
Development (CPD). We hope wecan clarify some things for you inthis brief article.
In an interview with Rabia Latiffat the Wits CPD Office (a division of the Wits Health Consortium(Pty) Ltd, a wholly owned sub-sidiary of the University of theWitwatersrand), I got clarity on theissue of who pays for the capture ofCPD points: “There is no direct costto the physiotherapist, except inthose cases where a course providerissues a certificate rather than keepsan attendance register, in whichcase the physio will have to sendthe original or a certified copy of an Attendance Certificate throughto Wits CPD Office his or herself,and pay the cost of capturing theCPD points.” Where an attendanceregister is kept, it is the provider’sresponsibility to send it through andpay for the capture of the points(undoubtedly the minimal cost will then be incorporated into thecourse fee). “Before you attend acourse, find out if the provider hashad the event or activity properlyaccredited, and if they will be issuing certificates of attendance or keeping an attendance register,”says Rabia. When CPD points areoffered for reading a journal, youwill be asked to submit a completedquestionnaire to the Journal, and itis the publisher’s responsibility tomark and assess the questionnaires;where the person has qualified forCPD points, the provider - in thiscase the publisher - must electro-nically forward the relevant CPD
points to the Wits CPD Office tocapture the points. (The accreditedprovider of these points will beresponsible for payment for thepoints.)
Physiotherapists do need to be alittle savvy about accreditation toavoid any mix-ups and muddles.Please note that it is not theprovider or the lecturer which isaccredited, but rather the event,course or lecture. The provider - the people responsible for adminis-trating the course, such as - theUniversity of the Free State,Clinical Solutions, Medunsa, orwhoever - must have applied tohave the course or event accredited.This is to ensure uniformity. “If wewere to just accredit the lecturer orprovider, then we would have noassurance of how each course wasgiven - the same lecturer could do atwo-day course in Cape Town andone day in Pretoria. It is also verydifficult to check and log points.Always ensure that the event isaccredited; if not, request that theprovider has the event accredited to avoid any confusion and assistby sending them the relevant con-tact details of the Wits CPD Office,which will gladly help with accredi-tation and requirements to processan application for approval andaccreditation.”
If you are concerned about yourCPD points and want to check upon them, nothing could be simpler.CPD Points will be available on theWeb once they’ve been captured.Just log in to: www.witshealth.co.za• Select CPD button• Select - Register for CPD Points• Enter your PT number
• Select own password• Answer a question and click on
submit• Select - Log in and view your
points.• Type your PT number and pass-
wordORE-mail - [email protected]
CONTACT DETAILSRabia Latiff:CPD Accreditation(011) 717-2862E-mail: [email protected]
Tatum Swanevelder:CPD Services and Points Logging(011) 717-2863E-mail:[email protected]
Jennifer Bryce-BorthwickCPD Administrator(011) 717-2864Email:[email protected]
Janine Pringle & Rose Mary RobsonE-mail:[email protected] CPD Points Logging CPD Sales andMarketing(011) 717-2880, 083 653 6675Fax: (011) 717-2860
Physical Address:Healthcare Park27 Eton RoadParktown 2193Postal Address:Suite 189, Private Bag X 2600Houghton 2041
On the following pages, we’veprinted the official Wits CPDCategories and Points Allocationform, which shows you whatpoints you will receive for differentactivities.
In our next issue, we’ll take a lookat the requirements for providers.
Point systemWe keep you updated on CPD
T
The Accreditor will evaluate the applications according to the criteria and guidelines for accre-ditation as provided by the Health Professions Council of South Africa (HPCSA)
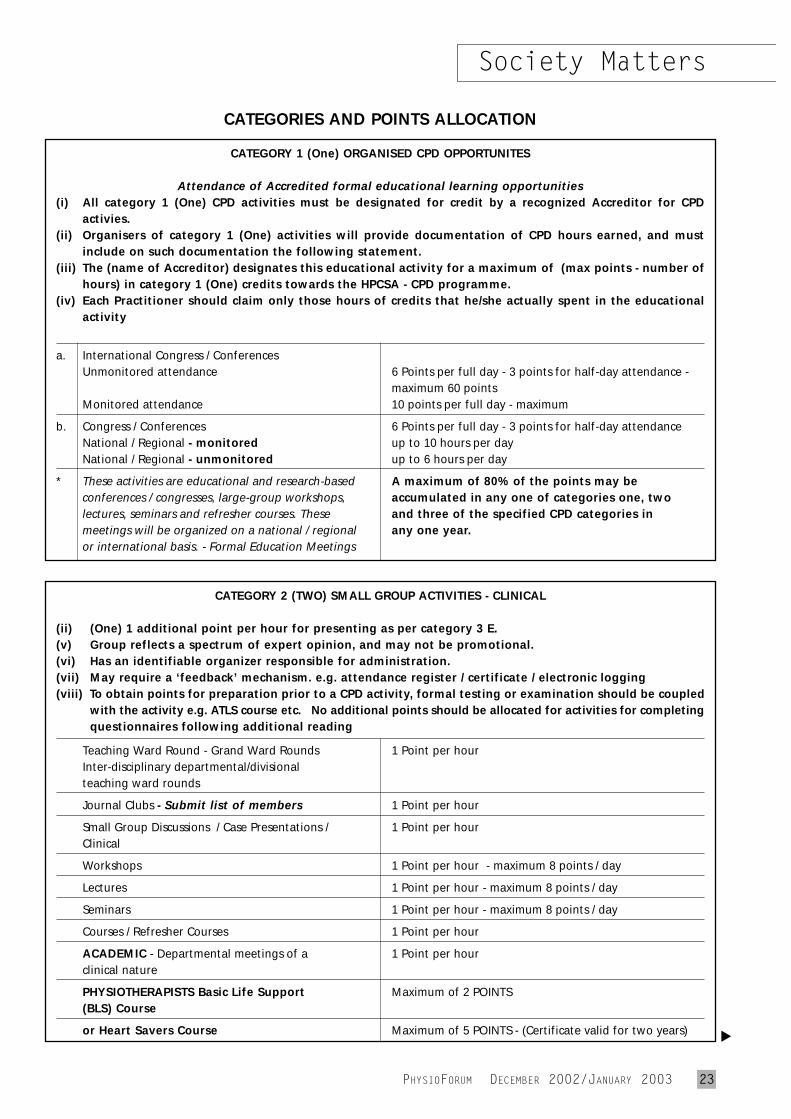
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 23
Society Matters
CATEGORIES AND POINTS ALLOCATION
CATEGORY 1 (One) ORGANISED CPD OPPORTUNITES
Attendance of Accredited formal educational learning opportunities(i) All category 1 (One) CPD activities must be designated for credit by a recognized Accreditor for CPD
activies.(ii) Organisers of category 1 (One) activities will provide documentation of CPD hours earned, and must
include on such documentation the following statement.(iii) The (name of Accreditor) designates this educational activity for a maximum of (max points - number of
hours) in category 1 (One) credits towards the HPCSA - CPD programme. (iv) Each Practitioner should claim only those hours of credits that he/she actually spent in the educational
activity
a. International Congress / ConferencesUnmonitored attendance 6 Points per full day - 3 points for half-day attendance -
maximum 60 pointsMonitored attendance 10 points per full day - maximum
b. Congress / Conferences 6 Points per full day - 3 points for half-day attendanceNational / Regional - monitored up to 10 hours per dayNational / Regional - unmonitored up to 6 hours per day
* These activities are educational and research-based A maximum of 80% of the points may beconferences / congresses, large-group workshops, accumulated in any one of categories one, twolectures, seminars and refresher courses. These and three of the specified CPD categories inmeetings will be organized on a national / regional any one year.or international basis. - Formal Education Meetings
CATEGORY 2 (TWO) SMALL GROUP ACTIVITIES - CLINICAL
(ii) (One) 1 additional point per hour for presenting as per category 3 E.(v) Group reflects a spectrum of expert opinion, and may not be promotional. (vi) Has an identifiable organizer responsible for administration.(vii) May require a ‘feedback’ mechanism. e.g. attendance register / certificate / electronic logging(viii) To obtain points for preparation prior to a CPD activity, formal testing or examination should be coupled
with the activity e.g. ATLS course etc. No additional points should be allocated for activities for completingquestionnaires following additional reading
Teaching Ward Round - Grand Ward Rounds 1 Point per hourInter-disciplinary departmental/divisionalteaching ward rounds
Journal Clubs - Submit list of members 1 Point per hour
Small Group Discussions / Case Presentations / 1 Point per hourClinical
Workshops 1 Point per hour - maximum 8 points / day
Lectures 1 Point per hour - maximum 8 points / day
Seminars 1 Point per hour - maximum 8 points / day
Courses / Refresher Courses 1 Point per hour
ACADEMIC - Departmental meetings of a 1 Point per hourclinical nature
PHYSIOTHERAPISTS Basic Life Support Maximum of 2 POINTS(BLS) Course
or Heart Savers Course Maximum of 5 POINTS - (Certificate valid for two years) ▲
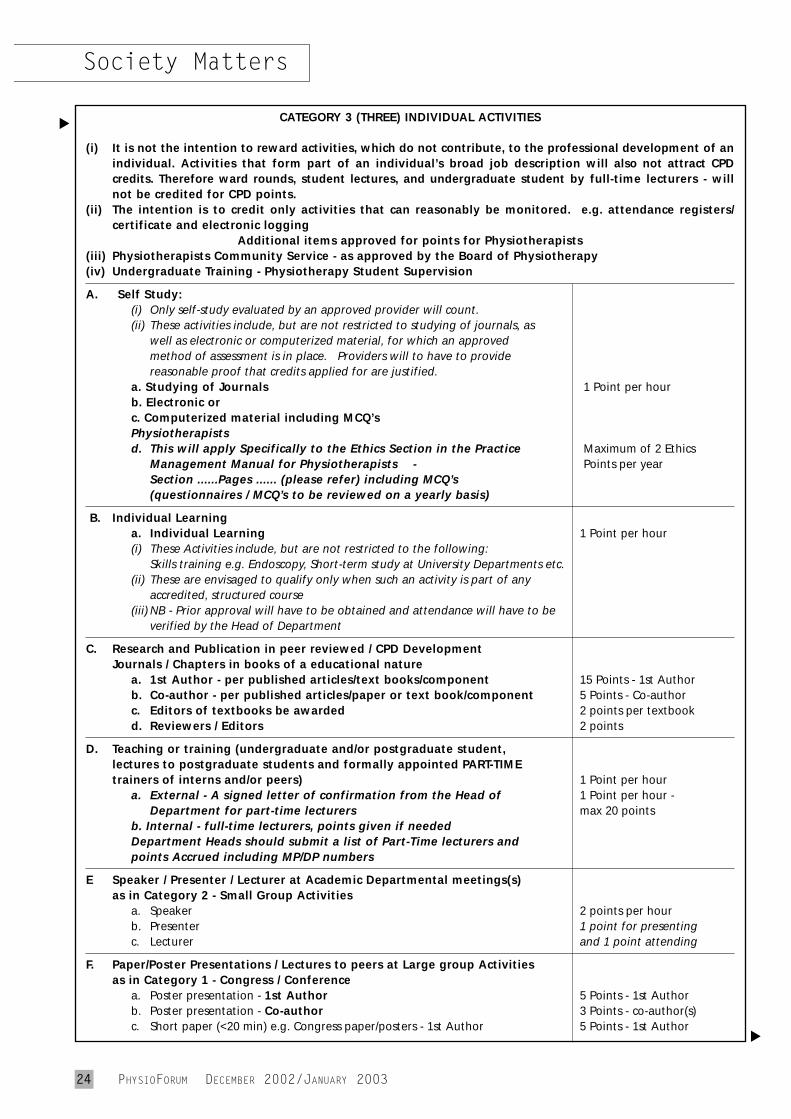
24 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
CATEGORY 3 (THREE) INDIVIDUAL ACTIVITIES
(i) It is not the intention to reward activities, which do not contribute, to the professional development of anindividual. Activities that form part of an individual’s broad job description will also not attract CPDcredits. Therefore ward rounds, student lectures, and undergraduate student by full-time lecturers - willnot be credited for CPD points.
