Embed Size (px)
Citation preview

DOI: 10.1016/j.athoracsur.2006.10.064 2007;83:1059-1066 Ann Thorac Surg
H. Sodeck, Roman Gottardi, Christian Loewe and Johannes Lammer Maria Schoder, Martin Czerny, Manfred Cejna, Thomas Rand, Alfred Stadler, Gottfried
True and False Lumen Diameter ChangesEndovascular Repair of Acute Type B Aortic Dissection: Long-Term Follow-Up of
http://ats.ctsnetjournals.org/cgi/content/full/83/3/1059located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2007 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 4, 2013 ats.ctsnetjournals.orgDownloaded from

EDLMACDU
taf
dsc(paidtg
s
Utihgpptrstttw
rrs
A
AIGm
©P
CA
RD
IOV
ASC
ULA
R
ndovascular Repair of Acute Type B Aorticissection: Long-Term Follow-Up of True and Falseumen Diameter Changesaria Schoder, MD, Martin Czerny, MD, Manfred Cejna, MD, Thomas Rand, MD,lfred Stadler, MD, Gottfried H. Sodeck, MD, Roman Gottardi, MD,hristian Loewe, MD, and Johannes Lammer, MD
epartments of Angiography and Interventional Radiology, Cardio-Thoracic Surgery, and Emergency Medicine, Medical
niversity of Vienna, Vienna, AustriaPaafdIwlot
ssgl
Background. The aim of this study was to determinehe technical success after endovascular treatment ofcute type B aortic dissections and to evaluate true andalse lumen diameter changes at long-term follow-up.
Methods. Twenty-eight patients with acute type B-issection who were treated by stent graft repair pre-ented with rupture (n � 1), contained rupture (n � 2),ompromised branch vessels (n � 14), pleural effusionn � 11), rapid aortic diameter progression (n � 5),ersistent pain (n � 3), refractory hypertension (n � 10),nd an aortic diameter of more than 4 cm (n � 4). Takingnto account the perfusion status of the false lumen,iameter changes were monitored in the thoracic aorta at
he level of the stented segment (L1), distal to the stentraft (L2), and at the level of the celiac trunk (L3).Results. Severe complications in 9 patients (32%) re-
ulted in 3 deaths for a 30-day mortality rate of 10.7%.
landot[
oafn
M
PFaryaa
iuertel 18-20, A-1090 Vienna, Austria; e-mail: [email protected].
2007 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
rimary sealing of the entry tear was achieved in 86%. Atll levels, the true lumen diameter increased significantlyfter stent graft placement. At the 1-year follow-up, thealse lumen in L1 was thrombosed in 90% and the meanifference of diameter reduction was highly significant.n L2, complete false lumen thrombosis occurred in 60%ith a significant diameter decrease. In L3, the false
umen thrombosed in only 22%, and the mean differencef false lumen diameter increase reached significance athe 2-year follow-up.
Conclusions. Ninety percent of patients were treateduccessfully with thrombosis of the false lumen in thetented segment. False lumen perfusion distal to the stentraft resulted in diameter increase in several patientseaving these segments an area of concern.
(Ann Thorac Surg 2007;83:1059–66)
© 2007 by The Society of Thoracic Surgeonsntil recently, acute uncomplicated Stanford type Bdissections were preferably managed by conserva-
ive medical treatment; however, complications includ-ng rupture, visceral or lower limb ischemia, refractoryypertension, continuing pain, and aortic diameter pro-ression occur in 5% to 20% of patients during the acutehase [1–5]. Furthermore, a considerable number ofatients without acute complications experience dissec-
ion-related adverse events during the chronic phase thatemain a treatment challenge [2, 3, 5]. A more aggressiveurgical approach is therefore advocated by some au-hors [6]. Despite technical advances, the surgical mor-ality rate in complicated acute dissections remains 14%o 31% [4, 7–10], with a remarkable increase in patientsith end-organ ischemia [7, 10–12].Closure of the primary entry tear by endovascular
epair may lead to thrombosis of the false lumen withemodelling of the true lumen in the acute and chronicetting. Furthermore, lowering the pressure in the false
ccepted for publication Oct 24, 2006.
ddress correspondence to Dr Schoder, Department of Angiography andnterventional Radiology, Medical University of Vienna, Waehringer
umen may restore the perfusion in the compromisedortic branch vessels. In recent years, encouraging tech-ical results after endovascular repair of acute type Bissection have been reported [13–21]; however, reportsn the true and false lumen changes after endovascularherapy during a longer-term follow-up remain limited13, 20, 22, 23].
The purpose of this study was to assess the clinicalutcome and technical success in endovascular repair ofcute type B aortic dissections. The significance of true andalse lumen diameter changes in the thoracic and abdomi-al aorta was also evaluated at the long-term follow-up.
aterial and Methods
atient Populationrom March 2000 to June 2005, 5 women and 23 men withcute type B aortic dissections were treated by stent graftepair. Mean age of patients was 57 years (range, 33 to 83ears). All patients stated an acute onset of chest pain atdmission. One patient was hemodynamically instablend 1 patient had paraplegia.Endovascular repair of thoracic aortic diseases was
ntroduced at Medical University of Vienna as an alter-
0003-4975/07/$32.00doi:10.1016/j.athoracsur.2006.10.064
by on June 4, 2013 als.org
n1afImi
e(
Zrfic(i
b(
T
1
1
1
11
1111
1
22
222
E
1060 SCHODER ET AL Ann Thorac SurgENDOVASCULAR REPAIR OF ACUTE TYPE B DISSECTION 2007;83:1059–66
CA
RD
IOV
ASC
ULA
R
ative treatment to surgical repair in high-risk patients in996. The local Institutional Review Board gave approvalnd consent for this retrospective study. Written in-ormed consent was obtained from all conscious patients.n one unconscious patient, the treatment decision was
ade collaboratively with cardiothoracic surgeons andnterventional radiologists.
