Embed Size (px)
Citation preview

Correlation of Histology With Biomarker Status AfterPhotodynamic Therapy in Barrett Esophagus
Ganapathy A. Prasad, MD1, Kenneth K. Wang, MD1, Kevin C. Halling, MD, PhD2, Navtej S.Buttar, MD1, Louis-Michel Wongkeesong, MD1, Alan R. Zinsmeister, PhD3, Shannon M.Brankley, BS2, Wytske M. Westra, MD1, Lori S. Lutzke, LPN1, Lynn S. Borkenhagen, MSN,NP1, and Kelly Dunagan1
1Barrett Esophagus Unit, Division of Gastroenterology and Hepatology, Mayo Clinic College of Medicine,Rochester, Minnesota.
2Department of Laboratory Medicine and Pathology, Mayo Clinic College of Medicine, Rochester,Minnesota.
3Division of Biostatistics, Mayo Clinic College of Medicine, Rochester, Minnesota.
AbstractBACKGROUND—Currently, histology is used as the endpoint to define success withphotodynamic therapy (PDT) in patients with high-grade dysplasia (HGD). Recurrences despite‘successful’ ablation are common. The role of biomarkers in assessing response to PDT remainsundefined. The objectives of the current study were 1) to assess biomarkers in a prospective cohortof patients with HGD/mucosal cancer before and after PDT and 2) to correlate biomarker status afterPDT with histology.
METHODS—Patients who underwent PDT for HGD/mucosal cancer were studied prospectively.All patients underwent esophagogastroduodenoscopy, 4-quadrant biopsies every centimeter,endoscopic mucosal resection of visible nodules, and endoscopic ultrasound. Cytology samples wereobtained by using standard cytology brushes. Biomarkers were assessed by using fluorescence insitu hybridization (FISH). The biomarkers that were assessed included loss of 9p21 (site of thep16 gene) and 17p13.1 (site of the p53 gene) loci; gains of the 8q24(c-myc), 17q (HER2-neu), and20q13 loci; and multiple gains. Patients received PDT 48 hours after the administration of sodiumporfimer. Demographic and clinical variables were collected prospectively. Patients were followedwith endoscopy and repeat cytology for biomarkers. The McNemar test was used to comparebiomarker proportions before and after PDT.
RESULTS—Thirty-one patients were studied. The median patient age was 66 years (interquartilerange [IQR], 56–73 years), and 28 patients (88%) were men. The mean Barrett segment length was5 cm (standard error of the mean, 0.5 cm). Post-PDT biomarkers were obtained after a medianduration of 9 months (IQR, 3–12 months). There was a statistically significant decrease in theproportion of several biomarkers assessed after PDT. Six patients without HGD after PDT still hadpositive FISH results for 1 or more biomarkers: of these, 2 patients (33%) developed recurrent HGD.
CONCLUSIONS—In this initial study, histologic downgrading of dysplasia after PDT wasassociated with the loss of biomarkers that have been associated with progression of neoplasia in
Address for reprints: Kenneth K. Wang, MD, Barrett Esophagus Unit, Alfred Main-Gastrointestinal Diagnostic Unit, St. Mary’s Hospital,Mayo Clinic, 200 First Street SW, Rochester, MN 55905; Fax: (507) 255-7612; E-mail: [email protected] patent has been filed for the fluorescence in situ hybridization (FISH) probe set described in this study. Dr. Kevin C. Halling, Dr.Kenneth K. Wang, Shanon M. Brankley, and the Mayo Clinic have the potential to receive royalties from the sale of this product.
NIH Public AccessAuthor ManuscriptCancer. Author manuscript; available in PMC 2009 February 5.
Published in final edited form as:Cancer. 2008 August 1; 113(3): 470–476. doi:10.1002/cncr.23573.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Barrett esophagus. Patients with persistently positive biomarkers appeared to be at a higher risk ofrecurrent HGD. These findings should be confirmed in a larger study.
KeywordsBarrett esophagus; biomarkers; photodynamic therapy; response; esophageal carcinoma
Barrett esophagus (BE) predisposes patients to esophageal adenocarcinoma, a cancer with oneof the fastest rising incidence rates over the past decade and a highly lethal malignancy onceit is symptomatic.1,2 It is believed that esophageal adenocarcinoma arises as the final step ofa postulated sequential change in the metaplastic epithelium, progressing from low-gradedysplasia (LGD), to high-grade dysplasia (HGD), and finally carcinoma. HGD on histologicsamples has been used as the most reliable clinical biomarker of potential carcinogenesis, withstudies reporting variable rates of progression to esophageal carcinoma (range, 16%–59%).3–5 Interruption of the metaplasia-dysplasia-carcinoma sequence by ablating or resecting thisat-risk mucosa has been proposed as a strategy to reduce the incidence of esophagealadenocarcinoma and has served as the rationale for the recommendation of esophagectomy forpatients with HGD.