(ii) The intention is to credit only activities that can reasonably be monitored. e.g. attendance registers/certificate and electronic logging
Additional items approved for points for Physiotherapists(iii) Physiotherapists Community Service - as approved by the Board of Physiotherapy(iv) Undergraduate Training - Physiotherapy Student Supervision
A. Self Study: (i) Only self-study evaluated by an approved provider will count. (ii) These activities include, but are not restricted to studying of journals, as
well as electronic or computerized material, for which an approvedmethod of assessment is in place. Providers will to have to providereasonable proof that credits applied for are justified.
a. Studying of Journals 1 Point per hour b. Electronic orc. Computerized material including MCQ’sPhysiotherapistsd. This will apply Specifically to the Ethics Section in the Practice Maximum of 2 Ethics
Management Manual for Physiotherapists - Points per yearSection ......Pages ...... (please refer) including MCQ’s(questionnaires / MCQ’s to be reviewed on a yearly basis)
B. Individual Learninga. Individual Learning 1 Point per hour(i) These Activities include, but are not restricted to the following:
Skills training e.g. Endoscopy, Short-term study at University Departments etc.(ii) These are envisaged to qualify only when such an activity is part of any
accredited, structured course(iii) NB - Prior approval will have to be obtained and attendance will have to be
verified by the Head of Department
C. Research and Publication in peer reviewed / CPD DevelopmentJournals / Chapters in books of a educational nature
a. 1st Author - per published articles/text books/component 15 Points - 1st Authorb. Co-author - per published articles/paper or text book/component 5 Points - Co-authorc. Editors of textbooks be awarded 2 points per textbookd. Reviewers / Editors 2 points
D. Teaching or training (undergraduate and/or postgraduate student,lectures to postgraduate students and formally appointed PART-TIMEtrainers of interns and/or peers) 1 Point per hour
a. External - A signed letter of confirmation from the Head of 1 Point per hour -Department for part-time lecturers max 20 points
b. Internal - full-time lecturers, points given if needed Department Heads should submit a list of Part-Time lecturers andpoints Accrued including MP/DP numbers
E Speaker / Presenter / Lecturer at Academic Departmental meetings(s)as in Category 2 - Small Group Activities
a. Speaker 2 points per hourb. Presenter 1 point for presentingc. Lecturer and 1 point attending
F. Paper/Poster Presentations / Lectures to peers at Large group Activitiesas in Category 1 - Congress / Conference
a. Poster presentation - 1st Author 5 Points - 1st Authorb. Poster presentation - Co-author 3 Points - co-author(s)c. Short paper (<20 min) e.g. Congress paper/posters - 1st Author 5 Points - 1st Author
Society Matters▲
▲
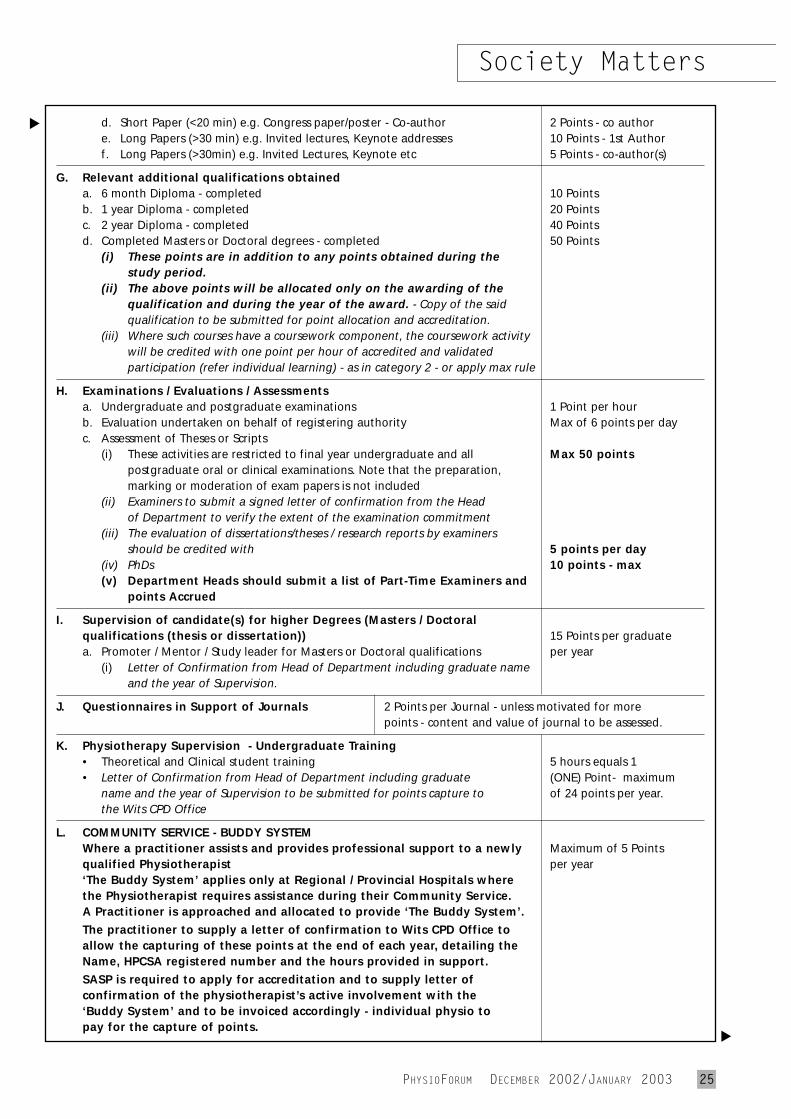
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 25
Society Matters
d. Short Paper (<20 min) e.g. Congress paper/poster - Co-author 2 Points - co authore. Long Papers (>30 min) e.g. Invited lectures, Keynote addresses 10 Points - 1st Authorf. Long Papers (>30min) e.g. Invited Lectures, Keynote etc 5 Points - co-author(s)
G. Relevant additional qualifications obtaineda. 6 month Diploma - completed 10 Pointsb. 1 year Diploma - completed 20 Pointsc. 2 year Diploma - completed 40 Pointsd. Completed Masters or Doctoral degrees - completed 50 Points
(i) These points are in addition to any points obtained during thestudy period.
(ii) The above points will be allocated only on the awarding of thequalification and during the year of the award. - Copy of the saidqualification to be submitted for point allocation and accreditation.
(iii) Where such courses have a coursework component, the coursework activitywill be credited with one point per hour of accredited and validatedparticipation (refer individual learning) - as in category 2 - or apply max rule
H. Examinations / Evaluations / Assessmentsa. Undergraduate and postgraduate examinations 1 Point per hourb. Evaluation undertaken on behalf of registering authority Max of 6 points per dayc. Assessment of Theses or Scripts
(i) These activities are restricted to final year undergraduate and all Max 50 pointspostgraduate oral or clinical examinations. Note that the preparation,marking or moderation of exam papers is not included
(ii) Examiners to submit a signed letter of confirmation from the Headof Department to verify the extent of the examination commitment
(iii) The evaluation of dissertations/theses / research reports by examinersshould be credited with 5 points per day
(iv) PhDs 10 points - max(v) Department Heads should submit a list of Part-Time Examiners and
points Accrued
I. Supervision of candidate(s) for higher Degrees (Masters / Doctoralqualifications (thesis or dissertation)) 15 Points per graduatea. Promoter / Mentor / Study leader for Masters or Doctoral qualifications per year
(i) Letter of Confirmation from Head of Department including graduate nameand the year of Supervision.
J. Questionnaires in Support of Journals 2 Points per Journal - unless motivated for morepoints - content and value of journal to be assessed.
K. Physiotherapy Supervision - Undergraduate Training• Theoretical and Clinical student training 5 hours equals 1 • Letter of Confirmation from Head of Department including graduate (ONE) Point- maximum
name and the year of Supervision to be submitted for points capture to of 24 points per year.the Wits CPD Office
L. COMMUNITY SERVICE - BUDDY SYSTEMWhere a practitioner assists and provides professional support to a newly Maximum of 5 Pointsqualified Physiotherapist per year‘The Buddy System’ applies only at Regional / Provincial Hospitals wherethe Physiotherapist requires assistance during their Community Service.A Practitioner is approached and allocated to provide ‘The Buddy System’.
The practitioner to supply a letter of confirmation to Wits CPD Office toallow the capturing of these points at the end of each year, detailing theName, HPCSA registered number and the hours provided in support.
SASP is required to apply for accreditation and to supply letter ofconfirmation of the physiotherapist’s active involvement with the‘Buddy System’ and to be invoiced accordingly - individual physio topay for the capture of points. ▲
▲
26 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
PROFESSIONAL ETHICS (MEDICAL / DENTAL)• 1 point per hour - Two points per year in professional (medical / dental) ethics will be required from
all practitioners. - NON-CLINICAL BUT HEALTH RELATED ACTIVITIES
• Health Care related but not necessarily clinically related - 1 Point per hour. A maximum of 5 points may beobtained in non-clinical but health related activities in any one year.
• A maximum of 5 points may be allocated to non-clinical degrees/diplomas• A Maximum of 5 points may be obtained in non-clinical but health related activities in any one year. This
restriction relates primarily and specifically to business practice and activities related to administration and management. Clinical - defined broadly as
(ii) ‘Pertaining to or founded on actual observation and treatment of patients, as distinguished from theoretical or basicsciences’
(iii) Activities specifically associated with the SPECIALITIES of community health and community dentistry. (iv) Activities, which may in the assessment of the Accreditor, be clinically relevant to participating practitioners, will be
considered.(v) A maximum of 5 points limitation for non-clinical, but health related activities is not applicable in activities provided
by a department of Community Health and which involves primary health care.
▲
Society Matters
SmileA Christmas
taleused to love Christmas when I was a little girl. We always had a real pine tree, shedding needles andthe sharp smell of resin; the pressies under the tree
were few (we weren’t very well off), but that madethem all the more exciting; and Mom used to bring outthe whitest of table cloths, shiny good silver, and candles for a feast of turkey, home-made Christmaspudding and artery-clotting brandy butter. It was atime for family; a time for going to church and givingas much as you could for those less fortunate than you;a time for being thankful. Even if you didn’t believe inthe biblical Christmas story, living out the ancient tra-ditions associated with the time of year filled you withthat spirit of generosity and love.
Am I just an awful cynic for thinking that the spirithas gone out of Christmas? It seems to all be spend,spend, spend, eat, eat, eat, drink, drink, drink... That’swhy I and my husband try to get away into the coun-tryside, at this time, away from the madding crowds, sowe can try to experience some of the old spirit in thecompany of those we love.
And I do hope that your Christmas is rich in love andall good things, but meanwhile the cynic in me offersyou some carols for our era:
Deck the boards with food so stodgyFalalalala lala la la‘Tis the season to get podgyFalalalala lala la laChristmas pudding, brandy butterFalalalala lala la laThen we’ll moan because we’re fatterFalalalala lala la la!
IGod rest ye merry, gentlemen, let nothing you dismayYour wives are doing all the work upon this festive dayThe stuffing of the turkey and the washing up, oh boy!What tidings of comfort and joy (for you anyway)Oh tidings of comfort and joy!
While parents wrapped their gifts by night, all seated round the treeA little angel stole downstairs, and oh, what did he see?“Old Santa Claus is just a joke, I know the truth,” he cried“‘Tis Mom and Dad who dish the gifts, ‘tis them I have espied!”
Away in a cluster, no room for a pineThe tree is pink plastic with a luminous shineThe holly is fabric, the mistletoe too,And the cottonwool snow is stuck on with some glue.
Oh, come, all ye wealthy, joyful and triumphantOh, bring all your bonuses to spend in the mall.You won’t behold us, poor and sick and starving,Oh come, let us be thoughtful, Oh come, let us be kindly,Oh come, let us be lovingOn Christmas Day!