Confirmation of dissection was based on contrast-nhanced computed tomography (CT) angiographyCTA) using a multidetector scanner (Somatom Volume
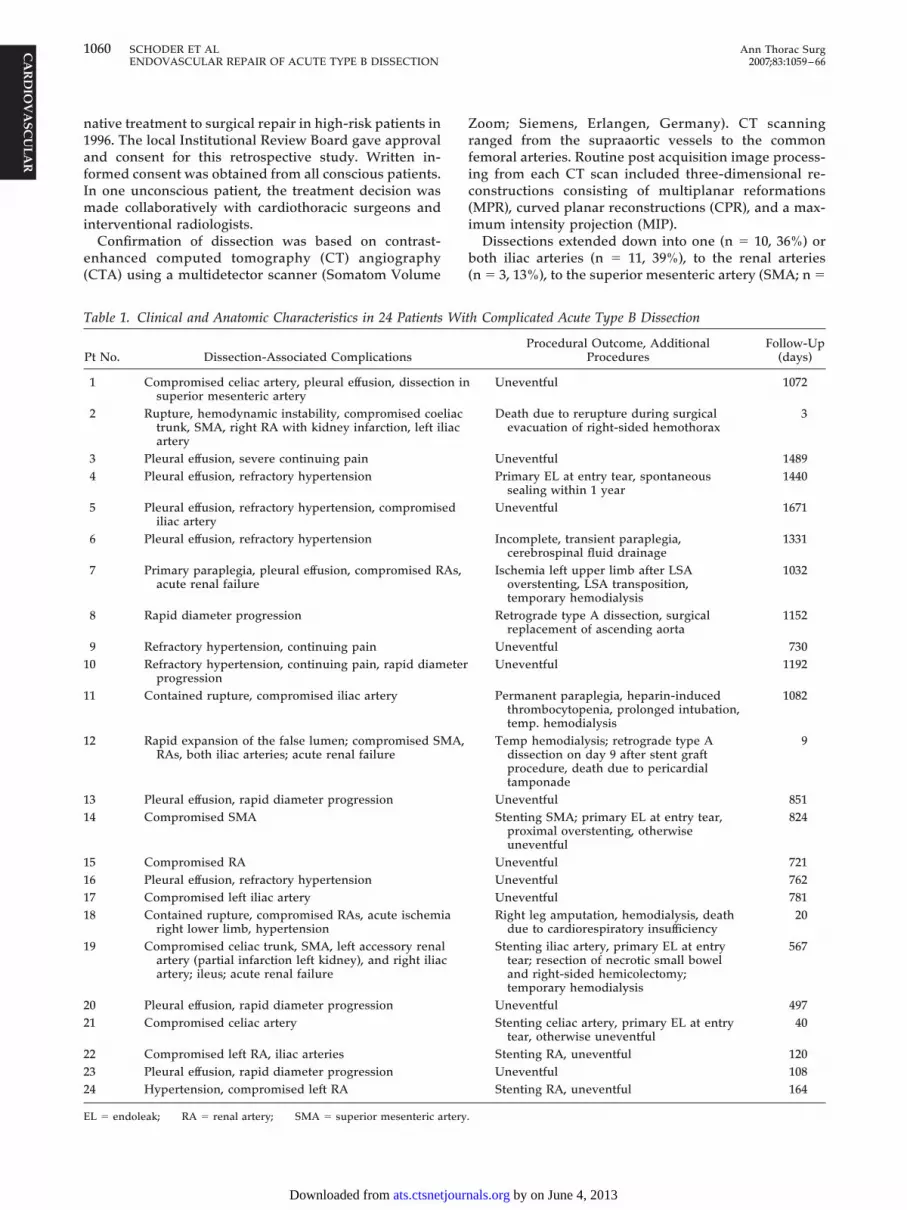
able 1. Clinical and Anatomic Characteristics in 24 Patients
Pt No. Dissection-Associated Complications
1 Compromised celiac artery, pleural effusion, dissectiosuperior mesenteric artery
2 Rupture, hemodynamic instability, compromised coetrunk, SMA, right RA with kidney infarction, left ilartery
3 Pleural effusion, severe continuing pain4 Pleural effusion, refractory hypertension
5 Pleural effusion, refractory hypertension, compromisiliac artery
6 Pleural effusion, refractory hypertension
7 Primary paraplegia, pleural effusion, compromised Racute renal failure
8 Rapid diameter progression
9 Refractory hypertension, continuing pain0 Refractory hypertension, continuing pain, rapid diam
progression1 Contained rupture, compromised iliac artery
2 Rapid expansion of the false lumen; compromised SMRAs, both iliac arteries; acute renal failure
3 Pleural effusion, rapid diameter progression4 Compromised SMA
5 Compromised RA6 Pleural effusion, refractory hypertension7 Compromised left iliac artery8 Contained rupture, compromised RAs, acute ischemi
right lower limb, hypertension9 Compromised celiac trunk, SMA, left accessory rena
artery (partial infarction left kidney), and right iliaartery; ileus; acute renal failure
0 Pleural effusion, rapid diameter progression1 Compromised celiac artery
2 Compromised left RA, iliac arteries3 Pleural effusion, rapid diameter progression4 Hypertension, compromised left RA
L � endoleak; RA � renal artery; SMA � superior mesenteric artery.
