Embed Size (px)
Citation preview
Early loading of implants with fixeddental prostheses in edentulousmandibles: 4.5-year clinical resultsfrom a prospective study
Stefanie SchwarzOlaf GabbertAlexander J. HasselMarc SchmitterChristiane SechePeter Rammelsberg
Authors’ affiliations:Stefanie Schwarz, Olaf Gabbert, Alexander J.Hassel, Marc Schmitter, Christiane Seche, PeterRammelsberg, Department of Prosthodontics,University of Heidelberg, Heidelberg, Germany
Correspondence to:Stefanie SchwarzDepartment of ProsthodonticsUniversity of HeidelbergIm Neuenheimer Feld 40069120 HeidelbergGermanyTel.: þ 49 6221/566 052Fax: þ 49 6221/565 371e-mail: [email protected]
Key words: early loading, edentulous mandible, fixed dental prosthesis, implants, survival
Abstract
Aim: The purpose of this study was to evaluate the survival and success of early-loaded
implants placed in the intraforaminal area of the edentulous mandible, and the survival of
the implant-supported fixed dental prostheses (FDP).
Material and methods: Thirty-seven patients (18.9% male, mean age 64.5 years) with
edentulous lower jaws were treated with implant-supported FDPs in the mandible. One
hundred and eighty-five screw-type implants were placed in the intraforaminal area of the
symphysis (five implants per patient). Immediately after implant placement, a framework
was fabricated and the FDP was manufactured on the framework. Within 2 weeks, the
implants were rigidly connected and loaded with the implant-retained FDP.
Results: During the 1–8-year observation period (mean 4.5 years), a total of 32 implant-
retained complications occurred. Nineteen implants were lost in 10 patients, resulting in a
cumulative survival of 89.7%. Nine implants in five patients did not osseointegrate.
Although these implants were not removed, because stability within the connective tissue
was acceptable and inflammation was absent, they were recorded as unsuccessful.
Consequently, the cumulative success declined to 84.9%. Four implants in three patients
had clinical signs of periimplantitis (2.2% of all implants). Denture-related complications
included one complete failure, when one FDP had to be removed after the last of five
implants had been replaced. Furthermore, 10 fractures of the framework occurred in six
patients, three FDPs had to be adapted or modified, and the facing of the FDP had to be
repaired 16 times in 11 patients.
Conclusion: Although one-stage early-loaded implants functioned well for most patients
with edentulous mandibles, immediate loading is associated with a larger number of
implant-related complications than in other studies investigating delayed loading. Because
of the substantial prosthetic complications and aftercare, this procedure cannot be
generally recommended.
Patients edentulous in the mandible fre-
quently experience problems with their
dentures. These problems can encompass
lack of stability and lack of retention,
which are associated with reduced chewing
ability (van Waas 1990). Insertion of im-
plants may improve the situation, leading
to better chewing ability and better
oral-health-related quality of life (Meijer
et al. 1999). The implant-based rehabilita-
tion procedure has been well documented
and reviewed, and is a successful treatment
option for edentulous jaws (Gomez-Roman
et al. 1997). The intraforaminal area of the
mandible, in particular, is described as a
preferred region for implant insertion. This
Date:Accepted 6 August 2009
To cite this article:Schwarz S, Gabbert O, Hassel A J, Schmitter M, Seche C,Rammelsberg P. Early loading of implants with fixeddental prostheses in edentulous mandibles: 4.5-yearclinical results from a prospective study.Clin. Oral Impl. Res. 21, 2010; 284–289.doi: 10.1111/j.1600-0501.2009.01843.x
284 c� 2010 John Wiley & Sons A/S

is especially true in cases of long-term
edentulous jaws associated with distinct
atrophy.
In addition to current literature discus-
sions about aspects of the osseointegration,
design, and surface of implants, there is
still much controversy about whether
immediate or early implant loading is
associated with higher failure than con-
ventional loading. Traditional implant
procedures for the lower jaw recommend
a two-stage surgical procedure, total pros-
theses abstention for 2 weeks after surgery,
and a rest period of at least 3 months before
applying load from masticatory forces to
the implants and surrounding bone via the
prostheses (Branemark et al. 1977).
Clinical studies focusing on immediate
loading of mandibular implants document
the high success of this treatment proce-
dure, however (Schnitman et al. 1997;
Tarnow et al. 1997; Chiapasco & Gatti
2003). The first results were published as
early as 1979 by Ledermann, who inserted
four TPS screws into the intraforaminal
region of an edentulous mandible and
placed a functionally loaded, bar-supported
overdenture on the same day as the surgery
(Ledermann 1979). After 12 years of use,
no implant failed and bone–implant con-
tact was approximately 70–80% at the
interface. The author confirmed the valid-
ity of this treatment concept if a minimum
of four implants was inserted into the
interforaminal area of the symphysis and
if these implants were rigidly splinted with
a bar (Ledermann et al. 1998). Uribe et al.
