Embed Size (px)
Citation preview
Reruseitatkni, 17 (1989) 173- 182 Elsevier Scientific Publishers Ireland Ltd.
173
ELECTROMECHANICAL DISSOCIATION: SIX YEARS PREHOSPITAL EXPERIENCE
HARLAN A. STUEVEN*, TOM AUFDERHEIDE, ELIZABETH M. WAITE and JAMES R. MATEER
Section of lpmuma and Emergency Medicine, Medical College of Wiseon.+ Milwaukee County Medical Complex, 8700 W. Wisconsin Avenue, Milwaukee WI 55226 K%S.A.I
(Received January 20tb, 1988) (Revision received June l&h, 1988) (Accepted June 2&h, 1988)
SUMMARY
Electromechanical dissociation (EMD) is the presenting rhythm in approximately 17% of all prehospital cardiorespiratory arrests. Yet, we know comparatively little about the demographic profile of these patients. The pur- pose of this study was to review historical and resuscitative parameters to help create a demographic profile. For a 6-year period of time from January 1st 1980 to December 31st, 1985,503 adult patients presented to a prehospital system in non-traumatic, nonpoisoned, cardiorespiratory arrest with an initial rhythm of electromechanical dissociation. The overall average response time was 6.1 -c 3.2 mini Sixty percent of the patients were witnessed arrests and 65W had bystander initiated CPR. Forty-six percent of the patients had a cardiac his- tory: myocardial infarction 13%, CHF 11% and other 21%. Other pertinent past medical history included diabetes 15%. COPD 10% and seizures 3O/b. The average age was 69.8 f 13.7 years. Fifty-seven percent were male. Forty-three percent were on cardiac medication including: digoxin, 24%; nitroglycerin, 12%; potassium supplements, 9%; propranolol, 8O,k1; isordil, 6%; quinidine, 3%; nitropaste, 3%: and other cardiac medications, 15%. One hundred forty-eight (29W) patients developed a pulse at some time during resuscitative efforts, of these 17 (3.4%) patients responded with a pulse immediately after intubation. The mean time of resuscitation to sustaining pulse was 20 f 11 min and the mean resuscitation time to sustaining pressure was 22 f 11 min. Nineteen per- cent were successfully resuscitated, defined as a conveyance of a patient with a pulse and a rhythm to an emergency department. Four point four percent were saved, defined as a patient discharged alive from the hospital. Approximately 53% of the successfully resuscitated patients and 45% of the save patients were determined to have a probable respiratory event as the primary etiology
*Author to whom reprint requests should be sent.
0300-9572/89/$08.50 0 1989 Elsevier Scientific Publishers Ireland Ltd. Priited and Published in Ireland
174
of their arrest. This study attempts to provide some insight into the demographic profile of the patients in EMD.
Key words: Electromechanical dissociation - Prehospital cardiac arrest
INTRODUCTION
Electromechanical dissociation (EMD) is the initial presenting rhythm in 19.6% of patients who are monitored at the onset of cardiac arrest and 16.5% of patients who present to a prehospital system in full cardiac arrest [l]. A variety of potentially reversible mechanisms have been implicated in the cause of EMD: tension pneumothorax, pericardial tamponade, hypovolemia, pulmonary embolism, anoxialsevere ischemia, severe electrolyte abnormalities and cardiac outlet obstruction. The American Heart Association’s Advanced Cardiac Life Support (ACLS) manuals recommended approach to the therapy of EMD is given with the admonition to rule out these reversible causes first. The recom- mended approach to drug therapy for EMD is, unfortunately, very generic. The 1980 ACLS guidelines recommended epinephrine, bicarbonate and, if ineffec- tive, calcium chloride or vasopressors. The 1986 ACLS guidelines recom- mended epinephrine with consideration given to bicarbonate therapy [2]. The purpose of this study was to review our prehospital experience with EMD, eval- uate historical parameters, and create a demographic profile.
