Embed Size (px)
Citation preview

Effect of Diclofenac on Corneal Haze after Photorefractive Keratectomy in Rabbits
Belquiz A Nassaralla, MD, Karin Szerenyi, MD, Xun W. Wang, BS, T. Al Reaves, PhD, Peter]. McDonnell, MD
Purpose: To evaluate the ability of topical diclofenac to decrease corneal opacity after excimer laser photorefractive keratectomy (PRK).
Methods: Twenty New Zealand white rabbits underwent a unilateral193-nm excimer laser myopic photorefractive keratectomy to correct 5 diopters. There were four groups of five rabbits each. The first group of rabbits received postoperative topical treatment with placebo (Voltaren Ophthalmic vehicle), the second group received topical 0.1% diclofenac, the third group received topical corticosteroid (0.1% fluorometholone), and the fourth group received diclofenac and fluorometholone. In the first month, the topical drugs were applied four times daily, and in the second month twice daily. Corneal haze was graded from 0 (totally clear) to 4 (completely opaque cornea). Slit-lamp pictures were obtained at weeks 2, 4, and 8, and keratometry readings was performed at weeks 4 and 8. At week 8, the rabbits were killed, and the eyes were submitted for histologic examination.
Results: At week 8, there was less corneal haze in the diclofenac-treated animals and in the fluorometholone-treated animals than in the control group, but only in the diclofenac-treated group was the difference statistically significant. Combination treatment with diclofenac and fluorometholone did not result in a further decrease in haze.
Conclusions: These data suggest that diclofenac and fluorometholone may influence corneal wound healing in rabbits after excimer laser PRK and support a potential role for using topical nonsteroidal anti-inflammatory drugs in preventing the development of excessive corneal haze after excimer laser surgery. Ophthalmology 1995;102:469-474
In 1983, Trokel et al 1 described the use ofshort wavelength excimer laser to achieve precise and controlled reshaping of the anterior corneal surface. They applied 193-nm radiation to bovine corneas and noted that ( l) the laser damage was localized to the zone of ablation, which
Originally received: April 4, 1994. Revision accepted: July 12, 1994. From the Doheny Eye Institute and the Department ofOphthalmology, University of Southern California School of Medicine, Los Angeles. Supported by a grant from CIBA Vision Ophthalmics, Atlanta, Georgia, by National Eye Institute/ National Institute of Health core grant EY03040. Bethesda, Maryland, a grant from the Autry Foundation, Los Angeles, California, and by an unrestricted grant from Research to Prevent Blindness, Inc, New York, New York. Dr. McDonnell is a William and Mary Greve International Research Scholar. Reprint requests to Peter J. McDonnell, MD, Doheny Eye Institute, 1450 San Pablo St, Los Angeles, CA 90033.
showed no evidence of thermal effects and (2) that the edges of the incisions were parallel and straight, without histologic disorganization of the adjacent stromal lamellae or epithelial edge. Since that time, many studies have been performed to understand the pathology and the microstructural changes that follow excimer laser ablation of the cornea. The 193-nm excimer laser removes surface molecules by disrupting molecular bonds, with little transfer of heat to underlying tissue.2 Energy is delivered in discrete pulses (commonly at 10 pulses per second), so the amount of tissue excised potentially can be controlled, with limited or negligible effects on adjacent tissue. 3
Corneal wound healing after excimer laser photorefractive keratectomy (PRK) poses two problems: the preservation of optical clarity of the ablated area, and the predictability and stability of the refractive result. Epithelial hyperplasia, subepithelial collagen production, disconti
469

Ophthalmology Volume 102, Number 3, March 1995
nuity in interlamellar alignment, vacuole formation, or stromal regeneration all can occur in the ablated zone and can alter the calculated refractive correction or cause corneal opacification.4 Studies ofhyperopic and myopic ablations in primates and humans have shown that an initial overcorrection occurs, followed by a partial loss of effect over time when corrections of 3 diopters (D) or greater are attempted. 3 Postoperative corneal clarity can range from completely clear to slightly hazy, or even to dense opacity, obscuring anterior chamber detail. 5
Modulation of the wound healing process to prevent excessive fibroblast proliferation, new collagen formation, and stromal ground substance, which are suspected to be the main causes of corneal haze after excimer laser ablation, would contribute greatly to improving the outcome of excimer laser PRK. Pharmacologic agents that inhibit fibroblast proliferation and haze formation may prove useful in this respect.
