Embed Size (px)
Citation preview
5/2014
Proteomic analysis of human nasal mucosa: different expression profile in rhino-pathologic states
Shrimp allergy beyond Tropomyosin in Italy: clinical relevance of Arginine Kinase, Sarcoplasmic calcium binding protein and Hemocyanin
An unusual case of occupational asthma in a part time magician. He has got an allergy surprise from his top hat!
A plausible allergy to peanut revealed only by Immunoblot
A case of long-undiagnosed Common Primary Immunodeficiency in adulthood
European Annalsof Allergy and
Clinical Immunology
Issn 1764-1489 Volume 46 n. 5/2014 – september 2014
THE OFFICIAL JOURNAL OF AAITO | ASSOCIAZIONE ITALIANA ALLERGOLOGI IMMUNOLOGI TERRITORIALI E OSPEDALIERI
THE OFFICIAL JOURNAL OF SPAIC | SOCIEDADE PORTUGUESA DE ALERGOLOGIA E IMUNOLOGIA CLINICA
Senza titolo-2 1 10/07/14 15:34
GOCERCA Un potente ICS* ed il LABA** più rapido in associazione1
X
1 - Bodzenta-Lukaszyk A et al., Efficacy and safety profile of fluticasone/formoterol combination therapy compared individual components administered concurrently in asthma: a randomised controlled trial. Curr Med Res Opin. 2013 Feb 20.2 - Flutiformo® - Riassunto delle caratteristiche di prodotto3 - Dissanayake S et al., Fluticasone/formoterol: a new single-aerosol combination therapy for patients with asthma.
Respiratory Medicine (2012) 106(S1), S20–S28
CLASSE A
Flutiformo® 50 µg / 5 µg 31,35 €Indicato negli adulti e negli adolescenti al di sopra dei 12 anni
Flutiformo® 125 µg / 5 µg 47,66 €Indicato negli adulti e negli adolescenti al di sopra dei 12 anni
Flutiformo® 250 µg / 10 µg 70,28 €Indicato SOLO negli adulti, al di sopra dei 18 anni
Dosaggi e prezzo al pubblicoal netto degli sconti obbligatori di legge
* IC
S= co
rtico
stero
ide
inal
ator
io
** LA
BA=b
ronc
odila
tato
re a
lung
a du
rata
d’a
zione
RCP
in a
llega
to
Dep
osito
AIFA
in d
ata
11/0
6/20
13
FL
U 20
PER LA PRIMA VOLTA IN ASSOCIAZIONE(3)
Ora associati in un unicoinalatore aerosol (1)
Fluticasone ha un potentee sostenuto effetto antiinfiammatorioe formoterolo fornisceuna rapida broncodilatazione (3)
Inalatore con indicatore di dose (2)
NOVITÀ
C
M
Y
CM
MY
CY
CMY
K
ADV Flutiformo 21x27.pdf 1 30/05/14 09.16
SUBSCRIBE NOW! www.eurannallergyimm.com• 6 print issues per year• full access to www.eurannallergyimm.com,
featuring all current and archived issues
European Annals of Allergy and Clinical Immunologyis a bimonthly peer-reviewed publication• The official Journal of the “Associazione Italiana Allergologi Immunologi Territoriali
e Ospedalieri” (Italian Association of Hospital Allergists and Immunologists - AAITO)and the “Sociedade Portuguesa de Alergologia e Imnunologia Clinica” (Portuguese Societyof Allergology and Clinical Immunology - SPAIC)
• indexed in PubMed and Scopus
• collects reviews, original works and case reports concerning etiology,diagnosis and treatment of allergic and immunological disorders
• includes a section of information comingfrom the main international health associations and authorities.
Italy SubScrIptIon only 60,00 Euro
InternatIonal SubScrIptIon
only 85,00 Euro
To submit your paper go to http://eaaci.edmgr.com
AbbAAITO210x270.indd 1 02/07/14 14.21
EDITORS IN CHIEFR. Asero (Milano – Italy)
M.Morais - Almeida (Lisbon – Portugal)
HONORARY EDITORA. Sabbah (Angers – France)
ASSOCIATE EDITORSS. Bonini (Roma – Italy), A. Tedeschi (Milano – Italy)
EDITORIAL BOARDM.B. Bilò (Ancona – Italy)
F. Bonifazi (Ancona – Italy)L. Cecchi (Firenze – Italy)
L. Delgado (Oporto – Portugal)P. Demoly (Montpellier – France)
G. D’Amato (Napoli – Italy)M. Drouet (Angers – France)
M. Fernandez-Rivas (Madrid – Spain)A. Fiocchi (Milano – Italy)
D. Macchia (Firenze – Italy)F. Mastrandrea (Taranto – Italy)
D.A. Moneret-Vautrin (Nancy – France)M. Morais-Almeida (Lisbon – Portugal)
G. Moscato (Pavia – Italy)C. Nunes (Portimao – Portugal)
M. Olivieri (Verona – Italy)P. Parronchi (Firenze – Italy)
G. Passalacqua (Genova – Italy)G. Pauli (Strasbourg – France)
A. Perino (Torino – Italy)O. Quercia (Faenza – Italy)A. Romano (Roma – Italy)G. Senna (Verona – Italy)
A. Todo Bom (Coimbra – Portugal)S. Voltolini (Genova – Italy)
SCIENTIFIC COMMITTEEL. Antonicelli (Italy)
A. Bener (Qatar)H. Bazin (Belgium)
J. Bellanti (USA)C. Geller-Bernstein (Israel)
S. Bonini (Italy)G.W. Canonica (Italy)
M. Cugno (Italy)B. David (France)
S. Durham (London)R. de Marco (Italy)
G.P. Girolomoni (Italy)R. Jarish (Austria)
S.G.O. Johansson (Sweden)F. Levi-Shaffer (Israel)
C. Lombardi (Italy)P. Lowenstein (Denmark)
J.L. Malo (Canada)A.G. Palma-Carlos (Portugal)
G. Scadding (London)G. Scadding (LondonE. Stevens (Belgium)
R. van Ree (Amsterdam)
FOUNDER AND CORRESPONDING MEMBERG.M. Halpern (USA)
Editors in ChiefRiccardo AseroMário Morais-Almeida
Publishing DirectorNicola Miglino
Publishing EditorChiara [email protected]. 02 88184.257
Production ManagerWalter [email protected]. 02 88184.222
Sales & MarketingLudovico [email protected]. 02 88184.354
TrafficDonatella [email protected]. 02 88184.292
[email protected] - Tel. 02 88184.317 - Fax 02 88184.151Italy subscription: 60 euroWorld subscription: 85 eurowww.eurannallergyimm.com
PrintingProntoStampa SrlVia Praga, 1 - 24040 Verdellino (BG)
EDRA LSWR SpAVia G. Spadolini, 720141 Milano - ItalyTel. 0039 (0)2-88184.1Fax 0039 (0)2-88184.301www.edizioniedra.it
© 2014 Associazione Italiana Allergologi Immunologi Territoriali e Ospedalieri - AAITO. Published by EDRA LSWR SpA.All rights reserved.
The contents of this Journal are indexed in PubMed and SCOPUS®
European Annalsof Allergy and
Clinical ImmunologyTHE OFFICIAL JOURNAL OF AAITO
ASSOCIAZIONE ITALIANA ALLERGOLOGI IMMUNOLOGI TERRITORIALI E OSPEDALIERI
THE OFFICIAL JOURNAL OF SPAICSOCIEDADE PORTUGUESA DE ALERGOLOGIA E IMUNOLOGIA CLINICA
AAITOAssociazione Italiana Allergologi Immunologi Territoriali e Ospedalieri
Directory BoarD
PresidentMaria Beatrice Bilò
Designate PresidentAntonino Musarra
Vice PresidentsRiccardo AseroFrancesco Murzilli
TreasurerOliviero Quercia
Honorary PresidentFloriano Bonifazi
MembersLorenzo CecchiDomenico GarganoGiuseppina ManzottiLionello Muratore Susanna Voltolini Marcello Zambito

162 Author Guidelines
European Annals of Allergy and Clinical Immunology will accept for publication suitable manuscripts dealing with the ae-tiology, diagnosis, and treatment of allergic and immunologic diseases. These might include the study of methods of con-trolling immunologic and allergic reactions, human and ani-mal models of hypersensitivity and other aspects of basic and applied clinical allergy in its broadest sense.We encourage case reports that focus on topic(s) of extreme contemporary interest. Paper reporting the results of drug trials will be considered.European Annals of Allergy and Clinical Immunology also publishes solicited and usolicited review articles on subjects of topical interest to clinical and experimental allergy.
Manuscript
We request that all manuscripts should be submitted online through our web-based peer review system.Submitted contributions are accepted for publication on the ba-sis of scientific interest and relevance, at the final discretion of the Editors in Chief, who will have blinded written evaluations from at least two anonymous reviewers. Once a manuscript has been accepted for publication, Authors will receive an electronic page proof for review and approval, following which the manuscript is published in the print jour-nal and on the journal website.Following acceptance, Authors are also requested to return both completed and signed Journal Publishing Agreement and Con-flict of interest disclosure forms by e-mail to: [email protected]
Full Authors Guidelines, online Submission System link, Jour-nal Publishing Agreement and Conflict of interest forms are available on Journal website: www.eurannallergyimm.comTyped manuscripts at 30 lines per page: maximum lenght 10 pages, around 300 lines.Manuscripts should be typewritten (double spacing) on one side of the paper; on a separate sheet, should bear the title of the paper, name, postal and e-mail address of the Author, together with the name of institution where the work was done.Generally, papers should be divided into the following parts and in the order indicated:1. Summary and key words: english, limited to 15 lines.2. Introduction: containing the reasons for doing the work.3. Materials and methods.4. Results: these should be given concisely; the use of tables
and figures to illustrate the same results will only rarely be allowed.
5. Discussion: the presentation of results should be separated from a discussion of their significance.
6. References.
Units and Abbreviations
European Annals of Allergy and Clinical Immunology rec-ognizes the adoption of the International Systems of Units (SI-Units). Abbreviations to be put in a glossary at the foot of page 1 on the text.
References
References should be in the order:• the order number corresponding with that of appearance in
the text;• the author’s name(s), followed by initial or first name;• the title of the work, in the original language;• for journals: usual title abbreviations according to interna-
tional nomenclature and in the order: year, volume number, issue number (in parenthesis), first and last page numbers of the work.
For example:Bodtger U, Linnegerg A. Remission of allergic rhinitis: An 8-year observational study. J Allergy Clin Immunol 2004; 114(6): 1384-8.• for books: name of the author/editor, title, publisher/institu-
tion, town where published, year of publication, first and last page numbers of the work.
For example:Paupe J, Scheinman P (Eds.). Allergologie Pédiatrique. Flam-marion, Paris, 1988: 324-42.
Illustrations
• Figures always on separate numbered sheets and legends on the back in pencil
• Figures always saved on separate numbered files• Figures, diagrams: JPG, 300 dpi minimum• Radiographs: JPG, 300 dpi minimum
All tables, figures, radiographs, etc. must be referenced in the text.Legends should be put on a separate sheet, saved on a separate file and have the same numbers as the figures.
The “pdf ” of the article will be sent to the author by e-mail.
EDRA LSWR SpAVia Spadolini, 720141 Milano - ItalyTel. 0039 (0)2-88184.1Fax 0039 (0)2-88184.301www.eurannallergyimm.com

Original ArticlesProteomic analysis of human nasal mucosa: different expression profile in rhino-pathologic states . . 164M. GelarDi, r.a. Siciliano, F. PaPa, M. F. Mazzeo, e. De nitto, n. Quaranta, r. liPPoliS
Shrimp allergy beyond Tropomyosin in Italy: clinical relevance of Arginine Kinase, Sarcoplasmic calcium binding protein and Hemocyanin . . . . . . . . . . . . . . . . . . . . . . 172M.G. GiuFFriDa, D. Villalta, G. MiStrello, S. aMato, r. aSero
Case ReportsAn unusual case of occupational asthma in a part time magician. He has got an allergy surprise from his top hat! . . . . . . . . . . . . . . . . . . . . . . . . . . 178G. liccarDi, l. Billeri, M. FoGlia, c. SaPio, M.a.r. De GiGlio, G. D’aMato
A plausible allergy to peanut revealed only by Immunoblot . . . . . . . . . . . . . . . . . . . . 181c. richarD, S. JacQuenet, D.a. Moneret-Vautrin
A case of long-undiagnosed Common Primary Immunodeficiency in adulthood . . . . . . . . . . 184D. tirotta, V. Durante
tAble of Contents
O R I G I N A L A R T I C L E S Eur Ann AllErgy Clin immunol Vol 46, n 5, 164-171, 2014
SummaryBackground. Rhinitis comprises several diseases with varying causes and different clinical manifestations and pathological features, but treated as a single clinical disorder. As heteroge-neous disease, proper differential diagnosis is useful to delineate appropriate therapeutic inter-vention. Comparative proteomic investigation was aimed to provide information for specific differentially expressed proteins in rhino pathologic state, that could be used for diagnostic purpose and therapeutic monitoring. Methods. Proteins extracted from nasal mucosa cells of patients with different features of rhinitis and from control subjects, were separated by 2-DE. Proteins differentially expressed were identified by mass spectrometry (MS). Results. Compar-ative proteomic analyses led to the identification of eighteen proteins differentially expressed in patients with rhinitis, mainly related to cell defense and innate and acquired immunity. From that, at least one protein can be a possible candidate as biomarker of disease.
Corresponding author Dr. Rosa LippolisInstitute of Biomembranes and Bioenergetics (IBBE)National Research Council (CNR)c/o Department of Basic Medical SciencesNeurosciences and Sense OrgansP.zza Giulio Cesare 1170124 Bari, ItalyPhone: +39 080 5448531Fax: +39 080 5448538E-mail: [email protected]
Key Words
Human nasal mucosa; rhinitis; two-dimensional electrophoresis; mass spectrometry; proteomics
1Department of Basic Medical Sciences, Neurosciences and Sense Organs, University of Bari, Italy 2Institute of Food Sciences, Italian National Research Council (CNR), Avellino, Italy3Institute of Biomembranes and Bioenergetics, Italian National Research Council, (CNR) Bari, Italy
M. GelarDi1, r.a. Siciliano2, F. PaPa1, M. F. Mazzeo2, e. De nitto1, n. Quaranta1, r. liPPoliS3
Proteomic analysis of human nasal mucosa: different expression profile in rhino-pathologic states
Introduction
The nasal mucosa tissue is a complex organ responsible for several functions of the nasal airway and, together with the osteo-meatal complex, is regarded as the critical area of the na-sal cavity in the pathogenesis and treatment of various patho-logic conditions. Rhinitis is one of the most common health care problems affecting a high percentage of the population and having a significant adverse effect on life quality and daily functioning (1). Historically treated as a single clinical dis-order, rhinitis comprises several diseases with varying causes, each one characterized by distinct clinical manifestations and pathological features. These include allergic rhinitis affecting
30% of the population, non-allergic vasomotor rhinitis “cel-lular” (NARES, NARMA, NARESMA) affecting less than 15% of the population and nasal polyposis affecting 4% of the population (2-3). Many aspects of disease pathophysiol-ogy still remain unknown. Currently, clinical diagnosis and determination of the therapeutic effects mainly depend on the observation of nasal mucosal changes as clinical presentations, cellular and molecular characteristics. As it is a heterogeneous disease, proper differential diagnosis is required to delineate appropriate therapeutic intervention. This aspect includes methods for defining disease-specific differences. Proteomics is a modern approach aimed at decoding information con-

165Proteomic analysis of human nasal mucosa: different expression profile in rhino-pathologic states
Skin prick test and nasal cytology
Allergic sensitization was assessed by skin prick test (4) using a definite panel of allergens (100 IR/mL), including house dust mites (Dermatophagoides farinae and Dermatophagoides pteron-yssinus); cat; dog; grass mix; Compositae mix; Parietaria judaica; birch, hazel and olive trees; Alternaria tenuis; Cladosporium; and Aspergilli mix) (Stallergenes, Milan, Italy). Equivocal skin test results were further investigated by a CAP-RAST assay (Phadia, Uppsala, Sweden). Endoscopic examina-tion was performed with a 3.4 mm diameter of flexible fiber-scope ENT 2000 (Vision Sciences®, USA). Patients were rated according to the following objective criteria: 1. Presence of intranasal anatomic alterations (septal deviation,
cartilaginous spurs, Concha bullosa, intranasal tumors). 2. Mucosal appearance (hyperemia, edema, atrophy, areas of
de-epithelialization). 3. Type of secretions (serous, mucous, pus, hematic, exudate-clot-
ted scabs) on the basis of the prick test and nasal cytology.
Nasal cytology was performed by anterior rhinoscopy. Nasal mucosa cells were collected from the middle portion of the in-ferior turbinate by a non-invasive scraping procedure (5). An aliquot of samples was placed on a glass slide, fixed by air-drying and then stained by the May-Grunwald Giemsa method (Car-lo Erba, Milan, Italy). The slide was observed under a Nikon E600 light microscope (Nikon, Canada) equipped with a digital camera (Nikon “Coolpix 3:34”) for the acquisition of micro-scopic images. Cell preparations were qualitatively evaluated to confirm the collection of a sufficient number of intact cells and the absence of evident contamination by blood cells caused by
tained in genomic sequences in terms of protein structures and functions as well as in the control of biological processes and pathways. In the biomedical field, the comprehensive study of the cell proteome is providing insight into the molecular mechanisms of a variety of physiopathological processes and disease states. The potential of proteomics in identifying dis-ease biomarkers is promising. However, this potential has yet to be explored across different subsets of patients with rhinitis. In this respect, a comprehensive analysis of protein compo-nents of nasal mucosa cells could be useful for evaluating the protein factors that are altered in pathologic states. In the present study, comparative proteomics was applied to characterize the nasal mucosal proteome and identify protein differentially expressed in nasal mucosa cells of patients affected by different rhino-pathologic diseases.
Materials and methods
Demographics and sample collection
A case-control study was performed in the Rhinology Clinic of the Otolaryngology Unit of the University of Bari (Italy). Eth-ical approval and informed consent were obtained from partic-ipating institutions and individuals, respectively. In total eight volunteers, four patients with rhinitis and four control subjects were recruited for sample collection. The patient’s history was taken to determine the presence of a familiar disease (atopy, asthma and ASA sensibility). The medical case history was also determined to gain suitable information on asthma, aspirin al-lergy, headache and/or facial pain, nasal obstruction, type of rhi-norrhea, itch, sneezing, daytime or night-time cough, halitosis, postnasal drip and fever.
Table 1 - Clinical and cytological characteristics of the subjects examined.
Control Subjects Age Sex Prick test Nasal Cytology Diagnosis
Control 1 59 F Neg. Neg. Negative
Control 2 24 F Neg. Neg. Negative
Control 3 25 M Neg. Neg. Negative
Control 4 55 M Neg. Neg. Negative
Rhino-pathologic subjects
Patient 1 32 F Neg. E++++/Mas+++++ NARESMA
Patient 2 23 F Neg. E+++ NARES
Patient 3 34 M Parietaria. Cypress. N+++E+/Mast+
Allergic rhinitis
Patient 4 26 M Olive, Cypress, Ep. Cat N+++E++++/Mast++++
Allergic rhinitis withNasal polyposis
166 M. Gelardi, R.A. Siciliano, F. Papa, M. F. Mazzeo, E. De Nitto, N. Quaranta, R. Lippolis
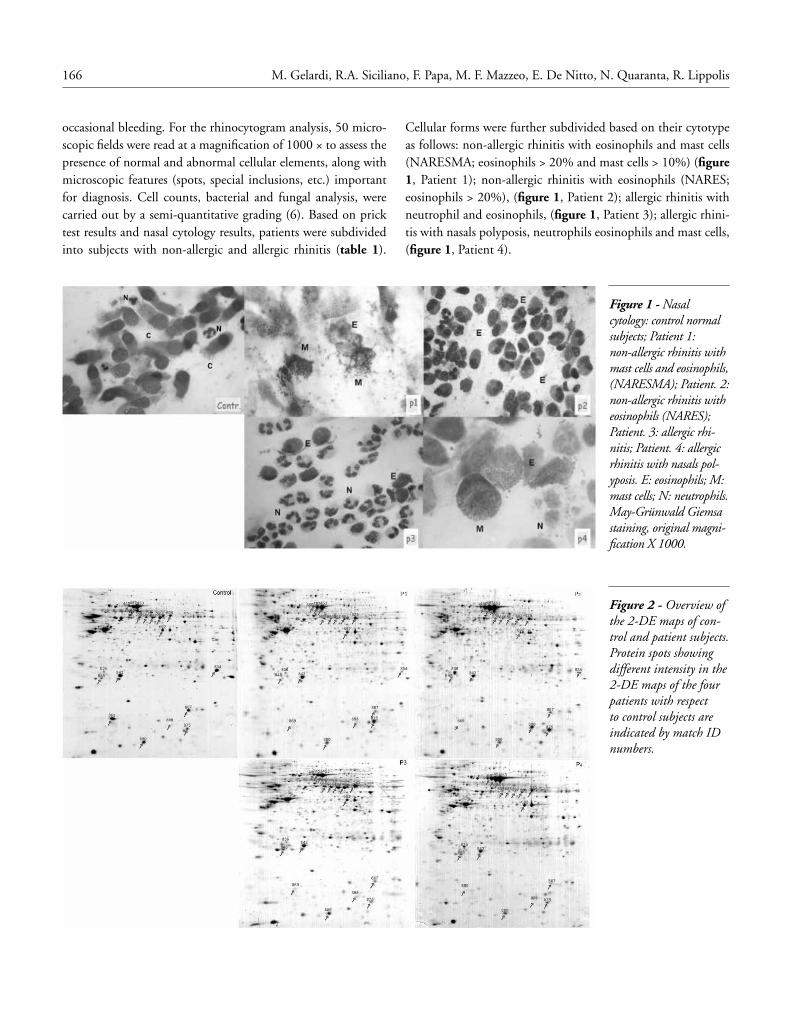
Cellular forms were further subdivided based on their cytotype as follows: non-allergic rhinitis with eosinophils and mast cells (NARESMA; eosinophils > 20% and mast cells > 10%) (figure 1, Patient 1); non-allergic rhinitis with eosinophils (NARES; eosinophils > 20%), (figure 1, Patient 2); allergic rhinitis with neutrophil and eosinophils, (figure 1, Patient 3); allergic rhini-tis with nasals polyposis, neutrophils eosinophils and mast cells, (figure 1, Patient 4).
occasional bleeding. For the rhinocytogram analysis, 50 micro-scopic fields were read at a magnification of 1000 × to assess the presence of normal and abnormal cellular elements, along with microscopic features (spots, special inclusions, etc.) important for diagnosis. Cell counts, bacterial and fungal analysis, were carried out by a semi-quantitative grading (6). Based on prick test results and nasal cytology results, patients were subdivided into subjects with non-allergic and allergic rhinitis (table 1).
Figure 1 - Nasal cytology: control normal subjects; Patient 1: non-allergic rhinitis with mast cells and eosinophils, (NARESMA); Patient. 2: non-allergic rhinitis with eosinophils (NARES); Patient. 3: allergic rhi-nitis; Patient. 4: allergic rhinitis with nasals pol-yposis. E: eosinophils; M: mast cells; N: neutrophils. May-Grünwald Giemsa staining, original magni-fication X 1000.
Figure 2 - Overview of the 2-DE maps of con-trol and patient subjects. Protein spots showing different intensity in the 2-DE maps of the four patients with respect to control subjects are indicated by match ID numbers.
167Proteomic analysis of human nasal mucosa: different expression profile in rhino-pathologic states
in lysis buffer containing 7 M urea, 2 M thiourea, 4% (w/v) 3-[(3-cholamidopropyl)dimethylammonio]-1-propanesul-fonate (CHAPS), 50 mM 1,4-dithio-DL-threitol (DTT) and protease inhibitors cocktail (Sigma-Aldrich, St. Louis, MO, USA). Cell lysis was achieved by sonication cycles on ice (10 × 10 s pulses with a 30 s interval between each ultrasonic cycle). The
Protein extraction from nasal mucosa cells
Three samples of mucosa cells from each subject were collected separately during the pollen season. Immediately after scrap-ing, recovered cells were washed with ice-cold PBS, pelleted and preserved at -80°C until analysis. To prepare soluble pro-tein fractions, pelleted cells were thawed on ice and suspended
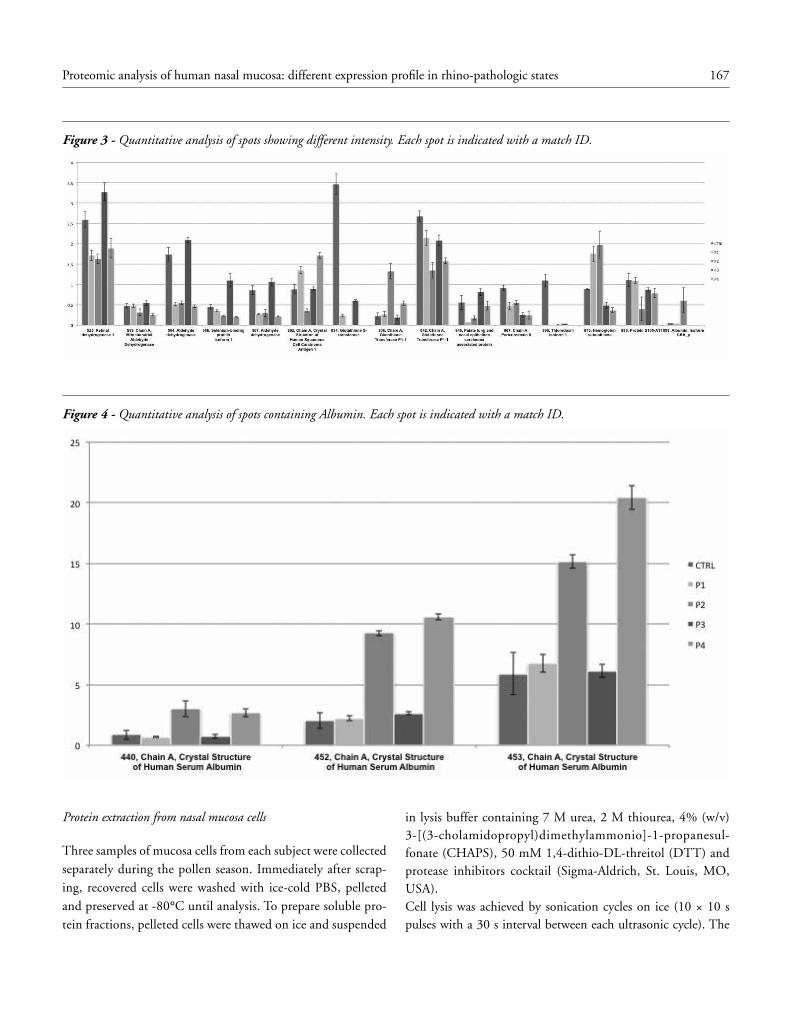
Figure 3 - Quantitative analysis of spots showing different intensity. Each spot is indicated with a match ID.
Figure 4 - Quantitative analysis of spots containing Albumin. Each spot is indicated with a match ID.

