Embed Size (px)
Citation preview

1
Original PaPer
ENC training reduces perinatal mortality in Karnataka, India
Shivaprasad S. goudar1, Sangappa M. Dhaded1, elizabeth M. McClure2, richard J. Derman3, Vishwanath D. Patil1, niranjana S. Mahantshetti1 roopa M. Bellad1, Bhala Kodkany1, Janet Moore2, linda l. Wright4 & Waldemar a. Carlo5 on behalf of the study investigators*
1Jawaharlal Nehru Medical College, Belgaum, India, 2Research Triangle Institute, North Carolina, USA, 3Christiana Care Health Services, Delaware, USA, 4Eunice Kennedy Shriver National Institute of Child Health and Human Development, Maryland, USA, and 5University of Alabama at Birmingham, Alabama, USA
The Journal of Maternal-Fetal and Neonatal Medicine
2011
00
00
000
000
© 2011 Informa Healthcare USA, Inc.
10.3109/14767058.2011.584088
1476-7058
1476-4954
The Journal of Maternal-Fetal and Neonatal Medicine, 2011, 1-7, Early OnlineCopyright © 2011 Informa Healthcare USA, Inc.ISSN 1476-7058 print/ISSN 1476-4954 onlineDOI: 10.3109/14767058.2011.584088
Correspondence: Shiva S. Goudar, Jawaharlal Nehru Medical College, Belgaum, India. Email: [email protected]
Objective: To evaluate the effect of World Health Organization Essential Newborn Care course and the American Academy of Pediatrics Neonatal Resuscitation Program training on perinatal mortality in rural India. Methods: This study was part of a multi-country prospective, community-based cluster randomized controlled trial. Birth, 7-day and 28-day neonatal outcomes for all women with pregnancies greater than 28 weeks in the 26 study communities in Karnataka, India were included. Mortality rates pre- and post-Essential Newborn Care training were collected prospectively and then communities randomized to either receive neonatal resuscitation or refresher newborn care training in the control clusters. Results: Consent was obtained on 99% of the 25,096 births. Perinatal mortality for infants ≥500g decreased from 52 to 36/1000 after newborn care training (RR 0.7; 95% CI 0.5, 0.9); stillbirth decreased from 23 to 14/1000 (RR 0.62; 95% CI 0.46, 0.83) and early neonatal mortality decreased from 29 to 22/1000 (RR 0.74; 95% CI 0.53, 1.03). Mortality was not reduced further with resuscitation training. Conclusions: Using a pre–post design, World Health Organization Essential Newborn Care community birth attendant training resulted in a significant reduction in perinatal mortality. In low-resource settings, the newborn care training package appears to be an effective intervention to decrease perinatal mortality.
Keywords: Perinatal mortality, essential newborn care, India
Worldwide, the largest numbers of perinatal deaths occur in the Southeast Asia region with an estimated 1.4 million newborn deaths and 1.3 million stillbirths each year[1–6]. In India, where more than half of the births occur at home, often unattended by skilled birth attendants, the major causes of perinatal deaths are estimated to be birth asphyxia, sepsis and low birth weight/prematurity[3].Evidence-based low-cost interventions, which can be introduced as a neonatal and postnatal care package, have been found to be effective in reducing death due to these major causes[7–10]. Estimates suggest that about one-half to two-thirds of the peri-natal deaths could be prevented with universal coverage of essen-tial maternal, newborn, and child care packages[8–10].One training package of newborn interventions is the Essential Newborn Course (ENC) developed by the World Health Organization (WHO)[11]. The ENC course includes evidence-based guidelines for routine care and initial management of
neonates following birth and during the first week after birth, including routine neonatal care, initiation of breathing and resus-citation, thermoregulation, early and exclusive breastfeeding, skin-to-skin care, care of the small baby, counseling on baby care and danger signs, and recognition and initial management of complications.One study found that training and implementation of the ENC significantly reduced early neonatal mortality in a low-risk population delivering in community health centers in Lusaka, Zambia[12,13]. But, in Belgaum district of Karnataka, India, about one-third of the deliveries occur at home, and these deliv-eries are attended only by a traditional birth attendant (TBA) or member of the family, who may have little or no training. Training TBAs has been shown to be possible, especially as a link in the health system, and may contribute to improvements in perinatal mortality in developing countries[11]. Although the ENC course has been used in several parts of the world, its clinical effectiveness has not been demonstrated in population-based studies in low-income countries[12,13]. The American Academy of Pediatrics (AAP) Neonatal Resuscitation Program (NRP) is among the most widely used program for teaching resuscitation; but it also has had only limited evaluation in low-resource settings[14]. Important questions remain about which type of training is most effective to reduce perinatal mortality in low-resource settings such as India.To address the need for effective interventions which can be delivered in home and community settings, we implemented ENC training for physicians, nurse midwives, and TBAs in 26 rural communities in Karnataka, India, as part of a larger Global Network trial on ENC and NRP, the FIRST BREATH Trial, whose major outcomes and methods have been reported elsewhere[13]. This trial (NCT00136708) is registered with a clinical trials database (www.ClinicalTrials.gov). We evaluated the impact of ENC and NRP training in one of the Indian sites, the largest site participating in the Global Network trial, to evaluate the specific impact and potential modifying factors, in one state of India. We hypothesized that ENC and NRP would result in decreased perinatal mortality as well as stillbirths and all cause 7-day (early) neonatal mortality in rural communities in India.
