Embed Size (px)
Citation preview

doi:10.1006/cyto.2002.1996
EFFECTS OF INTERLEUKIN-8 ON THEDEVELOPING HUMAN INTESTINE
Akhil Maheshwari,1 Wenge Lu,1 Atilano Lacson,2 Aaron A. Barleycorn,1
Sheila Nolan,1 Robert D. Christensen,1 Darlene A. Calhoun1
The human fetal/neonatal gastrointestinal tract is exposed to biologically significant concen-trations of interleukin (IL)-8 swallowed with amniotic fluid and human milk. We hypothesizedthat IL-8 has a physiologic function in the developing human intestine. IL-8 was measured inpreterm and term human milk, tested for stability under conditions simulating neonatal gastricand proximal small intestinal digestion, and its receptors were sought in human fetal bowel. Theeffect of IL-8 was then measured on intestinal cells in vitro. We observed that IL-8 is present insignificant concentrations in human milk and that it is stable under conditions simulatingdigestion. Both IL-8 receptors, CXCR1 and CXCR2, are expressed extensively in the fetalintestine. When human fetal and adult intestinal cells are treated with rhIL-8 in vitro, there is aconsistent increase in cell migration, proliferation, and differentiation. IL-8 also protectsintestinal cells against chemical injury. These results suggest that besides its better-known roleas a neutrophil chemoattractant, IL-8 has a trophic function in the developing human intestine.
� 2003 Elsevier Science Ltd. All rights reserved.
From the 1Division of Neonatology, Department of Pediatrics,University of South Florida College of Medicine, Tampa,FL, USA and the All Children’s Hospital, Saint Petersburg,FL, USA; 2Department of Pathology, All Children’s Hospital,Saint Petersburg, FL, USA
Correspondence to: Akhil Maheshwari, MD, 140 7th Ave S, CRI2006, Saint Petersburg, FL 33701, USA Tel: +(727) 553-1220;Fax: +(727) 553-1231. E-mail: [email protected]
Received 6 August 2002; revised 19 October 2002; accepted forpublication 4 November 2002
1043–4666/03/$-see front matter � 2003 Elsevier Science Ltd. Allrights reserved.
KEY WORDS: breastmilk/chemokine/fetal /interleukin-8/intestine
The human fetal/neonatal gastrointestinal tract isexposed to significant concentrations of interleukin(IL)-8 swallowed with, initially, amniotic fluid (AF),and later, human milk (HM).1–13 IL-8 is a potentchemotactic cytokine for neutrophils, and is viewed asa pro-inflammatory mediator and a marker of inflam-mation.14 High AF IL-8 levels occur in preterm labor,prolonged rupture of membranes, and intra-amnioticinfection, and these concentrations parallel other pro-inflammatory cytokines like IL-6.4,10,11,15–22 Elevatedhuman milk concentrations of IL-8 have also beendemonstrated in subclinical or overt mastitis.23–26 Inthe neonate, elevated serum IL-8 concentrations havebeen observed in sepsis, necrotizing enterocolitis, andvarious other inflammatory states.27–32
Concerns exist that exposure to high AF concen-trations of pro-inflammatory cytokines such as IL-8might predispose the fetus to adverse immediate and
256
long-term outcomes. Intra-uterine exposure to higherIL-8 and other pro-inflammatory cytokines present inAF is associated with an increased risk of chronic lungdisease,33–35 and adverse neurodevelopmental out-come.36 Although its effect on the fetal intestine is notknown, there are suggestions that the immature fetalgastrointestinal system may be less capable of regulat-ing the pro-inflammatory cascades, and thus may be ata higher risk of necrotizing enterocolitis with a varietyof etiologic insults. Gut tissue IL-8 levels have beenproposed as a marker of such inflammation.37
Despite concerns about potential adverse effects,evidence suggests that IL-8 has a physiologic role in theintestinal mucosa. Pro-inflammatory cytokines maystimulate DNA synthesis and induce mitogenic activityin small intestinal cells.38,39 Wilson and colleaguesshowed that IL-8 can stimulate migration of adulthuman colonic epithelial cells in vitro.40 Thus, itremains unclear whether increased local expressionof IL-8 upon exposure to infectious agents amplifiesdamage, or may have some protective function.
Since the fetal tissues are exposed to significantconcentrations of IL-8 in AF and extra-embryoniccoelomic fluid from very early in gestation,1 andbecause of the effects on intestinal cells, we hypoth-esized that IL-8 has a physiologic function in thedeveloping human intestine. To test this, we measuredIL-8 concentrations in human milk, tested this forstability in neonatal gastric and proximal smallintestinal conditions, sought IL-8 receptors in human
CYTOKINE, Vol. 20, No. 6 (21 December), 2002: pp 256–267

IL-8 and developing human intestine / 257
fetal bowel, and measured the effect of IL-8 on fetalintestinal cells.
RESULTS
Figure 1. IL-8 concentrations in human milk depicted as a function of days postpartum.
Milk IL-8 concentrations were measured by ELISA on clear supernatants following centrifugation. The data points in this scatter-plot conformto a linear regression model IL-8 concentration=1501.39–26.34 *Day postpartum. (F=9.53, r2=0.12; P=0.003).
IL-8 ELISAThe IL-8 ELISA was standardized for milk
samples. A quenching effect of milk was observed, suchthat 69–88% of the added rhIL-8 was measured.Thirty-two women donated a total of 75 milk samples,including 13 having donated more than one. Eighteenof these women had delivered preterm (mean�SD=29�2 weeks), while the other fourteen had delivered atterm (38�0.5 weeks). These women were enrolled inthe study at 3–65 days following delivery (median=7.5 days), and donated weekly samples 3–95 daysfollowing delivery.
IL-8 was detectable in most milk samples providedby all of the participating mothers (median 124 pg/ml;
range: <10–12 472 pg/ml). The concentrations werehighest in the immediate postpartum period, anddecreased significantly after the first week (median1212 pg/ml, range 81–12 472 pg/ml in the first week vsmedian 71 pg/ml, range: <10–926 pg/ml in latersamples; P<0.001). Time postpartum was nega-tively correlated with IL-8 concentrations in milk(Spearman’s r5�0.737, P<0.001) (Fig. 1). In samplesprovided by three of the participating women, the IL-8concentrations decreased to below the lower limit ofdetection (two of these women started with lowerinitial concentrations (81 and 282 pg/ml, respectively,compared to the first week median 1212 pg/ml;P<0.001), while in the third case, the concentrationsdecreased progressively and became undetectable 88days postpartum.
IL-8 concentrations were significantly higher inpreterm human milk (median 325 pg/ml; range:<10–12 472 pg/ml) as compared to term (median229 pg/ml; range 35–7210 pg/ml) (P=0.047). As the

258 / Maheshwari et al. CYTOKINE, Vol. 20, No. 6 (21 December, 2002: 256–267)
term samples were all within the first 28 days oflife, preterm samples collected only during a similarperiod were used for comparison (time elapsed post-partum being a significant determinant of milk IL-8concentration, vide supra).
We compared IL-8 concentrations in simul-taneous milk and serum samples (n=5). The two setswere significantly different (means�SD=38�9 pg/mlvs 83�18 pg/ml, respectively; P=0.001) and correlatedpoorly (r=0.73, P=0.155). IL-8 concentrations weresimilar in fore- and hind-milk samples (means�SD=41�8 pg/ml and 40�11 pg/ml, respectively), andcorrelated significantly (r=0.89, P=0.04).
