Embed Size (px)
Citation preview

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/authorsrights

Author's personal copy
Pharmacological Research 80 (2014) 21– 35
Contents lists available at ScienceDirect
Pharmacological Research
jo ur nal ho me page: www.elsev ier .com/ locate /yphrs
Review
Diabetic peripheral neuropathy: Current perspective and futuredirections
Randhir Singh ∗, Lalit Kishore, Navpreet KaurM.M. College of Pharmacy, Maharishi Markandeshwar University, Mullana-Ambala, Haryana 133207, India
a r t i c l e i n f o
Article history:Received 26 August 2013Received in revised form26 November 2013Accepted 16 December 2013
Keywords:Diabetic peripheral neuropathyHyperglycemiaTherapeutic approachesHerbal intervention
a b s t r a c t
Diabetic neuropathy is a heterogeneous group of disorders with extremely complex pathophysiologyand affects both somatic and autonomic components of the nervous system. Neuropathy is the mostcommon chronic complication of diabetes mellitus. Metabolic disruptions in the peripheral nervous sys-tem, including altered protein kinase C activity, and increased polyol pathway activity in neurons andSchwann cells resulting from hyperglycemia plays a key role in the development of diabetic neuropathy.These pathways are related to the metabolic and/or redox state of the cell and are the major sourceof damage. Activation of these metabolic pathways leads to oxidative stress, which is a mediator ofhyperglycemia induced cell injury and a unifying theme for all mechanisms of diabetic neuropathy. Thetherapeutic intervention of these metabolic pathways is capable of ameliorating diabetic neuropathy buttherapeutics which target one particular mechanism may have a limited success. Available therapeu-tic approaches are based upon the agents that modulate pathogenetic mechanisms (glycemic control)and relieve the symptoms of diabetic neuropathy. This review emphasizes the pathogenesis, presentlyavailable therapeutic approaches and future directions for the management of diabetic neuropathy.
© 2013 Elsevier Ltd. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222. Pathophysiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 223. Conventional therapies for DPN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
3.1. Glycemic control . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 243.2. Mechanism based therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
3.2.1. Aldose reductase Inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 243.2.2. PKC inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 243.2.3. Agents acting on hexosamine pathway . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 243.2.4. Agents acting on AGE pathway . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 243.2.5. ROS inhibitors. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
3.3. Symptomatic treatment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 253.3.1. Tricyclic and tetracyclic agents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 253.3.2. Selective serotonin reuptake inhibitors (SSRI) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 253.3.3. Serotonin–norepinephrine reuptake inhibitors (SNRI) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 273.3.4. Anticonvulsants . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Abbreviations: 3-DG, 3-deoxyglucosone; AGEs, advanced glycation end products; AMPA, �-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid; AR, aldose reduc-tase; CML, N�-(carboxymethyl) lysine; DAG, diacylglycerol; DPN, diabetic peripheral neuropathy; DPP-IV, dipeptidyl peptidase-IV; FDA, food and drug administration; GIP,glucose-dependent insulinotropic polypeptide; GlcNAc, UDP-N-acetylglucosamine; GLP-1, glucagon-like peptide-1; GSH, reduced glutathione; MAPK, mitogen-activatedprotein kinase; MG, methylglyoxal; MNCV, motor nerve conduction velocity; MOR-NRI, �-opioid receptor agonist-norepinephrine reuptake inhibitor; NADPH, nicotinamideadenine dinucleotide phosphate; NCV, nerve conduction velocity; NF-�B, nuclear factor-�B; NGF, nerve growth factor; NMDA, N-methyl-d-aspartate; NNR, neuronal nico-tinic acetylcholine receptor; NNT, number needed to treat; NO, nitric oxide; PDE-3A, phophodiesterase-3A; PHN, post-herpetic neuralgia; PKC, protein kinase C; PTB,N-phenacylthiazolium bromide; RCT, randomized clinical trials; ROS, reactive oxygen species; SNCV, sensory nerve conduction velocity; SNRI, serotonin–norepinephrinereuptake inhibitor; SOD, superoxide dismutase; SR-A, scavenger receptor class A; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic and tetracyclic antidepressant;TNF-�, tumor necrosis factor-�.
∗ Corresponding author. Tel.: +91 9896029234/8059930172.E-mail addresses: dahiya [email protected], [email protected] (R. Singh).
1043-6618/$ – see front matter © 2013 Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.phrs.2013.12.005

Author's personal copy
22 R. Singh et al. / Pharmacological Research 80 (2014) 21– 35
4. Future directions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284.1. Potential targets for management of DPN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
4.1.1. DPP-IV inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284.1.2. Hsp90 inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284.1.3. N-methyl-d-aspartate (NMDA) receptor antagonists . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284.1.4. Cannabinoid CB1 receptor antagonist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284.1.5. �-opioid receptor agonist-norepinephrine reuptake inhibitors (MOR-NRI) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284.1.6. Topical agents. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284.1.7. Vasopeptidase inhibition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 284.1.8. �4 �2 neuronal nicotinic acetylcholine receptor agonist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 294.1.9. PDE-5 inhibitor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 294.1.10. I�B phosphorylation inhibitor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 294.1.11. P13K/Akt signaling pathway . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 294.1.12. Galanin receptor-1 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
4.2. Other potential contributors for managing DPN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 295. Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
1. Introduction
Chronic diabetes mellitus is associated with various complica-tions such as retinopathy, neuropathy, nephropathy, cardiomyopa-thy, vasculopathy, dermatopathy and encephalopathy [1]. Diabeticneuropathy has been defined as the presence of symptoms and/orsigns of peripheral nerve dysfunction in diabetics after exclusion ofother causes (e.g. hereditary, traumatic, compressive, metabolic,toxic, nutritional, infectious, immune mediated, neoplastic andsecondary to other systemic illnesses) [2,3]. Diabetic peripheralneuropathy (DPN) is characterized by pain, paraesthesia, sensoryloss and affects approximately 50% of people with considerablemorbidity, mortality and diminished quality of life. The TorontoConsensus Panel on diabetic neuropathy recently defined DPN asa ‘symmetrical, length-dependent sensorimotor polyneuropathyattributable to metabolic and microvessel alterations resultingfrom chronic hyperglycemia and cardiovascular risk covariates [4].
Painful symptoms such as burning, tingling (‘pins and needles’or paraesthesia), shooting (like electric shock) or lancing (stab-bing) are present in around one third of patients with DPN andaround 20% of all diabetic patients [4,5]. DPN starts in the toesand gradually moves proximally. Once it is well established in thelower limbs, it affects the upper limbs, with sensory loss followingthe typical ‘glove and stocking’ pattern of distribution. Significantmotor deficits are not common in the early stages of DPN [4]. Thesesymptoms are generally worse at night and disturb sleep [6]. Anabnormality of nerve conduction tests, which is frequently subcli-nical, appears to be the first quantitative indication of the condition[7]. The patient does not typically complain of weakness, but whensymptoms are present, they tend to be sensory in nature. Symp-tomatic muscle weakness tends to develop later in the diseasecourse. Moreover, DPN is also associated with substantial morbid-ity including depression, susceptibility to foot or ankle fractures,ulceration and lower-limb amputations [8–11].
2. Pathophysiology
The pathogenesis of DPN has remained the subject of researchas well as controversy because of multifactorial underlying causeof diabetic neuropathy. It is the result of various biochemicalperturbations. Chronic hyperglycemia seems to be the major cul-prit in the initiation of various metabolic events underlying DPN.Increased free fatty acids develop insulin resistance and deteriora-tion of �-cell function in the context of concomitant hyperglycemia.Several studies suggested that insulin or C peptide deficienciesor both as such contribute to severe DPN [12]. Combinationof direct axonal injury due to the metabolic consequences of
hyperglycemia, insulin resistance, toxic adiposity, endothelialinjury and microvascular dysfunctions leads to nerve ischemia.Diabetes causes functional deficits in nitric oxide (NO) and alter-ations in endothelial derived relaxing factor (EDRF) resulting inmicrovascular reactivity and structural microangiopathy, whichadds to the worsening of DPN [13]. Hyperglycemia activates sev-eral major, well-characterized biochemical pathways that includeactivation of the polyol pathway [14], increased advanced gly-cation end products (AGEs) and their receptors [15], activationof protein kinase C (PKC) [16], mitogen-activated protein kinases(MAPK) [17] and inducible nitric oxide synthase [18]. Furthermore,hypoxia and ischemia [19], elevate cytokines such as tumor necro-sis factor (TNF)-� [20] and IL-6 [21], nerve growth factor (NGF)deficiency [22] also play significant etiologic role in DPN. One mech-anism that has been recognized to play a significant role in thepathogenesis of sensory neuron damage, is the process of reactivedicarbonyls forming AGEs due to hyperglycemia [23]. Hyper-glycemia leads to production of AGEs, which damage target cellsby three mechanisms. First, AGEs modify the intracellular proteins;hence their function is altered. Second, AGEs modify extracellularmatrix components, which interact abnormally with the recep-tors for matrix proteins (integrins) on cell. Third, plasma proteinsmodified by AGE precursors bind to AGE receptors on endothelialcells [24], mesangial cells, microglia and macrophages, inducingreceptor-mediated production of reactive oxygen species (ROS).This AGE receptor ligation activates transcription factor nuclearfactor-�B (NF-��), leading to pro-inflammatory gene expression[25]. It includes expression of cytokines and growth factors bymacrophages and mesangial cells (IL-1�, IGF-1, TNF-�, TGF-�,macrophage-colony-stimulating factor, granulocyte-macrophage-colony-stimulating factor and platelet-derived growth factor) andexpression of pro-coagulatory and pro-inflammatory molecules byendothelial cells (thrombomodulin, tissue factor and VCAM-1). Theactivation of NF-�� pathway by hyperglycemia also induces apo-ptosis in neuronal cells [26,27].
There is convincing experimental and clinical evidence that thegeneration of ROS increases in both types of diabetes and theonset of diabetes is closely associated with oxidative stress [28].The disease arises from a combination of microvascular and neu-ronal deficits. Oxidative stress can contribute significantly to thesedeficits as a direct result of prolonged hyperglycemia [29]. The tran-sient receptor ankyrin 1 ion channel on primary afferent nervefibers is involved in the pathogenesis of DPN due to sustainedactivation by reactive compounds, generated in diabetes melli-tus [30]. The AGE, polyol, PKC and hexosamine pathways directlyalter the redox capacity of the cell either through direct forma-tion of ROS or by depletion of necessary components of glutathione

Author's personal copy
R. Singh et al. / Pharmacological Research 80 (2014) 21– 35 23
Fig. 1. Sequential events leading to diabetic neuropathy. The metabolic abnormalities induced by hyperglycemia and insulin C peptide deficiencies are multifold and appearto occur in a temporal sequence and are commonly interactive and mutually perpetuating. They lead to unpaired nerve function and decreased blood flow, which initiallyare readily reversible. As structural changes emerge and progress, the functional abnormalities become increasingly less responsive to metabolic interventions. PKC/DAG,protein kinase C/Diacy (glycerol EDRF endothelial derived growth factor; NO, nitric oxide; PGI, prostaglandin I; AGE, advanced glycation end-product; HDL, high densitylipoprotein; LDL, low density lipoprotein; TG, triglyceride; MNCV, motor nerve conduction velocity; SNCV, sensory nerve conduction velocity.
recycling. These pathways always triggers damage through expres-sion of inflammation proteins which leads to impaired neuralfunction and finally apoptosis of neurons, Schwann and glial cells ofperipheral nervous system [31]. The possible sources of oxidativestress in diabetes might include auto-oxidation of glucose, shifts inredox balances, decreased tissue concentrations of low molecularweight antioxidants, such as reduced glutathione (GSH) and vita-min E, and impaired activities of antioxidant defense enzymes suchas superoxide dismutase (SOD) and catalase (CAT) [32].
The redox imbalance caused by chronic elevation of glucoselevel in diabetes causes oxidative stress and together leads toprotein oxidation and glycation [33], and dyslipidemia [elevatedplasma levels of total cholesterol (TC), low density lipoprotein-cholesterol (LDL-c) and triglycerides (TG) and low concentrationof high density lipoprotein cholesterol (HDL-c)]. Dyslipidemia, inboth type I and type II diabetes, plays a significant role in the mani-festation and development of premature atherosclerosis leading todecreased blood flow which impairs nerve perfusion and further tonerve dysfunction [34,35].
Various pathogenic mechanisms involved in the clinical courseof the disease thereby affect the structure and function of nerve(Fig. 1). In the early course of diabetes, activation of the polyol path-way, with a consequent impairment of neural Na+/K+-ATPase, leadsto impairment of endoneurial blood flow and micro- and macrovas-cular reactivity. Endoneurial hypoxemia secondary to impairedendoneurial blood flow contributes to impaired nerve perfusionand further to nerve dysfunction. One of the earliest detectablestructural changes in myelinated fibers is nodal and paranodalaxonal swelling which is associated to other abnormalities ofcytoskeletal structure leading to perturbated axonal transport andprogressive axonal atrophy [36].
Functional abnormalities like slowing of sensory nerve conduc-tion velocity (SNCV) and motor nerve conduction velocity (MNCV),hyperalgesia and allodynia are found to develop in early monthsof inception of hyperglycemia. As the disease progresses, signs ofaxonopathy, demyelination, nerve degeneration and hypoalgesiacan be detected [36]. Thermal hyperalgesia appears progressivelyduring the course of disease damaging small myelinated A-� andunmyelinated C-fibers and finally results in profound C-fiber loss[37]. The pathology of DPN is characterized by progressive nervefiber loss that gives rise to positive and negative clinical signs andsymptoms such as pain, numbness, paraesthesia and loss of sensa-tion. The most common morbidities related to DPN are recurrentfoot infections, ulcers and amputations, and Charcot’s joints [3].
3. Conventional therapies for DPN
The duration of time required for treatment of DPN is difficultto predict because of variable course of painful DPN and the rate ofpain recurrence is unknown [38]. Ideally, treatment should be ini-tiated when patients identify that painful neuropathy is impairingactivities of daily living and quality of life. The goal of treatment issymptom resolution, not a specific medication dose. There are fewtreatment principles that can be helpful for both the patient andclinician when initiating therapy for neuropathic pain. Firstly, it isimportant to establish realistic treatment goals and expectationsbecause therapies typically do not result in complete resolution ofsymptoms. Secondly, medication dosing must be tailored for theindividual patient. Thus, it is important to use the lowest effectivedose for an individual. Further titration can be considered, but mustbe weighed against an increased risk of side effects. Finally, there

