Embed Size (px)
Citation preview
CONTRACEPTION
ESTROGEN-PROGESTOGEN ONCE-A-MONTH INJECTABLE
CONTRACEPTIVES AND SERUN PROLACTIN
J. Garza-Flores, V.M. Alba, M.C. Cravioto, L. Hernandez, G. Perez-Palacios
Departamento de Biologia de la Reproduccibn Instituto National de la Nutricibn S. Zubirgn
Mexico City, Mexico
G. Alvarado, R. Rivera
Instituto de Investigacibn Cientifica Universidad Jugrez de1 Estado de Durango
Durango, Mexico
R. Recio, S. Basso1
Departamento de Biologia de la Reproducci& Hospital Universitario
Universidad Autonoma de Coahuila Torreen, Coahuila, Mexico
Abstract
To assess the effect of hormonal monthly injectable contraceptives upon the serum values of immunoreactive prolactin (Prl), three groups of women of reproductive age exposed to different estrogen-progestogen injectable formulation for a minimum of one year were studied. The first group (n=lO) received dihydroxyprogesterone acetophenide 150 mg and estradiol enanthate 10 mg (DHPA/E2- EN), Group 2 (n=21) received medroxyprogesterone acetate 25 mg and estradiol cypionate 5 mg (MPA/E2-C) and Group 3 (n=19) was exposed to norethisterone enanthate 50 mg and
Reprint requests and address for correspondence:
J. Garza-Flores; Department of Reproductive Biology, National Institute of Nutrition S. Zubiran; Vasco de Quiroga No. 15 Tlalpan, 14000 Mexico City, Mexico
Submitted for publication February 13, 1989 Accepted for publication February 24, 1989
MAY 1983 VOL. 39 NO. 5 519
CONTRACEPTION
estradiol valerate 5 mg (NET-EN/E2-V). A group of IUD users (n=16) served as the control group. Serum Prl and 17p- estradiol (E2) concentration were determined in blood samples (0 and 15 min.) on days 0 (day of last injection), 10, 20 and 30 after last contraceptive injection. The results demonstrated a slight though not significant increase (p ~0.05) in serum Prl in the three experimental groups as compared with the IUD control group. This increase in Prl levels observed on day 10 post-last injection never exceeded the upper limits of the normal range (20 ng/ml). Overall, the data demonstrated that the chronic administration of these estrogen/progestogen once-a- month injectable contraceptives does not affect the Prl baseline secretion in women.
Introduction
It is well known that estrogen administration results in significant increase in prolactin (Prl) secretion in different mammalian species including rodents (1,2), bulls and non-human primates (3-6). The studies carried out in normal women using estrogen-containing contraceptive agents have produced conflicting results; thus, some reports have suggested significant increases in serum Prl concentrations (7,8) and modified episodic pattern of Prl release in women during hormonal oral contraceptive administration (9).
Other reports, however, show normal Prl levels in subjects taking the same preparation (lO,ll), and no hyperprolactinemia in women with normal menstrual cycles after discontinuing the use of combined oral contraceptives has been found (12,13); this could be related to the antiestrogenic activity of progestins contained in the pill (14).
The change in prolactin levels during the menstrual cycle has been investigated, but the results are controversial since some revealed increased Prl levels at midcycle and during the luteal phase (15), while other studies did not reveal any cycle-related variations (16).
The apparent lack of correlation between the data obtained from animal studies as compared with the effect in women and the fact that there are countries where, in addition to the pill, once-a-month injectable contraceptives have been used for a number of years (17), it was decided to undertake a study aimed at assessing the effects of combined once-a-month injectable contraceptives on Prl serum levels in chronically exposed women.
520 MAY 1989 VOL. 39 NO. 5
CONTRACEPTION
subjects and Methods
Fifty healthy women of reproductive age entered this comparative study after being informed and written consent obtained. They had been receiving combined once-a-month injectable contraceptives for more than one year. Medical history was taken on admission and a complete gynecological examination including Papanicolaou smear was performed.
