Embed Size (px)
Citation preview

i 087
Gd-DTPA-Enhanced MR Imagingof Spinal Tumors
Paul M. Parizel12Danielle Bal#{233}naux1Georges Rodesch1
Chnstoph Segebarth3Benjamin Lalmand’
Catherine Chnstophe3Marc Lemort�
Philippe Haesendonck3H. Peter Niendorf
J. Flament-Durand5Jacques Brotchi6
This article appears In the March/April 1989issue of AJNR and the May 1989 Issue of AJR.
Received March 21, 1988; accepted after revi-sion July 20, 1988.
Presented in part at the annual meeting of theAmerican Society of Neuroradiology, New YorkCity, May 1987.
1 Department of Radiology, Clinic of Neurora-
diology, H#{244}pitalErasme, Uiiversit#{232}Ubre do Brux-elles, Route do Lennik 808, B-1070 Brussels, Bel-gium. Address reprint requests to 0. Bal#{233}rlaux.
2 Present address: Department of Radiology,
Antwerp University Hospital, B-2520 Edegem, Bel-
glum.
3 Magnetic Resonance Unit, H#{244}pitaIErasme,1k�iversit#{233}Libre do Bruxelles, B-i 070 Brussels,Belgium.
4 Department of Aadiology, FB Medizin, Scher-ingAG, P.O. Box6503 ii, D-i000BerIin6S,W.Germany.
5 Department of Pathology. H#{212}pitaIErasme,lkvversit#{233} Ubre do Bruxelles, 8-1070 Brussels,Belgium.
6 Department of Neurosurgery, HOpitai Erasme,
Universit#{233}Ubre do Bruxelles, B-1070 Brussels,Belgium.
AJR 152:1087-1096, May 19890361-803x/89/1 525-1 087C American Roentgen Ray Society
Forty-eight Gd-DiVA-enhanced MR examinations of the spine were performed in 40
patients referred for MR because of clinically suspected spinal tumor or for furtherevaluation of an expanded cord. The study group consisted of 32 patients with spinal
tumors (seven ependymomas; seven astrocytomas; four hemangioblastomas; twoartenovenous malformations; two unidentified intramedullary neoplasms; four meningi-omas; and single cases of metastatic breast carcinoma, cavernous hemangioma withassociated hematomyelia, neurinoma, angiolipoma, drop metastasis from medulloblas-toma, and epidermoid with diastematomyelia). In the remaining eight patients, otherdiagnoses were established: thoracic disk herniation (two patients), lumbosacral men-ingocele (one), syringomyelia secondary to arachnoiditis (four), and expanded cordsecondary to gliotic tissue (one). All but two diagnoses were proved histologically bybiopsy, surgery, or autopsy; in the two patients with arteriovenous malformations, thedefinitive diagnosis was made by spinal angiography. Contrast enhancement occurred
in 30 of the 32 spinal tumors, and Gd-DTPA-enhanced Ti-weighted images provedhelpful in defining and outlining intra- and extramedullary spinal neoplasms. All open-dymomas and astrocytomas (including low-grade astrocytomas) enhanced. In meningi-omas, an immediate and uniform contrast uptake was demonstrated. Additional advan-tages of Gd-DTPA MR include the differentiation of solid tumor components vs syrinx orcyst or pseudotumoral areas of cord expansion, and the differentiation of residual orrecurrent tumor from scar tissue in postoperative patients.
Our resufts suggest that IV-injected Gd-DTPA improves MR sensitivity and specificityin the evaluation of spinal lesions.
Increasingly, MR imaging has become the method of choice in viewing the normaland diseased spinal cord. Although the effectiveness of MA imaging in the neuro-radiologic evaluation of spinal tumors has been well documented, several problemsremain unsolved: the low specificity of noncontrast MA, tumor vs edema differen-tiation, accurate delineation of the lesion, recognition of solid tumor nodule vsassociated syrinx, and study of the postoperative spine. Several recent reportshave indicated the usefulness of the paramagnetic MR contrast agent gadolinium-DTPA-dimeglumine (Gd-DTPA) in outlining spinal neoplasms [1 -i 0]. The purposeof the present study of 40 patients was to determine to what extent the use of Gd-DTPA increases both the MR sensitivity in defining and localizing spinal tumorsand the MR specificity in the diagnosis of spinal lesions.
Subjects and Methods
Forty-eight Gd-DTPA-enhanced MR examinations of the spine were performed in 40patients with suspected spinal neoplasm (six patients had Gd-DTPA-enhanced studies bothbefore and after surgery; one patient had three examinations). All patients were referred forMR, either because of clinically suspected spinal tumor or for further investigation of anexpanded cord as detected by myelography, CT, or CT-myelography; spinal arteriographywas performed in two patients. The patient population included 1 9 males and 21 females,
14-72 years old (mean age, 44.8).