By examining the response ofpolymorphonuclear leukocytes to superficial corneal injury induced by chemical, mechanical, and PRK de-epithelialization methods, we have shown previousll that the 193-nm excimer laser induces substantial acute stromal inflammation in the rabbit cornea and that short-term use of anti-inflammatory agents may be appropriate after PRK. We noted also that topical diclofenac effectively reduces the postoperative inflammation in rabbit corneas by inhibiting the release of prostaglandin E2 , which is a chemoattractant for inflammatory cells. 7
Topical corticosteroids are used routinely in treating a number of ocular inflammatory conditions, and some topical nonsteroidal anti-inflammatory agents offer the possibility of even better treatment because they lack many of the systemic and ocular side effects ofsteroids.
Diclofenac is a nonsteroidal anti-inflammatory agent currently available for topical ophthalmic use. We report our findings in a masked, controlled study perfoqned in rabbits and compare the anti-inflammatory effects of0.1% diclofenac and 0.1% fluorometholone on the development of corneal haze after PRK.
Materials and Methods
Animals Twenty adult New Zealand white rabbits (20 eyes) were used in this study. All procedures were performed on anesthetized rabbits (ketamine hydrochloride [40 mg/kg] and xylazine [7 mg/kg]). Biomicroscopic examination was done on all rabbits preoperatively.
The animals ·used in this study were maintained in animal care facilities fully accredited by the American Association of Laboratory Animal Science, and all animal studies were done in accordance with the AR VO Statement for the Use of Animals in Ophthalmic and Vision Research.
Excimer Laser Ablations Laser ablation of rabbit cornea was performed with a commercially available 193-nm argon-fluoride excimer
laser (Twenty-Twenty excimer laser; VISX Inc, Santa Clara, CA).
In the right eye of each rabbit, a photorefractive keratectomy with a fluence of 160 mJ/cm2 and a pulse rate of 6 Hz in a 6-mm diameter with a central depth of 66 11m was done to correct 5 diopters of myopia after an ablation of 30 11m to remove the epithelium.
Drug Treatments and Regimen
After surgery, the rabbits were immediately randomized into one of four groups of five animals; each group received one ofthe following medications: placebo (Voltaren Ophthalmic vehicle), 0.1% diclofenac sodium, 0.1% fluorometholone, and a combination of diclofenac and fluorometholone. Drops were administered four times daily for the first month, and then two times daily for the second month.
Under general anesthesia, biomicroscopic examinations were performed immediately after and every 2 weeks after surgery; hyperemia, keratitis, and any amount of inflammation were recorded. Slit-lamp pictures documented the corneal wound healing at 2, 4, and 8 weeks. Keratometry readings were obtained at 4 and 8 weeks to measure any changes in the corneal curvature during the process of wound healing. All measurements were taken by the same masked observer.
The following criteria were used by the masked observer to grade the density ofcorneal haze: grade 0, totally clear cornea with no opacity seen by any method of microscopic slit-lamp examination; grade 0.5, trace or faint corneal haze seen only by indirect broad tangential illumination; grade 1, haze of minimal density seen with difficulty with direct and diffuse illumination; grade 2, mild haze easily visible with direct focal slit illumination; grade 3, moderate opacity that partially obscures details of the iris; and grade 4, severe opacity that completely obscures the details of intraocular structures. 8·9
A follow-up examination at 8 weeks was selected because we had previously10 shown that haze in these rabbits is maximal at 3 to 4 weeks after surgery, and then decreases.