Patients and methodsThis study was conducted in 26 clusters of Karnataka, India, between March 2005 and March 2008. The communities were
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 21
0.21
2.19
3.2
on 0
7/27
/11
For
pers
onal
use
onl
y.

2 S. S. Goudar et al.
The Journal of Maternal-Fetal and Neonatal Medicine
selected to be representative of rural areas, to be geographically distinct, and to have at least 300 births per year. The study included all births that occurred within the defined communities, and all deliveries at the public and private health centers, regardless of the presence of a trained birth attendant at delivery.
For baseline data, a registry of pregnant women was developed for each community with the goal of identifying all pregnancies by 28 weeks gestation and a detailed tracking system facilitated data collection. Study data were verified with government data and a house-to-house survey of expectant mothers. Maternal, pregnancy, delivery, and neonatal outcomes were collected. In addition, data were collected regarding existing newborn care and resuscitation practices in the community.
A trainer-of-trainers model was developed using a variety of teaching methods for participant learning including didactic presentations, clinical practice sessions and demonstrations. Experienced trainers (WAC, EMC; data collection; O. Lincetto, MD from WHO for ENC) trained a lead investigator (SSG) and two site coordinators (VDP, SMD) as national trainers. These national trainers, assisted by two more trainers (NSM, RMB), trained and one or more Cluster Coordinators (CC) per commu-nity. The CCs were Primary Health Center Medical Officers, who then trained all active birth attendants within each community. Birth attendants included nurses and physicians Auxiliary Nurse Midwives (ANMs), TBAs and other community birth attendants (practicing birth attendants with no formal government training). Data collection, ENC, and NRP training, were each 1–5 day courses held at different times.
The baseline training incorporated assessment of newborns for gestational age, Apgar scores and completion of the data forms (pictorial for TBAs). The ENC training focused on adoption of clean delivery practices, assisting the newborn to breathe by bag and mask ventilation, establishing skin-to-skin contact, and early initiation of breastfeeding. Training of the CC was for 5 days, the ANMs and TBAs were trained for 3 days and the physicians for one day. The training of the CCs and physicians was done centrally in Belgaum, conducted by the pediatric trainers while the training of the ANMs, TBAs and other community birth attendants was done in the community by the CCs with support and monitoring by the central research team.
All birth attendants were provided bags and masks and simple suction devices following the ENC training. Delivery kits were provided for all births throughout the trial. Kits included soap, sterilized disposable gloves, gauze, cotton balls, antiseptic solution, ties for clamping the umbilical cord and a blade. Stethoscopes, UNICEF spring Salter baby weighing Scales (UNICEF model 145555), and stop watches were also provided at the training.
Community birth attendants obtained consent and collected all data on standardized data forms, using numbered patient identifiers under the supervision of a CC who also performed the neurological exams on the seventh day after birth. Data forms were reviewed for accuracy by the CCs before submission to the local research office for data entry and transmission to the data coordinating center. Data were collected for 3 to 7 month pre-ENC and 4 to 6 months post-ENC training.
Clusters which had a minimal neonatal mortality rate and were within the identified geographic area were eligible for inclusion in the trial. A detailed description and sample size for the parent trial is described elsewhere[13]. The clusters were randomized to early or late Neonatal Resuscitation Program training using a stratified block design. For purposes of this analysis, we limited it to those which were in the trial in the Karnataka District. The first 16 clusters started baseline data collection in April to June 2005, and an additional 10 clusters joined the study in March
2006. During the parent trial, First Breath, investigators identified the need for additional study clusters. Thus, 10 additional clusters were included at the Karnataka site; a benefit was that the addition of these clusters ensured that the majority of births occurring in the Karnataka district during the period of the trial were included in this trial. The original clusters trained for ENC in November-December 2005 and the birth attendants in the additional clusters were trained in June 2006.
Following post-ENC data collection, communities were randomized to NRP training or control (the control community birth attendants received refresher ENC training). The NRP course contents included an in-depth hands-on training in basic knowledge and skills of initial resuscitation steps, and bag and mask ventilation. Chest compressions, endotracheal intubation, and other advanced contents were not taught. The NRP interven-tion training and data collection were completed between July 2006 and August 2008 (exact dates varied by cluster).
Community involvement and approvals
In these communities, government officials and leaders facilitated the training of all birth attendants in the protocol, data collection, and ENC course and allowed birth attendants to obtain consent and data collection. The study was approved by the institutional review boards at Jawaharlal Nehru Medical College (JNMC), University of Missouri at Kansas City, University of Alabama at Birmingham and RTI. Informed consent was obtained from the mothers. An independent Data Monitoring Committee appointed by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) reviewed recruitment and adverse events during the entire data collection period.
The primary outcome, perinatal mortality was defined as stillbirth or death within 7 days after birth. Secondary outcomes were stillbirth and early neonatal mortality rates, changes in both desirable newborn practices such as the (establishment of skin-to skin contact and putting the baby to breast in the first hour of life), and undesirable newborn practices (holding the baby upside down, sprinkling the baby with water, and blowing in the ear and mouth). Births <1500 g were excluded from the analyses.
