Embed Size (px)
Citation preview
Contents lists available at ScienceDirect
Can J Diabetes 38 (2014) 205e211
Canadian Journal of Diabetesjournal homepage:
www.canadianjournalofdiabetes.com
Original Research
D-WISE: Diabetes Web-Centric Information and SupportEnvironment: Conceptual Specification and Proposed Evaluation
Samina Abidi PhD, MBBS, MSc a,*, Michael Vallis PhD, R Psych b, Syed Sibte Raza Abidi PhD, MS, BE c,Helena Piccinini-Vallis MD, MSc, CCFP e, Syed Ali Imran MBBS, FRCP, FRCPC d
aMedical Informatics Program, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, CanadabCDHA Behaviour-Change Institute, QEII Health Sciences Center, Halifax, Nova Scotia, CanadacNICHE Research Group, Faculty of Computer Science, Dalhousie University, Halifax, Nova Scotia, CanadadDivision of Endocrinology and Metabolism, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, CanadaeDepartment of Family Medicine, Faculty of Medicine, Dalhousie University, Halifax, Nova Scotia, Canada
a r t i c l e i n f o
Article history:Received 7 March 2014Received in revised form23 March 2014Accepted 24 March 2014
Keywords:behaviour changeclinical decision supportdiabetes self-managementhealthcare knowledge modeling
* Address for correspondence: Samina Abidi, PhDmatics Program, Division of Medical Education, FacUniversity, 5849 University Avenue, PO Box 15000, HCanada.
E-mail address: [email protected]
1499-2671/$ e see front matter � 2014 Canadian Diahttp://dx.doi.org/10.1016/j.jcjd.2014.03.006
a b s t r a c t
Objective: To develop and evaluate Diabetes Web-Centric Information and Support Environment(D-WISE) that offers 1) a computerized decision-support system to assist physicians to A) use theCanadian Diabetes Association clinical practice guidelines (CDA CPGs) to recommend evidence-informedinterventions; B) offer a computerized readiness assessment strategy to help physicians administerbehaviour-change strategies to help patients adhere to disease self-management programs; and 2) apatient-specific diabetes self-management application, accessible through smart mobile devices, thatoffers behaviour-change interventions to engage patients in self-management.Methods: The above-mentioned objectives were pursued through a knowledge management approachthat involved 1) Translation of paper-based CDA CPGs and behaviour-change models as computerizeddecision-support tools that will assist physicians to offer evidence-informed and personalized diabetesmanagement and behaviour-change strategies; 2) Engagement of patients in their diabetes care bygenerating a diabetes self-management program that takes into account their preferences, challengesand needs; 3) Empowering patients to self-manage their condition by providing them with personalizededucational and motivational messages through a mobile self-management application. The theoreticalfoundation of our research is grounded in behaviour-change models and healthcare knowledgemanagement.We used 1) knowledge modelling to computerize the paper-based CDA CPGs and behaviour-changemodels, in particular, the behaviour-change strategy elements of A) readiness-to-change assessments;B) motivation-enhancement interventions categorized along the lines of patients’ being ready, ambiva-lent or not ready; and C) self-efficacy enhancement. The CDA CPGs and the behaviour-change models aremodelled and computerized in terms of A) a diabetes management ontology that serves as the knowl-edge resource for all the services offered by D-WISE; B) decision support services that use logic-basedreasoning algorithms to utilize the knowledge encoded within the diabetes management ontology toassist physicians by recommending patient-specific diabetes-management interventions and behaviour-change strategies; C) a mobile diabetes self-management application to engage and educate diabetespatients to self-manage their condition in a home-based setting while working in concert with theirfamily physicians.Results: We have been successful in creating and conducting a usability assessment of the physiciandecision support tool. These results will be published once the patient self- management application hasbeen evaluated.Conclusions: D-WISE will be evaluated through pilot studies measuring 1) the usability of the e-Healthinterventions; and 2) the impact of the interventions on patients’ behaviour changes and diabetes control.