METHODS
The prehospital care system studied is comprised of a two-tier response sys- tem with first responder EMT-basics provided by private ambulance services or fire department services. The average EMT-basic response time is two min- utes. Advanced life support is provided by strategically located paramedic units, staffed by EMT-P’s (paramedics) who are trained in rhythm recognition, i.v. access, endotracheal intubation, selected drug therapy, pericardiocentesis, thoracentesis and application of MAST trousers. The average paramedic response time is approximately 5 min [l].
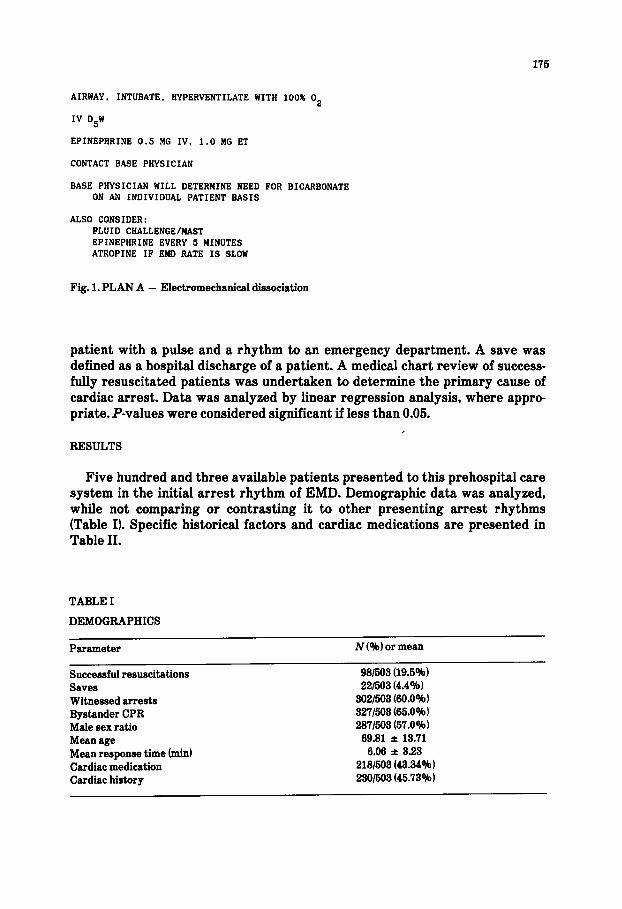
Upon arrival at the scene of a cardiac arrest, the paramedics operate under written medical protocol. The protocol for EMD includes: CPR, airway control, the establishment of an intravenous line and the administration of epinephrine (Fig. 1). Contact is then made with the paramedic base station, which is staffed by ACLS certified physicians, from which additional therapy may be ordered.
EMD was defined as a discernible electrical complex, excluding ventricular fibrillation and ventricular tachycardia, with no palpable pulse. Resuscitation time begins upon paramedic arrival at the scene until the patient develops an initial pulsatile rhythm. The time to sustaining pulse measures the same inter- val, but is longer for patients who transiently lose their initial perfusing rhythm. Successful resuscitation (SR) was defined as the conveyance of a
176
AIRWAY, INTUBATE. HYPERVENTILATE WITH 100% O2
IV D5W
EPINEPHRINE 0.5 BG IV, 1.0 MG ET
CONTACT BASE PHYSICIAN
BASE PHYSICIAN WILL DETERMINE NEED FOR BICARBONATE ON AN INDIVIDUAL PATIENT BASIS
ALSO CONSIDER: FLUID CHALLENGE/MAST EPINEPHRINE EVERY 5 MINUTES ATROPINE IF BMD RATE IS SLOW
Fig. 1. PLAN A - Electromechanical dissociation
patient with a pulse and a rhythm to an emergency department. A save was defined as a hospital discharge of a patient. A medical chart review of success- fully resuscitated patients was undertaken to determine the primary cause of cardiac arrest. Data was analyzed by linear regression analysis, where appro priate. P-values were considered significant if less than 0.05.
I RESULTS
Five hundred and three available patients presented to this prehospital care system in the initial arrest rhythm of EMD. Demographic data was analyzed, while not comparing or contrasting it to other presenting arrest rhythms (Table Il. Specific historical factors and cardiac medications are presented in Table II.
