Embed Size (px)
Citation preview
AUS DEM SCHWEIZERISCHEN TROPENINSTITUT BASEL
UND DER UNIVERSITÄTS-HAUTKLINIK
DER ALBERT-LUDWIGS-UNIVERSITÄT FREIBURG I.BR.
EFFICACY OF TRICLOSAN SOAP AGAINST SUPERFICIAL DERMATOMYCOSES AND SCABIES - A PLACEBO-
CONTROLLED STUDY AMONG 228 PRIMARY SCHOOL CHILDREN IN KILOMBERO DISTRICT, MOROGORO REGION,
TANZANIA
INAUGURAL-DISSERTATION
ZUR ERLANGUNG DES MEDIZINISCHEN DOKTORGRADES
DER MEDIZINISCHEN FAKULTÄT DER ALBERT-LUDWIGS-UNIVERSITÄT
FREIBURG I.BR.
VORGELEGT 2005 VON ALMUTH DINKELA
GEBOREN IN ROTENBURG (WÜMME)

DEKAN PROF. DR. C. PETERS
1. GUTACHTER PD DR. C. HATZ 2. GUTACHTER PROF. DR. L. BRUCKNER-TUDERMAN JAHR DER PROMOTION 2006
STUDIENKOORDINATOR:
PD DR. MED. C. HATZ LEITENDER ARZT MEDIZIN UND DIAGNOSTIK SCHWEIZERISCHES TROPENINSTITUT
UNIVERSITÄT BASEL SCHWEIZ MITGLIEDER DES DISSERTATIONSKOMITEES: PROF. DR. MED. L. BRUCKNER-TUDERMAN GESCHÄFTSFÜHRENDE DIREKTORIN
UNIVERSITÄTS-HAUTKLINIK ALBERT-LUDWIGS-UNIVERSITÄT FREIBURG I.BR. DEUTSCHLAND
PD DR. MED. P. SCHMID-GRENDELMEIER LEITENDER ARZT DER ALLERGIESTATION DERMATOLOGISCHE KLINIK UND POLIKLINIK
UNIVERSITÄTSSPITAL ZÜRICH SCHWEIZ DR. W. BASCHONG SCIENTIFIC LIASONS & BIOLOGICAL STUDIES HOME AND PERSONAL CARE SEGMENT CIBA SPECIALTY CHEMICALS INC. SCHWEIZ PROF. DR. PHIL. M. TANNER
INSTITUTSVORSTHER SCHWEIZERISCHES TROPENINSTITUT UNIVERSITÄT BASEL
SCHWEIZ
STUDIENKOORDINATOR AM IHRDC, IFAKARA/TANZANIA:
DR. B. IDINDILI
FACHARZT FÜR DERMATOLOGIE AM SFDDH, IFAKARA/TANSANIA:
DR. M. MBATA
UNTERSTÜTZUNG DER STATISTISCHEN AUSWERTUNG:
DR. T. A. SMITH, DR. P. VOUNATSOU

FÜR MEINE ELTERN
“song of lawino – song of ocol” Ring-worm sometimes eats up A little girl’s hair And this is terrible; But when hot porridge Is put on the head And a dance is held Under the sausage-fruit tree And the youths have sung
You, Ring-worm, Who is eating Duka’s hair, Here is your porridge, Then the girl’s hair Begins to grow again, And the girl is pleased.
Okot p’Bitek
LIST OF ABBREVIATIONS – IN ALPHABETICAL ORDER ............................................15
ACKNOWLEDGEMENTS – IN ALPHABETICAL ORDER ...............................................16
SUMMARY ........................................................................................................................17
ZUSAMMENFASSUNG.....................................................................................................18
INTRODUCTION ...............................................................................................................19
1. Superficial dermatomycoses ......................................................................................19 1.1 Tinea versicolor (synonym: Pityriasis versicolor) ................................................................................................. 19 1.2 Dermatophyte infections (synonym: Ringworm infections) .................................................................................. 22 1.2.1 Tinea capitis ........................................................................................................................................................ 22 1.2.2 Tinea corporis ..................................................................................................................................................... 24 1.2.1 and 1.2.2 Diagnosis............................................................................................................................................. 24 1.2.3 Tinea pedis .......................................................................................................................................................... 25 1.2.5 Tinea manuum .................................................................................................................................................... 26 1.2.6 Tinea unguium .................................................................................................................................................... 26
1.3 Scabies .......................................................................................................................27
2. Information about Triclosan .......................................................................................28 2.1 Properties ............................................................................................................................................................... 29 2.2 Triclosan-containing products currently in use in Africa....................................................................................... 32

METHODS.........................................................................................................................33
1. Study Area....................................................................................................................33
2. Selection of Primary Schools .....................................................................................34
3. Screening Examinations .............................................................................................34
4. Admission to the Study...............................................................................................37 4.1 Inclusion Criteria ................................................................................................................................................... 37 4.2 Excludsion Criteria ................................................................................................................................................ 37
5. Case Definitions...........................................................................................................38
6. Degree of Infection ......................................................................................................40
7. Randomisation.............................................................................................................41
8. Follow-up Examinations..............................................................................................42
9. Evaluation of Effectiveness - Dermatomycoses .......................................................43 9.1 General................................................................................................................................................................... 43 9.2 Pruritus................................................................................................................................................................... 43 9.3 Clinical and Microscopic Resolution ..................................................................................................................... 44 9.4 Definition of Evaluation Categories at Second Follow-up .................................................................................... 44
10. Evaluation of Effectiveness - Scabies......................................................................46
11. Assessment of Soap Use (Compliance) ..................................................................46
12. Determination of Minimal Inhibitory Concentrations (MIC’s) of Placebo Soap and of Triclosan ......................................................................................................................48
13. Data Entry and Analysis............................................................................................49
14. Additional Information...............................................................................................50

RESULTS..........................................................................................................................51
1. GENERAL INFORMATION...........................................................................................51
2. EPIDEMIOLOGY OF SUPERFICIAL DERMATOMYCOSES .......................................51
2.1 Prevalence rates ........................................................................................................51
2.2 Prevalence rates and degree of infection according to sex...................................52 2.2.1 Tinea versicolor .................................................................................................................................................. 52 2.2.2 Other superficial dermatomycotic infections ...................................................................................................... 53
2.3 Prevalence rates and degree of infection according to age groups .....................54 2.3.1 Tinea versicolor .................................................................................................................................................. 54 2.3.2 Other superficial dermatomycotic infections ...................................................................................................... 54
3. ASSESSMENT OF THE EFFECT OF SOAP ................................................................55
3.1 Assessment of the efficacy of Triclosan in soap....................................................55 3.1.1 Tinea versicolor infections.................................................................................................................................. 59 3.1.2 Other superficial dermatomycotic infections: Tinea capitis, corporis and pedis infections ................................ 67 3.2 Determination of minimal inhibitory concentrations (MIC’s) of placebo soap and of Triclosan .......................... 76
4. SCABIES.......................................................................................................................81 4.1 Epidemiology and Study population...................................................................................................................... 81 4.2 Assessment of the effect of soap and the efficacy of Triclosan ............................................................................. 81
DISCUSSION: ...................................................................................................................85
1. Epidemiology of superficial dermatomycoses..........................................................85 1.1 Tinea versicolor ..................................................................................................................................................... 85 1.2 Other superficial dermatomycotic infections ......................................................................................................... 86
2. Assessment of the effect of soap and the efficacy of Triclosan in soap ................87 2.1 Superficial dermatomycoses .................................................................................................................................. 87
3. Scabies .........................................................................................................................94 3.1 Epidemiology of scabies ........................................................................................................................................ 94 3.2 Assessment of the effect of soap............................................................................................................................ 95
4. Strength and Limitations.............................................................................................96 4.1 Physical examinations and photographic images................................................................................................... 96 4.3 Sample-taking and microscopic examination ........................................................................................................ 97 4.4 Quality control of microscopy and additional cultivation of fungi in Zürich......................................................... 97 4.5 Results during the first follow-up .......................................................................................................................... 98 4.6 Characteristics of the study population .................................................................................................................. 98 4.7 Spontaneous resolution and climatic influences .................................................................................................... 98
5. Conclusions .................................................................................................................99
6. Implications................................................................................................................100
BIBLIOGRAPHY .............................................................................................................101

APPENDIX: CALCULATION OF THE SAMPLE SIZE AND ASSUMED PREVALENCE RATES.............................................................................................................................113
APPENDIX A: TABLES (*NUMBER OF OBSERVATIONS, ROW PERCENTAGES AND COLUMN PERCENTAGES), SYMMETRY TABLES AND FIGURES ............................114
APPENDIX B: PHOTOGRAPHIC IMAGES ....................................................................146
APPENDIX C: 1. QUESTIONNAIRE (ENGLISH/KISWAHILI) ........................................161
Appendix D: 1. Informed Consent ................................................................................176
2. Information for the Parents – provided at school meeting ....................................178
3. Information for the Parents – about the skin diseases: Handouts for parents ....180
4. TREATMENT CARDS.................................................................................................184
5. ID CARD: DISTRIBUTED TO CHILDREN AT FIRST SOAP DISTRIBUTION............186


15
List of abbreviations – in alphabetical order A Isolates from Bacteriological or Veterinary Institutes
AD Almuth Dinkela
AIDS Acquired Immunodeficiency Syndrome
ATCC American Type Culture Collection
BBE Benzyl Benzoate Emulsion
BHI Brain Heard Infusion Agar
CI Confidence Interval
C.-G. Ciba Geigy
CITM Centre International de Distribution de Souches (Lausanne)
CM Charles Maswi
DEO District Educational Officer
DPT Dichlorodiphenyltrichlorethane
EKBB Ethik Komitee Beider Basel
ELM Epiluminescence Microscopy
FDA Food and Drug Administration
HHM Household Member
HIV Human Immunodeficiency Virus
IHRDC Ifakara Health Research and Development Centre
JF Julia Ferié
KCMC Kilimanjaro Christian Medical Centre
KOH potassium hydroxide
M Mycophil Agar
M-H Müller-Hinton Agar
MIC Minimal Inhibitory Concentration
MM Marco Mbata
NA Nutrient Agar
N.A. non-applicable
NCIB National Collection of Industrial Bacteria (U.K.)
NCTC National Collection of Type Cultures (London)
PCP Pneumocystis carinii pneumonia
PAS Periodic Acid Schiff
SFDDH St. Francis Designated District Hospital
SMA Sabouraud Maltose Agar
STI Swiss Tropical Institute, Basel
16
Acknowledgements – in alphabetical order I would like to express my deepest appreciations and gratefulness to the following persons. Without
their tremendous support and assistance it would not have been possible to carry out the field study,
analyse the data and write this dissertation.
Werner Baschong
Leena Bruckner-Tuderman
Dominique Bourgau
Julia Ferié
Armin Gemperli
Christoph Hatz
Boniphace Idindili
Nada Juricevic
Erik Krause
Charles Maswi
Marco Mbata
Jürg Meyer
Veronika Mkope
Charles Mayombana
Hassan Mshinda
Dietmar Ochs
Antonie Roll
Amanda Ross
Markus Schiltknecht
Peter Schmid-Grendelmeier
Marcel Schnyder
Thomas Smith
Marcel Tanner
Adriana Tami
Honorathy Urassa
Penelope Vounatsou
Many thanks also to other staff at STI and the IHRDC and last but not least, the pupils and teachers
of Lihami and Michenga Primary School.
17
SUMMARY Background: The present placebo-controlled double-blind study was performed to assess the
clinical efficacy of Triclosan against selected superficial dermatomycoses and scabies. The overall
effect of regular soap use was also evaluated. Methods: 820 Tanzanian primary school children
were examined for the presence of skin disorders. The clinical presentation of the dermatoses was
documented. Samples of suspected dermatomycoses were examined microscopically using KOH.
Quality control and culture were performed, and the MIC’s of placebo soap and Triclosan against
Malassezia spp. were assessed in vitro. The children with superficial dermatomycoses or scabies
were selected for this trial. They received either bar soap containing Triclosan (active group) or
placebo soap during a period of 8 weeks. They were followed-up after 1 and 2 months. Results:
Among the 820 examined children, superficial dermatomycoses were the most common diagnoses,
with a total prevalence rate of 33.9%. The prevalence rates of tinea versicolor, tinea capitis, corporis
and pedis were 26.2%, 5.5%, 2.6%, 3.2% respectively. Triclosan soap was not significantly more
effective against any of the selected dermatoses. Overall cure rates of tinea versicolor, tinea capitis,
corporis and pedis were 28.4%, 61.1%, 56.3% and 36.8% respectively. In tinea versicolor soap use
improved the overall degree of infection significantly (p = 0.000). The proportion of negative
microscopic results increased from 19.0 to 51.6%. Neither the placebo nor Triclosan were
efficacious against Malassezia spp. in vitro at relevant concentrations. In tinea capitis the overall
degree of infection also improved significantly (p = 0.001). The addition of Triclosan yielded only
slightly, non-significantly superior results. In the Triclosan group, the proportion of negative tinea
capitis samples increased from 22% to 64%, whereas it decreased from 57% to 53% in the placebo
group. In tinea corporis the size of the largest lesion decreased from 2.2 cm to 1.0 cm in the active
group whereas it increased in the placebo group. In tinea pedis the cure rate was non-significantly
higher for active than for placebo soap (86% versus 56%). The prevalence of scabies was 1.5%. All
6 children included in this study showed an overall tendency towards improvement with either soap.
Conclusions: In tinea versicolor the lack of superior efficacy of Triclosan soap is consistent with
the lack of in vitro efficacy of Triclosan. The overall improvement may be due to unspecific effects
associated with soap use such as a reduction of the amount of superficial skin lipids. In other
dermatomycoses, the overall improvement can be explained by the elimination of infectious
pathogens from the integument. The in vitro activity against certain dermatophyte spp. explains the
slight beneficial effect of Triclosan versus placebo soap. The lack of significance may be due to the
mode of application and the common use of vaseline. The results therefore confirm the usefulness
of soap, but do not justify the addition of Triclosan to treat superficial skin mycoses and scabies.
18
ZUSAMMENFASSUNG Einleitung: In der vorliegenden Placebo-Kontrollierten Doppelblindstudie wurden die klinische
Effektivität von Triclosan und der Gesamteffekt regelmäßigen Seifengebrauchs gegen ausgewählte
Dermatomykosen und Skabies ermittelt. Methoden: 820 tansanische Grundschüler wurden
bezüglich des Vorhandenseins von Hautkrankheiten untersucht. Bei klinisch vermuteten
Dermatomykosen wurden Proben von den Läsionsorten entnommen und mittels KOH
mikroskopisch untersucht. Eine Qualitätskontrolle, kulturelle Anzüchtung sowie die Ermittlung der
Minimal inhibitorischen Konzentrationen von Placeboseife und Triclosan gegen Malassezia spp. in
vitro wurden durchgeführt. Die an oberflächlichen Dermatomykosen oder Skabies leidenden
Schüler wurden für diese klinische Studie ausgewählt. Sie erhielten wöchentlich für 8 Wochen
entweder eine Triclosanseife oder eine Placeboseife. Nachuntersuchungen erfolgten nach 1 und 2
Monaten. Resultate: Die Dermatomykosen T. versicolor, capitis, corporis, pedis mit Prävelenzen
von 26,2%, 5,5%, 2,6%, 3,2% (Gesamt-Prävalenz: 33,9%) insgesamt die häufigsten Diagnosen.
Triclosanseife war gegen keine der Dermatosen signifikant wirksamer als das Placebo. Die
Gesamtheilungsraten von T. versicolor, T. capitis, corporis und pedis betrugen 28.4%, 61.1%,
56.3% und 36.8%. Der Schweregrad von T. versicolor verbesserte sich durch den Seifengebrauch
(Triclosan- und Placebogruppe zusammengefasst) signifikant (p = 0.000). Der Anteil der negativen
mikroskopischen Resultate erhöhte sich von 19,0 auf 51,6%. In vitro waren weder Triclosan noch
Placeboseife in relevanten Konzentrationen gegen Malassezia spp. aktiv. Der Schweregrad von T.
capitis verbesserte sich durch Seifengebrauch ebenfalls signifikant (p = 0,001). In der
Triclosangruppe erhöhte sich der Anteil negativer mikroskopischer Resultate von 22% auf 64%,
während er sich in der Placebogruppe von 57% auf 53% verringerte. Die durchschnittliche Größe
der Läsionen bei T. corporis verringerte sich in der Triclosangruppe von 2.2 cm auf 1.0 cm,
wohingegen er sich in der Placebogruppe vergrößerte. In der Triclosangruppe war die Heilungsrate
von T. pedis höher als in der Placebogruppe, wenn auch nicht signifikant (86% versus 56%). Die
Prävalenz von Skabies betrug 1,5%. Alle 6 in die Studie aufgenommen Kinder zeigten eine
deutliche Verbesserung ihrer Infektionen. Schlussfolgerungen: Dass Triclosanseife bei der
Behandlung von T. versicolor dem Placebo nicht überlegen war, korrespondiert mit der fehlenden
in-vitro-Aktivität der Substanz. Die Gesamtverbesserung könnte auf die durch den vermehrten
Seifenkonsum verringerten Hautlipide zurückzuführen sein. Die erwiesene in-vitro-Aktivität gegen
Dermatophyten konnte in dieser klinischen Studie nicht signifikant bestätigt werden. Die fehlende
Signifikanz könnte durch die Applikationsart und häufigen Gebrauch von Vaseline begründet sein.
Die Elimination infektiöser Partikel vom Integument erklärt die Gesamtverbesserung. Die Resultate
bestätigen die Nützlichkeit intensiven Seifengebrauchs, rechtfertigen aber den Zusatz von Triclosan
nicht, um Dermatomykosen und Skabies zu behandeln.
Introduction 19
Introduction Dermatomycoses such as dermatophyte infections and tinea versicolor are among the most common
human infections in the developing world (Ayaya et al., 2001; Sunenshine, 1998). Dermatophytoses
as well as scabies are known to be among the “dermatoses of poverty” (Schmeller et al., 2001;
Stingl, 2001).
Easy availability and affordability of treatment alone do not seem to be sufficient to reduce the
prevalence rates of these dermatoses in children. It seems to be necessary that standards of living,
health education and hygiene improve alongside with the provision of cheap and effective treatment
schemes (Schmeller, 1998).
The present study was performed in order to assess whether the antimicrobial agent “Triclosan”
contained in bar soap is clinically efficacious against selected superficial dermatomycoses and
scabies.
The overall effect of improved hygiene and regular soap use on signs and symptoms of these
diseases was also evaluated. A similar approach has, to this author’s knowledge, so far only been
reported from Nigeria, where a large proportion of fungal skin infections and scabies could be cured
through the application of soap (Alebiosu et al., 1994).
The availability of bar soap – medicated or non-medicated – proven to be clinically effective
against these common ailments would be a precious tool to treat and prevent the dermatoses that are
discussed in this study. This is true not only for the study participants, but also for those individuals
living in comparable settings, of which there are numerous throughout the world.
1. Superficial dermatomycoses
Fungal infections are usually divided into superficial mycoses located on the skin, hair, nails and
mucosal membranes, deep or subcutaneous mycoses affecting the subcutaneous tissues and
systemic mycoses primarily affecting internal organs (Svejgaard, 1986). The fungi causing
superficial mycoses belong to different parts of the taxonomic system: yeasts, dermatophytes and
moulds (Svejgaard, 1986).
Superficial fungal infections are a common diagnosis in everyday dermatological practice. They
constitute 10 – 20% of skin diseases treated in hospitals (Anezia, 1981), and are generally more
prevalent in developing than in developed countries (Canizares et al., 1993).
1.1 Tinea versicolor (synonym: Pityriasis versicolor)
This skin disorder is caused by Malassezia spp., which are human saprophytes. So far eleven
species have been described of which the majority are lipophilic (Gupta et al., 2003, Mirhendi et
al., 2005). Studies conducted within the past six years indicate that the pathogen most frequently
Introduction 20
associated with tinea versicolor may not be M. furfur but possibly M. globosa or M. sympodialis
(Gupta, 2002; Gupta et al., 2001, Nakabayashi et al., 2000).
Although tinea versicolor has a worldwide distribution, it is particularly common in hot and humid
tropical areas (Faergemann, 1994; Hay, 1996). Overall prevalence rates in tropical zones may reach
50% (Marples, 1950; Borelli, 1991). In contrast, only 0.5% of males and 0.3% of females were
found to suffer from tinea versicolor in the course of a population survey in Sweden (Hellgren et
al., 1983), and 1.9% of factory workers examined in central Turkey presented with tinea versicolor
lesions (Celik et al. 2003).
The majority of cases occur during adolescence. This may be because of hormonal changes and/or
increasing sebum production (Akpata et al., 1990). Among children tinea versicolor is generally
rare, although it may be found more commonly in this age group in tropical climates (Gupta, 2002;
Marples, 1950).
Studies have shown variable male to female ratios, but they appear to be nearly equal. In contrast to
dermatophyte infections, tinea versicolor is considered neither contagious nor is it due to poor
hygiene (Sunenshine, 1998). However, since this infection has been found to be associated with
malnutrition, the socio-economic status may indirectly play a role (Gupta, 2002).
The organism can be found in 90-100% of healthy subjects as part of the normal skin flora
(Canizares et al., 1993; Sunenshine, 1998; Schmidt, 1997; Leeming et al., 1989). Tinea versicolor
occurs when the yeast converts to its mycelial form due to certain predisposing factors, which can
be divided into endogenous and exogenous factors (Canizares et al., 1993). Endogenous factors
include malnutrition, use of oral contraceptives, use of systemic corticosteroids or
immunosuppressants, Cushing’s Syndrome, seborrhoeic dermatitis, or hyperhidrosis. According to
Sunenshine, hereditary factors might play a part since a positive family history in approximately
17% was confirmed by more than one study (Sunenshine, 1998; Burke, 1961). Hafez et al.
described a multifactorial inheritance, with a heridability of 22.2% in first-degree relatives (Hafez et
al., 1985). Immune deficiency disorders such as HIV/AIDS are believed to predispose to more
extensive infections, but Pityrosporum infections do otherwise not seem to differ from those in
HIV-negative subjects (Elmets, 1994; Schechtmann et al., 1995).
Exogenous factors include heat and moisture. Furthermore, lesions are most commonly found on
body areas covered by clothes which results in an altered pH range (Gupta, 20020; King et al.,
1978; Sunenshine, 1998). Exacerbation of the disease may also happen through the application of
creams or oils to the skin (Faergemann et al., 1982; Gupta, 2002).
The sites affected are usually those with the greatest density of sebaceous glands such as the upper
trunk, neck and face. Lesions on the face are more common in children than in adults (Gupta, 2002;
Sunenshine, 1998; aTerragni et al., 1991). Other common sites are the upper arms, but the disease
Introduction 21
may also occur on the scalp (Goncalves, 1963), the penis (Daneshvar et al. 1987), the neck and the
groin (Burkhart et al., 2000; Burke, 1961).
Apart from tinea versicolor, Pityrosporum yeasts may also cause pityrosporum folliculitis (Bäck, et
al., 1985). Besides, seborrhoeic dermatitis has been found to be associated with the colonization of
this yeast in sebum-rich areas (Gupta, 2002; McGinley et al., 1975).
Clinical diagnosis may be complicated due to the various forms of presentation. It is usually based
on the distribution, shape and appearance of the macules and patches. The furfuraceous scales can
be easily removed using the fingernails, which is called “fingernail test (Canizares et al., 1993).
Microscopic examination of skin scrapings obtained from the lesions is used to confirm the
diagnosis. The scales are usually placed on a microscopic slide, and 10-20% KOH solution is
applied to dissolve the keratin (Gupta, 2002). Staining with i.e. 1% methylene blue (Faergemann,
1994) or ink (Dominguez-Soto, 1994) may facilitate the diagnosis (Canizares et al., 1993).
Examination reveals round budding cells (spores) and hyphae or mycelia. This pattern is also
referred to as “spaghetti and meatballs” (Sunenshine, 1998). Additionally, the fungus may be
cultivated e.g. on Sabouraud’s agar rich in lipids. Bacterial growth and growth of moulds is
inhibited by addition of chloramphenicol and cycloheximide respectively (Gupta, 2002; Enweani,
1996).
The main complaint of the patient is cosmetic disturbance, but mild pruritus may be present (Gupta,
2002; Bélec, 1991).
Differential diagnosis includes vitiligo, leukoderma, chloasma, dermatophytoses, seborrhoeic
dermatitis, psoriasis pityriasis rosea, pityriasis alba, pityriasis rotunda, confluent and reticulate
papillomatosis of Gougerot-Carteaud, secondary syphilis, pinta, leprosy and erythrasma (Gupta,
2002; Sunenshine, 1998; Canizares, 1983).
Wood’s Light can help to distinguish tinea versicolor from dermatophytosis not caused by certain
fluorescing species such as Microsporum spp. or T. schoenleinii and from erythrasma, which
follows infection with Corynebacterium minutissimum (Cheesbrough, 1997). Ringworm lesions
caused by other Trichophyton spp., Epidermophyton spp. or few geophilic Microsporum spp.
generally do not fluoresce at all, and erythrasma would appear coral-red, whereas tinea versicolor
lesions show a yellow-green fluorescence (Gupta, 2002; Sunenshine, 1998).
There are various options to treat tinea versicolor, both topical or systemic variants may be
effective. Examples of topical agents are selenium sulfide, propylene glycol 50% in water
(Faergemann, 1994), ciclopiroxolamine or imidazoles (Gupta, 2002). Imidazoles are also effective
if administered orally, whereas terbinafine and griseofulvine are not (Gupta, 2002).
However, the treatment is associated with a relatively high rate of recurrence reaching 60 to 80%,
according to Arenas et al. (Arenas et al., 1982).
Introduction 22
1.2 Dermatophyte infections (synonym: Ringworm infections)
Dermatophyte infections are limited to the superficial layers of the epidermis and its appendices
such as the hair and nails (Shrum, 1994) and are able to invade these structures (Elewski, 1986).
They are classified according to genera, namely Trichophyton, Epidermophyton and Microsporum
(Canizares, 1983; Hay, 1996), according to ecology (antropophilic, geophilic or zoophilic
dermatophytes) (Shrum, 1994) and according to anatomic locations of infection (Weitzman et al.,
1995). Infections caused by geophilic or zoophilic fungi are generally more severe than those
caused by anthropophilic fungi (Canizares, 1983).
The prevalence of dermatophyte infections is higher in developing than in industrialized countries
because of prevailing poverty, overcrowding, sharing of fomites, poor hygiene and new drug
resistant pathogens (Ayaya et al., 2001; Canizares et al., 1993). Increasing use of
immunosuppressive therapy, chemotherapy, antibiotics and the HIV/AIDS pandemic, which affects
particularly the poorest areas of the world, further contribute to the emergence of these infections
(Ayaya et al., 2001; Elmets, 1994; Elewski, 2000).
Patients with AIDS may present with clinically atypical or more extensive lesions, but the incidence
is not higher than among immunocompetent individuals (Hay, 1996).
1.2.1 Tinea capitis
In the developing world tinea capitis remains the predominant clinical type among children (Welsh
et al., 2002; Al-Sogair, 1991; Porter, 1980; Shrum, 1994; Canizares, 1983). The spectrum of
causative agents is variable depending on the setting of the studies. Prevalence at primary schools
ranges between 11.3% in Ivory Coast (Hervé et al., 2002) and 33.3% in Kenya (Ayaya et al., 2001).
Tinea capitis may present with different symptoms (Shrum, 1994). The clinical manifestations can
be divided into three groups (Canizares et al., 1993):
1. One comprises scaly, dry, non-inflammatory lesions sometimes presenting grey patches or
“black dots”, which appear when hairs break off close to the hair follicle. This type usually
does not produce permanent alopecia. It is often caused by anthropophilic species and can
be subdivided into a microsporic and a trichophytic variety.
2. Another presentation is the more acute, wet, and inflammatory type with possible
suppuration or kerion formation (Shrum, 1994). Kerion celsi are characterized by
erythematous nodules, swelling, and regional lymphadenitis (Hussain et al., 1999) and
represents a hypersensitivity, often self-limiting, reaction to the invading pathogens
(Hussain et al., 1999; Weitzman et al., 1995; Canizares, 1983).
Introduction 23
3. The third type is dry, crusted, occasionally inflammatory and suppurative, caused mainly by
T. schoenleinii and other faviform fungi. This clinical picture is also referred to as “favus”.
It is characterized by yellow crusts which are referred to as scutulae (Canizares et al., 1993;
Canizares, 1983) (cup-shaped areas of densely interwoven mycelium, scales, and debris).
They may become confluent and appear as mats of honeycomb-like areas (Shrum, 1994)
leading to permanent alopecia (Canizares et al., 1993).
Bacterial superinfection and cervical lymphadenopathy may be present, and the patient may
develop an id reaction (Shrum, 1994; Canizares, 1983). Sometimes the infection may also be
accompanied by fever and malaise (Weitzman et al., 1995).
The differential diagnosis includes other disorders involving scaling and/or hair loss such as
seborrhoeic dermatitis, scalp psoriasis, alopecia areata and trichotillomania (Shrum, 1994).
Tinea capitis should be treated systemically as topical treatment is much less effective and in many
cases useless (P. Schmid-Grendelmeier, personal communication). Usually, topical antifungal
agents are recommended only as adjuncts to systemic treatment because they cannot penetrate into
hair follicules sufficiently (Chan et al., 2004; Canizares et al., 1993; Weitzman et al., 1995;
Schmeller, 1998).
The systemic application of griseofulvin has revolutionised treatment, especially of endothrix
infections. However, the dosage needed to cure tinea capitis has been slowly increasing over the
years (Gupta et al., 2003). Due to rapid elimination, long duration of therapy is necessary, which
may reduce patient compliance (Gupta et al., 2003). Newer antifungal drugs like terbinafine,
itraconazole or fluconazole are comparable in efficacy (Chan et al., 2004) and have longer retention
periods in the affected tissues (Gupta et al., 2003). In theory Terbafine is now available as an oral
formulation, but not in the study setting that is described in the present study. The newer agents are
generally more expensive than griseofulvin, which is still the only FDA-approved drug and for the
treatment of tinea capitis (Gupta et al., 2003), but have much less side effects. Even though in
temperate climates the drugs of choice are nowadays terbinafine or itraconazole, griseofulvin or
ketoconazole remain the first choice in the tropics (Welsh et al., 2002; P. Schmid-Grendelmeier,
personal communication).
Whitfield’s Ointment (5% benzoic acid, 5% salicylic acid and basic cream), tolfnaftate, haloprogin
and clotrimazole have been recommended for topical treatment. Besides, the application of topical
or systemic antibiotics or prednisolone may become necessary (Canizares et al., 1993). Apart from
drug treatment, general sanitation measures have to be taken to prevent the disease from spreading
(Canizares et al., 1993; Weitzman et al., 1995).
Taking these conditions into consideration, it can be concluded that a realistic approach to prevent
and reduce ringworm infections appears to be a change in hygiene behaviour. This has been
Introduction 24
achieved for example in Sri Lanka where the custom of frequent head baths with soap and water is
likely to be responsible for the relatively low prevalence of tinea capitis in certain studied
communities (Attapattu, 1989). Alebiousu et al. from Nigeria were able to cure more than half of
their study population with either tinea capitis or corporis by applying a soap containing plant-
derived ingredients for several weeks (Alebiosu et al., 2003).
1.2.2 Tinea corporis
This term usually describes all dermatophyte infections that do not involve the scalp, ear, face,
beard, axillae, hands, feet and groin (Shrum, 1994). In the present study, facial lesions are described
as tinea corporis lesions as well. Tinea corporis is common in children, but can also be found
frequently among adolescents and adults (Soyinka, 1978; Weitzman et al., 1995). Prevalence rates
in tropical regions such as Gambia have been reported to range between 3% in the wet season and
0.7% in the dry season (Porter, 1980); prevalence rates among primary schoolchildren were found
to be 2.7% in rural Ethiopia (Figueroa et al., 1996) and 0.8% in Nigeria (Soyinka, 1978). Tinea
corporis involves glabellar skin and presents with single or multiple oval, scaly patches with central
clearing, sometimes delineated by versicular borders (Weitzman et al., 1995; Canizares, 1983).
Especially in the tropics the presentation may be polymorphic (Canizares et al., 1993; Shrum,
1994). In case of invasion, the formation of “Majocchi’s Granuloma” may occur, usually after
minor trauma (Shrum, 1994). A distinct clinical type is tinea imbricata showing a polycyclic pattern
of the scaly lesions (Canizares et al., 1993; Shrum, 1994; Hay, 1996). As for tinea capitis, topical
treatment may not be sufficient and must then be supplemented by griseofulvin or ketoconazole or
other systemic agents (Shrum, 1994; Weitzman et al., 1995). However, in single lesions topical
treatment is mostly effective (P. Schmid-Grendelmeier, personal communication).
1.2.1 and 1.2.2 Diagnosis
Diagnosis for tinea corporis and capitis is made by microscopic examination of skin scrapings and
hair clippings (in case of tinea capitis) with KOH solution or by fungal cultures. Spores can be seen
either in or outside the hair (endothrix or ectothrix infection), depending on the causative species.
Besides, hyphae and mycelia may be found. The diagnostic test with best specifity is fungal culture
on Sabouraud’s agar; additionally, Wood’s Lamp or biopsy followed by PAS or silver staining can
be used (Shrum, 1994). Differential diagnosis of tinea corporis should include nummular eczema,
psoriasis, drug eruptions, mycosis fungoides and pityriasis versicolor (Gupta, 2002; Shrum, 1994).
Introduction 25
1.2.3 Tinea pedis
This disease, also known as “athlete’s foot”, is a common diagnosis in white urban populations
(Shrum, 1994; Canizares, 1983; Canizares et al., 1993). According to Shrum et al. it is a rare
condition in African populations, as well as in populations of other tropical regions (Shrum, 1994).
However, Soyinka found that the incidence of tinea pedis among secondary school children in
Nigeria was higher than that of other dermatomycoses (Soyinka, 1978). Another school survey in
Nigeria yielded a prevalence of 1.5% among the pupils (Enweani, 1996). Generally it is more
common among the older age groups (Shrum, 1994; Canizares, 1983).
Clinically, there are three varieties of tinea pedis (Canizares et al., 1993).
1. The first is the intertriginous type, with interdigital maceration, accompanied by whitish
thickening of the web spaces of the feet. It may extend to both the toes and the soles (Masri-
Fridling, 1996), pruritus and foul odour may be present.
2. The second type is the dishydrotic type with acute vesicular, bullous or vesiculo-bullous
lesions with erythema and fissuring. This type is usually located on the mid-sole.
3. The third form is the hyperkeratotic moccasin type, which tends to be chronic and presents
with scaling of the plantar surface (Shrum, 1994). Vesiculation is usually absent.
Asymptomatic infection is common in tinea pedis (Masri-Fridling, 1996), but severe cases
involving mixed infection by dermatophytes, candida and bacteria may also occur (Weitzman et al.,
1995; Hay, 1996). Bacterial superinfection is mostly noted in the interdigital type (Masri-Fridling,
1996). This feature is then referred to as “dermatophytosis complex” (Canizares et al., 1993; Odom,
1993). Diagnosis is made using KOH preparations and culture, as described above for the other
dermatophyte infections. Differential diagnosis includes psoriasis, contact dermatitis, dyshidrosis
and pompholyx (Shrum, 1994; Canizares, 1983). Candidiasis, erythrasma, acrodermatitis contiua,
pyodermas and secondary syphilis should also be considered (Masri-Fridling, 1996). Treatment
with topical fungistatic or fungicidal agents may be successful. Antibacterial soaps are
recommended in cases of mixed bacterial and fungal interdigital infections. Severe cases may
require the addition of systemic agents such as itraconazole or terbinafine and oral antibiotics
(Masri-Fridling, 1996).
1.2.4 Tinea cruris
This term describes dermatophyte infections of the groin, perianal and perineal areas and the upper
thighs. The infection is most common in adult men (Weitzman et al., 1995). Lesions usually appear
as erythematous or brown scaling patches. Involvement of the groins can be bilateral, and lesions
may present as annular patches, with active margins showing vesiculation and crusting (Weitzman
Introduction 26
et al., 1995; Canizares et al., 1996). It is more common in hot and humid climates, especially if the
standard of hygiene is low (Anezia, 1981). Differential diagnosis between tinea cruris caused by
dermatophytes, Erythrasma caused by Corynebacterium minutissimum, intertrigo, which may be of
bacterial origin, and candidiasis may be difficult if no microscopic diagnosis or fungal culture are
performed (Canizares, 1975). Wood’s light is a helpful device to identifiy C. minutissimum (also
see 1.1.1).
In this study, it was not in all cases possible to examine the inguinal or genital area. Furthermore,
only few samples could be obtained as privacy or an investigator of the same sex as the examined
child could not always be guaranteed. Since differential diagnosis could thus not be made, inguinal
lesions are referred to as “intertrigo”, summarizing all the above mentioned differential diagnoses
affecting the inguinal area.
1.2.5 Tinea manuum
Tinea manuum usually presents as unilateral diffuse hyperkeratotic lesions, localised in the
interdigital spaces or the palms (Weitzman et al., 1995; Canizares et al., 1993). Simultaneous
involvement of the feet is common (Canizares et al., 1993).
1.2.6 Tinea unguium
Dermatophytes may also invade nails. This infection is called tinea unguium. Infection of the nail
by non-dermatophytic fungi is referred to as onychomycosis. The invasion can be subungual or
superficial, which is also known as leukonychia trichophytica (Weitzman et al., 1995). T. rubrum
and T. mentagrophytes are the most common dermatophytes causing this infection (Weitzman et al.,
1995).
The management of fungal nail infections has greatly improved with the introduction of systemic
agents as well as topical nail polishes containing ciclopirox and amorolfine (Gupta et al., 2003).
1.2.7 Dermatomycoses caused by non-dermatophytic fungi
Primary infections of the skin and nails may also be caused by fungi other than dermatophytes or
Malassezia and Candida yeasts. These are for example Exophiala werneckii, Piedra hortae,
Trichosporon belgii, which cause tinea nigra palmaris, black piedra and white piedra respectively.
Aspergillus, Acremonium spp. and Scopulariopsis brevicaulis often invade nails and thus produce
onychomycosis (English et al., 1994; Elewski et al., 1989).
Other species such as Hendersonula toruloidea and Scytalidium hyalinum are non-dermatophyte
saprophytic moulds found in soil, water, air and on fomites (Masri-Fridling, 1996; Elewski et al.,
1991). These facultative pathogens may cause dermatomycoses mimicking the clinical picture of
Introduction 27
certain ringworm infections. Pathogenic moulds should be suspected if the infection is resistant to
standard antifungal treatment, if standard cultures fail to grow and if KOH preparations are
nevertheless positive (Masri-Fridling, 1996). Since species identification was not possible in all
cases in the present study, dermatomycoses other than tinea versicolor will be referred to as “other
superficial dermatomycotic infections”.
1.3 Scabies
Scabies remains a major public health problem in developing countries, especially because of the
HIV/AIDS pandemic (Usha et al., 2000; Green, 1989). The prevalence of scabies has been found to
be associated with similar factors as that of dermatophytoses, such as poverty, crowding in
households and poor hygiene (Inanir et al., 2002). Several further factors such as population
movements, wars, misdiagnosis, inadequate treatment, and changes in the immune status of the
population have been suggested to affect the epidemiology of scabies (Green, 1989). In 1962
Schaller found that between 11 and 57% of schoolchildren in various Ethiopian provinces were
infected (Schaller, 1969). Since 1990 prevalence rates ranging between 1.7% and 17% have been
reported from Nigeria and Ethiopia (Enweani, 1996; Figueroa et al., 1996).
Scabies is a contagious diseases, and its transmission is being favoured by warm closeness
(Canizares et al., 1993), thus affecting most likely the whole familiy at the same time (Anezib,
1981; White, 1996).
The infection is caused by the itch mite, Sarcoptes scabiei. The female parasites deposit their eggs
and faeces into burrows in the stratum corneum of the skin and die 14 days after fertilization. The
male parasites die immediately after fertilization. Larvae hatch after three to four days (Anezib,
1981; White, 1996). The six-legged larva passes through a nymphal state and finally turns into an
eight-legged adult (Canizares, 1983; Canizares et al., 1993).
Three features are diagnostic of scabies (Canizares, 1983).
1. Itching, the most characteristic symptom, starts between three days and six weeks after the
first infection, due to an Type IV hypersensitivity reaction against the mites and their
products (Burkhart et al., 2000). In subsequent infections pruritus appears within a few days.
Typically, pruritus is most severe at night.
2. Observing scabies burrows between the fingers or at other typical sites is pathognomonic for
the infestation (Burkhart et al., 2000). However, in children they may be difficult to find
(White, 1996). When opening a burrow, the mite can be extracted with a sharp instrument
and examined directly or microscopically (Canizares, 1983). Superficial scrapings from
ulcers may contain mites, scybala or eggs (White, 1996).
Introduction 28
3. The distribution of the lesions is characteristic. Burrows are typically localized in the webs
and on the sides of the fingers, wrists and ulnar border of the hands, elbows, anterior axillary
folds, areola of the breasts, umbilicus, waist, external genitalia and perineum, natal cleft,
thighs, knees, ankles and the palms and soles (Anezib, 1981). The distribution of the
urticarial rash does not necessarily correspond with the infestated sites (White, 1996).
In tropical environments scabies has to be distinguished from insect bites, papular urticaria, and
pediculosis. In immunocompromised individuals, crusted scabies may be found, involving profuse
crusting of the skin and the formation of hyperkeratotic plaques (White, 1996). Asymptomatic cases
of scabies have been reported (Jiminez-Lucho et al., 1995); some may be heavily infestated with
millions of mites but not show no crusted lesions (Estes et al., 1993). Scabies in children is often
atypical in appearance making differential diagnosis difficult at times. Differential diagnosis
includes eczema, pyoderma, and in the tropics also onchocerciasis (White, 1996).
Although scabies may not represent a major disease per se, it can be associated with secondary
complications such as bacterial superinfection, eczematisation and poststreptococcal
glomerulonephritis (White, 1996).
Systemical treatment of scabies with Ivermectin is effective (Terri et al., 1995), but topical
treatment also yields good results. 5% permethrin cream (Canizares et al., 1993), 0.3% lindane
cream, topical ivermectin, benzyl benzoate emulsion, crotaminon and sulfur are used as topical
agents (Pruksachatkunakorn et al., 2002; Pönnighaus, 1995; Anezib, 1981; Victoria et al., 2001). At
the dispensaries in and around Ifakara, scabies is usually treated with BBE (Benzyl benzoate
emulsion (Dr. M. Mbata, personal communication).
2. Information about Triclosan
The broad-spectrum antimicrobial agent Triclosan has been used worldwide for skin care products
during the last 30 years. It is a nonionic, off-white, odorless and tasteless powder. The chemical
name is 2,4,4’-trichloro-2’-hydroxy-diphenyl-ether (C12H17Cl3O2) (Jones et al., 2000). Triclosan
was originally developed by Ciba-Geigy Company, Basel, Switzerland, and has been used in the
United States since the 1960s in under-arm deodorants and bar soaps. In 1972 it was for the first
time introduced into health care as a surgical scrub (Jones et al., 2000). In many countries Triclosan
can nowadays be found in a wide range of further products apart from deodorants and soaps, such
as shower gels, health care personal hand washes, lotions, creams, toothpastes etc (© Ciba Specialty
Chemicalsb, 1998).
The chemical is currently distributed as IRGASAN® DP 300 for skin applications and
IRGACARE® MP for oral applications (Jones et al., 2000).
Introduction 29
2.1 Properties
2.1.1 Safety
IRGASAN® DP 300 / IRGACARE® MP is not toxic in acute toxicity tests when used in
formulations, not irritating to skin and eyes, non-sensitizing, non-carcinogenic, non-mutagenic, not
toxic to reproduction, non-teratogenic, completely eliminated and does not accumulate in organs or
tissues. It is well tolerated in humans (© Ciba Specialty Chemicalsb, 1999). Based on the broad
safety package and the long-term experience using this antimicrobial, IRGASAN® DP 300 /
IRGACARE® MP is considered to be safe for humans when used in the recommended
concentrations (Bhargava, et al., 1996).
2.1.2 Anti-inflammatory effect and anti-irritative effects
Triclosan was proven to be an effective inhibitor of cyclo-oxygenase and lipo-oxygenase, key
enzymes of the arachidonic acid metabolism, thus reducing the formation of pro-inflammatory
metabolites such as prostaglandin E2 and leukotriene B4 (Nissen et al., 1998). Triclosan is therefore
able to reduce inflammatory skin reactions and skin irritations (Kjaerheim et al., 1995; Skaare et al.,
1997; Barkvoll et al., 1994). Barkvoll and Rölla showed that Triclosan is capable of reducing skin
irritation caused by sodium lauryl sulphate (Barkvoll et al., 1994) as well as allergic reactions to
nickel in nickel sensitized patients (Barkvoll et al., 1995). In another study, Nissen and Ochs
demonstrated the concentration dependent anti-inflammatory efficacy on erythema caused by UV-
radiation (Nissen et al., 1998).
2.1.3 Broad-spectrum antimicrobial activity
Triclosan shows broad-spectrum antimicrobial activity against most gram-positive, gram-negative
bacteria, moulds and yeasts (Nissen et al., 1998). The antimicrobial spectrum and the speed of
activity of Triclosan have been documented both as various formulations and as an active ingredient
(Bhargava, et al., 1996; Larson, 1988; The Soap and Detergent Association and The Cosmetic,
Toiletry, and Fragrance Association, 1995; Jampani et al., 1998). These documentations include in
vivo as well as in vitro tests (The Soap and Detergent Association and The Cosmetic, Toiletry, and
Fragrance Association, 1995). Data collected in several in vitro tests with respect to the
antimicrobial efficacy against fungal pathogens are listed below (see Table 1).
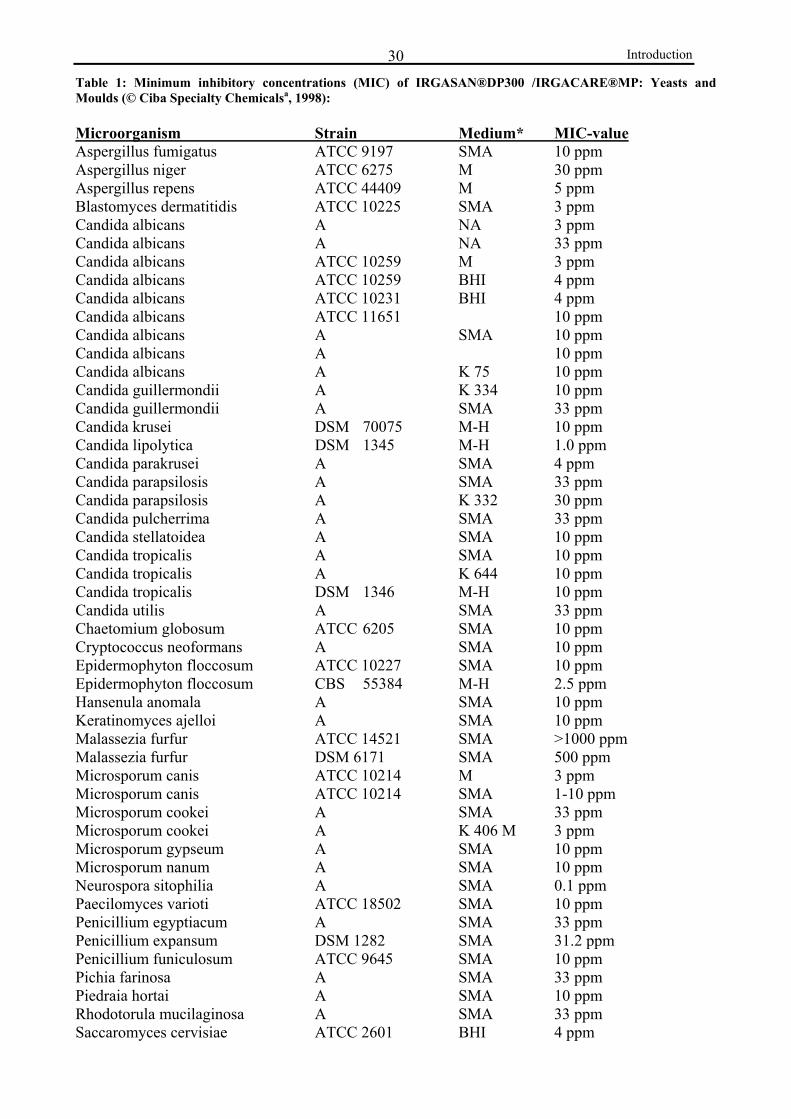
Introduction 30Table 1: Minimum inhibitory concentrations (MIC) of IRGASAN®DP300 /IRGACARE®MP: Yeasts and Moulds (© Ciba Specialty Chemicalsa, 1998): Microorganism Strain Medium* MIC-value Aspergillus fumigatus ATCC 9197 SMA 10 ppm Aspergillus niger ATCC 6275 M 30 ppm Aspergillus repens ATCC 44409 M 5 ppm Blastomyces dermatitidis ATCC 10225 SMA 3 ppm Candida albicans A NA 3 ppm Candida albicans A NA 33 ppm Candida albicans ATCC 10259 M 3 ppm Candida albicans ATCC 10259 BHI 4 ppm Candida albicans ATCC 10231 BHI 4 ppm Candida albicans ATCC 11651 10 ppm Candida albicans A SMA 10 ppm Candida albicans A 10 ppm Candida albicans A K 75 10 ppm Candida guillermondii A K 334 10 ppm Candida guillermondii A SMA 33 ppm Candida krusei DSM 70075 M-H 10 ppm Candida lipolytica DSM 1345 M-H 1.0 ppm Candida parakrusei A SMA 4 ppm Candida parapsilosis A SMA 33 ppm Candida parapsilosis A K 332 30 ppm Candida pulcherrima A SMA 33 ppm Candida stellatoidea A SMA 10 ppm Candida tropicalis A SMA 10 ppm Candida tropicalis A K 644 10 ppm Candida tropicalis DSM 1346 M-H 10 ppm Candida utilis A SMA 33 ppm Chaetomium globosum ATCC 6205 SMA 10 ppm Cryptococcus neoformans A SMA 10 ppm Epidermophyton floccosum ATCC 10227 SMA 10 ppm Epidermophyton floccosum CBS 55384 M-H 2.5 ppm Hansenula anomala A SMA 10 ppm Keratinomyces ajelloi A SMA 10 ppm Malassezia furfur ATCC 14521 SMA >1000 ppm Malassezia furfur DSM 6171 SMA 500 ppm Microsporum canis ATCC 10214 M 3 ppm Microsporum canis ATCC 10214 SMA 1-10 ppm Microsporum cookei A SMA 33 ppm Microsporum cookei A K 406 M 3 ppm Microsporum gypseum A SMA 10 ppm Microsporum nanum A SMA 10 ppm Neurospora sitophilia A SMA 0.1 ppm Paecilomyces varioti ATCC 18502 SMA 10 ppm Penicillium egyptiacum A SMA 33 ppm Penicillium expansum DSM 1282 SMA 31.2 ppm Penicillium funiculosum ATCC 9645 SMA 10 ppm Pichia farinosa A SMA 33 ppm Piedraia hortai A SMA 10 ppm Rhodotorula mucilaginosa A SMA 33 ppm Saccaromyces cervisiae ATCC 2601 BHI 4 ppm
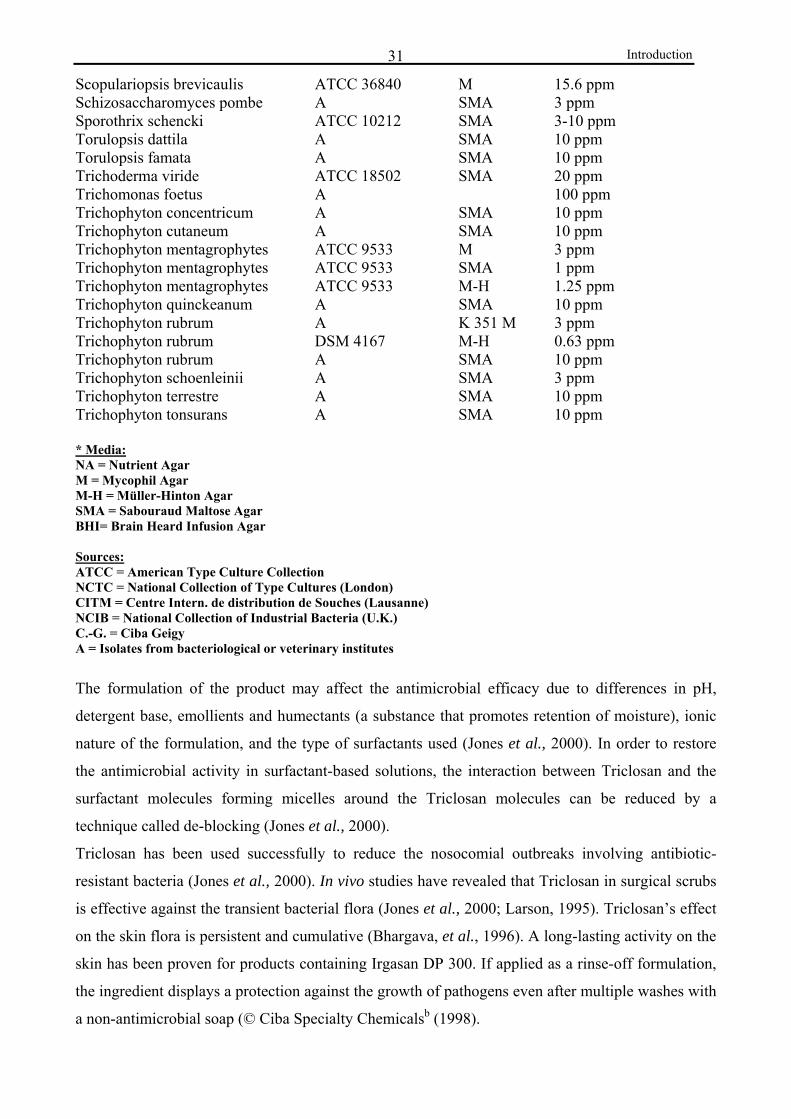
Introduction 31
Scopulariopsis brevicaulis ATCC 36840 M 15.6 ppm Schizosaccharomyces pombe A SMA 3 ppm Sporothrix schencki ATCC 10212 SMA 3-10 ppm Torulopsis dattila A SMA 10 ppm Torulopsis famata A SMA 10 ppm Trichoderma viride ATCC 18502 SMA 20 ppm Trichomonas foetus A 100 ppm Trichophyton concentricum A SMA 10 ppm Trichophyton cutaneum A SMA 10 ppm Trichophyton mentagrophytes ATCC 9533 M 3 ppm Trichophyton mentagrophytes ATCC 9533 SMA 1 ppm Trichophyton mentagrophytes ATCC 9533 M-H 1.25 ppm Trichophyton quinckeanum A SMA 10 ppm Trichophyton rubrum A K 351 M 3 ppm Trichophyton rubrum DSM 4167 M-H 0.63 ppm Trichophyton rubrum A SMA 10 ppm Trichophyton schoenleinii A SMA 3 ppm Trichophyton terrestre A SMA 10 ppm Trichophyton tonsurans A SMA 10 ppm * Media: NA = Nutrient Agar M = Mycophil Agar M-H = Müller-Hinton Agar SMA = Sabouraud Maltose Agar BHI= Brain Heard Infusion Agar Sources: ATCC = American Type Culture Collection NCTC = National Collection of Type Cultures (London) CITM = Centre Intern. de distribution de Souches (Lausanne) NCIB = National Collection of Industrial Bacteria (U.K.) C.-G. = Ciba Geigy A = Isolates from bacteriological or veterinary institutes
The formulation of the product may affect the antimicrobial efficacy due to differences in pH,
detergent base, emollients and humectants (a substance that promotes retention of moisture), ionic
nature of the formulation, and the type of surfactants used (Jones et al., 2000). In order to restore
the antimicrobial activity in surfactant-based solutions, the interaction between Triclosan and the
surfactant molecules forming micelles around the Triclosan molecules can be reduced by a
technique called de-blocking (Jones et al., 2000).
Triclosan has been used successfully to reduce the nosocomial outbreaks involving antibiotic-
resistant bacteria (Jones et al., 2000). In vivo studies have revealed that Triclosan in surgical scrubs
is effective against the transient bacterial flora (Jones et al., 2000; Larson, 1995). Triclosan’s effect
on the skin flora is persistent and cumulative (Bhargava, et al., 1996). A long-lasting activity on the
skin has been proven for products containing Irgasan DP 300. If applied as a rinse-off formulation,
the ingredient displays a protection against the growth of pathogens even after multiple washes with
a non-antimicrobial soap (© Ciba Specialty Chemicalsb (1998).
Introduction 32
Triclosan applied as a 1% formulation offers excellent immediate, broad-spectrum and persistent
antimicrobial activity combined with gentleness to the skin, even if applied frequently (Jones et al.,
2000).
2.1.4 Mechanism of action against dermatophytes, moulds and yeasts
The in vitro efficacy against many dermatophytes, moulds and yeasts can be explained by
interactions of the agent with the fungal cell membrane. Mainly unspecific effects such as
disorganization of the cytoplasmatic membrane and leakage of low molecular weight cellular
components as well as inhibition of nutrient uptake are considered to be important factors with
regard to the mode of action of Triclosan. The extent to which the inhibition of the enzyme enoyl
reductase, which is essential for synthesis of fatty acids and is an important target for Triclosan in
bacteria, particularly at low concentrations of Triclosan, plays a role in the activity against fungi is
not yet fully understood (Regös et al., 1974; D. Ochs, personal communication).
2.1.5 Concentrations currently in use
In cosmetic products Triclosan is usually available in concentrations ranging between 0.1 and 0.3%.
These products include under arm deodorants, deodorant bar and liquid soaps, liquid hand washes,
shower and bath products, lotions, creams, hair shampoos and shaving products.
If applied as a medical soap, the concentration of Triclosan has to be higher and reaches 1%. As a
rule, rinse-off formulations require higher concentrations than leave-on formulations.
2.2 Triclosan-containing products currently in use in Africa
There are several products currently available in East Africa, which contain Triclosan. Examples
are Protex® Antibacterial Soap (Colgate, Nairobi; Bodycare, Dar es Salaam), Lifebuoy®/Asespo®
Soap (Unilever Nairobi), Roberts® Antiseptic Soap (Cussons Nairobi), Familiy Medicated Soap®
(G&N Soap, Dar es Salaam), and Tropcial Deo® (Buyline, Nairobi).

