Embed Size (px)
Citation preview
DENTAL CARIES
CONTENTS INTRODUCTION EPIDEMIOLOGY DEFINITION CLASSIFICATION THEORIES OF CARIES CURRENT CONCEPTS IN CARIES
ETIOLOGY HISTOPATHOLOGY CONCLUSION
INTRODUCTION
EPIDEMIOLOGY
Pre-historic man have decreased caries prevalence
Decreased caries prevalence in African and Asian communities
Factors affecting caries prevalence:1. Race2. Age3. Sex 4. Familial
Current trends in caries incidence:
DEFINITION1. “Dental caries is a microbial disease of the
calcified tissues of the teeth, characterized by demineralization of the inorganic portion and destruction of the organic substance of the tooth” [Shaffer]
2. “Localized post eruptive pathologic process of external origin involving softening of the hard tissue and proceeding to the formation of a cavity” [WHO]
3. “An infectious microbiological disease of the teeth that results in localized dissolution and destruction of calcified tissues” [Sturdevant]
CLASSIFICATION
I. STURDEVANT
Based on - Location - Extent - Rate of progression
According to location: a. Primary caries b. Caries of pit and fissure origin c. Caries of enamel smooth surface origin d. Backward caries e. Forward caries f. Residual caries g. Root surface caries h. Secondary (recurrent) caries
• According to extent: a. Incipient (reversible) caries b. Cavitated (irreversible) caries
• According to rate of progression: a. Acute (rampant) caries b. Chronic (slow or arrested) caries
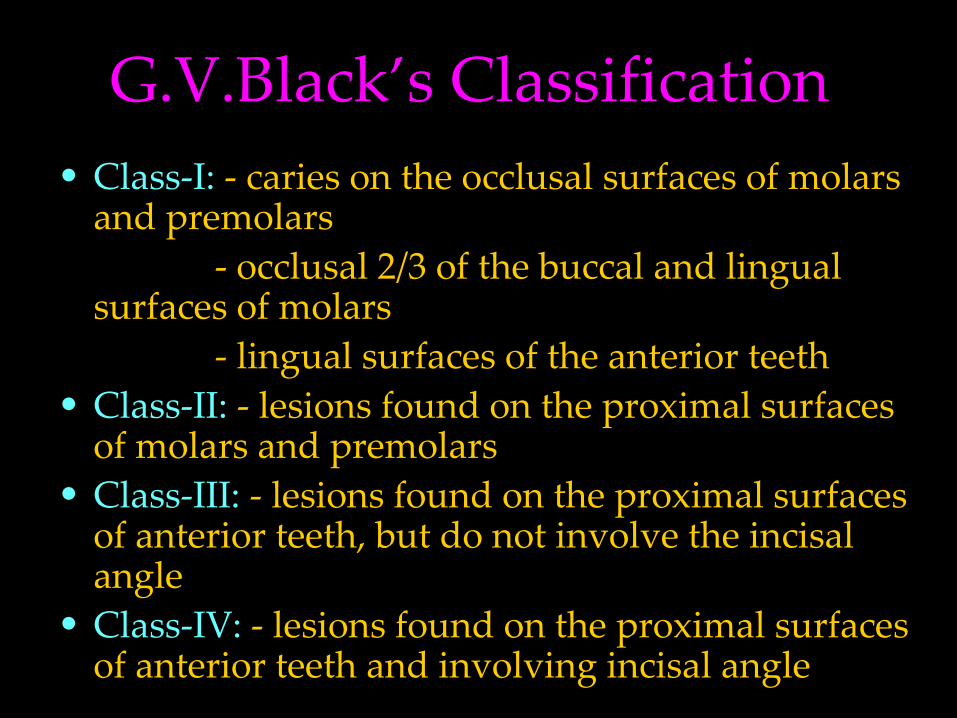
G.V.Black’s Classification • Class-I: - caries on the occlusal surfaces of molars
and premolars - occlusal 2/3 of the buccal and lingual
surfaces of molars - lingual surfaces of the anterior teeth• Class-II: - lesions found on the proximal surfaces
of molars and premolars• Class-III: - lesions found on the proximal surfaces
of anterior teeth, but do not involve the incisal angle
