Embed Size (px)
Citation preview

The LaryngoscopeLippincott Williams & Wilkins, Inc.© 2006 The American Laryngological,Rhinological and Otological Society, Inc.
Effect of Platelet Rich Plasma and FibrinSealant on Facial Nerve Regeneration in aRat Model
Tarik Y. Farrag, MD; Mohamed Lehar, MD; Pauline Verhaegen, MS; Kathryn A. Carson, ScM;Patrick J. Byrne, MD, FACS
Objective: To investigate the effects of plateletrich plasma (PRP) and fibrin sealant (FS) on facialnerve regeneration. Study Design: Prospective, ran-domized, and controlled animal study. Methods: Ex-periments involved the transection and repair of fa-cial nerve of 49 male adult rats. Seven groups werecreated dependant on the method of repair: suture;PRP (with/without suture); platelet poor plasma(PPP) (with/without suture); and FS (with/without su-ture) groups. Each method of repair was applied im-mediately after the nerve transection. The outcomesmeasured were: 1) observation of gross recovery ofvibrissae movements within 8-week period afternerve transection and repair using a 5-point scale andcomparing the left (test) side with the right (control)side; 2) comparisons of facial nerve motor action po-tentials (MAP) recorded before and 8 weeks afternerve transection and repair, including both thetransected and control (untreated) nerves; 3) histo-logic evaluation of axons counts and the area of theaxons. Results: Vibrissae movement observation: theinclusion of suturing resulted in overall improvedoutcomes. This was found for comparisons of the su-ture group with PRP group; PRP with/without suturegroups; and PPP with/without suture groups (P <.05). The PRP without suture group had a signifi-cantly greater degree of recovery than the PPP with-out suture group (P < .05), but it did not have betterperformance than suture group (P > .05). The move-ment recovery of the suture group was significantly
better than the FS group (P � .014). The recovery offunction of the PRP groups was better than that of theFS groups, although this did not reach statistical sig-nificance (P � .09). Electrophysiologic testing: therewas a significantly better performance of the suturegroup when compared with the PRP and PPP with-out suture groups in nerve conduction velocity (P <.05). The PRP with suture group had the best resultswhen compared with the suture as well as the PPPwith suture groups in duration and latency-2 of MAP(P < .05). For the FS groups, no results were founddemonstrating a biological effect. The PRP with su-ture group demonstrated the best performance in thelatency-2 and the area under the curve of MAP whencompared with the suture and FS with suture groups(P < .05). Histomorphometric analysis: PRP withsuture demonstrated the greatest increase in axoncounts when compared with suture, FS with suture,and PPP with suture groups (P < .05). There was nostatistically significant difference seen in axon diam-eter. Conclusion: The best results for the return offunction in our rat facial nerve axotomy models oc-curred when the nerve ends were sutured together.At the same time, the data demonstrated a measur-able neurotrophic effect when PRP was present, withthe most favorable results seen with PRP added tosuture. There was an improved functional outcomewith the use of PRP in comparison with FS or nobioactive agents (PPP). FS showed no benefit overconventional suturing in facial nerve regeneration.Our study provides the potential of a new clinicalapplication for PRP in peripheral nerve regenera-tion. Key Words: Facial nerve regeneration, plateletrich plasma, fibrin sealant.
Laryngoscope, 117:157–165, 2007
INTRODUCTIONPeripheral facial nerve palsy is a devastating condi-
tion. Restoration of function after transection of the facialnerve is poor, and occurrence of postparalytic sequelae isinevitable.1,2 Although epineural and fascicular suturingare the most widely used techniques for its repair,3 thereis a great deal of research being performed to search for
From the Department of Otolaryngology–Head and Neck Surgery(T.Y.F., M.L., P.J.B.), Johns Hopkins School of Medicine, Baltimore, Mary-land, U.S.A., Erasmus Medical School (P.V.), Rotterdam, The Netherlands,and the Department of Epidemiology (K.A.C.), Johns Hopkins BloombergSchool of Public Health, Baltimore, Maryland, U.S.A.
Editor’s Note: This Manuscript was accepted for publication Septem-ber 29, 2006.
This study was funded by a grant from Medtronics, Inc., U.S.A.Send correspondence to Dr. Patrick Joseph Byrne, Director of Facial
Plastic and Reconstructive Surgery, Department of Otolaryngology–Headand Neck Surgery, Assistant Professor, Johns Hopkins University Schoolof Medicine, 601 N. Caroline St. 6th Floor, Baltimore, MD 21287-0910,U.S.A. E-mail: [email protected]
DOI: 10.1097/01.mlg.0000249726.98801.77
Laryngoscope 117: January 2007 Farrag et al.: Platelet Rich Plasma/Fibrin Sealant in Facial Nerve Regeneration
157

improved techniques to enhance regeneration of injuredfacial nerve.4
Platelet rich plasma (PRP) is prepared by centrifuga-tion of the patient’s own blood.5 Platelets contain variousgrowth factors such as platelet-derived growth factor(PDGF), transforming growth factor-�, and vascular en-dothelial growth factor.5 When platelets are activated,they release these factors, which play important biologicalroles in various conditions.6 It has been demonstrated thatneurons express PDGF receptors7 and that PDGF-� hasbeen proven to be a mitogen and survival factor forSchwann cells with a trophic activity on neurons. Also, anaugmented PDGF-� expression in peripheral neurons hasbeen found after peripheral nerve injury,8 suggesting arole in peripheral nerve regeneration. These findings haveled some authors to investigate the effects of PDGF, whichhas been found to improve regeneration and remyelina-tion of the nervous system.9 Moreover, plasma, enrichedwith platelets provides a medium that allows for coagula-tion. The adhesive effect of this coagulation enabled theuse of PRP intraoperatively to help prevent or decreasesurgical bleeding.10,11 It is therefore hypothesized thatthe application of PRP to the transected peripheral nervecould better coapt the nerve ends, and at the same time, itprovides the nerve with a medium enriched with plateletgrowth factors to improve regeneration.
