Embed Size (px)
Citation preview
SOMERSET NHS FOUNDATION TRUST/
YEOVIL DISTRICT HOSPITAL NHS FOUNDATION TRUST
PUBLIC BOARD MEETINGS HELD IN COMMON A Public meeting of the Somerset NHS Foundation Trust and Yeovil District Hospital NHS Foundation Trust Boards will be held in common on Tuesday 1 March 2022 at 9.00am by way of a Microsoft Team meeting – below the link.
Join on your computer or mobile app
Click here to join the meeting
If you are unable to attend, would you please notify Mrs Ria Zandvliet, Secretary to the Trust at Somerset NHS Foundation Trust by email on [email protected] Yours sincerely COLIN DRUMMOND MARTYN SCRIVENS CHAIRMAN SFT CHAIRMAN YDH ___________________________________________________________________
A G E N D A
9.00 1. WELCOME AND APOLOGIES FOR ABSENCE
Joint
2. QUESTIONS FROM MEMBERS OF THE PUBLIC AND GOVERNORS
Joint
3. TO APPROVE THE MINUTES OF THE SOMERSET NHS FOUNDATION TRUST’S PUBLIC BOARD MEETING HELD ON 1 FEBRUARY 2022
SFT Enclosure A
4. TO APPROVE THE MINUTES OF THE YEOVIL DISTRICT HOSPITAL NHS FOUNDATION TRUST’S PUBLIC BOARD MEETING HELD ON 2 FEBRUARY 2022
YDH Enclosure B
5. TO REVIEW THE ACTION LOGS AND MATTERS ARISING
Joint Enclosure C
6. TO NOTE THE REGISTERS OF DIRECTORS’ INTERESTS AND RECEIVE ANY DECLARATIONS OF INTERESTS RELATING TO ITEMS ON THE AGENDA
Joint Enclosure D
7. TO NOTE THE CHAIRMEN’S REMARKS
Joint Verbal
9.20 8. TO RECEIVE THE CHIEF EXECUTIVE AND EXECUTIVE DIRECTORS’ REPORT
Joint Enclosure E
9.30 9. TO RECEIVE THE BOARD ASSURANCE FRAMEWORK PROGRESS REPORT
YDH Enclosure F
PATIENT STORY
9.45 10. MATERNITY SERVICES – WOMEN REQUIRING EXTRA NURTURING (WREN)
Joint Verbal
PERFORMANCE ITEMS
10.10 11. TO RECEIVE THE GROUP BOARD OVERVIEW QUADRANT – JANUARY 2022
YDH
Enclosure G
10.35 12. TO RECEIVE THE QUALITY AND PERFORMANCE REPORT
SFT
Enclosure H
10.50 Coffee
11.00 13. TO RECEIVE THE FINANCE REPORT
SFT Enclosure I
STRATEGIC ITEMS
11.15 14. TO APPROVE THE MINEHEAD MINOR INJURY UNIT - PERMANENT CHANGE TO OPENING TIMES REPORT
SFT Enclosure J
11.30 15. TO RECEIVE THE STAFFING ESTABLISHMENT REPORTS
YDH Enclosure K
SFT Enclosure L
12.00 16. TO RECEIVE THE SIX MONTHLY FREEDOM TO SPEAK UP PROGRESS REPORT
SFT Enclosure M
12.15 17. TO RECEIVE THE OCKENDEN PROGRESS REPORT AND MATERNITY SERVICES WORKFORCE PLANS
Joint Enclosure N
12.30 18. UPDATE ON THE MERGER BETWEEN SOMERSET NHS FOUNDATION TRUST AND YEOVIL DISTRICT NHS FOUNDATION TRUST
Joint Verbal
12.40 19. TO RECEIVE A REPORT DEVELOPING AN INCLUSIVE CULTURE
YDH Enclosure P
INFORMATION
12.50 20. TO RECEIVE ASSURANCE REPORTS OF THE FOLLOWING BOARD COMMITTEE MEETINGS:
• Audit Committee meeting held on 27 January 2022 - Somerset NHS Foundation Trust
• Quality and Performance Committee meeting held on 26 January 2022 - Somerset NHS Foundation Trust
• Financial Resilience Commercial Committee - Yeovil District Hospital NHS Foundation Trust
SFT
SFT
YDH
Enclosure Q Enclosure R Verbal
21. FOLLOW UP QUESTIONS FROM THE PUBLIC AND GOVERNORS
Joint
22. ANY OTHER BUSINESS
Joint
23. RISKS IDENTIFIED
Joint
24. EVALUATION OF THE EFFECTIVENESS OF THE MEETING
25. ITEMS TO BE DISCUSSED AT THE CONFIDENTIAL BOARD MEETINGS The items presented to the Confidential Board are items which are in draft format; are in pre submission stage; are related to specific patients or colleagues; are commercially sensitive (e.g contracts); are for strategic discussion; are otherwise required to be presented to the Confidential Board, e.g. due to regulatory requirements (approval of annual accounts and Quality Accounts); or the publicity on which would be prejudicial to the public interest. Every effort will be made to present items to the Public Board meeting.
26. WITHDRAWAL OF PRESS AND PUBLIC To move that representatives of the press and other members of the public be excluded from the remainder of the meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest.
1.10 27. DATE FOR NEXT MEETING 3 May 2022
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 1 - A
SOMERSET NHS FOUNDATION TRUST
MINUTES OF THE PUBLIC BOARD OF DIRECTORS MEETING HELD ON 1 FEBRUARY 2022 BY MS TEAMS
PRESENT Colin Drummond Chairman Jan Hull Non-Executive Director (Deputy Chairman) Barbara Gregory Non-Executive Director Kate Fallon Non-Executive Director Stephen Harrison Non-Executive Director Alexander Priest Non-Executive Director Sube Banerjee Non-Executive Director Martyn Scrivens Non-Executive Director Peter Lewis Chief Executive Phil Brice Director of Corporate Services Pippa Moger Chief Finance Officer Hayley Peters Chief Nurse (from item 9) Andy Heron Chief Operating Officer (Mental Health, Families and Neighbourhoods) Matthew Bryant Chief Operating Officer (Hospital Services) (from item 9) Daniel Meron Chief Medical Officer (from item 9) David Shannon Director of Strategy and Digital Development Isobel Clements Chief of People and Organisational Development Shelagh Meldrum Chief Officer - Partnerships and Collaboration IN ATTENDANCE Fiona Reid Director of Communications Graham Hughes Non-Executive Director, Yeovil District Hospital NHS Foundation Trust Meridith Kane Medical Director for Acute Hospitals Ian Hawkins Lead Governor Kate Butler Deputy Lead Governor Anna Baverstock Consultant Paediatrician and Wellbeing Lead (for item 14 only) Laura Walker Head of Patient Safety and Learning (for item 12 only) Harriet Jones Head of Inclusion (for item 13 only) Janet Fallon Guardian of Safe Working (for item 15 only) Lorna Stewart Consultant Clinical Psychologist, Lead for Colleague Psychological Health (for item 20) Ria Zandvliet Secretary to the Trust
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 2 - A
1. APOLOGIES In view of the current services pressures, it was noted that Daniel Meron (Chief Medical Officer), Matthew Bryant (Chief Operating Officer (Hospital Services)) and Hayley Peters (Chief Nurse) would join the meeting as soon after its start as possible. The Chairman confirmed that the meeting was quorate. The Chairman welcomed Shelagh Meldrum to the Executive Team and to her first Trust Board meeting.
2.
QUESTIONS FROM MEMBERS OF THE PUBLIC/GOVERNORS There were no questions from Members of the Public or Governors.
3. MINUTES OF THE SOMERSET NHS FOUNDATION TRUST’S PUBLIC BOARD MEETING HELD ON 2 NOVEMBER 2021 Stephen Harrison proposed, Kate Fallon seconded and the Board approved the minutes of the Somerset NHS Foundation Trust Public Board meeting held on 2 November 2021 as a correct record with the following amendment:
• page two – Chairman’s Remarks – seventh line – to replace “was a wholly owned” with “is a wholly owned”.
4. MINUTES OF THE SOMERSET NHS FOUNDATION TRUST’S PUBLIC BOARD MEETING HELD ON 11 JANUARY 2022 Stephen Harrison proposed, Barbara Gregory seconded and the Board approved the minutes of the Somerset NHS Foundation Trust Public Board meeting held on 11 January 2022 as a correct record.
5. TO REVIEW THE ACTION LOG AND MATTERS ARISING The Board received the action log and noted that all actions had been completed. Martyn Scrivens and Barbara Gregory also asked for an invite to a future Mental Health Act Committee. Action: Ria Zandvliet.
6. TO NOTE THE REGISTERS OF DIRECTORS’ INTERESTS AND RECEIVE ANY DECLARATIONS OF INTERESTS RELATING TO ITEMS ON THE AGENDA The Board received the Register of Directors’ interest. The Board noted the following changes to the register:
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 3 - A
• Martyn Scrivens – to remove “Chairman of SSL” and “Non Executive Director of Retail Money Market Limited (trading as RateSetter);
• Phil Brice – to add – “Non-Executive Director of SSL”;
• David Shannon - to add “Director of YEP Project Co Limited”;
• Pippa Moger - to add “Director of YEP Project Co Limited” and “Member of the Southwest Pathology Services (SPS) Board”;
• Jan Hull – to add “Non-Executive Director Yeovil District Hospital NHS Foundation Trust”;
It was noted that the executive directors’ declarations will need to be amended to include their appointment as an executive director at both Somerset NHS Foundation Trust and at Yeovil District Hospital NHS Foundation Trust. Kate Fallon declared an interest in relation to agenda item 15 as the Guardian of Safe Working for Junior Doctors Progress Report had been prepared and will be presented by her daughter.
7. CHAIRMAN’S REMARKS The Chairman advised that his remarks will be covered as part of the agenda items.
8. CHIEF EXECUTIVE AND EXECUTIVE DIRECTORS’ REPORT The Chief Executive presented the report which was received by the Board. The Chief Executive highlighted the areas of good news, including the Mental Health Trust of the Year awarded by the Health Service Journal; the Our People Awards and the accreditation as a Veteran Aware Trust. He further provided an update on the mandatory vaccination requirement and operational pressures:
• mandatory vaccination guidance – the content of the report was correct at the time of writing, but the Trust was pleased to hear the announcement by the Secretary of State for Health on 31 January 2021 that the vaccination requirement for healthcare staff will be reviewed. The Trust had subsequently received a letter from NHS England/ Improvement (NHSE/I) advising all trusts to pause their mandatory vaccination related work. It was noted that the requirement had not been removed as yet due to the Parliamentary process to be followed. The Chief Executive highlighted the amount of work which had taken place to support colleagues and the significant issues which had been identified as part of this support work. It was
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 4 - A
stressed that the majority of these issues were not related to strong anti vaccination views but related to personal issues. It was noted that the vaccination requirement had resulted in instances of division between groups of colleagues and any instances of poor behaviours will be addressed. Work was also taking place on the need for civility, kindness and respect. The Chief Executive advised that a large number of communications had been received from colleagues and from external sources querying the vaccination requirement and the steps taken, and to be taken, by the Trust. If the vaccination requirement had remained in place, the Trust would have been unable to employ colleagues in front line roles from 1 April 2022 but every possible support would have been provided to these colleagues. Further guidance on whether the vaccination requirement will be permanently removed was awaited. The Chief of People and Organisational Development advised that she had met with a group of colleagues who had not been vaccinated and their stories about the reasons for not being vaccinated and the impact of the vaccination requirement on their lives had been difficult to hear. She asked the Board to recognise the impact of the vaccination requirement and discussions on some colleagues. The change in guidance had been welcomed but it was recognised that the stress could have a longstanding impact and wellbeing support will continue to be provided as required;
• operational pressures update – bed capacity continued to deteriorate and as of 24 January 2022, the system had, for the first time, been in OPEL 4 escalation. This escalation level reflected the system wide bed capacity and patient flow issues and this escalation level was supported by the regional team. The Chief Executive highlighted the patient flow issues and advised that, as at 24 January 2022, care homes had a total of 66 empty beds which could not be used due to previous Covid-19 cases in these care homes and the requirement to stop admissions for a 14 day period. The Chief Executive highlighted the impact the lack of bedded care and the resulting delay in being able to discharge patients had on other services, including on the emergency department. It was noted that on occasions there had been in excess of 20 patients in the emergency department waiting for a bed and this pressure was now also affecting ambulance handover times. By way of example of the increase in pressures, the Chief Executive highlighted that on 3 January 2022 68 patients across Musgrove Park Hospital (MPH) and Yeovil District Hospital (YDH) experienced a delay for intermediate care
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 5 - A
support and on 31 January 2022 this number had increased to 130 patients. Trying to manage the winter demand with a reduction of 13/15% in bed base was challenging. To manage these pressures, it had unfortunately been necessary to cancel some surgeries. The pressures had an impact on patients admitted to an acute bed whilst they would be better placed in an intermediate care facility, but also had an impact on patients who could not be admitted. These areas of risk were reflected on the Board Assurance Framework and on the Corporate Risk Register. The Chief Operating Officer (Mental Health, Families and Neighbourhoods) advised that one of the key reasons for the discharge flow issues was the reduction in the domiciliary care labour market and the resulting lack of domiciliary care packages required to be able to discharge patients. In addition, there was also a shortage of care home staff. It was noted that innovative solutions were being explored and the improvement in domiciliary care staff pay and conditions, as agreed by the County Council, were starting to make a positive impact. Incentive schemes had been put in place to temporarily reassign colleagues from within the Trust to provide domiciliary care services. The Chief Operating Officer (Mental Health, Families and Neighbourhoods) highlighted that many of the same pressures as seen in acute services were also experienced in mental health services. It was noted that between 22 to 29 patients over the last week experienced a delay in discharge due to lack of social care facilities, private provider or out of area placements.
The Board discussed the report and commented/noted that:
• a number of student nurses who had not been vaccinated would, under the guidance, not have been allowed to undertake clinical placements, but in view of the change in guidance, they will now be allowed onto clinical placements;
• the impact of the change in guidance on the infection prevention measures was queried. It was noted that the infection control (IPC) arrangements had been put in place to be able to manage a strain of Covid-19 which was no longer the dominant strain. The IPC arrangements were not as effective against the Omicron strain and it was expected that the IPC guidance will change. It was highlighted that an earlier alignment of the IPC guidance might have avoided some of the current operational pressures;
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 6 - A
• the pressures were not just experienced in Somerset but were experienced across the country and Martyn Scrivens highlighted his personal experience of pressures in other systems. He queried whether the bank of vaccinators were being encouraged to support domiciliary care services. It was noted that a letter had been sent to all vaccinators before Christmas asking for their support but from the 700/800 vaccinators, only seven responses had been received. Although this was a small number, these colleagues still make a big difference. It was noted that a further communication will be sent to vaccinators and an incentive scheme will be put in place covering the next 12 weeks;
• the report included an overview of Executive Directors lead roles and the Chairman asked for an overview of the Non- Executive Directors lead roles to be attached to the March 2022 report. Action: Ria Zandvliet
The Board thanked the Executive Team for their hard work in managing the pressures and supported the Executive Team in the actions to be taken to mitigate risks.
9. RISK MANAGEMENT REPORT, INCLUDING BOARD ASSURANCE FRAMEWORK AND CORPORATE RISK REGISTER
The Director of Corporate Services presented the 2021/22 Board Assurance Framework and Corporate Risk Register progress report which was received by the Board.
The Board discussed the report and commented/noted that:
• objective 4 – safe, sustainable, effective, high quality, person-centred support in the most appropriate setting – and objective 9 – levels of performance in line with operational plan – remained the objectives with the highest risks due to the impact of the lack of domiciliary care and bedded care services on inpatient flow and bed capacity;
• the current risk for objective 8 – developing a workforce – had increased to 12 in view of the staffing issues and the reduction in resilience;
• the clinical objectives had been reviewed by the Quality and Governance Committee and the Committee was satisfied that the focus on these areas was appropriate but recognised that the operational pressures, particularly on bed-based care was impacting on delivery of the strategic aims for moving care closer to home;
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 7 - A
• three risks on the Corporate Risk Register had been rated 25 and these related to the overall Covid risk, system finances and intermediate care. It was noted that these risks had been discussed in detail at the Quality and Governance and the Finance Committee meetings respectively;
• the Board Assurance Framework and risks on the Corporate Risk Register reflected the challenges the Trust was facing;
• it was queried whether the difficulties faced by primary care were reflected in the Corporate Risk Register. It was noted that a risk relating to the wider primary care services had been included and this risk will be further discussed at the April 2022 Board Development Day;
• it was queried whether system OPEL 4 escalation should be reflected in the Corporate Risk Register or whether this was part of a number of risks. The Chief Executive advised that the OPEL 4 declaration reflected the escalation of a number of risks and the escalation level in itself was not a risk but an attempted mitigation. He advised that a number of metrics were being developed which will set the threshold for standing down the OPEL4 system escalation. It was stressed that the declaration did not signal a change in risk appetite. It was further queried whether there were any consequences of an OPEL 4 system declaration. The Chief Executive advised that the system declaration was reflective of internal and external recognition of the difficult position the Somerset system was in and the declaration enabled actions to be taken in a way which would otherwise not have been possible. One example was communicating with the public how they could support the Trust with some of the discharge arrangements etc. The tangible differences were not that great but it enabled a level of focus and recognition which was helpful. The declaration also indicated that the system itself needed support and some systems were receiving military support;
• the Chief Operating Officer (Hospital Services) advised that the declaration signalled the challenges faced but also demonstrated to teams at the most senior level that the Trust was listening and understood the gravity of the issues faced in all services. It enabled actions to be implemented at a greater speed and examples included requests for staff to work in domiciliary care for a certain number of weeks. The declaration recognised the level of risks not felt before and these risks impacted on the whole health and social care system. Work was taking place on a system wide basis to address the challenges faced;
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 8 - A
• it was queried what the hospital flow risks for patients were. The Chief Executive advised that there were a number of risks across the system as providers were unable to deliver care for every patient in the right place at the right time and a co-ordinated response was essential. The balance between the patient risks was assessed on a regular basis but not sufficient solutions were available to mitigate all risks. Holding three risks with a risk scoring of 25 was an unusual situation and this level of risk was not acceptable;
• the risks had been discussed at the recent Quality and Governance and Audit Committees and the Committees had acknowledged that the Board had recognised the enormous amount of work taking place whilst continue to deliver business as usual. One of the difficulties was that many of the factors influencing the position were external factors and this required actions on a system wide basis;
• the Chief Executive advised that it will be helpful to have a system wide communication to patients, families and other members of the public setting out the pressures and reasons for the pressures as it was not felt that the reasons were fully understood by members of the public;
• it was commented that the term OPEL 4 was not an outward facing term as members of the public did not understand this term. The term was part of an internal audit process and showed the seriousness and complexity of the challenges faced. There was the potential for a catastrophic incident with demonstrable harm to a patient which may not have occurred if the system had worked better together. The Chief Executive commented that the risk of a catastrophic incident was higher because of the current pressures but there could also be an adverse impact on other cohort of patients which may not be catastrophic but will still impact on the quality of patients’ life, e.g. by cancelling surgery, long waiting lists or patients not presenting for care, and these risks were less tangible and measurable;
• the Chief Operating Officer (Hospital Services) advised that population health will need to be a key area of focus going forward and the long term and intermediate care impact on patients will be an important aspect as part of that work;
• the Chief Nurse advised that delays in treatment will cause harm and e.g. patients not being able to access stroke care in a timely way can cause harm. Good teams and governance frameworks were in place to scan across all specialties to identify the deterioration of outcomes overall and to keep close oversight on patients at higher risk. Doubling patients up
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 9 - A
increased patient safety risks and although mitigation actions were being taken, this was still an area of high risk. The Chief Nurse highlighted the morale injury to clinical colleagues who carried the risk and who may have to work in less than ideal circumstances;
• in terms of risks, there were a range of risks, including patient experience, outcome and patient safety risks. In terms of patient safety risks, the balance was shifting in the wrong direction and, from a population perspective, the outcome was affected.
The Chairman advised that one of the key themes identified from the discussion related to communications with the public on a countywide basis so that members of the public know what the position is and how they can help by presenting in the right place for their needs. A further theme related to the need to support colleagues and this already had a high focus. The final theme was the need to work with local communities and although good progress was already being made, there was the potential to do more and mitigate risks at a granular level. It was recognised that there was a need to focus on areas with the highest risk.
The Board acknowledged the ongoing impact of the pandemic on services and colleagues and the pressures faced across the system.
10. QUALITY AND PERFORMANCE REPORT The Chief Finance Officer presented the report which was received by the Board. The Board noted the continued significant impact of Covid-19 on a range of access standards but also noted the areas in which performance had been sustained or notably improved. The Board discussed the report and commented/noted that:
• the reference to areas of good performance was welcomed;
• out of area placements – the graph was showing the number of patient days out of county and it was queried whether this could be reflected in a different way to avoid large variations due to the small number of patients involved. It was noted that the Trust was required to report performance on the basis of patient days and compared to neighbouring organisations, the Trust performed really well in terms of out of area placements;
• IAPT – it was queried whether the profile of patients accessing IAPT services had changed over the last two years. It was noted that detailed information was not to hand but it was expected that the profile had changed;
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 10 - A
• four of the 11 risks shown in the covering report related to staffing and three risks to capacity and it was queried whether the capacity risks also related to staffing. If related to staffing, it was suggested to be consistent in terms of referencing. It was noted that the risks as set out in the covering report reflected the wording on the Corporate Risk Register;
• finance performance – performance was monitored on an in-year basis only and both the Finance and Audit Committees had agreed that this was appropriate in view of the short planning horizons;
• mental health service performance overall was holding up well and the Board acknowledged this good performance;
• a number of indicators, e.g. falls, IAPT, cancer waits, in totality indicated an increase in harm but it was recognised that this was a complex picture. This will need to be further discussed at the next Quality and Governance Committee meeting to ensure that the Committee received assurance that everything possible was being done to understand the risks of harm and implement mitigating actions;
• the increase in cancer referrals was expected to be related to later presentation by patients and a backlog in primary care services. This was a population risk on which there was less clarity.
The Board agreed that performance remained challenging but also recognised the positive developments and actions taken to address the challenges where possible. The Board thanked the Executive Team for their dedication and commitment and thanked them for the actions taken to address the challenges faced.
11. FINANCE REPORT The Chief Finance Officer presented the report which was received by the Board. The Board noted that the finance report had been discussed at the recent Finance Committee meeting. The Board discussed the report and commented/noted that:
• the position as at 31 December 2021 showed a breakeven position in line with the plan for the period October 2021 to March 2022. It was anticipated that the forecast break even position as at 31 March 2022 will be delivered;
• the cost improvement programme for the period October 2021 to March 2022 required cost savings to the value of £8.4 million and £1.397 million savings had been delivered in month. The
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 11 - A
Board was assured that sufficient schemes had been identified to deliver the cost savings requirements for the remainder of the year;
• the capital programme was behind plan and this was due to a number of factors, including supply chains issues, workforce involved in the delivery of the schemes affected by Covid-19 and delays in building works. This position had been discussed in detail at the recent Finance Committee meeting. It was noted that the Trust had received additional capital funding for 2021/22 but due to the late notice of this funding, it will be challenging to spend the allocation. All possible efforts were being made to spend this additional funding as well as progress the capital programme, but it was noted that there was a risk of underspending on the capital programme. Particularly the AAH and Surgical Centre schemes were affected by the supply chains issues and a formal request had been made to the Department of Health and Social Care to delay the drawdown of £1 million for each of the schemes. Confirmation had not as yet been received;
• the majority of the planning guidance for 2022/23 guidance had been received on 24 December 2021 but some of the detailed financial guidance, particularly relating to the elective recovery funds, was still awaited. The guidance was currently being reviewed and a paper setting out the implications of the guidance will be presented to the February 2022 Finance Committee meeting. It was noted that a draft plan will need to be submitted on 17 March 2022 with the final plan to be submitted on 25 April 2022. Delegated authority for financial plan sign off by the Finance Committee will be requested at the March 2022 Board meeting;
• media announcements indicated that the New Hospital Programme had been oversubscribed and it was queried whether the Trust had received confirmation of funding. The Director of Strategy and Digital Development advised that the Trust was placed in cohort 4 of the existing New Hospital Programme. The business case had been signed off by the Board and submitted to the regional team. The business case was currently subject to the regional review process. Confirmation had been received that the Trust was placed in cohort 4 but decisions on the priorities within that cohort had not yet been made. In relation to the oversubscription of bids, this related to eight additional schemes in the next cohort and it was expected that a longlist for that cohort will be announced in the next few weeks;
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 12 - A
• it was queried whether the capital slippages will put pressure on capital scheme funding for 2022/23. The Director of Strategy and Digital Development advised that where slippage had been identified, every effort had been made to move projects scheduled for 2022/23 forward into 2021/22. The key financial risk related to externally funded schemes and this equated to a total value of £2 million.
12. QUARTERLY LEARNING FROM DEATHS FRAMEWORK: MORTALITY REVIEW PROGRESS REPORT Laura Walker, Head of Patient Safety and Learning, joined the meeting and presented the report which was received and noted by the Board. The Board discussed the report and commented/noted that:
• the Care Quality Commission had previously commented on the need to disseminate learning and considerable progress had been made in ensuring that learning was identified and disseminated. The examples of learning captured as well as the discussions at the Board and Quality and Governance Committee meetings showed the significant improvements made to the process;
• the last few months had been very challenging and Laura Walker extended her thanks to all teams for maintaining their mortality reviews, Learning for Deaths meetings, commitment to learning and engagement with the 72 hour reporting process;
• the HSMR coding issues were understood but it was queried how other, non integrated, trusts would manage mortality in community hospitals. Laura Walker advised that mortality in community hospitals was not measured in the same way as in acute hospitals. Community hospitals had always carried out robust reviews of any deaths and this will continue. The Chief Medical Officer advised that community trusts did not use HSMR as this was only a useful benchmarking tool for large number of similar patients. Community hospital mortality was significantly lower than in acute services and the profile of patients cared for in community hospitals was different. More helpful indicators were the number of mortality reviews carried out, the percentage of deaths in community hospitals which had been reviewed by the Medical Examiner, and the level 2 reviews. These indicators will provide the necessary assurance. A further source of assurance were the deep dives carried out to look at higher than expected HSMR data for community hospitals and these deep dives had not identified any concern but had concluded that the variation was due to a different patient mix;
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 13 - A
• the Trust used a number of bedded care facilities outside of acute and community hospital inpatient services and this bed base did not have the same level of scrutiny and those patients were not as visible to the Trust. It will be important to understand the outcomes for patients in care homes. It was noted that HSMR took account of 30 day post discharge mortality but this was less visible for patients in care homes. It was noted that a deep dive into the outcomes for patients placed in care homes had been carried after the Covid-19 wave one and no identified harm had been identified. It will be helpful to carry out a further exercise in the near future.
The Board thanked Laura Walker and the team for the diligence with which the learning from deaths process is being undertaken. Laura Walker left the meeting.
13. DEVELOPING AN INCLUSIVE CULTURE PROGRESS REPORT, INCLUDING THE EQUALITY DELIVERY SYSTEM EDS SELF ASSESSMENT Harriet Jones, Head of Inclusion, joined the meeting. Harriet Jones presented the reports which were received by the Board. Harriet Jones further set out the inclusion journey: reflections and next steps and highlighted:
• the principles which included: building on progress to date; a new approach - systemic change; and increasing our impact;
• inclusion maturity, which showed the journey from one off events (cup cake events) to more inclusive cultures;
• systemic change – systemic change referred to changing the systems, policies, processes and cultures that create or maintain inequality (fixing the system). It was stressed that systemic change did not relate to changing the people to fit the existing system;
• the key WDES, WRES and EDs findings;
• the systemic approach for WDEs, WRES and EDS which included: in depth data analysis; recruitment review; focus on work place culture and behaviours; and accountability for inclusion.
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 14 - A
The Board discussed the reports and presentation and commented/ noted that:
• the inclusion maturity table was very powerful and it was felt that the Trust was rightly focussed on a more inclusive culture;
• the joint working with Emma Symonds at YDH, was welcomed;
• it was important to ensure that all levels of staff were better represented;
• inclusion was not just about the way we treat each other but inclusion should be at the heart of everything we do. Questions to ask were “what does access mean” and “what does it mean to attend outpatient appointments” but this will be difficult to grasp;
• getting a change in the tone of conversations will be key and it was expected that the systemic approach will enable this to happen;
• the conceptual framework was very good and there was real value in getting it right, both for colleagues and patients. An inclusive workplace culture for colleagues will be fundamental for good quality care;
• it will be essential to ensure that culture will be tangible and mutable so that I can be changed. By operationalising this, colleagues can see what their responsibilities are and make changes;
• the reference to BAME was felt to be dismissive as people were worth more than just a four letter acronym and this acronym should therefore not be used. Harriet Jones agreed that the use of the term BAME was not productive but the use of this term was a Workforce Race Equality Standard (WRES) requirement;
• good progress had already been made and there was a clear strategic overall picture of the current position and the aspiring position. There was a huge opportunity working jointly with YDH to bring teams together across both trusts and to look at culture through an inclusion lens. Harriet Jones advised that this will be the approach when looking at the integration of teams and policies;
• there was also considerable work to be carried out at Non-Executive Director and Board level. A number of development
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 15 - A
sessions had taken place and outcomes had been variable but it was essential to continue this work;
• both trusts had made considerable progress in this area and it will be important to retain the areas of good practice in each of the trusts and ensure that there will be appropriate rising levelling up;
• the Board itself was not a diverse group and the impact of this lack of diversity on the rest of the organisation should be considered, as well as the areas of positive influence and ways to further improve those areas. This challenge was welcomed and it was agreed to continue this Board development work.
The Chairman thanked Harriet Jones for the excellent presentation and inclusion work. The challenge for the Board to look at its own diversity and inclusion was welcomed. The Chairman commented that people with disabilities were less talked about whilst they were severely affected by a lack of inclusion and it was hoped that the Trust will be able to make progress in this area. The Board thanked Harriet Jones for her excellent work. Harriet Jones left the meeting.
14. COLLEAGUE EXPERIENCE – CIVILITY Anna Baverstock, Consultant Paediatrician and Wellbeing Lead, joined the meeting. The Chief of People and Organisational Development advised that February 2022 had been dedicated as the civility month and this provided an excellent opportunity to focus on civility at the Board meeting. Continued efforts will be made to ensure that colleagues had the right environment to work in and to develop this work jointly with Yeovil District Hospital NHS Foundation Trust. Although it was felt that the Trust had developed a listening and learning culture, there was still feedback that communication was not right at all times and civility can address some of the communication issues. Anna Baverstock provided some powerful examples of uncivil conversations and set out the impact of rudeness on the person on the receiving end, but also on other colleagues who were in the same room. From the examples given it was clear that the impact went deeper than the two colleagues involved and this could result in a reduction in performance and willingness of colleagues to help others. The impact of uncivil behaviour was visible through Freedom to Speak Up feedback and complaints and PALS. The impact of bullying and harassment nationally had been calculated in terms of productivity, absenteeism and litigation etc and amounted to £2 billion a year across the NHS for a trust our size approx £2million.
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 16 - A
Anna Baverstock advised that the civility work had focussed on the Civility Saves Life Project and some of this focus had been on raising awareness from a baseline of 70% to 100%. The aim was to extend this work over the next year. The Maternity Civility Project went further and looked at how colleagues spoke to each other. A civility workshop had been added as a mandatory training requirement for relevant colleagues and this had resulted in a reduction in the amount of incivility reported from 70% to 50%. This was very positive and the Trust had been invited to write up a case study for NHSEI. Anna Baverstock highlighted the take away messages that words matter and that conversations and communications witnessed set the tone of the organisation from the top. Feedback from the workshops was that colleagues will be braver and stand up for themselves and for colleagues. Following on from the workshops, cup of coffee conversations had been held and the conversations had resulted in a higher respect for others. The Board discussed the story and commented/noted that:
• the story was powerful and it was helpful to reflect on our own behaviours;
• a proportion of colleagues may be on the autism spectrum and it was queried whether actions could be taken to raise awareness of the issues faced by these colleagues and how they interact with other colleagues. Anna Baverstock commented that the key issue was that colleagues (and people in general) often did not truly listen to each other. Usually people listen to hear when they can interrupt and were not truly listening;
• it was queried whether awareness should be raised early on in careers. It was noted that conversations were taking place in medical schools but this could be further improved;
• communications also took place in non face to face ways and it was queried what actions were being taken in relation to non face to face communications and improving colleagues’ experiences. Anna Baverstock advised that e.g. emails were not the best way of communicating as only 55% of the message would come through as intended and in phone calls this was 75%. Personal contact was therefore still the best way of communicating. The Trust had a good coaching culture and one of the key things Anna Baverstock had learned as a coach was to consider WAIT (Why Am I Talking) and questioning whether my talking is interrupting thinking time. She strongly recommended coaching through the organisation;
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 17 - A
• an increase in training will be helpful, but it will be essential to start at the top and encourage colleagues from the bottom. Any negative feedback from the top will however negatively affect this work. Clinical leads will need to be supported as they will be critical in ensuring a successful implementation throughout the organisation. Anna Baverstock commented that when realising that someone had been perceived to have been rude, it was important to be able to apologise. As leaders it will be important to more proactively seek out any incivility to be able to learn and feel included;
• civility will need to be at the heart of our work and support environment for colleagues. This work was interrelated to the Freedom to Speak Up and inclusion work and brings the whole people culture and organisational development agendas together;
• it was suggested to develop a civility programme specifically for Non-Executive Directors and this will be taken forward as part of the Board Development programme.
The Chief of People and Organisational Development advised that a proposal for a Civility Board as part of the People Committee structure was being developed and will be presented to a future People Committee meeting. The Chairman thanked Anna Baverstock for the excellent story and for her work on civility. Anna Baverstock left the meeting.
15. GUARDIAN OF SAFE WORKING FOR JUNIOR DOCTORS PROGRESS REPORT Janet Fallon, Guardian of Safe Working, joined the meeting and presented the report which contained both annual and quarterly data. The Board received the report. The Board discussed the report and commented/noted that:
• the implementation of Janet Fallon’s previous recommendations and additional investment had resulted in positive changes and this was evident in the data presented;
• the majority of exception reports were still from the medical directorate and this was as expected in view of the expansion in bed base and pressures faced by all clinical teams;
• the report was based on exception reporting only and did not take account of areas of good practice;
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 18 - A
• the introduction of the Hospital at Night programme had resulted in a reduction in exception reporting from the surgical directorate and no immediate safety concerns had been identified by the surgical directorate;
• the approach to exception reporting will need to be reviewed across the Trust as exception reporting still had a negative connotation particularly amongst junior doctors. Exception reporting did not have a high focus in medical training and Janet Fallon was working with the Deanery, trainees and the BMA on developing an education module;
• an e-rostering solution for medical rotas was being developed;
• structural changes had been made to the junior doctors rotas and it was queried whether this had led to the required improvements. Janet Fallon advised that the main driver for structural change over the last 18 months related to safety at night particularly in the surgical directorate and evidence showed that the safety at night issues had been mitigated and no immediate safety concerns in relation to safety at night had been raised;
• Hospital at Night work was essential and this will need to continue as it supported both non medical and medical roles at night time. The Hospital at Night work had been very effective and focussing on the robustness of the team and how hospital at night work was delivered across the Trust will be important. This will be reviewed through the Hospital at Night Committee. The Hospital at Night work made a real difference for non medical roles and not just for hospital at night nurses and co-ordinators;
• there had been a lack of Allied Health Professional (AHP) support over the Christmas period and it will be important to continue to focus on how AHPs are contributing to the overall on call system and not just to Hospital at Night;
• the planned expansion of the foundation training programme was encouraging and this will lead to more foundation trust doctors in the trust over the next four years.
The Chairman thanked Janet Fallon for her commitment to the Guardian of Safe Working work.
16. ASSURANCE REPORT FROM THE PEOPLE COMMITTEE MEETING HELD ON 7 DECEMBER 2021 Stephen Harrison, Joint Chair of the People Committee, presented the report and highlighted the areas of assurance received and the areas
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 19 - A
of concern. He advised that the Committee had not identified any issues to be reported to the Board or other Committees and no new risks had been identified. Jan Hull, Joint Chair of the People Committee, commented that the risks and concerns in relation to workforce were well known and understood. She highlighted the colleague story which had provided real insight into the work of the community and primary care directorate in supporting the health and wellbeing of their teams. This story provided considerable assurance and the whole range and breadth of work was heartening to hear. She further commented that the amount of joint work already taking place between both trusts was encouraging. The Board received the report.
17. ASSURANCE REPORT OF THE QUALITY AND GOVERNANCE COMMITTEE MEETING HELD ON 24 NOVEMBER 2021 Jan Hull, Chair of the Quality and Governance Committee, presented the report and highlighted the areas of assurance received and the areas of concern. She highlighted the following issue to be reported to the Board:
• hospital flow and capacity. Hospital flow and capacity had been discussed earlier in the Board meeting and the Board was well aware of the hospital flow and capacity challenges. Jan Hull advised that the patient safety strategy had been discussed at the December 2021 Planning meeting. The strategies were already well developed across both trusts and a further update will be provided to the March 2022 Committee meeting. It was noted that the Committee had also received assurance about the outstanding Care Quality Commission action plan and the digital solution for resus trolley checks. The Board received the report.
18. ASSURANCE REPORT OF THE MENTAL HEALTH ACT COMMITTEE MEETING HELD ON 15 DECEMBER 2021 Alexander Priest, Chairman of the Mental Health Act Committee, presented the report and highlighted the areas of assurance received and the areas of concern. It was noted that the Committee did not identify any new risks but agreed that the delay in the LPS guidance and the impact on the timetable for developing systems to manage LPS processes and develop training for staff; and the Mental Health Act training uptake remained areas of risk.
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 20 - A
The Chairman thanked Alexander Priest for taking over as Chairman of the Committee and for the seamless transition. The Chairman further commented that the assurance reports were very important and provided the Board with significant assurance. He thanked all Committees for their excellent work.
19. UPDATE ON THE MERGER BETWEEN SOMERSET NHS FOUNDATION TRUST AND YEOVIL DISTRICT HOSPITAL NHS FOUNDATION TRUST The Director of Strategy and Digital Development provided a verbal update and advised that the full due diligence reports and the findings of the checkpoint review will be presented to Part B of the Board meeting. He advised that the operational pressures continued to impact on the delivery of programmes and in particular on the development of the patient benefits case. Six areas for the patient benefits case had been identified but it had been challenging to progress these cases to the degree as anticipated. It was noted that the new transaction guidance will be implemented from April 2022 and the draft version of the guidance indicated a significant increase in engagement expectations and this will need to be taken into account. The Chairman advised that good progress had been made in the face of the operational pressures and the level of due diligence so early on in the process was remarkable. The Board received the verbal update.
20. WELLBEING GUARDIAN PROGRESS REPORT Dr Lorna Stewart joined the meeting for this agenda item. Stephen Harrison, Non-Executive Director Wellbeing Guardian, and Lorna Stewart provided an overview of the wellbeing work and highlighted:
• the background and the nine NHS wellbeing principles. Some of these principles will be difficult to measure, e.g. health and wellbeing of NHS people. Work was taking place on all principles but some of the principles will be challenging to implement;
• the programme level impacts and the 9 Principles Framework – Principle 1. This set out the work being undertaken and the measurements and the framework will be further populated to reflect all principles;
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 21 - A
• health and wellbeing – the problem, vision, aim, the wellbeing wheel, driver diagram and measures. A wellbeing strategy had been developed in April 2020 and this had evolved over time to ensure that the strategy remained dynamic. The vision was to move from a “wellbeing informed” to a “wellbeing infused” organisation. The aim was to influence and embed a culture of colleague health and wellbeing in order to reduce colleague sickness absence from 4.34% to 3.99%. The strategy was based on the wellbeing wheel which consisted of eight key domains and these eight domains were also reflected in the driver diagram;
• the project-level impacts in terms of the colleague support service dashboard – process measures – referrals to the colleague support service; SFT referrals, non SFT referrals, referral reasons to CSS and referrals by type of job role. It was noted that the main reasons for referrals related to: anxiety, mental health concerns, workplace stress, low mood and depression;
• the project-level impacts in terms of the colleague support service dashboard – outcome measures – GAD-7 and PHQ-9 scores from referral to and discharge from CSS; thinking pitstop (initial feedback, initial training survey (30 respondents); support provided by the Colleague Support Line and estimated cost avoidance as result of the support provided;
• the programme-level impacts – Model Health System – Wellbeing and People Promise Compartments. The Wellbeing Compartment covered six key themes whilst the People Promise Compartment covered five themes. The Trust scored well against the peer median and national median comparators and the work of the Trust was used as an exemplar;
• the Somerset system-level impacts and the academic partnership with Dundee University. The Trust had been successful in a number of bids and had recently been awarded £304,000 for 2022/2023 as well as a further £680,000 non recurrent funding to be allocated by April 2022 but to be spend in 2022/2023. Although funding was being received, not all funding was recurrent and difficult decisions will need to be made in future years what work can be supported on a recurrent basis;
• the next steps. The Board discussed the presentation and commented/noted that:
• the presentation was very encouraging and welcomed and both Stephen Harrison and Lorna Stewart were commended on their
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 22 - A
commitment to the wellbeing work and the granularity of the data;
• it was clear from the presentation that a lot of work could be carried out jointly between the Trusts;
• the referral by job role indicated that doctor referrals were low. It was queried whether this was correct – would doctors be less affected by stress and strains than others? It was therefore queried whether doctors were actively encouraged to use the service. Lorna Stewart confirmed that doctors were more reluctant to come forward and access mental health services. Doctors wellbeing areas had been set up to provide dedicated space for doctors and other avenues to access support were being made available and this included capacity for private psychological support;
• the Board meeting had seen a high focus on civility, inclusion and wellbeing and this focus was welcomed and provided assurance to the Board that joint work was taking place with YDH and with (some of) the wider system. Further work was required in relation to working with primary care services;
• the work taking place within the trusts provided significant assurance but the uptake from other parts of the system was disappointing. It was noted that the uptake from other system partners was lower and this was due to a number of different factors. Primary care had its own funded workstream and have found ways of supporting themselves partly through national schemes. The transition from national to local schemes had not yet been made. In relation to other system partners, it was difficult to reach everyone in the system but leaflets and posters had been distributed. System partners included care home providers;
• the topic of wellbeing will be raised as part of the leadership walkrounds.
The Board provided its support to becoming a “wellbeing infused” organisation.
21. FOLLOW UP QUESTIONS FROM THE PUBLIC AND GOVERNORS There were no follow up questions from the Public or Governors.
22. ANY OTHER BUSINESS There was no other business.
Minutes of the SFT Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 23 - A
23. RISKS IDENTIFIED The Board did not identify any new risks which had not as yet been included on the risk register but noted that a number of the risks, as discussed as part of the Board Assurance Framework and performance management agenda items, had increased in intensity and longer term plans will need to be developed to manage these risks.
24. EVALUATION OF THE EFFECTIVENESS OF THE MEETING The Board agreed that the meeting had been very effective with open and honest discussions and a good and appropriate focus on civility, wellbeing and inclusion. The Committee assurance reports showed excellent links between the Board and the Committees and provided the Board with significant assurance.
25. ITEMS FOR DISCUSSION AT CONFIDENTIAL BOARD MEETING The Chairman highlighted the items for discussion at the confidential Board meeting and set out the reasons for including these items on the Confidential Board agenda. These reasons related to contract confidentiality; commercially sensitive items; and draft reports.
26. WITHDRAWAL OF PRESS AND PUBLIC The Board moved that representatives of the press and other members of the public be excluded from the remainder of the meeting having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest.
27. DATE FOR NEXT MEETING 1 March 2022
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 1 -
Page | 1
B
BOARD OF DIRECTORS DRAFT Minutes of the Part 1 Board of Directors Meeting held on
Wednesday 2 February 2022 via MS Teams at Yeovil District Hospital
Present: Martyn Scrivens Jane Henderson Graham Hughes Paul Mapson Jan Hull Peter Lewis Isobel Clements Phil Brice Matthew Bryant Andy Heron Shelagh Meldrum Daniel Meron Pippa Moger Hayley Peters David Shannon
Chairman Non-Executive Director Non-Executive Director Non-Executive Director YDH & Somerset NHS FT Non-Executive Director Chief Executive Chief of People and Organisational Development Director of Corporate Services Chief Operating Officer - Hospital Services Chief Operating Officer - Neighbourhoods, Mental Health and Families Chief Officer – Partnerships and Collaboration Chief Medical Officer Chief Finance Officer Chief Nurse Director of Strategy and Digital Development
In Attendance: Bernice Cooke Stacy Barron-Fitzsimons Paul Foster Samantha Hann Merry Kane Mark Robinson Julie Reeve Virginia Membrey
Deputy Director of Quality Governance and Patient Safety & Patient Safety Specialist [items 1 - 5] Director of Operations YDH Site Medical Director Corporate Governance & Risk Manager Medical Director for Acute Hospitals Head of HR & Organisational Development [item 9] Staff Governor [Observer] Public Governor [Observer]
Apologies: Stephen Harrison Somerset NHS FT Non-Executive Director
Ref: No: Action
1-101/ 2122
1 1.1
WELCOME AND APOLOGIES FOR ABSENCE Martyn Scrivens welcomed everyone to the meeting including the new Executive Directors, Staff Governor Julie Reeve and Public Governor Virginia Membrey who are attending as Observers. Apologies were received as noted above.
1-102/ 2122
2 2.1
DECLARATIONS OF INTEREST The register containing the declarations of interests from members (voting and non-voting) of the Board was noted. Samantha Hann advised further changes will be made to the register to split out the voting and non-voting members of the Board. Phil Brice confirmed the register will be updated and presented at the next Board meeting.
SH / PB
1-103/ 2122
3 3.1
3.2
MINUTES/ACTIONS OF THE PREVIOUS MEETING The minutes of the meetings held on 3 November 2021 and 15 December 2021 were approved as a true and accurate record. With regard to actions and matters arising, Martyn Scrivens confirmed all actions have been completed. There were no matters arising raised.
1-104/ 2122
4 4.1
EXECUTIVE DIRECTOR REPORT Peter Lewis advised the Executive Director report had been circulated within the papers. He highlighted to the Board the appointment of Andrew Prowse as the Director of Pharmacy across YDH and Somerset Foundation Trust (SFT) NHS
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 2 -
B
4.2
4.3
4.4
4.5
4.6
4.7
4.8
Foundation Trust. He advised Andrew Prowse has experience of working across two Trusts which will be beneficial. When asked by Jan Hull for confirmation Andrew Prowse would not be continuing in the Chief Pharmacist role at Dorset County Hospital, Peter Lewis confirmed Andrew Prowse would only be working for YDH and SFT. Peter Lewis highlighted the leadership change in maternity services following the retirement of Sallyann Batstone. He advised a new structure has been put in place with Sallyann King in the post of Interim Director of Midwifery. There will be two Heads of Midwifery (HoM), one in each Trust. The recruitment of the YDH HoM is currently underway. In relation to mandatory vaccinations, Peter Lewis said the Executive Director report is now out of date due to a national announcement on Monday 31 January 2022. He advised NHS England and NHS Improvement wrote to all NHS organisations to ask them to pause the process to move to mandatory vaccinations by April 2022 and not to terminate contracts for members of staff until further notice. He said it was important to recognise the strain this has put on some relationships between staff members and their managers and the need to ensure staff continue to be supported. He advised a team brief session was held across YDH and SFT on 2 February 2022 to discuss this change with staff across both organisations. Peter Lewis updated the Board on the significant operational pressures across all services within the System including; increased demand and acuity of patients; insufficient capacity to discharge patients to care homes due to Covid-19 outbreaks; an increase in the numbers of patients waiting for ongoing care support rising rapidly from the beginning of January to the beginning of February 2022; and cancellation of planned care patients. He said the Somerset System declared for the first time, a System wide Opel 4 status on 24 January 2022. He advised that for a System to declare Opel 4, the regional team must sign off and support this decision. Peter Lewis highlighted the impact on patient safety and patient experience due to the operational pressures and advised the consequences of this would be a theme throughout the reports presented to the Board. Martyn Scrivens highlighted the discussion that took place at the SFT Board of Directors on 1 February 2022 in relation to the operational pressures. He said it was extremely unusual for a System to report an Opel 4 status and it was important to understand the significance of this. Peter Lewis said it was important to recognise how challenged the position is both internally for YDH and externally for the System. He advised that Somerset had been managing emergency care services well but the move to an Opel 4 System status is a declaration that the Somerset System is no longer able to safely manage the situation due to the operational challenges. He said it is important for the public to be aware of the pressures within the System and for them to be supportive of any family members who would leave hospital and be discharged home. Andy Heron advised the Board that SFT and YDH have launched an incentive scheme for staff to put themselves forward to support in domiciliary care for a period of 12 weeks for staff within non-clinical roles who have care experience. He said within 24 hours, 31 members of staff have come forward, with 14 of those who immediately meet the eligibility criteria.
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 3 -
B
4.9
4.10
4.11
4.12
4.13
4.14
Jan Hull referred to the discussion which took place at the SFT Board of Directors on 1 February 2022 stating it was important for the Board to understand the increased risk and the associated patient harm relating to the operational pressures. She said this is reflected in the reports presented to the Board Assurance Committees and the Board of Directors. The Board recognised the serious risk of harm to patients as a result of the operational pressures. The Board discussed the importance of understanding the wider population risk and the longer term implications of the risk which needs to be assessed and mitigating actions put in place. The Board agreed there is a need to review the longer term acute bed capacity and discharge arrangements within the Somerset System. It was acknowledged the factors which had compromised domiciliary care including; demand from the community; workforce challenges; impact of the pandemic; and outbreaks, need to be reviewed and resilience developed to support in the longer term. When asked for an update in relation to the number of planned care operations being cancelled, Stacy Barron-Fitzsimons advised 40 had been cancelled within the previous 7 days, with the majority of these being non-urgent operations. She advised the Trust reports to the regional team when urgent and/or cancer treatment has been cancelled and before treatment/operations are cancelled, the teams undertake a harm review and if patients are at risk, mutual aid is sought. Matthew Bryant spoke of the steps taken to support domiciliary care market in the run up to Christmas. He advised the problem has now shifted to issues within bedded care with 103 patients in the Acute Trusts who await bedded care. He said progress has been made to commission more bedded care beds but the workforce issues within domiciliary care are increasing again. Matthew Bryant praised the staff at YDH stating they are going above and beyond to respond to the challenges of the operational pressures including being creative in identifying solutions to address the challenges. He said feedback from the regional team for YDH, SFT and the Somerset System is complementary on how they are handling the challenges. Martyn Scrivens agreed with Matthew Bryant and on behalf of the Board, thanked the YDH staff for the work they do in challenging circumstances. He said they are dedicated and their extraordinary commitment was being demonstrated on a daily basis.
1-105/ 2122
5
5.1
5.2
5.3
BOARD ASSURANCE REPORTS Quarter 3 2021/22 Infection Prevention and Control (IPC) Board Assurance Report (BAF) Martyn Scrivens welcomed Bernice Cooke to the meeting to present the Quarter 3 2021/22 IPC BAF updates. Bernice Cooke advised that version 1.8 of the IPC BAF was released on 24 December 2022 replacing version 1.6. She said there has been no information provided to Trusts on the changes made to version 1.7. She confirmed version 1.6 and version 1.8 have been provided in full to the Governance and Quality Assurance Committee (GQAC) on 27 January 2022 and the Board of Directors. Bernice Cooke advised the IPC BAF is a self-assessment tool completed by Trusts. She said the framework identifies ten key lines of enquiry which fall
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 4 -
B
5.4
5.5
5.6
5.7
5.8
5.9
5.10
5.11
5.12
under the headings of intent; implement; and impact. She praised the work of Yvonne Thorne, Deputy Director of Infection Control to complete the document and provide assurance to the Trust on the robust IPC processes and procedures in place to meet the key lines of enquiries. In relation to the changes to version 1.8, Bernice Cooke highlighted the updated policies and Standing Operating Procedures but said the main focus in the updated version is the use of the terminology ‘hierarchy of controls’ which is a well-used risk assessment framework used in health and safety. An explanation of hierarchy of controls was provided and the most effective measures at each stage explained. Bernice Cooke provided an overview of the processes and arrangements in place at YDH to provide assurance against each of the key lines of enquiries including; risk assessments frequently updated; ward configurations; bed moves and site management; decision making at daily Executive Huddles; and implementation of new guidance. Bernice Cooke spoke of the work of the IPC Team advising it is a small team, who are flexible and agile and ensure there is a 7 day service despite the size of the team. Bernice Cooke updated the Board on a number of ongoing actions including; the establishment of a ventilation group that has been set up to support the work on the wards as ventilation has been an issue for the Trust; approval from the trade union is awaited for the implementation of the new software programme that is required for the new cleaning standards; testing of staff and patients; training and audits continue; alignment of policies and procedures with SFT where possible; and a review of the use of screens in the bays on the wards. Merry Kane advised a decision had been made on 1 February 2022 to remove the screens as these reduce air flow. Martyn Scrivens thanked Bernice Cooke for the helpful slides providing a concise overview of the comprehensive IPC BAF. Jane Henderson asked whether IPC measures are adversely affecting patient flow to which Hayley Peters advised the IPC team work closely with the patient flow team to safely manage the risks. She reflected that the national policy is focused on treating the Delta variant of Covid-19 in unvaccinated patients and there has been a national call for a change in the guidance which would give Trusts the ability to manage arrangements locally with less restrictions. The Board advised assurance could be taken from the presentation at GQAC and the Board of Directors meeting. Hayley Peters on behalf of the Board thanked the IPC team for their continued work and their flexibility to provide a 7 day service despite being a small team of less than 3 whole time equivalent members of staff. Quarter 3 2021/22 Freedom to Speak Up Guardian Report Isobel Clements presented the Quarter 3 2021/22 report advising this had been reviewed in detail at the QGAC on 27 January 2022. She advised 14 concerns had been raised within the Quarter which was significantly higher than previous Quarters. However she did note YDH still report lower numbers of concerns when compared to national figures but it was encouraging to see the numbers increasing. Isobel Clements advised that Debs Matthewson, Freedom to Speak up Guardian, had described at GQAC that the Guardians felt that knowledge had
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 5 -
B
5.13
5.14
5.15
5.16
5.17
5.18
5.19
5.20
5.21
increased amongst staff and with the new reporting portal in place, staff were starting to feel more confident to raise concerns. She said Guardians use information available to them to triangulate information. Isobel Clements updated the Board on the work that continues between SFT and YDH Guardians to review concerns raised and identify common themes and trends and discuss actions that can be taken to address the concerns raised. Graham Hughes provided an observation following the discussion at GQAC to say it was encouraging staff are reporting their concerns and YDH are no longer an outlier. He said the work across SFT and YDH was evident by the information provided by Debs Matthewson. Jane Henderson said Debs Matthewson had advised members of GQAC that none of the concerns raised within the Quarter had been raised as whistleblowing concerns. She said assurance had been provided of the processes in place to manage whistleblowing concerns and due to the considerable pressures the organisation and staff are under, it was acknowledged that this increases the risk of whistleblowing concerns being raised. Martyn Scrivens said that based on previous staff survey results, staff have always indicated they feel able to speak up and raise concerns which has not been reflected in the Freedom to Speak Up quarterly reports. He said he felt that the concerns being raised now were in relation to the current challenges staff faced. Matthew Bryant acknowledged Martyn Scrivens’ point and said he felt the increase in concerns being raised was due to the pressures staff are under but also as the improvements within the service have been made, and staff are more knowledgeable about the work of the Guardians and reporting has been made easier, this also impacted on the numbers of concerns being report. He said he felt assured by the discussion at GQAC. Matthew Bryant said it was important for the Executive Directors to listen and act upon the rich source of information included within the concerns raised and make necessary improvements accordingly and focus more on the detail within the concerns and what this is telling the Executive Directors, than the number being reported. Quarter 3 2021/22 Learning from Deaths Report Merry Kane provided an overview of the Learning from Deaths report advising the Trust’s Hospital Standardised Mortality Ratio (HSMR) and Summary Hospital Level Mortality Indicator (SHMI) data is as expected when the Covid-19 data is removed. She advised she had discussed at the Board meeting in November when the Quarter 2 report had been reviewed the reason why the Trust was below expected when the Covid-19 data is included. In relation to the HSMI data, Merry Kane said the weekday data is within the expected range and the Trust is not an outlier but there has been a steep rise in the weekend figures. She said this is likely to be confounded by the issues with discharges. The Clinical Outcomes Committee (CLOC) are undertaking a deep dive review into a subset of weekend deaths to review the data and identify any trends. Merry Kane advised that there have been two Cumulative Sum (CUSUM) alerts within the Quarter which relate to: occlusion or stenosis of precerebral arteries
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 6 -
B
5.22
5.23
5.24
5.25
5.26
5.27
5.28
with 1 death recorded compared to an expected zero figure; and diagnostic endoscopic procedures on lower GI tract - 6 observed compared to an anticipated 1.9. She advised CLOC are undertaking a review of the notes and checking the coding reported. She said that the Quarter 2 CUSUM alert in relation to Diabetes Mellitus remains ongoing with the deep dive continuing into the diabetes data. Learning will be discussed at CLOC and disseminated accordingly across the Trust in due course. Merry Kane said that within Quarter 3, the Medical Examiners scrutinised 33% of all inpatient deaths, a reduction compared to previous quarters due to the retirement of the main Medical Examiner at YDH. She advised that recruitment has taken place and two replacements have been appointed which will improve the numbers of deaths reviews. In relation to Coronial activity, Merry Kane advised that there had been 9 new instructions relating to deaths in Quarter 3 and one from a death in a previous Quarter. She said the increase in case numbers is reflected across the County and to date, none of the new instructions have identified a lapse in care. Merry Kane advised there had been one inquest held in the quarter requiring Trust attendance. Following from the inquest, the Trust received a Regulation 28 Prevention of Future Deaths direction with actions required to improve access to pre-hospital clinical information. She advised this inquest had included YDH, SFT and other services for a mental health patient. She said the joint working between organisations was working well and being led by Katalin Fernando and Janet Ebdon. She confirmed an action plan had been submitted in conjunction with SFT as there was learning for both Trusts. Merry Kane confirmed there had been no patients with a learning disability die within the Quarter and no deaths which met the criteria for review using the Perinatal Mortality Review Tool (PMRT). Merry Kane advised it has been noted from discussions with junior doctors that due to sickness, absence and operational pressures, there has been a perceived reduction in senior support. She advised steps have been taken to remedy this. When asked by Graham Hughes whether YDH has recruited GPs into the Medical Examiner roles, Merry Kane confirmed the Trust has, which will support the service in the longer term when Trusts are required to review community deaths. Merry Kane advised there is no confirmed date when this will commence but the Trust is preparing for this. She highlighted her concern that the capacity and workload within the service will need to be closely monitored as the introduction of reviewing community deaths will significantly impact on the service. Martyn Scrivens asked whether resources could be shared across YDH and SFT, to which Merry Kane advised that the Trusts are already working together. Dan Meron thanked Merry Kane for providing an overview of the report. He commended the teams involved for the work they continue to do in relation to learning from deaths despite the operational pressures. He thanked the teams for the joint working arrangements already in place which are working well. He acknowledged the concern Merry Kane raised and noted it will be a challenge for the Medical Examiner service to be scaled up to include community deaths but the team are committed to delivering the full service. He spoke of the additional learning that will be identified when the Trusts do review community deaths and how this learning can potentially support decision making within the Acute Trusts.
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 7 -
B
5.29
5.30
5.31
5.32
5.33
5.34
5.35
5.36
5.37
Jan Hull advised SFT received feedback from the Care Quality Commission (CQC) a number of years ago that learning from deaths could be improved and she noted it was interesting this had come up in the recent due diligence work within the clinical governance workstream. She advised this was not noted as a risk but an opportunity to link up clinical areas and improve the processes in place for learning. She said this is an important piece of work to take forward and ensure there are robust arrangements in place for learning to be identified, shared and disseminated across the two Trusts. Jan Hull and Merry Kane said this would be an area for QGAC to closely monitor and to link this work with peer reviews and Getting It Right First Time (GIRFT) as these also contribute to learning. Dan Meron agreed and said this also links to the national strategic move to the implementation of the Patient Safety Incident Response Framework (PSIRF). He advised every provider needs to develop a PSIRF plan bringing together all aspects of learning in a strategic plan. Phil Brice advised the Clinical Governance and Patient Experience teams are developing the PSIRF plans. He said these plans will be brought together as some of the actions stretch to 2025. Graham Hughes said this is an area where the merger of the two Trusts will have clear benefits for the population of Somerset. Martyn Scrivens said he was struck by the number of times during the meeting there had been good examples of working together across the two organisations and the difference this was already making. Quarter 3 2021/22 Guardian of Safeworking Report Merry Kane advised this is the first report since the change in Guardian of Safeworking Hours in December 2021. She highlighted slide 3 which demonstrated how the numbers of exception reports have reached pre-pandemic levels. She said this had been expected due to exception reports mirroring the operational pressures. In relation to the themes within the exception reports, Merry Kane advised the trends are; working hours; immediate patient safety issues; inadequate senior service support available to doctors; educational opportunities; and patterns of work. She advised actions are being taken to address the concerns raised in the reports including; additional support in place with Senior House Officers and Registrars in place; middle tier rota in place for Surgery; new rota to have the staff on site 24/7; and recruitment to vacant posts within medicine. Merry Kane said the majority of the exception reports are reported by the junior doctors within General Medicine and General Surgery. She said the themes of the exception reports and the specialities reporting the majority of the reports, are the same not only at SFT but nationally. Paul Foster advised that previously educational opportunities have not been exception reported by the Junior Doctors as this would normally be reported back through the Deanery. He advised that the Trust is working with the Junior Doctors and Consultants to find a balance between ensuring all areas are adequately staffed and providing educational opportunities at a time of increased absence and significant operational pressures. Matthew Bryant said the Junior Doctors have been very flexible and risen to the challenge in difficult circumstances. He reflected that the issues raised at YDH are the same issues raised at SFT and it is important for plans, short, medium
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 8 -
B
5.38
5.39
5.40
5.41
5.42
5.43
5.44
5.45
and longer term, to be developed across both Trusts, forming part of business case to deliver 7 day service working, increase the medical workforce; and expansion of non-clinical roles to support the clinician workforce. He highlighted the role of the Physician Associate role in the Emergency Department and how well the role works. Merry Kane advised Noella Rowton is working across both Trusts to undertake this piece of work. She advised the work will cover the medical workforce as well as Allied Health Professions. Matthew Bryant highlighted the need to meet the demand for the services but the need to be mindful of the cost and ensure the plans that are developed are financially effective and efficient for the workforce and delivery of patient care. Graham Hughes invited Julie Reeve to comment due to the work she is undertaking across the system. Julie Reeve advised she has met with Peter Lewis to discuss plans moving forward for the Trusts and the work of Health Education England in recruiting into workforce planning roles. She advised interviews have been arranged for the week commencing 7 February 2022 to support this piece of work. Quarter 3 2021/22 Board Assurance Framework (BAF) Samantha Hann presented the Quarter 3 BAF report. She advised the BAF had been reviewed by the Executive Directors who were in post in December 2021. It was noted that the Executive Directors had not been changed within the Quarter 3 report to reflect the new Executive Director appointments from 10 January 2022. Samantha Hann advised she had met with Phil Brice to reassign the principal risks on the BAF to the newly appointed single Executive Team. She confirmed each of the Executive Directors had been asked to review and refresh the principal risks under their remit. The changes would be reflected within the Quarter 4 2021/22 BAF report. In relation to the changes within Quarter 3, Samantha Hann advised that two of the principal risks, both under the remit of the Workforce Committee, had increased within the quarter, SR5 – development of a future workforce strategy; and SR6 – the Trust does not have an engaged workforce performing at the required level. Samantha Hann advised one principal risk decreased within the quarter, which was under the remit of the Governance and Quality Assurance Committee, SR13 - the Trust makes decisions that compromise quality and safety in order to achieve financial balance. She advised the remaining principal risks, including SR10 – ineffective partnership working slowing the development of the Integrated Care System – which was under the direct remit of the Board of Directors, had been reviewed and assessed with the same risk score for the Quarter. Samantha Hann confirmed the Quarter 3 2021/22 BAF had been reviewed within the Board Assurance Committees during the meetings held in January 2022. She advised the individual Board Assurance Committees received streamlined reports specific to the principal risks within their remit with the exception of the Executive Committee and Audit Committee that received the BAF report in full. Jane Henderson advised members of GQAC felt that the score for SR1 and SR3 no longer reflect the current position. She advised it lead to a discussion regarding whether the risk descriptions also need updating to reflect the current risk being faced and what is both within, and out of the control of the
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 9 -
B
5.46
5.47
5.48
5.49
5.50
5.51
5.52
5.53
5.54
organisation. She confirmed as the report covered Quarter 3, no changes to the report had been made in the meeting but it had been agreed to review and refresh the Principal risks during Quarter 4 by the Executive Directors. Martyn Scrivens said a similar discussion had taken place at Financial Resilience Commercial Committee (FRCC) in relation to the financial principal risks. Phil Brice confirmed the Executive Directors will undertake a review of the Principal risks during February 2022 as outlined by Samantha Hann. He said the conversations at the Assurance Committees had been helpful to support the Executives Directors with the review of the risks. It was agreed an updated BAF would be presented to the Board in March 2022. Phil Brice advised the Joint Board in April 2022 would set the strategic objectives for the new organisation and following this, the BAF and CRR report would be developed with the intention the BAF would be more dynamic. Martyn Scrivens said it was important to ensure the BAF reflects the increased risks faced by the organisation that are impacting on the Trust achieving its strategic objectives. He said there is significant assurance that risks are managed well within the organisation but it should be recognised that the BAF is not a fair reflection of the risks the Trust is facing of delivery of its strategic objectives within Quarter 4. Paul Mapson said he agreed a refresh is required but he was satisfied that the changes could be made as part of the alignment in risk management processes. He said some of the risks need to be increased and a review of whether the risks should be on the BAF or CRR should be undertaken. Andy Heron said the introduction of the joint single Executive Team will help to align risk management processes and ensure that mitigation is in place for the risks. He noted that as the single Executive Team have community services within their remit, even though these do not report through YDH at this stage, this will further help to bring the services together across the County and support with the mitigation of some of the risks to the strategic objectives. Martyn Scrivens summed up the discussion to advise the Board felt appropriate assurance was in place that risks are being well managed however the single Executive team were asked to take the opportunity to review and refresh the principal risks on the BAF in light of the operational pressures being faced during Quarter 4 2021/22. He noted the work that is underway on the alignment of risk management processes which should further enhance the risk management arrangements in place. Quarter 3 2021/22 Corporate Risk Register (CRR) Report Samantha Hann presented the Quarter 3 CRR report. She advised the individual Board Assurance Committees had received streamlined reports specific to the risks within their remit during the meetings held in January 2022 with the exception of the Executive Committee and the Audit Committee that receives the CRR report in full. She confirmed the CRR covers the YDH group including risks for YDH, SSL and SHS. Samantha Hann advised the risks on the CRR have been reassigned to the new Executive Directors in post. She confirmed that she is working with Phil Brice to review the full list of specialities included on the risk register and a piece of work
SH
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 10 -
B
5.55
5.56
5.57
5.58
5.59
5.60
5.61
would be undertaken to allocate all risks on the Trust’s risk register to the Executive Directors. Samantha Hann highlighted that SFT report all risks scoring 15 and above on their CRR which is different to YDH, who report all risks scoring 12 and above. She advised this will be one of the discussions the Joint Board of Directors for the new organisation will need to have and a decision on the threshold made, amongst other risk decisions. It was acknowledged that the Joint Board to Board meeting had agreed no changes would be made to either organisations Risk Management Strategy or risk management processes before April 2022 so all risks scoring 12 or above would form part of the CRR for YDH. Samantha Hann advised that there had been a significant increase in the amount of risks that form the CRR during Quarter 2, with a 59% increase since Quarter 1 2021/22. She said the risks on the CRR within Quarter 3 have decreased slightly decreasing from 51 risks in Quarter 2 to 48 risks in Quarter 3. She noted despite this reduction, when compared to Quarter 1 2021/22, there had been a 62.5% increase in the numbers of risks on the CRR and compared to Quarter 3 2020/21, there had been a 60.41% increase. She reflected this continues to demonstrate that risks are materialising as a result of the prolonged pandemic and the operational pressures the organisation is facing. It was highlighted by Samantha Hann the majority of the risks on the CRR fall within the category of ‘quality and governance’ risks. She noted however the numbers of risks categorised under continuity of service and compliance and performance are increasing as demonstrated within the circle heat map where the movement of all risks within the full risk register has been included. She said the majority of risks on the CRR now fall under the category of continuity of service risks. Within Quarter 3 2021/22, Samantha Hann advised there were eleven top risks to the organisation, which is an increase of three additional risks when compared to Quarter 2. She advised of the eleven top risks, none of these were under the direct remit of the Board of Directors. A summary of the four significant risks under the direct remit of the Board of Directors was provided by Samantha Hann which included; fire compartmentation breaches; delay in evacuating patients in the event of a fire on wards 6-9; lack of fire barrier containment; and loss of emergency power supply in the event of mains power cut. In relation to movement within the Quarter for risks directly under the remit of the Board of Directors, Samantha Hann said there had been no new risks added to the CRR, no risks had increased which added these to the CRR, no risks had reduced from the CRR and no risks had been archived. She advised the four risks under the direct remit of the Board of Directors had been reviewed as the same score during Quarter 3 but examples of the actions being taken to continue to mitigate the risks were provided. Following the joint Board to Board meeting on 21 July 2021, Samantha Hann confirmed work continues with SFT to align risk management processes by April 2022. She advised a second deep dive session with Phil Brice, Steve Thomson and Bernice Cooke had taken place on 20 January 2022 to outline the content of the presentation that would be delivered to the Board of Directors on 5 April 2022 during the Board development day. She said further meetings had been arranged in February and March 2022 to undertake the work required before April.
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 11 -
B
5.62
5.63
Samantha Hann advised the presentation would cover the proposed risk matrix; risk scoring; escalation of risks; risk appetite; risk tolerance; timeline of the implementation work; and the resource available. Martyn Scrivens thanked Samantha Hann for the update and noted the progress with the alignment of risk management processes as requested by the joint Board. He thanked Samantha Hann for her continued hard work and diligence. No questions were raised on the Quarter 3 2021/22 CRR report.
1-106/ 2122
6 6.1
6.2
6.3
6.4
6.5
6.6
6.7
YDH GROUP BOARD OVERVIEW QUADRANT The Board reviewed the YDH group overview quadrant. The following was discussed in more detail: Matthew Bryant advised the performance quadrant demonstrates the operational challenges and pressures YDH is under. He confirmed a number of the safety and patient experience items had already been discussed earlier in the meeting such as the IPC BAF and learning from deaths. He advised the number of falls remains within the expected range but these are increasing which the team are reviewing. He said it is expected that the number of falls and pressure ulcers would increase with the Trust working under such operational pressures. Matthew Bryant highlighted the rise in incident reporting which he reflected was positive as YDH has a high reporting culture. In terms of the serious harm incidents, complaints and readmission rates, he advised these remain steady and have not increased as may have been anticipated. In relation to the Sentinel Stroke National Audit Programme (SSNAP) results, Matthew Bryant advised a presentation was delivered to the Executive Committee and Governance and Quality Assurance Committee (GQAC) which covered the issues driving the performance rating which included ward configuration; pressures on patient flow; multi-disciplinary infrastructure; and workforce challenges. He said the mitigating actions in place had been discussed in detail during the meetings. Under the People section of the quadrant, Matthew Bryant advised the nursing workforce team remained in a good position. He highlighted the extensive work that had been done to achieve this position by the teams involved which he thanked. He noted the medical vacancies which he said drives the agency spend for the Trust. In relation to absences rates, Matthew Bryant advised these had been affected by Covid-19 absences. He confirmed mandatory training and appraisal rates remain consistent. He reminded the Board that the quadrant covers the YDH group position and noted that the appraisal rates are better within SHS than within YDH but he confirmed a review is underway to explore how compliance rates can be improved. Stacy Barron-Fitzsimons said the quadrant was a reflection of the operational position for the Trust. She advised routine operations and pathways are significantly below where the Trust would expect these to be. She said the number of cancelled operations have significantly increased due to the operational pressures. She said YDH is delivering more activity than in 2019/20. In relation to routine diagnostic activity, this is being impacted by emergency flows and acuity of the patients so routine patients are having to wait longer than they should.
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 12 -
B
6.8
6.9
6.10
6.11
6.12
6.13
6.14
6.15
Stacy Barron-Fitzsimons said there has been an increase in cancer referral rates and an increase in the numbers of diagnostic tests needed for patients on the cancer pathways. She said YDH are working with other Trusts to try and minimise the impact of patients. She praised the work of the teams who are working tirelessly to support the long wait patients. Martyn Scrivens thanked Matthew Bryant and Stacy Barron-Fitzsimons for the summaries of the position and said given the operational circumstances, there were no surprises within the performance pack. He commended the teams for the way they are managing the operational pressures. Jan Hull asked whether YDH is seeing the same increase in the numbers of cancer referrals as SFT are to which Stacy Barron-Fitzsimons confirmed this is the case. She said YDH have seen a 3% increase in January when compared to last year. She said this is across a wide range of different cancers. She noted the Trust is also seeing an increase in the numbers of late presentations for cancer which then requires additional investigations to manage these patients which further contributes to the wait times for all patients. She said there is a team of staff working on the cancer referrals and messaging is being communicated to patients to encourage them to seek medical attention early. Pippa Moger advised the financial element of the quadrant covers the month nine position. She said at a Group level, there will be 430k surplus in month and the Group are in line with the second half of the year plan which had been submitted to NHS England and NHS Improvement. She advised the agency spend is high but reflected on the discussion earlier in the meeting and said this was not surprising given the levels of sickness absence and vacancies. In relation to the cost improvement programme, Pippa Moger advised this is set to deliver in line with the revised plan which is promising. She said she is working with Ryan Garland, Deputy Chief Finance Officer, to understand the longer term cash forecast. She confirmed there are no concerns with the Trust delivering on the capital departmental expenditure limit but there is a challenge in relation to the Targeted Investment Fund (TIF). She advised YDH has received funding for the modular theatre and the outpatient improvements and the Trust will work closely with the System to maximise the capital available during the 2021/22 financial year. Pippa Moger advised the Group is forecast to break even by the end of the financial year. She said planning for 2022/23 is underway following the release of the planning guidance. It was noted that the detailed elective recovery funding guidance for 2022/23 had not yet been published and the challenges this presents was highlighted. She advised a detailed paper on the 2022/23 arrangements would be presented to the Financial Resilience and Commercial Committee (FRCC) in February 2022. David Shannon advised final approval for the TIF bids, which were submitted in September 2021, was received on 28 January 2022. The Board noted the frustration that it had taken longer for the approval process to be undertaken, than the NHS organisations now have to spend the funding and deliver the schemes. The Board acknowledged that all NHS organisations who have received funding will be in the same position as YDH. David Shannon advised weekly meetings have been established with SFT and the Somerset CCG to review the details and to ensure the schemes are delivered in time. He confirmed that the Trust would be in a position to provide a
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 13 -
B
6.16
6.17
more detailed update within the FRCC meeting in February 2022 and at the next Board of Directors meeting in March 2022. Martyn Scrivens asked whether there would be any help available from the region on how Trusts are expected to deliver against their schemes within a two month timeframe. David Shannon said to deliver against a deadline of 31 March will be incredibly difficult to manage for the scale and complexities for the schemes but the Tryst is utilising the resource it has, as best as it can, and working with the region on this. Martyn Scrivens thanked the teams involved for the hard work already undertaken and for the work that would be required to deliver the schemes to meet the deadline of the end of March 2022. He noted that the full guidance for 2022/23 was not yet available to the Finance team and the additional pressure this adds at an already challenging period of time.
1-107/ 2122
7 7.1
7.2
7.3
VACCINATION AND LATERAL FLOW REPORT Isobel Clements confirmed the report within the papers had been included as there is a requirement for the number of vaccinations and lateral flow tests (LFTs) to be reported to the Board. She thanked the Information Team for producing the report. Isobel Clements advised the report contains the breakdown of vaccinated staff (first, second and booster vaccines) and the numbers of staff who have submitted a LFT in the previous two weeks prior to the report being complete. Martyn Scrivens thanked Isobel Clements for the encouraging report. No questions were raised.
1-108/ 2122
8 8.1
FRIENDS AND FAMILY REPORT Phil Brice advised the report had been circulated within the papers. He said the report was overwhelming positive and the negative responses would be followed up on. He reflected the issues raised – communications and restrictions on visiting - were consistent with complaint and PALs data. It was noted that the response rate was lower than in previous years. No questions were raised by the Board in relation to the report.
1-109/ 2122
9 9.1
9.2
9.3
9.4
WELLBEING GUARDIAN REPORT Martyn Scrivens welcomed Mark Robinson to the meeting to support with the presentation of the Wellbeing Guardian report. Graham Hughes confirmed this is the second time the Wellbeing Guardian report has been presented to the Board for review. He confirmed he had been appointed the Wellbeing Guardian in 2021. He advised the reports presented at the SFT and YDH Boards are different and it had been agreed that the teams would work together to produce a report which would be more consistent in the format used. Graham Hughes highlighted the great work undertaken by the team which he said had been reflected within the staff survey and pulse survey results. He said actions are in place against each of the nine principles and the impact of the actions are being measured to identify further work that can be taken forward. Mark Robinson confirmed the joint working arrangements between the Trusts is increasing and the report will be developed and aligned before the next report to the Board of Directors. He said within the Quarter there has been a large
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 14 -
B
9.5
9.6
9.7
9.8
9.9
9.10
amount of activity and the team have ensured they are responsive to feedback and are committed to improving the experience for staff when at work. In relation to the most recent pulse survey results, Mark Robinson advised there were over 500 responses which represented approximately 20% of the workforce. He advised the national response rate is between 3-4% so YDH is performing well. Isobel Clements thanked Graham Hughes and Mark Robinson for their updates and she thanked the Health and Wellbeing team on behalf of the Board for their hard work and dedication. She said the results of the staff survey and the pulse survey demonstrate how important health and wellbeing is taken at YDH which she commended the Trust for. Martyn Scrivens said how encouraging the results from the staff survey and pulse surveys had been but he acknowledged staff resilience is one of the greatest risks to the Trust and it was important to maintain momentum and to keep identifying gaps and undertaking mitigating actions as this is a vital workstream for the Trust. When asked by Martyn Scrivens what support is provided to the GP Practices within SHS in relation to the health and wellbeing service, Shelagh Meldrum advised SHS have a good programme in place which is evident within their Practices. She said staff are good at sign posting other members of the teams to support. She said there is work within the wider primary care community, especially for GPs which she is currently reviewing. She said she has felt assured by the arrangements in place she has seen demonstrated since starting in her role as Chief Officer – Partnerships and Collaboration. Merry Kane advised that Doctors can be difficult to reach out and obtain help for themselves. She said the Trust ensures that health and wellbeing conversations are included at every opportunity including during the Clinical Directors meetings asking for them to ensure they cascade the message of support available. Martyn Scrivens thanked Shelagh Meldrum and Merry Kane for the updates and said how important it is for all staff groups to be captured and support to be provided. He thanked Graham Hughes for being the Non-executive Director Lead for Health and Wellbeing.
1-110/ 2122
10
10.1
10.2
10.3
COMMITTEE UPDATES AND MINUTES Audit Committee Paul Mapson confirmed the minutes from the meeting held on 26 October 2021 had been circulated within the papers. He highlighted that limited assurance had been provided on the work programme for the Transformation team with actions in place to address. Paul Mapson advised limited assurance had also been provided on the frailty service in the recent meeting held on 27 January 2022. He said the Audit Committee had asked the Executive Directors to review and take forward the recommendations from the Internal Audit report. Jan Hull asked whether the frailty service would be reviewed at GQAC, to which Jane Henderson confirmed an update would be requested at a future GQAC meeting. Paul Mapson said the draft Terms of Reference (ToR) had been updated to reflect the change in the Executive Directors and to bring the ToRs in line with
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 15 -
B
10.4
10.5
10.6
10.7
10.8
10.9
10.10
10.11
10.12
SFT and the Chief Executive would no longer need to attend the Audit Committee. The draft ToRs were approved by the Board of Directors. Governance and Quality Assurance Committee (GQAC) Jane Henderson confirmed the minutes from the meeting held on 26 October 2021 had been circulated within the papers. She advised the most recent GQAC meeting had been held on 27 January 2022. She highlighted to the Board the presentation on the SSNAP results advising of the deterioration in the YDH results for Quarter 2 2021/22 advising that the Trust normally receive a ‘B’ rating but this has deteriorated to a ‘C’ rating. Jane Henderson provided an overview of the presentation stating the Committee heard of the reasons for the deterioration, against each of the domains which had deteriorated which included; the impact of the pandemic; changes in ward configurations; turnover in stroke clinicians; operational pressures; and patient flow challenges. She said the team provided information on the actions that are in place to improve the Trust’s rating although it was acknowledged it might be some time before the rating would improve. Jane Henderson said the Committee took assurance from the presentation that was delivered by the Data Coordinator for Stroke Services and the General Manager for Internal Medicine, that the challenges identified were being addressed. She said it had been acknowledged the issues both within and outside of the Trust’s control and she highlighted the work between YDH and SFT to manage the service. The national and local shortfall in therapists, particularly physiotherapists and occupational therapists, was highlighted by Jane Henderson as an area discussed during GQAC and the impact this has on the SSNAP results. She advised a new Stroke Consultant has been appointed. The Board discussed stroke services at other Trusts within the region, noting the challenges and issues faced by other Trusts and the impacts on YDH and SFT as a result. Jane Henderson thanked Sallyann King for her first quarterly report since starting in post as Interim, Director of Midwifery. She said Sallyann King had congratulated the Midwifery team on the number of iCARE award nominations. She highlighted the challenges within the unit in relation to staff turnover and skill mix and the use of the supernumerary labour ward co-ordinator and the impact of this. Jane Henderson spoke of the joint working arrangements across YDH and SFT in relation to Safeguarding. She said the date for the implementation of Liberty Safeguards has not yet been announced. In relation to the remaining items discussed during the GQAC meeting on 27 January 2022, Jane Henderson advised these had already been covered during the Board meeting. She said the main theme is the increasing number of patient safety risks and the associated harm to patients. Jane Henderson said the draft Terms of Reference (ToRs) had been updated to reflect the change in the Executive Directors which has seen an increase in membership of the Committee and the change in name from the ‘Risk Assurance Committee’ to the ‘Quality Assurance Committee’. The draft ToRs were approved by the Board of Directors.
Minutes of the YDH Board of Directors meeting held on 2 February 2022 March 2022 Public Board - 16 -
B
10.13
10.14
10.15
10.16
10.17
10.18
Workforce Committee Graham Hughes highlighted the change in Guardian of Safer Working Hours in December 2021 advising that John McFarlane had taken on the role since the previous Guardian, Andrew Newton had left the Trust. He said the Committee had reviewed the Quarter 3 2021/22 report. In relation to the cultural maturity internal audit report, Graham Hughes said the report had been reviewed and he highlighted how positive the report was. Shelagh Meldrum agreed with Graham Hughes and said the report reflected how positive the YDH culture is. She said actions have been identified in relation to the merger which the Executive Directors will take forward. Graham Hughes advised the cultural maturity internal audits at YDH and SFT and the national staff survey results at both Trusts will be reviewed and actions developed. Graham Hughes advised the recommendation had been made for YDH to change the annual leave year from calendar year to financial year. He advised the reasons for the change had been discussed during the meeting and it had been agreed that no change would be made before 2023 and after further consideration. In relation to the ToRs, Graham Hughes said the first joint meeting of the Workforce Committee would be held in early March 2022 and the ToRs would be reviewed in light of these arrangements. He said the draft ToRs would be presented to the Board for approval by Spring 2022. Financial Resilience and Commercial Committee (FRCC) Martyn Scrivens advised the FRCC met on Monday 24 January 2022. He confirmed items relevant to the Part 1 Board meeting had been covered by Pippa Moger and David Shannon and there were no other items to bring to the attention of the Board. Executive Committee Phil Brice presented the draft Terms of Reference to the Board for approval advising minor changes had been made which had been detailed within the circulated papers which included; change to the Executive Directors; addition of the Deputy Chief Nurse; and the change to the name of the Quality Assurance Committee. The Board of Directors approved the revised Terms of Reference.
GH
1-111/ 2122
11 11.1
ANY OTHER BUSINESS No other items of business were raised.
1-112/ 2122
12 12.1
DATE OF NEXT MEETING 2 March 2022, MS Teams/Boardroom, Level 1, YDH
Action Notes from the SFT and YDH Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 1 - C
SOMERSET NHS FOUNDATION TRUST /YEOVIL DISTRICT HOSPITAL NHS FOUNDATION TRUST
SOMERSET NHS FOUNDATION TRUST
ACTION NOTES FROM THE PUBLIC BOARD OF DIRECTORS MEETING HELD ON 1 FEBRUARY 2022
AGENDA ITEM
ACTION BY WHOM DUE DATE PROGRESS
5. Action Log and Matters Arising
To arrange for Martyn Scrivens and Barbra Gregory to be invited to a future Mental Health Act Committee.
Ria Zandvliet March 2022 An invite has been sent.
8. Chief Executive and Executive Directors’ Report
To include an overview of Non Executive Directors’ lead roles in the report to the March 2022 Board meeting.
Ria Zandvliet March 2022 The overview has been included in the report.
Action Notes from the SFT and YDH Public Board of Directors meeting held on 1 February 2022 March 2022 Public Board - 2 - C
YEOVIL DISTRICT HOSPITAL NHS FOUNDATION TRUST
BOARD OF DIRECTORS – ACTION SHEET 1 March 2022
Minute Action Progress Due By
ACTIONS FROM 6 OCTOBER 2021
1-71/2122 (14.8) Joint Board to Board Seminar Session on equality, diversity and inclusion and WRES once the new Head of Inclusion is in post to be arranged
Scheduled for June 2022 Joint Board to Board Seminar
Session
June 2022 Samantha Hann
ACTIONS FROM 15 DECEMBER 2021
1-92/2122 (6.11) Cancer harm reviews presentation to be delivered to a future Joint SFT and YDH QGC/GQAC meeting
This has been added to the work programme for the Joint
GQAC/QGC meeting for 2022/23
April 2022 Samantha Hann
ACTIONS FROM 2 FEBRUARY 2022
1-102/2122 (2.1) Changes to be made to the Declaration of Interest Register to split out the voting and non-voting members of the Board
Complete February 2022 Phil Brice / Samantha Hann
1-105/2122 (5.47) Board Assurance Framework for Quarter 4 2021/22 to be presented to the Board of Directors in March 2022
Complete March 2022 Samantha Hann
1-110/2122 (10.16) Workforce Committee Terms of Reference to be revised and presented to the Board of Directors for approval
Not yet due May 2022 Graham Hughes
SFT and YDH Registers of Directors’ Interests
March 2022 Public Board - 1 –
D
Somerset NHS Foundation Trust / Yeovil District Hospital NHS Foundation Trust
REPORT TO: The Trust Board
REPORT TITLE: Registers of Directors’ Interests
SPONSORING EXEC: Director of Corporate Services
REPORT BY: Secretary to the Trust
PRESENTED BY: Chairman
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☒ For Assurance/
Discussion ☐ For Approval / Decision ☒ For Information
Executive Summary and Reason for presentation to Committee/Board
The Registers of Interests are presented to the Board at every meeting and reflect the interests of Board members as at 25 January 2022.
Recommendation The Board is asked to:
• note the Register of Interests;
• declare any changes to the Register of Interests;
• declare any conflict of interests in relation to the agenda items.
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☐ Care for our Population ☐ Develop our People
☐ Innovate and Collaborate ☐ Develop a Sustainable System
Somerset NHS FT
☐ Obj 1 Inclusive culture ☐ Obj 4 Safe services ☐ Obj 7 Improving outcomes
☐ Obj 2 Collaboration ☐ Obj 5 Self management ☐ Obj 8 Workforce
☒ Obj 3 Independent lives ☐ Obj 6 Value all people alike ☐ Obj 9 Performance
☐ Obj 10 Finance
Registers of Directors’ Interests
March 2022 Public Board - 2 – D
Implications/Requirements (Please select any which are relevant to this paper)
☐ Financial ☒ Legislation ☐ Workforce ☐ Estates ☐ ICT ☐ Patient Safety /
Quality
Details: Regulatory requirement to declare conflict of interests.
Equality The Trust wants its services to be as accessible as possible, to as many people as
possible. Please indicate whether the report has an impact on the protected characteristics
☒ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are no proposals or matters which affect any persons with protected characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
Not applicable
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
A report is presented to every Board meeting.
Reference to CQC domains (Please select any which are relevant to this paper)
☐ Safe ☐ Effective ☐ Caring ☐ Responsive ☒ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
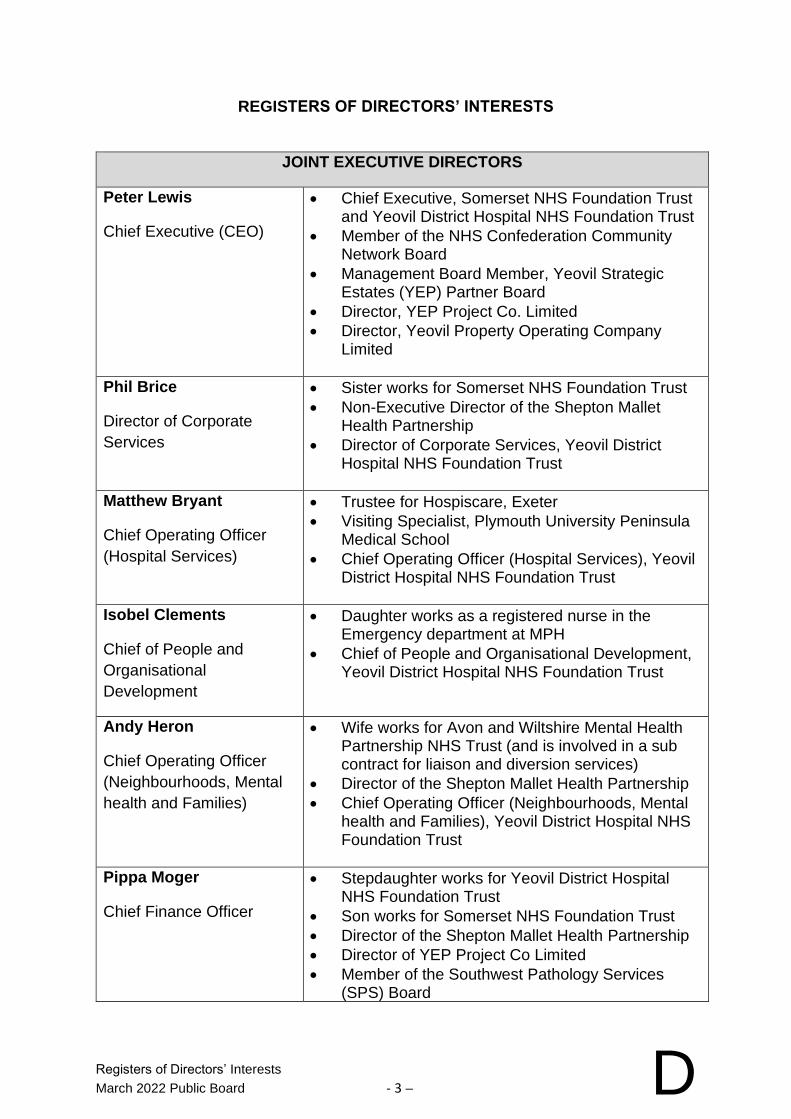
Registers of Directors’ Interests
March 2022 Public Board - 3 – D
REGISTERS OF DIRECTORS’ INTERESTS
JOINT EXECUTIVE DIRECTORS
Peter Lewis
Chief Executive (CEO)
• Chief Executive, Somerset NHS Foundation Trust and Yeovil District Hospital NHS Foundation Trust
• Member of the NHS Confederation Community Network Board
• Management Board Member, Yeovil Strategic Estates (YEP) Partner Board
• Director, YEP Project Co. Limited
• Director, Yeovil Property Operating Company Limited
Phil Brice
Director of Corporate
Services
• Sister works for Somerset NHS Foundation Trust
• Non-Executive Director of the Shepton Mallet Health Partnership
• Director of Corporate Services, Yeovil District Hospital NHS Foundation Trust
Matthew Bryant
Chief Operating Officer
(Hospital Services)
• Trustee for Hospiscare, Exeter
• Visiting Specialist, Plymouth University Peninsula Medical School
• Chief Operating Officer (Hospital Services), Yeovil District Hospital NHS Foundation Trust
Isobel Clements
Chief of People and
Organisational
Development
• Daughter works as a registered nurse in the Emergency department at MPH
• Chief of People and Organisational Development, Yeovil District Hospital NHS Foundation Trust
Andy Heron
Chief Operating Officer
(Neighbourhoods, Mental
health and Families)
• Wife works for Avon and Wiltshire Mental Health Partnership NHS Trust (and is involved in a sub contract for liaison and diversion services)
• Director of the Shepton Mallet Health Partnership
• Chief Operating Officer (Neighbourhoods, Mental health and Families), Yeovil District Hospital NHS Foundation Trust
Pippa Moger
Chief Finance Officer
• Stepdaughter works for Yeovil District Hospital NHS Foundation Trust
• Son works for Somerset NHS Foundation Trust
• Director of the Shepton Mallet Health Partnership
• Director of YEP Project Co Limited
• Member of the Southwest Pathology Services (SPS) Board
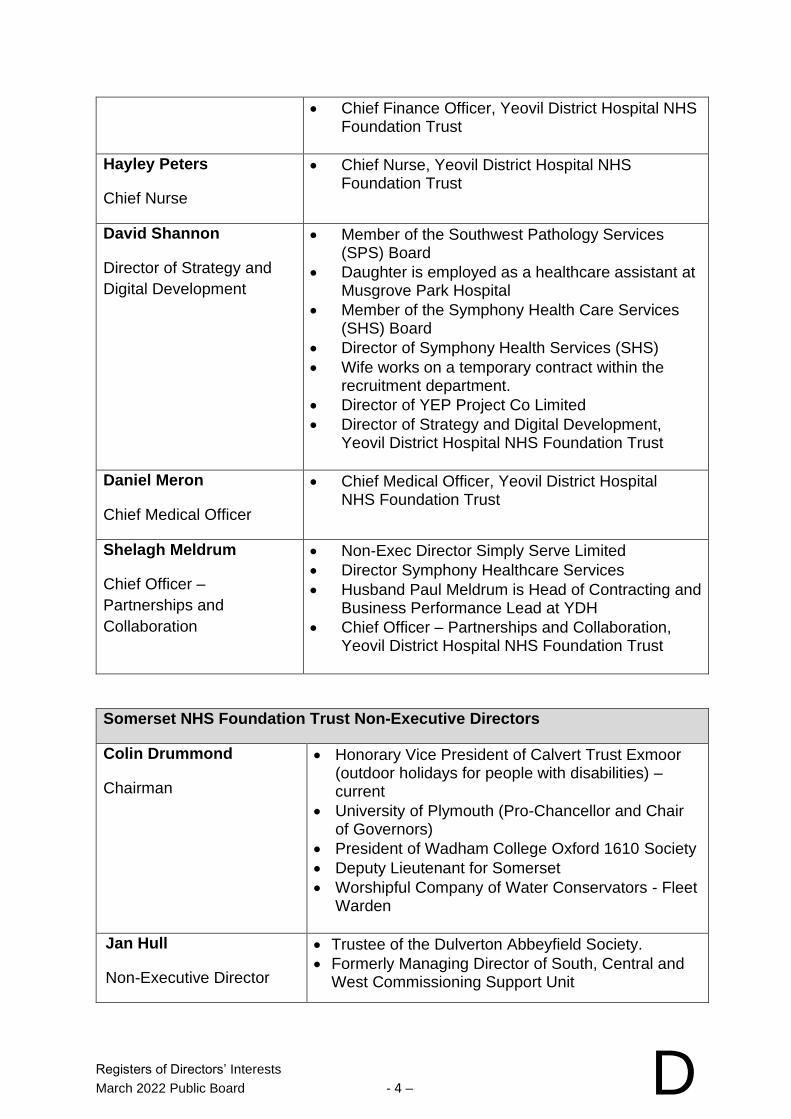
Registers of Directors’ Interests
March 2022 Public Board - 4 – D
• Chief Finance Officer, Yeovil District Hospital NHS Foundation Trust
Hayley Peters
Chief Nurse
• Chief Nurse, Yeovil District Hospital NHS Foundation Trust
David Shannon
Director of Strategy and
Digital Development
• Member of the Southwest Pathology Services (SPS) Board
• Daughter is employed as a healthcare assistant at Musgrove Park Hospital
• Member of the Symphony Health Care Services (SHS) Board
• Director of Symphony Health Services (SHS)
• Wife works on a temporary contract within the recruitment department.
• Director of YEP Project Co Limited
• Director of Strategy and Digital Development, Yeovil District Hospital NHS Foundation Trust
Daniel Meron
Chief Medical Officer
• Chief Medical Officer, Yeovil District Hospital NHS Foundation Trust
Shelagh Meldrum
Chief Officer –
Partnerships and
Collaboration
• Non-Exec Director Simply Serve Limited
• Director Symphony Healthcare Services
• Husband Paul Meldrum is Head of Contracting and Business Performance Lead at YDH
• Chief Officer – Partnerships and Collaboration, Yeovil District Hospital NHS Foundation Trust
Somerset NHS Foundation Trust Non-Executive Directors
Colin Drummond
Chairman
• Honorary Vice President of Calvert Trust Exmoor (outdoor holidays for people with disabilities) – current
• University of Plymouth (Pro-Chancellor and Chair of Governors)
• President of Wadham College Oxford 1610 Society
• Deputy Lieutenant for Somerset
• Worshipful Company of Water Conservators - Fleet Warden
Jan Hull
Non-Executive Director
• Trustee of the Dulverton Abbeyfield Society.
• Formerly Managing Director of South, Central and West Commissioning Support Unit
Registers of Directors’ Interests
March 2022 Public Board - 5 – D
(Deputy Chairman) • Non-Executive Director Yeovil District Hospital NHS Foundation Trust
Dr Kate Fallon
Non-Executive Director
(Senior Independent
Director)
• Daughter is a Consultant at Somerset NHS Foundation Trust
• Daughter has been appointed as the Guardian of Safe Working Hours for Junior Doctors
Stephen Harrison
Non-Executive Director
• Trustee, YMCA Brunel Group
• Trustee, Lawrence Centre, Wells
• Governor, Wookey Primary School
Barbara Gregory
Non-Executive Director
• RESEC Research into Elderly and Specialist Care Trustee.
• Deloitte Associate – with effect from 6 February 2018.
• Chair of the CNL (Chairs, Non Executive and Lay members) Faculty of HFMA
• Director of AGRF
Alexander Priest
Non-Executive Director
• Chief Executive Mind in Somerset
Sube Banerjee
Non-Executive Director
• Executive Dean, Faculty of Health, University of Plymouth
• Hon Consultant in Psychiatry, Plymouth University Hospitals NHS Trust (unremunerated)
• Visiting Professor, Brighton and Sussex Medical School (unremunerated)
• Trustee and Patron, Alzheimer’s Society (unremunerated)
• Editor-in-chief, The International Journal of Geriatric Psychiatry
• Director Cognitive Agility Ltd (personal consulting to governments and industry)
• Association Member BUPA (unremunerated)
• Trustee and Executive Board Member Medical Schools Council (unremunerated)
• Board member University of Plymouth Enterprise Limited (unremunerated)
Martyn Scrivens
Non-Executive Director
▪ Non-Executive Director Yeovil District Hospital NHS Foundation Trust
▪ Non Executive Director and Chair of Audit Committee of Hampshire Trust Bank Limited
▪ Wife works as a Bank Vaccinator for the Trust

Registers of Directors’ Interests
March 2022 Public Board - 6 – D
Yeovil District Hospital NHS Foundation Trust Non-Executive Directors
Martyn Scrivens
Interim Chairman
Non-Executive Director
▪ Non-Executive Director Yeovil District Hospital NHS Foundation Trust
▪ Non Executive Director and Chair of Audit Committee of Hampshire Trust Bank Limited
▪ Wife works as a Bank Vaccinator for the Trust
Jane Henderson
Non-Executive Director
Deputy Chairman
• Private Practice Therapeutic Counsellor
• Part-time, self-employed counsellor for Frome Birth Talk
Graham Hughes
Non-Executive Director
• Chairman of Simply Serve Limited
• Volunteer Advisor at Citizens Advice
• Parish Councillor of Babcary Parish Council
Paul Mapson
Non-Executive Director
• No declarations
Jan Hull
Non-Executive Director
• Trustee of the Dulverton Abbeyfield Society.
• Formerly Managing Director of South, Central and West Commissioning Support Unit
• Non-Executive Director Somerset NHS Foundation Trust
Chief Executive and Executive Directors’ Report March 2022 Public Board - 1 – E
Somerset NHS Foundation Trust / Yeovil District Hospital NHS Foundation Trust
REPORT TO: The Trust Board
REPORT TITLE: Chief Executive/Executive Director Report
SPONSORING EXEC: Chief Executive
REPORT BY: Executive Directors
PRESENTED BY: Chief Executive
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☐ For Assurance ☐ For Approval / Decision ☒ For Information
Executive Summary and Reason for presentation to Committee/Board
The purpose of the report is to update the Board on Chief Executive and Executive Director activities and/or points of note which are not covered in the standing business and performance reports and this update is for information. The report covers the period February 2022.
Recommendation To note the report.
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☒ Care for our Population ☒ Develop our People
☒ Innovate and Collaborate ☒ Develop a Sustainable System
Somerset NHS FT
☒ Obj 1 – Inclusive culture ☒ Obj 4 - Safe services ☒ Obj 7 – Improving outcomes
☒ Obj 2 - Collaboration ☒ Obj 5 - Self management ☒ Obj 8 – Workforce
☒ Obj 3 - Independent lives ☒ Obj 6 – Value all people alike ☒ Obj 9 - Performance
Implications/Requirements (Please select any which are relevant to this paper)
☐ Financial ☐ Legislation ☐ Workforce ☐ Estates ☐ ICT ☐ Patient Safety /
Quality
Details: N/A
Chief Executive and Executive Directors’ Report
March 2022 Public Board - 2 – E
Equality The Trust wants its services to be as accessible as possible, to as many people as
possible. Please indicate whether the report has an impact on the protected characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are no proposals or matters which affect any persons with protected characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
N/A
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
The report is presented to every Board meeting.
Reference to CQC domains (Please select any which are relevant to this paper)
☒ Safe ☒ Effective ☒ Caring ☒ Responsive ☒ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
Chief Executive and Executive Directors’ Report
March 2022 Public Board - 3 – E
CHIEF EXECUTIVE / EXECUTIVE DIRECTOR REPORT
JOINT ITEMS
1. MERGER UPDATE
1.1. The overarching aim of the merger is to provide better care for the population of Somerset and beyond, with everyone in our county enjoying access to the same high quality care and support no matter where they live in Somerset. Working with our partners, we want to improve access to preventative care that helps people stay well and out of hospital and ensure better outcomes from the treatment we provide. We also aim to develop stronger links between mental health and physical health services, so people get the care and support they need, from the right service, at the right time. The clinical strategy that we are developing is central to what we want to achieve as a new trust, and it is being developed with the input of teams across both trusts.
1.2. At our Trust Board meetings on 1 February 2022 both Trust Boards assessed our progress and our indicative timeline to complete the transaction. Both Boards agreed to plan to submit our business case to the regulator in October 2022, five months after we originally planned. This means we are planning to merge on 1 April 2023 if we receive the go ahead from the regulator.
1.3. We know how important it is to engage with colleagues as the best ideas for improvement come from those who work within our services. We are expecting new national guidance on merger transactions with an increased requirement to engage with colleagues, partners, patients, and the public. The new timeline will give us the extra time to ensure that we have meaningful discussions and act on feedback from them. The extra time will give teams, that are extremely stretched as a result of operational pressures, additional time to think through and plan the improvements that we can make as a result of integrating services and bringing our organisations together. We believe that this adjustment to the timeline is the right thing to do in recognition of the meaningful engagement that we want to have with colleagues, partners, patients and the public and the operational pressures teams are facing
1.4. We remain committed to bringing our trusts together. The work that our clinical and corporate teams are doing to integrate is already demonstrating the value of forming one organisation. We have responded to the extreme pressures that services in Somerset face this winter as a community, demonstrating that we are more resilient and better able to respond together.
Chief Executive and Executive Directors’ Report
March 2022 Public Board - 4 – E
2. GET INVOLVED – HELP US TO NAME OUR NEW ORGANISATION
2.1. As part of our preparations to merge our two trusts we need to agree what our merged trust will be called.
2.2. Our new, merged organisation will care for a population of more than half-a-million people living in Somerset and beyond, and employ around 12,000 colleagues, so it is important that we decide on a name which represents who we are and what we do, and which is meaningful to colleagues, partners, our patients and the public.
2.3. We want to identify a name for the trust which will be responsible for providing community-based services and mental health and learning disability services across Somerset; runs the county’s community hospitals and both acute hospitals (Yeovil Hospital and Musgrove Park Hospital) and manages a proportion of the county’s GP practices. The individual buildings themselves, from which we provide services such as A&E, maternity care, planned operations, mental health services, and minor injuries units, will retain their own names. For example, Yeovil Hospital will continue to be known by its name, our community hospitals and mental health sites will also keep their names, and Musgrove Park Hospital will continue to be called by its name.
2.4. Back in 2021 we asked for colleagues’ thoughts on the best name for our new organisation and nearly 200 of you gave us their thoughts. The joint executive team for both trusts has narrowed suggestions down to a shortlist of three which consists of names that fit the naming conventions for NHS provider trusts and incorporates those that were put forward by colleagues.
2.5. The shortlist is:
• Somerset Healthcare NHS Foundation Trust • Somerset County NHS Foundation Trust • Somerset NHS Foundation Trust
2.6. We want to hear from as many of you as possible. Please tell us anonymously which name you think is most appropriate and why via this survey before Sunday 20 March. Giving us your views will take just a few minutes. Our joint executive team will take all your feedback into account before putting forward a proposal to both Trust Boards for a decision.
3. COVID-19 UPDATE
Covid-19 Infection rate
3.1. The seven day Covid-19 infection rate per 100,000 population across Somerset as at 16 February 2022 stands at 816.80 - South Somerset
Chief Executive and Executive Directors’ Report
March 2022 Public Board - 5 – E
(822.10), Somerset West and Taunton (941.90), Mendip (686.10) and Sedgemoor (765.60).
3.2. Although the infection rate is high, the good news is that the proportion of people who are becoming seriously ill and needing to be admitted to hospital remains a small proportion of what it was at the start of the pandemic. 33 Covid-19 positive patients were admitted to the Trust’s inpatient services as at 16 February 2022 compared to 19 patients at YDH. For both trusts, this amounted to 5% of the total bed base.
4. HEALTH AND CARE IN SOMERSET IN HIGHEST LEVEL OF
ESCALATION 4.1. The health and social care system in Somerset declared OPEL 4 at the
end of January 2022. This level was the highest level of alert and enabling both trusts to take additional steps to ensure that we can continue to provide safe services for our patients. Both trusts continue to work very closely with other partners to improve patient flow through our services and support teams under pressures.
4.2. A series of sponsored social media adverts and videos have been created to help inform and manage public expectations. These focus on key areas such as: • supporting discharge; being ready to collect loved ones from
hospital as soon as they are medically well enough to leave can make a big difference. If you can provide some support for loved ones it will help us care for those people who are very unwell;
• a focus on emergency departments (EDs) across the county; choosing the right service for your healthcare needs, waiting times for non-urgent care, when to attend EDs and considering alternatives for minor illnesses;
• Promoting NHS 111;
• Promoting pharmacies;
• Promoting all healthcare services.
Operational pressures (as at 18 February 2022) 4.3. Both Musgrove Park Hospital (MPH) and Yeovil District Hospital have
been under severe pressures this week. At MPH increases in patients presenting to hospital through our Emergency Department resulted in an increase in waiting times for ambulance handovers and a severe knock on effect for the rest of the hospital at a time when capacity on our inpatient wards is already stretched and we are struggling to meet the demand. It led to us cancelling some elective surgery procedures and reviewing any other non-urgent services.
Chief Executive and Executive Directors’ Report
March 2022 Public Board - 6 – E
4.4. MPH and YDH are both in an internal critical incident and health and
care services in Somerset continue to be at system-wide operational pressure escalation level (OPEL) 4 – the highest possible.
4.5. Our teams continue to pull out all the stops to do their best for patients and ease the pressures within our services. The pressures have now eased, but we remain in the escalation levels described above.
4.6. We recognise that this pressure does have an effect emotionally, mentally and physically on colleagues and are reminding them of the wealth of wellbeing support that is available to them.
5. ADVICE TO COLLEAGUES, PATIENTS AND VISITORS FOLLOWING ENDING OF PLAN B COVID-19 RESTRICTIONS
5.1. The Government has lifted Plan B Covid-19 restrictions and we have reviewed our advice to colleagues, patients and visitors.
5.2. As part of that, we have reviewed visiting guidelines. Despite the increased pressures we are facing, we know how important seeing friends, family and carers is to our patients’ wellbeing and recovery. We have therefore made the decision to re-open responsible visiting. This means that visiting is now allowed at our hospitals and units again, but in a controlled manner to protect our patients, their families, and our colleagues delivering care.
5.3. Pre-booked visiting is allowed on most inpatient wards at out inpatient units, allowing one person at a time (or two if the visitor requires the support of a carer) to book a visiting slot. Further details are on our websites.
5.4. While Plan B restrictions are coming to an end, it is vital that we continue to do everything that we can to minimise the spread of Covid-19 within our services and on our sites. Mask wearing, regular gelling of hands and social distancing where possible remains in place on all our sites. We are also asking colleagues who can work successfully perform their roles from home, to continue working as you have been.
6. WORK STARTS ON NEW OPHTHALMIC DIAGNOSTIC CENTRES IN
SOMERSET
6.1 Ophthalmology patients in Somerset will soon be able to get an assessment at two brand new diagnostic centres in Yeovil and Taunton.
6.2 The multimillion pound project has been partly funded by NHS England
and both centres are expected to open for patients in Spring 2022.
Chief Executive and Executive Directors’ Report
March 2022 Public Board - 7 – E
6.3 The Yeovil centre will be based in the previous Monsoon retail unit on Middle Street in Yeovil Town Centre – opposite Boots Pharmacy and the Taunton centre will be located at Blackbrook Business Park – near Junction 25 of the M5.
6.4 The new centres will be able to carry out investigations for our retinal
and glaucoma patients. Between them they will have the capacity to see over 20,000 patients a year in a one stop shop where they will be able to have tests and images taken in the same appointment.
6.5 Ophthalmology is the highest volume outpatient specialty in the NHS
and demand for the treatment of eye care areas, such as glaucoma, cataract, retina and urgent care, is predicted to rise by 60 per cent in medical retina and 44 per cent in glaucoma over the next 20 years.
6.6 Operating these centres will help to tackle a growing waiting list and will
reduce the delays patients have experienced over the last two years as a result of the pandemic. It will also help to meet the challenge of the expected future demand on the service.
6.7 The work at both centres is being undertaken by Speller Metcalfe,
which completed Yeovil Hospital’s new residential accommodation for staff last year.
7. VACCINATION AND LATERAL FLOW TESTING COMPLIANCE 7.1. The trusts are required to report to the Board of Directors on the
vaccination and lateral flow testing compliance. The compliance rates for each of the trusts is set out below: Yeovil District Hospital NHS Foundation Trust
The % frontline staff C19 vaccinated are as follows:
• One dose – 94.7% (A decrease of 1.2% since the January report to the Board)
• Two doses – 93.1% (A decrease of 0.8% since the January report to the Board)
• Three doses - 81.1% (An increase of 0.7% since the January report to the Board)
The % all staff vaccinated 92.7% (at least two doses). This is a decrease of 1.3% since the January report to the Board.
34.3% of all staff (incl Bank/Locum) reported lateral flow tests at least once in last 2 weeks (947 staff) - the frontline split is not available. This is an increase of 7.8% since the January report to the Board.
Chief Executive and Executive Directors’ Report
March 2022 Public Board - 8 – E
65.0% of frontline staff have had their flu vaccinations with 65.1% of all staff receiving their flu vaccine. This is a slight decrease from the January report to the Board where there was 66.2% of frontline staff have had their flu vaccinations but a slight increase from 65.1% of all staff receiving their flu vaccine. Somerset NHS Foundation Trust
The percentage of all staff vaccinated is as follows:
• One dose – 93.7%
• Two doses – 92.3%
• Three doses - 81.6%
67.2% of frontline staff have had their flu vaccinations with 67.3% of all staff receiving their flu vaccine
YEOVIL DISTRICT HOSPITAL NHS FOUNDATION TRUST
8. WORLD CANCER DAY – A SPOTLIGHT ON YEOVIL HOSPITAL’S ONCOLOGY RESEARCH NURSES
8.1. Friday 4 February marked World Cancer Day, an annual event to bring communities together to raise awareness and take action against cancer.
