Embed Size (px)
Citation preview

5b
Diagnostic arthroscopy
R O B E R T W. IKE
In the early 20th century, physicians from Europe (Bircher, 1921), Asia (Takagi, 1933), and North America (Kreuscher, 1925; Geist, 1926; Burman et al, 1934) modified existing endoscopes to insert into diseased joints. For most of the ensuing years, endoscopy of joints--or arthroscopy--was undertaken mainly for diagnosis, usually to find an intra-articular derange- ment that might require a specific operation. The situation changed when development of motorized shavers and hand-operated instruments for cutting and grasping made it feasible to couple arthroscopic diagnosis with operative treatment. From the 1980s onwards, orthopaedists have adapted many procedures for arthroscopy that were once done through open arthrotomy, thus fuelling an explosive growth in arthroscopic surgery. Consequently, attention on arthroscopy as a diagnostic tool has been eclipsed by description and analysis of an ever expanding gamut of arthro- scopic interventions.
Whither diagnostic arthroscopy, then? Some rheumatologists explored uses of the technique when it re-entered Western medicine in the 60s and 70s, and recognized the potential value of directly observing intra-articular pathology (Jayson and Dixon, 1968; Yates and Scott, 1975; Altman, 1976). However, once arthroscopy had become a de facto tool of the orthopaedist, application to rheumatologic disorders mainly involved adaptations of pre- existing open procedures, notably 'debridement' for knee osteoarthritis (OA) (Burks, 1990) and synovectomy for rheumatoid arthritis (RA) and other inflammatory arthropathies (Ogilvie-Harris and Weisleder, 1995). Developments on several fronts have reawakened interest in performing arthroscopy to evaluate disorders that present to the rheumatologist: new instrumentation that permits arthroscopy to be used away from the operat- ing room (OR), observations from arthroscopy of joints affected by chronic rheumatic disorders, and re-emphasis on the need to document tissue effects of therapy. In addition, advances from bench research beg to be tested on clinical material. Thus, the role of arthroscopy in rheumatology, particularly as a diagnostic tool, is only beginning to emerge. An understanding of its evolving role rests on an appreciation of the arthroscopic technique as currently practised by rheumatologists, the nature of the information garnered at arthroscopy, the philosophy of diagnostic arthroscopy as applied to rheumatic disorders, and current clinical applications of arthroscopy.
Bailli~re's Clinical Rheumatology-- 495 Vol. 10, No. 3, August 1996 Copyright �9 1996, by BailliSre Tindall ISBN 0-7020-2183-0 All rights of reproduction in any form reserved 0950-3579/96/030495 + 23 $12.00/00
496 a.W. IKE
T E C H N I C A L ASPECTS OF ARTHROSCOPY: WHAT DO WE DO?
The basic schema for arthroscopic inspection of a knee has changed very little from that first described over 60 years ago (Burman et al, 1934). Fibreoptic illumination (replacing the tungsten bulb) has made the procedure safer, while multi-lens optics and videocameras have enhanced visual data quality and acquisition. Yet the goals of compartment-by- compartment inspection are achieved in the same manner, inspecting the joint through several entry sites while instilling and removing physiological fluid to clear the view of blood and other debris.
For reasons that have changed concomitant with its capabilities, arthroscopy has traditionally been done in an OR setting. Before arthro- scopic surgery was feasible, interested orthopaedists learned arthroscopy by inspecting the knees of patients slated for open procedures and com- paring arthroscopic findings with later direct observation, an exercise confined to the OR because of the open procedure. During the early days of arthroscopic surgery, an OR was deemed essential in case a thwarted arthroscopic intervention had to be converted to a more traditional open remedy. As arthroscopic surgery became routine, assured safety of potential arthrotomy faded as a practical concern, except for complex procedures such as cruciate ligament allografting, meniscal repair and transplantation, and combined arthroscopic/open repair procedures. Nevertheless, OR- based arthroscopy remained the norm, perpetuated by efficiency, con- venience, and habit. Recently, the reduced cost of arthroscopy done in an 'office' setting has been recognized (Halbrecht and Jackson, 1992; Small et al, 1994), hinting at a trend likely to grow in the current medical economic climate.
Regardless of cost savings, transition of arthroscopy to an 'office' setting would be unacceptable unless patient comfort could be assured. Fortunately, this is feasible for diagnostic arthroscopy, using local anaesthetic agents for puncture sites and intra-articular anaesthesia (Martin et al, 1989). To minimize soft tissue and joint trauma, smaller 'needle' arthroscopes have been developed. Unlike the conventional arthroscope of 4.0 mm diameter used in the OR (inserted through a 6-8 mm cannula), these instruments (1.6 to 2.7 mm in diameter) can indeed be inserted through large needle puncture. The first 'needlescope' was developed nearly 20 years ago (Figure la), but failed to attract much attention from those experi- menting with arthroscopy, as nearly all workers were committed to the OR setting. Current versions used for office-based arthroscopy are of two types (Wei et al, 1993; Yates, 1993). Pure fibreoptic systems (Figure lc), with camera and light source in a unit to which the fibreoptic cable is attached, are the easier to manoeuvre but lack angled-viewing capability and produce less clear pictures than conventional arthroscopes (Ike and O'Rourke, 1993; Denti et al, 1994). Glass-lens arthroscopes originally devised for ankles have been transformed by several instrument manufacturers into 'office' equipment for the knee. Attached to a small video-camera, these instru- ments are nearly as facile as the sleek fibreoptic 'wands'.

DIAGNOSTIC ARTHROSCOPY 497
(a)
(b)

498 R.W. IKE
(c)
Figure 1 (see also page 497). Evolution of diagnostic arthroscopy technique: (a) Mid-1970s: direct look through eyepiece of 2.2mm Dyonics Needlescope. (b) Mid-1980s: videoarthroscopy, with view projected to video screen through 100 gm Circon MicroSaticon tube camera (Circon Corporation, Santa Barbara, CA), coupled to eyepiece of 4.0 mm arthroscope (currently-used coupled chip-based video cameras measure approximated 1 • 3 cm and weigh <25 gm). (c) Mid-1990s: view of knee interior with 1.8 mm Medical Dynamics Arthrocatheter placed into joint through 12 gauge needle puncture; fibre- optic cable calxies light into joint and transmits image back to console, which contains light source and video camera (Medical Dynamics, Englewood, CO). ((a) Reproduced from Johnson (1977, Comprehensive Arthroscopic Evaluation of the Knee. St. Louis, MO: CV Mosby) with permission.
The equipment and personnel required for outpatient diagnostic arthroscopy can fit into a room having 80 square feet of floor area (Ike, 1993a). Space requirements increase if local practice standards mandate cardiorespiratory monitoring for patients who receive conscious sedation (vide infia). Vacuum suction is used for evacuating irrigation fluid from the joint and for suction-assisted biopsy instruments. All the major equipment dedicated to arthroscopy, i.e. arthroscope camera control unit, light source, video equipment (screen, printer or tape recorder) and motorized shaver control (if used), can be placed in a mobile lockable cart, thus freeing the space for other uses when arthroscopy is not being done. Certain reusable items must be sterilized before each procedure, including the ~i-throscope and its specific trochar/cannula set, instruments for probing intra-articular structures and retrieving tissue samples, and needle/trochar sets for penetrating and irrigating the joint. Single-use items, i.e. materials to prepare and maintain sterile fields for the joint area and instruments, tubing and fluids for joint lavage, supplies for arthrocentesis and local anaesthetic administration, are readily obtained hospital commodities. An experienced arthroscopist and well-trained assistant can carry out the procedure in this setting, although efficiency is promoted by a second assistant acting as a