� 2014 Canadian Diabetes Association
, MBBS, MSc, Medical Infor-ulty of Medicine, Dalhousiealifax, Nova Scotia B3H 4R2,
betes Association

S. Abidi et al. / Can J Diabetes 38 (2014) 205e211206
Mots clés :
changement du comportementaide à la décision cliniqueprise en charge autonome du diabètemodélisation des connaissances en matièrede soins de santér é s u m é
Objectif : Développer et évaluer le D-WISE (Diabetes Web-Centric Information and Support Environment)de manière à offrir : 1) un système informatisé d’aide à la décision qui contribuera à ce que les médecins :A) utilisent les lignes directrices de pratique clinique de l’Association canadienne du diabète (LDPC-ACD)en vue de proposer des interventions fondées sur des données probantes, B) offrent une stratégied’évaluation informatisée de la réceptivité au changement les aidant à gérer les stratégies de change-ment du comportement dans le but d’encourager les patients à s’inscrire aux programmes de prise encharge autonome de la maladie; 2) une application personnalisée pour la prise en charge autonome dudiabète qui sera ccessible à partir d’appareils mobiles intelligents et qui proposera des interventionsvisant à favoriser les changements du comportement dans le but d’encourager les patients à se prendreen charge de manière autonome.Méthodes : Les objectifs mentionnés ci-dessus ont été assurés par une approche de prise en charge desconnaissances qui faisait appel : 1) à la traduction des LDPC-ACD en format papier et aux modèles dechangement du comportement comme les outils informatiques d’aide à la décision qui aideront lesmédecins à offrir une prise en charge du diabète personnalisée et fondée sur des données probantes, etdes stratégies visant à favoriser les changements de comportement; 2) à la participation des patients àleurs soins de diabète en générant un programme de prise en charge autonome du diabète qui tientcompte de leurs préférences, leurs difficultés et leurs besoins; 3) à l’habileté des patients à prendre encharge de manière autonome leur affection en leur offrant des messages personnalisés éducatifs etmotivants à partir d’une application mobile sur la prise en charge autonome. Les fondements théoriquesde notre recherche reposent sur les modèles de changement du comportement et de gestion des con-naissances en matière de soins de santé.Nous avons utilisé : 1) la modélisation des connaissances pour informatiser les LDPC-ACD et les modèlesde changement du comportement, en particulier, les éléments de stratégie de changement du com-portement : A) les évaluations de la réceptivité au changement; B) les interventions d’amélioration de lamotivation catégorisées selon l’ambivalence ou la non réceptivité des patients au changement; C)l’amélioration de l’auto-efficacité. Les LDPC-ACD et les modèles de changement du comportement sontmodélisés et informatisés quant : A) à l’ontologie pour la prise en charge du diabète qui sert de ressourced’information pour tous les services offerts par le D-WISE; B) aux services d’aide à la décision qui uti-lisent les algorithmes sur le raisonnement logique pour exploiter les connaissances encodées dansl’ontologie pour la prise en charge du diabète afin d’aider les médecins en proposant des interventionspersonnalisées sur la prise en charge du diabète et des stratégies de changement du comportement; C) àune application mobile sur la prise en charge autonome du diabète pour encourager et éduquer lespatients diabétiques à prendre en charge de manière autonome la maladie dans le cadre de leur domiciletout en collaborant avec leur médecin de famille.Résultats : Nous avons réussi à créer et la réalisation d’une évaluation de la convivialité de l’outil d’aide àla décision du médecin. Ces résultats seront publiés une fois l’application d’auto-gestion des patients aété évaluée.Conclusions : Le D-WISE sera évalué par des études pilotes mesurant : 1) la convivialité des interventionsen télésanté; 2) l’effet des interventions sur les changements de comportement des patients et lamaîtrise de leur diabète.
� 2014 Canadian Diabetes Association
Introduction motivation is low (e.g. stages of change (8,9), theory of planned
The World Health Organization considers type 2 diabetes aglobal epidemic in which the prevalence in 2010 of 285 millionpeople is expected to grow to 438 million by 2030 (1). More than3 million Canadians live with diabetes and are at serious risk formorbidity, complications and mortality. According to the CanadianDiabetes Association (CDA), the personal costs of diabetes medi-cations and supplies is $1000 to $15,000 per year, and diabetes-related healthcare costs are estimated to grow to almost$17 billion by 2020 (2). Although the pathophysiology of diabetes iswell understood and is supported by effective interventions,effective diabetes self-management rests largely on the behaviourof the individuals (3,4). Optimal diabetes control requires ongoingadherence to medication and medical care, self-monitoring ofblood glucose, achieving a healthful weight, eating healthily, notsmoking, drinking moderately, being physically active and man-aging stress. The goal of the diabetes self-management interventionis to support the individual inmaking all of the behavioural changesrequired to achieve optimal diabetes control. Behavioural science isnow being integrated into diabetes self-management interventions(5e7) to better educate and engage individuals in self-managementof the condition. It involves theory-driven, evidence-basedapproaches a) to increase motivation to change when such
behaviour (10), social cognitive theory (11,12)), and b) motiva-tional interviewing (2,13) to support effective behaviour-changewhen motivation is present (14); and c) to address emotionaland relational barriers to change when they arise (15,16). Theseapproaches have been developed and applied to chronic-diseasemanagement in general and to diabetes control in particular.Our group, through the Behaviour Change Institute (BCI), hasdeveloped specialized behaviour-change training modules thatboth train and empower primary care providers, certified dia-betes educators (CDEs) and patients living with diabetes to usebehaviour-change methods to achieve clinical outcomes moreeffectively. Despite the availability of specialized behaviour-change interventions and evidence-based CDA clinical practiceguidelines (CPGs) (17) on diabetes management, the challenge isto translate these knowledge resources at the point of care suchthat family physicians (FPs) and CDEs can use them to offerevidence-informed behaviour-change support and diabetes man-agement to individuals with diabetes. Given that there are toofew training opportunities and significant barriers to the uptakeof intensive competency-based training programs, it is prudent toleverage technology-enabled mechanisms to deliver CDA CPGs-informed diabetes care and behaviour-change interventions tosupport FPs and CDEs in managing diabetes.

