Embed Size (px)
Citation preview

Acc
epte
d A
rtic
le
This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process which may lead to differences between this version and the Version of Record. Please cite this article as an 'Accepted Article', doi: 10.1111/jth.12555 This article is protected by copyright. All rights reserved.
Received Date : 08-Nov-2013
Accepted Date : 23-Feb-2014
Article type : Brief Report - Clinical Haemostasis and Thrombosis
Evaluation of a whole blood remote platelet function test for the diagnosis of mild bleeding
disorders
Short title: Remote platelet test for bleeding disorders
Natalia Dovlatova*,§, Marie Lordkipanidzé§, Gillian C. Lowe§, Ban Dawood§, Jane May*, Stan
Heptinstall*, Steve P. Watson§ and Susan C. Fox*, for the UK GAPP Study Group
*Cardiovascular Medicine, University of Nottingham, Queens Medical Centre, Nottingham, United
Kingdom
§Centre for Cardiovascular Sciences, Birmingham Platelet Group, University of Birmingham,
Birmingham, United Kingdom
Institution: The University of Nottingham and The University of Birmingham
Address for correspondence:
Natalia Dovlatova
Cardiovascular Medicine
D Floor, South Block

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Queen’s Medical Centre
Nottingham
NG7 2UH
United Kingdom
Tel +44 (0)115 8231019
Fax +44 (0)115 8231017
E-mail [email protected]
Abstract
Background: Mild platelet function disorders (PFDs) are complex and difficult to diagnose. The
current gold standard test, light transmission aggregometry (LTA), including lumi-aggregometry, is
time- and labour-intensive and blood samples must be processed within a limited time after
venepuncture. Furthermore, many subjects with suspected PFDs do not show a platelet
abnormality on LTA.
Objective: To assess the diagnostic potential of an easy-to-use remote platelet function test
(RPFT) as a diagnostic pre-test for suspected PFDs.
Methods: RPFT was compared to lumi-aggregometry in participants recruited to the Genotyping
and Phenotyping of Platelets study (GAPP, ISRCTN 77951167). For RPFT, whole blood was
stimulated with platelet agonists, stabilized with PAMFix and returned to the central laboratory
for analysis of P-selectin and CD63 by flow cytometry.
Results: In the 61 study participants (42 index cases and 19 relatives) there was a good agreement
between lumi-aggregometry and RPFT with diagnosis being concordant in 84% of cases
(kappa=0.668, p<0.0001). According to both tests, 29 participants were identified to have a
deficiency in platelet function and 22 participants appeared normal. There were 4 participants

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
where lumi-aggregometry revealed a defect but RPFT did not, and 6 participants where RPFT
detected an abnormal platelet response that was not identified by lumi-aggregometry.
Conclusion: This study suggests that RPFT could be an easy-to-use pre-test to select, which
participants with bleeding disorders would benefit from extensive platelet phenotyping. Further
development and evaluation of the test are warranted in a wider population of patients with
excessive bleeding and could provide informative screening tests for PFDs.
Keywords: bleeding, blood platelet disorders, platelet function tests, flow cytometry, platelets
Introduction
Mild platelet function disorders (PFDs) are complex, poorly understood, difficult to diagnose and
require extensive laboratory testing limited to specialised laboratories [1,2]. Lumi-aggregometry,
where dense granule secretion is assessed in parallel with traditional LTA [3-5] is informative, but
is time- and labour-intensive. It is performed on platelet-rich plasma and requires a considerable
volume of a fresh blood sample. In our previous study we demonstrated using lumi-aggregometry
that approximately 60% of participants with excessive clinical bleeding and a suspected
underlying inherited PFD have a demonstrable abnormality in platelet responses [5]. This suggests
that 40% of patients may have a platelet abnormality that is not detectable by lumi-aggregometry
or may have a defect in other components of the haemostatic pathway or a combination of mild
defects, which leads to a bleeding phenotype. These findings are in agreement with an earlier
study by Quiroga et al where approximately 60% of a slightly different patient population with
mild bleeding had no identified defect when assessed by LTA and serotonin and ATP release
measurements [6]. Accordingly, a simple and easy-to-perform preliminary test might be useful to
select patients with excessive bleeding for whom extensive platelet phenotyping using traditional
methodologies may be required for further characterisation. At present, there is no reliable easy-