DIAGNOSTIC ARTHROSCOPY 499
'circulator' (who transfers items to and from the arthroscopist and first assistant, who maintains sterile conditions).
The patient to be arthroscoped enters this setting awake, and remains conscious through the procedure. Mild sedating agents (e.g. alprazolam) can be given orally some time beforehand so that an adequate level can be attained by the time arthroscopy begins, or parenterally before and during the procedure, the level being adjusted to individual patient needs. The latter method, known as 'conscious sedation', is widely used for other forms of endoscopy, but is strictly regulated in some regions because of its theoretical potential for oversedation and adverse cardiorespiratory consequences. Some arthroscopists have patients wear headphones to hear music or other soothing audiotapes (Arnold, 1992; Wei et al, 1993). Arthrocentesis is followed by intra-articular instillation of local anaesthetic, preceding skin preparation and draping for arthroscopy to allow more time for the joint to become fully anaesthetized before being penetrated by larger instruments. Sites of entry portals for arthroscope and irrigation cannula are located by palpation, anaesthetized from skin to capsule, then enlarged with an appropriately sized needle and trochar, or knife blade. After inserting the arthroscope and irrigating cannula, the joint is lavaged with several exchanges of fluid to provide a clear view. A methodical compartment-by- compartment inspection assures that no pathology will be missed. Suspicious-looking structures can be palpated with a probe placed into the joint through another portal. Placing the scope in another portal can provide additional perspective on intra-articular pathology, particularly in those regions that can be difficult to inspect, such as the posterior horn of the medial meniscus. Tissue samples can be taken by forceps with grasping or hollow 'scoped' ends (Figure 2a). Suction-assisted devices, such as the hand-operated suction punch or the rotary shaver blade, designed for
(a)

5 0 0 R . W . IKE
(b)
(c)
Figure 2 (see also page 499). Instruments for retrieval of tissue at arthroscopy. (a) Scoop tip grasp- ing forceps. (b) DyoVac suction punch, 2.5 mm. (c) Motor drive and 3.5 mm rotary shaver blade. Tissue retrieved by (b) and (c) can be trapped in suction line attached to instrument while cutting end remains in joint (both by Smith and Nephew Dyonics, Andover, MA).

DIAGNOSTIC ARTHROSCOPY 501
powered use but also operable by hand (Ike, 1994a), can sample tissue from several sites within the same joint without having to remove and reinsert the instrument (Figures 2b,c). Commonly-used closed synovial biopsy needles, such as the Parker-Pearson (Schumacher and Kula, 1972) or the Tru-Cut TM (Forouzesh, 1982), are not as well suited to visually-directed biopsy, because the cutting segment of each is on the side rather than the tip. A considerable amount of tissue can be removed by the suction-assisted instruments, sometimes blurring the distinction between 'diagnostic' and 'therapeutic' arthroscopy (Moreland et al, 1995; Wei et al, 1995). Bleeding from vascular synovial tissue is minimized by using dilute epinephrine in the intra-articular anaesthetic mix, and can be reduced further by increas- ing the flow and pressure of joint lavage. Inspection and tissue retrieval can usually be completed in less than an hour. Puncture sites are closed with thin adhesive strips and dressed with sterile gauze. Activity proscriptions are dictated mainly by conscious sedation use, although patients who have had extensive tissue removal are advised to limit weight bearing activities for a few days. Post-arthroscopy pain is managed with mild narcotic analgesics and periodic application of ice packs.
Few complications have been noted following 'needle' arthroscopy. Some local discomfort is expected. Of 84 patients with knee OA who completed a questionnaire two weeks after needle arthroscopy with lavage, some (25%) had no pain, but 71% had sufficient pain to hamper their daily activities, often for a few days (<1 day, 44%; <2 days, 55%; <1 week, 79%); nevertheless, 90% of the patients tolerated the procedure well, and 82% considered their joint symptoms improved (Ayral et al, 1993). The overall rate of complications following needle arthroscopy was 1.7% in a mail survey of 16 physicians recounting 582 cases (Huff et al, 1992) and 11.5% in a retrospective review of four year's experience at two centres (Szachnowski et al, 1995). Minor complications included cellulitis, haemarthrosis, other effusions requiring arthrocentesis, vasovagal reactions, flare of crystal arthropatby, fluid extravasation, allergic reactions to skin preparation, and synovial sinus formation; most events occurred once or twice in each series. Intra-articular glucocorticoids and non- compliance with post-arthroscopy directions probably contributed to the sole major complication of culture-negative septic arthritis occurring two weeks after arthroscopy for severe knee OA (Szachnowski et al, 1995).
THE NATURE OF ARTHROSCOPIC INFORMATION: WHAT DO WE SEE?
Arthroscopic inspection provides qualitative information about intra- articular structures and their interrelationships. Development of systems to quantify the extent of pathology in some of these structures (e.g. hyaline cartilage and synovium) (Chapter 5a) should serve to promote arthroscopic data as reliable and useful outcome measures for interventional trials. However, clinical judgments to be made from arthroscopy still rest on qualitative observations. These can be considered according to tissues and