ats.ctsnetjournDownloaded from
oom; Siemens, Erlangen, Germany). CT scanninganged from the supraaortic vessels to the commonemoral arteries. Routine post acquisition image process-ng from each CT scan included three-dimensional re-onstructions consisting of multiplanar reformationsMPR), curved planar reconstructions (CPR), and a max-mum intensity projection (MIP).
Dissections extended down into one (n � 10, 36%) oroth iliac arteries (n � 11, 39%), to the renal arteries
n � 3, 13%), to the superior mesenteric artery (SMA; n �
h Complicated Acute Type B Dissection
Procedural Outcome, AdditionalProcedures
Follow-Up(days)
Uneventful 1072
Death due to rerupture during surgicalevacuation of right-sided hemothorax
3
Uneventful 1489Primary EL at entry tear, spontaneous
sealing within 1 year1440
Uneventful 1671
Incomplete, transient paraplegia,cerebrospinal fluid drainage
1331
Ischemia left upper limb after LSAoverstenting, LSA transposition,temporary hemodialysis
1032
Retrograde type A dissection, surgicalreplacement of ascending aorta
1152
Uneventful 730Uneventful 1192
Permanent paraplegia, heparin-inducedthrombocytopenia, prolonged intubation,temp. hemodialysis
1082
Temp hemodialysis; retrograde type Adissection on day 9 after stent graftprocedure, death due to pericardialtamponade
9
Uneventful 851Stenting SMA; primary EL at entry tear,
proximal overstenting, otherwiseuneventful
824
Uneventful 721Uneventful 762Uneventful 781Right leg amputation, hemodialysis, death
due to cardiorespiratory insufficiency20
Stenting iliac artery, primary EL at entrytear; resection of necrotic small boweland right-sided hemicolectomy;temporary hemodialysis
567
Uneventful 497Stenting celiac artery, primary EL at entry
tear, otherwise uneventful40
Stenting RA, uneventful 120Uneventful 108Stenting RA, uneventful 164
Wit
n in
liaciac
ed
As,
eter
A,
a
lc
by on June 4, 2013 als.org

1Tspdtaaota
oa2e�sd
Facfshath
EAsrEswm
Fs(fl
1061Ann Thorac Surg SCHODER ET AL2007;83:1059–66 ENDOVASCULAR REPAIR OF ACUTE TYPE B DISSECTION
CA
RD
IOV
ASC
ULA
R
, 4%), or were limited to the thoracic aorta (n � 3, 13%).he primary intimal tear was located just distal to the leftubclavian artery in 26 (93%) patients, whereas in 2atients, the entry tear was in the middle third of theescending aorta. The false lumen was patent in all pa-
ients. Thirty branch vessels were compromised by eithern exclusively dynamic process (n � 17) or a combination ofdynamic and a static process. In 12 patients (42.9%), eitherne branch vessel (renal artery in 10, celiac trunk in 1) orwo branch vessels (renal artery and superior mesentericrtery) originated from the false lumen.
Twenty-four symptomatic patients with more thanne complication were selected for endovascular ther-py because of rupture (n � 1), contained rupture (n �), compromised branch vessels (n � 14), pleuralffusion (n � 11), rapid aortic diameter progression (n
5), persistent pain (n � 3), and refractory hyperten-ion (n � 10). Specific patient characteristics with
ig 1. A 70-year old woman with acute renal failure caused by acutehows the entry tear located close to the left subclavian artery (LSA).C) Remarkable true lumen expansion after implantation of two Talenow in the abdominal branches and iliac arteries after stent grafting.
issection related complications are listed in Table 1. 2
ats.ctsnetjournDownloaded from
our clinically asymptomatic patients demonstratingn aortic diameter of more than 40 mm and markedompression of the true lumen were treated to preventurther aortic dilation. Owing to the severity of theirymptoms, 9 patients (32%) required emergent (withinours) stent graft implantation after CT diagnosis of ancute type B dissection. Another 11 patients werereated within 7 days. Mean time to treatment was 101ours (range, 1 to 312 hours).
ndovascular Prosthesis and Procedurell patients were treated with commercially available
tent grafts. A Talent endoprosthesis (Medtronic, Sun-ise, FL) was used in 18 patients, and the Thoracicxcluder (W. L. Gore & Assoc, Flagstaff, AZ) stent graftystem was used in 10. The diameter of the stent graftas calculated from the largest diameter of the proxi-al anchoring zone, and an oversizing factor of 10% to
B aortic dissection. (A) Angiogram before stent graft implantationompromised visceral, renal, and iliac arteries by a dynamic process.oprostheses with overstenting of the LSA. (D) Restoration of blood
type(B) Ct end
0% was added.
by on June 4, 2013 als.org

ittpbI(c
atGricSgagetiM
prtds
FC3ytse
SCscfmti(a
baltwta(
R
TIaaeps1itp1it
1fwpLf
Fdi
1062 SCHODER ET AL Ann Thorac SurgENDOVASCULAR REPAIR OF ACUTE TYPE B DISSECTION 2007;83:1059–66
CA
RD
IOV
ASC
ULA
R
All procedures were performed in an angiosuite thats equipped with digital subtraction angiography (Mul-istar T.O.P., Siemens, Erlangen, Germany). All pa-ients were under general anesthesia. Antibiotic pro-hylaxis was administered intravenously in all patientsefore the procedure. In patients without rupture, 5000U of heparin sodium was given after the access sitecommon femoral or external iliac artery) was surgi-ally exposed.