Women were grouped according to their previous use of monthly injectables or CUT 200 intrauterine device (IUD):
Group 1. Dihydroxyprogesterone acetophenide (DHPA) 150 mg + estradiol enanthate (EZ-EN) 10 mg (n=lO)
Group 2. Medroxyprogesterone acetate (MPA) 25 mg + estradiol cypionate (E2-C) 5 mg (n=21)
Group 3. Norethisterone enanthate (NET-EN) 50 mg + estradiol valerate (E2-V) 5 mg (n-19)
Group 4. IUD users (n=16)
Additionally, a control experiment was performed in 9 subjects on the effect of stress induced by direct venepuncture or through a cannula inserted 30 minutes prior on Prl levels. Subjects were randomly allocated and samples were taken on days 5 and 6 of a menstrual cycle.
In all women from the experimental groups, two blood samples were obtained from an antecubital vein with a 15- minute interval on days 0 (day of injection), 10, 20 and 30. In the control group, blood samples were taken on days 5, 15 and 25 of the menstrual cycle. The blood was allowed to clot and centrifuged, the stored at -2oOc
plasma separated and until analyzed. The Prl radioimmunoassay was
undertaken following the protocol provided by the Matched Reagent Programme of the World Health Organization (18). The antiserum was obtained from Dr. A.F. Parlow through the WHO. THe cross-reactivity of antiserum with growth hormone was 1.5%. The Prl standard used was IRP 751504. The separation of the bound and free fractions was performed by the second antibody technique. The sensitivity of the Prl assay was 1.1 ng/ml (37 mIU/l). Within-batch and between- batch coefficients of variation were 4.5 and 6.3%, respectively, at the dose of 12 ng/ml. The normal values for Prl, established in our laboratory, are from 3 to 19 ng/ml (97 to 617 mIU/l). The determination of 17l3-estradiol was carried out following the method and with reagents kindly provided by the WHO Matched Reagent Programme (18). The sensitivity of the E2 assay was 13 pg/ml (47.6 fmol/tube) . The intra- and interassay coefficients of
MAY 1989 VOL. 39 NO. 5 521
CONTRACEPTION
variation were 7.8 and 11.3%, respectively. The results are expressed in ng/ml for Prl and pg/ml for estradiol. Since it had been noticed that Prl levels in women were not normally distributed (lo), the results were expressed as the geometric mean with 95% confidence limits. The differences within each group among sampling days were calculated by analysis of variance followed by the Wilcoxon test.
Description of the Preparations:
Perlutal (Promeco, Mexico City) containing 150 mg dihydroxyprogesterone acetophenide (DAPA) (2$-methyl-2a- phenyl-16a,l7a-dioxolane-pregn-4-en-3,20 dione) and 10 mg estradiol enanthate (EZ-EN) (3,178-dihydroxyestra-1,3,5(10)- trien-17B-yl-heptanoate) dissolved in 1 ml benzyl benzoate.
Cycloprovera (Upjohn Company, Crawley, U.K.) containing 25 mg medroxyprogesterone acetate (MPA) (6a-methyl-3,20- dioxo-4-pregn-17a-yl-acetate) and 5 mg estradiol cypionate (E2-C) (3,17~-dihydroxy-1,3,5(lO)-trien-l7$-yl-(3-cyclo- pentyl)-propionate; manufactured as a 0.5 ml aqueous microcrystalline suspension.
HRP102 (Shering AG, Berlin) containing 50 mg norethisterone enanthate (NET-EN) (17a-ethynyl-178-hydroxy- 4-estren-3-one-178-yl-heptanoate) and 5 mg estradiol valerate (E2-V) (3-hydroxy-1,3,5(10)-trien-178-yl-valerate); manufactured as 1 ml oily solution.
The admission physical data of participating women are shown in Table I. Women from Groups 1 and 4 were older than those of Groups 2 and 3. The mean duration of usage in Group 1 was more than 3 years, whereas mean exposure in Groups 2 and 3 was 1 year.