502 R.w. IKE
structures normally found in the joint: synovium, hyaline cartilage, fibro- cartilage, ligaments, fat and bone. The discussion that follows pertains to the knee, but can be applied to other joints taking variations of intra- articular structure into account.
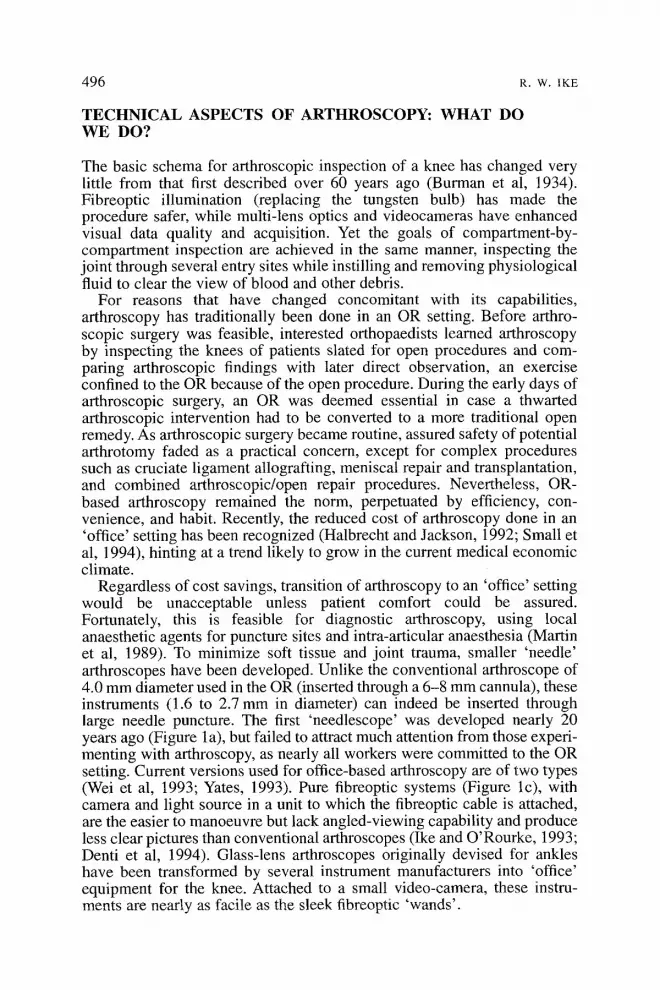
Synovium comprises only a portion of the knee joint, lining the capsule and outer rims of both menisci, while invaginating the cruciate ligaments to a variable extent. Reduplications of synovium can occur at sites where compartments of the knee were once separate during fetal development; such reduplications contribute to the synovium found around the cruciate ligaments and are found as folds, or plicae, adjacent to the patella on as many as three sides (medial, lateral, superior) (Johnson et al, 1993). Normal synovium is thin, translucent material through which a network of small blood vessels can be seen (Figure 3a). Early stages of synovial inflam- mation manifest hyperemia, in which the white or colourless area between vessels becomes pink, and increased vascularity, seen as an apparent increase in vessel number; proliferation of synovial tissue begins as protuberances into the joint space, recognized as villi when length exceeds width (Figures 3b-d) (Lindblad, 1988). The gross appearance of synovial villi can take several forms, documented by Watanabe over 30 years ago and similarly described today (Kurosaka et al, 1990). Synovium almost never becomes uniformly inflamed. Synovitis can be quite focal, and can vary considerably in macroscopic and microscopic intensity even when diffuse (Lindblad and Hedfors, 1985; Lindblad, 1988). Other pathological tissues can be found that probably originate in synovium (Ike, 1995). Fibrous tissue, or 'synovial scar' (sometimes quite dense), can develop after certain insults to the joint such as infection, trauma or previous surgery; occasionally, such tissue can be found in a knee affected by no previous insults other than RA or another idiopathic inflammatory
(a)
DIAGNOSTIC ARTHROSCOPY 503
(b)
(c)

504 R.w. IKE
~)
Figure 3 (see also pages 502 and 503). Examples of synovium findings at arthroscopy. (a) Normal synovium in lateral peripatellar region, left knee, of 46-year old man with refractory knee pain, swelling and mild radiographic OA. (b) Early villous synovitis without increased vascularity, from medial gutter adjacent to fibrillated area (not seen here) on medial femoral condyle, same patient. (c) Granular, hyper- vascular synovitis in medial gutter adjacent to normal-appearing femoral condyle, right knee, of 49-year old man with sporotrichosis and persistent sterile effusion following 4 months of treatment with itraconazole (culture of synovium also negative). (d) Villous, hypervascular synovitis overlying anterior horn of medial meniscus in left knee of 43-year old man with long-standing psoriatic arthritis and new knee pain and swelling (inflammatory fluid) that began several days after an on-the-job slip-and-fall; treated elsewhere as 'torn medial meniscus', but medial meniscus was normal at arthroscopy.
arthropathy. Pannus is defined macroscopically as synovial tissue that has become adherent to hyaline cartilage, menisci, or bone. Free-floating debris is common in chronically inflamed knees. Debris composed of fibrin and sloughed synovial villi tends to assume a shape reminiscent of rice grains, hence the common appellation of such debris as 'rice bodies' (Popert et al, 1982).
Hyaline cartilage lines the articulating surfaces of the tibial plateaux, femoral condyles, and patella. In the normal knee (Figure 4a), only the portion underlying the tibiofemoral meniscus is obscured from direct view, and these areas can be seen by lifting the edge of the meniscus and direct- ing the scope to the area underneath. Normal cartilage appears glistening white through the arthroscope, with dullness and discoloration as the earliest signs of pathology (Noyes and Stabler, 1989). Probe palpation detects softening as the first stage of physical disruption. Fragments of cartilage still adherent to the edges and base of the disrupted surface from which they arise are brought away from the surface by irrigating fluid, accentuating the appearance of fibrillation. Further surface disruption leads to ulceration, sometimes exposing bare bone. Ridges of cartilage (chondro-

DIAGNOSTIC ARTHROSCOPY 505
phytes) can develop at the edge of joint surface and can precede other features of OA. Damage to cartilage from pannus ingrowth can usually be appreciated only after removing the pannus, but can be inferred when soft synovium is found over an area where cartilage is expected.
A search for abnormalities of the fibrocartilagenous tibiofemoral menisci still accounts for most conventional knee arthroscopy. These structures cover about half the surface of each tibial plateau, composed mainly of type II collagen oriented circumferentially in all but the outer rim, which is penetrated by blood vessels and small crude nerve fibres (Wilson et al, 1969; Gronblad et al, 1985). A network of canaliculi in the avascular portion brings nutrients from the joint space to the inner matrix (Bird and Sweet, 1987). The generally-accepted terms to describe the various meniscal derangements found in the injured knee are based on the relation- ship of the tear to the circumferential fibres (Dandy, 1990). A tear from the central edge running perpendicular to the fibres, as if defining their radius, is a radial tear. A rent through the body of the meniscus running parallel to the fibres is a longitudinal tear. A split in the body of the meniscus that begins at the central edge but runs parallel to the tibial surface is a horizontal tear. Other descriptive terms supersede for tears that combine features of these three patterns; a tear that begins radially then extends longitudinally becomes aflap tear while a longitudinal tear that permits a large portion of the meniscus to become displaced while still anchored at each end of the tear is a bucket handle. However, such simple patterns are seldom found in knees being arthroscoped because they present a dilemma to the rheumatologist (Figure 4b). Yet, damage to menisci can result from processes other than major joint trauma, such as the altered biomechanics and repetitive microtrauma underlying OA (Ike, 1993a) or the direct and
(a)