IL-8 resistance to simulations of digestionThe stability of milk-borne rhIL-8 was evaluated
using simulated pre-prandial gastric, post-prandialgastric, and proximal small intestinal conditions. Theassays were performed in preterm and term subgroups:term or preterm human milk samples were incubatedwith pooled neonatal gastric secretions from thecorresponding defined gestational age group (n=5 ineach category). IL-8 concentrations did not changewith time in any of three simulated conditions (Fig. 2;one-factor repeated measures ANOVA, P=0.15–0.70).The assays were repeated with unspiked humanmilk samples (n=3) to identify any differences instability between recombinant and natural IL-8. The
concentrations did not differ significantly with time(P=0.72–0.93).
IL-8 receptorsReverse transcriptase polymerase chain (RT-
PCR) on human fetal intestinal samples consistentlyshowed the presence of a 200 bp electrophoretic band,corresponding to the PCR product of CXCR1 and/orCXCR2. This suggested that at least one of the twoIL-8 receptor genes was being transcribed in humanfetal intestinal tissue. Immunohistochemistry forCXCR1 and CXCR2 proteins individually confirmedthat both proteins are expressed extensively in humanfetal intestine at 20–24 weeks on the brush borderepithelium, lamina propria and the muscularis layers(Fig. 3). All the three cell lines (Caco-2, H4 andFHs-74-Int) also showed strong positive staining forboth CXCR1 and CXCR2.
Figure 2. Error bars showing simulations of neonatal gastric and proximal intestinal digestion.
Human milk samples were spiked with rhIL-8 and incubated with neonatal gastric secretions :(a) preterm and (b) term, in pre-prandial gastric(pH=3.2), post-prandial gastric (pH=5.8), and proximal intestinal (pH=7.4) conditions. Milk-borne IL-8 concentrations were measured byELISA. The error bars depict the means�S.E.M.
Effect of IL-8 on intestinal cell migrationThe cells migrating across the culture wound were
counted after treatment with rhIL-8 for 24 h (Fig. 4).Caco-2 cells showed significantly increased migrationat 0.01 (P=0.004), 1 (P=0.035), and 10 (P<0.001) nM.H4 cells showed a single peak at 100 nM (P<0.001).The FHs-74-Int cells showed increased migration at 1(P<0.001), 10 (P<0.001), and 100 (P<0.001) nM.

IL-8 and developing human intestine / 259
Effect of IL-8 on intestinal cell proliferationThe effect of IL-8 on cell proliferation was
measured by cellular BrdU incorporation (Fig. 5).Caco-2 cells showed significantly increased prolifer-ation at 0.1 (P=0.004) and 10 (P=0.003) nM ofrhIL-8. H4 cells showed increased proliferation at 0.01(P=0.012) and 10 (P=0.001) nM. The FHs-74-Int cellsshowed results similar to the H4 cell line, althoughthe optical density difference reached statisticalsignificance only at 10 nM (P<0.001).
Effect of IL-8 on intestinal cell differentiationThe effect of IL-8 on cell differentiation was
measured by cellular alkaline phosphatase expression(Fig. 6). The slide method was validated with ap-nitrophenyl phosphate tube assay; the results werequalitatively similar in terms of the enzyme expressionpeaks at various rhIL-8 concentrations. Caco-2 cellsshowed significantly increased AP expression at 0.01,
0.1, 1, 10, and 100 nM of rhIL-8 (all P values <0.001).H4 cells showed increased AP expression at 10(P<0.001) nM, while the FHs-74-Int cells showedincreased levels at 10 and 100 nM of rhIL-8 (P<0.001at both concentrations).
Figure 3. Immunohistochemistry for IL-8 receptors on fetal small intestine
Representative sections of human fetal small intestine (20–24 weeks gestation) showing (a) Negative control (b) CXCR1 (c) CXCR2immunoreactivity on the brush border epithelium (1), lamina propria (2), and the muscularis (3) layers. An enzyme-labeled biotin-streptavidintechnique was used with diaminobenzidine tetrahydrochloride as the chromogen (brown).
Protection against chemical injuryThe cytoprotective effect of IL-8 was quantified as
cell viability following exposure to tumour necrosisfactor alpha (TNF-�) and cydoheximide (CHI)(Fig. 7). When Caco-2 cells were pre-treated withrhIL-8 for 24 h prior to injury, they showed signifi-cantly increased viability at 0.1 (P=0.008) and 1(P=0.013) nM. When the cells were treated withrhIL-8 at the time of injury, higher viability wasobserved at 1 nM (P=0.002). For H4 cells, rhIL-8 hada protective effect at 0.1 nM (P=0.015) when added tothe medium 24 h prior to injury, and at 0.01 (P<0.001)and 0.1 (P=0.002) nM when added at the time of

260 / Maheshwari et al. CYTOKINE, Vol. 20, No. 6 (21 December, 2002: 256–267)
injury. The FHs-74-Int cells were protected at 0.01(P=0.007), 0.1 (P=0.004), and 1 (P=0.015) nM whenrhIL-8 was added 24 h before injury, and at 0.1 nM(P=0.008), when added at the time of injury.
Figure 4. Effect of IL-8 on intestinal cell migration in vitro.
Error-bar diagram showing the effect of rhIL-8 on intestinal cell migration in vitro: (a) Caco-2 cells (b) H4 cells (c) FHs-74–Int cells. The assayis based on the counts of migrating cells across wounds on culture monolayers (*P<0.05, **P<0.01, ***P<0.001). The error bars depict themeans�S.E.M.
Figure 5. Effect of IL-8 on intestinal cell proliferation in vitro.
Error-bar diagram showing the effect of rhIL-8 on intestinal cell proliferation in vitro: (a) Caco-2 cells (b) H4 cells (c) FHs-74-Int cells. Cellularproliferation was estimated by a cell ELISA for BrdU incorporation (*P<0.05, **P<0.01, ***P<0.001). The error bars depict themeans�S.E.M.
DISCUSSION
IL-8, the prototypal CXC chemokine in humans,is a potent neutrophil chemotactic factor. It is a crucialmediator in neutrophil-dependent acute inflammation,and elevated serum concentrations are associatedwith early and late-onset neonatal sepsis, necrotizingenterocolitis, and bronchopulmonary dysplasia.27–32
More recently, its actions are also being recognizedon cells of non-leukocytic lineage, and in regu-lation of epithelialization, tissue remodeling, andangiogenesis.14,48–52 It binds to two receptors, CXCR1
and CXCR2, which are both expressed in various fetaltissues since early stages of development.53,54
IL-8 is present in human milk, and the medianconcentrations we measured are comparable to thosereported by others.12,13,55 Our results, however, showa wider range (<10–12 472 pg/ml). Michie and col-leagues detected milk IL-8 concentrations of 500–6100 pg/ml,13 while Bottcher and coworkers reportedlevels of 100–5576 pg/ml.12 Although the reasons forthe inter-cohort differences remain unclear, variationin the incidence of subclinical mastitis (as reported inother studies in terms of markers such as milk sodiumconcentrations13 and sodium/potassium ratios56),concentrations of other immunomodulators such assoluble CD14,57 nutritional status, and ethnicity24,58
could be important factors. The effect of maternal drugtherapy, including steroids, may also be significant,and needs further study.