Over the past few years, endoscopic therapy has emerged as an alternative to esophagectomybecause of the significant mortality and morbidity associated with esophagectomy.6,7 Multiplemodalities, including photodynamic therapy (PDT),8 argon plasma coagulation,9 andmultipolar electrocoagulation10 in isolation and in combination with endoscopic mucosalresection (EMR),11,12 have been reported in the treatment of HGD. Variable success rateshave been reported (range, 75%–90%). A randomized multicenter trial compared PDT withsurveillance and treatment with omeprazole in patients with HGD. After a 24-month follow-up, complete ablation of HGD was noted in 77% of patients versus 39% in the omeprazolegroup. Thirteen percent of patients who received PDT plus omeprazole progressed to cancercompared with 28% of patients in the omeprazole group.13 This led to U.S. Food and DrugAdministration approval for the use of PDT for the treatment of HGD in BE. We recentlyreported that long-term outcomes (overall mortality and cancer-free survival) were comparablebetween patients who underwent esophagectomy and patients who received PDT.14
Several genetic alterations have been described in BE. These include loss of cell cyclecheckpoint genes, such as p16 and p53. Loss of these genes by allelic loss (deletions or lossof heterozygosity [LOH]), point mutations, or promoter hypermethylation (for p16) have beenobserved in a substantial number of patients with BE.15,16 Several other genetic alterationsthat involve gains/amplifications of proto-oncogenes (and growth factors/growth factorreceptors) as well as changes in DNA content (as assessed by flow cytometry and imagecytometry) also have been described.17,18
Currently, histology is used as the endpoint to define success with ablative therapy in HGD.However, recurrences and/or progression to cancer despite ‘successful’ ablation/resection arecommon. To our knowledge, predictors of recurrent dysplasia have not been defined. Fewstudies have assessed genetic alterations after ablation of BE19–21: those studies primarilyassessed patients with predominantly nondysplastic BE (a category for which ablation currentlyis not recommended) rather than HGD (in which endoscopic ablation is gaining acceptance asan alternative to esophagectomy) by using techniques that lack long-term data on successfulablation. Studies also have raised concern about the appearance of cancer-associatedbiomarkers after ablation (in patients with nondysplastic BE)20: however, data are lacking onthe clinical implication of this phenomenon in terms of the recurrence or progression ofdysplasia.
Prasad et al. Page 2
Cancer. Author manuscript; available in PMC 2009 February 5.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

The role of biomarkers in defining response to PDT remains unclear. The correlation betweenhistologic response and ‘biomarker response’ also is unknown. We hypothesized that patientswho remain positive for genetic alterations despite achieving a histologic response to PDTwould be at risk for recurrence of dysplasia. In this study, we used fluorescence in situhybridization (FISH) to characterize genetic alterations that were present in patients with HGDand mucosal cancer before treatment with PDT and compared them with the alterationsobserved after PDT. In addition, we assessed the recurrence of dysplasia after initial histologicresponse and correlated those findings with post-PDT genetic alterations assessed by FISH.
MATERIALS AND METHODSPatients with HGD and/or mucosal cancer (defined as carcinoma confined to the mucosawithout invasion of the submucosa) who were seen in the Barrett Esophagus Unit at St. Mary’sHospital, Rochester, Minnesota between 2002 and 2006 were included in this study. Inclusioncriteria were the presence of HGD/intramucosal carcinoma on biopsies, assessment ofbiomarkers using FISH before and after PDT, and treatment with PDT. Exclusion criteriaincluded patients with submucosal cancer on EMR (who were referred to surgery) and patientswho were unwilling or unable to consent to the study. Clinical, demographic, and endoscopicdata were extracted from a prospectively maintained database and included length of Barrettsegment, performance of EMR before PDT (including number of EMRs), number of PDTtreatments per application, results of post-PDT biopsies (classified as carcinoma, HGD, LGD,or non-dysplastic BE), and biomarkers obtained using FISH before and after PDT.
All patients underwent 4-quadrant biopsies every centimeter of the involved esophagus. Allpatients had their diagnosis of HGD or mucosal cancer confirmed by 2 experiencedgastrointestinal pathologists. Baseline assessments also included endoscopic ultrasound andEMR for any mucosal abnormalities. Computed tomography scans of the chest and upperabdomen were obtained in all patients.