Reprinted with kind permission from SkywaysDecember 2001
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 27
What’s Up
The Northern Cape Branch of theSASP, reports that members in theKimberley district recently provideda physiotherapy service and the SA Korfbal Tournament, which was held in Kimberley itself from 1-6 July.
“We would really like to thank Head Office for thewonderful promotionalitems and banner that wereceived in the week priorto the tournament. Theywere well used!” saysJanice Hall, chairman ofthe Northern Cape Branch(Janice can be seen withsome of the promotionalgoodies in these photos.)
“From our statistics,33% of the injuries we
treated were lateral ligament injuriesof the ankle, 16% were injuries to the finger joints, 14% wereAchilles tendon injuries, 10% patellatendinopathy. There were also indi-viduals with quadriceps, glutes andgastrocnemius injuries, as well as a neck injury.” Sounds like fun,huh!
FOR THEPROFESSION
If you are ever called upon to talk about the professionanywhere - for example, atCareers Night at your chil-dren’s school, or anything similar - it will surely interestyou to know that Head Officehas presentation materialsavailable about the scope ofthe profession, the require-ments, the qualifications andanything else you need toknow. Contact CEO Saira Khanon (011) 485-1467 if you’d liketo use this material.
Access-a-bus
Hands, knees, heels and ankles...
utco Limited is justifiably proudof one of its buses which travels
along the Pretoria, Mamelodi andShoshanguve routes on a dailybasis. The reason: the bus has beenspecially designed and adapted tocater for disabled passengers on itsPretoria routes.
The bus, designed and built locallyat Putco’s Dubigeon bus construc-tion plant in Brits, is the only suchroute-bus operating in this area. Thebus operates two routes in themorning: one from Mamelodi to thePretoria Academic Hospital, whichis next to a job centre where manyof the passengers are employed.
The second route, which carries a full load of 26 passengers, departs from Ruth First Road inShoshanguve and travels via thePretoria CBD, where many of thepassengers are employed, to thePretoria Academic Hospital. Thereis one afternoon route which trans-
ports all the passengers home toShoshanguve and Mamelodi.
“In order to render this service toPutco’s special passengers on the‘access bus’, two driver/conduc-tors are required for each leg of the journey. One driver/conductoroperates the wheelchair lift, assistswheelchair-bound passengers totheir seats, and also assists visuallyimpaired and blind passengers.The other driver/conductor drivesthe bus,” says Trevor Wickham,Mamelodi Strategic Business UnitManager: Putco Ltd.
The vehicle has an area wherewheelchairs can be anchored to the floor and a wheelchair storagearea for passengers who are able tosit on specially-designed seats. Thebus is driven by a specially-traineddriver, and regular passenger fairsare levied.
The main purpose for Putcoimplementing this service, Wickham
says, is to make public transportmore accessible to disabled peopleand to give them a greater degree ofindependence.
“The demand for such a serviceexceeds supply at the moment, butPutco is hoping to extend this ser-vice on some of its other routes inthe future,” says Mr Wickham.
SASP President-elect Zola Dantileattended the unveiling of the bus tothe media, and was very impressedby the service. This is the only busof its kind in South Africa so far,according to Wickham, althoughJoburg Metro does have a buswhich can lower its suspension -that is, bring its front door down tobe on the same level as the pave-ment, although obviously this doesnot make the service accessible towheelchair users.
It would be useful to develop adatabase of services like this whichare really helpful to people withdisabilities. Let us know if you haveany special services offered in yourarea by faxing (011) 674-3804 or e-mailing [email protected].
P
TEACHER I NEED YOU...
Do you teach a Back and Neckclass? You do? Then please get in touch with us! Lots of physiosdon’t, and many would like tosend their patients to classes - if only they knew who offeredthem... So we’re trying to collate a list of all Back and NeckClasses offered round the coun-try. Send details (name, contactnumbers, suburb and town, plustimes if possible) to us via fax at (011) 674-3804 or e-mail [email protected].
28 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
What’s Up
So in essence, among major membership categories, theincrease is barely discernable. An example is thatCategory A members currently pay R1720 (which is the basic fee, PhysioFocus subs, Website/Directoryaccess and Malpractice Insurance). In 2003, this cost isR1850.00. (Public Liability insurance is an add-on.)
For all the detail on the new fees, see the Fee StructureDiagram on page 29.
CPDOur negotiations with the HPCSA continue regardingcost-effective ways of obtaining CPD points. Further tothis, Professor Sielie Eales and I have been workingwith our web designers to provide our members withCPD Journal articles online. Watch this space for further information. You may ask, “What about physio-therapists who don’t have access to the Internet?” Wehave covered this as well. The Journal will have a questionnaire within it which you can complete andsubmit for CPD points.
All in all, we have had a hectic year at Head Office,but we are well on our way to attaining our objectiveswhich are:
a) Good accounting principles and accountability forfunds entrusted to our care.
b) A customer-orientated atmosphere, with emphasison rendering excellent service to our members.
c) A conducive work environment that will enable us toretain our staff and thus be more productive.
d) Contributing to the wellbeing of our profession andmembers by ensuring adequate and appropriate representation within the health care arena.
According to The Nando Times, 26 October 2002, a new study showsthat women describe very differentsymptoms from men when they’resuffering a stroke, a difference thatmay affect how female patients getemergency treatment.
“Overall, researchers found thatwomen were 62 percent more likelyto say they were feeling sensationsthat aren’t on the traditional list ofstroke symptoms.
Traditional stroke signs includesudden changes in sensation, walk-
ing ability, balance, motor functions(including paralysis of one side ofthe body), speech, language abilities,facial muscles, vision and dizziness.
Less familiar symptoms like face pain and limb pain; disorien-tation and change in consciousness; various neurologic symptoms likehiccups, nausea and general weak-ness; and symptoms that aren’tlikely to be brain-related, such aschest pain, shortness of breath andpalpitations are more likely to bereported by women.
News from Head Office - CEO Saira Khan reports
ead Office is busy streamlining processes to ensurethat we have, and adhere to, good accounting prin-
ciples. We have worked closely with the auditors to getcurrent and have been implementing good accountingprocesses to provide us with meaningful managementreports. We have appointed Yvonne Day as our book-keeper with effect from 1 November 2002. Lee Partingtonresigned at the end of August due to ill health.
We are also in the process of appointing a new secretaryfor the CEO and President, as Michelle Nair has movedon to greener pastures. We hope to have someone in byDecember or January 2003.
Americo Pinheiro was appointed in September 2002as the PR/Marketing Consultant for the Society. He hasbeen tasked with selling advertising space in our publications and on our website and will also beinvolved in the marketing and PR activities of theSociety. We welcome him to our organisation and aresure he will do very well. (Check the interview withhim on page 30 in our magazine).
MEMBERSHIP FEESThe membership fees have been finalised and we arepleased to announce that the increase has been kept toa minimum and further, that we now have a basicmembership fee with the malpractice insurance beingcompulsory, but also that our members now have thechoice of applying for benefits that pertain to their individual needs. We have opened up belonging toPhysioFocus because we believe that even one-manpractices who earn less but work independently are private practitioners.
We did not have an increase in 2002 and have left our income at virtually the same level as it was in 2002.
H
Gender differences in stroke presentation
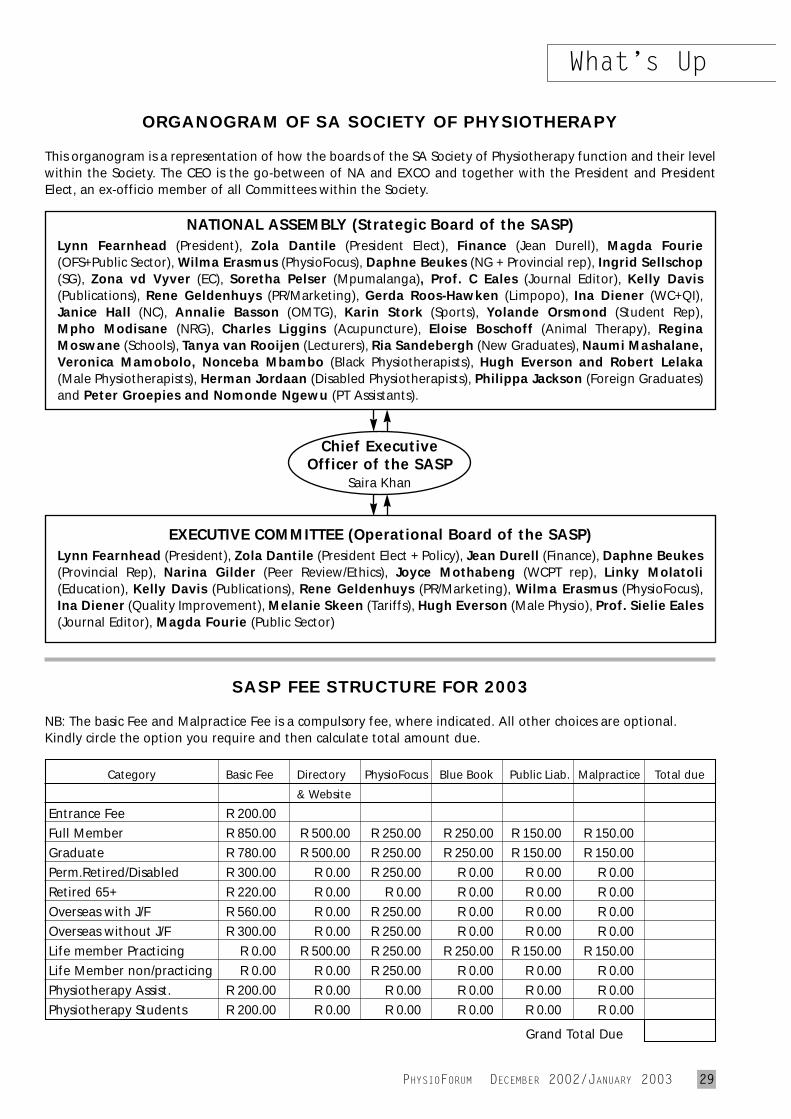
ORGANOGRAM OF SA SOCIETY OF PHYSIOTHERAPY
This organogram is a representation of how the boards of the SA Society of Physiotherapy function and their levelwithin the Society. The CEO is the go-between of NA and EXCO and together with the President and PresidentElect, an ex-officio member of all Committees within the Society.
SASP FEE STRUCTURE FOR 2003
NB: The basic Fee and Malpractice Fee is a compulsory fee, where indicated. All other choices are optional.Kindly circle the option you require and then calculate total amount due.