IL-8 and developing human intestine / 261
Figure 6. Effect of IL-8 on intestinal cell differentiation in vitro.
Error-bar diagram showing the effect of rhIL-8 on intestinal cell differentiation in vitro: (a) Caco-2 cells (b) H4 cells (c) FHs-74-Int cells. Celldifferentiation was studied with cellular alkaline phosphatase expression as a marker. The enzyme activity was assayed by using a modificationof the leukocyte alkaline phosphatase staining procedure and scoring for intracellular granules (table) (*P<0.05, **P<0.01, ***P<0.001). Theerror bars depict the means�S.E.M.
Figure 7. Protective effect of IL-8 on intestinal cells against chemical injury in vitro.
Clustered bar diagrams showing the effect of rhIL-8 on cell viability following exposure to TNF-� and cycloheximide: (a) Caco-2 cells (b) H4 cells(c) FHs-74-6Int cells. The three sets of bars represent control, effect of TNF-� and cycloheximide when cells were pre-treated with rhIL-8 for 24 h,and the effect when rhIL-8 was added at the same time as TNF-� and cycloheximide (*P<0.05, **P<0.01, ***P<0.001).
The differences we observed in IL-8 concen-trations between colostrum and mature human milkare similar to previously reported results.12,13 How-ever, previous studies have not reported the absence ofIL-8 in any milk samples, as compared to the negativeresults in some samples provided by three women inour cohort. Such variability is well known with otherchemokines such as RANTES (regulated on activation,normally T cell-expressed and secreted) and eotaxin,and with cytokines like IL-16 and IL-18.12,13,59 It isunclear if these negative samples represent a normalpostpartum decline of milk concentrations of IL-8alone, which started out lower, or if there is a sub-
population of women with subnormal milk concen-trations of multiple cytokines. We are currently study-ing the HM concentrations of other neutrophil-specificchemokines, which will shed some light on the mutualcorrelation between these levels.
We found higher IL-8 concentrations in humanmilk after preterm than after term deliveries. Michieand coworkers reported lower IL-8 concentrations inpreterm milk as compared to term.13 They alsodetected lower concentrations in preterm colostrum ascompared to mature preterm milk in the third week.This is different from our results where milk IL-8 levelscontinue to maintain a negative correlation with time
262 / Maheshwari et al. CYTOKINE, Vol. 20, No. 6 (21 December, 2002: 256–267)
elapsed postpartum in both the term and pretermsubgroups. These differences need to be studiedfurther, possibly in larger samples.
We also found a ‘‘quenching’’ effect of milk onconcentrations measured in ELISA.12,51,59 The reasonsfor this are unclear, although high fatty acid content ofmilk, which might result in decreased ligand-antibodybinding, has previously been incriminated.41
The discordance we observed between maternalserum and milk concentrations is consistent withcytokine secretion into milk being an active, localprocess of the mammary tissue.12,41,60,61 There is indi-rect support for this hypothesis from reports of intenseIL-8 immunoreactivity in the acinar epithelial cellsof normal mammary tissue, and also from studies onhuman mammary epithelial cells in culture.13,62
Our studies of simulated digestion suggest thatIL-8 is remarkably stable through the process of diges-tion in the neonate. These results are similar to thoseobtained with other cytokines such as erythropoietinand granulocyte-colony stimulating factor, and may berelated to the immature digestive capacity of the new-born infant and the presence of antiproteases in humanmilk.41–43,60 The assay is, however, somewhat limitedin the simulation of neonatal intestinal conditions andreproduces only the pH. The lack of neonatal smallintestinal secretions, for obvious ethical and logisticreasons, limits its validity in the distal small and largeintestinal conditions.
IL-8 receptors are expressed extensively on thefetal intestine, and the three cell lines used in this studyalso showed strong immunoreactivity for both CXCR1and CXCR2. As the morphologic differentiation of thefetal gut is nearly complete by 20 weeks of gestation,63
there is reason to believe that these findings can beextrapolated to the second half of gestation. This wasfurther indirect evidence that chemokines in AF andmilk may have a developmental role. We used estab-lished assays for cell migration, proliferation, differen-tiation and protection against cell injury to furtherdelineate these possibilities.
The migration of epithelial cells is an importantevent during development and in mucosal injuryrepair. Our data confirm the presence of a motogeniceffect of IL-8 on intestinal cells. However, fetal cellsmay be less sensitive than adult cells: with both H4 andthe FHs-74-Int cell lines, the results are tightly dose-dependent (at 1 and 10 nM). The motogenic effect onCaco-2 cells (which is an adult, malignant cell line)started at lower concentrations (0.01 nM), somewhatsimilar to the results reported by Wilson and colleagueswho also used a malignant adult colonic epithelial cellline, LIM 1215.40 The physiologic significance of thisdifference is not clear. The results with the adultepithelium may also need to be confirmed with aprimary cell line; any difference in adherence and
attachment properties of malignant cells is likely to actas a confounder.
Cell proliferation was studied using a BrdU-basedcolorimetric ELISA. We observed increased entero-cyte proliferation with IL-8, and the effects persistover a wide range of concentrations (0.01–10 nM).This is consistent with the findings of Zachrisson andcoworkers, who in their study on the effect of variouspro-inflammatory cytokines on intestinal cells reportedincreased DNA synthesis in the presence of 0.1 nMIL-8.39 The same authors, using adult duodenalexplants, reported increased metaphases in crypt cellsfollowing exposure to IL-8, suggesting that this effectof IL-8 persists beyond the neonatal period.38 It is alsointeresting that at very high doses, IL-8 seems to havean inhibitory effect on cultured enterocytes. Furtherstudies on the dose-response effects of IL-8 on theenterocyte cell-cycle are underway.
There was a consistent effect of IL-8 on cellularalkaline phosphatase expression, which is a marker ofcell differentiation.64,65 The effect in the two fetalprimary cell lines was most prominent at �10 nM, butthe effect was apparent at levels �0.01 nM withCaco-2 cells. While this dose-response difference couldbe due to a lower sensitivity of fetal intestinal cells, itcould have been confounded by the malignant natureof Caco-2 cells. More studies are needed to character-ize this effect further, focusing on brush border disac-charidases, transporter molecules, and intercellularjunctions.
We found a cytoprotective effect of IL-8 againstcell killing induced by co-treatment with TNF-� andCHI. This effect was examined when cells were pre-treated for 24 h, and also when IL-8 was added at thesame time as TNF-� and CHI. All the three cell lineswere protected at 0.01–1 nM. Since there is a protectiveeffect even in the subgroup with simultaneous IL-8treatment, it is likely that the higher number of viablecells in the IL-8 pre-treated group was not an artifactof its effect on cell proliferation. Furthermore, theprotective action seems to be centrally weightedaround 0.1 nM, which is different than the peaksobserved with cell proliferation. In further studies, itmay be interesting to examine the effect of IL-8 withother types of cell injury, such as with hypoxia orbacterial toxins.
These results point towards a wide range ofactions of IL-8 on fetal intestinal cells. These dose-response effects, however, need to be further quanti-tatively analysed with other experimental and animalmodels. Differences between various cell lines, artifactsinherent with log-fold increments (a peak effect at1 nM may actually be somewhere in 0.1–10 nM range,i.e., 800–80 000 pg/ml), and lack of concurrent effectsof other cellular and non-cellular elements preclude

IL-8 and developing human intestine / 263
direct extrapolation to the more complex developmen-tal matrix of a growing intestine. Further studies arealso needed to evaluate the specific activities andligand-binding affinity of CXCR1 and CXCR2 inenterocytes. Similarly, the effect of the simultaneouspresence of multiple CXC chemokine ligands onreceptor sensitivity also remains to be seen.