168 M. Gelardi, R.A. Siciliano, F. Papa, M. F. Mazzeo, E. De Nitto, N. Quaranta, R. Lippolis
Matrix Assisted Laser Desorption Ionization - Time of Flight - Mass Spectrometry (MALDI-TOF-MS) analyses performed on a Voyager DE PRO mass spectrometer (Applied Biosystems Foster City, CA) and database searches (12).
Results
Validation of nasal cell samples
Nasal mucosa cells samples from four controls and four rhi-no-pathologic patients with 34,75 years mean age (range 23-59 years) were obtained by a non-invasive nasal scraping pro-cedure followed by their quality evaluation by cytology (table 1). Control samples showed a normal cytology, characterized by numerous well-formed ciliated cells and some rare neutrophils (table 1 and figure 1, Control). The cytological analysis of nasal mucosa of the four rhino-pathologic patients showed a signifi-cant infiltration of inflammatory cells with variable percentages of neutrophils, eosinophil and mast cells (figure 1, P1, P2, P3, P4 and table 1).
Proteome analysis of nasal mucosa
Comparative proteomic analysis of the nasal mucosa cells from controls and rhino-pathologic subjects was performed integrat-ing 2-DE and mass spectrometric methodologies. Proteomic maps showed several hundreds of well-resolved protein spots distributed over a wide range of pI values and molecular masses (figure 2). The overall position and number of protein spots observed in the 2-DE maps were similar in the four control samples (476 ± 24, 458 ± 32, 470±19, 481± 57 for C1, C2, C3, and C4 respectively), and in the four patients samples (459 ± 37, 448 ± 43, 467 ± 83 and 489 ± 63 for P1, P2, P 3 and P4 respectively). For each subject, three biological samples were ob-tained and each sample was run in triplicate (figure 1-S and 2-S, in supplementary materials). The percent of matches between gels from the same class and from the five different classes was similar (around 65%). In order to analyze proteins differentially expressed in the four patient samples with respect to the con-trol samples, only the matched spots present in all gels were investigated. Among this group of spots, only those showing a different intensity with a P < 0.05 were considered for further mass spectrometric analyses. Using this constrained statistical analysis, no significant variation of spot intensity was revealed comparing the 2-DE maps of the four-control subjects that can be therefore considered as homogeneous reference to patholog-ical samples. Eighteen spots marked in figure 2, had different intensity in the 2-DE maps of the four patients samples com-pared to the control subjects. The data clearly indicated that differences in the proteome profile of the four patients samples were mostly affected by the specific pathology. Spots of interest
sample was clarified by centrifugation at 13 000 rpm for 10 min at 4°C to remove cellular debris. Protein concentration was determined using the Bio-Rad protein assay kit (Bio-Rad Lab-oratories, Hercules, CA, USA), according to the manufacturer’s instruction (7). Soluble protein samples were stored at -80°C until use.
Two-dimensional gel electrophoresis (2-DE)
Proteins were separated by 2-DE essentially as previously de-scribed (8,9). 250 μg of each protein sample, diluted in the IPG strip rehydration buffer, containing 8 M urea, 2% (w/v) CHAPS, 2% (w/v) DTT, was loaded on a 24-cm IPG strip with a linear 3-10 pH gradient. Isoelectric focusing was carried out at 20°C using the Ettan IPGphor Isoelectric Focusing System (GE Healthcare, Amersham Biosciences AB, Uppsala, Sweden) to 70 kVh. After isoelectric focusing the IPG strips were equilibrated for 15 min in the sodium dodecyl sulphate (SDS) equilibration buffer (50 mM Tris/HCl, pH 8.8, 6 M urea, 30% (v/v) glycer-ol, 2% (w/v) SDS, containing 1% (w/v) DTT) and for further 15 min in the same equilibration buffer containing 2.5% (w/v) iodoacetamide and trace of bromophenol blue. The second-di-mensional gel electrophoresis (SDS-PAGE) was carried out us-ing the vertical slab separation unit Ettan Dalt II System (GE Healtcare). Homogeneous 12,5% polyacrylamide gel was used in a Laemmli buffer system (10) at a constant current of 15 mA gel-1 and at 10°C. The gels were stained using Brilliant blue G-colloidal concentrate (Sigma, St. Louis, MO, USA) (11).
Image analysis of protein patterns
The coomassie-stained 2-DE gels were scanned with an image scanner at 300 dpi resolution to acquire gel images. Image anal-ysis was performed as reported (12), using Image Master 2-DE software v. 6.0 (GE Healthcare). Briefly, spot detection was car-ried out using the optimal values for spot intensity, spot area and saliency determined by applying real-time filters in order to minimize the detection of artefacts and to maximize the real spot detection. Three gels from each sample were used to create the five match sets with one gel included from each of three protein preparation repeats. Relative spot volume (% volume), i.e. digitized staining intensity integrated over the area of the in-dividual spot divided by the sum of volume of all spots in the gel and multiplied by 100, was used for spot quantification (13). The match identification number (ID) was used to identify all spots in a match. Spots present in all the gels of the five classes and exhibiting an intensity difference between the five samples with a P value < 0.05, using the two-tailored Student’s t-test, were considered to be differentially expressed. Spots of interest were excised from 2-DE gels and in-gel digest-ed using trypsin (14). Protein identification was achieved by
169Proteomic analysis of human nasal mucosa: different expression profile in rhino-pathologic states
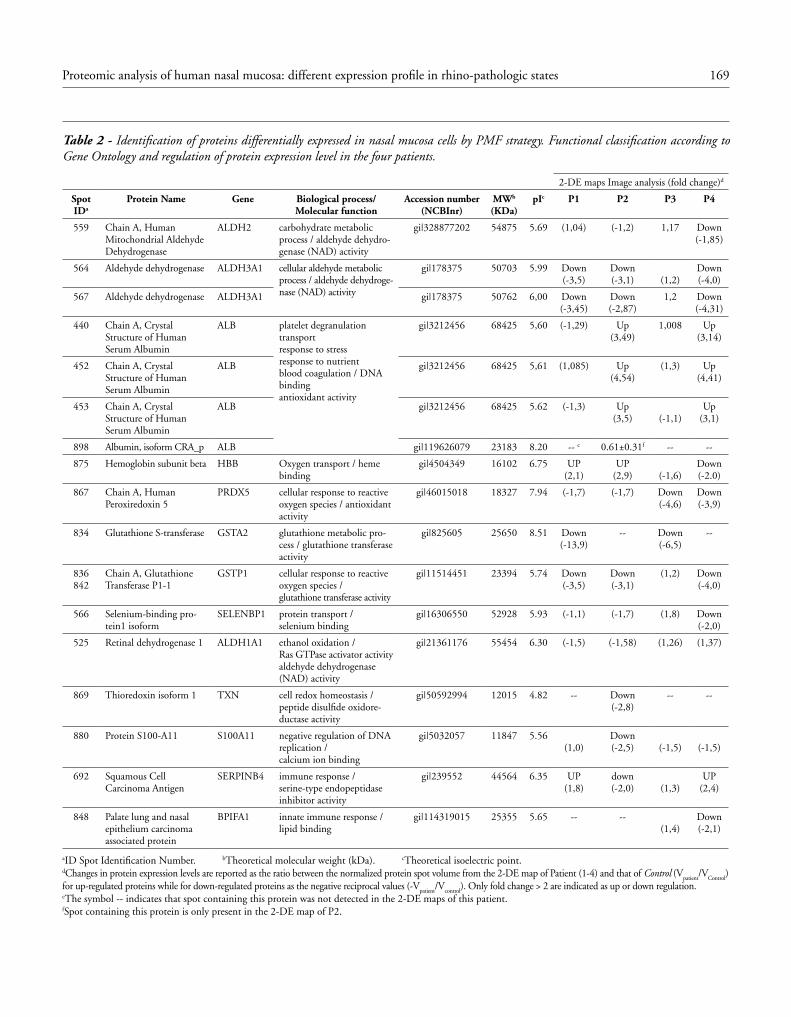
Table 2 - Identification of proteins differentially expressed in nasal mucosa cells by PMF strategy. Functional classification according to Gene Ontology and regulation of protein expression level in the four patients.
2-DE maps Image analysis (fold change)d
Spot IDa
Protein Name Gene Biological process/Molecular function
Accession number (NCBInr)
MWb (KDa)
pIc P1 P2 P3 P4
559 Chain A, Human Mitochondrial Aldehyde Dehydrogenase
ALDH2 carbohydrate metabolic process / aldehyde dehydro-genase (NAD) activity
gi|328877202 54875 5.69 (1,04) (-1,2) 1,17 Down(-1,85)
564 Aldehyde dehydrogenase ALDH3A1 cellular aldehyde metabolic process / aldehyde dehydroge-nase (NAD) activity
gi|178375 50703 5.99 Down(-3,5)
Down(-3,1) (1,2)
Down(-4,0)
567 Aldehyde dehydrogenase ALDH3A1 gi|178375 50762 6,00 Down(-3,45)
Down(-2,87)
1,2 Down(-4,31)
440 Chain A, Crystal Structure of Human Serum Albumin
ALB platelet degranulation transportresponse to stressresponse to nutrientblood coagulation / DNA bindingantioxidant activity
gi|3212456 68425 5,60 (-1,29) Up(3,49)
1,008 Up(3,14)
452 Chain A, Crystal Structure of Human Serum Albumin
ALB gi|3212456 68425 5,61 (1,085) Up(4,54)
(1,3) Up(4,41)
453 Chain A, Crystal Structure of Human Serum Albumin
ALB gi|3212456 68425 5.62 (-1,3) Up(3,5) (-1,1)
Up(3,1)
898 Albumin, isoform CRA_p ALB gi|119626079 23183 8.20 -- e 0.61±0.31f -- --
875 Hemoglobin subunit beta HBB Oxygen transport / heme binding
gi|4504349 16102 6.75 UP(2,1)
UP(2,9) (-1,6)
Down(-2.0)
867 Chain A, Human Peroxiredoxin 5
PRDX5 cellular response to reactive oxygen species / antioxidant activity
gi|46015018 18327 7.94 (-1,7) (-1,7) Down(-4,6)
Down(-3,9)
834 Glutathione S-transferase GSTA2 glutathione metabolic pro-cess / glutathione transferase activity
gi|825605 25650 8.51 Down(-13,9)
-- Down(-6,5)
--
836842
Chain A, Glutathione Transferase P1-1
GSTP1 cellular response to reactive oxygen species /glutathione transferase activity
gi|11514451 23394 5.74 Down(-3,5)
Down(-3,1)
(1,2) Down(-4,0)
566 Selenium-binding pro-tein1 isoform
SELENBP1 protein transport /selenium binding
gi|16306550 52928 5.93 (-1,1) (-1,7) (1,8) Down(-2,0)
525 Retinal dehydrogenase 1 ALDH1A1 ethanol oxidation /Ras GTPase activator activityaldehyde dehydrogenase (NAD) activity
gi|21361176 55454 6.30 (-1,5) (-1,58) (1,26) (1,37)
869 Thioredoxin isoform 1 TXN cell redox homeostasis /peptide disulfide oxidore-ductase activity
gi|50592994 12015 4.82 -- Down(-2,8)
-- --
880 Protein S100-A11 S100A11 negative regulation of DNA replication /calcium ion binding
gi|5032057 11847 5.56(1,0)
Down(-2,5) (-1,5) (-1,5)
692 Squamous Cell Carcinoma Antigen
SERPINB4 immune response /serine-type endopeptidase inhibitor activity
gi|239552 44564 6.35 UP(1,8)
down(-2,0) (1,3)
UP(2,4)
848 Palate lung and nasal epithelium carcinoma associated protein
BPIFA1 innate immune response /lipid binding
gi|114319015 25355 5.65 -- --(1,4)
Down(-2,1)
aID Spot Identification Number. bTheoretical molecular weight (kDa). cTheoretical isoelectric point. dChanges in protein expression levels are reported as the ratio between the normalized protein spot volume from the 2-DE map of Patient (1-4) and that of Control (V
patient/V
Control)
for up-regulated proteins while for down-regulated proteins as the negative reciprocal values (-Vpatient
/Vcontrol
). Only fold change > 2 are indicated as up or down regulation.eThe symbol -- indicates that spot containing this protein was not detected in the 2-DE maps of this patient. fSpot containing this protein is only present in the 2-DE map of P2.

170 M. Gelardi, R.A. Siciliano, F. Papa, M. F. Mazzeo, E. De Nitto, N. Quaranta, R. Lippolis
These proteins were expressed at high level in the normal na-sal mucosa, in line with its role in the first-line defense against foreign particles as well as in the differentiation of immune re-sponses (15). In patients affected by different kinds of rhinitis, the above mentioned proteins were differentially expressed. In particular ALDH, a carbohydrate metabolism related enzyme, was under expressed in patients P1, P2, and P4. ALDH plays a major role in the detoxification of exogenously and endogenous-ly generated aldehydes and has protective effects on cells during environmental stress. The protective action of ALDH is import-ant, as nasal mucosa is constantly exposed to stressors mainly in the form of cross-reacting substances. Our results could indicate a direct relation between eosinophil presence and under regu-lation of ALDH. It could be assumed that the pathologic state affects the expression level of this protein with a consequent de-creased ability of mucosa cells to react to environmental stress. Also, the expression level of GSTA2 and GSTP1, which play an important role in protecting cells from cytotoxic reactive oxygen species and carcinogenic agents (16), and PRDX5, an antioxi-dant enzyme (17), were under regulated in the four patients. This feature could affect the cell ability to counteract stressor action. The SERPINB4 was expressed at high level in patients P1 and P4 and was down-regulated in patient P2. This protein belongs to the serine proteinase inhibitor family. SERPINB4 has been reported as serological marker for more advanced squa-mous cell tumors of the cervix, lung, and oropharynx (18,19). High expression of SERPINB4, as in patient P1 and P4, could suggest the onset of a pathological process of the high and lower airways respiratory epithelium. This finding might pave the way to further characterization of this protein as a marker of the re-spiratory epithelium pathology and for therapeutic monitoring. PLUNC is a protein specifically expressed in the upper airways and nasopharyngeal regions. It has been suggested to be involved in in-flammatory responses to irritants and can play a role in innate im-mune responses (20). A decreased level of PLUNC was previously reported in the pooled nasal lavage fluid of current smokers when compared with non-smokers (21). Our results showed that this protein is expressed at very low level in the 2-DE maps of patients P1 and P2 while was detected in similar amount of the control subjects in patients P3 and P4. These distinct features could indi-cate a possible role of PLUNC in the pathogenesis of non allergic rhinitis, suggesting a decreased immune response to stressors and consequent increase of the inflammatory response of nasal mucosa cells in these patients. Two oxidoreductase enzymes were also differ-entially expressed: ALDH1A1, under expressed in patients P2, P3 and P4, and TXN-1, expressed at very lower amount in patient P2 and absent in the other three patients. ALDH1A1 can play a criti-cal role in the maintenance the mucociliary phenotype of epithelial cells in the upper respiratory tract (22), while TXN-1 is a hydro-gen donor for enzymes involved in reductive reactions and there-
were identified by Peptide Mass Fingerprint (PMF) strategy and results are summarized in table 2. The differentially expressed proteins were classified on the basis of their biological and mo-lecular functions by means of Gene Ontology and belonged to several functional categories as follows:(i) proteins involved in cell detoxification and cell defense: glutathione S-transferase A-2 (GSTA-2), spot ID 834, under expressed in all the four rhino pathologic subjects, glutathione transferase P1-1 (GSTP-1) spot ID 842, under expressed in P1, P2 and P4, chain A, human peroxiredoxin-5 (PRDX5), spot ID 867, under expressed in all the four pathologic samples, and selenium binding protein (SELENBP-1), spot ID 566, under expressed in P2 and P4;(ii) proteins related to immune responses: squamous cell car-cinoma antigen (SERPINB4), spot ID 692, under expressed in P2 and over expressed in P1 and P4, and palate lung and nasal epithelium carcinoma associated protein (spot ID 848), PLUNK, under expressed in P1, P2 and P4; (iii) Enzymes related to carbohydrate metabolism: chain A, hu-man mitochondrial aldehyde dehydrogenase (ALDH2), spot ID 559, aldehyde dehydrogenase (ALDH3A1), which migrates as pearl chains, spots ID, 564, 567, these two protein spots were under expressed in the P1, P2 and P4; (iv) oxidoreductase enzymes: retinal dehydrogenase (ALD-H1A1), spot ID 525, under expressed in P1 and P2 and thiore-doxin isoform 1 (TXN-1), spot ID 869, under expressed in all the four patients; (v) a calcium ion binding protein S100-A11 (spot ID 880), under expressed in P2; and, finally, (vi) proteins arising from the sys-temic compartment: chain A, crystal structure of human serum albumin (ALB) Spot ID. 440, 452, 453, over expressed in P2 and P4 and haemoglobin subunit beta (HBB) spot ID 875, overex-pressed in P1 and P2 and under expressed in P4. These results are shown in figure 2, 3 and 4 and summarized in table 2.
Discussion
The field of human proteomics has the potential to become a key tool in the characterization of disease biomarkers. In this report, we present a proteomic analysis of nasal mucosa in pa-tients with different rhinitis. Comprehensive proteomic profiles of nasal mucosa cells showed high resolution and high repro-ducibility of the protein pattern, and allowed to obtain prelimi-nary information about disease-related proteins. Our results revealed that several proteins were differentially expressed in each rhino-pathologic state (figure 2, 3 and 4). Eighteen proteins belonging to different functional categories were identified (table 2). The main functional groups included proteins related to cell defense as ALDH, GSTA-2, PRDX-5, SELENBP-1, and proteins associated with human immune re-sponse and inflammation marker as SERPINB4 and PLUNK.

