Embed Size (px)
Citation preview
229
Endocardial and Epicardial Ablation Guided byNonsurgical Transthoracic Epicardial Mapping
to Treat Recurrent Ventricular Tachycardia
EDUARDO SOSA. M.D.. MAURICIO SCANAVACCA, M.D., ANDRE D'AVILA. M.D.JOAO PICCIONI. M.D., OSVALDO SANCHEZ. M.D.. JOSE L. VELARDE, M.D.,
MARCIO SILVA, M.D., and BASILEO REOLAO, M.D.
From the Heart Institute, University of Sao Paulo Medical School, Sao Paulo, Brazil;
Nonsurgical Epicardial Ablation. Introduction: An epicardial site of origin of ventricu-lar tachycardia (VT) may explain unsuccessful endocardial radiofrequency (RF) catheter abla-tion. A new technique to map the epicardial surface of the heart through pericardial puncturewas presented recently and opened the possihility of u.sing epicardial mapping to guide endo-cardial ahlation or epicardial catheter ahlation. We report the efficacy and .safety of these twoapproaches to treat 10 consecutive patients with VT and Chagas' disease.
Methods and Results: Epicardial mapping was carried out with a regular steerable catheterintroduced into the pericardial space. An epicardial circuit was found in 14 of 18 mapahle VTsinduced in 10 patients. Epicardial mapping was used to guide endocardial ahlation in 4 pa-tients and epicardial ahlation in 6. The epicardial earliest activation site occurred 107 ± 60msec earlier than the onset of the QRS complex. At the epicardial site used to guide endocar-dial ahlation, earliest activation occurred 75 ± 55 msec hefore the QRS complex. Epicardialmid-diastolic potentials and/or continuous electrical activity were seen in 7 patients. After 4.8 ±2.9 seconds of epicardial RF applications, VT was rendered noninducihie. Hemopericardiumrequiring drainage occurred in 1 patient; 3 others developed pericardial friction without hemo-pericardium. Patients remain asymptomatic 5 to 9 months after the procedure. Interruptionduring endocardial pulses occurred after 20.2 ± 14 seconds (P - 0.004), hut VT was alwaysreinducihie and the patients experienced a poor outcome.
Conclusion: Epicardial mapping does not enhance the effectiveness of endocardial pulses ofRF. Epicardial applications of RF energy can safely and effectively treat patients with VT andChagas' disease. (J Cardlova.sc Electrophysiol. Vol. 9. pp. 229-239. March 199H)
ventricular tachycardia, catheter ablation, radiofrequency, mapping, eplcardium
Introduction
It has been suggested that 15% of isehemic ven-tricular tachycardias (VTs) have the crucial por-tion of the reentrant circuit located in a subepi-
Prcsenied in abstract form at ihe 70th Scientific Sessions of theAmerican Heart Association. Orlando, Florida, November 1997.
Address for correspondence: Edtiardo Sosa. M.D.. Institiito doCorav'ao. Grupo de ArHtniia. Av, Eneas de Carvaiho Aguiar, 44-Cerqueira Cesar. CEP 05403-000. Sao Pairlo. Brazil. Fax: 55-11-2822354; E-mail: [email protected]
Manuscript received 6 October 1997; Accepted for publication 14Januarv 1998.
cardial layer of viable muscle, which may makeendocardial pulses of radiofrequency (RF) en-ergy less effective and account for the disparity ofresults published by different investigators.' i-" There-fore, it became fundamental to differentiate an epi-cardial from an endocardial circuit during thisera of RF catheter ablation.
A new transthoracic technique to perform ex-tensive epicardial mapping through pericardialpuncture in the eleclrophysiology (EP) laboratorywas described recently by our group.'^ Accord-ing to this methodology, it was possible to iden-tify different VTs related lo an epicardial circuitin a specific subset of patients with VT and Cha-

230 Journal of Cardiovascular Electrophysiology Vol. 9. No. 3. March 1998
gas' disease, opening the possibility of using epi-cardial mapping not only to guide endocardial ab-lation but also to pertonn nonsurgical. transtho-racic epicardial catheter ablation.
The two approaches seem worth investigating.Conventional endocardial RF ablation to treat epi-cardial circuits can be effective if the applicationallows the temperature at the epicardial surface ofthe heart to rise.'* However, based on the experi-ence obtained by other investigators using epicar-dial laser photocoagulation during VT stirgery,^^^it is tempting to speculate that the effectiveness ofcatheter ablation to treat an epicardial circuit willdepend on a technique that allows RF pulses to bedelivered safely to the epicardial surface of the heart.
Tbe aim of the present study is to report the ef-ficacy and safety of endocardial applications guidedby epicardiai mapping and of epicardial applica-tions of RF energy used to treat 10 consecutivepatients with VT and Chagas' heart disease.
Methods
Study Group
The study protocol was approved by the Sci-entific and Ethical Committee of tbe University ofSao Paulo, Sao Paulo, Brazil.
Between July 1995 and March 1996, 10 patientswith drug-refractory VT and Chagas* diseasewere referred to the Heart Institute of the Univer-sity of Sao Paulo Medical School for optimizationof tbeir tberapy. Tlie mean age of the patients was53 ± 10 years (range 39 to 67); there were fourwomen. All patients had a history of at least twodocumented episodes of sustained VT. which oc-curred during the previous 18 months despite theuse of oral amiodarone. VT was associated withpalpitations in 2 patients, near-syncope or syncopein 6 patients, and aboned sudden death in 2 patients.In one patient, incessant VT occurred 1 month af-ter implantation of an implantable cardioverter de-fibrillator (ICD). Five patients previously had un-dergone conventional endocardial RF ablation.