(2005) reported comparable results for im-
mediate loading in a review of articles from
1997 to 2002. The authors concluded that
the outcome of immediate loading is pre-
dictable if preconditions such as initial
stability (�32 N/cm), micro movement
of the implant (o150 mm), and adequate
implant length (410 mm) are fulfilled
(Uribe et al. 2005).
Besides the treatment option of immedi-
ate implant loading, other authors have
examined the early loading mode, which
was defined at the consensus meeting of
the Implants World Congress in Barcelona
in 2002. According to this definition, early
loading describes insertion of dentures
within a few days after surgery, whereas
immediate loading means inserting the
denture on the day of surgery (Aparicio
et al. 2003).
As a result, Raghoebar et al. (2003) con-
ducted a 3-year multicentre study on one-
stage implant surgery and early loading in
the edentulous mandible. A total of 170
implants were placed in 40 patients with
mandibular edentulism and were function-
ally loaded within 6 weeks with overden-
tures (n¼ 30) or fixed prostheses (n¼ 10).
Over the observation period of 3 years, no
implants were lost after the first year of
loading and implant survival was 93% for
both implants and prostheses (fixed or
removable). In 2007, Kawai and Taylor
reviewed the effect of loading time on the
success of mandibular implant overden-
tures and concluded that conventional
loading after a 3-month healing period
had not been proved to be the only accep-
table procedure (Kawai & Taylor 2007).
Sennerby and Gottlow (2008) also re-
viewed the literature on the clinical out-
come of immediate/early loading of dental
implants based on studies published up to
2005. They found six comparative studies
and reported that none of these revealed
any difference in survival or marginal bone
loss after 1–5 years (Sennerby & Gottlow
2008).
Time-saving implantology seems to be
preferred by dental surgeons, not at least to
accommodate patients’ needs – immediate
and early loading eliminate surgery for im-
plant exposure, and the time for prosthetic
rehabilitation is also minimized, and so
physical and financial strains on the pa-
tients are markedly reduced. Clinical trials
have already been conducted to study this
issue, but there are few studies showing
long-term results, especially for edentulous
mandibles restored with fixed dentures.
The objective of this study was, there-
fore, to evaluate the 4.5-year survival and
success of early-loaded implants placed in
the intraforaminal area of the edentulous
mandible. Special focus was placed on im-
plant survival and on prosthetic complica-
tions within a prospective study design.
Material and methods
Participants
The study included patients seeking treat-
ment at the Dental School of the Univer-
sity of Heidelberg. The 37 patients
recruited were long-term edentulous in
the mandible who had experienced
problems with their dentures, for example
lack of retention associated with reduced
chewing ability. Inclusion criteria for the
study were an edentulous mandible, ade-
quate dimensions of the intermentonian
region (vertically and horizontally at least
1 mm of bone around the implant), and
informed consent to the immediate loading
procedure (265/99, Heidelberg). Exclusion
criteria included drug and alcohol abuse,
uncontrolled diabetes, haemophilia, meta-
bolic disorders, and general contraindica-
tions, for example pregnancy at the time of
the planned implant insertion. Occasion-
ally, however, the study clinicians sus-
pected that, for example, alcohol abuse
might have occurred during the study.
These cases remained in the sample so
that the study results would not be over-
estimated. In case of loss of more than two
implants and subsequent reoperation
within the study, the respective patients
were excluded from further participation.
The initial clinical examination included
orienting assessment of alveolar crest mor-
phology by digital palpation, assessment of
mucosal conditions from pathological find-
ings, and assessment of maxillary dental
status. In the maxilla, 26 patients had
complete dentures, five had fixed dentures,
and six had removable partial dentures. All
available re-evaluations of the patients
within 8 years of service (mean 4.5 years)
were analysed (18.9% male, mean age 64.5
years, standard deviation 7.9). During the
first 16 months of observation, eight pa-
tients (21.6%) were lost to follow-up: one
patient had died, four patients were ex-
cluded from further participation in the
study because of reoperation after loss of
two or more implants, and three patients
did not attend the follow-up examination.
After the follow-up period of 3 years, 28
patients (75.7%) still participated and after
5 years 67.6% (25 patients) were still under
evaluation. The four patients were lost to
follow-up because of serious illness or
death (one each) and return of two patients
to their previous dentist.