8.2. This year Yeovil Hospital wanted to shine a light on the invaluable research that is conducted throughout the world, dedicated to finding a cure to more than 100 variations of cancer. At Yeovil Hospital there is a team of oncology research nurses that work incredibly hard with patients and teams across the hospital to provide vital information and data to research trials throughout the UK, all with the aim of a lasting cure for cancer.
8.3. To read Senior Oncology Research Nurse Kerry Rennie unique insight into her role click here.
8.4. If you would like to find out more about a career as a research nurse click here, or if you would like to know more about research currently being undertaken at Yeovil Hospital click here.
9. YDH GOVERNOR ELECTIONS
9.1. As an NHS Foundation Trust, the Trust has a Council of Governors
which is made up of elected Trust members, staff members and representatives from nominated and voluntary organisations.
9.2. The role of a Governor includes holding the Trust’s Non-Executive Directors to account for the performance of the Board. They also
Chief Executive and Executive Directors’ Report
March 2022 Public Board - 9 – E
play an important part in setting the Trust’s strategic plans and priorities and form a vital link to our local communities.
9.3. Governors are elected for a term of up to three years and a number of Governors’ term of office will end on 1 June or 1 September 2022.
9.4. The following governor seats will be vacant: Public Dorset – 2 seats Public Greater Yeovil – 1 seat Public South Somerset (South & West) – 2 seats Public South Somerset (North & East) – 1 seat Staff – 2 seats
9.5. The Trust are currently finalising the timetable arrangements for the elections and further information will be updated on the Trust’s website in due course.
SOMERSET NHS FOUNDATION TRUST 10. SECRETARY OF STATE FOR HEALTH AND CARE MR SAJID
JAVID VISITS MUSGROVE PARK HOSPITAL
10.1. On Thursday 17 February 2022, the Secretary of State for Health, Sajid Javid visited Musgrove Park Hospital as part of a visit to the NHS in the South West.
10.2. He visited our new £4.4 million eye care unit which opened late last year. The new unit means eye surgery can continue even when the hospital is at its busiest – which previously could have led to the postponement of planned surgery.
10.3. The unit has two ophthalmic theatre suites, dedicated changing rooms and private waiting rooms as well as rooms for anaesthetists and surgeons to speak confidentially to, and examine, patients before their operation.
10.4. Patients are able to access the unit direct from the car park without needing to walk through the main hospital building. The unit has also been designed to meet the needs of people with impaired vision.
10.5. Creating this facility enabled the expansion of the number of available critical care beds within our existing theatre complex, supporting the increased demand for beds and supporting our response to Covid-19. The NHS in the South West has some of the lowest numbers of critical care beds per head of population and this expansion is a stepping stone towards a further expansion of beds (up to 24) when the new surgical centre opens in 2024.
Chief Executive and Executive Directors’ Report
March 2022 Public Board - 10 – E
10.6. This new unit is in addition to an outpatient macular and glaucoma hub that opened at Chard Hospital in late 2020, which together will help patients get the excellent eye care they need, in a timely way.
10.7. While at Musgrove Park Hospital, the Secretary of State, met with Peter Lewis, Dan Meron, Hayley Peters, David Shannon and Matthew Bryant for a private discussion before he met with a group of colleagues from acute services, community and intermediate care, mental health and the Covid-19 vaccination service.
10.8. The visit was a great opportunity to show some of the development work taking place to improve facilities and services at the hospital, discuss our recovery plans and for colleagues to share some of the tremendous work they are doing across acute, community and mental health services to respond to the current pressures facing the NHS locally.
11. SFT GOVERNOR ELECTIONS
11.1. As an NHS Foundation Trust, the Trust has a Council of Governors
which is made up of elected Trust members, staff members and representatives from nominated and voluntary organisations.
11.2. The role of a Governor includes holding the Trust’s Non-Executive Directors to account for the performance of the Board. They also play an important part in setting the Trust’s strategic plans and priorities and form a vital link to our local communities.
11.3. Governors are elected for a term of up to three years and a number of Governors’ term of office will end on 1 April or 1 May 2022. The Trust will be starting the nomination process on 2 March 2022 and is looking for interested, enthusiastic members with a passion for healthcare to nominate themselves as a candidate in the elections.
11.4. The following governor seats will be vacant: Public Somerset West and Taunton – 2 seats Public Sedgemoor – 1 seat Public Mendip – 2 seats Public South Somerset – 5 seats Public Outside Somerset – 1 seat Public Dorset – 1 seat Staff – 2 seats
11.5. Our elections are managed by Civica Election Services (CES) and to stand in the elections, you will be required to complete a nomination form and this form is available from CES. Their contact details are set out below:
Chief Executive and Executive Directors’ Report
March 2022 Public Board - 11 – E
By phone Tel. 020 8889 9203 By email [email protected] Website www.cesvotes.com/somerset2022 By post Civica Election Services, The Election Centre, 33 Clarendon Road, London, N8 0NW 11.6. Information on the statutory role of Governors, the time commitment,
disqualification criteria, and the Trust’s Constitution is available on CES’ website above. The timetable for the elections is as follows
Nomination Process – opens 2 March and closes on 23 March 2022 Ballot papers will be issued on 12 April 2022 and the elections will close
on 5 May 2022
12. MUSGROVE PARK CHOSEN TO TRIAL NEW PAEDIATRIC CHARTS
12.1. It is widely accepted that Paediatric Early Warning Systems (PEWS)
can help to identify deteriorating children, allowing for early interventions which can improve patient outcomes.
12.2. A survey in 2018/19 showed that 100% of paediatric departments now use a form of PEWS, however there are many different versions in use across the country. This means that there is a wide variation in which, and how many, parameters contribute to a PEWS score.
12.3. Musgrove Park Hospital has been chosen as one of 40 sites that will pilot a new PEWS chart – the System Wide Paediatric Observation Tracking (SPOT) programme. The programme, created by a working group with members from NHS England, The Royal College of Paediatrics and Child Health, and The Royal College of Nursing, aims to provide a single, common language for organisations, to detect deterioration in patients. It would ensure the easy facilitation of referrals into other services, and is also an important safety feature, allowing staff moving between hospitals in rotations to all recognise a single system.
12.4. The pilot project will give the trust an opportunity to pioneer the use of the charts, improving our own recognition and escalation pathways, and by feedbacking back our experiences, we can also influence the charts final design.
12.5. The charts were launched at the start of February, and the pilot study will run for around three months – after which, the charts will continue to be in use until the amended version is released nationally.
13. WHISTLEBLOWING REPORT
13.1. No whistleblowing incidents have been reported since the February 2022 Board meeting.

Draft YDH Board Assurance Framework – Quarter 4 2021/22 – February 2022
March 2022 Public Board - 1 – F
Yeovil District NHS Foundation Trust
REPORT TO: Board of Directors
REPORT TITLE: Draft Board Assurance Framework – Quarter 4 2021/22 – February 2022
SPONSORING EXEC: Phil Brice, Director of Corporate Services
REPORT BY: Samantha Hann, Corporate Governance and Risk Manager
PRESENTED BY: Samantha Hann, Corporate Governance and Risk Manager
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☒ For Assurance/
Discussion ☐ For Approval / Decision ☐ For Information
Executive Summary and Reason for presentation to Committee/Board
The Board Assurance Committees carry out detailed monitoring and review of the principal risks that relate to the organisation’s strategic objectives and priorities. These risks shall be proactively managed and reported on as a minimum requirement quarterly to the Board Assurance Committees and to the Board of Directors through the BAF. The Board Assurance Committees provides assurance to the Board with regard to the continued effectiveness of the Trust’s system of integrated governance, risk management and internal control. Committees continue to review the extent to which they are assured by the evidence presented for each risk. The BAF includes all principal risks that represent higher levels of opportunity/threat, which may have a major, or long-term impact on benefits realisation or organisation objectives and which may also impact upon the strategic objectives and outcomes positively or negatively. This is a first draft of the Quarter 4 2021/22 BAF following review by the Joint Executive Directors who commenced in post on 10 January 2022. The principal risks have been reassigned to the Joint Executive Directors and the final version of the Quarter 4 2021/22 BAF will be presented to the Assurance Committees in April 2022 and the Board of Directors in May 2022.
Recommendation The Board is asked to note and discuss the report.
Draft YDH Board Assurance Framework – Quarter 4 2021/22 – February 2022
March 2022 Public Board - 2 – F
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☒ Care for our Population ☒ Develop our People
☒ Innovate and Collaborate ☒ Develop a Sustainable System
Somerset NHS FT
☐ Obj 1 Inclusive culture ☐ Obj 4 Safe services ☐ Obj 7 Improving outcomes
☐ Obj 2 Collaboration ☐ Obj 5 Self management ☐ Obj 8 Workforce
☐ Obj 3 Independent lives ☐ Obj 6 Value all people alike ☐ Obj 9 Performance
☐ Obj 10 Finance
Implications/Requirements (Please select any which are relevant to this paper)
☒ Financial ☒ Legislation ☒ Workforce ☒ Estates ☒ ICT ☒ Patient Safety /
Quality
Details:
Equality The Trust wants its services to be as accessible as possible, to as many people as
possible. Please indicate whether the report has an impact on the protected characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are no proposals or matters which affect any persons with protected characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
Not applicable.
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
The Board Assurance Framework is presented to the Board on a quarterly basis.
Reference to CQC domains (Please select any which are relevant to this paper)
☒ Safe ☒ Effective ☒ Caring ☒ Responsive ☒ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
Draft YDH Board Assurance Framework – Quarter 4 2021/22 – February 2022
March 2022 Public Board - 3 – F
Introduction The Department of Health provided guidance on Assurance Frameworks in 2003. The document states that, ‘the Assurance Framework provides organisations with a simple but comprehensive method for the effective and focused management of the principal risks to meeting their objectives’. The Board Assurance Framework (BAF) forms part of the Trust’s risk management strategy and is the framework for identification and management of strategic risks. In line with the Trust’s Risk Management Strategy and the revised monitoring arrangements therein, the Board will receive the BAF on a quarterly basis (April, July, October and January). The BAF provides evidence to support the Annual Governance Statement. Board Assurance Framework The Board Assurance Committees carry out detailed monitoring and review of the principal risks that relate to the organisation’s strategic objectives and priorities. These risks shall be proactively managed and reported on as a minimum requirement quarterly to the Board Assurance Committees and to the Board of Directors through the BAF. The Board Assurance Committees provides assurance to the Board with regard to the continued effectiveness of the Trust’s system of integrated governance, risk management and internal control. Committees continue to review the extent to which they are assured by the evidence presented for each risk. The BAF includes all principal risks that represent higher levels of opportunity/threat, which may have a major, or long-term impact on benefits realisation or organisation objectives and which may also impact upon the strategic objectives and outcomes positively or negatively. The identified high-level objectives for Yeovil District Hospital are:
▪ Care for our Population ▪ Develop our People ▪ Innovate and Collaborate ▪ Develop a Sustainable System.
Underneath each high-level objectives are various key priorities to be achieved. What is Assurance? Assurance: Provides: Evidence/Confidence/Certainty To: Board/Managers/Stakeholders That: Action is taken as required In order to make this assessment, Board Assurance Committees consider the following questions, based on the evidence provided on the BAF for each risk:
• To what extent are the key controls (i.e. existing controls) effective?
• What are the gaps in the controls, how significant are they in relation to the current risk score?
• What internal assurances and independent external assurances are in place? Are they sufficient/adequate and are there any gaps? Are additional assurances required?
• Are there any areas where assurance is duplicated, repeated or excessive when compared with the activity undertaken?
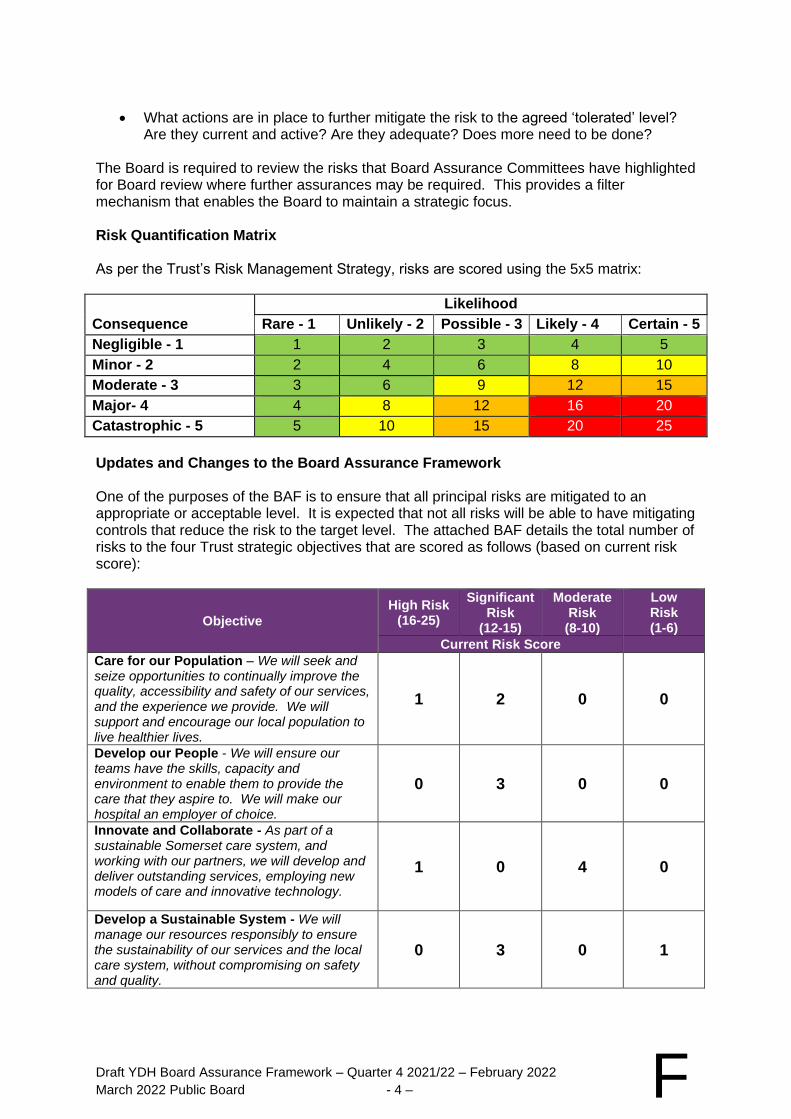
Draft YDH Board Assurance Framework – Quarter 4 2021/22 – February 2022
March 2022 Public Board - 4 – F
• What actions are in place to further mitigate the risk to the agreed ‘tolerated’ level? Are they current and active? Are they adequate? Does more need to be done?
The Board is required to review the risks that Board Assurance Committees have highlighted for Board review where further assurances may be required. This provides a filter mechanism that enables the Board to maintain a strategic focus. Risk Quantification Matrix As per the Trust’s Risk Management Strategy, risks are scored using the 5x5 matrix:
Likelihood
Consequence Rare - 1 Unlikely - 2 Possible - 3 Likely - 4 Certain - 5
Negligible - 1 1 2 3 4 5
Minor - 2 2 4 6 8 10
Moderate - 3 3 6 9 12 15
Major- 4 4 8 12 16 20
Catastrophic - 5 5 10 15 20 25
Updates and Changes to the Board Assurance Framework One of the purposes of the BAF is to ensure that all principal risks are mitigated to an appropriate or acceptable level. It is expected that not all risks will be able to have mitigating controls that reduce the risk to the target level. The attached BAF details the total number of risks to the four Trust strategic objectives that are scored as follows (based on current risk score):
Objective
High Risk (16-25)
Significant Risk
(12-15)
Moderate Risk (8-10)
Low Risk (1-6)
Current Risk Score
Care for our Population – We will seek and seize opportunities to continually improve the quality, accessibility and safety of our services, and the experience we provide. We will support and encourage our local population to live healthier lives.
1 2 0 0
Develop our People - We will ensure our teams have the skills, capacity and environment to enable them to provide the care that they aspire to. We will make our hospital an employer of choice.
0 3 0 0
Innovate and Collaborate - As part of a sustainable Somerset care system, and working with our partners, we will develop and deliver outstanding services, employing new models of care and innovative technology.
1 0 4 0
Develop a Sustainable System - We will manage our resources responsibly to ensure the sustainability of our services and the local care system, without compromising on safety and quality.
0 3 0 1
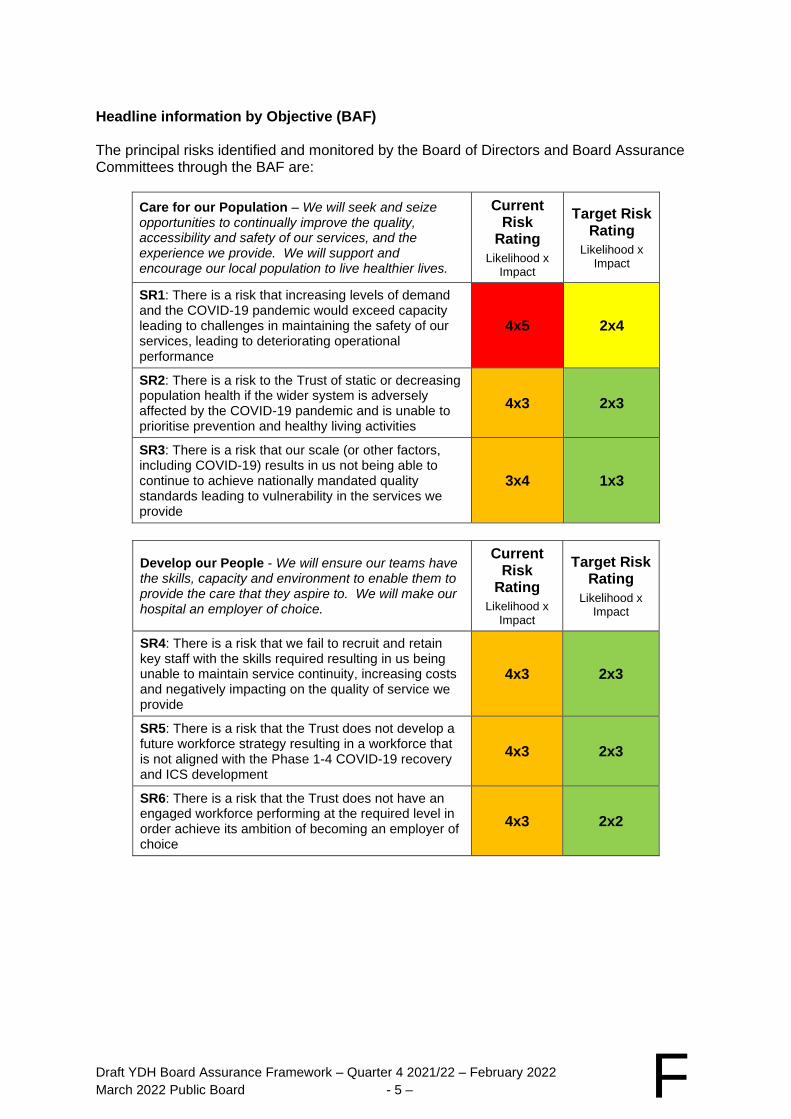
Draft YDH Board Assurance Framework – Quarter 4 2021/22 – February 2022
March 2022 Public Board - 5 – F
Headline information by Objective (BAF) The principal risks identified and monitored by the Board of Directors and Board Assurance Committees through the BAF are:
Care for our Population – We will seek and seize opportunities to continually improve the quality, accessibility and safety of our services, and the experience we provide. We will support and encourage our local population to live healthier lives.
Current Risk
Rating
Likelihood x Impact
Target Risk Rating
Likelihood x Impact
SR1: There is a risk that increasing levels of demand and the COVID-19 pandemic would exceed capacity leading to challenges in maintaining the safety of our services, leading to deteriorating operational performance
4x5 2x4
SR2: There is a risk to the Trust of static or decreasing population health if the wider system is adversely affected by the COVID-19 pandemic and is unable to prioritise prevention and healthy living activities
4x3 2x3
SR3: There is a risk that our scale (or other factors, including COVID-19) results in us not being able to continue to achieve nationally mandated quality standards leading to vulnerability in the services we provide
3x4 1x3
Develop our People - We will ensure our teams have the skills, capacity and environment to enable them to provide the care that they aspire to. We will make our hospital an employer of choice.
Current Risk
Rating
Likelihood x Impact
Target Risk Rating
Likelihood x Impact
SR4: There is a risk that we fail to recruit and retain key staff with the skills required resulting in us being unable to maintain service continuity, increasing costs and negatively impacting on the quality of service we provide
4x3 2x3
SR5: There is a risk that the Trust does not develop a future workforce strategy resulting in a workforce that is not aligned with the Phase 1-4 COVID-19 recovery and ICS development
4x3 2x3
SR6: There is a risk that the Trust does not have an engaged workforce performing at the required level in order achieve its ambition of becoming an employer of choice
4x3 2x2
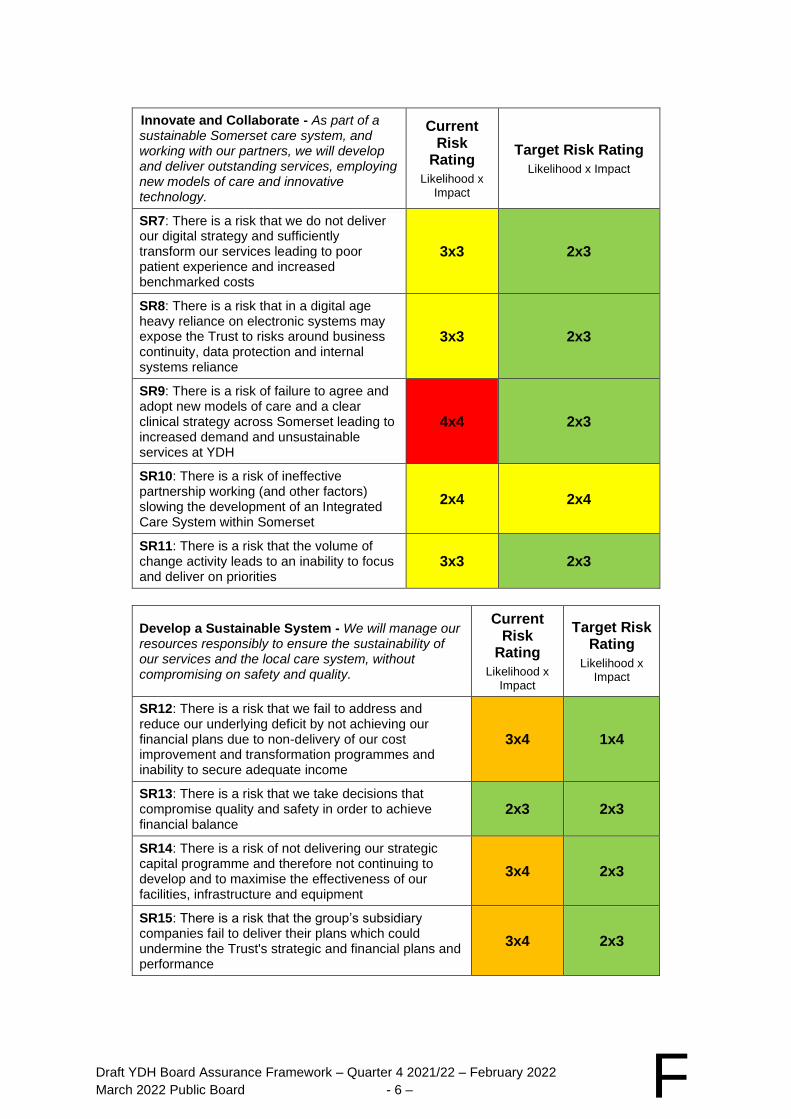
Draft YDH Board Assurance Framework – Quarter 4 2021/22 – February 2022
March 2022 Public Board - 6 – F
Innovate and Collaborate - As part of a sustainable Somerset care system, and working with our partners, we will develop and deliver outstanding services, employing new models of care and innovative technology.
Current Risk
Rating
Likelihood x Impact
Target Risk Rating
Likelihood x Impact
SR7: There is a risk that we do not deliver our digital strategy and sufficiently transform our services leading to poor patient experience and increased benchmarked costs
3x3 2x3
SR8: There is a risk that in a digital age heavy reliance on electronic systems may expose the Trust to risks around business continuity, data protection and internal systems reliance
3x3 2x3
SR9: There is a risk of failure to agree and adopt new models of care and a clear clinical strategy across Somerset leading to increased demand and unsustainable services at YDH
4x4 2x3
SR10: There is a risk of ineffective partnership working (and other factors) slowing the development of an Integrated Care System within Somerset
2x4 2x4
SR11: There is a risk that the volume of change activity leads to an inability to focus and deliver on priorities
3x3 2x3
Develop a Sustainable System - We will manage our resources responsibly to ensure the sustainability of our services and the local care system, without compromising on safety and quality.
Current Risk
Rating
Likelihood x Impact
Target Risk Rating
Likelihood x Impact
SR12: There is a risk that we fail to address and reduce our underlying deficit by not achieving our financial plans due to non-delivery of our cost improvement and transformation programmes and inability to secure adequate income
3x4 1x4
SR13: There is a risk that we take decisions that compromise quality and safety in order to achieve financial balance
2x3 2x3
SR14: There is a risk of not delivering our strategic capital programme and therefore not continuing to develop and to maximise the effectiveness of our facilities, infrastructure and equipment
3x4 2x3
SR15: There is a risk that the group’s subsidiary companies fail to deliver their plans which could undermine the Trust's strategic and financial plans and performance
3x4 2x3
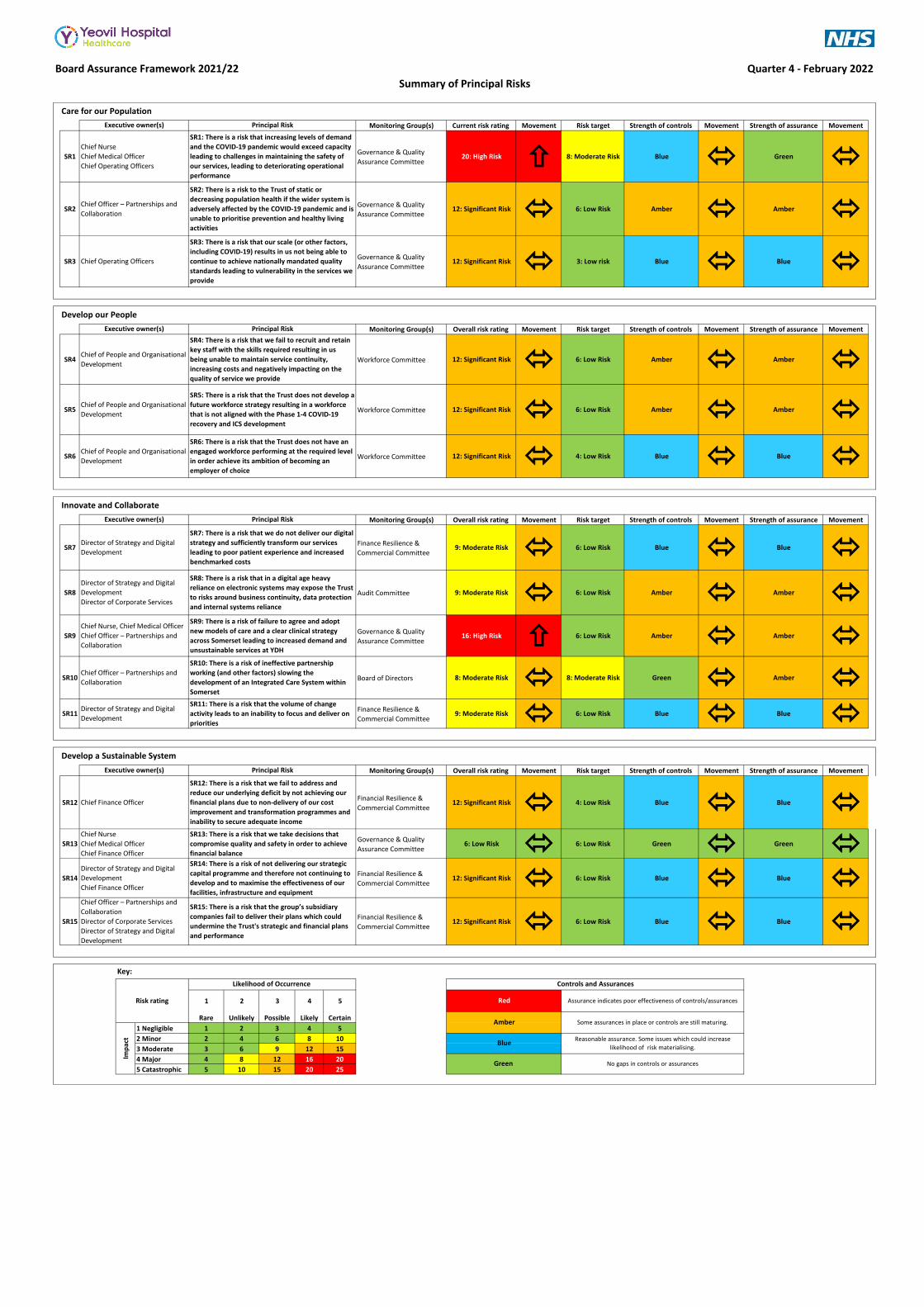
Board Assurance Framework 2021/22
Monitoring Group(s) Current risk rating Movement Risk target Strength of controls Movement Strength of assurance Movement
SR1Governance & Quality
Assurance Committee20: High Risk 8: Moderate Risk Blue Green
SR2Governance & Quality
Assurance Committee12: Significant Risk 6: Low Risk Amber Amber
SR3Governance & Quality
Assurance Committee12: Significant Risk 3: Low risk Blue Blue
Monitoring Group(s) Overall risk rating Movement Risk target Strength of controls Movement Strength of assurance Movement
SR4 Workforce Committee 12: Significant Risk 6: Low Risk Amber Amber
SR5 Workforce Committee 12: Significant Risk 6: Low Risk Amber Amber
SR6 Workforce Committee 12: Significant Risk 4: Low Risk Blue Blue
Monitoring Group(s) Overall risk rating Movement Risk target Strength of controls Movement Strength of assurance Movement
SR7Finance Resilience &
Commercial Committee9: Moderate Risk 6: Low Risk Blue Blue
SR8 Audit Committee 9: Moderate Risk 6: Low Risk Amber Amber
SR9Governance & Quality
Assurance Committee16: High Risk 6: Low Risk Amber Amber
SR10 Board of Directors 8: Moderate Risk 8: Moderate Risk Green Amber
SR11Finance Resilience &
Commercial Committee9: Moderate Risk 6: Low Risk Blue Blue
Monitoring Group(s) Overall risk rating Movement Risk target Strength of controls Movement Strength of assurance Movement
SR12Financial Resilience &
Commercial Committee12: Significant Risk 4: Low Risk Blue Blue
SR13Governance & Quality
Assurance Committee6: Low Risk 6: Low Risk Green Green
SR14Financial Resilience &
Commercial Committee12: Significant Risk 6: Low Risk Blue Blue
SR15Financial Resilience &
Commercial Committee12: Significant Risk 6: Low Risk Blue Blue
Key:
1 2 3 4 5
Rare Unlikely Possible Likely Certain
1 Negligible 1 2 3 4 5
2 Minor 2 4 6 8 10
3 Moderate 3 6 9 12 15
4 Major 4 8 12 16 20
5 Catastrophic 5 10 15 20 25
Chief of People and Organisational
Development
SR5: There is a risk that the Trust does not develop a
future workforce strategy resulting in a workforce
that is not aligned with the Phase 1-4 COVID-19
recovery and ICS development
SR15: There is a risk that the group’s subsidiary
companies fail to deliver their plans which could
undermine the Trust's strategic and financial plans
and performance
Director of Strategy and Digital
Development
Chief Finance Officer
SR14: There is a risk of not delivering our strategic
capital programme and therefore not continuing to
develop and to maximise the effectiveness of our
facilities, infrastructure and equipment
Chief Nurse, Chief Medical Officer
Chief Officer – Partnerships and
Collaboration
Chief Officer – Partnerships and
Collaboration
Director of Corporate Services
Director of Strategy and Digital
Development
Chief Nurse
Chief Medical Officer
Chief Finance Officer
SR13: There is a risk that we take decisions that
compromise quality and safety in order to achieve
financial balance
SR9: There is a risk of failure to agree and adopt
new models of care and a clear clinical strategy
across Somerset leading to increased demand and
unsustainable services at YDH
Chief Officer – Partnerships and
Collaboration
Director of Strategy and Digital
Development
SR11: There is a risk that the volume of change
activity leads to an inability to focus and deliver on
priorities
Principal Risk
SR12: There is a risk that we fail to address and
reduce our underlying deficit by not achieving our
financial plans due to non-delivery of our cost
improvement and transformation programmes and
inability to secure adequate income
Executive owner(s)
Chief Finance Officer
SR10: There is a risk of ineffective partnership
working (and other factors) slowing the
development of an Integrated Care System within
Somerset
Quarter 4 - February 2022
Summary of Principal Risks
Care for our Population
SR7: There is a risk that we do not deliver our digital
strategy and sufficiently transform our services
leading to poor patient experience and increased
benchmarked costs
SR8: There is a risk that in a digital age heavy
reliance on electronic systems may expose the Trust
to risks around business continuity, data protection
and internal systems reliance
Director of Strategy and Digital
Development
Chief Nurse
Chief Medical Officer
Chief Operating Officers
Executive owner(s) Principal Risk
SR1: There is a risk that increasing levels of demand
and the COVID-19 pandemic would exceed capacity
leading to challenges in maintaining the safety of
our services, leading to deteriorating operational
performance
SR2: There is a risk to the Trust of static or
decreasing population health if the wider system is
adversely affected by the COVID-19 pandemic and is
unable to prioritise prevention and healthy living
activities
SR3: There is a risk that our scale (or other factors,
including COVID-19) results in us not being able to
continue to achieve nationally mandated quality
standards leading to vulnerability in the services we
provide
Principal Risk
Chief Officer – Partnerships and
Collaboration
Chief Operating Officers
Director of Strategy and Digital
Development
Director of Corporate Services
Develop a Sustainable System
Develop our People
Principal Risk
SR4: There is a risk that we fail to recruit and retain
key staff with the skills required resulting in us
being unable to maintain service continuity,
increasing costs and negatively impacting on the
quality of service we provide
Innovate and Collaborate
Executive owner(s)
Chief of People and Organisational
Development
SR6: There is a risk that the Trust does not have an
engaged workforce performing at the required level
in order achieve its ambition of becoming an
employer of choice
Imp
act
Risk rating
Executive owner(s)
Chief of People and Organisational
Development
Likelihood of Occurrence
Red
Amber
Controls and Assurances
No gaps in controls or assurances
Blue
Green
Reasonable assurance. Some issues which could increase
likelihood of risk materialising.
Some assurances in place or controls are still maturing.
Assurance indicates poor effectiveness of controls/assurances
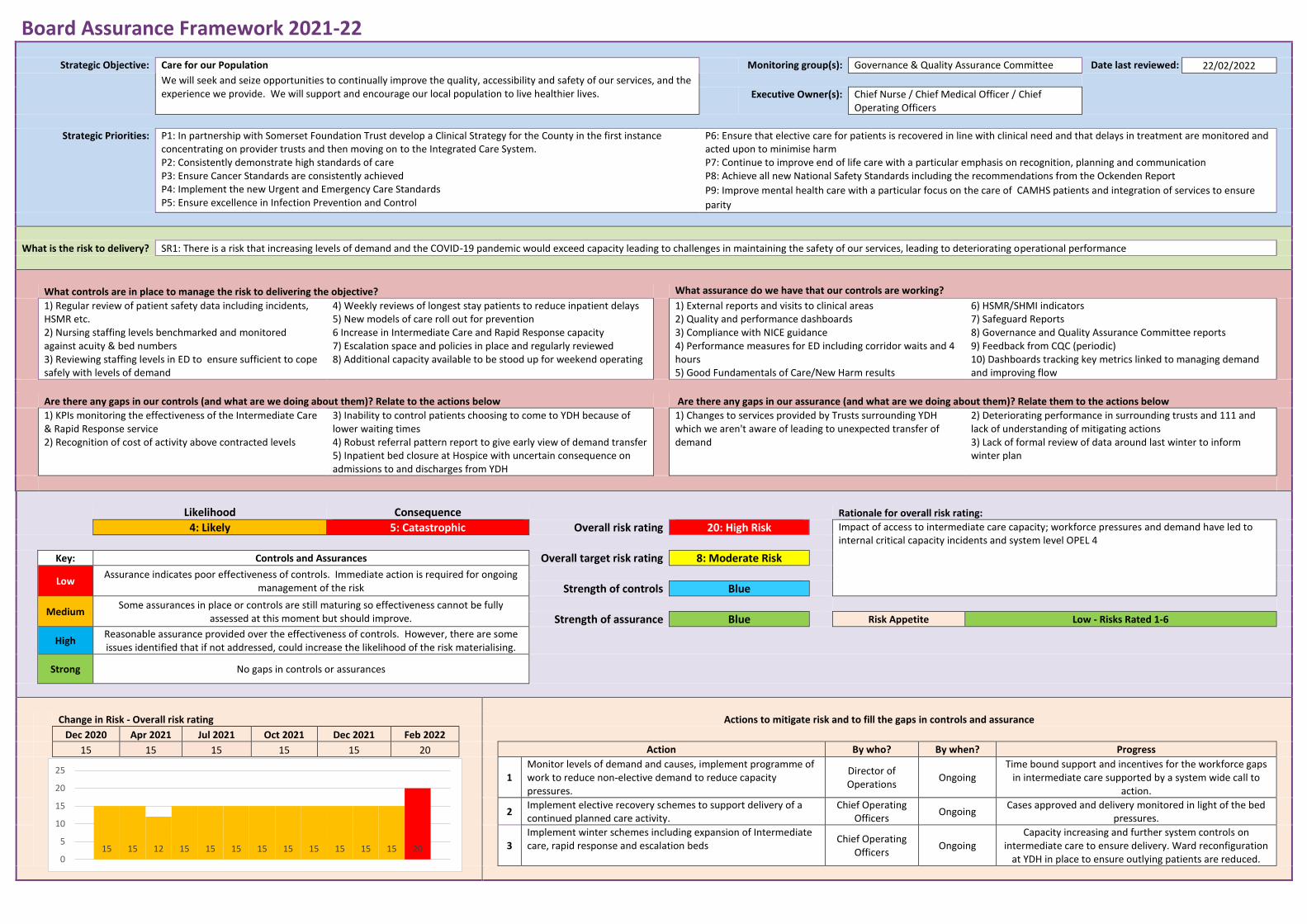
Board Assurance Framework 2021-22
Strategic Objective: Care for our Population Monitoring group(s): Governance & Quality Assurance Committee Date last reviewed: 22/02/2022
We will seek and seize opportunities to continually improve the quality, accessibility and safety of our services, and the experience we provide. We will support and encourage our local population to live healthier lives.
Executive Owner(s): Chief Nurse / Chief Medical Officer / Chief
Operating Officers
Strategic Priorities: P1: In partnership with Somerset Foundation Trust develop a Clinical Strategy for the County in the first instance concentrating on provider trusts and then moving on to the Integrated Care System. P2: Consistently demonstrate high standards of care P3: Ensure Cancer Standards are consistently achieved P4: Implement the new Urgent and Emergency Care Standards P5: Ensure excellence in Infection Prevention and Control
P6: Ensure that elective care for patients is recovered in line with clinical need and that delays in treatment are monitored and acted upon to minimise harm P7: Continue to improve end of life care with a particular emphasis on recognition, planning and communication P8: Achieve all new National Safety Standards including the recommendations from the Ockenden Report
P9: Improve mental health care with a particular focus on the care of CAMHS patients and integration of services to ensure
parity
What is the risk to delivery? SR1: There is a risk that increasing levels of demand and the COVID-19 pandemic would exceed capacity leading to challenges in maintaining the safety of our services, leading to deteriorating operational performance
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) Regular review of patient safety data including incidents, HSMR etc. 2) Nursing staffing levels benchmarked and monitored against acuity & bed numbers 3) Reviewing staffing levels in ED to ensure sufficient to cope safely with levels of demand
4) Weekly reviews of longest stay patients to reduce inpatient delays 5) New models of care roll out for prevention 6 Increase in Intermediate Care and Rapid Response capacity 7) Escalation space and policies in place and regularly reviewed 8) Additional capacity available to be stood up for weekend operating
1) External reports and visits to clinical areas 2) Quality and performance dashboards 3) Compliance with NICE guidance 4) Performance measures for ED including corridor waits and 4 hours 5) Good Fundamentals of Care/New Harm results
6) HSMR/SHMI indicators 7) Safeguard Reports 8) Governance and Quality Assurance Committee reports 9) Feedback from CQC (periodic) 10) Dashboards tracking key metrics linked to managing demand and improving flow
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) KPIs monitoring the effectiveness of the Intermediate Care & Rapid Response service 2) Recognition of cost of activity above contracted levels
3) Inability to control patients choosing to come to YDH because of lower waiting times 4) Robust referral pattern report to give early view of demand transfer 5) Inpatient bed closure at Hospice with uncertain consequence on admissions to and discharges from YDH
1) Changes to services provided by Trusts surrounding YDH which we aren't aware of leading to unexpected transfer of demand
2) Deteriorating performance in surrounding trusts and 111 and lack of understanding of mitigating actions 3) Lack of formal review of data around last winter to inform winter plan
Likelihood Consequence Rationale for overall risk rating:
4: Likely 5: Catastrophic Overall risk rating 20: High Risk Impact of access to intermediate care capacity; workforce pressures and demand have led to internal critical capacity incidents and system level OPEL 4
Key: Controls and Assurances Overall target risk rating 8: Moderate Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Blue
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Blue Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
15 15 15 15 15 20 Action By who? By when? Progress
1
Monitor levels of demand and causes, implement programme of work to reduce non-elective demand to reduce capacity pressures.
Director of Operations
Ongoing Time bound support and incentives for the workforce gaps
in intermediate care supported by a system wide call to action.
2
Implement elective recovery schemes to support delivery of a continued planned care activity.
Chief Operating Officers
Ongoing Cases approved and delivery monitored in light of the bed
pressures.
3
Implement winter schemes including expansion of Intermediate care, rapid response and escalation beds
Chief Operating Officers
Ongoing Capacity increasing and further system controls on
intermediate care to ensure delivery. Ward reconfiguration at YDH in place to ensure outlying patients are reduced.
15 15 12 15 15 15 15 15 15 15 15 15 200
5
10
15
20
25
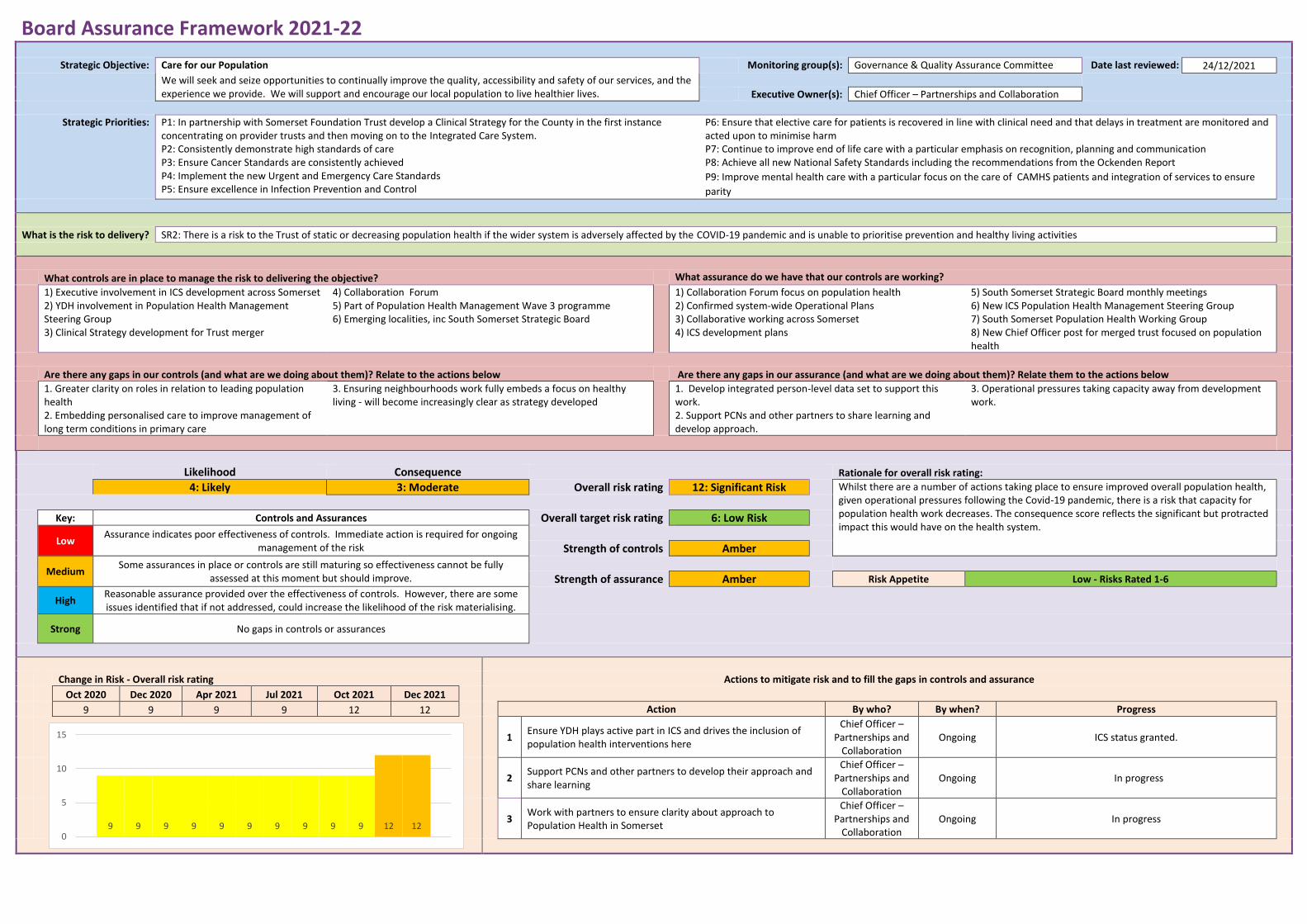
Board Assurance Framework 2021-22
Strategic Objective: Care for our Population Monitoring group(s): Governance & Quality Assurance Committee Date last reviewed: 24/12/2021
We will seek and seize opportunities to continually improve the quality, accessibility and safety of our services, and the experience we provide. We will support and encourage our local population to live healthier lives.
Executive Owner(s): Chief Officer – Partnerships and Collaboration
Strategic Priorities: P1: In partnership with Somerset Foundation Trust develop a Clinical Strategy for the County in the first instance concentrating on provider trusts and then moving on to the Integrated Care System. P2: Consistently demonstrate high standards of care P3: Ensure Cancer Standards are consistently achieved P4: Implement the new Urgent and Emergency Care Standards P5: Ensure excellence in Infection Prevention and Control
P6: Ensure that elective care for patients is recovered in line with clinical need and that delays in treatment are monitored and acted upon to minimise harm P7: Continue to improve end of life care with a particular emphasis on recognition, planning and communication P8: Achieve all new National Safety Standards including the recommendations from the Ockenden Report
P9: Improve mental health care with a particular focus on the care of CAMHS patients and integration of services to ensure
parity
What is the risk to delivery? SR2: There is a risk to the Trust of static or decreasing population health if the wider system is adversely affected by the COVID-19 pandemic and is unable to prioritise prevention and healthy living activities
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) Executive involvement in ICS development across Somerset 2) YDH involvement in Population Health Management Steering Group 3) Clinical Strategy development for Trust merger
4) Collaboration Forum 5) Part of Population Health Management Wave 3 programme 6) Emerging localities, inc South Somerset Strategic Board
1) Collaboration Forum focus on population health 2) Confirmed system-wide Operational Plans 3) Collaborative working across Somerset 4) ICS development plans
5) South Somerset Strategic Board monthly meetings 6) New ICS Population Health Management Steering Group 7) South Somerset Population Health Working Group 8) New Chief Officer post for merged trust focused on population health
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1. Greater clarity on roles in relation to leading population health 2. Embedding personalised care to improve management of long term conditions in primary care
3. Ensuring neighbourhoods work fully embeds a focus on healthy living - will become increasingly clear as strategy developed
1. Develop integrated person-level data set to support this work. 2. Support PCNs and other partners to share learning and develop approach.
3. Operational pressures taking capacity away from development work.
Likelihood Consequence Rationale for overall risk rating:
4: Likely 3: Moderate Overall risk rating 12: Significant Risk Whilst there are a number of actions taking place to ensure improved overall population health, given operational pressures following the Covid-19 pandemic, there is a risk that capacity for population health work decreases. The consequence score reflects the significant but protracted impact this would have on the health system.
Key: Controls and Assurances Overall target risk rating 6: Low Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Amber
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Amber Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Oct 2020 Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021
9 9 9 9 12 12 Action By who? By when? Progress
1
Ensure YDH plays active part in ICS and drives the inclusion of population health interventions here
Chief Officer – Partnerships and
Collaboration Ongoing ICS status granted.
2
Support PCNs and other partners to develop their approach and share learning
Chief Officer – Partnerships and
Collaboration Ongoing In progress
3
Work with partners to ensure clarity about approach to Population Health in Somerset
Chief Officer – Partnerships and
Collaboration Ongoing In progress
9 9 9 9 9 9 9 9 9 9 12 120
5
10
15
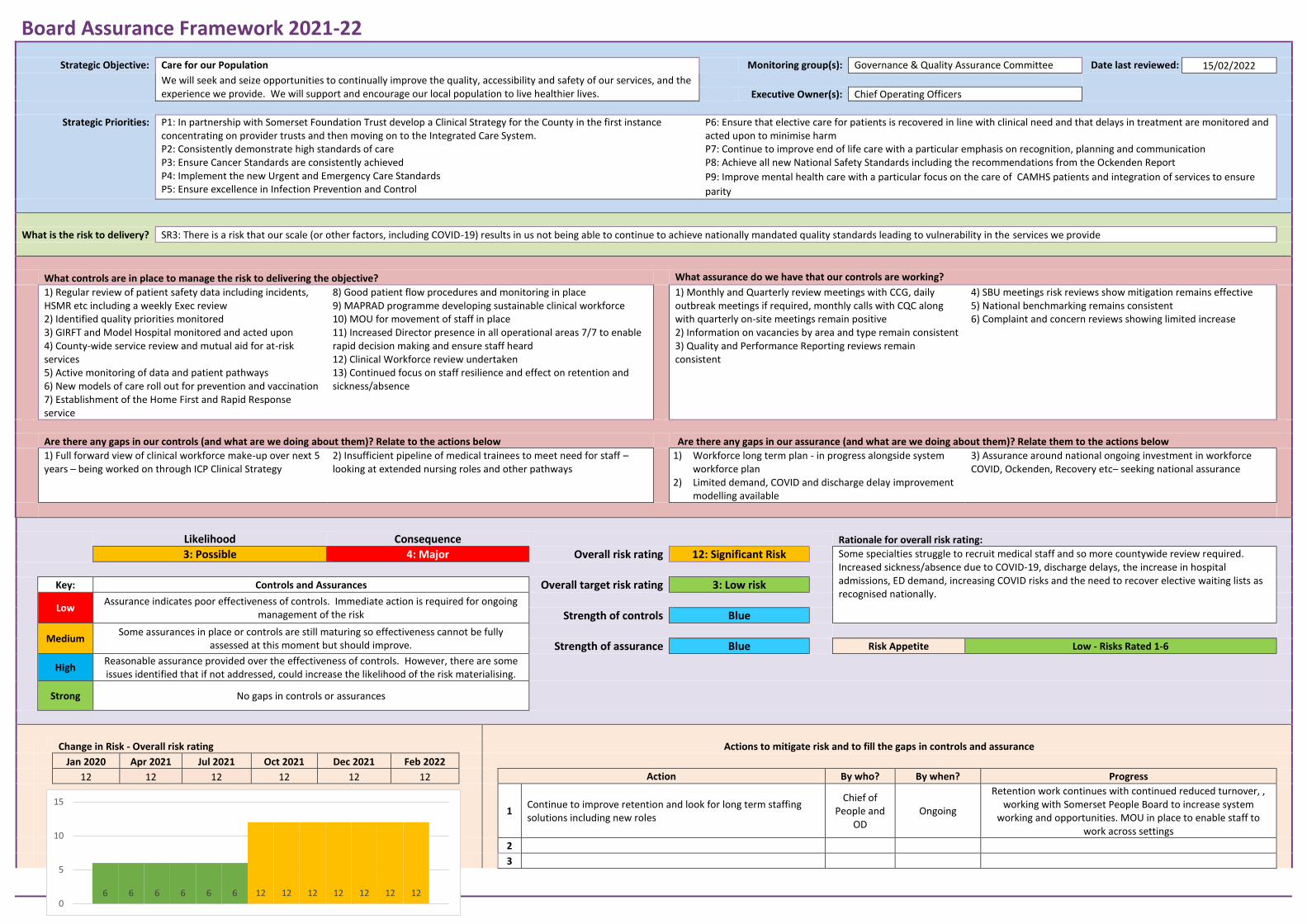
Board Assurance Framework 2021-22
Strategic Objective: Care for our Population Monitoring group(s): Governance & Quality Assurance Committee Date last reviewed: 15/02/2022
We will seek and seize opportunities to continually improve the quality, accessibility and safety of our services, and the experience we provide. We will support and encourage our local population to live healthier lives.
Executive Owner(s): Chief Operating Officers
Strategic Priorities: P1: In partnership with Somerset Foundation Trust develop a Clinical Strategy for the County in the first instance concentrating on provider trusts and then moving on to the Integrated Care System. P2: Consistently demonstrate high standards of care P3: Ensure Cancer Standards are consistently achieved P4: Implement the new Urgent and Emergency Care Standards P5: Ensure excellence in Infection Prevention and Control
P6: Ensure that elective care for patients is recovered in line with clinical need and that delays in treatment are monitored and acted upon to minimise harm P7: Continue to improve end of life care with a particular emphasis on recognition, planning and communication P8: Achieve all new National Safety Standards including the recommendations from the Ockenden Report
P9: Improve mental health care with a particular focus on the care of CAMHS patients and integration of services to ensure
parity
What is the risk to delivery? SR3: There is a risk that our scale (or other factors, including COVID-19) results in us not being able to continue to achieve nationally mandated quality standards leading to vulnerability in the services we provide
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) Regular review of patient safety data including incidents, HSMR etc including a weekly Exec review 2) Identified quality priorities monitored 3) GIRFT and Model Hospital monitored and acted upon 4) County-wide service review and mutual aid for at-risk services 5) Active monitoring of data and patient pathways 6) New models of care roll out for prevention and vaccination 7) Establishment of the Home First and Rapid Response service
8) Good patient flow procedures and monitoring in place 9) MAPRAD programme developing sustainable clinical workforce 10) MOU for movement of staff in place 11) Increased Director presence in all operational areas 7/7 to enable rapid decision making and ensure staff heard 12) Clinical Workforce review undertaken 13) Continued focus on staff resilience and effect on retention and sickness/absence
1) Monthly and Quarterly review meetings with CCG, daily outbreak meetings if required, monthly calls with CQC along with quarterly on-site meetings remain positive 2) Information on vacancies by area and type remain consistent 3) Quality and Performance Reporting reviews remain consistent
4) SBU meetings risk reviews show mitigation remains effective 5) National benchmarking remains consistent 6) Complaint and concern reviews showing limited increase
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) Full forward view of clinical workforce make-up over next 5 years – being worked on through ICP Clinical Strategy
2) Insufficient pipeline of medical trainees to meet need for staff – looking at extended nursing roles and other pathways
1) Workforce long term plan - in progress alongside system workforce plan
2) Limited demand, COVID and discharge delay improvement modelling available
3) Assurance around national ongoing investment in workforce COVID, Ockenden, Recovery etc– seeking national assurance
Likelihood Consequence Rationale for overall risk rating:
3: Possible 4: Major Overall risk rating 12: Significant Risk Some specialties struggle to recruit medical staff and so more countywide review required. Increased sickness/absence due to COVID-19, discharge delays, the increase in hospital admissions, ED demand, increasing COVID risks and the need to recover elective waiting lists as recognised nationally.
Key: Controls and Assurances Overall target risk rating 3: Low risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Blue
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Blue Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Jan 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
12 12 12 12 12 12 Action By who? By when? Progress
1 Continue to improve retention and look for long term staffing solutions including new roles
Chief of People and
OD Ongoing
Retention work continues with continued reduced turnover, , working with Somerset People Board to increase system
working and opportunities. MOU in place to enable staff to work across settings
2
3
6 6 6 6 6 6 12 12 12 12 12 12 12
0
5
10
15
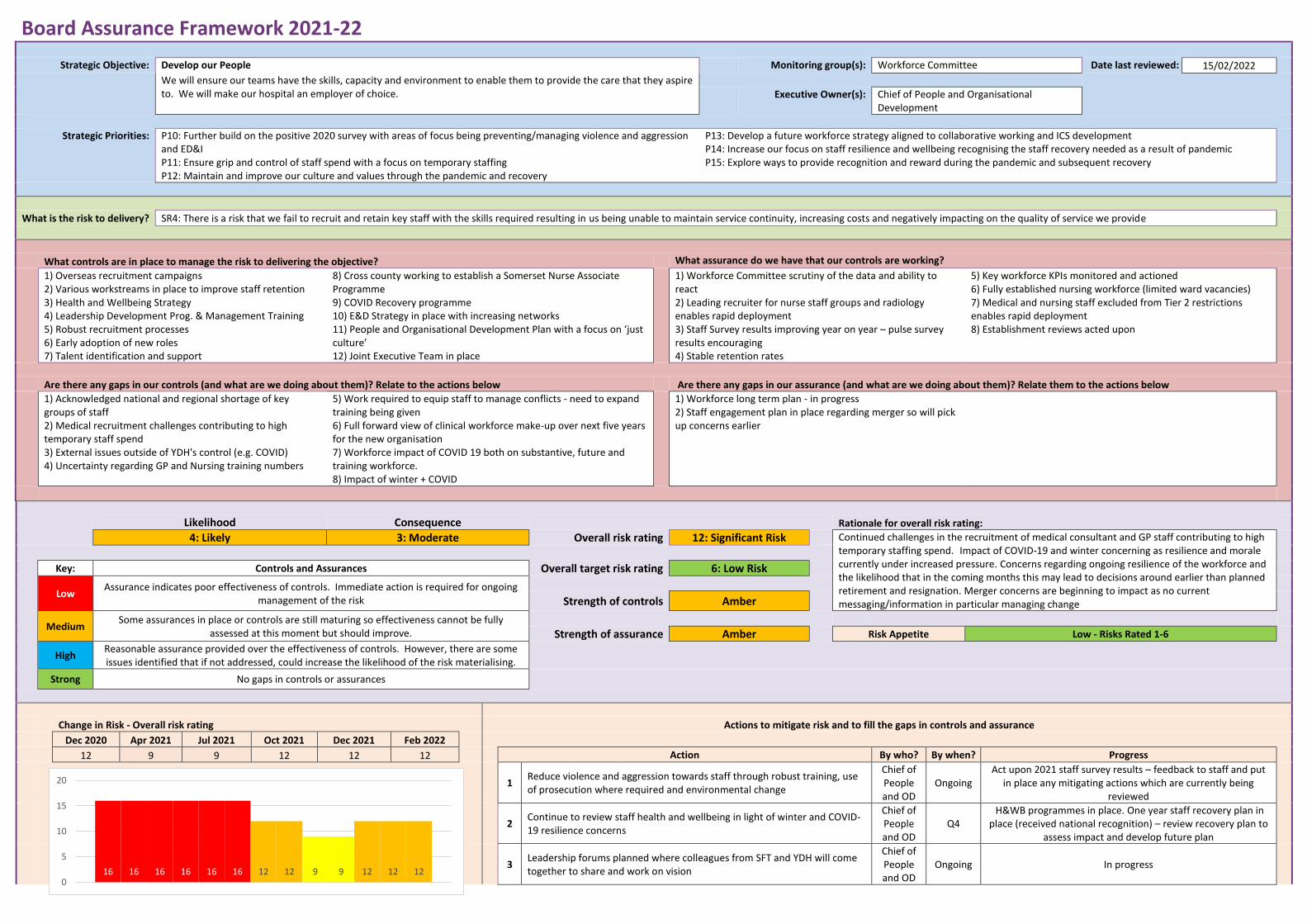
Board Assurance Framework 2021-22
Strategic Objective: Develop our People Monitoring group(s): Workforce Committee Date last reviewed: 15/02/2022
We will ensure our teams have the skills, capacity and environment to enable them to provide the care that they aspire to. We will make our hospital an employer of choice.
Executive Owner(s): Chief of People and Organisational
Development
Strategic Priorities: P10: Further build on the positive 2020 survey with areas of focus being preventing/managing violence and aggression and ED&I P11: Ensure grip and control of staff spend with a focus on temporary staffing P12: Maintain and improve our culture and values through the pandemic and recovery
P13: Develop a future workforce strategy aligned to collaborative working and ICS development P14: Increase our focus on staff resilience and wellbeing recognising the staff recovery needed as a result of pandemic P15: Explore ways to provide recognition and reward during the pandemic and subsequent recovery
What is the risk to delivery? SR4: There is a risk that we fail to recruit and retain key staff with the skills required resulting in us being unable to maintain service continuity, increasing costs and negatively impacting on the quality of service we provide
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) Overseas recruitment campaigns 2) Various workstreams in place to improve staff retention 3) Health and Wellbeing Strategy 4) Leadership Development Prog. & Management Training 5) Robust recruitment processes 6) Early adoption of new roles 7) Talent identification and support
8) Cross county working to establish a Somerset Nurse Associate Programme 9) COVID Recovery programme 10) E&D Strategy in place with increasing networks 11) People and Organisational Development Plan with a focus on ‘just culture’ 12) Joint Executive Team in place
1) Workforce Committee scrutiny of the data and ability to react 2) Leading recruiter for nurse staff groups and radiology enables rapid deployment 3) Staff Survey results improving year on year – pulse survey results encouraging 4) Stable retention rates
5) Key workforce KPIs monitored and actioned 6) Fully established nursing workforce (limited ward vacancies) 7) Medical and nursing staff excluded from Tier 2 restrictions enables rapid deployment 8) Establishment reviews acted upon
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) Acknowledged national and regional shortage of key groups of staff 2) Medical recruitment challenges contributing to high temporary staff spend 3) External issues outside of YDH's control (e.g. COVID) 4) Uncertainty regarding GP and Nursing training numbers
5) Work required to equip staff to manage conflicts - need to expand training being given 6) Full forward view of clinical workforce make-up over next five years for the new organisation 7) Workforce impact of COVID 19 both on substantive, future and training workforce. 8) Impact of winter + COVID
1) Workforce long term plan - in progress 2) Staff engagement plan in place regarding merger so will pick up concerns earlier
Likelihood Consequence Rationale for overall risk rating:
4: Likely 3: Moderate Overall risk rating 12: Significant Risk Continued challenges in the recruitment of medical consultant and GP staff contributing to high temporary staffing spend. Impact of COVID-19 and winter concerning as resilience and morale currently under increased pressure. Concerns regarding ongoing resilience of the workforce and the likelihood that in the coming months this may lead to decisions around earlier than planned retirement and resignation. Merger concerns are beginning to impact as no current messaging/information in particular managing change
Key: Controls and Assurances Overall target risk rating 6: Low Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Amber
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Amber Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
12 9 9 12 12 12 Action By who? By when? Progress
1
Reduce violence and aggression towards staff through robust training, use of prosecution where required and environmental change
Chief of People and OD
Ongoing Act upon 2021 staff survey results – feedback to staff and put
in place any mitigating actions which are currently being reviewed
2
Continue to review staff health and wellbeing in light of winter and COVID-19 resilience concerns
Chief of People and OD
Q4 H&WB programmes in place. One year staff recovery plan in
place (received national recognition) – review recovery plan to assess impact and develop future plan
3
Leadership forums planned where colleagues from SFT and YDH will come together to share and work on vision
Chief of People and OD
Ongoing In progress
16 16 16 16 16 16 12 12 9 9 12 12 120
5
10
15
20
4 Focused opportunities for colleagues on change management
Chief of People and OD
Ongoing In progress
5 Values and behaviours work which will involve 15% of combined workforce
Chief of People and OD
Q1 2022/23
Commences April 2022
6 Staff engagement focus groups planned for staff
Chief of People and OD
Ongoing In progress
7
Integration work ongoing for both clinical and non-clinical workstreams and staff
Chief of People and OD
Ongoing In progress
8 Develop operational model and plan
Chief of People and OD
Ongoing Early considerations of operational model and plan
commencing
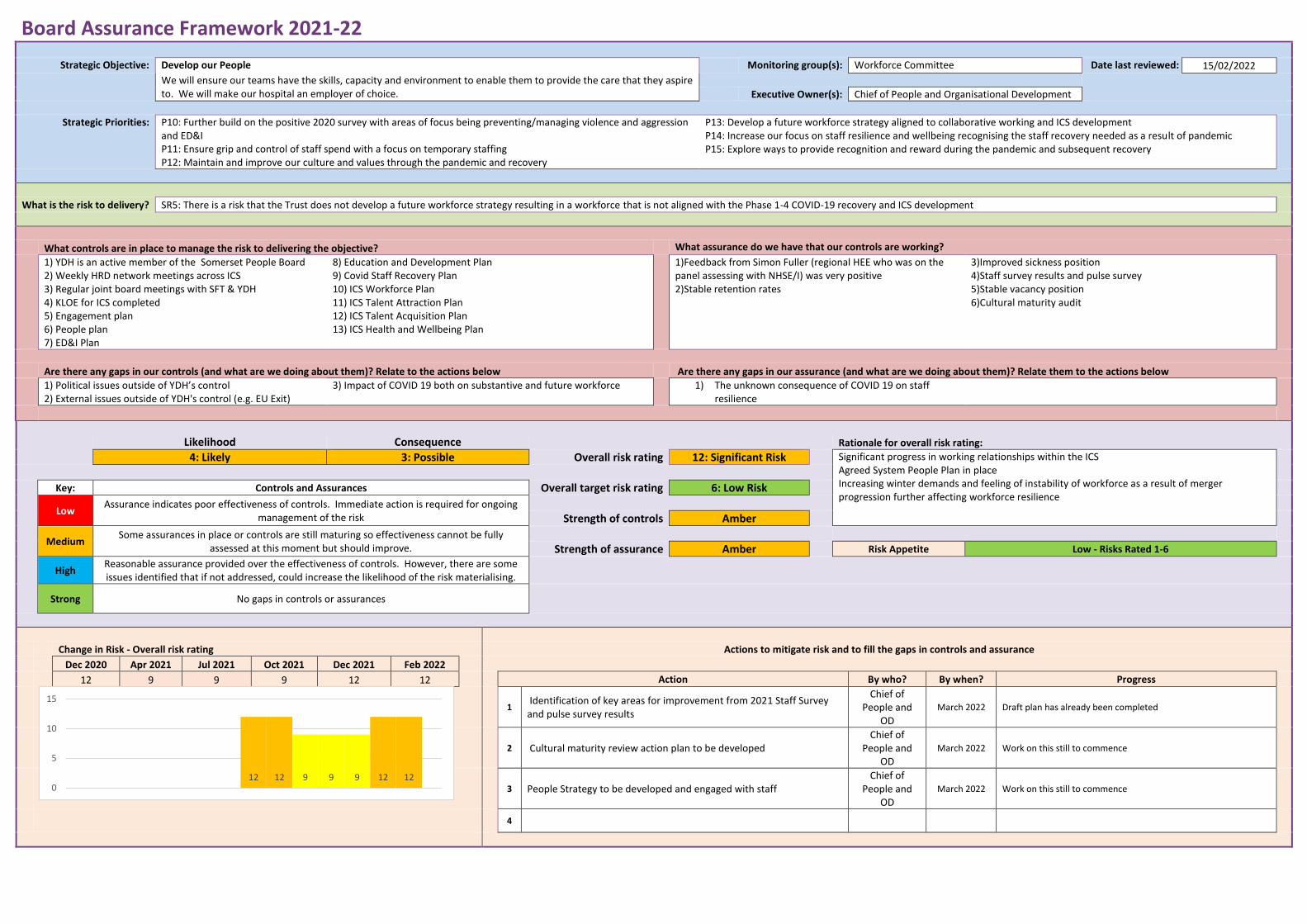
Board Assurance Framework 2021-22
Strategic Objective: Develop our People Monitoring group(s): Workforce Committee Date last reviewed: 15/02/2022
We will ensure our teams have the skills, capacity and environment to enable them to provide the care that they aspire to. We will make our hospital an employer of choice.
Executive Owner(s): Chief of People and Organisational Development
Strategic Priorities: P10: Further build on the positive 2020 survey with areas of focus being preventing/managing violence and aggression and ED&I P11: Ensure grip and control of staff spend with a focus on temporary staffing P12: Maintain and improve our culture and values through the pandemic and recovery
P13: Develop a future workforce strategy aligned to collaborative working and ICS development P14: Increase our focus on staff resilience and wellbeing recognising the staff recovery needed as a result of pandemic P15: Explore ways to provide recognition and reward during the pandemic and subsequent recovery
What is the risk to delivery? SR5: There is a risk that the Trust does not develop a future workforce strategy resulting in a workforce that is not aligned with the Phase 1-4 COVID-19 recovery and ICS development
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) YDH is an active member of the Somerset People Board 2) Weekly HRD network meetings across ICS 3) Regular joint board meetings with SFT & YDH 4) KLOE for ICS completed 5) Engagement plan 6) People plan 7) ED&I Plan
8) Education and Development Plan 9) Covid Staff Recovery Plan 10) ICS Workforce Plan 11) ICS Talent Attraction Plan 12) ICS Talent Acquisition Plan 13) ICS Health and Wellbeing Plan
1)Feedback from Simon Fuller (regional HEE who was on the panel assessing with NHSE/I) was very positive 2)Stable retention rates
3)Improved sickness position 4)Staff survey results and pulse survey 5)Stable vacancy position 6)Cultural maturity audit
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) Political issues outside of YDH’s control 2) External issues outside of YDH's control (e.g. EU Exit)
3) Impact of COVID 19 both on substantive and future workforce 1) The unknown consequence of COVID 19 on staff resilience
Likelihood Consequence Rationale for overall risk rating:
4: Likely 3: Possible Overall risk rating 12: Significant Risk Significant progress in working relationships within the ICS Agreed System People Plan in place Increasing winter demands and feeling of instability of workforce as a result of merger progression further affecting workforce resilience
Key: Controls and Assurances Overall target risk rating 6: Low Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Amber
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Amber Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
12 9 9 9 12 12 Action By who? By when? Progress
1 Identification of key areas for improvement from 2021 Staff Survey and pulse survey results
Chief of People and
OD
March 2022 Draft plan has already been completed
2 Cultural maturity review action plan to be developed
Chief of People and
OD
March 2022 Work on this still to commence
3 People Strategy to be developed and engaged with staff
Chief of People and
OD
March 2022 Work on this still to commence
4
12 12 9 9 9 12 120
5
10
15
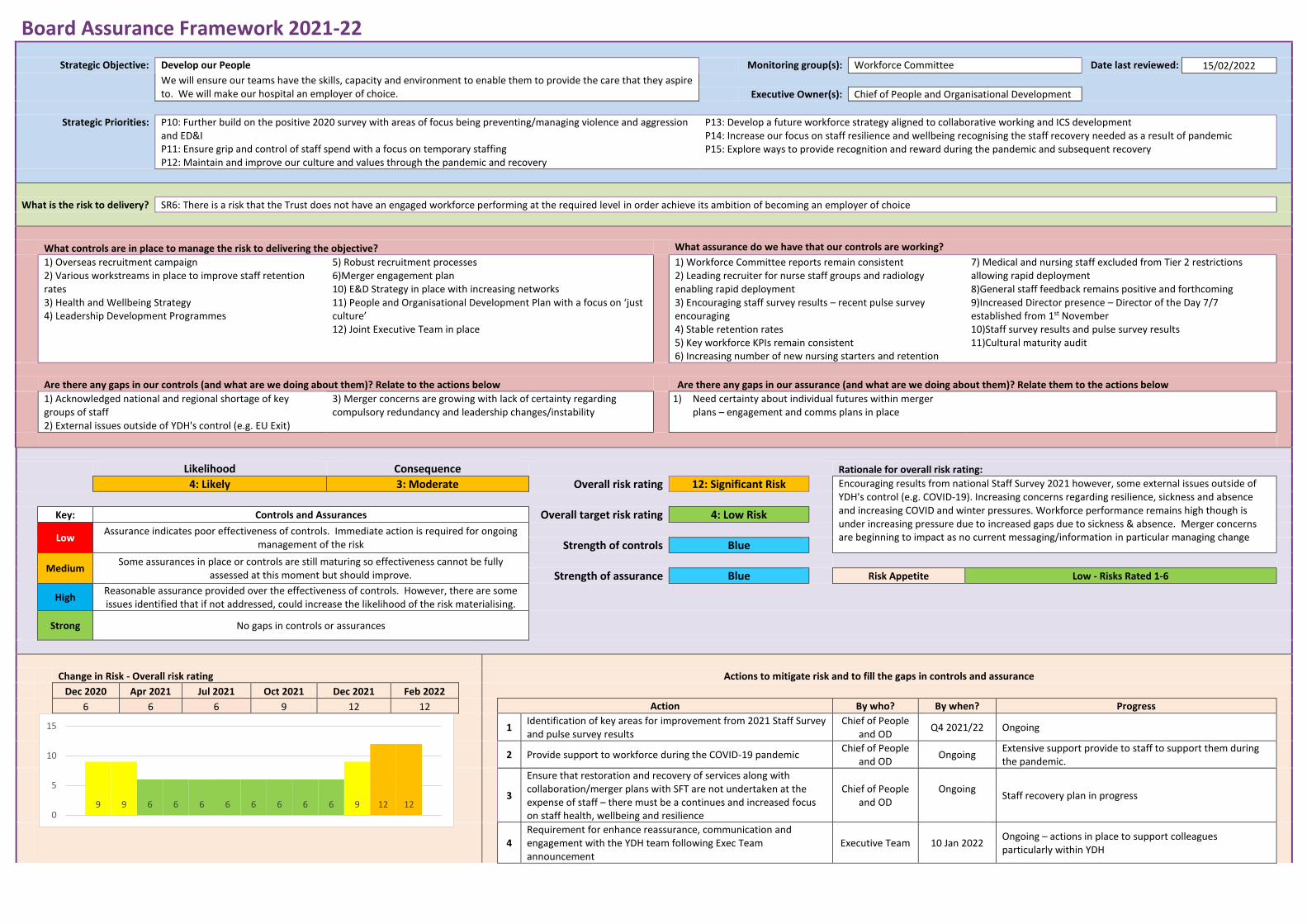
Board Assurance Framework 2021-22
Strategic Objective: Develop our People Monitoring group(s): Workforce Committee Date last reviewed: 15/02/2022
We will ensure our teams have the skills, capacity and environment to enable them to provide the care that they aspire to. We will make our hospital an employer of choice.
Executive Owner(s): Chief of People and Organisational Development
Strategic Priorities: P10: Further build on the positive 2020 survey with areas of focus being preventing/managing violence and aggression and ED&I P11: Ensure grip and control of staff spend with a focus on temporary staffing P12: Maintain and improve our culture and values through the pandemic and recovery
P13: Develop a future workforce strategy aligned to collaborative working and ICS development P14: Increase our focus on staff resilience and wellbeing recognising the staff recovery needed as a result of pandemic P15: Explore ways to provide recognition and reward during the pandemic and subsequent recovery
What is the risk to delivery? SR6: There is a risk that the Trust does not have an engaged workforce performing at the required level in order achieve its ambition of becoming an employer of choice
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) Overseas recruitment campaign 2) Various workstreams in place to improve staff retention rates 3) Health and Wellbeing Strategy 4) Leadership Development Programmes
5) Robust recruitment processes 6)Merger engagement plan 10) E&D Strategy in place with increasing networks 11) People and Organisational Development Plan with a focus on ‘just culture’ 12) Joint Executive Team in place
1) Workforce Committee reports remain consistent 2) Leading recruiter for nurse staff groups and radiology enabling rapid deployment 3) Encouraging staff survey results – recent pulse survey encouraging 4) Stable retention rates 5) Key workforce KPIs remain consistent 6) Increasing number of new nursing starters and retention
7) Medical and nursing staff excluded from Tier 2 restrictions allowing rapid deployment 8)General staff feedback remains positive and forthcoming 9)Increased Director presence – Director of the Day 7/7 established from 1st November 10)Staff survey results and pulse survey results 11)Cultural maturity audit
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) Acknowledged national and regional shortage of key groups of staff 2) External issues outside of YDH's control (e.g. EU Exit)
3) Merger concerns are growing with lack of certainty regarding compulsory redundancy and leadership changes/instability
1) Need certainty about individual futures within merger plans – engagement and comms plans in place
Likelihood Consequence Rationale for overall risk rating:
4: Likely 3: Moderate Overall risk rating 12: Significant Risk Encouraging results from national Staff Survey 2021 however, some external issues outside of YDH's control (e.g. COVID-19). Increasing concerns regarding resilience, sickness and absence and increasing COVID and winter pressures. Workforce performance remains high though is under increasing pressure due to increased gaps due to sickness & absence. Merger concerns are beginning to impact as no current messaging/information in particular managing change
Key: Controls and Assurances Overall target risk rating 4: Low Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Blue
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Blue Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
6 6 6 9 12 12 Action By who? By when? Progress
1
Identification of key areas for improvement from 2021 Staff Survey and pulse survey results
Chief of People and OD
Q4 2021/22 Ongoing
2 Provide support to workforce during the COVID-19 pandemic
Chief of People and OD
Ongoing Extensive support provide to staff to support them during the pandemic.
3
Ensure that restoration and recovery of services along with collaboration/merger plans with SFT are not undertaken at the expense of staff – there must be a continues and increased focus on staff health, wellbeing and resilience
Chief of People and OD
Ongoing
Staff recovery plan in progress
4
Requirement for enhance reassurance, communication and engagement with the YDH team following Exec Team announcement
Executive Team 10 Jan 2022 Ongoing – actions in place to support colleagues particularly within YDH
9 9 6 6 6 6 6 6 6 6 9 12 120
5
10
15
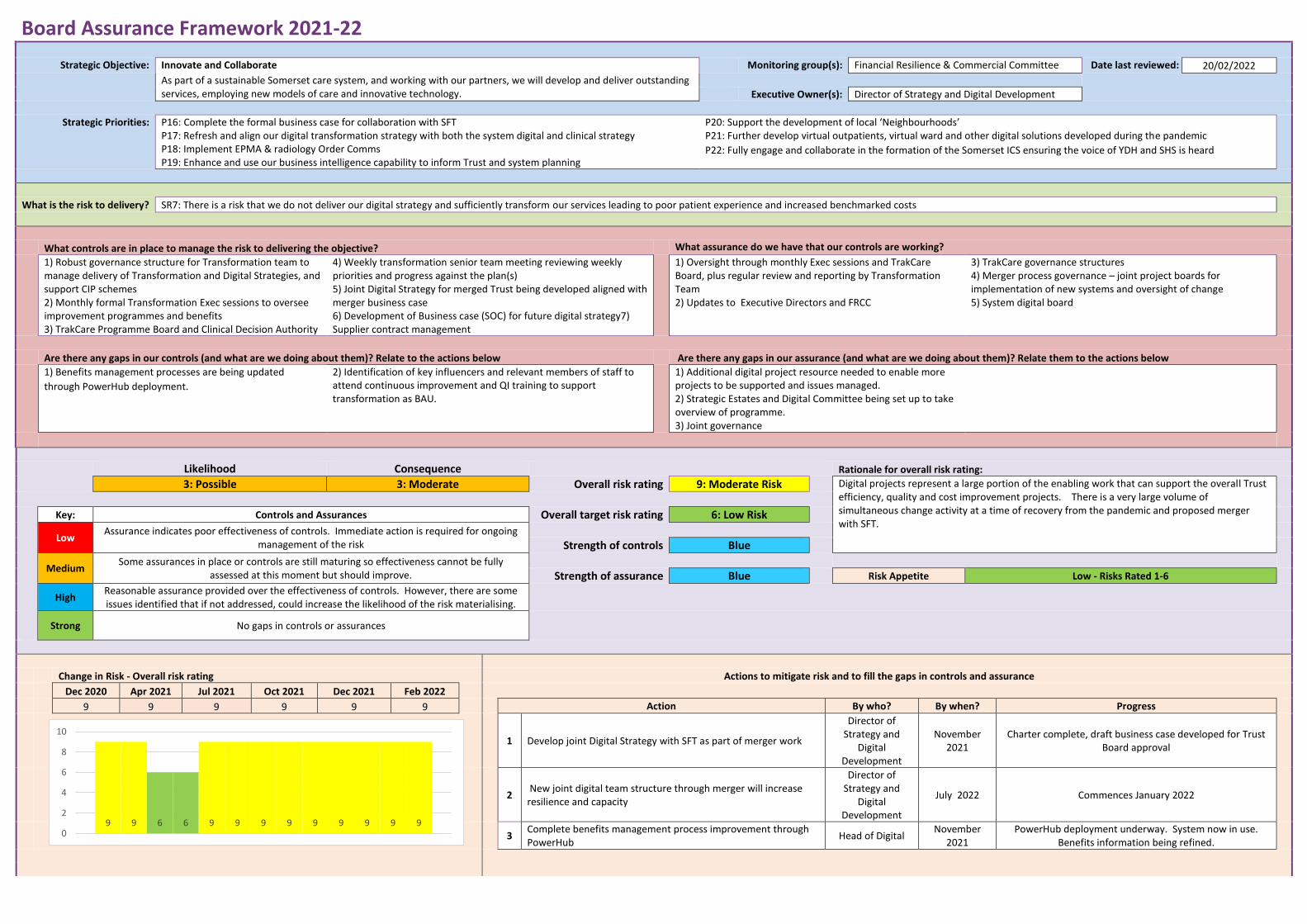
Board Assurance Framework 2021-22
Strategic Objective: Innovate and Collaborate Monitoring group(s): Financial Resilience & Commercial Committee Date last reviewed: 20/02/2022
As part of a sustainable Somerset care system, and working with our partners, we will develop and deliver outstanding services, employing new models of care and innovative technology.
Executive Owner(s): Director of Strategy and Digital Development
Strategic Priorities: P16: Complete the formal business case for collaboration with SFT P17: Refresh and align our digital transformation strategy with both the system digital and clinical strategy P18: Implement EPMA & radiology Order Comms P19: Enhance and use our business intelligence capability to inform Trust and system planning
P20: Support the development of local ‘Neighbourhoods’ P21: Further develop virtual outpatients, virtual ward and other digital solutions developed during the pandemic
P22: Fully engage and collaborate in the formation of the Somerset ICS ensuring the voice of YDH and SHS is heard
What is the risk to delivery? SR7: There is a risk that we do not deliver our digital strategy and sufficiently transform our services leading to poor patient experience and increased benchmarked costs
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) Robust governance structure for Transformation team to manage delivery of Transformation and Digital Strategies, and support CIP schemes 2) Monthly formal Transformation Exec sessions to oversee improvement programmes and benefits 3) TrakCare Programme Board and Clinical Decision Authority
4) Weekly transformation senior team meeting reviewing weekly priorities and progress against the plan(s) 5) Joint Digital Strategy for merged Trust being developed aligned with merger business case 6) Development of Business case (SOC) for future digital strategy7) Supplier contract management
1) Oversight through monthly Exec sessions and TrakCare Board, plus regular review and reporting by Transformation Team 2) Updates to Executive Directors and FRCC
3) TrakCare governance structures 4) Merger process governance – joint project boards for implementation of new systems and oversight of change 5) System digital board
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) Benefits management processes are being updated
through PowerHub deployment.
2) Identification of key influencers and relevant members of staff to attend continuous improvement and QI training to support transformation as BAU.
1) Additional digital project resource needed to enable more projects to be supported and issues managed. 2) Strategic Estates and Digital Committee being set up to take overview of programme. 3) Joint governance
Likelihood Consequence Rationale for overall risk rating:
3: Possible 3: Moderate Overall risk rating 9: Moderate Risk Digital projects represent a large portion of the enabling work that can support the overall Trust efficiency, quality and cost improvement projects. There is a very large volume of simultaneous change activity at a time of recovery from the pandemic and proposed merger with SFT.
Key: Controls and Assurances Overall target risk rating 6: Low Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Blue
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Blue Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
9 9 9 9 9 9 Action By who? By when? Progress
1 Develop joint Digital Strategy with SFT as part of merger work
Director of Strategy and
Digital Development
November 2021
Charter complete, draft business case developed for Trust Board approval
2 New joint digital team structure through merger will increase resilience and capacity
Director of Strategy and
Digital Development
July 2022 Commences January 2022
3
Complete benefits management process improvement through PowerHub
Head of Digital November
2021 PowerHub deployment underway. System now in use.
Benefits information being refined.
9 9 6 6 9 9 9 9 9 9 9 9 90
2
4
6
8
10
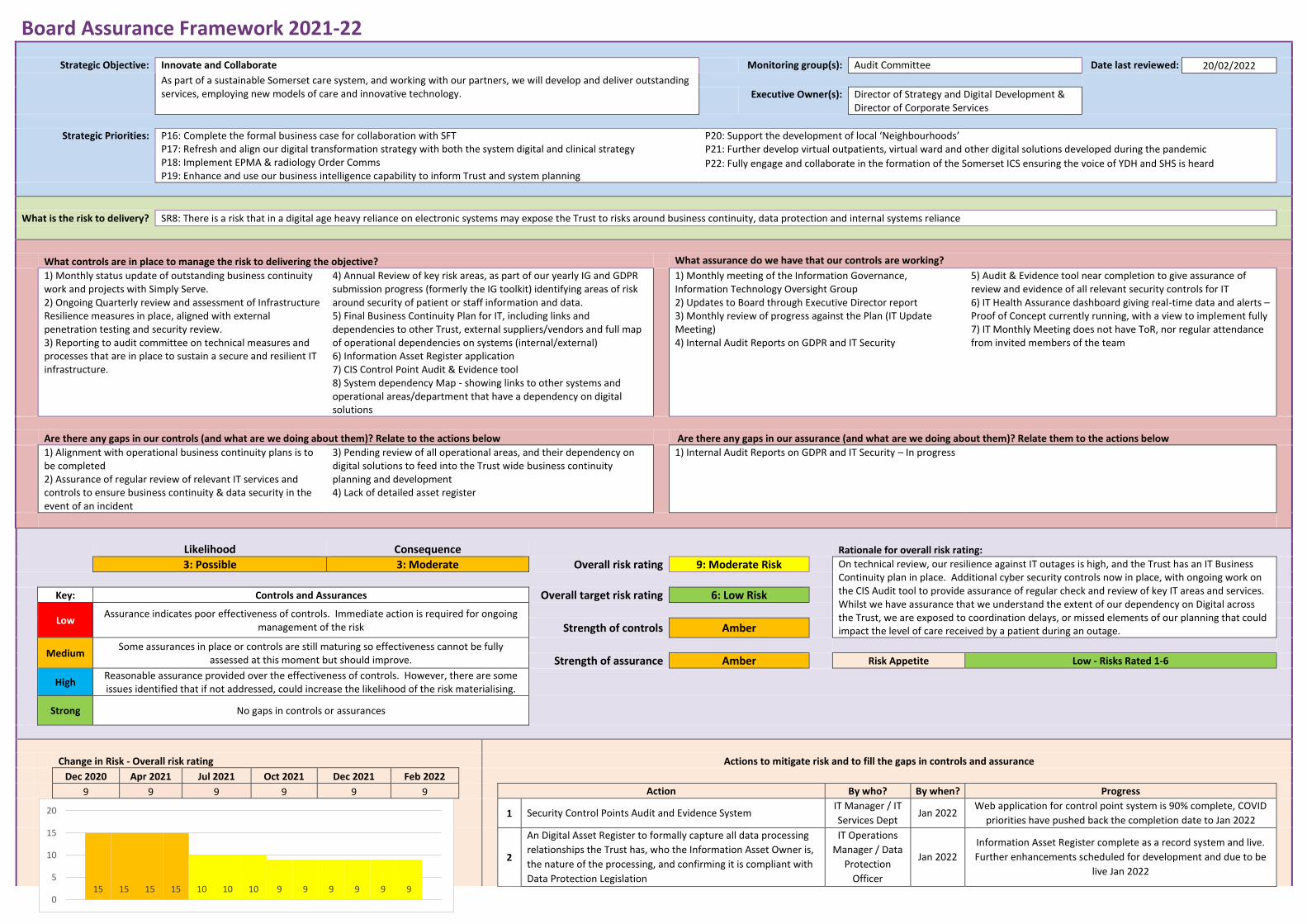
Board Assurance Framework 2021-22
Strategic Objective: Innovate and Collaborate Monitoring group(s): Audit Committee Date last reviewed: 20/02/2022
As part of a sustainable Somerset care system, and working with our partners, we will develop and deliver outstanding services, employing new models of care and innovative technology.
Executive Owner(s): Director of Strategy and Digital Development &
Director of Corporate Services
Strategic Priorities: P16: Complete the formal business case for collaboration with SFT P17: Refresh and align our digital transformation strategy with both the system digital and clinical strategy P18: Implement EPMA & radiology Order Comms P19: Enhance and use our business intelligence capability to inform Trust and system planning
P20: Support the development of local ‘Neighbourhoods’ P21: Further develop virtual outpatients, virtual ward and other digital solutions developed during the pandemic
P22: Fully engage and collaborate in the formation of the Somerset ICS ensuring the voice of YDH and SHS is heard
What is the risk to delivery? SR8: There is a risk that in a digital age heavy reliance on electronic systems may expose the Trust to risks around business continuity, data protection and internal systems reliance
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) Monthly status update of outstanding business continuity work and projects with Simply Serve. 2) Ongoing Quarterly review and assessment of Infrastructure Resilience measures in place, aligned with external penetration testing and security review. 3) Reporting to audit committee on technical measures and processes that are in place to sustain a secure and resilient IT infrastructure.
4) Annual Review of key risk areas, as part of our yearly IG and GDPR submission progress (formerly the IG toolkit) identifying areas of risk around security of patient or staff information and data. 5) Final Business Continuity Plan for IT, including links and dependencies to other Trust, external suppliers/vendors and full map of operational dependencies on systems (internal/external) 6) Information Asset Register application 7) CIS Control Point Audit & Evidence tool 8) System dependency Map - showing links to other systems and operational areas/department that have a dependency on digital solutions
1) Monthly meeting of the Information Governance, Information Technology Oversight Group 2) Updates to Board through Executive Director report 3) Monthly review of progress against the Plan (IT Update Meeting) 4) Internal Audit Reports on GDPR and IT Security
5) Audit & Evidence tool near completion to give assurance of review and evidence of all relevant security controls for IT 6) IT Health Assurance dashboard giving real-time data and alerts – Proof of Concept currently running, with a view to implement fully 7) IT Monthly Meeting does not have ToR, nor regular attendance from invited members of the team
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) Alignment with operational business continuity plans is to be completed 2) Assurance of regular review of relevant IT services and controls to ensure business continuity & data security in the event of an incident
3) Pending review of all operational areas, and their dependency on digital solutions to feed into the Trust wide business continuity planning and development 4) Lack of detailed asset register
1) Internal Audit Reports on GDPR and IT Security – In progress
Likelihood Consequence Rationale for overall risk rating:
3: Possible 3: Moderate Overall risk rating 9: Moderate Risk On technical review, our resilience against IT outages is high, and the Trust has an IT Business Continuity plan in place. Additional cyber security controls now in place, with ongoing work on the CIS Audit tool to provide assurance of regular check and review of key IT areas and services. Whilst we have assurance that we understand the extent of our dependency on Digital across the Trust, we are exposed to coordination delays, or missed elements of our planning that could impact the level of care received by a patient during an outage.
Key: Controls and Assurances Overall target risk rating 6: Low Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Amber
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Amber Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
9 9 9 9 9 9 Action By who? By when? Progress
1 Security Control Points Audit and Evidence System
IT Manager / IT
Services Dept Jan 2022
Web application for control point system is 90% complete, COVID
priorities have pushed back the completion date to Jan 2022
2
An Digital Asset Register to formally capture all data processing
relationships the Trust has, who the Information Asset Owner is,
the nature of the processing, and confirming it is compliant with
Data Protection Legislation
IT Operations
Manager / Data
Protection
Officer
Jan 2022
Information Asset Register complete as a record system and live.
Further enhancements scheduled for development and due to be
live Jan 2022
15 15 15 15 10 10 10 9 9 9 9 9 90
5
10
15
20
3
Further work on IT systems lists and Disaster Recovery / Business
Continuity ongoing, with consolidated list forming the basis of a
good understanding of inter-dependencies.
Head of IT Jan 2022 Nearing completion with a working model of interdependencies of
major IT systems and data across the Trust.
4
Online DR / BCP Action Cards to direct staff as to Immediate,
Follow-up and Final actions and notifications in specific
scenarios, providing a concise, easily accessed and understood,
standardised way to respond
Head of IT /
EPRR Manager Dec 2021
Pilot in place for IT Department, with population of action cards
ongoing. Roll out Trust-wide with appropriate approval and
adjustment to SOPs anticipated Dec 21
5
IT Health Assurance Dashboard and data application to enable
real-time view of various areas of IT risk including attacks,
patching, operating system updates, high-priority alerts and
network connections to be implemented, allowing detailed and
effective monitoring and proactive response to issues / scenarios
Head of IT /
Cyber Security
Manager
Sep 2021
POC in place and running, giving impressive oversight and
management of multiple areas. Business case for purchase of
system being drawn up, assuming approval system to be in place
by end of Sep 21
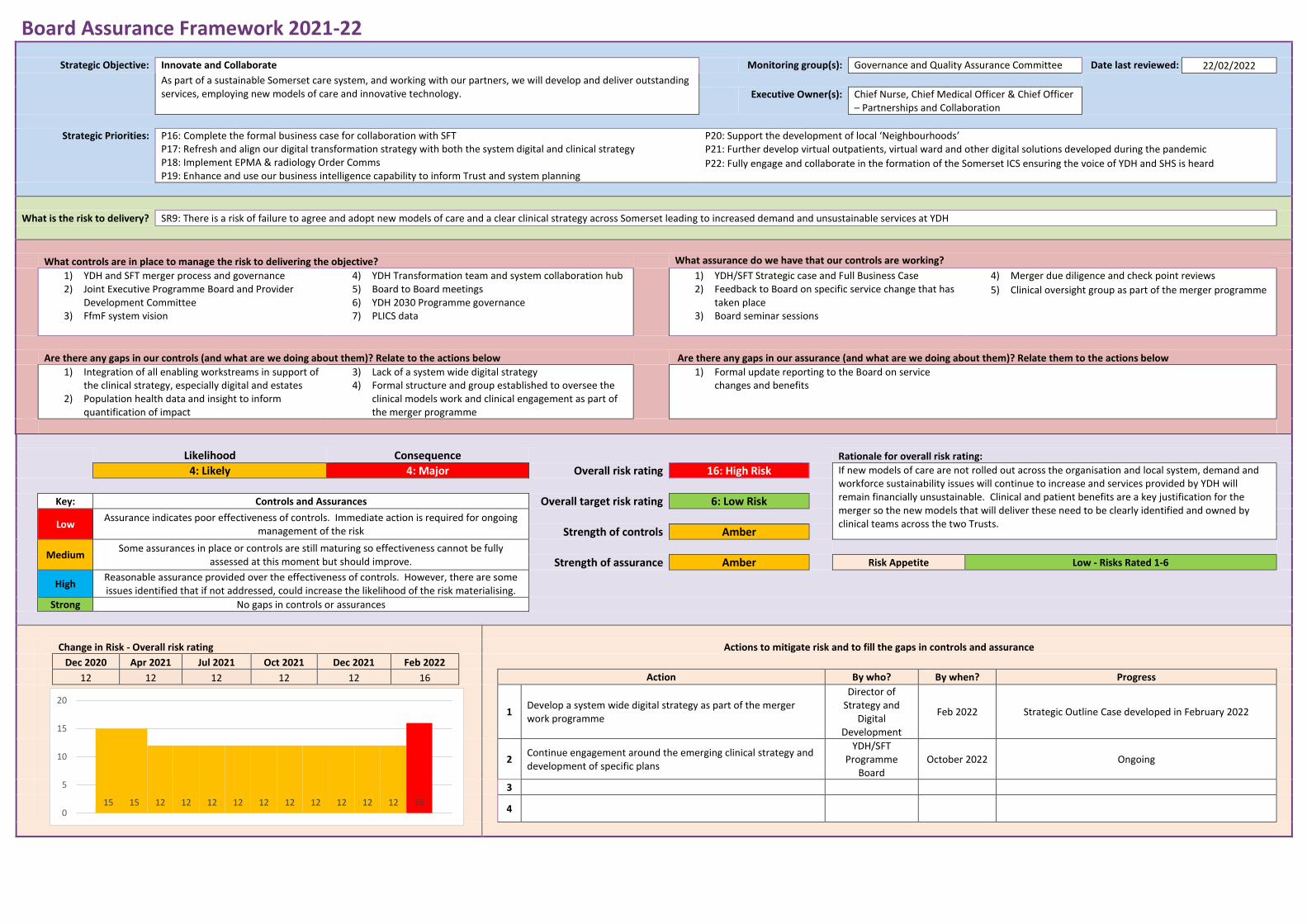
Board Assurance Framework 2021-22
Strategic Objective: Innovate and Collaborate Monitoring group(s): Governance and Quality Assurance Committee Date last reviewed: 22/02/2022
As part of a sustainable Somerset care system, and working with our partners, we will develop and deliver outstanding services, employing new models of care and innovative technology.
Executive Owner(s): Chief Nurse, Chief Medical Officer & Chief Officer
– Partnerships and Collaboration
Strategic Priorities: P16: Complete the formal business case for collaboration with SFT P17: Refresh and align our digital transformation strategy with both the system digital and clinical strategy P18: Implement EPMA & radiology Order Comms P19: Enhance and use our business intelligence capability to inform Trust and system planning
P20: Support the development of local ‘Neighbourhoods’ P21: Further develop virtual outpatients, virtual ward and other digital solutions developed during the pandemic
P22: Fully engage and collaborate in the formation of the Somerset ICS ensuring the voice of YDH and SHS is heard
What is the risk to delivery? SR9: There is a risk of failure to agree and adopt new models of care and a clear clinical strategy across Somerset leading to increased demand and unsustainable services at YDH
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) YDH and SFT merger process and governance 2) Joint Executive Programme Board and Provider
Development Committee 3) FfmF system vision
4) YDH Transformation team and system collaboration hub 5) Board to Board meetings 6) YDH 2030 Programme governance 7) PLICS data
1) YDH/SFT Strategic case and Full Business Case 2) Feedback to Board on specific service change that has
taken place 3) Board seminar sessions
4) Merger due diligence and check point reviews
5) Clinical oversight group as part of the merger programme
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) Integration of all enabling workstreams in support of the clinical strategy, especially digital and estates
2) Population health data and insight to inform quantification of impact
3) Lack of a system wide digital strategy 4) Formal structure and group established to oversee the
clinical models work and clinical engagement as part of the merger programme
1) Formal update reporting to the Board on service changes and benefits
Likelihood Consequence Rationale for overall risk rating:
4: Likely 4: Major Overall risk rating 16: High Risk If new models of care are not rolled out across the organisation and local system, demand and workforce sustainability issues will continue to increase and services provided by YDH will remain financially unsustainable. Clinical and patient benefits are a key justification for the merger so the new models that will deliver these need to be clearly identified and owned by clinical teams across the two Trusts.
Key: Controls and Assurances Overall target risk rating 6: Low Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Amber
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Amber Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
12 12 12 12 12 16 Action By who? By when? Progress
1 Develop a system wide digital strategy as part of the merger work programme
Director of Strategy and
Digital Development
Feb 2022 Strategic Outline Case developed in February 2022
2
Continue engagement around the emerging clinical strategy and development of specific plans
YDH/SFT Programme
Board October 2022 Ongoing
3
4
15 15 12 12 12 12 12 12 12 12 12 12 160
5
10
15
20
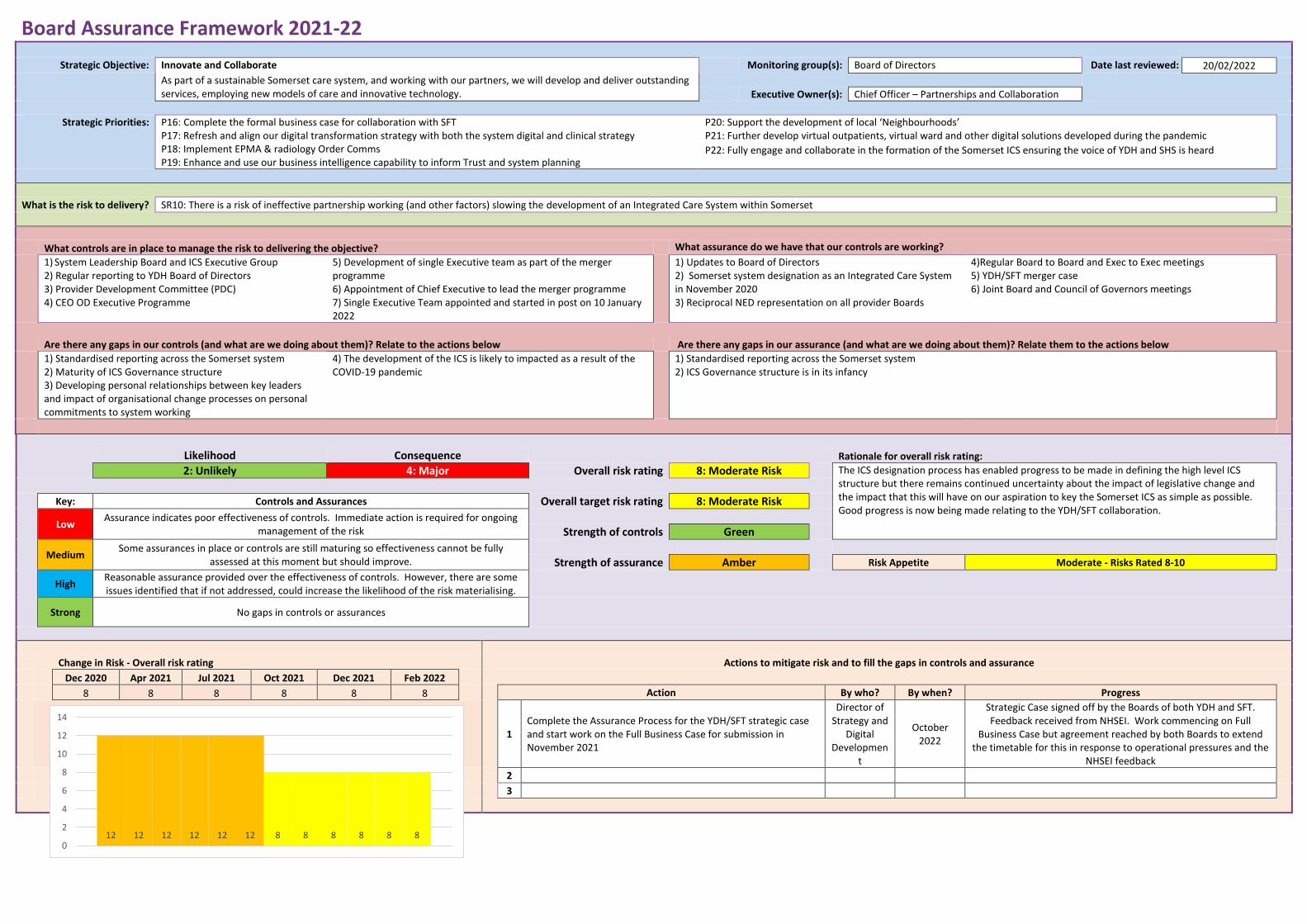
Board Assurance Framework 2021-22
Strategic Objective: Innovate and Collaborate Monitoring group(s): Board of Directors Date last reviewed: 20/02/2022
As part of a sustainable Somerset care system, and working with our partners, we will develop and deliver outstanding services, employing new models of care and innovative technology.
Executive Owner(s): Chief Officer – Partnerships and Collaboration
Strategic Priorities: P16: Complete the formal business case for collaboration with SFT P17: Refresh and align our digital transformation strategy with both the system digital and clinical strategy P18: Implement EPMA & radiology Order Comms P19: Enhance and use our business intelligence capability to inform Trust and system planning
P20: Support the development of local ‘Neighbourhoods’ P21: Further develop virtual outpatients, virtual ward and other digital solutions developed during the pandemic
P22: Fully engage and collaborate in the formation of the Somerset ICS ensuring the voice of YDH and SHS is heard
What is the risk to delivery? SR10: There is a risk of ineffective partnership working (and other factors) slowing the development of an Integrated Care System within Somerset
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) System Leadership Board and ICS Executive Group 2) Regular reporting to YDH Board of Directors 3) Provider Development Committee (PDC) 4) CEO OD Executive Programme
5) Development of single Executive team as part of the merger programme 6) Appointment of Chief Executive to lead the merger programme 7) Single Executive Team appointed and started in post on 10 January 2022
1) Updates to Board of Directors 2) Somerset system designation as an Integrated Care System in November 2020 3) Reciprocal NED representation on all provider Boards
4)Regular Board to Board and Exec to Exec meetings 5) YDH/SFT merger case 6) Joint Board and Council of Governors meetings
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) Standardised reporting across the Somerset system 2) Maturity of ICS Governance structure 3) Developing personal relationships between key leaders and impact of organisational change processes on personal commitments to system working
4) The development of the ICS is likely to impacted as a result of the COVID-19 pandemic
1) Standardised reporting across the Somerset system 2) ICS Governance structure is in its infancy
Likelihood Consequence Rationale for overall risk rating:
2: Unlikely 4: Major Overall risk rating 8: Moderate Risk The ICS designation process has enabled progress to be made in defining the high level ICS structure but there remains continued uncertainty about the impact of legislative change and the impact that this will have on our aspiration to key the Somerset ICS as simple as possible. Good progress is now being made relating to the YDH/SFT collaboration.
Key: Controls and Assurances Overall target risk rating 8: Moderate Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Green
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Amber Risk Appetite Moderate - Risks Rated 8-10
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
8 8 8 8 8 8 Action By who? By when? Progress
1 Complete the Assurance Process for the YDH/SFT strategic case and start work on the Full Business Case for submission in November 2021
Director of Strategy and
Digital Developmen
t
October 2022
Strategic Case signed off by the Boards of both YDH and SFT. Feedback received from NHSEI. Work commencing on Full
Business Case but agreement reached by both Boards to extend the timetable for this in response to operational pressures and the
NHSEI feedback
2
3
12 12 12 12 12 12 8 8 8 8 8 8
0
2
4
6
8
10
12
14
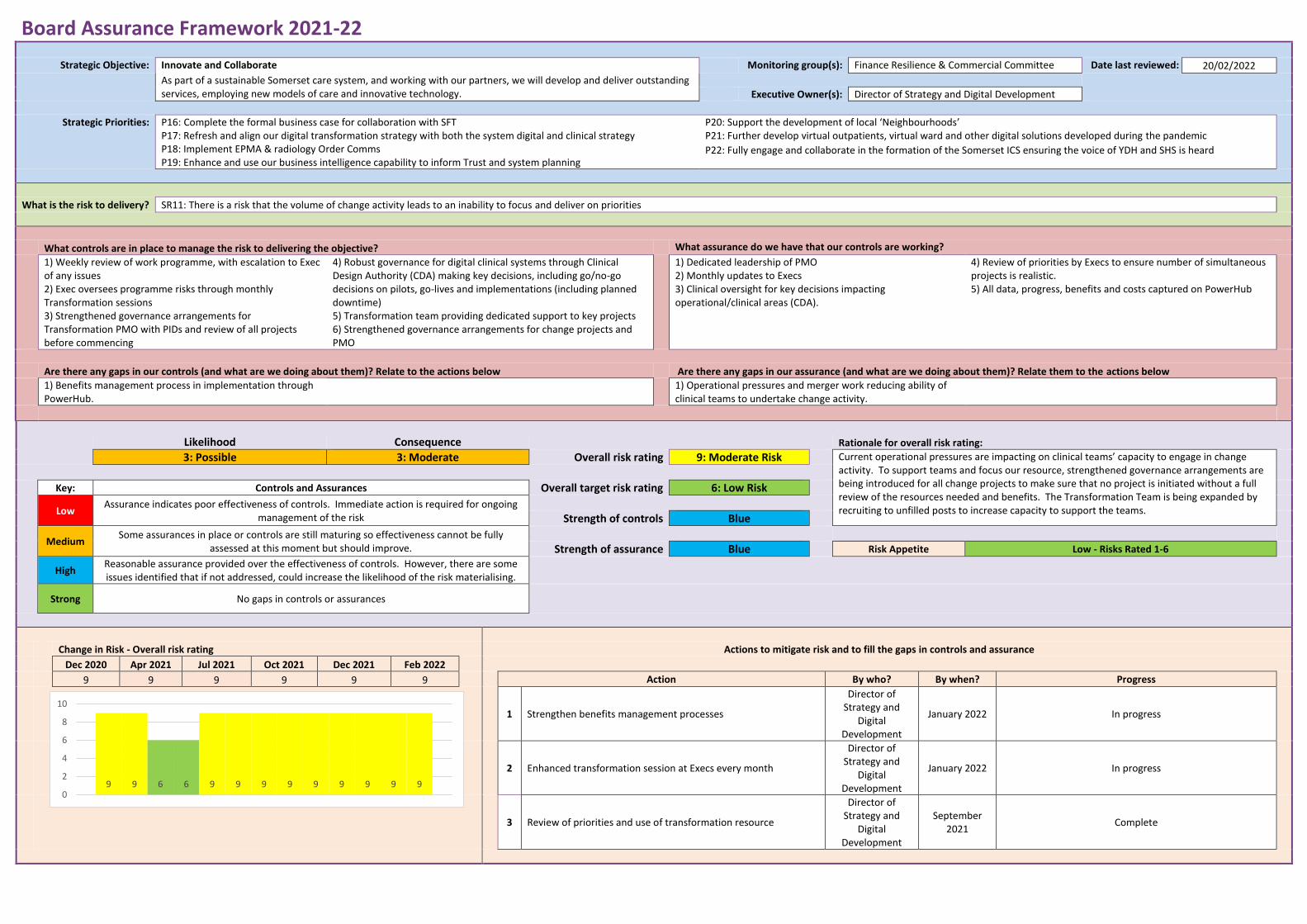
Board Assurance Framework 2021-22
Strategic Objective: Innovate and Collaborate Monitoring group(s): Finance Resilience & Commercial Committee Date last reviewed: 20/02/2022
As part of a sustainable Somerset care system, and working with our partners, we will develop and deliver outstanding services, employing new models of care and innovative technology.
Executive Owner(s): Director of Strategy and Digital Development
Strategic Priorities: P16: Complete the formal business case for collaboration with SFT P17: Refresh and align our digital transformation strategy with both the system digital and clinical strategy P18: Implement EPMA & radiology Order Comms P19: Enhance and use our business intelligence capability to inform Trust and system planning
P20: Support the development of local ‘Neighbourhoods’ P21: Further develop virtual outpatients, virtual ward and other digital solutions developed during the pandemic
P22: Fully engage and collaborate in the formation of the Somerset ICS ensuring the voice of YDH and SHS is heard
What is the risk to delivery? SR11: There is a risk that the volume of change activity leads to an inability to focus and deliver on priorities
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) Weekly review of work programme, with escalation to Exec of any issues 2) Exec oversees programme risks through monthly Transformation sessions 3) Strengthened governance arrangements for Transformation PMO with PIDs and review of all projects before commencing
4) Robust governance for digital clinical systems through Clinical Design Authority (CDA) making key decisions, including go/no-go decisions on pilots, go-lives and implementations (including planned downtime) 5) Transformation team providing dedicated support to key projects 6) Strengthened governance arrangements for change projects and PMO
1) Dedicated leadership of PMO 2) Monthly updates to Execs 3) Clinical oversight for key decisions impacting operational/clinical areas (CDA).
4) Review of priorities by Execs to ensure number of simultaneous projects is realistic. 5) All data, progress, benefits and costs captured on PowerHub
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) Benefits management process in implementation through PowerHub.
1) Operational pressures and merger work reducing ability of clinical teams to undertake change activity.
Likelihood Consequence Rationale for overall risk rating:
3: Possible 3: Moderate Overall risk rating 9: Moderate Risk Current operational pressures are impacting on clinical teams’ capacity to engage in change activity. To support teams and focus our resource, strengthened governance arrangements are being introduced for all change projects to make sure that no project is initiated without a full review of the resources needed and benefits. The Transformation Team is being expanded by recruiting to unfilled posts to increase capacity to support the teams.