Data edits, including inter- and intraform consistency checks, were performed upon data entry at each research site with addi-tional edits performed centrally by the data center. Multivariate logistic regression models with generalized estimating equa-tions adjusting for cluster were used to determine differences in maternal and neonatal characteristics between the pre- and post-ENC data and between the NRP intervention and control data. Adjusted relative risks (RR) and 95% confidence intervals (CI) using multivariate log-binomial models with generalized estimating equations adjusting for adjusting for intercluster are reported for the post- versus the precomparison of the effect of training in Essential Newborn Care and in the comparison of the Neonatal Resuscitation Program intervention versus post Neonatal Resuscitation Program control (ENC only) groups. The data were analyzed using SAS version 9.2 (Cary NC).
ResultsWithin the 26 community clusters, a total of 5,912 births occurred pre-ENC training and 6,163 births post-ENC training. Following randomization, 6,409 births were enrolled in the NRP control group and 6,386 births were enrolled in the NRP intervention group. Follow-up 7 days postbirth was obtained on >95% of infants enrolled in all groups. (Figure 1) Of the 1,234 area birth attendants, 973 (79 %) were active birth attendants trained in the ENC course, and 450 in the intervention group were trained
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 21
0.21
2.19
3.2
on 0
7/27
/11
For
pers
onal
use
onl
y.

ENC and NRP training in Karnataka 3
Copyright © 2011 Informa UK, Ltd.
in NRP. In each of the periods, the birth attendants consisted of 2-3% physicians and 20% ANMs. The remaining birth attendants were TBAs and other community birth attendants.
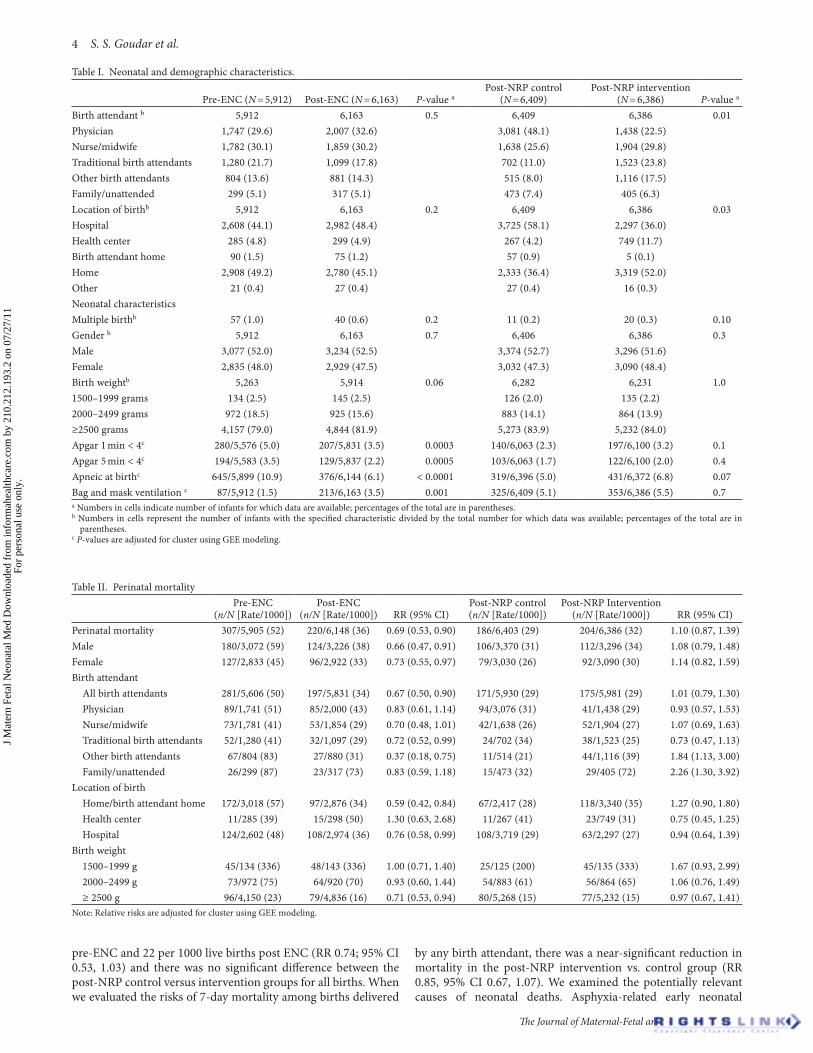
Table I shows the baseline neonatal characteristics of the pre- and post-ENC groups and post-NRP control and interven-tion groups. There were statistically significant differences in the distribution of birth attendants and birth location in the post NRP control vs. intervention groups. However, the groups were similar with respect to proportion of multiple births, birth weight and gender of infants. Compared to the pre-ENC group, there was a statistically significantly increase in the proportion of infants who received bag and mask ventilation in the post-ENC period compared (p = 0.001) but not a statistically significant difference in the post-NRP control vs. intervention group (p = 0.07).
The perinatal mortality rate during the pre-ENC period was 52 per 1000 compared to 36 per 1000 in the post-ENC period (RR 0.69, 95% CI 0.53, 0.90; Table II). There was no significant differ-ence in perinatal mortality rate in the post-NRP intervention clusters compared to the control clusters (RR 1.10; 95% CI 0.87,
1.39). The results were similar when the results were restricted to those births attended by birth attendants, although the perinatal mortality rates varied by type and presence of birth attendant. The highest perinatal mortality rates across all treatment groups were among those unattended or family attended deliveries. Finally, when we stratified by birth weight, the only significant decrease in perinatal mortality observed was from pre-ENC to post-ENC among infants ≥2500 g (RR 0.71; 95% CI 0.53, 0.94), although the total number of infants in the lower birth weight categories limited the power to detect a modest but clinically important differences. For perinatal mortality, the ICC was 0.001 and variance between clusters was 0.00004.
