Embed Size (px)
Citation preview
FUNDAMENTAL RESPIRATORY
WORKBOOK
Self Directed Learning Module(12 Hours)
Name: ______________________________________________Place of Work: ______________________________________________
______________________________________________Address ______________________________________________
____________________________________________________________________________________________
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 2
Table of Contents
Introduction ...................................................................................................................................... 3
Learning Outcomes ........................................................................................................................... 3
Module Assessment........................................................................................................................... 3
Module One Anatomy and Physiology of the Lungs ...................................................................... 4
Module Two National/International Guidelines.............................................................................31
Module Three Common Acute and Chronic Disorders of the Airways..............................................32
Module Four Smoking as a Respiratory Disorder (yet to be added) ..............................................38
Module Five Common Medications ..............................................................................................39
Module Six Nursing Assessment / Taking a Health History.........................................................44
Module Seven Ongoing care...........................................................................................................47
Respiratory Fundamentals Self Directed Test....................................................................................48
References ...............................................................................................................................57
Assessment and Feedback, Evaluation Form.....................................................................................58
This symbol links to web pages with reading materials
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 3
Introduction
Welcome to the Fundamental Respiratory Workbook. The aim of this module is to update yourknowledge, skills and understanding of common adult respiratory disorders and the impact these have onthe life of individuals and families. The Workbook aims to address the fundamental knowledge requiredby nurses when caring for adults with common respiratory disorders.
Learning Outcomes
All nurses, regardless of practice setting, are required to work collaboratively with the person withrespiratory disorders such as asthma and chronic obstructive airways pulmonary disease (COPD) toaddress their health needs.
At all stages of life, and at several points across the health continuum, people with chronic respiratorydisorders will require services from nurses in generalist settings such as general practice, diagnosticservices and general medical/surgical services. People with chronic respiratory disorders may also haveco-morbidities requiring identification, treatment and monitoring. All nurses need to be capable ofapplying generic nursing knowledge and skills to meet the health needs of these individuals.
In particular, all nurses should:
• work as part of a larger healthcare multidisciplinary team and understand their role in caring for apatient with chronic respiratory disorders
• practice nursing in a manner that the person with a chronic respiratory disorder determines asculturally safe
• role model the application of the Treaty of Waitangi principles in nursing practice
• assist individuals with (or at risk of developing) chronic respiratory disorders to accessresources/information
• lead or assist community health professionals with prevention initiatives as appropriate
• provide support to families of individuals living with a chronic respiratory disorder
• provide information and education to individuals and community groups
• be engaged in quality activities
• assess and interpret clinical indicators of general health status
• complete documentation of clinical assessment, care, recommendations and evaluation of responseaccurately
Module Assessment
1. Read the fundamental respiratory workbook and complete the self directed learning and questions
2. Return the workbook to the Nurse Educators for marking
3. A Certificate of Completion will be sent to you once you have completed the module and answered allthe questions correctly.
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 4
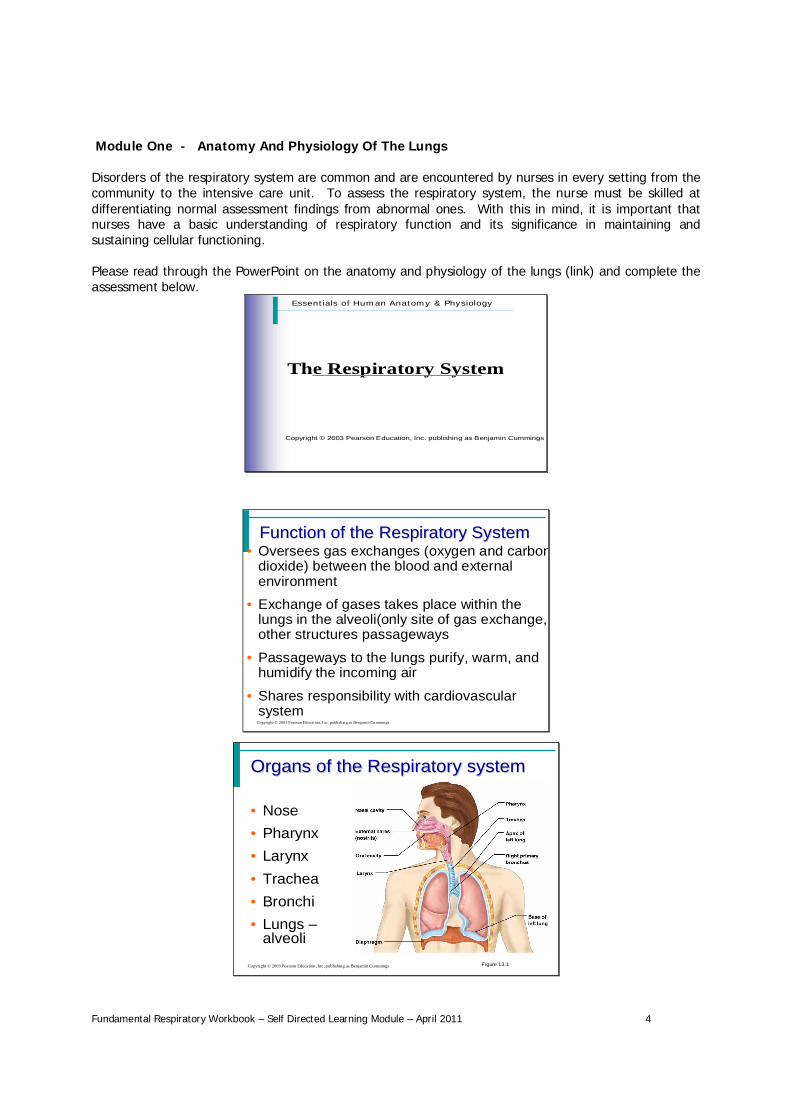
Module One - Anatomy And Physiology Of The Lungs
Disorders of the respiratory system are common and are encountered by nurses in every setting from thecommunity to the intensive care unit. To assess the respiratory system, the nurse must be skilled atdifferentiating normal assessment findings from abnormal ones. With this in mind, it is important thatnurses have a basic understanding of respiratory function and its significance in maintaining andsustaining cellular functioning.