During admission. 5 patients were in New YorkHeiirt Association (NYHA) functional Class I fordyspnea and 5 were in Class II. Mean left ven-tricuky ejection fraction determined by echocar-diography WILS 0.62 ± 0.08 (0.51 to 0.71). Twelve-lead ECG showed sinus rhythm in all patients andright bundle branch block in 5. Left superior fas-cicular block was seen in 8 patients and left bun-dle branch block was found in 1. No patient badobstructive coronary artery disease as shown by
coronary angiography, but left ventricular an-giography showed akinesia or dyskinesia of tbebasal inferolateral left ventriculaj' wall in all cases.Tbese are common findings in patients with re-current VT and Chagas' disease (Fig. 1).
EP Testing
Ail procedures were performed in the clinicalEP laboratory after verbal informed consent wasobtained from eacb patient. EP testing, endocar-dial and epicardial mapping, and ablation were car-ried out in patients deeply sedated with intravenousmidazolam and fentanyl.
A multipolar catheter was introduced under flu-oroscopic guidance through right femoral, anteriorjugular vein puncture and the right femoral artery;it was placed at the apex of the right ventricle,coronary sinus, and left ventricle. Jugular veinpuncture was avoided if the coronary sinus wasreached from tbe inferior vena cava. Ventricularstimulation was performed witb rectangular im-pulses of 2-msec duration at twice diastolic thresh-old. The stimulation protocol consisted of pro-grammed stimulation from the right ventriculai"apex and outflow tract at two different cycle lengthswith up to three premature extrastimuli. Endocar-dial and epicardial left ventricular stimulation wasused whenever necessary.
EP signals were recorded using a PC Electro-physiologic Measurement System (EMS 4.2, Uni-versity of Limburg, Limburg, The Netherlands)at a paper speed of 100 to 300 mm/sec. Tlie gainapplied to the endocardial and ECG signals was10 mm/mV, whereas the epicardial signals (coro-nmy sinus, intravenous, and epiciudial signals) wereregistered at 20 mm/mV and at a filter setting be-tween 50 and 500 Hz.
Endocardial Ablation Guided by EndocardialMapping
In the first four patients, a 7- or 8-Erencbquadripolar catheter witb a 4-mm distal electrodeand deflectable tip was used to perfonn endtK:ar-dial mapping and eventual ablation of ail inducedVTs. The catheter was introduced by right femoralartery puncture and passed retrogtadely across theaortic valve into the left ventricle. A 5(XX)-U bolusof heparin was administered intravenously followedby 10(X) U every hour while the catheter was inthe left ventricle. Catbeter positioning was guidedby fluoroscopy, and mapping sites were designatedaccording to the scbeme described by Josephson.'
Sosa. et al. Nonsurgical Epicardial Ablation 231
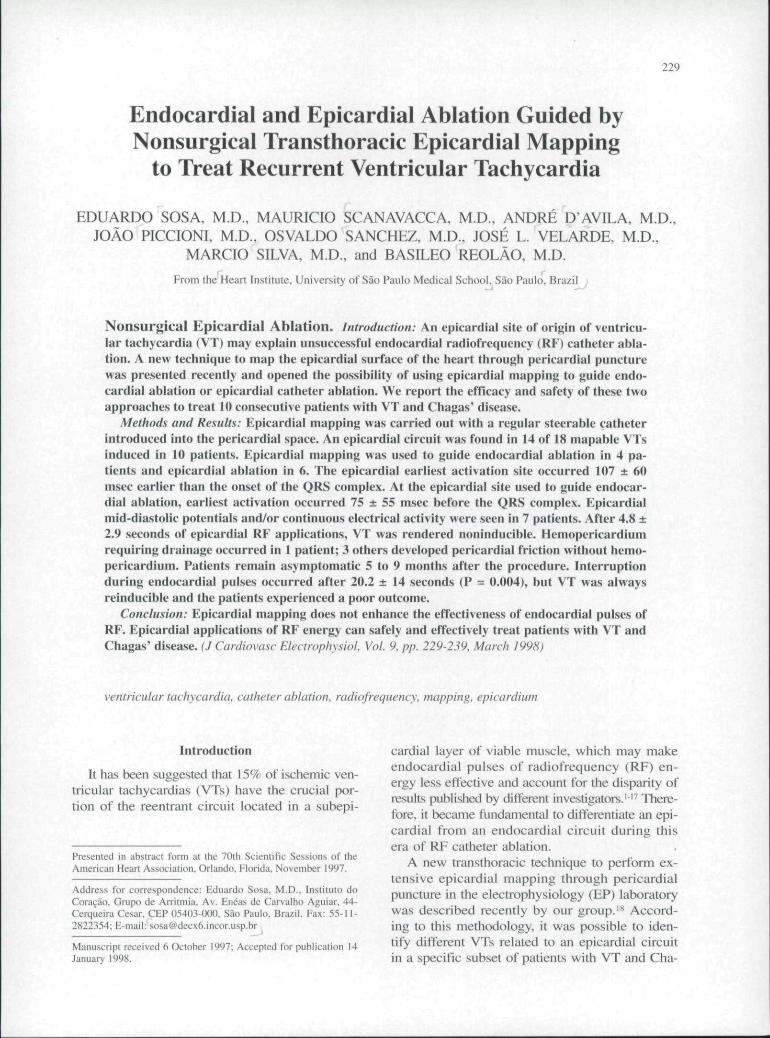
Figure 1. Contrast ventriculography from the 30° RAO view in a paficnr wiih Chagas' disease obtained during diastole (A)ami systole (B). An inferoUUeral aneiiiysm. whieh is the most common substrate for VT to occur in such patients, is .seen. Thetechnique used to peiform epicardiai mapping is summarized in panels C and D. Firsl. a soft floppy-tip guidewire is intro-duceJ hy pericardia! puncture into ihe pericardia! space (large arrow in panel C). The black arrows indicate the presence ofcontrast in the pericardial space. A 7-French regular steerable catheter is introduced gently into the pericardial sac and usedto perform epicardial mapping ami/or ablation. When an appropriate target for ablafion is found, contrast coronary artering-raphy can he obtained to assess the distance between the site of ablation and main coronary arteries and to evaluate the riskof coronary artery damage during RF application (panel D). CS = coronary sinus catheter: EP! = epicardial catheter; RV =right ventricular catheter.
