Embed Size (px)
Citation preview
Clin Perinatol 31 (2004) 743–764
Diagnosis and management of intrauterine
growth restriction
Ursula F. Harkness, MD, MPH*, Giancarlo Mari, MD
Division of Maternal Fetal Medicine, Department of Obstetrics and Gynecology,
University of Cincinnati, 231 Albert Sabin Way, PO Box 670526, Cincinnati, OH 45267-0526, USA
Normal growth on a cellular level is not homogeneous but rather follows a
pattern that shifts over time from rapid cellular duplication to rapid cellular
enlargement [1]. Early growth is characterized by an increase in cell number, and
this period has proportional increases in weight, protein, and DNA (phase of
hyperplasia). This phase is followed by one in which cell division slows and
existing cells enlarge (phase of hyperplasia and hypertrophy). During this time,
the increase in DNA is slower than the increase in protein and weight. During the
final phase, cell division decreases, and all further growth is due to enlargement
of cells (phase of hypertrophy). DNA does not continue to increase, although net
protein and weight do. The effects of stimuli that restrict growth may depend in
part on when in the sequence of cellular events they occur.
Fetal growth is determined by the mother, the fetus, and the placenta. Any
factor that affects one of these three environments can result in intrauterine
growth restriction (IUGR).
Dating the pregnancy
Accurate dating is the most important step in the prenatal management of
the IUGR fetus. Using the last menstrual period (LMP) to determine gestational
0095-5108/04/$ – see front matter D 2004 Elsevier Inc. All rights reserved.
doi:10.1016/j.clp.2004.06.006
* Corresponding author.
E-mail address: [email protected] (U.F. Harkness).
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764744
age is often unreliable. In one study, menstrual history could only be obtained
from 89.8% of the women enrolled, and 44.7% of these were unreliable because
of an unsure actual date of LMP, irregular menstrual cycles, recent oral
contraceptive use, or first-trimester bleeding [2]. Ultrasound performed before
18 weeks’ gestation was as good or better for prediction of estimated date of
confinement than even an optimal menstrual history—depending on the
gestational age at which the scan was performed [2].
In the first trimester, the crown-rump length (CRL) is used to estimate
gestational age. This measurement is highly accurate [3,4]. A longitudinal view
of the fetus is found, and the calipers are placed at the outer edge of the cephalic
pole and fetal rump with care not to include the yolk sac or fetal limbs. The
pregnancy should be dated by ultrasonography if there is a greater than 7-day
discrepancy between LMP and CRL [5].
In the second trimester, fetal biometry can be used to date a pregnancy
accurately. Chervenak et al [6] studied 152 singletons conceived through in vitro
fertilization. These authors used stepwise multiple linear regression to determine
the best equation for gestational age assessment using head circumference (HC),
biparietal diameter (BPD), femur length (FL), and abdominal circumference (AC)
alone or in combination. The most accurate single parameter was HC, which gave
a random error of 3.77 days. Adding AC and FL to HC slightly improved
prediction (random error 3.35 days). Based on this study, biometry should be
used to date the pregnancy if the discrepancy between LMP and ultrasound
dating is greater than 7 days in the absence of congenital anomalies and severe
growth delay.
The accuracy of a single ultrasonographic measurement for the detection of
gestational age decreases as gestational ages increases. The normal distribution of
measurements becomes wider as gestational age increases [7]. Serial ultrasound
should be performed at 3-week intervals when dating is to be determined using
third-trimester sonography.
Although precise sonographic assessment of gestational age in the third
trimester is not feasible in all cases based on fetal biometry alone, other sono-
graphic markers are currently used to estimate the gestational age. The ossi-
fication centers of various long bones are most commonly used in practice.
These centers become increasingly echo-dense and larger with advancing
gestational age. Although their presence does not give an exact gestational
age assessment, it can reassure the clinician that the pregnancy is relatively
late into the third trimester. The distal femoral epiphysis is noted at the distal
end of the femur in the plane of measurement of this bone. The distal femoral
epiphysis is never seen before 28 weeks, and it is observed in 72% of fetuses
at 33 weeks, 94% of fetuses at 34 weeks, and 100% of fetuses at 36 weeks
[8]. The proximal tibial epiphysis is seen adjacent to the head of the tibia
at its proximal end, in the plane of measurement of this bone. The proximal
tibial epiphysis is never seen before 34 weeks, and it is found in 35% of
fetuses at 35 weeks, 79% of fetuses at 37 weeks, and 100% of fetuses at
39 weeks [8]. Finally, if the proximal humeral epiphysis is greater than or equal
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764 745
to 1 mm, there is at least a probability of 0.69 that the pregnancy is at 40 to
42 weeks [9].
Estimating fetal weight
Many different formulae have been used to calculate gestational age. Two that
are commonly used are the Shepard and Hadlock formulae. The Hadlock formula
uses head circumference, abdominal circumference, and femur length to estimate
fetal weight [10]. The estimate of random error for this method is plus or minus
15% (2 standard deviations). The Shepard formula is based on BPD and AC [11].
The fetal weight estimate, once obtained, is compared with reference ranges.
A value between the 10th and 90th percentiles is usually considered normal.
These cut-offs are used in an attempt to identify fetuses at risk. Genetic and
environmental factors may influence growth, however, and thus different popu-
lations have different growth curves.
Definitions
The terms small for gestational age (SGA) and IUGR are often used inter-
changeably, although this is misleading. The growth-restricted fetus is a fetus that
fails to reach its growth potential and is at risk for adverse perinatal morbidity and
mortality. The American College of Obstetricians and Gynecologists (ACOG)
defines an IUGR fetus as a fetus with an estimated weight below the 10th
percentile [12]. Not all fetuses measuring less than the 10th percentile are at risk
for adverse perinatal outcome; many are just constitutionally small. IUGR refers
to the fetus who is SGA and displays other signs of chronic hypoxia or
malnutrition [5]. SGA is defined here as a fetus who measures less than the 10th
percentile for gestational age, whether it be because he is growth-restricted
(IUGR) or just constitutionally small. The authors will first discuss the fetus with
an estimated weight below the 10th percentile, then suggest ways to differentiate
the small fetus from the at-risk IUGR fetus and to manage the pregnancy
complicated by IUGR.
Traditionally, symmetric IUGR has been distinguished from asymmetric
IUGR [13]. The former is described as having an early onset. The insult affects
growth of skeletal, head, and abdominal measurements, because it occurs at a
time when fetal growth is affected primarily by cell division. Asymmetric IUGR,
by contrast, has its onset later in gestation, when fetal growth occurs secondary to
increases in cell size. Skeletal and head measurements are spared, but abdominal
circumference is small because of decreased liver size and subcutaneous fat.
More recently, the need to distinguish these entities has been questioned, because
it is unclear whether they can be associated with distinct causes or neonatal
outcomes [12]. One study demonstrated, however, that although the etiologies of
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764746
symmetrically and asymmetrically small fetuses overlap, the latter are at an
increased risk for neonatal and intrapartum complications [14].
Consequences of being small for gestational age
Short term
Estimated fetal weight below the 10th percentile is a leading risk factor for
fetal death [15]. As birth weight decreases from the 10th percentile to the first
percentile, perinatal morbidity and mortality increase markedly [16]. In term
infants, the rates of low 5-minute Apgars, severe acidemia, need for intubation in
the delivery room, seizures in the first 24 hours of life, sepsis, and neonatal death
increase significantly among infants at or below the third percentile for ges-
tational age [17]. In preterm infants, by contrast, there is no specific birth-weight
threshold below which neonatal morbidity and mortality are increased; rather,
respiratory distress (RDS) and neonatal death increase along a continuum with
decreasing birth weight percentile. In a retrospective review of more than
1.4 million deliveries, the risk of RDS, intraventricular hemorrhage (IVH), and
necrotizing enterocolitis (NEC) was found to increase significantly in IUGR
fetuses as compared with normally grown fetuses beginning at 34 to 35 weeks’
gestation [18]. (Because the IUGR group was found using an International
Classification of Diseases, Ninth Revision [ICD-9] code search of a large
state database, it is difficult to assess whether only IUGR or both IUGR and
SGA babies were included.)
The findings of the aforementioned study contrast with older studies that
reported that small neonates had a decreased incidence of RDS [19,20] and IVH
[20,21] when compared with appropriate-for-gestational-age preterm neonates,
suggesting that in small fetuses there is an adaptive reaction to intrauterine stress.
Another study using the Vermont Oxford Network database described a signifi-
cant increase in neonatal death, RDS, and NEC among babies whose birth weight
was less than the 10th percentile and who weighed between 500 and 1500 g, as
compared with appropriate-for-gestational-age (AGA) babies [22]. These authors
suggest that the inconsistency between their findings and those of earlier studies
may be due to the extent to which confounding variables are addressed and taken
into account.
