Embed Size (px)
Citation preview

Review
10.1517/14728214.13.1.145 © 2008 Informa UK Ltd ISSN 1472-8214 145
Oncologic, Endocrine & Metabolic
Emerging drugs for non-alcoholic fatty liver disease Alessandro Federico † , Marco Niosi , Camillo Del Vecchio Blanco & Carmela Loguercio †2nd University of Naples, Inter-University Research Center on Foods, Nutrition & Gastrointestinal Tract (CIRANAD), Gastroenterology Unit, Italy
Background : Non-alcoholic fatty liver disease (NAFLD) is a condition of emerging relevance that includes different forms of chronic liver damage, from a simple fatty infiltration (steatosis) of hepatocytes to steatohepatitis (NASH) with fibrosis. This last form may evolve to cirrhosis and hepato-cellular carcinoma. Objective : To discuss therapeutic management of NAFLD. Theoretically, only patients with non-alcoholic steatohepatitis (NASH) need to be treated, as only NASH may evolve to cirrhosis. Differentiation between steatosis and NASH currently requires a liver biopsy. Methods : We discuss different therapeutic approaches proposed in literature for patients with NAFLD. Results : The treatment of associated conditions leads to an improvement of NAFLD and NASH. No specific drug is actually present to treat liver steatosis or NASH. Conclusions : The treatment of NAFLD depends on the individual characteristics of each patient. Diet and physical exercise may be considered a basal universal approach. Future research will discover possible specific liver drugs.
Keywords: anti-oxidants , drugs , non-alcoholic fatty liver.
Expert Opin. Emerging Drugs (2008) 13(1):145-158
1. Background
Non-alcoholic fatty liver disease (NAFLD) is a clinical condition that includes various forms of chronic liver damage, from a simple fatty infiltration of the hepatocytes (steatosis) to steatohepatitis (NASH) that may progress to cirrhosis and hepatocellular carcinoma [1,2] . The clinical implications of NAFLD and NASH concern primarily the common occurrence of the condition in the general population as well as its progressive potential. In fact, NAFLD occurs in 14 – 30% of the general population, involving all age groups and ethnicities [3,4] , while the prevalence of NASH is about 3% [5] . Recent epidemiological studies in Italy have shown that the incidence of NAFLD is constantly increasing [6,7] . NASH has also been reported in children and is currently the most common hepatic disease among adolescents in North America [8] . The presence of fatty liver also negatively affects the course of other chronic liver diseases, such as those related to hepatitis C virus (HCV) infection and alcohol abuse [7] . A large number of reports in the literature clearly indicate that NAFLD is strongly associated with the metabolic syndrome and that obesity and diabetes are considered the two major risk factors for the development of NAFLD [9] . Patients with the metabolic syndrome and NAFLD present a higher risk of mortality from cardiovascular diseases compared with those without fatty liver [10,11] and NAFLD is a predictor factor for the onset of type 2 diabetes [12] . Therefore, the epidemiology of NAFLD and its potential evolution are both factors suggesting that treatment is mandatory.
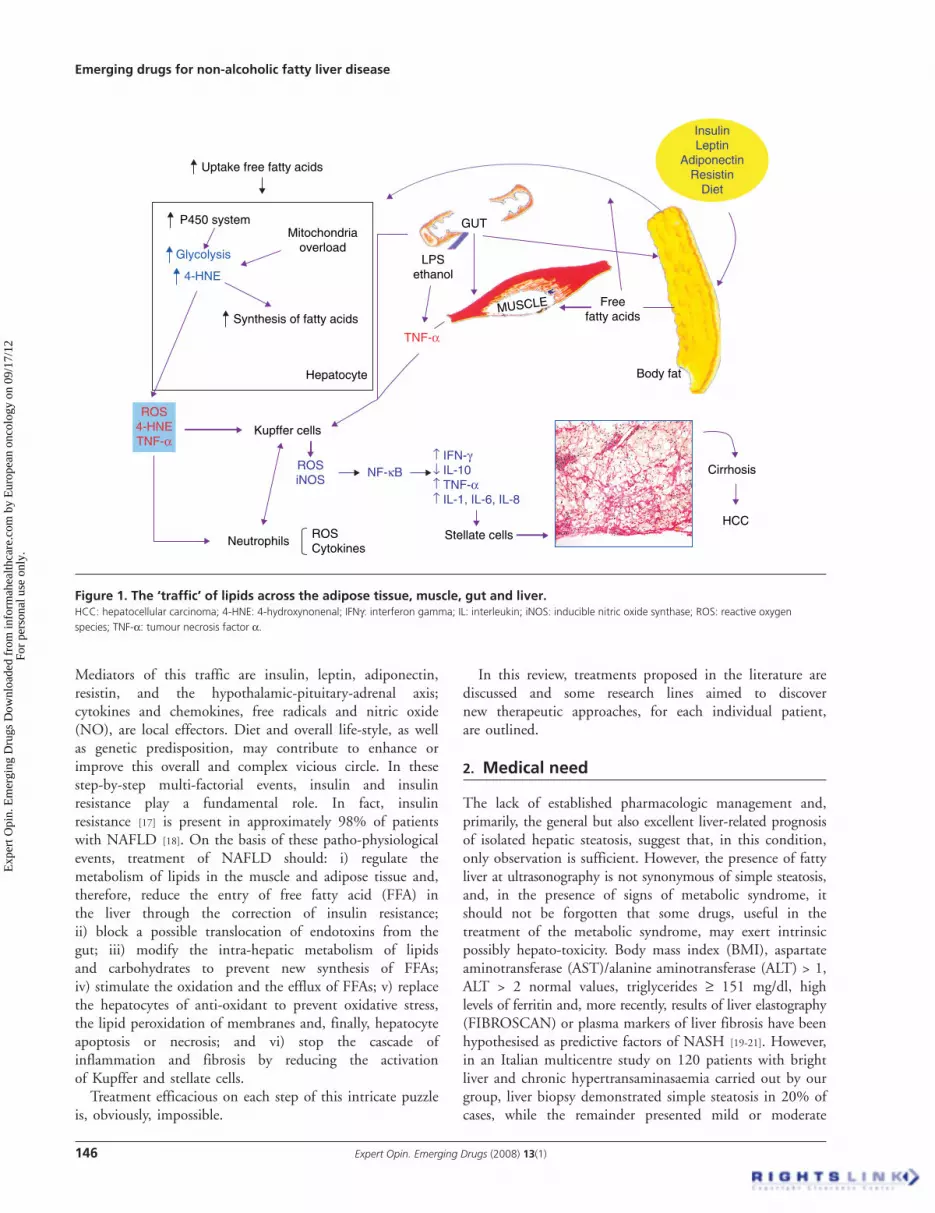
Fatty accumulation in the liver may be defined as a consequence of impaired ‘ traffic ’ of lipids in the adipose tissue, muscle, gut and liver ( Figure 1 ) [8,13-16] .
1. Background
2. Medical need
3. Existing treatment
4. Therapeutic class review
5. Current research goals and
scientifi c rationale
6. Competitive environment
7. Expert opinion and conclusions
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.
Emerging drugs for non-alcoholic fatty liver disease
146 Expert Opin. Emerging Drugs (2008) 13(1)
Mediators of this traffic are insulin, leptin, adiponectin, resistin, and the hypothalamic-pituitary-adrenal axis; cytokines and chemokines, free radicals and nitric oxide (NO), are local effectors. Diet and overall life-style, as well as genetic predisposition, may contribute to enhance or improve this overall and complex vicious circle. In these step-by-step multi-factorial events, insulin and insulin resistance play a fundamental role. In fact, insulin resistance [17] is present in approximately 98% of patients with NAFLD [18] . On the basis of these patho-physiological events, treatment of NAFLD should: i) regulate the metabolism of lipids in the muscle and adipose tissue and, therefore, reduce the entry of free fatty acid (FFA) in the liver through the correction of insulin resistance; ii) block a possible translocation of endotoxins from the gut; iii) modify the intra-hepatic metabolism of lipids and carbohydrates to prevent new synthesis of FFAs; iv) stimulate the oxidation and the efflux of FFAs; v) replace the hepatocytes of anti-oxidant to prevent oxidative stress, the lipid peroxidation of membranes and, finally, hepatocyte apoptosis or necrosis; and vi) stop the cascade of inflammation and fibrosis by reducing the activation of Kupffer and stellate cells.
Treatment efficacious on each step of this intricate puzzle is, obviously, impossible.
In this review, treatments proposed in the literature are discussed and some research lines aimed to discover new therapeutic approaches, for each individual patient, are outlined.
2. Medical need
The lack of established pharmacologic management and, primarily, the general but also excellent liver-related prognosis of isolated hepatic steatosis, suggest that, in this condition, only observation is sufficient. However, the presence of fatty liver at ultrasonography is not synonymous of simple steatosis, and, in the presence of signs of metabolic syndrome, it should not be forgotten that some drugs, useful in the treatment of the metabolic syndrome, may exert intrinsic possibly hepato-toxicity. Body mass index (BMI), aspartate aminotransferase (AST)/alanine aminotransferase (ALT) > 1, ALT > 2 normal values, triglycerides ≥ 151 mg/dl, high levels of ferritin and, more recently, results of liver elastography (FIBROSCAN) or plasma markers of liver fibrosis have been hypothesised as predictive factors of NASH [19-21] . However, in an Italian multicentre study on 120 patients with bright liver and chronic hypertransaminasaemia carried out by our group, liver biopsy demonstrated simple steatosis in 20% of cases, while the remainder presented mild or moderate
Figure 1 . The ‘ traffi c’ of lipids across the adipose tissue, muscle, gut and liver. HCC: hepatocellular carcinoma; 4-HNE: 4-hydroxynonenal; IFN γ : interferon gamma; IL: interleukin; iNOS: inducible nitric oxide synthase; ROS: reactive oxygen species; TNF- α : tumour necrosis factor α .