Neonatal monocytes appear to have a lowercapacity to express IL-8 mRNA and protein comparedwith adult cells.66 The developmental delay of chemo-kine production in the fetus and the neonate could inpart be compensated initially by the amniotic fluid, andlater, bridged by human milk. The evidence that IL-8survives gastric and proximal intestinal digestive pro-cesses, and has numerous local effects on the intestinalepithelium, suggests that besides its better known pro-inflammatory role as a neutrophil chemoattractant, itmay also have a crucial, local trophic function in thedeveloping intestine.
MATERIALS AND METHODS
SubjectsThe study was conducted at the University of South
Florida Children’s Research Institute, and the All Children’sHospital, St Petersburg, FL during the period January–May2002, after approval by the local Institutional ReviewBoard. A written informed consent was obtained from allparticipating mothers prior to enrollment in the study.
‘‘Term’’ gestation was defined as >37 completed weeks,and ‘‘preterm’’ as <34 completed weeks; discontinuousgestational ages were chosen so as to select representativesamples. Thirty-two lactating women donated weekly breast-milk samples for 6 weeks. Mothers with symptoms suggestiveof mastitis (local pain, swelling, redness with or withoutconstitutional symptoms), or any other febrile illness wereexcluded. Milk samples were collected with a sterile syringefrom pumped milk. Participating mothers were providedsterile disposable syringes and 2 ml polypropylene tubes forthis purpose. Samples were refrigerated until collection andtransported to the laboratory on ice, where these were storedat �80�C. All the milk samples were analysed in batchesduring the study period, and the average storage time wasless than a month.
Gastric secretionsGastric contents were collected from infants having an
existing indwelling oro-/nasogastric catheter, who were lessthan 3 days of age, and were not receiving any oral feedings.Secretions were pooled separately as ‘‘term’’ and ‘‘preterm’’,and frozen at �80�C. At the time of assay, they were clearedof particulate material by centrifugation at 14 000�g for10 min.
IL-8 concentrationIL-8 was estimated in the aqueous fraction of milk
using an Enzyme Linked Immunosorbent Assay (ELISA)(Quantikine�, R & D Systems, Minneapolis, MN, USA).
The assay requires 50 �l of sample and detects 10–3000 pg/mlof IL-8. The intra- and inter-assay precision for milk sampleswas comparable (pilot testing) to figures reported by themanufacturer for serum and cell-culture supernatants.
The ELISA was also performed to identify any differ-ences in IL-8 concentrations in fore- and hind-milk samples(defined as the first and the last 5 min of pumping), and alsoon paired milk and maternal serum samples.
A standard curve was obtained using duplicate measure-ments of the standard solutions provided with the ELISA,and separate curves were generated using milk samples‘‘spiked’’ with recombinant IL-8 to assess the ELISA func-tion in milk. The curve generated using spiked samples wascompared to the standard curve to record any ‘‘quenching’’effects of milk.41 All samples with IL-8 concentrations atextremes of the observed range were re-tested to confirm theresults. Concentrations beyond the linear range of the assaywere confirmed by testing in dilution.
Simulations of digestionThe susceptibility of IL-8 to degradation in human milk
was evaluated with an in vitro simulation of neonatal diges-tion.42,43 Pooled, thawed, and cleared gastric secretions fromterm and preterm neonates were collected in two separategroups, and simulations were run for 0 (baseline degra-dation), 1, and 2 h. These intervals were selected becauseafter human milk feedings, maximal gastric acid proteolyticactivity occurs at 1 h, and although not continuous, gastricemptying generally occurs between 1 and 2 h. To approxi-mate neonatal gastrointestinal luminal conditions withoutinterfering with proteolytic activity, three incubation bufferswere used in standard reaction mixtures.42 The buffers con-sisted of: (1) 0.1 M glycine at pH 3.2 to simulate preprandialgastric conditions, (2) 0.1 M maleate at pH 5.8 to simulatepostprandial gastric conditions, and (3) 0.01 M Triswith 6.7 mM CaCl2 at pH 7.4 to simulate proximal smallintestinal conditions. The standard reaction mixture includedone of the three buffers, neonatal gastric secretions, and thesubstrate (preterm or term human milk).
To ensure that endogenous enzymes were active for eachsimulation, 50 � l of each of the three pH buffers waspreincubated for 15 min at 37�C with 50 �l aliquots ofneonatal gastric secretions. To start the reaction, a 50 �laliquot of substrate was added and incubated at 37�C (150 �ltotal volume). Reaction mixtures were evaluated at each pHbuffer condition, on all substrates, for baseline, 1 h and 2 h at37�C. At the end of incubations, 5�l of 1 M Tris buffer, pH 8,was added to stop the reaction. Samples were then frozen at�80�C until assay.
The milk samples were spiked with rhIL-8 so as toachieve approximate concentrations of 1500 pg/ml, whichwas about midway through the range of observed IL-8 levelsin human milk. We included five samples in each gestationalage-based subgroup; the number was chosen to attainadequate statistical power (80% at an �=0.05), based on theassumption that digestive losses of up to 50% of the originalmay still leave biologically significant amounts of IL-8.
The in vitro digestion studies were repeated with milksamples (n=3) known to have high concentrations of IL-8, soas to identify any differences in the susceptibility of naturaland recombinant IL-8 to neonatal digestion.

264 / Maheshwari et al. CYTOKINE, Vol. 20, No. 6 (21 December, 2002: 256–267)
RT-PCRThis step was performed on human fetal (22–24 weeks
gestation) intestinal tissue (n=3). The gene expression of thetwo IL-8 receptors, CXCR1 and CXCR2 was detected usingthe CytoXpress� Multiplex PCR Kit (Biosource Inter-national, Camarillo, CA, USA). The primer pairs utilized inthe reaction are (1) CXCR1: 5�-CGACTGTGGGCGGATTCTTG-3�, 5�-AGACCGATACCATGTGCTCT-3�; CXCR2:5�-ACGCATGTTGCTGTCTCTGG-3� and 5�-TGTTGGTCCTAGGGCGTAG-3�. CXCR1 and CXCR2 produce asingle band at �200 bp, and hence, a positive result indicatedthe presence of at least one of the two receptors.
ImmunohistochemistryThe expression of the two individual IL-8 receptor
proteins was studied by immunohistochemistry on fetal intes-tinal tissue samples (n=3, 22–24 weeks gestation. We usedmonoclonal anti-human CXCR1 (IL-8 RA) (Sigma,St. Louis, MO, USA) and CXCR2 (IL-8 RB) (R&D). Theseare affinity-purified mouse IgG-2a antibodies, without anymutual cross-reactivity. Sections of fetal intestine wereimmunostained using an automated system utilizing anenzyme-labeled biotin-streptavidin technique (Ventana,NexES�, Tucson, AZ, USA) with diaminobenzidine tetra-hydrochloride (DAB) as the chromogen. A similar procedurewas used for immunostaining the three cell lines (vide infra)for CXCR1 and CXCR2 expression.