c�:r Age Gender Level Diagnosis (Histology) Enhancement
TiO-Ti 1
C6-C7C5-TiC7-T1C2-C5C2-C5Cl-TiCl -C5Cl -C3T9-T12
Conus medullarisCi -C4Conus medullarisT9-L1
C2-C3C4-C6
C4-C6C5-C6C4-C7
C7-T1 and T9-Ti 0T6T5-T6
C4-C6T7-T8
Ependymoma
Ependymoma (poorly differentiated)EpendymomaAstrocytoma (low grade)Astrocytoma (low grade)Astrocytoma (grade 2)Astrocytoma (grade 1)Astrocytoma (low grade)Astrocytoma (low grade)Astrocytoma (low grade)Unidentified intramedullary tumor + syrinxUnidentified intramedullary tumor (patient with neurofibromatosis)Metastasis from breast carcinomaHemangioblastoma + large syrinxHemangioblastoma + large syrinxMultiple hemangioblastomas + large syrinx (von Hippel-Lindau syndrome)Hemangioblastoma + associated syrinxCavernous hemangioma + hematomyeliaArteriovenous malformationArteriovenous malformation
C
+
. Schenng AG, Berlin, W. Germany.t Gyroscan Si 5, Philips Medical Systems, Eindhoven, Netherlands.
1088 PARIZEL ET AL. AJA:152, May 1989
TABLE 1: Histologic Diagnoses and Results of Gd-DTPA-Enhanced MR Imaging
Intramedullary tumors:1 27 M2 58 F3 58 M4 39 F5 40 M6 35 F7 47 F
8 21 M9 15 F
10 33 M11 68 M12 22 F13 28 F14 60 M15 64 F16 14 F17 48 F18 23 M19 38 M20 45 M21 72 M22 64 F23 29 M24 66 M
Extramedullary tumors:25 34 F C1-C326 66 M C1-C227 56 F T3-T428 57 F T3
29 50 F L3-L430 55 F Sacrum31 29 F T12-L532 37 F T4-T8
Other extramedullary lesions:33 20 F L5-sacrum34 55 F T8-T935 51 M T6-T7
Tumorlike conditions:
36 57 M T3-T1037 59 M T3-T738 62 M T5-L139 28 F T4-T840 62 M C1-C6
Ependymoma (grade 3)EpendymomaEpendymoma (grade 2)Ependymoma
MeningiomaMeningiomaMeningiomaMeningioma (psammomatous type)NeurinomaDrop metastasis from medulloblastomaEpidermoid + diastematomyeliaAngiolipoma (posterior extradural space)
Lumbosacral meningoceleDisk herniationDisk herniation
Syringomyelia secondary to arachnoiditisSyringomyelia secondary to arachnoiditisSyringomyelia secondary to arachnoiditisSyringomyelia secondary to arachnoiditisGliosis (unspecified)
++
++
++
+
+++++
++
+8
+8
+
++
++
++
++
+
+
+
a No definitive histology available.b In the two patients with arteriovenous malformations, the definitive diagnosis was made by spinal angiography. In the 38 other patients the diagnosis was
established histologically by biopsy, surgery, or autopsy.C The thoracic disk as such did not enhance, but enhancement of the posterior longitudinal ligament was observed, as well as triangular areas of contrast uptake
above and below the herniated disk. At surgery, these areas were found to correspond to engorged epidural veins with stagnant blood flow and vascular granulationtissue along the inflamed posterior ligament.
After obtaining written informed consent, a standard Gd-DTPA- sequences and in some instances a fast-field-echo technique. All
dimeglumine solution8 was injected IV in a dosage of 0.1 mmol/kg patients were examined within 5-40 minutes after administration ofbody weight. There is evidence that this is a well-tolerated and Gd-DTPA. The acquisition matrix was 256 x 256 with two to foureffective dose for MR imaging [1 1 -1 5]. All examinations were per- averages. The slice thickness was 5 mm in all instances. Patientformed on a superconductive unit,t initially operating at a 0.5 T field tolerance to the Gd-DTPA injection was excellent. There were nostrength (1 0 patients) and subsequently at 1 .5 T (30 patients). side effects during the MR examination or in the subsequent 24-48
Both Ti - and T2-weighted images were obtained before contrast hr. Patients with impaired renal and/or hepatic function were excludedadministration with the use of spin-echo sequences, 250-600/30 and from the study.
2000/30, 1 00 (TRITE), respectively. After IV Gd-DTPA injection,sequential Ti -weighted scans were obtained with short TR spin-echo Results
Our results are summarized in Table i . Spinal tumors wereidentified in 32 of 40 patients, including seven ependymomas

AJA:152, May 1989 Gd-DTPA MA OF SPINAL TUMORS 1089
(cases i -7); seven astrocytomas (cases 8-i 4); two uniden-tified intramedullary neoplasms (cases i 5 and i 6; case i 6was a patient with neurofibromatosis who presented with alarge posterior fossa meningioma and an unidentified cervicalintramedullary tumor); metastatic breast carcinoma (case 17);five hemangioblastomas with a large syrinx cavity (cases i 8-21); cavernous hemangioma with associated hematomyelia(case 22); two arteriovenous malformations (cases 23 and24); four meningiomas (cases 25-28); and single cases ofneurinoma (case 29), drop metastasis from posterior fossamedulloblastoma (case 30), epidermoid with associated dias-tematomyelia (case 31), and angiolipoma (case 32). All excepttwo diagnoses were established histologically (biopsy, defini-tive surgery, or autopsy). All tumors showed contrast en-hancement with Gd-DTPA, except for the epidermoid and thecavernous hemangioma.