Results
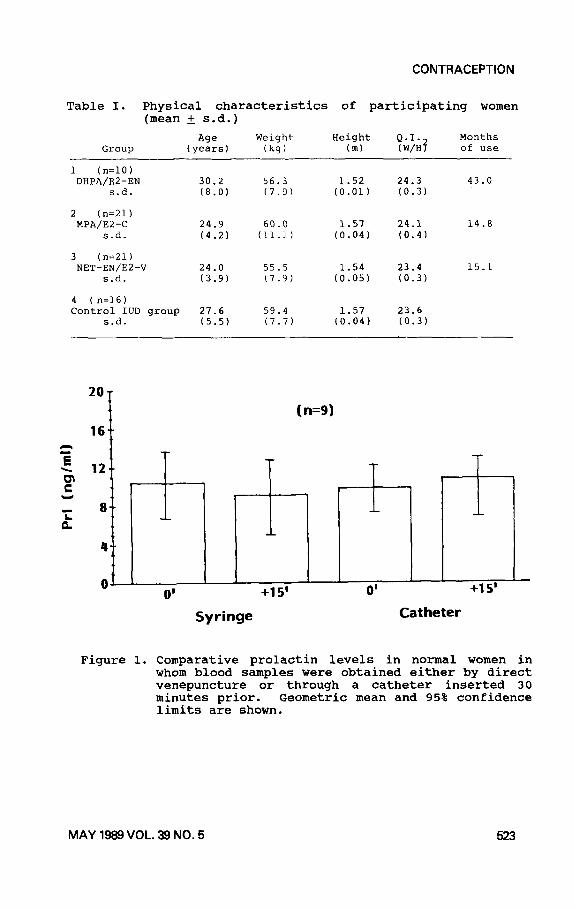
The results of Prl in normal women of reproductive age not exposed to contraception are shown in Figure 1. There were no significant differences between the women whose blood samples were taken with a syringe as compared with prior insertion of an intravenous catheter on day 5 or 6 of a menstrual cycle.
The Prl levels obtained before the last injection (day 0) of the once-a-month contraceptive groups were found within normal limits (3-19 ng/ml). All preparations tested were able to induce a moderate elevation in serum Prl, with maximum Prl levels observed 10 days after injection.
MAY 1989 VOL. 39 NO. 5
CONTRACEPTION
Table I. Physical characteristics of participating women (mean + s.d.)
Group We Weight Height Q.I. Months
(years) (kg) (m) (W/H? of use
1 (IFlO) DHPA/E2-EN 30.2 56.3 1.52 24.3 43.0
s.d. (8.0) (7.9) (0.01) (0.3)
2 (n=21) MPh/EZ-C 24.9 60.0 1.57 24.1 14.8
s.d. (4.2) (11.1) (0.04) (0.41
3 (n=21) NET-EN/E2-V 24.0 55.5 1.54 23.4 15.1
S.d. (3.9) (7.9) (0.05) (0.3)
4 (n=16) Control IUD group 27.6 59.4 1.57 23.6
s.d. (5.5) (7.7) (0.04) (0.3)
A
16
8
Figure 1.
(n=9)
Syringe Catheter
1 I-L +15’
Comparative prolactin levels in normal women in whom blood samples were obtained either by direct venepuncture or through a catheter inserted 30 minutes prior. Geometric mean and 95% confidence limits are shown.
MAY 1989 VOL. 39 NO. 5 523
CONTRACEPTION
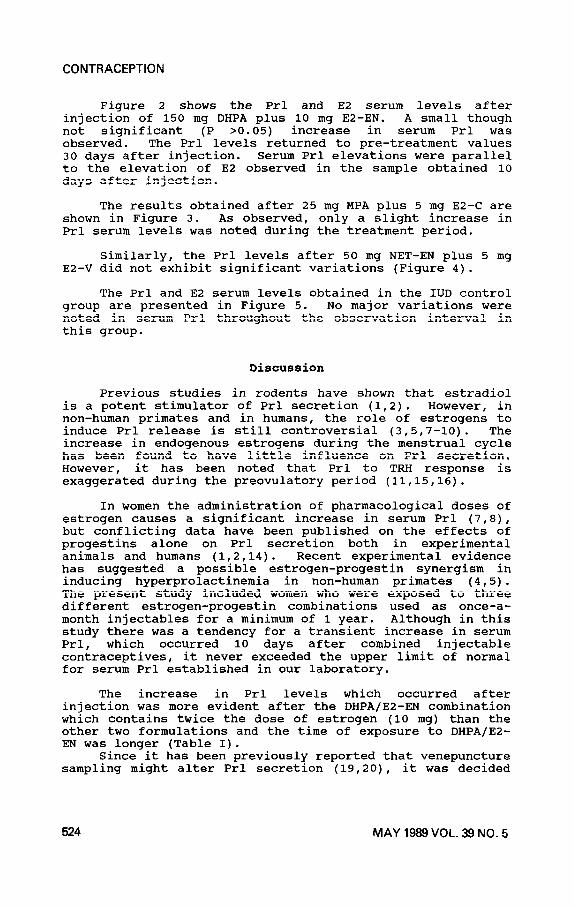
Figure 2 shows the Prl and E2 serum levels after injection of 150 mg DHPA plus 10 mg EZ-EN. A small though not significant (P >0.05) increase in serum Prl was observed. The Prl levels returned to pre-treatment values 30 days after injection. Serum Prl elevations were parallel to the elevation of E2 observed in the sample obtained 10 days after injection.