Cell cultureThe effects of IL-8 on the fetal intestine were further
studied in vitro utilizing cultured intestinal epithelial cells.We used two fetal intestinal cell lines (H4 cells, gifted byProf. W. Allen Walker, Harvard University, Boston, MA,and the FHs-74-Int cells, purchased from ATCC, Rockville,MD, USA) and compared these with Caco-2 cells (ATCC),which are an established model for human adult smallintestinal epithelium. The H4 cell line has been developedfrom fetal small intestinal epithelial cells at 20–22 weekgestation, whereas the FHs-74-Int is derived from a12–16 week human fetus.44
Caco-2 cell cultureCaco-2 cells were cultivated on 75 cm2 flasks (Beckman
Diagnostics, Franklin Lakes, NJ, USA) using Dulbecco’smodified Eagle medium (DMEM) (Sigma) containing 10%fetal bovine serum (FBS) (HyClone, Logan, UT, USA), 1%nonessential amino acids (GIBCO), 100 units/ml of penicil-lin, and 100 �g/ml streptomycin (GIBCO). Cells were main-tained on a controlled atmosphere at 37�C, 95% relativehumidity, and 5% CO2. Culture medium was changed everyother day for 5–6 days until cells reached 80–90% confluency.For all experiments cells with passage numbers 60–80 wereutilized.
H4 cell cultureH4 cells were cultivated using DMEM (Sigma) contain-
ing 10% FBS (HyClone), 1% nonessential amino acids(GIBCO), 1% HEPES (GIBCO), 100 units/ml of penicillin,and 100 �g/ml streptomycin (GIBCO), 1% Na pyruvate(GIBCO), 1% L-glutamine (GIBCO), and 0.2 U/ml insulin
(Humulin-R, Eli Lilly). Cells were maintained on a similarcontrolled atmosphere at 37�C, 95% relative humidity, and5% CO2. Culture medium was changed every 3–4 days.For all experiments cells with passage numbers 30–35 wereutilized.
FHs-74-Int cell cultureCells were cultivated using Hybricare (DMEM with 1%
non-essential amino acids, 0.5 mM sodium pyruvate, 1 mMoxaloacetic acid, 0.2 units/ml insulin, 10% FBS) (ATCC),with added 0.2% Na bicarbonate, 30 ng/ml human epidermalgrowth factor (Sigma), 100 units/ml of penicillin, and 100 �g/ml streptomycin (GIBCO). These cells were also maintainedin a controlled 37�C, 95% relative humidity, and 5% CO2
atmosphere. Culture medium was changed every 2–3 days.For all experiments, cells with passage numbers 13–15 wereutilized.
All the three culture media were assayed for IL-8 so as toavoid any unaccounted exposures through FBS. At the FBSconcentrations used, all the three media tested negative.
Cell migration studiesWe studied cell migration across wounded intestinal
epithelial monolayers, based on the model used by Ciacci andcoworkers.45,46 Each of the three cell lines was plated into60 mm dishes to achieve 80% confluence. After 24 h ofincubation, the cultures were ‘‘wounded’’ in triplicate using asterile 4 mm plastic edge. Immediately after wounding, thecultures were washed with PBS and the media replaced. Theplates were then incubated for an additional 24 h withlog-fold incremental concentrations of rhIL-8 (0, 0.01, 0.1, 1,10 and 100 nM). Cell migration was evaluated 24 h afterwounding. Cells were fixed with 10% formaldehyde for20 min, and then lightly stained with hematoxylin (Sigma).The number of nuclei that had migrated past the wound edgewere counted in four high-power fields in each of the threelines. Thus, there were 12 data points per culture dish. Thenumbers of cells migrating per wound were compared withcontrol.
Cell proliferation experimentsCells were plated in 96-well plates at a density of
1–2�104 cells per well. After the cells had been allowed toattach for 24 h, the media were changed to phenol-red freemedia containing 0, 0.01, 0.1, 1, 10 or 100 nM of rhIL-8 andincubated for 3 days. The cells were then labeled withBromodeoxyuridine (BrdU) for 24 h, and then subjected to acell proliferation ELISA (Roche Diagnostics, Indianapolis,IN, USA). The cells were fixed, and treated with a mousemonoclonal anti-BrdU antibody conjugated with peroxidase.BrdU incorporation was quantified by adding a color-forming tetramethyl benzidine (substrate) solution andmeasuring the absorbance at 450 and 690 nm. Theabsorbance is related logarithmically to cell number in thisassay.
Cell differentiation experimentsCells were plated on a chamber slide at a density of
5�104 cells per chamber, and allowed to attach for 24 h. Themedium was then changed and the cells were exposed to
IL-8 and developing human intestine / 265
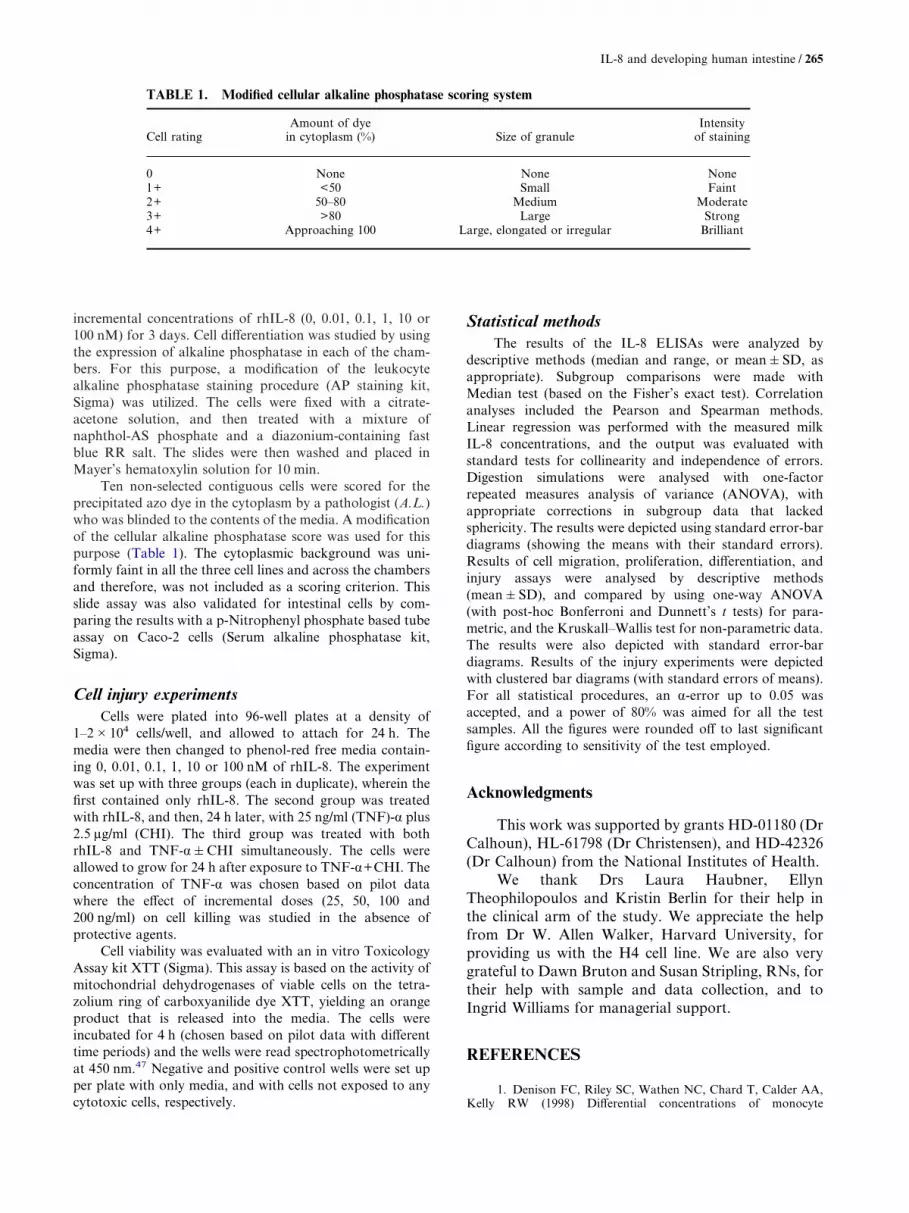
incremental concentrations of rhIL-8 (0, 0.01, 0.1, 1, 10 or100 nM) for 3 days. Cell differentiation was studied by usingthe expression of alkaline phosphatase in each of the cham-bers. For this purpose, a modification of the leukocytealkaline phosphatase staining procedure (AP staining kit,Sigma) was utilized. The cells were fixed with a citrate-acetone solution, and then treated with a mixture ofnaphthol-AS phosphate and a diazonium-containing fastblue RR salt. The slides were then washed and placed inMayer’s hematoxylin solution for 10 min.