Key: Controls and Assurances Overall target risk rating 6: Low Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Blue
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Blue Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
9 9 9 9 9 9 Action By who? By when? Progress
1 Strengthen benefits management processes
Director of Strategy and
Digital Development
January 2022 In progress
2 Enhanced transformation session at Execs every month
Director of Strategy and
Digital Development
January 2022 In progress
3 Review of priorities and use of transformation resource
Director of Strategy and
Digital Development
September 2021
Complete
9 9 6 6 9 9 9 9 9 9 9 9 90
2
4
6
8
10
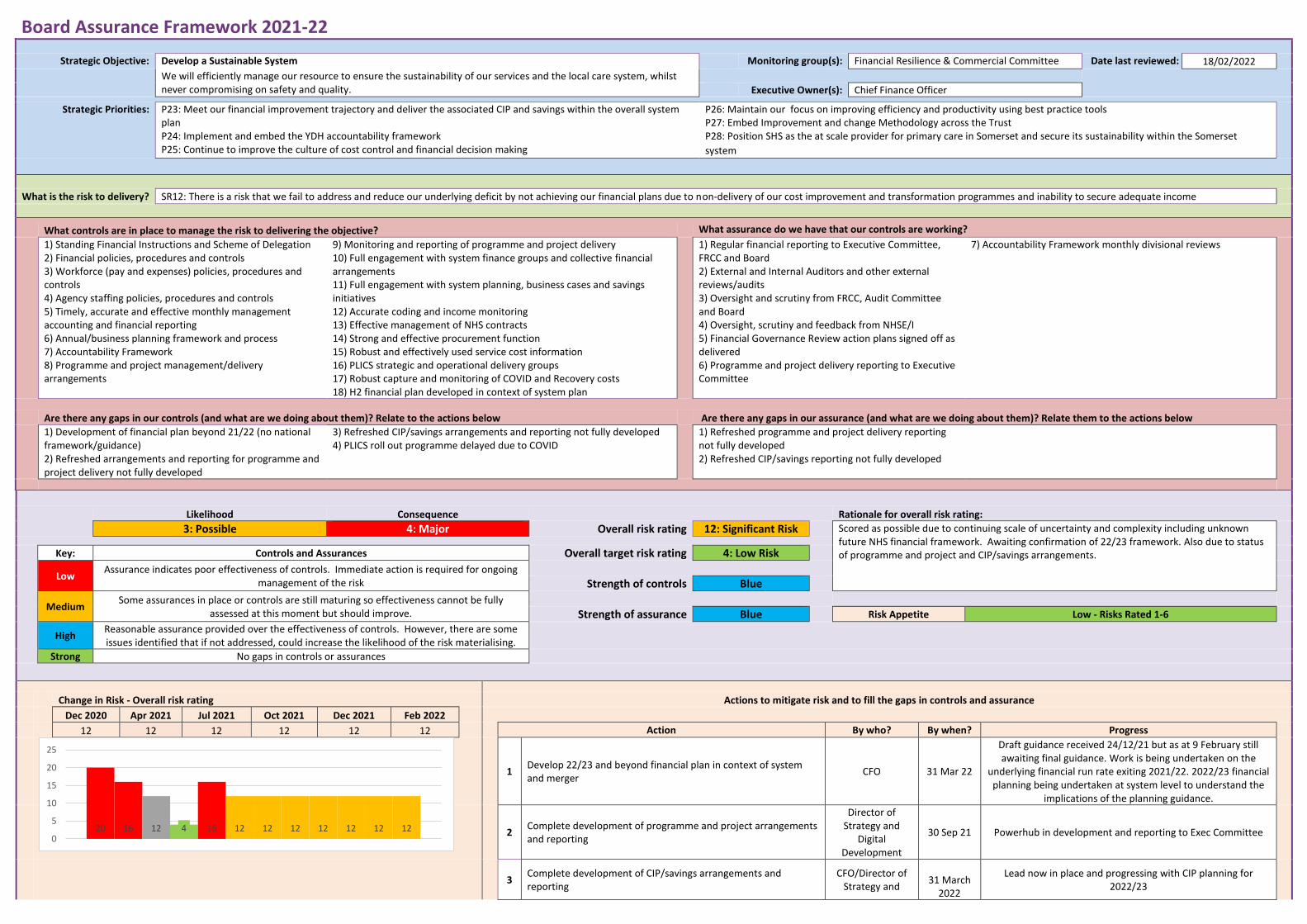
Board Assurance Framework 2021-22
Strategic Objective: Develop a Sustainable System Monitoring group(s): Financial Resilience & Commercial Committee Date last reviewed: 18/02/2022
We will efficiently manage our resource to ensure the sustainability of our services and the local care system, whilst never compromising on safety and quality.
Executive Owner(s): Chief Finance Officer
Strategic Priorities: P23: Meet our financial improvement trajectory and deliver the associated CIP and savings within the overall system plan P24: Implement and embed the YDH accountability framework P25: Continue to improve the culture of cost control and financial decision making
P26: Maintain our focus on improving efficiency and productivity using best practice tools P27: Embed Improvement and change Methodology across the Trust P28: Position SHS as the at scale provider for primary care in Somerset and secure its sustainability within the Somerset
system
What is the risk to delivery? SR12: There is a risk that we fail to address and reduce our underlying deficit by not achieving our financial plans due to non-delivery of our cost improvement and transformation programmes and inability to secure adequate income
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) Standing Financial Instructions and Scheme of Delegation 2) Financial policies, procedures and controls 3) Workforce (pay and expenses) policies, procedures and controls 4) Agency staffing policies, procedures and controls 5) Timely, accurate and effective monthly management accounting and financial reporting 6) Annual/business planning framework and process 7) Accountability Framework 8) Programme and project management/delivery arrangements
9) Monitoring and reporting of programme and project delivery 10) Full engagement with system finance groups and collective financial arrangements 11) Full engagement with system planning, business cases and savings initiatives 12) Accurate coding and income monitoring 13) Effective management of NHS contracts 14) Strong and effective procurement function 15) Robust and effectively used service cost information 16) PLICS strategic and operational delivery groups 17) Robust capture and monitoring of COVID and Recovery costs 18) H2 financial plan developed in context of system plan
1) Regular financial reporting to Executive Committee, FRCC and Board 2) External and Internal Auditors and other external reviews/audits 3) Oversight and scrutiny from FRCC, Audit Committee and Board 4) Oversight, scrutiny and feedback from NHSE/I 5) Financial Governance Review action plans signed off as delivered 6) Programme and project delivery reporting to Executive Committee
7) Accountability Framework monthly divisional reviews
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) Development of financial plan beyond 21/22 (no national framework/guidance) 2) Refreshed arrangements and reporting for programme and project delivery not fully developed
3) Refreshed CIP/savings arrangements and reporting not fully developed 4) PLICS roll out programme delayed due to COVID
1) Refreshed programme and project delivery reporting not fully developed 2) Refreshed CIP/savings reporting not fully developed
Likelihood Consequence Rationale for overall risk rating:
3: Possible 4: Major Overall risk rating 12: Significant Risk Scored as possible due to continuing scale of uncertainty and complexity including unknown future NHS financial framework. Awaiting confirmation of 22/23 framework. Also due to status of programme and project and CIP/savings arrangements.
Key: Controls and Assurances Overall target risk rating 4: Low Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Blue
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Blue Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
12 12 12 12 12 12 Action By who? By when? Progress
1 Develop 22/23 and beyond financial plan in context of system and merger
CFO 31 Mar 22
Draft guidance received 24/12/21 but as at 9 February still awaiting final guidance. Work is being undertaken on the
underlying financial run rate exiting 2021/22. 2022/23 financial planning being undertaken at system level to understand the
implications of the planning guidance.
2 Complete development of programme and project arrangements and reporting
Director of Strategy and
Digital Development
30 Sep 21 Powerhub in development and reporting to Exec Committee
3
Complete development of CIP/savings arrangements and reporting
CFO/Director of Strategy and
31 March
2022
Lead now in place and progressing with CIP planning for 2022/23
20 16 12 4 16 12 12 12 12 12 12 120
5
10
15
20
25
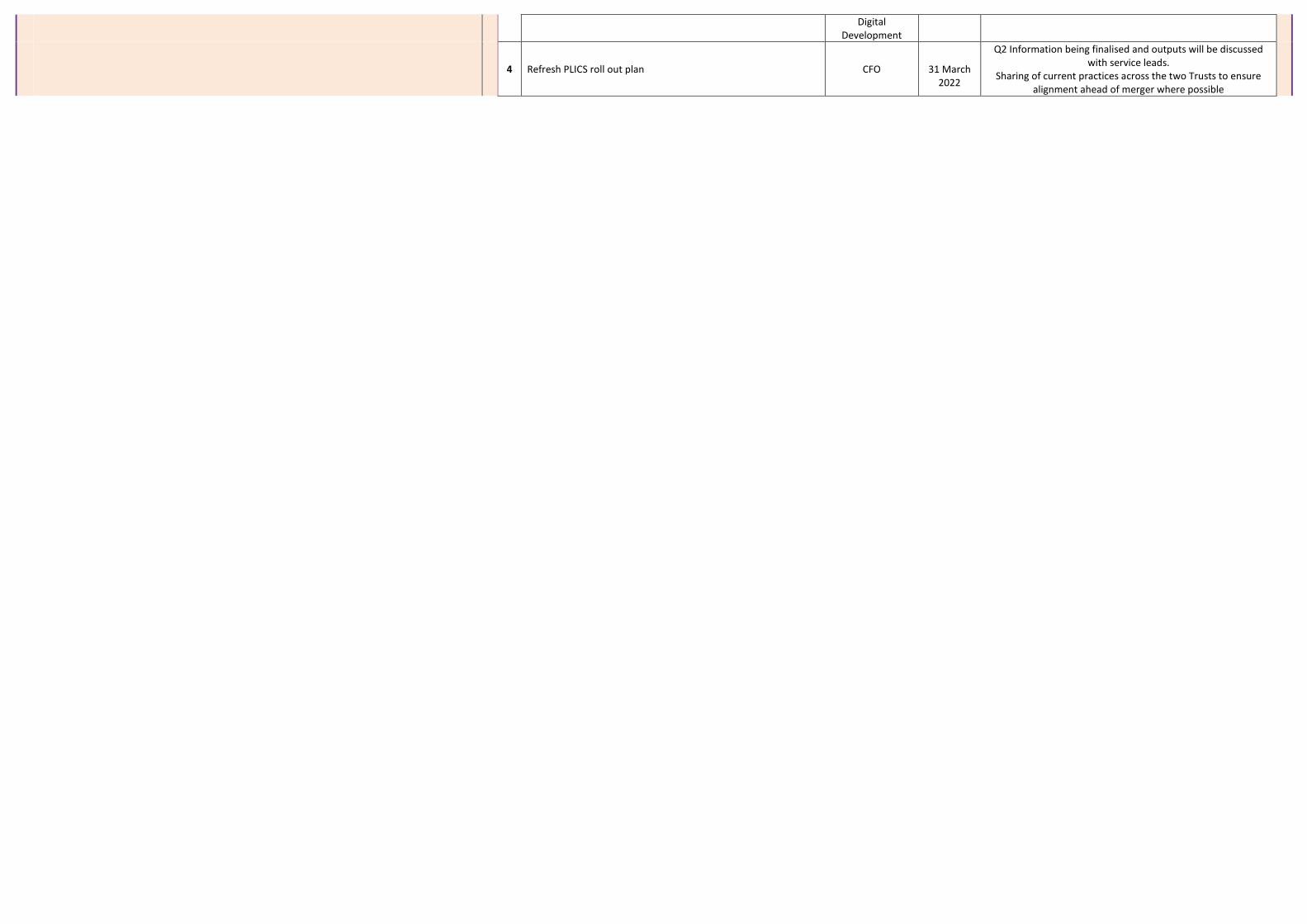
Digital Development
4 Refresh PLICS roll out plan CFO
31 March 2022
Q2 Information being finalised and outputs will be discussed with service leads.
Sharing of current practices across the two Trusts to ensure alignment ahead of merger where possible
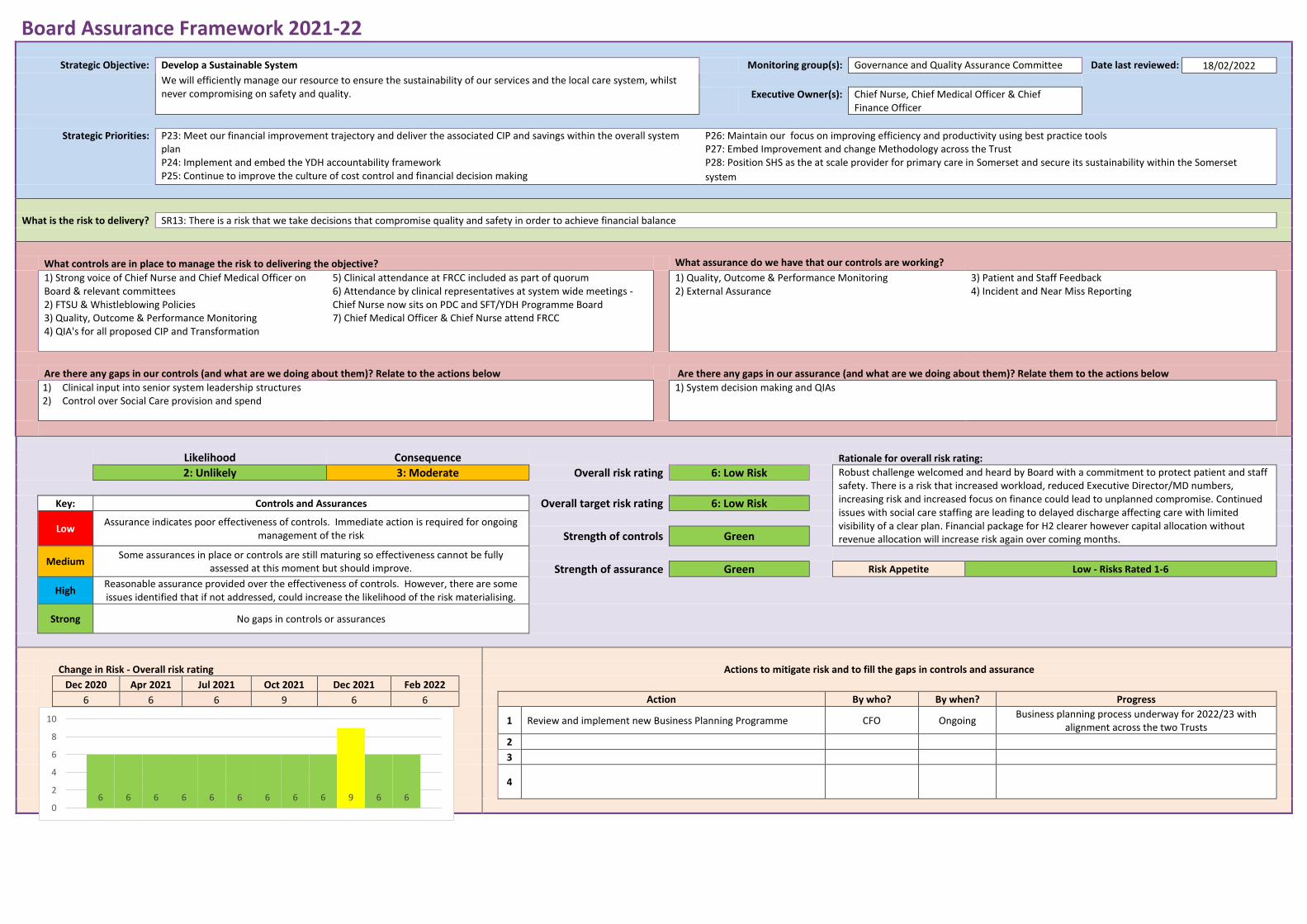
Board Assurance Framework 2021-22
Strategic Objective: Develop a Sustainable System Monitoring group(s): Governance and Quality Assurance Committee Date last reviewed: 18/02/2022
We will efficiently manage our resource to ensure the sustainability of our services and the local care system, whilst never compromising on safety and quality.
Executive Owner(s): Chief Nurse, Chief Medical Officer & Chief
Finance Officer
Strategic Priorities: P23: Meet our financial improvement trajectory and deliver the associated CIP and savings within the overall system plan P24: Implement and embed the YDH accountability framework P25: Continue to improve the culture of cost control and financial decision making
P26: Maintain our focus on improving efficiency and productivity using best practice tools P27: Embed Improvement and change Methodology across the Trust P28: Position SHS as the at scale provider for primary care in Somerset and secure its sustainability within the Somerset
system
What is the risk to delivery? SR13: There is a risk that we take decisions that compromise quality and safety in order to achieve financial balance
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) Strong voice of Chief Nurse and Chief Medical Officer on Board & relevant committees 2) FTSU & Whistleblowing Policies 3) Quality, Outcome & Performance Monitoring 4) QIA's for all proposed CIP and Transformation
5) Clinical attendance at FRCC included as part of quorum 6) Attendance by clinical representatives at system wide meetings - Chief Nurse now sits on PDC and SFT/YDH Programme Board 7) Chief Medical Officer & Chief Nurse attend FRCC
1) Quality, Outcome & Performance Monitoring 2) External Assurance
3) Patient and Staff Feedback 4) Incident and Near Miss Reporting
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) Clinical input into senior system leadership structures 2) Control over Social Care provision and spend
1) System decision making and QIAs
Likelihood Consequence Rationale for overall risk rating:
2: Unlikely 3: Moderate Overall risk rating 6: Low Risk Robust challenge welcomed and heard by Board with a commitment to protect patient and staff safety. There is a risk that increased workload, reduced Executive Director/MD numbers, increasing risk and increased focus on finance could lead to unplanned compromise. Continued issues with social care staffing are leading to delayed discharge affecting care with limited visibility of a clear plan. Financial package for H2 clearer however capital allocation without revenue allocation will increase risk again over coming months.
Key: Controls and Assurances Overall target risk rating 6: Low Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Green
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Green Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
6 6 6 9 6 6 Action By who? By when? Progress
1 Review and implement new Business Planning Programme CFO Ongoing
Business planning process underway for 2022/23 with alignment across the two Trusts
2
3
4
6 6 6 6 6 6 6 6 6 9 6 60
2
4
6
8
10
Board Assurance Framework 2021-22
Strategic Objective: Develop a Sustainable System Monitoring group(s): Financial Resilience and Commercial Committee Date last reviewed: 20/02/2022
We will efficiently manage our resource to ensure the sustainability of our services and the local care system, whilst never compromising on safety and quality.
Executive Owner(s): Director of Strategy and Digital Development &
Chief Finance Officer
Strategic Priorities: P17: Refresh and align our digital transformation strategy with both the system digital and clinical strategy P18: Implement EPMA & Radiology Order Comms P21: Further develop virtual outpatients, virtual ward and other digital solutions developed during the pandemic
P29: Refresh and align our estates strategy with the system strategic objectives and develop our case for major estate redevelopment
What is the risk to delivery? SR14: There is a risk of not delivering our strategic capital programme and therefore not continuing to develop and to maximise the effectiveness of our facilities, infrastructure and equipment
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) Capital governance structure with Capital Delivery Group (Capex), Strategic Estates and Digital Transformation Group (SETDG), Yeovil Estates Partnership Board and clear lines of accountability to Executive Team, FRCC and YDH Board 2) 3-5 year forward capital plan and YDH2030 plans 3) Estates Masterplan 4) Board approved annual capital plan 5) Standing Financial Instructions and Scheme of Delegation
6) Regular delivery and financial progress reporting to Capital Delivery Group, SEDTG and FRCC 7) Estates programme delivery arrangements 8) Digital programme delivery arrangements 9) Equipment programme delivery arrangements 10) Individual programme/project steering groups 11) System capital planning and prioritisation, access to shared expertise, and management of single system capital envelope
1) Regular reports to Capital Delivery Group, SEDTG, YEP Board, FRCC, Exec Committee and YDH Board 2) Internal audit reports on effectiveness of arrangements 3) Board owned annual capital plan with documented approval of material changes in year 4) NHSE/I monthly system capital assurance reviews 5) Shared system monitoring of use of system envelope
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) 3-5 year forward plan and YDH2030 plans not yet fully developed 2) Refreshed arrangements and reporting for digital
programme in infancy
3) Fully developed system single capital planning and prioritisation arrangements 4) Estates Masterplan refresh and Estates Strategy to be developed
Likelihood Consequence Rationale for overall risk rating:
3: Possible 4: Major Overall risk rating 12: Significant Risk Effective system working in place and improved internal capital planning and delivery. Risk due to scarcity of accessible capital funding for major projects.
Key: Controls and Assurances Overall target risk rating 6: Low Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Blue
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Blue Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
12 12 12 12 12 12 Action By who? By when? Progress
1 Fully develop YDH2030 plans in readiness for funding opportunities
Director of Strategy and
Digital Development
May 2022
Work programme in progress with system partner engagement. Expression of Interest submitted September. Updated and refreshed programme of work underway to
complete Strategic Outline Case.
2 Complete development of system prioritised 3-5 year forward plan
Director of Strategy and
Digital Development
31 Oct 21 Plan drafted and process in place for system prioritisation
3 Complete development of digital programme arrangements and reporting
Director of Strategy and
Digital Development
30 Sep 21 SEDTG now has oversight role. Powerhub in development
and reporting to Exec Committee. Updated governance
12 9 12 12 12 12 12 12 12 12 12 12 120
2
4
6
8
10
12
14
4 Refresh Estates Masterplan and develop Estates Strategy
Director Operations/ Director of Estates SSL
31 Dec 21 Master Plan and Estates Strategy review underway. Plan to
be developed as part of the Strategic Estates &DT Group work plan.
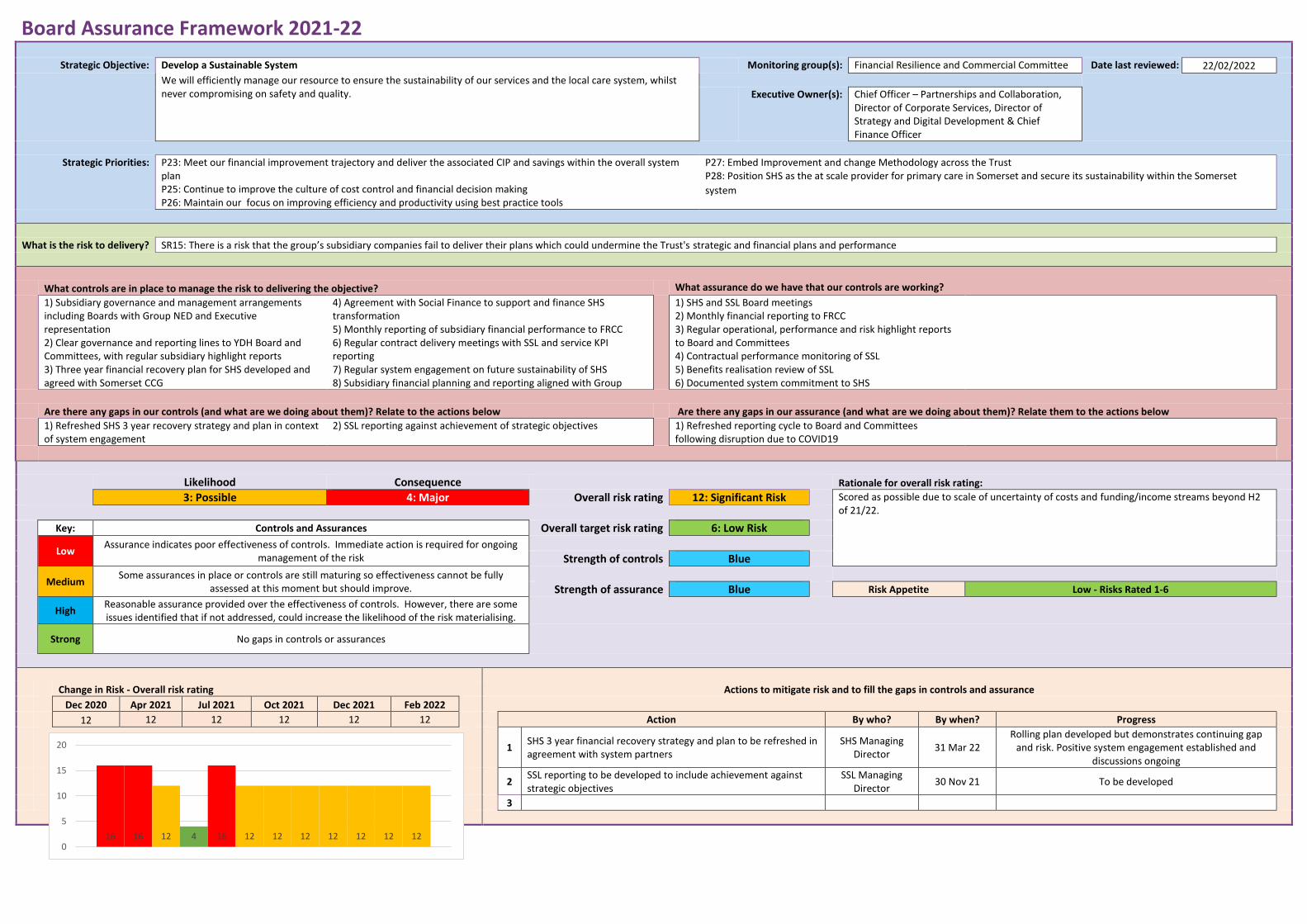
Board Assurance Framework 2021-22
Strategic Objective: Develop a Sustainable System Monitoring group(s): Financial Resilience and Commercial Committee Date last reviewed: 22/02/2022
We will efficiently manage our resource to ensure the sustainability of our services and the local care system, whilst never compromising on safety and quality.
Executive Owner(s): Chief Officer – Partnerships and Collaboration, Director of Corporate Services, Director of Strategy and Digital Development & Chief Finance Officer
Strategic Priorities: P23: Meet our financial improvement trajectory and deliver the associated CIP and savings within the overall system plan P25: Continue to improve the culture of cost control and financial decision making P26: Maintain our focus on improving efficiency and productivity using best practice tools
P27: Embed Improvement and change Methodology across the Trust P28: Position SHS as the at scale provider for primary care in Somerset and secure its sustainability within the Somerset
system
What is the risk to delivery? SR15: There is a risk that the group’s subsidiary companies fail to deliver their plans which could undermine the Trust's strategic and financial plans and performance
What controls are in place to manage the risk to delivering the objective? What assurance do we have that our controls are working?
1) Subsidiary governance and management arrangements including Boards with Group NED and Executive representation 2) Clear governance and reporting lines to YDH Board and Committees, with regular subsidiary highlight reports 3) Three year financial recovery plan for SHS developed and agreed with Somerset CCG
4) Agreement with Social Finance to support and finance SHS transformation 5) Monthly reporting of subsidiary financial performance to FRCC 6) Regular contract delivery meetings with SSL and service KPI reporting 7) Regular system engagement on future sustainability of SHS 8) Subsidiary financial planning and reporting aligned with Group
1) SHS and SSL Board meetings 2) Monthly financial reporting to FRCC 3) Regular operational, performance and risk highlight reports to Board and Committees 4) Contractual performance monitoring of SSL 5) Benefits realisation review of SSL 6) Documented system commitment to SHS
Are there any gaps in our controls (and what are we doing about them)? Relate to the actions below Are there any gaps in our assurance (and what are we doing about them)? Relate them to the actions below
1) Refreshed SHS 3 year recovery strategy and plan in context of system engagement
2) SSL reporting against achievement of strategic objectives 1) Refreshed reporting cycle to Board and Committees following disruption due to COVID19
Likelihood Consequence Rationale for overall risk rating:
3: Possible 4: Major Overall risk rating 12: Significant Risk Scored as possible due to scale of uncertainty of costs and funding/income streams beyond H2 of 21/22.
Key: Controls and Assurances Overall target risk rating 6: Low Risk
Low Assurance indicates poor effectiveness of controls. Immediate action is required for ongoing
management of the risk
Strength of controls Blue
Medium Some assurances in place or controls are still maturing so effectiveness cannot be fully
assessed at this moment but should improve.
Strength of assurance Blue Risk Appetite Low - Risks Rated 1-6
High Reasonable assurance provided over the effectiveness of controls. However, there are some issues identified that if not addressed, could increase the likelihood of the risk materialising.
Strong No gaps in controls or assurances
Change in Risk - Overall risk rating Actions to mitigate risk and to fill the gaps in controls and assurance
Dec 2020 Apr 2021 Jul 2021 Oct 2021 Dec 2021 Feb 2022
12 12 12 12 12 12 Action By who? By when? Progress
1
SHS 3 year financial recovery strategy and plan to be refreshed in agreement with system partners
SHS Managing Director
31 Mar 22 Rolling plan developed but demonstrates continuing gap
and risk. Positive system engagement established and discussions ongoing
2
SSL reporting to be developed to include achievement against strategic objectives
SSL Managing Director
30 Nov 21 To be developed
3
16 16 12 4 16 12 12 12 12 12 12 120
5
10
15
20
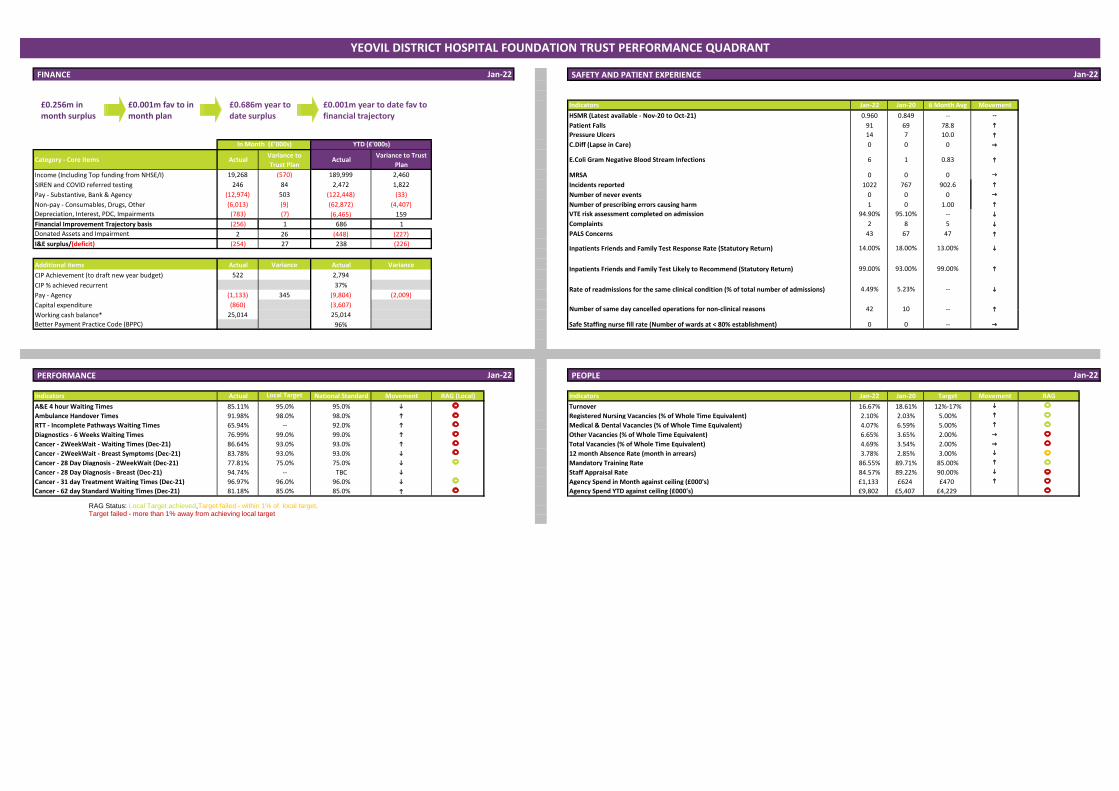
Jan-22 SAFETY AND PATIENT EXPERIENCE
Indicators Jan-22 Jan-20 6 Month Avg Movement
HSMR (Latest available - Nov-20 to Oct-21) 0.960 0.849 -- --
Patient Falls 91 69 78.8 h
Pressure Ulcers 14 7 10.0 h
C.Diff (Lapse in Care) 0 0 0 g
Category - Core items ActualVariance to
Trust PlanActual
Variance to Trust
PlanE.Coli Gram Negative Blood Stream Infections 6 1 0.83 h
Income (Including Top funding from NHSE/I) 19,268 (570) 189,999 2,460 MRSA 0 0 0 g
SIREN and COVID referred testing 246 84 2,472 1,822 Incidents reported 1022 767 902.6 h
Pay - Substantive, Bank & Agency (12,974) 503 (122,448) (33) Number of never events 0 0 0 g
Non-pay - Consumables, Drugs, Other (6,013) (9) (62,872) (4,407) Number of prescribing errors causing harm 1 0 1.00 h
Depreciation, Interest, PDC, Impairments (783) (7) (6,465) 159 VTE risk assessment completed on admission 94.90% 95.10% -- i
Financial Improvement Trajectory basis (256) 1 686 1 Complaints 2 8 5 i
Donated Assets and Impairment 2 26 (448) (227) PALS Concerns 43 67 47 h
I&E surplus/(deficit) (254) 27 238 (226)
Additional items Actual Variance Actual Variance
CIP Achievement (to draft new year budget) 522 2,794
CIP % achieved recurrent 37%
Pay - Agency (1,133) 345 (9,804) (2,009)
Capital expenditure (860) (3,607)
Working cash balance* 25,014 25,014
Better Payment Practice Code (BPPC) 96% Safe Staffing nurse fill rate (Number of wards at < 80% establishment) 0 0 -- g
PERFORMANCE Jan-22 PEOPLE
Indicators Actual Local Target National Standard Movement RAG (Local) Indicators Jan-22 Jan-20 Target Movement RAG
A&E 4 hour Waiting Times 85.11% 95.0% 95.0% i Turnover 16.67% 18.61% 12%-17% i
Ambulance Handover Times 91.98% 98.0% 98.0% h Registered Nursing Vacancies (% of Whole Time Equivalent) 2.10% 2.03% 5.00% h
RTT - Incomplete Pathways Waiting Times 65.94% -- 92.0% h Medical & Dental Vacancies (% of Whole Time Equivalent) 4.07% 6.59% 5.00% h
Diagnostics - 6 Weeks Waiting Times 76.99% 99.0% 99.0% h Other Vacancies (% of Whole Time Equivalent) 6.65% 3.65% 2.00% g
Cancer - 2WeekWait - Waiting Times (Dec-21) 86.64% 93.0% 93.0% h Total Vacancies (% of Whole Time Equivalent) 4.69% 3.54% 2.00% g
Cancer - 2WeekWait - Breast Symptoms (Dec-21) 83.78% 93.0% 93.0% i 12 month Absence Rate (month in arrears) 3.78% 2.85% 3.00% i
Cancer - 28 Day Diagnosis - 2WeekWait (Dec-21) 77.81% 75.0% 75.0% i Mandatory Training Rate 86.55% 89.71% 85.00% h
Cancer - 28 Day Diagnosis - Breast (Dec-21) 94.74% -- TBC i Staff Appraisal Rate 84.57% 89.22% 90.00% i
Cancer - 31 day Treatment Waiting Times (Dec-21) 96.97% 96.0% 96.0% i Agency Spend in Month against ceiling (£000's) £1,133 £624 £470 h
Cancer - 62 day Standard Waiting Times (Dec-21) 81.18% 85.0% 85.0% h Agency Spend YTD against ceiling (£000's) £9,802 £5,407 £4,229
i
h
Jan-22
Jan-22
Inpatients Friends and Family Test Likely to Recommend (Statutory Return) 99.00% 93.00% 99.00%
Number of same day cancelled operations for non-clinical reasons 42 10 --
Rate of readmissions for the same clinical condition (% of total number of admissions) 4.49% 5.23% --
In Month (£'000s) YTD (£'000s)
i
h
YEOVIL DISTRICT HOSPITAL FOUNDATION TRUST PERFORMANCE QUADRANT
FINANCE
Inpatients Friends and Family Test Response Rate (Statutory Return) 14.00% 18.00% 13.00%
RAG Status: Local Target achieved,Target failed - within 1% of local target, Target failed - more than 1% away from achieving local target
£0.686m year to date surplus
£0.001m year to date fav to financial trajectory
£0.256m in month surplus
£0.001m fav to in month plan
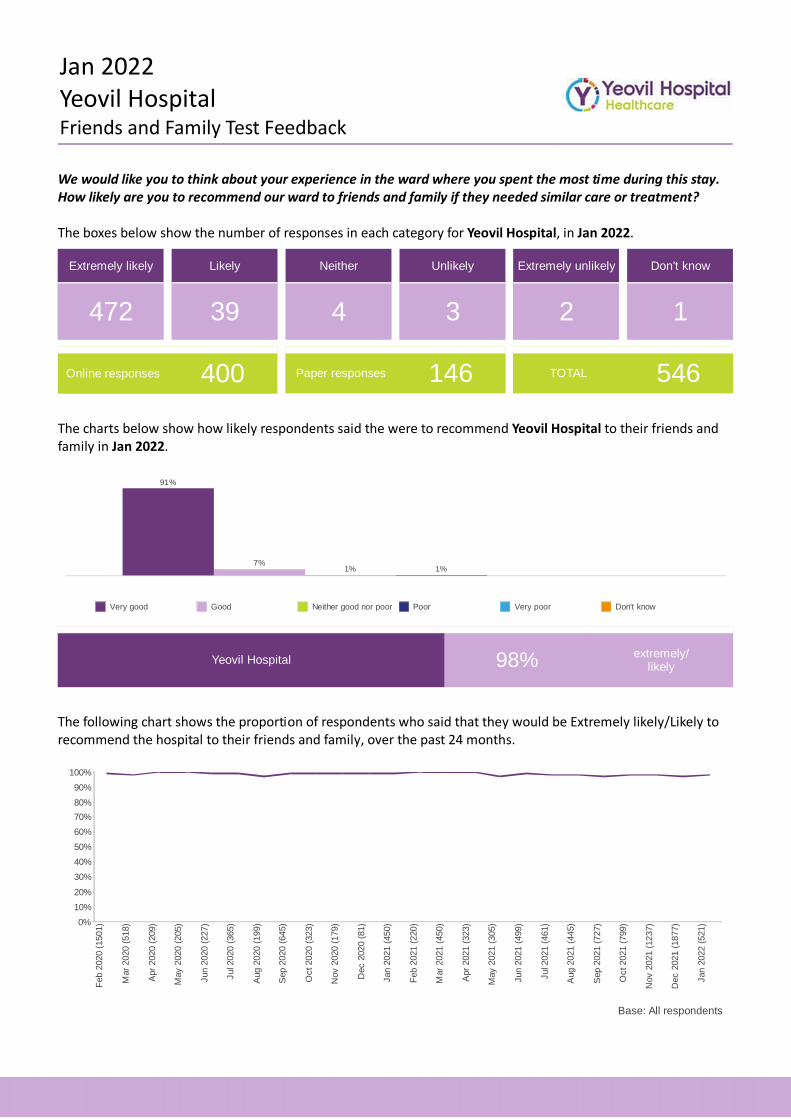
Jan 2022Yeovil HospitalFriends and Family Test Feedback
We would like you to think about your experience in the ward where you spent the most time during this stay. How likely are you to recommend our ward to friends and family if they needed similar care or treatment?
The boxes below show the number of responses in each category for Yeovil Hospital, in Jan 2022.
Extremely likely
472
Likely
39
Neither
4
Unlikely
3
Extremely unlikely
2
Don't know
1
Online responses 400 Paper responses 146 TOTAL 546
The charts below show how likely respondents said the were to recommend Yeovil Hospital to their friends and family in Jan 2022.
1%1%7%
91%
Very good Good Neither good nor poor Poor Very poor Don't know
Yeovil Hospital 98% extremely/likely
The following chart shows the proportion of respondents who said that they would be Extremely likely/Likely to recommend the hospital to their friends and family, over the past 24 months.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Feb
202
0 (1
501)
Mar
202
0 (5
18)
Apr
202
0 (2
09)
May
202
0 (2
05)
Jun
2020
(22
7)
Jul 2
020
(365
)
Aug
202
0 (1
99)
Sep
202
0 (6
45)
Oct
202
0 (3
23)
Nov
202
0 (1
79)
Dec
202
0 (8
1)
Jan
2021
(45
0)
Feb
202
1 (2
20)
Mar
202
1 (4
50)
Apr
202
1 (3
23)
May
202
1 (3
05)
Jun
2021
(49
9)
Jul 2
021
(461
)
Aug
202
1 (4
45)
Sep
202
1 (7
27)
Oct
202
1 (7
99)
Nov
202
1 (1
237)
Dec
202
1 (1
877)
Jan
2022
(52
1)
Base: All respondents
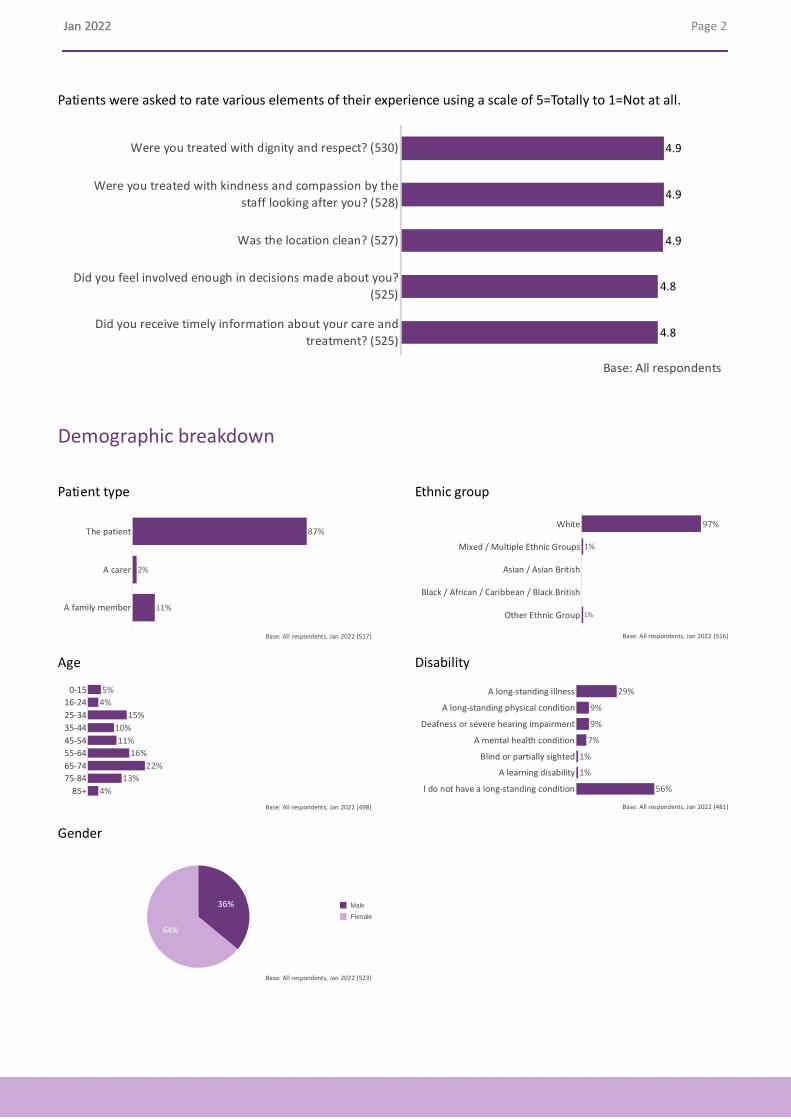
Jan 2022 Jan 2022 Page 2 .
Patients were asked to rate various elements of their experience using a scale of 5=Totally to 1=Not at all.
Were you treated with dignity and respect? (530)
Were you treated with kindness and compassion by the
staff looking after you? (528)
Was the location clean? (527)
Did you feel involved enough in decisions made about you?
(525)
Did you receive timely information about your care and
treatment? (525)
4.8
4.8
4.9
4.9
4.9
Base: All respondents
Demographic breakdown
Patient type Ethnic group
The patient
A carer
A family member
87%
2%
11%
Base: All respondents, Jan 2022 (517)
White
Mixed / Multiple Ethnic Groups
Asian / Asian British
Black / African / Caribbean / Black British
Other Ethnic Group
97%
1%
1%
Base: All respondents, Jan 2022 (516)
Age Disability
015
1624
2534
3544
4554
5564
6574
7584
85+
4%
13%
10%
4%
16%
11%
15%
22%
5%
Base: All respondents, Jan 2022 (498)
A longstanding illness
A longstanding physical condition
Deafness or severe hearing impairment
A mental health condition
Blind or partially sighted
A learning disability
I do not have a longstanding condition
9%
1%
56%
1%
9%
7%
29%
Base: All respondents, Jan 2022 (481)
Gender
36%
64%
Male
Female
Base: All respondents, Jan 2022 (523)
Qualiy and Performance Exception Report
March 2022 Public Board - 1 – H
Somerset NHS Foundation Trust
REPORT TO: The Trust Board
REPORT TITLE: Quality and Performance Exception Report
SPONSORING EXEC: Chief Finance Officer
REPORT BY:
Associate Director – Planning and Performance
Senior Performance Manager
Chief of People and Organisational Development
Deputy Chief Nurse
Director of Elective Care
PRESENTED BY: Chief Finance Officer
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☒ For Assurance/
Discussion ☐ For Approval / Decision ☒ For Information
Executive Summary and Reason for presentation to Committee/Board
Our Quality and Performance Exception Report sets out the key exceptions across a range of quality and performance measures, and the reasons for any significant changes or trends. Covid-19 continues to have a significant impact on a range of access standards, whilst restoration work is being undertaken to reduce the number of patients waiting and to shorten waiting times. As referrals recover to pre-Covid-19 levels this will also have an impact on services and numbers waiting. Urgent and emergency patients continue to be prioritised, to receive the treatments they need. Areas in which performance has been sustained or has notably improved include:
• performance against the 28-day faster cancer diagnosis standard;
• Compliance in respect of the 31 day wait from cancer diagnosis to first treatment;
Qualiy and Performance Exception Report
March 2022 Public Board - 2 –
H
• the percentage of IAPT (Talking Therapies) patients moving to recovery;
• vacancy levels;
• retention of colleagues. Areas in respect of which the contributory causes of, and actions to address, underperformance are set out in greater detail in this report include:
• the percentage of patients seen within four hours, in our accident and emergency department and minor injury units;
• the percentage of people waiting under 18 weeks from referral to treatment with our acute services;
• the percentage of people waiting under six weeks for a diagnostic test;
• the numbers of people waiting 18 weeks or more to be seen by our community physical health services, including our community dental service;
• sickness absence levels of colleagues.
Performance, across a broad range of indicators, is anticipated to continue to be adversely affected over the coming months, as a result of the necessary refocusing of priorities towards the effective management of Covid-19. Performance monitoring, and the provision of essential information to front line services, and for the purposes of governance and assurance, will continue. During the Covid-19 outbreak, NHS England/NHS Improvement wrote to all NHS Trusts to advise that changes had been implemented to governance and reporting arrangements, to reduce the burden of reporting and release capacity. This included the suspension of requirements to submit returns relating to a range of indicators, including the Friends and Family test and venous thromboembolism
Recommendation The Board is asked to discuss and note the report.
Qualiy and Performance Exception Report
March 2022 Public Board - 3 –
H
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☐ Care for our Population ☐ Develop our People
☐ Innovate and Collaborate ☐ Develop a Sustainable System
Somerset NHS FT
☒ Obj 1 Inclusive culture ☒ Obj 4 Safe services ☒ Obj 7 Improving outcomes
☐ Obj 2 Collaboration ☐ Obj 5 Self management ☒ Obj 8 Workforce
☒ Obj 3 Independent lives ☒ Obj 6 Value all people alike ☒ Obj 9 Performance
☐ Obj 10 Finance
Implications/Requirements (Please select any which are relevant to this paper)
☐ Financial ☒ Legislation ☒ Workforce ☐ Estates ☐ ICT ☐ Patient Safety /
Quality
Details:
The report provides an update on issues relating to staffing, in Section 1 and also in Appendix 4. (workforce)
The report provides an update, by exception, on the position relating to statutory Fire training, in Section 1. (legislation)
Equality The Trust wants its services to be as accessible as possible, to as many people as
possible. Please indicate whether the report has an impact on the protected characteristics
☒ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are no proposals or matters which affect any persons with protected characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
No recommendations are being made, other than to ask the Board to discuss and note the report.
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
Qualiy and Performance Exception Report
March 2022 Public Board - 4 –
H
A report is presented to every Board meeting.
Reference to CQC domains (Please select any which are relevant to this paper)
☒ Safe ☒ Effective ☒ Caring ☒ Responsive ☒ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
Qualiy and Performance Exception Report
March 2022 Public Board - 5 –
H
SOMERSET NHS FOUNDATION TRUST
QUALITY AND PERFORMANCE EXCEPTION REPORT: JANUART 2022
1. PURPOSE 1.1 Our Quality and Performance exception report sets out the key exceptions
across a range of quality and performance measures, and the reasons for any significant changes or trends.
1.2 The report presents information relating to the five key questions which the
Care Quality Commission considers when reviewing and inspecting services:
• Are they safe?
• Are they effective?
• Are they caring?
• Are they well-led?
• Are they responsive to people’s needs?
1.3 The exception reports include run charts, produced using Institute for Healthcare Improvement (IHI) methodology, and in consultation with the Academic Health Sciences Network. An explanation of how to interpret these charts is attached as Appendix 1.
1.4 A summary of our current Care Quality Commission ratings, which relate to our two predecessor organisations, is included as Appendix 2.
1.5 A summary of the monthly data and run charts for our key quality measures is attached as Appendix 3.
1.6 Our Corporate Balanced Scorecard is attached as Appendix 4. The measures included in the Corporate Balanced Scorecard may change during the year as new priority areas are identified.
1.7 Supporting information relating to referral levels, activity levels, lengths of stay, tumour-site-specific activity and performance, and other key measures for our services is included in Appendix 5.
Overview
The table below provides a summary of key successes, priorities, opportunities, risks and threats in relation to our current levels of
performance.
Successes Priorities
• during January 2022 we continued successfully to meet the challenges presented by COVID-19 to patients and colleagues.
• ‘Attend Anywhere’ technology continues to enable patients to be seen remotely and receive advice and support, and continues to be well received.
• urgent and emergency patients continue to receive the treatments they need.
• the percentage of patients waiting under six weeks for mental health services remains high.
• there has been a further reduction in the number of patients waiting over six weeks for a diagnostic test.
• our Talking Therapies (IAPT) service continues to maintain recovery rates which are significantly above the national standard.
• compliance in respect of mandatory training maintained despite the operational challenges faced by services.
• continue to maintain a safe service and making sure urgent patients are treated as quickly as possible within the context of the challenges the current coronavirus outbreak brings.
• continue to support the health and wellbeing, both physically and psychologically, of colleagues across the Trust, as they continue to deliver high quality care to patients whilst managing significant and ongoing pressures associated with COVID and rising levels of demand.
• continuing to restore and expand capacity above pre-COVID-19 levels, to address backlogs in routine elective work which has built-up.
• work with the Somerset system to encourage continued referrals and presentations at hospital where needed and appropriate, especially in respect of urgent or emergency care.
• continue the rollout of the mass vaccination programme.
Opportunities Risks and Threats
• continue to progress the health and wellbeing plans for our colleagues at pace; this includes the psychological support offered alongside practical aspects of support such as free car parking, accommodation provision, and nutrition.
• continue with new ways of working, particularly through the use of technology; this presents an opportunity for us to consider how we provide care appropriately and effectively to patients following the COVID-19 outbreak.
• continue to adapt our recruitment practice, developing more innovative arrangements and reducing time to hire significantly.
• develop reporting solutions to improve robustness of recording and reporting.
• COVID-19 will continue to have a significant impact on clinical capacity and the Trust’s ability to recover elective activity, which will continue to have a negative impact on waiting times for some time to come.
• delays in discharge of medically fit patients needing domiciliary care will result in further cancellations of surgery which will reduce the Trust’s capacity to treat long waiting patients.
• significantly increasing levels of demand, particularly for urgent care and mental health services, leading potentially to increased pressures on teams and longer waiting times.
• nursing vacancy levels remain challenging. Sickness / absence also presents a challenge for colleagues within some critical areas, and we need to ensure that we continue to support colleagues accordingly.
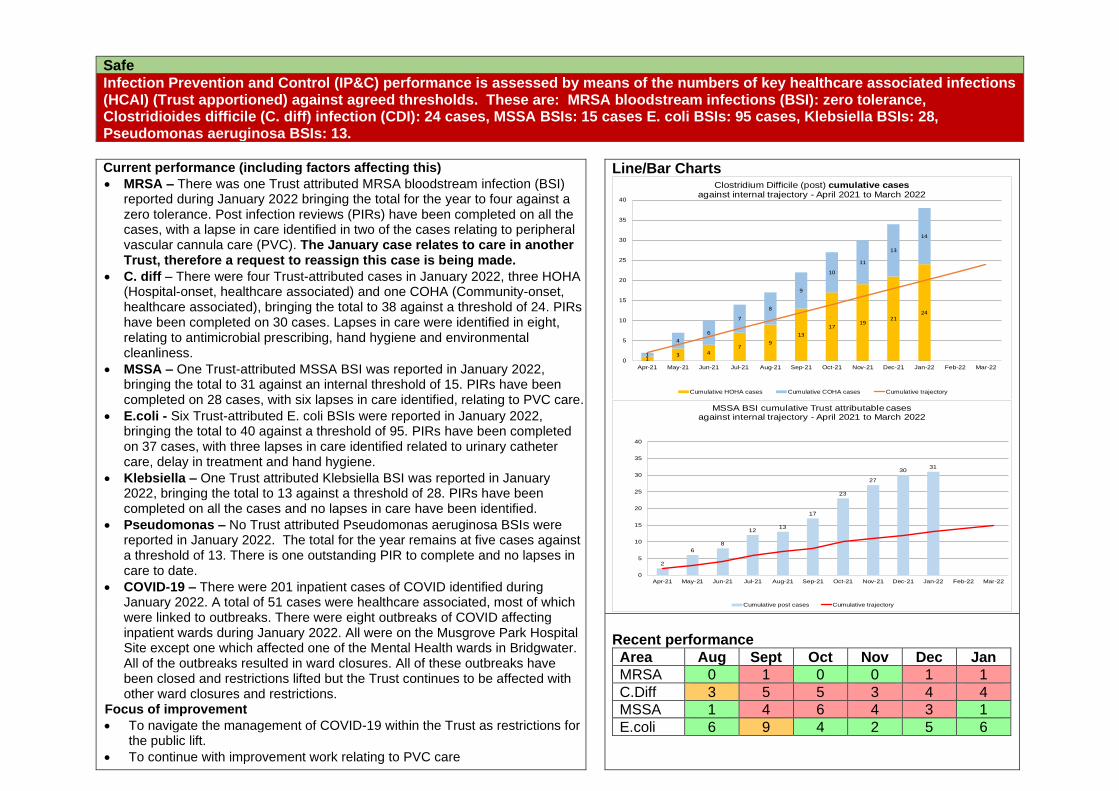
Safe
Infection Prevention and Control (IP&C) performance is assessed by means of the numbers of key healthcare associated infections (HCAI) (Trust apportioned) against agreed thresholds. These are: MRSA bloodstream infections (BSI): zero tolerance, Clostridioides difficile (C. diff) infection (CDI): 24 cases, MSSA BSIs: 15 cases E. coli BSIs: 95 cases, Klebsiella BSIs: 28, Pseudomonas aeruginosa BSIs: 13.
Current performance (including factors affecting this)
• MRSA – There was one Trust attributed MRSA bloodstream infection (BSI) reported during January 2022 bringing the total for the year to four against a zero tolerance. Post infection reviews (PIRs) have been completed on all the cases, with a lapse in care identified in two of the cases relating to peripheral vascular cannula care (PVC). The January case relates to care in another Trust, therefore a request to reassign this case is being made.
• C. diff – There were four Trust-attributed cases in January 2022, three HOHA (Hospital-onset, healthcare associated) and one COHA (Community-onset, healthcare associated), bringing the total to 38 against a threshold of 24. PIRs have been completed on 30 cases. Lapses in care were identified in eight, relating to antimicrobial prescribing, hand hygiene and environmental cleanliness.
• MSSA – One Trust-attributed MSSA BSI was reported in January 2022, bringing the total to 31 against an internal threshold of 15. PIRs have been completed on 28 cases, with six lapses in care identified, relating to PVC care.
• E.coli - Six Trust-attributed E. coli BSIs were reported in January 2022, bringing the total to 40 against a threshold of 95. PIRs have been completed on 37 cases, with three lapses in care identified related to urinary catheter care, delay in treatment and hand hygiene.
• Klebsiella – One Trust attributed Klebsiella BSI was reported in January 2022, bringing the total to 13 against a threshold of 28. PIRs have been completed on all the cases and no lapses in care have been identified.
• Pseudomonas – No Trust attributed Pseudomonas aeruginosa BSIs were reported in January 2022. The total for the year remains at five cases against a threshold of 13. There is one outstanding PIR to complete and no lapses in care to date.
• COVID-19 – There were 201 inpatient cases of COVID identified during January 2022. A total of 51 cases were healthcare associated, most of which were linked to outbreaks. There were eight outbreaks of COVID affecting inpatient wards during January 2022. All were on the Musgrove Park Hospital Site except one which affected one of the Mental Health wards in Bridgwater. All of the outbreaks resulted in ward closures. All of these outbreaks have been closed and restrictions lifted but the Trust continues to be affected with other ward closures and restrictions.
Focus of improvement
• To navigate the management of COVID-19 within the Trust as restrictions for the public lift.
• To continue with improvement work relating to PVC care
Line/Bar Charts
Recent performance
Area Aug Sept Oct Nov Dec Jan
MRSA 0 1 0 0 1 1
C.Diff 3 5 5 3 4 4
MSSA 1 4 6 4 3 1
E.coli 6 9 4 2 5 6
13 4
79
13
1719
2124
1
4
6
7
8
9
10
11
13
14
0
5
10
15
20
25
30
35
40
Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Feb-22 Mar-22
Clostridium Difficile (post) cumulative casesagainst internal trajectory - April 2021 to March 2022
Cumulative HOHA cases Cumulative COHA cases Cumulative trajectory
2
6
8
1213
17
23
27
3031
0
5
10
15
20
25
30
35
40
Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Feb-22 Mar-22
MSSA BSI cumulative Trust attributable cases against internal trajectory - April 2021 to March 2022
Cumulative post cases Cumulative trajectory
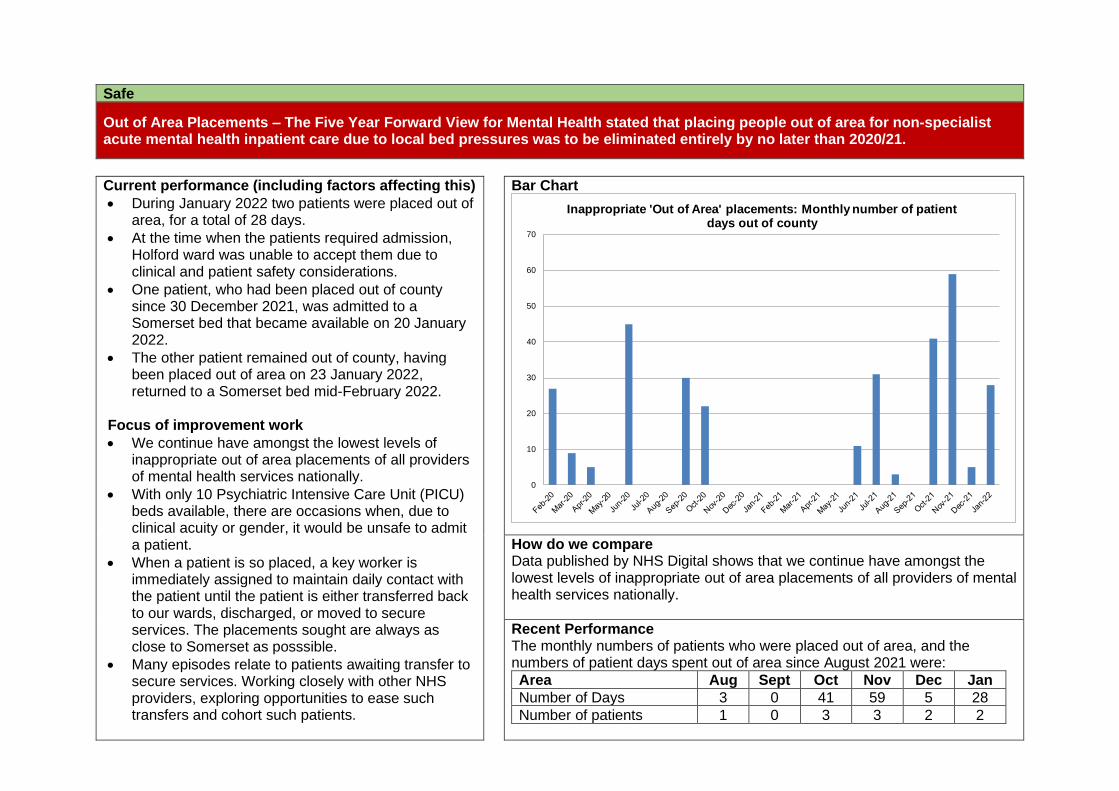
Safe
Out of Area Placements – The Five Year Forward View for Mental Health stated that placing people out of area for non-specialist acute mental health inpatient care due to local bed pressures was to be eliminated entirely by no later than 2020/21.
Current performance (including factors affecting this)
• During January 2022 two patients were placed out of area, for a total of 28 days.
• At the time when the patients required admission, Holford ward was unable to accept them due to clinical and patient safety considerations.
• One patient, who had been placed out of county since 30 December 2021, was admitted to a Somerset bed that became available on 20 January 2022.
• The other patient remained out of county, having been placed out of area on 23 January 2022, returned to a Somerset bed mid-February 2022.
Focus of improvement work
• We continue have amongst the lowest levels of inappropriate out of area placements of all providers of mental health services nationally.
• With only 10 Psychiatric Intensive Care Unit (PICU) beds available, there are occasions when, due to clinical acuity or gender, it would be unsafe to admit a patient.
• When a patient is so placed, a key worker is immediately assigned to maintain daily contact with the patient until the patient is either transferred back to our wards, discharged, or moved to secure services. The placements sought are always as close to Somerset as posssible.
• Many episodes relate to patients awaiting transfer to secure services. Working closely with other NHS providers, exploring opportunities to ease such transfers and cohort such patients.
Bar Chart
How do we compare Data published by NHS Digital shows that we continue have amongst the lowest levels of inappropriate out of area placements of all providers of mental health services nationally.
Recent Performance The monthly numbers of patients who were placed out of area, and the numbers of patient days spent out of area since August 2021 were:
Area Aug Sept Oct Nov Dec Jan
Number of Days 3 0 41 59 5 28
Number of patients 1 0 3 3 2 2
0
10
20
30
40
50
60
70
Inappropriate 'Out of Area' placements: Monthly number of patient days out of county
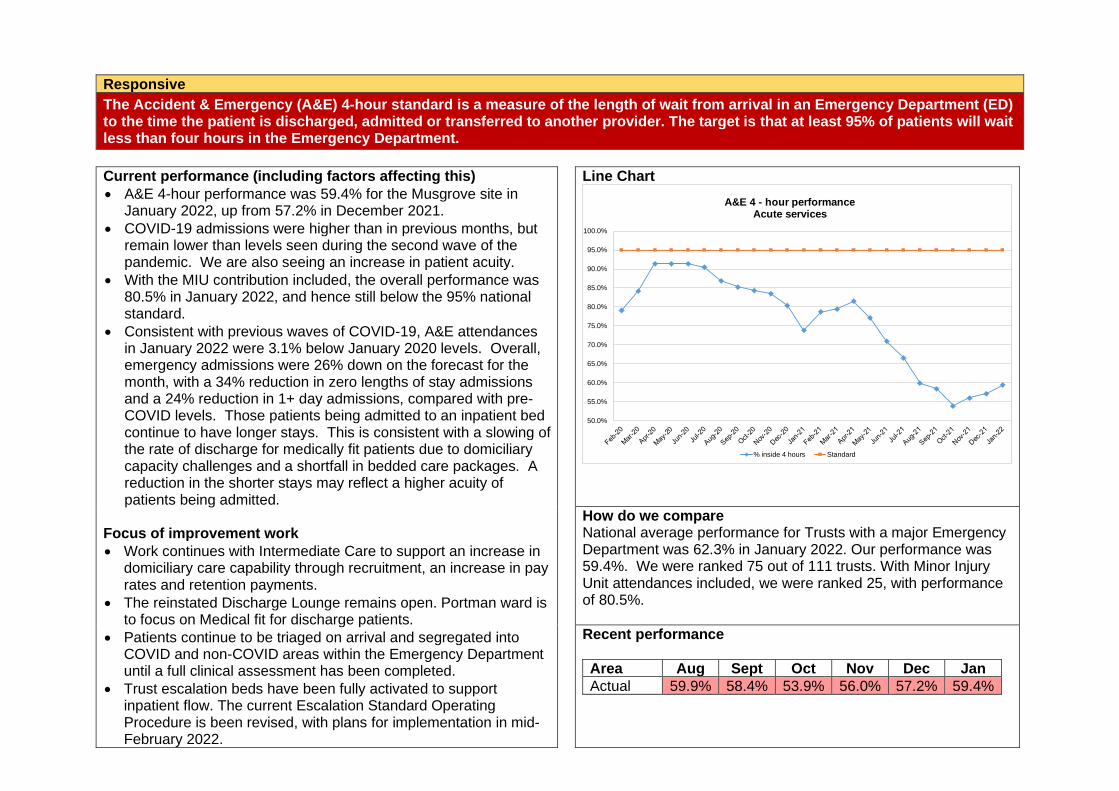
Responsive
The Accident & Emergency (A&E) 4-hour standard is a measure of the length of wait from arrival in an Emergency Department (ED) to the time the patient is discharged, admitted or transferred to another provider. The target is that at least 95% of patients will wait less than four hours in the Emergency Department.
Current performance (including factors affecting this)
• A&E 4-hour performance was 59.4% for the Musgrove site in January 2022, up from 57.2% in December 2021.
• COVID-19 admissions were higher than in previous months, but remain lower than levels seen during the second wave of the pandemic. We are also seeing an increase in patient acuity.
• With the MIU contribution included, the overall performance was 80.5% in January 2022, and hence still below the 95% national standard.
• Consistent with previous waves of COVID-19, A&E attendances in January 2022 were 3.1% below January 2020 levels. Overall, emergency admissions were 26% down on the forecast for the month, with a 34% reduction in zero lengths of stay admissions and a 24% reduction in 1+ day admissions, compared with pre-COVID levels. Those patients being admitted to an inpatient bed continue to have longer stays. This is consistent with a slowing of the rate of discharge for medically fit patients due to domiciliary capacity challenges and a shortfall in bedded care packages. A reduction in the shorter stays may reflect a higher acuity of patients being admitted.
Focus of improvement work
• Work continues with Intermediate Care to support an increase in domiciliary care capability through recruitment, an increase in pay rates and retention payments.
• The reinstated Discharge Lounge remains open. Portman ward is to focus on Medical fit for discharge patients.
• Patients continue to be triaged on arrival and segregated into COVID and non-COVID areas within the Emergency Department until a full clinical assessment has been completed.
• Trust escalation beds have been fully activated to support inpatient flow. The current Escalation Standard Operating Procedure is been revised, with plans for implementation in mid-February 2022.
Line Chart
How do we compare National average performance for Trusts with a major Emergency Department was 62.3% in January 2022. Our performance was 59.4%. We were ranked 75 out of 111 trusts. With Minor Injury Unit attendances included, we were ranked 25, with performance of 80.5%.
Recent performance
Area Aug Sept Oct Nov Dec Jan
Actual 59.9% 58.4% 53.9% 56.0% 57.2% 59.4%
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
A&E 4 - hour performance Acute services
% inside 4 hours Standard
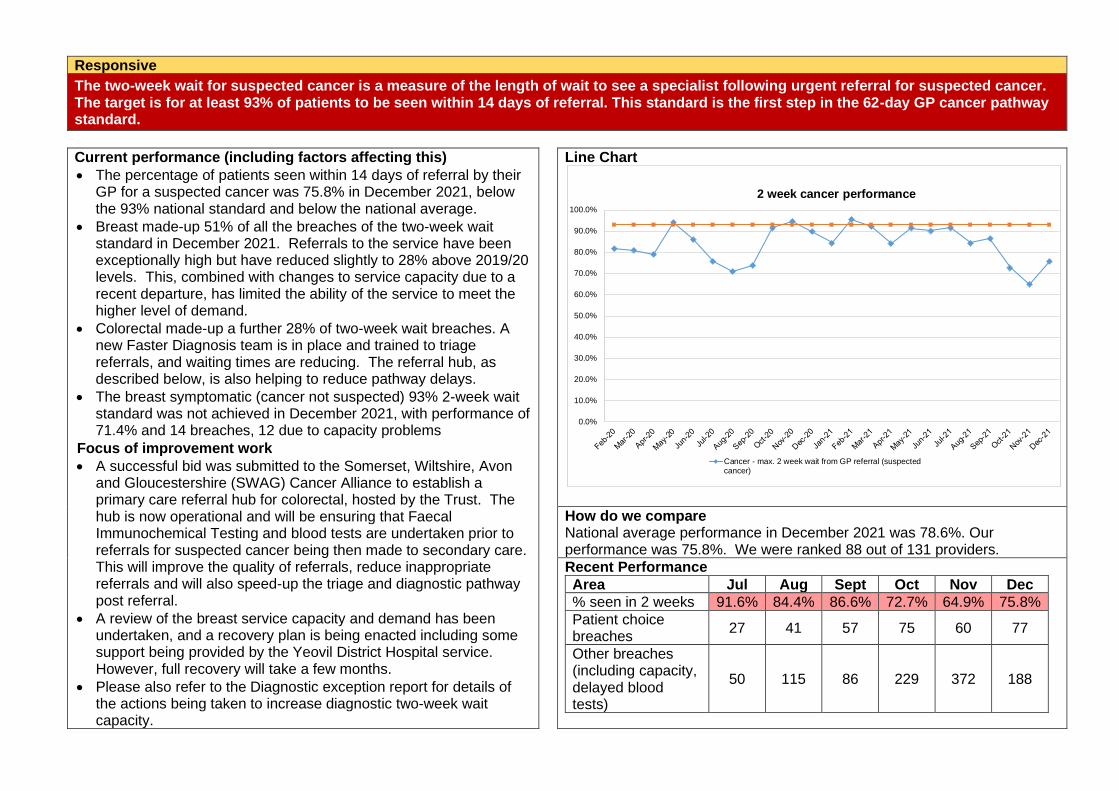
Responsive
The two-week wait for suspected cancer is a measure of the length of wait to see a specialist following urgent referral for suspected cancer. The target is for at least 93% of patients to be seen within 14 days of referral. This standard is the first step in the 62-day GP cancer pathway standard.
Current performance (including factors affecting this)
• The percentage of patients seen within 14 days of referral by their GP for a suspected cancer was 75.8% in December 2021, below the 93% national standard and below the national average.
• Breast made-up 51% of all the breaches of the two-week wait standard in December 2021. Referrals to the service have been exceptionally high but have reduced slightly to 28% above 2019/20 levels. This, combined with changes to service capacity due to a recent departure, has limited the ability of the service to meet the higher level of demand.
• Colorectal made-up a further 28% of two-week wait breaches. A new Faster Diagnosis team is in place and trained to triage referrals, and waiting times are reducing. The referral hub, as described below, is also helping to reduce pathway delays.
• The breast symptomatic (cancer not suspected) 93% 2-week wait standard was not achieved in December 2021, with performance of 71.4% and 14 breaches, 12 due to capacity problems
• Focus of improvement work
• A successful bid was submitted to the Somerset, Wiltshire, Avon and Gloucestershire (SWAG) Cancer Alliance to establish a primary care referral hub for colorectal, hosted by the Trust. The hub is now operational and will be ensuring that Faecal Immunochemical Testing and blood tests are undertaken prior to referrals for suspected cancer being then made to secondary care. This will improve the quality of referrals, reduce inappropriate referrals and will also speed-up the triage and diagnostic pathway post referral.
• A review of the breast service capacity and demand has been undertaken, and a recovery plan is being enacted including some support being provided by the Yeovil District Hospital service. However, full recovery will take a few months.
• Please also refer to the Diagnostic exception report for details of the actions being taken to increase diagnostic two-week wait capacity.
Line Chart
How do we compare National average performance in December 2021 was 78.6%. Our performance was 75.8%. We were ranked 88 out of 131 providers.
Recent Performance
Area Jul Aug Sept Oct Nov Dec
% seen in 2 weeks 91.6% 84.4% 86.6% 72.7% 64.9% 75.8%
Patient choice breaches
27 41 57 75 60 77
Other breaches (including capacity, delayed blood tests)
50 115 86 229 372 188
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
2 week cancer performance
Cancer - max. 2 week wait from GP referral (suspectedcancer)
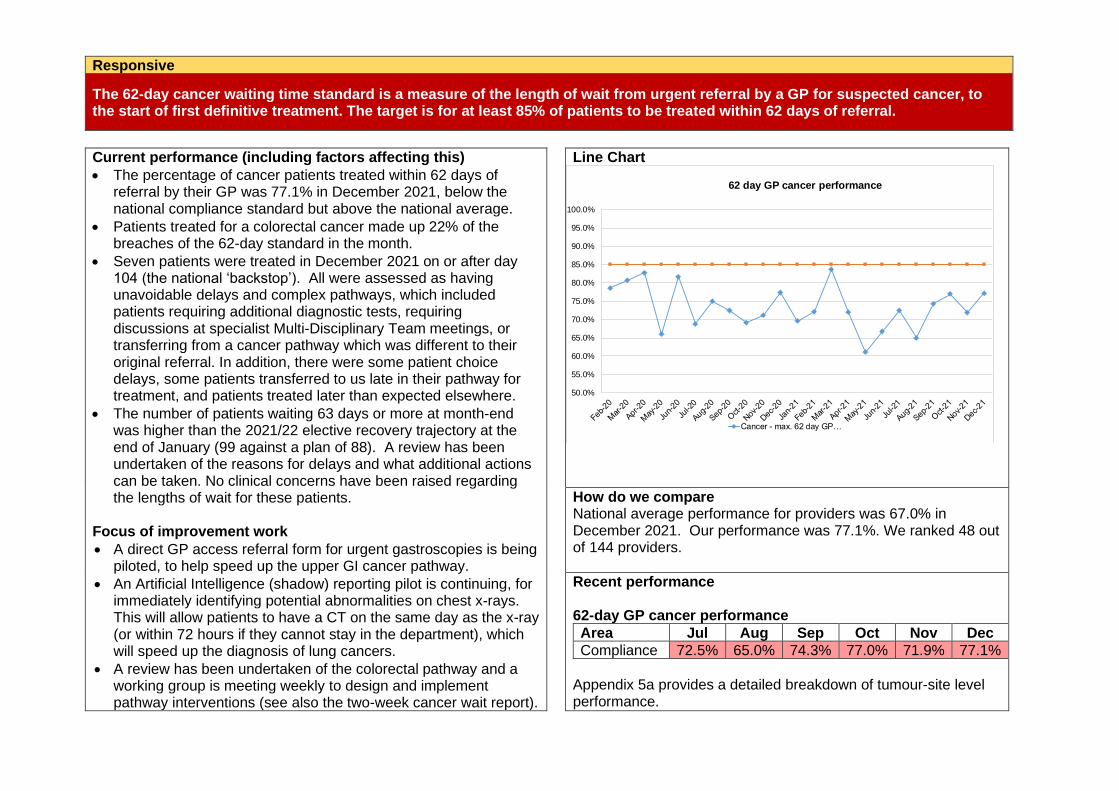
Responsive
The 62-day cancer waiting time standard is a measure of the length of wait from urgent referral by a GP for suspected cancer, to the start of first definitive treatment. The target is for at least 85% of patients to be treated within 62 days of referral.
Current performance (including factors affecting this)
• The percentage of cancer patients treated within 62 days of referral by their GP was 77.1% in December 2021, below the national compliance standard but above the national average.
• Patients treated for a colorectal cancer made up 22% of the breaches of the 62-day standard in the month.
• Seven patients were treated in December 2021 on or after day 104 (the national ‘backstop’). All were assessed as having unavoidable delays and complex pathways, which included patients requiring additional diagnostic tests, requiring discussions at specialist Multi-Disciplinary Team meetings, or transferring from a cancer pathway which was different to their original referral. In addition, there were some patient choice delays, some patients transferred to us late in their pathway for treatment, and patients treated later than expected elsewhere.
• The number of patients waiting 63 days or more at month-end was higher than the 2021/22 elective recovery trajectory at the end of January (99 against a plan of 88). A review has been undertaken of the reasons for delays and what additional actions can be taken. No clinical concerns have been raised regarding the lengths of wait for these patients.
Focus of improvement work
• A direct GP access referral form for urgent gastroscopies is being piloted, to help speed up the upper GI cancer pathway.
• An Artificial Intelligence (shadow) reporting pilot is continuing, for immediately identifying potential abnormalities on chest x-rays. This will allow patients to have a CT on the same day as the x-ray (or within 72 hours if they cannot stay in the department), which will speed up the diagnosis of lung cancers.
• A review has been undertaken of the colorectal pathway and a working group is meeting weekly to design and implement pathway interventions (see also the two-week cancer wait report).
Line Chart
How do we compare National average performance for providers was 67.0% in December 2021. Our performance was 77.1%. We ranked 48 out of 144 providers.
Recent performance 62-day GP cancer performance
Area Jul Aug Sep Oct Nov Dec
Compliance 72.5% 65.0% 74.3% 77.0% 71.9% 77.1%
Appendix 5a provides a detailed breakdown of tumour-site level performance.
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
62 day GP cancer performance
Cancer - max. 62 day GP…
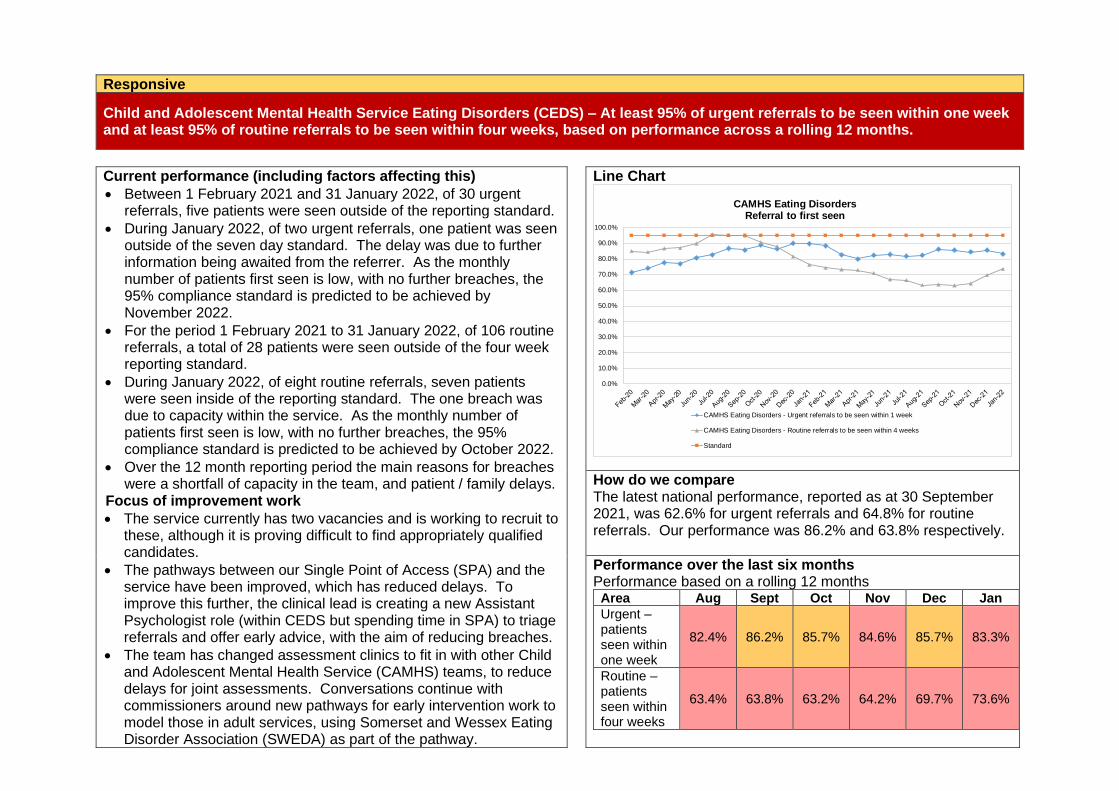
Responsive
Child and Adolescent Mental Health Service Eating Disorders (CEDS) – At least 95% of urgent referrals to be seen within one week and at least 95% of routine referrals to be seen within four weeks, based on performance across a rolling 12 months.
Current performance (including factors affecting this)
• Between 1 February 2021 and 31 January 2022, of 30 urgent referrals, five patients were seen outside of the reporting standard.
• During January 2022, of two urgent referrals, one patient was seen outside of the seven day standard. The delay was due to further information being awaited from the referrer. As the monthly number of patients first seen is low, with no further breaches, the 95% compliance standard is predicted to be achieved by November 2022.
• For the period 1 February 2021 to 31 January 2022, of 106 routine referrals, a total of 28 patients were seen outside of the four week reporting standard.
• During January 2022, of eight routine referrals, seven patients were seen inside of the reporting standard. The one breach was due to capacity within the service. As the monthly number of patients first seen is low, with no further breaches, the 95% compliance standard is predicted to be achieved by October 2022.
• Over the 12 month reporting period the main reasons for breaches were a shortfall of capacity in the team, and patient / family delays.
Focus of improvement work
• The service currently has two vacancies and is working to recruit to these, although it is proving difficult to find appropriately qualified candidates.
• The pathways between our Single Point of Access (SPA) and the service have been improved, which has reduced delays. To improve this further, the clinical lead is creating a new Assistant Psychologist role (within CEDS but spending time in SPA) to triage referrals and offer early advice, with the aim of reducing breaches.
• The team has changed assessment clinics to fit in with other Child and Adolescent Mental Health Service (CAMHS) teams, to reduce delays for joint assessments. Conversations continue with commissioners around new pathways for early intervention work to model those in adult services, using Somerset and Wessex Eating Disorder Association (SWEDA) as part of the pathway.
Line Chart
How do we compare The latest national performance, reported as at 30 September 2021, was 62.6% for urgent referrals and 64.8% for routine referrals. Our performance was 86.2% and 63.8% respectively.
Performance over the last six months Performance based on a rolling 12 months
Area Aug Sept Oct Nov Dec Jan
Urgent – patients seen within one week
82.4% 86.2% 85.7% 84.6% 85.7% 83.3%
Routine – patients seen within four weeks
63.4% 63.8% 63.2% 64.2% 69.7% 73.6%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
CAMHS Eating DisordersReferral to first seen
CAMHS Eating Disorders - Urgent referrals to be seen within 1 week
CAMHS Eating Disorders - Routine referrals to be seen within 4 weeks
Standard
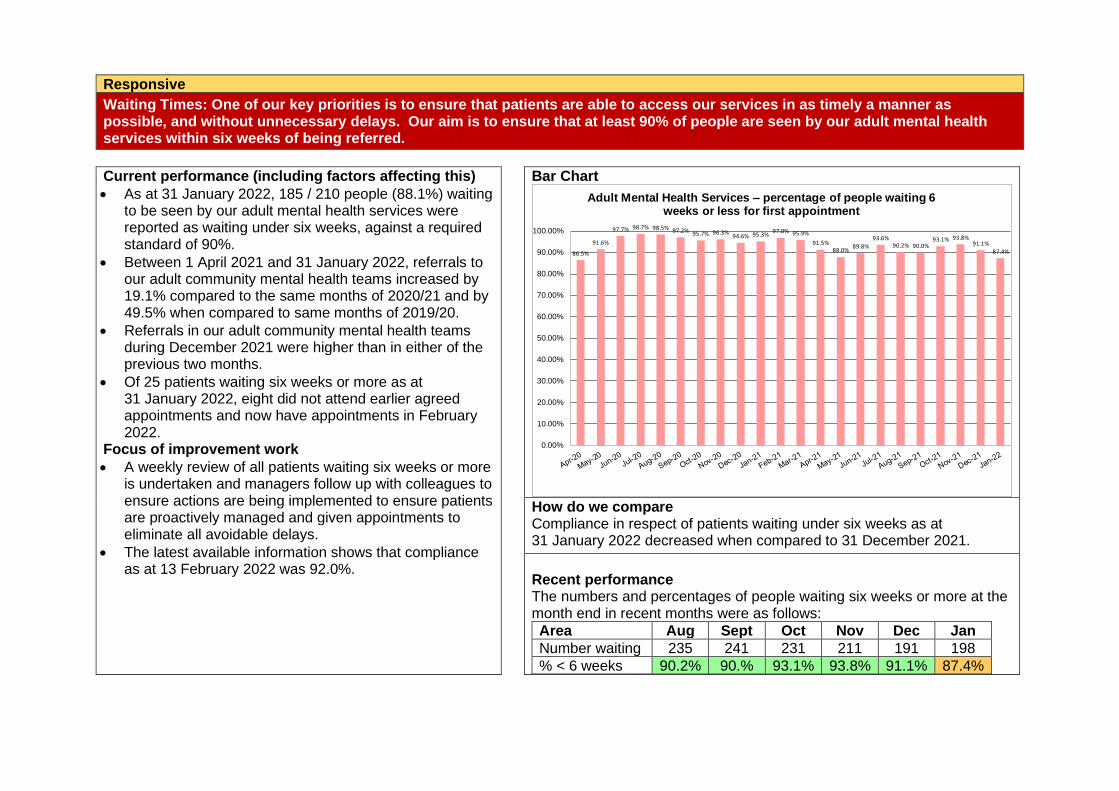
Responsive
Waiting Times: One of our key priorities is to ensure that patients are able to access our services in as timely a manner as possible, and without unnecessary delays. Our aim is to ensure that at least 90% of people are seen by our adult mental health services within six weeks of being referred.
Current performance (including factors affecting this)
• As at 31 January 2022, 185 / 210 people (88.1%) waiting to be seen by our adult mental health services were reported as waiting under six weeks, against a required standard of 90%.
• Between 1 April 2021 and 31 January 2022, referrals to our adult community mental health teams increased by 19.1% compared to the same months of 2020/21 and by 49.5% when compared to same months of 2019/20.
• Referrals in our adult community mental health teams during December 2021 were higher than in either of the previous two months.
• Of 25 patients waiting six weeks or more as at 31 January 2022, eight did not attend earlier agreed appointments and now have appointments in February 2022.
Focus of improvement work
• A weekly review of all patients waiting six weeks or more is undertaken and managers follow up with colleagues to ensure actions are being implemented to ensure patients are proactively managed and given appointments to eliminate all avoidable delays.
• The latest available information shows that compliance as at 13 February 2022 was 92.0%.
Bar Chart
How do we compare
Compliance in respect of patients waiting under six weeks as at 31 January 2022 decreased when compared to 31 December 2021.
Recent performance The numbers and percentages of people waiting six weeks or more at the month end in recent months were as follows:
Area Aug Sept Oct Nov Dec Jan
Number waiting 235 241 231 211 191 198
% < 6 weeks 90.2% 90.% 93.1% 93.8% 91.1% 87.4%
86.5%
91.6%
97.7% 98.7% 98.5% 97.2% 95.7% 96.3%94.6% 95.3%
97.0% 95.9%
91.5%88.0%
89.8%
93.6%90.2% 90.0%
93.1% 93.8%91.1%
87.4%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Adult Mental Health Services – percentage of people waiting 6 weeks or less for first appointment
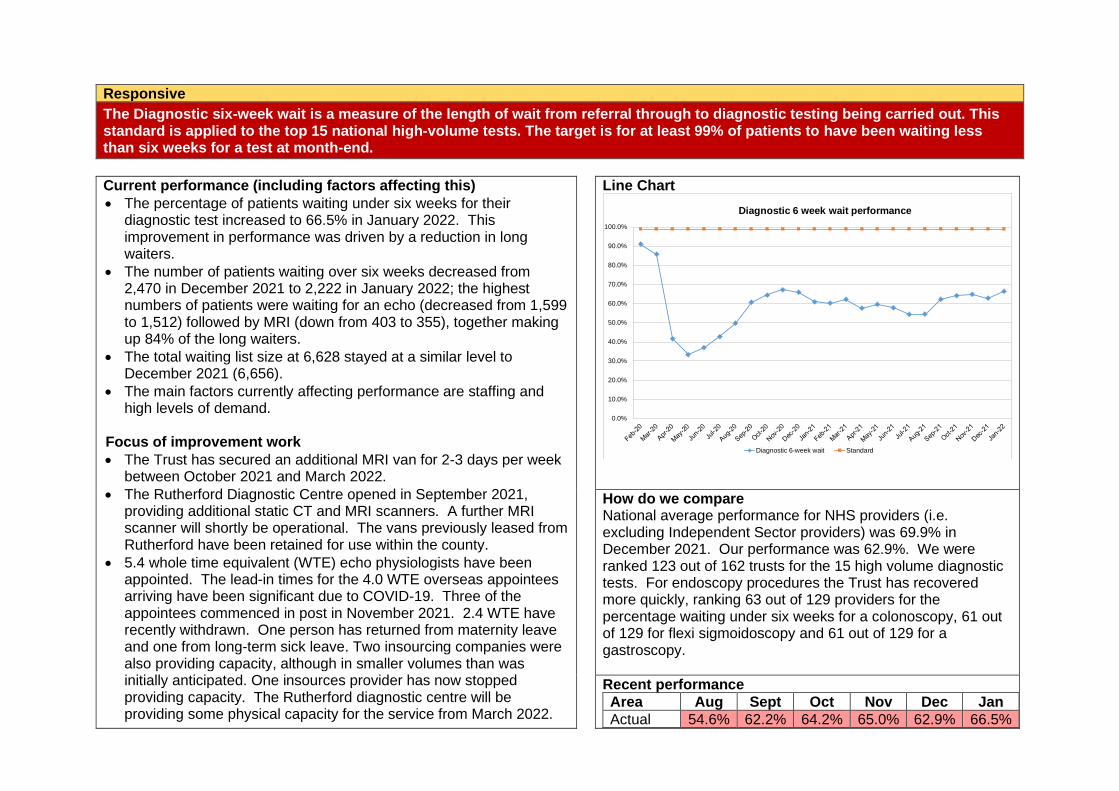
Responsive
The Diagnostic six-week wait is a measure of the length of wait from referral through to diagnostic testing being carried out. This standard is applied to the top 15 national high-volume tests. The target is for at least 99% of patients to have been waiting less than six weeks for a test at month-end.
Current performance (including factors affecting this)
• The percentage of patients waiting under six weeks for their diagnostic test increased to 66.5% in January 2022. This improvement in performance was driven by a reduction in long waiters.
• The number of patients waiting over six weeks decreased from 2,470 in December 2021 to 2,222 in January 2022; the highest numbers of patients were waiting for an echo (decreased from 1,599 to 1,512) followed by MRI (down from 403 to 355), together making up 84% of the long waiters.
• The total waiting list size at 6,628 stayed at a similar level to December 2021 (6,656).
• The main factors currently affecting performance are staffing and high levels of demand.
Focus of improvement work
• The Trust has secured an additional MRI van for 2-3 days per week between October 2021 and March 2022.
• The Rutherford Diagnostic Centre opened in September 2021, providing additional static CT and MRI scanners. A further MRI scanner will shortly be operational. The vans previously leased from Rutherford have been retained for use within the county.
• 5.4 whole time equivalent (WTE) echo physiologists have been appointed. The lead-in times for the 4.0 WTE overseas appointees arriving have been significant due to COVID-19. Three of the appointees commenced in post in November 2021. 2.4 WTE have recently withdrawn. One person has returned from maternity leave and one from long-term sick leave. Two insourcing companies were also providing capacity, although in smaller volumes than was initially anticipated. One insources provider has now stopped providing capacity. The Rutherford diagnostic centre will be providing some physical capacity for the service from March 2022.
Line Chart
How do we compare National average performance for NHS providers (i.e. excluding Independent Sector providers) was 69.9% in December 2021. Our performance was 62.9%. We were ranked 123 out of 162 trusts for the 15 high volume diagnostic tests. For endoscopy procedures the Trust has recovered more quickly, ranking 63 out of 129 providers for the percentage waiting under six weeks for a colonoscopy, 61 out of 129 for flexi sigmoidoscopy and 61 out of 129 for a gastroscopy.
Recent performance
Area Aug Sept Oct Nov Dec Jan
Actual 54.6% 62.2% 64.2% 65.0% 62.9% 66.5%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Diagnostic 6 week wait performance
Diagnostic 6-week wait Standard
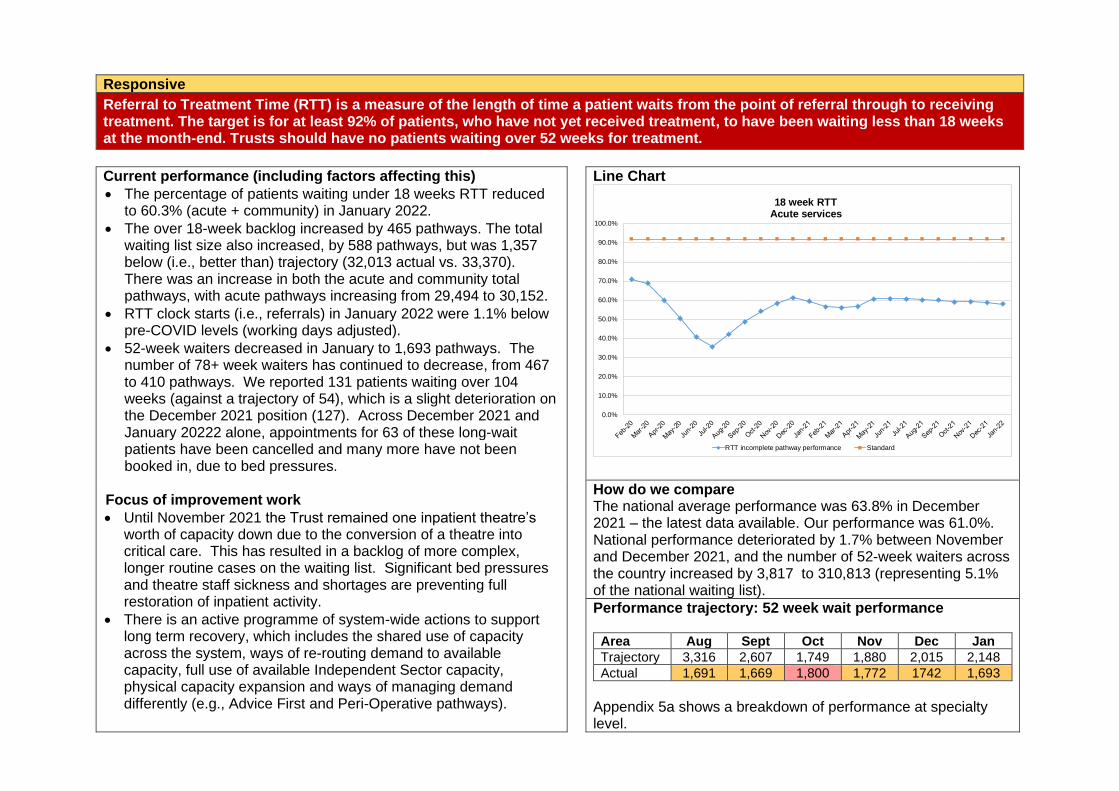
Responsive
Referral to Treatment Time (RTT) is a measure of the length of time a patient waits from the point of referral through to receiving treatment. The target is for at least 92% of patients, who have not yet received treatment, to have been waiting less than 18 weeks at the month-end. Trusts should have no patients waiting over 52 weeks for treatment.
Current performance (including factors affecting this)
• The percentage of patients waiting under 18 weeks RTT reduced to 60.3% (acute + community) in January 2022.
• The over 18-week backlog increased by 465 pathways. The total waiting list size also increased, by 588 pathways, but was 1,357 below (i.e., better than) trajectory (32,013 actual vs. 33,370). There was an increase in both the acute and community total pathways, with acute pathways increasing from 29,494 to 30,152.
• RTT clock starts (i.e., referrals) in January 2022 were 1.1% below pre-COVID levels (working days adjusted).
• 52-week waiters decreased in January to 1,693 pathways. The number of 78+ week waiters has continued to decrease, from 467 to 410 pathways. We reported 131 patients waiting over 104 weeks (against a trajectory of 54), which is a slight deterioration on the December 2021 position (127). Across December 2021 and January 20222 alone, appointments for 63 of these long-wait patients have been cancelled and many more have not been booked in, due to bed pressures.
Focus of improvement work
• Until November 2021 the Trust remained one inpatient theatre’s worth of capacity down due to the conversion of a theatre into critical care. This has resulted in a backlog of more complex, longer routine cases on the waiting list. Significant bed pressures and theatre staff sickness and shortages are preventing full restoration of inpatient activity.
• There is an active programme of system-wide actions to support long term recovery, which includes the shared use of capacity across the system, ways of re-routing demand to available capacity, full use of available Independent Sector capacity, physical capacity expansion and ways of managing demand differently (e.g., Advice First and Peri-Operative pathways).
Line Chart
How do we compare The national average performance was 63.8% in December 2021 – the latest data available. Our performance was 61.0%. National performance deteriorated by 1.7% between November and December 2021, and the number of 52-week waiters across the country increased by 3,817 to 310,813 (representing 5.1% of the national waiting list).
Performance trajectory: 52 week wait performance
Area Aug Sept Oct Nov Dec Jan
Trajectory 3,316 2,607 1,749 1,880 2,015 2,148
Actual 1,691 1,669 1,800 1,772 1742 1,693
Appendix 5a shows a breakdown of performance at specialty level.
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
18 week RTTAcute services
RTT incomplete pathway performance Standard
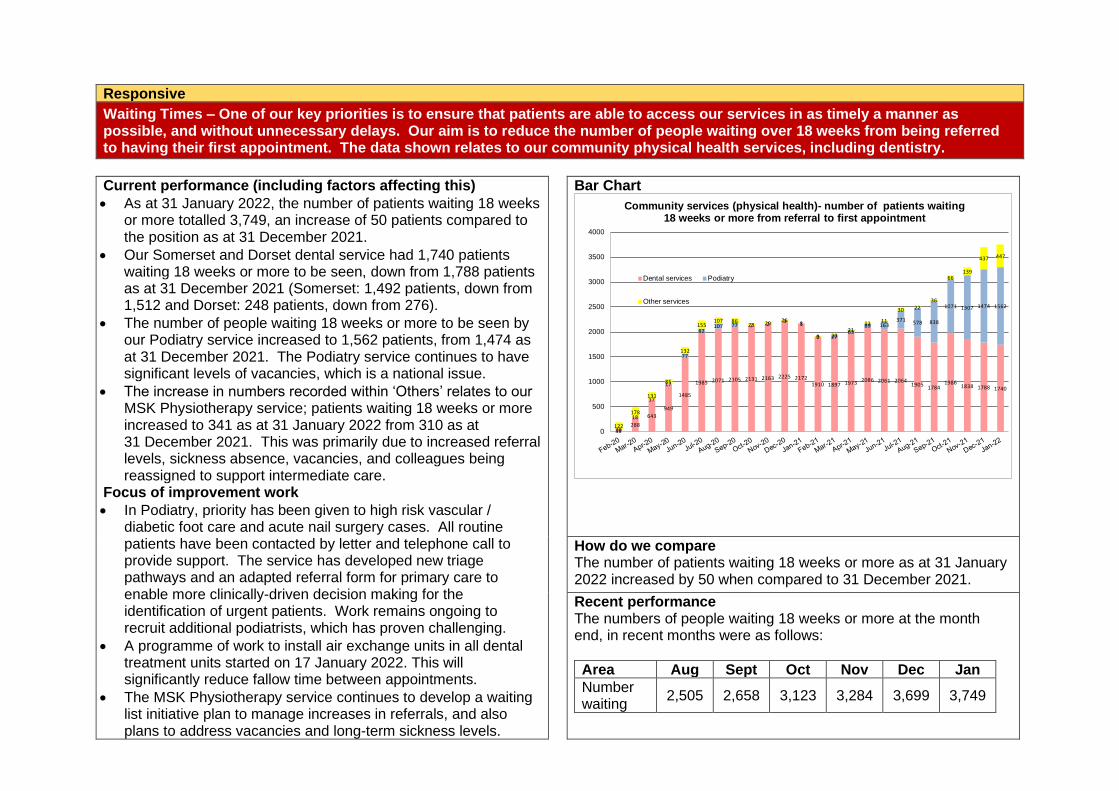
Responsive
Waiting Times – One of our key priorities is to ensure that patients are able to access our services in as timely a manner as possible, and without unnecessary delays. Our aim is to reduce the number of people waiting over 18 weeks from being referred to having their first appointment. The data shown relates to our community physical health services, including dentistry.
Current performance (including factors affecting this)
• As at 31 January 2022, the number of patients waiting 18 weeks or more totalled 3,749, an increase of 50 patients compared to the position as at 31 December 2021.
• Our Somerset and Dorset dental service had 1,740 patients waiting 18 weeks or more to be seen, down from 1,788 patients as at 31 December 2021 (Somerset: 1,492 patients, down from 1,512 and Dorset: 248 patients, down from 276).
• The number of people waiting 18 weeks or more to be seen by our Podiatry service increased to 1,562 patients, from 1,474 as at 31 December 2021. The Podiatry service continues to have significant levels of vacancies, which is a national issue.
• The increase in numbers recorded within ‘Others’ relates to our MSK Physiotherapy service; patients waiting 18 weeks or more increased to 341 as at 31 January 2022 from 310 as at 31 December 2021. This was primarily due to increased referral levels, sickness absence, vacancies, and colleagues being reassigned to support intermediate care.
Focus of improvement work
• In Podiatry, priority has been given to high risk vascular / diabetic foot care and acute nail surgery cases. All routine patients have been contacted by letter and telephone call to provide support. The service has developed new triage pathways and an adapted referral form for primary care to enable more clinically-driven decision making for the identification of urgent patients. Work remains ongoing to recruit additional podiatrists, which has proven challenging.
• A programme of work to install air exchange units in all dental treatment units started on 17 January 2022. This will significantly reduce fallow time between appointments.
• The MSK Physiotherapy service continues to develop a waiting list initiative plan to manage increases in referrals, and also plans to address vacancies and long-term sickness levels.
Bar Chart
How do we compare The number of patients waiting 18 weeks or more as at 31 January 2022 increased by 50 when compared to 31 December 2021.
Recent performance The numbers of people waiting 18 weeks or more at the month end, in recent months were as follows:
Area Aug Sept Oct Nov Dec Jan
Number waiting
2,505 2,658 3,123 3,284 3,699 3,749
38288
643
949
1485
1985 2071 2105 2131 2163 2225 21721910 1897 1973 2086 2061 2064
19051784
19861838 1788 1740
20
18
17
17
77
82107 77 7 2
3 1
0 2763
89 163371 578 838
1071 1307 1474 1562
122
178
131
85
132
155107 86
23 2926
8
9 2021
11 11
30 22
36
66139
437 447
0
500
1000
1500
2000
2500
3000
3500
4000
Community services (physical health)- number of patients waiting 18 weeks or more from referral to first appointment
Dental services Podiatry
Other services
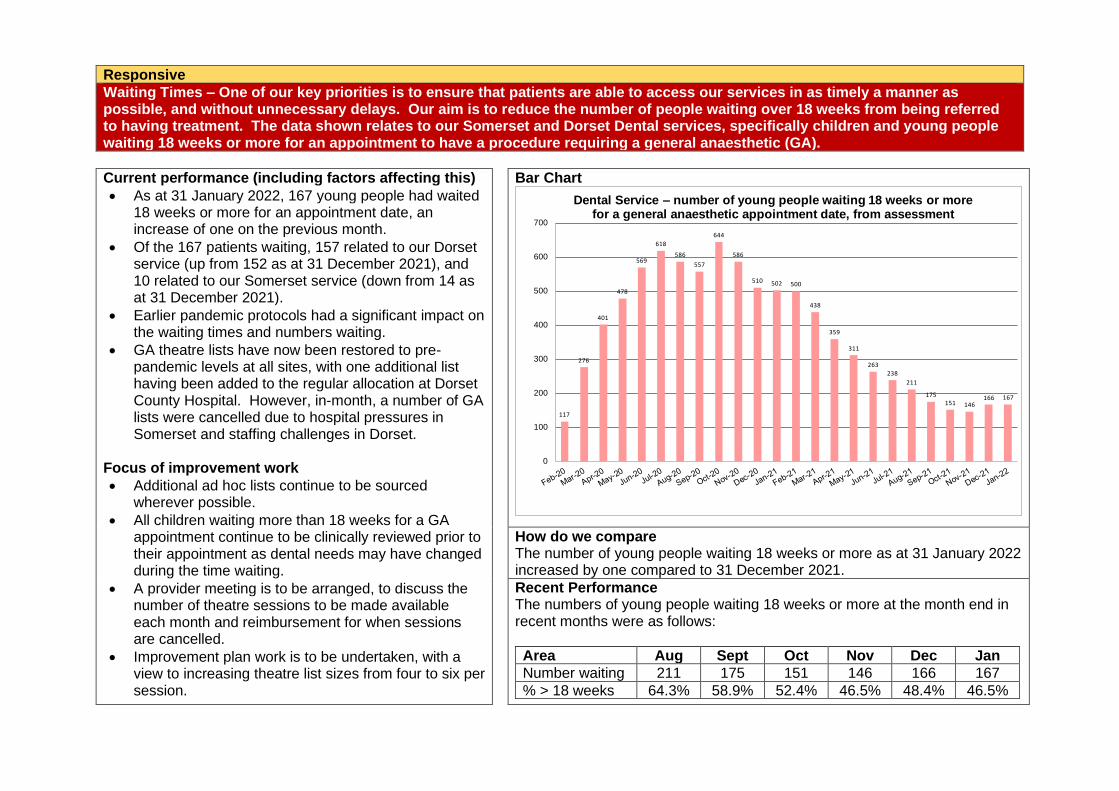
Responsive
Waiting Times – One of our key priorities is to ensure that patients are able to access our services in as timely a manner as possible, and without unnecessary delays. Our aim is to reduce the number of people waiting over 18 weeks from being referred to having treatment. The data shown relates to our Somerset and Dorset Dental services, specifically children and young people waiting 18 weeks or more for an appointment to have a procedure requiring a general anaesthetic (GA).
Current performance (including factors affecting this)
• As at 31 January 2022, 167 young people had waited 18 weeks or more for an appointment date, an increase of one on the previous month.
• Of the 167 patients waiting, 157 related to our Dorset service (up from 152 as at 31 December 2021), and 10 related to our Somerset service (down from 14 as at 31 December 2021).
• Earlier pandemic protocols had a significant impact on the waiting times and numbers waiting.
• GA theatre lists have now been restored to pre-pandemic levels at all sites, with one additional list having been added to the regular allocation at Dorset County Hospital. However, in-month, a number of GA lists were cancelled due to hospital pressures in Somerset and staffing challenges in Dorset.
Focus of improvement work
• Additional ad hoc lists continue to be sourced wherever possible.
• All children waiting more than 18 weeks for a GA appointment continue to be clinically reviewed prior to their appointment as dental needs may have changed during the time waiting.
• A provider meeting is to be arranged, to discuss the number of theatre sessions to be made available each month and reimbursement for when sessions are cancelled.
• Improvement plan work is to be undertaken, with a view to increasing theatre list sizes from four to six per session.
Bar Chart
How do we compare The number of young people waiting 18 weeks or more as at 31 January 2022 increased by one compared to 31 December 2021.
Recent Performance The numbers of young people waiting 18 weeks or more at the month end in recent months were as follows:
Area Aug Sept Oct Nov Dec Jan
Number waiting 211 175 151 146 166 167
% > 18 weeks 64.3% 58.9% 52.4% 46.5% 48.4% 46.5%
117
276
401
478
569
618
586
557
644
586
510 502 500
438
359
311
263
238
211
175151 146
166 167
0
100
200
300
400
500
600
700
Dental Service – number of young people waiting 18 weeks or more for a general anaesthetic appointment date, from assessment
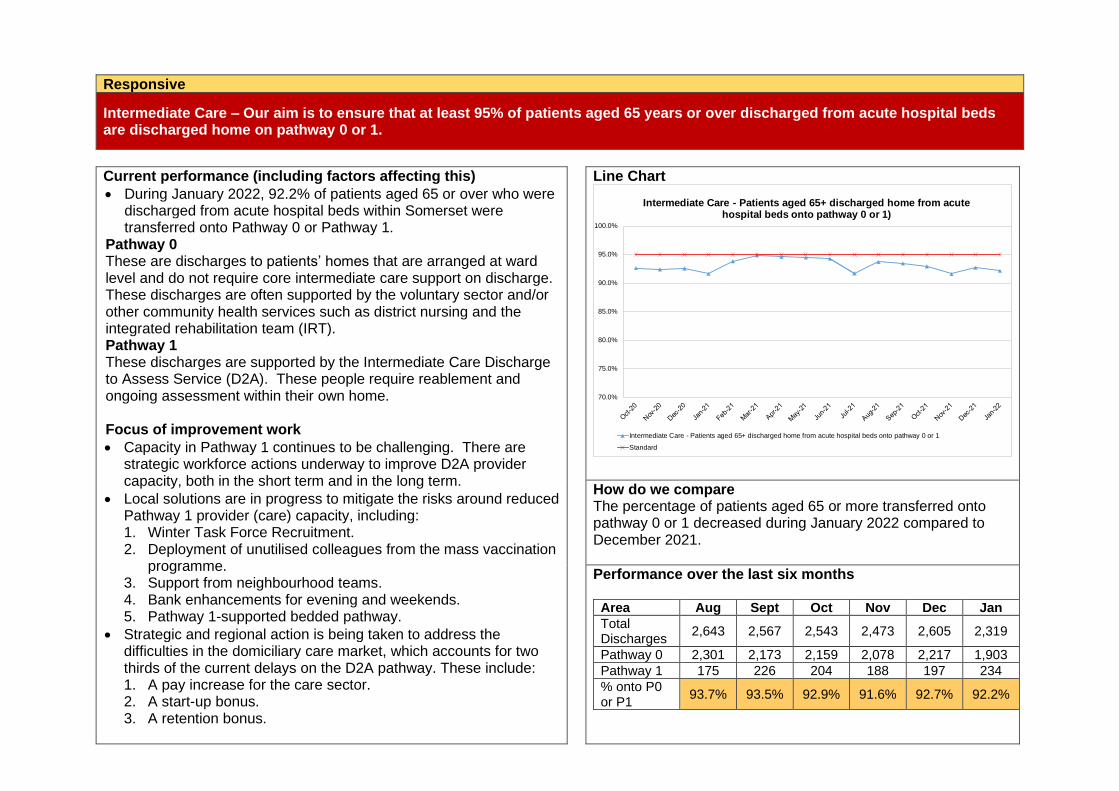
Responsive
Intermediate Care – Our aim is to ensure that at least 95% of patients aged 65 years or over discharged from acute hospital beds are discharged home on pathway 0 or 1.
Current performance (including factors affecting this)
• During January 2022, 92.2% of patients aged 65 or over who were discharged from acute hospital beds within Somerset were transferred onto Pathway 0 or Pathway 1.
Pathway 0 These are discharges to patients’ homes that are arranged at ward level and do not require core intermediate care support on discharge. These discharges are often supported by the voluntary sector and/or other community health services such as district nursing and the integrated rehabilitation team (IRT). Pathway 1 These discharges are supported by the Intermediate Care Discharge to Assess Service (D2A). These people require reablement and ongoing assessment within their own home. Focus of improvement work
• Capacity in Pathway 1 continues to be challenging. There are strategic workforce actions underway to improve D2A provider capacity, both in the short term and in the long term.
• Local solutions are in progress to mitigate the risks around reduced Pathway 1 provider (care) capacity, including: 1. Winter Task Force Recruitment. 2. Deployment of unutilised colleagues from the mass vaccination
programme. 3. Support from neighbourhood teams. 4. Bank enhancements for evening and weekends. 5. Pathway 1-supported bedded pathway.
• Strategic and regional action is being taken to address the difficulties in the domiciliary care market, which accounts for two thirds of the current delays on the D2A pathway. These include: 1. A pay increase for the care sector. 2. A start-up bonus. 3. A retention bonus.
Line Chart
How do we compare The percentage of patients aged 65 or more transferred onto pathway 0 or 1 decreased during January 2022 compared to December 2021.