Thoracic disk herniations were found in two patients (cases34 and 35) and a large lumbosacral meningocele was foundin one patient (case 33).
The remaining five patients had tumorlike conditions (wid-ening of the cord on nonenhanced MA scans), but no evidence
of an underlying neoplastic lesion was found. This group
included four patients (cases 36-39) with a syrinx cavity andirregular thickening of the cord secondary to arachnoiditis,initially believed to represent an intramedullary neoplasm. Thelesions did not enhance. The diagnosis was surgically con-firmed in all four patients. One patient (case 40) was diag-nosed as having an infiltrating intramedullary tumor on non-enhanced MA; there was heterogeneous contrast enhance-ment throughout the cervical spine. A surgical biopsy revealeddiffuse gliosis, without evidence of a true neoplasm.
Discussion
Intramedullary Tumors
The diagnostic usefulness of paramagnetic contrast agentssuch as Gd-DTPA in the evaluation of intraaxial (i.e., intra-medullary) gliomas is based on the fact that they do not crossthe intact blood-brain barrier (BBB). Thus, in order for a tumorto enhance, there must be an active breach of the BBB.Because the hydrophilic contrast agent, which has a highmolecular weight, leaks out of the vascular compartment intothe interstitial spaces, progressive contrast enhancement isto be expected. This gradual increase in signal intensityproduced by Gd-DTPA on Ti -weighted images reaches aplateau and then signal intensity drops slowly. This patternhas been well established in brain tumors [i 6]. Variations intime-dependent contrast enhancement have also been de-scribed in spinal tumors [17].
In summary, Gd-DTPA is a marker for alterations of theBBB, like a conventional CT contrast agent.
Ependymomas (n = 7) are seen on plain MA studies asareas of widening of the cord. On Ti -weighted images, epen-dymomas are isointense with respect to the spinal cord;therefore, their boundaries are difficult to define, unless theyare outlined, as is sometimes the case, by syrinx cavitiescapping the upper and lower poles of the tumor. On T2-
weighted sequences, ependymomas may have a multinodular
appearance, but the differentiation of tumor vs surroundingedema is virtually impossible, since both have prolonged T2relaxation times, presumably reflecting increased water con-tent.
The use of Gd-DTPA allows better definition of the upperand lower limits of these intramedullary tumors. In our expe-rience, ependymomas as a rule showed intense, homogene-ous, and sharply marginated focal enhancement (Fig. 1). Theytend to occupy the whole width of the spinal cord in theaffected segment, which is consistent with a centrifugal ex-pansion originating in the ependymal cells lining the centralcanal or in cellular components scattered in the white matterof the spinal cord.
In some instances, ependymomas have intratumoral cavi-ties. In these cases, Gd-DTPA not only brings out superbtumor-border definition but is also highly accurate in thedelineation of central low-signal-intensity components, corre-sponding to intratumoral cysts [1]. These areas of cysticdegeneration were identified after Gd-DTPA injection in threeof seven ependymomas in our series and subsequently con-firmed at surgery.
Conversely, astrocytomas (n = 7) tend to enhance in amore patchy, irregular way, consistent with a more diffuselyinfiltrating tumor. All astrocytomas, even low-grade astrocy-tomas, did enhance. The areas of contrast enhancement areoften eccentrically located ( usually in the posterior aspect ofthe spinal cord) and are less well defined with slightly fuzzymargins; they may be separated by regions of low signalintensity consistent with areas of necrosis or cystic change(Fig. 2). In addition, in some astrocytomas an exophytic tumorcomponent may be identified as an area of contrast enhance-ment, which could be verified readily at surgery.
These slightly different patterns of contrast uptake hadinitially suggested that Gd-DTPA might prove to be a usefultool in predicting the histology of intraspinal neoplasms. How-
ever, there is considerable overlap. Of particular interest aresome of the errors we made when using our own criteria asdescribed above. Figure 3 illustrates the case of a 28-year-old woman with a tumor at the level of the conus medullansthat showed marked, homogeneous, and sharply marginatedcontrast enhancement both on sagittal and coronal Se-quences. The tumor appeared very well defined. We expectedthis tumor to be an ependymoma, especially since ependy-momas (particularly of the myxopapillary type) are commonin this location. Surgery revealed an infiltrating intramedullarylesion; there was no clear cleavage plane and the tumor couldnot be completely resected. Pathologic examination showeda well-differentiated (low-grade) astrocytoma. A follow-up Gd-DTPA-enhanced MR scan was clearly superior to plain MRin the delineation of residual tumor tissue (Figs. 3E and 3F).
