Embed Size (px)
Citation preview

Annals of Human Biology, July–August 2010; 37(4): 536–553
ORIGINAL ARTICLE
Growth trends in body, fat, circumferential andphysiological traits during adolescence among Rajputfemales of Theog, Shimla District (Himachal Pradesh),India
INDU TALWAR, KRISHAN SHARMA & SAMTA KAPUR
Department of Anthropology, Punjab University, Chandigarh, India
(Received 21 April 2009; accepted 29 September 2009)
AbstractBackground: Information on growth status of a population is essential to establish the health status ofthe population and administer any health intervention programmes.Aims: The study aimed to examine growth patterns in body, fat and physiological traits duringadolescence in the light of various hypotheses and other studies.Subjects and methods: Cross-sectional data on a sample of 220 Rajput girls aged 11–17 years werecollected from Theog tehsil, Shimla District in Himachal Pradesh.Results: Mean body height and weight increased by 11% and 45.5%, respectively, from age 11 to17 years. The first marked growth in height took place between 11 and 12 years, while the maximumannual increment was witnessed between 13 and 14 years. ANOVA revealed significant differences inanthropometric traits between various adolescent age groups. Waist–hip ratio (WHR) decreased from0.77 at age 11 to 0.72 at age 17 years to attain gynoid pattern of body fat. Mean systolic and diastolicblood pressure increased from 106.92 and 66.48 mm Hg to 111.74 and 72.89 mm Hg, respectively.Conclusion: Although the girls in the present study did not suffer from any severe malnutrition, they hadlower dimensions than their Western counterparts when they entered the adolescence phase and alsolater on. In contrast to height deficits, increase in weight deficits was greater. There is no indication ofany compensatory or catch-up growth during adolescence. The present study does not support thehypothesis that lower nutritional stage during childhood affects the timing of adolescent take-off, age atpeak height and weight velocity. The data lend support to the hypothesis of saltatory patterns withintervening periods of stasis. BMI, %fat and FM were significantly correlated with diastolic bloodpressure but non-significantly correlated with systolic blood pressure.
Keywords: Adolescent growth, blood pressure, body fat, menarche
Correspondence: Prof. Indu Talwar, Department of Anthropology, Punjab University, Chandigarh 160014, India.E-mail: [email protected]
ISSN 0301-4460 print/ISSN 1464-5033 online � 2010 Informa UK Ltd.DOI: 10.3109/03014460903448040
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

Introduction
The beginning of biological growth and development during adolescence is signified by theonset of puberty, which is often defined as the physical transformation of a child into an adultand is marked by production of gonadal hormones that stimulate growth and maturation.Puberty, in fact, is a neuroendocrinological event controlling sexual maturation that occursbefore the start of the adolescent growth spurt. A number of biological changes occur duringpuberty, including sexual maturation, increases in height and weight, completion of skeletalgrowth accompanied by a marked increase in skeletal mass, and changes in body compo-sition. Although the succession of these events during puberty is consistent among adoles-cents, there can be a great deal of variation in the age of onset, duration, and tempo of theseevents between and within individuals and between and within populations. For this reason,adolescents of the same chronological age can vary greatly in physical appearance. Conse-quently, it has been recommended that sexual maturation should be used to assess the extentof biological growth and development and the individual nutritional needs of adolescents inplace of chronological age (Stang and Story 2005).
Weight and height measurements are often used in the literature to study adolescentgrowth (see Ulijaszek et al. 1998). Anthropometric indices are also used in the assessment ofnutritional status of adolescents including height-for-age, weight-for-age, body mass index(BMI)-for-age, and triceps and subscapular skinfold thicknesses-for-age. NCHS/WHOreference data (WHO 1983a) are used for this evaluation (Benefice et al. 2004; Jaswaland Jaswal 2005) although WHO has not explicitly recommended this for adolescents. Insome cases, local reference data may be required or other local factors must be considered.NCHS/WHO values are available up to 18 years of age for each sex. Cole et al. (2000, 2007)developed age- and sex-specific body mass index cut-offs to define thinness in children andadolescents from data derived from six countries (India not included) across severalcontinents. These charts extrapolate risks from adult experience to children. These cut-off points are recommended for use in international comparisons of prevalence ofoverweight and obesity. Studies on affluent Indian children have also been carried outto provide growth norms (Agarwal et al. 1992, 2001).
It is also necessary to examine changes in other physical dimensions especially in relationto spurt in height as stature growth has significance in the assessment of adolescent growth.The study of body composition gives an additional physiological dimension to classicalresearch of age changes during growth and development. It promotes further understandingof intra- and inter-group variability and plays an important role in applied research forassessing nutritional differences, or those connected with disease, physical activity and otherfactors influencing growth.
India is a vast country having about 5000 different breeding isolates living in diverseecological settings and thus providing a perfect study design for anthropological investiga-tions. A large body of data exists on population variations in growth patterns among Indianpopulations. These variations are determined by both genetic and environmental factors.Anthropometric measurements have been used to assess nutrition assessment, obesity andgrowth patterns. Singh (2008) has recently reviewed trends and perspectives ofanthropometric studies of growth based on Indian populations. A large number of studieson body fat patterning estimated by anthropometric traits, including skinfolds, have beencarried out on adolescent children belonging to different populations including those livingin the same geographical area of Northwest India, in the states of Punjab, Himachal Pradeshand Haryana and belonging to the middle socio-economic group and living in differentgeographical regions (Talwar and Kaur 1999; Talwar et al. 2001; Jaswal and Jaswal
Growth trends in adolescent females of Himachal Pradesh 537
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

2005; Talwar and Bajwa 2005; Sharma and Shandilya 2005; Sinha and Kapoor2005; Sharma and Aggarwal 2007; Singh and Gaur 2007 to quote some recent references).
Among several bioelectrical methods, bioelectrical impedance analysis (BIA) is a widelyused for measurement. It is based on differences in human body tissue resistance(impedance) to a small electrical current. The apparatus sends an extremely weakelectrical current through the hands, rather than the feet, to the body to determine theamount of body fat. This weak current is not perceptible by the subject when theinstrument is in operation. Adipose tissue has much higher resistance compared to thosetissues that contain a lot of water (extracellular fluid, blood, muscle, etc.) and comprisesthe major part of fat-free mass (Baumgartner 1996). The BIA technique is popular inanthropological studies as it is non-invasive and applicable for field research. It can beapplied technically to all subjects irrespective of their ethnicity, age, and sex and healthstatus. However, in practice, BIA studies of body composition in children are notnumerous due to methodological problems connected with the changing quantity ofwater in a growing organism, technical problems of placing electrodes on small hands andfeet, etc. (Baumgartner 1996).
Racial differences in body adiposity during adolescence are well documented (Kimm et al.2001). Garn and Haskell (1959) reported that lower thoracic fat, as measured on serial chestplates of 259 children in Ohio (USA), increased in girls, between ages 6.5 and 14.5 yearsand, in boys, between ages 6.5 and 11.5 years. No evidence for a marked loss of ‘baby’ fat inadolescence or for ‘waves’ of fattening around the time of puberty was found. Using the BIAmethod, Godina et al. (2007) studied fat mass (FM) and fat-free-mass (FFM) amongadolescent Russian children. They found high correlation between the two body compo-nents, which are supposed to have an independent variability. They also found that estimatesof fat components obtained by BIA and anthropometric methods were highly correlatedboth in boys and in girls: 0.85–0.88. They further reported, on the basis of multipleregression analysis between BIA estimates and anthropometric and functional traits, ahigher correlation in boys than in girls, with the exception of skinfolds, which possiblyreflected the importance of adipose tissue for the development of typical somatic character-istics in girls during puberty.
Variation in blood pressure has been the subject of extensive recent research because highblood pressure is a common risk factor for cardiovascular and renal disease (Kaplan andOpie 2006). Several factors such as, ethnicity, maturation, body size, obesity, genetic,endocrine and renal factors, physical activity, diet, noise, other social and psychologicalfactors are known to be related to blood pressure among children (WHO 1983b; Hohn et al.1994; Harshfield and Treiber 1999; Monyeki et al. 2005). Adolescence is an important lifestage in developing central body fat patterning among individuals that predisposes them tocoronary heart disease in their later lives (Kemper et al. 1999). Consequently, growthstudies are increasingly including blood pressure and other physiological traits to studychanges in these traits during childhood and adolescence (Talwar et al 2003; Rao et al.2005; Tripathy and Gupta 2007). Keeping these contemporary trends in mind, the presentgrowth study included anthropometric traits, estimation of body fat by BIA and otherphysiological traits following specific objectives: to report growth patterns in body, fat andphysiological traits during adolescence among Himalayan Rajput girls; to compare weightand height measurements of the present sample with those of affluent Indians, other samplesfrom the same area and NCHS values to study general nutritional adequacy; inter-traitcorrelation trends during adolescence; to determine the age at menarche and to test thevalidity of various known hypotheses on adolescent growth patterns reported on the basis ofother studies.
538 I. Talwar et al.
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