Category Basic Fee Directory PhysioFocus Blue Book Public Liab. Malpractice Total due
& Website
Entrance Fee R 200.00Full Member R 850.00 R 500.00 R 250.00 R 250.00 R 150.00 R 150.00Graduate R 780.00 R 500.00 R 250.00 R 250.00 R 150.00 R 150.00Perm.Retired/Disabled R 300.00 R 0.00 R 250.00 R 0.00 R 0.00 R 0.00Retired 65+ R 220.00 R 0.00 R 0.00 R 0.00 R 0.00 R 0.00Overseas with J/F R 560.00 R 0.00 R 250.00 R 0.00 R 0.00 R 0.00Overseas without J/F R 300.00 R 0.00 R 250.00 R 0.00 R 0.00 R 0.00Life member Practicing R 0.00 R 500.00 R 250.00 R 250.00 R 150.00 R 150.00Life Member non/practicing R 0.00 R 0.00 R 250.00 R 0.00 R 0.00 R 0.00Physiotherapy Assist. R 200.00 R 0.00 R 0.00 R 0.00 R 0.00 R 0.00Physiotherapy Students R 200.00 R 0.00 R 0.00 R 0.00 R 0.00 R 0.00
Grand Total Due
EXECUTIVE COMMITTEE (Operational Board of the SASP)Lynn Fearnhead (President), Zola Dantile (President Elect + Policy), Jean Durell (Finance), Daphne Beukes(Provincial Rep), Narina Gilder (Peer Review/Ethics), Joyce Mothabeng (WCPT rep), Linky Molatoli(Education), Kelly Davis (Publications), Rene Geldenhuys (PR/Marketing), Wilma Erasmus (PhysioFocus),Ina Diener (Quality Improvement), Melanie Skeen (Tariffs), Hugh Everson (Male Physio), Prof. Sielie Eales(Journal Editor), Magda Fourie (Public Sector)
Chief ExecutiveOfficer of the SASP
Saira Khan
NATIONAL ASSEMBLY (Strategic Board of the SASP)Lynn Fearnhead (President), Zola Dantile (President Elect), Finance (Jean Durell), Magda Fourie(OFS+Public Sector), Wilma Erasmus (PhysioFocus), Daphne Beukes (NG + Provincial rep), Ingrid Sellschop(SG), Zona vd Vyver (EC), Soretha Pelser (Mpumalanga), Prof. C Eales (Journal Editor), Kelly Davis(Publications), Rene Geldenhuys (PR/Marketing), Gerda Roos-Hawken (Limpopo), Ina Diener (WC+QI),Janice Hall (NC), Annalie Basson (OMTG), Karin Stork (Sports), Yolande Orsmond (Student Rep), Mpho Modisane (NRG), Charles Liggins (Acupuncture), Eloise Boschoff (Animal Therapy), ReginaMoswane (Schools), Tanya van Rooijen (Lecturers), Ria Sandebergh (New Graduates), Naumi Mashalane,Veronica Mamobolo, Nonceba Mbambo (Black Physiotherapists), Hugh Everson and Robert Lelaka(Male Physiotherapists), Herman Jordaan (Disabled Physiotherapists), Philippa Jackson (Foreign Graduates)and Peter Groepies and Nomonde Ngewu (PT Assistants).
What’s Up
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 29

30 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
What’s Up
TENNIS ELBOW, FOOTBALL KNEE?Agnes Wenham has sent us a translation of a German article:Those who play football end up bow-legged. Althoughthis might be obvious, it has never been the subject ofscientific investigations till now. Thanks to a study byBrik Witrouw of Gent University, we now have proof.Five hundred footballers were tested and found to be10 times more prone to being bowlegged than the general population. Every fourth footballer showed acharacteristic bend to the outer leg muscles. From theage of 13, there is an increase in bow-leggedness as wellas in the degree of deformation. The cause for thechange, according to Witrouw, is an asymmetrical pullon the knee joints.The inner muscles infootball players arestronger and shorterthan in non-players,and as a result abanana-shaped sil-houette appears to be present when run-ning. Players with severe conditions are more likely tosuffer from injuries. “We don’t want to cause panic,”says Witrouw. “Playing football can be wonderful too.”Nevertheless he recommends that players should takepreventative measures. The inner thigh muscles(adductors) should be stretched frequently and theouter thigh muscles (abductors) should be strengthenedby special exercises.
JUST STRETCH - NOT!Reuters Health reported on 30 August that “Contrary towidely held beliefs, stretchingbefore or after exercising doesnot prevent muscle soreness,according to a report byAustralian researchers. ‘Wefound clear evidence thatstretching...does not preventmuscle soreness,’ lead authorRob D. Herbert, from theUniversity of Sidney, toldReuters Health. ‘There is alsoquite strong evidence that
stretching does not reduce injury risk- although thegenerality of this finding is unclear,’ he added.
The authors reviewed English language studies published between 1949 and 2000 that investigated theeffects of stretching before and after exercise on musclesoreness, risk of injury and athletic performance.
Have a heart - walkPostmenopausal women whowalk regularly lower their heartdisease risk just as much aswomen who do more vigorousexercise, according to research published in the September 5thissue of The New England Journalof Medicine.
Dr JoAnn E. Manson, fromHarvard Medical School in Boston,and colleagues asked 73,743 women between the agesof 50 and 79, about the amount and types of physicalactivity they engaged in each week. None of thewomen had cancer or cardiovascular disease at the out-set. Over the next three years, 345 of the women devel-oped heart disease, but those who either walked orexercised regularly were less likely than others to devel-op cardiovascular disease, the investigators found, andboth activities were associated with the same reductionin risk. A brisk pace was the most beneficial, but evenslowcoaches who ‘covered 1 mile in 15 to 20 minutes’were protected.
However, sitting for prolonged periods undid someof the protective effect; women who did the same levelof exercise but sat for longer during the day were morelikely than others to develop cardiovascular disease.
PROFILE
Renaissanceman!
Americo Pinheiro, who joinedus in September as the PR/Marketing Consultant, bringsa very varied working expe-rience to bear on the job.Born in Germiston, Americo completed his schoolingat Germiston High and went on to study Videoand Film Technology at the Pretoria Technikon.He also earned himself a diploma in advertisingfrom Birnam Business College.Among the jobs he has held since then are: areamanager for a gun shop, manager of an art galleryand auction house, salesman of granite kitchencounters and manager of a bait-and-tackle shop!Americo is single, has no children, and is, he insists,well-behaved. He plays action soccer on Fridaynights, clubs away the weekends, cheers for theLions whenever they play and plays the oddround of golf.
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 31
Bio-Oil Ad to go on this page
Full Page AdBlack & White and 1 spot colour: orange
32 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
start of the World Cricket Cup andwill overlap with the 2nd WorldCongress of Science and Medicinein Cricket, which will also be heldat the Spier Estate.
FIMS, the International SportsMedicine Federation, will be
holding their Executive Meeting in conjunction with the SASMACongress, and international opinionleaders from the cricket medicinefraternity and from FIMS will participate in the SASMA Congressas guest speakers.
The SASMA Congress academicprogramme will include scientificpaper presentations, poster presen-tations and workshops on topics ofclinical significance. The followinginternational speakers have alreadybeen confirmed;
• Professor Karim Khan - co-authorof the best-selling textbookClinical Sports Medicine.
• Professor Roger Barlett - Directorof the Centre for Sport andExercise Science at HallamUniversity, Sheffield.
• Dr Sandy Gordon - NationalChair of the Australian Collegeof Sports Psychologists
• Dr Paul Hodges - AssociateProfessor in the Department ofPhysiotherapy at the Universityof Queensland.
• Dr Sam Headley - AssociateProfessor of Exercise Physiologyat the Springfield College inMassachusettes
• Professor K M Chan - Presidentof the International SportsMedicine Federation
• Professor Walter Fontera -Secretary General of theInternational Sports MedicineFederation
For further information contact;
The congress organiser: The Marketree on tel 083 753 2937,fax 011 896 2979, e-mail [email protected] OR The congress secretary:Miss Desiree Sellner ontel. 031 201 6653, fax 031 201 6653,e-mail [email protected] ORVisit the SASMA websitewww.sasma.org.za
for people with disabilities.This is the first WCPT Congress
to be planned by an InternationalScientific Committee, and the first to be managed centrally byWCPT, in collaboration with thehost organisation. More than 2400abstracts have already been sub-mitted for presentation at theCongress, ensuring that the care-fully selected programme will bevaried and of the highest quality.
“The fact that so many people areprepared to present material to thisCongress in itself indicates that theprofession is achieving new levelsof confidence,” says Elizabeth Ellis,Chair of the WCPT InternationalScientific Committee. “The Congresswill be a rare opportunity for cli-nicians to stop what they’re doing,and take a long hard look at wherewe’ve come from and where we aregoing.”
Further information is available onthe WCPT website: www.wcpt.orgor contact WCPT direct:WCPT, 46-48 Grosvenor Gardens,London SW1W 0EB.Tel: 44 (0) 20 7881 9234.Fax: 44 (0) 20 7881. 9239.E-mail: [email protected]: www.wcpt.orgRegistration deadline:31st December 2002 for ‘early bird’reduced fees, 20th May 2003 finaldeadline.
ver 3000 physical therapists willgather in Barcelona on 7th-
12th June 2003 for World PhysicalTherapy 2003 - the internationalcongress of the World Confederationfor Physical Therapy (WCPT).Delegates will have a uniqueopportunity to debate the clinicaland professional issues that willforge the profession’s global future,establish links with colleaguesaround the world and experiencethe sites and culture of this bea-utiful city.
“This will be totally differentfrom the sort of national conferencesmany physical therapists aroundthe world have experienced,” saysElizabeth Ellis, who has headed theprogramme planning process. “Itwill be truly international, chartingthe global agenda for physical therapy - so it will be relevant andimportant whatever part of theworld you come from.”
Highlights will include:• A series of symposia and panel
discussions, where experts andopinion leaders will explore current issues in lively debates
• Focused workshops examiningareas of special interest
• Key presentations examining thefuture direction of physical the-rapy, the implications of new disability classifications for healthprofessionals, and human rights
O
INTERNATIONAL EXPERTS FOR SA SPORTS MEDICINE CONGRESS
he 10th Biennial Congress of the South African Sports
Medicine Association will be heldat the Spier Estate in Stellenboschfrom February 9-11, 2003. The timing of this congress will coin-cide with the Official Opening and
14th WCPT International Congress -you’ve got to be there!
The opportunity of a lifetime
T
What’s Up
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 33
It is fully within the right and competence of physiotherapistsand podiatrists registered with theCouncil to issue sick-leave certifi-cates to their patients in appropri-ate circumstances, according to theExecutive Committee of Council.
This finding follows recom-mendations by the ProfessionalBoard for Physiotherapy and theProfessional Board for Podiatry.The Executive Committee said inits ruling that it was “within therights of a physiotherapist and a
podiatrist to indicate whether apatient was unable to work, pro-vided this related to the scope ofphysiotherapy or of podiatry.
The above ruling has recentlybeen confirmed by Council.(Bulletin. NUMBER 16. OCTOBER 1993, p. 4)
PHYSIOTHERAPISTS AND PODIATRISTS MAY ISSUE SICK CERTIFICATES
IN MEMORIAM
BARBARA TYRREL THOMPSON31st March 1934 - 1st September 2002
Barb (also known as Thompie to the hockey fraternity)was born in Uitenhage and educated in Pretoria andPietermaritzburg. She always wanted to be an accoun-tant and spent the first ten years of her working lifewith the railways as a bookkeeper before leaving forPretoria to study physiotherapy.
She qualified in 1965 and worked off her NPA con-tract at Edendale hospital on the outskirts of Pieter-maritzburg. In 1969 she opened a private practice withRuth Odams in the first medical centre. In 1988 shejoined Sheila Blackwood’s practice at Westville hospitalas administrative partner until her retirement in 1993.
Barb represented the Natal Midlands branch of theSASP at numerous council meetings and held the postof branch secretary from 1965 to 1969. When the PPAnational executive moved to KZN from 1978 to 1982Barb served as treasurer for this period. Her contri-bution to the SASP will live on in the lives of the manybranch treasurers and secretaries she trained and men-tored. Although a very shy person, Barb was always veryvocal in her support of the underdog and fought manybattles with medical aids on behalf of her patients.
Barb was a keen hockey player and played for theNatal B side. She later became the manager of thisteam and then turned her talents to umpiring. She was well respected for her fair and unbiased blowing.One of her proudest moments was receiving her greenand gold Springbok blazer when she umpired her firsttest match.
In between these activities Barb also became involvedin the administrative side of women’s’ hockey. Shebecame fixtures secretary for Pietermaritzburg andlater served as their chairperson as well. Barb also heldthe post of Natal chairperson for a number of yearsbefore moving on to become treasurer for the All SouthAfrica Women’s Hockey Association.
Barb will be sadly missed as a person as well as for thelarge contribution she made to the SASP, and the NatalMidlands branch in particular, with her accounting andadministrative skills.
Physiotherapy Intervention for High
Performance ProgrammeThe Sports Science and Medical Committee (SSMC), a joint committee consisting of representatives from the South African Sports Commission (SASC), HighPerformance Programme and the Medical Commissionof the National Olympic Committee of South Africa(NOCSA) is presently in the process of establishing anational database for physiotherapy service providers.
Physiotherapy intervention was recently included inthe High Performance Programme and will coveraspects of preventative, therapeutic and rehabilitativeservices, which an athlete will derive benefit from tooptimise his/her performance.
