Embed Size (px)
Citation preview
ELDERLY PREFERENCES FOR
&'FERNATIVE CARE SE-GS
Stephanie Stewart
A thesis submitted in confonnity with the requirements
for the degree of Master of Science
Graduate Department of HeaW Administration
University of Toronto
Cc) Copyright by Stepfianie Stewart 200 1
Acquisitions and Acquisitions et Bibliog raphic Services seiuices bibliograp hques
395 WeUington Street 395, rue Wdiurglon OttawaON K l A W -ON K1AûN4 Canada CaMda
The author has granted a non- exclusive licence dowing the National Lhay of Canada to reproduce, loan, distn'bute or seil copies of this thesis in microform, paper or electronic formats.
The author retains ownership of the copyright in this thesis. Neither the thesis nor substantid extracts fiom it may be printed or otherwise reproduced without the author's permission.
L'auteur a accordé une licence non exclusive pemettant à la Bibliothèque nationale du Canada de reproduire, prêter, distribuer ou vendre des copies de cette thèse sous la forme de microfiche/film, de reproduction sur papier ou sur format électronique.
L'auteur conseme la propriété du droit d'auteur qui protège cette thèse. Ni la thèse ni des extraits substantiels de celle-ci ne doivent être imprimks ou autrement reproduits sans son autorisation.
Abstract
This paper identifies the udertying p r e w fot two distnict LTC sdîhgs for persons with cfvonic heaith probkms. A timdnuk off (TïO) p d k n c c elicitation technique was used to determine the relative pmfèrence for home-based care cornpareci to kility-based carc for forty elderiy pcrsons cuniently m reccipt of home- based care for chrobic healîh probkms in North York, Ontano- Tbe variation m relative prefere~ce~ for home-bad care in thip study popuhaion wuld not be explaked by age, gender, wairing Jist staîus, livmg arrangemen& infbmal care, housing type, housing owaership, incorne kvel or own hcakh perception. Most of the variation was driven by bealth sgaus m an unexpacted diredion -a sbrongcr preference for home-basad cart wss associaiai with ltss heaithy participants. Exphnations include a preférençe for the home as a piace to die, risk attitudes or the meaning o f home and place. Further raxwch to confirm this riesuit is wananted-
KEY WORDS - prefhms, home-basai care, bng-term care, Gcili-based care, elderly, tirne trade 0% planning, therapaitic landacapc, sais of p b
Acknowledgemenb
1 would m e to dcnowkdge a numba of people who have coatnbutcd to the completion of this thesis- Thanlc you to my thesis sugervisor, Dr. Pder C. Co*, for boîh your supervision of my degree a d for pushùig me to work at an extra0rdrniu-y pace. Thank you also to Dr. Aud y Laporte fOr p u r ckir-hsded, constructive comments abng the way and for pur constant nitaest m othcr parts of m y M.
A special adcnowledgement is extended to the North York Community Cbrc Access Centre for k i r particÎpathn m this m h . In p t i c u k , thank you Linda Stark and each of the case managers at the NYCCAC - without you this study would not have been possible- I gnaly apprcciated p u r efforts to racniit study participis for this thesis, In addition thenk you to each of the study participuits for sbaring your time and your stories with me.
Thank you to my fàmily, my mother Sôelagh Gordon, my fidmer William Stewart and m y stepmotkr Syivia OaMs - you have crrh ôecn mcredibiy mtcrestcd and supportive. A speciai tbnk you to my amt, Jantt Stewart - 1 know 1 owe you more than a few martinii for all tbat you have done to inthence my education,
Finally, tbank you Chris - for your love and encouragement-
Table of Contenîs
List of TabIes vi
List of Figures vu
List of Appendices viii
1 -0 Introduction 1
2.0 Literature Review 4
2.1 Background 4 22 Search Strategy 5 2 3 LTC Planning Models 9 2.4 CareSe#ingsinOn&rio I l 2 5 Prefermce Theory and Measurnent 21 2.6 Ekierly Preferences for Care Settings 28 2-7 Chapter Summary 34
3.0 Methods 35
Study Type 35 Study Population 35
32-1 Recniitment 35 322 uiclusion Criteria 37
Data CoUection 38
3 3.1 Metbod Selection 42 3.3.2 The Time T ' r a d e 43 3 3 3 Final Daia Collection Methods 45
Analysis Strategy 46 Chapter Sunimary 50
4.0 R e s ~ l t s 51
4.1 Study Population 51 4 2 Health Relaîed Characteristics: EutoQol EQ-SD 56 4.3 Preferience Measurement Results 57 4.4 Regriession Mode1 59
5.0 Discussion Part 1 66
5.1 Limitations 67 5 2 Relation of the Result to the Literaniir and Methods 71 5.3 Altenrative Potential Explanations 76
5 3 .1 Rkk Aversion 76 53 2 Location for Death 82 53.3 The Signi6icance of the Horne 84
5.4 Chapter Summary 84
6.0 Discussion Part II 86
6.1 Therapeutic Landscapes 89 6 2 Sense of Place a d Home 93 6.3 Ecological and Structurai Aspects of the Home 102 6.4 Chapter Summmy 107
7.0 Conclusion and Future Reseatch Directkm 110
7.1 Conclusion 110 7 2 Future R-h Directions 112
7 1 Amendments to i m p v e the Mode1 113 722 Amenciments to Impmve the Interpretation 1 14
7.3 Chapter and Thesis Surnrnary 115
References 117
Appendix 138
List of Tables
Table 2-1 : Estimated Utib!bn of LTC Facues in -0, 1999 16 Table 22: Home-Based Services O f k d by the NYCCAC, 200 1 18 Table 2-3: Estimated Utilization of Home Care by Age
and Gender m Ontario, 1995 20 Table 3- 1 : Estimaîed Utüizaîion of LTC Facilities in Ontario, 1999 47 Tabie 3 2: Estimaîed Utilization of Home Carc by Age
and Gendcr in Ontario, 1995 47 Table 4.1 : Summary of Care Recipient Participants and Non-Participants 52 Table 4.2: Summary of Interview Respondcnts 53 Table 4.3: Personal Charrideristics of Gare Racipkîs 54 Table 4 . 3 ~ Age 54 Table 4.3 b: Gender 54 Table 4.3~: Marital Status 54 Table 4.3d: LWmg Arrangements 54 Table 4.3e: Accommodation 55 Table 4-3fi E d u d n Level 55 Table 4.3g: Incorne 55 Table 4.3h: Waiting List Status 55 Table 4.3i: Infonnd Caregivcr Time 56 Table 4.4: Summary of the Number of Responscs (96) m m h EuroQol Damam -56 Table 4.5: Summary of the Overall EuroQol Score and VAS Score 57 Table 4.6: Summary of the Priefaence Meas- One: D i Question 58 Table 4.7: Summary of the Prefance Meas- Two: Tiie Trade-On 58 Table 4.8: Relative Preference Scores for Horne-Basui Care 58 Table 4-9: Raw Variables Entemi in Mictosoft 0 Excel 61 Table 4. IO: Full Regression Models 62 Table 4-1 1: Variables Creaîed for EuroQol ïhmains 64 Table 4.12: Final Regression Models 65
List of Figures
Figure 2-1 : The Ti Tnde-OfF 26 Figure 3-1 : The Tirne TradeOEApplication 44 Figure 5.1 : Utiiity of Cam SeÉtiogs Function for the Study Participants 78 Figure 5.2: The Ut~lity of the Currcnt Care Sctting 79 Figure 53: Risk Aversion to Faciiity-Bascd Carie 80
List of Appeidkcs
Appendix I: Table of Relevaut Websites 138 Appendix II: Summary of Search Resuhs 140 Appendix III: Tekphoae Recniitment Protocol for Preference Interview 141 Appendix N: Telephone Recniibnent Protocol for Rekmce Int-ew B 142 Appendix V: Script: Introduction to interview 143 Appendix W P r e h c e Interview Consent Form 1 4 4 Appendix EuroQol EQjD 146 Appendïx Vm: Initial Rcfèrence ElEcitation 148 Appendk TX: TT0 Mettiod= Home-based Care Preferred to Facility-based Care -149 Appendix X: TïO Method: Facility-based Cart Prekrd to Homabaseci Carc -152 Appendix Xi: TT0 Mettiod: When care mipient unwilling to trade a year of üft_lSS Appendk W. Socio-Demographic Survey for Cam Reciphts and Caregivers-158 Appendix Xm: EuroQol E Q 5 D Scoring Fonaula 161 Appendix MV: TïO: Cakulation of Relative Preferc~lce for Home-Based Chce-163 Appendix XV: The The Trade-OEViual A'd 164 Appendix XVI: niank You to Study Participants 165 Appendk SAS Regtession Rcsults 1 66 Appendïx X W : Finai Rtgression Mode1 180
viii
Chapter 1
1.0 Introduction
Long-term care (LTC) in Ontario reflects a range of heaith, social and
personal care sewkes offéred a m s s shrrnaive care oem0igs1 Fonnal LTC services
in Ontario are fàcility-based, such as n d g homes and homes for the aged, and
community-based, such as home nurshg, bornemaking and supportive bousing.'" In
1998, there were approximately 55,882 Ontario residents in facili*.-brsed LTC' and
380,3 1 6 cücnts served by Ontario's Cwmiunity Care Access Centres6
The past two decades have been characterized by a shift in care k m the acute
hospital and tkiiii-based LTC sectors to the community, ofteri with goals to i n c m
economic efficiency and better meet the needs aad prefe tem of care recipients.'*'
Such a shift has resuiteû in an annuai gmwth of public home Gare expenditures of
approximately 20% suice 1975.' Nonethekss, it is uncertain mat tbe shift to the
community has resuited in more efficient use of resources and it is unhown whether
the needs and preferences of both care reciplenl and caregivers have been met bythis
shift. This uncertainty is in part due to the lack of a comprehensive mode1 that
properly identifies the d s and preferences o f the population for LTC.
Frefetences are important for LTC plannmg because they influence the
decision to seek and accept are. uideed, such pretèrences influence the type and
range of services uscd as well as the settiags in which such services are sou&
delivered and received. Consequentiy, one important driver of cunrent and ftture
patterns of he!aith service utilizrrtion art the underiying (and cbmguig) prtferenccs for
the type of LTC and the setting in which care is received by both care recipients and
caregivers8 Using c u m t utilmition rates as a means to forecast f î r e needs -out
a discussion of the underlying (and potentially changing) prefèrençes Unpkitly
assumes that prctèmces are e a b a invariant to c b g e or unïinportea9 inclusion of
care recipient and caregiver prefercnces in LTC planning removes this naïve
assumption.
While LTC planauig models have irnplicitly discussed the importance of pure
(or ha îe ) preferences for particular care &ngs, none of the planning models
reviewed in Chapter 2.0 obtained care recipieats or caregiver preferences for LTC
planning pur pose^.'^'^ h a , these models rcly on tbe miplkit assumptioa thet
people prefer autonomy over dependence, and that autonomy is achieved by
reniainhg In one's own home as long as possible* It is unErm>wn ifthis assumption
adequately captures the preferences for LTC, The most comprehensive LTC planning
mode1 would be one that explicitly incorporates the purit prekrences of care recipicnts
and caregivers by directly asking these îndividuats about their preferred settings for
LTC-
Pute (or innate) preferences refet to the uad-ng prefkences exhibited by
care recipients and caregivers with respect to the type and range of LTC services.
Holding d l other ktors constant, it is anticipatcd that a particular care settmg may be
preferred to other settings by care recipients and caregivers, and thaî ifasked, both
care recipients and caregivers might reveai this prcfercnce.t '* '' This is important for
LTC planning because if pure prefe~ences were not included in a p Ianaing mode!
there may be a mismatch betwem the type and amount of cam provided and the
amount of care sought by carie recipients and caregivers,
This thesis identified elderly preferences for tong-tenn arc. The specific
objective of this thesis was to rneasure and assess the underlying or innate preferences
for two distinct long-tmn c a ~ c &gs for petsons wIth chronic health pmbleais. The
end result was a mode1 that quantified preferences for two alternative long-tenu case
settmgs that may be used for planning LTC m Ontario- That said, this research
question required laiowledge of ütemtwe m a wide range of disciplines. As such this
thesis is not ody of inttxest to long-term care planncrs and decision-makers but also
to gerontobgists, home tare mearchers, health and social service workers, and
econornists-
Chapter 2
2.0 Literatun Review
2.1 Background
This chapter reviews the krature relevant to the study of underiyhg or innate
preferences for LTC settings. The chapter demonstrates that a mix of policy,
planning, economics and heakh services testarch shrrpe dris topic, While it begins in
Section 2 2 , with a desc~l~ption of the search strategy used to identift what çonstitutes
LTC and LTC plauning in Ontario and what is biown about priefcrrnœs for LTC
exhibited by the elderly, it is in the following f i e sections of this chapter that the
literature is shown to reflect the multidisciphary nature of this riesearch question.
Moteover, the chapter demonstrates that despite extensive research invested in heaith
services, gemntology, and economics, ftrthcr research on prefmces for LTC in
Ontario is warrantecl.
Section 2-3 reviews the LTC plannmg literature and estab tishes that
preferences are a factor important to decision-making. Nonedieless, in this section, it
is argued that preferences for heaith cate settings have been absent in planning models
despite the political rhetorïc tbaî pretieffnces are of utmost importance. An
understanding of LTC planning in Ontario is grounded in knowledge of the services
thaî consthte LTC. As such, Section 2.4 briefly d e s c r i i the array LTC services
onered in Ontario- In particular, the section fixus is home-based and facility-based
care, which were the tufo distinct care s h g s used to answer the mearch question.
Section 2.5 explains why underlying (or innate) prefèrences influence the type
and range of heaith and social care savices that carc rccipients will seek and acccpt.
The section outlines how basic economic theory explains the behaviour of the cart
recipient- From the viewpoht that undedying or mnate p r c f i condition the
behaviour of the care recipient, identifying prtîèrcnces for the two aheniative care
settings is warranted- Thus, preference dieory, as Section 2.5 descrr'bes, is concerned
with the ways and mems to quanti@ such prcfkmces-
Section 2.6 reviews studies that specükaiiy relate to the i d e n m e o n and
measurement of preferences held by the elderiy for heaiîh and social care semices-
The section dernonsirates the lack o f -dies thaî quant@ preferences held by the
elderly for alternative scttings. in particular, the section demonstrates the lack o f
studies that use methods deveioped expressfy for quantimg p r e h c e s for heahh
and social care evaluation- Section 2.6 argues that this thesis takes the first step
toward fWng this void.
Final comments are &en m Section 2.7. The cornments summarize the four
goals of this chapter 1) To show preferel~ces bave a place m planning alternative LTC
setîings; 2 ) To review the aiternative LTC d n g s in Ontario; 3) To demonstraîe that
because prefe~ences condition behaviour, there is value m measuring prefereuces;
and, 4) To show that quantitative methods to measure underlybg (or innate)
preferences, hereafler referred to as preferences, have not previously k e n employed
for two distinct care settings for persons wiîh chmnic heaith problems. To the extent
that these goals are met, this study is justüied-
2.2 Search Strategy
There were two distinct reviews for this thesis, The first review was
conducted to idenw the assumptions made by diffierient juridictions to forecast
demands for home and facility-based care for the elderly. This review was initiaily
conducted for the Ontario Ministry of Htahh and bng-Tcnn Care (MOII) h m June
2000 - September 2000 and a final report was written in Daember 2000.) S-h
strzttegies for this review were varieci and are explaineci below. The second distinct
review was conductecf specificdy to dent@ undettying (or innate) p t e f i for
care settings- This m k w took place throughout the mondis of Septcmber 2000 to
February 200 1. The straîegy of the second rcview is also discussed bebw,
Two rnam stratcgies were used initiai& m the search h r assumptions made by
diffetent jurisdictions to plan LTC: a scarch ofpubIlshed and "gry I i r e " and
contact with key stakeholders in LTC. A d e m i c iiterature was reviewed following
this îïrst "cenvVonmental sçan." Due to this author's Iïmited knowledgc of eithcr LTC
or health Gare p l M g in the early stages of the project, it was mggesteci that a search
of the "grey literaî~re~~ and identincation of key s&keholders was appropriate and
ükely to genemte the most rekvant literature? Reievant Iiterature was also forwarded
at the start of the MOH pmject, h m the Primary Investigator of the MOH pmject, to
this author. This literaaire was used to identify other sources.
The search for "grty literasure" began at the Home Care Evaluation and
Researçh Centre (HCERC) a& the University of Toronto. HCERC is, " a joint initiative
of the Faculty of Nursing and the Department of Health Admmisîmîïon, Facuity of
Medicine at the University of T'oronto?"~~~ is physically located in the Faculty
of Nur~mg at the University of Toronto and houses a p w i n g body of literahlre
devoted not only to home carie but also an array of othet settings for heaM and social
Gare. In addition to library resources, HCERC maintains a website
(www.hcerc.utomnto.ca) that pmvided usefiil links for building a foundation o f
knowiedge on LTC and LTC plammg, Websites Iinked to the HCERC website were
reviewed as were an array of other websites h m health and social care ministries and
organizations. Names and website addresses am appended (Appendix 1). The "grey
literature" search h d two outcornes. First, it belped identifY relevant articles that
provided sources for the review and second, it htiped id- kcy sî.&ebokfm
organizations to contact.
Key stakehokiers were identifid both h m a review of rielevant websites ami
by the Primary Investigator of the MOH pro* Alf organizations, identifiai in
Appendix I, were contacted via e-mai1 and a rcquest was made for documents or other
resources that relateci to LTC planning in theu respective j~sdict ioas . This method
of search was productive and documents were both suggtsted and forwarded. Not al1
of the organizations or key stakeholders responded and not aU of the documents were
relevant for a review of the assumptions used in planning LTC for the fhil eldaly. In
particular, there wem no explicit pianning models forwarded or identikd fiom
jurisdictions outside of Canadu within the tMic ûame o f this project. Subsequentty.
while LTC Iiterature from an array of jurisdictions was reviewed, the planning
M e w o r k advanced uas compared oniy to otha Canadian LTC planning models.
Seven Canadian LTC planning models were reviewed, as was the vast stock of
papers that related to LTC. Sixty-five diffèrent sources were used in the final paper
wriüen in December 2000. This represents only a f W o n of the litemture that coufâ
have been used for this pmject- Suffiœ it to say thai titis is a growing ares of reseatch
of that has produced, and is stiU producing, multi-disciplinary and rnuiti-national
studies. That ail the relevant literature could not be included within the t h e fkne
was a limitation of the final paper, m particular, the omission of other planning
models in jurisdictions outside of Canada was noteda
The second distinct review was conducted s p e c W i y to identi@ prefmces
for care settings. Eight databases were searched, The databases include. PreMedlme
" In awokhop M d Febmmy 13,2001, the lrdrofintanitiami MiYM in the fhd pepr fot the MOH was idaitifid niis aiticiam is &id. Whik m -kit plrurùrg mrdds in j\Pisdiaiom OutsideCanadawue ~ i n t b t t i r n t ~ i t i s I i W y t h r t h y & a 9 s t , 'Ihisjustificsfirrd# research. Furiha, this warrants ini- such as the HCERC, to kiild alliinices with otha jutisdiaiais and tkcby ammmgc cx@icnt d i m m of- Md i d i o n .
and Mediine (Ovid Technologies Version, 1966 - Mar& 200 l), EMBASE (Ovïd
Technologies Version, 1 980 - March 200 1), HealthStar (Ovid Technologies Version,
1 975 - March 200 l), CINAHL (Ovid Technologies Version, 1982 - Marrh 200 1),
EconLÎt (Cambridge Scientific Version, 1969 - March 2001), The Science Citation
index (Expanded) (Web of Science, 1993 -March 2001), The Social Science Citation
index (Expanded) (Web of Sciencey 1993 - March 200 1) and AgeLk (Siiver Platter
Version, 197% - Marcb 200 1)- Al1 of these databases were available to students and
faculty at the University of Toronto at the time of the review. Six diffèrent keyword
searches were used- pref-, p x d k a c e + heaith, preferences + health + care,
preferences + home + care, prefereaces + "borne arey' and pteferences + "long term
tare"- A p p d i x II sumarizes the resuk of each
The keyword 'preferences' search was omitted for al1 of the dstabases because
it was too broad (evidenced by the total 91,009 "Ms" combined). The keywords
'preferences + health' searich h m The Science Citation Index combinecf wïîh The
Social Science Citation Index was also omitted for similar iieasons (99 1 %its")- AU
other searches were considered. Titles and abstracts were read and relevant articles
were identifieci!' The inclusion criteria were broad- An article was included i f it
rneasured preferenax for location of care regard iess o f the age cohort studied. Both
qualitative and quantitative methoâs for measuring pre-ces were accepted- in
total, 66 articles were retained. niese articles provided additional refemces for this
study. The final list of tekences, at the end of this paper, is a result of the two search
strategies descn'bed above.
2.3 LTC Phaning Modeb
Preferences held and acted upon by both care reclpients and caregivers are
important to irtcorpomte in LTC p l d g modeis as they influence the decisionsi to
se& and accept LTC as well as the setting in which such case is receivd. An
assessrnent o f the trends m and the detenninants of such prefe~ences would provide a
more complete understanding of the ktors required to forecast the demand for LTC.
Holding d other mors constant, it is anticipated tbat a particular care setting may be
preferred to other settings by care recipients and caregivers, and that ifasked, both
care recipients and carrgivers might mved ihis prefmncc.L2 This is important for
LTC planning because if pure prekemes were not included m a pfanning mode1
tiiere may be a mismatch beniifeen the type and amount of care provided and the
amount of care sougtit by care mcipients and mgivem.
A systematic and curnprehensive long-tem care (LTC) planning h e w o r k to
aid decision-making shouki therefore include ckierfy prehences for particuiar care
settings? Nonetheless, examination of the LTC plannmg models4 - ' ' that were
reviewed for a psper to identifjr asumptions for plaMmg LTC' showcd that while
preferences heu by the eklerly were considerd important pure preferences were
rarely, ifever, quanti6Ted for forecasting fiiture LTC nceds.
Of the models identified and subsequentiy reviewed here, the Policy Advisory
Cornmittee of the Long-Term Lare Review for AIberta (1 999) paper made the best
attempt to include preferences in theu LTC planning madel? This study determined
the impact of shiftlng resources h m the facile-basad sysfem to the community
under three different assumptions that represmted abmaiive intensities of shifting
resources to the community. It was arguai that the shifts rcûectai contuiuing care
developmentts and trends such as, mcressed choice of cart settaig. AAcr f o m
were made ofthe impact - on sewke volumes and on costs - focus groups were
conducted, that included key stakeholders, to dctcrmhe the " p r e f e d direction for
the continu@ care systaa in Atberta-" Indeed, this study mat fUrthcr ttum others4-
"-" in idcntiflmg prefénaces in the LTC p b i n g rnodel but still did not attempt to
ask care recipienîs and their caregivers for their own prefkrences for alternative care
settings.
Another gmup also examined the impact of three dtemative shifk of
resources fiom LTC fbcilities to the community by crnpbyaig the same methodology
as the Alberta group? Aithough the authors uscd identicel m*hods, th& final report
was tess explicit ai identifjhg a d e for pref- than the teport by the Policy
Advisory C o m b e of the Long Term Care Review for Alberta (1 999), and again,
there is no evidenœ that puce prefmces have been idcntified exptessly for inclusion
into the LTC planning model,
A third mode! used a combination of setting target ratios for LTC M s per
1,000 population, using population projections and determinhg friture needs for
faciMy and community services for the contiming care and tesource allocation
fiamework in British ~olurnbia~ The only disaission of prefèrences in this mode1 is
to consider the use of needs-based demand forecasting- Unfôctunately, the needs-
based approach was lim ited to surveyhg Long-Tcnn Cam Assessors/Case Managers
@. 10 1) for their opinion of how many clients couM be cated fOr in the community.
At the time the fnmework was implemented, thcre was an expressed mterest to move
more care into die community b m the fiicility-based system but it is unclear that this
was m any way motivated by eldedy preferences,
The remainmg reports 4,6.7,10.11 do not discuss pmihmccs in an expliiit or
quanMve mamer- If prefërcnces were mentioned, comments were hitcd to
conventionai wisdoms and the belief that peopk wlsh to remah in their uwn homes as
long as possible,
Indeed, whiie CTC plannmg models have implicitfy dîscussed the importance
of pure preferences fot particular care scttings, none of the planning rnodels identifkd
by Coyte et al (2000) and subsequently reviewed hem obtahed a r e recipients or
caregiver pceferences for LTC planning purposs.41' Iastad, these models reliexi on
the implicit assumption that peopk prefet autonorny over dependence, and that
autonomy is achieved by riemainhg in ones own home as long as possible. It is
unknown if this assumption adequatety captures the pteferiences for LTC. Coyte et al
(2000), suggested that the most comprehensive LTC planning model wouM be one
that explicitly incorporated the pure preferences of carie recipients and carcgivers by
diractly asking these individuds about their preferred settings for LTC? This pilot
study, to elicit preferences for ahenrative LTC settings, was a preliminary step to
quanti@ preferences for the purposes of LTC planning in Ontario. This step is
particularly important given thaî LTC pol iy in Ontario is based on the premise that
the elderly want to remam in their own homes as long as possible and assumes both
implicit1y and explicitiy that ageing in place provides autonomy:
2.4 Cam Settiags in Ontario
Long-tenn care (LTC) m Ontario reflects a range of heahh, social and
persona1 care services offered across altemative are settings.l2 Forma1 LTC services
in Ontario are fafility-basai, such as nursmg homes and homes for the a@, and
comunity-baseci, such ss home nUrSiLIg, homemaking d supportive h~usin~.'~-'~ In
1998, then were approrrimately 55,882 midents in fncilïty-based LTC" in Ontario
and approxhmtely 380,3 1 6 clïenîs serval by ontmïo's Community Care Access
Centres.'7
To determine elderly prefèrmces ibr LTC settmgs for this study, the
alternatives were limiteci to f'sciiity-bas& LTC and home-based LTC. Of course
other care settmgs such as supportive housing are availab~e.~ Moreover, dinical and
social care needs can be, and are, met both focmally and mforrnaUy through social
networks in the community and the community (or comrnunity centres, or cburch, or
bowling alley etc.) is alsu a care sethg that is d B i t h m the home. Indeed
Informal cariegivers, a major part of a care ircipiart's social network, are also the
major care pronders to eiderly Canadiad as an estimateci 75% of the 3.4 million
Canadians older dian sixty five years of age =ive assistance h m an infomal
~ a r e ~ i v e r . ' ~ Despite this not kignifrrit form of care (and arguaMy tare snting),
facility-based aud hornebased LTC were chosen because these two care s d g s
represent the formal LTC available m Ontario. Supportive housing is d l useful but
for brevity and to simpliQ the anaiysis a stylized cornparison was used here. Thus, a
description of formal f'acZlity-based and formal home-based LTC o f f d in Ontario,
follows.
Long-Tenn Care facilities in Ontario are known as nutsing homes. homes for
the aged, rest homes and charitable iwthitions?* These homes provide assistance and
care to people who can no longer live mdependently d o r who cm no longer lïve in
their own homes and/or who may dm need 24-hout nursing and personal cardo
Regardless of differençes in their aamts fou types of homw m dicory, provide 8
simiiar LTC setting- This is impkit m the operational dekitions of each provided m
the Niasng Homes A&, the HomesBr the Aged und Rest Hiomes ACP. and the
Charitable ~rii~tihrtiom ~ c t ? ~ These Acts gïve the fbllowiog descriptions for tscility-
The definitions above offer simiiat descriptions of kility-based c m . Of
course, it is unlikely that any kility-based centre is identical in character to another.
Tt is not the purpose of this study to provide a critique of sQecific kiiity-based LTC
or their p hysical, psychologïcai, social, cuttural and spiritual diftèrences.' Rather î t is
the underlying idea, demonstrateci by the three Acts, thaî die philomphy of each
facility is gou us, t h provides the inpetus for includhg di types into ont
aitemative - tacriity-ôased LTC - m this study,
The assumption that esch fac~lity, rrgsrdkss of num, csn bc pookd bto a
single alternative is fiirîhcr supporteci by provmciaily detcrmmed and locaüy
operabiondized digiiility quimnents that are oimiiar for îhese hciüties." Variation
in eligi'bility requirements, hoidmg constant underlying p d è m x e s for the type and
range of LTC services, will aiter tbe observed LTC sceking bchaviours of the a r e
recipients and caregivers- Indeed, the care mipient or categiver might be more or les
willing to seeklaccept care as a resuk of a change m eligiôiiity ribquiiwnents, out-of-
pocket costs or availability of LTC services; however, the amount and type of care
thaî the carie recipient and the caregiva wüi seeW~cccpt depends on the underlying
(or innate) prefefences for LTC. Because variation in eligibility requirements across
the faciiities is h i t e d by the legislaaion imposed by the Province of Ontario the
grouping of %ornes" mto 'Taciiity-bad" c a ~ e is j d e d for diis study-
Wh& the forernost con- of this study is to determine underlying
preferences for alternative LTC settings, it is nonetheless worthwhile to detail the
etigi'bility requirements for forma1 LTC in Ontario. k i n g so provides a mom
complete understanding of fàcility-based and home-based care because the care
recipient's decision betwec~l the two alternatives should be understood m the political
context. Because this study assumes that the elderly either prefer to live pennanently
in a fàcility or, aiternativeS., prefa to receive homebaseci care, the particuk
eligibility requirements of interest with respect to facility-based aire are r e W to an
application for a long stay admission. These eligibitity mquircments are that:
A "Lang Stay" the appiicsuit mmst bt:
Faciiity-based care is not "fiiee'' at pint of service in Ontario- Consequentiy,
there are vaging mtes charged to care recipients across fonnal LTC facilities,
However, i f the appiicant metts the formal eligiitlity mquitcments the ktlity is
Iimited to charging a monthly maximum of $1,277.95 for a '%asic" room, $1 ,S2 t .28
for a "semi-private" m m , and 5 1,825.6 for a "private r00rn.'"~
Table 2.1 provides a snapshot of who used LTC fàciiities in Ontario in 1 999
by showing the estimated utilhiion of LTC fàcilities, by 5-year age cohort. The
nurnbers demonstrate uiat while only approximately 3.7% of the population over 65
years of age used LTC fàcilities m Ontario in 1999,7.3% of those over 75 years of
age and 17.6% of those over 85 years of age used f à c i l i i - b d LTC.
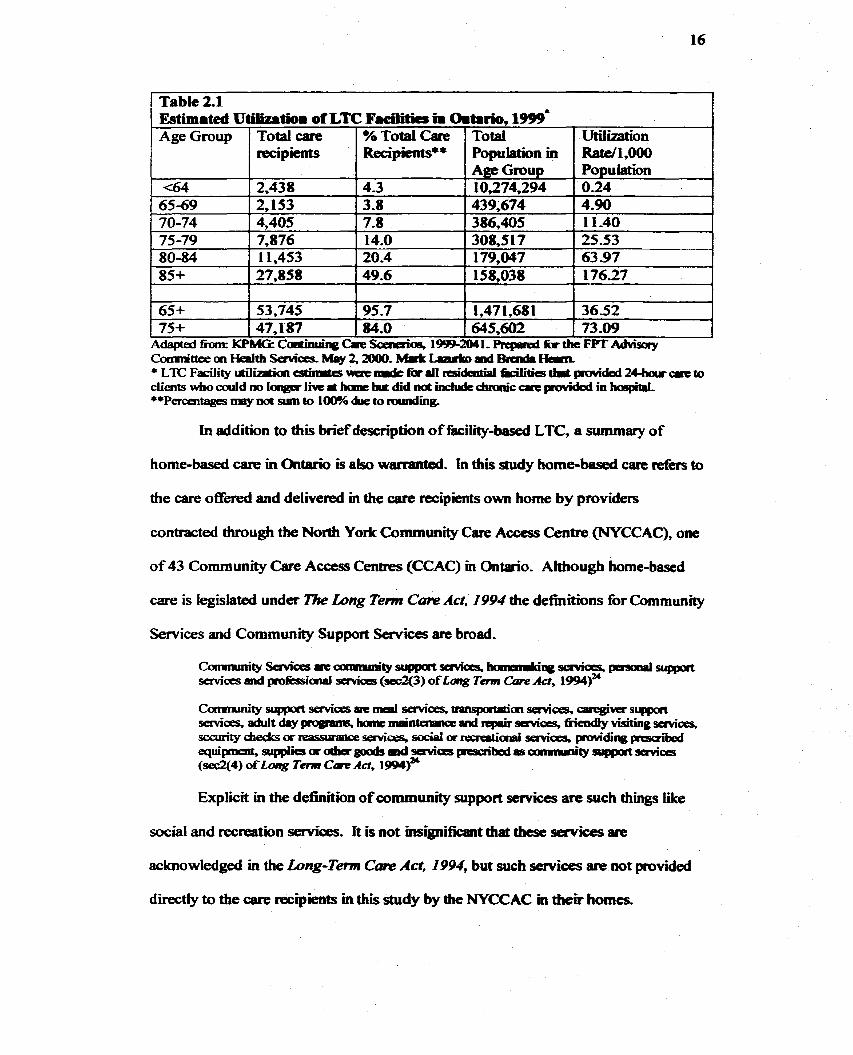
In addition to this brief description of faciiity-hased LTC, a summary of
home-based care in Ontario is also warranteû. In this study home-based care refers to
the care offered and delivered in the cate recipients own home by pmviders
contracteci through the North York Community Care Access Centre (NYCCAC), one
of 43 Community Care Access Centres (CCAC) in Ontario. Altbough home-based
care is Iegislated under The Long Tem C m Act, 1994 the definitions for Community
-ces and Community Support Services are broad.
Table 2.1 Estimated Utilivtiom of LTC Facioaa ii Omhrïo, 199)' -
Explicit in the definition of comrnunity support semices are such things Like
social and recreation services. It is not hignificant diat these services me
Age Group
(64
acknowledged in the Long-Tenn Cam Act, 1994, but such services are not provided
directly to the care recipients in this study by the NYCCAC m theu homes.
Total Population in Age Gmup 10,274,294 439,674 386,405
Utilizaîion Rate/1,000 Population 0.24 4.90 1 1-40
Total case reci pients
2,438
25.53 63 -97 176.27
36.52 73 .O9
% Total Care RecSpients8*
4.3 .
65-69 ( 2,153 70-74 4,405
AâaptedfhtmKrpMGsCadinubqgCaeScaiaios, l~ tW1-RcpRdîktheFVïAdvisay C o m i i i t t e e o n ~ t h ~ k i l o y 2 , ~ . ~ ~ a l d & a i d i H a m - *LTCFaEilityrailW~cstirnts\iiiiehnr&farJ1ddaitiplbcilities11i3~dad2Choucri:m ciients w b o d d n o l ~ l i v e ~ h a a t i n ~ t d i d n d i n c l u d t d i n i n i c ~ p u v i d d inho6pit.l, **~er~entages may net srim to 100.~ due to rauiding,
3-8 7.8
75-79 7,876 14.0 20-4 49.6
80-84 85+
308,s 1 7 179,047 158,038
1 1,453 27,858
1,47 1,68 1 645,602
65+ 75+
I 53,745 95.7 47,187 84.0
Acwrdingly, in this study, the km homebased carc is sdopted to difikentiate a
community settlog h m a home setting d to tiefèr s p e c ~ y to in-home care
currently pmvided to the care recipient by the NYCCAC wherein home means a
community dwellmg,
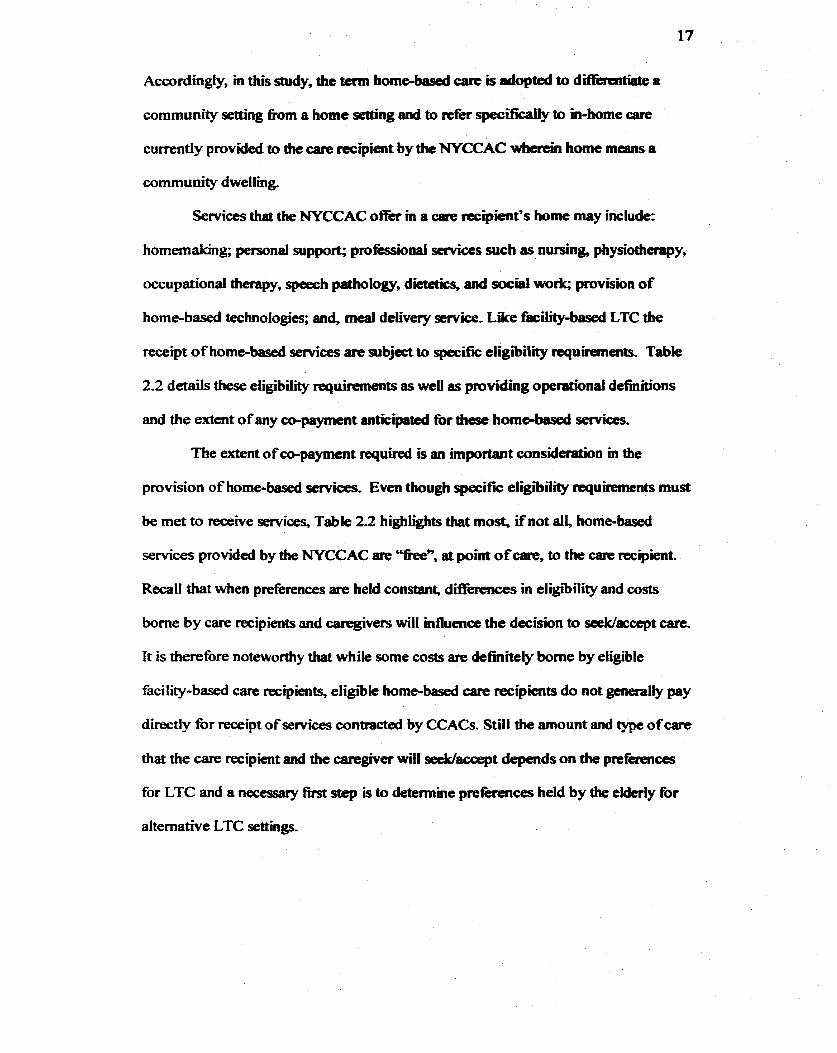
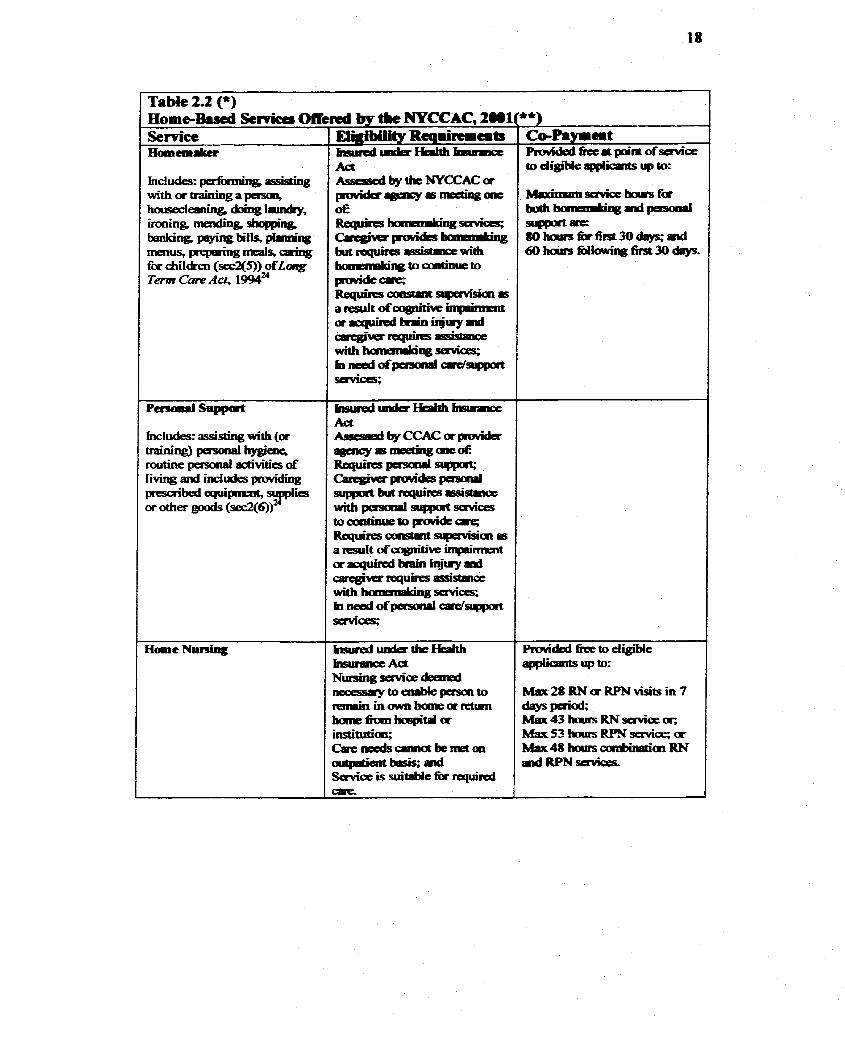
Senrices that the NYCCAC offer in a care recipient's home may include:
homemabg; personal support; proféssionai servÏces sucb as nursing, physiotherapy,
occupational therapy, speech pathology, dietetics and social work; provision of
home-based technologies; and, meai delivery service, Like fâcility-based LTC the
receipt of home-based services are subject to specifjc eligiiility requirements. Table
2.2 details these eügibility requirements as well as pmviding operational d e w o n s
and the extent of any ca-payment antkipated for thest horne-based services.
The extent of co-payment required is an importaot considefafion in the
provision of home-based semices, Even though specifk eligr'bility wu' uiements must
be met to receive services, Table 2 2 highlights that most, ifnot dl, home-basai
services provideci by the NYCCAC are '%een, at point of care, to the care rccipient.
RecaU tbat when preferences are held constant, d i B e m e s in eligibitity and costs
borne by care recipients and caregivers ml1 mfluencc the decision to seeWaccept c m .
Tt is therefore noteworthy that Mile some costs are definitely borne by eligible
facility-based care recipients, eligiÏie home-based a r e recipients do not generally pay
directly for receipt o f services contractai by CCACs. Still the amount and type of care
that the care mipient and the caregivet wifl seeWaccept depends on the preferences
for LTC and a necessary fmt step is to determine preferences held by the elderly for
alternative LTC settings.
1 Table 2.2 (3 H o r n ~ ~ %rvicg Oti Service
Includes= performing w i n g with or training a housecleania domg lamdcy, ironing, mendiag, shopping t J = l c e P P e n % h'lls, mq? =us,pepPinl3~%cairig for children (sec2(5)) of Long Term Care Act, 199p
Rnvided fice to eligiie applicants up to:
''objective is to financialïy sssst . - . residents to o&ah [needed) devices - . - interaded to giw people inaeased indepawlarcre and caitrd O= their W. Theymayallowthantoavad costly institutid seuüQp ad remain in a -ty living arrangaraa-a
I 1
(*) Sources: Law-Tent C m A& ; h m i o Minïstry ofHeaith ad -Tarn Cae Webïte. Available: !ltwxJ/urww- ; Fedeal-Pnmïacial-Ttxritaial Adn'say Cumüttep rn Health Serviœs (ACHS) Waking Group on Cmtinuing Cae- (May 2000)- Tbe Ideotificaticm and Analysis ofhceutks aad Disllioenim aad Caa-Efffdivmcss ofvarkus Fuding Apprraches fa Continuhg Gare- Tdmical Repart 5: An Oumkw ofcaitinuing Care services in Canala Hdlander Anaifid Suvices, Vidorr-a B.C. (**) This tabîe is specinc to the NYCCAC k a m e sane di- betuneen this CCAC and othas may exïst to the aaart that scmre services are adngemt ai the fùndraising aatity of the CCAC. Fm scanple, Meals on WheeIs is a p q p m pnivided besed ai availabk fiinds fiun the MOH and baEed on the fündmking ability of the portiailar CCAC.
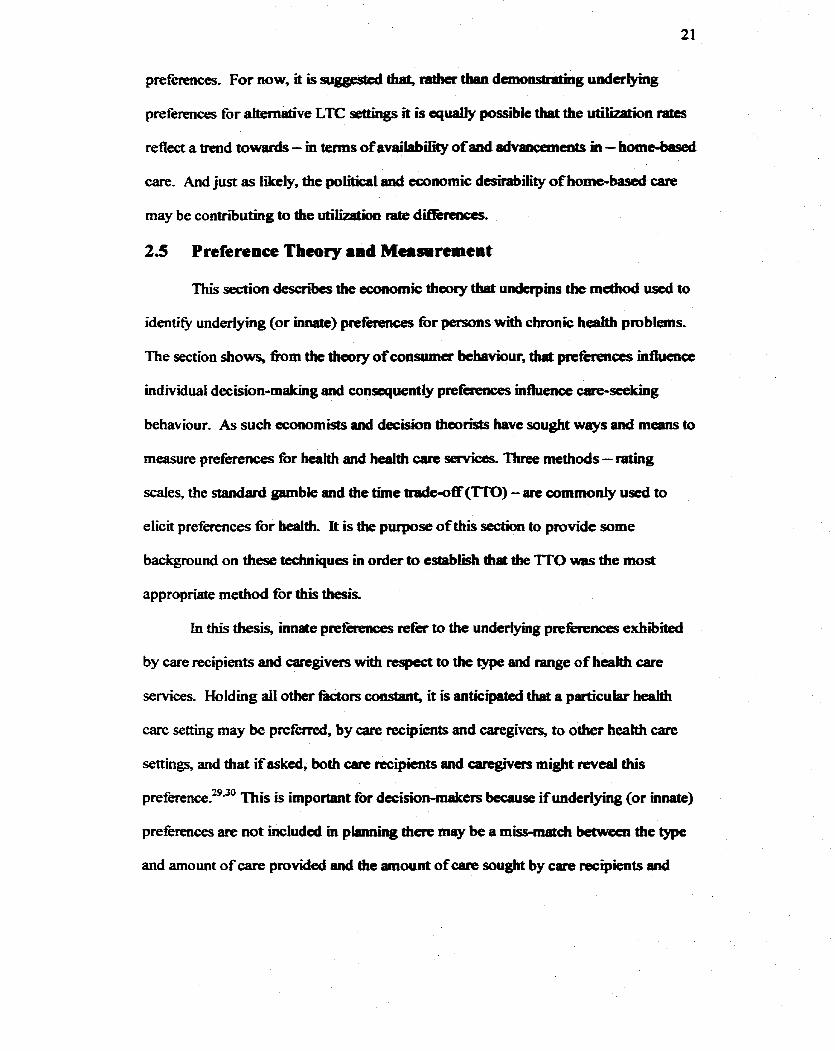
It is relevant to examine the utili7arinn of home care in Ontario- Table 2.3
provides a picture of who used home care in Ontario in 1995 and differs h m Table
2.1 in that it gives home care utilkation rates by both age and gender cohorts. Table
2.3 shows an increase in use of home care with age for both males and fernalies over
the age of 65. Similar to the iàcility-based care uscrs, the highest utilization of home
care occurs in the oldest (85+) age cohort (for both maies and fernales), The rate of
utilization of facüity-based care 1,000 population, in 1999, for those over 85 pars of
age was approximately 176 and the home caille utiiization rate per 1,000 population for
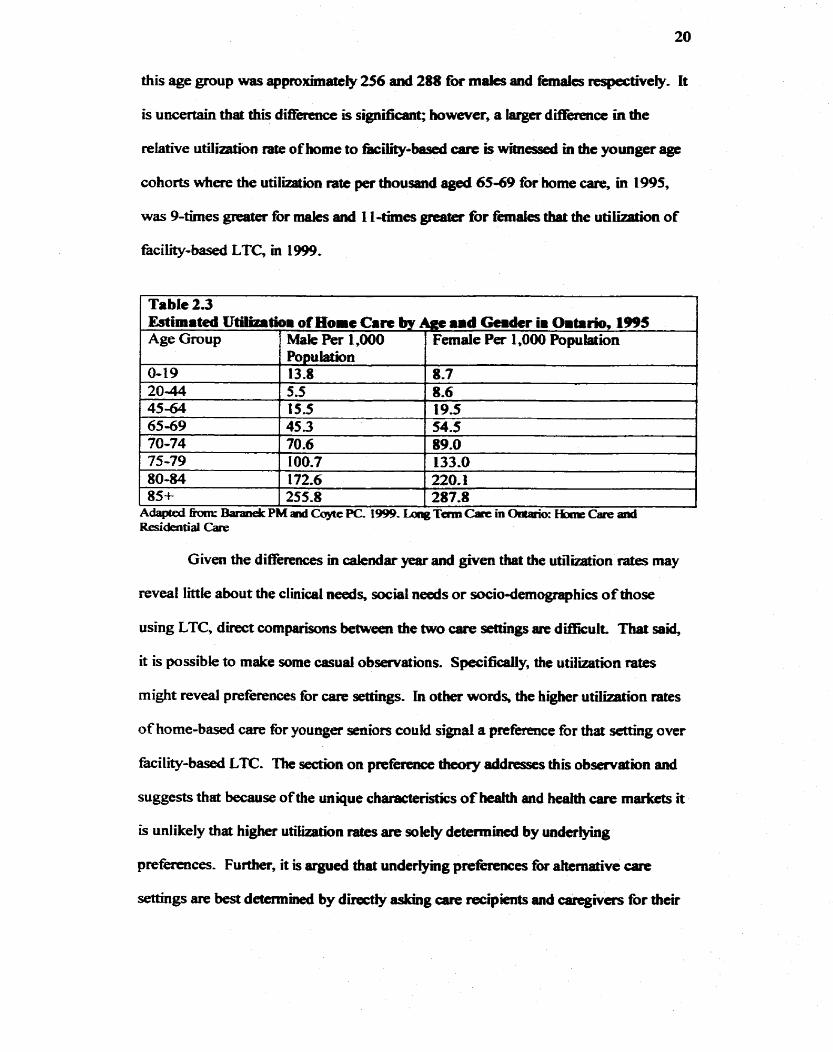
this age group was approrrimatcly 256 and 288 for males and fernales respectivefy, It
is uncertain haî this difference is significant; however, a larger diffhmce in the
relative utilinrtion rate of home to îàciiïty-based cart is witnessed in the younger age
cohorts where the utiiiization rate per tbousand aged 65-69 for home are , in 1995,
was 9-times for males and 1 l-times greater for fernales tbaî the ut iMon of
fâcility-based LTC, m 1999.
Given the differences m calendar year and given that the u w o n rates may
1
reveal Iittie about the c l i n i d needs, social needs or socio-dernographics of those
using LTC, direct cornparisons beniveen the two care settings are difficult. That said,
Table 2.3 Estimateà Utilizrtiom of Home Ca- bv Agc .id Gemdcr im Oitario, 1995
it is possible to make some casual observations. Specifiaiiy, the utiiization rates
Age Group
0-19 20-44 45-64 65-69 70-74 75-79 80-84
might reveal preferences for cane settllrgs. in other words, the higher utiIization rates
of home-based care for younger seniors could signal a prefaence for that sethg over
85+ I 255.8 I 287.8 I
Male Per 1,000 Female P a 1,000 Population
facility-bad LTC The section on preference dreory addresses this observation and
suggests that because of the unique chatacteristics of health and heaith care markcts it
is unlikely that higher utiiization ntco are mkty dctamined by underlying
preferences. Fu&-, it is argued that undermg prekences fbr ahernative care
settings are best determird by directly asking arc mcipients and caregivas for their
Population 13.8 5.5 15.5 45.3 70.6 100.7 172.6
8-7 8-6 19.5 54.5 89.0 133.0 220.1
preferences For now, it is suggesttd that, mtkc tbm demonstrraing underlylng
preferences for aitemaiive LTC &ngs it is equaily possible that the utilkaibn rates
reflect a trend towards - m tetms of availabiiity of and dvancemeats m - home-based
care. And just as Iikely, the political and tcommic dcsiraôility of homebased care
may be contributing to the utilization rate ditlérnices.