Material and methods
The present cross-sectional study is based on a sample of 220 Rajput girls aged 11–17 yearsbelonging to Theog tehsil of Shimla District in Himachal Pradesh. The data were collectedfrom four different schools of the Theog tehsil. Care was taken to include only those subjectswho were apparently healthy and normal. Dates of births of subjects were obtained frominstitutional records and cross checked with the students.
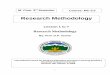
Theog tehsil extends from Kufri to Kandal 8 km short of Narkanda on National Highway,22 km from Khara Pathar of Shimla District, in the east of Summi sub-division onthe southern side of Shimla District. A location map of the study area is shownin Figure 1. The area is mountainous and the altitude varies from 915 to 2440 metresabove sea level. The temperature varies from –2�C to 29�C with an average rainfall of 140cm. The upper areas experience moderate to heavy snowfall during winter.
A total of 14 anthropometric measurements and two physiological parameters were takenfrom each subject. Anthropometric measurements included were: weight, stature, sevencircumferences (upper arm, wrist, waist, abdomen, hip, thigh and ankle) and five skinfoldsthickness (biceps, triceps, subscapular, suprailiac and medial calf).Various anthropometricinstruments used to take these measurements included Martin’s anthropometer for takingheight, spring balance for body weight, steel tape for taking circumferences and GPM-makeskinfold caliper to measure skinfolds. Mean skinfold refers to the average of the five aboveskinfolds. The physiological variables studied were blood pressure (systolic and diastolic) andpulse rate. Standard techniques recommended by Weiner and Lourie (1969) were employedfor taking various measurements. Abdomen circumference was measured at umbilical level.Waist circumference was measured midway between umbilicus and xiphoid. Thigh circum-ference was measured at gluteal fold. A mercury sphygmomanometer was used to measureblood pressure. All the measurements were taken on the left arm; subjects being in a seatedposition, with lower end of the arm resting on the table top. Subjects were asked to relax andrest for 10 min before the pressure measurements were taken. Systolic blood pressure (SBP)was recorded as the first Korotkov sound (phase I). Diastolic blood pressure (DBP) was takenas the disappearance of theKorotkov sounds (phaseV). Pulse ratewasmeasured by palpitatingthe radial artery at the wrist with the help of three middle fingers the number of beatsoccurring in half a minute and then doubled to obtain the rate per minute using a stop watch.Data on menarche status were calculated by the status quomethod. Since all the measurementswere taken by the same trained postgraduate student of anthropology, there were no inter-observer technical errors of measurement (TEM). Random checks were made to find outtechnical error of measurements. In all such checks, it was found to be less than 1%. Intra-observer error for stature was 0.3–1 cm. For body weight, it was between 0 and 0.5 kg; for girthmeasurements, values ranged from 0.1 to 0.3 cm; for skinfolds the range was between 0.5 and 1mm; for body fat error values ranged0.1–0.2; for bloodpressure values raged from1 to 5mmHg.
A body fat analyser (Omron HBF 302-Japanese Model) based on the bioelectricalimpedance method was used to calculate total body fat mass and % body fat. Derivedmeasures like body mass index (BMI = Body weight (kg)/Stature2 (m2)), waist–hip ratio(WHR) and appendicular to central circumference ratio (A/C = sum of upper arm, wrist,thigh and ankle circumferences/sum of hip, waist and abdomen circumferences) werecomputed from the anthropometric measurements for each individual. The whole yearmean annual increments were calculated by subtracting the mean of the preceding age groupfrom that of the succeeding group (Tanner 1962).
Socio-economic status (SES) of the subjects was measured in terms of the educationalattainment and occupation of their parents and this information was calculated through
Growth trends in adolescent females of Himachal Pradesh 539
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

interview schedule. Results of this analysis are given in Table I. Most of the parents of thesubjects were literate and had education through various levels: primary (9.6% fathers,30.5% mothers), high school (68.6% fathers and 56% mothers), and graduation/postgraduation (18.6% fathers and 4.5% mothers). Only 3.2% fathers and 8.6% mothers ofthe subjects were illiterate. The majority of the mothers (79%) were housewives. Fathers’major professions included farming (37.3%), service (32.3%) and business (16.9%). Theypredominantly belonged to the middle socio-economic group. No attempt was made to
Figure 1. Location of the Himachal Pradesh State in India and the study area in Shimla District.
540 I. Talwar et al.
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

exclude any subject on the basis of these parental attributes. The data so generated werestatistically analysed to obtain measures of central tendencies, dispersion and correlationcoefficient. Median age of menarche was calculated by probit analysis. One-way-analysis ofvariance (ANOVA) was performed for each variable to study to study age trends.
The staple diet of the subjects included wheat, rice, pulses, and seasonal vegetables. Themeals varied from two to three a day depending upon the distance between their residenceand school. On holidays, they took three meals a day. They took one glass of milk per daybesides seasonal fruits.
Results
Descriptive statistics of various anthropometric, bioelectric impedance analyses (BIA) of bodyfat and physiological traits are given in Table II. The mean body height increased by 11% from140.3 cm at age 11 to 155.7 cm at age 17 years. The maximum annual gain in stature occurredbetween 13+ and 14+ years, though first initial accelerated growth in height occurred between11+ to 12+ years. From 11 to 14 years, 8.6% increase in stature was noted and thereafter only2.2% increase was recorded from 14 to 17 years. The cut-off age between these two agecategories coincided with median age at menarche, which was 13.70 ± 0.92 years.
Growth trend for body weight was slightly different. Mean body weight increased from35.4 kg to 45.7 kg from 11 to 17 years and the total gain was 45.5% as compared to 11% forstature. The maximum mean annual gain took place around the median age of menarchebetween 13+ to 14+ years. The circumferential measurements also showed progressiveincrease in the mean value from 11 to 17 years. The maximum annual mean increment wasobserved between 13 and 14 years as for body weight.
The growth trend of various skinfolds of upper extremity was different from those for trunkand lower extremity. Mean biceps skinfold decreased from 11 to 14 years and there afterincreased with increase in age. Triceps, medial calf, suprailiac and subscapular skinfoldsincreased with increase in age except for an initial dip between 11 and 12 years in triceps andsubscapular skinfolds. Mean BMI, fat mass and % body fat values increased duringadolescence. The maximum mean annual increment occurred between 13 and 14 years.
Table I. Educational and occupational status of parents.
No. of fathers % of fathers No. of mothers % of mothers
Educational levelIlliterate 7 3.18 19 8.64Primary 21 9.55 67 30.45Matriculate 69 31.36 91 41.36Higher Secondary 82 37.27 33 15.00Graduate 17 7.73 6 2.73Postgraduate and above 24 10.90 4 1.82Occupational statusFarming 82 37.27 22 10.00Housewife – – 176 79.09Services 76 32.27 11 5.00Business 37 16.82 1 0.46Teacher 13 5.91 8 3.64Professional 6 2.73 1 0.46Army 6 2.73 – –
Head of village – – 1 0.46Any other 2 0.91% – –
Growth trends in adolescent females of Himachal Pradesh 541
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