Guidelines on intervention:• The cost of physiotherapy intervention will be borne
by SASC/NOCSA provided that:- The physiotherapist is accredited by the SSMC.- The fees are charged according to the scale of bene-fit (RAMS) and guidelines as laid down by the Boardof Healthcare Funders. - A detailed report on the evaluation, treatment andrecommendations accompanies the account. - Prior approval is obtained from the relevant accre-dited testing centre.
• Intervention will be provided to athletes based ontheir performance-based categorization, the need forsuch intervention, and with the recommendation ofthe regional medical coordinator.
• All service providers must be registered with theHealth Professionals Council of South Africa and theSouth African Society of Physiotherapy. In order to objectively accredit and categorize service
providers in the various regions, interested physiothe-rapists are requested to complete the attached accre-ditation form and return it to: Dr Nicola AppelcrynHigh Performance Programme, SA Sports CommissionP O Box 11239, Centurion 0157Tel: 012 - 677 9735 / 082 411 6148Fax: 012 - 677 9858 / 663 6410E-mail: [email protected]
What’s Up

34 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
he tiny babies lie side by sidein their transparent cots in St Mary’s Hospital’s high-care
nursery. A little mouth gasps forair; two little noses have tubes upthem. One baby pulls up her pencil-thin legs, stomach taut with pain.
Pain is one of the few thingsthese babies will know well beforethey succumb to infections such aspneumonia, gastro-enteritis, tuber-culosis and meningitis, their bodies’immunity immobilised by the ram-pant HI virus passed on to them by their mothers.
There are no last rites for thosetoo small to speak. They die quickly,wordlessly at a rate of about five aweek. One dies while I am there.Their mothers, huddled besidethem, bowed over and silent, knowthat their babies are on death row.Sister Philomena Pakade, whoheads the paediatric ward of thehospital, is so burdened by thisknowledge that it makes her wishshe were young enough to changeprofessions.
“Children are dying like flies,more especially the very smallbabies,” says Pakade heavily, show-ing me the list of ‘RIPs’ noted downin a small brown exercise book. “InJuly, we had a death almost everyday. These little ones suffer somuch. They have just come into theworld and the world is so cruel tothem.”
Around three-quarters of the 200children admitted each month areHIV-positive. “We get so excitedwhen we get an HIV-negativechild,” says Pakade. “We sit withthe mother and talk and educateher about HIV and prevention.”
Elsewhere in the busy paediatric
ward, toddlers scream from theircots. Skin conditions are endemic -one child’s entire face is coveredwith angry red pustules of impetigo,or veld sores.
“We didn’t used to see impetigothis bad,” says Dr Douglas Ross,superintendent of the Marianhill-based hospital that is owned by theCatholic Missionary Sisters of thePrecious Blood. Ironically, now theprecious blood of most of theirpatients is infected with HIV, andthis is causing unusual presenta-tions in a number of diseases fromimpetigo to TB.
SEXUAL ABUSEA 10-year-old girl lies on her side ina corner of the ward, staring outinto the room. Too big to have beeninfected at birth, Ross suspects she is being sexually abused by afamily member.
“This year we have noticed a bigincrease in HIV-positive childrenbetween the ages of four and 10. We suspect it is because of sexualabuse,” says Pakade.
The 234-bed St Mary’s serves apopulation of about 750 000 peoplein the west of Durban’s vastmetropolis, 250 000 of whom areestimated to be living with HIV. Itgets an 84% state subsidy and noone is turned away from the spot-less hospital although the patientload has increased considerably asthe HIV epidemic has turned intoan AIDS epidemic.
“Our patients are much sickernow than they were 10 years ago,and 50% of them are going to die,” says Ross, who has been at St Mary’s for seven years. “We havehad to change our expectations
about who is going to get better,and also start to pay attention tocaring for the carers.”
The hospital soon realised itcould never deal with the demand,and has thus become heavilyinvolved in community outreach.Its outreach team has trained a network of about 200 volunteers tohelp families to care for their dyingrelatives at home.
Preparation for death has becomeroutine at the hospital too, and aRotary-sponsored palliative careward for those at the end of theirlives came into operation at the end of October. This will be run byvolunteers, and serve patients whocannot get home-based care.
The mounting deaths have pre-sented a new challenge. “We have a problem of abandoned bodiesrather than babies,” says Ross, withan ironic laugh. “We have to crematethe unclaimed bodies as there’s nospace left in the city for paupers’burials and this cost the hospitalabout R48 000 last financial year.”
But while death is now routine, it still takes its toll. “There is a high level of staff burnout,” saysRoss. “Staff have to deal with anincreased workload, dying patientsand, at a personal level, with theeffects of HIV in their own families.Every four or five months, one ofmy staff members dies.”
Increasing pressure on St Mary’smakes it feel at times as if the hos-pital is like the little boy in theDutch fable who is trying to stop aleak in a massive dyke with histhumb, says Ross.
Nevertheless, the hospital has theremarkable ability to attract funds -and everything from furniture to
An island of hope in a sea of need
Kerry Cullinan of health-e news visits St Mary’s Hospital
T
Feature

PHYSIOFORUM DECEMBER 2002/JANUARY 2003 35
Feature
incubators seems to have beendonated. It has also managed toattract a number of other organisa-tions to its premises to start smallbut promising initiatives aimed atfighting back against the tidal waveof HIV/AIDS.
REACHING MOMSSt Anne’s Clinic on the hospitalpremises is at the heart of these initiatives. The Catholic MedicalMission Board runs a prevention of‘parent-to-child’ HIV transmissionprogramme. Headed by a straight-talking nun, Sister Christa MaryJones, the programme is trying toreach the 6 000 mothers who deliverbabies each year in the district toensure that their little ones don’tend up dying in Pakade’s paedia-tric ward.
A recent MRC survey found that54% of pregnant women in the district were HIV positive andJones’s record book is a mass ofred-pen positive entries.
“It’s a scary number and we’vehad our sadnesses,” Jones acknow-ledges. “But we are planning forthe future with the HIV-positivemums. They get ongoing coun-selling and they feel so bondedwith the counsellors they are likelimpet mines! We can really see theeffects of a positive message ontheir health.”
In the clean, bright ante-natalclinic, counsellors spend an entirehour counselling a patient (thenational average is 20 minutes)before the HIV test. During thistime, they explain how HIV istransmitted and prepare them forthe results. If positive, the womenare encouraged to get the anti-AIDSdrug nevirapine for themselves andtheir babies and to breastfeedexclusively for six months and thenwean rapidly. [Breastfeeding is stillthe preferred option where cleanwater is not available and womencan not afford formula, but babiesdo risk infection, so they must be weaned as soon as it is possible.Ed] Since the project’s launch in
January, the four-person staff hasreached around 900 women and anastounding 96% have agreed totake the test.
Next door, the University ofNatal and Harvard Medical Schoolare in the process of launching aclinical study to explore the effectsof short courses of anti-retroviral(ARVs) drugs to boost the long-term immunity of babies with HIV.
POSITIVE BABIES“St Mary’s is ideal because it istruly a community-based hospitaland this presents an opportunity tonot only treat individuals but toreach out to a community,” saysHarvard’s Dr Krista Dong.
Thirty babies will be enrolledfrom St Mary’s ante-natal clinic.After confirming that they are HIV-infected, 10 babies will have anti-retroviral treatment delayed untilthey start presenting with AIDS-related symptoms.
Ten will start ARVs immediatelyafter diagnosis (shortly after birth)and ten will also start immediatelybut the drugs will be given at setintervals with breaks in treatment,called ‘structured treatment inter-ruption’ (STI).
The idea behind the STI study,says Dong, is to get the babieswhen their immune systems arestill intact and to teach theirimmune systems to recognise thevirus and develop an immuneresponse to keep it in check.
The three-year trial will have ayear of treatment followed by twoyears of close clinical monitoring ofthose on the STI arm. The year oftreatment will be interrupted threetimes. Throughout the treatment
and interruptions, each baby willbe monitored intensively, and thedrugs will be restarted as soon asthe HIV in the babies’ blood risesabove a certain level.
Once the scheduled treatment isover, if any of the babies developsymptoms of AIDS, their motherswill have the option to restart themon ARVs. Their parents will also beable to access care through theIthemba Centre, which is beingplanned alongside the STI study.
ARV PROJECTThe Ithemba Centre is the brain-child of the hospital’s Dr Kay Ajao,a gregarious young doctor given to big hand gestures and aims tooffer 1 000 adults anti-retroviraldrugs within two years.
Patients will be drawn from fourgroups: hospital staff, communityoutreach volunteers and peoplefrom the households they serve,outpatients and parents of babieswho have been through SisterJones’s ante-natal clinic.
“We aim to start in the next sixweeks with 20 people,” says Ajao.“We have managed to get moneyfrom the Doris Duke Foundation andthe San Francisco AIDS Foundationis getting the drugs donated.”
Ross says the centre only hasabout half the money it needs, butthey’re starting it anyway and hopeto raise the balance as they goalong.
Ithemba, which means hope inisiZulu, also plans to offer ongoingcounselling and support to thoseliving with HIV, providing a homefor those who feel as if they are outcasts because of the stigma asso-ciated with AIDS.
Tiny and embattled, St Mary’scelebrates its 75th anniversary thismonth at a time when Ross is tryingto raise R3-million for the operatingcosts that no one wants to fund.Despite few role models and a seaof need, the hospital staff and itssupporters are fighting back with aquiet but dogged determinationthat is inspirational.
36 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
pring is in the air and in thehearts of the seven eagerrepresentatives from the fol-
lowing universities: University ofCape Town, University of Durban-Westville, University of the FreeState, University of Pretoria,University of Stellenbosch,University of the WesternCape, University of theWitwatersrand.
The first annual meeting ofthe National PhysiotherapyStudent Council (NPSC) 2002/2003 was held in Pretoria from20-22 September 2002. It is agreat privilege for physiothe-rapy students nationwide tohave a national student body,which allows them to have avoice at National Assembly.
Various matters were dis-cussed during the weekend.The NPSC meeting gave thestudents the opportunity todiscuss the structure (andpotential problems and issues)of the physiotherapy course ateach university. Communityservice is still quite a thornyissue for all parties involved, andall the chairpersons said it was apriority to keep the students fromthe respective universities properlyinformed.
At the end of the weekend, thechairpersons voted for which port-folio within the NPSC would beallocated to each of them. Goodluck to all with this extra respon-sibility; may you make it worth-while. Yoland Orsmond (TUKS) wasNPSC chairperson for 2001/2002and was responsible for organizingthe whole weekend and taking thechair during the meetings. A sincereword of appreciation to Yoland: her continuous effort during her2001/2002 term ensured that the
NPSC of 2002/2003 got off to asmooth start.
Just a quick glimpse into theactivities of all the well-balancedphysiotherapy students at therespective universities!
UNIVERSITY OF CAPE TOWN (UCT)
Lauren Walker is the chairperson of UCT’s Physiotherapy StudentCouncil; and being an extra skilledgirl, she was also elected as chair-person of the National Physiothe-rapy Student Council (NPSC) for2002/2003 - congratulations!
The physiotherapy studentsplayed an active role in manysporting events such as the TwoOceans Marathon, Argus Cycle Tour,South African Veteran’s TennisTournament, Artscape Dancing Per-formance and UCT rugby matches.UCT is affiliated with New Balance- selected third and fourth year students offer their services at the
events sponsored by New Balancesuch as the Men’s Health Surf SkiSeries and the Milkwood and SADMarathons. New Balance has kindlyagreed to manufacture all the UCTphysiotherapy uniforms in 2003.
The first year students arefocused on creating a studentroom, a long awaited dreamsoon to be realised. The secondyears are responsible for theFirst Year Welcome, which is a social evening where thenew students are introducedand a large amount of pizza is consumed! The third yearsorganised an amazing Physio-therapy Formal, which wasattended by staff and studentsand thoroughly enjoyed byall. They also organise cham-pagne and snacks for thefourth year pre-graduationcelebration. The mentoringsystem was introduced thisyear where third and fourthyear students were each allo-cated eight first years, whowere able to contact theirmentors at any time with any
queries or problems.There were two events which
gave the students a feeling of prideand accomplishment: the first wasthe strapping competition. For thefirst time in many years, UCT madeit to the finals! Congratulations toUDW for winning the competition:we look forward to seeing youagain next year!