In these patients, either RF pulses delivered atthe best site found did not succeed, or endocardialelectrograms obtained during ventricular mappingwere not considered good enough to justify RF ap-plication. Patients then were scheduled for a newEP evaluation at which time combined endocar-dial and epicardiai mapping was performed.
Transthoracic Epicardial Mapping
Epicardial mapping was perfonned in all pa-tients according to a previously described tech-nique.-*' The skin was prepared in an asepticfashion and ane.sthetized with 1 % lidocaine. Anintroducer needle used to perform epidural anes-thesia (Tuohy-17-^gr., effective length 79.4 mm.overall 101.6 mm. O.D. 1.5 mm, Abbott I/No.
E622 lAbbott Ireland Ltd., Sligo, Ireland]) was ad-vanced under fluoro.scopic guidance until light neg-ative pressure was felt. Two milliliters of contrastmedium was injected to determine the location ofthe needle tip. The appearance of layering of thecontrast medium around the heart silhouette indi-cated that the needle was positioned correetly. Asoft floppy-tip guidewire then was passed throughthe hollow needle and its tip lay within the peri-cardial space, as confirmed by fluoroscopy. A 7-French introducer was advanced, the guidewire re-moved, and a 7-French deflectable catheter with a4-mm tip introduced into the pericardial space un-der fluoroscopy {Fig. I). During VT. ventricularstimulation bipolar pacing with rectangular im-pulses of 2-msec duration at twice diastolic thresh-old obtained during endocardial stimulation was

232 Journal of Cardiovascular Electrophysiology Vol. 9, No. 3. March 1998
used to attempt ventricular capture. If capture wasnot possible, the output was increased progressivelyup to 10 mA and pulse duration up to 3.5 m.sec(maximum output of our device). Unipolar pacingwas never used in this study.
face as compared to the endocardial electrogram,and concealed entrainment with a similar returningcycle, mid-diastolic potentials, or continuous elec-trical activity was obtained only in the epicardiumand RF application rendered VT noninducible.
Endocardial Ablation Guided by TransthoracicEpicardial Mapping
Transthoracic epicardial mapping was used toguide endocardial catheter positioning in the firstfour patients in whom an appropriate signal wasnot obtained during endocardial mapping. In thesecases, a regular 7-French deflectable catheter wasintroduced into the pericardial space before hepa-rin administration. Information thus obtained wasused to guide positioning of the endocardial cath-eter. When a possible epicardial reentrant circuitwas found, the endocardial catheter was positionedin front of the epicardial catheter and RF energywas delivered between the distal tip of the endo-cardial catheter and an indifferent patch electrodelocated on the patient's back.
Epicardial Ablation
Epicardial mapping was used to guide epicar-dial ablation in six patients (patients 5 through 10).A 7-French quadripolar Marinr^^ (Medtronic Car-diorhythm [Minneapolis. MN, USA|) multicurvecatheter with 2-5-2 mm electrtxle spacing. 40- to60-nim curve range, lateral deflector ring, and 4-mm tip electrode was used in all patients. Epicar-dial RF energy was applied with a MedtronicAtakr®' generator, and applications were deliveredbetween the distal tip of the epicardial catheter andan indifferent 110-cm- cutaneous patch electrodelocated on the patient's left scapula. A tempera-ture setting of 60" was used and RF energy de-livered for 30 seconds at each apparently successfulsite. Application was discontinued within 10 sec-onds if VT was not inteniipted. A successful ap-plication was defined as the one producing inter-ruption of VT not preceded by ventricular pre-mature beats, rendering the VT noninducible afterventricular stimulation from the right ventricularapex and outflow tract at two different cycle lengthswith up to three premature extrastimuli prior toand after infusion of intravenous isoproterenol.
Definition of an Epicardial Circuit
VT was classified as epicardial when the earli-est activation site was located at the epicardial sur-
Selection of Target Sites for RF Ablation
Criteria to map VT related to a reentrant circuitas suggested by Stevenson et al." were used for en-docardial and epicardial mapping in the followingsequence. During sinus rhythm, the ablating cath-eter was positioned in the area most likely to bethe site of origin of VT according to analysis of theQRS complex in the 12-lead ECG recorded duringclinical VT. At that site, attempts were made to ob-tain perfect pace mapping. When a good matchingmorphology was found, VT was induced and thecatheter gently moved until an isolated mid-dia-stolic potential or diastolic continuous electrical ac-tivity was found. Pacing maneuvers were performedat these sites during ongoing VT at cycle lengths40 to 100 msec shorter than the VT cycle lengthto allow demonstration of concealed entrainmentand measurement of the returning cycle after in-terruption of epicardial pacing. When ventricularcapture was not possible due to a high stimulationthreshold, the presence of an isolated mid-diastolicpotential or continuous electrical activity was con-sidered an adequate target for ablation.
Avoiding Damage to Coronary Arteries DuringEpicardial RF Applications
In patients in whom epicardial ablation was per-fonned. special attention was given to the distancebetween the coronary arteries and the distal elec-trode of the ablating catheter. Theoretically, thecloser the catheter, the higher tbe risk of damag-ing an epicardial vessel during application of RFenergy. The distance was estimated by one of thefollowing: (1) analyzing the distance between theablating catheter, the coronary sinus catheter, andthe apex of the heart as major epicardial vesselsare unlikely to be present close to the apex; (2)observing the distance between the ablating cath-eter and a coronary artery during left coronaryarteriography (Fig. 1); and (3) observing the dis-tance between the ablating catheter and epicar-dial veins of the heart during retrograde injectionof contrast media into the coronary sinus. It wasassumed tbat in addition to a major epicardial vein,there sbould be an important coronary artery orone of its main branches.