2.5 Preference Theory and Measirement
This section desai- the economic theory that underpins the mcthod d to
identie undermg (or ùurate) preferences for persons with chronic heahh problems.
The section shows, k m the ttieory ofconsumu behaviour, that preftrences influence
individuat decision-mahg and conquentiy prefcrences influence are-seeking
behaviour. As such economists and decision thcorists have sought ways and means to
measure preferences for heahh and health Gare services- Thtee methods - rating
scales, the standard gamble and the tirne tnde-off m) - are commoniy used to
elicit preferences for health. It is the purpose of thiï section to provide some
background on these techniques in order to cstablish th& the TfO was the most
appropriate method for this thesis.
In this thesis, Uiaate preferierices refer to the underfying preferiences exhibiteci
by care recipients and caregïvers with respect to the type and range of health Gare
services. Holding all other &tors consian& it is anticipated thaî a particular heah
care setting rnay be preferred, by care recipients and caeegivers, to 0th- heakh care
settings, and thaî if asked, both aue recipients and caregjvers might meal this
preferenceY0 'This is important for decision-maicers because if underlying (or innaîe)
preferences are not included m plinining th- rnay be a mismatch beâweea the type
and amount of care provided and the amount of care sought by care recipients and
caregivers- The idea that underiyhg prcf-es influence behaviour wdcrpins
consumer theory.
Consumer theory descriii and explains consumer behaviour. In it's simplest
fom, demand aad suppIy of goods and services, are d e s c n i via the market
mechanism. On the demand side, a consumer will choost those goods and services
that maximiz his or her utility - or dsfiiction - subject to his or her budget
constraint. On the supply side, a supplier will offer those goods and services tbaî
rnaximize profits subject to his or her cost wnstraint, In a market, prices act as
signais to demanders and to suppkcs because prices provide bot. infiormation and
incentives A market will equiliirate wherc the quantity demandai by consumers at
some price is exactiy equal to the quantity supplied ri the pame In a market
widi no imperfections, consumer preferences are revealed through changes in prias
of goods and serviœs.'
Preferences are reveaIed in the market only given a set of strict assumptions;
consequently, deviations h m this mode1 imply that preferences might not be
transparent- Because the market for health and health care do deviate h m the
"perfectly cornpetitive market," other models for analyshg the demand for heahh can
also be used to describe consumer behaviow.
An exampb of a model for evaluating the demand for heaith and health care is
found in Grosman's ll~eory of Ckalth ~a~ i ta l . ) * Gmssman uses consuma theory as
the foundation for a fhnework to understand an individual's investment in heaïth- In
the Grossrnan model heaith is a durable capital asset, not vaiued for itselfbut rather
'The foliowing conditions are ne- homogeneous pmdm large number of buyers and seIlers; ûwdom of cntry and exit; pcrfèct Sonnation; transadions of any one f'um is smali relative to the marlcet; no collusion smong buygs and s e k , consumers maximize utility anà seliers nriuumi profits; tbe commodity is transferable?
for me consumption and mvestment ôenents tbst flow h m heakl13~ In otbgr words,
heaith care is analogous to a washmg machine -one invests in a washmg machine not
for the washing machine k i f b u t because the washing machine ckais our clothes-
Accordhg to Grossman, people invest m berilth care services because of the
consumption bene% - people are bappy wfien they arc h&y - and because of the
invesûnent bene66 - better heaith enhances a person's productive capacity.
in a sirnpWed Grossnan modei, defined over two periods, consumers seek to
maximize their own u t i l i This utiiity is given by the h c t i o n 2- 1 below-
(2.1) U = f@i1,m,X1,~2 Iprefernices)
The utility fiinction 2.1, above, impiies that utility, a function of heatth state
(Hl ; H2) and consumption bundles -1 ; X2), is conditwned by one 's preferences-
Moreover, this irnp lies that two individuals with identical heahh States and
consumption bundles might stüi behave d i f f i t i y ifeach individd has different
under lymg preferences.
Even though a thorough description of the Grossman mode1 is beyond the
scope of this paper, the very simple exphnation provide- is sufficient to show that
underlying preferences are not absent in this model of care seeking behaviour of
individuais. Further, the example of tbe Grossman model demonstrates that a
h e w o r k , that does not require a direct trade in "health", for andysing the demand
for health care services does not dismiss preferences despite the fâct that pret'iietences
for health are no longer revded in the market. It remains diat the decision to invest
in h d (and seek and accept heah and social care services) is made by mdividuals
who maxirnizle utile; thmefore, it remains îhat behaviour is conditionad by
underlying preferences.
24
Preferences for heahh arc reveakd in the market via individuais' decisions to
purchase investment as opposai to consumption goods and consequentty alternative
means of measuring preferieaces have been developed. Pref-ccs have becn
measwed ùi health services reseamh for both cliiical decision-making and for heaith
program evaluotion." Program evaluatïon is, "the use of sociai rrserrch proecdurcs to
systematically investïgate die effectiveaess of social intervention programs that is
adapted to their political and organipit'ional cnvironments and designcd to inform
social action in ways thaî improve social oodition~-"~~erence measuremmt
might be considered a social resecirch procedure that can inform heahh and social care
decisions and actions.
Indeed, rneasuring preferences is advocated for evaluating cost-effectiveness
of heahh poiicy options? Consequmtiy, in heaiîh program evakiatiai the use of
preferences is moa evident in efficiency evaluaiion~.-'~ Refacnce values in this type
of evaluation are used as outcomcs and o h the focus is to determine the prefemce
for particular heaith states diat might be realizRd as a result of the heatth intervention
or program? Becaus preferience mcssunment is endorsecl,' there is a growing body
of literature concemed with " . -. the study of individual preferences - specifically
n27 how they can be rneasured and how they should be used m reaching decisions . . , , or preference tfieory, and at the heart of this theory is " -. - that peoples' preferences
should count in machmg decisions mit wül a f k t themla7
Preference theory is subject to debate. A compdensive review of each issue
in measuring preferenœs is beyond the scope of this papcr. niat said, some of the
debated issues are implicit in the next fèw paragraphs and explicit in Chapter 3-0:
Methods. Key debates include whose prcfa~nces should be mcaciirad, what
rneasurement tooi shoukf be used and what (a prefermce, a u t i l e or a value) the
chosen rneasurernent tao1 is i n e a ~ u c i ~ l ~ ? ~ ~ ~ ~ ~ The h main tools for meamring
health sbte preferences - rating scales, standard gamble and the-traie off - and their
respective measuns are d e s c n i ia turn, below.
A mting scaie can be used to rneasure pref-ces for beaith States.
Respondents are shown a picturc or similar visual aid of a I h e , with ckarly defined
endpoints, and instnicted to piace the heahh state of interest on the scale. A rating
scale is -y to admmister and conceptualiy easy for the riespondent to understand-
Rathg scales do not requk the respondent to make a choice bctween alternatives.
Consequentiy, rating d e s masure and value pref- by ranking die heaith
states but they do not produce "utilitics" per se. 37.39,40.42,43
The sbndard gambk is aiso commoniy used to elicit ptcferc~lces for health
states. In generaf, the standad gamble offers a choice between alternative 1 that 1 4 s
to a certain outcome, usually a chronic heghh state for the remabder o f WC, and
alternative 2 that leads to an uncertain outcome - ideal tieatth with probability, p, or
death with pmbabiiity, 1-p. The probabiLity, p, is varied until the tespondeut is
indifferent between the two aitematives- At indifference this probability, p, represents
the preferenœ, numeriçally, of the chronic heahh state. To ovemrne problems that
respondents have with understanding probability" rcscaichers have developed and
modified visual aids such as chance b o d s and probabüity wheels? &cause of the
standard garnble's foundations in expected utility theory the ptefecence values are
believed to numericaiiy rcpresent "utilityn. 43-45
The TT0 rnethod is the thiid common methd discussed here. The TT0
rnethod was developed specificalfy for use in htâhh evaluation and is one of three
main methods ernployed to determine pnfercnces for h a h h dates? '* 43*46 In a heaW
state application of the 'ïï0, p~ferences fbr heaiîh states are determincd indirectly by
asking the respondent to cboose between two certain health states; usually, a cbronic
health state and an ideai health stak The respondent is ofhed eitber chronic hedth
for the remainder of his or her We, TT, or ideal heahh for some tirne, X, les than T.
The respondent "trades" t h e for the more prcferred health state (ideal heahh). The
ITO for a chronic health state and en ideal hdth state is Uustrated in Figure 2.1
be Iow.
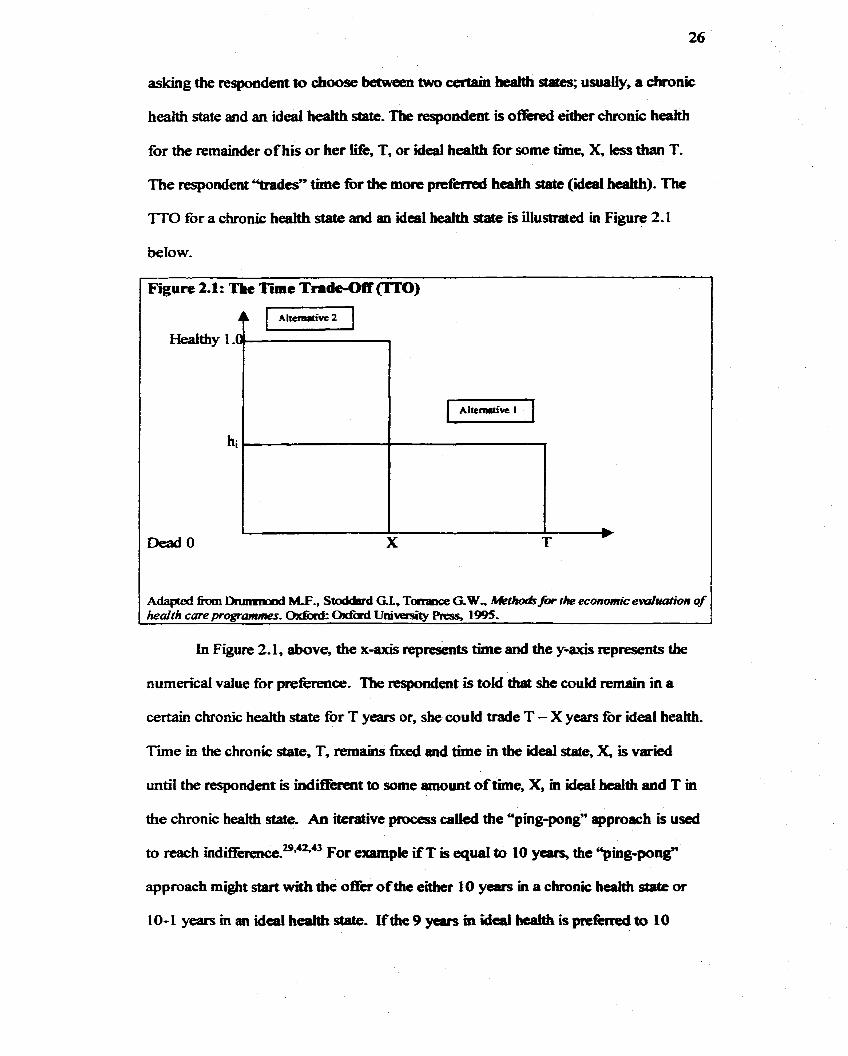
A@Hd fiioai Dnmmmd M., Stoddard GL, Torrance G-W, Meth& for the economic evoluation of healrh careprogrmrnes- Wrd Univasity PrPss, 1995.
Figure 2.1 : The Time Trade-Off 0)
In Figure 2.1, above, the x-axis reprekts t h e and the y& represents the
Healthy 1 ,Cm
numerical value for preference- The respondent is told that she could remab in a
Aherait-vc 2
certain chronic heaith state for T years or, she could trade T - X years for ideal heaîth.
T m e m the chronic state, T, remains fixed and time in the ideal date, X, is varied
'0
untiI the tespondent is indinkrent to some amount of tïme, X, m ideal hcaith and T in
hi
the chronic heahh state- An iterative process c a M the "'ping-pong" approach is used
to reach Ïndi~erience?*~~' For exampie XT is quai to 10 y- the "ping-pong?
pzzz-1
approach might start with the O& of the either 10 years in a chronic heaith state or
X T b
10-1 years m an ideal health state. If tbc 9 years m idcal hea1t.h is preftrred to IO
years in the chronic health sta5e then the next offa might be citha 10 years m a
chronic heatth state or 1 year in ideal M. If 10 years ia the chronic h& state is
preferred to f year in ideal hedth then the next O* mighî be 10 years m a chronic
health state or 8 years m ideal h d . Again, the iterative proces continues until
indifference is reached- I n d i f f i c e oocuts wben the mispondent will no longer trade
any years of lifè for ideal h&,
When mdiffince is reached it is possibie to vaiue the prefbmx for the
chronic health state.29*42*43 The vaiue for prefericnce is @en by die ratio X/T, Because
X is less than T the value of the chronic heahh state (state 1 in the figure) is less than
1 .O (unless the individual will not trade any time for the health state). Numefical
preference vaiues am ascertained for a @en heahh stase by assigning a vaiue of 1.0 to
ideal health, For example, if an individual is indifferent behween 5 years of ideal
health and 10 years in a c h n i c heaith state, his or k p r e f m value for this heakh
state is 5/10 or 0.5. When several diffèrent heahh ssates are valucd with the TT0 it is
possible to compare which states are more or kss preferrcd by comparing the values
of the TT0 score. The closer the value is to 1 .O the more preferred the heaith state.
This section has briefly descriid three pmference measurement techniques
that are used to detemine underlying (or innate) prefmces for bcakh and heahh
are , Each technique star& h m the proposition that prefetences c m be rneasured-
Preference measurement is important ifone ascn'bes to the theory that care recipieuts'
behaviour is conditioned by underiying (or innate) preferences. Prefetwlce
measurernent is therefore grounded in tbe assumption that cam recipiaits behave m a
way that maximizes their utility and consequently satisfïes prefcrences. If p r e h c e s
are unknown the care seeking behaviour of individuais mi@ not be properiy
anticipated by decision-makers and a miss--ch of services might resuk Ine desire
to match the services delivered to the care mipient with the services mught by the
Gare tecipient underiines the importance of determinihg preferences-
2.6 Elderïy Preferences for Cam Settings
Section 2 2 described a iiterature review search strategy that identifiai
underlying (or innrrte) prrfecences for a r e seüings, This section, eldedy preftrcnœs
for care settings, relates to the specific fïndings of that review. An array of studies
were identified that reiaîed to pretère~œs for care settnigs For example, studies
measured prefmnces for location of d s f - l i f k care,47~51"7*75 prefettnces for hospital
care vs- home care, 47-5134*55*76 prefirmces for âriliity-based a r e vs. homebaseci
-,52>6a and preferences for -ans of care other than a home-based care or
facility-based care or without such a cornparison!1*65*68~74 D i f l i n t , but d l relevant,
were studies that relatai to elderly perceptions of carenw7' and, otudies of elderly
az-ar.as.as-n preferences for trtabnent or health states-
The review of this literature identifies three things that support the present
study. First, it was diûïcult to fÏnd a study that rekted specifidy to elderly,
chronically ill, home care recipients. Second, none of the papas reviewed used the
method empioyed hem, the 'ITO, to messure the relative preferences for home-based
and facility-based care. fnstead, the studies that evaluated the prefmnces of home-
based and fafility-bacied care with scakd rrspoasess25738860 qualitative 8ssessment,"
or a b i n q response? And third, a kck of Canadian -dies was evident - oniy fow
of the studies Klentified onginated in Camda.50"wn-78 No twithstanding the d i f f i c ç s
in both the study questions and the snidy populations, some of the studies'
conclusions do inform this sbdy. Diffêreaces and relevant conclusions are discussed
bebw, with the conclusion that the lack of studies reiaîïng to prefemces for
alternative LTC settings primariiy m e s to underscore the importance of this paptr.
There w-ere a number o f -dies ideiitintd diat measured prefermces for
location of end-oGWe are^"^'*^'='^ Most of these studies evaiuated the prefèrence for
either death at home or, de& m the hospitd a d none evaluaîed a long-term kility-
based care option- Furthet, the majority of these studies eücited preferences for the
location of de& h m acute c m recipients and not h m those receiving home-based
care for a chronic illness. For exampk, Pritchard etal, (1 998) and Covinsky &al.
(2000), both studied the preferred location for de& - hospita1 or home - in paîïents
with acute Wilson (2ûûû), considemi the elderty preferences for location
of death in a study population that had experience carhg for a seriousiy iU individual
prior to that person's and McWhimKy etal. (1 995), and Dudgeon and
Kristjanson (1 999, retrospeaivefy examine and discuss whether preference for
Iocation of death was consistent with actual place of deah. 50.5 1
Two things are worth noting mgading the papers on prefcned location of
de&- First, it was evident that home death was preferred by care recipients to
hospital death in these study populations and second, there was evidence to suggest
that this preference was not known by physicians and/or sumgates such sis, a spouse
or child. Similar results wete found m Mattimore etal. (1997) where only 37%
(n=M 1 8) of surrogates and 25% (n= 1 067) of physicians knew exactly what the
preferences of the patients w e d 2 And in Mouton etd. (1 997), a lack of discussion,
and therefore knowledge, o f treatrnent prefetences with physicians was also
confimied?' Moreover, there was evidenœ that even wben the prrference was biown,
the location of death took place more often in the least preferred care setting. Suffice
it to say thai, if care rscipients prefeffnces are unbiown by fàmily and fami&
physicians, preferences for care settings are likely misunderstood by poticy makeis as
weil, This emphasiaes the importance o f includmg arc recipietits p r e b c e s m
evaluative research aud in planning for LTC.
References for hospitaï cart or home-based care have also been evahmted
whereùi the prefefence was for location of acute care rather than a prefereme for
location of deaîhc Coley etai, (1996), for instance, evaluated prefemices for
outpatient (home) care versus hospital care." Unfortunately, this study was not
lirnited to the elderly and was limited to iadiriduals with community-acquired
pneurnonia; thus, evaluating a younger population witb acute rather dren chronic
ihess- Freid etal- (1 W8), is more promismg in tbat the authors interview 29 petsons
aged 65-89 for the* feelings on home-based care versus hospital care; stili, the
question relates to a smgk mute episode?
The focus of Fried et-ai. (1998) was unrelated to the prefcrence for fâcility-
based care, but it is worth noting that prcferences did relate to belie) held by study
participants. In particular, prefmes were infïuenced by beliefs about what care
was possible in the home. In fàct, beliefk about wbaî wuid actually be d e l i v d in the
home coufd not be overcome even with given interviewers providing detailed
descriptions of available are . This illustrates the power of experience md knowledge
in forming preferences and signals to health rescarchers that it is possibIe for even the
best atternpts at de~criiing unfâmiliar services, to be in vain until the services are
actually available and in use.
Not al1 studies have restricted the location of interest to the home or the
hospitai- In fact, six said-ks were identifid that ciaimcd to assess the pmferiences for
homebased cane and fkiiii-based tare.'*- in geaeral, these papcrs identify the
iàcîlity as a 'hursing horne" and in one instance as a %est home". While nursing
homes are included in the definition of fàcility here, kility-based care is not limited
to the nursîng home and m thk swse these studk dïd not captue the prcfèrence fbr
facilîîy-based care that is of intexest m this paper- And dl, there are additional
difletences between these *dies a d the pment evduaaion.
For example, Mattimore et- al, (1997) exammed the wilüngness of seriously iil
patients to Iive m nursïng homes! nie ahanaive are locations wcre one's omi
home and a nwsùig home and the choice presented was similai. to the TT0 exercise
employed here - a move to a nursing home or eartiadeath. While this seems simiiar,
the differeaçe is subtle, Mattimore etal, assumed thrct m forma1 home care would be
avaiiable because it was not clinifalh. relevant to the study population to expect that
care could be provided- In this sense, the prefmce could be thought as prefmce
for care or no a r e . In contrast, it is of interest in the present shidy to determine, the
choice between home-based care and fàciüty-based care for elderiy p h t s - who
rnay be S ~ ~ O U S ~ Y il1 - without daciding whether the cboice was clmically relevant.
Instead it is assumed that the c u m t h e m state of tôe care recipient can be managed
in either care setting,
Chiu etal. (1998), were also mterested in the prefetences for living in a
nursing home but in contrast to Mattimore etal. (1998), provided the choice between
home are, as opposed to home with no ~arr, .ad nursing home 'Zhe study
population and study question m Chiu differs h m the study population and study
question of interest in ttiis paper because it is limitai to caregivers of stmke victims of
al1 ages.
Keysor et-al- (1999)' provides another exampk of a study that look at the
preference for LTC location in their evaluation of home-based care versus ricst home
ciire:' The study by Keysot etai. a p q particularly reknm to chis study for it's
attempt to understand what tkct0x-s predict a certain preference for location of c m -
Yet, in con- to this study, the primary focus of Kcysor etal, is the degrce to which
changes in disabif@ d a t e to pref'erence fbr location of LTC. While disability is a
f&or that is included here, disability is assumai to m a i n constant for each
individual and each care settïng. Evaluating disabiiity diffetences is instesd l i t e d to
the differences that exist across individuals-
The remahhg three studies rwiewed Illustrate -the dearth of studies
relevant to elderly preferences for LTC in Ontario. To Merstand pref-es for
LTC, held by consumers in the United States (US), Martin Gibla etal. (1997)
evaluated coasumers' understandmg of LTC ahernatives availabk in the US?' Whik
it is interestmg diat the authors conclude th& LTC is negativeiy and narrowly
perceived as 'hursing homes", that "maay" desired m-home care, and that most
people do not have a good understanding of the options, iî is unknown ifthis
perception would be identicaI in Chtario where the options for LTC are not the sanie.
SimilarIy, anotber LTC setîing study by Porter etal, (2000), examuled the preférence
for in-home service fkom the penpective of one 94-year old, rural, black woman
which is not illustrative of what is of interest in this study." And finally, McCusker
reports on the development o f a scaie tbat measutes preferences for home care
without specifically focussïng on the question of wht the p n h a s actu~üy are6"
The studies that evaluate preferences for the home-based and c~l i ty"-based
alternatives do contain some i n m g and potentiaily relevant results not the l e m of
which is that home-bad care was most often preferred to faciüty-based care. For
example, of thos mtervicwedg (n=3262) by MstiUnore etal., only 26% were eitha
very willing or sornewhat willmg to live in a nursmg home wbile 37% were somewtiat
unwiliing or very unwillmg to livc in a nursing home aad a fbrther 30./0 responded
The study panicipents were not living in a nirsiag bant at the tim ofthe interview ôut wuc inten?iewed in hosptal fdlowing admissicm fiir seriam illness.
that they would ratha die, The remaming 6% ~esponded that tbey did not laiow.
W e this might impiy that people prefer home-based care to hcifity-based carie (and
does ünply thaî people m those sfudies p~~ home care to ncvsing a nursing home
or to a rest home) this conclusion needs to be confînned for îhe elderly population in
Ontario,
Researchas have extensiveiy employed the fonnal methods fôr measwing
pre ferences discussed in Section 2.5. A review o f the studies that detennine
preferences for health or health care using fbrmal quantitative rnethods is beyond the
scope of this paper! That said., three cornmon measurement techniques - ratmg
scaies, the standard gamble and the time îde-off - werc considered prbr to seiection
of the TT0 method used to masure underlying (or innate) preferences for two
distinct care settmgs, nie jdfication for the choice of tht TïO is *en m Chapter 3:
Methods. The point made here is thaî formal methods appear hfkquently in the
studies used to determine prefeFenœs for location of case. I n d d this could be
related to the infkquency o f detmnining p r e h c e s for location of care but it
remains that the formal methods for determinhg p&kences are rare@, ifever, used,
in fàct, preferences for location of tare, in the -dies identified to have
mestsured sucb a preferience, asked only for a single response to a simple question and
it was not uncommon to fhd the use of qualitatbe, rather than quantitative methods to
descrii preferences. It m a i n s to be determined ifelderly pritferences for home-
b d and facility-based mue can be BSCerf8ined usmg the TT0 rnethod.
h n i c f f e i n ~ ~ a m i r e t ~ r i c v i c w d t b e q p l i a t i o n a f ~ m r r a r i r m m c t o o l s ~ i s o f k d here should sec Brapkra al Cl-), Dnainmd d al (lm and Gdd a d (1995). BrrP'a et al p.ovi& a oamprdiensivP m*w of the t dmkpm d a Ydariy oonpebaishe iist of to the techniques devtlqment ad qplidm Bah Ikunmiad (lm in C b @ u 6, Cow-Utiüty Anaiysis and M d et al (1995) in Cb@u4, Idaitiwng ad Valuing lis rcfkmm 50r this topic.
2.7 Chapter Sammary
This section had fbur goals. The fkt was to show that prekmwes for
alternative care settings have a "place" in pIanning LTC for the elderly because they
are often cited but rarely opcrationalizcd. It undermines the efforts to indude
preferences i f these prekemces are unlmown; thus, meeting the fïrst goal justitis the
relevance of this study for LTC planning aod policy.
The second goal was to review tbe litcraîure pertaming to care setting~ home-
based care and faciiity-based car% duit are relevant to this thesis- The
estab lihed why home-based care and hility-based care WWR appropriate aitematives
for this pilot study. The third goal was to danonstrate îhaî prefèreces
influence care seeking khaviour and can be measured. Therefore, accomplishing this
goal serves to justie using quantitative m a s for elicitmg prcîèremxs h m the
elderly population in this study.
The finai goal was to show tbat there is a de& of information rclating
spcifically to elderly prefetences for heahh care settings. Aibugh some simiiar
studies exist, it remains uncertain thaî their m h s art applicable to Ontano.
Achieving tfiis goal not on& justifies the foIlowing study but also UndetScotes its
necessity. In sum, ifelderty prefkmces were to appear in LTC planning rnethods and
elderly preferences can be quantitatively measured, then a determination of
preferences held by the elderly n d s to be dertaken. This is the goai of the pilot
study that follows.
Chapter 3
3.0 Methods
This chapter describes the methods u d in this study to measurit the
underlying or innate prtferences for two distinct sue settings for persons with chronic
health pro blems, The cbapter outlines, m fo w sections, the study type, die study
population, the data colkction methods and the anaiysis sSratcgy.
3.1 Study Type
This is a pilot saidy to measurc the undertying or uuiak preferwices for two
distinct care settuigs for persons witb cbronic heab problems. A pilot study is, a
small-scale test o f the methods and procedures to be used on a larger scale ifthe pilot
study were to dernonstrate that these methods and procedures can worlc.' A püot
study was justifhi tor this research b s e underlying or innate preferences wem
measured using the the trade-off method which had not been used to answer a
similar research question.
3.2 Study Population
This section outlines the meùiods used to identw and m i t the study
population intervieweci to measure underlying or innate preferences for two distinct
care settings. The section d e s c r i i in detaïi the recruitment process and the mclusion
criteria.
3.2.1 Recruitmcnt
Snidy participants were recruited h m the North York Comrnunity O r e
Access Centre (NYCCAC) m Toronto, Ontario, Canada Upon approval for this
study fiom the University o f Toronto ethics cornmittee in January 200 1, the Director
of Client Services at the NYCCAC was conîaeted m order to help idmtifjr potential
participants. A meeLing was held with the m b r of C k t Services to explain the
purpose of the study and the inclusion criteria- After this meeting, the Director
of Clients Services held an addihionsi meeting with case managers at the NYCCAC.
The case managers were presented the study protocol and inclusion criteria and asked
to idente potentiai participants fot this study, Rccmitment occurred over a two-
month period m Febniary and March 200 1,
Recruitment and consent to participate rcquired t h e steps. Fïcst, potedial
participants, defined in Section 3.2.2 were contacteci by tciephone by their case
managers. This initial step was mandatory because of cüent c o n ~ t i a i ï t y and a
NYCCAC policy tbaî ail requats for care riecipient participation in research are made
first by a care recipient's case managed Case managas me &en a tekphone
recruitment script (Appendix i ) to assist with the seiection of study participants, Only
if the care riecipient gave verbal conseat to participate to his or her case manager, did
his or her name, phone number, and address get forwarded to the author-
The second step in recniitmcnt and consent was to telephone al1 care recipients
who had agreed to participate after the M M phone call. Potentid participants were
telephoned a second t h e by the author to conf'um verbal consent and arrange an
inteMew date and time (Appendix II). At this point, care recipients were fke to
decline and received no fbrther contact-
The fhal step in recmitrnent and consent iequired that the participants sign a
d e n consent fonn (Appendix m). nie consent form was given to participants, by
the author, at the start of each inteMew. A11 participants read the consent form, had a
caregiver read the consent fonn or were read the consent fonn by the author. ifcare
recipients signed the consent fonn, die intaview continucd and the carie mipient was
included in the study- If the care recipients reftsed to sign the consent form, they
were thanked for dreu the, and the mterview was termniated - no fiirther data was
coliected on those who r e f i d to consent- Ihe author conducteci al1 interviews-
3.2.2 Iiclwioir Criteria
This study is concerned with measuring underlyïng or h a t e preferences of
persons with chronic heaith problans, Therefore, case managers were responsbk for
identifjhg potential participants who were not receivrng home-based care for either a
terminal iliness or a postgcute episode, In addition, c a ~ e recipmits wcre included if
they were over 65 years of age and Englïsh speaking and oognitively intaict AWugh
care recipients who are < 65 ycars of age tiepresent over 50% of the clicnt care base at
the NYCCAC, it is the prefkences of the elderly that were o f interest here. A gtasp
of the English language and no cognitive impairment were necessary because the
consent forms, surveys and personal interviews were dl required and adrnïnistered in
Engiisb. Care recipients wem disthguished on the basis of LTC waiting lkt status, i.e-
either on a waiting list for a LTC fiicility or not. Care recipicnts were dso
disthguished on the basis of their approximare number of limitations in Activities o f
Daily Living ( A m ) - eitber less than 3 ADL or 2 3 ADL.
ADLs are a rneasure o f fhctional disabiiity associated with the perrôrmance
of activities of daily living, such as walking, washing, bathing and gmoming, and
ushg the t o ü d In general, the pater the nurnkr of ADL mtrietiom the more
severe the level of disability although even one limitation in ADL has been used as a
proxy measure of severe disability? nie case managers who wen most fhmiiiar with
the care recipient were asked to estimate disability accordhg to the number of ADLs.
Because ADLs are aot officially documented in the NYCCAC it was not
possible to deâermine an exact number of limitations for a care recipient2 Case
managers were asked to specifj. it, m their opinion, the cam mipient had eidier kss
t h d q u a l to or, more than 3 ADLs but this daîa was not used m the analysis. The
request to estimate the number o f ADLs was used to ensure variation m heahh astus
in a sample that was not randomly sclected. Acîual h e m status was rne8sured with
the EuroQoI EQ-SD. The limitations of this are discussed in Chapter 5 and 6.
3 3 Data Coiiection
This section describes and justifies uie methods and sources used to collect the
data. The section rnirrors the chronological order of the personal mterview and data
coiiection. Prirnary data was collected on age, gender, waiting list (for hciiiibased
a r e ) statu% marital statu% tivi~g arrangements, availabiIity and tirne cornmitment of
a live-in informa1 caregiver, housing type, housing ownash'i, income, c u m t h d t h
status, own perception of health and prefkence for home-based or fàcirity-based are.
There were two p r h a y data sources for this study -the NYCCAC and personal
interviews,
Data was colkted f k t h m the NYCCAC and then h m the personal
interview. Age, gender, waïting list status and approximate nwnber of ADLs were
provided by the NYCCAC. All other variables were obtained dunng the personal
interview with the care recipient, The personal mterview begm a h an explmation
of the study purpose (Appendix LV) and after the care recipients signed the consent
fonn (Appendix V). The interview then assesed hea2efi stahis using the EuroQol EQ-
5D (Appendix VI), elicited preferences using both direct questionkg (Appendix VE)
and the tirne trade-offm) m e t h i (Appeadix VIII), and gathered remaining socio-
demographic data with a survey (Appendix TX). Each instrument is d e s c n i in turn.
The first phase of the personal intcmew detennimd care recipients' current
health * tus and own perception of health. Health staais and own perception of
health cm be measured using a standardised heahh s~atus measutement instrument
that asesses a pcrson's hcahh m s s brod categorics such as physicsl hctioning or
mental well-king.' In ais hdy, halth stshis and own perception of health wcre
measured with the EuroQol EQSD.
The EuroQol EQ-SD is a two-part tool that was designed m 1990 by a group
in Western Europe as a staadardistd, non-diseasespccific instrument to m m
different health s ta td The orst part dctcnnims heahb sts<us and the second part
detemines own perception of heahh, When fïrst introduced, the EuroQol assessed
health stanis within six domains - mobility, seLfkare, main activity, social
relationships, pain and mood.' Since 1990, the EuroQol has been reviscd to We
domains and now includes mobility, seIf-, usuai activity, paiddismmfort and
anxiety/depmsion? Within each domain thcm arc thra possibk rrsponses tha
reflect in general, no probiems, some probiems or extreme probiems within each
domah A single index for heah s~ate can be genetated from a fonnula - that was
based on tirne trade-off prcfe~ence scores - for 243 possibk health statedO*"
The second part of the EuroQol E Q 4 D is the visual analogue scale (VAS) to
masure own perception of health, At the bottom is the worst imaginable heslth state
(given a numerical value of O) a d at the top is the best imaginable beafth state (given
a numerical value of 100).'~ For this part of the EumQol EQ5D, the respoadent is
asked to mark his or her own health state diriectly on the scsle, The numetical value at
which the respondent marks his or her health represents the overall perçeption of
one's own health.
The EuroQol EQ-SD was scIected for this study because it is, generic, easy to
administer, short, ~Iiable and v ~ l i d ? ~ ~ ~ * ' ~ In addition, it is appropriate to present a
single weighted score h m the EuroQol EQ-SD and to diFactly interpret the VAS
score as a meanire of seIf-rated hahh." Theriefore, eima nurnber could potcntiilly
be included in the regession mode1 as a proxy for heahh status and self-ratcd heahh.
A fidl description of botb psrts ofthe EuroQol EQ-SD was given to each to
each study participant. Study participants were then asked to complete the EuroQul
EQ-SD. if the care recipient was unable to compkte the EuroQol EQ-SD, due for
example to blindness or an inability to write, then tbe interviewer conducted an oral
interview- Alteniatively, if a caregiver was p-t for the interview, he or sbe couid
help the care recipient cornplete the EmQol in the presence of the interviewer.
The next phase of the mtervicw was preferaice clicitatioa. Data on
preferences for health care settings wem elicited ushg two techniques: a direct
question and the 'ITO method. The direct question method prtsented descriptions of
home-based care and ki'lity-based care and asked care recipients to state which LTC
setting was preferred. Botb descriptions ulnere read abud to care recipients by the
interviewer and the p~efkrred care m g response was recordeci-
The primary reason for the first p r e f m question was to determine which
care setting to use as the anchor (analogous to a chronic b i t h m e ) in the TT0
method (the justification for this follows). That said, other researchers have asked a
single, direct question of elderly preference for care setting and found that more
respondents preferred home-based Tt was hypothcsised that the fjrst
pre ference question couki, secondarily, c o n h or refite a preknce for home-based
care in this study population.
The second mettrod for collecting data on pmf-ces was the t h e trade-off
(TTO). The TïO method was descn'bcd m Chapter 2.0, Section 2.6, above. Indeed,
preferences for health states can be, and have becn, meamred with other
Two commoa methods for masuriag prcfaaces include the rating
scale and the standard gsmbie whicb were d e s c n i in Chaptcr 2.0, Section 2.6,
above. These descriptions pmvided the foundations for explaming the selection of the
T T 0 method over either the rating scale or the standard gambk In the fbllowing
paragraphs it is made clear that the time trade off was appropriate for the second
prefèrence measure uscd in this saidy-
in an extensive rcview of iieahh sûttus measures used in economic evaluation,
Brazier -ai, (1999), cornpanxi and contmsted the techniques for eliciting preferences.
Rathg sales, the standard gamble and the TT0 were ail ptactical, acceptable and
reliable. However, the more cornplex the technique, the lower the completion rate.
The standard gamble and the TT0 demonstrated sirniiar completion rates to each
other and both were slightly less successfùl on ampletion, than the rating scale.
That said, the ratmg scale was based on p s y ~ h o r n ~ c s and psychophysics and is
theoretically inf&or to the standard gamble on the basis of econornic theory and the
TT0 on the basis that the TïO involves a choice betwecn altemathes, Even though
the standard gambIe is more grounded m economic theory than the TTO, the standard
gamble was still not considered superior to the ïTOI
in fact, no single method was found to outpedonn another with enough
consistency or over enough criteria to be riecommendeci as the ultimaîe measurement
tool. This conclusion was consistent with the recommendations for cost-effectiveness
evaluations made by Goki etal. (1 9wU, but is diffèrent h m Torrance (1989)~ and
Mehrez and G d i (1991)~' who bod~ endoRed the standard gambk, and W o b n
et.al. ( 1 9 8 2 ) ~ and Richardson (1994)'~ who both supportcd the TM. Given that no
"gold-s tdd" exists, the TïO method was sclected over the standard gamble and
the rating scale because it was more easily adapteci to measure the underfying or
innate prefetences for two distinct care settings -as opposed to heolth states - of persons with chronic health pmblerns.
Until now, tbere bas been no refetence to the u x of a measurement tool that
elicits preferences for aitemative care s&gs rather dran alternative heaith states. It
shoufd be noted that al1 of the tools mi@ be applied for this purpose - the lack of
explanation was intentional. As al1 of the techniques have performed well, the dioie
of technique was ultimately determined by considering how each might be used to
measure pref-ces for two distnict carie settings.
3.3.1 MetLod S&dioi
The ITO was considered the best choice to d e t e m i the preference for
home-based and facility-bad care. The rating scaie was not appropriate because it
would have required that some care setting anchor the top and a dinerent care setîing
anchor the bottom. This would have ixnposed a ' k s i? and "worst" care sctting with
the care recipient valuing home-based and kility-based care somewhere between the
two. While it seems reasonable that ideal health and death anchor the rating scale for
eliciting preferences for chronic heahh states, it was not reasonab le to make sirnilar
assumptions about alteniathe h& and social case settiags. This ruied out the rating
s d e .
The standard garnble was also rejected because Lke the ratmg scale, it required
some care sethg analogous to ideal healdi. The care settings of interest, home-based
or fàcility-based care, would be analogous to the chroniç hcalth state. Again, there
was a problem with determining the appropriate carc setting to use.
The standard gamble was also considered inappropriate beicause it required a
choice between alternaîivcs with outcomes. This was pmbkmatic in light of the
fol Iowing example: Suppose the choice offetcd waq home-based care or the "ideal"
care setting with probability, p, and death with probability 1-p? This question
demonstrated a problern with appiyÏng the standard gamble to tbe research question in
tbis study - heahh outcornes are not considered here- In the case o f a chronic healtb
state aitemative 1 was, for example, a new treatmeat while altemative 2 was, for
example, do-nothing. The trie9nnent Is uncer&Ui and th= is some ri& of death. b
other words each aitemative has a heafth outcome -one is certain and one is
uncertain- In this study, the alternatives were homebaseà and kiiity-based care and
the outcomes were both certain in the sense thaî eiuiet one p r e f d home-bad c m
or one preferred fàciiity-based tare No fùrther health outcornes tbat resuh h m the
care setîing were considemi,
3.3.2 Tbe T i c TrrbOPT
The TT0 method circumvented tbe problems identifiai with the rating scale
and the standard gambie. The ïTO rnethod detennmes pref- for two certain
alternatives and was therefore appropriate for determining the prefetenœ for either
homebased care or kility-based catt when heaith outcomes were not considered.
Further, the TT0 used in this study did not requke that some care setting was an
"ideal" care setting. I n d , a p r e f d care sethg was establishd by d k t i y
askÏng which, home-based care or fbcitity-based care, was preferred. The care setting
that was least preferred was analogous to the chronic healtn state and the respondent
traâed years of life for the more preferred care setting. The application of the TT0
method is üiustrated in Figure 3-1, below.
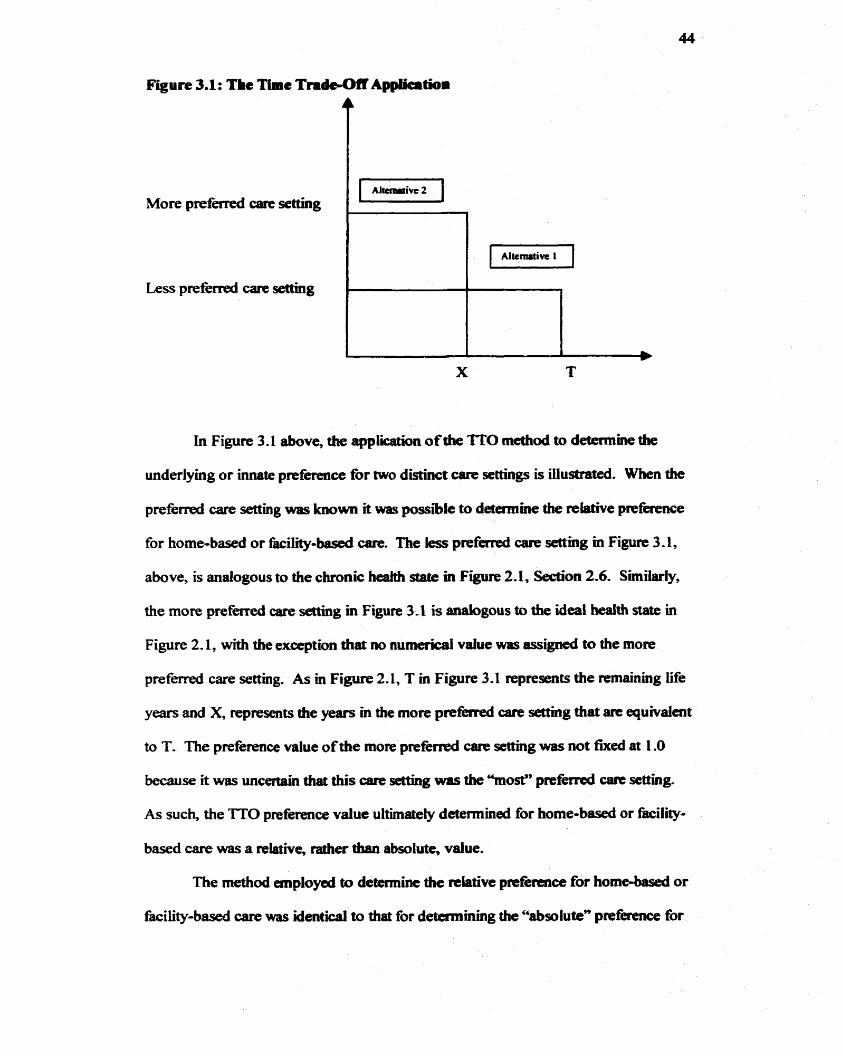
Figure 3.1 : The Time Tndc-on Applicitioa
More p r e f d care setting
L e s prefkrred care setting
In Figure 3.1 above, the application of the 'ITO method to determine the
underlying or uuiate preference for two distinct care settings is iilustrated. When the
preferred care setting was known it was possible to detemme the relotive prefacnce
for home-baseci or facility-based care. The less preferred care setting in Figure 3.1,
above, is analogous to the chronic heaith in Figure 2.1, Section 2.6. Similarly,
the more preferred care setting m Figure 3-1 is analogous to the i d e - Mth state in
Figure 2.1, with the exception that no numerical value was assigned to the more
preferred care setting. As in Figure 2.1, T in Figure 3.1 represents the remaining me
years and X, represents the years m the more p r e f d care d g that arc equivdent
to T. The preference value of the more p r e f ê d care setting was not fixeci at 1 .O
because it was uncertain that uiis care setting was the "most" p r e f d mue setting.
As such, the T T 0 preference value ultimately dctennined for home-based or fàcility-
based care was a relative, rather than absolute, value-
The rnethod employai to determine the relative preferaice for home-based or
faciiity-based care was identica) to that for detemrining the c'absolute" prefèrence for
a chronic health state. The care m-pient was offeffd the less p r c f d seüing for T
years or the more preferred care settuig for some amount of time, X < T and the
iterative "ping-pong" approach was uscd to mach indifkmce- T, the rernaining life
years, was detenniacd hm, Life T'dies Cuuds and ~mvinces. 1980-1982~' prior to
the personal iutervi*ew- Knowing T and deteminhg X widi the TT0 fàcilitated the
determination of the relative preference for either home-based or hiiïty-based are.
The m0 was employed on each carie recipient a d o r dieir carcgiver with the
help of a visual aid (Appendix XV). Al1 aire riecipients andor caregivers were shown
the visual aid and asked to tmde y- of life for the more preferred a r e settins Tbe
ITO rnethod was directed to the care recipient; however, consultation betwœn the
care recipient and the camgiver during the TT0 mcthod was alloweâ. if consensus
between the care recipient and a g i v e r wes not achieved, the care recipient's
response was recordeci. The TT0 was direct& to the caregiver o d y if die care
recipient was unable to responâ, for example if the care recipient was too sick (n =8).
The indflerence point was rccorded when the a re recipient wouM no longer trade
any more tirne, in years, for the more preferred care &g. AppendÏx Vm d e l s the
TT0 method whea the p r e h e û care seuïng was home-bascd case and Appendix PX
details the TT0 rnethod when îhe preferred care setting was the kiiity-based care
setting-
3.33 Find Ihta Colkdioi MetLods
The final phase of die pasonal interview was a survey (Appendix XI). The
survey comprised seven questions related to tbe socio-demographic data considerd m
the sîudy. Maritai -tus, living arrangements, availability and time oommitment of a
live-in informal caregiver, housing type, housing ownclship and incornes wexe
addressed. Thest variables as well as age, gender and waiting (for facility-based care)
list status, were chosen becaus thcy rcpriesented factors that are important to planning
L T ~ " ~ and because they r e M data tblt is known at a regionai kvel h m the
Census of ~opulation~~, the National Popul.tioa Hedh ~urvcy)''~, the Hcrkh and
Activity Limitation ~ u z y t q ? ~ * ~ and The CPMdian Community Health survey." It
was anticipateci that ifdie model were prcdictïve, the model could bc uscd at a
regional level so it was important to sekct variables diat were either the same as those
at a regional Ievei or that could proxy variables lawiwn at a regional level-
The personal niterview was concluded when the care tecipient and caregiver
had completed the sucvey. Ail ïndividuals wem t)uuiked for tb& participation at tbat
tune and subsequently sent a thank-you Ïn the mail (Appendix XVI). ind~iduds
were not financiaUy compensated fbr their participation.
3.4 Analysis Stmtegy
This section demonstratts why and how petsonal chsracteristics, independent
variables, were selected. Primary data was couected on age, gender, wai-ting list (for
façility-based care) status, marital status, Iivmg arrangements, availability and time
cornmitment of an informa) caregiver, housing type, housing ownership, income,
current health stanis and own perception of health. Each characteristic is considered in
tuni, This section then outlines the analysis strategy for the relative preference for
home-based care, the dependent variable, for this study.
The chmenstic was age- Age was necessary for the T T 0 method but
was also inctuded because it has been considered in other prieference studies with
uiconclusive results. Studies have found that age both is4' and is not significant in
predicring elderiy p~f i rraccP for location or type of csn."*'8"3" Age is aiso
positiveiy associateci with the utiiization of LTC in Ontano and because prefemces
have been fouad to predict utiüntion etsewhere* it was of interest to dctermme if-
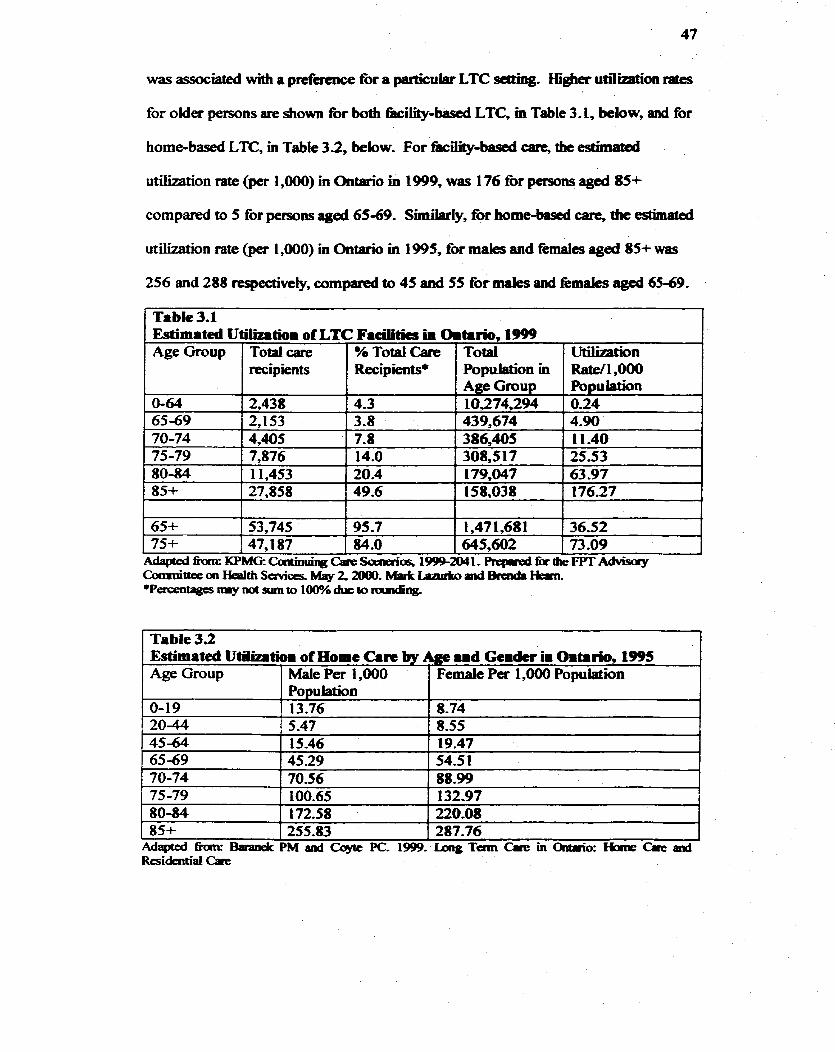
was associaîed with a prcfacaçe for a particuiar LTC seaing. fiigher utlli;catl*on rates
for oMer persons are shown for bodi k i i i t y -bad LTC, ni Table 3.1, below, and for
home-based LTC, in Table 3.2, below. For ~ ~ - b a s e d c m , the estimatcd
utilization rate (pet 1,000) in Ontario in 1999, was 176 for persons aged 85+
comparai to 5 for persoas aged 65-69. Sunilariy, for home-basai care, estimate-
utilizaîion rate (per 1,000) in Ontario in 1995, for males and fèmales aged 85+ was
256 and 288 respectively, compared to 45 and 55 for maies and fernales aged 65-69.
I
Table 3.1 Esfimated Utiüzlrtioi of LTC Facilitics in OiCirio, 1999
1 Table 3.2 1
Age Group
0-64 65-69 70-74 75-79 80-84 85+
1
65+ 75+
Estimated Utilizrtioi of Home Can by Age .id Geidcr u Oitario, 1995 Age Group 1 Mak Fer 1,000 1 Femaie Pa 1,000 Population
Total care recipient s
2,438 2,153 4,405
AdaptedfiomrKPMG:CartioriingC;neScaiaios, 1~2041.Repired*theFPrAdvisoy Comaiaee cm Health Services. May 2, îüûû- Mark ïamb a d Ikarcla Hiam. *Percmtagcsttieymtsumto 1w/oduetoniundiiig.