A 5F pigtail catheter was positioned into the ascendingorta through right-sided percutaneous brachial accesso perform an angiogram before stent graft deployment.aining access to the true lumen from the iliac route
equired adjunctive maneuvers in 2 patients. Approach-ng from the true lumen via brachial access, a pigtailatheter was advanced down to the aortic bifurcation.ubsequently, a 260-cm-long steerable hydrophilicuidewire (Terumo Europe N.V., Leuven, Belgium) wasdvanced to the iliac artery and snared with an Amplatzooseneck snare (ev3, Plymouth, MN). A diagnostic cath-ter was then introduced from the femoral site over thehrough-and-through wire up to the aortic arch to facil-tate placement of the superstiff guidewire (Back-up
eier, Boston Scientific, Natick, MA).After deployment of the device, an angiogram was
erformed to evaluate the position of the stent graftelative to supraaortic arch vessels, to confirm closure ofhe proximal entry tear, to ascertain the true lumeniameter along the aorta, and to document the perfusiontatus of the branch vessels.
ollow-up ImagingTA examinations were routinely performed withindays after the procedure, at 3, 6, and 12 months, and
early thereafter. To assess the extent of the dissection,he diameter of the true and false lumen, and the perfu-ion status of the false lumen and the branch vessels, thentire aorta and the iliac arteries were included.
tatistical Analysisontinuous variables are expressed as means and �
tandard deviation. For exact analysis of diameterhanges of the true and false lumen, preprocedural andollow-up CT examinations were reevaluated. Measure-
ents were obtained at the same levels perpendicular tohe line of the intimal flap and at the maximum diametern three selected aortic segments: stented aortic segmentL1), thoracic aorta distal to the stent graft (L2), and thebdominal aorta at the level of the celiac trunk (L3).Diameter changes were evaluated for significance
etween the preprocedural and first postprocedural im-ges. For statistical analysis of diameter changes forong-term follow-up, a 1-year and 2-year CTA examina-ion was required. Differences of aortic measurementsere tested for significance using the �2 test for propor-
ions. Significance level was set at p � 0.05. Statisticalnalysis was performed using SPSS 13 statistical software
SPSS Inc, Chicago, IL). (ats.ctsnetjournDownloaded from
esults
echnical Resultsn 7 patients, complete overstenting of the left subclavianrtery (LSA) was required to close the entry tear. Tovoid vertebrobasilarly symptoms after intentional cov-ring of the LSA, transposition was performed in 4atients with a dominant left vertebral artery before thetent graft procedure. The LSA was partially covered in9 patients, and 2 patients could be treated with anchor-ng of the stent graft distal to the LSA. Eight patients werereated with 1 endoprosthesis, 18 patients with 2, and 2atients with 3. Length of the covered aortic segment was0 to 21 cm. Deployment of the stent grafts was successfuln all patients; however, in 4 patients (14.3%), the entryear could not be sealed during the first procedure.
Proximal overstenting led to sealing of the entry tear inpatient, and in the second patient, the perfusion of the
alse lumen from the entry tear decreased steadily andas sealed completely at the 1-year follow-up. Twoatients (patient 19 and 21) with partial covering of theSA demonstrated residual flow into the false lumen
rom the proximal entry tear at the last follow-up. For
ig 2. Box plots show the differences of (A) true and (B) false lumeniameter changes between the preprocedural computed tomographymaging and the 1-year follow-up at the level of the stented segment
L1).by on June 4, 2013 als.org

fcptdc
ri(ab
SSdddordacsa
twpdpwvestfirhs
FMde
Fdi
T2
L
L
L
a
1063Ann Thorac Surg SCHODER ET AL2007;83:1059–66 ENDOVASCULAR REPAIR OF ACUTE TYPE B DISSECTION
CA
RD
IOV
ASC
ULA
R
urther proximal overstenting, transposition of the leftommon carotid artery would be necessary in these 2atients. One of these patients refused further interven-
ions, and the second patient has a stable thoracic aorticiameter. Consequently, these patients remain underlose observation.