We next examined the components of perinatal mortality, stillbirth and <7-day mortality, separately. As shown in Table III, the stillbirth rate declined significantly pre-to post ENC training, from 23 per 1000 to 14 per 1000 (RR 0.62; 95% CI 0.46, 0.83), among both macerated and fresh stillbirths and male and female fetuses. Table 4 shows the analyses of 7-day neonatal mortality. The 7-day neonatal mortality rates were 29 per 1000 live births
Figure 1. Consort flowchart.
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 21
0.21
2.19
3.2
on 0
7/27
/11
For
pers
onal
use
onl
y.
4 S. S. Goudar et al.
The Journal of Maternal-Fetal and Neonatal Medicine
pre-ENC and 22 per 1000 live births post ENC (RR 0.74; 95% CI 0.53, 1.03) and there was no significant difference between the post-NRP control versus intervention groups for all births. When we evaluated the risks of 7-day mortality among births delivered
by any birth attendant, there was a near-significant reduction in mortality in the post-NRP intervention vs. control group (RR 0.85, 95% CI 0.67, 1.07). We examined the potentially relevant causes of neonatal deaths. Asphyxia-related early neonatal
Table I. Neonatal and demographic characteristics.
Pre-ENC (N = 5,912) Post-ENC (N = 6,163) P-value aPost-NRP control
(N = 6,409)Post-NRP intervention
(N = 6,386) P-value a
Birth attendant b 5,912 6,163 0.5 6,409 6,386 0.01Physician 1,747 (29.6) 2,007 (32.6) 3,081 (48.1) 1,438 (22.5) Nurse/midwife 1,782 (30.1) 1,859 (30.2) 1,638 (25.6) 1,904 (29.8) Traditional birth attendants 1,280 (21.7) 1,099 (17.8) 702 (11.0) 1,523 (23.8) Other birth attendants 804 (13.6) 881 (14.3) 515 (8.0) 1,116 (17.5) Family/unattended 299 (5.1) 317 (5.1) 473 (7.4) 405 (6.3) Location of birthb 5,912 6,163 0.2 6,409 6,386 0.03Hospital 2,608 (44.1) 2,982 (48.4) 3,725 (58.1) 2,297 (36.0) Health center 285 (4.8) 299 (4.9) 267 (4.2) 749 (11.7) Birth attendant home 90 (1.5) 75 (1.2) 57 (0.9) 5 (0.1) Home 2,908 (49.2) 2,780 (45.1) 2,333 (36.4) 3,319 (52.0) Other 21 (0.4) 27 (0.4) 27 (0.4) 16 (0.3) Neonatal characteristicsMultiple birthb 57 (1.0) 40 (0.6) 0.2 11 (0.2) 20 (0.3) 0.10Gender b 5,912 6,163 0.7 6,406 6,386 0.3Male 3,077 (52.0) 3,234 (52.5) 3,374 (52.7) 3,296 (51.6) Female 2,835 (48.0) 2,929 (47.5) 3,032 (47.3) 3,090 (48.4) Birth weightb 5,263 5,914 0.06 6,282 6,231 1.01500–1999 grams 134 (2.5) 145 (2.5) 126 (2.0) 135 (2.2) 2000–2499 grams 972 (18.5) 925 (15.6) 883 (14.1) 864 (13.9) ≥2500 grams 4,157 (79.0) 4,844 (81.9) 5,273 (83.9) 5,232 (84.0) Apgar 1 min < 4c 280/5,576 (5.0) 207/5,831 (3.5) 0.0003 140/6,063 (2.3) 197/6,100 (3.2) 0.1Apgar 5 min < 4c 194/5,583 (3.5) 129/5,837 (2.2) 0.0005 103/6,063 (1.7) 122/6,100 (2.0) 0.4Apneic at birthc 645/5,899 (10.9) 376/6,144 (6.1) < 0.0001 319/6,396 (5.0) 431/6,372 (6.8) 0.07Bag and mask ventilation c 87/5,912 (1.5) 213/6,163 (3.5) 0.001 325/6,409 (5.1) 353/6,386 (5.5) 0.7a Numbers in cells indicate number of infants for which data are available; percentages of the total are in parentheses.b Numbers in cells represent the number of infants with the specified characteristic divided by the total number for which data was available; percentages of the total are in
parentheses.c P-values are adjusted for cluster using GEE modeling.