1
0-19 20-44
% TotalCare Recipients*
53,745 47,187
1 1 1,47 1,68 1 1 36.52 95.7
84.0 645,602
Population 13.76 5.47
25-53 63 -97 176.27
Total Population in Age Group
7,876 1 14.0 1 1,453 1 20.4 27,858 f 49.6
I
73 .O9
8.74 8.55
. * Wtbation R a t d ,000 Population
308,517 179,047 158,038
0.24 4.90 1 l -40
4-3 [ 10374,294 3.8 7-8
439,674 386,405
A second personal cbaractcristic was geader. Table 3.2, above, dernonstrates
gender differences in home-based care in Ontano la 1995, Women m ab age
categories, with the exception of those aged 0-19, reportad gr#rtet u o i n of home
care services than men. In addition, though not reported in Table 2, women in ail age
groups over 45 reported a grcater intensity of home care utilization (morie per
home care recipient) thn men in Ontario in 1995:' This hpliks that not on& were
more women reporting a grieater p r o p i t y to use home care scrvicq womcn were
also using and receiving more Servjces than theu male counterparts? It was of
interest here to determine ifrelative pref- like utilizatioh, were iafluencod by
gender. In addition, gender has been a variable included ia other prefetence studies
where, Iïke age, gender has been both a s igdj~ant~~ and insignioclat firror.'8-u*'6
Marital status, living arrangements and availability and time cornmiunent of
an inforna1 caregïver each relate to the extent of mfonnd are available to the çare
recipient. informai care is defined as "diat cate pmvided by h i l y and fiknds,
neighbours and . . . volunteer agencks - . .@J)~?'*'' Infomal care dBers f h n fomaf
care in that t h m is no formal client-agency relationship? The Diforna1 care sector
accounts for the greatest portion of cam providers withm the LTC continuum - it has
been estimateci that almost 75% of the 3.4 million Canadians older than sixty five
years of age receivc assistance h m an mfomai -ver!' Given the extent that
those over 65 years of age rely on informa1 care, variation in the availability of an
informal caregiver was hypotbesized to influence the prefericnœ for care se#uigs.
Indeed, marital status, living arrangements and the availability o f informal care have
al1 been associated with a p r e h c e for location of c ~ . " * ' * ~ ~
Houshg type and housing O-p arr included b s e housmg is an
integral componeat to the production o f health. An assurnption that is ïmplicitly made
where there have been shifts away fbm the acute care scctor to the community is that
appropriate housing circumstances exist to enable that shift; however, most homes,
even the h e s t homes, were not designed to be the satng for the provision of LTC."
Housing policy m Canada may not be respoading appropriately to the changes in the
LTC sector or to the changes in the agemg Moreover, no study, to
measure a preference for location of care, included dris variable in a modeL
Therefore, it was of interest to determine if boushg type and o d p influmced
preferences for home-based or tàciiity-based care.
Education and incorne level are also variables that fàcüitate the use o f LTC
services. Because utiIization o f health care services difTets across socio-economic
(SES) groups," it is o f mterest to consider if preferences also differ by SES. Socio-
economic status is relaîed not only to incorne leveis but also to education Ieveis
because higher levels o f education are associated with better employment, and
Lifetime opportunities and knowledge. Therefore, the mode1 included data both on
incornes and education levels. Education and incorne have been wtisidered m other
investigations. No support was found for any significant relationship h e e n
incornes and preferences for M o n of are.''-'^ In con- therr is both supportM"
and opposition"*18 that education is associateâ with a pmferellce for location of are.
Current health status and own perception of h d t h were also included m the
analysis. As discussed, in Section 3.3, both cumnt health status and own perception
of heaIth were rneasud with the EuroQol EQSD. Currcnt beiW stanis is likeiy to
influence the p r e f e m œ for care s&g which is evidenced by studies that showcd a
change m halth stahis changed preféremes tor are-"^*"" Thmfore, cumnt
healtk stanis, measured the EuroQot EQLSD was mchided- Sirnilariy, aüiû~dcs and
beliee rnight shape tare recipients' and czuegivers' p r e h c e s for LTC and proxy
measures of attiîudmaf hiaors bave becn invesboguted with respect to health and social
care services utilization with mixed resub, L's6-s8 Tt was hypotheSiOCd tbt o m health
perception, messurad by a reliabk end valid tool such as the EuroQol EQ-SD, rnight
influence the preference for borne-based tare- As such this measure of own health
perception wss mcluded hcrt-
3.5 Chapter Sumiiury
This chapter has d e s c n i and ju- the metbods and instruments used to
detemine the underlying or inuate prefètences for two distinct care settings- This was
a pilot study condudcd on a populetion of elder&, chronically ill home carie recipients
of the North York Community Care Access Centre. Scientific decisions made prior to
data collection kluded the choice of heahh status measurement tml and the choice
of preference elicitation rnethod. h addition, alI mdepmdent vanables were
considered for both theu potential mfluence on preference for alternative Gare settings
and for their potentiai application to regional data. Data was collected h m the
NYCCAC and k m personal interviews. This data was aaalyaed usmg tegression
techniques. The resuits of regression aaalysis are presented in the next chapter.
Chapter 4
4.0 Resulb
This chapter sumarilies the iesuhs of the data to identifil the underiying (or
innate) preerences for two distinct are st#ings for pasons with chronic heahb
problerns, The cfiapter is dïvided into four sections- Section 4.1, descri- the
personal characteristics of the finai mdy population. In die ncxt section, Section 4.2,
the results h m the EuroQol EQ-SD for die final study popubtion are given, The
third section, Section 4.3, summatiaes the responscs h m the direct pricfcrrnœ
question and the TT0 method and the final section, Section 4.4, summarizcs the
resuits fiom a regression rinalysis of die relative pmf- fbr home-baseâ care. in
Chapter 5: Discussion Part i, and Chapter 6: Discussion Part LI, the results are
interpreted,
4.1 Sbdy PopuIation
From the sample of 52 care recipknts identifieci by case manage= at t&e
NYCCAC for this study, 42 study participants cornpleted the mterview. The reasons
for non-completion are given m Table 4.1, below- Four a r e rccipients declined an
mterview wtien telephoned the second time by the author. One care recipht agreed
to an interview and subsequently declined to sign a written consent form. Two care
recipients were identified who did not meet the inclusion criteria - one was under the
age of 65 and the other was receivnig home cart for a post-acute probiem. Three tare
recipients coutd not be wntacted or were not availabk during the interview period,
Febmary 200 1 - March 200 1.
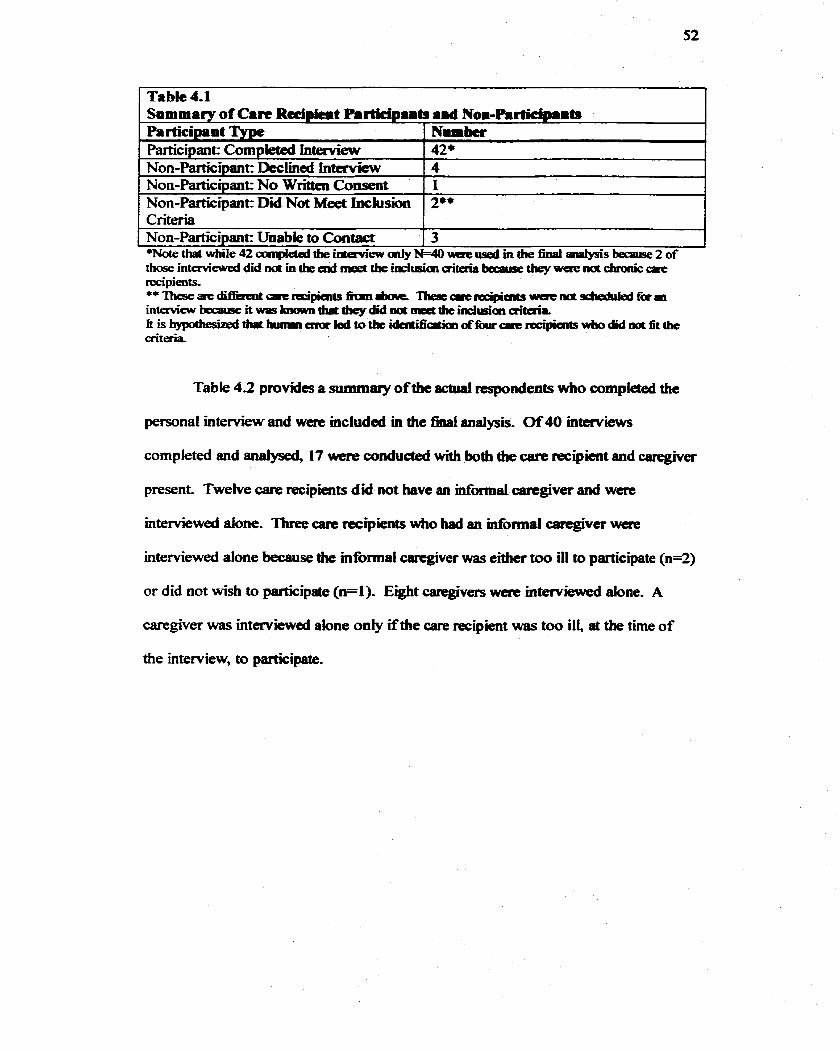
Table 4.1 Summary of C.n Rdpicrt P.rtidp8ib .id Nom-hrticipaits Participant Nmmber Partichant Corndeted interview 42+ on-~attici~ant: -&clined Tntervicw 14 Non-Participant No Written Consent ' 1 Non-Participant Did Not Meet Inclusion 2** Criteria Non-Partici~ant= Unabie to Contact 3
Table 4.2 provides a summary of the actuai respondents who compIered the
persona1 interview and wére mcluded m the finai analysisc Of40 interviews
completed and andysed, 17 were conducted with both die care recipht and caregiver
present- Twelve a m recipients did not have an infiormal caregiver aad were
interviewai done- Three cart rccipients who had an niformal caregiver were
intervieweci aione because the informa! carcgiver was either too to participate (n=2)
or did not wish to participate (n=l). Eight caregivers were mterviewed alone. A
caregiver was interviewed alone oniy if the care recipient was too ill, at the time of
the interview, to participate.
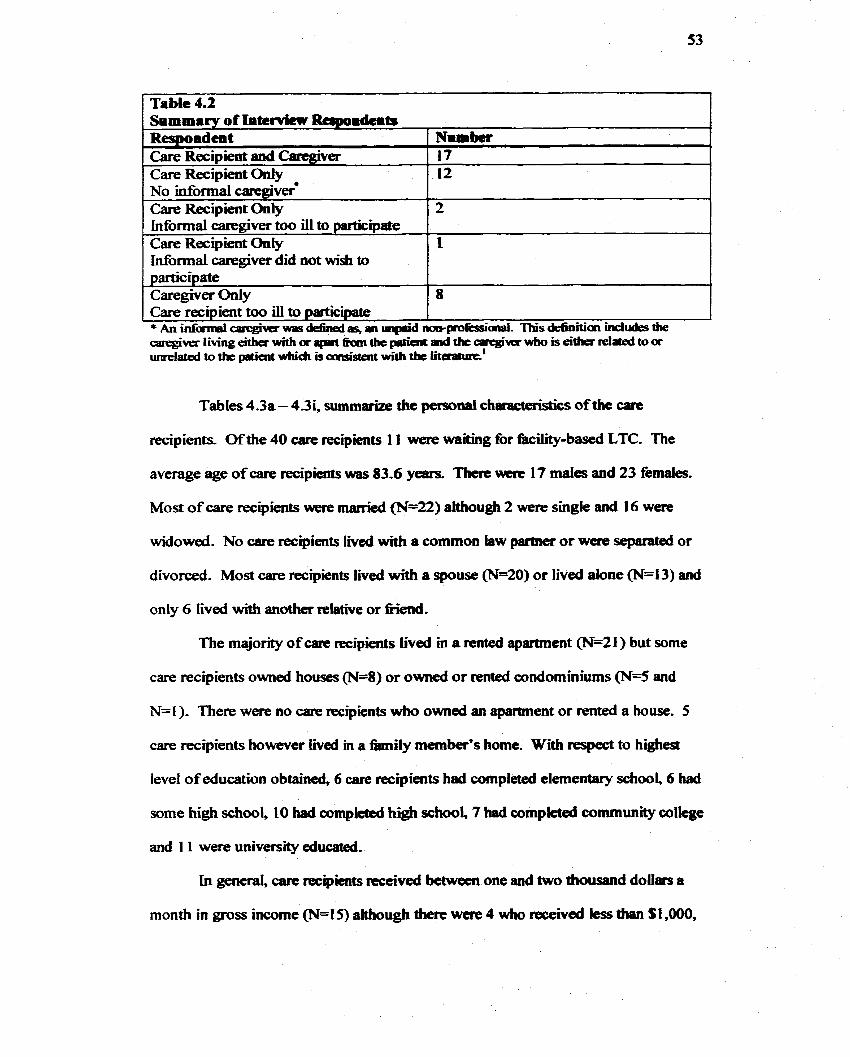
Table 4.2 Summary of Intervicn Reqmmdcib Respondent Care Recipient and CaregÏver Care Recipient Ody
Informa1 &@ver il1 to participate Care Recipient Only lnformal caregiver did not wish to partic ipate Caregiver Only
1 ~arerezipient too ill to participate 1 1
Tables 4.3a - 4 3 , s u m m e the personai chamcteristics of the care
recipients. Ofthe 40 care recipients 1 1 were waiting for kility-based LTC. The
average age of care recipîents was 83.6 years. There ulwt 17 males and 23 fernales.
Most of care recipients were married (N=22) although 2 were single and 16 were
widowed. No care recipients lived with a cornmon law partner or wcre separated or
divorced. Most care recipients lived with a spouse (N=20) or lived alone (N=13) and
only 6 tived with another relative or niend.
The majority of care recipients Lived m a rented apartment @=21) but some
care recipients owned houses (N=8) or owned or nmted wndommiums (N4 and
N=I ). There were no aire recipients who owned an a p m e n t or rented a house. 5
care recipients however l ied in a h i l y member's home. Wi respect to highest
level of education obtained, 6 care recipients had completed elernentary school, 6 bad
some high school, 10 had compkted hi@ school, 7 had cornpietai comrnunity colkge
and I 1 were university educated.
in gencral, care recipients rcceived betweicn one and two thousand doiiars a
month in gross incorne (N=l5) although there were 4 wbo received less then $1,000,
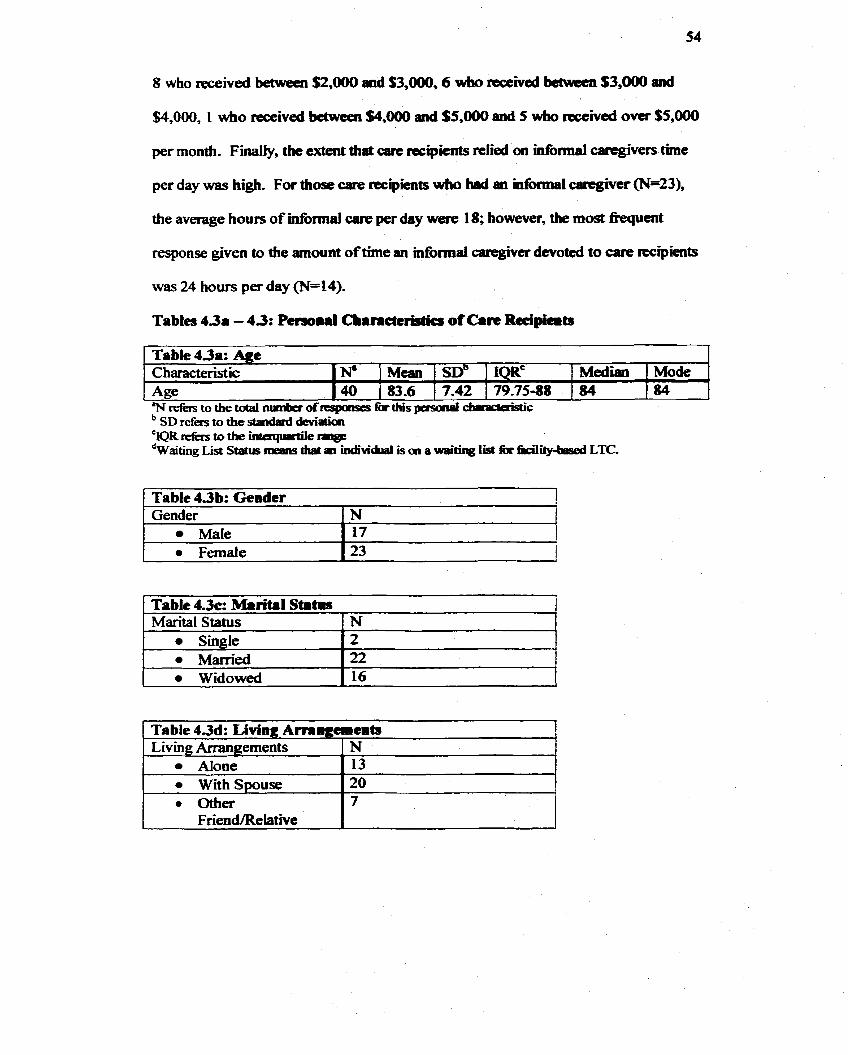
$4,000, 1 wtio received bctween $4,000 and $3,000 and 5 wbo reccivcd ovcr $5,000
per month. FinaUy, the extent that carc recipimts reliai on informal caregivers tirne
per day was hi&. For those care recipients who bad an mformal C8CtgiVer w=23),
the average hours of niformal care pet day were 1 8; however, the most muent
response given to the amount of time an mformal caregivcr devotcd to care irccigients
was 24 hours per day (N=14).
Tables 43. - 4.3: Persoral Cbamctcrgtics of Car+ Reciplcib
/ Table 4.3 b: Gendcr 1
Tabie 43a: Agt
Table 4.3~: Mkrital S t a m Marital Status 1 N
Mode 84
-
Gender Male
'N refers to the tdal nunba of rrsponse~ fàr this p e r d diiraaaistic
Characteristic Age
N 17
1 Widowed ( 16 1
N8 40
Single Married
Median .
84 Mean 1 SDB 83.6 1 7-42
2 22
79-75-88
--
~abkmd: Living Ammgaem* I Living Arrangements
Atone with Smuse
N 13 20
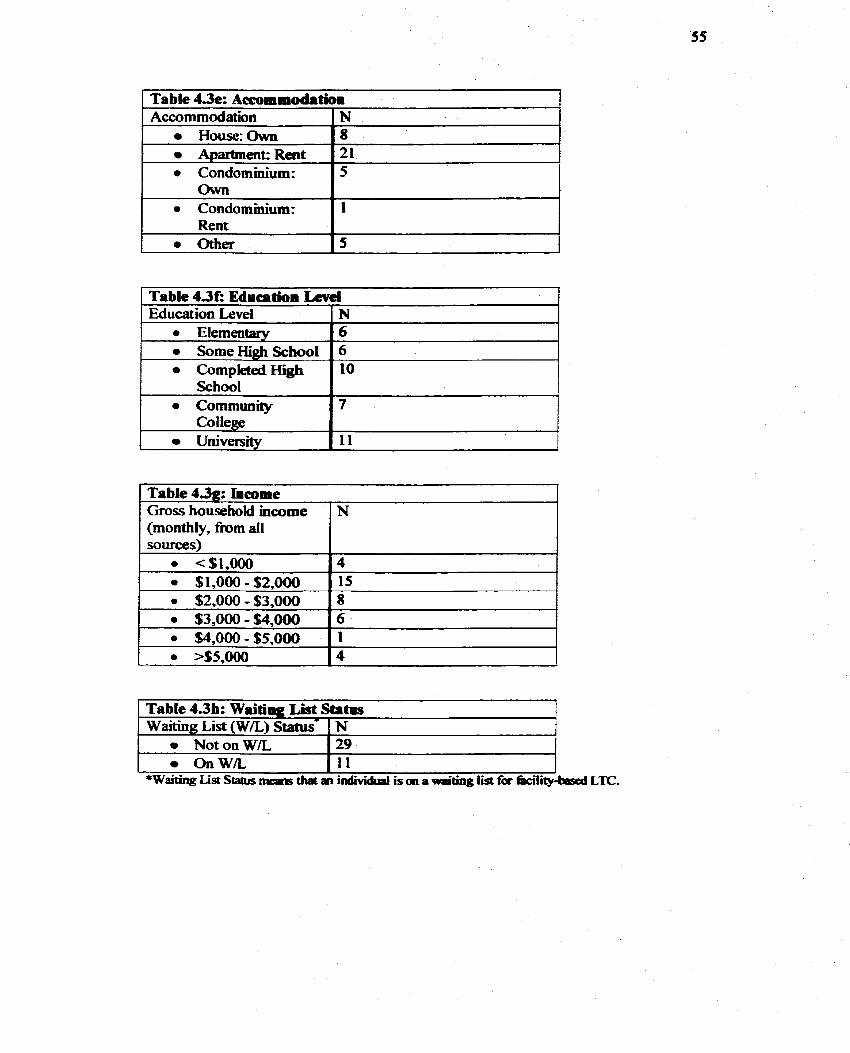
1 a Condominium: Chvn I '
Table 4.3e: Accommodatioi
Table 4.3E Education Wei Education Level 1 N
Accommodation House:Own
i Abartment: Rent
N 8 21
a Elemeutary 0 SorneHigh School 0 Completed High
6 6 10
College University 11
Table 4.3g: Incorne Gros household incorne (monthly, h m d l
Table 4.3b: Waîting List Statps
N
Waiting List (W/L) tat tus- Not on W/L Onw5
N 29 11
*Waiting List Status n r e ~ s that a iridividual is an sr wsiting lis& for facility-bd LTC,
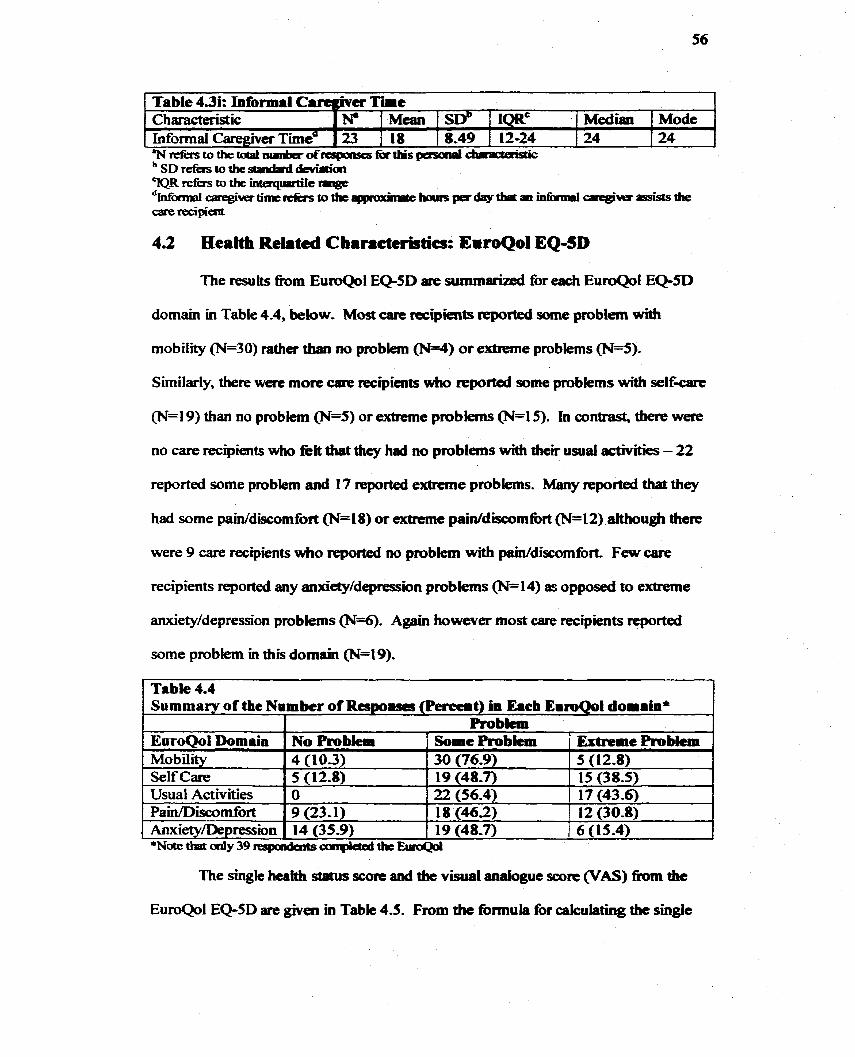
4.2 Health Reiated Characte~cs: EiroQol EQ-SD
Table 4.3i: Informal CarCgner T h e
The resuhs h m EuroQol EQ-SD are summarïzed for each EuroQol EQ-SD
domain in Table 4-4, below- Most care tecipieab reported sorne pmblem with
Characteristic Informal Caregivet Tmea
Similarly, thete were more a r e nxipients who reported some pmblems with self-
. * " N r e f k r s t o t h e t d a l n u n b a o f ~ k t h i s g e s r r i p t ~
N. Mean 1 SW 23 [ 18 1 8-49
IQRc 12-24
(N=19) than no problem @=5) or extrieme problems (N=15). In contrast, tkre were
Median 1 Mode 24 1 24
no care recipients wtio kit that dicy had no problems with theu usual activities - 22
reported some problem and 17 reported extmne problems. Many reported that they
had some paWdiscomfort (N=l8) or extrcme paiddiscomtort (N=12) ztithough there
were 9 care recipients wbo reported no ptobiexn with pain/discomfort, Few care
anxiety/depression problems (N=6). Again however most care recipients mported
some probfem in this domain (N=19).
Table 4.4 Summary of the Number of Respoam (Percent) in Eacb EumQol domain*
The single heatth status score and the visual mafogut score (VAS) fiom the
EuroQol Domain Mobility Self Care Usual Activiies Pain/Discomfort Anxiety/Depression
EuroQol EQ-SD are given in Table 4.5. From the formula for calculating the single
*Natethatdy39respondaitsconpktadthtE~r0Qd
No Probiem 1 Somc Probkm ' Extrpme Probkm 5 (12-8) 15 (38.5) 17 (43.6)
4 (103) 5 (12.8)
30 (76.9) 19 (48.7)
9 (23 - 1) 14 (35.9)
18 (46.2) 12 (30.8) 19 (48-7) 6 (15-4) .
O 22 (56.4)
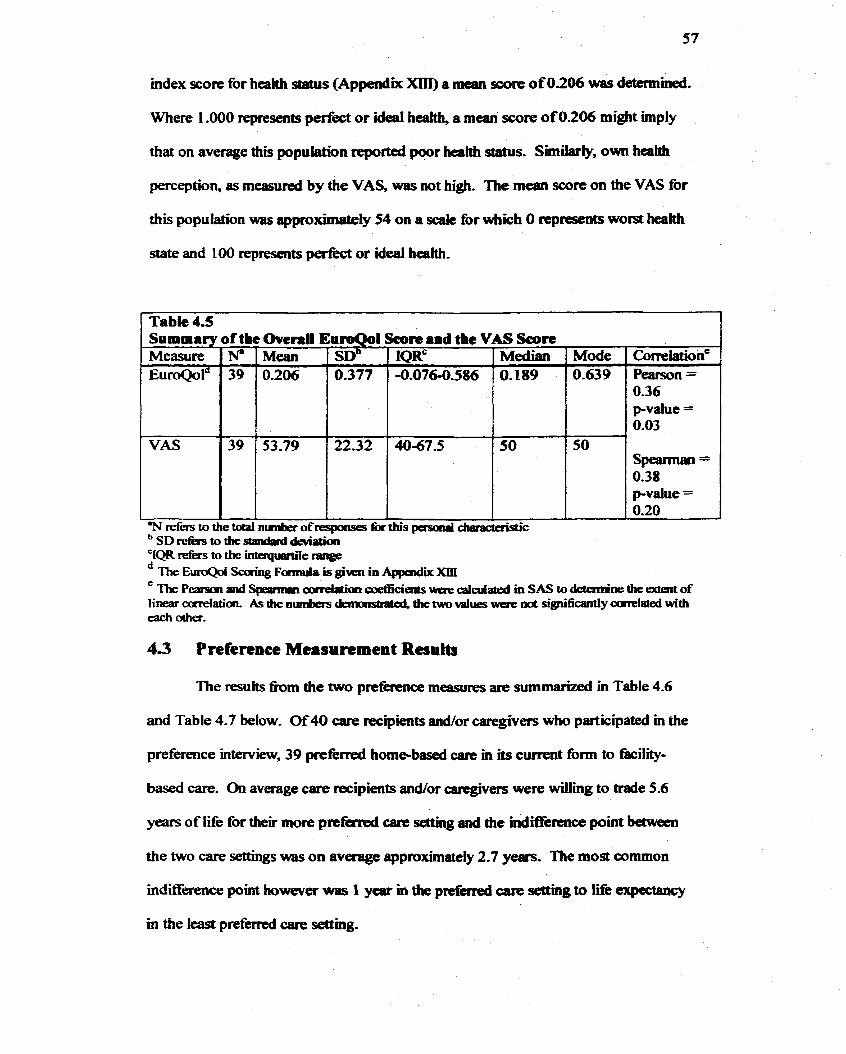
mdex score for heahh status (Appendix Xm) a mean score of 0.206 was determined.
Where 1 .O00 represents perfèct or ideal heatth, a mean score o f 0.206 might hp ly
that on average this population rcpocted poor health status. Similady, own heehh
perception, as measured by the VAS, was not high. The mean score on the VAS for
this population was approximately 54 on a scak for which O represents worst bealth
state and 100 represents perfect or ideal health.
The P- and Speaniian arrPlatim were calai id in SAS to detern.ae the aderit of I k cmnAatiari. As the numbas dainristrated, the two values wcre mt significantly ccrrelated wiîh each ocher.
- -
Table 4.5 Summary of t k OvcrrU ErroQol Score .id the VAS Soore
4.3 Prefertnce Measurement Results
The resuits b m the two preferenœ measures are summari-ted in Table 4.6
CorreWone Pearson = 0.36 p-value = 0.03
Speannan = 0.38 pvalue = 0.20
and Table 4.7 below. Of 40 care recipients andior caregivers who participated in the
'N cefers to the totd nrimber ofreqomes tor this pasaial draradaistic SD r e h to the standard deviatim 1QR refe i s to the inîeqmde range
Measure EuroQold
VAS
preference interview, 39 p r e f d home-based care in its cwrent form to îàcility-
N' 39
39
based care. On average care recipients andor carcgivers were willing to trade 5.6
Mode 0.639
years of Iife for their more prtfcrred car- settng and the indifkence point between
Mean 0.206
the two care settings was on average approximatefy 2.7 years. The most common
IQRc -0.076-0.586
' S D ~ 0.377
indifference point tiowever was I ytsr m the preferred care setthg to lifi: expeaamy
Median O. 189
53.79
m the ieast preferred care samg.
4067.5 2232 50 50
- *
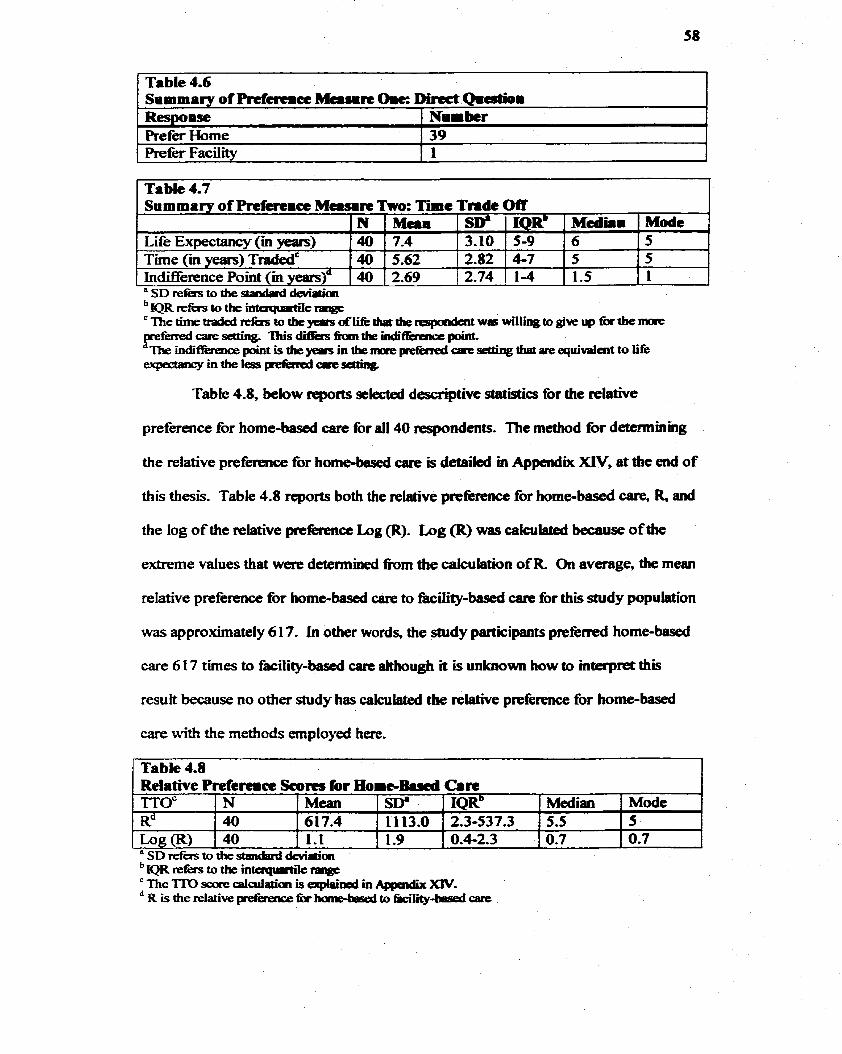
1 Tabk 4.7 1
Table 4.6 Summary of Prrt&remcc Ma~n Or= Direct Q m d i Respoase 1 -ber I
Refer Home Prefer FaciWy
Table 4.8, below reports seiected descriptive da î îs t i~ for the relative
preference for home-based care for al1 40 respondents. The mediod for determinhg
the relative preferience for home-based care is detailed in Appendix XIV, at the end o f
this thesis. Table 4.8 reports both the relative prefèrence for h o m e - b d care, R and
the log of the relative pttfecence Log (R). h g (R) was cakuiateû because of die
extreme values that were detennined h m the cakulation of R On average, the mean
relative preference for home-based carie to fàcility-based care for this study population
39 1
Siimmtry of Preferrict Mcrw~rt Tm: T i c Tnde Otr
was approximately 6 1 7. In other words, the study participants prefèrred home-based
care 6 17 tirnes to facility-bad tare ahhough it is unlcnown how to interpret thii
Mode 5 5 1
result because no other study bas cakulated the relative preference for home-based
a SD refërs to the standprd *aiai
Life Errpectancy (in years)
çate with the methods employed here.
IQR' 5-9 4-7 1-4
M d h i 6 5 1.5
3.10 N .40
Table 4.8 Relative Prefemcc Scom for HomeBami Cari
2.82 2.74 .
M a n 7.4 5-62 2.69
Tirne cm years) TdedC Inciifference Point (m years).
Mode 5 0.7
TTOc R" h g ( R )
,4û 40
" SD refàs to the sEandaFd deviath IQR d k s to b intuqudk range ' The 'ITO sare calculaion is e x p h i d in XIV. R is the relative peférence fu hame-bised to Gcility-besed care
N 40 40
Mean 61 7.4
- 1.1
Sw 11 13.0 1.9
IQRb Median 2.3-537.3 1 5.5 0.4-2.3 1 0.7
Data collected k m the NYCCAC and the persod hterview was enterad m
Microsoft ~xcel? A hl1 list of variables entacd in Excel is @en in Table 4-9 As
Table 4.9 demonstrates, dim were several dummy variables in this model. Al1
d u m y variables were transfomecl m Excd to O or 1 values. AU regressions were
run ushg SAS Version 8.1 ~ofhivare.'" Usbg SAS, a total of h r -ans models
were initially tested that included al1 of the variables coUected fiom the NYCCAC
and fiom the petsonal interviews. The fh& four regcession models are shown in
Table 4.1 0,
Linear regression is a statÏstical technique that is used to explain the influence
that an independent variable, or set of independent variables, has on a dependent
variabIe, Ushg linear tegression and tests of signifi~ce, it is possible to detennine
the extent (how much) and the d-on (positive or negative) that each independent
variable specified in the model has on tbe dependent variable. For example, suppose
the coefficient on the independent variable is - 2.5, and is significant, In this
example, the model predicts that a unit change m the independent variable wiil yield,
holding other diings constant, a reduction of 2.5 uaits in the dependent variabk.
In this thesis, regression techniques were employed ushg the SAS cornrnand
PROC REG. The output generated by this procedure provides not on@ parameter
estimates and their respective tests of signifkance but also an andysis of variance for
the regression model. The analysis of variance includes a goodness of fit measure, R-
squared, that nidicates how closely the independent variables account for variations in
the dependent variable, with a higher R - s q u d indicative of a "beüei' fit- A test for
correlation may be conducted in the event that there are no, or relative@ few,
significant independent variables g e n d by the regression. Iftwo independent
variables were corrtiaîed with one amthCr, it would be digicult to asœrfah the
unique contribution of each variabk to the proscn'bed model. A correlation test may
be conducted in SAS ushg tk PROC CORR corntuand.
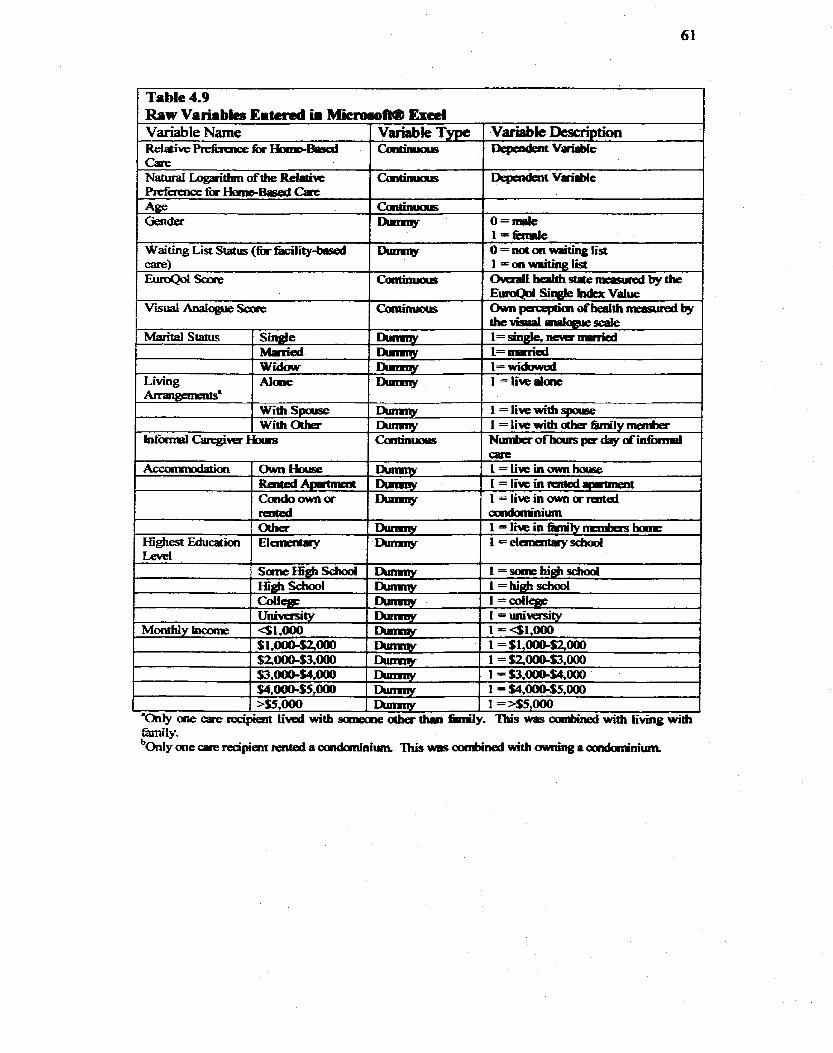
Table 4.9 Raw Varirbies Eitcrcd U Miemmoft@ Excd
Variable Description aepadeavorirble
aepaident VmBn8bie
o=niale 1 1 =fiinile O = notat -ting bst
Variable Name Reiaive PrefBaioe k r Hmd3ad a r e Naturai LogarithmoftheReldvc PrefaaicefffbBiisedGue Age Gencier
Waiting List Status (fà hiIity-birsed
Vanable Type
Caitinuas
Cantinu01s ~)umny
f>lrnmy
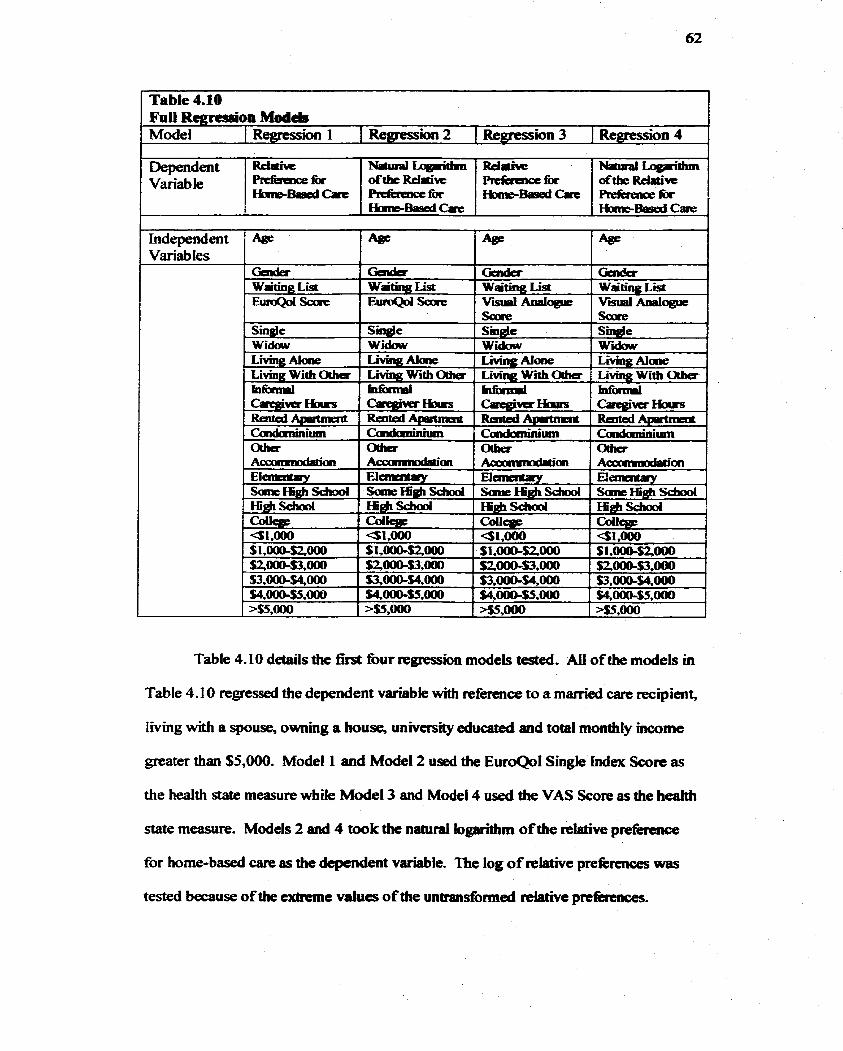
--
Table 4.10 FUN RcgressSon Models Mode1 1 Rearessim 1 1 Remesion 2 1 k~ression 3 1 Remesion 4
Dependent Variable
Genda Waiting List E u r o Q d a
L f i g Ahle 1 LM= 1 LiVin~: Alorie 1 Lhfhg luaie Living Wth Otha 1 L e With OUw 1 Lmng With OLha 1 Living With Odia
Reliai= PrrfirrncefOr ~ B p p C d C a r c
Sin&Ic Widcw
Table 4-10 details the first four regtession models tested. AU of the models in
Table 4.10 regressed the dependent variable with rieference to a married care recipient,
living with a spouse, ownmg a house, university educated and total monthly incorne
greater than $5,000. Model 1 and Model 2 used the EuroQol Single Index Score as
the health state measure wtiile Model 3 and Model 4 used the VAS Score as the health
state measure. Models 2 and 4 took the naairal logarithm of the relative prefèmnce
for home-bad care as the dependent variable. The log of relative prekences was
tested because of the extreme values of the untransforrned rektiive prefénnces.
Independent Variab les
Geda Wating List EutoQol Sare
1 S i d e
i Widclw
NariPalT~~@dun ofthe Rielatiwe RelEraKE1a bBasedCari=
NatrrralLquïthn of* -rive Rpfirenccfor Haiib8asadcn
Gader Wating List V d Analogue
Rd- -for b B a ! d c i m e
4~ 4~
Ciada Wgting List V d Aoalogue
Saire Single -,
Wïdmu
4~
saxe Smgie Widow
Age, gender, waitaig list status, living arrangements, accommodation and
incorne were not signifiaint in any of the regression models given ia Table 4.10.
Simiiarly, health perception measurcd by die visual analogue score and k l u d e d in
Model 3 and Mode1 4 was insigdcant Heaith state, rneasufed by the EutoQol
Singie Index Score, was signifbmt m Mode1 1 and Model2. Bemg widoured was
significant in Model 1 and Mode13 but not in the other two models. Completion of
high school was s i g n h t in M d e l I and Mode12 but insignifiant m Model 3 and
4. SAS Analysis of Variance and the Parameter Estimaies for the four models are
appended (Appendix XVII).
At fim glana, it appeared that heahh state was dxiving the result however a
negative sign on health state was uncxpcted. Tiie negaîive sign implied that the
relative preference for bomebased carie to kility-base. cate was lower if a care
recipient was in better health. In odier words, the sicker a care recipient was the more
the care recipient prefèrred home-basai care to fàcility-based care and the heahhier a
care recipient was the more wülig the care mipient would be to move ta a faciri.
A correlation mai& was used to check whether correlation bctween the variables led
to this unusual resutt. None of the variables proved to be correlateci to a degree that
would have af%cted the result, As such a new series of modek were tested for each
individual EuroQol domain- Table 4.1 1, below, shows the variab les that were created
for each domain-
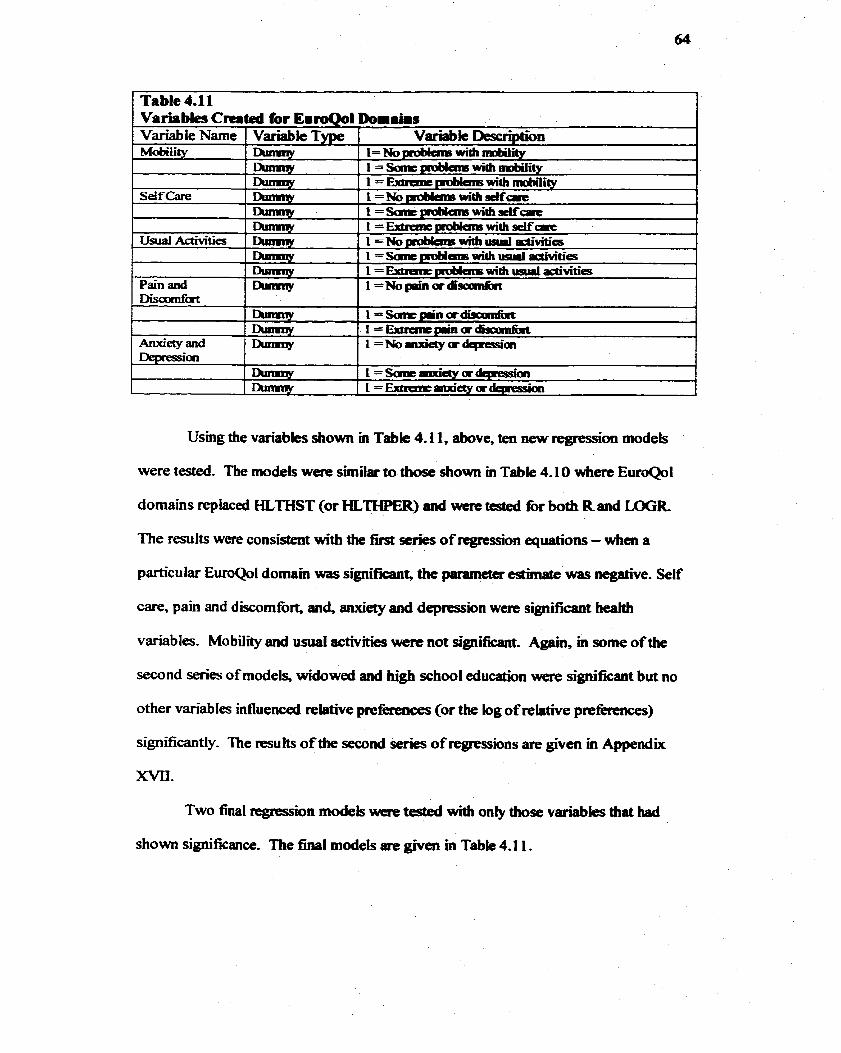
1 Table 4.11 1 Variabies Cnrted for EmroQol Doiiahs
Variable Descnbtbn
were tested. The models were simiiar to those show in Table 4.1 0 where EutoQol
domains replaced HLTHST (or HLTHPER) and were tested for both Rand LOGR
The results were consistent with the fitst series of regression equtions - when a
partîcular EuroQoI domam was significant, the parameter estirnate was negative. Self
care, pain and discornfort, anci, anxiety and depression w m significant heahb
variables. MobilÏty and usual activities were not sipificant. Agam, m some of the
second series of models, widowed and high school education were signifiaint but no
other vanables influenceci relative preférences (or the log of relative prefermçes)
significantly. The resuhs of the second series of regrcssions are given in Appendix
m.
Two final regression models were tested with oniy those variables that had
s h o w significance. The final models are given in Table 4.1 1.
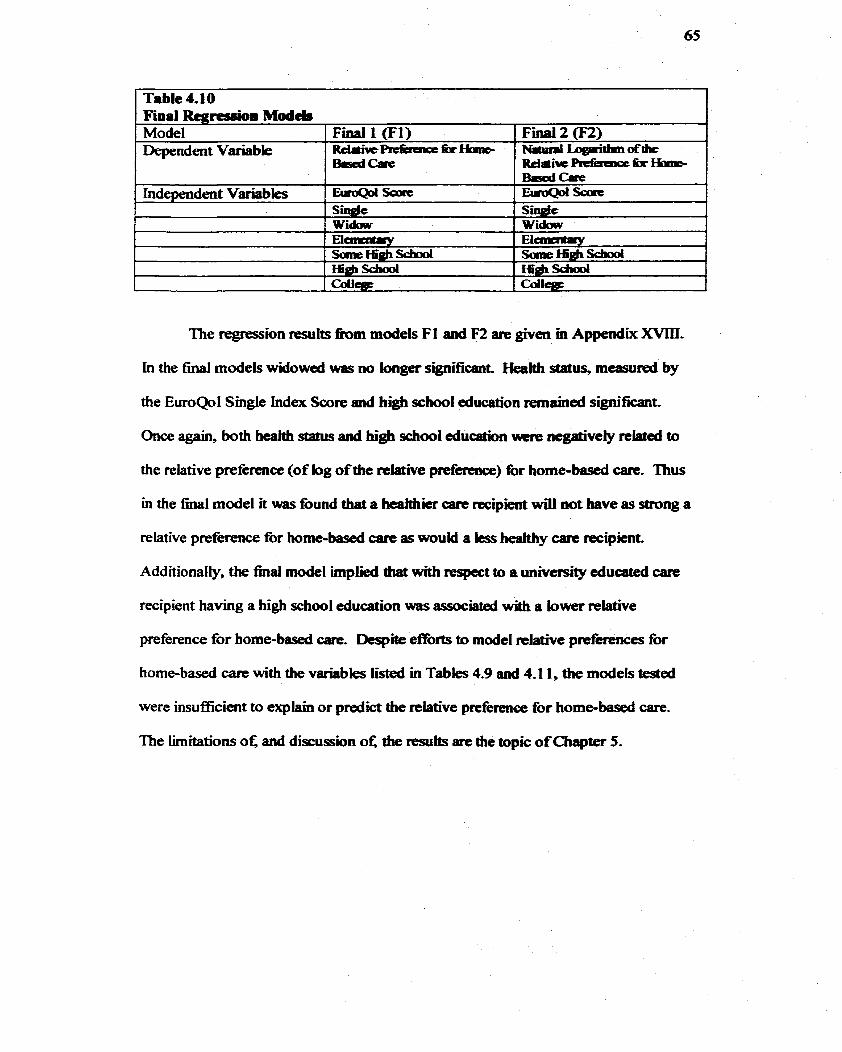
1 Tabk 4.LO 1
The regtession results f b m models FI and F2 are givm m Appendk XMIl.