In addition, fibrin sealant (FS) has been used fornerve repair. All preparations of FS mimic the final com-mon pathway of the coagulation cascade in which fibrin-ogen is converted to fibrin in the presence of thrombin andcalcium.12,13 There is debate in the literature with regardto the effect of FS on peripheral nerve regeneration. Someauthors report better results than suturing after transec-tion of peripheral nerves.4,13 In contrast, others reportbetter results with suturing than FS3 or no appreciabledifference between the two techniques.14
Studies exist comparing the effects of FS and PRP,primarily in oral and maxillofacial surgery.11 In the cur-rent study, we report our findings on the effects of PRPand FS on facial nerve regeneration after its transectionin a rat model.
METHODSApproval for performing this study was obtained from the
institutional animal care and use committee.
AnimalsExperiments were carried out on 49 male Sprague-Dauley
rats weighing 250 to 300 g.
Surgical TechniquesAll rats underwent two procedures: first, a survival surgery
(left side) and second, a nonsurvival surgery (right and left sides),performed 8 weeks after the first surgery. All surgical procedureswere performed under aseptic conditions. Rats were anesthetizedwith xylazine hydrochloride (3 mg/kg) and ketamine hydrochlo-ride (100 mg/kg) by intramuscular injection. The microsurgicaltechniques were performed using a Zeiss operating microscope(Carl Zeiss, Inc., Thornwood, NY). In the first surgery, the leftfacial nerve trunk was exposed and transected midway betweenthe point of its exit from the stylomastoid foramen and the pointof its bifurcation, and then it was followed by immediate re-anastomosis. The animals were categorized into four main groupsaccording to the method of re-anastomosis:
● Suture: 11 rats, using 2 perineural 9–0 microsutures(Ethicon Inc, Somerville, NJ);
● PRP: 10 rats, (a) without suturing, 5 rats; (b) with sutur-ing, 5 rats.
Fig. 1. Pretreatment normal evoked muscle action potential (MAP)(top) compared with 8 weeks after transection and repair (bottom).There is decreased amplitude (bottom, represented by horizontalmarkers) and a prolonged initial latency period (until first verticalmarker). Distances between stimulating and recording electrodeswere provided to program to calculate conduction velocity.
Fig. 2. (A) Sample of nerve (1/4 of nerve area) as outlined usingsoftware program “Stereo-investigator.” (B) Augmented view of onearea of A that shows “acceptance” (green) region (axons counted byprogram) and “rejection” (red) region (axons not counted). Axons arecounted in counting frame that has area of 625 ı̀m2 (25 � 25 �m).The dx-dy is 2,500 ı̀m2 (50 � 50 �m).
Laryngoscope 117: January 2007 Farrag et al.: Platelet Rich Plasma/Fibrin Sealant in Facial Nerve Regeneration
158

● Platelet poor plasma (PPP): 10 rats, (a) without suturing,5 rats; (b) with suturing, 5 rats.
● FS: 18 rats, (a) without suturing, 12 rats; (b) with sutur-ing, 6 rats.
The muscle layers and skin were closed with 6–0 silk su-tures. After an 8-week interval, the second (nonsurvival) surgerywas performed (right and left sides).
PRP and PPP PreparationPRP and PPP were obtained through a simplified closed
centrifugation system (Magellan Autologous Platelet Separator,Medtronics, Inc., Minneapolis, MN), which uses autologous anti-coagulated blood. Six rats were killed to obtain the rat blood.Each cycle required 30 mL of blood, and PRP or PPP were sepa-rated by the system. The device had a special software program toprocess rat blood.
FS PreparationA commercial FS was used for nerve re-anastomosis in the
FS group (Tisseel-VH, Two-component, Vapor heated Fibrin Seal-ant Kit, Baxter Health Care, Westlake Village, CA):
Fig. 3. Whiskers movements across groups. (A) Median time to startmovement. (B) Movement rating after 8 week period.
TABLE I.Percent of Rats in Each Whisker Rating Class After 8 Weeks by
Treatment Group.