171Proteomic analysis of human nasal mucosa: different expression profile in rhino-pathologic states
8. Weiss W, Görg A. High-resolution two-dimensional electrophore-sis. Methods Mol Biol. 2009;564:13-32.
9. Geiser L, Vaezzadeh AR, Deshusses JM, Hochstrasser DF. Shotgun proteomics: a qualitative approach applying isoelectric focusing on immobilized pH gradient and LC-MS/MS. Methods Mol Biol. 2011;681:449-58.
10. Laemmli UK. Cleavage of structural proteins during the assembly of the head of bacteriophage T4. Nature. 1970;227:680-5.
11. Neuhoff V, Taube AN, Ehrhardt WD. Improved staining of pro-teins in polyacrylamide gels including isoelectric focusing gels with clear background at nano grams sensitivity using Coomassie Bril-lant Blue G-250 and R-250. Electrophoresis. 1988:9:255-62.
12. Lippolis R, Gnoni A, Abbrescia A, et al. Comparative proteomic analysis of four Bacillus clausii strains: proteomic expression sig-nature distinguishes protein profile of the strains. J. Proteomics. 2011;74:2846-55.
13. Appel RD, Hochstrasser DF. Computer analysis of 2-D images. Methods Mol Biol. 1999;112:363-81.
14. Shevchenko A, Wilm M, Vorm O, Mann M. Mass spectromet-ric sequencing of proteins silver-stained polyacrylamide gels. Anal Chem. 1996:68;850-8.
15. Casado B, Pannell LK, Iadarola P, Baraniuk JN. Identification of human nasal mucous proteins using proteomics. Proteomics. 2005;5:2949-59.
16. Bostwick DG, Alexander EE, Singh R, et al. Antioxidant enzyme expression and reactive oxygen species damage in prostatic intraep-ithelial neoplasia and cancer. Cancer. 2000;89:123-34.
17. Fujii J, Ikeda Y. Advances in our understanding of peroxiredox-in, a multifunctional, mammalian redox protein. Redox Rep. 2002;7:123-30.
18. Yasumatsu R, Nakashima T, Kuratomi Y, et al. Serum squamous cell carcinoma antigen is a useful biologic marker in patients with inverted papillomas of the sinonasal tract. Cancer. 2002;1:152-8.
19. Matoušek P, Zeleník K, Šafarčík K, et al. Squamous cell carcinoma an-tigen as a marker of sinonasal inverted papilloma. European Archives of Oto-Rhino-Laryngology. 2013;Jun19. (Epub ahead of print).
20. Bingle CD, Craven CJ. PLUNC: a novel family of candidate host defence proteins expressed in the upper airways and nasopharynx. Hum Mol Genet. 2002;11:937-43.
21. Ghafouri B, Stahlbom B, Tagesson C, Lindahl M. Newly identified proteins in human nasal lavage fluid from nonsmokers and smok-ers using two-dimensional gel electrophoresis and peptide mass fingerprinting. Proteomics. 2002;2:112-20.
22. Million K, Tournier F, Houcine O, et al. Effects of retinoic acid receptor-selective agonists on human nasal epithelial cell differen-tiation. Am J Respir Cell Mol Biol. 2001;25:744-50.
23. Arnér ESJ, Holmgren A. Physiological functions of thioredoxin and thioredoxinreductase. Eur J Biochem. 2000;267:6102-9.
24. Saitoh M, Nishitoh H, Fujii M, et al. Mammalian thioredoxin is a direct inhibitor of apoptosis signal-regulating kinase (ASK) 1. EMBO J. 1998;17:2569-606.
25. Buckle FG, Cohen AB. Nasal mucosal hyperpermeability to mac-romolecules in atopic rhinitis and extrinsic asthma. Journal of Al-lergy and Clinical Immunology. 1975;55:4:213-21.
26. Takabayashi T, Kato A, Peters AT, et al. Excessive fibrin deposition in nasal polyps caused by fibrinolytic impairment through reduc-tion of tissue plasminogen activator expression. Am J Respir Crit Care Med. 2012;87:49-57.
fore can play a role in maintaining a reducing cell environment protecting from oxidative stress. (23). In addition, this protein has anti-apoptotic effect by binding to the apoptosis signal-regulating kinases (24). The expression level of TXN-1 is particularly import-ant in the determination of the pathophysiologic state of the cell, therefore, it could be a potential marker for diagnostic purposes and therapeutic monitoring of the diseases. It is worth to note the different expression level of ALB in the four patients. In fact, this protein was over expressed in patient P2, and P4. Diffusion of albu-min across the nasal mucosa has been shown in patients with rhini-tis (25), and plasma proteins, mainly albumin, could be involved in the initial nasal process of polyposis (26). In conclusion, our preliminary proteomic study revealed, for the first time, that rhinitis affected the expression levels of several na-sal mucosa proteins, mainly involved in cell defense and immuno-logical response. In addition, specific protein expression pattern was revealed for the different kind of pathologic states. Although additional studies are needed to assess the possibility to use some of these proteins as potential markers for diagnostic and thera-peutic purposes, the present study further confirms the key role of proteomics in providing information for a better characterization of proteins specifically involved in each rhino-pathological state.
Acknowledgments
The authors would like to acknowledge Professor Sergio Papa (Department of Basic Medical Sciences, Neurosciences and Sense Organs University of Bari) for comment and support.This work was supported by FIRB-MERIT ‘Molecular basis in ageing-related degenerative syndrome’, MIUR (RBNE08HWLZ).
References
1. Benninger MS, Ferguson BJ, Hadley JA, et al. Adult chronic rhi-nosinusitis: definitions, diagnosis, epidemiology, and pathophysi-ology. Otolaryngol Head Neck Surg. 2003;129:S1-32.
2. Bousquet PJ, Demoly P, Devillier P, et al. Impact of allergic rhinitis symptoms on quality of life in primary care. Int Arch Allergy Im-munol. 2012;160:393-400.
3. Gelardi M, Maselli Del Giudice A, Fiorella ML, et al. Non-allergic rhinitis with eosinophils and mast cells (NARESMA) constitutes a new severe nasal disorder. Int J Immunopathol Pharmacolol. 2008;23:325-31.
4. Academy of Allergology and Clinical Immunology: Skin tests used in type I allergy testing Position paper. Sub-Committee on Skin Tests of the European Academy of Allergology and Clinical Immu-nology. Allergy. 1989;44:1-59.
5. Gelardi M. Atlas of nasal cytology. Torino, Italy: Centro Scientifico Editore, 2006.
6. Meltzer EO, Jalowayski AA. Nasal cytology in clinical practice. Am J Rhinol. 1988;2:47-54.
7. Bradford MM. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of pro-tein-dye binding. Anal Biochem. 1976;72:248-54.
O R I G I N A L A R T I C L E S Eur Ann AllErgy Clin immunol
SummaryBackground. Little is known about the prevalence and clinical relevance of sensitization to shrimp allergens other than tropomyosin. Objective. We detected the prevalence of arginine kinase and sarcoplasmic calcium binding protein sensitization, and identified a high molecu-lar weight allergen that is frequently recognized by Italian shrimp-allergic patients. Methods. Sera from 40 shrimp-allergic patients underwent the detection of IgE specific for arginine kinase (rPen m 2) and sarcoplasmic calcium-binding protein (rPen m 4) by ISAC 112 Mi-croarray platform and immunoblot analysis. A high molecular weight shrimp allergen was identified by N-terminal amino acid sequencing. Results. IgE to rPen m 2 and rPen m 4 were found in 4/40 (10%) and 6/40 (15%) sera, respectively; two sera reacted to both allergens. Clinically, 6/8 Pen m 2 and/or Pen m 4 reactors experienced severe allergies to shrimp. On immunoblot, 4/6 rPen m 4-positive sera showed IgE reactivity at about 20 kDa, whereas no rPen m 2-positive serum reacted at about 40 kDa. Nineteen (47%) sera showed IgE reactivity at molecular weights > 60 kDa. Such profile was not associated with IgE reactivity to rPen m 2 or rPen m 4. N-terminal amino acid sequencing of the high molecular weight allergen led to the identification of hemocyanin. Conclusion. Shrimp arginine kinase and sarcoplasmic calcium-binding protein are minor allergens sensitizing only 10% -15% of Italian shrimp-al-lergic patients, but are clinically relevant. Hemocyanin is a clinically relevant high molecular weight shrimp allergen possibly cross-reacting to house dust mite.
Corresponding authorRiccardo Asero Ambulatorio di AllergologiaClinica San CarloVia Ospedale 2120037 Paderno Dugnano (MI), ItalyPhone: +39 02 990 38 470Fax: +39 02 990 38 223E-mail: [email protected]
Key Words
Food allergy; shrimp allergy; hemocyanin; sarcoplasmic calcium binding protein; arginine kinase; allergens
1Istituto Scienze Produzioni Alimentari CNR, c/o BioIndustry Park S. Fumero, Colleretto Giacosa, (TO), Italy2Allergologia e Immunologia Clinica, Dipartimento di Medicina di Laboratorio, A.O. “S. Maria degli Angeli”, Pordenone, Italy3Lofarma SpA, R & D, Milano, Italy4Ambulatorio di Allergologia, Clinica San Carlo, Paderno Dugnano (MI), Italy
M.G. GiuFFriDa1, D. Villalta2, G. MiStrello3, S. aMato3, r. aSero4
Shrimp allergy beyond Tropomyosin in Italy: clinical relevance of Arginine Kinase, Sarcoplasmic calcium binding protein and Hemocyanin
Introduction
Shrimp is a frequent cause of food allergy at all latitudes. Be-sides tropomyosin, a major allergen that was identified as long as 18 years ago (1-3), several other allergenic proteins have been detected in recent years, including arginine kinase (4,5), sarco-plasmic calcium binding protein (6,7), and myosin light chain (8). Very recently, hemocyanin was identified as one further al-lergen in a freshwater shrimp as well in other crustaceans (9,10) along with troponin C (10,11), triosephosphate isomerase (11), and fatty acid binding protein (FABP) (10). Little is known
about the prevalence of sensitization to these new allergens as well as about their clinical relevance. In a recent multi-centre study on more than 100 Italian shrimp-allergic adult patients investigated by immunoblot analysis and rPen a 1-specific IgE measurements, only 41% were tropomyosin reactors, whereas IgE reactivity at molecular weights > 60 kDa was detected in 52% of cases (12). In contrast, IgE reactivity at the molecu-lar weights of arginine kinase (Pen m 2; 40 kDa), sarcoplasmic calcium binding protein (Lit v 4; 20 kDa), myosin light chain (Lit v 3; 20 kDa), triosephosphate isomerase (Cra c 8; 27 kDa), troponin C (Cra c 6; 17 kDa), and fatty acid binding protein
Vol 46, n 5, 172-177, 2014
173Allergy to minor shrimp allergens in Italy
___SPT___ __CAP___ ____ISAC______
No. History Shrimp Mite Shrimp Pen a 1 Pen m 1 Pen m 2 Pen m 4
1 d Pos Pos 12,8 3,92 10 Neg Neg
2 ab Pos Pos 1,71 0,63 4,3 Neg Neg
3 X Pos Pos 9,95 Neg Neg 4 4,2
4 ab Pos Pos ND 0,24 0,7 Neg Neg
5 b Pos Pos ND Neg neg 0,8 neg
6 b Pos Pos ND 0,28 0,6 Neg Neg
7 b Pos Pos ND Neg Neg Neg 2,3
8 b Pos Pos ND Neg Neg Neg 0,8
9 ab Pos Pos ND Neg Neg Neg Neg
10 b Pos Pos ND Neg Neg Neg Neg
11 ab Pos Neg ND Neg Neg Neg 1
12 b Pos Pos ND Neg 0,4 Neg Neg
13 a Pos ND ND Neg Neg Neg Neg
14 a Pos Pos 1,69 Neg Neg 2,5 Neg
15 b Pos ND 13,2 0,75 2,6 Neg Neg
16 a Pos Pos 14,8 0,55 3 Neg Neg
17 x Pos Pos ND Neg Neg Neg Neg
18 x Pos Pos ND Neg Neg Neg Neg
19 x Pos Pos ND Neg Neg Neg Neg
20 b Pos Pos ND 56,2 77 Neg Neg
21 a Pos Neg ND 50,6 86 Neg Neg
22 a Pos Neg ND Neg Neg Neg Neg
23 b Pos Neg ND Neg Neg Neg Neg
24 b Pos Pos 3,12 Neg Neg 1,1 1,3
25 b Pos Pos 7,88 Neg Neg Neg Neg
26 b Pos Neg ND Neg Neg Neg Neg
27 b Pos Pos ND Neg Neg Neg Neg
28 b Pos Pos 0,18 Neg Neg Neg Neg
29 a Pos Pos ND Neg Neg Neg Neg
30 a Pos Pos ND Neg Neg Neg Neg
31 bd Pos Pos ND Neg Neg Neg Neg
32 a Pos Pos 0,71 Neg neg Neg Neg
33 a Pos Pos ND Neg Neg Neg Neg
34 b Pos Pos ND Neg Neg Neg Neg
35 a Pos ND 20,0 0,14 Neg Neg 0,6
36 bd Pos Pos ND Neg Neg Neg Neg
37 bd Pos Pos ND Neg Neg Neg Neg
38 a Pos Neg ND Neg Neg Neg Neg
39 a Pos Neg ND Neg Neg Neg Neg
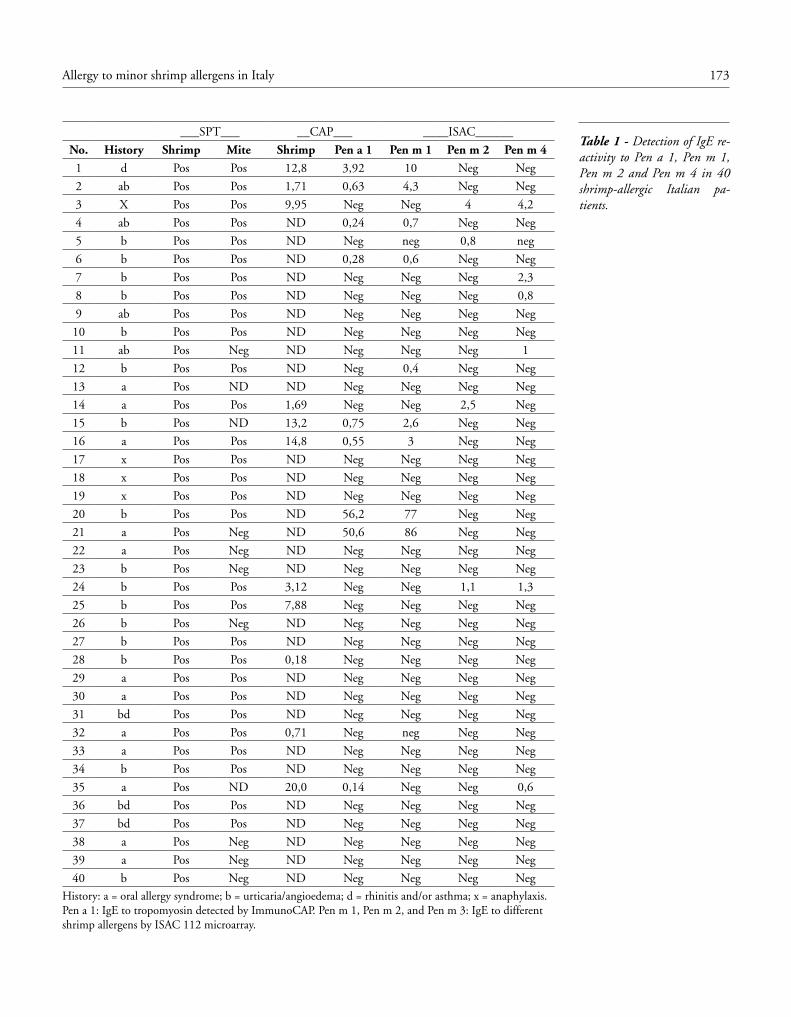
40 b Pos Neg ND Neg Neg Neg NegHistory: a = oral allergy syndrome; b = urticaria/angioedema; d = rhinitis and/or asthma; x = anaphylaxis. Pen a 1: IgE to tropomyosin detected by ImmunoCAP. Pen m 1, Pen m 2, and Pen m 3: IgE to different shrimp allergens by ISAC 112 microarray.
Table 1 - Detection of IgE re-activity to Pen a 1, Pen m 1, Pen m 2 and Pen m 4 in 40 shrimp-allergic Italian pa-tients.

174 M.G. Giuffrida, D. Villalta, G. Mistrello, S. Amato, R. Asero
with a fluorescence-labelled anti-human IgE for 30 min. After further washings, a laser scanner took fluorescence readings and results were transformed into numerical data by comparison with a reference serum standardized against ImmunoCAP IgE. As a consequence the results, expressed as ISAC standardized units (ISU/l), are indirectly linked to WHO IRP 75/502 IgE standard. Levels > than 0.3 ISU/l were regarded as positive, fol-lowing manufacturer’s recommendations.
Immunoblot analysis
Patients’ sera underwent immunoblot analysis at Lofarma Lab-oratories, Milan, Italy. Raw shrimp (Pandalus borealis) was ho-mogenized and extracted (5%) in 0.1 M phosphate-buffered saline (PBS), pH 7.4, under shaking for 2 hours at 4°C. The protein content, measured after Bradford method, was 1.2 mg/ml. Immunoblots were carried out under reducing conditions. The extract was mixed with LDS sample buffer (40% glycerol and 4% lithium dodecyl sulfate, to prevent adhesion of pro-teins to glassware and plastic, 4% Ficoll-400, 0.8 M trietha-nolamine-Cl, pH 7.6, 0.025% phenol red, 0.025% Coomassie G250, 2 mM EDTA disodium (Nupage Bis-Tris, Novex, Life Technologies, Milan) and 5% β-mercaptoethanol. The samples were then denaturated by heating at 100°C for 10 minutes.Electrophoresis of shrimp extract (25 μg/lane) was carried out in a 10% polyacrilamide precast gel (Nupage Bis-Tris, Novex, Life Technologies) at 180 mA for 1 h. The resolved proteins were transferred for 1 h onto a nitrocellulose membrane according to Towbin et al. (11). The membrane was saturated with 0.1 mol/L tris-buffered saline containing 5% fat-free milk powder and incu-bated for 16 h at 4°C with sera (dilution 1:1.5 in saturation buf-fer). After 3 washings, bound specific IgE were detected by perox-idase-conjugated anti-human IgE antibodies from goat (1:4000 in saturation buffer; Biospacific, Emeryville, CA, USA) and using an ECL western blotting kit (GE Healthcare) as substrate.
High molecular weight allergen identification
The high molecular weight allergen protein, detected by the use of a pool of sera reactive on immunoblot analysis (no. 17, 18, 19, 20, 26, 27 in table 1; figure 1), was identified by N-terminal amino acid sequencing technique. The selected band was excised from SDS-PAGE gel, passively eluted and the N-terminal amino acid sequence analysis was carried out on a Procise 492 protein se-quencer (Applied Biosystems, Foster City, CA, USA) as described by Pessione et al. (14). The amino acid sequence was searched using the MS-Homology software at Protein Prospector web site (http://prospector.ucsf.edu/prospector/) against both UniProt KB 2012.03.21 and NCBI nr. 2012.12.3 database. The param-eters used were: Order selected Decapoda, no limit for Protein MW, from 1 to 5 possible amino acid changes allowed.
(15 kDa) was rather rarely observed (13% altogether). Due to the absence of a routine assay able to detect IgE reactivity to the new minor allergens the analysis was not pursued further. Now, recombinant arginine kinase and sarcoplasmic calcium binding protein are available as a routine diagnostic means in ISAC mi-croarray assay (Thermofisher, Phadia, Uppsala, Sweden). Thus, we measured IgE specific for these two allergens in sera from a group of shrimp-allergic patients included in the previous study, in order to assess their prevalence and clinical relevance and to check whether the high molecular weight allergens de-tected in the previous study were polymers of Pen m 2 or Pen m 4. Further, since high molecular weight shrimp allergens are not currently available for in-vitro shrimp allergy diagnosis, the N-terminal sequencing of the high molecular weight allergen was carried out as well.
Patients and Methods
Patients
The clinical features of patients have been described in detail be-fore (12). Briefly, the starting population consisted of 116 adults who were selected in 15 Italian allergy centres from June to De-cember, 2009 based on unequivocal clinical history of shrimp allergy confirmed by positive skin prick tests (SPT) with fresh material and/or commercial shrimp extract. In most cases, pa-tients experienced systemic symptoms (urticaria with or without angioedema, asthma, or anaphylaxis) following the ingestion of shrimps. Since many of the participating centers were not suf-ficiently acquainted with emergency practice or did not have proper facilities to manage systemic allergic reactions, in view of the severity of many of the reported allergies, confirmative oral challenges (either blinded or open) were carried out only in doubt cases. Coded serum samples were kept at -20°C until in-vitro tests were carried out. 40 randomly selected serum samples out of 64 still available underwent the detection of IgE to arginine kinase and sarcoplasmic calcium binding protein. 28/40 patients had a history of systemic reactions. Nine were sensitized to tropomyo-sin (rPen a 1), as shown by IgE levels > 0.1 kU/l on ImmunoCAP (ThermoFisher, Uppsala Sweden) (table 1).
Detection of IgE to arginine kinase and sarcoplasmic calcium bind-ing protein
The ISAC 112 Microarray platform (Thermofisher, Phadia, Uppsala, Sweden) was used to detect serum IgE specific for arginine kinase (rPen m 2) and sarcoplasmic calcium-binding protein (rPen m 4) as such allergens are still unavailable in the ImmunoCAP as single allergens. Reactions sites were incubated with 30 μL of patients’ serum for 2 hours. After rinsing, wash-ing, and drying, allergen-specific IgE complexes were stained

175Allergy to minor shrimp allergens in Italy
mic calcium-binding protein and to tropomyosin was observed only in one case (#35, table 1).Clinically, 6 Pen m 2 and/or Pen m 4 reactors had a history of systemic allergic reactions to shrimp (anaphylaxis in 1 case, urticaria/angioedema in 5 cases), whereas 2 had a history of oral allergy syndrome. Interestingly, anaphylaxis occurred in one pa-tient co-sensitized to both allergens.
House dust mite tropomyosin hypersensitivity
Although the majority of patients (29/38 [76%]) showed a dou-ble reactivity to shrimp and house dust mite on skin tests, only 6 (21%) of these reacted to tropomyosin, an allergen that has been considered as the major cause of the cross reactivity be-tween house dust mite and shrimp. Other 6 mite/shrimp reac-tors were sensitized to either Pen m 2 and/or Pen m 4.Of the 8 shrimp-allergic patients not sensitized to house dust mite only 1 reacted to tropomyosin and another to Pen m 4.
Immunoblot analysis
Shrimp immunoblot analysis scored positive in 28/40 cases (fig-ure 2). Four out of 6 rPen m 4 reactors showed IgE reactivity at about 20 kDa; the two sera scoring negative at this M.W. were those showing the lowest rPen m 4 IgE levels on ISAC microarray (0.8 and 0.6 ISU, respectively). No one of the 4 rPen m 2-positive sera showed IgE reactivity at about 40 kDa on im-munoblot analysis; both co-sensitized patients showed an IgE reactivity at 20 kDa only. Nineteen sera showed IgE reactivity at molecular weights > 60 kDa. Such profile was not associated with IgE reactivity to rPen m 2 or rPen m 4.
Identification of the high molecular weight allergen
The sequence obtained by the N-terminal amino acid sequenc-ing matched with a high grade of homology with the hemocy-anin subunit 3 from Homarus americanus (the American lob-ster) (table 2). Sequences of other hemocyanins from different crustaceans further confirmed our identification.
Ethics
Since this study was an extension of a former one (12) which had been carried out with diagnostic purposes on patients who present-ed spontaneously in the clinics for clinical evaluation of their shrimp allergy and had already been approved by the local review boards, no further permission by a central ethical committee was required.
Results
IgE to arginine kinase and sarcoplasmic calcium-binding protein
Table 1 summarizes the shrimp-induced allergic reactions ex-perienced by study patients along with the skin reactivity to shrimp and house dust mite and the results of both Immuno-CAP and ISAC assays. A total of 8/40 (20%) patients scored positive for one of the two allergens studied. IgE to rPen m 2 and rPen m 4 were found in 4 (10%) and 6 (15%) cases, respec-tively; two sera contained IgE against both arginine kinase and sarcoplasmic calcium-binding protein. Although ISAC is only a semi-quantitative analysis, specific IgE levels ranged between 0.8 and 4.0 ISU for rPen m 2, and between 0.6 and 4.2 ISU for rPen m 4. Co-sensitization to arginine kinase and/or sarcoplas-
Figure 1 - Immunoreactive band submitted to N-terminal amino acid sequencing. Lane 1: molecu-lar weight markers; Lane 2: SDS-PAGE of shrimp extract; Lane 3: IgE reactivity to the high molec-ular shrimp allergen by a pool of sera from patients allergic to both shrimp and mites; Lane 4: negative control serum.
Figure 2 - Immunoblot analysis of sera from patients 1-28. Patients’ numbers correspond to those in table 1.

176 M.G. Giuffrida, D. Villalta, G. Mistrello, S. Amato, R. Asero
and Bolinus brandaris) but also to house dust mite were shown to co-recognize hemocyanin by direct RAST and inhibition as-says using commercial hemocyanin from Keyhole limpet (15). In a subsequent study (16), the same group detected a possible involvement of hemocyanin in house dust mite-allergic patients who experienced severe asthmatic reactions following the inges-tion of the terrestrial gasteropod snail. Much more recently, a study from Thailand identified hemocyanin as an allergen in a freshwater shrimp (9); in this study, the authors concluded that this allergen is not cross-reactive. Hemocyanin is an oxygen carrier protein representing 75-95% of total proteins in hemo-lymph of crustaceans (9). In the Decapoda order, hemocyanin is present in the predominant form of hexamers. There are three categories of crustacean hemocyanins called α (1 or A), β (2 or B) and γ (3 or C). We identified the hemocyanin C subunit as an allergen in our shrimp-allergic patients. Some crustacean hemocyanins are demonstrated to be glycosylated (17). Though hemocyanin subunits are reportedly species-specific (18-21), it cannot be excluded that some parts of the protein are phyloge-netically conserved and bear allergenic activity. In our previous study (12), we observed that many patients sensitized to high molecular weight shrimp allergens showed house dust mite hy-persensitivity as well, and clearly showed that HDM was able to strongly inhibit shrimp IgE reactivity in most cases. This find-ing is in keeping with that of the older study (15). Further, in a 2001 review article, Sidenius and co-workers (22) stated that “most often, more than one allergen is involved in the HDM snail cross-reactivity in a patient”. One further aspect that de-serves to be discussed is the different molecular weight of hemo-cyanin detected by Thai researchers (about 60-80 kDa; Ref 9) and by us (about 100 kDa). It is well known that the molecular weight of homologous proteins in different species may vary and that this could depend on a different degree of glycosila-tion. In our hands, hemocyanin appeared clinically relevant as
Discussion
One of the aims of the present study was to detect the prevalence of hypersensitivity to two recently described shrimp allergens, namely sarcoplasmic calcium binding protein and arginine ki-nase, in a group of allergic subjects, looking also at their associ-ation with tropomyosin sensitization, at their clinical relevance, and at their possible relationship with IgE reactivity against high M.W. shrimp allergens that was frequently observed in our previous study. We demonstrated that both proteins are minor allergens (i.e., recognized by < 50% of the allergic population), as in our population sensitization rate ranges between 10% and 15%. Both sarcoplasmic calcium protein sensitization and argi-nine kinase sensitization were independent on sensitization to the major allergen, tropomyosin, as only one case of co-sensiti-zation was recorded. Both allergens were found to be clinically relevant as sensitized patients experienced systemic symptoms in 7/8 cases, including one case of anaphylaxis. Finally, our investi-gations ruled out the possibility that the high molecular weight allergens frequently recognized by Italian shrimp-allergic were actually polymers of Pen m 2 or Pen m 4. The immunoblot as-says scored positive at about 20 kDa in most cases of sarcoplas-mic calcium-binding protein allergy, whereas no IgE reactivity was observed at about 40 kDa in patients sensitized to arginine kinase. The fact that shrimp extract was heated at 100°C for 10 min might have degraded the heat-sensitive arginine kinase, thus explaining the lack of reactivity at 40 kDa by immunoblot-ting for sera showing IgE against Pen m 2 in microarray.The second aim of the present study was to identify the high molecular weight shrimp allergen so frequently recognized by Italian allergic patients. N-terminal amino acid sequencing analysis led to the identification of this allergen as hemocyan-in. The first report of hemocyanin as a possible food allergen appeared as long as more than 20 years ago (15). In that study, patients allergic to different sorts of marine gasteropods (limpet
Table 2 - Identification of the immune reacting protein from fig. 2.
Species Amino acid sequences Protein name UniProt Entry
MW Homology
Pandalus borealis (our sequence)
1NVAQXQHDVNFL > 100,000 Da -
Homarus americanus 9NVAQKQHDVNFL Hemocyanin subunit 3 (fragment)
P82298 12,903 Da 92%
Cherax destructor 7SDAQKQHDVNYL Hemocyanin C chain (fragment)
P83172 13,513 Da 67%
Palinurus interruptus 12LLAQKQHDVNYL Hemocyanin C chain P80096 75,874 67%
Palinurus vulgaris 6DNAHKQHDVNHL Hemocyanin P80888 75,675 58%
X, amino acid not identified by the N-terminal amino acid sequencing; 1the database contains only the N-terminal part of the molecules.