Long term
The problems of the small fetus do not end at birth or soon after birth but
continue well into childhood and adulthood. Studies have shown that small
children have an increased rate of impaired school performance. One study
described significantly higher numbers of children with late entry into secondary
school and failure to pass or take the baccalaureate examination in the bsmallQ

U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764 747
group as compared with the AGA group, after controlling for maternal age,
maternal educational level, parental socioeconomic status, family size, and gen-
der [23]. Another large follow-up study of 14,189 full-term infants from the
United Kingdom showed that at 5, 10, and 16 years of age, individuals born with
a birth weight less than the fifth percentile had small but significant deficits in
academic achievement [24]. At 26 years of age, this same cohort of once SGA
babies showed lower levels of professional achievement, despite adjustment for
potential confounders.
Other studies have described an association between fetuses with weight or
height less than the 10th percentile and the development of hypertension,
hypercholesterolemia, impaired glucose tolerance, and diabetes in later life
[25–27]. In the United Kingdom, a follow-up study on 5654 men showed that
those with the lowest weight at birth and at 1 year of age had the highest death
rate from ischemic heart disease [28]. The bfetal originsQ hypothesis asserts thatchanges in the intrauterine nutritional or endocrine environment result in per-
manent alterations in structure, physiology, and metabolism that predispose the
affected individual to develop cardiovascular, metabolic, and endocrine disease
years later [26]. An endocrine-metabolic reprogramming occurs that enables
the small fetus to adapt to its adverse intrauterine environment; after birth,
nutrient abundance may lead to a metabolic syndrome and to the development of
the above-noted cardiovascular risk factors [25]. This theory is the so-called
bBarker’s hypothesis.Q
Screening for the small fetus
Fundal height assessment
Several studies have estimated that 41% to 86% of SGA babies could be
detected with routine use of symphysis-fundal height measurements [29–32].
Some of these studies used standard value curves, with the small fundal height
defined as that below the 10th percentile of standard values for gestational age.
The most common method in practice, however, uses the concept that, between
20 and 34 weeks, the fundal height in centimeters equals the gestational age in
weeks [33]. A measurement in centimeters is taken from the upper edge of the
symphysis pubis to the top of the uterine fundus. A measurement of 3 to 4 cm
below the expected number suggests inappropriate growth.
Ultrasonographic measurements
According to one meta-analysis of ultrasonographic measurements, AC and
estimated fetal weight (EFW) were the best predictors of fetal weight below the
10th percentile [34]. In high-risk populations, the sensitivity using AC of less
than the 10th percentile was 73% to 95%, whereas using EFW the sensitivity was
43% to 89%; in low-risk populations, the corresponding sensitivities were 48% to
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764748
64% for AC and 31% to 73% for EFW. In another study, AC measurements were
shown to predict small fetuses better than BPD, HC, or a combination of
parameters [35]. The sensitivity of a single AC measurement after 25 weeks for
the detection of fetuses with birth weight below the 10th percentile was 48%. In
the same study, a normal AC was found to exclude fetal growth restriction with a
false-negative rate of about 10%. Another study showed that a single AC
measurement for the detection of babies with birth weight less than the 10th
percentile was only slightly better than serial fundal height measurements
(sensitivity 83% versus 76%); the difference was not statistically significant [36].
Thus there is no clear evidence that routine ultrasound is a better screening
method for SGA than fundal height measurement in the general population.
Diagnosis of intrauterine growth restriction
The data already reported refer to fetuses with an estimated weight below the
10th percentile. When a fetus has an estimated weight below the 10th percentile
in the absence of congenital anomalies and in the presence of a normal amount of
amniotic fluid, Doppler velocimetry gives the most important information to
differentiate the truly growth-restricted fetus (IUGR) from the fetus that is
constitutionally small but otherwise normal.
Umbilical artery
Normal pregnancy is characterized by a low-resistance feto-placental system
with continuous forward flow throughout the cardiac cycle. Although several
indices to estimate vessel resistance as evaluated by Doppler ultrasonography
have been described, the most popular and the simplest of these is the systolic/
diastolic (S/D) ratio. This index is a ratio of the maximum systolic flow velocity
divided by the minimal end-diastolic flow velocity. Normal reference ranges
throughout pregnancy are reported in Fig. 1 [37]. In pregnancies complicated
by IUGR, there is a chronological process characterized by increased umbilical
artery resistance (increased S/D ratio), absent end-diastolic flow, and finally
reverse end-diastolic flow (Fig. 2). Various hypotheses have been proposed
to explain the pathophysiology of IUGR and abnormal umbilical artery Dopp-
ler velocimetry [38]: (1) reduced placental-stem artery number, (2) primary vil-
lus maldevelopment with small, hypovascular, and fibrotic terminal villi, and
(3) placental-stem vessel vasoconstriction.
Small fetuses with abnormal umbilical artery waveforms are admitted more
frequently to the neonatal intensive care unit and stay longer compared with those
small fetuses who have normal Doppler velocimetry in the umbilical artery
[39,40]. Studies have shown that the perinatal mortality rate in pregnancies
complicated by growth restriction or hypertension is higher in fetuses with
reversed end-diastolic flow (33% to 73%) or absent end-diastolic flow (9% to
41%) in the umbilical artery [41–43]. Finally, fetuses with absent and reverse
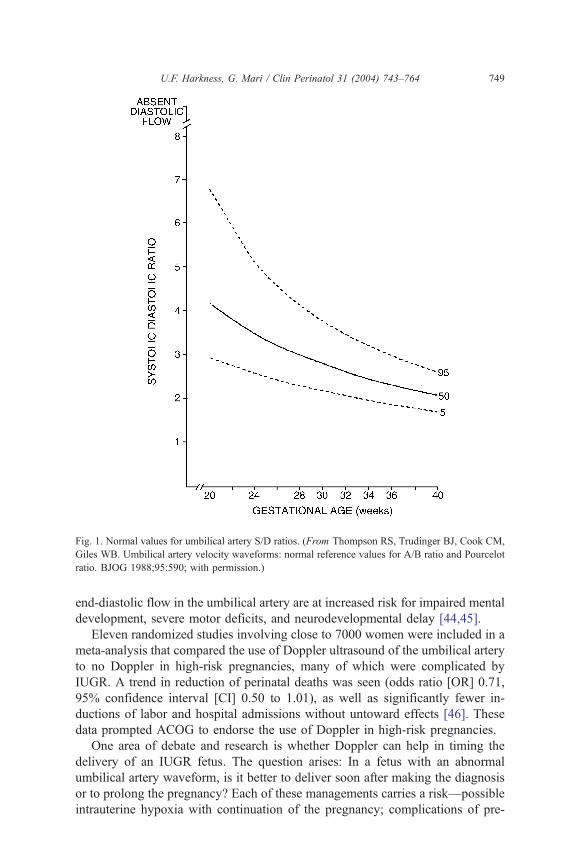
Fig. 1. Normal values for umbilical artery S/D ratios. (From Thompson RS, Trudinger BJ, Cook CM,
Giles WB. Umbilical artery velocity waveforms: normal reference values for A/B ratio and Pourcelot
ratio. BJOG 1988;95:590; with permission.)
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764 749
end-diastolic flow in the umbilical artery are at increased risk for impaired mental
development, severe motor deficits, and neurodevelopmental delay [44,45].
Eleven randomized studies involving close to 7000 women were included in a
meta-analysis that compared the use of Doppler ultrasound of the umbilical artery
to no Doppler in high-risk pregnancies, many of which were complicated by
IUGR. A trend in reduction of perinatal deaths was seen (odds ratio [OR] 0.71,
95% confidence interval [CI] 0.50 to 1.01), as well as significantly fewer in-
ductions of labor and hospital admissions without untoward effects [46]. These
data prompted ACOG to endorse the use of Doppler in high-risk pregnancies.
One area of debate and research is whether Doppler can help in timing the
delivery of an IUGR fetus. The question arises: In a fetus with an abnormal
umbilical artery waveform, is it better to deliver soon after making the diagnosis
or to prolong the pregnancy? Each of these managements carries a risk—possible
intrauterine hypoxia with continuation of the pregnancy; complications of pre-
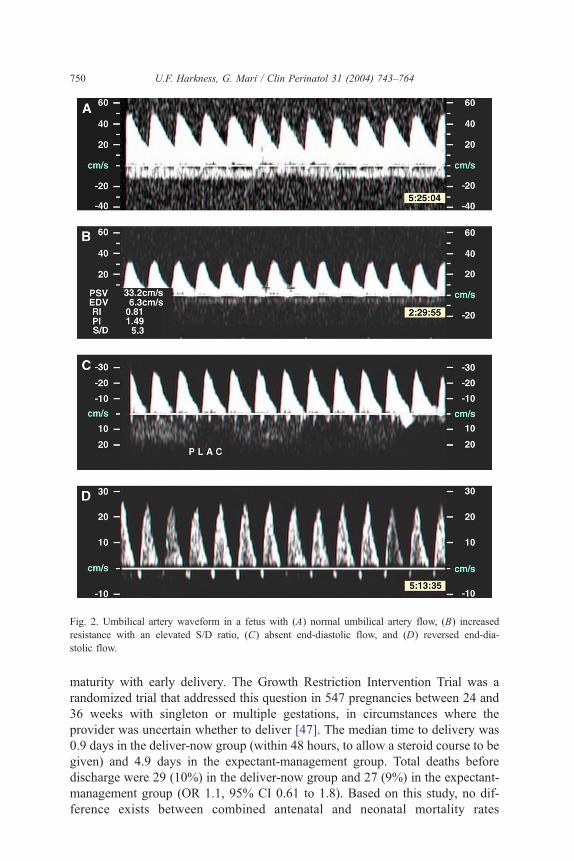
Fig. 2. Umbilical artery waveform in a fetus with (A) normal umbilical artery flow, (B) increased
resistance with an elevated S/D ratio, (C) absent end-diastolic flow, and (D) reversed end-dia-
stolic flow.