Please read through the PowerPoint on the anatomy and physiology of the lungs (link) and complete theassessment below.
Essentials of Human Anatomy & Physiology
The Respiratory System
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
Function of the Respiratory SystemFunction of the Respiratory System
Copyright © 2003 Pearson Educat ion, Inc. publish ing as Benjamin Cummings
• Oversees gas exchanges (oxygen and carbondioxide) between the blood and externalenvironment
• Exchange of gases takes place within thelungs in the alveoli(only site of gas exchange,other structures passageways
• Passageways to the lungs purify, warm, andhumidify the incoming air
• Shares responsibility with cardiovascularsystem
Organs of the Respiratory systemOrgans of the Respiratory system
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Nose• Pharynx• Larynx• Trachea• Bronchi• Lungs
alveoliFigure 13.1
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 5
Anatomy of the Nasal CavityAnatomy of the Nasal Cavity
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Olfactory receptors are located in themucosa on the superior surface
• The rest of the cavity is lined withrespiratory mucosa• Moistens air
• Traps incoming foreign particles
Pharynx (Throat)Pharynx (Throat)
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Muscular passage from nasal cavity tolarynx
• Three regions of the pharynx• Nasopharynx superior region behind
nasal cavity• Oropharynx middle region behind mouth• Laryngopharynx inferior region attached
to larynx• The oropharynx and laryngopharynx are
common passageways for air and food
Larynx (Voice Box)Larynx (Voice Box)
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Routes air and food into properchannels
• Plays a role in speech
• Made of eight rigid hyaline cartilagesand a spoon-shaped flap of elasticcartilage (epiglottis)
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 6
Trachea (Windpipe)Trachea (Windpipe)
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Connects larynx with bronchi
• Lined with ciliated mucosa• Beat continuously in the opposite direction of
incoming air
• Expel mucus loaded with dust and otherdebris away from lungs
• Walls are reinforced with C-shapedhyaline cartilage
Primary BronchiPrimary Bronchi
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Formed by division of the trachea
• Enters the lung at the hilus(medial depression)
• Right bronchus is wider, shorter,and straighter than left
• Bronchi subdivide into smallerand smaller branches
LungsLungs
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Occupy most of the thoracic cavity• Apex is near the clavicle (superior portion)
• Base rests on the diaphragm (inferiorportion)
• Each lung is divided into lobes by fissures
• Left lung two lobes
• Right lung three lobes
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 7
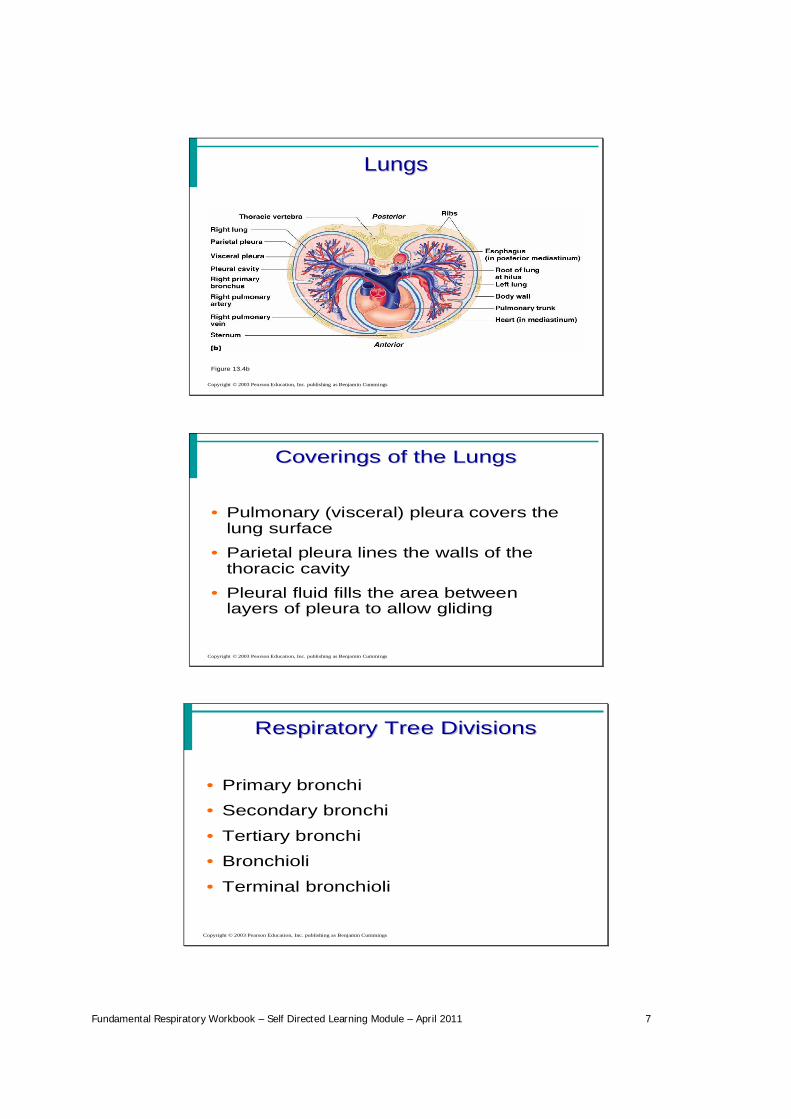
LungsLungs
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
Figure 13.4b
Coverings of the LungsCoverings of the Lungs
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Pulmonary (visceral) pleura covers thelung surface
• Parietal pleura lines the walls of thethoracic cavity
• Pleural fluid fills the area betweenlayers of pleura to allow gliding
Respiratory Tree DivisionsRespiratory Tree Divisions
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Primary bronchi
• Secondary bronchi
• Tertiary bronchi
• Bronchioli
• Terminal bronchioli
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 8
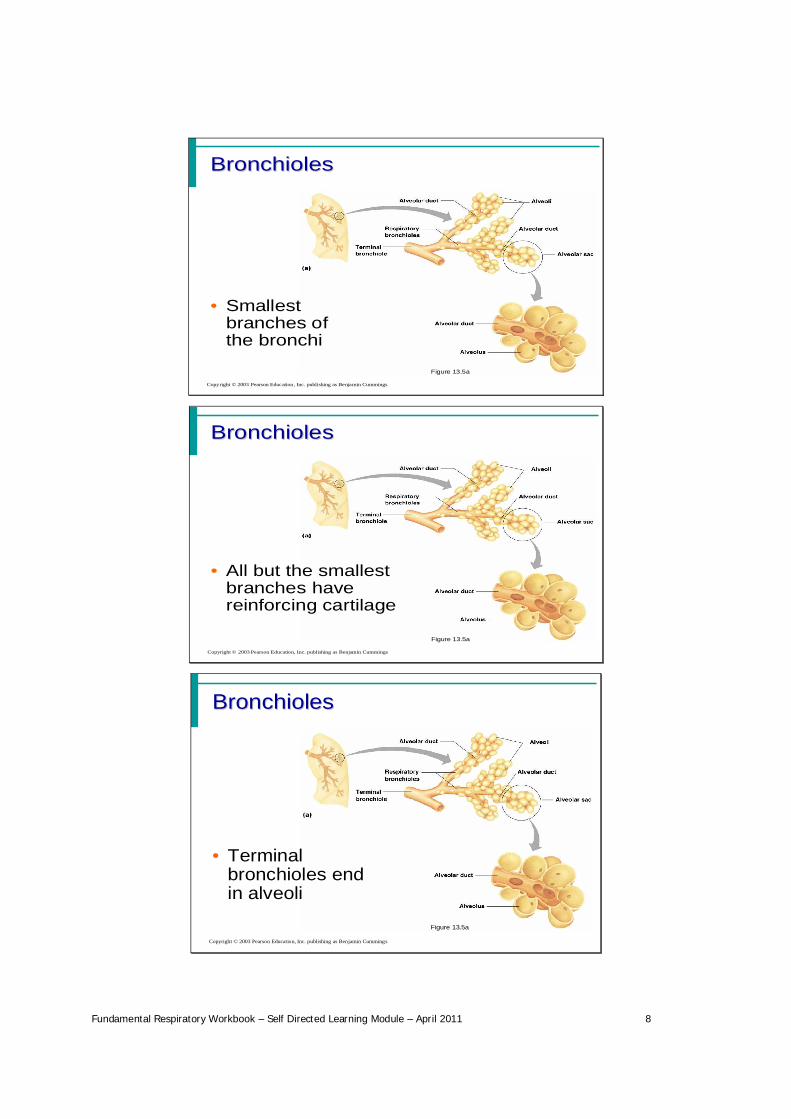
BronchiolesBronchioles
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
Figure 13.5a
• Smallestbranches ofthe bronchi
BronchiolesBronchioles
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
Figure 13.5a
• All but the smallestbranches havereinforcing cartilage
BronchiolesBronchioles
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Terminalbronchioles endin alveoli
Figure 13.5a
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 9
Respiratory ZoneRespiratory Zone
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Structures• Respiratory bronchioli
• Alveolar duct
• Alveoli
• Site of gas exchange
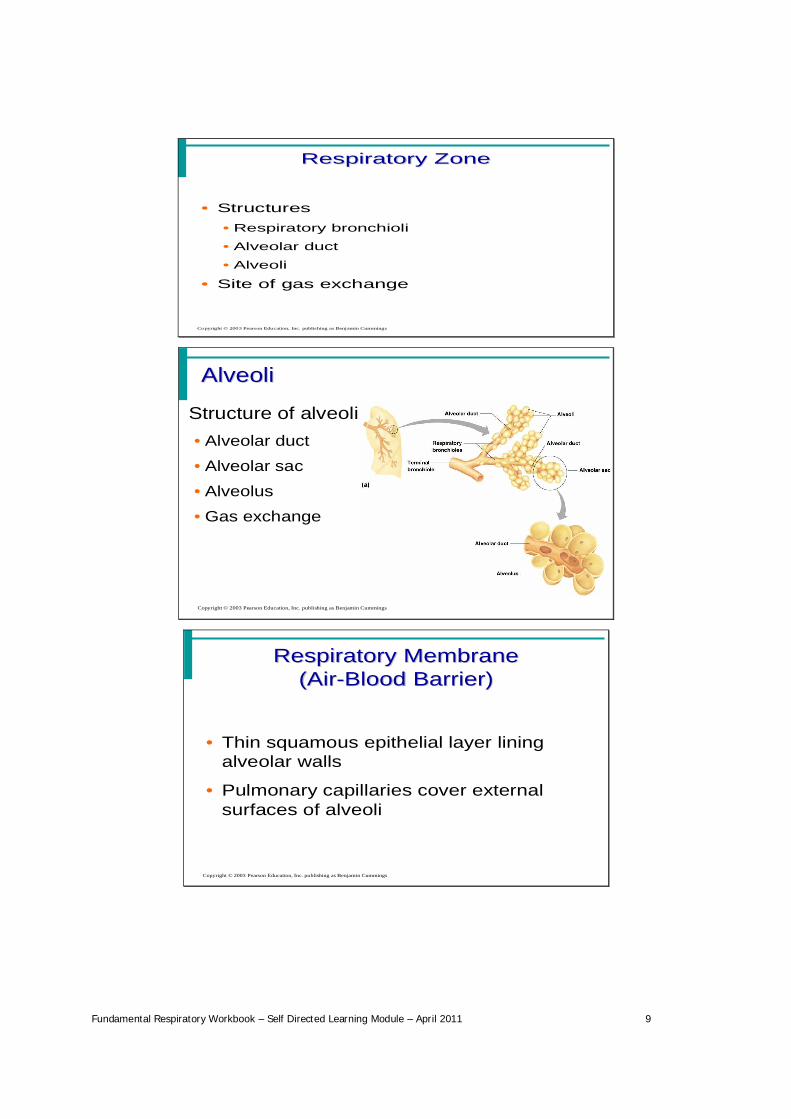
AlveoliAlveoli
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Structure of alveoli• Alveolar duct
• Alveolar sac
• Alveolus
• Gas exchange
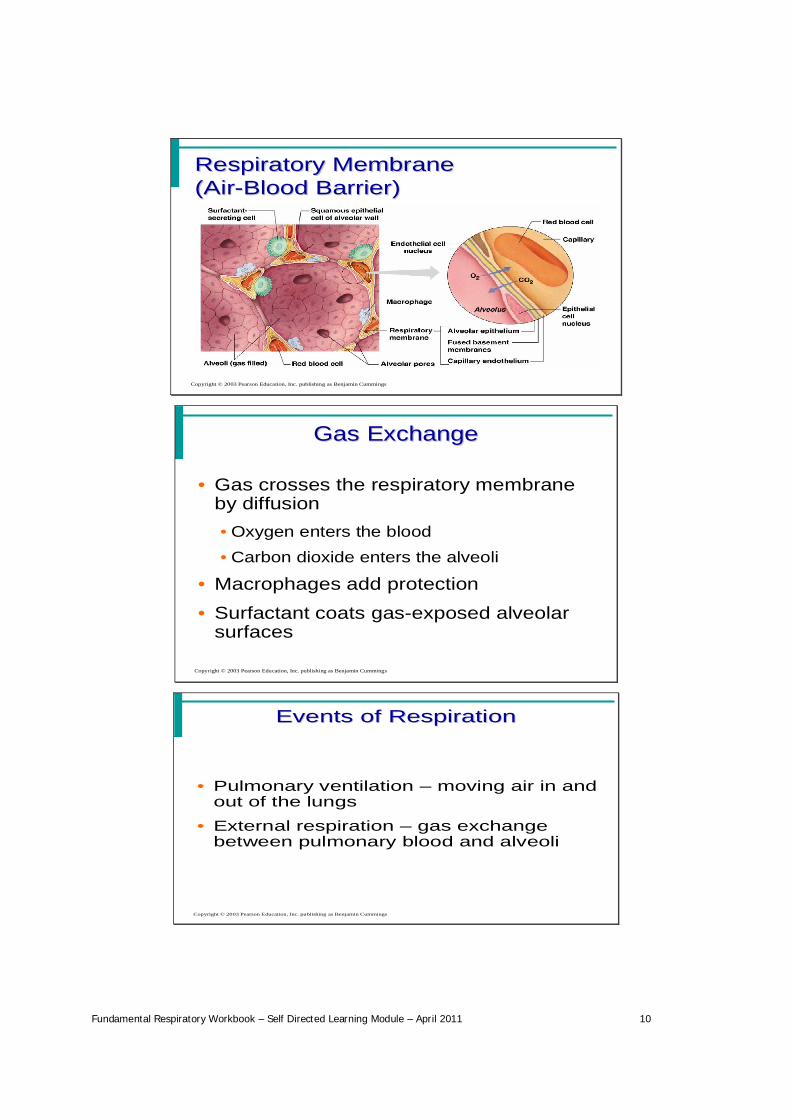
Respiratory MembraneRespiratory Membrane(Air(Air--Blood Barrier)Blood Barrier)
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Thin squamous epithelial layer liningalveolar walls
• Pulmonary capillaries cover externalsurfaces of alveoli
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 10
Respiratory MembraneRespiratory Membrane(Air(Air--Blood Barrier)Blood Barrier)
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
Gas ExchangeGas Exchange
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Gas crosses the respiratory membraneby diffusion•Oxygen enters the blood
•Carbon dioxide enters the alveoli
• Macrophages add protection
• Surfactant coats gas-exposed alveolarsurfaces
Events of RespirationEvents of Respiration
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Pulmonary ventilation moving air in andout of the lungs