Table II. Perinatal mortality
Pre-ENC
(n/N [Rate/1000])Post-ENC
(n/N [Rate/1000]) RR (95% CI)Post-NRP control (n/N [Rate/1000])
Post-NRP Intervention (n/N [Rate/1000]) RR (95% CI)
Perinatal mortality 307/5,905 (52) 220/6,148 (36) 0.69 (0.53, 0.90) 186/6,403 (29) 204/6,386 (32) 1.10 (0.87, 1.39)Male 180/3,072 (59) 124/3,226 (38) 0.66 (0.47, 0.91) 106/3,370 (31) 112/3,296 (34) 1.08 (0.79, 1.48)Female 127/2,833 (45) 96/2,922 (33) 0.73 (0.55, 0.97) 79/3,030 (26) 92/3,090 (30) 1.14 (0.82, 1.59)Birth attendant All birth attendants 281/5,606 (50) 197/5,831 (34) 0.67 (0.50, 0.90) 171/5,930 (29) 175/5,981 (29) 1.01 (0.79, 1.30) Physician 89/1,741 (51) 85/2,000 (43) 0.83 (0.61, 1.14) 94/3,076 (31) 41/1,438 (29) 0.93 (0.57, 1.53) Nurse/midwife 73/1,781 (41) 53/1,854 (29) 0.70 (0.48, 1.01) 42/1,638 (26) 52/1,904 (27) 1.07 (0.69, 1.63) Traditional birth attendants 52/1,280 (41) 32/1,097 (29) 0.72 (0.52, 0.99) 24/702 (34) 38/1,523 (25) 0.73 (0.47, 1.13) Other birth attendants 67/804 (83) 27/880 (31) 0.37 (0.18, 0.75) 11/514 (21) 44/1,116 (39) 1.84 (1.13, 3.00) Family/unattended 26/299 (87) 23/317 (73) 0.83 (0.59, 1.18) 15/473 (32) 29/405 (72) 2.26 (1.30, 3.92)Location of birth Home/birth attendant home 172/3,018 (57) 97/2,876 (34) 0.59 (0.42, 0.84) 67/2,417 (28) 118/3,340 (35) 1.27 (0.90, 1.80) Health center 11/285 (39) 15/298 (50) 1.30 (0.63, 2.68) 11/267 (41) 23/749 (31) 0.75 (0.45, 1.25) Hospital 124/2,602 (48) 108/2,974 (36) 0.76 (0.58, 0.99) 108/3,719 (29) 63/2,297 (27) 0.94 (0.64, 1.39)Birth weight 1500–1999 g 45/134 (336) 48/143 (336) 1.00 (0.71, 1.40) 25/125 (200) 45/135 (333) 1.67 (0.93, 2.99) 2000–2499 g 73/972 (75) 64/920 (70) 0.93 (0.60, 1.44) 54/883 (61) 56/864 (65) 1.06 (0.76, 1.49) ≥ 2500 g 96/4,150 (23) 79/4,836 (16) 0.71 (0.53, 0.94) 80/5,268 (15) 77/5,232 (15) 0.97 (0.67, 1.41)Note: Relative risks are adjusted for cluster using GEE modeling.
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 21
0.21
2.19
3.2
on 0
7/27
/11
For
pers
onal
use
onl
y.

ENC and NRP training in Karnataka 5
Copyright © 2011 Informa UK, Ltd.
deaths showed a non-significant reduction between the pre-and post-ENC periods (15.0 per 1000 pre-ENC vs. 11.0 per 1000 post ENC; RR 0.74; 95% CI 0.48–1.15) as well as the NRP intervention compared to control group (5.0 per 1000 post-NRP intervention vs. 7.0 per 1000 post-NRP control; RR 0.73; 95% CI 0.41–1.28; data not shown).
We also examined specific newborn care and resuscitation practices among those who were resuscitated (Table V). There were significant increases in the use of bag-and-mask resus-citation from pre-ENC to post-ENC (14 per 1000 to 48 per 1000, p < 0.0001), with a further increases observed in both groups, although there was not a significant difference between
the post-NRP intervention compared to control groups (88.1 per 1000 vs. 78.6 per 1000, p = 0.3). Skin-to-skin contact also increased significantly (50.2% to 81.7%, p < 0.0001) from pre-ENC to post-ENC and was even more in the NRP inter-vention clusters (83.7% vs. 92.2%, p = 0.004). Breastfeeding within one hour was significantly higher post-ENC compared to pre-ENC (88.4% vs. 73.1%, p < 0.0001). Finally, the analyses of the 7-day neurological evaluation showed no significant differences in the proportion of infants with impairment; 96.8% of the NRP intervention and 98.2% of those in the control group had a normal neurological examination (p = 0.5, data not shown).
Table III. Stillbirths.