Ten non-selected contiguous cells were scored for theprecipitated azo dye in the cytoplasm by a pathologist (A.L.)who was blinded to the contents of the media. A modificationof the cellular alkaline phosphatase score was used for thispurpose (Table 1). The cytoplasmic background was uni-formly faint in all the three cell lines and across the chambersand therefore, was not included as a scoring criterion. Thisslide assay was also validated for intestinal cells by com-paring the results with a p-Nitrophenyl phosphate based tubeassay on Caco-2 cells (Serum alkaline phosphatase kit,Sigma).
Cell injury experimentsCells were plated into 96-well plates at a density of
1–2�104 cells/well, and allowed to attach for 24 h. Themedia were then changed to phenol-red free media contain-ing 0, 0.01, 0.1, 1, 10 or 100 nM of rhIL-8. The experimentwas set up with three groups (each in duplicate), wherein thefirst contained only rhIL-8. The second group was treatedwith rhIL-8, and then, 24 h later, with 25 ng/ml (TNF)-� plus2.5 �g/ml (CHI). The third group was treated with bothrhIL-8 and TNF-��CHI simultaneously. The cells wereallowed to grow for 24 h after exposure to TNF-�+CHI. Theconcentration of TNF-� was chosen based on pilot datawhere the effect of incremental doses (25, 50, 100 and200 ng/ml) on cell killing was studied in the absence ofprotective agents.
Cell viability was evaluated with an in vitro ToxicologyAssay kit XTT (Sigma). This assay is based on the activity ofmitochondrial dehydrogenases of viable cells on the tetra-zolium ring of carboxyanilide dye XTT, yielding an orangeproduct that is released into the media. The cells wereincubated for 4 h (chosen based on pilot data with differenttime periods) and the wells were read spectrophotometricallyat 450 nm.47 Negative and positive control wells were set upper plate with only media, and with cells not exposed to anycytotoxic cells, respectively.
Statistical methodsThe results of the IL-8 ELISAs were analyzed by
descriptive methods (median and range, or mean�SD, asappropriate). Subgroup comparisons were made withMedian test (based on the Fisher’s exact test). Correlationanalyses included the Pearson and Spearman methods.Linear regression was performed with the measured milkIL-8 concentrations, and the output was evaluated withstandard tests for collinearity and independence of errors.Digestion simulations were analysed with one-factorrepeated measures analysis of variance (ANOVA), withappropriate corrections in subgroup data that lackedsphericity. The results were depicted using standard error-bardiagrams (showing the means with their standard errors).Results of cell migration, proliferation, differentiation, andinjury assays were analysed by descriptive methods(mean�SD), and compared by using one-way ANOVA(with post-hoc Bonferroni and Dunnett’s t tests) for para-metric, and the Kruskall–Wallis test for non-parametric data.The results were also depicted with standard error-bardiagrams. Results of the injury experiments were depictedwith clustered bar diagrams (with standard errors of means).For all statistical procedures, an �-error up to 0.05 wasaccepted, and a power of 80% was aimed for all the testsamples. All the figures were rounded off to last significantfigure according to sensitivity of the test employed.
Acknowledgments
This work was supported by grants HD-01180 (DrCalhoun), HL-61798 (Dr Christensen), and HD-42326(Dr Calhoun) from the National Institutes of Health.
We thank Drs Laura Haubner, EllynTheophilopoulos and Kristin Berlin for their help inthe clinical arm of the study. We appreciate the helpfrom Dr W. Allen Walker, Harvard University, forproviding us with the H4 cell line. We are also verygrateful to Dawn Bruton and Susan Stripling, RNs, fortheir help with sample and data collection, and toIngrid Williams for managerial support.
TABLE 1. Modified cellular alkaline phosphatase scoring system
Cell ratingAmount of dye
in cytoplasm (%) Size of granuleIntensity
of staining
0 None None None1+ <50 Small Faint2+ 50–80 Medium Moderate3+ >80 Large Strong4+ Approaching 100 Large, elongated or irregular Brilliant
REFERENCES
1. Denison FC, Riley SC, Wathen NC, Chard T, Calder AA,Kelly RW (1998) Differential concentrations of monocyte

266 / Maheshwari et al. CYTOKINE, Vol. 20, No. 6 (21 December, 2002: 256–267)
chemotactic protein-1 and interleukin-8 within the fluid compart-ments present during the first trimester of pregnancy. Hum Reprod13:2292–2295.
2. Santhanam U, Avila C, Romero R, Viguet H, Ida N,Sakurai S, Sehgal PB (1991) Cytokines in normal and abnormalparturition: elevated amniotic fluid interleukin-6 levels in womenwith premature rupture of membranes associated with intrauterineinfection. Cytokine 3:155–163.
3. Axemo P, Brauner A, Pettersson M, Eriksson L,Rwamushaija E, Bergstrom S (1996) Amniotic fluid interleukins inSwedish and Mozambican pregnant women. Gynecol Obstet Invest41:113–117.
4. Allbert JR, Naef RW, 3rd, Perry KG, Jr., Magann EF,Whitworth NS, Morrison JC (1994) Amniotic fluid interleukin-6 andinterleukin-8 levels predict the success of tocolysis in patients withpreterm labor. J Soc Gynecol Investig 1:264–268.
5. Hebisch G, Grauaug AA, Neumaier-Wagner PM,Stallmach T, Huch A, Huch R (2001) The relationship betweencervical dilatation, interleukin-6 and interleukin-8 during term labor.Acta Obstet Gynecol Scand 80:840–848.
6. Arntzen KJ, Kjollesdal AM, Halgunset J, Vatten L,Austgulen R (1998) TNF, IL-1, IL-6, IL-8 and soluble TNFreceptors in relation to chorioamnionitis and premature labor. JPerinat Med 26:17–26.
7. Dudley DJ, Hunter C, Mitchell MD, Varner MW (1994)Clinical value of amniotic fluid interleukin-6 determinations in themanagement of preterm labour. Br J Obstet Gynaecol 101:592–597.