TABLE I
DEMOGRAPHICS
Parameter iV (%I or mean
Successful resuscitations 981503 (19.5%) Saves 221603 (4.4Oh) Witnessed arrests 3021503 @O.O”~ 1 Bystander CPR 3271503 (66.0% 1 Male sex ratio 2871603 (57.0%) Mean age 69.81 * 13.71 Mean time response (min) 6.06 f 3.23 Cardiac medication 2181503 (43.34%) Cardiac history 2301603 (45.73%)
176
TABLE II
CARDIAC HISTORY, MEDICATION AND CHRONIC CONDITIONS
Parameter N(%)
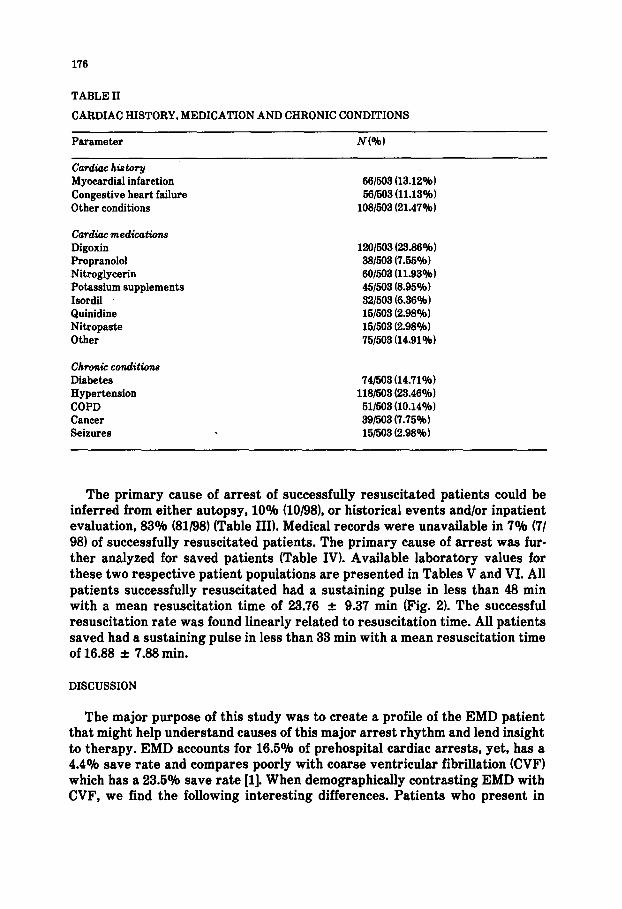
Car&kc his tosy Myocardial infarction Congestive heart failure Other conditions
Cardiuc medications Digoxin Propranolol Nitroglycerin Potassium supplements Isordil Quinidine Nitropaste Other
Chronic conditions
Diabetes Hypertension COPD Cancer Seizures .
66/563 (13.12%) 561593 (11.13%)
103/563 (21.47%)
1201563 (23.86%) 381593 (7.55%) 691563 (11.93%) 451593 (8.95%) 321503 (6.36%) 151603 (2.98%) 151503 (2.98%) 751503 (14.91%)
741563 (14.71%) lUl563 (23.46%)
61/563 (10.14%) 391563 (7.75%) 151563 (2.98%)
The primary cause of arrest of successfully resuscitated patients could be inferred from either autopsy, 10% (101981, or historical events and/or inpatient evaluation, 83% (81/98) (Table III). Medical records were unavailable in 7% (7/ 981 of successfully resuscitated patients. The primary cause of arrest was fur- ther analyzed for saved patients (Table IV). Available laboratory values for these two respective patient populations are presented in Tables V and VI. All patients successfully resuscitated had a sustaining pulse in less than 48 min with a mean resuscitation .time of 23.76 f 9.37 min (Fig. 21. The successful resuscitation rate was found linearly related to resuscitation time. All patients saved had a sustaining pulse in less than 33 min with a mean resuscitation time of 16.88 f 7.88 min.