• External respiration gas exchangebetween pulmonary blood and alveoli
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 11
Events of RespirationEvents of Respiration
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Respiratory gas transport transport ofoxygen and carbon dioxide via thebloodstream
• Internal respiration gas exchangebetween blood and tissue cells insystemic capillaries
Mechanics of BreathingMechanics of Breathing(Pulmonary Ventilation)(Pulmonary Ventilation)
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Completely mechanical process
• Depends on volume changes in thethoracic cavity
• Volume changes lead to pressurechanges, which lead to the flow ofgases to equalise pressure
Mechanics of BreathingMechanics of Breathing(Pulmonary Ventilation)(Pulmonary Ventilation)
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Two phases• Inspiration flow of air into lung• Expiration air leaving lung
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 12
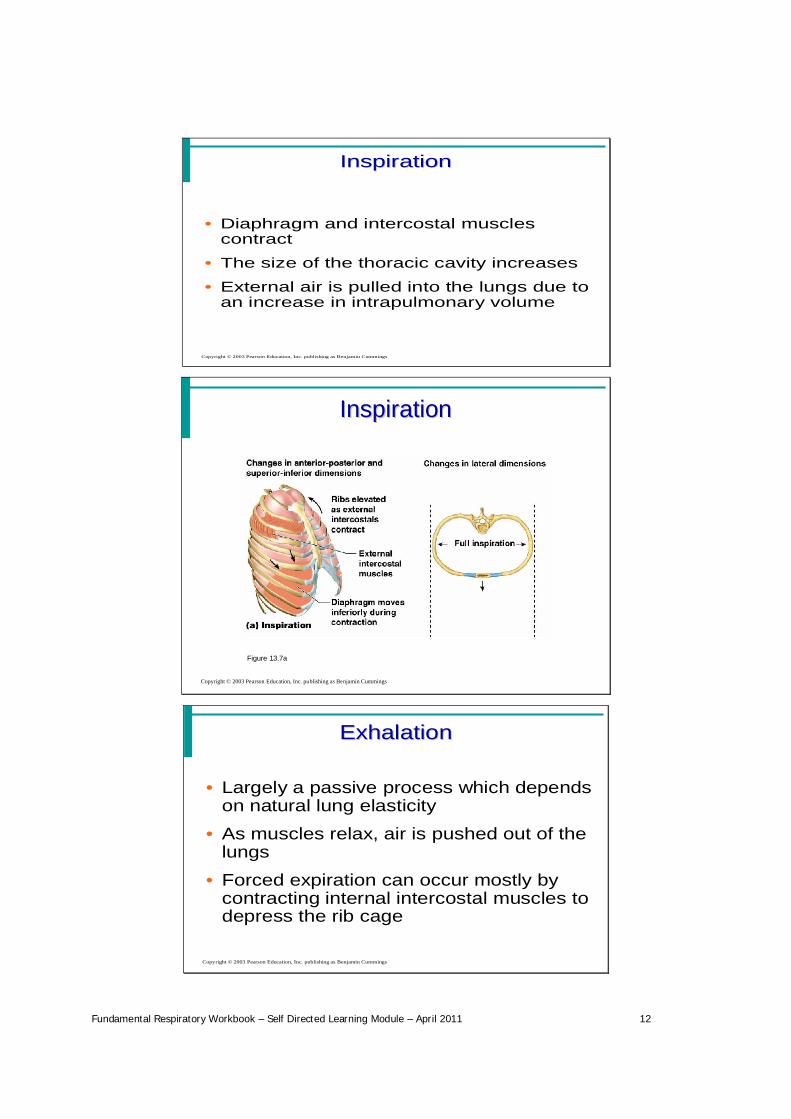
InspirationInspiration
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Diaphragm and intercostal musclescontract
• The size of the thoracic cavity increases
• External air is pulled into the lungs due toan increase in intrapulmonary volume
InspirationInspiration
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
Figure 13.7a
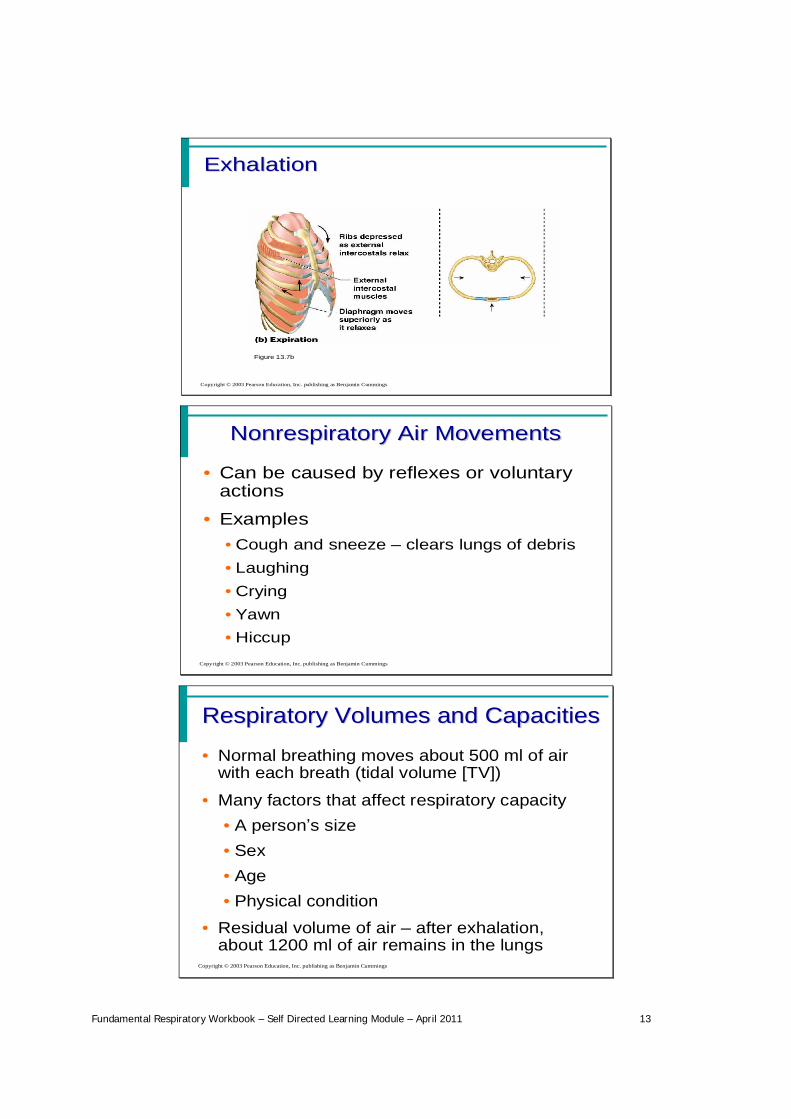
ExhalationExhalation
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Largely a passive process which dependson natural lung elasticity
• As muscles relax, air is pushed out of thelungs
• Forced expiration can occur mostly bycontracting internal intercostal muscles todepress the rib cage
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 13
ExhalationExhalation
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
Figure 13.7b
NonrespiratoryNonrespiratory Air MovementsAir Movements
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Can be caused by reflexes or voluntaryactions
• Examples•Cough and sneeze clears lungs of debris•Laughing•Crying•Yawn•Hiccup
Respiratory Volumes and CapacitiesRespiratory Volumes and Capacities
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Normal breathing moves about 500 ml of airwith each breath (tidal volume [TV])
• Many factors that affect respiratory capacity• A person s size• Sex• Age• Physical condition
• Residual volume of air after exhalation,about 1200 ml of air remains in the lungs
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 14
Respiratory Volumes and CapacitiesRespiratory Volumes and Capacities
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Inspiratory reserve volume (IRV)• Amount of air that can be taken in forcibly
over the tidal volume
• Usually between 2100 and 3200 ml
• Expiratory reserve volume (ERV)• Amount of air that can be forcibly exhaled
• Approximately 1200 ml
Respiratory Volumes and CapacitiesRespiratory Volumes and Capacities
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Residual volume• Air remaining in lung after expiration• About 1200 ml
Respiratory Volumes and CapacitiesRespiratory Volumes and Capacities
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Vital capacity• The total amount of exchangeable air• Vital capacity = TV + IRV + ERV• Dead space volume
• Air that remains in conducting zone andnever reaches alveoli
• About 150 ml
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 15
Respiratory Volumes and CapacitiesRespiratory Volumes and Capacities
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Functional volume• Air that actually reaches the respiratory
zone
• Usually about 350 ml
• Respiratory capacities are measuredwith a spirometer
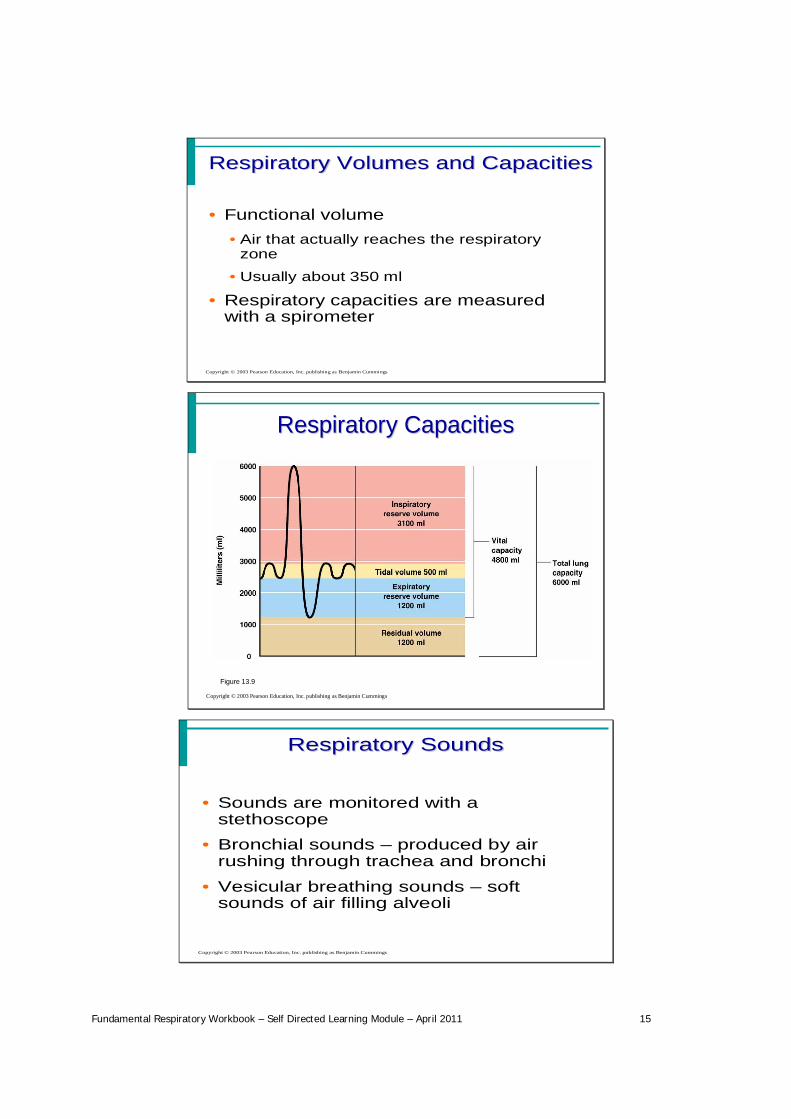
Respiratory CapacitiesRespiratory Capacities
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
Figure 13.9
Respiratory SoundsRespiratory Sounds
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Sounds are monitored with astethoscope
• Bronchial sounds produced by airrushing through trachea and bronchi
• Vesicular breathing sounds softsounds of air filling alveoli
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 16
External RespirationExternal Respiration
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Oxygen movement into the blood• The alveoli always has more oxygen than
the blood
• Oxygen moves by diffusion towards thearea of lower concentration
• Pulmonary capillary blood gains oxygen
External RespirationExternal Respiration
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Carbon dioxide movement out of theblood• Blood returning from tissues has higher
concentrations of carbon dioxide than air inthe alveoli
• Pulmonary capillary blood gives up carbondioxide
• Blood leaving the lungs is oxygen-richand carbon dioxide-poor
Gas Transport in the BloodGas Transport in the Blood
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Oxygen transport in the blood• Inside red blood cells attached to
hemoglobin (oxyhemoglobin [HbO2])
• A small amount is carried dissolved in theplasma
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 17
Gas Transport in the BloodGas Transport in the Blood
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