Body fat
Freefatty acids
MUSCLE
ROS4-HNETNF-α
LPSethanol
Kupffer cells
Neutrophils Stellate cells
InsulinLeptin
AdiponectinResistin
Diet
TNF-α
ROSiNOS
NF-κB
ROSCytokines
GUT
Cirrhosis
HCC
Uptake free fatty acids
4-HNE
P450 systemMitochondria
overload
Hepatocyte
↑ IFN-γ↓ IL-10↑ TNF-α↑ IL-1, IL-6, IL-8
Synthesis of fatty acids
Glycolysis
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.

Federico, Niosi, Blanco & Loguercio
Expert Opin. Emerging Drugs (2008) 13(1) 147
NASH and, in seven cases, unexpected cirrhosis was found [22] . Therefore, in the absence of a liver biopsy, it is impossible to reliably the liver pattern of fatty infiltration,
Accordingly, fatty liver should be treated because:
1. steatosis is not always a benign condition; in fact, it may evolve to steatohepatitis, and even to cirrhosis and hepatocellular carcinoma;
2. steatosis negatively affects the evolution of other types of chronic liver diseases, such as those related to chronic HCV infection or alcohol abuse;
3. a large number of patients with steatosis develop metabolic problems [23] ;
4. even if not clearly demonstrated, it is possible, on the basis of recent data in the literature, that steatosis could lead to an increase in mortality from cardiovascular diseases in patients with metabolic syndrome [10] ;
5. there is a possible association of steatosis with increased overall mortality and risk of cancer [24] .
3. Existing treatment
The main procedures suggested in the treatment of NAFLD are shown in Table 1 .
4. Therapeutic class review
4.1 Weight loss NAFLD is frequently, even if not always, associated with overweight or obesity. Overweight and obesity lead to the occurrence of other metabolic disorders, such as diabetes and or dyslipidaemia that are, in turn, predictive factors of NAFLD [12,25] . Even if, in the pathophysiology of NAFLD, greater importance is attached to visceral fat than to BMI, weight loss is usually recommended asfirst-line management for these patients [26] .
Weight loss could be achieved by diet restriction, physical exercise, anti-obesity drugs and/or surgery. The choice of modalities to obtain a significant weight loss is related to the age and general clinical conditions of each patient, to compliance, as well as to the entity of overweight.
4.1.1 Diet and physical exercise The American Gastroenterological Association recommends a target of 10% of baseline weight as an initial goal of weight loss if BMI exceeds 25 kg/m 2 and most trials have been carried out using a diet with an energy restriction and energy intake composed of 40 – 50% carbohydrates, 15 – 20% protein, and 25 – 40% predominantly unsaturated fats [27-29] .
Rapid weight loss, due to a very low energy diet (< 500 kcal day), has been associated with exacerbation of steatohepatitis in obese patients [30-32] and, in experimental animals, it has been demonstrated that excessive food deprivation is not tolerated by the mitochondria of fatty liver [33,34] .
Huang et al. [27] evaluated the histological features of steatohepatitis in patients submitted to biopsy before and after dieting, and found that, after 1 year of intense dieting, 9 out of 15 NASH patients who showed an improvement in liver histology, also showed an improvement in body weight (BW).
The optimal composition of diet for NAFLD patients is not yet known. Patients with NAFLD seem more likely to have a diet high in saturated fats and cholesterol and low in polyunsaturated fat, fibre and vitamins C and E [35] . Mono and poly-unsaturated fats may potentially improve insulin resistance and may be beneficial in improving hepatic steatosis [36] .
NAFLD patients tend to consume a large quantity of carbohydrates and vitamin A and, in agreement with others [27,35,37] , the intake of polyunsaturated fat is inversely related to the entity of liver steatosis. On the contrary, neither the total calories, nor the intake of total lipids are correlated with the entity of liver damage. These data are in keeping with those obtained in experimental animals, in which a diet poor in choline-methionine or rich in carbohydrates is used to induce fatty liver and NASH [38] . At present, foods suggested as damaging agents for NAFLD are fructose and saturated fatty acids, and asprotective omega-3, soya and coffee [39] . More recently, it has been documented that cysteine-enriched proteins improve oxidative stress and insulin resistance in NASH [40] .
Weight loss should be achieved by combining diet with constant physical exercise that should be selected on the basis of overweight, compliance and personal possibilities. It has been suggested that aerobic training would be the most effective in improving NAFLD.
Modifications in life-style (low-fat diet and exercise) are associated with an improvement in liver enzymes, inter-leukin (IL)-6, and hyaluronic acid plasma levels in patients with NASH [41] .
4.1.2 Anti-obesity drugs Orlistat is a lipase inhibitor that reduces fat absorption and promotes weight loss. A small pilot study showed an improvement in aminotransferases with a mean 10 kg weight loss after 6 months of orlistat [42] . A non-significant reduction in steatosis was seen.
Anorectic drugs, such as fenfluramine and phentermine, in addition to dietary and behavioural modifications were reported to improve aminotransferases levels in 11 obese patients [43] , but these drugs may induce cardiovascular and lung toxicity and they have been withdrawn from the market.
Sibutramine is widely used for the treatment of obesity and overweight patients with other cardiovascular risk factors, and is more efficacious than placebo in reducing BW, together with behavioural modifications, physical activity, and low calorie intake [44-46] .
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.

Emerging drugs for non-alcoholic fatty liver disease
148 Expert Opin. Emerging Drugs (2008) 13(1)
More recently, sibutramine has been associated with weight loss and improvement in aminotransferases over 6 months in 13 patients [47] . Histology was not assessed; however, regression of hepatic steatosis as determined by ultrasound, occurred in 11 patients.
4.1.3 Surgery Weight loss following placement of an adjustable gastric band leads to an improvement in lobular steatosis, liver inflammation and fibrosis [48-51] . Gastric bypass/banding appears to be beneficial for histological liver damage, while results for jejuno-ileal bypass are uncertain [52] : in fact, malabsorption and isolation of a significant portion of the gut may cause progressive liver damage. However, bariatric surgery is currently reserved, only for patients with BMI > 35 – 40, and, in several cases, severe NASH occurred following the drastic weight loss induced by this procedure [53] .
The main studies performed on weight loss and NAFLD are outlined in Table 2 . Even if in the majority of cases, trials are non-randomised, of short duration with limited numbers of participants, [28-30,53-57] , weight loss and modifi-cations of life-style should be encouraged because other than on NAFLD, they prevent metabolic syndrome and its consequences.
The following approach should be adopted:
1. Patient with overweight (BMI > 25): physical exercise + balanced diet for 1 year. In the absence of improvement on BW and liver damage tests, the addiction of anti-obesity drug should be performed
2. Patient with obesity (BMI > 30): diet + anti-obesity drugs 3. Patient with BMI > 40, if possible, surgery
4.2 Insulin sensitising drugs It is well established that insulin resistance is a common feature and a predictive factor of NASH in patients with NAFLD [58] .
In animals and man with fatty liver, metformin was able to improve hepatic steatosis and ALT levels [59,60] . However,
in a pilot trial, no significant differences were observed in ALT levels after 12 months ’ treatment with metformin, despite an initial improvement of liver enzymes at 3 months [61] . In 10 patients, in this trial, a liver biopsy was collected at the end of treatment; an improvement of steatosis was seen in one third of the patients, of inflammation in 20%, and of fibrosis in 10%. In a large study from Italy, the effect of metformin was compared to that of diet and vitamin E in NAFLD non-diabetic patients [62] . Metformin was more effective than vitamin E and diet in normalising ALT levels. Similar data were obtained for histological findings; in fact, in 17 of the 55 patients, assigned to metformin therapy, a significant improvement was found in steatosis, inflammation, and fibrosis, compared with baseline.
The thiozoladinediones, through the action on the peroxisome proliferators activated receptor γ (PPAR), improved insulin sensitivity and the redistribution of adipose tissue [63] . However, with thiozoladinediones, BW increases, because these drugs reduce the visceral, but enhance the subcutaneous adiposity. In animal models, PPAR γ agonists also have a protective effect against liver fibrosis by inhibiting the activation of hepatic stellate cells [64,65] . Despite promising results in a pilot trial [66] , troglitazone was removed from the market because its use was associated with liver toxicity [67] . The second generation of ‘ glitazones’ , rosiglitazone and pioglitazone, are structur-ally different from troglitazone and appear to be safer [68] . Two well designed pilot trials using pioglitazone and rosiglitazone showed an improvement in ALT, hepatic steatosis, and features of hepatic inflammation and fibrosis in patients with NAFLD [69,70] . Recently, Rosiglitazone was associated with a significant increase in the risk of myocardial infarction and of death from cardiovascular causes [71] . A randomised trial of 20 non-diabetic patients with NASH compared the effects of pioglitazone plus vitamin E vs. those of vitamin E alone: pioglitazone was more effective than vitamin E in improving hepatic inflammation [72] , even if no significant differences were observed for
Table 1 . Main treatments proposed for patients with NAFLD.