• Class-IV: - lesions found on the proximal surfaces of anterior teeth and involving incisal angle
• Class-V: - lesions found on the gingival third of the facial and lingual surfaces of anterior and posterior teeth.
• Class-VI: - were not included in Black’s classification
- proposed by Siomon - lesions on the incisal edge and
cusp tips of the teeth
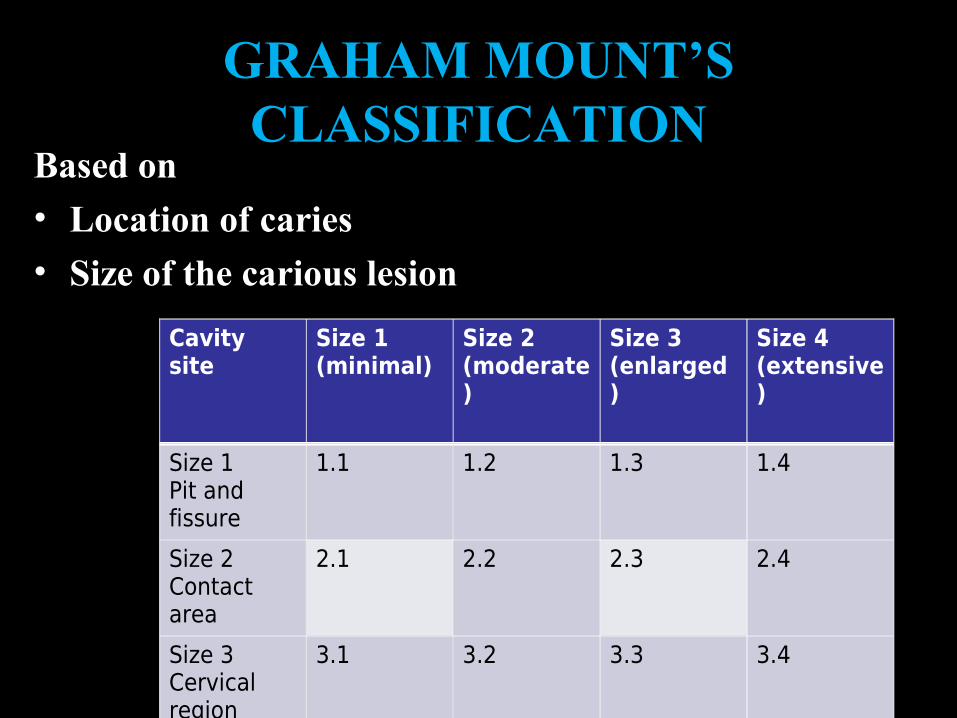
GRAHAM MOUNT’S CLASSIFICATION
Based on • Location of caries• Size of the carious lesion
Cavity site
Size 1(minimal)
Size 2(moderate)
Size 3(enlarged)
Size 4(extensive)
Size 1Pit and fissure
1.1 1.2 1.3 1.4
Size 2Contact area
2.1 2.2 2.3 2.4
Size 3Cervical region
3.1 3.2 3.3 3.4
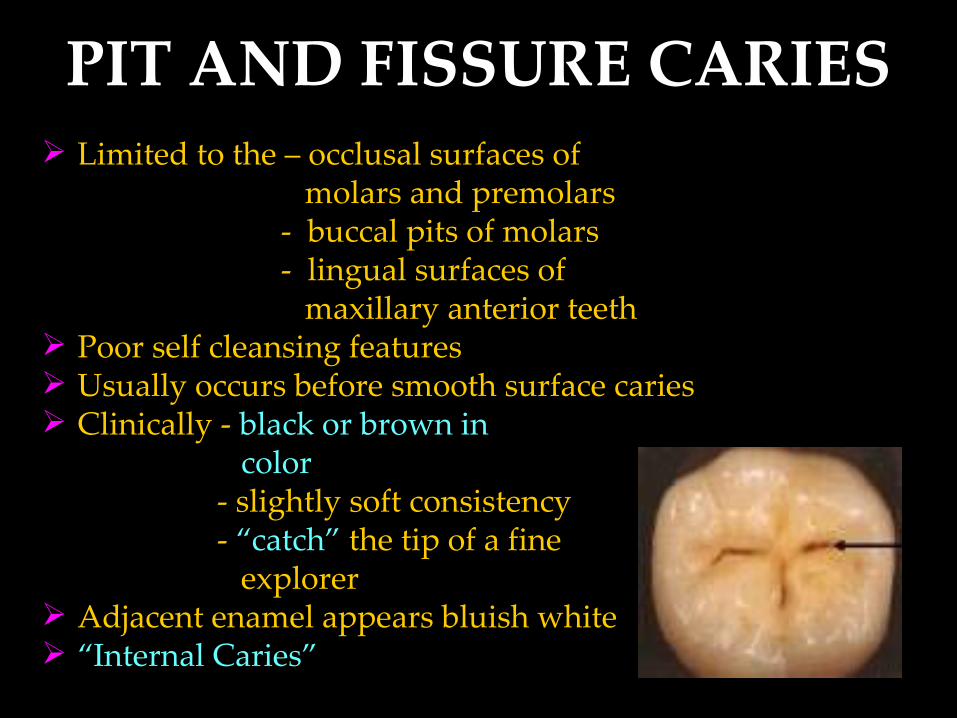
PIT AND FISSURE CARIES Limited to the – occlusal surfaces of molars and premolars - buccal pits of molars - lingual surfaces of maxillary anterior teeth Poor self cleansing features Usually occurs before smooth surface caries Clinically - black or brown in color - slightly soft consistency - “catch” the tip of a fine explorer Adjacent enamel appears bluish white “Internal Caries”
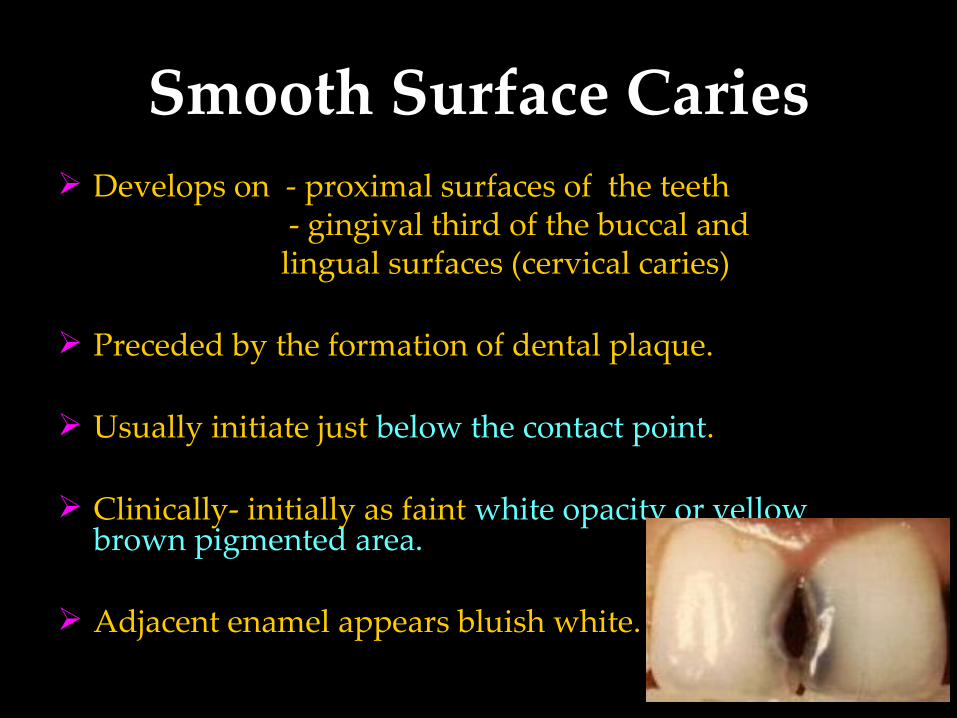
Smooth Surface Caries Develops on - proximal surfaces of the teeth - gingival third of the buccal and lingual surfaces (cervical caries)
Preceded by the formation of dental plaque.
Usually initiate just below the contact point.
Clinically- initially as faint white opacity or yellow brown pigmented area.
Adjacent enamel appears bluish white.
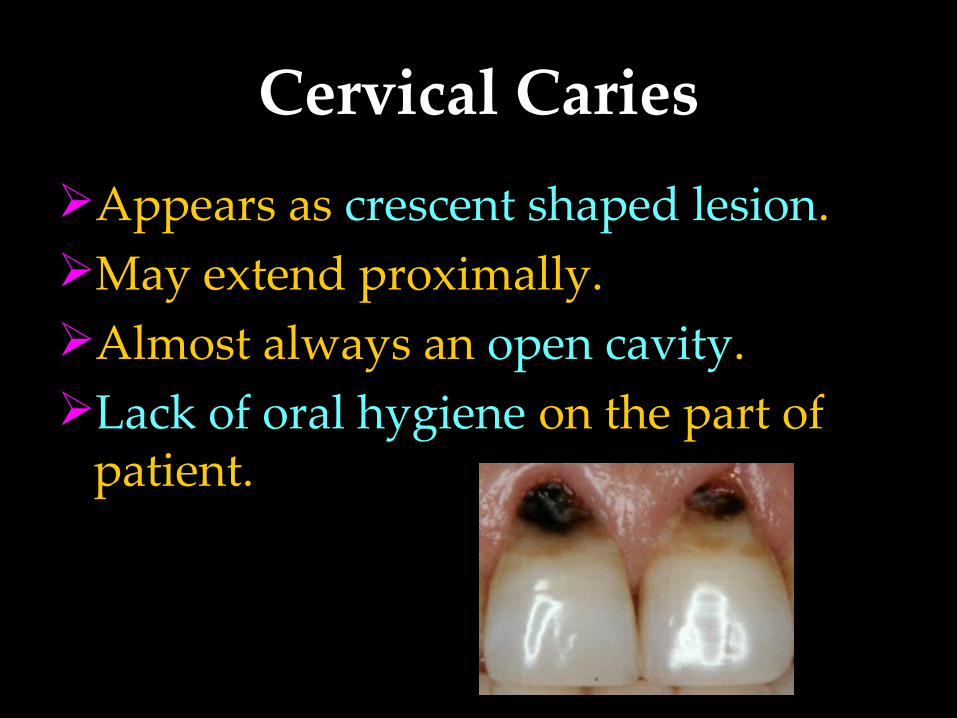
Cervical CariesAppears as crescent shaped lesion.May extend proximally.Almost always an open cavity.Lack of oral hygiene on the part of
patient.
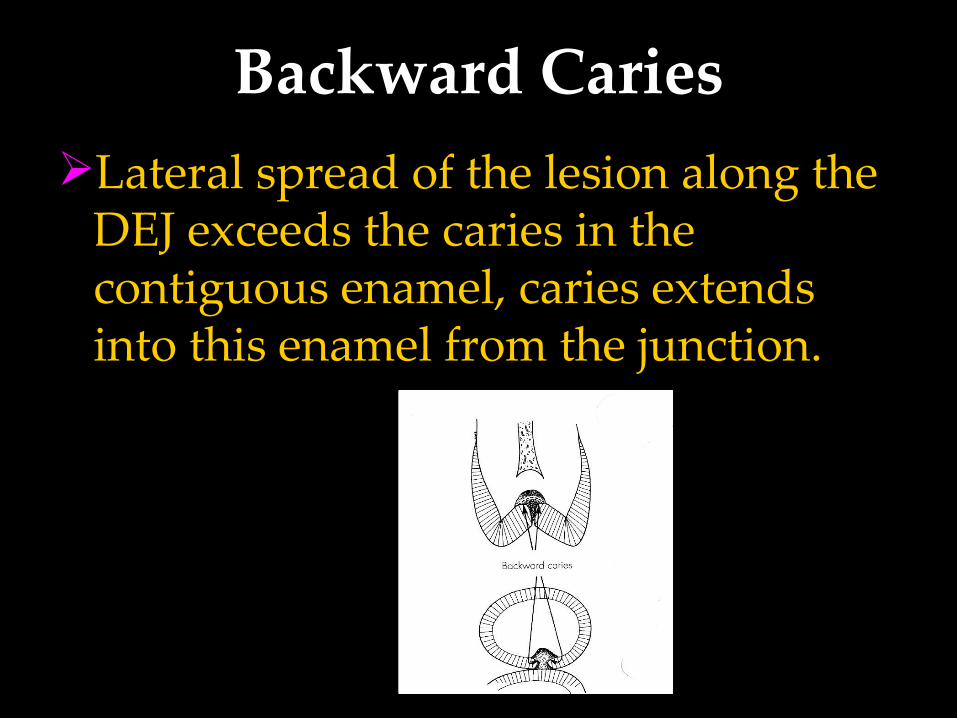
Backward CariesLateral spread of the lesion along the
DEJ exceeds the caries in the contiguous enamel, caries extends into this enamel from the junction.