Surgical procedure
Before surgery, a panoramic X-ray study,
Orthophos Plus, Sirona GmbH, Bensheim,
Germany of the initial situation and a
panoramic X-ray study (Orthophos Plus,
Sirona GmbH) with the drilling template,
to plan the ideal implant positions, were
Schwarz et al �Early-loaded implants
c� 2010 John Wiley & Sons A/S 285 | Clin. Oral Impl. Res. 21, 2010 / 284–289
performed in all cases (Fig. 1). Surgery
started with a triangular incision with a
trajectory over the alveolar crest and inci-
sions in the region of the first bicuspids.
Raising of the mucoperiostal layer was
followed by creation of notches in the
predetermined zones using rounded drills.
The sequence required for preparation of
the bone bed was completed using the
appropriate drills. Placement of five FRIA-
LOC-System implants (transgingival screw
implants, Friadent GmbH, Mannheim,
Germany) using a mechanical threading
drill followed. The torque of each implant
was controlled manually (demand:
50 N cm). The flap was sutured for open
healing of the implants. The choice of
inserted implants depended on bone di-
mensions; three lengths (10, 13, and
15 mm) and two diameters (3.5 and
4 mm) were used in the study.
Prosthetic procedure
All patients participating in this study were
treated with a fixed dental prosthesis
(FDP). Immediately after implant inser-
tion, the imprint posts of the system were
inserted. The open-impression technique
with polyether material (Impregum; 3M
ESPE, Seefeld, Germany) was used. After
removal of the posts, the healing caps were
positioned and a bite recording was taken.
The patients were reminded to abstain
from use of a prosthesis in the mandible
until insertion of the definitive FDP.
Within 24 h the dental technician made
the titanium metal framework of the
FDP. Clinical fitting of the framework
with monitoring of the passive fit was
then performed. Centric relation recording
was performed and middle line measure-
ments were taken. The next clinical step
was fitting of the waxing on the frame-
work. The FDP was inserted within
2 weeks. The FDP had artificial teeth
including the second bicuspid or the first
molars (shortened dental arch), depending
on the position of the most distal implant.
The limit for the cantilever was no more
than 1 cm distal to the most distal implant.
Subsequent to the passive fitting, the oc-
clusal concepts of the canine guidance
(upper jaw with fixed dentures or partial
removable denture) or the bilateral ba-
lanced occlusion (upper jaw with complete
denture) were ground away. The FDP were
rigidly screwed into the implants using a
torque of 14 N cm. An X-ray study was
performed to monitor the fit.
Re-evaluation
All re-evaluations were performed by den-
tists who had not fabricated the FDP, to
avoid the bias of overestimation of the
quality of their own work. The first clinical
procedure to eliminate possible pressure
sores was conducted 1–4 days after inser-
tion of the FDP. At this stage, the occlu-
sion was monitored again and strict
instructions were given on hygiene of the
implants and the FDP. Subsequent recalls
were performed after 3 months, 6 months,
and then at 1-year intervals. All follow-up
examinations included complete unscrew-
ing and clinical inspection of the implants
and the FDP. Loss of implants, implant
mobility, and signs of periimplantitis were
recorded, as also were fractures of the
framework and the facing. The torque
used to screw the FDP into the implants
was increased to 25 N cm. In addition to
the recall intervals, the patients were re-
quested to consult the clinic immediately
after recognition of any complication.
Therefore, it was possible to record the
real failure time.