In the final models widowcd was no longer significant. Health stahis, mcasured by
the EuroQol Smgle index Score and hi* school educaîion riemained signifiant-
Once again, both health status and hi& school education unrie negativeiy reked to
the relative preference (of log of the relative p~fcrençt) for home-based care. Thus
in the nnal mode1 it was found tbat a hcahhkr carc recipient wïii mt bave as strong a
relative preference fbr home-bad care as wouid a less heakhy carc recipient.
Additionaliy, tbe final mode1 implied tbat with respect to a univetsiîy educated care
recipient having a high school education was associated with a lower relative
preference for home-based care- Dcspite efforts to mode1 relative preferences for
homebased care with the vanables Iisted in Tabks 4.9 a d 4.1 1, the modek tested
were insuficient to explain or predict the relative prefhnce for home-based are.
The limitaîions oÇ and discussion ot; the resuits are the topic of Chapter 5.
Chapter 5
5.0 Discumion Part I
This chapter proviâes a discussion of the rtsults fimm this study to kientiIjl
underlying (or innate) prcferences tOr two distinct tarit scttings for persons with
chronic heaith pmblems. As such, this chaptu identifies the limitations of this
research and interprets the results, The d y limitations am discussed with respect to
the sample size and the selection of variables in Section 5.1. nien, in Section 5.2 the
results are discussed within the context of the 1- rtview, d e s c r i i in Chapter
2.0 and the metbods desmbed in Chaptcr 3 0. In Chapter 4.0, it was conduded that
the regression mode1 was insufficient at explainhg the relative prefhnce for home-
based care in this study population. To account for dris insuftlcieacy, Sect'mn 5.3,
below, provides duee aheniative hypothescs,
The fimi hypothesis, in Section 5.3, suggtsts that two things were
sllnultaneously changed - the site of cate and the type of care - when the offer of
home-based care or îàcility-based care was pilesented to the care recipient. It is not
possible to difkentiate the two effects and it is unknown ifthe preference for home-
based care related to a prefetence for the k m e or a preference for home c m . A
number of authors have suggested that the home is particularly significant to elderfy
persons.1-'4 It is possib k that the pnferenœ result represents an attacbmemt to the
home rather than a preference for homsbased are. Subsequcntly, in Chapter 6.0:
Discussion Part II the significance of the home to îhe elderly is considered in greater
detail,
This chaptet provides explanations fit the unanticipateci result that the dative
preference for home-based care was driven - negatively - by health statua As a pilot
study to identiQ underlying prefèrcnces for akmatïve LTC seüings for persons with
chronic health problems, it was not unanticïpated diat problems would a r k .
Therefore this Chapter also serves the purpose o f identi-g new questions and
amendments to the protocol that shouid be made. The h l chapter, Conclusion and
Future Research Directions, sumararizes these changes-
5.1 Limitations
There were a number of limitations in tbis study to iden* undermg (or
innate) preferences for two distinct care sttings for persons with chronic health
problems. Some limStations related to the inclusion cnteria but others resultcd h m a
smdl study population and recruitment probkms m the initial stages of the research!
Whiie a smaU sample was appropriate for a pilot study and a practicai mfes~ity: it
was a limitation. Further, the difncutty m recruiting care recipients rcqukd that the
original inclusion criteria be reiaxed. The impact of the inclusion criteria, a srna11
study populaîion and unanticipated m i t m e n t problems are dlscussed in this section.
The study population was not randomiy selecteâ. Instead, case managers at
the NYCCAC identikd potential participants. The non-random s e l d o n was
nece- not only because of client confidentiuiity but also because case managers,
most familiar with care tecipients', kmew which care recipients matched the inclusion
criteria. This was also intendeci to fàcilitate identifidon of appropriate study
participants within the two-month t h e h e - Nevertheless, non-random selection
Ieads to selection bias and a number of potentiai care rccipients xnight have been
excl~ded.'~ It was possible that care recipients wiîh good rapport with their case
managers were sekcted because they WOUM consent tO an interview. Furthtrmore, a
positive relationship between a are recipient and case manager migbt be associated
with a positive home cane experieace. Coclsequently, ifcase managas stlaaed care
recipients who baâ positive horne-based care experiencc for this study thcn the value
of the relative preferwce for home-based cart could be overrstimated- Ofcourse it is
unknown if this influenced the selection of potentid participants.
A similar probiem with the saniple selection was diat the study population was
liiited to ind~duals currently receiving home-bawxi care for a chronic hedth
condition- Indeed this M t s the abiliiy to generalk the results to a broder
popuiation. For example, it is unbiown w b t the relative prcference for home-based
care woufd be for iadividuals of s i m k ages who are mt currently receivhg publicty
fùnded home-based are. Similady, it is unlniown how the relative preferwices would
have differed if individuals in fàcilities M also been Ïncluded in this study.
The criterion that participants speak English was also a limitation. Because ail
interviews were conducted in En- this necessitattd the seiection of only English
speaking care recipients andior caregivers. A large percentage of the NYCCAC care
recipient population however is not ~ n g k i t - ~ p a a a g ' ~ a d m the initial rrcniitment
stages the English-spaknig crithon was probkmstie.' Consequentiy, the inclusion
criterion thai both the care recipient and the csregiver m u t sQeak English was
relaxed. ifa care recipient had an Englisb speakhg caregiver then the carie recipient
was considerd for the study? It is unknown how language influenced pteférences m
tbis shtdy.
69
Language was also Ianitaig in 81~)thcr capacity tbaî needs mention, nie
NYCCAC is committed to researcfi, which is evidenced by participation in other
researçh studies. The hi@ wst of hiring traaslators howcyer can be pmùiiitive to
researchers and as such most ofthis research is limited to English speaking clients.
This means that Engiish-speaking care recipients are repeatedly d e d for theü
participation and in the i n i i stages it was aclaiowledged that this population was
gettïng "tapped In tict, three are ~w:ipicat.s mcntioned, to the author, that
another student had m t i y interviewe- them on the same topic and one awe
recipient declined an interview with a similat explanation- Similarly, this wncern
was evidenced, in an interview* wtiere the tare recipient said, " - . . with al1 this
research, 1 feel like a guinea-pi&" It is unlarown how many care recipients were not
seiected or did nor consent based on having already or recently been involved with
research. Moreover, it is uncertaia ifprior involvement m mmrch mfluenced the
preferences determineci in this study population.
Related to langage are ethnicity and cuiturt. A small sarnple s k precluded
the selection of care recipients over an array of difEnmt ethic and cultural groups-
Yet, the population that the NYCCAC serves is diverse. The NYCCAC provides
information and refed, case managemmt, in-home health care services and access
to long-terni placement within the boundaries of the community of Nonh yorkt7 in
1996, North York had a total population of 589,653 of which approximately 53%
were non-Canadian bom and approximately 40.A werc visibk rninorities." ln
contrast, in the province of Ontano, immigrants and visible mmorities represented
approximateiy 26% and t 6% o f the population respxtively- Bacause ethnicity and
culture were not considerd it is not possible to conclude with certainty how ethnicity
70
and culture influenced the preferiences for alternative LTC scttïngs in this study. But,
the eEect of culture and ethnicity may bc particuIarty important m this population in
light of the composition ofNorth York and Ontario. W e culairP has been found to
influence the meanhg of home'g it has also km found insignifiant in predicting
heaith seNice uti1ization2~
The sample size also lunited the array of health conditions that could be
examineci- As such, the study population was not determmd by a given chronic
illness nor was any specifk chronic illness Ïdentified in the model. The s m d sample
size b i ted the extent to whiçh s u b p u p s could be considered so that an overail
heaith state was considered appropriate. As discussed m -ter 3, Methods, the
EuroQol EQ-SD was used to proxy overail htalth state. It is unkaown how the
preferences in this study were Wuenced by the particular chronic condition.
Similarly, health service use was ncittier a camponent of the inclusion criteria
nor a component of the model. Oaly c u m t receipt of service for a chronic condition
was used to identifY potential participants and not Intensity or type of heahh servke
and heaith service utilization variables were omitted- This omission of health services
utilization is a l'mitatioa because padculat services and providers wwere not
disthguished and therefore it is unknown how Feceipt of: for example home
physiotherapy, influences prefetences diffmntly h m receipt of homemaking. It is
not known how servie h m an array of providers would affect prefmnces in this
stud y. Like ethnicity, culture and chronic condition, an array of di£lterent services and
an array of differcnt service intensiu'es should be examineci with a larger sample than
was used for this study.
This section has s d d d Iimitations reiated to the study population.
However, there were also limitations to the methods employed to measure the
underlying {or baie) p r e h c e s for two distiact carc settnrgs tbr persons with
chronic heaith problenrs, In light of the result that home-based care was not o d y
preferred m this saidy population but also strongiy prefeRdd to fiaciiity-based carc the
rnethods of this study are reconsidered- Section 5 2, below, interprets the resutts by
chdenging the rnethods and the mseamh question, A rt-evaluaîion of the rnethods
and research question not only serves to explain the riesuiis but aiso identifies
potential fùture research important to policy t0rmation.
5.2 Relation of the Redt to the Litemtmre and Methods
This section discusses the result th& persons with cfvonic heahh problems
preferred home-based tare to kility-based care widiin the context of the Iiterature
review descriid m Chapter 2.0. In particuiar, the msults are discussed with respect
to Sectîon 2.4, Care Settings in Ontario and Section 2.5, Preference Theory and
Measurement. Chapter 3.0, Methods, also pertains to this section. It is suggested that
the results might have been mflueaced by knowledge (or lack) of alternative tare
setthgs, the eligibility rquirements for aiternative care settings or the CO-payments
required for aitemative care settmgs. S im~kly , c e f e n ~ ~ b u s assumptions
underlying the 'ITO exercise might also have influenced the result. To assume that
heahh *te, the home and the fàciiity were fixed may have been problematic. This
section highlights qualitative comments and observations recorded during the
interviews- It is bue that no qualitative mearch tool was used and comments are
offered only to highlight these influences rather than to c o n h that knowledge and
assumptions wem impactmg the msuits.
It is reasonable to assume that, as current recipients of home-based care, tbe
study participants haci some knowladge of the health and social care services o f f i
in the home- While not dl of the services d e s c r i i in Table 2.2 would be fauniliar ta
a care recipient it was not known if any of the LTC îàcilities descn'bed m Section 2-4
were h i l i ar . This unh~iliarity was reflected in tfiis comment made by ont of the
care recipients, "1 don't know much about t h e homes . - -" aad by this strirement
made by a caregiver, "Ibis is an iatmstmg question ifyou have not had expericnce
wïth a kility." Tbat said, some of tbe carie riecipicnts explicitly mehtioned
experience with facilities as they h d had spouses in fàcilities, volunttered in kilities
or worked in kilities. Unhiliarity with facility-based arey and similady
farnilianty, might have driven the result th most study participants preferred home-
based care. Indeed e-eaœ with different care s d g s and treatmcnts and
attitudes towards kilities have been found to influence preferences for location of
2 i -25 care. As experienœ with, or knowkdge of; a ki l i ty was not included in the study
no finn conclusions could be made.
in Section 2-4, it was noted that the care recipientys decision between the two
alternatives is understood in the p o l i i l context- in partjcuiar, eligibility
requirements might have ïnûuenced the result th* home-based care was most o h
preferred- Facility-based Gare is not 'W at point of service m Ontario, On the other
hand, even though spif ic eligibilÏty requirements must be met to receive home-
based services, most, if not dl, home-bssed services provided by the NYCCAC are
'WY, at point of care, to the care recipient, On more than one occasion during the
interviews a comment was made about the expense of moving to, and living in, a
facility. For example, one caregiver s&ted that, " .- - ri was] too expensive to put
ber] husband in a nursing home-" It is possiôle that the prefercnce resuk was driven
by ptacticai and financial considerations raîher than by an underiyhg prefbence for
home-based care per se.'
The number of mquests made by tbe study participants during the personai
interview for an increase in their home-bascd m*cts afso demonstmîcd that the
resuits rnight have been influencad by the political wntext. Certainiy tkre was an
awareness of eligibility quirements as study participants described conversasions
with th& case managers at the NYCCAC about requesting i n d service. It is not
impossible that sb-ong prefcrences for home-based carie wre articulated in hopes that
more home-based care would be providecl and change theù immediate circumstatices-
In Ikt, some study participants wre disappointed diat the personal interview would
not result in a change in tbeir current circumstances.
The study participants werc also aware o f requhents for fkiiii-based cate,
such as availabiiity, end discussed reasons that they were on waiting lists for
particuk LTC fàcilities. Most often, the study participants desaibed a prcference fbr
a particular fkility yet di, in cornparison to the home, even the particular facility of
their choice was not preferred- As Section 53, below, shows, a deiineation of the
meaning of the home and the home as a site for hedth and social care delivery might
be required to fiiiiy understand why, despite reveaimg a preferience to move to a
facility (in other words on a waithg list for a fiicility), theü underlying preference was
s t i U for home-based care.
Most study participants were eager to share theu feelings on alternative care
setîings and were positive about the policy implications o f the rcseamh. The study
participants h i 4 cornplaints but ako kit that home care was good- One enthusiastic
study participant stated that she ". . . loved home carie [and that] everyone tbat vis* is
great!" lndeed a sîudy that measured carc recipient satisfirct'in fin addition to other
variables) at the NYCCAC found that W! of 3 14 care recipients were satisfied with
the quaiity of homomaking and pasonal support ~ e r v j ~ t ~ ? Nevcrthekss one study
partkipant expresseci bis tbeimgs about tbc exteut to which the rcsearch might impact
governrnent sayïng tbat, " . , . realisticaiiy, it will not save tlsem money to have me at
home" and y& this same participant e x p d that, .. . there is no single answer to
health care."
Eleven of die forîy snidy participants were on a waiting list for tàcility-based
c m , yet ten of these participants, w k n asked, exprcssed a pref- for home-based
care, A possible explmation for puttïng one's name on a waiting List might be that a
change m health status was anticipsted. Uncertainty about health status might also
have influenced the preference result- Recall that m Section 2.5, Preference Theory
and Measurement, the TT0 was descriîed as a method that offcred two certain
alternatives? Indeed in the =O mdhod empbyed here two certain ean s*iings
were offered, AU k t o r s , including health status, wcre held constant and onIy the
care setting was changd. But it was endent that study participants had difficutty
with holding health status and the meanhg of various care settings constant. This
difficulty was refïected m the foiiowing comments,
'? wdd go to B.ycrest if my health got wast,"
"As long as I f d l ik this Imn fine in my awn ham ... ifmy h d t b chaigcs thai my answas wouid change."
The commena, above, showed that the mdy participants p r e f d home-
bas& care if their health status was kcpt constant and thus their undertying pref-ce
was home-based care. Nonetheless, the comrnents above, and in particular the iast
statement, also demonstnited that th& pmfbnces change. While stability bas
been considered elsewhere, it is unkiown m this study if prcièrences wiU bc stabk
over t i ~ ~ e ? " ~ Indeed pdkences might be UiaUenCdd by uncertanity of Iiealth status
or by health outcomcs m a pPrtÉuQr l o ~ i o n - ~ ' ' as much as by the uncerianty
O$ or knowledge oc a particukr carc settÏngmzu-' The prdè re~ l~e for home-based care
in this study populm-on was taken at a particuk pomt in time and Ï t is unknown if
changes in heahh status, for this population, would produce the same or snnilat
results.
While the assumption that hcaîth status was mastant might have influenceci
the result, the assumption was not the on@ methodological problem- Another
probIem was with the time incmncnts thrit wme offaed in the TT0 exmise- In the
original study protocol the trade off would start with years and then move to smaller
increments of time (months d days), Eariy on in the mterviews this proved
pmblematic as study participants became anxious at t h i d d g in tenns of days of Me.
This pro blem has been noteci elscwke in a study of pref-ces for tmûment for
Iung cancer." Afkr the firsî four interviews, the method was amended and only
discrete years were traded in the TT0 exercise, Smaller increments (mondis and
days) were offered oniy ifthe study participant would not even trade a single year of
life for the more preferred care setting or the study participant wuld trade al1 of their
life for the more preferred care setîing,
Al1 study participants were willing to trade some amount of tirne for the
preferred care setting yet more than half w e ~ willing to trade ahnost al1 of their
remaining Life years (would prefer home-based care fOr one year or less followed by
death) for the preferred care setting. in fàct 10 study participants responded that 1 day
in the p r e f d care setting was equivalent to living the rest of their life in the less
preferred car setting, It is possible that the riesponse was given to paci@ the
researcher but it is also possible that the respomie and its consecpence - that relative
preference for home-based care was negatively reîated to health status - can be
76
explained by risk aversion, prefèrence for location of death and the si-ce of the
home. These potentialiy consistent explanations for the negative relationship betweea
reIatïve preferience for home-basai care and health s&tus arc providai in the
following section.
5.3 Alternative Potenth1 Explrutions
Section 5 -1 and Section 5 2 , focussed on factors that hited the extent to
which variables could be considerd and cotlclusions couM be hm- indeed, the two
focussed on understanding die resuk tbat most (39 of 40) stiidy participants
preferred home-based care to &iMy based care and that the relative pref-e for
home-based care was strong (mean = homabascd care prekmd 61 7 tunes to fàcility-
based are)- This section focuses on the riesults of the regression model. In particulau,
this section provides thht potential explanatioas for the riesuit that tefative
preferences were negatively related to health status.
53.1 Risk Aversion
To iden@ the underlying (or innate) prieférences for two distinct care settings
for persons with chmnic heaith pmbtems the TïO p r e k c e elicMin rnethod was
used. As previously discussed in Sedon 2 -4, Refetence Theory and Measument,
and Chapter 3.0, Methods, the TfO technique offers a choice between two certain
alternatives- In this study the two certain alternatives wert home-based care and
&ciMy-based c m . Nonetheles, it was possible th& as current recipients of home-
based are, the study participants considerd the cboice as one between a certain
alternative (home-based care) and an unoertam abnative (f'aciiii-based mue).
Consequentiy, an expected utility maximizhg, ri& averst, study population might
explain the k t that one quarter of the sample was willtng to trade ahost al1 of theu
77
remaining life years for home-bssed amCIUt in fiict the choicc of f8cility-bascd carie
might be thought of as a major decision for which risk played an important d e .
Expected utility tbeory, mentioncd but not cxplained in Chapter 2.0, is usefil
for understanding the foie that rïsk might have played in this study. Expected utility
theory is a way of mderstanding how indiiiduals t . to betiave under u n d
44-47 conditions. Ushg expected utility theory as a fhmewok suppose tfiat the
decision requested h m the study participants was understood as maniing m a
certain care settins the home, or moving to an uncertain care setting, the hility.
Note that it is reasonable to assume that home-based carie was the riskiess alternative
because the study participants wcre currmt home care reciphts
To understand the shidy participants' choice between home-based a r e and
facility-based care begin with a set of aswmptions îhat derive in part h m the axioms
advanmi by von Neumann and Morgenstern and in part h m the sssumptions made
for risk aversion!57 Assume thai tht study participants' prcfaeaces were consistent
and can be descriied by a fûnction cakd 'Utility of Carie Settings," Assume that the
utility of care settings fiinction is mcreasing with "Benei' attributes of a heaith care
setting but that the fùnction is increasing at a demashg tate. in other words, a health
care setting with 'BeW aîtriiutes has a higher vdue of uti i i i than a carie setting
with "Worse" attributes but the incremental increase in utility wîth a unit change in
m'butes is smaller and srnaüer as tare settings get better and better- A fàciIityy or a
home, can only be so good; at some point no changes to the facility or home can
increase utilhy. Finaliy, assume that the study par&icipants were expected utility o f
care setting (E(U)) rnaximizers. The '2rtility of Care Satings" Itùnction is displayed
gmphicaily in Figure 5-1.
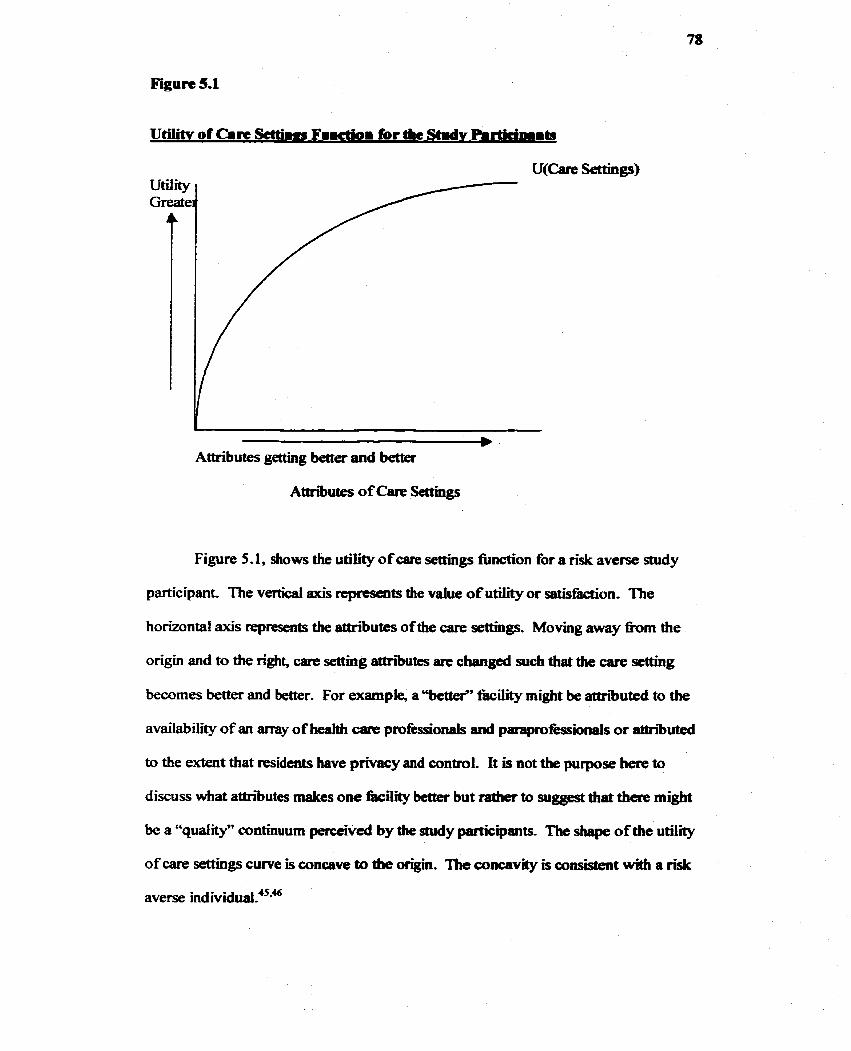
Figure 5.1
Attributes getting better and better
Attri'butes of Care Settiags
Figure 5.1, shows the utility o f care settings finction for a risk averse study
participant. The vertical axis tcpmsents the value of utility or satisiàction- The
horizontal axis represents the attributes of the care settiags. Moving away @om the
origin and to the right, care settiag ettributes are changed such that the care setîing
becornes better and better. For exampie, a "bette?' fàcility might be attriibuted to the
availability of an m y of heakh care pmfessionals and paapmfèssiinals or atcn'buted
to the extent that residents have privacy and control. It is not the purpose here to
discuss what attributes matces one fiicility better but rattier to suggest that there might
be a "qudity" continuum perccived by the study participants- The shape of the utility
of are settings cwve is concave to the origin. The concavity is consistent with a risk
averse indi~idual?**~
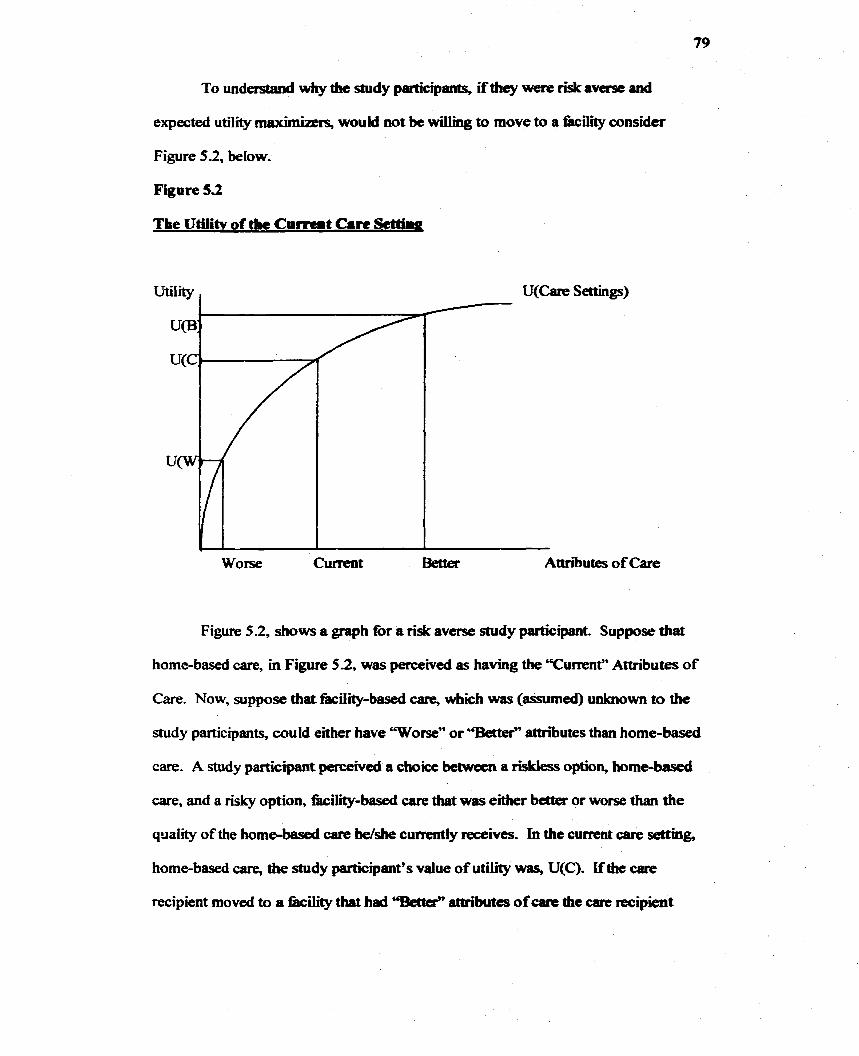
To understand why the snidy participants, ifthey were risk averse and
expected utility maximiaers, would not be wiIlimg to move to a kili ty consider
Figure 52 , below.
Figure 5.2
The Utilitv of the Corrent Cam &t't'hg
Worse Cuileat Better Attn'butes of Care
Figure 5 -2, shows a gmph for a risk averse stud y participant. Suppose that
home-based care, m Figure 5 2 , was perceiveci as having the Tument" Attributes of
Care. Now, suppose that kiiity-based care, which was (assumed) wilaiown to the
study participants, could either have Worse" or "Berter" attributes than home-based
carc A study participant perceivcd a choice between a riskless option, home-based
care, and a risky option, k i i i i b a s e û care that was either bctter or worse than the
qriality of the home-based care he/she cumntiy receives. h the current care setting,
home-based care, the study participant's value of utility was, U(C). If the care
recipient moved to a fiicility tbaî had "Betkr" attributes of care the care recipient
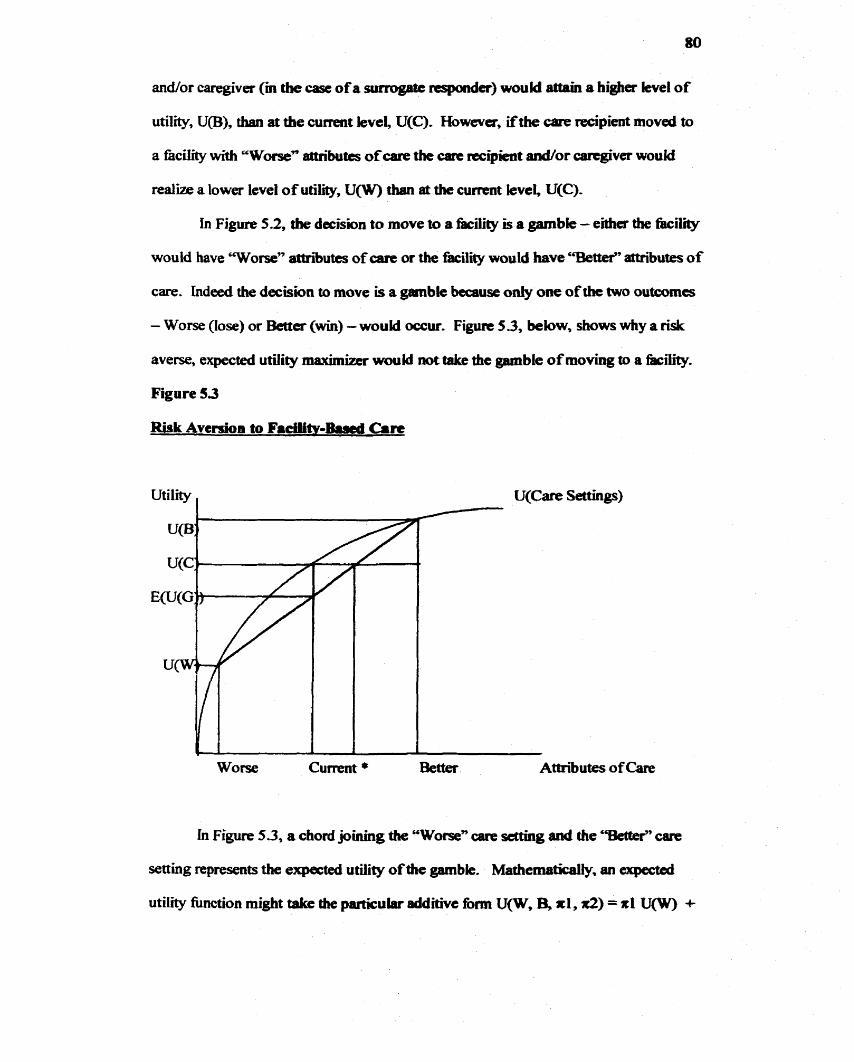
andior caregiver (in the case of a surrogatc rcsjm~Ier) would aüaia a higher kvel of
utility, U(B), than at the current levei, U(C). However, ifthe care recipient moved to
a facility with 'Worse" attributes of care the carie recipieut d o r csrtgiver would
realize a lower level of utility, UCW) than at the cwrent level U(C)-
in Figure 5 2 , the decision to move to a t'acility Is a gambie - either the fàcilii
wouki have 'Worse" attni'utes of care or the kilii would have c%dîef' attniutes of
Gare. I n d d the decision to move is a grimble b u s e oniy one of tbe two outcornes
- Worse (lose) or Better (win) - would occur. Figurit 5.3, below, shows why a risk
averse, expected utiiity maximizer would not take the gamble of moving to a fàc~lity-
Figure 53
Risk Aversion to Facllitv-M a r e
Utility , U(Cam Settings)
Worse Current * AtÉn'butes of C m
In Figure 5.3, a chord joining the "Wome" are senhg and the "£Wei' care
setting represents the errpected utility of the gamble. Mathem8ticaily, an ex@
utility fûnction might take the particuiar additive form U(W, B, xl , n2) = nl U(W) +
x2 U@), wfiere nl and ate the probabziity of outcornes W and B respectivdy.
Expeaed utility is therefore the weighted average of the two unccrilm choices4' and
simiiar1.y the expected vahie of the gamble beâwcxm moving to a "Worse" fiiciIlty and
a "Bettd' fàcility is the weighted average of the two mdependeat possibiiities-
Again, this is shown with a s&aïght h e phhg Worse" and "Bctter" in Figure 5-3,
above.
In Figure 5.3 the ex@ value ofdie gamble is E(U(G)) but is associated
with the same level of quality as the cwrent home care setting. The E(U(G)) h m
taking the gamble is lower than U(C), the current utiiity m the cemin care setting, the
home. in other wotds, the shidy pautkipant would expect a lower ievel of satisfbtbn
ifthe gab le of moving to a fàcility were takem The po& *, on the figure is the
expected attributes of cah that wouid make and indiviâual indifferent between the
current care and the gamble- A tisk averse, expected utility maximizing, individual
therefore would be unwilling to take the chance that facilïty-based care was Vorse"
than the current home-baseci care received.
It has been argued that the individuals are not errpected utility rnaxim~ers!~
A "veil of experience" or loss aversion is a h a potential exphmation for why the
study participants did not to takt the gaible.'9 It is possible that the study
participants preferred the status quo and that a loss in utility fiom giving up home-
based care is more significant than any potential gain h m "Better" fiicility-based
49 care. A Ioss averse snidy participant, as opposed to a nsk averse snidy participant,
would not gamble if aay loss (or a significant 10s) were anticipa&& For loss averse
study participants no gain is large enough to compensate for a potential los? Loss
aversion might also explain the ten study participants who were willing to trade
almost al1 of their rernainïng Lifé years to m a i n at home. Whether or not mdividuals
are in fàct expcted utiüty maximers is mt debaîcd bere. Rrdher, tisk aversion and
l o s aversion are offered as potentially consistent explamtbns for the resutts.
Expected utility thmry was prescnted berc as a hmeworlc to descni a
potentiaily consistent explenation for the uaanticipated resuit of the TT0 preference
elicitation and the subsequent unanticipated reg~ession rcsuit that relaîive preferences
were negaîively telated to health status. ïndeed there are dIfficulties with assuming
that individuals are expected utility rnaxirniaas? Expected uaili*. rnPrimhaîïon wms
an ex-pst explanation to highlight that the choice between two certain outcornes was
perceived as a choice between a fiskless outcorne and a risky outcorne. In fàct the
study participants may have betm too risk averse to gambie and thus preferred the
certain care setting, the home. In hindsight, it might have been possible to use the
standard gamble to value utiüty for the decision between home-based care and
potentially 'Worse" or 'mer" kiiity-based carie- Recall however that the standard
gambIe was not used in this study because it was not considerd appropriate to
assume that i'acitities were 'Worse",
53.2 Loatior for Duth
The purpose of this sû~dy was to determine the preferience for locatl'on of CTC
for persons with chronic heahh problms. hdeed the study participants were, on
average, quite unheafthy as demonstrated by the EuroQol Smgle index Scores and the
Visual Analogue Scale- It was anticipated that diose m poorer heaith States wouid
have a Iower relative prefance for homebascd are. Indeed it was anticipated that
individuals in poorer hedth states rnight prcfèr the type o f care offered in a facility. If
fàct the opposite result was determined for this study population - a worse heaitb
status imp tied a stronger preference fbr home-based tare.
A potential explmation fbr the unadcipetcd result rnight be tb~ those witb
the worst heaith were closer to death and that there was a prefërence to die at home.
In kt, other studies have confinnad a p h c e fm home death in elderly
persons?2-38 Thes audies, d i s c d m Chapter 2.0, evaluurted îhe prefércnce for
either death at home or, de& in the bospital - none cvaluated a long-tenn fkility-
based care option- For the most part, these -dies elicited prcferences for the location
of death h m acute care recipmits and not h m those receivmg homabascd care for
a chronic iilness. Whik it was evident that home death was p r e M to hospita1
death in ottier sudy popuhîhas, iî is unbiown if this prekmmce is gemmbble to a
population of chronhily ill home care recipients.
Stiii it is possible tbat the p r i t h c c for home-based care was a pmxy for
location of de&. in t'act several comments wre mdicative of a belief that the fàciüty
would lead to de&. The following comments show how a fkility/nursing home
might have been considered a place to die-
Care Recipient: "if1 went to a ûciiity, 1 w d d nd iivc for 5 yaus.''
Caregikr T I prefà bcime, why w d d 1 l i u l a i g a in a fh5lityY
Care Recipient: Y d d t to l i u m a hciiity 9 yam at ail!"
A strong preference for the home as the location for death coupled with very
poor he& is potentially consistent with the result tbat the relative preference for
home-based care was negatively related to heahh sîatus- It is suggested uiat if a
question had been included that asked about preference for place of de& the effect of
preference for home care could bave been disthguished h m the effect of p r e h c e
for dymg at home, As priekencc for location of deat& was not ekitcd in this a d y
no fïrm conclusions can be drawn.
533 m e Sïgmmaicc of the Home
A third potential explanation for the ~ l t tbat the relative prcf- for
home-based care was negativeiy reW to iuaith status mi@ be that the prefhnce
for the home couid not be difkrcntiated h m the preference for home-based carie.
Whiie the meaning of home is dBkuh to d i s ~ e n i ~ ~ ~ there have k e n studies thot
implied the home holds an exceptional signifiana to indi~iduals'-'~ Iadced, it has
been demonstrated that physical proximity was not necessary for a sense of home and
it has been recognizcd tbst horn~+~lre' can be aciüeved without maining in one's
"own" home.' Coascquently, thm are exampies of aitemative living ^placesw tbat
achieved the quplities of 6%ome"8-a" Despite the k t that a sense of home was
achieved in alternate care settings, the fkility in this study population might not have
been expected to be a home-place.
The interviews were uisufl6cient to conclude that the preference elicited in this
study was not for home-based care per se but raîher for mainhg in the home.
Nonetheless the possibility that the home is endowed with a particular meaning
deserved a more comprehensive exploration. An explanation, d E i t h m
econornic theory, is the topic of the fobwing chapter.
5.4 Chapter Summiry
This Chapter provided explanations for the unanticipated result that the
rehtive preference for home-based care was driven - negathely - by h d st;rtus. In
part, the resuit was attributed to a smali, non-random snidy population that limitecf the
extent to which variables could be selected and testeci. The resuh was also attnbuted
to the methodoiogy ernployed m the study- It was unlaiown what ex@ena sîudy
participants had wibi either home-baseci or fkcility-based carc - only that each study
participant was a current home care mipient It was sbiiertiy unimown vimether a
c m recipient had a mgdvc perception of eitber home-basai or --bascd m.
Assurning thai kdth state was fked and prefèrences were 6 was also a limitation.
Three additional explanations art advaacod that were potentially consistent
witfi the result that relaîive prcference for home-based care is negativtly related to
health status, Risk aversion, a pritkrence for home deah and a prefc~cnce for the
home rather than home-basai care might explab the uoanticipaîed resuhs, Ofcourse,
the hypotheses advanced require fbrther m g .
As a pilot study to iden* underS.mg p r e f m s for alternative LTC setîings
for persons with c h i c heahh problems, it was not unanticipated thaî probkms
might arise. Therefore, this Chapter sewed to iden* new queshns and
amendments to the pmtocol thaî should be d e . The final chapter, Concfusion and
Future Research M o n s , summwbs these changes.
Chapter 6
6.0 Discussion Part II
In ttiis chapter the results of research to dent* underlying or innate
preferences for two distinct tarit settings art (re)examined. This chapter, by turning
to the discourse of geography, interprets the result that ail but one of forty care
recipients prefërred home-based care, difkently h m the interpretaîion in the
previous chapter- While the former discussion f o c u d on the quantitative results of
the mode1 and the limitations in methods, diis chapter focuses on a broad
interpretation of home and pIucen to provide a comprehcnsive e x p l d o n for the
results and expand on Section 5-33, The Signifkmce of the Home-
The (re)examination uses the theoretical concept of a therapeutic landscape
and its elements of humanism, cuiturd ecology and stnicturaljsm. Therapeutic
landscape is a metaphor to descni a place in which healing, health and wellness
occur." It ernphasizes the idea that sense of p b a is as important as physical
location. Yet, mate îhan just kmking at the meaning of home (or place) or sense of
home (or place), the idea of theraQeutic landscapes kilitates lookïng at the home as a
place whcre heiiling, Mt. and weiiness occur (or do mt oc~ur).~' A subtle but
important meaning is tbat a therapeutic iandscape is an undetstood or taken-for-
granted place for heduig, hetilth and wellness.' The use of therapeutic landscapes as a
h e w o r k for understanding the home as a site for heahng, hdth and wellriess m
contrast to the fkiiity which might be a "toxic landscapc* is more eomprehensive
than s b p l y looking at the meaning of home-
Of course to fiiliy mtcrpret the tesult tbat elderiy petsons with h n î health
problems preferred homebased care to fkcility-based care, a step backwards is taken
by considering why the study participants would ahnost invariably have p n & d
home-based care. A s such the meanhg of home, specifidiy, the mtaning of home to
the elderly is considered au important haor in tight of the rtsult. SïmiIarly, it is
equally important to mflect on the meaning (and perception) of a fàcility to
understand die aversion to hciIity-based carie in this population. Aithougb there are
many understandings of the meaning of home, the primary focus here is the link
between home and sense of place. This focus hiflghts the maia &tors that made
the home and not the kility, for the study participants, a therapeutic landscape-
The concept of place, wbik impticit tbroughout this thesis, was takenofor-
granted: place was either the home or the frrcility- Even with this (re)examination, a
more comprehensive meaning of home or fàcility is insufficient to conclude that the
home was a place - or landsape - that was therapeutic. Despite that homes and
façilities are endowed with meaning, homes and fOLciüties me d l 1 physical landscapes
that rnay or rnay not be therapeutic. Whik no firm conclusions could be drawn fiom
this midy about what physical features contributcd to a therapeutic environment!'
some casuai observ&ons were made and upon reflection the (physical) homes were
quite varid. Besides understanding the (Pbysical) home within the concept of
therapeutic landscapes, the benefit of ident-g even incomplete physical features of
homes was fbr fùturc rcsearch w k e m tbe physical home rnight not be taken-for-
granted?
So why was the home taken-for-eted m this thesis? In part it was necessary
to shplitj. the preftrence elicitation but in part it might have been because home was
un&rstuod as "in Placen in the "Agiug in Place" philosophy o f health and social care
delivery for the elderfy,' In other words, it was assumeci that h& and social care
were delivered "in P18ce/Homem without understanding that "Place/Home" were
dynamic and variable.' The h e w o r k of tkrapeutic landscape additionaliy identifies
that social and poiitical structures lead to iandscapc as an udrstood place of heahh,
healing and wellness. Most importantfy considering the home within the concept of
therapeutic iandscapes in this chapter identifies a d S i n for fùture ce~e8cch on the
home as a place for heahh and social are deiivery-
This chapter is divided into four sections. The fkt , Section 6.1, describes the
concept of therapeutic landscapes. From there, Section 6.2 discusses sense of piaœ
and home and in psirticuiar how a sense of home might be especiaily signifkant to the
elderly. Section 6 3 examines how ecologicaJ and structural aspects might have
contrï'buted to a befief heu by this shidy populab'on that the home was a therapeutic
landscape. Finai& Section 6.4 provides a chapter surnmary and identifies fûture
researçh directions. The fùnire reseatch directions identified in this chapter together
with those imptied In the previous discussion are summarized in the final chapter of
this thesis.
6.1 Therapeatic Landrripes
The concept of therapeutic landscapes, maoduced in the openmg paragtaphs
of this chapter, offkm a îhneworlc that can be usecl to interpret the result ttiat home-
baseci care was p r e f è d to facility-based care m a population of chronically ilk home
care recipients. This section begins with a brief description of the "place" that
"therapeutic Iindsc~ipes" occupies in die fider dixipüne of geography- nie section
continues by addressing the rneaning of a therepeutic h d s c a ~ e as understood by
William Gesler and his foüowem to lay the fouodations for uaderststnding the home
within the context of a dierapeutic landscape-
It is suggested drat the home csn be "placed" within the theoy advmced by
Gesler. in other words, it is argued, but not wdümed, that the home is a tfierapeutic
landscape for the cate recipients in this study- Inde& diis section offers an
alternative and yet cornplimentary means of derstanding the resuk that most
chronicalty ill persons preferred home-based case and fobwing Gesler suggests, cc . . .
therapeutic landscape concepts can complement traditional heab care studies- What
is called for here is not an abandonment of work that has pmven its usefulness to
understanding and policy-making, but for new perspectives tbat parakt those in tbe
subfields of geography and the other social sciences @.744).'"
New perspectives in the field of geography (and sirnilarly in other social
sciences) m s e in the late 1960s as mearchers began to question the rok of positive
sciace and ernpiicism?ll As the, . . . pallid rational men thsory' and practice was
exposed for both its inteüecûJaf and existentid rigor rnortis (p.2),"'* humanistic
Thank you to Dr. Peux Coyte fa hiNighSing diit this -t is ibdidwe d a mi-g ofrat idity . indcsa"rrianilnm"isanewbo,fin~d~chrrPePtbt~ht
~eainciniicdefinitiaiofrtiamiismt~~llttosensiieoriasonibk.sthc statanentabrnrtmï@inply. A c h o i ~ ~ n r d t b y a n t ' i a t i a u l n m " ~ g ) r t b t a m @ U d y ~ toandherbutthisdocsnatinplythrtthtcha'awis~"irratidn.FiPtherrrt iditydaes not rule mt the passiiity o f d n g unique ù c h h u r -
geography, (re)emerged as a way of undersîading people and th& ~~I~*ooship to
landscape- Humanists concenid with, " . , . the separation of science aad man
(p.7),"10 inherent m positive science wught ~~~>nci l iat ion. AS such, hummist
geographm infused 8llfhfOpoce~ltticism iato their rrsarcl~.'~
The humanist geographer perspective b k s at humans as the centre of a
holistic world w k e peopk and place engage cocb oth~r.'~ One strum of humanist
research that developed as a conse~uenœ o f the 1960s questiooing o f ernpirical
science is the study o f perception and the idea that place is endowed mth rncaning."
PhiIosophies of meanmg countered the existing positivist mcthods and sense of place
studies, that explored the meaning of landscape through participant observation and
ethnography, domhatcd humanistic gcmgnphy.'*13 Simuftana>usly, field work was
advocated as an acceptable method to fiicilitate the " . .. exploration not of exotic,
fliraway lands but of thc cornpiex iandsapes of persoos' expxkntial wodds @.
1 74)?14
Humanist geographers focus on philosophies of meanhg and also ask for
specific meanings, values and interpretations that are given to a particular place or
landscape.' Quoting Gueke, (1 9743, Gesler writes, " . .. humanist geographers place
emphasis on the mind's interpretaîion of phenornena: one understaads a cultural
landscape by understandhg the diought behind it (Gesler, 1992 pg. 737 fiom Guelke
L- "An idealist alternative in human geopphy," Ann- As- A m Geog- 64, 193-202,
1974)." Indeed h m the literature on =se o f piace and humanistic geography
William Gesler, in 1995 coined îbe idea of a, %empmtk landscape." But for
Gesler, humanist, stucturatist aad cuhural ecology combined to fom the basis for
therapeutic lend~capes'~ and sirniiarly uns of phcc studies have considered p l e
attachent md L e social context in a geographic region.16
The humanist extension of the traditional way of thinkmg and descniing
landscape based on physifal form, to thmkmg of and desctr'bmg landsape hsed on
human and social idluences, infortnui Gesier's account of landscape- Nevertheless,
Gesler was aware diai too much of a humanistic view of sense of place might ignore
existing stmctures and constraints. While Gcskr identifiai specik human-
envuonment relations that wac hown heahg p ~ ' ~ 1 5 Gesler also incorporated
structuiaIism wittiin his concept of therapeutic landscape. Whiie ii is not the purpose
here to provide a history of each subdiscipline in gmgraphy it is important to
understand that Gesk, in ernphaskbg the =se of landscape, does not ignore
structural constraints. While structural constranits are not negiected below, humanisn
is emphasized here because the meaning of home in m~ular is consiâered
signifiant. 14.16.17
important here is that a landscape i~p iuce .~ A hdscape is both real and abstract - a
consequence of physical fonn and perception. Landscapcs are dynamic and shaped
by " . . - negotiation between, physical, individual and social fktors (p.743)."'
important because] people can bekve a place to be heahhy when, tiom their
perspective there is simply the absence of unhealthy elernents @-7)." But lwdscapn
are shaped also by historical events and changing dominant rnetaphor~~"~~ and it is
not -out purpose ttmî theraptutic laiidsaph itsclf a metaphor, was adopted.'
A therapeutic land-, d ï f k c d y than just a landscape, emphask that
healing ocms in a place. Building on the rneaning of landscape, a therapeutic
landscape then is one that i s p e m k d as hving haW a d baliDg pmperties.' A
therapeutic landscape is active in that it is a place that "heals", or maintas, but
therapeutic landscapes cm a h be associated the maintenance of heafth and
wellnedO and ". . . are places tht have achieved lashg reputations for providing
physicai, mentai, and spiritual hcaiing . , . [A therapeutic landscapes'] featuries include
. . . seme of place such as warmth, identity, rootedncss, or authenticity . . . (pg. 8)."
There are a growing number of studies that use the therapeutic landscape
concept to describe the heaith, M i n g and weli-bemg properties of specific p k s
and practices. La particuiar, a volume of papers h m The Sixth ïnteniatjonal
Symposium in Medical Geography (Portsmouth, England, 1996) refleds an array of
diverse places that have k e n und& using the thetapeutic landscape idea
Researchm have idcntified chikiren's camps,152' c h i k a ' s hospita~s,~ wildemess
cities and stmets, 2024"7 and ~pecifie medkaî prac&8 Win the context
of a therapeutic landsicape. Despite the range of examples provided hem, only one
was concemed with home-based care and the fwus was not on the therapeutic
iandscape of the home per se but rather on the therapeutic landsc~~pe of the city in
which home care workers tive. Thus the therapeutic landscape was a way to
understand health carc worker retention in an u n d m i c e c i cornrnunity?*
As suggested at the outset, the home (for the chronic tare zecipients in this
study) can be understood within the context of a therapeutic landscape. SpeciMly
the home can be undetstood by lookïng at the humanistic domain (sense of place), the
cuhiral ecological domain (the physical environment), and tôe sîructwal domain (the
social and poiiticaC). Eacb of h domains are d i i d with respect to the elderly,
and in particular the study participants, in the followtng sections.
6.2 Sense of Place and Home
It has been suggested above drat a major thaory underpindg die concept of a
therapeutic landscape is sense of place. As such Ït is important to provide a brief
discussion on sense of place and to explore the idea tbat tht home is a unique place
that also conveys a certain sense or meSnnrg. In particular, the sense of piace/home to
the elderly, as opposed to another subpopulation, is relevant to understanding the
result that the study participants p r e f d home-basad care and relevant to then using
the concept of therapeutic landscape as an akmate interprcgaion.
To @)examine the result that the elderiy prefèrred home-based care within the
concept of a therapeutic landscapc, it is necessary but not sufficient to suggest bat the
home had, or has, a w u l a r sense of place. It is as important to consider the sense
of the faciiity for these study participants. An undcrsümding of the meaning of the
facility is achieved both by considerhg relevant iiterature and by retrospectively
reviewing participant's comments. GÏven diat the orighai study did not empby
specific qualitative instmments there were notable ümits to this approach. Lndeed no
f3-m conclusions could be drawn h m the notes made during the mterviews because
no question on the meaning of kil ity (or home) was given in the interview. That
said certain comments were made tkquently enough to suggest that, while the home
might have conveyed a sense of place that was thetapeutic, the kility did not provide
a similm sense. In other words it is believed, by this rcsearicher, diaî the home and
the facility did not provide the sanie sense of place and that when contrasted with one
another the sense of home was more consistent widi the concept of a thetapcutic
landscape.
