Embed Size (px)
Citation preview

Losartan treatment, pre- peri- and post-MI 1
Effects of pre, peri and postmyocardial infarction treatment with Losartan in
rats: effect of dose on survival, ventricular arrhythmias, function and
remodeling
Ali Pourdjabbar 1; Thomas G. Parker 1; Quang Trinh Nguyen 2; Jean-Francois Desjardins 1; Nathalie Lapointe 2; James N. Tsoporis 1; Jean-Lucien Rouleau 3
1 Division of Cardiology and Department of Medicine, St. Michael’s Hospital, University of Toronto, Toronto, Ontario, M5B 1W8; 2 Division of Cardiology, University Health Network, Toronto, Ontario, M5G 2C4; and 3 Department of Medicine, Montreal Heart Institute, Montreal, Quebec, H1T 1C8.
Running head: Losartan treatment pre-, peri- and post-MI
Address correspondence and reprint requests to Dr. Thomas G. Parker, M.D. Division of Cardiology, St. Michael’s Hospital, Room 6-044 Queen Wing, 30 Bond Street, Toronto, Ontario; M5B 1W8, Canada. Tel: 416-864-5271; Fax: 416-864-6189; E-mail: [email protected]
Articles in PresS. Am J Physiol Heart Circ Physiol (November 11, 2004). doi:10.1152/ajpheart.00671.2004
Copyright © 2004 by the American Physiological Society.

Losartan treatment, pre- peri- and post-MI 2
Abstract
Angiotensin receptor blockers (ARBs) reduce post-MI adverse left ventricular (LV) remodeling, improve
LV function and survival when started post-myocardial infarction (MI). ARBs also reduce ventricular
arrhythmias during ischemia-reperfusion injury when started pre-MI. No information exists regarding
their efficacy and safety when started pre-MI and continued peri- and post-MI. We evaluated whether the
ARB, Losartan improves outcome when started pre-MI, and continued peri- and post-MI. Male Wistar
rats (n=502) were treated for 7 days pre-MI with Losartan high-dose, 30 mg/kg/day, or progressively
increasing dose, 3mg/kg/day (increased to 10mg/kg/day 10 days and 30mg/kg/day 20 days post-MI) or
no-treatment. Ambulatory systolic blood pressure and Holter monitoring were performed for 24-hours
post-MI. Echocardiography was done 30-days post-MI, and LV remodeling, cardiac hemodynamics and
fetal gene expression were assessed 38-days post-MI. High-dose Losartan reduced 24-hour post-MI
survival compared to progressive dose and control (21.9% vs. 36.6%, 38.1%, p=0.033 and p=0.009
respectively). This was associated with greater hypotension in high dose, and no change in ventricular
arrhythmias in all groups. In 24-hour post-MI survivors, the progressive dose group had reduced mortality
from 24hour to 38-days (8.5% vs. 28.6% for control vs. 38.9% for high dose, p=0.032 and p=0.01
respectively). Survivors of both Losartan groups demonstrated improved LV remodeling, cardiac
hemodynamics, preserved GLUT-4 and reduced cardiac fetal-gene expression. Pre-treatment with ARBs
does not reduce 24-hour post-MI ventricular arrhythmias or survival, and high doses increase mortality by
causing excessive hypotension. In 24-hour post-MI survivors, progressively increasing doses of Losartan
have multiple beneficial effects, including improved survival.
Keywords: Angiotensin II receptor blockers, Heart Failure, Infarction, Remodeling, Hypotension

Losartan treatment, pre- peri- and post-MI 3
Introduction
During the acute phase of a myocardial infarction (MI), ventricular arrhythmias are the principle cause of
death. Indeed, nearly 70% of patients dying of an acute MI die suddenly prior to arriving to hospital (10).
Safe and effective reduction in peri-MI arrhythmias is thus an essential strategy in improving peri-MI
survival. Once a patient reaches hospital, a major goal of therapy is re-establishing cardiac perfusion in
order to limit MI size. Once the MI is well established and the damage irreversible, it is important to limit
adverse left ventricular (LV) remodeling in order to reduce the risk of heart failure (HF). Indeed, the
extent of LV dilation is the most powerful predictor of long-term prognosis post-MI (22).
The acute phase of the MI is characterized by neurohumoral activation, a process that lasts for days then
generally subsides over days to weeks, unless HF develops, in which case there is chronic progressive
neurohumoral activation. The renin-angiotensin system, particularly angiotensin II (Ang II), is up-
regulated peri- and post-MI. Angiotensin receptor blockers (ARBs) have been shown to improve
outcome when started early post-MI (21). One of the proposed mechanisms for these beneficial effects is
improved LV remodeling (24), but other mechanisms are also possible (15) but not well worked out. It
is uncertain as to what effect the presence (pre-treatment) of an ARB would have in the setting of an acute
MI. One possibility is that it would exert a beneficial effect. In favor of this is a report of the ARB
Losartan decreasing peri-MI arrhythmias during cardiac ischemia-reperfusion (28). However, it is also
possible that they induce adverse effects due to excessive hypotension, as has been shown to occur with
the ACEi Enalapril (26).
In the two studies that compared ARBs to ACEi therapy, drugs were initiated in small doses in order to
avoid the adverse effects of excessive hypotension observed in the CONSENSUS II trial (26). The dose
was then progressively increased. In the OPTIMAAL trial, the ARB did not perform as well as the ACEi
(7). One proposed hypothesis is that the dose of the ARB was inadequate (6). Consistent with this
hypothesis, a larger dose of an ARB was found to be equivalent to an ACEi in the VALIANT trial (21).

Losartan treatment, pre- peri- and post-MI 4
Thus, avoiding excessively high doses of an ARB early post-MI and assuring the use of higher doses later
post-MI may be important in order to obtain the optimal effects of ARBs post-MI.
Thus, in the present study, we chose to mimic the proposed optimal clinical use of ARBs post-MI that is,
starting with smaller known effective doses and progressively increasing to a high dose of the ARB
losartan. We compared these effects to early and sustained high doses of losartan and to no treatment at
all. We compared early (24 hour) post-MI ventricular arrhythmias, systemic blood pressure and survival,
and late post-MI LV remodeling, function, MI size and fetal gene expression. We hypothesized that
progressive doses of losartan would exert beneficial effects that would be superior both control and early
a large doses of Losartan.
Materials and Methods
Animals and Drug-Regimen
Male Wistar rats (Charles River, St-Constant, Quebec, Canada) weighing 160-200 g were assigned to one
of three groups: Losartan (Merck Frosst, Montreal, Qc) at 30mg/kg/day (High-dose) or 3mg/kg/day with
an increase to 10mg/kg/day on day 10 post-MI, and to 30mg/kg/day on day 20 post-MI (progressive-
dose) or control. The low and high doses of Losartan were chosen based on a previous report
demonstrating cardio-protective effects in rats following a MI (5,24). The increasing dose of Losartan
over time post-MI was chosen to simulate the clinical situation where Losartan is started low and
increased post-large-MI. Losartan was administered in drinking water starting 7 days prior to MI surgery.
In order to assure adequate levels of Losartan peri and early post-MI, it was administered by oral gavage,
in high dose 15mg/kg (0.25ml) or low dose 1.5mg/kg (0.25ml) of Losartan or vehicle (0.9% saline) the
evening after the MI and again twice the next day, after which the medication was once again
administered in drinking water and continued for the duration of the specific protocol. All of the animal
experiments followed the guidelines of the Canadian Council on Animal Care and were approved by the
Animal Care Committee of the University Health Network (Toronto, ON).