Performance over the last six months
Area Aug Sept Oct Nov Dec Jan
Total Discharges
2,643 2,567 2,543 2,473 2,605 2,319
Pathway 0 2,301 2,173 2,159 2,078 2,217 1,903
Pathway 1 175 226 204 188 197 234
% onto P0 or P1
93.7% 93.5% 92.9% 91.6% 92.7% 92.2%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
Intermediate Care - Patients aged 65+ discharged home from acute hospital beds onto pathway 0 or 1)
Intermediate Care - Patients aged 65+ discharged home from acute hospital beds onto pathway 0 or 1
Standard
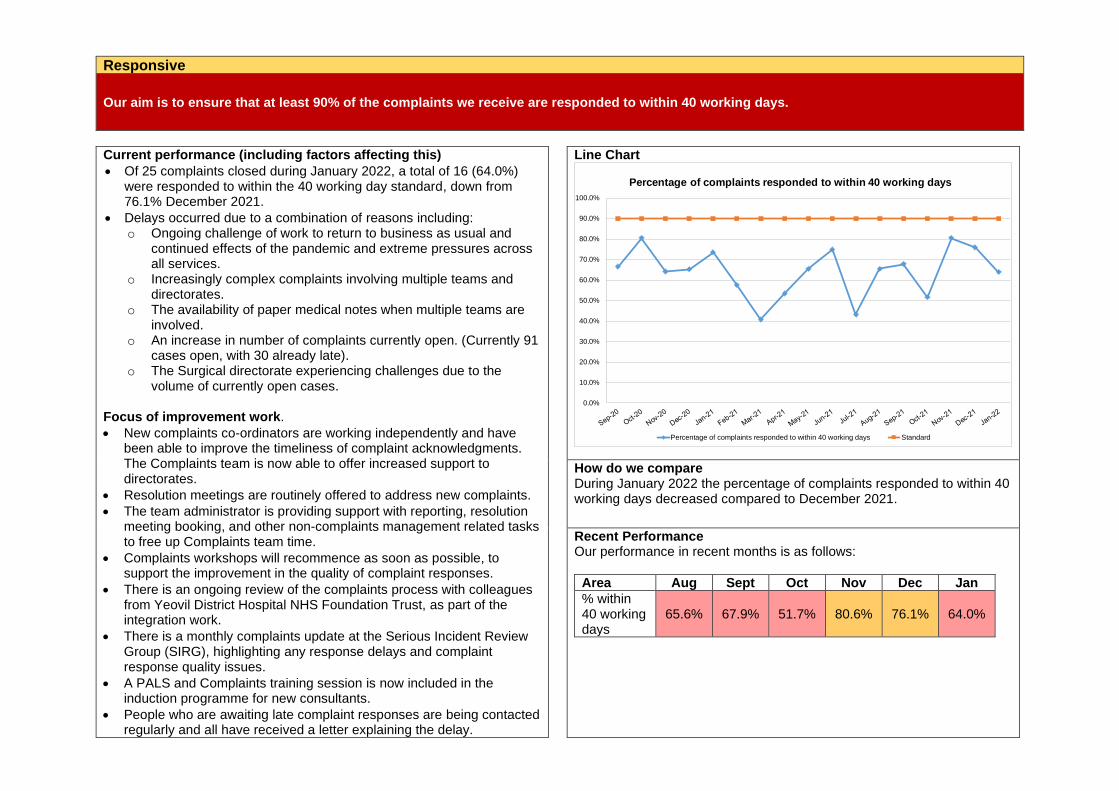
Responsive
Our aim is to ensure that at least 90% of the complaints we receive are responded to within 40 working days.
Current performance (including factors affecting this)
• Of 25 complaints closed during January 2022, a total of 16 (64.0%) were responded to within the 40 working day standard, down from 76.1% December 2021.
• Delays occurred due to a combination of reasons including: o Ongoing challenge of work to return to business as usual and
continued effects of the pandemic and extreme pressures across all services.
o Increasingly complex complaints involving multiple teams and directorates.
o The availability of paper medical notes when multiple teams are involved.
o An increase in number of complaints currently open. (Currently 91 cases open, with 30 already late).
o The Surgical directorate experiencing challenges due to the volume of currently open cases.
Focus of improvement work.
• New complaints co-ordinators are working independently and have been able to improve the timeliness of complaint acknowledgments. The Complaints team is now able to offer increased support to directorates.
• Resolution meetings are routinely offered to address new complaints.
• The team administrator is providing support with reporting, resolution meeting booking, and other non-complaints management related tasks to free up Complaints team time.
• Complaints workshops will recommence as soon as possible, to support the improvement in the quality of complaint responses.
• There is an ongoing review of the complaints process with colleagues from Yeovil District Hospital NHS Foundation Trust, as part of the integration work.
• There is a monthly complaints update at the Serious Incident Review Group (SIRG), highlighting any response delays and complaint response quality issues.
• A PALS and Complaints training session is now included in the induction programme for new consultants.
• People who are awaiting late complaint responses are being contacted regularly and all have received a letter explaining the delay.
Line Chart
How do we compare During January 2022 the percentage of complaints responded to within 40 working days decreased compared to December 2021.
Recent Performance Our performance in recent months is as follows:
Area Aug Sept Oct Nov Dec Jan
% within 40 working days
65.6% 67.9% 51.7% 80.6% 76.1% 64.0%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Percentage of complaints responded to within 40 working days
Percentage of complaints responded to within 40 working days Standard
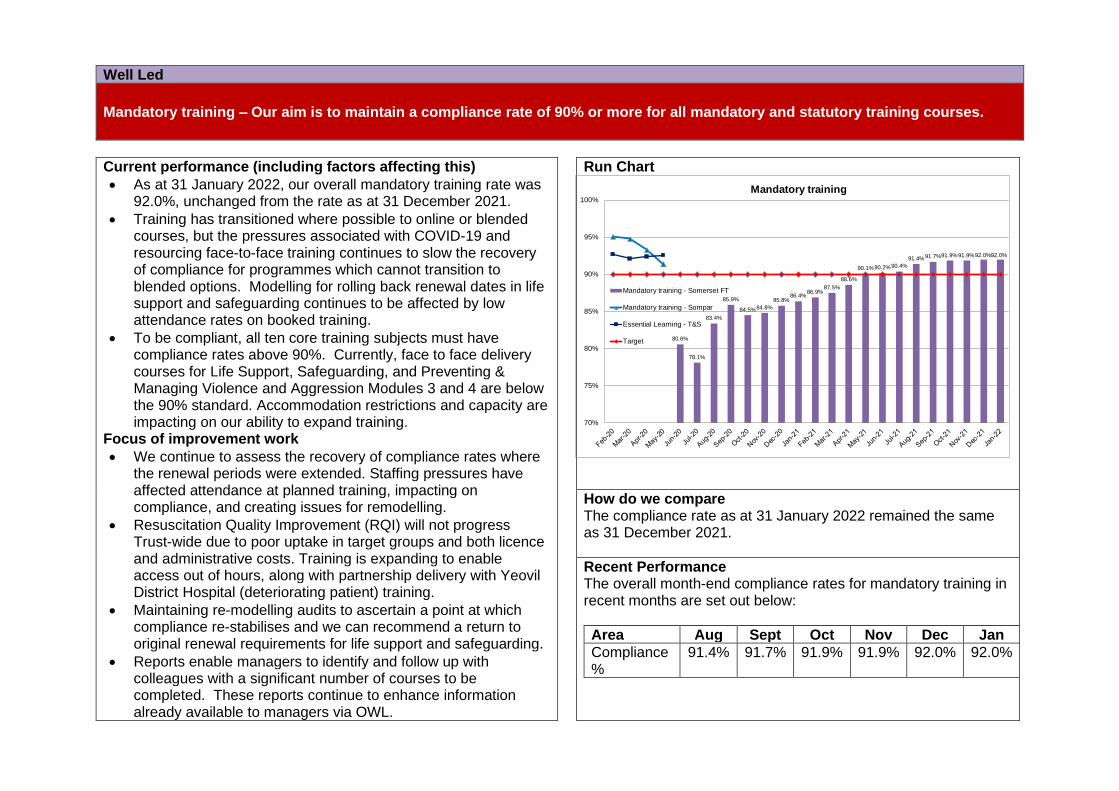
Well Led
Mandatory training – Our aim is to maintain a compliance rate of 90% or more for all mandatory and statutory training courses.
Current performance (including factors affecting this)
• As at 31 January 2022, our overall mandatory training rate was 92.0%, unchanged from the rate as at 31 December 2021.
• Training has transitioned where possible to online or blended courses, but the pressures associated with COVID-19 and resourcing face-to-face training continues to slow the recovery of compliance for programmes which cannot transition to blended options. Modelling for rolling back renewal dates in life support and safeguarding continues to be affected by low attendance rates on booked training.
• To be compliant, all ten core training subjects must have compliance rates above 90%. Currently, face to face delivery courses for Life Support, Safeguarding, and Preventing & Managing Violence and Aggression Modules 3 and 4 are below the 90% standard. Accommodation restrictions and capacity are impacting on our ability to expand training.
Focus of improvement work
• We continue to assess the recovery of compliance rates where the renewal periods were extended. Staffing pressures have affected attendance at planned training, impacting on compliance, and creating issues for remodelling.
• Resuscitation Quality Improvement (RQI) will not progress Trust-wide due to poor uptake in target groups and both licence and administrative costs. Training is expanding to enable access out of hours, along with partnership delivery with Yeovil District Hospital (deteriorating patient) training.
• Maintaining re-modelling audits to ascertain a point at which compliance re-stabilises and we can recommend a return to original renewal requirements for life support and safeguarding.
• Reports enable managers to identify and follow up with colleagues with a significant number of courses to be completed. These reports continue to enhance information already available to managers via OWL.
Run Chart
How do we compare The compliance rate as at 31 January 2022 remained the same as 31 December 2021.
Recent Performance The overall month-end compliance rates for mandatory training in recent months are set out below:
Area Aug Sept Oct Nov Dec Jan
Compliance %
91.4% 91.7% 91.9% 91.9% 92.0% 92.0%
80.6%
78.1%
83.4%
85.9%
84.5%84.8%
85.8%86.4%
86.9%87.5%
88.6%
90.1%90.2%90.4%
91.4%91.7%91.9%91.9%92.0%92.0%
70%
75%
80%
85%
90%
95%
100%
Mandatory training
Mandatory training - Somerset FT
Mandatory training - Sompar
Essential Learning - T&S
Target
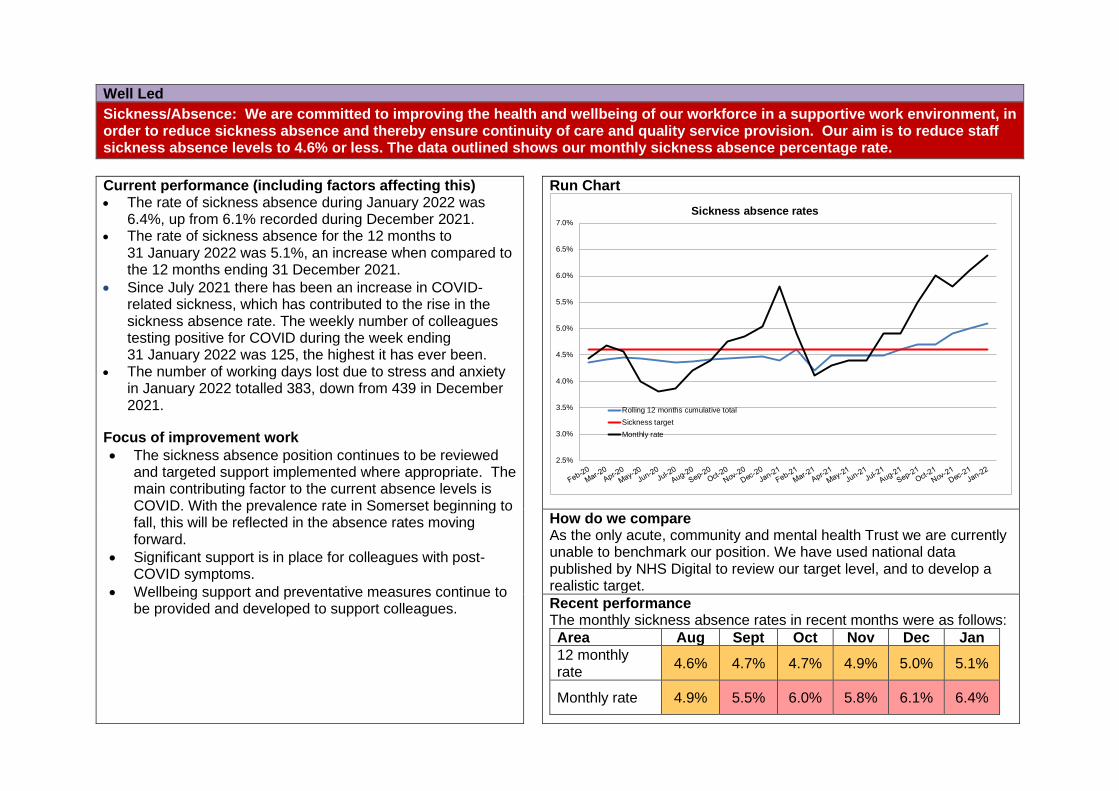
Well Led
Sickness/Absence: We are committed to improving the health and wellbeing of our workforce in a supportive work environment, in order to reduce sickness absence and thereby ensure continuity of care and quality service provision. Our aim is to reduce staff sickness absence levels to 4.6% or less. The data outlined shows our monthly sickness absence percentage rate.
Current performance (including factors affecting this) • The rate of sickness absence during January 2022 was
6.4%, up from 6.1% recorded during December 2021. • The rate of sickness absence for the 12 months to
31 January 2022 was 5.1%, an increase when compared to the 12 months ending 31 December 2021.
• Since July 2021 there has been an increase in COVID-related sickness, which has contributed to the rise in the sickness absence rate. The weekly number of colleagues testing positive for COVID during the week ending 31 January 2022 was 125, the highest it has ever been.
• The number of working days lost due to stress and anxiety in January 2022 totalled 383, down from 439 in December 2021.
Focus of improvement work
• The sickness absence position continues to be reviewed and targeted support implemented where appropriate. The main contributing factor to the current absence levels is COVID. With the prevalence rate in Somerset beginning to fall, this will be reflected in the absence rates moving forward.
• Significant support is in place for colleagues with post-COVID symptoms.
• Wellbeing support and preventative measures continue to be provided and developed to support colleagues.
Run Chart
How do we compare As the only acute, community and mental health Trust we are currently unable to benchmark our position. We have used national data published by NHS Digital to review our target level, and to develop a realistic target.
Recent performance The monthly sickness absence rates in recent months were as follows:
Area Aug Sept Oct Nov Dec Jan
12 monthly rate
4.6% 4.7% 4.7% 4.9% 5.0% 5.1%
Monthly rate 4.9% 5.5% 6.0% 5.8% 6.1% 6.4%
2.5%
3.0%
3.5%
4.0%
4.5%
5.0%
5.5%
6.0%
6.5%
7.0%
Sickness absence rates
Rolling 12 months cumulative total
Sickness target
Monthly rate
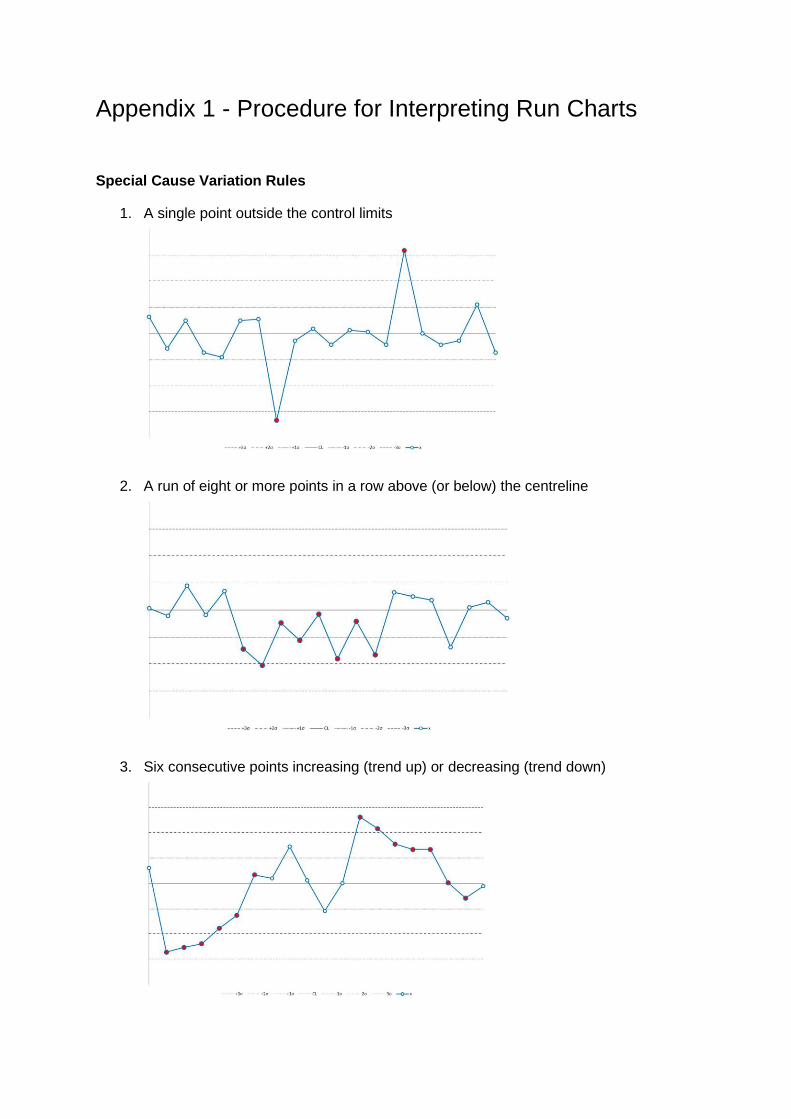
Appendix 1 - Procedure for Interpreting Run Charts
Special Cause Variation Rules
1. A single point outside the control limits
2. A run of eight or more points in a row above (or below) the centreline
3. Six consecutive points increasing (trend up) or decreasing (trend down)
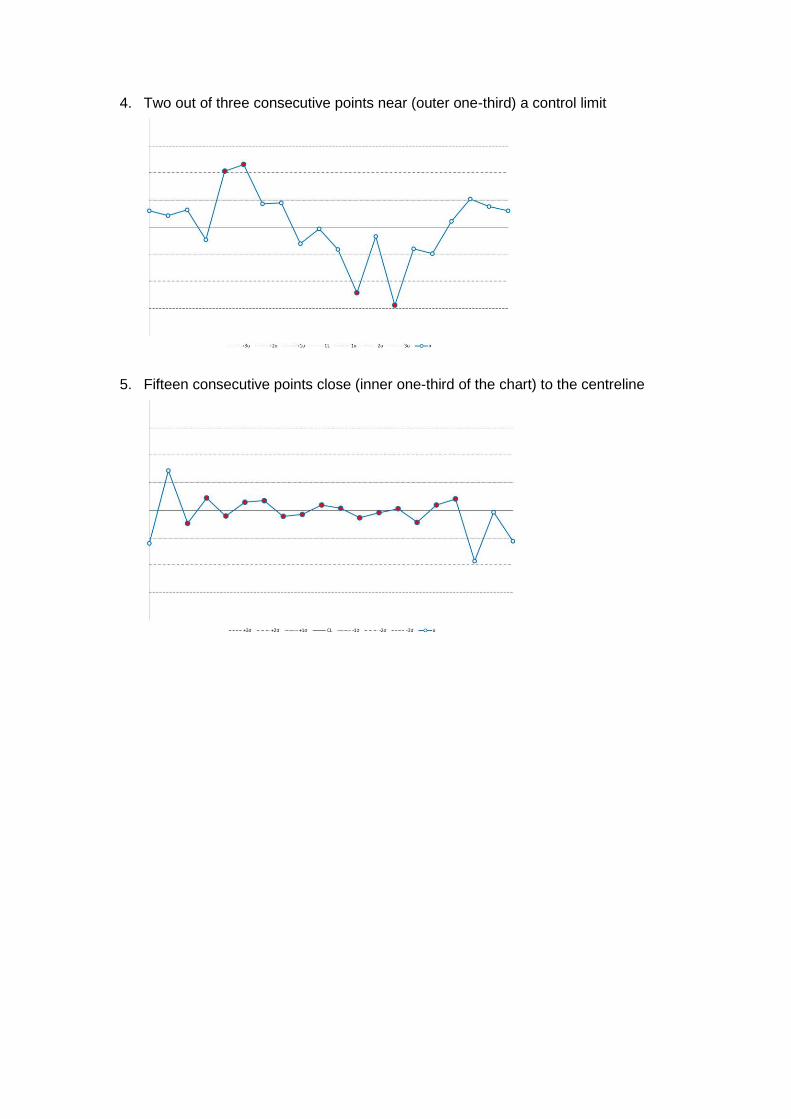
4. Two out of three consecutive points near (outer one-third) a control limit
5. Fifteen consecutive points close (inner one-third of the chart) to the centreline
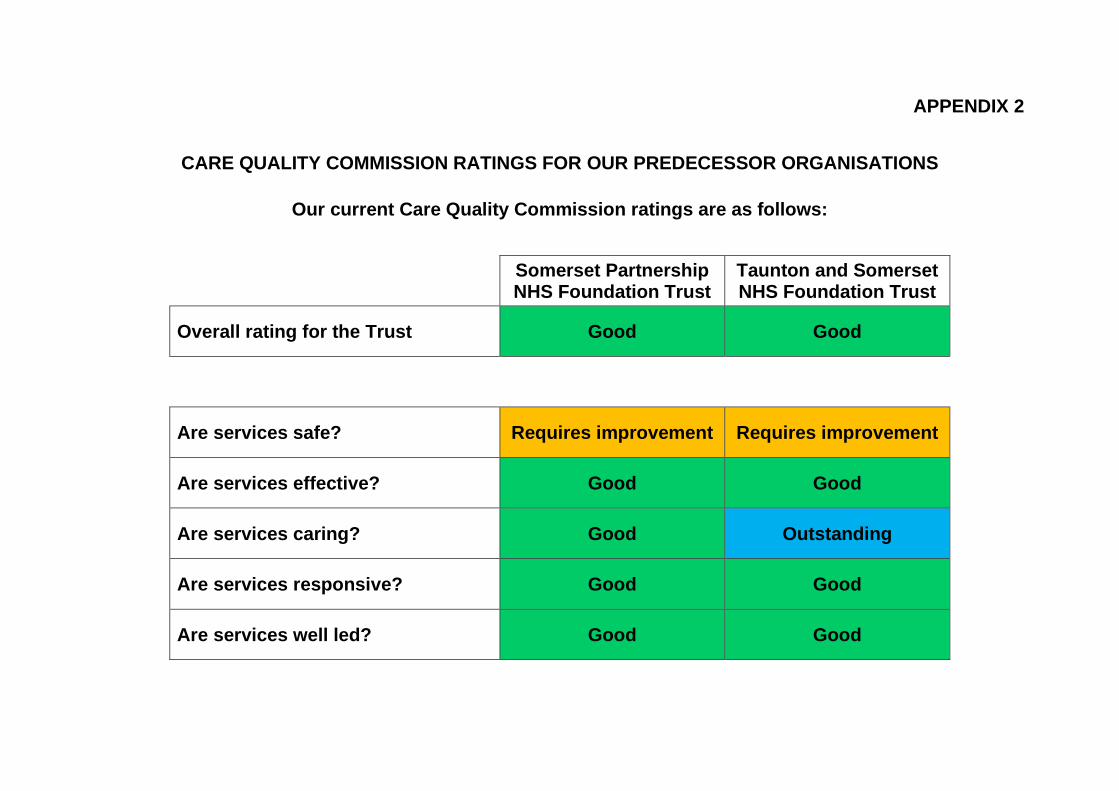
APPENDIX 2
CARE QUALITY COMMISSION RATINGS FOR OUR PREDECESSOR ORGANISATIONS
Our current Care Quality Commission ratings are as follows:
Somerset Partnership NHS Foundation Trust
Taunton and Somerset NHS Foundation Trust
Overall rating for the Trust Good Good
Are services safe? Requires improvement Requires improvement
Are services effective? Good Good
Are services caring? Good Outstanding
Are services responsive? Good Good
Are services well led? Good Good
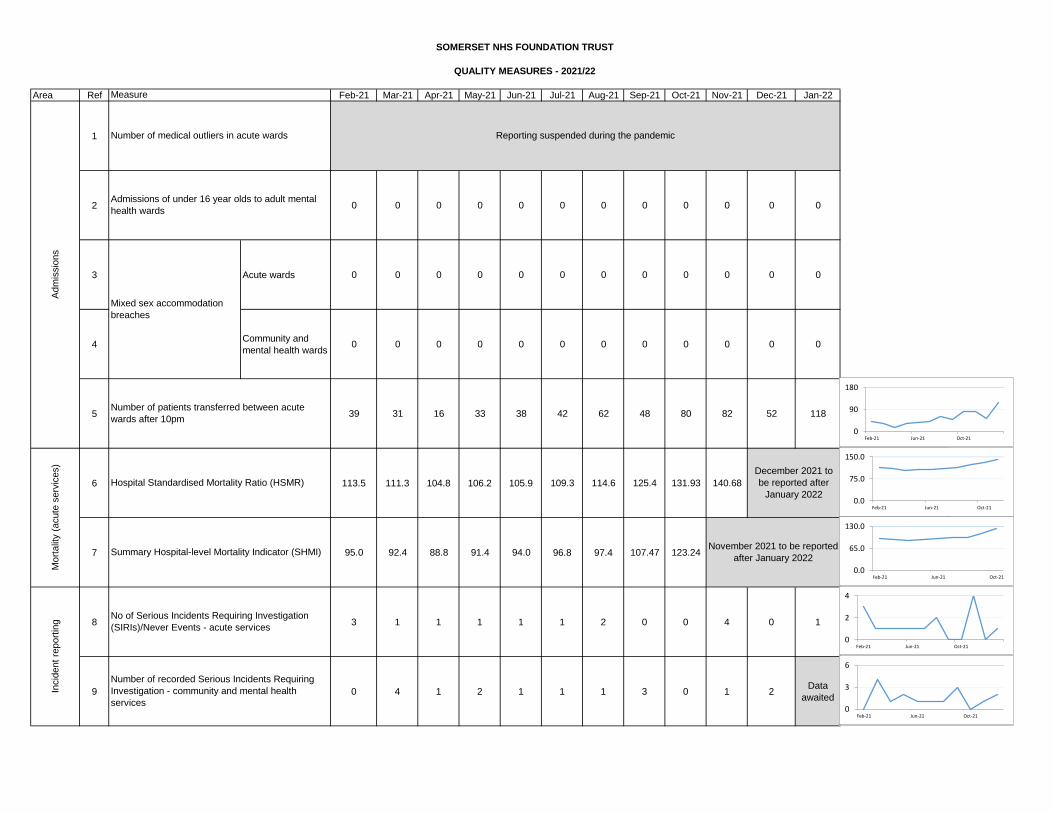
Area Ref Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22
1
2 0 0 0 0 0 0 0 0 0 0 0 0
3 Acute wards 0 0 0 0 0 0 0 0 0 0 0 0
4Community and
mental health wards0 0 0 0 0 0 0 0 0 0 0 0
5 39 31 16 33 38 42 62 48 80 82 52 118
6 113.5 111.3 104.8 106.2 105.9 109.3 114.6 125.4 131.93 140.68
7 95.0 92.4 88.8 91.4 94.0 96.8 97.4 107.47 123.24
8 3 1 1 1 1 1 2 0 0 4 0 1
9 0 4 1 2 1 1 1 3 0 1 2Data
awaited
Incid
ent
report
ing
Number of recorded Serious Incidents Requiring
Investigation - community and mental health
services
Reporting suspended during the pandemic
December 2021 to
be reported after
January 2022
November 2021 to be reported
after January 2022
SOMERSET NHS FOUNDATION TRUST
No of Serious Incidents Requiring Investigation
(SIRIs)/Never Events - acute services
Mort
alit
y (
acute
serv
ices)
Hospital Standardised Mortality Ratio (HSMR)
Summary Hospital-level Mortality Indicator (SHMI)
QUALITY MEASURES - 2021/22
Mixed sex accommodation
breaches
Number of patients transferred between acute
wards after 10pm
Measure
Number of medical outliers in acute wards
Adm
issio
ns
Admissions of under 16 year olds to adult mental
health wards
0
90
180
Feb-21 Jun-21 Oct-21
0
2
4
Feb-21 Jun-21 Oct-21
12
0
3
6
Feb-21 Jun-21 Oct-21
0.0
75.0
150.0
Feb-21 Jun-21 Oct-21
0.0
65.0
130.0
Feb-21 Jun-21 Oct-21
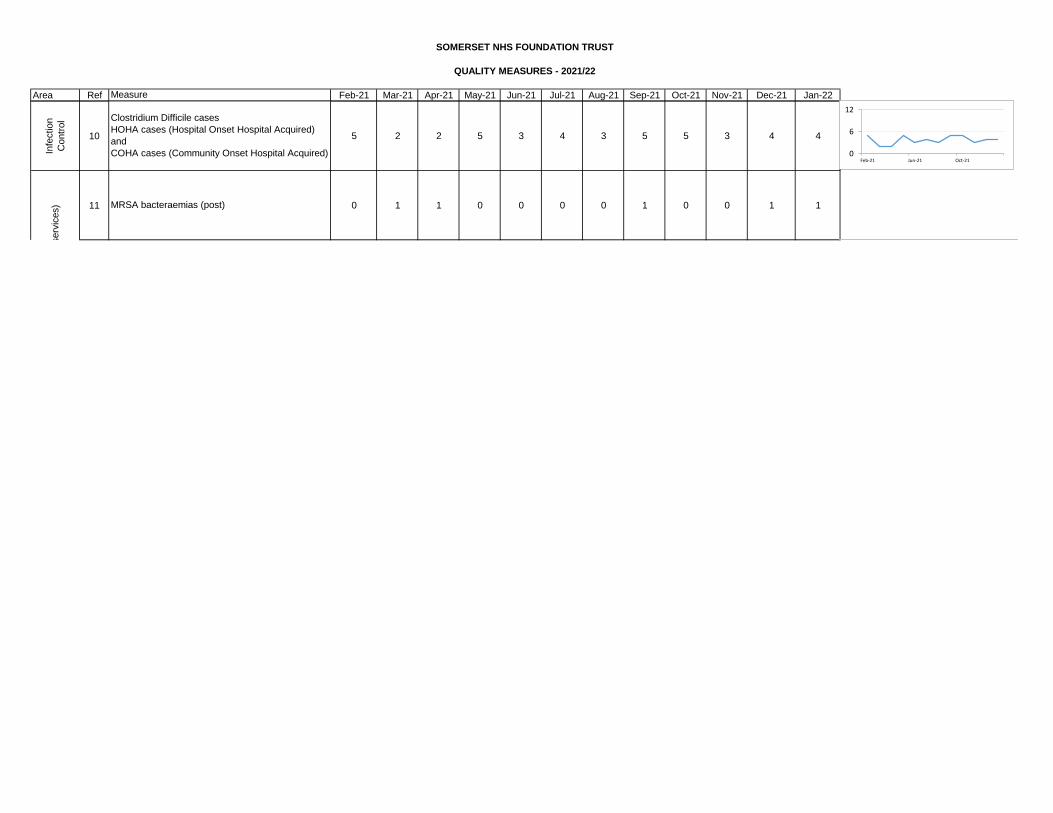
Area Ref Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22
SOMERSET NHS FOUNDATION TRUST
QUALITY MEASURES - 2021/22
Measure
Infe
ction
Contr
ol
10 5 2 2 5 3 4 3 5 5 3 4 4
11 0 1 1 0 0 0 0 1 0 0 1 1
Infe
ction C
ontr
ol (a
cute
serv
ices)
Clostridium Difficile cases
HOHA cases (Hospital Onset Hospital Acquired)
and
COHA cases (Community Onset Hospital Acquired)
MRSA bacteraemias (post)
0
6
12
Feb-21 Jun-21 Oct-21
10
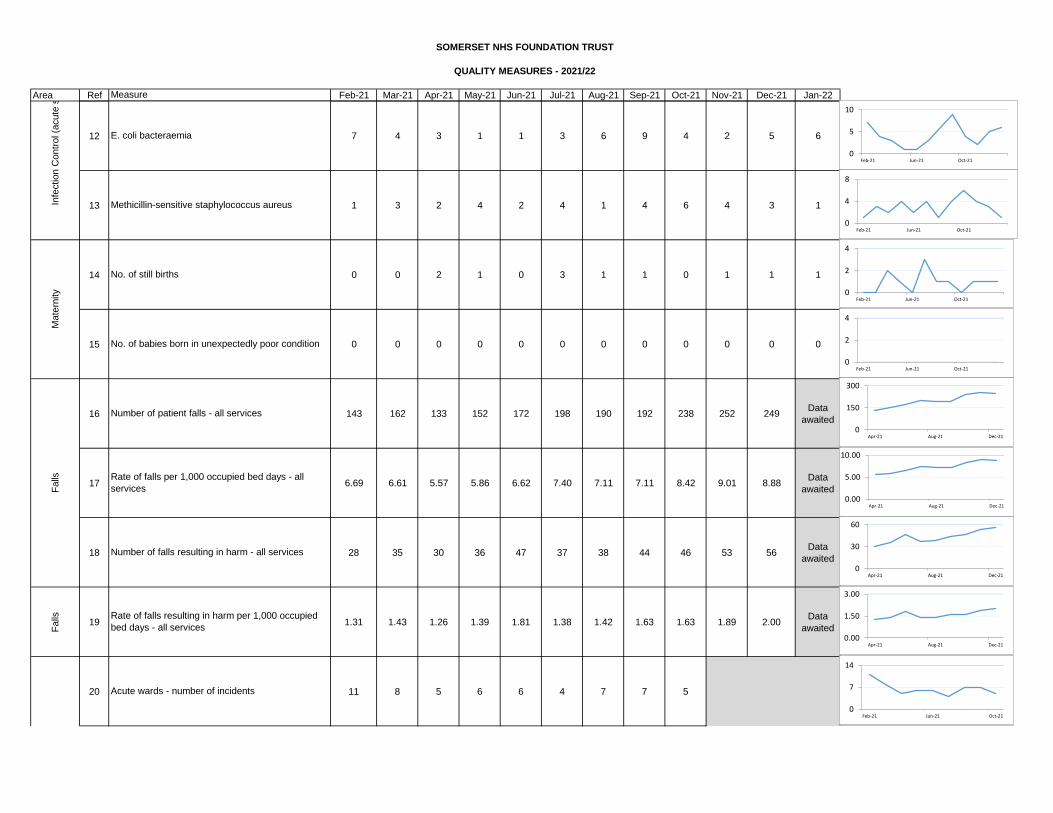
Area Ref Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22
SOMERSET NHS FOUNDATION TRUST
QUALITY MEASURES - 2021/22
Measure
12 7 4 3 1 1 3 6 9 4 2 5 6
13 1 3 2 4 2 4 1 4 6 4 3 1
14 0 0 2 1 0 3 1 1 0 1 1 1
15 0 0 0 0 0 0 0 0 0 0 0 0
16 143 162 133 152 172 198 190 192 238 252 249Data
awaited
17 6.69 6.61 5.57 5.86 6.62 7.40 7.11 7.11 8.42 9.01 8.88Data
awaited
18 28 35 30 36 47 37 38 44 46 53 56Data
awaited
Falls 19 1.31 1.43 1.26 1.39 1.81 1.38 1.42 1.63 1.63 1.89 2.00
Data
awaited
20 11 8 5 6 6 4 7 7 5
Number of patient falls - all services
Infe
ction C
ontr
ol (a
cute
serv
ices)
Number of falls resulting in harm - all services
Rate of falls resulting in harm per 1,000 occupied
bed days - all services
Pre
ssure
ulc
er
dam
age
Falls Rate of falls per 1,000 occupied bed days - all
services
Acute wards - number of incidents
Being validated
E. coli bacteraemia
Methicillin-sensitive staphylococcus aureus
Mate
rnity
No. of still births
No. of babies born in unexpectedly poor condition
0
2
4
Feb-21 Jun-21 Oct-21
0
2
4
Feb-21 Jun-21 Oct-21
0.80
0
7
14
Feb-21 Jun-21 Oct-21
0
5
10
Feb-21 Jun-21 Oct-21
0
4
8
Feb-21 Jun-21 Oct-21
0
150
300
Apr-21 Aug-21 Dec-21
0.00
5.00
10.00
Apr-21 Aug-21 Dec-21
0
30
60
Apr-21 Aug-21 Dec-21
0.00
1.50
3.00
Apr-21 Aug-21 Dec-21
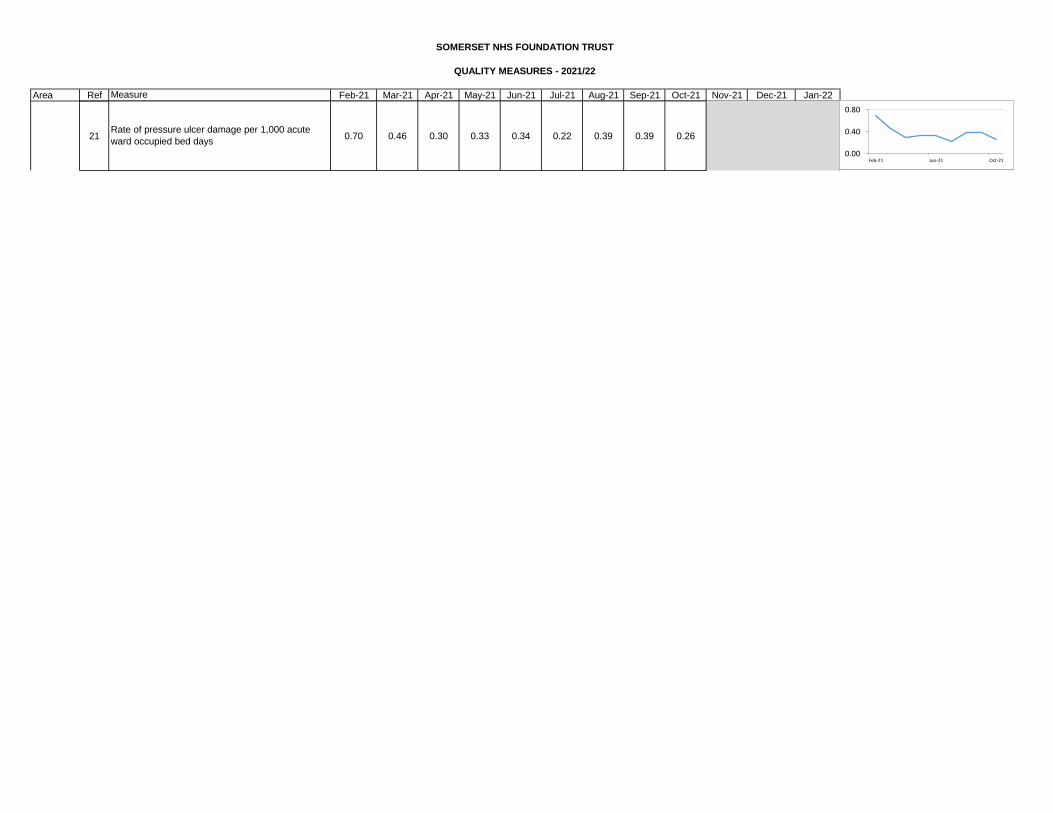
Area Ref Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22
SOMERSET NHS FOUNDATION TRUST
QUALITY MEASURES - 2021/22
Measure
21 0.70 0.46 0.30 0.33 0.34 0.22 0.39 0.39 0.26
Pre
ssure
ulc
er
dam
age
Rate of pressure ulcer damage per 1,000 acute
ward occupied bed days
Being validated
0.00
0.40
0.80
Feb-21 Jun-21 Oct-21
12
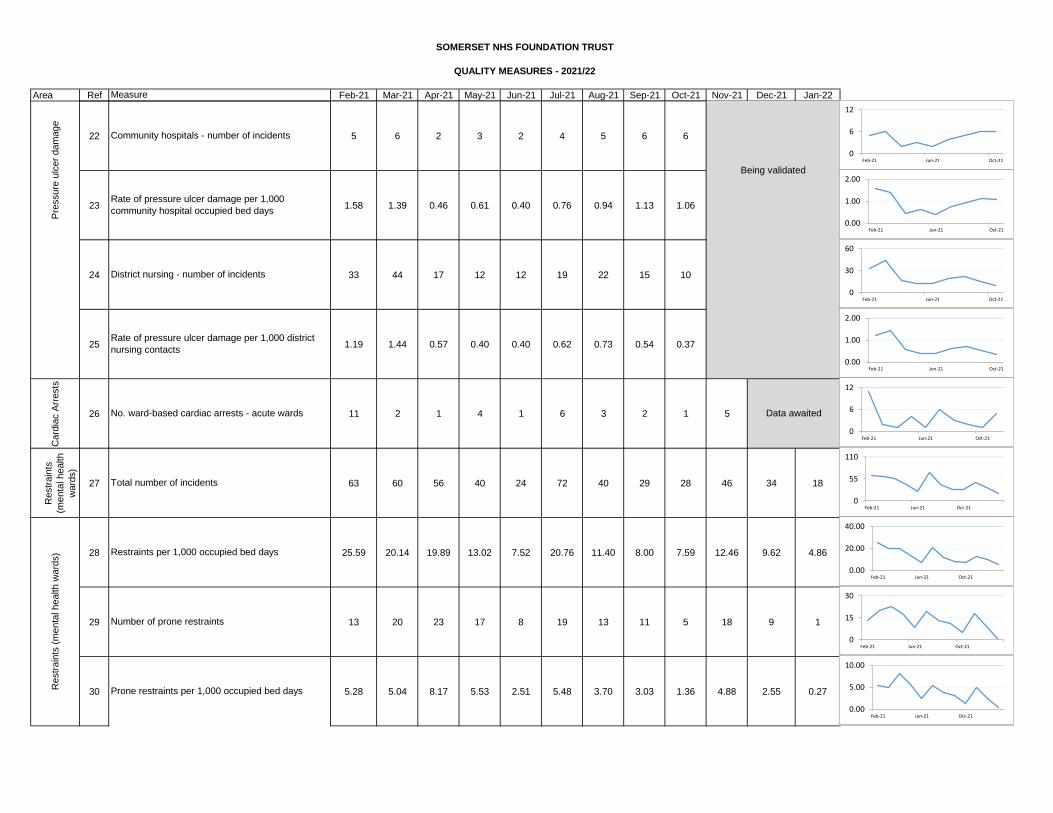
Area Ref Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22
SOMERSET NHS FOUNDATION TRUST
QUALITY MEASURES - 2021/22
Measure
22 5 6 2 3 2 4 5 6 6
23 1.58 1.39 0.46 0.61 0.40 0.76 0.94 1.13 1.06
24 33 44 17 12 12 19 22 15 10
25 1.19 1.44 0.57 0.40 0.40 0.62 0.73 0.54 0.37
Card
iac A
rrests
26 11 2 1 4 1 6 3 2 1 5
Restr
ain
ts
(menta
l health
ward
s)
27 63 60 56 40 24 72 40 29 28 46 34 18
28 25.59 20.14 19.89 13.02 7.52 20.76 11.40 8.00 7.59 12.46 9.62 4.86
29 13 20 23 17 8 19 13 11 5 18 9 1
30 5.28 5.04 8.17 5.53 2.51 5.48 3.70 3.03 1.36 4.88 2.55 0.27
Rate of pressure ulcer damage per 1,000
community hospital occupied bed days
Restr
ain
ts (
menta
l health w
ard
s)
Pre
ssure
ulc
er
dam
age
Total number of incidents
Restraints per 1,000 occupied bed days
Community hospitals - number of incidents
Prone restraints per 1,000 occupied bed days
No. ward-based cardiac arrests - acute wards
Rate of pressure ulcer damage per 1,000 district
nursing contacts
District nursing - number of incidents
Number of prone restraints
Data awaited
Being validated
0
6
12
Feb-21 Jun-21 Oct-21
0.00
1.00
2.00
Feb-21 Jun-21 Oct-21
0.00
1.00
2.00
Feb-21 Jun-21 Oct-21
0
30
60
Feb-21 Jun-21 Oct-21
0.00
20.00
40.00
Feb-21 Jun-21 Oct-21
0
6
12
Feb-21 Jun-21 Oct-21
0
55
110
Feb-21 Jun-21 Oct-21
0.00
5.00
10.00
Feb-21 Jun-21 Oct-21
0
15
30
Feb-21 Jun-21 Oct-21
150
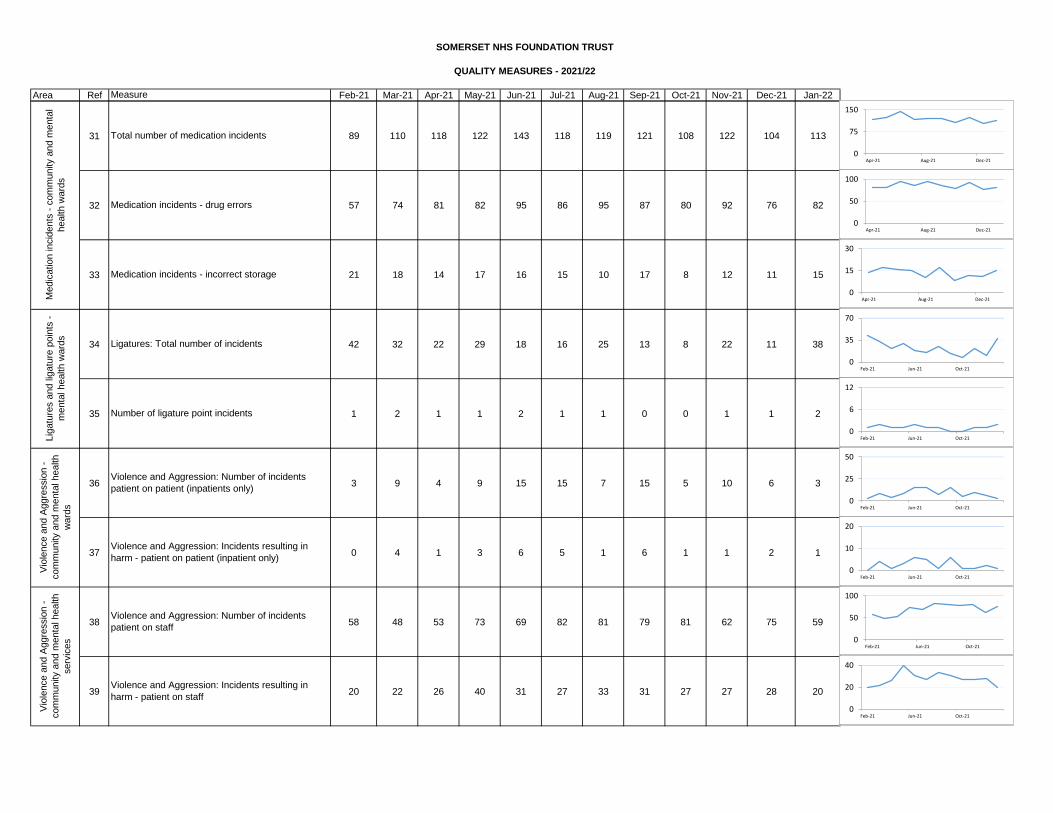
Area Ref Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22
SOMERSET NHS FOUNDATION TRUST
QUALITY MEASURES - 2021/22
Measure
31 89 110 118 122 143 118 119 121 108 122 104 113
32 57 74 81 82 95 86 95 87 80 92 76 82
33 21 18 14 17 16 15 10 17 8 12 11 15
34 42 32 22 29 18 16 25 13 8 22 11 38
35 1 2 1 1 2 1 1 0 0 1 1 2
36 3 9 4 9 15 15 7 15 5 10 6 3
37 0 4 1 3 6 5 1 6 1 1 2 1
38 58 48 53 73 69 82 81 79 81 62 75 59
39 20 22 26 40 31 27 33 31 27 27 28 20
Medic
ation incid
ents
- c
om
munity a
nd m
enta
l
health w
ard
s
Total number of medication incidents
Medication incidents - incorrect storage
Medication incidents - drug errors
Violence and Aggression: Incidents resulting in
harm - patient on staff
Lig
atu
res a
nd lig
atu
re p
oin
ts -
menta
l health w
ard
s
Vio
lence a
nd A
ggre
ssio
n -
com
munity a
nd m
enta
l health
ward
s
Vio
lence a
nd A
ggre
ssio
n -
com
munity a
nd m
enta
l health
serv
ices
Violence and Aggression: Number of incidents
patient on patient (inpatients only)
Number of ligature point incidents
Ligatures: Total number of incidents
Violence and Aggression: Incidents resulting in
harm - patient on patient (inpatient only)
Violence and Aggression: Number of incidents
patient on staff
0
75
150
Apr-21 Aug-21 Dec-21
0
15
30
Apr-21 Aug-21 Dec-21
0
35
70
Feb-21 Jun-21 Oct-21
0
6
12
Feb-21 Jun-21 Oct-21
0
25
50
Feb-21 Jun-21 Oct-21
0
10
20
Feb-21 Jun-21 Oct-21
0
50
100
Feb-21 Jun-21 Oct-21
0
20
40
Feb-21 Jun-21 Oct-21
10
0
50
100
Apr-21 Aug-21 Dec-21
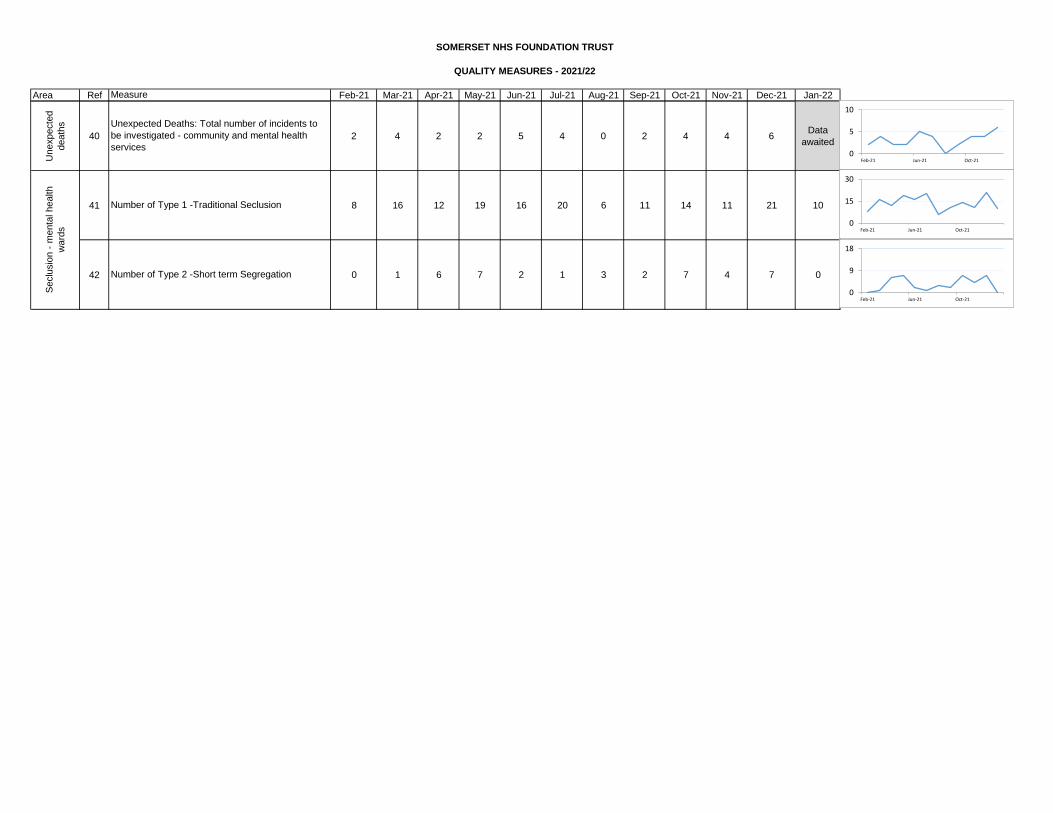
Area Ref Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22
SOMERSET NHS FOUNDATION TRUST
QUALITY MEASURES - 2021/22
Measure
Unexpecte
d
death
s
40 2 4 2 2 5 4 0 2 4 4 6Data
awaited
41 8 16 12 19 16 20 6 11 14 11 21 10
42 0 1 6 7 2 1 3 2 7 4 7 0Number of Type 2 -Short term Segregation
Seclu
sio
n -
menta
l health
ward
s
Unexpected Deaths: Total number of incidents to
be investigated - community and mental health
services
Number of Type 1 -Traditional Seclusion
0
5
10
Feb-21 Jun-21 Oct-21
0
15
30
Feb-21 Jun-21 Oct-21
0
9
18
Feb-21 Jun-21 Oct-21
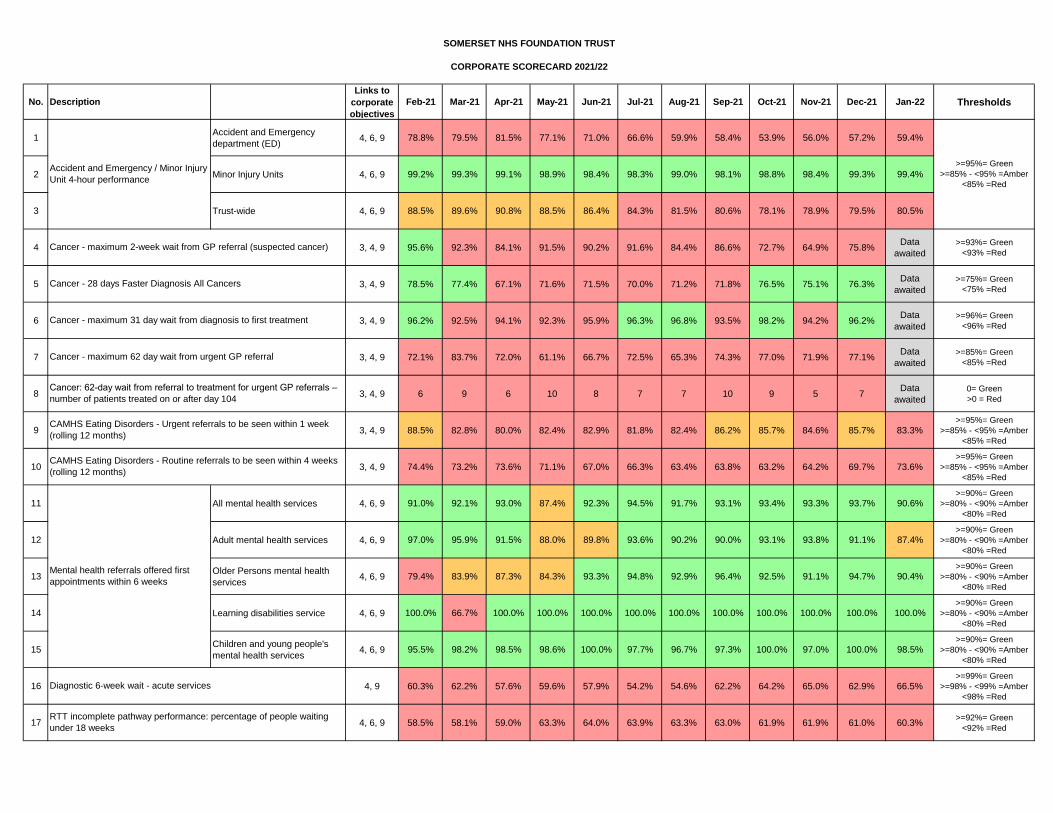
No. Description
Links to
corporate
objectives
Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Thresholds
1Accident and Emergency
department (ED)4, 6, 9 78.8% 79.5% 81.5% 77.1% 71.0% 66.6% 59.9% 58.4% 53.9% 56.0% 57.2% 59.4%
2 Minor Injury Units 4, 6, 9 99.2% 99.3% 99.1% 98.9% 98.4% 98.3% 99.0% 98.1% 98.8% 98.4% 99.3% 99.4%
3 Trust-wide 4, 6, 9 88.5% 89.6% 90.8% 88.5% 86.4% 84.3% 81.5% 80.6% 78.1% 78.9% 79.5% 80.5%
4 3, 4, 9 95.6% 92.3% 84.1% 91.5% 90.2% 91.6% 84.4% 86.6% 72.7% 64.9% 75.8%Data
awaited
>=93%= Green
<93% =Red
5 3, 4, 9 78.5% 77.4% 67.1% 71.6% 71.5% 70.0% 71.2% 71.8% 76.5% 75.1% 76.3%Data
awaited
>=75%= Green
<75% =Red
6 3, 4, 9 96.2% 92.5% 94.1% 92.3% 95.9% 96.3% 96.8% 93.5% 98.2% 94.2% 96.2%Data
awaited
>=96%= Green
<96% =Red
7 3, 4, 9 72.1% 83.7% 72.0% 61.1% 66.7% 72.5% 65.3% 74.3% 77.0% 71.9% 77.1%Data
awaited
>=85%= Green
<85% =Red
8 3, 4, 9 6 9 6 10 8 7 7 10 9 5 7Data
awaited
0= Green
>0 = Red
9 3, 4, 9 88.5% 82.8% 80.0% 82.4% 82.9% 81.8% 82.4% 86.2% 85.7% 84.6% 85.7% 83.3%>=95%= Green
>=85% - <95% =Amber
<85% =Red
10 3, 4, 9 74.4% 73.2% 73.6% 71.1% 67.0% 66.3% 63.4% 63.8% 63.2% 64.2% 69.7% 73.6%>=95%= Green
>=85% - <95% =Amber
<85% =Red
11 All mental health services 4, 6, 9 91.0% 92.1% 93.0% 87.4% 92.3% 94.5% 91.7% 93.1% 93.4% 93.3% 93.7% 90.6%>=90%= Green
>=80% - <90% =Amber
<80% =Red
12 Adult mental health services 4, 6, 9 97.0% 95.9% 91.5% 88.0% 89.8% 93.6% 90.2% 90.0% 93.1% 93.8% 91.1% 87.4%>=90%= Green
>=80% - <90% =Amber
<80% =Red
13Older Persons mental health
services4, 6, 9 79.4% 83.9% 87.3% 84.3% 93.3% 94.8% 92.9% 96.4% 92.5% 91.1% 94.7% 90.4%
>=90%= Green
>=80% - <90% =Amber
<80% =Red
14 Learning disabilities service 4, 6, 9 100.0% 66.7% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0%>=90%= Green
>=80% - <90% =Amber
<80% =Red
15Children and young people's
mental health services4, 6, 9 95.5% 98.2% 98.5% 98.6% 100.0% 97.7% 96.7% 97.3% 100.0% 97.0% 100.0% 98.5%
>=90%= Green
>=80% - <90% =Amber
<80% =Red
16 4, 9 60.3% 62.2% 57.6% 59.6% 57.9% 54.2% 54.6% 62.2% 64.2% 65.0% 62.9% 66.5%>=99%= Green
>=98% - <99% =Amber
<98% =Red
17 4, 6, 9 58.5% 58.1% 59.0% 63.3% 64.0% 63.9% 63.3% 63.0% 61.9% 61.9% 61.0% 60.3%>=92%= Green
<92% =Red
SOMERSET NHS FOUNDATION TRUST
Mental health referrals offered first
appointments within 6 weeks
Diagnostic 6-week wait - acute services
CAMHS Eating Disorders - Urgent referrals to be seen within 1 week
(rolling 12 months)
Cancer - maximum 62 day wait from urgent GP referral
CAMHS Eating Disorders - Routine referrals to be seen within 4 weeks
(rolling 12 months)
>=95%= Green
>=85% - <95% =Amber
<85% =Red
Accident and Emergency / Minor Injury
Unit 4-hour performance
Cancer - 28 days Faster Diagnosis All Cancers
Cancer - maximum 2-week wait from GP referral (suspected cancer)
Cancer - maximum 31 day wait from diagnosis to first treatment
Cancer: 62-day wait from referral to treatment for urgent GP referrals –
number of patients treated on or after day 104
CORPORATE SCORECARD 2021/22
RTT incomplete pathway performance: percentage of people waiting
under 18 weeks
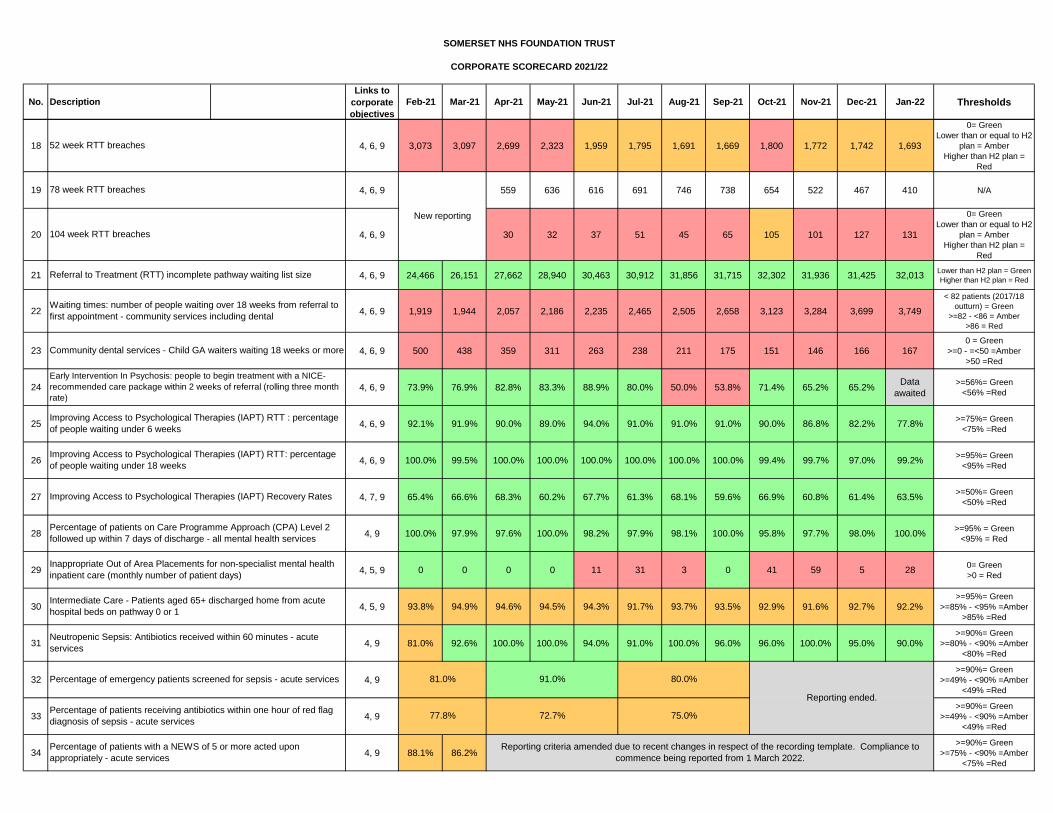
No. Description
Links to
corporate
objectives
Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Thresholds
SOMERSET NHS FOUNDATION TRUST
CORPORATE SCORECARD 2021/22
18 4, 6, 9 3,073 3,097 2,699 2,323 1,959 1,795 1,691 1,669 1,800 1,772 1,742 1,693
0= Green
Lower than or equal to H2
plan = Amber
Higher than H2 plan =
Red
19 4, 6, 9 559 636 616 691 746 738 654 522 467 410 N/A
20 4, 6, 9 30 32 37 51 45 65 105 101 127 131
0= Green
Lower than or equal to H2
plan = Amber
Higher than H2 plan =
Red
21 4, 6, 9 24,466 26,151 27,662 28,940 30,463 30,912 31,856 31,715 32,302 31,936 31,425 32,013Lower than H2 plan = Green
Higher than H2 plan = Red
22 4, 6, 9 1,919 1,944 2,057 2,186 2,235 2,465 2,505 2,658 3,123 3,284 3,699 3,749
< 82 patients (2017/18
outturn) = Green
>=82 - <86 = Amber
>86 = Red
23 4, 6, 9 500 438 359 311 263 238 211 175 151 146 166 1670 = Green
>=0 - =<50 =Amber
>50 =Red
24 4, 6, 9 73.9% 76.9% 82.8% 83.3% 88.9% 80.0% 50.0% 53.8% 71.4% 65.2% 65.2%Data
awaited
>=56%= Green
<56% =Red
25 4, 6, 9 92.1% 91.9% 90.0% 89.0% 94.0% 91.0% 91.0% 91.0% 90.0% 86.8% 82.2% 77.8%>=75%= Green
<75% =Red
26 4, 6, 9 100.0% 99.5% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 99.4% 99.7% 97.0% 99.2%>=95%= Green
<95% =Red
27 4, 7, 9 65.4% 66.6% 68.3% 60.2% 67.7% 61.3% 68.1% 59.6% 66.9% 60.8% 61.4% 63.5%>=50%= Green
<50% =Red
28 4, 9 100.0% 97.9% 97.6% 100.0% 98.2% 97.9% 98.1% 100.0% 95.8% 97.7% 98.0% 100.0%>=95% = Green
<95% = Red
29 4, 5, 9 0 0 0 0 11 31 3 0 41 59 5 280= Green
>0 = Red
30 4, 5, 9 93.8% 94.9% 94.6% 94.5% 94.3% 91.7% 93.7% 93.5% 92.9% 91.6% 92.7% 92.2%>=95%= Green
>=85% - <95% =Amber
>85% =Red
31 4, 9 81.0% 92.6% 100.0% 100.0% 94.0% 91.0% 100.0% 96.0% 96.0% 100.0% 95.0% 90.0%>=90%= Green
>=80% - <90% =Amber
<80% =Red
32 4, 9>=90%= Green
>=49% - <90% =Amber
<49% =Red
33 4, 9>=90%= Green
>=49% - <90% =Amber
<49% =Red
34 4, 9 88.1% 86.2%>=90%= Green
>=75% - <90% =Amber
<75% =Red
Percentage of emergency patients screened for sepsis - acute services
Percentage of patients receiving antibiotics within one hour of red flag
diagnosis of sepsis - acute services
Percentage of patients with a NEWS of 5 or more acted upon
appropriately - acute services
52 week RTT breaches
Improving Access to Psychological Therapies (IAPT) Recovery Rates
Improving Access to Psychological Therapies (IAPT) RTT : percentage
of people waiting under 6 weeks
Improving Access to Psychological Therapies (IAPT) RTT: percentage
of people waiting under 18 weeks
Waiting times: number of people waiting over 18 weeks from referral to
first appointment - community services including dental
Referral to Treatment (RTT) incomplete pathway waiting list size
Early Intervention In Psychosis: people to begin treatment with a NICE-
recommended care package within 2 weeks of referral (rolling three month
rate)
Inappropriate Out of Area Placements for non-specialist mental health
inpatient care (monthly number of patient days)
Percentage of patients on Care Programme Approach (CPA) Level 2
followed up within 7 days of discharge - all mental health services
New reporting
Reporting ended.
Reporting criteria amended due to recent changes in respect of the recording template. Compliance to
commence being reported from 1 March 2022.
104 week RTT breaches
78 week RTT breaches
Community dental services - Child GA waiters waiting 18 weeks or more
Neutropenic Sepsis: Antibiotics received within 60 minutes - acute
services
Intermediate Care - Patients aged 65+ discharged home from acute
hospital beds on pathway 0 or 1
75.0%
80.0%
72.7%
91.0%
77.8%
81.0%
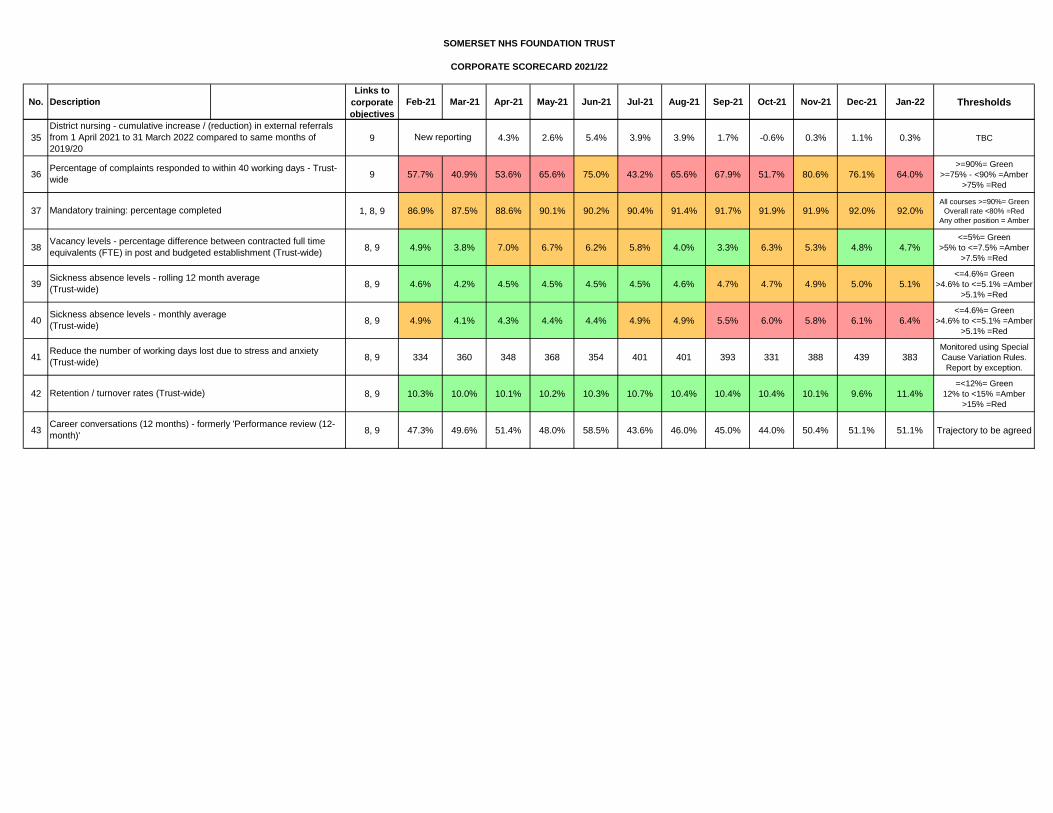
No. Description
Links to
corporate
objectives
Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Thresholds
SOMERSET NHS FOUNDATION TRUST
CORPORATE SCORECARD 2021/22
35 9 4.3% 2.6% 5.4% 3.9% 3.9% 1.7% -0.6% 0.3% 1.1% 0.3% TBC
36 9 57.7% 40.9% 53.6% 65.6% 75.0% 43.2% 65.6% 67.9% 51.7% 80.6% 76.1% 64.0%>=90%= Green
>=75% - <90% =Amber
>75% =Red
37 1, 8, 9 86.9% 87.5% 88.6% 90.1% 90.2% 90.4% 91.4% 91.7% 91.9% 91.9% 92.0% 92.0%All courses >=90%= Green
Overall rate <80% =Red
Any other position = Amber
38 8, 9 4.9% 3.8% 7.0% 6.7% 6.2% 5.8% 4.0% 3.3% 6.3% 5.3% 4.8% 4.7%<=5%= Green
>5% to <=7.5% =Amber
>7.5% =Red
39 8, 9 4.6% 4.2% 4.5% 4.5% 4.5% 4.5% 4.6% 4.7% 4.7% 4.9% 5.0% 5.1%<=4.6%= Green
>4.6% to <=5.1% =Amber
>5.1% =Red
40 8, 9 4.9% 4.1% 4.3% 4.4% 4.4% 4.9% 4.9% 5.5% 6.0% 5.8% 6.1% 6.4%<=4.6%= Green
>4.6% to <=5.1% =Amber
>5.1% =Red
41 8, 9 334 360 348 368 354 401 401 393 331 388 439 383Monitored using Special
Cause Variation Rules.
Report by exception.
42 8, 9 10.3% 10.0% 10.1% 10.2% 10.3% 10.7% 10.4% 10.4% 10.4% 10.1% 9.6% 11.4%=<12%= Green
12% to <15% =Amber
>15% =Red
43 8, 9 47.3% 49.6% 51.4% 48.0% 58.5% 43.6% 46.0% 45.0% 44.0% 50.4% 51.1% 51.1% Trajectory to be agreed
New reporting
Percentage of complaints responded to within 40 working days - Trust-
wide
District nursing - cumulative increase / (reduction) in external referrals
from 1 April 2021 to 31 March 2022 compared to same months of
2019/20
Sickness absence levels - monthly average
(Trust-wide)
Reduce the number of working days lost due to stress and anxiety
(Trust-wide)
Retention / turnover rates (Trust-wide)
Career conversations (12 months) - formerly 'Performance review (12-
month)'
Sickness absence levels - rolling 12 month average
(Trust-wide)
Mandatory training: percentage completed
Vacancy levels - percentage difference between contracted full time
equivalents (FTE) in post and budgeted establishment (Trust-wide)
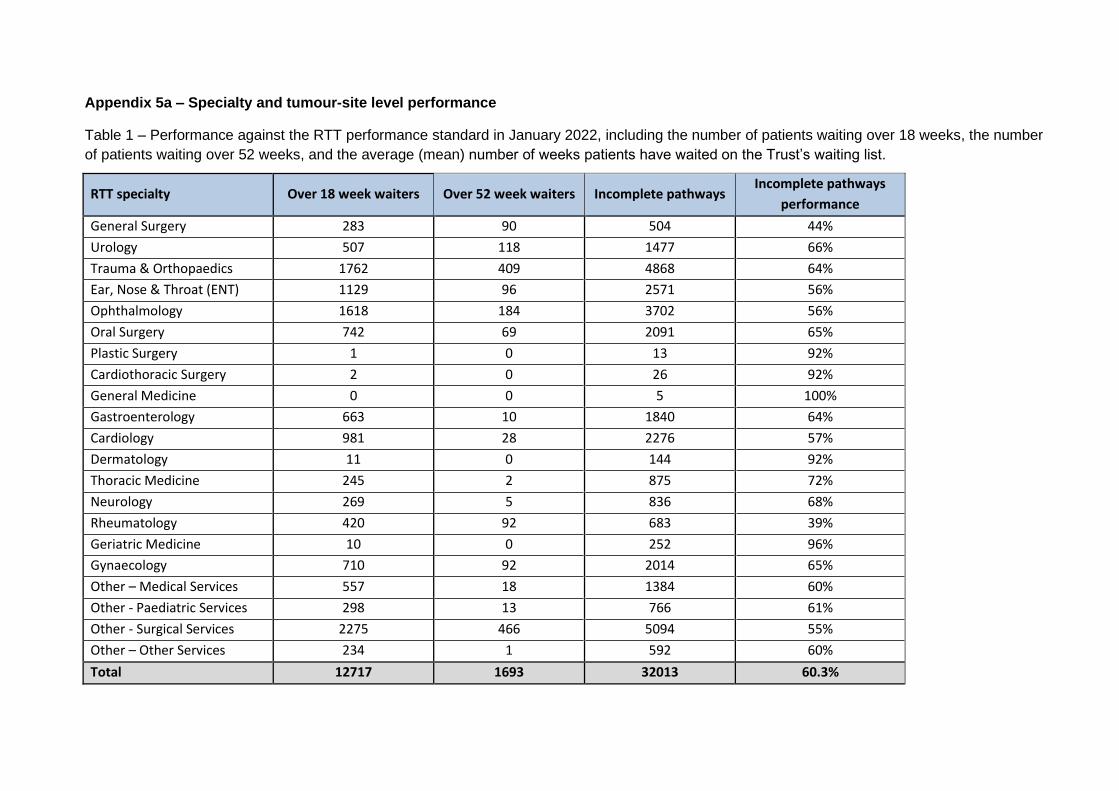
Appendix 5a – Specialty and tumour-site level performance
Table 1 – Performance against the RTT performance standard in January 2022, including the number of patients waiting over 18 weeks, the number
of patients waiting over 52 weeks, and the average (mean) number of weeks patients have waited on the Trust’s waiting list.
RTT specialty Over 18 week waiters Over 52 week waiters Incomplete pathways Incomplete pathways
performance
General Surgery 283 90 504 44%
Urology 507 118 1477 66%
Trauma & Orthopaedics 1762 409 4868 64%
Ear, Nose & Throat (ENT) 1129 96 2571 56%
Ophthalmology 1618 184 3702 56%
Oral Surgery 742 69 2091 65%
Plastic Surgery 1 0 13 92%
Cardiothoracic Surgery 2 0 26 92%
General Medicine 0 0 5 100%
Gastroenterology 663 10 1840 64%
Cardiology 981 28 2276 57%
Dermatology 11 0 144 92%
Thoracic Medicine 245 2 875 72%
Neurology 269 5 836 68%
Rheumatology 420 92 683 39%
Geriatric Medicine 10 0 252 96%
Gynaecology 710 92 2014 65%
Other – Medical Services 557 18 1384 60%
Other - Paediatric Services 298 13 766 61%
Other - Surgical Services 2275 466 5094 55%
Other – Other Services 234 1 592 60%
Total 12717 1693 32013 60.3%
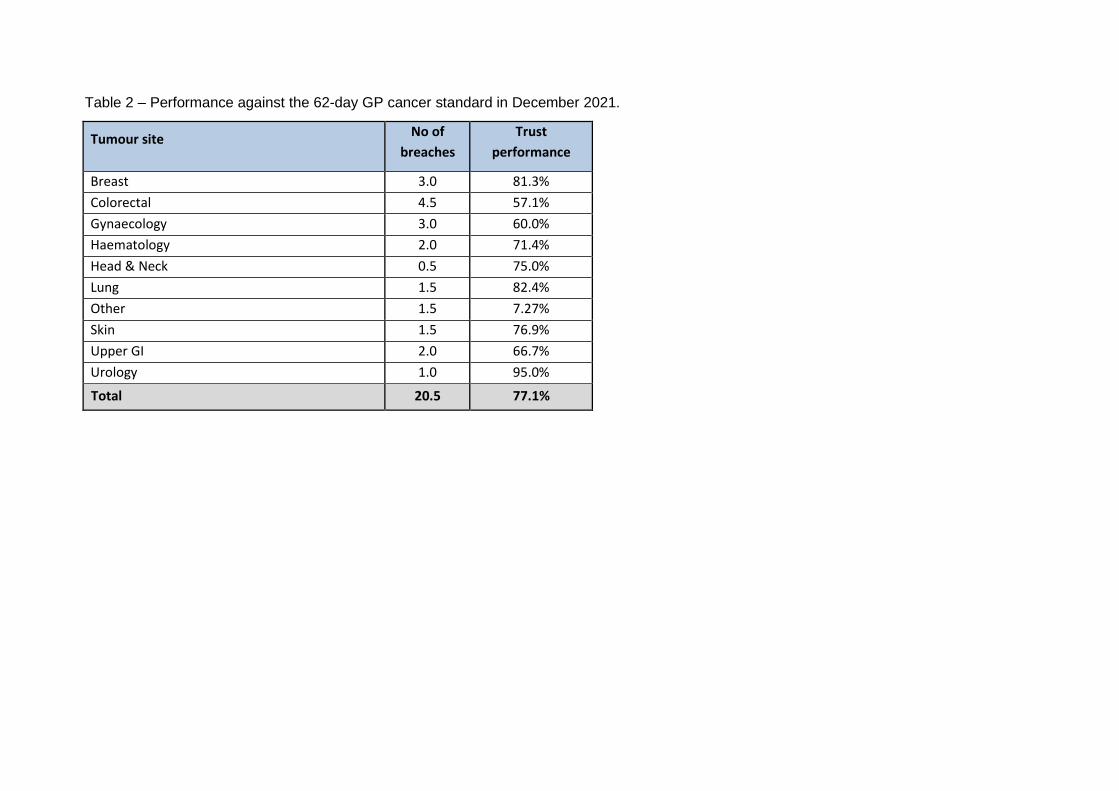
Table 2 – Performance against the 62-day GP cancer standard in December 2021.
Tumour site No of
breaches
Trust
performance
Breast 3.0 81.3%
Colorectal 4.5 57.1%
Gynaecology 3.0 60.0%
Haematology 2.0 71.4%
Head & Neck 0.5 75.0%
Lung 1.5 82.4%
Other 1.5 7.27%
Skin 1.5 76.9%
Upper GI 2.0 66.7%
Urology 1.0 95.0%
Total 20.5 77.1%
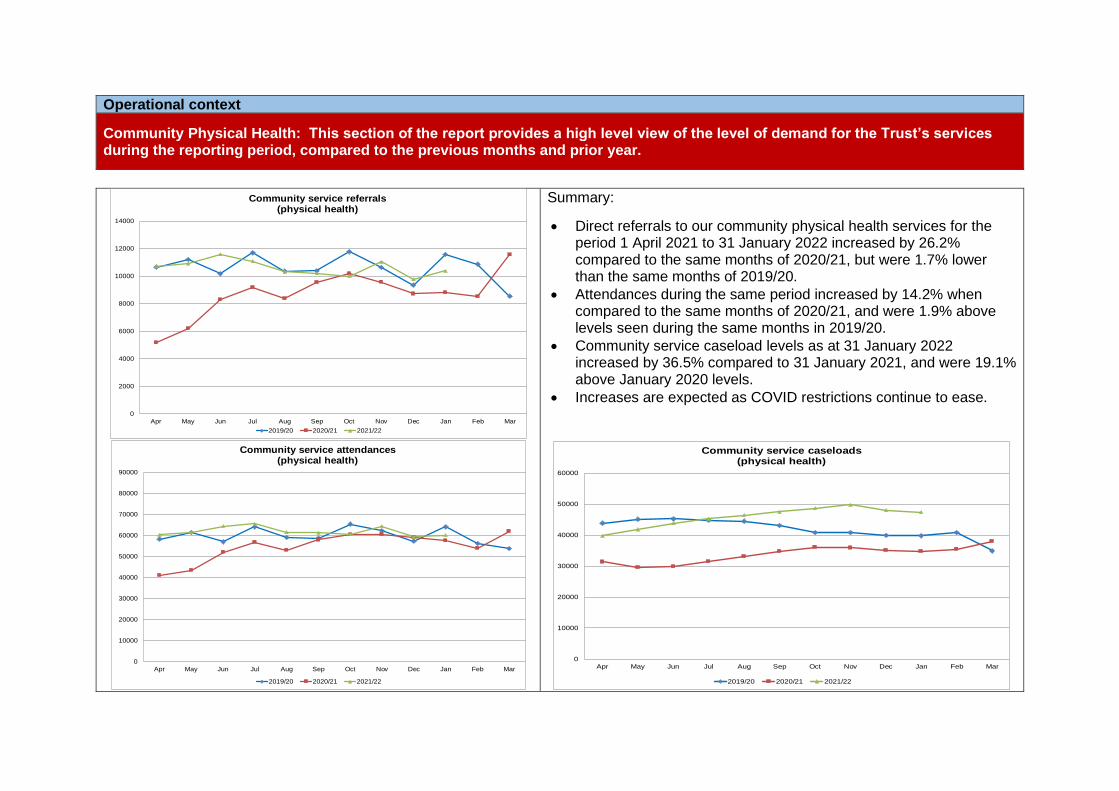
Operational context
Community Physical Health: This section of the report provides a high level view of the level of demand for the Trust’s services during the reporting period, compared to the previous months and prior year.
Summary:
• Direct referrals to our community physical health services for the period 1 April 2021 to 31 January 2022 increased by 26.2% compared to the same months of 2020/21, but were 1.7% lower than the same months of 2019/20.
• Attendances during the same period increased by 14.2% when compared to the same months of 2020/21, and were 1.9% above levels seen during the same months in 2019/20.
• Community service caseload levels as at 31 January 2022 increased by 36.5% compared to 31 January 2021, and were 19.1% above January 2020 levels.
• Increases are expected as COVID restrictions continue to ease.
0
2000
4000
6000
8000
10000
12000
14000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Community service referrals(physical health)
2019/20 2020/21 2021/22
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Community service attendances(physical health)
2019/20 2020/21 2021/22
0
10000
20000
30000
40000
50000
60000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Community service caseloads(physical health)
2019/20 2020/21 2021/22
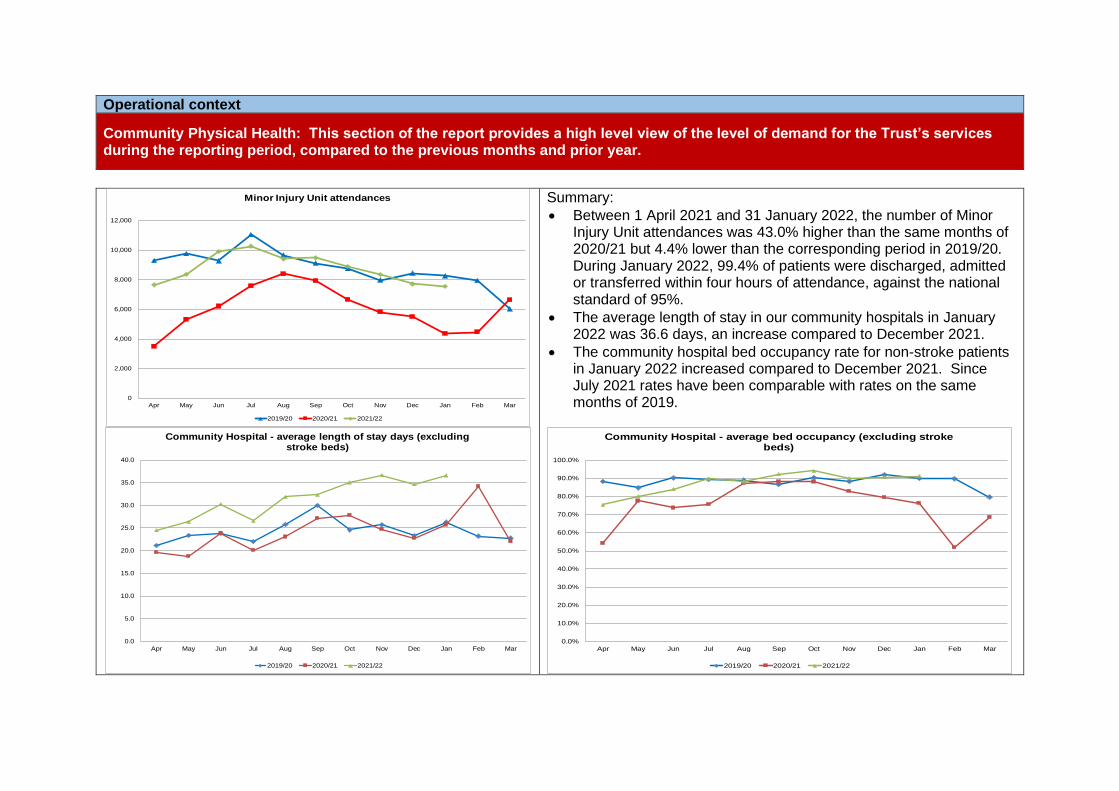
Operational context
Community Physical Health: This section of the report provides a high level view of the level of demand for the Trust’s services during the reporting period, compared to the previous months and prior year.
Summary:
• Between 1 April 2021 and 31 January 2022, the number of Minor Injury Unit attendances was 43.0% higher than the same months of 2020/21 but 4.4% lower than the corresponding period in 2019/20. During January 2022, 99.4% of patients were discharged, admitted or transferred within four hours of attendance, against the national standard of 95%.
• The average length of stay in our community hospitals in January 2022 was 36.6 days, an increase compared to December 2021.
• The community hospital bed occupancy rate for non-stroke patients in January 2022 increased compared to December 2021. Since July 2021 rates have been comparable with rates on the same months of 2019.
0
2,000
4,000
6,000
8,000
10,000
12,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Minor Injury Unit attendances
2019/20 2020/21 2021/22
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Community Hospital - average length of stay days (excluding stroke beds)
2019/20 2020/21 2021/22
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Community Hospital - average bed occupancy (excluding stroke beds)
2019/20 2020/21 2021/22
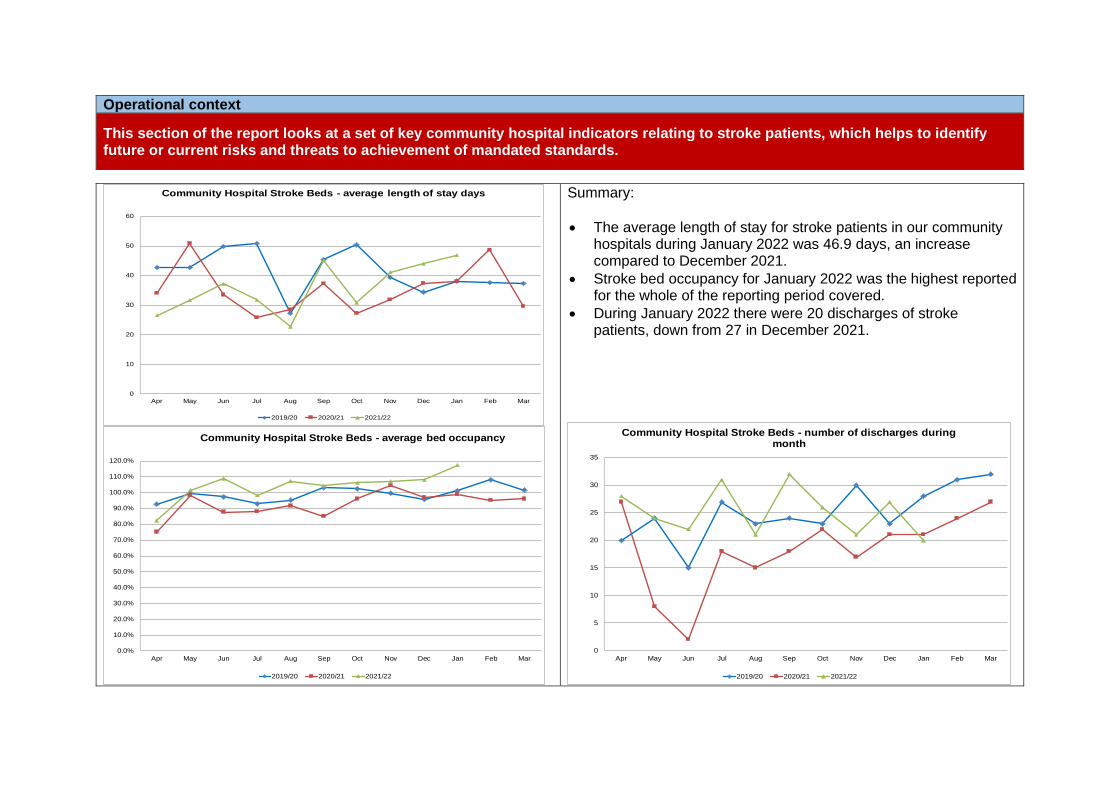
Operational context
This section of the report looks at a set of key community hospital indicators relating to stroke patients, which helps to identify future or current risks and threats to achievement of mandated standards.
Summary:
• The average length of stay for stroke patients in our community hospitals during January 2022 was 46.9 days, an increase compared to December 2021.
• Stroke bed occupancy for January 2022 was the highest reported for the whole of the reporting period covered.
• During January 2022 there were 20 discharges of stroke patients, down from 27 in December 2021.
0
10
20
30
40
50
60
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Community Hospital Stroke Beds - average length of stay days
2019/20 2020/21 2021/22
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
110.0%
120.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Community Hospital Stroke Beds - average bed occupancy
2019/20 2020/21 2021/22
0
5
10
15
20
25
30
35
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Community Hospital Stroke Beds - number of discharges during month
2019/20 2020/21 2021/22
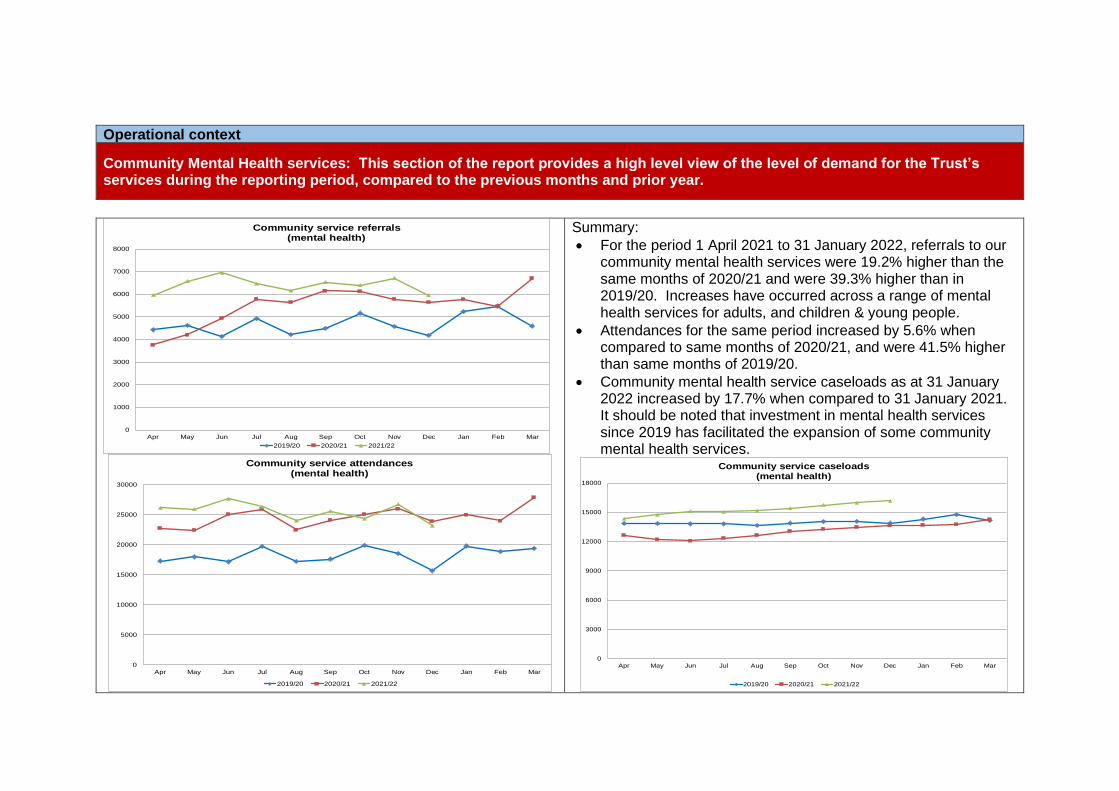
Operational context
Community Mental Health services: This section of the report provides a high level view of the level of demand for the Trust’s services during the reporting period, compared to the previous months and prior year.
Summary:
• For the period 1 April 2021 to 31 January 2022, referrals to our community mental health services were 19.2% higher than the same months of 2020/21 and were 39.3% higher than in 2019/20. Increases have occurred across a range of mental health services for adults, and children & young people.
• Attendances for the same period increased by 5.6% when compared to same months of 2020/21, and were 41.5% higher than same months of 2019/20.
• Community mental health service caseloads as at 31 January 2022 increased by 17.7% when compared to 31 January 2021. It should be noted that investment in mental health services since 2019 has facilitated the expansion of some community mental health services.
0
1000
2000
3000
4000
5000
6000
7000
8000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Community service referrals(mental health)
2019/20 2020/21 2021/22
0
5000
10000
15000
20000
25000
30000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Community service attendances(mental health)
2019/20 2020/21 2021/22
0
3000
6000
9000
12000
15000
18000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Community service caseloads(mental health)
2019/20 2020/21 2021/22
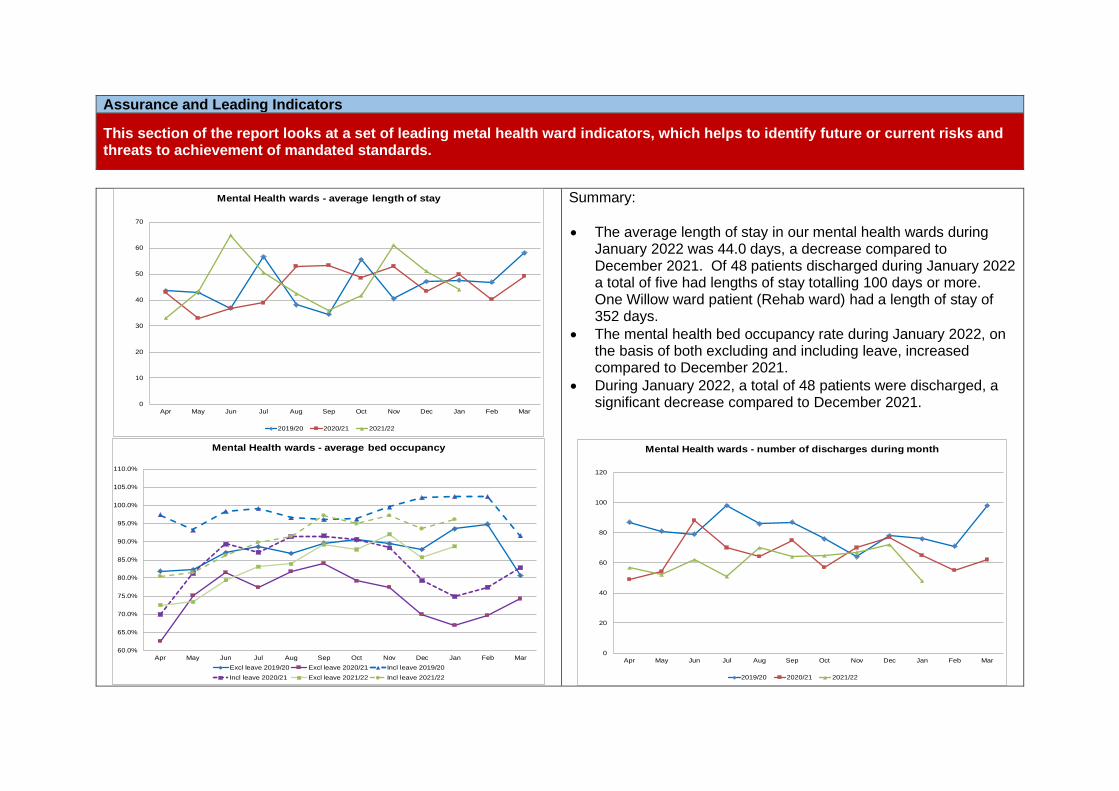
Assurance and Leading Indicators
This section of the report looks at a set of leading metal health ward indicators, which helps to identify future or current risks and threats to achievement of mandated standards.
Summary:
• The average length of stay in our mental health wards during January 2022 was 44.0 days, a decrease compared to December 2021. Of 48 patients discharged during January 2022 a total of five had lengths of stay totalling 100 days or more. One Willow ward patient (Rehab ward) had a length of stay of 352 days.
• The mental health bed occupancy rate during January 2022, on the basis of both excluding and including leave, increased compared to December 2021.
• During January 2022, a total of 48 patients were discharged, a significant decrease compared to December 2021.
0
10
20
30
40
50
60
70
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Mental Health wards - average length of stay
2019/20 2020/21 2021/22
60.0%
65.0%
70.0%
75.0%
80.0%
85.0%
90.0%
95.0%
100.0%
105.0%
110.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Mental Health wards - average bed occupancy
Excl leave 2019/20 Excl leave 2020/21 Incl leave 2019/20
Incl leave 2020/21 Excl leave 2021/22 Incl leave 2021/22
0
20
40
60
80
100
120
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Mental Health wards - number of discharges during month
2019/20 2020/21 2021/22
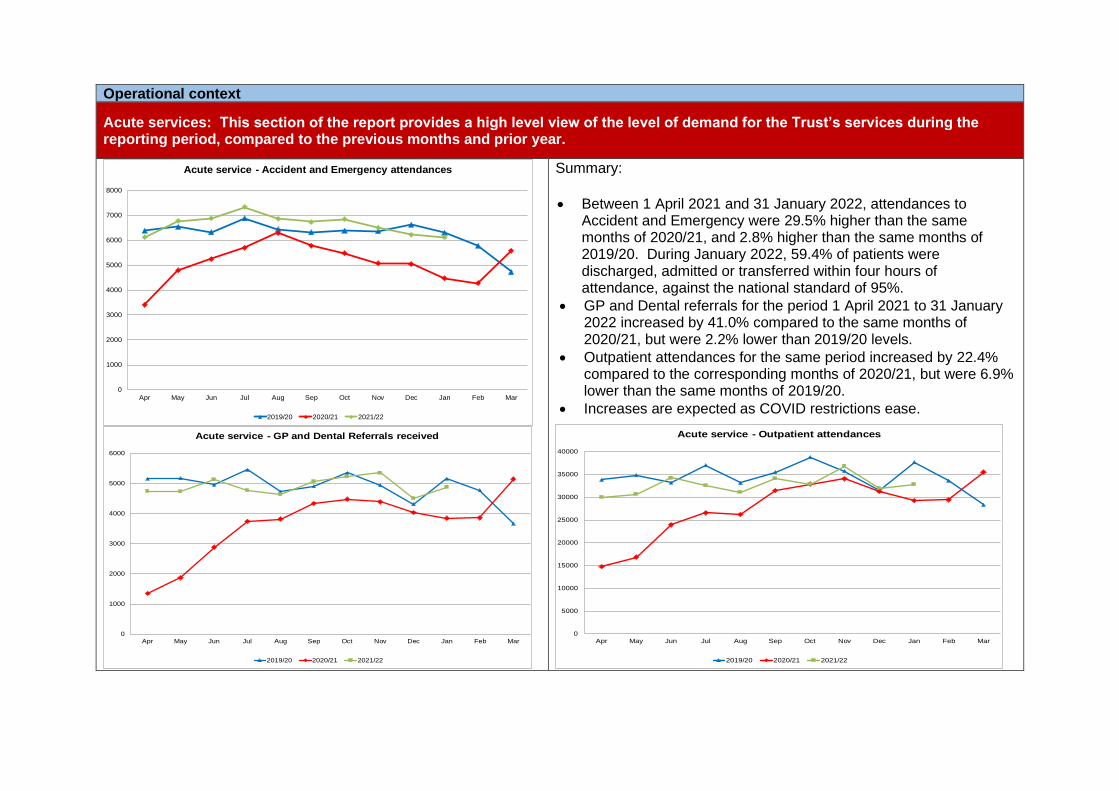
Operational context
Acute services: This section of the report provides a high level view of the level of demand for the Trust’s services during the reporting period, compared to the previous months and prior year.
Summary:
• Between 1 April 2021 and 31 January 2022, attendances to Accident and Emergency were 29.5% higher than the same months of 2020/21, and 2.8% higher than the same months of 2019/20. During January 2022, 59.4% of patients were discharged, admitted or transferred within four hours of attendance, against the national standard of 95%.
• GP and Dental referrals for the period 1 April 2021 to 31 January 2022 increased by 41.0% compared to the same months of 2020/21, but were 2.2% lower than 2019/20 levels.
• Outpatient attendances for the same period increased by 22.4% compared to the corresponding months of 2020/21, but were 6.9% lower than the same months of 2019/20.
• Increases are expected as COVID restrictions ease.
0
1000
2000
3000
4000
5000
6000
7000
8000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Acute service - Accident and Emergency attendances
2019/20 2020/21 2021/22
0
1000
2000
3000
4000
5000
6000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Acute service - GP and Dental Referrals received
2019/20 2020/21 2021/22
0
5000
10000
15000
20000
25000
30000
35000
40000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Acute service - Outpatient attendances
2019/20 2020/21 2021/22
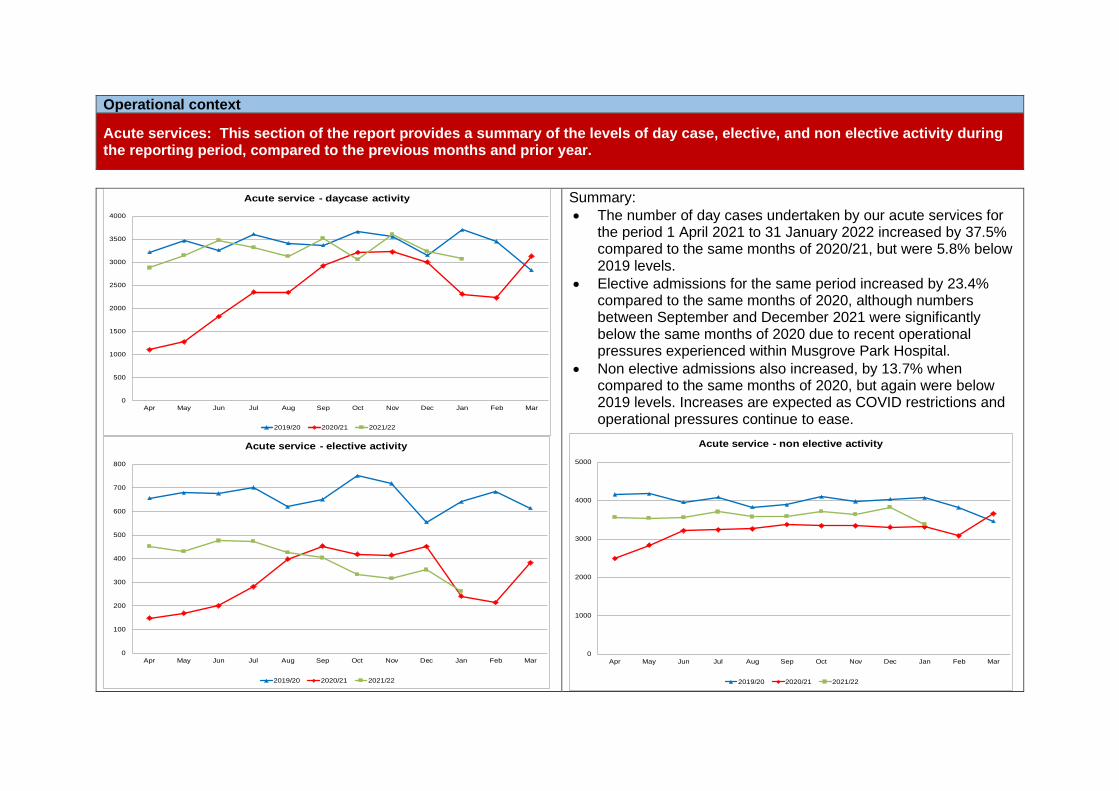
Operational context
Acute services: This section of the report provides a summary of the levels of day case, elective, and non elective activity during the reporting period, compared to the previous months and prior year.
Summary:
• The number of day cases undertaken by our acute services for the period 1 April 2021 to 31 January 2022 increased by 37.5% compared to the same months of 2020/21, but were 5.8% below 2019 levels.
• Elective admissions for the same period increased by 23.4% compared to the same months of 2020, although numbers between September and December 2021 were significantly below the same months of 2020 due to recent operational pressures experienced within Musgrove Park Hospital.
• Non elective admissions also increased, by 13.7% when compared to the same months of 2020, but again were below 2019 levels. Increases are expected as COVID restrictions and operational pressures continue to ease.
0
500
1000
1500
2000
2500
3000
3500
4000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Acute service - daycase activity
2019/20 2020/21 2021/22
0
100
200
300
400
500
600
700
800
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Acute service - elective activity
2019/20 2020/21 2021/22
0
1000
2000
3000
4000
5000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Acute service - non elective activity
2019/20 2020/21 2021/22
SFT Finance Report March 2022 Public Board - 1 - I
Somerset NHS Foundation Trust
REPORT TO: The Trust Board
REPORT TITLE: Finance Report
SPONSORING EXEC: Chief Finance Officer.
REPORT BY: Chief Finance Officer supported by Deputy Director of Finance.
PRESENTED BY: Chief Finance Officer
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☒ For Assurance/
Discussion ☐ For Approval / Decision ☐ For Information
Executive Summary and Reason for presentation to Committee/Board
The Finance report sets out the overall income and expenditure position for the Trust. It includes commentary on the key issues, risks and variances, which are affecting the financial position.
Recommendation The Board is requested to discuss the report.
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☐ Care for our Population ☐ Develop our People
☐ Innovate and Collaborate ☐ Develop a Sustainable System
Somerset NHS FT
☐ Obj 1 Inclusive culture ☐ Obj 4 Safe services ☐ Obj 7 Improving outcomes
☐ Obj 2 Collaboration ☐ Obj 5 Self management ☐ Obj 8 Workforce
☐ Obj 3 Independent lives ☐ Obj 6 Value all people alike ☐ Obj 9 Performance
☒ Obj 10 Finance
Implications/Requirements (Please select any which are relevant to this paper)
☒ Financial ☒ Legislation ☐ Workforce ☐ Estates ☐ ICT ☐ Patient Safety /
Quality
Details: Under the terms of its licence and NHS Improvement’s risk assessment framework the Trust has a duty to remain financially viable.
SFT Finance Report March 2022 Public Board - 2 - I
Equality The Trust wants its services to be as accessible as possible, to as many people as
possible. Please indicate whether the report has an impact on the protected characteristics
☒ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are no proposals or matters which affect any persons with protected characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
Not Applicable.
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
The report is presented to every Board meeting.
Reference to CQC domains (Please select any which are relevant to this paper)
☐ Safe ☒ Effective ☐ Caring ☐ Responsive ☒ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
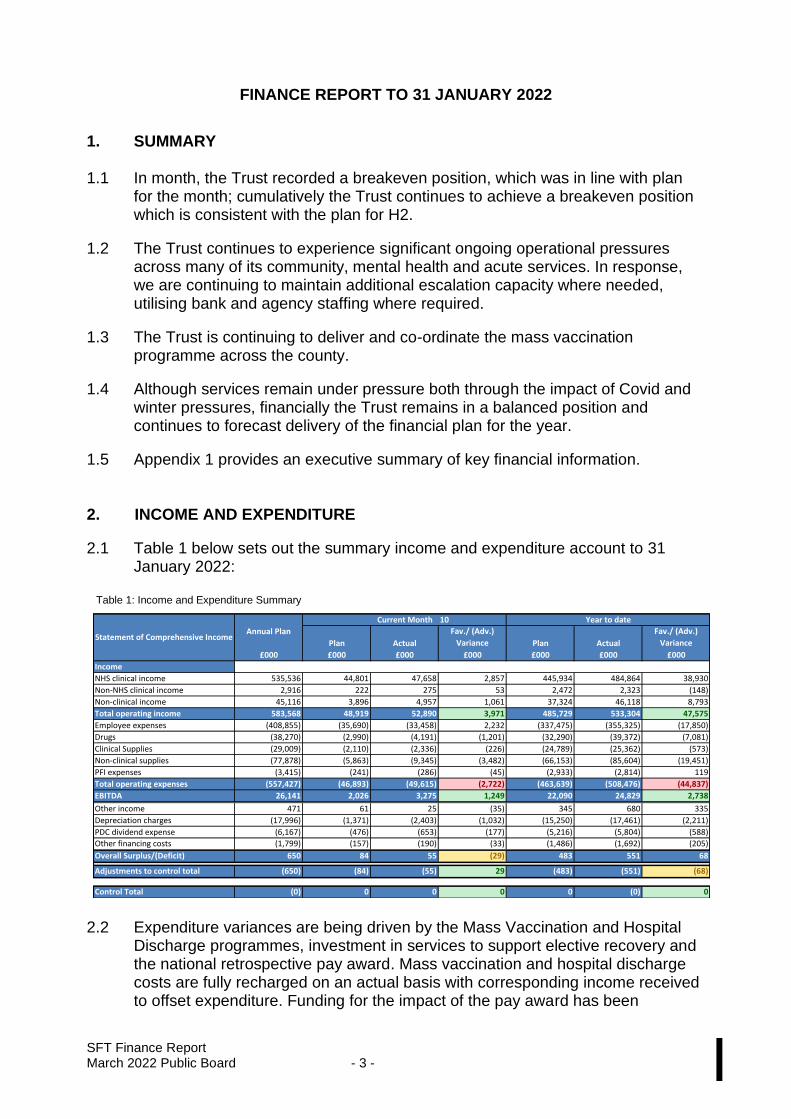
SFT Finance Report March 2022 Public Board - 3 - I
FINANCE REPORT TO 31 JANUARY 2022
1. SUMMARY 1.1 In month, the Trust recorded a breakeven position, which was in line with plan
for the month; cumulatively the Trust continues to achieve a breakeven position which is consistent with the plan for H2.
1.2 The Trust continues to experience significant ongoing operational pressures across many of its community, mental health and acute services. In response, we are continuing to maintain additional escalation capacity where needed, utilising bank and agency staffing where required.
1.3 The Trust is continuing to deliver and co-ordinate the mass vaccination programme across the county.
1.4 Although services remain under pressure both through the impact of Covid and winter pressures, financially the Trust remains in a balanced position and continues to forecast delivery of the financial plan for the year.
1.5 Appendix 1 provides an executive summary of key financial information.
2. INCOME AND EXPENDITURE
2.1 Table 1 below sets out the summary income and expenditure account to 31 January 2022:
Table 1: Income and Expenditure Summary
2.2 Expenditure variances are being driven by the Mass Vaccination and Hospital
Discharge programmes, investment in services to support elective recovery and the national retrospective pay award. Mass vaccination and hospital discharge costs are fully recharged on an actual basis with corresponding income received to offset expenditure. Funding for the impact of the pay award has been
10
Plan Actual
Fav./ (Adv.)
Variance Plan Actual
Fav./ (Adv.)