177Allergy to minor shrimp allergens in Italy
tein identified as a new shrimp allergen. J Allergy Clin Immunol 2009;124:114-20.
8. Ayuso R, Grishina G, Bardina I, Carrillo T, Blanco C, Ibanez MD, Sampson HA, Beyer K. Myosin light chain is a novel shrimp aller-gen Lit, v 3. J Allergy Clin Immunol 2008; 122: 795-802.
9. Piboonpocanun S, Jirapongsananuruk O, Tipayanon T, Boon-choo S, Goodman RE. Identification of hemocyanin as a novel non-cross-reactive allergen from the giant freshwater shrimp Mac-robrachium rosenbergii. Mol Nutr Food Res. 2011;55:1492-8.
10. Ayuso R, Grishina G, Pascal M et al. Hemocyanin, Troponin C and Fatty Acid binding protein (FABP) may be cross-reactive aller-gens between crustaceans, cockroach and dust mites. J Allergy Clin Immunol. 2011;127(2S)AB235.
11. Bauermeister K, Wangorsch A, Garoffo LP, Reuter A, Conti A, Taylor SL et al. Generation of a comprehensive panel of crustacean allergens from the North Sea Shrimp Crangon crangon. Mol Im-munol. 2011;48:1983-92.
12. Asero R, Mistrello G, Amato S, Ariano R, Colombo G, Conte ME, et al. Shrimp allergy in Italian adults; a multi center study showing a high prevalence of sensitvity to novel high molecular weight aller-gens. Int Arch Allergy Immunol. 2012;157:3-10.
13. Towbin H, Staehelin T, Gordon J. Electrophoretic transfer of pro-teins from polyacrylamide gels to nitrocellulose sheets. Procedure and some applications. Proc Natl Acad Sci. 1979;76:4350-4.
14. Pessione E, Giuffrida MG, Prunotto L, Barello C, Mazzoli R, For-tunato D, Conti A, Giunta C. Membrane proteome of Acineto-bacter radioresistens S13 during aromatic exposure. Proteomics. 2003;3:1070-6.
15. Mistrello G, Falagiani P, Riva G, Gentili M, Antonicelli L. Cross-re-actions between shellfish and house dust mite. XV Congress of the EAACI. Paris, France 10-15 May 1992.
16. Kurokawa T, Wuhrer M, Lochnit G, Geyer H, Markl J, Geyer R. Hemocyanin from the keyhole limpet Megathura crenulata (KLH) carries a novel type of N-glycans with Gal(beta1-6)Man-motifs. Eur J Biochem. 2002;269:5459-73.
17. Van Ree R, Antonicelli L, Akkerdaas JH, Pajno GB, Barberio G, et al. Asthma after consumption of snails in house dust mite-allergic patients: a case of IgE cross-reactivity. Allergy. 1996;51:387-93.
18. Hodgson E, Spicer JI. Subunit compositions of crustacean hemo-cyanins are species-specific; evidence from non-decapod species. Comp Biochem Physiol. 2001;128A:873-88.
19. Giomi F, Beltramini M. The molecular heterogeneity of hemo-cyanin: its role in the adaptive plasticity of crustaceans. Gene. 2007;398:192-201.
20. Durstewitz G, Terwilliger NB. cDNA cloning of a developmental-ly regulated hemocyanin subunit in the crustacean Cancer magister and phylogenetic analysis of the hemocyanin gene family. Mol Biol Evol. 1997;14:266-76.
21. Sellos D, Lemoine S, Wormhoudt AV. Molecular cloning of hemo-cyanin cDNA from Penaeus vannamei (Crustacea, Decapoda): structure, evolution and physiological aspects. FEBS Lett. 1997; 407:153-8.
22. Sidenius KE, Hallas TE, Poulsen LK, Mosbech H. Allergen cross-reactivity between house dust mites and other invertebrates. Allergy. 2001;56:723-33.
most patients showing predominant reactivity against shrimp allergens > 90 kDa (# 17-20, 22, 23, 26-28 in figure 2) had a history of systemic reactions to shrimp, with anaphylaxis in 3 cases (table 1).In conclusion, we suggest that hemocyanin is a clinically rele-vant shrimp allergen and that it is possibly cross-reactive with shrimp and house dust mite.
Acknowledgements
The authors thank the following colleagues for selecting shrimp-al-lergic patients whose sera were used for the present study:R. Ariano, Ospedale di Bordighera, Bordighera (IM), Italy; M.E. Conte and G.E. Senna, U.O. Allergologia, Azienda Ospedaliera, Verona, Italy; M.A. Crivellaro, Servizio di Allergologia Dipartimento di Me-dicina Ambientale e Salute Pubblica, Università di Padova, Pa-dova Italy; M. de Carli, Dipartimento di Medicina Interna, Az Ospedalie-ro-Universitaria Santa Maria della Misericordia, Udine, Italy; F. della Torre, I.N.R.C.A.-I.R.C.C.S. U.O.C. Pneumologia generale, U.O. Allergologia, Casatenovo (LC), Italy; F. Lodi Rizzini, S.S.V.D. Allergologia - Spedali Civili, Brescia, Italy; D. Macchia, U.O. Allergologia Immunologia Clinica, Azienda Sanitaria Firenze, Firenze, Italy; F. Murzilli, UO Allergologia, Ospedale S.S. Filippo e Nicola, Avezzano (AQ), Italy.
References
1. Leung PS, Chu KH, Chow WK, Ansari A, Bandea CI, et al. Clon-ing, expression, and primary structure of Metapenaeus ensis tro-pomyosin, the major heat-stable shrimp allergen. J Allergy Clin Immunol. 1994;94:882-90.
2. Daul C, Slattery M, Reese G, et al. Identification of the major brown shrimp (Penaeus aztecus) allergen as the muscle protein tro-pomyosin. Int Arch Allergy Immunol. 1994;105:49-55.
3. Witteman AM, Akkerdaas JH, ven Leeuwen JA, van der Ze JS, Aalberse RC. Identifiction of a cross-reactive allergen (presumably tropomyosin) in shrimp, mite and insects. Int Arch Allergy Clin Immunol. 1994;105:56-61.
4. Yu CJ, Lin YF, Chiang BL, Chow LP. Proteomics and immuno-logical analysis of a novel shrimp allergen, Pen m 2. J Immunol. 2003;170:445-53.
5. Garcia-Orozco KD, Aispuro-Hernandez E, Yepiz-Plascencia G, Calderon de la Barca AM, Sotelo-Mundo RR. Molecular charac-terization of arginine kinase, an allergen from the shrimp Litope-naeus vannamei. Int Arch Allergy Immunol. 2007;144:23-8.
6. Shioni K, Sato Y, Hamamoto S, Mita H, Shimakura K. Sarcoplam-ic calcium-binding protein: identification of a new allergen of the black tiger shrimp Penaeus monodon. Int Arch Allergy Immunol 2008;146:91-8.
7. Ayuso R, Grishina G, Ibanez MD, Blanco C , Carrillo T, et al. Sarcoplasmic calcium-binding protein is an EF-hand-type pro-
C A S E R E P O R T S Eur Ann AllErgy Clin immunol
Summary statementRabbit constitutes a risk factor for occupational asthma in susceptible magicians.
SummaryIn this report we describe a case of respiratory allergy induced by an unusual occupational ex-posure to rabbit. The patient worked as a part-time magician in theatres and private parties and the most popular performance of his show was to pull out a white rabbit from a top hat. Unfortunately, a few minutes after the extraction of rabbit from top hat, the patient experienced the onset of upper and lower airway symptoms, and in some occasions he was forced to stop the show and to use short acting β
2 agonists and intramuscular steroids. The results of SPT and eval-
uation of serological specific IgE (ImmunoCAP and ImmunoCAP ISAC IgE) revealed allergic sensitization to rabbit (Oryctolagus cuniculus) dander as well as to Parietaria and dust mites. ImmunoCAP ISAC IgE excluded allergic sensitization to other cross-reacting animal allergens. Rabbit constitutes a reliable risk factor for allergic sensitization in individuals working as pro-fessional / part-time magicians or as animators in some recreational settings (resorts, parties, charity shows, etc).
Corresponding authorGennaro Liccardi, MDDepartment of Chest Diseases, Division of Pneumology and AllergologyHigh Speciality “A. Cardarelli” HospitalPiazzetta Arenella n. 7, 80128 Naples, ItalyPhone: +39 081 747 33 35-4-3Fax : + 39 081 747 33 31 E-mail: [email protected]
Key Words
Allergy; allergic rhinitis; allergic sensitization; bronchial asthma; magician; occupational asthma; rabbit; pet allergy
1Department of Chest Diseases, Division of Pneumology and Allergology. High Speciality “A. Cardarelli” Hospital, Naples, Italy 2 Department of Laboratory Medicine, University Hospital, Padova, Italy3 Laboratory of Clinical Pathology “A. Cardarelli” Hospital, Naples, Italy4Consultant in Preventive Medicine, “Federico II” University, Naples, Italy
An unusual case of occupational asthma in a part time magician. He has got an allergy surprise from his top hat!
G. liccarDi1, l. Billeri2, M. FoGlia3, c. SaPio4, M.a.r. De GiGlio1, G. D’aMato1
Introduction
Exposure to rabbit (Oryctolagus cuniculus) constitutes a well rec-ognized cause of occupational asthma for people in regular con-tact with this animal in occupational settings such as research laboratories, breeding, pet shops etc. (1,2). In recent years, rab-bits became more popular as pets to have at home, like dogs and cats, in Italy and in other countries. Although in Italy there are no official data on the overall number of rabbits living in do-mestic environments, some indirect indexes suggest a significant increase in the rate of rabbit ownership, and commercial sources indicate an increasing business in rabbit breeding as well as in production of rabbit-related materials such as food, accessories etc. In these non occupational settings, the prevalence of allergic sensitization is poorly known; we have shown that in Naples
area (3,4) as well as in Italy (5) the values of prevalence ranges between 2.65-4.9% and 0.65-4.72% respectively.In this report we describe a case of respiratory allergy induced by an unusual professional exposure to rabbit.
Case report
A 30-year-old man referred in our Allergy Centre for the onset of intermittent nasal and conjunctival symptoms; in addition he reported severe bronchial symptoms such as cough, wheezing and dyspnea in some particular circumstances.Family history was positive for atopy (his father suffered from allergic urticaria). Although he was a teacher, he worked as a part-time magician in theatres and private parties. Among the children, the most popular performance of his show was to pull
Vol 46, n 5, 178-180, 2014

179An unusual case of occupational asthma in a part time magician. He has got an allergy surprise from his top hat!
Discussion
This is the first documented case-report of a severe respiratory allergy induced by occupational exposure to rabbit in a part-time magician. Previously, only a brief correspondence contain-ing few sentences on this topic has been published (8). The high degree of cutaneous and serological sensitization to rabbit aller-gens as well as the lack of IgE antibodies against lipocalins and albumins indicates a selective allergy to rabbit induced by occu-pational exposure. In other words, the absence of any response to lipocalins or albumins likely exclude the possibility of a rabbit sensitization induced by cross-reaction mechanisms (9,10). Some considerations can be drawn from our case:1. Rabbit constitutes a reliable risk factor for allergic sensitiza-tion in individuals working as professional/part-time magicians or as animators in some recreational settings (resorts, parties, charity shows, etc.). This category of workers should avoid to use rabbits or other less common pets during their shows, if already sensitized to common pets (cats/dogs).2. Allergists should query patients regarding direct/indirect con-tact with any furry animal in addition to exposure to common pets (cats/dogs). Since keeping “exotic animals” as pets is in-creasing in all developed countries (11), theoretically all animals living at home or in strict contact with humans may induce allergic sensitization.3. Since it is likely that animal sensitized patients constitute an “allergic phenotype” (12), SPTs to furry animal allergens should be performed in all at high risk individuals already sensitized to cats and/or dogs before beginning an activity involving a strict contact with less common pets or furry animals, and in those who wish to own an “exotic” furry animal.
References
1. Baur X. A compendium of causative agents of occupational asth-ma. J Occup Med Toxicol. 2013;24:15.
2. Renstrom A, Olsson M, Hedren M, Johansson SG, van Hage M. Pet shop workers: exposure, sensitization, and work-related symp-toms. Allergy. 2011;66:1081-7.
3. Liccardi G, Piccolo A, Dente B, Salzillo A., Noschese P, Gilder JA, Russo M, D’Amato G. Rabbit allergens: a significant risk for aller-gic sensitization in subjects without occupational exposure. Respir Med. 2007;101:333-9.
4. Liccardi G, Salzillo A, Piccolo A, Russo M, D’Amato G. Sensi-tization to furry animals in an urban atopic population living in Naples, Italy. Allergy. 2011;66:1500-1.
5. Liccardi G, Passalacqua G, on behalf of the Allergy Study Group of the Italian Society of Respiratory Medicine (SIMeR). Sensitization to rabbit allergens in Italy - A multicentre study in atopic sub-jects without occupational exposure. Int Arch Allergy Immunol. 2006;141:295-9.
6. Liccardi G, D’Amato G, Canonica GW, Dente B, Passalacqua G. Severe respiratory allergy induced by indirect exposure to rabbit dander: a case report. Allergy. 2004;59;1237-8.
out a white rabbit from a top hat. Unfortunately, a few minutes after the extraction of the rabbit from top hat, the patient expe-rienced the onset of upper and lower airway symptoms and in some occasions he was forced to stop the show and to use short acting β
2 agonists and intramuscular steroids. It is important to
note that rabbit was not living in patient’s dwelling; the animal was taken just before the show (6). Patient denied any pet own-ership or direct exposure to other mammals. Skin-prick-test (SPT) was performed with commercial stan-dardized allergenic extracts (ALK- Abello Group and Lofarma Laboratories, Milan, Italy). The panel included the following extracts: house dust mites, Parietaria species, grasses, cat and dog dander, olive, birch, Alternaria alternata, Cladosporium her-barum and mugwort, plus a positive (1% histamine hydrochlo-ride) and negative (glycerinate solution) control. In addition, we used dander standardized extracts of other mammals (rabbit, mouse, rat, hamster, horse, guinea pig and cow). The SPT was carried out and interpreted according to international guide-lines (7), the result was read after 10 min and expressed as the major diameter of the wheal and its orthogonal. A skin reaction of 3 mm or greater was considered positive.A blood sample was taken for the measurement of total IgE and specific IgE to the same allergens of SPT panel by ImmunoCAP FEIA as well as by the micro-array technique ImmunoCAP ISAC (Thermofisher Scientific, Immuno-Diagnostics, Milan, Italy). A standard spirometry was also carried out.As monoclonal antibodies-based methods to measure the amount of rabbit allergen are not available in Italy, we cannot evaluate the degree of rabbit allergen contamination in patient’s indoor environments.The results of SPT revealed allergic sensitization to Oryctolagus cuniculus dander (the diameters of wheal were 10 x 12 mm), Parietaria (8 x 9 mm), Dermatophagoides pteronyssinus (9 x 10 mm), D. farinae (9 x 9 mm), positive control induced a wheal of 7 x 7 mm diameters. ImmunoCAP total IgE antibodies were 179 kU/L. The values of ImmunoCAP specific IgE antibodies were the following: Oryc-tolagus cuniculus dander (e82) - 45.80 kUa/L, Dermatophagoides pteronyssinus - 3.24 kUa/L, D. farinae - 2.95 kUa/L, Parietaria - 12.35 kUa/L. The values of ImmunoCAP ISAC IgE were the following: rPar j 2 - 28 ISU-E, nDer f 1 - 0.8 ISU-E, rDerf 2 - 2.5 ISU-E, nDer p 1 - 2.7 ISU-E, rDer p 2 - 2.9 ISU-E. No IgE were found against animal cross-reacting allergens such as lipocalins (Can f 1, Can f 2, Equ c 1, Fel d 4, Mus m 1) and albumins (Bos d 6, Can f 3, Equ c 3, Fel d 2). When examining, spirometry revealed normal respiratory values.The removal of rabbit, as well as an intensive cleaning of clothes / items used during the show and indoor environments where the patient rehearsed the show, resulted in a complete disappear-ance of all respiratory symptoms during performances.

180 G. Liccardi, L. Billeri, M. Foglia, C. Sapio, M.A.R. De Giglio, G. D’Amato
7. Dreborg S, Frew A. Editors. Position Paper: allergen standardiza-tion and skin tests. Allergy. 1993;48(Suppl14):49-82.
8. Miller JD. Magician’s asthma. J Allergy Clin Immunol. 2009;124:386.
9. Liccardi G, Asero R, D’Amato M, D’Amato G. Role of sensitiza-tion to mammalian serum albumin in allergic disease. Curr Allergy Asthma Rep. 2011;11:421-6.
10. Liccardi G, Dente B, Restani P, Senna GE, Falagiani P, Ballabio C, D’Amato G. Respiratory allergy induced by exclusive polysensiti-zation to serum albumins of furry animals. Eur Ann Allergy Clin Immunol. 2010;42:127-30.
11. Phillips JF, Lockey RF. Exotic pet allergy. J Allergy Clin Immunol. 2009;123:513-5.
12. Liccardi G, Passalacqua G, Salzillo A, Piccolo A, Falagiani P, Russo M, Canonica GW, D’Amato G. Is sensitization to furry animals an independent allergic phenotype in non occupationally exposed individuals? J Investig Allergol Clin Immunol. 2011;21:137-41.
C A S E R E P O R T S Eur Ann AllErgy Clin immunol
Corresponding author Christelle Richard Genclis, 15 rue du bois de la Champelle54500 Vandoeuvre-Lès-Nancy, FranceTel: +33 03 83 67 82 11 Fax: +33 03 83 67 89 99E-mail: [email protected]
1Genclis SAS, Vandoeuvre-Lès-Nancy, France 2Lorraine-University, Nancy. Durkheim Hospital, Epinal, France. AllergyVigilance Network, Vandoeuvre-Lès-Nancy, France
c. richarD1, S. JacQuenet1, D.a. Moneret-Vautrin2
A plausible allergy to peanut revealed only by Immunoblot
Peanut allergy is currently linked to sensitization to major al-lergens. Ara h 2 is the leading one and is the best predictor of allergy, since a level > 0.23 kU/L is observed in 93% of cases, with a specificity of 97% (1). A level of Ara h 2-specific IgEs > 0.55 kU/L has an absolute specificity and sensitivity of 93% of cases in adults (2). In young children aged less than 15 months, sensitivity and specificity have been calculated at 73% and 95% (3). Most peanut allergens are glycosylated. Sensitization to car-bohydrate determinants (CDD) is frequent in pollinic patients and cases of hymenoptera anaphylaxis (4,5). Such anti-CCD sIgE could explain positive ImmunoCAP to peanut, in peanut tolerant patients (6,7). It has been assumed that sensitization to CCDs is not clinically relevant (6-8). For this reason, we present a rare case of plausible peanut allergy characterized by a mo-no-sensitization to CCDs. A 49 years old female presented in 2012 with serious systemic reaction including abdominal pain, vomiting, erythema, verti-go and sudation, 2 hours after ingesting approximately 4 g of Curly® (containing 59% maize flour and 30% peanut flour), together with 2 glasses of rum-based cocktail and wine. She had a rather specific past history, since she was not atopic. Prick tests to 13 common aeroallergens were negative. However, she had semi-delayed anaphylaxis to mammal meats linked to sensitiza-tion to alpha-galactose that had been diagnosed in 2010. Recov-ery was obtained by avoidance diet, excluding mammal meats, pork and beef kidney and milk proteins with alcohol (9,10).
Specific IgEs gradually decreased (table 1). She also experienced anaphylaxis to wasp venom in 2011, linked to sensitization to Ves v 5. She had concurrently anti-CCD IgEs (table 1). She is treated by specific immunotherapy at present. Prick tests to natural roasted peanut, to peanut commercial ex-tract (Stallergenes), to maize flour and to soy were negative on a skin normally reacting to 9% codeine phosphate. Total IgEs were 149 kU/L. No IgEs were detected to peanut and recom-binant allergens: rAra h 1, rAra h 2, rAra h 3, rAra h 8, rAra h 9 (ImmunoCAP system, Thermo Fisher). Furthermore, sIgE to rAra h 6 and rAra h 7 were determined by ELISA test performed in the Genclis lab, and were negative. A basophil activation test to peanut extract (made from peanut flour, Byrd Mill) was then performed by flow cytometry identifying CD63 and was pos-itive with a stimulation index > 2 for three concentrations of peanut extract.The patient gave her informed consent for an open oral chal-lenge with Curly. She tolerated 14.3 g of the product (peanut protein equivalent 3.3 g). She refused our offer to repeat the test with alcohol. Protein extracts of peanut and Curly® were prepared. Specific IgE to CCDs were screened using FEIA CAP system (brome-lain and HRP), and DPC to ascorbate oxydase. Only CAP to bromelain was positive (4.84 kU/L). Three inhibition tests were performed using 100 to 1000 μg/mL of protein as inhibitors (figure 1). Specific IgE to bromelain were inhibited: 30% by
Vol 46, n 5, 181-183, 2014
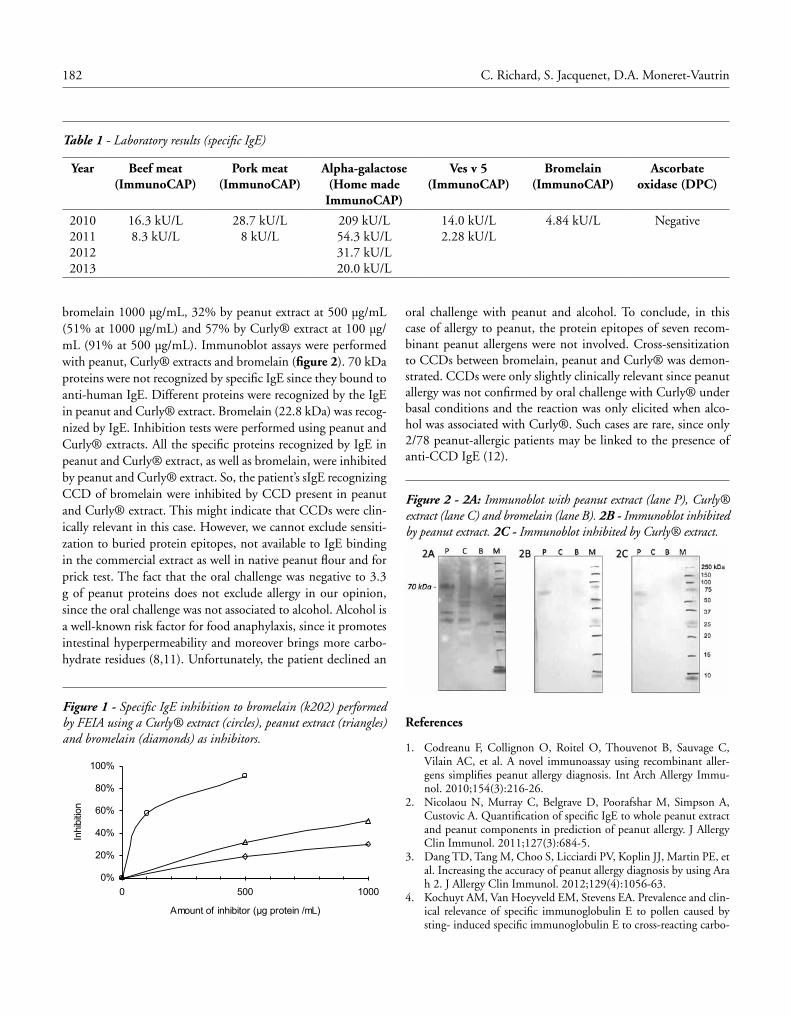
182 C. Richard, S. Jacquenet, D.A. Moneret-Vautrin
oral challenge with peanut and alcohol. To conclude, in this case of allergy to peanut, the protein epitopes of seven recom-binant peanut allergens were not involved. Cross-sensitization to CCDs between bromelain, peanut and Curly® was demon-strated. CCDs were only slightly clinically relevant since peanut allergy was not confirmed by oral challenge with Curly® under basal conditions and the reaction was only elicited when alco-hol was associated with Curly®. Such cases are rare, since only 2/78 peanut-allergic patients may be linked to the presence of anti-CCD IgE (12).
Figure 2 - 2A: Immunoblot with peanut extract (lane P), Curly® extract (lane C) and bromelain (lane B). 2B - Immunoblot inhibited by peanut extract. 2C - Immunoblot inhibited by Curly® extract.
References
1. Codreanu F, Collignon O, Roitel O, Thouvenot B, Sauvage C, Vilain AC, et al. A novel immunoassay using recombinant aller-gens simplifies peanut allergy diagnosis. Int Arch Allergy Immu-nol. 2010;154(3):216-26.
2. Nicolaou N, Murray C, Belgrave D, Poorafshar M, Simpson A, Custovic A. Quantification of specific IgE to whole peanut extract and peanut components in prediction of peanut allergy. J Allergy Clin Immunol. 2011;127(3):684-5.
3. Dang TD, Tang M, Choo S, Licciardi PV, Koplin JJ, Martin PE, et al. Increasing the accuracy of peanut allergy diagnosis by using Ara h 2. J Allergy Clin Immunol. 2012;129(4):1056-63.
4. Kochuyt AM, Van Hoeyveld EM, Stevens EA. Prevalence and clin-ical relevance of specific immunoglobulin E to pollen caused by sting- induced specific immunoglobulin E to cross-reacting carbo-
bromelain 1000 μg/mL, 32% by peanut extract at 500 μg/mL (51% at 1000 μg/mL) and 57% by Curly® extract at 100 μg/mL (91% at 500 μg/mL). Immunoblot assays were performed with peanut, Curly® extracts and bromelain (figure 2). 70 kDa proteins were not recognized by specific IgE since they bound to anti-human IgE. Different proteins were recognized by the IgE in peanut and Curly® extract. Bromelain (22.8 kDa) was recog-nized by IgE. Inhibition tests were performed using peanut and Curly® extracts. All the specific proteins recognized by IgE in peanut and Curly® extract, as well as bromelain, were inhibited by peanut and Curly® extract. So, the patient’s sIgE recognizing CCD of bromelain were inhibited by CCD present in peanut and Curly® extract. This might indicate that CCDs were clin-ically relevant in this case. However, we cannot exclude sensiti-zation to buried protein epitopes, not available to IgE binding in the commercial extract as well in native peanut flour and for prick test. The fact that the oral challenge was negative to 3.3 g of peanut proteins does not exclude allergy in our opinion, since the oral challenge was not associated to alcohol. Alcohol is a well-known risk factor for food anaphylaxis, since it promotes intestinal hyperpermeability and moreover brings more carbo-hydrate residues (8,11). Unfortunately, the patient declined an
Table 1 - Laboratory results (specific IgE)
Year Beef meat(ImmunoCAP)
Pork meat(ImmunoCAP)
Alpha-galactose(Home made ImmunoCAP)
Ves v 5(ImmunoCAP)
Bromelain(ImmunoCAP)
Ascorbate oxidase (DPC)
2010201120122013
16.3 kU/L 8.3 kU/L
28.7 kU/L 8 kU/L
209 kU/L 54.3 kU/L 31.7 kU/L 20.0 kU/L
14.0 kU/L2.28 kU/L
4.84 kU/L Negative
Figure 1 - Specific IgE inhibition to bromelain (k202) performed by FEIA using a Curly® extract (circles), peanut extract (triangles) and bromelain (diamonds) as inhibitors.
0%
20%
40%
60%
80%
100%
0 500 1000
Amount of inhibitor ( g protein /mL)
Inhi
bitio
n