Conversely, in one patient with an ependymoma, the slightlyinhomogeneous pattern of contrast enhancement as well asthe asymmetric appearance of the tumor led us initially to
consider a low-grade astrocytoma as the first differentialdiagnosis.
In summary, although we did find different patterns ofcontrast enhancement in some ependymomas and astrocy-
i 090 PARIZEL ET AL. AJA:i52, May 1989
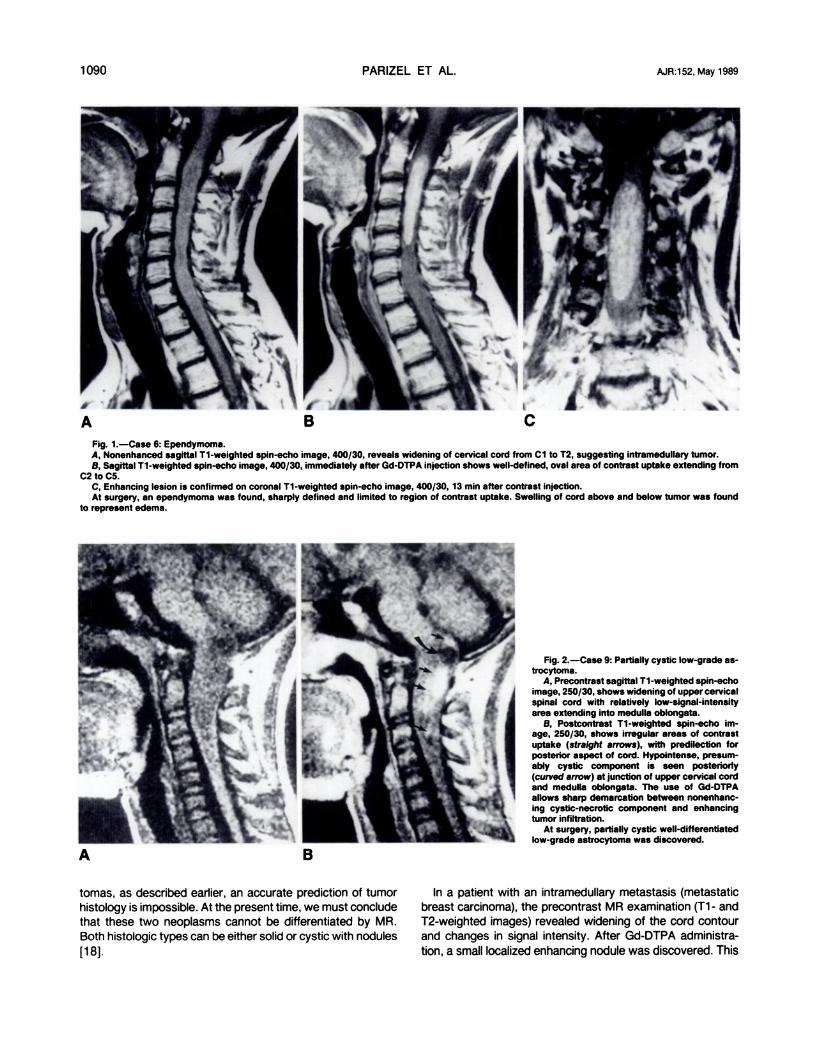
Fig. 1.-Case 6: Ependymoma.A, Nonenhanced sagittal TI-weighted spin-echo image, 400/30, reveals widening of cervical cord from Cl to T2, suggesting intramedullary tumor.B, Sagittal Ti-weighted spin-echo image, 400/30, immediately after Gd-DTPA injection shows well-defined, oval area of contrast uptake extending from
C2 to C5.C, Enhancing lesion is confirmed on coronal Ti-weighted spin-echo image, 400/30, 13 mm after contrast injection.At surgery, an ependymoma was found, sharply defined and limited to region of contrast uptake. Swelling of cord above and below tumor was found
to represent edema.
Fig. 2.-Case 9: Partially cystic low-grade as-trocytoma.
A, Precontrast sagittal Ti-weighted spin-echoimage, 250/30, shows widening of upper cervicalspinal cord with relatively low-signal-intensityarea extending into medulla oblongata.
B, Postcontrast Ti-weighted spin-echo im-age, 250/30, shows irregular areas of contrastuptake (straight arrows), with predilection forposterior aspect of cord. Hypointense, presum-ably cystic component is seen posterioriy(curved arrow) at junction of upper cervical cordand medulla oblongata. The use of Gd-DTPAallows sharp demarcation between nonenhanc-ing cystic-necrotic component and enhancingtumor infiltration.
At surgery, partially cystic well-differentiatedlow-grade astrocytoma was discovered.
tomas, as described earlier, an accurate prediction of tumorhistology is impossible. At the present time, we must concludethat these two neoplasms cannot be differentiated by MR.Both histologic types can be either solid or cystic with nodules
[i 8].