Sosa. et at. Nonsurgical Epicardial Ablation 233
Moreover, the ST-T segment was monitored dur-ing recording of the simultaneous 12-iead ECG af-ter VT interruption to detect any possible lesion inthe coronary arteries.
Postablation Management
Echocardiographic examination of the heart wasperformed just after withdrawal of the epiciirdialcatheter and on the day of hospital discharge. Cre-atine kinase and its MB fraction (CK-MB) weremeasured every 8 hours during the first 24 hoursafter the procedures. Patients were discharged 7days after the procedures if their elinical conditionallowed. They were followed-up in outclinic vis-its every week within the first month and every 3months thereafter.
Statistical Analysis
Statistical analysis was perfonned using the Sta-tistical Analysis System program (SAS InstituteInc., Ciiry, NC, USA). Descriptive data are pre-sented as mean ± SD. The Student's Mest was usedto assess differences between continuous variables.
Results
Eighteen mappable VTs were induced (1 to 4different morphologies per patient) in 10 patients.Electrophysiologic evidence of an epicardial cir-cuit was found in 14 of the VTs. The mean cyclelength of these mappable VTs was 305 ± 48 msec.Six other VTs were induced in 4 patients. Threeof the VTs degenerated into ventricular fibrillation;3 caused hemodynamic collapse and could not bemapped (Table I). When all patients were con-sidered, mean procedure duration was 187 min-utes, and mean radiation exposure time was 12minutes ot" pulsed fluoroscopy.
Endocardial Ablation Guided by EpicardialMapping Versus Epicardial Ablation
During ongoing VX the earliest site of activa-tion was found more frequently at the epicardialsurface of the heart (Table I). At these sites, epi-cardial stimulation was difficult to perform dueto a high threshold. Even with energy output of 10mA and pulse duration of 3.5 msec, only randomventricular capture could be obtained. Therefore,concealed entrainment was obtained in only twocases. In these patients, the returning cycle equaledVT cycle length, and RF application at these
sites interrupted and rendered VT noninducible.Epicardial mid-diastolic potentials and/or continu-ous electrical activity were seen in all patientsbut not in all morphologies (Figs. 2 through 4).
The earliest epicardial activation site occurredI07± 60 msec earlier than the onset of the QRScomplex. At the epicardial site used to guide en-docardial ablation, earliest activation occurred 75± 55 msec before the QRS complex. Time for VTinterruption differed according to the site of ap-plication. When RF energy was delivered to theepicardial surface, interruption occurred after 4.8± 2.9 seconds (Figs. 2 through 4), whereas endo-caidial applications interrupted VT after 20 ± 14seconds (P = 0.004). In patients 6 and 7, epicar-dial ablation of one and two different VTs renderedan additional moiphology noninducible in bothcases. These phenomena were not observed dur-ing endocardial applications guided by epicardialmapping (Table 1).
Endocardial Ablation Guided by TransvenousEpicardial Mapping
In patient 5, transvenous epicardial mapping de-tected several mid-diastolic potentials. At these epi-cardial sites, ventricular capture was not possibledue to a high stimulation threshold. The endocar-dial catheter was positioned in front of the elec-trode with the "best" potential, but endocardialstimulation failed to demonstrate concealed en-trainment. The "best" epicardial signal then waschosen to guide several 60-second endocardial ap-plications of RF.
VT was interrupted various times, usually af-ter 30 seconds of application, but the procedure
TABLE 1Results ol' Epiciirdial Mapping to Guide Endocardial
and Epicardial RF Ablation in 10 Consecutive Patientswith Chagas' Disease to Treat Recurrent Ventricular
Tachycardia Related to an Epicardial Circuit
Mapping CriteriaEarliesl ventricular
electrogram relativeto QRS
Mid-diastoiic potentialor CEA
Concealed entrainmentTime for intctruption*Reindiicibility after
interruption
EndocardialApplication(n = 4 VTs)
-75 ± 5 5 sec
2 VTs2 VTs20.2 ± 14 see
All VTs
EpicardialApplication
(n = 10 VTs)
- 107 ± 60 sec
5 VTs3 VTs
4.8 ± 2.9 sec
No reinduction
CEA = continuous electrical activity; RF = radiolrequency;VT = ventricular tachycardia. *P < 0.05.
234 Journal of Cardiovascular Electrophy.siology Vol. 9. No. 3, March 1998
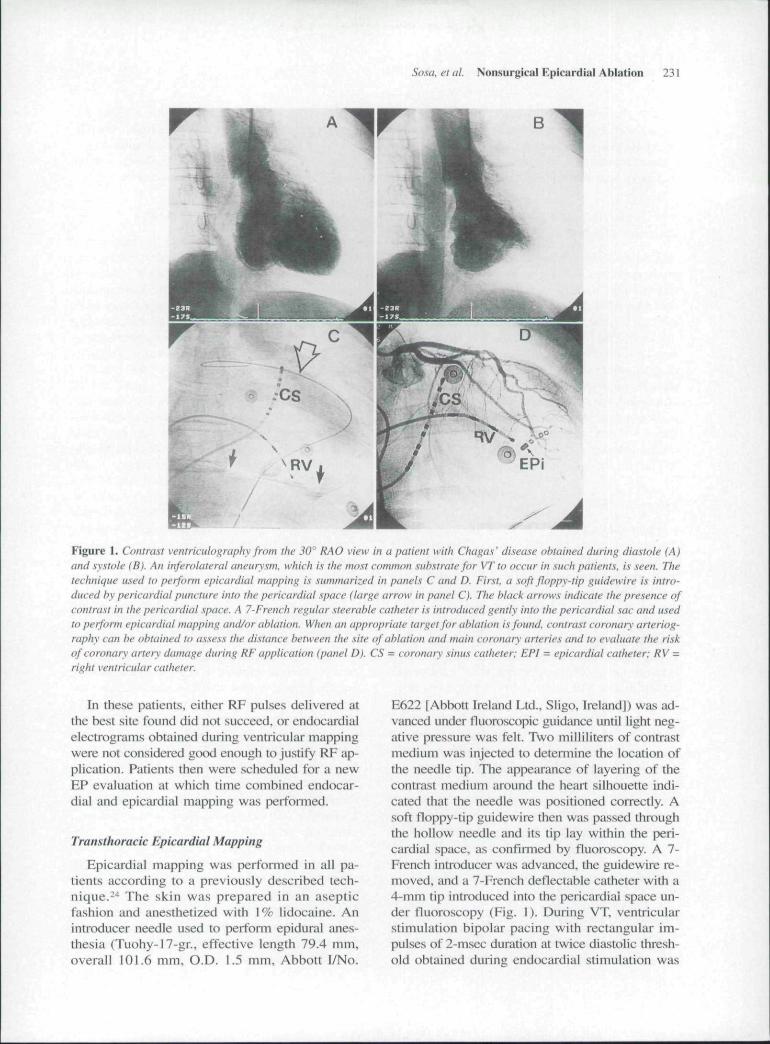
Figure 2. Activation mapping during VT obtained during transthoracic epicardial mapping. The epicardial electrogramsfound in EPi precedes ihe onset of the QRS complex hy 120 msec (upper panel}. At this site, epicardial application of RF in-terrupted VT within 4 seconds and rendered it noninducible (bollom panel). ECG leads I, II. Ill, V,, and V^ are shown. CS^ toCS = decapolar coronary sinus catheter: EPi = left venthcular epicardial catheter: HBE = His-bundle catheter.