The results obtained after 25 mg MPA plus 5 mg E2-C are shown in Figure 3. As observed, only a slight increase in Prl serum levels was noted during the treatment period.
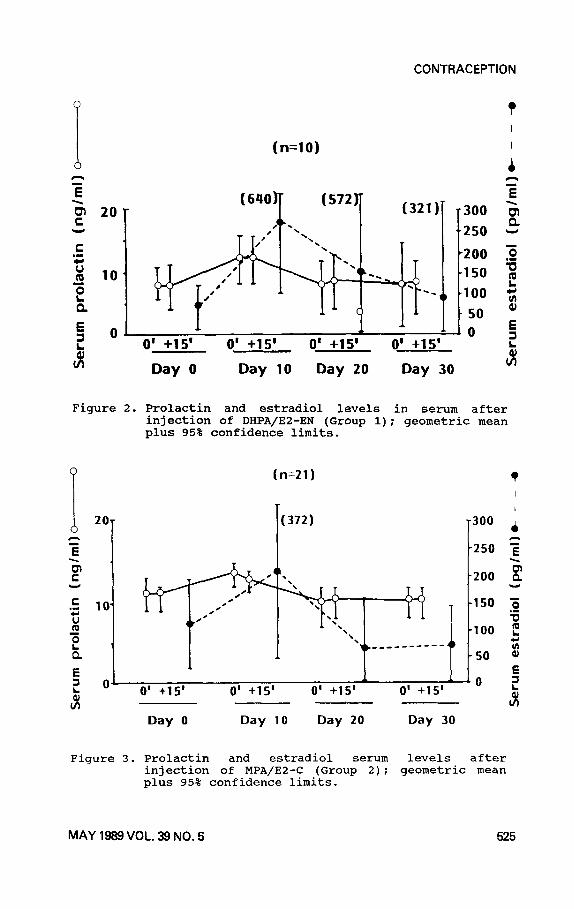
Similarly, the Prl levels after 50 mg NET-EN plus 5 mg E2-V did not exhibit significant variations (Figure 4).
The Prl and E2 serum levels obtained in the IUD control group are presented in Figure 5. No major variations were noted in serum Prl throughout the observation interval in this group.
Discussion
Previous studies in rodents have shown that estradiol is a potent stimulator of Prl secretion (1,2). However, in non-human primates and in humans, the role of estrogens to induce Prl release is still controversial (3,5,7-10). The increase in endogenous estrogens during the menstrual cycle has been found to have little influence on Prl secretion. However, it has been noted that Prl to TRH response is exaggerated during the preovulatory period (11,15,16).
In women the administration of pharmacological doses of estrogen causes a significant increase in serum Prl (7,8), but conflicting data have been published on the effects of progestins alone on Prl secretion both in experimental animals and humans (1,2,14). Recent experimental evidence has suggested a possible estrogen-progestin synergism in inducing hyperprolactinemia in non-human primates (4,5). The present study included women who were exposed to three different estrogen-progestin combinations used as once-a- month injectables for a minimum of 1 year. Although in this study there was a tendency for a transient increase in serum Prl, which occurred 10 days after combined injectable contraceptives, it never exceeded the upper limit of normal for serum Prl established in our laboratory.
The increase in Prl levels which occurred after injection was more evident after the DHPA/EZ-EN combination which contains twice the dose of estrogen (10 mg) than the other two formulations and the time of exposure to DHPA/E2- EN was longer (Table I).