Losartan treatment, pre- peri- and post-MI 5
Experimental Myocardial infarction
Rats were anaesthetized with an intra-muscular injection of a mixture of ketamine 50mg/kg (Rogar/STB,
Montreal, Qc), and xylazine 10 mg/kg (Bayer Canada, Etobicoke, ON). MI was induced by ligation of
the left anterior descending coronary artery as described previously by Nguyen et al. (19). Sham
operated rats underwent a similar procedure except the silk suture was not tied. Once awakened
following surgery, the rats were injected with buprenorphine HCl 0.01 mg/kg as described previously.
Twenty-Four Hour Protocol:
Ambulatory Electrocardiogram (ECG) and Blood Pressure Monitoring
Ten days prior to the MI, under ketamine and xylazine anesthesia, rats (n=48) had a transmitter
implanted in the peritoneal cavity and anchored to the abdominal musculature. The implants had a pair
of flexible stainless steel wires/leads (Data Sciences International, St-Paul, MN) implanted
subcutaneoulsy for continuous ECG monitoring, and a blood pressure catheter, which was inserted into
the descending aorta, as previously described (14). The body of the implant that contains the electronics
for signal handling and radio-transmission was placed in the peritoneal cavity. Rats were then housed in
an individual cage placed on a receiver that continuously captures the radio-frequency signal from the
transmitter and converts it into a serial bit stream (Dataquest A.R.T.2.2, DSI, St-Paul, Mn.). Ambient
barometric pressure was also measured and subtracted from the telemetered pressure by data collection
software to compensate for changes in atmospheric pressure.
Arrhythmia Analysis: Monitoring started 6-hours prior to MI until the time of death or 24-hours post-MI.
The observer classified all arrhythmic events on ambulatory electrocardiographic recordings according to
the guidelines provided by The Lambeth Conventions and Curtis and Walker (4) with minor
modifications as previously described by Lapointe et al (14). The average arrhythmia score was
calculated 6 h before MI, and for 4 post-MI time periods, 0-1 h, 1-6 h, 6-12 h, and 12-24 h.
Assessment of MI Size

Losartan treatment, pre- peri- and post-MI 6
Rats dying <4 hours post-MI were considered to have had a large-MI. Rats dying between 4 and 24-
hours or surviving 24-hours post-MI had their hearts removed for determination of infarct size by
triphenyl tetrazolium chloride (TTC). The LV was hand-cut into four slices before staining with TTC.
Tissue slices were stained by incubation in 1% TTC for 10 to 15 minutes at 37°C and pH 7.8. The tissue
was then bathed for 15 minutes in a 10% formalin phosphate buffer to enhance color contrast. For each
slice, the scarred area was photographed under a Leica M26 (Leica Microsystems Inc., Quebec, CA) and
its surface was determined by planimetry (Labtronics Inc., Guelph, ON). Sections were traced on a
calibrated digitizing tablet and morphologic variables calculated directly by computerized-planimetry
with the Sigma Scan Pro software (Labtronics Inc., Guelph, Ontario, Canada).
Thirty-Eight Day Protocol:
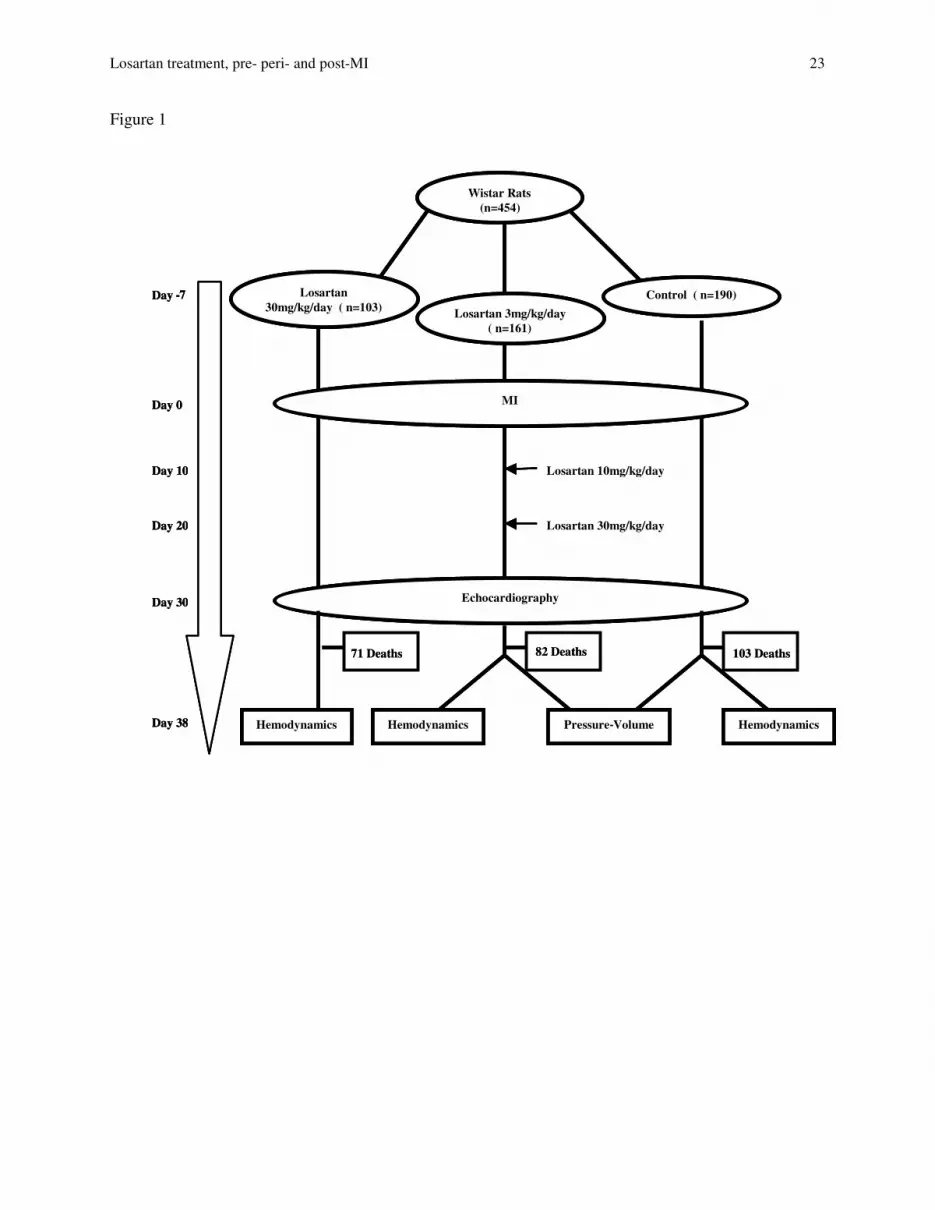
454 male Wistar rats were randomly assigned into 3 groups: Losartan High-dose (30mg/kg/day) (n=103),
Losartan Low-dose (3mg/kg/day increasing gradually to 30mg/kg/day) (n=161) or control (n=190),
administered as described above (Figure 1).
To verify if the low dose of Losartan chosen blocked the Angiotensin (Ang) II signaling pathway, a dose-
response curve to AngII 6.5ng/kg to 650ng/kg (Sigma, Lot# 31K51142) was constructed in 16 rats treated
with 3mg/kg/day of Losartan. The presser response to AngII was significantly attenuated for all doses of
Ang II as compared with control (results not shown).
Echocardiographic measurements:
Thirty days post-MI, cardiac function and geometry were evaluated with an echocardiographic system
equipped with a 15-MHz linear transducer (Acuson c256, Osiris Medical Inc., Toronto, ON). All studies
were performed with rats anaesthetized with 2% halothane (Halocarbon Laboratories, Riveredge, NJ)
using a vaporizer for halothane (Harvard Apparatus, Quebec, CA) and 0.2 l/min of oxygen. A
comprehensive 2-dimensional study was performed for the measurement of the LV circumference and
areas in both, systole and diastole. LV systolic diameter (LVSD), LV diastolic diameter (LVDD) were
measured in the short-axis M-mode as previously described (14).
Cardiac hemodynamic measurements