(a) (b)
(c) (d)
(e) (f)
(g)
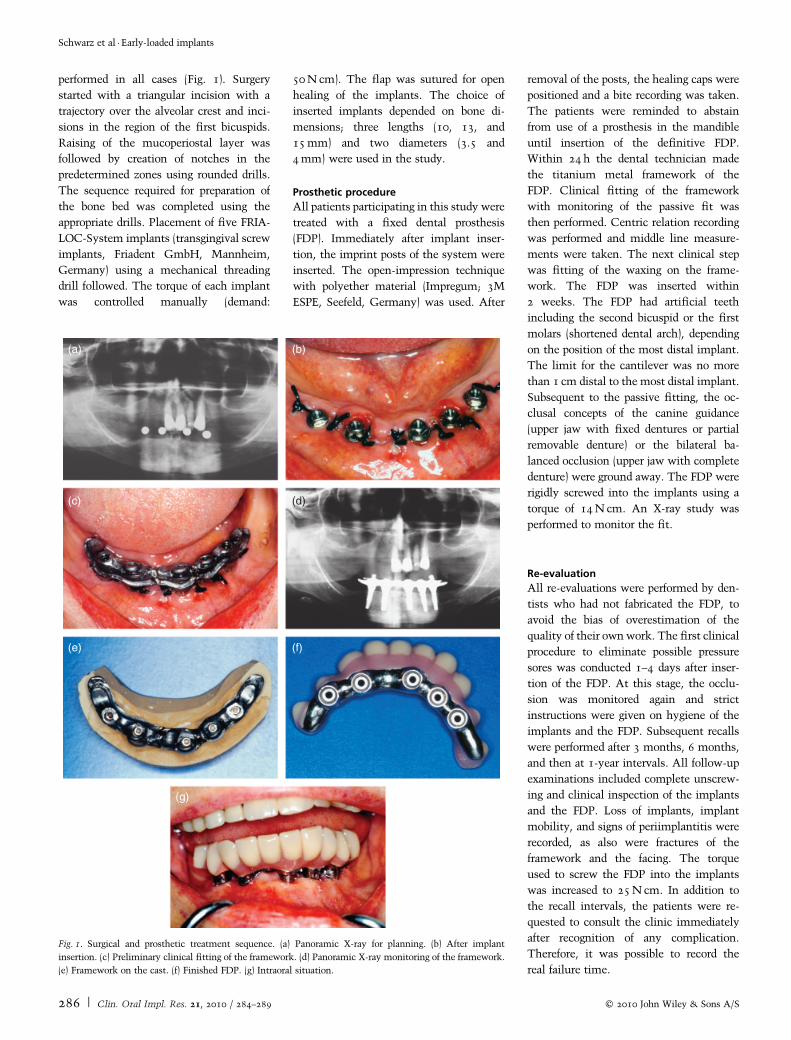
Fig. 1. Surgical and prosthetic treatment sequence. (a) Panoramic X-ray for planning. (b) After implant
insertion. (c) Preliminary clinical fitting of the framework. (d) Panoramic X-ray monitoring of the framework.
(e) Framework on the cast. (f) Finished FDP. (g) Intraoral situation.
Schwarz et al �Early-loaded implants
286 | Clin. Oral Impl. Res. 21, 2010 / 284–289 c� 2010 John Wiley & Sons A/S
Statistical procedures
All data were analysed using SPSS 16.0
(SPSS Inc., Chicago, IL, USA). The prob-
ability of survival was estimated using
Kaplan–Meier survival curves. The effects
of age, gender, the dental status of the
maxilla, and the localization of the im-
plants on the survival of the implants
were evaluated by General Estimation
Equation Model (binary logistic). The de-
pendent variable was implant success yes/
no, and the ID of the subjects was intro-
duced as a subject variable to take into
account that one patient had five implants.
Complications of the FDP were also eval-
uated graphically. The probability level for
statistical significance was set at a¼ 0.05.
Results
Implant-related complications
During the observation period of 1–8 years,
95 implants in 19 patients resulted in no
complication. In 18 patients (90 implants)
32 clinically relevant complications were
recorded. Nineteen implants were lost in
10 patients, resulting in a cumulative sur-
vival of 89.7% after 4.5 years. One patient
lost all five implants, two patients lost
three, one patient lost two, and six patients
lost one. Eleven of the lost implants were
removed within the first 3 months and
seven further implants within 10 months.
Nine implants in five patients, five im-
plants in one patient, and one implant in
four patients did not osseointegrate.