Expansion of the true lumen after stent graft deploymentesulted in a satisfactory perfusion of compromised vesselsn 83% (Fig 1). Additional stenting was necessary in five17%) arteries (2 visceral arteries, 2 renal arteries, 1 iliacrtery) to alleviate persistent obstruction of the true lumeny extension of the intimal flap beyond a vessel’s origin.
urvival and Complicationsevere complications in 9 (32%) patients resulted in 3eaths for 30-day mortality rate of 10.7%. One patientied from hemorrhage from a ruptured aortic dissectionuring surgical evacuation of the hemothorax. The sec-nd patient died from pericardial tamponade after aetrograde type A dissection on day 9. The third patientied as a result of cardiac and respiratory insufficiencyssociated with dissection-related acute ischemic compli-ations of the leg, followed by a massive reperfusionyndrome that required leg amputation. The survival ratet 1, 2, and 3 years was 89.3%.Further serious complications in the 25 surviving pa-
ients were spinal cord ischemia in 2 (7.1%). In patient 11,ho sustained permanent paraplegia, the LSA was com-letely overstented and the stent graft covered Th-8istally. In patient 6, who had incomplete transientaraplegia, the LSA was partially covered and the deviceas fixed distally at the level of the ninth thoracolumbar
ertebrae. Intentional occlusion of the LSA led to isch-mia of the left upper limb requiring secondary transpo-ition of LSA in 1 patient. A retrograde type A dissectionhat developed in another patient was treated success-ully with surgery. Dissection-related infarction of thentestines required a partial small bowel resection and aight-sided hemicolectomy in one patient. Temporaryemodialysis was necessary in 3 patients who had dis-
able 2. Mean Differences of Diameter Changes of the False-Year Follow-Upa
Thrombosed False Lumen
1 Year p Value 2 Year
1 (n) 18/20 14/14False lumen �11.6 � 8.2 �0.0001 �12.0 � 8.1Max diameter �4.3 � 7.9 0.36 �5.1 � 8.5
2 (n) 12/20 9/14False lumen �8.2 � 10.4 0.02 �5.7 � 11.2Max diameter �0.6 � 5.7 0.73 �0.9 � 6.6
3 (n) 4/18 4/13False lumen �8.5 � 8.0 0.12 �9.8 � 7.4Max diameter �1.3 � 5.9 0.698 �0.5 � 8.1
Data are presented in mm � standard error of the mean.
ection-related acute renal failure. d
ats.ctsnetjournDownloaded from
ollow-Up Analysis of the True and False Lumenean CT follow-up of surviving patients was 859 � 546
ays (range, 40 to 2107 days). The first postprocedural CTxamination was completed in 25 patients. Twenty pa-
ig 3. Box plots show the differences of (A) true and (B) false lumeniameter changes between the preprocedural computed tomographymaging and the 1-year follow-up in the thoracic aorta at the level
n and the Maximal Aortic Diameter at the 1-Year and
Patent False Lumen
p Value 1 Year p Value 2 Year p Value
2/20 0/14�0.0001 �1.0 � 5.7 0.844
0.42 �4.5 � 2.1 0.2058/20 5/14
0.17 �1.4 � 6.5 0.58 �6.2 � 5.2 0.0550.699 �4.9 � 3.8 0.0084 �9.4 � 3.4 0.0061
14/18 9/130.08 �2.9 � 4.9 0.058 �5.8 � 6.9 0.0370.91 �4.5 � 2.8 0.001 �7.6 � 5.1 0.002
Lume
istal of the stent-graft (L2).
by on June 4, 2013 als.org

ta3
L
dsl0m
twTpidwe
L
tf
ms
fcmf(f3l
L
pasa
odeidcpi
C
TdtiltadewdiItr
arl1ettpt
1lis
Fdi(
1064 SCHODER ET AL Ann Thorac SurgENDOVASCULAR REPAIR OF ACUTE TYPE B DISSECTION 2007;83:1059–66
CA
RD
IOV
ASC
ULA
R
ients were available for the 1-year CT follow-up analysis,nd 14 patients had CT examinations at 24 months, 8 at6, 4 at 48, and 2 at 60 months.
1-STENTED THORACIC AORTIC SEGMENT. At the first postproce-ural CT, a complete thrombosis of the false lumen waseen in 15 (60%) patients. The mean difference of trueumen diameter increase was highly significant (p �.0001) between the preprocedural and postproceduraleasurements (Fig 2, Table 2).Twelve month follow-up images demonstrated total
hrombosis of the false lumen in 18 patients (90%) alongith complete reabsorption of the thrombus in 9 (50%).he mean true lumen diameter between the initial post-rocedural CTA and 1-year follow-up increased further
n 16 patients (80%) and was stable in 4 (20%). Theiameter of the false lumen increased in 1 patient (5%)ith a patent false lumen. The mean false lumen diam-
ter in the remaining 19 patients (95%) decreased.
2-THORACIC AORTIC SEGMENT DISTAL OF THE STENT GRAFT. Athe first postprocedural CT a complete thrombosis of thealse lumen was observed in 5 patients (20%) and the
ig 4. Box plots show the difference of (A) true (B) and false lumeniameter changes between the preprocedural computed tomographymaging and the 1-year follow-up at the level of the celiac trunk
rL3).
ats.ctsnetjournDownloaded from
ean difference of true lumen diameter increase wastatistically significant (p � 0.0005; Fig. 3, Table 2).
At the 1-year follow-up, a complete thrombosis of thealse lumen was observed in 12 patients (60%), withomplete reabsorption of the thrombus in 4 (20%). Theean true lumen diameter between the first and 1-year
ollow-up increased in 14 patients (70%), was stable in 420%), and slightly decreased in 2 (10%). Conversely, thealse lumen decreased in 10 patients (50%), was stable in
(15%), and increased in 7 (35%) in whom the falseumen was patent.