Methods 33
Methods
1. Study Area
A placebo-controlled, double-blind clinical trial was carried out in Ifakara, Kilombero District,
Morogoro Region, in southern Tanzania, to assess the efficacy of Triclosan in soap against selected
dermatomycoses and scabies. The district is a rural area with an estimated population of
approximately 322,000 (United Republic of Tanzania, 2002). The district capital, Ifakara, is situated
in the river plain of Kilombero River, 270 m above sea level and 320 km southwest of Tanzania’s
largest city, Dar es Salaam. The estimated annual rainfall is 1350 mm/year. There are two rainy
seasons, from October to December and from February to May (Armstrong Schellenberg et al.,
2003). Ambient temperatures are highest in December and lowest in July (The management and
ecology of Tanzanian forests; 2001) (also see Table 1). Most inhabitants are subsistence farmers
who grow mainly rice, maize, cassava and bananas (aTanner et al., 1987). Other common
occupations are fishing and small-scale trading (Armstrong Schellenberg et al., 2002).
Figure 1: Tanzania (Source: SuperTravelNet.Com) Figure 2: Morogoro Region and Ifakara
© Acosta et al., 2001 Table 1: Overview of climatic conditions in Ifakara during the time of the study (Source: IPS Meteostar®)
Month Average High
(°C)
Average Low
(°C)
N° of days
with rain
April 30.6 25.0 11 Screening May 28.3 23.3 17 Follow-up 1 June 27.2 22.2 12
Exami- nation
Follow-up 2 July 26.2 21.6 12
The health situation in Kilombero District is still generally poor, prevalence rates of malnutrition
and communicable diseases are high, and availability of food, clean and safe water, and sound
environmental sanitation are limited. Common water sources are communal boreholes, natural
Methods 34
spring or river water, and hand-dug wells. The roads are unpaved and transport is difficult in the
rainy season. The public health in system is organized through dispensaries, health centres and
hospitals. Maternal and child health clinics are widely available (Armstrong Schellenberg et al.,
2002). The dermatologic outpatient department at Ifakara’s St. Francis Designated District Hospital
(SFDDH) with one dermatologist serves a population of over 600,000 of the whole diocese
(Kilombero and Ulanga District combined) (Kibatala, 2002).
According to the 1997 St. Francis Designated District Hospital’s (SFDDH) Annual Report, fungal,
parasitic and bacterial skin disorders in the rural population, are still highly prevalent among the
local population compared to the urban population (Kibatala, 1997).
2. Selection of Primary Schools
After the study protocol was approved by the ethical committees in Basel, Switzerland, (EKBB) and
in Tanzania (IHRDC), two primary schools (3 - 8 km from Ifakara town centre) were selected for
the study. This selection occurred in agreement between the local supervisor, Dr. B. Idindili, the
representative in charge of the District Medical Office and the District Educational Officer (DEO).
A written permission documenting this decision was obtained from the DEO. The field
investigators then introduced themselves to the teachers of the schools in order to explain the
concept and the procedures of the study and to present them the written permission. Both schools
agreed to take part in the study.
The screening examinations were started at Lihami Primary School and then continued at Michenga
Primary School until enough children could be recruited for the soap trial.
3. Screening Examinations
The screening examinations were performed at two primary schools (Lihami and Michenga Primary
Schools), 3 and 8 km from Ifakara town centre. All the physical examinations in the course of this
randomized, double-blind, prospective, placebo-controlled study were performed in Swahili by the
dermatologist of the local district hospital (SFDDH), Dr. M. Mbata (MM), a clinical officer, C.
Maswi (CM), and the medical students from the University Hospital Freiburg, Germany, Julia Ferié
(JF) and Almuth Dinkela (AD) (principal investigator of the soap trial). At Lihami Primary School
the interview and examination were carried out in two small rooms (each approximately 2.5 m2 x 2
m2) with two windows serving as light source. In Michenga, a larger room with a curtain generating
privacy was available. The first screening of each child consisted of four parts: (i) the examination
of the skin, (ii) written documentation of the history and clinical presentation of skin diseases
currently present, following standardized definitions and (iii) supported by digital photography, (iv)
Methods 35
sample-taking (skin scrapings and/or hair clippings) at the active borders of the lesions. These steps
were carried out as follows:
(i): The entire body surface, hairs and nails were examined. The examination of the genital region
was not possible in every child because privacy could not always be guaranteed depending on the
room in which the examinations were carried out. The largest diameter of the biggest lesion was
recorded.
(ii): Several questions concerning the hygiene behaviour and living conditions were asked. These
questions were evaluated in another study (For details please see Ferié, 2005). If during the physical
examination a skin disease was discovered, the history-taking and description of the skin disease
was documented using a standardized questionnaire in Kiswahili. In case that several diagnoses
were present, the “principal diagnosis” was described in detail and characteristic signs and
symptoms of the disease were assessed. The findings related to the other diagnoses were also
documented. In the case of dermatomycoses and scabies the characteristic parameters were
summarized in a clinical score to assess the degree of infection (see “Patients, Approaches and
Methods: 6. Degree of infection”).
In case of the presence of several diagnoses of interest for soap trial, the “principal diagnosis” was
selected according to the priorities of this study:
- if several superficial fungal infections were present, the order was as follows:
1. Tinea capitis
2. Tinea corporis
3. Tinea versicolor
4. Tinea pedis
- scabies was always the main disease
(iii): For each skin disease identified the main skin lesion was documented by digital photography.
In order to identify the child in the picture a piece of paper displaying the seven digit identification
number number of the child was placed beside the skin lesion. The attempt was to take pictures of
the same lesion during each of the three examinations. All uncertain and various representative
cases, were cross-checked by the expert dermatologist, PD Dr. P. Schmid-Grendelmeier in Zürich, a
fully trained dermatologist, skilled with experience in tropical skin diseases.
(iv): If tinea corporis, tinea capitis or tinea versicolor infection was suspected, a sample was taken at
the active borders of the lesions as described by Weitzman et al., and Gupta et al. and Stein
(Weitzman et al., 1996; Gupta, 2002; Gupta et al., 2001; Stein, 1983). In the case of tinea capitis,
apart from the skin scrapings, hair clippings or scrapings from hair stumps were taken if possible.
The samples were taken by using sterile surgical blades (n° 15). The scales were placed on pieces of
white paper, which were then folded, closed with stapler pins and stored in plastic envelopes, which
Methods 36
are normally used by the local pharmacies to store the pills to be sold. A new plastic envelope was
used for each child. If several samples were taken of one child, the different body sites were
documented on the piece of paper on which the scales were placed.
In the case of clinically diagnosed scabies, samples were taken from suspicious lesions with a sterile
surgical blade (n° 15) using immersion oil. They were directly placed on a microscopic slide,
covered with a cover slip and then preserved with clear polish and stored in a plastic envelope. All
samples were brought to the laboratory at IHRDC for microscopic examination on the same day or
after a maximum of two days. The microscopic examination was performed by AD and JF. The
fungal scales were put on a microscopic slide on which 20% potassium hydroxide solution had been
applied, and covered with a cover slip. After 20 minutes the samples were examined using 10 and
40 fold magnification. The result was regarded as positive if hyphae and/or mycelia and/or large
amounts of spores were seen. No sample was taken from tinea pedis lesions.
The scabies samples were examined with 10 fold magnification. The result was regarded as positive
if mites, scybala or eggs could be discovered. Quality control was ensured by controls performed by
H. Urassa, microbiologist and research scientist at IHRDC (Ifakara Health Research and
Development Centre).
In all cases of suspected fungal infections, particularly if differential diagnosis between tinea
corporis and tinea versicolor infections was difficult, additional skin samples were taken after one,
two and approximately three months after the baseline examination, stored in the plastic envelopes
in the usual manner and then transported to Zürich via air courier services to the laboratory of
mycology at the University Hospital Zürich. Here three drops of Congo Red solution were used
instead of KOH solution for microscopic diagnosis, six to seven pieces of scales were added and
covered with a coverslip. Examination of the samples was performed using a 20 to 40 fold
magnification. The remaining scales were placed on three different agars for culture (see Table 2).
Table 2: Composition of different media used for microscopic examination and culture Composition of Congo Red solution: Composition of Dixon Agar: SDS (sodium dodecyl sulphate) 5 g Bacto Malt Extract 5 mL Congo Red 0.5% in Ethanol 50% 5 mL Bacto oxygal 20 g Distilled water 1000 mL Bacto glycerol 2.5 mL Tween 40 10 mL
Distilled water 1000 mL Bacto Agar 15 g Chloramphenicol 50 mg Gentamycin 5 mg Cycloheximide + Aceton 0.4 g
Composition of Sabouraud Glucose Agar: Composition of Mycosel Agar (containing cycloheximide):
Glucose 40 g Mycosel Agar 54 g Neopeptone 10 g Distilled water 1500 ml Agar granulated 16 g Choramphenicol 50 mg Distilled water 1000 mL Gentamycin 5 mg Chloramphenicol 50 mg Gentamycin 5 mg

Methods 37
Dixon agar was used for cultivating Malassezia spp. Sabouraud Glucose Agar allows the growth of
dermatophytes, molds and yeasts apart from Malassezia spp. and contains chloramphenicol and
gentamycin to inhibit bacterial growth. Mycosel Agar is similar to the latter, but additionally
contains cyclohexmide to prevent the growth of molds. Cultures were left at about 20° C for 3 to 4
weeks. If Malassezia spp. cultivation on Dixon Agar was successful, a specimen of the culture was
stained using gram technique and observed under light microscope with a 100 fold magnification. If
dermatophytes were identified by colony morphology, two subcultures were prepared using Phenol
Red Agar and Potato Dextrose Agar. Specimens of cultures positive for dermatophytes were stained
with cotton blue and observed under a 40 fold magnification. A further identification technique was
that of the “hanging drop”.
4. Admission to the Study
4.1 Inclusion Criteria
The children were included in the study if they were diagnosed clinically at the screening
examination to suffer from tinea versicolor, tinea capitis, tinea corporis, tinea pedis or scabies.
The inclusion of cases of tinea cruris was not possible for two reasons. First, privacy and an
investigator of the same sex as the examined child could not be always guaranteed. Second, no
Wood Lamp was available, which would have facilitated the differential diagnosis between
erythrasma and tinea cruris. At both schools meetings were held during which the parents or
caretakers were informed about the procedures of the soap trial and were given the opportunity to
ask questions (see Appendix D 2.1 and 2.2). They were provided with information material
regarding the skin disorder their child was suffering from (see Appendix D 3.1.1 to 3.2.2). Besides,
they received a form sheet guaranteeing the access to free treatment for the skin disease which had
been the reason for admission to the study, if the study participant would not be cured after two
months of soap use or if he or she would suffer from any side-effects related to the soap use in the
course of the study (see Appendix D 4.1). At the end of these meetings the parents or caretakers
were asked to give their oral informed consent to let the child participate in the soap trial (see
Appendix D 1.1 and 1.2).
4.2 Excludsion Criteria
On admission children were excluded if the degree of their skin disorder was so severe they
required immediate treatment with either antifungal or antiscabietic drugs, which were then
administered directly after the screening examination. If the child explained in the course of the

Methods 38
history-taking that he or she had already been given any kind of standard treatment at other health
facilities participation in the present study was not possible.
During follow-up, study participants were excluded if they had decided they did not wish to
participate any longer; if they had received any of the above mentioned treatments other than the
soap since the first screening examination; if no more lesions were seen at the first soap
distribution; if they had received their soap less than four times or if they were not present at the
second follow-up examination. No child developed side-effects thus none had to be excluded for
this reason.
If the local dermatologist (Dr. M. Mbata) decided during the period of soap use that the infection
required urgent treatment, the children were excluded from the study and received a prescription for
free standard treatment (see 8. Follow-up Examinations) for their skin disorders from the
dermatologist.
5. Case Definitions
Tinea versicolor:
The following criteria characterize the clinical picture of tinea versicolor.
Shape and appearance of the lesions (Canizares et al., 1993; Sunenshine, 1998; Piamphongsant,
1983; Gupta, 2002):
• Multiform macules or patches
• Lesions may coalesce and/or be perifollicular
• Hypo- or hyperpigmented
• Fine, adherent scales (may be absent after the use of Vaseline)
• Pruritus may be present.
Typical localizations (Canizares et al., 1993):
Areas with the greatest density of sebaceous glands such as the upper trunk, neck and face,
sometimes on upper arms and abdomen. Rarely on other body parts.
Other superficial dermatomycoses (tinea capitis, corporis and pedis):
Species identification could not be performed in all cases. Apart from dermatophytes, yeasts or
moulds may have been among the etiologic fungi. Therefore cases of tinea capitis, corporis and
pedis will be referred to as “other superficial dermatomycoses”.
Tinea capitis:
One of the three clinical pictures has to be present for diagnosis.
Shape and appearance of the lesions (Canizares et al., 1993; Shrum, 1994; Weitzman et al., 1996):
Methods 39
• Scaly, dry, non-inflammatory lesions sometimes presenting grey patches or “black
dots”
• Acute, wet, and inflammatory lesions with possible suppuration or kerion formation
• Dry, crusted, occasionally inflammatory and suppurative lesions, yellow crusts (also
called “favus”). Folliculitis, bacterial superinfection, alopecia and scarring may
occur.
Pruritus may be present. Positive microscopy confirms diagnosis but is not regarded as mandatory
in this study.
Tinea corporis:
The following criteria characterize the clinical picture of tinea corporis. Shape and appearance of
the lesions (Canizares et al., 1993):
• Sharply demarcated round or oval scaly patch(es)
• Active vesicular border and central clearing may be present. Occasionally pustular
lesions
Pruritus may be present. Typical localizations (Canizares et al., 1993):
• Glabrous (=hairless) skin including non-hairy parts of face, neck, trunk, limbs (not
axillae, groins, interdigital spaces of hands or feet, palms or soles)
The aspect of the lesions may in some cases resemble those of tinea versicolor, especially if
multiple lesions are present. In these cases, the final diagnosis was based on the culture performed
in Zürich.
Tinea pedis:
One of the three clinical pictures has to be present for diagnosis.
Shape and appearance of the lesions (Canizares et al., 1993; Masri-Fridling, 1996; Shrum, 1994):
• Interdigital type with maceration. It may extend to both the toes and the soles
• Dishydrotic type with acute versicular, bullous or vesiculo-bullous lesions with
erythema, fissuring and sometimes bacterial superinfection. Usually located on the
mid-sole
• Hyperkeratotic moccasin type; tends to be chronic and presents with scaling of the
plantar surface. No vesiculation.
Pruritus may be present.
Scabies:
Four features are diagnostic of scabies (Canizares et al., 1993; Canizares, 19983; Van Hees, 2001;
Anezib, 1981; Haas , 2001; Burkhart, et al., 2000):
• Itching (most severe at night)
• Typical rash (small blisters and papules)

Methods 40
• Scabies burrows
• Common localization: sides of the fingers and hands, flexor sides of the wrists,
anterior parts of elbows, on the genitals and buttocks etc.
A history of contact with infestated persons supports the diagnosis.
6. Degree of Infection
Based on several other studies the degree of infection was assessed by using a separate symptom
score for tinea versicolor, tinea capitis, corporis and pedis as well as for scabies infection (Hira et
al., 1986; Lange et al., 1998; Hickman, 1996; Hussain et al., 1999; Martinez-Roig et al., 1988;
Gupta et al., 1998) (see Tables 3a and 3b).
This score reflects the degree of certain clinical signs and symptoms typical of each of the four
types of fungal infections. In order to calculate this score the appropriate parameters were chosen,
and score values were given by the four examiners on examination for each parameter (see Tables
3a and 3b; also see Appendix C Part 1.3). These score values were then added to yield the total
score.
Tables 3a and 3b: For each of these diseases the appropriate parameters were chosen, and separate score values were
added to a total score (based on Hira et al., 1986; Lange et al., 1998; Hickman, 1996; Hussain et al., 1999; Martinez-
Roig et al., 1988; Gupta et al., 1998). The score reflects the degree of certain clinical signs and symptoms typical of
each of the four types of fungal infections targeted for the study.
Table 3a: Score parameters and score values
Degree of pruritus
Number of lesions
Aspect of lesions
Size of largest lesion
Additional clinical signs
Diagnosis
Possible range of partial score according to parameter Total score
T. versicolor 0 to 3 0 to 8 0 to 14 N.A. N.A. 0 to 25
T. capitis 0 to 3 0 to 8 0 to 18 0 to 6 0 to 6 0 to 41 T.
corporis 0 to 3 0 to 8 0 to 12 0 to 6 N.A. 0 to 29
T. pedis 0 to 3 0 to 8 0 to 4 0 to 6 N.A. 0 to 21 Scabies 0 to 3 0 to 6* 0 to 16 N.A. N.A. 0 to 27
* number of common localizations (Pinkerton et al., 2003; Anezia, 1981)
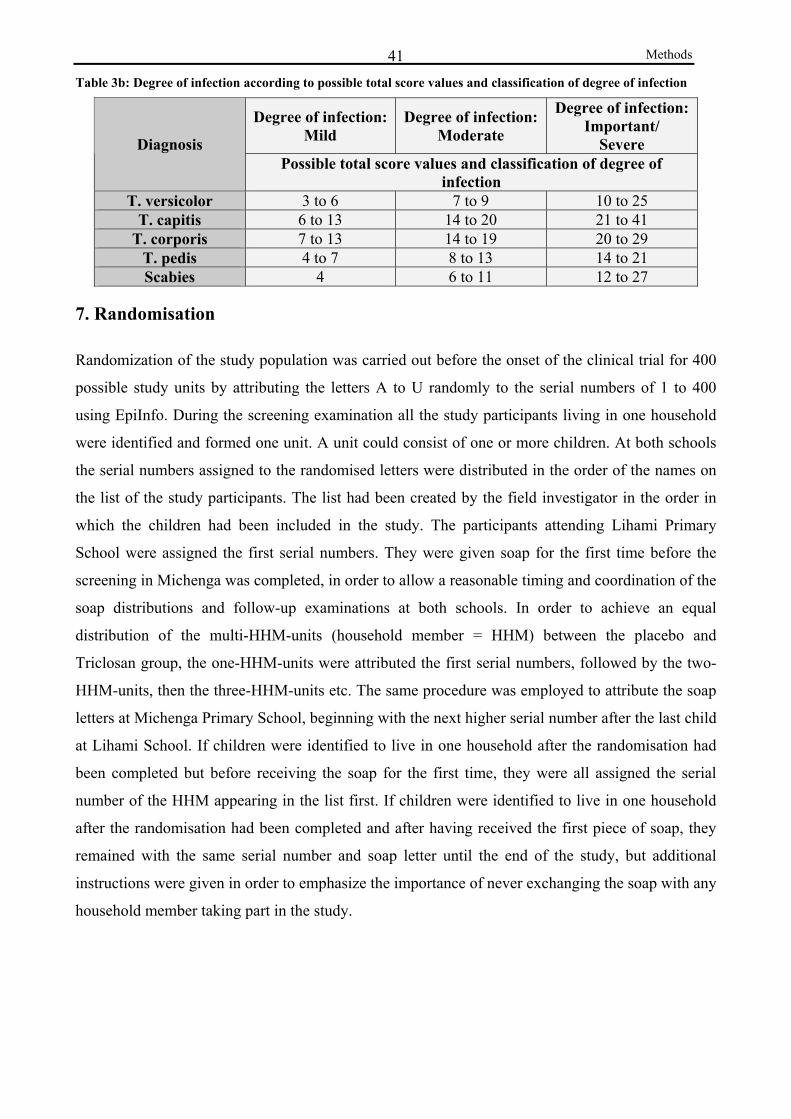
Methods 41Table 3b: Degree of infection according to possible total score values and classification of degree of infection
Degree of infection: Mild
Degree of infection: Moderate
Degree of infection: Important/
Severe Diagnosis Possible total score values and classification of degree of
infection T. versicolor 3 to 6 7 to 9 10 to 25
T. capitis 6 to 13 14 to 20 21 to 41 T. corporis 7 to 13 14 to 19 20 to 29
T. pedis 4 to 7 8 to 13 14 to 21 Scabies 4 6 to 11 12 to 27
7. Randomisation
Randomization of the study population was carried out before the onset of the clinical trial for 400
possible study units by attributing the letters A to U randomly to the serial numbers of 1 to 400
using EpiInfo. During the screening examination all the study participants living in one household
were identified and formed one unit. A unit could consist of one or more children. At both schools
the serial numbers assigned to the randomised letters were distributed in the order of the names on
the list of the study participants. The list had been created by the field investigator in the order in
which the children had been included in the study. The participants attending Lihami Primary
School were assigned the first serial numbers. They were given soap for the first time before the
screening in Michenga was completed, in order to allow a reasonable timing and coordination of the
soap distributions and follow-up examinations at both schools. In order to achieve an equal
distribution of the multi-HHM-units (household member = HHM) between the placebo and
Triclosan group, the one-HHM-units were attributed the first serial numbers, followed by the two-
HHM-units, then the three-HHM-units etc. The same procedure was employed to attribute the soap
letters at Michenga Primary School, beginning with the next higher serial number after the last child
at Lihami School. If children were identified to live in one household after the randomisation had
been completed but before receiving the soap for the first time, they were all assigned the serial
number of the HHM appearing in the list first. If children were identified to live in one household
after the randomisation had been completed and after having received the first piece of soap, they
remained with the same serial number and soap letter until the end of the study, but additional
instructions were given in order to emphasize the importance of never exchanging the soap with any
household member taking part in the study.

Methods 42Table 4: Composition of the placebo and active soaps
Placebo Soap: Active Soap: 0.2% Titanium Dioxide 0.2% Titanium Dioxide 0.023% Tetrasodium EDTA 0.023% Tetrasodium EDTA 3.0% Stearic Acid 3.0% Stearic Acid 0-5% Glycerine / Water 1:1 0-5% Glycerine / Water 1:1 q.s. Dye /Perfume q.s. Dye /Perfume ad 100.0% Soap Noodles* ad 100.0% Soap Noodles** 1.0% IRGASAN DP300 **Mettler Basic Soap:
80.0% Sodium tallowate 20.0% Sodium cocoate Through the attribution of the letter each child was assigned to receive his or her soap bar pieces
from one kind of box (labelled alphabetically, A to U) only. Each box contained 30 pieces of soap
(100g per piece). The letter printed on the boxes indicated if the soap contained Triclosan or not.
Until data entry and data cleaning was finished, all four field investigators were blind with regard to
who received Triclosan or the placebo (for composition of soap see Table 4). Considering the
possibility that the whole family would use the child’s soap, it was provided generously. The
prinicpal investigator (AD), assisted by MM, CM and JF, visited both schools weekly to distribute a
new soap bar per child.
8. Follow-up Examinations
Two follow-up examinations were performed, after the first and second month of soap use. Apart
from history-taking and questions concerning hygiene behaviour and living conditions, these
follow-up examinations involved the same steps as the first screening examination (also see Figure
3):
(i) examination of the skin, (ii) documentation of the skin lesions by digital photography, (iii) only
at the second follow-up examination: sample-taking if a superficial fungal infection (not in
candidiasis, tinea pedis or cruris infections) was present. The sample-taking was not repeated in the
case of scabies infections.
Three additional questions were introduced: (i) whether the child had experienced any improvement
of the skin disorder due to the soap consumption; (ii) if specifically the pruritus had improved; (iii)
and in case of tinea capitis infection if new hair growth was visible.
When possible, pictures were taken of the same lesion during each of the three examinations for
evaluation of improvement or resolution of symptoms during the follow-up examinations. On
comparison special attention was paid to the aspect of the lesions at the first and second follow-up.
The following parameters were assessed and summarised by classifying the result of the
comparison into “improvement”, “same” or “deterioration”:
Methods 43
• size of the lesion
• number of lesions
• presence of “active” lesions (see 5. Case definitions)
• presence of only residual hypopigmentation (Weitzman et al., 1996; Sunenshine,
1998) or postinflammatory hyperpigmentation
• presence of superinfection (in case of dermatophyte or scabies infection)
• new hair growth visible (in case of tinea capitis infection)
If a child was cured at the time of the first follow-up, no picture was taken. Samples were taken
during the second follow-up at the site of the former lesions, even if no one were present at this
stage. All children who were not cured by the end of the soap trial were given a presription from the
dermatologist Dr. M. Mbata to receive free treatment at the SFDDH dispensary. Drugs prescribed
were oral ketoconazole for tinea versicolor, tinea capitis, corporis or pedis; griseofulvine for tinea
capitis, corporis and pedis; clotrimazole cream or Whitfield’s Ointment for minor cases of tinea
versicolor, tinea capitis, corporis, or pedis and BBE to treat scabies. Terbinafine was provided to the
children who were severely affected by tinea capitis at the end of the soap trial.
9. Evaluation of Effectiveness - Dermatomycoses
9.1 General
In order to assess the effectiveness of the soap containing Triclosan, several endpoints (clinical
signs and symptoms typical of the disease) were evaluated during all examinations. The relative risk
of having these symptoms if receiving placebo versus active soap was calculated for the screening
and follow-up 2.
9.2 Pruritus
In order to improve the reliability of the answers of the children, the examiners asked twice during
the history-taking if the child had pruritus. Not all the children gave coherent answers. Therefore
the results may be sometimes contradictory, e.g. when compared with the degrees of pruritus.
The calculation of the relative risk combines answers provided at the two different stages of the
history- taking. If one of the two questions was answered positively, it was considered that pruritus
had been present.
Methods 44
9.3 Clinical and Microscopic Resolution
In order to decide whether the study participants were cured at time of the second follow-up seven
(five in case of tinea pedis) evaluation categories were defined, which combined clinical signs and
symptoms and the result of the microscopic examination (only clinical signs in the case of tinea
pedis). The Chi2 test or the Fisher’s exact test were used to find out if the evaluation categories
were equally distributed between active and placebo groups.
9.4 Definition of Evaluation Categories at Second Follow-up
9.4.1 Tinea versicolor
CATEGORY: DEFINITION:
Clinical and mycological resolution (based on Lange et al., 1998; Hickman, 1996):
1: clinical and microscopic resolution: score = 0, child cured
2: microscopic resolution: microscopy negative and few clinical symptoms:
Score < 4 (only if score had been > 4 at screening)
No resolution:
3: improvement: negative microscopic evidence with significant clinical
improvement: reduction of score to 5 or 6 & score at screening > 6
or reduction by 4 points & score at screening > 6
4: negative microscopic evidence with no significant clinical improvement
reduction of score to > 7
or reduction by < 4 points
or score at screening and at second follow-up = 4
5: positive microscopic evidence with significant clinical improvement:
reduction of score to 5 or 6 & score at screening > 6
or reduction by 4 points & score at screening > 6
6: lack of improvement: positive microscopy with a lack of significant clinical
improvement: score > 7 or reduction by < 4 points
7: deterioration: increased score
9.4.2 Tinea capitis
CATEGORY: DEFINITION:
Clinical and mycological resolution (based on Hussain et al., 1999; Gupta et al., 1998):
1: clinical and microscopic resolution: score = 0, child cured
Methods 45
2: microscopic resolution: microscopy negative and few clinical symptoms:
Score < 6
No resolution:
3: improvement: negative microscopic evidence with significant clinical
improvement: reduction of score to < 14 or reduction by > 6 points
4: negative microscopic evidence with no significant clinical improvement:
reduction of score to > 14 or reduction by < 6 points
5: positive microscopic evidence and clinical resolution with significant
clinical improvement: reduction of score to < 14 or reduction by > 6 points
6: lack of improvement: positive microscopy with a lack of significant clinical
improvement: reduction of score to > 14 or reduction by < 6 points
7: deterioration: increased score
9.4.3 Tinea corporis
CATEGORY: DEFINITION:
Clinical and mycological resolution: (based on Gooskens et al., 1994; Montero-Gei et al., 1992)
1: clinical and microscopic resolution: score = 0, child cured
2: microscopic resolution: microscopy negative and few clinical symptoms:
Score < 7
No resolution:
3: improvement: negative microscopic evidence with significant clinical
improvement: reduction of score to < 14 or reduction by > 6 points
4: negative microscopic evidence with no significant clinical improvement
reduction of score to > 14 or reduction by < 6 points
5: positive microscopic evidence and clinical resolution with significant
clinical improvement: reduction of score to < 14 or reduction by > 6 points
6: lack of improvement: positive microscopy with a lack of significant clinical
improvement: reduction of score to > 14 or reduction by < 6 points
7: deterioration: increased score
9.4.4 Tinea pedis
CATEGORY: DEFINITION:
Clinical resolution (abbreviations: N.A.= non-applicable)
1: clinical resolution: score = 0, child cured
no resolution:
Methods 46
2: improvement : score was reduced
3: lack of improvement: score remained the same
4: no resolution: score was N.A. at screening, but child was not cured at
second follow-up
5: deterioration: increased score
10. Evaluation of Effectiveness - Scabies
In order to assess the effectiveness of the soap containing Triclosan, several endpoints (certain signs
and symptoms typical of the disease) were evaluated during all the examinations. No significance
tests could be performed because the sample sizes were too small (only two children in the active
group).
Apart from the parameters used for the symptom score, the time of itching, involvement of other
family members, the localization of the lesions, and the result of the microscopic examination were
recorded. Burrows were hardly found during the baseline examination, which impaired the sample-
taking to a great extent. This procedure was therefore not repeated at the second follow-up.
11. Assessment of Soap Use (Compliance)
One piece of soap per week and child was distributed at the two schools. The availability of soap
was ensured for every study participant, by personal delivery through the field investigator, assisted
by MM, CM and JF at the two primary schools. The following additional tools for checking the use
of soaps were used:
1) Upon receipt of a new bar of soap, the remains of the former piece had to be returned.
2) If the child was not present in the school at the time of soap distribution, a student who
knew where the child lived was identified in order to deliver the soap to the child’s home, or
a teacher was given clearly labelled envelopes containing the soaps, which were then to be
delivered through him/her.
3) At each soap distribution a record was kept whether the child collected the soap him/herself
or who was selected as a courier instead.
4) If the child informed the investigator in advance that he/she would not be present for a
certain number of weeks, he or she received the appropriate number of soaps at the time
when the child was present.
5) During the second follow-up each child was asked if he/she received the soap the week
before and by whom.

Methods 47
6) After the last soap distribution, control visits lasting nine days in Lihami and seven days in
Michenga, were conducted by another field worker (professional nurse) at the homes of 10%
of the study participants who had been randomly selected. Before randomisation, two
clusters were independently formed at each school. One included children who had collected
the soap themselves at the last soap distribution while the other included children who had
been sent the soap by another person. The remaining pieces of soap had to be shown to the
field worker during her visit. This was done in order to check the presence of the study soap
pieces at the children’s homes. The field worker also questioned the child or the interviewed
household member about who had given the latest piece of soap to the child.
7) The field worker also asked how many pieces of soap the child had received in total and
how many people in the household had used the soap.
In the case of the 10% randomly selected study participants, this information was evaluated for
coherence. In case children had been delivered the soap at home, we calculated which proportion of
them could either show a piece of soap to the field worker or confirmed when asked in the course of
the second follow-up that they had received their piece of soap by someone else.
The tools employed to check the use of soaps proved that the measures taken to deliver the soaps
can be considered as reliable. Unlike originally planned, the children were given a new piece of
soap even if the remains of the former piece could not be returned, since most children had used the
whole piece or could not show it for other reasons. Their future soap consumption was regarded as
more likely if they were provided with a new piece of soap rather than being sent back home to
collect the old piece before obtaining the new one.
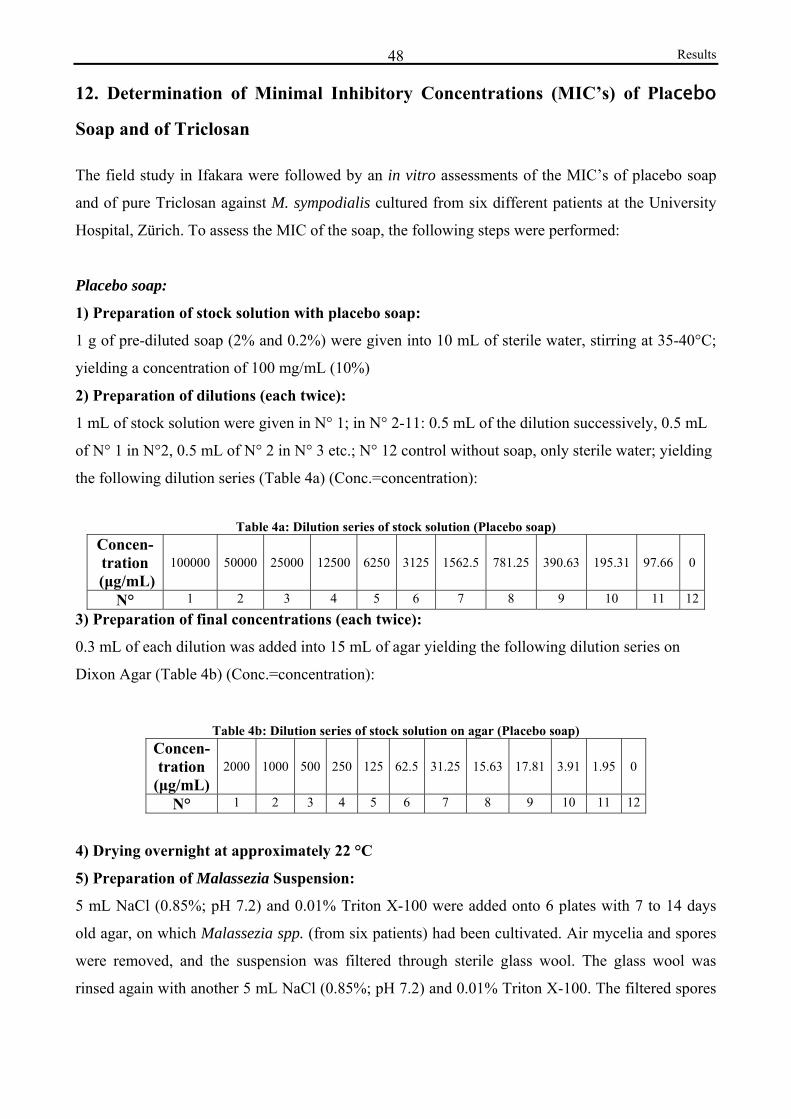
Results 48
12. Determination of Minimal Inhibitory Concentrations (MIC’s) of Placebo
Soap and of Triclosan
The field study in Ifakara were followed by an in vitro assessments of the MIC’s of placebo soap
and of pure Triclosan against M. sympodialis cultured from six different patients at the University
Hospital, Zürich. To assess the MIC of the soap, the following steps were performed:
Placebo soap:
1) Preparation of stock solution with placebo soap:
1 g of pre-diluted soap (2% and 0.2%) were given into 10 mL of sterile water, stirring at 35-40°C;
yielding a concentration of 100 mg/mL (10%)
2) Preparation of dilutions (each twice):
1 mL of stock solution were given in N° 1; in N° 2-11: 0.5 mL of the dilution successively, 0.5 mL
of N° 1 in N°2, 0.5 mL of N° 2 in N° 3 etc.; N° 12 control without soap, only sterile water; yielding
the following dilution series (Table 4a) (Conc.=concentration):
Table 4a: Dilution series of stock solution (Placebo soap) Concen- tration
(μg/mL) 100000 50000 25000 12500 6250 3125 1562.5 781.25 390.63 195.31 97.66 0
N° 1 2 3 4 5 6 7 8 9 10 11 123) Preparation of final concentrations (each twice):
0.3 mL of each dilution was added into 15 mL of agar yielding the following dilution series on
Dixon Agar (Table 4b) (Conc.=concentration):
Table 4b: Dilution series of stock solution on agar (Placebo soap) Concen- tration
(μg/mL) 2000 1000 500 250 125 62.5 31.25 15.63 17.81 3.91 1.95 0
N° 1 2 3 4 5 6 7 8 9 10 11 12
4) Drying overnight at approximately 22 °C
5) Preparation of Malassezia Suspension:
5 mL NaCl (0.85%; pH 7.2) and 0.01% Triton X-100 were added onto 6 plates with 7 to 14 days
old agar, on which Malassezia spp. (from six patients) had been cultivated. Air mycelia and spores
were removed, and the suspension was filtered through sterile glass wool. The glass wool was
rinsed again with another 5 mL NaCl (0.85%; pH 7.2) and 0.01% Triton X-100. The filtered spores
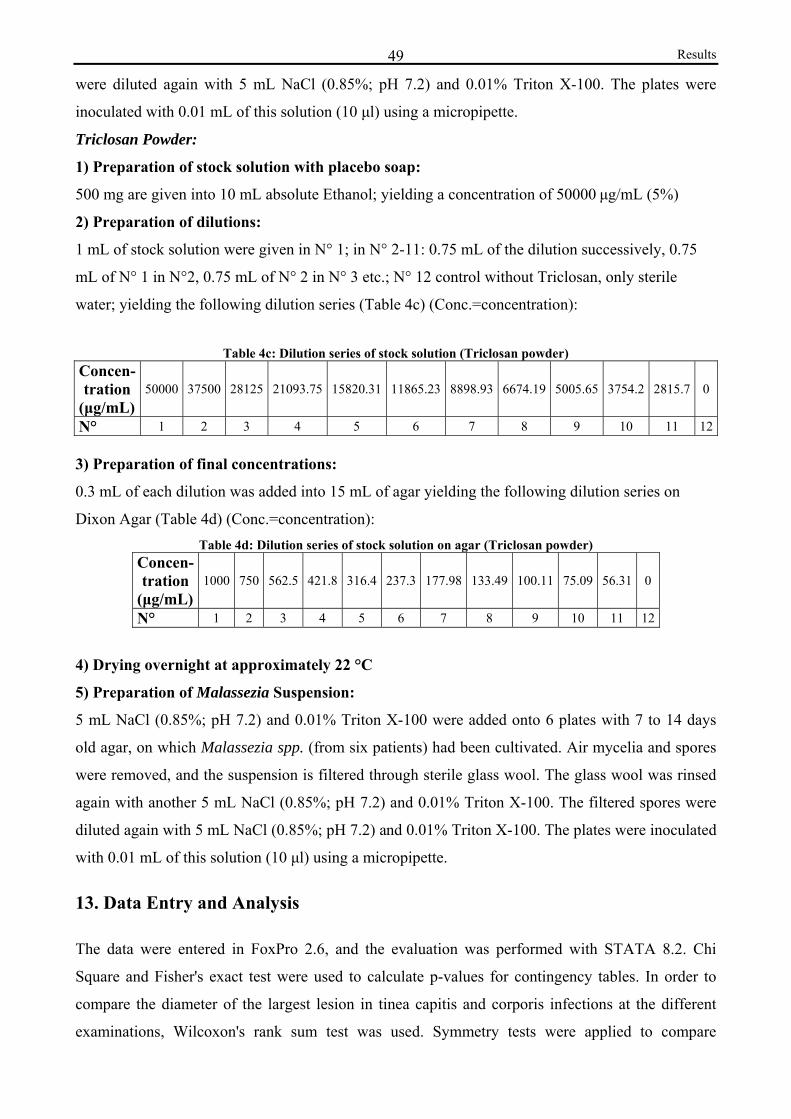
Results 49
were diluted again with 5 mL NaCl (0.85%; pH 7.2) and 0.01% Triton X-100. The plates were
inoculated with 0.01 mL of this solution (10 μl) using a micropipette.
Triclosan Powder:
1) Preparation of stock solution with placebo soap:
500 mg are given into 10 mL absolute Ethanol; yielding a concentration of 50000 μg/mL (5%)
2) Preparation of dilutions:
1 mL of stock solution were given in N° 1; in N° 2-11: 0.75 mL of the dilution successively, 0.75
mL of N° 1 in N°2, 0.75 mL of N° 2 in N° 3 etc.; N° 12 control without Triclosan, only sterile
water; yielding the following dilution series (Table 4c) (Conc.=concentration):
Table 4c: Dilution series of stock solution (Triclosan powder) Concen- tration
(μg/mL) 50000 37500 28125 21093.75 15820.31 11865.23 8898.93 6674.19 5005.65 3754.2 2815.7 0
N° 1 2 3 4 5 6 7 8 9 10 11 12 3) Preparation of final concentrations:
0.3 mL of each dilution was added into 15 mL of agar yielding the following dilution series on
Dixon Agar (Table 4d) (Conc.=concentration): Table 4d: Dilution series of stock solution on agar (Triclosan powder)
Concen- tration
(μg/mL) 1000 750 562.5 421.8 316.4 237.3 177.98 133.49 100.11 75.09 56.31 0
N° 1 2 3 4 5 6 7 8 9 10 11 12
4) Drying overnight at approximately 22 °C
5) Preparation of Malassezia Suspension:
5 mL NaCl (0.85%; pH 7.2) and 0.01% Triton X-100 were added onto 6 plates with 7 to 14 days
old agar, on which Malassezia spp. (from six patients) had been cultivated. Air mycelia and spores
were removed, and the suspension is filtered through sterile glass wool. The glass wool was rinsed
again with another 5 mL NaCl (0.85%; pH 7.2) and 0.01% Triton X-100. The filtered spores were
diluted again with 5 mL NaCl (0.85%; pH 7.2) and 0.01% Triton X-100. The plates were inoculated
with 0.01 mL of this solution (10 μl) using a micropipette.
13. Data Entry and Analysis
The data were entered in FoxPro 2.6, and the evaluation was performed with STATA 8.2. Chi
Square and Fisher's exact test were used to calculate p-values for contingency tables. In order to
compare the diameter of the largest lesion in tinea capitis and corporis infections at the different
examinations, Wilcoxon's rank sum test was used. Symmetry tests were applied to compare
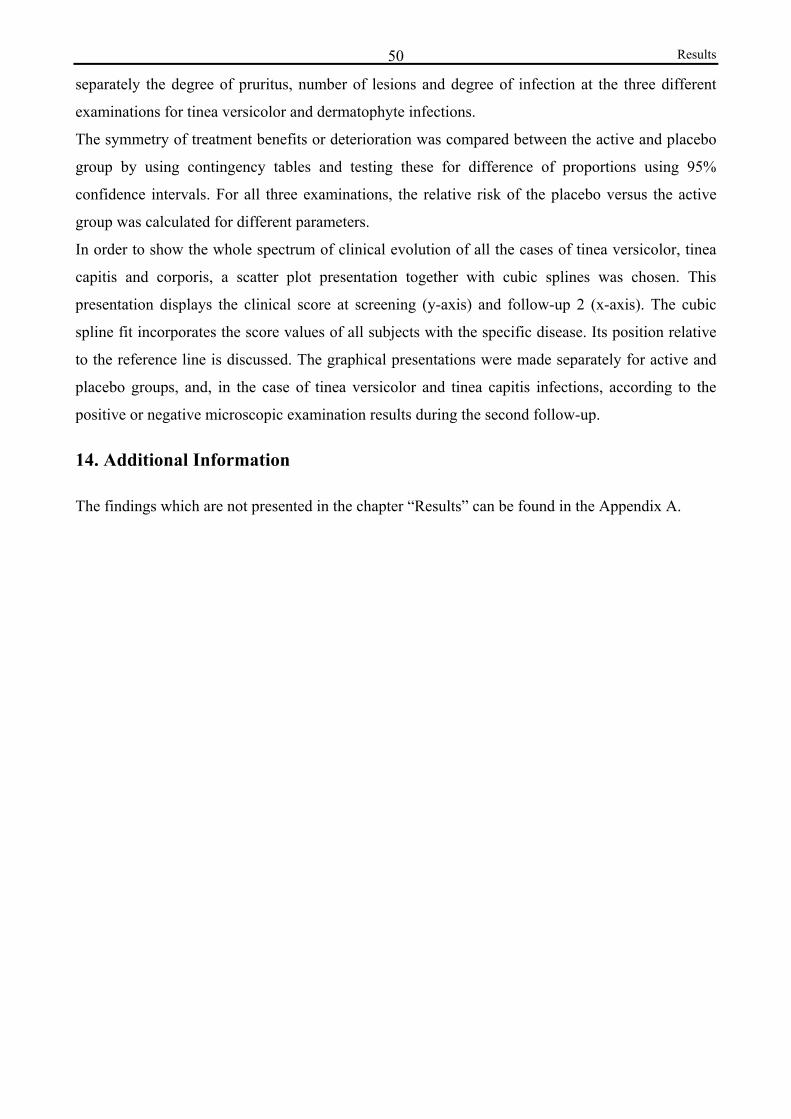
Results 50
separately the degree of pruritus, number of lesions and degree of infection at the three different
examinations for tinea versicolor and dermatophyte infections.
The symmetry of treatment benefits or deterioration was compared between the active and placebo
group by using contingency tables and testing these for difference of proportions using 95%
confidence intervals. For all three examinations, the relative risk of the placebo versus the active
group was calculated for different parameters.
In order to show the whole spectrum of clinical evolution of all the cases of tinea versicolor, tinea
capitis and corporis, a scatter plot presentation together with cubic splines was chosen. This
presentation displays the clinical score at screening (y-axis) and follow-up 2 (x-axis). The cubic
spline fit incorporates the score values of all subjects with the specific disease. Its position relative
to the reference line is discussed. The graphical presentations were made separately for active and
placebo groups, and, in the case of tinea versicolor and tinea capitis infections, according to the
positive or negative microscopic examination results during the second follow-up.
14. Additional Information
The findings which are not presented in the chapter “Results” can be found in the Appendix A.
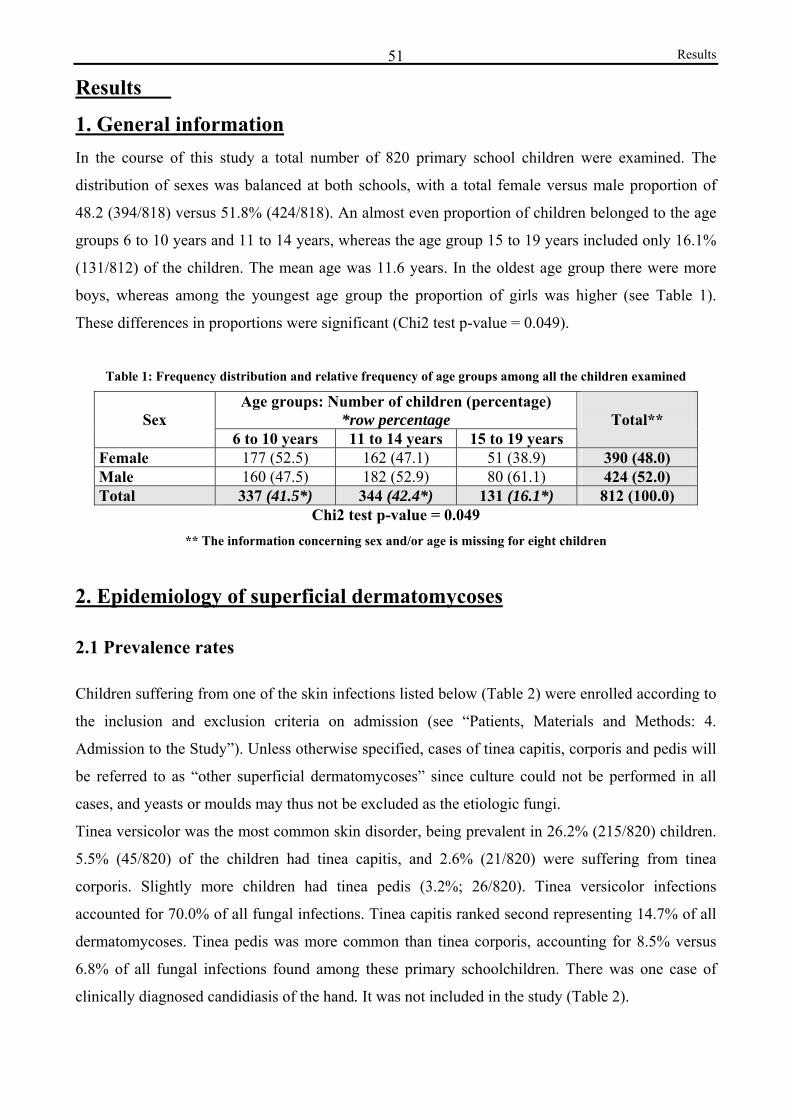
Results 51
Results
1. General information In the course of this study a total number of 820 primary school children were examined. The
distribution of sexes was balanced at both schools, with a total female versus male proportion of
48.2 (394/818) versus 51.8% (424/818). An almost even proportion of children belonged to the age
groups 6 to 10 years and 11 to 14 years, whereas the age group 15 to 19 years included only 16.1%
(131/812) of the children. The mean age was 11.6 years. In the oldest age group there were more
boys, whereas among the youngest age group the proportion of girls was higher (see Table 1).
These differences in proportions were significant (Chi2 test p-value = 0.049).
Table 1: Frequency distribution and relative frequency of age groups among all the children examined
Age groups: Number of children (percentage) *row percentage
Sex
6 to 10 years 11 to 14 years 15 to 19 years
Total**
Female 177 (52.5) 162 (47.1) 51 (38.9) 390 (48.0) Male 160 (47.5) 182 (52.9) 80 (61.1) 424 (52.0) Total 337 (41.5*) 344 (42.4*) 131 (16.1*) 812 (100.0)
Chi2 test p-value = 0.049 ** The information concerning sex and/or age is missing for eight children
2. Epidemiology of superficial dermatomycoses
2.1 Prevalence rates
Children suffering from one of the skin infections listed below (Table 2) were enrolled according to
the inclusion and exclusion criteria on admission (see “Patients, Materials and Methods: 4.
Admission to the Study”). Unless otherwise specified, cases of tinea capitis, corporis and pedis will
be referred to as “other superficial dermatomycoses” since culture could not be performed in all
cases, and yeasts or moulds may thus not be excluded as the etiologic fungi.
Tinea versicolor was the most common skin disorder, being prevalent in 26.2% (215/820) children.
5.5% (45/820) of the children had tinea capitis, and 2.6% (21/820) were suffering from tinea
corporis. Slightly more children had tinea pedis (3.2%; 26/820). Tinea versicolor infections
accounted for 70.0% of all fungal infections. Tinea capitis ranked second representing 14.7% of all
dermatomycoses. Tinea pedis was more common than tinea corporis, accounting for 8.5% versus
6.8% of all fungal infections found among these primary schoolchildren. There was one case of
clinically diagnosed candidiasis of the hand. It was not included in the study (Table 2).
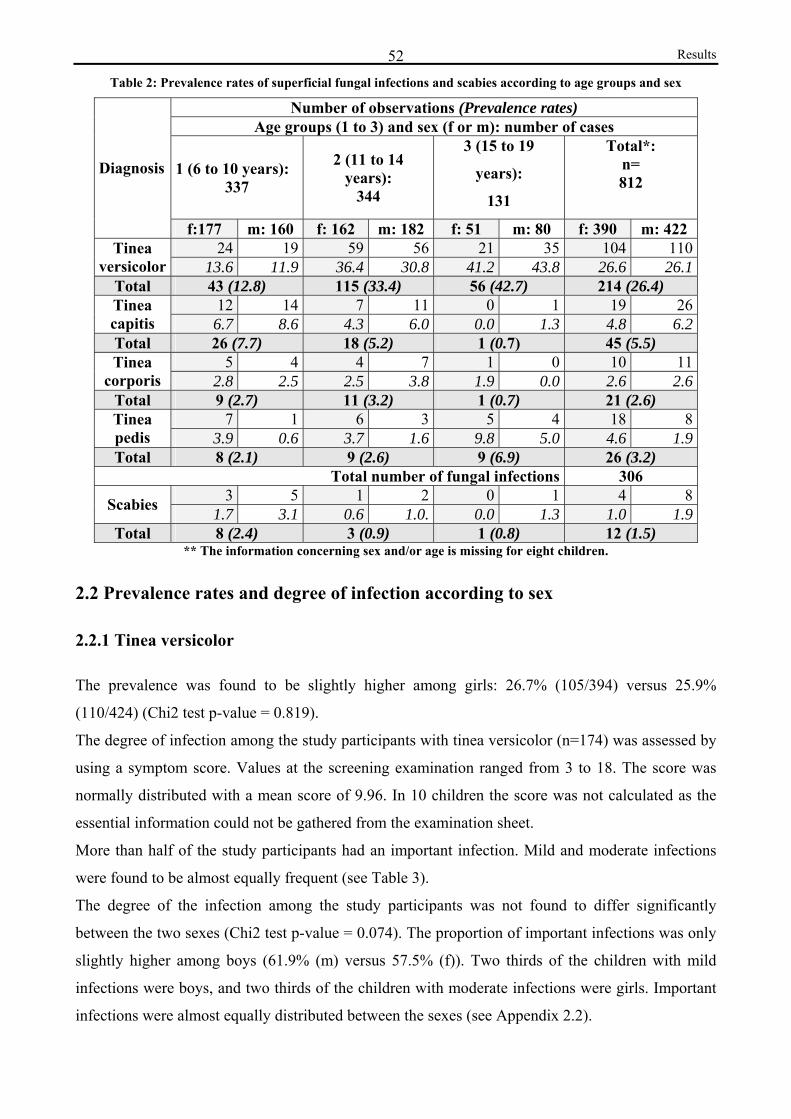
Results 52Table 2: Prevalence rates of superficial fungal infections and scabies according to age groups and sex
Number of observations (Prevalence rates) Age groups (1 to 3) and sex (f or m): number of cases
1 (6 to 10 years): 337
2 (11 to 14 years):
344
3 (15 to 19
years):
131
Total*: n= 812
Diagnosis
f:177 m: 160 f: 162 m: 182 f: 51 m: 80 f: 390 m: 422 24 19 59 56 21 35 104 110Tinea
versicolor 13.6 11.9 36.4 30.8 41.2 43.8 26.6 26.1Total 43 (12.8) 115 (33.4) 56 (42.7) 214 (26.4)
12 14 7 11 0 1 19 26Tinea capitis 6.7 8.6 4.3 6.0 0.0 1.3 4.8 6.2Total 26 (7.7) 18 (5.2) 1 (0.7) 45 (5.5)
5 4 4 7 1 0 10 11Tinea corporis 2.8 2.5 2.5 3.8 1.9 0.0 2.6 2.6
Total 9 (2.7) 11 (3.2) 1 (0.7) 21 (2.6) 7 1 6 3 5 4 18 8Tinea
pedis 3.9 0.6 3.7 1.6 9.8 5.0 4.6 1.9Total 8 (2.1) 9 (2.6) 9 (6.9) 26 (3.2)
Total number of fungal infections 306 3 5 1 2 0 1 4 8Scabies 1.7 3.1 0.6 1.0. 0.0 1.3 1.0 1.9
Total 8 (2.4) 3 (0.9) 1 (0.8) 12 (1.5) ** The information concerning sex and/or age is missing for eight children.
2.2 Prevalence rates and degree of infection according to sex
2.2.1 Tinea versicolor
The prevalence was found to be slightly higher among girls: 26.7% (105/394) versus 25.9%
(110/424) (Chi2 test p-value = 0.819).
The degree of infection among the study participants with tinea versicolor (n=174) was assessed by
using a symptom score. Values at the screening examination ranged from 3 to 18. The score was
normally distributed with a mean score of 9.96. In 10 children the score was not calculated as the
essential information could not be gathered from the examination sheet.
More than half of the study participants had an important infection. Mild and moderate infections
were found to be almost equally frequent (see Table 3).
The degree of the infection among the study participants was not found to differ significantly
between the two sexes (Chi2 test p-value = 0.074). The proportion of important infections was only
slightly higher among boys (61.9% (m) versus 57.5% (f)). Two thirds of the children with mild
infections were boys, and two thirds of the children with moderate infections were girls. Important
infections were almost equally distributed between the sexes (see Appendix 2.2).
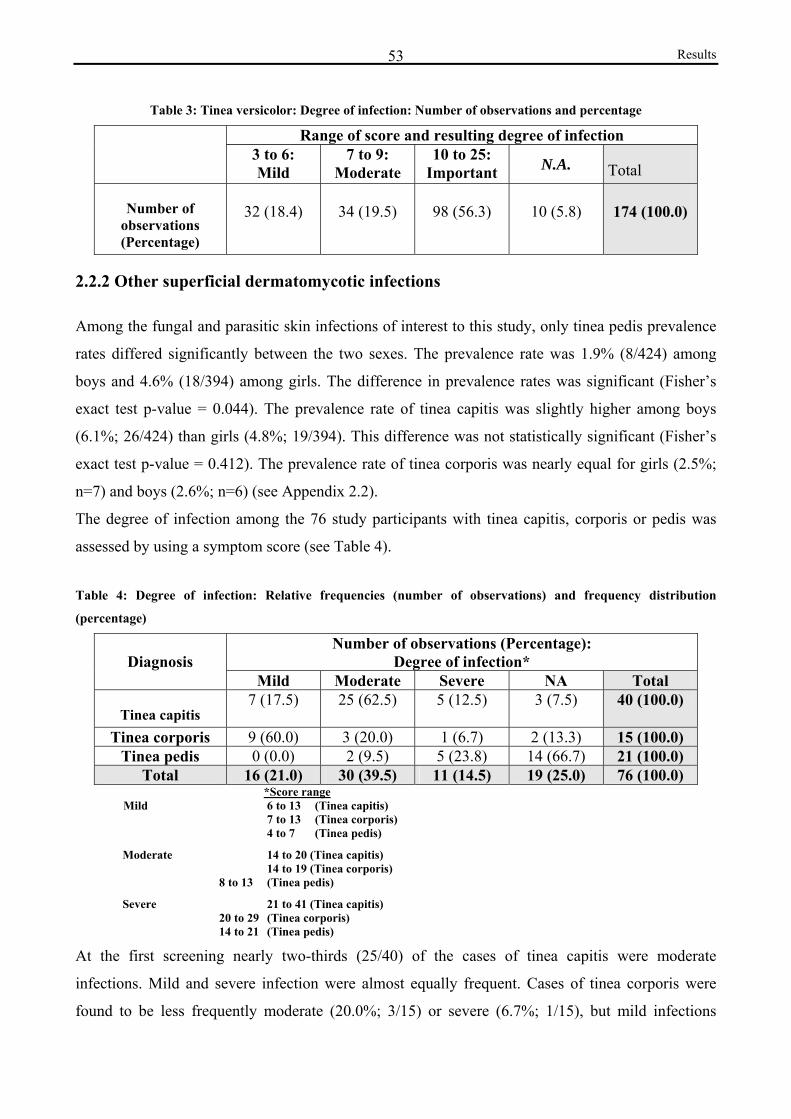
Results 53
Table 3: Tinea versicolor: Degree of infection: Number of observations and percentage
Range of score and resulting degree of infection 3 to 6:
Mild 7 to 9:
Moderate 10 to 25:
Important N.A. Total
Number of observations (Percentage)
32 (18.4)
34 (19.5)
98 (56.3)
10 (5.8)
174 (100.0)
2.2.2 Other superficial dermatomycotic infections
Among the fungal and parasitic skin infections of interest to this study, only tinea pedis prevalence
rates differed significantly between the two sexes. The prevalence rate was 1.9% (8/424) among
boys and 4.6% (18/394) among girls. The difference in prevalence rates was significant (Fisher’s
exact test p-value = 0.044). The prevalence rate of tinea capitis was slightly higher among boys
(6.1%; 26/424) than girls (4.8%; 19/394). This difference was not statistically significant (Fisher’s
exact test p-value = 0.412). The prevalence rate of tinea corporis was nearly equal for girls (2.5%;
n=7) and boys (2.6%; n=6) (see Appendix 2.2).
The degree of infection among the 76 study participants with tinea capitis, corporis or pedis was
assessed by using a symptom score (see Table 4).
Table 4: Degree of infection: Relative frequencies (number of observations) and frequency distribution
(percentage)
Number of observations (Percentage): Degree of infection* Diagnosis
Mild Moderate Severe NA Total
Tinea capitis 7 (17.5) 25 (62.5) 5 (12.5) 3 (7.5) 40 (100.0)
Tinea corporis 9 (60.0) 3 (20.0) 1 (6.7) 2 (13.3) 15 (100.0) Tinea pedis 0 (0.0) 2 (9.5) 5 (23.8) 14 (66.7) 21 (100.0)
Total 16 (21.0) 30 (39.5) 11 (14.5) 19 (25.0) 76 (100.0) *Score range
Mild 6 to 13 (Tinea capitis) 7 to 13 (Tinea corporis) 4 to 7 (Tinea pedis)
Moderate 14 to 20 (Tinea capitis) 14 to 19 (Tinea corporis)
8 to 13 (Tinea pedis)
Severe 21 to 41 (Tinea capitis) 20 to 29 (Tinea corporis) 14 to 21 (Tinea pedis)
At the first screening nearly two-thirds (25/40) of the cases of tinea capitis were moderate
infections. Mild and severe infection were almost equally frequent. Cases of tinea corporis were
found to be less frequently moderate (20.0%; 3/15) or severe (6.7%; 1/15), but mild infections
Results 54
accounted for 60% (9/15) of cases. The degree of the tinea capitis and corporis infection did not
differ significantly between the two sexes (Fisher’s exact test p-values > 0.05). No statement can be
made with regard to the whether the degree of tinea pedis infections depended on sex, since it the
score could only be calculated for one boy. For 14 out of 21 cases the score could not be calculated
(see Table 4). Only the interdigital, macerated type (see Background: 1.1.2.3 Tinea pedis) was
discovered among the examined primary school children.
2.3 Prevalence rates and degree of infection according to age groups
There were significant differences between prevalence rates among the three age groups for tinea
versicolor, tinea capitis and tinea pedis infections (Fisher’s exact test p-values = 0.000, 0.04 and
0.033 (Chi2 test p-value), respectively). The prevalence rates of tinea versicolor and tinea pedis
were found to increase with age, whereas the prevalence rates of tinea capitis and tinea corporis
(Fisher's exact test p-value = 0.295) were found to decrease with age.
2.3.1 Tinea versicolor
The degree of infection among the study participants was found to be significantly different for the
three age groups. (Fisher’s exact test p-value = 0.000). The proportion of children with severe
infection (81.4% of infections in this age group) was found to be highest in age group 3 (15 to 19
years; n=43) and lowest (48.8%) in age group 1 (6 to 10 years; n=29). Moderate infection was
found to be most frequent (29.4%) among the 11 to 14 year-old children (n=92), whereas mild
infections were most frequent (41.4%) among the 6 to 10 year-old children (see Appendix 2.3).
2.3.2 Other superficial dermatomycotic infections
The degree of tinea capitis and corporis infections was assessed according to two age groups (6 to
10 years; n=32, and >10 years; n=24). The degree of infection was not significantly different for the
two age groups (Fisher’s exact test p-values > 0.05). Severe infection was almost equally frequent
in both groups (see Appendix 2.3). The degree of the infection did not depend on the age group
(Fisher’s exact test p-value = 0.429). However, this statement is not reliable since the degree of
infection could only be determined for one third of the children.