was suspended as VT was always reinduced. Thepatient was discharged on 180 mg/day of oral so-talol., but VT recurred spontaneously 2 months later.The patient was readmitted and underwent a suc-ces.sful transthoracic epicardial ablation (Fig. 3).
Follow-Up
Clinical outcome was analyzed according to thetype of procedure the patient underwent.
Endocardial Ablation Guided by EpicardialMapping
Patients who underwent endocardial ablationguided by epicardial mapping had a poor long-term follow-up. All of the patients were discharged
on 400 mg of oral amiodarone, as VT was rein-duced after endocardial ablation. Patieni 1 had apoorly tolerated VT recurrence and was hospital-ized 16 months after the procedure, at whichtime a new unsuccessful endocardial ablative pro-cedure was attempted. The patient had a massivecerebral thromboembolism I day after the proce-dure and died 15 days later.
Patient 2 presented frequent palpitations butno spontaneous recurrence of VT 4 months afterthe piocedure. Patient 3 received an ICD and com-plained of frequent palpitations. In patient 4, VTbecame incessant 2 days after endocardial abla-tion. Although endocardial ablation rendered VTnoninducible during a second procedure, clinicalstatus degenerated and the patient died of bron-chopneumonia complicated by sepsis 36 days later
Sosa. et al Nonsurgical Epicardial Ablation 235
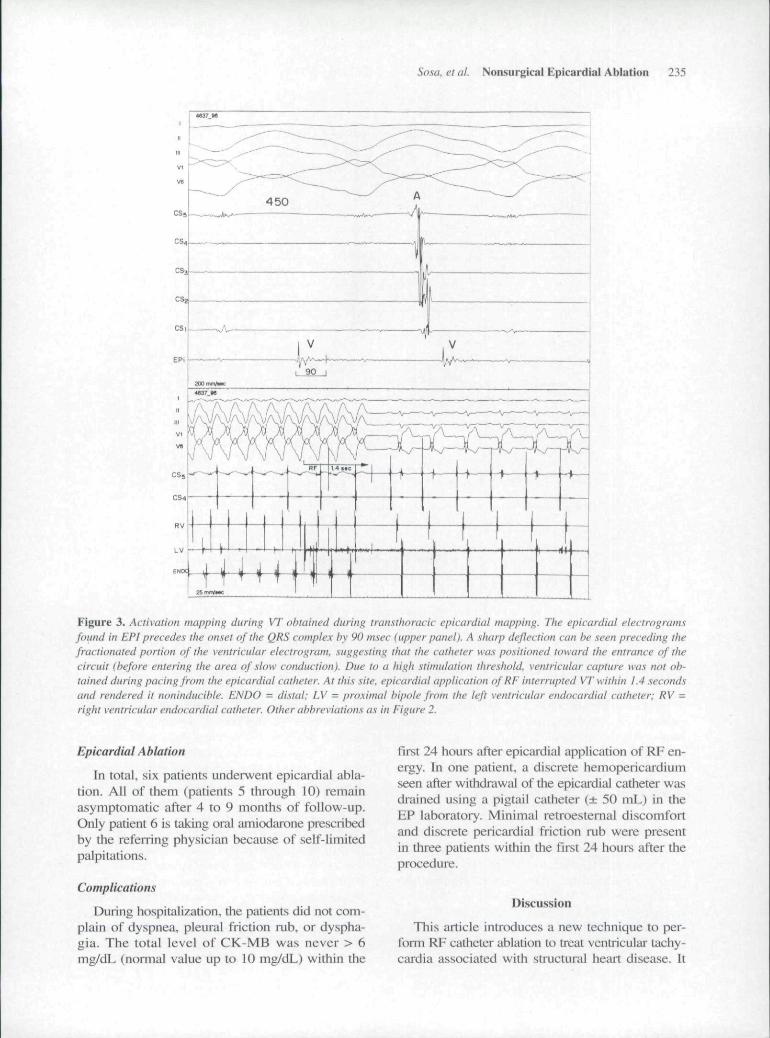
Figure 3, Activation mapping (hirinf> VT obtained during transthoracic cpicanlial mapping. The epicardial elecirogramsfotitid in EPI precedes the oiise! of the QRS cample.x by 90 msec (upper panel). A sharp deflection can be seen preceding thefractionated portion of the ventricular electrogram. .suggesting that the catheter was positioned toward the entrance of thecircuit {before entering the area of slow conduction). Due to a high stimulation threshold, ventricular capture was not ob-tained during pacing from the epicardial catheter. At this site, epicardial application ofRF interrupted VT within 1.4 .secondsand rendered it noninducible. ENDO = distal: LV = proximal hipole from the left ventricular endocardial catheter; RV =right ventricular endocardial catheter. Other abbreviations as in Eigure 2.