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764750
maturity with early delivery. The Growth Restriction Intervention Trial was a
randomized trial that addressed this question in 547 pregnancies between 24 and
36 weeks with singleton or multiple gestations, in circumstances where the
provider was uncertain whether to deliver [47]. The median time to delivery was
0.9 days in the deliver-now group (within 48 hours, to allow a steroid course to be
given) and 4.9 days in the expectant-management group. Total deaths before
discharge were 29 (10%) in the deliver-now group and 27 (9%) in the expectant-
management group (OR 1.1, 95% CI 0.61 to 1.8). Based on this study, no dif-
ference exists between combined antenatal and neonatal mortality rates

U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764 751
associated with immediate delivery and rates associated with expectant manage-
ment until the clinician is no longer uncertain that intervention is necessary.
Information on the developmental quotient of the survivors of this study at 2 years
of age will be available in the near future.
Many authors have suggested that small fetuses with normal umbilical artery
flow represent a group not at risk for adverse perinatal outcome. Most of these
babies are constitutionally small [48–50]. Recently, Baschat and Weiner [51]
reported on 308 women with ultrasonographic EFW less than the 10th percentile
or AC less than the 2.5th percentile for gestational age. Babies with abnormal
umbilical artery Doppler had increased rates of fetal distress associated with
chronic hypoxemia, RDS, and admission to a neonatal intensive care unit. The
authors suggested that antenatal surveillance may not be necessary in SGA babies
if the umbilical artery S/D ratio and amniotic fluid are normal.
One study of 167 women with small fetuses with normal umbilical artery
Dopplers randomly allocated participants to surveillance that occurred twice
weekly or every other week [52]. Although the two groups showed no differences
in neonatal morbidity, the more frequently tested group had a higher induction
rate. Unfortunately, this study did not have the power to detect clinically impor-
tant differences in neonatal outcome. These babies could not be assumed to be
simply small and healthy, because 32% were admitted to the neonatal special care
unit (range of stay 0 to 66 days, mean 4 to 5 days), 20% had hypoglycemia, and
40% had a low ponderal index at birth, despite the fact that the mean gestational
age at delivery was 38 weeks. However, 10% of the babies in this study had an
abnormal cerebral artery/umbilical artery resistance ratio, a finding that suggests
that some of them were growth-restricted babies with blood flow redistribution.
Evidence shows that umbilical artery Doppler can be used to distinguish
between the high-risk small fetus that is truly growth-restricted and the lower-risk
small fetus. A prospective randomized trial is needed to examine the question of
whether antenatal surveillance is necessary when fetal growth is less than the
10th percentile, but the umbilical artery S/D and AFI are normal.
Middle cerebral artery
The fetal response to chronic hypoxia is redistribution of blood flow to the
tissues that are most needed, such as the brain, myocardium, and adrenal glands.
This phenomenon has been called the bbrain-sparing effect.Q In this scenario,
oligohydramnios is thought to occur because of decreased renal perfusion.
Mari and Deter [53] described a parabolic pattern of middle cerebral artery
(MCA) pulsatility index ([peak systolic velocity � lowest diastolic velocity]/
mean velocity) in normal singletons across gestational age, with higher values
from 25 to 30 weeks (Table 1). These authors showed that SGA babies with
abnormal pulsatility indices were at a higher risk for perinatal death and neonatal
ICU stay of greater than 12 hours [53]. Fig. 3 demonstrates a normal MCA
waveform and one that suggests bbrain sparing.Q
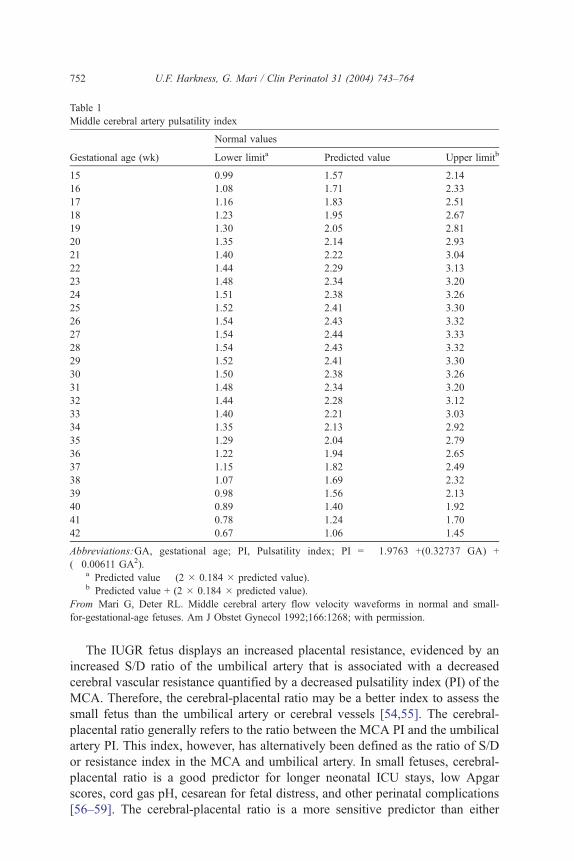
Table 1
Middle cerebral artery pulsatility index
Gestational age (wk)
Normal values
Lower limita Predicted value Upper limitb
15 0.99 1.57 2.14
16 1.08 1.71 2.33
17 1.16 1.83 2.51
18 1.23 1.95 2.67
19 1.30 2.05 2.81
20 1.35 2.14 2.93
21 1.40 2.22 3.04
22 1.44 2.29 3.13
23 1.48 2.34 3.20
24 1.51 2.38 3.26
25 1.52 2.41 3.30
26 1.54 2.43 3.32
27 1.54 2.44 3.33
28 1.54 2.43 3.32
29 1.52 2.41 3.30
30 1.50 2.38 3.26
31 1.48 2.34 3.20
32 1.44 2.28 3.12
33 1.40 2.21 3.03
34 1.35 2.13 2.92
35 1.29 2.04 2.79
36 1.22 1.94 2.65
37 1.15 1.82 2.49
38 1.07 1.69 2.32
39 0.98 1.56 2.13
40 0.89 1.40 1.92
41 0.78 1.24 1.70
42 0.67 1.06 1.45
Abbreviations:GA, gestational age; PI, Pulsatility index; PI = �1.9763 +(0.32737 GA) +
(�0.00611 GA2).a Predicted value � (2 � 0.184 � predicted value).b Predicted value + (2 � 0.184 � predicted value).
From Mari G, Deter RL. Middle cerebral artery flow velocity waveforms in normal and small-
for-gestational-age fetuses. Am J Obstet Gynecol 1992;166:1268; with permission.