Author's personal copy
24 R. Singh et al. / Pharmacological Research 80 (2014) 21– 35
are some data to support drug combinations in painful DPN but itis generally advisable to avoid poly-pharmacy when possible [39].
3.1. Glycemic control
Treatment of DPN is based on either pathogenetic mechanismsor symptomatic relief. A number of clinical trials have establishedsymptomatic treatment but for pathogenetic mechanisms, the onlyproven treatment strategy is strict glycemic control. As glycemicvariability leads to oxidative stress, therefore the therapeuticshaving ability to control glucose levels, holds potential for atten-uating DPN. Insulin and oral antihyperglycemic agents are alsoemployed to achieve glycemic control along with the agents reliev-ing neuropathic pain in the treatment of DPN. Orally administeredanti-diabetic agents (e.g. sulfonylureas, repaglinide, metformin, �-glucosidase inhibitors and thiazolidinediones) are used either aloneor in combinations. Insulin remains the only effective alterna-tive when oral antidiabetic drugs can no longer achieve adequateglycemic control in diabetes [40]. Oral antihyperglycemic agentsemployed in the treatment of DPN along with their mechanism ofaction are listed in Table 1.
3.2. Mechanism based therapy
The metabolic hypotheses for diabetic complications includepolyol pathway hyperactivity and related myo-inositol depletion,increased diacylglycerol-PKC cascade, oxidative stress and non-enzymatic glycation theory. It is the goal of existing and proposedtherapy to at least stabilize, or preferably attenuate DPN. Severalmechanism based approaches have been adopted for the manage-ment of diabetic complications.
3.2.1. Aldose reductase InhibitorsDuring hyperglycemia, the polyol pathway has increased activ-
ity. This pathway is responsible for the reduction of glucose tosorbitol via the enzyme aldose reductase, utilizing the cofactornicotinamide adenine dinucleotide phosphate (NADPH) [41]. Thisreduction reaction leads to increased sorbitol accumulation in thecells resulting in cellular and organ injury [42]. Additionally, exces-sive accumulations of sorbitol results in decrease of myo-inositolin peripheral nerves leading to decrease in Na+/K+-ATPase activity,which is essential for re-establishment of the resting electrochem-ical gradient [43]. As a result of the increased polyol pathwayactivity and the over-utilization of NADPH by the enzyme aldosereductase, a number of other homeostatic mechanisms are com-promised. NADPH depletion results in decreased (NO) and GSHproduction which cause reduced vasodilation and increased oxida-tive stress. The polyol pathway hyperactivity-induced reduction inglutathione causes increase in oxidative stress, leading to impairedendothelial cell function [44]. Thus, hyperglycemia and hyperactiv-ity of polyol pathway are the critical determinants of the severityof DPN [45].
Considering the role of polyol pathway in DPN, several drugshave been put forward for the management of DPN. Sorbinil iseffective in preventing neural dysfunction in diabetes. It reversessorbitol accumulation, accelerates the recovery of nerve myo-inositol content, improves nerve conduction velocity (NCV) to asmall extent and acts as an aldose reductase inhibitor [46–51]. Tol-restat, an aldose reductase inhibitor, restores defective NCV andimproves nerve regeneration [52]. Similarly, ponalrestat has beenfound to be efficacious in delaying the development of DPN. It nor-malizes NCV to a small extent and prevents impaired induction ofnerve ornithine decarboxylase [53–55]. Fidarestat induces matu-ration of immature regenerated nerve fibers, stimulates repair andhalts nerve fiber degeneration. It improves NCV and reduces oxida-tive stress [56–58]. Epalrestat prevents deterioration of median
MNCV and improves polyol pathway and suppresses production ofAGEs [59–61]. Zenarestat improves NCV and nerve morphology inDPN. It is discontinued due to renal toxicity, however prevents thealteration of endoneural blood flow resulting from impairment ofnitric oxide function [62,63]. Ranirestat in phase II trial has shownimprovement in sensory and motor nerve function, improvementin MNCV and reduction in sorbitol accumulation [64,65]. Myo-inositol prevents the genesis of early DPN and neural dysfunction[51].
3.2.2. PKC inhibitorsThe contribution of PKC in DPN still requires clarification. PKC
pathway is an additional mechanism by which hyperglycemia leadsto diabetic complications [66,67]. Elevated glucose level stimulatesdiacylglycerol (DAG) which in turn activates PKC. DPN is likely tooccur through its effects on vascular blood flow and microvasculardisease rather than directly in neuronal cells. Once PKC is activated,it activates MAPKs which further phosphorylates transcription fac-tors leading to the alteration of gene expression. Specifically, stressgenes such as heat-shock proteins and c-Jun kinases increases afterPKC activation and lead to apoptosis [17]. Increased PKC activationalso has been associated with changes in blood flow, basementmembrane thickening, extracellular matrix expansion, increasedvascular permeability and abnormal angiogenesis [68]. Inhibitionof PKC-� reduces oxidative stress and normalizes blood flow andnerve conduction deficits in diabetic rats [69,70]. High glucosecauses nuclear factor-�B (NF-kB) activation in endothelial cells,leading to ROS formation, and cellular activation, an effect whichis prevented in the presence of a PKC inhibitor [71]. Ruboxiastau-rin, a PKC-� inhibitor, appeared to be beneficial in the treatmentof neuropathy sensory symptoms and vibration sensation [72].Ruboxiastaurin improves endothelial and neural regulation of skinmicrovascular blood flow in patients with DPN, nerve fiber functionand quality of life [73–75].
3.2.3. Agents acting on hexosamine pathwayThe excessive flux of glucose or free fatty acids into a variety
of cell types results in the activation of the hexosamine biosyn-thetic pathway [76,77], which in turn leads to insulin resistanceand development of late complications of diabetes [78]. Shunt-ing of excess intracellular glucose into the hexosamine pathwaymight also cause several manifestations of diabetic complica-tions [79]. In this pathway, fructose-6-phosphate is diverted fromglycolysis to provide substrates for reactions which require UDP-N-acetylglucosamine (GlcNAc), such as proteoglycan synthesis andthe formation of O-linked glycoproteins. GlcNAc is a moleculethat attaches to the serine and threonine residues of transcrip-tion factors [24]. Hyperglycemic conditions create additional fluxthrough the hexosamine pathway, ultimately resulting in excessGlcNAc and abnormal modification of gene expression [24,79,80].Overexpression of plasminogen activator inhibitor-1 (PAI-1) pro-motes vascular smooth muscle cell mitosis which plays a rolein atherosclerosis [80]. Additionally, it was found that GlcNAcimpairs �-cell function by inducing oxidative stress [81]. Ben-fotiamine prevented the development of DPN demonstrated bymarked improvement in NCV in treatment group as comparedto placebo [82,83]. A 3-week randomized, controlled pilot studyalso demonstrated the therapeutic efficacy of benfotiamine inthe treatment of diabetic polyneuropathy [84]. Benfotiamine mayantagonize diabetes-induced cerebral oxidative stress through amechanism unrelated to AGEs, tissue factor and TNF-� [85,86].
3.2.4. Agents acting on AGE pathwayThe formation of AGEs and non-enzymatic glycation has been
shown to play a major role in the pathogenesis of diabeticcomplications. Tissue glucose level increases in hyperglycemia

Author's personal copy
R. Singh et al. / Pharmacological Research 80 (2014) 21– 35 25
Table 1Oral antihyperglycemic agents.
S. No. Drug class Drugs Mechanism of action
1. Sulphonylureas GlyburideGlipizideGlimipride
Stimulate pancreatic �-cells to increase first-phase insulin secretion
2. Biguanides Metformin Decreases excessive hepatic glucose production3. Meglitinides Rapeglinide
NateglinideIncreased secretion of insulin from �-cells by blocking ATP-sensitivepotassium channels
4. Thiazolidinediones RosiglitazonePioglitazone
Stimulates PPAR-� leading to increase in glucose uptake and decreasein insulin resistance
5. �-Glucosidase inhibitors AcarboseMiglitolVoglibose
Delays glucose absorption
6. Dipeptidyl peptidase IV inhibitors SitagliptinSaxagliptinvildagliptin
Decreases hepatic glucose production; decrease insulin resistance;increases insulin secretion
leading to the metabolism of glucose to give reactive dicar-bonyls like, 3-deoxyglucosone (3-DG), methylglyoxal (MG) andN�-(carboxymethyl) lysine (CML). They react with amino acids ofextracellular and intracellular proteins to produce AGEs. Increasedproduction of the reactive dicarbonyls or reducing detoxification bythe glyoxalase system or endogenous scavengers leads to a stateof carbonyl stress, acting as the major driving force for AGE for-mation and accumulation [15]. Along with the accumulation ofAGEs, receptors for AGE (RAGE) also add to the development of dia-betic complications. Galectin-3, scavenger receptor class A (SR-A),CD36, SR-BI and LOX-1 are the receptors of AGE [87]. Enhancedproduction of matrix metalloproteinase-2 (MMP-2) and matrixmetalloproteinase-9 (MMP-9) in diabetes leads to degradation ofextracellular matrix in blood vessels and leads to complications ofdiabetes. Minocycline in combination with aspirin shows signifi-cant protection in DPN by improving SNCV and MNCV, hot platelatency and tail flick latency. This improvement is due to amelio-ration of vascular structure by inhibition of MMP-2 and MMP-9,which prevents the development of experimental DPN and can bea potential approach for the treatment of DPN [88]. Aminoguani-dine prevents neural dysfunction and attenuated NCV slowing [51].N-phenacylthiazolium bromide (PTB) has been used to cleave AGEcross-links between albumin and collagen in vitro and recent stud-ies in diabetic rats have shown that PTB can prevent or reverse theaccumulation of AGEs in blood vessels [89].
3.2.5. ROS inhibitorsThere are convincing experimental and clinical evidence that
onset of diabetes is closely associated with oxidative stress andgeneration of ROS increases in type I and type II diabetes [28]. InDPN, AGE, polyol, PKC and hexosamine pathways directly alter theredox capacity of the cell through formation of ROS [31]. �-Lipoicacid prevents progression of neuropathic changes and amelioratesymptoms of distal sensorimotor polyneuropathy via inhibition ofROS generation [90,91]. Coenzyme Q10 inhibits oxidative stress anddown regulates pro-inflammatory factors [92,93]. Nicotinamideinhibits oxidative stress-PARP activation cascade [94]. Resvera-trol improves NCV, diabetic neuropathic pain and NF-�B inhibitoryaction contributing to neuroprotection [95,96]. Rutin prevents pro-tein glycation and prospects for controlling AGE-mediated diabeticpathological condition in vivo [97]. Taurine reduces oxidative andnitrosative stress in Schwann cells. It also reverses neurovasculardeficits and attenuates hyperalgesia [98–101]. Trigonelline amelio-rates hyperglycemia and reduces oxidative stress [102].
3.3. Symptomatic treatment
Control of pain symptoms is one of the most concerned issuesin the management of DPN. A careful history of the nature of
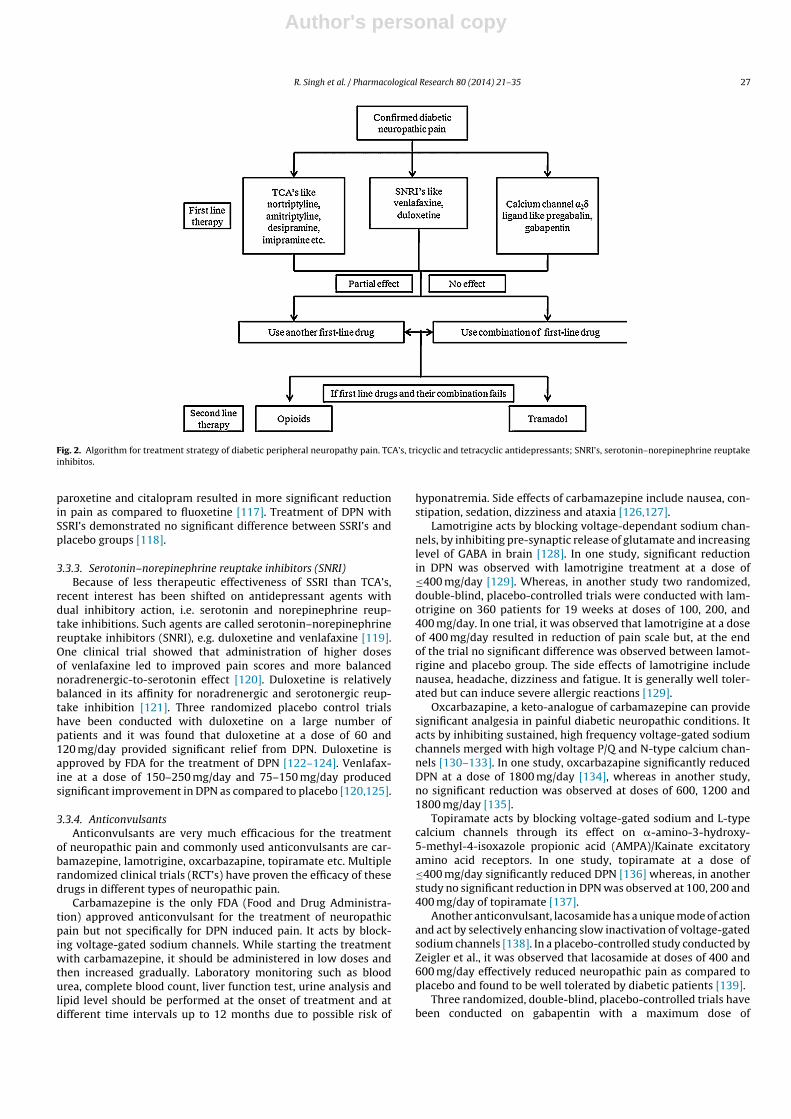
pain, exact location and detailed examination of lower limbs aremandatory to ascertain the causes of pain [103]. Various agents liketricyclic and tetracyclic antidepressants (TCA’s), selective serotoninreuptake inhibitors (SSRI’s), serotonin–norepinephrine reuptakeinhibitors (SNRI), anticonvulsants, opioids have been used by cli-nicians all over the world to provide symptomatic relief to thepatients (also see Fig. 2). Details of various clinical trials that havebeen conducted on these agents for preventing DPN are includedin Table 2.
3.3.1. Tricyclic and tetracyclic agentsThe TCA’s are considered as first line treatment for neuro-
pathic pain. Psychotropic agents like TCA’s have been extensivelyused over past three decades for the treatment of chronic painsyndrome. Putative mechanism of these agents includes inhibi-tion of norepinephrine or serotonin reuptake and antagonism ofN-methyl-d-aspartate (NMDA) mediated hyperalgesia and allo-dynia [104]. Amitryptline, imipramine and clomipramine are themost commonly used agents of this category. They induce nor-epinephrine and serotonine reuptake inhibition where as anotheragent desipramine is relatively selective toward norepinephrineinhibition [105]. TCA’s are therapeutically effective as well asaffordable but they should be used with caution as every 5th patientdiscontinues therapy due to adverse effects [106]. TCA’s are con-traindicated in patients with cardiac history including heart failure,myocardial ischemia, arrhythmia, orthostatic hypotension and nar-row angle glaucoma [107].
Two studies have been conducted on amitryptline at differentdoses of 25–75 and ≤150 mg/day, respectively, showing bet-ter results than placebo in the treatment of DPN [108,109]. Inanother phase III study, effect of amitryptline was compared withmaprotiline and placebo. It was found that amitryptline is moreeffective than maprotiline followed by placebo [110]. All thesestudies were conducted on small number of patients for short trialperiods. Therefore, the data interpretation is inefficient. Amitrypt-line has significant side effects like dry mouth, sedation and blurredvision. Studies on nortriptyline, desipramine, clomipramine andimipramine also suggest that they significantly reduced DPN ascompared to placebo [111–114].
3.3.2. Selective serotonin reuptake inhibitors (SSRI)Taking into consideration the relatively high adverse effects
and several contradictions of TCA’s, patients could alternativelybe treated with SSRI’s. These agents act by specifically inhibi-ting presynaptic reuptake of serotonin. Fluoxetine at a dose of40 mg/day was not found to be significantly useful in 46 patientsas compared to placebo in the treatment of DPN [112]. Paroxet-ine and citalopram at a dose of 40 mg/day produced better resultsas compared to placebo [115,116]. Moreover, treatment with