Epicardial Ablation
In total, six patients underwent epicardia! abla-tion. All of them (patients 5 through 10) remainasymptomatic after 4 to 9 months of follow-up.Only patient 6 is taking oral amiodarone prescribedby the referring physician because of self-limitedpalpitations.
Complications
During hospitalization, the patients did not com-plain of dyspnea, pleural friction rub. or dyspha-gia. The total level of CK-MB was never > 6mg/dL (normal value up to 10 mg/dL) within the
first 24 hours after epicardial application of RF en-ergy. Tn one patient, ii discrete hemopericardiumseen after withdrawal of tlie epicaidial catheter wasdrained using a pigtail catheter (± 50 mL) in theEP laboratory. Minimal retroesternal discomfortand discrete pericardial friction nab were presentin three patients within the first 24 hours after tbeprocedure.
Discussion
Tbis article introduces a new technique to per-fonn RF catheter ablation to treat ventricular tachy-cardia associated with structural heart disease. It
236 Journal of Cardiovascular Electrophysiology Vol. 9, No. 3. March 1998
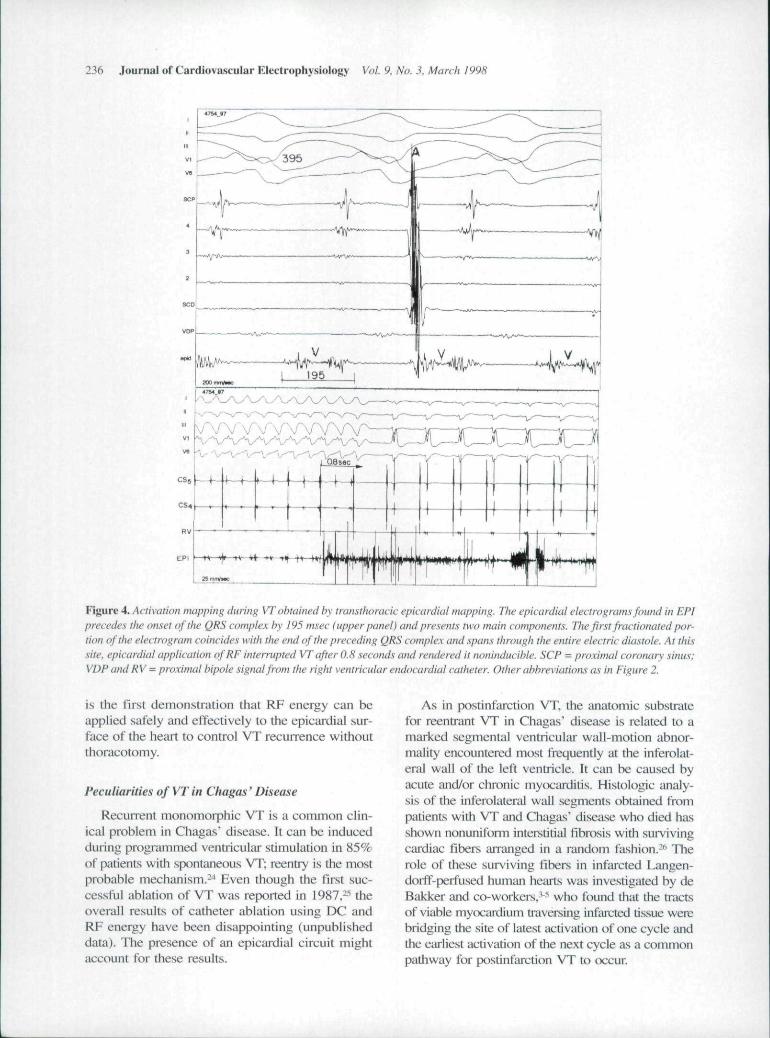
Figure 4. Activation mapping during VT obtained by transthoracic epicardial mapping. The epicardial electrograms found in EP!precedes the onset ofthe QRS complex hy 195 msec (upper panel) and presents two main components. The first fractionated por-tion ofthe electrogram coincides wilh the end ofthe preceding QRS complex and spans through the entire electric diastole. Ar this.site, epicardial application ofRF interrupted VT after 0.8 seconds and rendered it mminducihle. SCP = proximal coronary sinus;VDP and RV = proximal bipole signal from the right ventricular endocardial catheter Other abbreviations as in Figure 2.
is the first demonstration that RF energy can beapplied safely and effectively to the epicardial sur-face of the heart to control VT recurrence withoutthoracotomy.
Peculiarities of VT in Chagas' Disease
Recunent monomorphic VT is a common clin-ical problem in Chagas' disease. It can be inducedduring programmed ventricular stimulation in 85%of patients with spontaneous VT; reentry is the mostprobable mechanism.--* Even though the lust suc-cessful ablation of VT was reported in 1987,^'' theoverall results of catheter ablation using DC andRF energy have been disappointing (unpublisheddata). The presence of an epicardial circuit mightaccount for these results.
As in postinfarction VT, the anatomic substratefor reentrant VT in Chagas' disease is related to amarked segmental ventricular wall-motion abnor-tnality encountered most frequently at the inferolat-eral wall of the left ventricle. It can be caused byacute and/or chronic myocaniitis. Histologic analy-sis of the inferolateral wall segments obtained frompatients with VT and Chagas" disease who died hasshown nonuniform intei^stitial fibrosis with survivingcardiac fibers arranged in a random fashion.-** Therole of these sui"viving fibers in infarcted Langen-dorff-perfused human hearts was investigated by deBakker and co-workers,'-^ who found that the tractsof viable myocardium titiversing infarcted tissue werebridging the site of latest activation of one cycle andthe earliest activation of the next cycle as a commonpathway for postinfarction VT to occur.