Results 55
3. Assessment of the effect of soap
3.1 Assessment of the efficacy of Triclosan in soap
Study participants and dropouts:
248 children were enrolled in the study based on the inclusion and exclusion admission criteria. 20
had to be excluded after admission during the follow-ups. Before and after excluding these, the
number of children belonging to the placebo and active group was balanced (see Figure 1 and Table
5a).
Among the 228 study participants 48.3% were female and 51.7% male. The age distribution was
different from that of the originally examined children. 28.1% (64/228) were 6 to 10 years old,
51.3% (117/228) to the 11 to 14 years old, and 20.6% (47/228) were adolescents aged 15 to 19
years. Some study participants had two or more skin infections at the time of the screening
examination. They were regarded as separate cases of infection when dealing with the individual
diseases. Table 5a: Relative frequencies and frequency distribution of study participants (cases of infection) receiving
placebo versus active soap according to individual diagnoses – all dropouts excluded
Number of cases (Percentage)
Diagnosis Placebo Active Total
Tinea versicolor 82 (47.1) 92 (52.9) 174 Tinea capitis 21 (52.5) 19 (47.5) 40
Tinea corporis 7 (46.7) 8 (53.3) 15 Tinea pedis 11 (52.4) 10 (47.6) 21
Scabies 4 (66.7) 2 (33.3) 6 Total 125 (48.8) 131 (51.2) 256
Among the study participants 11 children had simultaneous tinea versicolor infection and tinea
capitis or and 10 had simultaneous tinea versicolor and tinea pedis infection (see Appendix 3.1 for
Table 5b).
Evaluation of follow-ups:
The data collected at the first follow-up were analyzed, but are listed only in the Appendix. The
emphasis placed on these results shall be small, since only 163 out of the 228 study participants
were present.
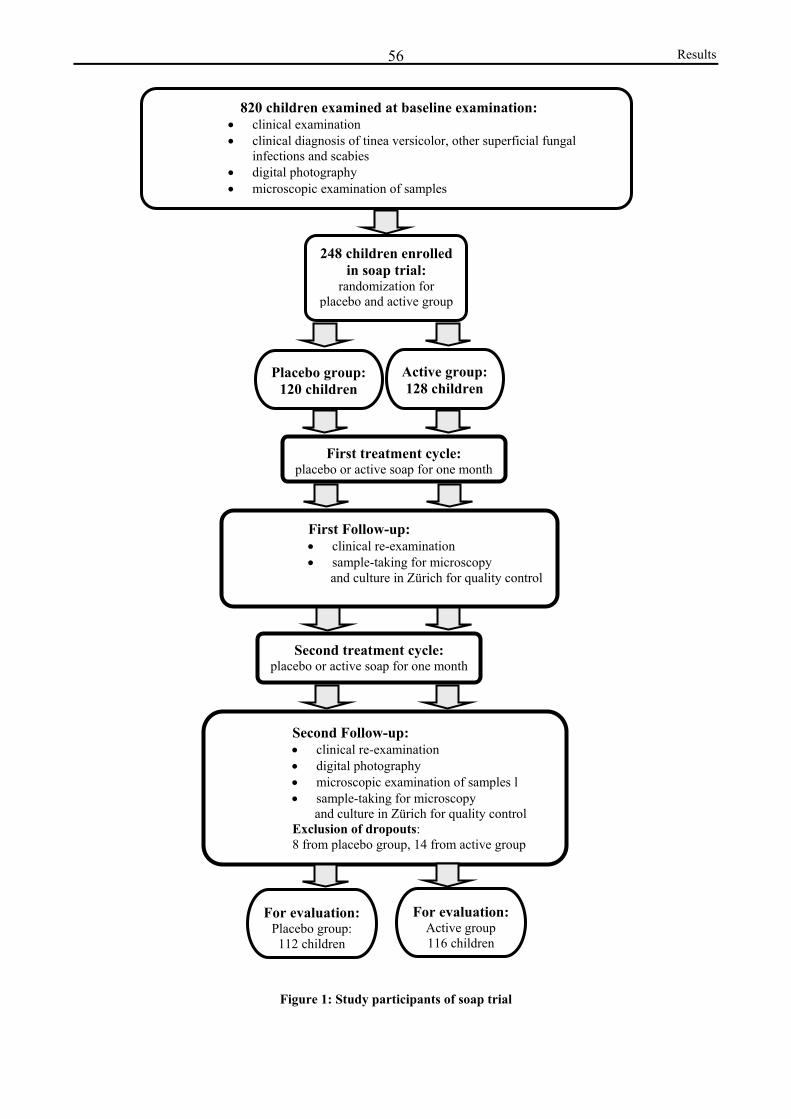
Results 56
Figure 1: Study participants of soap trial
248 children enrolledin soap trial:
randomization for placebo and active group
Placebo group:120 children
Active group:128 children
820 children examined at baseline examination: • clinical examination • clinical diagnosis of tinea versicolor, other superficial fungal
infections and scabies • digital photography • microscopic examination of samples
First treatment cycle: placebo or active soap for one month
First Follow-up: • clinical re-examination • sample-taking for microscopy
and culture in Zürich for quality control
Second treatment cycle: placebo or active soap for one month
Second Follow-up: • clinical re-examination • digital photography • microscopic examination of samples l • sample-taking for microscopy
and culture in Zürich for quality control Exclusion of dropouts: 8 from placebo group, 14 from active group
For evaluation:Placebo group: 112 children
For evaluation:Active group 116 children

Results 57
Table 6a:Characteristic Endpoints: Proportions at Screening and Follow-up 2 Placebo (P) versus Active soap (A) Tinea versicolor Tinea capitis Tinea corporis
n Number of
observations (percentage of n)
n Number of
observations (percentage of n)
n Number of observations (percentage of n)
Endpoints (clinical signs and
symptoms)
Exami- nation
P A P A P A P A P A P A
Screening 6 (7.9) 12 (14.0) 7 (100.0) 7 (100.0) 3 (25.0) 1 (20.0) Scaling Follow-up 2 76 86 3 (3.9) 3 (3.5) 7 7 5 (71.4) 4 (57.1) 7 6 0 (0.0) 0 (0.0) Screening 34 (55.7) 41 (56.2) 9 (81.8) 7 (77.8) 4 (80.0) 3 (60.0) Pruritus Follow-up 2 61 73 25 (40.1) 28 (38.4) 11 9 4 (44.4) 4 (44.4) 5 5 1 (20.0) 1 (20.0)
Pruritus improved Follow-up 2 82 90 12 (85.4) 23 (74.4) 21 18 19 (90.5) 16 (88.9) 8 6 7 (83.3) 6 (100.0)
Subjective impression: improved
Follow-up 2 53 59 49 (92.6) 57 (89.9) 20 17 18 (90.0) 17 (100.0) 6 8 6 (100.0) 8 (100.0)
Screening 73 (96.1) 80 (93.0) Hypo- pigmen-
tation Follow-up 2 76 86 54 (74.1) 65 (75.6)
Screening 4 (5.2) 9 (10.5) Hyper-pigmen-
tation Follow-up 2 77 86 4 (5.2) 8 (9.3)
Tinea capitis: The proportion of children with
occipital adenopathy increased in the active group, whereas it decreased in the placebo group. Besides, the child
with kerion lesions was not cured through the use of the active soap.
Screening 10 (61.1) 11 (62.5) Alopecia Follow-up 2 18 16 4 (22.2) 5 (31.3) Screening 6 (33.3) 2 (12.5) Occ./post.
cervical adenopathy Follow-up 2 18 16 3 (16.7) 4 (25.0)
Screening 1 (5.9) 3 (17.7) Grey patches Follow-up 2 17 17 0 (0.0) 0 (0.0)
Screening 3 (16.7) 5 (31.3) Black dots Follow-up 2 18 16 0 (0.0) 0 (0.0)
Screening 0 (0.0) 1 (6.3) Kerion Follow-up 2 18 16 0 (0.0) 1 (6.3) Screening 1 (5.9) 3 (17.7) Super-
infection Follow-up 2
Tinea versicolor: The proportion of children presenting the individual
endpoints was reduced from the screening examination to the
second follow-up apart from the proportion of children in the
placebo group with hyperpigmented lesions.
17 17 0 (0.0) 0 (0.0)
Tinea versicolor, tinea capitis and corporis: More than three quarters of all children in each group stated that pruritus had improved and that their infection in
general had improved in the course of the soap trial.
Table 6b: Clinical parameters: Number of observations according to diagnosis from Screening (SCR) to Follow-up 2 (Fu2):
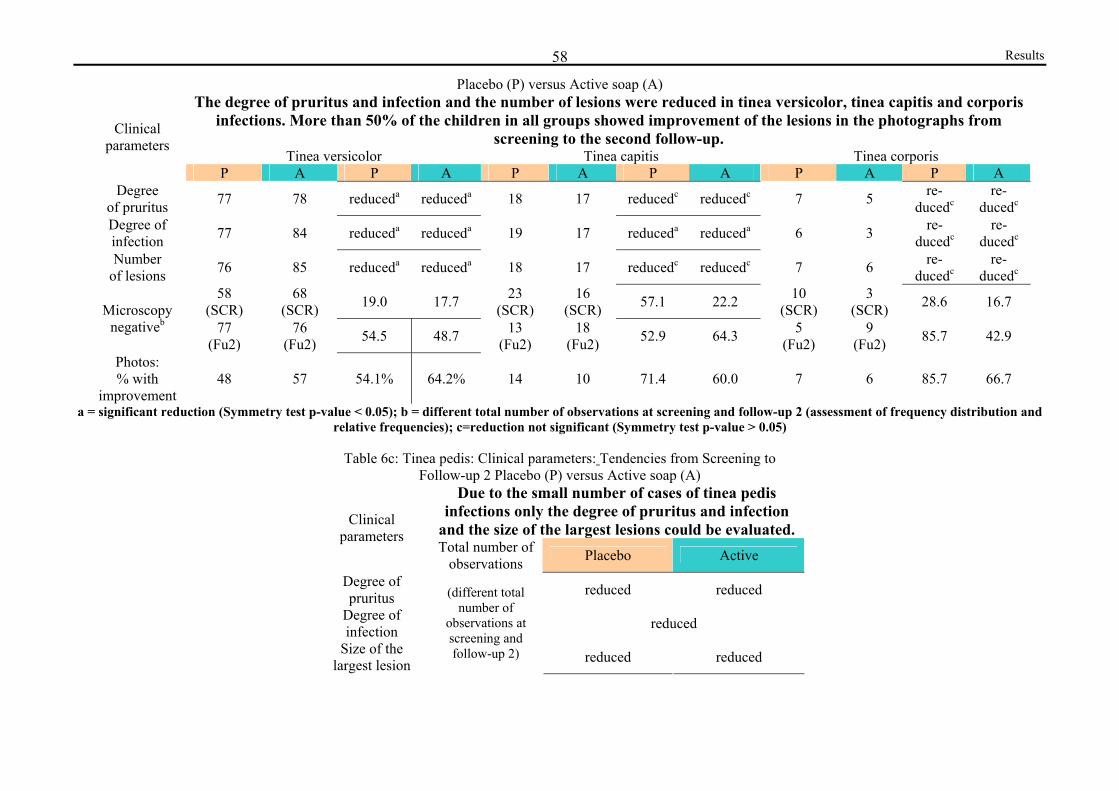
Results 58
Placebo (P) versus Active soap (A) The degree of pruritus and infection and the number of lesions were reduced in tinea versicolor, tinea capitis and corporis
infections. More than 50% of the children in all groups showed improvement of the lesions in the photographs from screening to the second follow-up.
Tinea versicolor Tinea capitis Tinea corporis
Clinical parameters
P A P A P A P A P A P A Degree
of pruritus 77 78 reduceda reduceda 18 17 reducedc reducedc 7 5 re-ducedc
re-ducedc
Degree of infection 77 84 reduceda reduceda 19 17 reduceda reduceda 6 3 re-
ducedc re-
ducedc
Number of lesions 76 85 reduceda reduceda 18 17 reducedc reducedc 7 6 re-
ducedc re-
ducedc
58 (SCR)
68 (SCR) 19.0 17.7 23
(SCR) 16
(SCR) 57.1 22.2 10 (SCR)
3 (SCR) 28.6 16.7 Microscopy
negativeb 77 (Fu2)
76 (Fu2) 54.5 48.7 13
(Fu2) 18
(Fu2) 52.9 64.3 5 (Fu2)
9 (Fu2) 85.7 42.9
Photos: % with
improvement 48 57 54.1% 64.2% 14 10 71.4 60.0 7 6 85.7 66.7
a = significant reduction (Symmetry test p-value < 0.05); b = different total number of observations at screening and follow-up 2 (assessment of frequency distribution and relative frequencies); c=reduction not significant (Symmetry test p-value > 0.05)
Table 6c: Tinea pedis: Clinical parameters: Tendencies from Screening to
Follow-up 2 Placebo (P) versus Active soap (A) Due to the small number of cases of tinea pedis
infections only the degree of pruritus and infection and the size of the largest lesions could be evaluated.
Clinical parameters
Total number of observations Placebo Active
Degree of pruritus reduced reduced
Degree of infection reduced
Size of the largest lesion
(different total number of
observations at screening and follow-up 2) reduced reduced
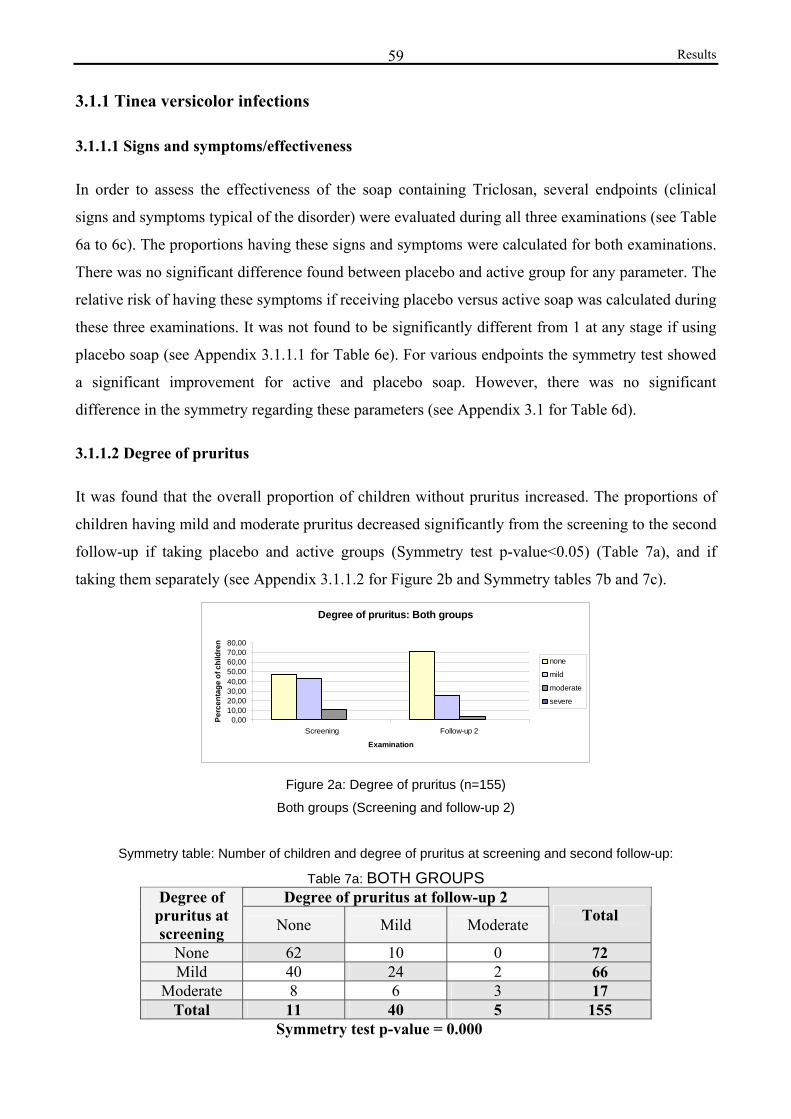
Results 59
3.1.1 Tinea versicolor infections
3.1.1.1 Signs and symptoms/effectiveness
In order to assess the effectiveness of the soap containing Triclosan, several endpoints (clinical
signs and symptoms typical of the disorder) were evaluated during all three examinations (see Table
6a to 6c). The proportions having these signs and symptoms were calculated for both examinations.
There was no significant difference found between placebo and active group for any parameter. The
relative risk of having these symptoms if receiving placebo versus active soap was calculated during
these three examinations. It was not found to be significantly different from 1 at any stage if using
placebo soap (see Appendix 3.1.1.1 for Table 6e). For various endpoints the symmetry test showed
a significant improvement for active and placebo soap. However, there was no significant
difference in the symmetry regarding these parameters (see Appendix 3.1 for Table 6d).
3.1.1.2 Degree of pruritus
It was found that the overall proportion of children without pruritus increased. The proportions of
children having mild and moderate pruritus decreased significantly from the screening to the second
follow-up if taking placebo and active groups (Symmetry test p-value<0.05) (Table 7a), and if
taking them separately (see Appendix 3.1.1.2 for Figure 2b and Symmetry tables 7b and 7c).
Degree of pruritus: Both groups
0,0010,0020,0030,0040,0050,0060,0070,0080,00
Screening Follow-up 2
Examination
Perc
enta
ge o
f chi
ldre
n
none
mild
moderate
severe
Figure 2a: Degree of pruritus (n=155)
Both groups (Screening and follow-up 2)
Symmetry table: Number of children and degree of pruritus at screening and second follow-up:
Table 7a: BOTH GROUPS Degree of pruritus at follow-up 2 Degree of
pruritus at screening None Mild Moderate Total
None 62 10 0 72 Mild 40 24 2 66
Moderate 8 6 3 17 Total 11 40 5 155
Symmetry test p-value = 0.000
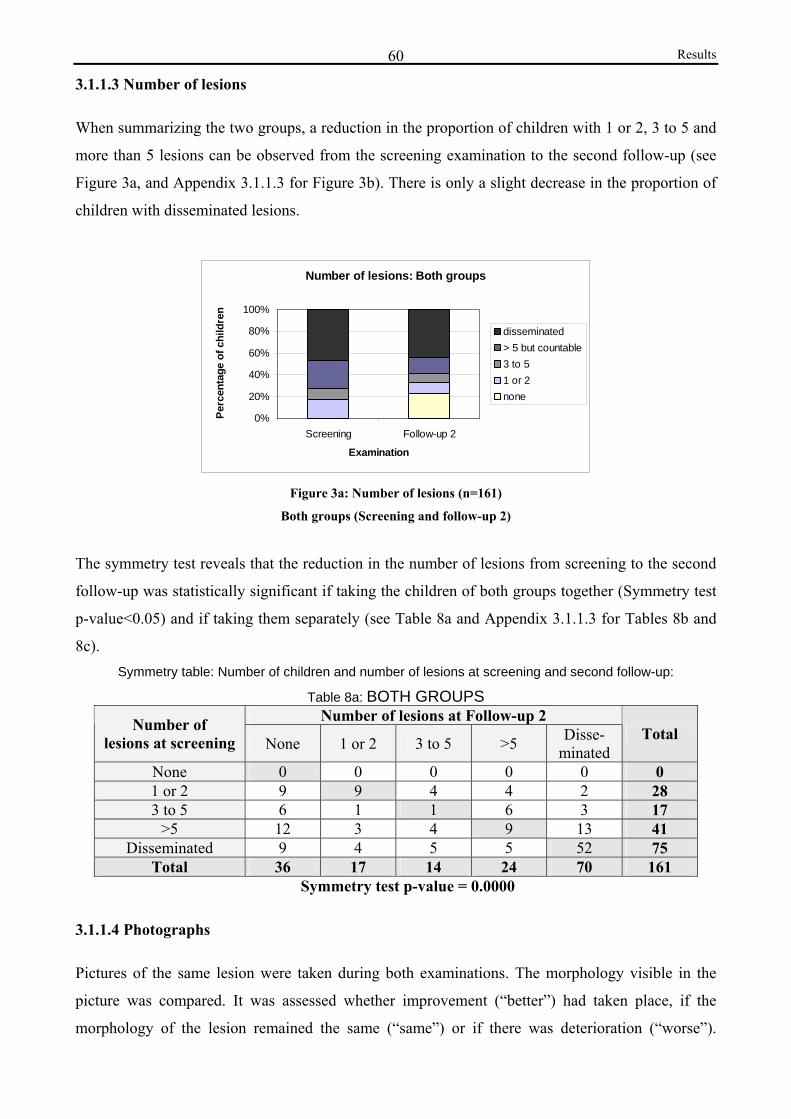
Results 60
3.1.1.3 Number of lesions
When summarizing the two groups, a reduction in the proportion of children with 1 or 2, 3 to 5 and
more than 5 lesions can be observed from the screening examination to the second follow-up (see
Figure 3a, and Appendix 3.1.1.3 for Figure 3b). There is only a slight decrease in the proportion of
children with disseminated lesions.
Number of lesions: Both groups
0%
20%
40%
60%
80%
100%
Screening Follow-up 2
Examination
Perc
enta
ge o
f chi
ldre
n
disseminated> 5 but countable3 to 51 or 2none
Figure 3a: Number of lesions (n=161)
Both groups (Screening and follow-up 2)
The symmetry test reveals that the reduction in the number of lesions from screening to the second
follow-up was statistically significant if taking the children of both groups together (Symmetry test
p-value<0.05) and if taking them separately (see Table 8a and Appendix 3.1.1.3 for Tables 8b and
8c). Symmetry table: Number of children and number of lesions at screening and second follow-up:
Table 8a: BOTH GROUPS Number of lesions at Follow-up 2 Number of
lesions at screening None 1 or 2 3 to 5 >5 Disse- minated
Total
None 0 0 0 0 0 0 1 or 2 9 9 4 4 2 28 3 to 5 6 1 1 6 3 17
>5 12 3 4 9 13 41 Disseminated 9 4 5 5 52 75
Total 36 17 14 24 70 161 Symmetry test p-value = 0.0000
3.1.1.4 Photographs
Pictures of the same lesion were taken during both examinations. The morphology visible in the
picture was compared. It was assessed whether improvement (“better”) had taken place, if the
morphology of the lesion remained the same (“same”) or if there was deterioration (“worse”).
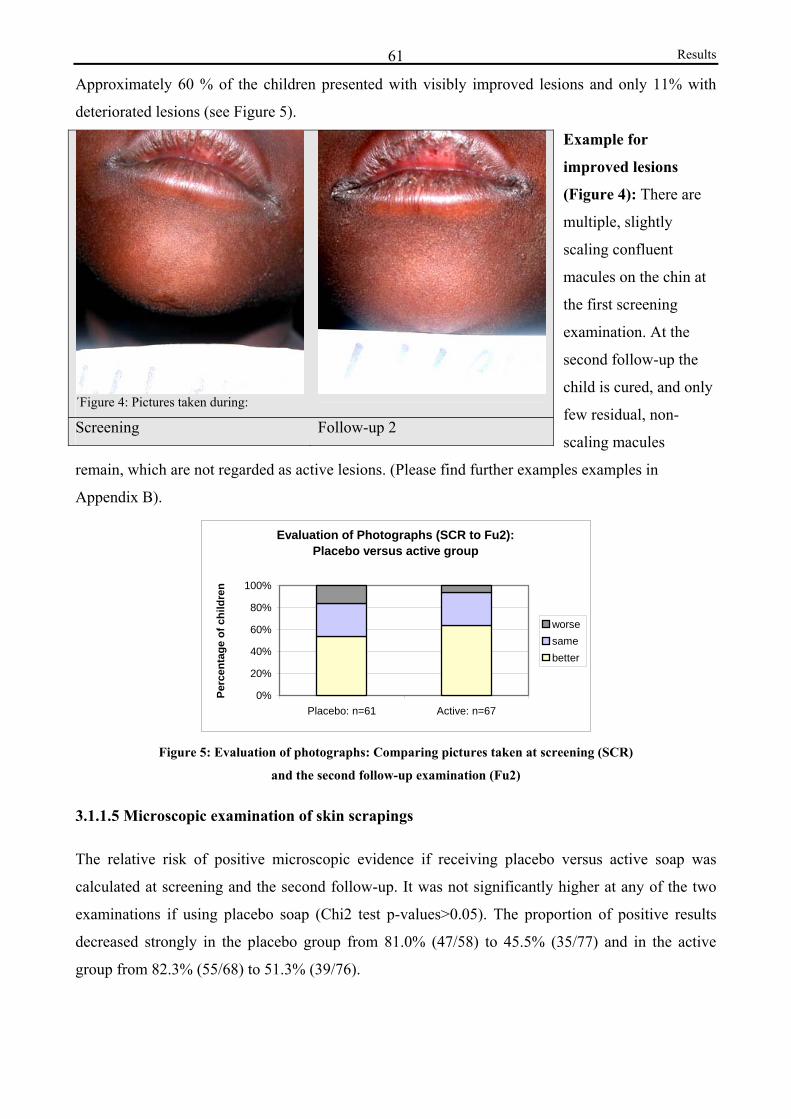
Results 61
Approximately 60 % of the children presented with visibly improved lesions and only 11% with
deteriorated lesions (see Figure 5).
Example for
improved lesions
(Figure 4): There are
multiple, slightly
scaling confluent
macules on the chin at
the first screening
examination. At the
second follow-up the
child is cured, and only
few residual, non-
scaling macules
remain, which are not regarded as active lesions. (Please find further examples examples in
Appendix B).
Evaluation of Photographs (SCR to Fu2):Placebo versus active group
0%
20%
40%
60%
80%
100%
Placebo: n=61 Active: n=67
Perc
enta
ge o
f chi
ldre
n
worsesame better
Figure 5: Evaluation of photographs: Comparing pictures taken at screening (SCR)
and the second follow-up examination (Fu2)
3.1.1.5 Microscopic examination of skin scrapings
The relative risk of positive microscopic evidence if receiving placebo versus active soap was
calculated at screening and the second follow-up. It was not significantly higher at any of the two
examinations if using placebo soap (Chi2 test p-values>0.05). The proportion of positive results
decreased strongly in the placebo group from 81.0% (47/58) to 45.5% (35/77) and in the active
group from 82.3% (55/68) to 51.3% (39/76).
´Figure 4: Pictures taken during: Screening Follow-up 2
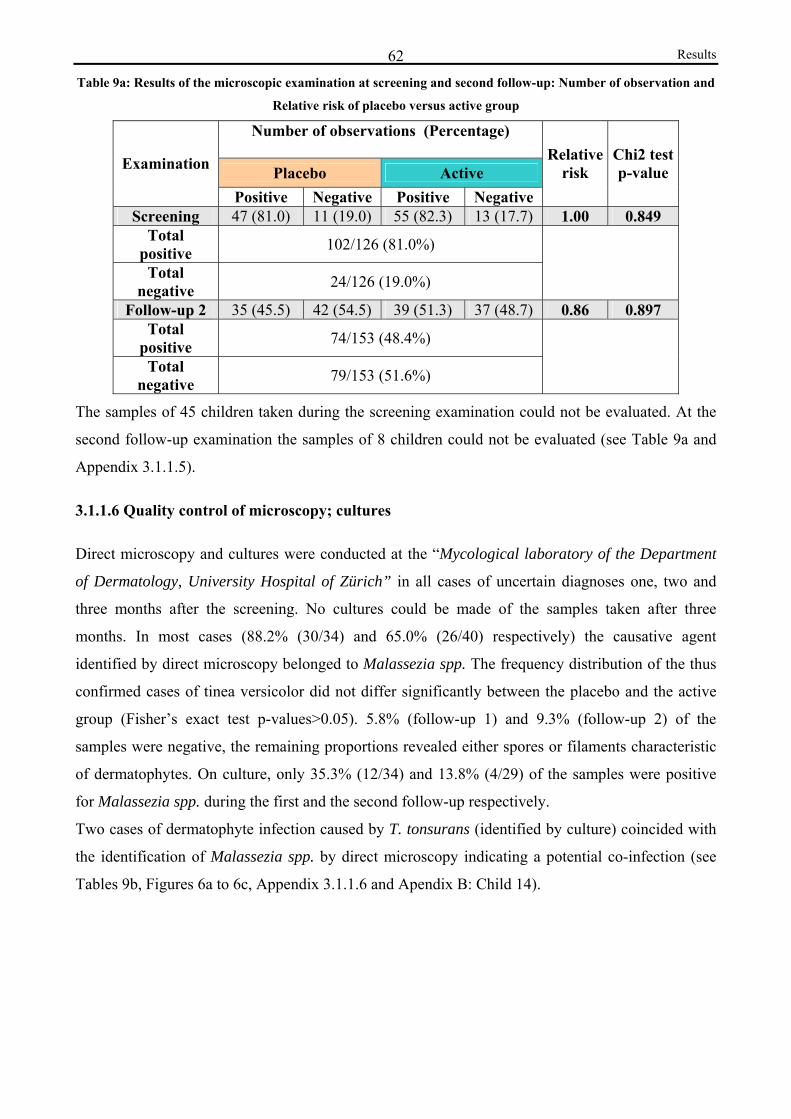
Results 62Table 9a: Results of the microscopic examination at screening and second follow-up: Number of observation and
Relative risk of placebo versus active group
Number of observations (Percentage)
Placebo Active Examination
Positive Negative Positive Negative
Relative risk
Chi2 testp-value
Screening 47 (81.0) 11 (19.0) 55 (82.3) 13 (17.7) 1.00 0.849 Total
positive 102/126 (81.0%)
Total negative 24/126 (19.0%)
Follow-up 2 35 (45.5) 42 (54.5) 39 (51.3) 37 (48.7) 0.86 0.897 Total
positive 74/153 (48.4%)
Total negative 79/153 (51.6%)
The samples of 45 children taken during the screening examination could not be evaluated. At the
second follow-up examination the samples of 8 children could not be evaluated (see Table 9a and
Appendix 3.1.1.5).
3.1.1.6 Quality control of microscopy; cultures
Direct microscopy and cultures were conducted at the “Mycological laboratory of the Department
of Dermatology, University Hospital of Zürich” in all cases of uncertain diagnoses one, two and
three months after the screening. No cultures could be made of the samples taken after three
months. In most cases (88.2% (30/34) and 65.0% (26/40) respectively) the causative agent
identified by direct microscopy belonged to Malassezia spp. The frequency distribution of the thus
confirmed cases of tinea versicolor did not differ significantly between the placebo and the active
group (Fisher’s exact test p-values>0.05). 5.8% (follow-up 1) and 9.3% (follow-up 2) of the
samples were negative, the remaining proportions revealed either spores or filaments characteristic
of dermatophytes. On culture, only 35.3% (12/34) and 13.8% (4/29) of the samples were positive
for Malassezia spp. during the first and the second follow-up respectively.
Two cases of dermatophyte infection caused by T. tonsurans (identified by culture) coincided with
the identification of Malassezia spp. by direct microscopy indicating a potential co-infection (see
Tables 9b, Figures 6a to 6c, Appendix 3.1.1.6 and Apendix B: Child 14).

Results 63Direct microscopy of Pityriasis versicolor (stained with Congo Red, original magnification: x40)
Pictures provided by the Mycological laboratory of the Department of Dermatology, University Hospital of Zürich
Figure 6a: Abundant large, round thick-walled spores and mycelia, “spaghetti and meatballs pattern”
Figure 6b: Hyphae forming groups of mycelia
Figure 6c: Few spores and short septate hyphae penetrating epidermal cells
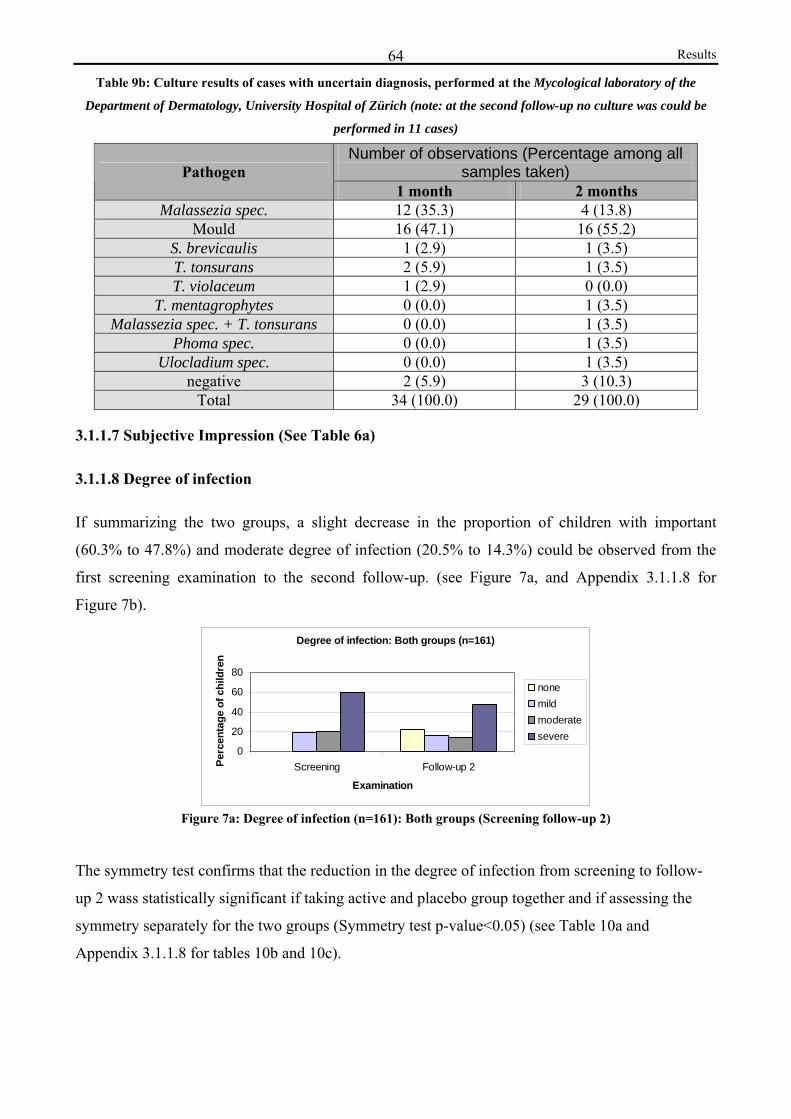
Results 64Table 9b: Culture results of cases with uncertain diagnosis, performed at the Mycological laboratory of the
Department of Dermatology, University Hospital of Zürich (note: at the second follow-up no culture was could be
performed in 11 cases)
Number of observations (Percentage among all samples taken) Pathogen
1 month 2 months Malassezia spec. 12 (35.3) 4 (13.8)
Mould 16 (47.1) 16 (55.2) S. brevicaulis 1 (2.9) 1 (3.5) T. tonsurans 2 (5.9) 1 (3.5) T. violaceum 1 (2.9) 0 (0.0)
T. mentagrophytes 0 (0.0) 1 (3.5) Malassezia spec. + T. tonsurans 0 (0.0) 1 (3.5)
Phoma spec. 0 (0.0) 1 (3.5) Ulocladium spec. 0 (0.0) 1 (3.5)
negative 2 (5.9) 3 (10.3) Total 34 (100.0) 29 (100.0)
3.1.1.7 Subjective Impression (See Table 6a)
3.1.1.8 Degree of infection
If summarizing the two groups, a slight decrease in the proportion of children with important
(60.3% to 47.8%) and moderate degree of infection (20.5% to 14.3%) could be observed from the
first screening examination to the second follow-up. (see Figure 7a, and Appendix 3.1.1.8 for
Figure 7b).
Degree of infection: Both groups (n=161)
0
20
40
60
80
Screening Follow-up 2
Examination
Perc
enta
ge o
f chi
ldre
n
nonemild moderatesevere
Figure 7a: Degree of infection (n=161): Both groups (Screening follow-up 2)
The symmetry test confirms that the reduction in the degree of infection from screening to follow-
up 2 wass statistically significant if taking active and placebo group together and if assessing the
symmetry separately for the two groups (Symmetry test p-value<0.05) (see Table 10a and
Appendix 3.1.1.8 for tables 10b and 10c).
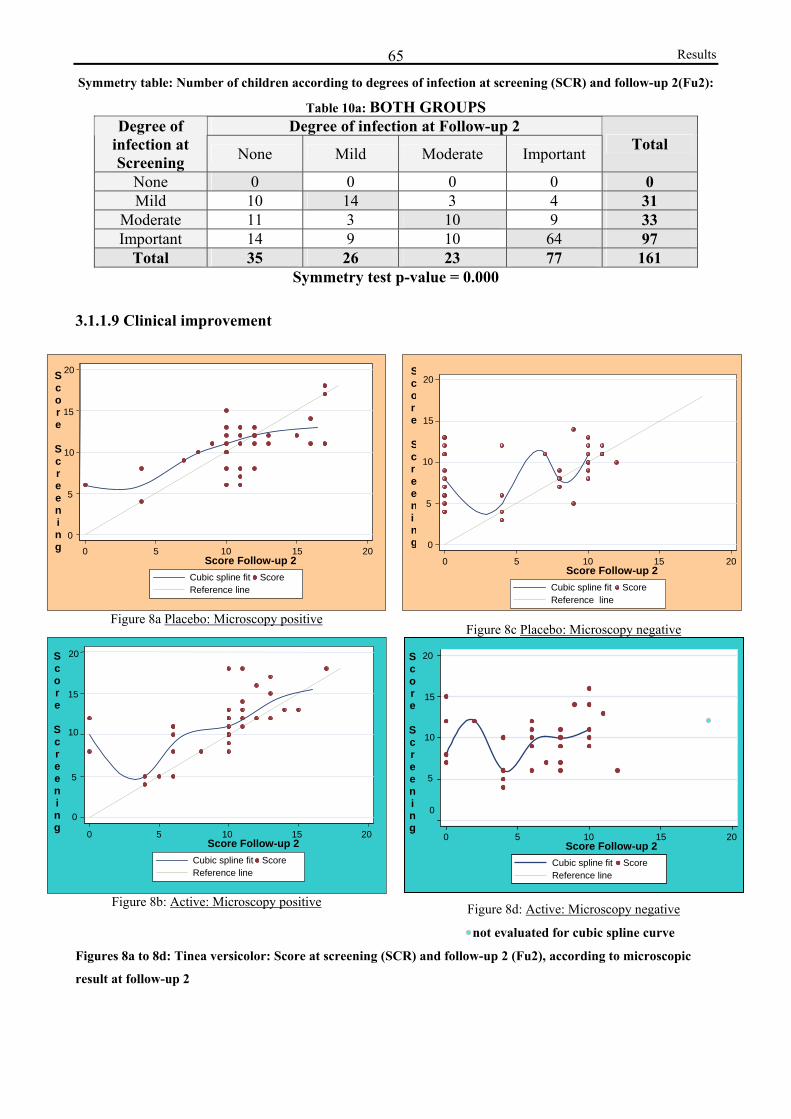
Results 65Symmetry table: Number of children according to degrees of infection at screening (SCR) and follow-up 2(Fu2):
Table 10a: BOTH GROUPS Degree of infection at Follow-up 2 Degree of
infection at Screening None Mild Moderate Important Total
None 0 0 0 0 0 Mild 10 14 3 4 31
Moderate 11 3 10 9 33 Important 14 9 10 64 97
Total 35 26 23 77 161 Symmetry test p-value = 0.000
3.1.1.9 Clinical improvement
Figure 8a Placebo: Microscopy positive Figure 8c Placebo: Microscopy negative
Figure 8b: Active: Microscopy positive
Figure 8d: Active: Microscopy negative
not evaluated for cubic spline curve
Figures 8a to 8d: Tinea versicolor: Score at screening (SCR) and follow-up 2 (Fu2), according to microscopic
result at follow-up 2
0
5
10
20
15
0 5 10 15 20Score Follow-up 2 Cubic spline fit Score
Reference line
S c o r e
S c r e e n i n g
0 5 10 15 20Score Follow-up 2 Cubic spline fit Score
Reference line
10
20
0
5
15
Score
Screening
0 5 10 15 20Score Follow-up 2 Cubic spline fit Score
Reference line
20
10
15
5
S c o r e
S c r e e n i n g
0
0 5 10 15 20Score Follow-up 2 Cubic spline fit Score
Reference line
20
15
10
5
0
S c o r e
S c r e e n i n g

Results 66
The overall improvement and the lack of superiority of active soap, as described in the paragraphs
3.1.1.1 to 3.1.1.8 above, can be confirmed when presenting the clinical score of each individual
stratified according to active and placebo group by using a scatter plot presentation. Figures 8a to
8d display the score at screening (y-axis) and follow-up 2 (x-axis).
It becomes evident that there was a marked improvement until follow-up 2, since the estimated
cubic spline, lies mostly above the reference line. The decrease in the score was slightly more
pronounced in the cases showing negative microscopic results during the second follow-up. In the
placebo group with positive microscopic results, the end of the fitted cubic spline curve, which was
an ascending slope, lies below the reference line. This indicates that cases which were more severe
at screening rather had a tendency to deteriorate. In the cases of negative microscopic results, the
cases of deterioration had been mild infections during the screening examination.
3.1.1.10 Clinical and microscopic resolution
Evaluation Categories at Follow-up2: Placebo versus active group
05
1015202530
1 2 3 4 5 6 7
Evaluation Categories
Perc
enta
ge o
f ch
ildre
n
PlaceboActive
* 1= resolution: child cured
2= microscopic resolution and only few clinical symptoms 3= improvement: negative microscopic evidence with significant clinical improvement
4= no significant clinical improvement but negative mycologic evidence 5= improvement: microscopy positive with significant clinical improvement 6= lack of improvement: positive mycologic evidence with no significant clinical improvement 7=
deterioration Figure 9: Proportions of children (placebo versus active soap) belonging to different evaluation categories (1 to
7) at the second follow-up examination (Fu2) after 2 months of soap use
There was no significant difference in the frequency distribution of the 7 evaluation categories
comprising the clinical signs and symptoms and the microscopic diagnosis between the placebo and
active group after 2 months. (Fisher’s exact test p-value= 0.194) (see Table 11 (Appendix 3.1.1.10)
and Figure 9).
The proportion of children showing resolution (category 1 plus category 2) is nearly identical for
the placebo versus active group: 28.0% (23/82) versus 28.9% (24/83) (Chi2 test p-value=1.000).
The overall cure rate was of 28.4% (47/165) (see Table 12). The proportion of children belonging to
category 2 (microscopic resolution but no complete clinical resolution) was greater in the active

Results 67
group. A larger proportion of children belonging to the active group had a positive microscopic
result. Lack of significant clinical improvement (category 4 plus 6) and deterioration (category 7)
was more common in the placebo group.
Table 12: Relative frequencies and frequency distribution of children with and without resolution (placebo
versus active) Number of observations (Percentage) Clinical and
microscopic resolution Placebo Active Total
Yes 23 (28.0) 24 (28.9) 47 (28.4) No 59 (72.0) 59 (71.1) 118 (71.5)
Total 82 (100.0) 83 (100.0) 165 (100.0) Fisher's exact test p-value = 1.000
3.1.2 Other superficial dermatomycotic infections: Tinea capitis, corporis and pedis
infections
3.1.2.1 Signs and symptoms/effectiveness
In order to assess the effectiveness of the soap containing Triclosan, several endpoints (clinical
signs and symptoms typical of the disease) were evaluated during all three examinations. The
proportions having these signs and symptoms were calculated for both examinations. There was no
significant difference found between placebo and active group for any parameter. The relative risk
of having these symptoms if receiving placebo versus active soap was calculated. It was not found
to be significantly different from 1 at any stage if using placebo soap (see Appendix 3.1.2.1). For
various endpoints the symmetry test showed a significant improvement for active and placebo soap.
However, there was no significant difference in the symmetry regarding these parameters (see
Appendix 3.1 for Table 6d).
3.1.2.2 Degree of pruritus
Tinea capitis, corporis and pedis infections
It was found that the proportion of children without pruritus increased, whereas the proportion of
children having mild, moderate or severe pruritus decreased significantly from the screening to the
second follow-up examination. This is if taking the two groups together (see Figure 10a) and if
taking placebo and active groups separately (see Appendix 3.1.2.2 for Figure 10b). If looking at the
three diagnoses separately, the degree of pruritus decreased significantly only for tinea capitis
infections (Symmetry test p-value = 0.0098) if both groups are summarized (see Appendix 3.1.2.2).
With regard to the other diagnoses the decrease was not significant.
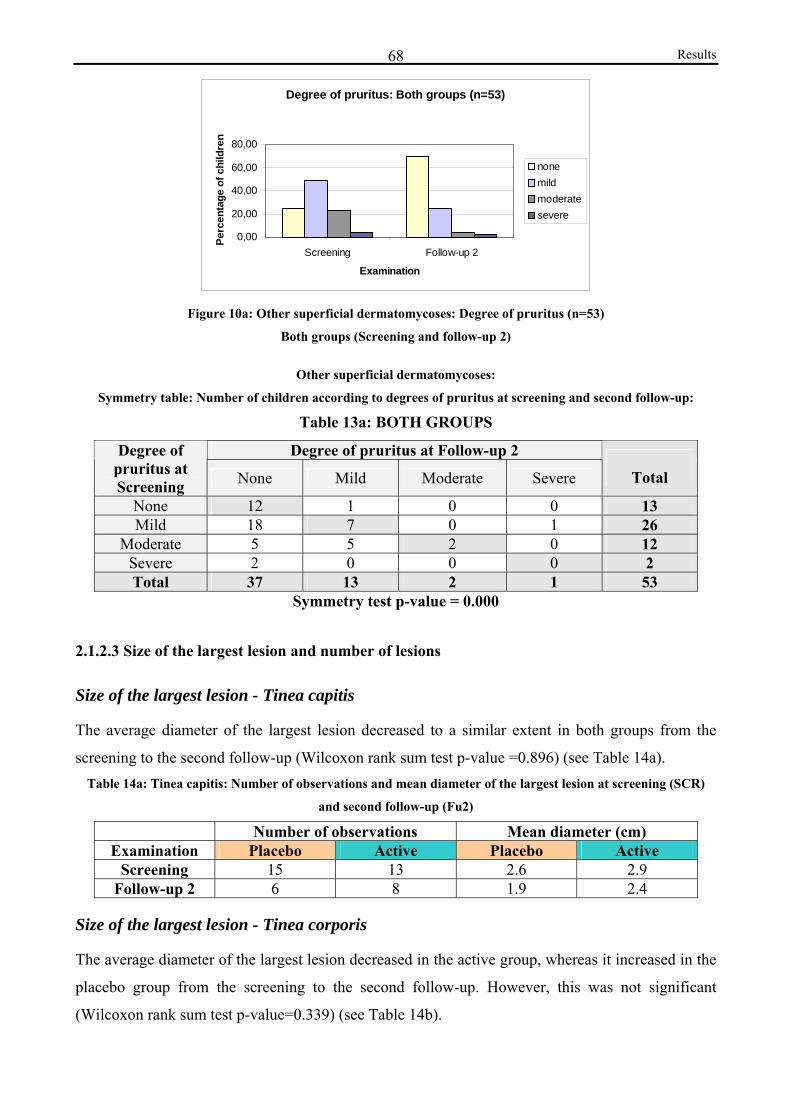
Results 68
Degree of pruritus: Both groups (n=53)
0,00
20,00
40,00
60,00
80,00
Screening Follow-up 2
Examination
Perc
enta
ge o
f chi
ldre
n
nonemildmoderatesevere
Figure 10a: Other superficial dermatomycoses: Degree of pruritus (n=53)
Both groups (Screening and follow-up 2)
Other superficial dermatomycoses:
Symmetry table: Number of children according to degrees of pruritus at screening and second follow-up:
Table 13a: BOTH GROUPS
Degree of pruritus at Follow-up 2 Degree of pruritus at Screening None Mild Moderate Severe
Total
None 12 1 0 0 13 Mild 18 7 0 1 26
Moderate 5 5 2 0 12 Severe 2 0 0 0 2 Total 37 13 2 1 53
Symmetry test p-value = 0.000
2.1.2.3 Size of the largest lesion and number of lesions
Size of the largest lesion - Tinea capitis
The average diameter of the largest lesion decreased to a similar extent in both groups from the
screening to the second follow-up (Wilcoxon rank sum test p-value =0.896) (see Table 14a). Table 14a: Tinea capitis: Number of observations and mean diameter of the largest lesion at screening (SCR)
and second follow-up (Fu2)
Number of observations Mean diameter (cm) Examination Placebo Active Placebo Active
Screening 15 13 2.6 2.9 Follow-up 2 6 8 1.9 2.4
Size of the largest lesion - Tinea corporis
The average diameter of the largest lesion decreased in the active group, whereas it increased in the
placebo group from the screening to the second follow-up. However, this was not significant
(Wilcoxon rank sum test p-value=0.339) (see Table 14b).

Results 69Table 14b: Tinea corporis: Number of observations and mean diameter of the largest lesion at screening (SCR)
and second follow-up (Fu2)
Number of observations Mean diameter (cm) Examination Placebo Active Placebo Active
Screening 7 5 2.1 2.2 Follow-up 2 4 7 3.1 1.0
Number of lesions - Tinea capitis
The symmetry test showed that there was a significant reduction in the number of lesions from
screening the second follow-up if taking the children of both groups together (Symmetry test p-
value = 0.0038), but not if taking the two groups separately (see Table 15a and Appendix 3.1.2.3 for
Tables 15b and 15c).
Table 15a: BOTH GROUPS
Number of lesions at Follow-up 2 Number of lesions at Screening None 1 or 2 3 to 5 >5 Disse-
minated Total
None 1 0 0 0 0 1 11 or 2 4 2 1 0 1 8 3 to 5 7 2 2 1 2 14
>5 6 0 0 0 2 8 Disseminated 2 1 0 0 1 4
Total 20 5 3 1 6 35 Symmetry test p-value = 0.0038
Number of lesions - Tinea corporis
The symmetry test reveals that there was a significant reduction in the number of lesions from
screening the second follow-up if taking the children of both groups together (Symmetry test p-
value 0.0460) but not if taking the two groups separately (see Table 15d and 15e and 15f
(Appendix)).
Table 15d: BOTH GROUPS Number of lesions Follow-up 2 Number of
lesions at Screening None 1 or 2 3 to 5 >5 Disse- minated
Total
None 0 0 0 0 0 0 1 or 2 5 3 0 0 0 8 3 to 5 0 1 0 0 0 1
>5 0 0 2 0 0 2 Disseminated 0 0 0 0 2 2
Total 5 4 2 0 2 13 Symmetry test p-value = 0.0460
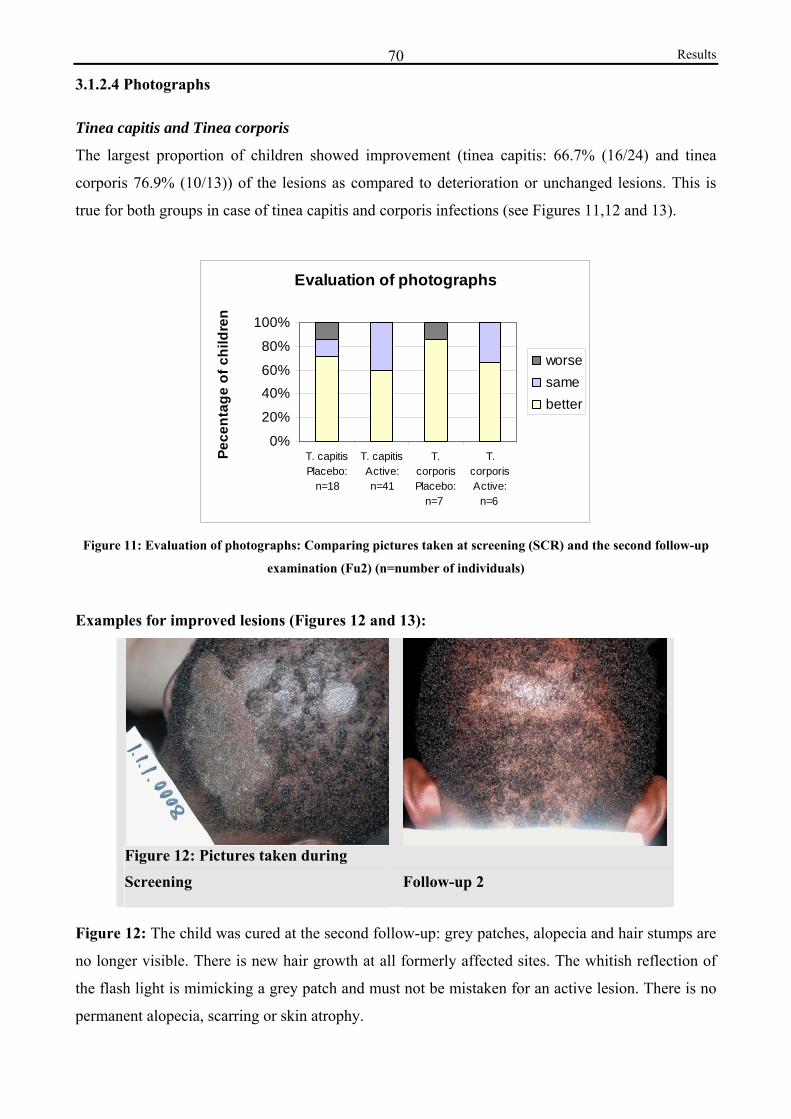
Results 70
3.1.2.4 Photographs
Tinea capitis and Tinea corporis
The largest proportion of children showed improvement (tinea capitis: 66.7% (16/24) and tinea
corporis 76.9% (10/13)) of the lesions as compared to deterioration or unchanged lesions. This is
true for both groups in case of tinea capitis and corporis infections (see Figures 11,12 and 13).
Evaluation of photographs
0%
20%
40%60%
80%
100%
T. capitisPlacebo:
n=18
T. capitisActive:n=41
T.corporisPlacebo:
n=7
T.corporisActive:
n=6
Pece
ntag
e of
chi
ldre
n
worsesamebetter
Figure 11: Evaluation of photographs: Comparing pictures taken at screening (SCR) and the second follow-up
examination (Fu2) (n=number of individuals)
Examples for improved lesions (Figures 12 and 13):
Figure 12: Pictures taken during
Screening Follow-up 2
Figure 12: The child was cured at the second follow-up: grey patches, alopecia and hair stumps are
no longer visible. There is new hair growth at all formerly affected sites. The whitish reflection of
the flash light is mimicking a grey patch and must not be mistaken for an active lesion. There is no
permanent alopecia, scarring or skin atrophy.
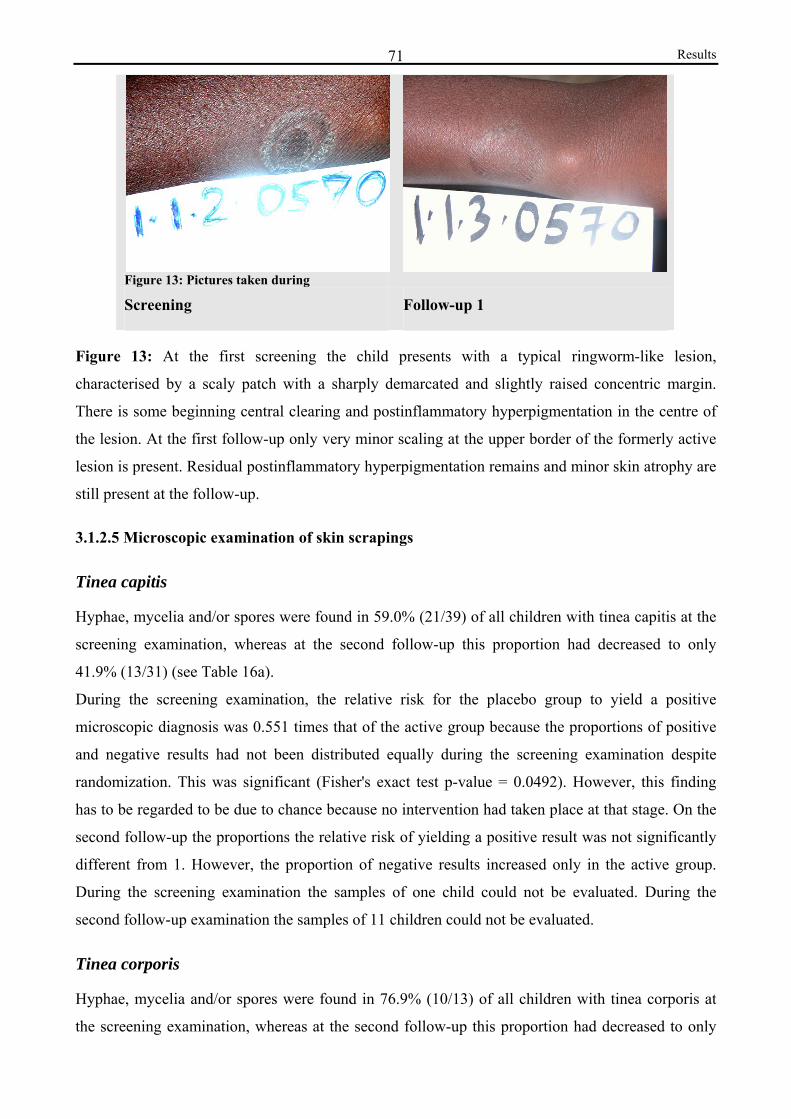
Results 71
Figure 13: Pictures taken during Screening Follow-up 1
Figure 13: At the first screening the child presents with a typical ringworm-like lesion,
characterised by a scaly patch with a sharply demarcated and slightly raised concentric margin.
There is some beginning central clearing and postinflammatory hyperpigmentation in the centre of
the lesion. At the first follow-up only very minor scaling at the upper border of the formerly active
lesion is present. Residual postinflammatory hyperpigmentation remains and minor skin atrophy are
still present at the follow-up.
3.1.2.5 Microscopic examination of skin scrapings
Tinea capitis
Hyphae, mycelia and/or spores were found in 59.0% (21/39) of all children with tinea capitis at the
screening examination, whereas at the second follow-up this proportion had decreased to only
41.9% (13/31) (see Table 16a).
During the screening examination, the relative risk for the placebo group to yield a positive
microscopic diagnosis was 0.551 times that of the active group because the proportions of positive
and negative results had not been distributed equally during the screening examination despite
randomization. This was significant (Fisher's exact test p-value = 0.0492). However, this finding
has to be regarded to be due to chance because no intervention had taken place at that stage. On the
second follow-up the proportions the relative risk of yielding a positive result was not significantly
different from 1. However, the proportion of negative results increased only in the active group.
During the screening examination the samples of one child could not be evaluated. During the
second follow-up examination the samples of 11 children could not be evaluated.
Tinea corporis
Hyphae, mycelia and/or spores were found in 76.9% (10/13) of all children with tinea corporis at
the screening examination, whereas at the second follow-up this proportion had decreased to only
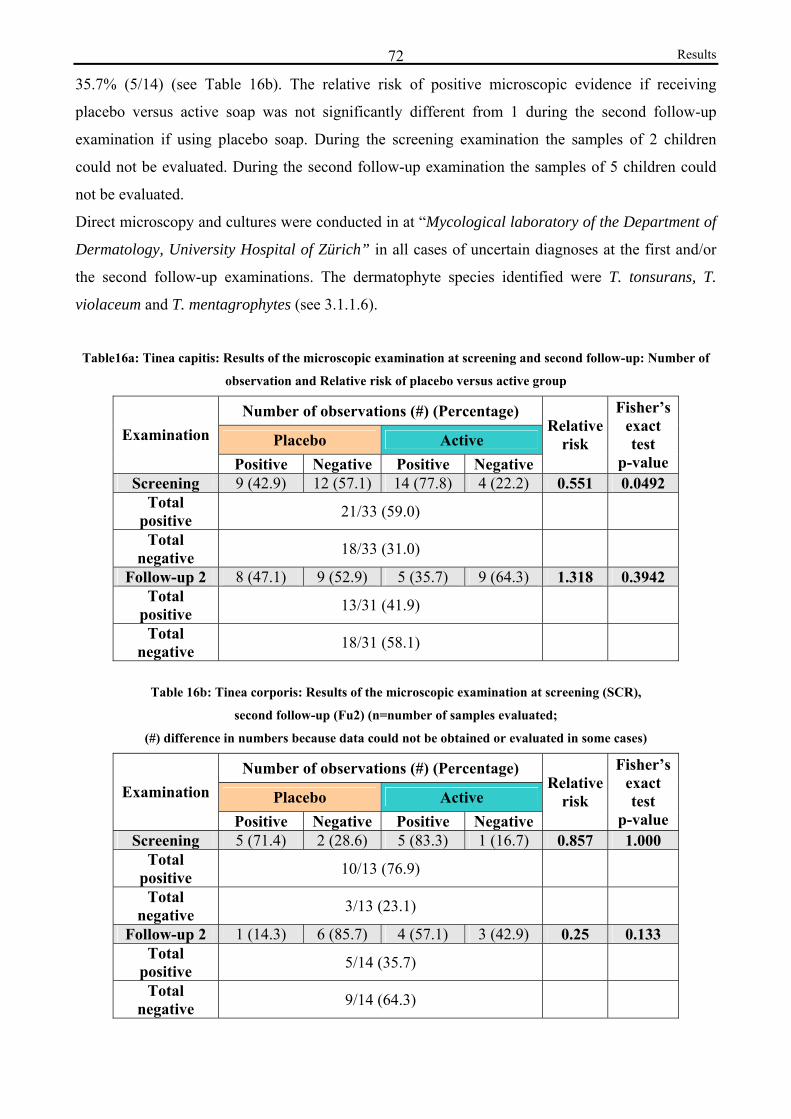
Results 72
35.7% (5/14) (see Table 16b). The relative risk of positive microscopic evidence if receiving
placebo versus active soap was not significantly different from 1 during the second follow-up
examination if using placebo soap. During the screening examination the samples of 2 children
could not be evaluated. During the second follow-up examination the samples of 5 children could
not be evaluated.
Direct microscopy and cultures were conducted in at “Mycological laboratory of the Department of
Dermatology, University Hospital of Zürich” in all cases of uncertain diagnoses at the first and/or
the second follow-up examinations. The dermatophyte species identified were T. tonsurans, T.
violaceum and T. mentagrophytes (see 3.1.1.6).
Table16a: Tinea capitis: Results of the microscopic examination at screening and second follow-up: Number of
observation and Relative risk of placebo versus active group
Number of observations (#) (Percentage)
Placebo Active Examination
Positive Negative Positive Negative
Relative risk
Fisher’s exact test
p-value Screening 9 (42.9) 12 (57.1) 14 (77.8) 4 (22.2) 0.551 0.0492
Total positive 21/33 (59.0)
Total negative 18/33 (31.0)
Follow-up 2 8 (47.1) 9 (52.9) 5 (35.7) 9 (64.3) 1.318 0.3942 Total
positive 13/31 (41.9)
Total negative 18/31 (58.1)
Table 16b: Tinea corporis: Results of the microscopic examination at screening (SCR),
second follow-up (Fu2) (n=number of samples evaluated;
(#) difference in numbers because data could not be obtained or evaluated in some cases)
Number of observations (#) (Percentage)
Placebo Active Examination
Positive Negative Positive Negative
Relative risk
Fisher’s exact test
p-value Screening 5 (71.4) 2 (28.6) 5 (83.3) 1 (16.7) 0.857 1.000
Total positive 10/13 (76.9)
Total negative 3/13 (23.1)
Follow-up 2 1 (14.3) 6 (85.7) 4 (57.1) 3 (42.9) 0.25 0.133 Total
positive 5/14 (35.7)
Total negative 9/14 (64.3)
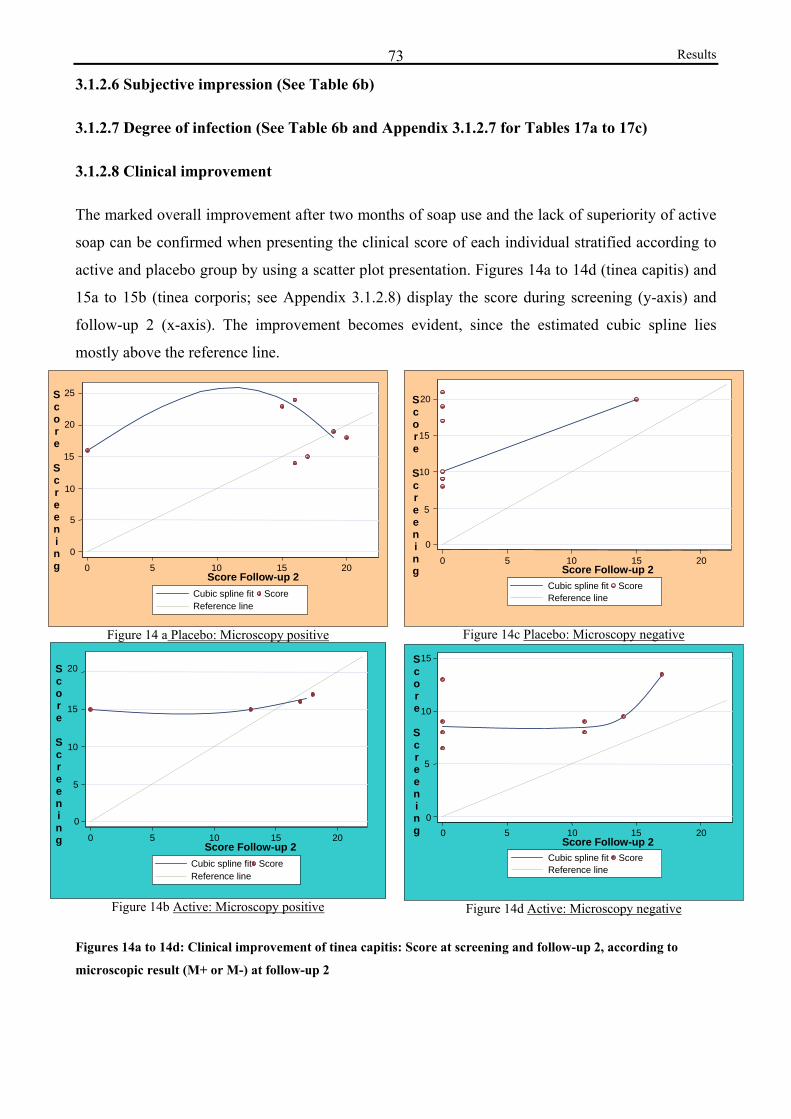
Results 73
3.1.2.6 Subjective impression (See Table 6b)
3.1.2.7 Degree of infection (See Table 6b and Appendix 3.1.2.7 for Tables 17a to 17c)
3.1.2.8 Clinical improvement
The marked overall improvement after two months of soap use and the lack of superiority of active
soap can be confirmed when presenting the clinical score of each individual stratified according to
active and placebo group by using a scatter plot presentation. Figures 14a to 14d (tinea capitis) and
15a to 15b (tinea corporis; see Appendix 3.1.2.8) display the score during screening (y-axis) and
follow-up 2 (x-axis). The improvement becomes evident, since the estimated cubic spline lies
mostly above the reference line.
Figure 14 a Placebo: Microscopy positive
Figure 14c Placebo: Microscopy negative
Figure 14b Active: Microscopy positive Figure 14d Active: Microscopy negative
Figures 14a to 14d: Clinical improvement of tinea capitis: Score at screening and follow-up 2, according to
microscopic result (M+ or M-) at follow-up 2
0 5 10 15 20Score Follow-up 2 Cubic spline fit
Score
Reference line
20
15
10
5
0
S c o r e
S c r e e n i n g 0 5 10 15 20
Score Follow-up 2 Cubic spline fit
Score Reference line
15
10
5
0
S c o r e
S c r e e n i n g
0 5 10 15 20Score Follow-up 2 Cubic spline fit
Score
Reference line
20
15
10
5
0
0 5 10 15 20Score Follow-up 2 Cubic spline fit Score
Reference line
25
20
15
10
5
0
S c o r e
S c r e e n i n g
S c o r e
S c r e e n i n g
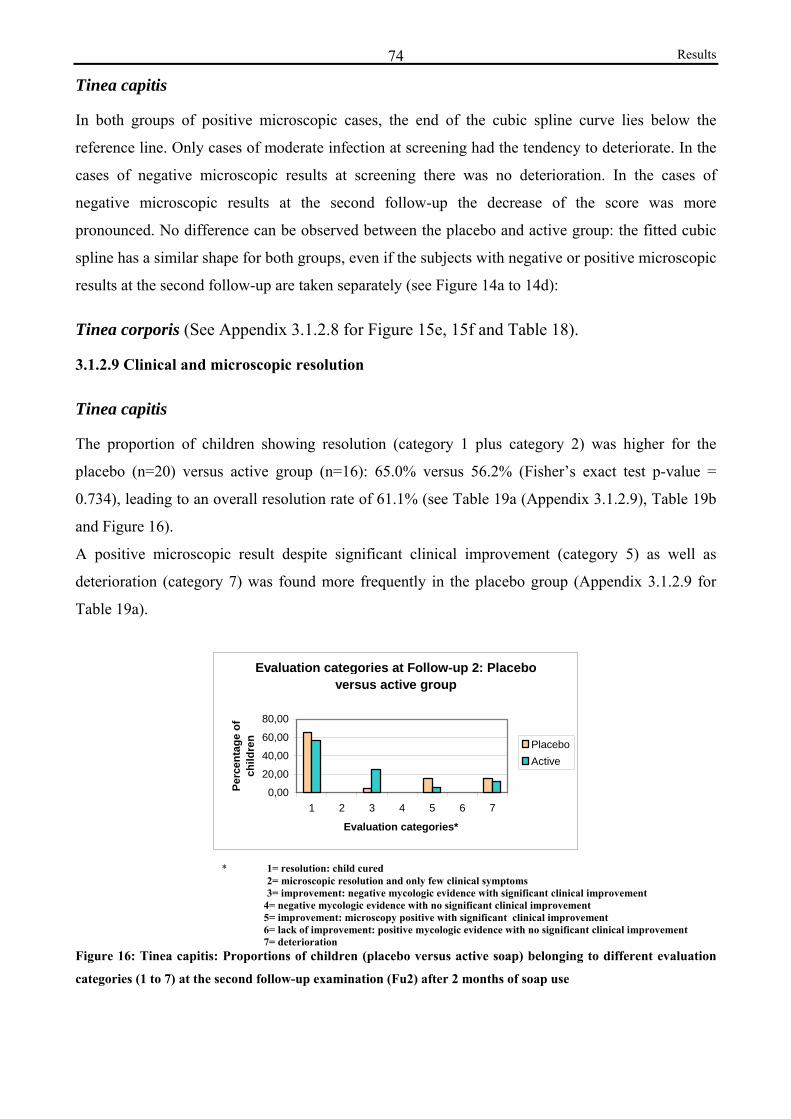
Results 74
Tinea capitis
In both groups of positive microscopic cases, the end of the cubic spline curve lies below the
reference line. Only cases of moderate infection at screening had the tendency to deteriorate. In the
cases of negative microscopic results at screening there was no deterioration. In the cases of
negative microscopic results at the second follow-up the decrease of the score was more
pronounced. No difference can be observed between the placebo and active group: the fitted cubic
spline has a similar shape for both groups, even if the subjects with negative or positive microscopic
results at the second follow-up are taken separately (see Figure 14a to 14d):
Tinea corporis (See Appendix 3.1.2.8 for Figure 15e, 15f and Table 18).
3.1.2.9 Clinical and microscopic resolution
Tinea capitis
The proportion of children showing resolution (category 1 plus category 2) was higher for the
placebo (n=20) versus active group (n=16): 65.0% versus 56.2% (Fisher’s exact test p-value =
0.734), leading to an overall resolution rate of 61.1% (see Table 19a (Appendix 3.1.2.9), Table 19b
and Figure 16).
A positive microscopic result despite significant clinical improvement (category 5) as well as
deterioration (category 7) was found more frequently in the placebo group (Appendix 3.1.2.9 for
Table 19a).
Evaluation categories at Follow-up 2: Placebo versus active group
0,00
20,00
40,00
60,00
80,00
1 2 3 4 5 6 7
Evaluation categories*
Perc
enta
ge o
f ch
ildre
n PlaceboActive
* 1= resolution: child cured 2= microscopic resolution and only few clinical symptoms 3= improvement: negative mycologic evidence with significant clinical improvement
4= negative mycologic evidence with no significant clinical improvement 5= improvement: microscopy positive with significant clinical improvement 6= lack of improvement: positive mycologic evidence with no significant clinical improvement 7= deterioration
Figure 16: Tinea capitis: Proportions of children (placebo versus active soap) belonging to different evaluation
categories (1 to 7) at the second follow-up examination (Fu2) after 2 months of soap use
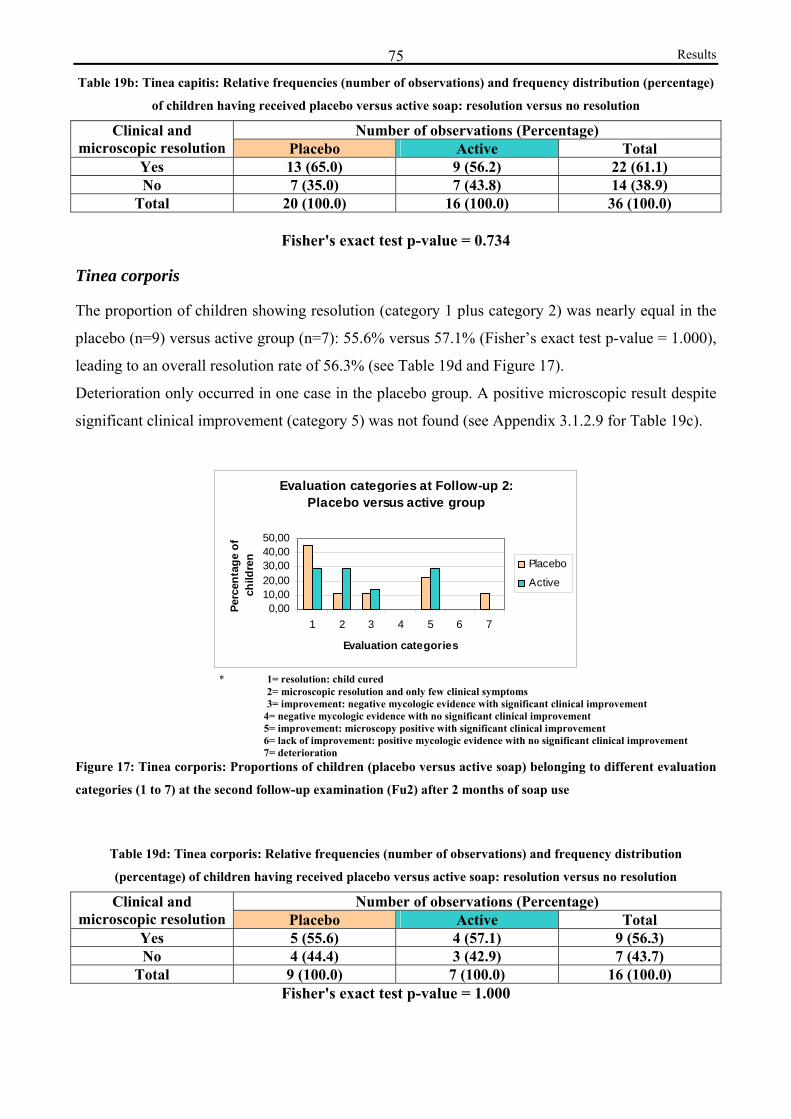
Results 75Table 19b: Tinea capitis: Relative frequencies (number of observations) and frequency distribution (percentage)
of children having received placebo versus active soap: resolution versus no resolution Number of observations (Percentage) Clinical and
microscopic resolution Placebo Active Total Yes 13 (65.0) 9 (56.2) 22 (61.1) No 7 (35.0) 7 (43.8) 14 (38.9)
Total 20 (100.0) 16 (100.0) 36 (100.0)
Fisher's exact test p-value = 0.734
Tinea corporis
The proportion of children showing resolution (category 1 plus category 2) was nearly equal in the
placebo (n=9) versus active group (n=7): 55.6% versus 57.1% (Fisher’s exact test p-value = 1.000),
leading to an overall resolution rate of 56.3% (see Table 19d and Figure 17).
Deterioration only occurred in one case in the placebo group. A positive microscopic result despite
significant clinical improvement (category 5) was not found (see Appendix 3.1.2.9 for Table 19c).
Evaluation categories at Follow-up 2: Placebo versus active group
0,0010,0020,0030,0040,0050,00
1 2 3 4 5 6 7
Evaluation categories
Perc
enta
ge o
f ch
ildre
n Placebo
Active
* 1= resolution: child cured 2= microscopic resolution and only few clinical symptoms 3= improvement: negative mycologic evidence with significant clinical improvement
4= negative mycologic evidence with no significant clinical improvement 5= improvement: microscopy positive with significant clinical improvement 6= lack of improvement: positive mycologic evidence with no significant clinical improvement 7= deterioration
Figure 17: Tinea corporis: Proportions of children (placebo versus active soap) belonging to different evaluation
categories (1 to 7) at the second follow-up examination (Fu2) after 2 months of soap use
Table 19d: Tinea corporis: Relative frequencies (number of observations) and frequency distribution
(percentage) of children having received placebo versus active soap: resolution versus no resolution Number of observations (Percentage) Clinical and
microscopic resolution Placebo Active Total Yes 5 (55.6) 4 (57.1) 9 (56.3) No 4 (44.4) 3 (42.9) 7 (43.7)
Total 9 (100.0) 7 (100.0) 16 (100.0) Fisher's exact test p-value = 1.000
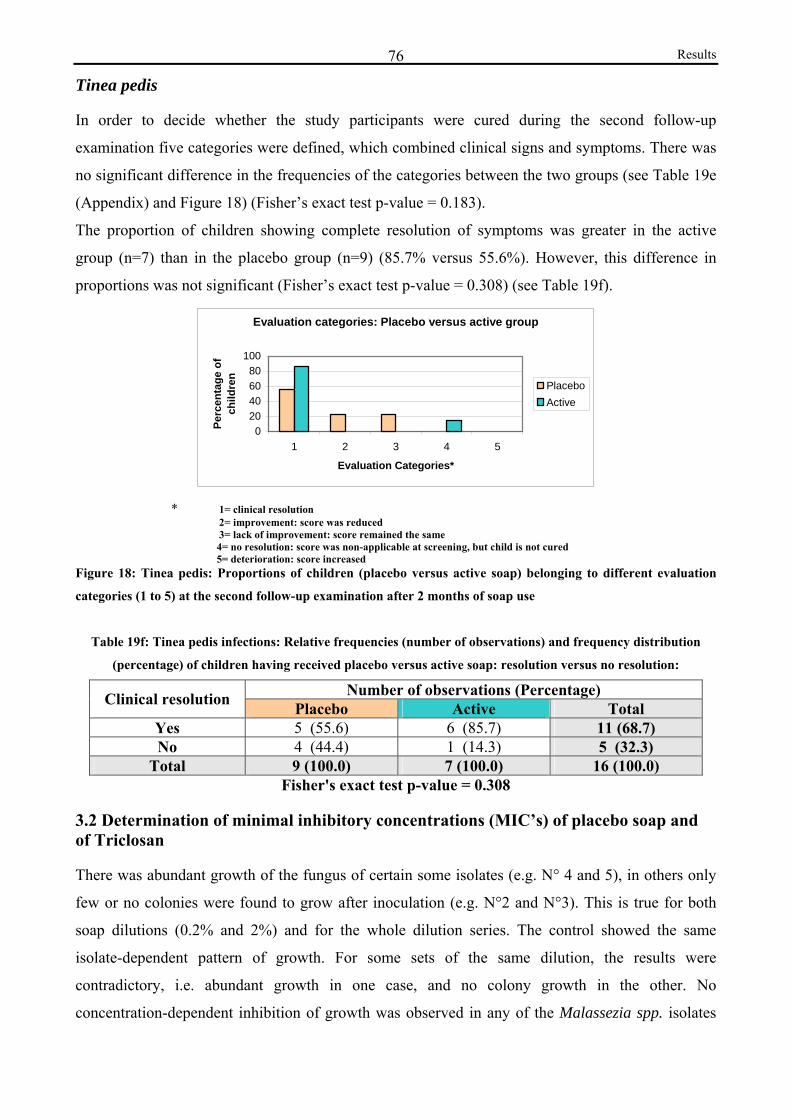
Results 76
Tinea pedis
In order to decide whether the study participants were cured during the second follow-up
examination five categories were defined, which combined clinical signs and symptoms. There was
no significant difference in the frequencies of the categories between the two groups (see Table 19e
(Appendix) and Figure 18) (Fisher’s exact test p-value = 0.183).
The proportion of children showing complete resolution of symptoms was greater in the active
group (n=7) than in the placebo group (n=9) (85.7% versus 55.6%). However, this difference in
proportions was not significant (Fisher’s exact test p-value = 0.308) (see Table 19f).
Evaluation categories: Placebo versus active group
020406080
100
1 2 3 4 5
Evaluation Categories*
Perc
enta
ge o
f ch
ildre
n
PlaceboActive
* 1= clinical resolution 2= improvement: score was reduced 3= lack of improvement: score remained the same
4= no resolution: score was non-applicable at screening, but child is not cured 5= deterioration: score increased
Figure 18: Tinea pedis: Proportions of children (placebo versus active soap) belonging to different evaluation
categories (1 to 5) at the second follow-up examination after 2 months of soap use
Table 19f: Tinea pedis infections: Relative frequencies (number of observations) and frequency distribution
(percentage) of children having received placebo versus active soap: resolution versus no resolution: Number of observations (Percentage) Clinical resolution Placebo Active Total
Yes 5 (55.6) 6 (85.7) 11 (68.7) No 4 (44.4) 1 (14.3) 5 (32.3)
Total 9 (100.0) 7 (100.0) 16 (100.0) Fisher's exact test p-value = 0.308
3.2 Determination of minimal inhibitory concentrations (MIC’s) of placebo soap and of Triclosan
There was abundant growth of the fungus of certain some isolates (e.g. N° 4 and 5), in others only
few or no colonies were found to grow after inoculation (e.g. N°2 and N°3). This is true for both
soap dilutions (0.2% and 2%) and for the whole dilution series. The control showed the same
isolate-dependent pattern of growth. For some sets of the same dilution, the results were
contradictory, i.e. abundant growth in one case, and no colony growth in the other. No
concentration-dependent inhibition of growth was observed in any of the Malassezia spp. isolates
Results 77
from the Department of Mycology, University of Zürich (see Table 20a and Appendix 3.2).
Therefore no MIC could be determined for placebo soap. For Triclosan an inhibition of growth was
only observed in the significant concentrations of 1000 to 562.5 μg/mL. In the successive dilutions,
no concentration dependent inhibition of growth could be found. As in placebo soap, the growth of
the fungus varied according to the isolate (see Table 20b).
Table20a: Growth of Malassezia spp. colonies on Dixon Agar inoculated with different concentrations of placebo
soap. Concentration of soap solution: 0.2%; for 2% soap solution see Appendix 3.2
Number of colony forming units (CFU) (### > 50 CFU) according to Malassezia spp. isolate (N°1 to 6)
Isolate 1
Isolate 2
Isolate 3
Isolate 4
Isolate 5
Isolate 6
Concentration of soap solution (0.2%) on agar (μg/mL) 1st
series 2nd
series 1st
series 2nd
series 1st
series 2nd
series 1st
series 2nd
series 1st
series 2nd
series 1st
series 2nd
series
400 ### 3 ### 0 0 0 ### ### ### ### ### 1 200 2 1 0 0 ### 0 ### ### ### ### ### ### 100 5 1 2 0 0 0 ### ### ### ### 0 0 50 10 2 0 0 0 0 ### ### ### ### ### 4 25 5 2 0 0 0 0 ### ### ### ### 9 2
12.5 5 3 1 0 ### 0 ### ### ### ### 0 1 6.25 2 2 0 0 0 0 ### ### ### ### ### ### 3.13 1 0 0 5 0 0 ### ### ### ### 2 ### 1.56 2 ### 0 3 0 0 ### ### ### ### ### ### 0.78 1 4 0 1 1 0 ### ### ### ### ### ### 0.39 1 ### 0 0 2 1 ### ### ### ### ### 1
0 2 4 0 2 1 0 ### ### ### ### ### 0
Table 20b: Growth of Malassezia spp. colonies on Dixon Agar inoculated with different concentrations Triclosan
Number of colonies according to Malassezia spp. isolate (1 to 6) Dilution series of Triclosan: Concentrations of Triclosan
on agar (μg/mL) Isolate
1 Isolate
2 Isolate
3 Isolate
4 Isolate
5 Isolate
6 1000 0 0 0 0 0 0 750 0 0 0 0 0 0
562.5 0 0 0 0 3 0 421.8 6 0 0 5 40 9 316.4 5 1 0 2 50 8 237.3 1 1 0 5 40 23
177.98 1 1 2 2 42 21 133.49 2 1 2 11 39 19 100.11 2 4 2 2 43 23 75.09 2 1 2 3 49 21 56.31 1 1 2 3 42 14
0 (only ethanol on agar) 4 2 2 2 40 19 Only agar 2 1 4 2 39 15
Results 81
4. Scabies
4.1 Epidemiology and Study population
Scabies infestation was a comparatively rare condition, with a prevalence of only 1.5% (12/820).
The prevalence was found to decrease with age, and boys were more often affected than girls.
Two of the 12 affected children were given Ivermectin because their infection was too severe to
take part in this study. Another two children were also not included because they had healing
scabies. One of them had already received BBE treatment.
The eight remaining study participants were pupils at Lihami Primary School. Two of them were
girls, six were boys. Seven children were between 6 and 10 years of age, one child was 13 years
old. The mean age was 9.25 years. After randomisation four children received placebo and four
children active soap.
4.2 Assessment of the effect of soap and the efficacy of Triclosan
4.2.1.2 Case descriptions Active Group
Screening
Diagnosis was made clinically. In one case microscopic examination of a skin sample was
successful. All four boys, who were aged between 8,8,9 and 10 years, had moderate infections (the
score ranged between 6 and 11). Their skin eruptions presented as typical papular pruritic rashes or
the characteristic primary lesions (burrows) on their forearms, hands and the anterior axillary folds.
Other localisations found were the umbilical and pubic region, the gluteal region and the thighs.
Three children complained about moderate pruritus, the child with the most severe infection in this
group about severe pruritus. In all four cases the itching was more severe at night. Other family
members were affected in 2 out of these four children.
Follow-up 2:
The two study participants aged 8 years had to be excluded from the study. One was lost to follow-
up, and the other one only came once to pick up his soap during the whole study. Nevertheless, this
child was cured. Only post-inflammatory excoriated lesions could be observed. The remaining two
boys showed a contrary evolution of their scabies infection. In one of them the infection got
significantly worse. The score had increased from 6 to 14. Some lesions had become superinfected.
The skin was dry and in some areas atrophic. Both entire arms including wrists and hands were
affected, and the infestation had spread to both anterior and posterior lower legs and the genital
region. Eight common localisations were affected. In the other boy, the signs of infection had