The rabbits were killed at the end of the eighth week. Documentary photographs of the experimental eyes were taken before the animals were killed.
Statistical Analysis Variables of the four groups were compared over time by analysis of variance. Group and time were considered as two within-subject effects. Pairwise comparisons were made by paired and unpaired Student's t test. All tests were two-tailed; P < 0.05 was considered significant. Data are reported as mean± standard deviation.
Results
All eyes showed mild hyperemia soon after surgery, but this resolved completely by 2 weeks. The degree ofkeratitis
470
Nassaralla et al · Diclofenac and Haze after PRK
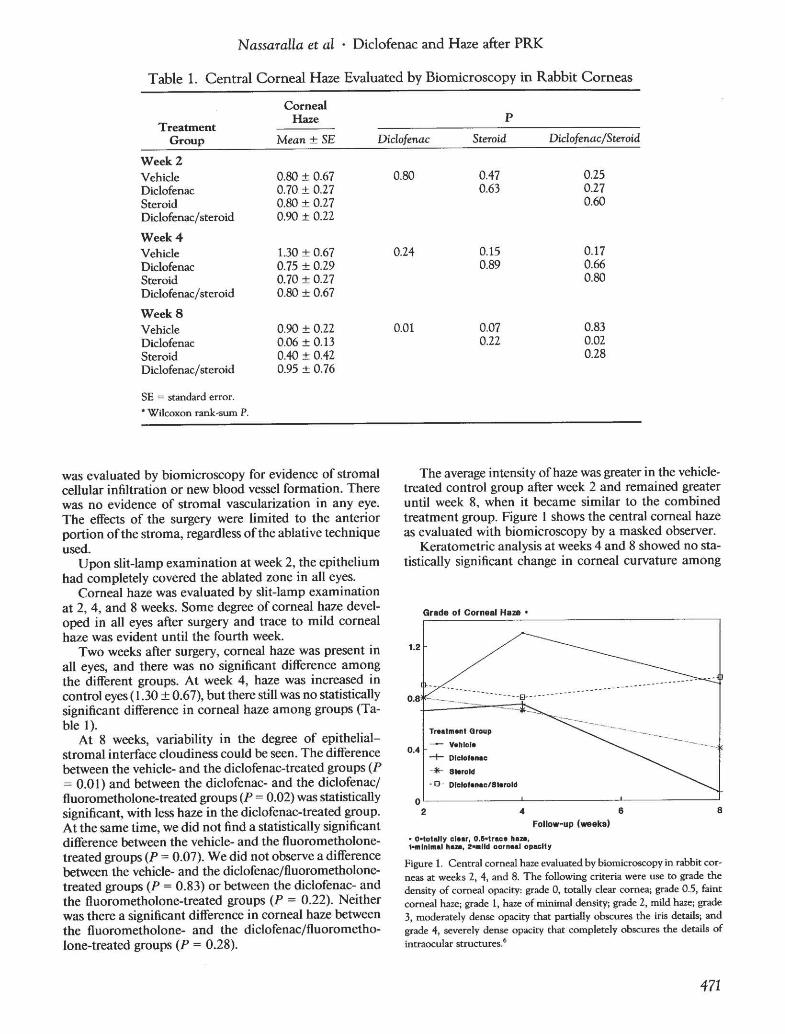
Table 1. Central Corneal Haze Evaluated by Biomicroscopy in Rabbit Corneas
Corneal pHaze
Treatment Group Mean± SE Diclofenac Steroid Diclofenac/Steroid
Week2 Vehicle Diclofenac Steroid Diclofenac/steroid
Week4 Vehicle Diclofenac Steroid Diclofenac/steroid
WeekS Vehicle Diclofenac Steroid Diclofenac/steroid
SE = standard error. *Wilcoxon rank-sum P.