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
to-use and sufficiently sensitive global platelet function test available for use as a screening tool in
subjects with suspected PFD [7].
We have developed a remote platelet function test (RPFT), in which a blood sample is
manipulated in a simple way that does not require specialised staff or equipment at the test site.
The sample is stabilised utilising a fixing solution, PAMFix, and sent to a flow cytometry fascility
for analysis [8], where the expression of the α-granule marker P-selectin and the dense granule
marker CD63 is measured. The samples treated with PAMFix are stable for up to 9 days at
ambient temperature. CD63 expression specifically evaluates dense granule secretion; analysis of
P-selectin expression is used as a marker of α-granule secretion and also as a general indicator of
platelet reactivity. Here we describe the evaluation of this new approach against traditional lumi-
aggregometry in patients with suspected inherited PFDs.
Methods
Study population
To assess the diagnostic potential of the RPFT in the diagnosis of PFDs, results were compared to
lumi-aggregometry in participants recruited to the Genotyping and Phenotyping of Platelets study
(GAPP, ISRCTN 77951167) from April 2012 to March 2013. We studied 61 participants (42 index
cases and 19 recruited relatives), 13 males (median age 13, range 5-45) and 48 females (median
age 39, range 2-77); all had a history of excessive bleeding with a suspected underlying inherited
PFD. These participants had normal coagulation parameters and a normal platelet count and were
referred from UK Comprehensive Care Haemophilia Centres. Patients with an existing diagnosis of
a known platelet defect were not included in this study. Bleeding symptoms in adult patients
(n=42) were assessed using the ISTH/SSC bleeding assessment tool (BAT) [9]. All the participants
presented with a significant bleeding history with a median bleeding score of 13 (interquartile
range: 8 – 16), whereas the 95th percentile within the healthy volunteer population was 4 [10].

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Platelet function was also assessed in 41 healthy volunteers recruited as controls, who had
no history of bleeding and had refrained from taking any medication known to affect platelet
function. All blood samples were either taken at or delivered by courier from several referring
centres (maximum distance 100 miles) to the central laboratory as previously described [5]. This
study was approved by the National Research Ethics Service Committee West Midlands –
Edgbaston (ref 06/MRE07/36). All participants provided written informed consent.
Assessment of platelet function
For the RPFT measurements, whole blood samples collected into sodium citrate were prewarmed
and stimulated at 37oC for 5 min without mixing. They were then fixed using PAMFix (Platelet
Solutions Ltd, Nottingham). Samples were then transported from the central laboratory to the
flow cytometry facility (60 miles) and routinely analysed within 3 days. For platelet stimulation
blood samples were treated with 1) saline alone to provide a baseline test; 2) adenosine
diphosphate (ADP) with U46619, a stable thromboxane A2 analogue (ADP/U4 10μM and 1μM
respectively); 3) thrombin receptor activating peptide (TRAP [SFLLRN] 20μM) and 4) arachidonic
acid with epinephrine (AA/EPI, 0.5mM and 100μM respectively). U46619 and epinephrine were
used as potentiating agents and were chosen based on previous studies where we investigated
optimal conditions for platelet activation in whole blood [11]. Intra- and inter-assay coefficients of
variation are 4.4% and 5.6% respectively.
Lumi-aggregometry was performed as previously described [5]. The results were considered
abnormal when they fell below the 5th percentile with reference to a bank of local healthy
volunteers (n=68).
Statistical analysis
Results of platelet function measurements are presented as individual data in median
fluorescence units (mf). To determine the ability of the RPFT to discriminate between subjects