It shouki be mted that die contras& hmeen home and nicility was sigaincant=
the home compared to the f4ciIity was a therapeutic landscape. It might not be tnre
that each of the homes were therapcutic in the physical seast, Had on@ the home
been considered, an awaceness of the characfcnstics - d and abstract - that made
one home therapeutic, w h i another was not, might instesd be understood- Thus
understanding what makes a particuiar home, a place for heahh, hediag and wcüness
is an area for fùture resead~
Sens of place studies are .ssocïated with phibsophies of meaaingL3 and are
concemed with the bonds that humans devebp wah ~pccific Sense of plire
studies have revealed a strong association between piace and, personal and cultural
identitytity3' Sense of piaœ bas been d e s c n i as taken-for-granteci a d
unarti~ulated.'~~' As such it is where the ftndamental values associatecf with
personal, social and symbolic experiences of places are chaüenged that the meaning
or sense of place bas been criticpliy ~emaed.)' For example, as people becPrne
more mobile as a result of changes in modes of trans~ortati~on the, "question of local
identity became po titicaiiy articulate (p. 168).'5' in this respe* this chapter criticaiiy
examines a sùnilar challenge to a sense of phce -the meaning of place for health and
social care delivery. Specifically it is the shiftmg of health and social care delwery to
the home and community (primarily) h m the acute sector and an emphasis on the
home as a site for LTC and as a place to die that are c u m t l y challenging the sense or
meaning o f home to Canadians and important@ the sense or meaniog of a site for
health and social care?
One of the ofbmentioned gcographers to examine sense of piace is Relph wtio,
in 1976, wrote, PIace and ~~aceiessrsess~~ a book that despite bemg d e n 25 years
ago is Uicreasingiy citeû in the lireraaue? Relph is considemi one of the first to
express that places not only be defineci by location but also thai places bt defÈad by
the rneaning bat they are given? Relph desaibat sense of phce as authentic or
inauthentic? Swm ofplace was authentic whca tha t was either fuU awirraess or
profound and unconscious identity widr place. Yet the most significant -or o f an
auîhentic sense of place wes, "insidedness" - " . -. belonging to p u r place both as an
individuai and as a member o f a comrnunity, and to know this without refleçting upon
it ( ~ . 6 5 ) - ' ~ ~
While sense of place concems mer scale physicaî locations such as &le
countrk, sense of place also concerns smaller scale physical locaîions such as the
home- indeed Relph devoted a portion of his book to, Wome places as profound
centres of human existence (p39)F2 Here Relph dcscrikd the "profound form" o f
home as an attachment to a place that is as necesary and unavoidable as the
attachent to people. La k t , " . . . if we am rcally mted m a place and atîached to it,
if this place is authentidiy our home, thcn ail these facets Cphysical appearance,
hdscape, awareness of a place through time, the fàct diat we laiow a place and are
known in a place, and, where we have had ow m m significant experiences] are
profoundly significant and inseparable, Such home places are indecâ foundations o f
man's existence, providing not oniy the confext for d l human activity, but also
securïty and identity for i n d ~ d u a l s and groups (p.41)-~'
Buttimer is another geographer d o has written about sense of place. Rather
than using the tenn, insidedness, Euttimer descriibed "centeredness" in her discussion
on home and "horimm o f reach."' Centering is an rtive proeess that involves phce
(or home) and d w e h g (or ceach)?' Lke Relph, Wmina emphasized that the
meaning of place was achieved thmugh a Iived, dynamic and reciprocal relationship
between people and locations. uidmduals were œnttbd if the home and reach o f their
Ofcourse Relph and Buttimer are not the only resesrchers to bave written on
sense of place." Rather than provide an exhaustive review o f sense of place, the
purpose was to highljght tbat sense of place and sitniiarly, home, was an active rather
than static concept. The discussions and ttieories advanceci by researchers lîke Relph
and Ehttimer on sense of phce have contriiuted to an understanding of the home, Iike
landscape, as a place that is more than a physical location and as a place drat
possesses rneaning for its iahabitants. hdeed understanding what contributes to a
sense of home rnight lead to creating home places that are aot ones ovm physical
home- Notwithstanding the contriiution of tbis riesearch the meanhg of home
remains indefinable. 29JW t For example, the Caaadian Oxford ~ictionary~' devotes
ahnost two pages to the dehition of home and it's variant^.^ SimiJariy, in ber review
of the concept of home Moore also presents a staggering account of tbe nurnber of
definitions for, and interpreîatiom oc home." It ans suggested thaï the even the most
comprehensive definition of home (see pg, 208) stil excluded culture and still
excluded the process behind the formation of home.29 Despite that the home has bcen
difficuk to define its meankg to the elderly haî been e ~ p l o r e d . ' ~ * ~ ~ ~
Rowles has been one of the major contributors to the literature specificaUy
relating sense of piace, the home and the e ldaf l in the early to mid-1970s Rowles
recognized that the, " . .. p r e v h t image of a pmgresively shrinking geographic
lifespace with advancing years attended by uicrccrsing aitachment to a local setting
I t w a s ~thratinicIinilti~pafudedradingevayscnscof~rocsndyd~afllll review of the sense of Pace Iitaaturr was na possible. -y seniinal book and arcïcics, fà exanple, Speçc and Plope by Y-F. TU^'* and, 'Ibc Pdcs ofSpct by G. ~iichclrrd6 are nr'ssing hthisdiscussioc~, "ItisndeYvOetfiy, f a r t h i s e , tbpta~~dtbedcnnitiom~dPdws,"miiistitiaionRirpasais needing czue, rest a rdùge"
was clearly a gross ovasimplinesiioa @. 176)"" and, d' smtkfkd with the la& of
studies thai explored the meaning of place to the elderly, conducteci a thme-year
experieutial study-
Experiential field work led Rowles i n i t i e to conclude that the clderly
experienoed piace dong four dimensions: 1 , action: physicd movement and
orientation, 2. orientation: cognitive interpretation of space, 3. fmling: emotional
interpretation of space and 4. ktasy: remmiScence of the pas& and projection onto the
contemporary ~andsespe.'~"' The fourth dimension, fantasy, received the most
attention fkom Rowles who observed that as the proximate space became smaller with
age, due to fùnctional declme, the role for geographical fàntasy beoame larged3
An additional observation on pmximate space, relevant to this discussion, was
that, as more tirne was spent at (physical) home - common with the elderly - there
was an mtensification of the importance of "pr0Xanat.e mncs." The two most
important ptoximate zones for the elderly became the home and a "surveillance zone"
surrounding the home. OCtiers have confimied that the home is particuhrly important
to the elderlyP649 For example, Sixmith (1990) concludeû mat older perwns are
more oriented to the home (home focusseci), th& oider persons are mom concemed
with the instrumental aspects of the home (independence), and, that older persons
have a deeper personal concm for their homes (attachmeat)?
On the home RowIes noted that, " -. , Horne, firlcnim of the lifeworld, was
possessed invio iab le space. Immediateiy outside, a narrow surveillance zone,
encornpassing the field of vision tkom the home, was disthguished by a sense of
partial control and waîchttl raiprociiy Mong acighbors (p. 59)."" Simüir to
Rowles' "hviolable space", Twigg noted that the home is a private space, süuctured
in tenns of privacy and inhacy and it is . . . [the] capacity to exclude - to &ut the
door on the outside world @. 384)," that &es tbe eldedy, or care rccipient, power
and contro~'~ Accordmg to Twigg, Wome is an almost universaiiy recognisd value
m modem society and its principle features , . ttie ethic of prhcy, the power to
exclude and the embodhent of identity - are highiy signifiant .. . (p. 3 ~ 4 ) n ' ~ In a
similar way, identÏty and controi were echoed in this statement by Abels and Kesrns:
Kontos (1 997) also highlighted the importance of control and personal
ideutity- Kontos m t e that, " . . . Home affords mdependence by defhing a space that
is controlled and is uniquely the domain of the individual. Home is a s p œ in which
to pursue personal hterests and also, as it is resonant with expetiences and
expectations, it is a vieal ficn of self-identity @. 179).'*' ïnterestingly, and diffamt
h m Rowles, Sixsmith and Twigg, the home that Kontos studied was a supportive
housing cornplex for the elderly and not 'lown" @hysical) homes. Nonetheless, the
key aspects - control, privacy, independence and identity - are the same and it is
signifiant that these key aspects could be achieved apart h m one's "own" home per
se. This idea, that a sense of home was not a consequeme of living in one's "own"
home, has also b- notai by ~ o w k d - ' "
Indeed Rowles reinterpreted his reçearch in the context of attachment to place.
The major idea was that attachrnent to place was Iinked to one's self-identity and tfiaî
this was particularly true for the oldest individu al^.^ Attachent to piace came h m a
" My emphasis Y ~~rsnith* and algo natc th.t ftrf.iiait to plpt is prriculahy inpaimc to cfie eldaly. Ehy explains a#arhnient additidly by -king the largth oftinr h o t a individuai i i d in a pœtiailor pi=
aw PWAY ml sua!-- =cy "~"!pam,, = aw P=P='P o w w q s 4 paou 4 ~ ~ 1 ! t y s mm &nywoqo == v w#ht p p 4 idsp 01 pue atmy
ay, oi w d ail, u i q ~ n ~ u o : , ~ o suas e qmyeur OJ '&ununum ptnr A p g qayl
01 uoynqguoa napr a31o~u1ai ot '=%cwq3 pqsAqd UMO n m j o @hy q %u@uolaqjo
a s u s B a-d q d 01 Supau1 a ~ d AI-a ayi Apuanbasuo:, pue3laçjo asus
8 0 3 pitirla sSaUp3Q!SU! p . l ~ ~ q o ) ~ '4-d~ ZsoW ,Fuog3g CKU%p -3
B 01 PUB ~ ~ ~ J ~ ~ s goq mga 01 w m q m ue 9 )aA pue 321 s,auo
u! =ql l ~ ~ p tir paiaq=- aq pin- =id au0 Dy) m 1- pJodrua, 8 peq osp
==paP!sn! 1=!q-olqo1nv - 4 w m d 4 mm!=!# aS arl%IUJ JBy, J Q F F ~ J ~
pqsAyd Aq p a m p ~ &=s==J 3~ - trrrl, = q d p 8 =& 11 * m ~ n q m u n
Pm patUBJ%-~o3-~ -Pw=! lwnl-oiqwrm P==P =IMo.tI
-auioq ,uih~, S,=O q SWJ Lps== i n o p a m q j o asuas a a ~ 3 g - p ~ ~ w
@nn mqi '- aT1 'SSaPpaP!~ mq-o!qol~ 4 ' W P u! 3! PaWsaP
pue N a m a aq, a q d o) w a ~ p a m j o uqsuauup a+nnom~d =ow aw 'Asmqj
aqy 'ssaripqsq pgdmSqqorniz parapsmm sapou -sapa- )sird pus w n a y d x a
~ - d j o q d :pgdaiso!qorne -c piie &!un-<» arp p ~ W u o p q j o
=as p m II-4 :pps -2 rpaanioq~ua JO amoq arp m ~S~U~IBME Apoq : p ~ A y d
-1 : S p ~ S W ~ p aWJ0 UO!WJy 833511 SPQaF lJ ! Pm , ~ P a p I S Y JO a s
home? indeed there are exampies of ahanative living "places" that achieved the
quaMeS of "home99-47;J".5'P W e not an exhaustive List home quahies inciude
fàmiliarity, pnvacy, independeme, control and proximity to fàmily and maîeriaf
possessions. Nevertheless, despite that a sense o f home is achieved in alternate
settings, the 'hursing home" has not been understood as a home-place.
The negative perception of a nursing homebb might be evidenced by an
unwillingness to rcbcaîe to a nursing home:3u a significantly h i g k percentage of
elderly with shilar disabiiitîes stiU living at or a fidl in nursing home
utiii~ation.~~ For example, whm eiderly pasoas wcre asked iftbey would be wiliing
to move to a nurshg home, 26% were very unwilling and 30% would &er die
(N=3,262). Qualitative studies also support a sense of nwsuig home thaî contrasts the
sense o f h ~ r n e . ~ ~ in Kontos <1997), an eldaly pmon expressed that, " . . - 1 am &id
of having to move to a nursmg home because it wouki b?l me (p. 174)?' Whik
home is a place of hova the nursing home it seems is a piace to die and it is true that
most persons who enter a nursing home do not transition back into the
community.lsS7
The Iast staternent, above, is subject to the criticism tbat it romanticiaes home
and it is noted that home is not necesSanIy a positive phçe?7;U*49 Again, because no
information was çollected on the &ors that made one home a place for heaith,
heahg and weliness, while another was not such a phce, the observation was that the
facility, cornpared to the hm, was not believed to be a place for heahh, healing and
wellness- A second criticism with the coacluding statement in the previous paragraph
is the use o f word, "nursing home", radier than facility, the term used in this study*
FÙciZity was chosen to avoid any negative associations with the terms nursing home,
Again, no speci6lc qualitative meastirement tools were used in this resesrch
and it is possible th& positive comments about the home were articulated but aot
recorded- But it is also possible that positive wmments about the fkility were
simiIarly not recordeci- The iack of explicit rcf-ces to one's own home might
mstead reflect the taken-for-granted notion of the home and the unarticulateci sense of
meaning that R o w k discuseeAt 14*42.43 And, in retmspcct, mmy unrecorded
comments paralleled tbe key tbemes in the üteraîure discussed above. For example,
control was rek ted in the comments made by several participants wtio spoke of
going to sleep, waking up and eaîing when ttiey wisbed. C t is unfortunate, in tight of
the one-sided result, that a q d ï v e instrument was not used to discern the fkctors
tha. related to the preference for the home-
Ultiruateiy the purpose of this section was to highlight that a certain sense of
place was asociated with the home for eMerly persons. In particular the ekterly had a
sense of home th& was dEerent h m their sense of a fkcility/nursing home. With
respect to the resuh that elderly pemns p r e f d home-based care to fâcility-based
care it is advanced here that this preference was, in part, related to the sense that home
could provide a place for healing and well-king that the facility could not - it
is advanced that the home, cornpareci to the fàcility, is a thetapeutic landscape-
6.3 Ecological and Structural Aspects of the Home
Aside h m a health, healing and weiSness sense of a place, it was undcrstood
that a thenpeutic landscape was a b the result o f physical and structural (social
political and economic) attniutes.' While the fwus of mis discussion has bem on the
pa.tticu1a.r meanhg of the home to the elderiy this author would be remiss to neglect
the physicai and siruchirat dimensions of the home and thcu relation to the concept of
therapeutic landscape. Again, it was unfortunate tbat no data was coiiected on die
physical fèatwes of a home other than the type - house, apartment, or condominium -
and because few notes about physical fcatures were made during the interviews no
lïrrn conclusions couid be drawn- On the other band, with respect to the s b u d
factors that made the home a therapeutic landscape, more could be said* The
structural factor thaî is the focus here is on the dommant philosophy, Ag- in Place,
which has been synonymous witb rernainiag in one's own home?
including concepts such as meenùig and sease in the definition of landscape
does not exclude the fbct that lamiscape has a physical component, It has hem
suggested that relatively little information was g a t h d on the physical atrriiutes of
the home however it is suggested now that wbat was gathetcd supports the argument
first thai the home was a "Iandscape'' and second thaî cerCsin physical features o f the
home added to the sense that the home was theripeutic.
That the home was a landxapc was evidenced by mmments made most ofken
when the interview was arrangeci, While interview times were not easy to schedule
with the care recipients, it was almost never because the person would not be home*
Rather, interview tirnes were difficult to schedule because the study participants were
for the most part unable or unwiilingdd to have both home tare and the interview on
the same day. Many study participants joked diat they were aiways around and never
went anywhere anpore. Some however refèrred to thanselves as "&ut-ins" and
were risibly upset thaî it had been weeks since they went outsiide of tkir own home.
On one occasion the lack o f mobility outside the home was relaîed to the weather,
The examples above supporteci that the home was the physical landscape for
the shidy participauts however they were insuffkient to show diat the landscape was
aiso therapeutic, Evidence that the physid fkatmes of tbe home were tberapeutic can
only be speculatd on here. It might be hypotbesized that the many h i l y portraits
and mementoes that wete shared tbughout the mt&ws indicaîed an attachment to
home and an autobiographical insidedness- Indeed these are physical items that have
been identifid in the literature."v42*43*46 Or else, the open display of cerbh physical
feaîures of the home rnight have been indicative of a therapeutic aspect of the home.
For example, several participants were keen to show off the aâaptations made to their
bathrwms and kitchew that helped them to manage theû functional d e ~ l i n e . ~
Sirnilarly, many participants discussed the move h m a house to an apartment as
k i n g necessitated by their inability to manage stairs-
A &ai provocative observation relates to Rowies' idea of ''proximate zones"
and the surveiUance area just outside of the home. Indeed, if a surveillance mne
becornes important and is indicative of a sense of control it was dernonstrated in the
dynamic processes then the home wuld be examincd as much tOr wbat made it
therapeutic as for what did not make it therapeutic,
The point d e h m is h î , the Aghg in Place philosophy supports the idea
that the home is the ideai place for the eldaiy to age. WhiIe aging m phce
philosophy has bem demonseaied ohde of one's own h~rne,"~*'~*"-" omt home stiu
dominates. As the Aging in P b phitosophy supports the ide8 to keep the elderly in
own home, heahh and sochi c m delivery and receipt in the home are cncouraged. In
this respect, home is an un&rstd, or taken-for-granted, therapeutic landsape
whether or not each 'dividual home is m k t d o w e d with dierapcutk qualities. It
is not the purpose here to siggest tbat Agmg in Place is a "ôad" philosophy but d e r
to imply that more can be b w n about what rnakes a home îherapeutic. I f it is taken-
for-granted that the home is therapeutic, one wonders bow many elderly persons are
not Aging in Place/Home at dl.
6.4 Chapter Summay
Places are lived and expericnced and even within one's "own homeg' a sense
of place can Vary. This dynarnic understanding of place has ben evident in the
concept of a thenpeutic landscape. The concept of a therapcutic landscape offered a
fhnework for understanding the home. Specincally, how elderly persons with
ctwnic heaith problems might petceive that the home was a therapeutic Wscape
was addressed. Within the concept of a therapeutic landscape, and with respect to
elderly persons with chronic health problms, th= dimensions were important: the
home had a particular meaning, the home had particular physical htures and the
home was an understood therapeutic environment. Each of the thme dimensions
contriiuted to the possibiiity that home, compawd to a fiicility, was a therapeutic
landxape for elderiy pasons with chronic h e m problems.
It was not inappropriate to use the thtmry of thcrapaitic land~cape~ Meed
Litva and Eyles state thaf " -. - difièrent theorks provide the concepts for describing
the same world but m dükent wayn Which theory we use should largely depend on
the type of researcb question we ask (p. 12)? Further the mm-age of a qualitative
theory with quantitative economk msearch has been eacoumged~* The specinc
knefit of using the thercrpeutic landsape concept in this paper was that it questioned
îhe origind underlying dekition and understendhg of die care setthgs (or places or
landscapes) used to determine the pref'erence for aitemative long-term care settings
for persons with chronic bealth problems, Because it is not enough to simply know
that location daers - how, why and the erdent to which difkrence -ers are equaliy
importad6- the concept of thempeutic land- also pmvided a fhmewodc to
consider meaning differences, physical differences, and sociai, political and econornic
differences-
It is acknowiedged that this research might have ekited a p r e h c e for the
taken-for-granfed therapeutk landscape, the borne, rather than a preference for the
home as a c~place/Iandscape" for heaith and social care delivery and receipt. In other
words piadandscape was fixeci and moreover oniy dlerapeutic with respect to a
faciMy!' To question whether a hwe is a tberapeutic landscqe ramer thai the home
rnight provide a differient interpretation for heaith and social care setting preferences.
This unique (re)exammaîion sbould not be understood to devalue the result
that etderly pemns with chronic health problems preferred h o m e - b d care but
instead should be understood to drive firture research. Indeed the resuits indicated a
strong prieference for home-based care for persons with chronic heahh probiems. The
next step is to undetstand ifa howe as aplace for health and socid care delivery is
II O f c o u r s e , f a c i l i r y i n h r n ~ g h t a s O ~ ~ a t l ~ b y t b t s a i d y p r c i u p n t ~ , d r m - ~ r ~
nor thaapeutic-
preferred- In other wods, rather tban take for gtanted that the home m a i n s constant
throughout, investigate how b k h and socid care delivery are iived and experiencad
in this piace and subsequedy ask by Iooknig at meanhg physical fé9turts and
structural factors, if there mains a p r e f m for home-based care-
TIiere are suggestions that fiture genedons of elderly might not have tbe
same preferences. 40.44.67 Of course wtiile it may bc tnie that kture generations wÏU
prefer a diffhnt landscape it is unkmwn how prie- for therapeutic landscapes
might change. The assertion that preferences change has been refated to sense of
place and the idea tbî an i n c d virnial and gen& worki might change our
attachent to and sense of "our home." The next phase m this investigation of
preferences for home as a p k e of heaiâh aad social care might bene& h m
c o n s i d e ~ g generation differençes, Whilc the nexi phase can put more emphasis on
qualitative investigation it should not be necessary to exclude a quantitative measum
such as the time trade-off- In fkct it is hypothcsmed that qualitative investigation
could Iead to a cornprefiensive understanding of the "care sc#ing descriptionsy' offercd
in the d e . As such preferences could be understood over a b d range of health
and social care services thaî are delivered and received over tirne m a home or a place
or a landscape.
Chapter 7
7.1 Conclusion
The purpose of this tfiesis was to iden- underlying (or innate) preferetlces
for two distinct LTC setthgs for persons with chronic health problems. At the outset
ir was argued that while p r e f ~ n c e s for atternative LTC setîings were important to
planning LTC in Ontario, p r e h c e s had not bum quantified with m economic
preference elkitaïion technique. It was hypottresizod that a technique such as the
TT0 could be used to mode1 the rchtive preièrences for home-based and fàcility-
based care for a study population of current home-based care mcipients, It was
hypothesized that dative prdêmces would be explained by a set of independent
variables that included heak statu% age, gender, waiting üst (for %il@-based care)
status, living arrangements, housmg type and ownership, extent of idionna1 care
available, education levei and incorne level.
A total of forty cwrent home-based came recipients d o t their caregivers
were inteM~ed- Ali but one of the study participants prefened home-based care
when giveo a choice between home-based cam and fàcility-based care. However the
relative preferences for home-based tare varied- On average home-based care was
preferred 61 7 times to kility-bas& care but îhe standard deviation for this resuït was
1 1 13 - The relative preferences for home-based a r e were modeiid ushg regression
techniques to understand which variables e x p l a i the variation in the relaîive
preferences for home-bssed care.
Several regression models were testcd to explain tbe variation in relative
preferences for home-based care in this study population. Despite the attempts to
mode1 relative preferences usmg several mdcpendent vatiables, only three variables
explained the variation. H d t h statu% megsurcd by the EuroQol EQ-SD, &eCtively
drove the resub. nie negative reiationship between dative prcferrnces fer home-
based Gare and heaith sfatus was unanticipamL It did not seem reasonable that those
study participants in the worst healdi would have a strongcr preference fbr home-
based tare- It was concluded that the regression model was insufficient to explain the
relative prefetence for borne-hieci tare.
Limitations in the study might have d h the unanticipaîed remit. Indeed the
sarnple was maIl and the inclusion cnteria may have becn Iimiting. The extent to
which variation amId be explaincd by the variables might have been gre!ater wiib a
Iarger and broader sampie, It was also possble that the methods employed in this
study were pmbïematic. For exampk, no questions were asked about the experiences
with aiternative care settings, yet, emence may have mfluenceà the mterview
responses. Inree alternative hypotheses were forwarded are that are potentially
consistent with the result that relative prefermces were negativciy related to heaW
StatuS.
It was advanced that if the study participants wete risk averse expected utiüty
maximizers, they would have been unwilling to take the gambie of rnoving to a
fàcility. Similady, if the study participants were los averters they might have been
unwilling to accept any amount of gain - m mental or social or physical health - if
there were even a minute chance of a loss.
it was also advanced diat die negative relationship between relative
preferences for home-based care and healui state was instead a negaîive relationship
between preference for location of death and heahh state. It was suggested that the
sicker a study @cipant, the closer that the snidy participant might have been to
death. If there were a strong preference to die d home, as opposed to a facility, the
relative preference for home-bssed care might have &en a proxy for location of
death. It was unknown ifthis was true because there was no question pertaining to
place of death,
Finally, it was advanced drat the cboice betwecn home-based carc and fàciüty-
bas& care vms a choice that mvoived a change m both the location and the type of
care. Unfortunately, it was not possible to difkentiatc the prcfkrence for location -
the home and the facility - h m the preference for the associaml service - home care
and facilm c m . it was possible thrit the prehnce for home-based care was a
preference for the home, as opposed to the hility. ifdeterioration in health wete
associami with a stronger pref-e for the home, as opposed to home care, thea the
worse a study participants' heahh the stronger the preference for the home. hdeed it
was possible tbt the relative pref- for home-based care wwt a proxy for the
relative preference for the home.
At first glance it might appear that this attempt to identifj., quanti@ and model
the underlying (or innaîe) preferences for aiternative LTC settings was unsuccessfiil.
On one band it is tnie th& the relative prefemces could not be modelled in this study.
On the other as a pilot study, the purpose was not only to attempt to mode1 the relative
preferences but also, to identiîy fùture research directions- A prefercnce for home-
based care was identifiai and a relative prieference for home-based tare to fàcility-
based care was quantifieci- In order to advance a predictive model further research is
warranteci. The final sectiton that fobws summarizes directions for friture research to
quanti@ preferences for atternative LTC d g s .
7.2 Future Research Directions
The discussion chapters detailad the limitations, rncthodological prioblems and
potentially consistent explanations for the unanticipaid muft that the relative
preference for home-based carie was negativeîy rielaîui to health status. in diis section
füture research d M o n s , implicit in the two cbapters, are highlighted- In thk section
changes to improve the mode1 are suggested dong with changes to improve the
capacity to explam the rcsults ifthe mode1 is stifl producing the riesuit tbat relative
preferences for home-based care are negativeiy associated with heaW status- Both
sub-dons below highlight a set of chaoges that will assist in fiturc msearch to
ident.6 underiying (or innate) p r e h c c s for LTC settings.
7.21 Amadmerb to larprove the Mo-
The first change to make in this study is to nimase the sampk s k e . A iarger
sample would not only increase the power but also allow for a more complete
examination of independent variables. For example, specific chronic health problerns
or ethnicity might be considered with a k g e r sarnple. A larger sampie might be
achieved by interviews with a greater number of home care recipients but it could also
be achieved by interviews with individuals who are not in receipt of home care.
interviews with those who are not currently, nor were not previously, receiving home-
based care might iden- different pretèrences b d on experience with home care.
Another change that might be made to the study protocol would be to measure
health status differentiy h m the method emptoyed here. While the EuroQol was
chosen for its simplicity and reliability it would be a bene& to the study to use 0 t h
measures of health status such as a measure of the ADLs. At Ieast one additional
measure seems important especially because the pceferences for home-based care
were driva by heaith status (as merrsud by the EuroQol singie index scom). Of
course, the benefit of a longer and more specific (to an elderly person with chronic
hesildi probbms) instrument needs to bc greater than the cost o f a longer interview
and i n d burden on the care recipient andor caregiver.
Tt might also be a possible to improve the mode1 with more comprehcnsive
descriptions of the care setîings, In this study the TTO exercise was completed
quickiy, perhaps because of a strong pritférence for own home, but per)raps because
an inadequate description of the kility was provided. in 0th- words, it is possible
that a more specifjc d-ption of the kiiity would lead study participants to rtflect
longer on their prefènmces for heahh and social Gare settings. In tum this could
influence the relative p r e f m for home-based care.
ImproWig the descriptions of the care settings might also mean conducting
more than one TT0 exercise, An additional TT0 exercise rnight be employai to
differentiate the attributes of fàcility-based (or h o m e - b d ) care. For example, one
kility might provide private rooms with kitchens while another docs not. R h
than change the attributes of the fkility (or home), a change to hcalth state can also
be made in additional TT0 exercists. In other words the descriptions of the hility
(or home) are nxed but the TT0 is conducted for current heahh state and potential
fùture health states. StiU, like introducing mother heah status measure, the benefits
of additionai T T 0 exercises must be weighed against the cost of a longer and more
burdensome interview.
Finally the addition of a question on the survey that relates to experience with
facility-based care might also improve the rnodel, It is hypothesized that experience
(or inexperience) with kility-based am might have infiuenced the relative
preference for home-based care. To test îhk hypothesis, mperience must be added as
an independent variable in this model.
7.2.2 Amendmeib to lmprow the Ioterprdation
Potentialiy consistent explanations were given in Cbapter 5 and Chapter 6 to
understand the unanticipated riesult of tôe qpss ion model. The previous section
a d d d some necessary changes to improve the predictive capacity of the modtl,
This section differeutly suggests that changes might be made to confirm the aheniate
exp tanations but also drat ncw avenues need to be c x p i o d in Sis m h thaî
pertain more specüidly to the home (or the îàciihy) as a place for heahh and social
care delivery and m i p t
The easier change to the interview is to address the prefereace for location of
death. Sy asking whem the study participant prefers to die - the home or the fàcility
- it would be possible to confirm ifthe prefemice for home-based carie werc a proxy
for facility-based arecate
The more difiicuit, but more provdve, change to the interview is to include
qualitative (and quantitative) measures of the study participants' semc of home and
sense of kil i ty. in other words, it is suggested that the next phase of this research
examine the home and the fircility within a fiamewrk lücc that of a therapeutic
landscape. The addition requires a cornprehensive understandmg of heafth care
settings as places that are dynamic, Lived and experienced. In this respect qualitative
(and quantitative) measutes n d to be employed that consider the physical and the
syrnbolic. Interviews might be recorded and certainly would be more d d l e d in
range and type of questions asked. It is hypothesized that the shift to understanding
what makes a home therapeutic (or not) rnight iden- a way that the prcference for
home can be satisfkd in LTC planning models- For exarnple, if the most "toxic"
aspect of a fàcility were the lack of privacy it might be part of a LTC plaMing mode1
to "build" a specific number of IBcilitii with private m m s .
73 Chapter and Thesis S imaa y
At the outset the study goal was to develop a predictive mode1 that could be
used for LTC plannmg in Ontario. It was known diat key LTC stakcholders in
Ontaritario vMmd prchnces a impomt but hi- uiuviihbk for phaniag-' Indecd
it would have been a siguikaut accompüshment to present a succffsfiil pradictive
mode1 and yet fàilure to do so oniy served to cal1 atîenth to an opporhmity to try
again. It is unlikely that the unanticipateci resuh was related to a unique study
population- It is more likely uiat the study population and the rneaning of place for
health and socid care delivery d e d to be beîter understood. It is hoped that this
thesis might encourage riesearch that continues to intelligent@ understand the
preferences for aitemative LTC settïngs for persans with chroiiic heahh pmblems-
References
Chapter 1: Iatroàuctioi
[II Baranek PM and Coyte PC- 1999- Long Tenn Care in Ontario: Home Care and Residential Care. Report pcepared for the Cokge of Physicians and Surgeons of Ontario, 1999.
[2] Federal-ProvinciaCTerrito~ Advisory Committet on Health Services (ACHS) Workmg Group on Continuhg Cart- (May 2000). The Identification and Analysis of Incentives and Disincentives and Cost-Effiictiveness of Various Fundhg Approaches for Continuing Care. Technical Report 5: An Ovecview of Coatuiuing Che Services in Canada. HoIlander A d y t î d Services- Victoria B.C-
[3] Heahh Canada- Home Cam Development, Provincial aad Territorhl Home Care Programs. June 1999,
[4] Long-Term Chre Act, 1994 Ontario Ministry of Health and Long-Term k.
151 Ontario Minisby of fiealth and Long-Tenn Care Website. Available:
[a Ontario Association of Community Carie Access Ceatres. Human Resources: A Looming Crisis in the Communiîy Cart System in Ontario. Position Paper June 30, 2000-
[A Federd-Provincial-Territorial Advisory Cornmittee on Heaith Services (ACHS) Workîng Group on Continuing Care. (May 2000). The Identifkation and Anaiysis of Incentives and Disincentives and Cost-EfEctiveness of Various Funding A p p d e s for Continuiag Care. Techical Report 2: Holiander A d y t i d Services- Victoria B.C,
[8] Aday, L. and Shortell, S.M. Indicaiors and Prcdictors of Health Service Utilization- In: introduction to H d Services Third Edition, Williams, S.J and Torrens, P R (eds.) John Wiley & Sons: New York. 1 988,
[9] Coyte, PC. 2000. Morne Care in Cd Passhg the Buck, unpublisheâ manuscript, Department of Heath Adrnmistration, University of Toronto.
[IO] H o M e r MJ and Pailan P- The British Columbia Contiauing Care System: Service delivery and resoume planning, Aging Clin. Exp. Res. 7: 94-109, 1995,
[11] Heaith Services Restructuring Co~nmission. RebuiMmg Ontario's bai th System: Interim Planning Guidelines and Implementation Strategics. A Diussion Papet July, 1997.
11 21 Health Stwkes Restniduring Commission. Ldchg Back Loolting Forward- A Legacy Report, March 2000.
[13] KPMG Report: Long-Tm Care Revimc Future ScenenOs: Coatinumg Cam SeBrice Needs in AIberta November 1999-
[14] KPMG: Continuing Care Scenerios, 1 999-SWl- Prepami for the FPT Advisory Cornmittee on Health Services. May 2,2000, Mark Laairlro and E3renda Hm.
1151 Manitoba Health, @raft) Piatmhg Fnunework for Long Tenn Care Beds m Manitoba November 30, 1999, Received h m : Bcvdy Kyle, Seniors Consuhot, Manitoba Health-
[I 61 Turner, Kathleen Department of H d î h and Cornmunity Services Program Development Division Govtinment of Newfoundland and Labrador. Persod Communication July 24 2000-
[17] Gold MX, Siegal JE., Russeil L.B. & Weinsteh M.C., Cost-Effectiveness in Healrh and Medicine, New York= Mord University Press, 1 996
1181 Varian, KR inîemedistt Microeconomics A Modern Approacb Thud Edition, W.W, Norton & Company: New York, 1993,
Chapter 2.0: Literatun Review
[l] Gold MX, Siegal JE., Russell L-B- & Weinstein MC, Cm?-Effeciiveness in HeaM and Medicine, New York: Oxfôrd Univmity Press, 1996
[A Vrtrian, H R Intermediate Microeconomics A Modem Approach Third Edition, W.W- Norton & Company: New York, 1993 - [3] Coyte PC, Laporte A, Stewart S: Identifj6ng the Assumptions Used by Various Jurisdictions to Forecas& Demands for Home and Facility-Bad Cate for the Eiderly. Report prepared under grant 02709 h m the Ministry of Healîh and Long-Tenn Care in Ontario to the University of Toronto, December, 2000.
[4] Kaminsky, B.A.: Continuing Cam Planning and Resource AUocation Model- A project conducted for the British Columbia M i & q of Healtb, Final Report, October 2985-
CS] Hollander MJ and Palian P- The British Columbia Continuing Care System: Service delivery and tesource ptanning. Aging Clin. Exp. Res. 7: 94- 109, 1995.
[6J Health Services Rtsbucturing Commissiin. Rebuilding Ontario's Heaitb System: interim Planning Guidelines and lmplementation Stratcgies. A Discussion Paper July, 1997,
[g Hea&th Services Restructuring Commission. IAK)king Back tooJcing Forward. A Legacy Report, March 2000.
[8] KPMG Report: Long-Tem Care Rtvicw: Future Sc& Continumg Gare Service Needs in Alberta. November 1999.
[9] KPMG: Contiming Care Scenerios, 1999-2041. Repaced for the FPT Advisory Committee on Health Services. May 2,2000- Mark L m w k o and Rmda Htani-
[IO] Manitoba Heahb. (Draft) Planning Framewotlc for Long Tenn Care Be& in Manitoba Novernber 30, 1999. Received h m : BeverIy Kyle, Seniors Consubt, Manitoba Health-
[L 11 Turner, Kathleen Deparbaent of Health and Community Services Rogram Bvelopment Division Governent of Newfoundlaad and Labrador, Pcrsonal Communication Juiy 24 2000.
Cl23 E3aranek PM and Coyte PC. 1999. Cong Tena Care in <)ntario: Home Care and Residentiiil Care. Repoit prepared for the College oQPhysicians and Surgeons of Ontario, 1999-
[13] Federal-Provincial-TemfOrial Advisory Committee on Health Services (ACHS) Working Group on Continuing Cam. (May 2000). The Identification and Analysis of Incentives and Disincentives and C o s t - E ~ e n e s s of Various Fundbg Approaches for Continunig Cam. Technical Rcport 5: An Overview of Continuing Carie Services in Canada. Hoilander Adytical Senrices. Victoria B.C-
1141 Health Canada Home Cam Development Provincial and Territorial Home Cart Programs, hne 1999-
[15] Long-Terxn Care Act, 1994 Ontario Ministry of Heahh and Long-Term Cam.
Cl 61 Ontario Mùustry of E-Leaith a d Long-Term Gate Website. Available: h m ~~www..aov,on.ca/heahh/engIish/pm~ rnn-hm1
[I 71 Ontario Association of Community Care Access Centres. Hümaa Resources: A Looming Crisis in the Community Carc System in atario. Position Paper June 30, 2000.
cl81 Keating, N, Fast, J, Frederkk, J, Cranswick, K and Pcnier, C. E i d m in Canada= Context, Content and Consequences. StaOistics Canada Housing and Social Statistics Division- Novernber 1999.
[19] Jenson, J. and Jacobtone, S. Care Allowances For the Frai1 Eldedy and Their Impact on Women Care-Givers. OECD Labour Market aad Social Policy - Occasional Paper No. 4 1 DEELSA/ELSAWq2000)2
[20] Ontario Minisiry of Health and Long-Tenn Care Website. Available:
12 1 ] Nursing Homes Act, Revised Statutes of Ontario, 1990, Chapter N-7, Available: httpiD09.195 - 107.57/ds.dlWom.isapi.dl.. ,--rd={ 17D4A) &soft@age=D wument, October 13,2000.

[22] Homes for the Aged and Rest f i m e s Act, Revised Statutes of Onîarh, 1990, Chapter 33-13, Availabk: http-J/209-19!5.107.57/cgi- builom_isapi.dl. _ .OOntanoBtrecord=~AC8 ~BCso~age=Document, Oictober 13, 2000.
f231 Chantable Institutions Act, Revised Statutes of i)atario, 1 990, Chapter C-9, Available: httpY/209.19S.lO7.57/cgi- büdom-isapi-dl.. .OOntariogrtecord={262A~ Btsof€@age=Docuiaent, Octo ber 13, 2000-
1241 Long-Tenn Carie Act, 1994 Ontario Mimistry o f Health and Long-Term Care.
[25) Ontano Ministry of Health and Long-Term Care Website- Availabie: h~~/~.aov.on.ca(heahh/eadishl~m~ad~/ado mn.htrn1
1261 Federal-Provinciai-Territorial Advisory Commitree on Health Services (ACHS) Working Group on Contiming Gare. M a y 2000). The Idmtification and Anaiysis of Incentives and Disincentives and Cost-Effectiveness of Various Funding Appmhes for Contmuing C m . Technical Report 2: Hollander Aaalytical Senrices. Victoria B.C.
[27l Meeting with Dr- Peter Coyte, May 24 2000-
[2S] Home Care Evaluation and Rcsearch Centre Website: www.hcerdutomnto.c
[29] Gold M.R, Siegd JE., Russell LB, & WeinstPin M.C., Cost-Eflectiveness in Health und Medicine, New Yotic: Oxford University Press, 19%
1301 Varian, HR Intermediate Micn>econornics A Modern Apptoach Third Edition, W.W- Norton & Company: New York, 1993.
[3 11 Blornqvist, A., Wonmcott, P., and R Womacott- An Introduction to Microeconornics, Third Canadian Edition (McGraw-Hill Ryemn: Toronto), 1990-
[32] Varian, HR htmediate Microeconomics A Modern Approach Third Edition, W.W. Norton & Company: New York, 1993-
[33] Lipsey, RG., Purvis, DD., and Steiner, P.O., Economics, Seventh Canadian Edition, ~ o ~ i n s Publishers: New York, 1991 -
1341 Pearce, D-W- (mi.), The MIT Dictionary o f Modem Economics. Fourth Edition, MIT Press: Cambridge, 1992.
[35] Grossman, M- (1972), "Oa the Concept of H a Capital and the Demand for HealW, Journal of the Political Economy, 80;2,223-255.
1361 Phelps, C E ., (1 !EU), Heaith EconORljCS (Harpcr Collais: Ncw York)
[3q Tomce, G. Preferences for health statcs: a mview of measurtmcnt methods- Mead Johnson Symposium on Perinataldê Developrnent Medicine. (20):3745, 1982.
[38] Rossi, P, Freeman, H. and Lipsey, M. (1998). Evalwation: A Systematic Appmach Sixth Edition, Thousand Oaks, Caiifomk Sage Publications
1391 Brazier, et.aL (1999). A review of the use of heahh status measures in economî evaluation, HiAth Tec hnobgy Assessment; 3(9)
1401 Hiwgreaves, WA., Shwnwmy, M-, )ai, T., and Cuftèl, B., Cost-Outcome Metbods for Mental Health, Academic Prrss: San Diego, 199%-
[4 11 Froberg, D.G., and Kane, RL., Methodoiogy for Measurnig Health-State Prefermces - Ik scaling method~ Clinical Journal of Epiderniology, 42: 459-92, 1989a
[42] Furlong et.d (IWO), Guide to Design and Development of Health-Staîe Utility Instrumentation, CHEPA Working Paper Series, 90-9
[43] Dnrmmond M.F., Stoddard GJ., Torrance G.W., Methodsjbr the economic evaluaiion of AeaIth care programmes. Oxfiord: O d o d University Press, 1995-
[44] Torrance G-W, Feeny, Dm, Furlong, WJ., Barr, RD., Zhang, Y., and Wang, Q., Multi i 'bute utility fùnctian for a comprefmisive hcalth status clasifkation systern. H d t h Utilities Index Mark 2, Medical C m , 34: 702-22,1996.
[45 J Gafhi, A., The standard gambk methoci: what is bemg measured and how it is interpreted, Heahh Services R m h , 29: 207-24, 1994.
[46] Torrance, G.W., Sacketâ, D L Thomas, W.K Utility Maximization Mode1 for Evduatian of Health Care Programs." Heaitis Scnkes Rescarch, 7(2):1184 33, 1972
[47 Pritchard etal. (1998). Influence of Patient Refmces and Lncal Hkdth System Characteristics on the Place of Derrth, J o u d of the American Geriatrics Society. Eblume 46. Number 10. October 198. 1242 - 1250.
1481 Covuisky, K.E., Fuller, J.D., Y&, K, Jouhnston, CB., b e l , M.B., Lynn, J., Teno, J. and Phillips, RS. Perspectives and Review of Support Findings, Communication and Decision-Making in Seriousiy Il1 Patients: Findings of the SUPPORT Project- Journal ofthe American Geriatrics Society Volume 48 Number 5 May 2000
1491 Wilson, D.M. Endsf-litè prefwnces of Canadian senior citizens with caregiving experience. Journal of Advancecl Nursmg, 2000,3 l(6): 1 4 16- 142 1.
[50] McWhinney, I.R, Bass, M.J. and Orr, V. Fadors Associated with Location of Death (Home or Hospital) of Patients Refirted to a Palliative Care Team CMAJ Volume 152(3), 1 Febniaryl995: 361-67
15 11 Dudgeon, DJ. and Kristjanson, L. Home Versus Hospital De&: Assessment of Preferences and Clnrical Chakges. CMAJ Volume l52(3) 1 February 1995: 337-340.
[52] Matbore et-al- (1997) Surrogatc and Physician Uliderstanding of Patients7 Preferences for Living Pezrnancntïy m a Nursing Home- Journal of the Ammicm Geriatrics Society Volume 45, Number 7 July L 197,8 18-824.
[53) Mouton, C, Teno, J.M., Mor, V, and Piette, J- Communication o f Preferences for Care Among Human IiumUIlOdC6ciency V i L n f e c t e d P-: Bmkm to W i e d Decisions? Archives of Family Medicine Volume 6(4) July/August 1992342-347
[54] Coley, CM-, Li, Y., Medsger, A.R, Marrie, TL, Fine, M, Kapoor, WN., Lave, J-R, Detsky, AS, Wemstein, MC., Smgcr, D.E. Refhnces for Horne vs. Hospital Care Arnong Low-Risk Paîknts With Commuaity-Acquued fneumonia, Archives of Intenial Medicine- Volume 1 56(14) 22Juîy 1996: 1 565-1 571
[55] Freid, T.R, van Dooni, C., Tine#i, M.E., and Drickamcr, MA. Older Petsons' Preferences for Site of Treaîment in Acute Illness Journal of G e n d intenial Medicine 1998; 13 522-527-
p6J Chui, L., Kwong-Yui, T, Yu-Hua, L, WoeKhetllg, S., Ta-Pang, C. a d Tcben- Ru, J-C. Consistency Between P r e h c e for Use of hg-Term Care Ammg Caregivers of Stmke Survivors- Public H d t h Nwsing. Volume 1 5. Number 5: 3 79- 386.1998
[57] K e p r J.J., Desai, T. and Mutran, EJ. Eiders' prefkeaces for can setting in short- and long-term disability scenerios, Gemtofogist 1999June;3!3(3):3344L
[58] Martin Gibler, KI, Lwnpkin, J.R and Moschis, G.P. Maîure Consumer Awateness and Attitudes Toward Retirement musmg and Long-Tm Care Aiteniatives. The Joumai of Consumer Atlàirs, Vo1.3 1, No.1, 1997:113-138
[59] Porter, EJ., Ganong, LH. and Armer, JM., The church hm@ and kin: An older nuaJ Biack woman7s support networlc and prefieffncts for carie providers, Qualitative Health Research; 1 O(4), juiî000:452-47OI
[60] McCusker, 1. Development of Scales to Measure Satidktbn and Refiirtnces Regardhg Long-Terni and Terrniiial Carie. Medical Care, May 1984, Vol. 22 N0.5:476-493
[61] Ryan, M. and Farrar, S., Using Conjoint Analysis to eticit preferences for headth care, British Medical Journal 320530-3,2000.
[62] Carmel, S. and Mutren, E J., Stability of e1derty ptrsons' exptessed prehmces regardhg the use of iüè-susîaining trieatments, Social Science & Medicine, 49303- 31 1,1990.
[63] Tilden, VP., Nelson, C.A., DUM, P.M., Donius, M., and Toile, S.W., Nursmg's Perspective on Irnproving Communication about Nursïng Home Residents' Preferences for Medicd Tceafments at End of L ' i Nuishg Outlook 48(3):109-115, 2000.
[W] Berger, J-T., and Majerovitz, D, Stability of Prekenœs for Traibnent Among Nursing Morne Residents, The Genintologkt, 38(2)217-233,1998-
[65] feek CM, Coward, RT.. Lee, G-R, and Zsembk, BA., The laauence of ComrnunÏty Context on the Ref-es of Older Adults for Entering a Nursing Home, The Gerontologist, 34(4)533-542, 1 997,
[Ml Michelson, C., Mulvhili, U, Hsu, M., and Olsoa, E., Eliciting Medical Care Preferences fbm Nursing Home Residents, The Gtrontologist, 3 l(L)gS 8-363, 199 1,
[67] Toile, S-W., Rosentkki, AG, Tildca, V.P, and Parit, Y, Oregon's Low In- Hospital Death Rates: What Detemines - People Die and ~s f iac t ion with Decisions on Piace of kath?, AiYiais of Intenial Medicmt, 13q8):681-685, 1999.
[68] Finlayson, S-RG., Bitirmeyer, JD., Tosteson, A.N.A, and Nease Jr., RF. Patient Preferences for Location of Care Impliçations for Regionabation. Medical Care 1999.37204-209.
[69] Tsevaî, JI, Dawson, N,V, Wu, A-W, Lym, J., Soukup, J.R, Cook, EX., Vidaillet, H-, and Phillips, RS., Health values of hospiÉalizcd patients 80 yam or older. HELP Investigators. Hospitalized Elderiy Longitudinal Pro@ JAMA. 1998 Feb4 ;S7!J(S):37 1-5
[70] Rodeid , KE., Wenger, N-S-, Phillips, RS., Connom AS., Dawson, N.V., Layde, P. C a l a RM., Liu, H., Lynn, J- and Oye, RK,, Factors Associatecl With Change in Resuscitation Prieference of Seriously III Pat'ients, Archives of Interna1 Medicine 1 S6(l4) 2Uuly 1996:155844
1711 Mazur, D. How OMer Patient Preferi~œs Are Idueaceci by Consideration of Future H e a b Outcornes. Journal of the American Geriatrics Society. Vohme 45 Number 6 June 1997.725-728
[72] Somogyi-Zalud, E., Zhong, 2, L ~ M , 3. and Hamel M.B, Patients Experiences as Death Approaches, Elderly Pcrsons' Last Six Montbs Of Life: Findings h m the Hospitaliaxi Elderly Longitudinal Project Jounal of the American Geriattics Society Volume 48 Number 5 May 2000
1731 Donald Sherbourne, C., Keeler, E., Unutzer, J., Lenert, L., md Wells, K., Relationship Between Age and Patients' Cwrient Health State References, The Gerontobgist, Vol 39. No, 3, 1 999271-278
[74] Lewis, CL., Wickstmm, G.C., Kolar, MM., Keyserling, TC., Bognar, B.A. DuPre, C.T. and Hayden, J., Patient Preferrences for Care by General Intemists and Specialists m the Ambulatory Setting, J o d of G e n d Internai Medicine 2000; l5:75-83.
[75] Freici, T.R, van Doom, C., O'Leary, LR, T i t t i , M.E., and Drickamer, M.A., Older Persons' Prefmnces for Site of Terminal Cam, Annsls of interna1 M d i c i i , 131(2):109-I 12, 1999,
[76] Freid, TOR, van ihorn, C., O'Leary, J& Timetti, MX, and DrIckamer, MA, Older Persons' Preferen~es fit Home vs. HosQital Cam m the TIie9tment of Acute Iliness, Archives of Interna1 Medicine, 1 60: 1 501 -lSO6,2OOO-
(771 Belle Brown, J., McWiams, C.L, and Mai, V., Barners and kilitators to seniors' independence, PecceptiOns of Seniors, carcgivers, and health care providers, Canadian Farnüy Physician, 43:469-475, 1997,
[78J McAUister, N., and Hollander, M.J., Seniors' Perceptions of and Attitudes To ward the British Columbia Continuhg Care System, Health Reports, 5(4):409-4 18, 1993-
Chapter 3.0: Methods
[Z 1 Last, J M , A Dictionary of Epidemiobgy, Third Edition, M o r d University Press: New Yotk, 1995.
[2] Stark, Linda Personal c o m m u ~ o n . November 2 1,2000-
[3] Chappe& N-L., Living Arrangements d soumes of caregiving, Jomai of Gerontology, 199 1 Jaa;46(1):Sl-8,
[4] Jacobmne, Stephane, Agemg and Cam For Frai1 Elderly Persons: An Overview of International Perspectives, Labour Market and Social Policy - Occasional Papers No, 38, OECD, April 1999.
[SI Jacobmae, S., Cambois, E., Cbaplain, E., and Robïne, J. Long Term Care Services to Older People, A PcTspBctive on Futwe Ne&- The Impact of An hpmving Heatth of OIder Persons- Ageiag Working Papers AWP 4.2. OECD 1 W8.
[q Jacobzone, S. Copnig Wi Aging: Intedonai Chalknges. Whaâ are the implications o f p a t e r iongevity and dcclhing disability levels? HaIth AfEiüs 19(3): May/June 2000-
[7j Brazier, et-al. (1999). A review of the use of health status measures in economic evaluaîion, H d t h Tec hnology Assessment; 3(9)
[8] EuroQol Group, EuroQol -a new fhciiity for the measurement o f health-related quality of life, Heakh Policy, 1 6: 1 99-208, 1 990.
193 Brooks, R with the EuroQol group- (1996). EuroQol: the current state of play. Health Policy, 37,53-72.
[t O] Dolan, P., Modeling Valuations for EuroQol He& States, Medical Care, 35(11): tO!W-llO8,l997.
[I 11 Drumtnond M.F., Stoddard GJ., Torrance G.W., Methods for the economic evaluation of heaith care programmes. Oxford: Mord University Press, 1995.