Losartan treatment, pre- peri- and post-MI 7
Thirty-eight days post-MI, rat were anesthetized with an intramuscular injection of ketamine (50 mg/kg),
and xylazine (10 mg/kg) mixture. The LV and right ventricular (RV) pressures were measured by a
Millar micro-tip catheter transducer, inserted into the right jugular vein and carotid artery and advanced to
the RV and LV, respectively. Systolic and diastolic arterial pressures were measured in the aorta before
being advanced to the LV. The maximum rate of pressure rise (+dP/dt) and decline (-dP/dt) were also
measured. The pressures were recorded on a Gould 2600S recorder (Gould, Cleveland, OH). Once the
hemodynamic measurements completed, rat were sacrificed and either used for assessment of LV
remodeling by passive pressure-volume relationship, or morphologic assessment of cardiac hypertrophy.
Morphological Assessment of Cardiac Hypertrophy
In rats surviving to 38-days, the heart was removed, rapidly rinsed in saline solution, and dissected into
atria, RV, LV, septum and scar. All portions of the heart, as well as the lungs, were then weighed
individually and frozen at -80ºC. MI size was assessed by measuring the surface area of the scar. Prior to
weighing, the scar was pinned on paper and its surface area measured by planimetry (Labtronics Inc.,
Guelph, ON). A large-MI was defined as an infarct size ≥ 0.8 cm2, a moderate MI was defined as an
infarct size < 0.8 cm2 and sham as no scar. A scar area of ≥ 0.8 cm2 is equivalent to an MI of ≥ 35% of
LV circumference in our experience (19). Rats dying later than 24-hours post-MI but prior to
hemodynamic monitoring had morphologic assessment for classification of MI size by assessing % of LV
circumference infracted, as previously described (3), but were not used for other measurements, except
for survival.
Passive Pressure-Volume Relationship and Ventricular Remodeling
Because the number of rats surviving the 38-days protocol in the high dose ARB group was low, only
control and low-dose Losartan groups were used for this protocol. Hearts were removed after cardiac
hemodynamic measurements, rinsed in a saline solution and then arrested in a supersaturated solution of
KCL, after which passive pressure volume was assessed as previously described (3). After the
assessment of the pressure-volume relationship, the hearts were filled with saline to a pressure of 15mm

Losartan treatment, pre- peri- and post-MI 8
Hg, sealed and fixed in 10% formalin phosphate solution for 24-hours. The heart was then cut halfway
between the base and apex, and 2 slices were obtained 1 mm above and below the middle cut and stained
with hematoxylin-phloxine saffron for assessment of MI size as previously described (3). Using this
method, a large-MI was defined as those having a LV scar of ≥35% of the ventricular cross-sectional
circumference, a moderate MI as having an LV scar<35%, and sham having no scar.
RNA Isolation and Purification
Total RNA was isolated from treated and untreated tissues from the septum of hearts, using TRIZOL
method. RNA samples were further subjected to RNase-free DNase I treatment at 37 °C for 30 min, then
purified with phenol chloroform and isoamyl alcohol, re-precipitated, and dissolved in nuclease-free
water. RNA was quantified with GeneQuant spectrophotometer (Amersham Pharmacia Biotech,
Piscataway, NJ) and RNA integrity was confirmed by running it on a formaldehyde gel. The isolated
total RNA was used in real-time quantitative RT-PCR experiments.
Real-Time Quantitative RT-PCR
Thermoscript one-step quantitative RT-PCR with platinum Taq kit was used in order to synthesize cDNA
and subsequent real-time quantitative RT-PCR (Applied Biosystems, Foster City, CA). The gene specific
sequences of oligonucleotide primers (100 nM final concentration of forward and reverse primers) were
used to check the expression of respective genes with a 1× final concentration of SYBR Green PCR
master mix (SYBR Green I Dye, AmpliTaq Gold DNA polymerase, dNTPs with UTP, passive reference,
and optimized buffer components), 0.25 U/mL multiscribe reverse transcriptase, 0.4 U/mL of RNase
inhibitor, and 10 ng of tissue RNA in a 50 µl PCR mixture according to the manufacturer’s protocol
(Applied Biosystems, Foster City, CA). The temperature profile included an initial 30 min, at 48 °C (for
cDNA synthesis), then denaturation at 95 °C for 10 min, in order to deactivate the RT and activate the
thermoscript taq polymerase. This was immediately followed by 40 cycles of denaturation at 95 °C for
15 s, 60 s at 60 °C annealing and elongation with optics on for fluorescence monitoring. The specificity
and purity of the amplification reaction was determined by performing a melting curve analysis. The

Losartan treatment, pre- peri- and post-MI 9
relative quantification of gene expression by real-time RT-PCR in a sample was determined by comparing
the target-amplified product against GAPDH (internal standard) within the same sample. GAPDH
mRNA expression was not significantly different among the various groups. Treated/control ratios were
tested for deviation from unity by calculation of confidence limits.
Statistical Analysis
All values were expressed as mean ± SEM. Results in figures 3 and 4 were analyzed by a
repeated- measures ANOVA across time post-MI and time prior to death and planned pairwise
comparisons (comparing 30mg dose to other conditions). A one-way ANOVA and Dunnett’s
Test were also used in figure 4A to compare mean arterial pressure prior to treatment and MI
procedure. Figure 5 was analyzed by a 2-way repeated measures ANOVA across volume by
dosage and condition (Large MI vs. sham). Lastly results within a given MI group and across
treatment groups in figure 6, and tables 1, 2 and 3 were analyzed by a one-way ANOVA and
Dunnett’s Test. Probability values of p< 0.05 were accepted as statistically significant. Kaplan-
Meier survival curves over the follow-up period were constructed and analyzed by the
generalized savage (Mantel-Cox) test.
Results
Survival
In the control group (n=190), 91 of 147 rats with a large-MI died within the first 24-hours (38.1%
survival), and 16 died over the following 37 days, leaving 40 survivors (27.2%) at the end of the 38-day
protocol. Of the rats receiving Losartan at 3mg/kg/day (n=161), 78 of 123 with a large-MI died within
the first 24-hours (36.6% survival) and 4 died over the following 37 days, leaving 41 survivors (33.3%).
Of the rats receiving Losartan at 30mg/kg/day (n=103), 64 of 82 with a large-MI died within 24-hours
(21.9% survival, p<0.01 vs. control and p<0.04 vs. Losartan low-dose). Of the remaining 18 rats, 7 died