Reduction of weight loss
Insulin-sensitising agents Lipid-lowering drugs Cytoprotective agents
Other drugs
Diet Metformin Clofi brate UDCA Probiotics
Physical exercise Pioglitazone Gemfi brozil Anti-oxidants Anti-TNF- α monoclonal antibodies
Surgery Bezafi brate Adiponectin
Anti-obesity drugs Atorvastatin Anti-hypertensive drugs
Probucol Pentoxifylline
Rosurvastatin Iron depletion
UDCA: Ursodeoxycholic acid.
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.

Federico, Niosi, Blanco & Loguercio
Expert Opin. Emerging Drugs (2008) 13(1) 149
ALT levels, steatosis and fibrosis stage between the two groups.
In a recent study, Belfort et al. [73] evaluated the effect of a hypocaloric diet plus pioglitazone or placebo on liver damage in patients with type 2 diabetes and obesity. Diet plus pioglitazone improved glycaemic control and glucose tolerance, normalised liver aminotransferase levels, decreased hepatic fat content, increased hepatic insulin sensitivity, improved ballooning necrosis and inflammation. These effects were statistically significant when compared with those obtained when treating patients with diet + placebo. The reduction of fibrosis, on the contrary, was similar in both groups. However, although obesity and diabetes are frequently associated with NASH, only one-third of patients with NASH have diabetes; in the placebo group, there is a slight reduction in BW; it is unclear whether the beneficial effect of pioglitazone occurs by way of an improvement in insulin sensitivity or through a direct anti-inflammatory effect of the drug on the liver, and, finally, in animals, the effect on the liver of pioglitazone occurs only in the presence of diabetes and obesity [70,72,73] . The main studies performed with antidiabetic/insulin-sensitising agents in patients with NASH are outlined in Table 3 .
In our opinion, insulin resistance should be corrected in patients with NAFLD and insulin resistance. However, the correction of insulin resistance does not necessarily indicate correction of liver damage, and in agreement with the Cochrane group [74] , we conclude that, at the present, we are unable to either support or refute the use of insulin-sensitising drugs in patients with NAFLD. The choice should be related to each individual patient, on the basis of general clinical and metabolic characteristics.
4.3 Lipid-lowering drugs Patients treated with clofibrate, compared to patients treated with ursodeoxycholic acid (UDCA) [75] , showed no significant improvement in clinical, biochemical and histological parameters of liver damage. Treatment with gemfibrozil [76] induced an improvement in serum levels of markers of liver damage, but not in liver histology. Atorvastatin [77] , administered for 6 months, leads to an improvement of BMI, serum aminotransferase levels,but not of histological parameters in 27 patients with biopsy-proven NASH. Pravastatin, given for 6 months, led to normalisation of liver enzymes and improved hepatic inflammation, in five patients with NASH [78] .
Probucol [79] significantly improved ALT and AST levels in patients; however, in that study liver histology was not evaluated. Ahmed recently proposed the use of rosuvastatin in the treatment of dyslipidaemia and NAFLD [80] , but not all NAFLD patients have dyslipidaemia.
Ekstedt [81] studied the effect of statins on hepatic histology in NAFLD patients; a significant reduction of steatosis was found and authors stressed the concept that statins may be prescribed in patients with NAFLD and elevated liver enzymes.
As dyslipidaemia is not always present and some of these drugs may have a liver toxicity, this class of drugs could be administered only in presence of a significant increase of triglycerides and/or cholesterol ( Table 4 ).
4.4 Cytoprotective agents 4.4.1 UDCA UDCA treatment improves liver enzymes and liver histology in patients with various hepato-biliary diseases [82] . However,
Table 2 . Main studies on the effect of weight loss in patients with NAFLD.
Treatment No. patients Duration (months ) Liver enzyme levels Histology Versus Ref.
Weight loss 14 6 Improved Not evaluated Baseline [28]
Weight loss 39 - Improved Not evaluated Baseline [54]
Weight loss 41 6 Improved Improved steatosis Baseline [30]
Weight loss 31 15 Improved Not evaluated - [55]
Weight loss + aerobic exercise
25 3 Improved Improved steatosis No treatment [29]
Weight loss + aerobic exercise
23 12 No change No change Baseline [27]
Weight loss + aerobic exercise
16 1.5 Improved Not evaluated - [41]
Orlistat 10 6 Improved Improved - [42]
Sibutramine 13 6 Improved Not evaluated Orlistat [47]
Weight loss (after surgery) 35 - Improved Improved steatosis - [50]
Weight loss (after surgery) 91 18 No change Improved steatosis Baseline [56]
Weight loss (after surgery) 69 27 Improved Improved steatosis Baseline [57]
Weight loss (after surgery) 36 26 Improved Improved steatosis Baseline [51]
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.

Emerging drugs for non-alcoholic fatty liver disease
150 Expert Opin. Emerging Drugs (2008) 13(1)
in a recent study [83] , it was clearly demonstrated that treatment with UDCA does not differ from that with placebo in patients with NASH.
4.4.2 Anti-oxidants The role of oxidative stress in the progression of NAFLD to NASH and cirrhosis is already well known [84-86] . Reactive oxygen and nitrogen species are normally generated during the oxidation of FFAs in mitochondria and particularly in cyto-chromes. When their production exceeds the capability of anti-oxidant systems, these high reactive species interact with lipids of membranes generating lipoperoxides and toxic aldehydes that may: i) induce apoptosis/necrosis of cells; ii) recruit neutrophils and macrophages; iii) enhance the production of inflammatory cytokines. These events trigger the inflammatory processes. Neutrophils per s è produce high amounts of radicals and these are also capable of activating nuclear transcrip-tional factors for cytokines in the hepatocytes in a vicious circle. Lipid peroxides, in turn, as well as apoptotic cells, are the main activators of stellate cells with a consequent induction of fibrosis [87] . On the basis of these pathogenic events, it is obvious to consider the use of anti-oxidants as a treatment of NAFLD and NASH. Anti-oxidants, in fact, should, in theory, act to reduce oxidative stress, to inhibit the inflammation and, finally, to block the fibrogenesis.
The cellular mechanisms in which free radicals and anti-oxidants are involved are very complex, and, in many cases, also useful for the overall function and metabolism of cells. Is the presence of ‘ oxidative stress ’ dangerous for cells, but it is impossible that a single anti-oxidant may reverse all cellular pathways related to an enhanced production of free radicals. In fact, anti-oxidant substances generally act in a complex cascade of events in which the oxidation/reduction reactions are mutually affected. In the absence of a clear spe-cific attack point by each anti-oxidant, the administration of generic substances with an anti-oxidant action, or of a generic mixture of various anti-oxidants, should produce any toxic effect on cells, because it is well known that more than one of these anti-oxidants also acts as pro-oxidant substances. This may explain, at least in part, the results of a recent meta-analysis that shows a lack of positive effects on health by various anti-oxidants [88] .
Despite these considerations, there are a series of clinical studies reporting positive effects of some anti-oxidant substances on NAFLD.
Betaine, a naturally occurring metabolite of choline, reduced biochemical and histological markers of liver disease, and particularly steatosis, in patients with NASH [89,90] .
In rats with NAFLD [91] , vitamins C and E prevented liver steatosis induced by a choline-deficient diet.
Table 3 . Main studies on the use of anti-diabetic/insulin-sensitising agents in patients with NAFLD.
Treatment No. patients Duration (months) Liver enzyme levels Histology Versus Ref.
Metformin 14 4 Improved Not evaluated Baseline [59]
Metformin 11 6 Improved Not evaluated Baseline [151]
Metformin 15 12 No change No change Baseline [61]
Metformin + weight loss 36 6 Improved Not improved Diet [152]
Metformin 110 12 Improved Improved Diet or vitamin E [62]
Metformin (children) 10 6 Improved Not evaluated Baseline [60]
Pioglitazone 18 11 Improved Improved Baseline [70]
Rosiglitazone 30 11 Improved Improved Baseline [69]
Vitamin E and Pioglitazone
20 6 Not reported Improved Vitamin E [72]
Diet and pioglitazone 55 6 Improved Improved Placebo [73]
Table 4 . Main studies on the use of anti-hyperlipidaemic agents in patients with NAFLD.
Treatment No. patients Duration (months) Liver enzyme levels Histology Versus Ref.
Clofi brate 16 12 Not improved Not improved Baseline [75]
Gemfi brozil 46 1 Improved Not improved Control group [76]
Atorvastatin 27 6 Improved Not improved UDCA [77]
Pravastatin 5 6 Improved Improved Baseline [78]
Probucol 30 6 Improved Not evaluated Placebo [79]
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.

Federico, Niosi, Blanco & Loguercio
Expert Opin. Emerging Drugs (2008) 13(1) 151
In man [15,41] , the addition of 800 IU/day of vitamin E to life-style modifications (low-fat diet and exercise) did not lead further improvement in the biochemical parameters of liver damage. On the contrary, a combination of α -tocopherol and vitamin C [92] in a prospective double-blind placebo-controlled trial induced a statistically significant improvement in the fibrosis score, but not in necroinflammatory activity. Hasegawa et al. [93] hypothesised that evaluation of plasma TGF- β 1, implicated in the development of liver fibrosis, represents a possible marker with which to discriminate between NASH (increased TGF- β 1 values) and NAFLD (normal TGF- β 1 values); α -tocopherol, given for 1 year, to patients with biopsy-proven NASH, inhibited the production of TGF -β 1 and also reduced liver steatosis, inflammation and fibrosis. In children [94] , serum amino-transferases decreased during vitamin E treatment. Very low plasma-free choline levels have been reported to be associated with liver steatosis and NASH in patients receiving long-term total parenteral nutrition [95] . Indeed, these patients, treated with lecithin supplementation, showed a significant and progressive decrease in hepatic fat.