Author's personal copy26
R.
Singh
et
al.
/
Pharmacological
Research
80 (2014) 21– 35
Table 2Pharmacological treatment of diabetic neuropathy.
Drug Number of patients Daily doses Duration Outcome NNT Reference
TCAsAmitriptyline 29 ≤150 mg crossover, 2 × 6 weeks Amitriptyline > placebo 2.1 [132]Nortriptyline 51 ≤100 mg Crossover 9 weeks Nortriptyline > placebo 2.4 [135]Desipramine 20 Avg. 201 mg crossover, 2 × 6 weeks Desipramine > placebo 2.2 [136]Imipramine 19 25–350 mg Crossover, 3 × 2 weeks Imipramine > placebo 4 [137]Clomipramine 18 50–200 mg Crossover, 3 × 2 weeks Clomipramine > placebo 4.5 [138]
SSRIsCitalopram 18 40 mg Crossover, 3 × 2 weeks Citalopram > placebo 3 [115]Paroxetine 26 40 mg Crossover, 3 × 2 weeks Paroxetine > placebo 5 [139]Fluoxetine 46 40 mg Crossover, 2 × 6 weeks Fluoxetine = placebo NA [136]
SNRIsVenlafaxine 244 150–225 mg Parallel, 6 weeks Venlafaxine > placebo 4.5 [119]Venlafaxine 60 75 mg, 150 mg Parallel, 8 weeks Venlafaxine > placebo – [124]Duloxetine 457 20, 60, 120 mg Parallel, 12 weeks Duloxetine (60 mg, 120 mg) > placebo 60 mg: 4.3;120 mg: 3.8 [121]Duloxetine 348 60 mg, 120 mg Parallel, 12 weeks Duloxetine (60 mg, 120 mg) > placebo 60 mg: 11; 120 mg: 5 [122]Duloxetine 334 60 mg, 120 mg Parallel, 12 weeks Duloxetine (60 mg, 120 mg) > placebo 60 mg: 6.3 120 mg: 3.8 [123]
AnticonvulsantsCarbamazepine 40 400 mg Crossovera, 2 weeks Carbamazepine > placebo 2.3 [200]Oxcarbazepine 146 <1800 mg Parallelb, 16 weeks Oxcarbazapine > placebo 6 [111]Lamotrigine 59 <400 mg Parallel, 8 weeks Lamotrigine > placebo 4 [106]Lamotrigine 360 ≤400 mg Crossover 19 weeks Lamotrigine > placebo – [201]Topiramate 323 <400 mg Parallel, 12 weeks Topiramate > placebo 7.4 [113]Lacosamide 513 400 and 600 mg day Parallel, 18 weeks Lacosamide > placebo – [127]Gabapentin 334 ≤2400 mg Parallel, 7 weeks Gabapentin > placebo – [140]Gabapentin 305 ≤2400 mg Crossover, 8 weeks Gabapentin > placebo – [141]Gabapentin 165 ≤3600 mg Parallel, 8 weeks Gabapentin > placebo 4 [125]Pregabalin 146 300 mg Parallel, 8 weeks Pregabalin > placebo 3.9 [202]Pregabalin 338 75, 300, 600 mg Parallel, 5 weeks Pregabalin (300, 600 mg) > placebo 300 mg: 3.6; 600 mg: 3.3 [143]Pregabalin 40 150, 300, 600 mg Parallel, 4 weeks Pregabalin > placebo 300 mg: 4.0; 600 mg: 3.3 [203]Pregabalin 395 150, 300, 600 mg Parallel, 12 weeks Pregabalin (600 mg) > placebo 6.3 [204]Pregabalin 246 150, 600 mg Parallel, 6 weeks Pregabalin (600 mg) > placebo 600 mg: 4.2 [205]
�-M receptor agonistsOxycodone CR 36 <80 mg Parallel, 4 weeks Oxycodone > placebo 2.6 [206]Oxycodone CR 159 10–100 mg Parallel, 6 weeks Oxycodone > placebo NA [207]Tramadol 127 100–400 mg Parallel, 6 weeks Tramadol > placebo 3.1 [208]
Topical agentClonidine 179 0.1% TDS Parallel, 12 weeks Clonidine > placebo – [209]
NKT receptor antagonistTKA731 87 150 mg Parallel, 2 weeks TKA731 = placebo – [210]
NNR agonistABT-594 266 300, 450, 600 �g Crossover 6 weeks ABT-594 > placebo – [163]
TCA: tricyclic and tetracyclic antidepressants, SSRIs: selective serotonin reuptake inhibitors, SNRIs: serotonin-Nor-epinephrine Reuptake Inhibitors, NNT: number needed to treat, NA: not available.a Crossover: a crossover study compares the results of a two treatment on the same group of patients.b Parallel: a parallel designed clinical trial compares the results of a treatment on two separate groups of patients.
Author's personal copy
R. Singh et al. / Pharmacological Research 80 (2014) 21– 35 27
Fig. 2. Algorithm for treatment strategy of diabetic peripheral neuropathy pain. TCA’s, tricyclic and tetracyclic antidepressants; SNRI’s, serotonin–norepinephrine reuptakeinhibitos.
paroxetine and citalopram resulted in more significant reductionin pain as compared to fluoxetine [117]. Treatment of DPN withSSRI’s demonstrated no significant difference between SSRI’s andplacebo groups [118].
3.3.3. Serotonin–norepinephrine reuptake inhibitors (SNRI)Because of less therapeutic effectiveness of SSRI than TCA’s,
recent interest has been shifted on antidepressant agents withdual inhibitory action, i.e. serotonin and norepinephrine reup-take inhibitions. Such agents are called serotonin–norepinephrinereuptake inhibitors (SNRI), e.g. duloxetine and venlafaxine [119].One clinical trial showed that administration of higher dosesof venlafaxine led to improved pain scores and more balancednoradrenergic-to-serotonin effect [120]. Duloxetine is relativelybalanced in its affinity for noradrenergic and serotonergic reup-take inhibition [121]. Three randomized placebo control trialshave been conducted with duloxetine on a large number ofpatients and it was found that duloxetine at a dose of 60 and120 mg/day provided significant relief from DPN. Duloxetine isapproved by FDA for the treatment of DPN [122–124]. Venlafax-ine at a dose of 150–250 mg/day and 75–150 mg/day producedsignificant improvement in DPN as compared to placebo [120,125].
3.3.4. AnticonvulsantsAnticonvulsants are very much efficacious for the treatment
of neuropathic pain and commonly used anticonvulsants are car-bamazepine, lamotrigine, oxcarbazapine, topiramate etc. Multiplerandomized clinical trials (RCT’s) have proven the efficacy of thesedrugs in different types of neuropathic pain.
Carbamazepine is the only FDA (Food and Drug Administra-tion) approved anticonvulsant for the treatment of neuropathicpain but not specifically for DPN induced pain. It acts by block-ing voltage-gated sodium channels. While starting the treatmentwith carbamazepine, it should be administered in low doses andthen increased gradually. Laboratory monitoring such as bloodurea, complete blood count, liver function test, urine analysis andlipid level should be performed at the onset of treatment and atdifferent time intervals up to 12 months due to possible risk of
hyponatremia. Side effects of carbamazepine include nausea, con-stipation, sedation, dizziness and ataxia [126,127].
Lamotrigine acts by blocking voltage-dependant sodium chan-nels, by inhibiting pre-synaptic release of glutamate and increasinglevel of GABA in brain [128]. In one study, significant reductionin DPN was observed with lamotrigine treatment at a dose of≤400 mg/day [129]. Whereas, in another study two randomized,double-blind, placebo-controlled trials were conducted with lam-otrigine on 360 patients for 19 weeks at doses of 100, 200, and400 mg/day. In one trial, it was observed that lamotrigine at a doseof 400 mg/day resulted in reduction of pain scale but, at the endof the trial no significant difference was observed between lamot-rigine and placebo group. The side effects of lamotrigine includenausea, headache, dizziness and fatigue. It is generally well toler-ated but can induce severe allergic reactions [129].
Oxcarbazapine, a keto-analogue of carbamazepine can providesignificant analgesia in painful diabetic neuropathic conditions. Itacts by inhibiting sustained, high frequency voltage-gated sodiumchannels merged with high voltage P/Q and N-type calcium chan-nels [130–133]. In one study, oxcarbazapine significantly reducedDPN at a dose of 1800 mg/day [134], whereas in another study,no significant reduction was observed at doses of 600, 1200 and1800 mg/day [135].
Topiramate acts by blocking voltage-gated sodium and L-typecalcium channels through its effect on �-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid (AMPA)/Kainate excitatoryamino acid receptors. In one study, topiramate at a dose of≤400 mg/day significantly reduced DPN [136] whereas, in anotherstudy no significant reduction in DPN was observed at 100, 200 and400 mg/day of topiramate [137].
Another anticonvulsant, lacosamide has a unique mode of actionand act by selectively enhancing slow inactivation of voltage-gatedsodium channels [138]. In a placebo-controlled study conducted byZeigler et al., it was observed that lacosamide at doses of 400 and600 mg/day effectively reduced neuropathic pain as compared toplacebo and found to be well tolerated by diabetic patients [139].
Three randomized, double-blind, placebo-controlled trials havebeen conducted on gabapentin with a maximum dose of