Losartan treatment, pre- peri- and post-MI 10
over the following 38-days, leaving only 11 survivors (13.4%, p<0.0001 vs. control and p<0.0001 vs.
Losartan low-dose) (figure 2A).
If one considers only rats with a large-MI that survived the first 24 h post-MI, over the following 37 days,
the group receiving low-dose Losartan with a gradual increase in dose had the best survival, 91.5% as
compared with 71.4% in the control group and 61.1% in Losartan high-dose (p<0.02 and p<0.01
respectively) (figure 2B).
24-Hour Protocol:
Incidence and Duration of Ventricular Arrhythmias: (figure 3)
No VT or VF was recorded during the 6-hour baseline recording prior to coronary artery occlusion.
There was no difference in average ventricular arrhythmia score between large-MI control rats and large-
MI rats receiving high-dose or low-dose Losartan.
Ambulatory Blood Pressure (figure 4A):
Mean arterial pressure (MAP) did not differ amongst the 3 treatment groups prior to Losartan
administration, but it was significantly lower after 7 days of Losartan treatment in the 30mg/kg/day
group. MAP decreased as a result of a large-MI in all 3 groups. Over the 24 hours post-MI period, MAP
differed significantly across treatment groups. Planned pairwise comparisons revealed that following a
large-MI, high dose treated animals had a lower MAP as compared to control and low-dose groups,
p=0.05 and 0.02, respectively. Following a large-MI the MAP of rats receiving Losartan 3mg/kg/day did
not significantly differ from those of control rats.
In high-dose Losartan rats with a large-MI that died in the first 24-hours post-MI, MAP was extremely
low prior to death. As compared with controls and low-dose rats with equivalent MI size, MAP was lower
over the 60-5 minutes time interval prior to death (both p<0.05), (figure 4B) suggesting that hypotension
played a role in the death.
38-Day Protocol:

Losartan treatment, pre- peri- and post-MI 11
Echocardiographic Measurements (Table 1)
In the sham-operated groups, Losartan in low or high-dose did not have a discernable effect on
echocardiographic measurements. In control large-MI, there was significant LV dilatation with LV
circumference and area in systole and diastole all increasing as compared to sham controls. There was
also significant thinning of both the anterior and posterior walls, an increase in LV diastolic and systolic
dimensions (LVDD and LVSD respectively), and impaired LV function as reflected by decreased LV
shortening fraction (LVSF) and LV ejection fraction (LVEF).
Losartan high and low-doses had similar effects. Following a large-MI, they attenuated LV dilatation and
helped preserve LV function as compared with control large-MI.
Hemodynamic Effects of Chronic Losartan Treatment (Table 2)
Thirty-eight days post-MI, in sham operated rats, in both Losartan groups (both were receiving 30
mg/kg/day at sacrifice) systolic and diastolic blood pressures were lower.
As compared with their sham counterparts, control large-MI rats had a decrease in LV systolic pressure
(LVSP), an increase in LV end diastolic pressure (LVEDP) and a decrease in all measured indices of
contractility and relaxation. These changes were accompanied by an increase in RV systolic pressure
(RVSP) and RV end diastolic pressure (RVEDP).
Both groups of Losartan large-MI rats had similar hemodynamic changes. Systemic arterial pressure as
well as LVSP decreased as compared with control animals with a large-MI. LVEDP, RVSP, and RVEDP
all increased less suggesting improved LV function. LV +dP/dt when corrected for LVSP also improved
as compared with control large-MI.
Morphological Measurements (Table 3)
In sham-operated rats, Losartan treatment had little effect, the only change being a reduction in LV mass
in the high-dose Losartan group. As compared with their sham counterparts, control large-MI rats had a
significant increase in RV, atrial and lung weights. In the two large-MI Losartan groups, the increase in
RV, septal, atrial and lung weights were less marked than in control large-MI.

Losartan treatment, pre- peri- and post-MI 12
Passive LV Pressure-Volume Relationship
Losartan treatment exerted a significant effect on the passive pressure-volume relationship (p<0.02). In
sham- operated rats, Losartan caused a slight leftward shift in the passive pressure-volume relationship.
A rightward shift in the passive pressure-volume relationships of all large-MI groups was observed,
however the rightward shift was less in the Losartan treated rats (Figure 5)
MI Size
Animals with a large infarct surviving the 38-day protocol used for real-time PCR had similar infarct
surface area, in the high dose group 1.05 ± 0.06 cm2 (n= 11) as compared to 1.21 ± 0.04 cm2 (n=31) and
1.24 ± 0.05 cm2 (n=14) in non-treated and low-dose treated animals respectively (p >0.05). No difference
in MI-size was also observed in animals who underwent passive LV pressure-volume assessment and had
their MI size calculated via HPS staining and computer planimetry in the non-treated (n= 9) and low-dose
treated (n=27) groups, 45.1 ± 1.8% vs. 41.6 ± 1.4% of the LV wall circumference, respectively, p=0.2.
Real-time PCR (Figure 6)
Losartan had no effect on LV target mRNA expression in sham-operated rats. In control-large-MI, there
was a significant reduction in GLUT-4 mRNA expression, and an increase in fetal gene expression
(SKACT, ANF, and β-MHC mRNA) as compared to sham-operated rats. Both Losartan large-MI groups
had significantly higher levels of GLUT-4 mRNA expression as compared to control large-MI, and LV
SKACT, ANF, and β-MHC mRNA expression were significantly less elevated than control large-MI.
Discussion:
The main findings of this study are 1) that the administration of the ARB Losartan in the pre- peri- and
post-large-MI period does not result in improved 38-day post-MI survival, and that the administration of
high-doses in the peri-MI period actually increases mortality due to excessive hypotension; 2) that
Losartan also does not reduce peri-MI (24 hours) arrhythmias in a meaningful way; 3) that Losartan has
beneficial effects on LV function remodeling and fetal gene expression, and that this results in improved