506 R. W, 1KE
(b)
(c)

DIAGNOSTIC ARTHROSCOPY 507
(a)
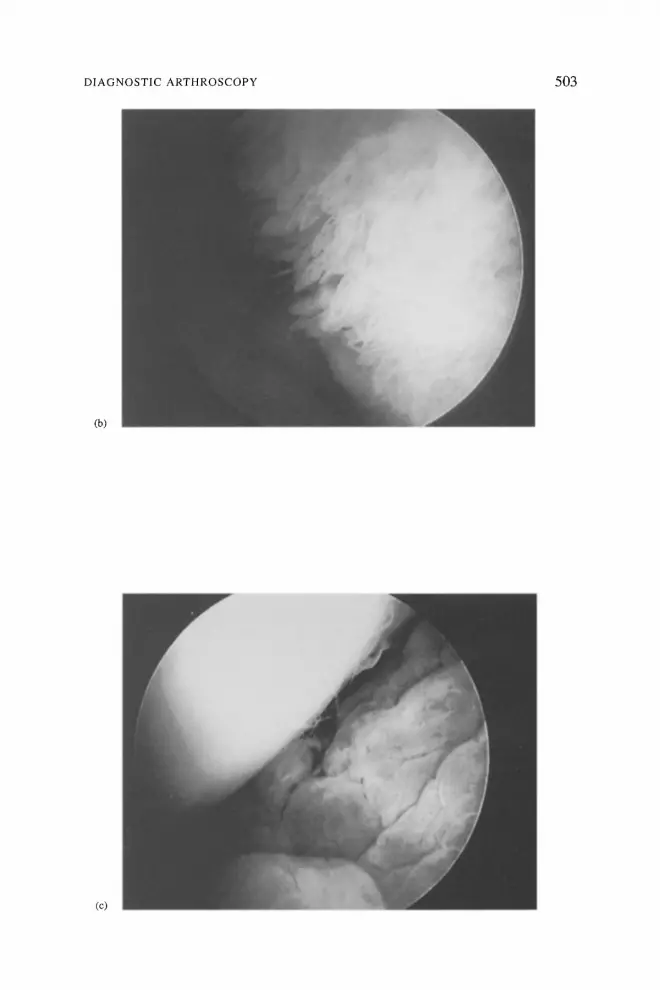
Figure 4 (see also pages 505 and 506). Examples of cartilage findings at arthroscopy. (a) Normal left knee femoral condyle, medial meniscus (posterior horn), and tibial plateau. (b) Complex tear of the medial meniscus, posterior horn; adjacent surfaces of femur and tibia are worn nearly to bone (seen in a middle aged man with left knee pain and bland effusion that had not responded to conventional medical therapy, including several intra-articnlar glucocorticoid injections). (c) Cartilaginous loose body being retrieved from posterior portion of medial tibiofemoral compartment in right knee of 36- year old man with recurrent knee locking and mild radiographic OA. (d) Extensive disruption of meniscus and extensively worn hyaline cartilage in lateral tibiofemoral compartment of 55-year old woman with refractory pain and swelling; X-ray showed only slight lateral joint space narrowing but no ehondrocalcinosis; note calcinosis of fibrocartilage (arrows at 9 o'clock) and hyaline cartilage (arrows at 7 o'clock); fragment of meniscus being removed with grasping forceps; synovial fluid was non-inflammatory and contained no crystals on polarized light microscopy.
indirect effects of chronic synovitis (Salisbury and Nottage, 1985). Menisci thus altered can often contribute to otherwise poorly explained clinical features.
Because their traumatic disruption is a major insult for which later repair is feasible, the eruciate ligaments are structures of major interest to the orthopaedist doing arthroscopy. The anterior cruciate spans the inter- condylar notch from the anterior horn of the medial meniscus to a posterior portion of the lateral femoral condyle The posterior cruciate is more difficult to see, although smaller 'needle' scopes that can be directed just medial to the posterior horn of the lateral meniscus, where the PCL originates, can see it easily. The cruciates may be obscured when invaginated by inflamed synovium. Chronic synovitis in the region of the cruciates can lead to weakening of the ligaments and eventual spontaneous disruption or disappearance (Salisbury and Nottage, 1985). Finding a disrupted cruciate in an OA knee could provide a clue to pathogenesis of the OA (Kannus and Jarvinen, 1989). Surgery to repair or augment

508 R.W. EKE
disrupted cruciates in such situations has not been especially useful for the few cases in which it was tried (Shelbourne and Wilckens, 1993). However, certain components of a physical therapy programme might be emphasized for a knee with chronic cruciate insufficiency (Giove et al, 1983).
The only intra-articular tendon seen in the knee is that from the popliteus muscle, penetrating the posterior horn of the lateral meniscus en route to attachment on the distal femur. The tendon resides in a synovial sheath inferior to the meniscus, and can sometimes be a resting place for loose bodies.
A fat pad between the tibia and the inferior patellar tendon is penetrated by the arthroscope placed through conventional anteromedial and antero- lateral portals, and thus is often not seen. A large fat pad can extend to the inferior portion of the patellofemoral articulation, but can be seen regard- less of size by directing the scope from a superior peripatellar portal to the region anterior to the tibiofemoral articulations. Whether the fat pad can produce symptoms when deranged, inflamed or entrapped, as implied by descriptions from the pre-arthroscopy era (Hoffa, 1904; Smilie, 1963), has not yet been clarified by arthroscopy (Ogilvie-Harris and Giddens, 1994).
Arthroscopy can detect several other phenomena in the abnormal knee that other imaging methods often miss. Various types of debris can cloud the arthroscopic view unless removed by lavage (Mori, 1979). Removal of this debris may underlie the clinical improvement often observed in knee arthritis (especially OA) following arthroscopy in which no intervention other than lavage is performed (Burnam et al, 1934; Ayral et al, 1993; lke, in press). Some particles of debris can become too large to pass through the cannulae used for arthroscopy. Debris of cartilagenous origin can grow into chondromata and cause intermittent mechanical symptoms (Figure 4c) (Kay et al, 1989). Aforementioned 'rice bodies' can perpetuate knee swelling. Removal with grasping forceps and motorized shavers is a feasible, if tedious, exercise. Mineral deposits in cartilage and synovium can be seen by the arthroscope long before they become apparent on X-ray (Figure 4d). They range from the shiny white deposits of calcium salts (CPPD, apatite, oxalate) (Altman, 1976; Spiera et al, 1995) to the rare black discoloration from homogentisic acid in alkaptonuria (Lurie and Musil, 1984).
Finally, arthroscopy shows relationships between the various abnor- malities found. For example, an area of synovitis adjacent to focal cartilage ulceration on a weight-bearing surface would imply the latter as the primary process; conversely, cartilage softening or erosion in a non-weight- bearing area adjacent to an expanse of synovitis would implicate the synovitis as a primary process. Analysing patellofemoral tracking can reveal the cause of disrupted retropatellar cartilage.
INTERPRETING ARTHROSCOPIC INFORMATION: WHAT DOES IT MEAN?
The orthopaedist uses information gathered at arthroscopy mainly to guide further surgical treatment, often delivered at the same setting although