Cytology Specimen AcquisitionCytology specimens for FISH were obtained during the endoscopy immediately before PDT.During endoscopy, a cytology brush (Hobbs Medical Inc., Stafford Springs, Conn) was sweptover the entire Barrett segment after the mucosal surface was sprayed with 10 mL of N-acetylcysteine (as a mucolytic). Then, the brush was placed in a vial that contained 20 mL ofPreservCyt solution (Cytyc Corp., Marlborough, Mass). Endoscopic brushing specimens wereprocessed by washing the brush with 40 mL of 3:1 methanol:glacial acetic acid fixativesolution. Cells were sedimented at ×800g for 8 minutes. The supernatant was removed, andthe cell pellet was resuspended in 10 mL of 3:1 methanol:glacial acetic acid fixative solution.Next, the cells were sedimented again at ×300g for 8 minutes. All but ≈100 µL of thesupernatant was removed. Finally, the cell pellet was resuspended, and the slides wereprepared.
Slide PreparationApproximately 3 µL of the cell pellet suspension were pipetted onto 3 etched 1-cm rings (GoldSeal, Portsmouth, NH), 1 ring for each of the 3 probe sets. Cellularity was assessed with aphase contrast microscope. Additional cell suspension was added to the slide until adequatecellularity was reached (ie, the highest number of cells possible per ring with minimal celloverlap) or until the cell pellet was exhausted. Table 1 describes the biomarkers that wereassessed prospectively in this study.
Prasad et al. Page 3
Cancer. Author manuscript; available in PMC 2009 February 5.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fluorescence In Situ HybridizationEsophageal brushing cells were harvested, fixed, and placed on a slide as described previously.22 Then, the following fluorescently labeled DNA probes were hybridized to the specimens:8q24.12–q24.13 (C-MYC), 9p21 (P16), 17p13.1 (p53), 17q11.2–q12 (HER-2), and 20q13.2(Abbott Molecular Inc., Des Plaines, Ill). Next, the slides were washed and stained with thenuclear counterstain 4′,6-diamidino-2-phenylindole (Abbott Molecular Inc.). Fluorescencemicroscopy was used with unique band filters that were specific for each of the probefluorophores to analyze and record all observed signal patterns for 100 (minimum, 50)consecutive, noninflammatory, nonsquamous cells. Enumeration was performed withoutknowledge of the patient’s clinical or histologic diagnosis. Details regarding the probes andthresholds for positivity are provided in Table 1.
Photodynamic TherapyPorfimer sodium (Photofrin; Axcan Pharma, Mont-St.-Hilaire, Quebec, Canada) was used asa photosensitizer at a dose of 2 mg/kg. Photofrin was administered intravenously 48 hoursbefore photoradiation, which was performed by using a bare cylindrical diffusing fiber. Thecylindrical diffusing fibers were either 2.5 cm or 5.0 cm in length (Fibers Direct, Andover,Mass). The cylindrical diffusing fiber was passed through the accessory channel of theendoscope and placed in the center of the esophageal lumen. The light was delivered from alaser (Lambda Plus [Coherent, Palo Alto, Calif ] or Diomed [Diomed Inc., Andover, Mass])that produced 630 nm light with an adjusted power output of 400 mW/cm fiber and delivereda total of 200 J/cm fiber energy to the mucosa.
Endoscopic Mucosal ResectionFocal, endoscopically visible lesions underwent EMR for diagnostic purposes to determinehistology and to exclude carcinoma. EMR was performed as described previously.23 PDT wasdelayed for a minimum of 4 weeks if a patient underwent EMR to allow healing of the EMRsite(s).
All patients were placed on twice a day proton pump inhibitor therapy after PDT at the standarddose for the pump. Patients were educated carefully regarding PDT and its complications,especially dysphagia and photosensitivity, by physicians, nurse practitioners, and clinicalcoordinators. Follow-up included endoscopic surveillance with biopsies and EMR, if indicated,every 3 months for 2 years, then every 6 months for 1 or 2 years if HGD was eliminated. IfHGD persisted, then patients were followed at 3-month intervals. If LGD was present, thenpatients were followed every 6 months. If only non-dysplastic Barrett mucosa or normalsquamous mucosa was present at 2 years, then patients were followed annually. Post-PDTcytology specimens were acquired at the first endoscopy after PDT (3 months after PDT), andthe results were correlated with histology obtained from biopsies that were taken at that visit.Repeat cytology samples were collected during subsequent endoscopy in patients whoconsented to repeat acquisition of cytology specimens and repeat FISH assays.