Table II. Means, standard deviations (SD) and ANOVA of anthropometric measurements, indices, body fat andphysiological variables in adolescent girls.
Age in years (n)
Variable11 12 13 14 15 16 17 ANOVA(25) (34) (35) (37) (30) (32) (27) F-ratio
Absolute measurementsWeight (kg)Mean 31.44 35.65 35.86 41.70 43.47 45.38 45.70 30.9**SD 5.54 5.92 5.82 4.54 4.16 6.03 5.28
Stature (cm)Mean 140.31 146.01 146.59 152.39 153.46 155.18 155.72 24.71**SD 7.26 6.95 8.01 4.18 4.70 5.61 4.26
Circumferences (cm)WaistMean 55.87 58.30 57.48 60.37 59.31 61.25 61.71 7.09**SD 3.64 5.17 5.10 4.24 3.45 3.88 3.29
HipMean 72.59 75.99 76.76 82.03 81.88 85.83 86.01 22.68**SD 5.57 7.05 5.91 3.92 7.06 5.40 5.30
AbdomenMean 60.12 62.98 61.79 66.23 66.98 68.72 68.94 12.25**SD 4.58 6.43 5.54 5.41 4.49 5.32 5.33
Upper armMean 17.87 18.99 18.66 20.09 20.75 21.25 21 14.52**SD 1.79 1.88 1.48 1.79 1.45 1.85 2.60
WristMean 13.39 13.84 13.86 14.42 14.44 14.61 14.82 11.68**SD 0.86 0.87 0.83 0.52 0.67 0.95 0.81
ThighMean 42.67 44.72 47.24 48.22 49.25 51.36 51.97 11.01**SD 4.86 6.01 5.56 5.02 5.49 5.01 5.75
AnkleMean 18.54 19.11 18.54 19.42 19.66 20.38 20.24 4.90**SD 1.63 1.71 1.83 1.09 1.54 3.04 1.35
Skinfolds (mm)BicepsMean 4.75 4.63 4.53 4.27 4.75 5.50 6.36 5.24**SD 1.48 1.46 1.72 1.52 2.06 2.14 1.58
TricepsMean 8.62 8.01 8.63 8.66 8.83 10.09 10.90 6.31**SD 2.59 1.64 2.12 2.44 1.35 2.51 2.46
SubscapularMean 8.10 7.71 8.14 9.45 9.82 11.02 11.07 13.42**SD 2.41 1.76 1.82 2.05 1.63 2.30 2.75
Supra-iliacMean 7.69 7.87 8.53 9.33 9.05 10.03 10.11 4.33**SD 2.37 2.41 2.27 2.48 2.40 3.05 2.59
CalfMean 10.04 10.76 10.55 12.01 11.51 12.99 13.18 6.41**SD 2.15 2.29 2.02 3.42 2.59 2.87 2.36
Mean skinfoldMean 7.87 7.80 8.08 8.74 8.79 9.93 10.33 12.03**SD 1.56 1.43 1.37 1.55 1.11 2.11 1.83
542 I. Talwar et al.
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

The waist–hip-ratio (WHR) growth trend showed a typical female pattern as it decreasedwith increase in age during adolescence from 0.77 at age 11 to 0.72 at age 17 years to achievegynoid pattern of body fat. But mean A/C index showed no age trend during adolescence asit remained constant around the value of 0.50 through all seven age groups. Mean SBP andDBP values increased with increase in age. On the contrary, as expected, mean pulse ratedecreased with increase in age. Results of one-way analysis of variance performed on eachvariable (Table II) show that there were significant age differences for most of the variableschosen for the study. However non-significant age differences were noted for A/C ratio, SBPand DBP as their F-ratios were not significant.
Table III shows the results of analysis of correlation coefficient between different traits.Body weight and stature showed significant positive correlations with each other through allage groups. Body weight was significantly correlated with BMI, mean skinfold and body fatthrough all age groups. Body fat was also very significantly associated with BMI. Fat masswas significantly negatively correlated with pulse rate. WHR was insignificantly correlatedwith about 36% of variables mainly including SBP and DBP, some skinfolds, % fat mass andA/C ratio. Pulse rate was poorly correlated with most of the anthropometric traits exceptwith BMI, %fat and FM with which it had significant negative correlation. SBP was
Table II (Continued)
Age in years (n)
Variable11 12 13 14 15 16 17 ANOVA(25) (34) (35) (37) (30) (32) (27) F-ratio
Body mass index (kg/m2)Mean 15.86 16.63 16.62 17.93 18.44 18.79 18.83 14.26**SD 1.62 1.91 1.88 1.57 1.26 1.81 1.85
Bioelectric impedance assessment (BIA)Fat mass (kg)Mean 5.28 6.87 6.64 8.77 10.19 10.90 9.36 23.83**SD 2.64 2.83 2.54 2.22 2.49 2.84 2.60
% Body fatMean 15.80 18.43 17.86 21.01 23.05 23.18 20.78 13.88**SD 5.20 4.77 4.79 3.35 3.40 3.23 4.08
Physiological variablesBlood pressure (BP)Systolic BPMean 106.92 106.44 109.20 109.22 110.53 111.16 111.74 1.15SD 7.34 8.05 8.94 9.51 9.46 10.80 16.46
Diastolic BPMean 66.48 72.37 74.15 70.57 71.23 71.06 72.89 1.75SD 10.10 9.18 8.60 11.46 7.66 9.56 10.69
Pulse rate (PR)Mean 86.32 82.35 79.29 78.49 73.40 80.88 81.74 3.51**SD 8.23 10.12 9.13 11.14 14.01 14.37 10.63
Other body indicesWaist hip ratio (WHR)Mean 0.77 0.77 0.75 0.74 0.73 0.71 0.72 7.80**SD 0.05 0.04 0.04 0.04 0.07 0.03 0.03
A/C ratioMean 0.45 0.49 0.50 0.49 0.50 0.50 0.50 1.20SD 0.03 0.02 0.03 0.03 0.04 0.03 0.03
**P < 0.01.
Growth trends in adolescent females of Himachal Pradesh 543
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