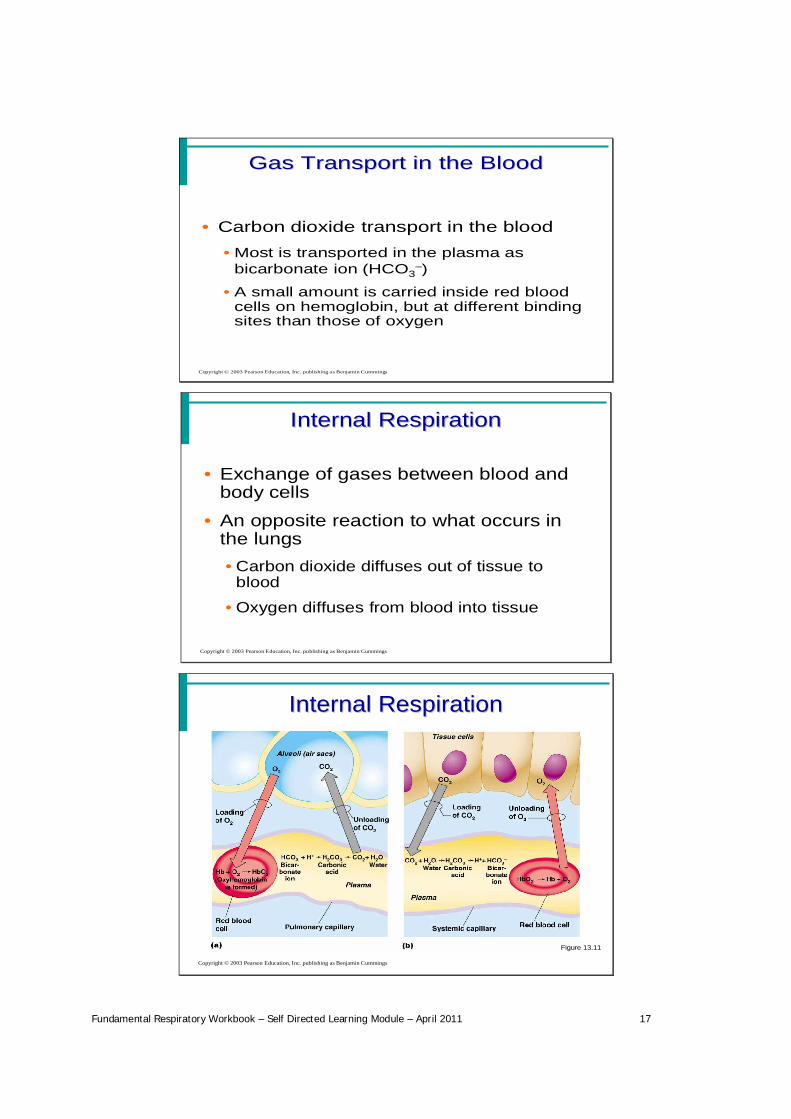
• Carbon dioxide transport in the blood• Most is transported in the plasma as
bicarbonate ion (HCO3 )
• A small amount is carried inside red bloodcells on hemoglobin, but at different bindingsites than those of oxygen
Internal RespirationInternal Respiration
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Exchange of gases between blood andbody cells
• An opposite reaction to what occurs inthe lungs•Carbon dioxide diffuses out of tissue to
blood
•Oxygen diffuses from blood into tissue
Internal RespirationInternal Respiration
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
Figure 13.11
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 18
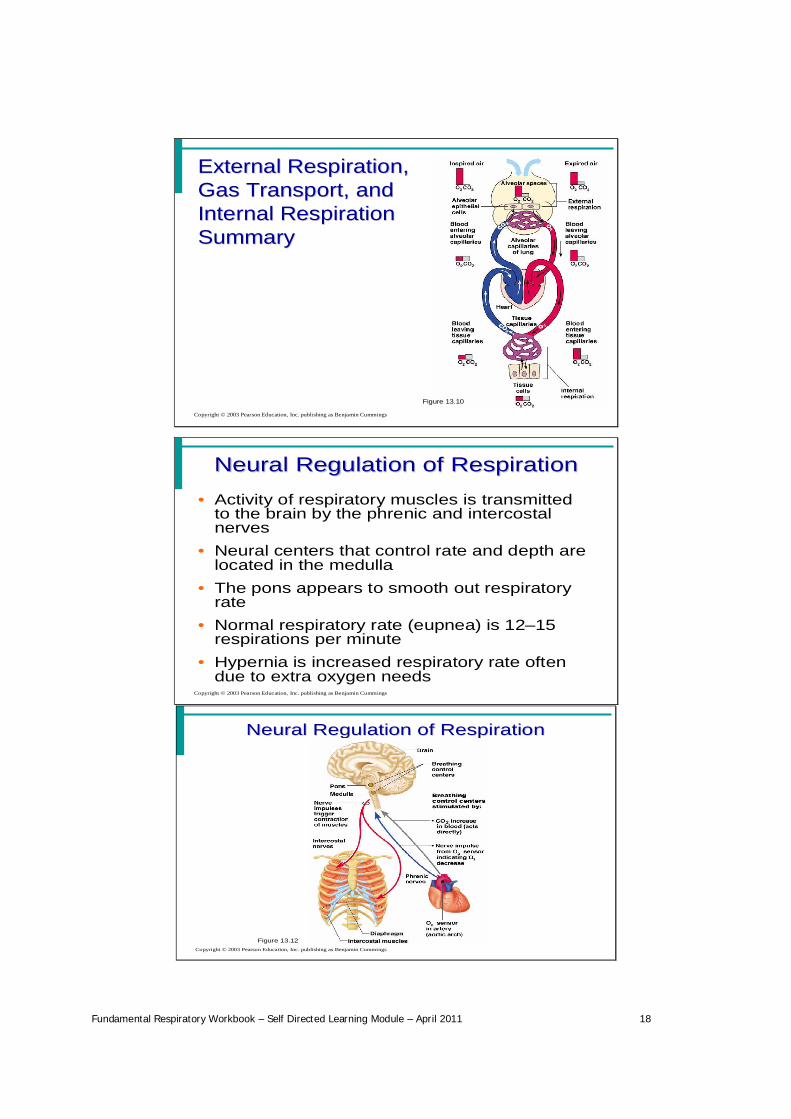
External Respiration,External Respiration,Gas Transport, andGas Transport, andInternal RespirationInternal RespirationSummarySummary
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
Figure 13.10
Neural Regulation of RespirationNeural Regulation of Respiration
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Activity of respiratory muscles is transmittedto the brain by the phrenic and intercostalnerves
• Neural centers that control rate and depth arelocated in the medulla
• The pons appears to smooth out respiratoryrate
• Normal respiratory rate (eupnea) is 12 15respirations per minute
• Hypernia is increased respiratory rate oftendue to extra oxygen needs
Neural Regulation of RespirationNeural Regulation of Respiration
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
Figure 13.12
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 19
Factors Influencing RespiratoryFactors Influencing RespiratoryRate and DepthRate and Depth
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Chemical factors• Carbon dioxide levels
• Level of carbon dioxide in the blood is themain regulatory chemical for respiration
• Increased carbon dioxide increasesrespiration
• Changes in carbon dioxide act directly onthe medulla oblongata
Factors Influencing RespiratoryFactors Influencing RespiratoryRate and DepthRate and Depth
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Chemical factors (continued)• Oxygen levels
• Changes in oxygen concentration in theblood are detected by chemoreceptors inthe aorta and carotid artery
• Information is sent to the medulla oblongata
Respiratory Disorders: ChronicRespiratory Disorders: ChronicObstructive Pulmonary DiseaseObstructive Pulmonary Disease
(COPD)(COPD)
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
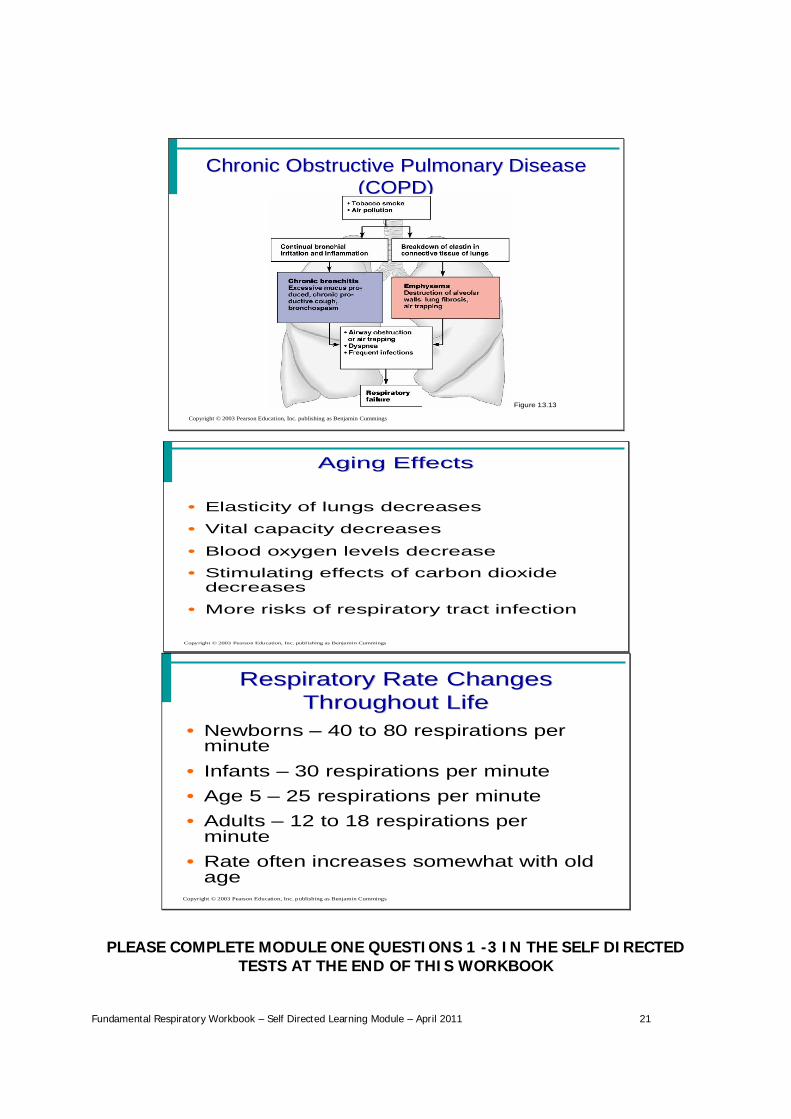
• Exemplified by chronic bronchitis andemphysema
• Major causes of death and disability inthe United States
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 20
Respiratory Disorders: ChronicRespiratory Disorders: ChronicObstructive Pulmonary DiseaseObstructive Pulmonary Disease
(COPD)(COPD)
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Features of these diseases• Patients almost always have a history of
smoking
• Labored breathing (dyspnea) becomesprogressively more severe
• Coughing and frequent pulmonaryinfections are common
EmphysemaEmphysema
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Alveoli enlarge as adjacent chambers breakthrough
• Chronic inflammation promotes lung fibrosis• Airways collapse during expiration• Patients use a large amount of energy to
exhale• Overinflation of the lungs leads to a
permanently expanded barrel chest• Cyanosis appears late in the disease
Chronic BronchitisChronic Bronchitis
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Mucosa of the lower respiratorypassages becomes severely inflamed
• Mucus production increases• Pooled mucus impairs ventilation and
gas exchange• Risk of lung infection increases• Pneumonia is common• Hypoxia and cyanosis occur early
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 21
Chronic Obstructive Pulmonary DiseaseChronic Obstructive Pulmonary Disease(COPD)(COPD)
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
Figure 13.13
Aging EffectsAging Effects
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Elasticity of lungs decreases
• Vital capacity decreases
• Blood oxygen levels decrease• Stimulating effects of carbon dioxide
decreases
• More risks of respiratory tract infection
Respiratory Rate ChangesRespiratory Rate ChangesThroughout LifeThroughout Life
Copyright © 2003 Pearson Education, Inc. publishing as Benjamin Cummings
• Newborns 40 to 80 respirations perminute
• Infants 30 respirations per minute• Age 5 25 respirations per minute• Adults 12 to 18 respirations per
minute• Rate often increases somewhat with old
age
PLEASE COMPLETE MODULE ONE QUESTIONS 1 -3 IN THE SELF DIRECTEDTESTS AT THE END OF THIS WORKBOOK
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 22
Module Two - National/International Guidelines
The New Zealand Diagnosis and Treatment of Adult Asthma Guidelines (2002) states that:
“The purpose of the Guidelines is to provide an evidence-based summary of the diagnosticmanagement and treatment options available for asthma in the adult population of New Zealand.This Guideline seeks to assist adults with asthma and their healthcare providers to evaluate thelatest evidence and make informed decisions to improve health outcomes.”