Whisker Rating
Group 0 1 2 3 4
Suture only 0 0 0 100 0
FS only 0 0 50 50 0
FS and suture 0 0 17 83 0
PRP only 0 20 80 0 0
PRP and suture 0 0 0 100 0
PPP only 0 100 0 0 0
PPP and suture 0 0 0 100 0
FS � fibrin sealant; PRP � platelet rich plasma; PPP � platelet poorplasma.
TAB
LEII.
Thre
e-W
ayC
omp
aris
onof
Sut
ure,
Pla
tele
tR
ich
Pla
sma
(PR
P)
Onl
y,an
dP
late
let
Poo
rP
lasm
a(P
PP
)O
nly
Gro
ups
(Med
ian
and
Ran
ge).
Rec
ord
ing
Left
PV
alue
Pos
ttre
atm
ent
PV
alue
Pos
ttre
atm
ent
Min
usP
retr
eatm
ent
Left
Min
usR
ight
Sut
ure
PR
PO
nly
PP
PO
nly
Sut
ure
PR
PO
nly
PP
PO
nly
Late
ncy-
1,m
s1.
2(�
0.1,
1.8)
1.1
(0.9
,1.7
)1.
7(1
.0,2
.6)
�.0
51.
3(0
.2,2
.0)
1.2
(0.6
,1.8
)1.
9(1
.2,2
.8)
�.0
5
Late
ncy-
2,m
s1.
1(0
.8,2
.2)
0.9
(0.9
,1.3
)1.
3(0
.9,1
.8)
�.0
51.
2(0
.9,2
.2)
1.0
(0.7
,1.7
)1.
3(1
.0,2
.1)
�.0
5
Dur
atio
n,m
s�
0.2
(�0.
6,2.
2)�
0.2
(�0.
5,0.
0)�
0.2
(�1.
1,�
0.1)
�.0
5�
0.1
(�0.
5,2.
0)�
0.3
(�0.
4,0.
2)�
0.3
(�0.
4,0.
0)�
.05
Am
plit
ude,
mA
�4.
7(�
5.0,
�3.
6)�
6.1
(�6.
1,�
3.1)
�5.
5(�
6.0,
�3.
8)�
.05
�4.
1(�
6.4,
�2.
4)�
3.9
(�7.
1,�
2.7)
�6.
3(�
6.8,
�5.
3)�
.05
Are
a,m
m2
�4.
1(�
5.1,
�3.
3)�
4.9
(�5,
�2.
9)�
4.8
(�5.
0,�
3.5)
�.0
5�
5.0
(�6.
0,�
3.8)
�3.
8(�
5.5,
�2.
7)�
4.8
(�5.
2,�
4.8)
�.0
5
CV
,m
/s�
11(�
15,�
7)�
12(�
14,�
11)
�17
(�18
,�13
)�
.05
�13
(�16
,�11
)�
14(�
17,�
6)�
16(�
20,�
15)
�.0
5
CV
�C
ond
uctio
nve
loci
ty.
Laryngoscope 117: January 2007 Farrag et al.: Platelet Rich Plasma/Fibrin Sealant in Facial Nerve Regeneration
159

● The fibrinogen concentration is 30 times that of humanblood, and it reproduces the last steps of the coagulationcascade (conversion of fibrinogen to fibrin).
● The contents are combined by using a double-syringeapplication system, with application then to the surgicalfield.
An amount of 0.3 to 0.5 mL from PRP, PPP, or FS was thenapplied to the equivalent group immediately after transection inbetween the two ends of the transected nerve while holding theperineurium of the nerve ends for an appropriate time beforewound closure (3–5 min). Application of PRP, PPP, or FS wasthrough double-syringe application system.
Methods of Functional Outcomes EvaluationSubjective vibrissae movement observation.The left-sided movements were assessed in comparison with
the right side using a 5-point scale: 0 � no movement, 1 � barelydetectable movement, 2 � less significant movement, 3 � signif-icant but asymmetric movement, and 4 � symmetric movement.Observed movement was recorded twice weekly for 8 weeks afterthe initial nerve transection and repair.
At the end of the 8-week period, the number of rats in eachtreatment group for each rating was counted and compared usingFisher’s exact test. Additional two-group and three-group com-parisons based on specific hypotheses were also performed usingFisher’s exact test.
Electrophysiologic testing.Electromyography recordings performed before axotomy (on
left side) and again 8 weeks after axotomy (on right “control” sideand posttreatment on left sides). The rats were anesthetized, andthe compound motor action potentials (MAPs) of the vibrissalpads were recorded by two monopolar needle electrodes insertedsubcutaneously at symmetric points in the vibrissal array. Themain trunk of the facial nerve was exposed and stimulated witha single electrode with a rectangular current pulse of 0.05 msduration delivered from a VikingQuest Portable 2-channel
Fig. 4. Median change in conduction velocity of muscle actionpotential across suture, platelet rich plasma only, and platelet poorplasma only groups. (A) Left side (posttreatment � pretreatment).(B) Posttreatment (left � right).
TAB
LEIII
.Th
ree-
Way
Com
par
ison
ofS
utur
e,P
late
let
Ric
hP
lasm
a(P
RP
)an
dS
utur
e,an
dP
late
let
Poo
rP
lasm
a(P
PP
)an
dS
utur
eG
roup
s(M
edia
nA
ndR
ange
).