8. Olah KS, Vince GS, Neilson JP, Deniz G, JohnsonPM (1996) Interleukin-6, interferon-gamma, interleukin-8, andgranulocyte- macrophage colony stimulating factor levels in humanamniotic fluid at term. J Reprod Immunol 32:89–98.
9. Stallmach T, Hebisch G, Joller H, Kolditz P, Engelmann M(1995) Expression pattern of cytokines in the different compartmentsof the feto-maternal unit under various conditions. Reprod FertilDev 7:1573–1580.
10. Saito S, Kasahara T, Kato Y, Ishihara Y, Ichijo M (1993)Elevation of amniotic fluid interleukin 6 (IL-6), IL-8 and granulocytecolony stimulating factor (G-CSF) in term and preterm parturition.Cytokine 5:81–88.
11. Laham N, Rice GE, Bishop GJ, Ransome C, Brennecke SP(1993) Interleukin 8 concentrations in amniotic fluid and peripheralvenous plasma during human pregnancy and parturition. ActaEndocrinol (Copenh) 129:220–224.
12. Bottcher MF, Jenmalm MC, Bjorksten B, Garofalo RP(2000) Chemoattractant factors in breast milk from allergic andnonallergic mothers. Pediatr Res 47:592–597.
13. Michie CA, Tantscher E, Schall T, Rot A (1998) Physio-logical secretion of chemokines in human breast milk. Eur CytokineNetw 9:123–129.
14. Mukaida N (2000) Interleukin-8: an expanding universebeyond neutrophil chemotaxis and activation. Int J Hematol 72:391–398.
15. Hitti J, Hillier SL, Agnew KJ, Krohn MA, Reisner DP,Eschenbach DA (2001) Vaginal indicators of amniotic fluid infectionin preterm labor. Obstet Gynecol 97:211–219.
16. Saji F, Samejima Y, Kamiura S, Sawai K, Shimoya K,Kimura T (2000) Cytokine production in chorioamnionitis. J ReprodImmunol 47:185–196.
17. Zhang W, Wang L, Zhao Y, Kang J (2000) Changes incytokine (IL-8, IL-6 and TNF-alpha) levels in the amniotic fluidand maternal serum in patients with premature rupture of themembranes. Zhonghua Yi Xue Za Zhi (Taipei) 63:311–315.
18. Gonzalez-Bosquet E, Cerqueira MJ, Dominguez C, GasserI, Bermejo B, Cabero L (1999) Amniotic fluid glucose and cytokinesvalues in the early diagnosis of amniotic infection in patients withpreterm labor and intact membranes. J Matern Fetal Med 8:155–158.
19. Hsu CD, Meaddough E, Aversa K, Hong SF, Lu LC, JonesDC, Copel JA (1998) Elevated amniotic fluid levels of leukemiainhibitory factor, interleukin 6, and interleukin 8 in intra-amnioticinfection. Am J Obstet Gynecol 179:1267–1270.
20. Hsu CD, Meaddough E, Aversa K, Copel JA (1998) Therole of amniotic fluid L-selectin, GRO-alpha, and interleukin-8 in the
pathogenesis of intraamniotic infection. Am J Obstet Gynecol178:428–432.
21. Cherouny PH, Pankuch GA, Romero R, Botti JJ, KuhnDC, Demers LM, Appelbaum PC (1993) Neutrophil attractant/activating peptide-1/interleukin-8: association with histologicchorioamnionitis, preterm delivery, and bioactive amniotic fluidleukoattractants. Am J Obstet Gynecol 169:1299–1303.
22. Puchner T, Egarter C, Wimmer C, Lederhilger F,Weichselbraun I (1993) Amniotic fluid interleukin-8 as a marker forintraamniotic infection. Arch Gynecol Obstet 253:9–14.
23. Semba RD, Kumwenda N, Taha TE, Hoover DR, Lan Y,Eisinger W, Mtimavalye L, Broadhead R, Miotti PG, Van DerHoeven L, Chiphangwi JD (1999) Mastitis and immunologicalfactors in breast milk of lactating women in Malawi. Clin Diagn LabImmunol 6:671–674.
24. Willumsen JF, Filteau SM, Coutsoudis A, Uebel KE,Newell ML, Tomkins AM (2000) Subclinical mastitis as a risk factorfor mother-infant HIV transmission. Adv Exp Med Biol 478:211–223.
25. Filteau SM, Lietz G, Mulokozi G, Bilotta S, Henry CJ,Tomkins AM (1999) Milk cytokines and subclinical breastinflammation in Tanzanian women: effects of dietary redpalm oil or sunflower oil supplementation. Immunology 97:595–600.
26. Barber MR, Yang TJ (1998) Chemotactic activities innonmastitic and mastitic mammary secretions: presence ofinterleukin-8 in mastitic but not nonmastitic secretions. Clin DiagnLab Immunol 5:82–86.
27. Schollin J (2001) Interleukin-8 in neonatal sepsis. ActaPaediatr 90:961–962.
28. Mehr SS, Doyle LW, Rice GE, Vervaart P, Henschke P(2001) Interleukin-6 and interleukin-8 in newborn bacterial infection.Am J Perinatol 18:313–324
29. Nupponen I, Andersson S, Jarvenpaa AL, Kautiainen H,Repo H (2001) Neutrophil CD11b expression and circulatinginterleukin-8 as diagnostic markers for early-onset neonatal sepsis.Pediatrics 108:E12.
30. Lacour AG, Gervaix A, Zamora SA, Vadas L, LombardPR, Dayer JM, Suter S (2001) Procalcitonin, IL-6, IL-8, IL-1receptor antagonist and C-reactive protein as identificators of seriousbacterial infections in children with fever without localising signs.Eur J Pediatr 160:95–100.
31. Edelson MB, Bagwell CE, Rozycki HJ (1999) Circulatingpro- and counterinflammatory cytokine levels and severity innecrotizing enterocolitis. Pediatrics 103:766–771.
32. Baier RJ, Loggins J, Kruger TE (2001) Monocyte chemo-attractant protein-1 and interleukin-8 are increased in broncho-pulmonary dysplasia: relation to isolation of Ureaplasmaurealyticum. J Investig Med 49:362–369.
33. Schmidt B, Cao L, Mackensen-Haen S, Kendziorra H,Klingel K, Speer CP (2001) Chorioamnionitis and inflammation ofthe fetal lung. Am J Obstet Gynecol 185:173–177.
34. Yoon BH, Romero R, Jun JK, Park KH, Park JD, GhezziF, Kim BI (1997) Amniotic fluid cytokines (interleukin-6, tumornecrosis factor-alpha, interleukin-1 beta, and interleukin-8) and therisk for the development of bronchopulmonary dysplasia. Am JObstet Gynecol 177:825–830.
35. Ghezzi F, Gomez R, Romero R, Yoon BH, Edwin SS,David C, Janisse J, Mazor M (1998) Elevated interleukin-8 concen-trations in amniotic fluid of mothers whose neonates subsequentlydevelop bronchopulmonary dysplasia. Eur J Obstet Gynecol ReprodBiol 78:5–10.
36. Yoon BH, Romero R, Park JS, Kim CJ, Kim SH, Choi JH,Han TR (2000) Fetal exposure to an intra-amniotic inflammationand the development of cerebral palsy at the age of three years. AmJ Obstet Gynecol 182:675–681.