Although these implants were not re-
moved, because stability within the con-
nective tissue was acceptable and
inflammation was absent, they were re-
corded as unsuccessful. Consequently, the
cumulative success declined to 84.9% after
4.5 years. Implants inserted into the most
posterior position were lost more fre-
quently than anterior implants [P¼0.028;
odds ratio (OR) 0.42]. Four implants in
three patients showed clinical signs of peri-
implantitis (2.2% of all implants). Implant
loss and implants without osseointegration
were evaluated as no success whereas signs
of periimplantitis were interpreted as com-
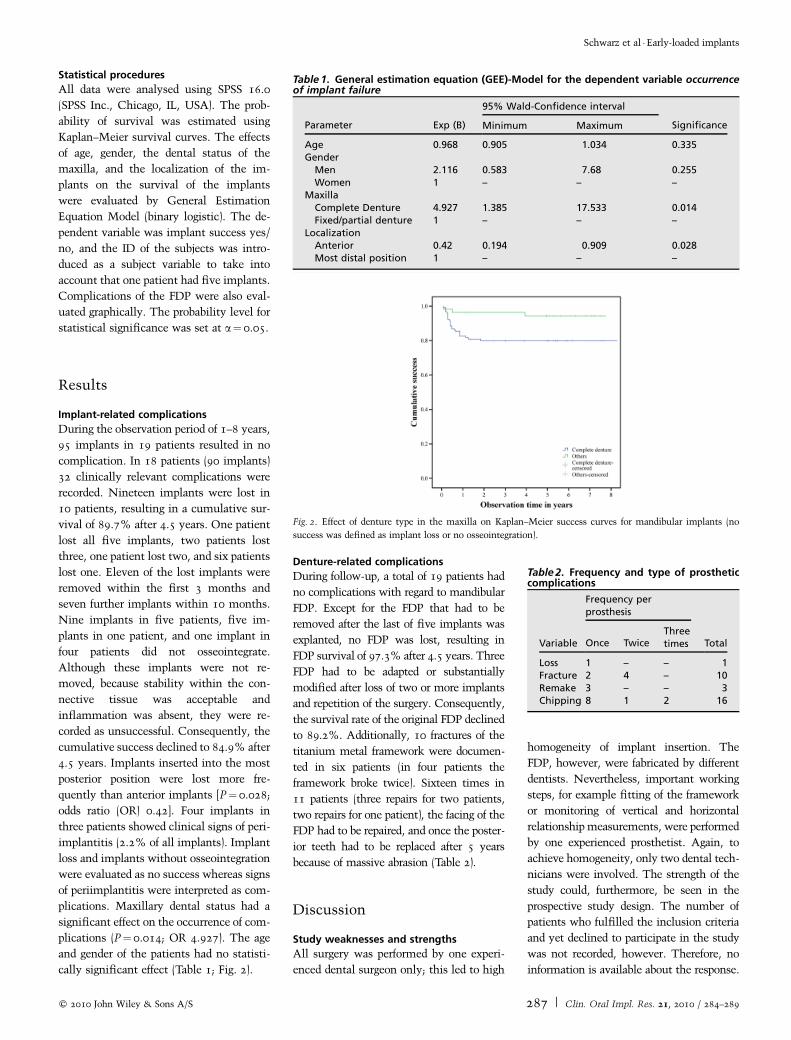
plications. Maxillary dental status had a
significant effect on the occurrence of com-
plications (P¼0.014; OR 4.927). The age
and gender of the patients had no statisti-
cally significant effect (Table 1; Fig. 2).
Denture-related complications
During follow-up, a total of 19 patients had
no complications with regard to mandibular
FDP. Except for the FDP that had to be
removed after the last of five implants was
explanted, no FDP was lost, resulting in
FDP survival of 97.3% after 4.5 years. Three
FDP had to be adapted or substantially
modified after loss of two or more implants
and repetition of the surgery. Consequently,
the survival rate of the original FDP declined
to 89.2%. Additionally, 10 fractures of the
titanium metal framework were documen-
ted in six patients (in four patients the
framework broke twice). Sixteen times in
11 patients (three repairs for two patients,
two repairs for one patient), the facing of the
FDP had to be repaired, and once the poster-
ior teeth had to be replaced after 5 years
because of massive abrasion (Table 2).
Discussion
Study weaknesses and strengths
All surgery was performed by one experi-
enced dental surgeon only; this led to high
homogeneity of implant insertion. The
FDP, however, were fabricated by different
dentists. Nevertheless, important working
steps, for example fitting of the framework
or monitoring of vertical and horizontal
relationship measurements, were performed
by one experienced prosthetist. Again, to
achieve homogeneity, only two dental tech-
nicians were involved. The strength of the
study could, furthermore, be seen in the
prospective study design. The number of
patients who fulfilled the inclusion criteria
and yet declined to participate in the study
was not recorded, however. Therefore, no
information is available about the response.
Table 1. General estimation equation (GEE)-Model for the dependent variable occurrenceof implant failure
Parameter Exp (B)
95% Wald-Confidence interval
SignificanceMinimum Maximum
Age 0.968 0.905 1.034 0.335Gender
Men 2.116 0.583 7.68 0.255Women 1 – – –
MaxillaComplete Denture 4.927 1.385 17.533 0.014Fixed/partial denture 1 – – –
LocalizationAnterior 0.42 0.194 0.909 0.028Most distal position 1 – – –
Fig. 2. Effect of denture type in the maxilla on Kaplan–Meier success curves for mandibular implants (no
success was defined as implant loss or no osseointegration).