Rec
ord
ing
Left
PV
alue
Pos
ttre
atm
ent
PV
alue
Pos
ttre
atm
ent
Min
usP
retr
eatm
ent
Left
Min
usR
ight
Sut
ure
PR
Pan
dS
utur
eP
PP
and
Sut
ure
Sut
ure
PR
Pan
dS
utur
eP
PP
and
Sut
ure
Late
ncy-
1,m
s1.
2(�
0.1,
1.8)
1.2
(1.0
,1.4
)1.
0(0
.7,1
.8)
�.0
51.
3(0
.2,2
.0)
0.9
(0.8
,1.3
)1.
4(0
.8,1
.6)
�.0
5
Late
ncy-
2,m
s1.
1(0
.8,2
.2)
0.6
(0.0
,1.0
)1.
3(0
.4,1
.7)
�.0
51.
2(0
.9,2
.2)
0.9
(0.2
,1.0
)1.
6(1
.0,2
.1)
�.0
5
Dur
atio
n,m
s�
0.2
(�0.
6,2.
2)�
0.6
(�0.
8,�
0.2)
�0.
1(�
0.3,
1.4)
�.0
5�
0.1
(�0.
5,2.
0)�
0.4
(�0.
6,�
0.1)
0.1
(0.0
,1.7
)�
.05
Am
plit
ude,
mA
�4.
7(�
5.0,
�3.
6)�
3.8
(�5.
2,�
3.7)
�3.
5(�
4.8,
�2.
6)�
.05
�4.
1(�
6.4,
�2.
4)�
3.6
(�4.
5,�
3.0)
�4.
9(�
6.8,
�3.
5)�
.05
Are
a,m
m2
�4.
1(�
5.1,
�3.
3)�
4(�
4.1,
�3.
3)�
3.4
(�4.
1,�
3.4)
�.0
5�
5.0
(�6.
0,�
3.8)
�3
(�4.
4,�
2.1)
�3
(�4.
8,�
2.2)
�.0
5
CV
,m/s
�11
(�15
,�7)
�14
(�17
,�12
)�
12(�
14,�
8)�
.05
�13
(�16
,�11
)�
14(�
15,�
9)�
15(�
18,�
11)
�.0
5
CV
�C
ond
uctio
nve
loci
ty.
Laryngoscope 117: January 2007 Farrag et al.: Platelet Rich Plasma/Fibrin Sealant in Facial Nerve Regeneration
160

electromyograph (Nicolet Biomedical, Madison, WI). The positionof stimulating electrodes was optimized to obtain an MAP thresh-old of less than 1.5 mA. All MAPs were obtained by supramaximalnerve stimulation and recorded with VikingQuest data-acquisitionsoftware. The program calculated the latencies of evoked MAPresponses, duration of MAP, peak-to-peak amplitude, conductionvelocity, and area under the curve for more estimation of re-innervated muscle fibers (Fig. 1).
Pretreatment recordings for the experimental (left) side pre-treatment were summarized by treatment group as medians andranges and compared across treatment groups. Difference inscores of posttreatment minus pretreatment for the experimentalside and also posttreatment for the experimental side minus thecontrol (right) side were calculated and summarized with medi-ans and ranges. Comparisons were made across all treatmentgroups using the nonparametric Kruskal-Wallis test. The sutureonly group was considered as a control treatment (standard of
care), and pair-wise comparisons were made for each of the othertreatment groups with the suture only group using the Wilcoxontwo-sample test. Additional two-group and three-group compari-sons based on specific hypotheses were also performed using theappropriate nonparametric test.
Histomorphometric analysis.Sacrifice was performed at the end of the end of the 8 week
period after the first surgery, and samples of facial nerve wereobtained. Two to 3 mm samples were obtained from the maintrunk of both sides at equivalent points, which was distal to thesite of transection. Fixation of the nerve biopsies was performedin 2% osmium tetroxide � 3% glut/4% paraformald at pH 7.4 for2 hours. The nerve was dehydrated and embedded in plastic(dodecenyl succinic anhydride and nadic methyl anhydride).Cross sections of 1 �m thickness were prepared, stained withtoluidine blue, and examined by light microscopy. The histologicanalysis of the facial nerve was performed digitally, and theaxons were counted and measured at a final magnification of�100 using a Nikon (Tokyo, Japan) camera with UPLAN oilimmersion objective. The observer was blinded in this evaluationof the different groups. Axon counts and the average area of theindividual axons were provided through software programs(Stereo Investigator and Neuro Explorer, MicroBright Field, Inc.,Williston, VT, U.S.A.) (Fig. 2). In this system, a two-dimensionalstereologic principle is used for the axons counts: an opticalfractionater, a sampling procedure that allows all axons to beequally represented. We have also used unbiased sampling sitesfor the morphometric analysis of the individual axons.