0.80 ± 0.67 0.70 ± 0.27 0.80 ± 0.27 0.90 ± 0.22
1.30 ± 0.67 0.75 ± 0.29 0.70 ± 0.27 0.80 ± 0.67
0.90 ± 0.22 0.06 ± 0.13 0.40 ± 0.42 0.95 ± 0.76
was evaluated by biomicroscopy for evidence of stromal cellular infiltration or new blood vessel formation. There was no evidence of stromal vascularization in any eye. The effects of the surgery were limited to the anterior portion ofthe stroma, regardless of the ablative technique used.
Upon slit-lamp examination at week 2, the epithelium had completely covered the ablated zone in all eyes.
Corneal haze was evaluated by slit-lamp examination at 2, 4, and 8 weeks. Some degree of corneal haze developed in all eyes after surgery and trace to mild corneal haze was evident until the fourth week.
Two weeks after surgery, corneal haze was present in all eyes, and there was no significant difference among the different groups. At week 4, haze was increased in control eyes ( 1.30 ± 0.67), but there still was no statistically significant difference in corneal haze among groups (Table l ).
At 8 weeks, variability in the degree of epithelialstromal interface cloudiness could be seen. The difference between the vehicle- and the diclofenac-treated groups (P = 0.0 l) and between the diclofenac- and the diclofenac/ fluorometholone-treated groups (P = 0.02) was statistically significant, with less haze in the diclofenac-treated group. At the same time, we did not find a statistically significant difference between the vehicle- and the fluorometholonetreated groups (P = 0.07). We did not observe a difference between the vehicle- and the diclofenac/fluorometholonetreated groups (P = 0.83) or between the diclofenac- and the fluorometholone-treated groups (P = 0.22). Neither was there a significant difference in corneal haze between the fluorometholone- and the diclofenacjfluorometholone-treated groups (P = 0.28).
0.80 0.47 0.63
0.24 0.15 0.89
0.01 0.07 0.22
0.25 0.27 0.60
0.17 0.66 0.80
0.83 0.02 0.28
The average intensity of haze was greater in the vehicletreated control group after week 2 and remained greater until week 8, when it became similar to the combined treatment group. Figure l shows the central corneal haze as evaluated with biomicroscopy by a masked observer.
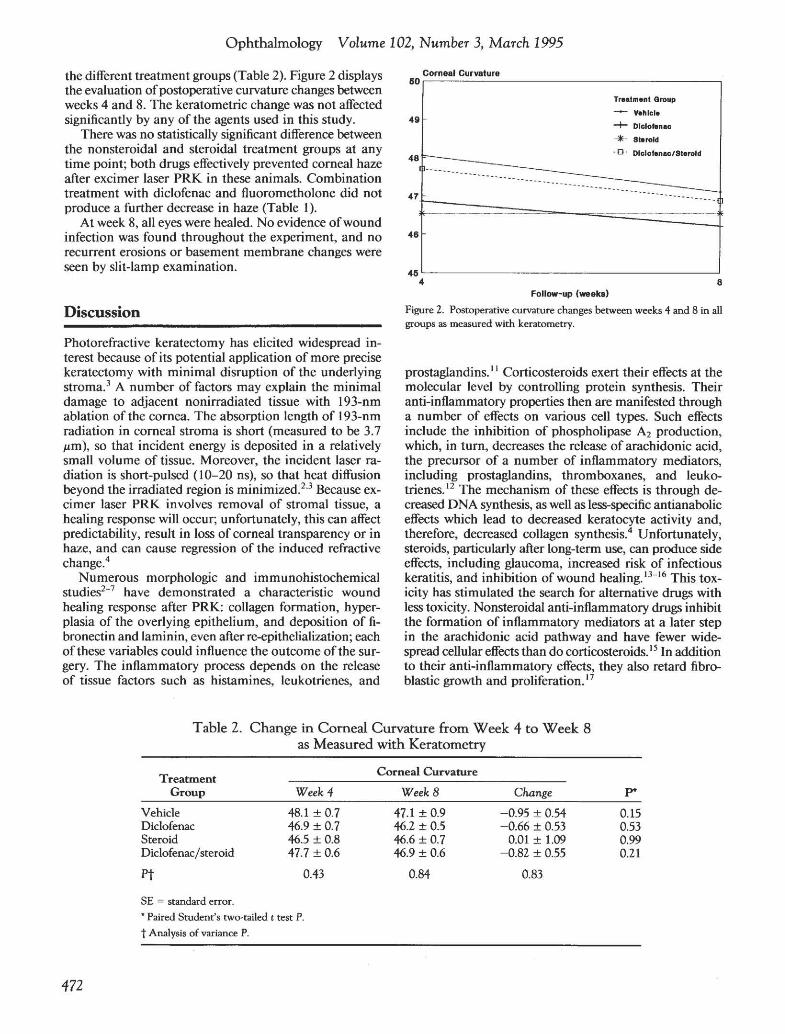
Keratometric analysis at weeks 4 and 8 showed no statistically significant change in corneal curvature among
Grade of Corneal Haze •
1.2
Treatment Qroup
_ - Vehicle 0 4 -+- Dlclolenac
-·*- Steroid
-0 ·
0~------------~------------~----------~
2 4 6 8 Follow-up l-eks)
• O•totally clear, O.D•trace hem, -lnlmal haa, 2..11d oorneal opacity