Table 2. Frequency and type of prostheticcomplications
Variable
Frequency perprosthesis
TotalOnce TwiceThreetimes
Loss 1 – – 1Fracture 2 4 – 10Remake 3 – – 3Chipping 8 1 2 16
Schwarz et al �Early-loaded implants
c� 2010 John Wiley & Sons A/S 287 | Clin. Oral Impl. Res. 21, 2010 / 284–289

Results and comparison with other studies
Extended integration periods and multiple
surgery are a challenge to patient accep-
tance of implant therapy in the treatment
of edentulous jaws. Early loading of oral
implants could potentially overcome these
problems. It is widely accepted that early
loading is a desirable procedure if outcomes
in terms of implant survival and success are
comparable with those of conventional
loading. In recent years, several reviews
have been published on early loading. The
conclusions were that early-loaded im-
plants resulted in no difference in survival
or marginal bone loss after 1–5 years com-
pared with the original two-stage concept
(Sennerby & Gottlow 2008) and that con-
ventional loading after a 3-month healing
period has not been proved to be the only
acceptable procedure (Kawai & Taylor
2007).
Randow and colleagues compared the
one-stage surgical procedure with the ori-
ginal two-stage concept and therefore
inserted 88 Branemark implants in
16 patients (experimental group) and 30
implants of the same kind in 11 patients
(control group). In the first group, the fixed
appliances were connected to the implants
within 20 days of implant installation
whereas the fixed appliances in the control
group were connected approximately
4 months after fixture installation. During
the 18-month observation period, no fix-
ture was lost in either of the two groups.
The implants under study and those in the
reference material were, at all observation
intervals, found to be clinically stable, and
so the authors concluded that it is, at least
on the basis of an 18-month observation
period, possible to successfully load tita-
nium dental implants early after installa-
tion via a permanent fixed rigid cross-arch
supraconstruction in the interforaminal
area of the edentulous mandible (Randow
et al. 1999). These results were substan-
tiated again in 2000 by the presentation of
stable long-term results from the same
study, based on a 5-year observation period
(Ericsson et al. 2000).
With a cumulative survival of 89.7%
and a cumulative success of 84.9% after
4.5 years of follow–up, the results of this
study are inferior to those described above.
The results are more comparable to
Friberg and colleagues, who evaluated the
5-year implant success of smooth-surface
Branemark-System implants when using a
1-stage surgical procedure with early load-
ing in edentulous mandible. One hundred
and seventy implants were placed in be-
tween the mental foramina, of which 120
implants in 30 patients were associated
with overdenture treatment and 50 im-
plants in 10 patients with fixed complete
dentures. Twelve implants failed in six
patients. The cumulative implant survival
rate was 92.9% after both 1 and 5 years of
follow-up. Another three implants were
recorded as mobile but still in function
when individually checked at the 5-year
visit, which resulted in a cumulative suc-
cess rate of 91% (Friberg et al. 2008). In
this study, implants without osseointegra-
tion were also evaluated as unsuccessful.
Nevertheless, they were not explanted be-
cause, although the patients were informed
of the need for explanting, they did not
agree to further surgery, arguing that the
implants were painless and not causing any
problems. Counting implants without os-
seointegration among the absolute compli-
cations might explain the lower success in
the present study.
In 2009, Eliasson et al. evaluated clinical
outcome and patient satisfaction with early
or delayed loading in patients treated with
fixed prostheses, using three different im-
plant systems. One hundred and nine con-
secutively treated patients received 490
implants supporting fixed prostheses. The
prostheses were placed within 2–3 weeks
in 55 patients; 54 patients underwent a
two-stage procedure. All patients had fixed
prostheses at follow-up with a mean ob-
servation time of 3.5 years. Cumulative
survival rates were 92.5% of prostheses
and 94.4% of implants for early loading,
and 98% and 97.9% for delayed loading.
With early loading, significantly more
prostheses (Po0.05) needed adjustment
or replacement (Eliasson et al. 2009).
Although factors affecting the success of
implants could be of a different origin, the
predominant factor affecting the survival of
early-loaded implants is believed to be im-
plant movement during the healing period.
When osseointegration was successful,
long-term results for early-loaded implants
were comparable with those for implants
inserted using the classical two-stage pro-
cedure (Petersson et al. 2001). This could
be interpreted as agreement with our re-
sults. Eleven of the lost implants were
explanted within the first 3 months, and
seven further implants within 10 months.
With the exception of one implant that
had to be removed after nearly 2 years,
no implant was lost in subsequent years.
In this case, however, the patient had
not attended the previous follow-up
examinations.