Statistical MethodsThe associations of baseline characteristics with response outcome were assessed forcontinuous variables by using the 2-sample t test or the Wilcoxon rank-sum test, depending onthe distribution of the baseline variable. The associations for baseline categorical data wereassessed by using the chi-square test (or the Fisher exact test when necessary because of smallindividual cell frequencies). Similarly, the association of response (no vs yes at the time ofrepeat biomarker assessment) and biomarker status was assessed by using the Fisher exact test.Continuous variables were summarized as the mean (±standard deviation [SD]) or median(interquartile range [IQR]), as warranted. A P value <.05 was considered statistically
Prasad et al. Page 4
Cancer. Author manuscript; available in PMC 2009 February 5.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

significant. The difference between the proportions of positive biomarkers (pre-PDT vs post-PDT) was examined only in patients who received PDT by using the McNemar test (exactbinomial distribution) at an α level of .05. Data management and statistical analysis were doneusing SAS software (1989–2002; SAS Institute Inc., Cary, NC).
RESULTSThirty-one of 71 patients who underwent PDT with biomarker assessment between 2002 and2005 at the Mayo Clinic, Rochester had biomarkers assessed after PDT. These patients wereyounger (aged 64.5 years vs 69.7 years; P = .03) than the patients who did not have repeatbiomarkers assessed, but they had a comparable sex distribution (88% men vs 95% men,respectively; P = .39), BE segment length (5 cm vs 5.9 cm, respectively; P = .25), and 3-monthfollow-up histology (chi-square statistic, 1.7; P = .74). The median age of the cohort that hadrepeat biomarker assessment was 66 years (IQR, 56–73 years). Twenty-eight patients weremen (88%). Twenty-five patients (78%) had HGD, and the remaining patients had mucosalcancer. Post-PDT biomarkers were obtained after a median duration of 6 months (IQR, 3–12months). Twenty-four patients (77%) had no evidence of HGD on biopsies at the time of repeatsampling for biomarkers. The distribution of biomarkers pre-PDT and post-PDT for the entirecohort is illustrated in Figure 1. There was a statistically significant decrease in the proportionof several biomarkers post-PDT. Data on p53 loss were available only on 17 patients becauseof nonavailability of the probes. Three patients had evidence of p53 loss before PDT, and nonehad p53 loss after PDT. The median follow-up of patients after PDT was 22 months (IQR,11.5–25 months).
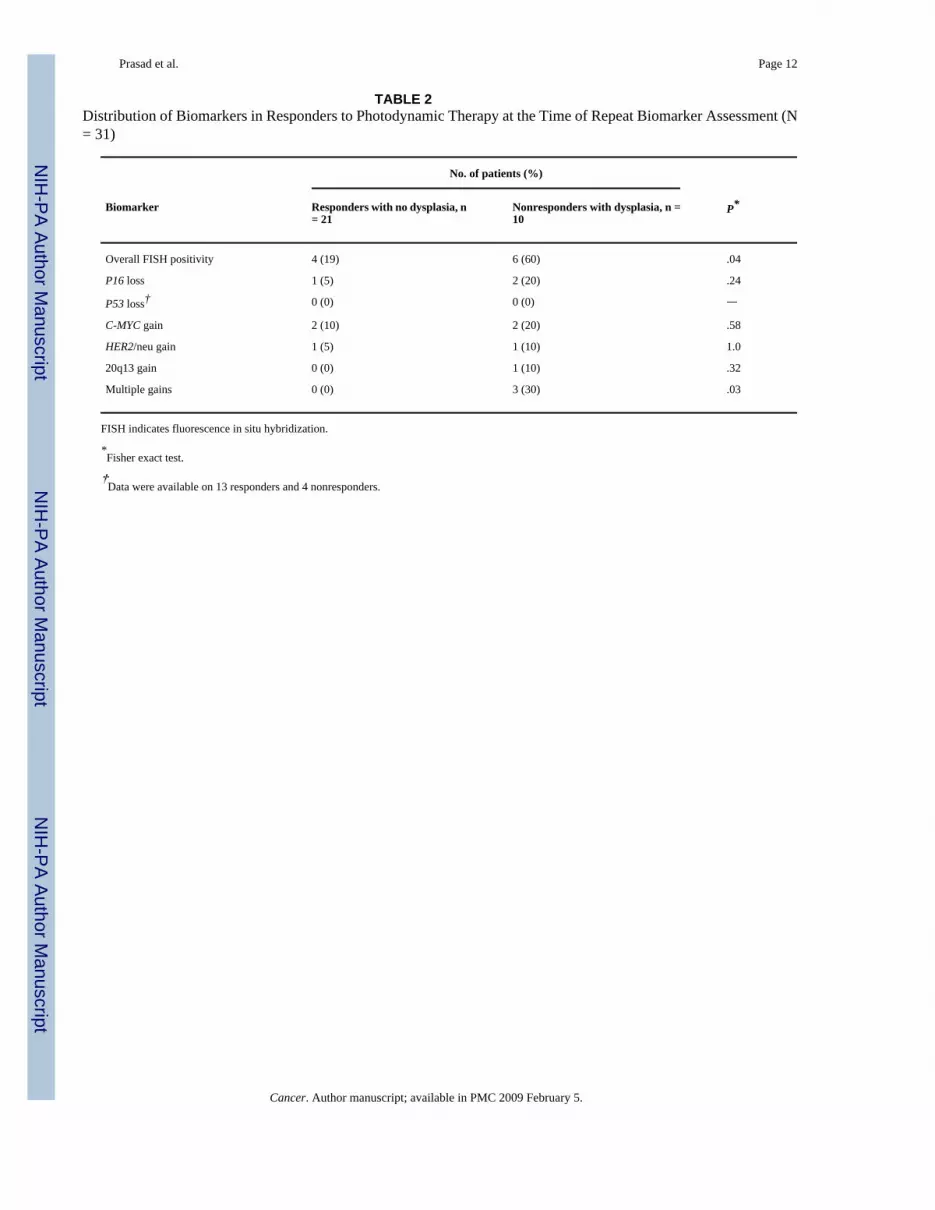
The frequency of FISH-positive results in ‘responders’ (with no evidence of dysplasia onsurveillance biopsies; n = 21) at the time of repeat biomarker assessment compared with‘nonresponders’ (n = 10) is shown in Table 2. Despite the elimination of dysplasia, a substantialminority of patients (5%–19%) remained positive by FISH, particularly for gains at oncogeneloci (8q24, 17q31.1). Multiple gains were observed in no responders compared with 30% ofnon-responders. This difference was statistically significant. The association between responsestatus and overall FISH positivity was significant (P = .04) (Table 2).
Follow-up histology of this cohort is described in Figure 2. In the subgroup of patients whohad an absence of HGD after PDT (N = 24), 6 patients remained FISH positive for 1 or morebiomarkers. Of those 6 patients, 2 patients (33%) developed recurrent HGD. One patientdeveloped HGD 9 months after PDT. He had evidence of amplification at the C-MYC locuson post-PDT FISH assessment. The second patient with recurrent HGD (which was detected10 months after PDT) had evidence of multiple gains on repeat FISH assessment. Both patientsdeveloped recurrent HGD after 2 intervening surveillance endoscopies without HGD, and bothwere treated endoscopically with EMR and remained free of HGD at the time of the currentreport. In contrast, none of the 18 patients with negative FISH studies after PDT developedrecurrent HGD over a median follow-up of 22 months (IQR, 11.5–25 months).