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764752
The IUGR fetus displays an increased placental resistance, evidenced by an
increased S/D ratio of the umbilical artery that is associated with a decreased
cerebral vascular resistance quantified by a decreased pulsatility index (PI) of the
MCA. Therefore, the cerebral-placental ratio may be a better index to assess the
small fetus than the umbilical artery or cerebral vessels [54,55]. The cerebral-
placental ratio generally refers to the ratio between the MCA PI and the umbilical
artery PI. This index, however, has alternatively been defined as the ratio of S/D
or resistance index in the MCA and umbilical artery. In small fetuses, cerebral-
placental ratio is a good predictor for longer neonatal ICU stays, low Apgar
scores, cord gas pH, cesarean for fetal distress, and other perinatal complications
[56–59]. The cerebral-placental ratio is a more sensitive predictor than either
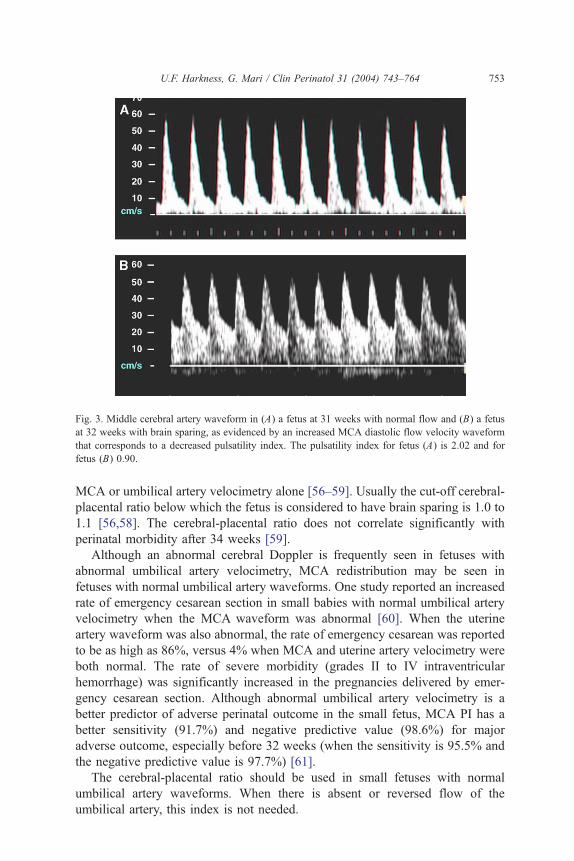
Fig. 3. Middle cerebral artery waveform in (A) a fetus at 31 weeks with normal flow and (B) a fetus
at 32 weeks with brain sparing, as evidenced by an increased MCA diastolic flow velocity waveform
that corresponds to a decreased pulsatility index. The pulsatility index for fetus (A) is 2.02 and for
fetus (B) 0.90.
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764 753
MCA or umbilical artery velocimetry alone [56–59]. Usually the cut-off cerebral-
placental ratio below which the fetus is considered to have brain sparing is 1.0 to
1.1 [56,58]. The cerebral-placental ratio does not correlate significantly with
perinatal morbidity after 34 weeks [59].
Although an abnormal cerebral Doppler is frequently seen in fetuses with
abnormal umbilical artery velocimetry, MCA redistribution may be seen in
fetuses with normal umbilical artery waveforms. One study reported an increased
rate of emergency cesarean section in small babies with normal umbilical artery
velocimetry when the MCA waveform was abnormal [60]. When the uterine
artery waveform was also abnormal, the rate of emergency cesarean was reported
to be as high as 86%, versus 4% when MCA and uterine artery velocimetry were
both normal. The rate of severe morbidity (grades II to IV intraventricular
hemorrhage) was significantly increased in the pregnancies delivered by emer-
gency cesarean section. Although abnormal umbilical artery velocimetry is a
better predictor of adverse perinatal outcome in the small fetus, MCA PI has a
better sensitivity (91.7%) and negative predictive value (98.6%) for major
adverse outcome, especially before 32 weeks (when the sensitivity is 95.5% and
the negative predictive value is 97.7%) [61].
The cerebral-placental ratio should be used in small fetuses with normal
umbilical artery waveforms. When there is absent or reversed flow of the
umbilical artery, this index is not needed.
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764754
Issues in management of intrauterine growth restriction
Ductus venosus
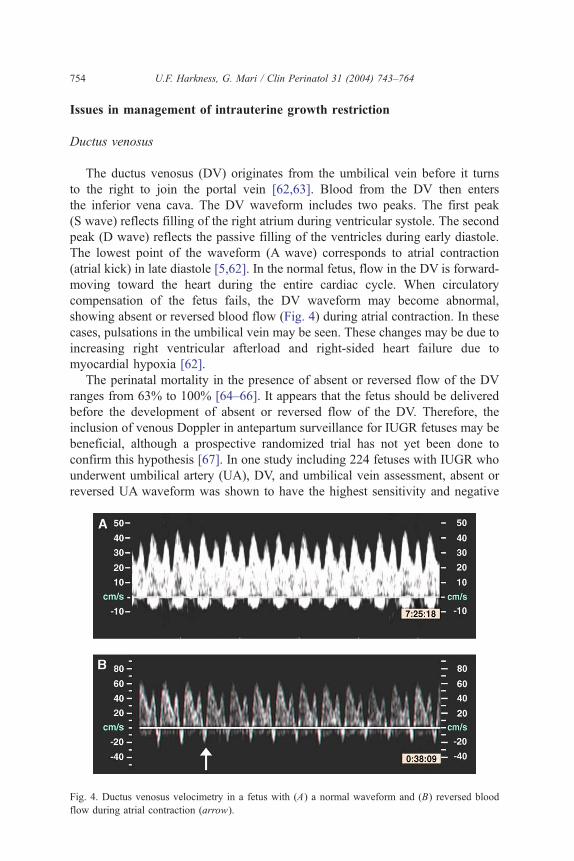
The ductus venosus (DV) originates from the umbilical vein before it turns
to the right to join the portal vein [62,63]. Blood from the DV then enters
the inferior vena cava. The DV waveform includes two peaks. The first peak
(S wave) reflects filling of the right atrium during ventricular systole. The second
peak (D wave) reflects the passive filling of the ventricles during early diastole.
The lowest point of the waveform (A wave) corresponds to atrial contraction
(atrial kick) in late diastole [5,62]. In the normal fetus, flow in the DV is forward-
moving toward the heart during the entire cardiac cycle. When circulatory
compensation of the fetus fails, the DV waveform may become abnormal,
showing absent or reversed blood flow (Fig. 4) during atrial contraction. In these
cases, pulsations in the umbilical vein may be seen. These changes may be due to
increasing right ventricular afterload and right-sided heart failure due to
myocardial hypoxia [62].
The perinatal mortality in the presence of absent or reversed flow of the DV
ranges from 63% to 100% [64–66]. It appears that the fetus should be delivered
before the development of absent or reversed flow of the DV. Therefore, the
inclusion of venous Doppler in antepartum surveillance for IUGR fetuses may be
beneficial, although a prospective randomized trial has not yet been done to
confirm this hypothesis [67]. In one study including 224 fetuses with IUGR who
underwent umbilical artery (UA), DV, and umbilical vein assessment, absent or
reversed UA waveform was shown to have the highest sensitivity and negative
Fig. 4. Ductus venosus velocimetry in a fetus with (A) a normal waveform and (B) reversed blood
flow during atrial contraction (arrow).
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764 755
predictive value for acidemia, asphyxia, stillbirth, and neonatal and perinatal
death [67]. Absent or reversed atrial systolic blood-flow velocity in the DV and
pulsatile flow in the umbilical vein, however, had the best specificity and positive
predictive values for prediction of the above outcomes. The authors suggested
that important intrauterine time can be gained for preterm fetuses who have
absent or reversed UA end-diastolic velocities but normal venous flows.
Results of a prospective multicenter longitudinal observational study also
suggested that Doppler velocimetry of the DV may be useful in timing the
delivery of the IUGR fetus [68]. Of 70 singleton IUGR fetuses delivered between
26 and 33 weeks’ gestation, DV PI was significantly higher, UA PI was sig-
nificantly higher, and short-term heart-rate variation (STV) was significantly
lower in the last 24 hours before delivery in babies with adverse outcomes. Poor
outcomes included perinatal death, cerebral hemorrhage of grade II or greater,
and bronchopulmonary dysplasia. Two to 7 days before delivery, only DV PI was
significantly higher. With logistic regression analysis, only DV waveform and
gestational age—not UA PI or STV—were predictive of adverse outcomes. Only
32% (6/19) of the infants with DV PI of 3 standard deviations or greater and 18%
(2/11) of the infants with absent or reversed DV A-wave flow in the 24 hours
before delivery had normal outcomes.
Although the results of these studies are promising for timing the delivery of
the IUGR fetus based on DV, data from randomized trials are not yet available to
support or refute its use. Currently, a multicenter prospective randomized trial is
being planned in Europe.
Other vessels
Many other vessels have been assessed by Doppler ultrasound in the AGA and
IUGR fetus [69–77]. Those studies have improved our understanding of fetal
physiology and the pathophysiology of the IUGR fetus. However, they do not
add much beyond the information given from assessment of the UA, MCA,
and DV.
Temporal sequence of Doppler changes
Recent longitudinal studies have described a Doppler temporal sequence in
the IUGR fetus before fetal distress. Hecher et al [78] reported findings from a
prospective observational multicenter study on 93 singleton pregnancies after
24 weeks complicated by IUGR. Amniotic fluid index and UA PI were the first
to become abnormal. These were followed by abnormalities of MCAvelocimetry,
aorta Doppler studies, STV of the fetal heart rate, DV waveforms, and inferior
vena cava Doppler studies. This trend appeared both before and after 32 weeks.
In the group delivered after 32 weeks, however, the probability of having any
given abnormality in Doppler velocimetry was lower, and the changes in actual
Doppler values and STV were less pronounced.