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
with and without abnormal platelet responses and to set optimal cut-off levels, receiver operator
characteristic (ROC) curve analysis was performed. For P-selectin measurements ROC curves were
generated using the subjects with and without any defect, as determined by lumi-aggregometry,
and for CD63 measurements, subjects with and without a secretion defect. Agreement between
the two tests was assessed using two-by-two analysis and Cohen’s kappa statistic. Analyses were
performed using the software packages SPSS 14.0 and GraphPad Prism 6.
Results
According to lumi-aggregometry, 33 of the 61 participants recruited to GAPP study were
considered to have an abnormality in platelet responses. The majority of these 33 participants
could be subdivided into three categories on the basis of their lumiaggregation profile [5] –
defects in dense granule secretion (n=9), Gi signalling (n=14) and the TxA2 pathway (n=3). The
remaining 7 participants had either a complex defect that was difficult to assign to any specific
group, presenting with reduced responses via several pathways (n=4), or a defect in the response
to collagen (n=1) or TRAP (n=2).
The area under the ROC curve for P-selectin (Figure 1a) and CD63 measurements (Figure 1b) with
different agonists varied between 0.72 and 0.99 (p<0.004). This confirmed that RPFT can
discriminate between individuals with excessive bleeding with and without abnormal platelet
responses as detected by lumi-aggregometry. Based on the ROC analysis, appropriate cut-off
levels for each parameter were chosen to provide the highest possible sensitivity of the RPFT to
minimise false negative results. Applying the chosen cut-offs in the group of healthy controls
indicated that 5 out of 41 participants presented with somewhat reduced platelet responses on
RPFT (Figure 2a). This small degree of overlap in platelet responsiveness between populations of
patients and healthy controls is also seen in other platelet function tests in addition to other tests
of haemostasis [6].