S. Abidi et al. / Can J Diabetes 38 (2014) 205e211 207
Rationale and Solution
Diabetes is managed by FPs in primary care settings and indiabetes management centres (DMCs) using health providersqualified by the CDA as CDEs. Although DMCs exist across thecountry, approximately 70% of individuals living with diabetes donot attend a DMC due to access limitations; rather, they mayreceive care from FPs (4,15). A number of Canadian (15,16,18) andinternational studies (19,20) have found suboptimal managementof type 2 diabetes in primary care settings, including suboptimalglycemic control (18,19,21) and failure to achieve CPGs-recommended targets for blood pressure and LDL cholesterol inpatients with type 2 diabetes (18e20). These studies suggest thatFPs’ knowledge of glycemic control does not necessarily translateinto action. The CDA CPGs recommend that an individual withdiabetesmanage the diseasewith the help of an integrated diabeteshealth team, employing a self-management model that blendsknowledge and skills development with cognitive behaviouralinterventions. Furthermore, individuals with diabetes (and theirfamilies) should be screened regularly for symptoms of psycho-logical distress, and preventive interventions, such as participativedecision making, feedback and psychological support, should beincorporated into diabetes self-management interventions. Thestate of affairs is that the recommendations proposed by the CDAare not being implemented in the diabetes care process currentlybecause of 1) lack of access to psychosocial resources within dia-betes medical servicesdFP and CDE are not well equipped tomanage behaviour change in individuals with low motivation orpsychosocial barriers to change; and 2) lack of incorporation of theCPGs in the care process at the family-practice level.
Given the above-mentioned challenges pertaining to the lack ofcare providers’ access to standardized behaviour-change strategiesand the CDA CPGs for diabetes control and, furthermore, the lack ofself-management and support for behaviour change by patients,we propose an e-Health solution to improve diabetes managementat the DMC, primary care and patient levels. This project aims toleverage e-Health technologies to develop the Diabetes Web-Centric Information and Support Environment (D-WISE) that fea-tures the following functionalities: 1) assessment of physicians’readiness to administer validated behaviour-change interventionswhen treating patients with diabetes; 2) educational support to FPsto help them offer behaviour-change interventions to patients withdiabetes; 3) access to evidence-based material, such as the CDACPGs; 4) development of personalized patient self-managementprograms to help diabetic patients achieve healthful behavioursso they can meet CDA targets for managing type 2 diabetes; 5)educational support for patients to help them in achieving behav-iour change; 6) monitoring patients’ progress in adhering to theirbehaviour-change programs and motivating them to be incompliance with their programs. D-WISE offers these functionsthrough an interactive web-based interface to physicians, whereasthe patients’ self-management programs and associated behaviourinterventions are delivered through smart mobile devices (phonesand tablets). A systematic review (21) of 42 controlled trials ofmobile technology interventions to improve healthcare deliveryprocesses indicated that some of these interventions are modestlyeffective. The review highlighted the need for more evaluations ofsuch interventions.
Research Approach
The research pursued in the D-WISE project is 2-fold: 1) toleverage theory-driven evidence-based behaviour-change modelsto enhance individuals’ self-efficacy in pursuing behaviour-change;and 2) to computerize and translate paper-based CPGs (in this caseCDA’s CPGs) as a point-of-care decision-support system so
physicians could discharge evidence-based care. The theoreticalfoundation of our research is grounded in the chronic care model(22), behaviour-change models (the knowledge content) (23,24)and healthcare knowledge management (the knowledge trans-lation method).
We suggest that health education and support for chronicdisease self-management should not focus solely on changingpatients’ awareness of the disease; rather, they should focus onempowering patients to make the right choices for achievingeffective disease management. In this regard, our researchapproach was to incorporate validated behaviour-change theories,in our case social cognition theory (25), so as to address individuals’self-efficacy expectations and perceived capabilities of learning andperforming self-care actions (25). Self-efficacy attainment has beenshown to influence individuals’ motivations, accomplishments,self-regulation, and efforts to perform self-care actions (25). Wenote that patient education programs grounded in self-efficacytheory have been shown to enhance patients’ adherence to self-care behaviour that has in turn been shown to improve clinicaloutcomes (26e29). Based on the principles of social cognitiontheory, our approach was to develop a specialized behaviour-change strategy that first assesses the physicians’ and patients’readiness to undertake behaviour-change interventions and then,in response to the physicians’ and patients’ readiness levels, stip-ulate a personalized behaviour-change program.
To computerize the CDA CPGs and the behaviour-change strat-egy, we have taken a healthcare-knowledgemanagement approachwhereby we have developed semantically rich knowledge modelsthat encapsulated the underlying knowledge resources. We havepursued ontology-based knowledge modelling to develop aknowledge model that represents diabetes-management conceptsand their relationships, constraints and rules. Ontology offers asemantically rich, unambiguous and executable representation ofheterogeneous healthcare knowledge sources by establishingsemantic relationships among knowledge elements. The knowl-edge represented within an ontology can be executed, using simpleif-then-else rules, to derive decision support around care actionsand recommendations in line with specific patients’ profiles(30e32). Ontologies have been used extensively to capture andrepresent medical knowledge because they allow human experts tovalidate the knowledge readily and intelligent computer systems toprocess the knowledge to derive knowledge-driven recommenda-tions. We are using OWL (Web Ontology Language), which is acomputational logic-based language to develop our ontologicalmodel.