DISCUSSIONBarrett esophagus is a major risk factor for esophageal adenocarcinoma. Esophagectomy24and PDT25 are accepted modalities of treatment for HGD in BE and produce comparable long-term results.14 In this prospective study, we observed a statistically significant decrease in theprevalence of all biomarkers after PDT. A minority of patients with a histologic ‘response’after PDT continued to show evidence of amplification at proto-oncogene loci: That group of‘responders’ appeared to be at a higher risk of recurrent HGD on follow-up. The absence ofgenetic alterations detected by FISH, in addition to histologic response, predicted a ‘durable’response to PDT.
Prasad et al. Page 5
Cancer. Author manuscript; available in PMC 2009 February 5.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

The specific chromosomal loci examined in this study were chosen based on a previous studyin which a panel of FISH probes to these loci was able to distinguish adenocarcinoma and HGDfrom lesser grades of dysplasia with a sensitivity and specificity of approximately 80%.22 Inaddition, we selected these probes for their reliable performance characteristics and becauseof the observation that gain/amplification at proto-oncogene loci may be a more specificindicator of neoplasia than chromosomal losses.22,26
Biomarker studies on squamous islands that appear in BE during prolonged treatment withproton pump inhibitors have reported the presence of increased proliferation and p53 staining.19 Some authors speculated that this may predict increased risk of progression to cancer. Theyassessed the presence of these biomarkers and cyclooxygenase 2 (COX-2) by usingimmunohistochemistry (IHC) in residual BE after ablation20 and observed evidence ofincreased Ki-67 staining, COX-2 staining, and p53 staining at the neosquamocolumnarjunction, raising concerns of neoplastic progression after incomplete ablation therapy. Thatreport was limited by the lack of histologic follow-up in patients with positive biomarkers, andthe poor accuracy of IHC for the p53 protein compared with gene sequencing. Hage et al.reported the biomarker status of 29 patients (including 8 patients with HGD) after ablativetreatment. 21 Markers that were assessed included Ki-67 antigen testing, p53 proteinexpression by IHC, and chromosome 1 ploidy by in situ hybridization. Those authors observedthat, despite the elimination of HGD in 70% of patients, the residual Barrett epitheliumcontinued to show evidence of increased proliferation,. Although the authors speculated thatthis increased the risk of progression of dysplasia, they did not provide information onrecurrence of HGD in these patients on follow-up. Moreover, the significance of increasedproliferation in residual epithelium after ablation has yet to be determined.27 In a follow-upstudy, the authors assessed genetic alterations by using gene sequencing in preablation andpostablation biopsy specimens.28 In their cohort, only 3 patients with HGD were included.They observed that the profile of biomarkers was not different before and after ablative therapydespite the absence of HGD on follow-up biopsies. This is in contrast to our finding of asignificant change (loss of biomarkers) in post-PDT surveillance cytology specimens. Thismay be attributable to the larger number of patients with HGD included in our study (3 patientsvs 31 patients) or perhaps because of the difference in techniques.