It was also shown that edentulous max-
illas with complete dentures had a signifi-
cant effect on implant success in this
study. Wearing complete dentures in the
maxilla was associated with greater failure
of implants in the mandible. This result is
supported by the findings of Falk and
colleagues and Lundgren and colleagues,
who observed increasing local closing and
chewing forces bilaterally in the distal
direction for mandibular implant-sup-
ported cross-arch prostheses occluding
with complete dentures. This was ex-
plained by the behaviour of the maxillary
complete denture during function. The
larger anterior resilience of the oral max-
illary mucosa probably causes hinging of
the denture base, thereby transferring more
load to the posterior area (Lundgren et al.
1989; Falk et al. 1990). Duyck et al. (2000)
also assumed that masticatory forces are
better distributed when the prosthesis is
antagonizing natural dentition or a fixed
restoration instead of a removable denture.
They registered maximum axial forces on
distal implants when the upper jaw was
provided with a removable denture,
although with lack of statistical signifi-
cance (Duyck et al. 2000).
With regard to survival of the FDP, it
was found that no FDP was lost for pros-
thetic-related reasons. One FDP was re-
moved after all implants had been
explanted, however, and three FDPs had
to be modified after reoperation, and so the
survival of the original FDP was 89.2%
only. During the 1–8-year observation per-
iod in this study, 19 patients had no com-
plication with regard to the FDP. The most
common complications were veneer or
resin fractures; the facing of the FDP had
to be repaired 16 times in 11 patients.
Fractures of the titanium metal frame
were observed in 16.2% of the patients,
and the framework broke twice in four
patients. The results of this study can be
seen to be in accordance with results from
studies reported in the literature. Ortorp
and Jemt compared 15-year retrospective
Schwarz et al �Early-loaded implants
288 | Clin. Oral Impl. Res. 21, 2010 / 284–289 c� 2010 John Wiley & Sons A/S

data for 72 of 155 implant-supported fixed
prostheses in the edentulous mandible pro-
vided with laser-welded titanium frame-
works (test) with data for gold-alloy
frameworks (control). The cumulative 15-
year survival of the original fixed pros-
theses was 89.2%. The most common
complications for titanium frameworks
within the follow-up of 15 years were resin
or veneer fractures. Fractures of the tita-
nium metal frame were observed in 15.5%
of the patients (Ortorp & Jemt 2008).
Conclusion
The results of this study showed that
one-stage early-loaded implants functioned
well for most patients with edentulous
mandibles. Early loading is, nevertheless,
associated with more implant-related
complications than in studies investigating
delayed loading, resulting in a greater need
for adaptation and modification of the
FDPs. Because of the substantial prosthetic
complications and aftercare, this procedure
cannot be generally recommended.
Acknowledgements: We thank Ian
Davies, copy editor, for language
revision. We also thank FRIADENT
GmbH, Mannheim, Germany, for
financial support.
References
Aparicio, C., Rangert, B. & Sennerby, L. (2003)
Immediate/early loading of dental implants: a
report from the Sociedad Espanola de Implantes
World Congress consensus meeting in Barcelona,
Spain, 2002. Clinical Implant Dentistry and
Related Research 5: 57–60.
Branemark, P.I., Hansson, B.O., Adell, R., Breine,
U., Lindstrom, J., Hallen, O. & Ohman, A. (1977)
Osseointegrated implants in the treatment of the
edentulous jaw. Experience from a 10-year period.
Scandinavian Journal of Plastic and Reconstruc-
tive Surgery and Hand Surgery 16: 1–132.
Chiapasco, M. & Gatti, C. (2003) Implant-retained
mandibular overdentures with immediate loading:
a 3- to 8-year prospective study on 328 implants.
Clinical Implant Dentistry & Related Research
5: 29–38.
Duyck, J., Van Oosterwyck, H., Vander Sloten, J.,
De Cooman, M., Puers, R. & Naert, I. (2000)
Magnitude and distribution of occlusal forces on
oral implants supporting fixed prostheses: an in
vivo study. Clinical Oral Implants Research 11:
465–475.
Eliasson, A., Blomquist, F., Wennerberg, A. &
Johansson, A. (2009) A retrospective analysis of
early and delayed loading of full-arch mandibular
prostheses using three different implant systems:
clinical results with up to 5 years of loading.
Clinical Implant Dentistry & Related Research
11: 134–148.
Ericsson, I., Randow, K., Nilner, K. & Peterson, A.
(2000) Early functional loading of Branemark
dental implants: 5-year clinical follow-up study.
Clinical Implant Dentistry & Related Research
2: 70–77.
Falk, H., Laurell, L. & Lundgren, D. (1990) Occlusal
interferences and cantilever joint stress in im-
plant-supported prostheses occluding with com-
plete dentures. International Journal of Oral &
Maxillofacial Implants 5: 70–77.