DIAGNOSTIC ARTHROSCOPY 509
sometimes postponed when more extensive arthroscopic or open inter- ventions seem indicated (such as cruciate ligament reconstruction, meniscal transplantation, or joint arthroplasty). However, most rheumatologists do not currently consider integrating information from arthroscopy into their diagnostic or therapeutic reasoning. Nevertheless, several clinical situations encountered by rheumatologists present diagnostic uncertainties or therapeutic frustrations that can be allayed by arthroscopy. A paradigm has been developed (O'Rourke and Ike, 1994) that presents arthroscopic applications to situations classified according to whether or not the knee condition can be considered 'inflammatory' (based on synovial fluid characteristics), or whether a rheumatic disease diagnosis has been rendered for the overall condition in which the knee problem has arisen. A fifth category was spun off from the 'inflammatory' arm of the paradigm for situations characterized by acute pyarthrosis, suggesting infection.
Arthroscopy is but one of several diagnostic imaging modalities that could be used to evaluate a perplexing knee. Choosing one to determine 'why does this knee hurt?' depends largely on which structures are suspected of being abnormal and causing pain. 'Pre-arthroscopic' compli- cations arise when diagnoses that cannot be established or treated by arthroscopy are neglected before choosing to arthroscope a problematic knee (Joyce and Mankin, 1983). Some, such as bursitis or tendonitis, can usually be established by physical examination. Others, notably osteonecrosis, can be confirmed only when suspicion is sufficient to seek the typical magnetic resonance imaging (MRI) features. Thus, careful consideration of the potential site(s) of pathology and the non-invasive tests that might be used to confirm or refute the anatomical diagnosis should occur before proceeding to arthroscopy.
Inflammatory arthropathies Whether involved in isolation, or with several other joints, the persistently inflamed knee for which no explaining diagnosis can be established provides an indication for arthroscopy and synovial biopsy. Unfortunately, diagnosis does not always ensue from the information obtained. Blocka and Sibley (1987) evaluated 38 patients with unexplained monarthritis (includ- ing 23 knees), and found that synovial tissue provided a diagnosis in just one case; a discrete diagnosis could be discerned in ! 1 other cases accord- ing to features discovered over time (e.g. sacroiliitis, rash, evolution of arthritis in other peripheral joints), and 16 cases persisted as unexplained monarthritis. Gibson et al (1985) established a diagnosis from synovial histopatbology in just 3 of 59 patients undergoing biopsy for knee monarthritis of unknown cause, finding one case each of tuberculosis, synovial chondromatosis, and pigmented villonodular synovitis. Closed- biopsy techniques failed to retrieve analysable synovial tissue in 6 of the 27 cases approached, whereas arthroscopic biopsy provided adequate tissue for all 32 cases in which it was used, illustrating that arthroscopically- directed synovial biopsy generally assures that an adequate amount of tissue will be obtained. Also, it assures that the tissue most likely to be

510 R.W. IKE
abnormal will be sampled. The variable distribution of abnormal synovium within the joint is well appreciated by experienced arthroscopists, but has not been extensively reported. Lindblad and Hedfors (1985) documented this variability, and found that macroscopic and microscopic features were strongly correlated. Hutton et al (1987), taking samples from the peri- patellar and tibiofemoral regions, found wide variability in intensity of inflammation from different sites. Finally, arthroscopy can demonstrate macroscopic features of synovium that can be diagnostic or highly suggestive of certain disorders (Table 1). The greatest utility of arthroscopy in this group of patients is its being able to detect chronic infection (e.g. tuberculosis, certain fungal infections, mycoplasma/ureoplasma species); hence, synovial specimens should be carefully stained and cultured using appropriate methodology to detect these organisms.
Knee symptoms sometimes persist in a patient with an established inflammatory arthropathy diagnosis despite conventional local therapy for the knee and adequate control of the systemic process. Potential causes of such symptoms include refractory local inflammation, intra-articular abnor- malities consequent to prior synovitis, or a combination of phenomena. Only some of these features dictate major operative intervention, with extensive bulky synovitis calling for synovectomy and widespread loss of articular cartilage identifying total joint arthroplasty as the only operation likely to relieve pain. Other problems have less drastic solutions. 'Rice bodies' can contribute to otherwise refractory joint swelling, and are removed by lavage. Several investigators have observed that pain and swelling diminish following needle arthroscopy (Wei et al, 1993; Sharma et al, in press), most likely as a result of the removal of intra-articular debris. Synovitis can persist focally, ranging from a small area that drives fluid- phase inflammation (and production of 'inflammatory' synovial fluid) to a mass collection that periodically interferes with joint motion (the 'synovial internal derangement') (Dorfmann, 1985); abnormal tissue can sometimes be removed by instruments used for biopsy. Finding that synovitis is very sparse or absent argues that local measures such as intra-articular cortico- steroids should not be continued. Attenuation or destruction of other intra- articular structures (e.g. ligaments, menisci) is addressed by tissue resection only when the remaining portion interferes with joint motion. Otherwise, modification of activities and a re-emphasis on physical therapy follow. Finally, synovial samples should always be cultured to detect the occa- sional case of indolent infection, to which such patients are predisposed (Hortas et al, 1988).
Bacterial septic arthritis needs to be considered in any patient with an acute pyarthrosis. Indeed, acute septic arthritis is the one clinical situation in which urgent arthroscopy may be justified (Smith, 1986); prudent practice, however, would dictate that more conservative measures (appro- priate antibiotics with repeated arthrocenteses), which are usually effective, be used first. Diagnostic arthroscopy is useful in those patients with suspected septic arthritis but negative synovial fluid cultures, as can occur in up to 15% of cases (yon Essen and Holtta, 1986). In such patients, arthro- scopically directed synovial biopsy for culture either leads to a diagnosis or,

DIAGNOSTIC ARTHROSCOPY 511
Table 1. Characteristic features of synovium in selected rheumatic diseases.
Diagnosis Macroscopic features Microscopic features
Crystalline diseases Calcium pyrophosphate disease Gout Hydroxyapatite arthropathy
Calcific deposits Refractile urate deposits Calcific deposits
lnJectious arthritis Bacterial and fnngal Adhesions, necrotic
synovium, cartilage discoloration
Chronic borreliosis (Lyme disease) -
Filiariasis Guinea worm Tuberculosis
Infiltrative diseases Amyloidosis
Fabry's disease
Inflammatory arthropathies Beh~et's disease Synovial 'slough' Post-venereal reactive
(Reiter's syndrome) Systemic lupus erythematosus
Malignancy Primary (e.g. synovioma) or
metastatic, leukaemia, lymphoma
Metabolic arthropathies Haemachromatosis
Ochronosis Black pigment, shards
Synovial disorders Pigmented villonodular synovitis (as name describes)
Synovial chondromatosis Cartilage in synovium
Other Haemangioma
Foreign body (e.g. plant thorn)
Multicentric reticulhistiocytosis -
Sarcoidosis Whipple's disease
Calcium pyrophosphate crystals Monosodium urate crystals Hydroxyapatite crystals (electron
microscopy); globular calcium- containing deposits (Von Kossa, Alizarin S stains)
Organisms; intense polymorpho- nuclear infiltrate
B. burgdorferi spirochete (silver stain)
Caseating granulomata with acid-fast bacilli
Amyloid deposition (Congo red stain)
Foam cells in vessel walls
Chlamydial bodies (with special immunofluorescent agents)
Haematoxylin bodies
Malignant ceils
Blue hue predominantly of synovial lining cells (due to iron deposition)
Fragments of pigmented cartilage
Villous hypertrophy with hemosiderin and giant cells
Islands of metaplastic cartilage
Excessive (often irregular or cavernous) blood vessels
Birefringent plant material; granulomatous reaction
Histiocytes and mulfinucleated giant cells
Noncaseating granulomata Periodic acid Scbiff-positive
macrophages
Reproduced from O'Rourke and lke (1994, Rheumatic Diseases Clinics of North America 20: 321-342) with permission.