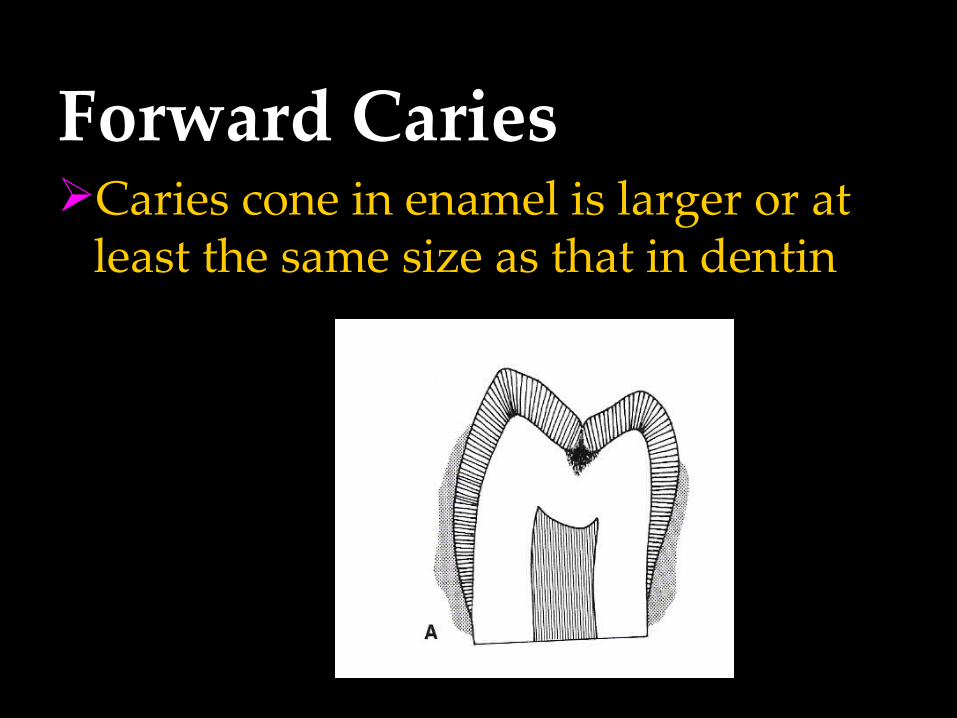
Forward CariesCaries cone in enamel is larger or at
least the same size as that in dentin
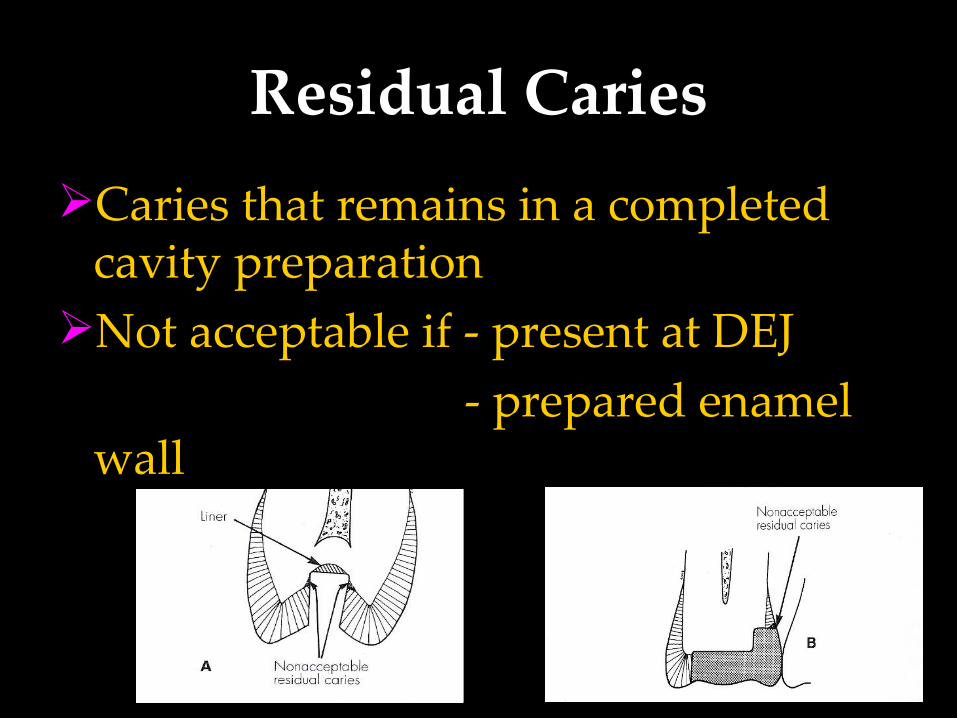
Residual CariesCaries that remains in a completed
cavity preparationNot acceptable if - present at DEJ - prepared enamel
wall
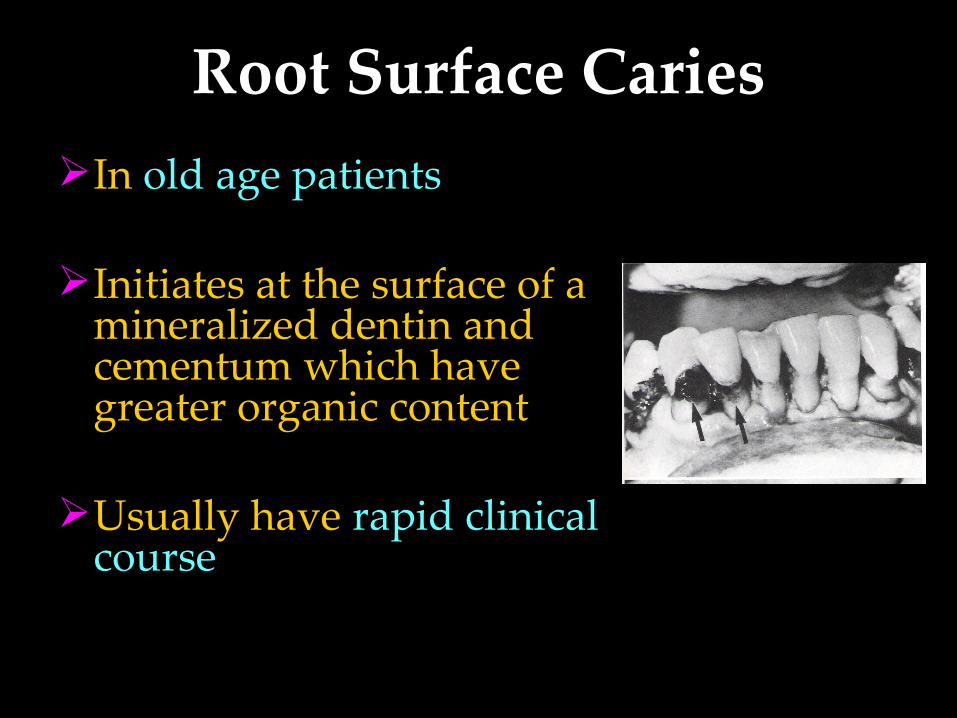
Root Surface CariesIn old age patients
Initiates at the surface of a mineralized dentin and cementum which have greater organic content
Usually have rapid clinical course
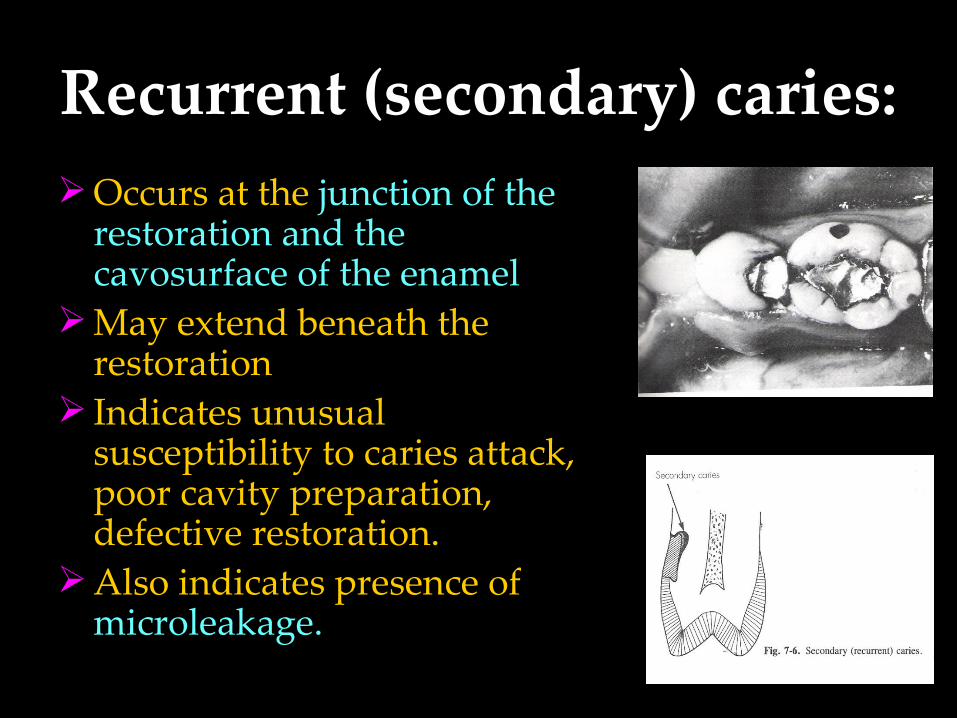
Recurrent (secondary) caries:Occurs at the junction of the
restoration and the cavosurface of the enamel
May extend beneath the restoration
Indicates unusual susceptibility to caries attack, poor cavity preparation, defective restoration.