Therefore the Guidelines are an essential tool on which to base the treatment and management of theadult with asthma. It is important, as a healthcare provider, that the registered nurse has knowledge ofand an understanding of how to access and use the Guidelines.
Please click on the link below to access the New Zealand Guidelines and open the folder marked NewZealand Guidelines Group
www.asthmanz.co.nz/nz_guidelines
Read Sections 4 and 5 – Diagnosis of Asthma.
Click on the link below to access the GINA Asthma Pocket Guide.
http://www.ginasthma.com/download.asp?filename=GINA_PG_2010.pdf
Please complete Module Two Questions 1 - 4 relating to the guidelines mentioned above
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 23
Module Three - Common Acute And Chronic Disorders Of The Airways
Please read the following articles
articles\Asthma IQ.pdf
articles\Coping with COPD.pdf
Differentiating between Asthma and Chronic Obstructive Pulmonary Disease (COPD)
Although challenging, it is important to be able to differentiate between asthma and COPD so treatmentcan be managed appropriately and optimised to allow the best outcome for the patient. Although bothare associated with chronic inflammation of the respiratory tract, the inflammatory cells and mediatorsinvolved in the disease process differ significantly even though many of the presenting symptoms, such ascough and shortness of breath are similar (Medscape: 2010).
Please read through the case study below downloaded 03/02/11 fromwww.medscape.org./viewarticle/72544
Nicola A. Hanania, MD, MS
This is the case of Debra, who is a 55-year-old woman who presents with shortness of breath over thelast 2 years. She noticed a recent limitation in her exercise tolerance especially when she plays golf.Previously she used to walk while golfing, but now she has to use a golf cart to get around the course.
Debra has also been having daily morning cough with some sputum production but denies any wheezing.As a child, Debra had several episodes of "bronchitis," and three years ago she was told she had a touchof asthma. She was given an inhaler to use when needed, but has not been taking any regularmedications. Her medical history is notable for allergies, hypertension, and osteoporosis. Herhypertension is controlled by salt restriction, and she does not currently require treatment for herallergies. Of note, Debra used to be a heavy smoker, smoking approximately one pack a day for 20years, but stopped five years ago. Her mom had diabetes and died from heart failure at age of 70, andher father had lung cancer and died from lung cancer. Both her mom and dad were also heavy smokers.
On physical examination, Debra is not in any distress. She has some decreased breath sounds and somescattered wheezing, but otherwise her examination is unremarkable.
Medscape: In the case of Debra, how would a clinician go about distinguishing whether shehas a diagnosis of COPD or asthma?

Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 24
Dr. Hanania
Debra's case is actually fairly common and is very characteristic of COPD. However, we as clinicians hadfor many years the tendency to label a woman presenting with symptoms such as Debra's as havingasthma rather than COPD because we erroneously thought of COPD as a disease limited to old men. Nowwe know that that is not correct. Debra's onset of symptoms has largely occurred later in life. She ismiddle-aged, and her heavy smoking history should tip off the clinician to the possibility of a diagnosis ofCOPD. Certainly her history of "bronchitis" as a child and allergies should also trigger a potential diagnosisof asthma.
So, by history alone, it is sometimes hard to confirm a diagnosis of COPD. Items that favour COPD inDebra's history are the age of onset of her symptoms and the progressive nature of her symptoms,including the cough and the sputum. If Debra were a 20-year-old woman when her symptoms developed,we would be less suspicious of a diagnosis of COPD. COPD symptoms rarely start in individuals who areless than 40 years of age, although certainly loss of lung function may be occurring before then. Sosymptom onset during middle age in this patient who was a heavy smoker favours a diagnosis of COPD.Could she have had asthma as a child? Sure, she could have had asthma, and in fact people with asthmaare not immune from getting COPD if they are heavy smokers. In fact, some epidemiologic studiessuggest that those with asthma may be at higher risk for COPD developing if they are exposed to smokethan the general population, although this remains a controversial issue.[2]
Another fact that may help a clinician differentiate between asthma and COPD is obviously the longsmoking history. Not to say that people with asthma don't smoke -- in fact about one quarter of thosewith asthma have a history of smoking [3] -- but the heavy smoking history usually favours a diagnosis ofCOPD. In general, a smoking history of greater than 20 pack-years favours the possibility of COPD.However, one has to keep in mind that 10%-20% of patients with COPD do not report smoking history, afact that makes the diagnosis more difficult to confirm.[1]
Loss of exercise tolerance and activity limitation can be seen in patients with either COPD or asthma;however, the progressive nature of her symptoms favours COPD. Patients with asthma usually reportepisodic symptoms, with wheezing and cough. Debra is having daily cough and sputum, and this isclassic of what we see in smokers with the chronic bronchitis form of COPD.
However, if a patient reports symptoms starting in childhood or early in life and if a history of allergies ora family history of asthma is present, a diagnosis of asthma may be favoured. Certainly, triggers ofasthma are usually prominent in such a case and these include environmental exposures such indoor andoutdoor allergen exposures as well as exposure to irritants such as environmental tobacco smoke.[4]
Obviously, not every patient who reports shortness of breath or exercise limitation has asthma or COPD;there are other potential diagnoses that need to be considered (Figure 1). Being a pulmonologist, I alwaysthink about lung disease first. But one should always rule out the presence of cardiac disease such asheart failure because it can also present with shortness of breath on exercise. However, it's sometimesvery hard to completely be sure, and further workup of the patient, including a physical examination andlung function tests like spirometry, is usually needed.

Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 25
Figure 1. Diagnoses associated with chronic dyspnea. COPD = chronic obstructive pulmonary disease
Medscape: Many myths exist surrounding the use of spirometry in the diagnosis of asthmaand COPD. Could you discuss its use in confirming a diagnosis of asthma and COPD?
Dr. Hanania: Both asthma and COPD are obstructive airway diseases, which can be demonstrated withspirometry. Therefore, the presence of airway obstruction does not favour a diagnosis of one over theother.[5]
Often we talk about a patient's acute bronchodilator response when doing spirometry. In the past, wethought that a patient's significant bronchodilator response -- that is, having significant reversible airwayobstruction (change in FEV1 by 12% and 200 mL from baseline) -- confirmed a diagnosis of asthma andruled out COPD.[1] However, we now know that this is not accurate and that it may lead to underdiagnosis of many patients with COPD. Studies have now demonstrated that acute bronchodilatorreversibility does not really help differentiate asthma from COPD because a substantial number of patientswith COPD may actually demonstrate acute bronchodilator response.[6] A postbronchodilator FEV1/FVCratio of < 0.7 favours the diagnosis of COPD.[1] In Debra's case, spirometry revealed a predicted FEV1 of60% and FEV1/FVC of 0.56 but did not demonstrate significant acute bronchodilator reversibility. In fact,her response after the bronchodilator decreased by 8%, which is in line with a diagnosis of COPD.However, to be clear, even if Debra had a significant postbronchodilator response to Salbutamol, thiswould not have ruled out a diagnosis of COPD.
The point here is the diagnostic implication using spirometry. Yes, it is important, so why do we dospirometry here for both asthma and COPD? We do spirometry to confirm airway obstruction but also tostage the disease. We don't do it to differentiate asthma and COPD. Staging asthma and COPD severity isvery important to guide management of both these diseases.
Medscape: Debra received a diagnosis of moderate (stage II) COPD and was started on long-acting beta-agonists. How would Debra's treatment plan have differed if she had received adual diagnosis of asthma and COPD?
Dr. Hanania: Debra was diagnosed with moderate disease on the basis of her history and spirometryvalue. Current guidelines advocate using inhaled long-acting bronchodilators (e.g., long-acting beta 2-agonists or anticholinergics) as first-line therapy in such a case.
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 26
On the other hand, if her diagnosis was asthma, inhaled corticosteroids should be considered as first-linetreatment of her disease and these should be instituted as early as possible in all patients with mild-to-persistent disease.[7] The response to inhaled steroids in asthma and COPD is different based on the factthat airway inflammation in asthma is generally eosinophilic in nature (steroid responsive) whileneutrophils play a major role in airway inflammation in COPD and the response to inhaled steroids is notas significant.
Although there is a major role for inhaled corticosteroids in COPD, they are usually added onto a long-acting bronchodilator.[1] Therefore, a major distinction between asthma and COPD regarding therapy isthat in asthma the platform for treatment is inhaled corticosteroids; then one should consider adding thelong-acting beta 2-agonists if the patient doesn't adequately respond to inhaled corticosteroids alone.[5] InCOPD, the platform for treatment is an inhaled long-acting bronchodilator, and inhaled corticosteroids areusually advocated in patients with severe disease, like those with an FEV1 of < 50% and in those patientswith history of recurrent exacerbations.[1]
However, if a clinician cannot easily differentiate between asthma and COPD in a patient, currentguidelines suggest treating such a patient as a case of asthma and advocate using inhaled corticosteroidsearly.[1] In the case of Debra, we have the confirmation that she has moderate COPD and thus it is notunreasonable to start treating her with an inhaled long-acting bronchodilator. However, on follow-up, ifshe starts experiencing flare-ups (i.e., exacerbations), then we should consider adding an inhaledcorticosteroid to her long-acting bronchodilator at that point.
Medscape: What other strategies should clinicians use to reduce the patient's risk forexacerbation and/or hospitalisation?
Dr. Hanania: In Debra's case, she had stopped smoking. If she hadn't, that would have been the firstand most important thing that we would have worked on. Debra also needs to be educated to avoidsecond-hand exposure to smoke and to any irritants to her airway.
Respiratory infections are very important triggers for exacerbations and even hospitalizations in patientswith COPD. We thus advocate that all patients with COPD get vaccinated against the flu every year andagainst pneumococcal pneumonia once every 7-10 years.
Treatment-wise, drugs that have been demonstrated to reduce exacerbations include long-actingbronchodilator medications such as tiotropium or long-acting beta 2-agonists (LABAs) and thecombination of an inhaled corticosteroid with a long-acting beta-agonist.[1]
Debra also needs to maintain a good exercise program. She is golfing right now, but she's minimizing heractivity because of her symptoms. Hopefully, with initiating her treatment her activity level will increase.We encourage all patients with COPD to continue being active, such as walking and other daily exercise.In patients who are severely limited, we refer them for pulmonary rehabilitation, which can improveexercise tolerance and quality of life and decreases their symptoms.
Other avenues that also need to be considered are nutritional and dietary counselling. Unfortunately,muscle wasting and nutritional depletion is not uncommon in COPD. Whereas improving or optimizingnutrition may help in some, it may be ineffective in patients with severe muscle wasting; it's really hard tobring that back, even by giving them nutritional supplementation.
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 27
A very important component in the management of both asthma and COPD is to remember to educatepatients about their disease. Numerous studies demonstrate the benefits of building up patients' self-management techniques (meaning to educate them about what they should expect with their disease,how to use their inhaler device, why they are sick, and what happened to their airway) in improvingpatient outcomes.[1] Educating them about recognizing exacerbation symptoms is also very important; ifthey start coughing more or start producing different-coloured sputum or getting more short of breathbeyond the day-to-day changes that they usually have, they need to give their clinician a call.