In rats [96] with liver damage induced by the hepato- and pneumo-toxin monocrotaline, β -carotene protected the liver parenchyma from inflammation, steatosis and septal fibrosis.
N -acetylcysteine (NAC), a precursor of glutathione, inhibits DNA synthesis and the expression of platelet-derived growth factor (PDGF) receptor β and SM α -actin with a consequent decrease in the deposit of collagen fibres, in cultured rat hepatic stellate cells; in rats [97] , NAC prevents liver damage and steatosis and decreases serum AST and ALT levels [98] .
There are numerous reports concerning the in vitro and in vivo anti-oxidant and protective effects of silymarin on liver cells and cirrhotic patients [99,100] . Silybin, the main component of silymarin, acts both as an anti-oxidant and an antifibrotic agent [101,102] . In fact, it inhibits the production of TNF- α , IFN- γ , IL-2 and IL-4, reduces the expression of TIMP-1, up-regulates the mRNA expression of TGF- β , and suppresses the proliferation of hepatic stellate cells, while itincreases the expression of IL10, iNOS [103] , and matrix metalloproteinases [104] . It has recently been demonstrated that silybin inhibits the activation of IKK- β , which is a crucial mediator of insulin signalling induced by excessive exposure of tissue to FFAs [105] . In rats with experimentally induced NASH, a complex silybin + vitamin E + phospholipids reduces lipid peroxidation and liver damage, as well as BMI [106] . Similar data were obtained by us in a preliminary pilot study in man, in which this complex with silybin was able to reduce insulin resistance, plasma markers of liver fibrosis and liver damage tests [107] .
Even if the reported, or other possible, antioxidants with a large spectrum of action should be considered as an alternative or a complementary therapeutic strategy in patients with NAFLD, the Cochrane group, at the moment, concludes that there are insufficient data to either support or refute the use of anti-oxidants in these patients [74] .
The effects of cytoprotective agents in patients with NAFLD are outlined in Table 5 .
The use of well-known anti-oxidant substances or mixtures, on the basis of data in the literature, is suggested both in NAFLD and NASH patients, by considering the cost and the compliance, and by excluding substances not known or not experimentally tested.
4.5 Other drugs 4.5.1 Probiotics In animals and man with NAFLD, there is an increased endogenous production of ethanol and acetaldehyde from carbohydrate oxidation by intestinal bacteria [108,109] and gut-derived bacteria and/or endotoxins significantly affect the progression of alcoholic liver disease by activating Kupffer cells and cytokine production [110] . In animal models of alcoholic fatty liver disease, the manipulation of intestinal microflora with antibiotics and/or lactobacilli inhibits the development of steatohepatitis [111,112] . In an experimental animal model of NAFLD, treatment with VSL#3, which is a mixture of bifidobacteria , lactobacilli and S. thermophilus , improved liver histology, reduced hepatic total fatty acid content and decreased serum ALT levels [113] . In apreliminary study by our group, the same mixture improved plasma levels of ALT levels and of markers of lipid peroxidation [114] in patients with NAFLD.
4.5.2 Anti-TNF- a antibodies In animals with experimentally-induced NASH, treatment with anti-TNF- α antibody improved liver histology, reduced hepatic total fatty acid content and decreased ALT levels [113] . No data are available, at present, in humans, probably because this therapeutic approach is not free from possible deleterious effects.
4.5.3 Adiponectin Fat mass plays a role in the regulation of glucose and insulin metabolism through the release of adipocytokines (leptin, adiponectin and resistin). Various studies support the important role of adiponectin in the pathogenesis of NAFLD and confirm the close correlation between reduced adiponectin production by adipose tissue, steatosis, insulin resistance and metabolic syndrome [115-117] . Experimental studies on animals suggest [118] that adiponectin may protect against NASH by reducing the production of TNF- α and other pro-inflammatory cytokines.
4.5.4 Resistin The role of resistin in man is still uncertain. Various authors have demonstrated that serum resistin levels are increased in patients with type 2 diabetes and that the decrease in plasma resistin is positively correlated with a decrease in hepatic fat [119-123] . However, at the moment, no data are available regarding the use of drugs able to modulate resistin production and action in animals or man with NAFLD, in clinical practice.
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.

Emerging drugs for non-alcoholic fatty liver disease
152 Expert Opin. Emerging Drugs (2008) 13(1)
4.5.5 Anti-hypertensive drugs The role of angiotensin-converting enzyme (ACE) inhibitors is currently being investigated, as the renin-angiotensin system plays a role in the development of metabolic syndrome-associated conditions. Besides the well-known anti-hypertensive properties, ACE inhibitors display steichio-metric features similar to PPAR γ ligands, a property useful in improving insulin sensitivity in patients with metabolic syndrome [124] . For these reasons ACE inhibitors were tested in hypertensive patients presenting with NAFLD. In NASH patients, losartan decreased plasma levels of TGF- β 1, ferritin and transaminases as well as the entity of liver fibrosis [125,126] . In animals, also candesartan displayed an antifibrotic effect [127] , while telmisartan improved carbohydrate and lipid metabolism in patients with metabolic syndrome [128] .
4.5.6 Pentoxifylline A methylxanthine compound, pentoxifylline has been employed to treat vascular diseases. The compound inhibits TNF- α [129] , which is increased in patients with NASH [130] . NASH patients presented improved biochemical parameters of liver damage after treatment with pentoxiphylline for 6 – 12 months. A recent study reported an improvement in biochemical markers and liver histology (steatosis/necroinflamation) in NASH patients with diabetes mellitus taking low-dose pentoxifylline [126] .
4.5.7 Iron depletion Hyperferritinaemia is frequently observed in NAFLD. Iron depletion by phlebotomy has been reported to decrease insulin resistance more than nutritional counselling alone, indepen-dently of changes in BMI, baseline HOMA-R, and the presence of the metabolic syndrome in NAFLD patients [131] .
5. Current research goals and scientifi c rationale
A series of pharmacological agents are currently being inves-tigated for treatment in patients with NAFLD/NASH. The main scientific aims of these treatments are: i) to prevent steatosis by correcting parameters of metabolic syndrome; ii)
to inhibit the progression of steatosis to steato-hepatitis by reducing or blocking the cascade of inflammationand fibrosis.
Rimonabant, the selective endocannabinoid CB1 receptor antagonist [132] , is a novel promising anorectic agent for the simultaneous treatment of obesity and metabolic syndrome. In obese mice, it activates thermogenesis and increases oxygen consumption [133] , improves glucose homeostasis [133] and increases FFA oxidation.
Other recent drugs, such as incretins, and particularly glucagon-like peptide-1 (GLP1), have been proposed in the treatment of overweight and insulin resistance, but, at present, no data are available in patients with NAFLD [134] .
Among the new promising agents, agonists of PPAR λ (thioglitazones) and PPAR α (fibrates) act synergistically to improve insulin sensitivity and up-regulate hepatic FFA oxidation thus decreasing hepatic steatosis, and both have shown promising results in a pilot trial in NAFLD patients. Combination dual PPAR γ and PPAR α agonists (muraglitazar, tesaglitazar) would, therefore, appear to be attractive candi-dates in the treatment of NAFLD. Phase II clinical trials are currently underway to examine the influence of these agents on cardiovascular risk factors [135] .
Other promising new targets, in the treatment of NAFLD/NASH, are aquaglyceroporins [136,137] . AQP3, is expressed in human liver and is up-regulated during hepatic steatosis [138] . AQP7 is responsible for adipocyte glycerol permeability and regulates adipocyte size and fat accumulation [139-143] . AQP9 mediates the uptake of sinusoidal blood glycerol into the hepatocyte [144] , and regulates its metabolism by interacting with PPAR α [145,146] whereas adipocyte AQPap is controlled by PPAR γ [147] . Finally, AQP7 and AQP9 are down-regulated at a transcriptional level by insulin [148] , suggesting their possible involvement in insulin resistance.
In rats with experimentally induced NASH, ciprofibrate decreases the severity of fatty change and hepatitis [149] while bezafibrate acts as a PPAR pan-agonist ( α , δ ) by improving fatty acid β -oxidation and directly preventing inflammation [150] .
Two large trials are in progress in US and Italy on complexes with Silybin, which should act by reducing the
Table 5 . Main studies on the use of cytoprotective agents in patients with NAFLD.
Treatment No. patients Duration (months) Liver enzyme levels Histology Versus Ref
Betaine 10 12 Improved Improved Baseline [89]
Betaine 96 1.5 Improved Not evaluated Placebo [90]
Vitamin E and C 45 6 Not improved Improved (only steatosis) Placebo [92]
Vitamin E 22 6 Improved Improved Baseline [93]
Vitamin E (children) 11 5 Improved Not evaluated Baseline [94]
UDCA 166 24 Not improved Not improved Placebo [83]
UDCA 24 12 Improved Improved (only steatosis) Clofi brate [75]
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.

Federico, Niosi, Blanco & Loguercio
Expert Opin. Emerging Drugs (2008) 13(1) 153
progression of steatosis to steatohepatitis as well as by blocking fibrogenesis.
6. Competitive environment
In addition to the drugs previously mentioned, there are other molecules that are being developed with other indications but that may have NAFLD as a potential indication ( Table 6 ).