Variance
£000 £000 £000 £000 £000 £000 £000
Income
NHS clinical income 535,536 44,801 47,658 2,857 445,934 484,864 38,930
Non-NHS clinical income 2,916 222 275 53 2,472 2,323 (148)
Non-clinical income 45,116 3,896 4,957 1,061 37,324 46,118 8,793
Total operating income 583,568 48,919 52,890 3,971 485,729 533,304 47,575
Employee expenses (408,855) (35,690) (33,458) 2,232 (337,475) (355,325) (17,850)
Drugs (38,270) (2,990) (4,191) (1,201) (32,290) (39,372) (7,081)
Clinical Supplies (29,009) (2,110) (2,336) (226) (24,789) (25,362) (573)
Non-clinical supplies (77,878) (5,863) (9,345) (3,482) (66,153) (85,604) (19,451)
PFI expenses (3,415) (241) (286) (45) (2,933) (2,814) 119
Total operating expenses (557,427) (46,893) (49,615) (2,722) (463,639) (508,476) (44,837)
EBITDA 26,141 2,026 3,275 1,249 22,090 24,829 2,738
Other income 471 61 25 (35) 345 680 335
Depreciation charges (17,996) (1,371) (2,403) (1,032) (15,250) (17,461) (2,211)
PDC dividend expense (6,167) (476) (653) (177) (5,216) (5,804) (588)
Other financing costs (1,799) (157) (190) (33) (1,486) (1,692) (205)
Overall Surplus/(Deficit) 650 84 55 (29) 483 551 68
Adjustments to control total (650) (84) (55) 29 (483) (551) (68)
Control Total (0) 0 0 0 0 (0) 0
Statement of Comprehensive IncomeAnnual Plan
Current Month Year to date
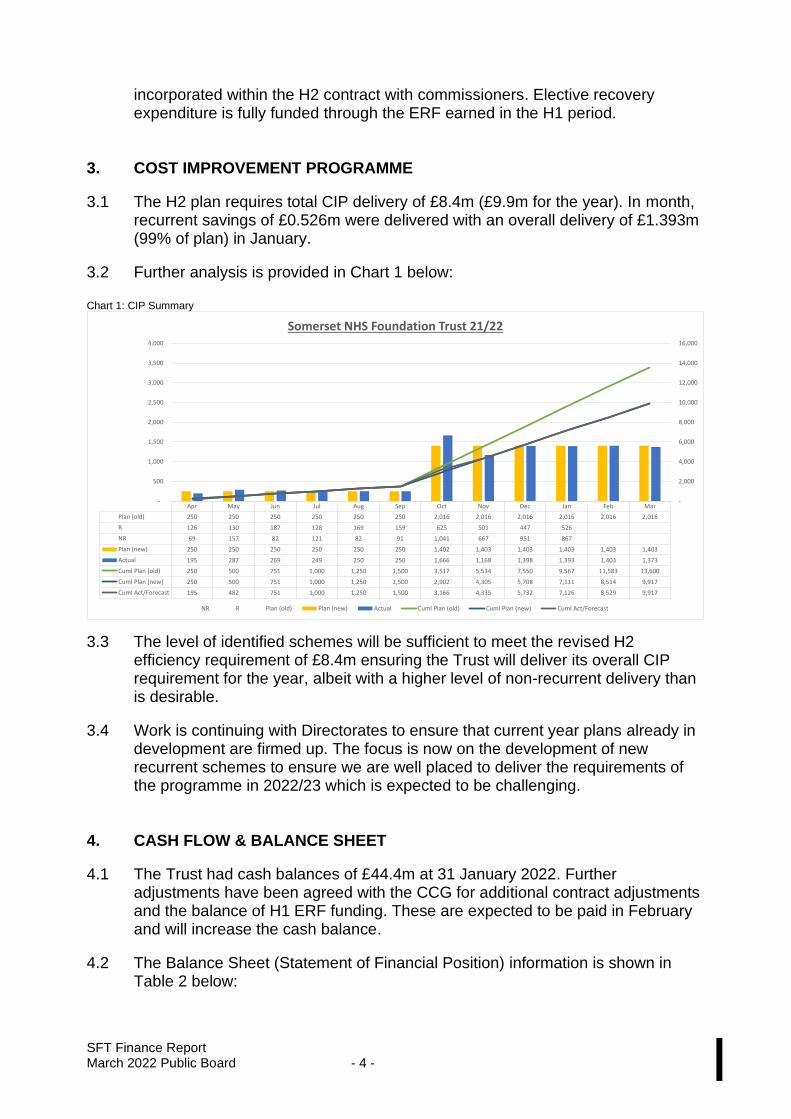
SFT Finance Report March 2022 Public Board - 4 - I
incorporated within the H2 contract with commissioners. Elective recovery expenditure is fully funded through the ERF earned in the H1 period.
3. COST IMPROVEMENT PROGRAMME
3.1 The H2 plan requires total CIP delivery of £8.4m (£9.9m for the year). In month, recurrent savings of £0.526m were delivered with an overall delivery of £1.393m (99% of plan) in January.
3.2 Further analysis is provided in Chart 1 below:
Chart 1: CIP Summary
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Plan (old) 250 250 250 250 250 250 2,016 2,016 2,016 2,016 2,016 2,016
R 126 130 187 128 169 159 625 501 447 526
NR 69 157 82 121 82 91 1,041 667 951 867
Plan (new) 250 250 250 250 250 250 1,402 1,403 1,403 1,403 1,403 1,403
Actual 195 287 269 249 250 250 1,666 1,168 1,398 1,393 1,403 1,373
Cuml Plan (old) 250 500 751 1,000 1,250 1,500 3,517 5,534 7,550 9,567 11,583 13,600
Cuml Plan (new) 250 500 751 1,000 1,250 1,500 2,902 4,305 5,708 7,111 8,514 9,917
Cuml Act/Forecast 195 482 751 1,000 1,250 1,500 3,166 4,335 5,732 7,126 8,529 9,917
-
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
-
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
Somerset NHS Foundation Trust 21/22
NR R Plan (old) Plan (new) Actual Cuml Plan (old) Cuml Plan (new) Cuml Act/Forecast
3.3 The level of identified schemes will be sufficient to meet the revised H2 efficiency requirement of £8.4m ensuring the Trust will deliver its overall CIP requirement for the year, albeit with a higher level of non-recurrent delivery than is desirable.
3.4 Work is continuing with Directorates to ensure that current year plans already in development are firmed up. The focus is now on the development of new recurrent schemes to ensure we are well placed to deliver the requirements of the programme in 2022/23 which is expected to be challenging.
4. CASH FLOW & BALANCE SHEET
4.1 The Trust had cash balances of £44.4m at 31 January 2022. Further adjustments have been agreed with the CCG for additional contract adjustments and the balance of H1 ERF funding. These are expected to be paid in February and will increase the cash balance.
4.2 The Balance Sheet (Statement of Financial Position) information is shown in Table 2 below:
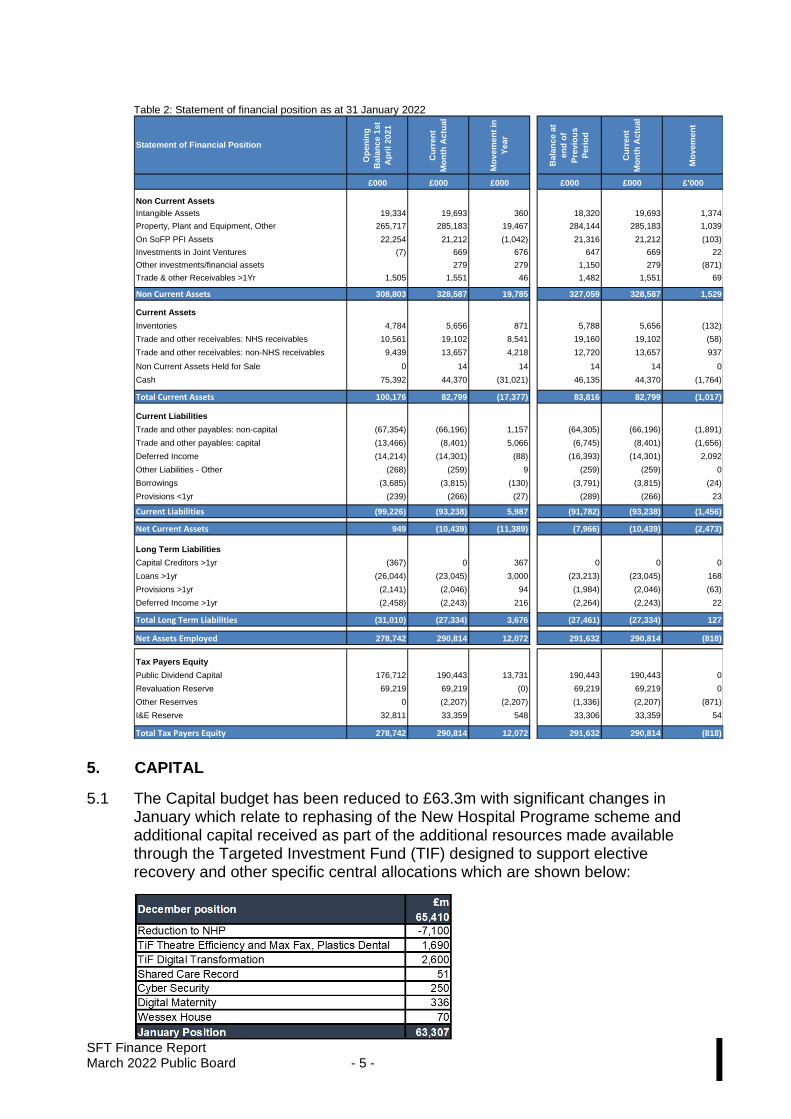
SFT Finance Report March 2022 Public Board - 5 - I
Table 2: Statement of financial position as at 31 January 2022
Op
en
ing
Bala
nc
e 1
st
Ap
ril 20
21
Cu
rre
nt
Mo
nth
Actu
al
Mo
vem
en
t in
Year
Ba
lan
ce a
t
en
d o
f
Pre
vio
us
Pe
rio
d
Cu
rre
nt
Mo
nth
Actu
al
Mo
ve
men
t
£000 £000 £000 £000 £000 £'000
Non Current Assets
Intangible Assets 19,334 19,693 360 18,320 19,693 1,374
Property, Plant and Equipment, Other 265,717 285,183 19,467 284,144 285,183 1,039
On SoFP PFI Assets 22,254 21,212 (1,042) 21,316 21,212 (103)
Investments in Joint Ventures (7) 669 676 647 669 22
Other investments/financial assets 279 279 1,150 279 (871)
Trade & other Receivables >1Yr 1,505 1,551 46 1,482 1,551 69
Non Current Assets 308,803 328,587 19,785 327,059 328,587 1,529
Current Assets
Inventories 4,784 5,656 871 5,788 5,656 (132)
Trade and other receivables: NHS receivables 10,561 19,102 8,541 19,160 19,102 (58)
Trade and other receivables: non-NHS receivables 9,439 13,657 4,218 12,720 13,657 937
Non Current Assets Held for Sale 0 14 14 14 14 0
Cash 75,392 44,370 (31,021) 46,135 44,370 (1,764)
Total Current Assets 100,176 82,799 (17,377) 83,816 82,799 (1,017)
Current Liabilities
Trade and other payables: non-capital (67,354) (66,196) 1,157 (64,305) (66,196) (1,891)
Trade and other payables: capital (13,466) (8,401) 5,066 (6,745) (8,401) (1,656)
Deferred Income (14,214) (14,301) (88) (16,393) (14,301) 2,092
Other Liabilities - Other (268) (259) 9 (259) (259) 0
Borrowings (3,685) (3,815) (130) (3,791) (3,815) (24)
Provisions <1yr (239) (266) (27) (289) (266) 23
Current Liabilities (99,226) (93,238) 5,987 (91,782) (93,238) (1,456)
Net Current Assets 949 (10,439) (11,389) (7,966) (10,439) (2,473)
Long Term Liabilities
Capital Creditors >1yr (367) 0 367 0 0 0
Loans >1yr (26,044) (23,045) 3,000 (23,213) (23,045) 168
Provisions >1yr (2,141) (2,046) 94 (1,984) (2,046) (63)
Deferred Income >1yr (2,458) (2,243) 216 (2,264) (2,243) 22
Total Long Term Liabilities (31,010) (27,334) 3,676 (27,461) (27,334) 127
Net Assets Employed 278,742 290,814 12,072 291,632 290,814 (818)
Tax Payers Equity
Public Dividend Capital 176,712 190,443 13,731 190,443 190,443 0
Revaluation Reserve 69,219 69,219 (0) 69,219 69,219 0
Other Reserrves 0 (2,207) (2,207) (1,336) (2,207) (871)
I&E Reserve 32,811 33,359 548 33,306 33,359 54
Total Tax Payers Equity 278,742 290,814 12,072 291,632 290,814 (818)
Statement of Financial Position
5. CAPITAL
5.1 The Capital budget has been reduced to £63.3m with significant changes in January which relate to rephasing of the New Hospital Programe scheme and additional capital received as part of the additional resources made available through the Targeted Investment Fund (TIF) designed to support elective recovery and other specific central allocations which are shown below:
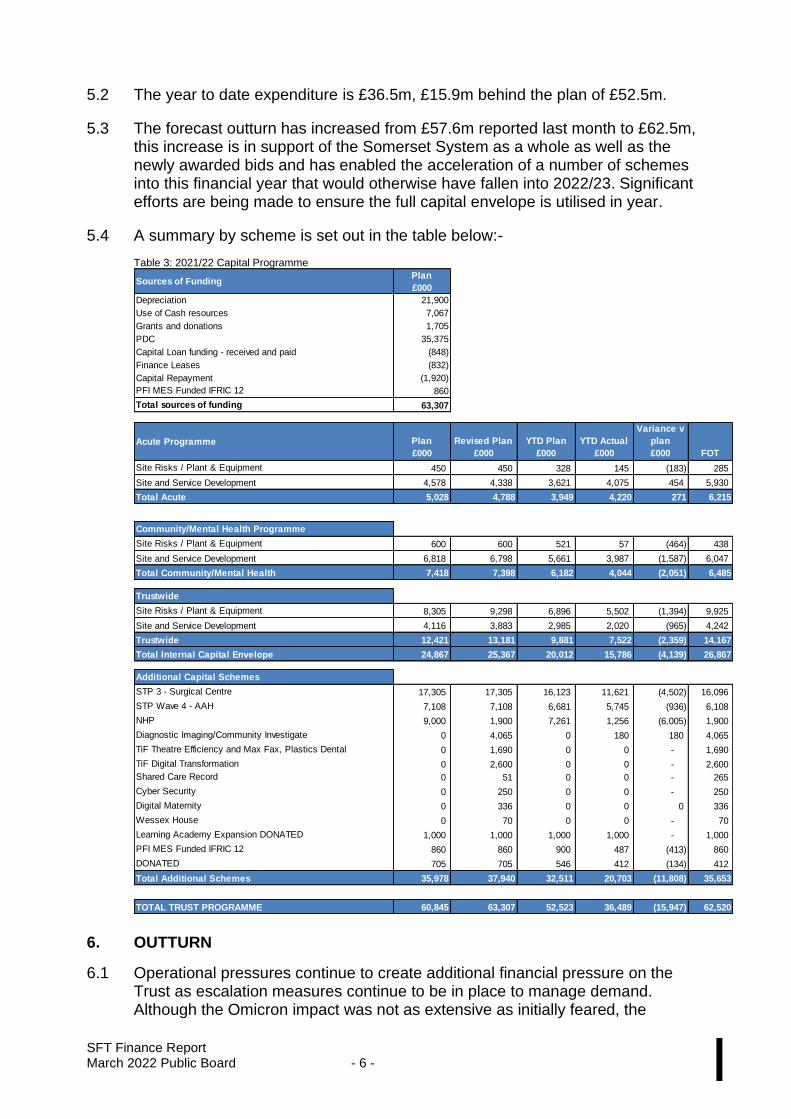
SFT Finance Report March 2022 Public Board - 6 - I
5.2 The year to date expenditure is £36.5m, £15.9m behind the plan of £52.5m.
5.3 The forecast outturn has increased from £57.6m reported last month to £62.5m, this increase is in support of the Somerset System as a whole as well as the newly awarded bids and has enabled the acceleration of a number of schemes into this financial year that would otherwise have fallen into 2022/23. Significant efforts are being made to ensure the full capital envelope is utilised in year.
5.4 A summary by scheme is set out in the table below:-
Table 3: 2021/22 Capital Programme
Sources of FundingPlan
£000
Depreciation 21,900
Use of Cash resources 7,067
Grants and donations 1,705
PDC 35,375
Capital Loan funding - received and paid (848)
Finance Leases (832)
Capital Repayment (1,920)
PFI MES Funded IFRIC 12 860
Total sources of funding 63,307
Acute Programme Plan
£000
Revised Plan
£000
YTD Plan
£000
YTD Actual
£000
Variance v
plan
£000 FOT
Site Risks / Plant & Equipment 450 450 328 145 (183) 285
Site and Service Development 4,578 4,338 3,621 4,075 454 5,930
Total Acute 5,028 4,788 3,949 4,220 271 6,215
Community/Mental Health Programme
Site Risks / Plant & Equipment 600 600 521 57 (464) 438
Site and Service Development 6,818 6,798 5,661 3,987 (1,587) 6,047
Total Community/Mental Health 7,418 7,398 6,182 4,044 (2,051) 6,485
Trustwide
Plan
£000
YTD Plan
£000
YTD Actual
£000
Variance
£000
Site Risks / Plant & Equipment 8,305 9,298 6,896 5,502 (1,394) 9,925
Site and Service Development 4,116 3,883 2,985 2,020 (965) 4,242
Trustwide 12,421 13,181 9,881 7,522 (2,359) 14,167
Total Internal Capital Envelope 24,867 25,367 20,012 15,786 (4,139) 26,867
Additional Capital Schemes
Plan
£000
YTD Plan
£000
YTD Actual
£000
Variance
£000
STP 3 - Surgical Centre 17,305 17,305 16,123 11,621 (4,502) 16,096
STP Wave 4 - AAH 7,108 7,108 6,681 5,745 (936) 6,108
NHP 9,000 1,900 7,261 1,256 (6,005) 1,900
Diagnostic Imaging/Community Investigate 0 4,065 0 180 180 4,065
TiF Theatre Efficiency and Max Fax, Plastics Dental 0 1,690 0 0 - 1,690
TiF Digital Transformation 0 2,600 0 0 - 2,600
Shared Care Record 0 51 0 0 - 265
Cyber Security 0 250 0 0 - 250
Digital Maternity 0 336 0 0 0 336
Wessex House 0 70 0 0 - 70
Learning Academy Expansion DONATED 1,000 1,000 1,000 1,000 - 1,000
PFI MES Funded IFRIC 12 860 860 900 487 (413) 860
DONATED 705 705 546 412 (134) 412
Total Additional Schemes 35,978 37,940 32,511 20,703 (11,808) 35,653
TOTAL TRUST PROGRAMME 60,845 63,307 52,523 36,489 (15,947) 62,520
6. OUTTURN
6.1 Operational pressures continue to create additional financial pressure on the Trust as escalation measures continue to be in place to manage demand. Although the Omicron impact was not as extensive as initially feared, the
SFT Finance Report March 2022 Public Board - 7 - I
ongoing pressures within the urgent care system, high occupancy and ED attendances continue to place huge pressure on Trust services.
6.2 It is anticipated that we can continue to manage the resultant financial impact of these operational pressures within the overall funding envelope available and we remain on track to deliver a balanced H2 position in line with the plan.
7. RECOMMENDATION
7.1 The Board is requested to note the financial performance for the month ending 31 January 2022.
CHIEF FINANCE OFFICER
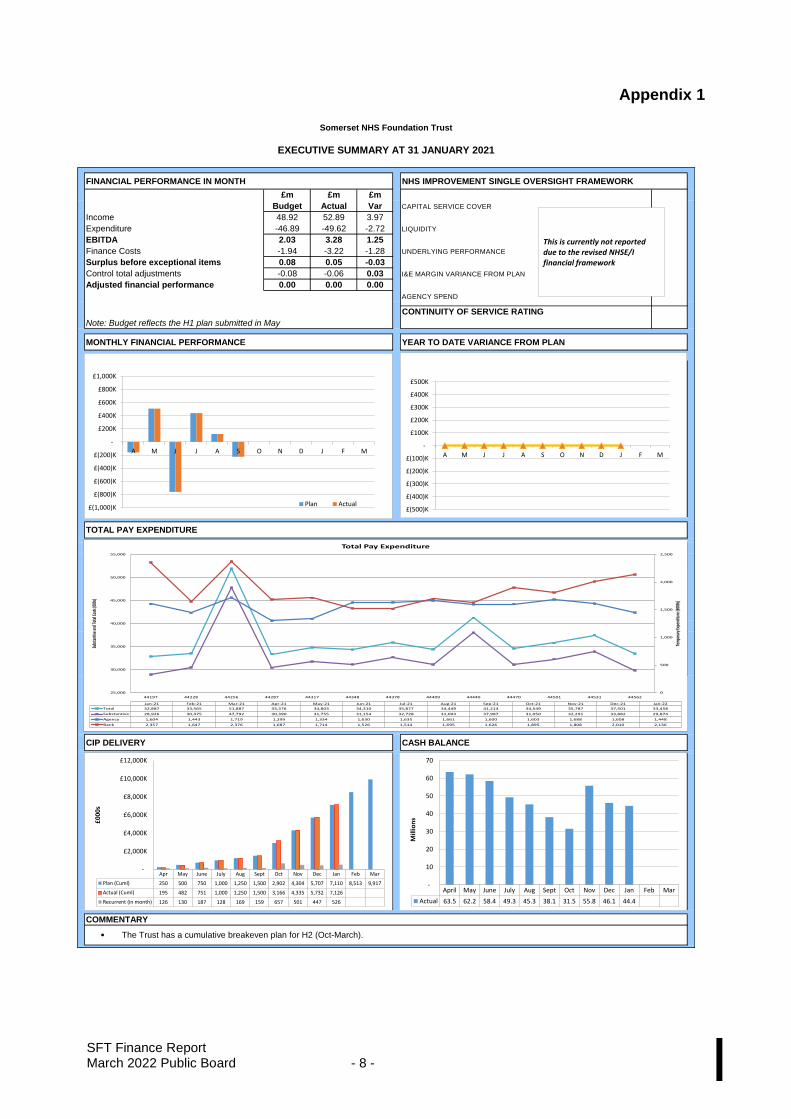
SFT Finance Report March 2022 Public Board - 8 - I
Appendix 1
FINANCIAL PERFORMANCE IN MONTH NHS IMPROVEMENT SINGLE OVERSIGHT FRAMEWORK
£m £m £m
Budget Actual Var CAPITAL SERVICE COVER
Income 48.92 52.89 3.97
Expenditure -46.89 -49.62 -2.72 LIQUIDITY
EBITDA 2.03 3.28 1.25
Finance Costs -1.94 -3.22 -1.28 UNDERLYING PERFORMANCE
Surplus before exceptional items 0.08 0.05 -0.03
Control total adjustments -0.08 -0.06 0.03 I&E MARGIN VARIANCE FROM PLAN
Adjusted financial performance 0.00 0.00 0.00
AGENCY SPEND
CONTINUITY OF SERVICE RATING
MONTHLY FINANCIAL PERFORMANCE YEAR TO DATE VARIANCE FROM PLAN
`
`
305023.8
CIP DELIVERY CASH BALANCE
COMMENTARY
.
Somerset NHS Foundation Trust
EXECUTIVE SUMMARY AT 31 JANUARY 2021
Note: Budget reflects the H1 plan submitted in May
TOTAL PAY EXPENDITURE
The Trust has a cumulative breakeven plan for H2 (Oct-March).
£(500)K
£(400)K
£(300)K
£(200)K
£(100)K
-
£100K
£200K
£300K
£400K
£500K
A M J J A S O N D J F M
£(1,000)K
£(800)K
£(600)K
£(400)K
£(200)K
-
£200K
£400K
£600K
£800K
£1,000K
A M J J A S O N D J F M
Plan Actual
April May June July Aug Sept Oct Nov Dec Jan Feb Mar
Actual 63.5 62.2 58.4 49.3 45.3 38.1 31.5 55.8 46.1 44.4
-
10
20
30
40
50
60
70
Mill
ion
s
This is currently not reported due to the revised NHSE/I financial framework
Apr May June July Aug Sept Oct Nov Dec Jan Feb Mar
Plan (Cuml) 250 500 750 1,000 1,250 1,500 2,902 4,304 5,707 7,110 8,513 9,917
Actual (Cuml) 195 482 751 1,000 1,250 1,500 3,166 4,335 5,732 7,126
Recurrent (in month) 126 130 187 128 169 159 657 501 447 526
-
£2,000K
£4,000K
£6,000K
£8,000K
£10,000K
£12,000K
£0
00
s
0
500
1,000
1,500
2,000
2,500
25,000
30,000
35,000
40,000
45,000
50,000
55,000
44197 44228 44256 44287 44317 44348 44378 44409 44440 44470 44501 44531 44562
Tem
pora
ry Ex
pend
iture
(£00
0s)
Subs
tant
ive an
d Tot
al Co
sts (0
00s)
Jan-21 Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22
Total 32,887 33,565 51,887 33,376 34,803 34,310 35,877 34,449 41,214 34,549 35,787 37,501 33,458
Substantive 28,926 30,475 47,792 30,390 31,755 31,154 32,728 31,093 37,987 31,050 32,291 33,882 29,874
Agency 1,604 1,443 1,719 1,299 1,334 1,630 1,635 1,661 1,600 1,603 1,688 1,608 1,448
Bank 2,357 1,647 2,376 1,687 1,714 1,526 1,514 1,695 1,626 1,895 1,808 2,010 2,136
Total Pay Expenditure
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 1 – J
Somerset NHS Foundation Trust
REPORT TO: The Trust Board
REPORT TITLE: Minehead Minor Injury Unit permanent change to opening times
SPONSORING EXEC:
Matthew Bryant, Chief Operating Officer – Hospital Services
Phil Brice, Director of Corporate Services
REPORT BY: Deirdre Molloy, Service Manager Urgent and Emergency Care
PRESENTED BY: Deirdre Molloy, Service Manager Urgent and Emergency Care
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☐ For Assurance/
Discussion ☒ For Approval / Decision ☐ For Information
Executive Summary and Reason for presentation to Committee/Board
Minehead Minor Injury Unit (MIU) has been temporarily closed during the night-time hours of 9pm – 8am for 4 months to investigate safety concerns that had been raised. During this time a review of the impact on the night- time closure was undertaken and included engagement with the public, staff and wider stakeholders. The findings of the review were reported to the SFT Trust board in November 2021 where a further extension to the night-time closure of MIU was approved to provide additional time to address the reports recommendations. In response to the identified need for improved access to same day urgent and emergency care services steps have been taken to bring all organisations together to determine a future urgent care model for Minehead and West Somerset area with Somerset CCG taking the lead. Since November, a task & finish group has been formed with meetings have been held with the stakeholder group extending to include local council and transport services. As per report recommendations a communications campaign has been undertaken with the Trust
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 2 – J
communications team working closely with the CCG. This is building on the current health messages and Choose Well campaign. Minehead MIU continues to provide a service between 8am and 9pm supporting the daytime activity and demand. During the agreed extension the impact of the night-time closure has continued to be monitored. There has been no further serious safety incidents associated with the night- time closure and there has been no discernible impact noted at Minehead MIU or across other healthcare services during this time. Somerset NHS FT has not been made aware of any significant adverse incidents as a result of the service not being available overnight during this period.
Recommendation • It is recommended that the temporary closure of Minehead MIU overnight is made permanent reducing the service provision from 24 hours to the new opening time of 8am – 9pm This change will align Minehead MIU with all similar and larger sized MIUs provided by Somerset Foundation Trust.
• The MIU service is required as a daytime service 7 days a week, where there is a significant demand for the treatment of minor injuries and common minor illness from both the local population and holidaymakers.
• Somerset CCG will continue to progress the development of an urgent care model that best addresses the urgent and emergency care needs of the local population of Minehead and West Somerset with partnership working across all health care providers. The development of this model will be informed by a further programme of patient and public engagement to ensure it takes into account the widest possible range of views on the needs of the local population
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☐ Care for our Population ☐ Develop our People
☐ Innovate and Collaborate ☐ Develop a Sustainable System
Somerset NHS FT
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 3 – J
☐ Obj 1 Inclusive culture ☐ Obj 4 Safe services ☐ Obj 7 Improving outcomes
☐ Obj 2 Collaboration ☐ Obj 5 Self management ☐ Obj 8 Workforce
☐ Obj 3 Independent lives ☐ Obj 6 Value all people
alike ☐ Obj 9 Performance
☐ Obj 10 Finance
Implications/Requirements (Please select any which are relevant to this paper)
☐ Financial ☐
Legislation ☒ Workforce ☐ Estates ☐ ICT
☐ Patient Safety /
Quality
Details:
Equality
The Trust wants its services to be as accessible as possible, to as many people as possible. Please indicate whether the report has an impact on the protected
characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are no proposals or matters which affect any persons with protected characteristics
☒ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities.
A copy of the Equality Impact Assessment is appended to the report.
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
During the period of the temporary closure, the Trust undertook colleague engagement and patient and public engagement, a copy of the report from which is appended to the report.
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
An update was provided to the February 2022 Part 2 Board meeting.
Reference to CQC domains (Please select any which are relevant to this paper)
☒ Safe ☒ Effective ☒ Caring ☒ Responsive ☐ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 4 – J
SOMERSET NHS FOUNDATION TRUST
MINEHEAD MINOR INJURY UNIT CHANGE OF OPENING TIMES (From 24-hour service to an 8am – 9pm service – aligned with all other Trust MIU
opening times)
1. BACKGROUND AND PURPOSE 1.1 Somerset NHS Foundation Trust (SFT) temporarily closed Minehead
Minor Injury Unit (MIU) overnight in July 2021 in response to concerns about the safety of the service. During this time the Trust reviewed the MIU service and worked with partners, patients, and public representatives to look at how we address these safety concerns, quantify, and meet the overnight needs of the local area within our available resources, and propose a way forward that is safe, sustainable, and operationally robust.
1.2 A report outlining the findings of the review and engagement undertaken
was presented to Trust board in November 2021. The report concluded that there were no significant safety risks identified following the closure of the MIU and no discernible impact on the surrounding healthcare services that could have been more appropriately managed had the MIU been opened at night.
1.3 The report highlighted that the local public had concerns about access to
urgent and emergency care as a whole in both Minehead and the West Somerset area with concerns identified in primary care provision, 999 ambulance and 111 responsiveness. Many respondents to the engagement exercise felt that the MIU acted as a ‘safety net’ for the local population in the event of urgent and emergency healthcare need. However, the report concluded that the role of any MIU could not deliver the level of urgent and emergency care as described i.e., ‘safety net’, “local Accident & Emergency service” and would attribute further safety concerns for the Trust.
1.4 Further recommendations were proposed to address the concerns
highlighted in the report approved by the Trust board to support final decision making. This included:
• Continued monitoring of impact of temporary closure of MIU overnight service on both the community and surrounding healthcare services.
• Somerset NHS Foundation Trust, local GPs, SWAST and Somerset CCG to work together to agree a model that will best respond to the urgent and emergency health care needs of the local population.
• A communication campaign was also supported to reinforce the role and service available within the MIU and how it differs to that of an Emergency Department.
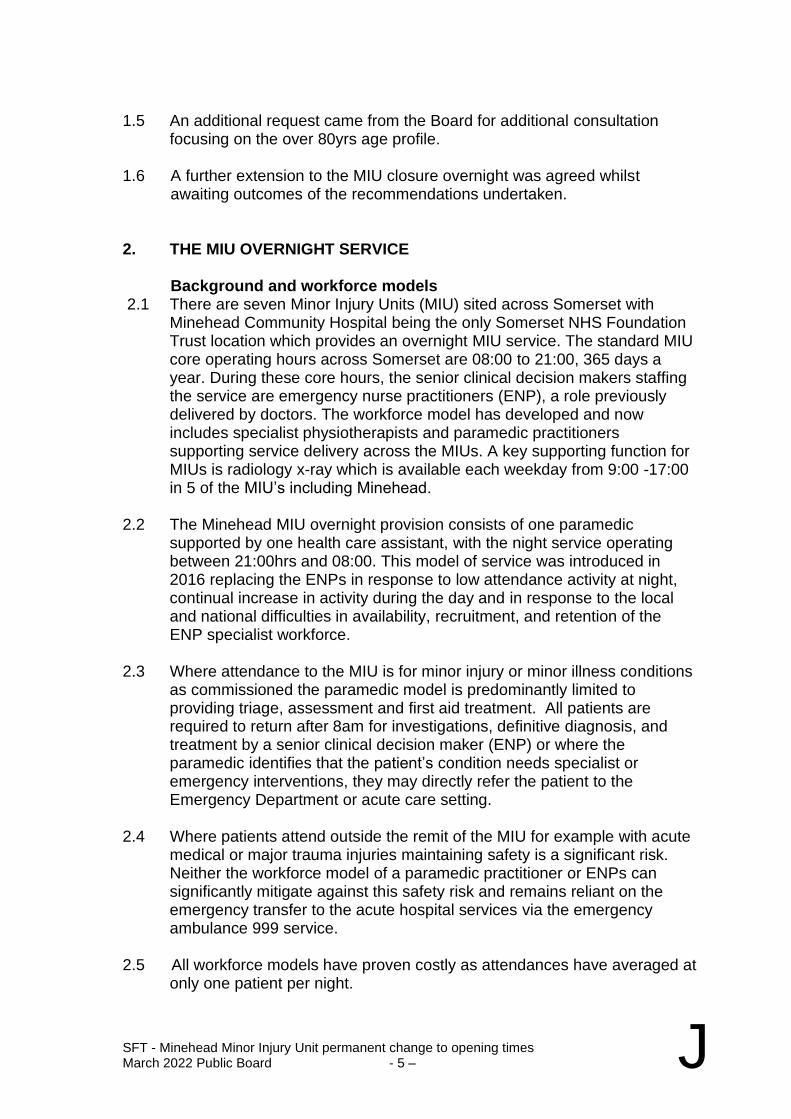
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 5 – J
1.5 An additional request came from the Board for additional consultation
focusing on the over 80yrs age profile.
1.6 A further extension to the MIU closure overnight was agreed whilst awaiting outcomes of the recommendations undertaken.
2. THE MIU OVERNIGHT SERVICE Background and workforce models 2.1 There are seven Minor Injury Units (MIU) sited across Somerset with
Minehead Community Hospital being the only Somerset NHS Foundation Trust location which provides an overnight MIU service. The standard MIU core operating hours across Somerset are 08:00 to 21:00, 365 days a year. During these core hours, the senior clinical decision makers staffing the service are emergency nurse practitioners (ENP), a role previously delivered by doctors. The workforce model has developed and now includes specialist physiotherapists and paramedic practitioners supporting service delivery across the MIUs. A key supporting function for MIUs is radiology x-ray which is available each weekday from 9:00 -17:00 in 5 of the MIU’s including Minehead.
2.2 The Minehead MIU overnight provision consists of one paramedic
supported by one health care assistant, with the night service operating between 21:00hrs and 08:00. This model of service was introduced in 2016 replacing the ENPs in response to low attendance activity at night, continual increase in activity during the day and in response to the local and national difficulties in availability, recruitment, and retention of the ENP specialist workforce.
2.3 Where attendance to the MIU is for minor injury or minor illness conditions
as commissioned the paramedic model is predominantly limited to providing triage, assessment and first aid treatment. All patients are required to return after 8am for investigations, definitive diagnosis, and treatment by a senior clinical decision maker (ENP) or where the paramedic identifies that the patient’s condition needs specialist or emergency interventions, they may directly refer the patient to the Emergency Department or acute care setting.
2.4 Where patients attend outside the remit of the MIU for example with acute
medical or major trauma injuries maintaining safety is a significant risk. Neither the workforce model of a paramedic practitioner or ENPs can significantly mitigate against this safety risk and remains reliant on the emergency transfer to the acute hospital services via the emergency ambulance 999 service.
2.5 All workforce models have proven costly as attendances have averaged at
only one patient per night.
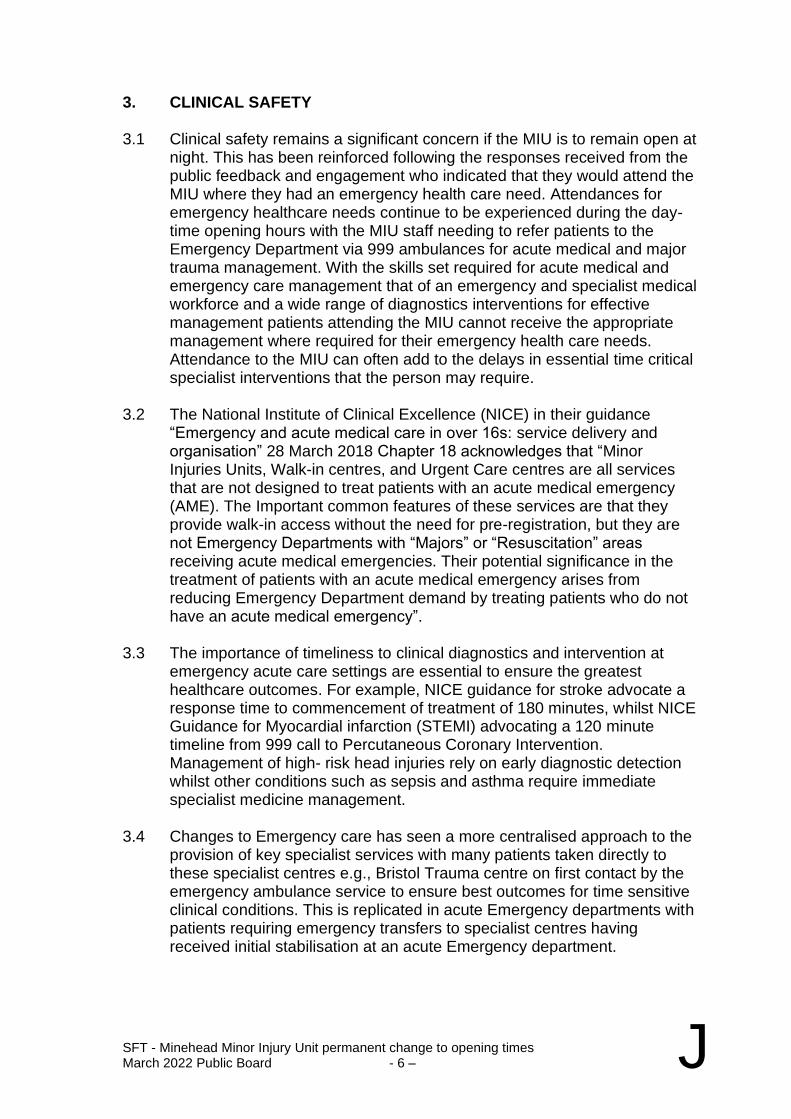
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 6 – J
3. CLINICAL SAFETY
3.1 Clinical safety remains a significant concern if the MIU is to remain open at night. This has been reinforced following the responses received from the public feedback and engagement who indicated that they would attend the MIU where they had an emergency health care need. Attendances for emergency healthcare needs continue to be experienced during the day- time opening hours with the MIU staff needing to refer patients to the Emergency Department via 999 ambulances for acute medical and major trauma management. With the skills set required for acute medical and emergency care management that of an emergency and specialist medical workforce and a wide range of diagnostics interventions for effective management patients attending the MIU cannot receive the appropriate management where required for their emergency health care needs. Attendance to the MIU can often add to the delays in essential time critical specialist interventions that the person may require.
3.2 The National Institute of Clinical Excellence (NICE) in their guidance “Emergency and acute medical care in over 16s: service delivery and organisation” 28 March 2018 Chapter 18 acknowledges that “Minor Injuries Units, Walk-in centres, and Urgent Care centres are all services that are not designed to treat patients with an acute medical emergency (AME). The Important common features of these services are that they provide walk-in access without the need for pre-registration, but they are not Emergency Departments with “Majors” or “Resuscitation” areas receiving acute medical emergencies. Their potential significance in the treatment of patients with an acute medical emergency arises from reducing Emergency Department demand by treating patients who do not have an acute medical emergency”.
3.3 The importance of timeliness to clinical diagnostics and intervention at emergency acute care settings are essential to ensure the greatest healthcare outcomes. For example, NICE guidance for stroke advocate a response time to commencement of treatment of 180 minutes, whilst NICE Guidance for Myocardial infarction (STEMI) advocating a 120 minute timeline from 999 call to Percutaneous Coronary Intervention. Management of high- risk head injuries rely on early diagnostic detection whilst other conditions such as sepsis and asthma require immediate specialist medicine management.
3.4 Changes to Emergency care has seen a more centralised approach to the provision of key specialist services with many patients taken directly to these specialist centres e.g., Bristol Trauma centre on first contact by the emergency ambulance service to ensure best outcomes for time sensitive clinical conditions. This is replicated in acute Emergency departments with patients requiring emergency transfers to specialist centres having received initial stabilisation at an acute Emergency department.
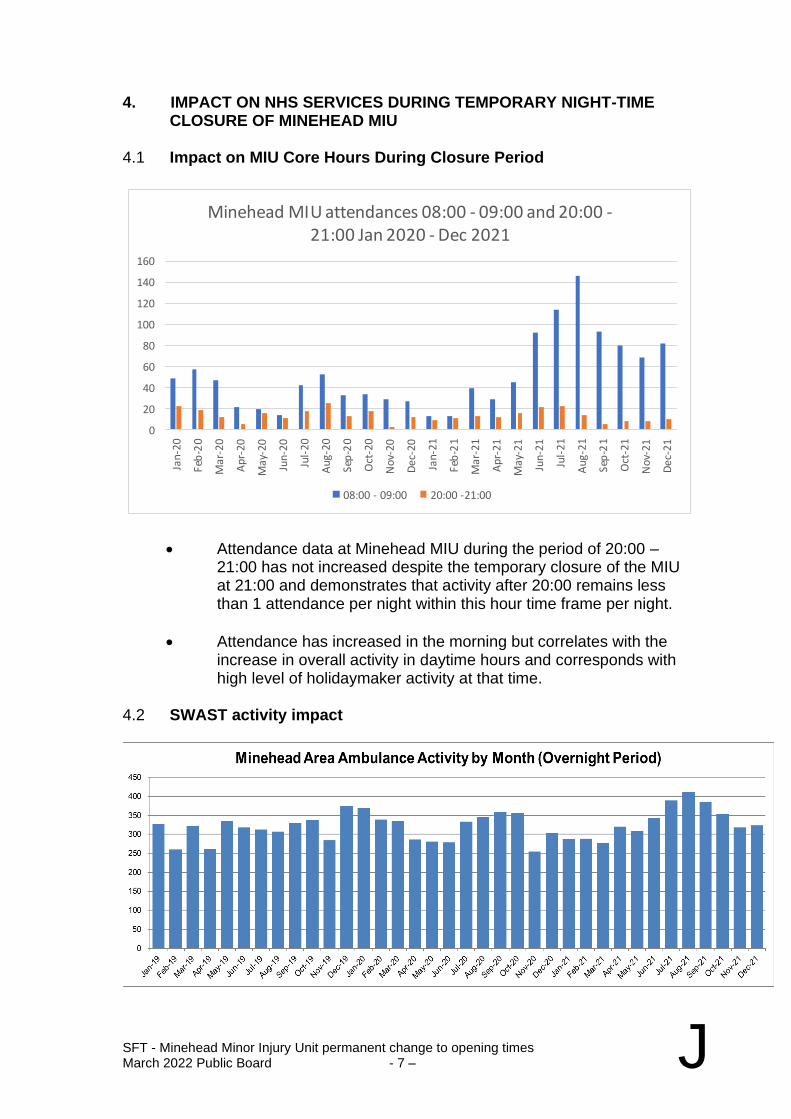
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 7 – J
4. IMPACT ON NHS SERVICES DURING TEMPORARY NIGHT-TIME CLOSURE OF MINEHEAD MIU
4.1 Impact on MIU Core Hours During Closure Period
0
20
40
60
80
100
120
140
160
Jan
-20
Feb
-20
Mar
-20
Ap
r-2
0
May
-20
Jun
-20
Jul-
20
Au
g-2
0
Sep
-20
Oct
-20
Nov
-20
Dec
-20
Jan
-21
Feb
-21
Mar
-21
Ap
r-2
1
May
-21
Jun
-21
Jul-
21
Au
g-2
1
Sep
-21
Oct
-21
Nov
-21
Dec
-21
Minehead MIU attendances 08:00 - 09:00 and 20:00 -21:00 Jan 2020 - Dec 2021
08:00 - 09:00 20:00 -21:00
• Attendance data at Minehead MIU during the period of 20:00 – 21:00 has not increased despite the temporary closure of the MIU at 21:00 and demonstrates that activity after 20:00 remains less than 1 attendance per night within this hour time frame per night.
• Attendance has increased in the morning but correlates with the increase in overall activity in daytime hours and corresponds with high level of holidaymaker activity at that time.
4.2 SWAST activity impact
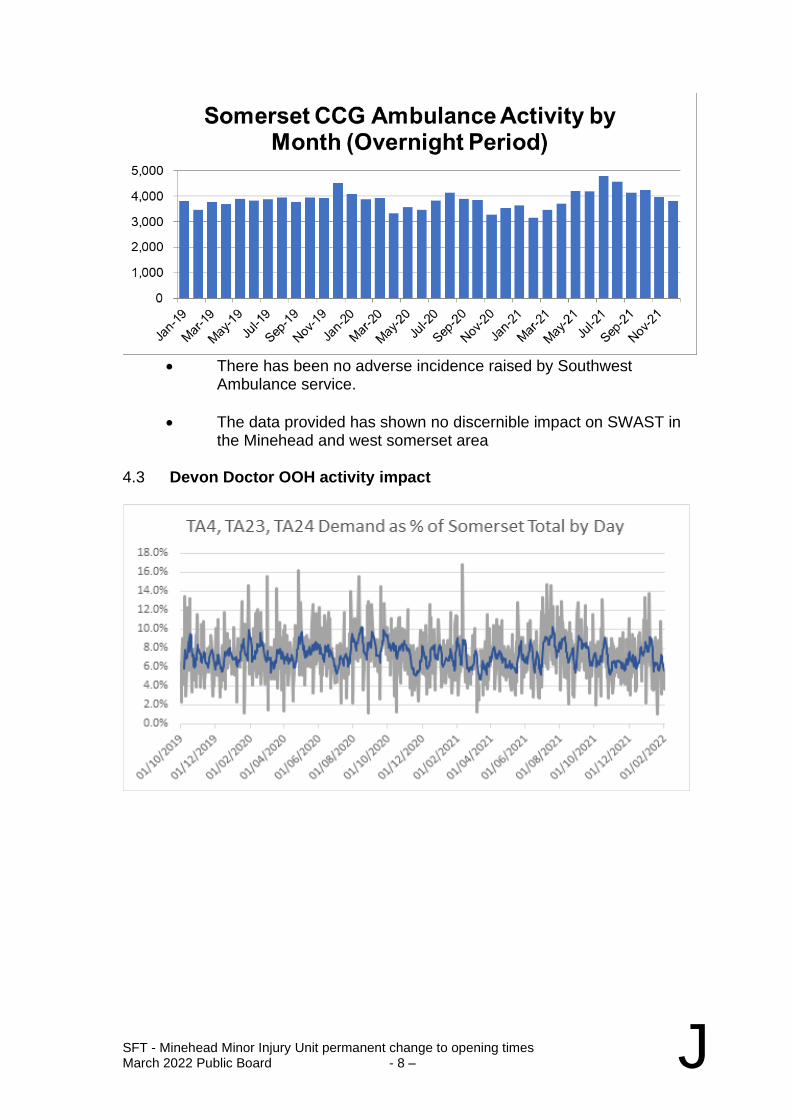
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 8 – J
• There has been no adverse incidence raised by Southwest
Ambulance service.
• The data provided has shown no discernible impact on SWAST in the Minehead and west somerset area
4.3 Devon Doctor OOH activity impact
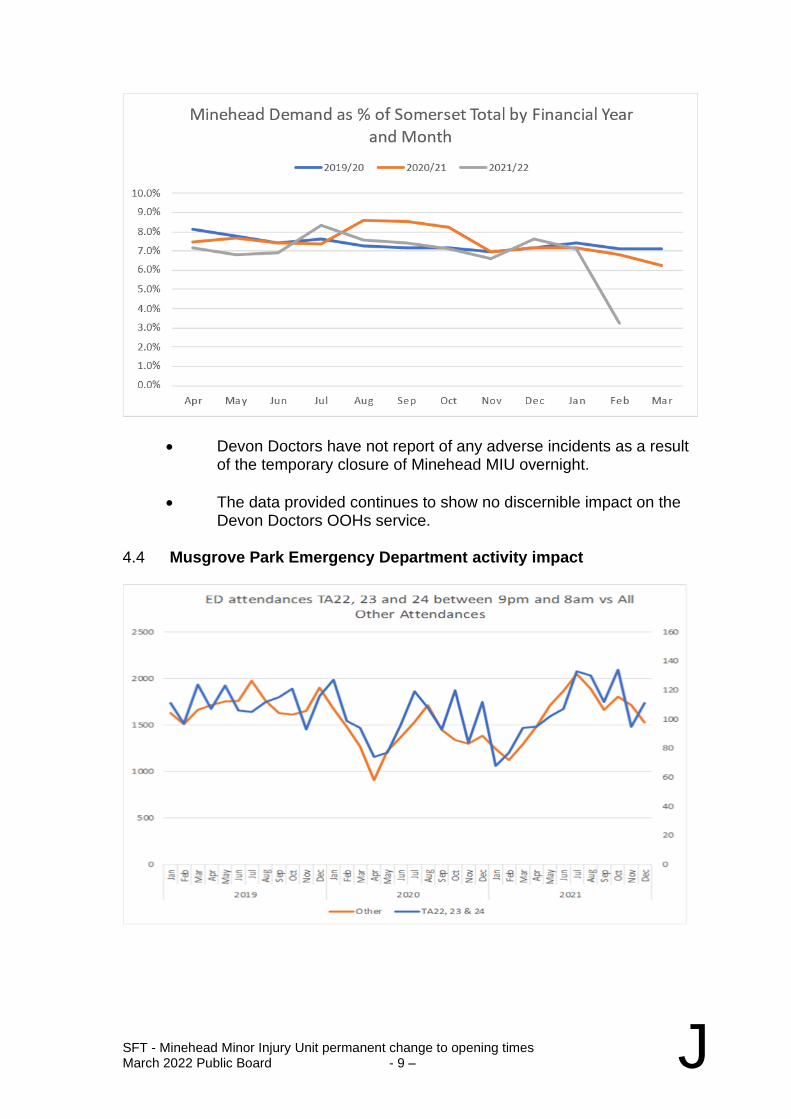
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 9 – J
• Devon Doctors have not report of any adverse incidents as a result of the temporary closure of Minehead MIU overnight.
• The data provided continues to show no discernible impact on the Devon Doctors OOHs service.
4.4 Musgrove Park Emergency Department activity impact
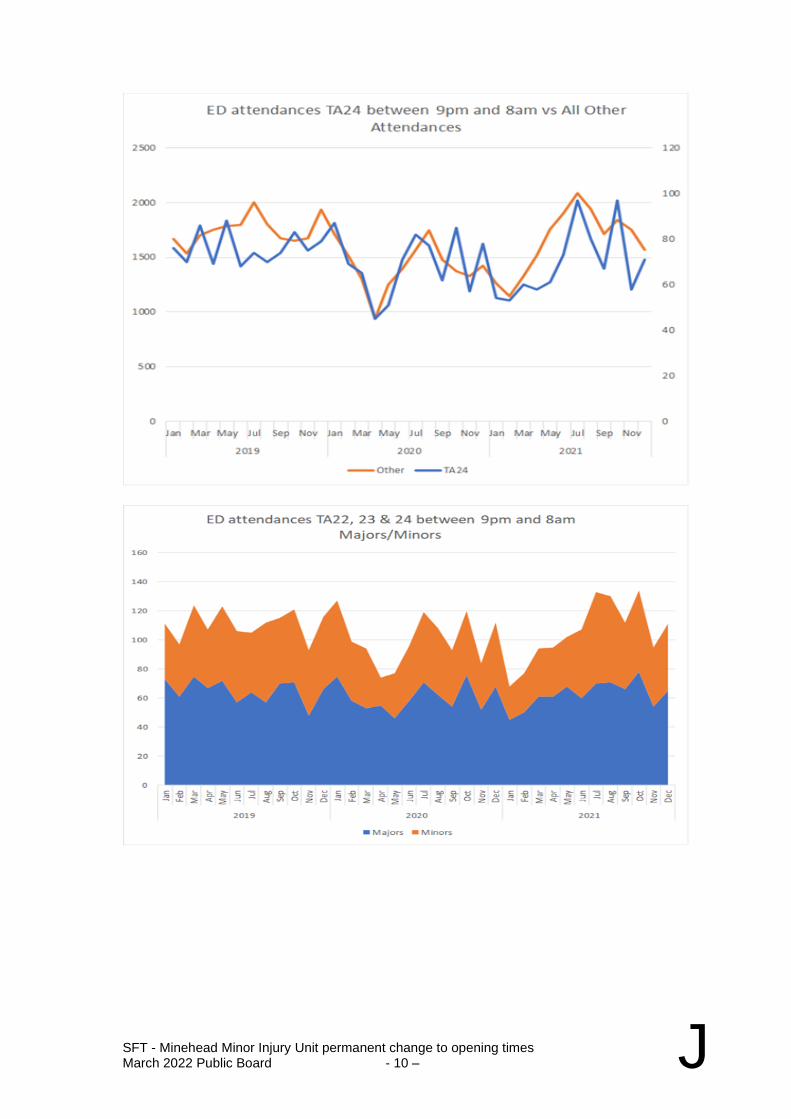
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 10 – J
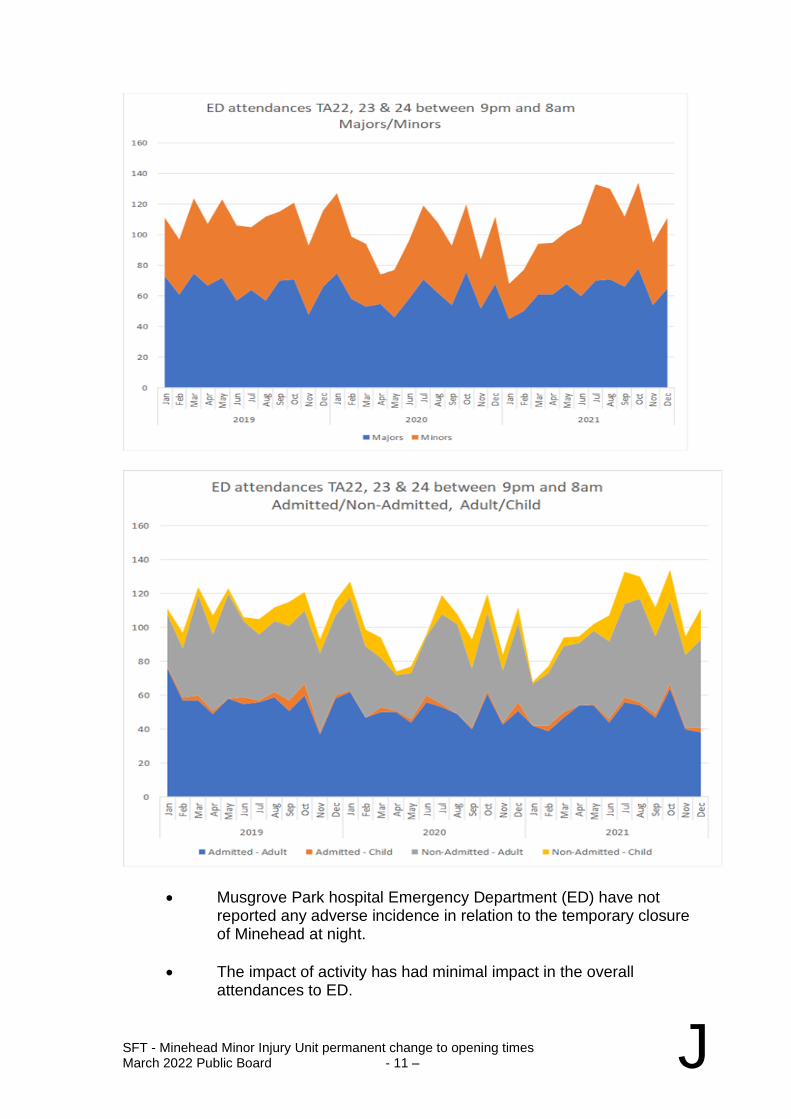
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 11 – J
• Musgrove Park hospital Emergency Department (ED) have not reported any adverse incidence in relation to the temporary closure of Minehead at night.
• The impact of activity has had minimal impact in the overall attendances to ED.
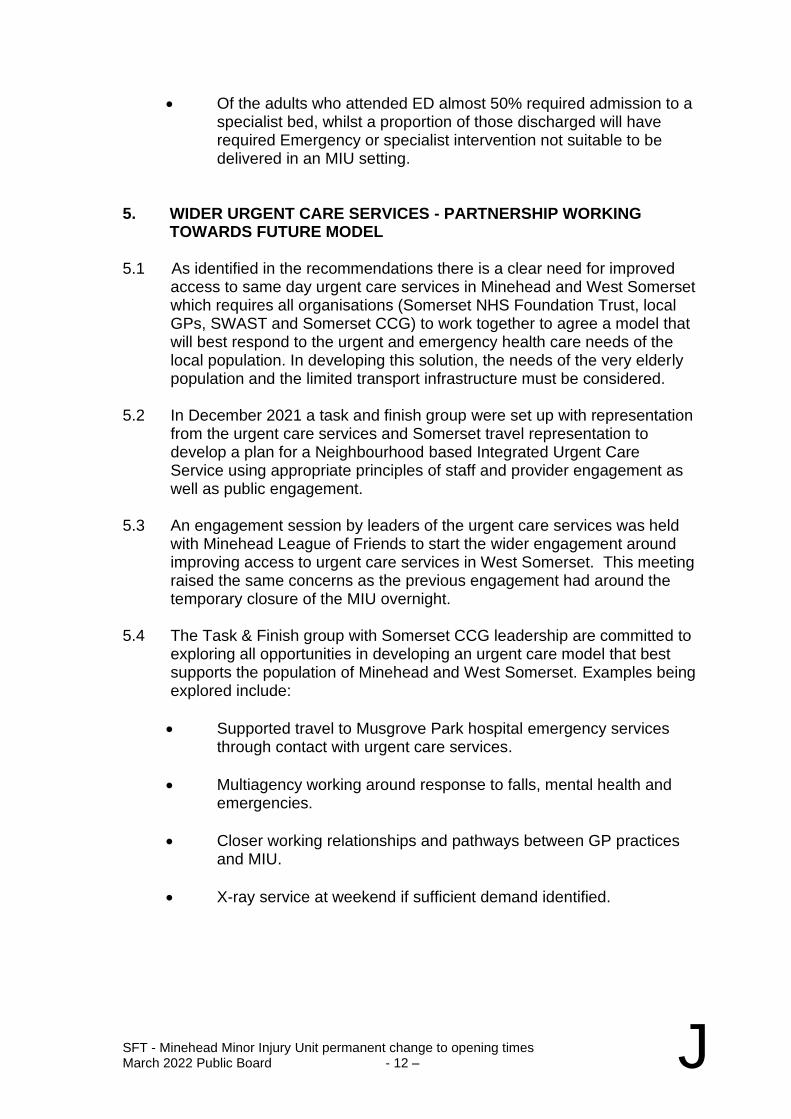
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 12 – J
• Of the adults who attended ED almost 50% required admission to a specialist bed, whilst a proportion of those discharged will have required Emergency or specialist intervention not suitable to be delivered in an MIU setting.
5. WIDER URGENT CARE SERVICES - PARTNERSHIP WORKING
TOWARDS FUTURE MODEL 5.1 As identified in the recommendations there is a clear need for improved
access to same day urgent care services in Minehead and West Somerset which requires all organisations (Somerset NHS Foundation Trust, local GPs, SWAST and Somerset CCG) to work together to agree a model that will best respond to the urgent and emergency health care needs of the local population. In developing this solution, the needs of the very elderly population and the limited transport infrastructure must be considered.
5.2 In December 2021 a task and finish group were set up with representation
from the urgent care services and Somerset travel representation to develop a plan for a Neighbourhood based Integrated Urgent Care Service using appropriate principles of staff and provider engagement as well as public engagement.
5.3 An engagement session by leaders of the urgent care services was held
with Minehead League of Friends to start the wider engagement around improving access to urgent care services in West Somerset. This meeting raised the same concerns as the previous engagement had around the temporary closure of the MIU overnight.
5.4 The Task & Finish group with Somerset CCG leadership are committed to
exploring all opportunities in developing an urgent care model that best supports the population of Minehead and West Somerset. Examples being explored include:
• Supported travel to Musgrove Park hospital emergency services through contact with urgent care services.
• Multiagency working around response to falls, mental health and emergencies.
• Closer working relationships and pathways between GP practices and MIU.
• X-ray service at weekend if sufficient demand identified.
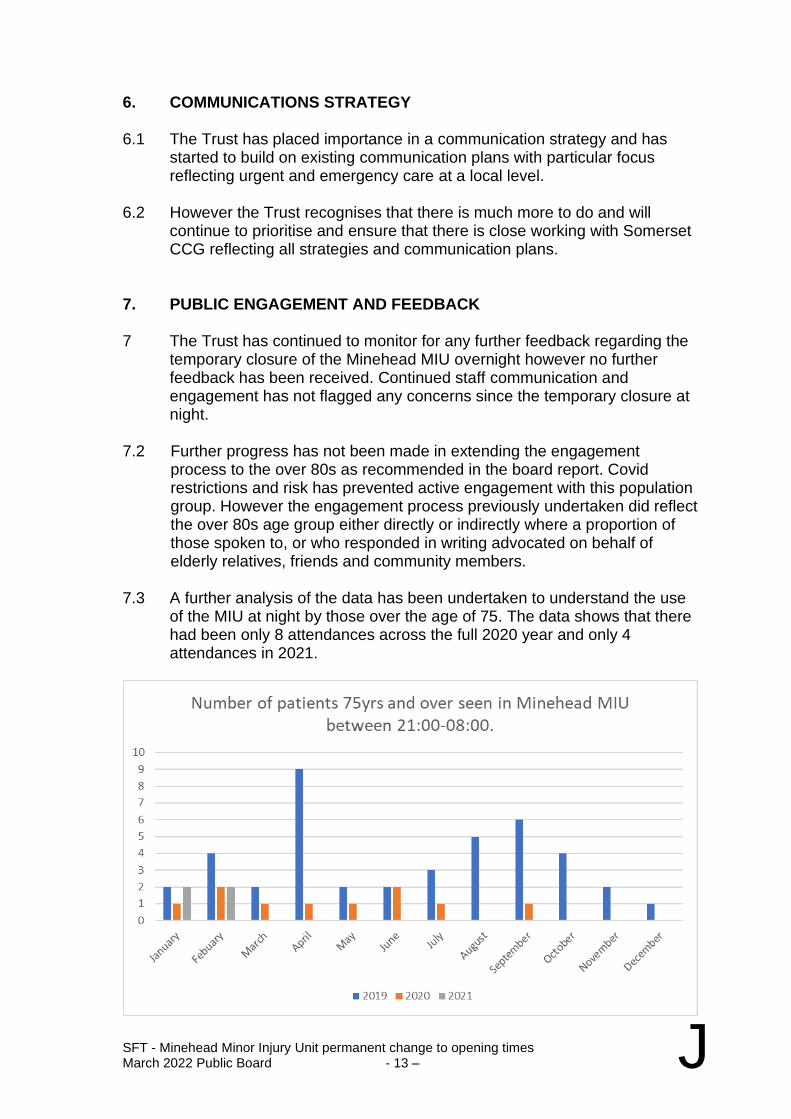
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 13 – J
6. COMMUNICATIONS STRATEGY 6.1 The Trust has placed importance in a communication strategy and has
started to build on existing communication plans with particular focus reflecting urgent and emergency care at a local level.
6.2 However the Trust recognises that there is much more to do and will
continue to prioritise and ensure that there is close working with Somerset CCG reflecting all strategies and communication plans.
7. PUBLIC ENGAGEMENT AND FEEDBACK 7 The Trust has continued to monitor for any further feedback regarding the
temporary closure of the Minehead MIU overnight however no further feedback has been received. Continued staff communication and engagement has not flagged any concerns since the temporary closure at night.
7.2 Further progress has not been made in extending the engagement process to the over 80s as recommended in the board report. Covid restrictions and risk has prevented active engagement with this population group. However the engagement process previously undertaken did reflect the over 80s age group either directly or indirectly where a proportion of those spoken to, or who responded in writing advocated on behalf of elderly relatives, friends and community members. 7.3 A further analysis of the data has been undertaken to understand the use
of the MIU at night by those over the age of 75. The data shows that there had been only 8 attendances across the full 2020 year and only 4 attendances in 2021.
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 14 – J
8. CONCLUSIONS
8.1 The current model of a Paramedic and HCA overnight in Minehead MIU presents a number of clinical safety concerns. These concerns have been reinforced based on the feedback from the public with many seeing the MIU as a “safety net” were they to have the misfortune to experience an emergency care need. Continued emergency attendances to the MIU during the day reaffirms this safety concern and risk.
8.2 To resource the MIU service to an appropriate level would mean replacing
the current model with at minimum of 2 ENPs and a receptionist. Unfortunately, the limited availability of trained ENP workforce and an increasing market for this specialist workforce means recruitment and retention of appropriately qualified ENPs remains very difficult both locally and nationally. Adhoc closures due to workforce constraints will remain an issue creating further safety risk.
8.3 It is evident that the MIU service in Minehead Community Hospital is well
used during day- time hours and is respected and valued by those in the local community. Activity reduces significantly to slightly less than 1 patient per night between 8pm and 9pm and further reduces to less that 1 person overnight between the hours of 9pm and 8am.
8.4 Temporary closure of the MIU overnight has had no discernible impact on
other healthcare services and providers with no significant incidents or risks reported.
8.5 Somerset CCG in partnership with urgent and emergency health care
providers have formed a task and finish group and are progressing in developing plans of an urgent care model that reflects the needs of the population of Minehead and West Somerset.
9. RECOMMENDATION 9.1 It is recommended that the temporary closure of Minehead MIU overnight
is made permanent reducing the service provision from 24 hours to the new opening time of 8am – 9pm This change will align Minehead MIU with all similar and larger sized MIUs provided by Somerset Foundation Trust.
9.2 The MIU service is required as a daytime service 7 days a week, where
there is a significant demand for the treatment of minor injuries and common minor illness from both the local population and holidaymakers.
9.3 Somerset CCG continue to progress the development of an urgent care
model that best addresses the urgent and emergency care needs of the local population of Minehead and West Somerset with partnership working across all health care providers. The development of this model will be informed by a further programme of patient and public engagement to ensure it takes into account the widest possible range of views on the needs of the local population

SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 15 – J
9.4 The Board is asked to discuss and approve the above recommendations.

SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 16 – J
Appendices
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 17 – J
Appendix 1 – Engagement Report
Patient and Public Engagement Report
September 2021
Minehead Minor Injury Unit (MIU) Overnight Service
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 18 – J
CONTENTS
1. Introduction and Methodology
2. Summary of Key Themes
3. Other Feedback, Email, Care Opinion
4. Conclusions
5. Recommendations
Appendix 1 Survey form
Appendix 2 Detailed Survey Findings
Appendix 3 Canvassing event comments

SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 19 – J
1. INTRODUCTION AND METHODOLOGY
Introduction
Somerset NHS Foundation Trust temporarily closed Minehead Minor Injury Unit (MIU) overnight from 9pm until 8am for four months from Thursday 1 July following concerns about the safety of the overnight service. The service continues to remain open from 8am – 9pm, seven days a week. During this period the Trust is monitoring the impact of the temporary closure, reviewing the service and working with partners and public representatives to look at how it can address the safety concerns, quantify and meet the overnight needs of the local area within available resources, and propose a way forward that is both safe and operationally robust. During August and September 2021, we sought views of local patients and the public on their experiences of using the MIU overnight; their expectations of the service and any concerns they had about the unavailability of the MIU overnight. Our figures show that while the MIU provides a well-used service during the day with an average of 32 patients per day pre pandemic, it is used much less overnight with less than one patient a night (0.9) seen by the overnight service on average over the last 3 years. Nevertheless, we want to understand people’s use of the service, what alternatives they would use overnight and to understand any concerns they have. This report provides an overview of the public engagement undertaken by the Trust and outlines the key themes of the feedback provided by the public in Minehead and the wider community.
Methodology
The engagement including a survey was publicised through local press, Somerset Foundation Trust public website, social media including local social media groups with promotions, advertisement within Minehead hospital. The public in Minehead town centre were canvassed for their views over 4 sessions during August and September. In the first week it was more difficult to speak to local people as there were still many holidaymakers around but during week 2 many more locals were willing to share their views. Most local people were aware of the temporary closure and expressed concern, though many referred to the MIU as an ‘Accident and Emergency Department’ rather than a Minor Injury Unit. An email address was available for people to share their views. The survey questions are in Appendix 1.

SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 20 – J
A drop-in session took place every Thursday for 5 weeks for people to attend in person to share their views, this was supported by the Patient Experience team and was also advertised widely in local press, on Social media and on the Trust website.
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 21 – J
2. SUMMARY OF KEY FINDINGS
The key themes identified in the responses to our survey and the drop-in sessions were: ATTENDANCE: Of those who responded to the survey 89% had attended the MIU during daytime hours. However, 36% had never attended the MIU overnight and 31% said they had used the overnight service once in the last year. (The attendances for April to March 2020-21 seen overnight by a paramedic were 65). The majority of those who attended had used the service for acute, emergency care or for unwell children. Although many had not used the service at night, they were more reassured in the knowledge that the MIU was open overnight if they had a need for urgent or emergency health care. The majority of respondents who had attended, said they had decided themselves to attend the MIU overnight. 31% said they had been directed there by NHS 111 and 8% said they had been directed there by a pharmacy or GP. 15% said they had attended because they could not get a GP appointment. WHAT I LIKE: When asked what they liked about the MIU service, the most common reasons given were that it was “close to where I live” (85%) and that it was a “walk-in service” (72%). ALTERNATIVE SERVICES: If the overnight MIU was unavailable, half of respondents (50%) said they would have gone to A&E instead. 48% said they would contact NHS 111. 9% said they would see a GP or pharmacist in the morning and 12% would return when the MIU was open. TRAVEL: 86% of those who had attended the overnight MIU said they had travelled fewer than 10 miles. EQUALITY: When asked which people in their community a closure might affect most, the main answer given was the elderly. We did not receive any responses to the survey from people over 85. People also identified those who did not have access to a car, as public transport is very limited. CONCERNS: The overwhelming majority expressed concerns about the long distance to travel to Musgrove Park Hospital for urgent or emergency health care, with very limited public transport available in the evenings and none overnight. People also cited challenges and delays in accessing alternative services generally, including NHS 111, GP appointments and delays in ambulance responses to 999 calls.
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 22 – J
3. OTHER FEEDBACK, EMAILS, CARE OPINION
The trust received 6 emails via [email protected] and one post regarding the closure on Care Opinion. There was a mixed response via these routes but issues were raised with regard to ensuring as wide a response as possible could be achieved to understand the full impact of any changes; that the holiday season may present more need for the overnight service; and the particular issues posed by the rurality and elderly population of the West Somerset area. A sample of the feedback. "With regard to the MIU closure I would comment as follows. The closure during the evenings only affects people when they have a problem. How can anyone know when they might have a minor injury, or a minor emergency that may require attendance. Also, how can a consultation by visiting Minehead town centre on weekdays give a proper representation of need. People have changed their shopping habits, and most of the people are holiday makers. Also, where in your consultation do you consider the people who may need an MIU when on holiday? The area has a high volume of holiday makers. We need an MIU with the facilities to deal with those minor injuries. If you have a MIU surely you also need an X Ray department which is open (or at the very least on call to deal with a possible broken bone.)" Minehead resident "Thanks for the opportunity to respond in this way. I find the rationale for closing the night provision a little flawed. Having spent 43 years of my life working in our wonderful NHS which I value immensely. Much of it spent at a senior level both Executive and Non-Executive. The impact of the loss of something does not arise until it is no more! Whilst I recognise the financial pressures the NHS is constantly challenged by; it is in my opinion great Value for Money when you look at the % of GDP allocated compared to other G7 Countries and major economies throughout the World. This consultation exercise is weak in its structure and process as the people who rely on it or need it will not be walking the streets or able to get to a Portakabin to participate properly or in an informed way. I live in Minehead now and have several health challenges and I am noticing clinic services beginning to be centralised at Musgrove Hospital.
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 23 – J
It seems that and I quote “You can measure the Cost of everything but the Value of nothing. Don’t jeopardise your reputation with flawed solutions that will certainly jeopardise the health and well-being of Minehead residents and visitors in the future if you damage the service model of Minehead Community Hospital which is what you will do if you continue to constrain the services it provides to us. Please think again” Feedback received from Minehead League of Friends in a letter to Peter Lewis Chief Executive Somerset Foundation Trust expressed that “There is a good case for arguing that this area warrants a levelling UP of services, not a further reduction. Our predominantly low-income, elderly and rural communities are significantly disadvantaged when compared with the superior services available to larger town and city dwellers” “I live in Minehead and have some very robust opinions regards the current proposed strategy. I am very much for the proposals which I see as a common sense approach to ongoing national difficulties not least the serious unacceptable financial burden to the NHS…Ultimately there has to be a business case as well as one which will serve Minehead community. We must also remember that some people on Exmoor would probably be closer to Taunton than Minehead anyway!!! I know a lot about this subject both personally and as a Governor” Minehead resident and Trust Governor
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 24 – J
4. CONCLUSIONS
The engagement exercises identified some clear themes and issues in relation to the MIU and wider urgent care services in Minehead and West Somerset. It is evident that the MIU service in Minehead Community Hospital is widely respected and valued by those in the local community. The daytime service is well used and should be maintained. 1. Safety Net: The overnight service is, unsurprisingly, significantly less
well-used but often cited as a necessary ‘safety net’ for local people because of the perceived limited availability, access and responses from other health care services including primary care, NHS111 and 999 Ambulance services. This concern around all aspects of access to same day urgent care in West Somerset needs to be addressed as part of the solution to the current issues in the overnight MIU service.
2. Travel times: This position is compounded by the travel distance to the nearest Accident and Emergency which for many will be at Musgrove Park Hospital, Taunton. For those who do not have ready access to private transport, access to urgent care can only be via ambulance or taxi – which can be prohibitively expensive. Any service solution must take account of the limited transport infrastructure in West Somerset.
3. Awareness of the limitations of the overnight service: Of those who had concerns with the temporary overnight closure, few had indicated that they had required the service at night during the period of closure. Night-time usage was mainly linked to emergency conditions or unwell children. There was a common and strong perception that by attending the MIU for serious health events, such as heart attacks, strokes or with acutely ill children, especially at night, those patients would have better survival outcomes. Consideration needs to be given as to how to raise awareness of the services offered at the MIU and where people in the area can best access the services they need.
4. Equality: A variety of methods were used to support widespread engagement and feedback from the local population within Minehead and the surrounding healthcare community. Although a good response was received from the public including public representatives it is important that this number needs to be viewed in the context of the total population of Minehead and surrounding health community. The age range of responders covered a wide spectrum with exception of the over 85-year age group. However, a number of responders expressed that they were also providing responses as a voice for older relatives or indeed for those within their care e.g., nursing home providers. Consideration must be given, when determining the most effective same day urgent care services, to the needs and voice of the very elderly community in West Somerset.
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 25 – J
5. RECOMMENDATIONS
1. The MIU service is required as a daytime service 7 days a week, where
there is a significant demand for the treatment of minor injuries and common minor illness from both the local population and holidaymakers.
2. There is a need for a communication campaign to reinforce the role and
service available within the MIU during its opening hours and how it differs from an Accident and Emergency Department. This should build on the existing ‘Choose Well’ campaigns but focus on the Minehead and West Somerset areas, including particularly where contacting 999 emergency service is the most appropriate action to take and addressing the ‘safety net’ misconception identified in the engagement exercise.
3. There is a clear need for improved access to same day urgent care
services in Minehead and West Somerset which requires all organisations (Somerset NHS Foundation Trust, local GPs, SWAST and Somerset CCG) to work together to agree a model that will best respond to the urgent and emergency health care needs of the local population. In developing this solution, the needs of the very elderly population and the limited transport infrastructure must be taken into account.
4. As part of that work, any future patient and public engagement should
ensure it captures the views and voice of the very elderly, as far as possible and seek to engage with those other communities who may not have been heard in this first engagement exercise.
5. The currently configured MIU overnight service does not meet the
identified needs of the local population at night with low level attendance and reasons for attending most commonly associated with urgent and emergency healthcare needs often requiring onward referral to Taunton Musgrove Park Hospital. The need to develop a same day urgent care service that does address those needs will take time to engage agencies, stakeholders and the local community. It is recommended that the current temporary closure if extended for a further period to allow that work to take place.
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 26 – J
Appendix 1 - Survey
Minehead Overnight Minor Injuries Unit Service 21.00 - 08.00 Patient Feedback If you have used the Minehead MIU we would be grateful for your feedback For each question, please tick all that apply. This survey is anonymous. Please do not include personal information that might identify you. 1) I am a
Patient
Carer or family member of a patient
Other 2) If you selected other, please state below 3) In the last year on average, how many times have you attended the MIU during core hours? – 08.00 – 21.00
More than once a month
Between 1-4 months
Between 4-6 months
Once a year
I have never attended before 4) In the last year on average, have many times have you attended the MIU overnight? – 21.00 – 08.00
More than once a month
Between 1-4 months
Between 4-6 months
Once a year
I have never attended before If you have used the MIU overnight, please answer the following questions: 5) If you used the MIU service overnight which service directed you to attend the MIU?
Advice from NHS 111 Advice from a pharmacy Advice from a GP surgery I was unable to access an appointment with my GP I made the decision myself to attend Other
6) If you selected other, please state below
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 27 – J
7) What did you like about the overnight MIU service?
Walk-in service Close to where I live Sort waiting times Free parking Friendly, professional skilled staff Other
8) If you selected other, please state below 9) If you needed healthcare overnight and the MIU was closed what did you use?
Called NHS 111/ used NHS 111 online Waited to see a Pharmacist in the morning Waited to see a GP in the morning Attended A&E Returned to the MIU in the morning Did nothing- wait and see
10) Explain the reason for your decision- Optional
11) How far did you travel to get to the MIU
Less than 5 miles 5-9 miles 9-14 miles 14-19 miles 20-30 miles
12) Please let us know the first part of your postcode -Optional About you You do not have to answer these questions but doing so will help us ensure that our decision takes into account the different groups of people that may be affected by these proposals. This information will be used for a report called an ‘Equality Impact Assessment’. You are welcome to answer as many or as few questions as you like.
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 28 – J
13) What is your gender
Male
Female
Unspecified 14) What is your age
Under 25
24-44 years old
45-64 years old
65-84 years old
85 years or older 15) Do you feel you have been treated unfairly for any of these reasons?
A disability
Your racial or ethnic background
Your sexual orientation
Your religion
Your gender
Your age
Another reason
None of these 16) If so please tell us more
17) Are you a carer (for a relative, spouse or friend)
Yes
No
I don't know 18) Do you consider that you have a disability
Yes
No
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 29 – J
I don't know 19) If you answered yes to the above question, how would you describe your disability
Sensory
Learning
Mental Health
Physical
Other
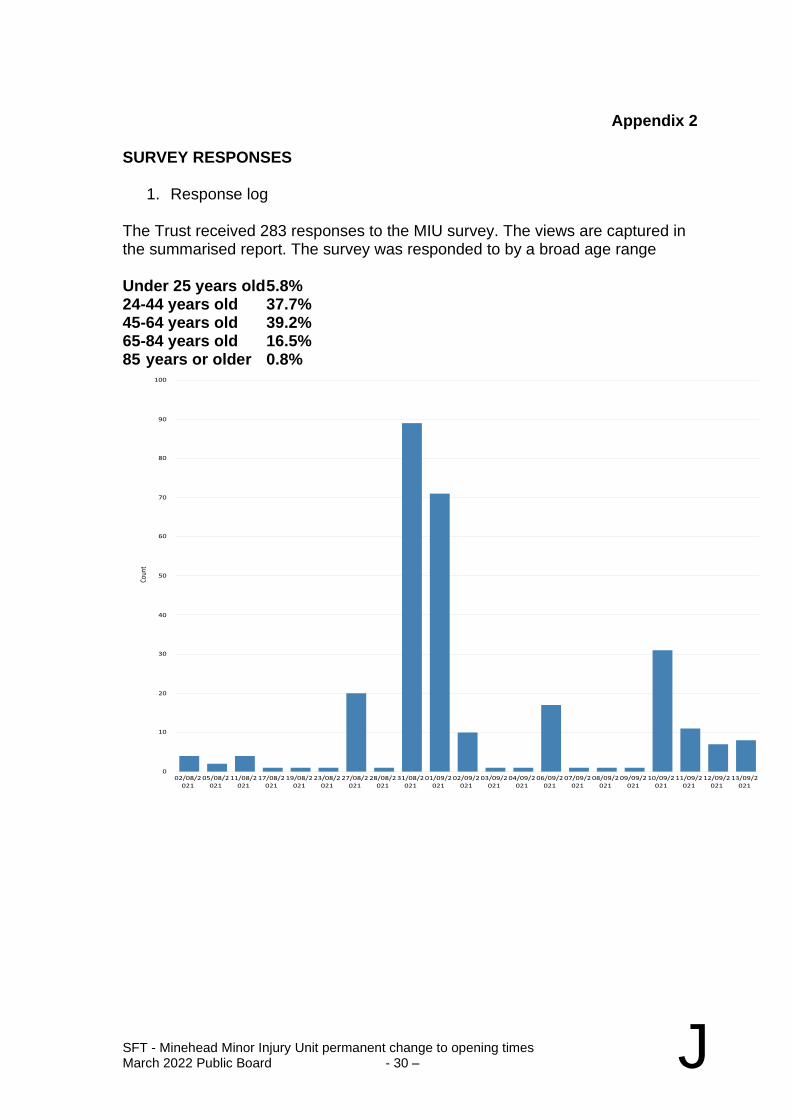
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 30 – J
Appendix 2
SURVEY RESPONSES
1. Response log The Trust received 283 responses to the MIU survey. The views are captured in the summarised report. The survey was responded to by a broad age range Under 25 years old 5.8% 24-44 years old 37.7% 45-64 years old 39.2% 65-84 years old 16.5% 85 years or older 0.8%
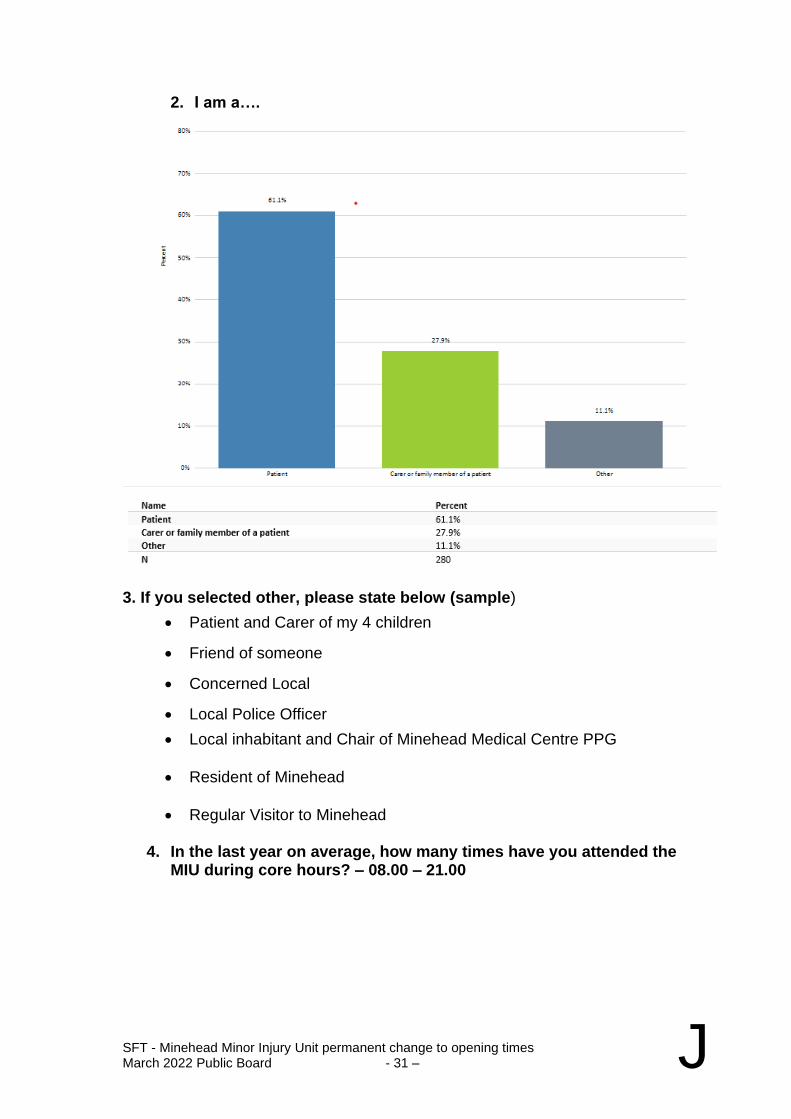
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 31 – J
2. I am a….
3. If you selected other, please state below (sample)
• Patient and Carer of my 4 children
• Friend of someone
• Concerned Local
• Local Police Officer
• Local inhabitant and Chair of Minehead Medical Centre PPG
• Resident of Minehead
• Regular Visitor to Minehead 4. In the last year on average, how many times have you attended the
MIU during core hours? – 08.00 – 21.00
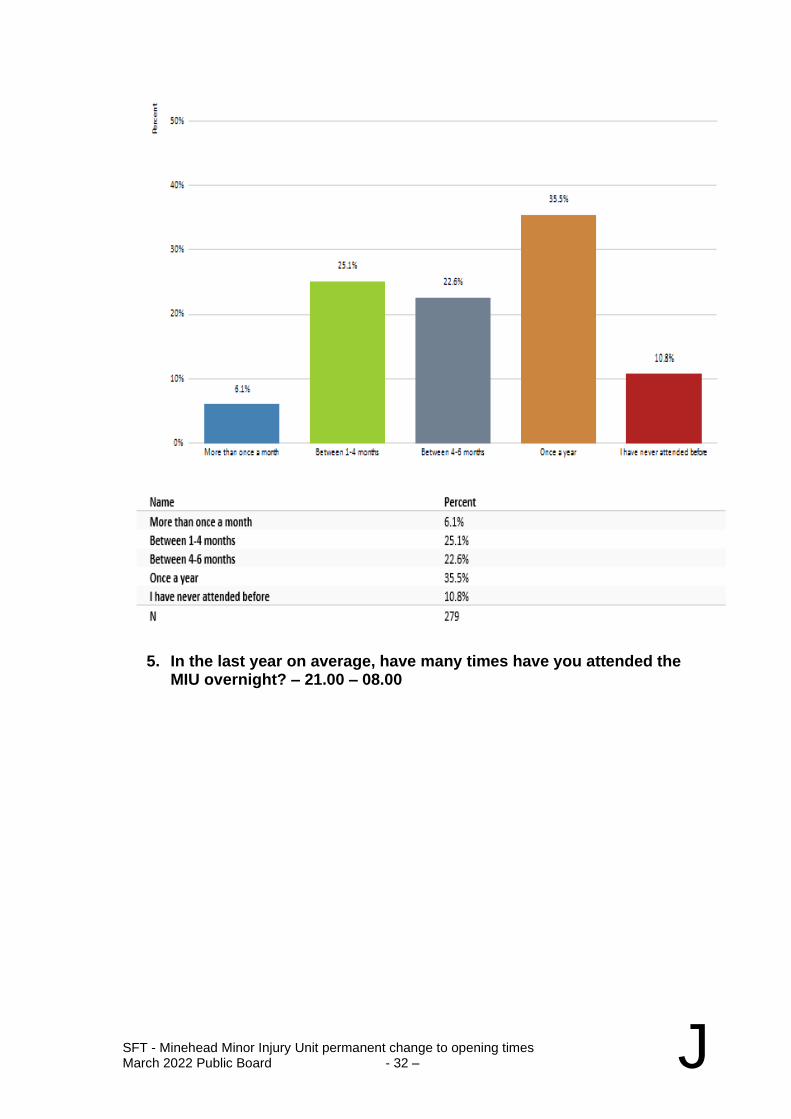
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 32 – J
5. In the last year on average, have many times have you attended the MIU overnight? – 21.00 – 08.00
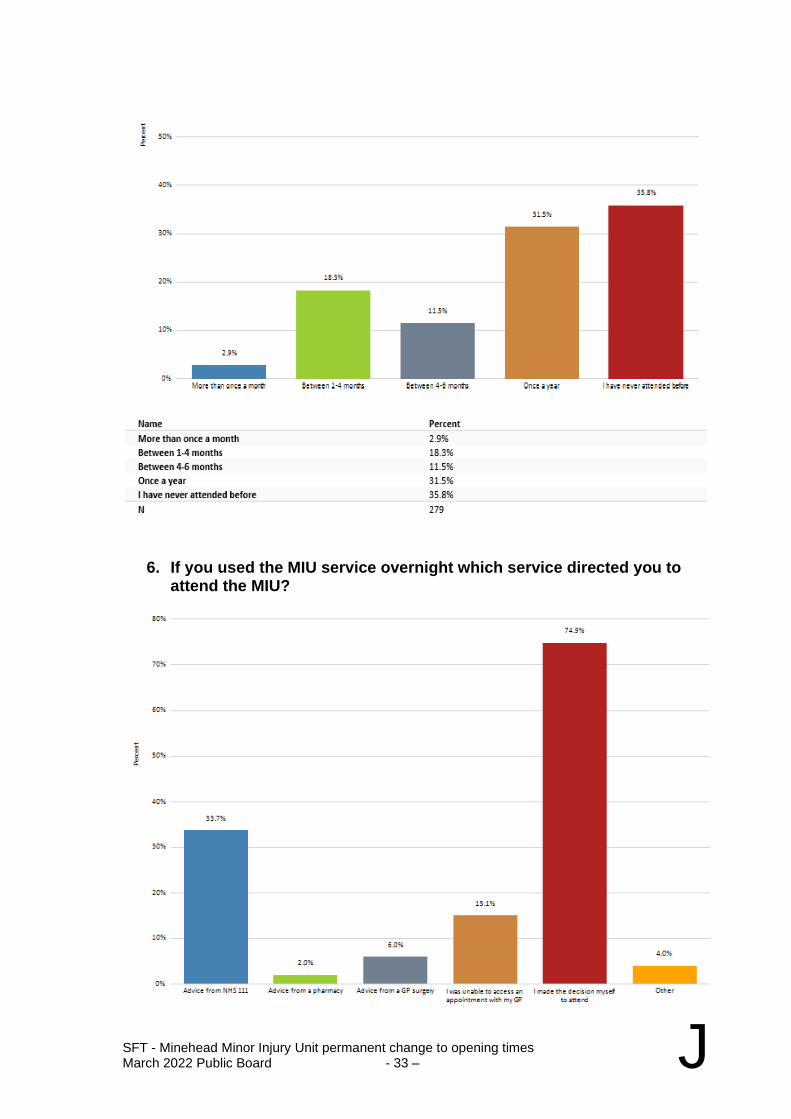
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 33 – J
6. If you used the MIU service overnight which service directed you to attend the MIU?
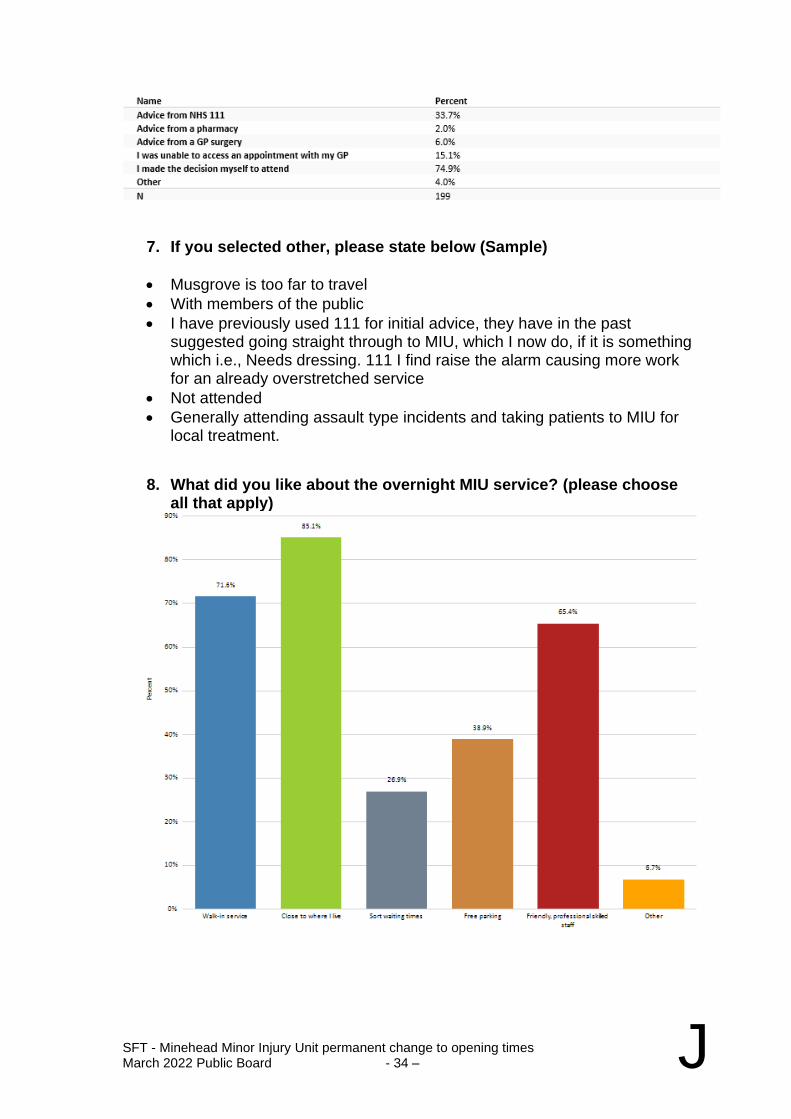
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 34 – J
7. If you selected other, please state below (Sample)
• Musgrove is too far to travel
• With members of the public
• I have previously used 111 for initial advice, they have in the past suggested going straight through to MIU, which I now do, if it is something which i.e., Needs dressing. 111 I find raise the alarm causing more work for an already overstretched service
• Not attended
• Generally attending assault type incidents and taking patients to MIU for local treatment.
8. What did you like about the overnight MIU service? (please choose all that apply)
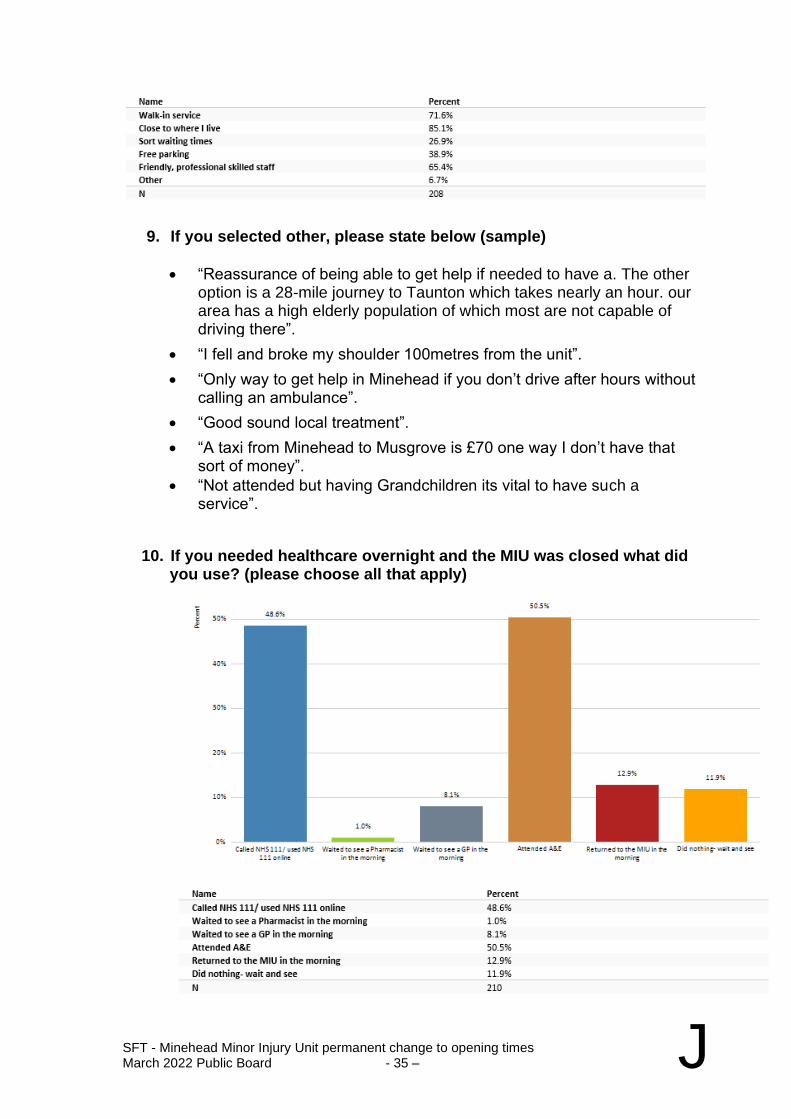
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 35 – J
9. If you selected other, please state below (sample)
• “Reassurance of being able to get help if needed to have a. The other option is a 28-mile journey to Taunton which takes nearly an hour. our area has a high elderly population of which most are not capable of driving there”.
• “I fell and broke my shoulder 100metres from the unit”.
• “Only way to get help in Minehead if you don’t drive after hours without calling an ambulance”.
• “Good sound local treatment”.
• “A taxi from Minehead to Musgrove is £70 one way I don’t have that sort of money”.
• “Not attended but having Grandchildren its vital to have such a service”.
10. If you needed healthcare overnight and the MIU was closed what did
you use? (please choose all that apply)
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 36 – J
11. Explain the reason for your decision- Optional (Sample)
• “Fortunately, the only time we've needed overnight MIU for our child, it was open Very nice staff helped us and got us an ambulance to Musgrove”.
• “Local dept for us, too far to go to Taunton. Always friendly and helpful”.
• “Couldn’t wait till morning child was very poorly spent week in Musgrove”.
• Nowhere else to go so It was either 111 or A&E which is 28 miles away plus don’t drive so had to pay out for a taxi!!!”
• “I had to drive 40-50mins to the nearest emergency health care facility, even though it wasn’t an emergency! MIU always acted as an intermediary between A&E and a local GP. Patients are at risk since this closure. We hear all the time about not using A&E unless necessary, but because this has closed, the definition of necessary has changed, and now attending A&E is much more necessary, even though MIU could have handled it”.
• “As we have hardly any doctor at local surgery everytime I phone GP I get told to go to MIU. When I’ve been to MIU I get told GP sending most people there and most appointments I get I have to go Musgrove as there isn't any for Minehead”.
• “Minehead is a very secluded area and the nearest service after 9pm is Taunton. For someone who doesn't drive and relies on transport links which do not run after 6pm it's extremely worrying that if something severe happened that the likelihood of something tragic happening is inevitable especially when you've waited over 3 hours for an ambulance 999 call. There is nowhere else to go. I feel taking away such a vital piece of medical help and support during certain hours is just a death wish waiting to happen so many people that could have had the support and medical advice immediately are sat at home waiting for an ambulance or advise from the 111 service”.
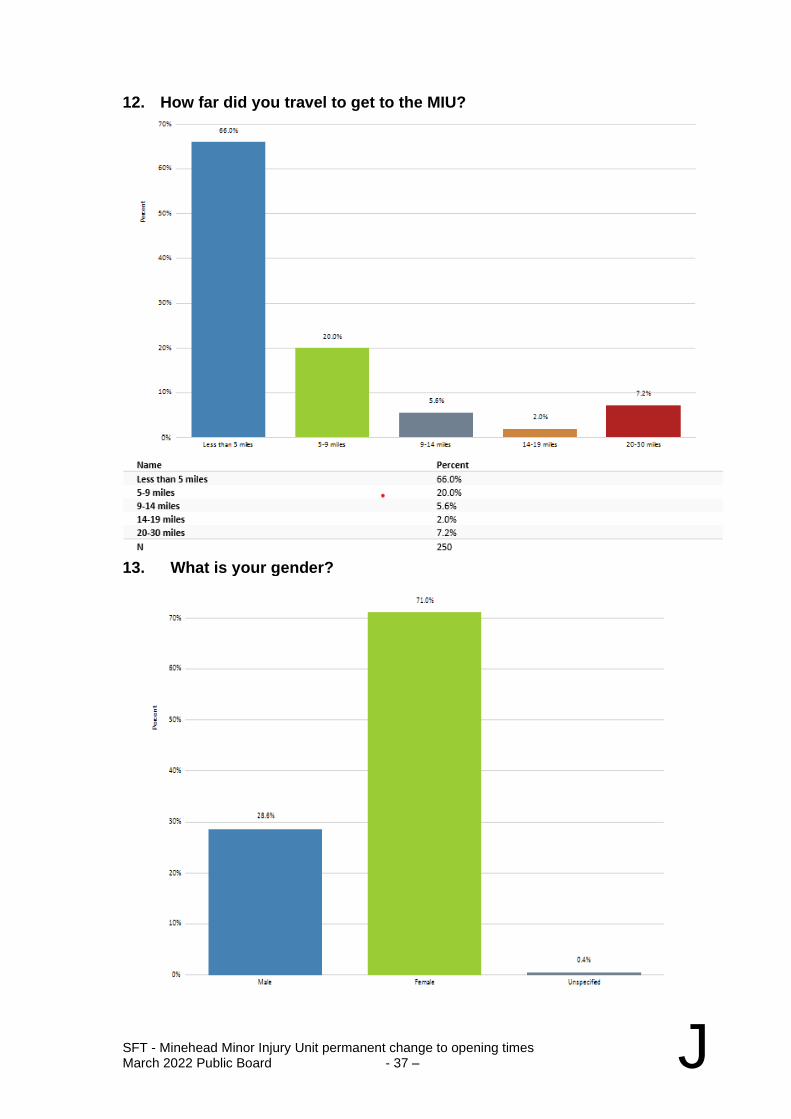
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 37 – J
12. How far did you travel to get to the MIU?
13. What is your gender?
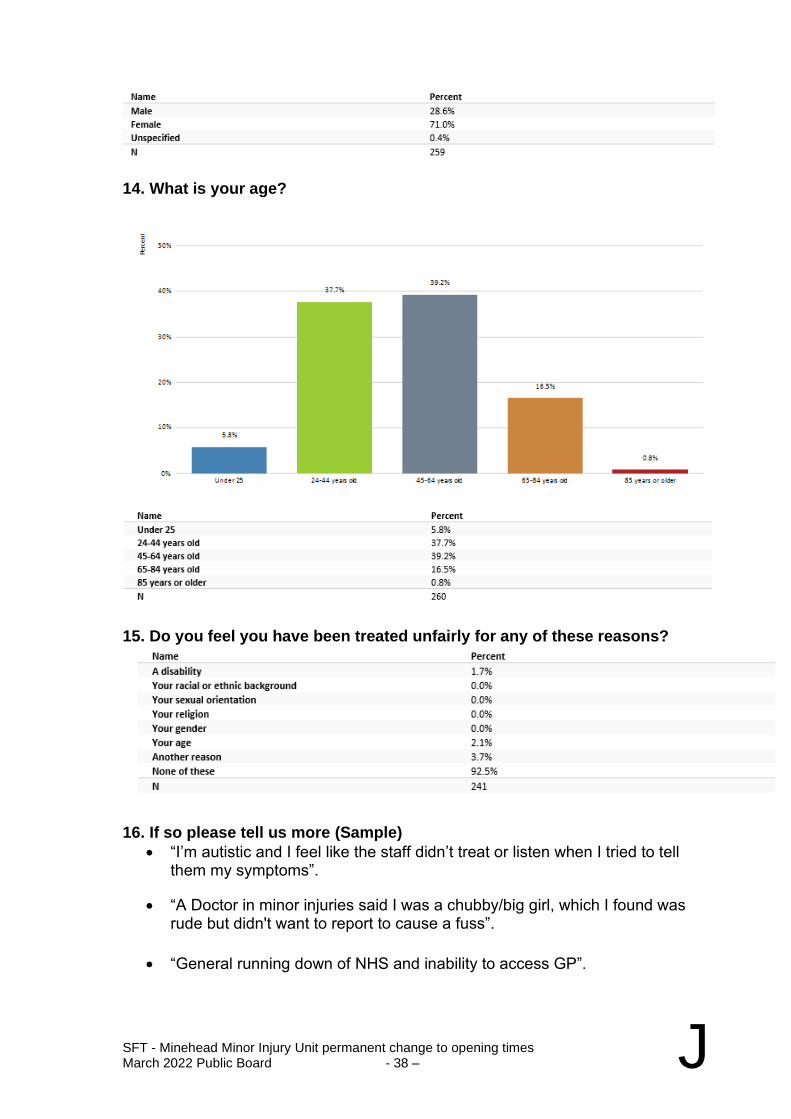
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 38 – J
14. What is your age?
15. Do you feel you have been treated unfairly for any of these reasons?
16. If so please tell us more (Sample)
• “I’m autistic and I feel like the staff didn’t treat or listen when I tried to tell them my symptoms”.
• “A Doctor in minor injuries said I was a chubby/big girl, which I found was rude but didn't want to report to cause a fuss”.
• “General running down of NHS and inability to access GP”.
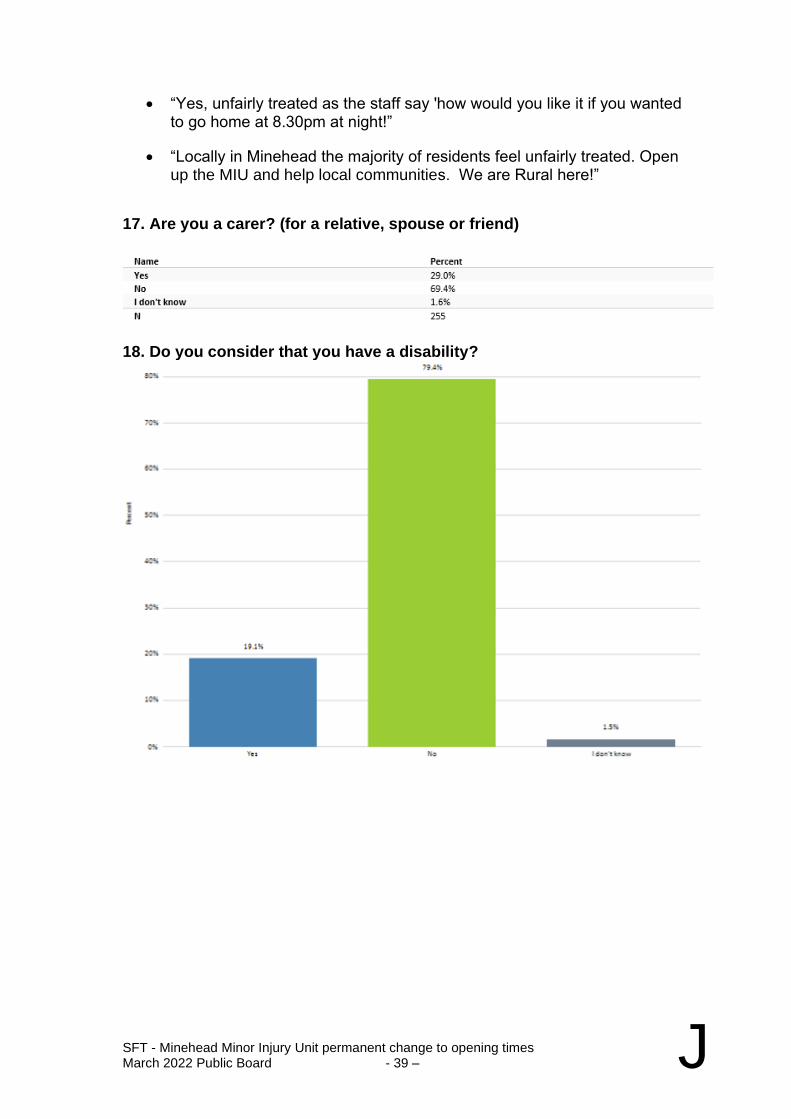
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 39 – J
• “Yes, unfairly treated as the staff say 'how would you like it if you wanted to go home at 8.30pm at night!”
• “Locally in Minehead the majority of residents feel unfairly treated. Open up the MIU and help local communities. We are Rural here!”
17. Are you a carer? (for a relative, spouse or friend)
18. Do you consider that you have a disability?
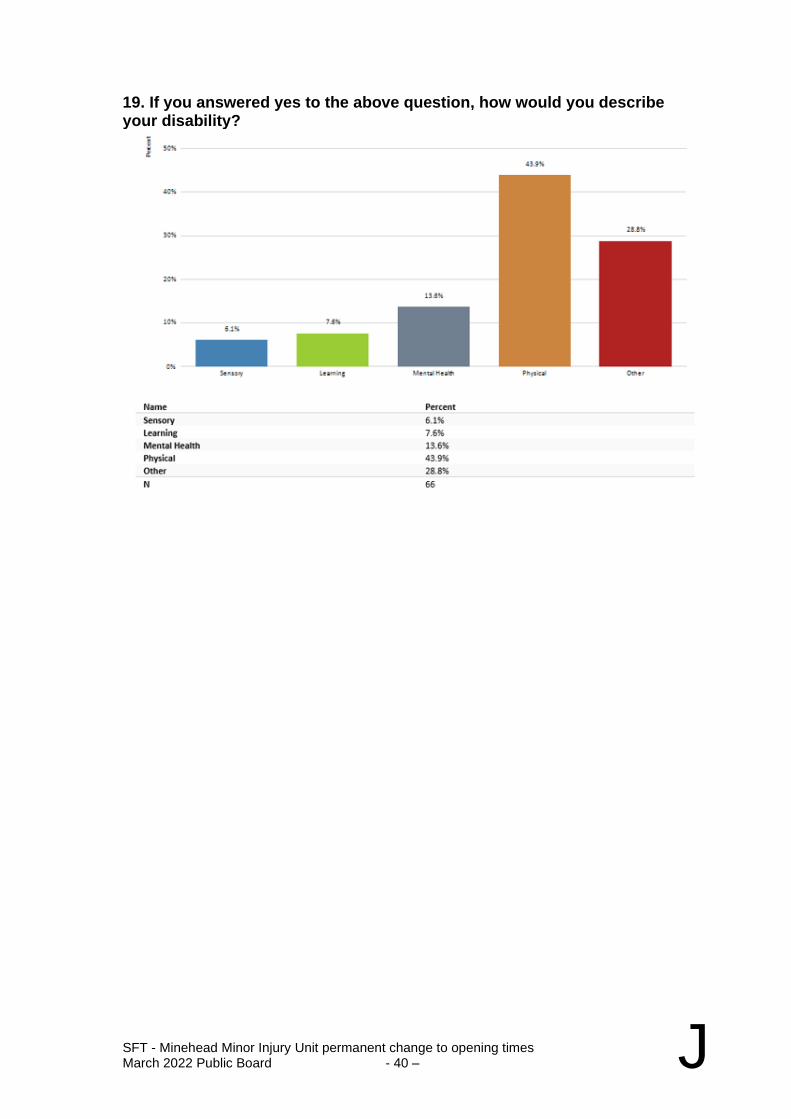
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 40 – J
19. If you answered yes to the above question, how would you describe your disability?
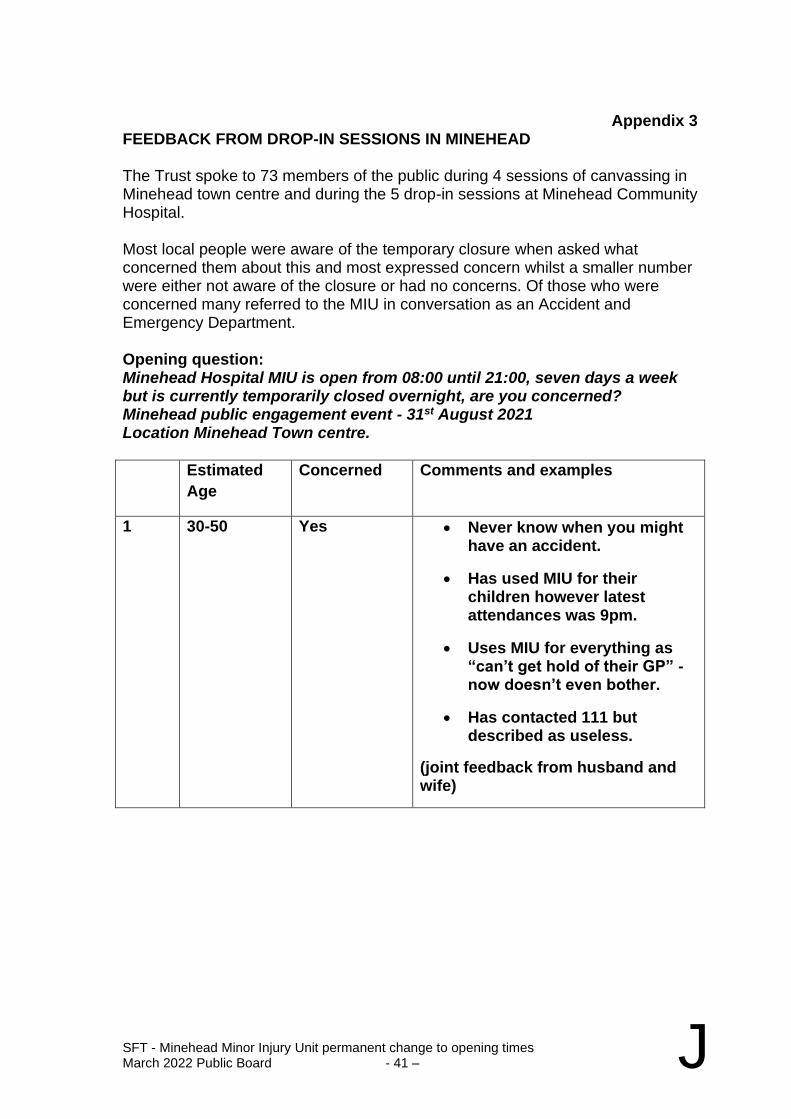
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 41 – J
Appendix 3
FEEDBACK FROM DROP-IN SESSIONS IN MINEHEAD The Trust spoke to 73 members of the public during 4 sessions of canvassing in Minehead town centre and during the 5 drop-in sessions at Minehead Community Hospital. Most local people were aware of the temporary closure when asked what concerned them about this and most expressed concern whilst a smaller number were either not aware of the closure or had no concerns. Of those who were concerned many referred to the MIU in conversation as an Accident and Emergency Department. Opening question: Minehead Hospital MIU is open from 08:00 until 21:00, seven days a week but is currently temporarily closed overnight, are you concerned? Minehead public engagement event - 31st August 2021 Location Minehead Town centre.