Unfortunately, many patients underreport their exacerbations because they don't know what anexacerbation is, a fact that further deteriorates their quality of life.[8]
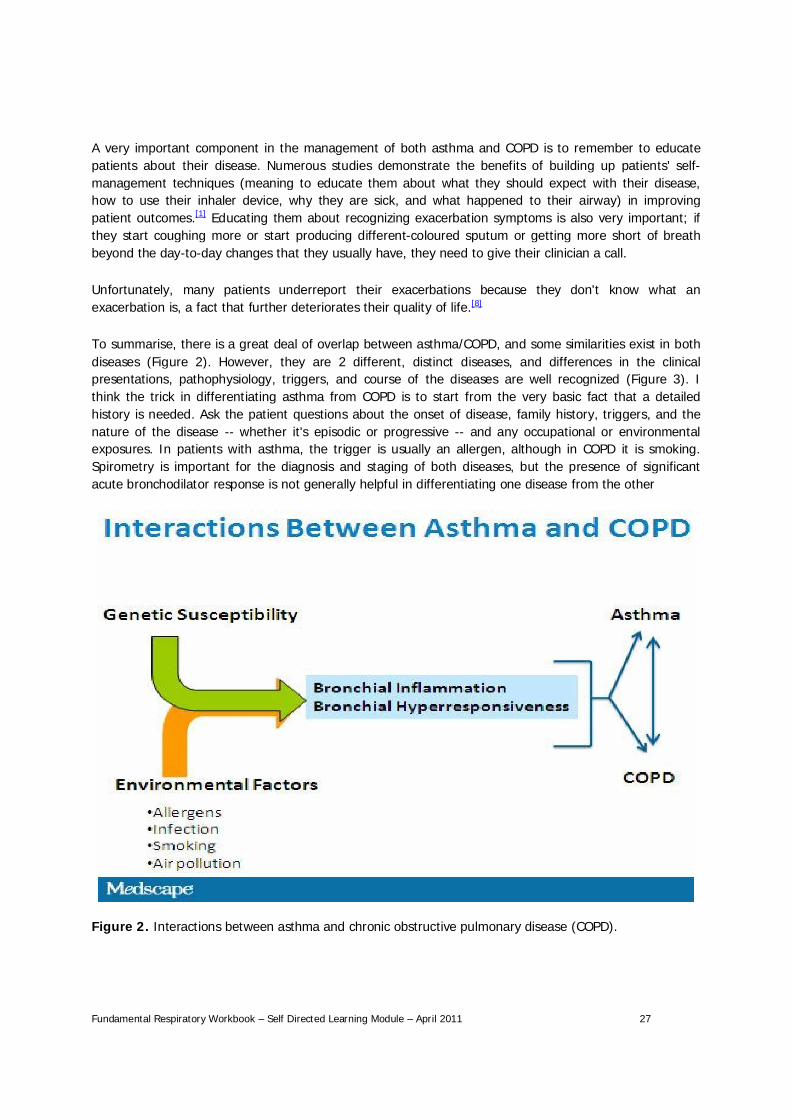
To summarise, there is a great deal of overlap between asthma/COPD, and some similarities exist in bothdiseases (Figure 2). However, they are 2 different, distinct diseases, and differences in the clinicalpresentations, pathophysiology, triggers, and course of the diseases are well recognized (Figure 3). Ithink the trick in differentiating asthma from COPD is to start from the very basic fact that a detailedhistory is needed. Ask the patient questions about the onset of disease, family history, triggers, and thenature of the disease -- whether it's episodic or progressive -- and any occupational or environmentalexposures. In patients with asthma, the trigger is usually an allergen, although in COPD it is smoking.Spirometry is important for the diagnosis and staging of both diseases, but the presence of significantacute bronchodilator response is not generally helpful in differentiating one disease from the other
Figure 2. Interactions between asthma and chronic obstructive pulmonary disease (COPD).
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 28
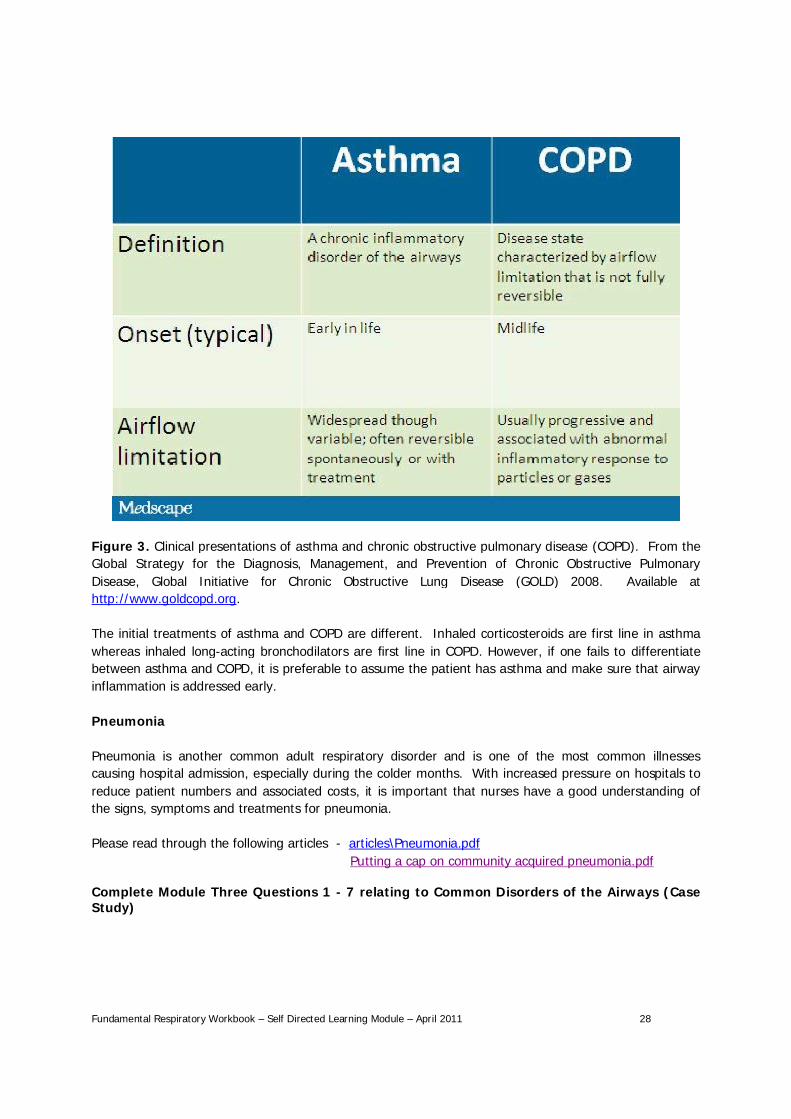
Figure 3. Clinical presentations of asthma and chronic obstructive pulmonary disease (COPD). From theGlobal Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive PulmonaryDisease, Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2008. Available athttp://www.goldcopd.org.
The initial treatments of asthma and COPD are different. Inhaled corticosteroids are first line in asthmawhereas inhaled long-acting bronchodilators are first line in COPD. However, if one fails to differentiatebetween asthma and COPD, it is preferable to assume the patient has asthma and make sure that airwayinflammation is addressed early.
Pneumonia
Pneumonia is another common adult respiratory disorder and is one of the most common illnessescausing hospital admission, especially during the colder months. With increased pressure on hospitals toreduce patient numbers and associated costs, it is important that nurses have a good understanding ofthe signs, symptoms and treatments for pneumonia.
Please read through the following articles - articles\Pneumonia.pdfPutting a cap on community acquired pneumonia.pdf
Complete Module Three Questions 1 - 7 relating to Common Disorders of the Airways (CaseStudy)

Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 29
Module Four - Smoking as a Respiratory Disorder (yet to be added)
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 30
Module Five - Common Medications
Medications play a vital role in helping patients with disorders of the airways to manage symptoms andmaintain control of the disorder. The type of medication prescribed will depend of the type and severityof the disorder and the effect it has on the day to day functioning of the patient. Please read through thefollowing section on respiratory medications prepared by the WDHB Pharmacy.
Respiratory Medications
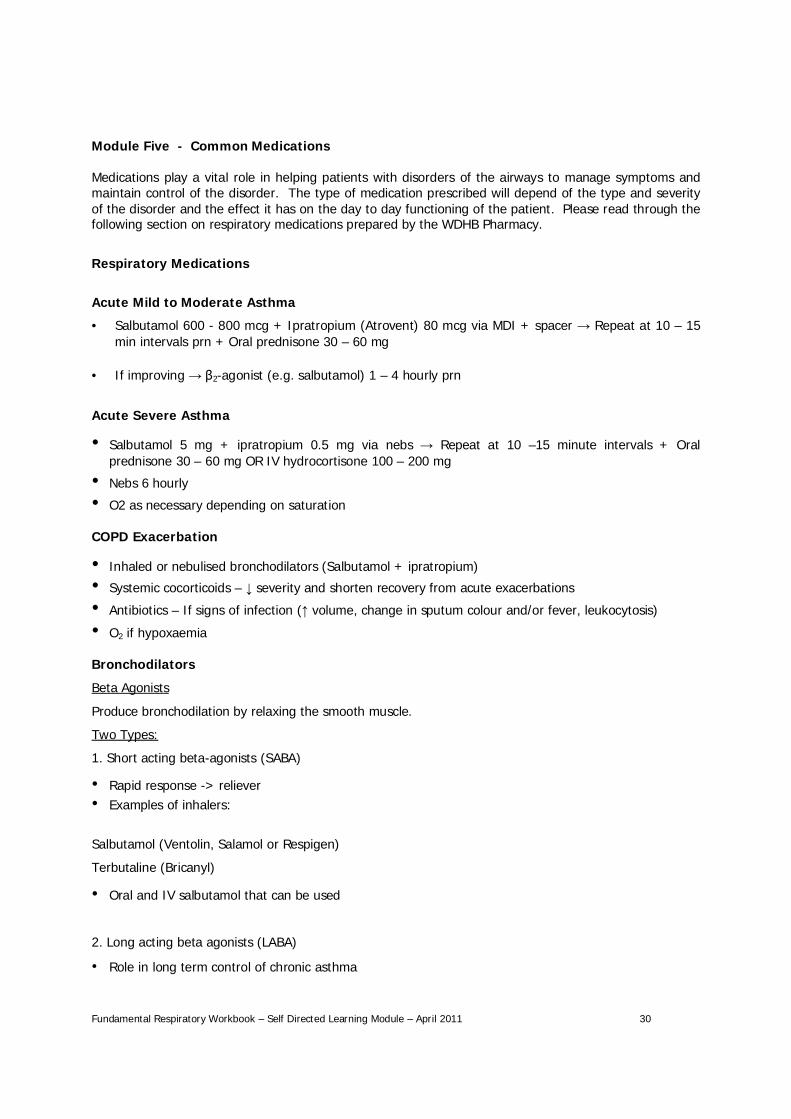
Acute Mild to Moderate Asthma
• Salbutamol 600 - 800 mcg + Ipratropium (Atrovent) 80 mcg via MDI + spacer Repeat at 10 – 15min intervals prn + Oral prednisone 30 – 60 mg
• If improving 2-agonist (e.g. salbutamol) 1 – 4 hourly prn
Acute Severe Asthma
Salbutamol 5 mg + ipratropium 0.5 mg via nebs Repeat at 10 –15 minute intervals + Oralprednisone 30 – 60 mg OR IV hydrocortisone 100 – 200 mg
Nebs 6 hourly
O2 as necessary depending on saturation
COPD Exacerbation
Inhaled or nebulised bronchodilators (Salbutamol + ipratropium)
Systemic cocorticoids – severity and shorten recovery from acute exacerbations
Antibiotics – If signs of infection ( volume, change in sputum colour and/or fever, leukocytosis)
O2 if hypoxaemia
Bronchodilators
Beta Agonists
Produce bronchodilation by relaxing the smooth muscle.