In a patient with an intramedullary metastasis (metastaticbreast carcinoma), the precontrast MA examination (Ti - andT2-weighted images) revealed widening of the cord contourand changes in signal intensity. After Gd-DTPA administra-tion, a small localized enhancing nodule was discovered. This

AJR:152, May 1989 Gd-DTPA MA OF SPINAL TUMORS 1091
Fig. 3.-Case 13: Low-grade astrocytoma.A and B, Nonenhanced coronal (A) and sag-
thaI (B) TI-weighted spin-echo Images, 400/30,of thoracolumbar spine. Mass lesion Is clearlyidentified (arrows). Tumor is appended to conusmedullaris and is lateralized to left, displacingupper part of cauda equlna to right.
C and D, After Gd-DiVA administration, cor-onal (C) and sagfttal (D) Ti-weighted spin-echoImages, 400/30, show sharply defined, homo-geneous contrast uptake throughout tumor (ar-rowheads). At surgery, a low-grade astrocytomawas partially resected; there was no cleavageplane.
E, Nonenhanced sagfttal Ti-weighted image3 months after surgery shows Increased diame-ter of conus medullaris (arrows), with heteroge-neous signal Intensity.
F, After Gd-DTPA injection, residualtumor ap-pears as sharply marginated area of contrastuptake (arrowheads), clearly outlined fromconus medullaris.

1092 PARIZEL ET AL. AJA:152, May 1989
finding indicates that much of the cord enlargement is due toperifocal edema.
In the patients with hemangioblastoma (n = 5, in fourpatients), noncontrast MA displayed irregular and diffusewidening of an apparently infiltrated spinal cord in its cervicaland thoracic segments. The intrinsic cord signal was hetero-geneous, with low-intensity areas supposedly representing avast syrinx cavity, alternating with isointense areas of thick-
ening of the cord. In one patient, the syrinx extended fromthe upper cervical to the lower thoracic cord.
The use of IV-administered Gd-DTPA allows accurate rec-
ognition of the highly vascular tumor nidus within a large areaof cystic change, thus providing the neurosurgeon with veryuseful information and directing surgery to the level of thesolid tumor component. Some authors have described howthe signal characteristics of a tumor nodule may be separatedfrom those of the cyst by using long TA and long TE se-quences, since the T2 of the cyst is usually longer [8, 18].However, in our experience, T2-weighted pulse sequencesalso are more apt to show artifacts and often are of poorerquality; the Gd-DTPA-enhanced Ti -weighted image was su-perior in highlighting a vascular tumor nodule within an asso-ciated cyst. In our limited experience, the association of astrongly enhancing solid tumor nodule within a vast syrinx isvery suggestive of hemangioblastoma.
In the patient with a cavernous hemangioma, plain MRrevealed an ovoid intramedullary lesion with heterogeneoussignal characteristics. A large area of hematomyelia extendedbelow the lesion. The mixed high- and low-signal-intensitycomponents of cavernous hemangiomas presumably indicatethe presence of mixed subacute and chronic hemorrhage[1 9]. After IV Gd-DTPA administration, no definite contrastuptake could be seen. It is likely that in this patient thecharacteristic crescent-shaped high-signal-intensity hemor-magic focus (as a result of the formation of methemoglobin)and the surrounding low-signal rim (important concentrationof hemosiderin) may mask an area of contrast uptake [8].
The arteriovenous malformations (n = 2) had a markedlyheterogeneous appearance, both on the pre- and postcon-trast MA examinations, due to the presence of old hemor-rhagic components and calcifications. The lesions containedserpiginous areas of signal void, reflecting vascular structureswith rapidly flowing blood. There was some contrast uptakeafter Gd-DTPA injection. The final diagnosis was made byspinal angiography.
Extramedullary Intradura! Tumors
The mechanism of contrast enhancement in extraaxial tu-mors is different, since these lesions have no BBB. Therefore,the degree of Ti shortening after IV injection of Gd-DTPA isa function of tumor vascularization, in much the same waythat highly vascular extraaxial tumors such as meningiomasand neurinomas will enhance on CT. Theoretically, one mightpredict a more immediate contrast enhancement, as opposedto the progressive contrast enhancement in intraaxial gliomas,which is based on the gradual leaking of Gd-DTPA moleculesthrough a ruptured BBB.
Meningiomas (n = 4) most often appear isointense withrespect to the spinal cord on nonenhanced Ti -weightedimages and may have a slightly higher signal intensity on T2-weighted images [20, 21 ]. The isointense mass may be seenin a typical extramedullary intradural location displacing andcompressing the cord.
After IV injection of Gd-DTPA, and with the use of a fast-field-echo technique to obtain rapid sequential scans, wecould demonstrate immediate and uniform contrast enhance-ment, as evidenced by marked Ti shortening (Fig. 4). Indeed,because meningiomas are highly vascular extraaxial lesionsand have no BBB, they are ideal candidates for enhancementwith a paramagnetic contrast agent [22, 23]. This type ofcontrast uptake is similar to what is reported in the CTliterature.
Our series included one patient with a neurinoma, at theleft L3-L4 level. After injection of Gd-DTPA, the lesion en-hanced homogeneously.