DISCUSSION
The major purpose of this study was to create a profile of the EMD patient that might help understand causes of this major arrest rhythm and lend insight to therapy. EMD accounts for 16.5% of prehospital cardiac arrests, yet, has a 4.4% save rate and compares poorly with coarse ventricular fibrillation (CVF) which has a 23.5% save rate [l]. When demographically contrasting EMD with CVF, we find the following interesting differences. Patients who present in
177
TABLE III
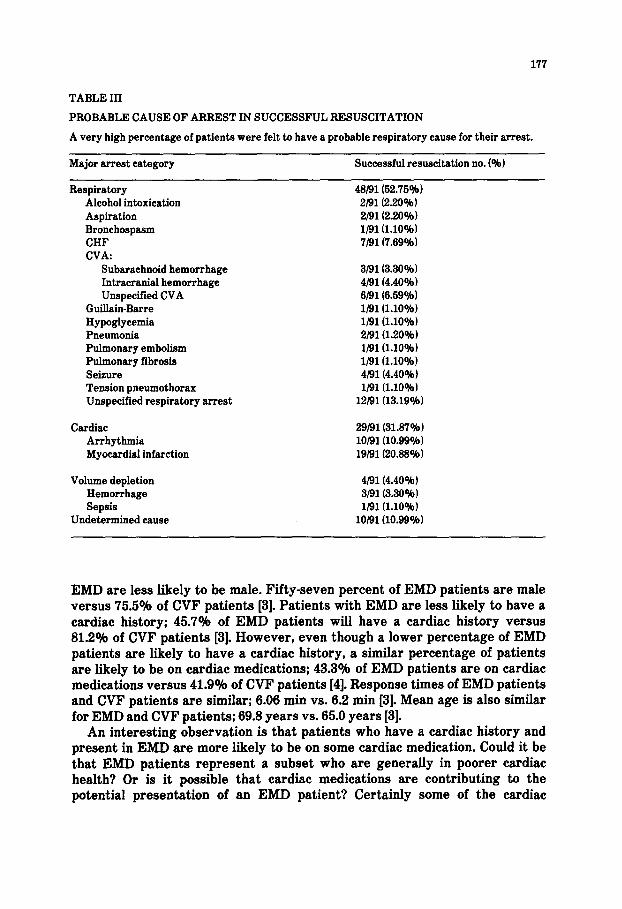
PROBABLE CAUSE OF ARREST IN SUCCESSFUL RESUSCITATION
A very high percentage of patients were felt to have a probable respiratory cause for their arrest.
Major arrest category Successful resuscitation no. (%I
Respiratory Alcohol intoxication Aspiration Bronchospasm CHF CVA:
Subarachnoid hemorrhage Intracranial hemorrhage Unspecified CVA
Guiilain-Barre Hypoglycemia Pneumonia Pulmonary embolism Pulmonary fibrosis Seizure Tension pneumothorax Unspecified respiratory arrest
48/91(52.‘75%) 2/91(2.20%) 2/91(2.20%) l/91 (1.10%) 7/91(7.69%)
3/91(3.36%) 4/91(4.40%) 6/91(6.59%) l/91 (1.10%) l/91 (1.10%) 21910.20%) l/91 (1.10%) l/91(1.10%) 4/91(4.40%) lj91(1.10%)
12/91(13.19%)
Cardiac Arrhythmia Myocardial infarction
29/91(31.87%) 10/91(10.99%) 19/91(20.88%)
Volume depletion Hemorrhage Sepsis
Undetermined cause
4/91(4.40%) 3/91(3.30%) l/91(1.10%)
10/91(10.99%)
EMD are less likely to be male. Fifty-seven percent of EMD patients are male versus 75.5O,41 of CVF patients [3]. Patients with EMD are less likely to have a cardiac history; 45.7% of EMD patients will have a cardiac history versus 81.2% of CVF patients [3]. However, even though a lower percentage of EMD patients are likely to have a cardiac history, a similar percentage of patients are likely to be on cardiac medications; 43.3% of EMD patients are on cardiac medications versus 41.9% of CVF patients [4]. Response times of EMD patients and CVF patients are similar; 6.06 min vs. 6.2 min [3]. Mean age is also similar for EMD and CVF patients; 69.8 years vs. 65.0 years [3].