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764756
Baschat et al [79] longitudinally studied 44 IUGR fetuses with elevated
umbilical artery PI who had a final biophysical profile of less than 6/10 before
delivery. In 42 fetuses (95.5%), one or more vascular parameters changed. UA
and DV indices markedly increased at a median of 4 days before the biophysical
score deteriorated. Fetal breathing movements declined beginning 2 to 3 days
before delivery; the following day, amniotic fluid volume dropped. Loss of fetal
movement and tone occurred on the day of delivery. In 70.5% of these fetuses,
Doppler deterioration was complete 24 hours before the biophysical profile
changed. Three patterns of Doppler deterioration were described in this study.
The majority of fetuses (72.7%) displayed a sequence of worsening of the UA
PI, development of brain sparing, then venous changes. Another group of fetuses
showed venous changes before brain sparing. Finally, some fetuses demonstrated
changes in the DV without ever showing Doppler changes consistent with
brain sparing.
Ferrazzi et al [80] evaluated 26 IUGR fetuses with abnormal uterine and UA
Doppler velocimetry. A temporal sequence of abnormal Doppler changes was
described. Early changes, assumed to reflect increased placental vascular resist-
ance and hypoxia, included absent end-diastolic flow in the UA and an abnormal
MCA PI. Half the fetuses showed these changes 15 to 16 days before delivery.
Late changes, thought to indicate circulatory collapse, were reverse flow in the
UA and abnormal DV, aortic, and pulmonary outflow tract velocimetry. Half the
fetuses were affected by these late changes 4 to 5 days before delivery. These late
Doppler changes correlated significantly with perinatal death.
Significantly, not all fetuses appear to follow the same pattern of circulatory
deterioration [79]. In addition, near-term fetuses may not show the same
progression of circulatory changes [79]. These differences need to be considered
when using Doppler velocimetry in the antenatal surveillance of the IUGR fetus.
Nonstress test
The heart rate of the fetus that is not affected by acidosis or neurologic de-
pression will accelerate in response to fetal movement. This reaction is the basis
of the nonstress test (NST). Although abnormal fetal heart-rate patterns are
related to impaired fetal oxygenation and subsequent neurologic outcome, these
are late changes. Ideally, the fetus should be delivered before evidence of
hypoxemia is noted on fetal heart-rate monitoring to avoid subsequent handicap
[81]. However, the NST remains the most common test used in evaluation of
pregnancies complicated by an IUGR fetus.
Biophysical profile
The biophysical profile (BPP) is based on the fact that the fetal central nervous
system initiates and regulates biophysical activity. Neuronal centers deprived of
oxygen have decreased or absent output, which results in alterations in fetal
movement, tone, and breathing. Systemic hypoxia is assumed to be absent as
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764 757
long as brain activity is normal, because the brain is one of the most oxygen-
dependent tissues [82].
The BPP is a widely used antepartum testing modality. A significant decrease
in perinatal mortality is seen in high-risk pregnancies managed with BPP as
opposed to those managed with untested historical controls. The perinatal mor-
tality in one study was 1.86 per 1000 in those tested, compared with 7.69 per
1000 in those not tested, for a decrease of 76% [83]. In a large retrospective study
of 26,290 high-risk fetuses who received BPP testing and 58,659 fetuses who
did not receive BPP testing, there was a very significant inverse exponential
relationship between BPP before delivery and incidence of cerebral palsy [84].
The incidence of cerebral palsy when the last BPP score before delivery was
normal (10/10, 8/10, or 8/8) was 0.7 per 1000, whereas with a score of 0/10 the
incidence of cerebral palsy was 333 per 1000. In the same study, these same
high-risk fetuses were compared with mixed low-risk and high-risk patients not
followed by BPP; the rate of cerebral palsy was 4.74 per 1000 in the untested
population and 1.33 per 1000 in the tested group, a significant difference.
Although the mean birth weight is noted to be smaller in the tested population,
the actual number of SGA or IUGR fetuses in this study is unknown.
The authors of a review assessing the effects of BPP on perinatal outcome
conclude that there is currently inconclusive evidence from randomized
controlled trials to support or argue against the use of BPP as a test of fetal
well-being in high-risk pregnancies, including those with IUGR [85]. Surpris-
ingly, however, the number of patients enrolled in randomized trials using this
method of antepartum testing is small (2839).
Corticosteroids
One important consideration regarding the use of the BPP in the management
of high-risk pregnancies is the effect of corticosteroids on fetal behavior and thus
on the score itself. In a study of 35 women at risk for preterm delivery without
IUGR and between 28 and 34 weeks, BPPs and Doppler velocimetry of the UA
and MCA were performed daily before a first dose of betamethasone and for
120 hours afterward [86]. Though none of the BPPs were less than or equal to 6 at
baseline, at 24, 48, and 72 hours poststeroids, 13.3%, 76.7%, and 16.7% were
less than or equal to 6, respectively (P b 0.05). The change in BPP was due to
decreased fetal movement, decreased fetal breathing, and more frequent
nonreassuring heart-rate tracing. The alteration in BPP in these healthy fetuses
was transient. Doppler indices were not affected by corticosteroid administration.
Another prospective study showed findings of decreased fetal breathing and
decreased fetal limb and trunk movements 48 hours from a first dose of beta-
methasone, with return to baseline at 96 hours; again, Doppler velocimetry of
the MCA and UA remained unchanged [87]. These effects should be considered
in managing women with IUGR after steroids have been administered.
The efficacy of antenatal corticosteroids for the preterm fetus with IUGR has
not been well studied. One study showed no significant difference in short-term
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764758
morbidity between infants with growth restriction delivered between 26 and
31 weeks who received corticosteroids and those who did not, but it did demon-
strate a significantly higher survival without disability or handicap in the steroid
group [88]. Another study reported no difference between growth-restricted
fetuses of less than 1750 g given steroids and AGA infants for several neonatal
outcomes, including RDS and intraventricular hemorrhage/periventricular leu-
komalacia [89].
However, a very recent study demonstrated that of 19 fetuses with absent or
reversed end-diastolic flow (ARED) in the UA, 10 developed transient forward
end-diastolic flow after betamethasone injection, whereas nine fetuses showed
persistent ARED [90]. Although some babies respond to steroids with vaso-
dilation of the fetoplacental circulation and decreased vascular resistance, other
babies respond with an increase in vascular resistance that may lead to fetal
deterioration. The persistent ARED group had more frequent acute fetal deterio-
ration. The two patients with a fetal demise and the two patients with severe
acidosis were in the persistent ARED group. The authors suggest performing
Doppler studies the day after steroid administration in IUGR fetuses with ARED.
If no forward end-diastolic flow is seen, the fetal venous circulation should be
examined, and delivery should be considered if abnormalities exist. The response
of IUGR fetuses to corticosteroid administration should be studied further.
Prediction of intrauterine growth restriction
Uterine artery
IUGR and pre-eclampsia have been associated with abnormal velocimetry of
the uterine arteries. The uterine artery is typically measured using color Doppler
where it crosses over the external iliac artery. In the normal pregnancy, the normal
waveform shows high flow throughout diastole. An abnormal waveform is
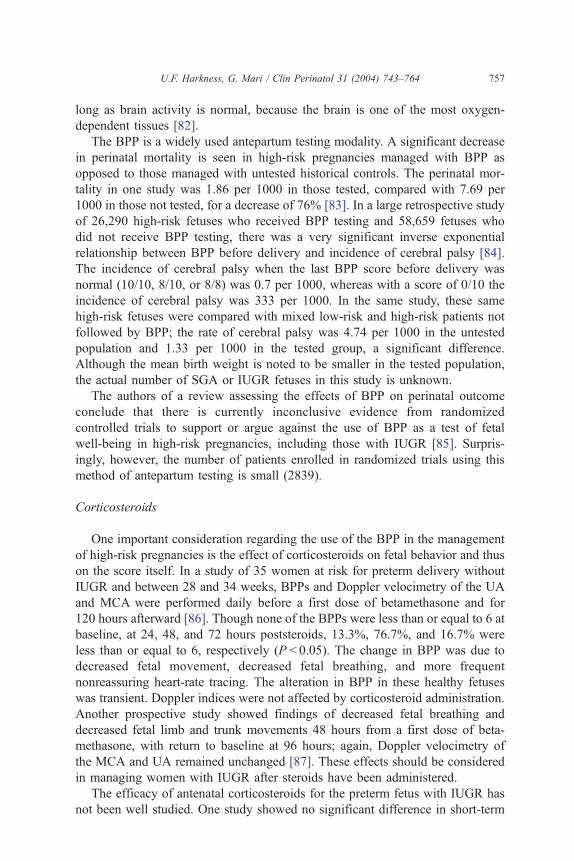
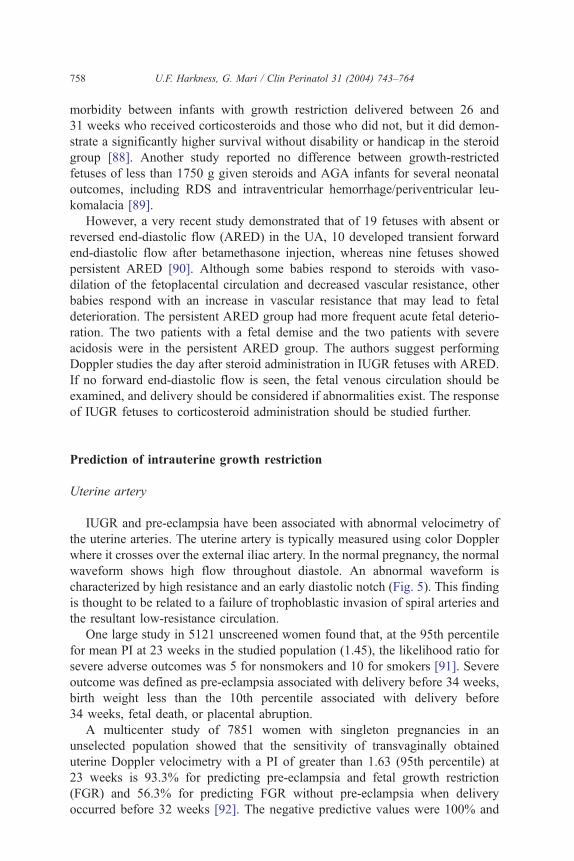
characterized by high resistance and an early diastolic notch (Fig. 5). This finding
is thought to be related to a failure of trophoblastic invasion of spiral arteries and
the resultant low-resistance circulation.