Losartan treatment, pre- peri- and post-MI 13
survival starting 24-hours post-MI. Thus, during the peri-MI period, as has been found with ACEi in the
clinical setting, large doses of ARBs should be avoided. Rather, ARBs should be given at lower doses
early post-MI and increased progressively over time. A similar progressive dosing schedule of ARBs in
the peri- and early post-MI settings should form the basis of the administration of ARBs in further
experimental studies in the field.
Peri-MI effects of Losartan: concerns regarding hypotension:
In animals with a large-MI, higher dose of Losartan given peri-MI resulted in an increase in 24-hour post-
MI mortality. Careful analysis of MAP in rats dying during the first 24-hours post-MI, revealed that rats
receiving the higher dose of Losartan more frequently had marked hypotension the hour prior to death
suggesting that hypotension contributed to their death. In these rats, MAP within 1-hour of dying ranged
between 50 and 60 mmHg, much lower than the 75-90 mmHg in rats dying in the control and lower dose
Losartan groups, suggesting a possible relationship between the hypotension caused by Losartan and
increased mortality. Persistent hypotension post-MI is a serious concern since it has been linked to the
occurrence of tachy-arrhythmias and ventricular fibrillation leading to sudden death (8). It must
nevertheless be noted that the lower dose of Losartan used in this study resulted in partial AT1 receptor
blockade as reflected by the rightward shift in Ang-II dose-response curve that it caused. In the
CONSENSUS II trial, a high dose of the ACEi, Enalapril, started within the first 24-hours following an
acute-MI resulted in a significantly higher incidence of hypotension and a trend towards increased
mortality within 6 months following the initial infarction (26). Worrisome hypotension has also been
reported in other clinical trials were ACE inhibition was initiated within the first day of a MI (1,2).
The idea of delaying therapy in order to reduce the onset of hypotension is a controversial one given that
infarct expansion and remodeling is initiated within hours of a MI. In favor of an early aggressive
approach is the HEART study by Pfeffer et al., where patients were randomized to early (within 24 hours)
low dose Ramipril, early higher dose (progressive dose increase), and delayed Ramipril use. The low
dose of Ramipril chosen for this study did not normally have hemodynamic effects, but did have mild
hemodynamic effects in the acute MI setting (20). Of the three treatment groups, the early high dose

Losartan treatment, pre- peri- and post-MI 14
group had the best effects on LV remodeling suggesting that adequate doses of an ACEi early post MI is
important. In the present study, the initial dose of losartan used, 3 mg/kg/day was proportionately greater
than the dose used in the HEART study. In pilot studies we showed this dose to cause a significant
rightward shift of the Ang-II dose-response relationship, and in a previous study, this dose that has been
shown to have significant beneficial effects in the post-MI setting (4). The dose was then rapidly
increased to 10 mg/kg/day, a larger dose also shown to be useful post-MI (12), and finally to 20 then 30
mg/kg/day. The results of the present study thus support the early use of lower doses of an ARB post-MI
with up-titration to full doses early, as the HEART study did in with ACEi.
The findings of this study, contrast previous reports that have demonstrated beneficial outcomes with the
use of ARBs administered pre- or early post-MI at doses similar to or higher than the 30mg/kg/day, used
in this study. In a study by Zhu et al., the authors reported that pre-treatment with Losartan at
40mg/kg/day for 10 weeks followed by 17-minutes of ischemia and two hours of reperfusion (IR),
resulted in decreased ventricular arrhythmias, decreased MI size, and decreased 2 hour post-MI mortality
(28). Surprisingly, the authors failed to show any hemodynamic modification with this high dose of
Losartan. The explanation for these differences is not clear, but may have resulted from a combination of
the experimental protocol (IR), the short follow-up period, and the anesthesia used in their study, our rats
were awake and mobile most of the 24hour follow-up period. In another study, Ruzicka et al., who
started Losartan treatment (15mg/kg/day) 3 days prior to MI and continued for 4 weeks post-MI, also did
not report any early detrimental effects, but also did not report mortality following LAD ligation (23).
Effects of Losartan on Ventricular Arrhythmias:
Losartan was not found to modify ventricular arrhythmias during the first 24-hours post-MI in either low
or high doses. In IR, results from Zhu et al would suggest that pre-treatment with Losartan at
40mg/kg/day, decreases ventricular arrhythmias in a rat model of IR (28). In another paper, the same
group found that longer duration of pre-treatment (i.e. 4 weeks) was more cardio-protective than shorter
periods (i.e. one week and one day) of pre-treatment prior to IR in rats (27), suggesting that longer pre-

Losartan treatment, pre- peri- and post-MI 15
treatment in our study may have resulted in different findings. Alternatively, it may be that Losartan
affects the arrhythmic properties in IR differently than it does in trans-mural MI, the mechanisms
involved in both being quite different (17). It may also be that the lack of hypotension associated with IR
combined with high doses of Losartan is both necessary for its anti-arrhythmic effects to occur. In the
study by Zhu et al, despite large doses, Losartan did not modify systolic blood pressure throughout the
study (28), while in ours, the hypotension associated with the MI and high dose Losartan may have
negated its anti-arrhythmic effects.
Beneficial post-MI effects of Losartan:
Losartan treatment in rats surviving the acute (24-hours) MI period with a low-dose, followed by timed,
gradual increase in the dosing regimen resulted in dramatic improvement in survival over the next 37-
days of the protocol. This improvement in survival was accompanied by an improvement in LV
remodeling and function, a finding compatible with previous experimental post-MI studies using ARBs in
rats (5,13,16,24,25), and more importantly, compatible with the results of the VALIANT study that found
the ARB Valsartan to be as effective as the ACEi Captopril post large-MI (21). Animals in both high and
progressive dose groups that survived the 38-day protocol, also presented similar improvements in LV
remodeling and function reported by others, suggesting that in survivors both dosing regimens are equally
cardio-protective. Our findings are supported by a previous study by Nakamura et al. who demonstrated
that chronic low and high dose ARB treatment following a MI in rats are equally beneficial in terms of
LV remodeling and function (18). In our study, the observed improvement in LV remodeling and
function was accompanied by attenuation in fetal gene re-expression, and in preservation of the cardiac
expression of the glucose transporters, GLUT-4. Our study confirms the results of Hanatani et al that
have previously reported attenuation of fetal gene expression in a shorter post-MI study with another
ARB in the post-MI setting (9). This is, however the first report of preservation of the glucose transporter
GLUT-4 in the post-MI setting. Greater expression of GLUT-4 could result in improved glucose
utilization in the failing heart, and thus improved cardiac energetics.

Losartan treatment, pre- peri- and post-MI 16
We also documented a significant improvement in right ventricular function as well as a reduction in
pulmonary congestion. Zornoff et al. have reported that RV dysfunction is a very important predictor of
survival (29). Thus, Losartan’s beneficial effects on RV hypertrophy, pressure and function could at least
partially be responsible for the observed improvement in survival in our study.
Despite these improvements we were unable to show a reduction in infarct size with Losartan pre- and
post-MI treatment, which has been previously reported by (25). Once again our findings contrasts with
the findings of Zhu et al. demonstrating that pre-treatment with 40mg/kg/day of Losartan decreased MI
size, but again the results of Zhu et al were in the setting of 17 minutes of ischemia then 2 hours of
reperfusion, a setting in which they found no reduction in systolic blood pressure with losartan (28).
This is the first time that the pre-, peri-MI effects of Losartan have been combined with their long-term
post-MI effects. Why the combined peri-and post-MI use of Losartan did not result in improved survival
is not clear, but an early detrimental effect of Losartan, even in the smaller dose, cannot be excluded.
Alternatively, because no early harm could be documented acutely (<24-hours) with the lower dose, this
lack of overall benefit may have resulted from inadequate sample size and power to detect a difference.
A study by Hu et al. has also reported that Losartan, at 10mg/kg/day; started early post-MI did not
attenuate structural dilatation following coronary occlusion in rats (11). At this time, no other study
evaluating the peri-MI effects of an ARB exists to evaluate consistency with our results.
Limitations:
Animals were anesthetized at the time of surgery. This may have influenced arrhythmias and survival in
the first two hours post-MI. Thereafter rats were awake and unrestrained for the next twenty-two hours of
monitoring. A number of rats died during the study, which may have influenced hemodynamic
measurements at the end of the study. In order to minimize problems related to loss of rats during the
study, we classified rats according to MI size. Finally, because we did not include a low dose group
without progressive up-titration, it is possible that it was unnecessary to progressively increase the dose.
This does not, however, change the clinical implications of our findings, that high doses of an ARB