Table III. Age-wise and total correlation coefficient (r) between variables.
Age (years)
Variables 11 12 13 14 15 16 17 Total
Weight vs stature 0.833** 0.738** 0.709** 0.608** 0.696** 0.681** 0.508** 0.820**Weight vs BMI 0.859** 0.862** 0.761** 0.863** 0.639** 0.690** 0.885** 0.856**Weight vs WHR –0.120 –0.160 0.091 0.061 –0.089 –0.056 –0.282 –0.323**Weight vs mean skinfold 0.556** 0.591** 0.610** 0.430* 0.381* 0.517** 0.515** 0.635**Weight vs % fat –0.031 0.592** 0.664** 0.729** 0.331 0.596** 0.709** 0.665**Weight vs fat mass 0.114 0.409* 0.822** 0.874** 0.870** 0.740** 0.747** 0.791**Weight vs SBP 0.045 0.430* 0.355* –0.001 –0.028 0.287 –0.018 0.221**Weight vs DBP 0.246 0.296 0.270 0.220 –0.002 0.050 0.390* 0.193**Weight vs pulse rate –0.328 –0.218 0.200 –0.194 0.052 –0.080 –0.073 –0.160*Stature vs BMI 0.437* 0.299 0.089 0.127 –0.106 0.033 0.051 0.431**Stature vs WHR 0.047 –0.234 –0.236 –0.242 –0.095 –0.104 –0.292 –0.360**Stature vs mean skinfold 0.503* 0.258 0.250 0.482** 0.211 0.047 –0.074 0.429**Stature vs % fat 0.009 0.372* 0.033 0.177 0.144 0.024 0.026 0.398**Stature vs fat mass 0.202 0.336 0.259 0.413* 0.443* 0.279 0.092 0.562**Stature vs SBP 0.115 0.333 0.167 0.266 0.079 0.015 0.168 0.212**Stature vs DBP 0.289 0.127 0.127 0.272 0.213 0.005 0.327 0.181**Stature vs pulse rate –0.226 –0.230 0.348* 0.001 0.230 0.084 –0.130 –0.078BMI vs WHR –0.220 –0.045 0.371** 0.225 –0.029 0.180 –0.176 –0.181*BMI vs mean skinfold 0.418 0.643** 0.651** 0.221 0.316 0.703** 0.644** 0.641**BMI vs % fat –0.041 0.587** 0.926** 0.799** 0.311 0.787** 0.802** 0.719**BMI vs fat mass –0.003 0.353* 0.924** 0.826** 0.720** 0.793** 0.825** 0.759**WHR vs mean skinfold 0.099 –0.086 0.080 –0.159 0.182 0.148 –0.112 –0.180**WHR vs % fat 0.101 –0.034 0.371* 0.165 0.154 0.047 –0.145 –0.118WHR vs fat mass 0.230 –0.012 0.234 0.160 –0.051 0.163 –0.095 –0.200**SBP vs DBP 0.675** 0.597** 0.383* 0.328* 0.153 0.236 0.376 0.358**SBP vs pulse rate –0.263 –0.060 0.081 –0.005 –0.090 0.159 –0.195 –0.056SBP vs BMI –0.057 0.349* 0.349* –0.158 –0.111 0.361* –0.105 0.171*SBP vs WHR –0.214 0.075 0.295 0.187 0.092 –0.038 –0.435 –0.074SBP vs mean skinfold 0.352 0.112 0.322 0.117 –0.145 0.182 –0.237 0.137*SBP vs % fat 0.087 0.319 0.223 –0.043 –0.109 0.184 –0.138 0.129SBP vs fat mass 0.029 0.322 0.263 –0.028 –0.086 0.250 –0.112 0.162*DBP vs pulse rate –0.412 –0.294 0.041 –0.091 0.420* –0.329 –0.236 –0.127DBP vs BMI 0.113 0.308 0.268 0.117 –0.236 0.092 0.286 0.158*DBP vs WHR –0.212 0.236 0.115 0.243 0.188 0.041 –0.495 0.028DBP vs mean skinfold 0.612** 0.342* 0.045 0.023 –0.009 0.113 0.164 0.159*DBP vs % fat 0.238 0.389* 0.280 0.184 –0.034 0.135 0.059 0.191**DBP vs fat mass 0.277 0.319 0..284 0.185 0.084 0.125 0.176 0.189**Pulse rate vs BMI –0.337 –0.136 –0.055 –0.242 –0.167 –0.224 –0.019 –0.208**Pulse rate vs WHR 0.181 –0.271 –0.324 0.008 0.234 0.033 0.277 0.093Pulse rate vs mean skinfold –0.158 –0.079 0.052 0.021 –0.067 –0.021 0.174 –0.025Pulse rate vs % Fat –0.374 –0.063 –0.065 –0.190 0.043 –0.229 0.000 –0.194**Pulse rate vs fat mass –0.085 –0.215 0.015 –0.165 –0.027 –0.200 –0.006 –0.197**Mean skinfold vs % fat 0.049 0.225 0.674** 0.291 0.336 0.671** 0.584** 0.475**Mean skinfold vs fat mass 0.249 0.247 0.686** 0.415* 0.380* 0.695** 0.519** 0.560**AC ratio vs SBP 0.388 –0.077 0.007 –0.151 0.230 0.267 0.122 0.114AC ratio vs DBP 0.382 0.173 0.025 0.060 0.050 0.016 0.066 0.098AC ratio vs BMI 0.374 0.144 –0.146 –0.330* 0.094 0.253 0.098 0.060AC ratio vs WHR –0.204 0.013 –0.137 –0.338* 0.632** –0.040 –0.330 0.008AC ratio vs pulse rate 0.165 0.120 –0.135 –0.128 0.271 0.072 –0.229 0.165AC ratio vs mean skinfold 0.374 0.120 0.201 0.258 0.138 0.315 0.115 0.208**AC ratio vs % fat –0.161 –0.006 –0.182 –0.293 0.188 0.227 –0.015 –0.004AC ratio vs fat mass –0.163 –0.162 –0.219 –0.286 0.077 0.253 –0.019 –0.001
*p< 0.05, **<0.01.
544 I. Talwar et al.
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

significantly but weakly correlated with a number of anthropometric traits; while for DBPcorrelations in pooled age groups ranged from 0.17 to 0.21 in significantly correlated traits.Blood pressure was insignificantly correlated with PR, WHR and A/C ratio.
The above correlation analysis results revealed significant association between bloodpressure and some body traits. To rule out the possibility that age might be a common causeof variation between them resulting in inflated correlation values, partial correlation(partial r) analysis was done by keeping age as a constant variable and results are presentedin Table IV. Both SBP and DBP were significantly correlated with BMI, FM and % fat in thetotal pooled data and ranged from 0.13 to 0.19. But after partial correlation analysis,significant change was noticed in SBP’s correlation values with BMI, FM and % fat; theirvalues decreased from 0.17, 0.13 and 0.16 to 0.09, 0.06 and 0.08, respectively, changingsignificant associations into non-significant ones suggesting that age was the common causebehind the correlation between SBP and BMI, % fat and fat mass. But no such results wereobserved for DBP although partial r values slightly decreased to 0.13, 0.17, and 0.17 from0.16, 0.19, and 0.17, respectively but remained statistically significant.
Discussion
As growth during adolescence contributes significantly to the attainment of final adult size ofan individual, the investigation of patterns of linear growth during adolescence is essential.
Table IV. Partial correlations along with their significance levels (p) and degree of freedom (d.f.) by keeping age as acontrol variable.
Variable Weight Stature SBP DBP BMI % fat FM
WeightR 1.000 0.693 0.144 0.186 0.827 0.540 0.661p – 0.000 0.034 0.006 0.000 0.000 0.000d.f. 0 216 216 216 216 216 216
StatureR 0.693 1.000 0.135 0.165 0.181 0.158 0.310p 0.000 – 0.046 0.014 0.007 0.020 0.000d.f. 216 0 216 216 216 216 216
SBPR 0.144 0.135 1.000 0.349 0.094 0.056 0.075p 0.034 0.046 – 0.000 0.166 0.408 0.269d.f. 216 216 0 216 216 216 216
DBPR 0.186 0.165 0.349 1.000 0.134 0.171 0.173p 0.006 0.014 0.000 – 0.047 0.012 0.011d.f. 216 216 216 0 216 216 216
BMIR 0.827 0.181 0.094 0.134 1.000 0.631 0.655p 0.000 0.007 0.166 0.047 – 0.000 0.000d.f. 216 216 216 216 0 216 216
% fatR 0.540 0.158 0.056 0.171 0.631 1.000 0.800p 0.000 0.020 0.408 0.012 0.000 – 0.000d.f. 216 216 216 216 216 0 216
Fat mass (FM)R 0.661 0.310 0.075 0.173 0.655 0.800 1.000p 0.000 0.000 0.269 0.011 0.000 0.000 –
d.f. 216 216 216 216 216 216 0
Growth trends in adolescent females of Himachal Pradesh 545
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