Results 82
improved. The score was reduced to 4 points. Lesions were found at common localisation only.
There was no more superinfection. Both boys reported that pruritus had improved.
4.2.1.3 Case descriptions Placebo Group
Screening
This group consisted of two girls, who were sisters and living together and of two boys, who were
brothers and also staying together in the same house. They were between 8 and 13 years of age.
Diagnosis was made clinically. No mites could be detected on microscopic examination of the skin
scrapings. Both girls had severe infection with score values of 13 and 19 respectively, whereas the
degree of infection of the two boys was moderate with score values of 6 and 9. Typical papular
pruritic rash on forearms, hands, knees and the umbilical region was observed. Besides, macules,
burrows, crusts and generalized lichenification could also be observed. In her sister some lesions
were excoriated, and most lesions were pink in colour. There was bacterial superinfection, which
was treated with a five day course of cloxacillin. The number of common localisations affected
varied between 1 and 5 in all four children. Bacterial superinfection was present in three of the four
children. The two boys complained about moderate pruritus. The child with the severest infection in
this group described her pruritus as only mild. Her sister had severe pruritus. In all four cases the
itching was more severe at night.
Follow-up 2
Both girls were completely cured, and the infestation of the boys had improved. The younger boy
was nearly cured, with only some residual signs and mild degree of infection (score=3). Most of the
lesions were now healing; active lesions were found in the genital region. Residual
postinflammatory hyperpigmentation was still found on the right anterior and posterior upper arm,
chest, abdomen and the genital region. Pruritus was no longer present. His brother had only
improved slightly. However, the score was reduced markedly to 11 because there was no more
bacterial superinfection or thick crusts. His skin showed generalized lichenification and was in
some areas atrophic. The lesions were not sharply demarcated and disseminated over nine common
localisations. Pruritus was now mild. In three children the improvement of the skin disease could be
confirmed by the photographs taken at the first screening examination and the second follow-up.
Deterioration of the lesions was seen in case of the 13 year-old boy from screening to the first
follow-up.
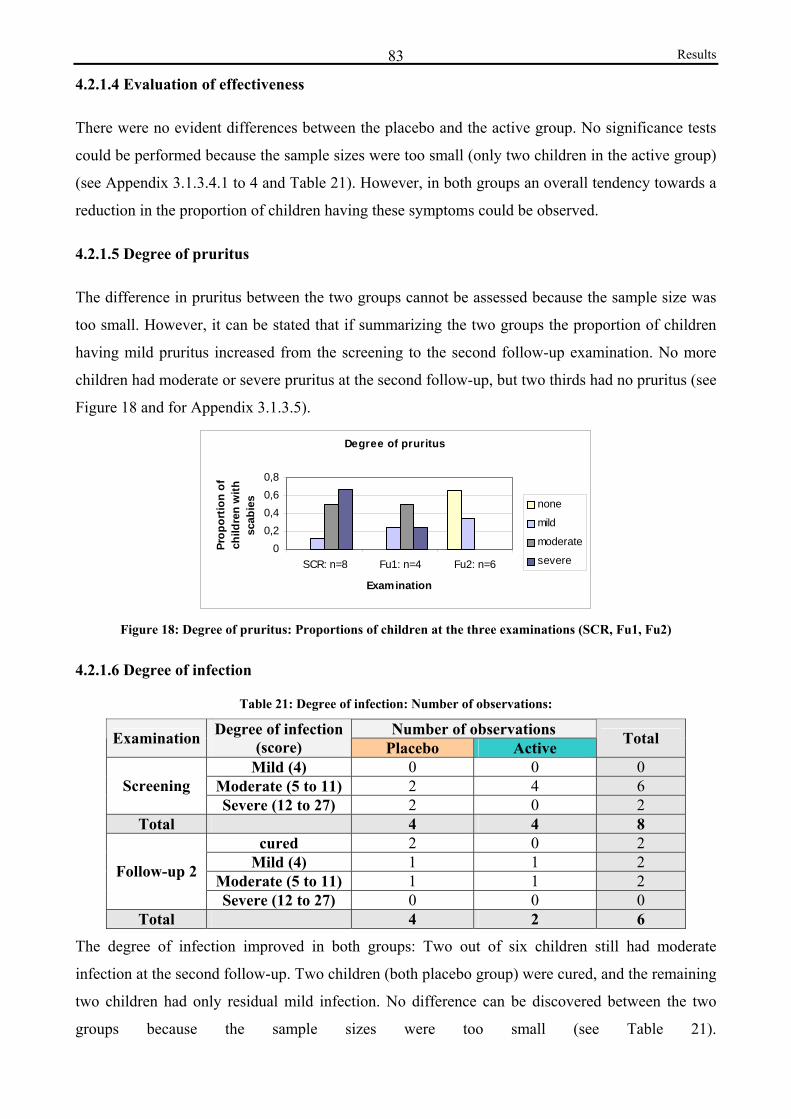
Results 83
4.2.1.4 Evaluation of effectiveness
There were no evident differences between the placebo and the active group. No significance tests
could be performed because the sample sizes were too small (only two children in the active group)
(see Appendix 3.1.3.4.1 to 4 and Table 21). However, in both groups an overall tendency towards a
reduction in the proportion of children having these symptoms could be observed.
4.2.1.5 Degree of pruritus
The difference in pruritus between the two groups cannot be assessed because the sample size was
too small. However, it can be stated that if summarizing the two groups the proportion of children
having mild pruritus increased from the screening to the second follow-up examination. No more
children had moderate or severe pruritus at the second follow-up, but two thirds had no pruritus (see
Figure 18 and for Appendix 3.1.3.5).
Degree of pruritus
00,20,40,60,8
SCR: n=8 Fu1: n=4 Fu2: n=6
Examination
Prop
ortio
n of
ch
ildre
n w
ith
scab
ies none
mild
moderate
severe
Figure 18: Degree of pruritus: Proportions of children at the three examinations (SCR, Fu1, Fu2)
4.2.1.6 Degree of infection
Table 21: Degree of infection: Number of observations:
Number of observations Examination Degree of infection (score) Placebo Active Total
Mild (4) 0 0 0 Moderate (5 to 11) 2 4 6 Screening Severe (12 to 27) 2 0 2
Total 4 4 8 cured 2 0 2
Mild (4) 1 1 2 Moderate (5 to 11) 1 1 2 Follow-up 2
Severe (12 to 27) 0 0 0 Total 4 2 6
The degree of infection improved in both groups: Two out of six children still had moderate
infection at the second follow-up. Two children (both placebo group) were cured, and the remaining
two children had only residual mild infection. No difference can be discovered between the two
groups because the sample sizes were too small (see Table 21).

Discussion 85
Discussion:
1. Epidemiology of superficial dermatomycoses
1.1 Tinea versicolor
In the present study the prevalence of tinea versicolor was found to be 26.2% and accounted for
70% of all dermatomycoses. A proportion of tinea versicolor infections among primary
schoolchildren as high as in the present study, and therefore relatively low proportion of tinea
capitis infections (14.7%), has to this author’s knowledge not been reported so far from Tanzania or
another sub-Saharan African country (Satimia et al., 1998; Schmeller, 1998; Schmeller et al.,
2001). This pattern cannot be easily explained, and only few assumptions shall be presented here.
Tinea versicolor is not regarded as a contagious disease, and Malassezia yeasts were also isolated
from healthy individuals (Gupta, 2002; Faergemann, 1994; Schmidt, 1997; Leeming et al., 1989).
The growth conditions present among the individuals in Ifakara must therefore have been highly
favourable for Malassezia yeasts thus leading to a successive overgrowth and shift to the pathogenic
filamentous form. This might at the same time have inhibited the growth of dermatophytes
competitively.
Certain predisposing factors for tinea versicolor infections might play an important role, e.g.
endogenous factors such as malnutrition, hyperhidrosis, a positive family history and
immunodeficiency possibly due to HIV infection. There is no information available with regard to
the actual rate of HIV positive children in Kilombero District, but in Ifakara 13.6% of the general
population are believed to be infected (Source: IHRDC, 2003). However, the proportion of HIV
positive children attending primary school may be relatively low. This is is due to the fact that those
infected during pregnancy, delivery or through breastfeeding usually die before reaching the school
age because of their increased susceptibility towards the effects of malnutrition and infectious
diseases like PCP or tuberculosis (Dr. B. Idindili, personal communication). The presence of any of
the above mentioned endogenous factors was not assessed in the course of this study.
Exogenous factors include heat, moisture and occlusion through clothes or vaseline, palm oil or
cocoa butter. Occlusion may increase CO2 production resulting in an altered microbiologic flora and
a change in the pH of the skin (Pontash et al., 1989; Dave et al., 1987; aTerragni et al., 2001; bTerragni et al., 2001; Bouassida et al., 1998). In the region where the present study was performed,
the application of vaseline – called “mafuta” is a very common procedure as shiny greasy skin is
looked at as being very attractive (P. Schmid-Grendelmeier, personal communication). During
history-taking and physical examination, this feature was not assessed in a systematic way, but our
observations confirmed the statement. Increased susceptibility of African in comparison to
Discussion 86
Caucasian children has also been discussed to play a part (bTerragni et al., 2001; Borelli, 1985). The
influence of the age distribution among the study population should not be neglected. 58.5% of the
children were older than 11 years. The group of adolescents was slightly over-represented thus
increasing the overall prevalence rate.
1.2 Other superficial dermatomycotic infections
In the Study Proposal of the present study, the prevalence rate of tinea capitis and/or tinea corporis
had been assumed to be approximately 15%. This assumption was based on studies conducted in
various comparable settings. In Ivory Coast 11.3% of the examined pupils (Hervé et al., 2002) had
tinea capitis infections whereas 16.9% (Melake et al., 1990) were in infected in north-west Ethiopia,
29% in south-west Ethiopia (Figueroa et al., 1997) and in Zimbabwe (Robertson, 1990) and another
study in even 33.3% (Ayaya et al., 2001) in Kenya. Figueroa et al. identified 24% of school
children as asymptomatic dermatophyte carriers (Figueroa et al., 1997). It is noteworthy that in the
present study samples were only taken from symptomatic children. The possibility that many
children were not identified to be infected with tinea capitis or corporis should be considered.
In the present study, 5.5% of the children showed clinical signs of tinea capitis infection, 3.2% of
tinea pedis and 2.6% of tinea corporis infections. The prevalence rate of 2.6% of tinea corporis was
similar to those described by Enweani et al. (1996) and Figueroa (1996) who discovered rates of
2.7% for Nigerian and Ethiopian schoolchildren respectively. It also coincides with the prevalence
described for children aged 6 to 14 years in various Tanzanian districts (approx. 1 to 4%) (KCMC,
unpublished data).
Tinea pedis infections were slightly more frequent in the pupils from Ifakara (3.2%) than in pupils
from Nigeria (1.5%) (Enweani, 1996) and from Turkey (0.5%) (Inanir et al., 2002). The prevalence
rate compares more closely to the average infection rate of 3.7% among British pupils as described
by English et al. (English et al. , 1959).
It remains uncertain whether hygiene conditions, health education and access to treatment were
better as compared to the other studies thus explaining the relatively low prevalence rate of tinea
capitis. Furthermore, it is possible though not very likely that the children attending the two primary
schools in Ifakara have less contact with animals, dust, contagious fomites or infected individuals.
The fact that all children attending standard 1 and 2 at any of the Ifakara Primary Schools had to
have short hair may protect them from tinea capitis infections.
Discussion 87
2. Assessment of the effect of soap and the efficacy of Triclosan in soap
Large proportions of cases of dermatomycoses were cured during two months of regular soap use.
Cure rates of tinea versicolor, tinea capitis, corporis and pedis were 28.4%, 61.1%, 56.3% and
36.8% respectively (overall cure rate for dermatomycoses: 36.0%).
2.1 Superficial dermatomycoses
2.1.1 Tinea versicolor infections
No significant differences were found between the active and placebo soap for any of the observed
parameters in any of the selected dermatoses. Some parameters were supportive of a slightly
superior effectiveness of Triclosan soap. It has to be concluded that Triclosan is not clinically
effective against Malassezia spp.
However, for both placebo and active soap significant tendencies towards improvement and
resolution could be identified (see Tables 6a and 6b). The fact that the proportion of children
presenting the following parameters: scaling, pruritus, and hypopigmentation; decreased from the
first examination to the second follow-up supports this statement. Severe extensive cases showed
less improvement than milder ones.
Triclosan as an inhibitor of cyclo-oxygenase and lipo-oxygenase has an anti-inflammatory and anti-
irritative properties (Nissen et al., 1998). However, since there was no difference in pruritus
between the Triclosan and the placebo group, it has to be concluded that Triclosan alone was
probably not responsible for the overall decrease of the degree of pruritus over two months. The
lacking of the additional effect by Triclosan might be explained by the fact that in spite of the long-
lasting antimicrobial efficacy of all products containing Triclosan, the anti-inflammatory or anti-
irritative effect is not as strong in rinse-off-formulations as in leave-on-formulations (M. Schnyder,
personal communication). The leave-on time might therefore have been too short for a more
pronounced anti-irritative effect of Triclosan to become evident.
The decrease in the intensity of pruritus could be explained by the procedure of intense and regular
washing which was promoted in the course of this study. Controlled soap use per se thus seems to
have had a beneficial effect on the degree of pruritus. The soap consumption during the study
period has probably been higher than normally, leading to a reduction of dust and other irritative
particles on the skin surface. The decrease in the intensity of pruritus is also associated with the
decrease in the overall degree of infection. Climatic conditions may have influenced the degree of
pruritus indirectly, since, according to Faergemann (1993) it seems to depend on the degree of
sweating.
Discussion 88
The overall proportion with disseminated lesions remained nearly the same. The soap might thus be
able to reduce the extension of the lesions, if lesions have not been disseminated before. In these
cases complete resolution may take longer to occur or may not at all be achieved by regular soap
use.
Regular soap use has strongly reduced the overall proportion of positive microscopic results from
81.0% during the screening to 48.4% during the second follow-up examination (see Results for
Table 10a). There was no significant difference between active and placebo group. Early changes in
the aspects of the filaments that may have taken place due to the use of the soap may not have even
been visible by light microscopy. McDaniel et al. have shown that already shortly after the onset of
treatment, the fungal cells may appear wrinkled and disorganized. These changes might have been
visible using electronmicroscopic techniques thus underlining even more the effectiveness of the
soap (McDaniel et al., 1984; Gupta, 2002). On the other hand it has to be considered that a very
thorough and frequent mode of washing of the skin may obscure a microscopic diagnosis, thus
producing some false negative results on microscopic examination (Faergemann, et al., 1982). This
may be the case in the present study, but would affect both groups to a similar extent.
In the present in vivo study Triclosan was not found to be mycologically more effective against
Malassezia spp. than the placebo. This coincides with in vitro experiments, which have shown that
Triclosan is not effective against M. furfur (MIC>1000 ppm) (© Ciba Specialty Chemicalsa, 1998).
Even though no efficacy of Triclosan could be proven for M. furfur, it is important that this species
may represent only 1 to 10% of all the species isolated. According to Gupta et al. the epidemiology
of Malassezia yeasts depends on the geographic region (Gupta et al., 2003).
The results of the microscopic examination and cultivation of fungi performed for quality control at
the “Mycological laboratory of the Department of Dermatology, University Hospital of Zürich”
revealed that, in nearly 90% of uncertain differential diagnoses between tinea versicolor and tinea
corporis, the lesions were caused by Malassezia spp. This implies that the clinical picture of tinea
versicolor shows a great variety of presentations. An over-diagnosis of tinea corporis may be the
consequence and should be considered as a possible source of bias.
In the placebo and active group the majority had experienced improvement at both follow-up
examinations. In conclusion, the subjective assessment shows that on a subjective level the soap use
was well-accepted and regarded as effective in reducing pruritus or the cosmetic disturbance, which
are the most relevant complaints of the children.
A significant improvement of the degree of infection could be achieved through the application of
both soaps (see Results for Figure 7a and 7b). There are several possible explanations for this.
First, the amount of oily or sebaceous substances on the skin surface might be reduced due to the
regular use of soap thus making the growth of the lipophilic yeasts more difficult.
Discussion 89
Second, less occlusion of skin through oily substances might provoke a decrease of CO2
concentration and an increase of the pH value on the skin surface.
Third, the change of season between the screening and the follow-up examinations, bringing less
heat and humidity than before (see Table 1, Patients, Approaches and Methods), also has to be
considered. These climatic factors are believed to contribute largely to the high prevalence in
tropical regions (Gupta, 2002; Taplin et al., 1965) by promoting the shift to the pathogenic mycelial
form. Miskeen et al. have described in India a marked increase in the number of cases during the
hot and humid summer months and a sudden decrease during the cooler and drier winter months
(Miskeen et al., 1984). Kamalam et al. found that the incidence of tinea versicolor in Madras was
highest in May (month of highest maximum temperatures) and October (month of most extensive
rainfalls) and lowest in January (month of lowest minimum temperatures) (Kamalam, et al., 1981).
In Venezuela a significantly higher prevalence rate of tinea versicolor was found in the semi-arid in
comparison to the sub-humid zone (Perez Blanco et al., 1990). Porter et al. also reported a markedly
higher prevalence during the rainy season from a Gambian village (Porter, 1979). According to him,
this decrease can be attributed to the higher hydration level of the stratum corneum associated with
the greater dispersal of sebum during the hot and humid season.
It is possible that in the present study vigorous scrubbing with soap and water, as recommended by
Canizares (1982) as an adjunct to further topical treatment, contributed to the overall improvement
seen. Spontaneous resolution is not believed to occur frequently (Canizares et al., 1993). However,
it is not possible to prove whether the improvement in the degree of infection in the present study,
representing a tendency towards resolution of the disorder over time, was due to the soap use or the
climatic conditions, as no control group could be included in the study for ethical reasons.
The scatter plot presentation (see Results for Figures 8a to 8d) allows the reader to visualize that a
large proportion of children showed improvement of their lesions. Important cases with positive
microscopy during the second follow-up rather had the tendency to deteriorate than cases that were
mild during the screening examination. This finding underlines that regular soap use was not
effective in more important cases particularly if spores and filaments could not be eliminated. These
cases would thus require other forms of topical or even systemic treatment.
Determination of minimal inhibitory concentrations (MIC’s) of placebo soap and of Triclosan
In order to further understand the possible mycological effectiveness of placebo soap against tinea
versicolor after all the analyses had been performed, it was attempted to assess the MIC’s of
placebo soap and of pure Triclosan against Malassezia species isolated in Zürich. For the Triclosan
dilution series, only the significant concentrations were able to inhibit growth. For relevant
concentrations (<10 (μg/mL) and for both dilution series of placebo soap, the growth of the fungus
Discussion 90
depended only on the properties of the isolate and was very irregular. The results provided no
explanation for the improvement found in vivo, since they do not allow any quantitative
conclusions. However, they support the hypothesis that the improvement seen is rather associated
with unspecific aspects related to regular soap use, and not a specific effectiveness of either the
soap or Triclosan against Malassezia spp. It has to be concluded that neither placebo soap nor
Triclosan soap inhibit the growth of Malassezia spp. at relevant concentrations.
2.1.2 Other superficial dermatophytic infections
There was an overall tendency towards improvement and resolution of the other dermatomycotic
infections during the two months of controlled soap use (see Results for Table 6a and 6b). The
proportion of children presenting the characteristic parameters decreased in both groups from the
screening to the second follow-up. It can be stated that Triclosan did not prove to be clinically
effective against tinea capitis, corporis or pedis infections, since both soaps seem to have had the
same overall curative effect (see Appendix 3.1.2.1).
The degree of pruritus decreased significantly in both groups. In the case of tinea pedis infections
the decrease was very striking. Only mild pruritus was still present in only one fifth of the children.
Controlled soap use per se seemed to have a beneficial effect on the degree of pruritus. Possible
explanations are analogous to those discussed with regard to the degree of pruritus in case of tinea
versicolor infections.
Calculation of the average diameter of the largest lesion can be regarded as an important tool to
assess the clinical effectiveness of the active and placebo soaps. For tinea capitis there was a similar
decrease in both groups: in the active group from 2.9 cm to 2.4 cm, and in the placebo group from
2.6 cm to 1.6 cm (see Results for Table 14a). For tinea corporis in the active group the mean
diameter of the largest lesion decreased from the screening to the second follow-up from 2.2 cm to
1.0 cm, whereas it increased in the placebo group (see Results for Table 16b). This finding is one of
the few parameters in favour of the active soap even though the difference was not significant.
Nevertheless this finding may rather be due to unspecific variation than a better effectiveness of
active soap.
The importance of the number of lesions when assessing the degree of the skin disorder should not
be overemphasized, because these two features do not necessarily coincide, since in severe and
extensive cases multiple lesions may coalesce to form one large patch.
On interpretation of the series of photographs, visible deterioration of the morphology of the lesions
only occurred in the placebo group (see Results for Figure 10). Nevertheless, improvement of tinea
capitis as well as tinea corporis infections was also found more frequently in the placebo group than
in the active group. Triclosan soap might thus prevent deterioration better than placebo soap.
Discussion 91
However, these differences were not significant, and one has to keep in mind, that the number of
children for whom the pictures could be evaluated was unbalanced: altogether 18 children in the
active and 41 in the placebo group.
The mycological effectiveness of Triclosan against some dermatophyte pathogens has been proven
in vitro (© Ciba Specialty Chemicalsa, 1998) (see Background: Information about Triclosan), but
this finding could not be reliably confirmed in the present clinical trial, since the relative risk did
not differ significantly. Both soaps seemed to have a certain mycological effectiveness against
dermatophytes, which may be due to the alkaline pH of the soap (pH=10), which itself displays an
antimicrobial effect (D. Ochs, personal communication). The effectiveness of Triclosan may have
become more evident if the treatment period had been longer. It should also be considered that the
filaments that were seen during the second follow-up might have been dead hyphae in some cases
(Gooskens et al., 1994). In tinea capitis this decrease of positive results occurred only in the active
group, which may be considered as supportive of the findings made in vitro.
In the scatter plot presentation for tinea capitis the overall improvement is even more striking than
in the cases of tinea versicolor infections. Increases of score values occurred in seven cases and
only resulted in an increase in the degree of in infection in one case. In all cases with negative
microscopic results the clinical score was reduced. This confirms that the score used in this study is
useful in reflecting the clinical course of the infections.
Overall improvement of tinea capitis and corporis:
There are different possible explanantions for the overall improvement of the cases of tinea capitis
and corporis infections included in the study. First, this might be due to the elimination of the
pathogens from the lesion sites simply through the washing process, supported by the antimicrobial
properties of the soap. Figueroa et al. have suggested that the burden of the dermatophytes may
determine the clinical stages of tinea capitis infections among Ethiopian schoolchildren (Figueroa et
al., 1997). In the present study, elimination of the pathogens from the scalp and glabrous skin have
also have reduced the chance of spreading from asymptomatic sites, which may simply be
contaminated or sites of asymptomatic infection, as well as the chance of re-infection. A protective
as well a curative effect of soap use have been described by other authors. Attapattu has reported
from Sri Lanka, that the custom of daily head baths of young children with water and soap may
account for the low prevalence of tinea capitis in the community he observed in spite of poverty and
overcrowding (Attapattu, 1989). More than half of the study participants with fungal infections
were cured by using a soap containing certain plant derivates during a study conducted by Alebiosu
et al. in Nigeria (Alebiosu et al., 2003).
Second, many children might have shown spontaneous resolution (Schmeller, 1998; Weitzman et
al., 1996). Resolution of the infection occurs more rapidly due to cell-mediated immunity if a

Discussion 92
severe primary infection has taken place before, which is very likely for most children in this study
(Canizares, 1982). Neither the incidence nor the prevalence among untreated children was assessed
at the time of the second follow-up and no control group was included. Therefore it is not possible
to determine whether resolution occurred spontaneously.
Third, the change of season from the screening (hot, rainy season) to the second follow-up
examination (cooler and drier; see also Table 1, Patients, Approaches and Methods) might have
influenced the overall improvement of the degree of infection (Canizares, 1982). Porter et al.
reported an increase in the prevalence rates of tinea coporis from the wet to the dry season in a
Gambian village, whereas the prevalence of tinea capitis decreased significantly (Porter, 1979).
Abu-Elteen et al. found that in a hot, semi-arid region at the north-eastern part of the Jordanian
desert, tinea capitis and corporis infections occurred predominantly in the spring and winter months
(Abu-Elteen et al., 1999). However, other authors believe that the growth of dermatophytes is
generally favoured by heat and humidity (Abu-Elteen et al., 1999; Hay, 1996; Kamalam et al.,
1981). Investigations by Kamalam in Madras confirmed that tinea capitis and corporis infections
were correlated with minimum and maximum temperatures as well as rainfall (Kamalam et al.,
1981). It is not possible to draw conclusions as to whether the prevalence rates in Ifakara also
changed due to the change of the season, since no control group without any treatment was
examined and because the numbers of cases were very small in the case of tinea corporis infections.
The rates of clinical and microscopic resolution are comparable to the clinical success rates reported
by Alebiosu et al. from Nigeria (Alebiosu et al., 2003), who treated 446 individuals with fungal
infections and 64 subjects with scabies with either “Toto Soap”, “Toto Ointment”, soap and
ointment or sulphur ointment for five to twelve weeks. “Toto Soap” is comparable to the placebo
soap used in the present study. It contains palm oil (Butyrosporum paradoxum oils and Elaeis
guineesis) as a plant derivate that has acclaimed medical value and a chlorinated phenol, which
might also have acted as the active substance. Out of 107 patients with fungal infections treated
with Toto soap alone, 51.4% of the patients with dermatomycoses could be cured after a median
period of five weeks. All five patients with scabies receiving Toto soap were cured. The authors
emphasize that even better effectiveness could be achieved by combining the soap with the
ointment. Both studies strongly suggest that regular soap use may have an important effectiveness
against these dermatoses, which are common in tropical Africa.
Effectiveness of Triclosan:
Triclosan is known to show in vitro effectiveness against a wide range of dermatophyte species (©
Ciba Specialty Chemicalsa, 1998). Among the pathogens that could be identified through cultures in
Zürich, Triclosan has been proven to be effective against T. mentagrophytes and T. tonsurans, with
minium inhibitory concentrations ranging between 1 and 10 ppm. Because of these in vitro findings,
Discussion 93
one might have expected a more pronounced mycological effectiveness of the active soap against
these dermatophytes. It is possible that in the present study pathogens which were not identified
through culture in Zürich are more resistant to topical treatment with Triclosan. This might explain
the lack of superior efficacy in most cases.
The assumption that the leave-on time of the soap might have been too short to produce any effect
at all, cannot explain the findings. Triclosan displays a long-lasting antimicrobial efficacy, even if
applied as a rinse-off formulation (Ciba Specialty Chemicalsa, 1999). Active dermal concentrations
can be detected after 24 hours, and the substance accumulates on the skin after repeated use.
However, the mycological effectiveness of Triclosan against the dermatophyte species might have
been influenced by certain interactions with vaseline applied onto the skin. It was observed during
the trial that many children used vaseline regularly. Excessive application of this substance after the
soap use might have reduced the amount of Triclosan that could accumulate on the skin, since
Triclosan is a lipophilic molecule, which would therefore be deposited in vaseline to a great extent.
If vaseline was applied before washing, an emulsion might be formed during the washing process,
which would be easliy rinsed off, thus reducing the long-term efficacy (Dr. W. Baschong, M.
Schnyder, personal communication).
It should also be mentioned that in the tropics a large proportion of dermatomycoses may be caused
by yeasts such as Candida spp. or by moulds, against which Triclosan is not highly effective (e.g.
MIC of C. albicans is 33 ppm). These fungi might have been among the causative species
particularly in the cases in which the samples could be evaluated.
It is important that apart from one case of tinea corporis infection caused by T. mentagrophytes, all
pathogens cultivated in Zürich either from tinea corporis or capitis lesions were T. tonsurans or T.
violaceum, which cause endothrix infections (see Results for Tables 9b and 9c). It can be assumed
that they were the most common causative species among the schoolchildren in Ifakara. Topical
treatment of tinea capitis probably is probably not capable of eliminating hyphae in the deeper parts
of the follicle or penetrate hair shafts (Schmeller, 1998; Hussain et al., 1999; Chan et al., 2004).
Therefore many authors doubt whether topical treatment e.g. with Whitfield’s Ointment is effective,
especially in cases of endothrix infections (Ayaya et al., 2001; Gooskens et al., 1994; Canizares et
al., 1993).
Weitzman et al. recommend that topical agents may be used as adjuncts to eliminate viable material
from the lesions and thus prevent further spreading (Weitzman et al., 1996). In the future, an
effective antifungal soap available for the majority of the population might fulfill this purpose better
than any other sort of topical treatment, which would only be used by patients who are aware of
their disease. With this kind of soap, asymptomic carriers (Weitzman et al., 1996; Figueroa et al.,
1997) as well as non-infected individuals could be “treated” effectively at the same time.
Discussion 94
Tinea pedis: The proportion of children showing complete resolution of symptoms was greater in
the active than in the placebo group (85.7% versus 55.6%) (see Results for Tables 19e and 19f). For
all remaining uncured children in the active group there is no information concerning the degree of
infection at the screening examination. Active soap might therefore have been clinically more
effective, but this assumption cannot be reliably proven by significance tests.
The possibly superior efficacy of Triclosan may be explained by the pathomechanism particularly
common in interdigital tinea pedis infections, which was the only type discovered in the present
study population: After destruction of the barrier role of the stratum corneum by the dermatophyte,
bacterial overgrowth at the expense of the dermatophyte may occur, especially under favourable
conditions such as occlusion and humidity. Bacterial organisms commonly isolated from these
“dermatophytosis complex” lesions include gram-positive species such as S. aureus or C.
minutissimum, and gram-negative bacteria such as Pseudomonas and Proteus spp. (Masri-Fridling,
1996), against all of which Triclosan is effective, apart from Pseudomonas spp. (Ciba Specialty
Chemicalsa, 1998).
In the present study the total number of observations was very small, and for 13 children the clinical
score could not be evaluated at the second follow-up. An overall proportion of 36.8% showed
clinical resolution at the second follow-up. The possibilities that this has occurred spontaneously or
was due to the change of season cannot be ruled out. Reports which investigate the influence of
seasonal changes on the prevalence of tinea pedis infections are slightly contradictory in their
findings. A decrease of the incidence of tinea pedis among Korean children in the cooler season of
the year has been described by Jang et al. (Jang et al., 2000). However, Kamalam found the highest
incidence rates in the months of medium temperatures and lowest rainfalls. The incidence rate was
lowest in November, when humidity is highest and rainfalls are abundant (Kamalam et al., 1981).
Abu-Elteen et al. described the highest incidence of tinea pedis for the summer months (Abu-Elteen
1999).
3. Scabies
3.1 Epidemiology of scabies
In the Study Proposal of the present study, the prevalence rate of ectoparasitoses (scabies and/or
pediculosis) had been assumed to be 10%. This assumption was based on the reports by bTanner et
al. (1987), Henderson (1992), Schmeller (1998), Figueroa et al. (1996) and Heukelbach et al.
(2003). Surveys in various districts of Tanzania revealed overall prevalence rates between 4 and
30.4% among the general population (KCMC, unpublished data). According to Tanner et al.,
Discussion 95
between 1982 and 1984 scabies was the third most common reason to seek treatment at any level of
the health care delivery system in Kilombero District (bTanner et al., 1987).
Considering a drop-out-rate of 40%, the minimum sample size calculated in the Proposal was 127
children in order to observe significant differences between active and placebo group.
This aim could not be achieved since none of the 820 examined children were suffering from
pediculosis and only 1.5% had scabies. Therefore only a descriptive analysis of the eight cases was
possible.
3.2 Assessment of the effect of soap
3.2.1 Assessment of the efficacy of Triclosan in soap
The difference in pruritus between the two groups could not be assessed because the sample size
was too small. As in the case of fungal infections, the soap may be able to relieve pruritus since it
reduces the amount of dust and irritative substances on the skin, and also has antimicrobial
properties. This effect does not appear to be due to Triclosan, but the sample is too small to verify
this assumption (see Results for Figure 18).
Both soaps have displayed a curative effect on the signs and symptoms of scabies (see Results for
Table 21). With regard to complete resolution of scabies, it is surprising that it only occurred in the
placebo group. Since the number of cases was very small, possible explanations are speculative.
The children with severe infestations, even though otherwhise instructed by the principal
investigator, may have sought further medical help at local health facilities. It is also possible that
other affected family members had been provided with the necessary medication and had been
instructed to include the whole family in the treatment. However, the possibility that the soap has
been effective should not be neglected. Due to the antimicrobial properties of the soap base,
particularly bacterial superinfection may have been reduced. Alebiosu et al. were able to cure all
five patients with scabies whom they treated with “Toto Soap" (Alebiosu et al., 2003 ). It is not
clear whether the active ingredients (Butyrospermum paradoxum oils and Elaesis guineesis) are
responsible for the resolution of scabies or whether the soap base itself produced this effect.
Lesions may have improved or even resolved spontaneously. Seasonal variation of the incidence
has been discussed. Most authors indicate a higher incidence in fall and winter (Christophersen,
1978; Mimouni et al., 2003). However, Porter et al. found no difference in prevalence rates between
the wet and dry season in Gambia (Porter, 1979). Any possible association between climatic
conditions and point prevalence rates does not seem to be an appropriate explanation for the
decrease in the degree of infection in the present study, since the second follow-up was performed
during the drier and cooler period of the year.

Discussion 96
Due to the small number of cases, it is difficult to make any statements regarding the possible
superior efficacy of the active soap. However, Triclosan did not prove to be strongly effective
against scabies infestations, and regardless of possible minor benefits such as anti-inflammtory
effects and antibacterial effectiveness (Ciba Specialty Chemicalsa, 1998 ) it should not be used as
the only therapy of scabies, but possibly as an adjunct to standard treatments. In a study conducted
in central Tanzania, Henderson et al. have shown that the addition of soap and scabicidal ointment
to standard BBE treatment schemes led to a significant rise in cure rates (Henderson et al., 1992).
The soap may be beneficial in supporting the prevention of re-infections from untreated relatives
and improve the hygiene conditions in the children’s homes.
4. Strength and Limitations
4.1 Physical examinations and photographic images
Poor illumination therefore affected to a certain extent the physical examinations in the classrooms.
At Lihami Primary School the illumination of the examination room was better during the two
follow-ups, as it had been possible to shift to a larger classroom. Since the conditions were not
exactly the same at the different examinations, it is possible that minor lesions had not been visible
in their full extension during the first screening. Some pictures taken at the first screening could not
be evaluated. The illumination was better at Michenga Primary School since a brighter room with a
curtain generating privacy could be used during the whole trial.
A strength of the study of the study is the fact that all examinations were performed by the same
four investigators. Since the clinical experience of the two medical students (Almuth Dinkela and
Julia Ferié) was still limited at the beginning of the study, each finding was briefly presented to Dr.
M. Mbata, who is a fully trained local dermatologist (Assistant Medical Officer). At a later stage all
unclear findings were still discussed with him. Quality control of the diagnosis was furthermore
ensured by the assessment of the digital photographs by the expert dermatologist in Zürich.
4.2 Design of questionnaires
The documentation system used in the questionnaires only allowed the examiners to describe
lesions due to the defined principal diagnosis in full detail. Further skin disorders could only briefly
be recorded. Open questions might have yielded more reliable information with regard to the
subjective description of the symptoms by the study participants. However, an unstructured
interview would have exceeded the language skills of the European investigators (AD and JF).
Discussion 97
4.3 Sample-taking and microscopic examination
The paper, scalpel or envelope may have become contaminated in some cases, since there was no
possibilty to store them in clean places during the whole examination period. Many samples could
not be evaluated because not enough material had been taken.
It was not possible to cultivate the fungi at the laboratory facilities available at IHRDC in Ifakara
itself. The identification of all the pathogens by culture or other techniques might have contributed
to answering some of the questions which this study has raised. Maybe Triclosan would have
proven to be effective against certain species. Furthermore, mere microscopic examination did not
allow us to distinguish between dead and viable material, which might have been important since
the study period lasted only two months and effects might not have been so evident yet.
Tinea pedis infections were not confirmed by microscopic diagnosis since they were not one of the
diseases that were to be evaluated with priority in the soap trial. Only clinical improvement was
assessed. However, one should bear in mind that, apart from dermatophytes, the infections might be
caused by many different species such as Candida spp., S. brevicaulis, H. toruloidea and Fusarium
spp. (Masri-Fridling, 1996). The number of cases was very small, and reliable statements can only
be made to a very little extent.
Only in one case a mite was detected on microscopic examination and thus allowed the
confirmation of clinically diagnosed scabies. Eggs were not seen in any case. Detection of scybala
was complicated by dirt. The sample-collection may have failed because burrows were hardly found
due to scratch effects and superinfection. Sample-taking was therefore not performed at the follow-
up examinations and the diagnosis was thus based on clinical findings.
4.4 Quality control of microscopy and additional cultivation of fungi in Zürich
Quality control of the microscopic examinations performed in Ifakara was not possible in all cases.
In case of dermatophyte infections, species identification in all cases would have been desirable to
explain the lack of efficacy of Triclosan.
Isolation of Malassezia yeasts from human skin does not necessarily indicate tinea versicolor
infections there is also skin colonization by this fungus without resulting skin pathology (Gupta,
2002; Roberts, 1969). Gupta et al. therefore postulate that the characteristic micromorphology of
fungal elements in the skin is identified to confirm the diagnosis, which could not be done with the
means available in Ifakara (Gupta et al., 2001). However, as the skin samples were taken from
affected skin and no other fungal elements were cultured, Malassezia spp. seem to be responsible
for the observed skin lesions in our patients.

Discussion 98
4.5 Results during the first follow-up
The first follow-up fell into the period of school holidays when many children moved with their
family into the far away “shamba (field) house”. Only 136 children came to this examination and
few to the soap distributions, even though attendance and compliance were promoted with the help
of the local Balozi leaders.
Even though an overall improvement could be observed for all diagnoses (Tinea verisocolor, tinea
capitis, corporis and pedis, and scabies), some results at the first follow-up (see Appendix) do not
reflect this tendency. Maybe these observations are due to unspecific variance. Irritation or
exacerbation under treatment would be another possible explanation. Furthermore, the assessment
may not have been as exact as at the second follow-up.
4.6 Characteristics of the study population
As Lihami Primary School could not provide the examiners with complete and up – to – date class
lists, it was difficult to check which children had already been seen. It is possible that some children
were not examined at all and that other children who otherwise would not have attended school
preferred to come to school to be examined.
Information obtained from the younger children with regard to the subjective impression of the skin
disorder and the degree of pruritus might not have been reliable, since they might have felt
pressured to provide the answer they believe to be expected to give. This has maybe hampered the
assessment of any possibly existing difference between the two groups. One may assume that the
compliance during these two months of the soap trial was good. Nevertheless, a longer study period
and maybe even greater amounts of soap distributed per week would have been required to reduce
the chance that the soap was used for other purposes or exchanged, possibly even between the study
participants.
4.7 Spontaneous resolution and climatic influences
It is not possible to determine whether resolution of the dermatoses occurred spontaneously. Neither
the incidence nor the prevalence among untreated children was assessed during the second follow-
up. Besides, a control group would have allowed us to draw conclusions as to whether the
prevalence rates in Ifakara also changed due to the change of the season.
Discussion 99
5. Conclusions
• Among 820 children aged 6 to 19 years, 277 children (33.9%) presented with fungal
infections and only 12 (1.5%) with scabies.
• Among the 306 cases of dermatomycoses, 214 (70.0%) were due to tinea versicolor, proven
by microscopy in 81.0%, 45 (14.7%) were due to tinea capitis, 21 (6.8%) to tinea corporis
and 26 (8.5%) to tinea pedis.
• In tinea versicolor, controlled soap use has resulted in significant improvement of the degree
of infection as well as an increase of in the proportion with negative microscopic results
from 19.0% to 51.6%. 28.4% of all individuals were cured; however there was no additional
effect if Triclosan was added to the soap. This is consistent with the lack of efficacy in vitro
of Triclosan against Malassezia spp. reported in the literature (© Ciba Specialty Chemicalsa,
1998) and found at the “Mycological laboratory of the Department of Dermatology,
University Hospital of Zürich”.
• In tinea capitis, corporis and pedis, a significant improvement was also observed after
controlled soap use, with or without Triclosan. Cure rates ranged from 36.8% to 61.1%.
There was no significant difference between placebo and active group. However, a decrease
of the average lesion size in tinea corporis only occurred in the active group, whereas it
increased in the placebo group. In tinea capitis the proportion of negative microscopic
findings decreased only if Triclosan soap was used.
• The mild beneficial effect of Triclosan can be explained by its known in vitro activity
against dermatophytes such as T. rubrum or mentagrophytes. The lack of a stronger efficacy
of Triclosan could be explained by the used rinse-off application instead of leave-on and the
additional use of petrolatum (vaseline).
• The group of patients with scabies was too small to allow any statistical analysis. The use of
soap seemed to be beneficial regarding resolution and pruritus, but there was no difference
when the soap contained Triclosan.
• In summary, the controlled use of soap over two months showed a beneficial effect against
tinea versicolor, other superficial dermatomycotic infections and scabies. While there is no
additional effectiveness of Triclosan against tinea versicolor, Triclosan may be useful
against superficial dermatomycotic infections if other application modes are used.
Our results argue for the use of soap, but are not sufficient to support the addition of Triclosan to
treat superficial skin mycoses and scabies. However, the fact that Triclosan is highly effective
against bacterial infections - also playing an important role in a tropical setting -, and its putative
beneficial effects do not argue against the addition of this agent.

Discussion 100
6. Implications
In low-income countries such as Tanzania, treatment options for benign but very common skin
disorders such as fungal and parasitic skin infections are poor, since numerous life-threatening
conditions have higher priority.
Nevertheless, the provision of safe, effective and inexpensive treatment of common skin diseases is
essential for successful tropical primary health care, since those diseases may lead to severe
cosmetic disfigurement, permanent alopecia or secondary bacterial superinfection including
complications such as poststreptococcal glomerulonephritis.
The prevention and treatment of the most relevant skin disorders should include the training of
paramedical personnel, care-takers, teachers and the children themselves, and also the availability
of cheap prevention measures and effective treatment options such as an effective topical agent
applied as bar soap.
More information is needed on the efficacy of Triclosan and improved hygiene compared to
established topical antifungals and antiscabietic drugs on a long-term basis. Control groups should
be included to assess the likelihood of spontaneous resolution or improvement due to seasonal
changes. However, it can be concluded from our findings that just the regular use of soap has lead
to a substantial improvement of superficial fungal infections of the skin, namely tinea versicolor,
tinea capitis, corporis and pedis among the study group in the investigated area of Tanzania.
© PHOTO COSMOS
© Photo: Cosmos Popperfoto