Results of the axons counts and the area of axons weresummarized as medians and ranges. Difference in scores of con-trol (right) side minus test (left) side were compared across alltreatment groups using a nonparametric Kruskal-Wallis test. Inaddition, the pair-wise comparisons were made for each of theother treatment groups to the suture only group using the Wil-
Fig. 5. Median change in muscle action potential latency-2 acrosssuture, platelet rich plasma and suture, and platelet poor plasmaand suture. (A) Left (posttreatment � pretratment). (B) Posttreat-ment (left � right).
Fig. 6. Median change in muscle action potential area under thecurve posttreatment (left � right) across fibrin sealant (FS) andsuture and FS only groups.
TABLE IV.Two-Group Comparison of Fibrin Sealant (FS) and Suture and FS Only (Median and Range).
Recording
Left
P Value
Posttreatment
P Value
Posttreatment Minus Pretreatment Left Minus Right
FS and Suture FS Only FS and Suture FS Only
Latency-1, ms 1.1 (1.0, 1.6) 1.2 (0.8, 2.3) �.05 1.1 (0.8, 1.6) 1.3 (0.8, 2.3) �.05
Latency-2, ms 1.2 (0.9, 1.5) 1.4 (0.2, 2.2) �.05 1.0 (0.8, 1.4) 1.5 (0, 2.4) �.05
Duration, ms 0.0 (�0.1, 0.4) 0.2 (�0.6, 0.6) �.05 �0.1 (�0.5, 0.6) 0.3 (�0.1, 0.9) �.1
Amplitude, mA �4.0 (�4.9, �3.2) �4.8 (�6.2, �2.9) �.05 �3.6 (�4.6, �2.8) �5.2 (�7.0, �3.2) �.1
Area, mm2 �3.2 (�4.3, �2.4) �3.2 (�5.3, �2.4) �.05 �3.2 (�3.8, �1.3) �4.5 (�5.4, �3.8) �.05
CV, m/s �14 (�17, �11) �14 (�17, �4) �.05 �14 (�17, �12) �13 (�20, �10) �.05
CV � Conduction velocity.
Laryngoscope 117: January 2007 Farrag et al.: Platelet Rich Plasma/Fibrin Sealant in Facial Nerve Regeneration
161

coxon two-sample test. Additional two-group and three-groupcomparisons based on specific hypotheses were also performedusing the appropriate nonparametric test. Statistical analysis ofthis study was performed using SAS version 9.1.3 (SAS Institute,Inc., Cary, NC). All P values are two sided.
RESULTS
Vibrissae Movement ObservationTime to onset of recovery.The PPP without suture group was the slowest group
to demonstrate recovery of movement after transectionand re-anastomosis. The suture groups, as well as thePRP and suture groups, were the earliest groups to startrecovery (Fig. 3A).
Final recovery (after 8 wk).
● PRP: inclusion of suturing resulted in an overall im-proved outcomes; this was in comparison with thefollowing groups: 1) suture versus PRP without su-ture groups (P � .05); 2) PRP with suture versus PRPgroups (P � .05); 3) PPP with suture versus PPPwithout suture groups (P � .05). The PRP with su-ture group did not have better performance com-pared with the suture group (P � .05). In addition,the PRP without suture group had a significantly
Fig. 7. Median change in latency-2 of muscle action potential acrosssuture, platelet rich plasma and suture, and fibrin sealant and suturegroups. (A) Left side (posttreatment � pretreatment). (B) Posttreatment(left � right).
TAB
LEV
.Th
ree-
Gro
upC
omp
aris
onof
Sut
ure,
Pla
tele
tR
ich
Pla
sma
(PR
P)
and
Sut
ure,
and
Fib
rinS
eala
nt(F
S)
and
Sut
ure
Gro
ups
(Med
ian
and
Ran
ge)
Rec
ord
ing
Left
PV
alue
Pos
ttre
atm
ent
PV
alue
Pos
ttre
atm
ent
Min
usP
retr
eatm
ent
Left
Min
usR
ight
Sut
ure
PR
Pan
dS
utur
eFS
and
Sut
ure
Sut
ure
PR
Pan
dS
utur
eFS
and
Sut
ure
Late
ncy-
1,m
s1.
2(�
0.1,
1.8)
1.2
(1.0
,1.4
)1.
1(1
.0,1
.6)
�.0
51.
3(0
.2,2
.0)
0.9
(0.8
,1.3
)1.
1(0
.8,1
.6)
�.0
5
Late
ncy-
2,m
s1.
1(0
.8,2
.2)
0.6
(0.0
,1.0
)1.
2(0
.9,1
.5)
�.0
51.
2(0
.9,2
.2)
0.9
(0.2
,1.0
)1.
0(0
.8,1
.4)
�.0
5
Dur
atio
n,m
s�
0.2
(�0.
6,2.
2)�
0.6
(�0.
8,�
0.2)
0.0
(�0.
1,0.
4)�
.05
�0.
1(�
0.5,
2.0)
�0.
4(�
0.6,
�0.
1)�
0.1
(�0.
5,0.
6)�
0.05
Am
plit
ude,
mA
�4.
7(�
5.0,
�3.
6)�
3.8
(�5.
2,�
3.7)
�4.
0(�
4.9,
�3.
2)�
.05
�4.