In the present sample, the adolescence phase from age 11 to 17 years contributed 11%increase in height and 45% increase in body weight. It has been believed that adolescenceprovides a second opportunity for growth as it facilitates catch-up growth for childrenexperiencing nutritional deficits in their early life. A key question that has been asked is towhat extent a growth-retarded child catches-up. Two contradictory view points have beenforwarded. Tanner (1989) opined that the undernourished child would slow down and waitfor better times. But it is generally observed that a child usually remains in the environmentwhich led to stunting. Consequently, there is no improvement in growth status.However, Adair (1999) has described catch-up between 2 and 12 years of age in Filipinochildren staying in the same environment and stunting of early years was reduced during thelater catch-up growth. On the contrary, Martorell et al. (1994) hold the view that stuntingarises from events early in life, and once present it remains for life.
It is commonly believed that children from developing countries have lower body weightand stature when compared with their Western counterparts. Pawloski (2002) reported thatMalian girls from the Segou Region are shorter and lighter than their US female counter-parts and these delays in growth are due to poor nutrient intakes and high-energyexpenditures. Pawloski et al. (2004) have reported delayed growth and development amongNicaraguan girls at most ages. Similarly people in poor communities from India havecharacteristically low body weights and substandard stature. Agarwal et al. (1987) found45–90% Indian children to be undernourished. Nearly one-third of neonates born in Indiahave low birth weight (ICMR 2003) and a large percentage of them are small for gestationalage (SGA). These preterm small for gestational age children have been found to be shorter,lighter and have the smallest head circumference (Chaudhari et al. 2008). Children bornsmall for gestational age have a seven fold increased risk of growth failure (Karlberg et al.1995) and their final height is said to contribute to 20% of the short adult population.
Genetic and/or environmental factors are believed to underlie the above differences in sizeattainments between children from Western and developing countries. Before jumping toany conclusion, it may be appropriate to compare the growth status of the present samplewith affluent Indian data (Agarwal et al. 1992) to see if nutritional factors had any impact onthe growth status of adolescent girls of the present study or not. The comparison of heightand weight data through different age groups has been done in Table IV. Girls of the presentsample did have lower mean values for height and weight than the affluent Indian girls. Butthe differences were statistically significant in two of seven age groups for height. For bodyweight, differences were significant in five of seven age groups, i.e. from 12 through 16 years.From this it can be concluded that stature is less affected than body weight by differences insocio-economic factors. In Table V, another comparison has been made with Rajput girlsliving in the same state and belonging to same socio-economic status, but living at slightlylower altitude in the District of Solan (Talwar et al. 2003). In comparison to Solan Rajputgirls, the girls of the present study had higher mean stature and weight; the differencesbetween the two samples were statistically significant in four age groups for stature and innone for body weight.
After ascertaining that there was some evidence of nutritional inadequacy in the presentsample, their height and weight data are compared with NCHS data to further explore theseaspects (WHO 1983a) given in Table V. As compared to NCHS reference data, mean statureof the present sample was deficient by about 2.69% (near the 30th centile) at age 11 and thisdeficiency increased to 4.82% (near 15th centile) at age 17 years. In contrast to deficiency instature, body weight deficiency was higher and increased further from childhood to adult-hood. Mean body weight was 14.1% lower (20th centile) at age 11 and 19.3% lower (near the7th centile) at age 17 years. To express these results another way, 70% of 11-year-old US girls
546 I. Talwar et al.
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

are taller and 80% of them are heavier than average Theog Rajput girls of the same age. At age17, the percentage of taller and heavier US girls rises to 85% and 93%. Similar trends are alsofound in other populations of the world (see Norgan 2002). As per WHO (1983a) recom-mendations, Theog Rajput girls of the present study, on average, were not severelymalnourished on the basis of their mean values as WHO (1983a) recommended cut-offpoint of –2 SD (< 3rd centile) for malnourished children. Hence on the basis of the above
Table V. Comparison of stature and body weight of the present study with affluent Indian and Rajput girls of thesame state.
Age (years)
Variables 11 12 13 14 15 16 17
StaturePresent study (PS)n 25 34 35 37 30 32 27Mean 140.31 146.04 146.59 152.39 153.46 155.80 155.72SD 7.26 6.95 8.01 4.18 4.70 5.61 4.26
Affluent Indian (AI)n 503 435 455 391 291 176 116Mean 141.30 146.70 151.40 153.60 155.0 155.10 157.10SD 7.16 6.66 5.96 5.73 5.62 5.03 5.91
Solan Rajput girls (SR)n 25 25 25 25 25 25 25Mean 137.71 139.39 146.20 149.38 153.80 152.30 152.70SD 7.93 11.21 7.08 6.09 3.65 4.69 4.55
Comparison of meanst-test values:PS vs AI 0.67 0.55 3.53* 1.25 1.44 –0.08 2.97*PS vs SR 1.18 2.74* 0.15 2.24* –0.28 3.74* 2.43*
WeightPresent study (PS)n 25 34 35 37 30 32 27Mean 31.44 35.65 35.86 41.70 43.41 45.38 45.70SD 5.55 5.92 5.82 4.54 4.16 6.03 4.28
Affluent Indian (AI)n 503 435 455 391 291 176 116Mean 34.30 38.70 42.60 45.70 48.0 49.20 49.0SD 8.06 8.54 8.52 8.88 9.19 9.12 7.74
Solan Rajput girls (SR)n 25 25 25 25 25 25 25Mean 28.96 33.06 34.10 40.14 41.32 43.60 44.52SD 6.09 6.61 6.40 4.92 4.43 3.86 4.01
Comparison of meanst-test values:AI vs PS 1.75 2.05* 4.58* 2.70* 2.63* 2.27* 0.21PS vs SR 1.47 1.55 1.72 1.26 1.82 1.26 0.88
NCHS StandardsStature50th 144.2 151.5 157.1 160.4 161.8 162.4 163.6–1 SD 137.3 144.7 150.5 153.7 155.0 155.7 157.5
Weight50th 36.6 41.5 46.1 50.3 53.7 55.8 56.6–1 SD 30.4 34.5 38.4 42.3 45.5 47.7 48.9
*P <0.05.
Growth trends in adolescent females of Himachal Pradesh 547
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