One large study in 5121 unscreened women found that, at the 95th percentile
for mean PI at 23 weeks in the studied population (1.45), the likelihood ratio for
severe adverse outcomes was 5 for nonsmokers and 10 for smokers [91]. Severe
outcome was defined as pre-eclampsia associated with delivery before 34 weeks,
birth weight less than the 10th percentile associated with delivery before
34 weeks, fetal death, or placental abruption.
A multicenter study of 7851 women with singleton pregnancies in an
unselected population showed that the sensitivity of transvaginally obtained
uterine Doppler velocimetry with a PI of greater than 1.63 (95th percentile) at
23 weeks is 93.3% for predicting pre-eclampsia and fetal growth restriction
(FGR) and 56.3% for predicting FGR without pre-eclampsia when delivery
occurred before 32 weeks [92]. The negative predictive values were 100% and
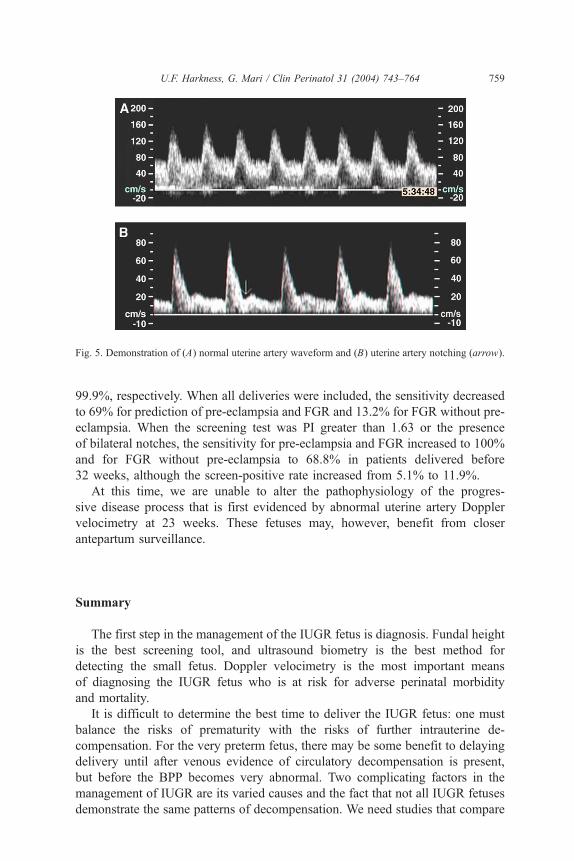
Fig. 5. Demonstration of (A) normal uterine artery waveform and (B) uterine artery notching (arrow).
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764 759
99.9%, respectively. When all deliveries were included, the sensitivity decreased
to 69% for prediction of pre-eclampsia and FGR and 13.2% for FGR without pre-
eclampsia. When the screening test was PI greater than 1.63 or the presence
of bilateral notches, the sensitivity for pre-eclampsia and FGR increased to 100%
and for FGR without pre-eclampsia to 68.8% in patients delivered before
32 weeks, although the screen-positive rate increased from 5.1% to 11.9%.
At this time, we are unable to alter the pathophysiology of the progres-
sive disease process that is first evidenced by abnormal uterine artery Doppler
velocimetry at 23 weeks. These fetuses may, however, benefit from closer
antepartum surveillance.
Summary
The first step in the management of the IUGR fetus is diagnosis. Fundal height
is the best screening tool, and ultrasound biometry is the best method for
detecting the small fetus. Doppler velocimetry is the most important means
of diagnosing the IUGR fetus who is at risk for adverse perinatal morbidity
and mortality.
It is difficult to determine the best time to deliver the IUGR fetus: one must
balance the risks of prematurity with the risks of further intrauterine de-
compensation. For the very preterm fetus, there may be some benefit to delaying
delivery until after venous evidence of circulatory decompensation is present,
but before the BPP becomes very abnormal. Two complicating factors in the
management of IUGR are its varied causes and the fact that not all IUGR fetuses
demonstrate the same patterns of decompensation. We need studies that compare
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764760
NST, BPP, and Doppler surveillance to one another and to management strategies
that combine them. Perhaps an integration of the testing modalities that reflect
central nervous system phenomena (NST, BPP) and circulatory phenomena
(Doppler velocimetry) will emerge as the best antepartum method of testing fetal
well-being.
References
[1] Winick M. Cellular changes during placental and fetal growth. Am J Obstet Gynecol 1971;
109:166–76.
[2] Campbell S, Warsof SL, Little D, Cooper DJ. Routine ultrasound screening for the prediction
of gestational age. Obstet Gynecol 1985;65:613–20.
[3] Robinson HP, Fleming JE. A critical evaluation of sonar bcrown-rump lengthQ measurements.
Br J Obstet Gynaecol 1975;82:702–10.
[4] Drumm JE, Clinch J, MacKenzie G. The ultrasonic measurement of fetal crown-rump length
as a method of assessing gestational age. Br J Obstet Gynaecol 1976;83:417–21.
[5] Ville Y, Nyberg DA. Growth, Doppler and fetal assessment. In: Nyberg DA, McGahan JP,
Pretorius DH, Pilu G, editors. Diagnostic imaging of fetal anomalies. Philadelphia7 Lippincott,
Williams & Wilkins; 2003. p. 31–58.
[6] Chervenak FA, Skupski DW, Romero R, Myers MK, Smith-Levitin M, Rosenwaks Z, et al.
How accurate is fetal biometry in the assessment of fetal age? Am J Obstet Gynecol 1998;
178:678–87.
[7] Manning F. Intrauterine growth restriction: diagnosis, prognostication, and management based
on ultrasound methods. In: Fleischer AC, Manning F, Jeanty P, Romero R, editors. Sonography
in obstetrics and gynecology: principles and practice. 6th edition. New York7 McGraw-Hill;
2001. p. 615–35.
[8] Goldstein I, Lockwood C, Belanger K, Hobbins J. Ultrasonographic assessment of gesta-
tional age with the distal femoral and proximal tibial ossification centers in the third trimester.
Am J Obstet Gynecol 1988;158:127–30.
[9] Goldstein I, Reece EA, O’Connor TZ, Hobbins JC. Estimating gestational age in the term
pregnancy with a model based on multiple indices of fetal maturity. Am J Obstet Gynecol
1989;161:1235–8.
[10] Hadlock FP, Harrist RB, Sharman RS, Deter RL, Park SK. Estimation of fetal weight with
the use of head, body and femur measurements—a prospective study. Am J Obstet Gynecol
1985;151:333–7.
[11] Shepard MJ, Richards VA, Berkowitz RL, Warsof SL, Hobbins JC. An evaluation of two
equations for predicting fetal weight by ultrasound. Am J Obstet Gynecol 1982;142:47–54.
[12] American College of Obstetricians and Gynecologists. Intrauterine growth restriction. ACOG
practice bulletin no. 12. Washington, DC7 American College of Obstetricians and Gynecolo-
gists; 2000.
[13] Resnik R. Intrauterine growth restriction. Obstet Gynecol 2002;99:490–6.
[14] Dashe JS, McIntire DD, Lucas MJ, Leveno KJ. Effects of symmetric and asymmetric fetal
growth on pregnancy outcomes. Obstet Gynecol 2000;96:321–7.
[15] Fretts RC, Boyd ME, Usher RH, Usher HA. The changing pattern of fetal death, 1961–1988.
Obstet Gynecol 1992;79:35–9.
[16] Manning FA. Intrauterine growth retardation. In: Manning FA, editor. Fetal medicine: principles
and practice. Norwalk (CT)7 Appleton and Lange; 1995.