An interesting observation is that patients who have a cardiac history and present in EMD are more likely to be on some cardiac medication. Could it be that EMD patients represent a subset who are generally in poorer cardiac health? Or is it possible that cardiac medications are contributing to the potential presentation of an EMD patient? Certainly some of the cardiac
178
TABLE IV
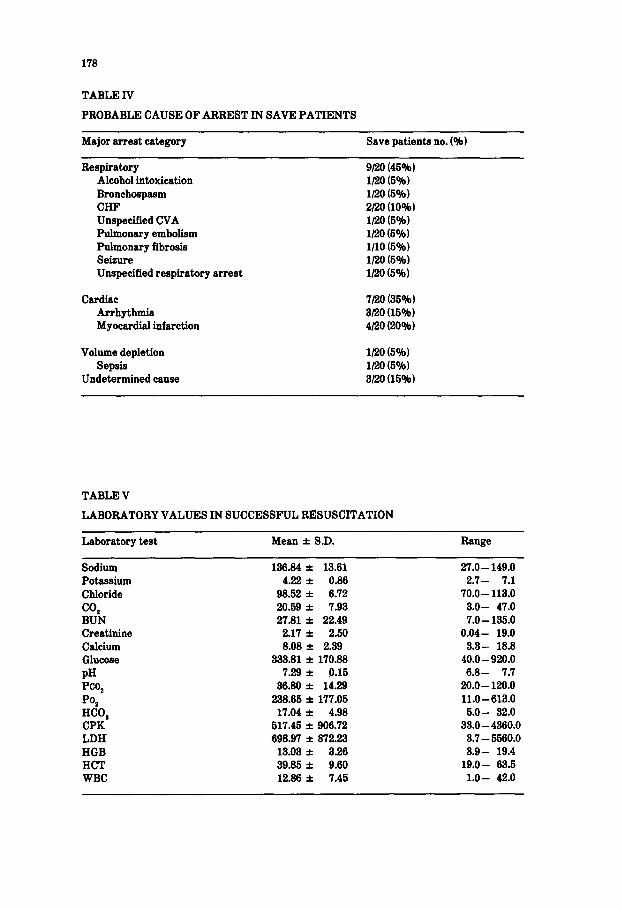
PROBABLE CAUSE OF ARREST IN SAVE PATIENTS
Major arrest category Save patients no. (%I
Respiratory Alcohol intoxication Bronchospasm CHF Unspecified CVA Pulmonary embolism Pulmonary fibrosis Seizure Unspecified respiratory arrest
Cardiac Arrhythmia Myocardiai infarction
Volume depletion Sepsis
Undetermined cause
9no (45%) 1120 (5%) 1120 (5%) 2120 (10%) l/20 (5%) l/20 (5%) 1110 (5%) 1120 (5%) l/20 (5%)
7120 (35%) 3/20 (15%) 4120 (20%)
l/20 (5%) l/20 (5%) 3120 (15%)
TABLE V
LABORATORY VALUES IN SUCCESSFUL RESUSCITATION
Laboratory test Mean f SD. Range
Sodium 136.84 f 13.61 27.0 - 149.0 Potassium 4.22 f 0.86 2.7- 7.1 Chloride 98.52 f 6.72 70.0 - 113.0 CO* 20.59 f 7.93 3.0- 47.0 BUN 27.81 f 22.49 7.0- 135.0 Creatinine 2.17 f 2.50 0.04- 19.0 Calcium 8.08 f 2.39 3.3- 18.8 Glucose 333.81 f 170.88 40.0 -920.0 PH 7.29 f 9.15 6.8- 7.7 Pco, 36.80 * 14.29 20.0- 120.0 PO* 238.65 f 177.05 11.0-613.0 HCO, 17.04 f 4.98 5.0- 32.0 CPK 517.46 f 906.72 33.0 - 4360.0 LDH 698.97 k 87223 3.7 - 5560.0 HGB 13.03 f 3.26 3.9- 19.4 HCT 39.85 f 9.60 19.0- 63.5 WBC 12.86 f 7.45 l.O- 42.0