Sosa, et al. Nonsurgical Epicardial Ablation 237
Interestingly, Svenson and colleagues-" - re-ported that 90% of all patients requiring epicardiallaser photocoagulation after endocardial photoco-agulation failed had either a right or left circum-flex coronary artery-re I ated inferior myocardial in-farction. One then could speculate that failure toablate VT related to an inferolateral aneurysm inChagas' disease possibly is due to the presence ofsurviving myocardial tracts traversing infarcted tis-sue located epicardially. Endocardial applicationof RF energy may fail to cure these ventricular ar-rhythmias, because it likely will not increasetemperature up to 50°C in deeper epicardial tis-sues. More recently, Pfeiffer et al.-' also suggestedthat mid-diastolic potentials are more frequentlyand better recorded from the epicardium than fromthe endocardium in postinfarction VT They usedtliese epicardial potentials to guide suT ical Nd:YAGlaser pholocoagulation of VT and speculated thattheir impressive success rate was because laser cre-ates a transmural lesion, destroying an epicardialas well as a possible endocardial circuit. However,taking into account that in our series VT inter-lTiption occurred within a few seconds of RE ap-plication, a transmural lesion might not be neces-sary to successfully treat patients with VT. Ac-cordingly, epicardial circuits may be more commonthan has been hypothesized.
Epicardial Mapping in the EP Laboratory
The ability of a given technique to localize anddestroy the surviving bundles determines the suc-cess rate of an ablative procedure. Therefore, dif-ferentiation of epicardial and endocardial sites oforigin is crucial. Until now, the only way to ob-tain extensive mapping of both right and left ven-tricular epicardial surfaces was during open chestcardiac surgeiy. Currently, however, coronary si-nus mapping and epicardial vein or intracoronai^artery catheters have been used to obtain epicar-dial signals in the EP laboratory. However, theseapproaches have several limitations. Eirst, the ex-tension of mapping is limited inexorably to thenumber of vessels and their distribution. Thesemetliods are useful only if the target site is kx:atedclose to either the AV ring or an epicardial ves-sel. Furthermore, the possibility of damaging acoronary artery may prevent an RE pulse from be-ing delivered even when the target site is found.
The new technique presented here has some ad-vantages when compared to previously publishedapproaches.-^-'^ Eirst, the catheter is introducedsafely because the needle being used is designed
especially to approach a virtual space. Subxiphoidpuncture allows it to reach the heart close to theventricuUir apex, fai' from the main coronary ar-teries. Once inside the pericardial space, the pos-sibility of provoking coronary vessel injury prob-ably is low.
As a virtual space, the pericardial sac is well lu-bricated, which permits the catheter tip to slip eas-ily. The only obstacles to catheter manipulation arepericiirdial reflections located aiound the vena cava,great vessels (pulmonary artery and aorta), and pul-monary veins. Excluding those regions, the entiresurface of both ventricles can be covered easilyand mapped using standard catheters.
Epicardial Versus Endocardial Mapping ofthe LeftVentricle
Epicardial mapping also presents advantageswhen compared to conventional endocardial map-ping. Despite the Iiirge experience gained with en-docardial mapping in centers dealing with VTablation, submitral valve apparatus, papillary mus-cle, and endocavitary thrombus can sporadicallyprevent adequate catheter manipulation and posi-tioning. Moreover, reduction of the left ventricu-laj- cavity during systole can displace the cathetertip away from a good site obtained after arduouswork. When the catheter is placed into the peri-cardial space, it tends to move following, notagainst, ventricular wall motion. Finally, heparininfusion is not necessary during epicardial map-ping and ablation.
Safety of Epicardial RF Ablation
The possibility of provoking lung and esopha-geal lesions was assessed from a clinical stand-point. Although small pulmonai"y lesions can beanticipated, they also have proved to be of no clin-ical significance in our study, as no complaints ofdyspnea, pleural friction rub, or dysphagia werereported by the patients during hospitalization andfollow-up. The need for 24-hour pericardialdrainage using a pigtail conventional catheter inone patient was the only complication of the pro-cedure. However, its important to emphasize thatit did not result in deleterious long-term conse-quences to this patient.
Apart from that, the potential risk of damagingmajor coronary aileries is minimized by analysisof the distance between the distal tip and the coro-nary vessels themselves. Position ofthe epicardialvessels can be determined by either contrast
238 Journal of Cardiovascular Electrophysiology Vol. 9, No. 3, March 1998
coronary arteriography or retrograde injection ofcontrast into the coronary sinus and. thus, one canevaluate how risky an application is. However, theminimal distance between the catheter tip and ma-jor coronaiy vessels that allows safe applicationremains to be determined.
Conclusion
These preliminary data suggest tbat tbere is ahigh prevalence of epicardial circuits in patientswith VT and Chagas" disease. Epicardial mappingdoes not enhance the effectiveness of endocardialapplications of RF. but epicardial mapping can ac-curately guide epicardial applications, which canbe used safely and effectively to treat this subsetof patients.
Avknowted^ments: The authors thank Ana Clara Tude Rodrigues.M.D.. and Cristian E. Zuagg. Ph.D.. for their comments and assis-tance during preparation ofthe manuscripl.
References
1. Josephson ME: Recurrent ventricular tachycardia. InJosephson ME, eds: Clinical CardiacElectrophysiology. Second Edllioii. Lea & Febiger.Philadelphia. 1993, pp. 417-615.
2. Stevenson GW: Veiilricuiar tachycardia after myociirdialintarctioii. J Cardiovasc Electrophysiol I995;6:942-9.5O.
3. de Bakker JMT, Coronel R, Tasseron S, et al:Venlrictilar tachycardia in the infarcted, Langendorff-perfused human heart: Role of the arrangement of sur-viving cardiac fibers. J Am Coll Cardiol 199O;I5:K'>94-1607.