1(�
6.4,
�2.
4)�
3.6
(�4.
5,�
3.0)
�3.
6(�
4.6,
�2.
8)�
.05
Are
a,m
m2
�4.
1(�
5.1,
�3.
3)�
4(�
4.1,
�3.
3)�
3.2
(�4.
3,�
2.4)
�.0
5�
5.0
(�6.
0,�
3.8)
�3
(�4.
4,�
2.1)
�3.
2(�
3.8,
�1.
3)�
.05
CV
,m
/s�
11(�
15,�
7)�
14(�
17,�
12)
�14
(�17
,�11
)�
.05
�13
(�16
,�11
)�
14(�
15,�
9)�
14(�
17,�
12)
�.0
5
CV
�C
ond
uctio
nve
loci
ty.
TABLE VI.Median of Difference of Test (Left) Minus Control (Right) Sides ofHistologic Evaluation of Facial Nerve Main Trunk Among Suture,Platelet Rich Plasma (PRP) and Suture, and Platelet Poor Plasma
(PPP) and Suture Groups.
Suture PRP and Suture PPP and Suture P Value
Axon counts �400 19312 10366 �.05
Area of axon(�m2)
�13.09 �13.84 �12.06 �.05
Laryngoscope 117: January 2007 Farrag et al.: Platelet Rich Plasma/Fibrin Sealant in Facial Nerve Regeneration
162

better recovery than the PPP without suture group(P � .05).
● FS: the suture group had a significantly better recov-ery than the FS without suture group (P � .05).
● PRP versus FS: recovery of function of the PRPwithout suture group was better than the FS with-out suture group, although this did not reach sta-tistical significance (P � .1) (Table I) (Fig. 3B).
Electrophysiologic testing.Initial recordings were obtained on the left (transected)
side of each rat pre-axotomy (pretreatment). The medianin the recorded values for latencies, duration, amplitude,area, and conduction velocity were compared between thegroups. There was no statistically significant differencesin the comparisons across the groups in their pre-axotomyrecordings (P � .05).
After 8 weeks, recordings were obtained on the treatedleft (transected) side and the untreated right (control ornontransected) side, where differences between left andright sides were calculated. In addition, pre- and posttreat-ment recordings on the left side were also calculated. Record-ings were then compared across the different groups.
● PRP, evaluation of the “adhesive” effect of PRP:there was a significantly better performance of thesuture group when compared with the PRP andPPP without suture groups in nerve conductionvelocity (P � .05); also, the PPP only group had theworst performance (Table II) (Fig. 4).
● PRP, evaluation of the “neurotrophic” effect ofPRP: the PRP with suture group had the best re-sults compared with the suture and PPP with su-
ture groups in duration and latency-2 of MAP (P �.05), (Table III) (Fig. 5).
● FS: the only parameter that met statistical signif-icance in which the FS with suture group had bet-ter performance than the FS only group was thearea under the curve of MAP in comparing thedifference between the posttreatment recordings ofthe left and right sides (P � .05) (Table IV) (Fig. 6).
● PRP versus FS: the PRP with suture group signif-icantly had the best performance in latency-2 andarea under the curve of the action potentials whencompared with the suture and FS with suturegroups (P � .05) (Table V) (Fig. 7).
Histomorphometric analysis.
● PRP: the PRP and suture group demonstrated thegreatest increase in the axon counts after treat-ment when compared with the suture and the PPPwith suture groups (P � .05) (Table VI) (Fig. 8A).
● FS: the histomorphometric analysis did not dem-onstrate any statistically significant findings incomparing the FS, FS with suture, and suturegroups.
● PRP versus FS: the PRP with suture group dem-onstrated the greatest increase in the axon countsafter treatment when compared with the sutureand the FS with suture groups (P � .05) (Table VII)(Fig. 8B).
DISCUSSIONThe obstacles to successful facial reanimation after
transection are formidable. Although repair of the injurednerve is often possible with a microsurgical technique, theresults are typically disappointing. The reasons for thisare complex. On the one hand, the effectiveness of axonalregeneration is often poor. On the other hand, synkinesis,the aberrant regeneration with subsequent disorderedmovement, inevitably occurs with significant regenera-tion. Progress in this regard will require more effectiveregeneration. Not only will axonal regeneration need to beenhanced, but this process will also need to be more accu-rate as well. This study was intended to investigate justone component of such a strategy, which is the potentialfor increasing axonal regeneration through the applica-tion of readily available, autogenous growth factors.
Our results demonstrate a measurable neurotrophiceffect of PRP on facial nerve regeneration after transec-tion in a rat model. This was particularly true when thePRP was used in conjunction with conventional suturing.
Fig. 8. Median difference in axon counts of test (left) minus control(right) sides of histologic evaluation of main trunk of facial nerveacross different groups.
TABLE VII.Median of Difference of Control (Right) Minus Test (Left) Sides ofHistologic Evaluation of Facial Nerve Main Trunk Among Suture,Platelet Rich Plasma (PRP) and Suture, and Fibrin Sealant (FS)
and Suture Groups.