An innovative aspect of our research approach is the modellingof the knowledge and workings of the BCI in terms of an ontology-based knowledge model, thus enabling the translation of thisspecialized knowledge to nonspecialists. In this regard, the D-WISEproject is developing an integrated knowledge model that willentail sections of the CDA CPGs pertaining to the management ofglycemic control and elements of BCI’s behaviour-change strategy,including assessments of readiness to change; motivation-enhancement interventions categorized along the lines ofpatients’ being ready, ambivalent or not ready; and self-efficacyattainment and self-management.
Research objectives
The broad objective of this research program is to develop aninnovative diabetes web-centric information and support envi-ronment (D-WISE) using state-of-the-art e-Health technologies inorder to:
S. Abidi et al. / Can J Diabetes 38 (2014) 205e211208
1. Assist FPs and CDE through web-based decision-support aidsthat will coach them on how to apply standardized behaviour-change strategies and evidence-based clinical guidelines
2. Empower patients with the skills and knowledge to self-manage and monitor their diabetes through planned, person-alized and pervasive chronic disease self-management andbehaviour-change strategies delivered via smart mobiledevices according to the behaviour changes (23).
Proposed Research Methodology
Our proposed research methodology comprises the followingstages:
1. Knowledge modelling to formalize and computerize the CDAdiabetes CPGs, behaviour-change models and behaviour-changestrategies practiced by the BCI in terms of ontology-basedknowledge models that will serve as the knowledge base forD-WISE
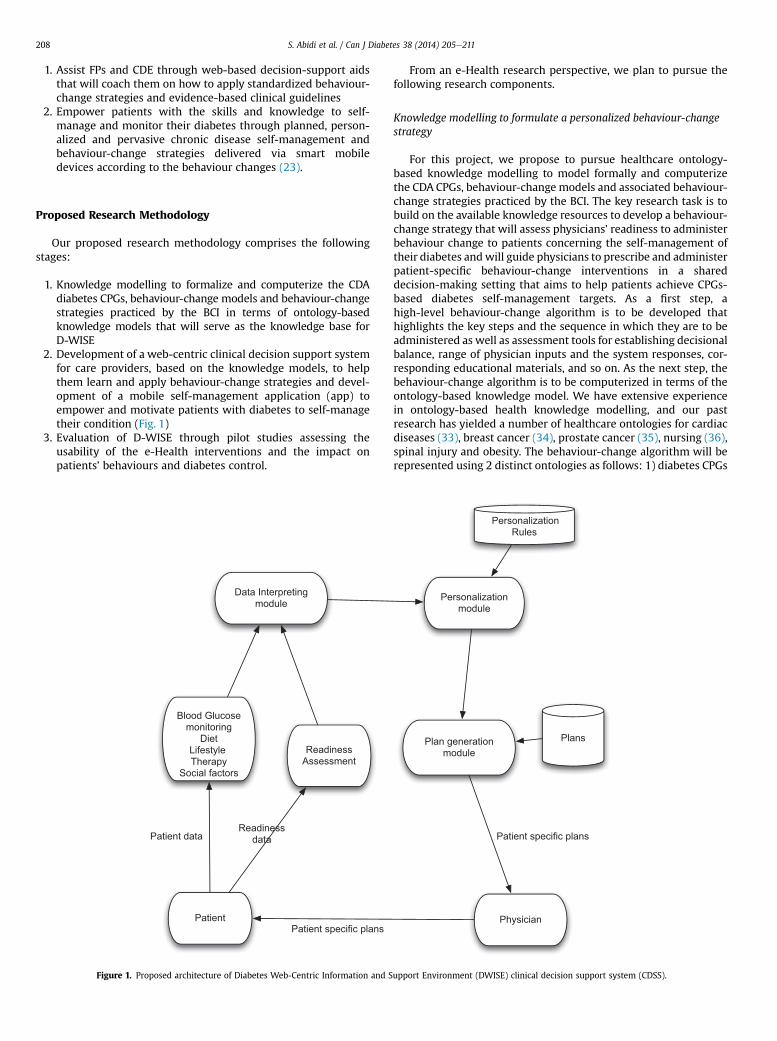
2. Development of a web-centric clinical decision support systemfor care providers, based on the knowledge models, to helpthem learn and apply behaviour-change strategies and devel-opment of a mobile self-management application (app) toempower and motivate patients with diabetes to self-managetheir condition (Fig. 1)
3. Evaluation of D-WISE through pilot studies assessing theusability of the e-Health interventions and the impact onpatients’ behaviours and diabetes control.
Patient
Blood Glucose monitoring
DietLifestyleTherapy
Social factors
Readiness Assessment
Patient data
Patient specific plans
Readiness data
Data Interpreting module
Figure 1. Proposed architecture of Diabetes Web-Centric Information and S
From an e-Health research perspective, we plan to pursue thefollowing research components.