183A plausible allergy to peanut revealed only by Immunoblot
hydrate determinants in Hymenoptera venoms. Clin Exp Allergy. 2005;35(4):441-7.
5. Mari A. IgE to cross-reactive carbohydrate determinants: analysis of the distribution and appraisal of the in vivo and in vitro reactiv-ity. Int Arch Allergy Immunol. 2002;129(4):286-95.
6. Guilloux L, Morisset M, Codreanu F, Parisot L, Moneret-Vautrin DA. Peanut allergy diagnosis in the context of grass pollen sensi-tization for 125 patients: roles of peanut and cross-reactive car-bohydrate determinants specific IgE. Int Arch Allergy Immunol. 2009;149(2):91-7.
7. van der Veen MJ, van Ree R, Aalberse RC, Akkerdaas J, Koppel-man SJ, Jansen HM, et al. Poor biologic activity of cross-reactive IgE directed to carbohydrate determinants of glycoproteins. J Al-lergy Clin Immunol. 1997;100(3):327-34.
8. Vidal C, Vizcaino L, Diaz-Peromingo JA, Garrido M, Gomez-Rial J, Linneberg A, et al. Immunoglobulin-E reactivity to a glycosylat-ed food allergen (peanuts) due to interference with cross-reactive carbohydrate determinants in heavy drinkers. Alcohol Clin Exp Res. 2009;33(8):1322-8.
9. Jacquenet S, Moneret-Vautrin DA, Bihain BE. Mammalian meat-induced anaphylaxis: clinical relevance of anti-galactose-al-pha-1,3-galactose IgE confirmed by means of skin tests to cetux-imab. J Allergy Clin Immunol. 2009;124(3):603-5.
10. Morisset M, Richard C, Astier C, Jacquenet S, Croizier A, Beaudouin E, et al. Anaphylaxis to pork kidney is related to IgE antibodies specific for galactose-alpha-1,3-galactose. Allergy. 2012;67(5):699-704.
11. Moneret-Vautrin DA. [Drugs as risk factors of food anaphylaxis in adults]. Med Sci (Paris). 2010;26(8-9):719-23.
12. Moverare R, Ahlstedt S, Bengtsson U, Borres MP, van Hage M, Poorafshar M, et al. Evaluation of IgE antibodies to recombinant peanut allergens in patients with reported reactions to peanut. Int Arch Allergy Immunol. 2011;156(3):282-90.
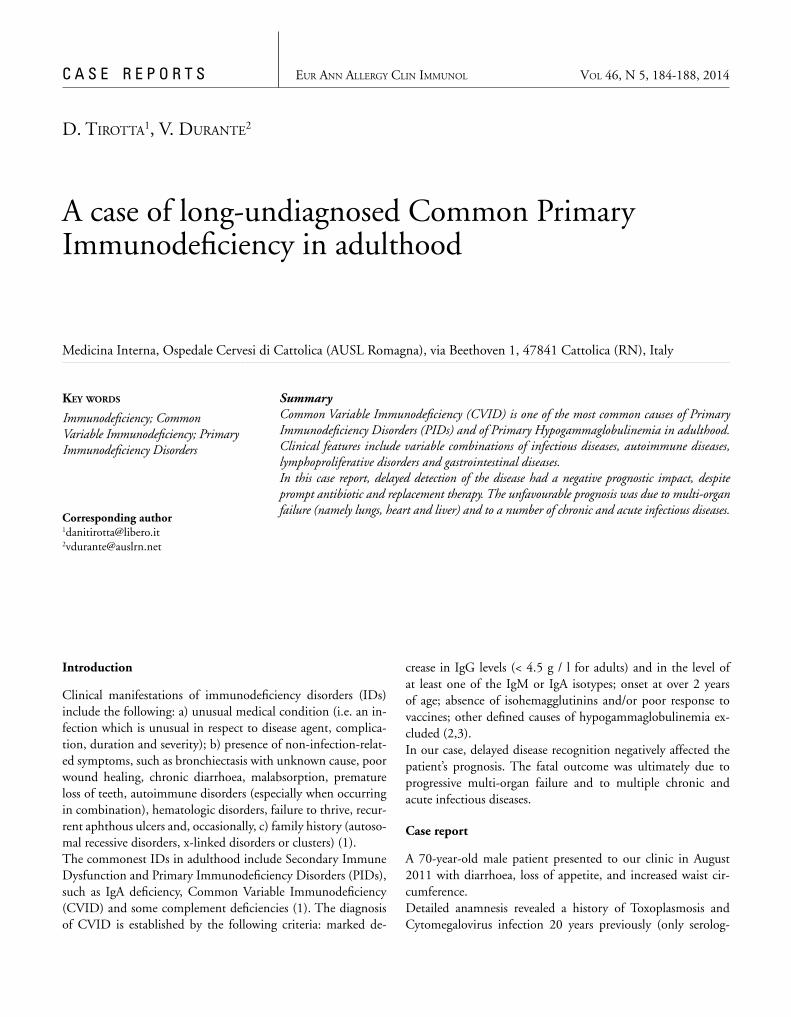
C A S E R E P O R T S Eur Ann AllErgy Clin immunol
SummaryCommon Variable Immunodeficiency (CVID) is one of the most common causes of Primary Immunodeficiency Disorders (PIDs) and of Primary Hypogammaglobulinemia in adulthood. Clinical features include variable combinations of infectious diseases, autoimmune diseases, lymphoproliferative disorders and gastrointestinal diseases.In this case report, delayed detection of the disease had a negative prognostic impact, despite prompt antibiotic and replacement therapy. The unfavourable prognosis was due to multi-organ failure (namely lungs, heart and liver) and to a number of chronic and acute infectious diseases.
Corresponding [email protected] [email protected]
Key Words
Immunodeficiency; Common Variable Immunodeficiency; Primary Immunodeficiency Disorders
Medicina Interna, Ospedale Cervesi di Cattolica (AUSL Romagna), via Beethoven 1, 47841 Cattolica (RN), Italy
D. tirotta1, V. Durante2
A case of long-undiagnosed Common Primary Immunodeficiency in adulthood
Introduction
Clinical manifestations of immunodeficiency disorders (IDs) include the following: a) unusual medical condition (i.e. an in-fection which is unusual in respect to disease agent, complica-tion, duration and severity); b) presence of non-infection-relat-ed symptoms, such as bronchiectasis with unknown cause, poor wound healing, chronic diarrhoea, malabsorption, premature loss of teeth, autoimmune disorders (especially when occurring in combination), hematologic disorders, failure to thrive, recur-rent aphthous ulcers and, occasionally, c) family history (autoso-mal recessive disorders, x-linked disorders or clusters) (1).The commonest IDs in adulthood include Secondary Immune Dysfunction and Primary Immunodeficiency Disorders (PIDs), such as IgA deficiency, Common Variable Immunodeficiency (CVID) and some complement deficiencies (1). The diagnosis of CVID is established by the following criteria: marked de-
crease in IgG levels (< 4.5 g / l for adults) and in the level of at least one of the IgM or IgA isotypes; onset at over 2 years of age; absence of isohemagglutinins and/or poor response to vaccines; other defined causes of hypogammaglobulinemia ex-cluded (2,3).In our case, delayed disease recognition negatively affected the patient’s prognosis. The fatal outcome was ultimately due to progressive multi-organ failure and to multiple chronic and acute infectious diseases.
Case report
A 70-year-old male patient presented to our clinic in August 2011 with diarrhoea, loss of appetite, and increased waist cir-cumference.Detailed anamnesis revealed a history of Toxoplasmosis and Cytomegalovirus infection 20 years previously (only serolog-
Vol 46, n 5, 184-188, 2014

185A case of long-undiagnosed Common Primary Immunodeficiency in adulthood
70-80; CD19 B lymphocytes: 3% [90/mmc], range: 5-15; CD4 T lymphocytes: 8 % [242/mmc], range: 35-55; CD8 T lym-phocytes: 79% [2394/mmc], range: 20-35; CD4/CD8 ratio 0.1, range: 0.8/5; NK lymphocytes: 6%, range: 8-22%. Both ELISA and p24 antigen test were negative for HIV. The clinical scenario now changed to humoral immune and lymphocyte deficiency (predominantly B-cells CD19+ and T-cells CD4+) associated with hepatosplenomegaly. Taking into account the patient’s age, we formulated the following two diag-nostic hypothesis: a) primary immunodeficiency (CVID); and b) immune deficiency secondary to lymphoproliferative disease, drug intake (especially corticosteroids), or excess loss (nephrotic syndrome, exudative enteropathy, skin loss). The patient underwent additional laboratory analyses. Com-plement C3 and C4 levels were within normal limits, while chest X-ray and chest-abdomen CT showed bronchiectasis with bibasal mucus, paratracheal adenopathy (1.2 cm diame-ter), chronic liver disease with caudate and left lobe hypertro-phy, ascites, and enlarged, inhomogeneous spleen (figure 1). Bone marrow aspiration identified inadequate erythroid mat-uration, whereas bone marrow biopsy showed maturing tri-lineage hematopoiesis, moderate CD8+T lymphocytosis, and significant reduction of plasma cells. Abdominal US revealed liver with nodular cirrhosis, portal vein ectasia, splenomegaly (14,1 cm) and moderate ascites (figure 2). Qualitative viral load tests for HCV RNA and quantitative HBV DNA assays were negative, as determined by real-time PCR. Antibody-spe-cific serological assays were also negative (ANA, AMA, ASMA, LKM: IFI test; minor hepatotropic viruses: PCR for CMV e EBV DNA). Paracentesis showed ascitic fluid lymphocytosis (4L evacuation: 425/μl WBC, 21% neutrophils, 70% lym-phocytes, 1% eosinophils). To rule out peritoneal TBC we planned a laparoscopic peri-toneal biopsy, followed by EGDS. Quantiferon was negative, while gastroscopy showed duodenal ulcer and biopsies were negative for lymphoma (MALToma). Based on laboratory tests results, we diagnosed CVID (Common Variable Immunodefi-ciency). The patient was put on immunoglobulin replacement therapy (0.5 g/Kg) administered monthly in a day-hospital regimen.From February to March 2012, the patient was again admitted to our department for hemorrhagic shock following paracente-sis. He also presented left pneumonia, with sputum testing pos-itive for Pseudomonas aeruginosa, and reported a new episode of diarrhoea. At analysis, stool specimens were strongly positive for Giardia lamblia. Pneumonia was treated with cephalosporin and peritoneal biopsy was suspended due to the patient’s overall clinical condition.On a subsequent admission to hospital, from April to May 2012, the patient showed the following:
ical markers had been tested for positivity: no DNA analysis had been carried out directly on the pathogens). The patient also reported multiple hospitalisations and outpatient visits for pneumonia (including necrotising pneumonia) and bronchitis, Chronic Obstructive Pulmonary Disease (COPD) with flare-up episodes associated with bronchiectasis, Secondary Chronic Pulmonary Heart Disease (NYHA III), Chronic Respiratory Failure and Permanent Atrial Fibrillation (AF) treated with an-ticoagulants. In two cases upon admission to hospital, bron-choalveolar lavage and sputum tested positive for Pseudomonas aeruginosa, Atypical mycobacteria, and Haemophylus. Family history for immune deficiencies was negative. In 1994, the patient underwent medical examinations for mod-erate leukopenia, severe hypogammaglobulinemia and recurrent respiratory infections. US abdomen, bone marrow aspiration and biopsy were negative. Flow cytometry analysis of periph-eral blood lymphocyte subsets showed mild CD4+ lymphocyte depletion (Total CD3 T lymphocytes: 87%, range: 70-80; CD 19 B lymphocytes: 5%, range: 5-15; CD4 T lymphocytes: 25%, range: 35-55; CD8 T lymphocytes: 67%, range: 20-35%).In August 2008, the patient had episodes of diarrhoea, which resolved spontaneously after 10 days. Colonoscopy was negative in this case. In June 2011, the subject was treated unsuccessfully with metronidazole for persistent diarrhoea and fever secondary to Giardia lamblia infection. Upon observation, he showed ca-chexia, rhonchi, basilar crackles, and AF (rate: 78 bpm).On to hospital admission, laboratory tests revealed the follow-ing: mild microcytic anemia (Hb 13.1 g/dl, MCV 65 fl), nor-mal white blood cell and platelet counts (PLT 271000/mmc, WBC 8190/mmc, N 4360/mmc, L 3030/mmc, M 740/mmc, E 50/mmc, B 10/mmc), high prothrombin time (PT 3.67), hy-pokalemia (2.7 mM/l), cholestasis (ALP U/l 237 vs. 129 U/l, GammaGT 82 U/l vs. 61 U/l), moderate inflammatory syn-drome (CRP 34.8 mg l vs. 5 mg/ll), low protein levels (48 g/l vs. 60 g/l), and Giardia lamblia in stools.The manifestations requiring medical attentions were in our view: cachexia, chronic diarrhoea secondary to Giardia lam-blia infection, recurrent respiratory infections associated with hepatomegaly, splenomegaly, ascites, cholestasis, and altered coagulation. We formulated two diagnostic hypothesis: a) im-munodeficiency secondary to liver cirrhosis, lymphoprolifera-tive disorder or viral infection (HIV); or b) primary immune deficiency with splenomegaly. Immunodeficiency tests revealed severe hypogammaglobulin-emia (gamma globulin: 2.4%, range: 11.1-18.8). Immunoglob-ulin values were of particular interest: IgA < 0.05 g/l (range: 0.7-4); IgG 0.72 g/l (range: 7-16); IgM 0.09 g/l (range: 0.4-2.3), tests were negative for both Bence Jones protein and alkaline phosphatase bone isoenzyme. Analysis of peripheral blood lym-phocyte subsets showed: Total CD3 T lymphocytes: 92%, range:

186 D. Tirotta, V. Durante
tomegalovirus and Toxoplasma gondii infection was determined on the basis of serological positivity alone, as the DNA of those pathogens had not been tested.The patient’s clinical history was characterised by progressive decline secondary to recurrent respiratory infections and by abnormal findings in the digestive tract and liver. As reported in the literature, the clinical phenotype is heterogeneous and includes (2,7,8,9) (table 1):• infectious diseases (over 90% of CVID patients had bacterial
pathogens in the upper and lower airways and in the gastro-intestinal tract) (2);
• autoimmune diseases (accounting for 20% of CVID cases);• lymphoproliferative disorders and gastric cancer (approxi-
mately 40-50% of CVID cases, possibly due to carcinogenic pathogens such as Helicobacter pylori and Epstein Barr vi-rus, or to impaired tumour cell surveillance);
• gastrointestinal symptoms: enteritis (Giardia lamblia, Sal-monella, Campylobacter), both non-bloody (sprue-like) and bloody (chronic inflammatory bowel disease) diarrhoea, asymptomatic or unformed stools (nodular lymphoid hy-perplasia of the duodenum and ileum), cholestasis (nodu-lar regenerative hyperplasia or granulomatous hepatitis with portal hypertension);
• rarely absent complications.
In our case, the unfavourable course could most likely be as-cribed to chronic, non-infectious complications. In literature, the prognosis for CVID is seen as depending on a number of causes, ranging from bronchiectasis, to enteropathy and auto-immunity and from B cell percentage to Ig and T cell response (9, 10). Interestingly, the risk of death is also 11 times higher for patients with non-infectious complications (lymphoma, chron-ic hepatitis, structural lung disease and chronic gastrointestinal disease) (7-10).A delayed diagnosis (from 1994 to 2011) was in the present case a negative prognostic factor. Indeed, several studies document that age at diagnosis has a significant impact on the outcome of the disease (7). The existing literature also suggests that Ig thera-py (administered either intravenously or subcutaneously) reduc-es the recurrence of infections, delays the onset of pulmonary complications (such as bronchiectasis and respiratory failure), and allows early detection of other complications (especially lymphomas and solid tumours) by approximately 10% (9,10). In conclusion, taking into account the patient’s history, as well as any signs and symptoms of recurrent infections, is of critical importance for a successful management of the disease. Specifi-cally, primary immunodeficiencies, most notably CVID, cannot be ruled out in adulthood, particularly when unusual infections (or unusual infection manifestations) should occur.
• Watery diarrhoea with stools testing positive for Giardia lamblia (subject to therapy with metronidazole 250 mg x 3 followed by albendazole 400 mg x 3) and for Clostridium difficile (remission 1 month from the start of therapy with oral vancomycin).
• Persistent left pneumonia with sputum testing positive for several types of bacteria (namely, Corynebacterium striatum, Stenotrophomonas maltophila and Pseudomonas aeruginosa).
Based on antibiogram results, the patient was intravenously in-jected with ceftazidime and levofloxacin, showing signs of clin-ical improvement. However, persistent radiographic infiltrates were also detected.In November 2012, the patient presented again to our depart-ment with the following symptoms:• Severe weight loss and cachexia;• Dyspnea, cough, global respiratory failure. Chest X-ray
showed bilateral edema, disatelectatic zones, apical fibrosis and infiltrates in the right upper pulmonary lobe. Bronchoal-veolar lavage was positive for multidrug-resistant Pseudomo-nas aeruginosa and S. Aureus, while sputum was positive for acid-alcohol resistant bacilli (negative BK PCR).
• Diarrhoea with negative stool specimens;• AF with high ventricular response.
The patient was kept in isolation and treated with high-flow oxygen, diuretics and antibiotics (imipenem 550 mg x 4 and levofloxacin750 mg, injected intravenously).Death occurred in November 2012 from acute pulmonary edema.
Discussion
Incidence of CVID is estimated between 1:10.000 and 1:50.000. The age of onset is usually in the second or third de-cade of life (3).At a first glance, there appeared to be an obvious mismatch between our patient’s age and diagnosis of CVID. However, a review of the literature suggests that CVID can indeed occur at any age (4). The French DEFI study group also identified a subset of CVID, referred to as ‘late onset combined immu-nodeficiency’ (LOCID), characterised by clinically relevant T-cell insufficiency and accounting for approximately 8.9% of CVID cases. The inclusion criteria set by the DEFI group were: CD4+ T cells below 200/μl and evidence of opportunis-tic infections (4-6). In the present case, a history of Cytomegalovirus and Toxo-plasma gondii infection and the absence of common clinical manifestations of LOCID at the time of hospitalisation, such as lymphopenia in bone marrow biopsies and in the blood stream, and absence of sarcoid-like granulomas (included pulmonary granulomas), argued against this diagnosis. The presence of Cy-
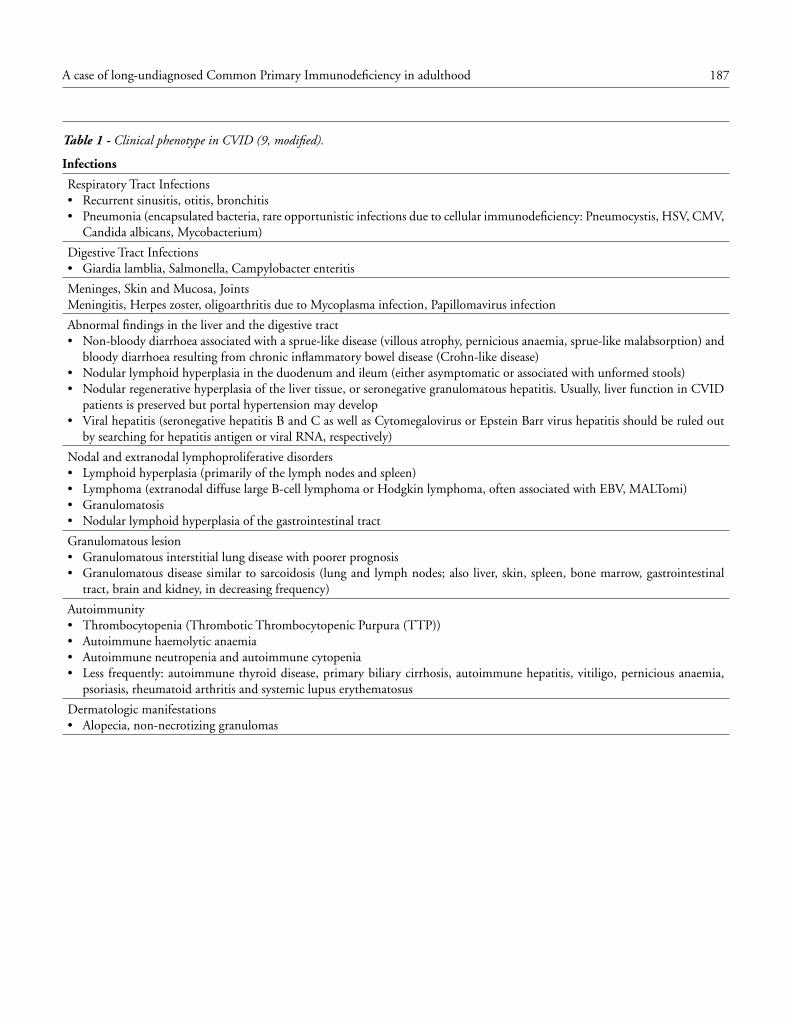
187A case of long-undiagnosed Common Primary Immunodeficiency in adulthood
Table 1 - Clinical phenotype in CVID (9, modified).
Infections
Respiratory Tract Infections• Recurrent sinusitis, otitis, bronchitis • Pneumonia (encapsulated bacteria, rare opportunistic infections due to cellular immunodeficiency: Pneumocystis, HSV, CMV,
Candida albicans, Mycobacterium)
Digestive Tract Infections • Giardia lamblia, Salmonella, Campylobacter enteritis
Meninges, Skin and Mucosa, JointsMeningitis, Herpes zoster, oligoarthritis due to Mycoplasma infection, Papillomavirus infection
Abnormal findings in the liver and the digestive tract• Non-bloody diarrhoea associated with a sprue-like disease (villous atrophy, pernicious anaemia, sprue-like malabsorption) and
bloody diarrhoea resulting from chronic inflammatory bowel disease (Crohn-like disease)• Nodular lymphoid hyperplasia in the duodenum and ileum (either asymptomatic or associated with unformed stools)• Nodular regenerative hyperplasia of the liver tissue, or seronegative granulomatous hepatitis. Usually, liver function in CVID
patients is preserved but portal hypertension may develop• Viral hepatitis (seronegative hepatitis B and C as well as Cytomegalovirus or Epstein Barr virus hepatitis should be ruled out
by searching for hepatitis antigen or viral RNA, respectively)
Nodal and extranodal lymphoproliferative disorders• Lymphoid hyperplasia (primarily of the lymph nodes and spleen)• Lymphoma (extranodal diffuse large B-cell lymphoma or Hodgkin lymphoma, often associated with EBV, MALTomi)• Granulomatosis• Nodular lymphoid hyperplasia of the gastrointestinal tract
Granulomatous lesion• Granulomatous interstitial lung disease with poorer prognosis • Granulomatous disease similar to sarcoidosis (lung and lymph nodes; also liver, skin, spleen, bone marrow, gastrointestinal
tract, brain and kidney, in decreasing frequency)
Autoimmunity• Thrombocytopenia (Thrombotic Thrombocytopenic Purpura (TTP))• Autoimmune haemolytic anaemia• Autoimmune neutropenia and autoimmune cytopenia• Less frequently: autoimmune thyroid disease, primary biliary cirrhosis, autoimmune hepatitis, vitiligo, pernicious anaemia,
psoriasis, rheumatoid arthritis and systemic lupus erythematosus
Dermatologic manifestations• Alopecia, non-necrotizing granulomas
188 D. Tirotta, V. Durante
References
1. Azar AE, Zuhair K.B. Evaluation of the Adult with Suspect-ed Immunodeficiency. The American Journal of Medicine. 2007;120,764-8.
2. Resnick ES, Moshier EL, Godbold JH, et al. Morbidity and mor-tality in common variable immunedeficiency over 4 decades. Blood. 2012;119:1650-7.
3. Salzer U., Chapel HM, K. Warnatz, H H Peter. Common vari-able immunodeficiency - an update. Arthritis Research & Therapy. 2012;14:223.
4. Malphettes M, Gérard L, Carmagnat M et al. Late-onset combined immune deficiency: a subset of common variable immunodeficiency with severe T cell defect. Clin Infect Dis. 2009;Nov1;49(9):1329-38.
5. Aslam A, Chapel H. Dissecting the group of common variable im-munodeficiency disorders. Clin Infect Dis. 2009;Nov1;49(9):1339-40. Comment on Clin Infect Dis. 2009;Nov1;49(9):1329-38.
6. Bussone G, Mouthon L. Late onset of primary immune deficien-cies. Presse Med. 2010;Feb;39(2):196-207.
7. Fieschi C, Malphettes M, Galicier L et al. Hypogammaglobulinemies primitives decouvertes a l’age adult. Presse Med. 2006;35:887-94.
8. Gathmann B, Grimbacher B, Beauté J et al. The European in-ternet-based patient and research database for primary immuno-deficiencies: results 2006-2008. Clin Exp Immunol. 2009;Sep;-157Suppl1:3-11.
9. Chapel H, Lucas M, Lee M et al. Common variable immunodefi-ciency disorders: division into distinct clinical phenotypes. Blood. 2008;112(2):27.
10. Sahn S, Mayer l et al. Treatment and prognosis of common variable immunodeficiency. Uptodate 2012 on line: www.uptodate.com.
Figure 1 - US abdomen of patient: splenomegaly. Figure 2 - Chest CT of patient.

Riassunto delle caratteristichedel prodotto
1. DENOMINAZIONE DEL MEDICINALEFlutiformo® 50 microgrammi/5 microgrammi per erogazione, so-spensione pressurizzata per inalazione.Flutiformo® 125 microgrammi/5 microgrammi per erogazione, so-spensione pressurizzata per inalazione.Flutiformo® 250 microgrammi/10 microgrammi per erogazione,sospensione pressurizzata per inalazione.
2. COMPOSIZIONE QUALITATIVA E QUANTITATIVAOgni dose erogata (dalla valvola dosatrice) contiene:• 50 microgrammi di fluticasone propionato e 5 microgrammi di for-
moterolo fumarato diidrato. Questo equivale ad a una dose inalata(dall’erogatore) di circa 46 microgrammi di fluticasone propionato/4,5microgrammi di formoterolo fumarato diidrato.
• 125 microgrammi di fluticasone propionato e 5 microgrammidi formoterolo fumarato diidrato. Questo equivale ad una doseinalata (dall’erogatore) di circa 115 microgrammi di fluticasonepropionato/ 4,5 microgrammi di formoterolo fumarato diidrato.
• 250 microgrammi di fluticasone propionato e 10 microgrammidi formoterolo fumarato diidrato. Questo equivale ad una doseinalata (dall’erogatore) di circa 230 microgrammi di fluticasonepropionato/9,0 microgrammi di formoterolo fumarato diidrato.
Per l’elenco completo degli eccipienti, vedere paragrafo 6.1.
3. FORMA FARMACEUTICASospensione pressurizzata per inalazione. La bomboletta contieneuna sospensione liquida di colore bianco-biancastro. La bombolettaè contenuta in un erogatore di colore bianco con indicatore delladose integrato di colore grigio e un cappuccio di protezione del boc-caglio di colore grigio chiaro.
4. INFORMAZIONI CLINICHE4.1 Indicazioni terapeutiche
Questa combinazione a dose fissa di fluticasone propionato e for-moterolo fumarato (Flutiformo®) è indicata per il trattamento rego-lare dell’asma quando l’uso di un prodotto di associazione(corticosteroide per via inalatoria e b2-agonista a lunga durata d’a-zione) è appropriato, ovvero:• in pazienti non adeguatamente controllati con corticosteroidi per via
inalatoria e b2-agonisti a breve durata d’azione “al bisogno”oppure• in pazienti già adeguatamente controllati sia con corticosteroidi per via
inalatoria che con b2-agonisti a lunga durata d’azione.Flutiformo® 50 microgrammi/5 microgrammi per erogazione è in-dicato negli adulti e negli adolescenti al di sopra dei 12 anni.Flutiformo® 125 microgrammi/5 microgrammi per erogazione èindicato negli adulti e negli adolescenti al di sopra dei 12 anni.Flutiformo® 250 microgrammi/10 microgrammi per erogazione èindicato solo negli adulti.
4.2 Posologia e modo di somministrazionePosologiaPer uso inalatorio.Occorre mostrare ai pazienti come utilizzare l’inalatore e che un me-dico valuti regolarmente la loro asma in modo che il dosaggio di Flu-tiformo® sia sempre ottimale e venga modificato solo dietro consigliomedico. La dose deve essere titolata alla dose minima che permettedi mantenere un efficace controllo dei sintomi. Una volta raggiuntoil controllo dell’asma con il dosaggio minimo di Flutiformo® sommi-nistrato due volte al giorno, occorre rivalutare il trattamento pren-dendo in considerazione l’eventualità di modificare la terapiapassando ad un corticosteroide inalatorio da solo. Come regola ge-nerale, la dose deve essere titolata alla dose minima che permettedi mantenere un efficace controllo dei sintomi. È estremamente im-portante controllare regolarmente i pazienti durante la riduzionedella terapia. Non sono disponibili dati sull’uso di Flutiformo® in pa-zienti con BPCO. Pertanto Flutiformo® non deve essere usato in que-sta tipologia di pazienti. Il dosaggio di Flutiformo® deve contenerela dose di fluticasone propionato adatta alla gravità della malattia.Nota: Flutiformo® 50 microgrammi/5 microgrammi per erogazionenon è appropriato per adulti e adolescenti con asma grave. I mediciprescrittori devono essere consapevoli che nei pazienti con asma, ilfluticasone propionato è efficace quanto altri steroidi per via inala-toria, se ne viene somministrata circa metà della dose giornaliera to-tale (in microgrammi). Qualora un paziente necessiti di dosi al difuori del regime posologico raccomandato, occorre prescrivere dosiadatte del b2-agonista e del corticosteroide per via inalatoria in ina-latori separati oppure dosi adatte del solo corticosteroide per via
inalatoria. Flutiformo® viene erogato attraverso un inalatore pres-surizzato predosato (pMDI) con indicatore della dose integrato. Ogniinalatore fornisce almeno 120 erogazioni (60 dosi).Flutiformo® 50 microgrammi/5 microgrammi per eroga-zione, sospensione pressurizzata per inalazioneDose raccomandata per adulti e adolescenti al di sopradei 12 anniFlutiformo® 50 microgrammi/5 microgrammi per erogazione, sospen-sione pressurizzata per inalazione: due inalazioni (puff) due volte algiorno, assunte normalmente alla mattina e alla sera. Se il pazientecontinua a presentare asma scarsamente controllata, la dose gior-naliera totale del corticosteroide inalatorio può essere aumentatasomministrando questo prodotto di associazione a un dosaggio suc-cessivo più elevato, ovvero Flutiformo® 125 microgrammi/5 micro-grammi per erogazione, sospensione pressurizzata per inalazione,due inalazioni (puff) due volte al giorno.Solo per adultiSe il paziente continua a presentare asma scarsamente control-lata, la dose giornaliera totale può essere ulteriormente aumen-tata somministrando questo prodotto di associazione al dosaggiomassimo, ovvero Flutiformo® 250 microgrammi/10 microgrammiper erogazione, sospensione pressurizzata per inalazione, due ina-lazioni (puff) due volte al giorno. Il dosaggio massimo va usatosolo negli adulti, non deve essere somministrato ad adolescential di sopra dei 12 anni.Bambini al di sotto dei 12 anniL’esperienza nei bambini al di sotto dei 12 anni è limitata (vedereparagrafi 4.4, 4.8, 5.1 e 5.3). L’uso di Flutiformo® sospensione pres-surizzata per inalazione a qualsiasi dosaggio non è raccomandatonei bambini al di sotto dei 12 anni.In questo gruppo d’età Flutiformo® non deve essere usato.Flutiformo® 125/5 microgrammi per erogazione, sospen-sione pressurizzata per inalazioneDose raccomandata per adulti e adolescenti al di sopradei 12 anniFlutiformo® 125 microgrammi/5 microgrammi per erogazione, so-spensione pressurizzata per inalazione: 2 inalazioni (puff) due volteal giorno, assunte normalmente alla mattina e alla sera. In caso diasma adeguatamente controllata è possibile passare i pazienti aldosaggio minimo di questo prodotto di associazione, ovvero Flu-tiformo® 50 microgrammi/5 microgrammi per erogazione. La doseper un paziente deve essere titolata alla dose minima che consentedi mantenere un efficace controllo dei sintomi.Solo per adultiSe il paziente continua a presentare asma scarsamente controllata,la dose giornaliera totale può essere aumentata somministrandoquesto prodotto di associazione al dosaggio massimo, ovvero Flu-tiformo® 250 microgrammi/10 microgrammi per erogazione, sospen-sione pressurizzata per inalazione, due inalazioni (puff) due volte algiorno. Il dosaggio massimo va usato solo negli adulti, non deve es-sere somministrato ad adolescenti al di sopra dei 12 anni.Bambini al di sotto dei 12 anniNon sono disponibili dati sull’impiego di Flutiformo® a questo do-saggio nei bambini. L’esperienza nei bambini al di sotto dei 12 anniè limitata (vedere paragrafi 4.4, 4.8, 5.1 e 5.3). L’uso di Flutiformo®
sospensione pressurizzata per inalazione a qualsiasi dosaggio nonè raccomandato nei bambini al di sotto dei 12 anni.In questo gruppo d’età Flutiformo® non deve essere usato.Flutiformo® 250 microgrammi/10 microgrammi per eroga-zione, sospensione pressurizzata per inalazioneDose raccomandata per adultiFlutiformo® 250 microgrammi/10 microgrammi per erogazione, so-spensione pressurizzata per inalazione: 2 inalazioni (puff) due volteal giorno, assunte normalmente alla mattina e alla sera. In caso diasma adeguatamente controllata è possibile passare i pazienti a undosaggio inferiore di questo prodotto di combinazione, ovvero Flu-tiformo® 125 microgrammi/5 microgrammi per erogazione o, even-tualmente, Flutiformo® 50 microgrammi/5 microgrammi. La dose perun paziente deve essere titolata alla dose minima che consente dimantenere un efficace controllo dei sintomi.Bambini e adolescenti al di sotto dei 18 anniNon sono disponibili dati sull’impiego di Flutiformo® a questo do-saggio nei bambini o negli adolescenti. L’esperienza nei bambini èlimitata (vedere paragrafi 4.4, 4.8, 5.1 e 5.3). L’uso di Flutiformo® sospensione pressurizzata per inala-zione a qualsiasi dosaggio non è raccomandato nei bambinial di sotto dei 12 anni.In questo gruppo d’età Flutiformo® non deve essere usato.Flutiformo® 250 microgrammi/10 microgrammi per eroga-zione non deve essere usato negli adolescenti.Tuttavia i dosaggi inferiori (50 microgrammi/5 microgrammi per ero-gazione o 125 microgrammi/5 microgrammi per erogazione) pos-sono essere usati negli adolescenti.Gruppi speciali di pazientiNon sono necessari aggiustamenti della dose nei pazienti anziani.Non sono disponibili dati sull’uso di Flutiformo® in pazienti con com-promissione epatica o renale (vedere paragrafo 5.2). Questi pazienti
devono essere monitorati regolarmente da un medico per garantireuna titolazione alla dose minima che permette di mantenere un ef-ficace controllo dei sintomi. Poiché le frazioni di fluticasone e for-moterolo che raggiungono la circolazione sistemica sono eliminateprincipalmente per via epatica, è possibile attendersi un aumentodell’esposizione nei pazienti con grave insufficienza epatica. Informazioni generaliLa monoterapia con corticosteroidi inalatori rappresenta il tratta-mento di prima linea per la maggior parte dei pazienti. Flutiformo®
non è indicato per il trattamento iniziale dell’asma di grado lieve.Per i pazienti con asma grave la terapia con corticosteroidi per viainalatoria deve essere istituita prima di prescrivere un prodotto dicombinazione a dose fissa. Occorre richiamare l’attenzione dei pa-zienti sul fatto che Flutiformo® deve essere utilizzato quotidiana-mente per trarne il massimo beneficio, anche in assenza di sintomi.Per nessun motivo i pazienti che usano Flutiformo® possono utiliz-zare altri b2-agonisti a lunga durata d’azione. Qualora i sintomidell’asma si manifestino nell’intervallo tra le dosi, per un sollievo im-mediato occorre assumere un b2-agonista a breve durata d’azioneper via inalatoria. Per i pazienti attualmente trattati con corticoste-roidi per via inalatoria a dosi moderate-alte, con gravità della ma-lattia tale da giustificare chiaramente due terapie di mantenimento,la dose iniziale raccomandata corrisponde a due inalazioni due volteal giorno di Flutiformo® 125 microgrammi/5 microgrammi per ero-gazione. Per pazienti che hanno difficoltà a sincronizzare l’eroga-zione aerosol con l’inspirazione si raccomanda l’impiego di undistanziatore con Flutiformo®. L’unico distanziatore raccomandatoper l’uso con Flutiformo® è AeroChamber Plus®. I pazienti devonoessere istruiti all’uso corretto e alla manutenzione dell’inalatore edel distanziatore, verificando la loro tecnica inalatoria per assicurarela distribuzione ottimale del farmaco inalato ai polmoni. Con l’usodi un distanziatore occorre sempre ri-titolare il farmaco alla dose mi-nima efficace.Modo di somministrazionePer garantire la corretta somministrazione del medicinale, un medicoo altri professionisti sanitari devono mostrare al paziente come uti-lizzare l’inalatore. L’utilizzo corretto dell’inalatore pressurizzato pre-dosato (pMDI) è essenziale per il successo del trattamento. Si deveconsigliare al paziente di leggere con attenzione il Foglio illustrativoe di seguire le istruzioni per l’uso e le figure ivi riportate. L’erogatoreè dotato di un indicatore della dose integrato che conta il numerodi erogazioni (puff) rimanenti. Quando il numero si avvicina a zero,occorre avvisare il paziente di contattare il medico prescrittore perrichiedere un nuovo inalatore. L’inalatore non deve essere utilizzatose l’indicatore della dose mostra uno “0” (zero).Attivazione dell’inalatorePrima di usare l’inalatore per la prima volta o se l’inalatore non èstato usato per 3 giorni o più o è stato esposto a temperature freddeo vicine allo zero (vedere paragrafo 6.4), è necessario attivarlo.• Togliere il cappuccio di protezione dal boccaglio e agitare bene l’i-
nalatore.• Erogare una dose (puff) tenendo l’inalatore lontano dal viso. Que-
sto passaggio deve essere ripetuto 4 volte.• L’inalatore deve sempre essere agitato immediatamente prima dell’uso.Ogni qualvolta sia possibile, i pazienti devono essere in piedi o sedutiin posizione eretta quando effettuano l’inalazione.Passaggi da seguire quando si utilizza l’inalatore1. Togliere il cappuccio di protezione dal boccaglio e controllare che
il boccaglio sia pulito e privo di polvere e sporcizia. Agitare l’ina-latore immediatamente prima di ogni erogazione (puff).
2. Espirare completamente e il più lentamente e profondamentepossibile.
3. Tenere la bomboletta in senso verticale, con il corpo dell’erogatorerivolto verso l’alto, e collocare il boccaglio tra le labbra. Tenere l’i-nalatore in posizione verticale con il/i pollice/i alla base del boc-caglio e l’indice/gli indici sulla parte superiore dell’inalatore. Nonmordere il boccaglio.
4. Al tempo stesso inspirare lentamente e profondamente dallabocca. Dopo aver iniziato a inspirare, premere la parte superioredell’inalatore per erogare una dose (puff) e continuare a inspirarein modo costante e profondo.
5. Continuare a trattenere il respiro il più a lungo possibile senzasforzarsi (idealmente per circa 10 secondi), quindi espirare lenta-mente. Non espirare nell’inalatore.
6. Tenere l’inalatore in posizione verticale per circa mezzo minuto,agitarlo, quindi ripetere i passaggi da 2 a 5.
7. Dopo l’uso riporre il cappuccio di protezione sul boccaglio.IMPORTANTE: i passaggi da 2 a 5 non devono essere eseguititroppo velocemente.Si può consigliare ai pazienti di esercitarsi davanti a uno specchio.Se dopo l’inalazione si osserva una nebbiolina fuoriuscire dall’i-nalatore o dai lati della bocca, occorre ripetere la procedura dalpassaggio 2. Per pazienti con una presa debole può essere più fa-cile tenere l’inalatore con entrambe le mani appoggiando gli indicisulla parte superiore della bomboletta ed entrambi i pollici allabase dell’inalatore.
FLUTIFORMO-Pagina ADV-RCP 210x270-maggio 2014_Layout 1 30/05/14 09.28 Pagina 1
Dopo ogni inalazione i pazienti devono risciacquarsi la bocca, faregargarismi con acqua o lavarsi i denti ed espellere eventuali residuiper minimizzare il rischio di candidosi orale o disfonia.PuliziaPer le istruzioni sulla pulizia dell’inalatore occorre avvisare i pazientidi leggere attentamente il Foglio illustrativo.L’inalatore deve essere pulito una volta alla settimana.• Togliere il cappuccio di protezione dal boccaglio.• Non estrarre la bomboletta dall’alloggiamento in plastica.• Pulire l’interno e l’esterno del boccaglio e l’alloggiamento in pla-
stica con un panno o fazzoletto asciutto.• Riporre il cappuccio di protezione sul boccaglio rispettando l’o-
rientamento corretto.• Non immergere la bomboletta metallica in acqua.Occorre informare i pazienti che necessitano di un distanziatore Ae-roChamber Plus® di leggere le istruzioni del produttore per assicu-rarsi di conoscere le procedure corrette per l’uso, la pulizia e lamanutenzione del dispositivo.
4.3 ControindicazioniIpersensibilità ai principi attivi o ad uno qualsiasi degli eccipienti (ve-dere paragrafo 6.1).
4.4 Avvertenze speciali e precauzioni di impiegoLa gestione dell’asma deve generalmente avvenire secondo un pro-gramma graduale, monitorando la risposta dei pazienti medianteesami clinici e test di funzionalità polmonare. Flutiformo® non deveessere usato nel trattamento dei sintomi acuti dell’asma che ne-cessitano di un broncodilatatore a breve durata e rapida insor-genza d’azione. Occorre avvisare i pazienti di portare sempre consé il farmaco di emergenza che utilizzano in caso di attacco asma-tico acuto. L’uso profilattico di Flutiformo® in caso di asma da eser-cizio fisico non è stato studiato. Per tale uso è consigliabile ricorrerea un differente broncodilatatore a rapida insorgenza d’azione. Oc-corre ricordare ai pazienti di assumere la dose di mantenimentocome prescritto, anche in assenza di sintomi. I pazienti non devonoiniziare il trattamento con Flutiformo® durante un’esacerbazioneo in caso di peggioramento significativo o deterioramento acutodell’asma. Durante il trattamento con Flutiformo® possono mani-festarsi esacerbazioni o eventi avversi seri correlati all’asma. È ne-cessario chiedere ai pazienti di continuare il trattamentoavvisandoli tuttavia di consultare un medico qualora non riescanoa controllare i sintomi dell’asma o essi peggiorino dopo l’avviodella terapia con Flutiformo®. Flutiformo® non deve essere usatocome trattamento di prima linea per l’asma. Qualora sia necessarioun uso più intenso di broncodilatatori a breve durata d’azione perattenuare i sintomi dell’asma oppure qualora l’efficacia di tale te-rapia si riduca o i sintomi dell’asma persistano, i pazienti devonoessere visitati da un medico quanto prima poiché tali segni pos-sono essere indicativi di un deterioramento nel controllo dell’asmae può essere necessario modificare la terapia. Un deterioramentoimprovviso e progressivo nel controllo dell’asma è potenzialmentefatale e il paziente deve essere visitato in urgenza, valutando l’op-portunità di aumentare la terapia corticosteroidea. Il paziente deveessere visitato anche qualora il dosaggio corrente di Flutiformo®
non permetta un controllo adeguato dell’asma, prendendo in con-siderazione l’introduzione di terapie corticosteroidee aggiuntive.Una volta ottenuto il controllo dei sintomi dell’asma, occorre sop-pesare l’eventualità di ridurre gradualmente la dose di Flutiformo®.È importante controllare regolarmente i pazienti durante la ridu-zione della terapia. Flutiformo® deve essere utilizzato alla dose mi-nima efficace (vedere paragrafo 4.2). Dato il rischio diesacerbazione, nei pazienti con asma il trattamento con Flu-tiformo® non deve essere interrotto bruscamente bensì sospesogradualmente sotto la supervisione del medico prescrittore. Un’e-sacerbazione dei sintomi clinici dell’asma può essere provocata daun’infezione batterica acuta del tratto respiratorio che necessitadi una terapia antibiotica appropriata, con un aumento della dosedei corticosteroidi per via inalatoria e un breve ciclo di corticoste-roidi orali. Come farmaco di emergenza va utilizzato un broncodi-latatore per via inalatoria a rapida insorgenza d’azione. Come tuttii medicinali contenenti corticosteroidi, Flutiformo® deve esseresomministrato con cautela a pazienti con tubercolosi polmonare,tubercolosi quiescente o infezioni delle vie aeree di origine mico-tica, virale o di altro tipo. Tali infezioni devono sempre essere ade-guatamente trattate se si utilizza Flutiformo®. Occorre cautela nelsomministrare Flutiformo® a pazienti con tireotossicosi, feocromo-citoma, diabete mellito, ipokaliemia non corretta o pazienti conpredisposizione a bassi livelli sierici di potassio, a cardiomiopatiaostruttiva ipertrofica, stenosi aortica sottovalvolare idiopatica, iper-tensione grave, aneurismi o altri gravi disturbi cardiovascolari comecardiopatia ischemica, aritmie cardiache o grave insufficienza car-diaca. Dosi elevate di b2-agonisti possono provocare un’ipokalie-mia potenzialmente grave. La somministrazione concomitante dib2-agonisti e farmaci in grado di indurre o potenziare un effettoipokaliemico, p.es. derivati della xantina, steroidi e diuretici, puòpotenziare un possibile effetto ipokaliemico del b2-agonista. Siraccomanda particolare cautela con l’uso variabile di broncodila-
tatori di emergenza in quadri di asma instabile, di asma graveacuto (poiché l’ipossia può aumentare il rischio associato) e in altrecondizioni accompagnate da una maggiore probabilità di insor-genza di effetti avversi a causa dell’ipokaliemia. In tali circostanzeè opportuno monitorare i livelli sierici di potassio. Occorre cautelacon i pazienti che presentano un prolungamento dell’intervalloQTc. Formoterolo può indurre un prolungamento dell’intervalloQTc. Come per tutti i b2-agonisti, occorre valutare l’opportunitàdi sottoporre i pazienti diabetici a controlli aggiuntivi della glice-mia. Occorre cautela quando si effettua il passaggio alla terapiacon Flutiformo®, in particolare se vi sono motivi per credere cheuna precedente terapia steroidea sistemica abbia compromesso lafunzionalità surrenalica. Come per altre terapie inalatorie, dopol’assunzione può verificarsi broncospasmo paradosso a causa diun aumento immediato del respiro sibilante e della dispnea. Ilbroncospasmo paradosso risponde a un broncodilatatore a rapidainsorgenza d’azione per via inalatoria e deve essere trattato im-mediatamente, interrompendo subito la terapia con Flutiformo®,visitando il paziente e istituendo, se necessario, una terapia alter-nativa. I corticosteroidi inalatori, in particolare se assunti a dosielevate e per periodi protratti, possono provocare effetti sistemici,con probabilità comunque molto inferiori rispetto ai corticosteroidiorali. I possibili effetti sistemici includono sindrome di Cushing,segni Cushingoidi, soppressione surrenalica, ritardo di crescita inbambini e adolescenti, riduzione della densità minerale ossea, ca-taratta, glaucoma e, in casi più rari, una serie di effetti psicologicie comportamentali inclusi iperattività psicomotoria, disturbi delsonno, ansia, depressione o aggressività (soprattutto nei bambini).Pertanto è importante controllare regolarmente il paziente e ridurrela dose di corticosteroidi per via inalatoria alla dose minima chepermette di mantenere un efficace controllo dell’asma. Il tratta-mento prolungato con corticosteroidi inalatori a dosi elevate puòprovocare soppressione surrenalica e crisi surrenalica acuta. Sonoparticolarmente a rischio i bambini e gli adolescenti al di sotto dei16 anni trattati con dosi elevate di fluticasone propionato (tipica-mente ≥ 1.000 microgrammi/die). Casi molto rari di soppressionesurrenalica e crisi surrenalica acuta sono stati descritti anche inpazienti trattati con fluticasone propionato a dosi comprese tra500 e <1.000 microgrammi. Gli eventi che potrebbero potenzial-mente scatenare una crisi surrenalica acuta includono traumi, in-terventi chirurgici, infezioni o qualsiasi rapida riduzione deldosaggio. I sintomi di presentazione sono tipicamente vaghi e pos-sono comprendere anoressia, dolore addominale, calo ponderale,stanchezza, cefalea, nausea, vomito, ipotensione, riduzione dellostato di coscienza, ipoglicemia e crisi convulsive. In periodi di stresso in caso di intervento chirurgico d’elezione occorre valutare l’op-portunità di somministrare un trattamento aggiuntivo con cortico-steroidi sistemici. I benefici di fluticasone propionato per viainalatoria dovrebbero minimizzare la necessità di assumere steroidiorali, ma i pazienti che passano dagli steroidi orali a fluticasonepropionato possono essere a rischio di compromissione della ri-serva surrenalica per lungo tempo. Anche i pazienti che in passatohanno già avuto bisogno di una terapia corticosteroidea di emer-genza ad alte dosi possono essere a rischio. Questa possibile com-promissione deve sempre essere tenuta presente in situazioni diurgenza ed elettive che possono provocare stress e occorre valutarel’opportunità di un trattamento corticosteroideo appropriato. A se-conda dell’entità della compromissione surrenalica può essere ne-cessario un consulto specialistico prima di sottoporre il paziente aprocedure elettive. Con una possibile compromissione della fun-zionalità surrenalica occorre monitorare regolarmente il funziona-mento dell’asse ipotalamo-ipofisi-surrene (HPA). La somministrazione combinata di fluticasone propionato con po-tenti inibitori del CYP3A4 comporta un maggior rischio di effettiindesiderati sistemici (vedere paragrafo 4.5). Occorre richiamarel’attenzione del paziente sul fatto che questo inalatore contenenteun prodotto di combinazione a dose fissa è una terapia profilatticae come tale deve essere utilizzato regolarmente, anche in assenzadi sintomi, per trarne un beneficio ottimale. L’uso di un distanzia-tore può comportare un possibile aumento nei depositi polmonarie un potenziale aumento dell’assorbimento sistemico e di eventiavversi sistemici. Poiché le frazioni di fluticasone e formoterolo cheraggiungono la circolazione sistemica sono eliminate principal-mente per via epatica, è possibile attendersi un aumento dell’e-sposizione nei pazienti con grave insufficienza epatica. I pazientidevono essere avvisati che Flutiformo® contiene una piccola quan-tità di etanolo (circa 1,00 mg per erogazione) che tuttavia è irriso-ria e non pone rischi per la loro salute.Popolazione pediatricaSi raccomanda di monitorare regolarmente la statura dei bambiniche ricevono un trattamento con corticosteroidi per via inalatoriaprotratto nel tempo. In caso di rallentamento della crescita, è neces-sario rivedere la terapia allo scopo di ridurre la dose dei corticoste-roidi inalatori, se possibile, alla dose minima che permette dimantenere un efficace controllo dell’asma. Va inoltre valutata l’e-ventualità di indirizzare il paziente a un pediatra specialista in di-sturbi respiratori.
Sono disponibili solo dati limitati sull’impiego di Flu-tiformo® in bambini al di sotto dei 12 anni.Si raccomanda di NON utilizzare Flutiformo® in bambini aldi sotto dei 12 anni fino a quando non saranno disponibiliulteriori dati.
4.5 Interazioni con altri medicinalied altre forme di interazioneNon sono stati effettuati studi formali di interazione con Flutiformo®.Flutiformo® contiene sodio cromoglicato a livelli non farmacologi-camente rilevanti. I pazienti non devono sospendere eventuali far-maci contenenti cromoglicato. Fluticasone propionato, uno deiprincipi attivi di Flutiformo®, è un substrato del CYP3A4. La co-som-ministrazione di potenti inibitori del CYP3A4 (p.es. ritonavir, ataza-navir, claritromicina, indinavir, itraconazolo, nelfinavir, saquinavir,ketoconazolo, telitromicina) e Flutiformo® per brevi periodi di tempoprovoca effetti di rilevanza clinica secondaria, ma occorre cautela incaso di trattamento a lungo termine evitando, se possibile, la co-somministrazione con tali farmaci. Occorre in particolare evitare lasomministrazione concomitante con ritonavir a meno che i beneficisiano superiori al maggior rischio di effetti indesiderati sistemici as-sociato ai glucocorticoidi. Non vi sono dati su questa interazione peril fluticasone propionato per via inalatoria, ma si prevede un marcatoaumento dei livelli plasmatici di fluticasone propionato. Sono statisegnalati casi di sindrome di Cushing e di soppressione surrenalica.Le alterazioni del tracciato ECG e/o l’ipokaliemia che possono deri-vare dalla somministrazione di diuretici non risparmiatori di potassio(come i diuretici d’ansa o tiazidici) possono essere aggravate in mi-sura acuta dai b-agonisti, in particolare se si supera la dose racco-mandata di questi farmaci. Benché la rilevanza clinica di questi effettisia sconosciuta, si consiglia cautela nella somministrazione conco-mitante di b-agonisti e diuretici non risparmiatori di potassio. I de-rivati della xantina e i glucocorticosteroidi possono potenziare ilpossibile effetto ipokaliemico dei b-agonisti. Inoltre, L-dopa, L-ti-roxina, ossitocina e alcol possono compromettere la tolleranza car-diaca ai b2-simpaticomimetici. Il trattamento concomitante coninibitori delle monoaminossidasi, compresi agenti con proprietà similicome furazolidone e procarbazina, può provocare reazioni iperten-sive. I pazienti sottoposti ad anestesia concomitante con idrocarburialogenati sono esposti a un alto rischio di aritmie. L’uso concomi-tante di altri farmaci b-adrenergici può avere un effetto potenzial-mente additivo. L’ipokaliemia può aumentare il rischio di aritmie inpazienti trattati con glicosidi digitalici. Come altri b2-agonisti, for-moterolo fumarato deve essere somministrato con estrema cautelaa pazienti trattati con antidepressivi triciclici o inibitori delle monoa-minossidasi, sia durante il periodo di trattamento che nelle due set-timane successive alla sua sospensione, o con altri farmaci cheprolungano l’intervallo QTc come antipsicotici (incluse le fenotiazine),chinidina, disopiramide, procainamide e antistaminici. I farmaci dicui è noto l’effetto di prolungamento dell’intervallo QTc possono au-mentare il rischio di aritmie ventricolari (vedere paragrafo 4.4). Qua-lora sia necessario somministrare per qualsiasi via farmaciadrenergici aggiuntivi, occorre procedere con cautela in quanto pos-sono potenziare gli effetti farmacologicamente prevedibili di formo-terolo a carico del sistema nervoso simpatico. La somministrazioneconcomitante di antagonisti dei recettori beta-adrenergici (b-bloc-canti) e formoterolo fumarato può avere un effetto di inibizione re-ciproca sull’azione dei due farmaci. I beta-bloccanti possono inoltreprovocare un quadro di grave broncospasmo in pazienti asmatici.Pertanto, in questa popolazione non devono essere usati. È impor-tante notare che i b-bloccanti sono contenuti nei colliri per il tratta-mento del glaucoma. Tuttavia, in determinate circostanze, p.es. comeprofilassi in seguito a infarto del miocardio, è possibile che non visiano altre alternative accettabili. In questo caso si potrebbe valutareun trattamento con b-bloccanti cardioselettivi, benché la loro som-ministrazione richieda cautela.
4.6 Fertilità, gravidanza e allattamentoGravidanzaI dati relativi all’uso di fluticasone propionato e formoterolo fuma-rato, somministrati sia singolarmente che in associazione ma in ina-latori separati, o di questo prodotto di combinazione a dose fissa,Flutiformo®, in donne in gravidanza sono in numero limitato. Glistudi sugli animali hanno mostrato una tossicità riproduttiva (vedereparagrafo 5.3). La somministrazione di Flutiformo® durante la gra-vidanza non è raccomandata e deve essere presa in considerazionesolo se il beneficio previsto per la madre è superiore ai possibili rischiper il feto. In tal caso, si deve usare la dose minima efficace che per-mette di mantenere un adeguato controllo dell’asma. Visto il poten-ziale di interferenza dei b-agonisti con la contrattilità uterina, l’usodi Flutiformo® per la gestione dell’asma durante il travaglio da partodeve essere limitato alle pazienti per le quali il beneficio risulta su-periore ai rischi.AllattamentoNon è noto se fluticasone propionato o formoterolo fumarato venganoescreti nel latte materno. Il rischio per i lattanti non può essere escluso.Pertanto occorre decidere se interrompere l’allattamento o la sommini-strazione di Flutiformo®/astenersi dalla terapia con Flutiformo® tenendo
FLUTIFORMO-Pagina ADV-RCP 210x270-maggio 2014_Layout 1 30/05/14 09.28 Pagina 2