Bibliography 101
Bibliography Abu-Elteen KH, Malek MA (1999) Prevalence of dermatophytoses in the Zarqua district of Jordan.
Mycopathologia 145: 137-142
Acosta CJ, Galindo CM, Kimanrio J, Senkoro K, Urassa H, Casals C, Corachán M, Eseko N,
Tanner M, Mshinda H, Lwilla F, Vila J,. Alonso PL (2001) Cholera Outbreak in Southern
Tanzania: Risk Factors and Patterns of Transmission. Ermerg Infect Dis 7(3): 583-587
Akpata LE, Gugnani HC Utsalo SJ (1990) Pityriasis versicolor in school children in Cross River
State of Nigeria. Mycoses 33(11/12): 549-551
Alebiosu CO, Ogunledun A, Ogunleye DS (2003) A report of clinical trial conducted on Toto
ointment and soap products. J Natl Med Assoc 95(1): 95-105
Al-Sogair SM (1991) Fungal infection as a cause of skin disease in the Eastern Province of Saudi
Arabia: prevailing fungi and patterns of infection. Mycoses 34: 333-337
Anezi N Okoroa (editor and author) (1981) Fungal Infections. In: Pictorial Handbook of Common
Skin Diseases. 1st edition, Macmillan International College Editions, pp. 49-62
Anezi N Okorob (editor and author) (1981) Infestations by Animal Parasites: Scabies. In: Pictorial
Handbook of Common Skin Diseases 1st edition. Macmillan International College Editions, pp. 33-
36
Arenas R, García Jaramillo JA, Estrada R (1982) Pityriasis versiolcor: Etudes de 100 cas
mexicains. Bull Soc Franc Myc Med 11(1): 65-68
Armstrong Schellenberg JRM, Nathan R, Abdulla S, Mukasa O, Tanya J. Marchant TJ, Tanner
M, Lengeler C (2002) Risk factors for child mortality in rural Tanzania. Trop Med Int Health 7(6):
506–511
Armstrong Schellenberg JRM, Victora CG, Mushi A, de Savigny D, Schellenberg D, Mshinda H,
Bryce J (2003) Inequities among the very poor: health care for southern Tanzania. Lancet,
published online http://image.thelancet.com/extras/02art2280web.pdf
Bibliography 102
Attapattu MC (1989) A study of Tinea capitis in Sri Lanka. J Med Vet Mycol 27(1): 27-32
Ayaya SO, Kamar KK (2001) Aetiology of Tinea capitis in school children. East Afr Med J 10:
531-535
Bäck O, Faergemann J, Hörnqvist R (1985) Pityrosporum folliculitis: a common disease of the
young and middle-aged. J Am Acad Dermatol 12: 56-61
Barkvoll P, Rölla G (1994) Triclosan protects the skin against dermatitis caused by sodium lauryl
sulphate exposures. J Clin Periodontol 21: 717-719
Barkvoll P, Rölla G (1995) Triclosan reduces the clinical symptoms of allergic patch test reaction
(APR) elicited with 1% nickel sulphate in sensitized patients. J Clin Peridontol 22: 485-487
Bélec L (1991) Pityriasis versicolor in the Central African Republic: a randomized study of 144
cases. Journal of Medical and Veterinary Mycology 29: 323-329
Bhargava HN, Leonard PA (1996) Triclosan: applications and safety. AJIC Am J Infect Control
24: 209-218
Borelli D (1991) Tinea versicolor: Epidemiologic, clinical, and therapeutic aspects. J Am Acad
Dermatol 25: 300-305
Borelli D (1985) Epidemiology, ecology and treatment of pityriasis versicolor in Latin America
(Venezuela). In: Oral therapy in dermatomycoses: A step forward. Proceedings of Symposium held
in Frankfurt: 111-115
Bouassida S, Boudaya S, Ghorbel R, Meziou TJ, Marrekchi S, Turki H, Zahaf A (1998) Pityriasis
versicolor in children: a retrospective study of 164 cases. Ann Dermatol Venereol 125(9): 581-584
Burke RC (1961) Tinea versicolor: susceptibility factors and experimental infection in human
beings. J Invest Dermatol 36: 389-402
Burkhart CG, Burkhart CN, Burkhart KM (2000) An epidemiologic and therapeutic reassessment
of scabies. Cutis 65(4): 233-240
Bibliography 103
Canizares O, Harman RRM (1993) Cosmopolitan Superficial Fungal Infections of Tropical
Importance. In: Clinical Tropical Dermatology, 2nd edition. Boston, Blackwell Scientific
Publications, pp 22-40
Canizares O (author and editor) (1975) The neck, axillae and the groins. In: A manual of
dermatology for developing countries. Oxford Medical Publications, p. 419a
Canizares O (author and editor) (1982) Superficial fungal infections. In: A manual of dermatology
for developing countries. Oxford Medical Publications, pp. 84-100
Celik E, Ilkit M, Tanir F (2003) Prevalence and causative agents of superficial mycoses in a textile
factory in Adana, Turkey. Mycoses 46(8): 329-333
Cheesbrough M (1987) Mycology 47:1-14. In: Butterworth-Heinemann (publishers) Medical
Laboratory Manual for Tropical Countries, pp. 372-391
Christophersen J (1978) The epidemiology of scabies in Denmark, 1900 to 1975. Arch Dermatol
114(5): 747-750
© Ciba Specialty Chemicalsa (1998) IRGASAN® DP 300 /I RGACARE® MP / IRGACIDE LP®
General information on chemical, physical and microbiological properties; No. 2520
© Ciba Specialty Chemicalsb (1998) IRGASAN® DP 300 / IRGACARE® MP Antimicrobial
active ingredient for personal care products; No. 2523
© Ciba Specialty Chemicalsa (1999) Irgasan in rinse-off products. 1041-1/Version 6-99
© Ciba Specialty Chemicalsb (1999) Toxicological and ecological data/Official registrations;
No.2521
Daneshvar SA, Hashimoto K (1987) An unusual presentation of tinea versicolor in an
immunosuppressed patient. Journal of the American Academy of Dermatology. Vol 17(2 pt 1): 304-
305
Bibliography 104
Dave VK, Roberts MM, Butterfield W (1987) Pityriasis versicolor and sunscreens containing
coconut oil. Lancet 2(8560): 685-686
Degremont A, Lwihula GK, Mayombana C, Burnier E, de Savigny D, Tanner M (1987)
Longitudinal study on the health status of children in a rural Tanzanian community: comparison of
community-based clinical examinations, the diseases Fn at village health posts and the perception of
health problems by the population. Acta Trop 44(2): 175-190
Dominguez-Soto L (1994) Pigmentary Problems in the tropics. Contemporary Tropical
Dermatology 12(4): 777-779
Elewski BE (2000) Tinea capitis: a current perspective. J Am Acad Dermatol 42(1 Pt 1):1-20; quiz
21-24
Elewski BE, Greer DL (1991) Hendersonula toruloidea and Scytalidium hyalinum. Arch Dermatol
127: 1041-1044
Elewski BE, Hazen PG (1989) The superficial mycoses and the dermatophytes. J Am Acad
Dermatol 21(4 Pt 1): 655-673
Elmets CA (1994) Management of common superficial fungal infections in patients with AIDS. J
Am Acad Dermatol 31(3 Pt 2): 60-63
English MP, Atkinson R (1994) Onychomycosis in elderly chiropody patients. Br J Dermatol
91(1): 67-72
English MP, Gibson MD (1959) Studies in the epidemiology of tinea pedis. I. Tinea pedis in school
children. Br Med J 15(5135): 1442-1446
Enweani IB (1996) Dermatophytosis in schoolchildren in Ekpoma, Nigeria: Mycoses 39: 303-305
Estes SA, Estes J (1993) Therapy of scabies: nursing homes, hospitals, and the homeless. Semin
Dermatol 12(1): 26-33
Bibliography 105
Faergemann J (1993) Pityriasis versicolor. Seminars in Dermatology Semin Dermatol 12(4): 276-
279
Faergemann J (1994) Pityrosporum infections. J Am Acad Dermatol 31: 18-20
Faergemann J, Frederiksson T (1982) Tinea Versicolor: Some New Aspects on Etiology,
Pathogenesis, and Treatment. In J Dermatol 21: 8-11
Ferié, J. (2005) Skin Disorders among Primary School Children in Rural Tanzania and an
Assessment of Contributing Factors and Therapeutic Needs. Inaugural Dissertation
Figueroa JI, Fuller LC, Abraha A, Hay RJ (1996) Prevalence of Skin Disease Among School
Children in Rural Ethiopia- A Preliminary Assessment of Dermatologic Needs (1996). Pediatric
Dermatology 13(5): 378-381
Figueroa JI, Hawranek T, Abraha A, Hay RD (1997) Tinea capitis in south-western Ethiopia: a
study of risk factors for infection and carriage. Int J Dermatol 36: 661-668
Goncalves AP (1963) Unusual locations of Pityriasis versicolor with particular reference to scalp
lesions. Dermatol Trop Ecol Geogr 15:211-216
Gooskens V, Pönnighaus, Clayton Y, Mkandawire P, Sterne JA (1994) Treatment of superficial
mycoses in the tropics: Whitfield’s Ointment versus Clotrimazole Cream. Int J Dermatol 33(10):
738-742
Green MS (1989) Epidemiology of scabies. Epidemiol Rev 11: 126-150
Gupta AK (2002) Pityriasis versicolor. JEADV (2002) 16: 19-33
Gupta AK, Batra R, Bluhm R, Faergemann J (2003) Pityriasis versicolor. Dermatol Clin 21(3):
413-429, v-vi
Gupta AK, Hofstader S (1998) Treatment of tinea capitis with itraconazole capsule pulse therapy. J
Am Acad Dermatol 39: 216-219
Bibliography 106
Gupta AK, Kohli Y, Faergemann J, Summerbell RC (2001) Epidemiology of Malassezia yeasts
associated with pityrisasis versicolor in Ontario, Canada. Med Mycol 39:199-206
Gupta AK, Ryder JE, Nicol K, Cooper EA (2003) Superficial fungal infections: an update on
pityriasis versicolor, seborrheic dermatitis, tinea capitis, and onychomycosis. Clin Dermatol 21(5):
417-425
Hafez M, El-Shamy S (1985) Genetic susceptibility in Pityriasis versicolor. Dermatologica 171: 86-
88
Hay RJ (author), Cook GC (editor) (1996) Fungal Infections. In: Manson’s Tropical Diseases, 20th
edition, Saunders, pp. 1048-1084
Hellgren L, Vincent J (1983) The incidence of tinea versicolor in central Sweden. J Med Microbiol
16: 501-502
Henderson CA, Nykia M (1992) Treatment of scabies in rural east Africa--a comparative study of
two regimens. Trop Doct 22(4): 165-167
Hervé Ménan EI, Zongo-Bounou O (2002) Tinea capitis in schoolchildren from Ivory coast
(western Africa). A 1998-1999 cross-sectional study. Int J Dermatol 41:204-207
Heukelbach J, van Haeff E, Rump B, Wilcke T, Moura RC, Feldmeier H (2003) Parasitic skin
diseases: health care-seeking in a slum in north-east Brazil. Trop Med Int Health 8(4): 368-373
Hickman JG (1996) A double-blind, randomized, placebo-controlled evaluation of short-term
treatment with oral itraconazole in patients with tinea versicolor. J Am Acad Dermatol 34: 785-787
Hira SK, Abraham MS (1986) Naftfine Solution (1%) in the Treatment of Pityriasis versicolor in
Zambia. Mykosen 29(8): 378-381
Hussain I, Muzaffar F, Rashid T, Ahmad TJ, Jahangir M, Haroon TS (1999) A randomized,
comparative trial of treatment of kerion celsi with griseofulvin plus oral prednisolone vs.
griseofulvin alone. Med Mycol 37; 97-99
Bibliography 107
Inanir I, Sahin MT (2002) Prevalence of Skin Conditions in Primary School Children in Turkey:
Differences Based on Socioecenomic Factors. Pediatr Dermatol 19(4): 307-311
Jampani H, Lee A, Newman J, Jones RA (1998) A comprehensive comparison of the in vitro and
in vivo antimicrobial effectiveness of triclosan, chlorhexidine, alcohol/chlorhexidine, and
poloxamer iodine topical formulations [abstract]. AJIC Am J Infect Control 26:186
Jang KA, Chi DH, Choi JH, Sung KJ, Moon KC, Koh JK: Tinea pedis in Korean children. Int J
Dermatol 39(1): 25-27
Jimenez-Lucho VE, Fallon F, Caputo C, Ramsey K (1995) Role of prolonged surveillance in the
eradication of nosocomial scabies in an extended care Veterans Affairs medical center. Am J Infect
Control 23(1): 44-49
Jones RD, Jampani HB, Newman,JL, Lee AS (2000) Triclosan: A review of effectiveness and
safety in health care settings. AJIC Am J Infect Control 28: 184-196
Kamalam A, Thambiah AS, Bagavandas M, Govindaraju S (1981) Mycoses in India--study in
Madras. Trans R Soc Trop Med Hyg 75(1): 92-100
Kane J, Leavitt E, Summerbell RC, Krajden S, Kasatiya SS (1988) An outbreak of Trichophyton
tonsurans dermatophytosis in a chronic care institution for the elderly. Eur J Epidemiol 4(2): 144-
149
Kibatala P (1997) Annual Report SFDDH
King RD, Cunico RL, Maibach HI, Greenberg JH, West ML, Jeppsen (1978) The effect of
occlusion on carbon dioxide emission from human skin. Acta Derm Venereol 58(2):135-138
Kjaerheim V, Barkvoll P, Waaler SM, Rölla G (1995) Triclosan inhibits histamine-induced
inflammation in human skin. J Clin Peridontol 22: 423-426
Lange DS, Richards HM (1998) Ketokonazole 2% shampoo in the treatment of tinea versicolor: A
multicentre, randomized, double-blind, placebo-controlled trial. J AM Acad Dermatol 39: 944-950
Bibliography 108
Larson EL (1988) American Practitioners of Infection Control guidelines for infection control
practice: guidelines for use of topical antimicrobial agents. AJIC Am J Infect Control 16: 253-266
Leeming JP, Notman FH, Holland KT (1989) The distribution and ecology of Malassezia furfur
and cutaneous bacteria on human skin. J Appl Bacteriol;67(1):47-52
Marples MJ (1950) The incidence of certain skin diseases in Western Samoa: A preliminary
survey. Trans R Soc Trop Med Hyg 44: 319-322
Martinez- Roig A, Torres-Rodriguez JM (1988) Double blind study of ketoconazole and
griseofulvin in dermatophytoses. Pediatr Infect Dis J 7: 37-40
Masri-Fridling GD (1996) Dermatophytosis of the feet. Dermatol Clin 14(1): 33-40
McDaniel DH, Welton WA (1984) Scanning electron microscopic evaluation of tinea versicolor.
Effects of treatment with miconazole nitrate and clotrimazole. Arch Dermatol 120(8): 1057-1058
McGinley KJ, Leyden JJ, Marples RR, Kligman AM (1975) Quantitative microbiology of the scalp
in non-dandruff, dandruff, and seborrheic dermatitis. J Invest Dermatol 64(6): 401-405
Mimouni D, Ankol OE, Davidovitch N, Gdalevich M, Zangvil E, Grotto I (2003) Seasonality
trends of scabies in a young adult population: a 20-year follow-up. Br J Dermatol 149(1): 157-159
Mirhendi H, Makimura K, Zomorodian K, Yamada T, Sugita T, Yamaguchi H (2005) A simple
PCR-RFLP method for identification and differentiation of 11 Malassezia species. J Microbiol
Methods 61 (2005) 281-284
Miskeen AK, Kelkar SS, Shroff HJ (1984) Pityriasis versicolor in children. Indian J Dermatol
Leprol 50:144-146
Montero-Gei F, Perera A (1992) Fungal infections in normal hosts: Therapy with fluconazole for
Tinea Capitis, Tinea Corporis, Tinea Cruris, and Tinea Pedis. Clin Infect Dis 14 (1): 77-81
MSD (Merck Sharp & Dohme) (1988) Poison Control Monograph. Ivermectin. Division of Merck
& Co Ltd, West Point, Pennsylvania, 18. pp
Bibliography 109
Nakabayashi A, Sei Y, Guillot J (2000) Identification of Malassezia species isolaed from patients
with seborrheic dermatitis, atopic dermatitis, pityriasis versicolor and normal subjects. Medical
Mycology 38: 337-341
Nissen HP, Ochs D (1998) Triclosan An antimicrobial acitve ingredient with anti-inflammatory
activity. Cosmetics & Toiletries® Magazine 113: 61
Odom R (1993) Pathophysiology of dermatophyte infections: J Am Acad Dermatol 28(5 Pt 1): 2-7
Perez Blanco M, Urbina de Guanipa O, Fernandez Zeppenfeldt G, Richard de Yegres N (1990)
Effect of temperature and humidity on the frequency of pityriasis versicolor. Epidemiological study
in the state of Falcon, Venezuela. Invest Clin 31(3): 121-128
Piamphongsant T (1983) Pityriasis pigmentosa. J Dermatol 10(4): 355-360
Pinkerton M, Ward S, Durvic M (2003) A perplexing pruritc papular rash. Dermatology Online
Journal 9(3): 9
Pönnighaus J (1995) Dermatology. In: Krawinkel M and Renz-Polster H (Editors): Medical
Practice in Developing Countries 1st edition Jungjohann to fit pocket, Neckarsulm, Lübeck, Ulm, pp
570-580
Pontash MJ, Kyanko ME, Brodell RT (1989) Tinea Versicolor of the Face in Black Children in a
Temperate Region. Cutis 43: 81-84
Porter MJ (1980) Seasonal change and its effect on the prevalence of infectious skin disease in a
Gambian village. Transactions of the Royal Society of Tropical Medicine and Hygiene 74(2): 162-
168
Pruksachatkunakorn C, Damrongsak M (2002) Sulfur for Scabies Outbreaks in orphanages. Ped
Dematol 19(5): 448-453
Regös J, Hitz HR (1974) Investigations on the mode of action of Triclosan, a broad spectrum
antimicrobial agent. Zentralbl Bakteriol 226(3): 390-401
Bibliography 110
Roberts SO (1969) Pityriasis versicolor: a clinical and mycological investigation. Br J Dermatol
81(5): 315-26
Robertson VJ (1990) A survey of tinea capitis in primary school children in Harare, Zimbabwe.
Journal of Tropical Medicine and Hygiene 93: 419-422
Satimia FT, McBride SR, Leppard B (1998) Prevalence of skin disease in rural Tanzania and
factors influencing the choice of health care, modern or traditional. Arch Dermatol 134(11): 1363-
1366
Schaller KF (1962) Skin diseases in rural Ethiopia. Hautarzt13: 289-298
Schechtman RC, Midgley G, Hay RJ (1995) HIV disease and Malassezia yeasts: a quantitative
study of patients presenting with seborrhoeic dermatitis. Br J Dermatol 133: 694-698
Schmeller W (1998) Community health workers reduce skin disease in East African children. Int J
Dermatol 37: 370-377
Schmeller W, Dzikus A (2001) Skin diseases in children in rural Kenya: long-term results of a
dermatology project within the primary health care system. Br J Dermatol 144(1):118-124
Schmidt A (1997) Malassezia furfur: a fungus belonging to the physiological skin flora and its
relevance in skin disorders. Cutis 59: 21-24
Shrum JP (1994) Superficial fungal infections in the tropics. Contemporary Tropical Dermatology
0733-9635/94: 687-693
Skaare AB, Kjaerheim V, Barkvoll P and Rölla G (1997) Does the nature of the solvent affect the
antiinflammatory capacity of triclosan ?: an experimental study, J Clin Periodontol 24: 124-128
Soyinka F (1978) Epidemiologic study of dermatophyte infections in Nigeria. Mycopatholpgia 63:
99-103
Stein DH (1983) Superficial fungal infections. Pediatr Clin North Am 30(3): 545-561
Bibliography 111
Stingl P (1987) Skin diseases in Sierra Leone. Hautarzt 38(3): 146-154
Sunenshine PJ (1998) Tinea versicolor. Int J Dermatol 37: 648-656
Svejgaard E (1986) Epidemiology and clinical features of dermatomycoses and dermatophytoses.
Acta Derm Venerol (Stockh); Suppl. 121: 19-26
Tanner Ma, Degremont A, de Savigny D, Freyvogel TA, Mayombana C, Tayari S (1987)
Longitudinal study on the health status of children in Kikwawila village, Tanzania: study area and
design. Acta Tropica 44: 119-136
bTanner M, de Savigny D (1987) Longitudinal study on the health status of children in a rural
Tanzanian community: comparison of community-based clinical examinations, the diseases seen at
village health posts and the perception of health problems by the population; Acta Tropica 44: 175-
190
Taplin D, Zaias N, Rebell G (1965) Environmental influences on the microbiology of the skin.
Arch Environ Health 11(4): 546-550
aTerragni L, Lasagni A, Oriani A (1991) Pityriasis versicolor of the face. Mycoses 34: 345-347
bTerragni L, Lasagni A, Oriani A, Gelmetti C (1991) Pityriasis versicolor in the Pediatric Age.
Pediatr Dermatol 8(1): 9-12
Terri L, Meinking TL, Taplin D, Hermida JL, Pardo R, Kerdel FA (1995) The Treatment of
Scabies with Ivermectin. N Engl J Med 333: 26-30
The management and ecology of Tanzanian forests (2001). Morogoro Region. Copyright ©
2001. The Centre for Ecology Law and Policy, The Environment Department, The University of
York, York, UK
The Soap and Detergent Association and The Cosmetic, Toiletry, and Fragrance Association
(1995) Letter to W. Gilbertson and attachments. FDA Public Pocket 75N-183H. Mar 15, June 13,
June 13, Dec 14
Bibliography 112
United Republic of Tanzania (2002) Population and Housing Census
Usha V, Gopalakrishnan N (2000) A comparative study of oral ivermectin and topical permethrin
cream in the treatment of scabies. J Am Acad Dermatol 42: 236-240
Van Hees C, Naafs B (2001) Scabies. In: Van Hees C, Naafs B (Ed.) Common skin diseases in
Africa. An illustrated guide. Produced by the author and the printer on a non-profit basis. p.83.
Victoria J, Trujillo R (2001) Topical ivermectin: a new successful treatment for scabies. Pediatr
Dermatol 18(1): 63-65
Weitzman I, Summerbell RC (1995) The Dermatophytes. Clinical Microbiological Reviews 8(2):
240-259
Welsh O, Schmid-Grendelmeier P, Stingl P, Hafner J, Leppard B, Mahé A (2002) Tropical
Dermatology. Part II. J Am Acad Dermatol 46(5): 748-763

113
Appendix: Calculation of the sample size and assumed prevalence rates (Excerpt from the Study Proposal) “We assume the prevalence rate of Tinea capitis to be 15% among the children, and of
ectoparasitoses to be 10%. The confidence interval is 95%, the power 80%. In order to proof the
effectiveness the prevalence of Tinea capitis within the group treated with the Triclosan-containing
soap has to be reduced from 100% to at least 40%, making a difference of at least 60% significant.
In the placebo group we expect the ordinary soap to reduce the prevalence from 100% to about
70%. When comparing the two groups after two months the superior efficacy of the Triclosan-
containing soap is proven if the prevalence rate is at least 30% smaller than in the group treated
with the placebo soap.
Both groups affected by Tinea capitis have to consist of 48 children each. Considering a drop-out-
rate of 40% during the study this sample size has to be at least 160 children (2*48+40%=160).
When comparing placebo and the verum group after two months the superior efficacy of the
Triclosan-containing soap on ectoparasitoses is significant if the prevalence rate is at least 30%
smaller than in the group treated with the placebo soap. The placebo and the verum group have to
consist of 38 children each. Considering the drop-out-rate of 40% this sample size has to consist of
at least 127 children (2*38+40%=126.6). Adding the two sample sizes, approx. 287 children will be
included in the study population.”
The prevalence rates assumed in the Study Proposal were 15% and 10% for dermatophytoses and
ectoparasitoses respectively.
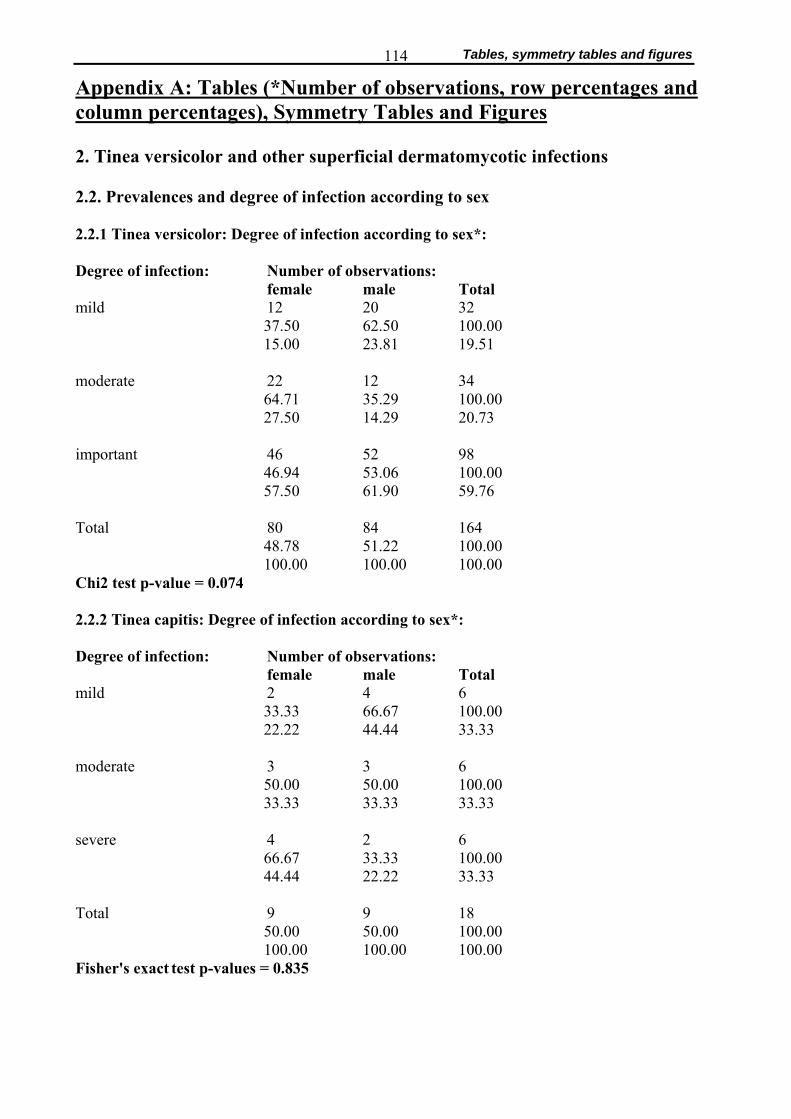
Tables, symmetry tables and figures 114
Appendix A: Tables (*Number of observations, row percentages and column percentages), Symmetry Tables and Figures 2. Tinea versicolor and other superficial dermatomycotic infections 2.2. Prevalences and degree of infection according to sex 2.2.1 Tinea versicolor: Degree of infection according to sex*: Degree of infection: Number of observations: female male Total mild 12 20 32
37.50 62.50 100.00 15.00 23.81 19.51
moderate 22 12 34
64.71 35.29 100.00 27.50 14.29 20.73
important 46 52 98
46.94 53.06 100.00 57.50 61.90 59.76
Total 80 84 164
48.78 51.22 100.00 100.00 100.00 100.00
Chi2 test p-value = 0.074 2.2.2 Tinea capitis: Degree of infection according to sex*: Degree of infection: Number of observations: female male Total mild 2 4 6
33.33 66.67 100.00 22.22 44.44 33.33
moderate 3 3 6
50.00 50.00 100.00 33.33 33.33 33.33
severe 4 2 6
66.67 33.33 100.00 44.44 22.22 33.33
Total 9 9 18
50.00 50.00 100.00 100.00 100.00 100.00
Fisher's exact test p-values = 0.835
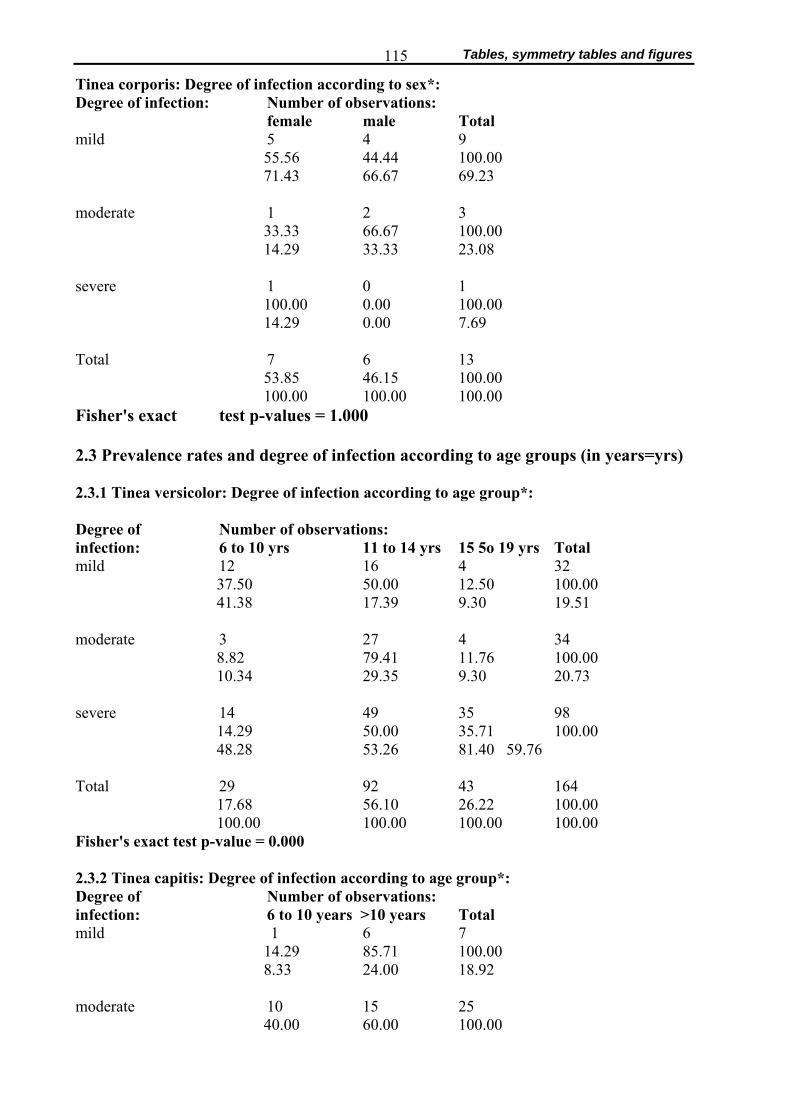
Tables, symmetry tables and figures 115
Tinea corporis: Degree of infection according to sex*: Degree of infection: Number of observations: female male Total mild 5 4 9
55.56 44.44 100.00 71.43 66.67 69.23
moderate 1 2 3
33.33 66.67 100.00 14.29 33.33 23.08
severe 1 0 1
100.00 0.00 100.00 14.29 0.00 7.69
Total 7 6 13
53.85 46.15 100.00 100.00 100.00 100.00
Fisher's exact test p-values = 1.000 2.3 Prevalence rates and degree of infection according to age groups (in years=yrs) 2.3.1 Tinea versicolor: Degree of infection according to age group*: Degree of Number of observations: infection: 6 to 10 yrs 11 to 14 yrs 15 5o 19 yrs Total mild 12 16 4 32
37.50 50.00 12.50 100.00 41.38 17.39 9.30 19.51
moderate 3 27 4 34
8.82 79.41 11.76 100.00 10.34 29.35 9.30 20.73
severe 14 49 35 98
14.29 50.00 35.71 100.00 48.28 53.26 81.40 59.76
Total 29 92 43 164
17.68 56.10 26.22 100.00 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.000 2.3.2 Tinea capitis: Degree of infection according to age group*: Degree of Number of observations: infection: 6 to 10 years >10 years Total mild 1 6 7
14.29 85.71 100.00 8.33 24.00 18.92
moderate 10 15 25
40.00 60.00 100.00
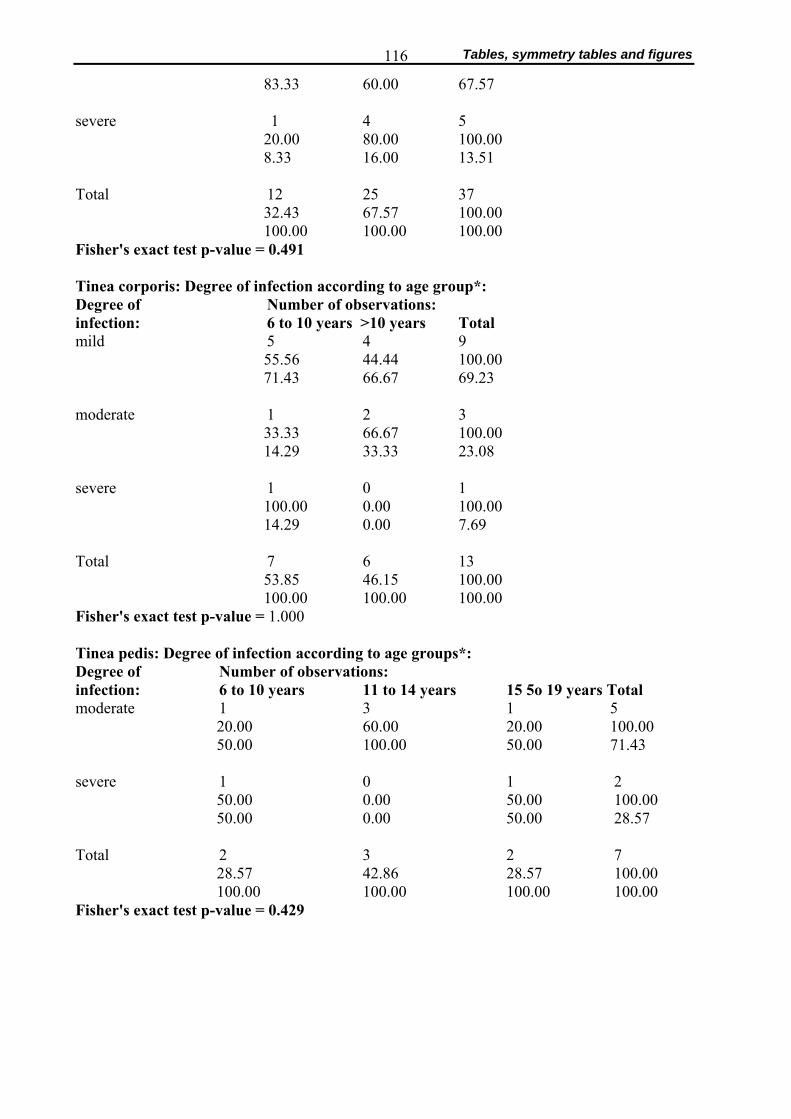
Tables, symmetry tables and figures 116
83.33 60.00 67.57 severe 1 4 5
20.00 80.00 100.00 8.33 16.00 13.51
Total 12 25 37
32.43 67.57 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.491 Tinea corporis: Degree of infection according to age group*: Degree of Number of observations: infection: 6 to 10 years >10 years Total mild 5 4 9
55.56 44.44 100.00 71.43 66.67 69.23
moderate 1 2 3
33.33 66.67 100.00 14.29 33.33 23.08
severe 1 0 1
100.00 0.00 100.00 14.29 0.00 7.69
Total 7 6 13
53.85 46.15 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 1.000 Tinea pedis: Degree of infection according to age groups*: Degree of Number of observations: infection: 6 to 10 years 11 to 14 years 15 5o 19 years Total moderate 1 3 1 5
20.00 60.00 20.00 100.00 50.00 100.00 50.00 71.43
severe 1 0 1 2
50.00 0.00 50.00 100.00 50.00 0.00 50.00 28.57
Total 2 3 2 7
28.57 42.86 28.57 100.00 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.429
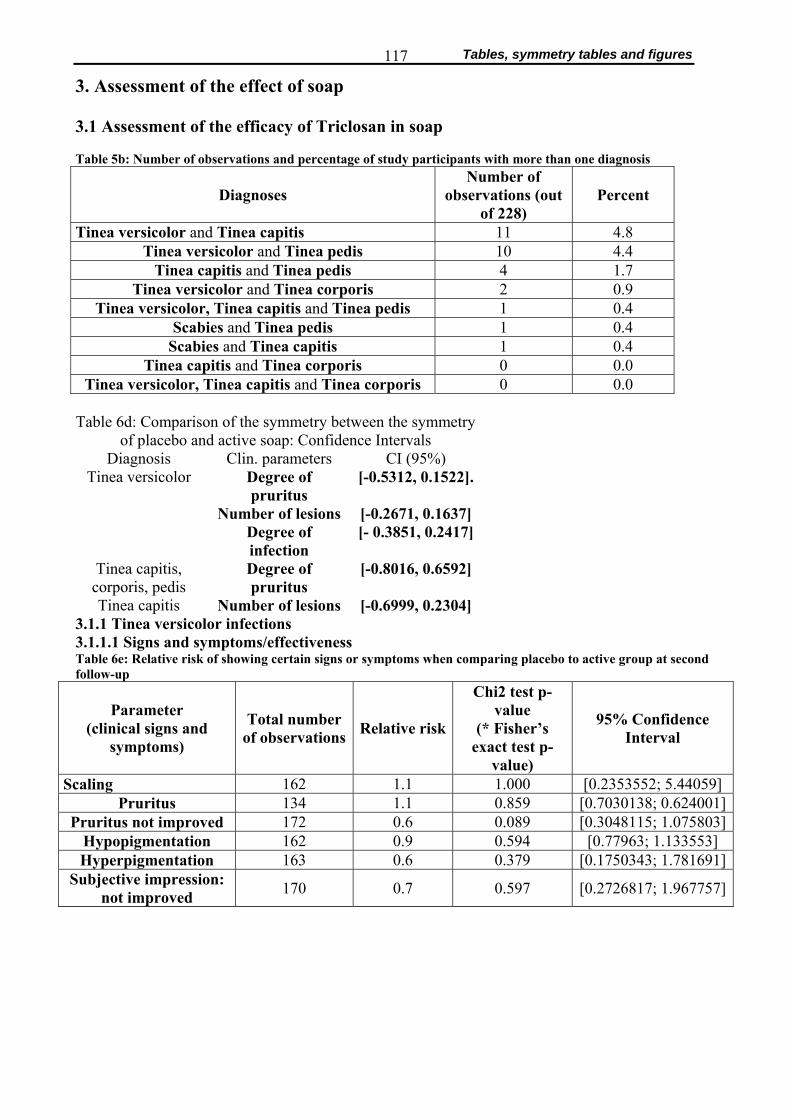
Tables, symmetry tables and figures 117
3. Assessment of the effect of soap 3.1 Assessment of the efficacy of Triclosan in soap Table 5b: Number of observations and percentage of study participants with more than one diagnosis
Diagnoses Number of
observations (out of 228)
Percent
Tinea versicolor and Tinea capitis 11 4.8 Tinea versicolor and Tinea pedis 10 4.4
Tinea capitis and Tinea pedis 4 1.7 Tinea versicolor and Tinea corporis 2 0.9
Tinea versicolor, Tinea capitis and Tinea pedis 1 0.4 Scabies and Tinea pedis 1 0.4
Scabies and Tinea capitis 1 0.4 Tinea capitis and Tinea corporis 0 0.0
Tinea versicolor, Tinea capitis and Tinea corporis 0 0.0 Table 6d: Comparison of the symmetry between the symmetry
of placebo and active soap: Confidence Intervals Diagnosis Clin. parameters CI (95%)
Degree of pruritus
[-0.5312, 0.1522].
Number of lesions [-0.2671, 0.1637]
Tinea versicolor
Degree of infection
[- 0.3851, 0.2417]
Tinea capitis, corporis, pedis
Degree of pruritus
[-0.8016, 0.6592]
Tinea capitis Number of lesions [-0.6999, 0.2304] 3.1.1 Tinea versicolor infections 3.1.1.1 Signs and symptoms/effectiveness Table 6e: Relative risk of showing certain signs or symptoms when comparing placebo to active group at second follow-up
Parameter (clinical signs and
symptoms)
Total number of observations Relative risk
Chi2 test p-value
(* Fisher’s exact test p-
value)
95% Confidence Interval
Scaling 162 1.1 1.000 [0.2353552; 5.44059] Pruritus 134 1.1 0.859 [0.7030138; 0.624001]
Pruritus not improved 172 0.6 0.089 [0.3048115; 1.075803]Hypopigmentation 162 0.9 0.594 [0.77963; 1.133553] Hyperpigmentation 163 0.6 0.379 [0.1750343; 1.781691]
Subjective impression: not improved 170 0.7 0.597 [0.2726817; 1.967757]

Tables, symmetry tables and figures 118
3.1.1.2 Degree of pruritus Tables for Figure 2a: Tinea versicolor: Degree of pruritus at screening* Degree of pruritus: Number of observations (and percentages): Placebo Active Total none 35 37 72 48.61 51.39 100.00 45.45 47.44 46.45 mild 37 29 66 56.06 43.94 100.00 48.05 37.18 42.58 moderate 5 12 17 29.41 70.59 100.00 6.49 15.38 10.97 Total 77 78 155 49.68 50.32 100.00 100.00 100.00 100.00 Fisher's exact test p-value = 0.140 Tinea versicolor: Degree of pruritus at follow-up 2*: Degree of pruritus: Number of observations (and percentages): Placebo Active Total none 52 58 110 47.27 52.73 100.00 67.53 74.36 70.97 mild 22 18 40 55.00 45.00 100.00 28.57 23.08 25.81 moderate 3 2 5 60.00 40.00 100.00 3.90 2.56 3.23 Total 77 78 155 49.68 50.32 100.00
100.00 100.00 100.00 Fisher's exact test p-value = 0.626
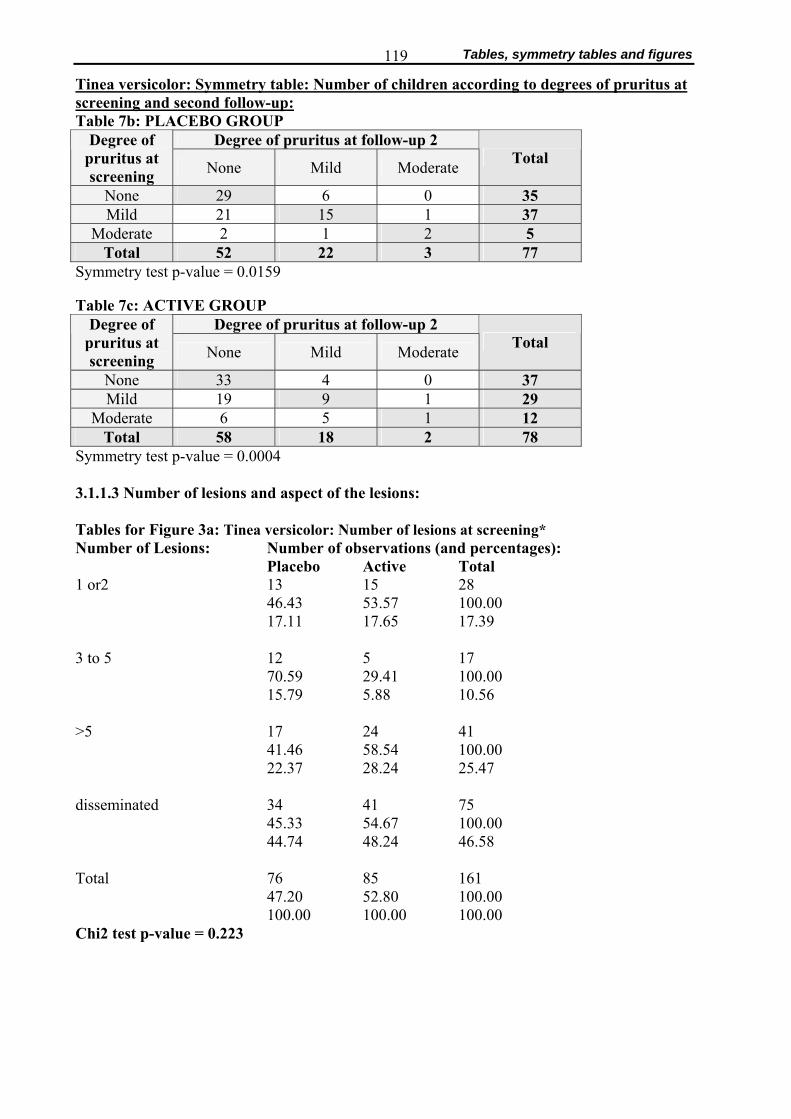
Tables, symmetry tables and figures 119
Tinea versicolor: Symmetry table: Number of children according to degrees of pruritus at screening and second follow-up: Table 7b: PLACEBO GROUP
Degree of pruritus at follow-up 2 Degree of pruritus at screening None Mild Moderate Total
None 29 6 0 35 Mild 21 15 1 37
Moderate 2 1 2 5 Total 52 22 3 77
Symmetry test p-value = 0.0159 Table 7c: ACTIVE GROUP
Degree of pruritus at follow-up 2 Degree of pruritus at screening None Mild Moderate Total
None 33 4 0 37 Mild 19 9 1 29
Moderate 6 5 1 12 Total 58 18 2 78
Symmetry test p-value = 0.0004 3.1.1.3 Number of lesions and aspect of the lesions: Tables for Figure 3a: Tinea versicolor: Number of lesions at screening* Number of Lesions: Number of observations (and percentages): Placebo Active Total 1 or2 13 15 28 46.43 53.57 100.00 17.11 17.65 17.39 3 to 5 12 5 17 70.59 29.41 100.00 15.79 5.88 10.56 >5 17 24 41 41.46 58.54 100.00 22.37 28.24 25.47 disseminated 34 41 75 45.33 54.67 100.00 44.74 48.24 46.58 Total 76 85 161 47.20 52.80 100.00 100.00 100.00 100.00 Chi2 test p-value = 0.223
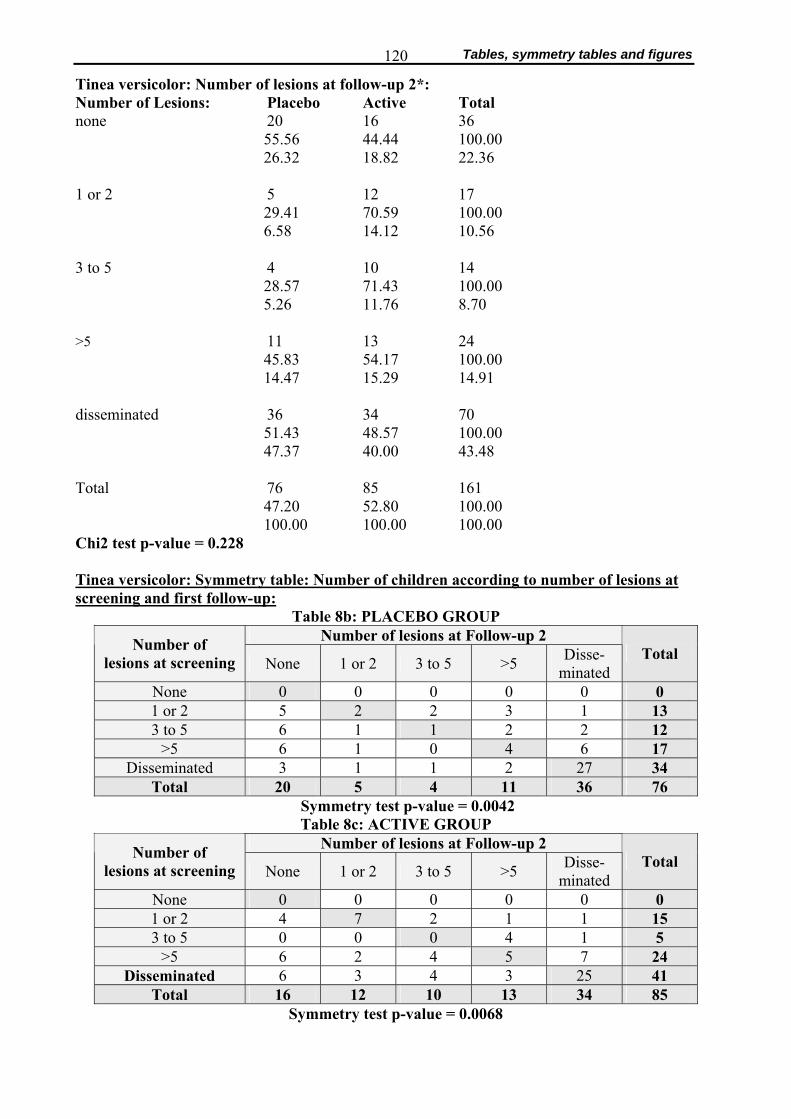
Tables, symmetry tables and figures 120
Tinea versicolor: Number of lesions at follow-up 2*: Number of Lesions: Placebo Active Total none 20 16 36
55.56 44.44 100.00 26.32 18.82 22.36
1 or 2 5 12 17
29.41 70.59 100.00 6.58 14.12 10.56
3 to 5 4 10 14
28.57 71.43 100.00 5.26 11.76 8.70
>5 11 13 24
45.83 54.17 100.00 14.47 15.29 14.91
disseminated 36 34 70
51.43 48.57 100.00 47.37 40.00 43.48
Total 76 85 161
47.20 52.80 100.00 100.00 100.00 100.00
Chi2 test p-value = 0.228 Tinea versicolor: Symmetry table: Number of children according to number of lesions at screening and first follow-up:
Table 8b: PLACEBO GROUP Number of lesions at Follow-up 2 Number of
lesions at screening None 1 or 2 3 to 5 >5 Disse- minated
Total
None 0 0 0 0 0 0 1 or 2 5 2 2 3 1 13 3 to 5 6 1 1 2 2 12
>5 6 1 0 4 6 17 Disseminated 3 1 1 2 27 34
Total 20 5 4 11 36 76 Symmetry test p-value = 0.0042 Table 8c: ACTIVE GROUP
Number of lesions at Follow-up 2 Number of lesions at screening None 1 or 2 3 to 5 >5 Disse-
minated Total
None 0 0 0 0 0 0 1 or 2 4 7 2 1 1 15 3 to 5 0 0 0 4 1 5
>5 6 2 4 5 7 24 Disseminated 6 3 4 3 25 41
Total 16 12 10 13 34 85 Symmetry test p-value = 0.0068

Tables, symmetry tables and figures 121
Tinea versicolor: Morphology of lesions at screening*: a: 1= sharply deliniated (possibly with central healing)
2= grey patches 3= both
Aspect of Lesionsa: Number of observations (and percentages): Placebo Active Total None/ N.A. 62 57 119
52.10 47.90 100.00 67.39 69.51 68.39
1 17 15 32
53.13 46.88 100.00 18.48 18.29 18.39
2 10 8 18
55.56 44.44 100.00 10.87 9.76 10.34
3 3 2 5
60.00 40.00 100.00 3.26 2.44 2.87
Total 92 82 174
52.87 47.13 100.00 100.00 100.00 100.00
Fisher's exact test p-value =0.990 Tinea versicolor: Aspect of lesions at follow-up 2*: a: 1= sharply deliniated (possibly with central healing)
2= grey patches 3= both
Aspect of lesionsa: Placebo Active Total None/ N.A. 77 75 152
50.66 49.34 100.00 82.80 88.24 85.39
1 9 3 12
75.00 25.00 100.00 9.68 3.53 6.74
2 2 3 5
40.00 60.00 100.00 2.15 3.53 2.81
3 5 4 9
55.56 44.44 100.00 5.38 4.71 5.06
Total 93 85 178
52.25 47.75 100.00 100.00 100.00 100.00
Fisher's exact test p-value =0.377
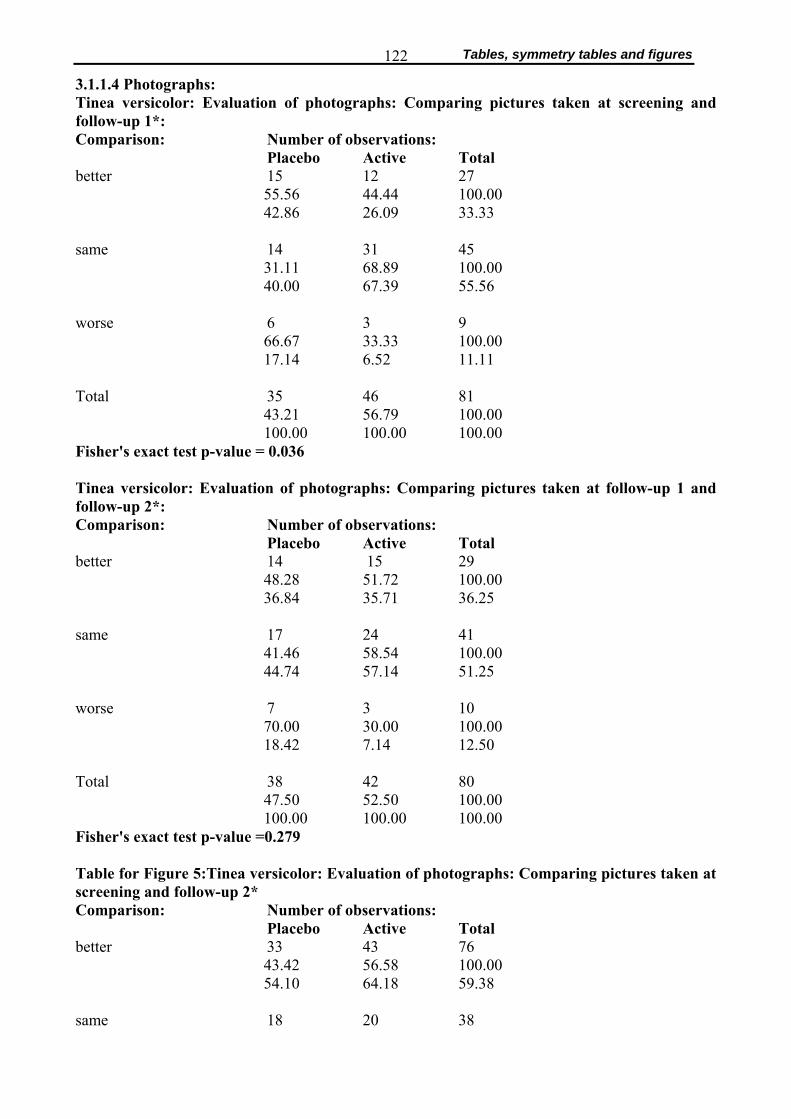
Tables, symmetry tables and figures 122
3.1.1.4 Photographs: Tinea versicolor: Evaluation of photographs: Comparing pictures taken at screening and follow-up 1*: Comparison: Number of observations:
Placebo Active Total better 15 12 27
55.56 44.44 100.00 42.86 26.09 33.33
same 14 31 45
31.11 68.89 100.00 40.00 67.39 55.56
worse 6 3 9
66.67 33.33 100.00 17.14 6.52 11.11
Total 35 46 81
43.21 56.79 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.036 Tinea versicolor: Evaluation of photographs: Comparing pictures taken at follow-up 1 and follow-up 2*: Comparison: Number of observations:
Placebo Active Total better 14 15 29
48.28 51.72 100.00 36.84 35.71 36.25
same 17 24 41
41.46 58.54 100.00 44.74 57.14 51.25
worse 7 3 10
70.00 30.00 100.00 18.42 7.14 12.50
Total 38 42 80
47.50 52.50 100.00 100.00 100.00 100.00
Fisher's exact test p-value =0.279 Table for Figure 5:Tinea versicolor: Evaluation of photographs: Comparing pictures taken at screening and follow-up 2* Comparison: Number of observations:
Placebo Active Total better 33 43 76
43.42 56.58 100.00 54.10 64.18 59.38
same 18 20 38
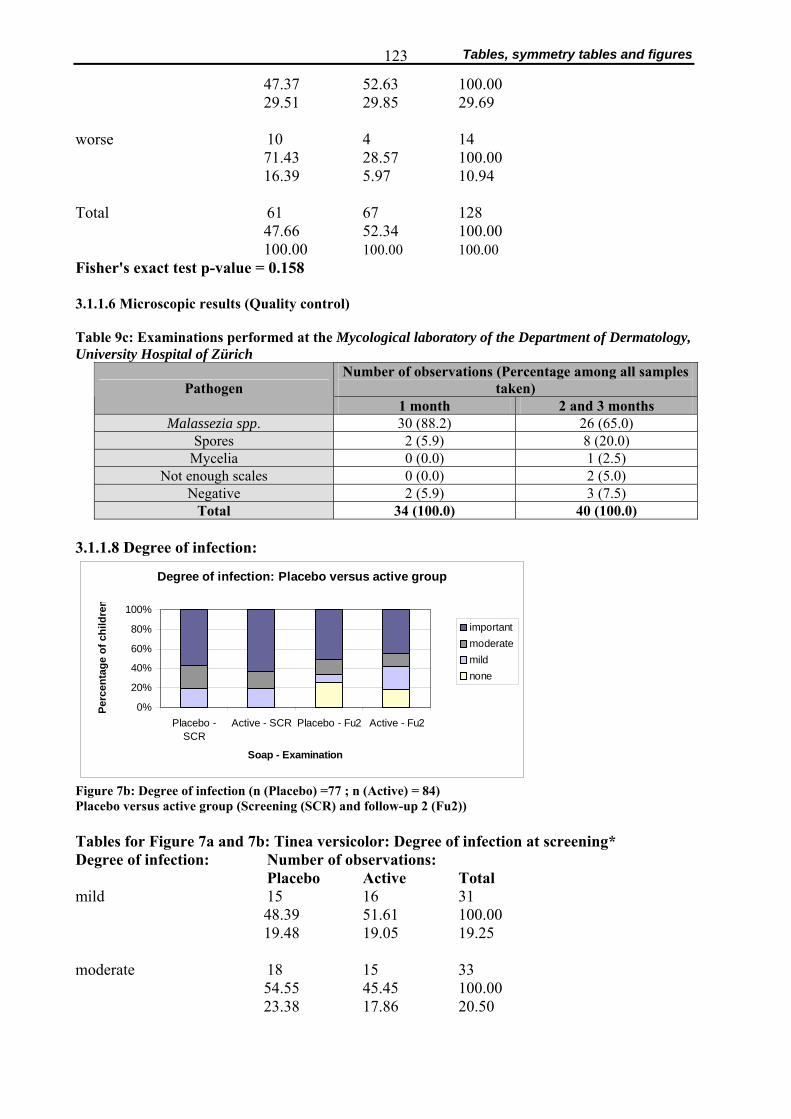
Tables, symmetry tables and figures 123
47.37 52.63 100.00 29.51 29.85 29.69
worse 10 4 14
71.43 28.57 100.00 16.39 5.97 10.94
Total 61 67 128
47.66 52.34 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.158 3.1.1.6 Microscopic results (Quality control) Table 9c: Examinations performed at the Mycological laboratory of the Department of Dermatology, University Hospital of Zürich
Number of observations (Percentage among all samples taken) Pathogen
1 month 2 and 3 months Malassezia spp. 30 (88.2) 26 (65.0)
Spores 2 (5.9) 8 (20.0) Mycelia 0 (0.0) 1 (2.5)
Not enough scales 0 (0.0) 2 (5.0) Negative 2 (5.9) 3 (7.5)
Total 34 (100.0) 40 (100.0) 3.1.1.8 Degree of infection:
Degree of infection: Placebo versus active group
0%
20%
40%
60%
80%
100%
Placebo -SCR
Active - SCR Placebo - Fu2 Active - Fu2
Soap - Examination
Perc
enta
ge o
f chi
ldre
n
importantmoderatemildnone
Figure 7b: Degree of infection (n (Placebo) =77 ; n (Active) = 84) Placebo versus active group (Screening (SCR) and follow-up 2 (Fu2)) Tables for Figure 7a and 7b: Tinea versicolor: Degree of infection at screening* Degree of infection: Number of observations:
Placebo Active Total mild 15 16 31
48.39 51.61 100.00 19.48 19.05 19.25
moderate 18 15 33
54.55 45.45 100.00 23.38 17.86 20.50
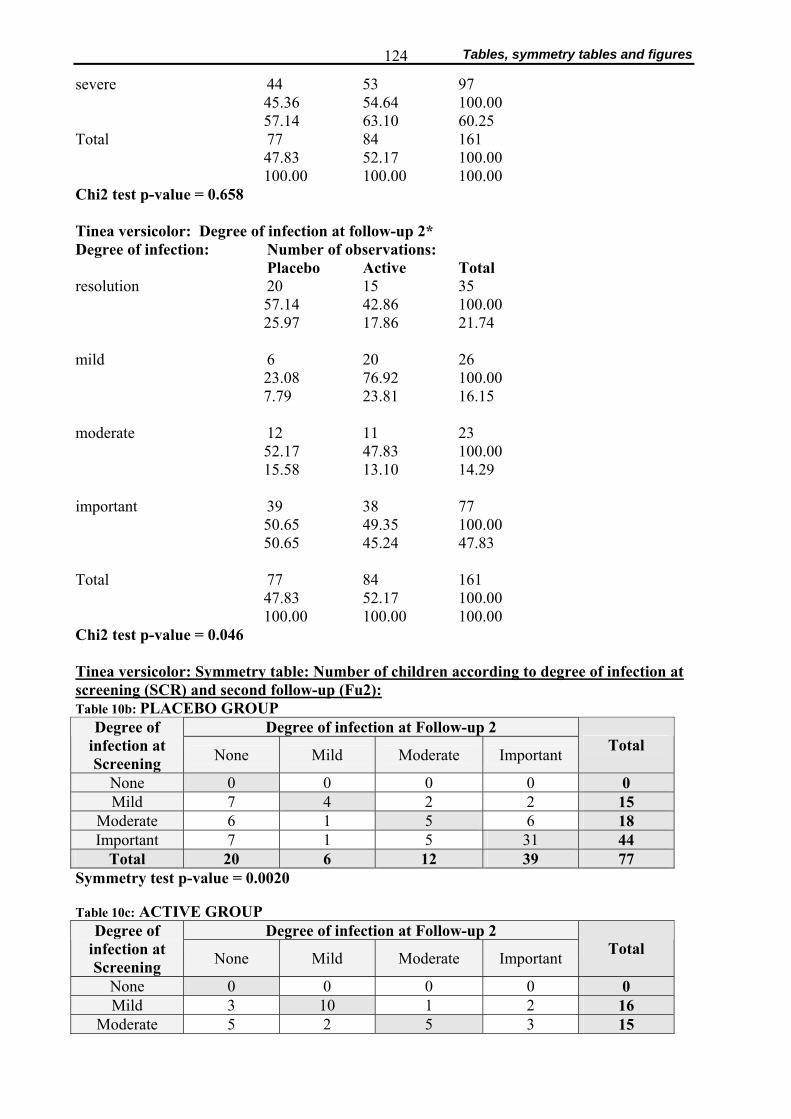
Tables, symmetry tables and figures 124
severe 44 53 97 45.36 54.64 100.00 57.14 63.10 60.25
Total 77 84 161 47.83 52.17 100.00 100.00 100.00 100.00
Chi2 test p-value = 0.658 Tinea versicolor: Degree of infection at follow-up 2* Degree of infection: Number of observations:
Placebo Active Total resolution 20 15 35
57.14 42.86 100.00 25.97 17.86 21.74
mild 6 20 26
23.08 76.92 100.00 7.79 23.81 16.15
moderate 12 11 23
52.17 47.83 100.00 15.58 13.10 14.29
important 39 38 77
50.65 49.35 100.00 50.65 45.24 47.83
Total 77 84 161
47.83 52.17 100.00 100.00 100.00 100.00
Chi2 test p-value = 0.046 Tinea versicolor: Symmetry table: Number of children according to degree of infection at screening (SCR) and second follow-up (Fu2): Table 10b: PLACEBO GROUP
Degree of infection at Follow-up 2 Degree of infection at Screening None Mild Moderate Important Total
None 0 0 0 0 0 Mild 7 4 2 2 15
Moderate 6 1 5 6 18 Important 7 1 5 31 44
Total 20 6 12 39 77 Symmetry test p-value = 0.0020 Table 10c: ACTIVE GROUP
Degree of infection at Follow-up 2 Degree of infection at Screening None Mild Moderate Important Total
None 0 0 0 0 0 Mild 3 10 1 2 16
Moderate 5 2 5 3 15
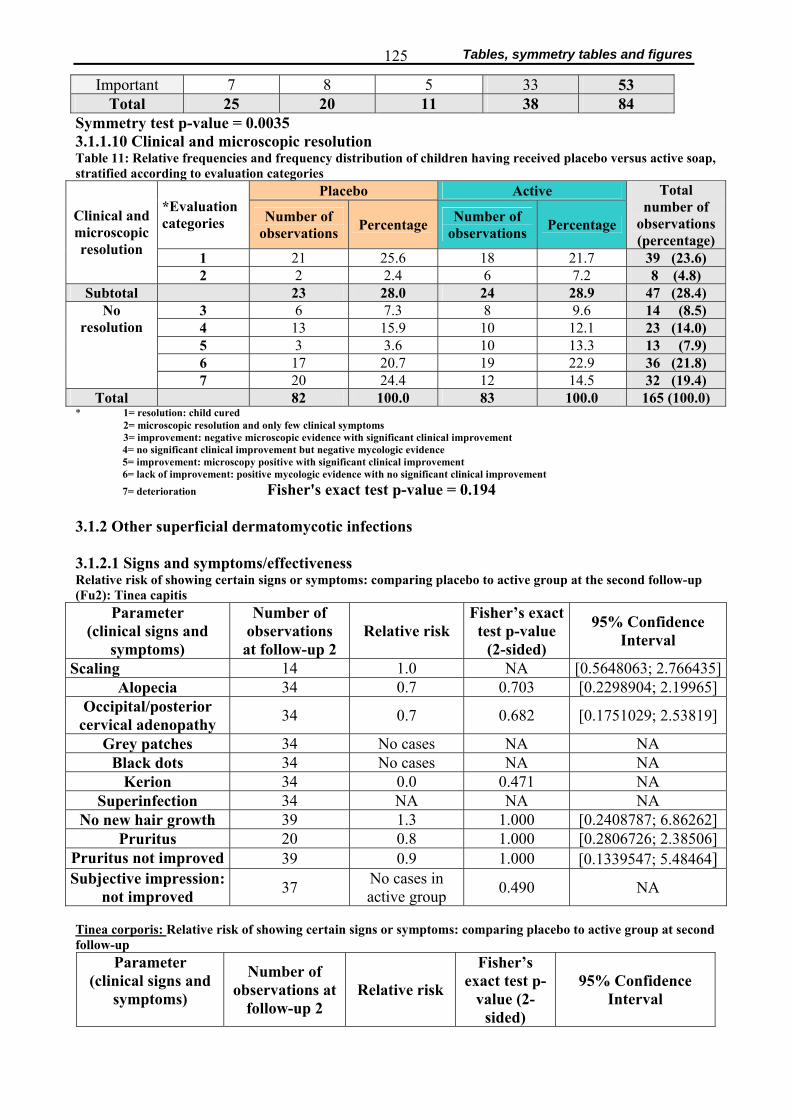
Tables, symmetry tables and figures 125
Important 7 8 5 33 53 Total 25 20 11 38 84
Symmetry test p-value = 0.0035 3.1.1.10 Clinical and microscopic resolution Table 11: Relative frequencies and frequency distribution of children having received placebo versus active soap, stratified according to evaluation categories
Placebo Active *Evaluation categories Number of
observations Percentage Number of observations Percentage
Total number of
observations (percentage)
1 21 25.6 18 21.7 39 (23.6)
Clinical and microscopic resolution
2 2 2.4 6 7.2 8 (4.8) Subtotal 23 28.0 24 28.9 47 (28.4)
3 6 7.3 8 9.6 14 (8.5) 4 13 15.9 10 12.1 23 (14.0) 5 3 3.6 10 13.3 13 (7.9) 6 17 20.7 19 22.9 36 (21.8)
No resolution
7 20 24.4 12 14.5 32 (19.4) Total 82 100.0 83 100.0 165 (100.0)
* 1= resolution: child cured 2= microscopic resolution and only few clinical symptoms 3= improvement: negative microscopic evidence with significant clinical improvement
4= no significant clinical improvement but negative mycologic evidence 5= improvement: microscopy positive with significant clinical improvement 6= lack of improvement: positive mycologic evidence with no significant clinical improvement 7= deterioration Fisher's exact test p-value = 0.194
3.1.2 Other superficial dermatomycotic infections 3.1.2.1 Signs and symptoms/effectiveness Relative risk of showing certain signs or symptoms: comparing placebo to active group at the second follow-up (Fu2): Tinea capitis
Parameter (clinical signs and
symptoms)
Number of observations at follow-up 2
Relative risk Fisher’s exact
test p-value (2-sided)
95% Confidence Interval
Scaling 14 1.0 NA [0.5648063; 2.766435]Alopecia 34 0.7 0.703 [0.2298904; 2.19965]
Occipital/posterior cervical adenopathy 34 0.7 0.682 [0.1751029; 2.53819]
Grey patches 34 No cases NA NA Black dots 34 No cases NA NA
Kerion 34 0.0 0.471 NA Superinfection 34 NA NA NA
No new hair growth 39 1.3 1.000 [0.2408787; 6.86262] Pruritus 20 0.8 1.000 [0.2806726; 2.38506]
Pruritus not improved 39 0.9 1.000 [0.1339547; 5.48464] Subjective impression:
not improved 37 No cases in active group 0.490 NA
Tinea corporis: Relative risk of showing certain signs or symptoms: comparing placebo to active group at second follow-up
Parameter (clinical signs and
symptoms)
Number of observations at
follow-up 2 Relative risk
Fisher’s exact test p-
value (2-sided)
95% Confidence Interval
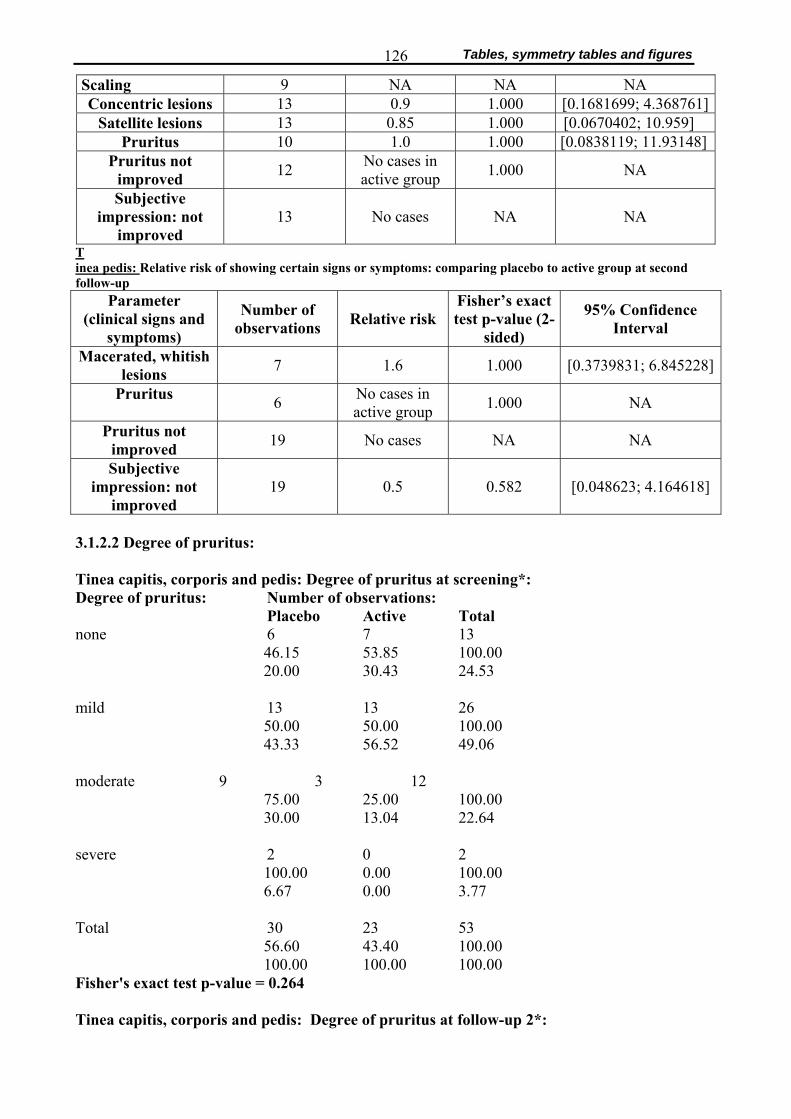
Tables, symmetry tables and figures 126
Scaling 9 NA NA NA Concentric lesions 13 0.9 1.000 [0.1681699; 4.368761]
Satellite lesions 13 0.85 1.000 [0.0670402; 10.959] Pruritus 10 1.0 1.000 [0.0838119; 11.93148]
Pruritus not improved 12 No cases in
active group 1.000 NA
Subjective impression: not
improved 13 No cases NA NA
T inea pedis: Relative risk of showing certain signs or symptoms: comparing placebo to active group at second follow-up
Parameter (clinical signs and
symptoms)
Number of observations Relative risk
Fisher’s exact test p-value (2-
sided)
95% Confidence Interval
Macerated, whitish lesions 7 1.6 1.000 [0.3739831; 6.845228]
Pruritus 6 No cases in active group 1.000 NA
Pruritus not improved 19 No cases NA NA
Subjective impression: not
improved 19 0.5 0.582 [0.048623; 4.164618]
3.1.2.2 Degree of pruritus: Tinea capitis, corporis and pedis: Degree of pruritus at screening*: Degree of pruritus: Number of observations:
Placebo Active Total none 6 7 13
46.15 53.85 100.00 20.00 30.43 24.53
mild 13 13 26
50.00 50.00 100.00 43.33 56.52 49.06
moderate 9 3 12
75.00 25.00 100.00 30.00 13.04 22.64
severe 2 0 2
100.00 0.00 100.00 6.67 0.00 3.77
Total 30 23 53
56.60 43.40 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.264 Tinea capitis, corporis and pedis: Degree of pruritus at follow-up 2*:
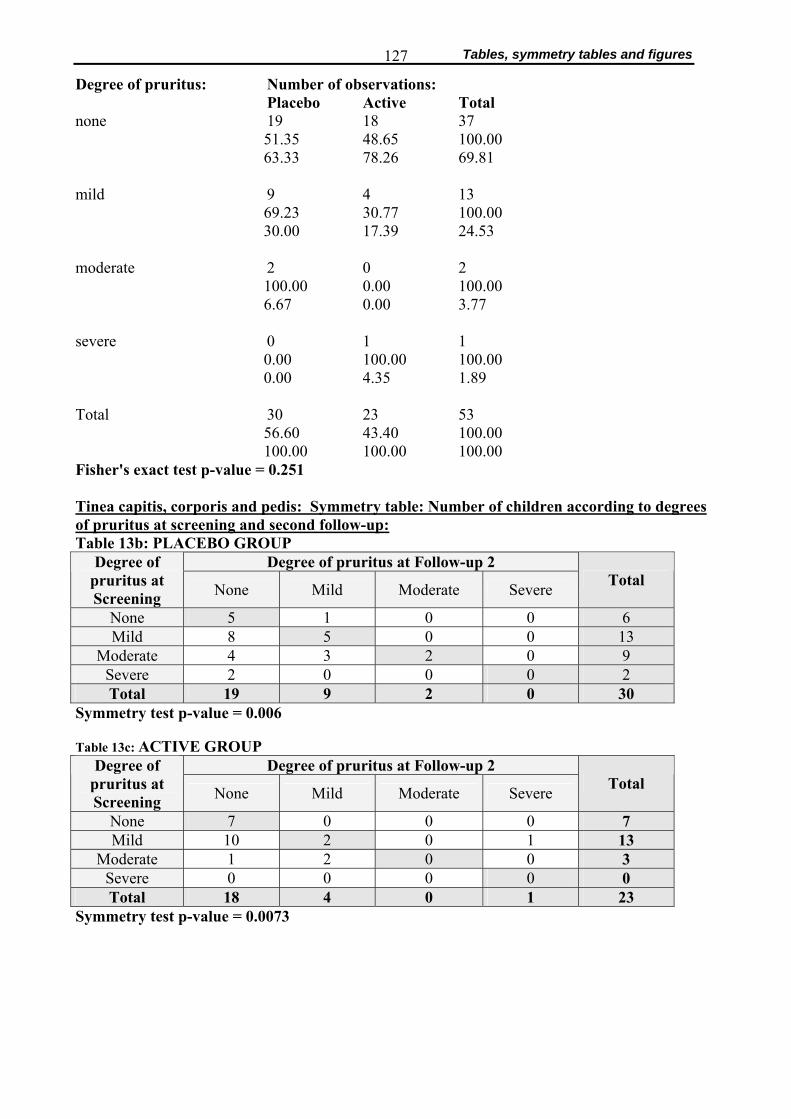
Tables, symmetry tables and figures 127
Degree of pruritus: Number of observations: Placebo Active Total
none 19 18 37 51.35 48.65 100.00 63.33 78.26 69.81
mild 9 4 13
69.23 30.77 100.00 30.00 17.39 24.53
moderate 2 0 2
100.00 0.00 100.00 6.67 0.00 3.77
severe 0 1 1
0.00 100.00 100.00 0.00 4.35 1.89
Total 30 23 53
56.60 43.40 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.251 Tinea capitis, corporis and pedis: Symmetry table: Number of children according to degrees of pruritus at screening and second follow-up: Table 13b: PLACEBO GROUP
Degree of pruritus at Follow-up 2 Degree of pruritus at Screening None Mild Moderate Severe Total
None 5 1 0 0 6 Mild 8 5 0 0 13
Moderate 4 3 2 0 9 Severe 2 0 0 0 2 Total 19 9 2 0 30
Symmetry test p-value = 0.006 Table 13c: ACTIVE GROUP
Degree of pruritus at Follow-up 2 Degree of pruritus at Screening None Mild Moderate Severe Total
None 7 0 0 0 7 Mild 10 2 0 1 13
Moderate 1 2 0 0 3 Severe 0 0 0 0 0 Total 18 4 0 1 23
Symmetry test p-value = 0.0073
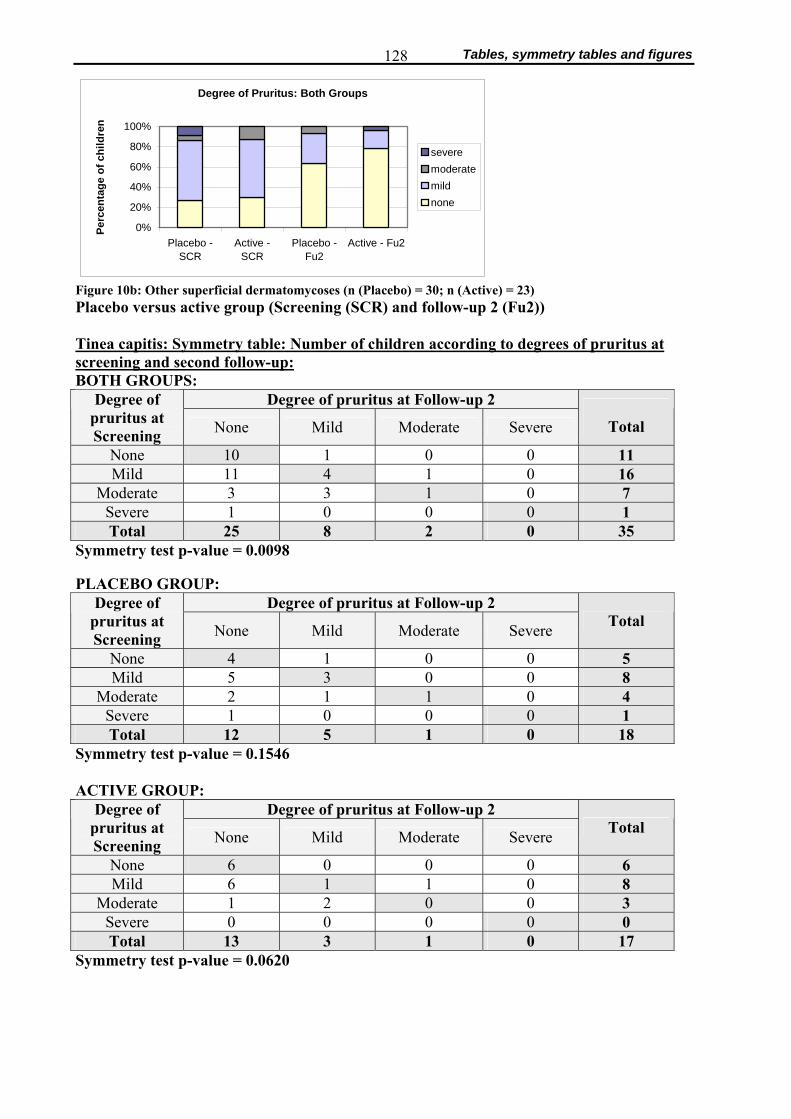
Tables, symmetry tables and figures 128
Degree of Pruritus: Both Groups
0%
20%
40%
60%
80%
100%
Placebo -SCR
Active -SCR
Placebo -Fu2
Active - Fu2
Perc
enta
ge o
f chi
ldre
n
severemoderatemildnone
Figure 10b: Other superficial dermatomycoses (n (Placebo) = 30; n (Active) = 23) Placebo versus active group (Screening (SCR) and follow-up 2 (Fu2)) Tinea capitis: Symmetry table: Number of children according to degrees of pruritus at screening and second follow-up: BOTH GROUPS:
Degree of pruritus at Follow-up 2 Degree of pruritus at Screening None Mild Moderate Severe
Total
None 10 1 0 0 11 Mild 11 4 1 0 16
Moderate 3 3 1 0 7 Severe 1 0 0 0 1 Total 25 8 2 0 35
Symmetry test p-value = 0.0098
PLACEBO GROUP: Degree of pruritus at Follow-up 2 Degree of
pruritus at Screening None Mild Moderate Severe Total
None 4 1 0 0 5 Mild 5 3 0 0 8
Moderate 2 1 1 0 4 Severe 1 0 0 0 1 Total 12 5 1 0 18
Symmetry test p-value = 0.1546 ACTIVE GROUP:
Degree of pruritus at Follow-up 2 Degree of pruritus at Screening None Mild Moderate Severe Total
None 6 0 0 0 6 Mild 6 1 1 0 8
Moderate 1 2 0 0 3 Severe 0 0 0 0 0 Total 13 3 1 0 17
Symmetry test p-value = 0.0620