Author's personal copy
28 R. Singh et al. / Pharmacological Research 80 (2014) 21– 35
2400 mg/day in two studies and 3600 mg/day in another study. Allthese studies have shown significant reduction in DPN as comparedto placebo [140–142]. Gabapentin and pregabalin have been shownto be very effective in treatment of DPN as compared to anticon-vulsants and TCA’s. Gabapentin and pregabalin decreased calciuminflux via binding to �2� site of L-type voltage-gated calcium chan-nels and produced a strong analgesic effect in the treatment ofDPN. Common side effects of these drugs are dizziness, somno-lence, peripheral edema and dry mouth with a similar frequencyfor both drugs. Five randomized, double-blind, placebo-controlledstudies have been conducted on different doses of pregabalin ran-ging from 75 to 600 mg/day and pregabalin have shown significantreduction in DPN than placebo. Pregabalin is approved by FDA fortreatment of DPN [143,144].
4. Future directions
4.1. Potential targets for management of DPN
For the past couple of years, tremendous efforts have been madefor the identification of novel target sites and therefore numerousagents have been explored for their therapeutic potential in thetreatment of DPN (Table 3).
4.1.1. DPP-IV inhibitorsDipeptidyl peptidase-IV (DPP-IV) incretin hormones are
released by gut endocrine cells and plays an important role inglucose homeostasis primarily by regulating blood glucose levelthrough stimulating glucose-dependent insulin secretion, reducingglucagon secretion and slowing gastric emptying. DPP-IV degradesand inactivates glucagon-like peptide-1 (GLP-1) and glucose-dependent insulin-tropic polypeptide (GIP) in vivo [145,146]. Thedegradation of these peptides by DPP-IV is responsible for theirshort half life in circulation [145,147]. Alogliptin, a DPP-IV inhibitor,has been evaluated for its effect on vascular and neural compli-cations in STZ-induced diabetic male Sprague-Dawley rats. After12 weeks of treatment, alogliptin significantly improved MNCVand thermal response latency. SNCV was marginally improvedin diabetic rats but the treatment did not improve the decreasein intraepidermal nerve fiber density [148]. Bianchi et al. (2012)conducted a study on a novel vidagliptin analogue PKF 275-055to evaluate the effect of compound on prevention, protectionand treatment of DPN in STZ-induced diabetic rats and it wasfound that PKF275-055 completely averted the decrease of Na+/K+-ATPase activity and partially counteracted the NCV deficit observedin untreated diabetic rats. PKF275-055 shows an anabolic effect,improved oral glucose tolerance, and counteract the alterationsin Na+/K+-ATPase activity, NCV and nociceptive thresholds in dia-betic rats [149]. The studies suggested that DPP-IV inhibitors canimprove some of the vascular and neural complications related todiabetes.
4.1.2. Hsp90 inhibitorsKU-32 is a novel novobiocin-based Hsp90 inhibitor which can
protect against neuronal cell death in vitro with minimal cytotox-icity on neuronal cells. An in vitro test conducted by Farmer et al.(2012) on human islet cells indicated that treating human isletswith KU-32 for 24 h shows no toxicity as assessed using the alamarBlue assay. Confocal microscopy confirms that with a minimumof 2-day exposure, KU-32 improves cellular viability by block-ing apoptosis. Functionally, isolated human islets release moreglucose-stimulated insulin when pre-incubated in KU-32 [150].
4.1.3. N-methyl-d-aspartate (NMDA) receptor antagonistsMK801, a N-methyl-d-aspartate (NMDA) receptor antagonist: in
a study conducted by Hwang et al. (2011), the change over time of
p35/p25 protein level in the spinal cord compared with behavioralresponses to thermal and mechanical stimulation in STZ-induceddiabetic rats was evaluated. It was found that electro-puncturecombined with MK-801 prolongs anti-hyperalgesia, increases p35expression, and decreases the cleavage of p35 to p25 during dia-betic neuropathic pain [151].
4.1.4. Cannabinoid CB1 receptor antagonistNabilone, a synthesized CB1 predominant receptor agonist,
has been used for neuropathic pain relief based upon anecdotalevidence and uncontrolled case series [152]. Toth et al. (2012),performed a single-center, randomized, double-blind, placebo-controlled, flexible dose study with an enriched enrollmentrandomized withdrawal design. Subjects achieving P30% pain relief(26/37) were then randomized and treated with either flexibledosing of nabilone 1–4 mg/day (n = 13) or placebo (n = 13) in afurther 5-week double-blind treatment period. Flexible dosing ofnabilone 1–4 mg/day effectively relieved DPN symptoms, improveddisturbed sleep, quality of life, and overall patient status. Nabilonewas well tolerated and successful as adjuvant in patients with DPN[153]. Rimonabant, the CB1 receptor antagonist increase skin bloodflow and reduce TNF-� level in diabetic rats suggesting that it canbe beneficial for the treatment of DPN, possibly due to its potentialrole in micro- and macro-vessel protection and anti-inflammatoryproperty [154].
4.1.5. �-opioid receptor agonist-norepinephrine reuptakeinhibitors (MOR-NRI)
Tapentadol ER represents a new class of centrally acting anal-gesic agent, MOR-NRI [155], and analgesic activity results fromcontribution of both mechanisms of action [156,157]. Afilalo andMorlion (2013) found that tapentadol ER (100–250 mg, b.i.d.) pro-vided comparable pain relief related to DPN up to one year oftreatment. Tapentadol ER treatment has been associated with bet-ter gastrointestinal tolerability and compliance with therapy thanoxycodone CR, which suggests that tapentadol ER may be a betteroption for the long-term management of chronic pain [158].
4.1.6. Topical agentsNGX-4010, a capsaicin 8% dermal patch, is licensed in the Euro-
pean Union for the treatment of peripheral neuropathic pain (PNP)in non-diabetic adults and in the United States for the treatmentof neuropathic pain associated with post-herpetic neuralgia (PHN)[159]. A multicenter, randomized, open-label design study wasconducted by Martini et al. (2012) to evaluate the effect of cap-saicin 8% in 91 patients with painful DPN. This study was aimed toevaluate the tolerability and efficacy of 1–4 high concentration cap-saicin (640 �g/cm2) patches, preceded by the topical application oflidocaine 4%. Pain score reduced in capsaicin 8% treated patientsand this mode-based approach allows analysis and optimization oftreatment for patients suffering from chronic pain conditions [160].Another open-label, multicenter study was conducted by Web-ster et al. (2012) in 117 patients with PHN, HIV-associated distalsensory polyneuropathy and painful DPN. Patients received a pre-treatment of lidocaine 4% or Topicaine® gel or Betacaine EnhancedGel 4 for 60 min followed by a 60–90 min NGX-4010 application for12 weeks. The treatment was found to be safe, well tolerated andresulted in approximately 30% reduction in neuropathic pain [161].
4.1.7. Vasopeptidase inhibitionAVE 7688 protects vascular and neural function by preven-
ting degradation of vaso- and neuro-active peptides and reducingoxidative stress. AVE 7688 (Ilepatril) prevented neural complica-tions including slowing of NCV, thermal hypoalgesia and decreased

Author's personal copy
R. Singh et al. / Pharmacological Research 80 (2014) 21– 35 29
Table 3Novel target sites for the management of diabetic neuropathy.
S. No. Drug Mechanism of action
1. Alogliptin DPP IV inhibitors2. PKF 275-0553. KU-32 Hsp90 inhibitor which can protect against neuronal cell death4. MK801 N-methyl-d-aspartate (NMDA) receptor antagonist5. Nabilone Cannabinoid CB1 predominant receptor
agonist6. Rimonabant7. Tapentadol ER �-opioid receptor agonist-norepinephrine reuptake inhibitor8. NGX-4010 Substance P depletion from nociceptors9. AVE7688 (Ilepatril) Vasopeptidase inhibition
10. ABT-594 �4 �2 neuronal nicotinic receptor agonist11. ABT-89412. Sildenafil PDE-5 inhibitor13. BAY 11-7082 I�B phosphorylation inhibitor14. Thymosin �4 Acts on P13K/Akt signaling pathway to preserve and/or restore vascular function in the sciatic nerve
intraepidermal nerve fiber density in STZ-induced diabetic mice[162].
4.1.8. ˛4 ˇ2 neuronal nicotinic acetylcholine receptor agonistABT-594 is a neuronal nicotinic acetylcholine receptor (NNR)
agonist that exhibits potent analgesic activity in preclinical mod-els of acute, chronic and neuropathic pain. ABT-594 was evaluatedclinically for the treatment of neuropathic pain, particularly thosetargeting the �4 �2 NNR subtype [163]. Analgesic efficacy andsafety of the highly selective �4 �2 NNR agonist ABT-894 wasevaluated in two separate randomized, double-blind, multicenter,placebo-controlled clinical trials in patients with DPN pain. In bothtrials, none of the ABT-894 treated groups showed efficacy com-pared to placebo. The failure of the highly selective �4 �2 NNRagonist ABT-894 indicates that selectively targeting �4 �2 NNR maynot be a viable approach to treating neuropathic pain [164].
4.1.9. PDE-5 inhibitorHyperglycemia up-regulates PDE-5 in Schwann cells and
reduces their proliferation, migration and expression of brain-derived neurotrophic factor (BDPNF). Blockage of PDE-5 withsildenafil increased cyclic guanosine monophosphate (cGMP) andcompletely abolished the effect of hyperglycemia on Schwann cells.These data indicate that hyperglycemia substantially up-regulatesPDE-5 expression and cGMP/PKG signaling pathway activated bysildenafil mediates the beneficial effects on DPN [165].
4.1.10. I�B phosphorylation inhibitorIn DPN, there is elevated expression of NF-�B (p65), I�B and
p-I�B along with increased levels of IL-6, TNF-� and inducibleenzymes (COX-2 and iNOS) resulting in deficits in nerve func-tions. Furthermore, there is an increase in oxidative stress anddecrease in Nrf/HO-1 expression. BAY 11-7082, an I�B phosphory-lation inhibitor reduced the levels of IL-6, TNF-�, COX-2 and iNOSin the sciatic nerve and ameliorated the increase in expressionof NF-�B, I�B and p-I�B, attenuated DPN by modulating neuro-inflammation and improving antioxidant defense [166].
4.1.11. P13K/Akt signaling pathwayThymosin �4 acts on endothelial and Schwann cells via
P13K/Akt signaling pathway to preserve and/or restore vascu-lar function in the sciatic nerve which facilitates improvementof peripheral nerve function in DPN. Therefore, thymosin �4 haspotential for the treatment of DPN [167]. Xanthine oxidase is animportant source of ROS which contributes to neurovascular dys-function in experimental diabetes. Inhibition of xanthine oxidaseby allopurinol could be a potential therapeutic approach to DPN[168].
4.1.12. Galanin receptor-1Reduced expression of galanin receptor-1 in spinal dorsal horn
exerts analgesic effect in diabetic rats with neuropathic pain. Thisreceptor could be the potential therapeutic target for diabetic neu-ropathic pain sensation [169]. The exact mechanism underlying theantinociceptive effect of galanin via galanin receptor 1 in spineis unclear but recent data may shed some light, indicating thatgalanin receptor 1 is preferentially expressed in a subpopulationof glutamatergic interneurons [170,171]. Over-activation of glu-tamate receptors contributes to axonal degeneration or axonalinjury [172,173]. Galanin release from both sensory and interneu-ron nerve endings in diabetic rats could then act on galanin receptor1-containing glutamatergic interneuron, resulting in attenuation ofglutamatergic activation of pain projection neurons and antinoci-ception [169].
4.2. Other potential contributors for managing DPN
Recently, numerous herbal interventions have been identifiedto possess the potential to ameliorate the progression of DPN(Table 4). The phenolic glucoside, gastrodin, is a main constituentof the Chinese herbal medicine Gastrodia elata Blume. Intraperi-toneal administration of gastrodin effectively attenuated boththe mechanical allodynia and thermal hyperalgesia induced bySTZ [174]. Diabetes induces prominent enhancement of INaT anddecreases potassium currents, especially slowly inactivating potas-sium currents (IAS). These effects were found to be completelyreversed by gastrodin in dose-dependent manner. The study pro-vided a cellular basis for the peripheral analgesic action of gastrodinfor the treatment of chronic pain, including DPN. An Ayurvedicnerve tonic herb Centella asiatica (CAST) was evaluated for its safetyand therapeutic effects in diabetic neuropathic patients. CAST orplacebo capsules were administered to 33 DPN subjects, in a ran-domized double-blind, placebo-controlled study. The dose of CASTwas escalated from 60 to 240 mg/day over the first 12 weeks, fol-lowed by a stable dose of 240 mg/day for the remaining 40 weeks.From the study it was concluded that CAST is stable and well tol-erated up to 240 mg/day. Moreover, CAST significantly improvessymptoms in diabetes neuropathic subjects [175].
Neuragen PN® is a FDA registered homeopathic drug contain-ing a blend of six homeopathic substances and five plant-basedessential oils. The six homeopathic substances are Hypericum perfo-ratum, Aconitum napellus, Lycopodium clavatum, Phosphorus, Rhustoxicodendron and Secale cornutum. A randomized, double-blind,placebo-controlled study on Neurogen PN® was conducted by Li(2010) on 60 participants with plantar cutaneous pain due to DPN.Each subject received one of the two treatments, Neuragen PN® orplacebo, per week in crossover design and acute spontaneous painlevel was assessed. The study revealed that Neurogen PN® provided