Two Types:
1. Short acting beta-agonists (SABA)
Rapid response -> relieverExamples of inhalers:
Salbutamol (Ventolin, Salamol or Respigen)
Terbutaline (Bricanyl)
Oral and IV salbutamol that can be used
2. Long acting beta agonists (LABA)
Role in long term control of chronic asthma
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 31
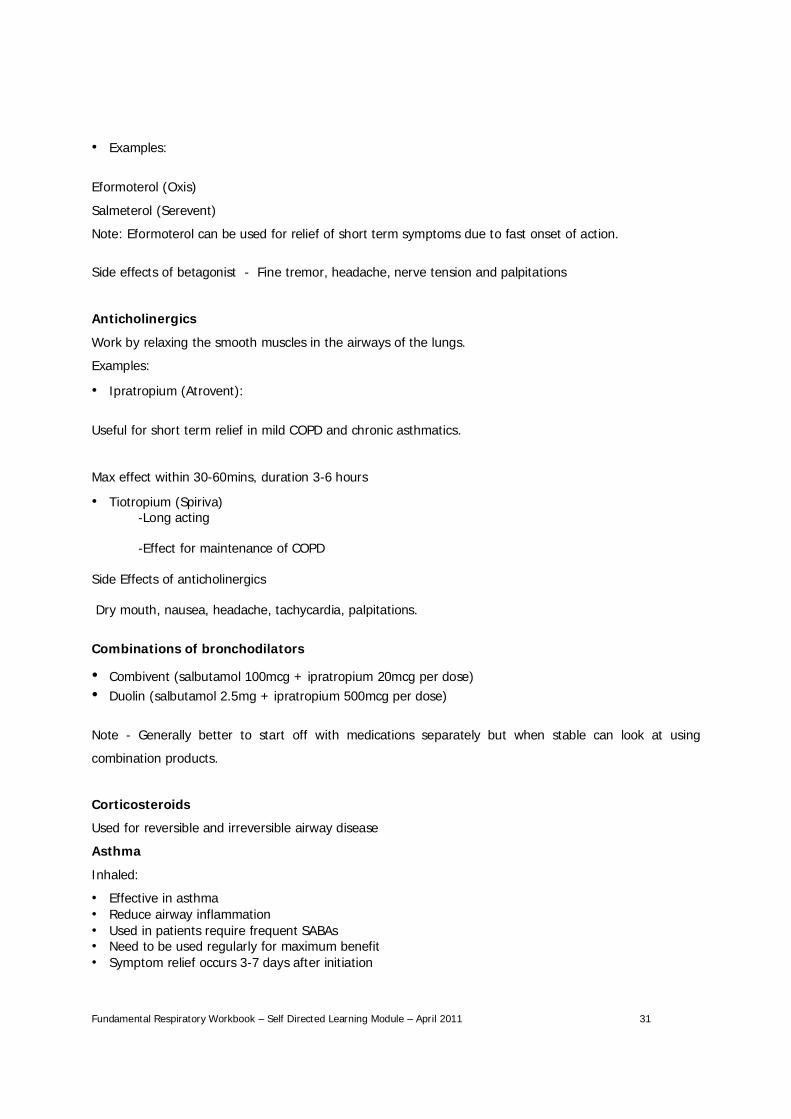
Examples:
Eformoterol (Oxis)
Salmeterol (Serevent)
Note: Eformoterol can be used for relief of short term symptoms due to fast onset of action.
Side effects of betagonist - Fine tremor, headache, nerve tension and palpitations
Anticholinergics
Work by relaxing the smooth muscles in the airways of the lungs.
Examples:
Ipratropium (Atrovent):
Useful for short term relief in mild COPD and chronic asthmatics.
Max effect within 30-60mins, duration 3-6 hours
Tiotropium (Spiriva)-Long acting
-Effect for maintenance of COPD
Side Effects of anticholinergics
Dry mouth, nausea, headache, tachycardia, palpitations.
Combinations of bronchodilators
Combivent (salbutamol 100mcg + ipratropium 20mcg per dose)Duolin (salbutamol 2.5mg + ipratropium 500mcg per dose)
Note - Generally better to start off with medications separately but when stable can look at using
combination products.
Corticosteroids
Used for reversible and irreversible airway disease
Asthma
Inhaled:
Effective in asthmaReduce airway inflammationUsed in patients require frequent SABAsNeed to be used regularly for maximum benefitSymptom relief occurs 3-7 days after initiation
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 32
Oral:
Acute attack -> 40-50mg prednisone daily for a few daysUsually quick response
IV:
Used in emergency situations for severe asthma
COPD
Inhaled:
May reduce exacerbationsConsider if expiratory volume in 1 second is less than 50% of predicted value and patient has had >2exacerbations in a year
Oral:
30mg for 7-14 days.Can be stopped abruptlyProlonged treatment generally of no benefit
Examples of Inhaled corticoids – “Preventers”
Beclomethasone (Beclazone®)
Budesonide (Pulmicort®)
Fluticasone (Flixotide®) – twice as potent
Symbicort® (Budesonide/Eformoterol)
Vannair® (Budesonide/Eformoterol)
Seretide® (Fluticasone/Salmeterol)
Side effects of corticosteriods
Inhaled:
Fewer S/EsIncreased doses = increase chance of SEsExamples: adrenal suppression, decrease bone mineral density.
Oral:
Generally occur more with long term treatmentInclude: psychiatric reaction, hypertension, sodium &water retention, Cushing’s Syndrome
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 33
Theophyline
Bronchodilator and pulmonary vasodilatorUsed for both asthma and COPDNarrow therapeutic range -> require TDMConsiderable variation in plasma-theophyline concentrations between patients
Side-effects
Tachycardia, palpitations, nausea, headache, insomnia
Other Treatments
Mast Cell Stabilisers:
E.g. Sodium cromoglycateCould be of value in asthmatics with an allergic basis
Leukotriene Receptor Antagonist:
E.g. MontelukostMay be of benefit in exercise induced asthma
Both classes not proven more effective than corticosteroids
Types of inhalers
Pressurised Metered Dose inhalers (MDIs):
Pressurised gas propels a set doseRelease by pressing the top of the inhalerCo-ordination needed
E.g. Flixotide, Seretide, Ventolin
Dry powder inhalers
Each dose contains a tiny amount of drug in a powder form that you suck inNeed to be able to breathe fairly hard to get powder in to lungsE.g.: Bricanyl, Symbicort, Pulmicort, Oxis, Spiriva
Inhaler Helper Tools
Spacers
Used with metered dose inhalers
Less co-ordination needed
Increased amount of drug reaching lungs
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 34
Haleraid
For patient who have difficulty pressing metered dose inhalers
Smoking cessation
Really important to stop disease progressionLots of smoking cessation aids
Influenza Vaccinations
Help prevent exacerbations, hospitalisations and death in COPD
Pneumonia Antibiotics:
E.g. penicillins, cephalosporins, roxithromycin usually IV 3-5 days po
Oxygen:
Treated as a drug - to decrease the work of breathing
Please also read the following:
Note: The drug referred to as Albuterol in several of the readings is referred to as Salbutamol inNew Zealand
articles\Asthma IQ.pdf Treatments section
articles\Coping with COPD.pdf Treament section
www.asthmanz.co.nz/nz_guidelines section 6 Principles of Pharmacutical Therapy
Complete Module Five Questions 1 - 4 relating to Common Medications
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 35
Module Six - Nursing Assessment/Taking a Health History
Taking a health history forms the basis of the nursing assessment and focuses on the physical andfunctional problems of the patient and the effect these problems have on his or her life. The reason thepatient with an airways disease is seeking healthcare is often related to problems such as shortness ofbreath (dyspnea), wheezing, cough, pain, sputum production, hemoptysis and general fatigue.
It is also important to identify other key points such as:
• when the symptoms started• how long they lasted• what makes it worse, what makes it better• precipitating factors• duration• severity• associated symptoms• risk factors• family history
Functional ability is also assessed to determine the impact the signs and symptoms have on the patient’sability to:
• perform normal activities of daily living• carry out a normal days’ work• participate in family and social functions
Psychosocial factors such as anxiety, role changes, family relationships, financial problems andemployment status are also taken into consideration.
Many respiratory diseases are chronic and progressively debilitating. Therefore, ongoing assessment ofthe patient’s physical abilities, psychosocial supports and quality of life is needed to plan appropriateinterventions. Performing a thorough assessment will enable you to develop a plan of care to meet yourpatient’s needs. The following is a brief overview of the different categories for assessment of a patientwith a respiratory disorder.
Health Status Examination
• Orthopnea (shortness of breath when lying down). Ask the patient how many pillows he or she usesat night. Ask them to describe the severity of orthopnoea
• Cough. Ask your patient – when did the cough start, does it produce phlegm, has it changedrecently. If so, how. What makes it better, what makes it worse, what medications are being taken
• Sputum. What time of day do they cough most, colour and amount
• Wheeze. What time of day does it occur, what makes it worse, is it loud enough for others to hear,what makes it better
• Chest Pain. Where is the pain exactly, what does it feel like, how long doe sit last, what causes it tooccur, what makes it better
• Previous Health History. Other respiratory disorders e.g. childhood asthma & eczema, dermatitis,allergic rhinitis
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 36
• Family history. Cancer, diabetes, heart disease, chronic illness such as asthma or emphysema
• Lifestyle patterns. Community and other environmental factors e.g. housing, workplace, type ofwork, smoking and drug habits, interpersonal relationships, mental status, stress management,coping style
Physical Examination
Physical examination involves four steps:
1. Inspection2. Palpation3. Percussion4. auscultation
1. Inspection. Look for chest wall symmetry, breathing rate and pattern, rise and fall of chest, skincolour especially around the mucous membranes and nail beds, clubbing of finger nails.
2. Palpation. Gentle palpation of the chest will reveal any symptoms such as painful areas, crepitusunder the skin, vibrations etc.
4. Percussion. Allows you to assess different sounds in different areas of the chest.
5. Auscultation. Helps to determine the condition of the alveoli and surrounding pleura. As air movesthrough the bronchi, sounds may change as they pass through fluid, mucus and narrowed airways.Each sound should be classified according to its intensity, location, pitch, duration and characteristicsand noting if it occurs on inspiration or expiration.
Diagnostic Tests
Diagnostic tests will help identify and evaluate any dysfunctions found on examination. Tests mayinclude:
• Pulse oxymetry• Peak flow recordings• Spirometry• Arterial blood gas analysis• Sputum analysis• Bronchoscpy• Chest xray
Performing a complete and thorough examination will aid in making an accurate diagnosis of your patientand allow you to plan nursing interventions to aid in treating symptoms as they arise. It is important fornurses to understand, use, incorporate and perform each of these assessment skills when caring for thepatient with a respiratory disorder. For further information on auscultation, Spiromety, peakflowmeasurements and pulse oxymetry please read the flowing:
articles\Auscultation.pdf
articles\Interpretation and evaluation of pulmonary function tests..pdf
articles\NZ Asthma guidelines.pdf Section 7 ‘Management of Asthma in the M ori Communit
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 37
Module Seven - Ongoing Care
Nurses play a key role in supporting the patient with a respiratory disease. Teaching is an essentialcomponent of nursing and reaches across the continuum of care from admission to discharge and beyond.Patient and family/whanau member’s knowledge and comfort level in coping needs to be assessed andconsidered when providing instructions about self-management strategies.