Figure 1. Central corneal haze evaluated by biomicroscopy in rabbit cor· neas at weeks 2, 4, and 8. The following criteria were use to grade the density of corneal opacity: grade 0, totally clear cornea; grade 0.5, faint corneal haze; grade 1, haze of minimal density; grade 2, mild haze; grade 3, moderately dense opacity that partially obscures the iris details; and grade 4, severely dense opacity that completely obscures the details of intraocular structures.6
471
Ophthalmology Volume 102, Number 3, March 1995
the different treatment groups (Table 2). Figure 2 displays the evaluation ofpostoperative curvature changes between weeks 4 and 8. The keratometric change was not affected significantly by any of the agents used in this study.
There was no statistically significant difference between the nonsteroidal and steroidal treatment groups at any time point; both drugs effectively prevented corneal haze after excimer laser PRK in these animals. Combination treatment with diclofenac and fluorometholone did not produce a further decrease in haze (Table I).
At week 8, all eyes were healed. No evidence ofwound infection was found throughout the experiment, and no recurrent erosions or basement membrane changes were seen by slit-lamp examination.
Discussion
Photorefractive keratectomy has elicited widespread interest because of its potential application of more precise keratectomy with minimal disruption of the underlying stroma.3 A number of factors may explain the minimal damage to adjacent nonirradiated tissue with 193-nm ablation of the cornea. The absorption length of 193-nm radiation in corneal stroma is short (measured to be 3.7 J.Lm), so that incident energy is deposited in a relatively small volume of tissue. Moreover, the incident laser radiation is short-pulsed ( 10-20 ns), so that heat diffusion beyond the irradiated region is minimized?3 Because excimer laser PRK involves removal of stromal tissue, a healing response will occur; unfortunately, this can affect predictability, result in loss of corneal transparency or in haze, and can cause regression of the induced refractive change.4
Numerous morphologic and immunohistochemical studies2-7 have demonstrated a characteristic wound healing response after PRK: collagen formation, hyperplasia of the overlying epithelium, and deposition of fibronectin and laminin, even after re-epithelialization; each of these variables could influence the outcome of the surgery. The inflammatory process depends on the release of tissue factors such as histamines, leukotrienes, and
Corneal Curvature 60.---------------------------------------.