Author's personal copy
30 R. Singh et al. / Pharmacological Research 80 (2014) 21– 35
Table 4Potential herbal interventions to have ameliorative effect in the progression of DPN.
S. No. Herbal interventions Mechanism of action Clinical benefit
1. Gastrodin [174] Inhibits sodium currents (INaT) It provides peripheral analgesic effect in the treatment ofchronic pain, including DPN
2. Centella asiatica [175] – Improves diabetic neuropathic symptoms.3. Neurogen PN® [176] – Relieves plantar cutaneous pain due to peripheral
neuropathy4. Olea europea L. [177] Inhibits caspase 3 activation and decreased BaX/Bcl2
ratioInhibits high glucose induced neural damage andsuppresses diabetes induced thermal hyperalgesia
5. Emblica officinalis Gaertn. [178] Modulates oxidative–nitrosative stress Attenuates diabetic neuropathic pain6. PMI-5011 [183] Blunts sciatic nerve and spinal cord
12/15-lipoxygenase activation andoxidative–nitrosative stress
Alleviates DPN
7. Momordica charantia L. [184] Modulates hyperglycemia and decreasing generationof ROS
Attenuates aggravated ischemia–reperfusion inducedneuronal injury and subsequent neurological functions
8. DA-9801 [185] Exhibits NGF-agonistic activity Produces neuroprotective effect against DPN9. Diosgenin [186] Possess NGF-agonistic activity Reverses functional and ultrastructural changes and
induces neural regeneration in a DPN model10. Fenugreek (Trigonella
foenum–graecum L.) [187]– Protects against thermal hyperalgesia and deranged motor
function test scores restores MNCV and thus effective inpainful DPN
11. Baicalein [188] Counteracts diabetes-associated p38 MAPKphosphorylation, oxidative–nitrosative stress, and12/15-lipoxygenase overexpression and activation
Prevents DPN
12. Tocotrienol [189] Modulates oxidative–nitrosative stress, inflammatorycytokine release, and caspase-3 in diabetic rats
Attenuates the diabetic condition and also reversesneuropathic pain13. Sesamol [190]
14. Lycopene [191] Shows inhibitory action in NO and TNF-� release Attenuates diabetic neuropathic pain
significant relief from neuropathic pain in all neuropathic groups[176]. Leaf extract of olive (Olea europea L.) was investigated forits effect in DPN pain. Olea europea leaf extract treatment inhibitedcaspase 3 activation and decreased BaX/Bcl2 ratio. The results sug-gested that olive leaf extracts inhibited high glucose induced neuraldamage and suppressed diabetes induced thermal hyperalgesia.The mechanism of these effects may be due to reduced neuronalapoptosis suggesting attenuation of DPN [177].
Emblica officinalis Gaertn. extract not only attenuated thediabetic condition but also reversed neuropathic pain throughmodulation of oxidative–nitrosative stress in diabetic rats [178].PMI-5011, an ethanolic extract of Artemisia dracunculus L., hasbeen reported to improve insulin and insulin receptor signaling[179], inhibit aldose reductase [180], oxidative stress [181], andNF-�B regulated inflammatory mechanisms [182]. Moreover, PMI-5011 alleviated DPN by blunting sciatic nerve and spinal cord12/15-lipoxygenase activation and oxidative–nitrosative stress,without ameliorating hyperglycemia or reducing sciatic nerve sor-bitol pathway intermediate accumulation [183]. Administration ofMomordica charantia L. in diabetic mice has been noted to attenu-ate aggravated ischemia–reperfusion induced neuronal injury andsubsequent neurological functions by modulating hyperglycemiaand decreasing generation of ROS. These results validate the tra-ditional use of Momordica charantia L. against diabetes and itscomplications [184]. DA-9801, a mixture extract of Dioscoreajaponica Thunb. and Dioscorea nipponica Makino, exhibits NGF-agonistic activity which may contribute to their neuroprotectiveeffect against DPN [185]. Diosgenin, a major sapogenin obtainedfrom Dioscorea nipponica, reverses functional and ultrastructuralchanges and induces neural regeneration in a DPN model throughinduction of NGF [186]. Fenugreek (Trigonella foenum–graecumL.) offered sustained protection against thermal hyperalgesia andderanged motor function test scores, restored MNCV and foundto be effective in painful DPN [187]. The flavonoid baicalein(5,6,7-trihydroxyflavone) counteracted diabetes-associated p38MAPK phosphorylation, oxidative–nitrosative stress, and 12/15-lipoxygenase overexpression and activation, but not glucoseor sorbitol pathway intermediate accumulation. These findingsprovide rationale for using hydroxyflavones as potential agentsfor the treatment of DPN [188]. The combination of insulin with
sesamol (natural phenol obtained from sesame oil) and tocotrienolnot only attenuated the diabetic condition but also reversed neu-ropathic pain through modulation of oxidative–nitrosative stress,inflammatory cytokine release and caspase-3 in diabetic rats andthus it may find clinical application to treat neuropathic pain in thediabetic patient [189,190]. Lycopene, a caratenoid mostly found intomatoes and its products, attenuated diabetic neuropathic painpossibly through its inhibitory action in NO and TNF-� release[191]. Taken together, these studies suggest that herbal drugs mayprovide a new therapeutic alternative for the treatment of DPN[192].
5. Summary
Hyperglycemia directly impacts multiple pathways and addi-tional indirect mechanisms also get involved along with theprogression of the disease, which may not respond merely toglycemic control. As glycemic control is the only proven approach,therefore the pharmacological approaches that attempt to miti-gate biochemical aberrations inducing neuronal damage are alsoof great importance. Therapeutic management of DPN is very com-plex and it depends on exploration of the pathogenetic mechanismsresponsible for the disease. One challenge in the development ofthese targeted therapies is the multifactorial nature of DPN. Var-ious metabolic pathways like AGE pathway, polyol pathway, PKCpathway and hexosamine pathway directly or indirectly alter theredox capacity of the cell and increase the production of ROS. Thisincreased oxidative stress leads to impaired neural function, grad-ually heading to apoptosis of neurons, Schwann and glial cells ofperipheral nervous system.
Preventing oxidative stress by enhancing antioxidant defenseis another logical therapeutic approach for preventing DPN. Addi-tional research is clearly needed to firmly establish whether eitherthe reduction of ROS formation activated by hyperglycemia and ele-vated free fatty acids level and/or the blockade of the ROS-inducedstress pathways will result in improved insulin action and/or secre-tion. Although small clinical trials on antioxidants like, �-lipoicacid, resveratrol, taurine, rutin etc., have proved their contributiontoward neuroprotection in diabetic patients [97,100,101,193,194]

Author's personal copy
R. Singh et al. / Pharmacological Research 80 (2014) 21– 35 31
Nonetheless, the totality of available data provides support for con-ducting more extensive clinical studies evaluating the effectivenessof antioxidant treatment.
Many areas of research into DPN are yet to be explored but thereare certain promising lines of investigation that can lead to theeffective management of the disease. Initially, DPN is diagnosedby making use of some simple diagnostic tools and the therapybegins with appropriate glycemic control which remains the foun-dation of prevention and pre-requisite of adequate treatment. Thus,an improved therapeutic response may be achieved by specificallytargeting the underlying pathogenesis of the disease manifesta-tions [195]. In management of DPN, TCA’s, SNRI’s and calciumchannel �2�-ligands are the first line medications but, if partialor no pain relief is achieved by a single drug, combinations areoften used. Due to lack of controlled studies, the rationale of suchtherapy was mainly based on theory, but now supported by RCTs.The best evidence is the combination of a TCA or an opioid withgabapentin. [196,197]. Anticonvulsant drugs do not act directly onthe underlying pathology of DPN but relieves diabetic neuropathicpain through indirect mechanism. Therefore, use of these symp-tom modifying drugs should also be considered in the managementof DPN to improve the quality of life for those who may respond[198]. In an evidence-based review on clinical data, it was estab-lished that pregabalin is effective in treating diabetic neuropathicpain. Also venlafaxine, duloxetine, gabapentin, amitriptyline, opi-oids and capsaicin can be effective and should be considered inpatients who are not responding to pregabalin [199].
Although several therapeutic approaches have been introducedin clinical practice but the pharmacological treatment of DPNremains a challenge for clinicians. Potential targeting sites shouldbe discovered which directly ameliorate DPN. In future, novel ther-apeutic agents working at the level of mitochondrial metaboliccontrol are likely to further improve the management of DPN. Nat-ural sources, for the treatment of DPN, should be explored in orderto provide safe and cost effective treatment to the patients. Alter-ation of metabolic pathways is directly involved in the pathogenesisof DPN, thus exploration of drugs acting through these pathwaysand conducting extensive clinical trials, may lead to evolution ofcurative therapy for DPN rather than a symptomatic relief withconventional therapy available.
References
[1] Balakumar P, Arora MK, Ganti SS, Reddy J, Singh M. Recent advances inpharmacotherapy for diabetic nephropathy: current perspectives and futuredirections. Pharmacol Res 2009;60:24–32.
[2] Vinik AI, Park TS, Stansberry KB, Pittenger GL. Diabetic neuropathies. Dia-betologia 2000;43:957–73.
[3] Edwards JL, Vincent AM, Cheng HT, Feldman EL. Diabetic neuropathy: mech-anisms to management. Pharmacol Ther 2008;120:1–34.
[4] Tesfaye S. Recent advances in the management of diabetic symmetrical poly-neuropathy. J Diabet Invest 2010;2:33–42.
[5] Davies M, Brophy S, Williams R, Taylor A. The prevalence, severity and impactof painful diabetic peripheral neuropathy in type 2 diabetes. Diabet Care2006;29:1518–22.
[6] Quattrini C, Tesfaye S. Understanding the impact of painful diabetic neurop-athy. Diabet Metab Res Rev 2003;19:S2–8.
[7] Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kempler P, et al. Dia-betic neuropathies: update on definitions, diagnostic criteria, estimation ofseverity and treatments. Diabet Care 2010;33:2285–93.
[8] Athans W, Stephens H. Open calcaneal fractures in diabetic patients withneuropathy: a report of three cases and literature review. Foot Ankle Int2008;29:1049–53.
[9] Veves A, Backonja M, Malik RA. Painful diabetic neuropathy: epidemi-ology, natural history, early diagnosis, and treatment options. Pain Med2008;9:660–74.
[10] Obrosova IG. Diabetic painful and insensate neuropathy: pathogenesis andpotential treatments. Neurotherapeutics 2009;6:638–47.
[11] Gandhi RA, Marques JL, Selvarajah D, Emery CJ, Tesfaye S. Painful diabeticneuropathy is associated with greater autonomic dysfunction than painlessdiabetic neuropathy. Diabet Care 2010;33:1585–90.
[12] Sima AA, Sugimoto K. Experimental diabetic neuropathy: an update. Dia-betologia 1999;42:773–88.
[13] Smith AG, Singleton JR. Diabetic neuropathy. Continuum Lifelong LearningNeurol 2012;18:60–84.
[14] Oates PJ. Polyol pathway and diabetic peripheral neuropathy. Int Rev Neuro-biol 2002;50:325–92.
[15] Toth C, Rong LL, Yang C, Martinez J, Song F, Ramji N, et al. Receptor foradvanced glycation end products (RAGEs) and experimental diabetic neu-ropathy. Diabetes 2008;57:1002–17.
[16] Xia P, Kramer RM, King GL. Identification of the mechanism for the inhi-bition of Na+, K(+)-adenosine triphosphatase by hyperglycemia involvingactivation of protein kinase C and cytosolic phospholipase A2. J Clin Invest1995;96:733–40.
[17] Tomlinson DR. Mitogen-activated protein kinases as glucosetransducers fordiabetic complications. Diabetologia 1999;42:1271–81.
[18] Vareniuk I, Pavlov IA, Obrosova IG. Inducible nitric oxide synthasegene deficiency counteracts multiple manifestations of peripheral neurop-athy in a streptozotocin-induced mouse model of diabetes. Diabetologia2008;51:2126–33.
[19] Low PA, Lagerlund TD, McManis PG. Nerve blood flow and oxygen deliv-ery in normal, diabetic, and ischemic neuropathy. Int Rev Neurobiol1989;31:355–438.
[20] Yamakawa I, Kojima H, Terashima T, Katagi M, Oi J, Urabe H, et al. Inactivationof TNF-� ameliorates diabetic neuropathy in mice. Am J Physiol EndocrinolMetab 2011;301:E844–52.
[21] Cameron NE, Cotter MA. Pro-inflammatory mechanisms in diabetic neu-ropathy: focus on the nuclear factor kappa B pathway. Curr Drug Targets2008;9:60–7.
[22] Leinninger GM, Vincent AM, Feldman EL. The role of growth factors in diabeticperipheral neuropathy. J Peripher Nerv Syst 2004;9:26–53.
[23] Jack M, Wright D. Role of advanced glycation endproducts and glyoxalase I indiabetic peripheral sensory neuropathy. Transl Res 2012;159:355–65.
[24] Brownlee M. Biochemistry and molecular cell biology of diabetic complica-tions. Nature 2001;414:813–20.
[25] Schmidt AM, Yan SD, Wautier JL, Stern D. Activation of receptor for advancedglycation endproducts: a mechanism for chronic vascular dysfunction in dia-betic vasculopathy and atherosclerosis. Circ Res 1999;84:489–97.
[26] Mastrocola R, Restivo F, Vercellinatto I, Danni O, Brignardello E, Aragno M,et al. Oxidative and nitrosative stress in brain mitochondria of diabetic rats. JEndocrinol 2005;187:37–44.
[27] Somfai GM, Knippel B, Ruzicska E, Stadler K, Toth M, Salacz G, et al. Solublesemicarbazide-sensitive amine oxidase (SSAO) activity is related to oxidativestress and subchronic inflammation in streptozotocin-induced diabetic rats.Neurochem Int 2006;48:746–52.
[28] Johansen JS, Harris AK, Rychly DJ, Ergul A. Oxidative stress and the use ofantioxidants in diabetes: linking basic science to clinical practice. CardiovascDiabetol 2005;4:5.
[29] Baydas G, Nedzvetskiib VS, Nerushc PA, Kirichenkob SV, Yoldasd T. Alteredexpression of NCAM in hippocampus and cortex may underlie memory andlearning deficits in rats with streptozotocin-induced diabetes mellitus. LifeSci 2003;73:1907–16.
[30] Koivisto A, Hukkanen M, Saarnilehto M, Chapman H, Kuokkanen K, Wei H,et al. Inhibiting TRPA1 ion channel reduces loss of cutaneous nerve fiberfunction in diabetic animals: sustained activation of the TRPA1 channel con-tributes to the pathogenesis of peripheral diabetic neuropathy. PharmacolRes 2012;65:149–58.
[31] Leinninger GM, Edwards JL, Lipshaw MJ, Feldman EL. Mechanisms of dis-ease: mitochondria as new therapeutic targets in diabetic neuropathy. NatClin Pract 2006;2:620–8.
[32] Niedowicz DM, Daleke DL. The role of oxidative stress in diabetic complica-tions. Cell Biochem Biophys 2005;43:289–330.
[33] King GL, Loeken MR. Hyperglycemia-induced oxidative stress in diabetic com-plications. Histochem Cell Biol 2004;122:333–8.
[34] Wilson Tang WH, Maroo A, Young JB. Ischemic heart disease and con-gestive heart failure in diabetic patients. Med Clin North Am 2004;88:1037–61.
[35] American Diabetes Association. Diagnosis and classification of diabetes mel-litus. Diabet Care 2005;28:S37–42.
[36] Dobretsov M, Romanovsky D, Stimers JR. Early diabetic neuropathy: triggersand mechanisms. World J Gastroenterol 2007;13:175–91.
[37] Sigaudo-Roussel D, Fromy B, Saumet JL. Diabetic neuropathy in animal mod-els. Drug Discov Today 2007;4:39–44.
[38] Huizinga MM, Peltier A. Painful diabetic neuropathy: a management-centeredreview. Clin Diabetes 2007;25:6–15.
[39] Hovaguimian A, Gibbons CH. Clinical approach to the treatment of painfuldiabetic neuropathy. Ther Adv Endocrinol Metab 2011;2:27–38.
[40] Bailey CJ. Potential new treatments for type 2 diabetes. Trends Pharmacol Sci2000;21:259–65.
[41] Brownlee M, Aiello LP, Cooper ME, Vinik AI, Nesto RW, Boulton AJM. Com-plications of diabetes mellitus. In: Kronenberg HM, Melmed S, Polonsky KS,Larsen PR, editors. Williams textbook of endocrinology. Philadelphia: Saun-ders Elsevier; 2008. p. 1417–501.
[42] Oyama T, Miyasita Y, Watanabe H, Shirai K. The role of polyol pathwayin high glucose-induced endothelial cell damages. Diabet Res Clin Pract2006;73:227–34.
[43] Oka M, Kato N. Aldose reductase inhibitors. J Enzym Inhib 2001;16:465–73.