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
In the patient group, the overall agreement between lumi-aggregometry and RPFT was
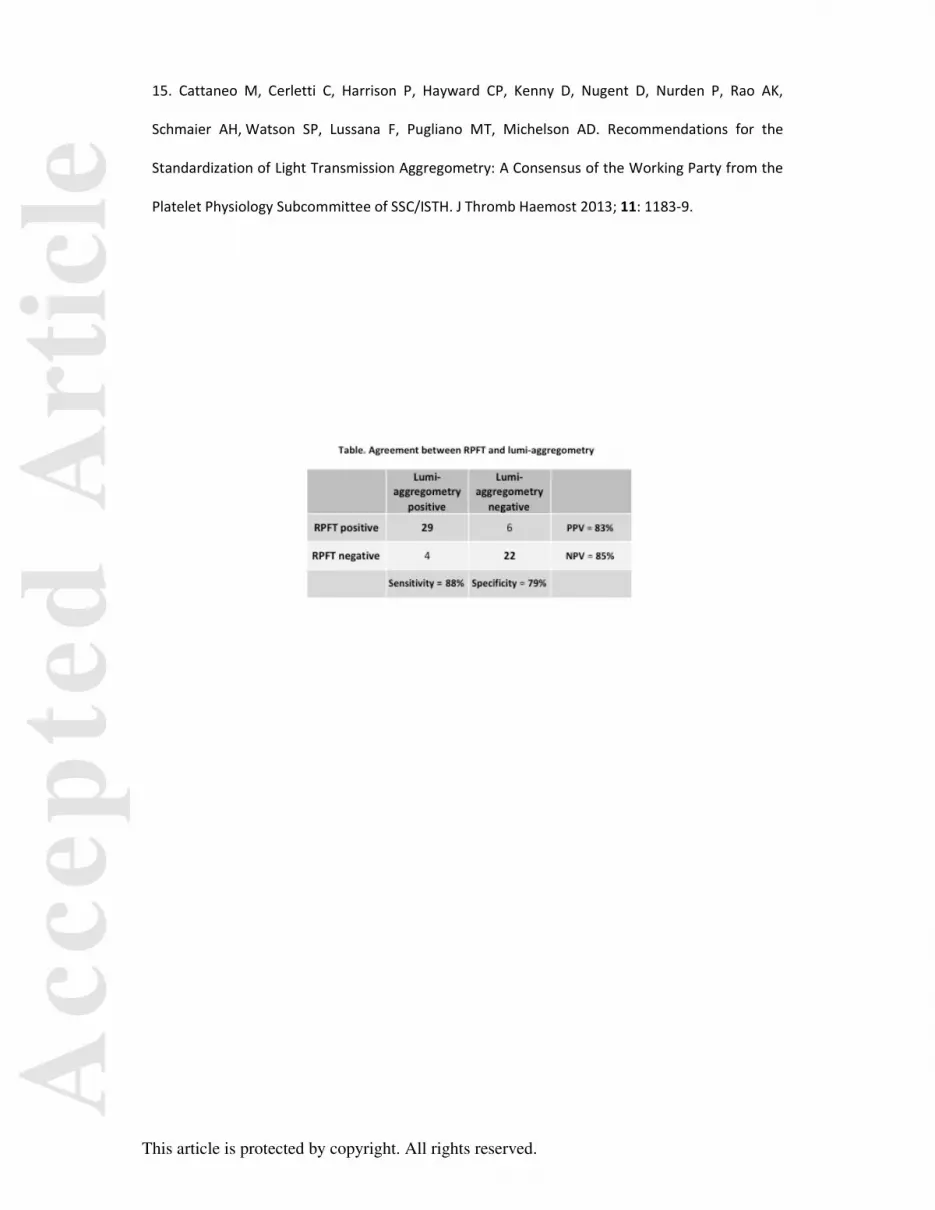
good, with the diagnosis being concordant in 84% of cases (kappa=0.668, p<0.0001) (Table). All
participants who presented with a dense granule secretion defect (Figure 2b) or a defect in the
TxA2 pathway (Figure 2c) on lumi-aggregometry were also classified as having a platelet
abnormality on the RPFT with at least one parameter falling below the normal range. Out of the
14 participants who presented with a defect in Gi signalling based on lumi-aggregometry (Figure
2d), 11 also showed abnormal platelet responses on RPFT, while 3 subjects were considered
normal. It should be noted that presentation of the Gi-type platelet defect on lumi-aggregometry
is variable, overlaps considerably with corresponding measurements in healthy volunteers (Figure
3) and is based on interpretation of kinetic information not available in endpoint assays. The
remaining case that was missed on RPFT presented with a reduced response to collagen on lumi-
aggregometry and was considered to have a potential defect in GPVI.
Six participants with normal responses on lumi-aggregometry presented with an abnormal
response on RPFT suggesting that this test may have an increased sensitivity. One of these
patients had normal aggregation and dense granule secretion on both tests, but markedly
reduced P-selectin expression in response to all agonists, indicative of impaired α-granule
secretion.
Discussion
Here we evaluated the performance of a novel remote platelet function test alongside lumi-
aggregometry in patients presenting with bleeding symptoms suggestive of an inherited PFD. The
new test directly assesses both α- and dense granule secretion in response to platelet stimulation
with several agonists in whole blood. The RPFT was able to discriminate between patients with
and without an abnormality in platelet function as detected by lumi-aggregometry, and showed
good levels of agreement with this reference test.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
All the participants identified by lumi-aggregometry to have a defect in dense granule
secretion or in the TxA2 pathway also presented with an abnormality on RPFT. Among the
participants with a defect in dense granule secretion, one had almost absent ATP release on lumi-
aggregometry and low CD63 expression on RPFT and was later identified to have Hermansky-
Pudlak syndrome-7 [12]. Interestingly, two other participants from the same group of defects
(highlighted in Figure 2b) presented with reduced P-selectin expression, but elevated CD63
expression even at baseline, and were later identified to have Hermansky-Pudlak syndrome-2,
which is known to be associated with impaired sorting of CD63 and its accumulation in the plasma
membrane rather than granule membrane [13].
Three individuals who were diagnosed with a defect in Gi signalling with lumi-aggregometry
appeared normal on RPFT. Their phenotype was relatively mild and the diagnosis was based
mainly on the kinetic information, with transient rather than sustained aggregation being
observed, or with delayed aggregation or secretion.
The RPFT identified 6 participants with reduced platelet reactivity that was not detected by
lumi-aggregometry. One of these participants had reduced P-selectin but normal CD63 expression
in response to all agonists, suggesting impaired α-granule secretion, which is reminiscent of Gray
Platelet Syndrome, a defect that would not be detected with lumi-aggregometry. These results
confirm that the absence of a platelet abnormality on traditional testing cannot eliminate the
possibility of a platelet defect.
There is considerable variability in methodology of LTA with a historical lack of
standardisation of aggregation [14]. Recently, the Platelet Physiology Scientific and
Standardization Committee of the International Society of Thrombosis and Haemostasis has
begun to standardise light transmission aggregometry [15] to improve the comparability of results
between laboratories. However, there remain many analytical and pre-analytical variables, which
render the application of lumi-aggregometry to a large population challenging. The main
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
advantage of the RPFT is the use of whole blood. Furthermore, the analysis is performed on fixed
samples and thus can be done remotely without the need for immediate processing of the blood
sample. This offers the potential for standardisation and improved accessibility of platelet
function testing, which is currently restricted to specialised laboratories.
The performance of the RPFT in this study indicates that if it had been used as a pre-test,
the time and labour intensive lumi-aggregometry approach could have been avoided in over one
third of participants in whom no abnormality was detected using the traditional testing. Further
development of the RPFT should include the measurement of glycoprotein receptors and their
function, including GPVI, and platelet procoagulant function, which could improve the sensitivity
of this test and would add to the measurements that are lacking in traditionally available
methodologies [2]. These additions would require extra flow cytometry analyses, but would not
add complexity at the point-of-care.
We conclude that, while the RPFT would not be suitable for the comprehensive diagnosis of
PFDs, due to the limited number of agonists and absence of kinetic information, we believe it has
a role as a pre-test to identify subjects with a potential defect who would benefit from further
detailed platelet phenotyping. In subjects with a minimal history of excessive bleeding, it may also
help to identify those who are unlikely to have a defect in platelet function detectable by lumi-
aggregometry and thus do not require such testing. Further development of the RPFT and
research in the utility of this assay as a first-line screening test in a wider population of individuals
with bleeding symptoms is warranted.
Funding sources: Birmingham-Nottingham Strategic Collaboration Fund, British Heart Foundation
(RG/09/007/27917; PG/10/36/02) and Wellcome Trust (093994).