512 R.W. IKE
if negative, identifies the case as 'pseudoseptic' and spares the patient prolonged hospitalization, unnecessary parenteral antibiotics and repeated drainage procedures. The latter clinical situation can occur in a patient with an established inflammatory arthropathy, e.g. rheumatoid arthritis or a spondyloarthropathy (Singleton et al, 1991; Ho, 1994, who presents with the sudden onset of monarthritis with purulent synovial fluid, resembling acute bacterial septic arthritis, but has culture-negative synovial fluid and synovium, bland chronic synovitis on arthroscopic inspection, and lacks macroscopic features (fibrinous adhesions, yellowing of articular cartilage, friable synovium) that would suggest bacterial infection.
Arthroscopy can be used to treat established bacterial septic arthritis when clinical features dictate the need for more extensive drainage than can be provided by repeated arthrocenteses. An OR environment might be required when extensive resection of fibrous adhesions and prolifera- tive synovium is necessary, as in cases where initiation of treatment has been delayed. However, closed lavage less extensive than that delivered at needle arthroscopy can provide effective drainage in some cases (Ike, 1993b) and needle arthroscopy with limited tissue removal has been described as effective in other cases (Moreland et al, 1995). Occasion- ally, culture-negative inflammatory effusions persist long after bacterio- logical 'cure', probably as a persistent synovial response to non-viable bacterial remnants (J/irvinen et al, 1990). Arthroscopy can identify this situation as non-infectious, and sometimes direct the removal of focal synovitis.
'Non-inflammatory' arthropathy The painful knee with non-inflammatory synovial fluid and normal X- rays often prompts a search for some sort of offending 'internal derange- ment', even when no traumatic event has occurred. Of the various intra-articular pathologies that might be detected, most are not amenable to surgical correction. The common practice of using MRI to detect deranged menisci or ligaments before proceeding to operative arthroscopy (Ruwe et al, 1992; Gluckert et al, 1992; Hutchinson and Wojtys, 1995) assigns undue weight to abnormal meniscal signals, which can be found in asymptomatic knees (Negedank et al, 1990; LaPrade et al, 1994), while ignoring pathologies that might be missed by MRI. Most important ,among these are various forms of primary synovitis that begin focally and initially produce 'non-inflammatory' fluid, and softened fibrillated weight- bearing cartilage ('early' OA). In addition, mineral salt deposits can sometimes be found in synovium or cartilage before they become evident in synovial fluid or X-rays (Spiera et al, 1995). Occasionally, no abnor- malities can be detected. Long-term prognosis for such cases is excellent as regards function, although symptoms persist for some (Mariana et al, 1987: Schlepckow et al, 1994). For all the aforementioned possibilities, it is far more feasible to minimize patient expectations for clinical improvement from the procedure when arthroscopy with diagnostic intent is done away from the OR.

DIAGNOSTIC ARTHROSCOPY 513
Osteoarthritis
When X-rays show osteophytes and joint space narrowing, OA is diagnosed. For the OA knee with only mild or moderate X-ray features, arthroscopy, usually with 'dtbridement', has become a popular intervention for those cases which have not responded to conventional medical therapy (Burks, 1990). However, controlled studies have failed to demonstrate a benefit from dtbridement beyond that achieved with lavage (Alistair Gibson et al, 1992; Moseley et al, 1996), sometimes delivered without an arthroscope (Chang et al, 1993). Many symptomatic OA knees harbour meniscal abnormalities (/ke, 1993a), but which types should be resected remain to be determined. Thus, using needle arthroscopy to inspect and lavage the otherwise troublesome OA knee provides one component of arthroscopy agreed to be therapeutic on occasion (lavage) while avoiding more extensive operative interventions of dubious value. Not infrequently, finding that hyaline cartilage pathology is more extensive than a clinical and radiographical assessment had predicted expedites consideration of total joint arthroplasty.
DIAGNOSTIC ARTHROSCOPY'S FUTURE: WHAT'S NEXT?
Since the pathologies of rheumatic disorders are expressed in many joints other than the knee, arthroscopic detection of these features would seem to be a logical goal for expansion of rheumatologic diagnostic capabilities (Ike, 1994b). Many joints besides the knee have been arthroscoped with therapeutic intent, usually so as to perform arthroscopically adapted surgical interventions that had previously required open arthrotomy. The shoulder has drawn considerable interest, particularly as effective inter- ventions for chronic suprapinatus tendonitis due to impingement have been developed (Green, 1995). For the elbow and ankle, debridement procedures for arthritis have become popular (O'Driscoll and Morrey, 1992; Ogilvie- Harris and Sekyi-Otu, 1995). The ligamentous pathology of the wrist is well discerned by arthroscopy (Vanden Eynde et al, 1994). Unexpected soft tissue pathology, including loose bodies and fibrous bands, have been disclosed by hip arthroscopy (Villar, 1995). Bursae of the subacromial, olecranon, prepatellar, and infrapatellar regions have been arthroscoped (Verdonk et al, 1988; Kerr and Carpenter, 1990; Klein, 1996). The temporomandibular joint has drawn the interest of many oral surgeons, with lavage and debridement the goal of most interventions (Nitzan et al, 1990). While arthroscopy of the small joints of the hands and feet is feasible (Watanabe, 1985), only a few descriptions of therapeutics have appeared (Vaupel and Andrews, 1985; Wilkes, 1987; Declercq et al, 1994).
Perhaps the rheumatologist should approach this array of possibilities by focusing on simple joints commonly affected by rheumatic disorders, such as the smaller joints of the band and forearm. These joints are easily entered using the currently available 'needle' arthroscopes, a task that should become even easier as arthroscopes shrink further. When detection and

514 R.w. ~KE
differentiation of 'early' disease states becomes a more widespread clinical goal, it will be important to examine sites commonly affected by these diseases.
Significance of arthroscopic observations will be further extended when features of joint tissues examined with techniques from 'the bench' prove to have diagnostic or prognostic implications. Ongoing cooperation between arthroscopists and basic investigators should foster this eventuality. In the meantime, collaboration among those who arthroscope joints affected by various rheumatic processes should serve to bring about a common language by which these findings might be discussed, including the quantification of arthroscopic data when possible.
SUMMARY
Arthroscopy has served a diagnostic role for most of this century, but found widespread popularity only when operative interventions were coupled with the procedure. The untapped potential inherent in directly observing the pathoanatomy underlying various rheumatologic disorders is being unlocked by developments on several fronts that have taken arthroscopy away from the operating room environment. Information from arthroscopy can influence diagnosis and treatment in certain non-traumatic knee disorders, particularly when the cause of synovitis is not evident from other clinical features and when knee symptoms are accompanied by bland synovial fluid and X-rays that are normal or show only minimal changes of osteoarthritis. Other joints can now be arthroscoped, which may prove use- ful for rheumatological diagnosis and evaluation, particularly for the smaller joints of the upper extremity commonly affected in 'early' disease states.
REFERENCES
Alistair Gibson JN, White MD, Chapman VM & Strachan RK (1992) Arthroscopic lavage and dei3ridement for osteoarthritis of the knee. Journal of Bone and Joint Surgery 74B: 534-537.
Altman RD (1976) Arthroscopic findings of the knee in patients with pseudogout. Arthritis and Rheumatism 19: 286-292.
Arnold WJ (1992) Office-based arthroscopy. Bulletin of the Rheumatic Diseases 41: 3 4 . Ayral X, Dougados M, Listrat Vet al (1993) Chondroscopy: A new method for scoring chondropathy.
Seminars in Arthritis and Rheumatism 22: 289-297. Bircher E (1921) Die arthroendoskopie. Zentrablattfiir Clzirurgie 48: 1460-1461. Bird MDT & Sweet MBE (1987) A system of canals in semilunar menisci. Annals of the Rheumatic
Diseases 46: 670-673. Blocka KLH & Sibley JT (1987) Undiagnosed chronic monarthritis. Clinical and evolutionary profile.
Arthritis and Rheumatism 30:1357-1361. Burks RT (1990) Arthroscopy and degenerative arthritis of the knee: a review of the literature.
Arthroscopy 6: 43-47. Burman MS, Finkelstein FH & Mayer L (1934) Arthroscopy of the knee joint. Journal of Bone and
Joint Surgery 16: 255-268. Chang RW, Falconer J, Stulberg SD et al (1993) A randomized, controlled trial of arthroscopic surgery
versus closed-needle joint lavage for patients with osteoarthritis of the knee. Arthritis and Rheumatism 36: 289-296,