Author's personal copy
32 R. Singh et al. / Pharmacological Research 80 (2014) 21– 35
[44] Tesfamariam B. Free radicals in diabetes endothelial cell dysfunction. FreeRadic Biol Med 1994;16:383–91.
[45] Yagihashi S, Yamagishi SI, Wada R-I, Baba M, Hohman TC, Yabe-Nishimura C,et al. Neuropathy in diabetic mice overexpressing human aldose reductaseand effects of aldose reductase inhibitor. Brain 2001;124:2448–58.
[46] Judzewitsch RG, Jaspan JB, Polonsky KS, Weinberg CR, Halter JB, Halar E, et al.Aldose reductase inhibition improves nerve conduction velocity in diabeticpatients. N Engl J Med 1983;308:119–25.
[47] Young RJ, Ewing DJ, Clarke BF. A controlled trial of sorbinil, an aldose reductaseinhibitor, in chronic painful diabetic neuropathy. Diabetes 1983;32:938–42.
[48] Lewin IG, O’Brien IA, Morgan MH, Corrall RJ. Clinical and neurophysiologicalstudies with the aldose reductase inhibitor, sorbinil, in symptomatic diabeticneuropathy. Diabetologia 1984;26:445–8.
[49] Cameron NE, Leonard MB, Ross IS, Whiting PH. The effects of sorbinil onperipheral nerve conduction velocity, polyol concentrations and morphologyin the streptozotocin-diabetic rat. Diabetologia 1986;29:168–74.
[50] Whiting PH, Ross IS. Increased nerve polyol levels in experimental diabetesand their reversal by Sorbinil. Br J Exp Pathol 1988;69:697–702.
[51] Coppey LJ, Gellett JS, Davidson EP, Dunlap JA, Yorek MA. Effect of treat-ing streptozotocin-induced diabetic rats with sorbinil, myo-inositol oraminoguanidine on endoneurial blood flow, motor nerve conduction veloc-ity and vascular function of epineurial arterioles of the sciatic nerve. Int J ExpDiabet Res 2002;3:21–36.
[52] Raccah D, Coste T, Cameron NE, Dufayet D, Vague P, Hohman TC. Effectof the aldose reductase inhibitor tolrestat on nerve conduction velocity,Na/K ATPase activity, and polyols in red blood cells, sciatic nerve, kiDP-Ney cortex, and kiDPNey medulla of diabetic rats. J Diabet Complications1998;12:154–62.
[53] Sima AA, Prashar A, Zhang WX, Chakrabarti S, Greene DA. Preventive effect oflong-term aldose reductase inhibition (ponalrestat) on nerve conduction andsural nerve structure in the spontaneously diabetic Bio-Breeding rat. J ClinInvest 1990;85:1410–20.
[54] Pekiner C, McLean WG. Impaired induction of nerve ornithine decarboxylaseactivity in the streptozotocin-diabetic rat is prevented by the aldose reductaseinhibitor ponalrestat. Br J Pharmacol 1990;101:978–80.
[55] Cameron NE, Cotter MA. Dissociation between biochemical and functionaleffects of the aldose reductase inhibitor, ponalrestat, on peripheral nerve indiabetic rats. Br J Pharmacol 1992;107:939–44.
[56] Hotta N, Toyota T, Matsuoka K, Shigeta Y, Kikkawa R, Kaneko T, et al. Clin-ical efficacy of fidarestat, a novel aldose reductase inhibitor, for diabeticperipheral neuropathy: a 52-week multicenter placebo-controlled double-blind parallel group study. Diabet Care 2001;24:1776–82.
[57] Kuzumoto Y, Kusunoki S, Kato N, Suzuki T, Yagihashi S. Effect of the aldosereductase inhibitor fidarestat on experimental diabetic neuropathy in the rat.Diabetologia 2006;49:3085–93.
[58] Zotova EG, Christ GJ, Zhao W, Tar M, Kuppam SD, Arezzo JC. Effects offidarestat, an aldose reductase inhibitor, on nerve conduction velocity andbladder function in streptozotocin-treated female rats. J Diabet Complications2007;21:187–95.
[59] Hotta N, Akanuma Y, Kawamori R, Matsuoka K, Oka Y, Shichiri M, et al.Long-term clinical effects of epalrestat, an aldose reductase inhibitor,on diabetic peripheral neuropathy: the 3-year, multicenter, comparativealdose reductase inhibitor-diabetes complications trial. Diabet Care 2006;29:1538–44.
[60] Matsuoka K, Sakamoto N, Akanuma Y, Hotta N, Shichiri M, Toyota T, et al.A long-term effect of epalrestat on motor conduction velocity of diabeticpatients: ARI-Diabetes Complications Trial (ADCT). Diabet Res Clin Pract2007;77:S263–8.
[61] Kawai T, Takei I, Tokui M, Funae O, Miyamoto K, Tabata M, et al. Effectsof epalrestat, an aldose reductase inhibitor, on diabetic peripheral neu-ropathy in patients with type 2 diabetes, in relation to suppression ofN(�)-carboxymethyl lysine. J Diabet Complications 2010;24:424–32.
[62] Greene DA, Arezzo JC, Brown MB. Effect of aldose reductase inhibitionon nerve conduction and morphometry in diabetic neuropathy. Neurology1999;53:580–91.
[63] Kihara M, Mitsui Y, Shioyama M, Hasegawa T, Takahashi M, Takakura S, et al.Effect of zenarestat, an aldose reductase inhibitor, on endoneurial blood flowin experimental diabetic neuropathy of rat. Neurosci Lett 2001;310:81–4.
[64] Bril V, Buchanan R. Long-term effects of ranirestat (AS-3201) on peripheralnerve function in patients with diabetic sensorimotor polyneuropathy. DiabetCare 2006;29:68–72.
[65] Matsumoto T, Ono Y, Kurono M, Kuromiya A, Nakamura K, Bril V. Ranirestat(AS-3201), a potent aldose reductase inhibitor, reduces sorbitol levels andimproves motor nerve conduction velocity in streptozotocin-diabetic rats. JPharmacol Sci 2008;107:231–7.
[66] Borghini I, Ania-Lahuerta A, Regazzi R, Ferrari G, Gjinovci A, Wollheim CB, et al.Alpha, beta I, beta II, delta, and epsilon protein kinase C isoforms and com-pound activity in the sciatic nerve of normal and diabetic rats. J Neurochem1994;62:686–96.
[67] Roberts RE, McLean WG. Protein kinase C isozyme expression in sciaticnerves and spinal cords of experimentally diabetic rats. Brain Res 1997;754:147–56.
[68] Evcimen ND, King GL. The role of protein kinase C activation and the vascularcomplications of diabetes. Pharmacol Res 2007;55:498–510.
[69] Ishii H, Koya D, King GL. Protein kinase C activation and its role in the develop-ment of vascular complication in diabetes mellitus. J Mol Med 1998;76:21–31.
[70] Cameron NE, Cotter MA. Effects of protein kinase C � inhibition on neu-rovascular dysfunction in diabetic rats: interaction with oxidative stress andessential fatty acid dysmetabolism. Diabet Metab Res Rev 2002;18:315–23.
[71] Srivastava AK. High glucose-induced activation of protein kinase signalingpathways in vascular smooth muscle cells: a potential role in the pathogenesisof vascular dysfunction in diabetes. Int J Mol Med 2002;9:85–9.
[72] Vinik AI, Bril V, Kempler P, Litchy WJ, Tesfaye S, Price KL, et al. Treatmentof symptomatic diabetic peripheral neuropathy with the protein kinase Cbeta-inhibitor ruboxistaurin mesylate during a 1-year, randomized, placebo-controlled, double-blind clinical trial. Clin Ther 2005;27:1164–80.
[73] Casellini CM, Barlow PM, Rice AL, Casey M, Simmons K, Pittenger G, et al.A 6-month, randomized, double-masked, placebo-controlled study evaluat-ing the effects of the protein kinase C-beta inhibitor ruboxistaurin on skinmicrovascular blood flow and other measures of diabetic peripheral neurop-athy. Diabet Care 2007;30:896–902.
[74] Brooks B, Delaney-Robinson C, Molyneaux L, Yue DK. Endothelial and neuralregulation of skin microvascular blood flow in patients with diabetic periph-eral neuropathy: effect of treatment with the isoform-specific protein kinaseC beta inhibitor, ruboxistaurin. J Diabet Complications 2008;22:88–95.
[75] Boyd A, Casselini C, Vinik E, Vinik A. Quality of life and objective measures ofdiabetic neuropathy in a prospective placebo-controlled trial of ruboxistaurinand topiramate. J Diabet Sci Technol 2011;5:714–22.
[76] Marshall S, Garvey WT, Traxinger RR. New insights into the metabolic regula-tion of insulin action and insulin resistance: role of glucose and amino acids.FASEB J 1991;5:3031–6.
[77] Boden G, Chen X, Ruiz J, White JV, Rossetti L. Mechanisms of fatty acid-inducedinhibition of glucose uptake. J Clin Invest 1994;93:2438–46.
[78] Schleicher ED, Weigert C. Role of the hexosamine biosynthetic pathway indiabetic nephropathy. Kidney Int Suppl 2000;58:S13–8.
[79] Kolm-Litty V, Sauer U, Nerlich A, Lehmann R, Schleicher ED, et al. High glucose-induced transforming growth factor beta1 production is mediated by thehexosamine pathway in porcine glomerular mesangial cells. J Clin Invest1998;101:160–9.
[80] Sayeski PP, Kudlow JE. Glucose metabolism to glucosamine is necessary forglucose stimulation of transforming growth factor-alpha gene transcription.J Biol Chem 1996;271:15237–43.
[81] Kaneto H, Xu G, Song KH, Suzuma K, Bonner-Weir S, Sharma A, et al.Activation of the hexosamine pathway leads to deterioration of pancreaticbeta-cell function through the induction of oxidative stress. J Biol Chem2001;276:31099–104.
[82] Stracke H, Lindemann A, Federlin K. A benfotiamine–vitamin B combina-tion in treatment of diabetic polyneuropathy. Exp Clin Endocrinol Diabetes1996;104:311–6.
[83] Stracke H, Gaus W, Achenbach U, Federlin K, Bretzel RG. Benfotiaminein diabetic polyneuropathy (BENDIP): results of a randomised, doubleblind, placebo-controlled clinical study. Exp Clin Endocrinol Diabetes2008;116:600–5.
[84] Haupt E, Ledermann H, Kopcke W. Benfotiamine in the treatment of diabeticpolyneuropathy—a three-week randomized, controlled pilot study (BEDIPstudy). Int J Clin Pharmacol Ther 2005;43:71–7.
[85] Wu S, Ren J. Benfotiamine alleviates diabetes-induced cerebral oxidativedamage independent of advanced glycation end-product, tissue factor andTNF-alpha. Neurosci Lett 2006;394:158–62.
[86] Balakumar P, Rohilla A, Krishan P, Solairaj P, Thangathirupathi A. The multi-faceted therapeutic potential of benfotiamine. Pharmacol Res 2010;61:482–8.
[87] Wada R, Yagihashi S. Role of advanced glycation end products and theirreceptors in development of diabetic neuropathy. Ann N Y Acad Sci2005;1043:598–604.
[88] Bhatt LK, Veeranjaneyulu A. Minocycline with aspirin: a therapeutic approachin the treatment of diabetic neuropathy. Neurol Sci 2010;31:705–16.
[89] Cooper ME, Thallas V, Forbes J, Scalbert E, Sastra S, Darby I, et al. The cross-linkbreaker, N-phenacylthiazolium bromide prevents vascular advanced glyca-tion end-product accumulation. Diabetologia 2000;43:660–4.
[90] McIlduff CE, Rutkove SB. Critical appraisal of the use of alpha lipoic acid (thioc-tic acid) in the treatment of symptomatic diabetic polyneuropathy. Ther ClinRisk Manage 2011;7:377–85.
[91] Ziegler D, Low PA, Litchy WJ, Boulton AJ, Vinik AI, Freeman R, et al. Efficacyand safety of antioxidant treatment with �-lipoic acid over 4 years in diabeticpolyneuropathy: the NATHAN 1 trial. Diabet Care 2011;34:2054–60.
[92] Shi TJ, Zhang MD, Zeberg H, Nilsson J, Grunler J, Liu SX, et al. Coenzyme Q10prevents peripheral neuropathy and attenuates neuron loss in the db−/db−
mouse, a type 2 diabetes model. Proc Natl Acad Sci U S A 2013;110:690–5.[93] Zhang YP, Eber A, Yuan Y, Yang Z, Rodriguez Y, Levitt RC, et al. Prophylactic
and antinociceptive effects of coenzyme Q10 on diabetic neuropathic pain ina mouse model of type 1 diabetes. Anesthesiology 2013;118:945–54.
[94] Negi G, Kumar A, Kaundal RK, Gulati A, Sharma SS. Functional and biochemicalevidence indicating beneficial effect of melatonin and nicotinamide alone andin combination in experimental diabetic neuropathy. Neuropharmacology2010;58:585–92.
[95] Sharma SS, Kumar A, Arora M, Kaundal RK. Neuroprotective potential ofcombination of resveratrol and 4-amino 1,8 naphthalimide in experimen-tal diabetic neuropathy: focus on functional, sensorimotor and biochemicalchanges. Free Radic Res 2009;43:400–8.
[96] Kumar A, Sharma SS. NF-kappaB inhibitory action of resveratrol: a prob-able mechanism of neuroprotection in experimental diabetic neuropathy.Biochem Biophys Res Commun 2010;394:360–5.