179
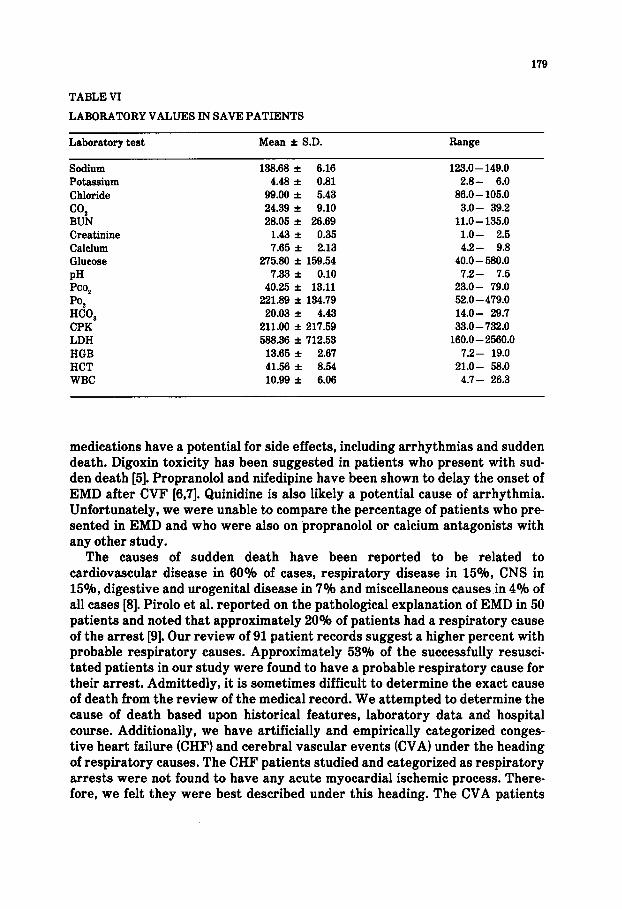
TABLE VI
LABORATORY VALUES IN SAVE PATIENTS
Laboratory test Mean f S.D. Range
Potassium Chloride
CO* BUN Creatinine Calcium Glucose PH Pco,
PO, HCO, CPK LDH HGB HCT WBC
138.68 f 6.16 4.48 f 0.81
99.00 f 5.43 24.39 + 9.10 28.05 f 26.69
1.43 f 0.35 7.65 f 2.13
275.80 f 159.54 7.33 * 0.10
40.25 f 13.11 221.89 f 134.79
20.03 f 4.43 211.00 + 217.59 588.36 f 712.53
13.65 f 2.67 41.56 f 8.54 10.99 f 6.06
123.0 - 149.0 2.8- 6.0
86.0 - 105.0 3.0- 39.2
11.0-135.0 l.O- 2.5 4.2- 9.8
40.0 - 580.0 7.2- 7.5
23.0- 79.0 52.0- 479.0 14.0- 29.7 33.0 - 732.0
160.0 - 2560.0 7.2- 19.0
21.0- 58.0 4.7- 26.3
medications have a potential for side effects, including arrhythmias and sudden death. Digoxin toxicity has been suggested in patients who present with sud- den death [5]. Propranolol and nifedipine have been shown to delay the onset of EMD after CVF [6,7]. Quinidine is also likely a potential cause of arrhythmia. Unfortunately, we were unable to compare the percentage of patients who pre- sented in EMD and who were also on propranolol or calcium antagonists with any other study.