results, Theog Rajput girls, as a population, cannot be described as suffering from stuntedgrowth and wasting when they entered adolescence. This conclusion is further strengthenedwhen height and weight data of affluent Indian children, who did not ever suffer from any foodinadequacy, were compared with NCHS data (see Table V). The results were really verycurious, intriguing and interesting as even affluent Indian children (Agarwal et al. 1992) hadstature near 30th centile and weight near 20th centile in all adolescent age groups. So it isunlikely that the large divergence observed between Indian adolescent girls andUS girls couldbe simply attributed to nutritional inadequacies. On the contrary, Bhandari et al. (2002) are ofthe opinion that that growth performance of affluent Indian children is similar to that indeveloped countries.
The growth studies reveal that growth during adolescence is less affected by environ-mental factors than growth during the previous stages and is said to be more under geneticcontrol. Growth studies of Indian and Kenyan children have shown that catch-up growthduring adolescence compensates growth disruption during childhood that had occurred dueto nutritional inadequacy (Little et al. 1983; Satyanaryana et al. 1989). If this hypothesis isuniversally true, then the compensatory or catch-up growth during adolescence among thegirls of the present study should have also compensated deficiencies in growth that occurredduring an earlier stage due to nutritional inadequacy. Contrary to the above reports, no suchcompensatory growth took place in the present study sample. On the contrary, in these6 years, the increase in height and weight during adolescence was 100% lower than theirWestern counterparts. This further slowing of growth during adolescence may be referred toas growth faltering without any sign of catch-up growth, assuming no differences betweenaffluent Indian children and those of developed countries as per observations of Bhandariet al. (2002). In a recent report on Thai girls, Pawloski et al. (2008) found them to be heavierthan the reference girls at ages 11–13 years but in later age groups of 14–17 years found themto be shorter and lighter. To explain the results of the present study, it can be argued that thelifestyle on hills required a lot of walking, which resulted in higher energy expenditure, andhence the exhibited growth faltering trend during adolescence might be a local adaptation tothose particular environments pressures to have a body type that would require lower energyexpenditure. It has been argued that a slowing of growth is a healthy adaptation to a habitatwith limited resources (Seckler 1980). It may be interesting to study such patterns in otherpopulations living at higher altitudes than plains from the developing countries.
Another question that can be raised here is whether lower nutritional stage duringchildhood also affects the timing of adolescent take-off; age at peak height and weightvelocity and the amount of annual gain at the maximum adolescent increment. Biologicalmaturation also varies in timing and tempo in each individual. On average Western girls gainapproximately 8.3 kg per year during peak rates of weight gain at 12.5 years of age (Barnes1975; Wong et al. 1995). In the present study, the maximum annual increment in bodyweight was of 5.8 kg and occurred between 13 and 14 years of age. The reported averageweight gain during adolescence among Western females is 17.5 kg (Barnes 1975; Wong et al.1995) as compared to 14.26 kg in the present study from 11 to 17 years. On the contrary,Satyanarayana et al. (1989) have shown that growth increments of Indian children between5 and 18 years may match Western children.
Regarding age at peak-height velocity (PHV), though the first marked growth in height inthe present sample took place between 11 and 12 years, yet maximum annual increment waswitnessed between 13 and 14 years. Incidentally the median age at menarche in the presentsample was 13.7 years. Growth studies have shown that most girls reach peak heightvelocity when their breasts are in stage 3 and before the start of menstruation (Marshalland Tanner 1986). Menarche is considered to be a marker of physiological maturity in
548 I. Talwar et al.
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

female adolescents. In the present sample, the age at PHV as well as the median age atmenarche is later than many European and Indian studies. Median age at menarche in Baniagirls of Mandi Gobindgarh, Punjab has been reported as 12.88 years (Talwar and Kaur1999). Sharma and Sharma (2005) reported median age of menarche among Punjabi ruraland urban girls as 12.06 years and 12.74 years, respectively. Sharma (1990) reviewed Indianstudies on age at menarche prior to 1990 and concluded that populations living at higheraltitude had later menarcheal age than populations living at lower altitude. Median age atmenarche among Rajput girls of Solan District in Himachal Pradesh was found to be13.00 years by Talwar and Bajwa (2005). Mokha et al. (2006) reported an earlier mean ageat menarche among urban Punjabi Jat Sikh girls (13.31 years) than rural girls (13.62 years)from Ludhiana. Sharma and Shandilya (2005) reported 13.40 years as the median age ofmenarche in an under privileged community of Scheduled Caste girls from Naraingarh,Haryana. As compared to all these studies, the menarcheal age in the present sample ofNorth Indian girls from Himalayas was found to be relatively late at an age of 13.7 years.However Dakshyani et al. (2007) found 13.93 ± 1.6 years as mean age of menarche amongIrulinga tribal girls of Karnataka in South India, which was even later than the presentsample.
The most extensive data summary of the reported age at menarche in populations aroundthe world based on the status quo method and probit analysis is provided by Eveleth andTanner (1990). About 60% of the median ages at menarche range between 12.50 and13.49 years. PHV in European females takes place between 12 and 13 years; and menarcheoccurs on an average a little more than a year after PHV between 13 and 14 years (see Malina1978). A similar trend has been reported among adolescent scheduled castes girls fromNaraingarh (Haryana) who belonged to relatively under-privileged communities of North-west India (Sharma and Shandilya 2005). In some countries, the age of menarche differswidely between social groups (see Marshall and Tanner 1986). However, in Europe, thegeographical variation in mean menarcheal age could not be explained on the basis of socio-economic factors alone, as a tendency was observed for menarche to occur later in countrieswith a high per capita gross domestic product (GDP) than countries with low GDP and viceversa (Danker-Hopfe 1986).
Due to the above peculiarities of the growth status of the present sample and to test theuniversality of some known hypotheses, it was considered necessary to compare and discussthe present study growth trends with other reported studies. Khond tribal children fromSouth-East Indian States of Orissa and Andhra Pradesh are known to suffer from rampantpoor nutrition during childhood. Khond girls have been reported to be shorter and lighterwith broader head and chest circumferences than ICMR (1989) standards and much shorterand lighter than Western standards and thus having dimensions lower than the presentsample. The adolescent growth spurt among Khond girls in stature and in circumferencessuch as head, chest, abdominal, upper arm, calf and in skinfolds such as suprailiac,abdominal and forearm have been observed to be attained between 9+ and 10+ yearsand 2 years later for bodyweight and skinfolds such as triceps, biceps and subscapular, i.e. 12+ and 13+ years (Rao et al. 2005). This means that PHV in Khond adolescent femalesoccurred about 1 year earlier than their Western counterparts in whom PHV is observedbetween 11 and 12 years (see Malina 1978). So the hypothesis that lower nutritional stageduring childhood affects the timing of adolescent take-off, age at peak height and weightvelocity and ultimately their final attained height and weight is not consistently true in allpopulations.
The characteristic growth spurts during adolescence may show saltatory patterns withintervening periods of stasis (Lampl et al. 1992). Though these temporal characteristics of
Growth trends in adolescent females of Himachal Pradesh 549
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

saltation and stasis patterns of growth are difficult to study by methods of moving averages ina cross-sectional study, yet the present series of data do give an indication of its presence.These saltation episodes reflect as interaction between cell-intrinsic information and centralneural signals mediated by endocrine, paracrine and cytocrine cascades (Lampl 2002). Inthe present study, the first marked spurt occurred between 11 and 12 years followed by aperiod of stasis. The next age group, i.e. 13–14, witnessed the maximum increment ofsomatic growth. The age of onset of puberty in the present sample seems to lie between 10and 11 years, resulting in the first spurt between 11 and 12 years.
Following the two component model of body composition the body is divided into the fatmass (FM) and fat-free mass (FFM) components, such that body mass is equal to the sum ofthese two components. It has been observed that body composition changes significantlyamong females during puberty due to rapid increase in FM that results in decrease in therelative proportion of FFM. In the present study, the relative contribution of average FFMto total body mass in females fell from 83.2% at age 11–76% at age 16 years; while averagecontribution of FM levels increased from 16% to 23% during the same duration. Femalesexperienced a 46.7% increase in body fat during this age span. On average, in the presentstudy females acquired approximately 0.94 kg of body fat mass as compared with 1.14 kg peryear in Western females (Frisch 1983) during puberty. The accretion of body fat mass is anormal phenomenon during adolescence, physiologically an essential process. The totalincrease in body fat mass from 11 to 16 years in the present study was 100%. Pawloski et al.(2008) found on the basis of BMI that Thai adolescent girls were thinner after menarchethan before, but no such trend was seen in the present sample. The findings of Sinha andKapoor (2005) and Talwar et al. (2005) were also compatible with our results as theyreported consistent increase in different skinfold measures with increase in age amongadolescent girls from Northwest India.
In the present cross-sectional sample (average altitude of about 2000 m), there is, as usual,an increase in blood pressure with increase in age and these values are similar to thosereported by Tripathy and Gupta (2007) for Tibetan adolescent girls living at a low-altitude(1000 m). At lower altitude, SBP and DBP among Tibetan girls increased from 105.26 and64.20 at age 10–11 years to 109.84 and 70.55, respectively, while at higher altitude (3000 m)these values increased from 98 and 55.56 to 104.75 and 61.17, respectively. From theseresults it can be concluded that blood pressure values among Theog adolescent Rajput girlsof the present study were comparable to those of the populations living on plains or at loweraltitude. There are many contradictory reports in the literature on these aspects. There arereports indicating that both SBP and DBP are lower in the populations living at higheraltitude than those at the lower altitude (Clegg et al. 1976; Frisancho 1979; Hanna 1999).A few other studies showed just the opposite relationship, that is, high-altitude residentsshowing higher blood pressure (Ethiopia: Harrison et al. 1969 and Clegg et al. 1976; Tibetanin comparison to Han: Sun 1986).
The results of the present study reveal a weak association between blood pressure andBMI, skinfolds and fat mass among the adolescent girls. Partial r value between SBP and fatmeasures was insignificant when age factor was kept constant. However DBP was signif-icantly but weakly associated with fat measures in the present study. Our results arecompatible with Stallones et al. (1982) who also reported a weak association betweencentral fat patterning and SBP in 13- to 17-year-old white females. Contrary to the aboveresults, Tripathy and Gupta (2007) have found that measures of adiposity includingskinfolds, BMI, and weight are strongly correlation with blood pressure among Tibetanchildren, adolescents, and adults. A significant association of blood pressure has also beenfound with fat-pattern ratios in girls showing signs of early menarche by van Lenthe et al.
550 I. Talwar et al.
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