Also indicates presence of microleakage.
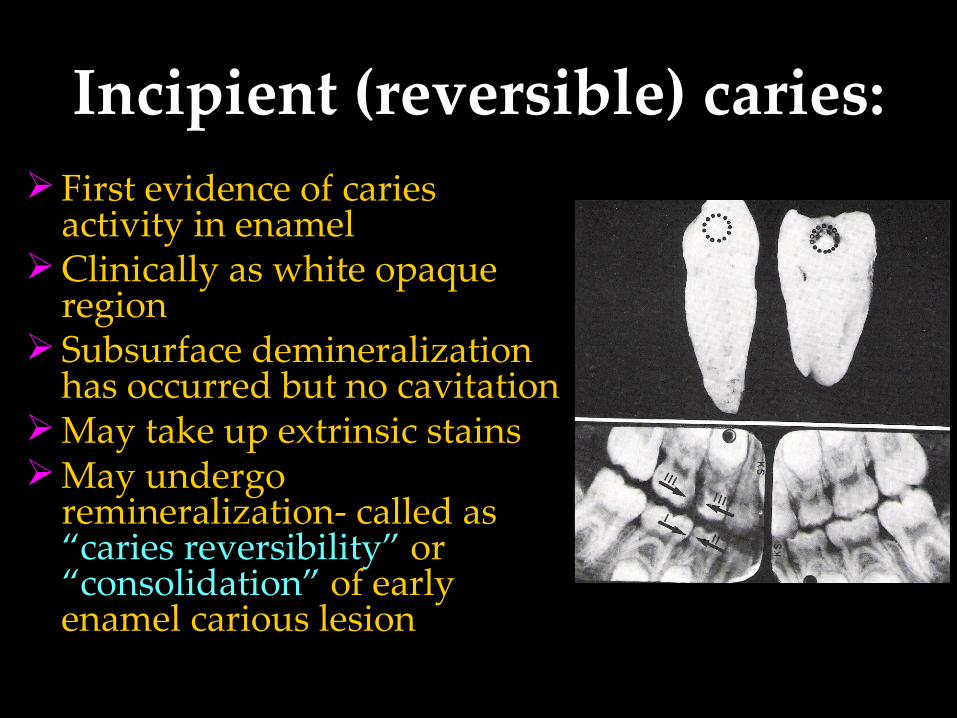
Incipient (reversible) caries:First evidence of caries
activity in enamelClinically as white opaque
region Subsurface demineralization
has occurred but no cavitationMay take up extrinsic stains May undergo
remineralization- called as “caries reversibility” or “consolidation” of early enamel carious lesion
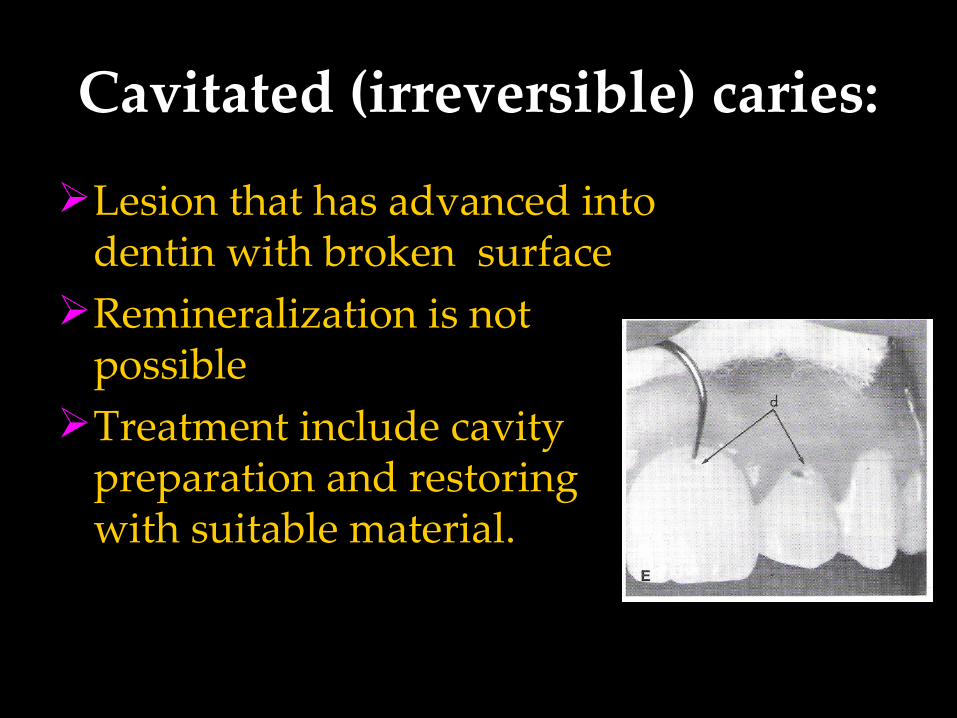
Cavitated (irreversible) caries:
Lesion that has advanced into dentin with broken surface
Remineralization is not possible
Treatment include cavity preparation and restoring with suitable material.
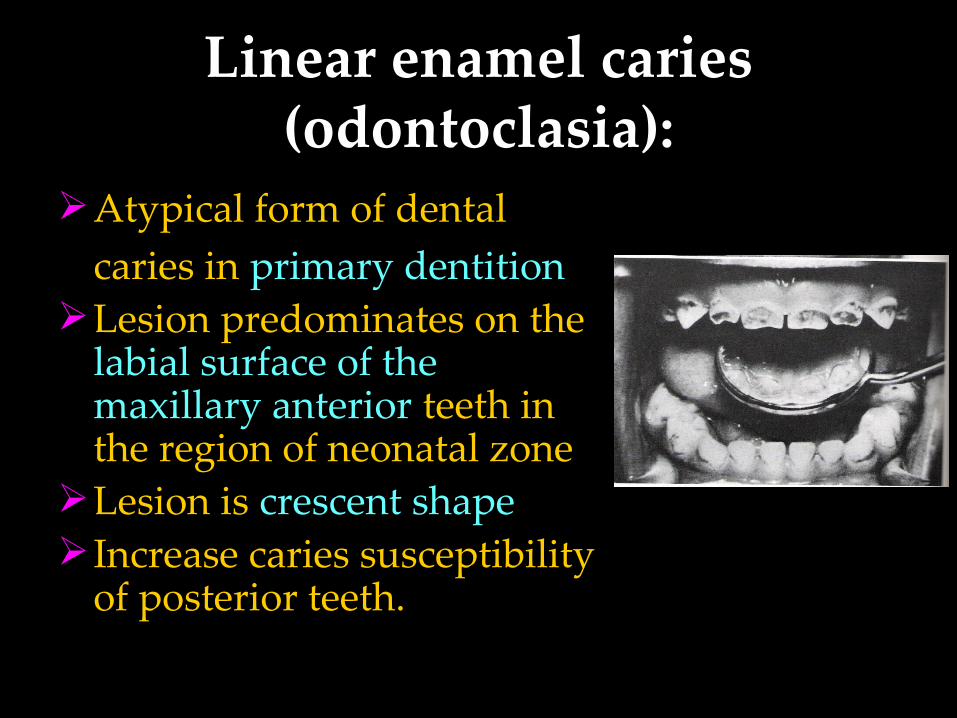
Linear enamel caries (odontoclasia):
Atypical form of dental caries in primary dentition
Lesion predominates on the labial surface of the maxillary anterior teeth in the region of neonatal zone
Lesion is crescent shape Increase caries susceptibility
of posterior teeth.