The causes of sudden death have been reported to be related to cardiovascular disease in 60% of cases, respiratory disease in 15%, CNS in 15% digestive and urogenital disease in 7% and miscellaneous causes in 4% of all cases [8]. Pirolo et al. reported on the pathological explanation of EMD in 50 patients and noted that approximately 20% of patients had a respiratory cause of the arrest [9]. Our review of 91 patient records suggest a higher percent with probable respiratory causes. Approximately 53% of the successfully resusci- tated patients in our study were found to have a probable respiratory cause for their arrest. Admittedly, it is sometimes difficult to determine the exact cause of death from the review of the medical record. We attempted to determine the cause of death based upon historical features, laboratory data and hospital course. Additionally, we have artificially and empirically categorized conges- tive heart failure (CHF) and cerebral vascular events (CVA) under the heading of respiratory causes. The CHF patients studied and categorized as respiratory arrests were not found to have any acute myocardial ischemic process. There- fore, we felt they were best described under this heading. The CVA patients
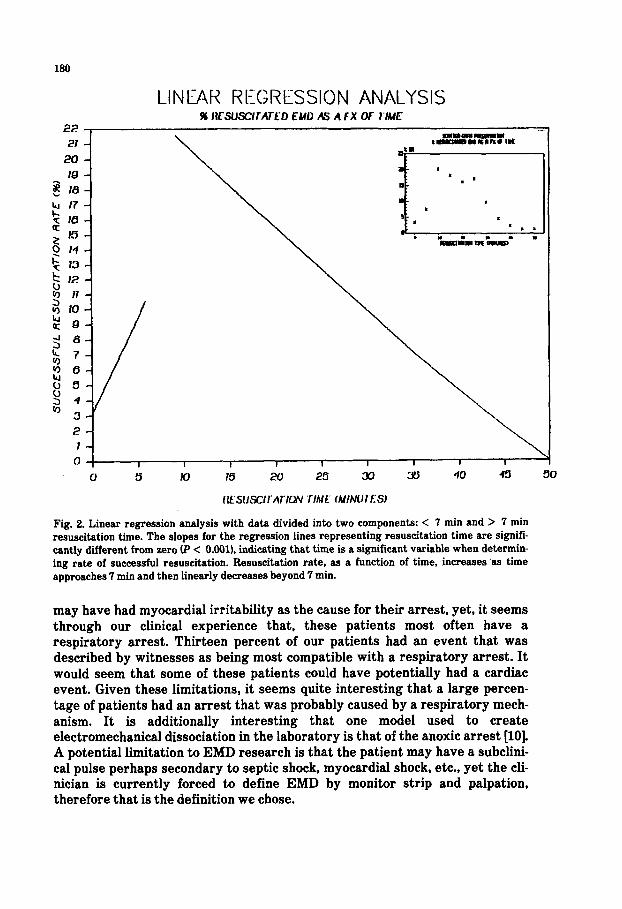
Fig. 2. Linear regression analysis with data divided into two components: < 7 min and > 7 min resuscitation time. The slopes for the regression lines representing resuscitation time are signifi- cantly different from zero P < O.OOl), indicating that time is a significant variable when determin- ing rate of successful resuscitation. Resuscitation rate, as a function of time, increases ‘as time approaches 7 min and then linearly decreases beyond 7 min.
may have had myocardial irritability as the cause for their arrest, yet, it seems through our clinical experience that, these patients most often have a respiratory arrest. Thirteen percent of our patients had an event that was described by witnesses as being most compatible with a respiratory arrest. It would seem that some of these patients could have potentially had a cardiac event. Given these limitations, it seems quite interesting that a large percen- tage of patients had an arrest that was probably caused by a respiratory mech- anism. It is additionally interesting that one model used to create electromechanical dissociation in the laboratory is that of the anoxic arrest [lo]. A potential limitation to EMD research is that the patient may have a subclini- cal pulse perhaps secondary to septic shock, myocardial shock, etc., yet the cli- nician is currently forced to define EMD by monitor strip and palpation, therefore that is the definition we chose.
181
We have previously reported that when EMD is independently analyzed in patients receiving bystander/first responder CPR compared to delayed CPR, the save rate is improved with bystander/first responder CPR [l]. This finding is in contrast to the lack of difference in save rate between those subgroups of CVF and/or asystole noted in the same study. Is it possible that this selective responsiveness of EMD to CPR represents the ventilation compound of CPR? Pirolo et al. [9] reported that 44% of EMD patients had myocardial ischemia, 6% had systemic shock secondary to sepsis, 20% had pulmonary vascular com- promise (pulmonary embolism and tension pneumothorax), and 12% had unde- termined causes. Our study showed a lower percentage of patients with documented myocardial ischemialinfarction (210~1, and an approximately equal percentage of patients with volume depletion (4.4%) and undetermined causes (11%). A major difference between our study and that of Pirolo’s was that we were able to determine probable cause of arrest in only successfully resusci- tated patients, whereas, his data represents all patients who were autopsied. It is possible that the patients who were not successfully resuscitated represent a different subset with a different percentage of causes.