The second - the main fundraisingevent - was the UCT Physio GolfDay in aid of the ‘Hear Fanie deVilliers Foundation’ for cochleaimplants. It was a highly successfulday which ended with a prize-giving and dinner. The planned2003 Golf Day promises to be evenmore spectacular!
Physio phunWhat did the students do last year, and what are their plans for 2003?
S
From left to right - Back: Henriëtte Tredoux,Elet Steyn and Lauren Walker.
Front: Marlize Jordaan and Adele Geldenhuys.
Student News

PHYSIOFORUM DECEMBER 2002/JANUARY 2003 37
Student News
2003 looks busy and excitingalready and includes new ideassuch as working at the ComradesMarathon and creating awarenessof the SASP in the hope that all students will participate activelyand join the SASP.
Finally, in acknowledgement ofhis hard work and determination, asincere thanks to Heath Matthews,Head Student 2002, for being thefounder of the UCT PhysiotherapyStudents Council.
UNIVERSITY OFDURBAN-WESTVILLE (UDW)
Melusi Mtshali, National AssemblyOfficer of the NPSC, was elected toserve as Chairperson of the appro-ximately 165 students who studyphysiotherapy at the University ofDurban-Westville. The studentcouncil consists of a chairperson,vice-chairperson, general secretary,treasurer, fundraising officer, publicrelations officer, sport and enter-tainment coordinator and a com-munity enrichment project officer.
The physiotherapy students atUDW are quite fortunate to be ableto participate in quite a number ofsporting events in the Durban area,such as the Newlands Marathon42.2km, the Thomas Moore run/walk, the tour Durban Cycle race,the Dusi marathon, Craven week,and the Comrades marathon.
Community involvement is a priority as well. The fourth yearsgive presentations during theirclinical community block on topicssuch as burns, the effects of cigarettesmoking, HIV/AIDS, ante-natal carean haemophilia - a total of eighttopics are covered and will be puttogether in a booklet. This bookletwill then be handed out in the ruralcommunities who have not yetbeen exposed to physiotherapy.
An annual Physiotherapy Balland a fun day before the firstsemester examinations are the twomain social events that dominatedthe 2002 calender - even more exciting events are proposed for2003, so be prepared.
Academic support for all physio-therapy students is in place, andspecial attention is given to firstyears who need to cope with thedemands of University student life.
UNIVERSITY OF THE FREE STATE (UFS)
Henriëtte Tredoux, secretary of theNPSC, is the more than capablechairperson of the UFS Physio-therapy Student Council. There arefive people on the PhysiotherapyStudent Council with her: vice-chairperson, secretary, treasurer/academics, fundraiser/entertain-ment, social/community/sport, andnewspaper/sponsors. Meetings areheld once a month. A departmentget-together is organized everyterm to keep the spirits high! Theyear-end function was on 4 October2002 and it was out of this world.
The Department is very proud of its newspaper (“Die Kruk”) and newsletters (“Die Kieriekie”),which provide all the students with information, jokes and all thegossip in the department.
Every year group plays an essen-tial part in the organizing of events.The fourth years have to orientatethe first years and make them feel part of the physio family. Thisday-long event, which includes arefreshing splash pool, takes placeat the department, ending with dinner and drinks. The fourth yearsare also responsible for presents for the lecturers at the annual year-end function.
The third years are responsiblefor the annual formal function atthe end of the year. This includesorganising farewell-presents forevery fourth year. The second years organise the annual informalfunction.
Each year, the fourth years havethe opportunity of working at the Comrades Marathon and theVisrivier Canoe Marathon.
Every second year a tour for thethird and fourth years is organised- in 2002 UFS paid a visit to CapeTown. Special schools, rehabilitation
centres and hospitals were visited. The Physiotherapy Student
Council’s main aims for 2003 are:implement the ‘buddy system’;obtain and provide informationconcerning community service toall the students; create awarenessabout Back Week; and implementan evaluating system for lecturersand clinical personnel to give stu-dents a chance to review standardsof classes.
UNIVERSITYOF PRETORIA
(TUKS)Elet Steyn, PRO of the NPSC, is theChairperson of the PhysiotherapyHouse Committee (HC) - as thePhysiotherapy Student Council isknown at TUKS.
The following portfolios areshared between the five othermembers on the HC: vice-chair-person, sport, treasurer, marketing,academic, projects, publications,secretary, social, culture, first yearmentor, clothing, RAG and commu-nity projects.
TUKS Physiotherapy values itspartnership with the North-Gautengbranch of the SASP and TUKS students participate in Back Weekand the SuperSport Show. Studentswho study non-medical courseswere the target group during BackWeek 2002: posters were put up,flyers handed out, advertisementmade on Radio TUKS, and the students were also available at acentral point on campus to giveadvice on taking care of back pain.The SuperSport Show was held atthe university’s sport grounds, andwilling students from TUKS andMEDUNSA helped with demon-strations such as stretching, Pilateson the ball and strapping.
To ensure good communicationbetween lecturers and students,there are specific ways to handlecomplaints. There is also a HCmember with the ‘academic’ port-folio, who takes care of such mat-ters. The chairperson also attendsstaff meetings.

38 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
The HC strives to maintain andimprove the relationship betweenstudents and parents, too. A‘mother-and-physio’ breakfast and‘father-and-physio’ golf day washeld in 2002. Needless to say, theseevents provided us with livelychatter and ample opportunity tochuckle (especially at some people’sgolf skills!).
Social, cultural and sport activi-ties are organised for the studentsduring the course of the year. TheGraduandi Ball (formal dinner), theinformal house dance, a picnic andkaraoke evening are just a few of
the social events that were heldduring the previous year. The livelymusical, CATS, was attended bythe majority of the students, andsome also went to the university’sown musical, GREASE.
The Physiotherapy Hockey teammade it to the final for the first timein years, and will definitely aim todo so again in 2003. The studentsalso competed against the hostelsin badminton, indoor-hockey, andnetball. The annual physio sportsday, where the year groups competeagainst each other and the lecturers,
was a huge success. In 2002 theannual volleyball tournament alsoincluded a jumping castle - much tothe delight of all involved!
At the Comrades Marathon,Hartebeespoort ‘Om die Dam’Marathon, the hostels’ rugby leagueand various other sporting events,the TUKS students offer their services. Then, of course, there’s themassaging of the champion BlueBulls-team...
The first years are well lookedafter. They have a first year mentor(‘Ienkvoog’) who ensures that theyfeel at home as soon as possible.
Each year in February, a first yearcamp is organised.
The HC strives to make a differ-ence in the community: in 2002 aTENS-machine was bought for oneof the old age homes in Eersterust,where the third year students work.
The ‘Grapevine’, a newsletter, iscirculated twice a year. A magazinewith stories and photos of all theactivities of the year was printed inJuly 2002.
The 2003 HC aims to maintainand if possible, improve, the excep-tional standards that were set by
From left to right - Front: Lauren Walker (UCT) Chairperson, Henriëtte Tredoux(UFS) Secretary, Marlize Jordaan (USSPS) Vice-chairperson & secretary, Elet Steyn(TUKS) PRO, Melusi Mtshali (UDW) National Assembly Officer.Back: Adele Geldenhuys (WITS) Treasurer, Warren Caesar (UWC) PRO.
the 2002 HC. Improving relation-ships between lecturers and stu-dents; making a difference in thecommunity; ensuring that all thestudents are well informed aboutcommunity service and making surethere is ample opportunity for thestudents to attend social, culturaland sport events are some of theaims.
UNIVERSITY OFSTELLENBOSCH (USSPS)
Marlize Jordaan, vice-chairpersonand secretary of the NPSC, is incharge of leading the enthusiasticbunch of students of the Stellen-bosch Physiotherapy StudentCouncil. They will be working hardto achieve at least as much successas the committee in 2001/2002.
All events organised during2001/2002 received overwhelmingsupport. This reflected the hardwork of every single committeemember, who did an outstandingjob. The marketing and advertisinghas improved incredibly, with creative and eye-catching postersgrabbing attention.
A few exciting events were intro-duced during the past year andbecause of their success, they arehere to stay!
A massage-a-thon was organisedto raise funds towards upgradingthe facilities and equipment atselected Community Health Centreswhere some of the students work.A farewell function was held for allthe fourth years and a Cheese andWine function was organised for all the staff and students of thePhysiotherapy Department - bothan end-of-year celebration and anopportunity for the Department toacknowledge the many achieve-ments of the talented students. Thewhole department also had theopportunity to bid the final yearclass farewell.
Then there are other activitiesorganised during the year, whichencourage greater awareness of the Student Council and greaterparticipation by the students. The
Student News

PHYSIOFORUM DECEMBER 2002/JANUARY 2003 39
annual summer fruit festival, aphysio braai at the Hippo Club andthe infamous Physio Dance whichwas held at the Paarl Stadsaal withpre-drinks at Simonsvlei are just afew of the social events which areorganised.
The students also offer their assistance at sporting events: theArgus Cycle Race, the Two OceansMarathon and the SAD half mara-thon.
The 2003 committee has greatplans to expand on the foundationswhich were so well established lastyear. All of their events will aim toencourage greater participationand spirit within the department.The fourth year class also plan onoffering their assistance at theComrades marathon.
UNIVERSITY OF THEWESTERN CAPE (UWC)
Warren Caesar, PRO of the NPSC, is the chairperson of UWC for the2002/2003 term.
Not only will he be leading thePhysiotherapy Student Council,but he will also approach sponsorsfor future projects and maintainbursaries for students in thePhysiotherapy Department.
The ‘Public Relations Officer’ willbe running a project in conjunctionwith AJAX Cape Town - a premiersoccer club. This is, needless to say,a great opportunity for physiothe-rapy students to get involved inprofessional soccer, one of the lead-ing sports in the country.
The primary objective of the port-folio of ‘Sport and Community’ isto create awareness in the commu-nity about the role of the physio-therapist. Porposed projects includea massage week and lectures oncorrect posture when studying. TheCape Argus Cycle Race and theComrades Marathon are the twomain events where the studentswould like to offer their services.They also aim to correct myths indifferent sports codes.
The ‘Equipment Officer’ (thisportfolio was only created recently)
will be responsible for drawing upan inventory of all the equipmentin the department and inform the Head of Department aboutdamaged equipment. He will alsoinvestigate new equipment on themarket, and ensure that there isawareness about it.
The ‘Education Officer’ needs tocreate awareness about the NPSCand the SASP. The mentor pro-gramme of the third year studentsis running successfully. One long-term goal is to have a library at thedepartment - this is rather a lengthyproject as it will rely mostly ondonated books. The possibility ofhaving a small computer centre atthe physiotherapy department isalso being investigated.
UNIVERSITY OF THEWITWATERSRAND (WITS)
The WITS Physiotherapy StudentCouncil consists of 12 members, whoare elected by their fellow students.The chairperson for 2002/2003 isAdele Geldenhuys. She is also thetreasurer of the NPSC.
The council of 2001/2002 got offto a very rocky start. Due to pro-blems that were experienced in theprevious year, they really had theirwork cut out for them.
The first event on our agenda wasthe karaoke evening held just beforethe end of year exams in 2001-which made it clear why we arephysiotherapy students and notentertainers :-).
We kicked off on a high note in2002 with the Annual Golf Day inaid of our charity organisation,‘The Avril Elizabeth Home’. Theday was a great success and all theplayers enjoyed the day of play aswell as the massages afterwards.Sponsors gave wonderful prizes,which were greatly appreciated bythe deserving winners.
Sport took the limelight fromMarch to June, as the third year students worked at the St. Johnsand KES Rugby Festival, The 702Spin-a-thon, KES WaterpoloChampionships, St. Mary’s Hockey
Tournament, SA Rowing Champion-ship as well as the U/21 RugbyWorld Cup. Some of the studentsalso had the opportunity to assistthe physios working with the CATS and LIONS rugby teams.This was a wonderful experience.