Treatment Group
~ Vehicle 49 -+- Dlclolenac
··*-· Steroid
• 0 · Dlclofonac/Storold48
47
46
45L-------------------------------------~ 4 8
Follow-up (weeks)
Figure 2. Postoperative curvature changes between weeks 4 and 8 in all groups as measured with keratometry.
prostaglandins. 11 Corticosteroids exert their effects at the molecular level by controlling protein synthesis. Their anti-inflammatory properties then are manifested through a number of effects on various cell types. Such effects include the inhibition of phospholipase A2 production, which, in turn, decreases the release of arachidonic acid, the precursor of a number of inflammatory mediators, including prostaglandins, thromboxanes, and leukotrienes.12 The mechanism of these effects is through decreased DNA synthesis, as well as less-specific antianabolic effects which lead to decreased keratocyte activity and, therefore, decreased collagen synthesis.4 Unfortunately, steroids, particularly after long-term use, can produce side effects, including glaucoma, increased risk of infectious keratitis, and inhibition of wound healing. 13- 16 This toxicity has stimulated the search for alternative drugs with less toxicity. Nonsteroidal anti-inflammatory drugs inhibit the formation of inflammatory mediators at a later step in the arachidonic acid pathway and have fewer widespread cellular effects than do corticosteroids. 15 In addition to their anti-inflammatory effects, they also retard fibroblastic growth and proliferation. 17
Table 2. Change in Corneal Curvature from Week 4 to Week 8 as Measured with Keratometry
Treatment Group Week4
Corneal Curvature
WeekS Change P*
Vehicle Diclofenac Steroid Diclofenac/ steroid
Pt
48.1 ± 0.7 46.9 ± 0.7 46.5 ± 0.8 47.7 ± 0.6
0.43
47.1 ± 0.9 46.2 ± 0.5 46.6 ± 0.7 46.9 ± 0.6
0.84
-0.95 ± 0.54 -0.66 ± 0.53
0.01 ± 1.09 -0.82 ± 0.55
0.83
0.15 0.53 0.99 0.21
SE = standard error. • Paired Student's two-tailed t test P. t Analysis of variance P.
472

Nassaralla et al · Diclofenac and Haze after PRK
Fluorometholone belongs to the class of corticosteroids that have been shown to induce production of lipomodulin, 18 a glycoprotein that functions as a specific phospholipase A2 inhibitor. Inhibition of phospholipase A2 leads to a decrease in arachidonic acid, and, consequently, to a reduction in lipoxygenase and cyclooxygenase metabolites. Diclofenac sodium, a phenylacetic acid derivative, has a well-defined ability to disrupt the function of cyclo-oxygenase, and hence the production ofprostaglandins. 19 It can reduce the availability of intracellular arachidonic acid by enhancing its uptake into triglyceride pools, and thus influences the production oflipoxygenase as well as cyclo-oxygenase products.20
Fibroblastic activity is part of the normal wound-healing process that involves an inflammatory response. Given the complex cellular, immunologic, and biochemical interactions involved in wound repair, anti-inflammatory agents theoretically could influence the rate and quality of wound healing.
Nguyen and Lee13 evaluated four commonly used topical cyclo-oxygenase inhibitors (diclofenac, flurbiprofen, piroxicam, and suprofen) for their potential use as antifibrotic agents after glaucoma filtration surgery. The attachment and proliferation of fibroblasts from human Tenon's capsule were studied. Diclofenac was the most effective agent in inhibiting fibroblast proliferation. Another study by the same authors14 compared the ability of a corticosteroid (dexamethasone sodium phosphate), a cyclooxygenase inhibitor (piroxicam), a lipoxygenase inhibitor (ferulic acid), and a dual cyclo/lipoxygenase inhibitor (phenidone) to inhibit Tenon's capsule fibroblast proliferation in culture. Phenidone was the only drug that showed inhibition in low doses and anti-inflammatory range in vivo. This nonsteroidal anti-inflammatory agent had antiproliferative activity comparable to or better than that of the steroids tested.