Tables, symmetry tables and figures 129
Tinea corporis: Symmetry table: Number of children according to degrees of pruritus at screening and second follow-up: BOTH GROUPS:
Degree of pruritus at Follow-up 2 Degree of pruritus at Screening None Mild Moderate Severe
Total
None 2 0 0 0 2 Mild 5 1 0 1 7
Moderate 1 1 1 0 3 Severe 0 0 0 0 0 Total 8 2 1 1 12
Symmetry test p-value = 0.0916 PLACEBO GROUP:
Degree of pruritus at Follow-up 2 Degree of pruritus at Screening None Mild Moderate Severe Total
None 1 0 0 0 1 Mild 3 0 0 0 3
Moderate 1 1 1 0 3 Severe 0 0 0 0 0 Total 5 1 1 0 7
Symmetry test p-value = 0.1718 ACTIVE GROUP:
Degree of pruritus at Follow-up 2 Degree of pruritus at Screening None Mild Moderate Severe Total
None 1 0 0 0 1 Mild 2 1 0 1 4
Moderate 0 0 0 0 0 Severe 0 0 0 0 0 Total 3 1 0 1 5
Symmetry test p-value = 0.2231
Tinea pedis: Symmetry table: Number of children according to degrees of pruritus at screening and second follow-up: BOTH GROUPS:
Degree of pruritus at* Follow-up 2
*Screening None Mild Moderate Severe
Total
None 0 0 0 0 0 Mild 1 2 0 0 3
Moderate 1 1 0 0 2 Severe 1 0 0 0 1 Total 3 3 0 0 6
Symmetry test p-value = 0.406
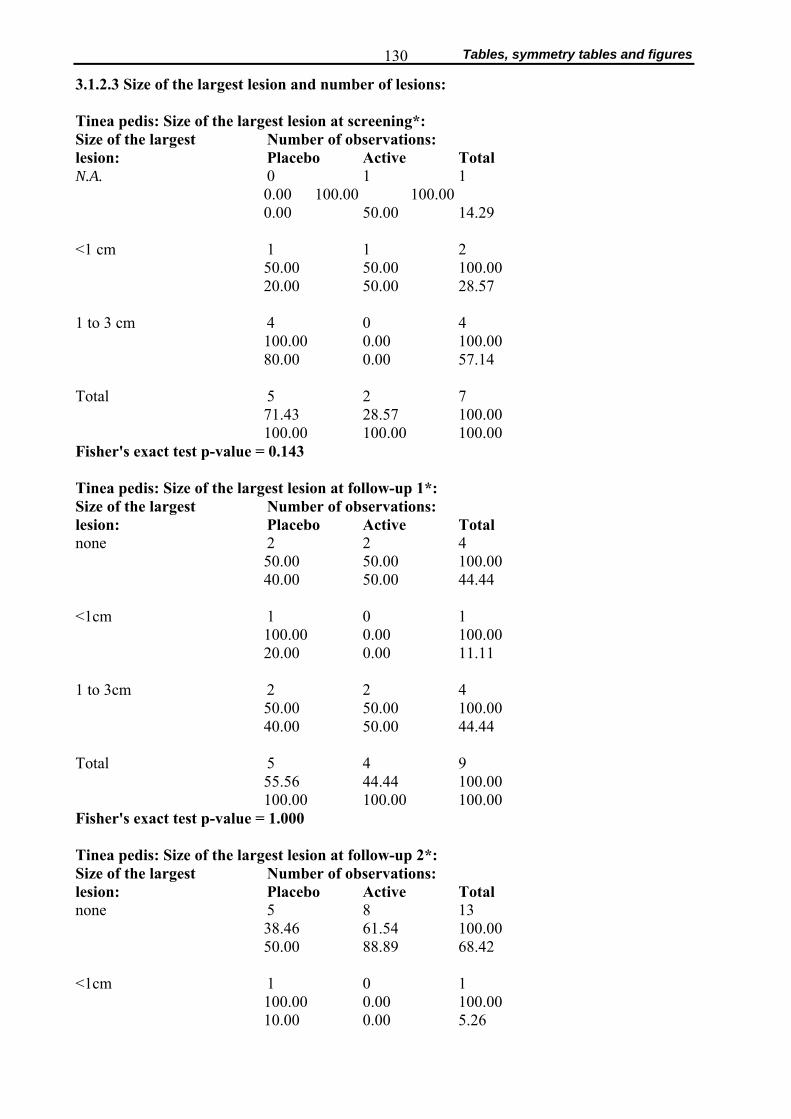
Tables, symmetry tables and figures 130
3.1.2.3 Size of the largest lesion and number of lesions: Tinea pedis: Size of the largest lesion at screening*: Size of the largest Number of observations: lesion: Placebo Active Total N.A. 0 1 1
0.00 100.00 100.00 0.00 50.00 14.29
<1 cm 1 1 2
50.00 50.00 100.00 20.00 50.00 28.57
1 to 3 cm 4 0 4
100.00 0.00 100.00 80.00 0.00 57.14
Total 5 2 7
71.43 28.57 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.143 Tinea pedis: Size of the largest lesion at follow-up 1*: Size of the largest Number of observations: lesion: Placebo Active Total none 2 2 4
50.00 50.00 100.00 40.00 50.00 44.44
<1cm 1 0 1
100.00 0.00 100.00 20.00 0.00 11.11
1 to 3cm 2 2 4
50.00 50.00 100.00 40.00 50.00 44.44
Total 5 4 9
55.56 44.44 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 1.000 Tinea pedis: Size of the largest lesion at follow-up 2*: Size of the largest Number of observations: lesion: Placebo Active Total none 5 8 13
38.46 61.54 100.00 50.00 88.89 68.42
<1cm 1 0 1
100.00 0.00 100.00 10.00 0.00 5.26
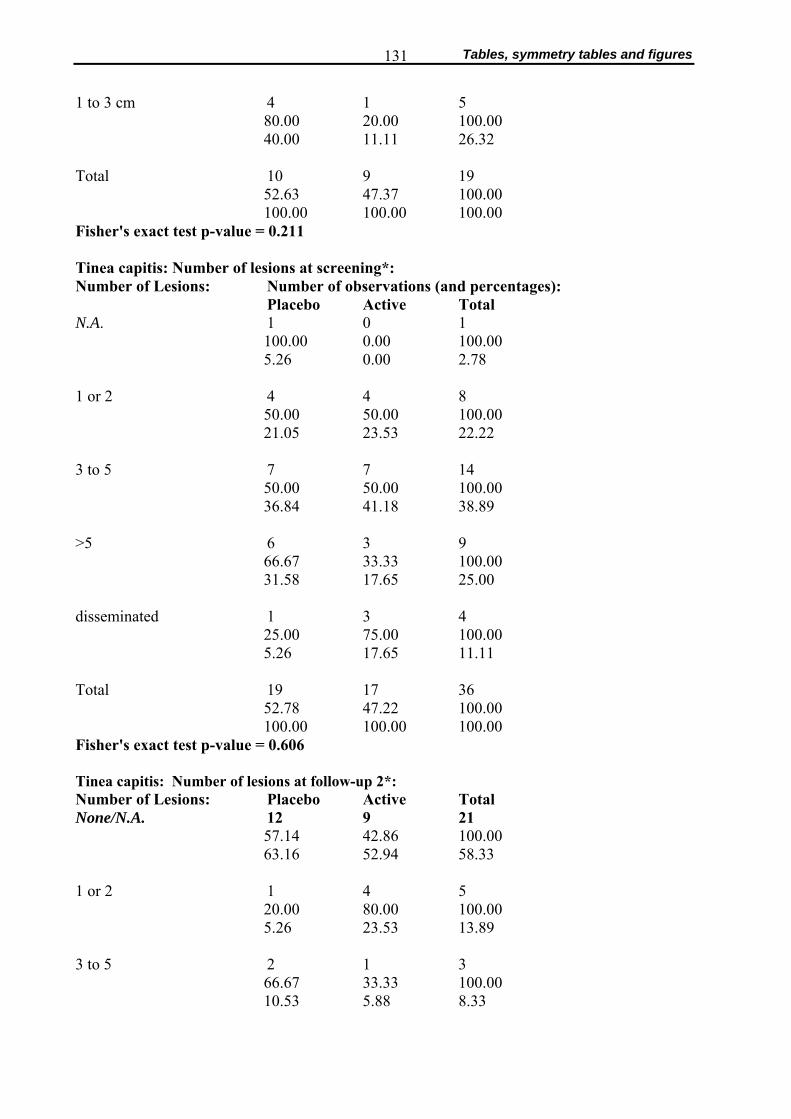
Tables, symmetry tables and figures 131
1 to 3 cm 4 1 5
80.00 20.00 100.00 40.00 11.11 26.32
Total 10 9 19
52.63 47.37 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.211 Tinea capitis: Number of lesions at screening*: Number of Lesions: Number of observations (and percentages): Placebo Active Total N.A. 1 0 1
100.00 0.00 100.00 5.26 0.00 2.78
1 or 2 4 4 8
50.00 50.00 100.00 21.05 23.53 22.22
3 to 5 7 7 14
50.00 50.00 100.00 36.84 41.18 38.89
>5 6 3 9
66.67 33.33 100.00 31.58 17.65 25.00
disseminated 1 3 4
25.00 75.00 100.00 5.26 17.65 11.11
Total 19 17 36
52.78 47.22 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.606 Tinea capitis: Number of lesions at follow-up 2*: Number of Lesions: Placebo Active Total None/N.A. 12 9 21
57.14 42.86 100.00 63.16 52.94 58.33
1 or 2 1 4 5
20.00 80.00 100.00 5.26 23.53 13.89
3 to 5 2 1 3
66.67 33.33 100.00 10.53 5.88 8.33
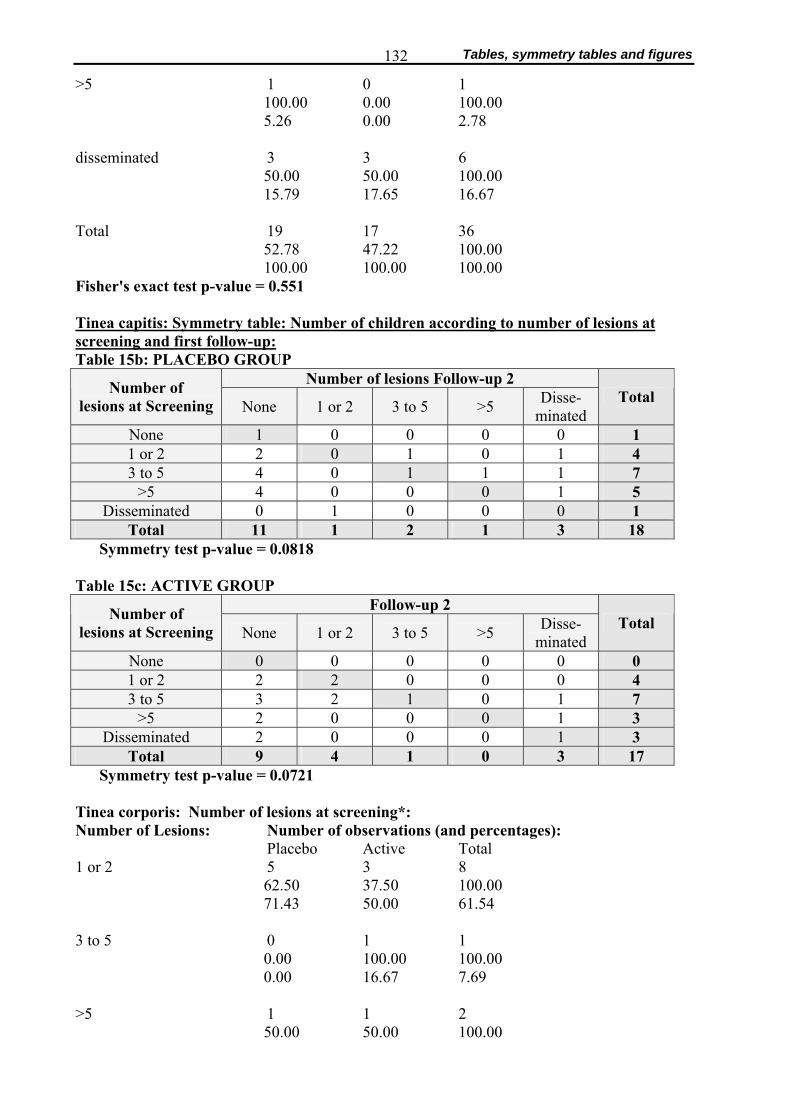
Tables, symmetry tables and figures 132
>5 1 0 1 100.00 0.00 100.00 5.26 0.00 2.78
disseminated 3 3 6
50.00 50.00 100.00 15.79 17.65 16.67
Total 19 17 36
52.78 47.22 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.551 Tinea capitis: Symmetry table: Number of children according to number of lesions at screening and first follow-up: Table 15b: PLACEBO GROUP
Number of lesions Follow-up 2 Number of lesions at Screening None 1 or 2 3 to 5 >5 Disse-
minated Total
None 1 0 0 0 0 1 1 or 2 2 0 1 0 1 4 3 to 5 4 0 1 1 1 7
>5 4 0 0 0 1 5 Disseminated 0 1 0 0 0 1
Total 11 1 2 1 3 18 Symmetry test p-value = 0.0818
Table 15c: ACTIVE GROUP Follow-up 2 Number of
lesions at Screening None 1 or 2 3 to 5 >5 Disse- minated
Total
None 0 0 0 0 0 0 1 or 2 2 2 0 0 0 4 3 to 5 3 2 1 0 1 7
>5 2 0 0 0 1 3 Disseminated 2 0 0 0 1 3
Total 9 4 1 0 3 17 Symmetry test p-value = 0.0721
Tinea corporis: Number of lesions at screening*: Number of Lesions: Number of observations (and percentages): Placebo Active Total 1 or 2 5 3 8
62.50 37.50 100.00 71.43 50.00 61.54
3 to 5 0 1 1
0.00 100.00 100.00 0.00 16.67 7.69
>5 1 1 2
50.00 50.00 100.00
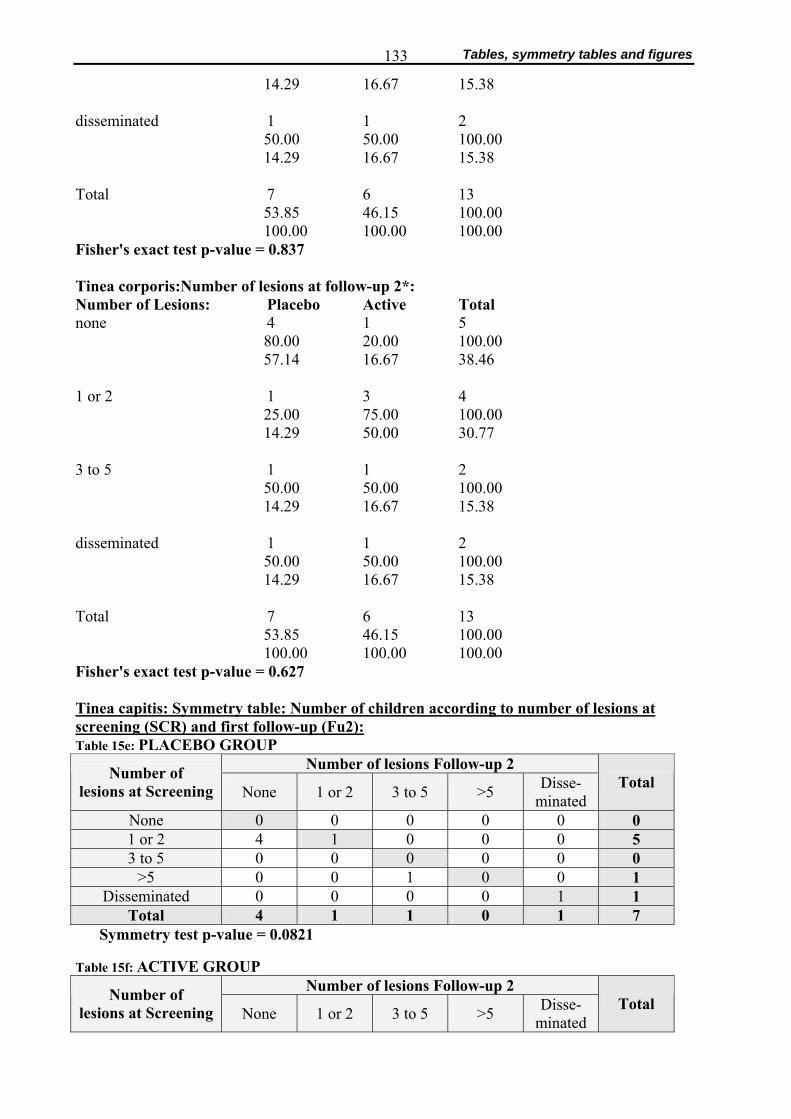
Tables, symmetry tables and figures 133
14.29 16.67 15.38 disseminated 1 1 2
50.00 50.00 100.00 14.29 16.67 15.38
Total 7 6 13
53.85 46.15 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.837 Tinea corporis:Number of lesions at follow-up 2*: Number of Lesions: Placebo Active Total none 4 1 5
80.00 20.00 100.00 57.14 16.67 38.46
1 or 2 1 3 4
25.00 75.00 100.00 14.29 50.00 30.77
3 to 5 1 1 2
50.00 50.00 100.00 14.29 16.67 15.38
disseminated 1 1 2
50.00 50.00 100.00 14.29 16.67 15.38
Total 7 6 13
53.85 46.15 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.627 Tinea capitis: Symmetry table: Number of children according to number of lesions at screening (SCR) and first follow-up (Fu2): Table 15e: PLACEBO GROUP
Number of lesions Follow-up 2 Number of lesions at Screening None 1 or 2 3 to 5 >5 Disse-
minated Total
None 0 0 0 0 0 0 1 or 2 4 1 0 0 0 5 3 to 5 0 0 0 0 0 0
>5 0 0 1 0 0 1 Disseminated 0 0 0 0 1 1
Total 4 1 1 0 1 7 Symmetry test p-value = 0.0821
Table 15f: ACTIVE GROUP Number of lesions Follow-up 2 Number of
lesions at Screening None 1 or 2 3 to 5 >5 Disse- minated
Total
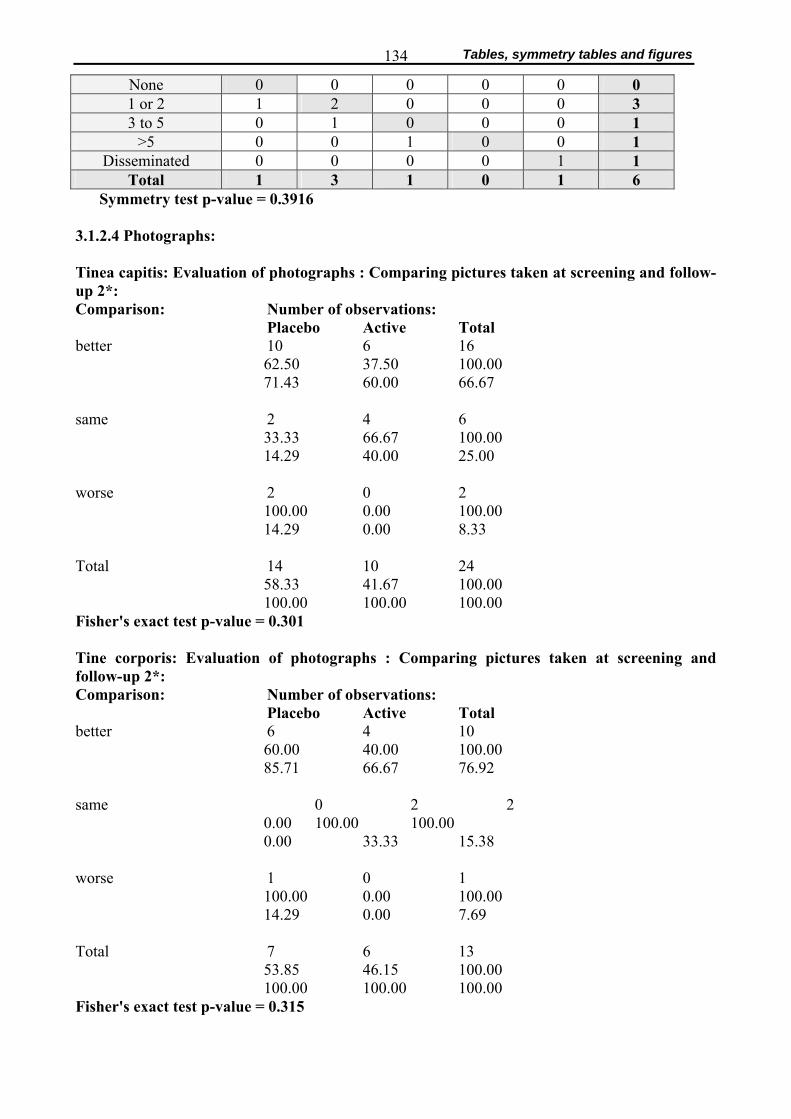
Tables, symmetry tables and figures 134
None 0 0 0 0 0 0 1 or 2 1 2 0 0 0 3 3 to 5 0 1 0 0 0 1
>5 0 0 1 0 0 1 Disseminated 0 0 0 0 1 1
Total 1 3 1 0 1 6 Symmetry test p-value = 0.3916
3.1.2.4 Photographs: Tinea capitis: Evaluation of photographs : Comparing pictures taken at screening and follow-up 2*: Comparison: Number of observations:
Placebo Active Total better 10 6 16
62.50 37.50 100.00 71.43 60.00 66.67
same 2 4 6
33.33 66.67 100.00 14.29 40.00 25.00
worse 2 0 2
100.00 0.00 100.00 14.29 0.00 8.33
Total 14 10 24
58.33 41.67 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.301 Tine corporis: Evaluation of photographs : Comparing pictures taken at screening and follow-up 2*: Comparison: Number of observations:
Placebo Active Total better 6 4 10
60.00 40.00 100.00 85.71 66.67 76.92
same 0 2 2
0.00 100.00 100.00 0.00 33.33 15.38
worse 1 0 1
100.00 0.00 100.00 14.29 0.00 7.69
Total 7 6 13
53.85 46.15 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.315
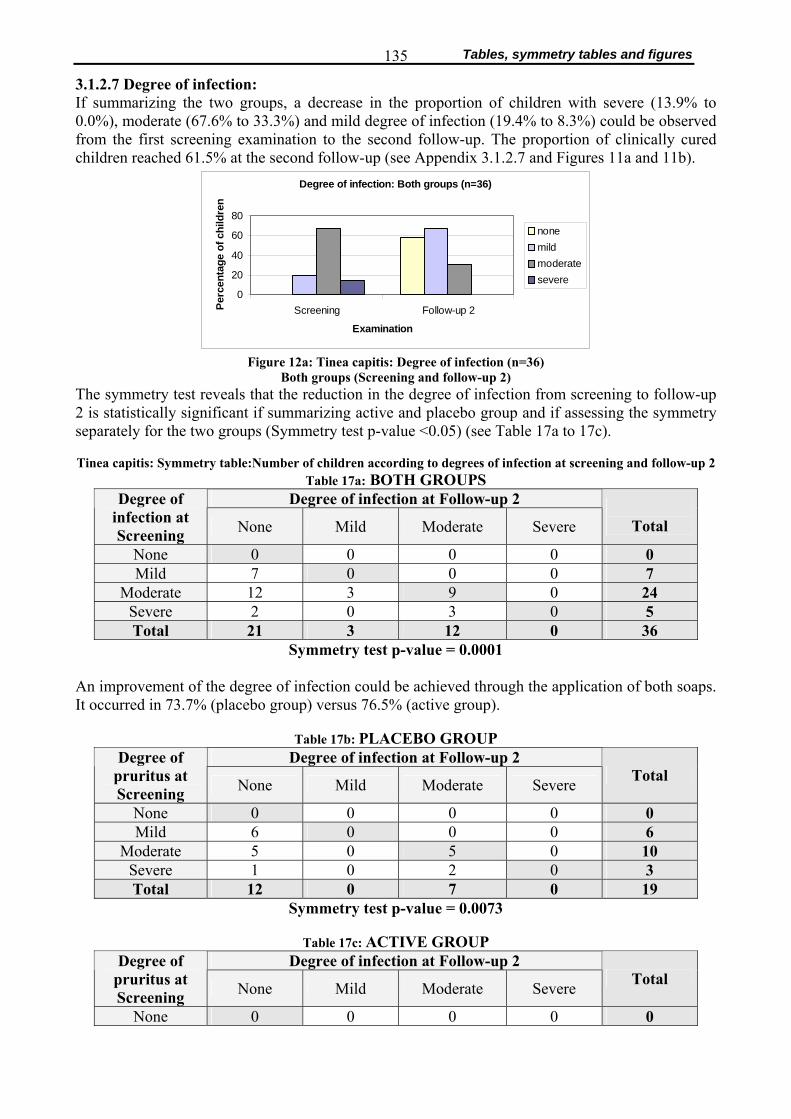
Tables, symmetry tables and figures 135
3.1.2.7 Degree of infection: If summarizing the two groups, a decrease in the proportion of children with severe (13.9% to 0.0%), moderate (67.6% to 33.3%) and mild degree of infection (19.4% to 8.3%) could be observed from the first screening examination to the second follow-up. The proportion of clinically cured children reached 61.5% at the second follow-up (see Appendix 3.1.2.7 and Figures 11a and 11b).
Degree of infection: Both groups (n=36)
0
20
40
60
80
Screening Follow-up 2
Examination
Perc
enta
ge o
f chi
ldre
nnonemildmoderatesevere
Figure 12a: Tinea capitis: Degree of infection (n=36)
Both groups (Screening and follow-up 2) The symmetry test reveals that the reduction in the degree of infection from screening to follow-up 2 is statistically significant if summarizing active and placebo group and if assessing the symmetry separately for the two groups (Symmetry test p-value <0.05) (see Table 17a to 17c).
Tinea capitis: Symmetry table:Number of children according to degrees of infection at screening and follow-up 2
Table 17a: BOTH GROUPS Degree of infection at Follow-up 2 Degree of
infection at Screening None Mild Moderate Severe
Total
None 0 0 0 0 0 Mild 7 0 0 0 7
Moderate 12 3 9 0 24 Severe 2 0 3 0 5 Total 21 3 12 0 36
Symmetry test p-value = 0.0001 An improvement of the degree of infection could be achieved through the application of both soaps. It occurred in 73.7% (placebo group) versus 76.5% (active group).
Table 17b: PLACEBO GROUP
Degree of infection at Follow-up 2 Degree of pruritus at Screening None Mild Moderate Severe Total
None 0 0 0 0 0 Mild 6 0 0 0 6
Moderate 5 0 5 0 10 Severe 1 0 2 0 3 Total 12 0 7 0 19
Symmetry test p-value = 0.0073
Table 17c: ACTIVE GROUP Degree of infection at Follow-up 2 Degree of
pruritus at Screening None Mild Moderate Severe Total
None 0 0 0 0 0
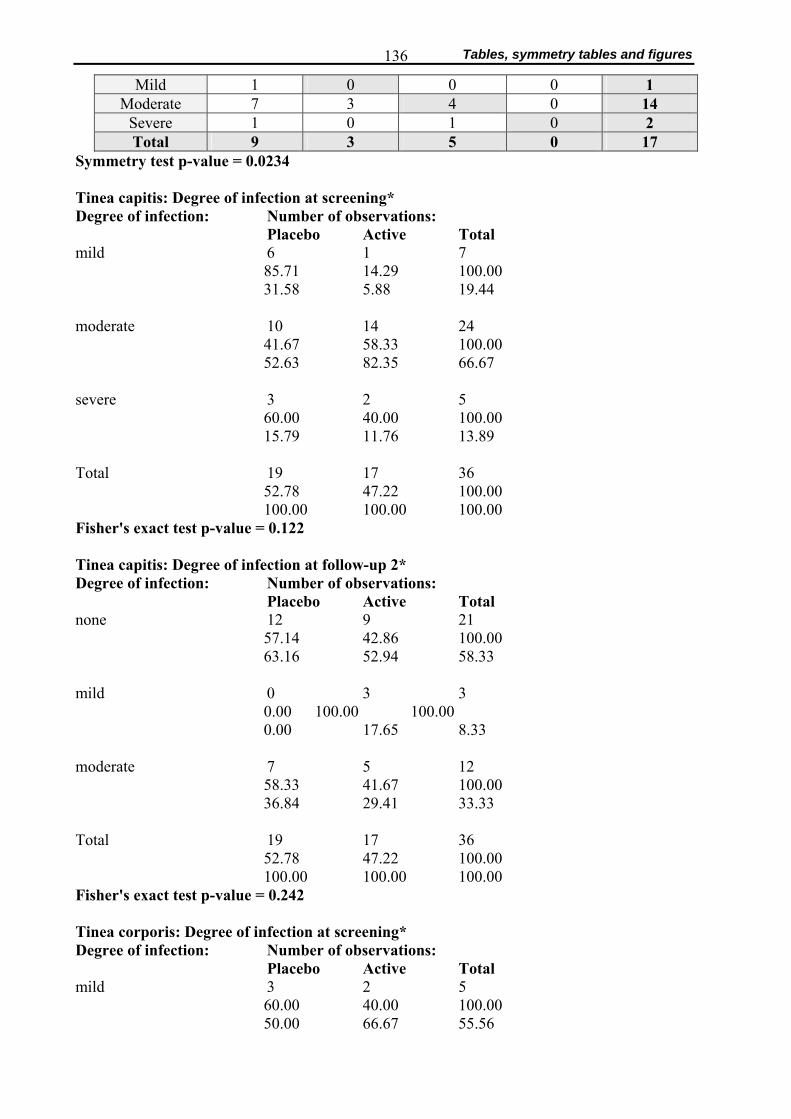
Tables, symmetry tables and figures 136
Mild 1 0 0 0 1 Moderate 7 3 4 0 14
Severe 1 0 1 0 2 Total 9 3 5 0 17
Symmetry test p-value = 0.0234 Tinea capitis: Degree of infection at screening* Degree of infection: Number of observations:
Placebo Active Total mild 6 1 7
85.71 14.29 100.00 31.58 5.88 19.44
moderate 10 14 24
41.67 58.33 100.00 52.63 82.35 66.67
severe 3 2 5
60.00 40.00 100.00 15.79 11.76 13.89
Total 19 17 36
52.78 47.22 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.122 Tinea capitis: Degree of infection at follow-up 2* Degree of infection: Number of observations:
Placebo Active Total none 12 9 21
57.14 42.86 100.00 63.16 52.94 58.33
mild 0 3 3
0.00 100.00 100.00 0.00 17.65 8.33
moderate 7 5 12
58.33 41.67 100.00 36.84 29.41 33.33
Total 19 17 36
52.78 47.22 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.242 Tinea corporis: Degree of infection at screening* Degree of infection: Number of observations:
Placebo Active Total mild 3 2 5
60.00 40.00 100.00 50.00 66.67 55.56
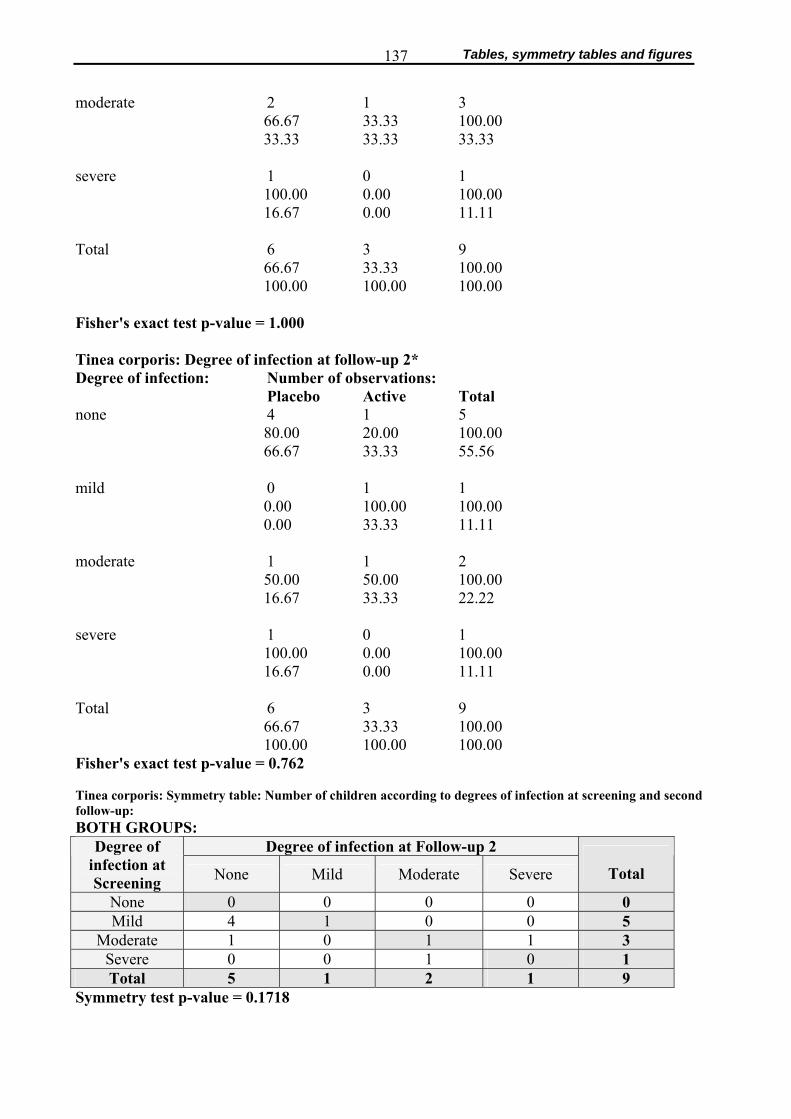
Tables, symmetry tables and figures 137
moderate 2 1 3
66.67 33.33 100.00 33.33 33.33 33.33
severe 1 0 1
100.00 0.00 100.00 16.67 0.00 11.11
Total 6 3 9
66.67 33.33 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 1.000 Tinea corporis: Degree of infection at follow-up 2* Degree of infection: Number of observations:
Placebo Active Total none 4 1 5
80.00 20.00 100.00 66.67 33.33 55.56
mild 0 1 1
0.00 100.00 100.00 0.00 33.33 11.11
moderate 1 1 2
50.00 50.00 100.00 16.67 33.33 22.22
severe 1 0 1
100.00 0.00 100.00 16.67 0.00 11.11
Total 6 3 9
66.67 33.33 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 0.762
Tinea corporis: Symmetry table: Number of children according to degrees of infection at screening and second follow-up: BOTH GROUPS:
Degree of infection at Follow-up 2 Degree of infection at Screening None Mild Moderate Severe
Total
None 0 0 0 0 0 Mild 4 1 0 0 5
Moderate 1 0 1 1 3 Severe 0 0 1 0 1 Total 5 1 2 1 9
Symmetry test p-value = 0.1718
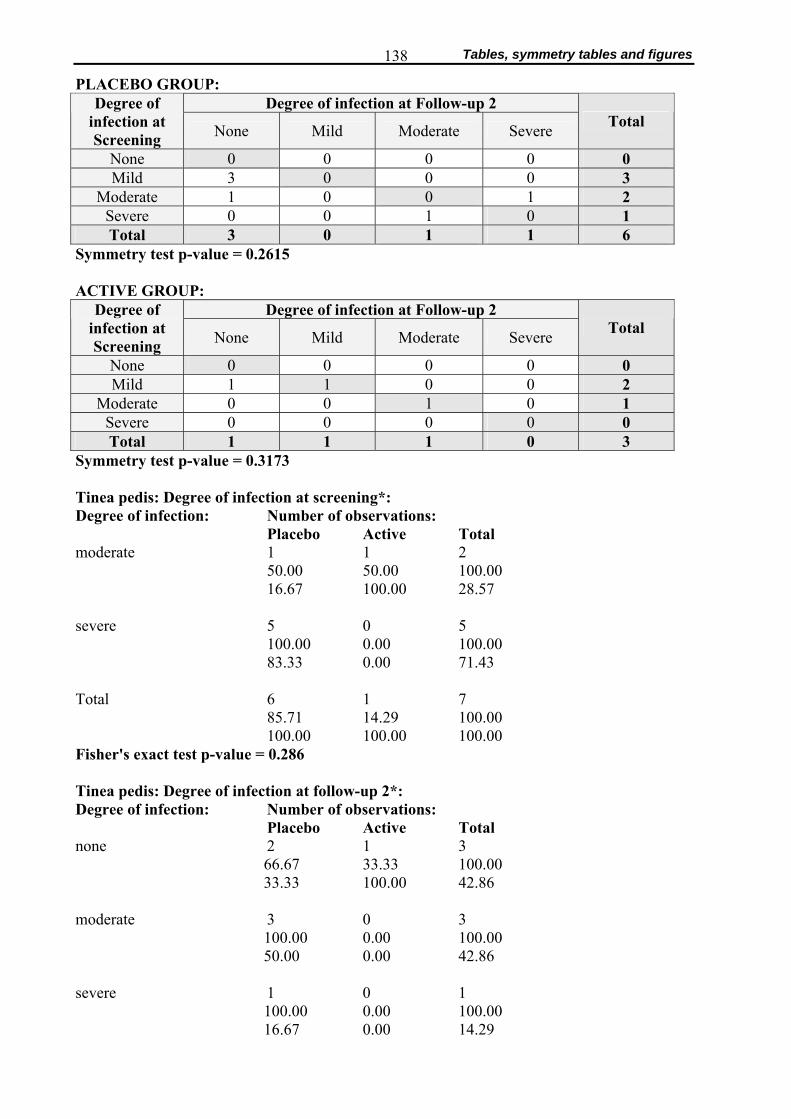
Tables, symmetry tables and figures 138
PLACEBO GROUP: Degree of infection at Follow-up 2 Degree of
infection at Screening None Mild Moderate Severe Total
None 0 0 0 0 0 Mild 3 0 0 0 3
Moderate 1 0 0 1 2 Severe 0 0 1 0 1 Total 3 0 1 1 6
Symmetry test p-value = 0.2615 ACTIVE GROUP:
Degree of infection at Follow-up 2 Degree of infection at Screening None Mild Moderate Severe Total
None 0 0 0 0 0 Mild 1 1 0 0 2
Moderate 0 0 1 0 1 Severe 0 0 0 0 0 Total 1 1 1 0 3
Symmetry test p-value = 0.3173 Tinea pedis: Degree of infection at screening*: Degree of infection: Number of observations:
Placebo Active Total moderate 1 1 2 50.00 50.00 100.00 16.67 100.00 28.57 severe 5 0 5 100.00 0.00 100.00 83.33 0.00 71.43 Total 6 1 7 85.71 14.29 100.00 100.00 100.00 100.00 Fisher's exact test p-value = 0.286 Tinea pedis: Degree of infection at follow-up 2*: Degree of infection: Number of observations:
Placebo Active Total none 2 1 3
66.67 33.33 100.00 33.33 100.00 42.86
moderate 3 0 3
100.00 0.00 100.00 50.00 0.00 42.86
severe 1 0 1
100.00 0.00 100.00 16.67 0.00 14.29

Tables, symmetry tables and figures 139
Total 6 1 7
85.71 14.29 100.00 100.00 100.00 100.00
Fisher's exact test p-value = 1.000 3.1.2.8 Clinical Improvement Tinea corporis: Score at screening (SCR) and follow-up 2 (Fu2)
Figure 13e: Placebo: Microscopy positive (M+)/ Microscopy negative (M-)
Figure 13f: Active: Microscopy positive (M+)/ Microscopy negative (M-)
Table 18: Clinical improvement of tinea corporis: Change of score (placebo versus active group) from screening to follow-up 2, according to positive (M. pos) or negative (M. neg.) microscopic result at the second follow-up. Score N.A.: No score value available for follow-up 2, but child not cured.
Number of children
Cured: Score at follow-up 2
= 0
Reduc-tion of score
In-creased score
Score N.A. Total
M. pos. 1 0 0 2 3 Placebo M. neg. 2 1 1 1 5 Subtotal Placebo 3 1 1 3 8
M. pos. 0 1 0 1 2 Active M. neg. 0 3 0 0 3 Subtotal Active 0 4 0 1 5
Grant Total 3 5 1 4 13 3.1.2.9 Clinical and microscopic resolution Table 19a: Tinea capitis: Relative frequencies (number of observations) and frequency distribution (percentage)
of children having received placebo versus active soap, stratifies according to evaluation Placebo Active
*Evaluation categories
Number of observations
Percentage
Number of observations
Percentage
Total number of
observations (percentage)
1 13 65.0 9 56.3 22 (61.1)
Clinical and
microscopic resolution
2 0 0.0 0 0.0 0 (0.0) Subtotal 14 65.0 10 56.3 22 (61.1)
3 1 5.0 4 25.0 5 (13.9) No resolution 4 0 0.0 0 0.0 0 (0.0)
0 5 10 15 20 25Score Fu2
Cubic spline fit
Score: M-Reference line
25
20
15
10
5
0
S c o r e
S C R
Score: M+
0 5 10 15 20 25
Score Fu2 Cubic spline fit
Score: M-
Reference line
20
15
10
5
0
25 S c o r e
S C R
Score: M+

Tables, symmetry tables and figures 140
5 3 15.0 1 6.3 4 (11.1) 6 0 0.0 0 0.0 0 (0.0)
7 3 15.0 2 12.4 5 (13.9) Total 20 100.0 16 100.0 36 (100.0)
* 1= resolution: child cured 2= microscopic resolution and only few clinical symptoms 3= improvement: negative mycologic evidence with significant clinical improvement
4= negative mycologic evidence with no significant clinical improvement 5= improvement: microscopy positive with significant clinical improvement 6= lack of improvement: positive mycologic evidence with no significant clinical improvement 7= deterioration
Fisher's exact test p-value = 0.420
Table 19c: Tinea corporis: Relative frequencies (number of observations) and frequency distribution (percentage) of children having received placebo versus active soap, stratifies according to evaluation categories
Placebo Active *Evaluation categories
Number of observations
Percentage
Number of observations
Percentage
Total number of
observations (percentage)
1 4 44.8 2 28.6 6 (37.5)
Clinical
and microscopic resolution
2 1 11.1 2 28.6 3 (18.8) Subtotal 5 55.9 4 57.2 9 (56.3)
3 1 11.1 1 14.3 2 (12.5 4 0 0.0 0 0.0 0 (0.0) 5 2 22.2 2 28.6 4 (25.0) 6 0 0.0 0 0.0 0 (0.0)
No resolution
7 1 11.1 0 0.0 1 (6.25) Total 9 100.0 7 100.0 16 (100.0)
Fisher's exact test p-value = 0.937
Table 19e: Tinea pedis: Relative frequencies (number of observations) and frequency distribution (percentage)
of children having received placebo versus active soap, stratifies according to evaluation categories Placebo Active
*Evaluation categories
Number of observations
Percentage
Number of observations
Percentage
Total number of
observations (percentage)
Clinical resolution
1 5 55.6 6 85.7 11 (68.8) 2 2 22.2 0 0.0 2 (12.5) 3 2 22.2 0 0.0 2 (12.5) 4 0 0.0 1 14.3 1 (6.2)
No resolution
5 0 0.0 0 0.0 0 (0.0) Total 9 100.0 7 100.0 16 (100.0)
* 1= clinical resolution 2= improvement: score was reduced 3= lack of improvement: score remained the same
4= no resolution: score was non-applicable at screening, but child is not cured 5= deterioration: score increased

Tables, symmetry tables and figures 141
3.2 Determination of minimal inhibitory concentrations (MIC’s) of placebo soap and of Triclosan Table 1: Growth of Malassezia spp. colonies on Dixon Agar inoculated with different concentrations of placebo soap. Concentration of soap solution: 2.0%
Number of colony forming units (CFU) (### > 50 CFU) according to Malassezia spp. isolate (N°1 to 6)
Isolate 1
Isolate 2
Isolate 3
Isolate 4
Isolate 5
Isolate 6
Concentration of soap solution (0.2%) on agar (μg/mL) 1st
series 2nd
series 1st
series 2nd
series 1st
series 2nd
series 1st
series 2nd
series 1st
series 2nd
series 1st
series 2nd
series
400 11 ### 4 0 0 0 ### ### ### ### 5 ### 200 7 ### 0 0 0 0 ### ### ### ### 2 ### 100 0 3 0 0 0 0 ### ### ### ### 1 2 50 1 4 0 0 0 0 ### ### ### ### 6 ### 25 1 1 1 0 0 0 ### ### ### ### 0 0
12.5 1 0 1 0 0 0 ### 1 ### ### 0 0 6.25 0 2 0 3 0 0 ### ### ### ### 9 0 3.13 5 3 0 ### 0 0 ### ### ### ### 8 ### 1.56 4 1 2 0 0 0 ### ### ### ### 0 ### 0.78 2 2 2 1 2 0 ### ### ### ### ### ### 0.39 2 6 4 1 0 0 0 ### ### ### ### 0
0 0 9 0 0 0 0 ### ### ### ### ### 0 Table 2: Growth of Malassezia spp. colonies on Dixon Agar inoculated with different concentrations of Triclosan (* colony growth visible, but number of colonies was not counted), after 7 and 14 days
Number of colony forming units (CFU) according to Malassezia spp. isolate (5 to 8) 7 days 14 days 7 days 14 days 7 days 14 days 7 days 14 days
Concentration of Triclosan in
stocking solution (μg/mL)
Concentration of Triclosan in
Dixon Agar (μg/mL)
Isolate 5
Isolate 6
Isolate 7
Isolate 8
1 50 000 1000 0 0 0 0 0 0 0 0 2 25 000 500 0 7 1 2 7 11 1 34 3 12 500 250 30 29 9 6 24 34 50 55 4 6 250 125 23 34 7 8 24 40 60 38 5 3 125 62.5 19 25 5 9 28 40 56 44 6 1562.5 31.25 24 23 4 4 21 44 53 53 7 781.24 15.63 12 16 2 4 19 39 46 52 8 390.63 7.81 10 23 1 1 9 33 50 45 9 195.31 3.91 10 20 3 4 8 36 51 47
10 97.66 1.95 13 20 0 2 10 30 51 47 11 48.83 0.98 9 19 1 6 11 28 45 51 12 24.41 0.49 6 20 1 3 10 41 51 54 13 12.21 0.24 13 17 1 4 15 32 54 47 14 6.10 0.12 9 15 2 3 5 23 45 42 15 3.05 0.06 9 23 1 1 9 30 45 34 16 1.53 0.03 11 16 1 2 7 27 35 40 17 0.08 0.015 6 15 1 1 2 24 40 35 18 0.04 0.008 2 9 2 3 1 19 42 41 19 0.02 0.004 6 11 3 4 3 41 43 43
20 Control (only ethanol) * * * * * * * *
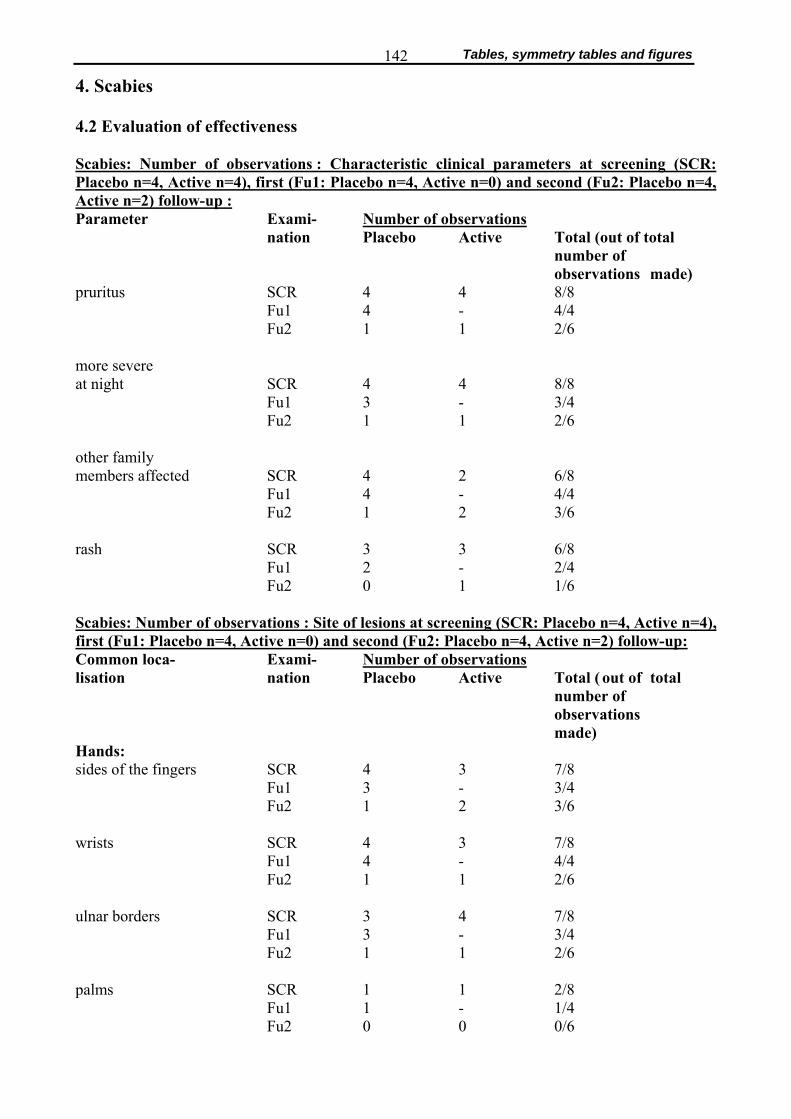
Tables, symmetry tables and figures 142
4. Scabies 4.2 Evaluation of effectiveness Scabies: Number of observations : Characteristic clinical parameters at screening (SCR: Placebo n=4, Active n=4), first (Fu1: Placebo n=4, Active n=0) and second (Fu2: Placebo n=4, Active n=2) follow-up : Parameter Exami- Number of observations nation Placebo Active Total (out of total number of observations made) pruritus SCR 4 4 8/8 Fu1 4 - 4/4 Fu2 1 1 2/6
more severe at night SCR 4 4 8/8 Fu1 3 - 3/4 Fu2 1 1 2/6
other family members affected SCR 4 2 6/8 Fu1 4 - 4/4 Fu2 1 2 3/6 rash SCR 3 3 6/8 Fu1 2 - 2/4 Fu2 0 1 1/6 Scabies: Number of observations : Site of lesions at screening (SCR: Placebo n=4, Active n=4), first (Fu1: Placebo n=4, Active n=0) and second (Fu2: Placebo n=4, Active n=2) follow-up: Common loca- Exami- Number of observations lisation nation Placebo Active Total ( out of total number of observations made) Hands: sides of the fingers SCR 4 3 7/8 Fu1 3 - 3/4 Fu2 1 2 3/6 wrists SCR 4 3 7/8 Fu1 4 - 4/4 Fu2 1 1 2/6 ulnar borders SCR 3 4 7/8 Fu1 3 - 3/4 Fu2 1 1 2/6 palms SCR 1 1 2/8 Fu1 1 - 1/4 Fu2 0 0 0/6
Tables, symmetry tables and figures 143
Other parts: anterior parts of elbows SCR 3 4 7/8 Fu1 2 - 2/4 Fu2 1 0 1/6 anterior axillary folds SCR 0 2 2/8 Fu1 2 - 2/4 Fu2 1 1 2/6 umbilical region SCR 1 2 3/8 Fu1 2 - 2/4 Fu2 2 1 3/6 external genitali, peri- neum, glans penis SCR 0 2 2/8 Fu1 1 - 1/4 Fu2 2 1 3/6 areloae SCR 0 0 0/8 Fu1 1 - 1/4 Fu2 0 1 1/6
gluteal region SCR 0 1 1/8 Fu1 1 - 1/4 Fu2 1 0 1/6 waist SCR 0 1 1/8 Fu1 1 - 1/4 Fu2 1 0 1/6 thighs SCR 0 1 1/8 Fu1 1 - 1/4 Fu2 0 0 0/6 knees SCR 1 0 1/8 Fu1 1 - 1/4 Fu2 0 1 1/6
ankles SCR 0 0 0/8 Fu1 3 - 3/4 Fu2 1 1 2/6 soles SCR 0 0 0/8 Fu1 3 - 3/4 Fu2 0 0 0/6 abdominal region SCR 1 1 2/8 Fu1 1 - 1/4 Fu2 0 1 1/6
Tables, symmetry tables and figures 144
others: SCR 4 4 8/8 . Fu1 1 - 1/4 Fu2 1 1 2/6 Scabies: Number of observations : Number of lesions at screening (SCR: Placebo n=4, Active n=4), first (Fu1: Placebo n=4, Active n=0) and second (Fu2: Placebo n=4, Active n=2) follow-up: Number of loca- Exami- Number of observations lisation nation Placebo Active Total ( out of total number of observations made) none SCR N.A. N.A. N.A.
Fu1 1 - 1/4 Fu2 2 0 2/6 1 to 3 SCR 2 1 2/8 Fu1 2 - 2/4 Fu2 1 1 2/6 4 to 6 SCR 1 1 2/8 Fu1 1 - 1/4 Fu2 1 0 1/6 >6 SCR 1 0 5/8 Fu1 2 - 2/4 Fu2 1 1 2/6 Scabies: Number of observations : Aspect of lesions at screening (SCR: Placebo n=4, Active n=4), first (Fu1: Placebo n=4, Active n=0) and second (Fu2: Placebo n=4, Active n=2) follow-up: Aspect of lesions Exami- Number of observations nation Placebo Active Total ( out of total number of observations made) none SCR N.A. N.A. N.A. Fu1 0 - 0/4 Fu2 1 0 1/6 papules, macules, burrows SCR 3 4 7/8 Fu1 4 - 4/4 Fu2 1 2 3/6 crusts, generalized lichenification SCR 1 0 1/8 Fu1 4 - 4/4 Fu2 1 1 2/6