3-ABDOMINAL AORTA-LEVEL OF CELIAC ARTERY. At the firstostprocedural CT, none of the 22 patients demonstratedthrombosis of the false lumen; however, the true lumen
howed a statistically significant mean difference of di-meter increase (p � 0.0009; Fig 4, Table 2).At the 1-year follow-up, thrombosis of the false lumen
ccurred in 4 (22%) of 18 patients and the thrombus wasissolved completely in one. The mean true lumen diam-ter between follow-up examinations increased furthern 11 patients (61%), was stable in 4 (22%), but slightlyecreased in 3 (17%). Conversely, the false lumen de-reased only in 6 (33%), and was stable in 2 (11%). In 10atients (56%), the diameter of the patent false lumen
ncreased.
omment
he current indications for intervention in acute type Bissections involve rupture or signs of impending rup-
ure, rapid diameter progression malperfusion of abdom-nal or peripheral vessels, persisting pain, and uncontrol-able hypertension, and 24 (85.7%) of our patients methese criteria. Medical management of uncomplicatedcute dissections remains the preferable treatment mo-ality. However, several studies showed that adversevents during the clinical course were strongly correlatedith a patent false lumen and a maximal thoracic aorticiameter of 40 mm or more [2, 3, 5]. Both predictive
ndicators were present in the 4 asymptomatic patients.n addition, these patients had a marked compression ofhe true lumen that led us to undertake urgent stent graftepair.
The effectiveness of surgical or endovascular repair forortic dissection is dependent on closure of the entry tear,eexpansion of the true lumen, and clotting of the falseumen. Our experience, as well as that in other studies [13,5, 16, 18, 19, 21, 24], indicates that stent graft repair is anffective approach even in the emergent treatment of pa-ients with a complicated acute type B dissection. In addi-ion to relief of acute symptoms, stent graft placement mayrevent aneurysmal degeneration of the thoracic aorta by
hrombus formation in the false lumen.The in-hospital mortality rate in this patient series was
0.7%, which is similar to the 7% to 20% reported initerature [13, 16, 18, 19, 24, 25]. Although these datandicate a superior survival compared with surgery, theerious condition of this category of patients is also
eflected in a complication rate of up to 36% as reportedby on June 4, 2013 als.org

boa
mfscrprlpte
rtHsasaM[otassiTlvt
ssflvpdopdgedIltbiw
ctchr
pdaleatletoci
rat((calsms
iwl[ptfaiLstt
dHtcrtcsia
MA
R
1065Ann Thorac Surg SCHODER ET AL2007;83:1059–66 ENDOVASCULAR REPAIR OF ACUTE TYPE B DISSECTION
CA
RD
IOV
ASC
ULA
R
y Kato and colleagues [25] and in the 30% occurrence inur patients, corresponding to the study by Eggebrechtnd colleagues [20].As a procedure-related complication, we observed per-anent paraplegia in 1 (3.6%) patient. This compares
avorably with reported rates in patients who underwenturgery [8, 9, 26]. Another serious procedure-relatedomplication was a retrograde type A dissection occur-ing in 2 patients who were treated with a Talent endo-rosthesis with a free flow design on the proximal cage,esulting in one death. The cause may be related to theimited flexibility of the currently available devices thatroduce forced wall stress at the outer curvature leading
o intimal injuries, which is also reported in previousxperiences [24, 27, 28].Intentional overstenting of the LSA without previous
evascularization is described as a feasible and well-olerated procedure in a few series [17, 21, 29, 30].
owever, 1 of our 3 patients with complete LSA occlu-ion, without previous revascularization, sustained acuterm ischemia that necessitated LSA transposition. Non-erious ischemic arm symptoms in 13.6% of patients werelso reported in the study of Görich and associates [29].oreover, in the series of Tiesenhausen and colleagues
31], 3 (37.5%) of 8 patients with partial or completecclusion of the LSA sustained vertebrobasilar symp-oms. As reported in the literature, bilateral vertebralrtery occlusion, which can be also simulated by over-tenting of a dominant LSA and an additional severelytenotic or hypoplastic right vertebral artery, causedrreversible neurologic problems in 23% of patients [32].herefore, to rule out patients for whom LSA revascu-
arization might be essential, both the carotid andertebral arteries should be evaluated before inten-ional overstenting.
Branch vessels may be compromised by a dynamic ortatic obstruction, or a combination of both [13, 33]. In atudy by Dake and colleagues [13], restoration of bloodow was sufficient after stent graft repair in all branchessels that were compromised exclusively by a dynamicrocess. In vessels also affected by a static component,eployment of an uncovered stent within the true lumenf the obstructed artery was necessary in 60% of theatients. In accordance with this, all our patients with aynamic obstruction of arteries could be treated by stentrafting alone. An additional stent deployment was nec-ssary in five vessels (17%) with an obstruction caused byirect extension of the flap beyond the vessel’s origin.
nfradiaphragmatic vessels originating from the falseumen did not suffer from malperfusion after occlusion ofhe entry tear. An adequate blood supply was providedy existing natural fenestrations of the intimal flap allow-
ng communication between the true and false lumen,hich has also been shown in other series [13, 34].Recent studies have reported patient outcome during the
hronic phase in type B dissections that have only beenreated with medical therapy [2, 5]. Akutsu and associatesoncluded [2] that patients with a thrombosed false lumenad a significantly better outcome in terms of dissection-
elated death and dissection-related events in the chronicats.ctsnetjournDownloaded from
hase. In addition, they found that a higher incidence ofissection-related death in patients with the most dilatedortic segment located at the distal arch. Marui and col-eagues [5] reported that during the chronic phase, thevent-free rate at 1 year was 97% in type B dissections withthrombosed false lumen and an aortic diameter of less
han 40 mm. Conversely, dissections with a patent falseumen and an aortic diameter of 40 mm or more had anvent-free rate of only 43% at the same instant. With respecto these findings, the advantage of endovascular treatmentf acute type B dissections is not limited to treatment ofomplications, but might also prevent adverse events dur-ng the chronic phase.