DIAGNOSTIC ARTHROSCOPY 515
Dandy DJ (1990) The arthroscopic anatomy of symptomatic meniscal lesions. Journal of Bone and Joint Surgery 72B: 628-633.
Declercq G, Schmitgen G & Verstreken J (1994) Arthroscopic treatment of metacarpophalangeal arthropathy in haemochromatosis. Journal of Hand Surgery 19B: 212-214.
Denti M, Arosio A & Trevisan C (1994) Comparison of 'catheter' and conventional arthroscopy in the diagnosis of knee derangements. A rthroscopy 10:6 l 4-617.
Dorfmann H (1985)Arthroscopic recognition of synovial disorders. Contemperary Orthopedics 10: 19-29.
Forouzesh S (1982) Closed synovial biopsy. Technique using Tru-Cut | disposable needle. Ortho- paedic Review 11: 139-140.
Geist ES (1926) Arthroscopy: preliminary report. Journal--Lancet 46: 306-307. Gibson T, Fagg N, Highton J e t al (1985) The diagnostic value of synovial biopsy in patients with
arthritis of unknown cause. British Journal of Rheumatology 24: 232-241. Glove TE Miller JM II], Kent BE et al (1983) Non-operative treatment of the tom anterior cruciate
ligament. Journal of Bone and Joint Surgery 65A: 184-192. Gluckert K, Kladny B, Blank-Schal A & Hofmann G (1992) MRI of the knee joint with a 3-D gradient
echo sequence. Equivalent to diagnostic arthroscopy? Archives of Orthopedics and Trauma Surgery 112: 5-14.
Green A (1995) Arthroscopic treatment of impingement syndrome, Orthopedic Clinics of North America 26:631-641.
Gronblad M, Korkala O, Liesi P & Karaharju E (1985) Innervation of synovial membrane and meniscus. Aeta Orthopaedica Scandinavica 56: 484-486.
Halbrecht JL & Jackson DW (1992) Office arthroscopy: a diagnostic alternative. Arthroscopy 8: 320-326. Ho G Jr (1994) Pseudoseptic arthritis. Rhode lsland Medicine 77: 7-9. Hoffa A (1904) Influence of adipose tissue with regard to the pathology of the knee joint. Journal of
the American Medical Association 43: 795-796. Homas C, Ferreiro JL & Galdo B (1988) Tuberculous arthritis of peripheral joints in patients with
previous inflammatory rheumatic disease. British Journal of Rheumatology 27: 65-67. Huff JP, Segueira W, Harris CA et al (1992). Survey of physicians doing office-based arthroscopy.
Arthritis and Rheumatism 35 (supplement): $292. Hutchinson CH & Wojtys EM (1995) MRI versus arthroscopy in evaluating knee meniscal pathology.
American Journal of Knee Surgery 8: 93-96. Hutton CW, Hinton C & Dieppe PA (1987) Intra-articular variation of synovial changes in knee
arthritis: biopsy study comparing changes in patellofemoral synovium and the medial tibio- femoral synovium. British Journal of Rheumatology 26: 5-8.
Ike RW (1993a) The role of arthroscopy in the differential diagnosis of osteoarthritis of the knee. Rheumatic Diseases Clinics of North America 19: 673-696.
Ike RW (1993b) Tidal irrigation in septic arthritis of the knee: a potential alternative to surgical drainage. Journal of Rheumatology 20:2104-2 l l 1.
]ke RW (1994a) Synovial biopsy using a manua/ly-operated rotary shaver blade: a low-cost technique for arthroscopically-guided and Closed approaches. Arthritis and Rheumatism 37 (supplement): $416.
Ike RW (1994b) Arthroscopy in rheumatology: a toot in search of a job (editorial). Journal of Rheumatology 21: 1987-1989.
Ike RW (1995) Arthroscopy: an outcome measure of synovitis? Rheumatology in Europe 24 (supple- ment 2): 134-138.
Ike RW (in press) Joint Lavage. In Brandt KD, Doherty M & Lohmander S (eds) Textbook on Osteoarthritis. Oxford: Oxford University Press.
Ike RW & O'Rourke KS (1993) Detection of intra-articular abnormalities in osteoarttaritis of the knee: a pilot study comparing needle arthroscopy with standard arthroscopy. Arthritis and Rheumatism 36: 1353-1363.
J/irvinen P, von Essen R & Nissil/i M (1990) Intraarticular osmic acid in postinfectious arthritis persisting after treated bacterial arthritis. Journal of Rheumatology 17: 1704-1706.
Jayson MI & Dixon AS (1968) Arthroscopy of the knee in rheumatic diseases. Annals of the Rheumatic Diseases 27:503-511.
Johnson DP, Eastwood DM & Witherow PJ (1993) Symptomatic synovial plicae of the knee. Journal of Bone and Joint Surgery 75A: 1485-1496.
Joyce MJ & Mankin HJ (1983) Caveat arthroscopos: extraarticular lesions of bone simulating intra- articular pathology of the knee. Journal of Bone and Joint Surgery 65A: 289-292.