Gd-DTPA has also been reported to be helpful in theevaluation of metastatic disease of the spine, including lep-tomeningeal tumor spread, where contrast-enhanced MRscans were far superior to examinations performed withoutcontrast agents [24-26]. Our series included one patient witha drop metastasis from a vermian medulloblastoma (Fig. 5).The lesion is identified on Ti -weighted images as a masslesion within the sacral canal, encasing and narrowing thedistal caudal sac. There is marked destruction of the sacrum.The T2-weighted images reveal heterogeneous signal inten-sity within the tumor. After Gd-DTPA injection, areas of Tishortening are identified; at surgery they are found to be richlyvascularized parts of an otherwise highly vascular drop me-tastasis of a medulloblastoma. The areas of enhancementcorrelate well with the regions of prolonged T2 on T2-weighted images.
No contrast enhancement was seen in a single patient withan intradural epidermoid (with associated diastematomyelia)in the lumbar spine. These congenital tumors with associatedbony malformations are essentially avascular in nature andtherefore do not enhance.
Extradural Lesions
Marked contrast uptake was present in a patient with alarge tumor in the posterior extradural space, extending fromT4 to T8. At surgery this lesion was found to be an angioli-poma.
In two patients with suspected spinal tumor, thoracic diskherniations were found. The herniated disk material as suchdid not enhance. However, in both patients we observedtriangular areas of contrast uptake above and below theherniated disk, as well as enhancement of the posteriorlongitudinal ligament. At surgery they were found to corre-spond to engorged epidural veins with stagnant blood flowand vascular granulation tissue along the inflamed posteriorlongitudinal ligament.
Tumor/ike Conditions
Of particular interest were four cases of syringomyeliasecondary to arachnoiditis. In these patients, nonenhanced

AJR:i52, May 1989 Gd-DTPA MA OF SPINAL TUMORS i 093
Fig. 4.-Case 26: Menlngloma.A, Nonenhanced sagfttal Ti-weighted Image,
600/30, cervIcal spine shows soft-tissue mass(arrowheads), which is slightly hypointense withrespect to spinal cord.
B-D, After IV Injection of Gd-DiVA, sagfttal(B), coronal (C), and axial (D) Ti-weIghted Im-ages, 600/30, reveal rapid, Intense, and home-geneous contrast uptake, providing superior dis-crimination between tumor and cord. Note en-hancement of thickened dura behInd C2vertebral body (B). Tumor has typical intraduralextramedullary topography. SpInal cord is flat-tened and dIsplaced posteriorly and to the right(arrows).
The lesion was a meningloma at Ci-C2.
MA was highly suggestive of intramedullary tumor: focalswelling of the spinal cord and central low-signal area com-patible with an area of necrotic/cystic change (Fig. 6). How-ever, whereas in our experience the majority of intramedullarytumors did enhance, no Ti shortening was seen in thesecases after Gd-DTPA injection. In two patients (cases 36 and37), the arachnoiditis was presumed to be secondary to anepisode of tuberculous meningitis many years before; onepatient (case 38) had a history of spinal trauma. The patientillustrated in Figure 6 (case 39) was clinically asymptomaticand underwent the MR examination as a “normal” volunteer.Surgical exploration revealed an area of adhesive arachnoid-itis covering the cord, with a subjacent syrinx, but no tumorcould be identified. No specific cause for the arachnoiditiswas identified. This early experience suggests that Gd-DTPAcan help to distinguish neoplastic from benign disease.
In one patient MR was suggestive of an intramedullarytumor. There was minimal heterogeneous contrast enhance-ment throughout the cervical spine. A surgical biopsy revealed
what was broadly defined as “gliotic tissue,” but no trueneoplasm could be found (case 40).
No contrast enhancement was present in a lumbosacralmeningocele that initially was misdiagnosed as a spinal tumor,because the cyst fluid had signal characteristics different fromthose of CSF.
In conclusion, paramagnetic contrast agents such as Gd-DTPA offer a means of positive contrast enhancement ofspinal tumors, as opposed to the displacement of contrastmaterial in myelography and CT-myelography. There is littledoubt that Gd-DTPA-enhanced MR imaging is superior toplain MA (Ti - and T2-weighted images) in the diagnosis andanatomic definition of spinal lesions and in assessing tumor
vascularity [4, 5, 7, 9, 1 0]. The increased sensitivity of Gd-DTPA-enhanced MA examinations of the spine is the resultof several factors: greater inherent tissue contrast with im-proved tumor border definition, possibility of lesion vs edemadifferentiation, identification of foci of necrosis, and intratu-moral cystic components.

1094 PARIZEL ET AL. AJR:152, May 1989
Fig. 5-Case 30: Drop metastasis from pos-terior fossa medulloblastoma.
A, Nonenhanced sagfttal Ti-weighted Image,400/30, displays mass lesion with large anteriorcomponent infiltrating in sacral canal and do-straying bone (large arrows) and smaller poste-dor component (small arrows).
B, Moderately T2-weighted image, 2000/50,reveals heterogeneous signal intensities withintumor. Posterior component (small arrows) andinferior portion of Intrasacral lesion (large ar-rows) are markedly hyperintense.