37. Nanthakumar NN, Fusunyan RD, Sanderson I, WalkerWA (2000) Inflammation in the developing human intestine: Apossible pathophysiologic contribution to necrotizing enterocolitis.Proc Natl Acad Sci USA 97:6043–6048.
38. Zachrisson K, Neopikhanov V, Wretlind B, Uribe A (2001)Mitogenic action of tumour necrosis factor-alpha and interleukin-8on explants of human duodenal mucosa. Cytokine 15:148–155.doi:10.1006/cyto.2001.0917.

IL-8 and developing human intestine / 267
39. Zachrisson K, Neopikhanov V, Samali A, Uribe A (2001)Interleukin-1, interleukin-8, tumour necrosis factor alpha and inter-feron gamma stimulate DNA synthesis but have no effect onapoptosis in small-intestinal cell lines. Eur J Gastroenterol Hepatol13:551–559.
40. Wilson AJ, Byron K, Gibson PR (1999) Interleukin-8stimulates the migration of human colonic epithelial cells in vitro.Clin Sci (Lond) 97:385–390.
41. Juul SE, Zhao Y, Dame JB, Du Y, Hutson AD, ChristensenRD (2000) Origin and fate of erythropoietin in human milk. PediatrRes 48:660–667.
42. Kling PJ, Sullivan TM, Roberts RA, Philipps AF,Koldovsky O (1998) Human milk as a potential enteral source oferythropoietin. Pediatr Res 43:216–221.
43. Calhoun DA, Lunoe M, Du Y, Staba SL, Christensen RD(1999) Concentrations of granulocyte colony-stimulating factor inhuman milk after in vitro simulations of digestion. Pediatr Res46:767–771.
44. Sanderson IR, Ezzell RM, Kedinger M, Erlanger M, XuZX, Pringault E, Leon-Robine S, Louvard D, Walker WA (1996)Human fetal enterocytes in vitro: modulation of the phenotype byextracellular matrix. Proc Natl Acad Sci USA 93:7717–7722.
45. Ciacci C, Lind SE, Podolsky DK (1993) Transforminggrowth factor beta regulation of migration in wounded rat intestinalepithelial monolayers. Gastroenterology 105:93–101.
46. Sato Y, Tsuboi R, Lyons R, Moses H, Rifkin DB(1990) Characterization of the activation of latent TGF-beta byco-cultures of endothelial cells and pericytes or smooth muscle cells:a self- regulating system. J Cell Biol 111:757–763.
47. Juul SE, Joyce AE, Zhao Y, Ledbetter DJ (1999) Why iserythropoietin present in human milk? Studies of erythropoietinreceptors on enterocytes of human and rat neonates. Pediatr Res46:263–268.
48. Gillitzer R, Goebeler M (2001) Chemokines in cutaneouswound healing. J Leukoc Biol 69:513–521.
49. Gimbrone MA, Jr., Obin MS, Brock AF, Luis EA, HassPE, Hebert CA, Yip YK, Leung DW, Lowe DG, Kohr WJ (1989)Endothelial interleukin-8: a novel inhibitor of leukocyte-endothelialinteractions. Science 246:1601–1603.
50. Salcedo R, Resau JH, Halverson D, Hudson EA, DambachM, Powell D, Wasserman K, Oppenheim JJ (2000) Differentialexpression and responsiveness of chemokine receptors (CXCR1-3)by human microvascular endothelial cells and umbilical veinendothelial cells. Faseb J 14:2055–2064.
51. Strieter RM, Polverini PJ, Kunkel SL, Arenberg DA,Burdick MD, Kasper J, Dzuiba J, Van Damme J, Walz A, MarriottD, et al. (1995) The functional role of the ELR motif in CXCchemokine-mediated angiogenesis. J Biol Chem 270:27348–27357.
52. Koch AE, Volin MV, Woods JM, Kunkel SL, ConnorsMA, Harlow LA, Woodruff DC, Burdick MD, Strieter RM (2001)Regulation of angiogenesis by the C-X-C chemokines interleukin-8
and epithelial neutrophil activating peptide 78 in the rheumatoidjoint. Arthritis Rheum 44:31–40.
53. Dame JB, Juul SE (2000) The distribution of receptors forthe pro-inflammatory cytokines interleukin (IL)-6 and IL-8 in thedeveloping human fetus. Early Hum Dev 58:25–39.
54. Maheshwari A, Gersting JA, Richards BE, Christensen RD,Calhoun DA (2001) Developmental expression of chemokinereceptor genes in the human fetus. Pediatr Res 49:59A.
55. Palkowetz KH, Royer CL, Garofalo R, Rudloff HE,Schmalstieg FC, Jr., Goldman AS (1994) Production of interleukin-6 and interleukin-8 by human mammary gland epithelial cells.J Reprod Immunol 26:57–64.
56. Flores M, Filteau S (2002) Effect of lactation counselling onsubclinical mastitis among Bangladeshi women. Ann Trop Paediatr22:85–88.
57. Vidal K, Labeta MO, Schiffrin EJ, Donnet-Hughes A(2001) Soluble CD14 in human breast milk and its role in innateimmune responses. Acta Odontol Scand 59:330–334.
58. Filteau SM, Rice AL, Ball JJ, Chakraborty J, Stoltzfus R,de Francisco A, Willumsen JF (1999) Breast milk immune factorsin Bangladeshi women supplemented postpartum with retinol orbeta-carotene. Am J Clin Nutr 69:953–958.
59. Takahata Y, Takada H, Nomura A, Ohshima K,Nakayama H, Tsuda T, Nakano H, Hara T (2001) Interleukin-18 inhuman milk. Pediatr Res 50:268–272.
60. Goldman AS, Chheda S, Garofalo R, Schmalstieg FC(1996) Cytokines in human milk: properties and potential effectsupon the mammary gland and the neonate. J Mammary Gland BiolNeoplasia 1:251–258.
61. Bottcher MF, Jenmalm MC, Garofalo RP, Bjorksten B(2000) Cytokines in breast milk from allergic and nonallergicmothers. Pediatr Res 47:157–162.
62. Basolo F, Conaldi PG, Fiore L, Calvo S, Toniolo A (1993)Normal breast epithelial cells produce interleukins 6 and 8 togetherwith tumor-necrosis factor: defective IL6 expression in mammarycarcinoma. Int J Cancer 55:926–930.
63. Lebenthal A, Lebenthal E (1999) The ontogeny of the smallintestinal epithelium. JPEN J Parenter Enteral Nutr 23:S3–6.
64. Hinnebusch BF, Ma Q, Henderson JW, Siddique A, ArcherSY, Hodin RA (2002) Enterocyte response to ischemia is dependenton differentiation state. J Gastrointest Surg 6:403–409.
65. Mariadason JM, Velcich A, Wilson AJ, Augenlicht LH,Gibson PR (2001) Resistance to butyrate-induced cell differentiationand apoptosis during spontaneous Caco-2 cell differentiation.Gastroenterology 120:889–899.
66. Chang M, Suen Y, Lee SM, Baly D, Buzby JS, Knoppel E,Wolpe S, Cairo MS (1994) Transforming growth factor-beta 1,macrophage inflammatory protein-1 alpha, and interleukin-8 geneexpression is lower in stimulated human neonatal compared withadult mononuclear cells. Blood 84:118–124.





