Knowledge modelling to formulate a personalized behaviour-changestrategy
For this project, we propose to pursue healthcare ontology-based knowledge modelling to model formally and computerizethe CDA CPGs, behaviour-change models and associated behaviour-change strategies practiced by the BCI. The key research task is tobuild on the available knowledge resources to develop a behaviour-change strategy that will assess physicians’ readiness to administerbehaviour change to patients concerning the self-management oftheir diabetes andwill guide physicians to prescribe and administerpatient-specific behaviour-change interventions in a shareddecision-making setting that aims to help patients achieve CPGs-based diabetes self-management targets. As a first step, ahigh-level behaviour-change algorithm is to be developed thathighlights the key steps and the sequence in which they are to beadministered as well as assessment tools for establishing decisionalbalance, range of physician inputs and the system responses, cor-responding educational materials, and so on. As the next step, thebehaviour-change algorithm is to be computerized in terms of theontology-based knowledge model. We have extensive experiencein ontology-based health knowledge modelling, and our pastresearch has yielded a number of healthcare ontologies for cardiacdiseases (33), breast cancer (34), prostate cancer (35), nursing (36),spinal injury and obesity. The behaviour-change algorithm will berepresented using 2 distinct ontologies as follows: 1) diabetes CPGs
Physician
Plan generation module
Personalization module
Plans
PersonalizationRules
Patient specific plans
upport Environment (DWISE) clinical decision support system (CDSS).

S. Abidi et al. / Can J Diabetes 38 (2014) 205e211 209
ontology to computerize the CDA CPGs, which will encapsulatediabetes-management knowledge; 2) behaviour model ontology tocomputerize the behaviour-change models and the specific stra-tegies used by the BCI, which will encapsulate the behaviour-change knowledge and expertise present in the research team.
Our approach is to model the diabetes-management andbehaviour-change knowledge as 2 separate ontologies so that theknowledge models are scalable and reusable across multipleapplications. During operation we will integrate these 2 distinctknowledge sources according to the behaviour-change algorithm.The integrated knowledge model for behaviour change will beevaluated for knowledge accuracy by experts and semantic accu-racy to ensure logical consistency (37).
Clinical decision support system for family physicians and diabeteseducators
We plan to develop a web-enabled diabetes-managementdecision-support system using the above-mentioned knowledgemodel so as to assist providers in delivering evidence-baseddisease-management recommendations and behaviour-changestrategies. In operation, the decision-support system care pro-viders will use the web-based clinical decision support system(CDSS) while engaging with their patients in a shared decision-making setting to develop a personalized behaviour-change strat-egy, akin to behaviour-change consultations performed at the BCI.The research will involve the dynamic generation of patient-specific disease management and behaviour-change strategies byoperationalizing the above-mentioned computerized behaviour-change algorithm based on patients’ current disease and behav-iour profiles.
We will leverage our existing research in semantic web tech-nologies for integrating multiple ontologies (38) and exploit ourOWL-based reasoning methods (39) to infer a dynamically gener-ated patient-specific behaviour-change strategy. The knowledgemanagement and behaviour-change expertise in the team willmanage the CDSS development.
Mobile self-management application for diabetes patients
This research project is targeting patient-centred e-Health so-lutions for self-management of diabetes in a home-based setting.For patients with diabetes, D-WISE will offer a diabetes messaging,monitoring and management mobile app for patients to self-manage their diabetes and achieve self-efficacy in attainingbehaviour change (40) through their smartphones and tablets.Based on the patients’ self-management and behaviour-changegoals, the mobile app will deliver to patients 1) self-efficacyattainment, behaviour-change (goal setting, behaviour shaping,stimulus control and reinforcement management) strategies(27,41); 2) context-aware motivational and behaviour-changeeducational messages; 3) diaries for capturing vitals, diet, exer-cise, stress and mood; 4) communication with care providers; and5) proactive alerts and reminders. We recognize the existence ofmobile apps for diabetes; however, existing apps offer only patient-data capture functions (42), whereas we propose an intelligentdiabetes app that uses behaviour models to offer personalizeddiabetes management. The apps will be developed for the Androidplatform with provisions for a future iOS-based apps. We will useour experience in developing web-based personalized patient-education programs (43) and mobile health apps, whereas thehealth team members will guide the content and clinical usabilityof the app. Data security and privacy regulations will be followed;no patient data will reside on the app, and only encrypted patientidentification and data will be communicated to and stored at asecure backend server, which is a computer resource that has not
been exposed to the Internet and thereforewill not directly interactwith the users. No personal identifiers will be stored on the server.