GSK-677954 is a PPAR pan-agonist, under development by GlaxoSmithKline (GSK) for the treatment of type 2 diabetes, insulin resistance, dyslipidaemia and metabolic syndrome associated with type 2 diabetes. It is already in Phase II trials, in patients with type 2 diabetes, and in pre-clinical studies in those with dyslipidaemia (Company pipeline, GSK, February 2007).
KD-3020 is an orally-active, non-thiazolidinedione selective PPAR δ agonist, under development by Kalypsys for the treatment of dyslipidaemia and diabetes (Company Web Page, Kalypsys, 2 February 2007).
7. Expert opinion and conclusions
In our opinion, the identification of NAFLD as a serious pathological condition of the liver is fairly recent, and several of the pathogenic mechanisms involved in its progression are until unclear. Liver steatosis is a dangerous substrate also when liver disease is dependent on other known causes of liver damage, it is present in relatively young patients, likely to present other liver impairments during
their lifetime (drugs, environmental toxic substances, etc.). Finally, it could be a predictive factor of death from cardio-vascular diseases other than hepatocellular carcinoma, as well as of the onset of type 2 diabetes, also in children. These considerations strongly indicate the need to treat each stage of NAFLD.
However, at present, no treatment is available which would be beneficial for all patients with NAFLD and the choice of individual treatment, in clinical practice, must be evaluated in terms of the evidence of efficacy and the potential for toxicity. Obese patients need to reduce BW, insulin sensitisers are necessary in those with diabetes and dyslipidaemia should be specifically treated. These approaches correct the conditions related to NAFLD but only indirectly improve, at least in theory, liver damage. However, the major alarm signals are in the liver, and in all phases free radicals are the main mediators of both metabolic and toxic reactions. In this key, future research should be aimed at establishing whether it is better to block some metabolic pathways able to enhance free-radical production (e.g., by blocking endotoxins, cytokines, intra-hepatocyte receptors, nuclear transcription factors) or to replace anti-oxidants, or both in the liver. Therefore, the future of treatment of NAFLD is strictly related to the future further researches on the pathophysiology of the liver damage.
Declaration of interest
The authors state no conflict of interest and have received no payment in preparation of this manuscript.
Table 6 . Compounds in development that could be indicated for patients with NAFLD.
Compound Company Structure Indication Development stage
Mechanism of action
Netoglitazone Mitsubishi Pharma
2,4-Thiazolidinedione, 5-[[6-[(2-fl uorophenyl)methoxy]-2-naphthalenyl]methyl]-[CAS]
Type 2 diabetes Phase II clinical trial PPAR α , δ and γ agonist
GSK-677954 GSK Type 2 diabetes and insulin resistance, hyperglycaemia and dyslipidaemia associated with type 2 diabetes and metabolic syndrome
Phase II clinical trial PPAR α , δ and γ agonist
KD-3020 Kalypsys dyslipidaemia and diabetes Pre-clinical Selective PPAR- δ agonist
GSK: GlaxoSmithKline; PPAR: Peroxisome proliferator-activated receptor.
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.

Emerging drugs for non-alcoholic fatty liver disease
154 Expert Opin. Emerging Drugs (2008) 13(1)
Bibliography Papers of special note have been highlighted as either of interest (•) or of considerable interest (••) to readers.
1. Ludwig J, Viggiano RT, McGill DB, et al. Non-alcoholic steatohepatitis. Mayo Clinic experience with a hitherto unnamed disease. Mayo Clin Proc 1980 ; 55 : 342 -8
•• Historical paper on the fi rst observation of NASH.
2. Caldwell SH, Crespo DM, Kang HS, Al-Osaimi AM. Obesity and hepatocellular carcinoma. Gastroenterology 2004 ; 127 : S97 -103
3. Browning J, Szczepaniak L, Dobbins R, et al. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology 2004 ; 40 : 1387 -95
4. Nomura H, Kashiwagi S, Hayashi J, et al. Prevalence of fatty liver in a general population of Okinawa, Japan. Jpn J Med 1988 ; 27 : 142 -9
5. Hilden M, Cristoffersen P, Juhl E, Dalgaard JB. Liver histology in a normal population - examinations of 503 consecutive fatal traffi c casualties. Scand J Gastroenterol 1977 ; 12 : 593 -7
6. Stroffolini T, Sagnelli E, Mele A, et al.The aetiology of chronic hepatitis in Italy: results from a multicentre national study. Dig Liver Dis 2004 ; 36 : 829 -33
7. Sagnelli E, Stroffolini T, Mele A, et al. The importance of HCV on the burden of chronic liver disease in Italy: a multicenter prevalence study of 9,997 cases. J Med Virol 2005 ; 75 : 522 -7
8. James O, Day C. Non-alcoholic steatohepatitis. Another disease of affl uence. Lancet 1999 ; 353 : 1634 -6
9. Clark JM, Brancati FL, Diehl AM. The prevalence and etiology of elevated aminotransferase levels in the United States. Am J Gastroenterol 2003 ; 98 : 960 -7
10. Brea A, Mosquera D, Martin E, et al. Nonalcoholic fatty liver disease is associated with carotid atherosclerosis: a case-control study. Arterioscler Thromb Vasc Biol 2005 ; 25 : 1045 -50
11. Schindhelm RK, Diamant M, Heine RJ. Nonalcoholic fatty liver disease and cardiovascular disease risk. Curr Diab Rep 2007 ; 7 (3): 181 -7
12. Targher G, Bertolini L, Padovani R, et al. Prevalence of nonalcoholic fatty liver disease and its association
with cardiovascular disease among type 2 diabetic patients. Diabetes Care 2007 ; 30 (5): 1212 -8
13. Festi D, Colecchia A, Sacco T, et al. Hepatic steatosis in obese patients: clinical aspects and prognostic signifi cance. Obes Rev 2004 ; 5 : 27 -42
14. Portincasa P, Grattagliano I, Palmieri VO, Palasciano G. Nonalcoholic steatohepatitis: recent advances from experimental models to clinical management. Clin Biochem 2005 ; 38 : 203 -17
15. Ramesh S, Sanyal AJ. Evaluation and management of non-alcoholic steatohepatitis. J Hepatol 2005 ; 42 : S2 -12
16. Luyckx FH, Lefebvre PJ, Scheen AJ. Non-alcoholic steatohepatitis: association with obesity and insulin resistance, and infl uence of weight loss. Diabetes Metab 2000 ; 26 : 98 -106
17. Sanyal AJ, Campbell-Sargent C. Nonalcoholic steatohepatitis: association of insulin resistance and mitochondrial abnormalities. Gastroenterology 2001 ; 120 : 1183 -92
18. Chitturi S, Farrell GC. Etiopathogenesis of nonalcoholic steatohepatitis. Semin Liver Dis 2001 ; 21 : 27 -41
19. Lydatakis H, Hager IP, Kostadelou E, et al. Non-invasive markers to predict the liver fi brosis in non-alcoholic fatty liver disease. Liver Int 2006 ; 26 (7): 864 -71
20. Miele L, Forgione A, Gasbarrini G, Grieco A. Noninvasive assessment of fi brosis in non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH). Transl Res 2007 ; 149 (3): 114 -25.
21. Kim Km, Choi Wb, Park SH, et al. Diagnosis of hepatic steatosis and fi brosis by transient elastography in asymptomatic healthy individuals: a prospective study of living related potential liver donors. J Gastroenterol 2007 ; 42 (5): 382 -8
22. Loguercio C, De Simone T, D’Auria MV, et al. Non-alcoholic fatty liver disease: a multicentre clinical study by the Italian Association for the Study of the Liver. Dig Liver Dis 2004 ; 36 : 398 -405
•• Epidemiological survey in Italy depicting the essential clinical features of patients with laboratory, ultrasonographic and histological evidence of NAFLD/NASH.
23. Friis-Liby I, Aldenborg F, Jerlstad P, et al. High prevalence of metabolic complications in patients with
non-alcoholic fatty liver disease. Scand J Gastroenterol 2004 ; 39 (9): 864 -9
• Exhaustive paper on the importance of fatty liver in the evolution of liver disease.
24. Smedile A, Bugianesi E. Steatosis and hepatocellular carcinoma risk. Eur Rev Med Pharmacol Sci 2005 ; 9 (5): 291 -3
25. Solga SF, Clark JM, Alkhuraishi AR, et al. Race and comorbid factors predict nonalcoholic fatty liver disease histopathology in severely obese patients. Surg Obes Relat Dis 2005 ; 1 (1): 6 -11
26. American Gastroenterological Association Medical Position Statement. Nonalcoholic fatty liver disease. Gastroenterology 2002 ; 123 : 1702 -4
27. Huang MA, Greenson JK, Chao C, et al. One-year intense nutritional counseling results in histological improvement in patients with non-alcoholic steatohepatitis: a pilot study. Am J Gastroenterol 2005 ; 100 : 1072 -81
28. Okita M, Hayashi M, Sasagawa T, et al. Effect of a moderately energy-restricted diet on obese patients with fatty liver. Nutrition 2001 ; 17 : 542 -7
29. Ueno T, Sugawara H, Sujaku K, et al. Therapeutic effects of restricted diet and exercise in obese patients with fatty liver. J Hepatol 1997 ; 27 : 103 -7
30. Andersen T, Gluud C, Franzmann MB, Christoffersen P. Hepatic effects of dietary weight loss in morbidly obese subjects. J Hepatol 1991 ; 12 : 224 -9
31. Luyckx FH, Scheen AJ, Desaive C, et al. Effects of gastroplasty on body weight and related biological abnormalities in morbid obesity. Diabetes Metab 1998 ; 24 : 355 -61
32. Drenick EJ, Simmons F, Murphy JF. Effects on hepatic morphology of treatment of obesity by fasting, reducing diets and small-bowel bypass. NEJM 1970 ; 282 : 829 -34
33. Dumas JF, Roussel D, Simard G, et al. Food restriction affects energy metabolism in rat liver mitochondria. Biochim Biophys Acta 2004 ; 1670 : 126 -31
34. Tirosh O, Aronis A, Zusman I, et al. Mitochondrion-mediated apoptosis is enhanced in long-lived alpha-MUPA transgenic mice and calorically restricted wild-type mice. Exp Gerontol 2003 ; 38 : 955 -63
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.