Tables, symmetry tables and figures 145
superinfection SCR 2 0 2/8 Fu1 1 - 1/4 Fu2 0 1 1/6 thick crusts SCR 0 0 0/8 Fu1 1 - 1/4 Fu2 0 0 0/6 4.2.1.5 Degree of pruritus: Scabies: Number of observations : Degree of pruritus at screening (SCR: Placebo n=4, Active n=4), first (Fu1: Placebo n=4, Active n=0) and second (Fu2: Placebo n=4, Active n=2) follow-up: Degree of Exami- Number of observations pruritus nation Placebo Active Total ( out of total number of observations made) none SCR 0 0 0/8 Fu1 0 - 0/4 Fu2 3 1 4/6 mild SCR 1 0 1/8 Fu1 1 - 1/4 Fu2 1 1 2/6 moderate SCR 1 3 4/8 Fu1 2 - 2/4 Fu2 0 0 0/6 severe SCR 2 1 3/8 Fu1 1 - 1/4 Fu2 0 0 0/6 pruritus improved Fu1 2 - 2/4 Fu2 0 0 0/6
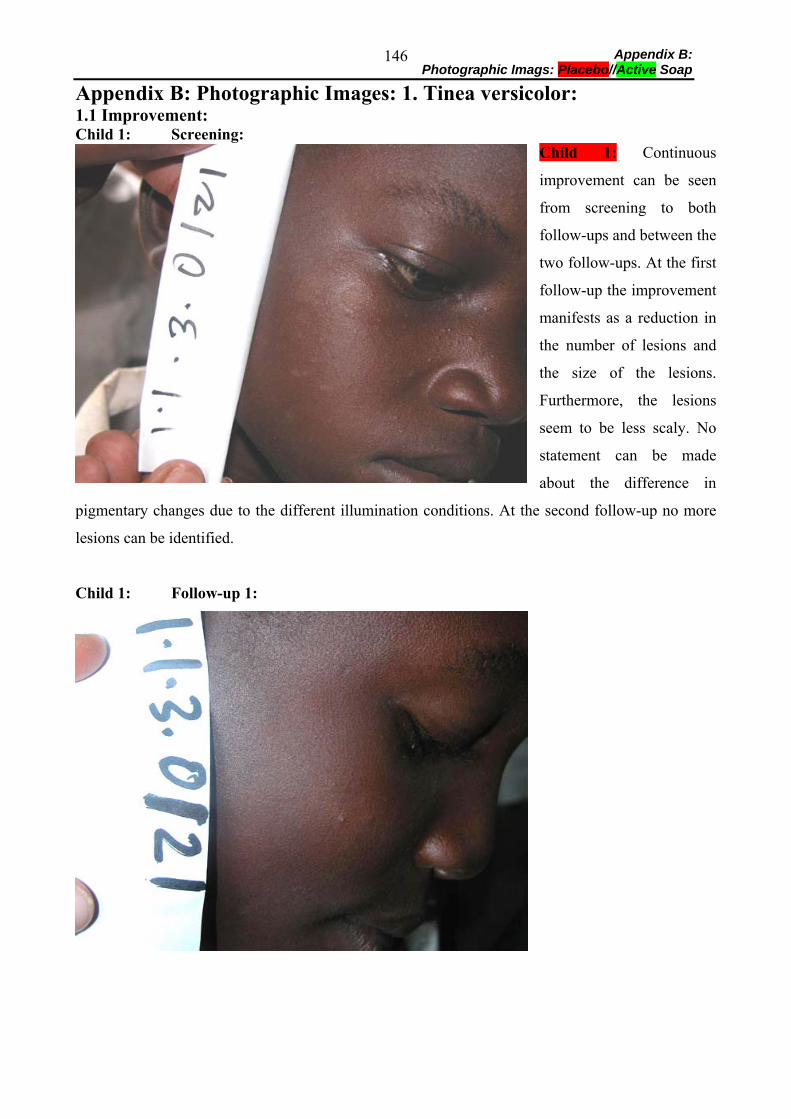
Appendix B: Photographic Imags: Placebo//Active Soap
146
Appendix B: Photographic Images: 1. Tinea versicolor: 1.1 Improvement: Child 1: Screening:
Child 1: Continuous
improvement can be seen
from screening to both
follow-ups and between the
two follow-ups. At the first
follow-up the improvement
manifests as a reduction in
the number of lesions and
the size of the lesions.
Furthermore, the lesions
seem to be less scaly. No
statement can be made
about the difference in
pigmentary changes due to the different illumination conditions. At the second follow-up no more
lesions can be identified.
Child 1: Follow-up 1:
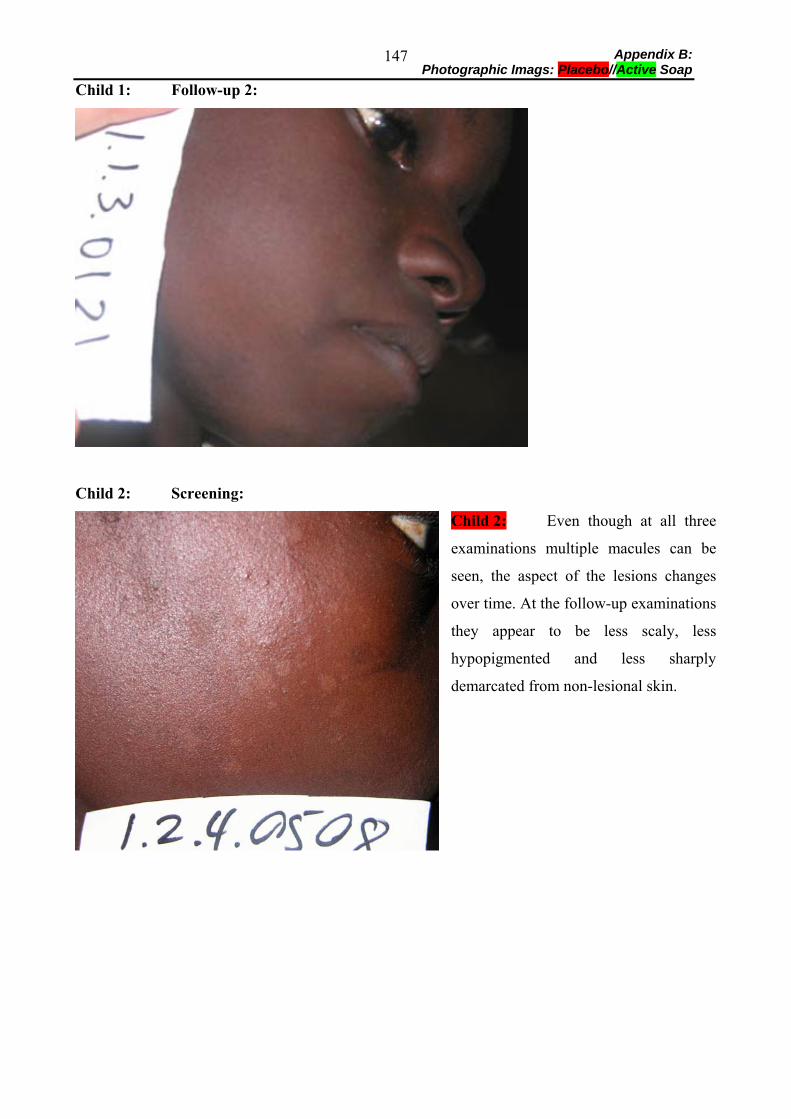
Appendix B: Photographic Imags: Placebo//Active Soap
147
Child 1: Follow-up 2:
Child 2: Screening:
Child 2: Even though at all three
examinations multiple macules can be
seen, the aspect of the lesions changes
over time. At the follow-up examinations
they appear to be less scaly, less
hypopigmented and less sharply
demarcated from non-lesional skin.
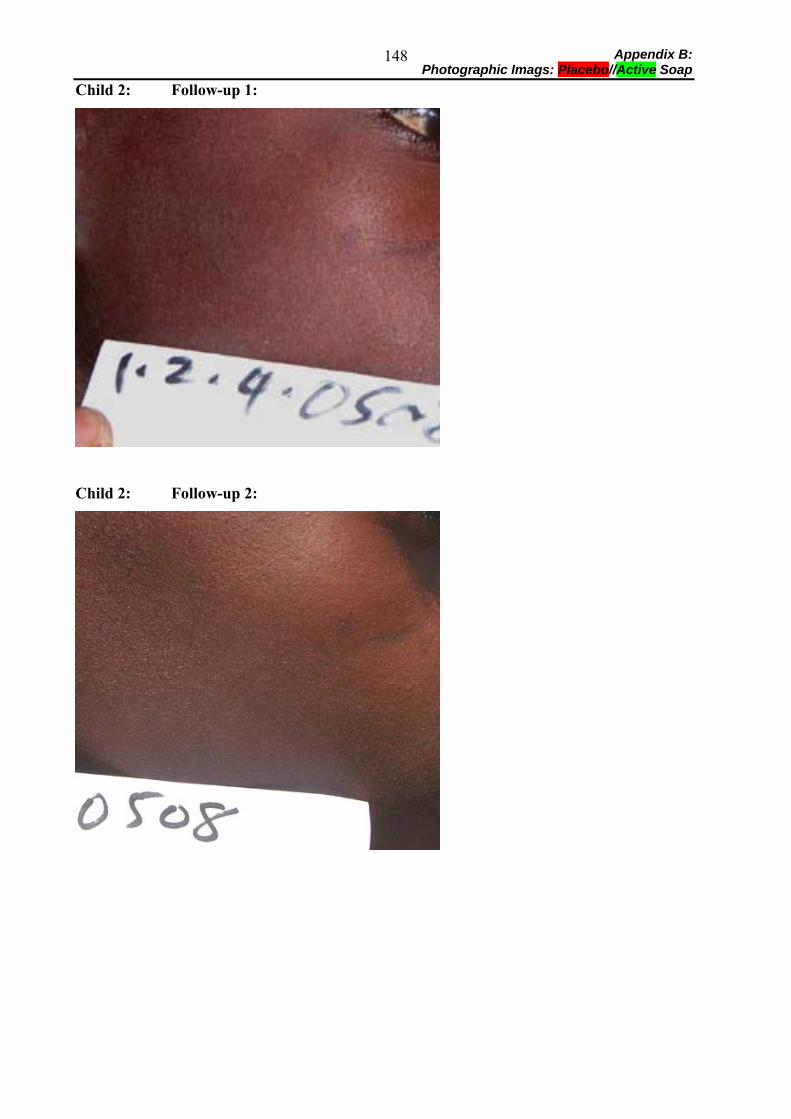
Appendix B: Photographic Imags: Placebo//Active Soap
148
Child 2: Follow-up 1:
Child 2: Follow-up 2:
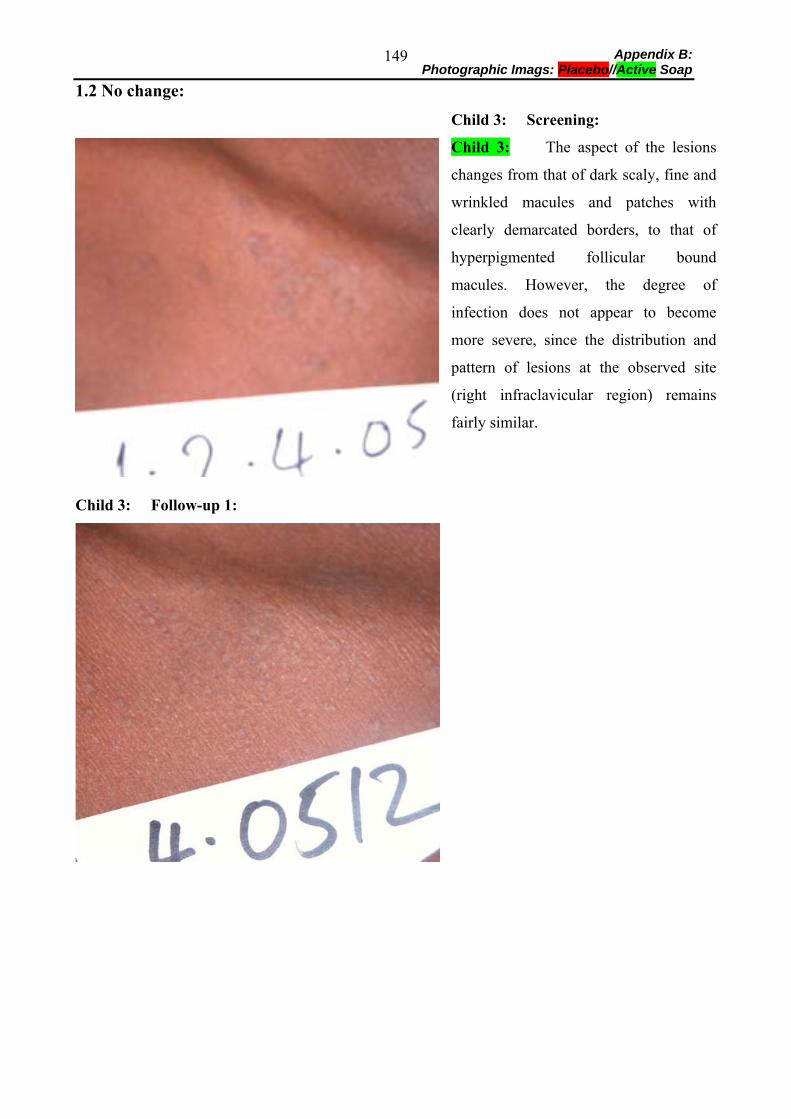
Appendix B: Photographic Imags: Placebo//Active Soap
149
1.2 No change:
Child 3: Screening:
Child 3: The aspect of the lesions
changes from that of dark scaly, fine and
wrinkled macules and patches with
clearly demarcated borders, to that of
hyperpigmented follicular bound
macules. However, the degree of
infection does not appear to become
more severe, since the distribution and
pattern of lesions at the observed site
(right infraclavicular region) remains
fairly similar.
Child 3: Follow-up 1:
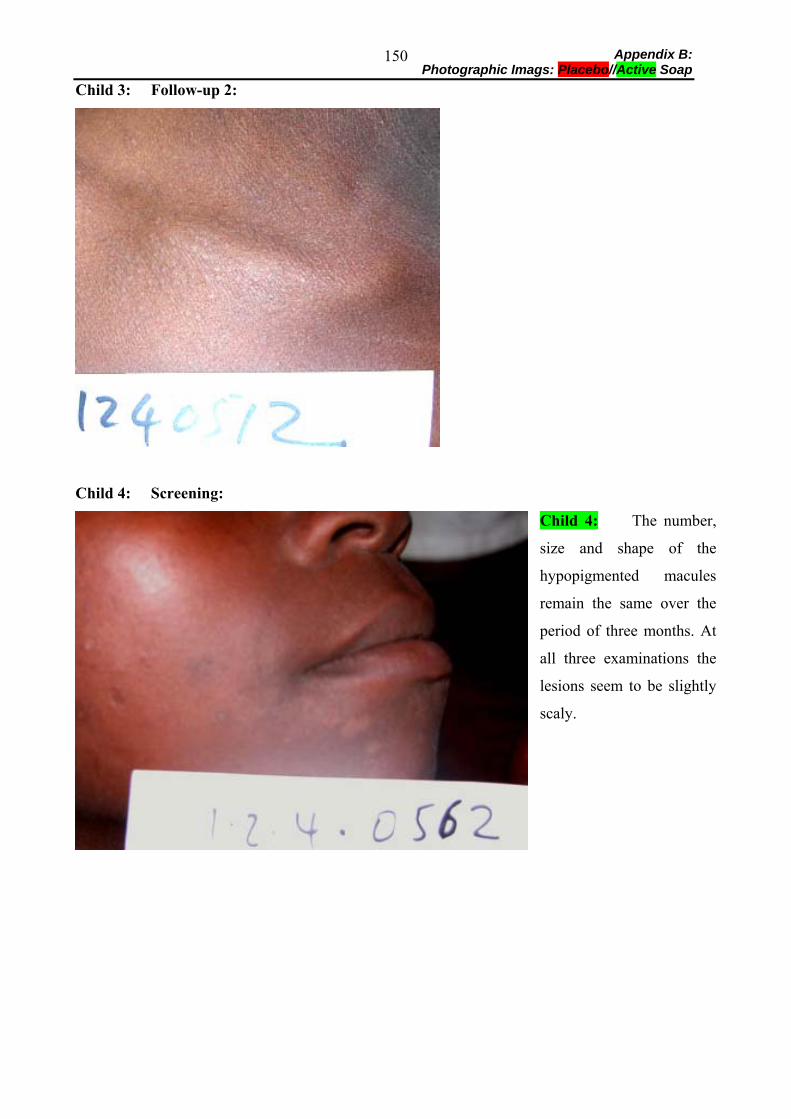
Appendix B: Photographic Imags: Placebo//Active Soap
150
Child 3: Follow-up 2:
Child 4: Screening:
Child 4: The number,
size and shape of the
hypopigmented macules
remain the same over the
period of three months. At
all three examinations the
lesions seem to be slightly
scaly.
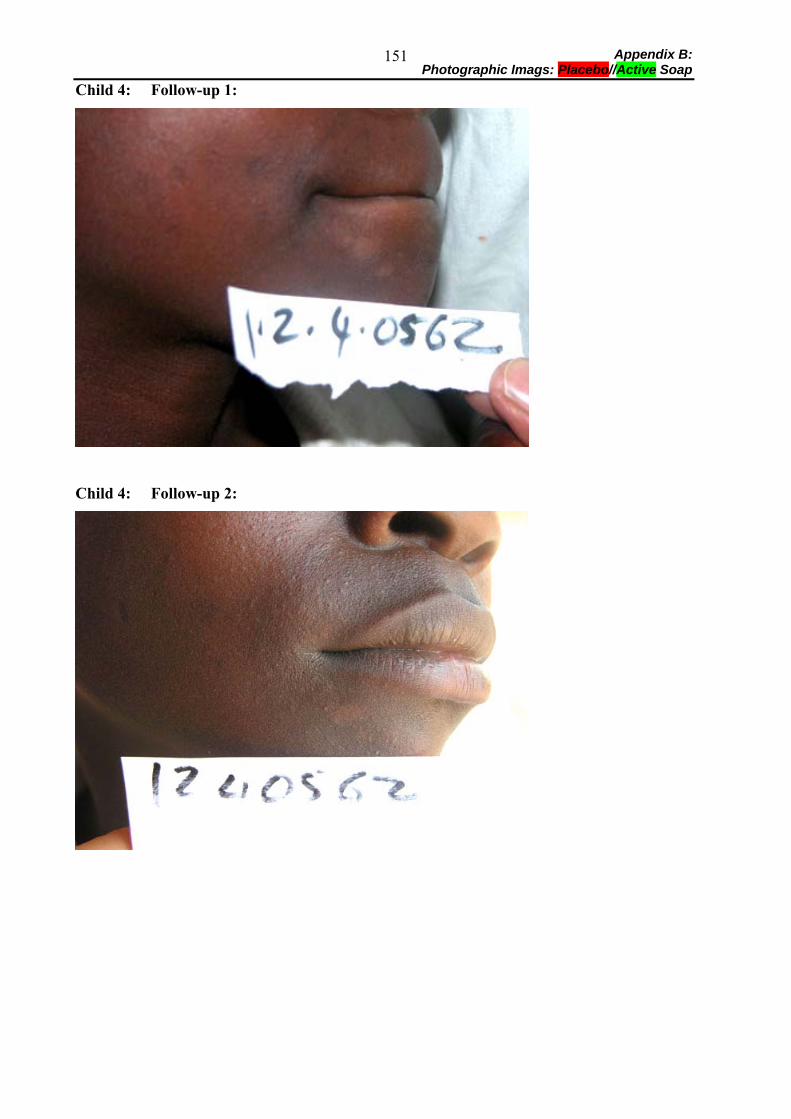
Appendix B: Photographic Imags: Placebo//Active Soap
151
Child 4: Follow-up 1:
Child 4: Follow-up 2:
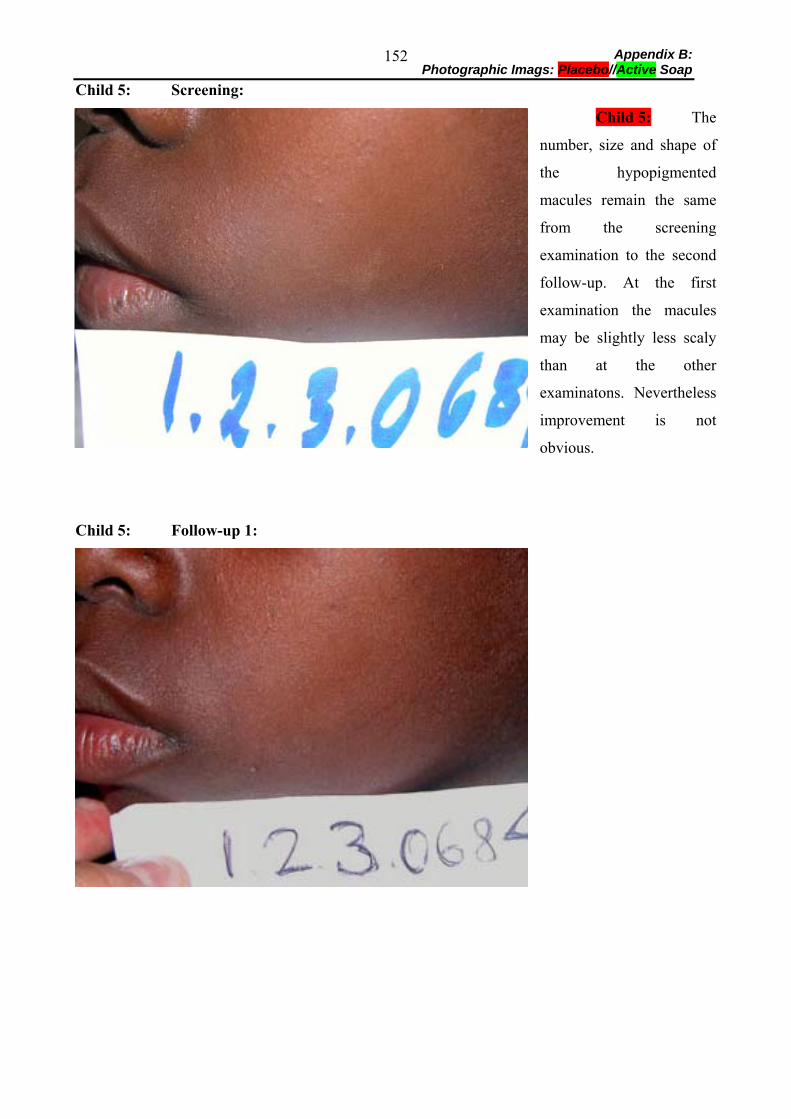
Appendix B: Photographic Imags: Placebo//Active Soap
152
Child 5: Screening:
Child 5: The
number, size and shape of
the hypopigmented
macules remain the same
from the screening
examination to the second
follow-up. At the first
examination the macules
may be slightly less scaly
than at the other
examinatons. Nevertheless
improvement is not
obvious.
Child 5: Follow-up 1:
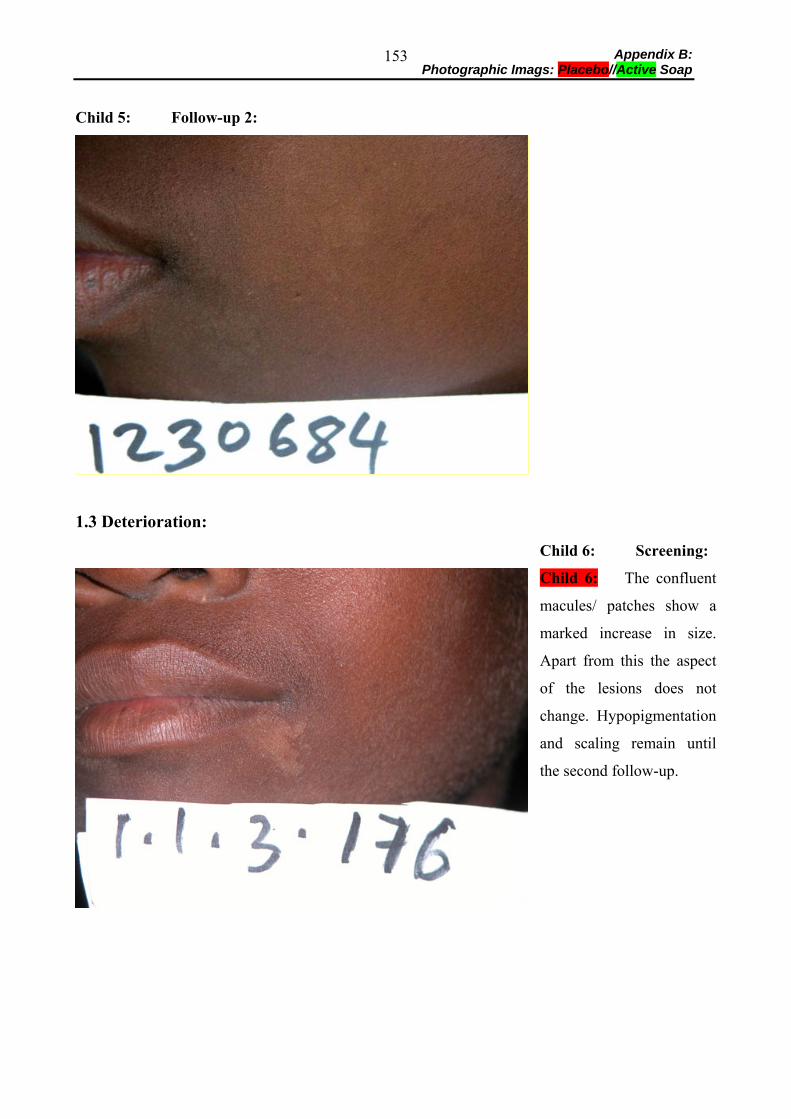
Appendix B: Photographic Imags: Placebo//Active Soap
153
Child 5: Follow-up 2:
1.3 Deterioration:
Child 6: Screening:
Child 6: The confluent
macules/ patches show a
marked increase in size.
Apart from this the aspect
of the lesions does not
change. Hypopigmentation
and scaling remain until
the second follow-up.
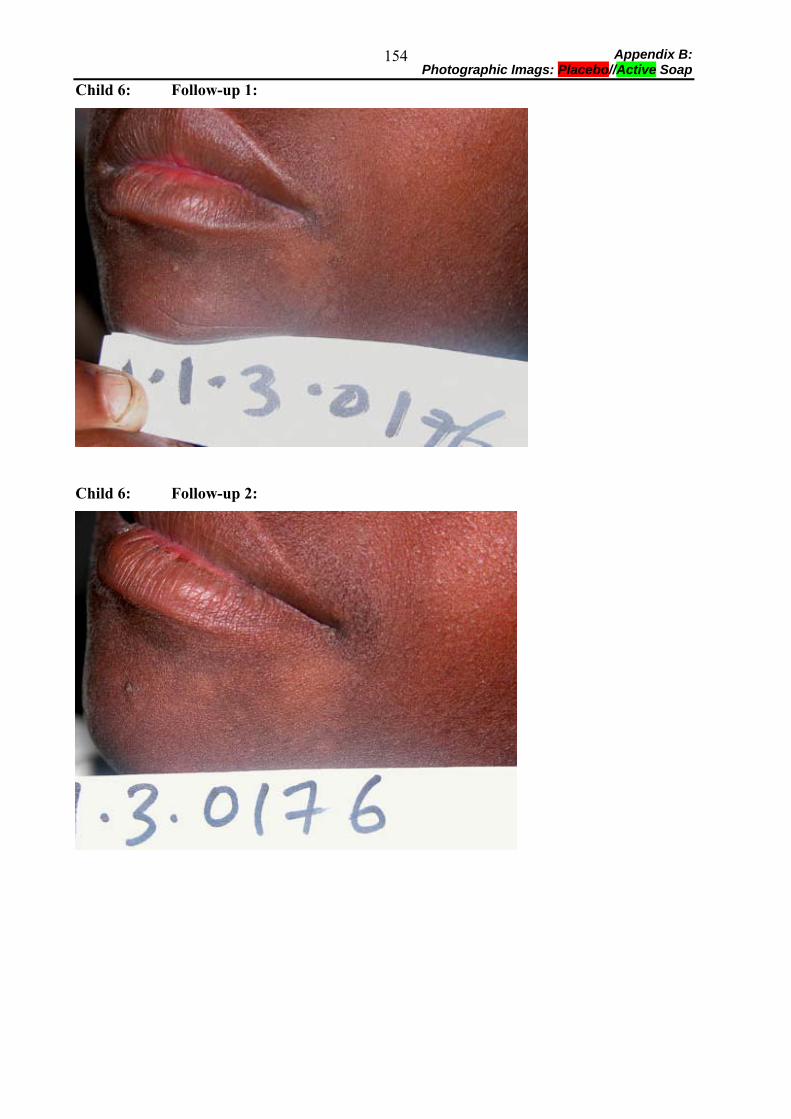
Appendix B: Photographic Imags: Placebo//Active Soap
154
Child 6: Follow-up 1:
Child 6: Follow-up 2:
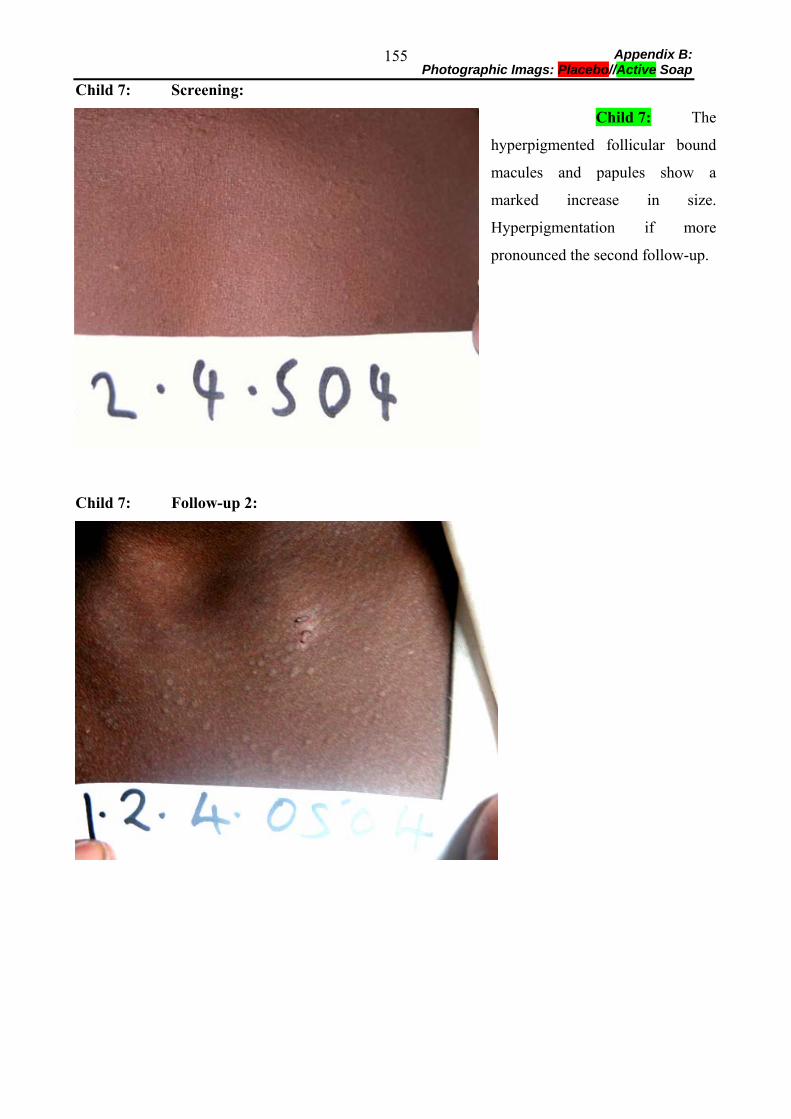
Appendix B: Photographic Imags: Placebo//Active Soap
155
Child 7: Screening:
Child 7: The
hyperpigmented follicular bound
macules and papules show a
marked increase in size.
Hyperpigmentation if more
pronounced the second follow-up.
Child 7: Follow-up 2:
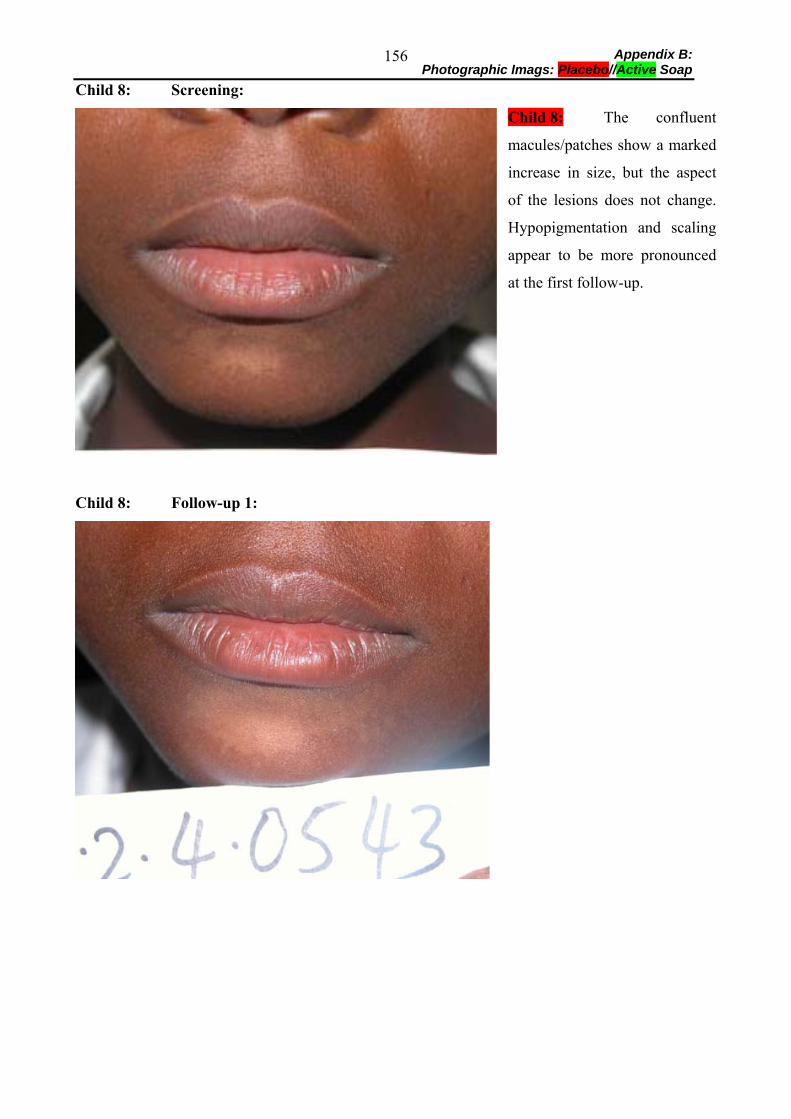
Appendix B: Photographic Imags: Placebo//Active Soap
156
Child 8: Screening:
Child 8: The confluent
macules/patches show a marked
increase in size, but the aspect
of the lesions does not change.
Hypopigmentation and scaling
appear to be more pronounced
at the first follow-up.
Child 8: Follow-up 1:
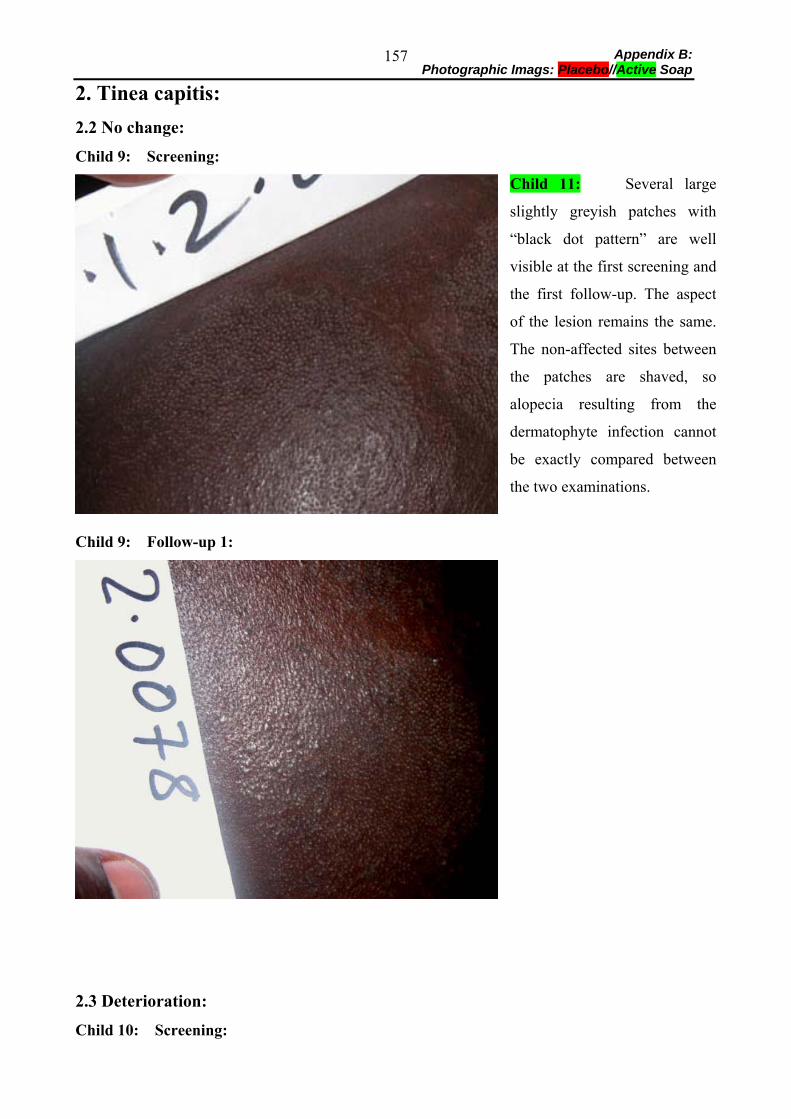
Appendix B: Photographic Imags: Placebo//Active Soap
157
2. Tinea capitis: 2.2 No change:
Child 9: Screening:
Child 11: Several large
slightly greyish patches with
“black dot pattern” are well
visible at the first screening and
the first follow-up. The aspect
of the lesion remains the same.
The non-affected sites between
the patches are shaved, so
alopecia resulting from the
dermatophyte infection cannot
be exactly compared between
the two examinations.
Child 9: Follow-up 1:
2.3 Deterioration:
Child 10: Screening:
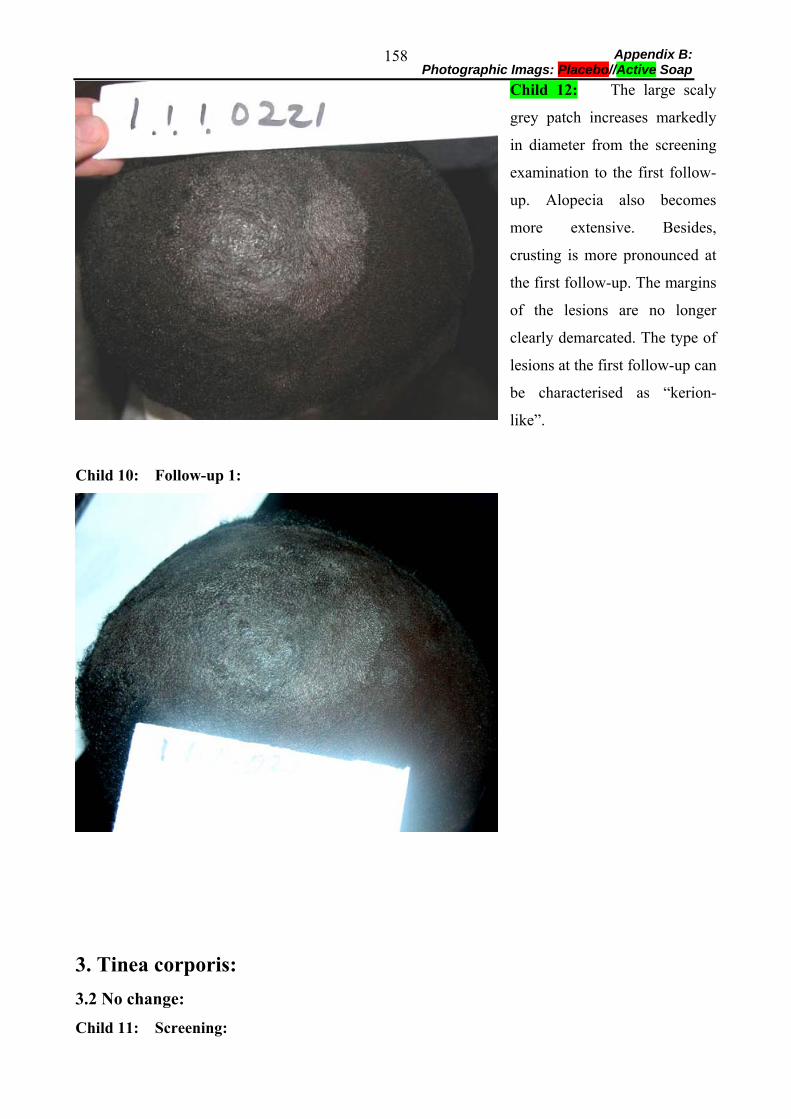
Appendix B: Photographic Imags: Placebo//Active Soap
158
Child 12: The large scaly
grey patch increases markedly
in diameter from the screening
examination to the first follow-
up. Alopecia also becomes
more extensive. Besides,
crusting is more pronounced at
the first follow-up. The margins
of the lesions are no longer
clearly demarcated. The type of
lesions at the first follow-up can
be characterised as “kerion-
like”.
Child 10: Follow-up 1:
3. Tinea corporis: 3.2 No change:
Child 11: Screening:
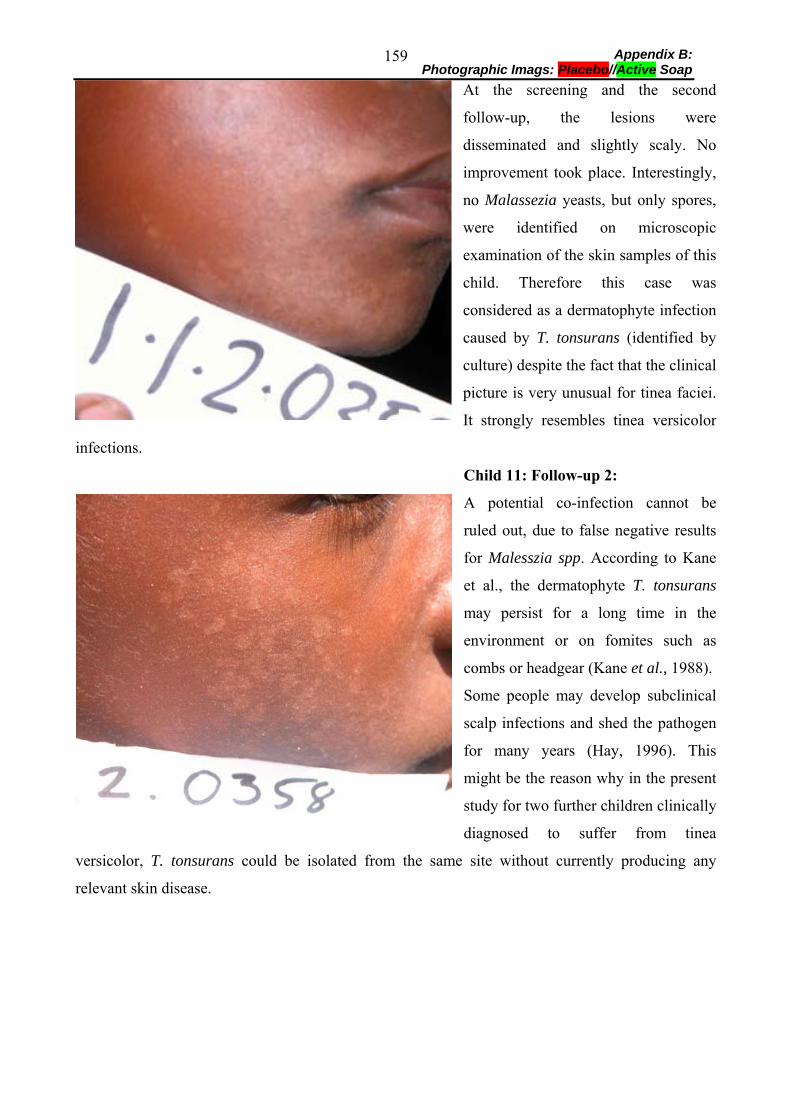
Appendix B: Photographic Imags: Placebo//Active Soap
159
At the screening and the second
follow-up, the lesions were
disseminated and slightly scaly. No
improvement took place. Interestingly,
no Malassezia yeasts, but only spores,
were identified on microscopic
examination of the skin samples of this
child. Therefore this case was
considered as a dermatophyte infection
caused by T. tonsurans (identified by
culture) despite the fact that the clinical
picture is very unusual for tinea faciei.
It strongly resembles tinea versicolor
infections.
Child 11: Follow-up 2:
A potential co-infection cannot be
ruled out, due to false negative results
for Malesszia spp. According to Kane
et al., the dermatophyte T. tonsurans
may persist for a long time in the
environment or on fomites such as
combs or headgear (Kane et al., 1988).
Some people may develop subclinical
scalp infections and shed the pathogen
for many years (Hay, 1996). This
might be the reason why in the present
study for two further children clinically
diagnosed to suffer from tinea
versicolor, T. tonsurans could be isolated from the same site without currently producing any
relevant skin disease.
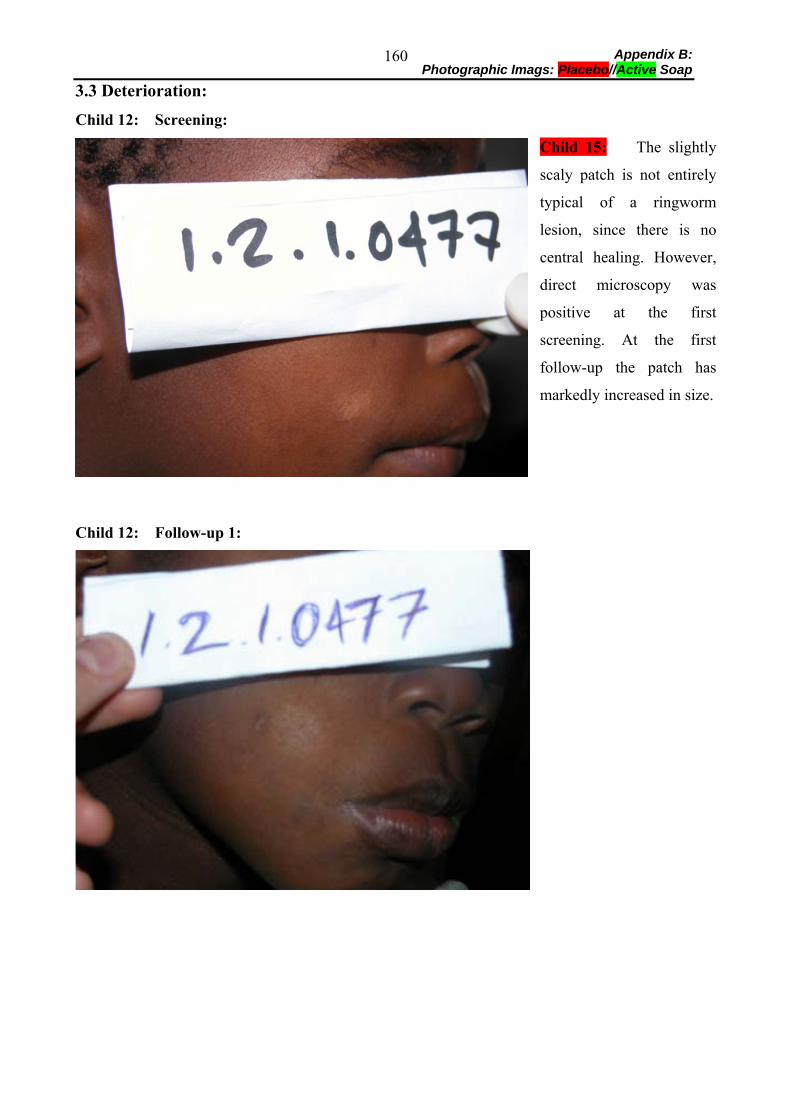
Appendix B: Photographic Imags: Placebo//Active Soap
160
3.3 Deterioration:
Child 12: Screening:
Child 15: The slightly
scaly patch is not entirely
typical of a ringworm
lesion, since there is no
central healing. However,
direct microscopy was
positive at the first
screening. At the first
follow-up the patch has
markedly increased in size.
Child 12: Follow-up 1:
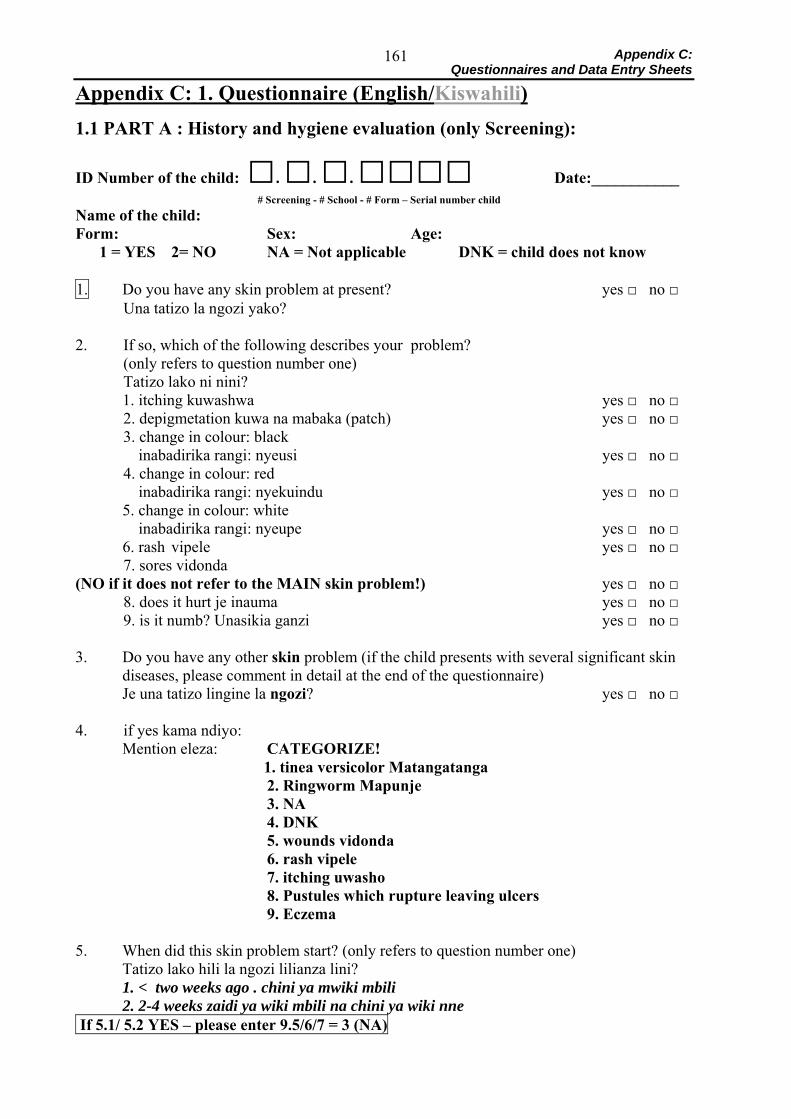
Appendix C: Questionnaires and Data Entry Sheets
161
Appendix C: 1. Questionnaire (English/Kiswahili) 1.1 PART A : History and hygiene evaluation (only Screening):
ID Number of the child: □. □. □. □□□□ Date:___________ # Screening - # School - # Form – Serial number child Name of the child: Form: Sex: Age:
1 = YES 2= NO NA = Not applicable DNK = child does not know
1. Do you have any skin problem at present? yes □ no □ Una tatizo la ngozi yako?
2. If so, which of the following describes your problem? (only refers to question number one) Tatizo lako ni nini?
1. itching kuwashwa yes □ no □ 2. depigmetation kuwa na mabaka (patch) yes □ no □ 3. change in colour: black
inabadirika rangi: nyeusi yes □ no □ 4. change in colour: red
inabadirika rangi: nyekuindu yes □ no □ 5. change in colour: white inabadirika rangi: nyeupe yes □ no □ 6. rash vipele yes □ no □
7. sores vidonda (NO if it does not refer to the MAIN skin problem!) yes □ no □ 8. does it hurt je inauma yes □ no □ 9. is it numb? Unasikia ganzi yes □ no □ 3. Do you have any other skin problem (if the child presents with several significant skin
diseases, please comment in detail at the end of the questionnaire) Je una tatizo lingine la ngozi? yes □ no □
4. if yes kama ndiyo: Mention eleza: CATEGORIZE!
1. tinea versicolor Matangatanga 2. Ringworm Mapunje 3. NA 4. DNK 5. wounds vidonda 6. rash vipele 7. itching uwasho
8. Pustules which rupture leaving ulcers 9. Eczema 5. When did this skin problem start? (only refers to question number one)
Tatizo lako hili la ngozi lilianza lini? 1. < two weeks ago . chini ya mwiki mbili 2. 2-4 weeks zaidi ya wiki mbili na chini ya wiki nne
If 5.1/ 5.2 YES – please enter 9.5/6/7 = 3 (NA)