Evaluation
We plan a pilot study of the functional usability of D-WISE froma care-provider perspective. We propose to use a cognitive andusability engineering framework (44) to establish whether D-WISEmeets the functional goals, content suitability and comprehen-siveness and usability needs of care providers. The study willincorporate background and postinteraction questionnaires inaddition to think-aloud protocol methods (45) to record the users’actual interactions with D-WISE. The qualitative think-aloud datawill be analyzed using the grounded theory method (46). Ethicsapproval from the Dalhousie University Health Sciences ResearchEthics Board will be sought. For this study we plan to recruit 10 careproviders; the sample size is estimated based on the evidence that70% of severe usability problems can be uncovered through the first5 users and up to 85% by the eighth user (44). The observations willbe used to improve D-WISE. We plan another pilot study to assessthe short-term impact of D-WISE on patient behaviour and asso-ciated health parameters. We plan to recruit a sample of 25individuals with type 2 diabetes from the Capital Health DiabetesPrograms with the aid of the knowledge user. The participants willuse the mobile app for 4 weeks, following a 2-week run-in periodthat will serve as a comparison stage. We will collect the followingdata: 1) frequency of app use; 2) frequency and timing of glucosemonitoring and glucose values (the frequency of glucose moni-toring and average daily glucose levels will be compared withpre-tool to post-tool use values; 3) self-reported adherence datagathered using the Morisky Medication Adherence Scale (47) andthe Summary of Diabetes Self-Care Activities Scale (48); and 4) self-reported diabetes distress based on the Diabetes Distress Scale (49)and the Diabetes Empowerment Scale-Short Form (50). Partici-pants will complete these self-report batteries at enrolment(pre-post tool use), again at the end of the 2-week run-in period,and again at the end of the 4-week evaluation period to allow forcomparisons.
Expected Contribution and Significance
E-Health technologies have been used effectively for healthinformation collection, information utilization and sharing solu-tions. E-Health apps can incorporate evidence-based healthcareknowledge to provide evidence-informed decisions. The incorpo-ration of evidence-based CPGs within computerized decision sup-port systems is a major challenge because CPGs are notdocumented in a manner that clearly articulates the clinicaldecision-making process. The significance of this research programis that it will provide a unique e-Health solution to translatecomplex healthcare knowledgedi.e. guidelines, clinical workflows,behaviour models, educational content and long-term careplansdin terms of easy-to-use, evidence-informed, point-of-caredecision aids for both care providers and patients. From a clinicalstandpoint, the contribution of this project is the translation ofspecialized behaviour-change knowledge to primary care providersand diabetes educators, thus enabling them to offer behaviour-change interventions to a larger population of diabetes patientsdatpresent only one-third of Canadians with diabetes receivediabetes educational programs. From the patients’ perspective,the contribution is a self-management program that engages andempowers them to manage their condition in home-based andprimary-care settings as opposed to specialist clinics. The uniqueaspect of this research is the demonstration of the synthesis ofpaper-based medical knowledge, behaviour-change models,healthcare knowledge management methods, and mobile

S. Abidi et al. / Can J Diabetes 38 (2014) 205e211210
technologies to develop intelligent and adaptive mobile patient-centred solutions that are customizable to specific care contextsand users’ knowledge and interests. The project will contribute ageneric e-Health strategy and technology based on theoreticalmodels that can be applied to a range of medical conditions todeliver intelligent and ubiquitous health educational and decisionaids.
Conclusions and Future Directions
This research program has long-term implications for themanagement of chronic disease and the engagement of patientsleveraging state-of-the-art e-Health technologies. This project willdevelop and demonstrate the potential of e-Health technologies fordiabetes self-management. The knowledge-modelling methodsand decision-support technologies being developed are both scal-able and generic in nature, such that they can be applied readily tocomputerize CPGs for other chronic diseases so as to develop low-cost decision-support aids that can standardize the care of chronicdiseases and comorbidities at the level of primary care. In the longterm, we plan to extend the research to other chronic diseaseswhere we will account for different disease-specific contextualfactors. In the medium term, wewill augment the research scope toincorporate other related metabolic conditions that are character-ized by hyperglycemia such as prediabetes. In the next stage, weplan to clinically evaluate D-WISE for its effectiveness and safety inprimary care settings, with the intent of disseminating it across theprovince of Nova Scotia. Through D-WISE, we plan to strengthenour linkages with public health, national and international agenciesresponsible for the dissemination of diabetes education and self-management strategies among diabetic patients. In a globalhealth setting, working with our collaborators in low- and middle-income countries, we plan to adapt and introduce D-WISE as alow-cost evidence-based intervention for patient-centred self-management of chronic conditions.
Author Disclosures
A Canadian Institute of Health Research (CIHR), E-Health Inno-vation (Catalyst) Grant has supported this research financially.
Author Contributions
SA was responsible for the healthcare knowledge modelling andcomputerization; MV led the research in formalizing the behaviour-change knowledge content and the application of behaviour-changestrategies; SSRA led the technical development and deployment ofthe e-Health infrastructure for D-WISE; SAI contributed to thedevelopment of subject matter related to diabetes management,especially regarding the application of clinical guidelines; HP servedas the primary-care specialist to help develop the interventions andassist in the evaluation of the study; SA, MV, and HPV drafted theoriginal manuscript with inputs from the other authors.
References
1. World Health Organization Fact Sheet #312, August 2011; IDF DiabetesAtlas (4th ed. 2009). http://www.who.int/mediacentre/factsheets/fs312/en/.Accessed October 10, 2012.