(1996). These contradictory results indicate that a large number of local environmental and/or biological factors including ethnicity, food habits, physiology, altitude, activity along withmany others may be responsible for these variable results as both genetic and environmentalfactors are known to contribute to individual differences in ambulatory blood pressurepatterns.
Conclusions
The study shows slowing of growth during adolescence when compared with NCHSreference data, and no catch-up or compensatory growth was seen during period. Thisgrowth slowing can not be attributed to nutritional factors, as well nourished Indianchildren have also shown a similar trend. From ages 11 to 16 years, the relative contributionof FFM decreased while that of FM increased. The growth spurt during adolescence showedsaltatory patterns with intervening periods of stasis. Lower nutritional status during child-hood does not seem to affect the timing of adolescent take-off, age at peak height and weightvelocity. SBP was insignificantly correlated with FM, while DBP was significantly thoughweakly correlated with fat mass.
Declaration of interest: The authors report no conflicts of interest. The authors alone areresponsible for the content and writing of the paper.
References
Adair LS. 1999. Filipino children exhibit catch up growth from age 2 to 12 years. J Nutr 129:1140–1148.Agarwal DK, Agarwal KN, Upadhyay SK, Mittal R, Prakash R, Rai S. 1992. Physical and sexual growth pattern of
affluent children from 5 to 18 years of age. Indian Paediatr 29:1203–1283.Agarwal DK, Upadhyay SK, Tripathy AM, Agarwal KN. 1987. Nutritional status, physical work capacity and
mental function in school children. New Delhi: Nutritional Foundation of India. Scientific Reports 6:1–4.Agarwal KN, Saxena A, Bansal AK, Agarwal DK. 2001. Physical growth assessment in adolescence. Indian Pediatr
38:1217–1235.Barnes HV. 1975. Physical growth and development during puberty. Med Clinics N America 59:1305–1317.Baumgartner RN. 1996. Electrical impedance and total body electrical conductivity. In: Roche AF, Heymsfield SB,
Lohman TG, editors. Human body composition. Human Kinetics, Champaign, IL, pp. 79–108.Benefice E, Garnier D, Ndiaye G. 2004. Nutritional status, growth and sleep habits among Senegalese adolescent
girls. Eur J Clin Nutr 58:292–301.Bhandari N, Bahl R, Taneja S, de Onis M, Bhan MK. 2002. Growth performance of affluent Indian children is
similar to that in developed countries. Bull World Health Organ 80:189–195.Chaudhari S, Otiv M, Hoge M, Pandit A, Mote A. 2008. Growth and sexual maturation of low birth weight infants
at early adolescence. Indian Pediatr 45:191–198.Clegg EJ, Jeffries DL, Harrison GA. 1976. Determinants of blood pressure at high and low altitudes in Ethiopia.
Proc R Soc London B 194:63–81.Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. 2000. Establishing a standard definition for child overweight and
obesity worldwide: International survey. BMJ 320:1240–1243.Cole TJ, Flegal KM, Nicholls D, Jackson AA. 2007. Body mass index cut offs to define thinness in children and
adolescents: International survey. BMJ 335:194–201.Danker-Hopfe H. 1986. Menarcheal age in Europe. Yearbook Phys Anthropol 29:81–112.Dakshyani B, Satish CM, Gangadhar MR. 2007. Menarche and menopause among the Iruliga tribal girls.
Anthropologist 9:255–256.Eveleth PB, Tanner JM. 1990. Worldwide variation in human growth. Cambridge: Cambridge University Press,
pp. 222–240.Frisancho AR. 1979. Human adaptation: A functional interpretation. Saint Louis, MO: Mosby.Frisch RE. 1983. Fatness, puberty and fertility: The effects of nutrition and physical training on menarche and
ovulation. In: Brooks-Gunn J, Peterson AC, editors. Girls at puberty: Biological and psychosocial perspectives.New York: Plenum, pp. 29–49.
Growth trends in adolescent females of Himachal Pradesh 551
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