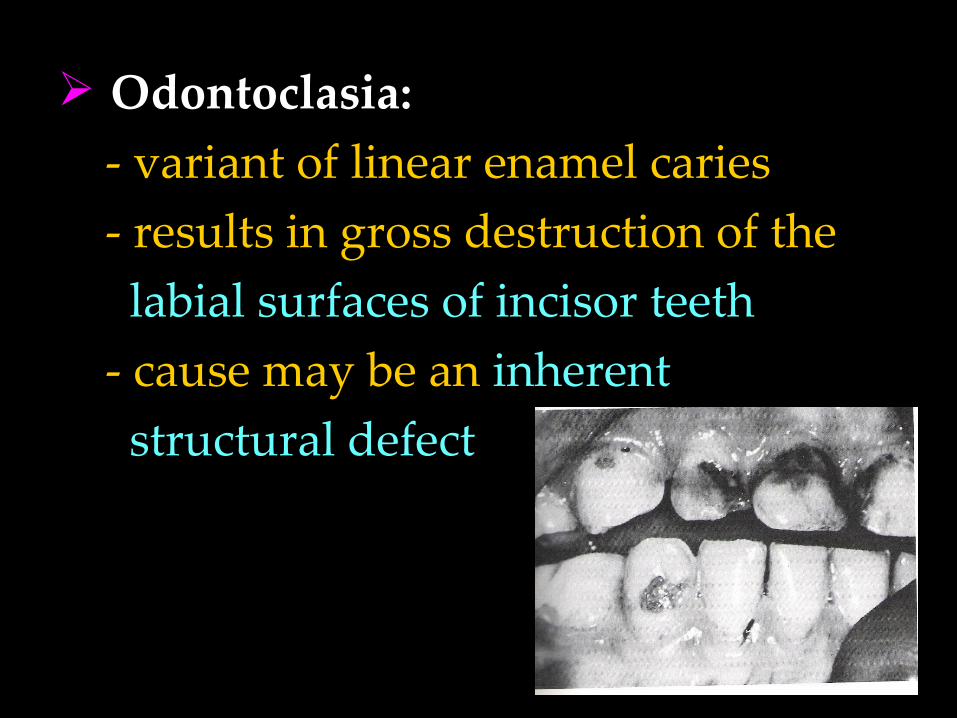
Odontoclasia: - variant of linear enamel caries - results in gross destruction of the labial surfaces of incisor teeth - cause may be an inherent structural defect
Acute dental caries:Rapid clinical course resulting in early
pulp involvementFrequently in children and young adultsEntry of lesion remains small while rapid
spread along the DEJClinically appears light yellow in colourPain is often present
Chronic dental cariesSlowly progressive lesion that
involves pulp much later Common in adultsLarge entrance of the lesionDentin is stained deep brown Moderate lateral spread of caries at
DEJPain is not a common clinical finding.

Rampant caries:Sudden and rapid onset
and almost uncontrollable destruction of teeth
Involves teeth that are ordinarily caries free (mandibular incisors)
Ten or more new increments of carious lesion in one year
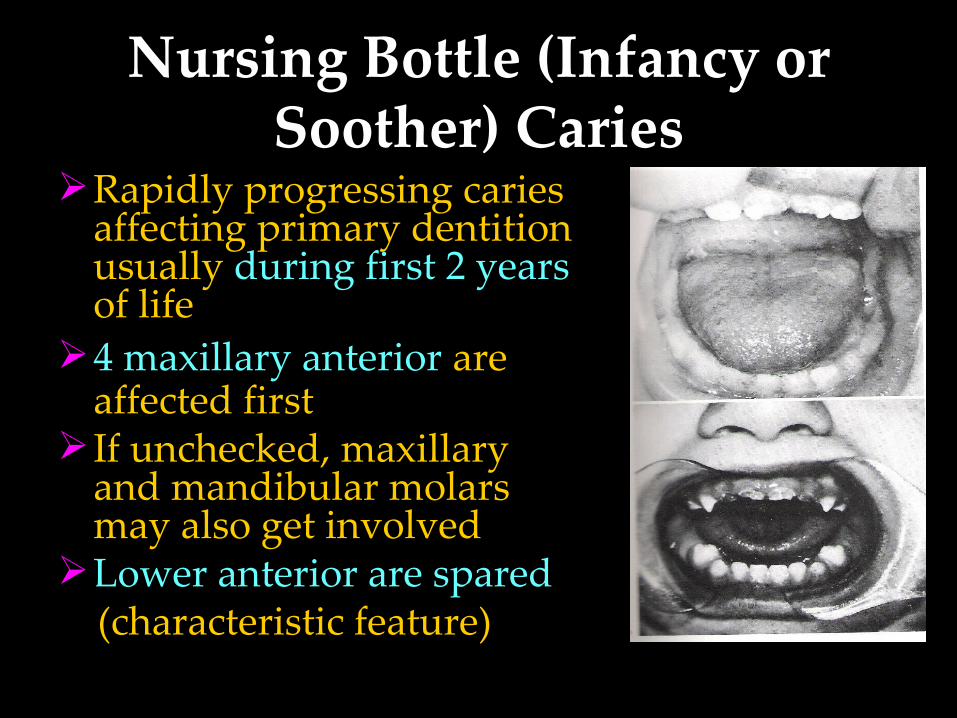
Nursing Bottle (Infancy or Soother) Caries
Rapidly progressing caries affecting primary dentition usually during first 2 years of life
4 maxillary anterior are affected first
If unchecked, maxillary and mandibular molars may also get involved
Lower anterior are spared (characteristic feature)
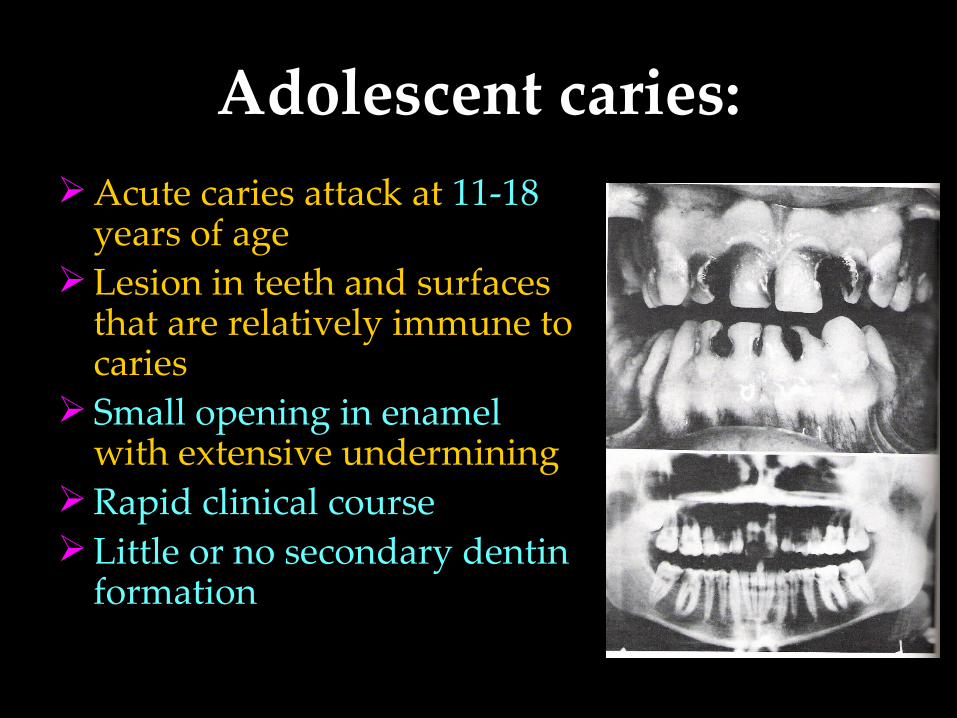
Adolescent caries:Acute caries attack at 11-18
years of ageLesion in teeth and surfaces
that are relatively immune to caries
Small opening in enamel with extensive undermining
Rapid clinical courseLittle or no secondary dentin
formation
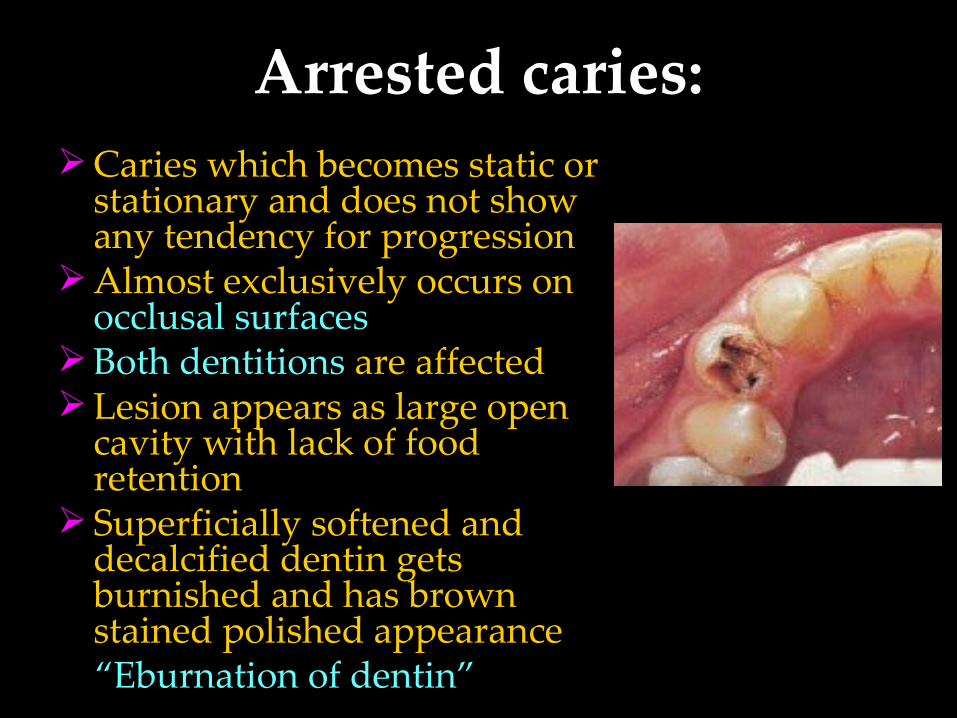
Arrested caries:Caries which becomes static or
stationary and does not show any tendency for progression
Almost exclusively occurs on occlusal surfaces
Both dentitions are affectedLesion appears as large open
cavity with lack of food retention
Superficially softened and decalcified dentin gets burnished and has brown stained polished appearance
“Eburnation of dentin”
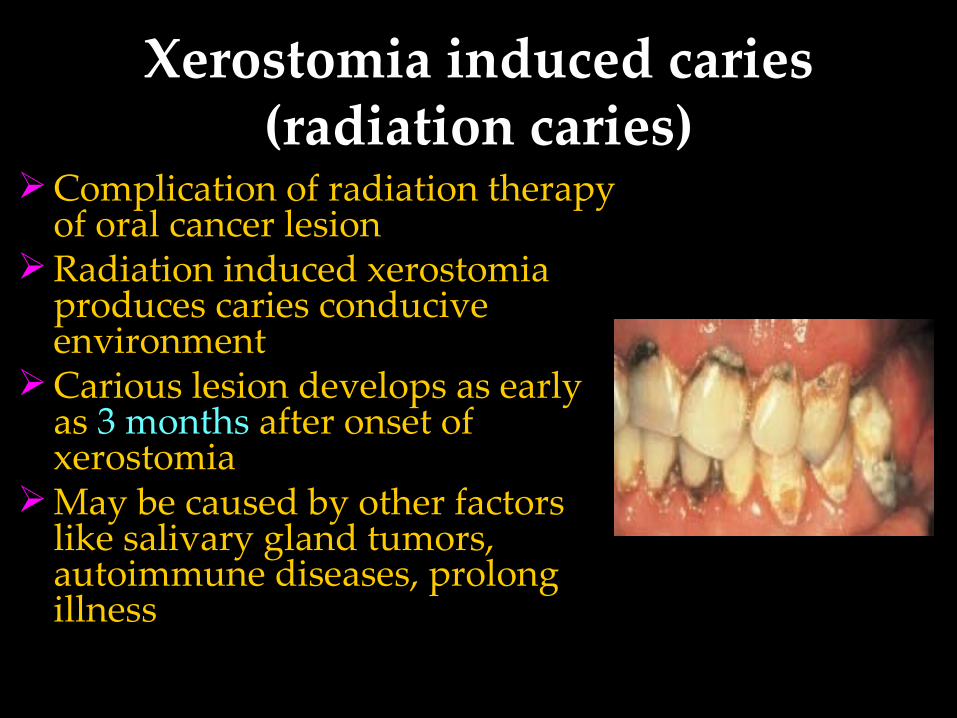
Xerostomia induced caries (radiation caries)
Complication of radiation therapy of oral cancer lesion
Radiation induced xerostomia produces caries conducive environment
Carious lesion develops as early as 3 months after onset of xerostomia
May be caused by other factors like salivary gland tumors, autoimmune diseases, prolong illness
Senile CariesCaries activity that spurts up during
the old age.They are located exclusively on the
root surfaces of the teeth.Also seen in association with partial
denture clasps.Causes: gingival recession, decreased
salivary secretion, poor oral hygiene.
Occult Caries / Hidden Caries
• Not clinically diagnosed, but detected only on radiograph.
• Seen in persons with low caries index suggestive of increased fluoride exposure.
• Also called as fluoride bombs or fluoride syndrome
1. Simple caries: one surface is involved
2. Compound caries: two surfaces are involved
3. Complex caries: three or more surfaces are involved
ETIOLOGICAL THEORIES
Early theories
Endogenous theories
Exogenous theories
EARLY THEORIES1. The Legend of the Worm:• According to an ancient Sumerian text, tooth