Losartan treatment, pre- peri- and post-MI 17
should be avoided early post-MI because they result in excessive hypotension and death. The combined
results of the OPTIMAAL and VALIANT studies have established the need to up-titrate post-MI.
Conclusions:
This study indicates that pre- and peri- MI treatment with the ARB Losartan exerts no beneficial effect on
survival and ventricular arrhythmias in the acute period post-MI, and high doses may even be detrimental
due to excessive hypotension. Losartan does not have early anti-arrhythmic properties, but, when given in
progressively increasing doses, results in improved LV remodeling and function, which in 24-hour post-
MI survivors, results in improved survival, reduced fetal gene expression, and preserved cardiac GLUT-4
expression despite no difference in infarct size.
Acknowledgement
The assistance of Aurora Mendelsohn on the statistical analysis of this study is gratefully acknowledged.
Ali Pourdjabbar is a recipient of The Government of Ontario/ Heart and Stroke Foundation of Ontario
Graduate Scholarship. This work was supported by the Canadian Institute of Health Research and Merck
Frosst Canada.
Reference
1. ISIS-4: a randomised factorial trial assessing early oral captopril, oral mononitrate, and
intravenous magnesium sulphate in 58,050 patients with suspected acute myocardial infarction.
ISIS-4 (Fourth International Study of Infarct Survival) Collaborative Group. Lancet 345:669-
85.1995.
2. Ambrosioni E, Borghi C, Magnani B. The effect of the angiotensin-converting-enzyme
inhibitor zofenopril on mortality and morbidity after anterior myocardial infarction. The Survival

Losartan treatment, pre- peri- and post-MI 18
of Myocardial Infarction Long-Term Evaluation (SMILE) Study Investigators. N Engl J Med
332:80-5.1995.
3. Belichard P, Savard P, Cardinal R, Nadeau R, Gosselin H, Paradis P, Rouleau JL. Markedly
different effects on ventricular remodeling result in a decrease in inducibility of ventricular
arrhythmias. J Am Coll Cardiol 23:505-13.1994.
4. Curtis MJ, Walker MJ. Quantification of arrhythmias using scoring systems: an examination of
seven scores in an in vivo model of regional myocardial ischaemia. Cardiovasc Res 22:656-
65.1988.
5. Daniels MC, Keller RS, de Tombe PP. Losartan prevents contractile dysfunction in rat
myocardium after left ventricular myocardial infarction. Am J Physiol Heart Circ Physiol
281:H2150-8.2001.
6. Dickstein K. What did we learn from the OPTIMAAL trial? What can we expect from
VALIANT? Am Heart J 145:754-7.2003.
7. Dickstein K, Kjekshus J. Effects of losartan and captopril on mortality and morbidity in high-
risk patients after acute myocardial infarction: the OPTIMAAL randomised trial. Optimal Trial in
Myocardial Infarction with Angiotensin II Antagonist Losartan. Lancet 360:752-60.2002.
8. Franciosa JA, Heckel R. Significance of hypotension preceding fatal ventricular
tachyarrhythmias in post-coronary obstruction sudden death. Am Heart J 101:421-7.1981.
9. Hanatani A, Yoshiyama M, Kim S, Omura T, Toda I, Akioka K, Teragaki M, Takeuchi K,
Iwao H, Takeda T. Inhibition by angiotensin II type 1 receptor antagonist of cardiac phenotypic
modulation after myocardial infarction. J Mol Cell Cardiol 27:1905-14.1995.
10. Heart and Stroke Foundation of Canada., Laboratory Centre for Disease Control (Canada). The
changing face of heart disease and stroke in Canada. Ottawa: Heart and Stroke Foundation of
Canada; 1999.
11. Hu K, Gaudron P, Anders HJ, Weidemann F, Turschner O, Nahrendorf M, Ertl G. Chronic
effects of early started angiotensin converting enzyme inhibition and angiotensin AT1-receptor

Losartan treatment, pre- peri- and post-MI 19
subtype blockade in rats with myocardial infarction: role of bradykinin. Cardiovasc Res 39:401-
12.1998.
12. Jain M, Liao R, Ngoy S, Whittaker P, Apstein CS, Eberli FR. Angiotensin II receptor
blockade attenuates the deleterious effects of exercise training on post-MI ventricular remodelling
in rats. Cardiovasc Res 46:66-72.2000.
13. Kim S, Yoshiyama M, Izumi Y, Kawano H, Kimoto M, Zhan Y, Iwao H. Effects of
combination of ACE inhibitor and angiotensin receptor blocker on cardiac remodeling, cardiac
function, and survival in rat heart failure. Circulation 103:148-54.2001.
14. Lapointe N, Nguyen QT, Desjardins JF, Marcotte F, Pourdjabbar A, Moe G, Calderone A,
Rouleau JL. Effects of pre-, peri-, and postmyocardial infarction treatment with omapatrilat in
rats: survival, arrhythmias, ventricular function, and remodeling. Am J Physiol Heart Circ Physiol
285:H398-405.2003.
15. McMurray JJ. Angiotensin receptor blockers for chronic heart failure and acute myocardial
infarction. Heart 86:97-103.2001.
16. Milavetz JJ, Raya TE, Johnson CS, Morkin E, Goldman S. Survival after myocardial
infarction in rats: captopril versus losartan. J Am Coll Cardiol 27:714-9.1996.
17. Muders F, Elsner D. Animal models of chronic heart failure. Pharmacol Res 41:605-12.2000.
18. Nakamura Y, Yoshiyama M, Omura T, Yoshida K, Izumi Y, Takeuchi K, Kim S, Iwao H,
Yoshikawa J. Beneficial effects of combination of ACE inhibitor and angiotensin II type 1
receptor blocker on cardiac remodeling in rat myocardial infarction. Cardiovasc Res 57:48-
54.2003.
19. Nguyen QT, Cernacek P, Calderoni A, Stewart DJ, Picard P, Sirois P, White M, Rouleau
JL. Endothelin A receptor blockade causes adverse left ventricular remodeling but improves
pulmonary artery pressure after infarction in the rat. Circulation 98:2323-30.1998.
20. Pfeffer MA, Greaves SC, Arnold JM, Glynn RJ, LaMotte FS, Lee RT, Menapace FJ, Jr.,
Rapaport E, Ridker PM, Rouleau JL, Solomon SD, Hennekens CH. Early versus delayed