Garn SM, Haskell JA. 1959. Fat and growth during childhood. Science 130:1711–1712.Godina E, Khomyakova I, Purundzhan A, Zadorozhnaya L. 2007. Some differences in body composition in
Moscow adolescent children according to the level of their physical activity: comparison of anthropometric andbioelectrical impedance methods of assessment. In: Singh SP, Gaur R, editors. Human body composition.Human Ecology Special Issue No. 15:63–74.
Hanna JM. 1999. Climate, altitude, and blood pressure. Hum Biol 71:553–582.Harrison GA, Kuchemann CF, Moore MAS, Boyce AJ, Baju T, Mourant AE, Godber MJ, Glasgow BG, Kopec
AC, Tills D, et al. 1969. The effects of altitudinal variation in Ethiopian populations. Phil Trans R Soc Lond B256:147–182.
Harshfield GA, Treiber FA. 1999. Racial differences in ambulatory blood pressure monitoring-derived 24 h patternsof blood pressure in adolescents. Blood Press Monitor 4:107–110.
Hohn AR, Dwyer MK, Dwyer JH. 1994. Blood pressure in youth from four ethnic groups: The PasadenaPrevention Project. J Pediatr 125:368–373.
ICMR. 1989. Growth and physical development of Indian infants and children. Technical Report series no. 18.New Delhi: ICMR.
ICMR. 2003. National Neonatal–Perinatal Database NNPD Network. 2002–2003: 25. New Delhi: Indian Councilof Med Research.
Jaswal IJS, Jaswal S. 2005. Physical growth and nutritional status of rural children of Western Sub-HimalayanRegion. Indian J Phys Anthrop Hum Genet 24:123–134.
Kaplan NM, Opie LH. 2006. Controversies in hypertension. Lancet 367:168–176.Karlberg J, Albertsson-Wikland K. 1995. Growth in full term small for gestational age infants: From birth to final
height. Pediatr Res 38:733–739.Kemper HC, Post GB, Twisk JW, van Mechelen W. 1999. Lifestyle and obesity in adolescence and young
adulthood: results from the Amsterdam Growth and Health Longitudinal Study (AGAHLS). Int J Obes RelatMetab Disord 23 (Suppl): S34–S40.
Kimm SYS, Barton BA, Obarzanek E, McMahon RP, Sabry ZI, WaclawiwMA, Schreiber GB, Morrison JA, SimiloS, Daniels SR. 2001. Racial divergence in adiposity during adolescence: the NHLBI growth and health study.Pediatrics 107. Available at: http://www.pediatrics.org/cgi/content/full/107/3/e34.
Lampl M. 2002. Saltation and stasis. In: Cameron N, editor. Human growth and development. Amsterdam:Academic Press.
Lampl M, Veldhuis JD, Johnson ML. 1992. Saltation and stasis. A model of human growth. Science 158:801–803.Little MA, Galvin K, Mugambi M. 1983. Cross-sectional growth of nomadic Turkana pastoralists. Hum Biol
55:811–830.Malina RM. 1978. Adolescent growth and maturation; selected aspects of current research. Yearbook Phys
Anthropol 21:63–95.Marshall WH, Tanner JM. 1986. Puberty. In Falkner F, Tanner JM (eds): Human Growth, vol. 2. New York,
Plenum Press, pp. 171–203.Martorell R., Kettel KL, Schroeder DG. 1994. Reversibility of stunting: epidemiological findings in children from
developing countries. Eur J Clin Nutr 48 (Suppl 1): S45–S57.Mokha R, Anuradha IK, Kaur N. 2006. Age at menarche in urban–rural Punjabi Jat Sikh girls. Anthropologist
8:207–209.Monyeki KD, Kemper HCG, Makgae PJ. 2005. The association of fat patterning with blood pressure in rural
South African children: the Ellisras Longitudinal Growth and Health Study. Int J Epidemiol 35:114–120.Norgan NG. 2002. Nutrition and growth. In Cameron N, editor. Human growth and development. Amsterdam:
Academic Press, pp. 139–164.Pawloski LR. 2002. The growth and development of adolescent girls from the Segou Region of Mali (West Africa).
Am J Phys Anthropol 117:364–372.Pawloski LR, Moore JB, Lumbi L, Rodriguez CP. 2004. A cross-sectional analysis of growth indicators from
Nicaraguan adolescent girls: A comparison of anthropometric data from their Guatemalan counterparts. AnnHum Biol 31:647–659.
Pawloski LR, Ruchiwit M, Pakapong Y. 2008. A cross-sectional examination of growth indicators from Thaiadolescent girls: Evidence of obesity among Thai youth. Ann Hum Biol 35:378–385.
Rao VLN, Rao BD, Rao CS, Busi BR. 2005. Patterns of growth and physiological variables among Khond tribalpopulation of Visakhapatnam District, Andhra Pradesh. Anthropologist 7:237–245.
Satyanaryana K, Radhaiah G, Murlimohan KR, Thimmayamma BVS, Pralhad Rao N, Narsinga Rao BS, Akleta S.1989. The adolescent growth spurt of height among rural Indian boys in relation to childhood nutritionalbackground; an 18 year longitudinal study. Ann Hum Biol. 16:289–300.
Seckler D. 1980. ‘Malnutrition’, an intellectual Odyssey. Western J Agricult Econ 5:219–227.
552 I. Talwar et al.
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.

Singh R. 2008. Trends and perspectives of anthropometrical research: Some methodological illustrations. In PrasadA, Mukherjee R, Ekka BA, editors. Social research methodologies in action, volume 1. Conceptual andTheoretical Concerns in Social Research. Ranchi: Xavier Institute of Social Service, pp. 207–227.
Singh SP, Gaur R. (editors). 2007. Human body composition. Human Ecology Special Issue No. 15. Delhi: KamlaRaj Enterprises, 117 pp.
Sharma K. 1990. Age at menarche in Northwest Indian females and a review of Indian data. Ann Hum Biol17:159–162.
Sharma K, Sharma P. 2005. Adolescent girth trends in urban and rural Punjabi girls from Gurdaspur. South AsianAnthropol 5:209–216.
Sharma K, Shandilya S. 2005. Growth patterns of human pelvis and body traits, menarcheal status, menstrualpatterns and nutritional status of adolescent scheduled castes girls from Naraingarh (Haryana). Indian J PhysAnthropol Hum Genet 24:153–168.
Sharma K, Aggarwal R. 2007. Patterns of body and abdominal adiposity growth in relation to menarche status inurban and rural Punjabi adolescent females. In: Sharma K, Pathak RK, Mehta S, Talwar I (eds) Genes,environment and health: anthropological perspectives. New Delhi: Serials Publications, pp. 105–114.
Sinha R, Kapoor S. 2005. Fat patterning among Indian adolescent boys and girls. Indian J Phys Anthropol HumGenet 24:135–141.
Stallones L, Mueller WH, Christensen BL. 1982. Blood pressure, fatness, and fat patterning among USAadolescents from two ethnic groups. Hypertension 4:483–486.
Stang J, Story M.2005. Adolescent growth and development. In: Stang J, Story M, editors. Guidelines forAdolescent Nutrition Services. Center for Leadership, Education and Training in Maternal and ChildNutrition. Division of Epidemiology and Community Health, School of Public Health, University ofMinnesta, MN, 63, pp. 1–8. http://www.epi.umn.edu/let/pubs/adol_book.shtm.
Sun SF. 1986. Epidemiology of hypertension on the Tibetan Plateau. Hum Biol 58:507–515.Talwar I, Kaur M. 1999. Growth pattern and age at menache in Bania girls of Mandi Govindgarh. Anthropologist
1:145–178.Talwar I. 2001. Fatness and fat patterning among Jat adolescent females. In: Bhasin MK, Malik SL, editors. The
science of man in service of man. Delhi: Department of Anthropology, University of Delhi, pp. 103–108.Talwar I, Bajwa P, Kaur P. 2003. Age changes in physiological variables and their relationship with anthropometric
traits among Rajput boys and girls. In Kalla AK, Bhattacharya DK, editors. Understanding people of India:Anthropological insight. Delhi: Department of Anthropology, University of Delhi, pp. 132–142.
Talwar I, Bajwa P. 2005. Age at menarche in relation to body size and physiological variables among Rajput girls.Punjab. University Res J (Science), 55:1–5.
Talwar I, Vasudha, Bajwa P. 2005. Fatness and regional distribution of body fat among adolescent Brahmin girls.Indian J Phys Anthrop Hum Genet 24:143–151.
Tanner JM. 1962. Growth at adolescence, 2nd edn. London: Oxford Blackwell Scientific.Tanner JM. 1989. Foetus into man. Physical growth from conception to maturity. Cambridge, MA: Harvard
University Press.Tripathy V, Gupta R. 2007. Blood pressure variation among Tibetans at different altitudes. Ann Hum Biol
34:470–483.Ulijaszek SJ, Johnston FE, Preece MA. 1998. The Cambridge encyclopedia of Human growth and development.
Cambridge: Cambridge University Press. pp. 497.van Lenthe FJ, Kemper HCG, van Mechelen W, Twisk, JWR. 1996. Biological maturation and the distribution of
subcutaneous fat from adolescence into adulthood: the Amsterdam Growth and Health Study. Int J ObesityRelated Metab Disord 20:121–129.
Weiner JS, Lourie JA. 1969. Human biology: A guide to field methods. Oxford: Blackwell.Wong DL, Wilson D, Whaley LF. 1995. Whaley & Wong’s nursing care of infants and children, 5th ed. St Louis,
MO: Mosby.WHO. 1983a. Measuring change in nutritional status. Geneva: World Health Organization.WHO. 1983b. Blood pressure studies in children. Geneva: World Health Organization, pp. 5–37.
Growth trends in adolescent females of Himachal Pradesh 553
Ann
Hum
Bio
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
IBI
Cir
cula
tion
- A
shle
y Pu
blic
atio
ns L
td o
n 08
/02/
10Fo
r pe
rson
al u
se o
nly.