Hersh et al 15 studied the effects on corneal wound healing of two topical nonsteroidal anti-inflammatory agents, flurbiprofen sodium (0.03%) and diclofenac sodium (0.1%), and the topical corticosteroid, prednisolone sodium phosphate ( 1%). They found that both the topical nonsteroidal anti-inflammatory agents and the corticosteroid decreased early epithelialization of corneal scrape wounds, but that they had no apparent effect on healing of the corneal stroma. Previous studies in our laboratory7 showed that topical application of diclofenac after photorefractive keratectomy caused a significant decrease in prostaglandin E2 levels. Fluorometholone treatment, on the other hand, did not significantly alter prostaglandin E2 levels, but did markedly inhibit leukocyte infiltration.
In a study of 285 eyes that underwent PRK and that were followed for up to 18 months, Caubet4 found that haze was maximal at 3 months, and then decreased. He noted also that the haze was greater in eyes that received increased application of laser energy and ablations less than 4.5 mm in diameter. All of his patients with significant haze acknowledged discontinuing the use of corticosteroids. He reported that the maximum cellular activity
occurred at the second or third postoperative month and its decrease correlated with a return to normal visua{ acuity and corneal clarity. Fantes et al8 in a study of29 rhesus monkey corneas that were followed up for 9 months after PRK, noted that the density of subepithelial fibroblasts was three times greater than normal at 3 weeks, but returned to normal by 9 months. At 6 weeks, mild to moderate subepithelial haze was apparent in 93% of the corneas, but progressive clearing occurred, and by 6 to 9 months 92% of the corneas were completely clear or had only a trace of haze.
In the current study, we compared the inhibitory effects of topical anti-inflammatory steroidal and nonsteroidal drugs on the development ofcorneal haze after photoablative keratectomy. Both drugs reduced the corneal haze, but did not influence refractive outcome. It is unclear why no additive effect was obtained by combining the drugs. This could have been due to toxicity of cumulative effect of preservatives or drug interactions (effect of combination). Because these issues have not been studied extensively in the clinical context, additional laboratory studies are necessary to better define the optimal dose interval, the toxicity of drug delivery vehicles, and the interactions between these drugs. Currently, we believe it is common for patients to be given both drugs after surgery: nonsteroidal anti-inflammatory drugs for a few days and a corticosteroid for a few weeks to months.
These results suggest that diclofenac and fluorometholone each may have beneficial effects on both postoperative inflammation and postoperative wound healing. Because diclofenac does not have the potential side effects ofcorticosteroids (including elevated intraocular pressure, increased viral infection, and cataractogenesis), the use of topical nonsteroidal anti-inflammatory drugs may be appropriate to prevent excessive fibroblast proliferation after excimer laser surgery.
Keratocytes are believed to play an important role in the synthesis and secretion ofcollagen, proteoglycans, and other extracellular proteins.21 Because diclofenac inhibits fibroblastic activity and corneal haze formation during wound healing, it may have an influence on keratocytes during corneal wound healing.
The value of corticosteroid therapy in humans after excimer photorefractive keratectomy has been questioned in recent randomized trials,4
•6•7
•22 and it may be that con
flicting reports on experimental studies reflect a difference between species in the response of the corneal wound healing process to anti-inflammatory therapy. Thus, further studies in humans will be necessary to evaluate pharmacologic manipulation of wound healing after photorefractive keratectomy.
Acknowledgments. The authors thank Laurie LaBree, MS, Department ofPreventive Medicine, University ofSouthern California School of Medicine, who performed the statistical analysis.
References
I. Trokel SL, Srinivasan R, Braren B. Excimer laser surgery ofthe cornea. Am J Ophthalmol 1983;96:710-15.
473
Ophthalmology Volume 102, Number 3, March 1995
2. Krauss JM, Puliafito CA, Steinert RF. Laser interactions with the cornea. Surv Ophthalmol 1986;31:37-53.
3. Del Pero RA, Gigstad JE, Roberts AD, et al. A refractive and histopathologic study of excimer laser keratectomy in primates. Am J Ophthalmol 1990;109:419-29.