Cl23 Kind, P., Dolan, P, Gudes C. and W i i A, Vaiatioas m populatioa hdth status: resuhs k m a United Kingdom naioiiPt questioanairt survey, British Mdical Journal, 3 16: 73641,1998-
Cl31 Brazier, J., Jones, N, Kind, P., Testing thc vahalidity of the EuroQol and cornparhg it with the SF-36 hahh s u ~ y questionnaire. Qiplity o f Life Resea~~h 1993 ;39: 169-80,
[14] Essink-Bot, M-L, Krabbe, P., Bonsel, G., Aaronson, N., An empirical cornparison of four gmcrif heaW statuo maourrs: thc Nottingham bciW pro* tht medical outcornes study 36-item short-form heahh survey, the COOPWONCA ch-, and the EutoQol Instrument, Medical Gare, 1997;35:522-37.
Cl51 Hwst, NP., Kind, P., Ruta, D, Himtcr, M., and Stubbings, A, Measuring Heaith-Reiated QuaEty of Life m Rbeumatoid Ardintis: Vaiidity, Respo11siVc11tss and Reliability of EuroQol CEQSD), British J o d of Rheumatoiogy 1997;36:551-559.
[16J Peek, C.W., Coward, RT., Le, G.R, and Zsembüc, BA., The Influence of Comrnunity Context on the Prefhmes of OIder Aduits for Entcring a Nursmg Home, The Gerontologist, 34(4)533-542,1997-
11 71 Keysor J.J., I)esai T. and Mutran, EJ. EIders' preferences for case setting in short- and long-tenn disobiMy sccnerios, Gezpntologist 1999June;39(3)334-44.
Il81 Chui, L., Kwoag-Yuï, T., Yu-Hua, L., Woei-chang, S., Ta-Pans C. and Tchen- Ru, J-C. Consistency &twecn Refirrncc 6 r Use of long-Tm Cam Among Caregivers of Strroke Survivurs. Rib tic Heaith Nwsing. Volume 1 5. Number 5: 379- 386. 1998
[19] Torrance, G.W, Sackett, DL, Thorn- W H Utility Maximization Model for Evaluation of Health Care Rograms." HeaW !kn&s Research, 7(2): 1 1 8- 13 3, 1972
[20] Torrance, G. Pieferences for heahh states: a revkw of measurement methods, Mesd Johnson Symposium on Perinatal & Development Medicine. (20)37-45, 1982.
[2 1 '] Furlong et .al. (1 990), Gu ide to Design and Development of Health-State Utility Instrumentation, CHEPA Working Paper Scries, 90-9
[22] Gold M.R, Siegal J E , Russell L.B. & Weinstein MC., Cost-Effectiveness in Heahh and Medicine, New Yotk: Mord University Press, 1996
[23] Torrance G. W., and Feeny, D. UtiIities and quality-adjusted lifê years, International Journal of Technology Assessrnent m Hcalth Care, 5:559-75, 1989.
1241 Mehrez A., and M i A., The heahhy-years equivalents: bow to measure dieni using the standard gamb k a p p m h, Medical Dscision M&hg 1 1 : 2 87-92, 1 99 1.
[25] Woifkn, AD., Sinciair, A J., Bombardier C, and McGner A., Prefcre~lct Measurements for FunctiOLIB( Status m Strokc Patitnts: I n t e and InterLachnique
cornpanSous, in: Kane, RL., aad Kane, RA, eds- Vahies and Long Term Care, Lexington Books: hdasachu- 1982: 194-21 4.
[2q Richardson, J., Cost-utility Adysis: what should be measwed? Social Science & Medicine, 39: 7-21, 1994-
[27]Statistics Canada, Heaitb Division, Life tables, Canada aad provinces 1980-82, Minister or Suppty and Services Canada, 19û4.
1281 Coyte PC, Laporte A, Stewart S: I d e n m g the Assumptions Used by V d u s Junsdictions to Forecast Demamis for Home and Faciüty-Basxi Care for the Elderly. Report pre@ under grant 02709 h m the Mini- of HeaW and Long-Term Carie in Ontario to tbe University of Toronto, December, 2000-
1291 Kaminsky, B A : Continuhg Care P h h g and Resource AUocation Modet. A project conducted for the British Columbia Ministry of Heaith, Final Report, October 1985.
[30] HoIlander MJ a ~ d Pallan P. The B&sh Coiumbia Continumg Che System: Service del ~ e r y and resourct plaunmg. Aging Clin. Exp. Res. 7: 94-109, 1995-
[3 11 Health Services Restnictwing Commission. Rebuildmg Ontario's Heaith System: Interim Planning Guidelines and lmpIementatbn Strategies. A Discussion Paper July, 1997.
[33] KPMG Report: Long-Tetm Care Revitw: Future Scenerios: Continubg Care Service Needs in Albe- November 1999.
[34] KPMG: Continuing Gare Scenerios, 1999-2041. RepaFed fOr the FPT Advisory Cornmittee on Health Services. May 2,2000- Mark Lazrrrko and mnda Hm.
[3 51 Manitoba Health. (Drafi) Plannuig Frarnework for Long Term Care Beds in Manitoba November 30, 1999. Received t'rom: Beverly Kyle, Seniors Consultant, Manitoba Health,
[36] Turner, Kathleen Department of HeaIth and Community Services Program Development Division Goverment ofNis~60~11dland and Labrador. Personai Communication July 24 2000.
[37] Statistics Crniada, Census of Population Census Questions, Availabk httpY/www.statcan.ca, J m u q 1 7,200 1 - [38] Statistics Canada, 1998 National Population Health Survey Content for June, 1 998, October 2 1, 1 998, Availabk b t î ~ ~ l w w w . ~ . c a , Jaauazy 1 7,200 1.
C391 Gudex, C., and Laforhine, G,, An InventMy of Health and Disabiiity-Reiatclcr Suxveys in OECD Countries, Labour Mariret and Socid Pol& -Occasional Papers No. 44,2000-
1401 Statistics Canada, )Iealdi and Activity Limitation Survey, 1991
[4 1 ] Statistics Canada, nie Canadian Community Mealth Sumcy, Availabk: httpr//www.statcan-ca, January 1 7,200 1
[42] Covinsky, LE., Fukr, J.O., Y*, K, Jouhnston, C-B., k e l , M.B., Lynn, J., Teno, J. and Phillips, RS. Perspectives rmd Rcvicw of Support Findings, C ~ r n m u n ~ o n and Decision-Making in Seriowly IU Patients: Fmdmgs of the SUPPORT Project. Journal of the American Genatncs Society Volume 48 Numbcr 5 May 2000
1431 Coley, CM. , Li, Y., Medsger, A.R., Marrie, TJ., Fme, M., Kapoor, W.N., Lave, J.R, Detsky, AS., Weinstein, MC., Singer, DE. Pttfbemes fOr Home vs- Hospital Care Among Low-Risk Paîhts With Communjfy-Acqukai Pncumonia Archives of Interna1 Medicine, Volume l5ql4) 2SJuty1996: lS6S-lS7l
[44] McAllister, N, and HoIIander, ML, Seniors' Perçeptions of and Attitudes Toward the British Columbia Contiming Carc System, Heaith Reports, 5(4):409418, 1993.
[45] Baranek PM and Coyte PC- 1999, Long Term Care in Ontario: Home Care and Residential Gare. Report ptepared for the College of Physicisns and Surgeons of Ontario, 1999,
[46] FUilayson, SKG., Biieyer, ID., Tosteson, ANA. and Nesse Jr., RF- fatitnt Preferences for Location of Carr Implications for Regionaihaîion. Medical Cam 1999.37204-209-
1471 Jenson, J, and Jacobzooe, S. Care Albwances For the Frai1 Elderly and Theu Impact on Women Care-Givers. OECD Labour Market and Social P o k y - Occasional Paper No. 4 1 DEELSA/ELSA/WD(2000)2
1481 Williams A- L996. The Development of Ontario's Home Care Program: A Critical Geographical Anaîysis. Social Science and Medicine Vol. 42 (6): 937-948. (p. 945)
[49] Keating, N, Fast, J, Fderick, J, CCBIISYYiCk, K and fenicr, C, Eldemare in Canada: Context, Content and Consequenoes. Statktks Canada Housing and Social Staîistics Division. Novcrnbcr 1999.
[SOI Freid, T.R, van Doorn, C., O'Leary, J E , Ti, ME., and Drickamer, M.A., Older Persons' EMèrellces for Home vs. Hospital Care m the Treatment of Acute mess, Archives of Internai Medicine, 160: 150 1 - ISO6,2OW.
[5 11 Coyte, PC- 2000. Home Carie m Canaâa: Passing tbe Buck, unpublished manuscript, Department of Healtti Administration, University of Toronto.
CS21 Bri& S- Housing the Fraii Elderiy m Canada- In Housing Frai1 Eiders, International Policies, PCTSPeCfiVcs, and Prospects, Jon Pynoos and Phoebe S. Liebig (eds.)Johns Hopkins UnRcmity Prws: Bnitimore 1995 pp. 163-186-
[53] Dualop, S., Coyte, P-C. and MC- W. Soci-aomic staus anâ the utilisation of physicians' serviccs= resuits b m the Cadian National Population Healt h Survey. Social Science & Medicine 5 1 (2000): 1 16-13 3
1543 Freid, TOR, van Doorn, C., T M , M.E., and Micamer, M.A. M e r Persoas' Preferences for Site of Treatment m Acute ntness. J o u d of Gaierai Iateniaf Medicine 1998; 1 3:522-527-
[55] Manu, D, How OIder Patient hferences Are Influenced by Consideraîion of Future Health Outcornes. Joumai of the American Geriatrics Society. Volume 45 Number 6 June 1997- 725-728
156) Linden, M., Horgas, A L , GElber& R, Steinhagen-Ineissen, E., Predicting beaW care u t r l ï n in the very old- The role of physical hdh , mental heaitb, attitudinal and social factors, Journal of Aging, 1997, Fcb;9(1)3-27.
[571 Tsevat, J,, Dawson, N-V., W u AM., Lynn, L, Souhp, J R , Cook, EX, Vidaillet, R and Pbiliips, RS., Wth Values of hospitaliaxi patients 80 years or older. HELP Investigators. Hospitalized Elderly Longitudinal bject, JAMA, 1998 Feb 4;279(5):3 7 1-5.
1581 Wilson, DM- End*f-lifk prcf- of Canadian senior citians with caregivmg experience. Journal of Advanced Nursing, 2000,3 1(6): 1416-1421.
Chapter 4.0: Results
[l ] Brouwer, W.B.F., van Exel N.J.A., Koopmanshap M.A. & Rutten, F.F.H., The Valuation of Idtomal Care m Economic Appraisal. InlernutÈomi Jourmal of Technology Assessrnent m Heuith Cam, 1 999, 1 5,147- 160.
[2] MicrosoW Excel2000. Copyright 1985-1999 Microsoft Corporaîion-
[3] SAS@ Software Version 8-1 Copyright (c) 1999-2000 by SAS Instiaite Inc., Cary, NC, USA. Licensed to University of Toronto Computing & Comrnunieatioas Site 00089870,
[4] Cody, M., and Smith, JX., Applied Statistics and the SAS@ Rogramming Language, Fourth Edition, New Jersey: Rentice Hall. 1997.
Chapter 5.0: Discussion Part 1
Cl] Rowles, GD., (1993), EvoWmg lmages of?& in Aging and "Aging in Ptace', Generations, Spring/Sumiacr 1993 : 65-70.
[2] Rowles, G.D., (1978), Reflections on Experientiai Field Work, Cbapter 1 1 m Humanistic Geogniphy: Prospects and Problems, Ley, D. and Samuels, M.S. (eds-), Maaroufà Press, Iac.: Chicago, 1978
[3] Rowles, G.D., (1983), Geographical dimensions of social support in nual AppaIacbia, m Rowks G.D., and Ohta, RJ. (Eds.), Aging and Milieu. Environmental Perspectives on Growing Old, Academic Press New Yotk= 1 1-130.
[43 Rowes, GD., (1983), Place and Personal Identity in OId Age: Observations for Appalachia, Journal of Environmental Psychology, 3: 2B-3 1 3-
[5] Rowles, G D , (2000), Habiîuation a d Bemg in Place, The Ckcupational Tberapy Journal of Research, 20Supplemm~ 52S-67S.
[6] S'Yrsmith, A.J., (1990), The meanïng and experience of 'home' in hîer lifè, in Bytheway, B, and Johnson, J., (Eds.), W e W and the Ageing Experience, Alciersbot: Gower, 1 72- 192.
[7J Kontos, P.C., (1998), Resisting IasritutionalVatinn: Constructing Old Age and Negotiating Home, Journal of Aging Studies, 12(2): 1 67- 184-
181 Kontos, P.C., (1999), Local Biilogy: bodies of differenœ in agehg studies, Ageing and Society, 677-689,
[9] Twigg, J., (1999), The spatial ordering of came: public and private in bathmg support at home, Sociology of Heah & Illness, 2 1 (4): 3 8 1 -400-
[l O] Hay, R, (1998), A mted sense of place in cms-cultural m v e , Canadian Geographer, 42(3): 245-266.
[Il] &y, R, (1998), Sense of P b in Developmental Contexî, Journal of Environmental Psychology, 1 8: 5-29.
(121 Chapin, R, and Dobbs-Kepper; D., (2001), Aging in place in assisted Living: Philosophy versus policy, The Gerontologist, 4 1 (1): 43-50 -
[13] Marek, K.D., and Rantz, ML, (2ûûû), Aging in Place: A New Model For Long- Tenn Care, Nursmg Administration QurirterS(, 24(3): 1-1 1 ,
1141 Filioa, P, Wister, A., and Coblew E.J., (1992), Subjective Diais ions of Environmental Adaptation Among the Elderly A Challenge to Models of busmg Policy, Journal of Housing fbr the Elderly, lO(112): 3-3 1.
11 51 Pagano, M., and Gauweau, K., Principks of B~~&UISWS, . . Second Edition, Dwbury Thomson Leaniing: California, 2000.
1161 Personai communication with Linda S- January 1 1 2001 -
1171 North York Commhty Care Access Centre Website, www.nvccac.on.ca Available: March 8,200 1 - [18] Statisîics Canada Website, htti>J/cc~asûûcao.Câ/enolish/be0W Availabk March
[ 191 Giles, W., (1 997), Re/Mernberiag the Portuguese Household in Toronto: Cutture, Contradictions and Resistance, Women's Stud-s Interoational Forum, 2û(3): 387- 396.
1201 Chappell, N L and Lai, D, (1998), Hwlth c r ~ r service use by Chinese seniors m British Columbia, Canada, Jouraal of Crodulairal Gerontology, 1 3: 2 1 -37.
f2 1) Wilson, D.M. End-of-life prefereaces of lanadian senior c h s with caregiving experience- Journal of Advanced Nursing, 2000,3 l(6): 1416- 142 1 -
1223 Freid, T-R, van Dooni, C, T i i ME., and Drickamer, MA, Older Persons' Prefemces for Site of Treatment m Acutc IUness J o d of General htcmal Medicine 1 998; 13 522-527-
1233 Freid, T-R, van Doorn, C., O ' ~ , J.R, Tiitti, M.E., and Drickamer, MA-, Older Persons' Preferem for Home vs. Hospital Cart in the Treatment of Acute Illness, Archives of Interna1 Medicine, 160: 150 1-1 506,2000.
[24] Sih- G., Pritchard, R, and Wekb, H.G., (1 998), Prefèmwes for chernotherapy in paîknts wiidi advanced non-mal1 ce11 hmg cancer dcwiptive study based on scripteci interviews, British Medical Journal, 3 17: 771-775.
1251 Keysor JI., Desai, T. and Mutra~, EJ. Eiâers' prefèrences for care setting in short- and long-term disability -OS, Gerontologist 1999June;39(3)334-44-
1261 Jagial, S., (2000), Impact of In-Home Service Adjustments on Clients m the North York CCAC Program, Report to the Board of the North York Comrnunity Care Access Centre.
[27] Torrance, G. Refemces for htalth states: a review of mtasurement mefhods Mead Johnson Symposium on Perinatsldk Developrncnt Medicine. (20)s 745,1982.
[28] Cannet, S., and Mutran, EJ., (1999), Stability of e k l y persons' e x p d prefèrences regacding the use of Me-sustainhg treatments, Social Science & Medicine, 49: 303-3 1 1.
[29] Ekrger, J.T., and Majerovitz, D., (1998), Stability ofRefirences for Treatment Among Nursing Home Residents, Rie Gerontologist, 3q2): 21 7-223.
[3O J Rosenfeld, K E ., et a1 (1996), Factors Associatal With C b g e in Resuscitation Preference of Seriousiy I11 Patients, Archives of lntanai Medicine, 1 Sql4): 155& 1564,
13 11 M a , I), How OMer Patient References Are Infiuenced by Consideration of Future Heakh Outcornes. Joumai of the American Geriatrics Society- Volume 45 Number 6 June 1997- 725-728-
[32] Pritchard e u . (1998). Influence of -nt Preferences d Local Heghh System Characteristics on the Place of Deatb- J o u d of the American Gcriatncs
- - Society. Bolume 46. Number 10. October 198, 1242 - 1250.
[33] Covinsky, K.E., Fuller, J.D., Yaffie, K, Jouhnston, Ca., Hamel, M.B., Lycm, JI, Teno, J. and Phillips, RS- Perspectives and Review of Support Findings, Communication and Decision-Making in Seriously PU Patients: Findmgs of the SUPPORT Roject. Journal of the American Genatrics
- - Society Volume 48 Number 5
May 2000
[34] Wilson, DM. End-of-Mie preferences of Canadian senior citîzens with caregiving expenDençe, Journal of Advanced Nursing, 2000,3 l(6): 1 4 16-1 42 1 - [3S] McWhinney, LR, Bass, MJ. and Orr, V- Factors AssocintPA with Location of Death morne or Hospital) of Patients Referred to a Palliative Gare Team- CMAJ Volume 1 S2(3), 1 February1995: 361 -67
1361 Dudgeon, DL and Knstjanson, L, Home Versus Hospital Death: Assesment of Prefetences and Clinical Challenges, CMAJ Volume 1 52(3) IFebruary 1995: 337-340.
[37] Tolle, S.W., Rodeld, A.G., Tikien, V.P., and Y, Oregon's Low In- Hospital Death Rates: What Detamines Where People Die and Satisfiiction with Decisions on Place of Death?, Annals of intemal Medicine, l30(8):68 1-683, 1999-
[38] Freid, T-R, van Doom, C-, O'Leary, J-R, Thetti, M.E., and Drickamet, MA, OMer Persons' Preferences for Site of Terminal Care, Annals of Intemal Medicine, 13 1(2):109-112, 1999.
1391 Moore, J., (2000), Placing Home m conte* Journal of Environmental Psychology, 20: 207-2 1 7.
[40] Bowlby, S., Gregory, S., and McKie, L., (1 997), 'l)oing Hume": Patriarr:hy, Caruig, and S pace, Women's Studies international Forum, 20(3): 343-3 50.
14 11 Case, D., (1 9%), Contributions of Joumeys Away to the Dennition of &me: An Empirical Study of A Dialectical Proces, J o u d of Environmental Psycbology, 16: 1-15.
[42] Douglas, M., (1 99 1), The Idea of a Home: A Kmd of Space, Social Research, 58(1): 287-307.
[43] Gurney, CM, (1997), ". . .HaifOfMc Was Wïsfk#"' MdEing Seose of Home Through Episodic Ethnographies, Women's Studies Intemaibnal Forum, 2q3): 373- 386.
w] Pearce, D-W- (ed.), The MiT Dictioaary of Modem Economics- Fowth Edition, MIT Press: Cambridge, 1 992-
[45] Varian, H K Intermediate Micmamnomics A Modem Appruacb mird Edition, W. W. Norton & Company: New York, 1993 -
1461 Friedman, M, and Savage, L.J., (1948), The Utility Analysis of Choices hvolving Risk, The J o u d of Political Econorny, Volume LVI, Number 4: 279 - 304.
[47] Alchian, a., (1953), The Meanhg of Utility Measuremmt, hnefican Econornk Review, 42: 26-50.
1481 Rabin, M, and Thaler, RH., (2001), Anomak: Risk Aversion, The J o d of Economic Perspectives, 1 5(1): 2 19-232-
1493 SaUcetd, G., Ryan, M., and Short, L., (2000), The Veil of Expericnce: So Consumers Refèr What They Know Best?, Htahh Economics, 9: 267-270,
Chapter 6.0: Discussion Part II
[ 1 ] Gesler, W, (1 MZ), Thetapeutic Landscapcs: Medical Issues In Light Of Ohe New Cultural Geography, Social Sciena & Medicine, 34(7): 735-746-
[2] Williams A., (1 999), Introduction, in W d l i A(ed), Therspeutic Landscapes: The Dynamic Between Piace and Wellness. New York University Ress of Amerka-
[4] 'The Hitting Home" hject, inhmation Available: w w w ~ . u t o m n t o ~ c a , April9 200 1.
[5] Coyte, P.C., McKeever, P., Behrens, D., et ai, (1999), Place in Health Care: Sites, Roles, Rights and Responsibilities. Report Rcpareû under the Auspices of a SSHRCfCHRSF Hkahh Insb'tute Design Grant.
[q Ontario Association of Community Cure Access Centres, (Sûûû), Human Resources: A Looming Cn'sis in the Conunuaity Care System in &tario, Position Paper.
[7J Ontario Mmistry of He& and Long Tarn Cam, Avatlabk:
[8] Co*, P.C, (2000), Home Care m Cansda: Passing the Wlclc, Report Repared fw the Dialogue in HeaM Reform,
[91 Abel, S., and Keams, R A , (199 1 ), Birth Places-. A gmgraphical perspective on pfanned home births in New Zesland, Social Science & Medicine, 33(7):%25-834-
[l O] Ley D., and Samuels M.S., (1 978), Introduction: Contexts of Modem Humanism in Geography, in Humanistic Geopphy: Rospats and Pmblexns, Ley, D. and Samuels, M.S. (eds,), Maaroufà Press, Inc.: Chkago, 1978
CI I l Pile, S., (1992), Human Agency and Hunan Geography Revisited: A Critique of 'New Models' of the Self; Transwtions of the Instiaitc of British Geographers, 18:122-139.
El 23 Lipsey, KG., Ruvis, D.D., and Steiner, P.O., Economics, Sevenh Canadian Edition, HarperCollhs Publishcts: New Yo& 1991-
[ 1 31 Ley, D., (1 !Ji%), Beâavioral geography and the philosophies of meanmg, Chaptcr 9 in Sehavioral Robkms in Wgraphy Revisitad, Cox, K-R, and Goîleâge, RG., (eds.), Methuen & Co.: New York, 1978.
1141 Rowles, G.D., (1 978), Reflections on Experiential Field Work, Chapter 1 1 in Humanistic Geogtaphy Rospects and Robiems, tey, D. and Samuels, M.S. (eds.), Maaroufâ Press, Inc.: Chicago, 1978
Cl 51 Keams, RA., and Colihs, D.C., (2000), New Zealand childreu's heahh camps: therapeutic laridscapes rneet the contract state, Social Science & Medicine, 5 1: 1047- 1059.
[I 61 Hay, R, (1 998), Sense of Place in Developmaital Context, Journal of Environmental Psychology, 18: 5-29.
[t 71 Kems, RA., (1997), Narrative aad metaphor in health geographies, Progress in Human Geography, 2 l(2): 269-277-
Cl%] Geores, M., (1998), S u ~ v u i g on metaphor= how 'heaith=hot sp~gs' created and sustained a tom, in Kearns, R, and Gesler, W., (Eds.), Futring Heaith into Place: Landscape* Identity, and WeiLBemg, Syracuse University Pms: Syracuse.
1191 Gesler, W., (1999), Words in wards: language, heaith and phce, He&h & P b , 5: 13-25.
[20] Williams, A., (1 999), P b Identity and Therapeutic Landscapes: The case of home care workers in a rnedicaiiy underserviced area, in Williams A.(&), Therapeutic Landscapes: The Dynamî Between Place and Weüness. New York University Press of Arnerica,
[21] Thurber, C., and Malinowski, J ., (1999), Surnmer camp as a thenputic hdscape, in Williams A.(ed), Therapeutic Landsaps: Ine D-ic Betwaen Place and Wehess. New Yo*: University Press of Amerka
[22] Keams, RA, and Barne#, J K , (1999), Adclad's SPcship Enterprise: Pkmg metaphor in chddren's hospital, in Williams A.(ed), Thetapeutic Landscapes: 'Ihe Dynamic i3etween Place and Weiiness. New Yorlc University Priess of AmcriCa,
[23] Palka, E., (199% Accessl'ble Wildeniess as a Therapcutic Lendscape: ExWencmg the Nature of I)enali Nationai Alaska, m Wïiiirims A.(cd), Thaapeutic Landsapes: The Dyamic Between P b and Wellness- New Yorlc UiGversity Press of America
[24] Bell, M, (1999), Rehabiiitating Middle England: htqpthg Ecology, Aesthetics, and Ethics, m Williams A.(ed), Tberapeutic Lendscapes: The Dynamic Between Place and WeUness. New York University Press of America.
[25] Geores, M., and Gesler W., (1999), Compromised Space: Coatîests over the Provision of a Th- Environment for People with Mental Ilhiess, in Williams A.(&), Therapeutic Laodscapes: The Dynemic Between Place and Welness- New York: University Press of America
1261 Parr,W., (1999), Mental Heakh and the Tbempeutic Geographies of the City: Individu al and Collective Negotiations, in Williams A.(ed), Therapeutic Landscapes: The Dynamic Between Place and W e t h . New Yorlc: University Ress of Amerka,
[27] Gesler, W., (1999), Bath's Reputath as a tEenling P w in Keams, R, and Gesler, W., (Ecis.), Puttmg Healtb into Place: Laodscagt, Identity* and Well-=mg, Syracuse University Press: Syrzccuse.
[28] Wii tiams, A., (1 W8), Therspeutic Landscapes in Holistic Medicine, Social Science & Medicine, 46(9): 1 193-1203.
[29] Moore, J., (2000), Plscing Home in context, Journal of Environmental Psychology, 20: 207-21 7.
[30] Buttimer, A., (1 980), Introduction, in Buttimer, A., d Seamon, Dm (Eds-), The Human Experienœ and Sense of Place, Billing and Sons Limited: Guilford.
[3 11 Buttimer, A., (1 980), Home, Reach, and the Sense of Place, in Buttirna, A., and Seamon, D. (Eda), The Human Experience and Sense of Place, Billing and Sons Limited: Guilford.
[32] Relph, E, (1 976), P b and Placekssness, Pion Limited: London.
[33 J Gold, J.R, (2000), Classics m human geography revisited: Cornmentary 1, Progress in Human Geogtrrphy, 24(4): 61 3-61 5.
[34] Stock, M., (2000). Classics in human geography revis'i: Commcntary 2, Progress in Human Geogtaphy, 24(4): 6 15-6 16.
1351 Tuan, W., (1 977), Space end Place: The Perspective of Experience, North Central Publishing Company Mianesota
[ 3 q Bachelard, G., (1958), The Poetics of Splice* Johs M (Tfa~l~), Boa6n: &acon Press-
[37] Bowlby, S., Gregory, S., and McKie, L., (1 997),'?)oing Home": Patriarçhy, Carin% and Space, Women's Studies Infernationai Forum, 20(3): 343-350.
[38] Case, D., (1996), Contriiutions ofJouraeys Amy to die Definition of Horne: An Empmcal Study of A D & d d Rocess, J o u d of Enviromeotd Psyichobgy, 16: 1-15.
1391 Douglas, M., (199 l), Tbe Idea of a Home: A Kind of Spsce, Social Research, 58(l): 287-307.
[40] Giles, W., (1 997), Re/Membering the Portugucse Household in Toronto: Culture* Contradictions and Resistance, Women's Studies Internationai Forum, 2q3): 387- 396.
141 ] Gmey, C.M., (1 997), ". . . M O f Me Was Satisfied": Making Sense of Home Through Episodic Ethnographies, Women's Studies International Fonun, 20(3): 373- 386-
[42 3 Rowles, G.D., (1983), Geographiml dimensions of social support m d Appdachia, in Rowks GD., and Ohta, R I (Eds.), Agmg and Milieu. Environmental Perspectives on Growiag Old, Acadernic Press: New York= 1 1-130.
[43] Rowles, G.D., (19831, P h and Pemd Identity m OH Age: Obsendons fbr Appalachia, Journal o f Environmental Psychology, 3: 299-3 1 3 - [44] Rowles, G.D., (1 993), Evolvhg Images of Place in Aging and 'Aging in Place', Generations, Sprmg.Summer 1993: 65-70.
1451 Rowles, GD, (2000), Habituation and king in Place, Tbe Occupcrtiod Therapy Journal of Researich, 20Supplement 52S47S.
[46] Sixsrnith, AL, (1990), The meanmg and experience of 'home' in later Iife, in Bytheway, B., and Johnson, J., Eds.), Welfhre and the Ageing Experience, Aldershot: Gower, 1 72- 1 92.
- . 1471 Kontos, P.C., (1998), Resistlng Institutiondmûon: Consûuctaig OU Age and Negotiatmg Home, J o u d of Agmg Studies, 12(2): 167-1 84-
1481 Kontos, P.C., (1 999, L o d Biokgy: bodies of diffère- in ageing studks, Ageing and Society, 677489.
[49] Twigg, J., (1 999), The s p W ordering of care: public and prïvaîe m bathing support at home, Sociobgy of H d h & Illness, 21(4): 381 -400-
[S il Chapïn, R, and Dobbs-Kepper, D., (2001), A@g in piace in assisted livhg: Philosophy versus policy, The Gaontologist, 4 1 (1): 43-50.
CS21 Marek, KiD-, and M.J., (Zûûû), Aging in P b . A New Mode! fer Long- Tenn Care, Nursing Administration Quarteriy, 24(3): 1-1 1.
[53] Mattunorie etai. (1 997) Surrogate and Physiciriri Understandmg of Patients' Preferences for Civmg Permanently m a N u r e g Hime. Journal of the American Gerïatncs Society. Volume 45, Number 7 July 1997,8 18-824.
1541 Filion, P, Wister, A., and Coblenz, EJ., (1 992), Subjective Dimaisions of Environmental Adaptation Among tbt Elderly: A Challenge to Models of Housing Policy, Journal of Housing for the EMerly, 10(1/2): 3-31.
[55] Tmttier, H., Martel L., Houk, C., Berthcbt, M., and Lé&, J, (2000), Living at home or in an institution: What makes die dia- for seniors?, Health Reports, 1 1(4): 49-61,
[56] Bishop, CE., (1999), Whcre Are The MÏssing Elders? The Dedine In Nursing Home Use, 1985 And 1995, Hegtth A m i 18(4): 146-155.
1571 Kelman, H R , and Thomas, C,, (199û), Transitions Between Comrnuaity and Nursing Home Residence In An Uhan EMeriy Population, Journal of Community Hdth, 15(2): 105-122.
[58] m e k , P.M., and Coyte, P.C., (1999), Long T m Care in Ontario: Home Care and Residential Care, March 30, 1999.
[59] Nurshg Homes Act, RS.O., 1990 Available: h#pi/ www.e- laws.~ov.on.ca/home - E.am?lan-n April9 2001.
[60} Homes for the Aged and Rest hmes Act, RS-O., 1990, Available: httpr// www.e-laws-aov-on.ca/home - E.asm?lann=en A p d 9 200 1.
[6 l ] Charitabk h t i t h m s Act, RS-O., 1990, Available; hW/ www-e- laws.~ov.on.ca/horne E.asp?hn-- Apnl9 200 1.
1621 EuroQol Group, (1 !BO), Eu-1- a new fàcility for the masurement of health- related quality of life, Health Policy, 16: 199-208-
[63] Dnrmmond M.F., Stoddard G.I., Torrance G-W., (1995), Methods for the economic evaluaîbn of heahh care programmes. OKford: Mord University Pms.
[64] Litva, A., and Eyles, J., (1995), Coming Out exposing social theory m medical geography, Heahh & Place, l(1): 5- 14,
1653 Coast, J., (1999), nie Appmptiate Use of Qualitative Metbods in Hcdîh Econornics, Health Economics, 8(4): 345-353-
14563 M m , G., (1995), (Re)placidg rcserrrch on heahh a d h e a h care, Ekah & Place, l(1): 1-4.
[6TJ Relph, E., (2000), Classics in human geography revis'ted: Author's response: Place and Piacelessness in a aew context, Rogress in Human Geography, 24(4): 6 17- 619.
1681 The Canadian Mord Dictionary, Kasberine Barber cd., Oxford University Press: Toronto, 1 998.
Chapter 7.0: Coaciasion and Future Research Dircetions
[l] Coyte, P.C., and Batan* PM-, (îûûl), 1dent;ft;ng the Assumptions Used by Various Jurisdictions to Forccast b a n d s for Home and Facility-Bad Care for the Elderiy. Report to the Ontario Mmisüy of Heaith and Long-Tenn Case, prepared under grant 02709 to the University of Tomnto, March 200 1 -
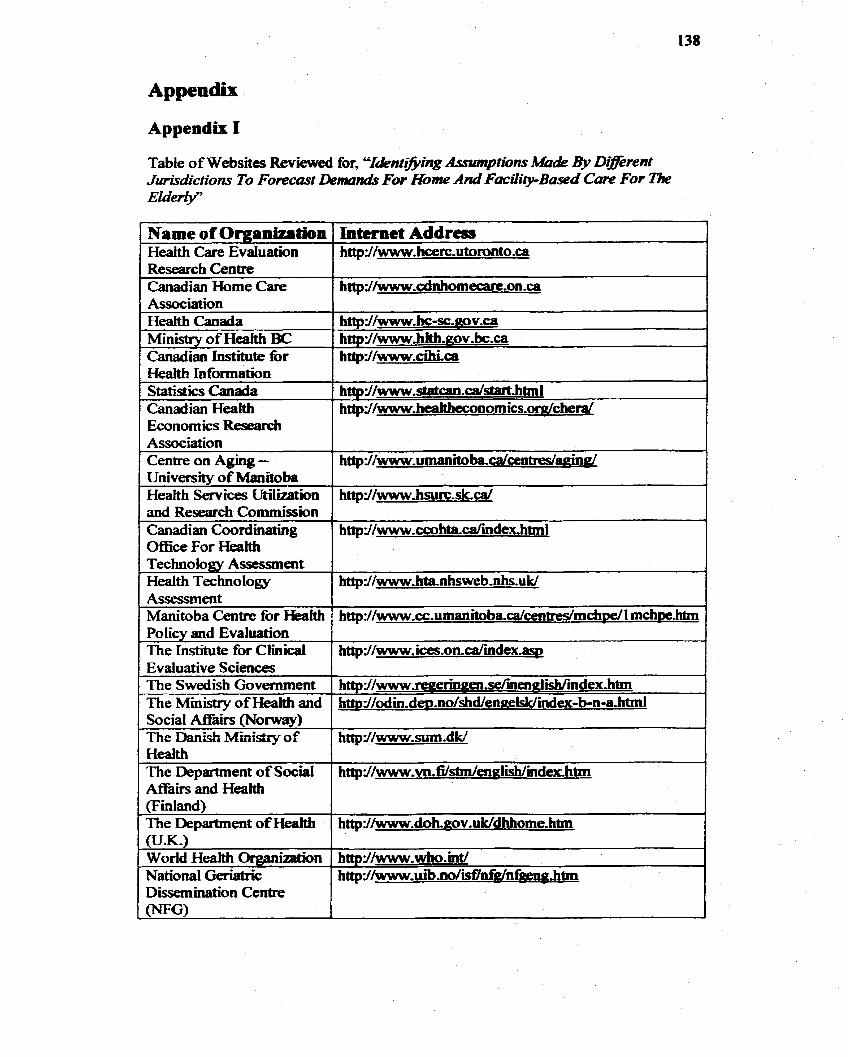
Appendix
Appendir 1
Table of Websiîes Reviewed for, CCI&ntz~mg Assmptions Ma& 9) D@e~nt JÙriSdictiom To Forecost Deman& For Home And F s c i l i p B e d Care For ï k Elderw
Research Centre Canadian Home Care
1 Statistics Canada 1 htfp~/~.stat~8~1.C8/start~htmI
httpd/www-cdnhomecazt-on .ça
Health Canada Ministry of Hedth BC Canadian Institute for Health Information
httpdIwwwhc-sc.aov.ca http d/wwwhith.gov- bc-ca htfpd/www.cihi.ca
Association Cenîre on Aging - University of Manitoba Healt h Services Ut i l i i on and Research Commission Canadian Cwrdùiating OfEce For Heatth
http~/www~umanitoba.ca/cenWaain~
httpd/www~hsurc.sk.ca~
http~~~~~kl~.ccohtadmdemhtml
Technology Assessment Health Technotogy
The Institute for Clmical httpY/w\ivw.~.on.ca/index.~ Evaluative Sciences 1
httpi/\~vww~hta-nhsweb,nhs.uk/ Assesment 1
1 The Swedish Governent 1 ht lp=/ /~~&nai .drnenal iUmdex.htm
Manitoba Centre for Health Policv and Evaluation
' hap~/~~~~cc.um~aitoba.dcentres/mchDe/I mch~e.htm
Social A f l k h (Norway) The Danish Ministry of Health The Department of Social Afiàirs and He&
httpY/www..sum.dk.
http~/~~~.~i.Wsbn/en~Iish/'mde~.htni
(F inland) The Department of H d httpr(/~.doh.nov.uk/dhhome.htm 0J.K-1 World He& Organiition National Geriaîrk
httprl/www.who.int/ http~/~~uibm/idnf~/nf~~.h6n
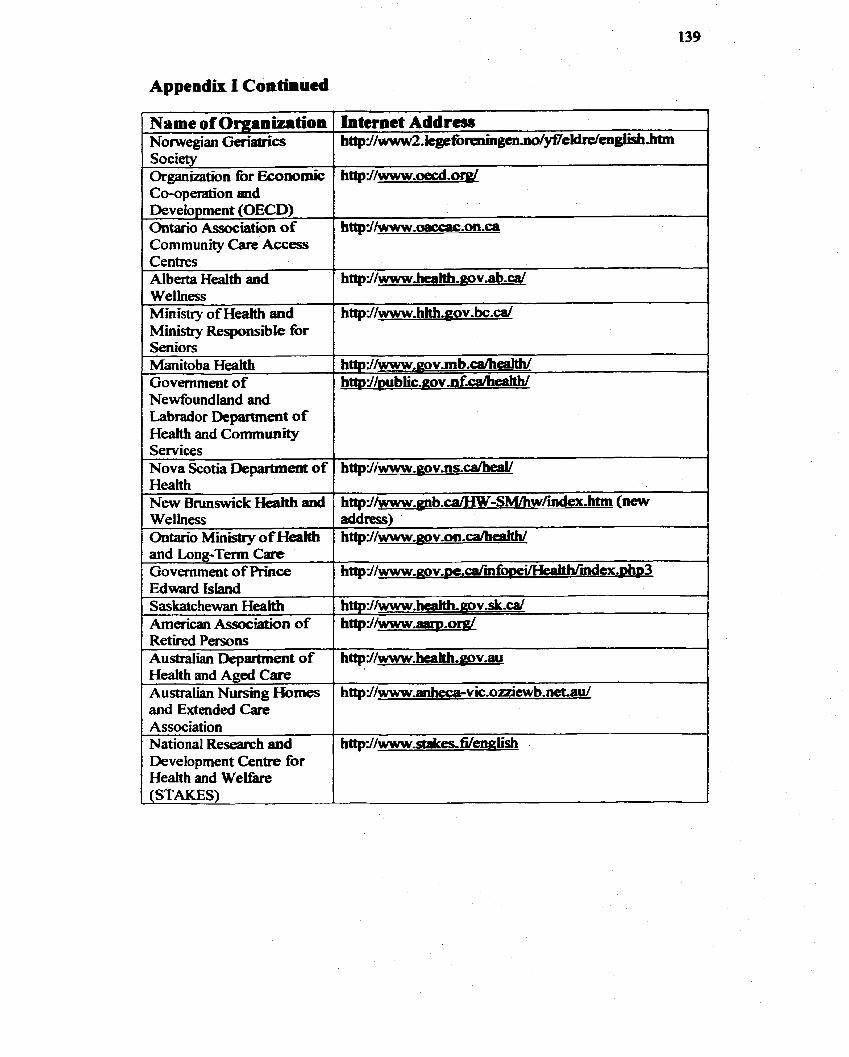
1 Cosperation and Deve fopment (OECD) Ontario Association of Community Care Access
Alberta Health aad
Mmistry o f Hedth and Ministry Responsible for Seniors Manitoba Heakh Govenunent of Newfoundland and Labrador Department of Health and Commuaity Services Nova Scotia Department of
and Long-Tenn Care Government of Pnnce
American Association of Retired Persons Australian Department of He& and Aged Care Australian Nursing Homes and Extendeci Care Association National Research and Development Centre for Heaith and W e b
h~Jhvww.enb.cajHW-SM/hwfurdex,htm (new address) h t t p I / w w w . g o v . o a . ~
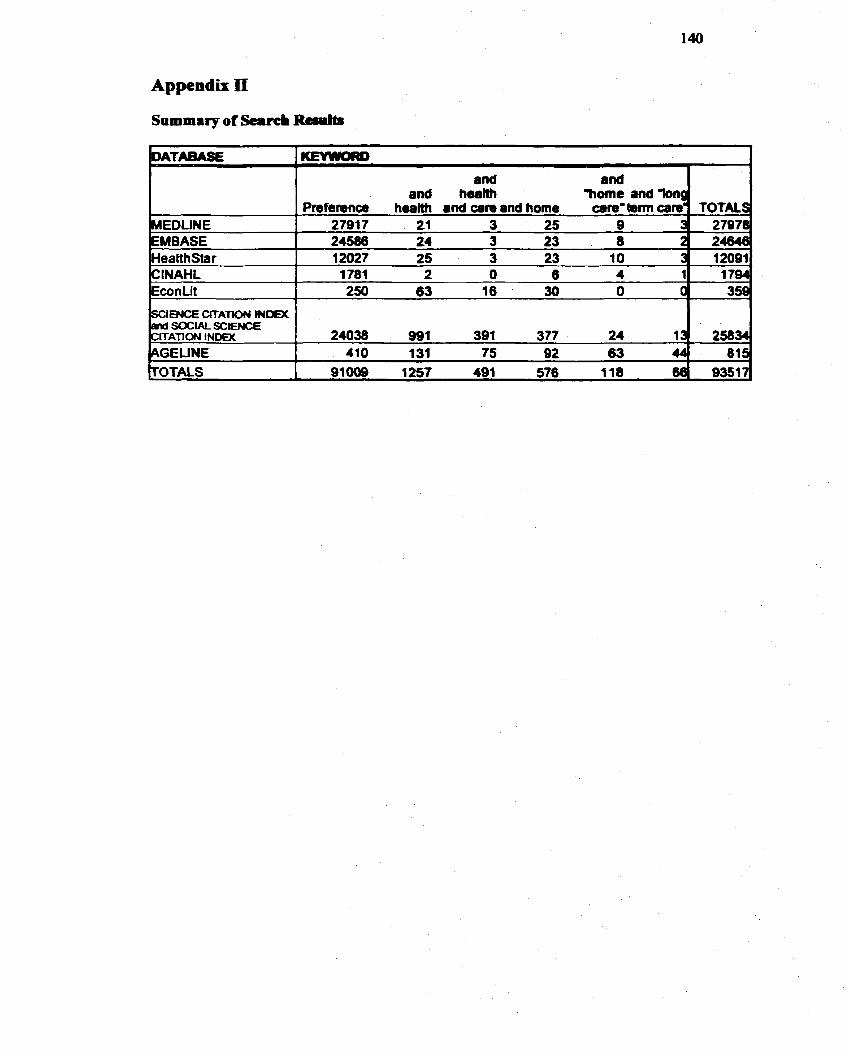
Appendix II
Sammrry of S a r c i R+riilts - --
and health
HEDLINE 27917 21 3 25 9 EMBASE 24586 24 3 23 8 HealthStar 12027 25 3 23 10 3 12081 Cl NA HL 1781 2 O 6 4 1 1 704
SOCW SCIENCE ITATlON INDM 1 24038 991 391 377 24 1 258
Appendh III Telephone Recnitmest Protocd for Fmf-ia Iifcnicrir
Telephone Script
Helb, this is (narne ofNYCCAC case manager)-
I am phoning with regards to a study bemg conducted at tbe UniversÏîy of Toronto. The cesearchers are tryaig to determine what type of carie setting, eidier home-based or fàcifity-based, is prcferrad by current home care recïpients.
For the study an interview wiii be cobducted in the home that will ask you and your pNnary caregiver to give your prefcrtnces for borne-based and fhcility-based c m .
The interview wüi take bctween 30 and 60 minutes.
Thete are no risks anticipated h m participaîion in the study.
Should you agree to participe in this study, yow c ~ n f i d ~ a i i t y wiü be respected and no information that discbses your identity will be ricieased witbout consent. Your name will not be mcorded on any of the forms. Only code numbcrs MI be usai to iden- the information tbat you p h d e . Your answers to the questions and aU submitted maîerial will remain c o ~ e n t i d - You will not be identined in any report or presentation that may aise h m this study- You can refuse to mswer any questions and can withâraw than the study at any t h e widiout palty. nie data collecteci will be housed in a secure, k k e d place in the m h office at the University of Toronto, and only resca~ch personnel will have access to the confidentid data.
Are you willing to participate m the study?
If no: Thank you for your time. Wouid you mmd teMing me why?
if yes: T h a d you. Stephanie Stewart will be conducting aii o f the home interviews fiom Monday January 15 until Wednesday January 3 1. Stephanie will be cailing you in the next couple of days to set up your interview date and t h e .
Appendix IY
Telephoae Rccrritmat Rotoco# for Prrkremce IntcRkrP B
Telephoae Script
Hello, my name is Stephanie Stewart and 1 am working on a study conductd by Dr- Peter Coyte, who is a professor in the Deparanent of EEestdi Admmistrau'on, Faculty o f Medicme at the University of Toronto, to determine what type of care d g , either home-based or fhciiity-bssed, is p r e f d by current home care tecipicnts- At this point I am inviting individuais who are currentiy reccivùig care tiom the North York Community Care Access Centre to participate in the study.
For this study 1 am conducting mtcrvjews that will ask home tare clients and their caregivers to staîe theu prcfknces fot home-based and fibciiîty-basad care-
The interview wiii take between 30 and 60 minutes.
Should you agree to participate in this saidy, your coafidentiality will be respected and no information th* disdoses yout identity or pteferenœs wiil be releascd without consent. Your name will not be ribcorded on any of the fonns. Only code numbers will be used to identm the information tôat you provide- Your ammers to the questions and al1 submitted material will remah conadential. You wiil not be identifid in any teport or prcsentation that may arise h m this study. You cari refiise to answer any questions and can withdraw h m tbe study at any time widiout penalty- Further, your current care witl not be afkted in any way. The data coUected will be housed in a secure, 1ocked p h in the research at the University of Toronto, and on@ myselfand Dr. Peter Coyte will have access to the confidential dam
Are you willing to participate in the study?
I f no: Thank you for your thee
Ifyes: Thank you- 1 would tike to interview you in your home at a t h e convenient for you. 1 will be conducting interviews h m Monday January 15 until Wednesday January 3 1,
1s there a day o f the week that is most wnvenient for you? (Suggest a date)
1s a moming, aftenioon or evening interview best for you? (Suggest a time)
m e n interview date and tirne are sekted): Thank you 1 will corne to your home on . I f 1 could c u h that your address is
? 1 would like to give you my contact number in case y w have any questions or ifyou must cancel die interview for any remon. Agah, my Nune is Stephanie Stewart and my contact phone number is 489-81 28-
"1 am interesteci m knowing what peopk, Wrt yourseE thllik about dBkent long- term care settings, When 1 d e r to a long-term care sctting, 1 am refi:rring to the plsce where you receive assistancc wEth daily ad* aadfOr where you receive heatth related carie. As a currait home cart rccipmit, your hg-term cere setting is the home-"
%or to beginning the interview, 1 wouid like you to please read caretiilly and sign this consent fom. Ifyou have any questions fael k to ask me. Let me know when you are kished a d we will procecd with the mtervicw. Ifyou w d d like me to rwd the consent forrn b you, 1 would bc bappy to do m."
(When fonn is signed) "Ibank you. To begm, 1 want to emphasize that 1 am conductùig thïs mterview for researcb purposes only. Nothing that 1 desaibe to you or that you tell me will in any way affect the carie that you are currentiy meiving fiom any care provider-"
Preference Liitcrvicrv Coiscit Fora
Interview Consent Form:
& , understand that 1 am king asked to consent to patticipate in a research study f h d d by the Ontario Ministry of Health to identi@ m y p r e f m for home-bascd and fiilcility-bascd long tena care,
1 understand that participation m the study will mean that 1 wii be anmuerhg questions about
HowIam fëeiing; M y preference for home-bascd or fircitity-based carc; and, My background such as my level of education.
1 understand tbat the interview will take 30-60 minutes and will occur at a çonvenient time and place. 1 understand that by sgreeing to tuke part m this study I am also permWig the invdgaîor to record intonnalion h m my Commuaity Care Access Centre record,
1 understand that it is a voluntary chok to participate in this study- 1 understand that 1 will be asked to compkte a strucnued survey at the interview. I understand that 1 wiii be asked to respond to queabns on my prr&rcnccs for homebased and faclity- based care settings.
Confidenüality and Privacy
My confidentiality will be respectai and no information that discloses my identity wdi be released without consent. 1 understand tbî my name wiiî not be recorded on any of the fonns, nor will1 be identifid as the source of additional suggestions fbr participants. Oaly code numbers wiIl be used to identifi. the infionnation that 1 have provided. 1 understand that my ~LL~SW~ZS to the questions and ai1 submitted material wîll rernain confidentid, 1 also understand tbat I will not be identifiai in any report or presentation that may arise h m this study, 1 understand tbat I am refùst to answer any question and that I can wittidraw h m the stdy at any thne without penahy- 1 understand that the data collected will be hoW in a secure, locked place m the research office at the University of Toronto, a d only the principal investigator of this amendment to the sub-study (Stephanie Stewart) and the principal mvcstigator of tbe overall study (Dr. Peter Coyte) wüï have acœss to this confidenial data
Appendù V Continucd
1 understand that if I choose to volunîariiy participate in this study, I will not benefit directly k m tbis study. 1 h understand that îhere are no nsks anticipateû h m my participation in this study, but some questions may be upsetting, If1 have questions or wncerns, either beforc or foliowing my particrpotion, I c m c d Ik. Pdcr Coytc (Principal Investigaîor) at 416-9784369- 1 bave been pmvided with a mpy of this consent fortn,
1 understand what this study invohtes and I agme to take part in this study.
Signature of Participant Name @k print)
Signature of Wiaiess Name (please print)
Date
Ifyou have any questions or concems, please do not hesitaîe to contact the Study Principai Investigatot: Dr. Peter Coyte at (4 16) 978-8369.