Author's personal copy
R. Singh et al. / Pharmacological Research 80 (2014) 21– 35 33
[97] Muthenna P, Akileshwari C, Saraswat M, Bhanuprakash Reddy G. Inhibitionof advanced glycation end-product formation on eye lens protein by rutin. BrJ Nutr 2012;107:941–9.
[98] Li F, Obrosova IG, Abatan O, Tian D, Larkin D, Stuenkel EL, et al. Taurine replace-ment attenuates hyperalgesia and abnormal calcium signaling in sensoryneurons of STZ-D rats. Am J Physiol Endocrinol Metab 2005;288:E29–36.
[99] Li F, Abatan OI, Kim H, Burnett D, Larkin D, Obrosova IG, et al. Taurine reversesneurological and neurovascular deficits in Zucker diabetic fatty rats. Neuro-biol Dis 2006;22:669–76.
[100] Askwith T, Zeng W, Eggo MC, Stevens MJ. Oxidative stress and dysregulationof the taurine transporter in high-glucose-exposed human Schwann cells:implications for pathogenesis of diabetic neuropathy. Am J Physiol EndocrinolMetab 2009;297:E620–8.
[101] Askwith T, Zeng W, Eggo MC, Stevens MJ. Taurine reduces nitrosativestress and nitric oxide synthase expression in high glucose-exposed humanSchwann cells. Exp Neurol 2012;233:154–62.
[102] Zhou JY, Zhou SW. Protection of trigonelline on experimental diabetic periph-eral neuropathy. Evid Based Complement Alternat Med 2012;2012:164219.
[103] UKPDS. Intensive blood-glucose control with sulphonylureas or insulin com-pared with conventional treatment and risk of complications in patients withtype 2 diabetes (UKPDS 33). Lancet 1998;352:837–53.
[104] Ulugol A, Karadag HC, Tamer M. Involvement of adenosine in the anti-allodynic effect of amitriptyline in streptozotocin-induced diabetic rats.Neurosci Lett 2002;328:129–32.
[105] Finnerup NB, Otto M, McQuay HJ, Jensen TS, Sindrup SH. Algorithm for neuro-pathic pain treatment: an evidence based proposal. Pain 2005;118:289–95.
[106] Saarto T, Wiffen PJ. Antidepressants for neuropathic pain. Cochrane DatabaseSyst Rev 2007;4:CD005454.
[107] Simmons Z, Feldman EL, Williams R, et al. Treatment of diabetic neuropathy.The evidence base for diabetes care. West Sussex, England: John Wiley & Sons;2002. p. 555–76.
[108] Max MB, Culnane M, Schafer SC, Gracely RH, Walther DJ, Smoller B, et al.Amitriptyline relieves diabetic neuropathy pain in patients with normal ordepressed mood. Neurology 1987;37:589–96.
[109] Vrethem M, Boivie J, Arnqvist H, Holmgren H, Lindstrom T, Thorell LH. Acomparison a amitriptyline and maprotiline in the treatment of painful poly-neuropathy in diabetics and nondiabetics. Clin J Pain 1997;13:313–23.
[110] Morello CM, Leckband SG, Stoner CP, Moorhouse DF, Sahagian GA. Ran-domized double-blind study comparing the efficacy of gabapentin withamitriptyline on diabetic peripheral neuropathy pain. Arch Intern Med1999;159:1931–7.
[111] Hammack JE, Michalak JC, Loprinzi CL, Sloan JA, Novotny PJ, Soori GS,et al. Phase III evaluation of nortriptyline for alleviation of symptoms ofcisplatinum- induced peripheral neuropathy. Pain 2002;98:195–203.
[112] Max MB, Lynch SA, Muir J, Shoaf SE, Smoller B, Dubner R. Effects ofdesipramine, amitriptyline, and fluoxetine on pain in diabetic neuropathy.N Engl J Med 1992;326:1250–6.
[113] Sindrup SH, Gram LF, Skjold T, Froland A, Beck-Nielsen H.Concentration–response relationship in imipramine treatment of diabeticneuropathy symptoms. Clin Pharmacol Ther 1990;47:509–15.
[114] Sindrup SH, Gram LF, Skjold T, Grodum E, Brosen K, Beck-Nielsen H.Clomipramine vs desipramine vs placebo in the treatment of diabetic neu-ropathy symptoms. A double-blind cross-over study. Br J Clin Pharmacol1990;30:683–91.
[115] Sindrup SH, Gram LF, Brosen K, Eshoj O, Mogensen EF. The selective sero-tonin reuptake inhibitor paroxetine is effective in the treatment of diabeticneuropathy symptoms. Pain 1990;42:135–44.
[116] Sindrup SH, Bjerre U, Dejgaard A, Brosen K, Aaes-Jorgensen T, Gram LF. Theselective serotonin reuptake inhibitor citalopram relieves the symptoms ofdiabetic neuropathy. Clin Pharmacol Ther 1992;52:547–52.
[117] Argoff CE, Backonja MM, Belgrade MJ, Bennett GJ, Clark MR, Cole BE, et al.Diabetic peripheral neuropathic pain: consensus guidelines for treatment. JFam Pract 2006:1–19.
[118] Collins SL, Moore RA, McQuayHJ, Wiffen P. Antidepressants and anticon-vulsants for diabetic neuropathy and postherpetic neuralgia: a quantitativesystematic review. J Pain Symptom Manage 2000;20:449–58.
[119] Kajdasz DK, Iyengar S, Desaiah D, Backonja MM, Farrar JT, Fishbain DA, et al.Duloxetine for the management of diabetic peripheral neuropathic pain:evidence-based findings from post hoc analysis of three multicenter, ran-domized, double-blind, placebo-controlled, parallel-group studies. Clin Ther2007;29:2536–46.
[120] Rowbotham MC, Goli V, Kunz NR, Lei D. Venlafaxine extended release in thetreatment of painful diabetic neuropathy: a double-blind, placebo-controlledstudy. Pain 2004;110:697–706.
[121] Sultan A, Gaskell H, Derry S, Moore RA. Duloxetine for painful diabetic neu-ropathy and fibromyalgia pain: systematic review of randomised trials. BMCNeurol 2008;8:29.
[122] Goldstein DJ, Lu Y, Detke MJ, Lee TC, Iyengar S. Duloxetine vs. placebo inpatients with painful diabetic neuropathy. Pain 2005;116:109–18.
[123] Raskin J, Pritchett YL, Wang F, D’Souza DPN, Waninger AL, Iyengar S, et al.A double-blind, randomized multicenter trial comparing duloxetine withplacebo in the management of diabetic peripheral neuropathic pain. Pain Med(Malden, MA) 2005;6:346–56.
[124] Wernicke JF, Pritchett YL, D’Souza DPN, Waninger A, Tran P, Iyengar S, et al. Arandomized controlled trial of duloxetine in diabetic peripheral neuropathicpain. Neurology 2006;67:1411–20.
[125] Yucel A, Ozyalcin S, Koknel, Kiziltan E, Yucel B, Andersen OK, et al. The effect ofvenlafaxine on ongoing and experimentally induced pain in neuropathic painpatients: a double blind, placebo controlled study. Eur J Pain 2005;9:407–16.
[126] Wiffen PJ, McQuay HJ, Moore RA. Carbamazepine for acute and chronic pain.Cochrane Database Syst Rev 2005;3:CD005451.
[127] East Hanover NJ. Tegretol (carbamazepine) [package insert]. NovartisPharmaceuticals Corporation; 2008 http://www.pharma.us.novartis.com
[128] Lamictal (lamotrigine) tablets prescribing information.Research Triangle Park, NC: GlaxoSmithKline; 2004http://www.fda.gov/downloads/Drugs/DrugSafety/UCM152835.pdf
[129] Eisenberg E, Lurie Y, Braker C, Daoud D, Ishay A. Lamotrigine reducespainful diabetic neuropathy: a randomized, controlled study. Neurology2001;57:505–9.
[130] Ichikawa K, Koyama N, Kiguchi S, Kojima M, Yokota T. Inhibitory effectof oxcarbazepine on high frequency firing in peripheral nerve fibers. Eur JPharmacol 2001;420:119–22.
[131] Ambrosio AF, Soares-Da-Silva P, Carvalho CM, Carvalho AP. Mechanisms ofaction of carbamazepine and its derivatives, oxcarbazepine, BIA 2-093 andBIA 2-024. Neurochem Res 2002;27:121–30.
[132] Fox A, Gentry C, Patel S, Kesingland A, Bevan S. Comparative activityof the anti-convulsants oxcarbazepine, carbamazepine, lamotrigine andgabapentin in a model of neuropathic pain in the rat and guinea-pig. Pain2003;105:355–62.
[133] Kiguchi S, Imamura T, Ichikawa K, Kojima M. Oxcarbazepine antinociceptionin animals with inflammatory pain or painful diabetic neuropathy. Clin ExpPharmacol Physiol 2004;31:57–64.
[134] Dogra S, Beydoun S, Mazzola J, Hopwood M, Wan Y. Oxcarbazepine in painfuldiabetic neuropathy: a randomized, placebo-controlled study. Eur J Pain2005;9:543–54.
[135] Beydoun A, Shaibani A, Hopwood M, Wan Y. Oxcarbazepine in painfuldiabetic neuropathy: results of a dose-ranging study. Acta Neurol Scand2006;113:395–404.
[136] Raskin P, Donofrio PD, Rosenthal NR, Hewitt DJ, Jordan DM, Xiang J, et al. Top-iramate vs placebo in painful diabetic neuropathy: analgesic and metaboliceffects. Neurology 2004;63:865–73.
[137] Thienel U, Neto W, Schwabe SK, Vijapurkar U. Topiramate in painful diabeticpolyneuropathy: findings from three double-blind placebo-controlled trials.Acta Neurol Scand 2004;110:221–31.
[138] Errington AC, Stohr T, Heers C, Lees G. The investigational anticonvulsantlacosamide selectively enhances slow inactivation of voltage-gated sodiumchannels. Mol Pharmacol 2008;73:157–69.
[139] Ziegler D, Hidvégi T, Gurieva I, Bongardt S, Freynhagen R, Sen D, et al. Effi-cacy and safety of lacosamide in painful diabetic neuropathy. Diabet Care2010;33:839–41.
[140] Backonja M, Beydoun A, Edwards KR, Schwartz SL, Fonseca V, Hes M, et al.Gabapentin for the symptomatic treatment of painful neuropathy in patientswith diabetes mellitus: a randomized controlled trial. J Am Med Assoc1998;280:1831–6.
[141] Rice ASC, Maton S, Postherpetic Neuralgia Study Group. Gabapentin in pos-therpetic neuralgia: a randomised, double blind, placebo controlled study.Pain 2001;94:215–24.
[142] Serpell MG, Neuropathic Pain Study Group. Gabapentin in neuropathicpain syndromes: a randomised, double-blind, placebo-controlled trial. Pain2002;99:557–66.
[143] Wiffen PJ, McQuay H, Edwards J, Moore RA. Gabapentin for acute and chronicpain. Cochrane Database Syst Rev 2005;3:CD005452.
[144] Lesser H, Sharma U, La Moreaux L, Poole RM. Pregabalin relieves symptomsof painful diabetic neuropathy: a randomized controlled trial. Neurology2004;63:2104–10.
[145] Lee B, Shi L, Kassel DB, Asakawa T, Takeuchi K, Christopher RJ. Pharmacoki-netic, pharmacodynamic, and efficacy profiles of alogliptin, a novel inhibitorof dipeptidyl peptidase-4, in rats, dogs, and monkeys. Eur J Pharmacol2008;589:306–14.
[146] Neumiller JJ, Wood L, Campbell RK. Dipeptidyl peptidase-4 inhibitors for thetreatment of type 2 diabetes mellitus. Pharmacotherapy 2010;30:463–84.
[147] Lam S, Saad M. Saxagliptin: a new dipeptidyl peptidase-4 inhibitor for type 2diabetes. Cardiol Rev 2010;18:213–7.
[148] Davidson EP, Coppey LJ, Dake B, Yorek MA. Treatment of streptozotocin-induced diabetic rats with alogliptin: effect on vascular and neuralcomplications. Exp Diabet Res 2011:8104–69.
[149] Bianchi R, Cervellini I, Porretta-Serapiglia C, Oggioni N, Burkey B, Ghezzi P,et al. Beneficial effects of PKF275-055, a novel, selective, orally bioavailable,long-acting dipeptidyl peptidase IV inhibitor in streptozotocin-induced dia-betic peripheral neuropathy. J Pharmacol Exp Ther 2012;340:64–72.
[150] Farmer K, Williams SJ, Novikova L, Ramachandran K, Rawal S, Blagg BS,et al. KU-32, a novel drug for diabetic neuropathy, is safe for humanislets and improves in vitro insulin secretion and viability. Exp Diabet Res2012:6716–73.
[151] Hwang HS, Yang EJ, Lee SM, Lee SC, Choi SM. Antiallodynic effects ofelectroacupuncture combined with MK-801 treatment through the reg-ulation of p35/p25 in experimental diabetic neuropathy. Exp Neurobiol2011;20:144–52.
[152] Beaulieu P. Effects of nabilone, a synthetic cannabinoid, on postoperative pain.Can J Anaesth 2006;53:769–75.
[153] Toth C, Mawani S, Brady S, Chan C, Liu C, Mehina E, et al. Anenriched-enrolment, randomized withdrawal, flexible-dose, double-blind,