Since it has been previously reported that venepuncture sampling might alter Prl secretion (19,20), it was decided
524 MAY 1989 VOL. 39 NO. 5
CONTRACEPTION
(n=lO) I
A A
z
5 a. V
Day 0 Day 10 Day 20 Day 30 ci
Figure 2. Prolactin and estradiol levels in serum after injection of DHPA/EZ-EN (Group 1); geometric mean plus 95% confidence limits.
P (n=21) 0
20- (372) -300
-250
Day 0 Day 10 Day 20 Day 30
Figure 3. Prolactin and estradiol serum levels after injection of MPA/E2-C (Group 2); geometric mean plus 95% confidence limits.
MAY 1989 VOL. 39 NO. 5 525
CONTRACEPTiON
P (n=19)
T
d -(440) I
20 - -300
;
ii 2 ‘250 z
V -200 i V
l E lo- -150
i
‘ij ._
-. .,
e ~ --__ --__ -100
P *
; oi I * 7:
0 -_
50 2
0 5
91 0’ +15’ 0’ +15’ 0’ +15’ 0’ +15’ - r. Ji
Figure 4
Day 0 Day 10 Day 20 Day 30
Prolactin levels and estradiol serum levels after injection of NET-EN/E2-V (Group 3): geometric mean plus 95% confidence limits.
(n=l6)
(309) -
5 0
i 0’ +15’ 0’ +15’ 0’ +15’ 0’ +15’
Day 5 Day 15 Day 25 Day 5
? I
I
300 & A
250 z
5 200 5
150 5 ‘e
100 ;
50 ii
0 4
i
Figure 5. Prolactin and estradiol serum levels in IUD users (Group 4); geometric mean plus 95% confidence limits.
526 MAY 1969VOL. 39 NO. 5
CONTRACEPTION
to compare the effects of direct venepuncture and intravenous catheter on Prl levels in a group of non- contraceptive users. The results obtained did not show major differences in the two forms of blood collection and therefore, for the purposes of this study, direct venepuncture was chosen. Since diurnal variations in Prl secretion have been reported (10,16,21,22), in this study sampling time was confined from 10:00 a.m. to 12:00 p.m.
Assessment of the safety of existing as well as new once-a-month estrogen-progestin formulations has been considered important in view of the wide acceptance by some cultures of this method of contraception (17,23-26).
Overall, the data presented herein indicate that there is no tendency to hyperprolactinemia in normal women chronically exposed to combined once-a-month injectable contraceptives. These results underscore the safety of this method of fertility regulation in women.
Acknowledgements
This work was supported by the Special Programme of Research Training in Human Reproduction (Geneva, Switzerland). The assistance of Miss Guadalupe Alarcon is appreciated.
1.
2.
3.
4.
5.
References
Chen CL, Meites J. Effects of estrogen and progesterone on serum and pituitary prolactin levels in ovariectomized rats. Endocrinology 1970;86:503-05.
Kalra PS, Fawcett CP, Krulich L, McCann SM. The effect of gonadal steroids on plasma gonadotropins and prolactin in the rat. Endocrinology 1973;92:1256-68.
Milmore JE. Influence of ovarian hormones on prolactin release in the rhesus monkey. Biol Reprod 1978;19:593- 96.
Williams RF, Gianfortoni JG, Hodgen GD. Hyperprolactinemia induced by an estrogen-progesterone synergy: quantitative and temporal effects of estrogen priming in monkeys. J Clin Endocrinol Metab 1985;60:126-32.
Williams RF, Barber DL, Cowan BD, Lynch A, Marut EL, Hodgen GD. Hyperprolactinemia in monkeys: induction by an estrogen-progesterone synergy. Steroids 1981;38:321-31.
MAY 1989 VOL. 39 NO. 5 527
CONTRACEPTION
6. Schams D, Rehinhardt V, Karg H. The immediate response of the plasma prolactin level to oestrogen and progesterone infusions in bulls. Acta Endocrinologia 1974;76:242-47.
7. Badawy SZA, Rebscher F, Kohn L, Wolfe H, Oates RP, Moses A. The relation between oral contraceptive use and subsequent development of hyperprolactinemia. Fertil Steril 1981;36:464-67.
8.
9.
Abu-Fadil S, De Vane G, Siler TM, Yen SSC. Effects of oral contraceptive steroids on pituitary prolactin secretion. Contraception 1976;13:79-85.