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Addendum
N. Dovlatova, M. Lordkipanidzé and G. C. Lowe contributed to the concept and design of the
study, collection, analysis and interpretation of data, critical writing and final approval of the
manuscript. B. Dawood and J. May contributed to the collection and analysis of data. S
Heptinstall, S. P. Watson and S. C. Fox contributed to the concept and design of the study, critical
writing and revising the intellectual content and final approval of the version of manuscript to be
published.
Acknowledgements
We would like to thank Dr Paul Harrison for his critical advice on the interpretation of the study
results and for constructive comments on the manuscript. We are also grateful to Milan Fernando
and Marko Benner for their technical support.
Legends
Figure 1. Receiver operating characteristic curves for P-selectin (a) and CD63 (b) expression
measurement with RPFT. Receiver operating characteristic curves demonstrating the relationship
between defects in platelet function as determined by lumi-aggregometry and a) P-selectin and b)
CD63 expression measurements with three conditions of platelet stimulation.
Table. Two-by-two analysis of the agreement between lumi-aggregometry and the RPFT.
«Positive» indicates the presence of an abnormality in platelet function and «negative» indicates
normal platelet responses. PPV and NPV stand for positive and negative predictive values
respectively.

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
Figure 2. Performance of the RPFT in healthy subjects and in participants with platelet function
defects as determined by lumi-aggregometry. a) P-selectin and CD63 measured with RPFT in
healthy volunteers at baseline and after stimulation. For P-selectin cut-offs were 899 (ADP/U4),
991 (TRAP) and 1006 (AA/EPI), and for CD63 – 103 (ADP/U4), 120 (TRAP) and 112,5 (AA/EPI),
expressed as median fluorescence units; b) dense granule secretion defect (the two highlighted
participants are discussed in the text); c) defect in the TxA2 pathway and d) defect in Gi signalling.
Horizontal lines indicate cut-offs determined for each parameter using ROC curve analysis.
Figure 3. Platelet aggregation assessed by LTA in healthy volunteers (filled symbols) and in
patients with a defect in Gi signalling (open symbols). Platelet aggregation was assessed by LTA
in response to ADP (10 and 30μM, final aggregation) and epinephrine (10 and 30μM) in
participants with defect in Gi signalling. Horizontal lines indicate cut-offs determined as 5th
percentile of the corresponding measurement in healthy volunteers.
References
1. Watson SP, Lowe GC, Lordkipanidzé M, Morgan NV; on behalf of the GAPP consortium.
Genotyping and phenotyping of platelet function disorders. J Thromb Haemost 2013; 11 (Suppl 1):
351-63.
2. Quiroga T, Mezzano D. Is my patient a bleeder? A diagnostic framework for mild bleeding
disorders. Hematology Am Soc Hematol Educ Program 2012; 2012: 466-74.
3. Miller JL. Platelet function testing: an improved approach utilizing lumi-aggregation and an
interactive computer system. Am J Clin Pathol 1984; 81: 471-6.
4. Nieuwenhuis HK, Akkerman JW, Sixma JJ. Patients with a prolonged bleeding time and
normal aggregation tests may have storage pool deficiency: studies on one hundred six
patients. Blood 1987; 70: 620-3.