ache was caused by a worm that drank the blood of the teeth and fed on the roots of the jaws
• Antony Van Leeuwenhock (1700) the father of modern microscopy wrote a letter to the Royal Society of London describing little worms taken out of a corrupt tooth and said that they caused the pain in tooth ache.
ENDOGENOUS THEORY• Humoral Theory “dental caries is produced by internal
action of acid and corroding humors”.• Four elemental fluids of the body-blood, phlegm, black bile and yellow bile
• Vital Theory “tooth decay originated, like bone
gangrene, from within the tooth itself”
EXOGENOUS THEORY
• Chemical (Acid) theory: “ teeth are destroyed by acids formed in the
oral cavity ”
• Parasitic (Septic) theory: “ microorganisms are associated with
carious process ”
Acidogenic Theory Proposed by W.B.Miller 1890, most accepted “Acids formed due to the fermentation of dietary
carbohydrates by oral bacteria leads to progressive decalcification of tooth structure with subsequent disintegration of organic matrix.”
He isolated micro-organisms from his experiments & stated that many were involved in the carious process.
3 important factors which can influence process of tooth destruction in process of dental caries:
Dietary carbohydrates, micro-organisms and acid
• Limitations– Did not explain sub-surface
demineralization
– Failed to justify rampant caries
– Did not explain caries in impacted
tooth
– Phenomenon of arrested caries is
not explained
– Smooth surface caries is not
accounted in this theory
Proteolytic Theory Proposed by Gottlieb in 1941. “formation of dental caries is essentially
proteolytic process. Bacteria present produce hydrolytic enzymes and cause proteolysis leading to the dissolution of organic substance.”
Microorganisms invade the organic substance first.
He did admit that, acid formation accompanied the proteolysis.
Yellow pigmentation of dental caries is because of pigment production by proteolytic organism.
Caries is initiated at slightly alkaline pH.
Limitations:In vitro studies didn’t prove the
proteolytic process of caries.Proteolytic bacteria are uncommon in oral
cavity.Didn’t explain about the role of sucrose,
pH and fluoride in dental caries.Protein content of enamel is 0.6%. So,
initiation of caries by proteolytic process is questionable.
Proteolytic-chelation Theory Proposed by Schwatz in 1955. Stated that two processes are involved in caries –
proteolysis & chelation. Chelation is a process involving complexing of
ions into a complexing substance by covalent bond which results in a highly stable, poorly dissociated and weekly ionized compound called chelate.
Bacterial attack on enamel is initiated by keratolytic microorganisms.
Eg: citrates, lactates Chelates are always –ve.
Limitations: Fails to make a mention of sugar and acid
production. Scientists proved that chelates are weak
and can not cause de calcification. Schwatz said, carbohydrates does not cause
acid production but it stimulates proteolysis, which is not true.