Pre-ENC
(n/N [Rate/1000])Post-ENC
(n/N [Rate/1000]) RR (95% CI)Post-NRP control (n/N [Rate/1000])
Post-NRP intervention (n/N [Rate/1000]) RR (95% CI)
Stillbirth 138/5,912 (23) 89/6,163 (14) 0.62 (0.46, 0.83) 86/6,409 (13) 112/6,386 (18) 1.31 (0.88, 1.95)Fresh stillbirth 104/5,912 (18) 71/6,163 (12) 0.65 (0.46, 0.93) 73/6,409 (11) 91/6,386 (14) 1.25 (0.81, 1.93)Macerated stillbirth 34/5,912 (6) 18/6,163 (3) 0.51 (0.28, 0.93) 13/6,409 (2) 21/6,386 (3) 1.62 (0.60, 4.35)Male 82/3,077 (27) 52/3,234 (16) 0.60 (0.41, 0.88) 48/3,374 (14) 61/3,296 (19) 1.30 (0.77, 2.19)Female 56/2,835 (20) 37/2,929 (13) 0.64 (0.45, 0.91) 38/3,032 (13) 51/3,090 (17) 1.32 (0.81, 2.15)Birth attendant All birth attendants 125/5,613 (22) 78/5,846 (13) 0.60 (0.43, 0.83) 81/5,936 (14) 98/5,981 (16) 1.20 (0.78, 1.85) Physician 39/1,747 (22) 40/2,007 (20) 0.89 (0.56, 1.41) 40/3,081 (13) 27/1,438 (19) 1.45 (0.70, 2.98) Nurse/midwife 32/1,782 (18) 18/1,859 (10) 0.54 (0.29, 0.99) 22/1,638 (13) 30/1,904 (16) 1.17 (0.66, 2.08) Traditional birth attendants 26/1,280 (20) 9/1,099 (8) 0.40 (0.19, 0.84) 15/702 (21) 20/1,523 (13) 0.61 (0.36, 1.05) Other birth attendants 28/804 (35) 11/881 (13) 0.36 (0.17, 0.75) 4/515 (8) 21/1,116 (19) 2.42 (0.70, 8.43) Family/unattended 13/299 (44) 11/317 (35) 0.80 (0.39, 1.65) 5/473 (11) 14/405 (35) 3.27 (0.99, 10.80)Location of birth Home/birth attendant home 75/3,019 (25) 36/2,882 (12) 0.50 (0.37, 0.69) 33/2,417 (14) 63/3,340 (19) 1.38 (0.87, 2.19) Health center 4/285 (14) 8/299 (27) 1.91 (0.64, 5.67) 7/267 (26) 10/749 (13) 0.51 (0.20, 1.29) Hospital 59/2,608 (23) 45/2,982 (15) 0.67 (0.44, 1.01) 46/3,725 (12) 39/2,297 (17) 1.37 (0.73, 2.60)Birth weight (g) 1500–1999 g 16/134 (119) 22/145 (152) 1.27 (0.75, 2.15) 7/126 (56) 29/135 (215) 3.87 (1.14, 13.06) 2000–2499 g 35/972 (36) 27/925 (29) 0.81 (0.50, 1.31) 25/883 (28) 28/864 (32) 1.14 (0.65, 2.02) ≥2500 g 29/4,157 (7) 21/4,844 (4) 0.62 (0.37, 1.04) 34/5,273 (6) 36/5,232 (7) 1.07 (0.60, 1.90)Note: Relative risks are adjusted for cluster using GEE modeling.
Table IV. Seven-day neonatal mortality.
Pre-ENC
(n/N [Rate/1000])Post-ENC
(n/N [Rate/1000]) RR (95% CI)Post-NRP control (n/N [Rate/1000])
Post-NRP intervention (n/N [Rate/1000]) RR (95% CI)
Seven-day neonatal mortality 169/5,767 (29) 131/6,059 (22) 0.74 (0.53, 1.03) 100/6,317 (16) 92/6,274 (15) 0.93 (0.73, 1.17)Male 98/2,990 (33) 72/3,174 (23) 0.69 (0.46, 1.05) 58/3,322 (17) 51/3,235 (16) 0.90 (0.63, 1.30)Female 71/2,777 (26) 59/2,885 (20) 0.80 (0.57, 1.13) 41/2,992 (14) 41/3,039 (13) 0.98 (0.64, 1.51)Birth attendant All birth attendants 156/5,481 (29) 119/5,753 (21) 0.73 (0.52, 1.02) 90/5,849 (15) 77/5,883 (13) 0.85 (0.67, 1.07) Physician 50/1,702 (29) 45/1,960 (23) 0.78 (0.55, 1.12) 54/3,036 (18) 14/1,411 (10) 0.56 (0.33, 0.95) Nurse/midwife 41/1,749 (23) 35/1,836 (19) 0.81 (0.51, 1.30) 20/1,616 (12) 22/1,874 (12) 0.95 (0.51, 1.76) Traditional birth attendants 26/1,254 (21) 23/1,088 (21) 1.02 (0.65, 1.61) 9/687 (13) 18/1,503 (12) 0.91 (0.46, 1.82) Other birth attendants 39/776 (50) 16/869 (18) 0.37 (0.15, 0.90) 7/510 (14) 23/1,095 (21) 1.53 (0.71, 3.30) Family/unattended 13/286 (46) 12/306 (39) 0.86 (0.53, 1.41) 10/468 (21) 15/391 (38) 1.80 (0.85, 3.80)Location of birth Home/birth attendant home 97/2,943 (33) 61/2,840 (21) 0.65 (0.40, 1.05) 34/2,384 (14) 55/3,277 (17) 1.18 (0.74, 1.86) Health center 7/281 (25) 7/290 (24) 0.97 (0.36, 2.61) 4/260 (15) 13/739 (18) 1.14 (0.55, 2.39) Hospital 65/2,543 (26) 63/2,929 (22) 0.84 (0.59, 1.20) 62/3,673 (17) 24/2,258 (11) 0.63 (0.39, 1.01)Birth weight 1500–1999 g 29/118 (246) 26/121 (215) 0.87 (0.56, 1.35) 18/118 (153) 16/106 (151) 0.99 (0.44, 2.25) 2000–2499 g 38/937 (41) 37/893 (41) 1.02 (0.52, 1.99) 29/858 (34) 28/836 (33) 0.99 (0.64, 1.53) ≥2500 g 67/4,121 (16) 58/4,815 (12) 0.74 (0.52, 1.06) 46/5,234 (9) 41/5,196 (8) 0.90 (0.60, 1.34)Note: Relative risks are adjusted for cluster using GEE modeling.
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 21
0.21
2.19
3.2
on 0
7/27
/11
For
pers
onal
use
onl
y.