June hosted the long awaitedComrades marathon, and 43 eagerfourth years set off to Durban tomake us proud. As one of themsaid, “It’s an experience I’ll neverforget”.
July was culture time, and wehosted 250 guests at Running Riot at The Civic Theatre inJohannesburg - just what the doctorordered to help us through thechilly winter. We also hosted amovie evening, which was orga-nised by our second year students.They sold 270 tickets and providedsnacks. This was a great success,much enjoyed by all who attended.
8 August 2002 finally came, andthe Annual Graduation Ball. Aftera lot of hard work from all thecouncil members, the evening waswell worth the wait. With goodfood and brilliant music the stu-dents and lecturers partied wellinto the early hours of Fridaymorning.
Our proudest moment was whenthe fourth year strapping teammade it through to the final, whichwas held on 27 September 2002.Congratulations to these five stu-dents!
The new council was announcedat the ball and the hard work started two weeks later.
Our proposed projects for 2003are: First year braai, Spin-a-thon,Golf Day, Strapping competition,Sporting Events, Comrades, MovieEvening, Theatre Evening andGraduation Ball.
On behalf of the WITS PSC Iwould like to thank Christine, ourchairperson 2001/2002, and wishall the other PhysiotherapyCouncils the best of luck for theupcoming exams and for 2003.
Adele Geldenhuys. (Chairperson2002/2003)
Student News
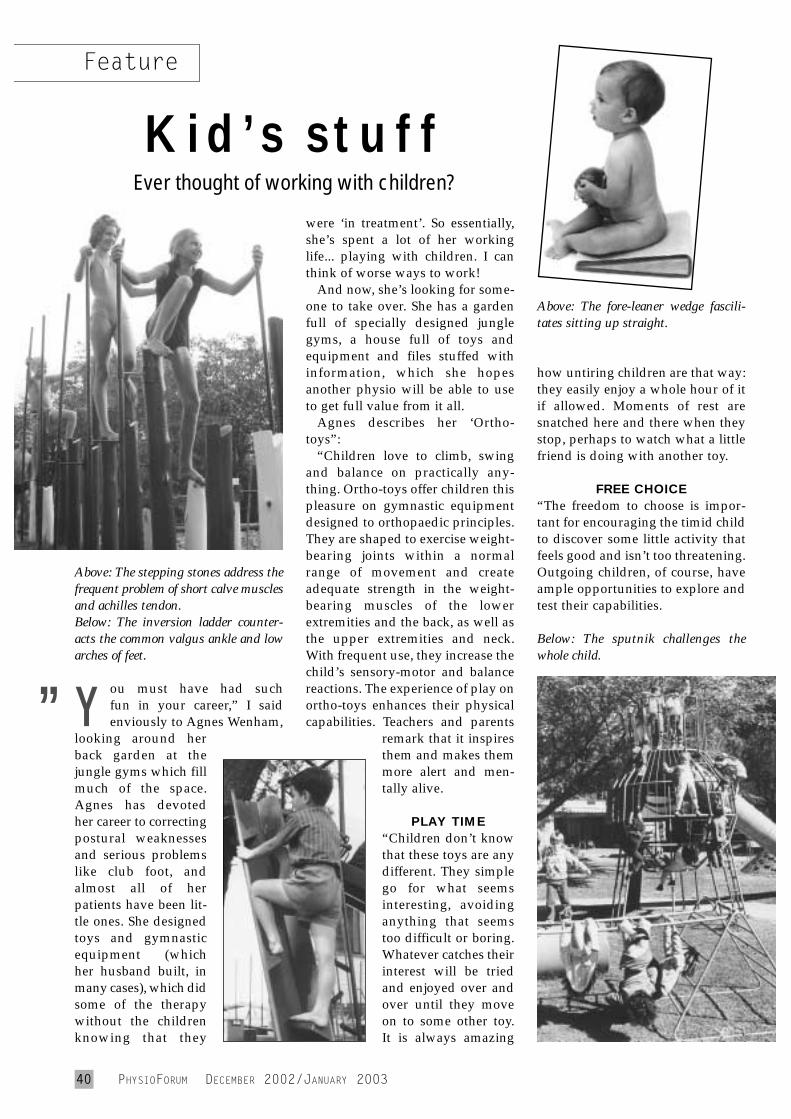
40 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
ou must have had such fun in your career,” I saidenviously to Agnes Wenham,
looking around herback garden at thejungle gyms which fillmuch of the space.Agnes has devotedher career to correctingpostural weaknessesand serious problemslike club foot, andalmost all of herpatients have been lit-tle ones. She designedtoys and gymnasticequipment (which her husband built, inmany cases), which didsome of the therapywithout the childrenknowing that they
were ‘in treatment’. So essentially,she’s spent a lot of her workinglife... playing with children. I canthink of worse ways to work!
And now, she’s looking for some-one to take over. She has a gardenfull of specially designed junglegyms, a house full of toys andequipment and files stuffed withinformation, which she hopesanother physio will be able to useto get full value from it all.
Agnes describes her ‘Ortho-toys”:
“Children love to climb, swingand balance on practically any-thing. Ortho-toys offer children thispleasure on gymnastic equipmentdesigned to orthopaedic principles.They are shaped to exercise weight-bearing joints within a normalrange of movement and create adequate strength in the weight-bearing muscles of the lowerextremities and the back, as well asthe upper extremities and neck.With frequent use, they increase thechild’s sensory-motor and balancereactions. The experience of play onortho-toys enhances their physicalcapabilities. Teachers and parents
remark that it inspiresthem and makes themmore alert and men-tally alive.
PLAY TIME“Children don’t knowthat these toys are anydifferent. They simplego for what seemsinteresting, avoidinganything that seemstoo difficult or boring.Whatever catches theirinterest will be triedand enjoyed over andover until they moveon to some other toy.It is always amazing
Kid’s stuffEver thought of working with children?
Above: The stepping stones address thefrequent problem of short calve musclesand achilles tendon. Below: The inversion ladder counter-acts the common valgus ankle and lowarches of feet.
Above: The fore-leaner wedge fascili-tates sitting up straight.
Below: The sputnik challenges thewhole child.
how untiring children are that way:they easily enjoy a whole hour of itif allowed. Moments of rest aresnatched here and there when theystop, perhaps to watch what a littlefriend is doing with another toy.
FREE CHOICE“The freedom to choose is impor-tant for encouraging the timid childto discover some little activity thatfeels good and isn’t too threatening.Outgoing children, of course, haveample opportunities to explore andtest their capabilities.
”Y
Feature
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 41
THE TEACHER“On ortho-playgrounds, teachers find relief from thepressure to plan, organise and lead physical therapysessions. Their personal interests and sensitive approachto each child will bring out the best in him. The teacherplays a mainly passive role - very few suggestions shouldbe made so the children can use their own imaginations.Respect the child’s hesitations, and praise where praiseis due - this will help develop self-esteem and encour-age pleasure in physical activities lifelong.
PHYSICAL SHORTCOMINGS“Experience shows that nearly all common posturalfaults are inherited and often seem to run in families.Mild versions of faults like bandy legs can be improvedsimply through frequent play with ortho-toys. Moresevere weaknesses require physiotherapy. The earlier aweakness is spotted, the better and quicker are theresults achieved. Daily practising can then be greatlyenhanced by the right choice of a therapeutic ortho-toy.It helps the child to pinpoint the concentration onsomething concrete and interesting, and is extra helpfulfor the correction.”
If you are interested in working with children andwith ortho-toys, please contact Agnes.
Physiotherapists are required for posture promoting andposture correcting exercises on Ortho-toys - gymnasticequipment for indoor and outdoor use, designed onorthopaedic principles. There is a need for leaders in thissubject.Contact Agnes Wenham,27 6th Ave, Parktown North, JohannesburgTel early or late, at (011) 788-5028, or fax (011) 497-5333.
Feature
Thinking of Relocating toAustralia?
A diverse and vibrant, multi-practitionerPhysiotherapy Practice available for saleor lease in beautiful Hobart, Tasmania.
■ Long established & well equipped.■ Excellent, experienced staff.■ Extensive client base.■ Walking distance to CBD.■ Potential for expansion.
Premises also available for sale or lease.
Expressions of interest to:
■ PM Hunn7 Byard StreetMt StuartTasmania 7000
EXCITING NEW OPPORTUNITY
We require physiotherapists whowould like to specialize in the treatment of sportsinjuries, although GP and unsurance referrals also apply.
* Full & part time positions available
* 3 month start up retainer + patient percentage
* Accommodation & transport provided for Floaters
5 years experience requiredOMT1 preferable
Top Rates
Traci Glen: 082 436 6484Interviews will take place in JHB/DBN/CTend Feb early MarchPlease mail c.v’s to: [email protected]
Physiotherapy & Sports Injury ClinicsSartorius Clinics (UK)
IBITA ADULT HEMIPLEGIA COURSE(BOBATH CONCEPT).Instructor: Michele Gerber
(Senior instructor Switzerland)Assisted by Mary Riley
Date: 6 - 24 January 2003Venue: South Rand HospitalCost: R2200.00Enquiries/Applications: Caren Anderson
(011) 485 3794
42 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
CHECK OUTTHE SASP’S
WEBSITEAT
www.physiosa.org.za
HOLD THEPRESSES!
Get your classified ads intothe February issue NOW!
Closing date: 13 January 2003
(Non-SASP members) PUBLICATIONS LOCAL OVERSEAS SA Journal of Physiotherapy 4 issues - Mar, May, Aug, Nov. R220.00 R420.00 PhysioForum 7 issues - Feb, Apr, June, July, Sep, Oct, Dec. R220.00 R420.00SA Journal of Physiotherapy and PhysioForum (11 issues per year) R440.00 R860.00 (Renewal on subscriptions must be taken out for: February 2003 - December 2003)
Prices include postage costs. SASP members receive the South African Journal of Physiotherapy and PhysioForum as part oftheir membership package. NB Should you wish to receive any publication airmail, please fax us for a quote.
Name ....................................................................................................................................................................
Postal address........................................................................................................................................................
..............................................................................................................................................................................
..............................................................................................................................................................................
..............................................................................................................................................................................
Postal code....................................................................Country...........................................................................
Tel (H) ...........................................................................(W)..................................................................................
Signature .......................................................................
Cheque/Postal order must accompany order form R.................................. Date ..................................................
Please print order form and send with payment to: Physiotherapy Publications,PO Box 92125, Norwood, 2117, South Africa. Fax (011) 485-1613. Attention: Americo
SUBSCRIPTION ORDER FORM FOR FEBRUARY - DECEMBER 2003
Course Notes
INTERNATIONAL COURSES IN JHB: CRANIOSACRAL THERAPY (CST1) UPLEDGER INSTITUTE UK.A world renowned educational and research organization. CranioSacral Therapy is used to treat headaches and migraines, neck and back pain, TMJ dysfunction, chronic fatigue and motor co-ordination problems,hyperactivity, dyslexia, colic, feeding and sleeping problems, difficult-to-treat cases. March 8-11, 2003. Limited numbers R5800.00.
STOTT PILATES INTERNATIONAL CERTIFICATION COURSES FROM TORONTO, CANADA.Intensive Mat, Advanced Mat, Reformer, Advanced Reformer, Injuries and Special Populations & day workshops. June 2-25, 2003. Contact: Riverclub Physiotherapy and Pilates Clinic.
Joanne Enslin or Rina (011) 706-9159/60 or fax (011) 706-7259.
PHARMACOLOGY FOR PHYSIOTHERAPISTSMedications can impact on an individual’s response to rehabilitation. To effectively and successfully work intoday’s health care community, physiotherapists must be familiar with their patient’s drug regimens.