Federico, Niosi, Blanco & Loguercio
Expert Opin. Emerging Drugs (2008) 13(1) 155
35. Musso G, Gambino R, De Michieli F, et al. Dietary habits and their relations to insulin resistance and postprandial lipemia in nonalcoholic steatohepatitis. Hepatology 2003 ; 37 : 909 -16
36. Fernandez MI, Torres MI, Gil A, et al. Steatosis and collagen content in experimental liver cirrhosis are affected by dietary monounsaturated and polyunsaturated fatty acids. Scand J Gastroenterol 1997 ; 32 : 350 -6
37. Solga S, Alkhuraishe AR, Clark JM, et al. Dietary composition and nonalcoholic fatty liver disease. Dig Dis Sci 2004 ; 49 : 1578 -83
38. Koteish A, Mae Diehl A. Animal models of steatohepatitis. Best Pract Res Clin Gastroenterol 2002 ; 16 : 679 -90
39. Cave M, Deaciuc I, Mendez C, et al. Nonalcoholic fatty liver disease: predisposing factors and the role of nutrition. J Nutr Biochem 2007 ; 18 (3): 184 -95
40. Blouet C, Mariotti F, Azzout-Marniche D, et al. Dietary cysteine alleviates sucrose-induced oxidative stress and insulin resistance. Free Radic Biol Med 2007 ; 42 (7): 1089 -97
41. Kugelmas M, Hill DB, Vivian B, et al. Cytokines and NASH: a pilot study of the effects of lifestyle modifi cation and vitamin E. Hepatology 2003 ; 38 : 413 -9
42. Harrison SA, Fincke C, Helinski D, et al. A pilot study of orlistat treatment in obese, non-alcoholic steatohepatitis patients. Aliment Pharmacol Ther 2004 ; 20 : 623 -8
43. Kazi M, De Meo M, Mikolaitis S. Effects of weight loss on abnormal liver function test (LFT) in obese patients. FASEB J 1997 ; A600 : 3466
44. Luque CA, Rey JA. Sibutramine: a serotonin-norepinephrine reuptake-inhibitor for the treatment of obesity. Ann Pharmacother 1999 ; 33 : 968 -78
45. Filippatos TD, Kiortsis DN, Liberopoulos EN, et al. A review of the metabolic effects of sibutramine. Curr Med Res Opin 2005 ; 21 : 457 -68
46. Li Z, Maglione M, Tu W, et al. Meta-analysis: pharmacologic treatment of obesity. Ann Intern Med 2005 ; 142 : 532 -46
47. Sabuncu T, Nazligul Y, Karaoglanoglu M, et al. The effect of sibutramine and orlistat on the ultrasonographic fi ndings, insulin resistance and liver enzyme levels in obese patients with nonalcoholic steatohepatitis. Rom J Gastroenterol 2003 ; 12 : 189 -92
48. Jaskiewicz K, Raczynska S, Rzepko R, Sledzinski Z. Nonalcoholic fatty liver disease treated by gastroplasty. Dig Dis Sci 2006 ; 51 : 21 -6
49. Stratopoulos C, Papakonstantinou A, Terzis I, et al. Changes in liver histology accompanying massive weight loss after gastroplasty for morbid obesity. Obes Surg 2005 ; 15 : 1154 -60
50. Barker KB, Palekar NA, Bowers SP, et al. Non-alcoholic steatohepatitis: effect of Roux-en-Y gastric bypass surgery. Am J Gastroenterol 2006 ; 101 : 368 -73
51. Dixon JB, Bhathal PS, Hughes NR, O’Brien PE. Nonalcoholic fatty liver disease: Improvement in liver histological analysis with weight loss. Hepatology 2004 ; 39 : 1647 -54
52. Dixon JB. Surgical treatment for obesity and its impact on non-alcoholic steatohepatitis. Clin Liver Dis 2007 ; 11 (1): 141 -54
53. Elder KA, Wolfe BM. Bariatric surgery: a review of procedures and outcomes. Gastroenterology 2007 ; 132 (6): 2253 -71
54. Palmer M, Schaffner F. Effects of weight reduction on hepatic abnormalities in overweight patients. Gastroenterology 1990 ; 99 : 1408 -13
55. Hickman IJ, Jonsson JR, Prins J, et al. Modest weight loss and physical activity in overweight patients with chronic liver disease results in sustained improvements in alanine aminotransferase, fasting insulin, and quality of life. Gut 2004 ; 53 : 413 -9
56. Silverman EM, Sapala JA, Appelman HD. Regression of hepatic steatosis in morbidly obese persons after gastric bypass. Am J Clin Pathol 1995 ; 104 : 23 -31
57. Luyckx FH, Desaive C, Thiry A, et al. Liver abnormalities in severely obese subjects: effects of drastic weight loss after gastroplasty. Int J Obes Relat Metab 1998 ; 2 : 222 -6
58. Dixon JB, Brathal PS, O ’ Brien PE. Nonalcoholic fatty liver disease: predictors of nonalcoholic steatohepatitis and liver fi brosis in severely obese. Gastroenterology 2001 ; 121 : 91 -100
59. Marchesini G, Brizi M, Bianchi G, et al. Metformin in nonalcoholic steatohepatitis. Lancet 2001 ; 358 : 893 -4
60. Schwimmer JB, Middleton MS, Deutsch R, Lavine JE. A phase 2 clinical trial of metformin as a treatment for non-diabetic paediatric non-alcoholic
steatohepatitis. Aliment Pharmacol Ther 2005 ; 21 : 871 -9
61. Nair S, Diehl AM, Wiseman M, et al. Metformin in the treatment of non-alcoholic steatohepatitis: a pilot open label trial. Aliment Pharmacol Ther 2004 ; 20 : 23 -8
62. Bugianesi E, Gentilcore E, Manini R, et al. A randomized controlled trial of metformin versus vitamin E or prescriptive diet in nonalcoholic fatty liver disease. Am J Gastroenterol 2005 ; 100 : 1082 -90
63. Shadid S, Jensen MD. Effects of pioglitazone versus and exercise on metabolic health and fat distribution in upper body obesity. Diabetes Care 2003 ; 26 : 3148 -52
64. Kawaguchi K, Sakaida I, Tsuchiya M, et al. Pioglitazone prevents hepatic steatosis, fi brosis, and enzyme-altered lesions in rat liver cirrhosis induced by a choline-defi cient L-amino acid-defi ned diet. Biochem Biophys Res Commun 2004 ; 315 : 187 -95
65. Yuan GJ, Zhang ML, Gong ZJ. Effect of PPAR γ agonist pioglitazone on rat hepatic fi brosis. World J Gastroenterol 2004 ; 10 : 1047 -51
66. Caldwell S, Hespenheide EE, Redick JA, et al. A pilot study of a thiazolidinedione, troglitazone, in nonalcoholic steatohepatitis. Am J Gastroenterol 2001 ; 96 : 519 -25
67. Menon KVN, Angulo P, Lindor KD. Severe cholestatic hepatitis from troglitazone in a patient with nonalcoholic steatohepatitis and diabetes mellitus. Am J Gastroenterol 2001 ; 96 : 1631 -4
68. Marcy TR, Britton ML, Blevins SM. Second-generation thiazolidinediones and hepatotoxicity. Ann Pharmacother 2004 ; 38 : 1419 -23
69. Neuschwander-Tetri BA, Brunt EM, Wehmeier KR, et al. Improved nonalcoholic steatohepatitis after 48 weeks of treatment with the PPAR-gamma ligand rosiglitazone. Hepatology 2003 ; 38 : 1008 -17
70. Promrat K, Lutchman G, Uwaifo GI, et al. A pilot study of pioglitazone treatment for nonalcoholic steatohepatitis. Hepatology 2004 ; 39 : 188 -96
71. Nissen SE. Effect of Rosiglitazone on the risk of myocardial infarction and death from cardiovascular causes. NEJM 2007 ; 356 (24): 2457 -71
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.