in considerazione il beneficio dell’allattamento per il bambino e quellodel trattamento per la madre.FertilitàNon vi sono dati relativi agli effetti della somministrazione di Flu-tiformo® sulla fertilità. Negli studi sugli animali non sono emersi ef-fetti sulla fertilità in seguito alla somministrazione individuale deidue principi attivi a dosi clinicamente rilevanti (vedere paragrafo 5.3).
4.7 Effetti sulla capacità di guidare veicolie sull’uso di macchinariFlutiformo® non altera o altera in modo trascurabile la capacità diguidare veicoli o di usare macchinari.
4.8 Effetti indesideratiGli effetti indesiderati associati all’uso di Flutiformo® durante lo sviluppoclinico sono riportati nella tabella seguente, elencati per classe sistemico-organica e classificati in base alle seguenti categorie di frequenza: moltocomune (≥1/10); comune (da ≥1/100 a <1/10); non comune (da≥1/1.000 a <1/100); rara (da ≥1/10.000 a <1/1.000), molto rara(<1/10.000) e non nota (la frequenza non può essere definita sulla basedei dati disponibili). All’interno di ciascuna classe di frequenza, gli effetti indesideratisono riportati in ordine decrescente di gravità.
Come per altre terapie inalatorie, può insorgere broncospasmo para-dosso con un aumento immediato del respiro sibilante e della dispneadopo la somministrazione. Il broncospasmo paradosso, che rispondea un broncodilatatore per via inalatoria a rapida insorgenza d’azione,deve essere trattato immediatamente, la terapia con Flutiformo® deveessere sospesa e il paziente deve essere visitato istituendo, se neces-sario, una terapia alternativa. Poiché Flutiformo® contiene sia flutica-sone propionato che formoterolo fumarato, si può verificare lo stessoquadro di effetti indesiderati osservato in relazione ai due principi attivi.Gli effetti indesiderati elencati di seguito sono associati a fluticasonepropionato e formoterolo fumarato, ma non sono stati riscontrati du-rante lo sviluppo clinico di Flutiformo®. Fluticasone propionato: reazionidi ipersensibilità tra cui orticaria, prurito, angioedema (soprattutto fac-ciale e orofaringeo), reazioni anafilattiche. Possono manifestarsi effettisistemici dei corticosteroidi per via inalatoria, in particolare se sommi-nistrati a dosi elevate e per periodi di tempo prolungati, che includonosindrome di Cushing, segni Cushingoidi, soppressione surrenalica, ri-tardo di crescita in bambini e adolescenti, riduzione della densità mi-nerale ossea, cataratta e glaucoma, disturbi del sonno, contusioni,atrofia cutanea e predisposizione alle infezioni. La capacità di adatta-mento allo stress può risultare compromessa. Tuttavia, questi effettisistemici si verificano con probabilità molto inferiori in seguito a terapiacon corticosteroidi inalatori rispetto a corticosteroidi orali. Il tratta-mento protratto nel tempo con dosi elevate di corticosteroidi inalatoripuò portare a una soppressione surrenalica clinicamente significativacon crisi surrenalica acuta. Durante periodi di stress (traumi, interventichirurgici, infezioni) può essere necessaria una copertura aggiuntivacon corticosteroidi sistemici. Formoterolo fumarato: reazioni di iper-sensibilità (tra cui ipotensione, orticaria, edema angioneurotico, prurito,esantema), prolungamento dell’intervallo QTc, ipokaliemia, nausea,
mialgia, aumento dei livelli ematici di lattato. Il trattamento con b2-agonisti come formoterolo può provocare un aumento dei livelli ema-tici di insulina, di acidi grassi liberi, di glicerolo e di corpi chetonici.Reazioni di ipersensibilità sono state osservate in pazienti che utiliz-zano farmaci con sodio cromoglicato per via inalatoria come principioattivo. Benché il sodio cromoglicato sia un eccipiente di Flutiformo® esia presente solo in bassa concentrazione, non è noto se le reazioni diipersensibilità siano dipendenti dalla dose. Nell’eventualità poco pro-babile che Flutiformo® provochi una reazione da ipersensibilità, il trat-tamento deve basarsi sulle raccomandazioni standard per le reazionida ipersensibilità, con l’uso di antistaminici e altre terapie al bisogno.È possibile che Flutiformo® debba essere sospeso immediatamente in-staurando, se necessario, una terapia alternativa per l’asma. Disfoniae candidosi orale possono essere attenuati con gargarismi o risciacquidella bocca con acqua o lavandosi i denti dopo aver usato il prodotto.La candidosi sintomatica può essere trattata con una terapia antimi-cotica topica continuando il trattamento con Flutiformo®.
4.9 SovradosaggioNon sono disponibili dati ottenuti da studi clinici sul sovradosaggiodi Flutiformo®. Tuttavia, di seguito vengono riportati i dati sul sovra-dosaggio dei singoli principi attivi. Formoterolo fumaratoUn sovradosaggio di formoterolo provocherebbe probabilmenteun’esagerazione degli effetti tipici dei b2-agonisti. In tal caso po-trebbero verificarsi le seguenti reazioni avverse: angina, ipertensioneo ipotensione, palpitazioni, tachicardia, aritmia, prolungamento del-l’intervallo QTc, cefalea, tremore, nervosismo, crampi muscolari, sec-chezza delle fauci, insonnia, spossatezza, senso di malessere,convulsioni, acidosi metabolica, ipokaliemia, iperglicemia, nausea evomito. Il trattamento di un sovradosaggio di formoterolo prevedela sospensione del farmaco e l’istituzione di un’adeguata terapia sin-tomatica e/o di supporto. Può essere preso in considerazione un usoprudente di b-bloccanti cardioselettivi, tenendo presente il rischio dibroncospasmo associato a tali farmaci. Non vi sono evidenze suffi-cienti per stabilire se la dialisi possa avere effetti positivi in caso disovradosaggio di formoterolo. Si raccomanda di sottoporre il pa-ziente a monitoraggio cardiaco. Qualora sia necessario sospenderela terapia con Flutiformo® a causa di un sovradosaggio del b-ago-nista contenuto nel medicinale, si deve prendere in considerazioneun’adeguata terapia steroidea sostitutiva. Occorre monitorare i livellisierici di potassio in quanto può insorgere ipokaliemia e valutareeventualmente una terapia sostitutiva con potassio.Fluticasone propionatoUn sovradosaggio acuto di fluticasone propionato non costituisce ingenere un problema clinico. L’unico effetto dannoso provocato dal-l’inalazione di una dose elevata di farmaco in un breve periodo ditempo è la soppressione della funzione dell’asse ipotalamo-ipofisi-surrene (HPA) che generalmente si normalizza nell’arco di alcunigiorni, come documentato dalle misurazioni dei livelli di cortisoloplasmatico. Il trattamento con il corticosteroide inalatorio deve pro-seguire alla dose raccomandata per garantire il controllo dell’asma.Sono stati riferiti rari casi di crisi surrenalica acuta. Sono particolar-mente a rischio i bambini e gli adolescenti al di sotto dei 16 annitrattati con dosi elevate di fluticasone propionato (tipicamente ≥1.000 microgrammi/die). I sintomi di presentazione possono esserevaghi (anoressia, dolore addominale, calo ponderale, stanchezza, ce-falea, nausea, vomito e ipotensione). I sintomi tipici di una crisi sur-renalica comprendono una riduzione dello stato di coscienza,ipoglicemia e/o crisi convulsive. L’uso cronico di dosi molto elevatepuò provocare atrofia della corteccia surrenale con soppressionedell’asse HPA. Può essere necessario monitorare la riserva surrena-lica. I possibili effetti sistemici includono sindrome di Cushing, segniCushingoidi, soppressione surrenalica, ritardo di crescita in bambinie adolescenti, riduzione della densità minerale ossea, cataratta eglaucoma (vedere paragrafo 4.4). Nell’ambito della gestione di unsovradosaggio cronico, in situazioni di stress può essere necessariosomministrare corticosteroidi per via orale o sistemica. Tutti i pazienticonsiderati in sovradosaggio cronico devono essere trattati come sefossero dipendenti dagli steroidi somministrando loro una dose dimantenimento adeguata di un corticosteroide sistemico. Una voltastabilizzati, occorre continuare la terapia con un corticosteroide ina-latorio alla dose raccomandata per ottenere il controllo dei sintomi.
5. PROPRIETÀ FARMACOLOGICHE
5.1 Proprietà farmacodinamicheCategoria farmacoterapeutica: Formoterolo e altri medicinali per lemalattie ostruttive delle vie respiratorie.Codice ATC: R03AK07 Meccanismo di azione ed effetti farmacodinamiciFlutiformo® contiene sia fluticasone propionato che formoterolo fumaratoi cui meccanismi d’azione sono descritti separatamente di seguito. Questifarmaci appartengono a due classi differenti (uno è un corticosteroidesintetico, l’altro un agonista selettivo del recettore b2-adrenergico a lungadurata d’azione) e, come per altre combinazioni di corticosteroidi inalatorie agonisti b2-adrenergici a lunga durata d’azione, si osservano effetti ad-ditivi in termini di riduzione delle esacerbazioni asmatiche.
Fluticasone propionatoFluticasone propionato è un glucocorticoide sintetico trifluoruratoche, per via inalatoria, esercita una potente azione antinfiammatoriasui polmoni. Fluticasone propionato riduce i sintomi e le esacerba-zioni dell’asma ed è associato a un numero inferiore di effetti avversirispetto ai corticosteroidi sistemici.Formoterolo fumaratoFormoterolo fumarato è un agonista selettivo del recettore b2-adre-nergico a lunga durata d’azione. Se inalato, svolge localmente neipolmoni un’azione broncodilatatoria. L’effetto broncodilatatorio in-sorge rapidamente, nell’arco di 1-3 minuti e dura almeno 12 oredopo una dose singola.Flutiformo®
In studi clinici della durata di 12 settimane condotti su adulti eadolescenti l’aggiunta di formoterolo a fluticasone propionato hamigliorato i sintomi asmatici e la funzionalità polmonare, riducendole esacerbazioni. L’effetto terapeutico di Flutiformo® è risultato su-periore a quello del solo fluticasone propionato. Non esistono daticomparativi a lungo termine su Flutiformo® vs. fluticasone propio-nato. In uno studio clinico di 8 settimane su Flutiformo® l’effettodel medicinale sulla funzionalità polmonare è stato quantomenopari a quello della combinazione di fluticasone propionato e for-moterolo fumarato somministrati in due differenti inalatori. Nonsono disponibili dati comparativi a lungo termine su Flutiformo®
vs. fluticasone propionato e formoterolo fumarato. Gli studi clinicicon durata fino a 12 mesi, condotti su pazienti adulti e adolescenti,non hanno evidenziato segni di attenuazione degli effetti terapeu-tici di Flutiformo®. Sono emersi trend dose-risposta per Flutiformo®
per gli endpoint basati sui sintomi, con benefici incrementali perle dosi elevate rispetto alle basse più probabili nei pazienti conasma più grave.Popolazione pediatricaIn uno studio della durata di 12 settimane su pazienti pediatrici, conuna fase di estensione di 6 mesi tesa a valutare la sicurezza a lungotermine, 210 bambini nella fascia d’età 4-12 anni sono stati trattaticon una dose di mantenimento di Flutiformo® (2 inalazioni di 50/5microgrammi due volte al giorno) o con un comparatore a combina-zione fissa. Durante le 12 settimane dello studio la funzionalità pol-monare dei bambini trattati con Flutiformo® è risultata quantomenoidentica a quella dei bambini trattati con il comparatore. Dopo lostudio principale era possibile partecipare a una fase di estensionedi 6 mesi, completata da 205 pazienti trattati con Flutiformo®, du-rante la quale il farmaco è risultato sicuro e ben tollerato.
5.2 Proprietà farmacocineticheFluticasone propionatoAssorbimentoL’assorbimento sistemico di fluticasone propionato assunto per viainalatoria avviene principalmente attraverso i polmoni e mostra unacorrelazione lineare con la dose nell’intervallo di 500-2.000 micro-grammi. L’assorbimento è inizialmente rapido, poi prolungato. Glistudi pubblicati sul dosaggio orale del farmaco approvato vs. nonapprovato hanno dimostrato che la biodisponibilità assoluta siste-mica orale di fluticasone propionato è trascurabile (<1%) per la com-binazione di due fattori: un assorbimento incompleto dal trattogastrointestinale e un esteso metabolismo di primo passaggio.DistribuzioneFluticasone propionato assunto per via endovenosa è ampiamentedistribuito nell’organismo. La fase iniziale di eliminazione è rapida ecoerente con la sua elevata solubilità lipidica e la capacità di legametissutale. Il volume di distribuzione corrisponde mediamente a 4,2l/kg. La percentuale di fluticasone propionato legato alle proteineplasmatiche umane è in media del 91%. Fluticasone propionato pre-senta un legame debole e reversibile con gli eritrociti e non è legatoin misura significativa alla transcortina umana.MetabolismoFluticasone propionato presenta un’elevata clearance totale (media:1.093 ml/min), di cui la clearance renale rappresenta meno dello0,02%. Questo tasso molto elevato indica un’ampia clearance epa-tica. L’unico metabolita circolante rilevato nell’uomo è il derivatoacido 17b-carbossilico di fluticasone propionato, formato mediantela via della sottofamiglia dell’isoforma 3A4 del citocromo P450(CYP3A4). Rispetto al composto parentale questo metabolita pre-senta in vitro un’affinità inferiore (ca. 1/2.000) per il recettore glu-cocorticoide del citosol polmonare nell’uomo. Altri metaboliti rilevatiin vitro da colture cellulari di epatoma umano non sono stati riscon-trati nell’uomo.EliminazioneL’87-100% di una dose orale viene escreto nelle feci, fino al 75%come composto parentale. È inoltre presente un metabolita maggiorenon attivo. Fluticasone propionato somministrato per via endovenosamostra una cinetica con andamento poliesponenziale e ha un’emivitaterminale di circa 7,8 ore. Una percentuale inferiore al 5% di una doseradiomarcata è escreta nelle urine sotto forma di metaboliti, il restoviene escreto nelle feci come composto parentale e metaboliti.Formoterolo fumaratoI dati sulla farmacocinetica plasmatica di formoterolo sono stati rac-colti su volontari sani in seguito all’inalazione di dosi superiori al-
Classe sistemico-organica Evento avverso Frequenza
Infezioni e infestazioni Candidosi oraleSinusite acuta
Rara
Disturbi del metabolismoe della nutrizione
Iperglicemia Non comune
Disturbi psichiatrici Sogni anomaliAgitazioneInsonnia
Iperattività psicomotoria, ansia,depressione, aggressione,modificazioni comportamentali(prevalentemente nei bambini)
Rara
Non nota
Patologie del sistema nervoso CefaleaTremoreCapogiriDisgeusia
Non comune
Patologie dell’orecchioe del labirinto
Vertigini Rara
Patologie cardiache PalpitazioniExtrasistolia ventricolare
Angina pectorisTachicardia
Non comune
Rara
Patologie vascolari Ipertensione Rara
Patologie respiratorie, toraciche e mediastiniche
Esacerbazione dell’asmaDisfoniaIrritazione della gola
DispneaTosse
Non comune
Rara
Patologie gastrointestinali Secchezza delle fauci
DiarreaDispepsia
Non comune
Rara
Patologie della cutee del tessuto sottocutaneo
Rash Rara
Patologiedel sistema muscoloscheletricoe del tessuto connettivo
Spasmi muscolari Rara
Patologie sistemichee condizioni relative alla sededi somministrazione
Edema periferico
Astenia
Non comune
Rara
FLUTIFORMO-Pagina ADV-RCP 210x270-maggio 2014_Layout 1 30/05/14 09.28 Pagina 3