Primary closure of the entry tear after stent grafting waseported in 89% to 100% [16, 17, 19, 21, 24, 35] and waschieved in 85.7% of our patients. In our series, completehrombosis of the false lumen in the stented aortic segmentL1) as well as in the thoracic aorta distally to the stent graftL2) was observed in 90% and 60%, respectively. A signifi-ant reduction of the false lumen diameter was alsochieved in these patients. In dissections with a patent falseumen in L2, the false lumen increased without reachingtatistical significance at the 2-year follow-up. However, theaximal aortic diameter increased significantly over the
ame time period.Thrombosis of the false lumen occurred in the abdom-
nal aorta (L3) in 22% of our patients, a rate consistentith the findings of other studies that reported false
umen thrombosis in the abdominal aorta in 0% to 10%13, 20, 36]. This circumstance can be explained by theresence of reentries, as mentioned previously. In con-
rast to the results of Czermak and associates [23], whoound no substantial volume change in the abdominalorta, we showed that the mean difference of diameterncrease of a patent false lumen was remarkable at the3 level at the 1-year follow-up and reached statisticalignificance at the 2-year follow-up. There was a clearendency for diameter decrease at this level with ahrombosed false lumen.
A limitation of this study is the small sample size, whichid not allow us to draw final conclusions from our results.owever, closure of the entry tear and stabilization of the
rue lumen presents a promising alternative treatment toonventional surgery for relief of life-threatening dissectionelated complications. Furthermore, aortic segments with ahrombosed false lumen had no substantial diameterhanges during the follow-up period. False lumen perfu-ion distal of the stent graft resulted in substantial diameterncrease in several of our patients leaving these segmentsn area of great concern.
edtronic sponsored a research grant for the Department ofngiography and Interventional Radiology.
eferences
1. Sueyoshi E, Sakamoto I, Hayashi K, Yamaguchi T, Imada T.Growth rate of aortic diameter in patients with type B aortic
dissection during the chronic phase. Circulation 2004;110:II256–61.by on June 4, 2013 als.org

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
1066 SCHODER ET AL Ann Thorac SurgENDOVASCULAR REPAIR OF ACUTE TYPE B DISSECTION 2007;83:1059–66
CA
RD
IOV
ASC
ULA
R
2. Akutsu K, Nejima J, Kiuchi K, et al. Effects of the patent falselumen on the long-term outcome of type B acute aorticdissection. Eur J Cardiothorac Surg 2004;26:359–66.
3. Onitsuka S, Akashi H, Tayama K, et al. Long-term outcomeand prognostic predictors of medically treated acute type Baortic dissections. Ann Thorac Surg 2004;78:1268–73.
4. Hagan PG, Nienaber CA, Isselbacher EM, et al. The Inter-national Registry of Acute Aortic Dissection (IRAD): newinsights into an old disease. JAMA 2000;283:897–903.
5. Marui A, Mochizuki T, Mitsui N, Koyama T, Kimura F,Horibe M. Toward the best treatment for uncomplicatedpatients with type B acute aortic dissection. Circulation1999;100:II275–80.
6. Palma JH, Almeida DR, Carvalho AC, Andrade JCS, BuffoloE. Surgical treatment of acute type B aortic dissection usingan endoprosthesis (elephant trunk). Ann Thorac Surg 1997;63:1081–4.
7. Lauterbach SR, Cambria RP, Brewster DC, et al. Contempo-rary management of aortic branch compromise resultingfrom acute aortic dissection. J Vasc Surg 2001;33:1185–92.
8. Elefteriades JA, Lovoulos CJ, Coady MA, Tellides G, KopfGS, Rizzo JA. Management of descending aortic dissection.Ann Thorac Surg 1999;67:2002–5.
9. Gysi J, Schaffner T, Mohacsi P, Aeschbacher B, Althaus U,Carrel T. Early and late outcome of operated and non-operated acute dissection of the descending aorta. EurJ Cardiothorac Surg 1997;11:1163–70.
0. Fann JI, Sarris GE, Mitchell RS, et al. Treatment of patientswith aortic dissection presenting with peripheral vascularcomplications. Ann Surg 1990;212:705–13.
1. Cambria RP, Brewster DC, Gertler J, et al. Vascular compli-cations associated with spontaneous aortic dissection. J VascSurg 1988;7:199–209.
2. Laas J, Heinemann M, Schaefers HJ, Daniel W, Borst HG.Management of thoracoabdominal malperfusion in aorticdissection. Circulation 1991;84:20–4.
3. Dake MD, Kato N, Mitchell RS, et al. Endovascular stent-graft placement for the treatment of acute aortic dissection.N Engl J Med 1999;340:1546–52.
4. Shimono T, Kato N, Yasuda F, et al. Transluminal stent-graftplacements for the treatments of acute onset and chronicaortic dissections. Circulation 2002;106:I241–7.
5. Beregi JP, Haulon S, Otal P, et al. Endovascular treatment ofacute complications associated with aortic dissection: mid-term results from a multicenter study. J Endovasc Ther2003;10:486–93.