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
5. Dawood BB, Lowe GC, Lordkipanidzé M, Bem D, Daly ME, Makris M, Mumford A, Wilde
JT, Watson SP. Evaluation of participants with suspected heritable platelet function
disorders including recommendation and validation of a streamlined agonist panel. Blood
2012; 120: 5041-9.
6. Quiroga T, Goycoolea M, Panes O, Aranda E, Martínez C, Belmont S, Muñoz B, Zúñiga P,
Pereira J, Mezzano D. High prevalence of bleeders of unknown cause among patients with
inherited mucocutaneous bleeding. A prospective study of 280 patients and 299 controls.
Haematologica. 2007; 92: 357-65.
7. Harrison P, Mackie I, Mumford A, Briggs C, Liesner R, Winter M, Machin S; British Committee
for Standards in Haematology. Guidelines for the laboratory investigation of heritable disorders
of platelet function. Br J Haematol 2011; 155: 30-44.
8. Fox SC, May JA, Heptinstall S. WO 2008107724 A2 University of Nottingham, patent application
number PCT/GB2008/050169, stabilisation of biological cell markers. 2008
9. Rodeghiero F, Tosetto A, Abshire T, Arnold DM, Coller B, James P, Neunert C, Lillicrap D;
ISTH/SSC joint VWF and Perinatal/Pediatric Hemostasis Subcommittees Working Group.
ISTH/SSC bleeding assessment tool: a standardized questionnaire and a proposal for a new
bleeding score for inherited bleeding disorders. J Thromb Haemost 2010; 8: 2063-5.

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
10. Lowe GC, Lordkipanidzé M, Watson SP, on behalf of the UK GAPP study group. Utility of the
ISTH Bleeding Assessment Tool in predicting platelet defects in participants with suspected
inherited platelet function disorders. J Thromb Haemost 2013; 11: 1663-8.
11. Fox SC, May JA, Shah A, Neubert U, Heptinstall S. Measurement of platelet P-selectin for
remote testing of platelet function during treatment with clopidogrel and/or aspirin.
Platelets 2009; 20: 250-9.
12. Lowe GC, Sánchez Guiu I, Chapman O, Rivera J, Lordkipanidzé M, Dovlatova N, Wilde J, Watson
SP, Morgan NV; UK GAPP collaborative. Microsatellite markers as a rapid approach for
autozygosity mapping in Hermansky-Pudlak syndrome: Identification of the second HPS7
mutation in a patient presenting late in life. Thromb Haemost 2013; 109: 766-8.
13. Dell'Angelica EC, Shotelersuk V, Aguilar RC, Gahl WA, Bonifacino JS. Altered trafficking of
lysosomal proteins in Hermansky-Pudlak syndrome due to mutations in the beta 3A subunit of the
AP-3 adaptor. Mol Cell 1999; 3: 11-21.
14. Cattaneo M, Hayward CP, Moffat KA, Pugliano MT, Liu Y, Michelson AD. Results of a
worldwide survey on the assessment of platelet function by light transmission
aggregometry: a report from the platelet physiology subcommittee of the SSC of the ISTH.
J Thromb Haemost 2009; 7: 1029.
Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.
15. Cattaneo M, Cerletti C, Harrison P, Hayward CP, Kenny D, Nugent D, Nurden P, Rao AK,
Schmaier AH, Watson SP, Lussana F, Pugliano MT, Michelson AD. Recommendations for the
Standardization of Light Transmission Aggregometry: A Consensus of the Working Party from the
Platelet Physiology Subcommittee of SSC/ISTH. J Thromb Haemost 2013; 11: 1183-9.

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.

Acc
epte
d A
rtic
le
This article is protected by copyright. All rights reserved.





