l’intervallo raccomandato e su pazienti con BPCO in seguito all’ina-lazione di dosi terapeutiche.AssorbimentoIn volontari sani che hanno inalato una singola dose da 120 micro-grammi, formoterolo fumarato è stato assorbito rapidamente nel pla-sma e ha raggiunto la concentrazione massima di 91,6 pg/ml entro 5minuti dall’inalazione. In pazienti con BPCO trattati per 12 settimanecon formoterolo fumarato alla dose di 12 o 24 mg due volte al giornosono state osservate concentrazioni plasmatiche in intervalli compresitra 4,0 e 8,9 pg/ml e 8,0 e 17,3 pg/ml rispettivamente a 10 minuti ea 2 e 6 ore post-inalazione. Studi sull’escrezione urinaria cumulativadi formoterolo e/o dei suoi enantiomeri RR e SS hanno evidenziato unaumento lineare dell’assorbimento correlato alla dose in seguito a ina-lazione di polvere secca (12-96 microgrammi) o erogazione di formu-lazioni aerosol (12-96 microgrammi). Dopo 12 settimane disomministrazione di formoterolo in polvere alla dose di 12 o 24 mi-crogrammi due volte al giorno, l’escrezione urinaria di formoterolo im-modificato è aumentata del 63-73% in pazienti adulti con asma, del19-38% in pazienti adulti con BPCO e del 18-84% in pazienti pedia-trici. Questo dato è indicativo di un accumulo modesto e autolimitantedi formoterolo nel plasma in seguito a somministrazione ripetuta. DistribuzioneFormoterolo ha una capacità di legame con le proteine plasmatichedel 61-64% (del 34% prevalentemente con l’albumina). Non si os-serva saturazione dei siti di legame nell’intervallo di concentrazioneraggiunto con le dosi terapeutiche. Le concentrazioni di formoteroloutilizzate per valutare la capacità di legame con le proteine plasma-tiche sono risultate superiori a quelle osservate nel plasma in seguitoall’inalazione di una dose singola da 120 microgrammi.MetabolismoL’eliminazione di formoterolo avviene principalmente attraverso ilmetabolismo. La glucuronidazione diretta è la principale via di bio-trasformazione, un’altra via è la O-demetilazione seguita da un’ul-teriore glucuronidazione. Le vie minori di eliminazione includono lasolfoconiugazione e la deformilazione seguita da solfoconiugazione.Isoenzimi multipli catalizzano la glucuronidazione (UGT1A1, 1A3,1A6, 1A7, 1A8, 1A9, 1A10, 2B7 e 2B15) e la O-demetilazione (CYP2D6, 2C19, 2C9 e 2A6) di formoterolo, pertanto formoterolo pre-senta un basso potenziale di interazione metabolica con altri farmaci.A concentrazioni terapeuticamente rilevanti il farmaco non ha inibitogli isoenzimi del citocromo P450. Formoterolo presenta un profilocinetico simile dopo somministrazione singola e ripetuta, il che indical’assenza di autoinduzione o di inibizione del metabolismo. EliminazioneIn pazienti asmatici e pazienti con BPCO trattati per 12 settimanecon formoterolo fumarato alla dose di 12 o 24 microgrammi duevolte al giorno, rispettivamente il 10% e il 7% circa della dose sonostati recuperati nelle urine come formoterolo immodificato. Questapercentuale è risultata pari al 6% circa della dose in pazienti pedia-trici asmatici che hanno ricevuto più dosi da 12 o 24 microgrammi.Gli enantiomeri RR e SS rappresentano rispettivamente il 40% e il60% del recupero urinario di formoterolo immodificato in seguitoalla somministrazione di dosi singole (12-120 microgrammi) a vo-lontari sani e di dosi singole e ripetute a pazienti asmatici. Dopo unasingola dose orale di 3H-formoterolo, il 59-62% della dose è statorecuperato nelle urine e il 32-34% nelle feci. La clearance renale diformoterolo è pari a 150 ml/min. In seguito a inalazione, i dati sulprofilo cinetico plasmatico e sulla velocità di escrezione urinaria diformoterolo in volontari sani indicano un’eliminazione bifasica, conemivite terminali pari rispettivamente a 13,9 e 12,3 ore per gli enan-tiomeri RR e SS. Il picco di escrezione viene raggiunto rapidamente,entro 1,5 ore. Il 6,4-8% circa della dose è stato recuperato nelleurine sotto forma di formoterolo immodificato, con gli enantiomeriRR e SS responsabili rispettivamente del 40% e del 60%.Flutiformo® (combinazione di fluticasone propionato/formoterolofumarato)Una serie di studi ha indagato le caratteristiche farmacocinetiche di flu-ticasone propionato e formoterolo fumarato valutati individualmente ri-spetto alla loro associazione in Flutiformo®, somministrati siaseparatamente che in combinazione. Questi studi presentano tuttaviaun’elevata variabilità inter- e intrastudio. In generale emerge una tendenzache indica che l’esposizione sistemica a fluticasone e formoterolo in com-binazione fissa è inferiore a quella dei due componenti individuali som-ministrati in combinazione. Non è stata dimostrata l’equivalenzafarmacocinetica tra Flutiformo® e i suoi componenti individuali. Non sonodisponibili dati comparativi a lungo termine su Flutiformo® vs. fluticasonepropionato e formoterolo fumarato (vedere paragrafo 5.1). AssorbimentoFlutiformo® – fluticasone propionatoIn seguito all’inalazione di una singola dose da 250 microgrammi di flu-ticasone propionato ottenuta da 2 erogazioni di Flutiformo® 125 micro-grammi/5 microgrammi in volontari sani è stato osservato un rapidoassorbimento plasmatico, con una concentrazione massima media di32,8 pg/ml entro 45 minuti dall’inalazione. In pazienti asmatici trattaticon dosi singole di fluticasone propionato ottenuto dall’inalazione diFlutiformo®, le concentrazioni plasmatiche massime medie di 15,4 pg/mle di 27,4 pg/L sono state raggiunte rispettivamente entro 20 minuti e
30 minuti dalla somministrazione di 100 microgrammi/10 microgrammi(2 erogazioni di Flutiformo® 50 microgrammi/5 microgrammi) e di 250microgrammi/10 microgrammi (2 erogazioni di Flutiformo® 125 micro-grammi/5 microgrammi). In studi che hanno valutato la somministrazionedi dosi multiple a volontari sani, con dosi di Flutiformo® pari a 100 mi-crogrammi/10 microgrammi, 250 microgrammi/10 microgrammi e 500microgrammi/20 microgrammi sono state raggiunte concentrazioni pla-smatiche massime medie di fluticasone pari rispettivamente a 21,4, 25,9-34,2 e 178 pg/ml. I dati relativi alle dosi da 100 microgrammi/10microgrammi e 250 microgrammi/10 microgrammi sono stati generatiutilizzando un nebulizzatore privo di distanziatore, quelli relativi alla doseda 500 microgrammi/20 microgrammi sono stati generati utilizzandoun nebulizzatore dotato di distanziatore. In volontari sani l’uso di un di-stanziatore AeroChamber Plus® aumenta la biodisponibilità sistemicamedia di fluticasone (equivalente all’assorbimento polmonare) del 35%rispetto alla somministrazione di Flutiformo® mediante un dispositivopMDI privo di distanziatore. In volontari sani l’uso di un distanziatoreAeroChamber Plus® diminuisce la biodisponibilità sistemica media diformoterolo del 25% rispetto alla somministrazione di Flutiformo® me-diante un dispositivo pMDI privo di distanziatore. Ciò è probabilmentedovuto a una riduzione dell’assorbimento gastrointestinale con l’utilizzodel distanziatore, che compensa il previsto aumento corrispondentenell’assorbimento polmonare.Flutiformo® - formoterolo fumaratoIn seguito alla somministrazione di una dose singola di Flutiformo®
a volontari sani, una dose da 20 microgrammi di formoterolo fuma-rato ottenuta con 2 erogazioni di Flutiformo® 250 microgrammi/10microgrammi ha prodotto una concentrazione plasmatica massimamedia di 9,92 pg/ml entro 6 minuti dall’inalazione. Con dosi multipledi 20 microgrammi di formoterolo fumarato ottenuti con 2 eroga-zioni di Flutiformo® 250 microgrammi/10 microgrammi è stata rag-giunta una concentrazione plasmatica massima media di 34,4 pg/ml.DistribuzioneNon esistono attualmente dati sulla capacità di legame con le pro-teine plasmatiche specifici per fluticasone propionato o formoterolofumarato contenuti in Flutiformo®.MetabolismoNon esistono attualmente dati sul metabolismo di fluticasone pro-pionato o formoterolo fumarato rispetto all’inalazione di Flutiformo®.EliminazioneFluticasone propionatoFluticasone propionato assunto con l’inalazione di 2 erogazioni diFlutiformo® 250 microgrammi/10 microgrammi ha un’emivita ter-minale di circa 14,2 ore.Formoterolo fumaratoFormoterolo fumarato assunto con l’inalazione di 2 erogazioni diFlutiformo® 250 microgrammi/10 microgrammi ha un’emivita ter-minale di circa 6,5 ore. Una percentuale inferiore al 2% di una sin-gola dose di formoterolo fumarato inalato con Flutiformo® vieneescreta nelle urine.
5.3 Dati preclinici di sicurezzaLa tossicità osservata negli studi sugli animali con formoterolo fu-marato e fluticasone propionato, somministrati separatamente o incombinazione, consiste principalmente in effetti associati a un’atti-vità farmacologica esagerata. Gli effetti sul sistema cardiovascolaresono correlati alla somministrazione di formoterolo e comprendonoiperemia, tachicardia, aritmie e danno miocardico. La co-sommini-strazione dei due principi attivi non ha provocato né un aumentodella tossicità né l’insorgenza di reperti inattesi. Gli studi sulla ripro-duzione condotti con Flutiformo® su ratti e conigli hanno confermatoi noti effetti embrio-fetali dei due componenti individuali, tra cui ri-tardo di crescita fetale, ossificazione incompleta, letalità embrionale,palatoschisi, edema e alterazioni scheletriche. Tali effetti sono statiosservati a esposizioni inferiori a quelle attese usando la dose mas-sima clinica raccomandata. Un’esposizione sistemica molto alta aformoterolo ha provocato un certo calo della fertilità in ratti maschi.Test standard in vitro e in vivo condotti individualmente sui due com-ponenti non hanno evidenziato genotossicità. Non sono stati con-dotti studi sulla cancerogenicità della combinazione. Non è emersoun potenziale cancerogeno per fluticasone propionato. In seguitoalla somministrazione di formoterolo è stato osservato un lieve au-mento nell’incidenza di tumori benigni del tratto riproduttivo nellefemmine di topo e ratto. Tale riscontro è considerato un effetto diclasse nei roditori esposti, per periodi protratti, a dosi elevate di b2-agonisti e non è indicativo di un rischio potenziale di cancerogenicitànell’uomo. Studi preclinici su HFA 227 non rilevano rischi particolariper l’uomo sulla base di studi di tossicità a dosi ripetute, genotossi-cità, cancerogenicità e tossicità della riproduzione.
6. INFORMAZIONI FARMACEUTICHE6.1 Elenco degli eccipienti
Sodio cromoglicato Etanolo anidro Eptafluoropropano HFA 227
6.2 IncompatibilitàNon pertinente.
6.3 Periodo di validità2 anni. Validità della confezione aperta: 3 mesi dall’apertura dellabustina di alluminio.
6.4 Precauzioni particolari per la conservazioneConservare a temperatura non superiore a 25°C. Non refrigerare ocongelare. Se l’inalatore viene esposto a temperature vicino allo zero,occorre avvisare il paziente che deve lasciarlo a temperatura am-biente per 30 minuti e riattivarlo prima dell’uso (vedere paragrafo4.2). La bomboletta contiene un liquido pressurizzato. Non esporrea temperature superiori a 50°C. Non forare, rompere o bruciare,anche se apparentemente vuota.
6.5 Natura e contenuto del contenitore120 erogazioni per inalatore.L’erogatore è di colore bianco con un indicatore della dose integratodi colore grigio e un cappuccio di protezione del boccaglio di coloregrigio chiaro.La sospensione è contenuta in una bomboletta pressurizzata di al-luminio sigillata con una valvola dosatrice standard. La bombolettaè inserita in un erogatore predosato dotato di copriboccaglio (en-trambi in polipropilene) e un indicatore della dose integrato che se-gnala il numero di erogazioni (puff) rimanenti. Ogni contenitoreeroga 120 dosi. L’inalatore assemblato è avvolto in un foglio lami-nato di alluminio all’interno di una scatola in cartone.Confezioni:1 inalatore (120 erogazioni)Confezione multipla da 3 inalatori (120 erogazioni).È possibile che non tutte le confezioni siano commercializzate
6.6 Precauzioni particolari per lo smaltimentoe la manipolazioneNessuna istruzione particolare.Per istruzioni dettagliate sull’uso del medicinale vedere paragrafo4.2 (Posologia e modo di somministrazione).
7. TITOLARE DELL’AUTORIZZAZIONEALL’IMMISSIONE IN COMMERCIOMundipharma Pharmaceuticals SrlVia G. Serbelloni, 4 - 20122 Milano, Italia
8. NUMERO(I) DELL’AUTORIZZAZIONEALL’IMMISSIONE IN COMMERCIO AIC n.042294013Flutiformo 50 microgrammi/5 microgrammi1 inalatore da 120 erogazioniAIC n.042294025Flutiformo 125 microgrammi/5 microgrammi1 inalatore da 120 erogazioniAIC n.042294037Flutiformo 250 microgrammi/10 microgrammi1 inalatore da 120 erogazioniAIC n. 042294049Flutiformo 50 microgrammi/5 microgrammi3 inalatori da 120 erogazioniAIC n. 042294052Flutiformo 125 microgrammi/5 microgrammi3 inalatori da 120 erogazioniAIC n. 042294064Flutiformo 50 microgrammi/5 microgrammi3 inalatori 120 erogazioni
9. DATA DELLA PRIMA AUTORIZZAZIONE/RINNOVODELL’AUTORIZZAZIONE13/05/2013
10. DATA DI REVISIONE DEL TESTO03/2014
Dosaggi e prezzo al pubblicoal netto degli sconti obbligatori di legge
Flutiformo® 50 / 5 µg 31,35 €Indicato negli adulti e negli adolescential di sopra dei 12 anni
Flutiformo® 125 / 5 µg 47,66 €Indicato negli adulti e negli adolescential di sopra dei 12 anni
Flutiformo® 250 / 10 µg 70,28 €Indicato SOLO negli adulti,al di sopra dei 18 anni
CLASSE A
FLUTIFORMO-Pagina ADV-RCP 210x270-maggio 2014_Layout 1 30/05/14 09.28 Pagina 4

GOCERCA Un potente ICS* ed il LABA** più rapido in associazione1
X
1 - Bodzenta-Lukaszyk A et al., Efficacy and safety profile of fluticasone/formoterol combination therapy compared individual componentsadministered concurrently in asthma: a randomised controlled trial. Curr Med Res Opin. 2013 Feb 20.
2 - Flutiformo® - Riassunto delle caratteristiche di prodotto3 - Dissanayake S et al., Fluticasone/formoterol: a new single-aerosol combination therapy for patients with asthma.
Respiratory Medicine (2012) 106(S1), S20–S28
CLASSE A
Flutiformo® 50 µg / 5 µg 31,35 €Indicato negli adulti e negli adolescenti al di sopra dei 12 anni
Flutiformo® 125 µg / 5 µg 47,66 €Indicato negli adulti e negli adolescenti al di sopra dei 12 anni
Flutiformo® 250 µg / 10 µg 70,28 €Indicato SOLO negli adulti, al di sopra dei 18 anni
Dosaggi e prezzo al pubblicoal netto degli sconti obbligatori di legge
* IC
S= co
rtico
stero
ide
inal
ator
io
** LA
BA=b
ronc
odila
tato
re a
lung
a du
rata
d’a
zione
RCP
in a
llega
to
Dep
osito
AIFA
in d
ata
11/0
6/20
13
FL
U 20
PER LA PRIMA VOLTA IN ASSOCIAZIONE(3)
Ora associati in un unicoinalatore aerosol (1)
Fluticasone ha un potentee sostenuto effetto antiinfiammatorioe formoterolo fornisceuna rapida broncodilatazione (3)
Inalatore con indicatore di dose (2)
NOVITÀ
C
M
Y
CM
MY
CY
CMY
K
ADV Flutiformo 21x27.pdf 1 30/05/14 09.16
SUBSCRIBE NOW! www.eurannallergyimm.com• 6 print issues per year• full access to www.eurannallergyimm.com,
featuring all current and archived issues
European Annals of Allergy and Clinical Immunology is a bimonthly peer-reviewed publication• The official Journal of the “Associazione Italiana Allergologi Immunologi Territoriali
e Ospedalieri” (Italian Association of Hospital Allergists and Immunologists - AAITO)and the “Sociedade Portuguesa de Alergologia e Imnunologia Clinica” (Portuguese Societyof Allergology and Clinical Immunology - SPAIC)
• indexed in PubMed and Scopus
• collects reviews, original works and case reports concerning etiology,diagnosis and treatment of allergic and immunological disorders
• includes a section of information comingfrom the main international health associations and authorities.
Italy SubScrIptIon only 60,00 Euro
InternatIonal SubScrIptIon
only 85,00 Euro
To submit your paper go to http://eaaci.edmgr.com
AbbAAITO210x270.indd 1 02/07/14 14.21
5/2014
Proteomic analysis of human nasal mucosa: different expression profile in rhino-pathologic states
Shrimp allergy beyond Tropomyosin in Italy: clinical relevance of Arginine Kinase, Sarcoplasmic calcium binding protein and Hemocyanin
An unusual case of occupational asthma in a part time magician. He has got an allergy surprise from his top hat!
A plausible allergy to peanut revealed only by Immunoblot
A case of long-undiagnosed Common Primary Immunodeficiency in adulthood
European Annalsof Allergy and
Clinical Immunology
Issn 1764-1489 Volume 46 n. 5/2014 – september 2014
THE OFFICIAL JOURNAL OF AAITO | ASSOCIAZIONE ITALIANA ALLERGOLOGI IMMUNOLOGI TERRITORIALI E OSPEDALIERI
THE OFFICIAL JOURNAL OF SPAIC | SOCIEDADE PORTUGUESA DE ALERGOLOGIA E IMUNOLOGIA CLINICA
Senza titolo-2 1 10/07/14 15:34





