6 S. S. Goudar et al.
The Journal of Maternal-Fetal and Neonatal Medicine
DiscussionThis study conducted in rural communities in India found that ENC training significantly reduced perinatal mortality, while subsequent NRP training did not provide further reductions in mortality. There are limited data on the effectiveness of training community birth attendants including TBAs in low-income countries[9,15–17]. Our findings are consistent with a commu-nity trial which estimated a 30% reduction in neonatal mortality in Nepal in clusters exposed to different community-based interventions[16] and by training TBAs in Pakistan[17]. These and other studies have suggested that reducing mortality beyond a certain level requires access to facility care where emergency obstetrical and neonatal care services can be obtained[9,18,16]. However, to date, randomized trials have not evaluated the impact of ENC or NRP training programs on mortality rates which, despite their widespread use worldwide, have had limited evaluation in a community setting[11,17,19–21].
Our study included training of a wide variety of birth atten-dants, who both conducted home and hospital deliveries in the area. While we saw an increase in babies born in the hospital and delivered by physicians in the post-ENC period, this alone is unlikely to explain the mortality decreases because the largest decreases in perinatal mortality and stillbirth rates occurred for babies delivered at home and by TBAs. Stillbirth rates were unchanged in the hospitals. Although there were no significant reductions in perinatal mortality overall, when we examined the mortality rates among those with a physician present, the NRP training group had a significant reduction in mortality. These results, however, must be interpreted with caution as there may be other factors involved.
One of the strengths of this study was the comprehensive system established to register all women during pregnancy. In addition, all births in the community were included in the study outcome, regardless of the presence of a trained birth attendant at the delivery, to account for a potential shift in delivery loca-tion or attendant over time. The rigorous training using master instructors, the use of local trainers to train the birth attendants, the use of pregnancy/birth registries to capture all births, the high consent rate, and the high 7-day follow-up rate were addi-tional strengths. This is among the first effectiveness studies of a neonatal care package, the ENC and NRP, conducted at scale
in a large population-based study in India[22]. We found that a training package with a train-the-trainer mechanism can reduce overall perinatal mortality rates in geographic areas with high baseline rates.
One of the limitations of the study include that clusters were not randomized to receive the ENC training. Although this may have improved the internal validity of the study, this study was undertaken as part of a larger study to examine the effects of NRP and for ethical reasons and uniformity of comparison, we chose to use ENC as a run-in intervention before the NRP education was provided.
We speculate that the ENC focus on birth preparedness, resuscitation, breastfeeding, clean delivery, cord care, and hypothermia prevention will need to be supplemented with other programs in the community for the early recognition and treatment of sepsis in the newborn as well as manage-ment of low and very low birth weight babies in order to reduce neonatal mortality rates further. Future research should include determinations of other effective community interventions in addition to ENC training to reduce neonatal mortality rates. Furthermore, our study also examined factors among communities that might have impacted the variation in mortality after the ENC. This analysis may help other countries, or sites as these programs are expanded. Our data provide evidence that newborn outcomes can be influenced by the ENC implemented in community based settings within the existing health care infrastructure with a wide variety of birth attendants. We present this as one way to improve survival of newborns in developing countries.
Acknowledgements*The authors are grateful to the contributions of additional study investigators: Vidya Sharma MD; University of Missouri at Kansas City, USA, and Hrishikesh Chakraborty, Research Triangle Institute, USA.
Declaration of interest: The Bill and Melinda Gates Foundation and the US National Institute of Child Health and Human Development (NICHD), under a cooperative agreement with the grantees supported the trial (U01 HD043464, U01 HD040607,
Table V. Newborn care and resuscitation practices.
Pre-ENC (n/N [%]) Post-ENC (n/N [%]) P-Value
Post-NRP control (n/N [%])
Post-NRP intervention (n/N [%]) P-value
Number resuscitated 622 440 407 396 Bag and Mask 87 (14.0) 212 (48.2) < 0.0001 320 (78.6) 349 (88.1) 0.3Mouth to Mouth 129 (20.7) 51 (11.6) 0.06 10 (2.5) 6 (1.5) 0.7Chest Compression 278 (44.7) 90 (20.5) < 0.0001 20 (4.9) 18 (4.5) 0.9Skin to Skin Contact 2,902 (50.2) 4,999 (81.7) < 0.0001 5,341 (83.7) 5,832 (92.2) 0.004Baby Put to Breast in 1st Hour 4,196 (73.1) 5,401 (88.4) < 0.0001 5,671 (88.9) 5,901 (93.3) 0.08Received Resuscitation 622 (10.5) 440 (7.1) < 0.0001 407 (6.4) 396 (6.2) 0.9Resuscitation Practices 622 440 407 396 Baby upside down 39 (6.3) 12 (2.7) 0.007 1 (0.2) 0 (0.0) —Blowing in ear and mouth 18 (2.9) 1 (0.2) 0.008 0 (0.0) 1 (0.3) —Cleaning oral cavity 25 (4.0) 7 (1.6) 0.09 0 (0.0) 0 (0.0) —Nasal stimulation 9 (1.4) 1 (0.2) < 0.0001 0 (0.0) 0 (0.0) —Oxygen 26 (4.2) 24 (5.5) 0.5 8 (2.0) 0 (0.0) —Sprinkling with water 82 (13.2) 11 (2.5) < 0.0001 1 (0.2) 0 (0.0) —Suction 70 (11.3) 76 (17.3) 0.07 63 (15.5) 4 (1.0) 0.001Tactile stimulation 68 (10.9) 40 (9.1) 0.7 3 (0.7) 11 (2.8) 0.1Note: P-values are adjusted for cluster using GEE modeling.