Estimated
Age
Concerned Comments and examples
1 30-50 Yes • Never know when you might have an accident.
• Has used MIU for their children however latest attendances was 9pm.
• Uses MIU for everything as “can’t get hold of their GP” - now doesn’t even bother.
• Has contacted 111 but described as useless.
(joint feedback from husband and wife)
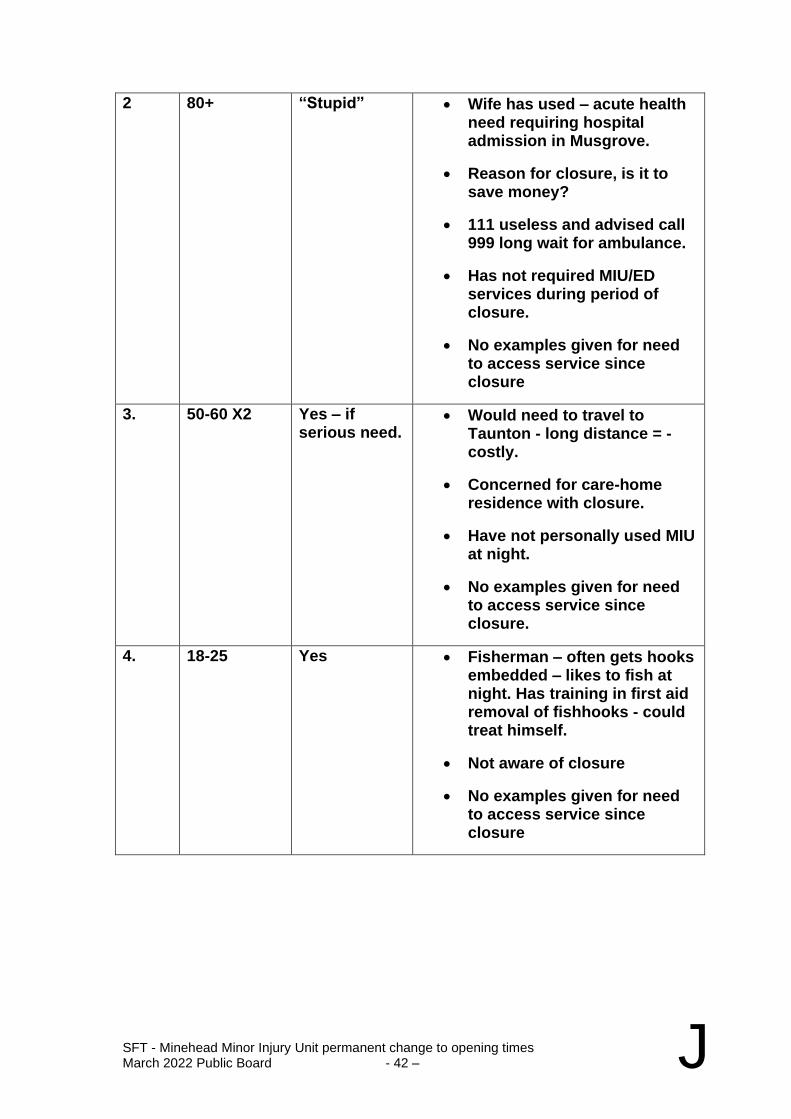
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 42 – J
2 80+ “Stupid” • Wife has used – acute health need requiring hospital admission in Musgrove.
• Reason for closure, is it to save money?
• 111 useless and advised call 999 long wait for ambulance.
• Has not required MIU/ED services during period of closure.
• No examples given for need to access service since closure
3. 50-60 X2 Yes – if serious need.
• Would need to travel to Taunton - long distance = - costly.
• Concerned for care-home residence with closure.
• Have not personally used MIU at night.
• No examples given for need to access service since closure.
4. 18-25 Yes • Fisherman – often gets hooks embedded – likes to fish at night. Has training in first aid removal of fishhooks - could treat himself.
• Not aware of closure
• No examples given for need to access service since closure
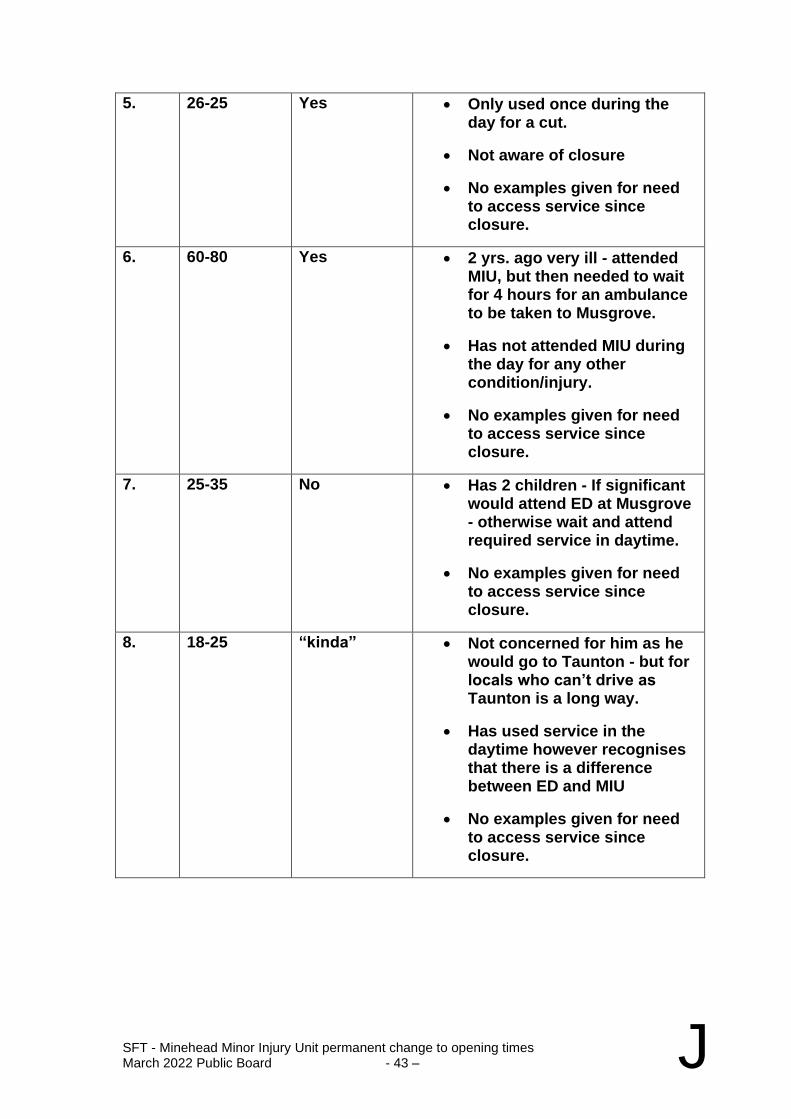
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 43 – J
5. 26-25 Yes • Only used once during the day for a cut.
• Not aware of closure
• No examples given for need to access service since closure.
6. 60-80 Yes • 2 yrs. ago very ill - attended MIU, but then needed to wait for 4 hours for an ambulance to be taken to Musgrove.
• Has not attended MIU during the day for any other condition/injury.
• No examples given for need to access service since closure.
7. 25-35 No • Has 2 children - If significant would attend ED at Musgrove - otherwise wait and attend required service in daytime.
• No examples given for need to access service since closure.
8. 18-25 “kinda” • Not concerned for him as he would go to Taunton - but for locals who can’t drive as Taunton is a long way.
• Has used service in the daytime however recognises that there is a difference between ED and MIU
• No examples given for need to access service since closure.
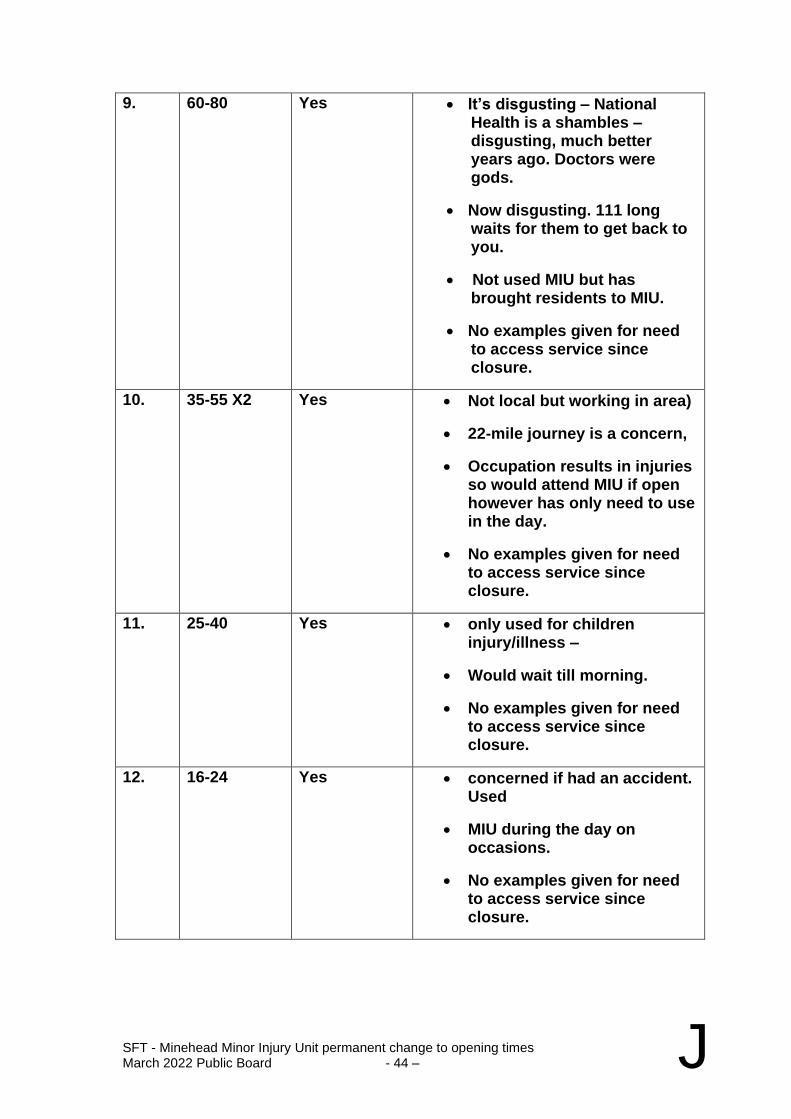
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 44 – J
9. 60-80 Yes • It’s disgusting – National Health is a shambles – disgusting, much better years ago. Doctors were gods.
• Now disgusting. 111 long waits for them to get back to you.
• Not used MIU but has brought residents to MIU.
• No examples given for need to access service since closure.
10. 35-55 X2 Yes • Not local but working in area)
• 22-mile journey is a concern,
• Occupation results in injuries so would attend MIU if open however has only need to use in the day.
• No examples given for need to access service since closure.
11. 25-40 Yes • only used for children injury/illness –
• Would wait till morning.
• No examples given for need to access service since closure.
12. 16-24 Yes • concerned if had an accident. Used
• MIU during the day on occasions.
• No examples given for need to access service since closure.
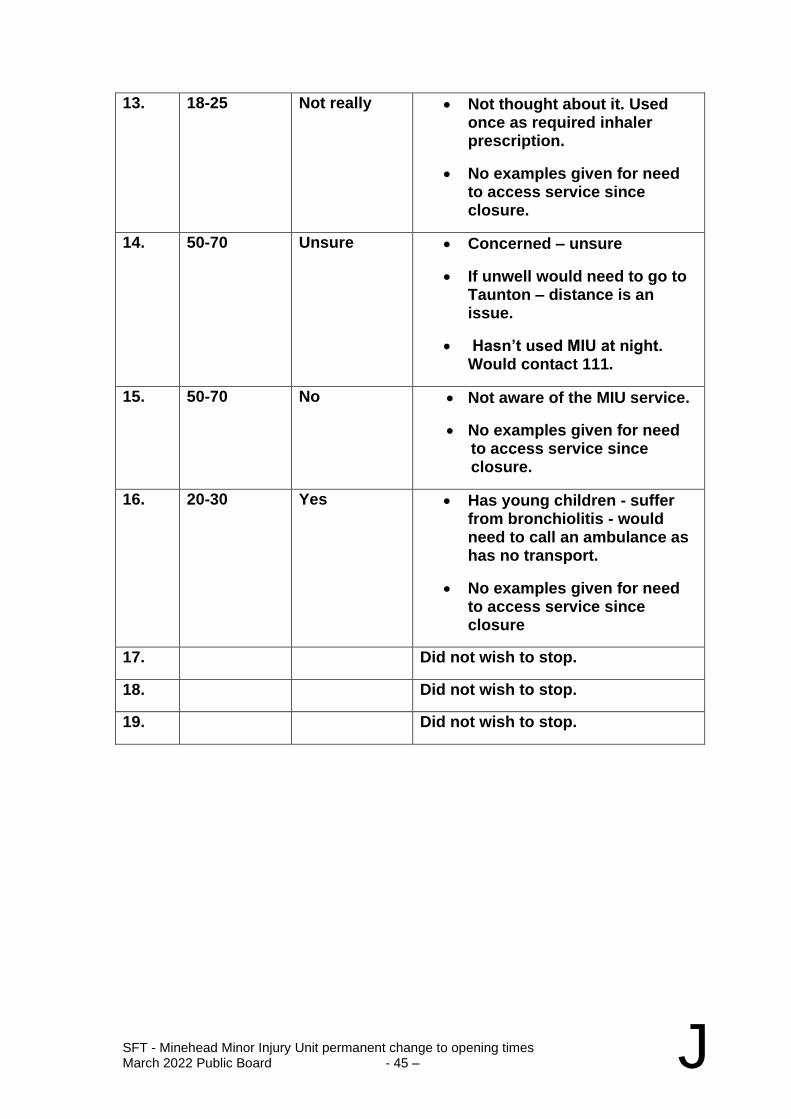
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 45 – J
13. 18-25 Not really • Not thought about it. Used once as required inhaler prescription.
• No examples given for need to access service since closure.
14. 50-70 Unsure • Concerned – unsure
• If unwell would need to go to Taunton – distance is an issue.
• Hasn’t used MIU at night. Would contact 111.
15. 50-70 No • Not aware of the MIU service.
• No examples given for need to access service since closure.
16. 20-30 Yes • Has young children - suffer from bronchiolitis - would need to call an ambulance as has no transport.
• No examples given for need to access service since closure
17. Did not wish to stop.
18. Did not wish to stop.
19. Did not wish to stop.
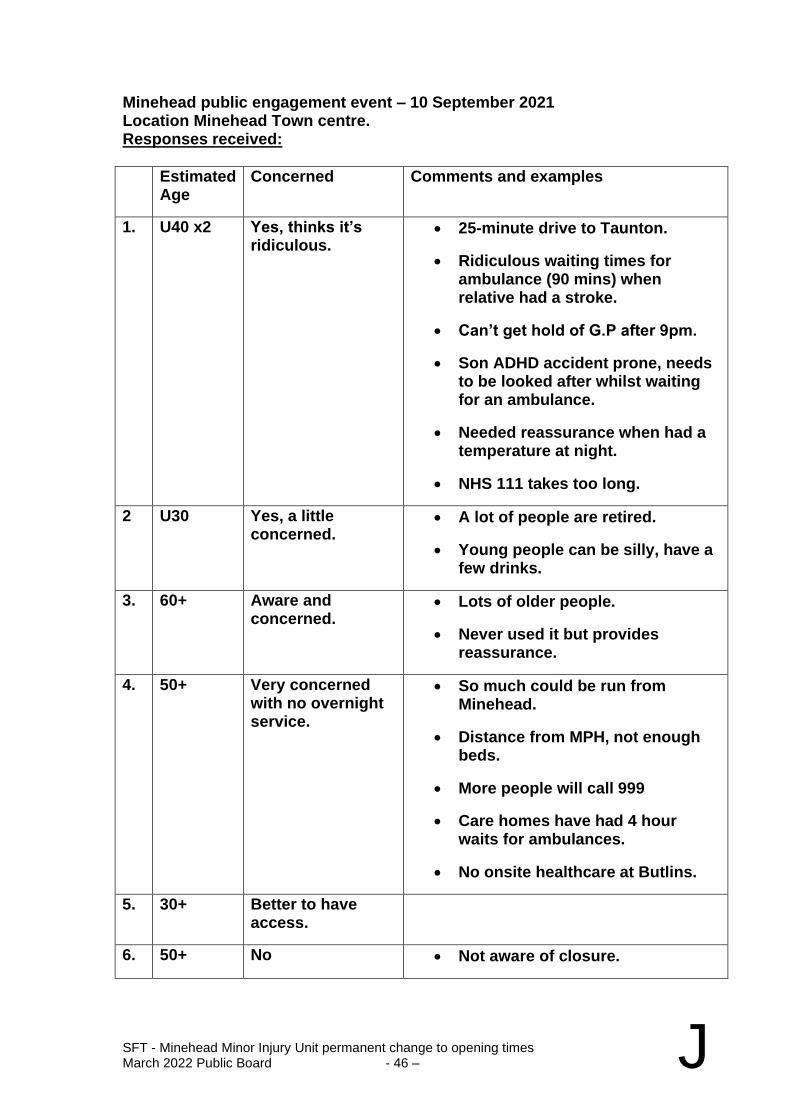
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 46 – J
Minehead public engagement event – 10 September 2021 Location Minehead Town centre. Responses received:
Estimated Age
Concerned Comments and examples
1. U40 x2 Yes, thinks it’s ridiculous.
• 25-minute drive to Taunton.
• Ridiculous waiting times for ambulance (90 mins) when relative had a stroke.
• Can’t get hold of G.P after 9pm.
• Son ADHD accident prone, needs to be looked after whilst waiting for an ambulance.
• Needed reassurance when had a temperature at night.
• NHS 111 takes too long.
2 U30 Yes, a little concerned.
• A lot of people are retired.
• Young people can be silly, have a few drinks.
3. 60+ Aware and concerned.
• Lots of older people.
• Never used it but provides reassurance.
4. 50+ Very concerned with no overnight service.
• So much could be run from Minehead.
• Distance from MPH, not enough beds.
• More people will call 999
• Care homes have had 4 hour waits for ambulances.
• No onsite healthcare at Butlins.
5. 30+ Better to have access.
6. 50+ No • Not aware of closure.
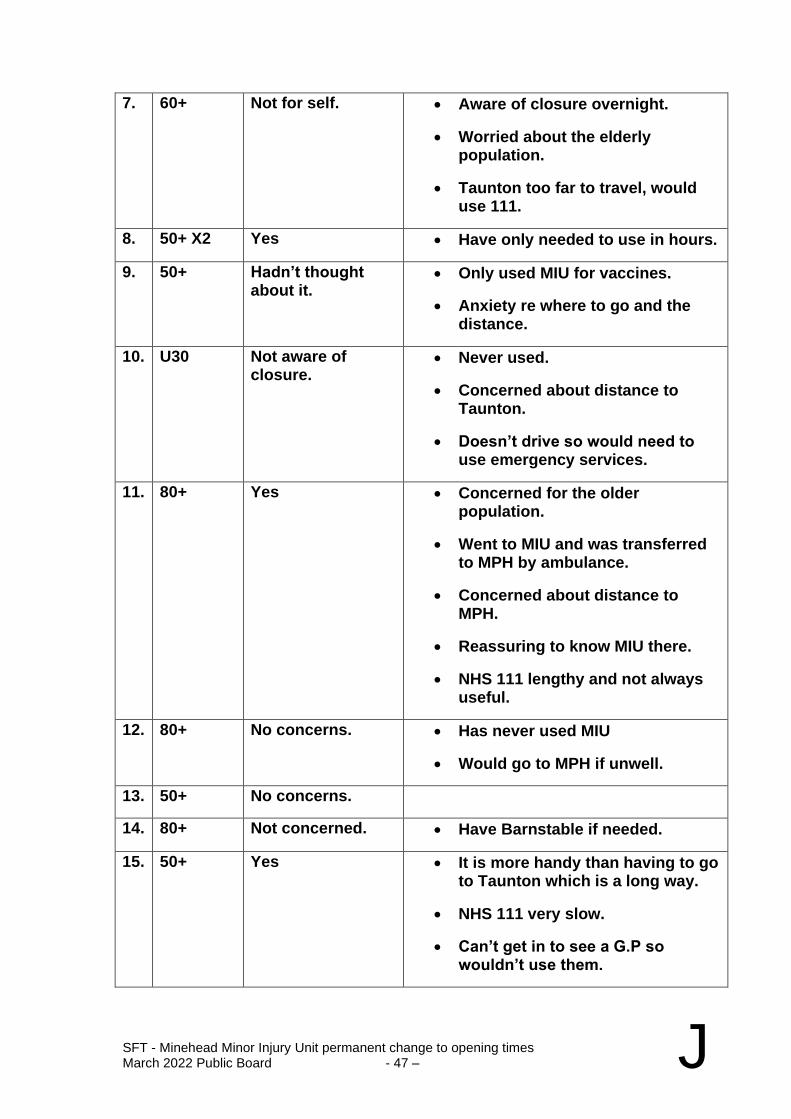
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 47 – J
7. 60+ Not for self. • Aware of closure overnight.
• Worried about the elderly population.
• Taunton too far to travel, would use 111.
8. 50+ X2 Yes • Have only needed to use in hours.
9. 50+ Hadn’t thought about it.
• Only used MIU for vaccines.
• Anxiety re where to go and the distance.
10. U30 Not aware of closure.
• Never used.
• Concerned about distance to Taunton.
• Doesn’t drive so would need to use emergency services.
11. 80+ Yes • Concerned for the older population.
• Went to MIU and was transferred to MPH by ambulance.
• Concerned about distance to MPH.
• Reassuring to know MIU there.
• NHS 111 lengthy and not always useful.
12. 80+ No concerns. • Has never used MIU
• Would go to MPH if unwell.
13. 50+ No concerns.
14. 80+ Not concerned. • Have Barnstable if needed.
15. 50+ Yes • It is more handy than having to go to Taunton which is a long way.
• NHS 111 very slow.
• Can’t get in to see a G.P so wouldn’t use them.
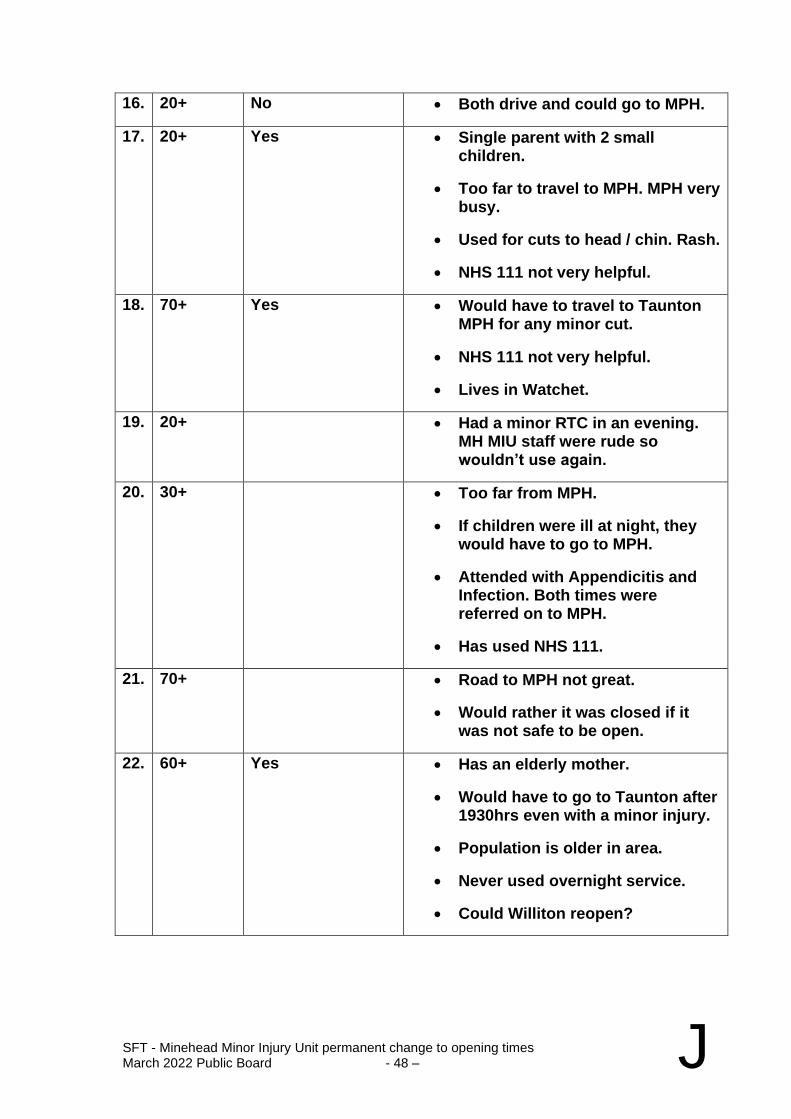
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 48 – J
16. 20+ No • Both drive and could go to MPH.
17. 20+ Yes • Single parent with 2 small children.
• Too far to travel to MPH. MPH very busy.
• Used for cuts to head / chin. Rash.
• NHS 111 not very helpful.
18. 70+ Yes • Would have to travel to Taunton MPH for any minor cut.
• NHS 111 not very helpful.
• Lives in Watchet.
19. 20+ • Had a minor RTC in an evening. MH MIU staff were rude so wouldn’t use again.
20. 30+ • Too far from MPH.
• If children were ill at night, they would have to go to MPH.
• Attended with Appendicitis and Infection. Both times were referred on to MPH.
• Has used NHS 111.
21. 70+ • Road to MPH not great.
• Would rather it was closed if it was not safe to be open.
22. 60+ Yes • Has an elderly mother.
• Would have to go to Taunton after 1930hrs even with a minor injury.
• Population is older in area.
• Never used overnight service.
• Could Williton reopen?
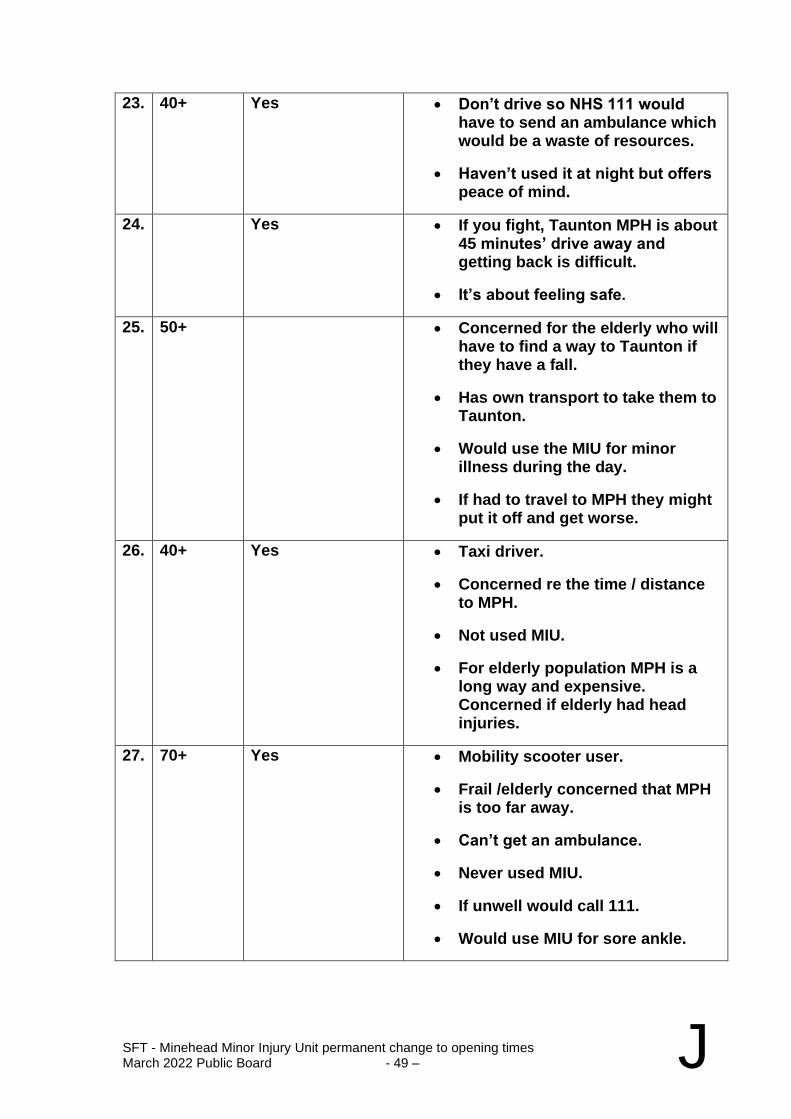
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 49 – J
23. 40+ Yes • Don’t drive so NHS 111 would have to send an ambulance which would be a waste of resources.
• Haven’t used it at night but offers peace of mind.
24. Yes • If you fight, Taunton MPH is about 45 minutes’ drive away and getting back is difficult.
• It’s about feeling safe.
25. 50+ • Concerned for the elderly who will have to find a way to Taunton if they have a fall.
• Has own transport to take them to Taunton.
• Would use the MIU for minor illness during the day.
• If had to travel to MPH they might put it off and get worse.
26. 40+ Yes • Taxi driver.
• Concerned re the time / distance to MPH.
• Not used MIU.
• For elderly population MPH is a long way and expensive. Concerned if elderly had head injuries.
27. 70+ Yes • Mobility scooter user.
• Frail /elderly concerned that MPH is too far away.
• Can’t get an ambulance.
• Never used MIU.
• If unwell would call 111.
• Would use MIU for sore ankle.
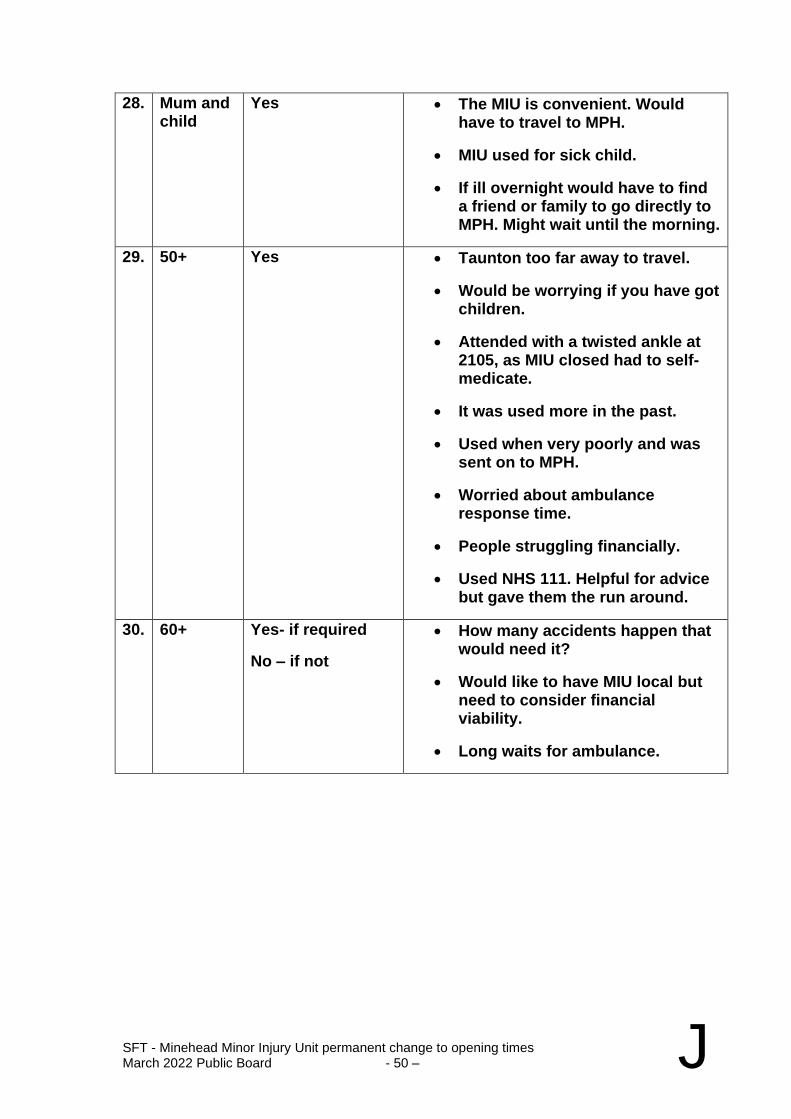
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 50 – J
28. Mum and child
Yes • The MIU is convenient. Would have to travel to MPH.
• MIU used for sick child.
• If ill overnight would have to find a friend or family to go directly to MPH. Might wait until the morning.
29. 50+ Yes • Taunton too far away to travel.
• Would be worrying if you have got children.
• Attended with a twisted ankle at 2105, as MIU closed had to self-medicate.
• It was used more in the past.
• Used when very poorly and was sent on to MPH.
• Worried about ambulance response time.
• People struggling financially.
• Used NHS 111. Helpful for advice but gave them the run around.
30. 60+ Yes- if required
No – if not
• How many accidents happen that would need it?
• Would like to have MIU local but need to consider financial viability.
• Long waits for ambulance.
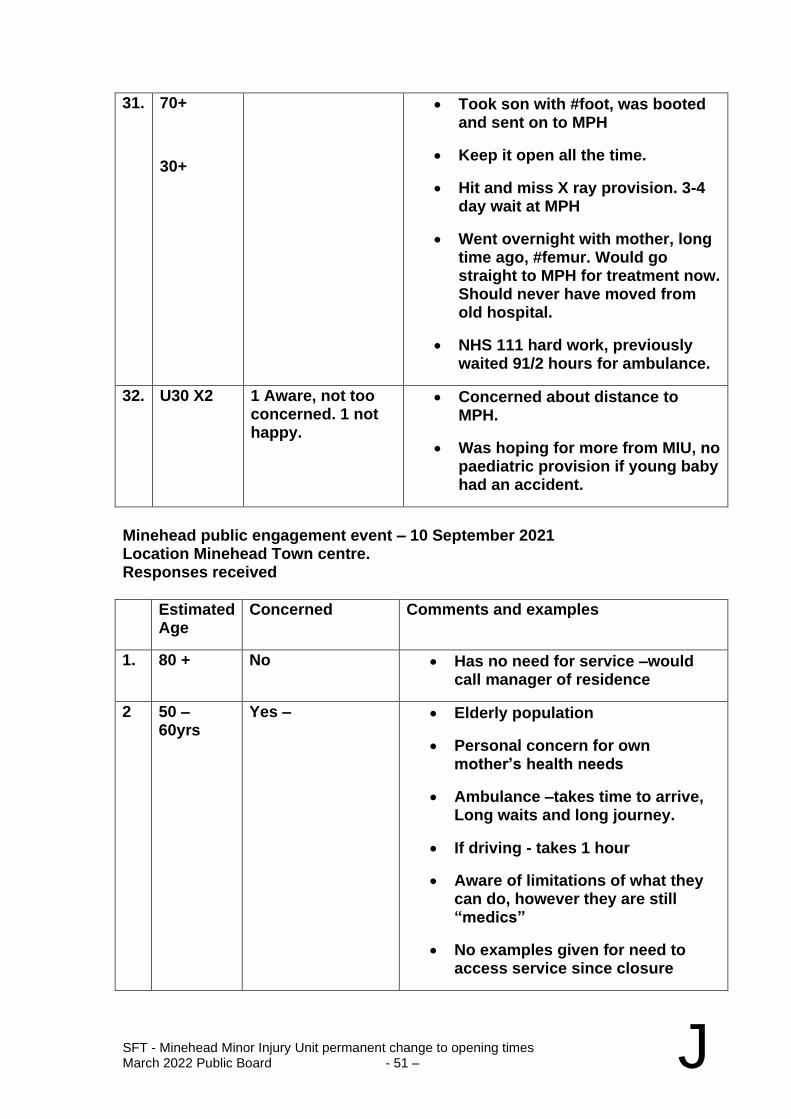
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 51 – J
31. 70+
30+
• Took son with #foot, was booted and sent on to MPH
• Keep it open all the time.
• Hit and miss X ray provision. 3-4 day wait at MPH
• Went overnight with mother, long time ago, #femur. Would go straight to MPH for treatment now. Should never have moved from old hospital.
• NHS 111 hard work, previously waited 91/2 hours for ambulance.
32. U30 X2 1 Aware, not too concerned. 1 not happy.
• Concerned about distance to MPH.
• Was hoping for more from MIU, no paediatric provision if young baby had an accident.
Minehead public engagement event – 10 September 2021 Location Minehead Town centre. Responses received
Estimated Age
Concerned Comments and examples
1. 80 + No • Has no need for service –would call manager of residence
2 50 – 60yrs
Yes – • Elderly population
• Personal concern for own mother’s health needs
• Ambulance –takes time to arrive, Long waits and long journey.
• If driving - takes 1 hour
• Aware of limitations of what they can do, however they are still “medics”
• No examples given for need to access service since closure
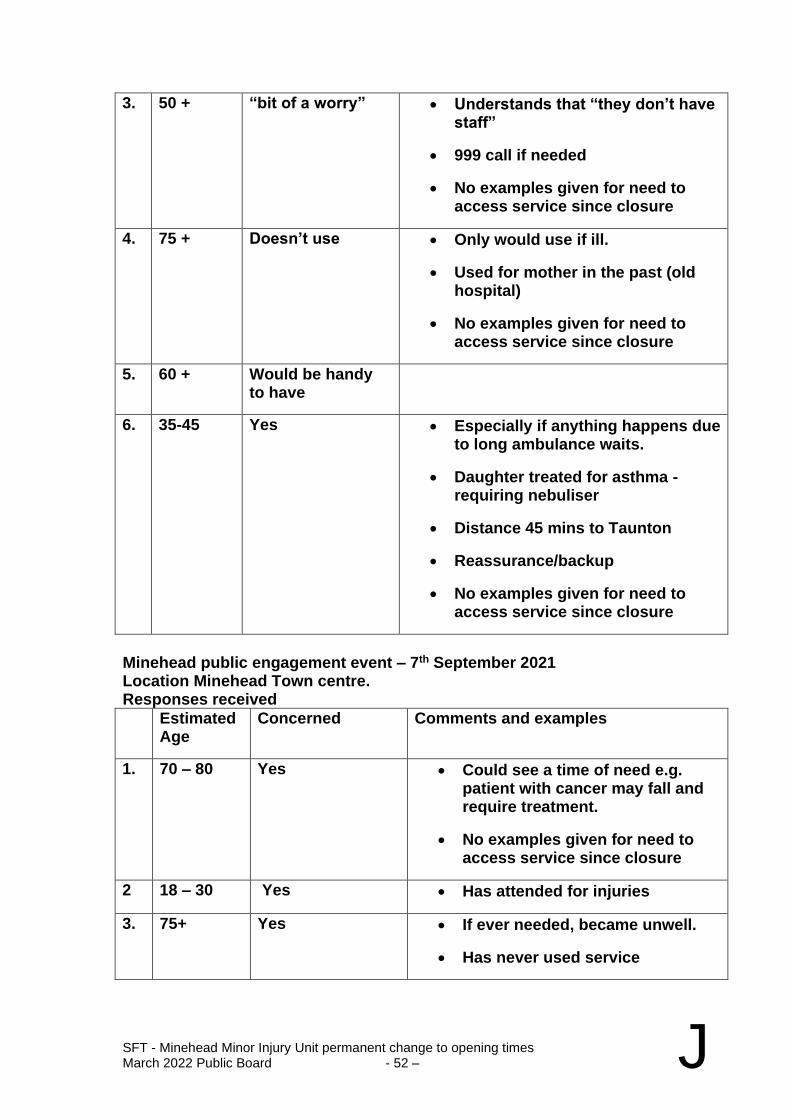
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 52 – J
3. 50 + “bit of a worry” • Understands that “they don’t have staff”
• 999 call if needed
• No examples given for need to access service since closure
4. 75 + Doesn’t use • Only would use if ill.
• Used for mother in the past (old hospital)
• No examples given for need to access service since closure
5. 60 + Would be handy to have
6. 35-45 Yes • Especially if anything happens due to long ambulance waits.
• Daughter treated for asthma - requiring nebuliser
• Distance 45 mins to Taunton
• Reassurance/backup
• No examples given for need to access service since closure
Minehead public engagement event – 7th September 2021 Location Minehead Town centre. Responses received
Estimated Age
Concerned Comments and examples
1. 70 – 80 Yes • Could see a time of need e.g. patient with cancer may fall and require treatment.
• No examples given for need to access service since closure
2 18 – 30 Yes • Has attended for injuries
3. 75+ Yes • If ever needed, became unwell.
• Has never used service
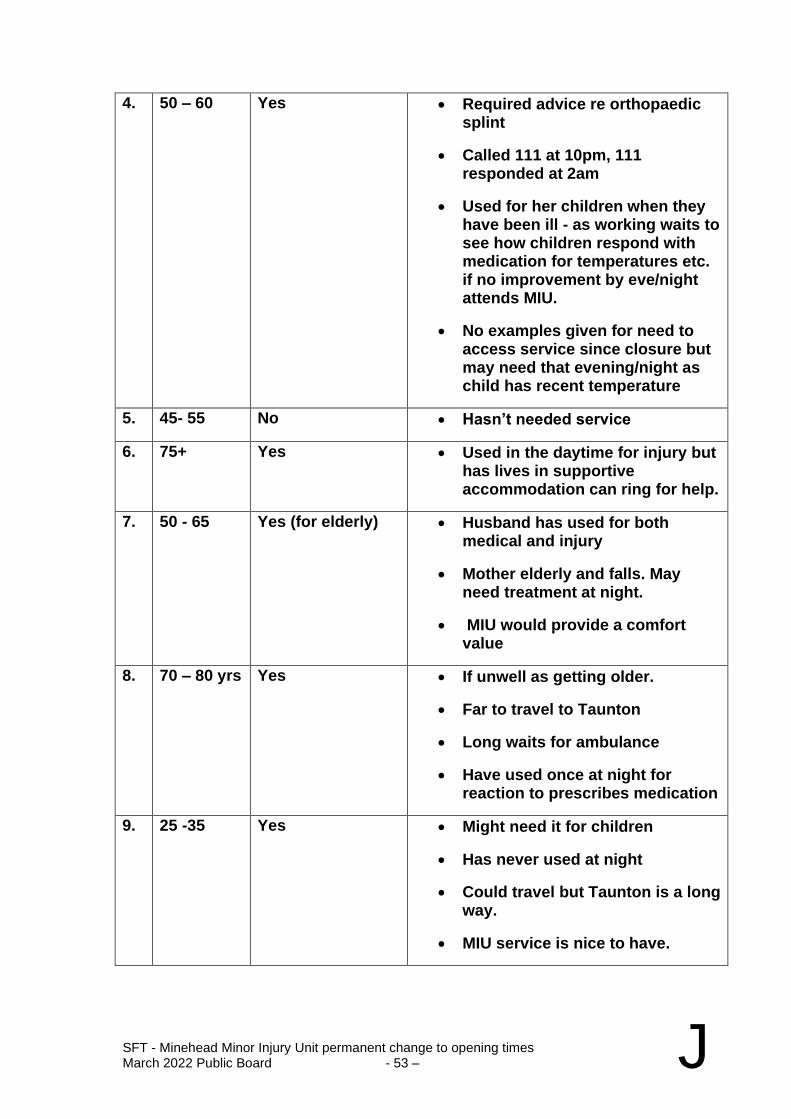
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 53 – J
4. 50 – 60 Yes • Required advice re orthopaedic splint
• Called 111 at 10pm, 111 responded at 2am
• Used for her children when they have been ill - as working waits to see how children respond with medication for temperatures etc. if no improvement by eve/night attends MIU.
• No examples given for need to access service since closure but may need that evening/night as child has recent temperature
5. 45- 55 No • Hasn’t needed service
6. 75+ Yes • Used in the daytime for injury but has lives in supportive accommodation can ring for help.
7. 50 - 65 Yes (for elderly) • Husband has used for both medical and injury
• Mother elderly and falls. May need treatment at night.
• MIU would provide a comfort value
8. 70 – 80 yrs Yes • If unwell as getting older.
• Far to travel to Taunton
• Long waits for ambulance
• Have used once at night for reaction to prescribes medication
9. 25 -35 Yes • Might need it for children
• Has never used at night
• Could travel but Taunton is a long way.
• MIU service is nice to have.
SFT - Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 54 – J
10. 60+ Yes • A lot of care homes in Minehead -
11-15
5 x individuals did not want to participate
Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 55 – J
Appendix 2 – Equality Impact Assessment
Somerset Equality Impact Assessment
Before completing this EIA please ensure you have read the EIA guidance notes – available from your Equality Officer
Organisation prepared for Somerset Foundation Trust
Version v. 1.2 Date Completed 04.02.22
Description of what is being impact assessed
Impact on temporary closure and proposed permanent change to service opening times of Minehead MIU from a 24-hour service to a reduced service time of 8am – 9pm
Evidence
What data/information have you used to assess how this policy/service might impact on protected groups? Sources such as the Office
of National Statistics, Somerset Intelligence Partnership, Somerset’s Joint Strategic Needs Analysis (JSNA), Staff and/ or area profiles,, should
be detailed here
Data from:
Somerset FT (Minehead MIU and Musgrove Park ED), South West Ambulance Service, Devon Doctors
NICE Guidance:
Stroke and transient ischaemic attack in over 16s: diagnosis and initial management NICE guideline [NG128]
Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 56 – J
Acute coronary syndromes in adults Quality standard [QS68]
Head injury: assessment and early management Clinical guideline [CG176] Sepsis: recognition, diagnosis and early management NICE guideline [NG51] BTS/SIGN British Guideline on the Management of Asthma
Sources: Staff, Patients, Public, local councillors & politicians, League of Friends, Social Media, Pals
Who have you consulted with to assess possible impact on protected groups? If you have not consulted other people, please explain
why?
During the temporary closure we have had an engagement process, this has included a questionnaire for the public, meeting with local politicians, Patient Liaison team in the hospital to speak to the public directly, visiting Minehead town and asking the public directly their opinions on the closure, and working with community social media groups to get feedback and opinions. We have continued to monitor any feedback, comments received through our PALs and complaints office but none has been received.
Minehead hospital or MIU have not received any further feedback since the engagement process.
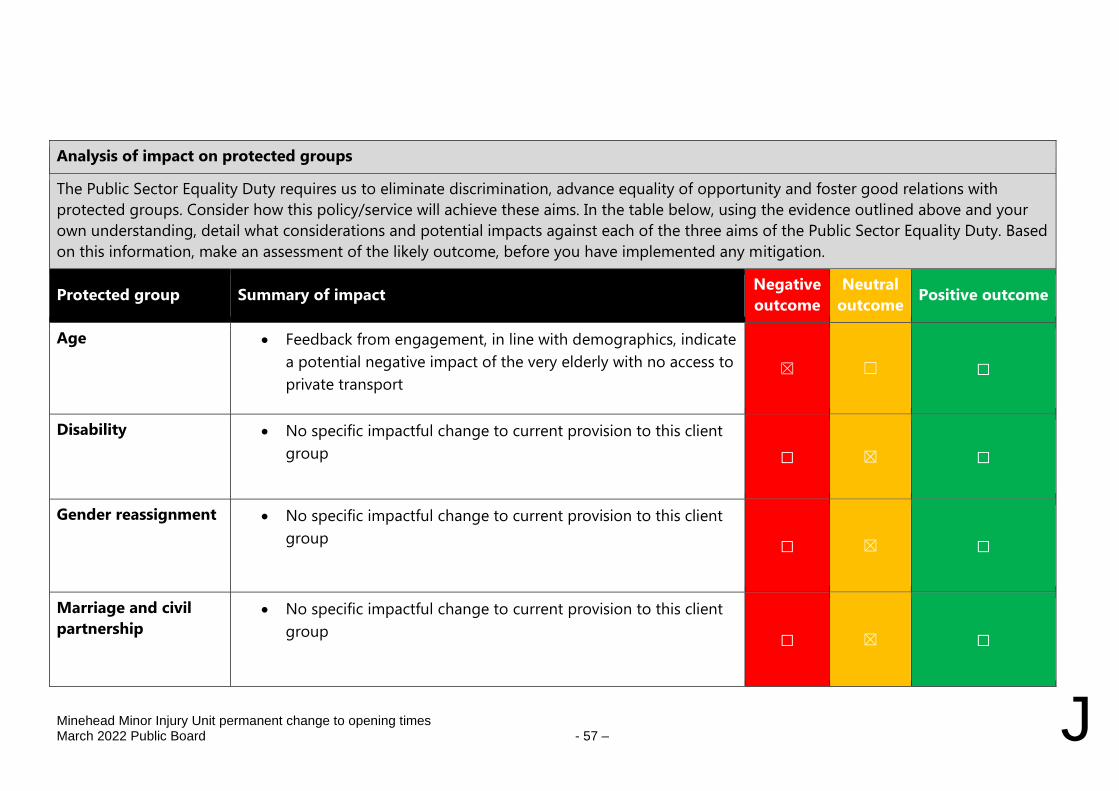
Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 57 – J
Analysis of impact on protected groups
The Public Sector Equality Duty requires us to eliminate discrimination, advance equality of opportunity and foster good relations with
protected groups. Consider how this policy/service will achieve these aims. In the table below, using the evidence outlined above and your
own understanding, detail what considerations and potential impacts against each of the three aims of the Public Sector Equality Duty. Based
on this information, make an assessment of the likely outcome, before you have implemented any mitigation.
Protected group Summary of impact Negative
outcome
Neutral
outcome Positive outcome
Age • Feedback from engagement, in line with demographics, indicate
a potential negative impact of the very elderly with no access to
private transport ☒ ☐ ☐
Disability • No specific impactful change to current provision to this client
group ☐ ☒ ☐
Gender reassignment • No specific impactful change to current provision to this client
group ☐ ☒ ☐
Marriage and civil
partnership • No specific impactful change to current provision to this client
group ☐ ☒ ☐
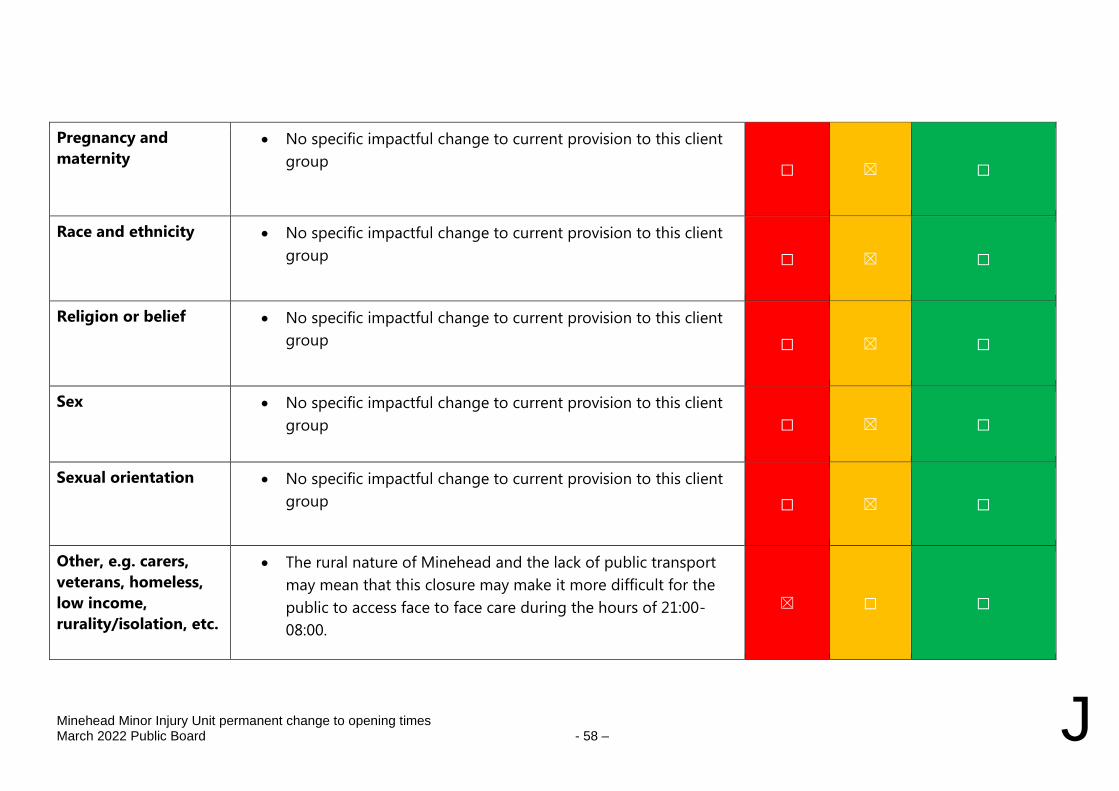
Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 58 – J
Pregnancy and
maternity • No specific impactful change to current provision to this client
group ☐ ☒ ☐
Race and ethnicity • No specific impactful change to current provision to this client
group ☐ ☒ ☐
Religion or belief • No specific impactful change to current provision to this client
group ☐ ☒ ☐
Sex • No specific impactful change to current provision to this client
group ☐ ☒ ☐
Sexual orientation • No specific impactful change to current provision to this client
group ☐ ☒ ☐
Other, e.g. carers,
veterans, homeless,
low income,
rurality/isolation, etc.
• The rural nature of Minehead and the lack of public transport
may mean that this closure may make it more difficult for the
public to access face to face care during the hours of 21:00-
08:00.
☒ ☐ ☐
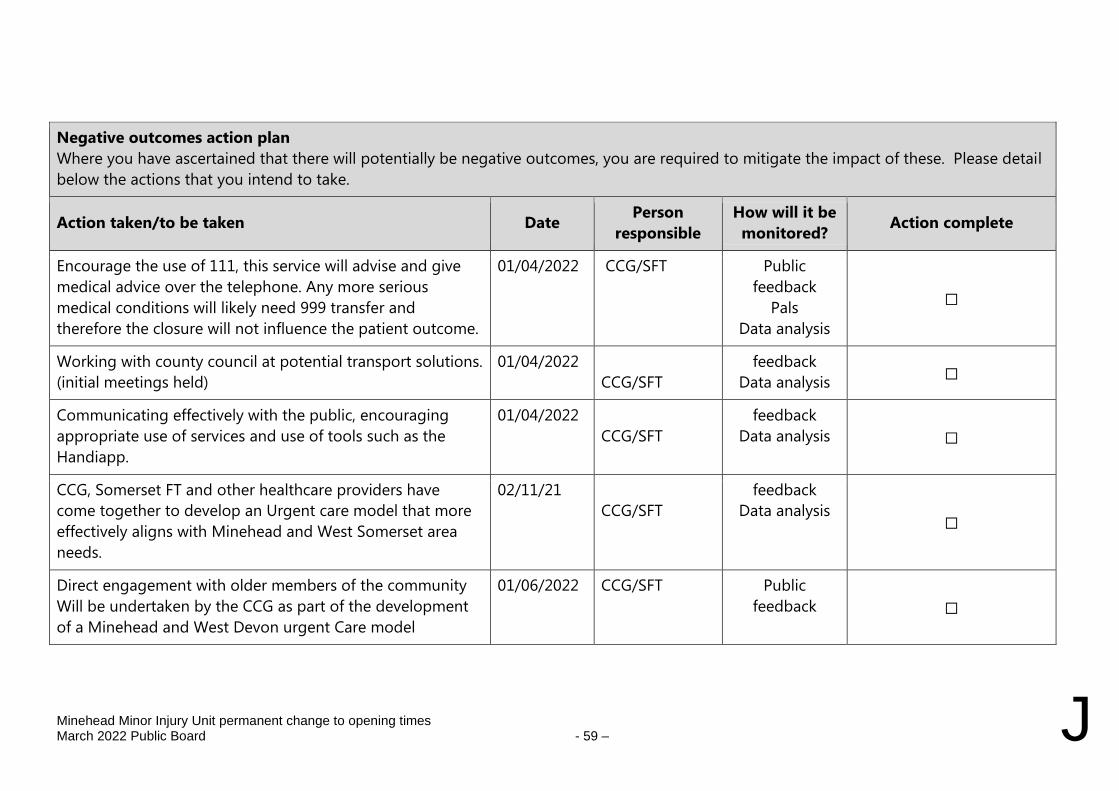
Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 59 – J
Negative outcomes action plan
Where you have ascertained that there will potentially be negative outcomes, you are required to mitigate the impact of these. Please detail
below the actions that you intend to take.
Action taken/to be taken Date Person
responsible
How will it be
monitored? Action complete
Encourage the use of 111, this service will advise and give
medical advice over the telephone. Any more serious
medical conditions will likely need 999 transfer and
therefore the closure will not influence the patient outcome.
01/04/2022 CCG/SFT
Public
feedback
Pals
Data analysis
☐
Working with county council at potential transport solutions.
(initial meetings held)
01/04/2022
CCG/SFT
feedback
Data analysis ☐
Communicating effectively with the public, encouraging
appropriate use of services and use of tools such as the
Handiapp.
01/04/2022
CCG/SFT
feedback
Data analysis ☐
CCG, Somerset FT and other healthcare providers have
come together to develop an Urgent care model that more
effectively aligns with Minehead and West Somerset area
needs.
02/11/21
CCG/SFT
feedback
Data analysis ☐
Direct engagement with older members of the community
Will be undertaken by the CCG as part of the development
of a Minehead and West Devon urgent Care model
01/06/2022 CCG/SFT Public
feedback
☐
Minehead Minor Injury Unit permanent change to opening times
March 2022 Public Board - 60 – J
If negative impacts remain, please provide an explanation below.
Completed by: Deirdre Molloy
Date 04/02/22
Signed off by: Julie Jones
Date O4/02/22
Equality Lead/Manager sign off date:
To be reviewed by: (officer name)
Review date:
YDH Safer Staffing Report
March 2022 Public Board - 1 –
K
Yeovil District NHS Foundation Trust
REPORT TO: Board of Directors
REPORT TITLE: Safer Staffing Report
SPONSORING EXEC: Hayley Peters Chief Nurse – SFT/YDH
REPORT BY: Mark Robinson, Deputy Chief Nurse - YDH
PRESENTED BY: Hayley Peters Chief Nurse - SFT/YDH
Mark Robinson Deputy Chief Nurse - YDH
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☒ For Assurance/
Discussion ☐ For Approval / Decision ☐ For Information
Executive Summary and Reason for presentation to Committee/Board
There is a requirement, following the publication of the Francis Report (February 2013, that NHS Boards receive a six monthly report on nursing and midwifery staffing. Subsequently, the NHS National Quality Board published new guidance, in November 2013, to support providers and commissioners to make the right decisions about nursing, midwifery and care staffing capacity and capability. In January 2018, the National Quality Board refreshed its’ guidance for safe, sustainable and productive staffing to provide a number of ward and department specific improvement resources. These resources have been utilised accordingly. The Board of Directors (BoD) received the previous staffing report in October 2021. This report highlights any significant changes in nursing and midwifery workforce; since the last report and provides the Board with an overview of key issues and changes to the nursing and midwifery establishment in response to the pandemic. Key issues to note include:
• The current elevation in some ward establishment,
Jasmine remaining open and other escalation areas being operationalised more frequently across the Trust, has significantly impacted on the Trust’s ability to cover

YDH Safer Staffing Report
March 2022 Public Board - 2 – K
vacant shifts with temporary bank staff and there has been an increased reliance on nurse agencies outside of national frameworks. The impact of lock downs, the need for some staff to continue to shield and continuing to manage higher than normal sickness levels, have also had a significant effect. In an attempt to mitigate the short fall and improve fill rates, the number of bank shifts offered with an additional incentive payment has continued and for specialist area such as ICU and ED further incentives were also offered.
• Despite these additional incentives it has been difficult to maintain the required levels of registered and unregistered healthcare professionals in clinical areas during the July to December 2021 period.
• Sickness rates in nursing have continued to run well above the 3.5% baseline and this has continued to impact on nursing teams and further increased the reliance on bank and agencies to keep staffing levels adequate. The average sickness rate for Nursing for July to December 2021 has been 6.65%, however with emergence of the Omicron variant there was a significant increase in sickness rates attributed to COVID during December although there was also an increase in non-COVID sickness. The number of shifts lost per day because of sickness has been between 6 – 12 registered and non-registered nurses a day.
• Nurse vacancies have improved significantly since the last report and as of 31 December 2021 there were no vacancies in ward areas. Theatres has continued to have difficulties recruiting staff despite support from the overseas recruitment programme the current vacancy factor is running at 12.18 wte. Midwifery vacancies have improved since the last report and as of the 31st December 2021 were only reporting 2 vacancies. Nursing, Midwifery and Theatres used above cap agency for RNs on 790 occasions in this reporting period. A total of 3104 RN shifts were covered through a combination extra shifts and bank shifts this is significantly lower than the previous 6 months despite additional incentives offered.
• Model Hospital data shows over the last 3 recorded data submissions the CHPPD are equal to or slightly below Peer and National Median. This means that we have less or equal RN time per patient as compared to other organisations.
YDH Safer Staffing Report
March 2022 Public Board - 3 – K
• New appointments of Registered Nurses during the period under review was 40 plus 35 overseas gained NMC registration are working as band 5 registered nurses. There are 44 Preceptorship Nurses currently in training and should successfully gain NMC registration in the coming months.
• There were 154 staffing shortage related incident forms completed during July to December 2021. 41 were related to maternity staffing. This report has been reviewed by the Chief Nurse who is satisfied that there are processes in place and provide assurance that during the pandemic, staffing has been managed appropriately in the last 6 months.
Recommendation The Board are asked to note the content of this report and be assured that senior nurses are reviewing staffing levels daily to ensure that there is sufficient nursing and midwifery capacity in line with national guidance, which will ensure a clinical workforce that will deliver safe, effective and compassionate care.
Key risks addressed:
Risk No: 342 – Registered nursing staffing levels-recruitment and retention
Risk No: 355 – Theatres staffing levels
Risk No: 705 - Inability to fill all vacant HCA shifts on wards
There are a number of Business cases pending approval that have been cited in this report:
EC11 ICU Band 7 Establishment EC63 Theatre education team and workforce transformation EC 62 6 Day Elective Operating EC 35 Improved provision of weekend staffing to support
Trauma and CEPOD
EC 64 Improved provision of staffing to improve utilisation and efficiency of Theatres
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☒ Care for our Population ☒ Develop our People
☐ Innovate and Collaborate ☒ Develop a Sustainable System
YDH Safer Staffing Report
March 2022 Public Board - 4 – K
Somerset NHS FT
☐ Obj 1 Inclusive culture ☐ Obj 4 Safe services ☐ Obj 7 Improving outcomes
☐ Obj 2 Collaboration ☐ Obj 5 Self management ☐ Obj 8 Workforce
☐ Obj 3 Independent lives ☐ Obj 6 Value all people alike ☐ Obj 9 Performance
☐ Obj 10 Finance
Implications/Requirements (Please select any which are relevant to this paper)
☐ Financial ☐ Legislation ☒ Workforce ☐ Estates ☐ ICT ☒ Patient Safety /
Quality
Details:
Equality The Trust wants its services to be as accessible as possible, to as many people as
possible. Please indicate whether the report has an impact on the protected characteristics
☐ This report has not been assessed against the Trust’s Equality Impact Assessment
Tool and there are no proposals or matters which affect any persons with protected characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
Senior staff are involved in the preparation of the report.
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
A report is presented to the Board of Directors on a regular basis.
Reference to CQC domains (Please select any which are relevant to this paper)
☒ Safe ☒ Effective ☒ Caring ☐ Responsive ☒ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
YDH Safer Staffing Report March 2022 Public Board - 1 – K
NURSING AND MIDWIFERY SAFER STAFFING
REPORT JULY TO DECEMBER 2021
1 Introduction
1.1 There is a requirement, following the publication of the Francis Report (February 2013, that NHS Boards receive a six monthly report on nursing and midwifery staffing. Subsequently, the NHS National Quality Board published new guidance, in November 2013, to support providers and commissioners to make the right decisions about nursing, midwifery and care staffing capacity and capability. In January 2018, the National Quality Board refreshed its’ guidance for safe, sustainable and productive staffing to provide a number of ward and department specific improvement resources. The recommendations can be summarised as follows:
• A systematic approach should be adopted to using an evidence-informed decision support tool, triangulated with professional judgement and comparison with relevant peers
• A strategic staffing review must be undertaken annually or sooner if changes to
services are planned
• Staffing decisions should be taken in the context of the wider registered multi-
professional team
• Consider of safer staffing requirements and workforce productivity should form
an integral part of the operational planning process
• Actions plans to address local recruitment and retention priorities should be in
place and subject to regular review
• Flexible employment options and efficient deployment of staff should be
maximised across the hospital to limit the use of temporary staff
• A local dashboard should be in place to assure stakeholders regarding safe and
sustainable staffing.
• Organisations should ensure they have an appropriate escalation process in
cases where staffing is not delivering the outcomes identified.
• All organisations should include a process to determine additional uplift
requirements based on the needs of the patients and staff
• All organisations should investigate staffing related incidents and their outcomes
on patients and staff, and ensure action and feedback.
1.2 This approach is aligned to the CNO’s Commitment 9 of Leading Change, Adding Value:
a framework for nursing, midwifery and care staff (May, 2016).
2 Purpose
2.1 The purpose of this paper is to provide the Board of Directors with assurance of
delivery of safe staffing levels for the period June 2020 to December 2020, which uses
recommended evidence based tools, triangulated with professional judgement, and
makes recommendations to any changes to establishments for the 2020/21 financial
year.
2.2 It provides an overview of nursing staffing capacity and compliance with the National
Institute for Clinical Excellence (NICE) Safe Staffing and NQB standards.
YDH Safer Staffing Report March 2022 Public Board - 2 – K
2.3 It provides a cumulative oversight of care hours per patient day (CHPPD) and cost per
care hour over the last 6 months. These new metrics replace the previously reported
planned and actual staffing and are published on NHS Choices.
3 Scope
3.1 This report focusses on all inpatient areas including:
• All inpatient adult wards including critical care
• Emergency admission areas including the Emergency Department and
Emergency Assessment Unit
• Inpatient paediatric wards including SCBU
• Maternity services
• Operating Theatres (excluding day case)
• Outpatient Department
3.2 This report does not include Macmillan or day case units.
4 National Nursing and Midwifery Staffing Context
4.1 Nationally workforce supply remains high on the agenda; in June 2019 NHSi published the NHS People Plan to ensure that culture, leadership, tackling the nursing challenge and delivering care in the 21st century are considered when developing a new operating model for the NHS workforce.
4.2 The Governments immigration white paper was presented to Parliament on 19th
December 2018. The paper set out the Government’s plans to create a single skills
based immigration system for when the UK leaves the European Union. The Home
Office has accepted the recommendation made by the Migration Advisory Committee
(MAC) January 2020 to remove the cap on numbers in the existing Tier 2 visa route
(for skilled workers) and make the sponsorship system less bureaucratic for
employers. It was also recommended a minimum salary threshold of £30,000 for
workers with intermediate skills. However, this threshold has now be lowered to
£26,600 for skilled workers and those paid in accordance with nationally agreed pay
scales are exempt from these thresholds and any migrant worker must be paid on
these scales, but cannot be paid less than £20,480. This includes all nurses working
in the NHS who are paid in accordance with the agenda for change pay scales. The
new Health and Care Visa which was launched last year has enabled fast track entry
with reduced visa fees, and a permanent suspension of the Immigration Health
Surcharge for health and care workers.
4.3 In ‘Closing the Gap, Key areas for action on the health and care workforce’, (The Health Foundation, The King’s Fund, Nuffield Trust, 2019), it is estimated that an additional 5,000 more nurses need to start in training by 2021. To achieve this, recommendations to Government include increases in financial support to nursing students such as ‘cost of living grants’ and covering the costs of tuition fees. The availability and quality of clinical placements also needs to be addressed. The report stipulates that, ‘whilst policy action and investment could transform the outlook for nurse staffing shortages over the next decade, the prospects until the end of parliament are much more worrying’. To avoid nurse staffing shortages acting as a major brake to the Long Term Plan, international recruitment will need to play a substantial role with an additional 5,000 internationally recruited nurses estimated to be needed each year until
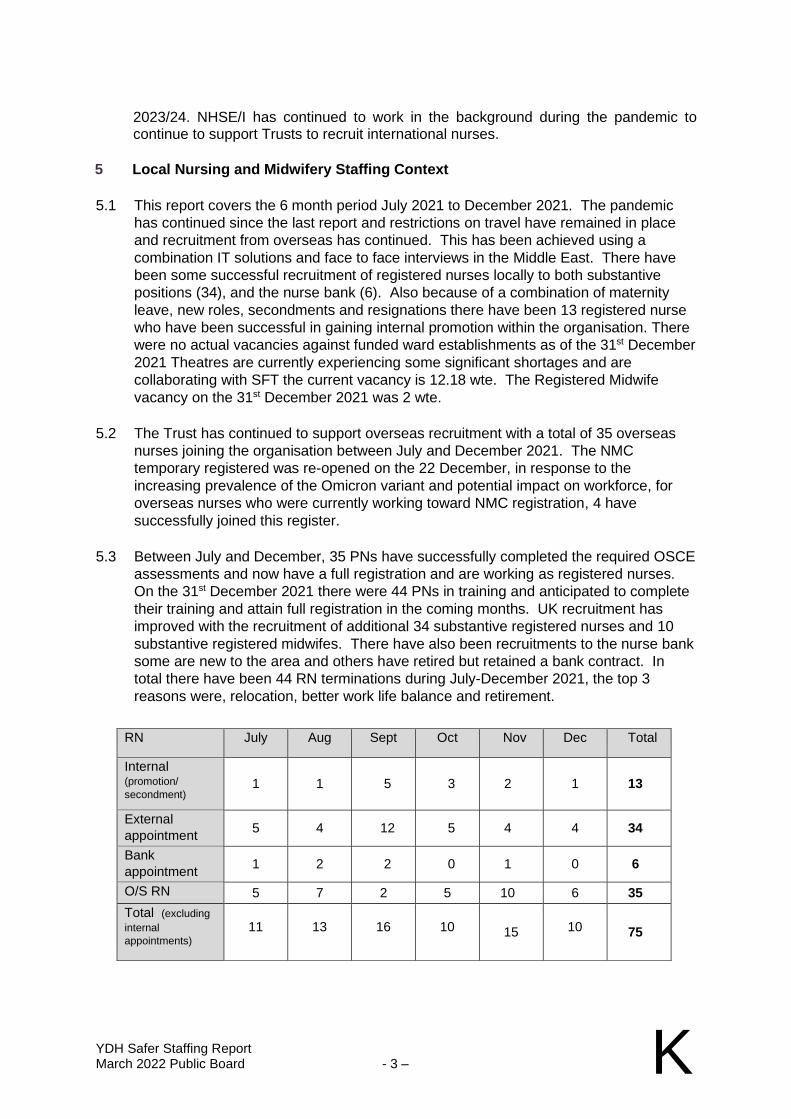
YDH Safer Staffing Report March 2022 Public Board - 3 – K
2023/24. NHSE/I has continued to work in the background during the pandemic to continue to support Trusts to recruit international nurses.
5 Local Nursing and Midwifery Staffing Context
5.1 This report covers the 6 month period July 2021 to December 2021. The pandemic
has continued since the last report and restrictions on travel have remained in place
and recruitment from overseas has continued. This has been achieved using a
combination IT solutions and face to face interviews in the Middle East. There have
been some successful recruitment of registered nurses locally to both substantive
positions (34), and the nurse bank (6). Also because of a combination of maternity
leave, new roles, secondments and resignations there have been 13 registered nurse
who have been successful in gaining internal promotion within the organisation. There
were no actual vacancies against funded ward establishments as of the 31st December
2021 Theatres are currently experiencing some significant shortages and are
collaborating with SFT the current vacancy is 12.18 wte. The Registered Midwife
vacancy on the 31st December 2021 was 2 wte.
5.2 The Trust has continued to support overseas recruitment with a total of 35 overseas
nurses joining the organisation between July and December 2021. The NMC
temporary registered was re-opened on the 22 December, in response to the
increasing prevalence of the Omicron variant and potential impact on workforce, for
overseas nurses who were currently working toward NMC registration, 4 have
successfully joined this register.
5.3 Between July and December, 35 PNs have successfully completed the required OSCE
assessments and now have a full registration and are working as registered nurses.
On the 31st December 2021 there were 44 PNs in training and anticipated to complete
their training and attain full registration in the coming months. UK recruitment has
improved with the recruitment of additional 34 substantive registered nurses and 10
substantive registered midwifes. There have also been recruitments to the nurse bank
some are new to the area and others have retired but retained a bank contract. In
total there have been 44 RN terminations during July-December 2021, the top 3
reasons were, relocation, better work life balance and retirement.
RN July Aug Sept Oct Nov Dec Total
Internal (promotion/
secondment) 1 1 5 3 2 1 13
External
appointment 5 4 12 5 4 4 34
Bank
appointment 1 2 2 0 1 0 6
O/S RN 5 7 2 5 10 6 35
Total (excluding
internal
appointments) 11 13 16 10 15 10 75
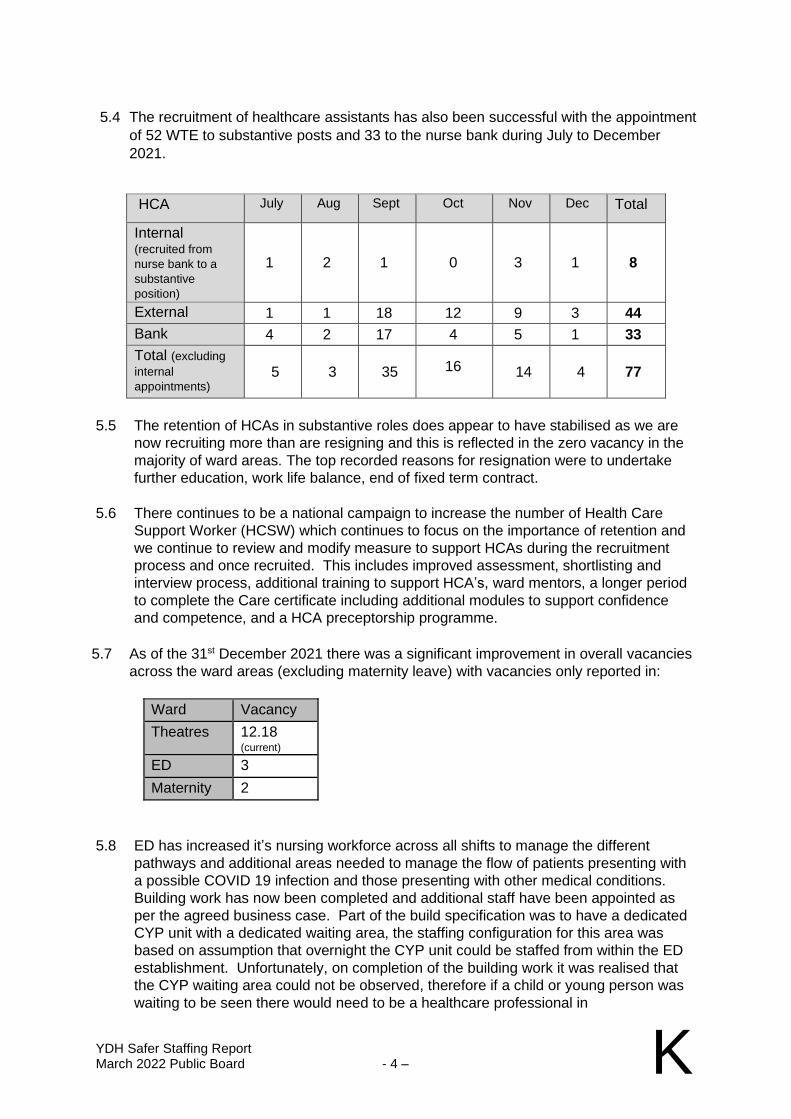
YDH Safer Staffing Report March 2022 Public Board - 4 – K
5.4 The recruitment of healthcare assistants has also been successful with the appointment
of 52 WTE to substantive posts and 33 to the nurse bank during July to December
2021.
HCA July Aug Sept Oct Nov Dec Total
Internal (recruited from
nurse bank to a
substantive
position)
1 2 1 0 3 1 8
External 1 1 18 12 9 3 44
Bank 4 2 17 4 5 1 33
Total (excluding
internal
appointments) 5 3 35 16 14 4 77
5.5 The retention of HCAs in substantive roles does appear to have stabilised as we are
now recruiting more than are resigning and this is reflected in the zero vacancy in the
majority of ward areas. The top recorded reasons for resignation were to undertake
further education, work life balance, end of fixed term contract.
5.6 There continues to be a national campaign to increase the number of Health Care
Support Worker (HCSW) which continues to focus on the importance of retention and
we continue to review and modify measure to support HCAs during the recruitment
process and once recruited. This includes improved assessment, shortlisting and
interview process, additional training to support HCA’s, ward mentors, a longer period
to complete the Care certificate including additional modules to support confidence
and competence, and a HCA preceptorship programme.
5.7 As of the 31st December 2021 there was a significant improvement in overall vacancies
across the ward areas (excluding maternity leave) with vacancies only reported in:
Ward Vacancy
Theatres 12.18 (current)
ED 3
Maternity 2
5.8 ED has increased it’s nursing workforce across all shifts to manage the different
pathways and additional areas needed to manage the flow of patients presenting with
a possible COVID 19 infection and those presenting with other medical conditions.
Building work has now been completed and additional staff have been appointed as
per the agreed business case. Part of the build specification was to have a dedicated
CYP unit with a dedicated waiting area, the staffing configuration for this area was
based on assumption that overnight the CYP unit could be staffed from within the ED
establishment. Unfortunately, on completion of the building work it was realised that
the CYP waiting area could not be observed, therefore if a child or young person was
waiting to be seen there would need to be a healthcare professional in
YDH Safer Staffing Report March 2022 Public Board - 5 – K
attendance, in case of deterioration. This was identified as a significant risk and
additional funding was agreed to mitigate this risk. On the 31st December 2021 ED
was reporting only 3 wte vacancy.
5.9 Theatre staffing has been a challenge and the team has been largely reliant on the
Overseas Recruitment and block agency bookings, despite a rolling local advert.
Overseas recruitment has extended the lead in period because staff need to be able to
function safely across all specialities and cover the on-call. The figure reported above
is the current (actual) vacancy and work has already started with SFT to look at a
system wide recruitment initiative. Some of the shortfall is currently covered by block
agency booking.
5.10 There has been no significant changes to ward configuration since the last report and
there have been no siginfacant changes to establishments in current run rate.
5.11 9A has continued to support patients needing additional respiratory support because
of COVID and stands up the Enhance Care Respiratory Unit (ECRU) when required.
This has supported the flow of patients into ICU and out of ICU, additionally the ward
is also the primary cohort ward and has had to manage a mix of surgical and medical
admissions. The complexities of managing a higher level of care and mixed
specialities necessitated that registered and non-registered nurse numbers have
increased on a number of shifts to support the early recognition in deterioration and
ensure that supportive treatments were put in place quickly.
5.12 The requirement for highly skilled staff both registered and non-registered has
continued to be challenge in the intensive care unit. The requirement to increase the
number of available staff has been dynamic and reactive during the pandemic to
deliver the levels of care required to critically ill patients. Whilst the numbers of
patients with COVID as reason for admission has reduced during this period there has
still been a high number of patients requiring highly invasive treatments. Recruitment
has continued, mainly from overseas which has presented some significant challenges
regard training and competency and there has been an increased reliance on agency
and bank nurses when acuity has been elevated.
5.13 There has been an agreement from the executive team that we could over recruit to
reduce the reliance on temporary staffing, unfortunately this was not achieved,
5.14 The COVID swabbing clinic is now firmly established and continues to support the
patient pathway for elective care and staff who report COVID symptoms or have been
in contact with others who may be infected. The allergy clinic for those patients who
needed to have their COVID vaccination in a hospital setting because of the risk of
moderate to severe allergy has continued this has been staffed using a combination of
bank shifts and redeployment from substantive rotas.
5.15 Jasmine ward has remained open and continues to support the care of those patients
who no longer require hospital care, but are unable to be discharged. The staffing of
Jasmine did present some significant challenge with an increase in incident reports
and lack of care continuity because there was no substantive workforce. Therefore,
we have substantively recruited some staff to the ward and also have a dedicated
ward manager which has made a significant difference.
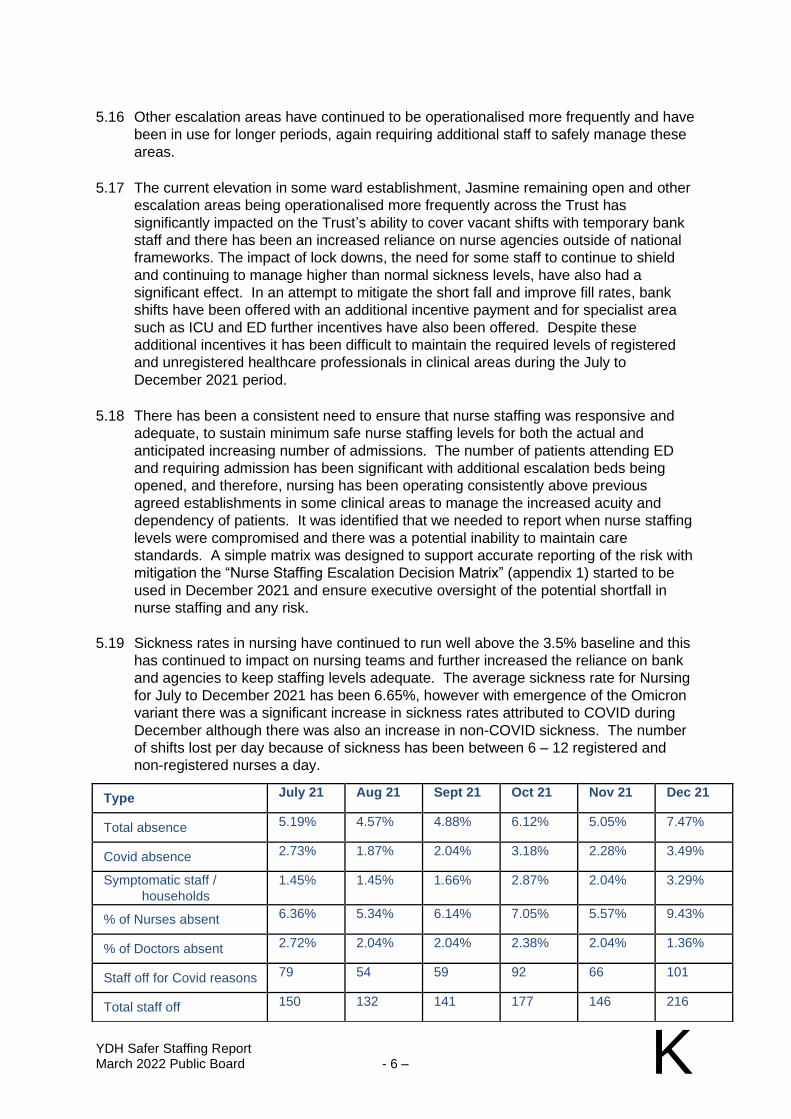
YDH Safer Staffing Report March 2022 Public Board - 6 – K
5.16 Other escalation areas have continued to be operationalised more frequently and have
been in use for longer periods, again requiring additional staff to safely manage these
areas.
5.17 The current elevation in some ward establishment, Jasmine remaining open and other
escalation areas being operationalised more frequently across the Trust has
significantly impacted on the Trust’s ability to cover vacant shifts with temporary bank
staff and there has been an increased reliance on nurse agencies outside of national
frameworks. The impact of lock downs, the need for some staff to continue to shield
and continuing to manage higher than normal sickness levels, have also had a
significant effect. In an attempt to mitigate the short fall and improve fill rates, bank
shifts have been offered with an additional incentive payment and for specialist area
such as ICU and ED further incentives have also been offered. Despite these
additional incentives it has been difficult to maintain the required levels of registered
and unregistered healthcare professionals in clinical areas during the July to
December 2021 period.
5.18 There has been a consistent need to ensure that nurse staffing was responsive and
adequate, to sustain minimum safe nurse staffing levels for both the actual and
anticipated increasing number of admissions. The number of patients attending ED
and requiring admission has been significant with additional escalation beds being
opened, and therefore, nursing has been operating consistently above previous
agreed establishments in some clinical areas to manage the increased acuity and
dependency of patients. It was identified that we needed to report when nurse staffing
levels were compromised and there was a potential inability to maintain care
standards. A simple matrix was designed to support accurate reporting of the risk with
mitigation the “Nurse Staffing Escalation Decision Matrix” (appendix 1) started to be
used in December 2021 and ensure executive oversight of the potential shortfall in
nurse staffing and any risk.
5.19 Sickness rates in nursing have continued to run well above the 3.5% baseline and this
has continued to impact on nursing teams and further increased the reliance on bank
and agencies to keep staffing levels adequate. The average sickness rate for Nursing
for July to December 2021 has been 6.65%, however with emergence of the Omicron
variant there was a significant increase in sickness rates attributed to COVID during
December although there was also an increase in non-COVID sickness. The number
of shifts lost per day because of sickness has been between 6 – 12 registered and
non-registered nurses a day.
Type July 21 Aug 21 Sept 21 Oct 21 Nov 21 Dec 21
Total absence 5.19% 4.57% 4.88% 6.12% 5.05% 7.47%
Covid absence 2.73% 1.87% 2.04% 3.18% 2.28% 3.49%
Symptomatic staff /
households
1.45% 1.45% 1.66% 2.87% 2.04% 3.29%
% of Nurses absent 6.36% 5.34% 6.14% 7.05% 5.57% 9.43%
% of Doctors absent 2.72% 2.04% 2.04% 2.38% 2.04% 1.36%
Staff off for Covid reasons 79 54 59 92 66 101
Total staff off 150 132 141 177 146 216
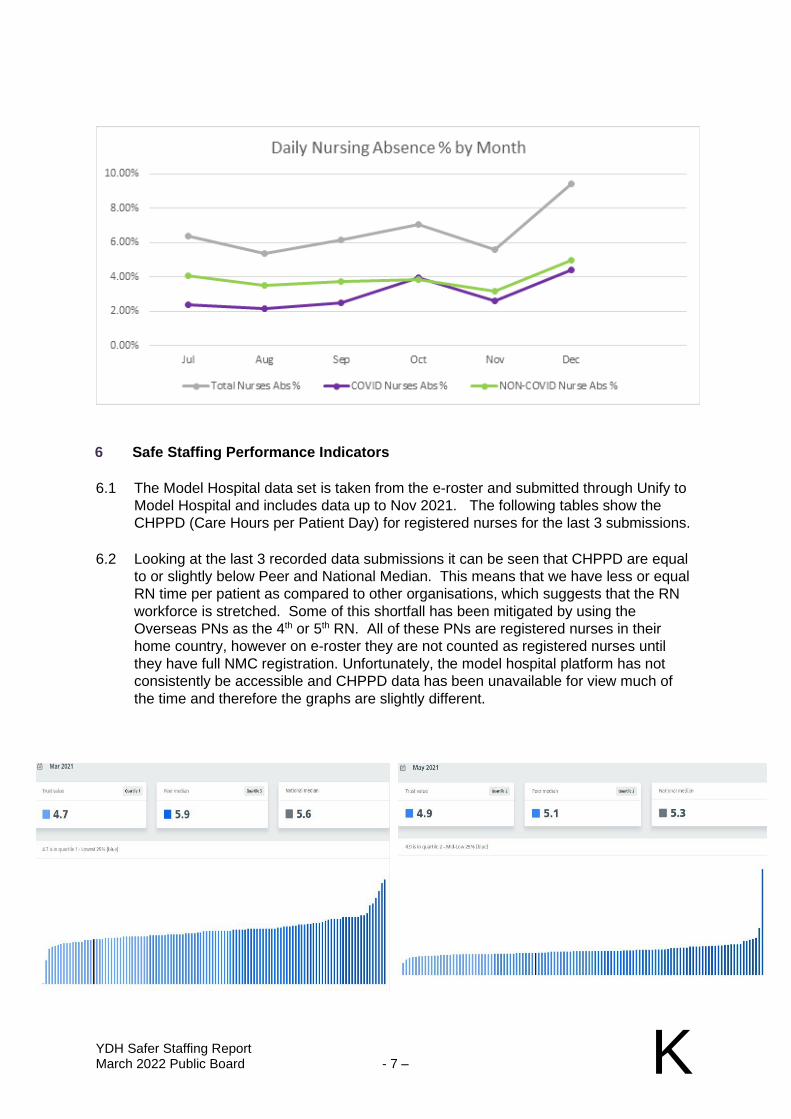
YDH Safer Staffing Report March 2022 Public Board - 7 – K
6 Safe Staffing Performance Indicators
6.1 The Model Hospital data set is taken from the e-roster and submitted through Unify to
Model Hospital and includes data up to Nov 2021. The following tables show the
CHPPD (Care Hours per Patient Day) for registered nurses for the last 3 submissions.
6.2 Looking at the last 3 recorded data submissions it can be seen that CHPPD are equal
to or slightly below Peer and National Median. This means that we have less or equal
RN time per patient as compared to other organisations, which suggests that the RN
workforce is stretched. Some of this shortfall has been mitigated by using the
Overseas PNs as the 4th or 5th RN. All of these PNs are registered nurses in their
home country, however on e-roster they are not counted as registered nurses until
they have full NMC registration. Unfortunately, the model hospital platform has not
consistently be accessible and CHPPD data has been unavailable for view much of
the time and therefore the graphs are slightly different.
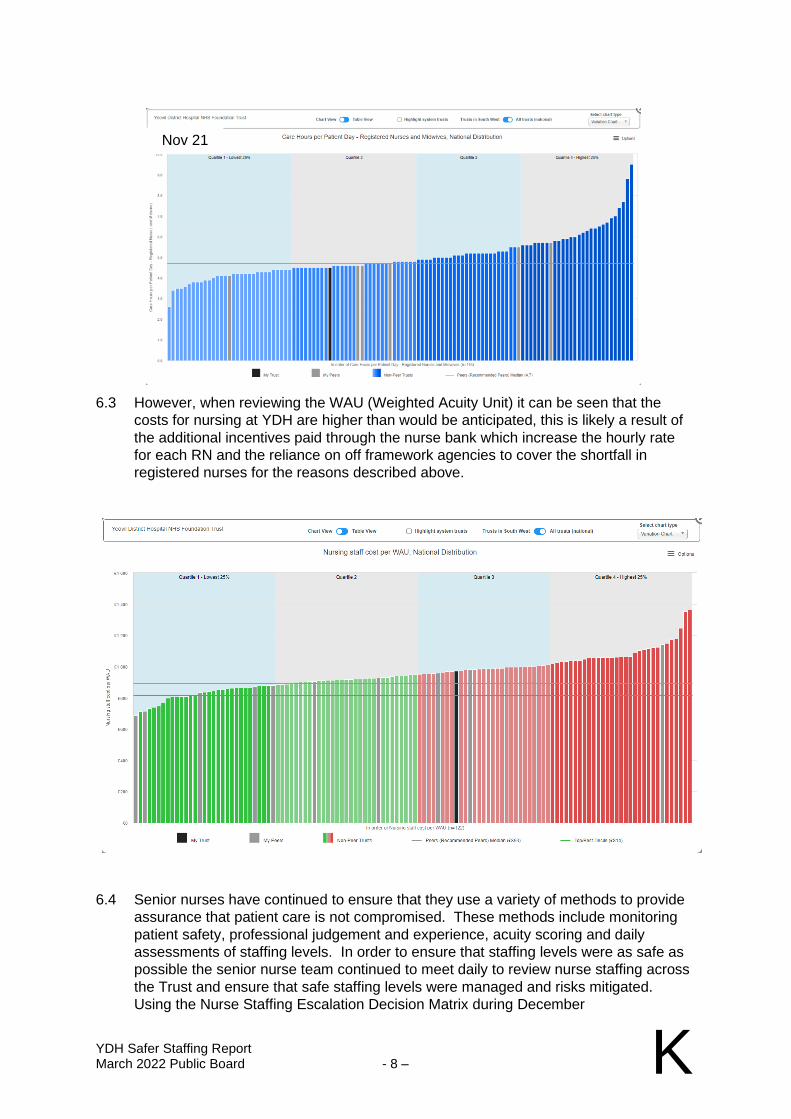
YDH Safer Staffing Report March 2022 Public Board - 8 – K
6.3 However, when reviewing the WAU (Weighted Acuity Unit) it can be seen that the
costs for nursing at YDH are higher than would be anticipated, this is likely a result of
the additional incentives paid through the nurse bank which increase the hourly rate
for each RN and the reliance on off framework agencies to cover the shortfall in
registered nurses for the reasons described above.
6.4 Senior nurses have continued to ensure that they use a variety of methods to provide
assurance that patient care is not compromised. These methods include monitoring
patient safety, professional judgement and experience, acuity scoring and daily
assessments of staffing levels. In order to ensure that staffing levels were as safe as
possible the senior nurse team continued to meet daily to review nurse staffing across
the Trust and ensure that safe staffing levels were managed and risks mitigated.
Using the Nurse Staffing Escalation Decision Matrix during December
Nov 21

YDH Safer Staffing Report March 2022 Public Board - 9 – K
demonstrates that there has still be a shortfall in the required numbers of registered
and unregistered nurses on a daily bases (there was no record for weekends or BHs)
6.5 It was noted in the last FRC meeting that there are still some significant challenges in
nursing including cost of ward configuration and associated increases in establishment
run rate, COVID swabbing clinic, allergy vaccination clinic and staffing of escalation
areas. The graph clearly shows the continuing impact of the pandemic as well the
effect of higher than normal sickness and the reliance on bank incentives and agency
to keep staffing levels at a safe level.
7 Staffing Review
7.1 Since the previous report the following changes have taken place:
• There has been a marked improvement in recruitment and breakeven position has been achieved in most inpatient areas now reporting no
0
1
2
Nurse Escalation Stage
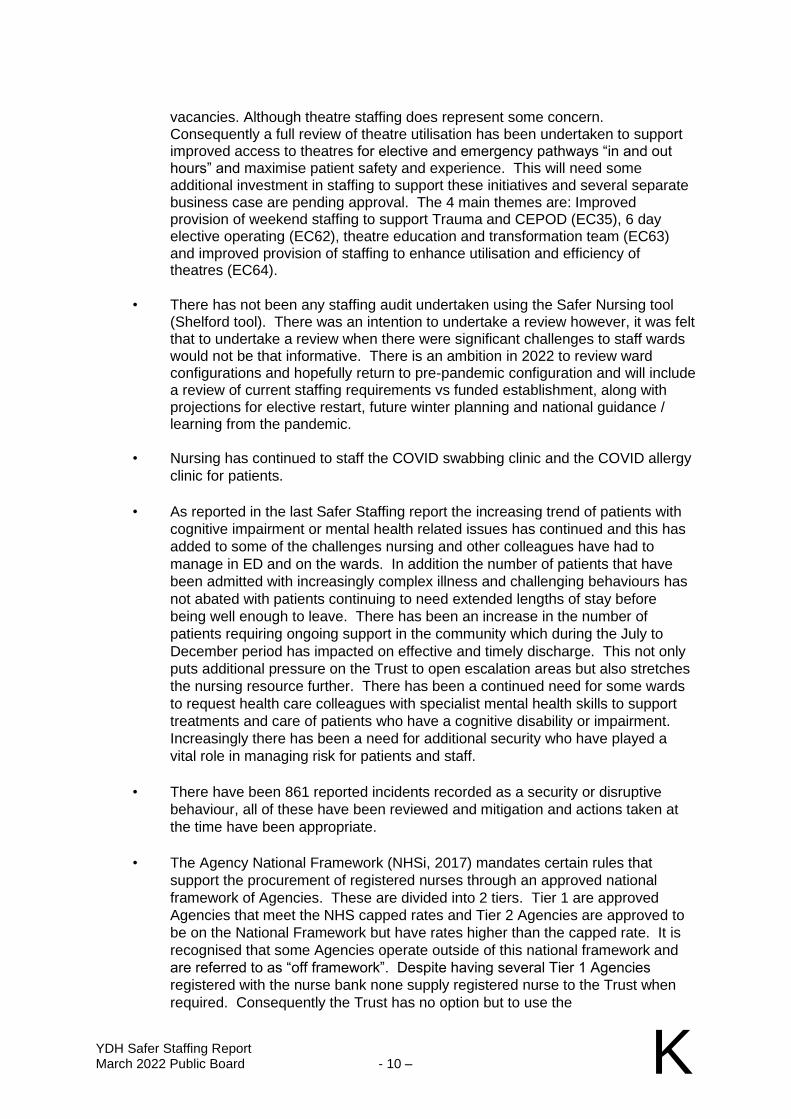
YDH Safer Staffing Report March 2022 Public Board - 10 – K
vacancies. Although theatre staffing does represent some concern. Consequently a full review of theatre utilisation has been undertaken to support improved access to theatres for elective and emergency pathways “in and out hours” and maximise patient safety and experience. This will need some additional investment in staffing to support these initiatives and several separate business case are pending approval. The 4 main themes are: Improved provision of weekend staffing to support Trauma and CEPOD (EC35), 6 day elective operating (EC62), theatre education and transformation team (EC63) and improved provision of staffing to enhance utilisation and efficiency of theatres (EC64).
• There has not been any staffing audit undertaken using the Safer Nursing tool (Shelford tool). There was an intention to undertake a review however, it was felt that to undertake a review when there were significant challenges to staff wards would not be that informative. There is an ambition in 2022 to review ward configurations and hopefully return to pre-pandemic configuration and will include a review of current staffing requirements vs funded establishment, along with projections for elective restart, future winter planning and national guidance / learning from the pandemic.
• Nursing has continued to staff the COVID swabbing clinic and the COVID allergy
clinic for patients.
• As reported in the last Safer Staffing report the increasing trend of patients with
cognitive impairment or mental health related issues has continued and this has
added to some of the challenges nursing and other colleagues have had to
manage in ED and on the wards. In addition the number of patients that have
been admitted with increasingly complex illness and challenging behaviours has
not abated with patients continuing to need extended lengths of stay before
being well enough to leave. There has been an increase in the number of
patients requiring ongoing support in the community which during the July to
December period has impacted on effective and timely discharge. This not only
puts additional pressure on the Trust to open escalation areas but also stretches
the nursing resource further. There has been a continued need for some wards
to request health care colleagues with specialist mental health skills to support
treatments and care of patients who have a cognitive disability or impairment.
Increasingly there has been a need for additional security who have played a
vital role in managing risk for patients and staff.
• There have been 861 reported incidents recorded as a security or disruptive
behaviour, all of these have been reviewed and mitigation and actions taken at
the time have been appropriate.
• The Agency National Framework (NHSi, 2017) mandates certain rules that
support the procurement of registered nurses through an approved national
framework of Agencies. These are divided into 2 tiers. Tier 1 are approved
Agencies that meet the NHS capped rates and Tier 2 Agencies are approved to
be on the National Framework but have rates higher than the capped rate. It is
recognised that some Agencies operate outside of this national framework and
are referred to as “off framework”. Despite having several Tier 1 Agencies
registered with the nurse bank none supply registered nurse to the Trust when
required. Consequently the Trust has no option but to use the
YDH Safer Staffing Report March 2022 Public Board - 11 – K
Agencies approved for Tier 2. The difference in cost between a Tier 1 and Tier 2
Agency
for a Band 5 registered nurse is approximately £13/hr. During the period under
review (July to December 2021) 790 RN shifts have been covered by a
combination of Tier 2 and off framework agencies. This is 164 more than the
January to June 2021 period.
• The highest number of registered agency staff used during this period was in ED
at 196, this is attributable to the need to staff CYP unit overnight, some long term
sickness, and maternity leave and because staffing numbers have been
increased during the day to support increases in acuity and activity. There is a
plan to step some of this additional support down during February/March 2022.
Despite this relatively high number of agency staff there were almost double this
number covered by bank staff or substantive staff working extra hours (374).
Overall there was less reliance on temporary staffing during the July to
December period than the previous 6 months, mainly because of the improved
vacancy position.
• ICU has relied more heavily on registered agency staff during July to December
period with 82 shifts being covered, compared to 37 in the previous 6 months.
However, the number of bank shifts covered for July to December period has
dropped considerably compared to the previous 6 months (199/356 respectively).
The reliance on additional agency staff has been because of increased levels of
COVID absence and increased activity and acuity of patients.
• The pandemic has identified some opportunities to strengthen the senior nurse
role in the management of the critical care patient pathway, improved decision
making, improved patient flow and shortening length of stay. In addition the
increase in a senior nurse presence across all shifts will support improvements in
sickness monitoring, performance management, staff education and training as
well as continuing to support health and well-being of the ICU team.
Consequently, a business case has been submitted and is pending approval:
ICU Band 7 establishment (EC11).
• Theatre usage of agency is also relatively high, essentially due to vacancy and
the need to block book and this is consistent with the previous 6 months.
• Maternity have also had to utilise agency midwifes more frequently this is has
mostly because of high levels of sickness attributable to the pandemic and some
vacancy.
• Interestingly, the overall number of shifts covered by bank staff has declined in
the July to December period (3104) when compared to the January to June
period (6220). This reduction is likely due to the impact of the pandemic on
overall resilience. This has also been evident in the number of shifts which have
remained uncovered with staff having to manage on less than optimal rotas.
• A total of 790 RN shifts were covered by Tier 2 agencies and off framework
agencies. There were 3104 RN shifts covered by a combination of extra shifts or
bank shifts during July to December 2021.
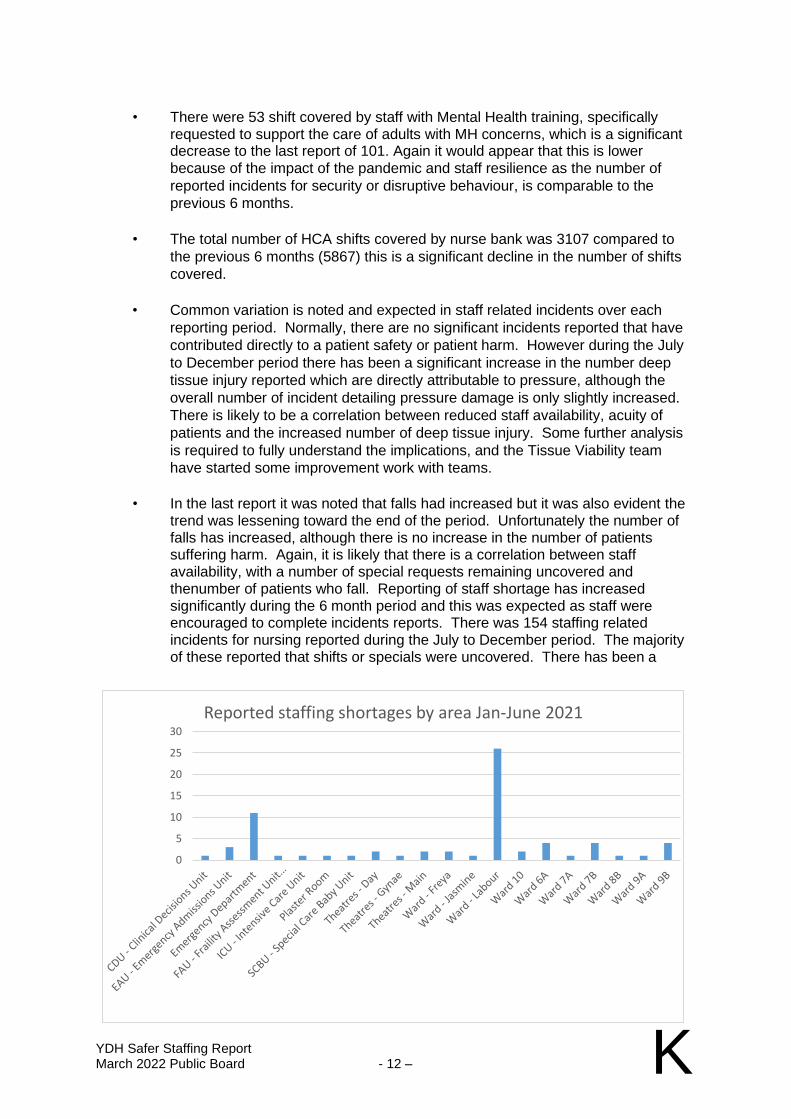
YDH Safer Staffing Report March 2022 Public Board - 12 – K
• There were 53 shift covered by staff with Mental Health training, specifically requested to support the care of adults with MH concerns, which is a significant decrease to the last report of 101. Again it would appear that this is lower
because of the impact of the pandemic and staff resilience as the number of
reported incidents for security or disruptive behaviour, is comparable to the
previous 6 months.
• The total number of HCA shifts covered by nurse bank was 3107 compared to
the previous 6 months (5867) this is a significant decline in the number of shifts
covered.
• Common variation is noted and expected in staff related incidents over each
reporting period. Normally, there are no significant incidents reported that have
contributed directly to a patient safety or patient harm. However during the July
to December period there has been a significant increase in the number deep
tissue injury reported which are directly attributable to pressure, although the
overall number of incident detailing pressure damage is only slightly increased.
There is likely to be a correlation between reduced staff availability, acuity of
patients and the increased number of deep tissue injury. Some further analysis
is required to fully understand the implications, and the Tissue Viability team
have started some improvement work with teams.
• In the last report it was noted that falls had increased but it was also evident the trend was lessening toward the end of the period. Unfortunately the number of falls has increased, although there is no increase in the number of patients suffering harm. Again, it is likely that there is a correlation between staff availability, with a number of special requests remaining uncovered and thenumber of patients who fall. Reporting of staff shortage has increased significantly during the 6 month period and this was expected as staff were encouraged to complete incidents reports. There was 154 staffing related incidents for nursing reported during the July to December period. The majority of these reported that shifts or specials were uncovered. There has been a
0
5
10
15
20
25
30
Reported staffing shortages by area Jan-June 2021
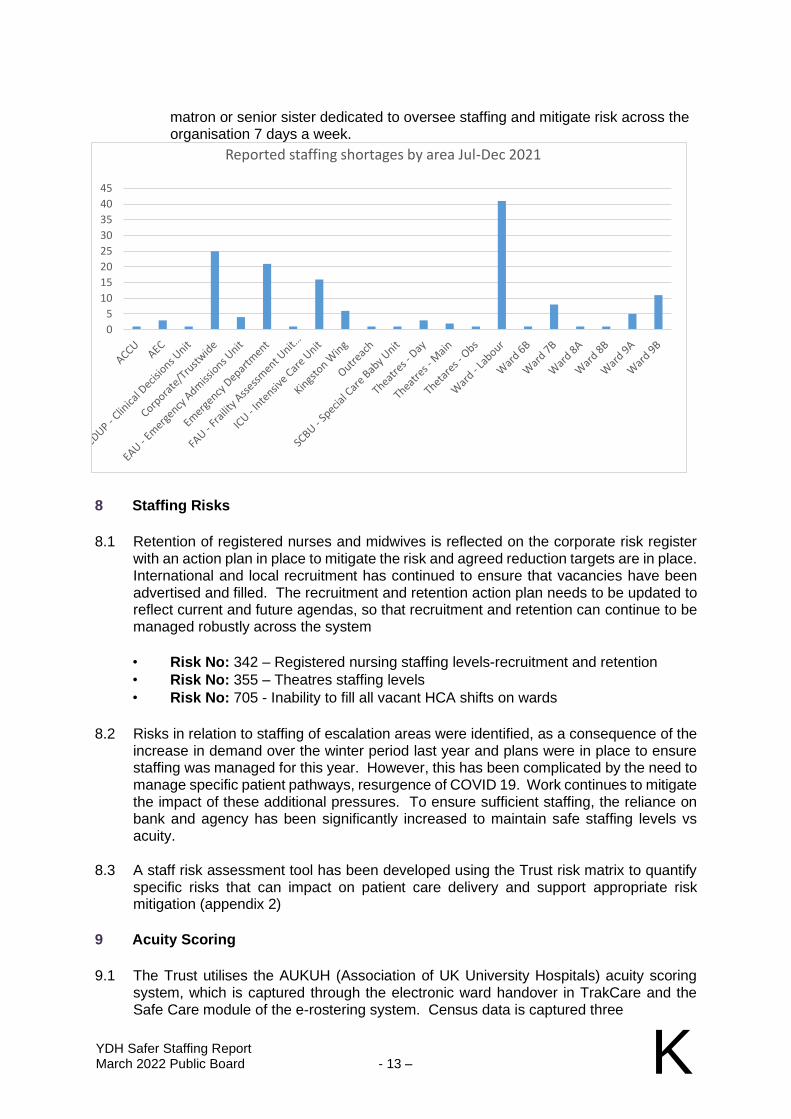
YDH Safer Staffing Report March 2022 Public Board - 13 – K
matron or senior sister dedicated to oversee staffing and mitigate risk across the organisation 7 days a week.
8 Staffing Risks
8.1 Retention of registered nurses and midwives is reflected on the corporate risk register with an action plan in place to mitigate the risk and agreed reduction targets are in place. International and local recruitment has continued to ensure that vacancies have been advertised and filled. The recruitment and retention action plan needs to be updated to reflect current and future agendas, so that recruitment and retention can continue to be managed robustly across the system
• Risk No: 342 – Registered nursing staffing levels-recruitment and retention
• Risk No: 355 – Theatres staffing levels
• Risk No: 705 - Inability to fill all vacant HCA shifts on wards
8.2 Risks in relation to staffing of escalation areas were identified, as a consequence of the increase in demand over the winter period last year and plans were in place to ensure staffing was managed for this year. However, this has been complicated by the need to manage specific patient pathways, resurgence of COVID 19. Work continues to mitigate the impact of these additional pressures. To ensure sufficient staffing, the reliance on bank and agency has been significantly increased to maintain safe staffing levels vs acuity.
8.3 A staff risk assessment tool has been developed using the Trust risk matrix to quantify specific risks that can impact on patient care delivery and support appropriate risk mitigation (appendix 2)
9 Acuity Scoring
9.1 The Trust utilises the AUKUH (Association of UK University Hospitals) acuity scoring system, which is captured through the electronic ward handover in TrakCare and the Safe Care module of the e-rostering system. Census data is captured three
0
5
10
15
20
25
30
35
40
45
Reported staffing shortages by area Jul-Dec 2021
YDH Safer Staffing Report March 2022 Public Board - 14 – K
times daily and staffing levels reviewed utilising a visual display together with professional judgement to allocate and deploy staffing to maintain safe levels. Ward level dashboards are in use to improve oversight of fill rates, vacancy and sickness, acuity levels and care hours per patient day (CHPPD). Looking at the data available in the safe care module it clearly shows in most areas the number CHPPD available on the ward areas are lower than what is required when matched to patient acuity. Over the next 6 months matrons will work with ward teams to ensure that this data accurately reflects what is happening on the wards and identify opportunities for working differently.
10 Quality Metrics
10.1 The Trust key performance indicators indicate that the overall standards of patient care have been maintained. There were no complaints specifically in relation to staffing levels reported during the period by patients or relatives, although there has been increase in the number concerns raised in regard to relatives receiving timely updates, answering of telephones and answering of call bells, it is likely that there is correlation with the reduced staffing levels as described above. There has been an increase in deep tissue damage as described above. There is also a delay in the timely recording of MUST scores and improvement work has started, additionally it also seem that there is a reporting error with is being investigated to identify how this can be resolved. Patient falls have increased slightly, even though during the last reporting period (January-June 2021) there was evidence of an improving trend. The continuance of the pandemic, the emergence of the Omicron variant and staff resilience have impacted on nurse staffing levels, coupled with increasing numbers of patients with dementia/delirium and general deconditioning have contributed to the number of falls reported. Thankfully there has been no increase in the number of patients suffer harm from a fall. Further information is available in the Quality Report.
11 Recruitment and Retention
12
11.1 Specialist areas continue to face some challenge especially Operating Theatres. Work is ongoing to recruit registered professionals into these areas with supervision and preceptorship programmes in place. Focused effort will be given to ensuring a continuous reduction in agency usage and workforce development for hard to fill posts over the next 6 to 12 months as we emerge from the pandemic.
11.2 The overseas nursing recruitment has been challenging this year although it is
anticipated that this will continue to ease as restrictions associated with the pandemic
ease.
11.3 A leadership development programme for band 5 registered nurses and newly appointed sisters/charge nurses has started with 15 staff being successfully given a place. Feedback so far from participants is very positive. There are plans to recruit a further cohort in 2022. Work continues to develop a modular course that could be available for all registered nurse to have an opportunity to apply for later this year. In addition we continue to support the training of Nurse Associates.