Suture PRP and Suture FS and Suture P Value
Axon counts �400 19312 4246 �.05
Area of axon(�m2)
�13.09 �13.84 �14.19 �.05
Laryngoscope 117: January 2007 Farrag et al.: Platelet Rich Plasma/Fibrin Sealant in Facial Nerve Regeneration
163
This is based on the statistically significant results thatwe found when transected facial nerve was treated withPRP with suture: 1): vibrissae movement evaluation ofthis group demonstrated a more rapid recovery; 2) elec-trophysiologic testing of this group demonstrated that itsMAP had the lowest prolongation of latency-2 after treat-ment; and 3) histologic evaluation of this group demon-strated the greatest increase in the axon counts aftertreatment. These findings are supported by previous stud-ies that documented a neurotrophic effect of plateletgrowth factors on neurons.7,8 It is also to be noted that weevaluated outcomes in our facial nerve rat model after 8weeks from transection and repair, which has been dem-onstrated to be optimal to obtain successful results.15
The results for the group with suture and PRP weresuperior to the PRP without suture group. The adhesiveeffect of PRP does not appear to be sufficient for facialnerve repair after transection. It was noted on the surgicalexploration of transection sites that the groups with PRPwithout suture often demonstrated poor coaptation andnerve end alignment. The meticulous coaptation of thenerve ends is critical to good outcomes, and the PRPwithout suture did not appear to accomplish this to anacceptable level. At the same time, the superior results ofthe PRP without suture when compared with the PPPwithout suture groups that were consistently demon-strated in our study demonstrate the neurotrophic valueof PRP in improving the functional outcome of facial nerveregeneration.
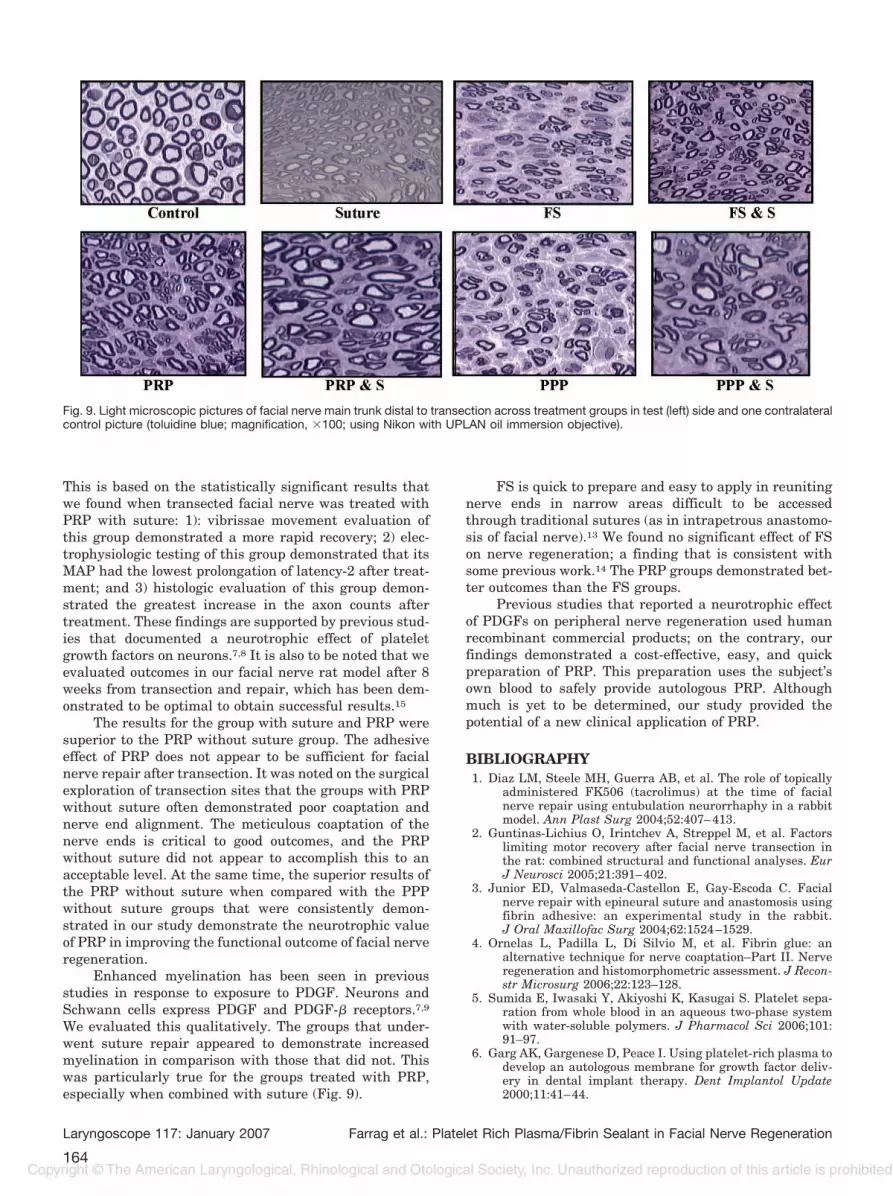
Enhanced myelination has been seen in previousstudies in response to exposure to PDGF. Neurons andSchwann cells express PDGF and PDGF-� receptors.7,9
We evaluated this qualitatively. The groups that under-went suture repair appeared to demonstrate increasedmyelination in comparison with those that did not. Thiswas particularly true for the groups treated with PRP,especially when combined with suture (Fig. 9).