Lactobacillus in dental caries is because of chelation and said that microorganisms are not involved in caries.
Sucrose Chelation Theory• If there is a very high concentration of
sucrose in mouth of a caries active individual, there can be formation of complexes like calcium saccharates, calcium complexing intermediaries, etc by action of phosphorylating enzymes
• These complexes cause release of Ca, P ions from enamel and result in DC
•Limitations Sucrose readily gets metabolized to
form acids, hardly any scope for
formation of calcium saccharates, etc.
Very high levels of pH required for
formation of Calcium saccharates,
which is no achievable in the oral cavity
Autoimmune Theory
Few odontoblast cells at specific sites within pulp of specific teeth are damaged by autoimmune mechanism
Due to this the defense capacity & integrity of of enamel and dentin in those specific areas are compromised and act as potential sites for caries development in future
Sulfatase Theory Proposed by Pincus in 1951. Bacterial sulfatases hydrolyses the
mucoitin sulfate of enamel and chondroitin sulfate of dentin producing sulfuric acid that in turn causes decalcification.
Limitation: Sulfated polysacharide in enamel is
very small and not readily accessible as a substrate for enzymatic degradation. So, this is highly unlikely hypothisis for the degragation of tooth enamel.
Levine’s theory Proposed by Levine in 1977. Established chemical relationship between
enamel, plaque and factors which favors the movement of minerals between them.
Also called as “SEW – SAW” mechanism. Said enamel demineralization and
remineralization is a continuous process. Movement of ions between enamel and plaque
occurs in both direction which depend upon - plaque ph - calcium and phosphate ions at the interface - fluoride ion concentration
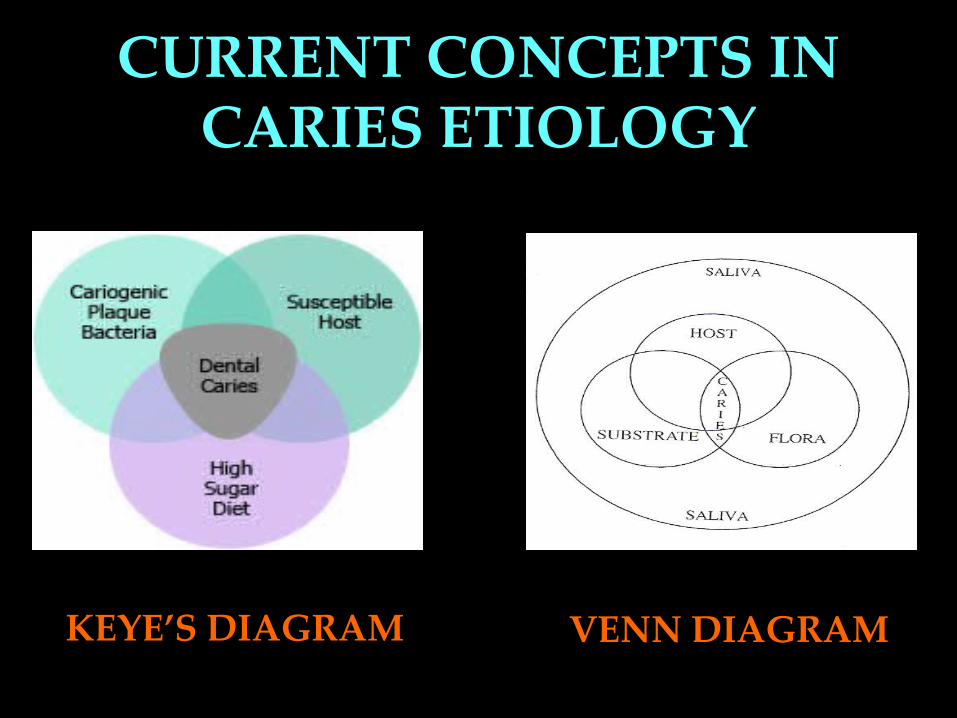
CURRENT CONCEPTS IN CARIES ETIOLOGY
KEYE’S DIAGRAM VENN DIAGRAM

Secondary Factors:
• Saliva• Other dietary
factors• Vitamins &
minerals• Hereditary
factors
Primary Factors: Teeth Diet Microorganisms
Etiological Factors:
1. Morphology:• Accentuated pits and fissures• Enamel hypoplasia• Mottled enamel• Bucco-lingual width of carious teeth2. Position:• Malpositioned teeth• Rotated teeth
TEETH
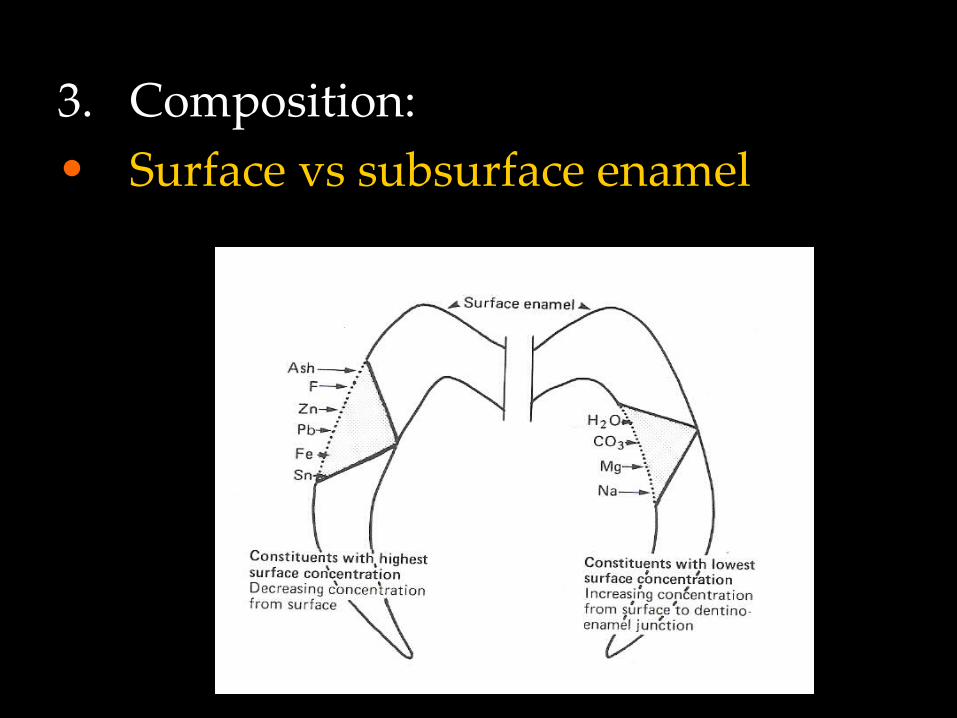
3. Composition: • Surface vs subsurface enamel
DIET• Carbohydrate is a cariogenic diet• Cariogenicity is based on1. Physical nature2. Chemical nature3. Mode of intake4. Clearance rate5. Frequency of intake 6. Other dietary factors
PLAQUE AND MICROORGANISMS
PLAQUE:• The concept about dental plaque was first
proposed by Williams in 1897• Consist of - salivary component- mucin - desquamated epithelial cells - microorganisms - calcium and phosphate
To produce caries, micro organisms should have following properties:
1. Should be acedogenic.2. Should be aceduric.3. Should posses attachment
mechanism.4. Should have the capacity to store
sucrose.5. Should be able to synthesize
extracellular glucans.