Losartan treatment, pre- peri- and post-MI 20
angiotensin-converting enzyme inhibition therapy in acute myocardial infarction. The healing and
early afterload reducing therapy trial. Circulation 95:2643-51.1997.
21. Pfeffer MA, McMurray JJ, Velazquez EJ, Rouleau JL, Kober L, Maggioni AP, Solomon
SD, Swedberg K, Van de Werf F, White H, Leimberger JD, Henis M, Edwards S,
Zelenkofske S, Sellers MA, Califf RM. Valsartan, captopril, or both in myocardial infarction
complicated by heart failure, left ventricular dysfunction, or both. N Engl J Med 349:1893-
906.2003.
22. Picard MH, Wilkins GT, Ray PA, Weyman AE. Natural history of left ventricular size and
function after acute myocardial infarction. Assessment and prediction by echocardiographic
endocardial surface mapping. Circulation 82:484-94.1990.
23. Ruzicka M, Yuan B, Leenen FH. Blockade of AT(1) receptors and Na(+)/H(+) exchanger and
LV dysfunction after myocardial infarction in rats. Am J Physiol 277:H610-6.1999.
24. Schieffer B, Wirger A, Meybrunn M, Seitz S, Holtz J, Riede UN, Drexler H. Comparative
effects of chronic angiotensin-converting enzyme inhibition and angiotensin II type 1 receptor
blockade on cardiac remodeling after myocardial infarction in the rat. Circulation 89:2273-
82.1994.
25. Sladek T, Sladkova J, Kolar F, Papousek F, Cicutti N, Korecky B, Rakusan K. The effect of
AT1 receptor antagonist on chronic cardiac response to coronary artery ligation in rats.
Cardiovasc Res 31:568-76.1996.
26. Swedberg K, Held P, Kjekshus J, Rasmussen K, Ryden L, Wedel H. Effects of the early
administration of enalapril on mortality in patients with acute myocardial infarction. Results of
the Cooperative New Scandinavian Enalapril Survival Study II (CONSENSUS II). N Engl J Med
327:678-84.1992.
27. Zhu B, Sun Y, Sievers RE, Browne AE, Lee RJ, Chatterjee K, Parmley WW. Effects of
different durations of pretreatment with losartan on myocardial infarct size, endothelial function,
and vascular endothelial growth factor. J Renin Angiotensin Aldosterone Syst 2:129-33.2001.

Losartan treatment, pre- peri- and post-MI 21
28. Zhu B, Sun Y, Sievers RE, Browne AE, Pulukurthy S, Sudhir K, Lee RJ, Chou TM,
Chatterjee K, Parmley WW. Comparative effects of pretreatment with captopril and losartan on
cardiovascular protection in a rat model of ischemia-reperfusion. J Am Coll Cardiol 35:787-
95.2000.
29. Zornoff LA, Skali H, Pfeffer MA, St John Sutton M, Rouleau JL, Lamas GA, Plappert T,
Rouleau JR, Moye LA, Lewis SJ, Braunwald E, Solomon SD. Right ventricular dysfunction
and risk of heart failure and mortality after myocardial infarction. J Am Coll Cardiol 39:1450-
5.2002.
Legends for Figures
Figure 1: Flow diagram of the various groups of rats according to treatment and the experimental design.
Figure 2A: Comparison of the 38-day survival of rats with a large-myocardial infarction (MI), in the
various treatment groups.
Figure 2B: Comparison of survival between day 1 and day 38 in rats with a large-myocardial infarction
(MI), in the various treatment groups.
Figure 3: Average arrhythmia score of rats with a large-myocardial infarction (MI), 24-hours following
the MI. Cont. = Control, L30 = Losartan at 30mg/kg/day, L3 = Losartan at 3mg/kg/day
Figure 4A: Continuously monitored mean arterial blood pressure of rats with a large myocardial
infarction (MI) starting post treatment, prior to the MI and 24-hours following the MI. ‡p<0.05 vs.
3mg/kg/day, † p=0.05 vs. control.

Losartan treatment, pre- peri- and post-MI 22
Figure 4B: The monitored mean arterial blood pressure of rats with large-myocardial infarction (MI) that
died during the first 24-hours post-MI. Cont = Control, L30 = Losartan at 30mg/kg/day, L3= Losartan at
3mg/kg/day. *p<0.05 vs. Control, ‡p<0.05 vs. 3mg/kg/day.
Figure 5: Passive left ventricular (LV) pressure-volume relations of rats 38-days following a sham
operation or a large-myocardial infarction (MI) according to treatment groups.
Figure 6(A-D): The relative mRNA expression of GLUT-4, Sk. α actin, ANF and β-MHC, after
adjusted to sham control 38-days post-MI. * = P<0.05 vs. Sham, # = P<0.05 vs. control LMI. LV = left
ventricle, Sk. α actin = skeletal α actin, ANF = atrial natriuretic factor, MHC = myosin heavy chain,
Losartan HD = Losartan at high dose (30mg/kg/day), Losartan LD = Losartan at progressive dose starting
at 3mg/kg/day.
Losartan treatment, pre- peri- and post-MI 23
Figure 1
Wistar Rats (n=455)
Losartan 30mg/kg/day ( n=103) Losartan 3mg/kg/day
( n=161)
Control ( n=191)
MI
Echocardiography
Hemodynamics Hemodynamics Pressure-Volume Hemodynamics
Day -7
Day 0
Day 30
Day 38
Losartan 10mg/kg/day
Losartan 30mg/kg/day Day 20
Day 10
71 Deaths 82 Deaths 103 Deaths
Wistar Rats (n=455)
Losartan 30mg/kg/day ( n=103) Losartan 3mg/kg/day
( n=161)
Control ( n=191)
MI
Echocardiography
Hemodynamics Hemodynamics Pressure-Volume Hemodynamics
Day -7
Day 0
Day 30
Day 38
Losartan 10mg/kg/day
Losartan 30mg/kg/day Day 20
Day 10
Wistar Rats (n=454)
Losartan 30mg/kg/day ( n=103) Losartan 3mg/kg/day
( n=161)
Control ( n=190)
MI
Echocardiography
Hemodynamics Hemodynamics Pressure-Volume Hemodynamics
Day -7
Day 0
Day 30
Day 38
Losartan 10mg/kg/day
Losartan 30mg/kg/day Day 20
Day 10
71 Deaths 82 Deaths 103 Deaths

Losartan treatment, pre- peri- and post-MI 24
Figure 2A
0 10 20 30 400
50
100Control (n=147)
Losartan (30mg/kg/day) (n=82)
Losartan (Progressive Dose) (n=123)
Time (Days)
Surv
ival
%
*
*
* P < 0.05 vs. 30mg/kg/day

Losartan treatment, pre- peri- and post-MI 25
Figure 2B
0 10 20 30 4050
75
100 Control (n=56)
Losartan 30mg/kg/d (n=18)
Losartan Progressive Dose (n=45)
Time (Days)
Surv
ival
%
*
*
* P<0.05 vs. Progressive dose Group