In response to requests, Prof P van der Bijl will present the above 2 day course focussing on the relationshipbetween pharmacology and physiotherapy, including basic principles of how drugs work, categories of therapeutic agents important to physiotherapy practice and agents used or recommended by to complementtreatment.Application for CPD points (6/day) has been made.Venue: Department of Physiotherapy, University of Stellenbosch Date: Saturday 5th April and Saturday 12th April 2003Time: 9:00am - 4:00pmCost: R300 per dayFurther information + course bookings, please ph Ms Annelene Dorman - Tel 938-9300.
PRACTICE FOR SALE
Blairgowrie: Well establishedclient base for sale. Contact:083 272-8225.
Killarney: Solo practice for sale inwell established medical centerwithin shopping mall. Many privateclinics in the area. Contact Preven,082 561-0042.
Cape Town: Well establishedorthopaedic practice in Tokai forsale. Call Estelle, (021) 712-7754.
Meyerton: Goed gevestigde prak-tyd te koop. Ongelooflike goeiegeleentheid om eie besigheid op‘n baie billike wyse te bekom.Kontak Laurika, 082 872-6571.
Midrand: Sports and orthopaedicpractice for sale. Owner moving toCape Town. Call Sarah, 083 308-9233.
ROOMS AVAILABLE
Cape Town: Premises availablenext to pharmacy and doctors’rooms in southern suburbs. Phone(021) 696-1532.
Amanzimtoti: Lovely spaciousrooms with built-in reception area, own toilet facilities andair conditioned. Adjoins busydoctors practice. Second handequipment also available.Excellent opportunity. ColleenPitchford, 082 653-3275.
Rivonia, Sandton: Room/s to letat exclusive personal fitness andrehabilitation private gym. RentalR2500 p/m. Established businesssince 1996. Contact Robyn on(011) 803-1124 or 082 993-0300.
CLASSIFIEDSCLASSIFIEDS
COURSE NOTESCOURSE NOTES
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 43
44 PHYSIOFORUM DECEMBER 2002/JANUARY 2003
Physio Connection: For apermanent or locum employmentconnection, please contact(011) 678-5212 or 476-3810.Reasonable once-off placement fee.
Springs: Dinamiese fisioterapeutbenodig. Kamers-/hospitaalwerk.Meestal ortopedies, sport enspinaal (Maitland). Kontak André,072 545-2585.
Somerset West: Part-time/full- time physiotherapist required.OMT an advantage. Futureprospects available. Opportunitiesfor academic and clinical pursuit.Contact: (021) 852-3458.
Pretoria/WilgersHospitaal:Middagpos/flexityd beskikbaar virhospitaal en kamerwerk. So gouas mootlik. Kontak Riana/Hanlie,(012) 807-0256/7.
Pretoria/Wilgers Hospitaal:Voldagpos beskikbaar vir hospitaalen kamerwerk. Vanaf Desember2002/Jan 2003. Goeie werksverskei-denheid en mededingende salaris.Kontak Hanlie/Riana, (012) 807-0256.
Florida Park: Afternoon physio-therapist required for privatepractice. To start mid January 2003.Contact Wilna 672-6159 (w),475-1030 (h) .
Cape Town: Full-time physio-therapist required in private practicein northern suburbs. Practiceinvolves outpatients, as well ashospital patients, (ICU, Orthopaedics,Surgery + Peadiatrics). FrancoisPretorius, (021) 595-1630 or082 415-2274.
Rosebank: Full-time and part-timeposts available for general roomsand hospital practice. Contact Fiona(o/h) 447-1815 or 880-5365.
Randburg: Multidisciplinarygeneral and sport medicine practiceseeks to employ experiencedphysiotherapists. E-mail CV [email protected] fax it to Dr Branfield at(011) 792 8906.
Cape Town/Claremont:Enthusiastic physioterapist forhospital/rooms, private practice.Starting January 2003. ContactGail/Denise, (021) 797-7396.
Bronkhorstspruit: Full-timephysiotherapist needed forSizanani Home for disabledchildren, mostly NDT work. ContactMatron Schilling, (013) 932-1904.
Pretoria: Full-day physiotherapistrequired. Both rooms and hospitalwork. To start ASAP. Phone Rina,083 263-4399.
Benoni: Full-time physiotherapistrequired in diverse orthopaedicpractice from Dec/Jan 2003.Contact Lauren/Caroline at849-3721 (w) or 083 227-2915.
Plettenberg Bay: Practice in privatehospital requires full-time physio-therapist for room and hospitalwork. To start ASAP. Please contactYolanda/Liza, 083 464-5092.
Sandton, Parkmore: Part-timephysiotherapist needed for friendlyorthopaedic practice. To start ASAP.Contact Carol at 883-1065 (a/h).
Pretoria: Dinamiese fisioterapeutbenodig vir besige praktyk. Hospitaalen kamerwerk. Poste onmiddelikbeskikbaar, maar verkieslik1 Januarie 2003. Kontak Charné,(012) 325-5690/1 of 082 375-1128.
Physio required for full- orhalf-day position at PhyllisBerger’s Pain Management andRehabilitation Centre. An interestin acupuncture, hydrotherapy andrehabilitation would be an asset.Please contact (011) 802-1275.
Sandton/Rivonia: Part-time physiorequired. Sport/orthopaedicpractice. Part-time Pilatesinstructor needed. Contact Jacqui,083 324-8424.
Port Elizabeth: Full-timephysiotherapist needed at hospitaland rooms practice. Contact FrancisEllis, Tel (041) 373-7082/373-5514.
SITUATIONS VACANT
Roodepoort: Fisioterapeut benodigin twee-man privaat praktyk.Kontak Melinda, 082 378-9373.Januarie 2003.
Rustenburg: Dinamiese buite-pasient praktyk het ’n pos beskikbaar vir fisioterapeute watbelangstel in muskuloskeletalekondisies, sportbeserings enalgemene fisioterapie. Uitstekendewerksomstandighede, vergoedingen professionele ontwikkelings-geleentheid. Vanaf Jan / Feb 2003.Marius de Bruyn, (014) 533-2070.
Sandton: Full-time physio fordynamic practice. Please call:083 600-1777.
Fourways: Physiotherapist invitedto join multi-disciplinary practice.Contact Alessia, (011) 705-1368.
Physiotherapist contracts inEngland. No agency registrationfees. Tel (012) 804-5397.E-mail: [email protected]
Ermelo: Sport, ortopediese enalgemene praktyk benodig voldagfisioterapeut so gou moontlik.Kontak Jacqueline, 082 920-1882of (017) 819 3405.
Boksburg: Voldagpos beskikbaarin privaatpraktyk vanaf 2003.Hospitaal en kamerswerk.Kompeterende gestruktureerdesalarispakket. Kontak 082 923-0113.
Physiotherapist needed atThe Headache Clinic. Packagenegotiable. Contact Gerda at(011) 484-0933.
Sunward Park/Boksburg: Physiorequired for mainly afternoons andweekends. Hospital and rooms.Good salary. Sonia, (011) 913 3602/3.
Durban: Full-time physiotherapistrequired for busy private practice.Pleasant working environment.From January 2003 (01.01.2003).Tel (031) 312-2308 or 082 260-0218.
Classifieds (Continued)
PHYSIOFORUM DECEMBER 2002/JANUARY 2003 45
CLASSIFIEDS COUPON 2002Please insert at R7,00 per word (or R8,00 to include on Website with immediateeffect), in the next available issue of PhysioForum or The South African Journal ofPhysiotherapy. (Note: a minimum of R65,00 will be charged for every advert). TheSASP request payment upfront for the placement of advertisements in our publications.
❑ PLEASE INCLUDE CLASSIFIED ADVERT ON THE WEBSITE (Tick if necessary)Please Note: No classifieds will be accepted without this coupon.
Any cancellation/alteration will only be accepted in writing.
Area:.............................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................Submission date: ...........................................................................................................Name:...............................................................................................................................Address: ........................................................................................................................................................................................................Code...................................................Telephone: Work (...........).................................Home (...........)
SASP Head Office - AdvertisingTel: (011) 485-1467, Fax: (011) 485-1613
E-mail: [email protected]
AGREEMENT OF PLACEMENT OF ADVERTISEMENT(S) 2002Please Note: No advert bookings will be accepted without this coupon.
Any cancellation/alteration will only be accepted in writing.
..............................................................................................................................Mr / Mrs / Miss / Me / Prof / Dr
Signed ........................................................................
on the ................................... Day of ......................................... 2001
Name: .............................................................................................................................Company:.........................................................................................................................Address: ..................................................................................................................................................................................................................................................................................................................................................Code...................................................Telephone: Work (...........).................................Home (...........) ...................................Submission date (Starting) .............................date (Ending): ...................................
SASP Head Office - AdvertisingTel: (011) 485-1467, Fax: (011) 485-1613
E-mail: [email protected]
Nelspruit: Voldag fisioterapeutbenodig in privaatpraktyk vir 2003.Uiteenlopende praktyk en hospitaal-werk wat naweekwerk insluit.Kontak Christa, 083 241-1900,Elmarie, 082 338-1360.
FULL-TIMEPHYSIOTHERAPY POSITIONLaunceston Tas, Australia:Private PracticeGreat life style, stimulating andinteresting job. Skills in sportsinjuries, muscle energy and corestability work desirable, ongoingtraining provided and encouraged. Drivers license essential. Able togain registration in Tasmania, or byalready having registration thatwould be recognised in Australia(e.g. Current New Zealand regi-stration). This position is recognisedfor sponsorship under currentAustralian immigration policy.A suitable applicant would be ableto apply for permanent residencestatus after completion of a twoyear contract.Contact Karl Thomas on0011 613 6331 3811Email: [email protected] Box 677, Launceston TAS 7250,Australia
FOR SALE
Pretoria: AKRON TRACTION for sale. Phone Douglas, Cell:083 234-1492, work (012) 845-1333.
Textbooks for sale: For list orview e-mail [email protected] fax (011) 704-0401 att.Joan van der Zee, or phone Karen(011) 485 3794.
Johannesburg: Chattanoogaultrasound, 183 MHZ. 1 year old. Lucy, 083 260-3247.
HOLD THE PRESSES!Get your classified
ads into the Februaryissue NOW!
Closing date:13 January 2003
NewMillenniumTime tothink of achange?
Sonja Lewis Quality Locums Cape TownTel: 021 4222895Fax: 021 4222899Email: [email protected]
Matt Wagner Quality Locums DurbanTel: 031 3091471 Fax: 031 3091382 Email: [email protected]
Quality Locums are looking for qualitypersonnel in all grades and specialitiesfor work in the UK. Eligibility for a visaor work permit would be an advantage, buteven if you are not eligible we would stilllike to hear from you as we may be able tohelp. Quality Locums are the largest independent Medical, Care andEducation Agency in the UK and we have branches in South Africa andAustralia. We need Medical Staff of all specialities, Social Workers andTeachers urgently to fill full and part time positions throughout Great Britainand Ireland. We are experts at helping you to take advantage of theopportunities in the UK. Why not call one of our managers today for aninformal discussion.
Canadian Opportunities
Alta-Sask Resolution Rehabilitation &Sports Physiotherapy has 2, full-timephysiotherapy positions available. We arelooking for energetic professionals whoare committed to continuing educationand providing high quality care in
Orthopedics, Sports Physiotherapy and IndustrialRehabilitation. We offer a very competitive salary, benefits package, education funding and a signing/relocation bonus is negotiable.
Our clinic is a private practice located in Lloydminster (a prairie city of 25,000 people). We feature a 4000 squarefoot facility, which includes a fully equipped gym/exercisearea. “Lloyd” is located a short distance betweenEdmonton, Alberta and Saskatoon, Saskatchewan. Itsupports a strong South African medical community.
Please direct inquires or applications to:Alta-Sask Resolution Rehab. & Sports Physio.#5, 4517 - 50th AvenueLloydminster, Saskatchewan, S9V OZ9Ph: (306) 825-2383 Fax: (306) 825-2292e-mail: [email protected]
NB: A clinic representative will be in South Africa frommid December to early January 2003 to meet with seriouscandidates.





