Emerging drugs for non-alcoholic fatty liver disease
156 Expert Opin. Emerging Drugs (2008) 13(1)
72. Sanyal AJ, Mofrad PS, Contos MJ, et al. A pilot study of vitamin E versus vitamin E and pioglitazone for the treatment of nonalcoholic steatohepatitis. Clin Gastroenterol Hepatol 2004 ; 2 : 1107 -15
73. Belfort R, Harrison S, Brown K, et al. A placebo controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. NEJM 2006 ; 355 : 2297 -307
74. Angelico F, Burattin M, Alessandri C, et al. Drugs improving insulin resistance for non-alcoholic fatty liver disease and/or non-alcoholic steatohepatitis. Cochrane Database Syst Rev 2007 ; 1 : CD 005166
75. Laurin J, Lindor KD, Crippin JS, et al. Ursodeoxycholic acid or clofi brate in the treatment of non-alcohol-induced steatohepatitis: a pilot study. Hepatology 1996 ; 23 : 1464 -7
76. Basaranoglu M, Acbay O, Sonsuz A. A controlled trial of gemfi brozil in the treatment of patients with nonalcoholic steatohepatitis. J Hepatol 1999 ; 31 : 384 -9
77. Kiyici M, Gulten M, Gurel S, et al. Ursodeoxycholic acid and atorvastatin in the treatment of nonalcoholic steatohepatitis. Can J Gastroenterol 2003 ; 17 : 713 -8
78. Rallidis LS, Drakoulis CK, Parasi AS. Pravastatin in patients with nonalcoholic steatohepatitis: results of a pilot study. Atherosclerosis 2004 ; 174 : 193 -6
79. Merat S, Malekzadeh R, Sohrabi MR, et al. Probucol in the treatment of non-alcoholic steatohepatitis: a double-blind randomized controlled study. J Hepatol 2003 ; 38 : 414 -8
80. Ahmed MH. Rosuvastatin as treatment for non alcoholic steatohepatitis (NASH) and highly active antiretroviral therapy (HAART)-dyslipidaemia: new treatment for global dangers. Med Hypotheses 2006 ; 66 (2): 440 -1
81. Ekstedt M, Franzen LE, Mathiesen UL, et al. Statins in non-alcoholic fatty liver disease and chronically elevated liver enzymes: a histopathological follow-up study. J Hepatol 2007 ; 47 (1): 135 -41
82. Trauner M, Graziadei IW. Mechanisms of action and therapeutic applications of ursodeoxycholic acid in chronic liver diseases. Aliment Pharmacol Ther 1999 ; 13 : 979 -96
83. Lindor KD, Kowdley KV, Heathcote JE, et al. Ursodeoxycholic acid for treatment of nonalcoholic steatohepatitis: results of a randomized trial. Hepatology 2004 ; 39 : 770 -8
84. Galli A, Svegliati-Baroni G, Ceni E, et al. Oxidative stress stimulates proliferation and invasiveness of hepatic stellate cells via a MMP2-mediated mechanism. Hepatology 2005 ; 41 : 1074 -84
85. Pessayre D, Fromenty B. NASH: a mitochondrial disease. J Hepatol 2005 ; 42 : 928 -40
86. Loguercio C, Federico A. Oxidative stress in viral and alcoholic hepatitis. Free Radic Biol Med 2003 ; 34 : 1 -10
87. De Villiers WJ, Song Z, Nasser MS, et al. 4-Hydroxynonenal-induced apoptosis in rat hepatic stellate cells: mechanistic approach. J Gastroenterol Hepatol 2007 ; 22 (3): 414 -22
88. Bjelakovic G, Nikolova D, Gluud LL, et al. Mortality in randomized trials of antioxidant supplements for primary and secondary prevention: systematic review and meta-analysis. JAMA 2007 ; 297 : 842 -57
89. Abdelmalek MF, Angulo P, Jorgensen RA, et al. Betaine, a promising new agent for patients with nonalcoholic steatohepatitis: results of a pilot study. Am J Gastroenterol 2001 ; 96 : 2711 -7
90. Miglio F, Rovati LC, Santoro A, Setnikar I. Effi cacy and safety of oral betaine glucuronate in non-alcoholic steatohepatitis. A double-blind, randomized, parallel-group, placebo-controlled prospective clinical study. Arzneimittelforschung 2000 ; 50 : 722 -7
91. Oliveira CP, Gayotto LC, Tatai C, et al. Vitamin C and Vitamin E in prevention of nonalcoholic fatty liver disease (NAFLD) in choline defi cient diet fed rats. Nutr J 2003 ; 2 : 9 -19
92. Harrison SA, Torgerson S, Hayashi P, et al. Vitamin E and vitamin C treatment improves fi brosis in patients with nonalcoholic steatohepatitis. Am J Gastroenterol 2003 ; 98 : 2485 -90
93. Hasegawa T, Yoneda M, Nakamura K, et al. Plasma transforming growth factor-beta 1 level and effi cacy of alpha-tocopherol in patients with non-alcoholic steatohepatitis: a pilot study. Aliment Pharmacol Ther 2001 ; 15 : 1667 -72
94. Lavine JE. Vitamin E treatment of nonalcoholic steatohepatitis in children: a pilot study. J Pediatr 2000 ; 136 : 734 -8
95. Buchman AL, Dubin M, Jenden D, et al. Lecithin increases plasma free choline and decreases hepatic steatosis in long-term
total parenteral nutrition patients. Gastroenterology 1992 ; 102 : 1363 -70
96. Baybutt RC, Molteni A. Dietary beta-carotene protects lung and liver parenchyma of rats treated with monocrotaline. Toxicology 1999 ; 137 : 69 -80
97. Nakano H, Nagasaki H, Barama A, et al. The effects of N-acetylcysteine and anti-intercellular adhesion molecule-1 monoclonal antibody against ischemia-reperfusion injury of the rat steatotic liver produced by a choline-methionine-defi cient diet. Hepatology 1997 ; 26 : 670 -8
98. Hiroko M, Kazuo I, Yuji N, et al. Sulfur-containing amino acids attenuate the development of liver fi brosis in rats throughdown-regulation of stellate cell activation. J Hepatol 2004 ; 40 : 917 -25
99. Saller R, Melzer J, Reichling J, et al. An updated systematic review of the pharmacology of silymarin. Forsch Komplementarmed 2007 ; 14 (2): 70 -80
100. Velussi M, Cernigoi AM, De Monte A, et al. Long-term (12 months) treatment with an anti-oxidant drug (silymarin) is effective on hyperinsulinemia, exogenous insulin need and malondialdehyde levels in cirrhotic diabetic patients. J Hepatol 1997 ; 26 : 871 -9
101. Kravchenko LV, Morozov SV, Tutel’Yan VA. Effects of fl avonoids on the resistance of microsomes to lipid peroxidation in vitro and ex vivo. J Hepatol 2003 ; 39 : 333 -40
102. Valenzuela A, Lagos C, Schmidt K, Videla LA. Silymarin protection against hepatic lipid peroxidation induced by acute ethanol intoxication in the rat. Biochem Pharmacol 1985 ; 34 : 2209 -12
103. Schumann J, Prockl J, Kiemer AK, et al. Silibinin protects mice from T cell-dependent liver injury. J Hepatol 2003 ; 39 : 333 -40
104. Jia JD, Bauer M, Cho JJ, et al. Antifi brotic effect of silymarin in rat secondary biliary fi brosis is mediated by downregulation of procollagen alpha1(I) and TIMP-1. J Hepatol 2001 ; 35 : 392 -8
105. McCarty MF. Potential utility of natural polyphenols for reversing fat-induced insulin resistance. Med Hypotheses 2005 ; 64 : 628 -35
106. Di Sario A, Bendie E, Taffetani S. Realsil, a new sylibin-phospatidylcoline complex,
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.
Federico, Niosi, Blanco & Loguercio
Expert Opin. Emerging Drugs (2008) 13(1) 157
reduces dimethylnitrosamine-induced hepatic fi brosis in the rat. J Hepatol 2003 ; 38 : P76
107. Federico A, Trappoliere M, Tuccillo C, et al. A new silybin - vitamin E - phospholipid complex improves insulin resistance and liver damage in patients with non alcoholic fatty liver disease: preliminary observations. Gut 2006 ; 55 : 901 -2
108. Nair S, Cope K, Risby TH, Diehl AM. Obesity and female gender increase breath ethanol concentration: potential implications for the pathogenesis of nonalcoholic steatohepatitis. Am J Gastroenterol 2001 ; 96 (4): 1200 -4
109. Solga SF, Diehl AM. Non-alcoholic fatty liver disease: lumen-liver interaction and possible role for probiotics. J Hepatol 2003 ; 38 (5): 681 -7
110. Nanji AA, Khettry U, Sadrzadeh SM. Lactobacillus feeding reduces endotoxiemia and severity of experimental alcoholic liver (disease). Proc Soc Exp Biol Med 1994 ; 205 (3): 243 -7
111. Adachi Y, Moore LE, Bradford BU, et al. Antibiotics prevent liver injury in rats following long-term exposure to ethanol. Gastroenterology 1995 ; 108 (1): 218 -24
112. Iimuro Y, Gallucci RM, Luster MI, et al. Antibodies to tumor necrosis factor alfa attenuate hepatic necrosis and infl ammation caused by chronic exposure to ethanol in the rat. Hepatology 1997 ; 26 (6): 1530 -7
113. Li Z, Yang S, Lin H, et al. Probiotics and antibodies to TNF inhibit infl ammatory activity and improve nonalcoholic fatty liver disease. Hepatology 2003 ; 37 (2): 343 -50
114. Loguercio C, Federico A, Tuccillo C, et al. Benefi cial effects of a probiotics VSL#3 on parameters of liver dysfunction in chronic liver diseases. J Clin Gastroenterol 2005 ; 39 (6): 540 -3
115. Mendez-Sanchez N, Chavez-Tapia NC, Villa AR, et al. Adiponectin as a protective factor in hepatic steatosis. World J Gastroenterol 2005 ; 11 : 1737 -41
116. Targher G, Bertolini L, Scala L, et al. Decreased plasma adiponectin concentrations are closely associated with nonalcoholic hepatic steatosis in obese individuals. Clin Endocrinol 2004 ; 61 : 700 -3
117. Pagano C, Soardo G, Esposito W, et al. Plasma adiponectin is decreased in
nonalcoholic fatty liver disease. Eur J Endocrinol 2005 ; 152 : 113 -8
118. Xu A, Wang Y, Keshaw H, et al. The fat-derived hormone adiponectin alleviates alcoholic and nonalcoholic fatty liver diseases in mice. J Clin Invest 2003 ; 112 : 91 -100
119. Hasegawa G, Ohta M, Ichida Y, et al. Increased serum resistin levels in patients with type 2 diabetes are not linked with markers of insulin resistance and adiposity. Acta Diabetol 2005 ; 42 : 104 -9
120. Ballantyne GH, Gumbs A, Modlin IM. Changes in insulin resistance following bariatric surgery and the adipoinsular axis: role of the adipocytokines, leptin, adiponectin and resistin. Obes Surg 2005 ; 15 : 692 -9
121. Banerjee RR, Rangwala SM, Shapiro JS, et al. Regulation of fasted blood glucose by resistin. Science 2004 ; 303 : 1195 -8
122. Bajaj M, Suraamornkul S, Hardies LJ, et al. Plasma resistin concentration, hepatic fat content, and hepatic and peripheral insulin resistance in pioglitazone-treated type II diabetic patients. Int J Obes Relat Metab Disord 2004 ; 28 : 783 -9
123. Muse ED, Obici S, Bhanot S, et al. Role of resistin in diet-induced hepatic insulin resistance. J Clin Invest 2004 ; 114 : 232 -9
124. Vitale C, Mercuro G, Castiglioni C, et al. Metabolic effect of telmisartan and losartan in hypertensive patients with metabolic syndrome. Cardiovasc Diabetol 2005 ; 4 : 6 -10
• Telmisartan and losartan could have a role in the prevention and treatment of metabolic syndrome.