C, Segfttal Ti-weighted spin-echo Image,400/30, 3 mm after IV injection of Gd-DTPA.Contrast uptake is seen to correspond to thoseregions that had a prolonged T2 (arrowheads).
D, 13 mm after Injection, degree of enhance-ment has diminished, but differences in contrastuptake between dIfferent parts of tumor remain.
Surgery revealed strongly vascularized dropmetastasIs from posterior fossa medulloblas-toma.
It has been suggested that precontrast T2-weighted imagesmight be more sensitive than postcontrast Ti -weighted im-ages, since the former identify all lesions with an increasedwater content, both with and without an active BBB break-down, whereas the contrast enhancement in the latter de-ponds on an active disruption of the BBB and a viable blood
supply. This may be true in the brain, but in the spine ourexperience shows that the Gd-DTPA-enhanced MA studieswere superior to scans obtained without contrast material.Indeed, even when the disease is obvious on a standard MA
scan and the lesion is clearly identified on the T2-weightedimage, a Gd-DTPA-enhanced study may still be useful inhelping to characterize the lesion or in tumor vs edemadifferentiation. In addition, the enhanced spin-echo Ti -
weighted images have shorter acquisition times and fewerartifacts than do the longer T2-weighted spin-echo images,thereby allowing more accurate visualization of spinal lesions.
The improved visualization and delineation of spinal tumorson the Gd-DTPA-enhanced MR examination often guides theneurosurgical approach [1 0]. We found this to be particularly

AJR:152, May 1989 Gd-DTPA MR OF SPINAL TUMORS 1095
Fig. 6.-Case 39: Adhesive arachnolditis withsyrinx.
A, Nonenhanced sagfttal Ti-weighted image,400/30, shows increased diameter of midtho-mole spinal cord with central area of cavitation.Posterior subarachnold spaces are partially do-Iterated. Intramedullary tumor was suspected.
B, After IV Injection of Gd-DTPA, no contrastuptakels seen within Intramedullary lesion (iden-ticalpulse sequence). Note enhancementof baa-ivertebral veins (arrows).
Surgical exploration revealed adhesive arach-noiditis, wIth syrinx cavity, believed to be see-ondary to arachnoidftls. There was no intramed-ullary tumor.
true for lesions with a solid enhancing tumor nodule within anassociated intramedullary cavity (e.g., hemangioblastoma).
Another very promising result appears to be the possibilityof differentiating residual or recurrent tumor from scar tissuein the postoperative spine [4, 7, 9].
We conclude that Gd-DTPA-enhanced MR imaging im-proves the reliability of spinal tumor diagnosis and increasesMR Sensitivity and specificity. It is still too early to concludewhether the pattern of enhancement may contain character-istic or even pathognomonic information regarding the differ-ential diagnosis of intramedullary tumors (ependymoma vsastrocytoma). On the other hand, our findings show thatcontrast enhancement does occur in the vast majority oftumors, enabling differentiation of cystic tumor from nontu-moral cyst or syrinx [6, 27, 28], including pseudotumoralsyringomyelia secondary to arachnoiditis. In this way, Gd-DTPA can help differentiate neoplastic tissue from benigndisease.
ACKNOWLEDGMENT
We thank J. Haustein for reviewing the manuscript and offeringbibliographic advice.
REFERENCES
1 . Bydder GM, Brown J, Niendort HP, Young lR. Enhancement of cervicalintraspinal tumors in MR imaging with intravenous gadolinium-DTPA. J
Comput Assist Tomogr 1985;9(5):847-8512. Yoshikawa K, Aoki S, Mornose T, et al. Gd-DTPA as contrast agent in MR
imaging of spinal intramedullary tumors. Presented at the annual meeting
of the Society of Magnetic Resonance in Medicine, Montreal, Canada,August 1986
3. Fenzl G, Ussner J, Heywang SH, et al. MR of spinal lesions with Gd-DTPA
as contrast medium. Presented at the annual meeting of the Society ofMagnetic Resonance in Medicine, Montreal, Canada, August 1986
4. Treisch J, Claussen C, Massih M, Kommesser W, Felix R. Intraspinaltumours in plaln and Gd-DTPA-enhanced magnetic resonance imaging.Presented at the annual meeting of the Society of Magnetic Resonance inMedicine, Montreal, Canada, August 1986