11.4 Also we have introduced changes to support the recruitment and retention of HCAs
which has been described earlier in this report.
13 Maternity Services
YDH Safer Staffing Report March 2022 Public Board - 15 – K
12.1 Midwifery staffing levels have been significantly challenged at times during the July to December period. There have been 10 successful appointments to vacancies, on the 31st December 2021 there was still 2 outstanding vacancies. The maternity unit has had some significant challenges with COVID related absence in hospital and community teams.
12.2 Senior midwifes have had to continually review staffing daily and have had to utilise on call midwifes, community teams to support the care of women in labour. In addition the supervisory coordinator has had to support women in labour and provide direct patient care. This has been identified as a “red flag” event by the NPSA and the supervisory status of the labour ward coordinator is considered a key criteria. There were 41 staffing incidents reported on Ulysses during July to December 2021 compared to only 26 in the previous 6 months.
12.3 The Trust assessment to the Ockenden IEA’s has now been reassessed and agreed with
the LMNS and Region. There is an ambition for the Trust to complete all required actions by March 2022, any actions that will not be achieved by the deadline need to be identified, an action plan is in place detailing actions required to achieve by a given date, to support the implementation of all IEA’s, pending 2nd Ockenden report in Spring 2022.
14 Recommendations
13.1 The Board of Directors is asked to note the information contained in this summary
report and the actions currently in place.
.
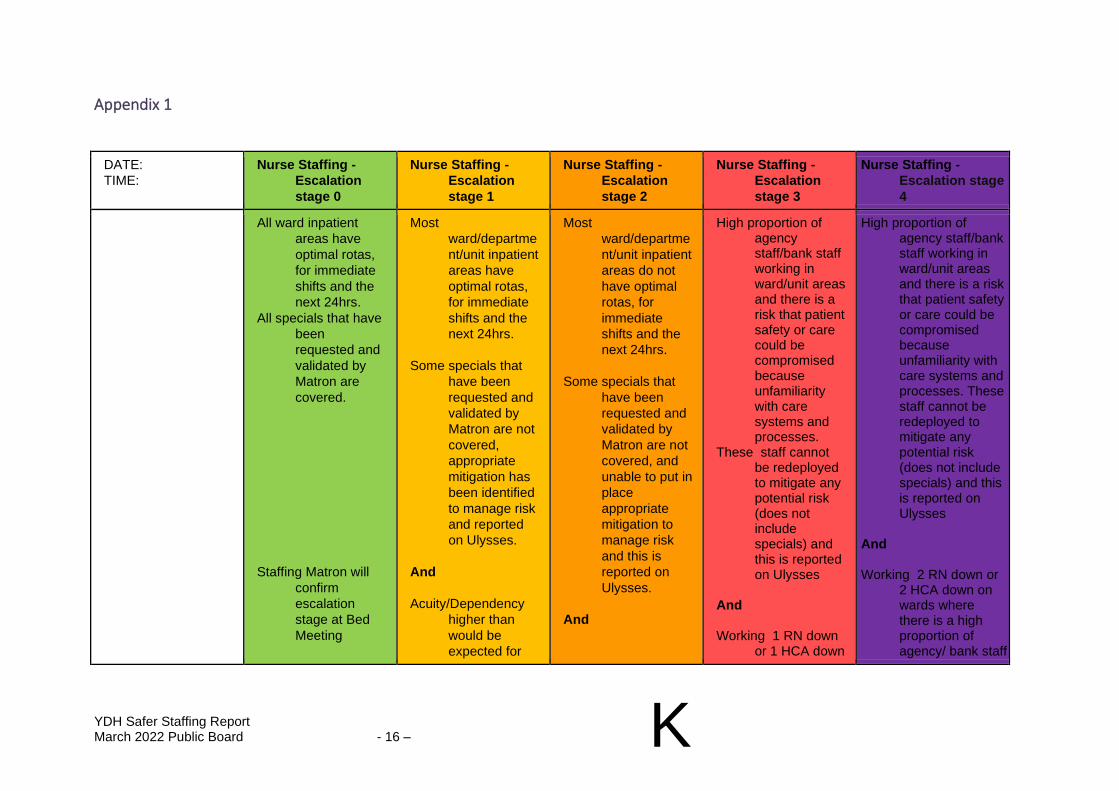
YDH Safer Staffing Report March 2022 Public Board - 16 – K
Appendix 1
DATE:
TIME:
Nurse Staffing -
Escalation
stage 0
Nurse Staffing -
Escalation
stage 1
Nurse Staffing -
Escalation
stage 2
Nurse Staffing -
Escalation
stage 3
Nurse Staffing -
Escalation stage
4
All ward inpatient
areas have
optimal rotas,
for immediate
shifts and the
next 24hrs.
All specials that have
been
requested and
validated by
Matron are
covered.
Staffing Matron will
confirm
escalation
stage at Bed
Meeting
Most
ward/departme
nt/unit inpatient
areas have
optimal rotas,
for immediate
shifts and the
next 24hrs.
Some specials that
have been
requested and
validated by
Matron are not
covered,
appropriate
mitigation has
been identified
to manage risk
and reported
on Ulysses.
And
Acuity/Dependency
higher than
would be
expected for
Most
ward/departme
nt/unit inpatient
areas do not
have optimal
rotas, for
immediate
shifts and the
next 24hrs.
Some specials that
have been
requested and
validated by
Matron are not
covered, and
unable to put in
place
appropriate
mitigation to
manage risk
and this is
reported on
Ulysses.
And
High proportion of agency staff/bank staff working in ward/unit areas and there is a risk that patient safety or care could be compromised because unfamiliarity with care systems and processes.
These staff cannot be redeployed to mitigate any potential risk (does not include specials) and this is reported on Ulysses
And Working 1 RN down
or 1 HCA down
High proportion of agency staff/bank staff working in ward/unit areas and there is a risk that patient safety or care could be compromised because unfamiliarity with care systems and processes. These staff cannot be redeployed to mitigate any potential risk (does not include specials) and this is reported on Ulysses
And Working 2 RN down or
2 HCA down on wards where there is a high proportion of agency/ bank staff
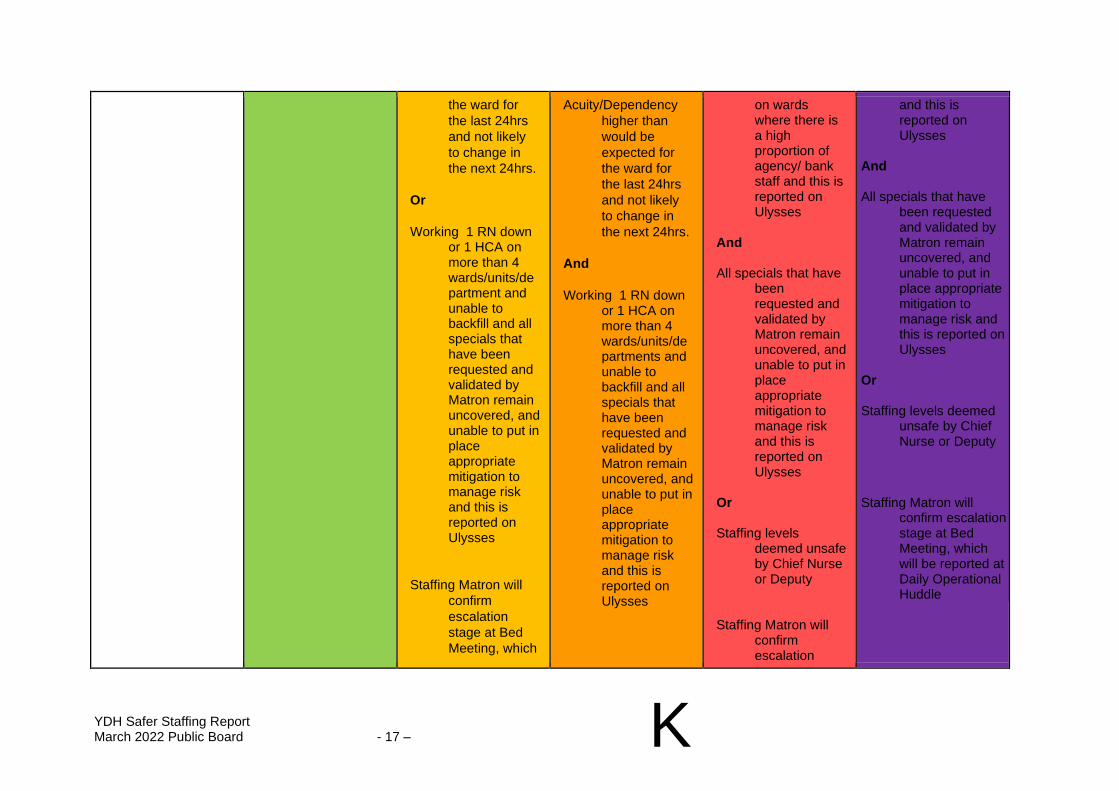
YDH Safer Staffing Report March 2022 Public Board - 17 – K
the ward for
the last 24hrs
and not likely
to change in
the next 24hrs.
Or
Working 1 RN down or 1 HCA on more than 4 wards/units/department and unable to backfill and all specials that have been requested and validated by Matron remain uncovered, and unable to put in place appropriate mitigation to manage risk and this is reported on Ulysses
Staffing Matron will
confirm
escalation
stage at Bed
Meeting, which
Acuity/Dependency
higher than
would be
expected for
the ward for
the last 24hrs
and not likely
to change in
the next 24hrs.
And
Working 1 RN down or 1 HCA on more than 4 wards/units/departments and unable to backfill and all specials that have been requested and validated by Matron remain uncovered, and unable to put in place appropriate mitigation to manage risk and this is reported on Ulysses
on wards where there is a high proportion of agency/ bank staff and this is reported on Ulysses
And All specials that have
been requested and validated by Matron remain uncovered, and unable to put in place appropriate mitigation to manage risk and this is reported on Ulysses
Or Staffing levels
deemed unsafe by Chief Nurse or Deputy
Staffing Matron will
confirm escalation
and this is reported on Ulysses
And All specials that have
been requested and validated by Matron remain uncovered, and unable to put in place appropriate mitigation to manage risk and this is reported on Ulysses
Or Staffing levels deemed
unsafe by Chief Nurse or Deputy
Staffing Matron will
confirm escalation stage at Bed Meeting, which will be reported at Daily Operational Huddle
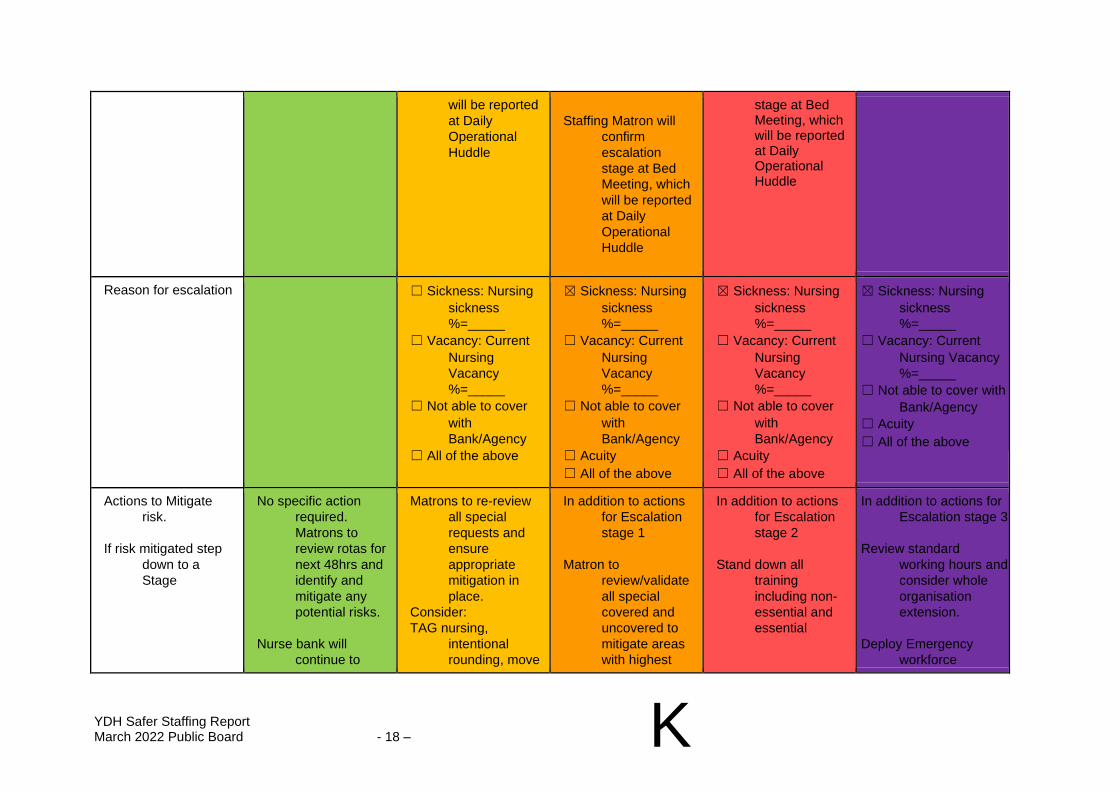
YDH Safer Staffing Report March 2022 Public Board - 18 – K
will be reported
at Daily
Operational
Huddle
Staffing Matron will
confirm
escalation
stage at Bed
Meeting, which
will be reported
at Daily
Operational
Huddle
stage at Bed Meeting, which will be reported at Daily Operational Huddle
Reason for escalation ☐ Sickness: Nursing
sickness
%=_____
☐ Vacancy: Current
Nursing
Vacancy
%=_____
☐ Not able to cover
with
Bank/Agency
☐ All of the above
☒ Sickness: Nursing
sickness
%=_____
☐ Vacancy: Current
Nursing
Vacancy
%=_____
☐ Not able to cover
with
Bank/Agency
☐ Acuity
☐ All of the above
☒ Sickness: Nursing
sickness
%=_____
☐ Vacancy: Current
Nursing
Vacancy
%=_____
☐ Not able to cover
with
Bank/Agency
☐ Acuity
☐ All of the above
☒ Sickness: Nursing
sickness
%=_____
☐ Vacancy: Current
Nursing Vacancy
%=_____
☐ Not able to cover with
Bank/Agency
☐ Acuity
☐ All of the above
Actions to Mitigate
risk.
If risk mitigated step
down to a
Stage
No specific action
required.
Matrons to
review rotas for
next 48hrs and
identify and
mitigate any
potential risks.
Nurse bank will
continue to
Matrons to re-review
all special
requests and
ensure
appropriate
mitigation in
place.
Consider:
TAG nursing,
intentional
rounding, move
In addition to actions
for Escalation
stage 1
Matron to
review/validate
all special
covered and
uncovered to
mitigate areas
with highest
In addition to actions
for Escalation
stage 2
Stand down all
training
including non-
essential and
essential
In addition to actions for
Escalation stage 3
Review standard
working hours and
consider whole
organisation
extension.
Deploy Emergency
workforce
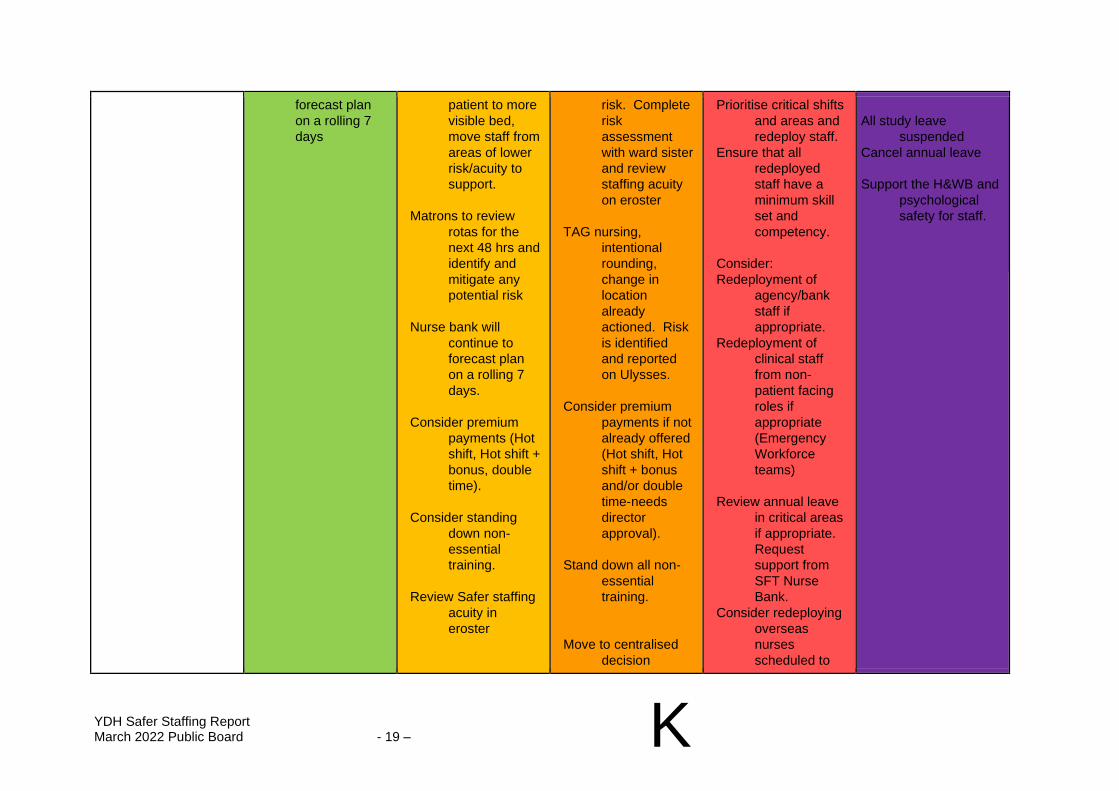
YDH Safer Staffing Report March 2022 Public Board - 19 – K
forecast plan
on a rolling 7
days
patient to more
visible bed,
move staff from
areas of lower
risk/acuity to
support.
Matrons to review
rotas for the
next 48 hrs and
identify and
mitigate any
potential risk
Nurse bank will
continue to
forecast plan
on a rolling 7
days.
Consider premium
payments (Hot
shift, Hot shift +
bonus, double
time).
Consider standing
down non-
essential
training.
Review Safer staffing
acuity in
eroster
risk. Complete
risk
assessment
with ward sister
and review
staffing acuity
on eroster
TAG nursing,
intentional
rounding,
change in
location
already
actioned. Risk
is identified
and reported
on Ulysses.
Consider premium
payments if not
already offered
(Hot shift, Hot
shift + bonus
and/or double
time-needs
director
approval).
Stand down all non-
essential
training.
Move to centralised
decision
Prioritise critical shifts
and areas and
redeploy staff.
Ensure that all
redeployed
staff have a
minimum skill
set and
competency.
Consider:
Redeployment of
agency/bank
staff if
appropriate.
Redeployment of
clinical staff
from non-
patient facing
roles if
appropriate
(Emergency
Workforce
teams)
Review annual leave
in critical areas
if appropriate.
Request
support from
SFT Nurse
Bank.
Consider redeploying
overseas
nurses
scheduled to
All study leave
suspended
Cancel annual leave
Support the H&WB and
psychological
safety for staff.
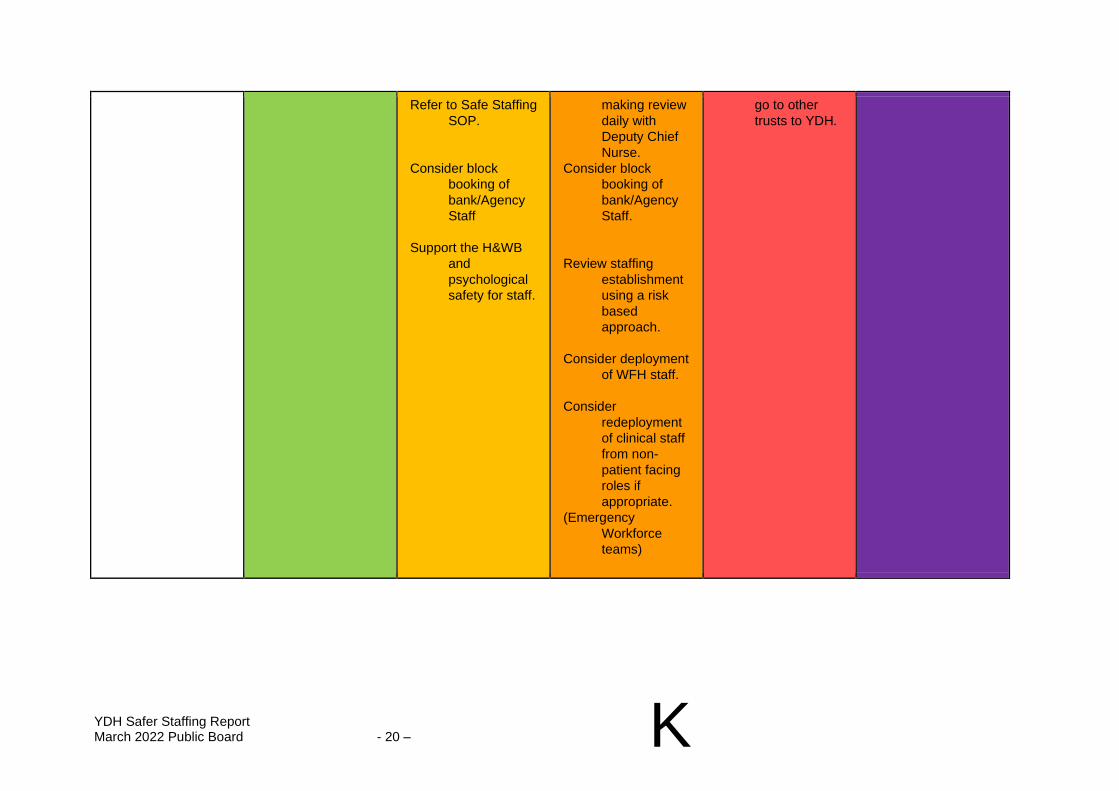
YDH Safer Staffing Report March 2022 Public Board - 20 – K
Refer to Safe Staffing
SOP.
Consider block
booking of
bank/Agency
Staff
Support the H&WB
and
psychological
safety for staff.
making review
daily with
Deputy Chief
Nurse.
Consider block
booking of
bank/Agency
Staff.
Review staffing
establishment
using a risk
based
approach.
Consider deployment
of WFH staff.
Consider
redeployment
of clinical staff
from non-
patient facing
roles if
appropriate.
(Emergency
Workforce
teams)
go to other
trusts to YDH.
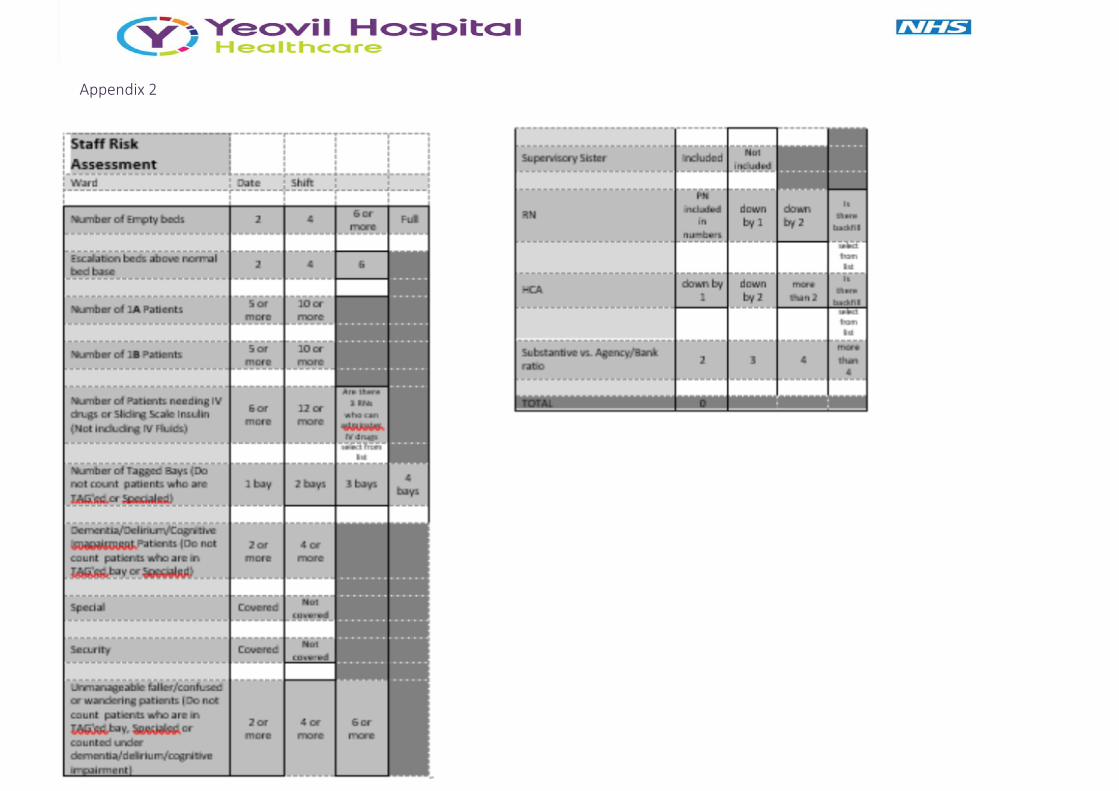
Appendix 2
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff
March 2022 Public Board - 1 – L
Somerset NHS Foundation Trust
REPORT TO: Board of Directors
REPORT TITLE: Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff
SPONSORING EXEC: Hayley Peters, Chief Nurse
REPORT BY:
Alison Wootton, Deputy Chief Nurse Paul Townsend, Director of Mental Health & Learning Disabilities Care Clare Boobyer-Jones, Director of Allied Health & Psychology Professions (AHPPs)
PRESENTED BY: Hayley Peters, Chief Nurse
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☒ For Assurance/
Discussion ☐ For Approval / Decision ☒ For Information
Executive Summary and Reason for presentation to Committee/Board
This paper provides the required assurance that SFT had safe nurse staffing levels across all in-patient ward areas as well as providing detail across broader services provided by the Trust. The paper provides assurance that appropriate systems have been in place to manage the capacity and demand. This report covers the reporting period for September 2021 – March 2022. The pandemic has exerted pressure on services across Somerset and SFT colleagues have been required to work in new ways and in different wards, departments and environments. At times, it has also required nursing and AHP colleagues to work in alternative clinical settings to support discharge and flow from hospital through D2A work, and support patient groups that may be unfamiliar to them. Colleagues have also been deployed to provide countywide Covid vaccination clinics in response to the pandemic. The NHSE/I principles and Nursing and Midwifery Council (NMC) regulatory guidance have been followed to support our response and maintain safe staffing measures. These have been detailed and outlined in the previous reports.
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff
March 2022 Public Board - 2 – L
This report is going to offer high level reassurance that safe staffing is regularly reviewed on a day-to-day basis and appropriate action is in place to support quality and care. The long-term impact of the pandemic on colleagues has not yet been seen, and it is possible that nursing and colleague retention plans require a review in response to the changing circumstances. The Trust’s improved well-being offer continues to provide relevant ongoing support to colleagues. As part of the merger, work needs to be undertaken to review and streamline a new safe staffing review and reporting process ready for the new organisation. This work will be led by the Chief Nurse over the coming months with the aim for a joint safe staffing report being presented. The board are asked to note:
• strategic work to develop a consistent pipeline for recruitment of colleagues locally, nationally, and internationally;
• where strategic risks exist around safe staffing that these have been discussed and explored at the quality and governance committee;
• that where business cases are linked to safe staffing and mentioned in this paper they have been through a robust review and challenge phase and assessed alongside all other business cases.
The local response to the national pandemic and general
system and winter pressures within the NHS has meant that
staffing has been affected in several ways, in particular:
• colleague absence due to COVID-19 symptoms or test results and self-isolation;
• the demands of providing colleagues to support and deliver the Somerset COVID-19 vaccination programme;
• changing bed capacity and service configuration to manage COVID-19;
• the change of ward functions and purpose to care and treat COVID-19;
• Increased capacity pressure within the system over an extended period.
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff
March 2022 Public Board - 3 – L
System delays to discharge and increased capacity pressures have required an unprecedented number of escalation beds to be opened. This has impacted on staffing levels and minimal or altered staffing operating procedures have often been implemented.
Recommendation The Board is asked to review and accept the report and note;
• that systems and processes are in place to review the required safe staffing levels on both a daily basis and to ensure there are plans in place to support any strategic changes in care requirements due to change in activity, acuity or dependency;
• that strategic plans are in place to support the required levels of recruitment to minimise vacancy in nursing and AHP groups;
• that risks around safe staffing issues are identified, risk assessed, and mitigation plans enacted. These risks are managed locally with support and review at corporate level where local mitigation is not able to control or reduce the risk to an acceptable level.
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☐ Care for our Population ☐ Develop our People
☐ Innovate and Collaborate ☐ Develop a Sustainable System
Somerset NHS FT
☐ Obj 1 Inclusive culture ☒ Obj 4 Safe services ☒ Obj 7 Improving outcomes
☐ Obj 2 Collaboration ☒ Obj 5 Self management ☒ Obj 8 Workforce
☐ Obj 3 Independent lives ☐ Obj 6 Value all people alike ☐ Obj 9 Performance
☐ Obj 10 Finance
Implications/Requirements (Please select any which are relevant to this paper)
☐ Financial ☒ Legislation ☒ Workforce ☐ Estates ☐ ICT ☐ Patient Safety /
Quality
Details:
Equality The Trust wants its services to be as accessible as possible, to as many people as
possible. Please indicate whether the report has an impact on the protected characteristics
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff
March 2022 Public Board - 4 – L
☒ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are no proposals or matters which affect any persons with protected characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
This report has involved the senior clinical leaders in each directorate to ensure that any / all issues are able to be raised to the board.
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
Previous safe staffing paper presented in September 2021.
Reference to CQC domains (Please select any which are relevant to this paper)
☒ Safe ☒ Effective ☒ Caring ☐ Responsive ☒ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 1 – L
SOMERSET NHS FOUNDATION TRUST
SIX MONTHLY ESTABLISHMENT REVIEW, NURSING, MIDWIFERY AND AHPP STAFF
1. BACKGROUND AND PURPOSE 1.1 This paper provides a six-month review of the Trust’s current status for the provision of nurse, midwifery and AHPP (Allied Health Professionals and Psychologists) safe staffing. It provides information on risk and current mitigations to offer oversight and reassurance of the ongoing work to maintain safe staffing levels. The review methodology ensures that local directorate services can review and escalate any areas of concern. 1.2 Direction from NHS Improvement ‘Developing workforce safeguards –
supporting providers to deliver high quality care through safe and effective staffing’ (October 2018) has built on the previous guidance to support organisations and boards to demonstrate that safe staffing levels have been reviewed for all clinical groups and that a robust governance framework is in place to support these reviews and any proposed changes in staffing level or skill mix.
1.3 The Trust Board is asked to:
• Note the on-going work to ensure compliance as far as possible with the national guidance surrounding safe staffing levels and, where possible, the implementation of a robust methodology in determining the correct levels and skill mix of colleagues.
• Consider and endorse the recommendations and proposed actions to be taken to address any issues that are highlighted in this report.
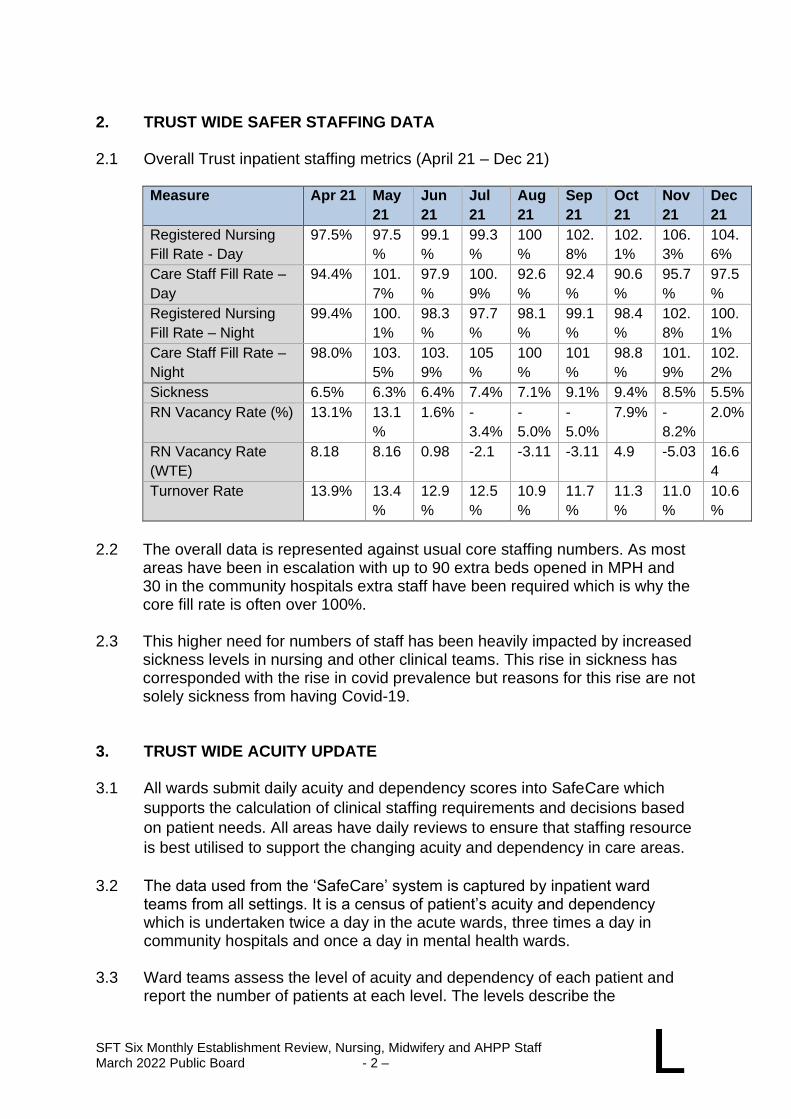
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 2 – L
2. TRUST WIDE SAFER STAFFING DATA 2.1 Overall Trust inpatient staffing metrics (April 21 – Dec 21)
Measure Apr 21 May
21
Jun
21
Jul
21
Aug
21
Sep
21
Oct
21
Nov
21
Dec
21
Registered Nursing
Fill Rate - Day
97.5% 97.5
%
99.1
%
99.3
%
100
%
102.
8%
102.
1%
106.
3%
104.
6%
Care Staff Fill Rate –
Day
94.4% 101.
7%
97.9
%
100.
9%
92.6
%
92.4
%
90.6
%
95.7
%
97.5
%
Registered Nursing
Fill Rate – Night
99.4% 100.
1%
98.3
%
97.7
%
98.1
%
99.1
%
98.4
%
102.
8%
100.
1%
Care Staff Fill Rate –
Night
98.0% 103.
5%
103.
9%
105
%
100
%
101
%
98.8
%
101.
9%
102.
2%
Sickness 6.5% 6.3% 6.4% 7.4% 7.1% 9.1% 9.4% 8.5% 5.5%
RN Vacancy Rate (%) 13.1% 13.1
%
1.6% -
3.4%
-
5.0%
-
5.0%
7.9% -
8.2%
2.0%
RN Vacancy Rate
(WTE)
8.18 8.16 0.98 -2.1 -3.11 -3.11 4.9 -5.03 16.6
4
Turnover Rate 13.9% 13.4
%
12.9
%
12.5
%
10.9
%
11.7
%
11.3
%
11.0
%
10.6
%
2.2 The overall data is represented against usual core staffing numbers. As most areas have been in escalation with up to 90 extra beds opened in MPH and 30 in the community hospitals extra staff have been required which is why the core fill rate is often over 100%.
2.3 This higher need for numbers of staff has been heavily impacted by increased
sickness levels in nursing and other clinical teams. This rise in sickness has corresponded with the rise in covid prevalence but reasons for this rise are not solely sickness from having Covid-19.
3. TRUST WIDE ACUITY UPDATE 3.1 All wards submit daily acuity and dependency scores into SafeCare which
supports the calculation of clinical staffing requirements and decisions based
on patient needs. All areas have daily reviews to ensure that staffing resource
is best utilised to support the changing acuity and dependency in care areas.
3.2 The data used from the ‘SafeCare’ system is captured by inpatient ward
teams from all settings. It is a census of patient’s acuity and dependency which is undertaken twice a day in the acute wards, three times a day in community hospitals and once a day in mental health wards.
3.3 Ward teams assess the level of acuity and dependency of each patient and
report the number of patients at each level. The levels describe the
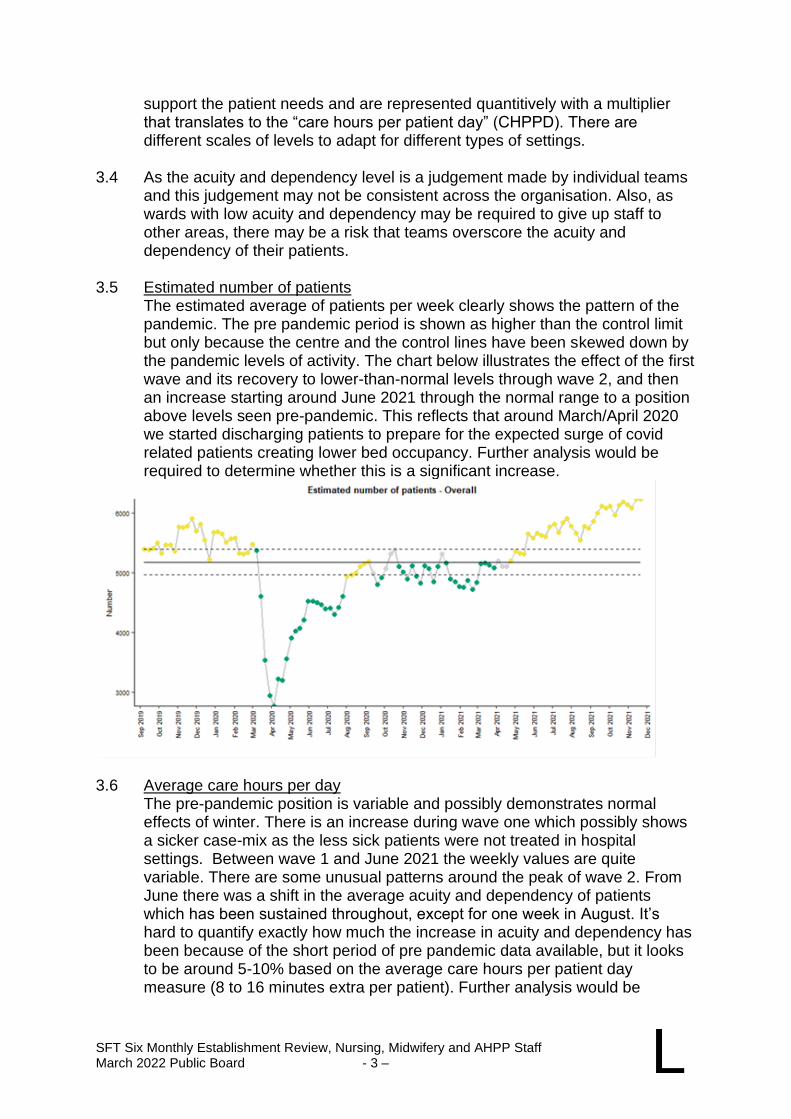
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 3 – L
support the patient needs and are represented quantitively with a multiplier that translates to the “care hours per patient day” (CHPPD). There are different scales of levels to adapt for different types of settings.
3.4 As the acuity and dependency level is a judgement made by individual teams
and this judgement may not be consistent across the organisation. Also, as wards with low acuity and dependency may be required to give up staff to other areas, there may be a risk that teams overscore the acuity and dependency of their patients.
3.5 Estimated number of patients
The estimated average of patients per week clearly shows the pattern of the pandemic. The pre pandemic period is shown as higher than the control limit but only because the centre and the control lines have been skewed down by the pandemic levels of activity. The chart below illustrates the effect of the first wave and its recovery to lower-than-normal levels through wave 2, and then an increase starting around June 2021 through the normal range to a position above levels seen pre-pandemic. This reflects that around March/April 2020 we started discharging patients to prepare for the expected surge of covid related patients creating lower bed occupancy. Further analysis would be required to determine whether this is a significant increase.
3.6 Average care hours per day
The pre-pandemic position is variable and possibly demonstrates normal effects of winter. There is an increase during wave one which possibly shows a sicker case-mix as the less sick patients were not treated in hospital settings. Between wave 1 and June 2021 the weekly values are quite variable. There are some unusual patterns around the peak of wave 2. From June there was a shift in the average acuity and dependency of patients which has been sustained throughout, except for one week in August. It’s hard to quantify exactly how much the increase in acuity and dependency has been because of the short period of pre pandemic data available, but it looks to be around 5-10% based on the average care hours per patient day measure (8 to 16 minutes extra per patient). Further analysis would be
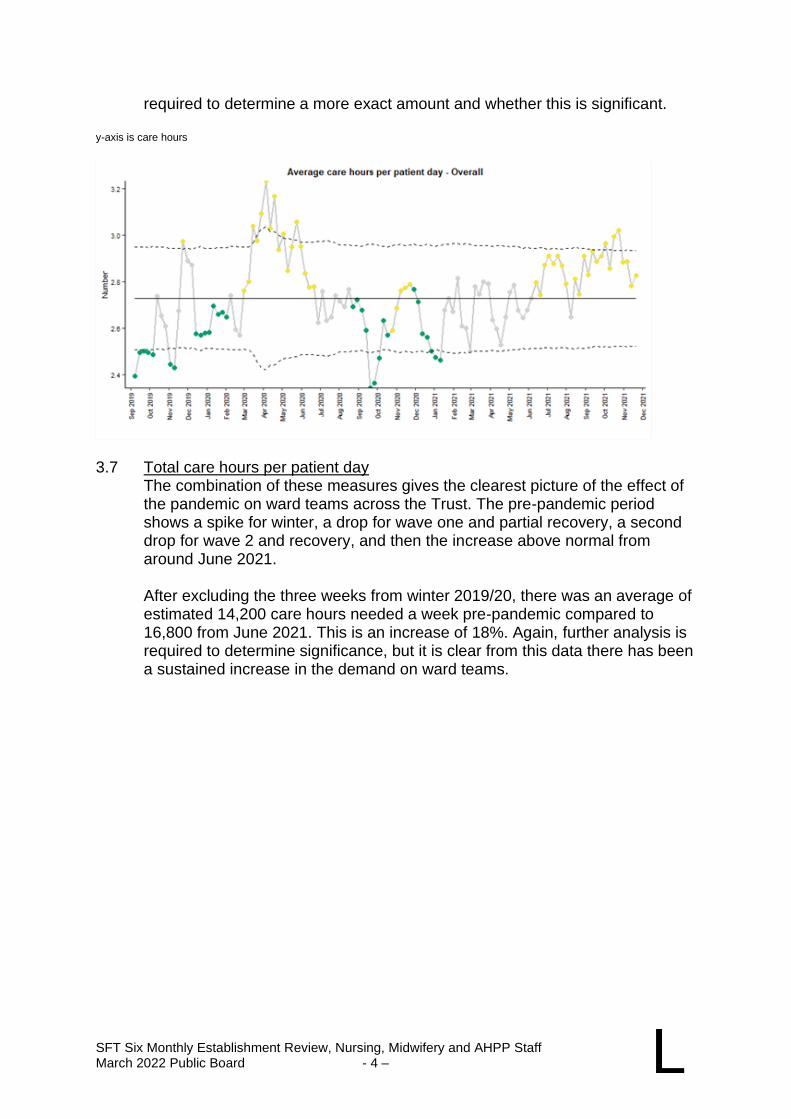
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 4 – L
required to determine a more exact amount and whether this is significant. y-axis is care hours
3.7 Total care hours per patient day
The combination of these measures gives the clearest picture of the effect of the pandemic on ward teams across the Trust. The pre-pandemic period shows a spike for winter, a drop for wave one and partial recovery, a second drop for wave 2 and recovery, and then the increase above normal from around June 2021. After excluding the three weeks from winter 2019/20, there was an average of estimated 14,200 care hours needed a week pre-pandemic compared to 16,800 from June 2021. This is an increase of 18%. Again, further analysis is required to determine significance, but it is clear from this data there has been a sustained increase in the demand on ward teams.
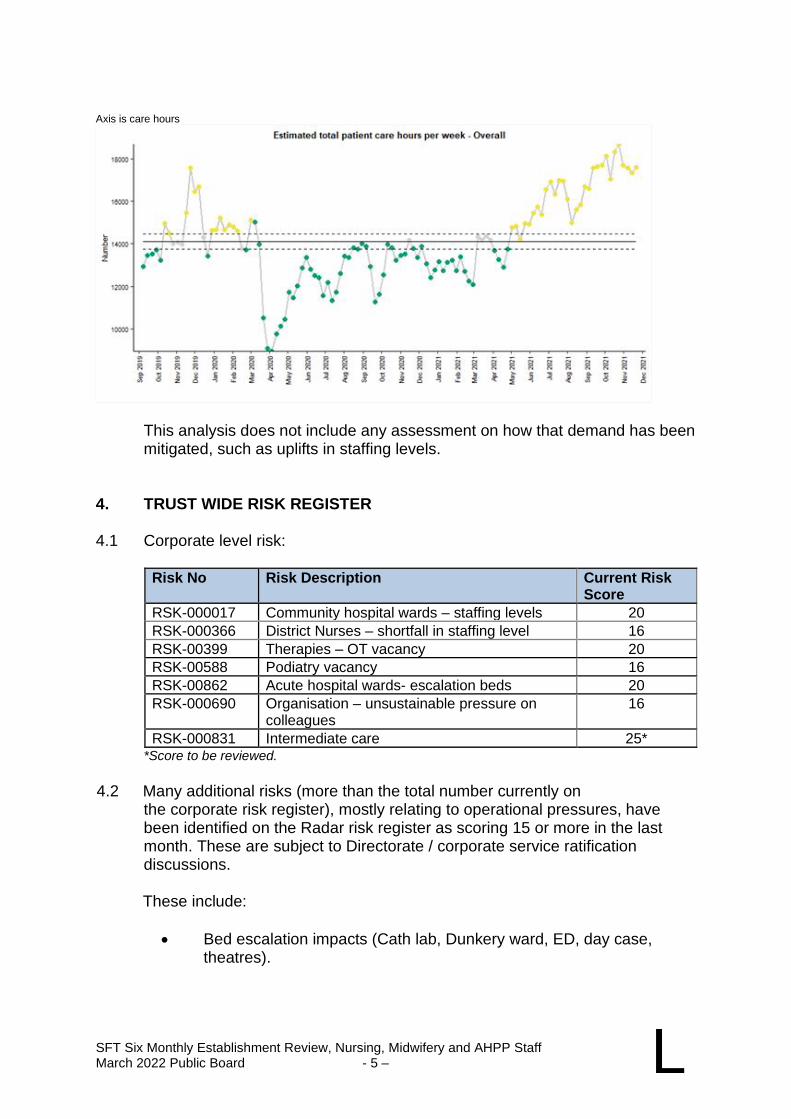
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 5 – L
Axis is care hours
This analysis does not include any assessment on how that demand has been mitigated, such as uplifts in staffing levels.
4. TRUST WIDE RISK REGISTER 4.1 Corporate level risk:
Risk No Risk Description Current Risk Score
RSK-000017 Community hospital wards – staffing levels 20
RSK-000366 District Nurses – shortfall in staffing level 16
RSK-00399 Therapies – OT vacancy 20
RSK-00588 Podiatry vacancy 16
RSK-00862 Acute hospital wards- escalation beds 20
RSK-000690 Organisation – unsustainable pressure on colleagues
16
RSK-000831 Intermediate care 25* *Score to be reviewed.
4.2 Many additional risks (more than the total number currently on
the corporate risk register), mostly relating to operational pressures, have been identified on the Radar risk register as scoring 15 or more in the last month. These are subject to Directorate / corporate service ratification discussions.
These include:
• Bed escalation impacts (Cath lab, Dunkery ward, ED, day case, theatres).
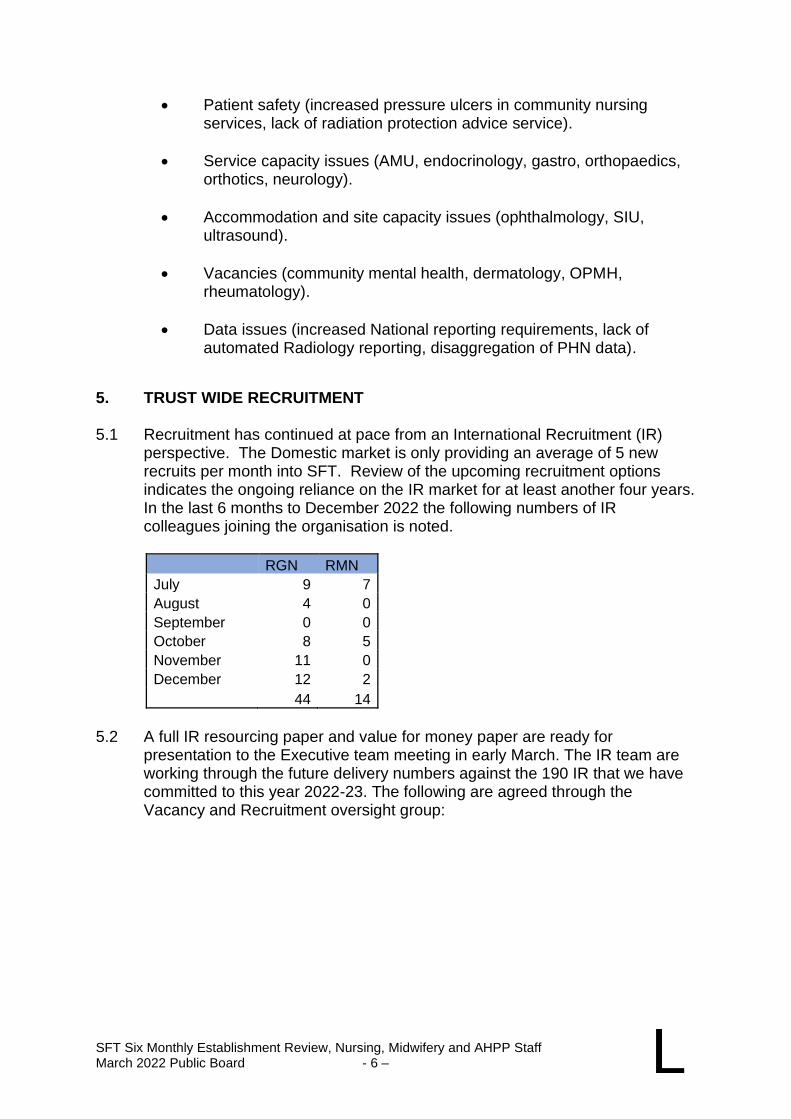
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 6 – L
• Patient safety (increased pressure ulcers in community nursing services, lack of radiation protection advice service).
• Service capacity issues (AMU, endocrinology, gastro, orthopaedics, orthotics, neurology).
• Accommodation and site capacity issues (ophthalmology, SIU, ultrasound).
• Vacancies (community mental health, dermatology, OPMH, rheumatology).
• Data issues (increased National reporting requirements, lack of automated Radiology reporting, disaggregation of PHN data).
5. TRUST WIDE RECRUITMENT 5.1 Recruitment has continued at pace from an International Recruitment (IR)
perspective. The Domestic market is only providing an average of 5 new recruits per month into SFT. Review of the upcoming recruitment options indicates the ongoing reliance on the IR market for at least another four years. In the last 6 months to December 2022 the following numbers of IR colleagues joining the organisation is noted.
RGN RMN
July 9 7
August 4 0
September 0 0
October 8 5
November 11 0
December 12 2
44 14
5.2 A full IR resourcing paper and value for money paper are ready for
presentation to the Executive team meeting in early March. The IR team are working through the future delivery numbers against the 190 IR that we have committed to this year 2022-23. The following are agreed through the Vacancy and Recruitment oversight group:
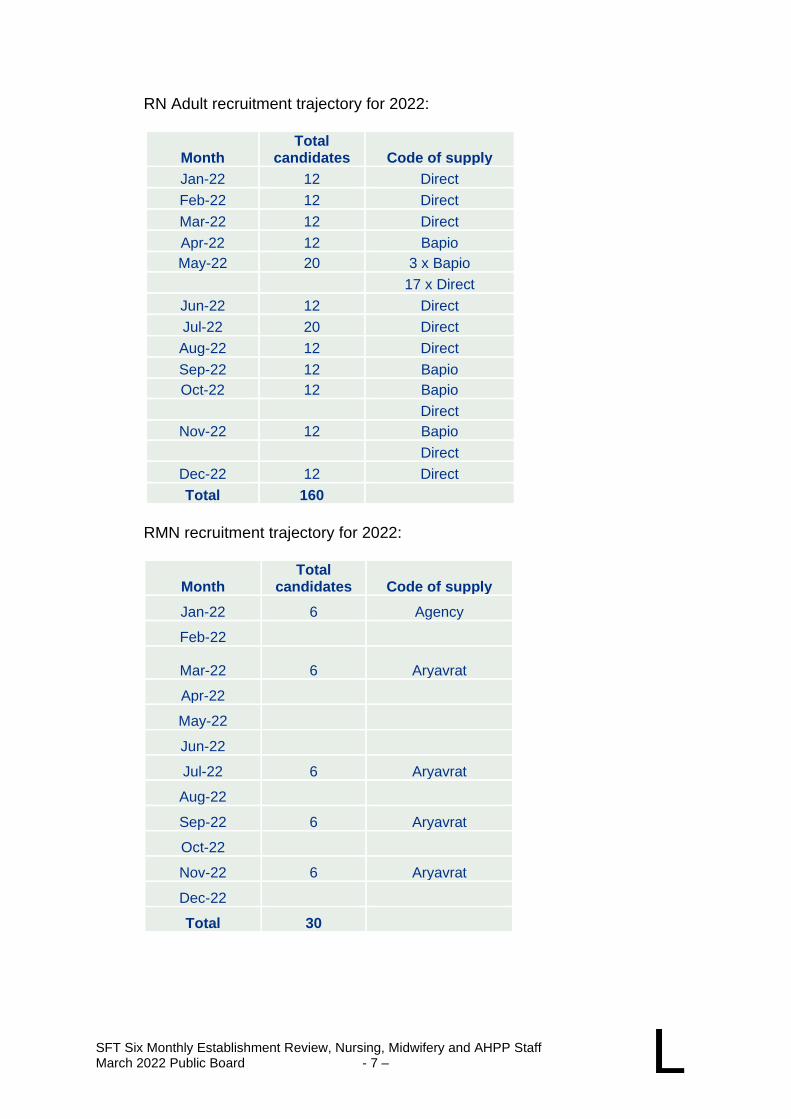
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 7 – L
RN Adult recruitment trajectory for 2022:
Month Total
candidates Code of supply
Jan-22 12 Direct
Feb-22 12 Direct
Mar-22 12 Direct
Apr-22 12 Bapio
May-22 20 3 x Bapio
17 x Direct
Jun-22 12 Direct
Jul-22 20 Direct
Aug-22 12 Direct
Sep-22 12 Bapio
Oct-22 12 Bapio
Direct
Nov-22 12 Bapio
Direct
Dec-22 12 Direct
Total 160
RMN recruitment trajectory for 2022:
Month Total
candidates Code of supply
Jan-22 6 Agency
Feb-22
Mar-22 6 Aryavrat
Apr-22
May-22
Jun-22
Jul-22 6 Aryavrat
Aug-22
Sep-22 6 Aryavrat
Oct-22
Nov-22 6 Aryavrat
Dec-22
Total 30
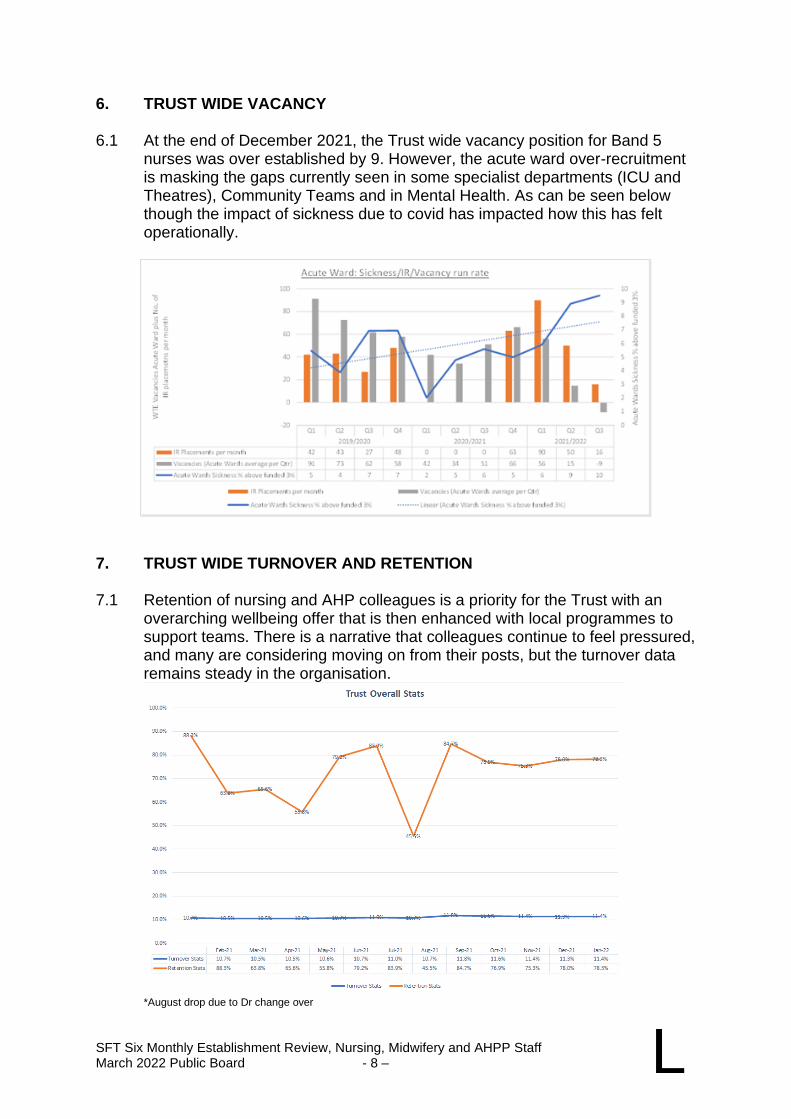
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 8 – L
6. TRUST WIDE VACANCY 6.1 At the end of December 2021, the Trust wide vacancy position for Band 5
nurses was over established by 9. However, the acute ward over-recruitment is masking the gaps currently seen in some specialist departments (ICU and Theatres), Community Teams and in Mental Health. As can be seen below though the impact of sickness due to covid has impacted how this has felt operationally.
7. TRUST WIDE TURNOVER AND RETENTION 7.1 Retention of nursing and AHP colleagues is a priority for the Trust with an
overarching wellbeing offer that is then enhanced with local programmes to support teams. There is a narrative that colleagues continue to feel pressured, and many are considering moving on from their posts, but the turnover data remains steady in the organisation.
*August drop due to Dr change over
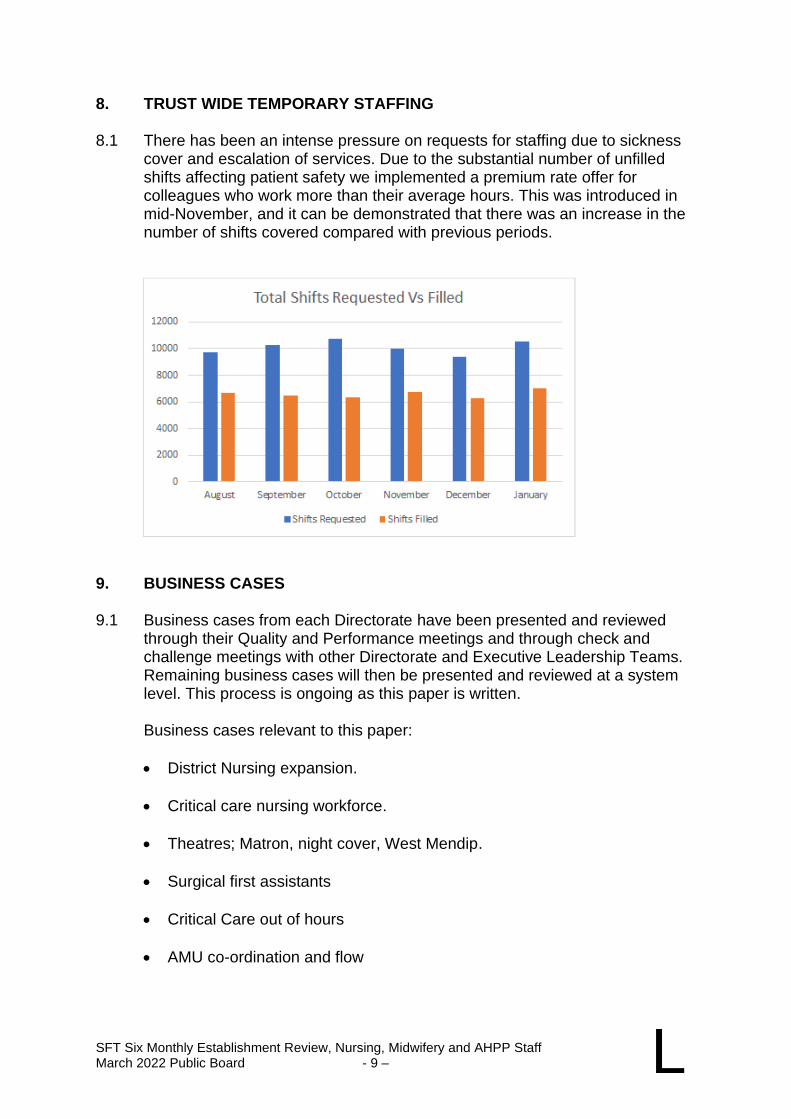
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 9 – L
8. TRUST WIDE TEMPORARY STAFFING 8.1 There has been an intense pressure on requests for staffing due to sickness
cover and escalation of services. Due to the substantial number of unfilled shifts affecting patient safety we implemented a premium rate offer for colleagues who work more than their average hours. This was introduced in mid-November, and it can be demonstrated that there was an increase in the number of shifts covered compared with previous periods.
9. BUSINESS CASES 9.1 Business cases from each Directorate have been presented and reviewed
through their Quality and Performance meetings and through check and challenge meetings with other Directorate and Executive Leadership Teams. Remaining business cases will then be presented and reviewed at a system level. This process is ongoing as this paper is written.
Business cases relevant to this paper:
• District Nursing expansion.
• Critical care nursing workforce.
• Theatres; Matron, night cover, West Mendip.
• Surgical first assistants
• Critical Care out of hours
• AMU co-ordination and flow
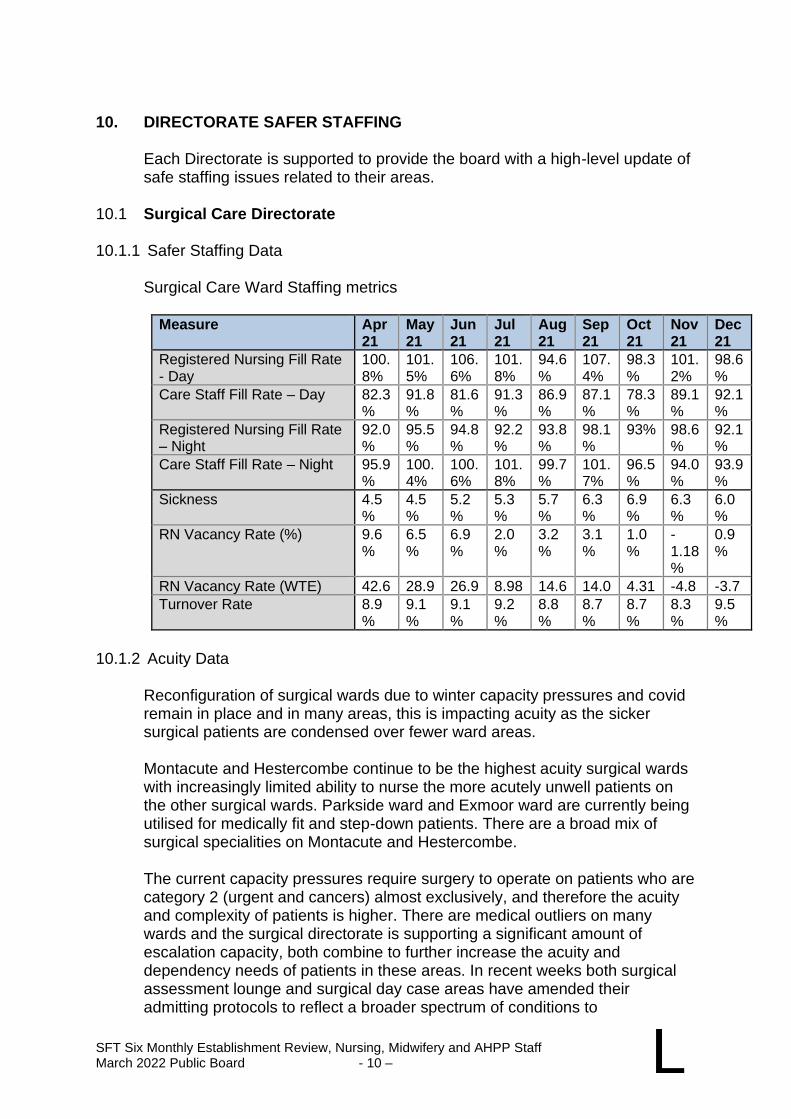
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 10 – L
10. DIRECTORATE SAFER STAFFING
Each Directorate is supported to provide the board with a high-level update of safe staffing issues related to their areas.
10.1 Surgical Care Directorate 10.1.1 Safer Staffing Data
Surgical Care Ward Staffing metrics
Measure Apr 21
May 21
Jun 21
Jul 21
Aug 21
Sep 21
Oct 21
Nov 21
Dec 21
Registered Nursing Fill Rate - Day
100.8%
101.5%
106.6%
101.8%
94.6%
107.4%
98.3%
101.2%
98.6%
Care Staff Fill Rate – Day 82.3%
91.8%
81.6%
91.3%
86.9%
87.1%
78.3%
89.1%
92.1%
Registered Nursing Fill Rate – Night
92.0%
95.5%
94.8%
92.2%
93.8%
98.1%
93% 98.6%
92.1%
Care Staff Fill Rate – Night 95.9%
100.4%
100.6%
101.8%
99.7%
101.7%
96.5%
94.0%
93.9%
Sickness 4.5%
4.5%
5.2%
5.3%
5.7%
6.3%
6.9%
6.3%
6.0%
RN Vacancy Rate (%) 9.6%
6.5%
6.9%
2.0%
3.2%
3.1%
1.0%
-1.18%
0.9%
RN Vacancy Rate (WTE) 42.6 28.9 26.9 8.98 14.6 14.0 4.31 -4.8 -3.7
Turnover Rate 8.9%
9.1%
9.1%
9.2%
8.8%
8.7%
8.7%
8.3%
9.5%
10.1.2 Acuity Data
Reconfiguration of surgical wards due to winter capacity pressures and covid remain in place and in many areas, this is impacting acuity as the sicker surgical patients are condensed over fewer ward areas.
Montacute and Hestercombe continue to be the highest acuity surgical wards with increasingly limited ability to nurse the more acutely unwell patients on the other surgical wards. Parkside ward and Exmoor ward are currently being utilised for medically fit and step-down patients. There are a broad mix of surgical specialities on Montacute and Hestercombe.
The current capacity pressures require surgery to operate on patients who are category 2 (urgent and cancers) almost exclusively, and therefore the acuity and complexity of patients is higher. There are medical outliers on many wards and the surgical directorate is supporting a significant amount of escalation capacity, both combine to further increase the acuity and dependency needs of patients in these areas. In recent weeks both surgical assessment lounge and surgical day case areas have amended their admitting protocols to reflect a broader spectrum of conditions to
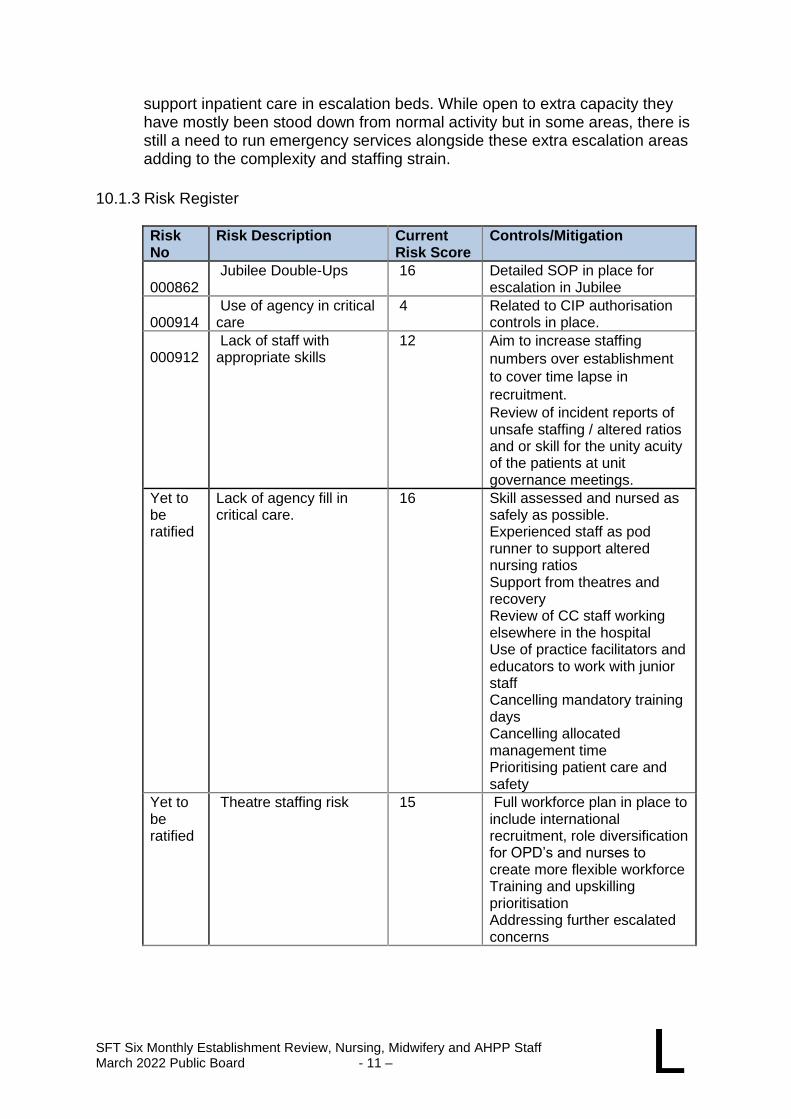
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 11 – L
support inpatient care in escalation beds. While open to extra capacity they have mostly been stood down from normal activity but in some areas, there is still a need to run emergency services alongside these extra escalation areas adding to the complexity and staffing strain.
10.1.3 Risk Register
Risk No
Risk Description Current Risk Score
Controls/Mitigation
000862
Jubilee Double-Ups 16 Detailed SOP in place for escalation in Jubilee
000914
Use of agency in critical care
4 Related to CIP authorisation controls in place.
000912
Lack of staff with appropriate skills
12 Aim to increase staffing
numbers over establishment
to cover time lapse in
recruitment.
Review of incident reports of unsafe staffing / altered ratios and or skill for the unity acuity of the patients at unit governance meetings.
Yet to be ratified
Lack of agency fill in critical care.
16 Skill assessed and nursed as safely as possible. Experienced staff as pod runner to support altered nursing ratios Support from theatres and recovery Review of CC staff working elsewhere in the hospital Use of practice facilitators and educators to work with junior staff Cancelling mandatory training days Cancelling allocated management time Prioritising patient care and safety
Yet to be ratified
Theatre staffing risk 15 Full workforce plan in place to include international recruitment, role diversification for OPD’s and nurses to create more flexible workforce Training and upskilling prioritisation Addressing further escalated concerns
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 12 – L
10.1.4 Recruitment
Wards position: The highest ward vacancy rate is within Surgical Assessment Unit with 7 outstanding RN Vacancies and 8 HCA vacancies. There is an active programme to recruit and induct colleagues to the ward.
Exmoor ward and Surgical Assessment Lounge currently trying to recruit over establishment to support ongoing additional escalation beds.
Hestercombe and Montacute ward are fully established with nurses for their 40-bed establishment however they are frequently increasing their bed bases to care for up to 50 patients due to ‘double up’ side rooms being utilised, additional nurse staffing is required, and agreement was made to over recruit to these wards for the winter, but this has not been achieved. Use of any available temporary staff and balancing a staff numbers across all wards is implemented to balance the risk. There are unfilled HCA vacancies at present however corporate HCA interviews are ongoing with allocations to wards as colleagues are recruited.
Critical Care Position: Critical care continues to recruit, induct, and train new colleagues as they have not yet filled the establishment required for the larger number of beds. Extra posts to support staff training and wellbeing are now in post and a post to support planned rehabilitation of patients is being advertised.
Theatres position: Nationally there is a shortage of appropriately trained and qualified theatre staff. Ongoing vacancy in this area has necessitated use of agency colleagues to fill essential gaps. As restoration of services will require enhanced activity through the theatre departments there is a growing risk that the right workforce may not be in place to support this. This is being assessed alongside the workforce plan to fully understand the possible mitigation and remaining risk.
Theatres is a highly specialised area with several areas that require enhanced training and competency and any recruitment programme needs to try and attract colleagues with these skills or provide training and support to develop them. Trust overseas recruitment programme has yielded some results over the last 2 years but here remain skills gaps as recruitment has been of nurses who have limited or no theatre experience. This leaves a higher level of the vacancy in the areas of specialist skill.
A ‘grow our own’ approach to ODP recruitment has been successful in developing HCA’s & Apprentices into registered practitioners. Further work is being undertaken to expand this, but it is unlikely to fill the requirement.
SFT theatres teams are working closely with the YDH theatres teams to have a joint understanding of need, recruitment plan and outstanding risk where there are gaps.
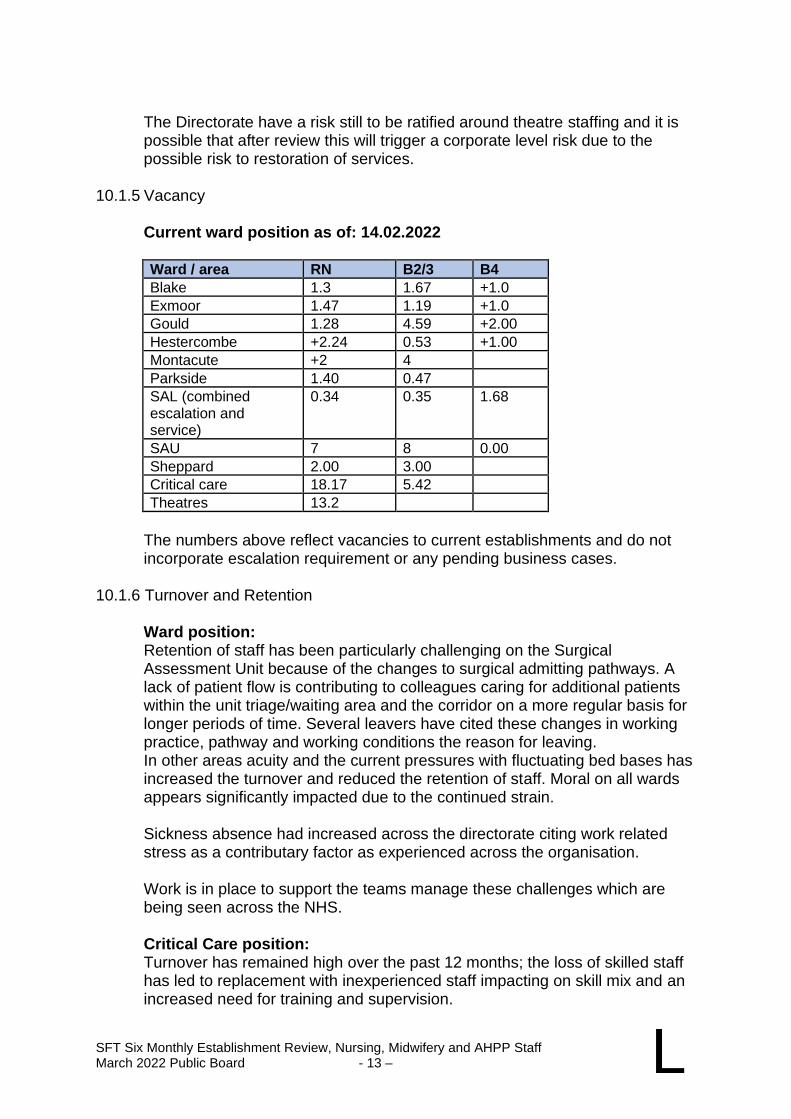
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 13 – L
The Directorate have a risk still to be ratified around theatre staffing and it is possible that after review this will trigger a corporate level risk due to the possible risk to restoration of services.
10.1.5 Vacancy
Current ward position as of: 14.02.2022
Ward / area RN B2/3 B4
Blake 1.3 1.67 +1.0
Exmoor 1.47 1.19 +1.0
Gould 1.28 4.59 +2.00
Hestercombe +2.24 0.53 +1.00
Montacute +2 4
Parkside 1.40 0.47
SAL (combined escalation and service)
0.34 0.35 1.68
SAU 7 8 0.00
Sheppard 2.00 3.00
Critical care 18.17 5.42
Theatres 13.2
The numbers above reflect vacancies to current establishments and do not incorporate escalation requirement or any pending business cases.
10.1.6 Turnover and Retention
Ward position: Retention of staff has been particularly challenging on the Surgical Assessment Unit because of the changes to surgical admitting pathways. A lack of patient flow is contributing to colleagues caring for additional patients within the unit triage/waiting area and the corridor on a more regular basis for longer periods of time. Several leavers have cited these changes in working practice, pathway and working conditions the reason for leaving. In other areas acuity and the current pressures with fluctuating bed bases has increased the turnover and reduced the retention of staff. Moral on all wards appears significantly impacted due to the continued strain.
Sickness absence had increased across the directorate citing work related stress as a contributary factor as experienced across the organisation.
Work is in place to support the teams manage these challenges which are being seen across the NHS.
Critical Care position: Turnover has remained high over the past 12 months; the loss of skilled staff has led to replacement with inexperienced staff impacting on skill mix and an increased need for training and supervision.
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 14 – L
In the past 12 months, the unit have recruited 27 B5 WTE to support the expansion to 16/18 beds. A significant part of this cohort were overseas colleagues who have required a more comprehensive induction.
There is still a significant challenge in appointing more senior and experienced staff.
Theatre's position: Unfortunately, due to multiple and complex factors theatres are experiencing some of the most significant retention issues within the directorate and staff turnover is high. Remedial action plans are underway.
Sickness levels are higher than average in many of our theatre areas. Support and development work is in place with a second theatre Matron being appointed to ensure higher levels of support for this area.
10.1.7 Temporary Staffing
Ward position: Bank and agency shifts are often unfilled and premium incentive shifts continue. The incentives offered have had a measured positive impact, but daily colleagues are moved to balance risk and core staffing levels are not consistently reached.
Critical Care position: Bank and agency are utilised to achieve required staffing numbers dependant on the number of patients on the unit. The number and complexity of patients can change rapidly. A reduced staffing standard operating procedure is planned, and, on some occasions, this is utilised.
Theatre's position: Use of bank and agency is ongoing and continued. A substantial number of shift requests go unfilled.
10.1.8 Business Cases
Critical care:
• Increase in establishment to staff 16 or 18 beds
• Operational B7
• Outreach – improved OOH capacity
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 15 – L
Theatres:
• Additional Matron
• Night theatres establishment
• Surgical First Assistants
• Minehead theatre staff
10.1.9 Summary of Key Issues
Ward position:
• Increased bed base on the Jubilee Wards (ward establishment does not meet service need.
• Increased acuity within all surgical wards apart from Exmoor Ward who have increased dependency due to high number of people with care medical care needs.
• Exmoor Ward currently operating as a mixed medical/surgical medically fit for discharge unit.
• SAU – large vacancies and lack of retention.
• SALS operating a dual service – escalation and SAL service.
• Increased sickness largely COVID and stress related issues ongoing as reasons for absence.
Critical care position:
• Lack of appropriately skilled staff internally to be able to promote so need to attract external interest.
• Need to stagger recruitment as cannot support large numbers of staff on induction and as trainees.
• Pressure on staffing due to increased bed use as escalation beds often used and higher levels of sickness.
Theatre position:
• The vacancy factor, poor retention and increased turnover are a significant risk for the organisation in terms of the elective recovery programme.
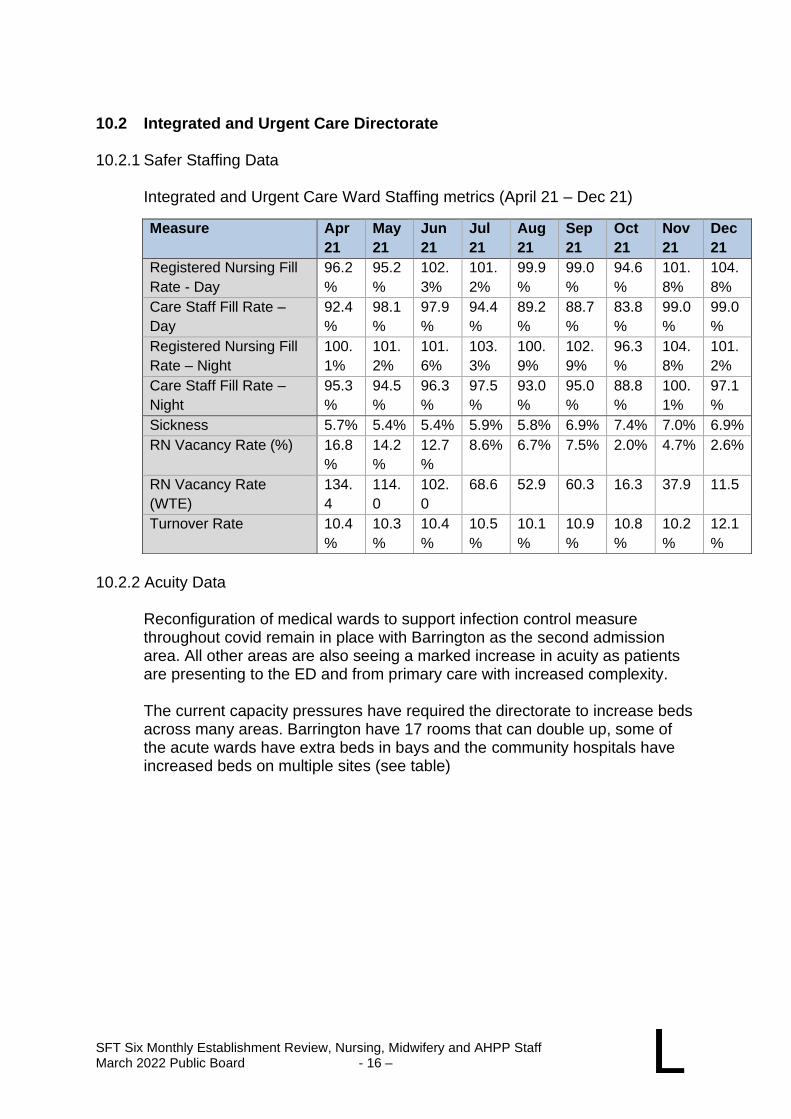
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 16 – L
10.2 Integrated and Urgent Care Directorate 10.2.1 Safer Staffing Data
Integrated and Urgent Care Ward Staffing metrics (April 21 – Dec 21)
10.2.2 Acuity Data
Reconfiguration of medical wards to support infection control measure throughout covid remain in place with Barrington as the second admission area. All other areas are also seeing a marked increase in acuity as patients are presenting to the ED and from primary care with increased complexity.
The current capacity pressures have required the directorate to increase beds across many areas. Barrington have 17 rooms that can double up, some of the acute wards have extra beds in bays and the community hospitals have increased beds on multiple sites (see table)
Measure Apr
21
May
21
Jun
21
Jul
21
Aug
21
Sep
21
Oct
21
Nov
21
Dec
21
Registered Nursing Fill
Rate - Day
96.2
%
95.2
%
102.
3%
101.
2%
99.9
%
99.0
%
94.6
%
101.
8%
104.
8%
Care Staff Fill Rate –
Day
92.4
%
98.1
%
97.9
%
94.4
%
89.2
%
88.7
%
83.8
%
99.0
%
99.0
%
Registered Nursing Fill
Rate – Night
100.
1%
101.
2%
101.
6%
103.
3%
100.
9%
102.
9%
96.3
%
104.
8%
101.
2%
Care Staff Fill Rate –
Night
95.3
%
94.5
%
96.3
%
97.5
%
93.0
%
95.0
%
88.8
%
100.
1%
97.1
%
Sickness 5.7% 5.4% 5.4% 5.9% 5.8% 6.9% 7.4% 7.0% 6.9%
RN Vacancy Rate (%) 16.8
%
14.2
%
12.7
%
8.6% 6.7% 7.5% 2.0% 4.7% 2.6%
RN Vacancy Rate
(WTE)
134.
4
114.
0
102.
0
68.6 52.9 60.3 16.3 37.9 11.5
Turnover Rate 10.4
%
10.3
%
10.4
%
10.5
%
10.1
%
10.9
%
10.8
%
10.2
%
12.1
%
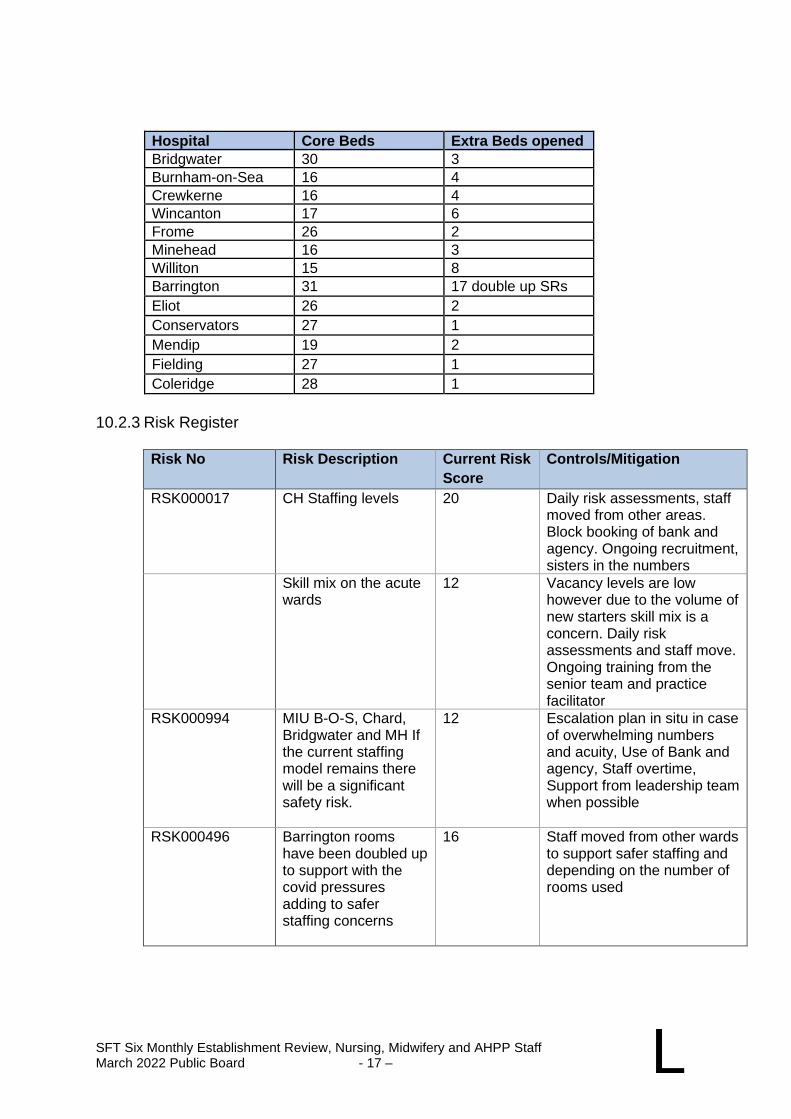
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 17 – L
Hospital Core Beds Extra Beds opened
Bridgwater 30 3
Burnham-on-Sea 16 4
Crewkerne 16 4
Wincanton 17 6
Frome 26 2
Minehead 16 3
Williton 15 8
Barrington 31 17 double up SRs
Eliot 26 2
Conservators 27 1
Mendip 19 2
Fielding 27 1
Coleridge 28 1
10.2.3 Risk Register
Risk No Risk Description Current Risk
Score
Controls/Mitigation
RSK000017
CH Staffing levels 20 Daily risk assessments, staff moved from other areas. Block booking of bank and agency. Ongoing recruitment, sisters in the numbers
Skill mix on the acute wards
12 Vacancy levels are low however due to the volume of new starters skill mix is a concern. Daily risk assessments and staff move. Ongoing training from the senior team and practice facilitator
RSK000994 MIU B-O-S, Chard, Bridgwater and MH If the current staffing model remains there will be a significant safety risk.
12 Escalation plan in situ in case of overwhelming numbers and acuity, Use of Bank and agency, Staff overtime, Support from leadership team when possible
RSK000496 Barrington rooms have been doubled up to support with the covid pressures adding to safer staffing concerns
16 Staff moved from other wards to support safer staffing and depending on the number of rooms used
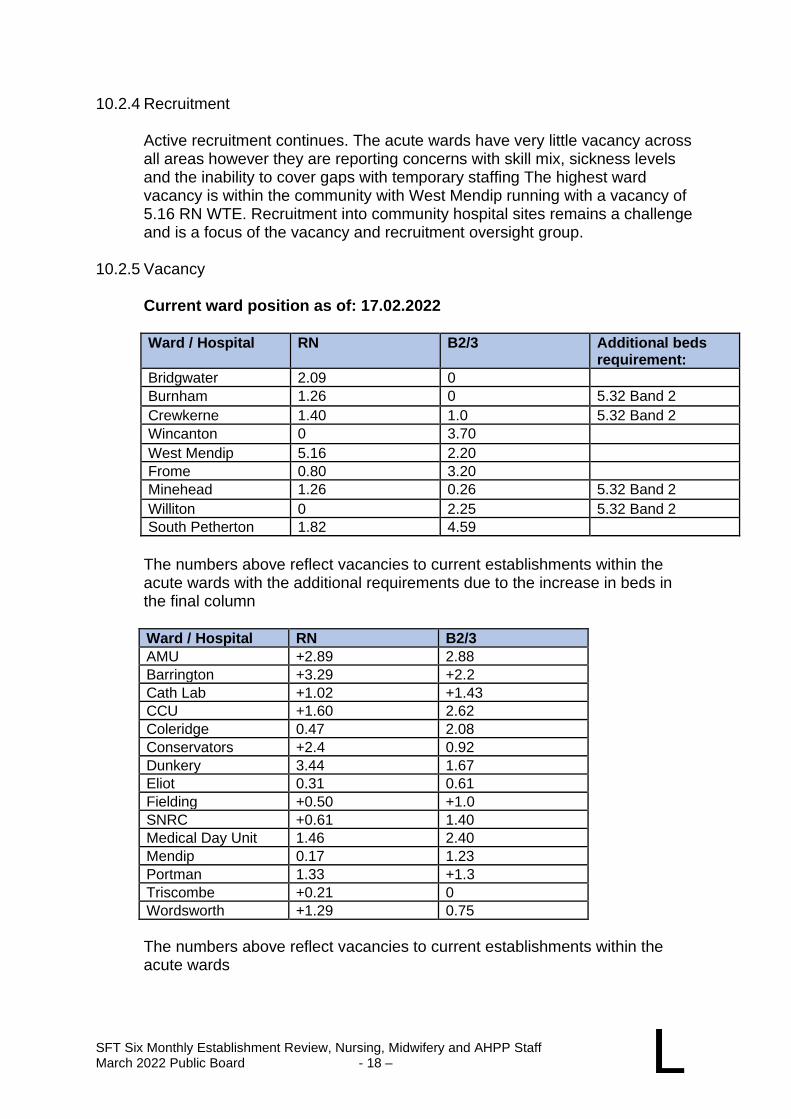
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 18 – L
10.2.4 Recruitment
Active recruitment continues. The acute wards have very little vacancy across all areas however they are reporting concerns with skill mix, sickness levels and the inability to cover gaps with temporary staffing The highest ward vacancy is within the community with West Mendip running with a vacancy of 5.16 RN WTE. Recruitment into community hospital sites remains a challenge and is a focus of the vacancy and recruitment oversight group.
10.2.5 Vacancy
Current ward position as of: 17.02.2022
Ward / Hospital RN B2/3 Additional beds
requirement:
Bridgwater 2.09 0
Burnham 1.26 0 5.32 Band 2
Crewkerne 1.40 1.0 5.32 Band 2
Wincanton 0 3.70
West Mendip 5.16 2.20
Frome 0.80 3.20
Minehead 1.26 0.26 5.32 Band 2
Williton 0 2.25 5.32 Band 2
South Petherton 1.82 4.59
The numbers above reflect vacancies to current establishments within the acute wards with the additional requirements due to the increase in beds in the final column
Ward / Hospital RN B2/3
AMU +2.89 2.88
Barrington +3.29 +2.2
Cath Lab +1.02 +1.43
CCU +1.60 2.62
Coleridge 0.47 2.08
Conservators +2.4 0.92
Dunkery 3.44 1.67
Eliot 0.31 0.61
Fielding +0.50 +1.0
SNRC +0.61 1.40
Medical Day Unit 1.46 2.40
Mendip 0.17 1.23
Portman 1.33 +1.3
Triscombe +0.21 0
Wordsworth +1.29 0.75
The numbers above reflect vacancies to current establishments within the acute wards
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 19 – L
10.2.6 Turnover and Retention
Retention of staff has been particularly challenging in the community hospitals with many staff stating that they are struggling with the increase in beds and acuity. We are also seeing high levels of sickness across our senior nursing team within these hospitals. In other areas acuity and demand remains high. We have seen increased sickness levels continuing for many months with stress being cited by many with a high background level of covid related illness.
10.2.7 Temporary Staffing
Bank and agency fill rate remains low, shifts especially last-minute sickness
often go unfilled. The premium incentive shifts have had a positive impact
and continue to be offered. Daily risk assessments are carried out by the
matrons and staff are moved around to balance the risk. This is much more
difficult across the Community sites due to geography and low numbers of
substantive staff.
10.2.8 Business Cases
AMU Outward flow coordinator Band 5 10.2.9 Summary of Key Issues
• It is difficult to meet the safer staffing levels required to support the Increased bed base on the wards.
• Increased acuity across all wards.
• Increased sickness largely COVID and stress related.
• Low numbers of bank and agency fill rate.
• Pockets of high vacancy rate which is proving difficult to recruit into across community hospitals.
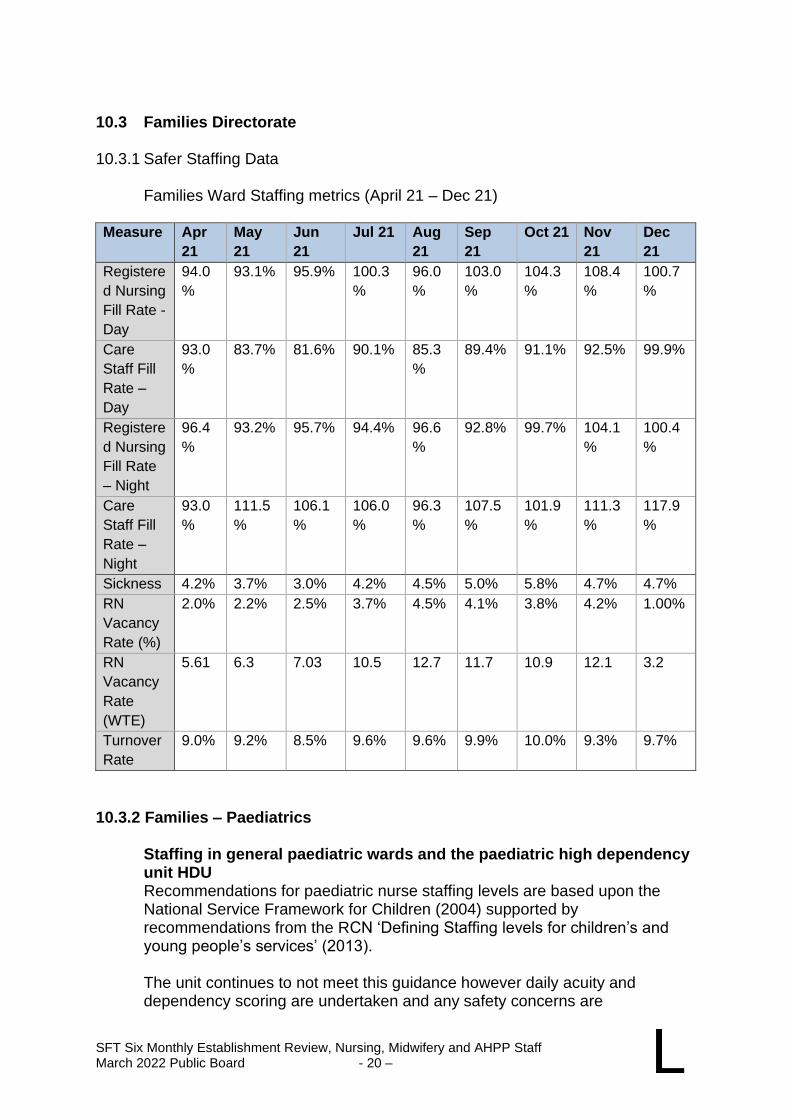
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 20 – L
10.3 Families Directorate 10.3.1 Safer Staffing Data
Families Ward Staffing metrics (April 21 – Dec 21) Measure Apr
21
May
21
Jun
21
Jul 21 Aug
21
Sep
21
Oct 21 Nov
21
Dec
21
Registere
d Nursing
Fill Rate -
Day
94.0
%
93.1% 95.9% 100.3
%
96.0
%
103.0
%
104.3
%
108.4
%
100.7
%
Care
Staff Fill
Rate –
Day
93.0
%
83.7% 81.6% 90.1% 85.3
%
89.4% 91.1% 92.5% 99.9%
Registere
d Nursing
Fill Rate
– Night
96.4
%
93.2% 95.7% 94.4% 96.6
%
92.8% 99.7% 104.1
%
100.4
%
Care
Staff Fill
Rate –
Night
93.0
%
111.5
%
106.1
%
106.0
%
96.3
%
107.5
%
101.9
%
111.3
%
117.9
%
Sickness 4.2% 3.7% 3.0% 4.2% 4.5% 5.0% 5.8% 4.7% 4.7%
RN
Vacancy
Rate (%)
2.0% 2.2% 2.5% 3.7% 4.5% 4.1% 3.8% 4.2% 1.00%
RN
Vacancy
Rate
(WTE)
5.61 6.3 7.03 10.5 12.7 11.7 10.9 12.1 3.2
Turnover
Rate
9.0% 9.2% 8.5% 9.6% 9.6% 9.9% 10.0% 9.3% 9.7%
10.3.2 Families – Paediatrics
Staffing in general paediatric wards and the paediatric high dependency unit HDU Recommendations for paediatric nurse staffing levels are based upon the National Service Framework for Children (2004) supported by recommendations from the RCN ‘Defining Staffing levels for children’s and young people’s services’ (2013).
The unit continues to not meet this guidance however daily acuity and dependency scoring are undertaken and any safety concerns are
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 21 – L
escalated and mitigated. The 2020 CQC report did not identify any staffing issues however this does not reflect the adverse effect that the COVID pandemic has had on the children and young people population.
In June 2018 the National Quality Board (NQB) published ‘Safe, sustainable and productive staffing’. An improvement resource for children and young people’s inpatient wards in acute hospital’s The NQB paper quotes the previous guidance and states that this is based on professional opinion but that it needs to be considered and triangulated against a variety of other outcome issues such as, patient and staff feedback, nursing quality metrics such as the children’s safety thermometer, throughput counting both day attenders and those requiring inpatient care, and robust use of an evidence-based acuity and dependency tool. The wards undertook training and reflection on the use of the SafeCare acuity and dependency measures as part of an assurance process to validate ward measurements and staffing levels. The Directorate has worked to produce a ‘dashboard’ to present throughout, acuity and dependency with outcome measures so that we can obtain an overview of activity and care on the unit. This is now operational and reviewed through the Directorate governance processes monthly.
The Paediatric Assessment Unit (PAU) has been running successfully for 2 years. Expected sick children can be seen in this area and, if possible, plans made to minimise admissions to hospital. The unit is currently staffed for weekdays only. As part of previous winter planning, we were hoping to open over the weekends if funding was agreed however funding was declined. As part of escalation plans for the expected RSV surge through this winter, funding had been agreed to extend opening to weekends, however this has not been required. The team will continue to frequently review the requirement of weekend opening.
We continue to see an ongoing increase of admissions for young people with
complex combined physical and mental health care requirements. Extra
resources have been invested to support this care with enhanced staffing and
hours of service from the CAMHS and psychiatry liaison service.
There is ongoing work to strengthen links between CAMHS and the paediatric
unit. We have commenced a rotation programme between the unit and
Wessex House for both trained nurses and HCAs. There are ongoing
discussions around the possibility of recruiting either and RMN or an RSCN
with mental health qualifications or experience to support our current
CYPSEMH (Children and Young People Social Emotional and Mental Health)
nurse.
With the increase in complex young people that the unit has seen, there has
also been an increase in incidents relating to violence and aggression
involving both staff and patients. This has led to discussions around the need
for staff to be appropriately trained in de-escalation techniques as well as
restraint to safely care for the complex needs of young people within an acute
paediatric unit.
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 22 – L
An application has been submitted to be in the first cohort of ‘We Can Talk’
which is a co-produced educational project utilising the experience and
expertise of children, young people, hospital staff and mental health experts to
improve mental health crisis support in acute hospital settings. The
programme aims to deliver sustainable changes in practice and hospital
culture to improve patient experience, reduce risk and improve outcomes for
C&YP. It is hoped that this QI programme will improve confidence and
competency to deal with C&YP presenting with emotional distress. For staff to
safely restrain in line with guidance there may be a need to increase staffing,
particularly on night shifts and weekends which are currently staffed on
reduced numbers.
There is a separate piece of work underway, exploring the provision of dedicated commissioned beds for children with eating disorders (CEDs) as an option. This work will take time and is ongoing but there is a growing need in this area.
The unit has successfully recruited a band 4 nursing associate and we are exploring the possibility of increasing our band 4 workforce. We now also have a successful rotation programme with ED.
We have secured funding for a fixed term clinical skills post in addition to our current practice educator to support the development of new and existing staff. Historically there has been a high ratio of band 6 nurses with varying job descriptions. To bring the unit in line with the rest of the acute trust, we are aiming to upskill our band 6 junior sisters to support leadership and management of the unit. Our long-term goal will be to reduce the amount of band 6s to increase band 4 and 5 nursing staff.
Paediatric High Dependency Unit (PHDU) Recommendations for PHDU nurse staffing is based upon the Paediatric Intensive Care Standards 2010. Children within PHDU are nursed at a level of 1:2. PHDU is staffed according to occupancy and the 1:2 ratios.
It is a requirement that all nursing staff allocated to care for a child receiving PHDU level of care should be Qualified in Specialty (QIS) in Paediatric High Dependency Nursing.
Currently there are 8 nursing staff who are allocated to work in this area. Across the unit there are 18 people who are QIS trained but they are not all actively working in this area but able to offer support in HDU if required and nurse higher dependency patients on the rest of the unit.
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 23 – L
Community Children’s Nursing The information regarding the growth in population of young people in Somerset also has an impact on the workload of the Community Children’s Nursing Team.
There is a known increase in survival rates for pre-term infants with complex long term multiple therapy needs. Following the experience of the pandemic the community children’s nursing team developed an on-call system to support children overnight who need occasional support from the nursing team. At the time this resulted in significant workload. The workload has now reduced although it remains a valuable service, leading to a reduction of attendance to the local ward.
In addition, the team continue to see increases in children referred ADHD and Epilepsy. A piece of work on the optimal pathway for ADHD across the county is in progress.
The team expanded into the East Mendip area and links with Royal United Hospital in Bath are progressing. However, there is an identified gap with patients receiving services via The Seahorse centre in Weston-Super-Mare.
Since the pandemic and alongside other external factors it has been noted that the recruitment for band 3 carers has been difficult. Throughout the pandemic and beyond it has been observed that the team has remained strong and supportive of each other, setting up various wellbeing tools such as WhatsApp groups and days out where allowed. Fatigue and concern about wellbeing has played a larger part in the service recently. This is an area of focus for the Team Leads.
All developments moving forward will focus on collaborative working with our YDH colleagues.
Children’s and Young Person’s Therapy Service (CYPTS) The significant increase in the diagnostic work for neurodevelopmental disorders such as ASD and ADHD has been recognised at a system level and new funding agreed including therapies. The service has deployed staff to cover this work, and external recruitment is now taking place.
Paediatric Psychology Historically, paediatric psychology posts have proved difficult to recruit into and the service has also found it hard to retain staff. Reasons are complex but include working across two different teams, and poor balance between realistic workload and time in the role.
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 24 – L
The current psychology department is small and therefore has limited capacity for working as a team. The split of the role between several clinical areas (Diabetes, CF, Oncology) may also result in frustration that insufficient effective provision can be given to any one service. There are many patients that cannot access paediatric psychology at all as no service is commissioned for certain groups. We are currently working with the CCG to improve the access to psychological services in paediatrics.
10.3.3 Families – Maternity
The integration of the maternity services in Somerset is now actively being developed as part of the SFT YDH merger. Ongoing service changes due to the COVID-19 pandemic are already aligning across the Somerset Local MatNeo Maternity System (LMNS) to continue supporting an equitable service for all users. There are 3 LMNS funded project roles currently working across the system to drive implementation of the National Maternity Service Review deliverables (Better Births 2015). This includes the maternity specific public health agenda and development of bereavement services aligned to the National Bereavement Care Pathway (NCBP).
SFT has undertaken the staffing assessment Birthrate plus using retrospective data from August to October 2020. The final report was sent in November 2021. The methodology used in this review draws upon a set of national assumptions and benchmarked data from other recent reviews. The data assessed that establishment met the requirement at the time of the data capture. Additional assessments were undertaken to calculate the number of midwives required to deliver continuity of care. Although indicating a reduction in birth rate, the report acknowledged a 23% rise in complexity of women accessing maternity care, both socially and medically. Maternal mental health and safeguarding concerns and referrals have seen a significant rise during the pandemic.
In the last 6 months midwifery numbers have fluctuated but overall, the establishment has remained within national recommendations for a 1:28 midwife to birth ratio. This ratio does not reflect the impact of the increased workload, because of different pathways and ways of working within the pandemic and the increased workload associated with increased complexity. Required compliance with the essential safety actions identified in the Ockenden report (Dec 20) has further impacted maternity service staffing requirements outside of the Birthrate Plus calculations.
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 25 – L
Midwife to Birth ratio July to December 2021
2021 Jul Aug Sep Oct Nov Dec
Midwife/birth ratio
(including maternity &
sick leave)
1:26 1:24 1:25 1:26 1:28 1:24
10.3.4 Acuity Data
The care acuity levels have remained low between 57 – 72%. Midwifery Red Flag events (NICE – safe staffing in Midwifery Settings 2015), have been impacted with a frequent delay in commencing induction of labour. There have been no reported safety incidents because of delays, although user feedback has reflected dissatisfaction with delays. Supernumerary labour ward co-ordinator and 1:1 care in labour ward remains 100%. The acuity assessment does not reflect workforce requirements outside of the obstetric led labour ward.
Red Flag Acuity Data July – December 2021
Acuity Supernumerary labour ward coordinator
1:1 care in labour (core delivery suite only)
July 57% 100% 100%
Aug 61% 100% 100%
Sept 58% 100% 100%
Oct 59% 100% 100%
Nov 58% 100% 100%
Dec 72% 100% 100%
10.3.5 Recruitment
A workforce review is ongoing to ensure each area has staffing and appropriate skill mix to support the changing national drivers. Provision of Continuity of Carer (CoC) using Better Births, remains a challenge and is dependent upon the workforce review being completed. The merging organisation needs to develop a working plan to ensure that as a Somerset system, CoC is the default care pathway for all pregnant women by March 2023, prioritising those most at risk of poor maternity outcomes. The concerns in achieving this has been raised with the Regional Chief Midwife and Nurse.
Active recruitment is in place for 10.0wte midwives and 5.0wte band 3 support workers. There is uncertainty if the midwifery vacancy will be filled with the continuing national shortage of midwives. Funding has been made available for the international recruitment of midwives. This is being actively pursued; however, this will only address the medium-term recruitment of midwives and sustainable future workforce feeds need to be pursued.
SFT Maternity has a small separate pool of bank staff and vacant shifts are generally covered by substantive staff working additional hours.
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 26 – L
The number of specialist maternity midwives is 9.32wte. This includes 1.28wte nursing associate. This is the lower end of the Birthrate plus recommendation wte which suggests 8-10% of the funded establishment.
The newborn hearing screening service is System wide. Despite the current issues with retention of staff, the service continues to provide an exceptional service meeting KPI’s and the top performing in the Southwest Region.
Somerset Neonatal Intensive Care Unit (SNICU)
SNICU is a Local Neonatal Unit (LNU) providing neonatal care for the catchment population of Somerset, except for the smallest and sickest babies. All categories of neonatal care are provided, but babies who require surgery, cooling and other complex or longer-term intensive care are transferred to a higher level NICU, generally in Bristol. Many babies over 27 weeks of gestation will usually receive their full care, including high dependency and short periods of intensive care, within SNICU. Transfers from other neonatal services in the network are accepted if these fall within the agreed work pattern
SNICU has 18 cots; eight designated intensive and high dependency care and ten special care, with transitional care supported on the post-natal ward. Transitional care is a model of care developed to keep some babies with parents in the post-natal ward areas rather than being admitted to NICU. The care is supported by both midwifery and neonatal staff to meet both the needs of mother and babies. This model aims to avoid unnecessary admission to the NICU and to keep mums and babies together and is evidenced to support good outcomes
Recommendations for neonatal nurse staffing are based upon the British Association of Perinatal Medicine (BAPM, 2010) guidelines, the ‘specialist commissioners’ service specification for Neonatal Critical Care (Intensive Care, HDU and Special Care), E08/S/a and the ‘Toolkit for High Quality Neonatal Services’ (DoH 2009) which states that nursing staffing levels should be as follows: Special care 1:4 staff to baby ratio, High dependency care 1:2 staff to baby ratio and Intensive care 1:1 staff to baby ratio and an additional nurse coordinator. These recommendations are based upon number of cots presuming there is 80% cot occupancy and one additional nursing coordinator per shift with an overview of the unit
The CQC report, in May 2016 and an external peer review, recognised that the Neonatal Unit did not fully meet trained nurse staff levels in accordance with BAPM guidance of 2011 because the ratio of staff to patient against acuity of care falls below the requirement of 1:1 and 1:2 nurses to baby care for the neonatal intensive and high dependency nursing care management of these babies and a ‘must do’ recommendation was made to review this level of staffing.
Following a review by the Quality and Governance Committee uplift in neonatal staffing was agreed with funding into registered nurse
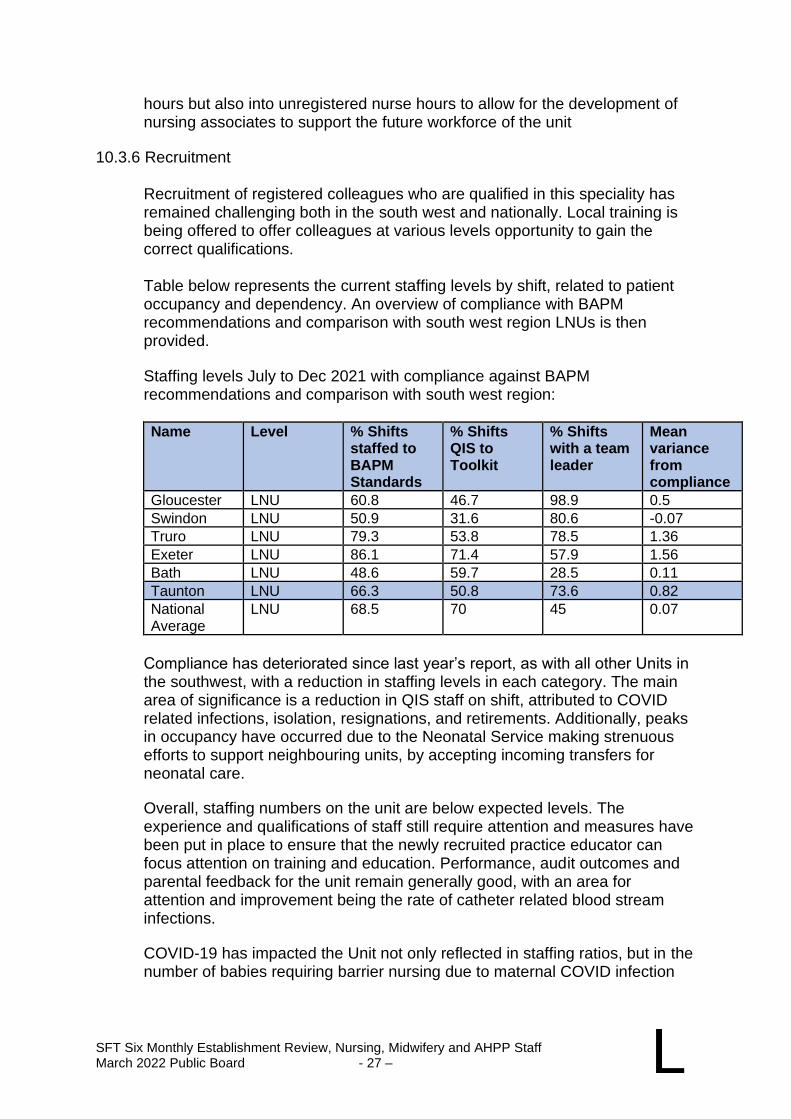
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 27 – L
hours but also into unregistered nurse hours to allow for the development of nursing associates to support the future workforce of the unit
10.3.6 Recruitment
Recruitment of registered colleagues who are qualified in this speciality has remained challenging both in the south west and nationally. Local training is being offered to offer colleagues at various levels opportunity to gain the correct qualifications.