FS is quick to prepare and easy to apply in reunitingnerve ends in narrow areas difficult to be accessedthrough traditional sutures (as in intrapetrous anastomo-sis of facial nerve).13 We found no significant effect of FSon nerve regeneration; a finding that is consistent withsome previous work.14 The PRP groups demonstrated bet-ter outcomes than the FS groups.
Previous studies that reported a neurotrophic effectof PDGFs on peripheral nerve regeneration used humanrecombinant commercial products; on the contrary, ourfindings demonstrated a cost-effective, easy, and quickpreparation of PRP. This preparation uses the subject’sown blood to safely provide autologous PRP. Althoughmuch is yet to be determined, our study provided thepotential of a new clinical application of PRP.
BIBLIOGRAPHY1. Diaz LM, Steele MH, Guerra AB, et al. The role of topically
administered FK506 (tacrolimus) at the time of facialnerve repair using entubulation neurorrhaphy in a rabbitmodel. Ann Plast Surg 2004;52:407–413.
2. Guntinas-Lichius O, Irintchev A, Streppel M, et al. Factorslimiting motor recovery after facial nerve transection inthe rat: combined structural and functional analyses. EurJ Neurosci 2005;21:391–402.
3. Junior ED, Valmaseda-Castellon E, Gay-Escoda C. Facialnerve repair with epineural suture and anastomosis usingfibrin adhesive: an experimental study in the rabbit.J Oral Maxillofac Surg 2004;62:1524–1529.
4. Ornelas L, Padilla L, Di Silvio M, et al. Fibrin glue: analternative technique for nerve coaptation–Part II. Nerveregeneration and histomorphometric assessment. J Recon-str Microsurg 2006;22:123–128.
5. Sumida E, Iwasaki Y, Akiyoshi K, Kasugai S. Platelet sepa-ration from whole blood in an aqueous two-phase systemwith water-soluble polymers. J Pharmacol Sci 2006;101:91–97.
6. Garg AK, Gargenese D, Peace I. Using platelet-rich plasma todevelop an autologous membrane for growth factor deliv-ery in dental implant therapy. Dent Implantol Update2000;11:41–44.
Fig. 9. Light microscopic pictures of facial nerve main trunk distal to transection across treatment groups in test (left) side and one contralateralcontrol picture (toluidine blue; magnification, �100; using Nikon with UPLAN oil immersion objective).
Laryngoscope 117: January 2007 Farrag et al.: Platelet Rich Plasma/Fibrin Sealant in Facial Nerve Regeneration
164

7. Eccleston PA, Funa K, Heldin CH. Expression of platelet-derived growth factor (PDGF) and PDGF alpha- and beta-receptors in the peripheral nervous system: an analysis ofsciatic nerve and dorsal root ganglia. Dev Biol 1993;155:459–470.
8. Oya T, Zhao YL, Takagawa K, et al. Platelet-derived growthfactor-b expression induced after rat peripheral nerve in-juries. Glia 2002;38:303–312.
9. Allamargot C, Pouplard-Barthelaix A, Fressinaud C. A singleintracerebral microinjection of platelet-derived growth fac-tor (PDGF) accelerates the rate of remyelination in vivo.Brain Res 2001;918:28–39.
10. Della Valle A, Sammartino G, Marenzi G, et al. Prevention ofpostoperative bleeding in anticoagulated patients undergo-ing oral surgery: use of platelet-rich plasma gel. J OralMaxillofac Surg 2003;61:1275–1278.
11. Whitman DH, Berry RL, Green DM. Platelet gel: an autolo-gous alternative to fibrin glue with applications in oral and
maxillofacial surgery. J Oral Maxillofac Surg 1997;55:1294–1299.
12. Sirieix D, Chemla E, Castier Y, et al. Comparative study ofdifferent biological glues in an experimental model of sur-gical bleeding in anesthetized rats: platelet-rich and -poorplasma-based glue with and without aprotinin versus com-mercial fibrinogen-based glue. Ann Vasc Surg 1998;12:311–316.
13. Bento RF, Miniti A. Comparison between fibrin tissue adhe-sive, epineural suture and natural union in intratemporalfacial nerve of cats. Acta Otolaryngol Suppl 1989;465:1–36.
14. Suri A, Mehta VS, Sarkar C. Microneural anastomosis withfibrin glue: an experimental study. Neurol India 2002;50:23–26.
15. Streppel M, Angelov DN, Guntinas-Lichius O, Neiss WF.Quantitative determination of specific reinnervation aftersuture of the facial nerve in the rat. HNO 1998;46:587–591.
Laryngoscope 117: January 2007 Farrag et al.: Platelet Rich Plasma/Fibrin Sealant in Facial Nerve Regeneration
165





