Although, to our knowledge, this is the largest study of its kind to date, the current study hassome potential limitations. The possibility cannot be excluded that the lack of HGD on biopsiesmay reflect sampling error. This sampling error also potentially may affect the correlation ofpost-PDT biopsies and FISH markers. The fairly long period of follow-up (median, 22 months)without HGD does make this less likely. The proportion of patients with P1615 and P53loss29,30 in our cohort is lower than that reported in the literature. Compared with geneanalysis, dual-probe FISH has moderate sensitivity (68.4%) but high specificity (95.8%).31However, FISH may be more sensitive in identifying allelic loss, because LOH analysestypically require the presence of ≥70% tumor cells in a sample to be able to detect LOH.31We also performed FISH on cytology specimens, because the use of tissue sections may leadto sectioning artifacts, which could compromise FISH results. Finally, only 31 patients (44%)underwent repeat FISH assessment after PDT, raising the possibility of selection bias. Patientswho did not have repeat biomarker assessments largely had demographic and clinicalcharacteristics that were comparable to those in patients who did have repeat biomarkerassessments. Finally, we recognize that, although this may have been the largest study to datein these patients, the sample size of the study was limited, and our results need to be validatedin a larger multicenter study.
In conclusion, the absence of HGD after PDT appears to be associated with a significantdecrease in the prevalence of biomarkers associated with the progression of neoplasia in BE.Patients with a histologic response (the absence of HGD) who have persistent genetic
Prasad et al. Page 6
Cancer. Author manuscript; available in PMC 2009 February 5.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

abnormalities appear to be a higher risk of developing recurrent HGD: This cohort of patientsmay merit closer and longer surveillance. In contrast, patients who have histologic and ‘genetic’responses may be at decreased risk of recurrence and may not require further mucosal therapy.
AcknowledgementsSupported by the following grants from the National Institutes of Health; R01 CA111603-01A1, R01CA097048, andR21CA122426-01 (all to Kenneth K. Wang).
REFERENCES1. Devesa SS, Blot WJ, Fraumeni JF Jr. Changing patterns in the incidence of esophageal and gastric
carcinoma in the United States. Cancer 1998;83:2049–2053. [PubMed: 9827707]2. Provenzale D, Schmitt C, Wong JB. Barrett’s esophagus: a new look at surveillance based on emerging
estimates of cancer risk. Am J Gastroenterol 1999;94:2043–2053. [PubMed: 10445526]3. Reid BJ, Levine DS, Longton G, Blount PL, Rabinovitch PS. Predictors of progression to cancer in
Barrett’s esophagus: baseline histology and flow cytometry identify low- and high-risk patient subsets.Am J Gastroenterol 2000;95:1669–1676. [PubMed: 10925966]
4. Schnell TG, Sontag SJ, Chejfec G, et al. Long-term nonsurgical management of Barrett’s esophaguswith high-grade dysplasia. Gastroenterology 2001;120:1607–1619. [PubMed: 11375943][seecomment].
5. Weston AP, Sharma P, Topalovski M, Richards R, Cherian R, Dixon A. Long-term follow-up ofBarrett’s high-grade dysplasia. Am J Gastroenterol 2000;95:1888–1893. [PubMed: 10950031]
6. Birkmeyer JD, Stukel TA, Siewers AE, Goodney PP, Wennberg DE, Lucas FL. Surgeon volume andoperative mortality in the United States. N Engl J Med 2003;349:2117–2127. [PubMed: 14645640]
7. Orringer MB, Marshall B, Stirling MC. Transhiatal esophagectomy for benign and malignant disease.J Thorac Cardiovasc Surg 1993;105:265–276. [PubMed: 8429654]discussion 276–277
8. Overholt BF, Panjehpour M, Haydek JM. Photodynamic therapy for Barrett’s esophagus: follow-upin 100 patients. Gastrointest Endosc 1999;49:1–7. [PubMed: 9869715][see comment].
9. Attwood SE, Lewis CJ, Caplin S, Hemming K, Armstrong G. Argon beam plasma coagulation astherapy for high-grade dysplasia in Barrett’s esophagus. Clin Gastroenterol Hepatol 2003;1:258–263.[PubMed: 15017666][see comment].