4. Caubet E. Course of subepithelial corneal haze over 18 months after photorefractive keratectomy for myopia. Refract Corneal Surg 1993;9(Suppl 2):S65-70.
5. McDonald M8, Frantz JM, Klyce SD, et al. Central photorefractive keratectomy for myopia. The blind eye study. Arch Ophthalmol 1990; I 08:799-808.
6. Campos M, Abed HM, McDonnell PJ. Topical fluorometholone reduces stromal inflammation after photorefractive keratectomy. Ophthalmic Surg 1993;24:654-7.
7. Phillips AF, Szerenyi K, Campos M, et al. Arachidonic acid metabolites after excimer laser corneal surgery. Arch Ophthalmol 1993;111:1273-8.
8. Fantes FE, Hanna KD, Waring GO Ill, et al. Wound healing after excimer laser keratomileusis (photorefractive keratectomy) in monkeys. Arch Ophthalmol 1990; 108: 665-75.
9. Campos M, Cuevas K, Garbus J, et al. Corneal wound healing after excimer laser ablation. Effects of nitrogen gas blower. Ophthalmology 1992;99:893-7.
I0. Campos M, Cuevas K, Shieh E, et al. Corneal wound healing after excimer laser ablation in rabbits: expanding versus contracting apertures. Refract Corneal Surg 1992;8:378-81.
II. Tahery MM, Lee DA. Review: pharmacologic control of wound healing in glaucoma filtration surgery. J Ocul Pharmacoll989;5:155-79.
12. Malmsten CL. Prostaglandins, thromboxanes, and leukotrienes in inflammation. Am J Med 1986;80(Suppl48)117.
13. Nguyen KD, Lee DA. In vitro evaluation ofantiproliferative potential of topical cyclo-oxygenase inhibitors in human Tenon's fibroblasts. Exp Eye Res 1993;57:97-105.
14. Nguyen KD, Lee DA. Effect of steroids and nonsteroidal antiinflammatory agents on human ocular fibroblast. Invest Ophthalmol Vis Sci 1992;33:2693-70 I.
15. Hersh PS, Rice 8A, 8aer JC, et al. Topical nonsteroidal agents and corneal wound healing. Arch Ophthalmol 1990; 108:577-83.
16. Miller D, Gruenberg P, Miller R, Bergamini MVW. Topical flurbiprofen or prednisolone. Effect on corneal wound healing in rabbits. Arch Ophthalmol 1981 ;99:681-2.
I7. Priestley GC. Effects of corticosteroids on the growth and metabolism of fibroblasts cultured from human skin. 8r J Dermatol 1978;99:253-61.
18. Hirata F, Schiffmann E, Venkatasubramanian K, et al. A phospholipase A2 inhibitory protein in rabbit neutrophils induced by glucocorticoids. Proc Natl Acad Sci USA 1980;77:2533-6.
19. Kantor TG. Current modalities in arthritic diseases. Am J Med 1987;83(Suppl 48):2-5.
20. Ku EC, Lee W, Kothari HV, Scholer DW. Effect of diclofenac sodium on the arachidonic acid cascade. Am J Med 1986;80(Suppl 48): 18-23.
21. Nishida T, Yasumoto K, Otori T, Desaki J. The network structure of corneal fibroblasts in the rat as revealed by scanning electron microscopy. Invest Ophthalmol Vis Sci 1988;29: 1887-90.
22. Gartry DS, Kerr Muir MG, Lohmann CP, Marshall J. The effect of topical corticosteroids on refractive outcome and corneal haze after photorefractive keratectomy. A prospective, randomized, double-blind trial. Arch Ophthalmol 1992;110:944-52.
474





