Vekemans M, Robyn C. The influence of exogenous estrogen on the circadian periodicity of circulating prolactin in women. J Clin Endocrinol Metab 1975;40:886-89.
10. Davis JRE, Selby C, Jeffcoate WJ. Oral contraceptive agents do not affect serum prolactin in normal women. Clin Endocrinol 1984;20:427-34.
11. Mishell DR Jr, Kletzky OA, Brenner PF, Roy S, Nicoloff J. The effect of contraceptive steroids on hypothalamic-pituitary function. Am J Obstet Gynecol 1977;128:60-74.
12. Jacobs HS, Knuth UA, Hull MGR, Franks S. Post-l'pill'l amenorrhoea, cause or coincidence? Brit Med J 1977;11:940-42.
13.
14.
Klein TA, Mishell DR Jr. Gonadotropin, prolactin and steroid hormone levels after discontinuation of oral contraceptives. Am J Obstet Gynecol 1977;127:585-89.
Sitruk-Ware R, Varian C, Clair F, Maugis E, Fermanian J, Mauvais-Jarvis P. In vivo effects of progestins on prolactin secretion. J Clin Endocrinol Metab 1985;60:575-78.
15. Vekemans M, Delvoye P, L'Hermite M, Robyn C. Serum prolactin levels during the menstrual cycle. J Clin Endocrinol Metab 1977;44:989-93.
16. Ehara Y, Siler T, Vandenberg G, Sinha YN, Yen SSC. Circulating prolactin levels during the menstrual cycle: Episodic release and diurnal variations. Am J Obstet Gynecol 1973;117:962-70.
17. Garza-Flores J, Hall PE. Once-a-month injectable contraceptives. In: Perez-Palacios G, Garza-Flores J, Hall PE, eds. Advances recientes en regulation de la fertilidad, Vol. 1. Mexico, Ed. Piensa, 1987;57-73.
528 MAY 1989 VOL. 39 NO. 5
CONTRACEPTION
18.
19.
20.
21.
22.
23.
24.
25.
26.
Sufi SB, Donaldson A, Jeffcoate SL. Method manual of matched assay reagent programme, 7th ed. Geneva: World Health Organization Special Programme of Research in Human Reproduction, 1983.
Corenblum B, Taylor PJ. Mechanisms of control of prolactin release in response to apprehension stress and anesthesia-surgery stress. Fertil Steril 1981;36:712-15.
Noel GL, Suh HK, Stone JG, Frantz AG. Human prolactin growth hormone release during surgery and other conditions of stress. J Clin Endocrinol Metab 1972;35:840-51.
Parker DC, Rossman LG, Vanderlaan EF. Sleep-related nyctohemeral and briefly episodic variation in human plasma prolactin concentrations. J Clin Endocrinol Metab 1973;36:1119-24.
Armeanu MC Frolich M, Lequin RM. Circadian rhythm of prolactin during the menstrual cycle. Fertil Steril 1986;46:315-16.
Recio R, Garza-Flores J, Schiavon R, Reyes A, Diaz- Sanchez V, Valles V, de la Cruz 0, Oropeza G, Perez- Palacios G. Pharmacodynamic assessment of dihydroxyprogesterone acetophenide plus estradiol enanthate as a monthly injectable contraceptive. Contraception 1987;33:579-89.
Schiavon R, Benavides S, Oropeza G, Garza-Flores J, Recio R, Diaz-Sanchez V, Perez-Palacios G. Serum estrogens and ovulation return in chronic users of a once-a-month injectable contraceptive. Contraception 1988;37:591-98.
Garza-Flores J, Rodriguez V, Perez-Palacios G, Virutamasen P, Tang-Keow P, Konaga Sayreepong R, Kovaks L, Koloszar S, Hall PE. A multicentred pharmacokinetic, pharmacodynamic study of once-a-month injectable contraceptives. I. Different doses of HRPll2 and Depoprovera. Contraception 1987;36:441-57.
World Health Organization Systemic
Task Force on Long-Acting Agents for Fertility Regulation. A
multicentred phase III comparative study of two hormonal contraceptive preparations given once-a-month by intramuscular injection. I. and side effects.
Contraceptive efficacy Contraception 1988;37:1-20.
MAY 1999 VOL. 39 NO. 5 529




