10. Kovacs BJ, Chen YK, Lewis TD, DeGuzman LJ, Thompson KS. Successful reversal of Barrett’sesophagus with multipolar electrocoagulation despite inadequate acid suppression. GastrointestEndosc 1999;49:547–553. [PubMed: 10228250]
11. Buttar NS, Wang KK, Lutzke LS, Krishnadath KK, Anderson MA. Combined endoscopic mucosalresection and photodynamic therapy for esophageal neoplasia within Barrett’s esophagus.Gastrointest Endosc 2001;54:682–688. [PubMed: 11726842]
12. Pacifico RJ, Wang KK, Wongkeesong LM, Buttar NS, Lutzke LS. Combined endoscopic mucosalresection and photodynamic therapy versus esophagectomy for management of earlyadenocarcinoma in Barrett’s esophagus. Clin Gastroenterol Hepatol 2003;1:252–257. [PubMed:15017665][see comment].
13. Overholt BF, Lightdale CJ, Wang KK, et al. International, multicenter, partially blinded, randomizedstudy of the efficacy of photodynamic therapy (PDT) using porfimer sodium (POR) for the ablationof high-grade dysplasia (HGD) in Barrett’s esophagus (BE): results of 24-month follow up [abstract].Gastroenterology 2003;124:153.Abstract 151
14. Prasad GA, Wang KK, Buttar NS, et al. Long-term survival following endoscopic and surgicaltreatment of high-grade dysplasia in Barrett’s esophagus. Gastroenterology 2007;132:1226–1233.[PubMed: 17408660]
15. Wong DJ, Paulson TG, Prevo LJ, et al. p16(INK4a) lesions are common, early abnormalities thatundergo clonal expansion in Barrett’s metaplastic epithelium. Cancer Res 2001;61:8284–8289.[PubMed: 11719461]
16. Prevo LJ, Sanchez CA, Galipeau PC, Reid BJ. p53-Mutant clones and field effects in Barrett’sesophagus. Cancer Res 1999;59:4784–4787. [PubMed: 10519384]
Prasad et al. Page 7
Cancer. Author manuscript; available in PMC 2009 February 5.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

17. Walch AK, Zitzelsberger HF, Bruch J, et al. Chromosomal imbalances in Barrett’s adenocarcinomaand the metaplasia-dysplasia-carcinoma sequence. Am J Pathol 2000;156:555–566. [PubMed:10666385]
18. Tselepis C, Morris CD, Wakelin D, et al. Upregulation of the oncogene c-myc in Barrett’sadenocarcinoma: induction of c-myc by acidified bile acid in vitro. Gut 2003;52:174–180. [PubMed:12524396]
19. Garewal H, Ramsey L, Sharma P, Kraus K, Sampliner R, Fass R. Biomarker studies in reversedBarrett’s esophagus. Am J Gastroenterol 1999;94:2829–2833. [PubMed: 10520829]
20. Dvorak K, Ramsey L, Payne CM, et al. Abnormal expression of biomarkers in incompletely ablatedBarrett’s esophagus. Ann Surg 2006;244:1031–1036. [PubMed: 17122630]
21. Hage M, Siersema PD, Vissers KJ, et al. Molecular evaluation of ablative therapy of Barrett’soesophagus. J Pathol 2005;205:57–64. [PubMed: 15586364]
22. Brankley SM, Wang KK, Harwood AR, et al. The development of a fluorescence in situ hybridizationassay for the detection of dysplasia and adenocarcinoma in Barrett’s esophagus. J Mol Diagn2006;8:260–267. [PubMed: 16645214]
23. Prasad GA, Wang KK, Lutzke LS, et al. Frozen section analysis of esophageal endoscopic mucosalresection specimens in the real-time management of Barrett’s esophagus. Clin Gastroenterol Hepatol2006;4:173–178. [PubMed: 16469677]
24. Headrick JR, Nichols FC 3rd, Miller DL, et al. High-grade esophageal dysplasia: long-term survivaland quality of life after esophagectomy. Ann Thorac Surg 2002;73:1697–1702. [PubMed: 12078755]discussion 1702–1703
25. Overholt BF, Lightdale CJ, Wang KK, et al. Photodynamic therapy with porfimer sodium for ablationof high-grade dysplasia in Barrett’s esophagus: international, partially blinded, randomized phase IIItrial. Gastrointest Endosc 2005;62:488–498. [PubMed: 16185958]
26. Sokolova IA, Halling KC, Jenkins RB, et al. The development of a multitarget, multicolorfluorescence in situ hybridization assay for the detection of urothelial carcinoma in urine. J Mol Diagn2000;2:116–123. [PubMed: 11229514]
27. Krishnadath KK, Wang KK, Taniguchi K, et al. Persistent genetic abnormalities in Barrett’sesophagus after photodynamic therapy. Gastroenterology 2000;119:624–630. [PubMed: 10982754]