4. de Bakker JMT, van Capelle FJL, Janse MJ. et al:Macroreentry in the infareted human heart: The mech-anism of ventricular tachycardias with a "focar' activa-tion pattem. J Am Coll Cardiol 1991:18:1005-1014.
5. de Bakker JMT, van Capelle FJL. Janse MJ. et al:Reentry as a cause of ventricular tachycardia in pa-tients with chronic ischemic heart disease:Electrophysiologic and anatomic correlation.Circulation I988;77:589-6O6.
6. Morady F. Harvey M, Kalbfleisch SJ, et al:Radiofrequency catheter ablation of ventricular tachy-cardia in patients with coronary artery disease.Circulation 1993;87:363-372.
7. Stevenson WG. Khan H, Sager P, et al: rdentifieationof reentry circuit sites during catheter mapping and ra-diofrequency ablation of VT late after myocardial in-farction. Circulation 1993:88:1647-1670.
8. Gonska BD, Cao K, Schaumann A, et al: Catheter ab-lation of ventricular tachycardia in 136 patients withcoronary artery disease: Results and long-term follow-up. J Am Coll Cardiol 1994:24:1506-1514.
9. Wilber D, Kail J. Kopp D. et al: Catheter ablation ofthemitral isthmus for ventricular tachycardia associated
with inferior infarction. Circulation 1995:92:3481-3489.10. Hadjis T. Stevenson WG. Friedman PL. et al:
Ventricular tachycardia after inferior wall myocardialinfarction: Predominance of locations for critical slowconduction zones. (Abstract) J Am Coll CardiolI995;25:IO8A.
11. Kottkamp H. Hindrieks G. Chen X. et al:Radiofrequency catheter ablation of sustained ventricu-lar tachycardia in idiopathic dilated cardiomyopathy.Circulation 1995:92:1159-1168.
12. Kim YH, Sosa-Suarez G. Trouton TG. et al: Treatmentof ventricular tachycardia by transcatheter radiofre-quency ablation in patients with ischemic heart disease.Circulation 1994:89:1094-1102.
13. Morady P. Kadish A, Rosenheck S. et al: Concealedentrainment as a guide for ventricular tachycardia inpatients with prior myocardial infarction. J Am CollCardiol 1991:17:678-689.
14. Trappe HJ. Klein H. Auricchio A. et al: Catheter abla-tion of ventricular tachycardia: Role of the underlyingetiology and the site of energy delivery. PACE 1992;15:411-424.
15. Fitzgerald DM, Friday KJ. Wat JAYL: Etectrogrampatterns predicting successful catheter ablation of ven-tricular tachycardia. Circulation 1988:77:806-814.
16. Kaltenbrunner W, Cardinal R. Dubuc M, et al:Epicardial and endocardial mapping of ventriculartachycardia in patients with myocardial infarction. Isthe origin of the tachycardia always subendocardiallylocalized'.' Circulation 1991:84:1058-1071.
17. d'Avila A, Nellens P. Anddes E. et al: Catheter abla-tion of ventricular tachycardia occurring late aftermyocardial infarction: A point-of-view. PACE 1994;17:532-541.
18. Sosa E. Scanavacca M. d'Avila A. et al: A new tech-nique lo perform epicardia! mapping in the electro-physiology laboratory. J Cardiovasc Electrophysioll996;7:53l-536.
!9. Sosa E. Scanavacca M, d'Avila A. et al:Radiofrequency catheter ablation of ventricular tachy-cardia guided by non-surgical epicardial mapping inchronic Chagasic heart disease. PACE 1998: (In press).
20. Svenson RH. Littmann L. Gallagher JJ. et al:Termination sequence of ventricular tachycardia withepicardial laser photocoagulation: A clinical compari-son with patients undergoing successful endocardialphotocoagulation alone. J Am Coll Cardiol1990; 15:163-170.
2L Svenson RH, Littmann L. Colavita PG, et al: Laserphotoablation of ventricular tachycardia: Correlation ofdiastolic activation times and photoablation effects oncycle length and termination: Observations supportinga macroreentrant mechanism. J Am Coll Cardiol 1992;19:607-613.
22. Littman L, Svenson RH, Gallagher JJ, et al: Functionalrole of ventricular tachycardia. Observations derivedfrom computerized epicardial activation mapping, en-trainment. and epicardial laser photoablation.Circulation I991;83:I577-159I.
Sosa, et al. Nonsurgical Epicardial Ablation 239
23. Pfeiffer D, Moosdorf R. Svenson RH: YAG laser pho-tocoagulation of ventricular tachycardia without ven-triculototny in patients after myociirdial infarction.Circulation 1996;94:322l-3225.
24. Scanavacca M. Sosa E: Electrophysiologic study inchronic Chagas' heart Jisea.se. Sao Paulo Med J 1995;113:841-850.
25. Sosa E, Scalabrini. Rati M. et ai: Successful catheterablation of the origin of recurrent ventricular tachycar-dia in chronic chagasic heart disease. J Electrophysiol1987:1:58-61.
26. Sosa E. Scanavacca M, Barbero Marciel M, et al:
Surgical treatment of cardiac arrhythmias. In CruzEilho FES, Maiii IG, ed.s: Elefrnfisiologia Cli'nica eIntervencionisra dci.s Arriimias Cardiacas. EditoraRevinter Ltda. Rio de Janeiro, 1997, pp. 443-455.
27. Arruda M, Chandrasekaran K, Reynolds D. et al:Idiopathic epicardial outflow tract ventricular tachycar-dia: Implications for RF catheter ablation. (Abstract)PACE 1996; 19:611.
28. de Paola AAV. Melo WDS, Tavora MZ. et al:Coronary venous mapping in patients wilh sustainedventricular tachycardia. (Abstract) J Am Coll CardiolI997;29:2O2A.
The King drinking. Serengetti Plain






