2. Canadian Diabetes Association. The prevalence and costs of diabetes: Facts,2009. http://www.diabetes.ca/diabetes-and-you/what/prevalence/. AccessedOctober 12, 2012.
3. Fisher EB, Fitzgibbon ML, Glasgow RE, et al. Behavior matters. Am PreventiveMed 2011;40:e15e30.
4. Glasgow RE, Fisher EB, Anderson BJ, et al. Behavioral science in diabetes:Contributions and opportunities. Diabetes Care 1999;22:832e43.
5. Packer TL, Boldy D, Ghahari S, et al. Self-management programs conductedwithin a practice setting: Who participates, who benefits and what can belearned? Patient Educ Couns 2012;87:93e100.
6. Jones H, Edwards L, Vallis TM. Changes in diabetes self-care behaviors make adifference to glycemic control: The Diabetes Stages of Change (DiSC) study.Diabetes Care 2003;26:732e7.
7. Vallis M, Ruggiero L, Greene G, et al. Stages of change for healthy eating indiabetes: relation to demographic, eating-related, health care utilization, andpsychosocial factors. Diabetes Care 2003;26:1468e74.
8. Nguyen MN, Potvin L, Otis J. Regular exercise in 30- to 60-year-old men:Combining the stages-of-change model and the theory of planned behavior toidentify determinants for targeting heart health interventions. J CommunHealth 1997;22:233e46.
9. King DK, Glasgow RE, Toobert DJ, et al. Self-efficacy, problem solving, andsocial-environmental support are associated with diabetes self-managementbehaviors. Diabetes Care 2010;33:751e3.
10. Mishali M, Omer H, Heymann AD. The importance of measuring self-efficacy inpatients with diabetes. Fam Pract 2011;28:82e7.
11. Miller WR, Rose GS. Toward a theory of motivational interviewing. Am Psychol2009;64:527e37.
12. Wing RR, Goldstein MG, Acton KJ, et al. Behavioral science research in diabetes:Lifestyle changes related to obesity, eating behavior, and physical activity.Diabetes Care 2001;24:117e23.
13. Soo H, Lam S. Stress management training in diabetes mellitus. J Health Psychol2009;14:933e43.
14. Fisher EB, Thorpe CT, Devellis BM, Devellis RF. Healthy coping, negative emo-tions, and diabetes management: A systematic review and appraisal. DiabetesEduc 2007;33:1080e103. discussion 1104-86.
15. Kirkman MS, Williams SR, Caffrey HH, Marrero DG. Impact of a program toimprove adherence to diabetes guidelines by primary care physicians. DiabetesCare 2002;25:1946e51.
16. Harrisa SB, Ekoéb J, Zdanowiczc Y, Webster-Bogaerta S. Glycemic control andmorbidity in the Canadian primary care setting (results of the diabetes inCanada evaluation study). Diabetes Res Clin Prac 2005;70:90e7.
17. Canadian Diabetes Association Clinical Practice Guidelines Expert Committee.Canadian Diabetes Association 2013 Clinical Practice Guidelines for the Pre-vention and Management of Diabetes in Canada. http://guidelines.diabetes.ca.Accessed January 12, 2014.
18. Braga MF, Casanova A, Teoh H, et al. Poor achievement of guidelines-recommended targets in type 2 diabetes: Findings from a contemporary pro-spective cohort study. Int J Clin Pract 2012;66:457e64.
19. Stein R, Aubart-Schuller M, Vandenberghe H. Evaluation and care of patientswith type II diabetes regarding recommendations concerning cardiovascularrisk factors and adherence to values in general medicine in the Grand Duchy ofLuxembourg. Bull Soc Sci Med Grand Duche Luxemb 2010;2:289e301.
20. Kirk JK, Huber KR, Clinch CR. Attainment of goals from national guidelinesamong persons with type 2 diabetes: A cohort study in an academic familymedicine setting. N C Med J 2005;66:415e9.
21. Free C, Phillips G, Watson L, et al. The effectiveness of mobile-health tech-nologies to improve health care service delivery processes: A systematic re-view and meta-analysis. PLoS Med 2013;10:e1001363.
22. Wagner EH, Austin BT, VonKorff M. Organizing care for patients with chronicillness. Milbank Q 1996;74:511e44.
23. Elder JP, Ayala GX, Harris S. Theories and intervention approaches to healthbehavior change in primary care. Am J Prevent Med 1999;17:275e84.
24. Taylor D, Bury M, Campling N, et al. A review of the use of the Health BeliefModel (HBM), the Theory of Reasoned Action (TRA), the Theory of PlannedBehavior (TPB) and the Trans Theoretical Model (TTM) to study and predicthealth related behavior change. www.nice.org.uk/nicemedia/live/11868/44524/44524.pdf. Accessed October 10, 2012.
25. Bandura A. Social foundations of thought and action: a social cognitive theory.Englewood Cliffs: Prentice Hall, 1986.