5. Stimac GK, Porter BA, Olson DO, Gerlach R, Genton M, Nelson S.
Gadolinium DTPA/dimeglumine-enhanced MR of spinal neoplasms: prelirn-nary experience. Presented at the annual meeting of the Society of
Magnetic Resonance in Medicine, New York City, August 19876. Jenkins JPR, Stack JP, Watson Y, Isherwood I. Magnetic resonance
imaging of spinal lesions: the role of gadolinium-DTPA. Presented at theannual meeting of the Society of Magnetic Resonance in Medicine, NewYork City, August 1987
7. Bal#{233}riauxD, Parizel PM, Niendorf HP, ROdeSCh GL, Segebarth C. Value
of intravenous Gd-DTPA contrast injection in the MRI evaluation of spinaltumors. Presented at the annual meeting of the American Society of
Neuroradiology, New York City, May 19878. Sigal R, Halimi Ph, Doyon D, Hurth M, Pigeau I, Thibault M. High-field MR
imaging of spinal cord tumors using contrast media. Presented at theannual meeting of the Radiological Society of North America, Chicago,November 1987
9. Dillon WP, Bolla K, Mark AS, Tsudura JS, Norman 0, Newton TH. Gd-DTPA MR imaging enhancement of spinal cord tumors. Presented at theannual meeting of the Radiological Society of North America, Chicago,November 1987
10. VaIk J. Gd-DTPA in MR of spinal lesions. AJNR 1988:9:345-350, AJRi988;i50:1163-1168
1 1 . Laniado M, Weinmann HJ, Schemer W. Felix A. Speck U. First use of Gd-DTPA/dimeglumine in man. Physiol Chem Phys Med NMR i984;1 6:157-1 65
12. Welnmann HJ, Laniado M, Mutzel W. Pharmacokinetics of Gd-DTPA/dimeglumine after intravenous injection into healthy volunteers. Physiol
ChemPhys MedNMR 1984;16:167-1721 3. Weinmann HJ, Brasch AC, Press WA, Wesbey GE. Characteristics of
gadohniurn-DTPA complex: a potential NMR contrast agent. AJRi984;142:619-624
14. Carr OH, Brown J, Bydder GM, et al. Gadolinium-OTPA as a contrast
agent in MRI: initial clinical experience in 20 patients. AJR i984;143:21 5-224

1096 PARIZEL ET AL. AJR:152, May 1989
15. Carr OH, Brown J, Bydder GM, et al. Intravenous chelated gadolinium as
a contrast agent in NMR Imaging of cerebral tumors. Lancet 1984;1:
484-486
16. SchomerW, Laniado M, N’IendOrfHP, Schubert C, Felix R. Time-dependentchanges in image contrast In brain tumors after gadollnium-DTPA. AJNR
1986;7:1013-102017. Laniado M, Kommesser W. TrelSch J, Felix R, Oelmllng M. Gd-DTPA-
enhanced fast magnetic resonance Imaging of brain and spinal tumors:
early clinical experience. In: Runge VM, et al., ed. Contrast agents inmagnetic resonance Imaging. Proceedings of an international workshop,
January 1986, San Diego, California. Amsterdam: Excerpts Medico,1986:136-140
18. Scoth G, Scialfa G, Colombo N, Landoni L. Magnetic resonance diagnosisof Intramedullary tumors of the spinal cord. Neuroradiology 1987;29:130-135
19. Fontaine 5, Melanson D, Cosgrove R, Bertrand G. Cavernous heman-giomas of the spinal cord: MR Imaging. Radiology i988;166:839-841
20. Scoth G, Scialfa G, Colombo N, Landoni L MR imaging of Intraduralextramedullary tumors of the cervical spine. J Comput Assist Tomogr
1985;9: 1037-104121 . Boisserie-Lacroix M, Klan P, CalVe JM. L’imagene des tumeurs intra-
durales et extra-medullaires: les neurinomes et les meningiomes. J Neu-roradioi 1987;14:66-81
22. Berry I, Brant-Zawadzki, Osaki L, Brasch AC, Murovic J, Newton TH. Gd-
DTPA in dinical MR imaging of the brain: 2. Extraaxial lesions and normal
structures. AJNR 1986;7:789-79323. Bydder G, Kingsley P, Brown J, Niendorf H, Young I. MR imaging of
meningiomas including studies with and without gadolinium-DTPA. J Corn-
put Assist Tornogr 1985;9:690-697
24. Sze G, Abramson A, Krol G, Zimmerman A, Deck MDF. Metastatic diseaseof the spine: MR evaluation with Gd-DTPA. Presented at the annualmeeting of the Radiological Society of North America, Chicago, Novem-bar 1987
25. Sze G, Abrarnson A, Krol G, et al. Gadolinium-OTPA in the evaluation ofleptorneningeal tumor spread in the spine. Presented at the annual meetingof the Society of Magnetic Resonance in Medicine, New York City,August 1987
26. Sze G, Abramson A, Krol G, et al. Gadolinium-DTPA in the evaluation ofmtradural extramedullary spinal disease. AJNR i988;9:153-163, AiR1988;150:91 1-921
27. Slasky BS, Bydder GM, NiendOrt HP, Young IA. MR imaging with gadolin-ium-DTPA in the differentiation of tumor, syrinx, and cyst of the spinal
cord.JCornputAssist Tornogr i987;11:845-85028. Slasky BS, Niendorf HP, Stelner RE, Bydder GM, Young IA. Does Gd-
DTPA help in separating tumor from syrinx or cyst in the spinal cord?
Presented at the annual meeting of the Radiological Society of NorthAmerica, Chicago, November 1987




