28. Hage M, Siersema PD, Vissers KJ, et al. Genomic analysis of Barrett’s esophagus after ablativetherapy: persistence of genetic alterations at tumor suppressor loci. Int J Cancer 2006;118:155–160.[PubMed: 16032707]
29. Wu TT, Watanabe T, Heitmiller R, Zahurak M, Forastiere AA, Hamilton SR. Genetic alterations inBarrett esophagus and adenocarcinomas of the esophagus and esophagogastric junction region. AmJ Pathol 1998;153:287–294. [PubMed: 9665490]
30. Neshat K, Sanchez CA, Galipeau PC, et al. p53 mutations in Barrett’s adenocarcinoma and high-grade dysplasia. Gastroenterology 1994;106:1589–1595. [PubMed: 8194706]
31. Wongsurawat VJ, Finley JC, Galipeau PC, et al. Genetic mechanisms of TP53 loss of heterozygosityin Barrett’s esophagus: implications for biomarker validation. Cancer Epidemiol Biomarkers Prev2006;15:509–516. [PubMed: 16537709]
Prasad et al. Page 8
Cancer. Author manuscript; available in PMC 2009 February 5.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

FIGURE 1.Comparison of biomarkers that were detected by fluorescence in situ hybridization (FISH) inpatients with high-grade dysplasia (HGD)/mucosal cancer before and after photodynamictherapy (PDT) (N = 3). *Statistically significant. NA indicates not available.
Prasad et al. Page 9
Cancer. Author manuscript; available in PMC 2009 February 5.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

FIGURE 2.Schematic representation of histologic diagnosis and fluorescence in situ hybridization (FISH)results during follow-up. PDT indicates photodynamic therapy; HGD, high-grade dysplasia;+, positive; −, negative.
Prasad et al. Page 10
Cancer. Author manuscript; available in PMC 2009 February 5.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Prasad et al. Page 11
TABLE 1Genetic Alterations Assessed Prospectively by Using Fluorescence In Situ Hybridization in Patients With High-gradeDysplasia or Mucosal Cancer in Barrett Esophagus
Biomarker* Definition of positive result
9q21/P16 status Loss
17p 13.1/P53 status Loss
8q 24/C-MYC status Gains
17q/HER-2 status Gains
20q13 status Gains
Cell ploidy Multiple gains†
*The cutoffs used for 8q (C-MYC), 9p21 (P16), 17q (HER2), and 20q were established by using receiver operating characteristic (ROC) curves. Based
on these ROC curves, a specimen was considered positive for P16 loss when ≥11% of cells exhibited hemizygous 9p21 loss, when ≥6% of cells exhibitedhomozygous 9p21 loss, or when ≥11% of cells exhibited a mixture of hemizygous and homozygous 9p21 loss. Thresholds for categorizing results aspositive for the other probes were as follows: ≥14% of cells exhibited p53 loss (cutoff for P53 loss was the average percentage of P53 loss ±3 standarddeviation observed in a normal value study) (unpublished observations), or ≥5% of cells demonstrated gains of 8q24, 17q11.2, or 20q13. ‘Multiple gains’were defined as gains of 2 or more of the 8q24, 17q11.2, or 20q13 loci by using previously defined thresholds.
†Defined as gains of 2 or more of the 4 probes in a patient.
Cancer. Author manuscript; available in PMC 2009 February 5.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Prasad et al. Page 12
TABLE 2Distribution of Biomarkers in Responders to Photodynamic Therapy at the Time of Repeat Biomarker Assessment (N= 31)
No. of patients (%)
Biomarker Responders with no dysplasia, n= 21
Nonresponders with dysplasia, n =10
P*
Overall FISH positivity 4 (19) 6 (60) .04
P16 loss 1 (5) 2 (20) .24
P53 loss† 0 (0) 0 (0) —
C-MYC gain 2 (10) 2 (20) .58
HER2/neu gain 1 (5) 1 (10) 1.0
20q13 gain 0 (0) 1 (10) .32
Multiple gains 0 (0) 3 (30) .03
FISH indicates fluorescence in situ hybridization.
*Fisher exact test.
†Data were available on 13 responders and 4 nonresponders.
Cancer. Author manuscript; available in PMC 2009 February 5.













![[Steven F. Barrett] Arduino Microcontroller Proces(Book ZZ org)](https://img.pdfslide.net/doc/110x75/634cf5843bdc8e8810071d9a/steven-f-barrett-arduino-microcontroller-procesbook-zz-org.jpg)