[17] McIntire DD, Bloom SL, Casey BM, Leveno KJ. Birth weight in relation to morbidity
and mortality among newborn infants. N Engl J Med 1999;340:1234–8.
[18] Gilbert WM, Danielsen B. Pregnancy outcomes associated with intrauterine growth restriction.
Am J Obstet Gynecol 2003;188:1596–601.
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764 761
[19] Gluck L, Kulovich MV. Lecithin/sphingomyelin ratios in amniotic fluid in normal and abnor-
mal pregnancy. Am J Obstet Gynecol 1973;115:539–46.
[20] Procianoy RS, Garcia-Prats JA, Adams JM, Silvers A, Rudolph AJ. Hyaline membrane disease
and intraventricular haemorrhage in small for gestational age infants. Arch Dis Child 1980;
55:502–5.
[21] Pena IC, Teberg AJ, Finello KM. The premature small-for-gestational-age infant during the
first year of life: comparison by birth weight and gestational age. J Pediatr 1988;113:1066–73.
[22] Bernstein IM, Horbar JD, Badger GJ, Ohlsson A, Golan A. For the Vermont Oxford Network.
Morbidity and mortality among very-low-birth-weight neonates with intrauterine growth
restriction. Am J Obstet Gynecol 2000;182:198–206.
[23] Larroque B, Bertrais S, Czernichow P, Leger J. School difficulties in 20-year-olds who were
born small for gestational age at term in a regional cohort study. Pediatrics 2001;108:111–5.
[24] Strauss RS. Adult functional outcome of those born small for gestational age: twenty-six-
year follow-up of the 1970 British Birth Cohort. JAMA 2000;283:625–32.
[25] Kanaka-Gantenbein C, Mastorakos G, Chrousos GP. Endocrine-related causes and consequences
of intrauterine growth retardation. Ann N Y Acad Sci 2003;997:150–7.
[26] Godfrey KM, Barker DJP. Fetal nutrition and adult disease. Am J Clin Nutr 2000;71(Suppl):
1344S–52S.
[27] Barker DJP. Fetal programming of coronary heart disease. Trends Endocrinol Metab 2002;
13:364–8.
[28] Barker DJP, Winter PD, Osmond C, Margetts B, Simmonds SJ. Weight in infancy and death
from ischaemic heart disease. Lancet 1989;2:577–80.
[29] Belizan JM, Villar J, Nardin JC, Malamud J, Sainz de Vicuna L. Diagnosis of intrauterine
growth retardation by a simple clinical method: measurement of uterine height. Am J Obstet
Gynecol 1978;131:643–6.
[30] Quaranta P, Currell R. Prediction of small-for-dates infants by measurement of symphysial-
fundal height. Br J Obstet Gynaecol 1981;88:115–9.
[31] Jensen OH, Larsen S. Evaluation of symphysis-fundus measurements and weighing during
pregnancy. Acta Obstet Gynecol Scand 1991;70:13–6.
[32] Walraven GE, Mkanje RJ, van Roosmalen J, van Dongen PW, van Asten AG, Dolmans WM.
Single pre-delivery symphysis-fundal height measurement as a predictor of birthweight and
multiple pregnancy. Br J Obstet Gynecol 1995;102:525–9.
[33] Cunningham FG, Gant NF, Leveno KJ, Gilstrap III LC, Hauth JC, Wenstrom KD. Prenatal care.
In: Williams obstetrics. 21st edition. New York7 McGraw Hill; 2001. p. 221–47.
[34] Chang TC, Robson SC, Boys RJ, Spencer JAD. Prediction of the small for gestational age
infant: which ultrasonic measurement is best? Obstet Gynecol 1992;80:1030–8.
[35] Warsof SLK, Cooper DJ, Little D, Campbell S. Routine ultrasound screening for antena-
tal detection of intrauterine growth retardation. Obstet Gynecol 1986;67:33–9.
[36] Pearce JM, Campbell S. A comparison of symphysis-fundal height and ultrasound as screen-
ing tests for light-for-gestational age infants. Br J Obstet Gynaecol 1987;94:100 – 4.
[37] Thompson RS, Trudinger BJ, Cook CM, Giles WB. Umbilical artery velocity waveforms:
normal reference values for A/B ratio and Pourcelot ratio. Br J Obstet Gynaecol 1988;95:
589–91.
[38] Sebire NJ. Umbilical artery Doppler revisited: pathophysiology of changes in intrauterine
growth restriction revealed. Ultrasound Obstet Gynecol 2003;21:419–22.
[39] Berkowitz GS, Mehalek KE, Chitkara U, Rosenberg J, Cogswell C, Berkowitz RL. Doppler
velocimetry in the prediction of adverse outcome in pregnancies at risk for intrauterine
growth retardation. Obstet Gynecol 1988;71:742–6.
[40] Gaziano EP, Knox E, Ferrera B, Brandt DG, Calvin SE, Knox GE. Is it time to reassess the
risk for the growth retarded fetus with normal velocimetry of the umbilical artery? Am J Obstet
Gynecol 1994;170:1734–41.
[41] Brar H, Platt LD. Reverse end-diastolic flow velocity on umbilical artery velocimetry in high
risk pregnancies: an ominous finding with adverse pregnancy outcome. Am J Obstet Gynecol
1988;159:559–61.
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764762
[42] Karsdorp VHM, van Vugt JMG, van Geijn HP, Kostense PJ, Arduini D, Montenegro N, et al.
Clinical significance of absent or reversed end diastolic velocity waveforms in umbilical artery.
Lancet 1994;344:1664–8.
[43] Zelop CM, Richardson DK, Heffner LJ. Outcomes of severely abnormal umbilical artery
Doppler velocimetry in structurally normal singleton fetuses. Obstet Gynecol 1996;87:434–8.
[44] Wienerroither H, Steiner H, Tomaselli J, Lobendanz M, Thun-Hohenstein L. Intrauterine
blood flow and long-term intellectual, neurologic, and social development. Obstet Gynecol
2001;97:449–53.
[45] Vogbeck S, de Camargo OK, Grab D, Bode H, Pohlandt F. Neonatal and neurodevelopmental
outcome in infants born before 30 weeks of gestation with absent or reversed end-diastolic
flow velocities in the umbilical artery. Eur J Pediatr 2001;160:128–34.
[46] Neilson JP, Alfirevic Z. Doppler ultrasound for fetal assessment in high risk pregnancies
(Cochrane Review). In: The Cochrane Library, Issue 1, 2004. Chichester (UK)7 John Wiley and
Sons; 2004.
[47] Hornbuckle J, Vail A, Spiegelhalter D, Levene M, Thornton JG, and GRIT study group.
A randomized trial of timed delivery for the compromised preterm fetus: short term outcomes
and Bayesian interpretation. Br J Obstet Gynaecol 2003;110:27–32.
[48] Nienhuis SJ, Vles JSH, Gerver WJM, Hoogland HJ. Doppler ultrasonography in suspected
intrauterine growth retardation: a randomized clinical trial. Ultrasound Obstet Gynecol 1997;
9:6–13.
[49] Burke G, Stuart B, Crowley P, Scanaill SN, Drumm J. Is intrauterine growth retardation
with normal umbilical artery blood flow a benign condition? BMJ 1990;300:1044–5.
[50] Ott WJ. Intrauterine growth restriction and Doppler ultrasonography. J Ultrasound Med
2000;19:661–5.
[51] Baschat AA, Weiner CP. Umbilical artery Doppler screening for detection of the small fetus
in need of antepartum surveillance. Am J Obstet Gynecol 2000;182:154–8.
[52] McCowan LME, Harding JE, Roberts AB, Barker SE, Ford C, Stewart AW. A pilot randomized
controlled trial of two regimens of fetal surveillance for small-for-gestational-age fetuses with
normal results of umbilical artery Doppler velocimetry. Am J Obstet Gynecol 2000;182:81–6.
[53] Mari G, Deter RL. Middle cerebral artery flow velocity waveforms in normal and small-
for-gestational-age fetuses. Am J Obstet Gynecol 1992;166:1262–70.
[54] Wladimiroff JW, Wijngaard JA, Degani S, Noordam MJ, Eyck J, Tonge HM. Cerebral
and umbilical arterial blood flow velocity waveforms in normal and growth-retarded preg-
nancies. Obstet Gynecol 1987;69:705–9.
[55] Arbeille P, Roncin A, Berson M, Patat F, Pourcelot L. Exploration of the fetal cerebral blood
flow by duplex Doppler–linear array system in normal and pathological pregnancies. Ultrasound
Med Biol 1987;13:329–37.
[56] Arbeille P. Fetal arterial Doppler—IUGR and hypoxia. Eur J Obstet Gynecol Reprod Biol
1997;75:51–3.