1. Pioneer / primary bacteria – initiate caries
• S.mutans (smooth surface caries)• Lactobacillus acidophilus (pit &
fissure caries)• Actinomyces (root surface caries)
1. Invaders / secondary bacteria• Staphylococcus, Veillonellae
Streptococci mutans:• Chief etiological agent in dental caries disease 1. it can produce low pH (acidogenic) 2. it can survive in low pH (acidouric) 3. utilize sucrose at a faster rate than other bacteria 4. can metabolize sucrose to synthesize glucan and fructan ( attachment mechanism ) 5. it can store intracellular glycogen amylopectin
type polysaccharides that act as a reservoir of substrate and prolongs its metabolic activity
Other Bacteria• Lactobacillus acidophilus
– Found in carious dentin & saliva of persons with high caries activity
– Release lactic acid• Actinomyces
– Found esp. in root caries– Acidogenic – Attachment to tooth by glycoprotein called
Lectin
Acids produced area) Lactic acid b) Acetic acidc) Butyric acid d) Propionic acide) Traces of formic acid• Lactic acid is the strongest acid
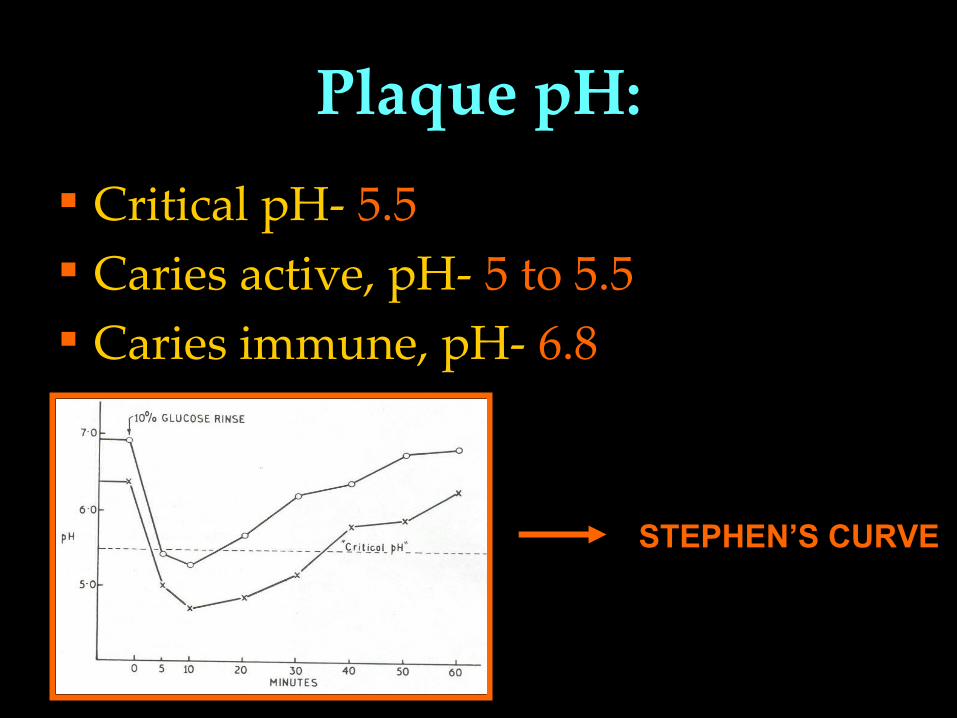
Plaque pH: Critical pH- 5.5 Caries active, pH- 5 to 5.5 Caries immune, pH- 6.8
STEPHEN’S CURVE
MINOR FACTORSI. SALIVA:
1. Flow rate2. Viscosity3. Buffering capacity4. Amount of saliva
Components of saliva:• Bicarbonates• Anti-bacterial agents• Ig-A• Salivary urea and bicarbonates
II. Dietary factor– Diet containing Phosphates decreases caries– Proteins & fat also prevents or decreases caries, as
they prevent attachment of carbohydrates to tooth– Trace elements of Vanadium & Molybdenum
decreases caries – Selenium increases risk of caries– Vitamin A & B are important in formation of hard
tissues. Thus if they are deficient, hypoplasia of teeth is seen, teeth more prone to caries
– Fibrous food help in cleansing of teeth, removal of lodged food
III. Hereditary factors:
HISTOPATHOLOGYImportant for:1. Research purpose2. To know the changes taking place in
dental caries Not important for diagnosis.Studied under: Light microscope Electron microscope Polarized microscope microradiographs
– Loss of inter-rod substance
– prominent enamel-rods
– Appearance of transverse striations of
enamel rods due to segmental
demineralization
– Accentuation of incremental striae of
Retzius
H/F of early enamel caries
H/F of Advanced enamel caries
Classified on the basis of pore volume and
mounting media used Zone 1 – Translucent zone
Zone 2 – Dark zone
Zone 3 – Body of lesion
Zone 4 – Surface zone
• These zones are from the dentin towards the outer
enamel surface
Translucent Zone• Is deepest & forms advancing front of
lesion• Not seen always, seen in 50% of cases.
When seen, appear clear due to mounting media which enters these big pores making them look clear/bright
• Pore volume is 1%, which is more than normal (0.1%)
• Zone cant be easily identified clinically / radiographically
Dark zone / positive zone• Dark zone as mounting media cant penetrate
this zone. Positive zone as it is always present• Pore volume – 2-4%. 2 types of pores seen here large & small
• Initially only large pores, later change to micro-pores. This change mainly due to demineralization occurring in deeper areas which release ions & there is remineralization of superficial areas
• This zone is narrower in rapidly advancing caries & wider in slowly advancing caries
Body of the lesion• Largest zone, between dark & surface zone• Greater amount of demineralization taking
place. Pore size – 5-25%• 5% variation is near periphery, 25% at
center• Prominent striae of Retzius due to
demineralization of inorganic minerals• Contains apatite crystals larger than that
found in normal enamel
Surface Zone
• Quite intact, appears radio-opaque
• Unaffected despite subsurface
demineralization; may be due to:
– surface remineralization by salivary ions
– More amount of fluoride
Dentinal Caries
• Once lesion spreads to DEJ, there is lateral
spread of caries
• Surface enamel gets unsupported enamel rods
enamel # greater cavitation
• Zones of dentinal caries
– Zones start from pulpal side towards dentinal side
1. Zone of Fatty Degeneration of Tomes’ process
2. Zone of Sclerosis
3. Zone of Decalcification without Bacterial
Invasion
4. Zone of Decalcification with Bacterial Invasion
5. Zone of Decomposed Dentin / Infected dentin
Fatty Degeneration of Tomes’ Process
• Innermost layer of dentinal caries towards pulp
• Due to deposition of fatty tissue in odontoblastic processes
• Seen usually in rapidly progressing caries• No crystals or bacteria in lumen of tubules• Intertubular dentin normal
Zone of Sclerosis/Sub-Transparent Dentin
As the microorganisms cause destruction to dentin, initially there is an attempt to stop the advancement of caries by depositing the minerals.
There is a deposition of mineral in intertubular dentin.
Zone is called “transparent zone” Odontoblasts are also start depositing dentin. At the periphery of sclerotic dentin, dead tracts
are present.
Zone of Decalcification without Bacterial Invasion /
Transparent Dentin• Decalcification is by bacterial acid diffusion
• Very narrow zone, softer than normal dentin
• Further loss of minerals from inter tubular
dentin
• Large crystals within lumen of dentinal
tubules
Zone of Decalcification with Bacterial Invasion / Turbid
Dentin• Initially only few tubules are involved & micro-
orgs also less
• These are acidogenic, pioneer bacteria
(initiators), present long before lesion is
clinically detected
• Bacteria multiply within tubules & are seen in
advancing front of lesion
• Walls of tubules are thin & when micro-orgs penetrate, they cause irregularities/distensions of walls ROSARY BEAD appearance
• Later, bacteria have proteolytic activity, areas of proteolysis appear as spaces containing necrotic material & bacteria
• These areas “Liquefaction Foci of Miller”.
• These areas vary in number & are parallel to dentinal tubules
Zone of Decomposed Dentin / Infected Dentin
• Outermost zone, large scale destruction of
dentin
• Foci of Miller join together
• Areas of dentin decomposition, occur
perpendicular to dentinal tubules
“Transverse Clefts”
• Mechanism of formation of Clefts - not known
– May follow course of incremental lines or
– May result from coalescence of liquefaction of
adjacent tubules
– Also may rise by extensive proteolytic activity
along interconnecting lateral branches of
odontoblastic processes
• Bacteria shift from dentinal tubules to the peri &
inter tubular dentin
Secondary / Reactionary dentin
• Protective mechanism to protect pulp
• Develops as a result of localized, non-specific
irritation to odontoblasts
• Hyper mineralized,less number of dentinal
tubules having irregular & torturous course
Root Caries / Cemental CariesHistopathology:• Outer surface of cementum – hyper mineralized,
thus more caries resistant• Resistance due to
– Reprecipitation of minerals from within– Precipitation of minerals from Plaque
• Clefts formed, through which bacteria penetrate & cause tooth structure destruction
• Penetration occurs along course of Sharpey's fibers
• Once cementum completely exposed & destroyed, underlying dentin is involved















![[Preventive strategies in the control of dental caries: a research synthesis]](https://img.pdfslide.net/doc/110x75/63571937dffe30f4b50c715f/preventive-strategies-in-the-control-of-dental-caries-a-research-synthesis.jpg)