516 R.W. IKE
Kannus P & Jarvinen M (1989) Posttraumatic anterior cruciate ligament insufficiency as a cause of osteoarthfitis in a knee joint. Clinical Rheumatology 8:251-260.
Kay PR, Freemont AJ & Davies DR (1989) The aetiology of multiple loose bodies. Snow storm knee. Journal of Bone and Joint Surgery 71B: 501-504.
Kerr DR & Carpenter CW (1990) Arthroscopic resection of olecranon and prepatellar bursae. Arthroscopy 6: 86-88.
Klein W (1996) Endoscopy of the deep infrapatellar bursa. Arthroscopy 12: 127-131. Kreuscher PH (1925) Semilunar cartilage disease: plea for early recognition by means of arthroscope
and early treatment of this condition. Illinois Medical Journal 47: 290-292. Kurosaka M, Ohno O & Hirohata K (1990) Arthroscopic evaluation of synovitis in the knee joints.
Arthroscopy 7:162-170. LaPrade RF, Burnett QM II, Veenstra MA & Hodgman CG (1994) The prevalence of abnormal
magnetic resonance imaging findings in asymptomatic knees. With correlation of magnetic resonance imaging to arthroscopic findings in symptomatic knees. American Journal of Sports Medicine 22: 739-745.
Lindblad S (1988) Recent progress in the study of synovitis by macroscopic and microscopic examination--a review. Scandinavian Journal of Rheumatology 76 (supplement): 27-32,
Lindbald S & Hedfors E (1985) Intraarticular variations in synovitis. Local macroscopic and micro- scopic signs of inflammatory activity are significantly correlated. Arthritis and Rheumatism 28: 977-986.
Lurie DP & Musil G (1984) Knee arthropathy in ochronosis: diagnosis by arthroscopy with ultra- stxuctural features. Jottrnal of Rheumatology 11: 101-103.
Mariani PP, Gigli C, Puddu G & Ferretto A (1987) Long-term assessment of negative arthroscopies. Arthroscopy 3: 53-55.
Martin RC, Brown DE, Zell B K & Lichtman DM (1989) Diagnostic and operative arthroscopy of the knee under local anesthesia with parenteral medication. American Journal of Sports Medicine 17: 436-439.
Moreland LW, Calvo-Al6n J & Koopman WJ (1995) Synovial biopsy of the knee joint under direct visualization by needle arthroscopy. Journal of Clinical Rheumatology 1: 103-108.
Mori Y (1979) Debris observed by arthroscopy of the knee. Orthopedics Clinics of North America 10: 559-563.
Moseley JB Jr, Wray NP, Kuykendall D et al (1996) Arthroscopic treatment of osteoarthritis of the knee: a prospective, randomized, placebo controlled trial. Results of a pilot study. American Journal of Sports Medicine 24: 28-34.
Negendank WG, Fernandez-Madrid FR, Heilbrun LK & Teitge RA (1990) Magnetic resonance imaging of meniscal degeneration in asymptomatic knees. Journal of Orthopedic Research 8: 311-320.
Nitzan DW, Dolwick MF & Heft MW (1990) Arthroscopic lavage and lysis of the temporomandibular joint: a change in perspective. Journal of Oral and Maxillofacial Surgery 48: 798-801.
Noyes FR & Stabler CL (1989) A system for grading articular cartilage lesions at arthroscopy. American Journal of Sports Medicine 17:505-513.
O'Driscoll SW & Morrey BF (1992) Arthroscopy of the elbow. Diagnostic and therapeutic benefits and hazards. Journal of Bone and Joint Surgery 74A: 84-94.
O'Rourke KS & Ike RW (1994) Diagnostic arthroscopy in the arthritis patient. Rheumatic Diseases Clinics of North America 20: 321-342.
Ogilvie-Harris D & Giddens J (1994) Hoffa's disease: arthroscopic resection of the infrapatellar fat pad. Arthroscopy 10: 184-187.
Ogilvie-Harris DJ & Sekyi-Otu A (1995) Arthroscopic debridemeut for the osteoarthritic ankle. Arthroscopy 11: 433-436.
Ogilvie-Harris DJ & Weisleder L (1995) Arthroscopic synovectomy of the knee: is it helpful? Arthroscopy 11: 91-95,
Popert A J, Scott DL, Wainwright AC et al (1982) Frequency of occurrence, mode of development, and significance of rice bodies in rheumatoid joints. Annals of the Rheumatic Diseases 41: 109-117.
Ruwe PA, Wright J, Randall RL et al (1992) Can MR imaging effectively replace diagnostic arthroscopy? Radiology 182: 335-339.
Salisbury RB & Nottage WM (1985) A new evaluation of gross pathologic changes and concepts of rheumatoid articular cartilage degeneration. Clinical Orthopedics and Related Research 199: 243-247.

DIAGNOSTIC ARTHROSCOPY 517
Schlepckow R Weber M & Hempel K (1994) Arthroscopy of the knee without pathological findings. Knee Surgery Sports Traumatology Arthroscopy 2: 85-87.
Schumacher HR Jr & Kula JP (1972) Needle biopsy of the synovial membrane, Experience with the Parker-Pearson technique. New England Journal of Medicine 286: 416-419.
Sharma A, Baethge BA, Acebes JC & Lisse JR (in press) Arthroscopic lavage in treatment of rheumatoid arthritis of the knee. Journal of Rheumatology.
Shelbourue KD & Wilckens JH (1993) Intraarticular anterior cruciate ligament reconstruction in the symptomatic at'thritic knee. American Journal of Sports Medicine 21: 685-688.
Singleton JD, West SG & Nordstrom DM (1991) 'Pseudoseptic' arthritis complicating rheumatoid arthritis: a report of six cases. Journal of Rheumatology 18: 1319-1322.
Small NC, Glogan AI, Berezin MA & Fafless BL (1994) Office operative arthroscopy of the knee: technical considerations and a preliminary analysis of the first 100 patients. Arthroscopy 10: 534-539.
Smilie IS (1963) Lesions of the infrapatellar fat pad and synovial fringes: Hoffa's disease. Acta Orthopaedica Scandinavica. 33:371-377.
Smith MJ (1986) Arthroscopic treatment of the septic knee. Arthroscopy 2: 30-34. Spiera RF, Mysler E, DiCarlo E & O'Brien SJ (1995) Diagnostic utility of small-bore arthoscopy and
guided synovial tissue biopsy in an academic medical center. Arthritis and Rheumatism 38 (supplement): $232.
Szachnowski P, Wei N, Arnold WJ, & Cohen LM (1995) Complications of office based arthroscopy of the knee. Journal of Rheumatology 22: 1722-1725.
Tagaki K (1933) Practical experience using Takatz's arthroscope. Journal of the Japanese Orthopedic Association 8: 132.
Vanden Eynde S, De Smet L & Fabry G (1994) Diagnostic value of arthrography and arthroscopy of the radiocarpal joint. Arthroscopy 10: 50-53.
Vaupel GL & Andrews JR (1985) Diagnostic and operative arthroscopy of the thumb metacarpo- phalangeal joint. A case report. American Journal of Sports Medicine 13: 139-141.
Verdonk R, Van Meirhaeghe J, Van Houcke H et al (1988) Shoulder bursoscopy. Acta Orthopaedica Belgica 54: 233-236.
Villar R (1995) Hip arthroscopy. Journal of Bone and Joint Surgery 77B: 517-518. yon Essen R & Holtta A (1986) Improved method of isolating bacteria from joint fluids by the use of
blood culture bottles. Annals of the Rheumatic Diseases. 45: 454-457. Watanabe M (1985) Arthroscopy of small joints. Tokyo: lgaku-Shoin. Wei N, Delauter SK & Eflichman MS (1993) Office knee arthroscopy: the first 100 cases,
Rheumatology Review 2: 151-158. Wei N, Delauter SK & Erlichman MS (1995) Office-based arthroscopy. Evolution of the procedure:
the second 100 cases. Journal of Clinical Rheumatology 1: 219-226. Wilkes LL (1987) Arthroscopic synovectomy in the rheumatoid metacarpophalangeal joint. Journal
of the Medical Association of Georgia 76: 638-639. Wilson AS, Legg PG & McNeur JC (1969) Studies on the innervation of the medial meniscus in the
human knee joint. Anatomic Record 165: 485-492. Yates DB & Scott JT (1975) Rheumatoid synovitis and joint disease. Relationship between arthro-
scopic and histologic changes. Annals of the Rheumatic Diseases 34: 1-6. Yates JW Jr (1993) Diagnostic office arthroscopy. Journal of the South Carolina MedicalAssociation
89: 329-331.





