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 21
0.21
2.19
3.2
on 0
7/27
/11
For
pers
onal
use
onl
y.

ENC and NRP training in Karnataka 7
Copyright © 2011 Informa UK, Ltd.
U01 HD040636, U01 HD042372). The authors declare that no conflict of interest.
References1. Lawn J, Shibuya K, Stein C. No cry at birth: global estimates of
intrapartum stillbirths and intrapartum-related neonatal deaths. Bull World Health Organ 2005;83:409–417.
2. McClure EM, Wright LL, Goldenberg RL, Goudar SS, Parida SN, Jehan I, Tshefu A, et al.; NICHD FIRST BREATH Study Group. The global network: a prospective study of stillbirths in developing countries. Am J Obstet Gynecol 2007;197:247.e1–247.e5.
3. WHO. The World Health Report 2005: make every mother and child count. 2006. http://www.who.int/whr/2005/en/
4. Lawn JE, Cousens S, Zupan J; Lancet Neonatal Survival Steering Team. 4 million neonatal deaths: when? Where? Why? Lancet 2005;365:891–900.
5. Murray CJ, Laakso T, Shibuya K, Hill K, Lopez AD. Can we achieve Millennium Development Goal 4? New analysis of country trends and forecasts of under-5 mortality to 2015. Lancet 2007;370:1040–1054.
6. Darmstadt GL, Bhutta ZA, Cousens S, Adam T, Walker N, de Bernis L; Lancet Neonatal Survival Steering Team. Evidence-based, cost-effective interventions: how many newborn babies can we save? Lancet 2005;365:977–988.
7. Haws RA, Thomas AL, Bhutta ZA, Darmstadt GL. Impact of packaged interventions on neonatal health: a review of the evidence. Health Policy Plan 2007;22:193–215.
8. Bhutta ZA, Darmstadt GL, Hasan BS, Haws RA. Community-based interventions for improving perinatal and neonatal health outcomes in developing countries: a review of the evidence. Pediatrics 2005;115:519–617.
9. Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS; Bellagio Child Survival Study Group. How many child deaths can we prevent this year? Lancet 2003;362:65–71.
10. WHO. Essential newborn care 1996. World Health Organization, Geneva: WHO/FRH/MSM/96.13
11. Carlo WA, Wright LL, Chomba E, McClure EM, Carlo ME, Bann CM, Collins M, Harris H. Educational impact of the neonatal resuscitation
program in low-risk delivery centers in a developing country. J Pediatr 2009;154:504–508.e5.
12. Chomba E, McClure EM, Wright LL, Carlo WA, Chakraborty H, Harris H. Effect of WHO newborn care training on neonatal mortality by education. Ambul Pediatr 2008;8:300–304.
13. Carlo WA, Goudar SS, Jehan I, Chomba E, Tshefu A, Garces A, Parida S, et al.; First Breath Study Group. Newborn-care training and perinatal mortality in developing countries. N Engl J Med 2010;362:614–623.
14. Kumar V, Mohanty S, Kumar A, Misra RP, Santosham M, Awasthi S, Baqui AH, et al.; Saksham Study Group. Effect of community-based behaviour change management on neonatal mortality in Shivgarh, Uttar Pradesh, India: a cluster-randomised controlled trial. Lancet 2008;372:1151–1162.
15. Manandhar DS, Osrin D, Shrestha BP, Mesko N, Morrison J, Tumbahangphe KM, Tamang S, et al.; Members of the MIRA Makwanpur trial team. Effect of a participatory intervention with women’s groups on birth outcomes in Nepal: cluster-randomised controlled trial. Lancet 2004;364:970–979.
16. Jokhio AH, Winter HR, Cheng KK. An intervention involving traditional birth attendants and perinatal and maternal mortality in Pakistan. N Engl J Med 2005;352:2091–2099.
17. McClure EM, Goldenberg RL, Bann CM. Maternal mortality, stillbirth and measures of obstetric care in developing and developed countries. Int J Gynaecol Obstet 2007;96:139–146.
18. Bang AT, Bang RA, Reddy HM, Deshmukh MD, Baitule SB. Reduced incidence of neonatal morbidities: effect of home-based neonatal care in rural Gadchiroli, India. J Perinatol 2005;25 Suppl 1:S51–S61.
19. Vidal SA, Ronfani L, da Mota Silveira S, Mello MJ, dos Santos ER, Buzzetti R, Cattaneo A. Comparison of two training strategies for essential newborn care in Brazil. Bull World Health Organ 2001;79:1024–1031.
20. Uxa F, Bacci A, Mangiaterra V, Chiaffoni GP. Essential newborn care training activities: 8 years of experience in Eastern European, Caucasian and Central Asian countries. Semin Fetal Neonatal Med 2006;11:58–64.
21. McClure EM, Carlo WA, Wright LL, Chomba E, Uxa F, Lincetto O, Bann C. Evaluation of the educational impact of the WHO Essential Newborn Care course in Zambia. Acta Paediatr 2007;96:1135–1138.
22. Kesterton AJ, Cleland J. Neonatal care in rural Karnataka: healthy and harmful practices, the potential for change. BMC Pregnancy Childbirth 2009;9:20.
J M
ater
n Fe
tal N
eona
tal M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y 21
0.21
2.19
3.2
on 0
7/27
/11
For
pers
onal
use
onl
y.





