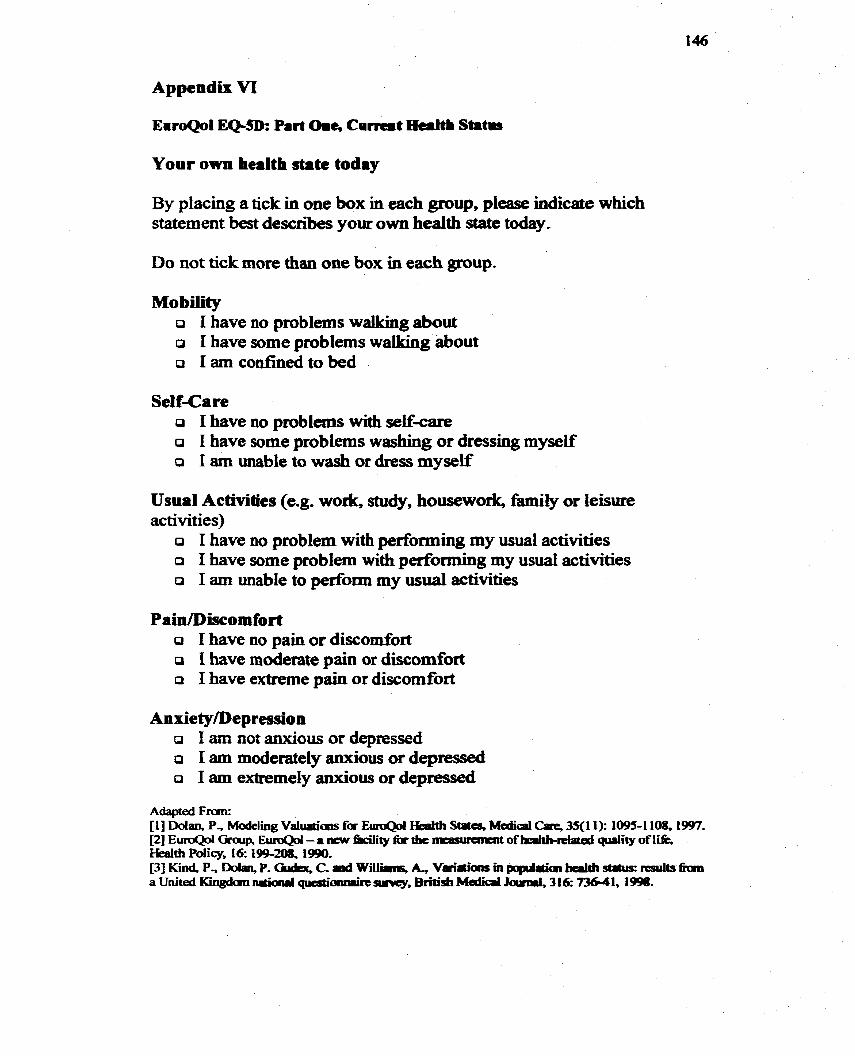
EaroQol EQ-SD= Part Orne Current malth Statms
Your own haïth *te today
By placing a tick in one box in each group, please indicate which statement best descri'bes your own health state today.
Do not tick more than one box in each group.
M o bility O I have no problems wallllrig about O 1 have some problems wallcing about O I am confinecl to bed
Sel f-Ca re a 1 have no problems with sewcare o 1 have sume problems washing or dressing myself o 1 am unable to wash or dress myself
Usual Activities (e.g. wodr, stuciy, housework, family or leisure ac tivït ies)
o 1 have no problem with performhg my usual activities a 1 have some problem with performing my usual activities O 1 am unable to perfomi my usual activities
Pain/l[)iscomfort o 1 have no pain or discomfoa O I have moderate pain or discomfort o 1 have extreme pain or discodort
AnxietylDepression a I am not anxious or depressed O 1 am moderately anxious or depressed
1 am extremely anxious or depressed
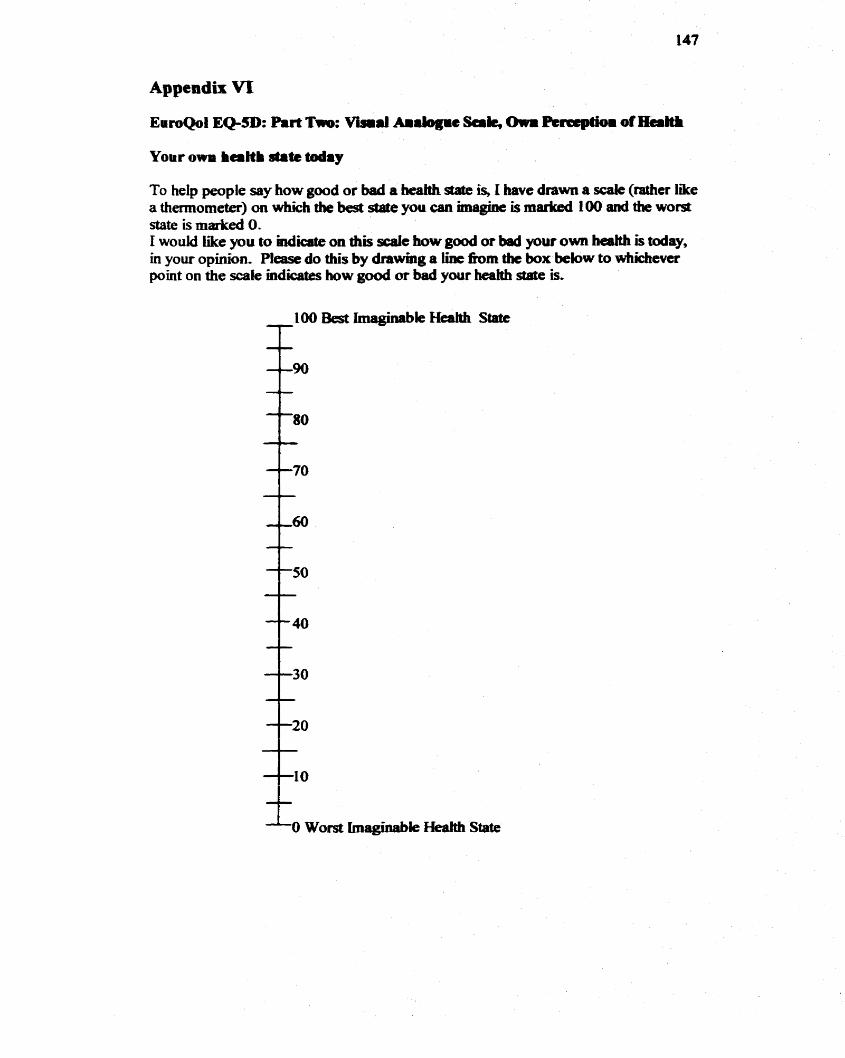
Appendix VI
Eu-1 EQ-SD: Part Tw: Visid Ai rbg ic Sak, Owm Perœpth of Ham
To help people say how good or bad a heaiîh state is, I have drawn a scale (raîher like a themorneter) on which tbe best state you can miagine is rnariced 1 0 and the worst state is matked O- 1 would like you to indicate on diis d e how good or bad yow own b& is May, in your opinion. Please do this by drawing a lint h m the box below to whkhever point on the scaIe indicates how good or bad your heaitb stade is.
'The two care settings 1 am gomg to ask you about are home-based are end kility- based tare- Here are brief descriptions of these scttings-"
Horne-based care is the care that you are currentiy receivmg in yout home h m the North York Commwtity Care Access Centre. In-bome services may include:
community support services such as mail services, transportation & caregiver support services or duit day support homernaking services; persond support services; and, professional services such as home nwsing.
Long-Term Care Centres are midentid homes thaî provide both care and assisiance that meet your health and social carr nds. Facility-t#rsed Long-Term Cane is available for people who are not abk to Iive independently or ï~ their own homes and who may require 24-hour nursing service to be availabie to mœt their nursing and personal care needs.
Y wouM like you to teU me, given your cwrent s&te of bcaith and cwrent care plan, if you would prefer
home-based care as y o u k currently receivhg or, O to move to a long-tenn care faciiity of your choice."
O HOMECARE
a FACILTY CARE
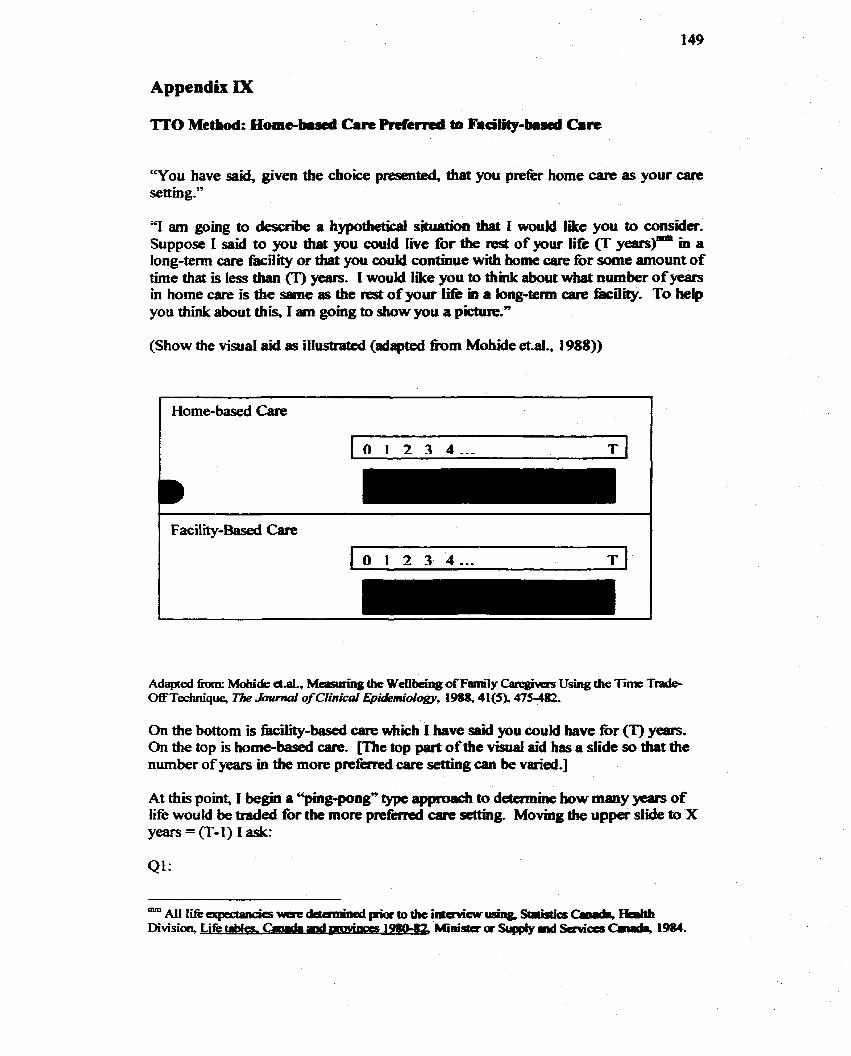
"You have said, given the chok presented, tbat you prefkt home carie as your care setting-"
Y am going to d e s n i a hypothetid situation duit 1 would like y w b consider. Suppose 1 sùd to you that you could live for the rest of p u r Iife (T y-)- h a long-term care fkility or that you could continue with home Gare for some amount of time that is les than (T) years- I would Iîke you to thhk about what number of years in home care is the sarne as the rest of your l e m a long-tenn care faciliîy. To help you diuik about this, 1 am gomg to show you a picaire." -
(Show the visual aid as illuscrated (adapted h m Mohide etal., 1988))
Adaptai 6nnn: Mohide etal., Measuring the Wenbeing ofFanri1y Categiwxs Using the Tim T& OfFTecfuu'que, The h u m d of Cfinicai Epidpmiollogy, 19ûû,41(5), 475-482,
On the bottom is fkciiity-based care which I have said you could have for (T) years. On the top is home-based care- me top part of the visual aid hss a slide so that the number of years m the more p r e f d cate senitig can be varied.]
At this point, I begin a *mg-pong" type approsdi to d e t c m k how many yeam of Life would be traded for the more p r e f d care sc#ing. Movhg tfie uppa slide to X years=(T-1) Iask:
Ql:
"Suppose you could live (T) years in f k i i i i - b a d care or Q-1) pars in ho=-based care, Which wouM you p m W
Ifthe individual prefers tbe Wiity-&id care setîbg then this mdividual wiU not trade a fùlt year of lik for home care and the exercisc is oontinued whereby the individual is given the option of trading a number of monttis for home-based aue. The proceâure is ailalogous to tradmg years of Miee The line of questioning that continues is gBren in Appendk X.
0 lfthe mdividual p r e h the home-based care setting the exericisc continues because this individual may be willmg to trade evm more years for the homo- based are-
42: "Suppose you could live (T) Yeats in fbcility-based Gare or 1 year in home are. Which wouM you prefer?
ifthe mdividual prefers the fàcility-based a r e setting the exercise continues,
If the individual prefers the home-based care sctting the exemk is completed and it is assumed thaî the mdividual is mdülierent betweem T years in a kility and 1 year in home-based care.
43: "Suppose you could live CT) years in kility-based care or (T-2) years in home carie. Which would you prefer?"
if the individual prefers the facility-based care setting the exercise is completed and it is assurnad thaî this individual is indifferent between T years in a f8ciity and (T-2) years m home-based WC.
Ifthe individual prefers the home-based axe sethg the exercise continues.
44: "Suppose you could live Cr) ylears in kility-basad care or 2 years in home care. Which would you prefèr?"
ifthe individuai prefers the iàcility-based Gare setting the exercise continues.
ifthe individual prefers the home-bd care setting the exercise is completed and it is assumed that the mdividud is m d b n t between T years in a fiacility and 2 years in homebased are.
Q5: "Suppose you couid iive (T) years m kility-based care or (T-3) years in home care. Which would you p r i e W
a If the individual prefers the f8cGty-based care setîhg the exercise is cornpleted and it is assumed that thjs individual is indifhmt between T years in a f'acility and 0 - 3 ) years m borne-based care.
If the individual ph tht home-based carc scftMg the cxercise continues.
46: "Suppose you could live CT) pars in fiicile-based care or 3 years in home care- Which would you p r e f e
0 I f die individual prefers the kility-bascd carie se#ing the exaise continues.
0 If the individual p r e h the home-based cab setîing the exercise is completed and it is assumed that the individual is indifferent between T years in a facility and 3 years ui homebased carc.
This iine of questionhg continues until the mdmdual is indifhmt between the home-based care seaing and dit ~ ~ b a s e d awe setting. When this point is determined, the feîiowing information wiil be noted:
m.#
More Preferred C m Setting: Home -Basci Care
Less Preferred Care Setting: Facilitv-Based Care
Life Expectancy (T):
Indifference Point OC):
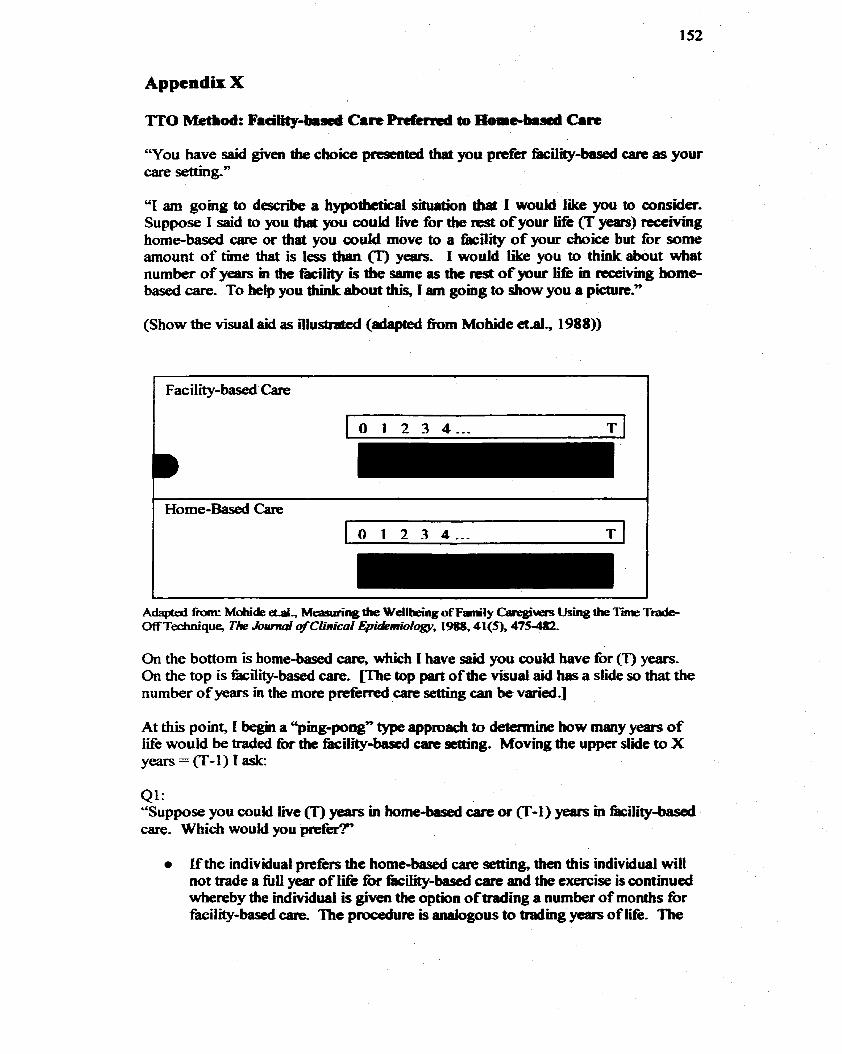
Appendu X
T o u have said given the choice presented ttiat you priefer fkciiity-based care as yow care setting-"
"1 am gomg to descn'be a hypodietical situation tbat 1 wouid like you to consider- Suppose 1 said to you dia you couid live for the rest of your Life (T years) receivmg home-based care or that you couM move to a facility of your choice but for some amount of time that is less than 03 years. 1 would like you to think about what number of years in the fàciiity i . the same as die Test of your iifk in ~eceiving home- based care- To heip you think about diis, 1 am going to show you a picture."
(Shaw the visual aid as illustmfed (adapted hm Mobide &.al, 1 988))
Fac iiity-based Care
Adapted ûortr Mohï& d., Wamrhg the Wdlbeing o fFmly Caregit~e~ Using îhe Ti Ttzub O£FTedmîque, T k hd of ClinicaI Epidemiologv, 1988,41(5), 475482
On the bottom is home-based care, which 1 have said you coukï have for (T) years- On the top is kility-based are. me top part of the visual aid has a slide so that the number of years in the more prdèrried care setiing can be varied.]
At this point, I begin a "ping-pong" type approach to determine how many years of Iifie would be traded for the fàcility-based cart setîing. Moving the upper slide to X yeats=(T-l)rask:
QI: "Suppose you could live (T) years in home-hieci care or F I ) years in fàcility-based care. Which would you p r e f H
ifthe individual prefers the home-based G a r e setting, then this individual will not d e a fiIl year of tife for f8cirity-based Gare and the exetcise is continued whereby the individuai is given the option of trading a number of months for &ciMy-based are. The procedure is analogous to tradmg years of iii. Tbe
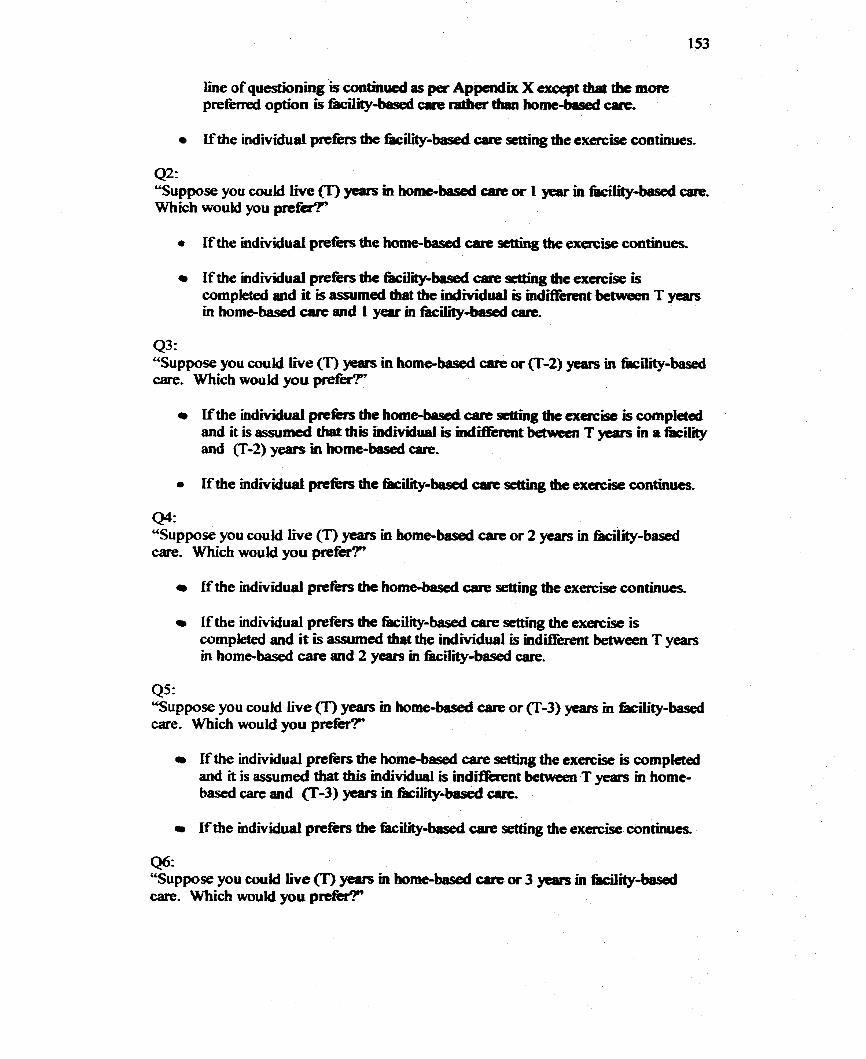
line of questionhg is continucd as pet Appendk X except duit the more preferred option is Wity-based care ratber tban home-bad care,
Lfthe individual pilltfèrs the fàcility-based cane sctting the exercise continues.
Q2: "Suppose you couki In(e (T) years in home-based care or 1 year in facility-based are- Which would you p r e W
O I f the mdividual prefers the home-based care setting the exaise continues.
m I f the individual p~~ die fric-basecl carie scüing the exercise is wmpleted md it is assumeci that the individual is indifkent between T years in home-based carr= and I year m fàciüty-based care,
4 3 : "Suppose you couid Live (T) pars in home-based care or (T-2) years in kility-based are. Which would you prefer?"
Ifthe individuai prefers the homeAnsxi cam setting the exercise is completad and it is assumeâ thaî this mdividual is indifltirent beîwecn T years in a facility and (T-2) years in home-based care.
44: "Suppose you couki iive (T) pars in home-based care or 2 years in fâcility-based Gare- Which wouki you p r e f e
m lf the individual p r e h the hombbised care nOUig the exercise continus
0 ifthe individual prefers the fàcility-based care seaing the exercise is completed and it is assumed that the individual is indifferent between T years in home-based c m and 2 yeats in fàciiity-based c m .
Q5: "Suppose you could Iive (T) ywvs m home-based care or (T-3) years in kility-based care. Which would you prefer?" - I f the individual prcfèn the home-based care settùig the exercise is compfeted
and it is a s s u d that this individual is indiffemt between T years in home- based care and fl-3) yeam in fhiliîybased arc. - If the individual p r d k the kiIity-based c8re setting the exercise continues.
46: ccSuppose you could Iive Cr) years in home-bsrsed care or 3 years m Wcility-basai are. Which wouM you prefetT
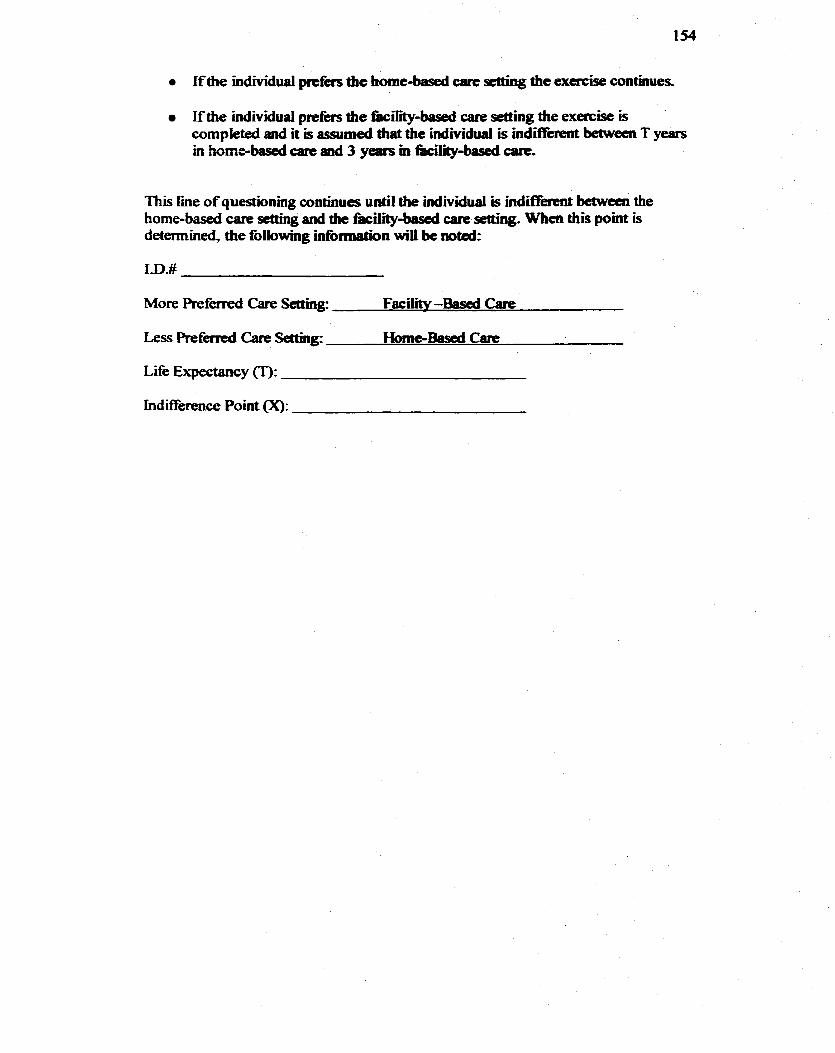
I f the individual prcfcrs the home-based care sc#uig the exercise continues.
ifthe individual p d x s the fki l i-based care setting the exercise is completed and it is assumed drat the individual is mdïtiiint betwecn T years in homebascd and 3 yean m fkciiity-based c a t c
This iine of questionhg continues until the individual is indBixent between the home-based care setîing and the kility-bascd care setting. Whcn this point is determineci, the foliowing information wiii bc notai:
More Preferred Carie Setting: Facility-Bascd Gue
Less Prefed Care Settuig: HomeBased Care
Life Expectancy Cr):
IndifKerence Point 0:
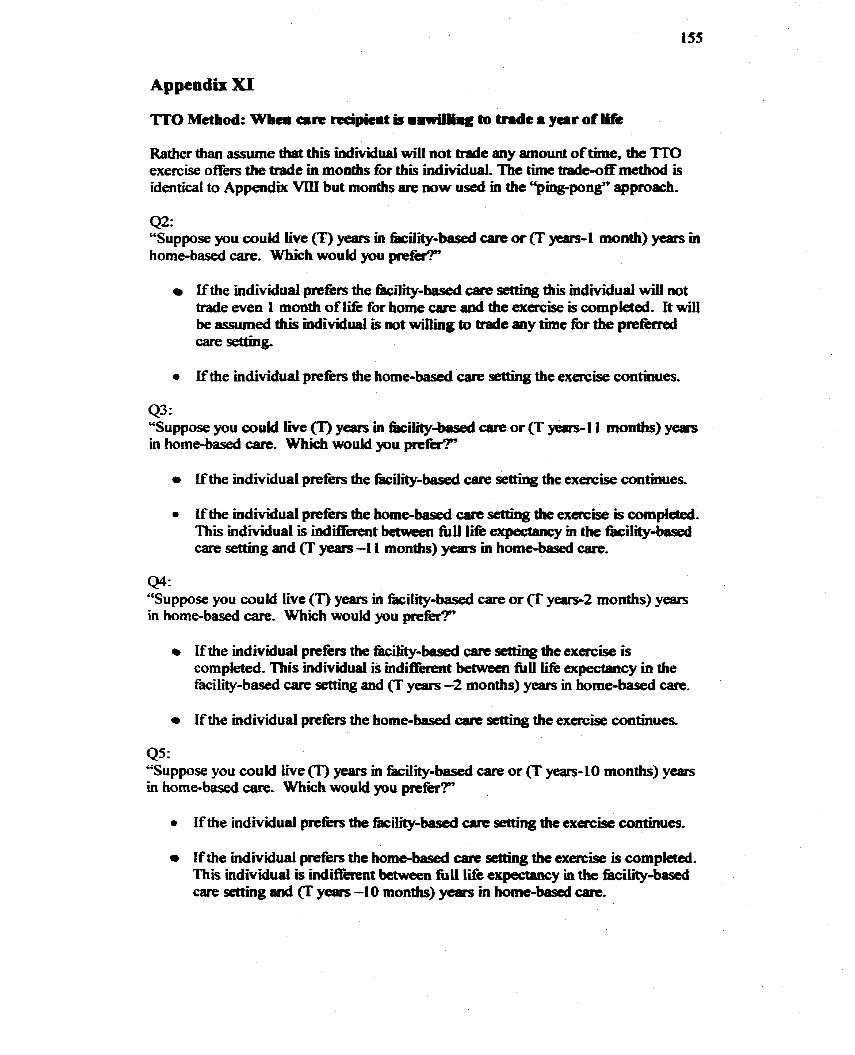
Appendk XI
TT0 Method: Wb- eue recipicit b o i w ü h g to tnde 8 y a r of l&
Rather than assume that this individual will not trade any amount of tirne, the TïO exercise offers the trade in months for this individual, The t h e de-off method Ïs identical to Appendk Vm but moaîhs are now used m the "ping-pong" approach.
42: "Suppose you could k e Cr) years in kiJÏty-based mue or (T yerirs-1 month) ytars m homebased care, Wbich woukl you prefg?"
ifthe individuai p r e k the kility-based are setting this mdividud will not trade even 1 month of M e for home care and the exmise is completed. It wiil be asswned this individual is not wiiling to trade any time for the pmfèrrd care settaig,
rn If the individual prefers the home-based care setting the exercise continues.
43: "Suppose you could live (T) years in &il@-ôased care or Cr years- 1 1 mont)is) years in home-based tare- Which would you prefer?"
ifthe individual prefers the fàcitiibasxi care setting the exercise continues.
Ifthe individuai prefèrs the home-based cart sethg the exercise is compleîed. This individual ïs ùrdWerent îmweea fiil1 lifk expectancy m the f8ciliibaseà care sethg and (T years -1 1 months) years in home-based care.
44: "Suppose you could live Cr) years in façility-based care or (T y e - 2 rnonths) years in home-based care- Which wouM you p r e W
O If the individual pmfers the fàcility-based care seîîing the exerciJe is completed. 'ibis individual is indifferent betwcen full lifè expectaucy in the fàcility-based a r e setting and (T years -2 months) years in home-based W.
I f the individual prefèrs the home-based tare setting the exercise contmues,
Q5r "Suppose you could live (T) years in kility-based Gare or (T years-10 months) years in home-based care, Which wouid p u prefer?"
If the individual ph the hiMy-based tare setting the exercisc continues,
o I f the individual preférs the home-based care setting the exercise is completed. This individual is indifkent b e e n full Iife eqeamcy in the fàciiity-bas& care setting and (T years -10 months) years m homebased care.
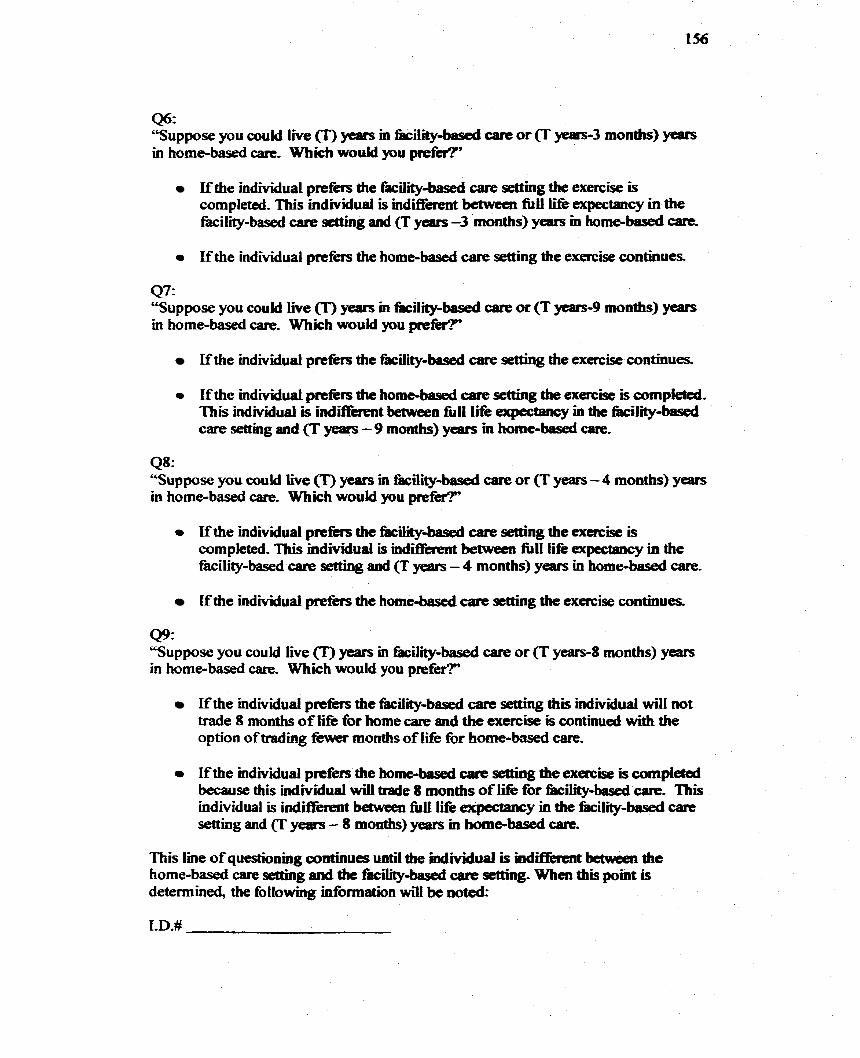
46: "Suppose you could Live (T) ye8rs m kility-based care or years-3 months) y- in homebased care. Which would you p r e W
If the individual prefits the Eicility-based care setîing the exercise is completed, This individual is indifferent bctween fÙU life expectancy in the fkcilÏty-based carie setting and (T years -3 months) years in home-based arc.
Ifthe individual prefers the home-based care setting the exercise continues
47: "Suppose you could live (T) years in kility-ôased care or fl y#irs-9 months) y- in home-based carg- Which would you prefér?"'
Ifthe individuai preférs the &il@-based care setthg the exercise contmues.
If the mdividuai prtfers the home-based care setting the exercisc is compieted. This individual is indifkmt between ftll Lifë expectancy in the nicility-based care sethg and (T years - 9 months) years m home-based are.
Q8: "Suppose you couM live CT) ycars m %il@-based are or (T years - 4 months) y- in home-based care. Which woukl you p r e f e
Ifthe individual p d b the Wiity-based are setting the exercise is cornpietecl, This mdividual is indift'iirent between f t U life expectancy in the facility-based a r e setting and (T years - 4 months) years in home-based care.
I f the individual prefers the home-bascd care setting the exercise continues.
Q9: "Suppose you could live (T) years in &ility-based care or (T years-8 months) years in home-based care. Which would you prefef?"'
Ifthe mdividual prefèrs the fàcility-based care setting this individual wZll not trade 8 months of life for home care and the exercise is contmud with the option of trading fewer months of Mie for home-bd care. - I f the individual prcfers the home-based cace se#ùig the exmise is wmpleted because this ind~idual wiil trade 8 months of life for f8ciW-based carie- This individual is uidifferent between fùll Iüé expectancy in dre fircility-based care setting and (T years - 8 months) years m hombbased are.
This line o f questionmg coatinues until the individual is indüièrcnt bctween the home-based care setting and the fhcility-baseci care setting- When this point is determined, the following information wili be noted:
More Preferred Carie Settins Home -Based Carie
Less Preferred Care Setting: Facilii-Based Care
Life Expectancy (t):
hdifference Point (x):
Appendix XIL
Soao-Demogripk Smmcy for Cire Recipka(. rmd Cireghem
Elderly Preferences for Care Setting
Care Recipient and Caregiver Survey
Please select the most appropriate response for each of the questions.
Your answers are confidentid. At no time will your identity be revealed.
There are no risks to you for participathg.
Tbank yoi for yoar participation.
1. What is your cmrent marital status? O Single O MarriedCommon Law O DivorcedSeparated O Widowed
2. What are your living arrangements? O Live Alone (go to question 5) O Live with spouse O Live with other relative or %end
3. Does your spouse, relative or fiend help you with your daily activities (for example, cooking. cleaning, grocery shopping)?
O No (go to question 5) O Yes Please speciw your relationship to this individual:
4. On average, how many hours per day does your spouse, Wend, relative provide help with your daily activities?
5. What is your type of living accommodation? O House
O Own O Rent
O Apartrnent P Own O Rent
O Condominium a Own O Rent
O Live in relative's or fiends home
6. What is your highest level of education? a Elementary School O Some High School O Completed High School a Comrnunity College P University O Other, please specify:
7. Which category cornes closest to your total monthly household income?
O ~$1 ,000 0 $1,000 -$2,000 O $2,000 - $3,000 o $3,000 - $4,000 o $4,000 - $5,000 CI > $5,000
Thank you for your participation. This completes Our interview.
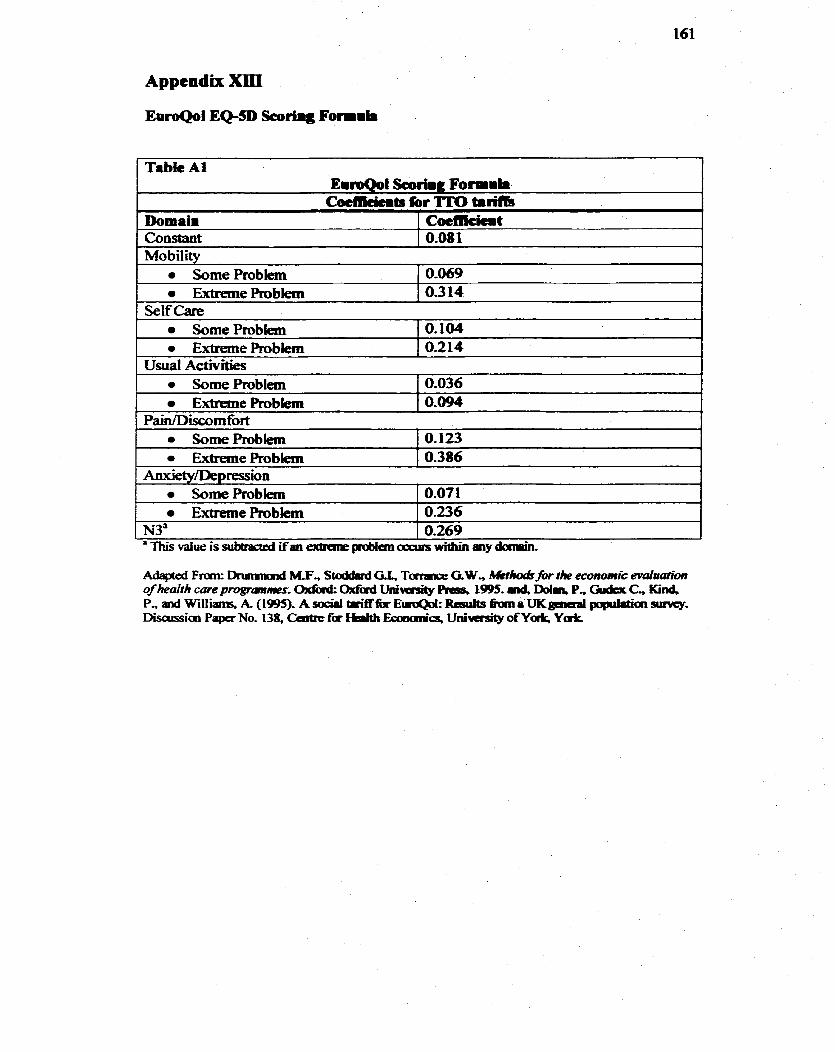
Appendîx XIII
EaroQol EQ-SD !Seorhg F o i i h
Tabk Al ErroQol Scoriig Formil. Cocmcicits for ITO trribnr
Domain Con~tmt
Some Problem Extreme Roblem
Cotmcicmt 0.08 1
0.104 0.2 14
Mobility
Usual Activities
S o m e h b l e m Extreme Problem
SornePmblem Extreme Problem
0.069 0.3 14
0.036 0.094
Self Care .
Pain/Discornfort SomePmbiem ExtremeProbiem
O. 123 0.386
Aaxiety/Depression SomePmbiem 1 0.071 I.Xtreme Problem
N3' 0.236 0-269
'ThisMiueissubtraaed ifaneirtraiiepmôfancxxxirswithïnanydaipin.
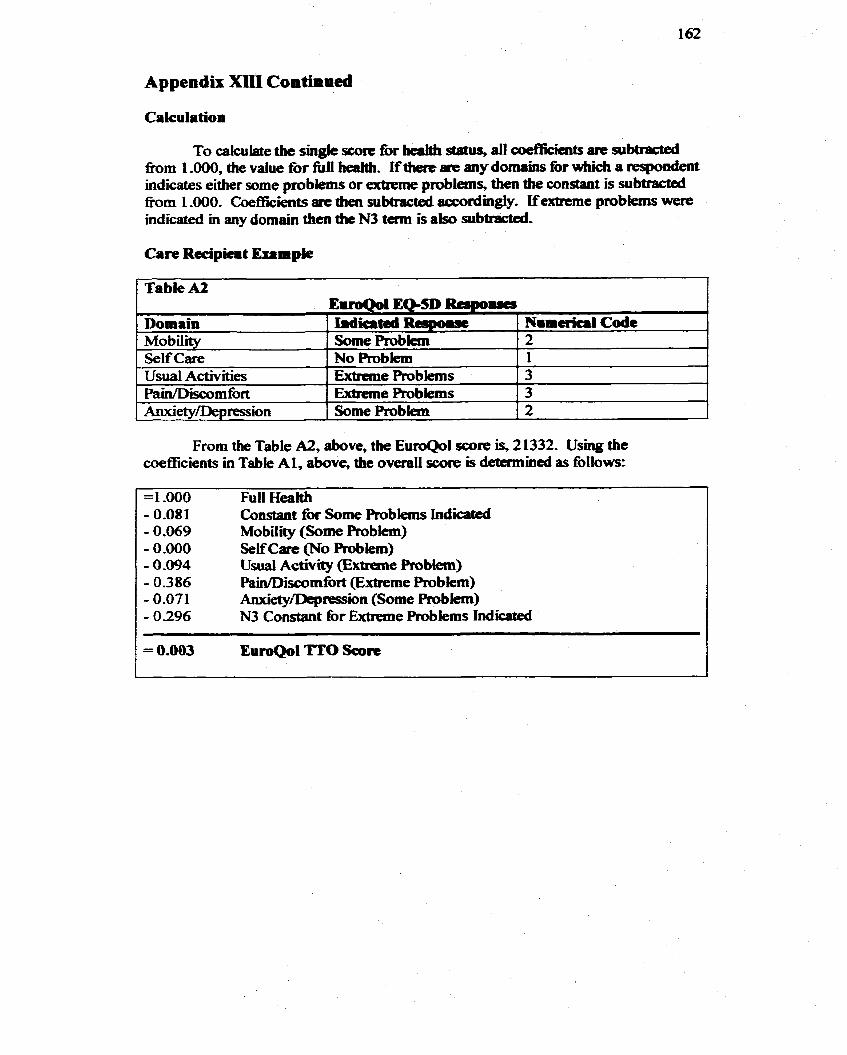
Appendu XlXI Confimacd
Ca kulation
To calculate tbe singk SCOL~C foc beaW s t a t ~ , di coe86ciaits are subbacted h m 1 .O, the value for f i I I heatth. Ifthen are any domains for which a riespondent indicrites either some problans or extreme problems, then the constant is subtmcted ffom 1,000. CoefEcients arc tben subtracted accocdingly, ifexûeme problems were indicated in any domain then the N3 term is also subtracted-
Care Recipicat Esample
1 Table A2 1
From the Table A2, above, the EuroQol score is, 2 1332- Using the coefficients in Table A 1, above, the overaii score is detcrmiaed as follows:
Mobiiity Some Probkm 2 Self Care No R o b h 1
Full H d Constant for Some R o b h Indicated Mo bility (Some Problem) Self Care (No Roblem) Usuai Activity (Extreme Pmblem) Pain/Discomfort (Extreme Prob lem) Anxiety/Depression (Some Problern) N3 Constant for Extreme h b l e m s Indkated
Usual Activities Pain/Discomfort Anxïetv/Denression
Extreme Problems Extreme Ptobiems Some Problem
3 3 2
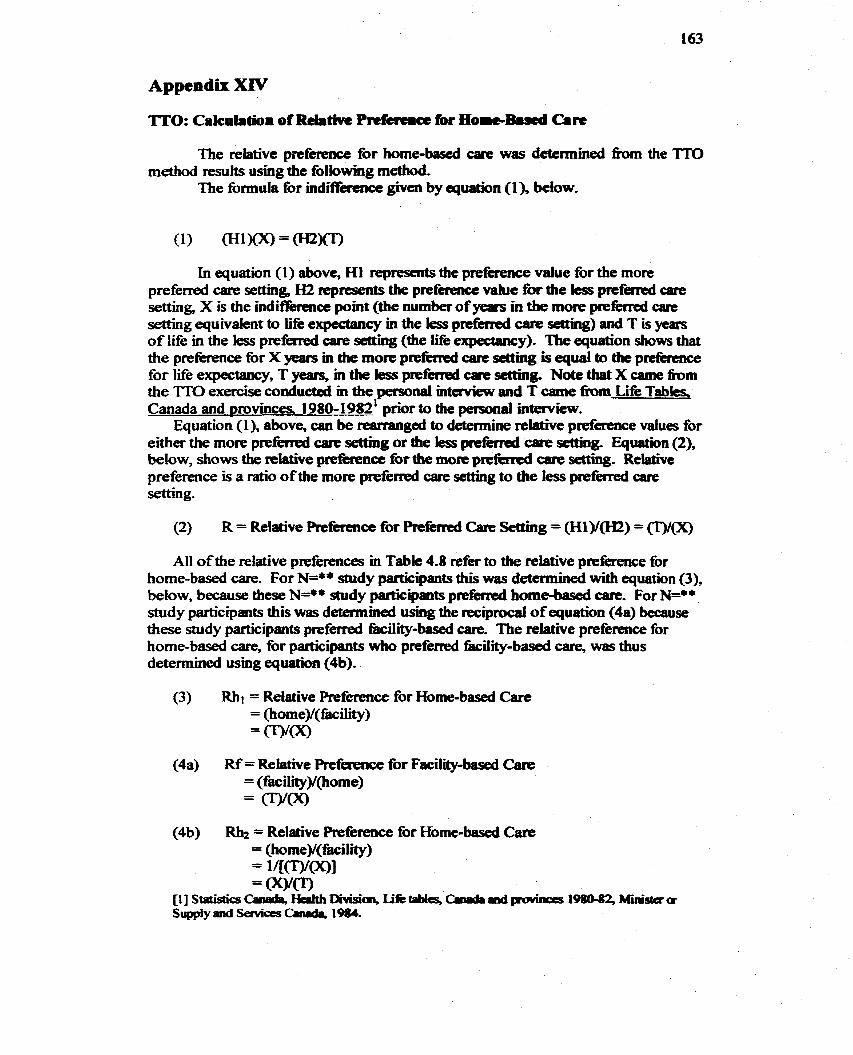
Appendu XIV
=O: CaIc~lafjOm of Relative Pnfereme for HomeBoscd Cln
The relative prefemnce for home-based c a ~ e was detcnnined the TT0 method resuits using the following rnethod-
The formula for mdiffercnce given by cquatjon (l), below-
In equaîion (1) above, Hl represcnts the pxefet.lence value for the more preferred am setîing H2 represents the prefereace value fw the les preferred care setting, X is the indif?kmœ point (the number of years in the more preferred care setting equivaient to Me expectprncy in the les preferred are setting) and T is yem of life in the less preferred care settiag (the lifé expectancy). The equation shows that the p r e h n œ fbr X yeam m the more prefkd carc scââing is equal to the p d h m c e for lifie expectancy, T years, in the less preférred care settins Note tbat X came h m the T'TO exercise conducted in the personal mtaview and T came h m Li& Tabks, Canada and provinces 1980-1982' prbr to the pasonal interview.
Equation (l), above, c m be m g e d to detemine relative prefererice values for either the moE p r i e f d a r e setting or the les preférred care setthg- Eqwthn (2), below, shows the relative prefhmœ for the more pritfèrrcd wre d g . Relative preference is a ratio of the more prefened care sc#ing to the less prefemd care setting .
(2) R = Relative Reference for Preferred Cam Setting = (Hl)/(H2) = CT)/(X)
Al1 of the relative preferences in Table 4.8 refer to the relative pteference for home-based are. For N=** study participants this was determined with equation (3), below, because these N=** study participants pmfierried home-based care- For N=** study participants this was determmed using the reciprocal of equation (4a) because these study participants p r e f d t8ciiity-based m. The relat'we prefèrence for home-based care, for participants who preferred fiicility-based are, was thus detennined usmg equation (4b)-
(3) Rhi = Relative Preference for Home-based Care = (horne)/(fàciiity) =mm
(4a) Rf = Relative Prefêrence for Fwility-based Care = (fàciiity)/(home) = ( W C X )
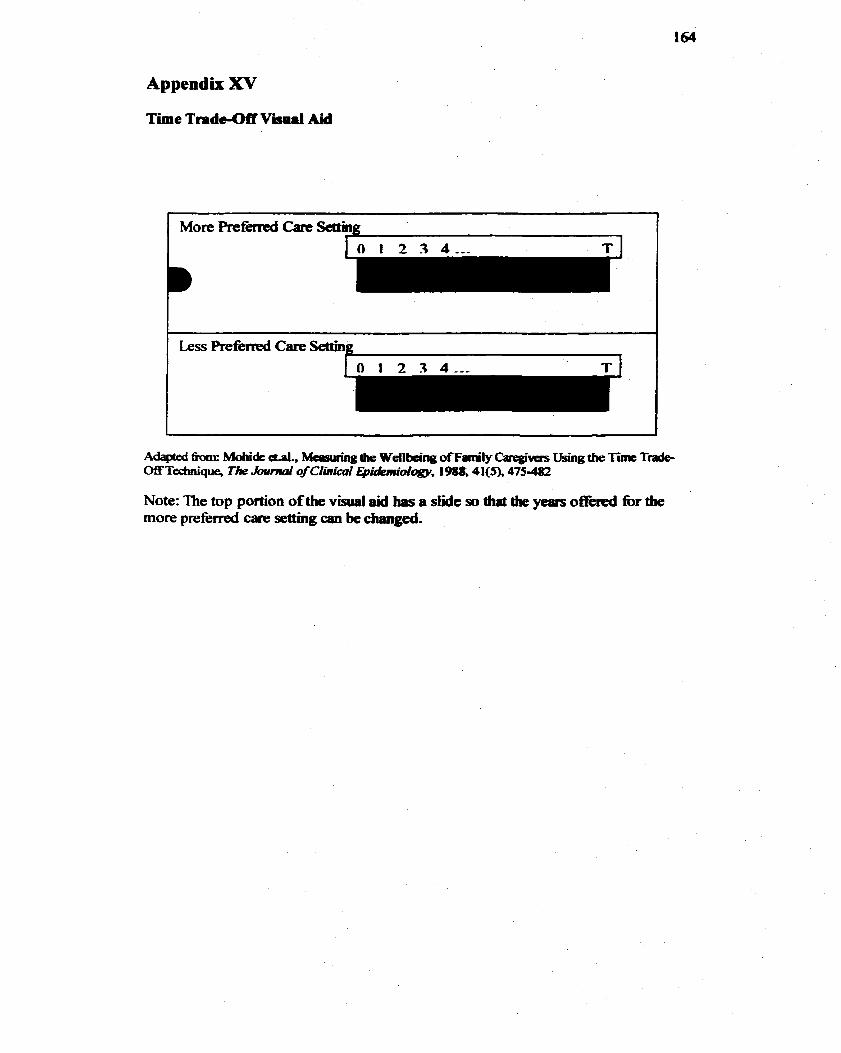
Appendix XV
T ï e Trpde-Off V i d Aid
Note: The top portion of the visual aid has a slide so diat the years offiricd for the more preferred care sethg can be czuuiged.