Friberg, B., Raghoebar, G.M., Grunert, I., Hobkirk,
J.A. & Tepper, G. (2008) A 5-year prospective
multicenter study on 1-stage smooth-surface
Branemark System implants with early loading
in edentulous mandibles. International Journal of
Oral & Maxillofacial Implants 23: 481–486.
Gomez-Roman, G., Schulte, W., d’Hoedt, B. &
Axman-Krcmar, D. (1997) The Frialit-2 implant
system: five-year clinical experience in single-
tooth and immediately postextraction applica-
tions. International Journal of Oral & Maxillofa-
cial Implants 12: 299–309.
Kawai, Y. & Taylor, J.A. (2007) Effect of loading
time on the success of complete mandibular
titanium implant retained overdentures: a sys-
tematic review. Clinical Oral Implants Research
18: 399–408.
Ledermann, P.D. (1979) Stegprothetische Versor-
gung des zahnlosen Unterkiefers mit Hilfe von
plasmabeschichteten Titan-schraubenimplanta-
ten. Deutsche Zahnarztliche Zeitung 34:
907–911.
Ledermann, P.D., Schenk, R.K. & Buser, D. (1998)
Long-lasting osseointegration of immediately
loaded, bar-connected TPS screws after 12 years
of function: a histologic case report of a 95-
year-old patient. The International Journal of Perio-
dontics and Restorative Dentistry 18: 553–563.
Lundgren, D., Falk, H. & Laurell, L. (1989) Influ-
ence of number and distribution of occlusal canti-
lever contacts on closing and chewing forces
in dentitions with implant-supported fixed
prostheses occluding with complete dentures.
International Journal of Oral & Maxillofacial
Implants 4: 277–283.
Meijer, H.J., Raghoebar, G.M., Van’t Hof, M.A.,
Geertman, M.E. & Van Oort, R.P. (1999) Im-
plant-retained mandibular overdentures compared
with complete dentures; a 5-years’ follow-up
study of clinical aspects and patient satisfaction.
Clinical Oral Implants Research 10: 238–244.
Ortorp, A. & Jemt, T. (2008) Early laser-welded
titanium frameworks supported by implants in
the edentulous mandible: a 15-year comparative
follow-up study. Clinical Implant Dentistry &
Related Research [Epub ahead of print].
Petersson, A., Rangert, B., Randow, K. & Ericsson,
I. (2001) Marginal bone resorption at different
treatment concepts using Branemark dental im-
plants in anterior mandibles. Clinical Implant
Dentistry & Related Research 3: 142–147.
Raghoebar, G.M., Friberg, B., Grunert, I., Hobkirk,
J.A., Tepper, G. & Wendelhag, I. (2003) 3-year
prospective multicenter study on one-stage im-
plant surgery and early loading in the edentulous
mandible. Clinical Implant Dentistry & Related
Research 5: 39–46.
Randow, K., Ericsson, I., Nilner, K., Petersson, A. &
Glantz, P.O. (1999) Immediate functional loading
of Branemark dental implants. An 18-month
clinical follow-up study. Clinical Oral Implants
Research 10: 8–15.
Schnitman, P.A., Wohrle, P.S., Rubenstein, J.E., Da
Silva, J.D. & Wang, N.H. (1997) Ten-year results
for Branemark implants immediately loaded with
fixed prostheses at implant placement. Interna-
tional Journal of Oral & Maxillofacial Implants
12: 495–503.
Sennerby, L. & Gottlow, J. (2008) Clinical out-
comes of immediate/early loading of dental im-
plants. A literature review of recent controlled
prospective clinical studies. Australian Dental
Journal 53: 82–88.
Tarnow, D.P., Emtiaz, S. & Classi, A. (1997) Im-
mediate loading of threaded implants at stage 1
surgery in edentulous arches: ten consecutive case
reports with 1- to 5-year data. International Jour-
nal of Oral & Maxillofacial Implants 12:
319–324.
Uribe, R., Penarrocha, M., Balaguer, J. & Fulgueiras,
N. (2005) Immediate loading in oral implants.
Present situation. Medicina oral, patologıa oral
y cirugıa bucal 10: 143–153.
van Waas, M.A. (1990) The influence of psychologic
factors on patient satisfaction with complete den-
tures. The Journal of Prosthetic Dentistry 63:
545–548.
Schwarz et al �Early-loaded implants
c� 2010 John Wiley & Sons A/S 289 | Clin. Oral Impl. Res. 21, 2010 / 284–289




