Pionkowski et al. [3] reported a least squares regression analysis of patients who were resuscitated from ventricular fibrillation. He demonstrated a linear drop off in the survival rate, as a function of resuscitation time, that reached a change in slope at approximately 20 min. Additionally, he noted some saves after as much as 60 min prehospital resuscitation time [3]. We attempted a simi- lar linear regression analysis and noted an increase in the successful resuscita- tion rates over time up to 7 min and then a linear reduction in resuscitation rate from 10 to 50 min. It would appear from this data that patients in EMD must be optimally resuscitated for a minimum of ten minutes prior to discontinuing efforts to achieve optimal resuscitation rates. Could this be because of a need to replace an oxygen debt? Beyond 50 min of resuscitation time there is little like- lihood of successful resuscitation. Additionally, it appears that all patients who were saved had a sustaining pulse in less than 33 min of resuscitation time. Given that this study represents a 6-year time period and 500 plus resuscitation attempts, we believe the clinician or the EMS medical director can feel confi- dent in discontinuing resuscitation efforts after 35- 50 min of total ACLS resuscitation efforts, providing the airway and vascular access have been secured.
CONCLUSION
EMD patients are less likely to be male, less likely to have a cardiac history and are more likely to be on cardiac medications. A high percentage of resusci- tated patients are found to have a probable respiratory cause for the arrest. Patients are rarely resuscitated after 35 min of ACLS and survival to hospital discharge was not found in our series of greater than 500 patients after 35 min of prehospital ACLS.

182
ACKNOWLEDGEMENTS
We would like to thank Charles Frodermann, Data Consults, Inc., for his assistance and support as our Revelations Systems Consultant.
REFERENCES
1
8
9
10
H. Stueven, P. Troiano. B. Thompson. JR. Mateer, E.H. Kastenson, D. Tonsfeldt. K. Hargar- ten, It. Kowalski, C. Aprahamian and J. Darin., Bystanderlfirst responder CPR: Ten years experience in a paramedic system, Ann. Emerg. Med., 16 (1986) 707- 710. American Heart Association, Textbook of Advanced Cardiac Life Support, American Heart Association (National Center), DaIlas. Texas, 1987. R.S. Pionkowski, B.M. Thompson, H.W. Gruchow, C. Aprahamian and J. Darin. Resuscitation time in ventricular fibrillation - a prognostic indicator, Ann. Emerg. Med., 12 (1988) 733-788. R. Kowalski, B.M. Thompson, L. Horwitx, H. Stueven, C. Aprahamian and J. Darin, Bystander CPR in prehospitai coarse ventricular fibrillation, Ann. Emerg. Med., 13 (1984) 1016- 1020. D.S. OIson, H.A. Stueven, J.L. Teresi, B.M. Thompson and A.S. Yee. Digoxin levels in prehospi- tai sudden-death syndrome, J. CIin. Pharmacol., 27 (1987) 184- 186. D.R. Kostreva, A. Castaner and J.P. Kampine, Role of autonomies in the initiation of electrome- chanical dissociation, Am. J. Physiol.. 2410981) R213-R221. G. Martin, J. Cosin, M. Such, A. Hernandez and P. Llamas, Relation between power spectrum time course during ventricular fibrillation and electromechanical dissociation. Effects of coro- nary perfusion and nifedipine. Eur. Heart J., 7 (1986) 660 - 669. KM McIntyre, A.J. Lewis, E.B.J. Winslow, M.R. Parker and W. Kaye. Sudden Cardiac Death. In: Textbook of Advanced Life Support, American Heart Association (National Center). Dailas, Texas, 1981, pp. II-1 - 11-10. J.S. Pirolo. G.M. Hutchins, and G.W. Moore, Electromechanicai dissociation: Pathologic expian- ations in 60 patients, Hum. Pathol., 16 (1985) 485- 487. J.S. Redding, R.R. Haynes and J.D. Thomas, Drug therapy in resuscitation from electrome chanical dissociation, Crit. Care Med., ll(1988) 681-684.





