Author's personal copy
34 R. Singh et al. / Pharmacological Research 80 (2014) 21– 35
placebo-controlled, parallel assignment efficacy study of nabilone as adju-vant in the treatment of diabetic peripheral neuropathic pain. Pain2012;153:2073–82.
[154] Liu WJ, Jin HY, Park JH, Baek HS, Park TS. Effect of rimonabant, the cannabi-noid CB1 receptor antagonist, on peripheral nerve in streptozotocin-induceddiabetic rat. Eur J Pharmacol 2010;637:70–6.
[155] Kress HG. Tapentadol and its two mechanisms of action: is there a new phar-macological class of centrally-acting analgesics on the horizon? Eur J Pain2010;14:781–3.
[156] Tzschentke TM, De Vry J, Terlinden R, Hennies HH, Lange C, Strassburger W,et al. Tapentadol HCl. Drugs Future 2006;31:1053–61.
[157] Tzschentke TM, Christoph T, Kögel B, Schiene K, Hennies H-H, EnglbergerW, et al. (−)-(1R,2R)-3-(3-Di- methylamino-1-ethyl-2-methyl-propyl)-phenol hydrochloride (tapentadol HCl): a novel �-opioid receptor ago-nist/norepinephrine reuptake inhibitor with broadspectrum analgesicproperties. J Pharmacol Exp Ther 2007;323:265–76.
[158] Afilalo M, Morlion B. Efficacy of tapentadol ER for managing moderate tosevere chronic pain. Pain Physician 2013;16:27–40.
[159] Peppin JF, Majors K, Webster LR, Simpson DM, Tobias JK, Vanhove GF. Toler-ability of NGX-4010, a capsaicin 8% patch for peripheral neuropathic pain. JPain Res 2011;4:385–92.
[160] Martini C, Yassen A, Olofsen E, Passier P, Stoker M, Dahan A. Pharmacodynamicanalysis of the analgesic effect of capsaicin 8% patch (QutenzaTM) in diabeticneuropathic pain patients: detection of distinct response groups. J Pain Res2012;5:51–9.
[161] Webster LR, Peppin JF, Murphy FT, Tobias JK, Vanhove GF. Tolerability ofNGX-4010, a capsaicin 8% patch, in conjunction with three topical anestheticformulations for the treatment of neuropathic pain. J Pain Res 2012;5:7–13.
[162] Coppey L, Davidson E, Lu B, Gerard C, Yorek M. Vasopeptidase inhibitorilepatril (AVE7688) prevents obesity- and diabetes-induced neuropathy inC57Bl/6J mice. Neuropharmacology 2011;60:259–66.
[163] Rowbotham MC, Duan WR, Thomas J, Nothaft W, Backonja MM. A ran-domized, double-blind, placebo-controlled trial evaluating the efficacy andsafety of ABT-594 in patients with diabetic peripheral neuropathic pain. Pain2009;146:245–52.
[164] Rowbotham MC, Arslanian A, Nothaft W, Duan WR, Best AE, Pritchett Y, et al.Efficacy and safety of the �4�2 neuronal nicotinic receptor agonist ABT-894in patients with diabetic peripheral neuropathic pain. Pain 2012;153:862–8.
[165] Wang L, Chopp M, Szalad A, Liu Z, Bolz M, Alvarez FM, et al. Phosphodiesterase-5 is a therapeutic target for peripheral neuropathy in diabetic mice.Neuroscience 2011;193:399–410.
[166] Kumar A, Negi G, Sharma SS. Suppression of NF-�B and NF-�B reg-ulated oxidative stress and neuroinflammation by BAY 11-7082 (I�Bphosphorylation inhibitor) in experimental diabetic neuropathy. Biochimie2012;94:1158–65.
[167] Wang L, Chopp M, Szalad A, Liu Z, Lu M, Zhang L, et al. Thymosin �4 promotesthe recovery of peripheral neuropathy in type II diabetic mice. Neurobiol Dis2012;48:546–55.
[168] Inkster ME, Cotter MA, Cameron NE. Treatment with the xanthine oxidaseinhibitor, allopurinol, improves nerve and vascular function in diabetic rats.Eur J Pharmacol 2007;561:63–71.
[169] Xu X, Liu Z, Liu H, Yang X, Li Z. The effects of galanin on neuropathic pain instreptozotocin-induced diabetic rats. Eur J Pharmacol 2012;680:28–33.
[170] Landry M, Liu HX, Shi TJ, Brumovsky P, Nagy F, Hokfelt T. Galaninergic mecha-nisms at the spinal level: focus on histochemical phenotyping. Neuropeptides2005;39:223–31.
[171] Landry M, Bouali-Benazzouz R, Andre C, Shi TJ, Leger C, Nagy F, et al. Galaninreceptor 1 is expressed in a subpopulation of glutamatergic interneurons inthe dorsal horn of the rat spinal cord. J Comp Neurol 2006;499:391–403.
[172] Ouardouz M, Coderre E, Basak A, Chen A, Zamponi GW, Hameed S, et al. Gluta-mate receptors on myelinated spinal cord axons: I. GluR6 kainate receptors.Ann Neurol 2009;65:151–9.
[173] Ouardouz M, Coderre E, Zamponi GW, Hameed S, Yin X, Trapp BD, et al.Glutamate receptors on myelinated spinal cord axons: II. AMPA and GluR5receptors. Ann Neurol 2009;65:160–6.
[174] Sun W, Miao B, Wang XC, Duan JH, Ye X, Han WJ, et al. Gastrodininhibits allodynia and hyperalgesia in painful diabetic neuropathy rats bydecreasing excitability of nociceptive primary sensory neurons. PLoS ONE2012;7:e73964.
[175] Soumyanath A, Dimitrova D, Arnold G, Belding H, Seifer N, Le N, et al. P02.186.CAST (Centella asiatica selected triterpenes): stability, safety, and effect ondiabetic neuropathy (DPN). BMC Complem Altern Med 2012;12:242.
[176] Li L. The effect of neuragen PN on neuropathic pain: a randomized, doubleblind, placebo controlled clinical trial. BMC Complem Altern Med 2010;10:22.
[177] Kaeidi A, Esmaeili-Mahani S, Sheibani V, Abbasnejad M, Rasoulian B, Hajial-izadeh Z, et al. Olive (Olea europaea L.) leaf extract attenuates early diabeticneuropathic pain through prevention of high glucose-induced apoptosis:in vitro and in vivo studies. J Ethnopharmacol 2011;136:188–96.
[178] Tiwari V, Kuhad A, Chopra K. Emblica officinalis corrects functional, biochem-ical and molecular deficits in experimental diabetic neuropathy by targetingthe oxido-nitrosative stress mediated inflammatory cascade. Phytother Res2011;25:1527–36.
[179] Wang ZQ, Ribnicky D, Zhang XH, Zuberi A, Raskin I, Yu Y, et al. An extractof Artemisia dracunculus L. enhances insulin receptor signaling and modu-lates gene expression in skeletal muscle in KK-A(y) mice. J Nutr Biochem2011;22:71–8.
[180] Logendra S, Ribnicky DM, Yang H, Poulev A, Ma J, Kennelly EJ, et al. Bioassay-guided isolation of aldose reductase inhibitors from Artemisia dracunculus.Phytochemistry 2006;67:1539–46.
[181] Watcho P, Stavniichuk R, Ribnicky DM, Raskin I, Obrosova IG. High-fatdiet-induced neuropathy of prediabetes and obesity: effect of PMI-5011,an ethanolic extract of Artemisia dracunculus L. Mediators Inflamm 2010:268547.
[182] Kheterpal I, Coleman L, Ku G, Wang ZQ, Ribnicky D, Cefalu WT. Regula-tion of insulin action by an extract of Artemisia dracunculus L. in primaryhuman skeletal muscle culture: a proteomics approach. Phytother Res2010;24:1278–84.
[183] Watcho P, Stavniichuk R, Tane P, Shevalye H, Maksimchyk Y, Pacher P, et al.Evaluation of PMI-5011, an ethanolic extract of Artemisia dracunculus L.,on peripheral neuropathy in streptozotocin-diabetic mice. Int J Mol Med2011;27:299–307.
[184] Malik ZA, Singh M, Sharma PL. Neuroprotective effect of Momordica charan-tia in global cerebral ischemia and reperfusion induced neuronal damage indiabetic mice. J Ethnopharmacol 2011;133:729–34.
[185] Kim N, Kim SH, Kim YJ, Kim JK, Nam MK, Rhim H, et al. Neurotrophicactivity of DA-9801, a mixture extract of Dioscorea japonica Thunb.and Dioscorea nipponica Makino, in vitro. J Ethnopharmacol 2011;137:312–9.
[186] Kang TH, Moon E, Hong BN, Choi SZ, Son M, Park JH, et al. Diosgeninfrom Dioscorea nipponica ameliorates diabetic neuropathy by inducing nervegrowth factor. Biol Pharm Bull 2011;34:1493–8.
[187] Morani AS, Bodhankar SL, Mohan V, Thakurdesai PA. Ameliorative effectsof standardized extract from Trigonella foenum-graecum L. seeds onpainful peripheral neuropathy in rats. Asian Pac J Trop Med 2012;5:385–90.
[188] Stavniichuk R, Drel VR, Shevalye H, Maksimchyk Y, Kuchmerovska TM, NadlerJL, et al. Baicalein alleviates diabetic peripheral neuropathy through inhi-bition of oxidative–nitrosative stress and p38 MAPK activation. Exp Neurol2011;230:106–13.
[189] Kuhad A, Chopra K. Tocotrienol attenuates oxidative–nitrosative stress andinflammatory cascade in experimental model of diabetic neuropathy. Neu-ropharmacology 2009;57:456–62.
[190] Chopra K, Tiwari V, Arora V, Kuhad A. Sesamol suppresses neuro-inflammatory cascade in experimental model of diabetic neuropathy. J Pain2010;11:950–7.
[191] Kuhad A, Sharma S, Chopra K. Lycopene attenuates thermal hyperalgesiain a diabetic mouse model of neuropathic pain. Eur J Pain 2008;12:624–32.
[192] Singh R, Kaur N, Kishore L, Kumar GK. Management of diabetic complica-tions: a chemical constituents based approach. J Ethnopharmacol 2013;150:51–70.
[193] Anjaneyulu M, Chopra K. Quercetin, a bioflavonoid, attenuates thermalhyperalgesia in a mouse model of diabetic neuropathic pain. Prog Neuropsy-chopharmacol Biol Psychiatry 2003;27:1001–5.
[194] Anjaneyulu M, Chopra K. Quercetin attenuates thermal hyperalgesia and coldallodynia in STZ-induced diabetic rats. Indian J Exp Biol 2004;42:766–9.
[195] Nickerson HD, Dutta S. Diabetic complications: current challenges and oppor-tunities. J Cardiovasc Trans Res 2012;5:375–9.
[196] Gilron I, Bailey JM, Tu D, Holden RR, Weaver DF, Houlden RL. Morphine,gabapentin, or their combination for neuropathic pain. N Engl J Med2005;352:1324–34.
[197] Gilron I, Bailey JM, Tu D, Holden RR, Jackson AC, Houlden RL. Nortriptyline andgabapentin, alone and in combination for neuropathic pain: a double-blind,randomised controlled crossover trial. Lancet 2009;374:1252–61.
[198] Hanna M, O’Brien C, Wilson MC. Prolonged-release oxycodone enhances theeffects of existing gabapentin therapy in painful diabetic neuropathy patients.Eur J Pain 2008;12:804–13.
[199] Finnerup NB, Sindrup SH, Jensen TS. Recent advances in pharmacologicaltreatment of neuropathic pain. F1000 Med Rep 2010;2:52.
[200] Rull JA, Quibrera R, Gonzalez-Millan H, Lozano Castaneda O. Symptomatictreatment of peripheral diabetic neuropathy with carbamazepine (Tegretol):double blind crossover trial. Diabetologia 1969;5:215–8.
[201] Vinik AI, Tuchman M, Safirstein B, Corder C, Kirby L, Wilks K, et al. Lamot-rigine for treatment of pain associated with diabetic neuropathy: results oftwo randomized, double-blind, placebo-controlled studies. Pain 2007;128:169–79.
[202] Rosenstock J, Tuchman M, LaMoreaux L, Sharma U. Pregabalin for thetreatment of painful diabetic peripheral neuropathy: a double-blind, place-bocontrolled trial. Pain 2004;110:628–38.
[203] Vranken JH, Dijkgraaf MG, Kruis MR, van der Vegt MH, Hollmann MW,Heesen M. Pregabalin in patients with central neuropathic pain: a random-ized, double-blind, placebo-controlled trial of a flexible-dose regimen. Pain2008;136:150–7.
[204] Tolle T, Freynhagen R, Versavel M, Trostmann U, Young Jr JP. Pregabalin forrelief of neuropathic pain associated with diabetic neuropathy: a randomized,double-blind study. Eur J Pain 2008;12:203–13.
[205] Richter RW, Portenoy R, Sharma U, Lamoreaux L, Bockbrader H, Knapp LE.Relief of painful diabetic peripheral neuropathy with pregabalin: a random-ized, placebo-controlled trial. J Pain 2005;6:253–60.
[206] Watson CP, Moulin D, Watt-Watson J, Gordon A, Eisenhoffer J. Controlled-release oxycodone relieves neuropathic pain: a randomized controlled trialin painful diabetic neuropathy. Pain 2003;105:71–8.

Author's personal copy
R. Singh et al. / Pharmacological Research 80 (2014) 21– 35 35
[207] Gimbel JS, Richards P, Portenoy RK. Controlled-release oxycodone forpain in diabetic neuropathy: a randomized controlled trial. Neurology2003;60:927–34.
[208] Harati Y, Gooch C, Swenson M, Edelman S, Greene D, Raskin P, et al. Double-blind randomized trial of tramadol for the treatment of the pain of diabeticneuropathy. Neurology 1998;50:1842–6.
[209] Campbell CM, Kipnes MS, Stouch BC, Brady KL, Kelly M, Schmidt WK, et al.Randomized control trial of topical clonidine for treatment of painful diabeticneuropathy. Pain 2012;153:1815–23.
[210] Sindrup SH, Graf A, Sfikas N. The NK1-receptor antagonist TKA731 inpainful diabetic neuropathy: a randomised, controlled trial. Eur J Pain2006;10:567–71.





