Appendix XVI
Thank You to StPày Puticipaits
Dear (participants name)
Thank you very much for your in my reseafch study on preferences for health car8 senings. One of the most enjoyabie parts of my thesis was getüng to hear not only your thoughts on home care and facility care but aiso your life stories. I know that aie short interview rnight not seem like much but I hope that you kmw how important your participation in research was.
Thanks again and best wishes.
Stephanie Stewart
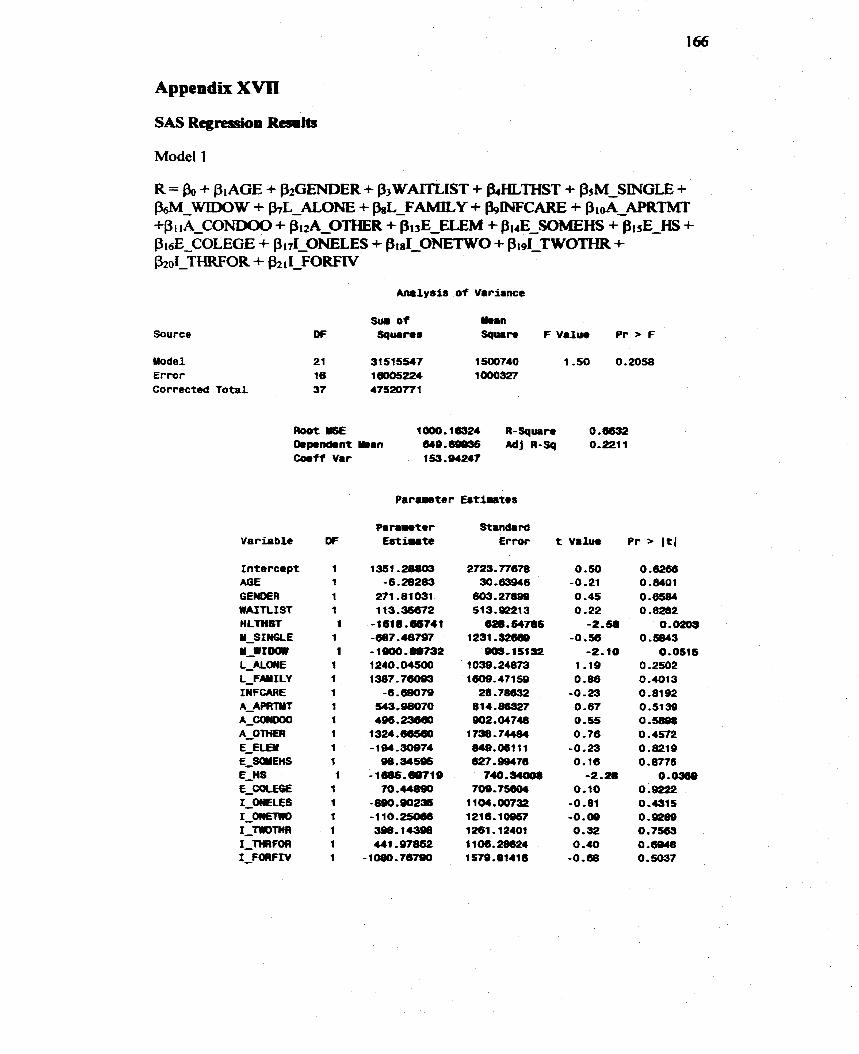
SAS Regressioa Resmhs
Model 1
A m l y s f s o f Variance
Source
Model Error Corrected Total
Sui, of YHn DF Squrins Sqwre F Value Pr F
RootMSE 1W.16324 CI-Square O.üS32 Oepenôent b a n 64@.éLW36 Adj R-Sq 0.2211 C o e f f Var
Variable
Intercept AGE G E N M R WAITLIST HLTHST Y-SINGLE u-wroar L-MCME L-FMILV INFCARE A - M W
A-- A-OTHER €-€Lai E - ~ E n S E-HS E_COLEGE 1-ONELES
1-- 1-niornt7 1-MFOCI 1-FORFI V
1 53.94247
Parameter Estintes
Standard Error

Source
Mode1 E r m r Correcthd T o t a l
Analysir o f Variance
Sur of min DF ~quir8~ Squan F Value P r r F
Root YSE 1.34274 R-Square 0.5320 Dapendent h a n 1,33365 Mj R-Sq -0.OB23 Wff Var 100-68168
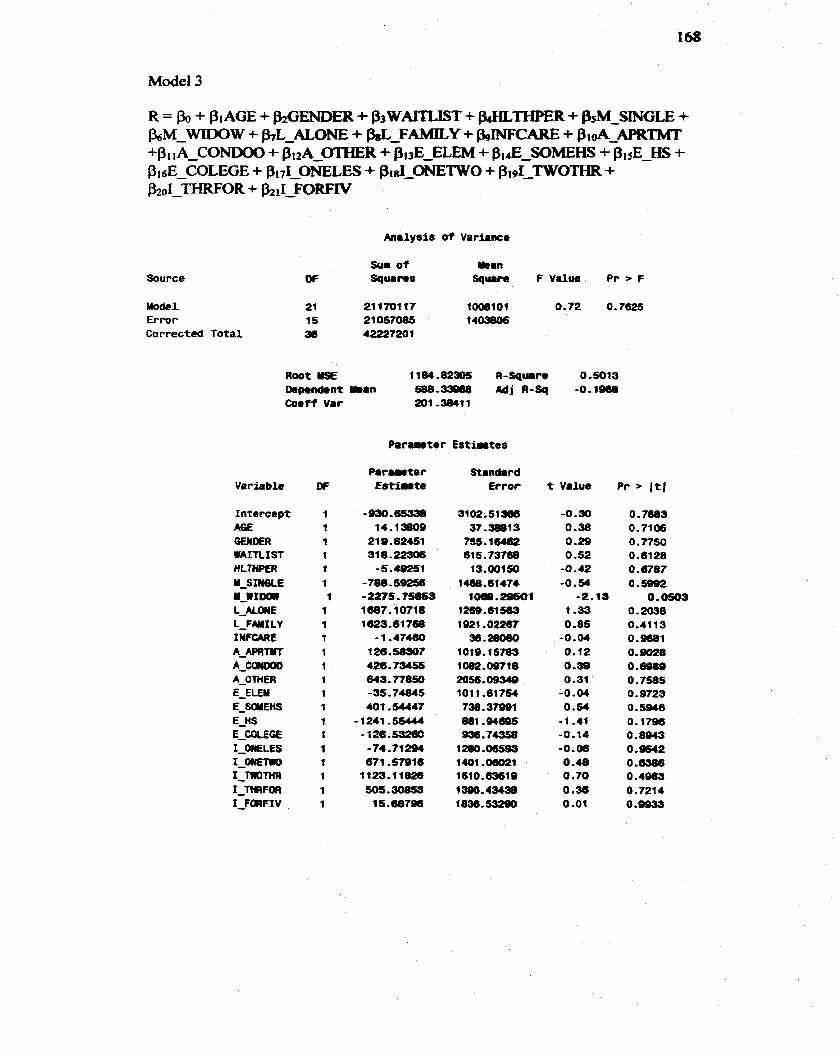
Source
Uodel Error Corrected Total
Sur of üean OF Squans Square F V d u e P r > F
Root üSE 1164.82r)5 R-Squir. 0.5013 ûep.nd.nt man Wû,- Mj A-Sq -0.196û Coeff Var 201 -3841 1
Standard Error t Vahe Pr > 1 t 1
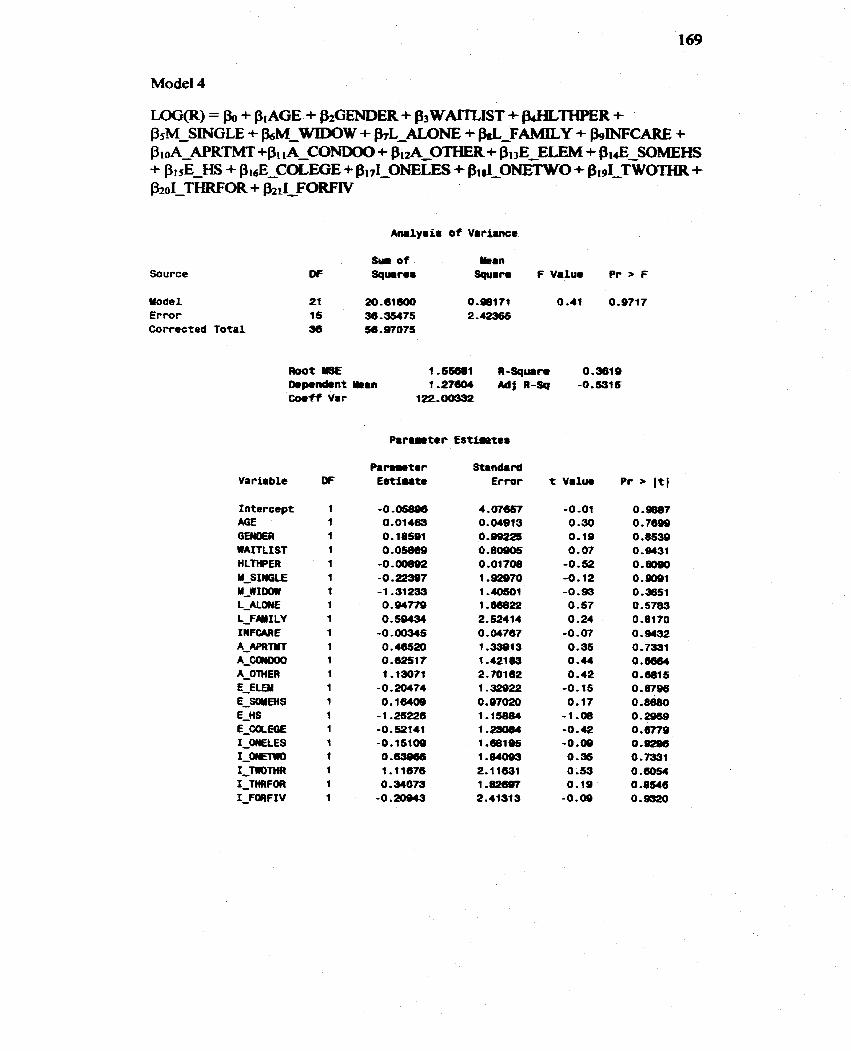
LOG@) = Bo + PIAGE + fhGEMlER + p3 WAULIST + B+HLTHPE3t + BsM-SINGLE + bM-WIDOW + &rL-ALOl?E + w-FAMILY + bINFCARE + ProA-AE'RT'MT +Pt 1A-CONDO0 + Pi2ANDOOOTHER+ P13E ELEM + Bi& SOMEHS + BI&-= + BisE-COLEGE + BIII-ONELES + $I~I-ON~TIKO + - TWOTHR + p2oI-THRFOR + &iI-FORFN
Source
Yodel Error Corrected Total
A m l y s i s of Variance
Sui o f &an OF Squares Square FValue P r r F
Variable ff
1 ntercept AG€ GEWOER WAITLIST HLTHPER Y-SINGLE M-WIoarr L-MONE L-FWI LY INFCARE A-APRTYT A-- A-OlHER E-ELDiI E-SûüEMS E-HS E_COLEQ€ 1-WLES 1,- 1-TIlOTHR 1-THRF OF1 1-FaRFIV
Paremeter Standard Est-te Error t Value Pr I t l
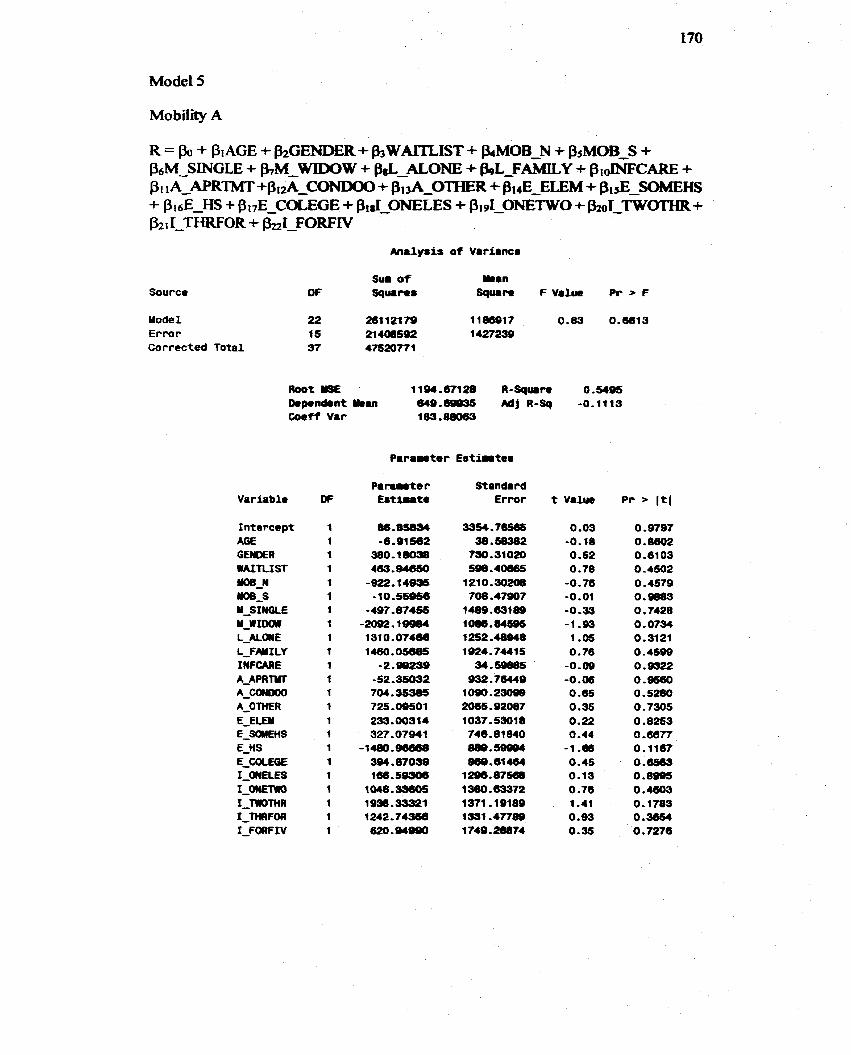
Analysis o f Variance
Source
Yodel E r m r Corrected Total
Root YQE 1194.67128 R - S q u i n 0.5495 [kpenôont man [email protected] Mf R-Sq -0,1118 Coef f Var
Variable
Intercept AG€ GENER WAITLIST
-_W -3 Y-SINGLE u-w1m L-ALWE L-FNILY IIYFCAAE A-APRM
A-- A-OTHER E-EiEU E_SdYEHS E-HS E-CûLEûE 1-OMELES L- I-monin 1-MFOR 1-FORFIV
Standard Error t Value
O .O3 -0.18 0.52 0 -78
-0.76 -0.01 -0-33 -1 .B3 1 .OS 0.76
-0.09 -0.06
O .6S 0.35 0.22 0.44
-1 .m 0.45 0.13 O .76 1.41 0.99 0.35
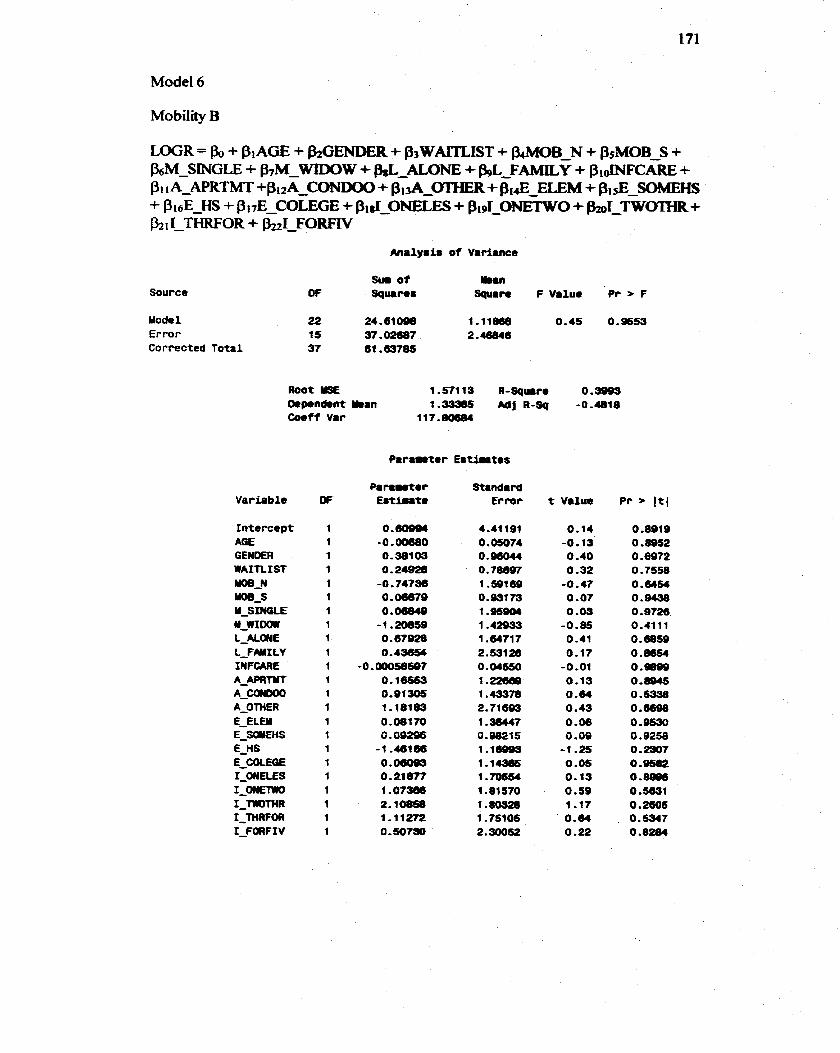
Antlysis o f Variance
Source
Mode1 Error Correctcd Tota l
Sur o f ban O F Sqmrus Square F Value P r > F
Root YSE 1.57119 R-Sqwro 0.9999 mponâent man 1.33385 Mj R-Çq -0,4818 Coeff Var
Panmotor Stinde rd E s t i u t e Error t Value P r > (t(
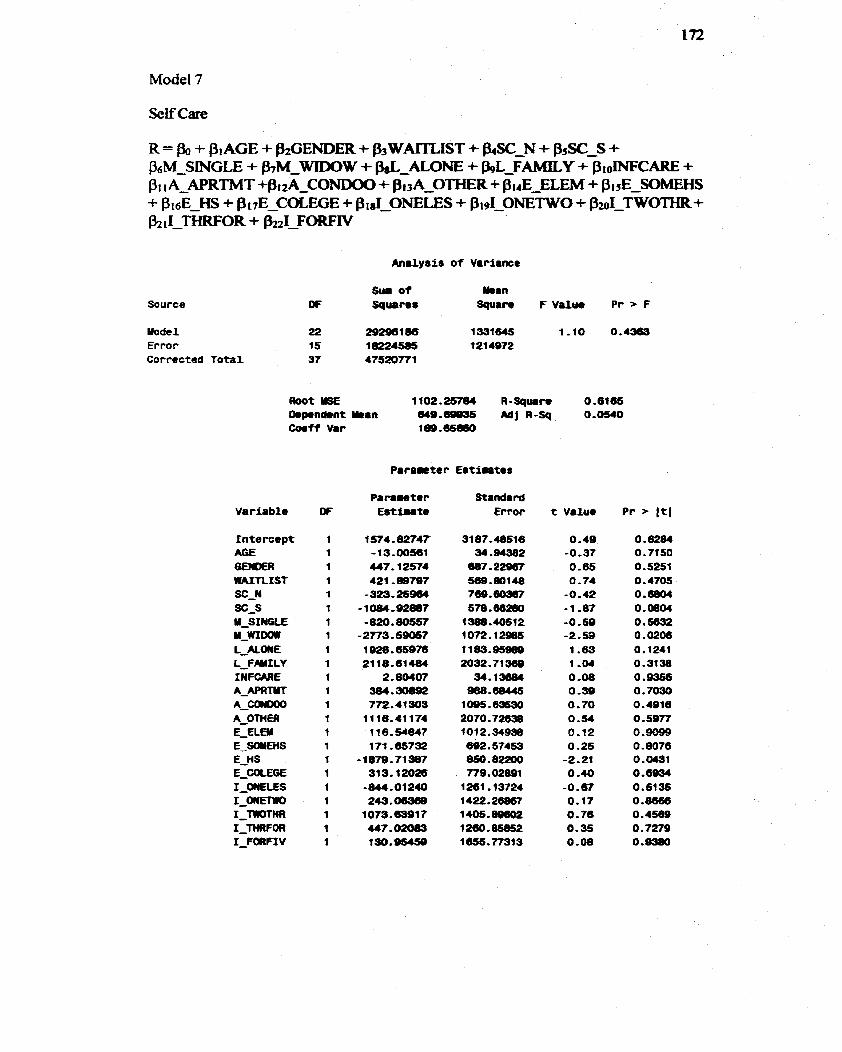
Analysis o f Variance
Source
Mode1 Error Correctcd Tota l
S u i o f Wrn O F Squares Square F Value Pr > F
Corff Var 1Be,65(n0
Parawter E r t i i i t e s
Standa rd Error t Value
0 -49 -0.37 0 -65 0.74
-0.42 -1 -87 -0.59 -2.53 1.63 1-04 0 -08 0 -30 0.70 O .SI 0-12 0.25
-2.21 O -40
-0.67 O. 17 0 -76 0.35 0 -08
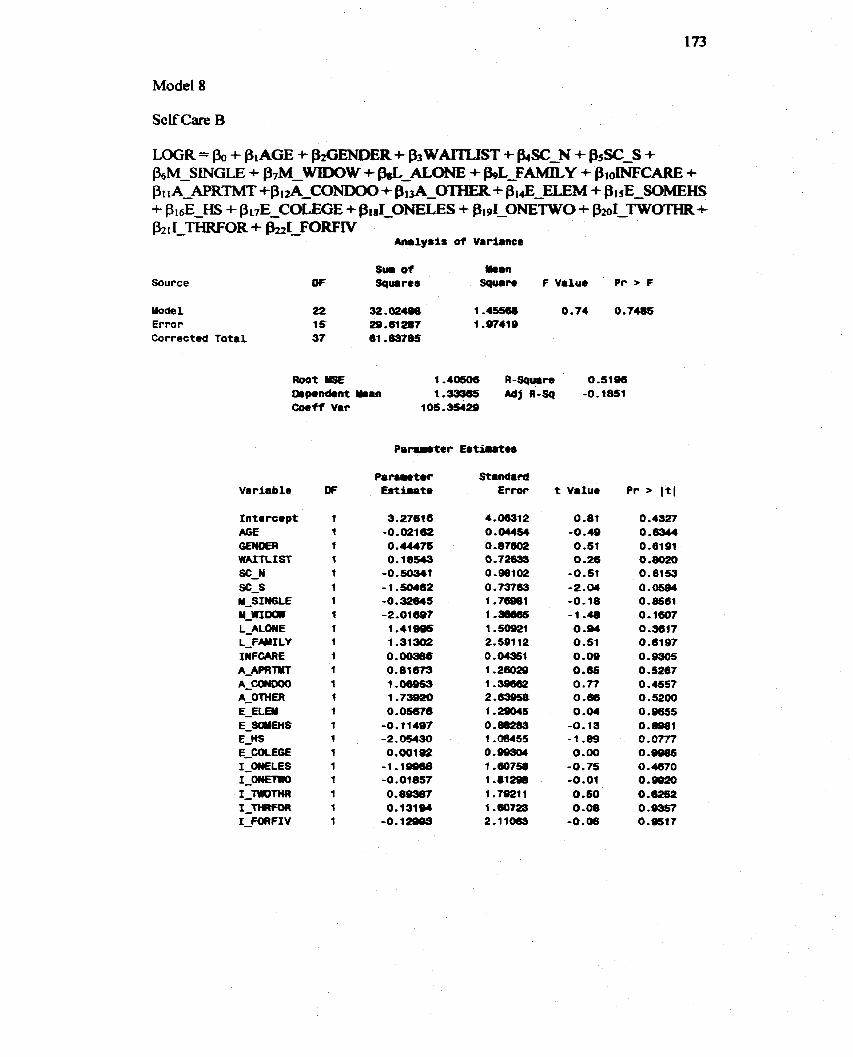
Self Care B
Source
Mode 1 Error Corrected Tota l
R ~ o t Y5E 1.40606 R-Spum 0.5iQû [kp.nd.nt h a n 1.33365 Adj R-Sq -0.1851 Coeff Var
Standard Error
4.06312 0 .Ws4 O. 87- 0,72633 0,98102 O. 73763 1 .76981 1 .- 1 ,50921 2.591 12 O.(W961 1 .26029 1.39682 2. 1.29045 O. 88283 1 .O8455 0.99304 1 .a758 1 -812m 1 .TOZlI 1 .m723 2.11063
t Value P r > I t (
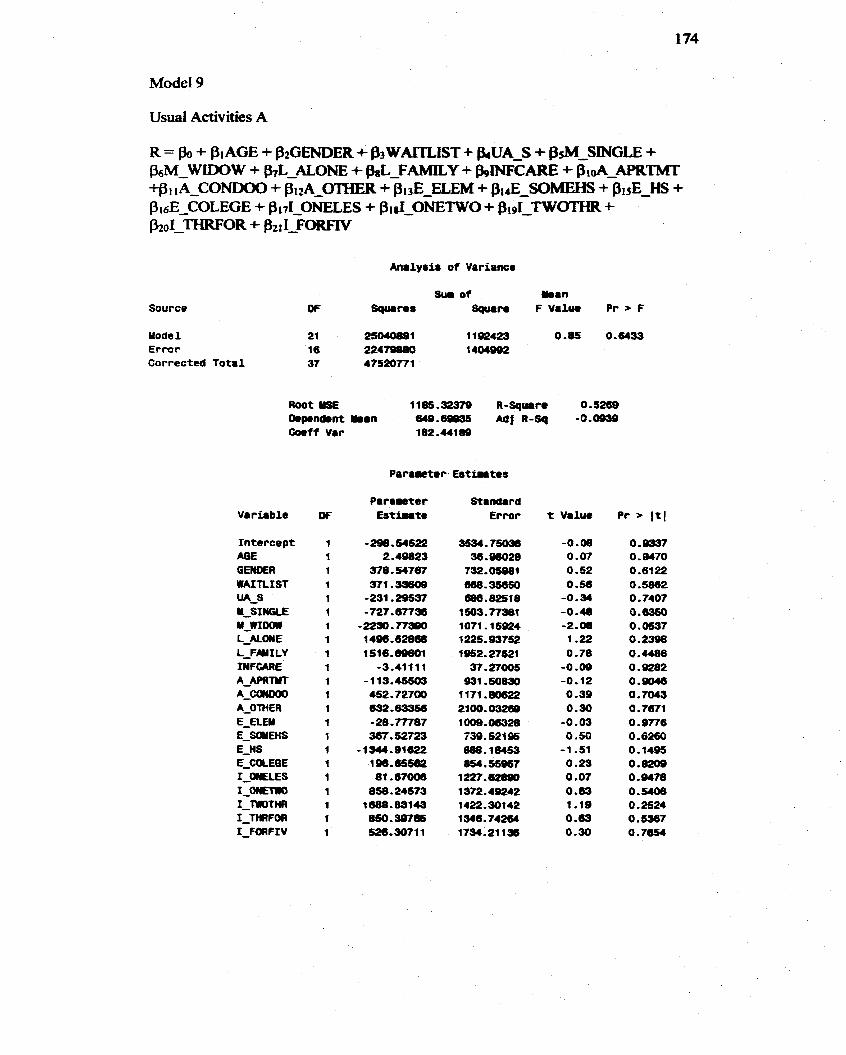
Usual Activities A
Analyriu of Variance
Source
Mode1 Error Corrected Total
Root US€ 11û5.32379 R-Square 0.5269 O.p.nâent Umm a 9 . M Mf R-SQ -0.0959 Cosff Var 182.44189
P a m r t o r Eut intes
Standard Error
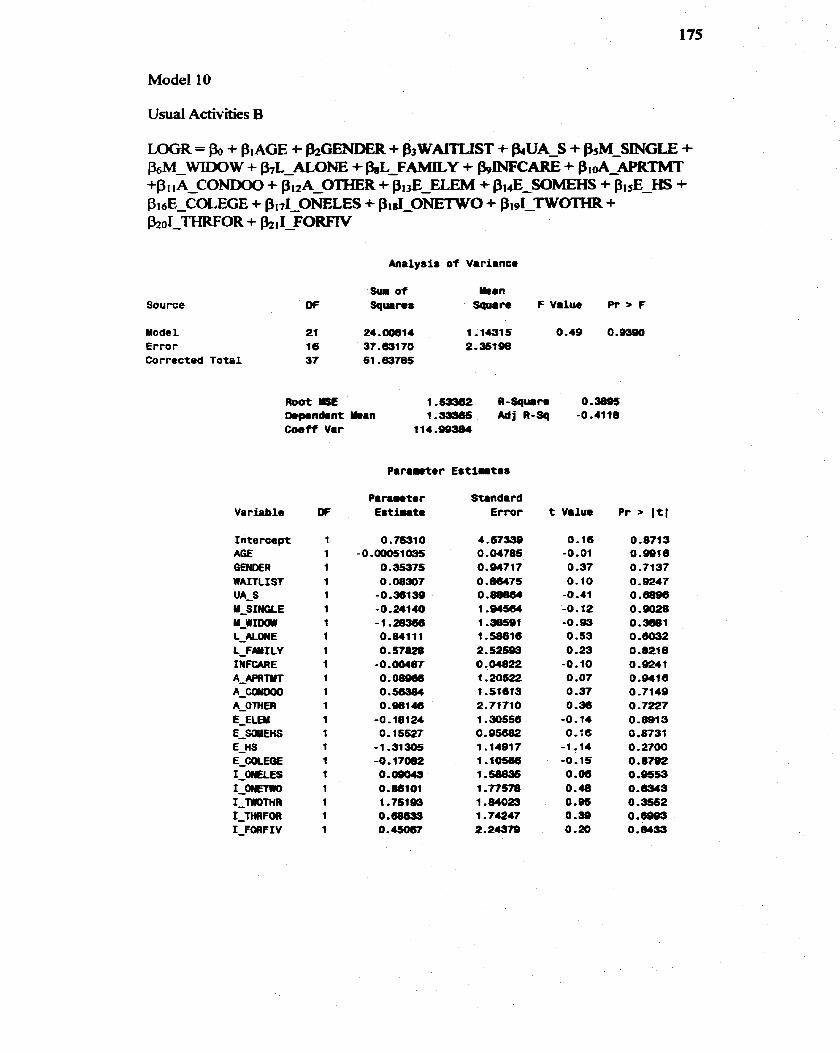
Analysis o f Variance
Source
Mode1 21 24.00814 1-1-15 0.49 0.9390 Ermr 16 37--170 2-35198 Corrected Total 37 61 -63785
Wt ILSE 1.53362 R-SqMare 0.38@$ -pondent man 1.- A d j R-Sq -0.4118 C o e f f Var
Variable
Intercept MIE GENûER WAfT LIST UA-S U-SINGLE u-w1m L-ALONE 1-FNI LY INFCARE A_APRiYT
A-- A-OTHER E-ELEM E_ÇQIEHS E-ns E_COCEW I-OM%ES 1-- I-mnm 1-MFCm 1-FORFIV
Parnuter Standard Est fute Ermr t Value
0.16 -0.01
O .37 0.10
-0.41 -0.12 -0.w
O -53 0.23
-0.10 0 .O7 0 -37 0 .a6
-0.14 0-16
-1 -14 -0.15 O -06 0-48 0.05 0 -99 0.20
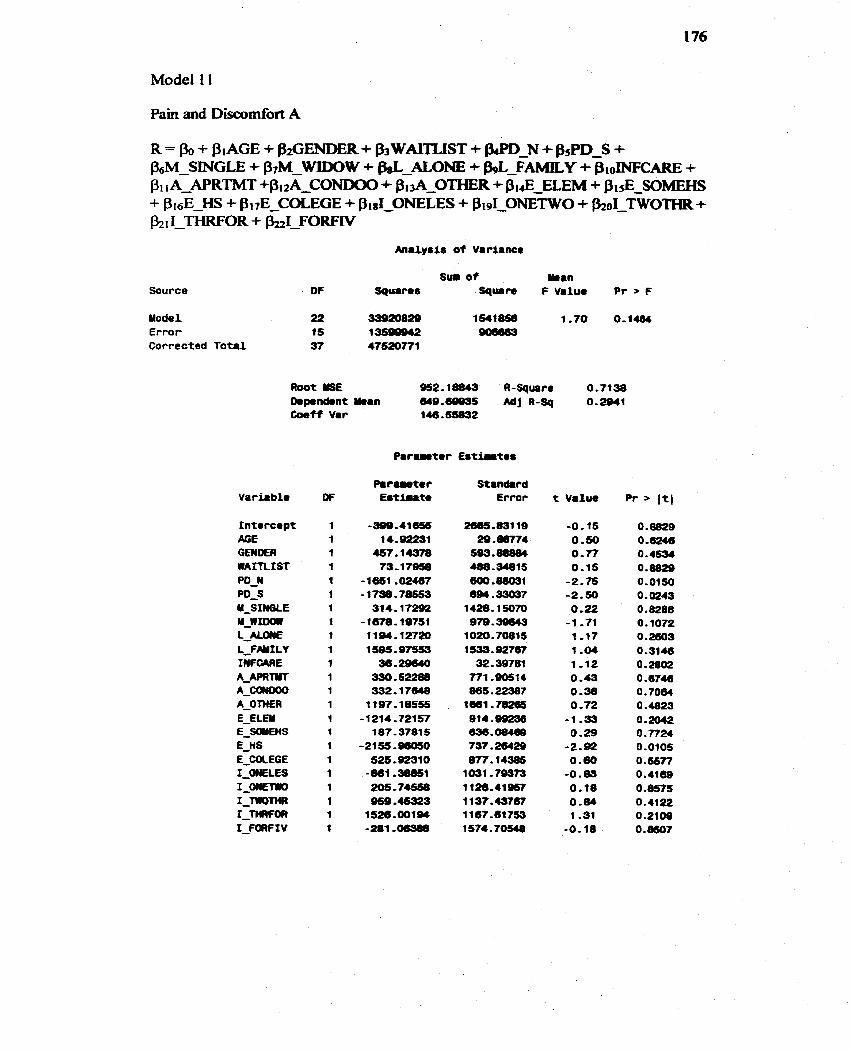
Source
Uodel Error Corrected T o t a l
S w o f man DF Sqmr8s Squm F Value P r > F
Root USE Q52.lûû43 R-Square 0.7138 6.p.ndrnt -an 649.æ9ss AdjR-Sq 0.2Q41 Coeff Var 146.55832
Standard Error t Value Pr > I t (
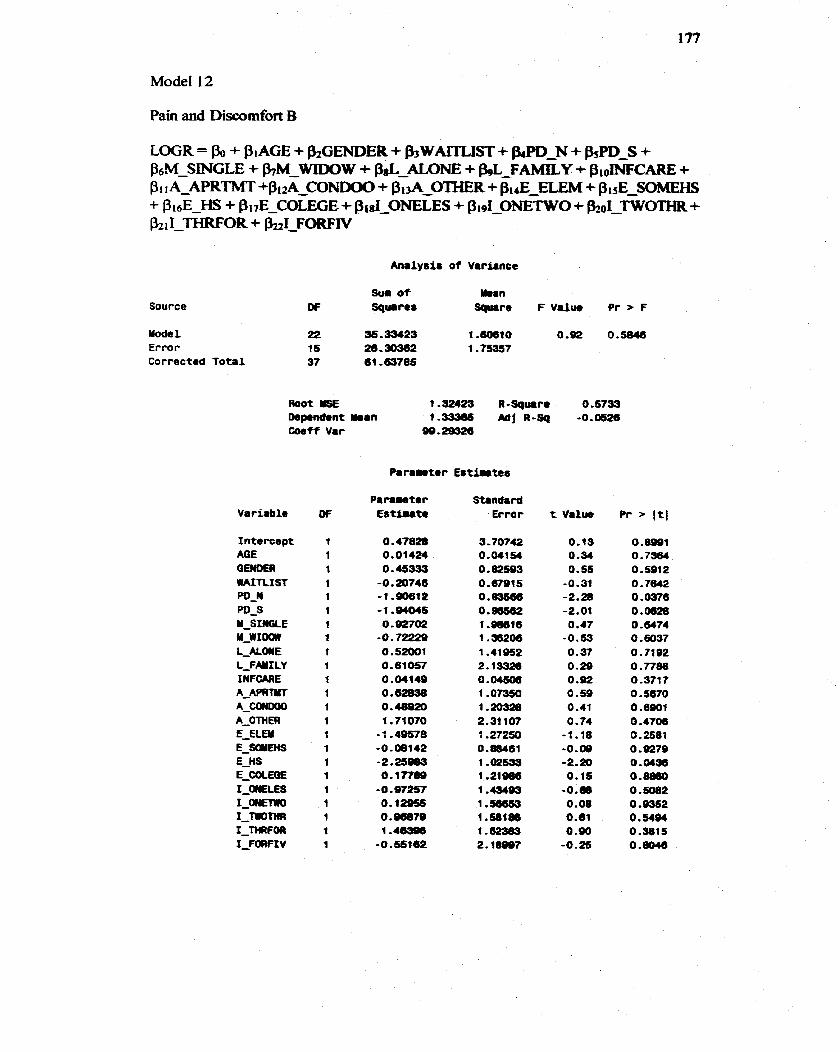
Pain and Discornfort B
Analyeiir o f Variance
Source
Yode 1 Error Corrected Tota l
S w o f W i n O F Squrres Squrre F Value Pr F
Root YSE 1 .a2423 R-Squire 0.6733 Dapendent man *-ma6 ~j R-sq -0.0026 &eff Var
Variable
Intercept AG€ GEMDER WAIftlST PO-N PD-S U-SINûLE u-w1m L - M a € L-FHILY I N F W E A - m n r
AL- A-OTHER E-ELEY E-SCMEHS E-HS E_COCEOE 1--LES 1-mm 1-mom 1-WFOR IFOCIFIV
Standard Er ro r
3 - 70742 0.01154 0.82593 0.67915 O.mse6 0.96562 1 .ml6 1.38206 1.41952 2.13326 O . M s a 1 .O- 1 -20328 2-31 107 1.27250 0.88461 1 ,02599 1.21= 1 .-a3 1 .sa653 1.5ble6 1.62383 2.1ôS@7
t Valus
0.19 0 -34 0.55
-0.31 -2.28 -2.01
O -47 -0.63 0.37 0.29 0.92 0.59 0.41 0 -74
-1.18 -0.09 -2.20 o. 15
-0.m 0.08 0.81 0.90
-0.2s
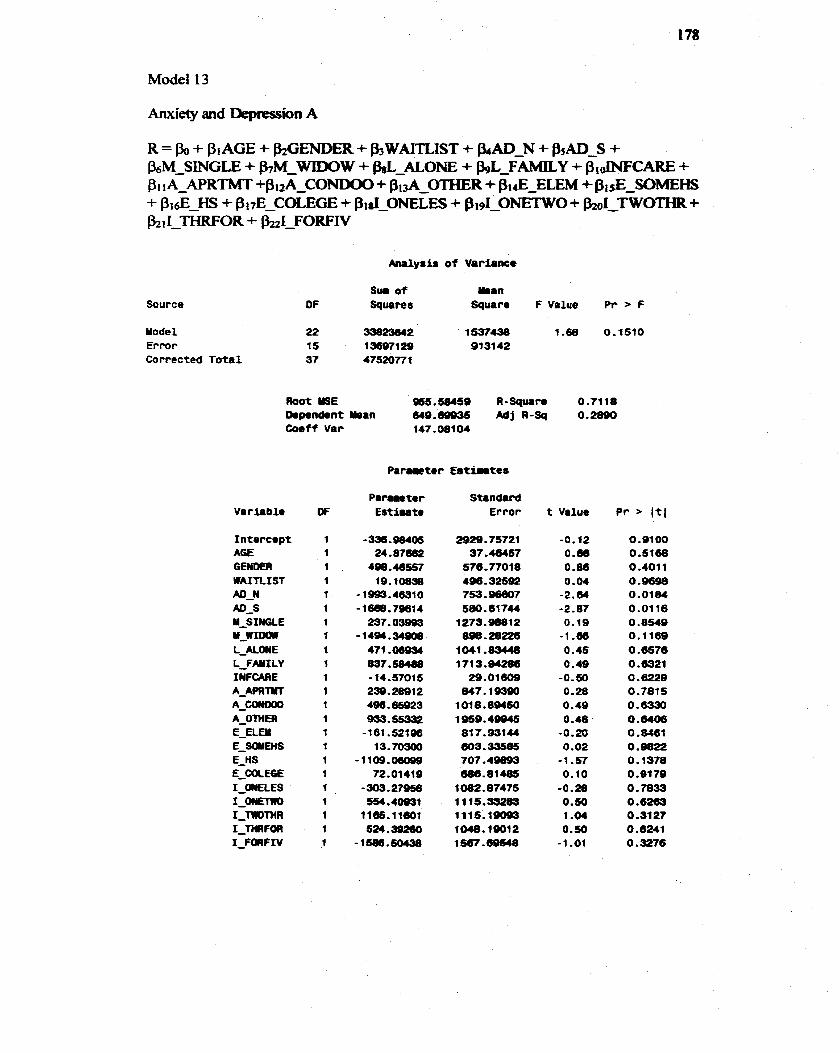
Anxieîy and Depression A
kialysir o f Variance
Source S w o f unan
OF Squares Square F Value P r > F
Mode1 22 33023642 1 537438 1.68 0,1510 Error 15 1 3697 1 29 933142 Corrected Total 37 47520771
Root S E 965.51WSQ A-Square O .?il8 Rprndont man cwB.ûQO3S Adj R-Sq O.28OO Caeff V a r 147.08104
Standard Error
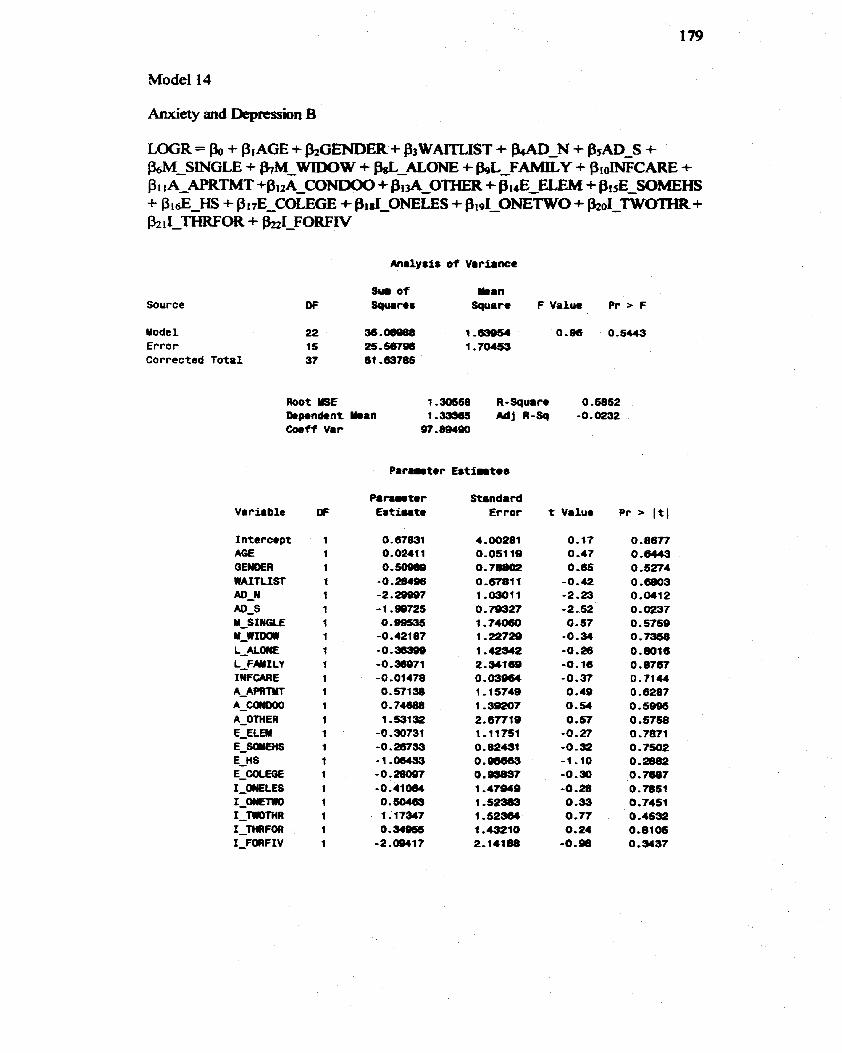
Model 14
Source Sum o f man
Of Square8 Square F Value Pr > F
Mode1 22 36.08888 1,63954 0.96 0.5443 Error 15 25 - 567- 1 ,70453 Corrected Total 37 61 - 63785
Coeff Var
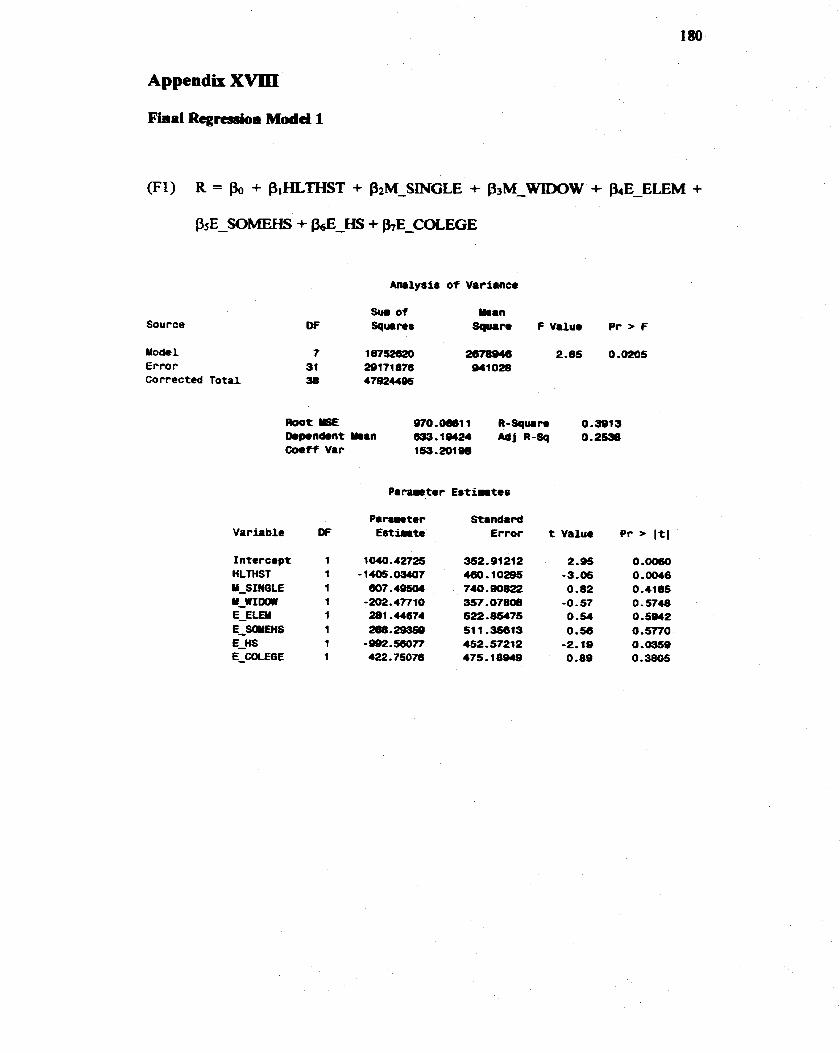
Appendix X W
Final Regressioa Modd 1
Amlysis o f Variance
Source Sw of Yi.n
O F Squrirer Squam F Value P r > F
Yodel 7 18752620 2678B46 2.85 O . M o 5 Error 31 29171876 941 028 Corrected Total 38 47924495
m o t Y5E 97O.Ml1 R - S q w n 0.9913 0.pond.nt man 1 2 A d j R - S q 0.2538 C o e f f Var 163.2ûlW
Pmnmetec Standard Variable O F Estimate Error t Value P r > I t l
Intercept HLTHST Y-SIMGLE u-w1m E-ELEU E_SOYUIS E-HS E_COCECiE
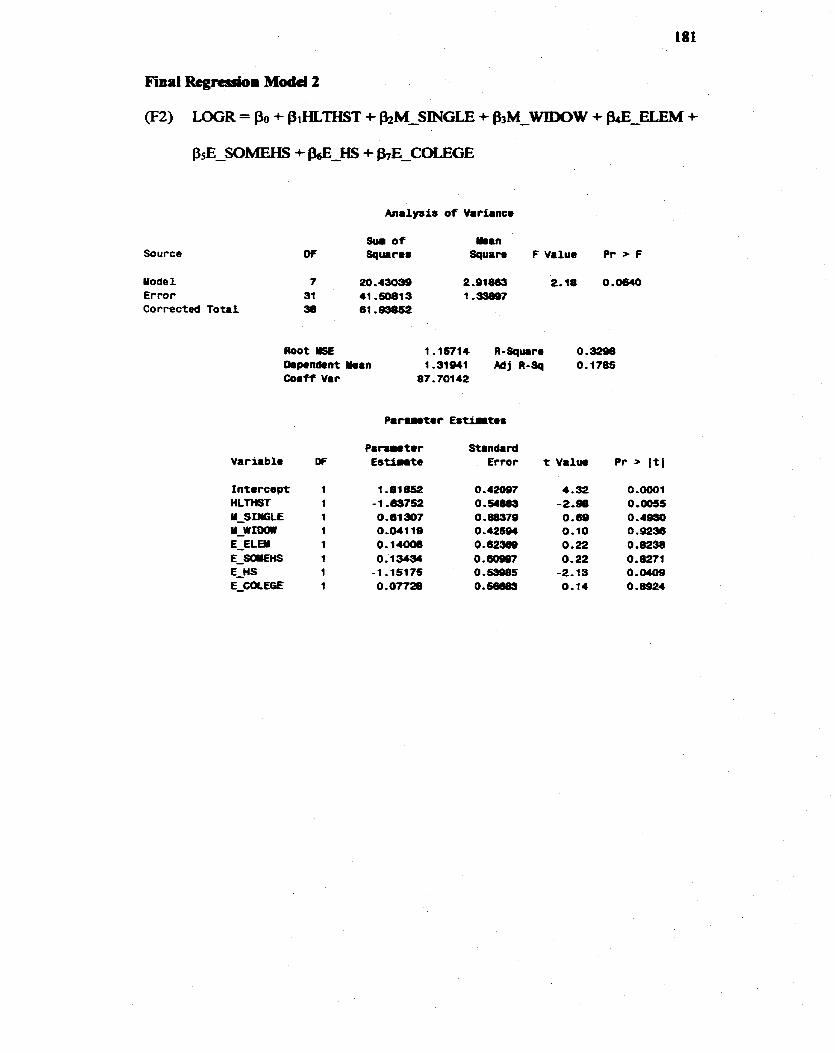
Source
Mode1 Er ro r Corrected Total
Sui o f W i n D f Squares Square F V a l u e P r - F
Root USE 1.15714 R-Squrirm 0 -3290 D.p.n&nt Man r.3le41 Mj R-Sq O-170s Coaf-f Var 87.701 42
P i n m e t e r Standard Variable DF E s t i n t e Error t V a l w Pr > I t 1
Intercept HLTHST U-SIm;tE u-wroclrr E-ELEN E-SaKnS E-HS E-UXEGE





