Losartan treatment, pre- peri- and post-MI 26
Figure 3
1-6 6-120
2
4
6 Cont n=20
L3 n=11
L30 n=17
Arr
hyth
mia
Sco
re
Hours Post-MI 0-1 12-24

Losartan treatment, pre- peri- and post-MI 27
Figure 4A
0 5 10 15 20 2540
50
60
70
80
90
100
110
Control (n=15)Losartan 30mg/kg/day (n=11) Losartan 3mg/kg/day (n=10)
Hours Post-MI
Mea
n A
rter
ial P
ress
ure
(m
mH
g)
‡ †

Losartan treatment, pre- peri- and post-MI 28
Figure 4B
45
50
55
60
65
70
75
80
85
90
95
Mea
n A
rter
ial P
ress
ure
(mm
Hg)
Time Prior to Death (minutes)
Control (n=9) Losartan 3mg/kg/day (n=6) Losartan 30mg/kg/day (n=9)
-60 -15 -5
* ‡

Losartan treatment, pre- peri- and post-MI 29
Figure 5
0
10
20
30
40
50
0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 1.1 1.2 1.3
Large MI+Losartan 3mg/kg/day (n=27)
Large MI+Control (n=9) SHAM+Losartan
3mg/kg/day (n=9) SHAM+Control (n=9)
Pas
sive
Dia
stol
ic P
ress
ure
(mm
Hg)
Volume (ml)

Losartan treatment, pre- peri- and post-MI 30
Figure 6
0.0
0.5
1.0
1.5 ControlLosartan LDLosartan HD
Rel
ativ
e m
RN
Aex
pres
sion
0
1
2
3
4ControlLosartan LDLosartan HD
Rel
ativ
e m
RN
Aex
pres
sion
0.0
2.5
5.0
7.5
10.0 ControlLosartan LDLosartan HD
Rel
ativ
e m
RN
Aex
pres
sion
0
1
2
3 ControlLosartan LDLosartan HD
Rel
ativ
e m
RN
Aex
pres
sion
LV Glut4 mRNA ExpressionLV Glut4 mRNA ExpressionFigure 6AFigure 6A
Sham LMISham LMI
Figure 6BFigure 6B
Sham LMISham LMI
Figure 6CFigure 6C
Sham LMISham LMI
Figure 6DFigure 6D
Sham LMISham LMI
LV SKLV SK--αα actin mRNA Expressionactin mRNA Expression
LV ANF mRNA ExpressionLV ANF mRNA Expression LV LV ββ−−MHC mRNA ExpressionMHC mRNA Expression
*
#
#
##
####
*
*
*

Ant W. (cm)
LVDD(cm)
Pos W.(cm)
LVSD(cm)
LVSF(%)
LVEF(%)
SHAM (n=20) 0.2±0.02 0.8±0.02 0.2±0.01 0.6±0.04 31±2 46±4SHAM + Losartan (30mg/kg/day) (n=10) 0.2±0.01 0.8±0.04 0.1±0.01 0.6±0.05 29±3 39±4SHAM + Losartan (3mg/kg/day) (n=16) 0.14±0.01 0.8±0.03 0.2±0.01 0.6±0.04 29±3 41±4
LMI (n=40) 0.1±0.01* 1.14±0.01* 0.1±0.0* 1.1±0.01* 8.1±0.6* 16±1.*LMI + Losartan (30mg/kg/day) (n=11) 0.1±0.01* 1.09±0.01*† 0.14±0.01* 0.95±0.03*† 12.4±2*† 21±3*LMI + Losartan (3mg/kg/day) (n=41) 0.1±0.01* 1.11±0.01* 0.12±0.01* 0.99±0.01*† 11±0.7*† 20±1*†
LMI = Large myocardial infarction; Ant W. = anterior wall thickness; LVDD = left ventricular diastolic dimension; Pos W. = posterior wall thickness; LVSD left ventricular systolic dimension in short axis, just below plane of mitral valve; LV SF = left ventricular shortening fraction; LV EF = left ventricular ejection fraction
Values are given as mean ± SEM. *P < 0.05, vs sham; †P < 0.05, vs control Large MI.
Table 1: Echocardiographic Measurements at 30 Days Post MI

Losartan treatment, pre- peri- and post-MI 32
SBP DBP HR RVSP RVEDP DP/DT(+)/RVSP LVSP LVEDP DP/DT(+)/LVSP(mmHg) (mmHg) (BPM) (mmHg) (mmHg) (mmHg) (mmHg)
SHAMControl n=15 123±4 92±2 274±14 28±1 2±0.5 69±3 120±5 4±1 70±3Losartan (30mg/kg/day) n=9 104±4† 78±4† 303±25 26±1 1±1 80±6 101±3† 3±0.5 73±4Losartan (3mg/kg/day) n=16 101±3† 75±3† 284±10 26±1 1±0.5 69±2 99±3† 6±1 73±2
Large MIControl n=37 102±3* 81±2* 289±8 43±2* 5±1 53±2* 97±3* 15±1* 57±1*Losartan (30mg/kg/day) n=11 96±4 73±3 273±7 32±4† 2±0.5† 63±3*† 93±4 10±2* 56±2*Losartan (3mg/kg/day) n=41 89±3*† 69±2† 301±13 31±1*† 2±0.3† 63±2*† 83±3*† 10±1*† 59±2
SBP = systolic blood pressure; DBP = diastolic blood pressure; HR = heart rate; RVSP = right ventricular systolic pressure; RVEDP = right ventricular end diastolic pressure; LVSP = left ventricular systolic pressure; LVEDP = left ventricular end diastolic pressure.
Values are given as mean ± SEM. *P < 0.05, vs sham; †P < 0.05, vs control Large MI.
Table 2: Hemodynamic Measurements at 38 Days Post MI

Losartan treatment, pre- peri- and post-MI 33
BW LV Total Septum RV Scar Atria Lungs(g) (g) (g) (g) (g) (g) (g)
SHAMControl n=10 430±9 0.83±0.03 0.27±0.02 0.25±0.01 0.1±0.01 1.6±0.05Losartan (30mg/kg/day) n=9 420±10 0.70±0.03† 0.24±0.02 0.22±0.01 0.07±0.003 1.6±0.04Losartan (Progressive) n=6 448±10 0.77±0.04 0.22±0.02 0.25±0.02 0.08±0.01 1.9±0.17
Large MIControl n=32 422±8 0.67±0.02 0.31±0.01 0.42±0.02* 0.1±0.01 0.20±0.01* 2.8±0.12*Losartan (30mg/kg/day) n=11 411±12 0.65±0.02 0.28±0.01 0.29±0.03*† 0.1±0.01 0.12±0.01*† 2.0±0.24†Losartan (Progressive) n=14 441±7 0.64±0.03 0.26±0.01† 0.32±0.03† 0.1±0.01 0.16±0.01*† 2.2±0.11†
BW = body weight; LV = left ventricle; RV = right ventricle; LV total = LV + septum
Values are given as mean ± SEM. *P < 0.05, vs sham; †P < 0.05, vs control Large MI
Table 3: Morphological Measurements at 38 Days Post MI






