Self-management strategies may include:
• adherence to prescribed therapy• preventative measures• attendance at follow up appointments• nutrition• correct use of inhalers• environment modifications• lifestyle modifications• coping measures• breathing exercises• patient and family understanding of complications and side effects of medication.• signs and symptoms of infection/complications/exacerbations of illness.
Referral to support networks is vital to ensure patients have the necessary guidance and support toenable self-management. Support networks include referral to:
o respiratory nurseo smoking cessation providero dieticiano rehabilitation programmeo support groups
Nurses work in partnership with patients with respiratory disorders to ensure they have achievable goalsand strategies to manage symptoms and to maintain quality of life. Please read the following:
articles\asthma update.pdf ‘Under your influence’ page 49
articles\Coping with COPD.pdf ‘Help your patients breathe’ page 48
articles\NZ Asthma guidelines.pdf section 10
Education, Self Management and Routine Clinical Care
Complete Module Six and seven: Case Study relating to Nursing Assessment/Taking a HealthHistory/Ongoing Care
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 38
RESPIRATORY FUNDAMENTALSSELF DIRECTED TEST
A mark of 80% must be achieved in all tests in order to receive a certificateand to proceed to the Advanced Respiratory Study Day
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 39
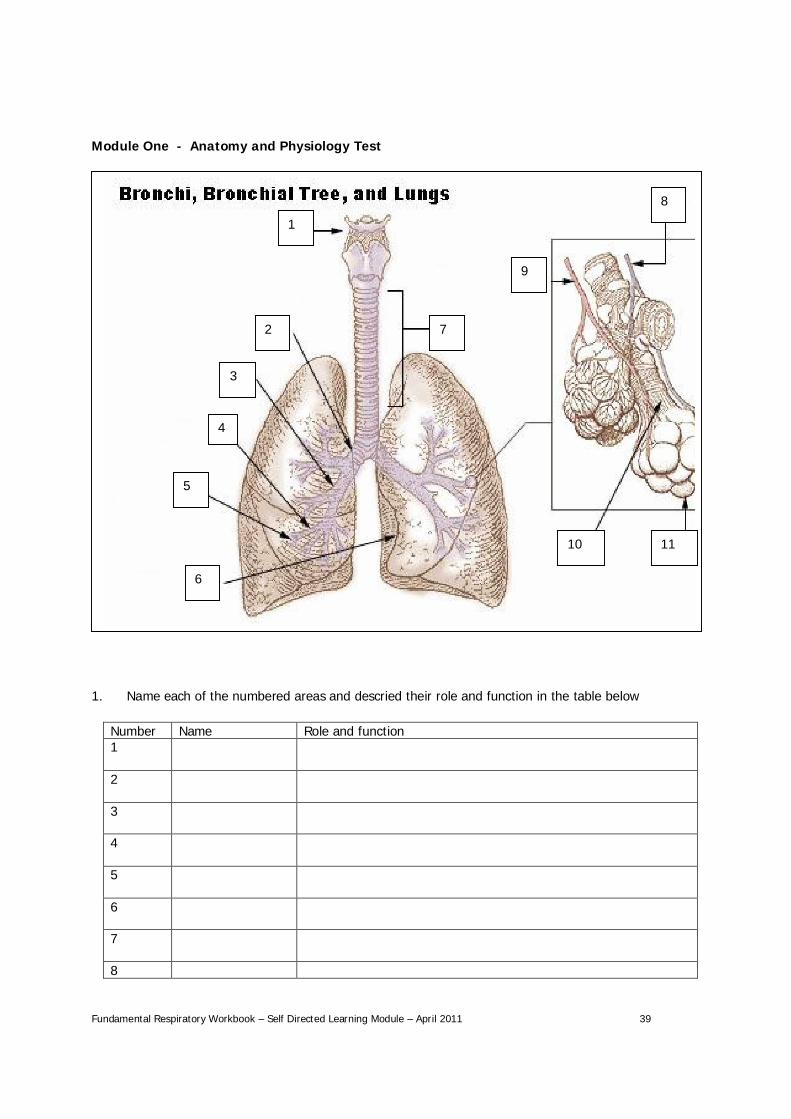
Module One - Anatomy and Physiology Test
1. Name each of the numbered areas and descried their role and function in the table below
Number Name Role and function1
2
3
4
5
6
7
8
1
6
2
3
4
5
7
8
9
10 11
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 40
9
10
11
2. What does TV+ IRV = ERV stand for and what does it measure?
____________________________________________________________________________________________________________________________________________________________________________
3. Explain the difference between internal and external respirations
Internal External
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 41
Module Two - National/International Guidelines Test
1. Name three key diagnostic indicators mentioned in Section 5______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
2. List five differences between asthma and COPD (page 23)__________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
3. How is the severity of asthma classified. (articles\Asthma IQ.pdf articles\asthma update.pdf mayhelp answer this question)
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Complete the following table - Severity Criteria in Asthma
Severity Clinical features Lung functionMild/intermittent
Moderate
Severe
4. Give an explanation of the value both of the guidelines and explain how these could support youin caring for a patient with asthma.
______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 42
Module Three - Disorders of the Airways Test
1. List five factors in Debra’s history that were used to help inform the clinician’s differential diagnosisbetween asthma and COPD
1
2
3
4
5
2. Were these factors alone sufficient to make a diagnosis? (Circle one only)
Yes No
3. Give a rationale for your answer to Question 2______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
4. What is the purpose of spirometry in aiding diagnosis?______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
5. If Debra’s diagnosis had been asthma, what is considered to be the first line of treatment?
ABCD
6. What other treatment is added when a diagnosis of COPD is made?______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 43
7. List six strategies used to reduce the patient’s risk for exacerbation and/or hospitalisations
1
2
3
4
5
6
8. Complete the following table
ASTHMA COPDDEFINITION
ONSET (TYPICAL)
AIRFLOW LIMITATION
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 44
Module Five - Common Medications Test
The treatment of asthma is based on the classification and severity of symptoms. Medications play a vitalrole in controlling symptoms and ensuring patients are self managing their care to prevent exacerbationsof both Asthma and COPD. Please complete the following section.
1. Please give a brief definition of:
A Reliever__________________________________________________________________________________________________________________________________________________________________
A Preventer__________________________________________________________________________________________________________________________________________________________________
2. Describe the aim of drug therapy:___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
3. Relievers are described as:______________________________________________________________________________________________________________________________________________________________
An example of a reliever is:_________________________________________________________
Preventers are described as: _________________________________________________________________________________ _________________________________________________________________________________
An example of a preventer is:_______________________________________________________
4. Answer true (T) or false (F) to the questions below
a) In hailed corticosteroids are considered the first line treatment patients with asthma andCOPD
b) Bronchodilators are only used in an emergency situation
c) Inhaled drug therapy is superior to oral therapy for short acting ß² agonists,antincholinergics, long acting ß² agonist and inhaled corticosteroids
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 45
Module Six and seven- Nursing Assessment/Taking a Health History/ Ongoing Care Putting It All Together.
Respiratory Scenario
Mary is a 48 year old Maori woman who works full time as an office administrator. She is married to Tomand they have four children. The youngest is 16 and is the only child living at home. Mary is a smokerwith a one pack (20) per day smoking history. She began smoking at the age of 15. Mary has had twochest infections every winter for the past three years. There is no family history of asthma and no othersignificant medical history. She denies breathlessness, cough or wheeze at night. She states she has a“smokers cough.” She presents today with breathlessness, fever and productive cough.
Initial Care
1. What would be your initial assessment involve?________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
2. What investigations should you arrange?________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
3. Name three differential diagnoses (what other problems might her symptoms suggest)?________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
4. During your assessment of Mary what factors would alert to her risk of having an acuterespiratory event?________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 46
Management of care
Mary has been diagnosed with ‘Acute exacerbation of COPD” and admitted to the medical ward
5. Provide a general care plan for Mary____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
6. What monitoring would you expect Mary to be having on a regular basis? Why?____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
7. What referrals would you make and why?________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
8. Name three factors that may impact on Mary’s management of her COPD.
___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 47
9. What are some lifestyle changes that Mary might have to consider?____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
10. Name two resources that you could use to help with you management of Mary’s condition._____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Ongoing Care: To ensure Mary is able to manage her condition at home, please describe thefollowing
1. What should be included in Mary’s education plan and who will be involved in formulating the plan?
_________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
2. Who is available to support Mary within the community and what is their role?
_________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
You have now completed all criteria of the workbook.Well done!
Please forward the completed workbook to:
Nurse EducatorsWhanganui District Health Board
Private Bag 3003Whanganui 4501
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 48
References
Booker, R (2008) Spirometry in primary care. Primary health care. 18,10 37-47
Coughlan, M. (2007) Coping with COPD. Nursing made Incredibly Easy November/Devember 2007, 40 -49.
Dunn, L (2005) pneumonia: classification, diagnsis and nursing management. Nursing Standard. 19, 042,50-54
Ferns, T & West, S (2008) The art of auscultation: evaluating a patient’s respiratory pathology. BristishJournal of Nursing, 17, 12, 772-777
Global Initiative for Asthma (2010) Pocket guide for asthma management and prevention. Downloadedfrom http://www.ginasthma.com/download.asp?filename=GINA_PG_2010.pdf. March 2010.
Kent, V (2011) put a cap on community acquired pneumonia. Nursing made Incredibly easy. March/April2011. 34-43.
McCormack, M. (2009) Boost your asthma IQ. Nursing made Incredibly easy. January/February 2009, 24-52
McCormack, M (20100 Asthma Update. Nursing made Incredibly Easy. March/April 2010. 43-51
New Zealand Guidelines Group (2002) The diagnosis and treatment of adult asthma. Downloaded fromwww.asthmanz.co.nz/nz_guidelines. march 2011
Pearson Education (2003) ‘The respiratory System.’ PowerPoint, downloaded March 2011
WDHB Pharmacy (2010) Respiratory Medications.
Fundamental Respiratory Workbook – Self Directed Learning Module – April 2011 49
Assessment and Feedback
Marker’s Name: _____________________________________
Date Module Received: _____________________________________
Date Module Marked: _____________________________________
Complete/Incomplete
Comments of Marker:______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
______________________________________________________________________________________
Evaluation Form
Please evaluate and assess the education provided which will assist in planning and implementing futureeducation programmes. We welcome your feedback to evaluate the value of the information provided
and the effectiveness of the methods used in presenting the information
1. How informative was the subject matter?1 2 3 4 5 6 7 8 9 10
LOW HIGH
Comments:
2. How relevant to practice was the education?1 2 3 4 5 6 7 8 9 10
LOW HIGH
Comments:
3. Was the education well researched?1 2 3 4 5 6 7 8 9 10
LOW HIGH
Comments:
4. Were your learning needs met?1 2 3 4 5 6 7 8 9 10
LOW HIGH
Comments:
5. Are there any other topics you would like to see included in this education?
6. What did you find the most valuable?
7. What did you find the least valuable?
8. Have you any suggestions for improvement?
Thank you for taking the time to complete this evaluation. We appreciate your feedback.





