6. Lonn L, Delle M, Falkenberg M, Thony F, Aubert A, Blin D.Endovascular treatment of type B thoracic aortic dissection.J Card Surg 2003;18:539–44.
7. Nienaber CA, Ince H, Weber F, et al. Emergency stent-graftplacement in thoracic aortic dissection and evolving rupture.J Card Surg 2003;18:464–70.
8. Bortone AS, De Cillis E, D’Agostino D, de Luca TupputiSchinosa L. Endovascular treatment of thoracic aorticdisease: four years of experience. Circulation 2004;110(11 Suppl 1):II262–7.
9. Leurs LJ, Bell R, Degrieck Y, Hobo R, Lundbom J;EUROSTAR; UK Thoracic Endograft Registry collaborators.Endovascular treatment of thoracic aortic diseases: com-
bined experience from the EUROSTAR and United King-ats.ctsnetjournDownloaded from
dom thoracic endograft registries. J Vasc Surg 2004;40:670–80.
0. Eggebrecht H, Herold U, Kuhnt O, et al. Endovascularstent-graft treatment of aortic dissection: determinants ofpost-interventional outcome. Eur Heart J 2005;26:489–97.
1. Palma JH, de Souza JA, Alves CM, Carvalho AC, Buffolo E.Self-expandable aortic stent-grafts for treatment of descend-ing aortic dissections. Ann Thorac Surg 2002;73:1138–42.
2. Kusagawa H, Shimono T, Ishida M, et al. Changes in falselumen after transluminal stent-graft placement in aorticdissections: six years’ experience. Circulation 2005;111:2951–7.
3. Czermak BV, Mallouhi A, Perkmann R, et al. Serial CTvolume and thrombus length measurements after endovas-cular repair of Stanford type B aortic dissection. J EndovascTher 2004;11:1–12.
4. Duebener LF, Lorenzen P, Richardt G, et al. Emergencyendovascular stent-grafting for life-threatening acute type Baortic dissections. Ann Thorac Surg 2004;78:1261–7.
5. Kato N, Shimono T, Hirano T, et al. Midterm results ofstent-graft repair of acute and chronic aortic dissection withdescending tear: the complication-specific approach. J Tho-rac Cardiovasc Surg 2002;124:306–12.
6. Nienaber CA, Fattori R, Lund G, et al. Nonsurgical recon-struction of thoracic aortic dissection by stent-graft place-ment. N Engl J Med 1999;340:1539–45.
7. Fattori R, Napoli G, Lovato L, et al. Descending thoracicaortic diseases: stent-graft repair. Radiology 2003;229:176–83.
8. Totaro M, Miraldi F, Fanelli F, Mazzesi G. Emergencysurgery for retrograde extension of type B dissection afterendovascular stent graft repair. Eur J Cardiothorac Surg2001;20:1057–8.
9. Görich J, Asquan Y, Seifarth H, et al. Initial experience withintentional stent-graft coverage of the subclavian arteryduring endovascular thoracic aortic repairs. J Endovasc Ther2002;9:39–43.
0. Hausegger KA, Oberwalder P, Tiesenhausen K, et al. Inten-tional left subclavian artery occlusion by thoracic aorticstent-grafts without surgical transposition. J Endovasc Ther2001;8:472–6.
1. Tiesenhausen K, Hausegger KA, Oberwalder P, et al. Leftsubclavian artery management in endovascular repair ofthoracic aortic aneurysms and aortic dissections. J Card Surg2003;18:429–35.
2. Steinberg GK, Drake CG, Peerless SJ. Deliberate basilar orvertebral artery occlusion in the treatment of intracranialaneurysms. J Neurosurg 1993;79:161–73.
3. Williams DM, Lee DY, Hamilton BH, et al. The dissectedaorta. Part III. Anatomy and radiologic diagnosis of branch-vessel compromise. Radiology 1997;203:37–44.
4. White RD, Ullyot DJ, Higgins CB. MR imaging of the aortaafter surgery for aortic dissection. Am J Radiol 1988;150:87–92.
5. Kato M, Matsuda T, Kaneko M, et al. Outcomes of stent-grafttreatment of false lumen in aortic dissection. Circulation1998;98:II305–12.
6. Lambrechts D, Casselman F, Schroeyers P, De Geest R,D’Haenens P, Degrieck I. Endovascular treatment of thedescending thoracic aorta. Eur J Vasc Endovasc Surg 2003;
26:437–44.by on June 4, 2013 als.org

DOI: 10.1016/j.athoracsur.2006.10.064 2007;83:1059-1066 Ann Thorac Surg
H. Sodeck, Roman Gottardi, Christian Loewe and Johannes Lammer Maria Schoder, Martin Czerny, Manfred Cejna, Thomas Rand, Alfred Stadler, Gottfried
True and False Lumen Diameter ChangesEndovascular Repair of Acute Type B Aortic Dissection: Long-Term Follow-Up of
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/83/3/1059including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/83/3/1059#BIBL
This article cites 36 articles, 13 of which you can access for free at:
Citations
shttp://ats.ctsnetjournals.org/cgi/content/full/83/3/1059#otherarticleThis article has been cited by 23 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/great_vessels Great vessels
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 4, 2013 ats.ctsnetjournals.orgDownloaded from




