26. McGowan P. The effect of diabetes patient education and self-managementeducation in type 2 diabetes. Can J Diabetes 2012;35:46e53.
27. Lorig KR, Holman H. Self-management education: History, definition, outcomesand mechanism. Ann Behav Med 2003;26:1e7.
28. Lorig KR, Sobel DS, Ritter PL, et al. Effect of self-management program onpatient with chronic disease. Effect Clin Pract 2001;4:256e61.
29. Norris SL, Lau J, Smith SJ, et al. Self-management education for adults with type2 diabetes: a meta-analysis of the effect of glycemic control. Diabetes Care2002;25:1159e71.
30. Peleg M, Tu SW. Design patterns for clinical guidelines. Artif Intell Med 2009;47:1e24.
31. Gooch P, Roudsari A. Computerization of workflows, guidelines, and carepathways: A review of implementation challenges for process-oriented healthinformation systems. J Am Med Inform Assoc 2011;18:738e48.
32. Riaño D, Real F, López-Vallverdú JA, et al. An ontology-based personalization ofhealth-care knowledge to support clinical decisions for chronically ill patients.J Biomed Inform 2012;45:429e46.
33. Abidi S, Cox J, Abidi SSR, Shepherd M. Using OWL ontologies for clinicalguidelines based comorbid decision support. Proceeding of the Forty FifthHawai’i International Conference on System Science. (HICCS-45). Los Alamitos:IEEE Press, pg. 3030-8.
34. Abidi SR, Abidi SS, Hussain S, Shepherd M. Ontology-based modeling of clnicalpractice guidelines: a clinical decision support system for breast cancer follow-up interventions at primary care settings. Stud Health Technology Inform2007;129(Pt 2):845e9.
35. Abidi S, Abidi SSR, Hussain S, Butler L. Ontology-based modeling and mergingof institution-specific prostate cancer clinical pathways. Knowledge
S. Abidi et al. / Can J Diabetes 38 (2014) 205e211 211
Management for Healthcare Procedures European Conference on Artificial In-telligence (ECAI) 2008 workshop, K4HeIP 2008, Patras, Greece, July 21 2008:Revised Selected Papers. Berlin: Springer; 2009.
36. Din M, Abidi SSR, Jafarpour B. Ontology based modeling and execution ofnursing care plans and practice guidelines. Proceeding of 13th Conference onArtificial Intelligence in Medicine, AIME 2011, Bled Slovenia, July 2-6 2011. MorPeleg, Nada Lavrac, Carlo Combi, Eds. Berlin: Springer; p. 307-11.
37. Gómez-Pérez A. Evaluation of ontologies. Int J Intell Sys 2001;16:391e409.38. Abidi SSR. Medical knowledge morphing: towards case-specific integration of
heterogeneous medical knowledge resources. Presented at the 18th IEEE In-ternational Symposium on Computer-Based Medical Systems. Trinity College,Dublin, Ireland: IEEE Computer Society; 2005.
39. Jafarpour B, Abidi S, Abidi SSR. Exploiting OWL reasoning services to executeontologically-modeled clinical practice guidelines. Knowledge Representationfor Health-Care - AIME 2011 Workshop KR4HC 2011, Bled, Slovenia, July 2-6,2011. Revised Selected Papers; 01/2011. Berlin: Springer Verlag.
40. Park MJ, Kim HS. Evaluation of mobile phone and internet intervention onwaist circumference and blood pressure in post-menopausal women withabdominal obesity. Int J Med Inform 2012;81:388e94.
41. Funnell MM, Anderson RM. Empowerment and self-management of diabetes.Clin Diabetes 2004;22:123e6.
42. Promoting the technology of health. http://thechronicleherald.ca/artslife/138423-promoting-the-technology-of-health. Accessed October 10, 2012.
43. Davis S, Abidi SSR, Stewart S. A compositional personalization approachfor designing personalized patient educational interventions for cardio-vascular risk management. Stud Health Technol Inform 2010;160(Pt 1):629e33.
44. Kushnirk AW, Patel VL. Cognitive and usability engineering methods for theevaluation of clinical information systems. J Biomed Informatics 2004;37:56e76.
45. Kushnirk AW, Patel VL. Cognitive evaluation of decision making processes andassessment of information technology in medicine. Int J Med Informatics 1998;51:83e90.
46. Glaser B. Conceptualization: on theory and theorizing using grounded theory.Inter J Qualitat Meth 2002;1:1e31.
47. Morisky DE, Ang A, Krousel-Wood M, Ward H. Predictive validity of a medi-cation adherence measure for hypertension control. J Clin Hypertens 2008;10:348e54.
48. Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care ac-tivities measure. Diabetes Care 2000;23:943e50.
49. Polonsky WH, Fisher L, Earles J, et al. Assessing psychosocial distress in dia-betes: development of the diabetes distress scale. Diabetes Care 2005;28:626e31.
50. Anderson RM, Funnell MM, Fitzgerald JT, Marrero DG. The diabetes empow-erment scale: a measure of psychosocial self-efficacy. Diabetes Care 2000;23:739e43.




