125. Yokohama S, Yoneda M, Haneda M, et al. Therapeutic effi cacy of an angiotensin II receptor antagonist in patients with nonalcoholic steatohepatitis. Hepatology 2004 ; 40 : 1222 -5
126. Georgescu EF, Georgescu M. Therapeutic options in non-alcoholic steatohepatitis (NASH). Are all agents alike? Results of a preliminary study. J Gastrointestin Liver Dis 2007 ; 16 : 39 -46
127. Yoshiji H, Kuriyama S, Yoshii J, et al. Angiotensin-II type 1 receptor interaction is a major regulator for liver fi brosis development in rats. Hepatology 2001 ; 34 : 745 -50
128. Kurtz TW. Treating the metabolic syndrome: telmisartan as a peroxisome
proliferator-activated receptor-gamma activator. Acta Diabetol 2005 ; 42 (1): S9 -16
129. Neuner P, Klosner G, Schauer E, et al. Pentoxifylline in vivo down-regulates the release of IL-1 beta, IL-6, IL-8 and tumour necrosis factor-alpha by human peripheral blood mononuclear cells. Immunology 1994 ; 83 : 262 -7
130. Wigg AJ, Roberts-Thomson IC, Dymock RB, et al. The role of small intestinal bacterial overgrowth, intestinal permeability, endotoxaemia, and tumour necrosis factor alpha in the pathogenesis of non-alcoholic steatohepatitis. Gut 2001 ; 48 : 206 -11
131. Valenti L, Fracanzani AL, Dongiovanni P, et al. Iron depletion by phlebotomy improves insulin resistance in patients with nonalcoholic fatty liver disease and hyperferritinemia: evidence from a case-control study. Am J Gastroenterol 2007 ; 102 (6): 1251 -8
132. Rinaldi-Carmona M, Barth F, Heaulme M, et al. SR141716A, a potent and selective antagonist of the brain cannabinoid receptor. FEBS Lett 1994 ; 350 : 240 -4
133. Liu YL, Connoley IP, Wilson CA, Stock MJ. Effects of the cannabinoid CB1 receptor antagonist SR141716 on oxygen consumption and soleus muscle glucose uptake in Lep(ob)/Lep(ob) mice. Int J Obes 2005 ; 29 : 183 -7
134. Rotella CM, Pala L, Mannucci E. Glucagon-like peptide 1 (GLP-1) and metabolic diseases. J Endocrinol Invest 2005 ; 28 (8): 746 -58
135. Tenenbaum A, Motro M, Fisman EZ. Dual and pan-peroxisome proliferator-activated receptors (PPAR) co-agonism: the bezafi brate lessons. Cardiovasc Diabetol 2005 ; 16 : 4 -14
136. Hara-Chikuma M, Verkman AS. Physiological roles of glycerol-transporting aquaporins: the aquaglyceroporins. Cell Mol Life Sci 2006 ; 63 : 1386 -92
137. Jeyaseelan K, Sepramaniam S, Armugam A, Wintour EM. Aquaporins: a promising target for drug development. Expert Opin Ther Targets 2006 ; 10 : 889 -909
138. Chiappini F, Barrier A, Saffroy R, et al. Exploration of global gene expression in human liver steatosis by high-density oligonucleotide microarray. Lab Invest 2006 ; 86 : 154 -65
139. Kishida K, Shimomura I, Kondo H, et al. Genomic structure and insulin-mediated repression of the aquaporin adipose
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.

Emerging drugs for non-alcoholic fatty liver disease
158 Expert Opin. Emerging Drugs (2008) 13(1)
(AQPap), adipose-specifi c glycerol channel. J Biol Chem 2001 ; 276 : 36251 -60
140. Maeda N, Funahashi T, Hibuse T, et al. Adaptation to fasting by glycerol transport through aquaporin 7 in adipose tissue. Proc Natl Acad Sci USA 2004 ; 101 : 17801 -6
141. Hara-Chikuma M, Sohara E, Rai T, et al. Progressive adipocyte hypertrophy in aquaporin-7-defi cient mice: adipocyte glycerol permeability as a novel regulator of fat accumulation. J Biol Chem 2005 ; 280 : 15493 -6
142. Hibuse T, Maeda N, Funahashi T, et al. Aquaporin 7 defi ciency is associated with development of obesity through activation of adipose glycerol kinase. Proc Natl Acad Sci USA 2005 ; 102 : 10993 -8
143. Marrades MP, Milagro FI, Martinez JA, Moreno-Aliaga MJ. Differential expression of aquaporin 7 in adipose tissue of lean and obese high fat consumers. Biochem Biophys Res Commun 2006 ; 339 : 785 -9
144. Carbrey JM, Gorelick-Feldman DA, Kozono D, et al. Aquaglyceroporin AQP9: solute permeation and metabolic control of expression in liver. Proc Natl Acad Sci USA 2003 ; 100 : 2945 -50
145. Rojek AM, Skowronski MT, Fuchtbauer EM,et al. Defective glycerol metabolism in aquaporin 9 (AQP9) knockout mice. Proc Natl Acad Sci USA 2007 ; 104 : 3609 -14
146. Patsouris D, Mandard S, Voshol PJ, et al. PPARalpha governs glycerol metabolism. J Clin Invest 2004 ; 114 : 94 -103
147. Kishida K, Shimomura I, Nishizawa H, et al. Enhancement of the aquaporin adipose gene expression by a peroxisome proliferator-activated receptor gamma. J Biol Chem 2001 ; 276 : 48572 -9
148. Kuriyama H, Shimomura I, Kishida K, et al. Coordinated regulation of fat-specifi c and liver-specifi c glycerol channels, aquaporin adipose and aquaporin 9. Diabetes 2002 ; 51 : 2915 -21
149. Rao MS, Papreddy K, Musunuri S, Okonkwo A. Prevention/reversal of choline defi ciency-induced steatohepatitis by a peroxisome proliferator-activated receptor alpha ligand in rats. In Vivo 2002 ; 16 : 145 -52
150. Nagasawa T, Inada Y, Nakano S, et al. Effects of bezafi brate, PPAR pan-agonist, and GW501516, PPARdelta agonist, on development of steatohepatitis in mice fed
a methionine- and choline-defi cient diet. Eur J Pharmacol 2006 ; 536 : 182 -91
151. Magalotti D, Marchesini G, Ramilli S, et al. Splanchnic haemodynamics in non-alcoholic fatty liver disease: effect of a dietary/pharmacological treatment. A pilot study. Dig Liver Dis 2004 ; 36 : 406 -11
152. Uygun A, Kadayifci A, Isik AT, et al. Metformin in the treatment of patients with non-alcoholic steatohepatitis.
Aliment Pharmacol Ther 2004 ; 19 : 537 -44
Affi liation Alessandro Federico † 1 ,2 MD PhD , Marco Niosi 1 MD , Camillo Del Vecchio Blanco 1 MD & Carmela Loguercio 1 MD †Author for correspondence 1 Via Alcide De Gasperi 80, 84018 Scafati (SA), ItalyTel: +39 0815666718 ; Fax: +39 0815666837 ; E-mail: [email protected] 2 2nd University of Naples, Inter-University Research Center on Foods, Nutrition & Gastrointestinal Tract (CIRANAD), Gastroenterology Unit, Italy
Exp
ert O
pin.
Em
ergi
ng D
rugs
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Eur
opea
n on
colo
gy o
n 09
/17/
12Fo
r pe
rson
al u
se o
nly.





