[57] Sterne G, Shields LE, Dubinsky TJ. Abnormal fetal cerebral and umbilical Doppler measure-
ments in fetuses with intrauterine growth restriction predict the severity of perinatal morbidity.
J Clin Ultrasound 2001;29:146–51.
[58] Gramellini D, Folli MC, Raboni S, Vadora E, Merialdi A. Cerebral-umbilical Doppler ratio
as a predictor of adverse perinatal outcome. Obstet Gynecol 1992;79:416–20.
[59] Bahado-Singh RO, Kovanci E, Jeffres A, Oz U, Deren O, Copel J, et al. The Doppler
cerebroplacental ratio and perinatal outcome in intrauterine growth restriction. Am J Obstet
Gynecol 1999;180:750–6.
[60] Severi FM, Bocchi C, Visentin A, Falco P, Cobellis L, Florio P, et al. Uterine and fetal cerebral
Doppler predict the outcome of third-trimester small-for-gestational age fetuses with normal
umbilical artery Doppler. Ultrasound Obstet Gynecol 2002;19:225–8.
[61] Fong KW, Ohlsson A, Hannah ME, Grisaru S, Kingdom J, Cohen H, et al. Prediction of
perinatal outcome in fetuses suspected to have intrauterine growth restriction: Doppler US
study of fetal cerebral, renal, and umbilical arteries. Radiology 1999;213:681–9.
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764 763
[62] Hecher K, Campbell S. Characteristics of fetal venous blood flow under normal circumstances
and during fetal disease. Ultrasound Obstet Gynecol 1996;7:68–83.
[63] Kiserud T, Eik-Nes SH. Doppler velocimetry of the ductus venosus. In: Maulik D, editor.
Doppler ultrasound in obstetrics and gynecology. New York7 Springer-Verlag; 1997. p. 403–22.
[64] Goncalves LF, Romero R, Silva M, Ghezzi F, Soto A, Munoz H, et al. Reverse flow in the
ductus venosus: an ominous sign. Am J Obstet Gynecol 1995;172:266.
[65] Ozcan T, Sbracia M, d’Ancona RL, Copel JA, Mari G. Arterial and venous Doppler velo-
cimetry in the severely growth-restricted fetus and associations with adverse perinatal outcome.
Ultrasound Obstet Gynecol 1998;12:39–44.
[66] Hecher K, Campbell S, Doyle P, Harrington K, Nicolaides K. Assessment of fetal compromise
by Doppler ultrasound investigation of the fetal circulation. Circulation 1995;91:129–38.
[67] Baschat AA, Gembruch U, Weiner CP, Harman CR. Qualitative venous Doppler waveform
analysis improves prediction of critical perinatal outcomes in premature growth-restricted
fetuses. Ultrasound Obstet Gynecol 2003;22:240–5.
[68] Bilardo CM, Wolf H, Stigter RH, Ville Y, Baez E, Visser GHA, et al. Relationship between
monitoring parameters and perinatal outcome in severe, early intrauterine growth restriction.
Ultrasound Obstet Gynecol 2004;23:119–25.
[69] Mari G. Arterial blood flow velocity waveforms of the pelvis and lower extremities in normal
and growth-retarded fetuses. Am J Obstet Gynecol 1991;165:143–51.
[70] Abuhamad AZ, Mari G, Bogdan D, Evans III AT. Doppler flow velocimetry of the splenic artery
in the human fetus: is it a marker of chronic hypoxia? Am J Obstet Gynecol 1995;172:820–5.
[71] Mari G, Abuhamad AZ, Uerpairojkit B, Martinez E, Copel JA. Blood flow velocity waveforms
of the abdominal arteries in appropriate- and small-for-gestational-age fetuses. Ultrasound
Obstet Gynecol 1995;6:15–8.
[72] Mari G, Deter RL, Uerpairojkit B. Flow velocity waveforms of the ductus arteriosus in
appropriate and small-for-gestational age fetuses. J Clin Ultrasound 1996;24:185–96.
[73] Uerpairojkit B, Chan L, Reece AE, Martinez E, Mari G. Cerebellar Doppler velocimetry in
the appropriate- and small-for-gestational-age fetus. Obstet Gynecol 1996;87:989–93.
[74] Mari G, Uerpairojkit B, Abuhamad AZ, Copel J. Adrenal artery velocity waveforms in the
appropriate and small-for-gestational age fetus. Ultrasound Obstet Gynecol 1996;8:82–6.
[75] Abuhamad AZ, Mari G, Cortina RM, Croitoru DP, Evans AT. Superior mesenteric artery Doppler
velocimetry and ultrasonographic assessment of fetal bowel in gastroschisis: a prospective
longitudinal study. Am J Obstet Gynecol 1997;176:985–90.
[76] Rhee E, Detti L, Mari G. Superior mesenteric artery flow velocity waveforms in small
for gestational age fetuses. J Matern Fetal Med 1998;7:120–3.
[77] Mari G, Wasserstrum N. Flow velocity waveforms of the fetal circulation preceding fetal
death in a case of lupus anticoagulant. Am J Obstet Gynecol 1991;164:776–8.
[78] Hecher K, Bilardo CM, Stigter RH, Ville Y, Hackeloer BJ, Kok HJ, et al. Monitoring of
fetuses with intrauterine growth restriction: a longitudinal study. Ultrasound Obstet Gynecol
2001;18:564–70.
[79] Baschat AA, Gembruch U, Harman CR. The sequence of changes in Doppler and bio-
physical parameters as severe fetal growth restriction worsens. Ultrasound Obstet Gynecol 2001;
18:571–7.
[80] Ferrazzi E, Bozzo M, Rigano S, Bellotti M, Morabito A, Pardi G, et al. Temporal sequence
of abnormal Doppler changes in the peripheral and central circulatory systems of the severely
growth-restricted fetus. Ultrasound Obstet Gynecol 2002;19:140–6.
[81] Visser GH. Abnormal antepartum fetal heart rate patterns and subsequent handicap. Baillieres
Clin Obstet Gynaecol 1998;2:117–24.
[82] Manning FA. Fetal biophysical profile. Obstet Gynecol Clin North Am 1999;26:557–77.
[83] Manning FA. Fetal biophysical profile scoring. In: Fetal medicine, principles and practice.
Norwalk (CT)7 Appleton & Lange; 1995. p. 237.
[84] Manning FA, Bondaji N, Harman CR, Casiro O, Menticoglou S, Morrison I, et al. Fetal
assessment by fetal biophysical profile score. VI. The incidence of cerebral palsy among
tested and non-tested perinates. Am J Obstet Gynecol 1998;178:696–706.
U.F. Harkness, G. Mari / Clin Perinatol 31 (2004) 743–764764
[85] Alfirevic Z, Neilson JP. Biophysical profile for fetal assessment in high risk pregnancies
(Cochrane Review). In: The Cochrane Library, Issue 1, 2004. Chichester (UK)7 John Wiley &
Sons; 2004.
[86] Deren O, Karaer C, Onderoglu L, Yigit N, Durukan T, Bahado-Singh RO. The effect of steroids
on the biophysical profile and Doppler indices of umbilical and middle cerebral arteries in
healthy preterm fetuses. Eur J Obstet Gynecol Reprod Biol 2001;99:72–6.
[87] Rotmensch S, Liberati M, Celentano C, Efrat Z, Bar-Hava I, Kovo M, et al. The effect
of betamethasone on fetal biophysical activities and Doppler velocimetry of umbilical and
middle cerebral arteries. Acta Obstet Gynecol Scand 1999;78:768–73.
[88] Schaap AH, Wolf H, Bruinse HW, Smolders-de Haas H, Van Ertbruggen I, Treffers PE. Effects
of antenatal corticosteroid administration on mortality and long-term morbidity in early
preterm, growth-restricted infants. Obstet Gynecol 2001;97:954–60.
[89] Elimian A, Verma U, Canterino J, Shah J, Visintainer P, Tejani N. Effectiveness of antenatal
steroids in obstetric subgroups. Obstet Gynecol 1999;93:174–9.
[90] Simchen MJ, Alkazaleh F, Adamson SL, Windrim R, Telford J, Beyene J, et al. The fetal
cardiovascular response to antenatal steroids in severe early-onset intrauterine growth restriction.
Am J Obstet Gynecol 2004;190:296–304.
[91] Lees C, Parra M, Missfelder-Lobos H, Morgans A, Fletcher O, Nicolaides KH. Individualized
risk assessment for adverse pregnancy outcome by uterine artery Doppler at 23 weeks. Obstet
Gynecol 2001;98:369–73.
[92] Papgeorghiou AT, Yu CKH, Bindra R, Pandis G, Nicolaides KH for the Fetal Medicine
Foundation Second Trimester Screening Group. Multicenter screening for preeclampsia and
fetal growth restriction by transvaginal uterine artery Doppler at 23 weeks of gestation.
Ultrasound Obstet Gynecol 2001;18:441–9.





