Table below represents the current staffing levels by shift, related to patient occupancy and dependency. An overview of compliance with BAPM recommendations and comparison with south west region LNUs is then provided.
Staffing levels July to Dec 2021 with compliance against BAPM recommendations and comparison with south west region:
Name Level % Shifts
staffed to BAPM Standards
% Shifts QIS to Toolkit
% Shifts with a team leader
Mean variance from compliance
Gloucester LNU 60.8 46.7 98.9 0.5
Swindon LNU 50.9 31.6 80.6 -0.07
Truro LNU 79.3 53.8 78.5 1.36
Exeter LNU 86.1 71.4 57.9 1.56
Bath LNU 48.6 59.7 28.5 0.11
Taunton LNU 66.3 50.8 73.6 0.82
National Average
LNU 68.5 70 45 0.07
Compliance has deteriorated since last year’s report, as with all other Units in the southwest, with a reduction in staffing levels in each category. The main area of significance is a reduction in QIS staff on shift, attributed to COVID related infections, isolation, resignations, and retirements. Additionally, peaks in occupancy have occurred due to the Neonatal Service making strenuous efforts to support neighbouring units, by accepting incoming transfers for neonatal care.
Overall, staffing numbers on the unit are below expected levels. The experience and qualifications of staff still require attention and measures have been put in place to ensure that the newly recruited practice educator can focus attention on training and education. Performance, audit outcomes and parental feedback for the unit remain generally good, with an area for attention and improvement being the rate of catheter related blood stream infections.
COVID-19 has impacted the Unit not only reflected in staffing ratios, but in the number of babies requiring barrier nursing due to maternal COVID infection
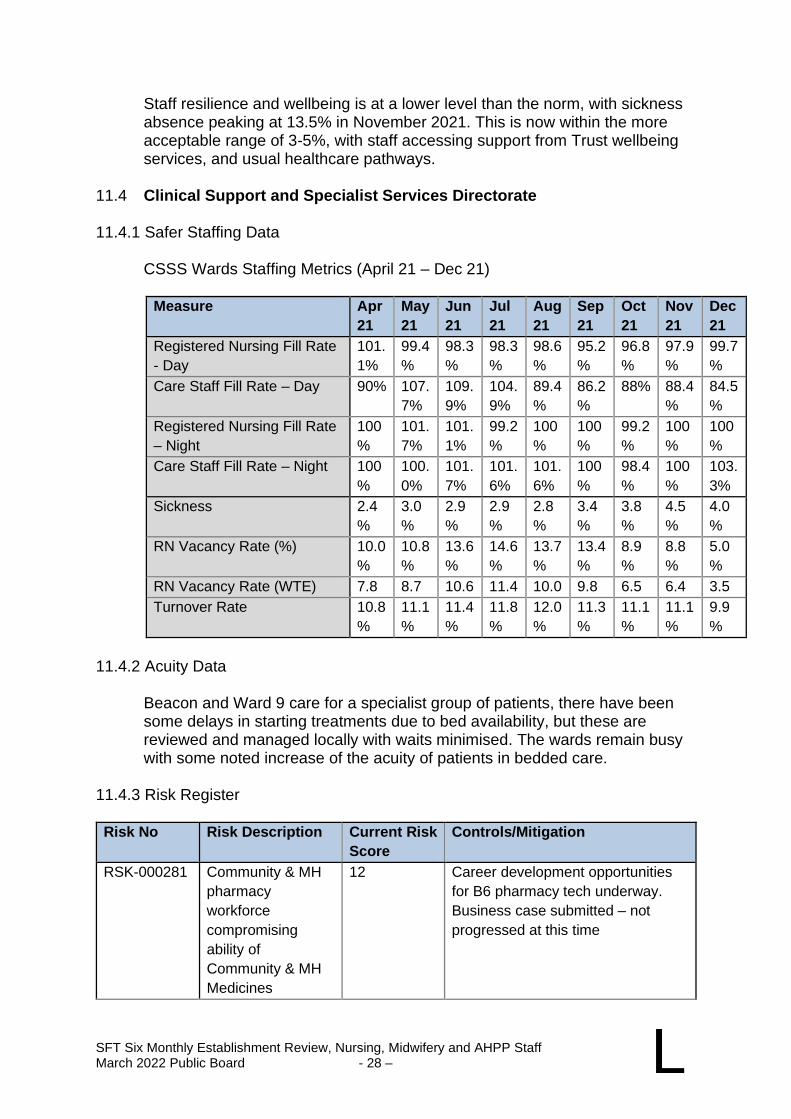
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 28 – L
Staff resilience and wellbeing is at a lower level than the norm, with sickness absence peaking at 13.5% in November 2021. This is now within the more acceptable range of 3-5%, with staff accessing support from Trust wellbeing services, and usual healthcare pathways.
11.4 Clinical Support and Specialist Services Directorate
11.4.1 Safer Staffing Data
CSSS Wards Staffing Metrics (April 21 – Dec 21)
Measure Apr
21
May
21
Jun
21
Jul
21
Aug
21
Sep
21
Oct
21
Nov
21
Dec
21
Registered Nursing Fill Rate
- Day
101.
1%
99.4
%
98.3
%
98.3
%
98.6
%
95.2
%
96.8
%
97.9
%
99.7
%
Care Staff Fill Rate – Day 90% 107.
7%
109.
9%
104.
9%
89.4
%
86.2
%
88% 88.4
%
84.5
%
Registered Nursing Fill Rate
– Night
100
%
101.
7%
101.
1%
99.2
%
100
%
100
%
99.2
%
100
%
100
%
Care Staff Fill Rate – Night 100
%
100.
0%
101.
7%
101.
6%
101.
6%
100
%
98.4
%
100
%
103.
3%
Sickness 2.4
%
3.0
%
2.9
%
2.9
%
2.8
%
3.4
%
3.8
%
4.5
%
4.0
%
RN Vacancy Rate (%) 10.0
%
10.8
%
13.6
%
14.6
%
13.7
%
13.4
%
8.9
%
8.8
%
5.0
%
RN Vacancy Rate (WTE) 7.8 8.7 10.6 11.4 10.0 9.8 6.5 6.4 3.5
Turnover Rate 10.8
%
11.1
%
11.4
%
11.8
%
12.0
%
11.3
%
11.1
%
11.1
%
9.9
%
11.4.2 Acuity Data
Beacon and Ward 9 care for a specialist group of patients, there have been some delays in starting treatments due to bed availability, but these are reviewed and managed locally with waits minimised. The wards remain busy with some noted increase of the acuity of patients in bedded care.
11.4.3 Risk Register Risk No Risk Description Current Risk
Score
Controls/Mitigation
RSK-000281
Community & MH
pharmacy
workforce
compromising
ability of
Community & MH
Medicines
12 Career development opportunities
for B6 pharmacy tech underway.
Business case submitted – not
progressed at this time
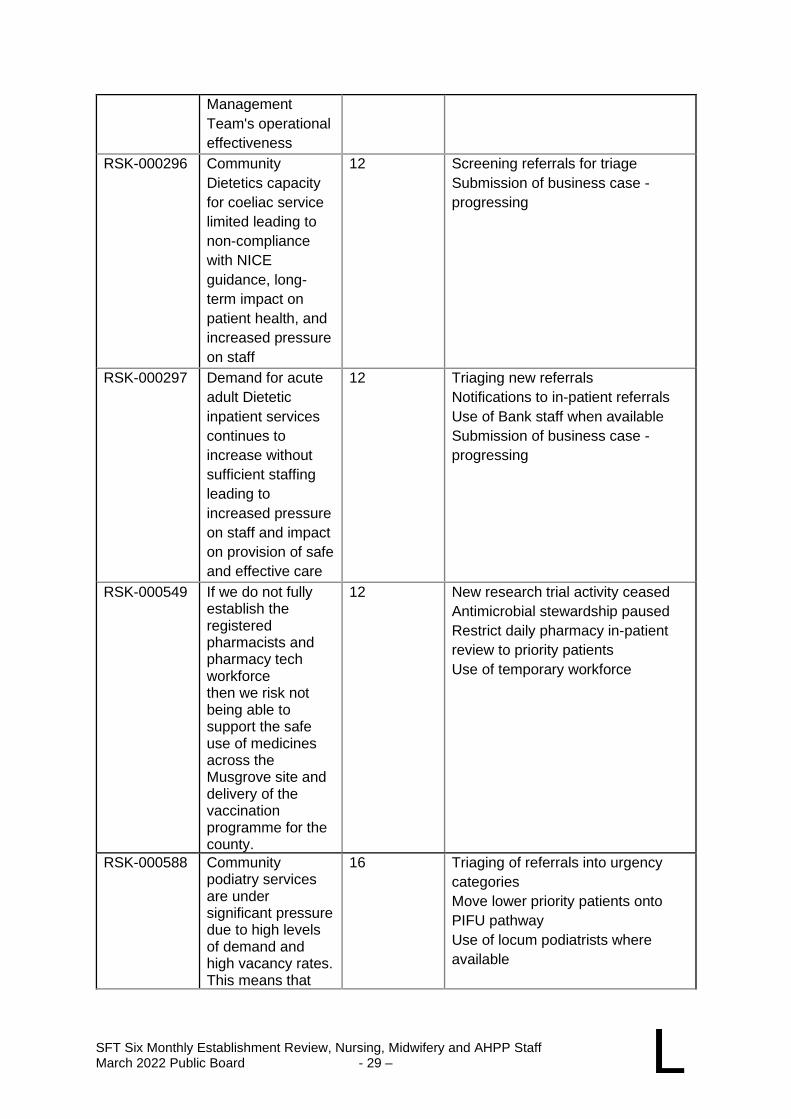
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 29 – L
Management
Team's operational
effectiveness
RSK-000296
Community
Dietetics capacity
for coeliac service
limited leading to
non-compliance
with NICE
guidance, long-
term impact on
patient health, and
increased pressure
on staff
12
Screening referrals for triage
Submission of business case -
progressing
RSK-000297
Demand for acute
adult Dietetic
inpatient services
continues to
increase without
sufficient staffing
leading to
increased pressure
on staff and impact
on provision of safe
and effective care
12 Triaging new referrals
Notifications to in-patient referrals
Use of Bank staff when available
Submission of business case -
progressing
RSK-000549
If we do not fully establish the registered pharmacists and pharmacy tech workforce then we risk not being able to support the safe use of medicines across the Musgrove site and delivery of the vaccination programme for the county.
12 New research trial activity ceased
Antimicrobial stewardship paused
Restrict daily pharmacy in-patient
review to priority patients
Use of temporary workforce
RSK-000588
Community podiatry services are under significant pressure due to high levels of demand and high vacancy rates. This means that
16 Triaging of referrals into urgency
categories
Move lower priority patients onto
PIFU pathway
Use of locum podiatrists where
available
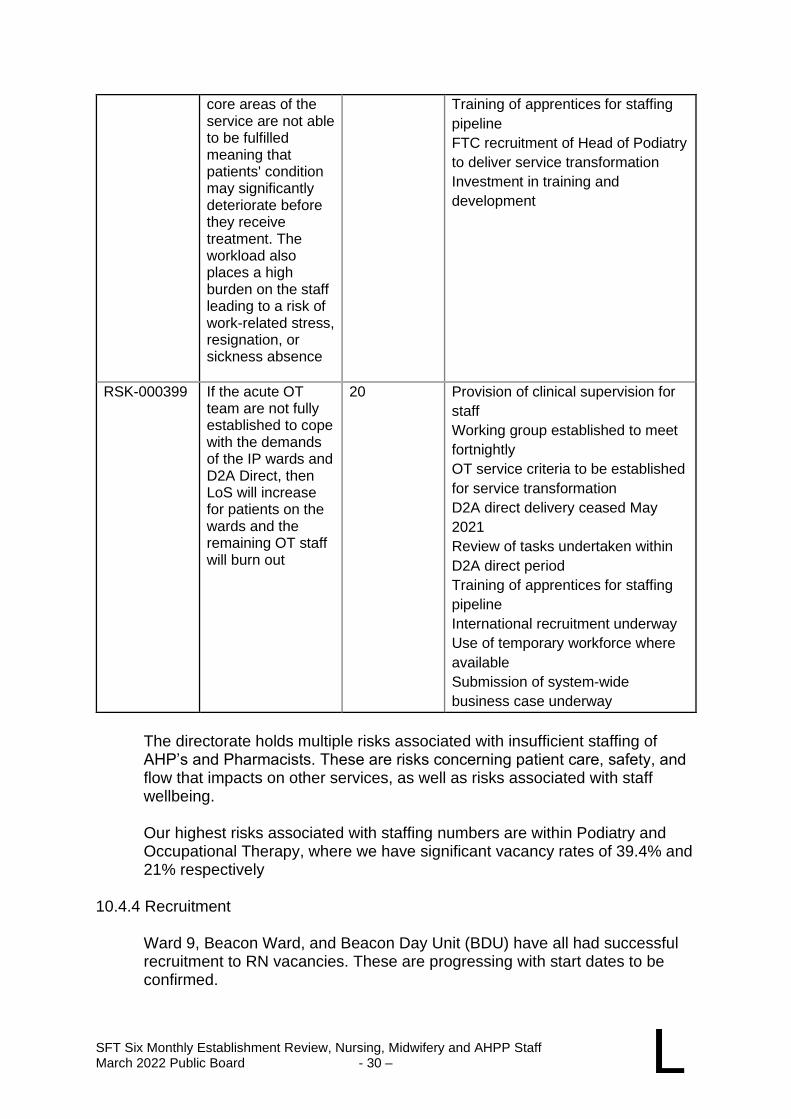
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 30 – L
core areas of the service are not able to be fulfilled meaning that patients' condition may significantly deteriorate before they receive treatment. The workload also places a high burden on the staff leading to a risk of work-related stress, resignation, or sickness absence
Training of apprentices for staffing
pipeline
FTC recruitment of Head of Podiatry
to deliver service transformation
Investment in training and
development
RSK-000399
If the acute OT team are not fully established to cope with the demands of the IP wards and D2A Direct, then LoS will increase for patients on the wards and the remaining OT staff will burn out
20 Provision of clinical supervision for
staff
Working group established to meet
fortnightly
OT service criteria to be established
for service transformation
D2A direct delivery ceased May
2021
Review of tasks undertaken within
D2A direct period
Training of apprentices for staffing
pipeline
International recruitment underway
Use of temporary workforce where
available
Submission of system-wide
business case underway
The directorate holds multiple risks associated with insufficient staffing of AHP’s and Pharmacists. These are risks concerning patient care, safety, and flow that impacts on other services, as well as risks associated with staff wellbeing.
Our highest risks associated with staffing numbers are within Podiatry and Occupational Therapy, where we have significant vacancy rates of 39.4% and 21% respectively
10.4.4 Recruitment
Ward 9, Beacon Ward, and Beacon Day Unit (BDU) have all had successful recruitment to RN vacancies. These are progressing with start dates to be confirmed.
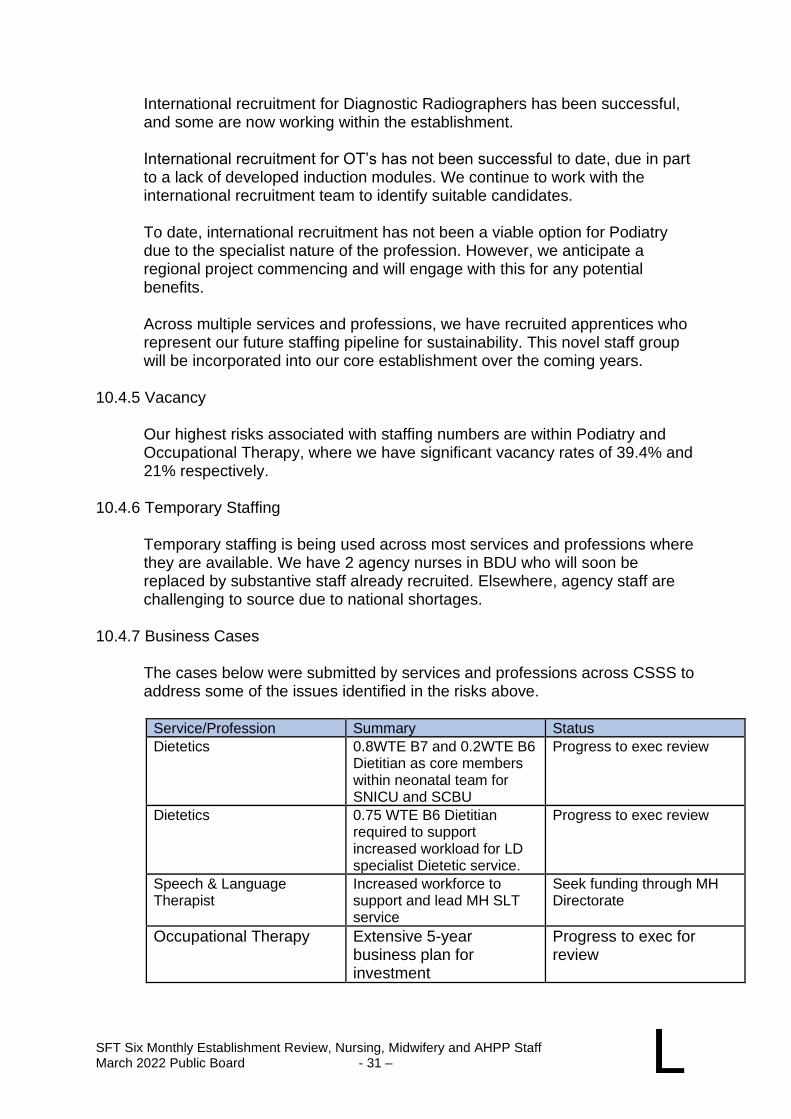
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 31 – L
International recruitment for Diagnostic Radiographers has been successful, and some are now working within the establishment.
International recruitment for OT’s has not been successful to date, due in part to a lack of developed induction modules. We continue to work with the international recruitment team to identify suitable candidates.
To date, international recruitment has not been a viable option for Podiatry due to the specialist nature of the profession. However, we anticipate a regional project commencing and will engage with this for any potential benefits.
Across multiple services and professions, we have recruited apprentices who represent our future staffing pipeline for sustainability. This novel staff group will be incorporated into our core establishment over the coming years.
10.4.5 Vacancy
Our highest risks associated with staffing numbers are within Podiatry and Occupational Therapy, where we have significant vacancy rates of 39.4% and 21% respectively.
10.4.6 Temporary Staffing
Temporary staffing is being used across most services and professions where they are available. We have 2 agency nurses in BDU who will soon be replaced by substantive staff already recruited. Elsewhere, agency staff are challenging to source due to national shortages.
10.4.7 Business Cases
The cases below were submitted by services and professions across CSSS to address some of the issues identified in the risks above.
Service/Profession Summary Status
Dietetics 0.8WTE B7 and 0.2WTE B6 Dietitian as core members within neonatal team for SNICU and SCBU
Progress to exec review
Dietetics 0.75 WTE B6 Dietitian required to support increased workload for LD specialist Dietetic service.
Progress to exec review
Speech & Language Therapist
Increased workforce to support and lead MH SLT service
Seek funding through MH Directorate
Occupational Therapy Extensive 5-year business plan for investment
Progress to exec for review
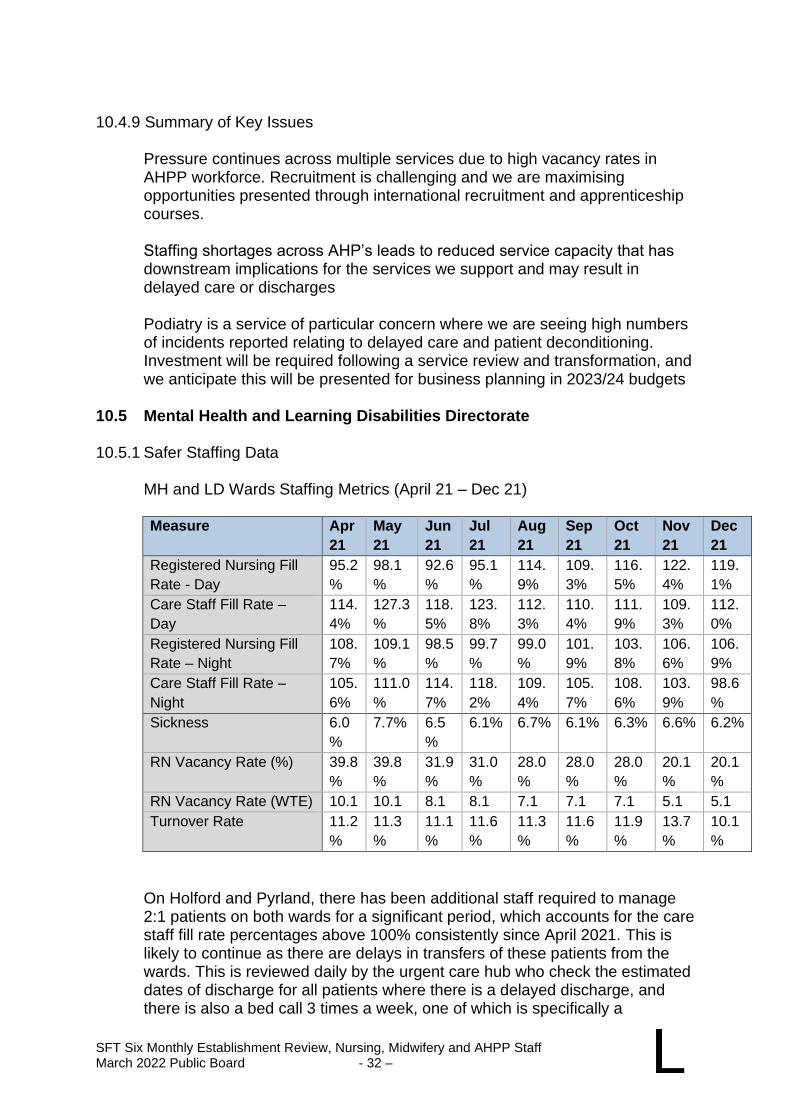
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 32 – L
10.4.9 Summary of Key Issues
Pressure continues across multiple services due to high vacancy rates in AHPP workforce. Recruitment is challenging and we are maximising opportunities presented through international recruitment and apprenticeship courses.
Staffing shortages across AHP’s leads to reduced service capacity that has downstream implications for the services we support and may result in delayed care or discharges
Podiatry is a service of particular concern where we are seeing high numbers of incidents reported relating to delayed care and patient deconditioning. Investment will be required following a service review and transformation, and we anticipate this will be presented for business planning in 2023/24 budgets
10.5 Mental Health and Learning Disabilities Directorate 10.5.1 Safer Staffing Data
MH and LD Wards Staffing Metrics (April 21 – Dec 21)
Measure Apr
21
May
21
Jun
21
Jul
21
Aug
21
Sep
21
Oct
21
Nov
21
Dec
21
Registered Nursing Fill
Rate - Day
95.2
%
98.1
%
92.6
%
95.1
%
114.
9%
109.
3%
116.
5%
122.
4%
119.
1%
Care Staff Fill Rate –
Day
114.
4%
127.3
%
118.
5%
123.
8%
112.
3%
110.
4%
111.
9%
109.
3%
112.
0%
Registered Nursing Fill
Rate – Night
108.
7%
109.1
%
98.5
%
99.7
%
99.0
%
101.
9%
103.
8%
106.
6%
106.
9%
Care Staff Fill Rate –
Night
105.
6%
111.0
%
114.
7%
118.
2%
109.
4%
105.
7%
108.
6%
103.
9%
98.6
%
Sickness 6.0
%
7.7% 6.5
%
6.1% 6.7% 6.1% 6.3% 6.6% 6.2%
RN Vacancy Rate (%) 39.8
%
39.8
%
31.9
%
31.0
%
28.0
%
28.0
%
28.0
%
20.1
%
20.1
%
RN Vacancy Rate (WTE) 10.1 10.1 8.1 8.1 7.1 7.1 7.1 5.1 5.1
Turnover Rate 11.2
%
11.3
%
11.1
%
11.6
%
11.3
%
11.6
%
11.9
%
13.7
%
10.1
%
On Holford and Pyrland, there has been additional staff required to manage 2:1 patients on both wards for a significant period, which accounts for the care staff fill rate percentages above 100% consistently since April 2021. This is likely to continue as there are delays in transfers of these patients from the wards. This is reviewed daily by the urgent care hub who check the estimated dates of discharge for all patients where there is a delayed discharge, and there is also a bed call 3 times a week, one of which is specifically a
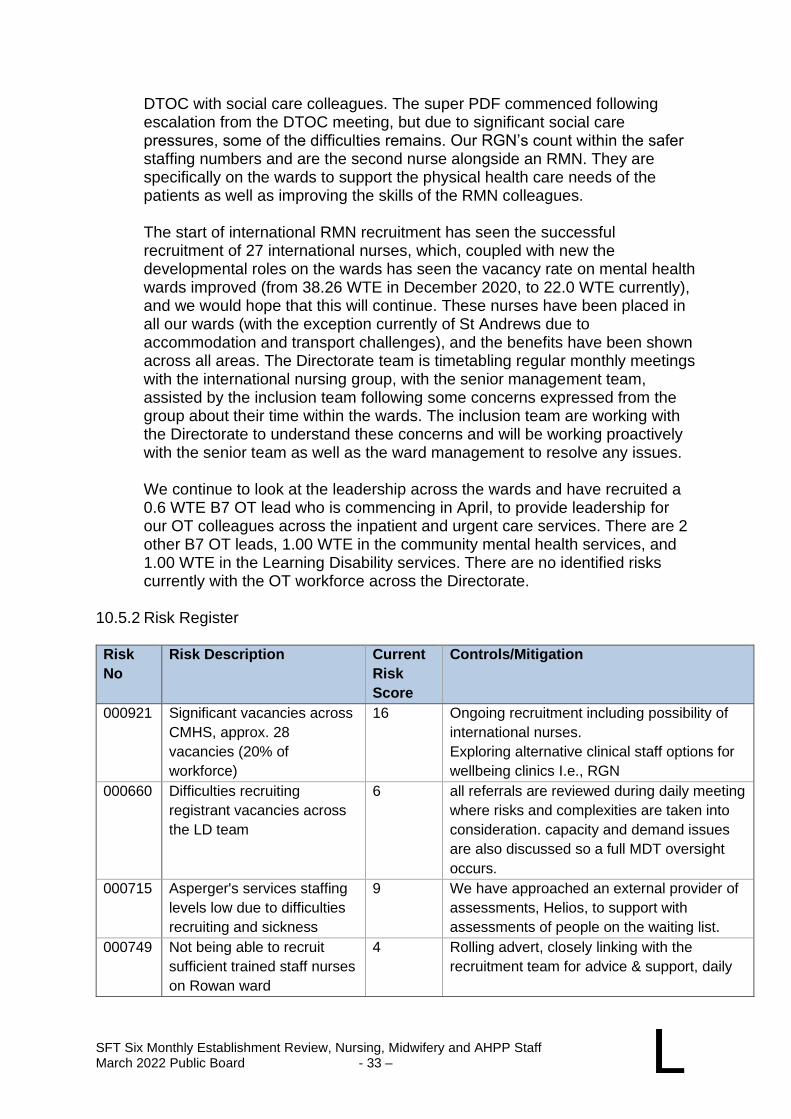
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 33 – L
DTOC with social care colleagues. The super PDF commenced following escalation from the DTOC meeting, but due to significant social care pressures, some of the difficulties remains. Our RGN’s count within the safer staffing numbers and are the second nurse alongside an RMN. They are specifically on the wards to support the physical health care needs of the patients as well as improving the skills of the RMN colleagues.
The start of international RMN recruitment has seen the successful recruitment of 27 international nurses, which, coupled with new the developmental roles on the wards has seen the vacancy rate on mental health wards improved (from 38.26 WTE in December 2020, to 22.0 WTE currently), and we would hope that this will continue. These nurses have been placed in all our wards (with the exception currently of St Andrews due to accommodation and transport challenges), and the benefits have been shown across all areas. The Directorate team is timetabling regular monthly meetings with the international nursing group, with the senior management team, assisted by the inclusion team following some concerns expressed from the group about their time within the wards. The inclusion team are working with the Directorate to understand these concerns and will be working proactively with the senior team as well as the ward management to resolve any issues.
We continue to look at the leadership across the wards and have recruited a 0.6 WTE B7 OT lead who is commencing in April, to provide leadership for our OT colleagues across the inpatient and urgent care services. There are 2 other B7 OT leads, 1.00 WTE in the community mental health services, and 1.00 WTE in the Learning Disability services. There are no identified risks currently with the OT workforce across the Directorate.
10.5.2 Risk Register Risk
No
Risk Description Current
Risk
Score
Controls/Mitigation
000921 Significant vacancies across
CMHS, approx. 28
vacancies (20% of
workforce)
16 Ongoing recruitment including possibility of
international nurses.
Exploring alternative clinical staff options for
wellbeing clinics I.e., RGN
000660 Difficulties recruiting
registrant vacancies across
the LD team
6 all referrals are reviewed during daily meeting
where risks and complexities are taken into
consideration. capacity and demand issues
are also discussed so a full MDT oversight
occurs.
000715 Asperger's services staffing
levels low due to difficulties
recruiting and sickness
9 We have approached an external provider of
assessments, Helios, to support with
assessments of people on the waiting list.
000749 Not being able to recruit
sufficient trained staff nurses
on Rowan ward
4 Rolling advert, closely linking with the
recruitment team for advice & support, daily
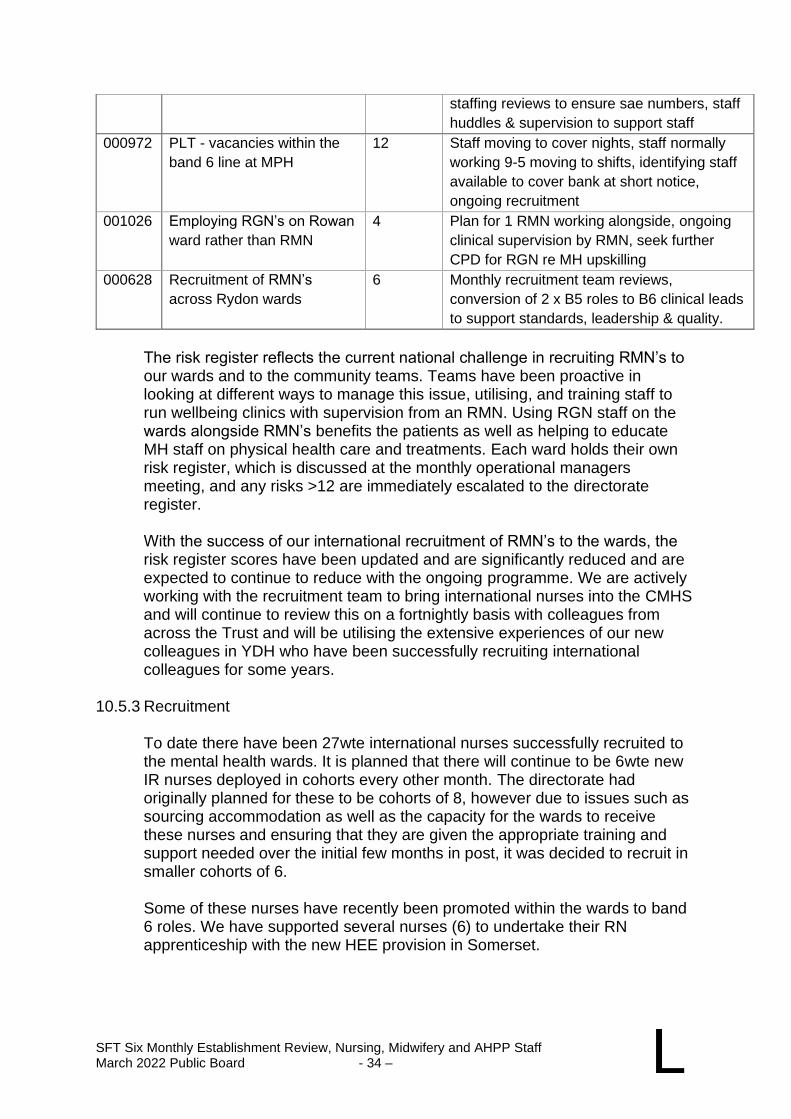
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 34 – L
staffing reviews to ensure sae numbers, staff
huddles & supervision to support staff
000972 PLT - vacancies within the
band 6 line at MPH
12 Staff moving to cover nights, staff normally
working 9-5 moving to shifts, identifying staff
available to cover bank at short notice,
ongoing recruitment
001026 Employing RGN’s on Rowan
ward rather than RMN
4 Plan for 1 RMN working alongside, ongoing
clinical supervision by RMN, seek further
CPD for RGN re MH upskilling
000628 Recruitment of RMN’s
across Rydon wards
6 Monthly recruitment team reviews,
conversion of 2 x B5 roles to B6 clinical leads
to support standards, leadership & quality.
The risk register reflects the current national challenge in recruiting RMN’s to our wards and to the community teams. Teams have been proactive in looking at different ways to manage this issue, utilising, and training staff to run wellbeing clinics with supervision from an RMN. Using RGN staff on the wards alongside RMN’s benefits the patients as well as helping to educate MH staff on physical health care and treatments. Each ward holds their own risk register, which is discussed at the monthly operational managers meeting, and any risks >12 are immediately escalated to the directorate register.
With the success of our international recruitment of RMN’s to the wards, the risk register scores have been updated and are significantly reduced and are expected to continue to reduce with the ongoing programme. We are actively working with the recruitment team to bring international nurses into the CMHS and will continue to review this on a fortnightly basis with colleagues from across the Trust and will be utilising the extensive experiences of our new colleagues in YDH who have been successfully recruiting international colleagues for some years.
10.5.3 Recruitment
To date there have been 27wte international nurses successfully recruited to the mental health wards. It is planned that there will continue to be 6wte new IR nurses deployed in cohorts every other month. The directorate had originally planned for these to be cohorts of 8, however due to issues such as sourcing accommodation as well as the capacity for the wards to receive these nurses and ensuring that they are given the appropriate training and support needed over the initial few months in post, it was decided to recruit in smaller cohorts of 6.
Some of these nurses have recently been promoted within the wards to band 6 roles. We have supported several nurses (6) to undertake their RN apprenticeship with the new HEE provision in Somerset.
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 35 – L
We are actively recruiting for a rotational band 5 post between Rowan, the HTT and the CMHS which will offer staff a varied experience and improve retention as well as sharing knowledge across the teams.
We have appointed an additional band 7 ward manager to support the two Pyrland wards, who provides further leadership and enabling further integration with other directorates.
We are planning a pilot around Advanced Nurse Practitioners (ANP) across our wards which will improve patient care and inspire staff to develop their careers within the inpatient services and have successfully supported our first ANP to achieve accreditation within the ADHD service.
11.5.4 Vacancy
There are currently 22wte RMN vacancies across the wards, and we continue
to work closely with the recruitment team to encourage applicants to apply to
the Trust. Winning the MH Trust of the Year, and the developments across
the MH directorate will hopefully be positive for recruitment, and an increase
in applicants has already been noted.
With significant new investment in community mental health provision, there
has been introduced a risk of ward staff moving to new roles in the community
services, and therefore we will be continuing to look at developing a pathway
for staff to remain on the wards and to progress with their inpatient career.
Across the community teams, recruitment of staff of all grades remains a
challenge, and affects our ability to meet the demand for care co-ordinators,
but to note that with the national implementation of the changes to CPA there
will not be a wait for care-coordination, but there may be a wait for a key
worker for an identified intervention. There are also difficulties recruiting for
staff for psychology/therapy interventions as well nurse cover for Depot and
Clozapine clinics, however the teams are looking at innovative ideas (such as
RGN recruitment) to manage these areas. Agency and bank staff are used to
manage these gaps in service currently, with the hope that the benefits from
the MH Trust of the year award will be realised. Band 5 roles are offered as
development posts which allows staff to improve skills and experiences within
the team, and they are then in a position to become band 6’s within a stated
period of between 1 year to 18 months.
Across the CMHS, there are 28.1wte vacancies, with a mixture of banding.
Within the CMHS some of the roles are generic, so are advertised as a mental
health worker which allows flexibility when deciding the more appropriate
registrant for each team (I.e., Nurse, OT, social worker).
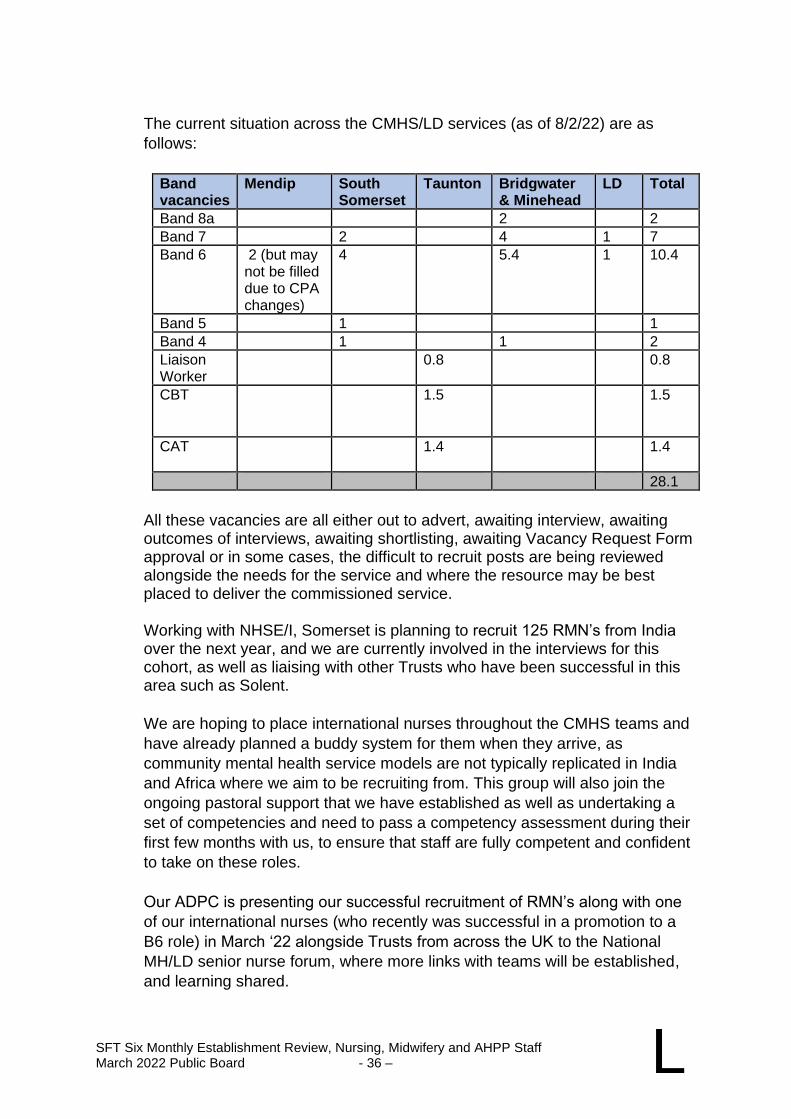
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 36 – L
The current situation across the CMHS/LD services (as of 8/2/22) are as
follows:
Band vacancies
Mendip South Somerset
Taunton Bridgwater & Minehead
LD Total
Band 8a 2 2
Band 7 2 4 1 7
Band 6 2 (but may not be filled due to CPA changes)
4 5.4 1 10.4
Band 5 1 1
Band 4 1 1 2
Liaison Worker
0.8 0.8
CBT
1.5 1.5
CAT 1.4
1.4
28.1
All these vacancies are all either out to advert, awaiting interview, awaiting outcomes of interviews, awaiting shortlisting, awaiting Vacancy Request Form approval or in some cases, the difficult to recruit posts are being reviewed alongside the needs for the service and where the resource may be best placed to deliver the commissioned service.
Working with NHSE/I, Somerset is planning to recruit 125 RMN’s from India over the next year, and we are currently involved in the interviews for this cohort, as well as liaising with other Trusts who have been successful in this area such as Solent.
We are hoping to place international nurses throughout the CMHS teams and
have already planned a buddy system for them when they arrive, as
community mental health service models are not typically replicated in India
and Africa where we aim to be recruiting from. This group will also join the
ongoing pastoral support that we have established as well as undertaking a
set of competencies and need to pass a competency assessment during their
first few months with us, to ensure that staff are fully competent and confident
to take on these roles.
Our ADPC is presenting our successful recruitment of RMN’s along with one
of our international nurses (who recently was successful in a promotion to a
B6 role) in March ‘22 alongside Trusts from across the UK to the National
MH/LD senior nurse forum, where more links with teams will be established,
and learning shared.
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 37 – L
10.5.5 Turnover and Retention
Turnover appears to be stable, and we are encouraging our ward managers to look at succession planning across their RMN team, and to actively support promotion where possible. We will continue to encourage staff with their professional development and utilise the CPD training monies to support this.
10.5.6 Temporary Staffing
We meet fortnightly with the temporary staffing leads to review the data relating to agency and bank staff fill rates, and to support the continued recruitment of bank staff. Indicators reviewed in Directorate Finance and Planning meetings suggest the improved staffing position on the wards is positively impacting on reduced agency usage and a reduction in associated costs.
10.5.7 Business Cases
No current business cases. 10.5.8 Summary of Key Issues
The Board are asked to note:
• Successful recruitment of 27 international MH nurses – cohorts of 6 every other month - next cohort due March’22.
• Ongoing programme of international recruitment, will start to focus on the CMHS as well as the wards.
• Working with the L&D team and recruitment to positively prepare these nurses for CMHS work, including skills training and competency assessments, buddying systems and wellbeing support.
• Award of MH Trust of the Year has potentially had a positive effect on applicants; 3 staff have applied for roles in Yeovil which has traditionally not attracted any applicants.
• Development of inpatient RMN’s using the CPD monies to aid retention on the wards to increase applications for vacant posts by improving our reputation as a dynamic and supportive place to work.
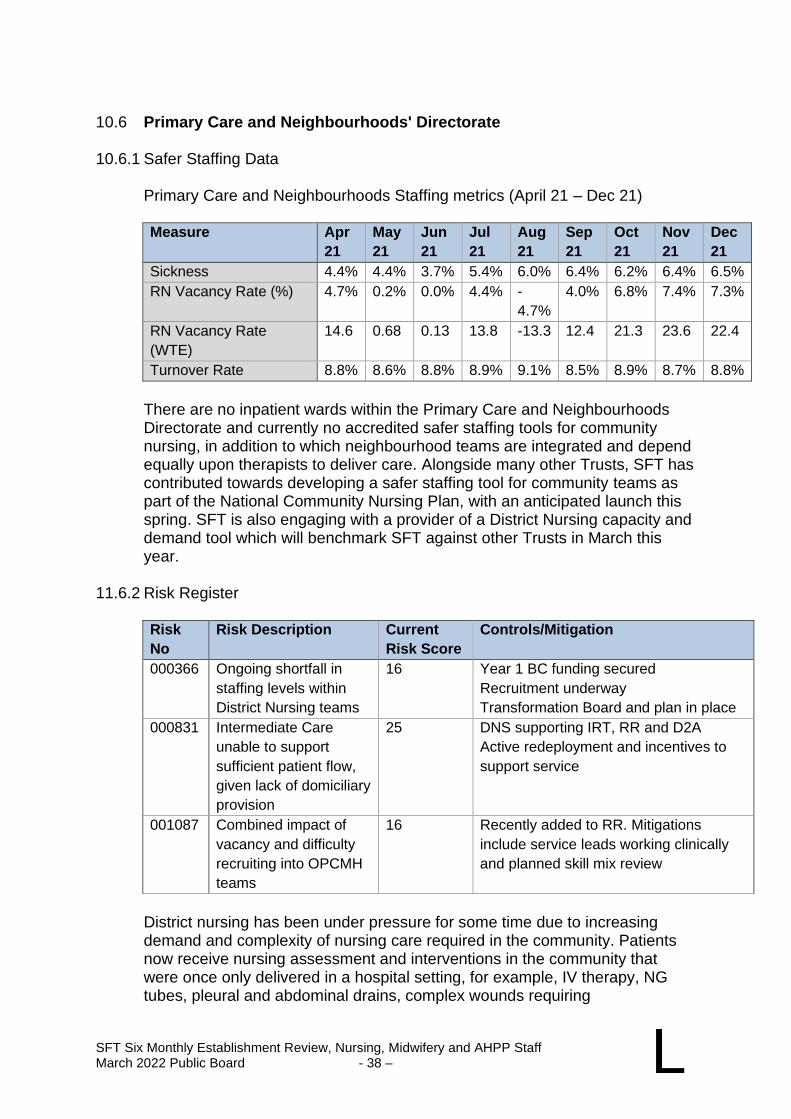
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 38 – L
10.6 Primary Care and Neighbourhoods' Directorate 10.6.1 Safer Staffing Data
Primary Care and Neighbourhoods Staffing metrics (April 21 – Dec 21)
Measure Apr
21
May
21
Jun
21
Jul
21
Aug
21
Sep
21
Oct
21
Nov
21
Dec
21
Sickness 4.4% 4.4% 3.7% 5.4% 6.0% 6.4% 6.2% 6.4% 6.5%
RN Vacancy Rate (%) 4.7% 0.2% 0.0% 4.4% -
4.7%
4.0% 6.8% 7.4% 7.3%
RN Vacancy Rate
(WTE)
14.6 0.68 0.13 13.8 -13.3 12.4 21.3 23.6 22.4
Turnover Rate 8.8% 8.6% 8.8% 8.9% 9.1% 8.5% 8.9% 8.7% 8.8%
There are no inpatient wards within the Primary Care and Neighbourhoods Directorate and currently no accredited safer staffing tools for community nursing, in addition to which neighbourhood teams are integrated and depend equally upon therapists to deliver care. Alongside many other Trusts, SFT has contributed towards developing a safer staffing tool for community teams as part of the National Community Nursing Plan, with an anticipated launch this spring. SFT is also engaging with a provider of a District Nursing capacity and demand tool which will benchmark SFT against other Trusts in March this year.
11.6.2 Risk Register
Risk
No
Risk Description Current
Risk Score
Controls/Mitigation
000366 Ongoing shortfall in
staffing levels within
District Nursing teams
16 Year 1 BC funding secured
Recruitment underway
Transformation Board and plan in place
000831 Intermediate Care
unable to support
sufficient patient flow,
given lack of domiciliary
provision
25 DNS supporting IRT, RR and D2A
Active redeployment and incentives to
support service
001087 Combined impact of
vacancy and difficulty
recruiting into OPCMH
teams
16 Recently added to RR. Mitigations
include service leads working clinically
and planned skill mix review
District nursing has been under pressure for some time due to increasing demand and complexity of nursing care required in the community. Patients now receive nursing assessment and interventions in the community that were once only delivered in a hospital setting, for example, IV therapy, NG tubes, pleural and abdominal drains, complex wounds requiring
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 39 – L
negative wound pressure therapy. The unique setting of working in the home environment demands a nursing workforce with specialist knowledge and skills and demands an elevated level of responsibility and risk management. A career pathway from band 2 to band 8a advanced clinical practice has been developed in district nursing to support the increasing demand and complexity of nursing care required in the community.
Detailed risk assessments outlining demand and capacity pressures are in place and the DNS has been on both directorate and corporate risk registers for some time. Given that context, the service adapted remarkably quickly in response to the pandemic which saw many other parts of primary care reduced/stood down and relying even more so on DNS. Despite which a high standard of care continued to be provided to prevent hospital admission, support patient flow, and support the care homes. This included using technology and skilling up support workers and carers to enable the registered nurses to concentrate their efforts on the more complex patients.
Year 1 funding of the 2021 DN business case (which was geographically targeted) has been secured and recruitment continues into the service but has proved difficult and is not yet complete. Full competency and skill mix review has been completed with recognition that transformation (involving more B4 roles) is required as well as additional band 6 and band 7 posts (to ensure adequate supervision and leadership). There is recognition of significant unmet need for restorative supervision across the whole service to support colleagues increasingly dealing with complex situations (DNs have been first on scene for collapse, suicide etc.). There has also been the increased acuity mentioned above as well as increased activity. To support increasing acuity, multidisciplinary and professional meetings are stood up within hours of referral to the service or on assessing a complex situation.
Unfortunately, staff are also reporting increased violence and aggression from families. Individual patient risks are recorded in their clinical records and on RADAR. Professional Nurse Advocate (PNA) training is underway and restorative supervision will be targeted/piloted within identified District Nursing teams to support this ongoing pressure. The DN teams also work closely with safeguarding colleagues, and this provide extra support in dealing with complex issues.
The service has supported other areas where shortfalls have impacted care of patients in the system with some of the team supporting intermediate care. has added additional pressure on an already stretched service. The service often has to review any planned and preventative visits, and some have had to be cancelled, with resource targeted at urgent care and end of life care.
Intermediate care is significantly impacted by current escalation and is supporting domiciliary care patients until care packages are in place to support flow in the acute hospitals by freeing up hospital beds. This is a capacity issue rather than purely a staffing issue and spans therapy as well as nursing roles. However, the service is under significant pressure and
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 40 – L
incentives have been offered to temporarily increase capacity during escalation.
Older Peoples Mental Health (OPMH) staffing within community teams has recently been added to the Directorate risk register because of significant vacancy, compounded by difficulties in recruiting registered staff. Service leads are currently mitigating by covering and further work is underway in relation to additional mitigation.
10.6.3 Recruitment
Work is underway to have a proactive rolling programme of recruitment, in line with transformation plans and workforce planning requirements. Recruitment of RN/RMNs has proved challenging and is further complicated as overseas placements have proved tricky as overseas colleagues do not necessarily have community experience or feel confident enough to gain that experience in a different country. Exploratory work around overcoming this with rotational experience has started, although has been on hold whilst the directorate is in escalation (supporting patient flow).
The directorate is re-attempting to recruit a clinical skills facilitator (first attempt resulted in no applicants) to work with learning and development teams and specifically support the DNS transformation programme through supporting the development of skills and competency in the band 3 and 4 support worker role. This will ensure that Registered Nurse time is concentrated on assessment and treatment of complex patients.
Therapy recruitment echoes the difficulties trust wide and the Directorate is part of the wider Trust workforce planning and recruitment for therapy teams. Recruitment is in progress for Advanced Care Practitioners for OPMH, to provide specialist leadership within teams. Alternative roles are continuously being explored, including Assistant Psychologists, who are successfully employed in memory assessment services.
10.6.4 Vacancy
The directorate has not seen significant increases in long term vacancy, but hotspots remain in district nursing teams (previously discussed) and more recently in OPMH teams, especially South Somerset, where a similar programme of workforce planning and transformation is underway, including linking with overseas recruitment programme.) and more recently in OPMH teams, where a similar programme of workforce planning and transformation is underway, including linking with overseas recruitment programme.
There are some key leadership posts in the directorate that have remined vacant for a significant period, hence, talent mapping and succession planning is a workforce priority, but again has been delayed by both the initial COVID response and more recently by the escalation status of the directorate/Trust.
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 41 – L
10.6.5 Turnover and Retention
Despite a higher than Trust average age profile, turnover in the directorate is lower than the trust average and is not currently identified as a risk within the directorate. However, as previously mentioned there is ongoing work around succession planning, talent mapping, developing advanced practice roles and clinical leadership, to offer career opportunities other than the traditional management routes.
Staff well -being is a significant concern for the directorate and as well as signposting colleagues to wider Trust well-being support, directorate level support has been targeted at specific teams where support needs have been identified.
10.6.6 Temporary Staffing
There is minimal usage of additional temporary/bank staffing in community as specific skill sets are required and because of the nature of the work (lone working, with driving involved) it is difficult to support/orientate temporary staff sufficiently. Existing workforce tends to cover as required, which has added to work overload/pressure that teams feel.
10.6.7 Business Cases
7 day working in District Nursing (year 2 funding). The paper outlines the proposal for Year Two of the Three Year District Nursing 7 Day Working Business Case submitted and approved in March 2021. The March 2021 paper describes the unique contribution that the District Nursing Service makes to the priorities of the NHS Long term Plan in the transformation of community services to build capacity to deliver more integrated care at home, support more people in the community for longer and improve hospital discharge.
10.6.8 Summary of Key Issues
Key non-medical staffing issues for the directorate have been highlighted as district nursing, OPMH and intermediate care capacity. None of which are registered nurse specific. Therapy and support staff as well as skill mix is equally important as RN establishments for neighbourhood teams. Transformation of services using skill mix, integrated teams and linking to apprentice and advanced practice role development is a priority Clinical and restorative supervision will be key to supporting colleague well- being as the Trust continues to move towards being an ICS, which inevitably requires more community-based capacity.
SFT Six Monthly Establishment Review, Nursing, Midwifery and AHPP Staff March 2022 Public Board - 42 – L
11. SUMMARY
The Board is asked to note that:
• safe staffing levels have been reviewed as laid out in this report and unless concern has been highlighted, they have been found to meet standards, guidance and to support good patient experience and outcomes.
• several areas have been described as raising some concern and these areas will be closely monitored and deficits responded to as required.
• the response to Covid-19 and ongoing system capacity pressures has had a profound effect on all colleagues. There is ongoing disruption of services which has meant that a priority focus has been towards a dynamic approach to monitor and oversee staffing. This has left many services in a vulnerable position that requires on going close monitoring and action and mitigation to support care delivery and adverse outcomes.
• some areas have required altered establishments to deliver care to an increased number of beds due to escalation.
• Vacancy is low in the nursing groups with a robust plan for ongoing international recruitment, but increased workload and elevated levels of sickness and absence have caused difficulty in sustainably maintaining safe staffing levels and altered or minimum staffing levels are put in to balance the risks.
• AHPPs are seeing a significant level of vacancy in many professions, and this is impacting on the services offered in many areas and raising some areas of risk.
SFT Six Monthly Freedom to Speak Up Progress Report
March 2022 Public Board - 1 –
M
Somerset NHS Foundation Trust
REPORT TO: The Trust Board
REPORT TITLE: Freedom to Speak Up Guardian Report
SPONSORING EXEC: Chief of People and Organisational Development
REPORT BY: Freedom to Speak Up Guardian
PRESENTED BY: Freedom to Speak Up Guardian
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☒ For Assurance/
Discussion ☐ For Approval / Decision ☐ For Information
Executive Summary and Reason for presentation to Committee/Board
All organisations which regulate or provide NHS healthcare should implement the principles and actions set out in the report Freedom to Speak Up: An independent review into creating an open and honest reporting culture in the NHS. This paper provides an update regarding FTSU activity in Somerset FT. It informs the Trust Board about the number of concerns received and the professional background of the colleagues contacting the service. It also outlines the themes of the concerns. It covers the period April 2021 – Dec 2021. 65 concerns were raised in Q1 2021 -22, 59 in Q2, and 55 in Q3. Data collected demonstrates that registered and non-registered nursing staff, AHPs and Admin / Ancillary colleagues have raised most of the concerns over the past year. Of the 179 concerns raised by colleagues during Q1-Q3, 8 were specifically related to Covid-19.
Recommendation The Board is asked to note and discuss the report.
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☐ Care for our Population ☐ Develop our People
SFT Six Monthly Freedom to Speak Up Progress Report
March 2022 Public Board - 2 – M
☐ Innovate and Collaborate ☐ Develop a Sustainable System
Somerset NHS FT
☐ Obj 1 Inclusive culture ☐ Obj 4 Safe services ☐ Obj 7 Improving outcomes
☐ Obj 2 Collaboration ☐ Obj 5 Self management ☒ Obj 8 Workforce
☒ Obj 3 Independent lives ☐ Obj 6 Value all people alike ☐ Obj 9 Performance
☐ Obj 10 Finance
Implications/Requirements (Please select any which are relevant to this paper)
☒ Financial ☐ Legislation ☒ Workforce ☐ Estates ☐ ICT ☐ Patient Safety /
Quality
Details:. N/A
Equality The Trust wants its services to be as accessible as possible, to as many people as
possible. Please indicate whether the report has an impact on the protected characteristics
☒ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are no proposals or matters which affect any persons with protected characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
Not applicable.
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
The Freedom to Speak Up six monthly progress report was presented to the September 2021 Board meeting.
Reference to CQC domains (Please select any which are relevant to this paper)
☒ Safe ☒ Effective ☒ Caring ☒ Responsive ☒ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
SFT Freedom to Speak Up Guardian Report March 2022 Public Board - 1 - M
1. INTRODUCTION 1.1 The joint speaking up model across Somerset Foundation Trust (SFT) is fully
embedded and work has commenced to align the services across SFT and Yeovil District hospital (YDH) in preparation for the merger. The service continues to grow both in terms of the number of cases raised and proactive work fulfilled, including service promotion and education around the FTSU concept. The model consists of a full-time lead guardian, Caroline Sealey, and a part-time (0.6wte) guardian, Kerry Coles.
1.2 Our vision is to create a culture of safety within Somerset FT where
colleagues are encouraged and empowered to speak up without experiencing detriment, regardless of their role.
2. NATIONAL DATA 2.1 Since the last Board report in September 2021, there has been no interim
data report published by the National Guardian’s Office (NGO). A reminder of the national picture from 1 April 2020 and 31 March 2021 is set out below*:
• 20,388 speaking up cases were raised, an increase of 26% on the previous year
• 18% of cases involved an element of patient safety / quality. This is a 5% reduction from 2019/20.
• 30.1% of cases involved an element of bullying and harassment. This is a 5.8% decrease from 2019/20 and continued downward trend since 2017/18.
• Almost 12% of cases were reported anonymously.
• Detriment for speaking up continued to decrease and was indicated in 3.1% of cases.
• Nurses and midwives accounted for the biggest proportion of cases raised (29%) followed by admin/clerical and ancillary colleagues (20.8%) and AHP’s (11.7%).
• 84.3% of those who gave feedback said they would speak up again.
* The Year of the Pandemic: A Summary of Speaking Up to Freedom To Speak Up Guardians; NGO, July 2021
Current regional conversations indicate that speaking up cases remain high and we are likely to see record numbers again for the year 1 April 2021 to 31 March 2022.
SOMERSET NHS FOUNDATION TRUST
FREEDOM TO SPEAK UP GUARDIAN REPORT
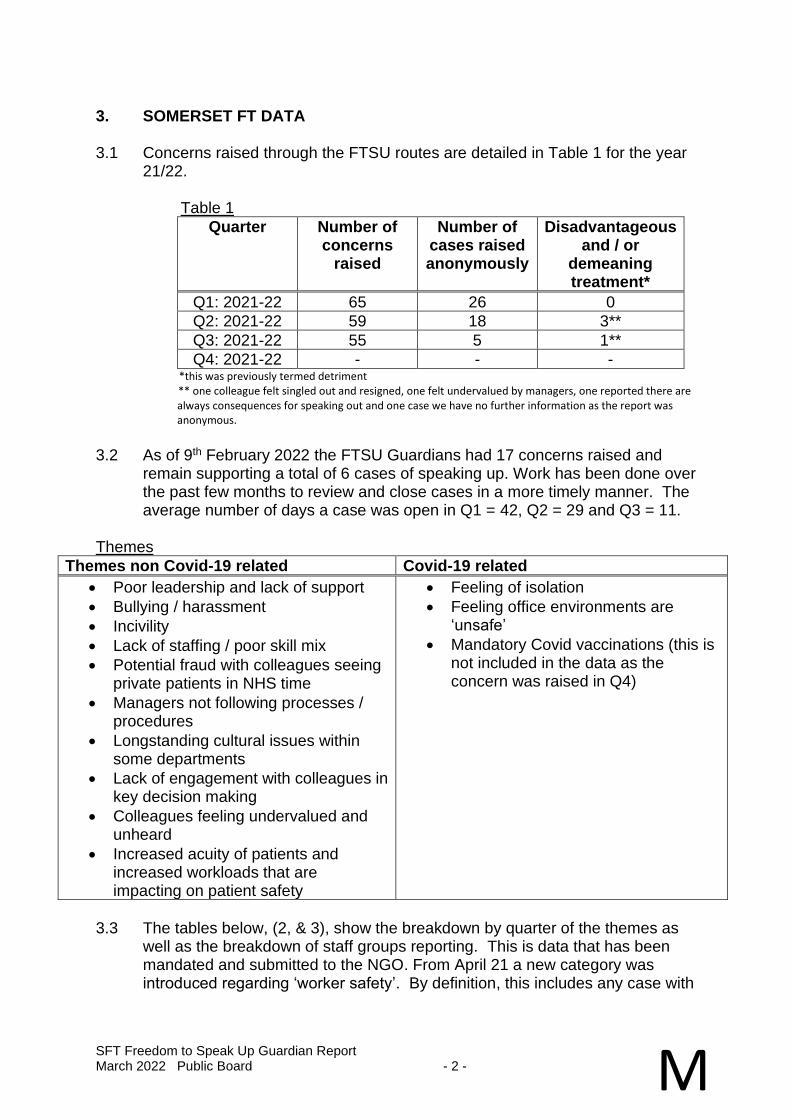
SFT Freedom to Speak Up Guardian Report March 2022 Public Board - 2 - M
3. SOMERSET FT DATA 3.1 Concerns raised through the FTSU routes are detailed in Table 1 for the year
21/22. Table 1
Quarter Number of concerns
raised
Number of cases raised anonymously
Disadvantageous and / or
demeaning treatment*
Q1: 2021-22 65 26 0
Q2: 2021-22 59 18 3**
Q3: 2021-22 55 5 1**
Q4: 2021-22 - - - *this was previously termed detriment ** one colleague felt singled out and resigned, one felt undervalued by managers, one reported there are always consequences for speaking out and one case we have no further information as the report was anonymous.
3.2 As of 9th February 2022 the FTSU Guardians had 17 concerns raised and
remain supporting a total of 6 cases of speaking up. Work has been done over the past few months to review and close cases in a more timely manner. The average number of days a case was open in Q1 = 42, Q2 = 29 and Q3 = 11.
Themes
Themes non Covid-19 related Covid-19 related
• Poor leadership and lack of support
• Bullying / harassment
• Incivility
• Lack of staffing / poor skill mix
• Potential fraud with colleagues seeing private patients in NHS time
• Managers not following processes / procedures
• Longstanding cultural issues within some departments
• Lack of engagement with colleagues in key decision making
• Colleagues feeling undervalued and unheard
• Increased acuity of patients and increased workloads that are impacting on patient safety
• Feeling of isolation
• Feeling office environments are ‘unsafe’
• Mandatory Covid vaccinations (this is not included in the data as the concern was raised in Q4)
3.3 The tables below, (2, & 3), show the breakdown by quarter of the themes as
well as the breakdown of staff groups reporting. This is data that has been mandated and submitted to the NGO. From April 21 a new category was introduced regarding ‘worker safety’. By definition, this includes any case with
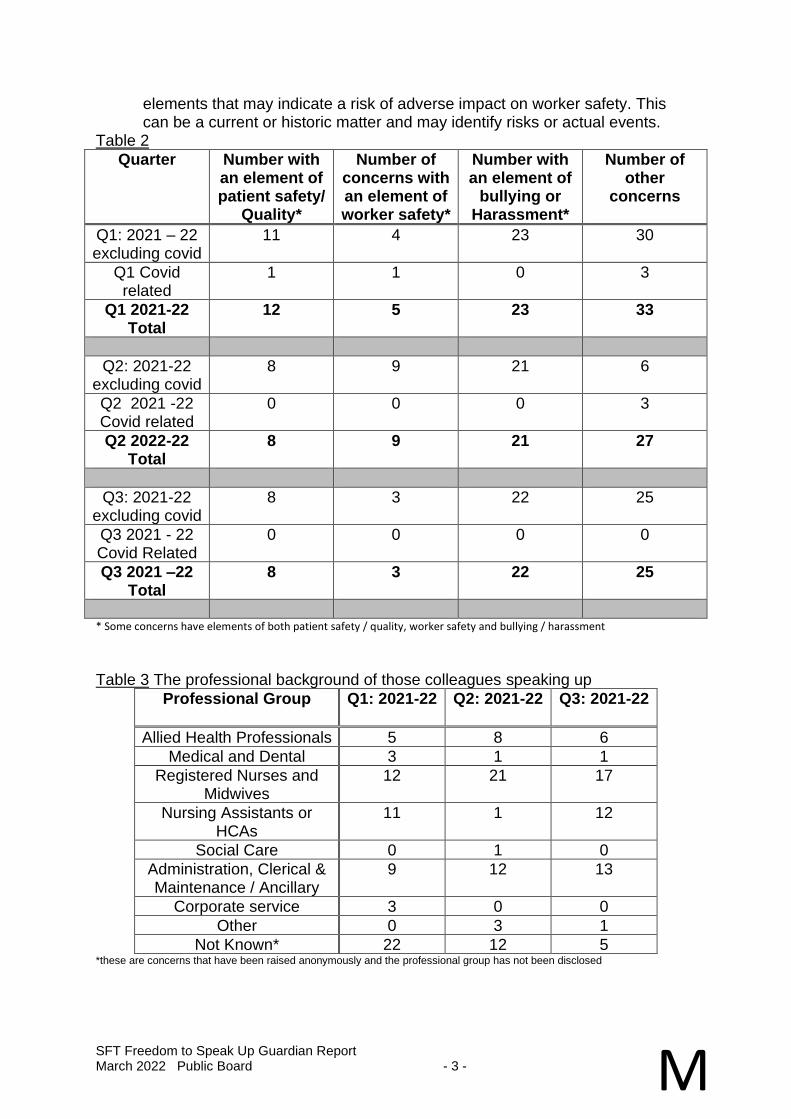
SFT Freedom to Speak Up Guardian Report March 2022 Public Board - 3 - M
elements that may indicate a risk of adverse impact on worker safety. This can be a current or historic matter and may identify risks or actual events.
Table 2
Quarter Number with an element of patient safety/
Quality*
Number of concerns with an element of worker safety*
Number with an element of
bullying or Harassment*
Number of other
concerns
Q1: 2021 – 22 excluding covid
11 4 23 30
Q1 Covid related
1 1 0 3
Q1 2021-22 Total
12 5 23 33
Q2: 2021-22 excluding covid
8 9 21 6
Q2 2021 -22 Covid related
0 0 0 3
Q2 2022-22 Total
8 9 21 27
Q3: 2021-22 excluding covid
8 3 22 25
Q3 2021 - 22 Covid Related
0 0 0 0
Q3 2021 –22 Total
8 3 22 25
* Some concerns have elements of both patient safety / quality, worker safety and bullying / harassment
Table 3 The professional background of those colleagues speaking up
Professional Group Q1: 2021-22 Q2: 2021-22
Q3: 2021-22
Allied Health Professionals 5 8 6
Medical and Dental 3 1 1
Registered Nurses and Midwives
12 21 17
Nursing Assistants or HCAs
11 1 12
Social Care 0 1 0
Administration, Clerical & Maintenance / Ancillary
9 12 13
Corporate service 3 0 0
Other 0 3 1
Not Known* 22 12 5 *these are concerns that have been raised anonymously and the professional group has not been disclosed
SFT Freedom to Speak Up Guardian Report March 2022 Public Board - 4 - M
3.4 Local data for Q1-Q2 2021/22 has shown:
• 61% increase in reported cases from Q3 – Q4 2020/21.
• 16% of the cases raised in this period contained and element of patient safety/quality compared to 18% for Q3 – Q4 2020/21.
• 35.5% of the cases raised in this period contained and element of bullying and harassment compared to 25.9% for Q3 – Q4 2020/21;
• 35.4% of cases were raised anonymously.
• Disadvantageous and / or demeaning treatment as a result of speaking up is 2.4% of cases.
• 26.6% of concerns raised came from Nursing and Midwifery, 16.9% from admin/clerical and ancillary colleagues, 10.5% from allied health professionals and 8.9% from nursing assistants and HCA’s.
• 89.3% of those who gave feedback said they would speak up again.
• Response time from first contact has been introduced as a monitoring metric. The agreed response time is within 3 working days. Data collection commenced at the start of Q2 and shows that 93% of concerns were responded to the same day, 5% within one working day and 2% within 2 working days for that quarter.
4. ACTIONS 4.1 To date great progress has been made to create a positive speaking up
culture across the organisation. This has been supported by the launch, in August 2021, of the mandatory training modules ‘Speak Up’ and ‘Listen Up’. Compliance across the Trust as of January 2022 was 67.3%.
The service collates feedback from service users and some of the feedback
received is detailed below:
• Prompt, polite, helpful, empathetic
• Quick comms good advice and follow up support
• Helpful, honest, responsive
• I was made to feel that I could express my concerns without being judged. It is a comfort to know that this service is available
SFT Freedom to Speak Up Guardian Report March 2022 Public Board - 5 - M
• I felt supported and I was not pushed to take action I wasn't comfortable with
• I felt that I was listened to and that my query was treated with respect and importance
• It is good to talk to someone not connected to the ward about worries and concerns
• I felt safe throughout their involvement. I felt able to express an honest view. I valued the objectivity and impartiality of their involvement as sometimes that can be hard to evaluate that you are achieving yourself when you are in the middle of a situation. They had the scope within their role to ask questions at all levels. I feel their involvement had an influence and raised the voice of concerns that although expressed through appropriate channels by people involved, didn't appear to have been otherwise heard.
4.2 The team will continue to build on the progress achieved to date supporting the creation of a culture where every colleague, irrespective of role, feels safe to speak up. Some of the work includes:
• Collaborative working with Wellbeing, Leadership & OD and Colleague Support Service as part of the Integrated People Support team. As a cohesive team we are able to:
✓ offer timely, bespoke, integrated support for individuals, teams and the organisation that can be tailored according to need and intensity
✓ identify areas in need and coordinate the appropriate support, reducing duplication and improving communication between us
✓ learn from areas of success and to run QI projects where we can
test the impact of a range of interventions
✓ This results in improved colleague experience and satisfaction, reduced sickness absence and a reduced complexity of cases
• Continuation of the training for wellbeing champions that is extending the reach and diversity of the FTSU service.
• Further promotion of the training videos: ‘Speak Up’ for all colleagues and ‘Listen Up’ for managers. This will help ensure that colleagues feel safe to speak up and it becomes business as usual, and managers respond appropriately. A further module ‘Follow Up’ will be produced and released in line with National Guidance later in the year.
SFT Freedom to Speak Up Guardian Report March 2022 Public Board - 6 - M
• Supporting teams with departmental / ward training either post incident or proactively.
• Continuation of the speaking up network meetings that brings all stakeholders together on a 6 weekly basis to share themes and triangulate information. This enables the Trust to address concerns in a robust way.
• Attendance at the Safety Action Group to allow triangulation of safety specific data and themes.
• Working in collaboration with our FTSU colleagues in YDH in preparation for the upcoming merger.
• Gap analysis of the service in line with the case review guidance from the NGO.
• Completion of the Board Self-Assessment Tool in conjunction with the Exec Lead.
Ockenden N Report
March 2022 Public Board - 1 –
N
Somerset NHS Foundation Trust/ Yeovil District NHS Foundation Trust
REPORT TO: Board of Directors
REPORT TITLE:
OCKENDEN: First report: Emerging Findings and Recommendations from the Independent Review of Maternity Services at the Shrewsbury and Telford Hospitals NHS Trust
SPONSORING EXEC: Chief Nurse
REPORT BY: Sallyann King, Interim Director of Midwifery for Somerset
PRESENTED BY: Sallyann King, Interim Director of Midwifery for Somerset
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☒ For Assurance/
Discussion ☐ For Approval / Decision ☐ For Information
Executive Summary and Reason for presentation to Committee/Board
It is a year since the release of the First Ockenden Report for maternity services and release of the seven Immediate and Essential Actions (IEA’s) for Trusts to action by 24 March 2022. Over the last year there have been two assessments of compliance when both Trusts independently submitted evidence through the NHS Futures portal. Submissions have been assessed and quality assured by the regional Chief Midwifery team. The Ockenden phase 2 compliance report was returned to both Trusts in December 2021 and identified an overall compliance of 81% at YDH and 74% at SFT. This was based on further evidence which was submitted in November 2021. Ongoing compliance with Trusts Action Plans is being monitored as a Somerset System through the Local Maternity/Neonatal System (LMNS). This is exception reported through the CCG quality and safety forums to the National team. Through collaborative working across sites, there has been a positive uplift in compliance. Overall compliance as of 18 Feb 2022 YDH = 88% SFT = 86%
Ockenden N Report
March 2022 Public Board - 2 – N
The National ambition is for all Trusts to be 100% complaint by 24 March 2022 in readiness for the new actions that will be a requirement of the full Ockenden Report and the anticipated Kirkup 2 Report to be released in June 2022.
All outstanding issues within the Trusts’ Action Plans will continue to be monitored through the Safety Subgroup of the LMNS. A local assessment forecasts that the Somerset system will be 95% compliant by 24 March 2022
Recommendation The Board is asked to note and discuss the progress made. u
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☒ Care for our Population ☐ Develop our People
☐ Innovate and Collaborate ☐ Develop a Sustainable System
Somerset NHS FT
☐ Obj 1 Inclusive culture ☒ Obj 4 Safe services ☒ Obj 7 Improving outcomes
☐ Obj 2 Collaboration ☐ Obj 5 Self management ☐ Obj 8 Workforce
☐ Obj 3 Independent lives ☐ Obj 6 Value all people alike ☐ Obj 9 Performance
☐ Obj 10 Finance
Implications/Requirements (Please select any which are relevant to this paper)
☐ Financial ☐ Legislation ☐ Workforce ☐ Estates ☐ ICT ☒ Patient Safety /
Quality
Details:
Equality The Trust wants its services to be as accessible as possible, to as many people as
possible. Please indicate whether the report has an impact on the protected characteristics
☒ This report has not been assessed against the Trust’s Equality Impact Assessment
Tool and there are no proposals or matters which affect any persons with protected characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
Not applicable.
Ockenden N Report
March 2022 Public Board - 3 – N
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
The findings from the Ockenden report were previously presented to the Board.
Reference to CQC domains (Please select any which are relevant to this paper)
☒ Safe ☐ Effective ☒ Caring ☒ Responsive ☐ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
Ockenden N Report
March 2022 Public Board - 4 – N
OCKENDEN: First report: Emerging Findings and Recommendations from the Independent Review of Maternity Services at the Shrewsbury and Telford
Hospitals NHS Trust
1. BACKGROUND 1.1. Donna Ockenden was the lead midwife appointed to undertake the
independent maternity review of Maternity Services at the Shrewsbury and Telford Hospitals NHS Trust. The review is about families who have suffered harm as a result of their NHS care during pregnancy and childbirth. The initial review was commissioned in response to concerns raised by 23 families dating from 2009. Since the review commenced there were a number of families who directly contacted the team with their own experiences of poor care and outcome, with more than 1800 families coming forward with experiences dating back to 2000.
1.2. At the outset of the review, themes were emerging which required urgent response and in December 2020 the Ockenden Report – Emerging Findings and Recommendations form the Independent Review of Maternity Services was released. This report contained seven Immediate and Essential Actions (IEA’s) which Trusts were asked to implement as a priority, pending the full report once the review completed.
1.3. Over the last year Trusts have been assessed on two occasions by the National team. Evidence to support compliance was assessed by the regional and national team. Financial support has been released to support services to meet the requirements at pace. In December 2021, the responsibility of ongoing monitoring was handed to the local LMNS who report to the Regional Maternity team.
1.4. The additional funding allocated to the Somerset LMNS was for both SFT and YDH maternity services.

Ockenden N Report
March 2022 Public Board - 5 – N
1.5. There is ongoing midwifery recruitment across the system, to reach the
midwifery workforce requirements. There are constant challenges with a lack of trained midwives available.
1.6. YDH will be fully established with obstetric consultants by April 2022, however
they are already fully compliant with the obstetric requirements of Ockenden. Additional postings will support the sustainability of this.
1.7. Additional obstetric recruitment is in progress at SFT. There is support in place with the use of Locum consultants. Non-compliance with Ockenden remains an outstanding issue.
2. ASSESSMENT
2.1. Current compliance
1) Enhanced Safety – 87%
a) A plan to implement the Perinatal Clinical Quality Surveillance Model
b) All maternity SIs are shared with Trust boards at least monthly and the LMS, in addition to reporting as required to HSIB
Outstanding actions
Further development and implementation of the Perinatal Quality Surveillance Tool
Funding Element
Funding Purpose Allocation
1 Total Midwifery Workforce (inc. MDT provision) 9.4 WTE
· To increase midwifery establishment by 7.6 WTE · To provide MDT training (1.8 WTE equivalent)
Total
£249,478 £57,345
£306,824 2 Total Obstetric Workforce (inc. MDT provision) 1.9 WTE
· To increase obstetric workforce by 1.6 WTE · To provide MDT training (0.3 WTE equivalent)
Total
£174,329 £32,283
£206,612 3 MDT Training for other staff groups working in maternity
£37,425
TOTAL ALLOCATION FOR 2021/22 £550,860
Payment timings: 66% to be paid in August 21 34% to be paid in December 21
Total
£363,568 £187,293 £550,860
Ockenden N Report
March 2022 Public Board - 6 – N
2) Listening to Women and their Families – 79% a) Evidence that you have a robust mechanism for gathering service
user feedback, and that you work with service users through your Maternity Voices Partnership (MVP) to coproduce local maternity services.
b) In addition to the identification of an Executive Director with
specific responsibility for maternity services, confirmation of a named nonexecutive director who will support the Board maternity safety champion bringing a degree of independent challenge to the oversight of maternity and neonatal services and ensuring that the voices of service users and staff are heard.
Outstanding actions MVP – co-produced plan needs to be developed and agreed
3) Staff Training and working together – YDH 94% SFT- 85%
a) Implement consultant led labour ward rounds twice daily (over 2
hours) and 7 days per week.
b) MDT training schedules in place.
c) Confirmation that funding allocated for maternity staff training is ringfenced and any CNST Maternity Incentive Scheme (MIS) refund is used exclusively for improving maternity safety
Outstanding actions Confirmation of ringfenced monies for training Attendance records
Implementation of twice daily ward rounds at SFT to the required specification of morning and evening – must be consultant led with the MD team who will be working over that period of time. Considerable challenges with the capacity to implement this and maintain the full service provision for Obstetrics and gynaecology. Additional consultant recruitment in progress. Will not meet compliance deadline of 24th March 2022 and risk of slippage to proposed date of 1st June.
4) Managing complex pregnancy – 86%
a) All women with complex pregnancy must have a named
consultant lead, and mechanisms to regularly audit compliance must be in place
b) Understand what further steps are required by your organisation
to support the development of maternal medicine specialist centres
Outstanding actions
Ockenden N Report
March 2022 Public Board - 7 – N
Notes audit Maternal medicine pathways – outside of local control. Regional centre contract has been awarded to Bristol. Will await guidance and pathways from regional teams. Will not meet compliance as of 24 March.
5) Risk Assessment throughout pregnancy – YDH – 87% SFT - 81% a) A risk assessment must be completed and recorded at every
contact. This must also include ongoing review and discussion of intended place of birth. This is a key element of the Personalised Care and Support Plan (PSCP). Regular audit mechanisms are in place to assess PCSP Compliance
Outstanding actions Audit of notes/digital records Implementation of personalised care plans – currently being agreed with MVP SFT - Evidence of ongoing risk assessments – dependant upon most recent maternity digital update.
6) Monitoring Fetal Wellbeing – 100% a) Implement the saving babies lives bundle. Element asking that a
second lead is identified so that every unit has a lead midwife and a lead obstetrician in place to lead best practice, learning and support. This will include regular training sessions, review of cases and ensuring compliance with saving babies lives care bundle 2 and national guidelines.
7) Informed Consent – 79%
a) Every trust should have the pathways of care clearly described, in
written information in formats consistent with NHS policy and posted on the trust website.
Outstanding actions Notes audit MVP action plan as in IEA 2
8) Workforce – 90% The safe delivery of maternity services is dependent on a Multidisciplinary Team approach. The Maternity Transformation Programme has implemented a range of interventions to deliver increases in healthcare professionals and support workers including: the development of the maternity support worker role, the expansion of midwifery undergraduate numbers, additional maternity placements and active recruitment.
Ockenden N Report
March 2022 Public Board - 8 – N
Outstanding actions Workforce planning as an ICS. This will be ongoing as part of the Maternity Transformation programme to include the merger.
3. RECOMMENDATIONS – FOR RESOLUTION OF EXCEPTION ISSUES 3.1. As a system there are two IEA’s which will be non-compliant on 24 March
2022. Non-compliance with IEA 3 will be SFT only.
IEA 3 – Twice daily consultant ward rounds morning and evening. There is extensive support from the executive team to the n supporting the implementation of this second ward round. Current mitigation includes a second ward round at 17:00 and a telephone Board round at 22:00. There is a need to re job plan consultant roles to meet the many requirements of obstetrics and gynaecology. There has been no formal demand and capacity of maternity services for many years and with the growing requirements of the Maternity Transformation program and Ockenden there is a concern that the planned consultant availability with the additional recruitment, will still leave a deficit in service demand. This may impact the ability to commence the twice daily ward rounds as planned in June. IEA 4 – Maternal Medicine Network and pathways This is being managed at a regional level and the hosting Trust has been appointed, however the pathways have not yet been agreed. This will fall outside of local management ability. Audit There are several changes to data capture process and therefore the timing of audits to evidence compliance need to allow the full implementation of new processes. This may delay the ability to complete audits by the 24th March. The combined Trusts will be launching a Maternity Transformation Programme Board in March which will provide ongoing support for all National maternity programmes, including Ockenden, Better Births and the anticipated Kirkup Report. Ongoing Trust Board oversight of this is recommended on a quarterly basis.
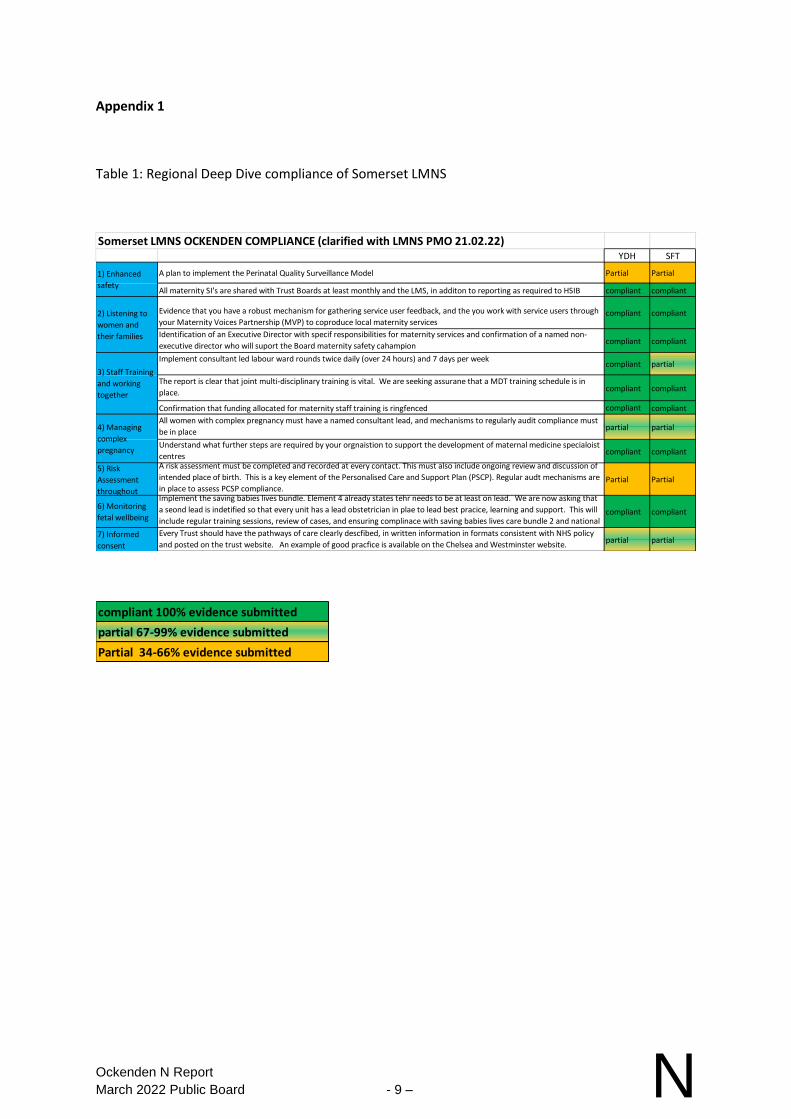
Ockenden N Report
March 2022 Public Board - 9 – N
Appendix 1
Table 1: Regional Deep Dive compliance of Somerset LMNS
Somerset LMNS OCKENDEN COMPLIANCE (clarified with LMNS PMO 21.02.22)YDH SFT
A plan to implement the Perinatal Quality Surveillance Model Partial Partial
All maternity SI's are shared with Trust Boards at least monthly and the LMS, in additon to reporting as required to HSIB compliant compliant
Evidence that you have a robust mechanism for gathering service user feedback, and the you work with service users through
your Maternity Voices Partnership (MVP) to coproduce local maternity servicescompliant compliant
Identification of an Executive Director with specif responsibilities for maternity services and confirmation of a named non-
executive director who will suport the Board maternity safety cahampioncompliant compliant
Implement consultant led labour ward rounds twice daily (over 24 hours) and 7 days per weekcompliant partial
The report is clear that joint multi-disciplinary training is vital. We are seeking assurane that a MDT training schedule is in
place. compliant compliant
Confirmation that funding allocated for maternity staff training is ringfenced compliant compliant
All women with complex pregnancy must have a named consultant lead, and mechanisms to regularly audit compliance must
be in placepartial partial
Understand what further steps are required by your orgnaistion to support the development of maternal medicine specialoist
centrescompliant compliant
5) Risk
Assessment
throughout
A risk assessment must be completed and recorded at every contact. This must also include ongoing review and discussion of
intended place of birth. This is a key element of the Personalised Care and Support Plan (PSCP). Regular audt mechanisms are
in place to assess PCSP compliance.Partial Partial
6) Monitoring
fetal wellbeing
Implement the saving babies lives bundle. Element 4 already states tehr needs to be at least on lead. We are now asking that
a seond lead is indetified so that every unit has a lead obstetrician in plae to lead best pracice, learning and support. This will
include regular training sessions, review of cases, and ensuring complinace with saving babies lives care bundle 2 and national compliant compliant
7) Informed
consent
Every Trust should have the pathways of care clearly descfibed, in written information in formats consistent with NHS policy
and posted on the trust website. An example of good pracfice is available on the Chelsea and Westminster website.partial partial
1) Enhanced
safety
2) Listening to
women and
their families
3) Staff Training
and working
together
4) Managing
complex
pregnancy
compliant 100% evidence submitted
partial 67-99% evidence submitted
Partial 34-66% evidence submitted
YDH Developing an Inclusive Culture
March 2022 Public Board - 1 –
P
Yeovil District NHS Foundation Trust
REPORT TO: Board of Directors
REPORT TITLE: Developing an Inclusive Culture
SPONSORING EXEC: Chief of People and Organisational Development
REPORT BY: Harriet Jones, Head of Inclusion
PRESENTED BY: Harriet Jones, Head of Inclusion
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☒ For Assurance/
Discussion ☐ For Approval / Decision ☐ For Information
Executive Summary and Reason for presentation to Committee/Board
The presentation outlines the advanced approach to inclusion being adopted across both trusts to accelerate its impact and progress towards an inclusive culture.
Recommendation The Board is asked to note the inclusion journey, reflections and next steps.
e
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☐ Care for our Population ☐ Develop our People
☒ Innovate and Collaborate ☐ Develop a Sustainable System
Somerset NHS FT
☒ Obj 1 Inclusive culture ☐ Obj 4 Safe services ☐ Obj 7 Improving outcomes
☐ Obj 2 Collaboration ☐ Obj 5 Self management ☐ Obj 8 Workforce
☐ Obj 3 Independent lives ☐ Obj 6 Value all people alike ☐ Obj 9 Performance
☐ Obj 10 Finance
Implications/Requirements (Please select any which are relevant to this paper)
☐ Financial ☐ Legislation ☒ Workforce ☐ Estates ☐ ICT ☐ Patient Safety /
Quality
Details:
Equality The Trust wants its services to be as accessible as possible, to as many people as
possible. Please indicate whether the report has an impact on the protected characteristics
YDH Developing an Inclusive Culture
March 2022 Public Board - 2 – P
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are no proposals or matters which affect any persons with protected characteristics
☒ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities
The inclusion work includes a focus on persons with protected characteristics.
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
Not applicable.
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
The presentation was presented to the SFT Board meeting held in February 2022 but it was felt useful to also present to the joint Board meeting.
Reference to CQC domains (Please select any which are relevant to this paper)
☐ Safe ☐ Effective ☒ Caring ☐ Responsive ☒ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
Our Inclusion Journey: Reflections and next steps
Harriet Jones, Head of Inclusion
Principles
Building on progress to date
A new approach -systemic change
Increasing our impact
2
3
Inclusion maturity
4
WHAT SYSTEMIC CHANGE IS
Changing the systems, policies, processes and cultures that create or
maintain inequality.
“Fixing the system”
WHAT SYSTEMIC CHANGE IS NOT
Changing the people to fit the existing system.
“Fixing the people”
What is systemic change?
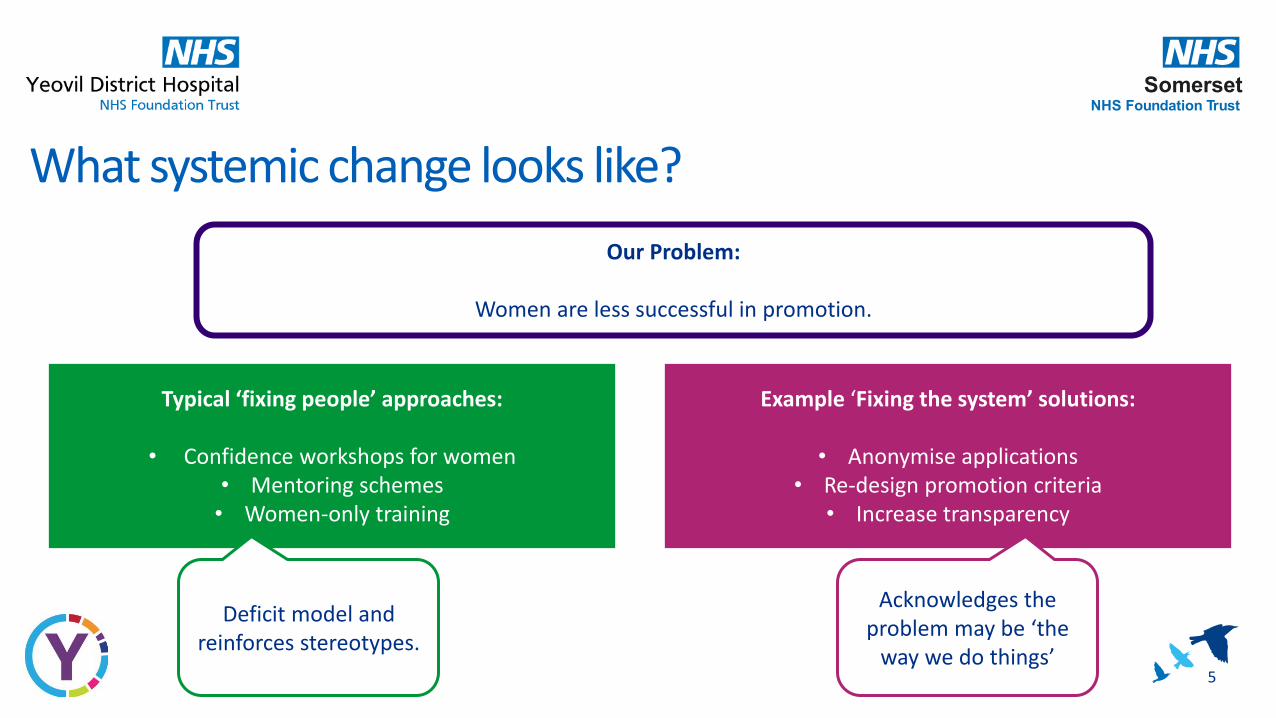
5
Our Problem:
Women are less successful in promotion.
Typical ‘fixing people’ approaches:
• Confidence workshops for women• Mentoring schemes • Women-only training
Example ‘Fixing the system’ solutions:
• Anonymise applications• Re-design promotion criteria
• Increase transparency
Deficit model and reinforces stereotypes.
Acknowledges the problem may be ‘the
way we do things’
What systemic change looks like?

A shift in focus
6
7
Data led
Research based
Collaboration & Influence
Empower others
How we work systemically
Assurance Report from the SFT Audit Committee meeting held on 27 January 2022
March 2022 Public Board - 1 –
Q
Somerset NHS Foundation Trust
REPORT TO: The Trust Board
REPORT TITLE: Assurance report from the Audit Committee meeting held on 27 January 2022
SPONSORING EXEC: Barbara Gregory, Chairman of the Audit Committee
REPORT BY: Secretary to the Trust
PRESENTED BY: Barbara Gregory, Chairman of the Audit Committee
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☒ For Assurance/
Discussion ☐ For Approval / Decision ☐ For Information
Executive Summary and Reason for presentation to Committee/Board
The attached report sets out the items discussed at the Audit Committee meeting held on 27 January 2022 and the assurance received by the Committee. The Committee identified a concern in relation to the findings of the Patient Deterioration audit report and agreed to ask the Quality and Governance Committee to review the findings of the audit report and follow up the actions with the executive leads.
Recommendation The Board is asked to note the assurance provided and the area of concern identified by the Audit Committee.
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☐ Care for our Population ☐ Develop our People
☐ Innovate and Collaborate ☐ Develop a Sustainable System
Somerset NHS FT
☒ Obj 1 Inclusive culture ☒ Obj 4 Safe services ☒ Obj 7 Improving outcomes
☒ Obj 2 Collaboration ☒ Obj 5 Self management ☒ Obj 8 Workforce
☒ Obj 3 Independent lives ☒ Obj 6 Value all people alike ☒ Obj 9 Performance
☐ Obj 10 Finance
Assurance Report from the SFT Audit Committee meeting held on 27 January 2022
March 2022 Public Board - 2 – Q
Implications/Requirements (Please select any which are relevant to this paper)
☐ Financial ☒ Legislation ☐ Workforce ☐ Estates ☐ ICT ☐ Patient Safety /
Quality
Details:
Equality The Trust wants its services to be as accessible as possible, to as many people as
possible. Please indicate whether the report has an impact on the protected characteristics
☒ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are no proposals or matters which affect any persons with protected characteristics
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
Not applicable.
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
The assurance report is presented to the Board after every meeting.
Reference to CQC domains (Please select any which are relevant to this paper)
☒ Safe ☒ Effective ☒ Caring ☒ Responsive ☒ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
Assurance Report from the SFT Audit Committee meeting held on 27 January 2022
March 2022 Public Board - 3 – Q
SOMERSET NHS FOUNDATION TRUST
AUDIT COMMITTEE MEETING HELD ON 27 JANUARY 2022 1. PURPOSE 1.1 The report sets out the items discussed at the meeting held on 27 January
2022, the assurance received by the Committee and any areas of concern identified.
2. ASSURANCE RECEIVED
Board Assurance Framework
2.1 The Committee discussed the Board Assurance Framework (BAF) and noted that the highest strategic risks related to objectives 4 (safe, sustainable, effective, high quality, person-centred support in the most appropriate setting) and 9 (to deliver levels of performance that are in line with our operational plans, system ambitions). The reasons for the heightened levels of these risks had previously been discussed at Board and Committee meetings and were well understood.
2.2 The Committee discussed the time period covered by the BAF and agreed that the BAF did not completely reflect the underlying positions but, in view of the short planning horizon, an in-year view was felt to be appropriate.
2.3 Having also reviewed the minutes in relation to BAF discussions at other Committee meetings and at the Board, the Committee felt assured that the BAF was a live document, that it supported the assurance process of the Trust, and that it reflected the current position.
2.4 The Committee noted that a review of the strategic objectives and the BAF will be undertaken at the April 2022 Joint Board Development Day. Internal audit progress report
2.5 The Committee received the 2021/22 internal audit progress report and noted the delays in some of the scheduled audits due to the impact of the Covid-19 pandemic on colleagues. It was noted that, with the exception of the complaints audit, the remaining audits on the audit plan will be presented to the April 2022 Audit Committee meeting. The Committee agreed to carry the complaints audit forward into the 2022/23 audit plan.
2.6 The Committee reviewed the work of the Committee and format of meetings against the national “Reducing the Burden” guidance and auditors agreed that the focus of the agenda and Committee meeting attendance was appropriate. Key Financial Systems (KFS) audit report
2.7 The Committee received the KFS audit report which provided substantial assurance for both design and operational effectiveness. The Committee noted that one low priority recommendation was made. The
Assurance Report from the SFT Audit Committee meeting held on 27 January 2022
March 2022 Public Board - 4 – Q
Committee agreed that the findings were exceptionally good and provided the Committee with significant assurance. Data Quality audit report
2.8 The Committee received the Data Quality audit report which provided substantial assurance for design and moderate assurance for operational effectiveness. The Committee noted that one medium and two low priority recommendations were made and the implementation of the recommendations will be monitored through the internal audit follow up process. The Committee agreed that the audit report provided good assurance. IT Strategy audit report
2.9 The Committee received the IT Strategy audit report which provided substantial assurance for design and moderate assurance for operational effectiveness. The Committee noted that one medium and one low priority recommendations were made and the implementation of the recommendations will be monitored through the internal audit follow up process. The Committee agreed that the audit report provided good assurance. Learning from Deaths audit report
2.10 The Committee received the Learning from Deaths audit report which provided substantial assurance for design and moderate assurance for operational effectiveness. The Committee noted that one medium and one low priority recommendations were made and the implementation of the recommendations will be monitored through the internal audit follow up process. The Committee agreed that the audit report provided good assurance. Internal audit follow up report
2.11 The Committee received the internal audit recommendations follow up report and agreed that the report provided the Committee with significant assurance about the timely implementation of the recommendations. Draft Audit Plan for 2022/23
2.12 The Committee received the draft audit plan for 2022/23 and noted that the plan included sufficient flexibility to be able to respond to requests for urgent audits during the year. Counter Fraud Progress Report
2.13 The Committee received the counter fraud progress report and particularly noted the national fraud initiative matching exercise and details of the ongoing counter fraud investigations. The Committee agreed that the report provided good assurance about the implementation of the counter fraud work plan. Counter Fraud Recommendation Tracker
2.14 The Committee received the counter fraud recommendations follow up report and the Committee agreed that the report provided significant assurance about the implementation of the recommendations.
Assurance Report from the SFT Audit Committee meeting held on 27 January 2022
March 2022 Public Board - 5 – Q
External audit report 2.15 The Committee received the external audit progress report and noted that
planning work for the 2021/22 annual accounts had been completed and that an interim audit was currently being undertaken. The Committee received technical updates in relation to: the DHSC Integrated Care Partnership (ICP) engagement document; the NHS environmental sustainability guidance map; switching activity targets to reward ‘clock stops’; the launch of the landmark review of health and social care leadership. External Audit Plan for 2021/22
2.16 The Committee received the external audit plan for 2021/22 and noted the impact of the implementation of IFRS16 on the balance sheet. Code of Conduct and Managing Conflict of Interest and Personal Conduct Policy
2.17 The Committee received the revised policy and approved the proposed changes to the policy. Losses and Special Payments
2.18 The Committee received the losses and special payments report and noted the reasons for the losses and special payments. Single Quotation/Tender Waiver Action report
2.19 The Committee received the single quotation/tender waiver action report and noted the single quotation and tender waiver actions and the reasons for these actions. Audit Committee Work Plan
2.20 The Committee discussed progress against its work plan and agreed that good progress was being made.
3. AREAS OF CONCERN/FOLLOW UP Patient Deterioration audit report
3.1 The Committee received the Patient Deterioration audit report which provided moderate assurance for design and limited assurance for operational effectiveness. The Committee noted that one high and five medium priority recommendations were made. The Committee noted that the high priority recommendation related to the use of handheld devices on acute inpatient wards and the implementation of this recommendation and the medium priority recommendations will be monitored through the internal audit follow up process.
3.2 The Committee expressed its concern about the audit findings but was assured by internal auditors that robust action plans were in place.
3.3 The Committee asked for a similar audit to be considered in community hospitals.
Assurance Report from the SFT Audit Committee meeting held on 27 January 2022
March 2022 Public Board - 6 – Q
4. RISKS 4.1 The Committee did not identify any new risks which had not already been
included on the risk register.
4.2 The Committee agreed to ask the Quality and Governance Committee to review the findings of the Patient Deterioration internal audit and follow up the actions with the executive leads.
CHAIRMAN OF THE AUDIT COMMITTEE
Assurance Report from the SFT Quality and Governance Committee meeting held on 26
January 2022
March 2022 Public Board - 1 – R
Somerset NHS Foundation Trust
REPORT TO: The Trust Board
REPORT TITLE: Assurance Report from the Quality and Governance Committee meeting held on 26 January 2022
SPONSORING EXEC: Director of Corporate Services
REPORT BY: Secretary to the Trust
PRESENTED BY: Jan Hull, Chairman of the Quality and Governance Committee
DATE: 1 March 2022
Purpose of Paper/Action Required (Please select any which are relevant to this paper)
☒ For Assurance/
Discussion ☐ For Approval / Decision ☐ For Information
Executive Summary and Reason for presentation to Committee/Board
The attached report sets out the items discussed at the Quality and Governance Committee meeting held on 26 January 2022. The Committee received assurance in relation to:
• Maternity Incentive Scheme (MIS)
• patient Experience, Complaints and PALS Update
• Leadership Quality Walkrounds 2021/22
• Quality and governance Committee Annual Workplan 2022/23
• Due diligence process The Committee identified the following areas of concern or for follow up:
• Corporate Risk Register – in particular the increase in risks and the three risks rated at 25. A review of the risks and mitigating actions will be undertaken at the February 2022 planning meeting
• Hospital Flow
Assurance Report from the SFT Quality and Governance Committee meeting held on 26
January 2022
March 2022 Public Board - 2 – R
• NHSE/I Mental Health Homicide and the commissioning of an external independent review
The Committee identified three areas to be reported to the Board or to other Committees:
• Hospital Flow and Capacity: to be reported to the Trust Board and included in the Committee Assurance report.
• Leadership Quality Walkrounds: to be reported to the People Committee to be sighted on some of the issues identified during the visits.
• Duty of Candour audit: Audit Committee to have oversight of the terms of reference.
Recommendation The Board is asked to note the assurance and areas of concern or follow up identified by the Quality and Governance Committee.
Links to Board Assurance Framework and Corporate/Directorate Risk Register (Please select any which are impacted on / relevant to this paper)
Yeovil District Hospital NHS FT
☐ Care for our Population ☐ Develop our People
☐ Innovate and Collaborate ☐ Develop a Sustainable System
Somerset NHS FT
☐ Obj 1 Inclusive culture ☒ Obj 4 Safe services ☒ Obj 7 Improving outcomes
☐ Obj 2 Collaboration ☒ Obj 5 Self management ☐ Obj 8 Workforce
☒ Obj 3 Independent lives ☒ Obj 6 Value all people alike ☐ Obj 9 Performance
☐ Obj 10 Finance
Implications/Requirements (Please select any which are relevant to this paper)
☒ Financial ☒ Legislation ☐ Workforce ☐ Estates ☐ ICT ☐ Patient Safety /
Quality
Details:
Equality The Trust wants its services to be as accessible as possible, to as many people as
possible. Please indicate whether the report has an impact on the protected characteristics
☒ This report has not been assessed against the Trust’s Equality Impact Assessment
Tool and there are no proposals or matters which affect any persons with protected characteristics
Assurance Report from the SFT Quality and Governance Committee meeting held on 26
January 2022
March 2022 Public Board - 3 – R
☐ This report has been assessed against the Trust’s Equality Impact Assessment Tool
and there are proposals or matters which affect any persons with protected characteristics and the following is planning to mitigate any identified inequalities
Public/Staff Involvement History
(Please indicate if any consultation/service user/patient and public/staff involvement has informed any of the recommendations within the report)
Not applicable.
Previous Consideration
(Indicate if the report has been reviewed by another Board, Committee or Governance Group before submission to the Board or is a follow up report to one previously
considered by the Board – eg. in Part B]
The assurance report is presented to the Board after each meeting.
Reference to CQC domains (Please select any which are relevant to this paper)
☒ Safe ☒ Effective ☒ Caring ☒ Responsive ☐ Well Led
Is this paper clear for release under the Freedom of Information Act 2000?
☒ Yes ☐ No
Assurance Report from the SFT Quality and Governance Committee meeting held on 26
January 2022
March 2022 Public Board - 4 – R
SOMERSET NHS FOUNDATION TRUST ASSURANCE REPORT FROM THE QUALITY AND GOVERNANCE COMMITTEE
MEETING 1. PURPOSE 1.1 The report sets out the items discussed at the formal meeting held on 26
January 2022, along with the assurance received by the Committee and any areas of concern identified. The meeting was conducted by video conference call.
2. ASSURANCE RECEIVED
Maternity Incentive Scheme (MIS)
2.1 The Committee received an update on the maternity incentive scheme and noted that the Trust was on track to meet the Safety Actions. The Committee signed off the detailed Safety Action 3: Avoiding Term Admissions into Neonatal Unit action plan.
2.2 The Committee agreed that the report provided significant assurance about
progress made in achieving the quality standards. Patient Experience, Complaints and PALS Update
2.3 The Committee received an update on patient experience, complaints and concerns. The Committee noted the achievements in relation to the time taken to acknowledge complaints and the recruitment to the team which had made a significant improvement to the complaints response times. The PALS service had seen some staffing challenges and there will be a focus on clearing the PALS backlog.
2.4 The Committee noted the reinstatement of the Family Liaison Team from October 2021 and the positive impact of the team on patient experience.
2.5 The Committee noted the challenges in relation to complaint investigation times and the quality of the information provided. Progress was being made and work was ongoing with specific directorates to improve response rates and the quality of the responses.
2.6 The Committee noted the key themes for complaints and PALS enquiries – communication, nursing/ general care, and attitude of staff – and further noted that training using patient videos to illustrate the patient experience was being developed and will be rolled out to wards. It was further hoped that the PALS team can reinstate their support for the Have Your Say meetings on mental health inpatient wards.
2.7 The Committee agreed that the update provided good assurance about progress made and plans in place to continue to address the backlogs.
Assurance Report from the SFT Quality and Governance Committee meeting held on 26
January 2022
March 2022 Public Board - 5 – R
Leadership Quality Walkrounds 2021/22
2.8 The Committee received the report from the Leadership Quality Walkrounds undertaken in December 2021 and noted that the issues identified during the walkrounds were in line with the expected findings e.g. staffing, recruitment, workforce challenges. In addition, there were some frustrations around the responsiveness for estates and IT issues.
2.9 The Committee noted that overall, the visits evidenced real positivity particularly from the teams in terms of how it felt to have the visits and the programme will be restarted as soon as possible and invitations extended to YDH Non-Executive Directors. The report provided the Committee with assurance that none of the reviewers had heard anything from the teams visited that did not align with the discussions in terms of risks and issues that the Trust was aware of. Quality and Governance Committee Annual Workplan 2022/23
2.10 The Committee approved their workplan for 2022/23 but noted that the workplan may need to be amended to take account of the move to joint Committee meetings with YDH. Due Diligence/Merger Update
2.11 The Committee noted that all Non-Executive Directors were working diligently through the details of the due diligence templates and these templates will be discussed with the workstream leads and Senior Responsible Officer(s) over the next few weeks.
3. AREAS OF CONCERN OR FOLLOW UP Corporate Risk Register
3.1 The Committee received the up-to-date Corporate Risk Register and noted that there were currently 17 risks on the risk register, three of which had been rated 25. The Committee asked for assurance that all actions had been taken to mitigate the risks and that there was an ongoing focus on identifying additional actions. The Committee received assurance that all the risks were closely monitored by the relevant Committee, Board or Executive Team, but in view of the increase in risks and the high rating of three of the risks, the Committee agreed to review the risks and mitigating actions at the February 2022 planning meeting, focusing on those relating to quality and patient safety.
3.2 The Committee received assurance in relation to the staffing risks and noted that all teams and services reviewed their staffing and resilience structures on a daily basis and a full resourcing update will be presented to the next People Committee meeting.
3.3 The Committee noted the position in relation to the unvaccinated colleagues and the work taking place to encourage unvaccinated colleagues to get vaccinated before the deadline.
Assurance Report from the SFT Quality and Governance Committee meeting held on 26
January 2022
March 2022 Public Board - 6 – R
3.4 The Committee further received an update on the alignment of the risk management processes across both trusts and the Committee noted that the strategic objectives and risk management processes will be discussed at the April 2022 Board Development Day. Hospital Flow Update
3.5 The Committee received a detailed update on the position in relation to hospital flows. The Committee noted that the number of ED attendances had stabilised but the number of patients waiting for an inpatient bed had increased resulting in patients being cared for in a sub-optimal clinical setting.
3.6 The Committee noted that the main issue related to delayed discharges from hospital and the number of patients waiting for discharge to supported pathways in Somerset continued to increase.
3.7 The Committee noted the workforce pressures in the intermediate care system and the positive impact of the actions taken to increase pay for domiciliary care staff. This had resulted in a decrease in patients waiting for domiciliary care but the number of patients waiting for bedded care had however increased.
3.8 The Committee further noted the impact of the bed pressures on planned care and the less than ideal environment in which care had to be provided. The Committee received assurance that elective recovery planning was an area of high focus.
3.9 The Committee received an update on the system response to the current pressures and the declaration of OPEL 4 on a system basis and noted the work taking place to secure additional bedded care and the work with the Care Quality Commission to shorten the time care homes have to close following a Covid-19 outbreak.
3.10 The Committee recognised the difficult position and the risks to patient and colleague safety.
3.11 The Committee further received an update on the number of Covid-19 patients in Musgrove Park Hospital and community and mental health settings noted that the morbidity profile of the Omicron variant was significantly different from previously variants with patients being less unwell. The data on hospital acquired Covid-19 showed that the Trust benchmarked well and had remained able to protect patients from hospital acquired infections.
3.12 The Committee received an overview of the ambulance handover times and noted that the Trust had decided to carry the risk of a patient having to be conveyed to the emergency department in house. This meant that patients were not held up in ambulances. Measures had been put in place to secure additional beds to hold patients waiting for ED or for admission.
3.13 The Committee agreed to invite the ED senior team to the March 2022 Committee meeting to highlight the work taking place to manage the pressures and the focus on the way forward.
Assurance Report from the SFT Quality and Governance Committee meeting held on 26
January 2022
March 2022 Public Board - 7 – R
3.14 Although the Committee received assurance from the update and actions
taken, the Committee agreed that hospital flow remained an area of concern.
NHSE/I Mental Health Homicide Independent Investigation 3.15 The Committee received the investigation report and noted the circumstances
of the homicide incident.
3.16 The Committee noted that NHSE/I will be commissioning an external independent review of the care and treatment provided to the perpetrator as well as of the Trust’s processes.
3.17 The Committee noted that a Duty of Candour internal audit had been commissioned.
4. RISKS AND ISSUES TO BE REPORTED TO THE BOARD OR OTHER
COMMITTEES
4.1 The Committee identified the following risks and issues to be reported to the Board and/or Board Committees:
• Hospital Flow and Capacity: to be reported to the Trust Board and included in the Committee Assurance report.
• Leadership Quality Walkrounds: to be reported to the People Committee to be sighted on some of the issues identified during the visits.
• Duty of Candour audit: Audit Committee to have oversight of the terms of reference.
5. BOARD ASSURANCE FRAMEWORK (BAF)
5.1 The objectives covered at the meeting related to:
• Objective 4, safe, high quality care - the detailed discussion regarding acute services and community services has provided us with positive and negative assurance. The Committee considered that the risk in relation to this objective had increased. The MIS provided positive assurance for this objective in relation to maternity services.
• Objective 1, learning organisation - assurance provided from the Leadership Quality Walkrounds report and the commitment in the Patient Experience presentation to improve response times.
Assurance Report from the SFT Quality and Governance Committee meeting held on 26
January 2022
March 2022 Public Board - 8 – R
5.2 The Board is asked to direct the Committee as to any future areas of deep dives relating to the above objectives.
Jan Hull CHAIRMAN OF THE QUALITY AND GOVERNANCE COMMITTEE





