Appendix C: Questionnaires and Data Entry Sheets
162
3. 2-6 months ago zaidi ya miwezi mibili na chini ya miwezi sita 4. <1 year ago mwaka 1 5. 2 years ago miaka 2 6. 3 years ago miaka 3 7. > years ago zaidi ya miaka mitatu
6. Where did this skin problem start? (only refers to question number one) Tatizo hili limeanzia wapi? 1. scalp ngozi ya kichwa yes □ no □ 2. face uso yes □ no □ 3. neck shingo yes □ no □ 4. chest kifua yes □ no □ 5. abdomen tumbo yes □ no □ 6. back mgongo yes □ no □ 7. axilla makwapa yes □ no □ 8. arms mkono yes □ no □ 9. hands viganjwa yes □ no □ 10. finger webs uwazi wa vidole yes □ no □ 11. genital region sehemu za siri yes □ no □ 12. thighs mapaja yes □ no □ 13. knees magoti yes □ no □ 14. lower leg miguu yes □ no □ 15. feet nyaao yes □ no □ 16. between the toes baina ya kidole cha miguu yes □ no □
7. Size Ukubwa:
1. Does it remain the same? Inabakia vilevile? 2. Is it increasing in size? Inaongezeka ukubwa?
3. Is it decreasing in size? Inapungua? 4. Is it varying in size? Inarudiarudia? 8. Does this skin disease itch (lesions described in question no. 1)? Je ugonjwa wako huu unawasha? yes □ no □ 9. When does it itch? Ni wakati gani unawasha zaidi? 1. in the hot sun jua kali yes □ no □ 2. in bed/sleeping kitandani/ unapolala yes □ no □
3. after bathing with hot water baada ya kuoga na maji joto yes □ no □ 4. after bathing with cold water maji baridi yes □ no □
IF Question No. 5.1/ 5.2 = YES: Please fill in 3 (NA) in Question No. 9.5/ 9.6/ 9.7 = 5. rainy season masika yes □ no □ 6. hot/dry season kiangazi yes □ no □ 7. cold season wakati wa baridi yes □ no □
13. Are there any others at home who have the same skin disease
or the same signs of the skin disease as you?
How many Taja wangapi: IF NO, PLEASE ENTER “0” □ 15. Apart from the skin problem(s) do you have another problem such as the following? Una tatizo lolote kati ya haya yafuatayo: 1. fever homa yes □ no □
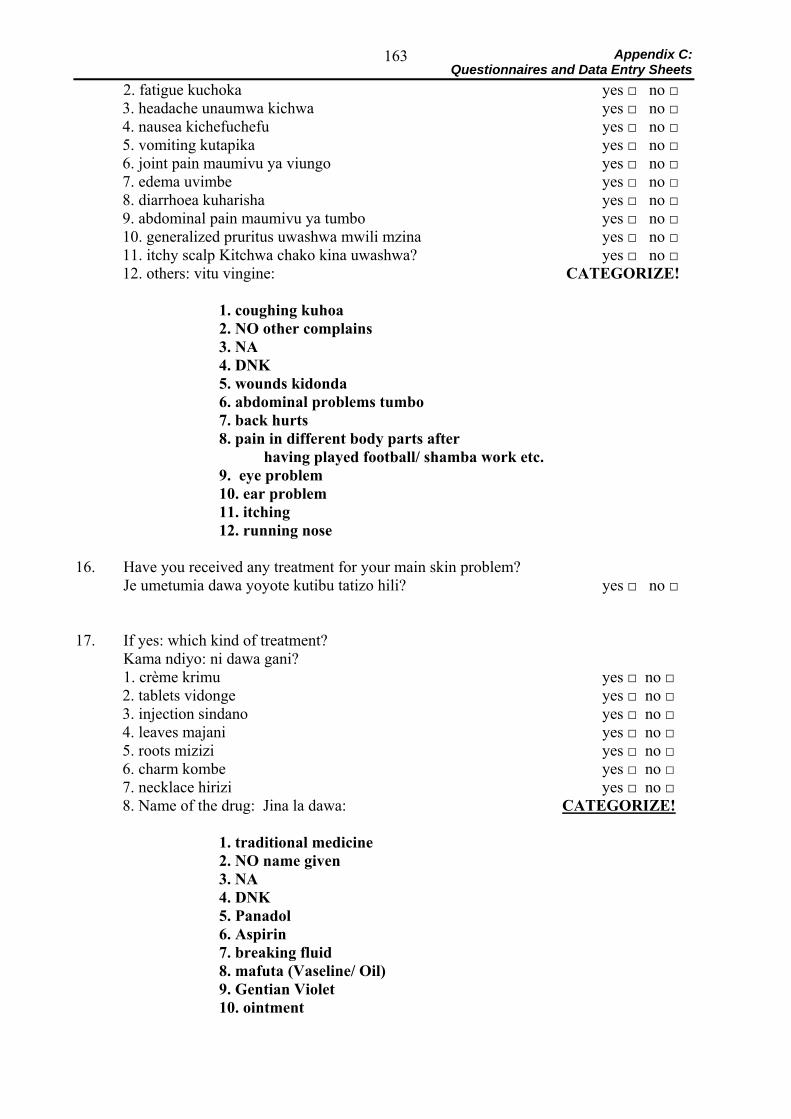
Appendix C: Questionnaires and Data Entry Sheets
163
2. fatigue kuchoka yes □ no □ 3. headache unaumwa kichwa yes □ no □ 4. nausea kichefuchefu yes □ no □ 5. vomiting kutapika yes □ no □ 6. joint pain maumivu ya viungo yes □ no □ 7. edema uvimbe yes □ no □ 8. diarrhoea kuharisha yes □ no □ 9. abdominal pain maumivu ya tumbo yes □ no □ 10. generalized pruritus uwashwa mwili mzina yes □ no □ 11. itchy scalp Kitchwa chako kina uwashwa? yes □ no □ 12. others: vitu vingine: CATEGORIZE! 1. coughing kuhoa 2. NO other complains
3. NA 4. DNK 5. wounds kidonda 6. abdominal problems tumbo 7. back hurts 8. pain in different body parts after
having played football/ shamba work etc. 9. eye problem 10. ear problem 11. itching 12. running nose
16. Have you received any treatment for your main skin problem? Je umetumia dawa yoyote kutibu tatizo hili? yes □ no □ 17. If yes: which kind of treatment? Kama ndiyo: ni dawa gani? 1. crème krimu yes □ no □
2. tablets vidonge yes □ no □ 3. injection sindano yes □ no □ 4. leaves majani yes □ no □ 5. roots mizizi yes □ no □ 6. charm kombe yes □ no □ 7. necklace hirizi yes □ no □ 8. Name of the drug: Jina la dawa: CATEGORIZE!
1. traditional medicine
2. NO name given 3. NA
4. DNK 5. Panadol 6. Aspirin 7. breaking fluid 8. mafuta (Vaseline/ Oil) 9. Gentian Violet 10. ointment
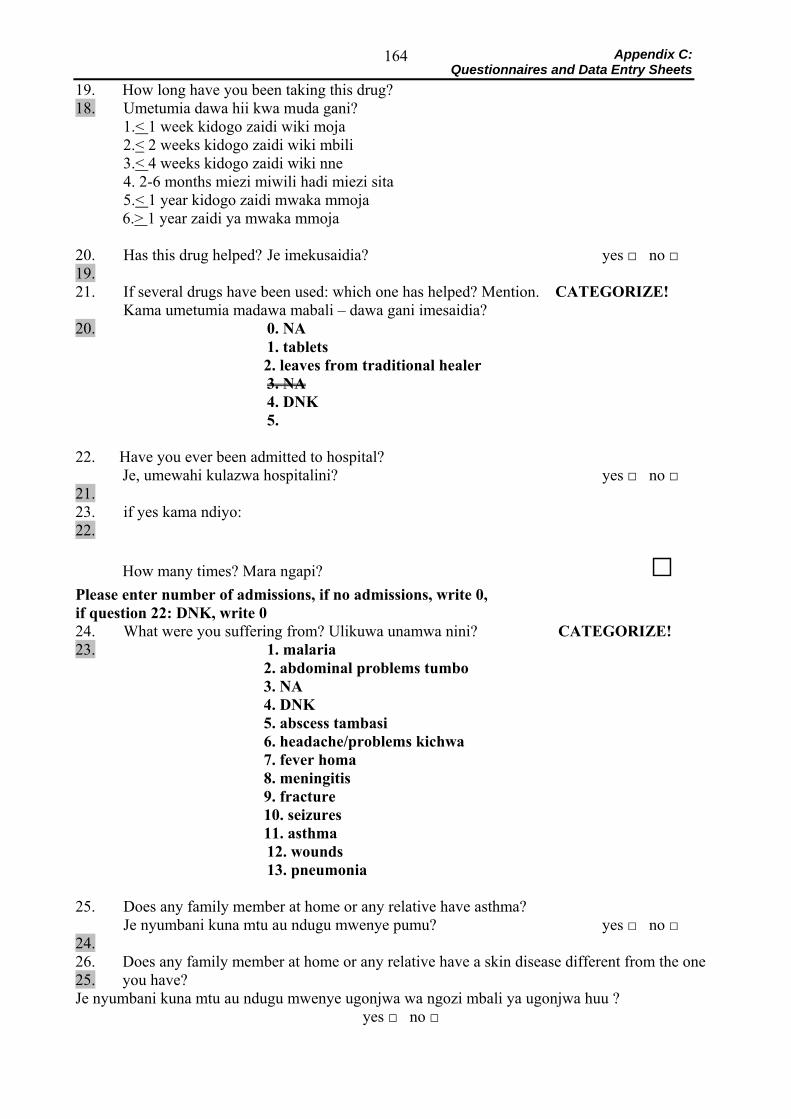
Appendix C: Questionnaires and Data Entry Sheets
164
19. How long have you been taking this drug? 18. Umetumia dawa hii kwa muda gani? 1.< 1 week kidogo zaidi wiki moja 2.< 2 weeks kidogo zaidi wiki mbili 3.< 4 weeks kidogo zaidi wiki nne 4. 2-6 months miezi miwili hadi miezi sita 5.< 1 year kidogo zaidi mwaka mmoja
6.> 1 year zaidi ya mwaka mmoja 20. Has this drug helped? Je imekusaidia? yes □ no □ 19. 21. If several drugs have been used: which one has helped? Mention. CATEGORIZE! Kama umetumia madawa mabali – dawa gani imesaidia? 20. 0. NA 1. tablets
2. leaves from traditional healer 3. NA
4. DNK 5.
22. Have you ever been admitted to hospital?
Je, umewahi kulazwa hospitalini? yes □ no □ 21. 23. if yes kama ndiyo: 22.
How many times? Mara ngapi? □ Please enter number of admissions, if no admissions, write 0, if question 22: DNK, write 0 24. What were you suffering from? Ulikuwa unamwa nini? CATEGORIZE! 23. 1. malaria
2. abdominal problems tumbo 3. NA 4. DNK 5. abscess tambasi 6. headache/problems kichwa 7. fever homa 8. meningitis 9. fracture 10. seizures 11. asthma
12. wounds 13. pneumonia
25. Does any family member at home or any relative have asthma? Je nyumbani kuna mtu au ndugu mwenye pumu? yes □ no □ 24. 26. Does any family member at home or any relative have a skin disease different from the one 25. you have? Je nyumbani kuna mtu au ndugu mwenye ugonjwa wa ngozi mbali ya ugonjwa huu ?
yes □ no □
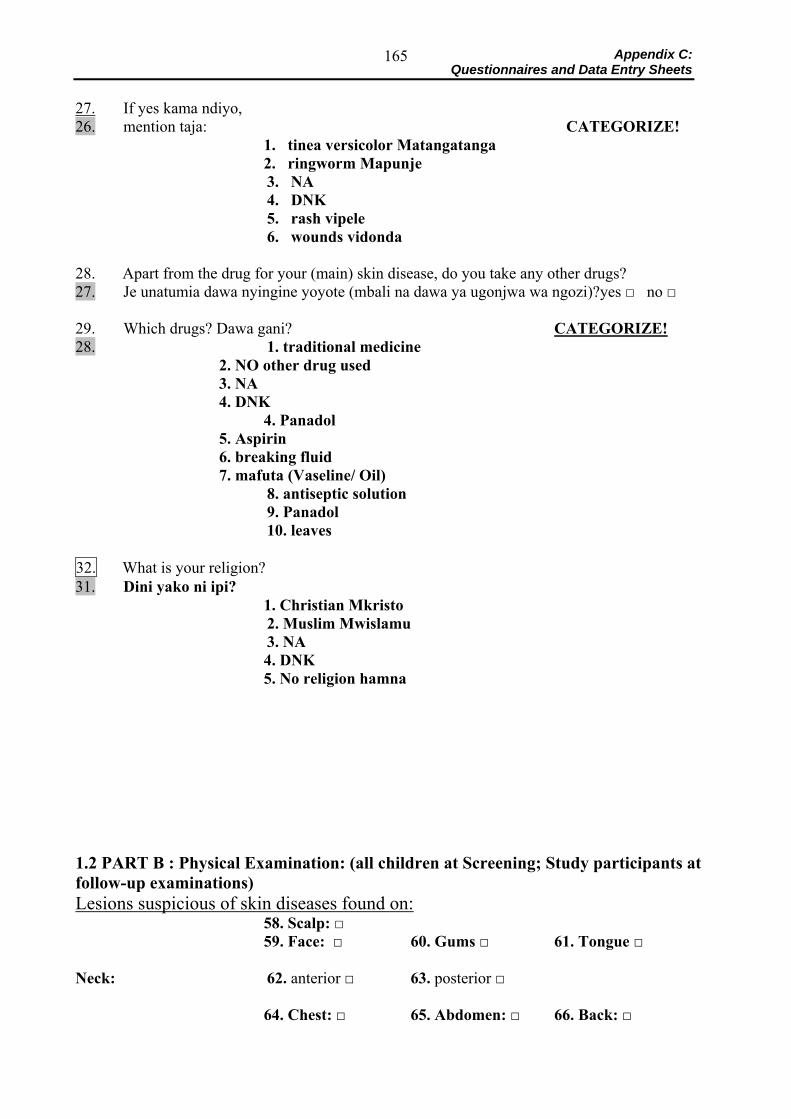
Appendix C: Questionnaires and Data Entry Sheets
165
27. If yes kama ndiyo, 26. mention taja: CATEGORIZE!
1. tinea versicolor Matangatanga 2. ringworm Mapunje
3. NA 4. DNK 5. rash vipele 6. wounds vidonda 28. Apart from the drug for your (main) skin disease, do you take any other drugs? 27. Je unatumia dawa nyingine yoyote (mbali na dawa ya ugonjwa wa ngozi)?yes □ no □ 29. Which drugs? Dawa gani? CATEGORIZE! 28. 1. traditional medicine
2. NO other drug used 3. NA 4. DNK
4. Panadol 5. Aspirin 6. breaking fluid 7. mafuta (Vaseline/ Oil)
8. antiseptic solution 9. Panadol 10. leaves
32. What is your religion? 31. Dini yako ni ipi?
1. Christian Mkristo 2. Muslim Mwislamu 3. NA
4. DNK 5. No religion hamna
1.2 PART B : Physical Examination: (all children at Screening; Study participants at follow-up examinations) Lesions suspicious of skin diseases found on:
58. Scalp: □ 59. Face: □ 60. Gums □ 61. Tongue □
Neck: 62. anterior □ 63. posterior □
64. Chest: □ 65. Abdomen: □ 66. Back: □
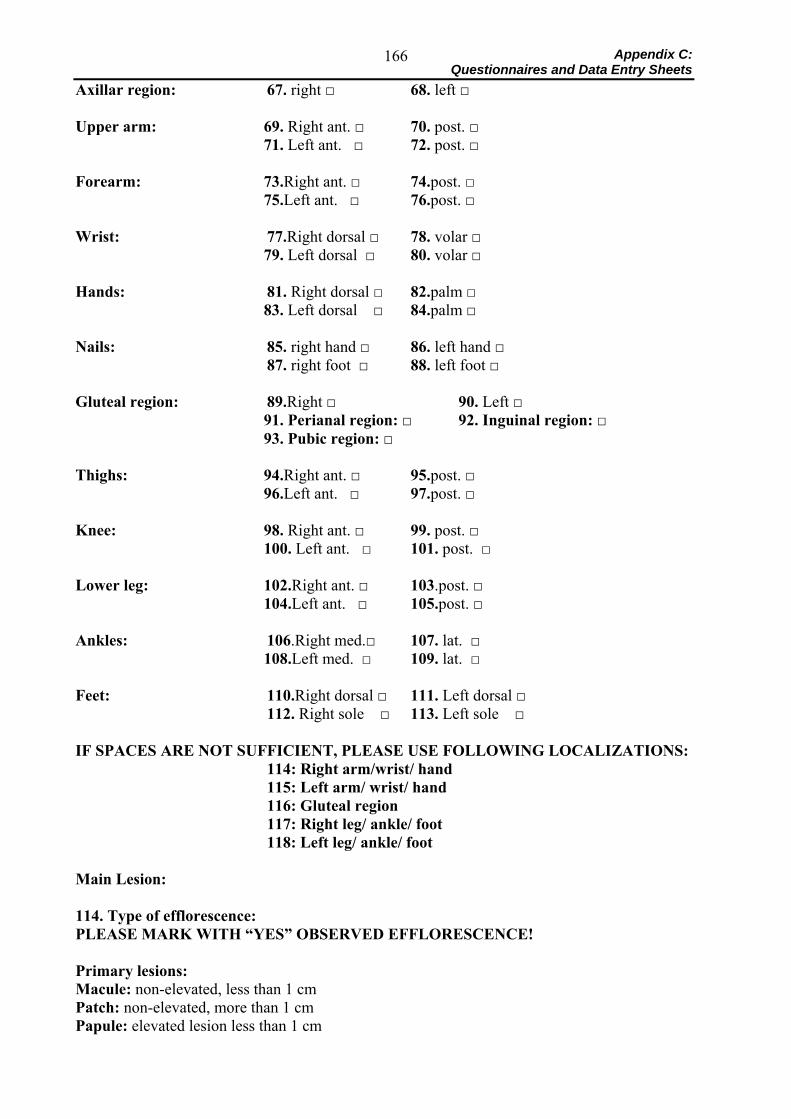
Appendix C: Questionnaires and Data Entry Sheets
166
Axillar region: 67. right □ 68. left □ Upper arm: 69. Right ant. □ 70. post. □
71. Left ant. □ 72. post. □ Forearm: 73.Right ant. □ 74.post. □
75.Left ant. □ 76.post. □ Wrist: 77.Right dorsal □ 78. volar □
79. Left dorsal □ 80. volar □ Hands: 81. Right dorsal □ 82.palm □
83. Left dorsal □ 84.palm □ Nails: 85. right hand □ 86. left hand □ 87. right foot □ 88. left foot □ Gluteal region: 89.Right □ 90. Left □
91. Perianal region: □ 92. Inguinal region: □ 93. Pubic region: □
Thighs: 94.Right ant. □ 95.post. □
96.Left ant. □ 97.post. □ Knee: 98. Right ant. □ 99. post. □
100. Left ant. □ 101. post. □ Lower leg: 102.Right ant. □ 103.post. □
104.Left ant. □ 105.post. □ Ankles: 106.Right med.□ 107. lat. □
108.Left med. □ 109. lat. □ Feet: 110.Right dorsal □ 111. Left dorsal □ 112. Right sole □ 113. Left sole □ IF SPACES ARE NOT SUFFICIENT, PLEASE USE FOLLOWING LOCALIZATIONS: 114: Right arm/wrist/ hand 115: Left arm/ wrist/ hand 116: Gluteal region 117: Right leg/ ankle/ foot 118: Left leg/ ankle/ foot Main Lesion: 114. Type of efflorescence: PLEASE MARK WITH “YES” OBSERVED EFFLORESCENCE! Primary lesions: Macule: non-elevated, less than 1 cm Patch: non-elevated, more than 1 cm Papule: elevated lesion less than 1 cm
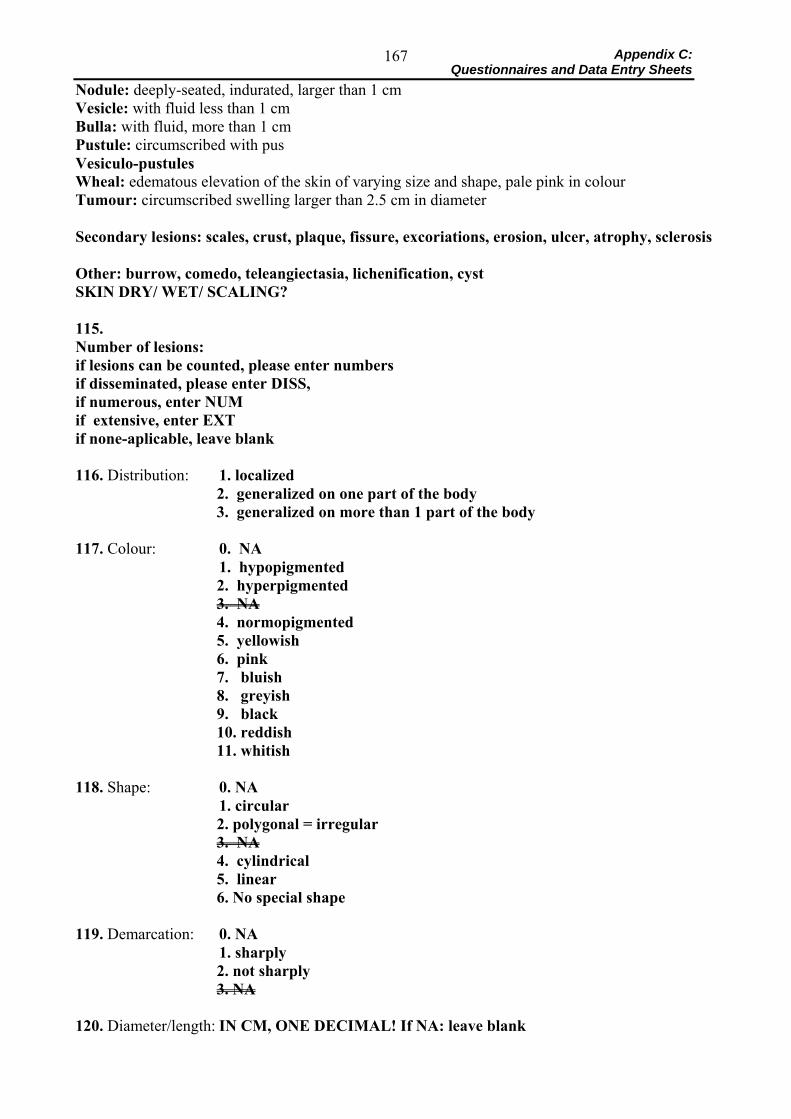
Appendix C: Questionnaires and Data Entry Sheets
167
Nodule: deeply-seated, indurated, larger than 1 cm Vesicle: with fluid less than 1 cm Bulla: with fluid, more than 1 cm Pustule: circumscribed with pus Vesiculo-pustules Wheal: edematous elevation of the skin of varying size and shape, pale pink in colour Tumour: circumscribed swelling larger than 2.5 cm in diameter Secondary lesions: scales, crust, plaque, fissure, excoriations, erosion, ulcer, atrophy, sclerosis Other: burrow, comedo, teleangiectasia, lichenification, cyst SKIN DRY/ WET/ SCALING? 115. Number of lesions: if lesions can be counted, please enter numbers if disseminated, please enter DISS, if numerous, enter NUM if extensive, enter EXT if none-aplicable, leave blank 116. Distribution: 1. localized
2. generalized on one part of the body 3. generalized on more than 1 part of the body
117. Colour: 0. NA 1. hypopigmented
2. hyperpigmented 3. NA 4. normopigmented 5. yellowish 6. pink 7. bluish 8. greyish 9. black 10. reddish 11. whitish
118. Shape: 0. NA 1. circular
2. polygonal = irregular 3. NA 4. cylindrical 5. linear 6. No special shape
119. Demarcation: 0. NA 1. sharply
2. not sharply 3. NA
120. Diameter/length: IN CM, ONE DECIMAL! If NA: leave blank
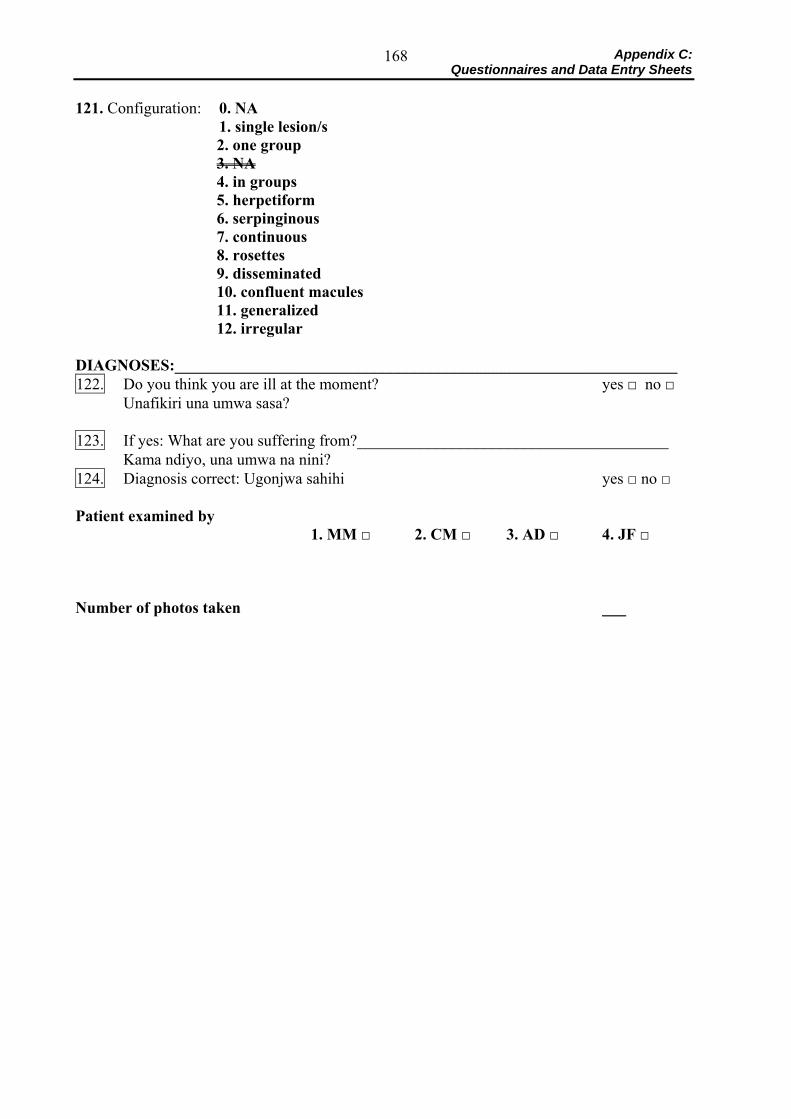
Appendix C: Questionnaires and Data Entry Sheets
168
121. Configuration: 0. NA 1. single lesion/s
2. one group 3. NA 4. in groups 5. herpetiform 6. serpinginous 7. continuous 8. rosettes 9. disseminated 10. confluent macules 11. generalized 12. irregular
DIAGNOSES:_______________________________________________________________ 122. Do you think you are ill at the moment? yes □ no □ Unafikiri una umwa sasa? 123. If yes: What are you suffering from?_______________________________________ Kama ndiyo, una umwa na nini? 124. Diagnosis correct: Ugonjwa sahihi yes □ no □ Patient examined by
1. MM □ 2. CM □ 3. AD □ 4. JF □ Number of photos taken ___
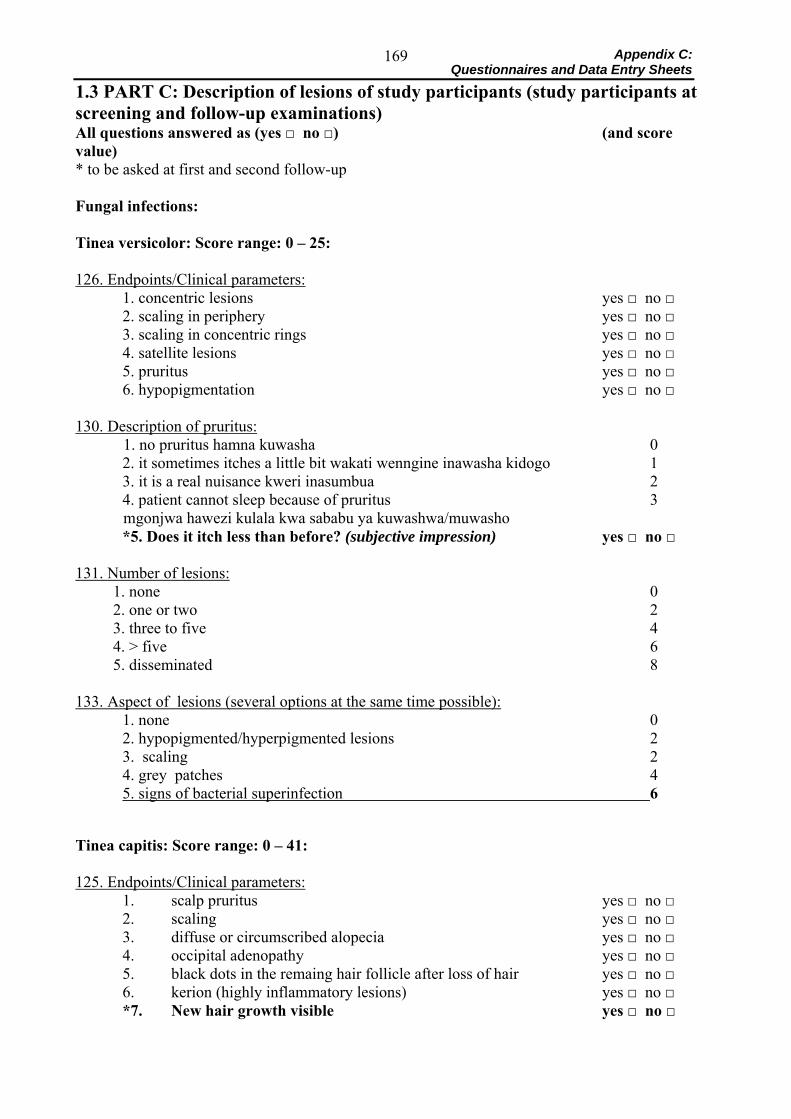
Appendix C: Questionnaires and Data Entry Sheets
169
1.3 PART C: Description of lesions of study participants (study participants at screening and follow-up examinations) All questions answered as (yes □ no □) (and score value) * to be asked at first and second follow-up Fungal infections: Tinea versicolor: Score range: 0 – 25: 126. Endpoints/Clinical parameters:
1. concentric lesions yes □ no □ 2. scaling in periphery yes □ no □ 3. scaling in concentric rings yes □ no □ 4. satellite lesions yes □ no □ 5. pruritus yes □ no □ 6. hypopigmentation yes □ no □
130. Description of pruritus: 1. no pruritus hamna kuwasha 0
2. it sometimes itches a little bit wakati wenngine inawasha kidogo 1 3. it is a real nuisance kweri inasumbua 2 4. patient cannot sleep because of pruritus 3
mgonjwa hawezi kulala kwa sababu ya kuwashwa/muwasho *5. Does it itch less than before? (subjective impression) yes □ no □
131. Number of lesions:
1. none 0 2. one or two 2 3. three to five 4 4. > five 6 5. disseminated 8
133. Aspect of lesions (several options at the same time possible): 1. none 0 2. hypopigmented/hyperpigmented lesions 2 3. scaling 2 4. grey patches 4 5. signs of bacterial superinfection 6
Tinea capitis: Score range: 0 – 41: 125. Endpoints/Clinical parameters:
1. scalp pruritus yes □ no □ 2. scaling yes □ no □ 3. diffuse or circumscribed alopecia yes □ no □ 4. occipital adenopathy yes □ no □ 5. black dots in the remaing hair follicle after loss of hair yes □ no □ 6. kerion (highly inflammatory lesions) yes □ no □ *7. New hair growth visible yes □ no □
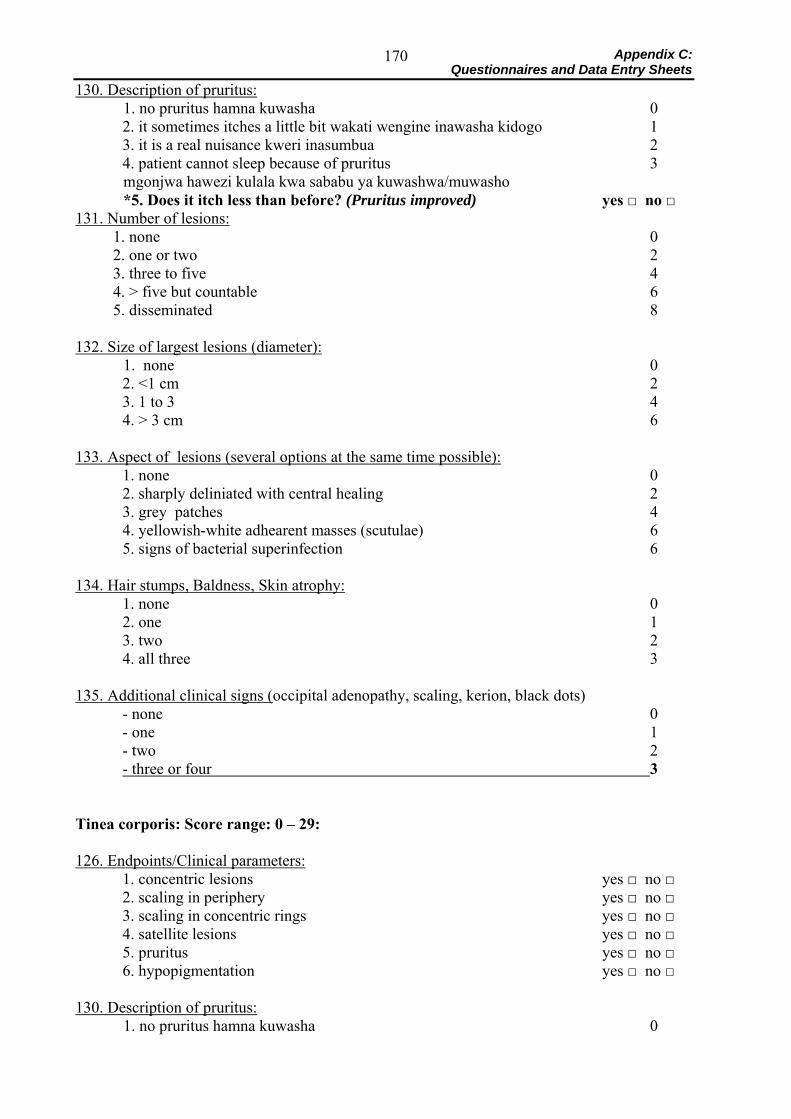
Appendix C: Questionnaires and Data Entry Sheets
170
130. Description of pruritus: 1. no pruritus hamna kuwasha 0
2. it sometimes itches a little bit wakati wengine inawasha kidogo 1 3. it is a real nuisance kweri inasumbua 2 4. patient cannot sleep because of pruritus 3
mgonjwa hawezi kulala kwa sababu ya kuwashwa/muwasho *5. Does it itch less than before? (Pruritus improved) yes □ no □ 131. Number of lesions:
1. none 0 2. one or two 2 3. three to five 4 4. > five but countable 6 5. disseminated 8
132. Size of largest lesions (diameter): 1. none 0
2. <1 cm 2 3. 1 to 3 4 4. > 3 cm 6
133. Aspect of lesions (several options at the same time possible): 1. none 0 2. sharply deliniated with central healing 2 3. grey patches 4 4. yellowish-white adhearent masses (scutulae) 6 5. signs of bacterial superinfection 6
134. Hair stumps, Baldness, Skin atrophy: 1. none 0 2. one 1 3. two 2 4. all three 3
135. Additional clinical signs (occipital adenopathy, scaling, kerion, black dots)
- none 0 - one 1 - two 2 - three or four 3
Tinea corporis: Score range: 0 – 29: 126. Endpoints/Clinical parameters:
1. concentric lesions yes □ no □ 2. scaling in periphery yes □ no □ 3. scaling in concentric rings yes □ no □ 4. satellite lesions yes □ no □ 5. pruritus yes □ no □ 6. hypopigmentation yes □ no □
130. Description of pruritus: 1. no pruritus hamna kuwasha 0
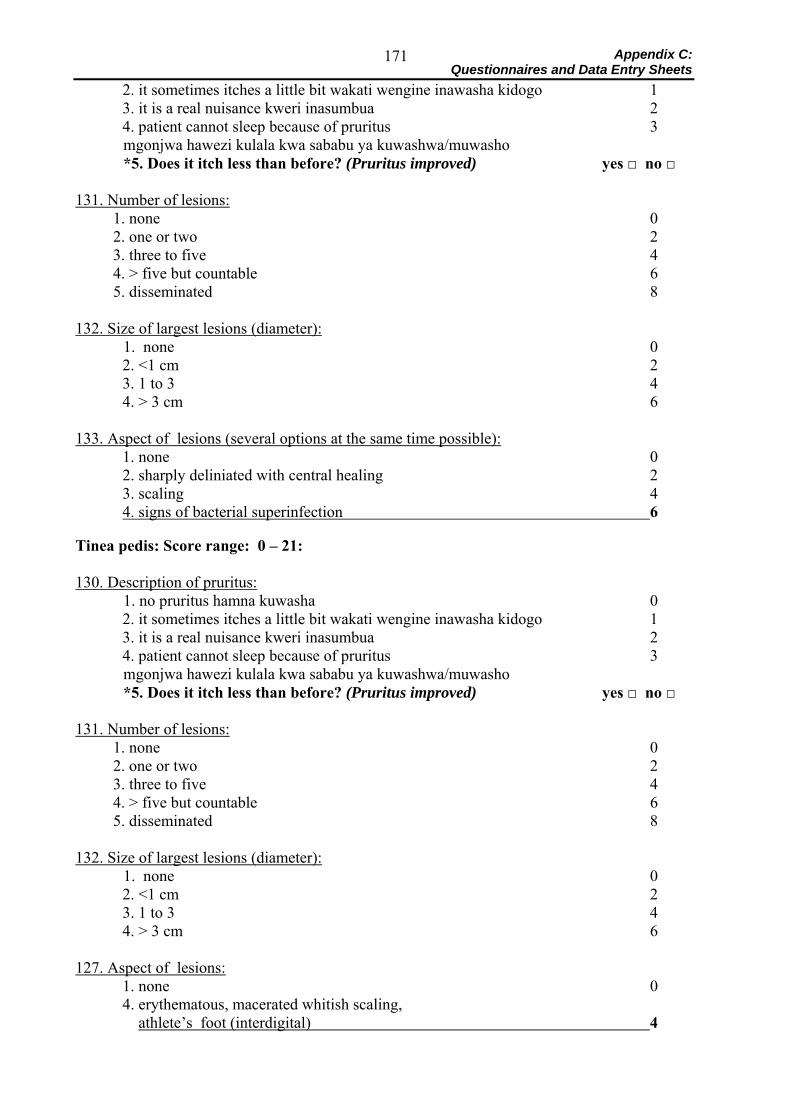
Appendix C: Questionnaires and Data Entry Sheets
171
2. it sometimes itches a little bit wakati wengine inawasha kidogo 1 3. it is a real nuisance kweri inasumbua 2 4. patient cannot sleep because of pruritus 3
mgonjwa hawezi kulala kwa sababu ya kuwashwa/muwasho *5. Does it itch less than before? (Pruritus improved) yes □ no □ 131. Number of lesions:
1. none 0 2. one or two 2 3. three to five 4 4. > five but countable 6 5. disseminated 8
132. Size of largest lesions (diameter): 1. none 0
2. <1 cm 2 3. 1 to 3 4 4. > 3 cm 6
133. Aspect of lesions (several options at the same time possible): 1. none 0 2. sharply deliniated with central healing 2 3. scaling 4 4. signs of bacterial superinfection 6
Tinea pedis: Score range: 0 – 21: 130. Description of pruritus: 1. no pruritus hamna kuwasha 0
2. it sometimes itches a little bit wakati wengine inawasha kidogo 1 3. it is a real nuisance kweri inasumbua 2 4. patient cannot sleep because of pruritus 3
mgonjwa hawezi kulala kwa sababu ya kuwashwa/muwasho *5. Does it itch less than before? (Pruritus improved) yes □ no □ 131. Number of lesions:
1. none 0 2. one or two 2 3. three to five 4 4. > five but countable 6 5. disseminated 8
132. Size of largest lesions (diameter): 1. none 0
2. <1 cm 2 3. 1 to 3 4 4. > 3 cm 6
127. Aspect of lesions: 1. none 0 4. erythematous, macerated whitish scaling, athlete’s foot (interdigital) 4
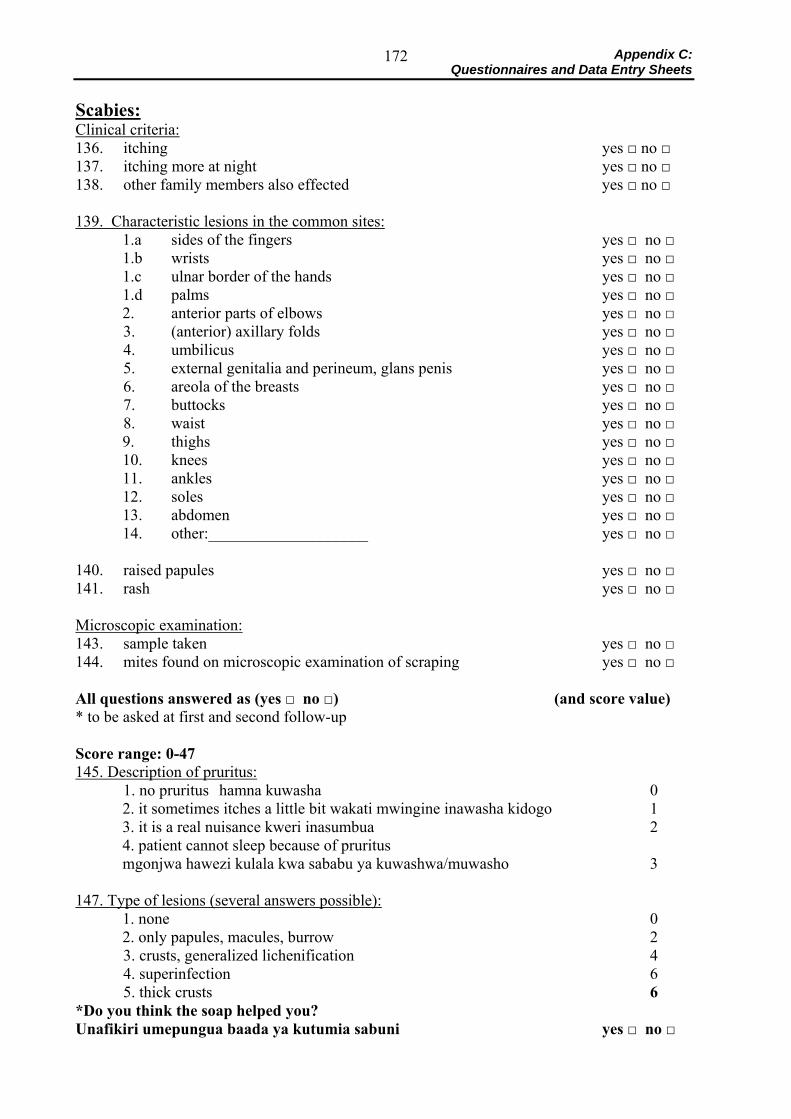
Appendix C: Questionnaires and Data Entry Sheets
172
Scabies: Clinical criteria: 136. itching yes □ no □ 137. itching more at night yes □ no □ 138. other family members also effected yes □ no □ 139. Characteristic lesions in the common sites:
1.a sides of the fingers yes □ no □ 1.b wrists yes □ no □ 1.c ulnar border of the hands yes □ no □ 1.d palms yes □ no □ 2. anterior parts of elbows yes □ no □
3. (anterior) axillary folds yes □ no □ 4. umbilicus yes □ no □ 5. external genitalia and perineum, glans penis yes □ no □ 6. areola of the breasts yes □ no □ 7. buttocks yes □ no □ 8. waist yes □ no □
9. thighs yes □ no □ 10. knees yes □ no □ 11. ankles yes □ no □ 12. soles yes □ no □ 13. abdomen yes □ no □ 14. other:____________________ yes □ no □
140. raised papules yes □ no □ 141. rash yes □ no □ Microscopic examination: 143. sample taken yes □ no □ 144. mites found on microscopic examination of scraping yes □ no □ All questions answered as (yes □ no □) (and score value) * to be asked at first and second follow-up Score range: 0-47 145. Description of pruritus: 1. no pruritus hamna kuwasha 0
2. it sometimes itches a little bit wakati mwingine inawasha kidogo 1 3. it is a real nuisance kweri inasumbua 2 4. patient cannot sleep because of pruritus mgonjwa hawezi kulala kwa sababu ya kuwashwa/muwasho 3
147. Type of lesions (several answers possible): 1. none 0 2. only papules, macules, burrow 2
3. crusts, generalized lichenification 4 4. superinfection 6 5. thick crusts 6 *Do you think the soap helped you? Unafikiri umepungua baada ya kutumia sabuni yes □ no □
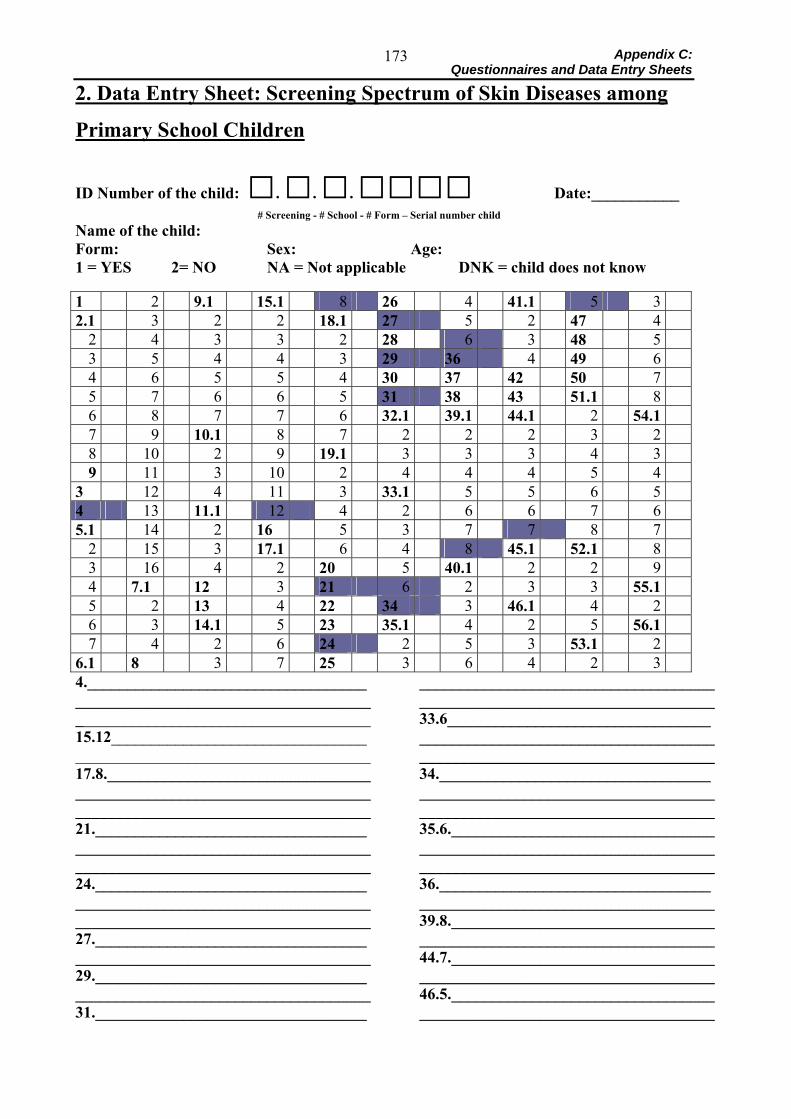
Appendix C: Questionnaires and Data Entry Sheets
173
2. Data Entry Sheet: Screening Spectrum of Skin Diseases among
Primary School Children
ID Number of the child: □. □. □. □□□□ Date:___________ # Screening - # School - # Form – Serial number child Name of the child: Form: Sex: Age: 1 = YES 2= NO NA = Not applicable DNK = child does not know 1 2 9.1 15.1 8 26 4 41.1 5 3 2.1 3 2 2 18.1 27 5 2 47 4
2 4 3 3 2 28 6 3 48 5 3 5 4 4 3 29 36 4 49 6 4 6 5 5 4 30 37 42 50 7 5 7 6 6 5 31 38 43 51.1 8 6 8 7 7 6 32.1 39.1 44.1 2 54.1 7 9 10.1 8 7 2 2 2 3 2 8 10 2 9 19.1 3 3 3 4 3 9 11 3 10 2 4 4 4 5 4
3 12 4 11 3 33.1 5 5 6 5 4 13 11.1 12 4 2 6 6 7 6 5.1 14 2 16 5 3 7 7 8 7
2 15 3 17.1 6 4 8 45.1 52.1 8 3 16 4 2 20 5 40.1 2 2 9 4 7.1 12 3 21 6 2 3 3 55.1 5 2 13 4 22 34 3 46.1 4 2 6 3 14.1 5 23 35.1 4 2 5 56.1 7 4 2 6 24 2 5 3 53.1 2
6.1 8 3 7 25 3 6 4 2 3 4._____________________________________________________________________________________________________________ 15.12_____________________________________________________________________ 17.8.______________________________________________________________________ _____________________________________ 21._______________________________________________________________________ _____________________________________ 24.____________________________________________________________________________________________________________ 27._______________________________________________________________________ 29._______________________________________________________________________ 31.__________________________________
_____________________________________ _____________________________________ 33.6___________________________________________________________________________________________________________ 34.____________________________________________________________________________________________________________35.6.___________________________________________________________________________________________________________36._______________________________________________________________________39.8.______________________________________________________________________44.7.______________________________________________________________________ 46.5.______________________________________________________________________
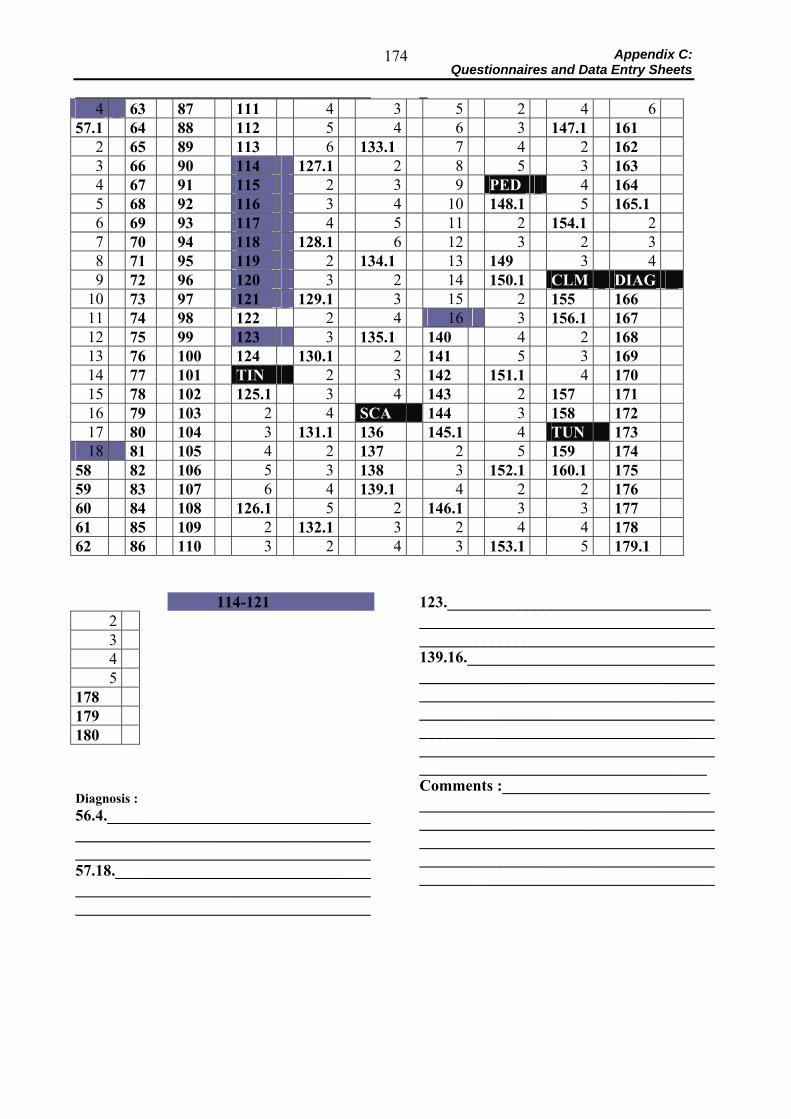
Appendix C: Questionnaires and Data Entry Sheets
174
_____________________________________ _ 4 63 87 111 4 3 5 2 4 6
57.1 64 88 112 5 4 6 3 147.1 161 2 65 89 113 6 133.1 7 4 2 162 3 66 90 114 127.1 2 8 5 3 163 4 67 91 115 2 3 9 PED 4 164 5 68 92 116 3 4 10 148.1 5 165.1 6 69 93 117 4 5 11 2 154.1 2 7 70 94 118 128.1 6 12 3 2 3 8 71 95 119 2 134.1 13 149 3 4 9 72 96 120 3 2 14 150.1 CLM DIAG
10 73 97 121 129.1 3 15 2 155 166 11 74 98 122 2 4 16 3 156.1 167 12 75 99 123 3 135.1 140 4 2 168 13 76 100 124 130.1 2 141 5 3 169 14 77 101 TIN 2 3 142 151.1 4 170 15 78 102 125.1 3 4 143 2 157 171 16 79 103 2 4 SCA 144 3 158 172 17 80 104 3 131.1 136 145.1 4 TUN 173 18 81 105 4 2 137 2 5 159 174
58 82 106 5 3 138 3 152.1 160.1 175 59 83 107 6 4 139.1 4 2 2 176 60 84 108 126.1 5 2 146.1 3 3 177 61 85 109 2 132.1 3 2 4 4 178 62 86 110 3 2 4 3 153.1 5 179.1
114-121
2 3 4 5
178 179 180 Diagnosis : 56.4.___________________________________________________________________________________________________________57.18.__________________________________________________________________________________________________________
123.___________________________________________________________________________________________________________139.16.____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Comments :___________________________________________________________________________________________________________________________________________________________________________________________________________________
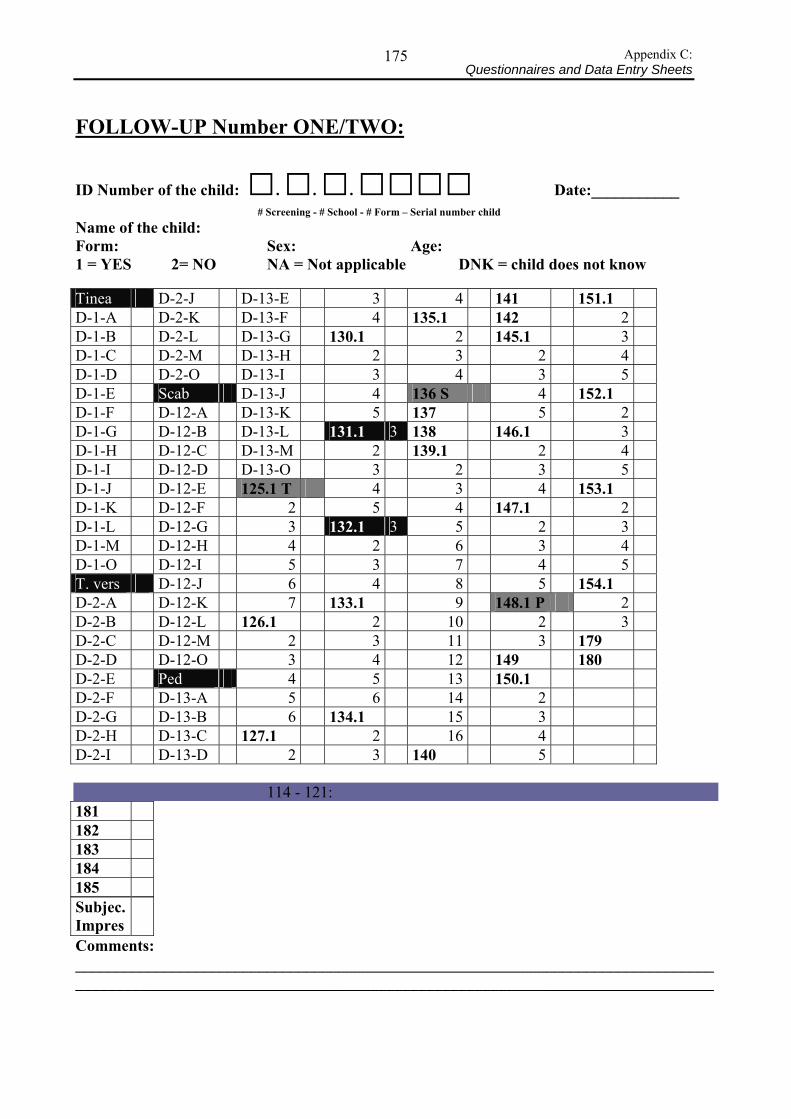
Appendix C: Questionnaires and Data Entry Sheets
175
FOLLOW-UP Number ONE/TWO:
ID Number of the child: □. □. □. □□□□ Date:___________ # Screening - # School - # Form – Serial number child Name of the child: Form: Sex: Age: 1 = YES 2= NO NA = Not applicable DNK = child does not know Tinea D-2-J D-13-E 3 4 141 151.1 D-1-A D-2-K D-13-F 4 135.1 142 2 D-1-B D-2-L D-13-G 130.1 2 145.1 3 D-1-C D-2-M D-13-H 2 3 2 4 D-1-D D-2-O D-13-I 3 4 3 5 D-1-E Scab D-13-J 4 136 S 4 152.1 D-1-F D-12-A D-13-K 5 137 5 2 D-1-G D-12-B D-13-L 131.1 3 138 146.1 3 D-1-H D-12-C D-13-M 2 139.1 2 4 D-1-I D-12-D D-13-O 3 2 3 5 D-1-J D-12-E 125.1 T 4 3 4 153.1 D-1-K D-12-F 2 5 4 147.1 2 D-1-L D-12-G 3 132.1 3 5 2 3 D-1-M D-12-H 4 2 6 3 4 D-1-O D-12-I 5 3 7 4 5 T. vers D-12-J 6 4 8 5 154.1 D-2-A D-12-K 7 133.1 9 148.1 P 2 D-2-B D-12-L 126.1 2 10 2 3 D-2-C D-12-M 2 3 11 3 179 D-2-D D-12-O 3 4 12 149 180 D-2-E Ped 4 5 13 150.1 D-2-F D-13-A 5 6 14 2 D-2-G D-13-B 6 134.1 15 3 D-2-H D-13-C 127.1 2 16 4 D-2-I D-13-D 2 3 140 5 114 - 121: 181 182 183 184 185 Subjec. Impres
Comments: ________________________________________________________________________________________________________________________________________________________________
Appendix D: Information for the study participants and parents 176
Appendix D: 1. Informed Consent 1.1 English version: Invitation for parents, addressed to Local Leaders (“Balozi”) Dear Balozi Leaders, My name is Almuth Dinkela, I am a medical student sent to Ifakara by the Swiss Tropical Institute in Basel (Switzerland). I am working for IHRDC here in Ifakara in order to do my Medical Doctor research project in Kilombero District. I am interested in two skin diseases that are a very common problem in this area: Ringworm and scabies. Together with the specialist of dermatology at St. Francis Designated District Hospital, SFDDH, Dr. M. Mbata, Dr. Charles Maswi and Julia Ferié, I examined all the children attending Lihami Primary School to find out which skin diseases they are suffering from. We have identified those who have fungal infections and scabies to take part in my study. On Monday, May 12th 2003, a meeting will we held at Lihami Primary School (Michenga Primary School). We would like to invite you and all the parents of these children to attend the meeting at -_____________. The parents will have the chance to ask questions about the study and will be asked for their permission to let their children participate. We would be very happy if you could inform the parents about this meeting. Thank you very much for your co-operation! Almuth Dinkela
Appendix D: Information for the study participants and parents 177
Kiswahili versicon: Invitation for parents, addressed to Local Leaders (“Balozi”):
Ndugu balozi, Mimi naitwa Almuth Dinkela. Mimi ni daktari mwanafunzi, nimekuja Ifakara kwa niaba ya kituo cha utafiti wa magonjwa katika nchi za joto cha uswisi, kilichopo Basel uswisi. Kwa hapa Ifakara nafanya kazi kituo cha utafiti wa magonjwa ya binadamu (IHRDC) ikiwa ni utafiti katika kufanikisha shahada yangu ya udaktari. Ninaangalia magonjwa mawili ya ngozi ambayo yameenea sana katika eneo hili, nayo ni mapunye/matangatanga na upele. Kwa kushirikiana na mtaalamu wa magonjwa ya ngozi toka hospitali ya mtakatifu Francis, Dr M. Mbata, na Charles Maswi na Julia Ferie, tumewapima watoto wote wanaosoma shule ya msingi Lihami ili kuona ni ugonjwa gani wa ngozi wanooumwa. Tumewatambua wale wenye mapunye/matangatanga na upele ambao ndio watakaoshiriki kwenye utafiti wangu. Jumanne tarehe 13/05/2003 kutakuwa na mkutano Lihami shuleni. Tunapenda kuwaalika wazazi wa watoto hawa kuhudhuria mkutanoni saa ___________. Wazazi watapewa fursa yakuuliza maswali yanayohusiana na utafiti huu, na tatawataka ruhusa ili watoto wao waweze kushiriki. Itakuwa ni furaha yetu kubwa kama utawataarifu iliwaweze kuhudhuria mkutanoni. Tunashukuru sana kwa ushirikiano wako. Almuth Dinkela
Appendix D: Information for the study participants and parents 178
2. Information for the Parents – provided at school meeting: 2.1 English version: Dear Parents, My name is Almuth Dinkela, I am a medical student sent to Ifakara by the Swiss Tropical Institute in Basel (Switzerland). I am working for IHRDC here in Ifakara in order to do my Medical Doctor research project in Kilombero District. I am interested in two skin diseases that are a very common problem in this area: Ringworm and scabies. Together with the specialist of dermatology at St. Francis Designated District Hospital, SFDDH, Dr. M. Mbata, Dr. Charles Maswi and Julia Ferié, I examined all the children attending Lihami Primary School. We found out that your child________________________________________________ is suffering from Ringworm/Scabies. Therefore he/she has been identified to take part in my study. What I am trying to find out: I would like to find out if regular body washing with soap can cure and prevent Fungal infetions/Scabies. There are two kinds of soap that I will be using. I would like to find out which of the two soap its more effective. One is a normal soap for washing the body, the other one contains an additional substance, called Triclosan. This drug has been used with great success in industrialised countries for more than 25 years to prevent and treat many skin diseases. The soap will contain it in the same concentration (1%) as soaps that are sold in the United States of America and Europe. What will happen during the study: The study will last for 2 months. During these 2 months your child will receive its soap for free. This soap has been produced in Switzerland for this study. Until the end of the 2 months you and I will not know which type of soap he/she has received because the two types of soap look the same. I will visit the school every week and distribute new soap bars. Your child can only receive a new bar, if he/she brings the remaining piece of the previous one back to school. If your child does not use the soap at least once per day, he/she will not receive any more bars. I will examine your child again after one month and after two months. If the skin disease of your child could not be cured by the soap, your child will receive free treatment of the skin disease at SFDDH. How your child has to use the soap: Your child has to use the soap every day. It must be used for washing the body only. All the body parts should be covered with foam, especially the parts where the skin is affected by the skin disease. The foam should be rinsed off with clear water afterwards. Eye contact with the soap or the foam should be avoided to prevent irritation. What is important for the child’s well-being:
• Triclosan has never had any severe or toxic side effects • If for some reason your child does not tolerate the soap, he/she does not have to use it any
longer and will be referred to SFDDH for treatment .Agreeing to participate in this study: It is entirely your choice whether you let the child participate in this study or not. A decision not to let him/her participate will not affect your rights to treatment at SFDDH. We will respect your decision. If you choose to let your child participate in the study, all the information collected in this study will remain confidential and will be used for research purposes only. Whenever you have questions about the study please contact any of the persons mentioned above or Dr. Boniphace Idindili from IHRDC.´ Thank you for your time and co-operation!
Appendix D: Information for the study participants and parents 179
2.2 Kiswahili version: Taarifa kwa wazazi Wazazi wapendwa, Mimi naitwa Almuth Dinkela. Mimi ni daktari mwanafunzi, nimekuja Ifakara kwa niaba ya kituo cha utafiti wa magonjwa katika nchi za joto cha uswisi, kilichopo Basel uswisi.Kwa hapa Ifakara nafanya kazi kituo cha utafiti wa magonjwa ya binadamu (IHRDC) ikiwa ni utafiti katika kufanikisha shahada yangu ya udaktari. Ninaangalia magonjwa mawili ya ngoziambayo yameenea sana ktika eneo hili, nayo ni mapunye/matangatanga na upele. Kwa kushirikiana na mtaalamu wa magonjwa ya ngozi toka hospitali ya mtakatifu Francis, Dr M. Mbata, Charles Maswi na Julia Ferie , tumewapima watoto wote wanaosoma shule ya msingi Lihami. Tumegundua kuwa watoto _____________________________________________________ wanaumwa upele. Kwa hiyo atakuwa mshiriki katika mradi huu. Ninachokiangalia: Ninajaribu kuangalia kama kuoga mwili kwa sabuni wakati wote kunaweza kutibu na kukinga upele. Kuna aina mbili za sabuni nitakazotumia. Ninataka kuangalia ni aina ipi ya sabuni kati ya hizo inasaidia zaidi. Ya kwamza ni sabuni ya kawaida ya kuogea, na nyingine ni sabuni iliyoongezwa dawa maalum inayoitwa Triclosan. Dawa hii imekuwa ikitumiwa kwa mafanikio makubwa katika nchi zilizoendelea kwa zaidi ya miaka 25 kutibu na kukinga magonjwa ya ngozi. Sabuni hii ina kiwango sawa cha 1%, kama sabuni zinazotumika marekani na ulaya. Kitakachofanyika katika utafiti huu: Utafiti huu utadumu kwa miezi miwili. Katika miezi hiyo watoto watapewa sabuni bure. Sabuni hizi zimetoka Uswiwi kwa ajili ya utafiti huu. Mwishoni mwa miezi hii miwili wewe na mimi hatutakuwa tukijua mtoto amepata aina ipi ya sabuni kwa maana sabuni zote mbili zinafanana. Nitatembelea shuleni kila wiki na kugawa sabuni mpya. Mtoto atapata sabuni mpya pale atakapoleta kipande cha sabuni iliyoisha shuleni. Kama mtoto atakuwa hatumii sabuni angalau mara moja kila siku , hatapewa sabuni nyingine. Nitampima tena mtoto baada ya mwezi mmoja na miwili. Kama uganjwa wake wa ngozi haujapona kwa sabuni, atatibiwa ugonjwa huo hospitalini St Francis bure. Namna mtoto atakavyotumia sabuni: Mtoto antakiwa kutumia sabuni yake kila siku. Itatumika kwa kuogea tu. Mwili mzima unatakiwa kupakwa sabuni na zaidi sehemu yenye ugonjwa wa ngozi. Povu la sabuni lapashwa kuondolewa kwa kuoga maji safi. Inabidi kujihadhari povu la sabuni lisiingie machoni ili kuepuka kuwashwa. Mambo muhimu katika afya ya mtoto.
• Triclosan hijawahi kuonyesha madhara yoyote. • Kama kwa sababu yoyote ile mtoto akiwa hapatani na sabuni hiyo anatakiwa kuiacha na
atapelekwa hospitalini kwa matibabu. Kukubali kushiriki kwenye utafiti: Una hiari ya kumruhusu mtoto kushiriki katika utafiti huu au la. Uamuzi wa kutomruhusu kushiriki kwenye utafiti huu hautamnyima haki yake ya kutibiwa hospitalini. Kama utamruhusu mtoto kushiriki kwenye utafiti huu, habari zote zitakazopatikana kwenye utafiti huu zitabaki kuwa siri na zitatumika kwa ajili ya utafiti tu. Wakati wowote ukiwa na maswaliyahusuyo utafiti huu wasiliana na Dr. Boniface Idindili kutoka IHRDC.
Tunashukuru kwa ushirikiano wako! Almuth Dinkela
Appendix D: Information for the study participants and parents 180
3. Information for the Parents – about the skin diseases: Handouts for parents 3.1.1 Ringworm: English version: Your child has been diagnosed to suffer from:
Ringworm:
This skin disease appears as small rings of raised skin. Ringworm itches. It is most often: • on the head • between the toes • in the groin
CAUSES: Ringworm is caused by a kind of germ called a fungus. Ringworm is not caused by a worm. The disease spreads by touching or other contacts with the infected skin. Ringworm can spread if a healthy person
• uses the brush, comb or used clothing of an infected person, or sleeps in a bed with an infected person.
Ringworm • on the head makes patches of hair come out and the skin can itch • between the toes can cause much itching
TREATMENT: Washing helps stop the disease:
• wash itchy places with soap and water and dry the places very well • wash the head with soap especially thoroughly and dry well after washing • wash between the toes with soap and dry well after washing • wash in the groins with soap and dry well after washing
But most important is cleanliness: Wear clean clothes – dirty socks and shoes help the disease to spread! PREVENTION: Ringworm and other fungus infection spread quickly:
• do not let a person with fungus infection sleep with others • do not use a comb or clothing of a person who has fungus infection unless the comb or
clothing are washed very well
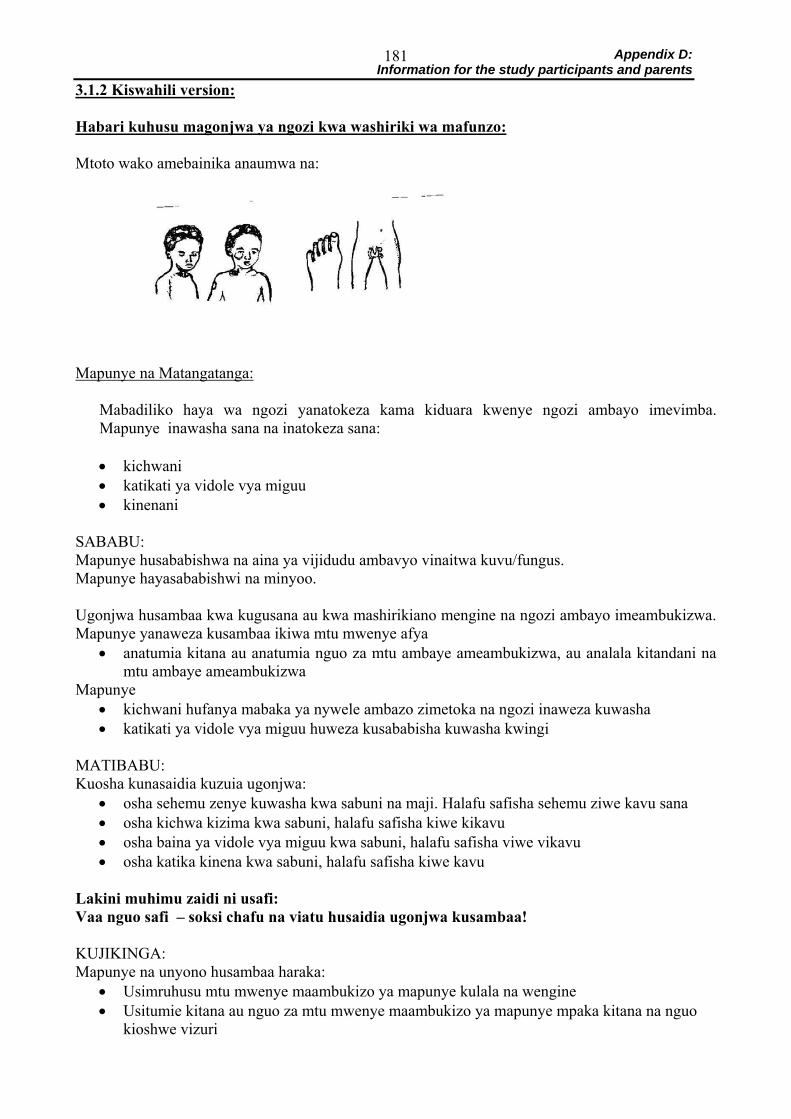
Appendix D: Information for the study participants and parents 181
3.1.2 Kiswahili version: Habari kuhusu magonjwa ya ngozi kwa washiriki wa mafunzo: Mtoto wako amebainika anaumwa na:
Mapunye na Matangatanga:
Mabadiliko haya wa ngozi yanatokeza kama kiduara kwenye ngozi ambayo imevimba. Mapunye inawasha sana na inatokeza sana: • kichwani • katikati ya vidole vya miguu • kinenani
SABABU: Mapunye husababishwa na aina ya vijidudu ambavyo vinaitwa kuvu/fungus. Mapunye hayasababishwi na minyoo. Ugonjwa husambaa kwa kugusana au kwa mashirikiano mengine na ngozi ambayo imeambukizwa. Mapunye yanaweza kusambaa ikiwa mtu mwenye afya
• anatumia kitana au anatumia nguo za mtu ambaye ameambukizwa, au analala kitandani na mtu ambaye ameambukizwa
Mapunye • kichwani hufanya mabaka ya nywele ambazo zimetoka na ngozi inaweza kuwasha • katikati ya vidole vya miguu huweza kusababisha kuwasha kwingi
MATIBABU: Kuosha kunasaidia kuzuia ugonjwa:
• osha sehemu zenye kuwasha kwa sabuni na maji. Halafu safisha sehemu ziwe kavu sana • osha kichwa kizima kwa sabuni, halafu safisha kiwe kikavu • osha baina ya vidole vya miguu kwa sabuni, halafu safisha viwe vikavu • osha katika kinena kwa sabuni, halafu safisha kiwe kavu
Lakini muhimu zaidi ni usafi: Vaa nguo safi – soksi chafu na viatu husaidia ugonjwa kusambaa! KUJIKINGA: Mapunye na unyono husambaa haraka:
• Usimruhusu mtu mwenye maambukizo ya mapunye kulala na wengine • Usitumie kitana au nguo za mtu mwenye maambukizo ya mapunye mpaka kitana na nguo
kioshwe vizuri
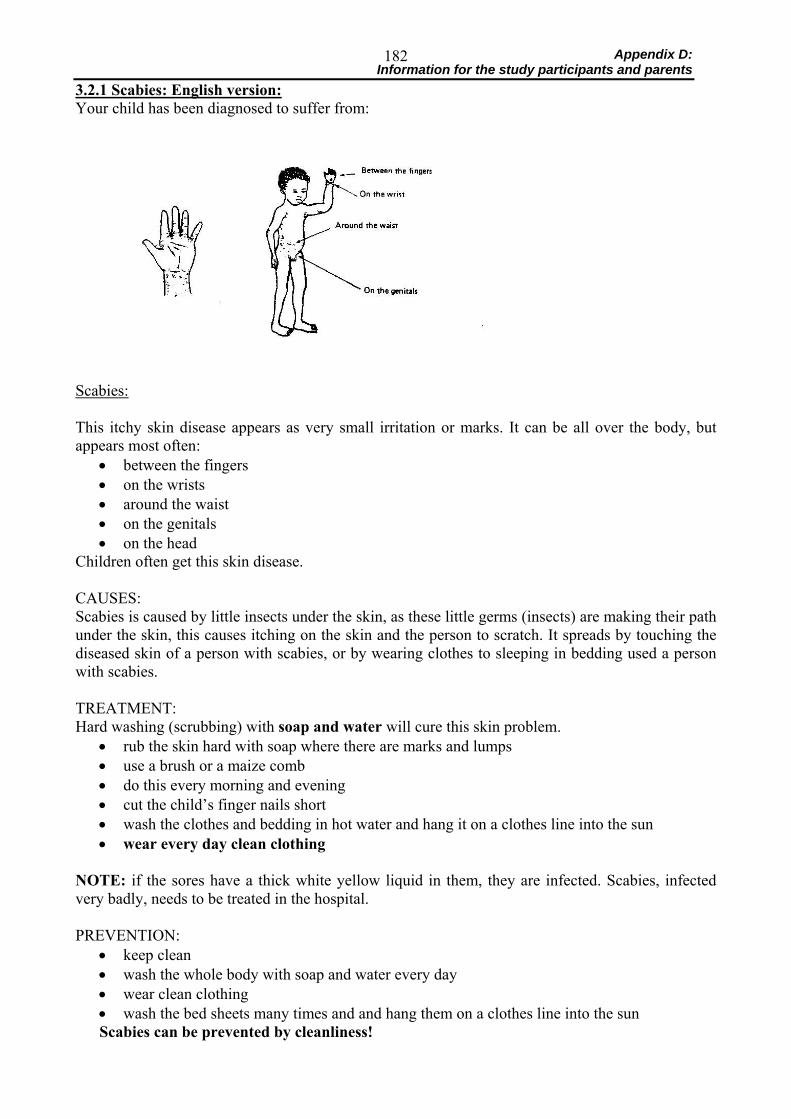
Appendix D: Information for the study participants and parents 182
3.2.1 Scabies: English version: Your child has been diagnosed to suffer from:
Scabies: This itchy skin disease appears as very small irritation or marks. It can be all over the body, but appears most often:
• between the fingers • on the wrists • around the waist • on the genitals • on the head
Children often get this skin disease. CAUSES: Scabies is caused by little insects under the skin, as these little germs (insects) are making their path under the skin, this causes itching on the skin and the person to scratch. It spreads by touching the diseased skin of a person with scabies, or by wearing clothes to sleeping in bedding used a person with scabies. TREATMENT: Hard washing (scrubbing) with soap and water will cure this skin problem.
• rub the skin hard with soap where there are marks and lumps • use a brush or a maize comb • do this every morning and evening • cut the child’s finger nails short • wash the clothes and bedding in hot water and hang it on a clothes line into the sun • wear every day clean clothing
NOTE: if the sores have a thick white yellow liquid in them, they are infected. Scabies, infected very badly, needs to be treated in the hospital. PREVENTION:
• keep clean • wash the whole body with soap and water every day • wear clean clothing • wash the bed sheets many times and and hang them on a clothes line into the sun Scabies can be prevented by cleanliness!

Appendix D: Information for the study participants and parents 183
3.2.2 Kiswahili version: Habari kuhusu magonjwa ya ngozi kwa washiriki wa mafunzo: Mtoto wako amebainika anaumwa na:
Upele: Mabadiliko haya ya vipele vya ngozi yanatokeza kama kiwasho au alama ndogo. Vinaweza kuwa mwili mzima, lakini hutokeza mara nyingi:
• Katikati ya vidole (between the fingers) • Kwenye viwiko (on the wrists) • Karibu na kiumo (around the waist) • Katika sehemu za siri (on the genitals) • Kichwani (on the head)
Watoto mara nyingi hupata ugonjwa huu wa ngozi. SABABU: Vipele husababishwa na vijidudu vidogo chini ya ngozi. Ilivyokuwa vijidudu hivi hufanya njia chini ya ngozi, vinasababisha kuwasha na mtu hujikuna. Husambaa kwa kugusa ngozi ya mgonjwa wa vipele au kwa kuvaa nguo na kulalia sehemu ambazo zilitumiwa na mgonjwa wa vipele. MATIBABU: Kusugua kwa sabuni na maji kutibu matatizo ya ngozi.
• Sugua ngozi sana kwa sabuni sehemu zenye alama au • Tumia brashi au kibunzi cha muhindi • Fanya hivi kila asubuhi na jioni • Kata kucha ya ziwe fupi • Fua nguo na mashuka kwa maji ya moto halafu anika kwenye kamba juani • Vaa nguo safi kila siku!
Angalia: Ikiwa vidonda vina ute wa majimaji yenye rangi ya manjano laini, kwa hivyo vidonda hivyo vimeambukizwa. Vipele ambayo vimeambukizwa sana, vinahitaji matibabu hospitalini. KUJIKINGA:
• Kuwa msafi • Oga mwili mzima kwa sabuni na maji kila siku • Vaa nguo safi • Fua mashuka mara nyingi na anika kwenye kamba juani
Upele unaweza kuzuwiwa kwa kuwa msafi!
Appendix D: Information for the study participants and parents 184
4. Treatment Cards: 4.1 Distributed to children at first soap distribution: IHRDC BOX 53 Ifakara This is to certify that the holder of this document NAME: ____________________________ ID-Number: ____________________________ has the right to receive free medical treatment at St. Francis Designated District Hospital for the skin disease mentioned below
• Tinea capitis • Tinea corporis • Tinea pedis • Tinea versicolor • Scabies
1) if the holder of this document has not been cured of these skin diseases after the Triclosan-
Soap study has officially been declared to be finished or if he/she cannot take part in the study any longer because of severe side effects
2) if the holder of this document shows any signs of intolerance towards the soap and requires
immediate treatment of these side effects All diagnoses have to be confirmed by Dr. M. Mbata before the treatment can be provided. This sheet has to be presented to prove the right to access free treatment for the conditions mentioned above. Dr. M. Mbata Charles Maswi Almuth Dinkela Julia Ferié
Appendix D: Information for the study participants and parents 185
4.2 Distributed to children after the trial to receive free treatment at SFDDH pharmacy:
St. Francis Hospital
KADI YA DAWA: PROJECT: TRICLOSAN SOAP STUDY
Issued on: Valid until: Name of the patient: ______________________________
ID-Number: Age: ____ Sex: ____ Diagnoses: 1)_____________________________ ______________________________ ______________________________ Prescription: 1)_____________________________ ______________________________ ______________________________ Signature: Please collect and store this card in the blue folder labelled “TRICLOSAN SOAP STUDY” at the SFDDH Dispensary after handing out the drug. THANK YOU!
Appendix D: Information for the study participants and parents 186
5. ID card: Distributed to children at first soap distribution:
Date Present Soap returned Name
ID Age Sex Age Soap letter Serial N° Comments:





























